Whole-Body 18F FDG Positron Emission Tomography/ Computed Tomography Evaluation of Patients With Uveal Metastasis PAYAL PATEL AND PAUL T. FINGER ● PURPOSE: To investigate the value of whole-body positron emission tomography/computed tomography (PET/CT) as a screening tool for patients with uveal metastasis. ● DESIGN: Retrospective observational case series. ● METHODS: SETTING: Clinical practice. STUDY POPULA- TION: Eighteen patients with uveal metastatic tumors were evaluated. Patients had no history of malignancy or a past medical history of malignancy without known active metastasis or known systemic cancer. INTERVEN- TION: Whole-body PET/CT was used as a screening tool to evaluate the intraocular tumor, to evaluate for multi- organ metastatic disease, and for cancer staging. MAIN OUTCOME MEASURES: Detection and PET/CT uptake of primary tumors and metastatic disease. ● RESULTS: PET/CT imaging uncovered previously oc- cult primary nonocular cancers (11/18, 61%), revealed progression of known primary systemic cancer (7/18, 39%), and confirmed multi-organ metastases in all cases (18/18, 100%). PET/CT findings were used to direct nonocular, confirmatory biopsy in 67% of cases (12/18). No uveal biopsies were required. PET/CT revealed lymph nodes and bone as the most common metastatic sites. The intraocular tumor was detectable in 28% of cases. Small, non-avid tumors and those within the hypermetabolic, PET-avid brain were falsely negative. ● CONCLUSION: This study suggests that whole-body PET/CT can be useful for clinical evaluation of patients with uveal metastases. It allowed for screening of the entire body and directed extraocular biopsy. Commonly used for tumor staging, PET/CT aided in the detection of the primary cancer in patients with metastatic uveal tumors. (Am J Ophthalmol 2012;153:661– 668. © 2012 by Elsevier Inc. All rights reserved.) M ETASTATIC CHOROIDAL TUMORS ARE THE MOST common intraocular malignancy. 1–4 Detection of the primary malignancy typically precedes ocular findings. 5 However, in a relatively small subset of these patients, ocular findings can be the first sign of metastatic disease. 5,6 These patients typically present to the ophthalmologist with foveal invasion or secondary macular retinal detachment with associated symptoms of blurred vision, metamorphopsia, and photopsia. There are 3 common clinical presentations for patients with uveal metastatic tumors. When uveal metastasis is clinically apparent in the setting of known disseminated metastatic disease, ophthalmic treatment can be initiated. When there exists a history of primary cancer without known metastatic disease, restaging is necessary. Lastly, when there is no known primary cancer and uveal metas- tasis is suspected, a systemic evaluation is also necessary. Given that most cases of uveal metastasis are from a breast primary in women and from lung in men, radio- graphic surveys have focused on these 2 areas. 4,7,8 How- ever, alternate primaries such as prostate, gastrointestinal, kidney, thyroid, and others have been described. 7–10 Fur- ther, multifocal nonocular sites may be overlooked by focal, limited radiographic imaging. Computed tomogra- phy (CT) allows for anatomic views that may not distin- guish between benign and malignant tumors. Positron emission tomography (PET) allows for physiological views with poor anatomic localization. 11,12 Magnetic resonance imaging (MRI) is associated with a number of contraindi- cations (including body size, metallic implants, and renal insufficiency) and has been shown to be inferior in staging of tumors when compared to PET/CT. 13 For these reasons, whole-body 18-fluoro-2-deoxyglucose (18F FDG) PET/CT is gaining worldwide use for the staging, screening, and management of patients with can- cer. 14 –19 PET/CT combines the functional metabolism revealed by PET with the anatomic characteristics found on CT, putting form and function on the same diagnostic page. In this study, we have evaluated PET/CT for initial staging of patients with uveal metastasis. METHODS A RETROSPECTIVE OBSERVATIONAL CASE REVIEW OF CON- secutive patients at a single clinical practice was per- formed. Entry criteria included a clinical diagnosis of uveal metastasis, and at the initial visit, patients had either no history of malignancy, a history of cancer thought to be in remission, or a known solitary nonocular metastasis. When Accepted for publication Sept 19, 2011. From the New York Eye Cancer Center and New York University School of Medicine, Department of Ophthalmology, New York, New York (P.P., P.T.F.). Inquiries to Paul T. Finger, the New York Eye Cancer Center, 115 East 61st St, New York, NY 10065; e-mail: pfi[email protected] © 2012 BY ELSEVIER INC.ALL RIGHTS RESERVED. 0002-9394/$36.00 661 doi:10.1016/j.ajo.2011.09.028

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

p(m
cp3(nNlsch
Pweutt©
o
Whole-Body 18F FDG Positron Emission Tomography/Computed Tomography Evaluation of Patients With
Uveal Metastasis
PAYAL PATEL AND PAUL T. FINGER
tfpgewicio
● PURPOSE: To investigate the value of whole-bodyositron emission tomography/computed tomographyPET/CT) as a screening tool for patients with uvealetastasis.
