1 © OLIVER WYMAN | CHI-HLC06101-046 HEALTH & LIFE SCIENCES HEALTH CARE 2020 ROADMAP – THE VOLUME TO VALUE REVOLUTION AOA Meeting San Antonio June 7, 2014 Jim Bonnette, MD Partner, Chief Medical Officer 1 © OLIVER WYMAN | CHI-HLC06101-046 1 Volume to Value Pre-Test • In a population pyramid what is the savings potential of patient centered care? – A. 5% – B. 10% – C. 15% • South Central Foundation has been providing population based care for how many years? – A. 10 – B. 20 – C. 30 • The top 1% of Medicare patients cost on average how much per year? – A. $75,000 – B. $125,000 – C. $200,000 • Efficient population health managers can reduce Medicare admissions – A. 25% – B. 35% – C. 50% 2 © OLIVER WYMAN | CHI-HLC06101-046 2 VOLUME TO VALUE REVOLUTION

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
© OLIVER WYMAN | CHI-HLC06101-046
HEALTH & LIFE SCIENCES
HEALTH CARE 2020 ROADMAP –THE VOLUME TO VALUE REVOLUTION
AOA Meeting San Antonio
June 7, 2014
Jim Bonnette, MDPartner, Chief Medical Officer
1© OLIVER WYMAN | CHI-HLC06101-046 1
Volume to Value Pre-Test• In a population pyramid what is the savings potential of patient centered care?
– A. 5%
– B. 10%
– C. 15%
• South Central Foundation has been providing population based care for how many years?
– A. 10
– B. 20
– C. 30
• The top 1% of Medicare patients cost on average how much per year?
– A. $75,000
– B. $125,000
– C. $200,000
• Efficient population health managers can reduce Medicare admissions
– A. 25%
– B. 35%
– C. 50%
2© OLIVER WYMAN | CHI-HLC06101-046 2
VOLUME TO VALUE REVOLUTION

2
3© OLIVER WYMAN | CHI-HLC06101-046 3
Momentum is building
Medicare
Employers Medicaid
Consumers
Across populations
Across geographies
Across health conditions
Easy
Personal
Integrated
Error free
Personalized
Mobile/social
Always available
