1 When Acute Pain Becomes Chronic – What Do We Know and How Can We Prevent It? Sean Mackey, M.D.,Ph.D. Chief – Pain Management Division Stanford University Department of Anesthesia Division of Pain Management http://paincenter.stanford.edu http://anesthesia.stanford.edu [email protected] Disclosures – funding sources National Institutes of Neurological Diseases and Syndromes (NINDS) R01 NS053961 National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) U01 DK082316 National Institutes of Drug Abuse (NIDA) K24 DA029262 R21 DA026092 K23 DA25152 (Carroll) Dodie and John Rosekrans Pain Research Endowment Chris Redlich Pain Research Endowment Overview Impact of acute pain transitioning to chronic pain Focus on low back pain and postsurgical pain Mechanisms and factors that predict the transition from acute pain to chronic pain Tools to prevent the transition

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
When Acute Pain
Becomes Chronic – What
Do We Know and How
Can We Prevent It?
Sean Mackey, M.D.,Ph.D.
Chief – Pain Management Division Stanford University
Department of Anesthesia
Division of Pain Management http://paincenter.stanford.edu
http://anesthesia.stanford.edu
Disclosures – funding sources National Institutes of Neurological Diseases and
Syndromes (NINDS)
R01 NS053961
National Institute of Diabetes and Digestive and Kidney
Diseases (NIDDK)
U01 DK082316
National Institutes of Drug Abuse (NIDA)
K24 DA029262
R21 DA026092
K23 DA25152 (Carroll)
Dodie and John Rosekrans Pain Research Endowment
Chris Redlich Pain Research Endowment
Overview
Impact of acute pain transitioning to chronic pain
Focus on low back pain and postsurgical pain
Mechanisms and factors that predict the transition from acute pain to chronic pain
Tools to prevent the transition

2
Impact of the Transition
from Acute to Chronic Pain
Low Back Pain and Perioperative Pain
as Models
Low Back Pain: Epidemiology 60%–90% lifetime prevalence
Second most common complaint
to prompt a medical evaluation
Leading cause of long-term work
disability
Estimated US direct and indirect costs: $30-50 billion/year
Disability and costs related to
pain, not to the disease process
Natural history non specific low
back pain (NSLBP)
80% of patients with first episode NSLBP will recover in 1 month
10% recover within 3 months
10% go on to CHRONIC PAIN
Recurrence rates high (5-80%) depending on study
Garcy P, Mayer T, Gatchel RJ, Spine 1996; 21(8):952-959
Rossignol M, Suissa S, Abenhaim L, Spine 1992;17(9):1043-1047
Von Korff M, Saunders K, Spine 1996;21:2833-2837
Nordin, et al. Proceedings of the 10th World Congress on Pain, Vol 24

3
Post Surgical Chronic Pain Thirty-four million Americans
undergo surgery each year.
Post operative chronic pain is
defined as pain that lasts longer
than 3 -6 months and is different in
quality and or location from pain
prior to surgery.
On average 10% of postsurgical
patients will develop chronic pain.
DeFrances, C.J. and M.N. Podgornik, 2004 National Hospital Discharge Survey. Advance Data from
Vital & Health Statistics of the National Center for Health Statistics, 2006(371): p. 1-19.
Persistent Postoperative Pain Thoracotomy: 30-60%*
Inguinal Hernia Repair: 6-11%1,2
Extremity Amputations: 30-80%
Cardiac Surgery
Caesarean section: 12% Additional 11% had discomfort or
abdominal skin sensitivity
Breast Surgery, especially with
dissection: 50%
Spinal Surgery
Orthopedic Surgery
Gallbladder surgery: 3-56%
Hysterectomy
Nephrectomy: 24%
Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. May 13 2006;367(9522):1618-
1625.*Maguire MF, Ravenscroft A, Beggs D, Duffy JP. A questionnaire study investigating the prevalence of the neuropathic
component of chronic pain after thoracic surgery. European Journal of Cardio-Thoracic Surgery. May 2006;29(5):800-805. 1.
