Wilms Tumor Wilms Tumor By Rasin Worawongsakul

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Wilms TumorWilms TumorBy Rasin Worawongsakul

Scope
• Introduction• Clinical presentation • Histopathology• Work-up• Management &
Staging COG/NWTS SIOP
• Bilateral Wilms tumor• Clear cell sarcoma of
kidney (CCSK)• Rhabdoid tumor of
kidney (RTK)• Radiation treatment
field• Treatment mortality &
morbidity

Epidemiology
• Most common renal malignancy in children
• 7 cases per million children in USA• Median age - 3.5yr• 2/3 diagnosis before 5 year-old• 95% diagnosed before 10 year-
old• M:F 0.92:1

Evolution of Wilms tumor therapy

Association syndromes
Syndromes Anomalies Genetic change Incidence of WT
WAGR Aniridia, Genitourinary anomalies,Metal retardation
Monoallelic deletion of WT1 gene at chromosome 11p13
>30%
Denys‐Drash Intersexual disorders (male pseudohermaphroditism), nephropaty
WT1 point mutation (8thor 9th exon)
>90%
Beckwith‐Wiedemann
Macroglossia, Organomegaly, Neonatal hypoglycemia, Gigantism
Duplication of paternal allele in chromosome 11p15.5 (WT2 gene)
<5%

Other syndromes and Genetics
https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0032528/?report=classic

Loss of Heterozygosity
Grundy PE et al. J Clin Oncol 2005; 23(29):7312-21

Gain of 1q
• Favorable histology – important prognostic factor Present in 25% of Wilms tumor patients Prognostic of OS in st. 1,4 and EFS in st. 1,3,4 1q gain maybe more important than LOH at
1p & 16q?
Gratias EJ et al. J Clin Oncol 2016; 34(26):3189-94.

Pattern of spreading
• Lymphatic spreading
Direct extension through Gerota’sfascia or renal sinus
Spread to peritoneal
Hematogenousmetastases lung (80%) Liver

Clinical presentation
• Asymptomatic abdominal mass (most common 83%)
• Abdominal pain (37%)• Fever (23%)• Hematuria (21%)• Hypertension (20%)
Pediatric Radiation Oncology. 5th edition; 2011.

Histopathology
• Gross Gray/tan-colored mass, may be cyst,
hemorrhage, necrosis surrounded by pseudocapsule
• Favorable histology (FH) - 87% Consist of three cell type of normal renal development
Blastemal cells : undifferentiated cells Stromal cells : immature spindle cells and heterologous
skeletal muscle, cartilage, osteoid, fat Epithelial cells : glomeruli and tubule

Benign renal blastema
Wilms tumor
Tubular differentiation
Undifferentiated blastema(tightly packed small blue cells)
Blastema
Stroma
Epithelial tubules

Histopathology
• Anaplasia > poor outcome -unfavorable histology (UH) Presence of multipolar polypoid mitotic figures
and marked nuclear enlargement with hyperchromasia

Anaplasia
Imaging work-up
• Ultrasound Origin of renal mass Identifies contralateral kidney Detect tumor extension into renal sinus or IVC Doppler USG may assess patent blood flow
• CXR Lung metastases Chest CT have more sensitivity – lung metastases
visible only on CT?

Imaging work-up
• CT or MRI of abdomen and pelvis MRI may help to distinguish nephrogenic rest
from Wilms tumor• Radionuclide bone scan (CCSK or RTK)• MRI brain (CCSK or RTK)

Large inhomogeneous renal mass Ruptured Wilms tumor
CT whole abdomen
Ultrasound whole abdomen

Laboratory work-up
• Urinalysis If proteinuria in Denys-Drash syndrome
• Serum Creatinine• Liver function test > liver metastasis• Hypercalcemia In rhabdoid tumor of kidney or congenital
mesoblastic nephroma• Coagulogram 8% in Wilms tumor have acquired vWD

MANAGEMENTCOG approachSIOP approach

COG vs SIOPCOG (USA) SIOP (European)

COG vs SIOP
COG/NWTS (USA)
• Upfront Surgery > adjuvant Rx
• Diagnosis and staging information known
• Collection of treatment naïve-biology materials
SIOP (European)
• Preoperative Rx > Surgery
• Decrease tumor spillage/rupture
• Response assessment• Down staging • Less children
receiving radiotherapy
COG vs SIOP
COG/NWTS (USA)
• Upfront Surgery > adjuvant Rx
• Diagnosis and staging information known
• Collection of treatment naïve-biology materials
SIOP (European)
• Preoperative Rx > Surgery
• Decrease tumor spillage/rupture
• Response assessment• Down staging • Less children receiving
radiotherapy

COG/NWTS APPROACH

Include tumor biopsy before definite surgery

NWTS-1
• Objectives To determine whether routine postoperative
RT was necessary with tumor confined to the kidney and completely resected To establish AMD, VCR, or the combination
more locally advanced stage To study efficacy of preoperative VCR in
metastatic tumor
D’Angio GJ et al. Cancer 1976; 38:633-46

Wilms tumor stage I, FH
• NWTS-1 RT not necessary for St. I with < 2 years old RT has benefit for St. I with ≥ 2 years old (***
CMT = AMD alone)
• NWTS-2 In St. I patients do not necessary when VCR was
added 6 mo was not inferior to 15 mo CMT (AMD+VCR)
– 3yr- RFS 89% vs 84%
D’Angio GJ et al. Cancer 1976; 38:633-46D’Angio GJ et al. Cancer 1981; 47:2302-11

