Clinical Pharmacokinetics of VANCOMYCIN WELLA AFRIANI WELLA AFRIANI 1111012041 1111012041

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Clinical Pharmacokinetics of VANCOMYCIN
WELLA AFRIANIWELLA AFRIANI11110120411111012041
Vancomycin—A glycopeptide
http://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?id=1399

INTRODUCTION• Inhibits bacterial cell wall synthesis• Time-dependent effect • Gram positive bacteria• Indications :– Documented infections:
• Methicillin/Cephalosporin-Resistant Staphycoccal infection.• Penicillin/Cephalosporin-Resistant Streptococcal infection.• Staphy./Strep. infection in patient allergic to penicillin.• Staphy. infection in patient with renal disease undergoing
hemodialysis. • Penicillin-Resistant Diphtheroid infection.• Severe antibiotic-associated enterocolitis.

• Indications (cont’) :
– Empiric Therapy:• Suspected MRSA nosocomial infection.• Meningitis in patient who had neurosurgery.• Neutropenic febrile patient not responding or allergic to
penicillin.• Suspected Staphy. infection in patient with renal disease
undergoing hemodialysis.
– Prophylaxis:• Endocarditis in patient allergic to penicillin.• Prosthetic valve placement in patient allergic to
penicillin.

Vancomycin• Volume of distribution: • An average value of 0.7 L/kg or • For patient older than 18 years:
V (L) = 0.17 (age in yr) + 0.22 (TBW in kg) + 15• Eliminated primarily by the renal route;
approximately 5% of the dose is metabolized (Vancomycin Cl ~ Clcr)
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.

Vancomycin• t1/2 elimination• Newborns: 6-10 hours• Infants & Children 3 months to 4 years: 4 hours• Children > 3 years: 2.2 – 3 hours• Adults: 5 – 11 hours; significantly prolonged with renal
impairment
Lexicomp Online, June 2012

ADVERSE DRUG REACTION• Ototoxicity (tinnitus, fullness in the ear)• Nephrotoxicity
• An increase in SrCr of 0.5mg/dL or greater, or as 50% increase from baseline.
• Occurs at a rate of 5% with Vancomycin alone and increase to 22% with addition of Aminoglycosides.
• Red-Man Syndrome (hypotension, upper body maculopapular rash)
• Cutaneous reaction (urticaria, angioedema, erythema)
• Neutropenia (within 15 – 30 days of drug initiation)• Fever
PHARMACOKINETIC CHARACTERISTICS
• Two- or three-compartment model.• Bioavailability– Per oral < 5%– Intravenous 100%
• Protein binding 30 – 55%• Excretion– Renal: >90% unchanged in urine

