Journal of Community Psychology Volume 18, January 1990 When Social Support Fails: The Homeless Andrea Solarz U.S. Congress Office of Technology Assessment G. Anne Bogat Michigan State University The social support networks of residents of a temporary shelter for the homeless were examined. Participants (N = 125) were interviewed to ob- tain detailed information concerning resources of support, specific types of support, and subjective appraisals of support. Seven meaningful subgroups of homeless persons were identified using a cluster analysis technique. These groups varied along the dimensions of transiency, psychiatric history, criminal victimization, and criminal activity. As expected, this population had relatively small social networks, although most clearly had some sources of support, particularly from family members. Few differences on social support variables were revealed between subgroups. The differences between the homeless and other nonclinical populations are discussed, and implica- tions for interventions are addressed. It is uncertain how many persons in this country are currently homeless (estimates range from 250,000 to 3 million; U.S. General Accounting Office, 1988); however, clear demographic shifts have occurred during the last decade. In the past, few women lived on the streets (Bahr, 1973; Blumberg, Shipley, & Barsky, 1978); today women comprise as much as a quarter of the homeless population (Arce & Vergare, 1984; Bachrach, 1984; Crystal, 1984; Stoner, 1983). There is also a broad consensus that the number of homeless families (most headed by single women) is increasing, and that children may be the fastest growing group of homeless individuals (U.S. Conference of Mayors, 1987). From the 1940s to the late 1960s, the mean age of the homeless steadily increased from about 45 (e.g., Sutherland & Locke, 1936) to the mid-50s (Bahr, 1973). The mean age of the homeless has now dropped to about 35 (e.g., Arce, Tadlock, Vergare, & Shapiro, 1983; Ball & Havassy, 1984; Depp & Ackiss, 1983; Lamb & Grant, 1983; Lipton, Sabitini, & Katz, 1983). Finally, greater numbers of the homeless are mentally ill (USGAO, 1988). Appleby and Desai (1985) suggested that the incidence of homelessness among the men- tally ill is at least three to four times that of the general population. Estimates of the numbers of homeless persons who are mentally ill range from 25% or lower (e.g., Segal, Baumohl, & Johnson, 1977) to 91% (Bassuk, Rubin, & Lauriat, 1984); a recent na- tional study reported that 20% of homeless adults had a history of psychiatric hospitaliza- tion (Burt & Cohen, 1988). A complex interplay of societal and individual factors creates a context in which homelessness may occur. Societal antecedents include inflation, unemployment, the gen- trification of urban areas, and the deinstitutionalization policies of the 1960s. These The views presented in this article are those of the authors and do not necessarily represent the official position of OTA. Please send reprint requests to G. Anne Bogat, Department of Psychology, Michigan State University,East Lansing, MI 48824. We would like to thank Richard Hillyer, Fred Rogosch, and Rich Amdur for their insightful comments on an earlier draft. This research was funded by dissertation research grants to the first author from the State of Michigan Department of Mental Health and the Urban Affairs Program, Michigan State University. 79

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Community Psychology Volume 18, January 1990
When Social Support Fails: The Homeless Andrea Solarz
U.S. Congress Office of Technology Assessment
G . Anne Bogat Michigan State University
The social support networks of residents of a temporary shelter for the homeless were examined. Participants ( N = 125) were interviewed to ob- tain detailed information concerning resources of support, specific types of support, and subjective appraisals of support. Seven meaningful subgroups of homeless persons were identified using a cluster analysis technique. These groups varied along the dimensions of transiency, psychiatric history, criminal victimization, and criminal activity. As expected, this population had relatively small social networks, although most clearly had some sources of support, particularly from family members. Few differences on social support variables were revealed between subgroups. The differences between the homeless and other nonclinical populations are discussed, and implica- tions for interventions are addressed.
It is uncertain how many persons in this country are currently homeless (estimates range from 250,000 to 3 million; U.S. General Accounting Office, 1988); however, clear demographic shifts have occurred during the last decade. In the past, few women lived on the streets (Bahr, 1973; Blumberg, Shipley, & Barsky, 1978); today women comprise as much as a quarter of the homeless population (Arce & Vergare, 1984; Bachrach, 1984; Crystal, 1984; Stoner, 1983). There is also a broad consensus that the number of homeless families (most headed by single women) is increasing, and that children may be the fastest growing group of homeless individuals (U.S. Conference of Mayors, 1987). From the 1940s to the late 1960s, the mean age of the homeless steadily increased from about 45 (e.g., Sutherland & Locke, 1936) to the mid-50s (Bahr, 1973). The mean age of the homeless has now dropped to about 35 (e.g., Arce, Tadlock, Vergare, & Shapiro, 1983; Ball & Havassy, 1984; Depp & Ackiss, 1983; Lamb & Grant, 1983; Lipton, Sabitini, & Katz, 1983). Finally, greater numbers of the homeless are mentally ill (USGAO, 1988). Appleby and Desai (1985) suggested that the incidence of homelessness among the men- tally ill is at least three to four times that of the general population. Estimates of the numbers of homeless persons who are mentally ill range from 25% or lower (e.g., Segal, Baumohl, & Johnson, 1977) to 91% (Bassuk, Rubin, & Lauriat, 1984); a recent na- tional study reported that 20% of homeless adults had a history of psychiatric hospitaliza- tion (Burt & Cohen, 1988).
A complex interplay of societal and individual factors creates a context in which homelessness may occur. Societal antecedents include inflation, unemployment, the gen- trification of urban areas, and the deinstitutionalization policies of the 1960s. These
The views presented in this article are those of the authors and do not necessarily represent the official position of OTA. Please send reprint requests to G . Anne Bogat, Department of Psychology, Michigan State University, East Lansing, MI 48824. We would like to thank Richard Hillyer, Fred Rogosch, and Rich Amdur for their insightful comments on an earlier draft. This research was funded by dissertation research grants to the first author from the State of Michigan Department of Mental Health and the Urban Affairs Program, Michigan State University.
79
80 SOLARZ AND BOGAT
global antecedents coupled with various stressful life events (e.g., eviction, destruction of homes by dilapidation or fire) precipitate individual instances of homelessness.
Although people become homeless for many reasons, an experience that all share is the lack of the type of social support afforded by a place of residence and, with it, a recognized place in the larger community. Alienated from relatives and friends after histories of mental illness, involvement in crime, or family disruption (e.g., divorce, death, abuse), individuals with limited economic resources easily exhaust the mainstays of informal support and can no longer stay with those on whom they may have former- ly depended. Once they enter the shelter system, the homeless may become geographically distant from their customary sources of community and personal support and thus fur- ther erode their social support networks. Formal support resources, too, can fail: For example, those released from either mental or penal institutions often experience inade- quate follow-up and aftercare; although they may technically have been released to a residence, this may in fact be substandard, strictly temporary, or simply manufactured by the client in an effort to meet the requirements for discharge.
Indeed, long before the term “social support” was coined, Sutherland and Locke (1936) discussed the isolation of the homeless from family and other groups. They noted that over half had little or no contact with their parental families, few had developed close personal relationships, and most had either never married or were currently isolated from their spouses.
Unfortunately, modern research has done little more than confirm these demo- graphic statistics. We can still say that most of the homeless are single (Bassuk et al., 1984; Bassuk, Rubin, & Lauriat, 1986; Burt & Cohen, 1988; Fischer, Shapiro, Breakey, Anthony, & Kramer, 1986; Kroll, Carey, Hagedorn, Fire Dog, & Benavides, 1986; Mowbray, Solarz, Johnson, Phillips-Smith, & Combs, 1986; Robertson, Ropers, & Boyer, 1985), although this is somewhat less true for women than for men (Crystal, 1984), and that they are isolated from their families: It is estimated that either one-third (Fischer, 1984), one-half (Cohen & Sokolovsky, 1983), or three-quarters (Bassuk et al., 1984) of the homeless have no family contact. Also, about one-quarter had no friends to provide support (Bassuk et al., 1984; Bassuk & Rosenberg, 1988), two-thirds had no confiding relationships (Fischer, 1984), and less than half had weekly contact with a friend (Mowbray et al., 1986). Bassuk and Rosenberg (1988) found that the networks of homeless mothers were smaller and more fragmented than those of domiciled mothers. Finally, there is some evidence that homeless persons with previous psychiatric hospitalizations, compared to those without such history, have even less support from both friends and family (Bassuk et al., 1984).