NWTS-1
Gr. I
Gr. II & III
Gr. IV
Regimen A: Sx + RT + AMDRegimen B: Sx + AMD (No RT)
Regimen A: Sx + RT + AMDRegimen B: Sx + RT + VCRRecimen C: Sx + RT + AMD + VCR
Regimen A: Sx + RT + AMD + VCRRegimen B: Pre‐op VCR ‐>Sx + RT
+ AMD + VCR
RANDOM
RANDOM
RANDOM
D’Angio GJ et al. Cancer 1976; 38:633-46

NWTS-2
Gr. I
Gr. II, III, IV
Regimen E: FollowRegimen B: AMD+VCR 9,12,15 mo
Regimen C: VCR 6,7,8 wk, AMD+VCR 3,6,9,12,15 mo
Regimen D: VCR 6,7,8 wk,ADR 6wk, 4.5,7.5,10.5,13.5 moAMD+VCR 3,6,9,12,15 mo
RANDOM
RANDOM
Sx + AMD +VCR para‐op 6wk, 3,6 mo
Sx + RT + AMD +VCR para‐op
D’Angio GJ et al. Cancer 1981; 47:2302-11

Wilms tumor stage II, FH

Wilms tumor stage III, FH

Spillage and biopsy
• NWTS-4 data shows inferior RFS for stage 2 patients -> re-classified as stage 3
• Biopsy? UKW3: biopsy vs no biopsyAny local relapse : 10.5% vs 5.7% (ss) Significant factor on univariate analysis but
not multivariate analysis

Biopsy
• Biopsy – adequate to identify UH? NWTS-4 – 0% of patients bilateral Wilms
tumor had anaplasia detected by needle biopsy
• Role of biopsy should be reserved for unresectable primaries or patients with concern for bilateral Wilms tumor
PMID: 25465191.
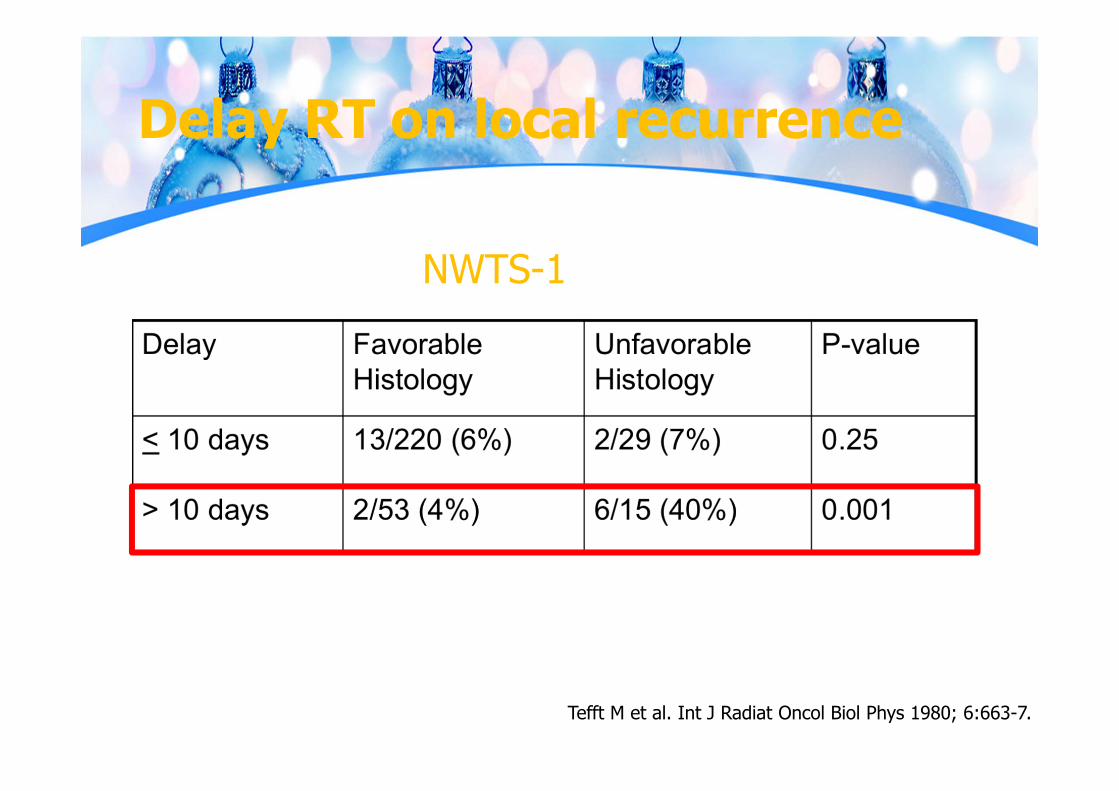
Delay RT on local recurrence
Tefft M et al. Int J Radiat Oncol Biol Phys 1980; 6:663-7.
NWTS-1

RT treatment delay
• Final pathology and stage needed within few days
• Need time to do simulation esp. younger children may need anesthesia

RT treatment delay (NWTS-3 & 4)
• 1226 children with st. II-IV who received flank or abdominal RT
• Mean RT delay: 10.9 d (median 9 d)• 59% had RT delay 8-12 d• Flank and abdominal recurrence rates for delay
>10 d vs ≥10 d were not signifcance
Kalapurakal JA et al. Int J Radiat Oncol Biol Phys 2003; 57:495-9.

