WEGENER'S GRANULOMATOSIS Granuloma of the nose with systemic polyarteritis nodosa By A. E. READ, M.D.(LOND.), M.R.C.P. and C. S. TREIP, M.D.(LOND.) Central Middlesex Hospital, London, N. W. Io Rose (1956), in an investigation of 66 cases of polyarteritis nodosa without lung involvement, found a preceding history of upper respiratory infection in I2 cases, i.e. i8 per cent. It may well be that infection rather than any drug used for its suppression may give rise to a state of hyper- sensitivity with the production of systemic poly- arteritis. There is much to support such a hypo- thesis from consideration of a particular group of cases of polyarteritis originally described by Klinger (193i) and Wegener (I937, I939). These cases are characterized by symptoms and signs of respiratory tract infection with the formation of granulomata and later by the development of polyarteritis, progressive renal involvement and death from uraemia. Since the original descriptions some 25 additional cases have been reported. Many of these reports are concerned with the pathological features for the very obvious reason that the diagnosis has, in the past, often been a post-mortem one. However, with increasing accuracy of recognition, the prob- lems of diagnosis and treatment are assuming a position of more importance. The variety of physical signs which may appear are of consider- able interest and the following case illustrates some of the more unusual features of Wegener's granulomatosis. Case Report Presenting Features An Irish girl, aged I9 years, was admitted to hospital on August 20, I955, with a complaint of one month's sweating, fever and headache. For two days she had also been vomiting. One week before admission she had attended another hospital because of a small crusted skin lesion which had appeared on the right temple. There was no sig- nificant past or family history. Physical examination revealed a pale, ill-looking girl with a puffy face and a slight saddle deformity of the nose (Fig. i). On the right temple there was ..:: .....'::: FIG. i.-The exophthalmos is now bilateral and more marked on the right, where there is considerable chemosis. The face has become far more puffy and the nasal deformity is more marked (before cortisone). a small crusted area. She ran an intermittent pyrexia up to ioo.60F. There were, at that time, no other physical signs. The blood pressure was 140/80 mm. Hg. Investigations X-ray film of chest-no abnormality. Blood copyright. on August 26, 2022 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.33.378.199 on 1 April 1957. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

WEGENER'S GRANULOMATOSISGranuloma of the nose with systemic polyarteritis nodosa
By A. E. READ, M.D.(LOND.), M.R.C.P.
and C. S. TREIP, M.D.(LOND.)Central Middlesex Hospital, London, N. W. Io
Rose (1956), in an investigation of 66 cases ofpolyarteritis nodosa without lung involvement,found a preceding history of upper respiratoryinfection in I2 cases, i.e. i8 per cent. It maywell be that infection rather than any drug used forits suppression may give rise to a state of hyper-sensitivity with the production of systemic poly-arteritis. There is much to support such a hypo-thesis from consideration of a particular group ofcases of polyarteritis originally described byKlinger (193i) and Wegener (I937, I939). Thesecases are characterized by symptoms and signs ofrespiratory tract infection with the formation ofgranulomata and later by the development ofpolyarteritis, progressive renal involvement anddeath from uraemia.
Since the original descriptions some 25 additionalcases have been reported. Many of these reportsare concerned with the pathological features forthe very obvious reason that the diagnosis has, inthe past, often been a post-mortem one. However,with increasing accuracy of recognition, the prob-lems of diagnosis and treatment are assuming aposition of more importance. The variety ofphysical signs which may appear are of consider-able interest and the following case illustrates someof the more unusual features of Wegener'sgranulomatosis.
Case ReportPresenting FeaturesAn Irish girl, aged I9 years, was admitted to
hospital on August 20, I955, with a complaint ofone month's sweating, fever and headache. Fortwo days she had also been vomiting. One weekbefore admission she had attended another hospitalbecause of a small crusted skin lesion which hadappeared on the right temple. There was no sig-nificant past or family history.
Physical examination revealed a pale, ill-lookinggirl with a puffy face and a slight saddle deformityof the nose (Fig. i). On the right temple there was
..::.....':::
FIG. i.-The exophthalmos is now bilateral and moremarked on the right, where there is considerablechemosis. The face has become far more puffy andthe nasal deformity is more marked (beforecortisone).
a small crusted area. She ran an intermittentpyrexia up to ioo.60F. There were, at that time,no other physical signs. The blood pressure was140/80 mm. Hg.
