REVIEW Wearable and implantable pancreas substitutes Leonardo Ricotti • Tareq Assaf • Paolo Dario • Arianna Menciassi Received: 8 March 2012 / Accepted: 27 August 2012 Ó The Japanese Society for Artificial Organs 2012 Abstract A lifelong-implanted and completely auto- mated artificial or bioartificial pancreas (BAP) is the holy grail for type 1 diabetes treatment, and could be a definitive solution even for other severe pathologies, such as pan- creatitis and pancreas cancer. Technology has made several important steps forward in the last years, providing new hope for the realization of such devices, whose feasibility is strictly connected to advances in glucose sensor tech- nology, subcutaneous and intraperitoneal insulin pump development, the design of closed-loop control algorithms for mechatronic pancreases, as well as cell and tissue engineering and cell encapsulation for biohybrid pancre- ases. Furthermore, smart integration of the mentioned components and biocompatibility issues must be addressed, bearing in mind that, for mechatronic pancreases, it is most important to consider how to recharge implanted batteries and refill implanted insulin reservoirs without requiring periodic surgical interventions. This review describes recent advancements in technologies and concepts related to artificial and bioartificial pancreases, and assesses how far we are from a lifelong-implanted and self-working pancreas substitute that can fully restore the quality of life of a diabetic (or other type of) patient. Keywords Artificial pancreas Á Bioartificial pancreas Á Artificial organs Á Diabetes management Á Pancreas substitutes Introduction Type 1 diabetes (T1D) is one of the fastest growing diseases globally [1]. It is mainly caused by a loss of functionality of pancreatic b cells, resulting in a lack of insulin production. Recent technological advances have led to a paradigmatic shift in diabetes treatment, involving the introduction of automatic and semi-automatic systems to replace traditional procedures, and relying solely on multiple daily insulin injections. In particular, the dream of achieving a lifelong- implanted fully automated artificial or bioartificial pancreas (BAP) that can fully replace the functionality of the endo- crine pancreas represents the holy grail for T1D treatment [2]. Indeed, such a device could also represent a solution for other severe pancreas-related pathologies, such as pancrea- titis and pancreas cancer, but it necessarily entails formida- ble interdisciplinary efforts, as it involves engineering, biological, physical, and medical issues. The desire and demand for an automated artificial pan- creas (AP) was generated by the discovery of insulin in 1921, but only around 1980 did the first commercial insulin pumps appear on the market [3]. Artificial automated devices for controlling glucose levels started to appear on the market and evolved with the discovery and application of novel technologies that could be utilized in their com- ponents—insulin pumps, glucose sensors, and control algorithms. These elements are the three pieces of the L. Ricotti (&) Á P. Dario Á A. Menciassi (&) The Biorobotics Institute, Scuola Superiore Sant’Anna, Viale Rinaldo Piaggio 34, 56025 Pontedera (Pisa), Italy e-mail: [email protected] A. Menciassi e-mail: [email protected] T. Assaf Á P. Dario Center for Micro-BioRobotics@SSSA, Italian Institute of Technology, Pontedera (Pisa), Italy T. Assaf Bristol Robotics Laboratory, University of Bristol, Avon, Bristol BS34 8QZ, UK 123 J Artif Organs DOI 10.1007/s10047-012-0660-6

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

REVIEW
Wearable and implantable pancreas substitutes
Leonardo Ricotti • Tareq Assaf • Paolo Dario •
Arianna Menciassi
Received: 8 March 2012 / Accepted: 27 August 2012
� The Japanese Society for Artificial Organs 2012
Abstract A lifelong-implanted and completely auto-
mated artificial or bioartificial pancreas (BAP) is the holy
grail for type 1 diabetes treatment, and could be a definitive
solution even for other severe pathologies, such as pan-
creatitis and pancreas cancer. Technology has made several
important steps forward in the last years, providing new
hope for the realization of such devices, whose feasibility
is strictly connected to advances in glucose sensor tech-
nology, subcutaneous and intraperitoneal insulin pump
development, the design of closed-loop control algorithms
for mechatronic pancreases, as well as cell and tissue
engineering and cell encapsulation for biohybrid pancre-
ases. Furthermore, smart integration of the mentioned
components and biocompatibility issues must be addressed,
bearing in mind that, for mechatronic pancreases, it is most
important to consider how to recharge implanted batteries
and refill implanted insulin reservoirs without requiring
periodic surgical interventions. This review describes
recent advancements in technologies and concepts related
to artificial and bioartificial pancreases, and assesses how
far we are from a lifelong-implanted and self-working
pancreas substitute that can fully restore the quality of life
of a diabetic (or other type of) patient.
Keywords Artificial pancreas � Bioartificial pancreas �Artificial organs � Diabetes management � Pancreas
substitutes
Introduction
Type 1 diabetes (T1D) is one of the fastest growing diseases
globally [1]. It is mainly caused by a loss of functionality of
pancreatic b cells, resulting in a lack of insulin production.
Recent technological advances have led to a paradigmatic
shift in diabetes treatment, involving the introduction of
automatic and semi-automatic systems to replace traditional
procedures, and relying solely on multiple daily insulin
injections. In particular, the dream of achieving a lifelong-
implanted fully automated artificial or bioartificial pancreas
(BAP) that can fully replace the functionality of the endo-
crine pancreas represents the holy grail for T1D treatment
[2]. Indeed, such a device could also represent a solution for
other severe pancreas-related pathologies, such as pancrea-
titis and pancreas cancer, but it necessarily entails formida-
ble interdisciplinary efforts, as it involves engineering,
biological, physical, and medical issues.
The desire and demand for an automated artificial pan-
creas (AP) was generated by the discovery of insulin in
1921, but only around 1980 did the first commercial insulin
pumps appear on the market [3]. Artificial automated
devices for controlling glucose levels started to appear on
the market and evolved with the discovery and application
of novel technologies that could be utilized in their com-
ponents—insulin pumps, glucose sensors, and control
algorithms. These elements are the three pieces of the
L. Ricotti (&) � P. Dario � A. Menciassi (&)
The Biorobotics Institute, Scuola Superiore Sant’Anna,
Viale Rinaldo Piaggio 34, 56025 Pontedera (Pisa), Italy
e-mail: [email protected]
A. Menciassi
e-mail: [email protected]
T. Assaf � P. Dario
Center for Micro-BioRobotics@SSSA, Italian Institute
of Technology, Pontedera (Pisa), Italy
T. Assaf
Bristol Robotics Laboratory, University of Bristol,
Avon, Bristol BS34 8QZ, UK
123
J Artif Organs
DOI 10.1007/s10047-012-0660-6

mechatronic puzzle constituting the basis of a completely
artificial pancreas, the development of which is strictly
related to future advances in micro- and nanotechnologies.
In parallel, the idea of replacing the lost physiological
activity of b cells by directly replacing a living organ or a
portion of it has been around since 1966, when the first
pancreas transplantation was performed [4]. Great advan-
ces in the field of living cell- and tissue-based artificial
pancreas will strongly depend on new discoveries in the
fields of biomaterials, tissue engineering, and stem cell
technology. These will allow us to resolve the various
problems currently associated with the bioartificial
approach, with the aim of achieving a safe, long-term, and
effective pancreas substitute.
The following sections will highlight the current status of
scientific research concerning the artificial pancreas and
BAP platforms developed and tested so far, along with the
results achieved and the drawbacks related to each solution.
Furthermore, recent ideas and future perspectives on the
two mentioned strategies will be analyzed and discussed.
The present review aims to provide the reader with a wide-
ranging (but at the same time concise and clear) view of the
significant number of systems, technologies, and approa-
ches that are currently used to replace the functions of the
pancreas. In comparison with other recent review articles on
this topic, which normally focus on specific issues (e.g.,
pancreas or islet transplantation, glucose sensor technolo-
gies, insulin pump development, implantable artificial sys-
tems, etc.), our work aims to report and compare the main
advantages and drawbacks of all existing strategies based
on completely artificial components as well as cell- or tis-
sue-based bioartificial devices. This will allow researchers
in the field of artificial pancreases or BAPs to identify the
strong and weak points of each strategy, facilitating an
integrated vision of the problem that overcomes current
limitations through a multitechnological approach.
