This article was downloaded by: [King's College London] On: 09 June 2012, At: 08:48 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Counselling and Psychotherapy Research: Linking research with practice Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/rcpr20 Women counsellors' experiences of personal therapy: A thematic analysis Karen Ciclitira a , Fiona Starr a , Lisa Marzano b , Nicola Brunswick a & Ana Costa c a Middlesex University, Psychology, Hendon b University of Oxford, Department of Psychiatry, Warneford Hospital, Oxford c Maudsley Hospital, Centre for Anxiety Disorders and Trauma, London, UK Available online: 06 Jan 2012 To cite this article: Karen Ciclitira, Fiona Starr, Lisa Marzano, Nicola Brunswick & Ana Costa (2012): Women counsellors' experiences of personal therapy: A thematic analysis, Counselling and Psychotherapy Research: Linking research with practice, 12:2, 136-145 To link to this article: http://dx.doi.org/10.1080/14733145.2011.645050 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This article was downloaded by: [King's College London]On: 09 June 2012, At: 08:48Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Counselling and Psychotherapy Research: Linking
research with practicePublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/rcpr20
Women counsellors' experiences of personal therapy:
A thematic analysis
Karen Ciclitira a , Fiona Starr a , Lisa Marzano b , Nicola Brunswick a & Ana Costa ca Middlesex University, Psychology, Hendonb University of Oxford, Department of Psychiatry, Warneford Hospital, Oxfordc Maudsley Hospital, Centre for Anxiety Disorders and Trauma, London, UK
Available online: 06 Jan 2012
To cite this article: Karen Ciclitira, Fiona Starr, Lisa Marzano, Nicola Brunswick & Ana Costa (2012): Women counsellors'experiences of personal therapy: A thematic analysis, Counselling and Psychotherapy Research: Linking research withpractice, 12:2, 136-145
To link to this article: http://dx.doi.org/10.1080/14733145.2011.645050
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form toanyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses shouldbe independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims,proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly inconnection with or arising out of the use of this material.

Women counsellors’ experiences of personal therapy: A thematicanalysis
KAREN CICLITIRA1*, FIONA STARR1, LISA MARZANO2, NICOLA BRUNSWICK1, &
ANA COSTA3
1Middlesex University, Psychology, Hendon, 2University of Oxford, Department of Psychiatry, Warneford Hospital, Oxford,
and 3Maudsley Hospital, Centre for Anxiety Disorders and Trauma, London, UK
AbstractBackground: Following recent moves to relax the requirements for clinical mental health trainees to undergo personaltherapy, this qualitative project explored the effects of personal therapy on volunteer counsellors. Method: Interviews wereconducted with 19 volunteer counsellors at a women’s community centre, and the data were analysed using thematicanalysis. Findings: Emerging themes included the importance of personal therapy for trainee development, key elements ofpersonal therapy and the idea that personal therapy is ‘a double-edged sword’. Discussion: Allowing for evidentmethodological difficulties in evaluating the impact of personal therapy on trainees, this study suggests that closeconsideration should be given to the potentially adverse effects of reducing requirements for personal therapy in clinicaltrainings.
Keywords: personal therapy; qualitative research; volunteer; counsellors; thematic analysis
Introduction
Personal therapy is generally perceived as an invalu-
able component in the training of psychotherapists,
counselling psychologists and counsellors. Research
conducted over the past four decades shows that
most clinicians consider it indispensable to their
personal lives (Mahoney, 1997; Stevanovic &
Rupert, 2004) and professional development
(Buckley, Karasu, & Charles, 1981; Pope & Tabach-
nick, 1994; Williams, Coyle, & Lyons, 1999).
Historically, psychotherapists were expected to be
sufficiently aware of their own difficulties to prevent
them from adversely affecting their clinical work
(Macaskill, 1988).
Research into clinicians’ use of personal therapy in
Britain and elsewhere is extensive (e.g. Atkinson,
2006; Rizq & Target, 2008). In a US study, 85% of
727 mental health workers cited personal reasons for
seeking therapy, only 5% identified training as their
main reason for seeking therapy, and over 90%
reported positive outcomes from therapy (Bike,
Norcross, & Schatz, 2009). In a study of 4000
therapists from 14 countries, personal therapy was
consistently ranked among the top three positive
influences on professional development, along with
direct experience with clients and formal case super-
vision (Orlinsky, Botermans, & Rønnestad, 2001).
Psychologists in Britain and America report learn-
ing lasting lessons from their own therapy, including
better understanding of the importance of empathy,
transference and countertransference, and the need
for patience (Norcross, Dryden, & DeMichele,
1992; Norcross, Strausser-Kirtland, & Missar,
1988). Clinicians’ therapeutic experiences were felt
to validate the supposition that change is possible,
and to help them develop their clinical techniques
through modelling the good and bad practice of their
therapists (Grimmer & Tribe, 2001).
In six studies involving more than 1400 American
and nearly 1000 British clinicians, over 90%
reported experiencing considerable personal im-
provement, and over 75% strong professional devel-
opment as therapists: they experienced improvements
in self-esteem,work functioning, social life, emotional
expression, characterological conflicts, and symptom
*Corresponding author. Email: [email protected]
Counselling and Psychotherapy Research, June 2012; 12(2): 136!145
ISSN 1473-3145 print/1746-1405 online # 2012 British Association for Counselling and Psychotherapy
http://dx.doi.org/10.1080/14733145.2011.645050
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

severity (Orlinsky, Norcross, Rønnestad, &Wiseman,
2005).