InvestigationsX-ray film of chest-no abnormality. Blood
copyright. on A
ugust 26, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.33.378.199 on 1 A
pril 1957. Dow
nloaded from

200 POSTGRADUATE MEDICAL JOURNAL April 1957
picture-haemoglobin 13.2 g. per ioo ml. (89 percent.); white blood cells, 6,900 per cu mm.;normal differential count; Wassermann reaction(blood) negative. Blood cultures sterile on severaloccasions. Blood urea, 20 mg. per ioo ml.Catheter specimen of urine-red blood cells,granular casts and albuminuria. Plasma proteins-normal total and differential levels. Bone marrow-no abnormality. Lumbar puncture-chemicallyand cytologically normal fluid under normalpressure. Cultures of nasal swabs produced agrowth of staph. pyogenes sensitive to tetracyclineand streptomycin.The only abnormality appeared to be micro-
scopic haematuria and cylinduria, which were con-sistently present.
Nasal Discharge and ExophthalmosA month after admission the patient had several
epistaxes and admitted that she had noticed a nasaldischarge and heavy nasal catarrh for the past threemonths. X-ray examination of the nasal sinusesshowed evidence of chronic nasal obstruction withfluid levels in both maxillary sinuses. She alsobegan to develop slight exophthalmos, at firstaffecting the right eye alone, but later bilateral andprogressive, with considerable chemosis, peri-orbital oedema and some patches of scleritisdeveloping (Fig. i). An ulcer also appeared on thehard palate, accompanied by increasing saddledeformity of the nose.
BiopsySpecimens were taken from the palatal ulcer,
the skin lesion and the nasal mucosa, examinationof the nose having revealed evidence of nasal sepsiswith considerable crusting of the mucous mem-brane.
i. Right temple. The epidermis was ulcerated,the floor of the ulcer being lined by fibroblasticgranulation tissue infiltrated by lymphocytes,eosinophils and plasma cells. The granulomabecame more extensive in the deeper layers of thecutis, where a central area of eosinophilic necrosiswas surrounded by numerous giant cells, some ofthe foreign body and some of the Langhans type.This inflammatory tissue extended into the sub-cutaneous fat.
Several arteries in the subcutis were involved bythe granuloma, all the coats were affected and thelumen was filled with granulomatous tissue (Fig.2), including giant cells. Elastic staining showedsplitting and partial disappearance of the elasticainterna (Weigert and van Gieson). Fibrinoidchanges were not seen (phosphotungstic acidhaematoxolyn).
2. Right middle turbinate-. The mucosa was
4
.
p
¼ -L -g.' -, A,
4-,,. 4-.4 4.,,,' .g4.%.4W ...
1..i
FIG. 2.-Right temple: (a) arteritis affecting all coats.The lumen is filled with granulation tissue. H. & E.x ISO.
ulcerated with conspicuous submucous oedema.More deeply there was an infiltration by neutro-phils, eosinophils and plasma cells; the- neutro-phils invaded the media of several 'small submucousarterioles. Centrally there was fibroblastic granula-tion tissue with giant cells, similar to that seen- inthe temple. Necrosis was not seen. Vascular lesionswere confined to small arterioles and did not affectlarger vessels.
3. Palate. The mucosal epithelium was partlyulcerated; where present, it was thickened withpeg-like prolongations into the stroma. Thestroma was mostly replaced by blood clot, pus andgranulation tissue containing many giant cells,some of the foreign body and some of the Lang-han's type. A blood vessel, probably a vein, withits media heavily infiltrated by neutrophils, was-surrounded by many giant cells. Fibrinoid changewas not seen.
Ziehl-Neelsen preparations were negative foracid-fast bacilli in all sections.The histological diagnosis was malignant granu-
loma of the nose.
copyright. on A
ugust 26, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.33.378.199 on 1 A
pril 1957. Dow
nloaded from

April I957 READ and TREIP: Wegener's Granulomatosis 20I
.4 ¾
~ L ~ i '
ME--.
FIG. 2.-(b) The elastic lamina is interrupted, andshows splitting. Weigert-van-Gieson x !So.