One reason that so little information exists about the support networks of the homeless is that all of the studies reported above (except for Cohen & Sokolovsky, 1983) have had only a peripheral interest in this topic. Hence, the questions about support have focused mainly on detailing support resources (specific persons who provide sup- port), ignoring the types of support the homeless receive and their subjective appraisals of this support. Most important, because the homeless are a heterogeneous population with an assortment of problems and life histories, it seems likely that summary statistics (e.g., means) that are reported for the sample as a whole may obscure real differences in how particular segments of the homeless use social support.
Again, there are almost no data to help us in identifying various subgroups of the homeless population. Arce et al. (1983) described three different types of homeless shelter residents: The “street people” lived on the street regularly for stretches lasting more than

SOCIAL SUPPORT AND THE HOMELESS 81
1 month at a time, were generally over the age of 40, and had a history of health and psychological problems; the “episodic homeless” were domiciled more often (their periods of street living generally lasting less than a month), were usually younger, did not have a history of prior hospitalization, and had sporadic contact with a number of different human service agencies; and the “situationally homeless” were living in the shelter because of an acute personal crisis.
Although this typology might be criticized because it was not empirically derived, its three broad categories nonetheless allow researchers to generate more sophisticated hypotheses about differences in support received by the homeless than would be possi- ble if that population were taken as a single homogeneous group. For example, some research indicates that persons suffering from severe psychological problems, such as schizophrenia, have little contact with family; their social networks are dominated by nonkin (e.g., Garrison, 1978). Therefore, one would expect street people, who had histories of severe psychological problems, to have nonkin-dominated networks. Iden- tification of types of homeless individuals and differences in their support networks may be a first step toward developing appropriate services for this population.
The objectives of the current study were to (a) provide detailed information con- cerning resources, specific types of support, and subjective appraisals of support for the homeless; (b) provide an empirical understanding of different types of homeless per- sons; and (c) compare these different types of homeless persons on various social sup- port measures. Data for this project were collected by interviewing residents of a shelter for the homeless.
Method Participants
Participants were randomly sampled from a roster of guests staying at a temporary shelter in a large midwestern city (population 1,089,OOO). The shelter is funded by several social and human service agencies and churches in the city. First opened in 1982, the shelter can accommodate 72 individuals each night. It was the largest shelter in the city at the time of the research study. Previous research on the homeless in this city indicated that this shelter had a very diverse clientele (Solarz & Mowbray, 1985).
Guests at the shelter include men, women, and families. They are referred by local social service agencies or through self-referrals. After their arrival at the shelter, guests work with a staff member to develop a plan to address their needs, especially the need to locate permanent housing. Once the service plan is successfully completed (or suffi- cient progress has been made), guests are discharged from the facility. However, sometimes guests are asked to leave the shelter because of their violent behavior or because they have broken the rules of the shelter.
Overall, 85.3% ( N = 125) of those approached to participate in the study agreed to be interviewed. A comparison of participants and nonparticipants on the variables of race, gender, and history of psychiatric hospitalization indicated that nonpartici- pants were more likely to be White, t(148) = 2.07, p < .05, and female, t(148) = 2.56, p < .05. There was no difference in the percentages of participants and nonparticipants with histories of psychiatric hospitalization based on State Department of Mental Health archival records.
The sample consisted of 79 males and 46 females with a mean age of 33.4 (range, 17-72). Twenty percent of the participants were White, 79% were Black, and 1070 were
82 SOLARZ AND BOGAT
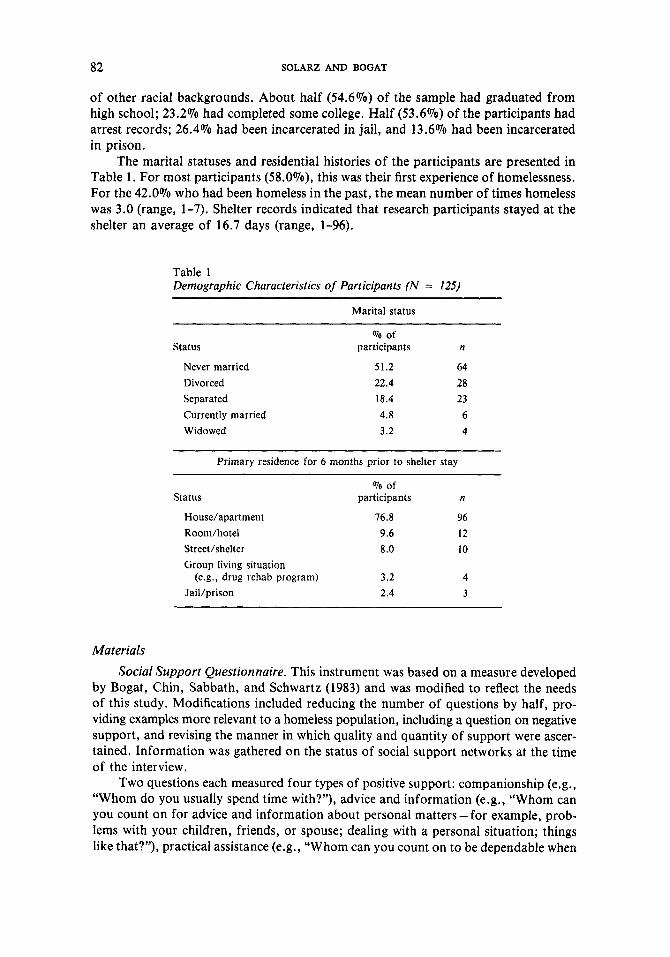
of other racial backgrounds. About half (54.6%) of the sample had graduated from high school; 23.2% had completed some college. Half (53.6%) of the participants had arrest records; 26.4% had been incarcerated in jail, and 13.6% had been incarcerated in prison.
The marital statuses and residential histories of the participants are presented in Table 1. For most participants (58.0%), this was their first experience of homelessness. For the 42.0% who had been homeless in the past, the mean number of times homeless was 3.0 (range, 1-7). Shelter records indicated that research participants stayed at the shelter an average of 16.7 days (range, 1-96).
Table 1 Demographic Characteristics of Participants (N = 125)
Marital status
Status
Never married Divorced Separated Currently married Widowed
To of participants n
51.2 64 22.4 28 18.4 23 4.8 6 3.2 4
Primary residence for 6 months prior to shelter stay
Status To of
participants n
House/apartment 76.8 96 Room/hotel 9.6 12 StreeUshelter 8.0 10 Group living situation
(e.g., drug rehab program) 3.2 4 Jail/prison 2.4 3
Materials Social Support Questionnaire. This instrument was based on a measure developed
by Bogat, Chin, Sabbath, and Schwartz (1983) and was modified to reflect the needs of this study. Modifications included reducing the number of questions by half, pro- viding examples more relevant to a homeless population, including a question on negative support, and revising the manner in which quality and quantity of support were ascer- tained. Information was gathered on the status of social support networks at the time of the interview.
Two questions each measured four types of positive support: companionship (e.g., “Whom do you usually spend time with?”), advice and information (e.g., “Whom can you count on for advice and information about personal matters - for example, prob- lems with your children, friends, or spouse; dealing with a personal situation; things like that?”), practical assistance (e.g., “Whom can you count on to be dependable when
SOCIAL SUPPORT AND THE HOMELESS 83
you need help?”), and emotional support (e.g.; “Who really cares about you?”). One question about negative support was also included (“Who makes your life difficult: such as someone who expects too much from you or makes too many demands on you, some- one who you wish would leave you alone, or someone whom you would like to avoid?”). Participants could list as many as 10 supporters for each of these nine questions. The variable “total network size” was calculated by summing the number of unique names nominated on the positive support questions.