Should all clinicians have personal therapy?
A minority of clinicians have negative experiences of
personal therapy in training. These include the
discomfort of attending therapy, the difficulties of
receiving therapy from their teachers, undergoing
types of therapy inappropriate to their needs, and
experiencing poor or harmful therapy. Some report
stress due to the constraints on time or money that
personal therapy entails (McEwan & Duncan,
1993). Other studies have found a small negative
effect on client outcomes (see Bike et al., 2009).
While personal therapy used to be generally
considered a prerequisite for clinical work, therapists
who do not undergo personal therapy often claim to
have ways of dealing with stress and to be able to
resolve their problems independently. The impor-
tance of personal therapy varies according to theo-
retical orientation; behavioural and cognitive
therapists are less likely to enter therapy than
therapists from other theoretical orientations (Bike
et al., 2009), and it may be that personal therapy is
more congruent with some therapeutic trainings
than others (Atkinson, 2006).
Personal therapy requirements for UK clinicians
The British Association for Counselling and Psy-
chotherapy’s (BACP) requirement for a minimum of
40 hours of personal therapy for newly accredited
members was waived in 2005; but the Division of
Counselling Psychology still requires chartered
counselling psychologists to have completed 40
hours of personal therapy during training, on the
grounds that interpersonal skills and the use of the
self are important for the therapeutic process
(Grimmer & Tribe, 2001). Regulatory requirements
for counsellors and psychotherapists in the UK are
changing. The government has announced that the
Council for Healthcare Regulatory Excellence will
be the new regulatory body. It seems likely that
requirements for personal therapy will continue to
depend on individual clinical trainings.
Impact of therapy on clinical practice
The impact of personal therapy on clinical outcomes
is difficult to measure. Personal therapy is only one
factor that may affect a therapist’s professional
development and potential to affect clients’ out-
comes. Other factors, including clients’ resources
and the vicissitudes of the therapeutic relationship,
make it difficult to conceptualise how one could
reliably determine the specific impact of a therapist’s
personal therapy on clients’ outcomes (Orlinsky
et al., 2005).
Research into the impact of personal therapy on
clinical practice has examined therapists’ own eva-
luation of personal therapy (Wiseman & Shefler,
2001) and measured client outcomes (Macran &
Shapiro, 1998). Experimental outcome studies have
examined therapists’ responses to analogous ther-
apeutic situations (McDevitt, 1987; Strupp, 1955,
1973), and process studies have examined within-
session client-therapist interactions (Wheeler, 1991).
Qualitative methods continue to offer a useful
alternative to explore therapists’ own therapy, and
this study aims to explore the views and experiences
of counsellors from diverse orientations working in
the voluntary sector.
Method
Research was carried out at a community health
centre which provides a range of low-cost treatments
for women ! including low-fee therapy, once a week
for up to two years ! in the South East of England.
Female volunteer counsellors from diverse theoreti-
cal orientations provide long-term counselling at the
Centre. Approximately half of these counsellors
require the practice hours for their training require-
ments; others work at the centre post-qualification.
This service differs from most National Health
Service (NHS) mental health services, which gen-
erally offer only short-term cognitive behavioural
therapy (CBT) in a medical setting (Cooper, 2008).
This article focuses on research with the service-
providers (i.e. the counsellors).
Design
This study sought to explore counsellors’ views and
experiences using a qualitative approach, since this is
capable of providing a rich and complex under-
standing of data (Braun & Clarke, 2006). Thematic
analysis was chosen as being compatible with a
constructionist paradigm, whereby meaning is
viewed as co-created by interviewer and participant.
The value of qualitative methodologies for exploring
the meanings of therapeutic change is recognised
as being particularly appropriate when research
Women counsellors’ experiences of personal therapy 137
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

questions are concerned with understanding pro-
cesses rather than outcomes (Rubin & Rubin, 1995;
Smith, 1996). This study was designed to address
desiderata for qualitative research outlined by
McLeod (2006) and Stiles (1993):
(1) Clarity and comprehensiveness, by giving suffi-
cient procedural detail.
(2) Adequacy of conceptualisation of data, by
acknowledging the provisional and open-ended
nature of the analysis.
(3) Credibility of researchers, through acknowled-
ging power differentials, and the researchers
meeting to consider difficulties and differences
throughout the research process.
(4) Sufficient contextualisation, by carrying out a
comprehensive literature review which enabled
the research to be historically and socially
located.
(5) Systematic consideration of competing inter-
pretations of data: the five researchers, with
differing views about the benefits of personal
therapy, systematically analysed the data indi-
vidually, in pairs, and again as a team.
(6) Experiential authenticity of the material, by
reporting participants’ rich and verbatim ac-
counts, offering participants copies of their
transcripts and asking two participants to com-
ment on the authenticity of the final draft. All
participants will have access to academic arti-
cles and reports resulting from this research.
Methodology
This study used qualitative methods to explore the
impact of personal therapy on clinical trainees. Most
research to date has not considered the role of
therapy in counsellors’ training, and relatively few
studies have used qualitative methods. One recent
study considered the impact of compulsory personal
therapy on counsellors’ personal and professional
development (van Haenisch, 2010).
