WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage

WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
ISBN 978-92-4-155015-4
© World Health Organization 2017
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there
the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such
reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Printed in Switzerland
Acknowledgements 1
Acronyms and abbreviations 2
Executive Summary 3
1. Background 5
2. Methods 6
3. Evidence and recommendation 11
4. Research implications 20
5. Dissemination and implementation of the recommendation 21
6. Applicability issues 22
7. Updating the recommendation 23
References 24
Annex 1. External experts and WHO staff involved in the preparation of the guideline 26
Annex 2. Critical and important outcomes for decision-making 29
Annex 3: Summary and management of declared interests from GDG members 30
Annex 4. Summary of the considerations related to the strength of the recommendations 32
Annex 5. GRADE Tables 33
Contents

WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
1
AcknowledgementsThe Department of Reproductive Health and Research of the World Health Organization gratefully acknowledges the contributions of many individuals and organizations to the updating of this recommendation. Work on this update was coordinated by Olufemi Oladapo, Joshua Vogel and A. Metin Gülmezoglu of the WHO Department of Reproductive Health and Research.
WHO extends sincere thanks to Edgardo Abalos, Yap-Seng Chong, Catherine Deneux-Tharaux, Bukola Fawole, Justus Hofmeyr, Caroline Homer, Pisake Lumbiganon, Suellen Miller, Ashraf Nabhan, Hiromi Obara, Zahida Qureshi, Rahat Qureshi and Helen West who served as members of the Guideline Development Group (GDG), and to James Neilson for chairing the technical consultation. We also thank Richard Adanu, Fernando Althabe, Sue Fawcus, Jamilu Tukur and Dilys Walker who were members of the External Review Group. WHO also gratefully acknowledges the contribution of the members of the Executive Guideline Steering Group.
the GRADE tables and drafted the narrative summary of evidence. Joshua Vogel and Olufemi Oladapo revised the narrative summaries and double-checked the corresponding GRADE tables. Joshua Vogel, Olufemi Oladapo, A. Metin Gülmezoglu and Mercedes Bonet commented on the draft document before it was reviewed by participants at the WHO technical consultation. The External Review Group peer-
We acknowledge the various organizations that were represented by observers
Agency for International Development), Kusum Thapa (Maternal and Child Survival Program/Jhpiego), Janna Patterson (Bill & Melinda Gates Foundation), Sally Tracy (International Confederation of Midwives), Gerard Visser (International Federation of Gynecology and Obstetrics) and Beverly Winikoff (Gynuity Health Projects). Haleema Shakur-Still (London School of Hygiene and Tropical Medicine) provided an overview
update – Mavjuda Babamuradova, Ramez Khairi Mahaini, Anoma Jayathilaka, Bremen De Mucio, Claudio Sosa, Mari Nagai and Léopold Ouedraogo.
The United States Agency for International Development and the Department of
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
2
Acronyms and abbreviations
trial
DOI Declaration of Interest
FIGO International Federation of Gynecology and Obstetrics
GDG Guideline Development Group
GRC Guideline Review Committee
GRADE Grading of Recommendations, Assessment, Development, and Evaluation
GSG Executive Guideline Steering Group
ICM International Confederation of Midwives
IPD individual participant data meta-analysis
LMIC low- and middle-income country
LY life-year
MCA WHO Department of Maternal, Newborn, Child and Adolescent Health
MPA Maternal and Perinatal Health & Preventing Unsafe Abortion (a team in
MPH maternal and perinatal health
NNT number needed to treat
PICO population (P), intervention (I), comparison (C), outcome (O)
PPH postpartum haemorrhage
RHR [WHO Department of] Reproductive Health and Research
RR relative risk
SDG Sustainable Development Goals
TXA tranexamic acid
UN United Nations
UNFPA United Nations Population Fund
USAID United States Agency for International Development
WHO World Health Organization
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
3
Executive Summary Introduction
more within 24 hours after birth, and it affects about 5% of all women giving birth around the world. Globally, nearly one quarter of all maternal deaths are associated with PPH, and in most low-income countries it is the main cause of maternal mortality.
Improving care for women around the time of childbirth to prevent and treat PPH is a necessary step towards achievement of the health targets of the Sustainable Development Goals (SDGs). Efforts to prevent and reduce PPH-associated morbidity and mortality can reduce the profound inequities in maternal health globally. To achieve this, healthcare providers, health managers, policy makers and other stakeholders need up-to-date and evidence-based recommendations to inform clinical policies and practices.
In 2017, the Executive Guideline Steering Group (GSG) on WHO maternal and perinatal health recommendations prioritized the updating of the existing WHO recommendation on the use of tranexamic acid (TXA) for PPH treatment in response to important new evidence on this intervention. This updated recommendation thus supersedes the previous recommendation on TXA for PPH treatment, which was issued in the 2012 WHO recommendations on prevention and treatment of PPH.
Target audienceThe primary audience includes health professionals who are responsible for developing national and local health protocols (particularly those related to PPH) and those directly providing care to pregnant women and their newborns, including midwives, nurses, general medical practitioners, obstetricians, managers of maternal and child health programmes, and relevant staff in ministries of health, in all settings.
Guideline development methodsThe updating of this recommendation was guided by standardized operating pro-cedures in accordance with the process described in the WHO handbook for guide-line development. The recommendation was initially developed using this process,
of the evidence, (iii) assessment and synthesis of evidence, (iv) formulation of the recommendation, and (v) planning for the dissemination, implementation, impact evaluation and updating of the recommendation.
Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) -
oritized question. WHO convened an online technical consultation on 29 August 2017 where an international group of experts – the Guideline Development Group (GDG) – formulated and approved the recommendation.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
4
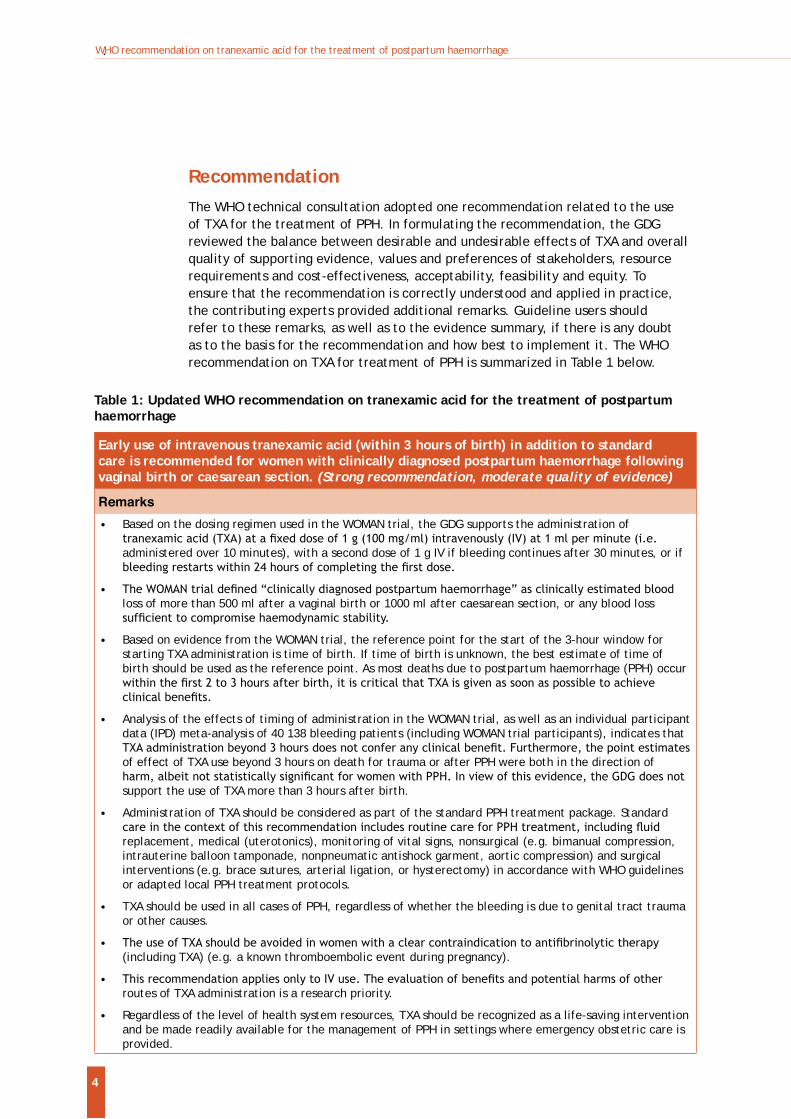
Table 1: Updated WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
Early use of intravenous tranexamic acid (within 3 hours of birth) in addition to standard care is recommended for women with clinically diagnosed postpartum haemorrhage following vaginal birth or caesarean section. (Strong recommendation, moderate quality of evidence)
Remarks
Based on the dosing regimen used in the WOMAN trial, the GDG supports the administration of
administered over 10 minutes), with a second dose of 1 g IV if bleeding continues after 30 minutes, or if
loss of more than 500 ml after a vaginal birth or 1000 ml after caesarean section, or any blood loss
Based on evidence from the WOMAN trial, the reference point for the start of the 3-hour window for starting TXA administration is time of birth. If time of birth is unknown, the best estimate of time of birth should be used as the reference point. As most deaths due to postpartum haemorrhage (PPH) occur
Analysis of the effects of timing of administration in the WOMAN trial, as well as an individual participant data (IPD) meta-analysis of 40 138 bleeding patients (including WOMAN trial participants), indicates that
of effect of TXA use beyond 3 hours on death for trauma or after PPH were both in the direction of
support the use of TXA more than 3 hours after birth.
Administration of TXA should be considered as part of the standard PPH treatment package. Standard
replacement, medical (uterotonics), monitoring of vital signs, nonsurgical (e.g. bimanual compression, intrauterine balloon tamponade, nonpneumatic antishock garment, aortic compression) and surgical interventions (e.g. brace sutures, arterial ligation, or hysterectomy) in accordance with WHO guidelines or adapted local PPH treatment protocols.
TXA should be used in all cases of PPH, regardless of whether the bleeding is due to genital tract trauma or other causes.
(including TXA) (e.g. a known thromboembolic event during pregnancy).
routes of TXA administration is a research priority.
Regardless of the level of health system resources, TXA should be recognized as a life-saving intervention and be made readily available for the management of PPH in settings where emergency obstetric care is provided.
RecommendationThe WHO technical consultation adopted one recommendation related to the use of TXA for the treatment of PPH. In formulating the recommendation, the GDG reviewed the balance between desirable and undesirable effects of TXA and overall quality of supporting evidence, values and preferences of stakeholders, resource requirements and cost-effectiveness, acceptability, feasibility and equity. To ensure that the recommendation is correctly understood and applied in practice, the contributing experts provided additional remarks. Guideline users should refer to these remarks, as well as to the evidence summary, if there is any doubt as to the basis for the recommendation and how best to implement it. The WHO recommendation on TXA for treatment of PPH is summarized in Table 1 below.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
5
1. Background
birth, and affects about 5% of all women giving birth around the world.1,2 Globally, nearly one quarter of all maternal deaths are associated with PPH, and in most low-income countries it is the main cause of maternal mortality.3
Severe maternal health conditions, such as organ dysfunction or death, generally occur following substantial blood loss that compromises maternal haemodynamic stability. Uterine atony is the most common cause of PPH and a leading cause of maternal mortality worldwide.3 Genital tract trauma (that is, vaginal or cervical lacerations), uterine rupture, retained placental tissue, or maternal bleeding disorders are frequently associated with PPH. Although the majority of women
labour and multiple gestation are obstetric conditions that are associated with an increased risk of bleeding after birth.4 In addition, anaemia is a common aggravating factor.
The majority of PPH-associated deaths could be avoided by the use of prophylactic uterotonics during the third stage of labour and appropriate treatment. Thus, improving health care for women during childbirth to prevent and treat PPH is a necessary step towards achievement of the health targets of the Sustainable Development Goals (SDGs). Furthermore, 99% of all maternal deaths occur in low- and middle-income countries (LMICs). Efforts to prevent and reduce PPH-associated morbidity and mortality can thus reduce the profound inequities in maternal health globally. In support of this, health workers at all levels of care (particularly in LMICs) need to have access to appropriate medications and training in relevant procedures. Healthcare providers, health managers, policy-makers and other stakeholders also need up-to-date, evidence-based recommendations to inform clinical policies and practices, in order to enable improved healthcare outcomes.
In 2012, WHO published 32 recommendations for the prevention and treatment of PPH, including a recommendation on the use of TXA for treatment of PPH.5 These recommendations were developed according to WHO guideline development standards, including synthesis of available research evidence, use of the GRADE methodology, and formulation of recommendations by a guideline panel of international experts.
In 2017, the Executive GSG on WHO maternal and perinatal health recommendations prioritized the updating of the existing WHO recommendation on the use of TXA for PPH treatment in response to important new evidence on this question. This updated recommendation thus supersedes the previous recommendation on TXA for PPH treatment, issued in the 2012 WHO recommendations on prevention and treatment of PPH.
Rationale and objectives TXA is a competitive inhibitor of plasminogen activation, and it can reduce bleeding
6 It is in routine clinical use for reduction of blood loss in surgery and trauma, and it is listed on the WHO Essential Medicines List for management of anticoagulation.7 At the time of
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
6
the GDG meeting on prevention and treatment of PPH in March 2012, there was no direct evidence on the effectiveness and safety of TXA when used for treatment of PPH. The GDG conditionally recommended the use of TXA for the treatment of PPH only when uterotonics fail to control the bleeding or when the bleeding is thought to be partly due to trauma. The GDG noted that a large, randomized controlled trial
administration of TXA on mortality, hysterectomy, and other morbidities in women with clinically diagnosed PPH – was ongoing.8 The WOMAN trial has now concluded,
9 In light of this new evidence, the Executive GSG prioritized the updating of the recommendation on TXA use for PPH treatment.
and practices, the Department of Reproductive Health and Research (RHR) has now updated the recommendation on the use of TXA for treatment of PPH. This recommendation provides a foundation for the sustainable implementation of the intervention globally.
Target audienceThe primary audience includes health professionals who are responsible for developing national and local health guidelines and protocols (particularly those related to PPH) and those directly providing care to women during labour and childbirth, including midwives, nurses, general medical practitioners, obstetricians, managers of maternal and child health programmes and relevant staff in ministries of health, in all settings.
This recommendation will also be of interest to professional societies involved in the care of pregnant women, nongovernmental organizations concerned with promotion of people-centred maternal care, and implementers of maternal and child health programmes.
Scope of the recommendationThe question for this recommendation was: in women with PPH (P), does administration of TXA for PPH treatment (I) compared to placebo, no treatment or other treatments (C), improve outcomes (O)? If so, what is the most appropriate period to administer TXA to improve outcomes? The population affected by this recommendation includes women who experience PPH in low-, middle- or high-income settings.
2. MethodsThis recommendation is an update of the existing recommendation relating to TXA use for PPH treatment, published in the WHO recommendations for prevention and treatment of postpartum haemorrhage (2012).5
in accordance with the process described in the WHO handbook for guideline development.10
question and critical outcomes, (ii) retrieval of the evidence, (iii) assessment and
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
7
synthesis of evidence, (iv) formulation of the recommendation, and (v) planning for the dissemination, implementation, impact evaluation and updating of the recommendation. The WHO recommendation on TXA use for treatment of PPH was
important evidence on this question.
Contributors to the guideline
Executive Guideline Steering Group (Executive GSG)
The Executive GSG is an independent panel of external experts and relevant stakeholders from the six WHO regions. This group advises WHO on the prioritization of new and existing questions in maternal and perinatal health for recommendation development or updating.