● DESIGN: Retrospective observational case series.● METHODS: SETTING: Clinical practice. STUDY POPULA-TION: Eighteen patients with uveal metastatic tumorswere evaluated. Patients had no history of malignancy ora past medical history of malignancy without knownactive metastasis or known systemic cancer. INTERVEN-TION: Whole-body PET/CT was used as a screening toolto evaluate the intraocular tumor, to evaluate for multi-organ metastatic disease, and for cancer staging. MAIN
OUTCOME MEASURES: Detection and PET/CT uptake ofprimary tumors and metastatic disease.● RESULTS: PET/CT imaging uncovered previously oc-ult primary nonocular cancers (11/18, 61%), revealedrogression of known primary systemic cancer (7/18,9%), and confirmed multi-organ metastases in all cases18/18, 100%). PET/CT findings were used to directonocular, confirmatory biopsy in 67% of cases (12/18).o uveal biopsies were required. PET/CT revealed
ymph nodes and bone as the most common metastaticites. The intraocular tumor was detectable in 28% ofases. Small, non-avid tumors and those within theypermetabolic, PET-avid brain were falsely negative.
● CONCLUSION: This study suggests that whole-bodyET/CT can be useful for clinical evaluation of patientsith uveal metastases. It allowed for screening of the
ntire body and directed extraocular biopsy. Commonlysed for tumor staging, PET/CT aided in the detection ofhe primary cancer in patients with metastatic uvealumors. (Am J Ophthalmol 2012;153:661–668.
2012 by Elsevier Inc. All rights reserved.)
M ETASTATIC CHOROIDAL TUMORS ARE THE MOST
common intraocular malignancy.1–4 Detectionof the primary malignancy typically precedes
cular findings.5 However, in a relatively small subset ofthese patients, ocular findings can be the first sign of
Accepted for publication Sept 19, 2011.From the New York Eye Cancer Center and New York University
School of Medicine, Department of Ophthalmology, New York, NewYork (P.P., P.T.F.).
Inquiries to Paul T. Finger, the New York Eye Cancer Center, 115 East
61st St, New York, NY 10065; e-mail: [email protected]© 2012 BY ELSEVIER INC. A0002-9394/$36.00doi:10.1016/j.ajo.2011.09.028
metastatic disease.5,6 These patients typically present tothe ophthalmologist with foveal invasion or secondarymacular retinal detachment with associated symptoms ofblurred vision, metamorphopsia, and photopsia.
There are 3 common clinical presentations for patientswith uveal metastatic tumors. When uveal metastasis isclinically apparent in the setting of known disseminatedmetastatic disease, ophthalmic treatment can be initiated.When there exists a history of primary cancer withoutknown metastatic disease, restaging is necessary. Lastly,when there is no known primary cancer and uveal metas-tasis is suspected, a systemic evaluation is also necessary.
Given that most cases of uveal metastasis are from abreast primary in women and from lung in men, radio-graphic surveys have focused on these 2 areas.4,7,8 How-ever, alternate primaries such as prostate, gastrointestinal,kidney, thyroid, and others have been described.7–10 Fur-her, multifocal nonocular sites may be overlooked byocal, limited radiographic imaging. Computed tomogra-hy (CT) allows for anatomic views that may not distin-uish between benign and malignant tumors. Positronmission tomography (PET) allows for physiological viewsith poor anatomic localization.11,12 Magnetic resonance
maging (MRI) is associated with a number of contraindi-ations (including body size, metallic implants, and renalnsufficiency) and has been shown to be inferior in stagingf tumors when compared to PET/CT.13
For these reasons, whole-body 18-fluoro-2-deoxyglucose(18F FDG) PET/CT is gaining worldwide use for thestaging, screening, and management of patients with can-cer.14–19 PET/CT combines the functional metabolismrevealed by PET with the anatomic characteristics foundon CT, putting form and function on the same diagnosticpage. In this study, we have evaluated PET/CT for initialstaging of patients with uveal metastasis.
METHODS
A RETROSPECTIVE OBSERVATIONAL CASE REVIEW OF CON-
secutive patients at a single clinical practice was per-formed. Entry criteria included a clinical diagnosis of uvealmetastasis, and at the initial visit, patients had either nohistory of malignancy, a history of cancer thought to be in
remission, or a known solitary nonocular metastasis. WhenLL RIGHTS RESERVED. 661
Original text:
givenname
Original text:
surname
Original text:
givenname
Original text:
surname
cNtbcs
6.6
necessary, nonocular systemic lesions were confirmed bybiopsy.
Ophthalmic examinations included a best-corrected vi-sual acuity, pupillary, ocular motor, and confrontationalvisual field assessment. Slit-lamp biomicroscopy and indi-rect ophthalmoscopy were performed. Ancillary testingincluded ultrasound imaging (USG), photography, fluores-cein angiography (FA), fundus autofluorescence (FAF),and optical coherence tomography (OCT). Once theclinical diagnosis of metastatic choroidal tumor was estab-lished, a whole-body 18F FDG PET/CT was obtained toevaluate the intraocular tumor, define the primary, anddiscover multi-organ metastatic disease.