Additional information was collected about each network member listed for the nine questions: the supporter’s relationship to the respondent (e.g., family, friend, pro- fessional), the gender of the supporter, the length of time the respondent had known the supporter (1 = 1 week or less to 6 = more than 5 years), the reciprocity of the relationship (supporter provides more support than respondent, supporter and respon- dent provide equal support, respondent provides more support than supporter), and the importance of the relationship with the supporter (1 = not at all important to 7 = extremely important).
Network members were also described as support “specialists” or “generalists” (cf. Bogat, Caldwell, Rogosch, & Kriegler, 1985). Network members were coded as specialists if they provided only one of the four types of positive support and as generalists if they provided two or more types of positive support.
Participants noted their satisfaction with the quality and quantity of each of the four types of support using a 7-point rating scale ranging from “terrible” (1) to “delighted” (7) (e.g., “In general, how do you feel about the quality of emotional support that you receive?” “In general, how do you feel about the amount of emotional support that you receive?”). In addition, there was a one-item measure of overall satisfaction with social support. These nine items were linearly combined to form a Satisfaction with Social Support Scale (Cronbach’s alpha = 38).
Last, descriptive data were gathered on marital status, family configuration, number of good friends, and number of relatives living in the area and the frequency of contact with them.
Background in formation. Information was collected on the demographic variables of race, gender, age, and education. Additional information was gathered on sources of income during the previous 6 months, including income from state and federal financial entitlement programs, work, family, selling plasma, or illegal activities.
Psychiatric history was assessed through self-report of past hospitalization and through a records search of the State Department of Mental Health data system. A self- report of general health status was obtained using a 4-point scale from “poor” (1) to “excellent” (4). Substance use was measured by reported frequency of use of alcohol, marijuana, and hard drugs.
Residential history data were gathered on types and numbers of places stayed during the previous 6 months. Shelter use history included number and recency of previous shelter visits.
Participants provided criminal history information: number of prior arrests, jail terms, and prison terms. Data from the State Department of Corrections records and the State Police computerized convictions register supplemented the self-report data.
Finally, data were gathered on criminal victimizations during the previous 6 months. Using questions based on the annually administered National Crime Survey (U.S. Dept. of Justice, 1983), information was obtained on the incidence of robbery, assault, threats of assault, and property theft.

84 SOLAR2 AND BOGAT
Procedure Trained, senior-level undergraduate and graduate students interviewed the par-
ticipants. Interviews, which lasted about 1 hour, were conducted at the shelter, in private. Respondents received a small remuneration for their participation. (Data were gathered in the context of a larger study, Solarz, 1986, that examined the effect of type of pay- ment and type of appointment card on return for a subsequent interview appointment.) Participation in the study was voluntary; written, informed consent was obtained from each respondent. Participants also signed consent forms allowing the researchers to search the State Department of Mental Health, police, court, State Department of Corrections, and shelter records.
Results Types of Support
The average total network size (number of unique positive supporters) was 6.0 (SD = 4.2, range, 1-24). Participants named the greatest number of supporters for emo- tional support (M = 3.4), followed by companionship (M = 2.8), practical assistance (M = 2.3), and advice and information (M = 2.1). Just under 5% (4.8%) of the par- ticipants claimed to have no positive supporters.
These networks consisted of half specialists and half generalists. The highest percen- tage of specialists was indicated for companionship (37.3%). This was followed by emo- tional support (29.7%), practical assistance (24.7%), and advice and information (21.3%).
Half of the participants provided names of negative supporters (M = 1.8; range, 1-6). About 14% of supporters provided both negative and positive support, whereas 8% of all supporters provided only negative support. The majority of supporters who provided negative support were relatives (64%); nearly all of these were nuclear family members (85%).
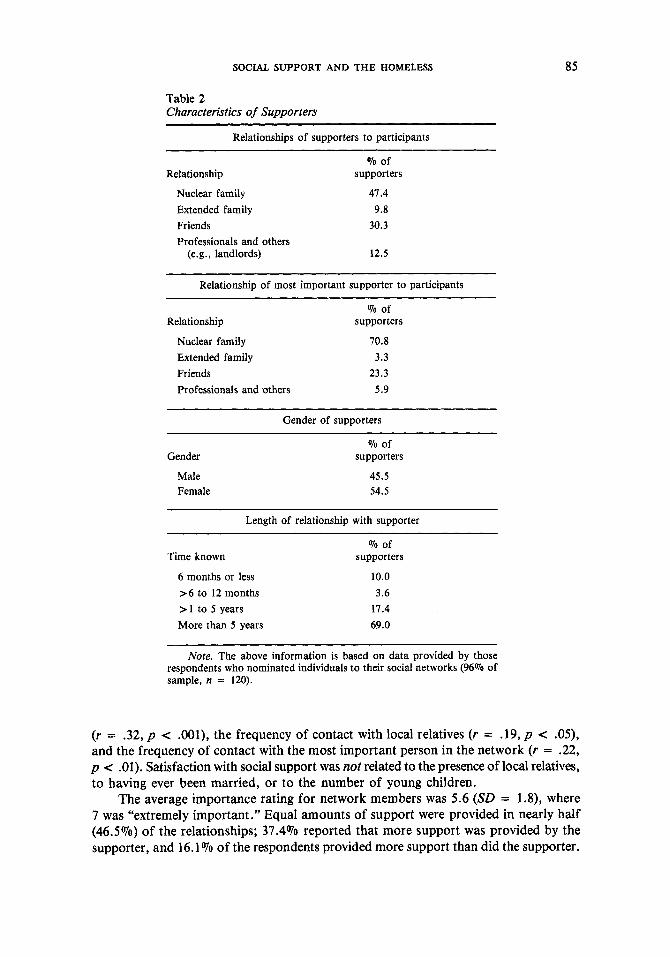
Support Resources Table 2 shows the types of relationships respondents had with their supporters.
The majority of participants (81.6%) had relatives in the area; 76.5% of these, or 62.4% of all respondents, had had contact with their local relatives at least once during the previous month.
Most of the participants (64.8%) had children. Compared to men, women were more likely to have children, t(123) = 2.86, p < .01, and were more likely to have their children with them at the shelter, t(79) = 5.33, p < .001.
Women tended to have a higher proportion of nuclear family members in their net- works than did men, 54.4% versus 39.8%; t(123) = 2.58, p < .05. This difference was not significant, however, when supporters who were children were excluded from the analysis. There were no differences between men and women in the percentages of their networks composed of friends or “other” members.
Subjective Appraisals of Support On the average, participants felt “mixed” to “mostly satisfied” about their social
support (M = 4.7, SD = 1.1); however, almost a quarter (23.2%) felt less positively. Satisfaction with social support was significantly and positively correlated with the
number of close friends (r = .25, p < . O l ) , the total number of positive supporters
SOCIAL SUPPORT AND THE HOMELESS 85
Table 2 Characteristics of Supporters
Relationships of supporters to participants
070 of Relationship supporters
Nuclear family Extended family Friends
47.4 9.8
30.3 Professionals and others
(e.g., landlords) 12.5
Relationship of most important supporter to participants
070 of Relationship supporters
Nuclear family 70.8 Extended family 3.3 Friends 23.3 Professionals and others 5.9
Gender of supporters
Gender
Male Female
Yo of supporters
45.5 54.5
Length of relationship with supporter
Time known
6 months or less >6 to 12 months >1 to 5 years More than 5 years
070 of supporters
10.0 3.6
17.4 69.0
~~ ~
Note. The above information is based on data provided by those respondents who nominated individuals to their social networks (96070 of sample, n = 120).
( r = .32, p < .001), the frequency of contact with local relatives (r = .19, p < .05), and the frequency of contact with the most important person in the network (r = .22, p < .01). Satisfaction with social support was not related to the presence of local relatives, to having ever been married, or to the number of young children.