Less invasive
Predictive/preventative
Accessible
Much better value
Population Health and Lifestyle Managers rotating over $1 TN
towards higher value
4CASECODE-FILENAME (YYYYMMDD Descriptor).ppt© Oliver Wyman � www.oliverwyman.com
Concepts driving change
�No matter what the regulatory or payment system, physicians and caregivers around the globe fundamentally deliver care the same way focusing on symptomatic treatment and acute care, not longitudinal care or prevention
�The age wave, extended longevity and new medical technologies are exacerbating the cost issue – and this will get significantly worse without change
�Current care systems are neither safe nor efficient, most care provided by physicians could be provided by those of a lesser skill level as part of a team
�Automating the current symptomatic treatment system through EHR’s is insufficient to drive the quality, cost and efficiency gains required to create an affordable and sustainable system
�Payment mechanism reforms alone are insufficient to put the healthcare system on a sustainable cost and quality track – and the economic weight of the current system could cripple the economic vitality of any country (and FFS is a problem)
�Providing more of the right services to the sickest of the sick actually reduces total cost
�Only when we change in a very fundamental fashion how we engage and manage patients will we significantly impact the safety, quality and cost
55© OLIVER WYMAN | CHI-HLC06101-046
Unleashing free market competition – What is possible
20% total cost reduction
5.5% trend reduction
25% consumer value improvement
$7 TN of cost reduction over ten years
$1 TN of value rotation
100X the diffusion rate
3
66© OLIVER WYMAN | CHI-HLC06101-046
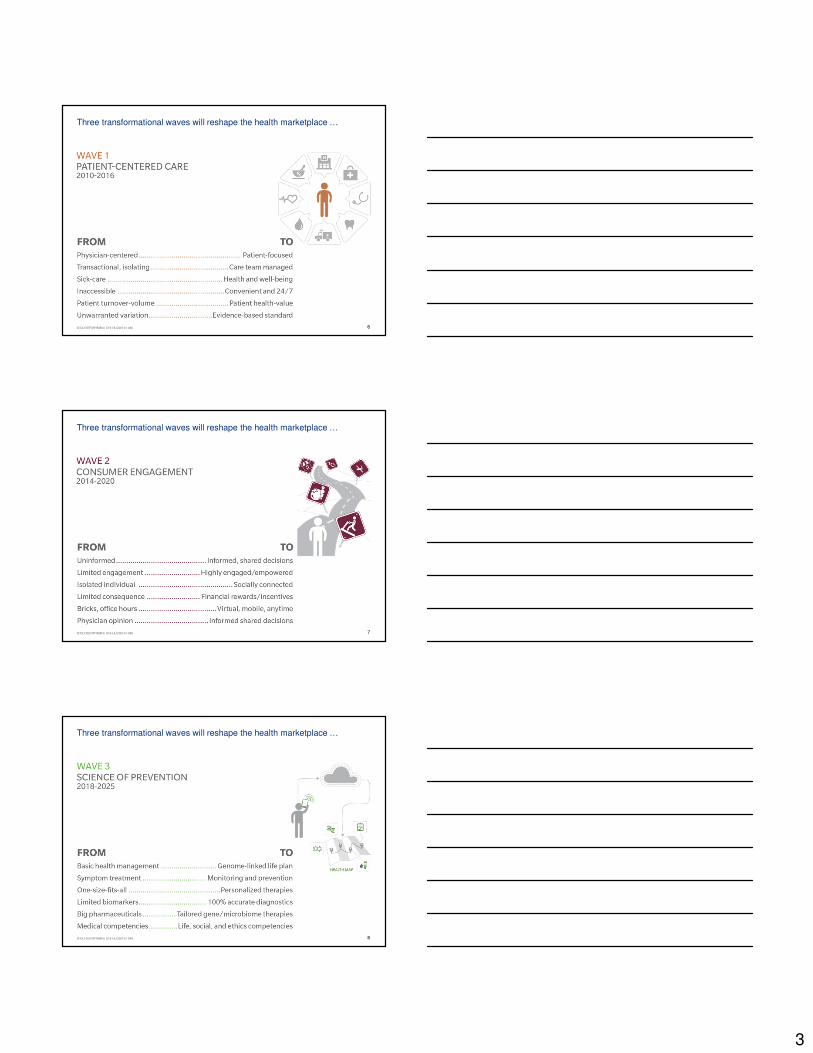