Aasvang EK. Bay-Nielsen M. Kehlet H. Pain and functional impairment 6 years after inguinal herniorrhaphy.Hernia. 10(4):316-21,
2006 Aug 2. Nienhuijs S, et al. Chronic Pain after Mesh Repair: a systemic review. The American Journal of Surgery 194 (2007)
394–400
How many of your surgeons consent
their patients for the possibility of
chronic pain?

4
Factors and Biomarkers that
Predict the Transition from Acute
to Chronic Pain
Transition from Acute to Chronic Low
Back Pain In prospective longitudinal studies,
catastrophizing and fear were associated with
increased risk of chronic back pain one year after
acute low back injury.
Catastrophizing over seven times more powerful
than any other predictor in predicting transition
from acute to chronic pain.
Pain-related fear causes patients with pain to
over-predict the severity of pain they will
experience. This leads to over-production of
avoidance behavior Burton, A.K., et al., Psychosocial predictors of outcome in acute and subchronic low back trouble. Spine, 1995. 20(6): p. 722-8.
Swinkels-Meewisse, I.E., et al., Fear of movement/(re)injury predicting chronic disabling low back pain: a prospective inception
cohort study. Spine, 2006. 31(6): p. 658-64.
McCracken, L.M., et al., Prediction of pain in patients with chronic low back pain: effects of inaccurate prediction and pain-related
anxiety. Behav Res Ther, 1993. 31(7): p. 647-52.
Effects of Depression and Anxiety 30-65% of patients with chronic pain have co-morbid depression, often with
anxiety
Longitudinal epidemiologic studies determine that patients with depression
and anxiety are between 2-5 times more likely to have a new chronic pain
problem at follow-up from 1 to 8 years later.
Patients with depression appear to be less sensitive to pain in response to
experimental noxious stimuli compared to healthy controls.
Suggests that depression and possibly anxiety may elevate the risk of
chronic pain by altering pain persistence rather than by altering pain
thresholds or pain severity.
1. Croft, P.R., et al., Psychologic distress and low back pain. Evidence from a prospective study in the general population. Spine, 1995. 20(24): p. 2731-2737.
2. Hotopf, M., et al., Temporal relationships between physical symptoms and psychiatric disorder. Results from a national birth cohort . The British journal of
psychiatry, 1998. 173: p. 255-261.
3. Currie, S.R. and J. Wang, More data on major depression as an antecedent risk factor for first onset of chronic back pain. Psychol Med, 2005. 35(9): p. 1275-82.
4. Carroll, L.J., J.D. Cassidy, and P. Côté, Depression as a risk factor for onset of an episode of troublesome neck and low back pain. Pain, 2004. 107(1-2): p.
134-139.
5. Von Korff, M., L. Le Resche, and S.F. Dworkin, First onset of common pain symptoms: a prospective study of depression as a risk factor. Pain, 1993. 55(2): p.
251-258.
6. Magni, G., et al., Prospective study on the relationship between depressive symptoms and chronic musculoskeletal pain. Pain, 1994. 56(3): p. 289-297.
7. Dworkin, R.H., W.C. Clark, and J.D. Lipsitz, Pain responsivity in major depression and bipolar disorder. Psychiatry Res, 1995. 56(2): p. 173-81.

5
Factor Predicting Postsurgical
Chronic Pain
Few studies have explored multiple
psychological and physiological factors that
influence a patients’ post-operative pain
course.
Even fewer studies addressed how these
factors contribute to the patients post
operative pain resolution and opioid and
analgesic cessation.
Factors Predicting Chronic Pain
Acute pain experience predicts chronic pain:
True for herpes zoster and postherpectic neuralgia
True for thoracotomy, hernia repair, and most surgical procedures
Nerve damaging operations are at greater risk for chronic pain
Extent of surgically induced nerve damage doesn’t correlate well with chronic pain
Postsurgical Chronic Pain 625 patients, mixed surgical procedure.