Progress and Further InvestigationsThe exophthalmos gradually progressed, the
nasal sepsis continued, and the urine persistentlycontained a deposit of red blood cells, pus cells andcasts. Examination of the serum proteins byelectrophoresis now revealed reversal of thealbumin-globulin ratio with an increased propor-tion of gamma-globulin. There was also increasingnitrogen retention (blood urea go mg. per cent.);persistent anaemia had developed (haemoglobin6o per cent.), as had moderate hypertension(-i6o/ioo mm. Hg.).
-Suspicion of Wegener's granulomatosis led -tobiopsy of a-specimen of muscle from the right thigh(Mr. J. B. -Hobbs).
Histology of Muscle BiopsySeveral small arteries showed an acute inflamma-
tion (Fig. 3), the adventitia and media beinginfiltrated by plasma cells, lymphocytes and poly-morpho-nuclears, among which eosinophils wereconspicuous. The media showed fibrinoid necrosis.There was some intimal proliferation. Elasticstaining showed in one vessel a complete destruc-tion of the elastica interna.
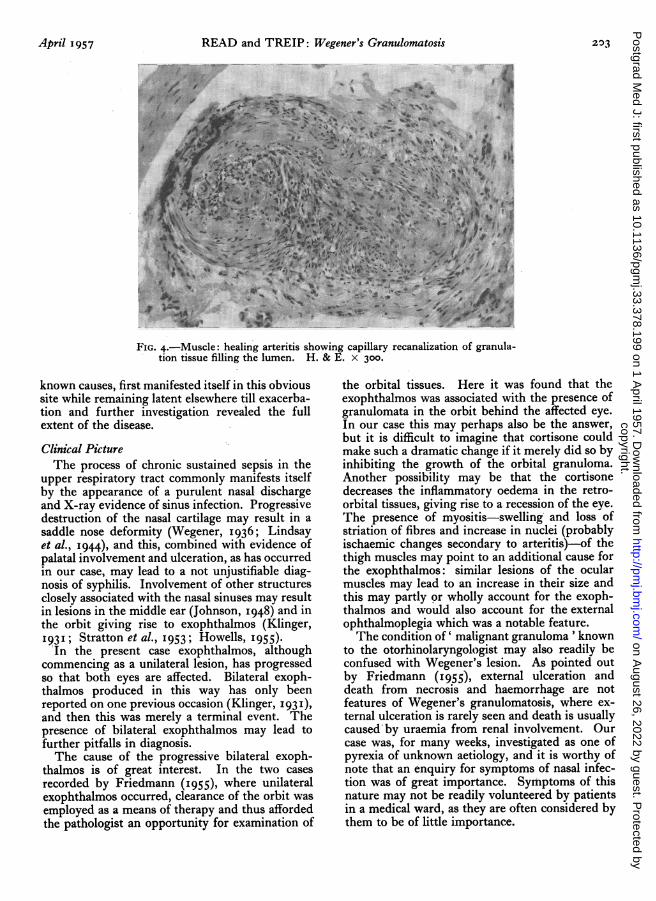
In other vessels there was an obliterative end-arteritis, the affected vessels being surrounded bya moderate amount of haemosiderin pigment. Thelumina of these vessels contained a cellular fibro-blastic tissue in which capillary recanalization wasseen (Fig. 4); the media and adventitia showed ascanty infiltration by neutrophils and eosinophilsand occasional granules of haemosiderin werepresent in these layers.There was moderate increase in inter-fascicular
nuclei with occasional lymphocytic collections. Apatchy degeneration of muscle was seen, the fibresbeing swollen with loss of staining reaction andstriation.The combined evidence of acute allergic arteritis
of the polyarteritis nodosa type and of a granulo-matous process in the nose confirmed the clinicaldiagnosis of Wegener's granulomatosis.
TreatmentCortisone. Dramatic improvement of the che-
mosis and exophthalmos followed cortisone therapyalone, and this has been a most notable featurethroughout. Temporary cessation of hormonetherapy always led to recurrence of the exoph-thalmos, which again improved with further corti-sone. The palatal ulcer also healed with thistherapy and there was no further vomiting.The patient's pyrexia, however, was not com-
pletely controlled. She was greatly distressed by acopious and foul nasal discharge and by the alarm-ing alteration in her face.