The average importance rating for network members was 5.6 (SD = 1.8), where 7 was “extremely important.” Equal amounts of support were provided in nearly half (46.5%) of the relationships; 37.4% reported that more support was provided by the supporter, and 16.1% of the respondents provided more support than did the supporter.
86 SOLARZ AND BOGAT
Typological Analysis Profile analysis procedures were used to identify distinct subgroups of homeless
that were internally consistent or similar to each other and that were dissimilar from other groups. Because this type of procedure has not been used previously with homeless populations, Tryon and Bailey’s (1 970) 0-Type analysis (BCTRY), which offers several useful features relative to other programs available to the researchers, was employed. BCTRY can automatically determine initial seed points for further subject clustering. (This is particularly useful when no empirical data exist on which to determine how to seed the computer.) Also, BCTRY uses an iterative procedure that iterates until there is optimal fit of respondents to clusters.
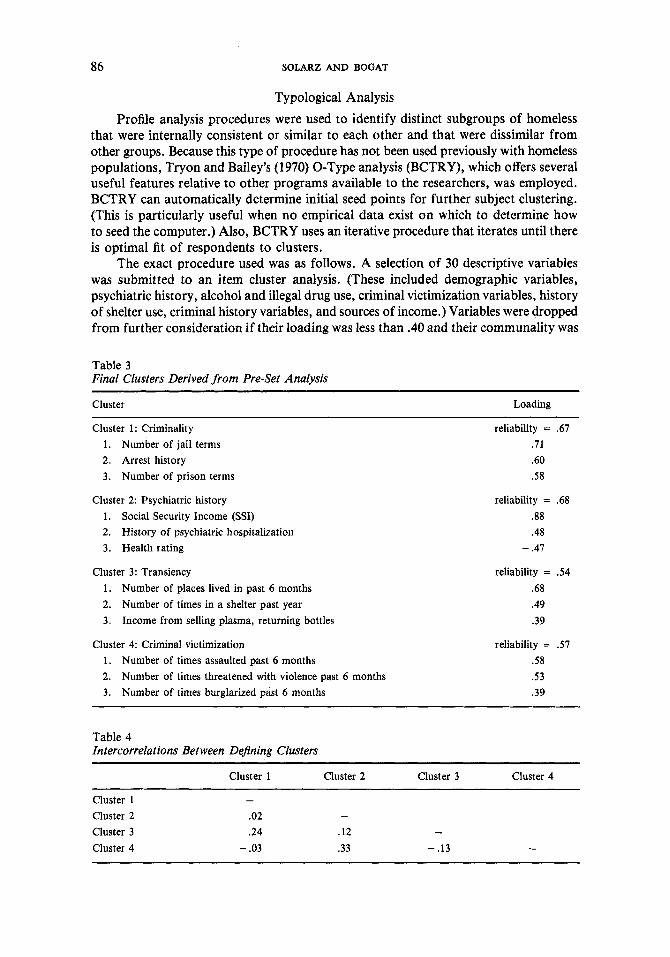
The exact procedure used was as follows. A selection of 30 descriptive variables was submitted to an item cluster analysis. (These included demographic variables, psychiatric history, alcohol and illegal drug use, criminal victimization variables, history of shelter use, criminal history variables, and sources of income.) Variables were dropped from further consideration if their loading was less than .40 and their communality was
Table 3 Final Clusters Derived from Pre-Set Analysis
Cluster Loading
Cluster 1: Criminality 1 . Number of jail terms 2. Arrest history 3. Number of prison terms
Cluster 2: Psychiatric history 1. Social Security Income (SSI) 2. History of psychiatric hospitalization 3. Health rating
Cluster 3: Transiency 1 . Number of places lived in past 6 months 2. Number of times in a shelter past year 3. Income from selling plasma, returning bottles
Cluster 4: Criminal victimization 1 . Number of times assaulted past 6 months 2. Number of times threatened with violence past 6 months 3. Number of times burglarized past 6 months
reliability = .67 .71 .60 .58
reliability = .68 .88 .48
- .47
reliability = 3 4 .68 .49 .39
reliability = .57 .58 .53 .39
Table 4 Intercorrelations Between DeJining Clusters
Cluster 1 Cluster 2 Cluster 3 Cluster 4
Cluster 1 - Cluster 2 .02 - Cluster 3 .24 .12 - Cluster 4 - .03 .33 - .13 -
SOCIAL SUPPORT AND THE HOMELESS 87
below .20. This item clustering procedure identified four empirical dimensions: criminal behavior, psychiatric history, transiency, and criminal victimization. These dimensions are described in Table 3. Table 4 shows the relative independence of these four dimensions.
Data were then submitted to a profile analysis that grouped respondents according to their patterns of scores on the four dimensions from the cluster analysis; a total of eight profiles (or O-Types), which accounted for 121 of the 125 participants, were iden- tified. BCTRY has an arbitrary threshold for dropping respondents from O-Types. Because three respondents' patterns of scores were very similar to existing O-Types, they were assigned to O-Types by the researchers. Thus, 124 of the 125 participants were categorized by the eight O-Types. The mean Euclidean distance between O-Types was 31.48; the mean distance between members and O-Type centers was 8.75.
The number of individuals in each O-Type ranged from 2 to 57. The O-Type with only 2 individuals was dropped from further analysis. The following O-Types (N = 122) were identified:
1. Lower Deviancy (n = 57)- low scores on all four clusters; 2. High Victimization (n = 13)- had experienced high rates of criminal victimiza-
3. High Transiency (n = 9)- were highly transient and exhibited low to moderate
4. High Psychiatric (n = 20)-exhibited high rates of psychiatric problems; 5 . High TransiencyiHigh Psychiatric (n = 5 ) - were highly transient and generally
6. High Criminality (n = 10)-showed high rates of criminal behavior; 7. High Criminality/High Transiency (n = 8)-showed high rates of criminal
behavior and were highly transient.