WHO Steering Group
The WHO Steering Group, comprising WHO staff members from the Departments of Reproductive Health and Research (RHR) and Maternal, Newborn, Child and Adolescent Health (MCA), managed the updating process. The Group drafted the key
guideline methodologist, as well as the guideline development and external review groups. In addition, the WHO Steering Group supervised the retrieval and syntheses of evidence, organized the Guideline Development Group meeting, drafted and
implementation and impact assessment. The members of the Steering Group are presented in Annex 1.
Guideline Development Group
stakeholders from the six WHO regions to constitute the WHO Maternal and Perinatal Health Guideline Development Group (MPH-GDG). This is a diverse group of experts who are skilled in critical appraisal of research evidence; implementation of evidence-based recommendations; guideline development methods; and clinical practice, policy and programmes relating to maternal and perinatal health. Members
expertise cuts across thematic areas within maternal and perinatal health.
From the MPH-GDG pool, 14 external experts and relevant stakeholders were invited to constitute the Guideline Development Group (GDG) for updating this recommendation. This wasis a diverse group of individuals with expertise in PPH research, guideline development methods, and clinical policy and programmes relating to PPH prevention and treatment.
The GDG members convened for this recommendation were selected in a way that ensured geographic representation and gender balance, and there were no
to inform the recommendation, advised on the interpretation of this evidence,
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
8
are presented in Annex 1.
External Review Group
and commented on clarity of the language, contextual issues and implications for implementation. The Group ensured that the decision-making processes have considered and incorporated contextual values and preferences of potential users of the recommendations, healthcare professionals and policy makers. They did not change the recommendation that was formulated by the GDG. The members of the External Review Group are presented in Annex 1.
Systematic review team and guideline methodologists
A Cochrane systematic review on this question was initiated, supported by the Cochrane Pregnancy and Childbirth Group. The WHO Steering Group reviewed and provided input into the protocol, and it worked closely with the Cochrane Pregnancy and Childbirth Group to appraise the evidence using the GRADE methodology. A representative of the Cochrane Pregnancy and Childbirth Group attended the GDG meeting to provide an overview of the available evidence and GRADE tables and to respond to technical queries from the GDG.
External partners and observers
Representatives of the United States Agency for International Development (USAID), the Maternal and Child Survival Programme (MCSP)/Jhpiego, the Bill & Melinda Gates Foundation (BMGF), the International Confederation of Midwives (ICM), the International Federation of Gynecology and Obstetrics (FIGO) and Gynuity Health Projects participated in the GDG meeting as observers. These organizations, with a long history of collaboration with the RHR Department in guideline dissemination and implementation, are implementers of the updated recommendation. In addition, one of the WOMAN trial co-ordinators from the London School of Hygiene
the WOMAN trial and responded to questions from the GDG, but did not participate in GDG deliberations nor revision of the recommendation. The list of observers who
The critical and important outcomes were aligned with the prioritized outcomes from the WHO recommendations on prevention and treatment of PPH (2012).5 These
published, systematic reviews and a prioritization of outcomes by the 2012 GDG panel. During the updating of this recommendation, a further two outcomes were
question: namely, maternal death (all causes) and maternal death due to bleeding.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
9
this document for evidence searching, retrieval, grading and formulation of the recommendation. The list of critical and important outcomes is provided in Annex 2.
by the Cochrane Pregnancy and Childbirth Group, as an offshoot of the existing Cochrane review of treatment for PPH.11 This systematic review12 was the primary source of evidence for this recommendation.
Randomized, controlled trials relevant to the key question were screened by the review authors, and data on relevant outcomes and comparisons were extracted
comparisons and outcomes (those that were not relevant to the recommendation
(GRADEpro) and GRADE criteria were used to critically appraise the retrieved
prepared for comparisons of interest, including the assessment and judgements for each outcome, and the estimated risks.
Quality assessment and grading of the evidence The quality assessment of the body of evidence for each outcome was performed using the GRADE approach.13 Using this approach, the quality of evidence for each
Study design limitationsindividual study and then across studies contributing to the outcome. For
by the majority of the studies contributing to the outcome.
Inconsistency of the results The similarity in the results for a given outcome was assessed by exploring the magnitude of differences in the direction and size of effects observed from different studies. The quality of evidence was not
overlapped, whereas quality was downgraded when the results were in different
Indirectness The quality of evidence was downgraded when there were serious or very serious concerns regarding the directness of the evidence, that is, whether there were important differences between the research reported and the context for which the recommendation was being prepared. Such differences were related, for instance, to populations, interventions, comparisons or outcomes of interest.
Imprecision This assessed the degree of uncertainty around the estimate of effect. As this is often a function of sample size and number of events, studies with
effect estimates, were downgraded for imprecision.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
10
Publication bias Quality rating could also be affected by perceived or statistical evidence of bias to underestimate or overestimate the effect of an intervention as a result of selective publication based on study results. We considered downgrading evidence by one level for strong suspicion of publication bias.
Formulation of recommendations
corresponding GRADE tables, other related documents for assessment of values and preferences, resource requirements and cost-effectiveness, acceptability, feasibility and equity were provided in advance to members of the GDG. The GDG members and other participants were then invited to attend an online technical consultation (see Annex 1 for the list of participants) organized by the Steering Group in Geneva, Switzerland, on 29 August 2017. During the technical consultation, the GDG members reviewed and discussed the balance between desirable and undesirable effects of TXA and the overall quality of supporting evidence, values and preferences of stakeholders, resource requirements and cost-effectiveness,
remarks.
Declaration of interests by external contributorsAccording to WHO regulations, all experts must declare their relevant interests prior to participation in WHO guideline development processes and meetings. All GDG members were therefore required to complete a standard WHO Declaration of Interest (DOI) form before engaging in the guideline development process and before participating in the guideline-related meeting. The WHO Steering Group
the guideline development process and recommendation. To ensure consistency,
interests in the WHO Handbook for Guideline Development for all experts. All
WHO DOI guidelines on a case-by-case basis and communicated to the experts.
to the guideline development process or reduce its credibility, the experts were only
no further actions were taken.
interest were managed by the Steering Group.
Decision-making during the technical consultationDuring the technical consultation, the GDG reviewed and discussed the evidence
desirable and undesirable effects of TXA and the overall quality of the evidence, the GDG applied additional criteria based on the GRADE evidence-to-decision framework to determine the direction and strength of the recommendation. These criteria
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
11
included values of stakeholders, resource implications, acceptability, feasibility and equity. Considerations were based on the experience and opinions of members of the GDG and supported by evidence from a literature search where available.
synthesis or detailed economic evaluation) were not performed to inform discussions on these criteria. Evidence-to-decision tables were used to describe and synthesize these considerations.
or more of the participants. None of the GDG members expressed opposition to the recommendation.
Document preparation Prior to the online technical consultation, the WHO Steering Group prepared a draft
relevant to the deliberation of the GDG. The draft documents were made available to the participants of the technical consultation two weeks before the meeting for
the deliberations and decisions of the participants. The draft document was sent
approval.
Peer review
involved in the guideline panel for peer review. The WHO Steering Group evaluated the inputs of the peer reviewers for inclusion in this document. After the technical
to the document were limited to correction of factual errors and improvement in language to address any lack of clarity.
3. Evidence and recommendationThe following section outlines the recommendation and the corresponding narrative summary of evidence for the prioritized question. The GRADE table is presented in Annex 5. The evidence-to-decision table, summarizing the balance between desirable and undesirable effects and the overall quality of the supporting evidence, values and preferences of stakeholders, resource requirements, cost-effectiveness, acceptability, feasibility and equity that were considered in determining the strength and direction of the recommendation, is presented in Annex 4.
The following recommendation was adopted by the GDG. Evidence on the effectiveness of the intervention was derived from one systematic review and was summarized in GRADE tables (Annex 5). The quality of the supporting evidence was
is correctly understood and appropriately implemented in practice, additional
recommendation.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
12
Early use of intravenous tranexamic acid (within 3 hours of birth) in addition to standard care is recommended for women with clinically diagnosed postpartum haemorrhage following vaginal birth or caesarean section. (Strong recommendation, moderate quality of evidence)
Remarks
Based on the dosing regimen used in the WOMAN trial, the GDG supports the
intravenously (IV) at 1 ml per minute (i.e. administered over 10 minutes), with a second dose of 1 g IV if bleeding continues after 30 minutes, or if bleeding restarts within 24
estimated blood loss of more than 500 ml after a vaginal birth or 1000 ml after
Based on evidence from the WOMAN trial, the reference point for the start of the 3-hour window for starting TXA administration is time of birth. If time of birth is unknown, the best estimate of time of birth should be used as the reference point. As
Analysis of the effects of timing of administration in the WOMAN trial, as well as an individual participant data (IPD) meta-analysis of 40 138 bleeding patients (including WOMAN trial participants), indicates that TXA administration beyond 3 hours does
beyond 3 hours on death for trauma or after PPH were both in the direction of harm,
GDG does not support the use of TXA more than 3 hours after birth.
Administration of TXA should be considered as part of the standard postpartum haemorrhage treatment package. Standard care in the context of this recommendation
(uterotonics), monitoring of vital signs, nonsurgical (e.g. bimanual compression, intrauterine balloon tamponade, nonpneumatic antishock garment, aortic compression) and surgical interventions (e.g. brace sutures, arterial ligation or hysterectomy) in accordance with WHO guidelines or adapted local PPH treatment protocols.
TXA should be used in all cases of PPH regardless of whether the bleeding is due to genital tract trauma or other causes.
The use of TXA should be avoided in women with a clear contraindication to
pregnancy).
harms of other routes of TXA administration is a research priority.
Regardless of the level of health system resources, TXA should be recognized as a life-saving intervention and be made readily available for the management of postpartum haemorrhage in settings where emergency obstetric care is provided.
A. Review Question For women with postpartum haemorrhage (P), does administration of
tranexamic acid in addition to standard care (I) compared to standard care alone (C), improve outcomes (O)?
If so, when is the most appropriate period to administer tranexamic acid to improve outcomes?
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
13
B. Assessment
Effects of the intervention
What are the anticipated effects of administration of TXA in addition to standard care for PPH treatment?
Research evidence
Evidence on the use of TXA for treatment of PPH was extracted from a forthcoming Cochrane systematic review of two trials (20 212 women).12 This
interventions other than TXA.
One multicentre trial was conducted in eight obstetric units in France with recruitment between 2005 and 2008.14 This trial randomized 152 women with PPH > 800 ml after a vaginal birth. The intervention group received a loading dose of 4 g TXA mixed with 50 ml saline, administered IV over 1 hour, followed by a maintenance dose of 1 g/hour for 6 hours. Women in the control group were given standard care only, as per the routine practice in participating facilities. The primary outcome was blood loss between randomization and 6 hours.
The second (WOMAN trial) was a multicountry, multicentre, placebo-controlled randomised trial of 20 060 women in 193 hospitals, across 21 high-, middle- and low-income countries conducted between March 2010 and April 2016.9 The trial
blood loss after a vaginal birth of > 500 ml, or > 1000 ml following a caesarean
where the clinician responsible for care was uncertain as to whether or not to use TXA. In addition to usual care, women in the experimental group were initially given 1 g TXA IV in a 10 ml solution, at an approximate rate of 1 ml/minute, as soon as possible after randomization. A second dose was used if bleeding continued after 30 minutes or if it stopped and restarted within 24 hours after
regimen. When the trial protocol was registered, the primary outcome was a composite of death from all causes or hysterectomy within 42 days. During the course of the study (but before results were available or any unblinding), the primary outcome was revised to maternal death due to bleeding, and the sample size increased.
Evidence regarding this intervention is almost entirely derived from the WOMAN trial.
Comparison: TXA (in addition to standard care) versus standard care alone
The effects of TXA on critical outcomes for all women with PPH, regardless of
described below.
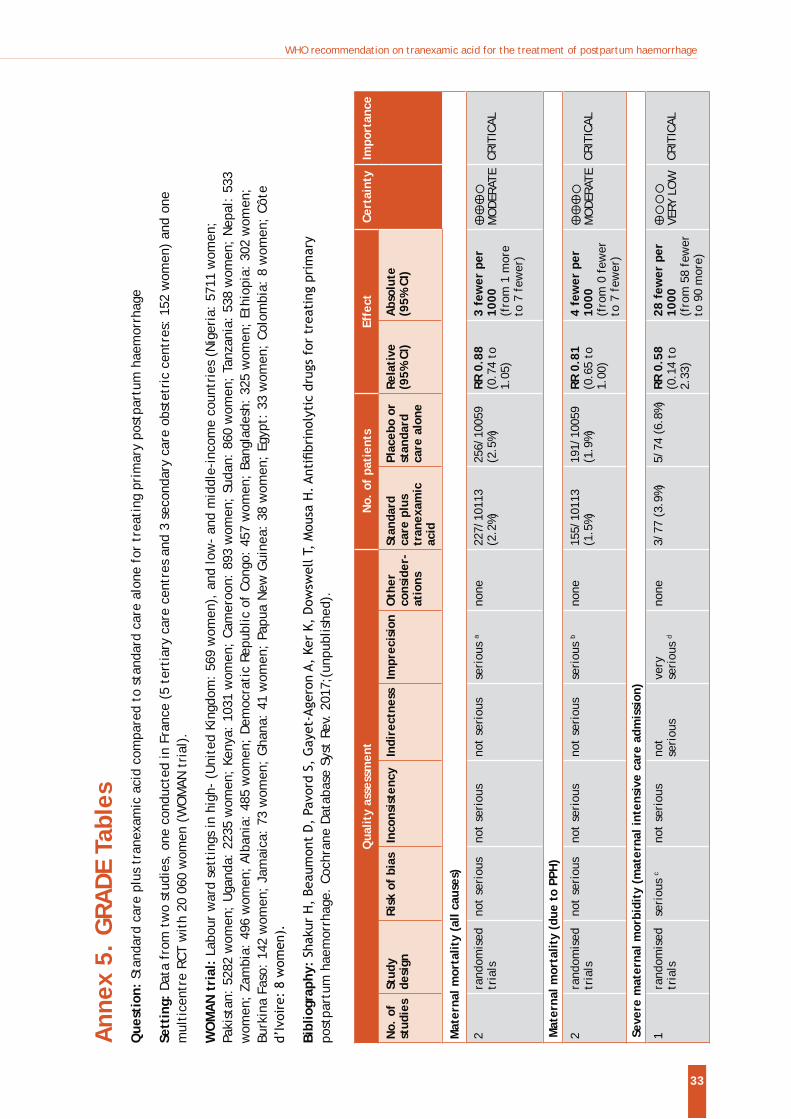
Maternal mortality (all causes): Moderate certainty evidence suggests slightly fewer deaths in the group receiving TXA although this difference was not statistically
RR 0.88, 95% CI 0.74 to 1.05).
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
14
Maternal mortality due to PPH: In both trials, clinicians were asked to record the primary cause of death. Moderate certainty evidence suggests that deaths that were considered to be due to bleeding were probably reduced in the TXA group (two studies, 20 172 women, 155/10 113 (1.5%) vs 191/10 059 (1.9%), RR 0.81, 95% CI 0.65 to 1.00). The number needed to treat (NNT) to prevent one maternal death due to bleeding is 258 (95% CI 133.2 to 4051.8).
Severe maternal morbidity: The French trial reported multiple organ failure; there were no events in either arm and very few admissions to intensive care (one study, 152 women, 3/77 (3.9%) vs 5/74 (6.8%), RR 0.58 (95% CI 0.14 to 2.33). The number of women suffering any severe morbidity was not reported in the WOMAN trial report,
or no difference between groups for any of morbidity outcomes reported (respiratory failure: RR 0.87, 95% CI 0.67 to 1.12; seizure: two studies; RR 0.76, 95% CI 0.49 to 1.20; hepatic failure RR 0.96, 95% CI 0.58 to 1.60; cardiac failure: RR 0.95, 95% CI 0.73 to 1.23; renal failure: two studies; RR 1.09, 95% CI 0.85 to 1.39).