Unfortunately, large doses of cortisone sooninduced a paranoid psychosis which necessitatedtermination of therapy.
Local X-ray Treatment. As withdrawal of corti-sone was followed by a return of pyrexia, vomitingand a worsening of the ocular manifestations, itwas decided to try a course of local X-ray therapy.This produced a temporary improvement in well-being, but the original exophthalmos soonreturned.
In January 1956 the patient took her own dis-charge, only to be readmitted three weeks laterwith a return of her symptoms and gross bilateralexophthalmos.
Combined Cortisone and Antibiotics. Treatmentwas recommenced with cortisone, ioo mg. dailyby mouth, and antibiotics in the form of tetra-cycline, 500 mg. q.d.s. Since this time therehas been an improvement in the patient's symp-toms: the nasal discharge has decreased, thepyrexia and vomiting have ceased and the exoph-thalmos is now non-progressive. The palatal ulcerhas remained healed and the degree of nitrogenretention has decreased (blood urea 4I mg. per100 ml.).
copyright. on A
ugust 26, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.33.378.199 on 1 A
pril 1957. Dow
nloaded from

202 POSTGRADUATE MEDICAL JOURNAL April 1957
DiscussionThe condition of systemic polyarteritis associated
with chronic sepsis and granuloma formation inthe respiratory tract is rare. Affecting both sexes,it is usually most common in the fourth or fifthdecades, although the age of onset has varied fromI2 years (Godman and Churg, I954) to 70 years(Ahlstr6m et al., I953) in the cases recorded. Fewof these cases have been reported in this country.Almost any portion of the respiratory tract can
be affected by the process of granuloma formation.Lesions are commonly found in the nose and-accessory sinuses, also in the pharynx and larynx,and in other cases granuloma formation hasoccurred in the lung parenchyma. Sometimeslesions are found in-both situations.
Criteria for DiagnosisGodman and Churg (1954) give three criteria
for the diagnosis of Wegener's granulomatosis:(i) necrotizing granuloma of the upper and/orlower respiratory tract; (2) generalized focalnecrotizing vasculitis; and (3) glomerulonephritis.In our case the first two of these criteria have beenestablished. The presence of glomerulonephritisis adduced by the persistence of haematuria andthe slow rise in the blood urea.Taken separately, the lesions of the nose and
palate in this case conform with descriptions of' malignant granuloma' or granuloma gangraen-escens of the upper respiratory tract (Ellis, 1955).The lesion on the temple in our patient may be anextension from an underlying involved nasal sinusor a cutaneous granuloma. The granulomata ofspecific infections, such as tuberculosis andbrucellosis, were at first suspected as the cause ofthe- temporal lesion, but the nasal symptomsrevealed the true nature of the condition and nospecific organisms could be demonstrated eitherbacteriologically or histologically.The generalized vasculitis found in Wegener's
granulomatosis may be ' hypersensitivity angiitis,'described by Zeek et al. (1948), or polyarteritisnodosa. In our case the generalized lesion isconsidered to be polyarteritis nodosa, despite theabsence of symptoms, because muscular arteriesand not veins are involved, and healing processes,usually absent in hypersensitivity angiitis, areprominent (recanalization of occluded arteries andhaemosiderin deposition). The lesions of the noseand temple accord more with the appearance ofhypersensitivity angiitis in that veins are involved,although the presence of granulomata in the luminaof arteries suggests the beginnings of healingfollowing thrombosis. It should be noted thatmuscle biopsy may be negative, though the con-dition is suspected clinically (McCallum, 1954).