Interview schedule
A semi-structured interview schedule was designed
following the biographical-interpretive approach of
Hollway and Jefferson (2000). Participants were
asked about the theoretical orientation of their
personal therapy and their clinical training, their
experience of long-term therapy, and how their own
therapy had impacted on their clinical practice.
Participants
Forty counsellors had worked at the Centre for more
than six months, and 19 of them volunteered to
participate. Their ages ranged from 32!63 years, and
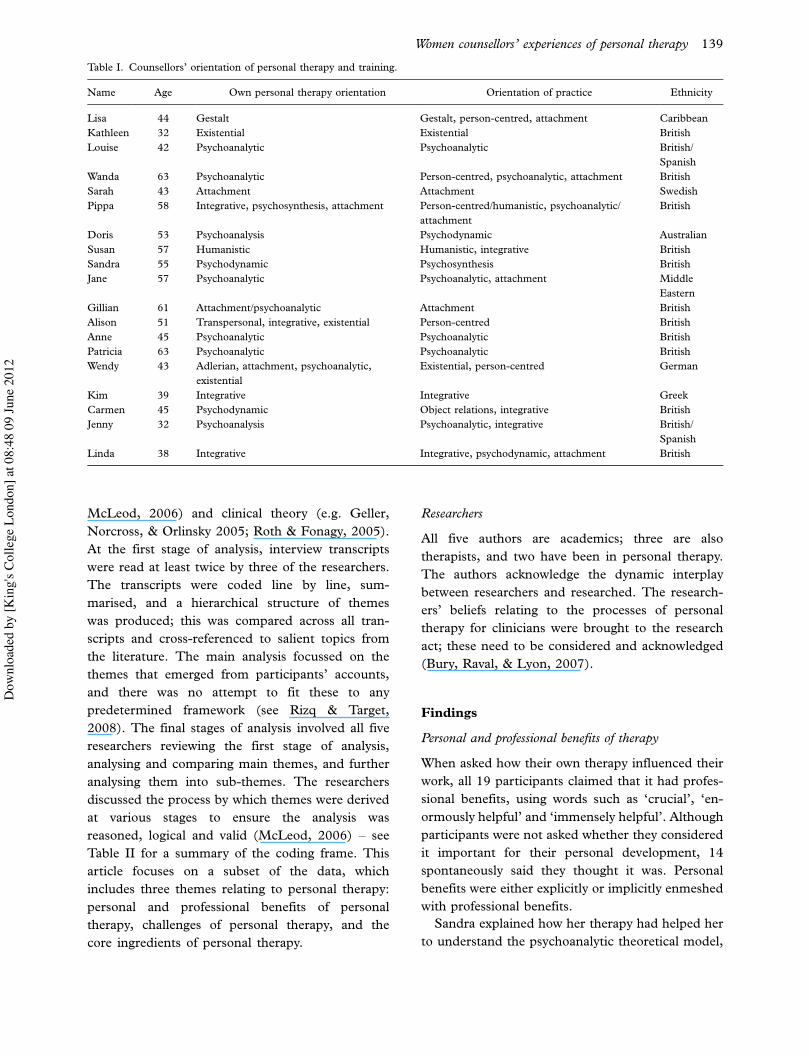
their theoretical orientations varied (see Table I). All
19 had been in personal therapy between one and
three times, and the frequency per week varied
between one and five times. Length of time spent
in therapy ranged from 3!21 years (mean"4.7
years). When interviewed, 12 of the participants
were undergoing personal therapy, and six of these
were in training. These women worked as unpaid
volunteers; nine had an income of less than £25,000
per annum, and four earned less than £10,000.
In order to work as a volunteer at the Centre, all
trainee counsellors are required to be in weekly
therapy, and all (including those who are qualified)
must attend clinical supervision with one of the
Centre’s four low-fee supervisors. As the participants
were all working as counsellors, a distinction was not
made between psychotherapists, counsellors, and
counselling psychologists; all are referred to here as
‘counsellors’.
Ethics
Participants gave signed consent to participate, and
for anonymised extracts of interviews to be pub-
lished. Participants’ pseudonyms have been provided
for the purpose of citing excerpts from their inter-
views. A university ethics committee gave ethical
approval for this study.
Data collection
One-to-one interviews were carried out by three
of the researchers. These interviews were
audio-recorded and took between 33 and 73 min-
utes. Interviews were transcribed verbatim, with
words underlined to indicate vocal emphasis by
participants. All participants were offered the op-
portunity to amend their transcripts; three requested
to read their transcripts and one made minor
amendments. At the end of each interview, partici-
pants were asked what they thought about the
research project and about their experiences of the
research process.
Analysis
The main theoretical influences on the analysis
were qualitative theory (Braun & Clarke, 2006;
138 K. Ciclitira et al.
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2
McLeod, 2006) and clinical theory (e.g. Geller,
Norcross, & Orlinsky 2005; Roth & Fonagy, 2005).
At the first stage of analysis, interview transcripts
were read at least twice by three of the researchers.