Three transformational waves will reshape the health marketplace …
77© OLIVER WYMAN | CHI-HLC06101-046
Three transformational waves will reshape the health marketplace …
88© OLIVER WYMAN | CHI-HLC06101-046
Three transformational waves will reshape the health marketplace …
4
99© OLIVER WYMAN | CHI-HLC06101-046
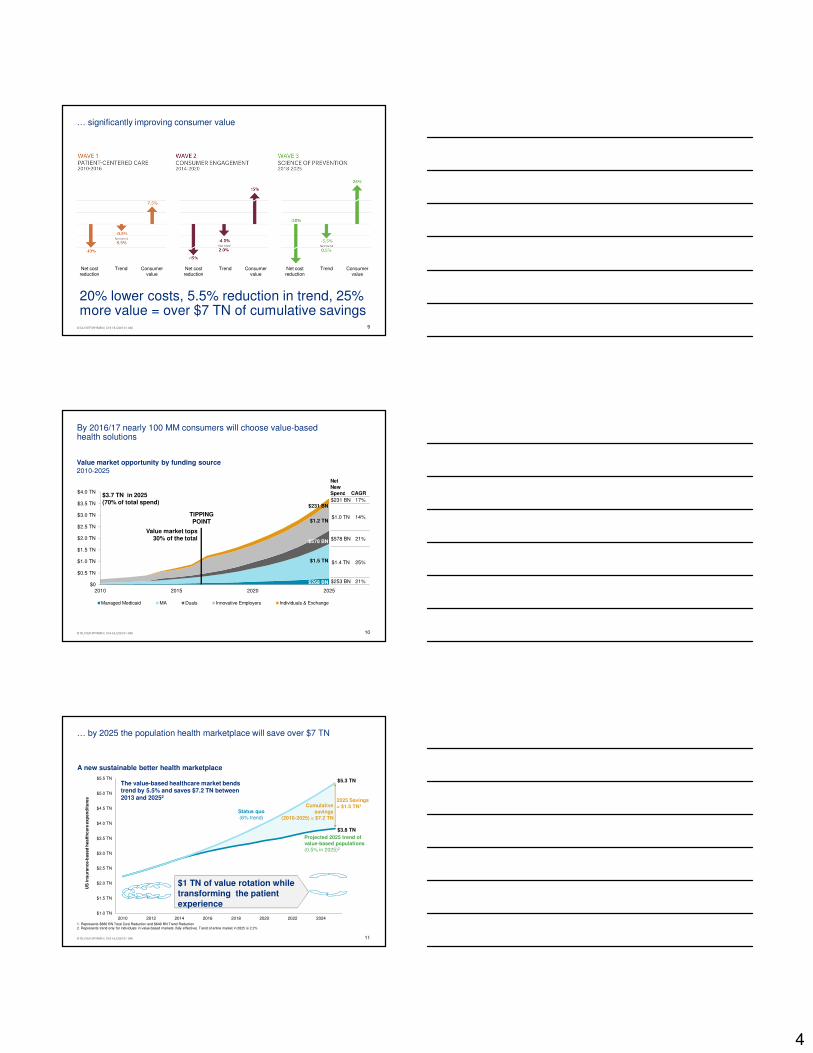
… significantly improving consumer value
20% lower costs, 5.5% reduction in trend, 25% more value = over $7 TN of cumulative savings
Net cost reduction
Trend Consumer value
Net cost reduction
Trend Consumer value
Net cost reduction
Trend Consumer value
10© OLIVER WYMAN | CHI-HLC06101-046 10
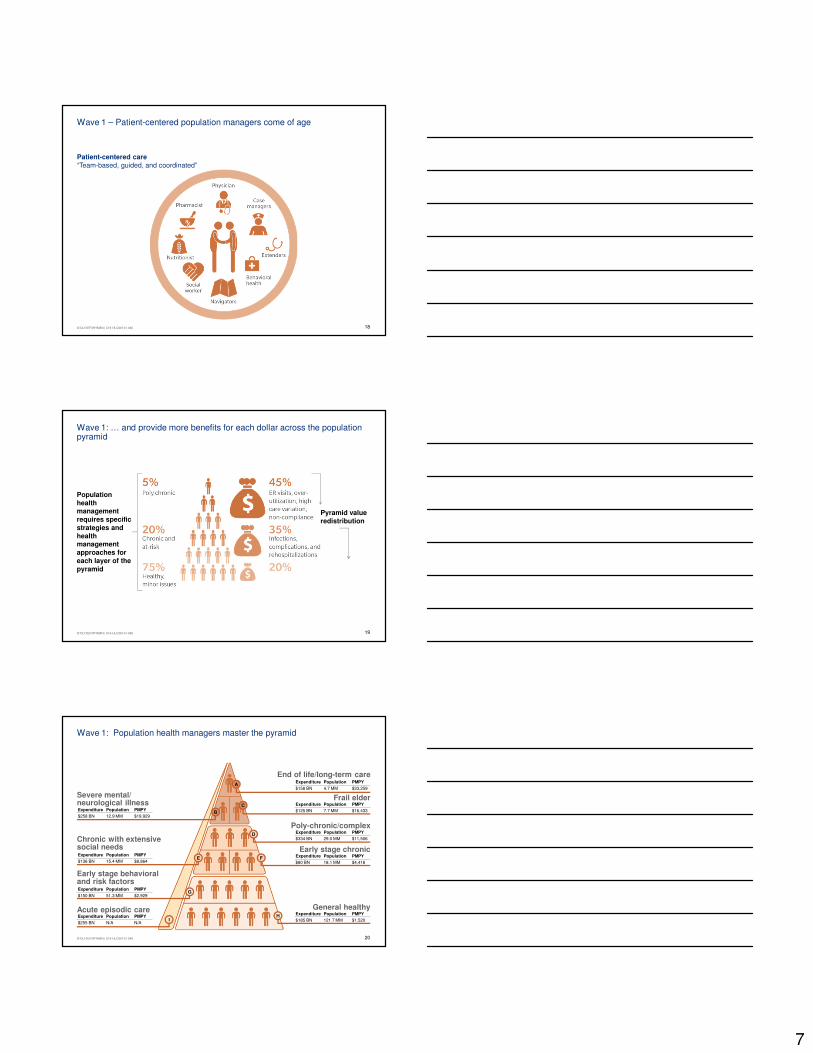
By 2016/17 nearly 100 MM consumers will choose value-based health solutions
$0
$0.5 TN
$1.0 TN
$1.5 TN
$2.0 TN
$2.5 TN
$3.0 TN
$3.5 TN
$4.0 TN
2010 2015 2020 2025
Managed Medicaid MA Duals Innovative Employers Individuals & Exchange
$268 BN
$1.5 TN
$578 BN
$1.2 TN
$231 BN
Value market opportunity by funding source2010-2025
NetNew Spend CAGR
$231 BN 17%
$1.0 TN 14%
$578 BN 21%
$1.4 TN 25%
$253 BN 21%
$3.7 TN in 2025(70% of total spend)
Value market tops 30% of the total
TIPPING POINT
11© OLIVER WYMAN | CHI-HLC06101-046 11
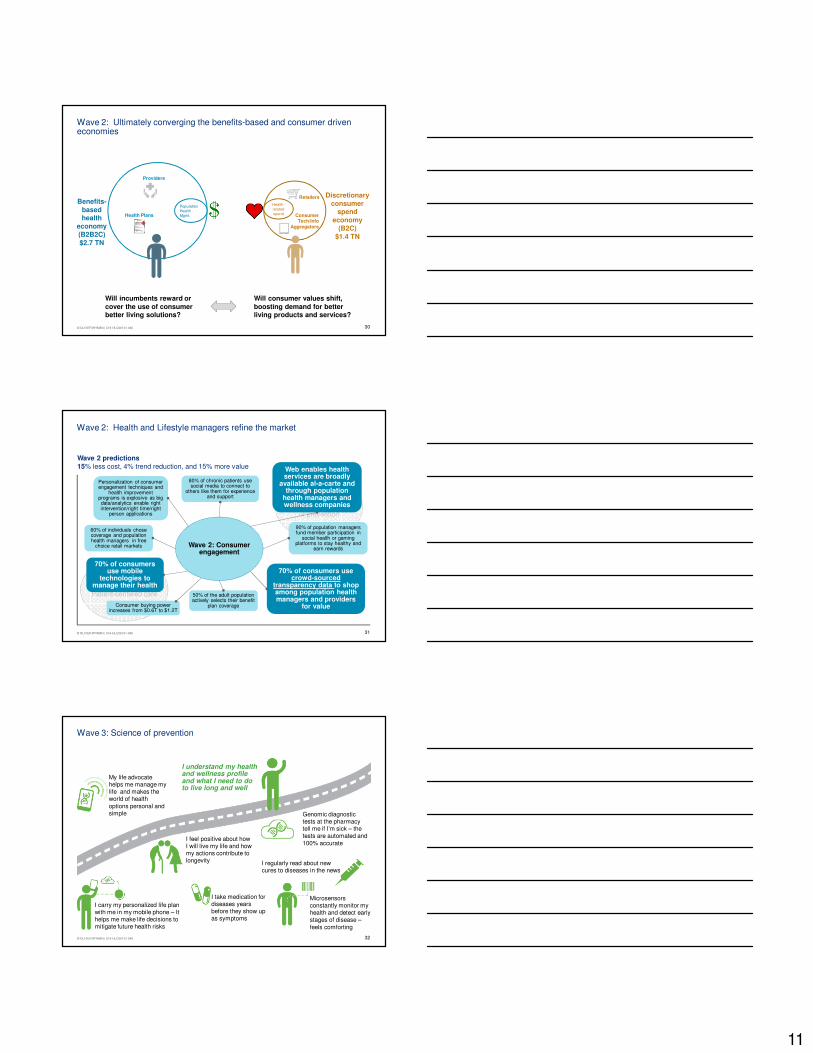
… by 2025 the population health marketplace will save over $7 TN
$1.0 TN
$1.5 TN
$2.0 TN
$2.5 TN
$3.0 TN
$3.5 TN
$4.0 TN
$4.5 TN
$5.0 TN
$5.5 TN
2010 2012 2014 2016 2018 2020 2022 2024
US
in
su
ran
ce-b
ased
healt
hcare
exp
en
dit
ure
s
Status quo(6% trend)
Projected 2025 trend of value-based populations(0.5% in 2025)2
2025 Savings = $1.5 TN1
The value-based healthcare market bends trend by 5.5% and saves $7.2 TN between 2013 and 20252
$5.3 TN
$3.8 TN
1. Represents $880 BN Total Cost Reduction and $640 BN Trend Reduction2. Represents trend only for individuals in value-based markets (fully effective). Trend of entire market in 2025 is 2.2%
