Welcome to I-TECH HIV/AIDS Clinical Seminar Series 9 April, 2009 Management of HIV-exposed Infant Perinatal TB Exposure Chris Mathews, MD

Welcome to I-TECH HIV/AIDS Clinical Seminar Series 9 April, 2009 Management of HIV-exposed Infant Perinatal TB Exposure Chris Mathews, MD.
Jan 03, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Welcome to I-TECH HIV/AIDS Clinical Seminar Series
9 April, 2009
Management of HIV-exposed Infant Perinatal TB Exposure
Chris Mathews, MD

Management of HIV-exposed Infant Perinatal TB Exposure
Chris Mathews, M.D.ITECH South AfricaUCSD Owen Clinic
2

Learning Objectives
• To review the risk of perinatal transmission of tuberculosis from HIV co-infected mother to neonate
• To review indications for empiric TB therapy in neonatal period
• To review indications for isoniazid preventive therapy in neonatal period
• To review use of BCG in TB and HIV exposed neonate
3
Case Presentation
• 25 year old woman with newly diagnosed HIV infection, unknown CD4 and viral load
• Presents in late 3rd trimester with smear positive pulmonary tuberculosis
• Initiates anti-TB therapy 3 days prior to delivery
• Prior TB history unknown
4

Questions Posed by Managing Doctor
• Should baby receive BCG?
• Should baby receive isoniazid preventive therapy?
• Should baby be treated for TB disease empirically?
5

Polling Question 1

What is the risk of perinatal TB transmission from smear + mother?
• Between April 1997 and July 1999, 107 pregnant women diagnosed with TB in KZN
• Of these, 82 (77%) were HIV-1 co-infected
• No statistically significant differences between HIV-1-infected and non-infected women in– distribution of bacteriologically proven TB disease– trimester of TB diagnosis– compliance with TB therapy
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69
7

What is the risk of perinatal TB transmission from smear + mother?
• The 107 mothers accounted for 114 births.
• All perinatal deaths were among HIV infected women– 6 stillbirths– 1 early neonatal death
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69 8

What is the risk of perinatal TB transmission from smear + mother?
• Overall perinatal mortality rate (PMR)of 85.4 per 1000 maternities in HIV-1-infected women with active TB.– PMR attributed to TB disease was
• 65.2/1000 in HIV-1-infected women • 0/1000 in the non-infected
• Maternal haemoglobin was lower in those with perinatal deaths– mean 8.2 g/dl vs. 9.8 g/dl, P 0.02
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69 9

What is the risk of perinatal TB transmission from smear + mother?
• Excluding the stillbirths, M. tuberculosis was detected in 16 neonates resulting in a transmission rate of 16%.
• Detection was by culture in 12, and smear microscopy in a further 4 that failed to grow on culture.
• In 12 cases, diagnosis based on samples submitted in 1st week of life, and a further 4 in the first 3 weeks after birth.
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69 10

What is the risk of perinatal TB transmission from smear + mother?
• These organisms grew from gastric washing and CSF samples obtained predominantly within the first week of life in mainly growth retarded, low birth weight newborns, and
• Therefore most likely reflects transplacental transmission in utero
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69 11
What is the risk of perinatal TB transmission from smear + mother?
• Less than half of the TB transmitting mothers were sputum smear microscopy or culture-positive, • although all of the mothers had clinical and
radiological signs suggestive of TB.
• Untreated TB disease was associated with detection of bacilli in the baby, suggesting that most of this transmission occurs close to delivery.
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69 12

What is the risk of perinatal TB transmission from smear + mother?
• Authors’ recommendation– Where the baby is symptomatic in the neonatal
period, it may be acceptable to institute empiric anti-tuberculosis treatment in the at-risk HIV-1-exposed baby whose mother has TB disease in pregnancy.
– This is primarily due to the long time toculture, and deaths from rapidly progressive HIV-1 disease while awaiting culture confirmation.
Pillay et al. INT J TUBERC LUNG DIS 2004; 8(1):59–69 13

Pillay et al. Lancet Infect Dis 2004; 4: 155–6514

Should BCG be given to HIV & TB exposed neonate?
• In resource-limited settings where compliance and follow-up is uncertain, the BCG vaccine should be administered to the newborn for the following reasons:– failure to administer BCG in the high-risk
neonate could result in the baby being at greater risk for miliary tuberculosis and tuberculosis meningitis
Pillay et al. Lancet Infect Dis 2004; 4: 155–65 15