Insulin delivery
Insulin delivery is the first function that must be provided
by an AP. Insulin pumps, if inserted in a proper closed-loop
system, allow automatic insulin delivery when the patient’s
blood glucose level increases. Such delivery can be per-
formed according to three possible approaches: an intra-
venous route, subcutaneous insulin infusion (SCII), or
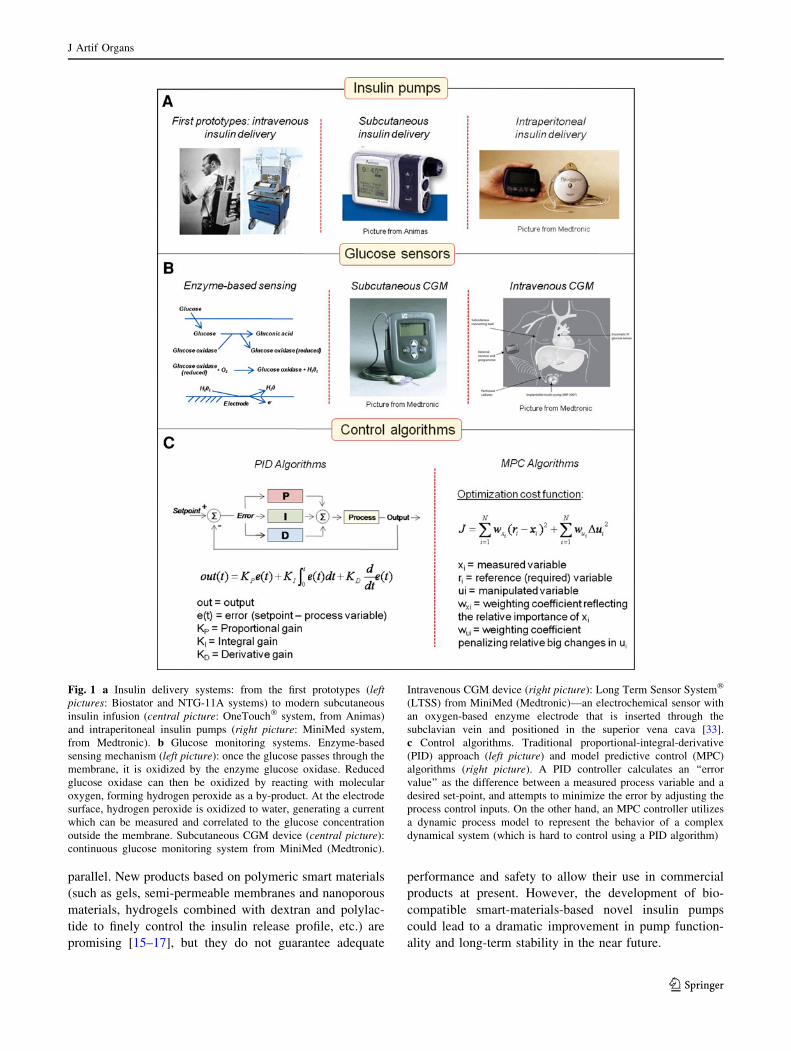
intraperitoneal insulin delivery (Fig. 1a).
History
The intravenous route was explored using implantable
insulin delivery devices from the 1970s up to the early
1990s [5], and good results were obtained in terms of the
restoration of near-normoglycemia, although some limita-
tions were also noted, which were mainly due to catheter
complications and blood clotting. This problem hindered
the further development of this route, such that other
methods became more favorable. SCII was introduced in
the late 1990s and is currently often used in insulin pump
therapy, even though it has many effectiveness and safety
issues due to delays in insulin absorption and action and
subcutaneously inserted catheter instability [6]. It has been
demonstrated that intraperitoneal insulin delivery allows
for more physiological plasma insulin profiles and more
stable implants, resulting in a dramatic reduction in severe
hypoglycemic events [7, 8].
Current trends
Current commercial pumps for subcutaneous insulin delivery
are small portable devices, and can even allow wireless
control of glycemic parameters. Examples are the IR 1200�,
OneTouch�, and Ping� insulin pumps from Animas Corpo-
ration [9], and the MiniMed Paradigm� REAL-Time Revel
System produced by Medtronic [10]. Implantable intraperi-
toneal insulin pumps are presently provided with a refillable
insulin reservoir. Refilling is a rather simple procedure that
involves inserting a syringe through the skin (by means of a
properly placed catheter) and delivering insulin into the
implanted device. An example is the Minimed 2007�
implantable insulin pump system from Medtronic.
Unsolved problems
As previously mentioned, the key issue with subcutaneous
insulin delivery remains the delay in action caused by the
time needed for subcutaneous absorption, resulting in late
insulin peaks that occur up to 120 min after the injection of
a subcutaneous bolus of regular insulin [11].
Concerning the intraperitoneal approach, the main lim-
itations are related to the high costs associated with this
technology, as well as surgical issues concerning intra-
peritoneal pump implantation and periodic substitution.
The clinical use of implantable programmable insulin
pumps has thus been limited, and there have even been
insulin aggregation issues [12] and increased production of
anti-insulin antibodies in some patients [13, 14] that have
impaired insulin action.
Future perspectives
Less invasive and cheaper implantable pumps for intra-
peritoneal insulin delivery have recently started to appear
on the market (e.g., DiaPort, Roche Diagnostics).
Mechanical insulin pumps have evolved in the last few
years, but alternative approaches have been investigated in
J Artif Organs
123
parallel. New products based on polymeric smart materials
(such as gels, semi-permeable membranes and nanoporous
materials, hydrogels combined with dextran and polylac-
tide to finely control the insulin release profile, etc.) are
promising [15–17], but they do not guarantee adequate
performance and safety to allow their use in commercial
products at present. However, the development of bio-
compatible smart-materials-based novel insulin pumps
could lead to a dramatic improvement in pump function-
ality and long-term stability in the near future.
Fig. 1 a Insulin delivery systems: from the first prototypes (leftpictures: Biostator and NTG-11A systems) to modern subcutaneous
insulin infusion (central picture: OneTouch� system, from Animas)
and intraperitoneal insulin pumps (right picture: MiniMed system,
from Medtronic). b Glucose monitoring systems. Enzyme-based
sensing mechanism (left picture): once the glucose passes through the
membrane, it is oxidized by the enzyme glucose oxidase. Reduced
glucose oxidase can then be oxidized by reacting with molecular
oxygen, forming hydrogen peroxide as a by-product. At the electrode
surface, hydrogen peroxide is oxidized to water, generating a current
which can be measured and correlated to the glucose concentration
outside the membrane. Subcutaneous CGM device (central picture):
continuous glucose monitoring system from MiniMed (Medtronic).
Intravenous CGM device (right picture): Long Term Sensor System�
(LTSS) from MiniMed (Medtronic)—an electrochemical sensor with
an oxygen-based enzyme electrode that is inserted through the
subclavian vein and positioned in the superior vena cava [33].
c Control algorithms. Traditional proportional-integral-derivative
(PID) approach (left picture) and model predictive control (MPC)
algorithms (right picture). A PID controller calculates an ‘‘error
value’’ as the difference between a measured process variable and a
desired set-point, and attempts to minimize the error by adjusting the
process control inputs. On the other hand, an MPC controller utilizes
a dynamic process model to represent the behavior of a complex
dynamical system (which is hard to control using a PID algorithm)
J Artif Organs
123

Glucose sensing
The second function of an AP is glucose measurement
(Fig. 1b). Many studies are currently focusing on contin-
uous glucose monitoring (CGM) and the development of
long-term-implantable subcutaneous, blood-stream, or
other kinds of glucose sensors. Such efforts are justified, as
glucose measurement is a key aspect of a closed-loop AP—
possibly the most challenging one.
History
Following the proposal, in 1967, of the first miniature
electrical transducer of glucose that could be implanted
into animals to monitor subcutaneous interstitial fluid
glucose continuously and remotely [18], electrochemical
biosensor-based glucose sensing evolved until the first
commercial CGM system, namely the CGMS�, was
developed by MiniMed [19, 20].
Concerning subcutaneously implantable sensors, despite
the fact that a considerable amount of technical effort has
been focused on this area, the good results obtained in in
vitro tests have not been replicated in vivo. In fact, after
implantation, the sensors exhibit a progressive loss of
function due to tissue reactions to the implanted device;
improvements in in vivo performance will be possible only
after a better understanding of the processes involved in
sensor inactivation has been gained [21].
Concerning glucose sensors placed directly in the blood
stream, chronic intravascular application of such sensors in
dogs revealed that they were stable for 7–108 days, and
that biocompatibility, enzyme lifetime, O2 availability, and
biochemical interference did not present a problem. Fur-
thermore, there was no need for recalibration during the
entire period of implantation [22]. This study highlighted
the potential for the longer-term application of this tech-
nology, thus suggesting its possible application in humans
by introducing a catheter-like sensor into the vena cava,
which would be retrieved and replaced every three months
in a nonsurgical procedure [23].
Current trends
Recently, some commercial sensors have been produced
by different companies and approved by the Food and Drug
Administration (FDA). These sensors include the Guardian�,
Guardian RT�, REAL-Time�, STS�, SEVEN PLUS�, and
FreeStyle Navigator�, whose accuracy was demonstrated in
several studies [24]. Developing a glucose sensor that is
designed to be implanted in the human body for long periods
may be the main challenge associated with the development
of a fully automated artificial pancreas, and current systems
are still quite far from achieving this goal.
Unsolved problems
Subcutaneously implanted sensors have inherent limita-
tions, as they measure the glucose concentration in inter-
stitium rather than blood. During rapidly changing
conditions (e.g., after a meal or during a hypoglycemic
episode), interstitial glucose and blood glucose can be
markedly different [25–27]. Therefore, CGM subcutaneous
devices require periodic calibration using multiple daily
blood glucose samples. Such calibration influences the
accuracy of CGM [28]. Clinical data acquired by Zucchini
et al. [29] recently highlighted that SCII is much more
effective than therapy based on sensor-augmented multiple
daily injections, although SCII does have some drawbacks
(e.g., mild hypoglycemic episodes can occur). In general,
despite such limitations, the current accuracy of subcuta-
neous CGM devices is considered adequate for AP closed-
loop control. In fact, this kind of sensor recently showed
only short physiological time lags (*3.28 min) in blood
glucose level detection during in silico trials [30], while
clinical trials revealed good accuracy when compared with
gold standard laboratory measurements [31]. However,
further advances in subcutaneous glucose sensor technol-
ogy (as well as in control algorithms) are needed before
they can be safely used for closed-loop glycemic control.