Many variables collected
At 6 months, patients with high levels of pain on postop day #4 and surgery longer than 3 hours: More pain
More functional restrictions
Poor “global recovery”
Worse quality of life
Preoperative fear of surgery negatively associated with more pain, poor global recovery, and worse quality of life 6 months later.
Optimism was associated with better recovery and higher quality of life.
Peters ML, et al, Somatic and psychologic predictors of long-term unfavorable outcome
after surgical intervention. Annals of Surgery. 245(3):487-94, 2007

6
Longitudinal Study to Characterize Post-
Surgical Pain Persistence
Table C1: Patient Characteristics (n=77)
Characteristic Mean Range
Age 59 18 - 85
Beck Depression Inventory Score 9.6 0 - 54
Fear of Pain Score 70 14 - 134
Anxiety Sensitivity Index Score 35.4 3 - 98
SOAPP 13.6 4 - 41
Gender (percent male) 26%
Positive PTSD symptomatology 21%
Pre - operative Opiate Use 20%
History of Unprescribed Opioid Use 9%
Surgery Type Number
Thoracotomy 20
Total Hip Replacement 15
Total Knee Replacement 15
Radical Mastectomy 17
Lumpectomy 10
Table C3: Multivariate Analysis of Factors Promoting Delayed Pain Resolution
Characteristic Hazard Ratio P - Value Positive PTSD Symptoms 0.35 0.04
Pain Severity: Post Operative Day 1 0.85 0.04 Self - Perceived Risk of Addiction 0.41 0.05
Beck Depression Inventory Score 0.99 0.97
Carroll, Mackey in revision
The Transition from Acute to
Chronic Pain
Every Surgical Procedure
Cuts nerves
Cuts tissues
Induces the injury response
Alters peripheral and central nervous system pain
processing
Can cause chronic pain
Note: Similarly, most chronic low back pain starts with
an acute pain episode

7
Peripheral vs Central Mechanisms of
Neuropathic Pain: Experimental Effects
Peripheral Effects Central Effects
• Ectopic and spontaneous
discharge
• Nonsynaptic conduction
• Alterations in ion channel
expression
• Collateral sprouting of primary
afferent neurons
• Sprouting of sympathetic neurons
in dorsal root ganglion
• Nociceptor sensitization
• Neurogenic inflammation
• Central sensitization
• Spinal reorganization
• Cortical reorganization
• Changes in inhibitory
pathways
• Changes in glial cell
functioning
1. Reprinted with permission from M. Lotze, MD. Inst of Medical Psychology & Behavioral Neurobiology, Univ. of Tübingen, Germany. Lotze M, et al. Brain. 2001;124(pt 11):2268-2277.
Right arm amputation below elbow Lip pursing and phantom limb pain (PLP):
Face Hand
Upper Arm
patients without PLP
patients with PLP
healthy controls
1.