Should BCG be given to HIV & TB exposed neonate?
– a uniform policy limits any nursing/medical confusion about who should and should not receive the vaccine in busy resource-restricted neonatal units
– evidence that isoniazid/rifampicin prophylaxis inhibits the immunogenicity of the BCG vaccine is not conclusive
Pillay et al. Lancet Infect Dis 2004; 4: 155–65 16

Should BCG be given to HIV & TB exposed neonate?
– in the symptomatic baby, whose mother is considered infectious for M tuberculosis, the risks of acquiring wild-type tuberculosis may outweigh the risks of disseminated BCG vaccine tuberculosis
Pillay et al. Lancet Infect Dis 2004; 4: 155–65 17

Should BCG be given to HIV & TB exposed neonate?: More Recent Data
Mak et al. Lancet. 2008 Sep 6;372(9641):786-7 18

Should BCG be given to HIV & TB exposed neonate?
• Risks outweigh benefits for BCG vaccination for infants who are known to be HIV infected with or without signs or reported symptoms of HIV infection.– These infants should not be immunized.
WHO. Wkly Epidemiol Rec. 2007 May 25;82(21):193-6Hesseling et al. Int J Tuberc Lung Dis. 2008;12(12):1376-9
19

Should BCG be given to HIV & TB exposed neonate?
• Risks usually outweigh benefits for BCG vaccination for infants whose HIV infection status is unknown but who have signs or reported symptoms suggestive of HIV infection and who are born to HIV-infected mothers. – These children should not be immunized.
WHO. Wkly Epidemiol Rec. 2007 May 25;82(21):193-6Hesseling et al. Int J Tuberc Lung Dis. 2008;12(12):1376-9
20

Should BCG be given to HIV & TB exposed neonate?
• However, this guideline will be applicable only to children who have not yet received BCG in the first few weeks of life, since clinical manifestations typically occur after 3 months of age.
• If infection status can be established with early virological testing, BCG may then be administered once HIV infection has been ruled out.WHO. Wkly Epidemiol Rec. 2007 May 25;82(21):193-6Hesseling et al. Int J Tuberc Lung Dis. 2008;12(12):1376-9
21
Should BCG be given to HIV & TB exposed neonate?
• A key implementation consideration is selectively delaying vaccination of HIV-exposed infants from birth until, for example, 10–14 weeks of age, following a negative HIVPCR testing result, e.g., at 4–6 weeks of age.
• This could be combined with alternative TB preventive strategies such as isoniazid preventive therapy in the intervening period.
WHO. Wkly Epidemiol Rec. 2007 May 25;82(21):193-6Hesseling et al. Int J Tuberc Lung Dis. 2008;12(12):1376-9
22

HIV-1 Infection in Infants Severely Impairs the Immune Response Induced by BCG
23Mansoor et al. J Infect Dis. 2009 Apr 1;199(7):982-990

HIV-1 Infection in Infants Severely Impairs the Immune Response Induced by BCG
24Mansoor et al. J Infect Dis. 2009 Apr 1;199(7):982-990

HIV-1 Infection in Infants Severely Impairs the Immune Response Induced by BCG
• Infection with HIV severely impairs the BCG-specific T cell response during the first year of life.
• BCG may therefore provide little, if any, vaccine-induced benefit in HIV-infected infants.
• Considering the significant risk of BCGosis, these data strongly support not giving BCG to HIV-infected infants.
25Mansoor et al. J Infect Dis. 2009 Apr 1;199(7):982-990

HIV-1 Infection in Infants Severely Impairs the Immune Response Induced by BCG
• How can protection against TB then be achieved in HIV+ infants? – One approach may be to initiate highly active
antiretroviral therapy as early as possible for these infants and thereafter vaccinate them with BCG.
– An alternative approach is to institute isoniazid prophylaxis in all HIV− infants.
– Ultimately, a novel TB vaccine, which is safer and hopefully more effective than BCG in HIV+ infants, will constitute the most sustainable intervention.
26Mansoor et al. J Infect Dis. 2009 Apr 1;199(7):982-990