* jX:*X}Y:}, wjjtp.::: :i'.: ::::.::. ': ?S:S:ill}::.8#:. S?S<w°?i ......... 3Ei.:*: : :: :. :} !:.:i +. . ::} ::: .......... sm se < . S}C s Bw w ss:: - l m -W.:. :: : . : ,. £ SS0.?=s?4st! Be3 C{RE ffi ffi i eX | ....... ! t!. -. >i ........... m? Scj °>?: S3 ,!|.>3 ........................... ... ?|111 k3.: .}:}::. :'. ....... YIS °>- :.o;..'.S?1:? ........... £#5S3 DiSS: B1= S8fSs ............ .. .S I-:: ::::}ow:: ':': :: £::.':S.?,O ;ff 23 ?i. !l! LX. FF i3...\.,, .ee ,. .,! s: .. , i,gsfflg- . . i :: * ? eX t s ? U S t e|.; Y^ 41 SE8> 8.8s-agS;- cefE Z ,ZiE ? .*e!>ffiffi$jfi :e..'x:^..twj.X;.'o:'.w#xixffi3i -@gP Z WFX: ?£e^4- §
s;X&e :8::a;:: 8?Ww< W-. iES::.wSw'i-w.?-i E15
i I |;t'9'ffi.?#:3as ; flRKi-o..:?#SOF:ii.nSp}S!!-?8>e?s?:e?wjU"S=w3xwwsewilk:}.{::i:zu d:'? li -mS.ge.?3eg | |W.@-. | J
YS2it{8W#]^gaW ,-ewlE isl--
's-||5W? i:'8'8sP.82.YS;' #'.eS !e. d::,R, : S. <. ?: XE: lz!..fNq-e g3gf 8:>R} ..: :.RE;: 'o :'c;X.?.g:.?: .:: -!-e-s >. .-
§zo?w S,Q#<ozm3.S.s xi lSfe?;=F ,fiiS;i?|-;=S!D--
a>e?gX ,xfy;.,fi=d?Sie.io;lg S. - :oRF: .e sq<3?S? f.R >, es4. ::et ,W£e3: s,eX<8 ^2s-eiaRwi-e .:¢s oNaS;^eEFS < w Es^s^e. £# : :°.?::?°.::F}::w-Pu=-.*o, Xfakus oX8t eR.o#aew::#s3|fi&qwx<: S<<.;;iSS?ii;Si w--RR?e-lie3°i.e. <: S? eS?w
NXaC.i... ..:: ..:saB<s wXlS?Ef>>xe}>de?>}S }X028eaE.-*R iEeSx:S .. <e:s? eyS °Xe --$ Se^::'8Mle?633F£.°BW: ^; we^ex Z'i;E? S ,;., S, -.::2w.-:.-: .-b?iiXw-i-
*:: ::^ >iEhze>.:. .°iU-... C-W.eX 3?. -SM!} (F.5lt dM5ox8r:aBX88?i -fiSB::S?.-S>. 'Ul''O.:::s?::W::!.,:3:. 8D.SSES-e. -:E1-Se88WH :'?;':- ..... e .2 .y,: q3ffi^X?lE °Xe <ffi?,KS?WiCK #-,?q,w.,-tw:9tt *''WBiWl# S ..' .:!.;:!..S§:.8-ffi.'{¢ } SY:es;xom-I-?K
*°.::^ ::. .' '. £::.: .: :::. .'':'..:.'. :<SAi: ..b}::?n§R} d¢^ xwxeo?ES?SSt: :.-E: .em°e.; < ; ... : e?.: : o<W r o; :"e@R:::8SrsFwxs?xwt' -l, .> ................................ -''u; . -U :t 9?c . .. :::i isxX-W>8e:£: :::. ........... 8 zX8e o i 'lllll,1niCHISWisEw3B;. ': :3F:: ::::}: .8i 8' :§'.'o:: .:Su ::= :.02 .N7^{...--*j3S ........ ... S wd.- ........ ^ :^ e: .. :.<e uaLMs w .fi ;s-<gi : 8 : : es.Xae8#isRllE8ressos:oiR:?¢ a ,8aw,-... . B * S.2 -.1 - :; - * ^^8. # lo; - ., ' -°^ -'w-FIG. 3.-Muscle: acute arteritis with fibrinoid necrosis
of media. H. & E. x 300.