KEY PARAMETERS• Ctarget Conventionally P = 40 – 50 mg/L
T = 10 – 15 mg/LContinuous infusion Cave
ss = 12 – 18 mg/L• F <0.05 PO• Vd 0.7 (0.5 – 1.0) (L/kg)
• CLVanco 0.65CLCr x 0.06 (L/H)• t½ 7 (H)• Ke 0.00083(CLCr) + 0.0044 (H-1)
*CLCr in ml/min
Some Useful PK Formulas• K = ln (C1 / C2 ) (t2 – t1)• K = Cl V• t1/2 = 0.693 / K
• For steady state, bolus model :Dose = (Css1 ) (V) (1- e-Kτ )
(e-Kt1 )
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.
Some Useful PK Formulas
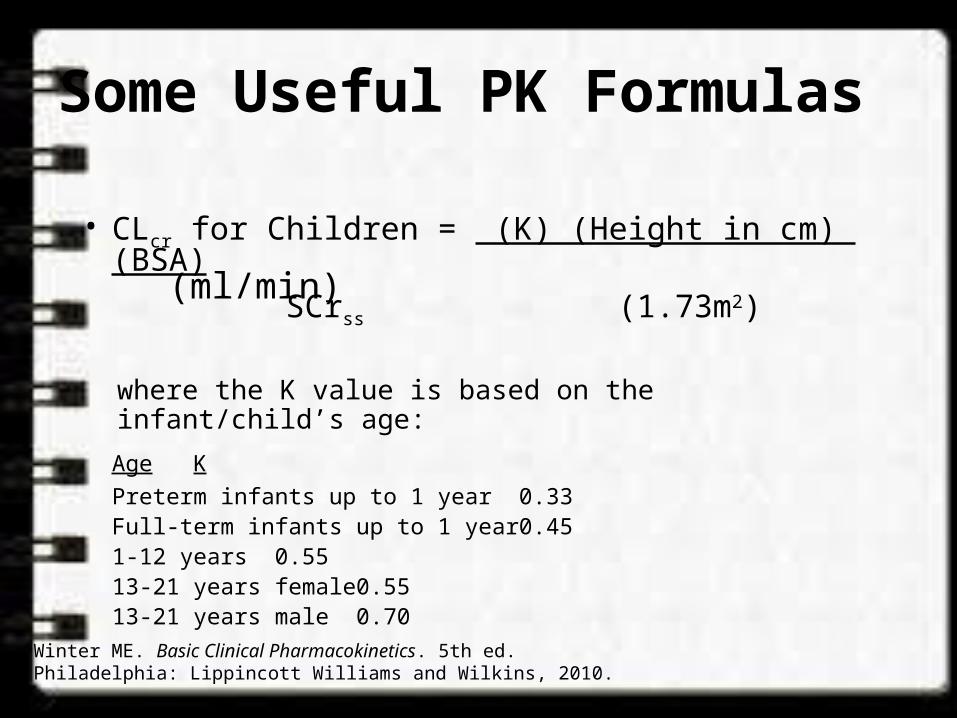
• CLcr for Children = (K) (Height in cm) (BSA) (ml/min) SCrss (1.73m2)
where the K value is based on the infant/child’s age:Age KPreterm infants up to 1 year 0.33Full-term infants up to 1 year 0.451-12 years 0.5513-21 years female 0.5513-21 years male 0.70
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.

Some Useful PK Formulas
• BSA in m2 = Patient’s weight in kg (1.73 m2)
• CLcr for males = (140 - Age) (Weight) (ml/min) (72) (SCrss)
• CLcr for females = (0.85) (140 - Age) (Weight) (ml/min) (72) (SCrss)
Winter ME. Basic Clinical Pharmacokinetics. 5th ed. Philadelphia: Lippincott Williams and Wilkins, 2010.
70 kg
0.7

Clinical Calculators• Clinical calculator available at LPCH Intranet:
Lane Library Specialty Portals Pharmacy-Calculators Drug Levels-Vancomycin & Aminoglycoside Pharmacokinetics•http://medcalc.com.laneproxy.stanford.edu/pk/•Other calculators available at Pharmacy Network: Pharmacy Network Pharmacokinetic Monitoring• CF Kinetics - by Dr. Carlos Milla• NICU Drug Kinetics - by Dr. William Benitz