● POSITRON EMISSION TOMOGRAPHY/COMPUTED TO-
MOGRAPHY IMAGING: Each patient in this study re-eived PET/CT imaging at different institutions in theew York area. Each imaging center was called to ensure
hat the protocols for PET/CT met the guidelines providedy the American College of Radiology. Briefly, the proto-ol was as follows and has been previously de-cribed.14,17,19,20 Imaging requires that patients refrain
from eating a carbohydrate-based dinner the night beforetesting and fast 4 to 6 hours before the injection of 18FFDG (radioactive tracer). These measures diminish phys-iological glucose utilization and reduce insulin serum levels
TABLE 1. Patient Charac
Patient
Age,
Years Sex History of Any Cancer
Ye
D
1 80 M None
2 52 F None
3 64 M None
4 71 M None
5 70 F None
6 55 M None
7 42 F None
8 69 M Multiple myeloma
9 78 M Cutaneous
melanoma
U
10 85 M Cutaneous
melanoma
11 41 M Colon
12 52 F Breast
13 63 F Breast
14 81 F Breast
15 70 M Pancreatic
16 73 M Lung
17 74 F Lung
18 57 F None
Mean 65.4 — —
to baseline.
AMERICAN JOURNAL OF662
Imaging was initiated approximately 60 minutes afterinjection of 18F FDG. The whole-body noncontrast CT isperformed first. The CT portion (General Electric Discov-ery ST, Discovery STE, Fairfield, Connecticut, USA) withBGO (bismuth germanate) consists of a multi-detectorhelical scanner. It is initiated at the top of the head andends at the bottom of the feet. Whole-body PETscanning is then performed. Patients are asked to lie in6 to 9 bed positions. The resolution of the PET scan is4 mm. The PET scan reconstructs the images and usesthe CT scan to correct for attenuation. Xeleris orAdvantage Workstation (General Electric software)computer software was used to fuse and display the PETand CT images simultaneously on 1 diagnostic page. Aradiologist who specializes in nuclear medicine at eachfacility evaluated the images. The data collection wasgathered from the reports.
Standardized maximum uptake (SUV) represents themetabolic activity of a lesion. Lesions that are SUVpositive are clinically correlated and evaluated for thesuspicion of malignancy vs benign causes. In all of thecenters in this study, tumors were graded as positivewith tracer uptake of 2.5 or more (comparison with thesurrounding structures). The standardized maximumSUV was calculated at each site by employing the
tics at Initial Presentation
ce
is Previous Treatment
Known
Metastasis
None None
None None
None None
None None
None None
None None
None None
None None
n Excision None
Excision None
Resection Lung
Mastectomy/chemotherapy/
radiation
None
Mastectomy None
Mastectomy/chemotherapy/
radiation
None
Chemotherapy Liver
Resection/chemotherapy Brain
Resection None
None None
— —
teris
ars Sin
iagnos
—
—
—
—
—
—
—
10
nknow
9
6
12
7
8
1
2
10
—
conventional formula using body weight normalization.
OPHTHALMOLOGY APRIL 2012
� re
RESULTS
EIGHTEEN PATIENTS (10 MALE AND 8 FEMALE) WITH A
mean age of 65.4 years (range 41– 85) diagnosed withintraocular metastatic tumors were screened withwhole-body PET/CT. Eight patients (44%) had no priorhistory of malignancy and 3 patients (17%) had ahistory of unrelated cancer. Seven patients (39%) hada history of cancer found to be metastatic to the eye; ofthese 7 patients, 4 were thought to be in remission and3 were thought to have a solitary nonocular lesion. In
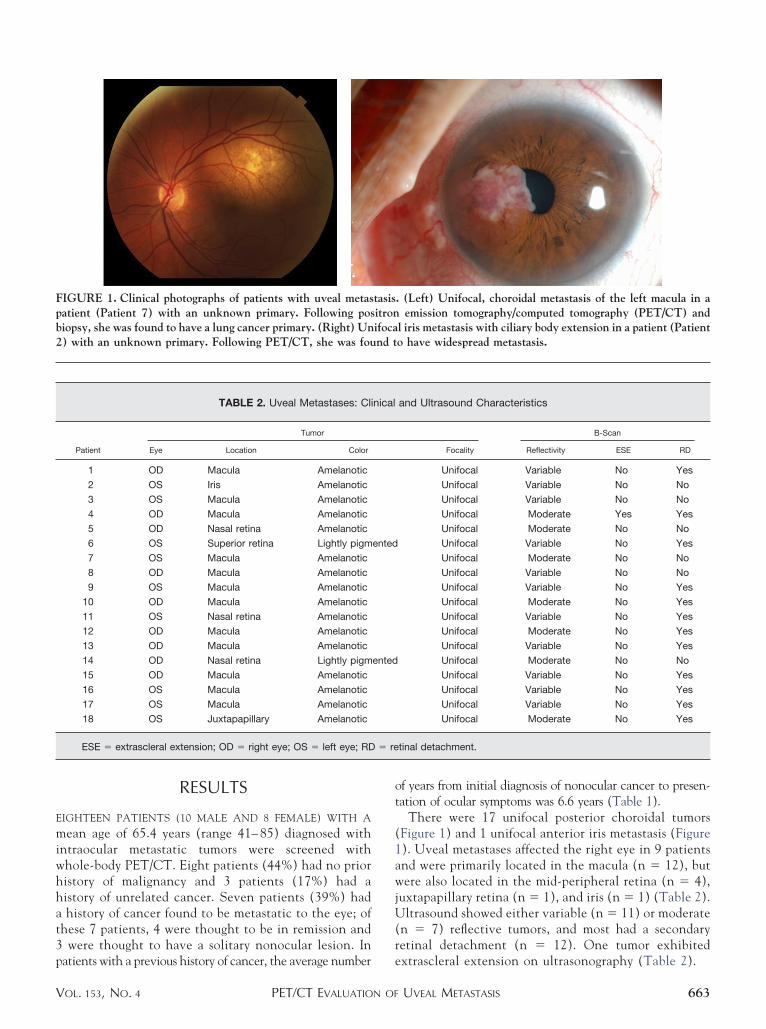
FIGURE 1. Clinical photographs of patients with uveal metaspatient (Patient 7) with an unknown primary. Following posbiopsy, she was found to have a lung cancer primary. (Right) Un2) with an unknown primary. Following PET/CT, she was fou
TABLE 2. Uveal Metastases: Cli
Tumor
Patient Eye Location Color
1 OD Macula Amelanotic
2 OS Iris Amelanotic
3 OS Macula Amelanotic
4 OD Macula Amelanotic
5 OD Nasal retina Amelanotic
6 OS Superior retina Lightly pigm
7 OS Macula Amelanotic
8 OD Macula Amelanotic
9 OS Macula Amelanotic
10 OD Macula Amelanotic
11 OS Nasal retina Amelanotic
12 OD Macula Amelanotic
13 OD Macula Amelanotic
14 OD Nasal retina Lightly pigm
15 OD Macula Amelanotic
16 OS Macula Amelanotic
17 OS Macula Amelanotic
18 OS Juxtapapillary Amelanotic
ESE � extrascleral extension; OD � right eye; OS � left eye; RD
patients with a previous history of cancer, the average number
PET/CT EVALUATION OFVOL. 153, NO. 4
of years from initial diagnosis of nonocular cancer to presen-tation of ocular symptoms was 6.6 years (Table 1).