Lung metastases (CT only?)
• CXR has traditionally been used for staging• CT scan – more sensitivity• Nodules could be other than metastases Infection Atelectasis Harmatoma Pseudotumor Intrapulmonary LN

Lung metastases (CT only)
• St Jude 11/124 (9%) – negative CXR with positive CT
chest -> treated as local stage (No lung RT) 4/11 (36%) – relapsed at lung
• NWTS-3 &4 No difference in EFS, OS for lung RT (N=37)
vs no lung RT (N=53)
Wilimas JA et al. J Clin Oncol 1988; 6:1144-6.Meisel JA et al. Int J Radiat Oncol Biol Phys 1999; 44:579-85.

Lung metastases (CT only)

Omission WLI?

AREN0533
• After 6 wk CMT -> central radiology review 58% of 279 isolated lung metastases had incomplete
response 3yr-EFS & OS – 88% & 92% (addition
cyclophosphamide/etoposide showed benefits) 60% had grade 3 or higher hematologic toxicity
39% of 391 pts -> CR 4yr-EFS & OS – 78% &95% (no statistically
significant difference when compared to historical treatment with lung RT)
May be alternative treatment approach
Dix DB et al. J Clin Oncol 32, 2014 (suppl; abstr 10001)

Omission adjuvant treatment?
• Dana Farber Cancer Institute/ Children’s hospital Boston pilot study Cassady tumor (very low risk tumor -> age <24 mo
with st. I, unilateral, total tumor/kidney weight <550g, FH)
5yr-OS 100%, 5yr-EFS 88% (N=8)
• NWTS-5 75 children with cassady tumor 2yr-os 100%, 5yr-DFS 86.5% 3pt developed metachronous tumor 8pt relapsed (lung = 5, abdomen =3)
Larsen E et al. Cancer 1990; 66:264-6.Green DM et al. J Clin Oncol 2001; 19:3719-24.

Risk adaptation for LOH 1p & 16q
• AREN 0532

Risk adaptive (สรปุ)

AREN0532- St. III FH
4yr-EFS & OS – 88% and 96%
Fernandez CV et al. J Clin Oncol 33, 2015 (suppl; abstr 10010)

Dix DB et al. J Clin Oncol 33, 2015 (suppl; abstr 10009)

AREN0532/AREN0533: 4yr-EFS
Dix DB et al. J Clin Oncol 33, 2015 (suppl; abstr 10009)
Regimen M improved EFS for St.III/IV FH with LOH 1p&16q compared to history Grade 3 or higher hematological toxicity was seen
60% Benefit DD4A for St.I/II FH LOH 1p&16q is less clear

COG guidelines (FH)

COG guidelines (FH)

COG guidelines (FH)

COG vs SIOP
COG/NWTS (USA)
• Upfront Surgery > adjuvant Rx
• Diagnosis and staging information known
• Collection of treatment naïve-biology materials
SIOP (European)
• Preoperative Rx > Surgery
• Decrease tumor spillage/rupture
• Response assessment• Down staging • Less children receiving
radiotherapy

SIOP APPROACH

SIOP staging

SIOP staging
• Stage I Limited to kidney or surrounded with fibrous
pseudocapsule Renal sinus may be minimally infiltrated, without any
vessel involvement. Intra-renal vessels may be involved Tumor may protrude into the pelvic system without
infiltrating the wall of the ureter Presence of necrotic tumor or chemotherapy-
induced changes in the renal sinus or soft tissue outside the kidney does not upstage the tumor provided it is completely excised
Neither FNA nor Trucut biopsy upstage the tumor

SIOP staging
• Stage II Tumor extends beyond kidney, but is completely
resected Tumor penetration of renal capsule, vessels or
adjacent organs, but completely resected Includes tumors with large core needle biopsies. May
include tumors with local tumor spillage confined to the flank

SIOP staging
• Stage III Incomplete excision (gross or microscopic) confined
to abdomen Includes cases with any of the following: Involvement of abdominal LN Diffuse peritoneal contamination (metastases
or spillage) Tumor thrombi at resected margin Residual tumor in abdomen Piecemeal resection Surgically biopsied prior to chemotherapy
Presence of necrotic tumor or chemotherapy-induced changes in LN or at resected margins -> St. III

Post-chemotherapy (SIOP 2001)

SIOP background
• SIOP 1 (1971-1974) Pre-surgery RT (RT-Sx-RT) vs Post-surgery RT (Sx-RT) St. 1 – 20Gy, St. 2-3 – 30Gy Pre-surgery RT reduces tumor rupture and
downstages tumor 5yr-RFS for ruptured tumor vs non-ruptured
tumor – 27% vs 51%
AMD 1 course vs 6 course No need for prolonged AMD after surgery

SIOP background
• SIOP 2 (1974-1976) – confirmed SIOP1 Pre-surgery RT (RT-Sx-RT) vs Post-surgery RT (Sx-RT) Pre-surgery RT reduces tumor rupture 5% vs 20%
(p = 0.0025)
AMD/VCR 9 mo vs 15 mo AMD/VCR 9 mo = 15 mo