Individual Differences in Pain
8
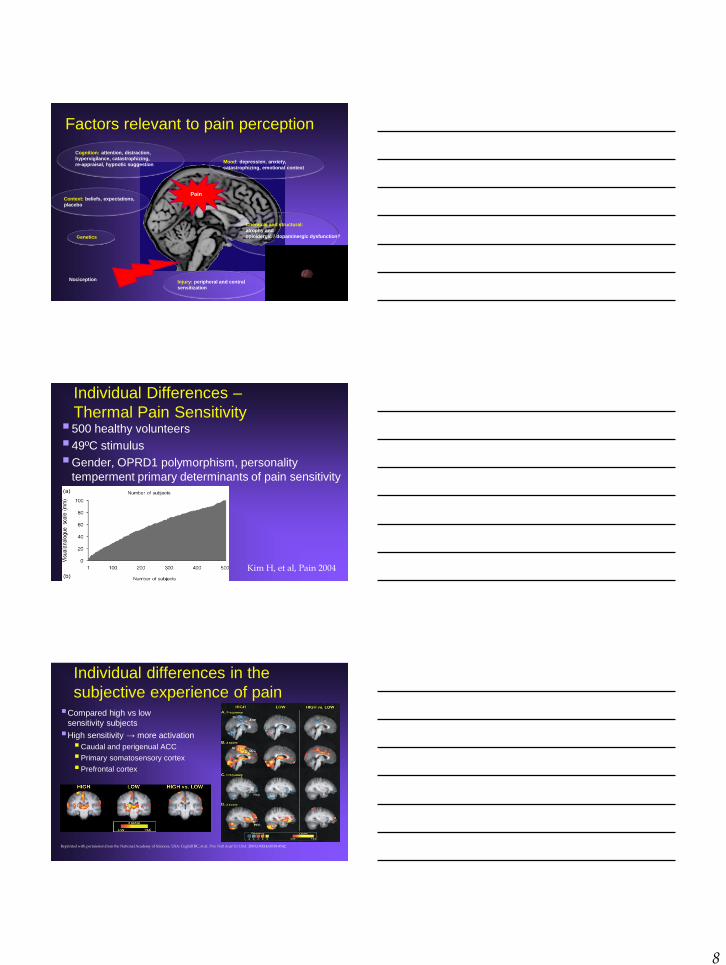
Factors relevant to pain perception
Cognition: attention, distraction,
hypervigilance, catastrophizing,
re-appraisal, hypnotic suggestion Mood: depression, anxiety,
catastrophizing, emotional context
Genetics
Injury: peripheral and central
sensitization
Chemical and structural:
atrophy and
opioidergic / dopaminergic dysfunction?
Context: beliefs, expectations,
placebo
Nociception
Pain
Individual Differences –
Thermal Pain Sensitivity 500 healthy volunteers
49ºC stimulus
Gender, OPRD1 polymorphism, personality
temperment primary determinants of pain sensitivity
Kim H, et al, Pain 2004
Individual differences in the
subjective experience of pain Compared high vs low
sensitivity subjects
High sensitivity → more activation
Caudal and perigenual ACC
Primary somatosensory cortex
Prefrontal cortex
Reprinted with permission from the National Academy of Sciences, USA: Coghill RC, et al. Proc Natl Acad Sci USA. 2003;100(14):8538-8542.

9
Pain - Fear and Anxiety
Individual’s anxiety about, and fear of, painful sensations
predicts physical complaints and treatment outcomes in
patients with chronic pain (McCraken, 1998, 1999)
Patients high in anxiety more likely to develop post-
herpetic neuralgia (Dworkin, 1992)
Preop gababentin improves functional recovery after knee
surgery, AND decreases anxiety (Menigaux C, Anesth
and Analg, 2005)
Psychological construct? But why? What are the
neurophysiological underpinnings?
Individual difference in pain – Effects of fear of pain
Right Lateral Orbitofrontal Cortex Right Lateral orbital frontal activation may reflect attempts by fearful individuals to evaluate and/or regulate possible responses to painful stimuli
Ochsner KN, et al. Pain. 2006;120(1-2):69-77.
Lateral Orbitofrontal Cortex
-0.8 -0.6 -0.4 -0.2 0.0 0.2 0.4 0.6 0.8 1.0
50 60 70 80 90 100 110
Fear of Pain Questionnaire Ratings
Para
mete
r E
stim
ate
s
r=0.912
Individual difference in pain – effects of somatic anxiety
Medial Prefrontal Gyrus: involved in self-focused elaboration of the negative personal implications of pain that may characterize individuals high in anxiety sensitivity
Ochsner KN, et al. Pain. 2006;120(1-2):69-77.