There were 17 unifocal posterior choroidal tumors(Figure 1) and 1 unifocal anterior iris metastasis (Figure1). Uveal metastases affected the right eye in 9 patientsand were primarily located in the macula (n � 12), butwere also located in the mid-peripheral retina (n � 4),juxtapapillary retina (n � 1), and iris (n � 1) (Table 2).Ultrasound showed either variable (n � 11) or moderate(n � 7) reflective tumors, and most had a secondaryretinal detachment (n � 12). One tumor exhibited
. (Left) Unifocal, choroidal metastasis of the left macula in aemission tomography/computed tomography (PET/CT) and
l iris metastasis with ciliary body extension in a patient (Patiento have widespread metastasis.
and Ultrasound Characteristics
B-Scan
Focality Reflectivity ESE RD
Unifocal Variable No Yes
Unifocal Variable No No
Unifocal Variable No No
Unifocal Moderate Yes Yes
Unifocal Moderate No No
Unifocal Variable No Yes
Unifocal Moderate No No
Unifocal Variable No No
Unifocal Variable No Yes
Unifocal Moderate No Yes
Unifocal Variable No Yes
Unifocal Moderate No Yes
Unifocal Variable No Yes
Unifocal Moderate No No
Unifocal Variable No Yes
Unifocal Variable No Yes
Unifocal Variable No Yes
Unifocal Moderate No Yes
tinal detachment.
tasisitronifocand t
nical
ented
ented
extrascleral extension on ultrasonography (Table 2).
UVEAL METASTASIS 663
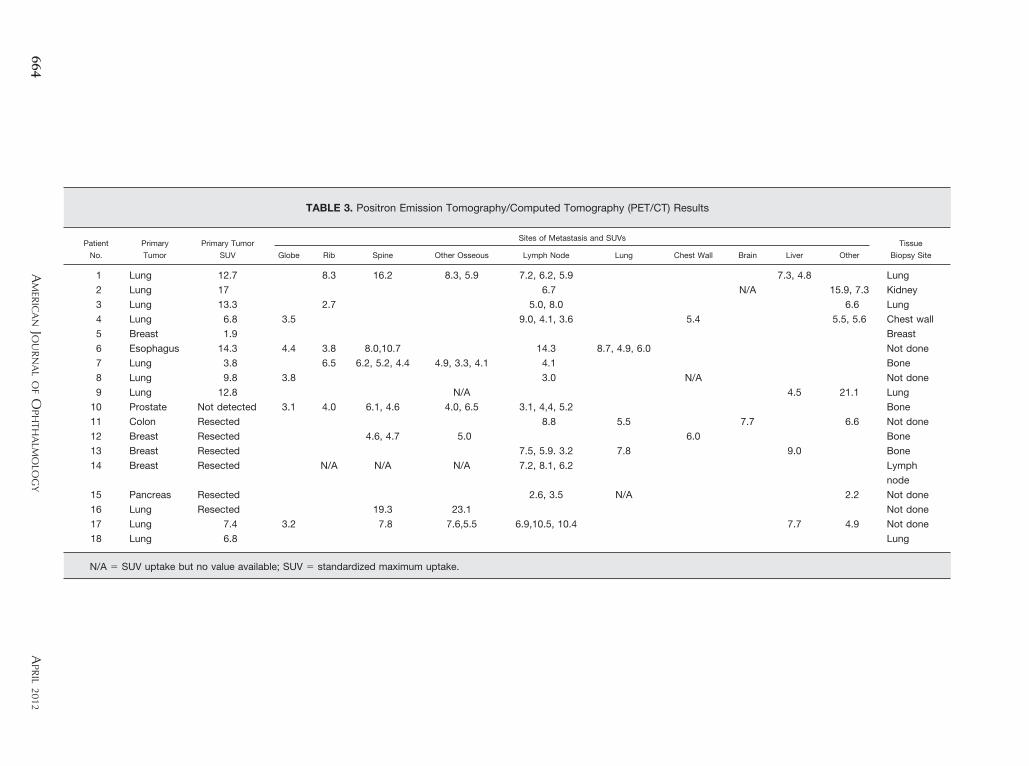
TABLE 3. Positron Emission Tomography/Computed Tomography (PET/CT) Results
Patient
No.