SIOP background
• SIOP 5 (1977-1979) Pre-operative AMD/VCR (4 wk) vs Pre-operative RT Pre-operative RT (20Gy pre- & 15Gy post-op) Post-operative RT only – 30Gy Pre-op AMD/VCR = Pre-op RT

SIOP background
• SIOP 6 (1980-1987) St. I – Adj. AMD/VCR long course (38 wk) vs short
course (17 wk) Short course = long course
St. 2(N0) – Adj. RT vs no RT No difference survival at 2yr & 5yr
St. 2(N+)/3 –Adj. intensive VCR vs Add Dox Doxorubicin improved 2yr-DFS (74% vs 49%) but
not OS

SIOP background
• SIOP 9 (1987-1991) 8wk pre-op CMT vs 4wk pre-op CMT 4wk pre-op CMT = 8 wk pre-op CMT 4wk pre-op CMT became standard in SIOP
protocol But 8wk pre-op CMT had further volume
decrease

SIOP background
• SIOP 93-01 (1993-1999) After pre-op CMT -> Sx (Intermediate risk &
anaplasia) Adj. 4wk CMT vs 18wk CMT Shorter CMT accepted Risk adapted therapy accepted

SIOP WT 2001
• Aim To assess post-op Doxorobucin can safely
remove from intermediate risk st. 2-3 after pre-op CMT and Sx
• St. 2 N+ will be re-assign to st. 3• New pathological risk classification• Central radiology and pathological review

SIOP WT 2001
• All pt get pre-op CMT Localised tumor: 4 wk pre-op CMT (AMD/VCR) Metastatic disease: 6 wk pre-op CMT (AMD/VCR/DOX) Bilateral: 2 drugs CMT 2-4 wk
• Lung metastasis are documented only CXR (CT if doubt)• Lung metastasis only seen on CT Rx as localized
disease• Post-op treatment according to local stage and histology

Post-chemotherapy (SIOP 2001)

Post-op treatment
** RT only for diffuse anaplasianot blastemal predominant
AV‐1 = AV 4wk
AV‐2 = AV 27wk
High‐risk = CCED 35wk

SIOP WT 2001
Kathy PJ et al. Lancet 2015; 386:1156-64.

SIOP WT 2001
Kathy PJ et al. Lancet 2015; 386:1156-64.
2yr‐EFS difference 4.4% but not exceed 10% predefined margin
No difference in OS
Doxorubicin does not need in treatment of stage 2‐3 intermediate risk Wilmstumor

SIOP WT 2001
• Outcome for blastemal type Wilms tumor Doxorubicin reduce risk
of relapse in blastemal-type Wilms tumor
OS benefit only seen in stage I
• 95% relapse distant
MM van den Heuvel-Eibrink et al. European J Cancer 2015; 51:498-506.

SIOP: RT dose
St. I St. 2 St.3
Low‐risk ‐ ‐ ‐
Intermediate‐risk ‐ ‐ • 14.4Gy + boost 10.8Gy• PAN+ should boost to
PANHigh‐risk ‐ • 25.2Gy/14F • 25.2Gy/14F
Whole-abdominal RT – diffuse spillage, peritoneal metastasis
14.4-21Gy (1.5Gy/F) Kids <1yr : 10-12Gy (1.25Gy/F)

SIOP: RT dose (metastatic site)
Disease site RT field RT doseLiver Incompletely resected
tumor + 2cm margin19.8Gy/11F
Brain Whole brain 25.5Gy/17F consider boost 4.5Gy/3F
Bone Disease visible on imaging + 3cm margin
30Gy/17F