The transcripts were coded line by line, sum-
marised, and a hierarchical structure of themes
was produced; this was compared across all tran-
scripts and cross-referenced to salient topics from
the literature. The main analysis focussed on the
themes that emerged from participants’ accounts,
and there was no attempt to fit these to any
predetermined framework (see Rizq & Target,
2008). The final stages of analysis involved all five
researchers reviewing the first stage of analysis,
analysing and comparing main themes, and further
analysing them into sub-themes. The researchers
discussed the process by which themes were derived
at various stages to ensure the analysis was
reasoned, logical and valid (McLeod, 2006) ! see
Table II for a summary of the coding frame. This
article focuses on a subset of the data, which
includes three themes relating to personal therapy:
personal and professional benefits of personal
therapy, challenges of personal therapy, and the
core ingredients of personal therapy.
Researchers
All five authors are academics; three are also
therapists, and two have been in personal therapy.
The authors acknowledge the dynamic interplay
between researchers and researched. The research-
ers’ beliefs relating to the processes of personal
therapy for clinicians were brought to the research
act; these need to be considered and acknowledged
(Bury, Raval, & Lyon, 2007).
Findings
Personal and professional benefits of therapy
When asked how their own therapy influenced their
work, all 19 participants claimed that it had profes-
sional benefits, using words such as ‘crucial’, ‘en-
ormously helpful’ and ‘immensely helpful’. Although
participants were not asked whether they considered
it important for their personal development, 14
spontaneously said they thought it was. Personal
benefits were either explicitly or implicitly enmeshed
with professional benefits.
Sandra explained how her therapy had helped her
to understand the psychoanalytic theoretical model,
Table I. Counsellors’ orientation of personal therapy and training.
Name Age Own personal therapy orientation Orientation of practice Ethnicity
Lisa 44 Gestalt Gestalt, person-centred, attachment Caribbean
Kathleen 32 Existential Existential British
Louise 42 Psychoanalytic Psychoanalytic British/
Spanish
Wanda 63 Psychoanalytic Person-centred, psychoanalytic, attachment British
Sarah 43 Attachment Attachment Swedish
Pippa 58 Integrative, psychosynthesis, attachment Person-centred/humanistic, psychoanalytic/
attachment
British
Doris 53 Psychoanalysis Psychodynamic Australian
Susan 57 Humanistic Humanistic, integrative British
Sandra 55 Psychodynamic Psychosynthesis British
Jane 57 Psychoanalytic Psychoanalytic, attachment Middle
Eastern
Gillian 61 Attachment/psychoanalytic Attachment British
Alison 51 Transpersonal, integrative, existential Person-centred British
Anne 45 Psychoanalytic Psychoanalytic British
Patricia 63 Psychoanalytic Psychoanalytic British
Wendy 43 Adlerian, attachment, psychoanalytic,
existential
Existential, person-centred German
Kim 39 Integrative Integrative Greek
Carmen 45 Psychodynamic Object relations, integrative British
Jenny 32 Psychoanalysis Psychoanalytic, integrative British/
Spanish
Linda 38 Integrative Integrative, psychodynamic, attachment British
Women counsellors’ experiences of personal therapy 139
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

and had allowed her to separate her own issues from
those of her clients:
I had the space of the therapy and the supervision
to do the work of separating out what was mine
and what was the client’s . . .My personal issues
were resonating with my client’s issues . . . It helpedme theoretically, it helped me in my learning as
well. It was helping me personally, but it was also
helping me understand the model as well and how
to be a therapist.
Patricia claimed that the influence of her therapy was
‘immense’:
It’s absolutely to do with the separation that has to
happen . . . I’m either taking responsibility for
something which isn’t mine which is going to
paralyse me, or I’m giving somebody else respon-
sibility for my own stuff which is going to paralyse
them.
Alison said how she thought personal therapy should
be mandatory for all clinical trainees:
It is absolutely crucial . . . It’s absolutely essential
that I deal with all my stuff in order to be able to
accompany my clients, partly so they don’t trigger
stuff off in me . . . I need to be able to learn how to
put all my stuff back. So it is absolutely crucial and
I can’t understand about the BACP saying that
trainee therapists don’t have to do it, it is
completely nuts.
Jenny described how her personal therapy helped her
to listen and think:
If this room were me, and I piled it full of rubbish,
the more I clear out the more space there is in
there, and the more space that I have the better
the capacity to think about what’s going on with
my clients . . .Those little moments when your
mind just drifts just for a couple of seconds and
you think ‘Oh god what was it they just said that
was so, I don’t want to hear that bit, I don’t want
to go to that place in myself.’ So the clearer my
space is the more I can do, the more I can listen,
the more I can help people.
Linda thought her own therapy enabled her to be
more emotionally resilient in her clinical work:
Having been in therapy, and confronted and
worked through some extremely traumatic and
difficult things means that I know they are
survivable. And so I am less likely to shut a client
down or flee from their own sense of chaos,
disaster, collapse whatever.
Carmen discussed how her training, supervision,
and personal therapy all contributed to her develop-
ing her own style:
Table II. A summary of the coding frame.