Primary
Tumor
Primary Tumor
SUV
Sites of Metastasis and SUVsTissue
Biopsy SiteGlobe Rib Spine Other Osseous Lymph Node Lung Chest Wall Brain Liver Other
1 Lung 12.7 8.3 16.2 8.3, 5.9 7.2, 6.2, 5.9 7.3, 4.8 Lung
2 Lung 17 6.7 N/A 15.9, 7.3 Kidney
3 Lung 13.3 2.7 5.0, 8.0 6.6 Lung
4 Lung 6.8 3.5 9.0, 4.1, 3.6 5.4 5.5, 5.6 Chest wall
5 Breast 1.9 Breast
6 Esophagus 14.3 4.4 3.8 8.0,10.7 14.3 8.7, 4.9, 6.0 Not done
7 Lung 3.8 6.5 6.2, 5.2, 4.4 4.9, 3.3, 4.1 4.1 Bone
8 Lung 9.8 3.8 3.0 N/A Not done
9 Lung 12.8 N/A 4.5 21.1 Lung
10 Prostate Not detected 3.1 4.0 6.1, 4.6 4.0, 6.5 3.1, 4,4, 5.2 Bone
11 Colon Resected 8.8 5.5 7.7 6.6 Not done
12 Breast Resected 4.6, 4.7 5.0 6.0 Bone
13 Breast Resected 7.5, 5.9. 3.2 7.8 9.0 Bone
14 Breast Resected N/A N/A N/A 7.2, 8.1, 6.2 Lymph
node
15 Pancreas Resected 2.6, 3.5 N/A 2.2 Not done
16 Lung Resected 19.3 23.1 Not done
17 Lung 7.4 3.2 7.8 7.6,5.5 6.9,10.5, 10.4 7.7 4.9 Not done
18 Lung 6.8 Lung
N/A � SUV uptake but no value available; SUV � standardized maximum uptake.
AM
ERIC
AN
JOU
RN
AL
OF
OPH
THA
LMO
LOG
Y664
APR
IL2012
e
PET/CT imaging revealed widespread metastasis (in-volving 2 or more metastatic foci) in 16 of 18 (89%)patients. The remaining 2 PET/CT scans (Patients 5and 18) revealed only the primary cancer but no othermetastatic lesions. The primary tumor was not visible in7 patients, 6 attributed to previous resection of thecancer and 1 because it was not detectable on PET/CT.The mean SUV for the primary tumor was 9.7, range1.9 –17 (Table 3).
Extraocular tissue biopsy was used to confirm theprimary tumor in 67% of patients (12/18). Fifty-sixpercent (10/18) were found to have metastatic lungcarcinoma (Figure 2), 22% (4/18) metastatic breastcarcinoma, and the other 22% had colon (n � 1),sophageal (n � 1), prostate (n � 1), and pancreatic
carcinomas (n � 1).The most common metastatic sites detected on PET/CT
were lymph node (13/18, 72%) and osseous (10/18, 56%)lesions (Figure 3). Less common metastatic sites werefound in the lung, brain, chest wall, and liver. Intraoculartumors were detected by PET/CT in 28% of cases (5/18)
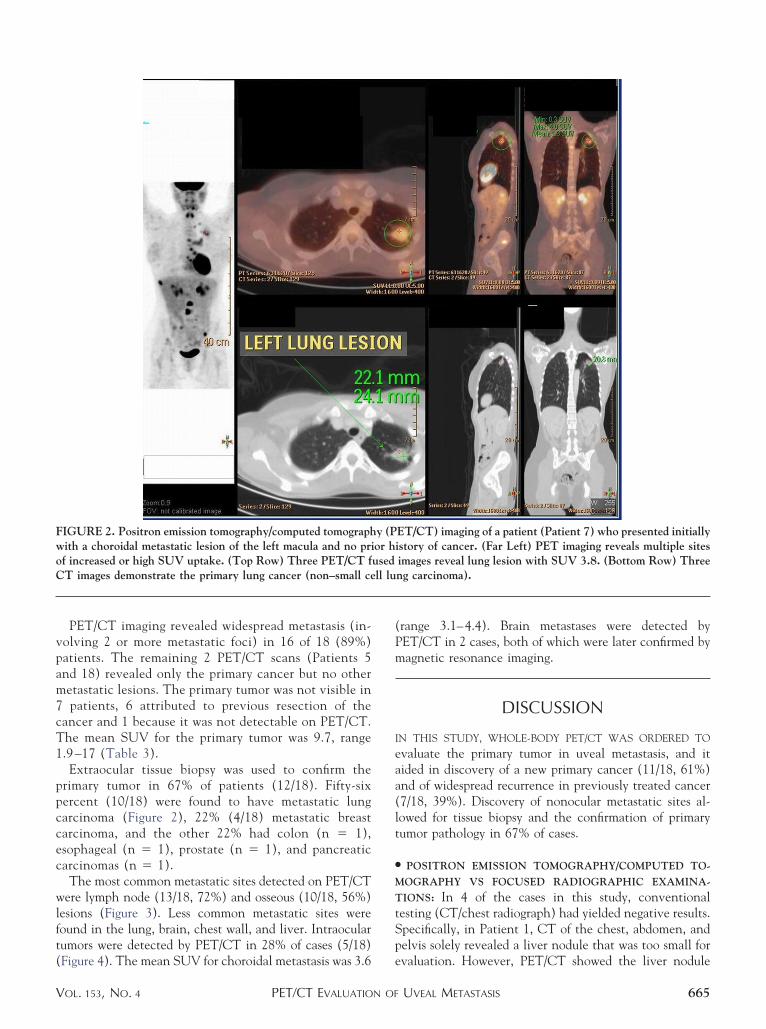
FIGURE 2. Positron emission tomography/computed tomographwith a choroidal metastatic lesion of the left macula and no priof increased or high SUV uptake. (Top Row) Three PET/CT fCT images demonstrate the primary lung cancer (non–small ce
(Figure 4). The mean SUV for choroidal metastasis was 3.6
PET/CT EVALUATION OFVOL. 153, NO. 4
(range 3.1–4.4). Brain metastases were detected byPET/CT in 2 cases, both of which were later confirmed bymagnetic resonance imaging.