Bilateral Wilms tumor
• 4-8% of Wilms cases• ESRD occurs 12% of cases -> major source of
morbiditySynchronous Metachronous
NWTS-1 33/606 (5.4%) 20/606 (3.3%)NWTS-2 & 3 145/3300 (4.4%)St. Jude 29/328 (8.8%) 7/328 (2.1%)SIOP 1. 2. 5 43/1043 (4.0%) 25/1043 (2.4%)
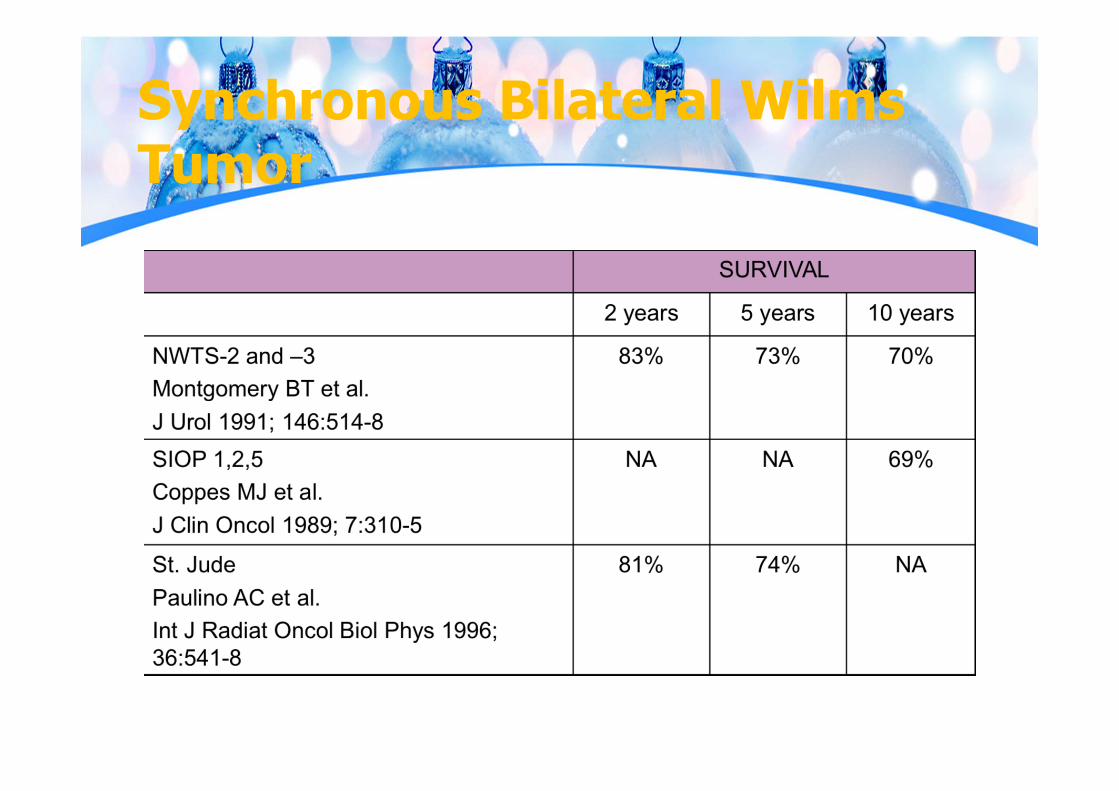
Synchronous Bilateral WilmsTumor

AREN0534

AREN0534
• Tumor response (N = 189)
Ehrlich P et al. Ann Surg, 2017.
Tumor Response
No. of pts (%)
CR 8 (4.2%)PR 121 (64.0%)SD 58 (30.7%)PD 2 (1.1%)
Histology No. of ptsFavorableHistology
167
Focal Anaplasia 7Diffuse Anaplasia 16

AREN0534
• Bilateral Wilms tumor 189 pts 163 (84%) – Definitive Sx by 12 wk(partial
or complete nephrectomy or wedge resection at least 1 kidney) 30% of 163 aim did by 6-week evaluation point
Ehrlich P et al. Ann Surg, 2017.
Surgical approach % of ptsUnilateral nephrectomy + contralateral partial nephrectomy
48
Bilateral partial nephrectomy 35Unilateral total nephrectomy 10.5Unilateral partial nephrectomy 4Bilateral total nephrectomy 2.5

AREN0534
• 4yr-EFS & OS - 82.1% & 94.9% (NWTS-5 56% & 80.8%)
• 23pt (12%) relapsed Median time to relapse
15.2 + 10.7 mo FH - 16/167 (9.5%), FA –
0/7 (0%), DA – 7/16 (43%)
• Toxicity No grade 5 toxicity 4 cases – VOD (received
DD4A postnephrectomy) but all recovered Ehrlich P et al. Ann Surg, 2017.

AREN0534
Ehrlich P et al. Ann Surg, 2017.

Anaplastic Wilms tumor
• Unfavorable histology (UH) – found 4-5% of NWTS & SIOP studies
• Uncommon in infants, but found 10% of >5year-old pt
• More relapse and poor survival

Anaplastic Wilms tumor
Faria P et al. Am J Surg Pathol 1996; 20:909-20.

Anaplastic Wilms tumor
• NWTS-4 St. I treated with AMD/VCR -> 2yr-OS 85.5-
93.3% (depends on AMD administration St. II-IV treated with AMD/VCR/DOX vs
AMD/VCR/DOX/CPM -> 4yr-OS 27.1% vs52.2% (p = 0.04)

Anaplastic Wilms tumor
• NWTS-5
Dome JS et al. J Clin Oncol 2006; 24:2352-8.