Blood products transfusion (all): Moderate certainty evidence suggests there is very little or no difference between groups for transfusion of blood products, with more than half of the women in both arms of the WOMAN trial receiving a transfusion (two studies; RR 1.00, 95% CI 0.97 to 1.03).
Additional blood loss: The French trial reported additional blood loss > 500 ml or > 1000 ml. Low-quality evidence suggests TXA probably reduces blood loss > 500 ml (RR 0.50, 95% CI 0.27 to 0.93, 151 women). Although the direction of effect was the
between groups (4/77 women versus 8/74).
Additional uterotonics: The vast majority of women in the WOMAN trial received uterotonics (99.3% vs 99.1%, two studies; RR 1.00, 95% CI 1.0 to 1.0).
Surgical interventions: High or moderate certainty evidence suggests there is probably little difference between groups for most surgical interventions to control bleeding (hysterectomy (all): two studies; RR 1.01, 95% CI 0.88 to 1.17; ligature: RR 0.88, 95% CI 0.74 to 1.05; embolization: RR 0.82, 95% CI 0.42 to 1.62). High certainty evidence suggests laparotomy to control bleeding is reduced for women in the TXA group (0.8% vs 1.3%) (RR 0.64, 95% CI 0.49 to 0.85) while brace sutures are increased (RR 1.19, 95% CI 1.01 to 1.41).
Invasive nonsurgical interventions: High certainty evidence suggests there is probably little or no difference in intrauterine tamponade (one study; RR 0.96, 95% CI 0.87 to 1.06) or manual removal of placenta: (one study; RR 0.95, 95% CI 0.87 to 1.04).
Procedure-related complications: Moderate certainty evidence suggests there is probably little or no difference between groups for thromboembolic events (any maternal thromboembolic event: RR 0.88, 95% CI 0.54 to 1.43; deep venous thrombosis: two studies; RR 0.62 95% CI 0.20 to 1.88; pulmonary embolism RR 0.85, 95% CI 0.44 to 1.61; myocardial infarction: RR 0.66, 95% CI 0.11 to 3.97; stroke: RR 1.33, 95% CI 0.46 to 3.82).
Neonatal adverse effects: Available neonatal outcome data were limited (data from WOMAN trial only). There were no neonatal thromboembolic events and no clear differences in deaths in breastfed neonates (eight deaths with TXA vs seven deaths with placebo) in the WOMAN trial.
Longer-term outcomes: Available data on longer-term outcomes was limited (data from the WOMAN trial only). Outcomes in the WOMAN trial were measured up to hospital discharge or 42 days if still in hospital. There was no information on longer-term outcomes in women or babies.
Subgroup analysis examining treatment effect by mode of birth (vaginal or caesarean) suggests no clear difference in effect on maternal death (all causes) and maternal death due to PPH for type of birth (moderate certainty of evidence).
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
15
Comparison: TXA (in addition to standard care) versus standard care alone, by timing of TXA administration
Evidence for this subgroup comparison was derived from a pre-planned subgroup analysis of the WOMAN trial.
Maternal mortality due to PPH: There are subgroup differences for the timing of drug administration. Women receiving TXA less than 1 hour after birth had reduced risk of
than 1 hour: RR 0.80, 95% CI 0.55 to 1.16). Women receiving TXA 1 to 3 hours after birth were at reduced risk of death from bleeding (1 to 3 hours: RR 0.60, 95% CI 0.41 to 0.88) compared with women where more than 3 hours had elapsed before TXA was administered (more than 3 hours: RR 1.07, 95% CI 0.76 to 1.51).
Maternal mortality (all cause): Compared to the control group, women receiving TXA less than 1 hour after birth had similar risks of death (any cause) (less than 1 hour: RR 0.98, 95% CI 0.72 to 1.33), as did women receiving TXA more than 3 hours after birth (more than 3 hours: RR 1.00, 95% CI 0.75 to 1.33). However, women receiving TXA 1 to 3 hours after birth were at reduced risk of death from all causes (1 to 3 hours: RR 0.69, 95% CI 0.49 to 0.96).
Death or hysterectomy: Compared to the control group, women receiving TXA less than 1 hour after birth had similar risks of death or hysterectomy (less than 1 hour: RR 1.08, 95% CI 0.91 to 1.28), as did women receiving TXA more than 3 hours after birth (more than 3 hours: RR 1.01, 95% CI 0.82 to 1.25). However, women receiving TXA 1 to 3 hours after birth were at reduced risk of death or hysterectomy (1 to 3 hours: RR 0.80, 95% CI 0.63 to 1.00).
Laparotomy for bleeding: Compared to the control group, women receiving TXA less than 1 hour after birth had reduced risk of laparotomy for bleeding (less than 1 hour: RR 0.48, 95% CI 0.29 to 0.79), as did women receiving TXA at 1 to 3 hours after birth (1 to 3 hours: RR 0.54, 95% CI 0.31 to 0.95). Women receiving TXA more than 3 hours after birth were not at reduced risk of laparotomy for bleeding (more than 3 hours: RR 0.89, 95% CI 0.59 to 1.35).
Desirable effects
How substantial are the desirable anticipated effects of TXA + standard care vs standard care alone?
Judgement
Varies
Trivial
Small
Moderate
Large
Undesirable effects
How substantial are the undesirable anticipated effects TXA + standard care vs standard care alone?
Judgement
Varies
Large
Moderate
Small
Trivial
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
16
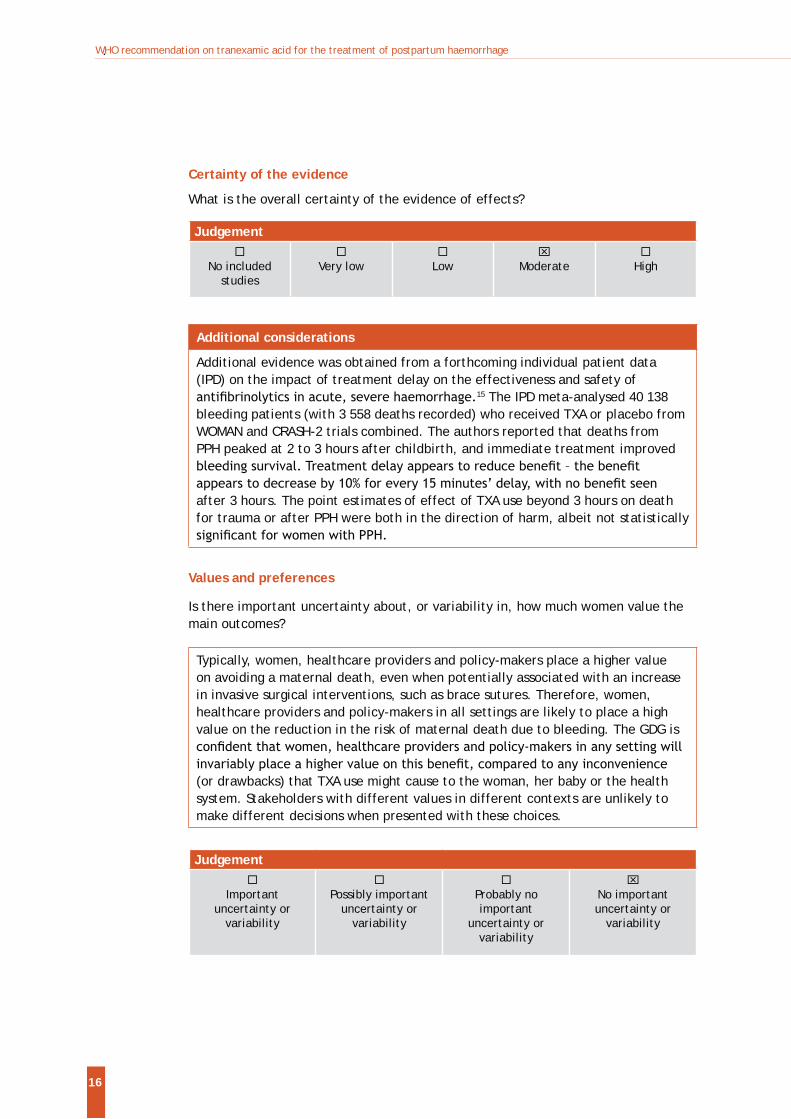
Certainty of the evidence
What is the overall certainty of the evidence of effects?
Judgement
No included studies
Very low
Low
Moderate
High
Additional considerations
Additional evidence was obtained from a forthcoming individual patient data (IPD) on the impact of treatment delay on the effectiveness and safety of
15 The IPD meta-analysed 40 138 bleeding patients (with 3 558 deaths recorded) who received TXA or placebo from WOMAN and CRASH-2 trials combined. The authors reported that deaths from PPH peaked at 2 to 3 hours after childbirth, and immediate treatment improved
after 3 hours. The point estimates of effect of TXA use beyond 3 hours on death for trauma or after PPH were both in the direction of harm, albeit not statistically
Values and preferences
Is there important uncertainty about, or variability in, how much women value the main outcomes?
Typically, women, healthcare providers and policy-makers place a higher value on avoiding a maternal death, even when potentially associated with an increase in invasive surgical interventions, such as brace sutures. Therefore, women, healthcare providers and policy-makers in all settings are likely to place a high value on the reduction in the risk of maternal death due to bleeding. The GDG is
(or drawbacks) that TXA use might cause to the woman, her baby or the health system. Stakeholders with different values in different contexts are unlikely to make different decisions when presented with these choices.
Judgement
Important uncertainty or
variability
Possibly important
uncertainty or variability
Probably no important
uncertainty or variability
No important uncertainty or
variability
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
17
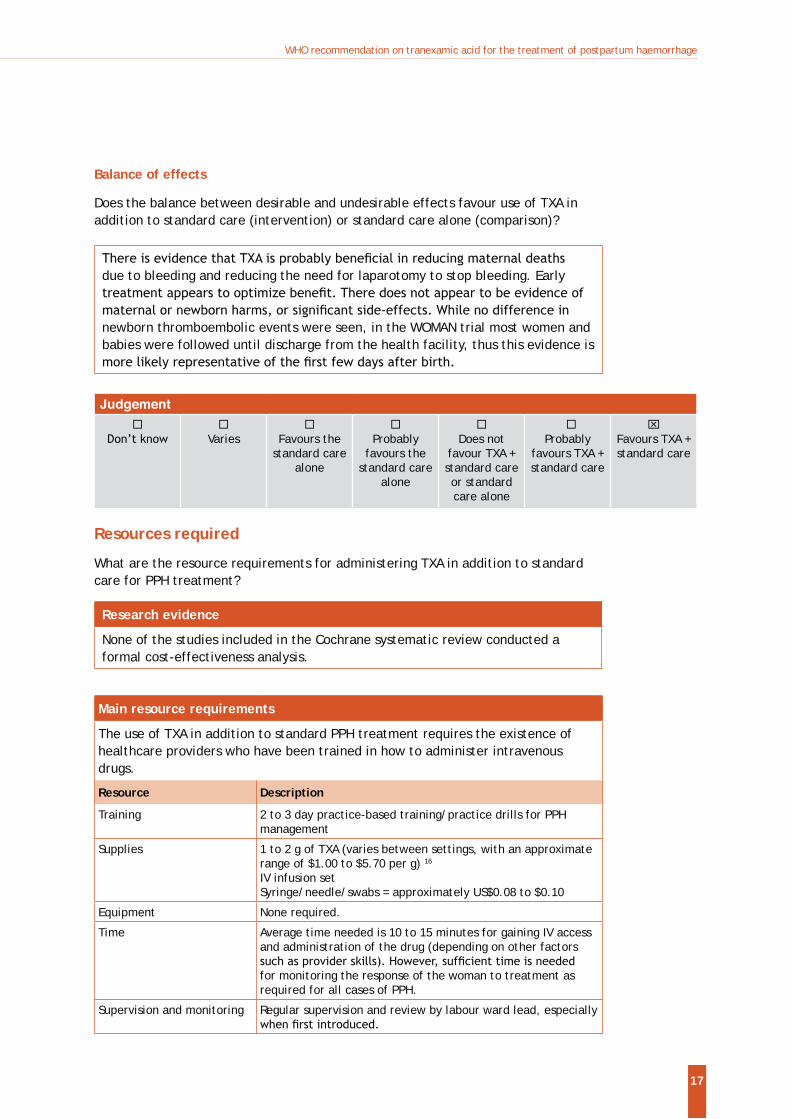
Balance of effects
Does the balance between desirable and undesirable effects favour use of TXA in addition to standard care (intervention) or standard care alone (comparison)?
due to bleeding and reducing the need for laparotomy to stop bleeding. Early
newborn thromboembolic events were seen, in the WOMAN trial most women and babies were followed until discharge from the health facility, thus this evidence is
Judgement
Varies
Favours the
standard care alone
Probably
favours the standard care
alone
Does not
favour TXA + standard care or standard care alone
Probably
favours TXA + standard care
Favours TXA + standard care
Resources required
What are the resource requirements for administering TXA in addition to standard care for PPH treatment?
Research evidence
None of the studies included in the Cochrane systematic review conducted a formal cost-effectiveness analysis.
Main resource requirements
The use of TXA in addition to standard PPH treatment requires the existence of healthcare providers who have been trained in how to administer intravenous drugs.
Resource Description
Training 2 to 3 day practice-based training/practice drills for PPH management
Supplies 1 to 2 g of TXA (varies between settings, with an approximate range of $1.00 to $5.70 per g) 16
IV infusion setSyringe/needle/swabs = approximately US$0.08 to $0.10
Equipment None required.
Time Average time needed is 10 to 15 minutes for gaining IV access and administration of the drug (depending on other factors
for monitoring the response of the woman to treatment as required for all cases of PPH.
Supervision and monitoring Regular supervision and review by labour ward lead, especially
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
18
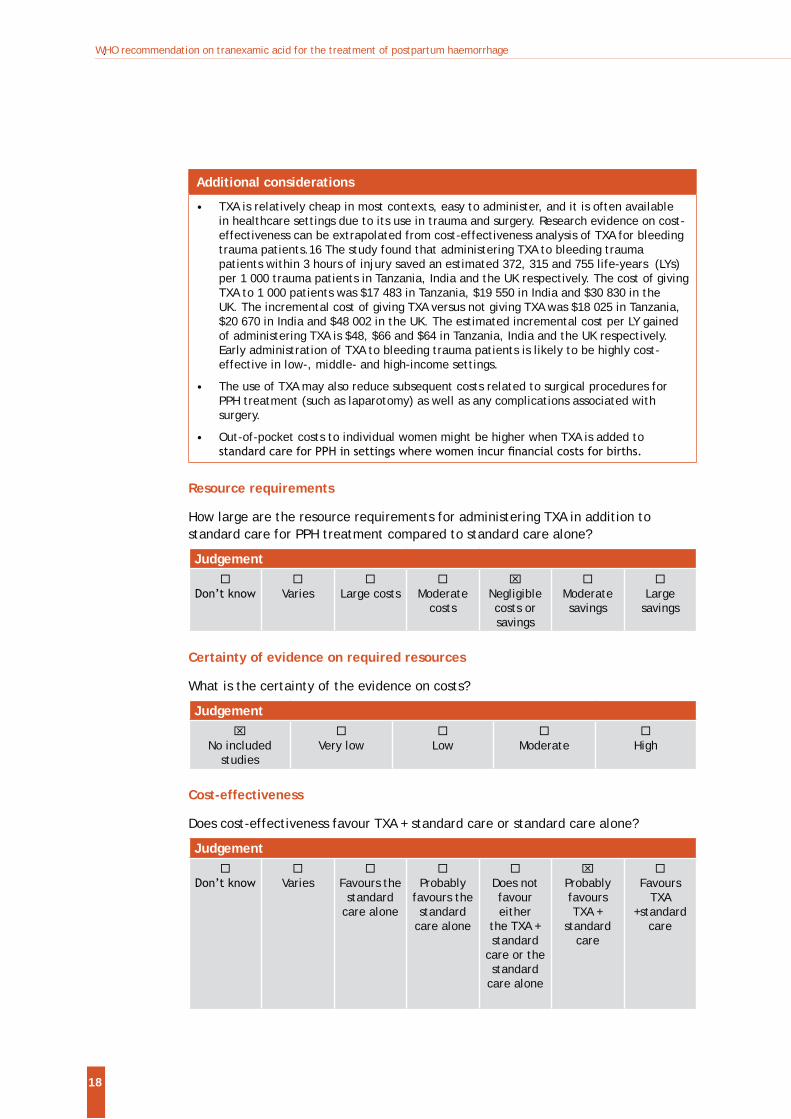
Additional considerations
TXA is relatively cheap in most contexts, easy to administer, and it is often available in healthcare settings due to its use in trauma and surgery. Research evidence on cost-effectiveness can be extrapolated from cost-effectiveness analysis of TXA for bleeding trauma patients.16 The study found that administering TXA to bleeding trauma patients within 3 hours of injury saved an estimated 372, 315 and 755 life-years (LYs) per 1 000 trauma patients in Tanzania, India and the UK respectively. The cost of giving TXA to 1 000 patients was $17 483 in Tanzania, $19 550 in India and $30 830 in the UK. The incremental cost of giving TXA versus not giving TXA was $18 025 in Tanzania, $20 670 in India and $48 002 in the UK. The estimated incremental cost per LY gained of administering TXA is $48, $66 and $64 in Tanzania, India and the UK respectively. Early administration of TXA to bleeding trauma patients is likely to be highly cost-effective in low-, middle- and high-income settings.