DISCUSSION
IN THIS STUDY, WHOLE-BODY PET/CT WAS ORDERED TO
evaluate the primary tumor in uveal metastasis, and itaided in discovery of a new primary cancer (11/18, 61%)and of widespread recurrence in previously treated cancer(7/18, 39%). Discovery of nonocular metastatic sites al-lowed for tissue biopsy and the confirmation of primarytumor pathology in 67% of cases.
● POSITRON EMISSION TOMOGRAPHY/COMPUTED TO-
MOGRAPHY VS FOCUSED RADIOGRAPHIC EXAMINA-
TIONS: In 4 of the cases in this study, conventionaltesting (CT/chest radiograph) had yielded negative results.Specifically, in Patient 1, CT of the chest, abdomen, andpelvis solely revealed a liver nodule that was too small for
ET/CT) imaging of a patient (Patient 7) who presented initiallyistory of cancer. (Far Left) PET imaging reveals multiple sitesimages reveal lung lesion with SUV 3.8. (Bottom Row) Threeng carcinoma).
y (Por husedll lu
evaluation. However, PET/CT showed the liver nodule
UVEAL METASTASIS 665
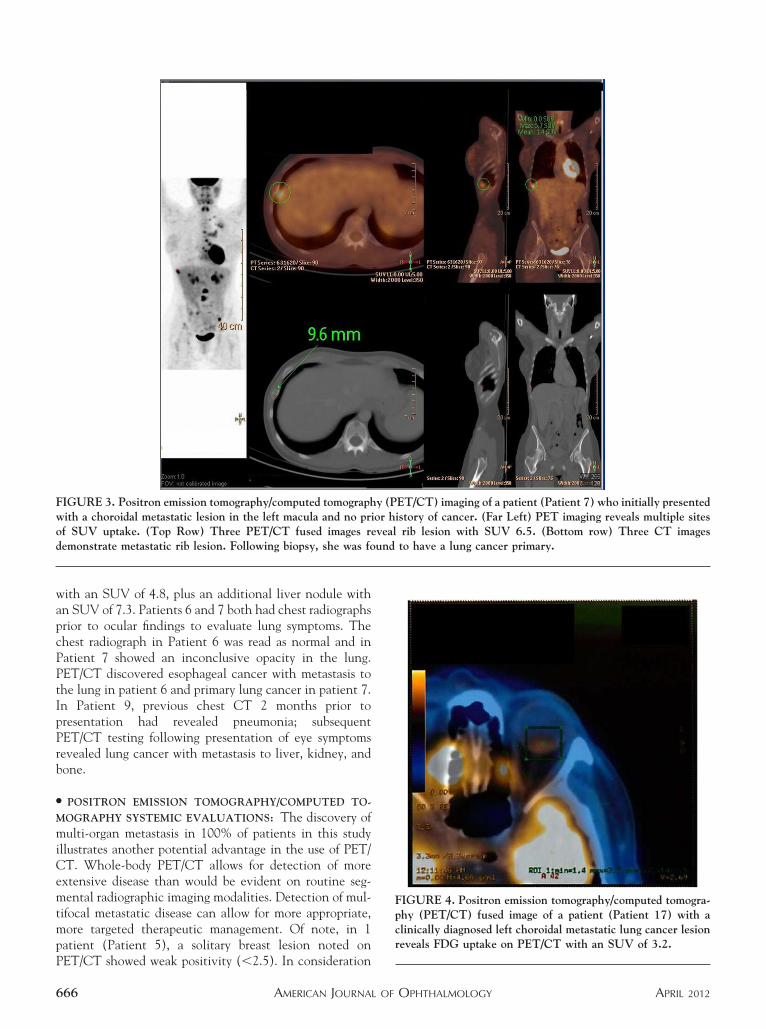
with an SUV of 4.8, plus an additional liver nodule withan SUV of 7.3. Patients 6 and 7 both had chest radiographsprior to ocular findings to evaluate lung symptoms. Thechest radiograph in Patient 6 was read as normal and inPatient 7 showed an inconclusive opacity in the lung.PET/CT discovered esophageal cancer with metastasis tothe lung in patient 6 and primary lung cancer in patient 7.In Patient 9, previous chest CT 2 months prior topresentation had revealed pneumonia; subsequentPET/CT testing following presentation of eye symptomsrevealed lung cancer with metastasis to liver, kidney, andbone.