Anxiety State Inventory Ratings
Medial Prefrontal Cortex
r=.890
1.5
1
0.5
0
-0.5
-1
-1.5
10 20 30 40
Para
mete
r E
stim
ate
s
Medial Prefrontal Gyrus

10
Tools to Prevent the Transition
from Acute to Chronic Pain
Everything mentioned is off-label
Gabapentanoids – Should we add
this to the drinking water?
Gabapentanoids – Gabapentin and Pregabalin Meta-analyses and systemic review: Helpful for postop pain.
Hurley RW, et al Reg Anesth Pain Med 2006.
Ho K-Y. Gan TJ. Habib AS. Pain. 126(1-3):91-101, 2006.
600 – 1200 mg preop decreases pain and/or opioid requirements: breast, hysterectomy, chole, spine, thyroid, nephrectomy, knee, tonsillectomy Menigaux et al Anesthesia & Analgesia 2005;
Turan et al Anesthesia & Analgesia 2005;
Pandey et al Can J Anaesthesia 2004;
Dirks et al Anesthesiology 2002,
Al-Mujadi H et al. Can J Anaesth 2005
Makes epidural analgesia work better Turan A et al Br J Anaesth 2006
Works pre/post incision nephrectomy Pandey CK et al Can J Aneasth 2005
Combined with COX-2 Inhibitor works better than either separately Gilron I et al Pain 2005
Two weeks of perioperative pregabalin reduces neuropathic pain at 3 and 6 months (0%, 0%) compared to placebo (8.7%, 5.2%) after TKA Buvanendran et al Anesthesia and Analgesia 2010
11
Is gabapentin working entirely as a
pain med?
Gabapentin has also been shown to reduce
anxiety in a variety of circumstances including
pre-operative anxiety
Menigaux, C., et al., Preoperative Gabapentin Decreases Anxiety and Improves Early Functional
Recovery from Knee Surgery. 2005. p. 1394-1399.
de-Paris, F., et al., Effects of gabapentin on anxiety induced by simulated public speaking. J
Psychopharmacol, 2003. 17(2): p. 184-8.
Mula, M., S. Pini, and G.B. Cassano, The role of anticonvulsant drugs in anxiety disorders: a critical
review of the evidence. J Clin Psychopharmacol, 2007. 27(3): p. 263-72
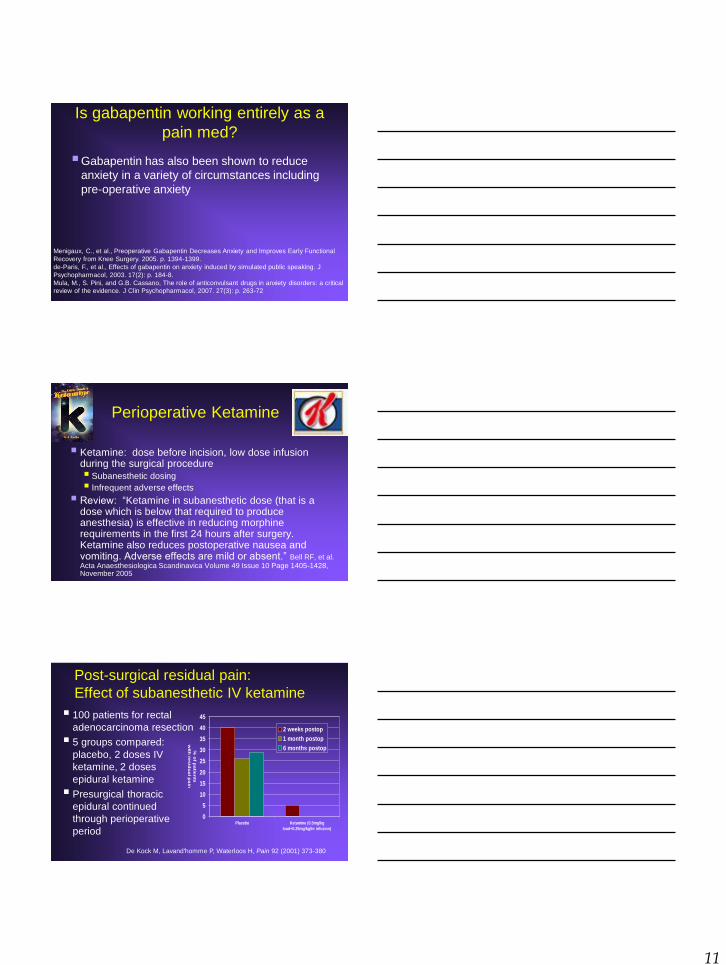
Perioperative Ketamine
Ketamine: dose before incision, low dose infusion during the surgical procedure Subanesthetic dosing
Infrequent adverse effects
Review: “Ketamine in subanesthetic dose (that is a dose which is below that required to produce anesthesia) is effective in reducing morphine requirements in the first 24 hours after surgery. Ketamine also reduces postoperative nausea and vomiting. Adverse effects are mild or absent.” Bell RF, et al.