Since the concept of a glucose sensor that is directly
placed in the blood stream was first introduced by Gough
and Armour in 1995, no dramatic advances in this kind of
glucose sensor have occurred: intravenous blood glucose
recording is not yet the gold standard or the most useful
approach for controlling insulin pumps. This is mainly due
to concerns over patient safety due to the possibility of clot
formation or vascular wall damage [32, 33].
Future perspectives
Despite their inherent limitations, CGM devices produce
rich data sets with frequent sampling (e.g., every
5–10 min), allowing them to serve as AP-enabling tech-
nology. Future CGM devices will display to patients their
rate of change in blood glucose in real time, alerting them
to potential upcoming episodes of hypo- or hyperglycemia.
Furthermore, technological advances and the use of micro-
and nanostructured functionalized smart materials will
lead to improvements in glucose sensor lifetime and
performances.
Closed-loop control
The third componentthat is needed by an AP is an auto-
mated control unit that uses algorithms which acquire
sensor input and generate treatment outputs (Fig. 1c). An
J Artif Organs
123

important aspect to consider is that an ‘‘automated’’ closed-
loop pancreas cannot approach the complexity of the native
human endocrine pancreas, which continuously takes data
from substrates, hormones, paracrine compounds, and
autonomic neural inputs and secretes hormones in
response. However, the perspectives for blood glucose
control in T1D patients have improved considerably in the
last few years.
Treatments based on multiple daily injections or con-
tinuous insulin infusion based on an open-loop approach
are associated with short- and long-term risks, as their
tendency to produce abnormally high or low glucose levels
is quite high. These approaches require human intervention
and a precise knowledge of the patient’s lifestyle (meals,
sport plans, etc.). The substantial advantage of closed-loop
control in the treatment of T1D is the opportunity to
decouple the treatment (which becomes automated) from
the patient’s daily life, but it also helps to reduce severe
complications, such as retinopathies, cardiovascular prob-
lems, and kidney failure. A purely closed-loop control
scheme determines whether to instantaneously deliver
insulin on the basis of CGM signal alone, but its use can
result in delays to the action of insulin on plasma glucose,
implying that corrections to the desired glucose levels may
arrive too late to prevent hyper- or hypoglycemic episodes.
History
It has been pointed out that a trade-off between nocturnal
regulation based on mild control actions and postprandial
regulation, characterized by prompt and energetic correc-
tion, must be achieved [34]. This can be done by means of
a closed-loop glucose control scheme combining feedfor-
ward and feedback actions [35], thus allowing prompt
compensation for meals (through the feedforward bolus) to
be coupled with the robustness of closed-loop control that
can adapt to unpredicted events, disturbances, and changes
in the patient’s dynamics. The deployment of a controller,
especially a closed-loop one, relies heavily on mathemat-
ical models. It is therefore clear that proper models of
glucose and insulin dynamics, as well as models that can be
used to predict near-future metabolic behavior, are man-
datory. Minimal models (describing the key components of
system functionality) and maximal models (nonlinear,
high-order models that provide a comprehensive descrip-
tion of metabolic regulation and include a large number of
parameters) have been well reviewed by Cobelli et al. [36],
who also described how to apply them in the most common
control strategies for AP development. Control algorithms
for AP applications have been also reviewed in [37–39].
Proportional-integral-derivative (PID) algorithms that are
used in industrial settings have also been used for closed-
loop controls. It has also been argued that the pancreatic
islets are actually controlled by proportional, derivative,
and integral factors [40]. While the PID approach is rela-
tively straightforward, and is able to mimic many typical
islet response phases using its three components, system
optimization is often difficult, with manual tuning required.
A drastically different approach is implemented by
model predictive control (MPC) algorithms, which rely on
the use of an internal model to predict future outcomes
based on past and current states and a mathematical model
called cost function minimization. This approach makes it
possible to find a sequence of control inputs that will lead
to the desired future outcomes.
Current trends
Many modern MPC algorithms are based on the minimal
model of glucose Kinetics, developed by Bergman et al.
[41] in 1979, and they represent a good solution for the
principal AP control dilemma: finding a trade-off between
slow-paced regulation, which is well suited to mild control
actions that can be applied to a quasi-steady state (e.g.,
overnight), and postprandial regulation, which calls for
prompt and energetic correction [42].
MPC has shown to be suitable for multivariate nonlinear
systems such as the human body, and it gives demonstrably
better performances than PID control with patient-specific
fine-tuned gains [43]. Nonlinear model predictive control
(NMPC) or linear model predictive control (LMPC) algo-
rithms can be used, and several successful clinical trials
using MPC were recently published [44–47]. MPC also
allows individualization using patient-specific parameters
[48].
Unsolved problems
The PID approach has inherent limitations due to
unavoidable time lags in glucose sensing (especially via the
subcutaneous route) and insulin action.
MPC algorithms are promising tools, but they face addi-
tional difficulties. One is inter- and intrapatient variability.
Fortunately, MPC algorithms can be ‘‘personalized’’ using
patient-specific model parameters. Another challenge is the
need to provide the algorithm with certain feedforward
capabilities—the ability to use a combination of feedforward
(e.g., patient-initiated) and feedback (controller-initiated)
insulin delivery—to address the dilemma of finding a suit-
able trade-off between slow-paced regulation in a quasi-
steady state and prompt correction for meals.
Future perspectives
Advanced MPC algorithms represent a promising solution
for closed-loop APs, above all due to the ability to set their
J Artif Organs
123

parameters in a patient-specific manner, thus overcoming
the issue of patient variability. Novel technologies are also
emerging, such as fuzzy logic algorithms and advanced
neural networks, which could foster the development of
effective and safe fully automated APs.
Totally artificial implantable pancreas
History
The first attempt to build an automated device to control
human blood glucose dates back to 1964: the concept was
based on continuous blood glucose sensing and delivering
insulin through a servomotor, as controlled by an ‘‘on–off’’
algorithm [49]. Obviously, such an approach was too
simplistic to provide good glycemic control, but this study
established many of the technical methods used by artificial
pancreas developers during the subsequent decade.
After this pioneering study, researchers continued to
tackle the technological challenge of creating an artificial
pancreas substitute, and good results were achieved around
1980 with the development of the Biostator (Ames Divi-
sion, Miles Laboratories, Elkhart, IN, USA), a device
combining a glucose oxidase membrane-based sensor for
CGM and a simple proportional-derivative algorithm to
control intravenous insulin delivery [50, 51]. The Biostator
was far from being an implantable device due to its bulk-
iness, limitations of the control algorithm, as well as a
problem with pump-induced insulin aggregation. STG-11A
and STG 22 (Nikkiso, Tokyo, Japan) were two bedside-
type commercial APs developed in the same period. These
consisted of an extracorporeal intravenous glucose sensor
with a blood-sampling double-lumen catheter, a propor-
tional-derivative control algorithm, and an intravenous
insulin and glucose delivery system. These devices were
used by Hoshino et al. [52, 53], who placed the glucose
sensor in the superior vena cavae of acutely ill severe
patients with glucose intolerance. However, the bulkiness
of these devices did not allow a normal lifestyle, as the
patient was obliged to lay in bed in order to monitor his/her
glycemia. Over the following 30 years, insulin pumps and
glucose sensors became smaller and more portable, thus
bringing such devices closer to the ideal of wearable or
implanted APs [54–60] (Table 1).
Current trends
Wearable systems have evolved considerably over the last
decade, and many commercial devices have been pro-
duced. In the framework of the project ADICOL
(ADvanced Insulin infusion using a COntrol Loop), funded
by the European Commission from 2000 to 2003, a wear-
able AP was developed which combined a microdialysis
system for sampling interstitial fluid (open flow microp-
erfusion) with an enzymatic sensor for measuring the fluid
glucose concentration and a closed-loop SCII, controlled
by an MPC algorithm [61, 62]. During 2008 and 2009, the
first multinational study comparing the use of a closed-loop
control artificial pancreas to state-of-the-art open-loop
therapy in adult T1D patients was completed [63]. A sub-
cutaneous glucose sensor (Freestyle Navigator�) detected
glycemia and sent the data to an MPC algorithm, actuating
a subcutaneous insulin pump (Deltec Cozmo). The trials
suggested that closed-loop delivery of insulin improved
overnight control of glucose levels and reduced the risk of
nocturnal hypoglycemia in comparison with traditional
insulin pump therapy. More recently, Bruttomesso et al.
[64] combined subcutaneous glucose sensing and contin-
uous SCII, as contolled with an MPC algorithm, for the
treatment of T1D patients in both Padova and Montpellier.
In particular, a Freestyle Navigator� CGM system and an
Omnipad� insulin pump were applied in each trial, and
resulted in good control of glycemia in the tested patients.
The safety and efficacy of overnight closed-loop insulin
delivery in comparison with traditional ‘‘open-loop’’ insu-
lin pump therapy in adult T1D patients was also demon-
strated by Hovorka et al. [65] in 2011, using again a
Freestyle Navigator� glucose sensor and a Deltec Cozmo
insulin pump.