Cumulative savings
(2010-2025) = $7.2 TN
$1 TN of value rotation while transforming the patient experience
A new sustainable better health marketplace

5
12© OLIVER WYMAN | CHI-HLC06101-046 12
The race to value will drive consolidation and convergence
Near-term population
risk arbitrage
Procedure
volume
PCPs
Payers
Hospitals
Diagnostics/Labs
Specialists
Ambulatory Facilities
Physical/Occupational Therapy
Long-term Care
Home Care
Behavioral Health
PBMs
Brokers/Distribution
Ethical Drugs
Devices/Equipments
Sales volume
(prescription)
Fitness/Nutrition
OTC
HIT
TPAs
CROs
Web-based consumer information
Commissions
Advertising
Sales volume
(consumer)
On-going revenue
streams for B2B service
Value Model Value Models
Long-term clinical risk arbitrage
Efficient episode management
On-demand al-a-carte services
Shared savings
Consumer subscriptions
B2B enablement
Product and service add-ons
App/gadget/software sales
Traditional siloed business designs Converged wellness health ecosystems
1313© OLIVER WYMAN | CHI-HLC06101-046
Next generation leaders / innovators will leverage the work of the pioneers
• 18% lower than average member costs
• 24% lower than average hospitalization rate
• 38% shorter than average hospital stays
• $2 MM savings for every 1,000 members
• Medicare readmission rates up to 30% lower than national average
• Leader in CA in patient satisfaction (top 10%)
• 50% drop in urgent care and ER utilization
• 40% drop in hospital admissions
• Patient and staff satisfaction over 90%
Founded: 1992
Whole-Pyramid Focus
Founded: 1997
Complex/Polychronic Focus
Founded: 1982
Whole-Pyramid Focus
Imp
act
Sources: WellPoint; http://www.gogreendps.com/HealthCarePartnersCommReport.htm; Southcentral Foundation - Nuka System of Care 09-05-12 V2; http://content.healthaffairs.org/content/30/3/416.extract