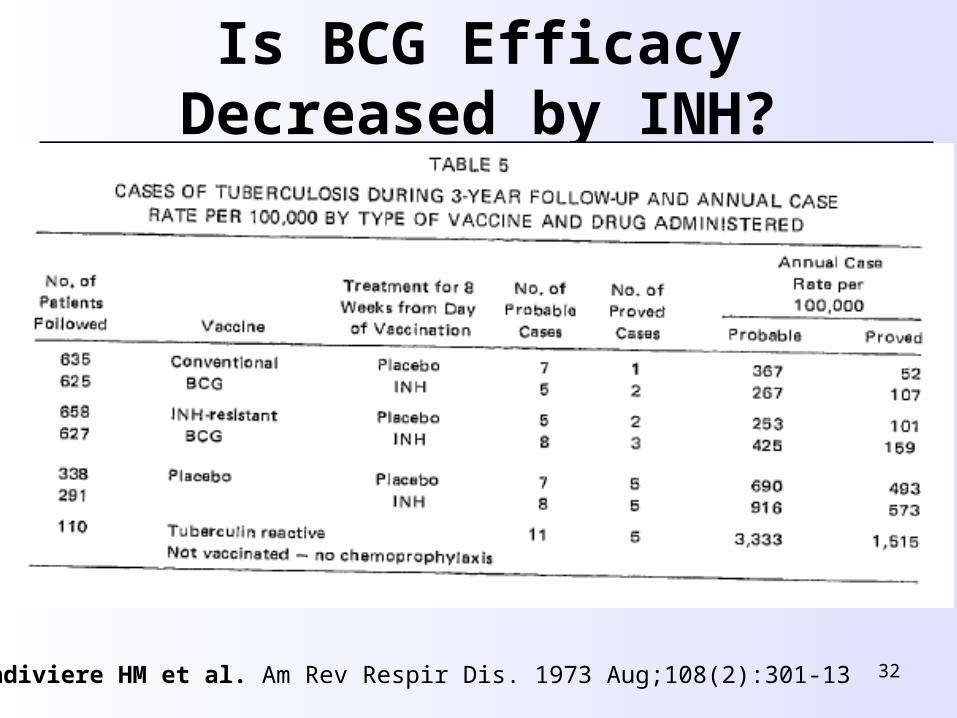
Is BCG Efficacy Decreased by INH?
• Vandiviere HM et al. Am Rev Respir Dis. 1973 Aug;108(2):301-13
• Dworski et al. Am Rev Respir Dis. 1973 Aug;108(2):294-300
• De Boer et al. Impaired immune response by isoniazid treatment during intravesical BCG administration in the guinea pig Prog Clin Biol Res. 1992;378:81-93
• Perinatal Prophylaxis of TB Lancet. 1990 Dec 15;336(8729):1479-80
27

Is BCG Efficacy Decreased by INH?
28
Vandiviere HM et al. Am Rev Respir Dis. 1973 Aug;108(2):301-13

Is BCG Efficacy Decreased by INH?
29
Vandiviere HM et al. Am Rev Respir Dis. 1973 Aug;108(2):301-13

Is BCG Efficacy Decreased by INH?
30
Vandiviere HM et al. Am Rev Respir Dis. 1973 Aug;108(2):301-13

Is BCG Efficacy Decreased by INH?
31Vandiviere HM et al. Am Rev Respir Dis. 1973 Aug;108(2):301-13
Is BCG Efficacy Decreased by INH?
32Vandiviere HM et al. Am Rev Respir Dis. 1973 Aug;108(2):301-13

Anti-Tuberculous Drugs in Infants
Pillay et al. Lancet Infect Dis 2004; 4: 155–6533

Breast milk transmission of Tuberculosis?
• The risk of transmission of tuberculosis to infants from breastfeeding exists, but is not quantified.
• Since tuberculosis is an airborne pathogen, unlike HIV, the risks of postnatal transmission from an infectious mother, with open pulmonary tuberculosis, to her baby remain, even if she is not breastfeeding.
Pillay et al. Lancet Infect Dis 2004; 4: 155–6534

Breast milk transmission of Tuberculosis?
• Provided the HIV-infected mother with TB disease is adequately treated for tuberculosis, and the baby at risk is appropriately given prophylaxis, the feeding choice should not be restricted by tuberculosis in the mother
• No evidence that this residual breast-milk transfer of antituberculosis therapy supports the emergence of drug-resistant strains of Mtuberculosis in infants.
Pillay et al. Lancet Infect Dis 2004; 4: 155–65
35

Polling Question 2

Mathews’ Recommendations
• Culture baby for TB: gastric washings
• Withhold BCG
• Start anti-TB therapy for baby
• At 6 weeks, perform DBS PCR for HIV and PPD
• At 8 weeks, if cultures negative and mother smear negative, stop TB therapy and complete IPT course
37


Welcome to I-TECH HIV/AIDS Clinical Seminar Series
Next session: 23 April, 2009
Roy Colven, MD
HIV Dermatology: Virtual Office Hours
Related Documents