Acta Anaesthesiologica Scandinavica Volume 49 Issue 10 Page 1405-1428, November 2005
Post-surgical residual pain:
Effect of subanesthetic IV ketamine
0
5
10
15
20
25
30
35
40
45
Placebo Ketamine (0.5mg/kg
load+0.25mg/kg/hr infusion)
% o
f pa
tien
ts
with
res
idu
al p
ain
2 weeks postop
1 month postop
6 months postop
De Kock M, Lavand'homme P, Waterloos H, Pain 92 (2001) 373-380
100 patients for rectal
adenocarcinoma resection
5 groups compared:
placebo, 2 doses IV
ketamine, 2 doses
epidural ketamine
Presurgical thoracic
epidural continued
through perioperative
period
12
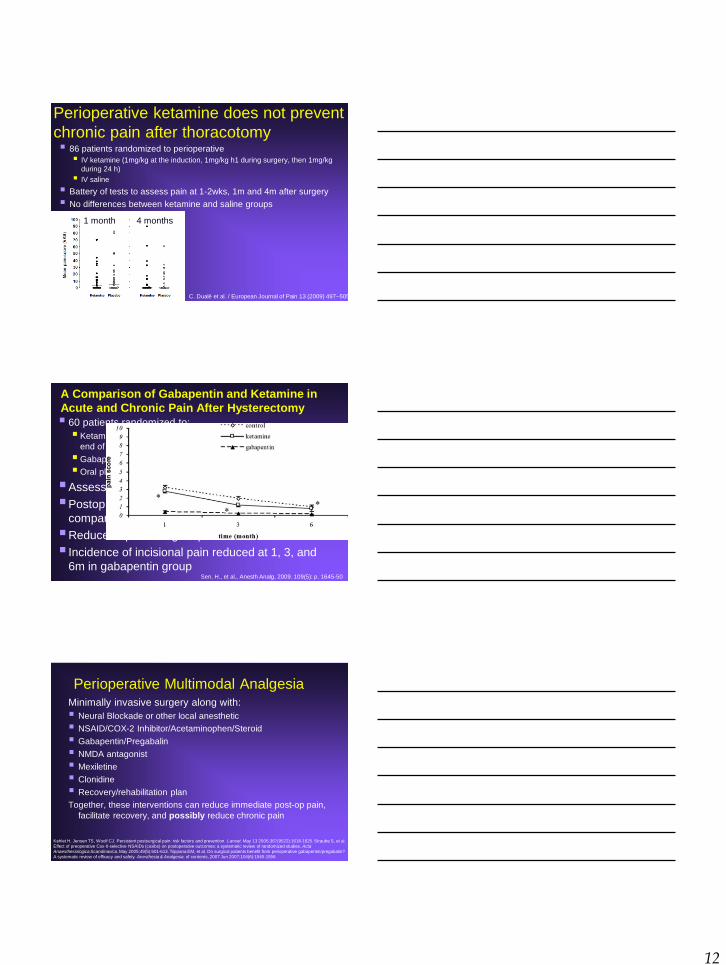
Perioperative ketamine does not prevent
chronic pain after thoracotomy 86 patients randomized to perioperative
IV ketamine (1mg/kg at the induction, 1mg/kg h1 during surgery, then 1mg/kg
during 24 h)
IV saline
Battery of tests to assess pain at 1-2wks, 1m and 4m after surgery
No differences between ketamine and saline groups
C. Dualé et al. / European Journal of Pain 13 (2009) 497–505
1 month 4 months
A Comparison of Gabapentin and Ketamine in
Acute and Chronic Pain After Hysterectomy
60 patients randomized to:
Ketamine – 0.3mg/kg IV bolus and 0.05mg/kg/hr infusion until
end of surgery, PO placebo
Gabapentin – PO1200mg, IV saline
Oral placebo, IV saline
Assessed 1, 3 and 6m after surgery
Postop pain decreased in gabapentin group
compared with ketamine and saline
Reduced opioids in gabapentin and ketamine
Incidence of incisional pain reduced at 1, 3, and
6m in gabapentin group Sen, H., et al., Anesth Analg, 2009. 109(5): p. 1645-50
Perioperative Multimodal Analgesia Minimally invasive surgery along with:
Neural Blockade or other local anesthetic
NSAID/COX-2 Inhibitor/Acetaminophen/Steroid
Gabapentin/Pregabalin
NMDA antagonist
Mexiletine
Clonidine
Recovery/rehabilitation plan
Together, these interventions can reduce immediate post-op pain,