… only better – open, social / mobile, scalable, portable, assimilative, personalized and always available
14© OLIVER WYMAN | CHI-HLC06101-046 14
From physician to patient (or will it be consumer) centered

6
15© OLIVER WYMAN | CHI-HLC06101-046 15
Today: Fee-for-Service (2013)
My doctor controls my referrals, and I don’t know who provides the best care
Doctor’s hours don’t match real life hours
I feel rushed during doctor visits
I only seek care when I have no other alternative
I am the only person coordinating my care –doctors don’t talk to each other and don’t think about me once I leave their office
I avoid my healthcare because it’s too confusing and inconvenient
I have no idea how my insurance works – it’s so confusing
I feel lost and overwhelmed
1616© Oliver Wyman | CHI-SRH01811-007
This is what we currently call “patient-centered” care
Payer Affiliated physicians Care/access programs FQHCs County/community services Collaboration Flow of funds Claims reimbursement Informal linkages
Additional resources include: psychiatrists for inpatient, social workers, palliative care, hospitalists, advanced practice providers, RNs/MAs, etc.
h
County programs
Lancaster General Health
Clinic A
Hospital A
Specialty Group
Superutilizers program
MH/MR/EI
Office of aging
Coalition to end homelessness
Drug & alcohol commission
Other county programs include: Children & Youth Agency, County Prison, Adult Probation & Parole Services, Veteran’s Affairs
Poverty assistance
FQHC
Medicaid
MedicaidFFS
Mobile psychiatric nursing
Mental Health MCO
FQHC BH Integration Project
Assertive Community Treatment (ACT)
Rehab/detox services
State
Treatment for serious mental illness
Food stamps, welfare, etc.