The use of TXA may also reduce subsequent costs related to surgical procedures for PPH treatment (such as laparotomy) as well as any complications associated with surgery.
Out-of-pocket costs to individual women might be higher when TXA is added to
Resource requirements
How large are the resource requirements for administering TXA in addition to standard care for PPH treatment compared to standard care alone?
Judgement
Varies
Large costs
Moderate costs
Negligible costs or savings
Moderate savings
Large
savings
Certainty of evidence on required resources
What is the certainty of the evidence on costs?
Judgement
No included studies
Very low
Low
Moderate
High
Cost-effectiveness
Does cost-effectiveness favour TXA + standard care or standard care alone?
Judgement
Varies
Favours the standard
care alone
Probably
favours the standard
care alone
Does not favour either
the TXA + standard
care or the standard
care alone
Probably favours TXA +
standard care
Favours
TXA +standard
care
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
19
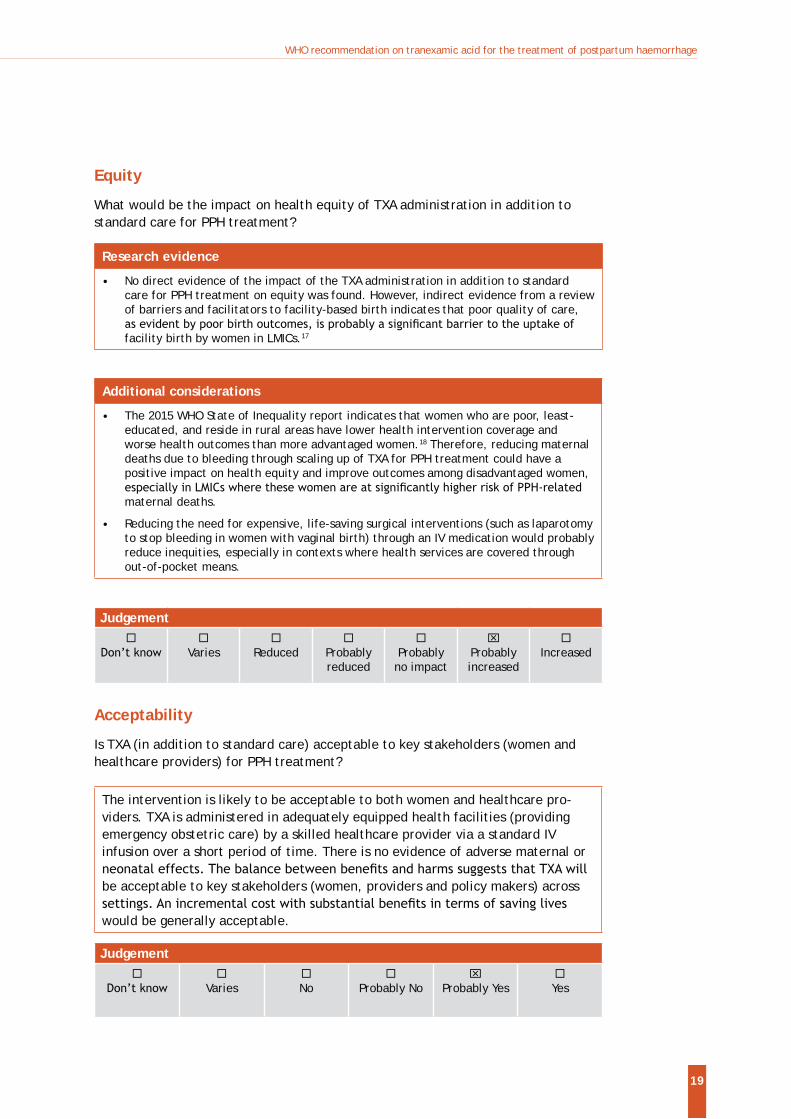
Equity
What would be the impact on health equity of TXA administration in addition to standard care for PPH treatment?
Research evidence
No direct evidence of the impact of the TXA administration in addition to standard care for PPH treatment on equity was found. However, indirect evidence from a review of barriers and facilitators to facility-based birth indicates that poor quality of care,
facility birth by women in LMICs.17
Additional considerations
The 2015 WHO State of Inequality report indicates that women who are poor, least-educated, and reside in rural areas have lower health intervention coverage and worse health outcomes than more advantaged women.18 Therefore, reducing maternal deaths due to bleeding through scaling up of TXA for PPH treatment could have a positive impact on health equity and improve outcomes among disadvantaged women,
maternal deaths.
Reducing the need for expensive, life-saving surgical interventions (such as laparotomy to stop bleeding in women with vaginal birth) through an IV medication would probably reduce inequities, especially in contexts where health services are covered through out-of-pocket means.
Judgement
Varies
Reduced
Probably reduced
Probably
no impact
Probably increased
Increased
Acceptability
Is TXA (in addition to standard care) acceptable to key stakeholders (women and healthcare providers) for PPH treatment?
The intervention is likely to be acceptable to both women and healthcare pro-viders. TXA is administered in adequately equipped health facilities (providing emergency obstetric care) by a skilled healthcare provider via a standard IV infusion over a short period of time. There is no evidence of adverse maternal or
be acceptable to key stakeholders (women, providers and policy makers) across
would be generally acceptable.
Judgement
Varies
No
Probably No
Probably Yes
Yes
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
20
Feasibility
Is TXA feasible to implement in addition to standard care for PPH treatment?
The use of IV TXA for treatment of PPH in healthcare facilities was regarded by the GDG as feasible. Standard IV infusion equipment is required, as well
infusions (similar to oxytocin infusion). Many hospitals already have access to TXA due to its common use for trauma and surgery. Available preparations are compatible with recommended dosing regimens for PPH treatment. In many healthcare facilities (including in LMICs) no (or minimal) additional resources, infrastructure or training is required to commence using TXA for this indication. Administration of TXA should be relatively easy to integrate into standard PPH treatment packages. It is listed on the WHO Model List of Essential Medicines under medicines affecting coagulation.
The successful implementation of the WOMAN trial in 193 hospitals in 21 countries, which recruited over 20 000 women, in itself can be considered a potential demonstration of the feasibility of implementing this intervention.9 The pragmatic nature of the trial, coupled with the variations in the capacities of participating institutions (from low to very high) also supports feasibility across low-, middle- and high-income settings. These hospitals are likely to implement a recommendation of TXA easily.
However, given that evidence currently supports IV TXA for treatment, the intervention may not be feasible in settings where IV administrations are restricted to doctors working in high-level or referral facilities.
Judgement
Varies
No
Probably No
Probably Yes
Yes
4. Research implications
of IV TXA for PPH treatment, other research priorities include:
What are the effects of TXA by other routes of administration (for example, oral, intramuscular, topical, buccal) when used for PPH treatment?
What is the cost-effectiveness of TXA when used for PPH treatment?
What is the optimal dosing regimen of TXA for PPH treatment?
What are the longer-term effects (on women and breastfed newborns) of TXA when used for PPH treatment?
What are the effects of oral or intravenous TXA when used for PPH prevention? 19
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
21
5. Dissemination and implementation of the recommendationDissemination and implementation of the recommendation is to be considered by all actors involved in the provision of care for pregnant women at the international, national and local levels. There is a vital need to increase access and strengthen the capacity of health centres to provide high quality services for all women giving birth. It is therefore crucial that this recommendation is translated into PPH treatment packages and programmes at country and health-facility levels.
Recommendation dissemination and evaluationThe recommendation will be disseminated through WHO regional and country
other United Nations agencies and nongovernmental organizations, among others. This recommendation will be also available on the WHO website and in the WHO Reproductive Health Library. To increase awareness of the recommendation, a short commentary will be published in a peer-reviewed journal. The recommendation
WHO staff. The executive summary will be translated into the six UN languages and
the six UN languages.
Implementation considerationsThe successful introduction of evidence-based policies (related to the prevention and management of PPH) into national programmes and healthcare services depends on well planned and participatory, consensus-driven processes of adaptation and implementation. These processes may include the development or revision of existing national guidelines or protocols based on this document. TXA should be included as part of the standard package for PPH treatment. It should therefore be available at all times in the labour room of facilities providing emergency obstetric care.
precautions and contraindications. TXA for injection may be mixed with most solutions for infusion, such as electrolyte solutions, carbohydrate solutions, amino acid solutions and dextran solutions.20 TXA should be administered as a bolus IV injection over 10 minutes, as there is a potential risk of transient lowering of blood pressure. TXA should not be mixed with blood for transfusion, solutions containing penicillin or mannitol.20 It can be administered via the same IV cannula used for IV hydration or uterotonic administration.
An enabling environment should be created for the use of TXA (for example, by widening its availability) in order to support changes in the behaviour of healthcare practitioners to enable the use of evidence-based practice. This includes technical support for local guideline implementers in the development of training manuals,
meetings. Local professional societies play important roles in this process, and an inclusive and participatory process should be encouraged.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
22
Health facilities where emergency obstetric care is provided need to have the necessary supplies and equipment, as well as the necessary training for staff attending births, so that TXA can be administered safely by IV infusion. The shelf life of TXA is generally three years, and can be stored at room temperature (15 to 30 degrees Celsius). The opened product must be used immediately. The
precedence.
The recommendation should be adapted into locally appropriate documents that are
6. Applicability issuesAnticipated impact on the organization of care and resourcesImplementing this evidence-based recommendation can be achieved without substantive additional resources. The GDG noted that updating training curricula and providing training on the updated recommendation would increase the
treatment by including this recommendation into existing packages of care can encourage healthcare provider behaviour change.
Monitoring and evaluating guideline implementationImplementation should be monitored at the health-service level as part of broader efforts to monitor and improve the quality of maternal and newborn care. For example, interrupted time series, clinical audits or criterion-based clinical audits can be used to obtain relevant data related to the management of PPH. Clearly
with locally agreed targets. These can be aligned with the standards and indicators described in the WHO document Standards for improving quality of maternal and newborn care in health facilities.21
In 2012, the GDG of the WHO recommendations on prevention and treatment of PPH strongly recommended the use of coverage of prophylactic uterotonics as a process indicator for the monitoring of PPH prevention.5 This indicator provides
recommendations on PPH prevention and treatment. The use of other locally agreed
uterotonics or use of TXA for PPH treatment) may be necessary to obtain a more complete assessment of the quality of care related to the prevention and treatment
severe maternal complications (including PPH) based on the near-miss and criterion-based clinical audit concepts.22
team, data on country and regional level implementation of the recommendation will be collected and evaluated in the short- to medium-term to evaluate the
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
23
Information on recommended indicators can also be obtained at the local level by interrupted time series or clinical audits.
7. Updating the recommendation
of maternal and perinatal health recommendations, and to prioritize new and existing questions for recommendation development and updating. Accordingly, the recommendation on TXA use for the treatment of PPH will be reviewed and prioritized by the Executive GSG. In the event that new evidence (that could
may be revalidated.
Following publication and dissemination of the updated recommendation, any concern about validity of the recommendation will be promptly communicated to the guideline implementers, in addition to plans to update the recommendation.
WHO welcomes suggestions regarding additional questions for inclusion in the updated recommendation. Please email your suggestions to [email protected].
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
24
References1. Souza JP, Gülmezoglu AM, Vogel J, et al. Moving beyond essential interventions
for reduction of maternal mortality (the WHO Multicountry Survey on Maternal and Newborn Health): a cross-sectional study. Lancet. 2013;381(9879):1747-55.
2. Carroli G, Cuesta C, Abalos E, Gulmezoglu AM. Epidemiology of postpartum haemorrhage: a systematic review. Best Pract Res Clin Obstet Gynaecol. 2008;22(6):999-1012.
3. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2(6):e323-33.
4. Oyelese Y, Ananth CV. Postpartum hemorrhage: epidemiology, risk factors, and causes. Clin Obstet Gynecol. 2010;53(1):147-56.
5. WHO recommendations for the prevention and treatment of postpartum haemorrhage. Geneva: World Health Organization, 2012.
6. National Center for Biotechnology Information PCD, CID=5526. Tranexamic acid – compound summary for CID 5526. 2017 (https://pubchem.ncbi.nlm.nih.gov/compound/5526, accessed 31 August 2017).
7. Report of the WHO Expert Committee on Selection and Use of Essential Medicines, 2017 (including the 20th WHO Model List of Essential Medicines and the 6th WHO Model List of Essential Medicines for Children). Geneva: World Health Organization, 2017.
8. Shakur H, Elbourne D, Gülmezoglu M, et al. The WOMAN Trial (World Maternal
haemorrhage: an international randomised, double blind placebo controlled trial. Trials. 2010:11:40.
9. WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet. 2017;389(10084):2105-16.
10. WHO handbook for guideline development (second edition). Geneva: World Health Organization; 2014.
for primary postpartum haemorrhage. Cochrane Database Syst Rev. 2014;(2):CD003249.
12. Shakur H, Beaumont D, Pavord S, Gayet-Ageron A, Ker K, Dowswell T, Mousa H.
Database Syst Rev. 2017;(unpublished).
13. Balshem H, Helfand M, Schünemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401-6.
14. Ducloy-Bouthors AS, Jude B, Duhamel A, et al. High-dose tranexamic acid reduces blood loss in postpartum haemorrhage. Crit Care. 2011;15(2):R117.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
25
15. Gayet-Ageron A, Prieto-Merino D, Ker K, Shakur H, Ageron F-X, Roberts I. Impact
severe haemorrhage: an individual patient data meta-analysis in 40 138 bleeding patients. Lancet. 2017; accepted for publication.
16. Guerriero C, Cairns J, Perel P, Shakur H, Roberts I, collaborators Ct. Cost-effectiveness analysis of administering tranexamic acid to bleeding trauma patients using evidence from the CRASH-2 trial. PLoS One. 2011;6(5):e18987.