PathogenesisFor the pathogenesis of the condition Williams
(I949) and Godman and Churg (I954) postulatethe following train of events: infection of therespiratory tract, hypersensitivity with granulomaformation developing in this easily sensitized locus.Later, generalized hypersensitivity occurs, withvasculitis and glomerulonephritis. In our caseconstitutional symptoms were present only onemonth after nasal symptoms, and haematuria andalbuminuria were present at the first examination,so that it is probable that generalized vasculitis andglomerulonephritis developed soon after, if notconcomitantly with, the nasal granuloma. Pagel(I95I, Case 3) has shown that tuberculoid giantcell granulomata involving blood vessels may, infact, occur in polyarteritis nodosa. It seems, then,that the nasal granulomata and the generalized andrenal lesions of Wegener's syndrome may all beslightly differing expressions of a single patho-logical process-in our case polyarteritis nodosa(Klinger, I93I). It may be that the polyarteritisis an expression of hypersensitivity to the chronicantral infection, but it is also possible that thegeneralized hypersensitivity, resulting from un-
copyright. on A
ugust 26, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.33.378.199 on 1 A
pril 1957. Dow
nloaded from
April 1957 READ and TREIP: Wegener's Granulomatosis 203
':
PA"P
........ !!X!IfFIG. 4.-Muscle: healing arteritis showing capillary recanalization of granula-
tion tissue filling the lumen. H. & E. x 300.
known causes, first manifested itself in this obvioussite while remaining latent elsewhere till exacerba-tion and further investigation revealed the fullextent of the disease.
Clintcal PictureThe process of chronic sustained sepsis in the
upper respiratory tract commonly manifests itselfby the appearance of a purulent nasal dischargeand X-ray evidence of sinus infection. Progressivedestruction of the nasal cartilage may result in asaddle nose deformity (Wegener, I936; Lindsayet al., I944), and this, combined with evidence ofpalatal involvement and ulceration, as has occurredin our case, may lead to a not unjustifiable diag-nosis of syphilis. Involvement of other structuresclosely associated with the nasal sinuses may resultin lesions in the middle ear (Johnson, 1948) and inthe orbit giving rise to exophthalmos (Klinger,I93I; Stratton et al., I953; Howells, I955).
'In the present case exophthalmos, althoughcommencing as a unilateral lesion, has progressedso that both eyes are affected. Bilateral exoph-thalmos produced in this way has only beenreported on one previous occasion (Klinger, 193 I),and then this was merely a terminal event. Thepresence of bilateral exophthalmos may lead tofurther pitfalls in diagnosis.The cause of the progressive bilateral exoph-
thalmos is of great interest. In the two casesrecorded by Friedmann (I955), where unilateralexophthalmos occurred, clearance of the orbit wasemployed as a means of therapy and thus affordedthe pathologist an opportunity for examination of
the orbital tissues. Here it was found that theexophthalmos was associated with the presence ofgranulomata in the orbit behind the affected eye.In our case this may perhaps also be the answer,but it is difficult to imagine that cortisone couldmake such a dramatic change if it merely did so byinhibiting the growth of the orbital granuloma.Another possibility may be that the cortisonedecreases the inflammatory oedema in the retro-orbital tissues, giving rise to a recession of the eye.The presence of myositis-swelling and loss ofstriation of fibres and increase in nuclei (probablyischaemic changes secondarv to arteritis)-of thethigh muscles may point to an additional cause forthe exophthalmos: similar lesions of the ocularmuscles may lead to an increase in their size andthis may partly or wholly account for the exoph-thalmos and would also account for the externalophthalmoplegia which was a notable feature.The condition of ' malignant granuloma ' known
to the otorhinolaryngologist may also readily beconfused with Wegener's lesion. As pointed outby Friedmann (I955), external ulceration anddeath from necrosis and haemorrhage are notfeatures of Wegener's granulomatosis, where ex-ternal ulceration is rarely seen and death is usuallycaused by uraemia from renal involvement. Ourcase was, for many weeks, investigated as one ofpyrexia of unknown aetiology, and it is worthy ofnote that an enquiry for symptoms of nasal infec-tion was of great importance. Symptoms of thisnature may not be readily volunteered by patientsin a medical ward, as they are often considered bythem to be of little importance.
copyright. on A
ugust 26, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.33.378.199 on 1 A
pril 1957. Dow
nloaded from

204 POSTGRADUATE MEDICAL JOURNAL April I957
TreatmentTreatment of this condition is difficult; few
clinicians have been afforded an opportunity totreat cases because of their rarity. The therapeuticproblems come under two main headings:
Control of respiratory sepsis. Respiratory sepsisseems to indicate a need for long-term antibiotictherapy supplemented by procedures such asantral drainage. Control of infection is of im-portance, not only because of the distressing com-plications associated with it, such as nasal de-formity and copious nasal discharge, but alsobecause the development of polyarteritis and itsseverity may be a direct consequence of thisinfection. However, the administration of anti-biotics may lead to further sensitization and it isof note that in one case (Walton and Leggatt,1956) the development of the syndrome has fol-lowed the use of streptomycin and PAS for thetreatment of a granulomatous lesion wronglysuspected as being tuberculous. In all probabilitysome product of infection is the cause of the hyper-sensitive state, but the classical experimental workof Rich and Gregory (I943) may serve as areminder of the theoretical dangers of antibioticadministration.