Table 1 Representative artificial pancreas systems and their characteristics
Artificial pancreas type Glucose sensing method Control algorithm Insulin delivery system Tested on References
Bedside Intravenous PD Intravenous Humans [50–53]
Wearable Interstitial MPC Subcutaneous Humans [61, 62]
Wearable Subcutaneous MPC Subcutaneous Humans [63–65]
Partially implanted Intravenous MPC Subcutaneous Pigs [67]
Partially implanted Intravenous MPC Subcutaneous Humans [68]
Partially implanted Subcutaneous PID Intraperitoneal Humans [69]
Totally implanted Intravenous PD Intraperitoneal Humans [66]
AP artificial pancreas, PD proportional-derivative control, PID proportional-integral-derivative control, MPC model predictive control
J Artif Organs
123

Implanted AP development would surely represent a
more challenging approach. Renard et al. [66] reported the
results obtained with a closed-loop system called the Long
Term Sensor System�, consisting of an intravenous long-
term enzymatic sensor, an implantable insulin pump
delivering insulin into the peritoneum, and a controller
with a PD algorithm. There was no harmful complication
related to the implants for an average duration of nine
months, and this remains the only closed-loop system to
utilize intravenous sensing and intraperitoneal insulin
delivery to date. Although this study demonstrated the
feasibility of a fully implantable AP, it also highlighted the
need to improve sensor structure, increase longevity, and
decrease sensor delay, effecting closed-loop control at meal
times. A bihormonal closed-loop system for glucose con-
trol was tested in 2009 by El-Khatib et al. [67] on thirteen
diabetic pigs. Blood glucose was sampled through an
implanted sensor in the vena cava, while insulin and glu-
cagon were provided subcutaneously by means of a 6 mm
cannula (Quick-set, Minimed Medtronic), and a generalized
predictive control (GPC) algorithm was implemented. The
study revealed the feasibility of bihormonal closed-loop
glycemic regulation using an implanted glucose detection
unit. The same group performed a similar study in humans
in 2010, using an intravenous blood glucose monitoring
system, a subcutaneous insulin and glucagon pump, and a
customized MPC algorithm [68], obtaining good results in
glycemic regulation. A subcutaneous glucose sensor and an
intraperitoneal insulin pump were used by Renard et al. [69]
in 2010 to test a new partially implanted AP model. This
approach developed from the observation that subcutaneous
insulin delivery from a portable pump guided by a subcu-
taneous glucose sensor encountered delays and variability
in insulin absorption. An implanted pump was therefore
tested (MMT-2007D, Medtronic) on eight adult T1D
patients for at least three months; the pump was controlled
by a PID algorithm receiving glycemic data from a subcu-
taneous glucose sensor (CGMS�, Medtronic). Results
demonstrated the feasibility of such an approach, and
encouraged further studies.
Unsolved problems
Together with other factors, the limited success of present
closed-loop wearable artificial pancreases is related to
psychological aspects, which have been demonstrated to be
a key issue in therapy success [70]. The present paradigm
for closed-loop artificial pancreases is based on glycemia
detection by means of subcutaneous glucose sensors and
insulin delivery by means of subcutaneous insulin pumps.
This implies the need for portable external devices, as well
as periodic replacement of catheters. A T1D patient is
therefore obliged to constantly pay attention to such
devices, avoiding certain daily life behaviors or modifying
them (sporting activity, showers, etc.). Furthermore, car-
rying devices (or transcutaneous gate accesses) on the body
can lead to body image issues, causing negative feelings of
shame and embarrassment (an especially important factor
in children and adolescents [71]). This goes against the aim
of an artificial pancreas—to fully replace the lost pancre-
atic functionality, allowing the patient to forget his/her
pathology and thus to fully restore their quality of life.
The main obstacle to the development of a working and
safe implantable AP is the current status of glucose sensors,
which are insufficiently accurate and cannot ensure long-
term stability. Furthermore, the following three main
complex implantability-related problems need to be
addressed: recharging the battery of the implanted device,
long-term insulin stability in the implanted reservoir, and
refilling the implanted insulin reservoir without the need
for periodic surgical interventions and possibly without
transcutaneous implanted gate accesses.
Infection-related issues
Modern medicine often takes advantage of an increasing
number of implantable medical devices, but their benefits
can be attenuated by the morbidity, mortality, and expense
associated with implant-derived infections. The presence of
foreign bodies in patients lowers their threshold to bacterial
infection and generates local immunosuppression. Oppor-
tunistic microorganisms can thus exploit this weakening in
the patient’s defenses. Furthermore, bacteria initially
adsorb onto the implant surface, often forming an adherent
biofilm that exhibits increased protection from host
defenses and enhanced resistance to antibiotic treatments
[72, 73]. Invasive medical implants, when infected, can
actually result in resistant chronic infections or tissue
necrosis. The design and development of a long-term-
implantable artificial pancreas must face these issues and
provide approaches that reduce or eliminate infections of
the implanted device.
Much research effort is currently focused on developing
strategies to prevent biofilm formation, including physio-
chemical modification of the biomaterial surface to create
antiadhesive surfaces, the incorporation of antimicrobial
agents into medical device polymers, mechanical design
alternatives, and the release of antibiotics. Biosurfactants
have also been reported to be a promising strategy, as they
effectively inhibit bacterial adhesion and retard biofilm
formation. Important recent reviews on this topic can be
found in [74, 75].
Bloom et al. reported interesting results concerning the
implantation of electronic devices using an antibacterial
envelope. This system was a polymer mesh that was able to
release two antibiotics (minocycline and rifampin) after
J Artif Organs
123

implantation, thus reducing the risk of infection [76]. The
use of protective envelopes in this manner could even be a
good solution for the implantation of an artificial pancreas,
but the device itself could be built from functionalized
materials that are able to release antimicrobial agents in a
controlled way, as suggested in recent literature [77–79].
Xu and Siedlecki [80] also suggested that certain nano-
structured surfaces can prevent bacterial adhesion, so
introducing patterned surface texturing could provide an
effective means to reduce biofilm formation and implant-
associated infections.
In the future, it is hoped, the sensitivity and accuracy of
new emerging methods such as those based on mass
spectroscopy [PCR-electrospray ionization (Ibis) and
matrix-assisted laser desorption ionization coupled with
time-of-flight analysis (MALDI-TOF)] for the diagnosis of
bacterial infections will be demonstrated in depth. These
improvements in diagnosis should be coupled with
advanced control strategies: anti-infective or infection-
resistant materials, biofilm agent disaggregation, comple-
mentary therapies, vaccines, and other preventive measures
resulting from progress in our knowledge of pathogenesis
and molecular epidemiology, which could revolutionize the
treatment of implant infections [81].
Future perspectives
Progress in AP development is expected to rely partly on
the outpatient setting. This step would require specific
elements, such as a server and communication tools for
remote monitoring as well as remote intervention. How-
ever, the dream is to achieve a fully automated closed-loop
long-term artificial system that is able to fully (i.e., no loss
of quality) replace endocrine pancreatic functionality for
the entire remaining lifetime of the patient. This ambitious
objective may be feasible in the not-so-distant future due to
novel and emerging technologies (micro- and nanotech-
nologies, novel biomaterials, miniaturized sensors and
actuators, etc.) that, if combined appropriately, would
allow the development of APs with unprecedented
performance.
The biohybrid approach
History
The path for research into pancreatic islet transplantation
was paved by the discovery of a collagenase-based method
of isolating islets [82], while the first examples of islet
transplantation—which made it possible to reverse diabetes
in rodents and primates—appeared in 1973 and 1975,
respectively [83, 84].
In 2001, a ground-breaking paper on human islet allo-
transplantation was published, describing the use of a novel
immunosuppressive regimen together with improved islet
isolation methods [85]. This technique yielded excellent
results and became the preferred islet transplantation
method for diabetic patients.
A smart alternative to transplantation procedures is
represented by bioartificial organs, which contain cells or
cell clusters within a synthetic biocompatible semiperme-
able membrane, thus separating the foreign tissue from the
host’s immune system [86, 87]. BAPs fully mimic the
behavior and function of a healthy pancreas, eliminating
the need for immunosuppressing drugs. The biocompatible
membrane allows the viability and functionality of cells to
be retained by providing them with access to nutrients,
oxygen, and stimulatory agents, while it also prevents
immune cells and antibodies (which have relatively high
molecular weights) from crossing the membrane. This can
be achieved by tailoring the membrane pore size appro-
priately. Several different BAP models have been studied
over the last few decades, but to be accepted as an alter-
native therapy a model must be biocompatible, its mem-
brane must exhibit good diffusional properties, the device
must be easy to retrieve or biodegradable, and it must be
able to maintain cell viability and functionality for long
periods of time. An extensive review of biocompatible
materials used in BAP devices is provided by [88].