17. Bohren MA, Hunter EC, Munthe-Kaas HM, Souza JP, Vogel JP, Gülmezoglu AM. Facilitators and barriers to facility-based delivery in low- and middle-income countries: a qualitative evidence synthesis. Reprod Health. 2014;11(1):71.
18. State of inequality: reproductive, maternal, newborn and child health. Geneva: World Health Organization; 2015.
19. Novikova N, Hofmeyr GJ, Cluver C. Tranexamic acid for preventing postpartum haemorrhage. Cochrane Database Syst Rev. 2015;(6):CD007872.
20. EMC. Cyclokapron Injection. 15 March 2016 (https://www.medicines.org.uk/emc/medicine/1489w5, accessed September 2017).
21. Standards for improving quality of maternal and newborn care in health facilities. Geneva: World Health Organization; 2016.
22. Evaluating the quality of care for severe pregnancy complications: The WHO near-miss approach for maternal health. Geneva: World Health Organization; 2011.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
26
Annex 1. External experts and WHO staff involved in the preparation of the guideline
A. Participants at the who technical consultation on TXA for the treatment of PPH
Guideline Development Group
Edgardo Abalos (unable to attend)Centro Rosarino de Estudios Perinatales (CREP)Rosario, Argentina
Yap-Seng ChongDepartment of Obstetrics and GynaecologyNational University HospitalSingapore
Catherine Deneux-TharauxInserm U1153Obstetrical, Perinatal and Pediatric Epidemiology Research Team Centre of Research in Epidemiology and Statistics Sorbonne Paris CitéUniversité Paris Descartes Paris, France
Bukola FawoleDepartment of Obstetrics & GynaecologyCollege of MedicineUniversity of IbadanIbadan, Nigeria
Justus HofmeyrUniversities of the Witwatersrand and Walter Sisulu/Eastern Cape Department of HealthEast London, South Africa
Caroline Homer (unable to attend)WHO Collaborating Centre for Nursing, Midwifery and Health DevelopmentFaculty of HealthUniversity of Technology Sydney, Australia
Pisake Lumbiganon Department of Obstetrics and GynaecologyFaculty of MedicineKhon Kaen UniversityKhon Kaen, Thailand
Suellen MillerDepartment of Obstetrics, Gynecology & Reproductive SciencesDirector, Safe Motherhood ProgramBixby Center for Global Reproductive Health San Francisco, United States
Ashraf NabhanDepartment of Obstetrics and GynecologyFaculty of MedicineAin Shams UniversityAbbasia, Cairo, Egypt
James Neilson
The University of Liverpool
Liverpool, United Kingdom
Hiromi ObaraJICA Health Policy Advisor
Zahida QureshiDepartment of Obstetrics and GynaecologySchool of MedicineUniversity of NairobiNairobi, Kenya
Rahat QureshiAga Khan UniversityDepartment of Obstetrics and GynecologyKarachi, Pakistan
Helen WestThe University of Liverpool
Liverpool, United Kingdom
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
27
Observers
Deborah ArmbrusterUnited States Agency for International Development (USAID)Bureau for Global HealthWashington DC, United States
Kusum Thapa MCSP/JhpiegoUSAID Grantee1776 Massachusetts Ave Washington DC, United States
Janna PattersonMaternal, Neonatal & Child HealthGlobal Development ProgramBill & Melinda Gates FoundationSeattle, Washington, United States
Haleema Shakur-StillLondon School of Hygiene and Tropical MedicineLondon, United Kingdom
Sally TracyInternational Confederation of Midwives (ICM) Sydney UniversitySydney, Australia
Gerard H.A. VisserInternational Federation of Gynecology and Obstetrics (FIGO)London, United Kingdom
Beverley WinikoffGynuity Health ProjectsNew York, United States
Systematic Review Team
Therese Dowswell
The University of Liverpool
Crown Street Liverpool, United Kingdom
Mavjuda Babamuradova Sexual and Reproductive HealthNoncommunicable diseases and life-course
Copenhagen, Denmark
Anoma Jayathilaka Family Health, Gender and Life Course
New Delhi, India
Ramez Khairi Mahaini (unable to attend)Reproductive and Maternal Health
Cairo, Egypt
Bremen De Mucio Sexual and Reproductive Health
Montevideo, Uruguay
Mari Nagai (unable to attend)Reproductive, Maternal, Newborn, Child and Adolescent Health Division of NCD and Health through Life-Course
Manila, Philippines
Léopold Ouedraogo (unable to attend)Reproductive HealthHealth Promotion Cluster (HPR)
Brazzaville, Republic of Congo
Claudio SosaSexual and Reproductive Health
Montevideo, Uruguay
WHO Secretariat
A. Metin GülmezogluCoordinator, RHR/MPAMaternal and Perinatal Health & Preventing Unsafe AbortionDepartment of Reproductive Health and Research
Mercedes Bonet
Maternal and Perinatal Health & Preventing Unsafe AbortionDepartment of Reproductive Health and Research
Olufemi T. Oladapo
Maternal and Perinatal Health & Preventing Unsafe AbortionDepartment of Reproductive Health and Research
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
28
Joao Paulo Souza (unable to attend)
Maternal and Perinatal Health & Preventing Unsafe AbortionDepartment of Reproductive Health and Research
Joshua P. Vogel
Maternal and Perinatal Health & Preventing Unsafe AbortionDepartment of Reproductive Health and Research
Maurice Bucagu (unable to attend)
Policy, Planning and ProgrammesDepartment of Maternal, Newborn, Child and Adolescent Health
Fran McConville (unable to attend)
Policy, Planning and ProgrammesDepartment of Maternal, Newborn, Child and Adolescent Health
Anayda Portela
Research and DevelopmentDepartment of Maternal, Newborn, Child and Adolescent Health
B. WHO Steering GroupA. Metin Gülmezoglu(WHO Department of Reproductive Health and Research)
Olufemi T. Oladapo (WHO Department of Reproductive Health and Research)
Anayda Portela (WHO Department of Maternal, Newborn, Child and Adolescent Health)
Joshua Vogel(WHO Department of Reproductive Health and Research)
C. External Review Group Richard M.K. AdanuSchool of Public HealthUniversity of GhanaAccra, Ghana
Fernando AlthabeDepartment of Maternal and Child Health Research Institute for Clinical Effectiveness and Health Policy Buenos Aires, Argentina
Sue Fawcus Department of Obstetrics and GynaecologyUniversity of Cape TownCape Town, South Africa
Jamilu Tukur Department of Obstetrics and GynaecologyBayero University Kano, Nigeria
Dilys WalkerDepartment of Obstetrics, Gynecology & Reproductive SciencesUCSF School of MedicineUniversity of CaliforniaSan Francisco, United States
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
29
Annex 2. Critical and important outcomes for decision-makingKey question Priority Outcomes
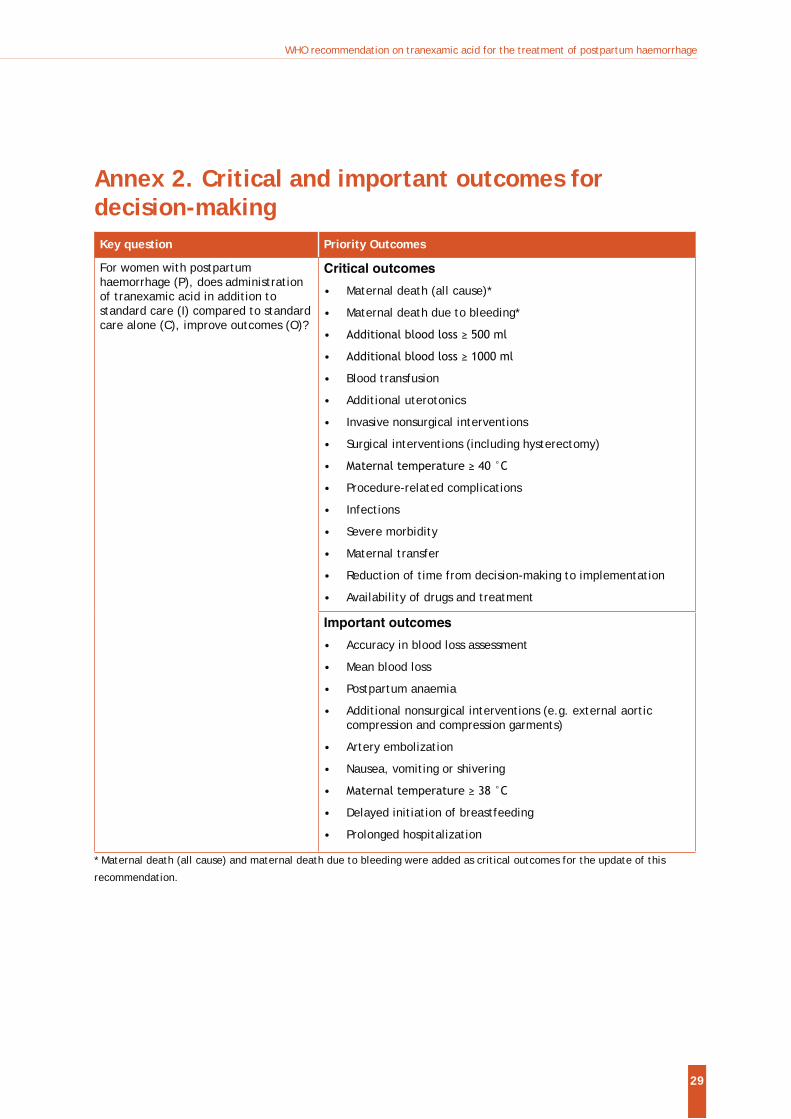
For women with postpartum haemorrhage (P), does administration of tranexamic acid in addition to standard care (I) compared to standard care alone (C), improve outcomes (O)?
Critical outcomes
Maternal death (all cause)*
Maternal death due to bleeding*
Blood transfusion
Additional uterotonics
Invasive nonsurgical interventions
Surgical interventions (including hysterectomy)
Procedure-related complications
Infections
Severe morbidity
Maternal transfer
Reduction of time from decision-making to implementation
Availability of drugs and treatment
Important outcomes
Accuracy in blood loss assessment
Mean blood loss
Postpartum anaemia
Additional nonsurgical interventions (e.g. external aortic compression and compression garments)
Artery embolization
Nausea, vomiting or shivering
Delayed initiation of breastfeeding
Prolonged hospitalization
* Maternal death (all cause) and maternal death due to bleeding were added as critical outcomes for the update of this
recommendation.
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
30
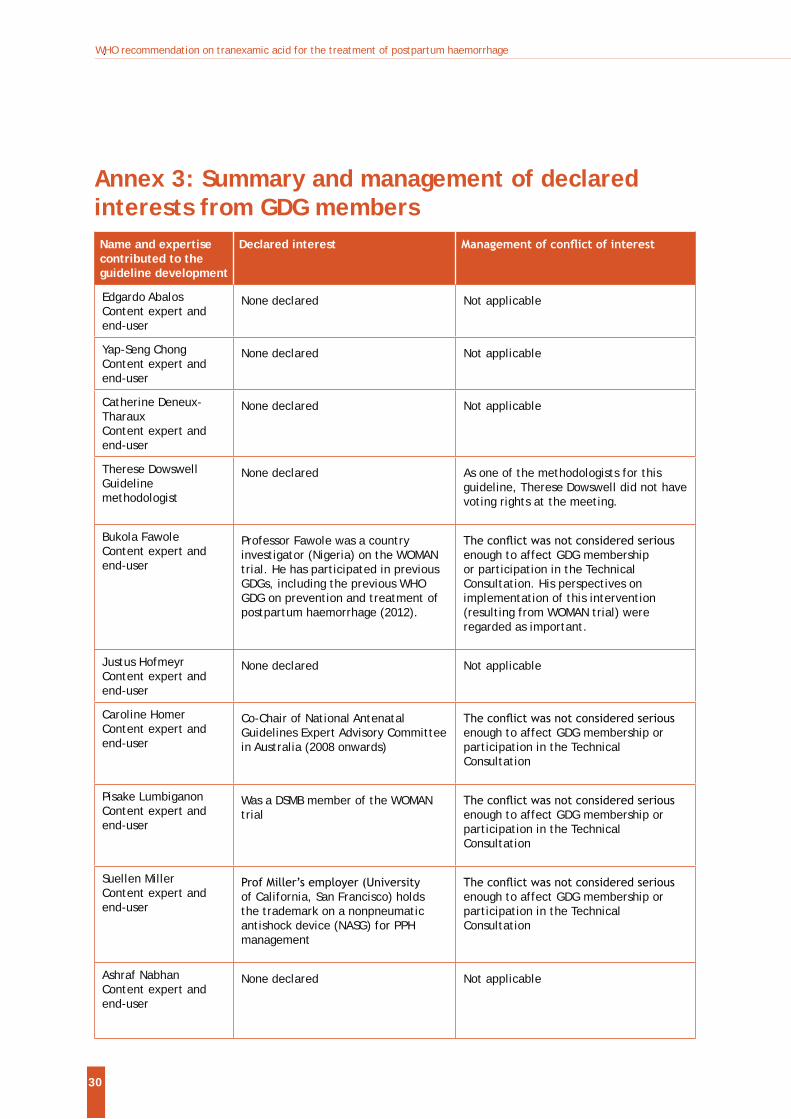
Annex 3: Summary and management of declared interests from GDG membersName and expertise contributed to the guideline development
Declared interest
Edgardo AbalosContent expert and end-user
None declared Not applicable
Yap-Seng ChongContent expert and end-user
None declared Not applicable
Catherine Deneux-TharauxContent expert and end-user
None declared Not applicable
Therese DowswellGuideline methodologist
None declared As one of the methodologists for this guideline, Therese Dowswell did not have voting rights at the meeting.
Bukola FawoleContent expert and end-user
Professor Fawole was a country investigator (Nigeria) on the WOMAN trial. He has participated in previous GDGs, including the previous WHO GDG on prevention and treatment of postpartum haemorrhage (2012).
enough to affect GDG membership or participation in the Technical Consultation. His perspectives on implementation of this intervention (resulting from WOMAN trial) were regarded as important.