● POSITRON EMISSION TOMOGRAPHY/COMPUTED TO-
MOGRAPHY SYSTEMIC EVALUATIONS: The discovery ofmulti-organ metastasis in 100% of patients in this studyillustrates another potential advantage in the use of PET/CT. Whole-body PET/CT allows for detection of moreextensive disease than would be evident on routine seg-mental radiographic imaging modalities. Detection of mul-tifocal metastatic disease can allow for more appropriate,more targeted therapeutic management. Of note, in 1patient (Patient 5), a solitary breast lesion noted on
FIGURE 3. Positron emission tomography/computed tomographwith a choroidal metastatic lesion in the left macula and no priof SUV uptake. (Top Row) Three PET/CT fused images redemonstrate metastatic rib lesion. Following biopsy, she was fo
y (PET/CT) imaging of a patient (Patient 7) who initially presentedor history of cancer. (Far Left) PET imaging reveals multiple sitesveal rib lesion with SUV 6.5. (Bottom row) Three CT imagesund to have a lung cancer primary.
PET/CT showed weak positivity (�2.5). In consideration
AMERICAN JOURNAL OF666
FIGURE 4. Positron emission tomography/computed tomogra-phy (PET/CT) fused image of a patient (Patient 17) with aclinically diagnosed left choroidal metastatic lung cancer lesionreveals FDG uptake on PET/CT with an SUV of 3.2.
OPHTHALMOLOGY APRIL 2012

socS
uai
tn
of our clinical diagnosis of uveal metastasis, this lesion wasbiopsied and ultimately proven to be breast cancer.
PET/CT is also particularly useful in detecting bonymetastasis, which was present in 10 of 18 of the patients inthis study. Osseous lesions are difficult to detect on CTalone and can be indistinguishable from benign lesions.18
PET/CT was found to be very helpful in detecting osseouslesions that later served as the source for tissue biopsy in 4cases.
● POSITRON EMISSION TOMOGRAPHY/COMPUTED TO-
MOGRAPHY INTRAOCULAR TUMOR IMAGING: In ourtudy, the intraocular tumor was PET/CT positive in 28%f cases. Reddy and associates investigated the SUV ofhoroidal melanoma and also found these tumors to beUV positive in 28% of patients.20 Of interest, the mean
apical height in that study was much larger (at 8.1 mm)than in the present study (2.8 mm). This indicates thatdespite their relatively small size, the uveal metastatictumors demonstrate a higher metabolic activity than largerprimary melanomas. Further, this suggests increased 18FDGptake in metastatic uveal tumors or higher metabolicctivity. This finding may be found helpful in distinguish-ng between metastatic and primary uveal malignancy.
● POSITRON EMISSION TOMOGRAPHY/COMPUTED TO-
MOGRAPHY DISADVANTAGES: One potential disadvan-age of PET/CT is the occurrence of false positives andegatives.18 FDG uptake is not specific for malignant cells
and false positives can occur in cases of inflammation,
infection, and trauma. Also, small non-avid tumors and447–451.
1
PET/CT EVALUATION OFVOL. 153, NO. 4
those within the hypermetabolic brain can be falselynegative. False-negative PET/CT findings were seen in 2patients: 1 had brain metastasis detected by MRI (Patient16), the other had a prostate cancer diagnosed to be theprimary source after biopsy of a distant bone metastasis(Patient 10).
The main disadvantages of PET/CT are often said to becost and limited availability. In review of this subject manyvariables must be considered. A wide range of prices arecharged for whole-body PET/CT imaging. PET/CT islikely to be more expensive than a single CT or magneticresonance imaging (MRI). However, the cost of total-bodyMRI or CT exceeds that of PET/CT alone. In addition,calculations of cost must take into account the expenseassociated with local treatments unnecessarily adminis-tered based on segmental imaging with missed lesions.Most important, there is the human cost of down-staging tumors because of lack of diagnosis. In sum, ifPET/CT can avoid the use of further imaging andtesting, as well as guide in accurate diagnosis andtreatment, it can prove cost-effective. Clearly, PET/CTcost is a complex issue that should be the subject of alarger prospective study.
In this series, whole-body PET/CT was found to be auseful investigative tool for patients with uveal metastases.However, a larger prospective study would be needed todetermine statistical proof of the efficacy of whole-bodyPET/CT vs other imaging modalities. Until such databecomes available, this study suggests that PET/CT can beused to locate a primary malignancy, to evaluate the
intraocular tumor, and to detect multi-organ metastasis.ALL AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OFInterest and none were reported. Publication of this article was supported by funding from The Eye Cancer Foundation, Inc, New York, New York,USA (http://eyecancerfoundation.net). Both authors (P.P., P.T.F.) were involved in design and conduct of the study; collection, management,analysis, and interpretation of the data; and preparation, review, or approval of the manuscript. Prospective Institutional Review Board (IRB)approval was obtained from the IRB of The New York Eye Cancer Center.