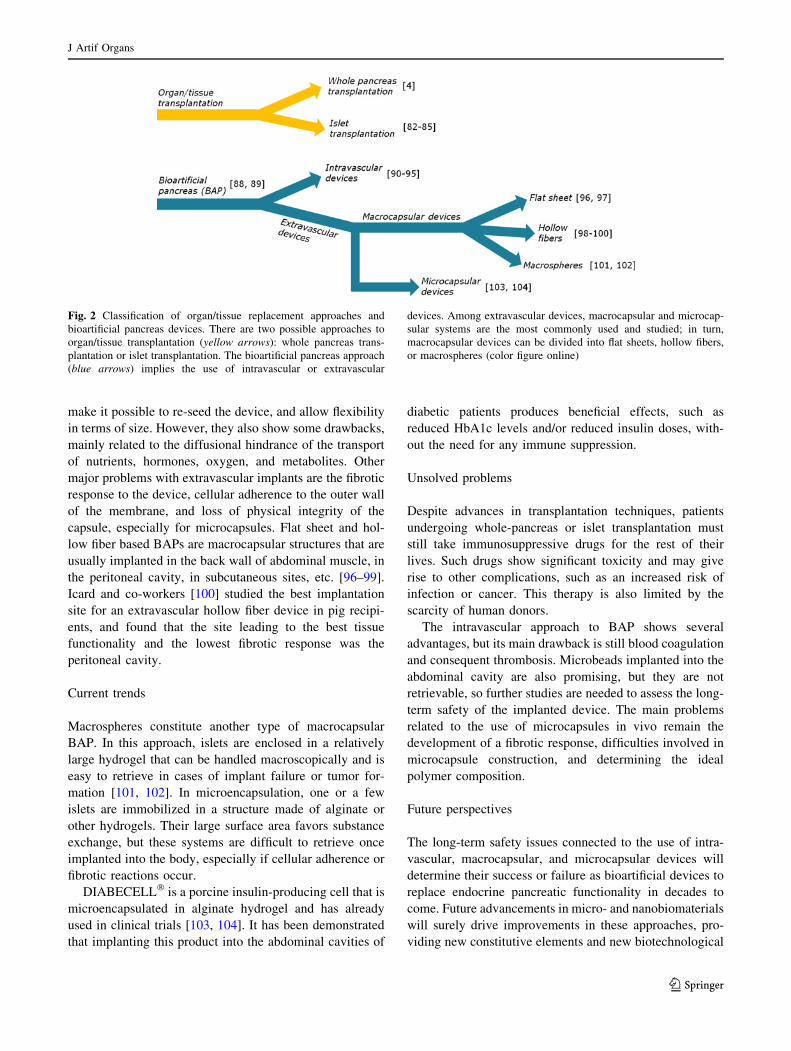
An overview of BAP classification is shown in Fig. 2.
Devices are mainly divided into two groups: intravascular
and extravascular devices. Intravascular devices are usually
made of hollow fiber membranes, and are blood perfusion
systems, inserted as an artery-to-vein shunt in the reci-
pient’s body [89]. Significant results were obtained by
Monaco et al., who used a device consisting of two con-
centric tubular membranes with one end anastomosed to an
artery and the other to a vein. The blood was allowed to
perfuse the lumen of the inner membrane, allowing the
transport of oxygen, nutrients, and signaling molecules to
the cells, which were placed in the annular space between
the two membranes [90]. Other similar devices were
transplanted in vivo into dogs [91, 92], and ex vivo into
monkeys [93, 94]. While the ex vivo implants showed good
functionality for several months, in vivo grafts never lasted
more than a few days, mainly due to blood coagulation
which led to to thrombosis. More recently, Ikeda et al. [95]
developed a new intravascular BAP that showed good
blood glucose control in pancreatectomized pigs, but strong
anticoagulation treatment was still necessary.
Extravascular BAPs can be classified into macrocap-
sular and microcapsular systems. Both approaches show
some advantages when compared with their intravascular
counterparts: they lead to a smaller risk from surgical
implantation, are easier to retrieve (for macrocapsules),
J Artif Organs
123
make it possible to re-seed the device, and allow flexibility
in terms of size. However, they also show some drawbacks,
mainly related to the diffusional hindrance of the transport
of nutrients, hormones, oxygen, and metabolites. Other
major problems with extravascular implants are the fibrotic
response to the device, cellular adherence to the outer wall
of the membrane, and loss of physical integrity of the
capsule, especially for microcapsules. Flat sheet and hol-
low fiber based BAPs are macrocapsular structures that are
usually implanted in the back wall of abdominal muscle, in
the peritoneal cavity, in subcutaneous sites, etc. [96–99].
Icard and co-workers [100] studied the best implantation
site for an extravascular hollow fiber device in pig recipi-
ents, and found that the site leading to the best tissue
functionality and the lowest fibrotic response was the
peritoneal cavity.
Current trends
Macrospheres constitute another type of macrocapsular
BAP. In this approach, islets are enclosed in a relatively
large hydrogel that can be handled macroscopically and is
easy to retrieve in cases of implant failure or tumor for-
mation [101, 102]. In microencapsulation, one or a few
islets are immobilized in a structure made of alginate or
other hydrogels. Their large surface area favors substance
exchange, but these systems are difficult to retrieve once
implanted into the body, especially if cellular adherence or
fibrotic reactions occur.
DIABECELL� is a porcine insulin-producing cell that is
microencapsulated in alginate hydrogel and has already
used in clinical trials [103, 104]. It has been demonstrated
that implanting this product into the abdominal cavities of
diabetic patients produces beneficial effects, such as
reduced HbA1c levels and/or reduced insulin doses, with-
out the need for any immune suppression.
Unsolved problems
Despite advances in transplantation techniques, patients
undergoing whole-pancreas or islet transplantation must
still take immunosuppressive drugs for the rest of their
lives. Such drugs show significant toxicity and may give
rise to other complications, such as an increased risk of
infection or cancer. This therapy is also limited by the
scarcity of human donors.
The intravascular approach to BAP shows several
advantages, but its main drawback is still blood coagulation
and consequent thrombosis. Microbeads implanted into the
abdominal cavity are also promising, but they are not
retrievable, so further studies are needed to assess the long-
term safety of the implanted device. The main problems
related to the use of microcapsules in vivo remain the
development of a fibrotic response, difficulties involved in
microcapsule construction, and determining the ideal
polymer composition.
Future perspectives
The long-term safety issues connected to the use of intra-
vascular, macrocapsular, and microcapsular devices will
determine their success or failure as bioartificial devices to
replace endocrine pancreatic functionality in decades to
come. Future advancements in micro- and nanobiomaterials
will surely drive improvements in these approaches, pro-
viding new constitutive elements and new biotechnological
Fig. 2 Classification of organ/tissue replacement approaches and
bioartificial pancreas devices. There are two possible approaches to
organ/tissue transplantation (yellow arrows): whole pancreas trans-
plantation or islet transplantation. The bioartificial pancreas approach
(blue arrows) implies the use of intravascular or extravascular
devices. Among extravascular devices, macrocapsular and microcap-
sular systems are the most commonly used and studied; in turn,
macrocapsular devices can be divided into flat sheets, hollow fibers,
or macrospheres (color figure online)
J Artif Organs
123

strategies to overcome the problems of thrombosis, fibrotic
response, and other unwanted body reactions to implanted
devices. In the near future, microelectromechanical systems
(MEMS) could also be integrated into bioartificial devices to
monitor cell status (by means of miniaturized sensors) or to
interfere with cell activity (via properly designed actuators).
This could allow the potential of a mechatronic approach
within a BAP to be exploited.
Recent ideas and promising technologies
Recent advances in micro- and nanotechnologies, together
with the development of new smart materials and plat-
forms, have allowed new generations of APs, BAPs, and
components to be developed.
If we consider artificial insulin pumps, some examples
include the polymer alloy membrane-based insulin pump
proposed by Uchiyama et al. [105] and the thin film Nitinol
pumps presented by Schetky et al. [106]. Recent approa-
ches to glucose sensing are represented, for instance, by
noninvasive measurements performed using near-infrared
spectroscopy [107], the novel highly responsive needle-
type sensor proposed by Ichimori et al. [108] and based on
polyimide, and the enzyme-free sensor developed by
Yoshimi and co-workers [109] using the gate effect of a
molecularly imprinted polymer. Research is also pro-
gressing in the field of control algorithms, with the gen-
eration of novel approaches such as adaptive, fuzzy logic,
and neural network based algorithms, with the aim being to
control blood glucose through automatic self-ameliorating
methods [110–112].
Recently, a new invention proposed a new implantable
AP with a wireless battery recharging system and a
noninvasive strategy for refilling the insulin reservoir based
on swallowing polymeric capsules [113]. Figure 3 depicts
this system.
A wireless energy transfer system exploiting nonradiative
energy transfer allows the implanted battery to be recharged
by simply wearing a belt (for example, overnight), [114,
115], while the insulin reservoir is refilled by swallowing
sensorized capsules. The system requires careful consider-
ation of surgical and long-term biocompatibility issues, but
those aside, it represents an interesting trade-off in the
development of a self-working implantable AP that can
completely restore T1D patients’ quality of life.
This technology could also open novel avenues for the
treatment of critically ill patients affected by other meta-
bolic pathologies, such as impaired glucose tolerance
(IGT), type 2 diabetes, and the combination of medical
disorders known as metabolic syndrome in general. The
possibility of implanting a reliable, lifelong-implanted
organ that is able to deliver specific substances, when
needed, into the peritoneal cavity or directly into the
bloodstream would allow closed-loop continuous drug
treatment capable of countering or even preventing the
negative effects of these metabolic alterations.
Concerning BAP evolution, progress in nanotechnology
will surely encourage the development of microencapsu-
lation techniques and membrane preparation, allowing
more precise control over pore size, and nanoscale-pat-
terned surfaces that permit selective adhesion of proteins or
signaling molecules. Together with advances in biocom-
patible materials, this will lead to enhanced safety and
functionality of implanted devices. Furthermore, future
insights into iPS cell differentiation will allow researchers
to obtain pancreatic-like tissue that functions in vitro and
can be used in combination with retrievable BAPs.