Justus HofmeyrContent expert and end-user
None declared Not applicable
Caroline HomerContent expert and end-user
Co-Chair of National Antenatal Guidelines Expert Advisory Committee in Australia (2008 onwards)
enough to affect GDG membership or participation in the TechnicalConsultation
Pisake Lumbiganon Content expert and end-user
Was a DSMB member of the WOMAN trial enough to affect GDG membership or
participation in the TechnicalConsultation
Suellen MillerContent expert and end-user
of California, San Francisco) holds the trademark on a nonpneumatic antishock device (NASG) for PPH management
enough to affect GDG membership or participation in the TechnicalConsultation
Ashraf NabhanContent expert and end-user
None declared Not applicable
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
31
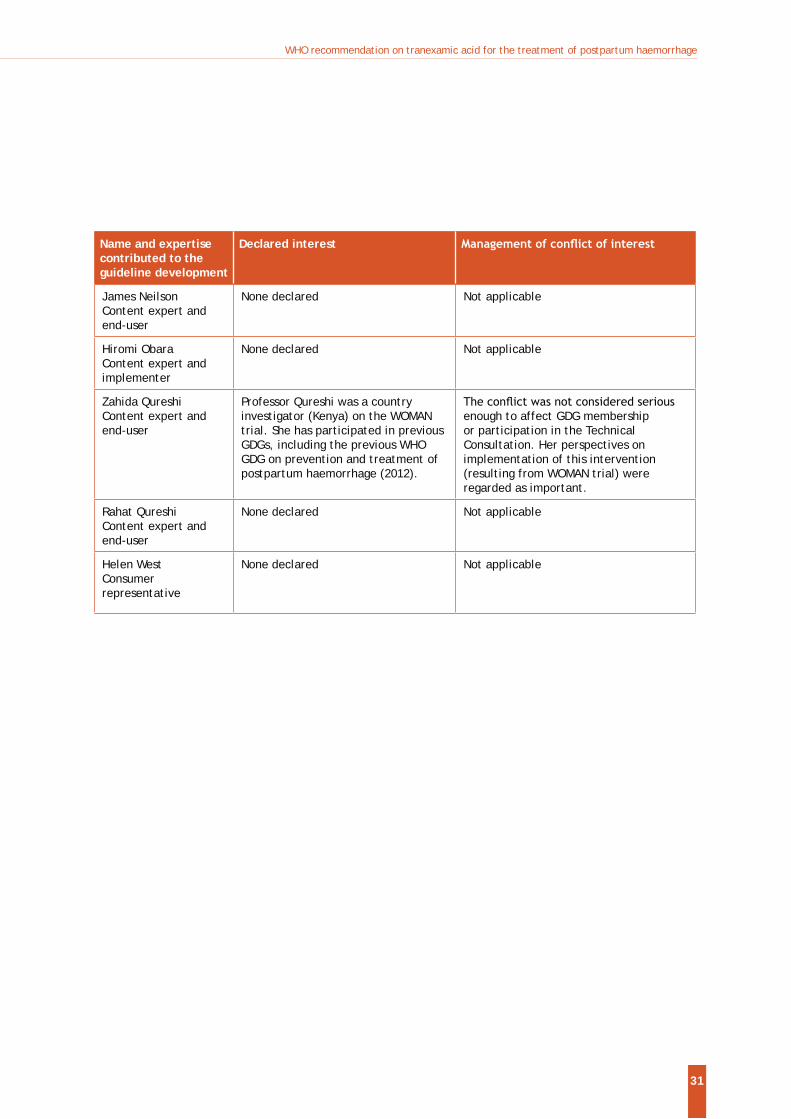
Name and expertise contributed to the guideline development
Declared interest
James NeilsonContent expert and end-user
None declared Not applicable
Hiromi ObaraContent expert and implementer
None declared Not applicable
Zahida QureshiContent expert and end-user
Professor Qureshi was a country investigator (Kenya) on the WOMAN trial. She has participated in previous GDGs, including the previous WHO GDG on prevention and treatment of postpartum haemorrhage (2012).
enough to affect GDG membership or participation in the Technical Consultation. Her perspectives on implementation of this intervention (resulting from WOMAN trial) were regarded as important.
Rahat QureshiContent expert and end-user
None declared Not applicable
Helen WestConsumer representative
None declared Not applicable
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
32
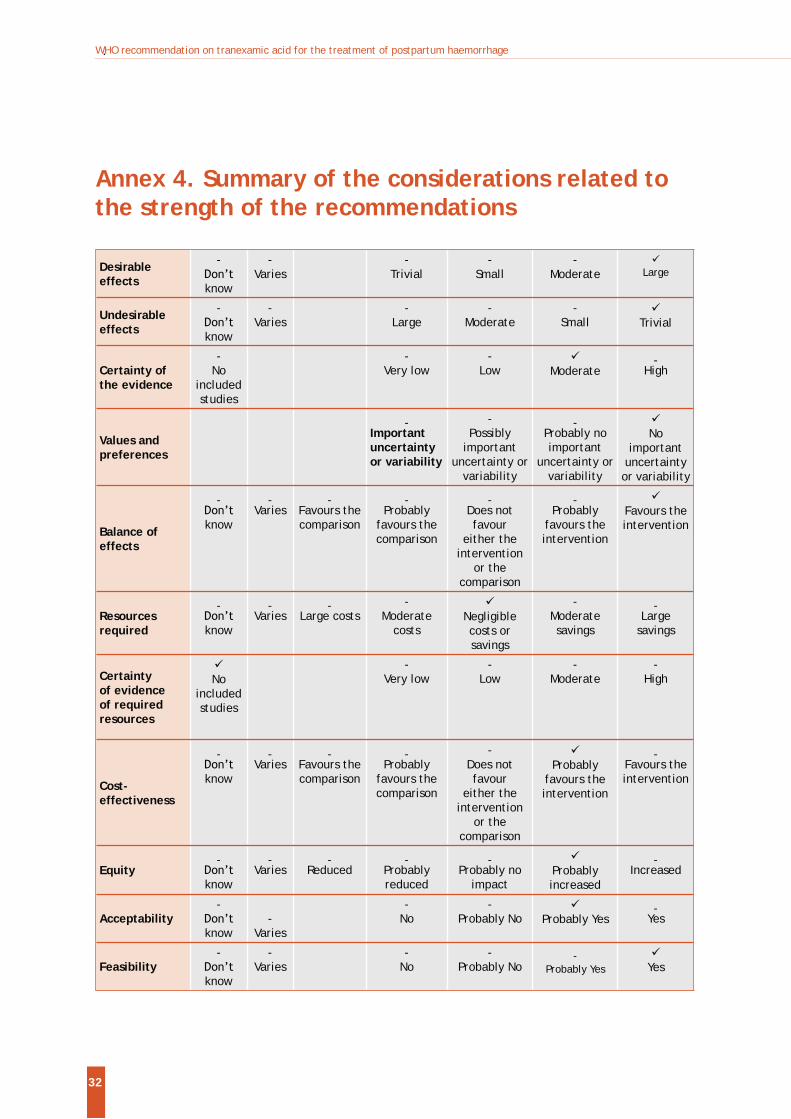
Annex 4. Summary of the considerations related to the strength of the recommendations
Desirable effects
-
know
-Varies
-Trivial
-Small
-Moderate Large
Undesirable effects
-
know
-Varies
-Large
-Moderate
-Small Trivial
Certainty of the evidence
-No
included studies
-Very low
-Low Moderate
-High
Values and preferences
-Important uncertainty or variability
-Possibly
important uncertainty or
variability
-Probably no important
uncertainty or variability
No important
uncertainty or variability
Balance of effects
-
know
-Varies
-Favours the comparison
-Probably
favours the comparison
-Does not favour
either the intervention
or the comparison
-Probably
favours the intervention
Favours the intervention
Resources required
-
know
-Varies
-Large costs
-Moderate
costsNegligible costs or savings
-Moderate savings
-Large
savings
Certainty of evidence of required resources
No included studies
-Very low
-Low
-Moderate
-High
Cost-effectiveness
-
know
-Varies
-Favours the comparison
-Probably
favours the comparison
-Does not favour
either the intervention
or the comparison
Probably favours the intervention
-Favours the intervention
Equity-
know
-Varies
-Reduced
-Probably reduced
-Probably no
impactProbably increased
-Increased
Acceptability-
know-
Varies
-No
-Probably No Probably Yes
-Yes
Feasibility-
know
-Varies
-No
-Probably No
-Probably Yes Yes
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
33
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Mat
erna
l mor
talit
y (a
ll ca
uses
)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
22
7/10
113
(2.2
%)
256/
1005
9 (2
.5%)
RR
0.8
8(0
.74
to
1.05
)
3 fe
wer
per
10
00(f
rom
1 m
ore
to 7
few
er)
MO
DER
ATE
CRIT
ICAL
Mat
erna
l mor
talit
y (d
ue t
o PP
H)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s b
none
15
5/10
113
(1.5
%)
191/
1005
9 (1
.9%)
RR
0.8
1(0
.65
to
1.00
)
4 fe
wer
per
10
00(f
rom
0 f
ewer
to
7 f
ewer
)
M
OD
ERAT
E CR
ITIC
AL
Seve
re m
ater
nal m
orbi
dity
(m
ater
nal i
nten
sive
car
e ad
mis
sion
)
1 ra
ndom
ised
tr
ials
se
riou
s c
not
seri
ous
not
se
riou
s ve
ry
seri
ous
dno
ne
3/77
(3.
9%)
5/74
(6.
8%)
RR 0
.58
(0.1
4 to
2.
33)
28 f
ewer
per
10
00(f
rom
58
few
er
to 9
0 m
ore)
VE
RY L
OW
CR
ITIC
AL
Ann
ex 5
. G
RAD
E Ta
bles
Que
stio
n: S
tand
ard
care
plu
s tr
anex
amic
aci
d co
mpa
red
to s
tand
ard
care
alo
ne f
or t
reat
ing
prim
ary
post
part
um h
aem
orrh
age
Sett
ing:
Dat
a fr
om t
wo
stud
ies,
one
con
duct
ed in
Fra
nce
(5 t
erti
ary
care
cen
tres
and
3 s
econ
dary
car
e ob
stet
ric
cent
res:
152
wom
en)
and
one
mul
tice
ntre
RCT
wit
h 20
060
wom
en (
WO
MAN
tri
al).
WO
MA
N t
rial
: La
bour
war
d se
ttin
gs in
hig
h- (
Uni
ted
King
dom
: 56
9 w
omen
), a
nd lo
w-
and
mid
dle-
inco
me
coun
trie
s (N
iger
ia:
5711
wom
en;
Paki
stan
: 52
82 w
omen
; U
gand
a: 2
235
wom
en;
Keny
a: 1
031
wom
en;
Cam
eroo
n: 8
93 w
omen
; Su
dan:
860
wom
en;
Tanz
ania
: 53
8 w
omen
; N
epal
: 53
3 w
omen
; Za
mbi
a: 4
96 w
omen
; Al
bani
a: 4
85 w
omen
; D
emoc
rati
c Re
publ
ic o
f Co
ngo:
457
wom
en;
Bang
lade
sh:
325
wom
en;
Ethi
opia
: 30
2 w
omen
; Bu
rkin
a Fa
so:
142
wom
en;
Jam
aica
: 73
wom
en;
Gha
na:
41 w
omen
; Pa
pua
New
Gui
nea:
38
wom
en;
Egyp
t: 3
3 w
omen
; Co
lom
bia:
8 w
omen
; Cô
te
Bibl
iogr
aphy
: po
stpa
rtum
hae
mor
rhag
e. C
ochr
ane
Dat
abas
e Sy
st R
ev.
2017
;(un
publ
ishe
d).
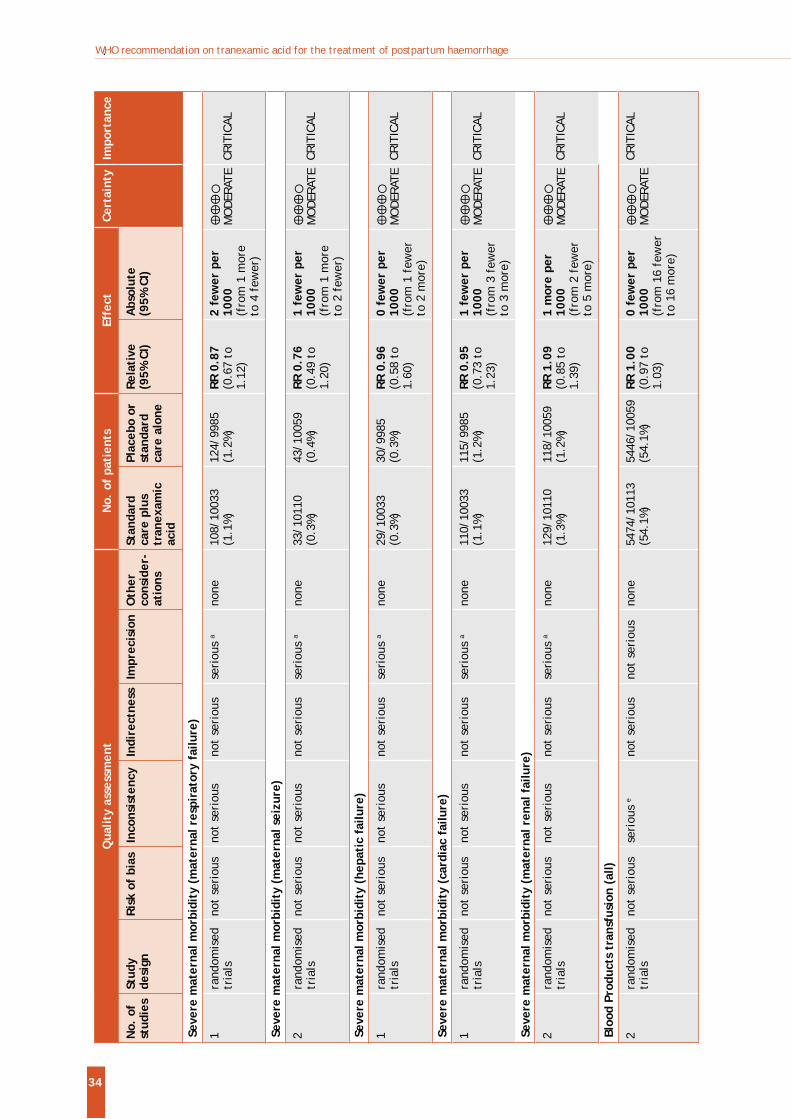
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
34
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Seve
re m
ater
nal m
orbi
dity
(m
ater
nal r
espi
rato
ry f
ailu
re)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
10
8/10
033
(1.1
%)
124/
9985
(1
.2%)
RR
0.8
7(0
.67
to
1.12
)
2 fe
wer
per
10
00(f
rom
1 m
ore
to 4
few
er)
M
OD
ERAT
E CR
ITIC
AL
Seve
re m
ater
nal m
orbi
dity
(m
ater
nal s
eizu
re)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
33
/101
10
(0.3
%)
43/1
0059
(0
.4%)
RR
0.7
6(0
.49
to
1.20
)
1 fe
wer
per
10
00(f
rom
1 m
ore
to 2
few
er)
M
OD
ERAT
E CR
ITIC
AL
Seve
re m
ater
nal m
orbi
dity
(he
pati
c fa
ilure
)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
29
/100
33
(0.3
%)
30/9
985
(0.3
%)
RR 0
.96
(0.5
8 to
1.