REFERENCES
1. Bloch RS, Gartner S. The incidence of ocular metastaticcarcinoma. Arch Ophthalmol 1971;85(6):673–675.
2. Albert DM, Rubenstein RA, Scheie HG. Tumor metasta-sis to the eye. I. Incidence in 213 adult patients withgeneralized malignancy. Am J Ophthalmol 1967;63(4):723–726.
3. Ferry AP, Font RL. Carcinoma metastatic to the eye andorbit. I. A clinicopathologic study of 227 cases. ArchOphthalmol 1974;92(4):276–286.
4. Ferry AP, Font RL. Carcinoma metastatic to the eye andorbit II. A clinicopathological study of 26 patients withcarcinoma metastatic to the anterior segment of the eye.Arch Ophthalmol 1975;93(7):472–482.
5. Solomon SD, Smith JH, O’Brien J. Ocular manifestations ofsystemic malignancies. Curr Opin Ophthalmol 1999;10(6):
6. Tang RA, Kellaway J, Young SE. Ophthalmic manifestationsof systemic cancer. Oncology 1991;5(1):59–66.
7. Shields CL, Shields JA, Gross NE, et al. Survey of 520eyes with uveal metastases. Ophthalmology 1997;104(8):1265–1276.
8. Soysal HG. Metastatic tumors of the uvea in 38 eyes. Can JOphthalmol 2007;42(6):832–835.
9. Kim CY, Ha CW, Lee SC. Vitreous and retinal metastasisfrom gastric cancer. Eur J Ophthalmol 2010;20(3):615–617.
10. Ahmadi MA, Nicholes D, Esmaeli B. Late choroidal metas-tasis secondary to papillary thyroid carcinoma. Am J Oph-thalmol 2001;132(5):796–798.
11. Cohade C, Osman M, Leal J, et al. Direct comparison of18F-FDG-PET and PET/CT in patients with colorectal car-cinoma. J Nucl Med 2003;44(11):1797–1803.
2. Messa C, Bettinardi V, Picchio M, et al. PET/CT indiagnostic oncology. Q J Nucl Med Mol Imaging 2004;48(2):
66–75.UVEAL METASTASIS 667

1
1
1
2
“ttut
S
13. Antoch G, Vogt FM, Freudenberg LS, et al. Whole body dualmodality PET/CT and whole body MRI for tumor staging inoncology. JAMA 2003;290(24):3199–3206.
14. Finger PT, Kurli M, Reddy S, Tena LB, Pavlick AC. Wholebody PET/CT for initial staging of choroidal melanoma. Br JOphthalmol 2005;89(10):1270–1274.
15. Schoder H, Larson SM, Yeung HWD. PET/CT in oncology:integration into clinical management of lymphoma, mela-noma, and gastrointestinal malignancies. J Nucl Med 2004;45(Suppl 1):72S–81S.
16. Freudenberg LS, Schueler AO, Beyer T, et al. Whole bodyfluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) in staging advanceduveal melanoma. Surv Ophthalmol 2004;49(5):537–540.
AJO History of OWilliam Moon’s Ta
Becoming blind himself by age 21, William Moon(1818-94) developed the first widely-used means oreading for the blind: a tactile reading system termed
Moon.” It is a simpler reading system than Braille and is easiero memorize. Its characters are bold and simple in outline andhus easy to distinguish by touch. Most characters are 9naltered or slightly-modified Roman letters in different posi-ions. These are easier to discern when fine motor skills are
ubmitted by Alice (Wendy) T. Gasch from the Cogan Ophth
AMERICAN JOURNAL OF668
7. Kurli M, Chin K, Finger PT. Whole-body 18 FDG PET/CTimaging for lymph node and metastatic staging of conjunctivalmelanoma. Br J Ophthalmol 2008;92(4):479–482.
8. Mawlawi O, Townsend DW. Multimodality imaging: anupdate on PET/CT technology. Eur J Nucl Med Mol Imaging2009:36(Suppl 1):S15–29.
9. Roe RH, Finger PT, Kurli M, Tena LB, Iacob CE. Whole-body positron emission tomography/computed tomographyimaging and staging of orbital lymphoma. Ophthalmology2006;113(10):1854–1858.
0. Reddy S, Kurli M, Tena LB, Finger PT. PET/CT imaging:detection of choroidal melanoma. Br J Ophthalmol2005;89(10):1265–1269.
halmology Seriesle Reading System
oor, or when finger tips are calloused from manual labor,umbed by peripheral neuropathy, or otherwise have lostensation. Thus, Moon is particularly helpful to blind, learn-g-disabled children and adults, and to print-readers who
ave lost their vision late in life. Sometimes, the latter useoon as a stepping-stone to learn Braille. Although Braille
as superseded Moon, it has not replaced it. Moon is widely-sed particularly in Great Britain.
phtcti
fpnsinhMhu
almic History Society.
OPHTHALMOLOGY APRIL 2012
Related Documents



![Tecniche di imaging tomografico non distruttivo in ... · Tecniche di imaging tomografico non ... Alcuni Traccianti PET • Metabolismo del glucosio [18F]FDG ... 18FDG-PET 18FDG-PET](https://static.cupdf.com/doc/110x72/5c6b2b7109d3f262278b69d2/tecniche-di-imaging-tomografico-non-distruttivo-in-tecniche-di-imaging-tomografico.jpg)