Main themes Sub-themes Sub-themes
1. Personal and professional
benefits of therapy
Personal benefits Working through personal issues ! separation of the personal from the
professional
Emotional resilience
Personal journey
Professional benefits Applying theory to practice
Therapist as role model
Mandatory therapy ! issues and tensions
The ‘art’ of therapy
2. The challenges of personal Boundaries and difficulties Learning from therapists’ practice ! positive and negative
therapy Boundaries ! benefits and limitations
Constraints ! financial and time
Double-edged sword of therapy ! disturbance, pain, rewards and
endings
3. The core ingredients of
therapy
Therapeutic relationship,
orientation and skills
Therapeutic relationships: learning through relating ! unconscious
processes, therapeutic change and empathy
Learning aspects of theory and skills through live observation
How it feels to be a client
140 K. Ciclitira et al.
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

It feels a little bit like when you learn to drive, and
your driving instructor has all these fixed things
like ‘mirror-signal-manoeuvre’, but then once
you’ve actually been driving for long enough you
do it your own way. You’ve worked out your own
style.
Some participants were emphatic about the impor-
tance of personal therapy. Doris noted:
I don’t think the training would have been nearly
as successful without the therapy . . . I can see what
analysis has done and the way it has totally
revolutionised my life.
One of the centre’s counselling co-ordinators em-
phasised the importance of personal therapy for
trainees:
What I’ve come to realise over time is that a key
factor in whether . . . they’re going to be a good
counsellor or not, is actually the amount of sort of
personal work they’ve done.
The challenges of personal therapy: boundaries and
difficulties
Five participants reported negative experiences such
as not getting on with their therapist, finding their
therapist unprofessional, or finding the process
frustrating. These experiences were, however, re-
ported as an aid to learning even when they were
anti-therapeutic, as Sarah’s comments indicate:
I think that she is arh very rigid, and not actually
very relational at all . . .Until I say, ‘Yes, you are
right, I am like that’, we’re not moving anywhere.
And since I’m not prepared to do that, so I think
she’s partly wrong at least . . . It’s one of those
times where you kind of learn from the negative
you know, so I’m being very wary of not being like
she is when I am the therapist . . . It’s all learning,it’s not pleasant in any kind of way but it is
teaching me I think good things.
Sarah also raised the challenges posed by personal
therapy being a training requirement as it could
make it difficult to change therapists:
Fingers crossed . . .The course has to make a
decision . . . as far as I understand; I will be given
the permission to, to finish.
Some therapists were thought to be ‘too rigid’, and
others too open about their personal lives. Pippa
raised the importance of boundaries in relation to
her new therapist:
She is very professional; she is a good role model
for me, because I’ve started supervising now. She
is very, very boundaried, and I had a very
unboundaried therapist for seven years, and I
knew so much about her.
Wendy had a more critical perspective about ther-
apeutic boundaries and the setting, having been a
client herself:
There’s one problem with counselling, which I
guess always happens with anything that becomes
institutionalised, regulated and all those
things . . . I can say all kinds of things and I could
cry or I could, you know but certain things I can’t
do. Like I can’t just take my clothes off or dance
around the room, or go into his kitchen and get a
bottle of beer, or even have a cigarette in the
session . . . certain things are just not possible and
however much we say ‘oh this is a space for you,
you can say anything’ it’s not true at all and it’s
very, very limited in what can happen, for good
reasons.
Undergoing personal therapy can create financial
strain and time constraints, particularly for unpaid
female volunteers who are also caregivers. Carmen
said:
I’m going twice a week and I find it a terrible
chore . . . I look after X (disabled child) for 40
hours a week, as well as these three placements. So
I think it’s the squeezing it in late in the evening
when you’re tired . . . It’s hugely useful and I
wouldn’t be without it, and I think it would be
unsafe to work without it.
Wendy noted being pleased to take a break from
therapy for financial reasons:
I had six months of no therapy, and I just couldn’t
get it together to sort it out and it seemed really
nice not to have to go, save some money.
Alison considered her therapy difficult but reward-
ing:
Women counsellors’ experiences of personal therapy 141
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

It is very, very challenging, well I find it very
challenging. We’re doing very, very good work.
Sandra described her therapeutic ‘journey’ as painful
but also useful:
I really felt that I had done this kind of a journey
and I had gone into what I needed to go into, my
life’s journey and looked at things and then come
out again . . .The intense pain and agony, and then
I came back up into the adult place again.
Jenny was finishing six years of therapy and dis-
cussed how experiencing her own personal challenge
of ending long-term therapy was a learning experi-
ence:
We spent a long time working towards an ending,
and actually that in and of itself, at the time,
wasn’t something particularly I wanted to do. But
I realised in the end it was something that was
quite important for me. It was just a big part of my
process, it’s not my favourite thing, ending.
The core ingredients of therapy: therapeutic relationship,
orientation and skills
Participants described learning about the core in-
gredients of therapy from their own therapists. Jane
discussed how her own therapy had enhanced her
understanding about relating and change:
My experience with my therapist allowed me to
see how I do relationships, and allowed me to
understand how we can project, how we can
assume and how change is possible when that is
thought about together and understood.
Wendy was doing an existential training, and
described the different ingredients required for a
beneficial therapeutic experience: the therapist’s
personality, openness, theoretical orientation, ther-
apeutic skills, and techniques. Her new therapist
was existential like herself, and she felt was better
able to help her explore difficulties than was her
previous psychoanalytic therapist. She noted:
It’s really good, I am really happy. It is much
more disturbing and intense than the other one
(previous therapist). I think it was partly to do
with her, as well, not maybe just the relation-
ship, but it felt like I was telling her about
something which has already happened . . . I
always had the sense that she had a certain view
about what is a healthy way to live or what is a
good way to be, or how I should end up after
successful therapy.