60)
0 fe
wer
per
10
00(f
rom
1 f
ewer
to
2 m
ore)
M
OD
ERAT
E CR
ITIC
AL
Seve
re m
ater
nal m
orbi
dity
(ca
rdia
c fa
ilure
)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
11
0/10
033
(1.1
%)
115/
9985
(1
.2%)
RR
0.9
5(0
.73
to
1.23
)
1 fe
wer
per
10
00(f
rom
3 f
ewer
to
3 m
ore)
M
OD
ERAT
E CR
ITIC
AL
Seve
re m
ater
nal m
orbi
dity
(m
ater
nal r
enal
fai
lure
)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
12
9/10
110
(1.3
%)
118/
1005
9 (1
.2%)
RR
1.0
9(0
.85
to
1.39
)
1 m
ore
per
1000
(fro
m 2
few
er
to 5
mor
e)
M
OD
ERAT
E CR
ITIC
AL
Bloo
d Pr
oduc
ts t
rans
fusi
on (
all)
2 ra
ndom
ised
tr
ials
no
t se
riou
s se
riou
s e
not
seri
ous
not
seri
ous
none
54
74/1
0113
(5
4.1%
) 54
46/1
0059
(5
4.1%
) RR
1.0
0(0
.97
to
1.03
)
0 fe
wer
per
10
00(f
rom
16
few
er
to 1
6 m
ore)
M
OD
ERAT
E CR
ITIC
AL
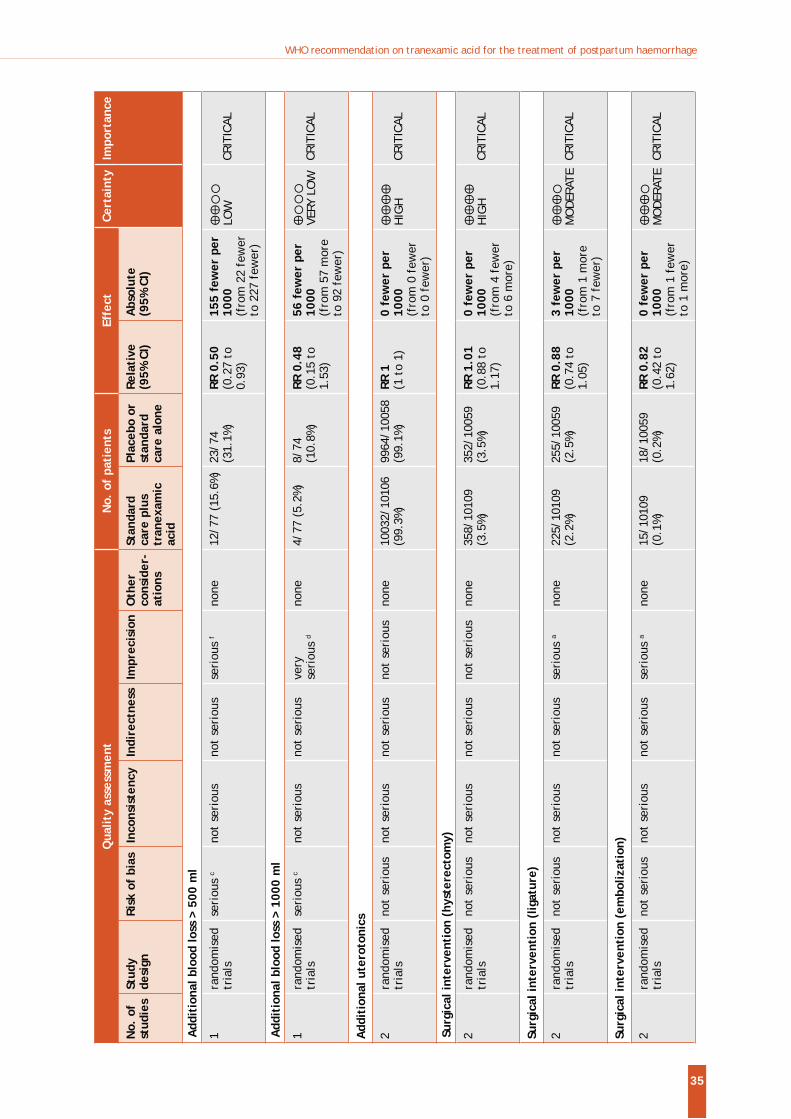
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
35
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Add
itio
nal b
lood
loss
> 5
00 m
l
1 ra
ndom
ised
tr
ials
se
riou
s c
not
seri
ous
not
seri
ous
seri
ous
fno
ne
12/7
7 (1
5.6%
) 23
/74
(31.
1%)
RR 0
.50
(0.2
7 to
0.
93)
155
few
er p
er
1000
(fro
m 2
2 fe
wer
to
227
few
er)
LO
W
CRIT
ICAL
Add
itio
nal b
lood
loss
> 1
000
ml
1 ra
ndom
ised
tr
ials
se
riou
s c
not
seri
ous
not
seri
ous
very
se
riou
s d
none
4/
77 (
5.2%
) 8/
74
(10.
8%)
RR 0
.48
(0.1
5 to
1.
53)
56 f
ewer
per
10
00(f
rom
57
mor
e to
92
few
er)
VE
RY L
OW
CR
ITIC
AL
Add
itio
nal u
tero
toni
cs
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
1003
2/10
106
(99.
3%)
9964
/100
58
(99.
1%)
RR 1
(1 t
o 1)
0
few
er p
er
1000
(fro
m 0
few
er
to 0
few
er)
H
IGH
CR
ITIC
AL
Surg
ical
inte
rven
tion
(hy
ster
ecto
my)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
358/
1010
9 (3
.5%)
35
2/10
059
(3.5
%)
RR 1
.01
(0.8
8 to
1.
17)
0 fe
wer
per
10
00(f
rom
4 f
ewer
to
6 m
ore)
H
IGH
CR
ITIC
AL
Surg
ical
inte
rven
tion
(lig
atur
e)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
22
5/10
109
(2.2
%)
255/
1005
9 (2
.5%)
RR
0.8
8(0
.74
to
1.05
)
3 fe
wer
per
10
00(f
rom
1 m
ore
to 7
few
er)
M
OD
ERAT
E CR
ITIC
AL
Surg
ical
inte
rven
tion
(em
boliz
atio
n)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
15
/101
09
(0.1
%)
18/1
0059
(0
.2%)
RR
0.8
2 (0
.42
to
1.62
)
0 fe
wer
per
10
00(f
rom
1 f
ewer
to
1 m
ore)
M
OD
ERAT
E CR
ITIC
AL
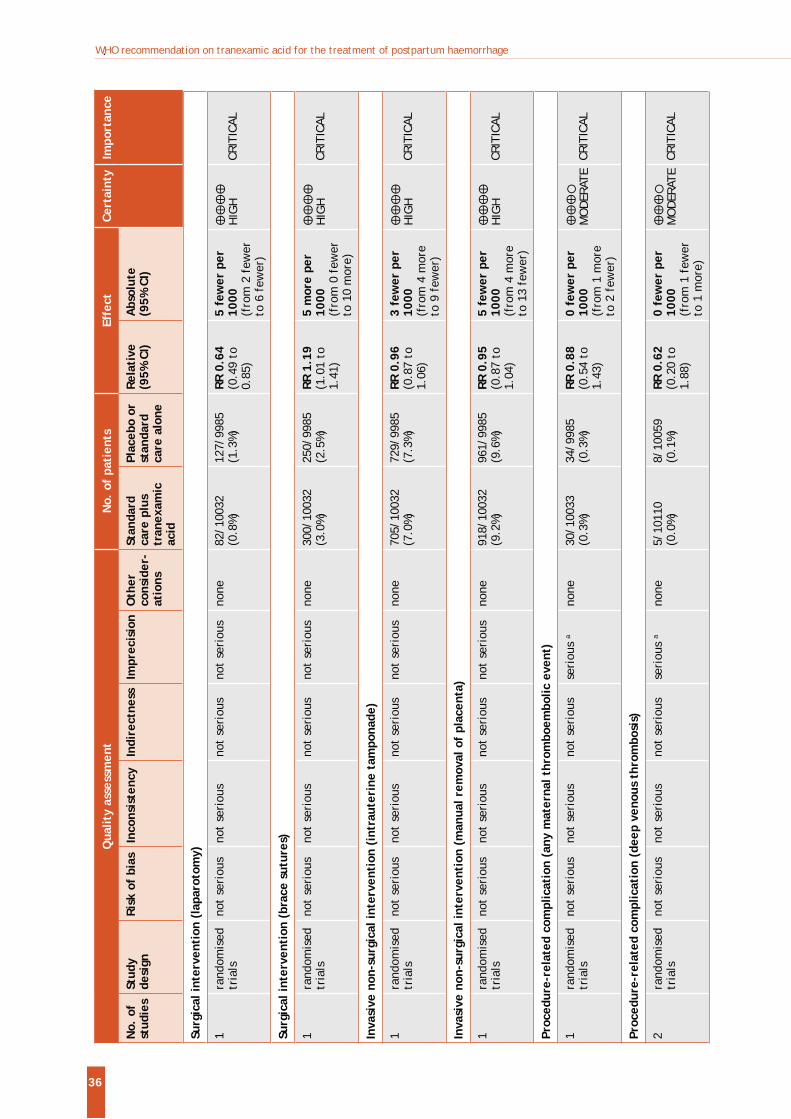
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
36
Surg
ical
inte
rven
tion
(la
paro
tom
y)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
82/1
0032
(0
.8%)
12
7/99
85
(1.3
%)
RR 0
.64
(0.4
9 to
0.
85)
5 fe
wer
per
10
00(f
rom
2 f
ewer
to
6 f
ewer
)
H
IGH
CR
ITIC
AL
Surg
ical
inte
rven
tion
(br
ace
sutu
res)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
300/
1003
2 (3
.0%)
25
0/99
85
(2.5
%)
RR 1
.19
(1.0
1 to
1.
41)
5 m
ore
per
1000
(fro
m 0
few
er
to 1
0 m
ore)
H
IGH
CR
ITIC
AL
Inva
sive
non
-sur
gica
l int
erve
ntio
n (i
ntra
uter
ine
tam
pona
de)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
705/
1003
2 (7
.0%)
72
9/99
85
(7.3
%)
RR 0
.96
(0.8
7 to
1.
06)
3 fe
wer
per
10
00(f
rom
4 m
ore
to 9
few
er)
H
IGH
CR
ITIC
AL
Inva
sive
non
-sur
gica
l int
erve
ntio
n (m
anua
l rem
oval
of
plac
enta
)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
918/
1003
2 (9
.2%)
96
1/99
85
(9.6
%)
RR 0
.95
(0.8
7 to
1.
04)
5 fe
wer
per
10
00(f
rom
4 m
ore
to 1
3 fe
wer
)
H
IGH
CR
ITIC
AL
Proc
edur
e-re
late
d co
mpl
icat
ion
(any
mat
erna
l thr
ombo
embo
lic e
vent
)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
30
/100
33
(0.3
%)
34/9
985
(0.3
%)
RR 0
.88
(0.5
4 to
1.
43)
0 fe
wer
per
10
00(f
rom
1 m
ore
to 2
few
er)
M
OD
ERAT
E CR
ITIC
AL
Proc
edur
e-re
late
d co
mpl
icat
ion
(dee
p ve
nous
thr
ombo
sis)
2 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
5/
1011
0 (0
.0%)
8/
1005
9 (0
.1%)
RR
0.6
2(0
.20
to
1.88
)
0 fe
wer
per
10
00(f
rom
1 f
ewer
to
1 m
ore)
M
OD
ERAT
E CR
ITIC
AL
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
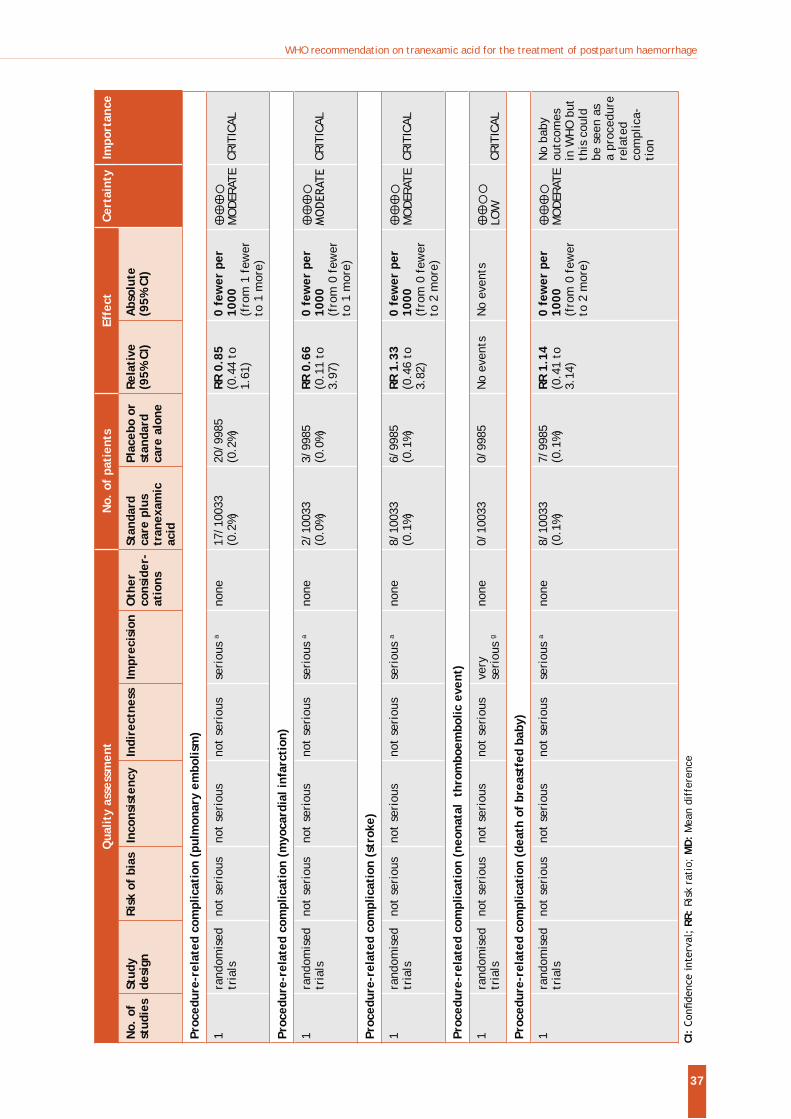
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
37
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Proc
edur
e-re
late
d co
mpl
icat
ion
(pul
mon
ary
embo
lism
)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
17
/100
33
(0.2
%)
20/9
985
(0.2
%)
RR 0
.85
(0.4
4 to
1.
61)
0 fe
wer
per
10
00(f
rom
1 f
ewer
to
1 m
ore)
M
OD
ERAT
E CR
ITIC
AL
Proc
edur
e-re
late
d co
mpl
icat
ion
(myo
card
ial i
nfar
ctio
n)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
2/
1003
3 (0
.0%)
3/
9985
(0
.0%)
RR
0.6
6(0
.11
to
3.97
)
0 fe
wer
per
10
00(f
rom
0 f
ewer
to
1 m
ore)
MODER
ATE
CRIT
ICAL
Proc
edur
e-re
late
d co
mpl
icat
ion
(str
oke)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
8/
1003
3 (0
.1%)
6/
9985
(0
.1%)
RR
1.3
3(0
.46
to
3.82
)
0 fe
wer
per
10
00(f
rom
0 f
ewer
to
2 m
ore)
M
OD
ERAT
E CR
ITIC
AL
Proc
edur
e-re
late
d co
mpl
icat
ion
(neo
nata
l th
rom
boem
bolic
eve
nt)
1ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s ve
ry
seri
ous
gno
ne
0/10
033
0/99
85
No
even
tsN
o ev
ents
LO
W
CRIT
ICAL
Proc
edur
e-re
late
d co
mpl
icat
ion
(dea
th o
f br
east
fed
baby
)
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
8/
1003
3 (0
.1%)
7/
9985
(0
.1%)
RR
1.1
4(0
.41
to
3.14
)
0 fe
wer
per
10
00(f
rom
0 f
ewer
to
2 m
ore)
M
OD
ERAT
E N
o ba
by
outc
omes
in
WH
O b
ut
this
cou
ld
be s
een
as
a pr
oced
ure
rela
ted
com
plic
a-ti
on
CI:
RR:
Risk
rat
io;
MD
: M
ean
diff
eren
ce
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
38
Expl
anat
ions
c. S
ingl
e st
udy
wit
h de
sign
lim
itat
ions
(no
blin
ding
)
e. M
oder
ate
stat
isti
cal h
eter
ogen
eity
and
may
be
clin
ical
het
erog
enei
ty
f. S
ingl
e st
udy
wit
h sm
all s
ampl
e si
ze
g. N
o ev
ents
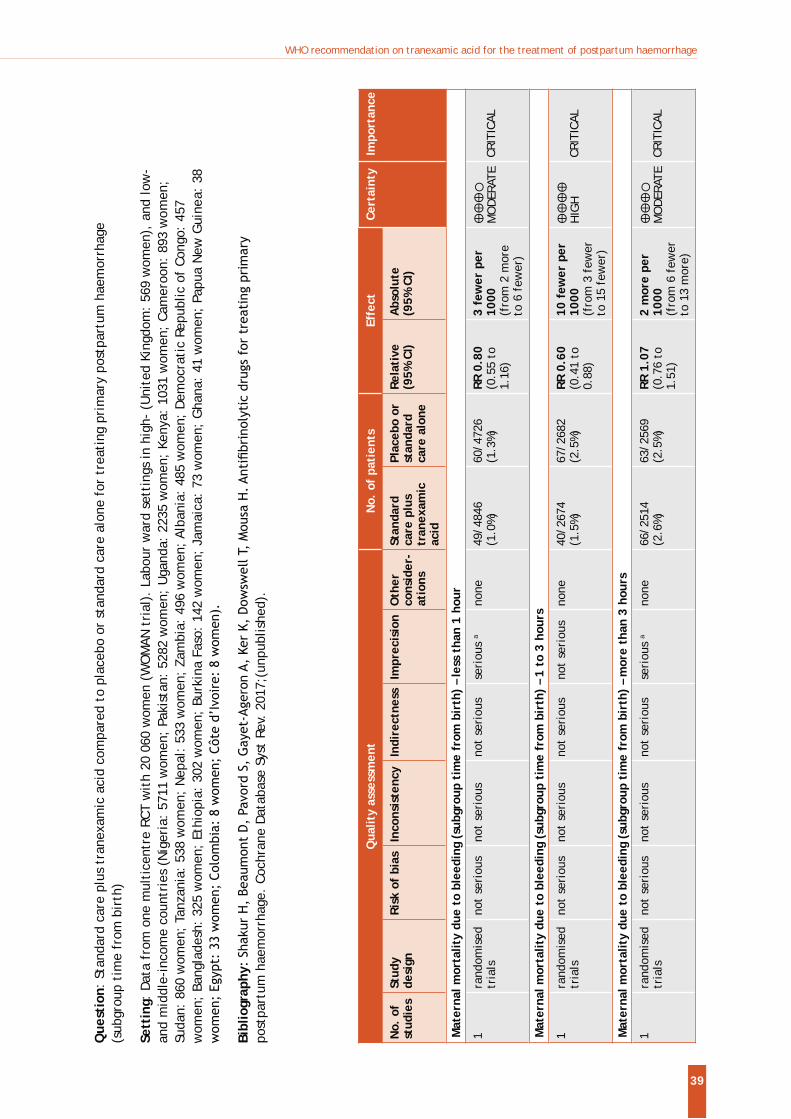
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
39
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Mat
erna
l mor
talit
y du
e to
ble
edin
g (s
ubgr
oup
tim
e fr
om b
irth
) –
less
tha
n 1
hour
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
49
/484
6 (1
.0%)
60
/472
6 (1
.3%)
RR
0.8
0(0
.55
to
1.16
)
3 fe
wer
per
10
00(f
rom
2 m
ore
to 6
few
er)
M
OD
ERAT
E CR
ITIC
AL
Mat
erna
l mor
talit
y du
e to
ble
edin
g (s
ubgr
oup
tim
e fr
om b
irth
) –
1 to
3 h
ours
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
40/2
674
(1.5
%)
67/2
682
(2.5
%)
RR 0
.60
(0.4
1 to
0.