Fig. 3 The implantable and refillable artificial pancreas architecture
[113]. A sensorized insulin capsule, once swallowed, reaches the
docking system at the stomach wall and docks with it. Insulin is then
transferred from the capsule to the implanted insulin reservoir. A
glucose sensor triggers the closure of the control loop with an
intraperitoneal insulin pump; an external receiver allows the status of
the implanted device to be monitored; and an external charging belt
allows wireless recharging of the implanted batteries
J Artif Organs
123

Conclusions
In the last few decades, considerable research effort has
been focused on two different approaches with the same
final aim: to restore the quality of life of diabetic patients
and, in general, of patients suffering from pancreas-related
pathologies. These two approaches are to develop a totally
artificial mechatronic wearable or implanted system or to
realize a bioartificial device containing insulin-producing
living cells. In this review, recent progress and scientific
advances in these two directions have been reported and
discussed, highlighting the advantages and drawbacks of
each strategy. The main bottleneck in the development of a
working and safe AP is represented by glucose sensors,
which are not yet sufficiently accurate and stable over the
long term to be used in APs. Furthermore, for implantable
APs, insulin stability, charging the battery of the implanted
device, and refilling the implanted insulin reservoir without
the need for periodic surgical interventions and possibly
without transcutaneous implanted gate accesses are the
other main issues to address. Also, none of the BAP
devices developed so far have managed to reduce the
associated fibrotic response to acceptable (i.e., negligible)
levels. Furthermore, diffusional limitations imposed by the
encapsulating material and the capsule size are crucial
issues to graft success. The use of new biomaterials and
new microcapsular designs have been attempted with some
degree of success, but BAPs still need considerable
improvement before they can be accepted routinely in the
clinical setting. Recent ideas in and future perspectives on
this field of research have been also described in this paper,
which has attempted to envision the directions that future
research efforts will take.
Acknowledgments The authors are deeply grateful to Professor
Claudio Cobelli, whose precious suggestions were of primary
importance during the preparation of this review article.
References
1. Onkamo P, Vaananen S, Karvonen M, Tuomilehto J. Worldwide
increase in incidence of type I diabetes—the analysis of the data
on published incidence trends. Diabetologia. 1999;42:1395–403.
2. Howorka R, Wilinska ME, Chassin LJ, Dunger DB. Roadmap to
the artificial pancreas. Diabetes Res Clin Pract. 2006;74:S178–82.
3. Steil GM, Panteleon AE, Rebrin K. Closed-loop insulin deliv-
ery—the path to physiological glucose control. Adv Drug Deliv
Rev. 2004;56:125–44.
4. Kelly WD, Lillehei RC, Merkel FK, Idezuki Y, Goetz FC.
Allotransplantation of the pancreas and duodenum along with
the kidney in diabetic nephropathy. Surgery. 1967;61:827–37.
5. Selam JL, Charles MA. Devices for insulin administration.
Diabetes Care. 1990;13:955–79.
6. Renard E. Insulin delivery route for the artificial pancreas:
subcutaneous, intraperitoneal, or intravenous? Pros and cons.
J Diab Sci Tech. 2008;2:735–8.
7. Broussolle C, Jeandidier N, Hanaire-Broutin H. French multi-
centre experience with implantable insulin pumps. The EVA-
DIAC Study Group. Lancet. 1994;343:514–5.
8. Renard E, Place J, Cantwell M, Chevassus H, Palerm CC.
Closed-loop insulin delivery using a subcutaneous glucose
sensor and intraperitoneal insulin delivery. Diabetes Care.
2010;33:121–7.
9. Animas� Corporation. Insulin pump product information
(updated March 8, 2012). http://www.animas.com.
10. Medtronic, Inc. Insulin pump product information (updated
March 8, 2012). http://www.medtronic.com.
11. Pickup J, Keen H. Continuous subcutaneous insulin infusion at
25 years: evidence base for the expanding use of insulin pump
therapy in type 1 diabetes. Diabetes Care. 2002;25:593–8.
12. Renard E, Bouteleau S, Jacques-Apostol S, Lauton D, Gibert-
Boulet F, Costalat G, Bringer J, Jaffiol C. Insulin underdelivery
from implanted pumps using peritoneal route. Diabetes Care.
1996;19:812–7.
13. Olsen CL, Chan E, Turner DS. Insulin antibody responses after
long-term intraperitoneal insulin administration via implantable
programmable insulin delivery systems. Diabetes Care.
1994;17:169–76.
14. Renard E, Costalat G, Chevassus H, Bringer J. Artificial beta-
cell: clinical experience toward an implantable closed-loop
insulin delivery system. Diab Metabol. 2006;32:497–502.
15. LaVan DA, McGuire T, Langer R. Small-scale systems for in
vivo drug delivery. Nat Biotechnol. 2003;21:1184–91.
16. Adiga SP, Curtiss LA, Elam JW, Pellin MJ, Shih CC, Shih CM,
Lin SJ, Su YY, Gittard SD, Zhang J, Narayan RJ. Nanoporous
materials for biomedical devices. J Min Met Mater Soc.
2008;60:26–32.
17. Cabral J, Moratti SC. Hydrogels for biomedical applications.
Future Med Chem. 2011;3:1877–88.
18. Updike SJ, Hicks GP. The enzyme electrode. Nature.
1967;214:986–8.
19. Mastrotaro JJ. The MiniMed continuous glucose monitoring
system (CGMS). J Pediatr Endocrinol Metab. 1999;12:751–8.
20. Mastrotaro JJ. The MiniMed continuous glucose monitoring
system. Diabetes Technol Ther. 2000;2:S13–8.
21. Gerritsen M, Jansen JA, Lutterman JA. Subcutaneously
implantable glucose sensors in patients with diabetes mellitus;
still many problems. Ned Tijdschr Geneeskd. 2002;146:1313–6.
22. Armour JC, Lucisano JY, McKean BD, Gough DA. Application
of chronic intravascular blood glucose sensor in dogs. Diabetes.
1990;39:1519–26.
23. Gough DA, Armour JC. Development of the implantable glu-
cose sensor. What are the prospects and why is it taking so long?
Diabetes. 1995;44:1005–9.
24. Skyler JS. Continuous glucose monitoring: an overview of its
development. Diabetes Technol Ther. 2009;11:S5–10.
25. Rebrin K, Steil GM, Van Antwerp WP, Mastrotaro JJ. Subcu-
taneous glucose predicts plasma glucose independent of insulin:
implications for continuous monitoring. Am J Physiol.
1999;277:E561–71.
26. Rebrin K, Steil GM. Can interstitial glucose assessment replace
blood glucose measurements? Diabetes Technol Ther.
2000;2:461–72.
27. Steil GM, Rebrin K, Hariri F, Jinagonda S, Tadros S, Darwin C,
Saad MF. Interstitial fluid glucose dynamics during insulin-
induced hypoglycaemia. Diabetologia. 2005;48:1833–40.
28. Buckingham BA, Kollman C, Beck R, Kalajian A, Fiallo-
Scharer R, Tansey MJ, Fox LA, Wilson DM, Weinzimer SA,
Ruedy KJ, Tamborlane WV. Evaluation of factors affecting
CGMS calibration. Diabetes Technol Ther. 2006;8:318–25.
29. Zucchini S, Scipione M, Balsamo C, Maltoni G, Rollo A,
Molinari E, Mangoni L, Cicognani A. Comparison between
J Artif Organs
123
sensor-augmented insulin therapy with continuous subcutaneous
insulin infusion or multiple daily injections in everyday life:
3-day analysis of glucose patterns and sensor accuracy in chil-
dren. Diabetes Technol Ther. 2011;13:1187–93.
30. Keenan DB, Grosman B, Clark HW, Roy A, Weinzimer SA,
Shah RV, Mastrotaro JJ. Continuous glucose monitoring con-
siderations for the development of a closed-loop artificial pan-
creas system. J Diabetes Sci Technol. 2011;5:1327–36.
31. Keenan DB, Mastrotaro JJ, Zisser H, Cooper KA, Raghavendhar
G, Lee WS, Yusi J, Bailey TS, Brazg RL, Shah R. Accuracy of
the Enlite 6-day glucose sensor with Guardian and Veo cali-
bration algorithms. Diabetes Technol Ther. 2012;14:225–31.
32. Renard E. Implantable continuous glucose sensors. Curr Diab
Rev. 2008;4:169–74.
33. Renard E, Shah R, Miller M, Kolopp M, Costalat G, Bringer J.
Sustained safety and accuracy of central IV glucose sensors
connected to implanted insulin pumps and short term closed-
loop trials in diabetic patients. Diabetes. 2003;52:A36.
34. Magni L, Forgione M, Toffanin C, Dalla Man C, De Nicolao G,
Kovatchev B, Cobelli C. Run-to-run tuning of model predictive
control for type I diabetic subjects: an in silico trial. J Diabetes
Sci. 2009;3:1091–8.
35. Lee H, Buckingham BA, Wilson DM, Bequette BW. A closed-
loop artificial pancreas using model predictive control and a
sliding meal size estimation. J Diabetes Sci Technol.
2009;3:1082–90.
36. Cobelli C, Cobelli C, Cobelli C, Cobelli C, Cobelli C, Kovat-
chev BP. Diabetes: models, signals, and control. IEEE Rev
Biomed Eng. 2009;2:54–96.
37. Bequette BW. A critical assessment of algorithms and chal-
lenges in the development of a closed-loop artificial pancreas.
Diabetes Technol Ther. 2005;7:28–47.
38. Teixeira RE, Malin S. The next generation of artificial pancreas
control algorithms. J Diabetes Sci Technol. 2008;2:105–12.