Other participants talked about the educational
benefits of having had more than one clinician, and
one of a different theoretical orientation. Carmen
said:
I like the variety of having . . .different insights
from each of the counsellors that I have seen.
Sandra argued that trainee clinicians should experi-
ence the same orientation of therapy and also
undertake sessions of the same frequency as that
offered to their clients:
I can’t imagine being a therapist without having
the experience of being in therapy. I think you
must have the experience of the type of therapy
you are going into. What I’m saying is if you do
weekly then you must have weekly, if you do
fortnightly or twice a week or whatever. I think
you have to actually experience that.
Being a client allowed participants to observe what
kinds of interventions seemed more or less helpful.
Lisa explained:
I find myself observing her and being . . .counselled by her at the same time, to see how
she, she deals with me and reacts to me. And
sometimes I find myself just asking things to see
what she says . . .Because she’s Gestalt as well.
And I’m supposed to be Gestalt too.
Wendy thought it was important for her clinical work
to have had the experience of being a client:
If you are just the therapist and you never have the
client’s role, it’s quite easy not to realise the basic
little things that can be awkward or difficult for the
clients.
She went on to describe how a particular experience
had affected her own responses to clients:
And he’s (therapist) just sitting there watching me
settling down and it felt really uncomfortable. I’ve
got a couple of clients who always apologise for
that and I, until it happened to me, I . . .didn’tunderstand why you know what are they saying.
142 K. Ciclitira et al.
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

Why don’t they just take their time? I’m quite
happy to sit there, but it’s because I was watching
them and um just things like that. Just to know
what it’s like to be in that role of silence.
Discussion
All 19 participants believed that their personal
therapy had professional benefits, and was an
integral part of their training. This concurs with
previous findings (Grimmer & Tribe, 2001; Orlinsky
& Rønnestad, 2005). Participants repeatedly noted
that therapy contributed to their professional devel-
opment, helped them deal with their own psycholo-
gical difficulties, and facilitated their ability to
distinguish clients’ issues from their own. However,
five participants also reported negative experiences
such as not getting on with their therapists. They
found their therapists either too rigid or too un-
boundaried, or the process emotionally and practi-
cally demanding. Other studies have drawn similar
conclusions (Grimmer & Tribe, 2001; Macaskill,
1988; Macaskill & Macaskill, 1992; Murphy, 2005).
Research has found that a good therapist!clientrelationship is one of the most important factors for
a successful client outcome (Roth & Fonagy, 2005).
One participant in this study (Patricia) said ‘the only
thing that matters is the kind of relationship you have
with somebody and not their theoretical model’.
Some participants suggested that their likes and
dislikes about their therapists were connected to
their therapists’ theoretical orientation: Wendy de-
scribed her psychoanalytic therapist as being like a
‘sphinx’, while Pippa preferred an attachment thera-
pist who was more boundaried than a psychosynth-
esis practitioner. In both cases the participants
preferred to be treated by a therapist trained in the
same theoretical model as themselves. In fact,
participants’ accounts of having more than one
therapist, and trying out therapists who used differ-
ent models, suggested that working with therapists
trained in the same orientation as themselves could
be of professional benefit for trainee clinicians.
Previous studies have suggested that by observing
the work of experienced therapists, therapist-patients
learn what might help or hinder their practice
(Norcross & Guy, 2005; Rizq & Target, 2008). In
this study participants also described how their
therapy had allowed them to experience for them-
selves the efficacy of specific therapeutic techniques,
and to model their own therapists. As in other
research, trainees who experienced therapeutic
incompetence did not think it invalidated therapy
itself (Grimmer & Tribe, 2001).
The view that personal therapy is effective for
clinicians is not novel (e.g. Orlinsky et al., 2001), but
there are many variables to be considered: the timing
of therapy, the motivation of a person to pursue
personal therapy, the mode(s) of intervention, the
theoretical orientation(s), the competence of the
therapist, and the therapeutic alliance (Roth &
Fonagy, 2005). The resulting dynamics are difficult
if not impossible to control, especially given hidden
contextual forces, life experiences, and the impreci-
sion of measurement criteria. Findings from this
study cannot be generalised, but may nonetheless
inform counsellor trainings and placements. This
topic is of particular interest at the current time
given the apparent reluctance of professional orga-
nisations such as the BACP and the British Psycho-
logical Society to insist or even recommend that
personal therapy should be mandatory for trainee
clinicians.
Without personal therapy, trainees may not con-
front in a systematic manner those areas of their own
personality which may be a potential source of
conflict in their work. These cannot be effectively
addressed by supervision alone. Furthermore, resis-
tance to enter into a process of self-exploration may
imply defensiveness detrimental to the therapeutic
process (Howell, 2009). It can be argued that
personal therapy improves the emotional functioning
of clinicians, allows a better understanding of
personal dynamics, interpersonal relationships, and
alleviates the emotional stresses inherent in the
practice of psychotherapy (see Orlinsky et al.,
2005). However, insistence for trainees to undertake
personal therapy, whether by a training organisation
or employer, can create resistance (Rizq & Target,
2008). Furthermore, this study highlighted the fact
that personal therapy can be a double-edged sword
for female volunteers. Research shows that unpaid
volunteers are generally women who often also have
the main household care-giving responsibilities (see
Bondi & Burman, 2001). Such women may need
personal therapy to deal with their own mental
health difficulties and to help them with their
professional development, but they may struggle to
find the time and money to do so.