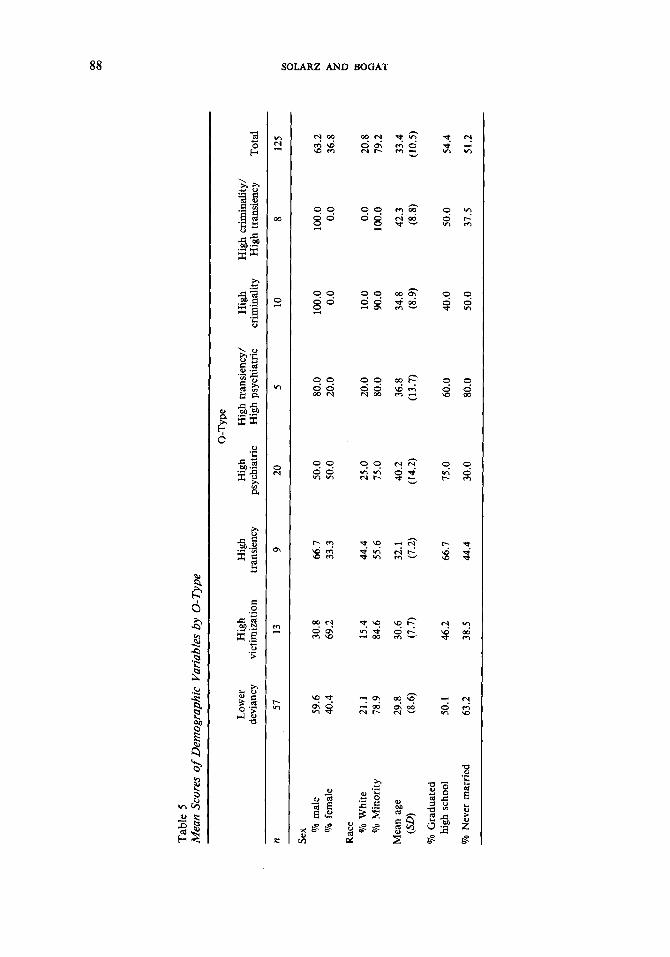
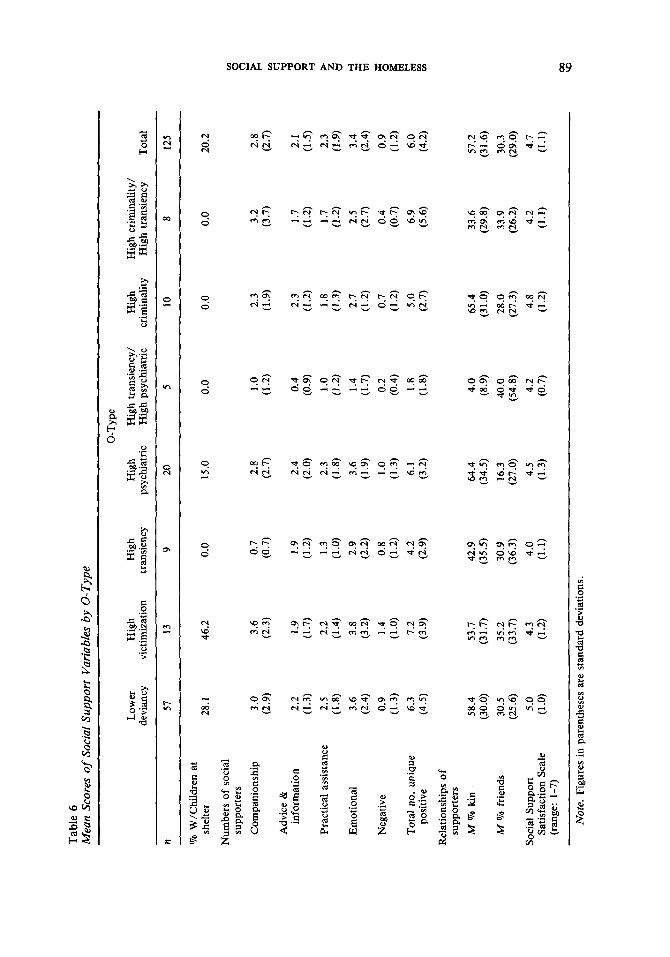
Analyses of variance were performed to determine whether O-Types differed significantly on selected social support variables: numbers of social supporters in each category of support, percentages of supporters who were relatives, percentages of sup- porters who were friends, and Satisfaction with Social Support Scale scores. Differences on a number of demographic characteristics were also examined using chi-square analyses (i.e., the respondent's gender, race, and age, and whether the respondent had ever mar- ried). (See Tables 5 and 6.)
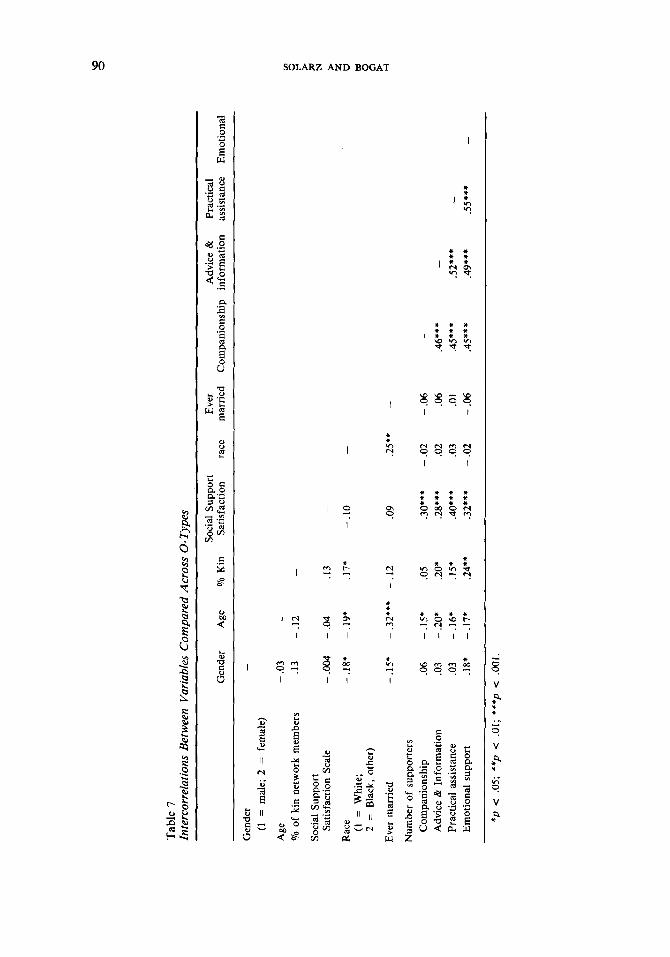
Intercorrelations between the selected social support variables and the demographic variables indicated 24 significant correlation coefficients (out of a possible 45), most less than .30. (See Table 7.) The relatively high intercorrelations between the four types of support may indicate that these are not discrete or independent variables.
There were significant gender differences between the seven O-Types, xL (6, N = 122) = 18.59, p < .005. A posttest contrast of means (McSweeney & Marascuilo, 1977) indicated that there were significantly more women in the high victimization and high psychiatric groups than there were in the high criminal, high transiency/high psychiatric, and high criminal/high transiency groups.
Group differences were also found for age, F(6, 115) = 4.27, p < .001. Scheffk post hoc comparisons indicated that members of the lower deviancy group were signi- ficantly younger than were the high psychiatric and high criminality/high transiency groups.
tion during the previous 6 months;
rates of criminal behavior and mental illness histories;
had psychiatric problems;
Tab
le 5
M
ean
Scor
es o
f D
emog
raph
ic V
aria
bles
by
0-T
ype
0-T
ype
devi
ancy
vi
ctim
izat
ion
trans
ienc
y ps
ychi
atric
H
igh
psyc
hiat
ric
crim
inal
ity
Hig
h tra
nsie
ncy
Tota
l Lo
wer
H
igh
Hig
h H
igh
Hig
h tr
ansi
ency
/ H
igh
Hig
h cr
imin
ality
/
n 57
13
9
20
5 10
8
125
Sex Qo
mal
e 59
.6
30.8
66
.7
50.0
80
.0
100.
0 10
0.0
63.2
N
* z U
% f
emal
e 40
.4
69.2
33
.3
50.0
20
.0
0.0
0.0
36.8
Rac
e
B %
Whi
te
21.1
15
.4
44.4
25
.0
20.0
10
.0
0.0
20.8
07
0 M
inor
ity
78.9
84
.6
55.6
75
.0
80.0
90
.0
100.
0 79
.2
% M
ean
age
29.8
30
.6
32.1
40
.2
36.8
34
.8
42.3
33
.4
(SO
(8
.6)
(7.7
) (7
.2)
(14.
2)
(13.
7)
(8.9
) (8
.8)
(10.
5)
high
sch
ool
50.1
46
.2
66.7
75
.0
60.0
40
.0
50.0
54
.4
% G
radu
ated
Vo N
ever
mar
ried
63.2
38
.5
44.4
30
.0
80.0
50
.0
31.5
51
.2
Tab
le 6
M
ean
Scor
es of
Soci
al S
uppo
rt V
aria
bles
by
0-T
ype
0-T
ype
devi
ancy
vi
ctim
izat
ion
trans
ienc
y ps
ychi
atric
H
igh
psyc
hiat
ric
crim
inal
ity
Hig
h tra
nsie
ncy
Tot
al
Low
er
Hig
h H
igh
Hig
h H
igh
tran
sien
cy/
Hig
h H
igh
crim
inal
ity/
n 57
13
9
20
5 10
8
125
% W
/Chi
ldre
n at
sh
elte
r
Num
bers
of
soci
al
supp
orte
rs
Com
pani
onsh
ip
Adv
ice
&
info
rmat
ion
Prac
tical
ass
ista
nce
Emot
iona
l
Neg
ativ
e
Tota
l no
. un
ique
po
sitiv
e
Rel
atio
nshi
ps o
f su
ppor
ters
M T
o ki
n
M T
o fr
iend
s
Soci
al S
uppo
rt
Satis
fact
ion
Scal
e (r
ange
: 1-
7)
28.1
3 .O
(2.9
)
2.2
(1.3
) 2.