NWTS-5 (UH results)
Dome JS et al. J Clin Oncol 2006; 24:2352-8.
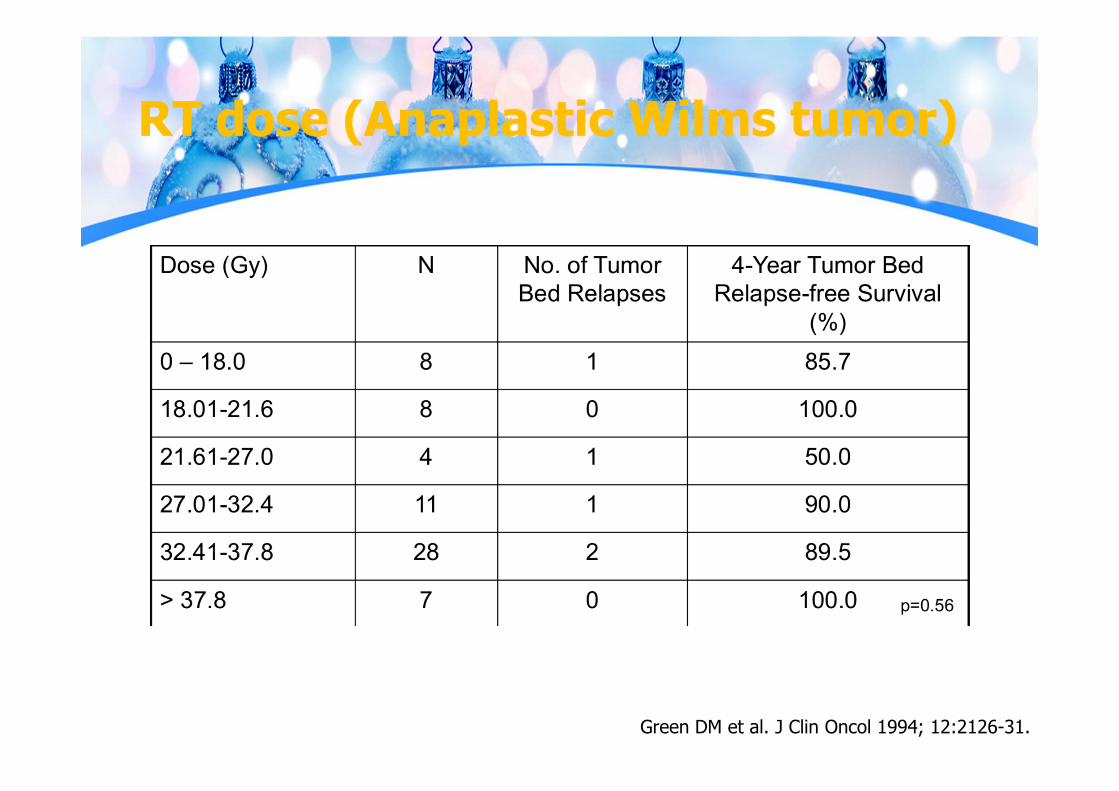
RT dose (Anaplastic Wilms tumor)
Green DM et al. J Clin Oncol 1994; 12:2126-31.

Prognosis (Anaplastic Wilmstumor)
https://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0032528/?report=classic
NCI PDQ summary

Clear cell sarcoma of Kidney (CCSK)• First reported by Kidd (1970)• Originally called “Bone-
metastasizing renal tumor of childhood” by Marsden (1978)
• 20 cases each year in USA• 4-5% of all renal tumors• M:F = 2:1• 29% LN metastasis at diagnosis• Most common sit of recurrence
Bone and lung Abdomen Brain
https://www.pathologyoutlines.com/imgau/kidneytumorclearcellsarcomarollins2.jpgArgani P et al. Am J Surg Pathol 2000; 24:4-18.
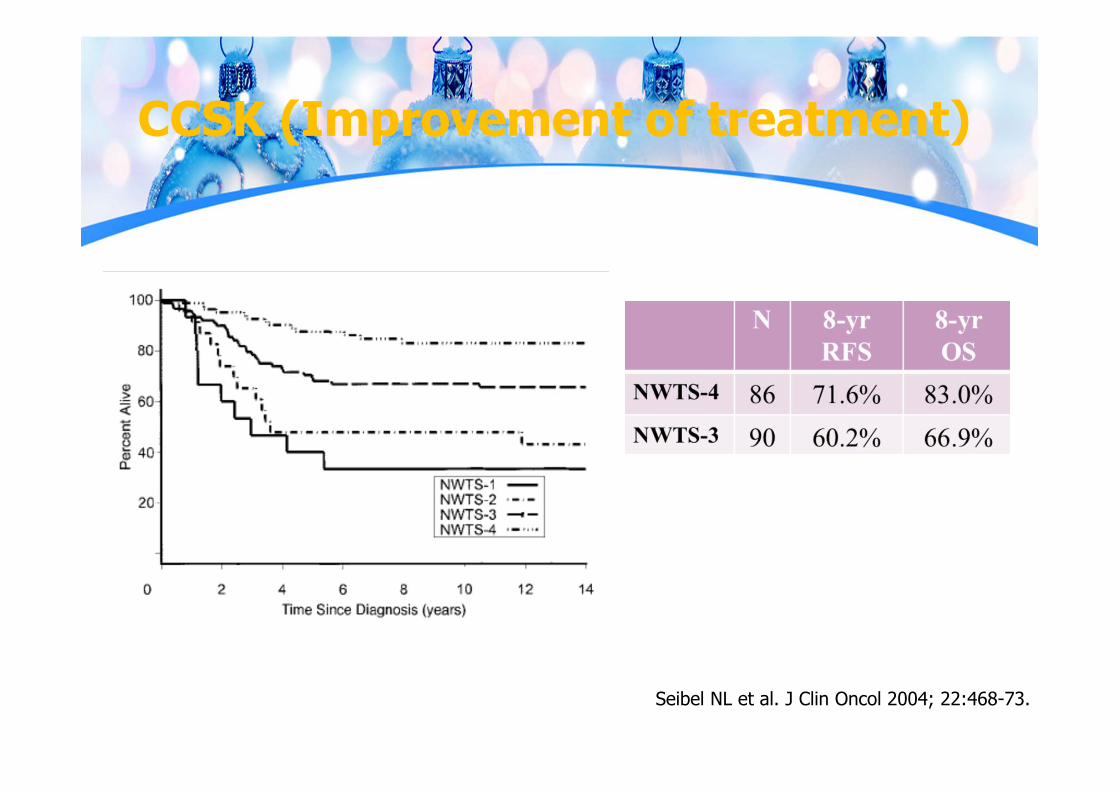
CCSK (Improvement of treatment)
Seibel NL et al. J Clin Oncol 2004; 22:468-73.