Macaskill (1988) proposes that personal therapy is
only likely to have a significant impact on client
outcomes when therapists are put under emotional
pressure from working with clients with complex
disorders. However, it is questionable whether a
Women counsellors’ experiences of personal therapy 143
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

connection between client outcomes and clinicians’
personal therapy or, for that matter, their super-
vision, is empirically verifiable (Mackey & Mackey,
1993). Studies into the effects of personal therapy
suffer from inevitable defects in sampling,
design and measurement (Ciclitira, Marzano,
Brunswick, Starr, & Berger, 2004).
The proliferation of CBT through the Improving
Access to Psychological Therapy (IAPT) scheme is
resulting in a significant reduction in requirements
for both supervision and personal therapy for
therapists (Department of Health/Mental Health
Programme/IAPT, 2008). The lack of empirical
evidence for the benefits of personal therapy for
trainees gives cause for concern in this evidence-
based assessment culture to which services and
training institutions are increasingly subject. The
fact that personal therapy is not mandatory for most
clinicians working in the NHS has uncertain con-
sequences for training undertaken and client out-
comes.
Acknowledgements
We would like to thank our participants and Sue
Berger. We gratefully acknowledge the support of
Middlesex University and the King’s Fund.
References
Atkinson, P. (2006). Personal therapy in the training of therapists.
European Journal of Psychotherapy and Counselling, 8 (4),
407!410.Bike, J., Norcross, J., & Schatz, D. (2009). Processes and
outcomes of psychotherapists’ personal therapy: Replication
and extension 20 years later. Psychotherapy Theory, Research,
Practice, Training, 46 (1), 19!31.Bondi, L., & Burman, E. (2001). Women and mental health: A
feminist review. Feminist Review, 68, 6!33.Braun, V., & Clarke, V. (2006). Using thematic analysis in
psychology. Qualitative Research in Psychology, 3 (2), 77!101.Buckley, P., Karasu, T.B., & Charles, E. (1981). Psychotherapists
view their personal therapy. Psychotherapy: Theory, Research and
Practice, 18, 299!305.Bury, C., Raval, H., & Lyon, L. (2007). Young people’s
experiences of individual psychotherapy. Psychology and
Psychotherapy: Theory, Research and Practice, 80 (1), 79!96.Ciclitira, K., Marzano, L., Brunswick, N., Starr, F., & Berger, S.
(2004). Theoretical and ethical issues in conducting research at
a women’s health centre. Psychology of Women Section Review,
6 (1), 60!69.Cooper, M. (2008). Essential research findings in counselling and
therapy. London: Sage.
Department of Health/Mental Health Programme/IAPT (2008).
Implementation plan: Curriculum for low-intensity therapies
workers. Department of Health Publishers.
Geller, J, Norcross, J., & Orlinsky, D. (2005). Research on
conducting psychotherapy with mental health professionals.
In J. Geller, J. Norcross & D.E. Orlinsky (Eds.), The
psychotherapist’s own psychotherapy. Patient and clinician
perspectives (pp. 345!364). Oxford: Oxford University Press.
Grimmer, A., & Tribe, R. (2001). Counselling psychologists’
perceptions of the impact of mandatory personal therapy on
professional development ! an exploratory study. Counselling
Psychology Quarterly, 14, 287!301.Hollway, W., & Jefferson, T. (2000). Doing qualitative research
differently: Free association, narrative and the interview method.
London: Sage.
Howell, R. (2009). BACP no longer requires mandatory personal
therapy as a prerequisite for accreditation. But is it appropriate
for therapists to work with clients if they have not walked a
similar path themselves? Therapy Today, April, 28!29.Macaskill, N. (1988). Personal therapy in the training of the
psychotherapist: Is it effective? British Journal of Psychotherapy,
4, 219!226.Macaskill, N., & Macaskill, A. (1992). Psychotherapists-in-
training evaluate their personal therapy: Results of a UK
survey. British Journal of Psychotherapy, 9, 133!138.Mackey, R.A., & Mackey, E.F. (1993). The value of personal
psychotherapy to clinical practice. Clinical Social Work Journal,
21, 1.
Macran, S., & Shapiro, D. (1998). The role of personal therapy
for therapists: A review. British Journal of Medical Psychology,
71, 13!25.Mahoney, M.J. (1997). Psychotherapists’ personal problems and
self-care patterns. Professional Psychology: Research and Practice,
28, 14!16.McDevitt, J. (1987). Therapists’ personal therapy and profes-
sional self awareness. Psychotherapy, 24 (4), 693!703.McEwan, J., & Duncan, P. (1993). Personal therapy in the
training of psychologists. Canadian Psychology, 34, 186!194.McLeod, J. (2006). Qualitative research in counselling and
psychotherapy. London: Sage.
Murphy, D. (2005). A qualitative study into the experience of
mandatory personal therapy during training. Counselling and
Psychotherapy Research, 5 (1), 27!32.Norcross, J.C., Dryden, W., & DeMichele, J.T. (1992). British
clinical psychologists and personal therapy: III. What’s good
for the goose? Clinical Psychology Forum, 44, 29!33.Norcross, J.C., & Guy, J. (2005). The prevalence and parameters
of personal therapy in the United States. In J.D. Geller,
J.C. Norcross & D.E. Orlinsky (Eds.), The psychotherapist’s
own psychotherapy: Patient and clinician perspectives (pp. 165!176). Oxford: Oxford University Press.