5 (1.8)
3.6
0.9
6.3
(4.5
)
(2.4
)
(1.3
)
58.4
(3
0.0)
30
.5
(25.
6)
5.0
(1 .O
)
46.2
3.6
(2.3
)
1.9
2.2
3.8
(3.2
) 1.
4 (1
.0)
(3.9
)
(1.7
)
(1.4
)
7.2
53.7
(3
1.7)
35
.2
(33.
7)
4.3
(1.2
)
0.0
0.7
(0.7
)
1.9
(1.2
) 1.
3 (1.0)
2.9
(2.2
) 0.
8 (1
.2)
4.2
(2.9
)
42.9
(3
5.5)
30
.9
(36.
3)
4.0
(1.1
)
15.0
2.8
(2.7
)
2.4
(2.0
) 2.
3 (1.8)
3.6
(1.9
) 1 .o
(1
.3)
6.1
(3.2
)
64.4
(3
4.5)
16
.3
(27.
0)
4.5
(1.3
)
0.0 1 .o
(1
-2)
0.4
1 .o
(1.2
) 1.
4
0.2
1.8
(1.8)
(0.9
)
(1.7
)
(0.4
)
4.0
(8.9
) 40
.0
(54.
8)
4.2
(0.7
)
0.0
2.3
(1.9
)
2.3
(1.2
) 1.
8 (1
.3)
2.7
(1.2
) 0.
7 (1
4
5 .O
(2.7
)
65.4
(3
1.0)
28
.0
(27.
3)
4.8
(1 .2
)
0.0 3.2
(3.7
)
1.7
(1.2
) 1.
7 (1
.2)
2.5
(2.7
) 0.
4
6.9
(5.6
)
(0.7
)
33.6
(2
9.8)
33
.9
(26.
2)
4.2
(1.1
)
20.2
2.8
(2.7
)
2. I
(1.5
) 2.
3 (1
.9)
3.4
(2.4
) 0.
9 (1
.2)
6.0
(4.2
)
57.2
(3
1.6)
30
.3
(29.
0)
4.7
(1.1
)
Not
e. F
igur
es i
n pa
rent
hese
s ar
e st
anda
rd d
evia
tions
.
Tab
le 7
In
terc
orre
latio
ns B
etw
een
Var
iabl
es C
ompa
red
Acr
oss
0- T
ypes
Soci
al S
uppo
rt
Ever
A
dvic
e &
Pr
actic
al
Gen
der
Age
'70
Kin
Sa
tisfa
ctio
n ra
ce
mar
ried
C
ompa
nion
ship
in
form
atio
n as
sista
nce
Em
otio
nal
Gen
der
(1 =
mal
e; 2
= f
emal
e)
Age
'70
of
kin
netw
ork
mem
bers
Soci
al S
uppo
rt
Rac
e Satis
fact
ion
Scal
e
(1 =
W
hite
; 2
= B
lack
, oth
er)
Ever
mar
ried
Num
ber
of s
uppo
rter
s C
ompa
nion
ship
A
dvic
e &
Inf
orm
atio
n Pr
actic
al a
ssist
ance
E
mot
iona
l sup
port
- .0
3 .1
3
- .0
04
- .1
8*
-.IS
*
.06
.03
.03
.18*
- - .I
2
- .04
-.19
*
- .3
2***
- .1
5*
- .2
0*
- .1
6*
- .1
7*
.I3
.17*
-
.12
.05
.20*
.1
5*
.24*
*
-
.10
-
.09
.25*
* -
.30*
**
-.02
-.
06
-
.28*
**
.02
.06
.46*
**
- .4
0***
.0
3 .0
1 .4
5***
.5
2***
-
.32*
**
-.02
-.
06
.4
5***
.4
9***
.5
5***
-
N
U
*p
< .0
5; *
*p <
.Of; *
**p
< .0
01

SOCIAL SUPPORT AND THE HOMELESS 91
Analysis of variance indicated group differences for the percentages of network members related to the respondent, F(6, 115) = 3.74, p < .01. Scheffk post hoc com- parisons indicated that members of the high transiency/high psychiatric group had significantly fewer kin in their networks than did those in the lower deviancy, high psychiatric, and high criminality groups.
Finally, there were group differences on the Satisfaction with Social Support Scale, F(6, 112) = 2.12, p < .05. However, post hoc Scheffk tests did not identify any signi- ficant between-groups differences.
Differences between O-Types were not found for any of the categories of positive social support: companionship, F(6, 115) = 1.68; advice and information, F(6, 115) = 1.38; practical assistance, F(6, 115) = 1.37; and emotional support, F(6, 115) = 1.18. Nor were significant differences found for race, ~ ’ ( 6 , N = 122) = 6.38; the percentage of net- work members who were friends, F(6, 115) = .92; or whether the respondent had ever married, ~ ’ ( 6 , N = 122) = 10.13.
Discussion The present study was able to classify 97% of the participants using subject clustering
procedures and thus provides a first step toward defining the different types of homeless persons who reside in shelters. Future research is needed to replicate this factor struc- ture with similar homeless populations as well as with those homeless who do not reside in this type of facility.
A common perception is that the homeless population is composed primarily of former mental patients or those who have become victims of deinstitutionalization policies. As mentioned previously, Bassuk et al. (1984) reported that as many as 90% of shelter guests need mental health treatment. In this study, one third of the participants had been hospitalized at some time for emotional problems. These rates are substan- tially higher than those for the general population (Taube & Barrett, 1985; U.S. Bureau of the Census, 1984); yet, the bulk of the homeless in this study had not been hospitalized.
Although “street people” comprised the largest group (43%) in the Arce et al. study (1983), the largest group in this study was the lower deviancy group (45.6%). This group had fewer problems, overall, than did the other groups (less criminal behavior, less psychiatric history, less transiency, and less criminal victimization). Members of this group were also younger and had somewhat more support from relatives when com- pared to several of the other groups. In this study, the group that best corresponds to the street people category in the Arce et al. study is the high transiency/high psychiatric O-Type. This group included only 4% of our participants.
Some of the discrepancies between our results and those of Arce et al. may be due to differences in populations and methodologies. The Arce et al. typology may be less comprehensive because it was not empirically derived. Further, the typologies may not have been based on a “typical” shelter population. The shelter from which the Arce et al. sample was drawn opened in response to a crisis caused by cold weather. Profes- sionals had searched the street to bring many of the homeless to the shelter; thus, that sample may have contained a particularly high proportion of “hard-core” homeless. The shelter in our study was a medium-sized family shelter providing services on an ongoing basis.
In generating an empirically derived typology of the homeless, we hoped to gain a more precise understanding of the various patterns of social support present among this population - knowledge that could inform relevant interventions. Although the data

92 SOLARZ AND BOGAT
from this study confirm and, more important, elaborate the current information con- cerning the support networks of the homeless, it found only one support difference among the seven 0-Types.
Past research has indicated that the homeless have very small social support net- works. Similarly, the social networks of the participants in this study were quite trun- cated. The mean number of supporters was six. In comparison, studies using a similar social support measure have found that undergraduate subjects report means of about 12 (Bogat et al., 1985), and a recent study of community adults indicated a mean of 19 (Habelow, 1987).
Studies comparing clinical and nonclinical populations indicated that the former group have significantly smaller networks (e.g., Cohen & Sokolovsky, 1978; Garrison, 1978). However, in this study, psychiatric history was not related to size of the network (there were no differences between the seven 0-Types on the number of supporters nominated for each of the four types of support): All respondents had small networks.