Additional Information
• Area Under the Curve (AUC) = area under the plasma drug concentration vs. time curve• AUC = dose administered/drug clearance• AUC (mg.hr/L)= C0 = initial concentration (mg/L)
k elimination rate constant (hr-1)
• Gentamicin and Tobramycin:• AUC24 = 70 – 100 mg.hr/L
• Cystic fibrosis patients: tobramycin AUC24 ~ 100 to 125
Prescott WA Jr, Nagel JL. Extended-interval once-daily dosing of aminoglycosides in adult and pediatric patients with cystic fibrosis. Pharmacotherapy 2010 Jan;30(1):95-108.
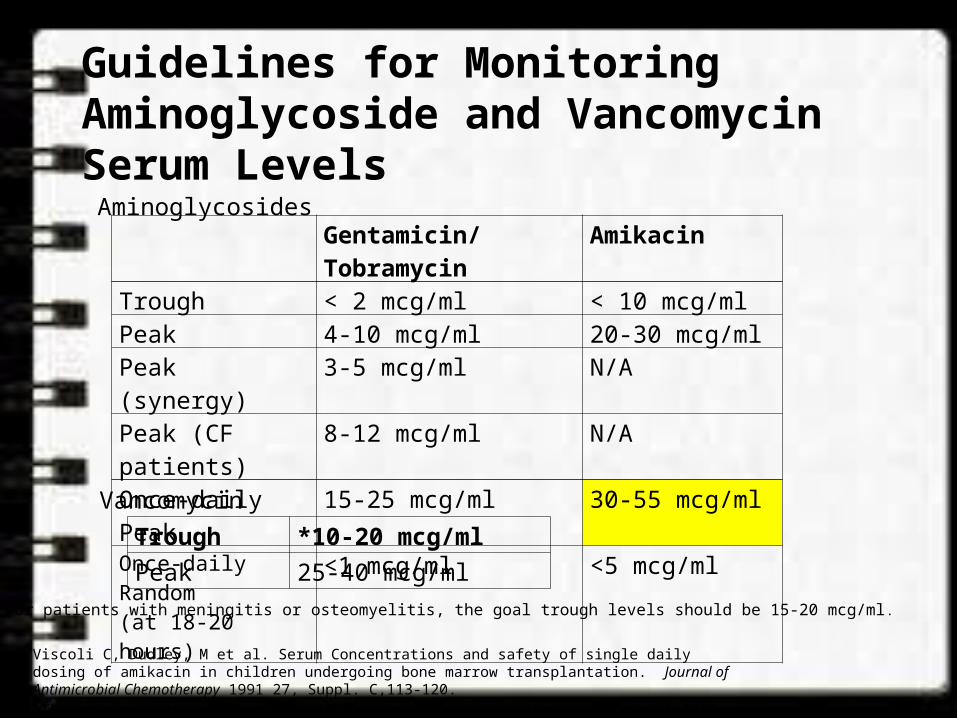
Guidelines for Monitoring Aminoglycoside and Vancomycin Serum Levels
Gentamicin/Tobramycin
Amikacin
Trough < 2 mcg/ml < 10 mcg/mlPeak 4-10 mcg/ml 20-30 mcg/mlPeak (synergy) 3-5 mcg/ml N/APeak (CF patients) 8-12 mcg/ml N/AOnce-daily Peak 15-25 mcg/ml 30-55 mcg/mlOnce-daily Random(at 18-20 hours)
<1 mcg/ml <5 mcg/ml
Trough *10-20 mcg/mlPeak 25-40 mcg/ml
Aminoglycosides
Vancomycin
*For patients with meningitis or osteomyelitis, the goal trough levels should be 15-20 mcg/ml.
Viscoli C, Dudley, M et al. Serum Concentrations and safety of single daily dosing of amikacin in children undergoing bone marrow transplantation. Journal of Antimicrobial Chemotherapy 1991 27, Suppl. C,113-120.Trujillo H, Robledo J et al. Single daily dose amikacin in paediatric patients with severe Gram-negative infections. Journal of Antimicrobial Chemotherapy 1991 27, Suppl. C, 141-147.
INITIATING VANCOMYCIN
• Cultures– Appropriate C&S obtain within 48hrs before
starting therapy.– Antibiotic therapy modified (if necessary) within
24hrs of the C&S results.• Renal Function– Estimated CLCr within 24hrs of initiating therapy.
– Monitoring CLCr every 3 – 5 days during therapy.

INITIATING VANCOMYCIN (CONT’)
• Dosage Regimen & Monitoring Needs– Conventional dosing• Peak & Trough concentration method
– Continuous infusion• Trough concentration method

INITIATING VANCOMYCIN (CONT’)
• Conventional Dosage Regimen– Initial per dose is between 10 – 15 mg/kg body wt– Dosage interval based on estimated CLCr.– Rate of infusion not more than 20 mg/min.– Adjustment based on measured levels.
• Serum Drug Concentration– Levels taken at steady-state.– If stable renal function, repeat trough levels once a
week.– Trough levels obtained if with other nephrotoxic drugs.– Trough and peak levels obtained if:
» Not responding to therapy.» Altered physiologic parameters