CCSK (NWTS-4)
Seibel NL et al. J Clin Oncol 2004; 22:468-73.

CCSK (NWTS-5)
• Median follow-up 4.6 yr• 5yr-EFS & OS – 79% & 89% (outcome similar as
NWTS-4, SIOP & UKCCSG)• 5yr-EFS for st.4(9/110) still low – 36%
Seibel NL et al. J Clin Oncol 24, 2006 (suppl; abstr 9000)

RT dose (CCSK)
Green DM et al. J Clin Oncol 1994; 12:2126-31.

Rhabdoid tumor of kidney (RTK)
• 2% of all renal tumors• Median age at diagnosis – 18
mo 80% found at age <2 yr
• M:F = 1.5:1• INI-1 gene mutation Associate with AT/RT
• Worst prognosis for renal tumors
https://www.webpathology.com/slides-13/slides/Kidney_Pediatric_Rhabdoid4.jpeg

Age at diagnosis (RTK)
Tomlinson GE et al. J Clin Oncol 2005; 23:7641-5.

Optimal RT dose
• Optimal RT dose is not known UKCCSG Second Wilms tumor study – 30Gy with
AMD/VCR/DOX 2- & 4-yr EFS (UKCCSG) – 36%
NWTS-5 – 10.8 Gy Tomlinson, et al. (2005) analyzed NWTS-1-5 for RTK ≥25Gy – improved 4yr-OS But when adjusted by age and stage – No longer
benefit of high dose RT
Mitchell Cet al. Br J Cancer 2000; 83:602-8.Tomlinson GE et al. J Clin Oncol 2005; 23:7641-5.

Risk adaptive (สรปุ)

Risk adaptive (สรปุ)

Current COG Guidelines

Current COG Guidelines

National Protocol for the treatment of childhood cancers 2016

THAI-POG (Bilat. Wilms tumor)
National Protocol for the treatment of childhood cancers 2016

Recurrence Wilms tumor
Adverse prognostic factor• Initial st. 4• UH• Early relapse
(<12 mo)• ≥2 relapses• Relapse in RT
field
Spreafico F et al. Expert Rev Anticancer Ther 2009.Grundy P et al. J Clin Oncol 1989; 7:638-47.
40‐60%
48‐73%

Recurrence Wilms tumor
Perez and Brady's Principles and Practice of Radiation Oncology. 6th edition; 2013.

Radiation field (Flank)
Perez and Brady's Principles and Practice of Radiation Oncology. 6th edition; 2013.
Pre-treatment tumor should be covered
*** Cover entire width of vertebral body with 1cm margin -> prevent scoliosis
Exclude as much of contralateral kidney as possible
Laterally, field encompasses abdominal wall
Superior-inferior : concern for breathing (at least 1cm )
Boost to residual: 1-2cm margin

Scoliosis & bone hypoplasia from RT
Paulino AC et al. Int J Radiat Oncol Biol Phys 2000; 46:1236-46.

Whole abdominal RT
• Sup – superior to diaphragm 1cm (block heart)
• Inf – lower border of obturatorforamen
• Lat – cover abdominal wall• Acetabulum & femoral head are
blocked• Remaining kidney should be blocked
after 10-12Gy• Gross residual disease boost with 1-
2cm margin
Perez and Brady's Principles and Practice of Radiation Oncology. 6th edition; 2013.
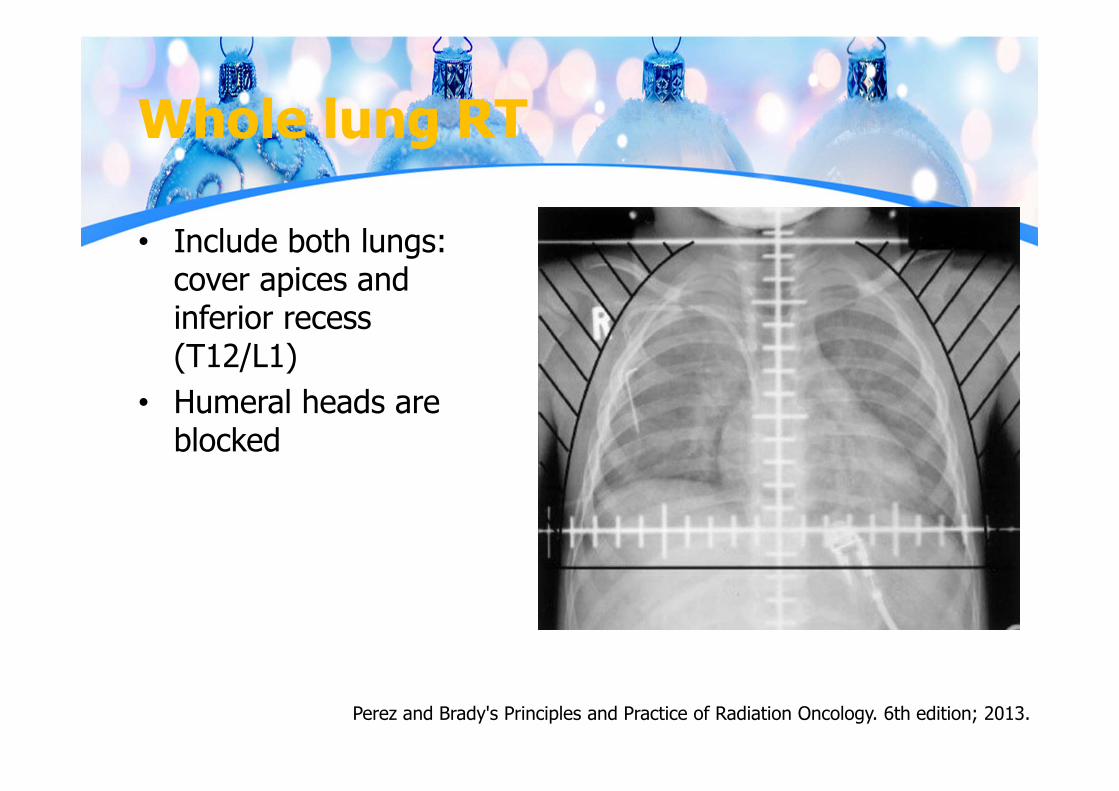
Whole lung RT
• Include both lungs: cover apices and inferior recess (T12/L1)
• Humeral heads are blocked
Perez and Brady's Principles and Practice of Radiation Oncology. 6th edition; 2013.