facilitate recovery, and possibly reduce chronic pain
Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. May 13 2006;367(9522):1618-1625. Straube S, et al.
Effect of preoperative Cox-II-selective NSAIDs (coxibs) on postoperative outcomes: a systematic review of randomized studies. Acta
Anaesthesiologica Scandinavica. May 2005;49(5):601-613. Tiippana EM, et al. Do surgical patients benefit from perioperative gabapentin/pregabalin?
A systematic review of efficacy and safety. Anesthesia & Analgesia. of contents, 2007 Jun 2007;104(6):1545-1556

13
Summary Most chronic pain started with an acute pain event
We are creating an epidemic of chronic pain with our surgeries
Factors have been identified to predict the transition of acute to
chronic pain in postsurgical patients and LBP
Preoperative and immediate postop pain
Fear, anxiety, depression, catastrophizing, PTSD
Exaggerated response to experimental pain stimuli
Tantalizing data that some anti-neuropathics, Coxibs, and
regional anesthesia may reduce this transition
We may learn much about the transition from acute to chronic
postsurgical pain by applying research from other chronic pain
conditions
Much more research needed.
Stanford Systems Neuroscience and Pain Lab (SNAPL) • Faculty
• Sean Mackey, MD, PhD
• Ian Carroll, MD, MS
• Jarred Younger, PhD
• Research Fellows
• Paul Nash, PhD
• Heather Chapin, PhD
• Kevin Johnson, PhD
• Jiang-Ti Kong, MD
• Elizabeth Stringer, PhD
• Lab Manager
• Rebecca McCue
• Research Assistants
• Epifanio Bagarinao, PhD
• Noorulain Noor
• Rachel Moericke
• Debra Clay, RN
• Laura Jastrzab, MS
• Hoameng Ung
• Graduate Students
• Justin Brown
• Administration
• Andrew Morrow
• Matthew Chen
• Undergraduate Student Research Assistants
• Juan-Carlos Foust
• J.C. Lopez
• Stephen Matzat
• Laura Pulido
• Gabriella Ruchelli
• Daniel Schwarz
Related Documents