Control of hypersensitive state. There seems nodoubt that when antibiotics are used their ad-ministration should be covered by cortisone andthere seems every reason to believe that antibioticsto combat the infective lesion plus cortisone tocontrol the hypersensitive state is the most success-ful form of therapy for this condition. Godman andChurg (I954) record survival for 39 months on thiscombined therapy in one patient, whereas, withfew exceptions, the disease usually runs a fullcourse to a fatal outcome in untreated cases in sixto io months.
In this case apparent control of pyrexia and ofother symptoms with a marked recession of theeyes and a lessening of nasal sepsis seems to havebeen obtained by the joint use of these drugs.Cortisone used alone appeared to produce an in-complete response and, in the presence of un-controlled infection, may, indeed, be dangerous.Similarly, X-ray therapy, although sometimes suc-cessful (Ellis, 1955) in cases of ' malignant granu-loma,' would seem to play little part in the treat-ment of this syndrome.One important feature throughout has been the
lack of symptoms referable to the systemic disease.It is perhaps worth remembering the presence ofthis condition when patients with chronic upperrespiratory tract infection, which fails to respondto the usual therapy, develop unusual featureseither locally or outside the respiratory tract.
SummaryI. A case of Wegener's granulomatosis is de-
scribed in which bilateral exophthalmos, palatalulceration and progressive saddle deformity of thenose developed.
2. An important feature was the absencethroughout the illness of symptoms and signs refer-able to the systemic disease, the diagnosis of whichhad to be confirmed by blind muscle biopsy.
3. The disease was controlled by combinedantibiotic and cortisone treatment; neither ofthese was completely successful when given alone.
4. This condition should be remembered in allcases of chronic nasal infection which developunusual features and do not respond to routinetreatment.
AeknowledgmentsWe would like to express our thanks to Dr.
Richard Asher for permission to publish detailsof this case, to Dr. Walter Pagel for his advice andhelpful criticism, and to Miss Y. Vincent for herphotography.
BIBLIOGRAPHYAHLSTROM, C. G., LIEDHOLM, K., and TRUEDSSON, E.
(1953), Acta. med. scand., 144, 323.ELLIS, M. (X955), Brit. med. 7., 1, 1251.FRIEDMANN, I. (I9SS), Y. Laryng., 69, 331.GODMAN, G. C., and CHURG, J. (1904), Arch. Path. (Chicago),
58, 533.HOWELLS, G. (i95S), J. Laryng., 69, 309.JOHNSON, S. (I948), Acta. path. microbiol. scand., 2S, 573.KLINGER, H. (I93I), Frankfurt. Z. Path., 42, 455.LINDSAY, S., AGGELER, P. M., and LUCIA, S. P. (1944),
Amer. 7. Path., 20, 1057.McCALLUM, A. G. (I9s4), J. LarYng., 68, 56o.PAGEL, W. (i9si), J. clin. Path., 4, I37.RICH, A. R., and GREGORY, J. E. (1942), Bull. 3ohns Hopkins
Hosp., 71,123.ROSE, G. (I956), personal communication.STRATTON, H. J. M., PRICE, T. M. L., and SKELTON, M. 0.
(1953), Brit. med. 3'., i, 127.WALTON, E. W., and LEGGATT, P. 0. (I956), Y. clin. Path.,
9, 31.WEGENER, F. (1936), Verh. dtsch. path. Ges., 29, 202.WEGENER, F. (1939), Beitr. path. Anat., i02, 36.ZEEK, P. M., SMITH, C. C., and WEETER, J. C. (1948), Amer.
.7. Path., 24, 889.
copyright. on A
ugust 26, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.33.378.199 on 1 A
pril 1957. Dow
nloaded from
Related Documents