Treatment related mortality
• 25yr Mortality 6% Cardiac cause Second malignancy (SMN)
• Cause for Mortality: 85% tumor, 15% late effects Year 1-5: 94% tumor, 1.3% SMN,
0.7% cardiac, 0.6% ESRD Year >5: 40% tumor, 17% SMN,
8.8% cardiac, 8.2% ESRD
• Trend to reduce late-effect mortality Cecilia AC et al. J Clin Oncol 2009; 27:1304-9.

Treatment related mortality
• Second malignancy 15yr: 1.6% (NWTS) 25yr: 3% (Mortality
6.1%)
• Predictors RT dose ≥35Gy Doxorubicin dose Treatment for relapse
AM Termuhlen et al. Pediatr Blood Cancer 2011; 57:1210-6.JM Lange et al. Cancer 2014.
Breast cancer risk at 40yr –4.5% Prior Chest RT: 14.8% Prior abdominal RT: 3.1% No RT: 0.3%

Treatment Morbidity
• Children Cancer Survival Study (CCSS) 25yr survival – chronic health problem: 65% any or 24% severe HR for CHF = 23.6, Renal failure = 50.7, HTN = 8.2
• CHF NWTS1-4: 4.4% at 20yr Predictors: cumulative doxorubicin dose, WLI, Lt abdominal RT,
female
AM Termuhlen et al. Pediatr Blood Cancer 2011; 57:1210-6.DM Green et al. J Clin Oncol 2001; 19:1926-34.
Treatment Morbidity
• Renal failure Unilateral WT: 1.3% at 20yr (0.6% without other syndrome) Increase risk in pt with WAGR syndrome, Denys-Drash & non-
syndromic bilateral Wilms tumor Associated with increase therapy, abdominal RT
• Pulmonary disease Cumulative incidence - 4% at 15yr Associated with lung RT (either primary treatment or relapse)
NE Breslow et al. J Urol 2005; 174:1972-5.DM Green et al. J Clin Oncol 2001; 19:1926-34.

Treatment Morbidity
• Fertility Previous flank radiated women
Increase risk offspring: low birth weight, prematurity Pregnancy outcomes: hypertension complicating pregnancy,
fetal malposition, preterm labor No significant trend with radiation dose in congenital
anomalies Flank RT dose >25Gy – more complication rates
DM Green et al. J Clin Oncol 2010; 28:2924-30.

John T. Lucas Jr. Presented in Educational session in ASTRO 2017
Take home
• Wilms tumor is most common renal malignancy in children• 2/3 diagnosed before 5 years old• High curable disease even in stage 4• Avoid biopsy before treatment – increase risk tumor spillage• Tumor rupture – increase risk intra-abdominal recurrence• Evaluation for pulmonary nodule with chest CT should not be used
routinely Used only in patient who was suspected lung metastasis from
CXR Data did not show benefit for WLI in CT only detected lung
nodule

Take home
• Management COG/NWTS approach: upfront surgery + adjuvant (risk
stratification) SIOP approach: Pre-op CMT then surgery + adjuvant (risk
stratification) THAI-POG: mainly use in Thailand (adapt from COG approach)
• Radiotherapy mainly use for At least stage 3, favorable histology Unfavorable histology Post neoadjuvant CMT with stage 3 disease or stage 2 with
anaplasia
Take home
• RT dose and volume – as protocol described• Delay RT >10 days should be aware, especially in unfavorable
histology• WLI can be omitted in lung metastatic patient with favorable biology
who response to CMT rapidly
• Bilateral Wilms tumor: goal is to spare at least 1 function kidney Pre-op CMT then sx within 12wk At least 1 nephron-sparing surgery with negative margin

Take home
• Late toxicity from treatment should be concerned Cover whole vertebral column + margin 1cm: uniform dose to
vertebral body to prevent scoliosis WAI: contralateral kidney, liver, heart doses should be concerned Second malignancy, CHF and ESRD can be cause of death apart
from primary disease Proton or IMRT may have role to reduce long-term toxicity

The End
Related Documents