One partial explanation for the small networks is that few respondents were living with a romantic partner; virtually none were married and living with their spouse, and only about 5 % had lived with a significant other prior to residing at the shelter. In con- trast, nearly 80% of adults in the general population have been married, and 60.6% are currently married (not separated) (US. Bureau of the Census, 1984). Similar figures for Blacks living in metropolitan areas, a comparison population more similar to this sample, indicate that 65.8% have been married and 38.7% are currently married (not separated). Thus, although the percentages of persons in this study who had married at some time were only moderately lower than figures for urban Blacks in general, a far greater proportion of their marriages had foundered. Not being married or involved in a significant, intimate relationship deprives an individual not only of the support of the significant other but also of the support from the relatives of that person (that is, the benefits of a larger extended kin network).
Although their social networks were small, the respondents in this study were nonetheless able to identify a range of support resources. For most participants, a relative was the most important person in their network; however, participants in this study reported less contact with relatives than do nonhomeless populations. Fischer (1984) notes that less than 10% of a general population sample did not maintain regular con- tact with relatives. In contrast, almost 40% of our participants indicated no contact with relatives during the previous month.
Participants had networks composed largely of relatives (57.2%). Given this fact, it is understandable that participants had generally known their supporters for at least a year.
Most research indicates that persons with severe mental health problems tend to have less family contact and rely primarily for support on nonfamily members (Froland, Brodsky, Olson, & Stewart, 1979; Garrison, 1978). One exception is a study by Tolsdorf (1976) in which schizophrenic men had a greater proportion of family members in their networks than did the control group. In our study, psychiatric history in and of itself was not related to the percentage of relatives in the support network. Only the high psychiatridhigh transiency group had a significantly lower percentage of relatives in their networks in comparison to the high psychiatric and high criminality groups. These results seem to lend support for both positions; that is, family-dominated networks can be associated with either positive or negative mental health. Information about the specific nature of the interactions between the homeless and their relatives would be useful.
SOCIAL SUPPORT AND THE HOMELESS 93
Research on a range of physical (e.g., Mohamed, Weisz, & Waring, 1978) and psychological problems (e.g., Vaughn & Leff, 1976) indicates that overinvolvement with family members can be damaging for the individual (Coyne & DeLongis, 1986).
Respondents frequently named friends as sources of support. However, other studies, with nonhomeless subjects, indicate that friends usually constitute a larger pro- portion of the network. For example, Shulman (1975), in a study of adults aged 18 to 65, found that friends comprised about 40% of the network. In this study, networks were composed of 30% friends, and there were no differences between O-Types on this variable. Even O-Types with a high psychiatric component showed no differences in friend support when compared to those O-Types without the high psychiatric factor. Given that persons with more severe psychological problems rely heavily on nonkin sources of support (e.g., Froland et al., 1979; Garrison, 1978), we had expected to find differences between O-Types on this variable.
Most of the homeless were able to identify supporters for the four different types of support (companionship, advice and information, practical assistance, and emotional support). About half of the supporters were support generalists; they provided more than one type of support. The numbers of supporters in each of the four types of sup- port did not differ among O-Types. This was surprising. For instance, one might expect that those who experience less transiency would also have more sources of all types of support. Clearly, we need to know more about how the experience of homelessness alters social relationships.
Belle (1983) points out the importance of recognizing that not all social ties pro- vide support. Some network members may actually constitute a drain on emotional and material resources. In this study, many relationships had some negative aspects, either by providing an unequal exchange of support or by making the lives of the respondents more difficult in some way.
In McFarlane, Neale, Norman, Roy, and Streiner’s (1981) study of a general popula- tion sample, 85.6% of support relationships were reciprocal; only 62.6% of the rela- tionships in this study were reciprocal. Similarly, approximately half of our respondents reported individuals who made their lives difficult. It is possible that some of these ratings would be different at a time when respondents were not in crisis; residence in a shelter signified to a certain extent that their social networks had failed. In fact, disagreement with family members or friends was a common reason for leaving the last residence. During interviews, some respondents expressed frustration and disappointment that family members had not been more helpful.
Many researchers have indicated that satisfaction with available support may be as important or more important than the amount of support. To date, few studies of the homeless have reported on subjective appraisals of support. Overall, participants in this study felt between “mixed” and “mostly satisfied” about their social support and social relationships (M = 4.7 on a 7-point scale). In comparison, Sarason, Levine, Basham, and Sarason (1983) reported that college undergraduates are very satisfied with their networks (A4 = 5.4 on a 6-point scale). Apparently the networks of the homeless are not meeting their support needs to the extent often reported by the general population.
Conclusions
As in most studies of the homeless, participants in this study were guests of a tem- porary shelter. Although the shelter used in the study was believed to house homeless persons who were representative of the shelter-using population of the city, its residents
94 SOLAR2 AND BOGAT
may not be representative of those who utilize “warehouse”-style shelters typical of some larger cities. Further, shelter users are not likely to be representative of all homeless people, particularly those who make a deliberate choice not to use these types of facilities (Burt & Cohen, 1988). Those who access shelters may be more willing than those who stay on the street to accept certain types of professional support and services, particularly those that require social interactions.
Past research has indicated that the homeless have deficient social support networks. The results of this study are less dismal than those of Bassuk et al. (1984) or Fischer (1984). Our findings suggest that many of the homeless had significant support resources available to them. In particular, many of the residents were able to identify family members as providers of support. Nonetheless, the support networks of the individuals in this study were clearly smaller and less satisfying than were those reported for domiciled populations.
The present study presents information that may guide future research on social support and homelessness as well as interventions for this group. In much social sup- port research, the presence of at least one supporter (often termed a confidant) is con- sidered sufficient support to reduce distress (e.g., Kahn & Antonucci, 1980; Lowenthal & Haven, 1968). This study clearly indicates that the simple presence or absence of sup- port is not the critical variable that prevents homelessness. Although prospective, longitudinal studies of this population are probably unrealistic (at least glven our cur- rent knowledge of homelessness), interviews that collect retrospective information about social relations and social networks at earlier points in the respondents’ lives are necessary to trace whether, in fact, social networks have deteriorated or whether the small net- works are a direct result of being homeless. For some, a current episode of homelessness reflects a life that has been highly disrupted by the ongoing stresses of poverty and family dysfunction (Bassuk & Rosenberg, 1988). For example, during the interviews we were struck with how many of the respondents (41.6%) had stopped living with at least one of their parents before the age of 16.
The support networks of the homeless in this study do not seem to corroborate some findings about social support (for example, the correlation between various pat- terns of support and mental illness). This suggests that the homeless are a unique popula- tion and support may function differently for them, or that the circumstance of homelessness results in changes in the way support functions for individuals. Studying the episodic homeless for an extended period of time would enable researchers to under- stand what factors precipitate periods of homelessness as well as how support is accessed and provided during periods of homelessness and domiciliation.
Such research would begin to elucidate the relative influence of diminished support on becoming homeless. For populations other than the homeless, Coyne and DeLongis (1986) have noted that “In some cases, a Oerceived lack of support may be secondary to other difficulties, and these difficulties may make it less likely that vulnerable persons will either seek or benefit from interventions designed to increase support” (p. 455). Before we can design effective interventions for the homeless, we need to know the contribu- tion of social support to homelessness vis-8-vis such factors as poverty, minority status, lack of affordable housing, or unemployment.
Although social support may not be the panacea for human problems that com- munity psychologists have suggested, it is a particularly compelling focus for interven- tions involving the homeless and those at risk of homelessness. For example, fostering the mending of estranged social networks may facilitate the re-entry of homeless per-

SOCIAL SUPPORT AND THE HOMELESS 95
sons into housing by increasing resources for child care, transportation, information, possible financial support, and emotional support.
Having adequate social support suggests an appropriate amount of connectedness with one’s world and the people in it. To have no home is to be unconnected to place and only minimally connected to persons. An appropriate goal for community psycholo- gists is to determine whether support can provide an avenue back to becoming domiciled.
References
Appleby, L., & Desai, P. (1985). Documenting the relationship between homelessness and psychiatric hospitalization. Hospital and Community Psychiatry, 36, 732-737.
