“What Makes Our Special Care Unit Special ?” Deer Lodge Centre Dementia Care Unit Maureen Chouinard, Manager of Resident Care Arlis Decorte, Clinical Resource Nurse Nancy Fiebelkorn, Social Worker

“What Makes Our Special Care Unit Special ?” Deer Lodge Centre Dementia Care Unit Maureen Chouinard, Manager of Resident Care Arlis Decorte, Clinical Resource.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

“What Makes Our Special Care Unit
Special ?”
Deer Lodge CentreDementia Care Unit
Maureen Chouinard, Manager of Resident CareArlis Decorte, Clinical Resource Nurse
Nancy Fiebelkorn, Social Worker

SCU – Tower, SCU-West
47 beds on two units Tower opened in 1988, West opened
in 2006 Higher staff to resident ratio Units address behaviours, care
needs Male or female; veterans or
community applications
Philosophy of Care
Equal, individualized, respectful and safe care
A person’s individuality is unique and does not change because of cognitive impairment
Staff are advocates A specialized environment is required
for dementia care Families have the right to be informed

Philosophy of Care (continued)
Specialized skills and abilities are essential
Interdisciplinary team approach End of life care Upholding Resident’s Bill of Rights Effective and efficient use of
available resources

SCU Admission Criteria
Age Primary and secondary diagnoses Environment Behaviours Risks

How to Access the Special Care Unit at
DLC WRHA Behavioral Panel Contact the panel secretary at 940-3600 Access Office is at 490 Hargrave St. Application should include an A/A form, a
Dependency Assessment Supplement and the Behavioral Assessment Supplement.
A brief summary of the resident/client will be submitted along with behavior maps, recent progress notes, consults and lab work.
Behavioural Panel Purpose:
To facilitate the management of individuals with challenging behaviors in the most appropriate care setting.
Behavioural Panel Guiding Principles:
Behaviors are not being managed in their current environments
Existing resources already accessed Information meets panel criteria and
standards Panel meets monthly Additional problem-solving may be
required to ensure placement in proper environment
Behavioural PanelWho Sits on the Panel?
Medical Director of the Rehab/Geriatrics Program Director of the LTC Access Centre or designate A representative from a PCH A representative from the Geriatric Mental
Health Team A CNS for the WRHA long term care program Access Coordinators Health care professionals/family who have been
integral to managing the individual’s care needs
Preadmission Visits
Purpose:• Confirm the information provided by panel• Meet needs of the applicant?• Plan for any special needs or equipment• Meet the applicant and family
Completed by the Social Worker and Unit Manager once accepted by Behaviour Panel
Visit usually within one week, at applicant’s current residence
The Interdisciplinary Approach
The SCU at Deer Lodge Centre utilizes an interdisciplinary approach to care.
Weekly meetings Goal is to review each resident on a
quarterly basis. Post-admission and Annual conferences All members of the team are available
to family Contact information provided
The Interdisciplinary Team Consists of:
The Resident and Family Attending Physician and Consultant
Psychiatrist Manager of Resident Care Clinical Resource Nurse The Nursing Team-RNs, RPNs, HCAs

The Interdisciplinary Team Consists of
(continued) : Social Worker Pharmacist Physiotherapist Occupational Therapist Dietician Recreation Facilitators Spiritual Care
What Gives Us a Sense of Well-being?
-The Bradford Dementia Group

Well-Being (continued)
What do we need to maintain a sense of well-being?
A sense of control A sense of who we are A feeling of safety and security The ability to communicate with others The feeling that we are socially
included
Well-Being (continued)
Having meaningful things to do Being taken seriously- do others
respect and recognize when we feel frustrated, angry, sad, anxious, tired/exhausted, confused, lonely, frightened?
Reactive Behaviours
Reactive Behaviour- the way in which a person responds to a specific set of conditions.
P.I.E.C.E.S. program
All residents on the Special Care Unit have a behavioural history which has made residing in a regular personal care home setting difficult or impossible.