39. El Youssef J, Castle J, Ward WK. A review of closed-loop
algorithms for glcemic control in the treatment of type 1 dia-
betes. Algorithms. 2008;2:518–32.
40. Steil GM, Rebrin K, Janowski R, Darwin C, Saad MF. Modeling
beta-cell insulin secretion-implications for closed-loop glucose
homeostasis. Diabetes Technol Ther. 2003;5:953–64.
41. Bergman RN, Ider YZ, Bowden CR, Cobelli C. Quantitative
estimation of insulin sensitivity. Am J Physiol. 1979;236:
E667–77.
42. Cobelli C, Renard E, Kovatchev B. Artificial pancreas: past,
present, future. Diabetes. 2011;60:2672–82.
43. Hovorka R. Continuous glucose monitoring and closed-loop
systems. Diabet Med. 2005;23:1–12.
44. Kovatchev BP, Cobelli C, Renard E. Multinational study of
subcutaneous model-predictive closed-loop control in type 1
diabetes mellitus: summary of the results. J Diab Sci Technol.
2010;4:1374–81.
45. Hovorka R, Allen JM, Elleri D, Chassin LJ, Harris J, Xing D,
Kollman C, Hovorka T, Larsen AMF, Nodale M, De Palma A,
Wilinska ME, Acerini CL, Dunger DB. Manual closed-loop
insulin delivery in children and adolescents with type 1 diabetes:
a phase 2 randomised crossover trial. Lancet. 2010;375:743–51.
46. El-Khatib FH, Russell SJ, Nathan DM, Sutherlin RG, Damiano
ER. A bi-hormonal closed-loop artificial pancreas for type 1
diabetes. Sci Transl Med. 2010;2:27ra27.
47. Castle JR, Engle JM, El Youssef J, Massoud RG, Yuen KC,
Kagan R, Ward WK. Novel use of glucagon in a closed-loop
system for prevention of hypoglycaemia in type 1 diabetes.
Diabetes Care. 2010;33:7.
48. Magni L, Raimondo DM, Bossi L, Dalla Man C, De Nicolao G,
Kovatchev B, Cobelli C. Model predictive control of type 1
diabetes: an in silico trial. J Diabetes Sci Technol. 2007;1:12.
49. Kadish AH. Automation control of blood sugar. A servomech-
anism for glucose monitoring and control. Am J Med Electron.
1964;3:82–6.
50. Fogt EJ, Dodd LM, Jenning EM, Clemens AH. Development
and evaluation of a glucose analyzer for a glucose controlled
insulin infusion system (Biostator). Clin Chem. 1978;24:
1366–72.
51. Clemens AH, Hough DL, D’Orazio PA. Development of the
Biostator glucose clamping algorithm. Clin Chem. 1982;28:
1899–904.
52. Hoshino M, Haraguchi Y, Hirasawa H, Sakai M, Saegusa H,
Hayashi K, Horita N, Ohsawa H. Close relationship of tissue
plasminogen activator-plasminogen activator inhibitor-1 com-
plex with multiple organ dysfunction syndrome investigated by
means of the artificial pancreas. Crit Care. 2001;5:88–99.
53. Hoshino M, Haraguchi Y, Mizushima I, Sakai M. Close rela-
tionship between strict blood glucose control, including sup-
pression of blood glucose variability, and mortality reduction in
acutely ill patients with glucose intolerance investigated by
means of a bedside-type artificial pancreas. J Artif Organs.
2010;13:151–60.
54. Jaremko J, Rorstad O. Advances toward the implantable artifi-
cial pancreas for the treatment of diabetes. Diabetes Care.
1998;21:444–50.
55. Klonoff DC, Cobelli C, Kovatchev B, Zisser HC. Progress in
development of an artificial pancreas. J Diabetes Sci Technol.
2009;3:1002–4.
56. Kumareswaran K, Evans ML, Hovorka R. Artificial pancreas: an
emerging approach to treat type 1 diabetes. Exp Rev Med Dev.
2009;6:401–10.
57. Hoshino M, Haraguchi Y, Mizushima I, Sakai M. Recent pro-
gress in mechanical artificial pancreas. J Artif Organs.
2009;12:141–9.
58. Dassau E, Atlas E, Phillip M. Closing the loop. Int J Clin Pract.
2011;65:20–5.
59. Gregory JM, Moore DJ. Can technological solutions for diabetes
replace islet cell function? Organogenesis. 2011;7:32–41.
60. Klonoff DC, Zimliki CL, Stevens A, Beaston P, Pinkos A, Choe
SY, Arreaza-Rubın G, Heetderks W. Innovations in technology
for the treatment of diabetes: clinical development of the arti-
ficial pancreas (an autonomous system). J Diabetes Sci Technol.
2011;5:804–26.
61. Schaller HC, Schaupp L, Bodenlenz M, Wilinska ME, Chassin
LJ, Wach P, Vering T, Hovorka R, Pieber TR. On-line adaptive
algorithm with glucose prediction capacity for subcutaneous
closed-loop control of glucose: evaluation under fasting condi-
tions in patients with type 1 diabetes. Diabet Med. 2006;23:
90–3.
62. Hovorka R, Canonico V, Chassin LJ, Haueter U, Massi-
Benedetti M, Orsini Federici M, Pieber TR, Schaller HC,
Schaupp L, Vering T, Wilinska ME. Nonlinear model predictive
control of glucose concentration in subjects with type 1 diabetes.
Physiol Meas. 2004;25:905–20.
63. Kovatchev B, Cobelli C, Renard E, Anderson S, Breton M,
Patek S, Clarke W, Bruttomesso D, Maran A, Costa S, Avogaro
A, Dalla Man C, Facchinetti A, Magni L, De Nicolao G, Place J,
Farret A. Multinational study of subcutaneous model-predictive
closed-loop control in type 1 diabetes mellitus: summary of the
results. J Diabetes Sci Technol. 2010;4:1374–81.
64. Bruttomesso D, Farret A, Costa S, Marescotti MC, Vettore M,
Avogaro A, Tiengo A, Dalla Man C, Place J, Facchinetti A,
Guerra S, Magni L, De Nicolao G, Cobelli C, Renard E, Maran
A. Closed-loop artificial pancreas using subcutaneous glucose
sensing and insulin delivery and a model predictive control
algorithm: preliminary studies in Padova and Montpellier.
J Diabetes Sci Technol. 2009;3:1014–21.
J Artif Organs
123
65. Hovorka R, Kumareswaran K, Harris J, Allen JM, Elleri D, Xing
D, Kollman C, Nodale M, Murphy HR, Dunger DB, Amiel SA,
Heller SR, Wilinska ME, Evans ML. Overnight closed-loop
insulin delivery (artificial pancreas) in adults with type 1 dia-
betes: crossover randomised controlled studies. Brit Med J.
2011;342:d1911–2.
66. Renard E. Clinical experience with an implanted closed-loop insulin
delivery system. Arq Bras Endocrinol Metabol. 2008;52:349–54.
67. El-Khatib FH, Jiang J, Damiano ER. A feasibility study of bi-
hormonal closed-loop blood glucose control using dual subcu-
taneous infusion of insulin and glucagon in ambulatory diabetic
swine. J Diabetes Sci Technol. 2009;3:789–803.
68. El-Khatib FH, Russell SJ, Nathan DM, Sutherlin RG, Damiano
ER. A bihormonal closed-loop artificial pancreas for type 1
diabetes. Sci Transl Med. 2010;2:2–27.
69. Renard E, Place J, Cantwell M, Chevassus H, Palerm CC.
Closed-loop insulin delivery using a subcutaneous glucose
sensor and intraperitoneal insulin delivery. Feasibility study
testing a new model for the artificial pancreas. Diabetes Care.
2009;33:121–7.
70. Aberle I, Scholz U, Bach-Kliegel B, Fischer C, Gorny M,
Langer K, Kliegel M. Psychological aspects in continuous
subcutaneous insulin infusion: a retrospective study. J Psychol
Inter Appl. 2009;143:147–60.
71. Hofer SE, Heidtmann B, Raile K, Frohlich-Reiterer E, Lilienthal
E, Berghaeuser MA, Holl RW. Discontinuation of insulin pump
treatment in children, adolescents, and young adults. A multi-
center analysis based on the DPV database in Germany and
Austria. Pediatr Diabetes. 2010;11:116–21.
72. Reid G. Biofilms in infection disease and on medical devices. Int
J Antimicrob Agents. 1999;11:223–6.
73. Schierholz JM, Beuth J. Implant infections: a haven for oppor-
tunistic bacteria. J Hosp Infect. 2001;49:87–93.
74. Francolini I, Donelli G. Prevention and control of biofilm-based
medical-device-related infections. FEMS Immunol Med
Microbiol. 2010;59:227–38.
75. Rodrigues LR. Inhibition of bacterial adhesion on medical
devices. Adv Exp Med Biol. 2001;715:351–67.
76. Bloom HL, Constantin L, Dan D, De Lurgio DB, El-Chami M,
Ganz LI, Gleed KJ, Hackett FK, Kanuru NK, Lerner DJ, Rasekh
A, Simons GR, Sogade FO, Sohail MR. Implantation success
and infection in cardiovascular implantable electronic device
procedures utilizing an antibacterial envelope. Pacing Clin
Electrophysiol. 2011;34:133–42.
77. Palchesko RN, McGowan KA, Gawalt ES. Surface immobili-
zation of active vancomycin on calcium aluminium oxide. Mater
Sci Eng C. 2011;31:637–42.