88)
10 f
ewer
per
10
00
(fro
m 3
few
er
to 1
5 fe
wer
)
H
IGH
CR
ITIC
AL
Mat
erna
l mor
talit
y du
e to
ble
edin
g (s
ubgr
oup
tim
e fr
om b
irth
) –
mor
e th
an 3
hou
rs
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
66
/251
4 (2
.6%)
63
/256
9 (2
.5%)
RR
1.0
7 (0
.76
to
1.51
)
2 m
ore
per
1000
(f
rom
6 f
ewer
to
13
mor
e)
M
OD
ERAT
E CR
ITIC
AL
Que
stio
n: S
tand
ard
care
plu
s tr
anex
amic
aci
d co
mpa
red
to p
lace
bo o
r st
anda
rd c
are
alon
e fo
r tr
eati
ng p
rim
ary
post
part
um h
aem
orrh
age
(sub
grou
p ti
me
from
bir
th)
Sett
ing:
Dat
a fr
om o
ne m
ulti
cent
re R
CT w
ith
20 0
60 w
omen
(W
OM
AN t
rial
). L
abou
r w
ard
sett
ings
in h
igh-
(U
nite
d Ki
ngdo
m:
569
wom
en),
and
low
- an
d m
iddl
e-in
com
e co
untr
ies
(Nig
eria
: 57
11 w
omen
; Pa
kist
an:
5282
wom
en;
Uga
nda:
223
5 w
omen
; Ke
nya:
103
1 w
omen
; Ca
mer
oon:
893
wom
en;
Suda
n: 8
60 w
omen
; Ta
nzan
ia:
538
wom
en;
Nep
al:
533
wom
en;
Zam
bia:
496
wom
en;
Alba
nia:
485
wom
en;
Dem
ocra
tic
Repu
blic
of
Cong
o: 4
57
wom
en;
Bang
lade
sh:
325
wom
en;
Ethi
opia
: 30
2 w
omen
; Bu
rkin
a Fa
so:
142
wom
en;
Jam
aica
: 73
wom
en;
Gha
na:
41 w
omen
; Pa
pua
New
Gui
nea:
38
Bibl
iogr
aphy
post
part
um h
aem
orrh
age.
Coc
hran
e D
atab
ase
Syst
Rev
. 20
17;(
unpu
blis
hed)
.
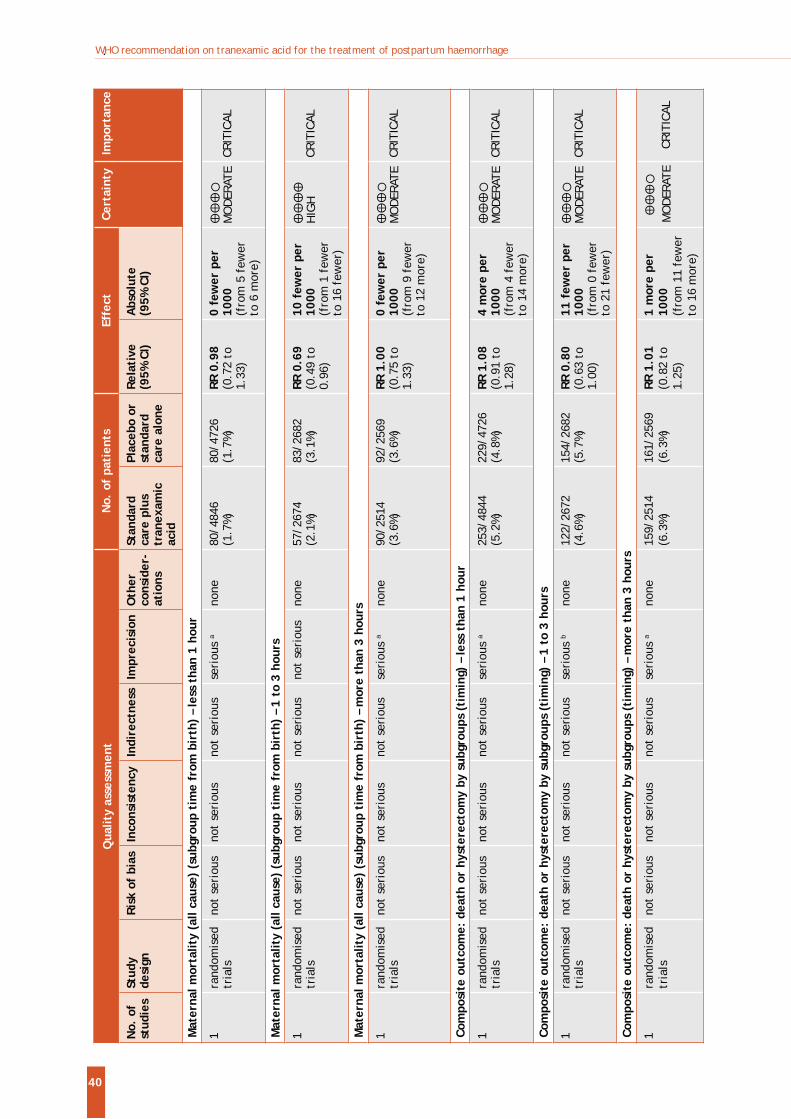
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
40
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Mat
erna
l mor
talit
y (a
ll ca
use)
(su
bgro
up t
ime
from
bir
th)
– le
ss t
han
1 ho
ur
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
80
/484
6 (1
.7%)
80
/472
6 (1
.7%)
RR
0.9
8(0
.72
to
1.33
)
0 fe
wer
per
10
00(f
rom
5 f
ewer
to
6 m
ore)
M
OD
ERAT
E CR
ITIC
AL
Mat
erna
l mor
talit
y (a
ll ca
use)
(su
bgro
up t
ime
from
bir
th)
– 1
to 3
hou
rs
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
57/2
674
(2.1
%)
83/2
682
(3.1
%)
RR 0
.69
(0.4
9 to
0.
96)
10 f
ewer
per
10
00(f
rom
1 f
ewer
to
16
few
er)
H
IGH
CR
ITIC
AL
Mat
erna
l mor
talit
y (a
ll ca
use)
(su
bgro
up t
ime
from
bir
th)
– m
ore
than
3 h
ours
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
90
/251
4 (3
.6%)
92
/256
9 (3
.6%)
RR
1.0
0(0
.75
to
1.33
)
0 fe
wer
per
10
00(f
rom
9 f
ewer
to
12
mor
e)
M
OD
ERAT
E CR
ITIC
AL
Com
posi
te o
utco
me:
dea
th o
r hy
ster
ecto
my
by s
ubgr
oups
(ti
min
g) –
less
tha
n 1
hour
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
25
3/48
44
(5.2
%)
229/
4726
(4
.8%)
RR
1.0
8 (0
.91
to
1.28
)
4 m
ore
per
1000
(f
rom
4 f
ewer
to
14
mor
e)
M
OD
ERAT
E CR
ITIC
AL
Com
posi
te o
utco
me:
dea
th o
r hy
ster
ecto
my
by s
ubgr
oups
(ti
min
g) –
1 t
o 3
hour
s
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s b
none
12
2/26
72
(4.6
%)
154/
2682
(5
.7%)
RR
0.8
0 (0
.63
to
1.00
)
11 f
ewer
per
10
00
(fro
m 0
few
er
to 2
1 fe
wer
)
M
OD
ERAT
E CR
ITIC
AL
Com
posi
te o
utco
me:
dea
th o
r hy
ster
ecto
my
by s
ubgr
oups
(ti
min
g) –
mor
e th
an 3
hou
rs
1 ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
15
9/25
14
(6.3
%)
161/
2569
(6
.3%)
RR
1.0
1 (0
.82
to
1.25
)
1 m
ore
per
1000
(f
rom
11
few
er
to 1
6 m
ore)
M
OD
ERAT
E
CRIT
ICAL
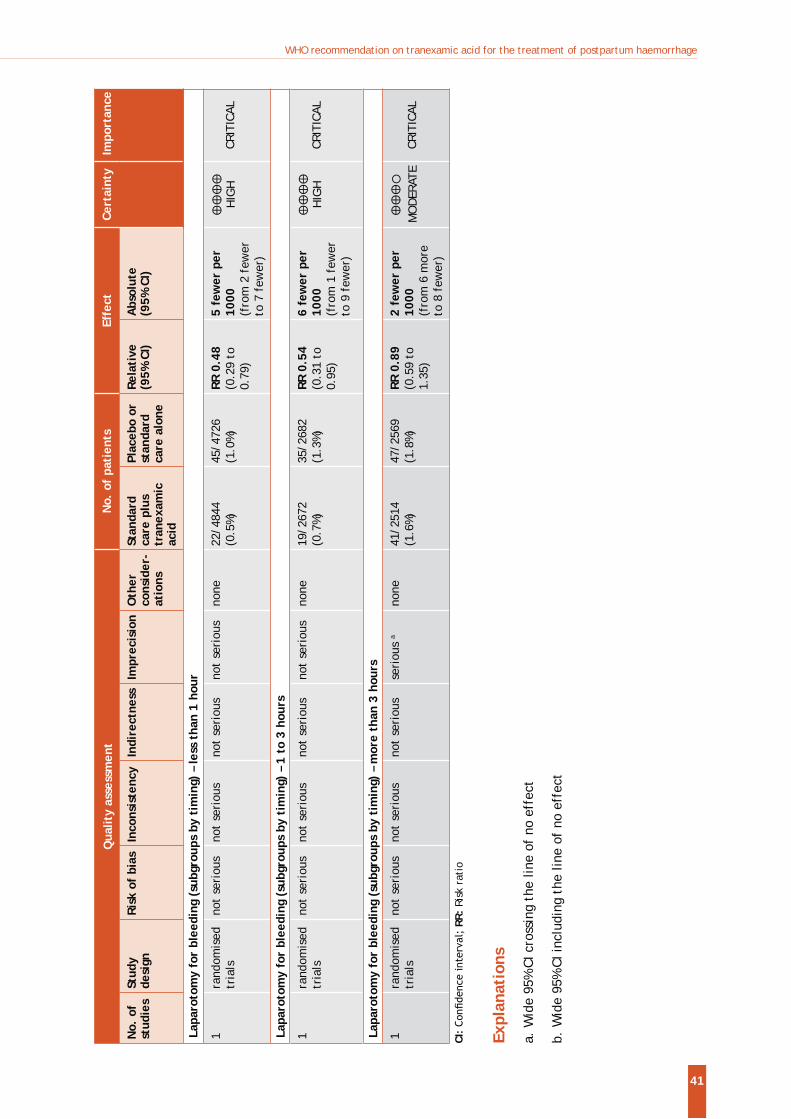
WHO recommendation on tranexamic acid for the treatment of postpartum haemorrhage
41
Qua
lity
asse
ssm
ent
No.
of
pati
ents
Effe
ctCe
rtai
nty
Impo
rtan
ce
No.
of
stud
ies
Stud
y de
sign
Risk
of
bias
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nO
ther
co
nsid
er-
atio
ns
Stan
dard
ca
re p
lus
tran
exam
ic
acid
Plac
ebo
or
stan
dard
ca
re a
lone
Rela
tive
(9
5% C
I)A
bsol
ute
(95%
CI)
Lapa
roto
my
for
blee
ding
(su
bgro
ups
by t
imin
g) –
less
tha
n 1
hour
1ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
22/4
844
(0.5
%)
45/4
726
(1.0
%)
RR 0
.48
(0.2
9 to
0.
79)
5 fe
wer
per
10
00
(fro
m 2
few
er
to 7
few
er)
H
IGH
CR
ITIC
AL
Lapa
roto
my
for
blee
ding
(su
bgro
ups
by t
imin
g) –
1 t
o 3
hour
s
1ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s no
t se
riou
s no
ne
19/2
672
(0.7
%)
35/2
682
(1.3
%)
RR 0
.54
(0.3
1 to
0.
95)
6 fe
wer
per
10
00
(fro
m 1
few
er
to 9
few
er)
H
IGH
CR
ITIC
AL
Lapa
roto
my
for
blee
ding
(su
bgro
ups
by t
imin
g) –
mor
e th
an 3
hou
rs
1ra
ndom
ised
tr
ials
no
t se
riou
s no
t se
riou
s no
t se
riou
s se
riou
s a
none
41
/251
4 (1
.6%)
47
/256
9 (1
.8%)
RR
0.8
9 (0
.59
to
1.35
)
2 fe
wer
per
10
00
(fro
m 6
mor
e to
8 f
ewer
)
M
OD
ERAT
E CR
ITIC
AL
CI:
RR:
Risk
rat
io
Expl
anat
ions
a.W
ide
95%
CI c
ross
ing
the
line
of n
o ef
fect
b.W
ide
95%
CI in
clud
ing
the
line
of n
o ef
fect
ISBN 978 92 4 155015 4
For more information, please contact:
Department of Reproductive Health and Research E-mail: [email protected]/reproductivehealth
Maternal, Newborn, Child and Adolescent HealthE-mail: [email protected]/maternal_child_adolescent
World Health Organization Avenue Appia 20, CH-1211 Geneva 27 Switzerland
Related Documents