Reactive Behaviours (continued)
Reactive behaviours may include: Restlessness Calling out
Wandering Hoarding Resistance to Care Agitation Anxiety Aggression Withdrawal Inappropriate Sexual Behaviour
Reactive Behaviours (continued)
Staff are encouraged and trained to monitor and document reactive behaviour:
Antecedents (Triggers) Behaviours Interventions Consequences
Reactive Behaviours (continued)
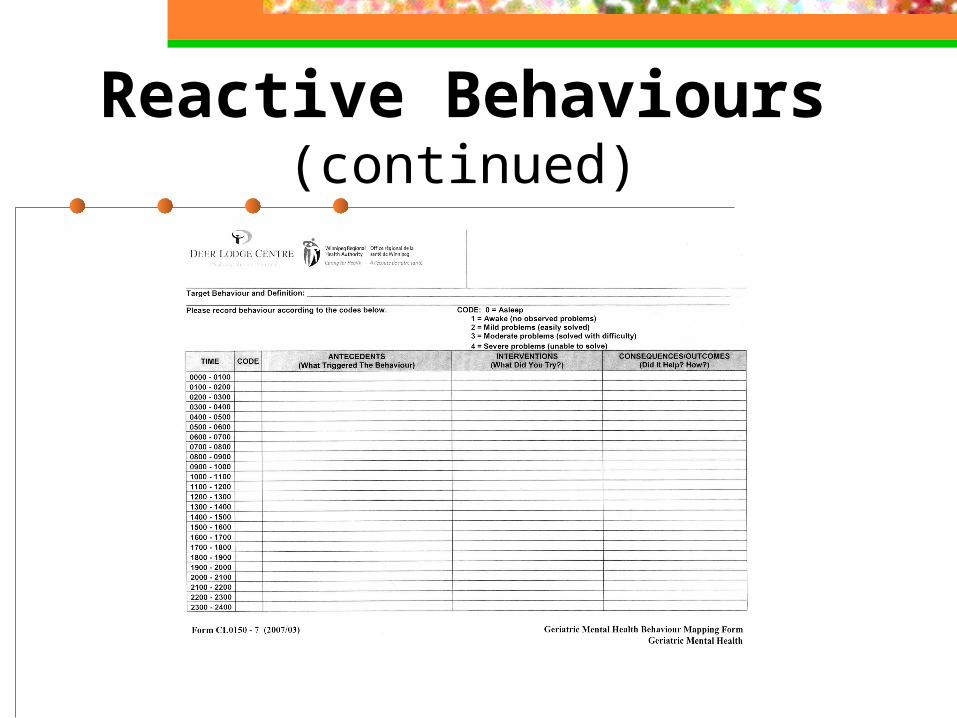
Reactive Behaviours (continued)
Key Elements of CareAlzheimer’s Australia, 2003
Assessment Individualized Care Interdisciplinary Team Approach Programming Relationships

Key Elements of Care (continued)
Key Elements of Care (continued)
Communication Skills Physical Environment Flexibility in Routines and Practices Staff Training and Education
Communication
Communication with persons who are cognitively impaired may be difficult and frustrating at times for both you and them
Remember that behaviour is a form of communication for residents that have impaired expressive ability
Communication Areas to focus on include:
Approach in a gentle manner and identify yourself by name
Maintain eye contact Provide gentle direction Do not make an issue of a mistake,
they happen Avoid asking facts

Communication Areas to focus on include
(continued): Reduction of distractions and
background noise Reorientation may not work Appropriate touch Items and illustrations to convey
messages
Visiting
May be difficult for families/caregivers – We, by nature, need something from our visits• Love• Reassurance• Support returned to us• Ease of guilt• Confirmation of our decisions• To feel that a connection remains

Visiting (continued)
Goals of Visiting Who should Visit When to Visit Where to Visit What to do when you Visit Why Visiting may be difficult Saying goodbye after your Visit When younger family members Visit

Caregiver Support Group
Informal group for families/friends that meet once a month
Connections for them, connections for us
Share questions and information about SCU
Supportive and safe environment Luncheons

Case Study
79 year-old gentleman residing on a general medical hospital ward.
dx of Alzheimer’s/Parkinson’s disease. hx of resistance and aggression during
care, occasionally towards co-residents. Poor response to psychotropics -
oversedation-minimal effect on behaviour.
Case Study Care Plan in General Hospital
Setting 6 staff to provide care Resident to be restrained on bed utilizing
4 staff, 2 staff to prepare and provide care.
Broda with lap table for meals and rest periods.
Current Rx • Carbamazepine 200mg bid• Trazodone 75 mg od 18:00

Case Study Care Plan on SCU - Goals
Gain the resident’s trust. Create a “resident-friendly” care
plan. Involve resident and family in care
planning-create an environment where resident and family have decision-making authority.
Ensure Consistency/reliability.

Case Study Care Plan on SCU -
Interventions ADL Care Broda chair and table for meals. “Bath-in-a-bag” products - no tub baths,
no showers Incontinent product-pullup/brief/overnight Monitoring behaviour on unit Plan all care -
Scheduled………..CONSISTENT

Case Study Care Plan on SCU (continued) Initially provide 4 staff for care and
safety “Normalized care”, bathroom routine When resident requires care, approach
and “be with” resident Reapproach after a “break period”, invite
him to attend his room with you, or simply walk to room with him.
If care required more urgently, need to be more “matter of fact”

Case Study Care Plan on SCU (continued)
Adjustment to medication following admission
Trazodone Rx on revised care plan: 07:00 - 25 mg. 12:00 - 50 mg. 17:00 - 50 mg.

Case Study Care Plan on SCU - Outcomes 2-3 staff to provide care, dependant
on mood - (do not provide care alone)
Aggression with co-residents Broda chair/table for meals ADL/Bathing Ongoing staff education The challenge of CONSISTENCY

End of Life Care
Advance Care Plan/Health Care Directive Care planning around a progressive illness What is Comfort Care and its focus?
• Pain• Difficulty Swallowing• Lack of Appetite• Labored Breathing• Skin Breakdown• Loving Presence
When the Resident No Longer Requires
SCU
Resident no longer requires the specialized programs of our unit.
Social Worker prepares the family Move to another unit in DLC or
another facility
Barriers to Discharge
Long Wait Lists History of reactive behavior Families reluctance to move Concerns of receiving facility
• Small unit vs large unit• Treatment unit vs long-term care unit
ConclusionWhat Have We Learned?
The value of the unit staff Admissions – need to try new things Environmental challenges
• Closed-in vs. open spaces, Wall protection, Decoration
Low stimulus is a great idea but…… Require a balance between
environment and pharmacological treatment
Related Documents