INITIATING VANCOMYCIN (CONT’)
• Continuous Infusion Regimen– Infusion rate is based on estimated CLCr and
targeted Cavess (15 mg/L).
– Rate of infusion, Ro (mg/H)
Ro = CLvancoCavess
= VdKeCavess
– Adjustment based on measured Cavess

INITIATING VANCOMYCIN (CONT’)• Lake’s Method– Target serum levels:
T = 5 – 10 mg/L (30 min before the next infusion)P = 20 – 30 mg/L (15 min after the end of infusion)
– Maintenance dose (per dose) = 8 mg/kg (LBW)– To be give at Q H interval:
CLCr (ml/min) (H) >90 6 70 – 89 8 46 – 69 12 30 – 45 18 15 – 29 24

• Rodvold’s MethodRodvold’s Method• Target serum levels:Target serum levels:
T = 5 – 10 mg/L (30 min before the next T = 5 – 10 mg/L (30 min before the next infusion)infusion)
P = 30 – 40 mg/L (15 min after the end of P = 30 – 40 mg/L (15 min after the end of infusion)infusion)
• Daily maintenance dose Daily maintenance dose Dose (mg/kg TBW per 24H) = (0.227(CLDose (mg/kg TBW per 24H) = (0.227(CLCrCr) + 5.67) + 5.67
• Interval:Interval:CLCLCrCr (ml/min) (ml/min) (H) (H) >65>65 8 8 46 – 65 46 – 65 12 12 20 – 39 20 – 39 24 24 10 – 19 10 – 19 48 48
INITIATING VANCOMYCIN (CONT’)
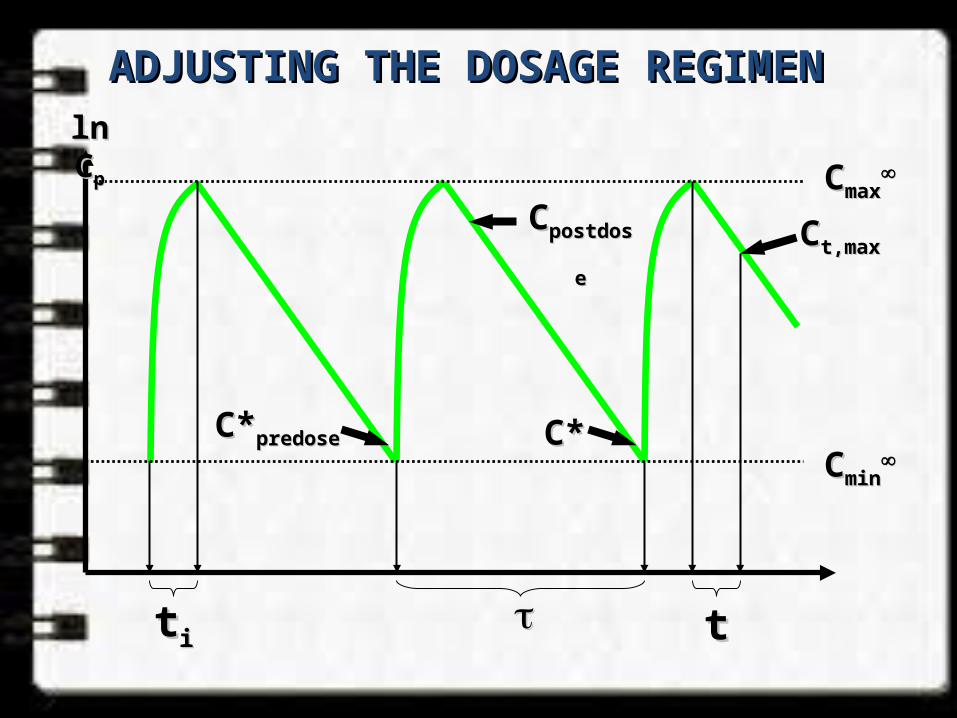
ADJUSTING THE DOSAGE REGIMEN ADJUSTING THE DOSAGE REGIMEN ln Cln Cpp
ttii tt
CCminmin
CCmaxmax
C*C*predosepredose C*C*
CCpostdosepostdose CCt,maxt,max