Norcross, J.C., Strausser-Kirtland, D., & Missar, C. (1988). The
process and outcomes of psychotherapists’ personal treatment
experiences. Psychotherapy, 25 (1), 36!43.Orlinsky, D.E., Botermans, J.F., & Rønnestad, M.H. (2001).
Towards an empirically grounded model of psychotherapy
training: Four thousand therapists rate influences on their
development. Australian Psychologist, 36 (2), 139!148.Orlinsky, D.E., Norcross, J. C., Rønnestad, M.H., & Wiseman,
H. (2005). Outcomes and impacts of the psychotherapist’s own
psychotherapy. In J.D. Geller, J.C. Norcross & D.E. Orlinsky
(Eds.), The psychotherapist’s own psychotherapy: Patient and
clinician perspectives (pp. 214!230). Oxford: Oxford University
Press.
144 K. Ciclitira et al.
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2

Orlinsky, D.E., & Rønnestad, M.H. (2005). How psychotherapists
develop: A study of therapeutic work and professional growth.
Washington, DC: American Psychological Association.
Pope, K.S., & Tabachnick, B.G. (1994). Therapists as patients: A
national survey of psychologists’ experiences, problems, and
beliefs. Professional Psychology: Research and Practice, 25, 247!258.
Rizq, R., & Target, M. (2008). ‘‘Not a little Mickey Mouse thing’’:
How experienced counselling psychologists describe the sig-
nificance of personal therapy in clinical practice and training.
Some results from an interpretive phenomenological analysis.
Counselling Psychology Quarterly, 21 (1), 29!48.Roth, A., & Fonagy, P. (2005). What works for whom? A critical
review of psychotherapy research, 2nd ed. New York: Guilford
Press.
Rubin, H., & Rubin, I. (1995). Qualitative interviewing: The art of
hearing data. Thousand Oaks, CA: Sage.
Smith, J.A. (1996). Qualitative methodology: Analysing partici-
pants’ perspectives. Current Opinion in Psychiatry, 9 (6), 417!421.
Stevanovic, P., & Rupert, P.A. (2004). Career-sustaining beha-
viours, satisfactions, and stress of professional psychologists.
Psychotherapy, 41, 301!309.Stiles, W.B. (1993). Qualitative control in qualitative research.
Clinical Psychology Review, 13, 593!618.Strupp, H. (1955). The effect of psychotherapists’ personal
analysis upon his techniques. Journal of Consulting Psychology,
19, 197!204.Strupp, H. (1973). The therapist’s performance: A comparison of
two professional groups. In H. Strupp (Ed.), Psychotherapy:
Clinical research and theoretical issues. New York: Jason Aronson.
Van Haenisch, C. (2010). How did compulsory personal therapy
during counsellor training influence personal and professional
development? Counselling and Psychotherapy Research, 11 (2),
148!155.Wheeler, S. (1991). Personal therapy: An essential aspect of
counsellor training, or a distraction from focusing on the client?
International Journal for the Advancement of Counselling, 14,
193!202.Williams, F., Coyle, A., & Lyons, E. (1999). How counselling
psychologists view their personal therapy. British Journal of
Medical Psychology, 72 (4), 545!555.Wiseman, H., & Shefler, G. (2001). Experienced psychoanalyti-
cally oriented therapists’ narrative accounts of their personal
therapy: Impacts on professional and personal development.
Psychotherapy: Theory, Research, Practice, Training, 38,
129!141.
Biographies
Karen Ciclitira is a practising psychotherapist
and a principal lecturer in psychology at Middlesex
University. Her research interests include clinical
research, evaluative- and practitioner-based research,
psychoanalysis, women’s health, gender, racism,
feminist research and qualitative methodologies.
Fiona Starr is a clinical psychologist and princi-
pal lecturer at Middlesex University. She works
clinically with adolescents, children and families.
She also carries out medico-legal work where there
are child protection concerns. Her research interests
include applied, clinical, evaluative- and practi-
tioner-based research.
Lisa Marzano is a postdoctoral researcher at the
Centre for Suicide Research, University of Oxford.
Her research interests include: suicide and self-harm
in prison, mental health provisions and understand-
ings in criminal justice settings, feminist methods and
theory in relation to women’s and men’s health, and
qualitative methodologies.
Nicola Brunswick has held post-doctoral posi-
tions at the Wellcome Department of Imaging
Neuroscience (UCL), the MRC Cognitive Develop-
ment Unit, and the Department of Epidemiology and
Public Health (UCL Medical School). Her research
interests include the cognitive neuropsychology of
language and specific learning difficulties, and health
psychology.
Ana Costa is a postdoctoral researcher at the
Maudsley Hospital. Her research interests include
eating disorders, body dysmorphic disorder, border-
line personality disorder, suicide, self-harm, and their
prevention and treatment. She has also worked as
a dialectical behavioural therapy psychotherapist,
dealing with individuals who self-harm.
Women counsellors’ experiences of personal therapy 145
Dow
nloa
ded
by [K
ing'
s Col
lege
Lon
don]
at 0
8:48
09
June
201
2
Related Documents