78. Braceras I, Azpiroz P, Briz N, Fratila RM, Oyarbide J, Ipinazar
E, Alvarez N, Atorrasagasti G, Aizpurua JM. Plasma polymer-
ized silylated ciprofloxacin as an antibiotic coating. Plasma
Process Polym. 2011;8:599–606.
79. Satishkumar R, Sankar S, Yurko Y, Lincourt A, Shipp J,
Heniford BT, Vertegel A. Evaluation of the antimicrobial
activity of lysostaphin-coated hernia repair meshes. Antimicrob
Agents Chemother. 2011;55:4379–85.
80. Xu LC, Siedlecki CA. Submicron-textured biomaterial surface
reduces staphylococcal bacterial adhesion and biofilm forma-
tion. Acta Biomater. 2012;8:72–81.
81. Arciola CR, Montanaro L, Costerton JW. New trends in diag-
nosis and control strategies for implant infections. Int J Artif
Organs. 2011;34:727–36.
82. Lacy P, Kostianovsky M. Method for the isolation of intact islets
of Langerhans from the rat pancreas. Diabetes. 1967;16:35–9.
83. Kemp C, Knight M, Scharp D, Lacy P, Ballinger W. Trans-
plantation of isolated pancreatic islets into the portal vein of
diabetic rats. Nature. 1973;244:7.
84. Scharp D, Murphy J, Newton W, Ballinger W, Lacy P. Trans-
plantation of islets of Langerhans in diabetic rhesus monkeys.
Surgery. 1975;77:100–5.
85. Ryan EA, Lakey JRT, Rajotte RV, Korbutt GS, Kin T, Imes S,
Rabinovitch A, Elliott JF, Bigam D, Kneteman NM, Warnock
G, Larsen I, Shapiro AMJ. Clinical outcomes and insulin
secretion after islet transplantation with the Edmonton protocol.
Diabetes. 2001;50:710–9.
86. Hunkeler D. Bioartificial organs transplanted from research to
reality. Nat Biotechnol. 1999;17:335–6.
87. Lanza RP, Sullivan SJ, Chick WL. Islet transplantation with
immunoisolation. Diabetes. 1992;41:1503–10.
88. Silva AI, Matos AN, Brons IG, Mateus M. An overview of the
development of a bio-artificial pancreas as a treatment of insu-
lin-dependent diabetes mellitus. Med Res Rev. 2006;26:
181–222.
89. Sumi S. Regenerative medicine for insulin deficiency: creation
of pancreatic islets and bioartificial pancreas. J Hepatobiliary
Pancreat Sci. 2011;18:6–12.
90. Monaco AP, Maki T, Ozato H, Carretta M, Sullivan SJ, Borland
KM, Mahoney MD, Chick WL, Muller TE, Wolfrum J, Solomon
B. Transplantation of islet allografts and xenografts in totally
pancreatectomized diabetic dogs using the hybrid artificial
pancreas. Ann Surg. 1991;214:339–62.
91. Orsetti A, Hagelsteen C, Zouari N. Temporary normalization of
blood sugar, in a totally pancreatectomized dog, after placing an
artificial insulin distributor. C R Seances Soc Biol Fil.
1977;171:858–64.
92. Orsetti A, Guy C, Zouari N, Deffay R. Implantation of a bio-
artificialinsulin distributor in dogs, using islets of Langerhans
from different animal species. C R Seances Soc Biol Fil.
1978;172:44–150.
93. Chick WL, Perna JJ, Lauris V, Low D, Galletti PM, Panol G,
Whittemore AD, Like AA, Colton K, Lysaght MJ. Artificial
pancreas using living b-cells: effects on glucose homeostasis in
diabetic rats. Science. 1977;197:780–2.
94. Sun AM, Parisius W, Healy GM, Vacek I, Macmorine HG. The
use, in diabetic rats and monkeys, of artificial capillary units
containing cultured islets of Langerhans (artificial endocrine
pancreas). Diabetes. 1977;26:1136–9.
95. Ikeda H, Kobayashi N, Tanaka Y, Nakaji S, Yong C, Okitsu T,
Oshita M, Matsumoto S, Noguchi H, Narushima M, Tanaka K,
Miki A, Rivas-Carrillo JD, Soto-Gutierrez A, Navarro-Alvarez
N, Tanaka K, Jun HS, Tanaka N, Yoon JW. A newly developed
bioartificial pancreas successfully controls blood glucose in
totally pancreatectomized diabetic pigs. Tissue Eng. 2006;12:
1799–809.
96. Ohgawara H, Miyazaki J, Karibe S, Katagiri N, Tashiro F,
Akaike T. Assessment of pore size of a semipermeable mem-
brane for immunoisolation or xenoimplantation of pancreatic B
cells using a diffusion chamber. Transplant Proc. 1995;27:
3319–20.
97. Kessler L, Jesser C, Belcourt A, Pinget M. Influence of acinar
tissuecontamination on encapsulated pancreatic islets: morpho-
logical and functional studies. Transplant. 1997;63:1537–40.
98. Tze WJ, Tai J, Cheung SS, Bissada N, Starzl TE. Prolongation
of pig islet xenograft survival in rats by local immunosuprres-
sion with FK 506. Transplant Proc. 1994;26:777–8.
99. Rivereau AS, Darquy S, Chaillous L, Maugendre S, Gouin E,
Reach G, Sai P. Reversal of diabetes in non-obese diabetic mice
by xenografts of porcine islets entrapped in hollow fibres com-
posed of polyacrylonitrile-sodium methallysulphonate copoly-
mer. Diabetes Metab. 1997;23:205–12.
100. Icard P, Penfornis F, Gotheil C, Boillot J, Cornec C, Barrat F,
Altman JJ. Tissue reaction to implanted bioartificial pancreas in
pigs. Transplant Proc. 1990;22:724–6.
J Artif Organs
123

101. Trivedi N, Keegan M, Steil GM, Hollister-Lock J, Hasenkamp
WM, Colton CK, Bonner-Weir S, Weir GC. Islets in alginate
macrobeads reverse diabetes despite minimal acute insulin
secretory responses. Transplant. 2001;71:203–11.
102. Wang W, Gu Y, Hori H, Sakurai T, Hiura A, Sumi S, Tabata Y,
Inoue K. Subcutaneous transplantation of macroencapsulated
porcine pancreatic endocrine cells normalizes hyperglycaemia
in diabetic mice. Transplant. 2003;76:290–6.
103. Macdonald RA. Presentation on behalf of Living Cell Tech-
nologies at Bio Investor Forum, October 2010. http://www.
lctglobal.com/Media-And-News/2010/Press-Releases/.
104. Elliott RB, Escobar L, Tan PL, Muzina M, Zwain S, Buchanan C.
Live encapsulated porcine islets from a type 1 diabetic patient 9.5
yr after xenotransplantation. Xenotransplant. 2007;14:157–61.
105. Uchiyama T, Watanabe J, Ishihara K. Pressure-induced change
in permeation of insulin through a polymer alloy membrane for
an implantable insulin pump. J Membr Sci. 2002;210:423–31.
106. Schetky LM, Jardine P, Moussy F. A closed loop implantable
artificial pancreas using thin film nitinol MEMS pumps. In:
Pelton AR, Duerig T (eds) Proceedings of SMST 2003. Menlo
Park, CA: SMST Society, Inc.; 2003.
107. Acosta GM, Henderson JR, Haj NAA, Ruchti TL, Monfre SL,
Blank TB, Hazen KH. Compact apparatus for noninvasive
measurement of glucose through near-infrared spectroscopy. US
Patent No. 7,133,710 B2; 2006.
108. Ichimori S, Nishida K, Shimoda S, Sekigami T, Matsuo Y,
Ichinose K, Shichiri M, Sakakida M, Araki E. Development of a
highly responsive needle-type glucose sensor using polyimide
for a wereable artificial endocrine pancreas. J Artif Organs.
2006;9:105–13.
109. Yoshimi Y, Narimatsu A, Nakayama K, Sekine S, Hattori K,
Sakai K. Development of an enzyme-free glucose sensor using
the gate effect of a molecularly imprinted polymer. J Artif
Organs. 2009;12:264–70.
110. El-Khatib FH, Jiang J, Damiano ER. Adaptive closed-loop
control provides blood-glucose regulation using dual subcuta-
neous insulin and glucagon infusion in diabetic swine. J Diabe-
tes Sci Technol. 2007;1:181–92.
111. Grant P. A new approach to diabetic control: fuzzy logic and
insulin pump technology. Med Eng Phys. 2007;29:824–7.
112. Wang Y, Dassau E, Doyle FJ III. Closed-loop control of artifi-
cial pancreatic b-cell in type 1 diabetes mellitus using model
predictive iterative learning control. IEEE Trans Biomed Eng.
2010;57:211–9.
113. Ricotti L, Assaf T, Stefanini C, Menciassi A. System for con-
trolled administration of a substance from a human-body-
implanted infusion device. PCT Patent No. WO2012/011132A1;
2012.
114. Chen C, Lin C, Hsu C. Wireless charging module and electronic
apparatus. US Patent No. 20090289595; 2009.
115. Vandevoorde G, Puers R. Wireless energy transfer for stand-
alone systems: a comparison between low and high power
applicability. Sens Actuat A Phys. 2001;92:305–11.
J Artif Organs
123
Related Documents