• Sawchuck-Zaske Method (Conventional/Multiple short infusion)
– Determine the t½Ke = ln (Cpeak/Ctrough) / (ttrough – tpeak) t½ = 0.693 / Ke
– Determine the Vd
Vd = Ro x 1 – e-Keti . Ke (Cmax – (Cmine-Keti)
*Ro = mg/H infusion– Determine the new
new = ln (Cmax desired / Cmin desired) + ti
Ke
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
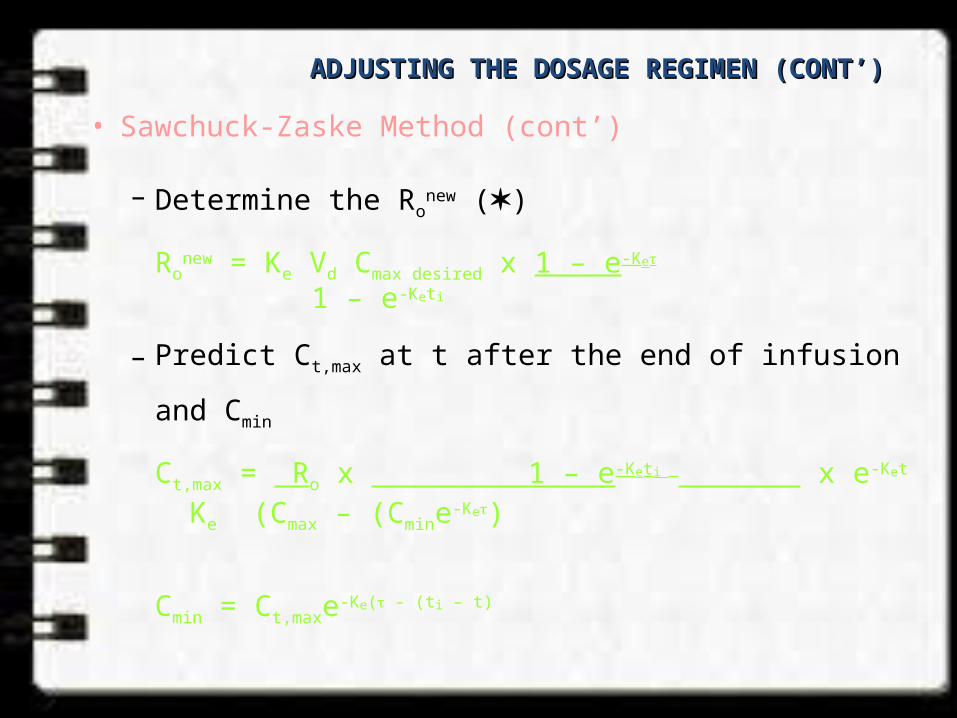
• Sawchuck-Zaske Method (cont’)
– Determine the Ronew ()
Ronew = Ke Vd Cmax desired x 1 – e-Ke
1 – e-Keti
– Predict Ct,max at t after the end of infusion and Cmin
Ct,max = Ro x 1 – e-Keti x e-Ket
Ke (Cmax – (Cmine-Ke)
Cmin = Ct,maxe-Ke( - (ti – t)
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)

• Continuous Infusion Method
– Determine the CLvanco
CLvanco* = Ro / achieved Cave
ss
– Determine the new Ro (mg/H)
Ro = CLvanco* x targeted Cave
ss
ADJUSTING THE DOSAGE REGIMEN (CONT’) ADJUSTING THE DOSAGE REGIMEN (CONT’)
THANK YOU
Related Documents

![Hw (1) - afriani sinaga [merencanakan hidup]](https://static.cupdf.com/doc/110x72/54037d188d7f72e04c8b4775/hw-1-afriani-sinaga-merencanakan-hidup.jpg)