Arce, A., Tadlock, M., Vergare, M., & Shapiro, S. (1983). A psychiatric profile of street people admitted to an emergency shelter. Hospital and Community Psychiatry, 34, 812-817.
Arce, A., & Vergare, M.(1984). Identifying and characterizing the mentally ill among the homeless. In H. R. Lamb (Ed.), Identtfying and characterizing the mentally ill among the homeless (pp. 75-89). Washington, DC: American Psychiatric Association.
Bachrach, L. (1984). Deinstitutionalization and women: Assessing the consequences of public policy. American Psychologist, 39, 171-177.
Bahr, H. (1973). Skid row: An introduction to disqffiliation. New York: Oxford University Press. Ball, F. L. B., & Havassy, B. (1984). A survey of the problems and needs of homeless consumers of acute
psychiatric services. Hospital and Community Psychiatry, 35, 917-921. Bassuk, E., & Rosenberg, L. (1988). Why does family homelessness occur? A case-control study. American
Journal of Public Health, 78, 783-788. Bassuk, E., Rubin, L., & Lauriat, A. (1984). Is homelessness a mental health problem? American Journal
of Psychiatry, 141, 1546-1550. Bassuk, E., Rubin, L., & Lauriat, A. (1986). Characteristics of sheltered homeless families. American Journal
of Public Health, 76, 1097-1101. Belle, D. (1983). The impact of poverty on social networks and supports. Marriage and Family Review, 5,
Blumberg, L., Shipley, T., & Barskey, S. (1978). Liquor andpoverty: Skidrow asa human condition. Rutgers: Rutgers Center of Alcohol Studies.
Bogat, G. A., Caldwell, R., Rogosch, F., & Kriegler, J. (1985). Differentiating specialists and generalists within college students’ social support networks. Journal of Youth and Adolescence, 14, 23-35.
Bogat, G. A., Chin, R., Sabbath, W., & Schwartz, C. (1983). Social support questionnaire. Unpublished instrument, Michigan State University, East Lansing, MI.
Burt, M., & Cohen, B. (1988). Feeding the homeless: Does the prepared mealprovision help? Washington, DC: The Urban Institute.
Cohen, C. I . , & Sokolovsky, J. (1978). Schizophrenia in social networks: Expatients in the inner city. Schizophrenia Bulletin, 4, 546-560.
Cohen, C., & Sokolovsky, J. (1983). Toward a concept of homelessness. Journalof Gemntology, 38, 81-89. Coyne, J. C., & DeLongis, A. (1986). Going beyond social support: The role of social relationships in adap-
Crystal, S. (1984). Homeless men and homeless women: The gender gap. Urban and Social Change Review,
Depp, F., & Ackiss, V. (1983, July). Assessing needs among sheltered homeless women. Paper presented at the conference “Homelessness: A Time for New Directions,” Washington, DC.
Fischer, P. (1984, August). Health and social characteristics of Baltimore homelesspersons. Paper presented at the meeting of the American Psychological Association, Toronto.
Fischer, P., Shapiro, S., Breakey, W., Anthony, J., & Kramer, M. (1986). Mental health and social characteristics of the homeless: A survey of mission users. American Journal of Public Health, 76, 519-524.
Froland, C., Brodsky, G., Olson, M., &Stewart, L. (1979). Social support and social adjustment: Implica- tions for mental health professionals. Community Mental Health Journal, 15, 82-93.
Garrison, V. (1978). Support systems of schizophrenic and non-schizophrenic Puerto Rican migrant women in New York City. Schizophrenia Bulletin, 4, 561-596.
Habelow, W. (1987). Social support in the marital relationship. Unpublished master’s thesis, Michigan State University, East Lansing, MI.
89-103.
tation. Journal of Consulting and Clinical Psychology, 54, 454-460.
17, 2-6.
96 SOLAR2 AND BOGAT
Kahn, R. L., & Antonucci, T. C. (1980). Convoys over the life course: Attachment, roles, and social sup- port. In P. B. Baltes & 0. Brim (Eds.), Life-span development and behavior (Vol. 3, pp. 254-286). Boston: Lexington Press.
Kroll, J., Carey, K., Haggedorn, D., Fire Dog, P., & Benavides, E. (1986). A survey of homeless adults in urban emergency shelters. Hospital and Community Psychiatry, 37, 283-286.
Lamb, R., & Grant, R. (1983). Mentally ill women in a county jail. Archives of General Psychiatry, 40,
Lipton, F., Sabitini, A., & Katz, S. (1983). Down and out in the city: The homeless mentally ill. Hospital and Community Psychiatry, 34, 817-821.
Lowenthal, M. F., & Haven, C. (1968). Interaction and adaptation: Intimacy as a critical variable. American Sociological Review, 33, 20-30.
McFarlane, A., Neale, K., Norman, G. , Roy, R., & Streiner, D. (1981). Methodological issues in develop- ing a scale to measure social support. Schizophrenia Bulletin, 7, 90-100.
McSweeney, M., & Marascuilo, L. (1977). Nonparametric and distribution- free methods for the socialsciences. Monterey, CA: BrooksKole.
Mohamed, S. N., Weisz, G . M., & Waring, E. M. (1978). The relationship of chronic pain to depression, marital adjustment, and family dynamics. Pain, 5, 285-292.
Mowbray, C., Solarz, A., Johnson, V. S., Phillips-Smith, E., & Combs, C. (1986). Mental health and homelessness in Detroit: A research study. Lansing: Michigan Department of Mental Health.
Robertson, M., Ropers, R., & Boyer, R. (1985). The homeless of Los Angeles County: An empirical evalua- tion. In The Federal response to the homeless crisis. Hearings before the Subcommittee of the Commit- tee on Government Operations, U.S. House of Representatives (pp. 984-1 108) (GPO Item No. 1106A, 1016B microfiche). Washington, DC: Government Printing Office.
Sarason, I., Levine, J., Basham, R., & Sarason, B. (1983). Assessing social support: The Social Support Questionnaire. Journal of Personality and Social Psychology, 44, 127-1 39.
Shulman, N. (1975). Life-cycle variations in patterns of close relationships. Journal of Marriage & the Family,
Solarz, A. (1986). Follow-up study in a temporary shelter for the homeless: A look at quality of life and
Solarz, A., & Mowbray, C. (1985, November). An examination of physical and mental health problems
Stoner, M. (1983). The plight of homeless women. Social Service Review, 57, 565-581. Sutherland, E., & Locke, H. (1936). Twenty thousand homeless men: A study of unemployed men in the
Taube, C., & Barrett, S. (Eds.). (1985). Mental health, United States, 1985 (DHHS Pub. No. ADM 85-1378).
Tolsdorf, C. (1976). Social networks, support and coping: An exploratory study. Family Process, 15, 407-418. Tryon, R., & Bailey, D. (1970). U S . Bureau of the Census. (1984). Maritalstatus and living arrangements: March 1983 (Current Popula-
tion Reports, Series P-20, No. 389). Washington, DC: Government Printing Office. US. Conference of Mayors. (1987). The continuing growth of hunger, homelessness andpoverty in America’s
cities: 1987. Washington, DC: Author. U.S. Department of Justice, Bureau of Justice Statistics. (1983). Criminal victimization in the United States,
1981: A National Crime Survey report (NCJ-90208). Washington, DC: Department of Justice. US. General Accounting Office. (1988). Homeless mentally ill: Problems and optionr in estimating numbers
and trends (GAOIPEMD-88-24). Washington, DC: Author. Vaughn, C. C., & Leff, J. (1976). The influence of family and social factors on the course of psychiatric
illness: A comparison of schizophrenic and depressed neurotic patients. British Journal of Psychiatry,
363-368.
37, 813-821.
social supports. Unpublished doctoral dissertation, Michigan State University, East Lansing, MI.
of the homeless. Paper presented at the meeting of the American Public Health Association.
Chicago shelters. Chicago: J . B. Lippincott.
Washington, DC: Government Printing Office.
Cluster analyses. New York: McGraw-Hill.
129, 125-137.
Related Documents