Safety net services for the frail elderly
Housing support and transitional assistance
Healthy beginnings+
Nurse family partnership
Geriatric house call
Heart failure/high risk clinic
MCO B
MCO A
MCO E
MCO D
MCO C
County A
County C
County B
County E
County D
Medical & dental center FQHC
Medical Group A
IPA A
HIV clinic
PCMH NCQA level 3 accreditation
PACE/program participation
Transportation programs
Inpatient psych
Emergency department
Urgent care
Rx assistance programs
Employment assistance
Home care providers
Support groups for drug &
alcohol
Inpatient rehabilitation
facilities
Crisis interventions
Case management
Support helplines
Food banks/stamps/
distribution
Child welfareProtective services
Pharmacies
Social rehabilitation
Low-income energy
assistance
Drug & alcohol outpatient centers
Domestic abuse support
services
Housing, shelters, missions
Unaffiliated healthcare providers
Outpatient center/clinic
Health express
Community resources
Other MH/BH networks
Emergency/transitional
housing
Support for the disabled
Counseling and legal services
IDN ACounty
project access
Member
Mental health collaborative
1717© OLIVER WYMAN | CHI-HLC06101-046
Wave 1: Patient-centered care
My care team truly cares about my holistic health –I am not alone
I work with my care team to improve my health and live better – we have a shared plan that is personalized to me
I believe that my healthiest days are ahead of me
My care team takes care of all my health needs
The system isworking for me
My substance abuse and depression are managed
My care team proactively motivates me to stick to my care plan
I monitor my health with tools to identify issues early
Care extends beyond my doctor’s office to my home and to local retailers
7
1818© OLIVER WYMAN | CHI-HLC06101-046
Wave 1 – Patient-centered population managers come of age
Patient-centered care“Team-based, guided, and coordinated”
1919© OLIVER WYMAN | CHI-HLC06101-046
Wave 1: … and provide more benefits for each dollar across the population pyramid
Population health management requires specific strategies and health management approaches for each layer of the pyramid
Pyramid value redistribution
2020© OLIVER WYMAN | CHI-HLC06101-046
Wave 1: Population health managers master the pyramid
Expenditure Population PMPY
$258 BN 12.9 MM $19,929
Expenditure Population PMPY
$136 BN 15.4 MM $8,864
Expenditure Population PMPY
$150 BN 51.3 MM $2,929
Expenditure Population PMPY
$255 BN N/A N/A
Expenditure Population PMPY
$158 BN 4.7 MM $33,259
Expenditure Population PMPY
$125 BN 7.7 MM $16,433
Expenditure Population PMPY
$334 BN 29.0 MM $11,506
Expenditure Population PMPY
$80 BN 18.1 MM $4,418
Expenditure Population PMPY
$185 BN 121.7 MM $1,520
C
D
F
HAcute episodic care
I
Severe mental/neurological illness
B
Chronic with extensive social needs
E
Early stage behavioral and risk factors
G
End of life/long-term careA
Frail elder
Poly-chronic/complex
Early stage chronic
General healthy

8
2121© OLIVER WYMAN | CHI-HLC06101-046
Wave 1: Population health managers grow at the expense today’s FFS profit centers
Inpatient
Outpatient
Emergency Department
Retail
Primary care hubs
Direct primary care
Virtual web based health models
Convenient care clinics
Diagnostics
Specialty care offices
Ambulatory center
LTC facilities
Behavioral health
Home health care
Outlook for traditional players in a value-based population management ecosystem
22CASECODE-FILENAME (YYYYMMDD Descriptor).ppt© Oliver Wyman � www.oliverwyman.com
The shift in patient care will drive practice revenue to PCPs and select specialties that play coordinating roles at the primary expense of surgical specialists
40%
27%
6%
7%
26%
23%
12%
13%
13%
12%
4%
3%
0%
20%
40%
60%
80%
100%
Current expenditures Future expenditures
with care models
Impact of care models on medical expenditures1
Hospitals
Rx
Med equip & non-durable med prod.
Legend
Nursing home / home health
Medical specialists
PCP
% change
(5%)
(10%)
10%
(10%)
20%
(32%)
(15%)
$2.0 T
$1.7 T
19% 23%
6%7%
14%15%
17%17%
3%2%11%
10%
10%8%
21% 14%
0%
20%
40%
60%
80%
100%
Current expenditures Future expenditures
with care models
Impact of care models on physician specialties
5% decrease
10% decrease
20% decrease
30% decrease
Legend
5% increase
10% increase
20% increase
Types of physicians
$597 B$574 B
1 Excludes other non-IHM spend (e.g., private insurance, dental, gov’t) which represent $0.3T in spend and are not impacted by care models
No change
�Internal medicine�Pediatrics
�Oncology�Pulmonology
�Cardiologist�Endocrinologist
�Neurology�ENT
�ER medicine
�Gastroent.�OB/GYN
�Cardio int. �Orthopedic surg
�Gen surg.�Radiology�CV surgery
Specialists 10% decline
PCP20% increase
Med
ical exp
en
dit
ure
s
23© OLIVER WYMAN | CHI-HLC06101-046 23
Wave 1: Population health managers redefine patient value
Wave 1: Patient-centered care
Wave 1 predictions 10% less cost, 0.5% trend reduction, 7.5% more value
Wave 3: The science
of prevention
Wave 2: Consumer engagement
Most patients love their population health manager and value thepatient experience
Multi-skilled health and wellness teams (social workers, nutritionist, coaches) are the norm
70% of provider visits are conducted virtually, or outside of normaloffice hours
75% of patients have a personal health record and a health management plan
75% of poly-chronic patients have their care coordinated across settings by a navigator
35 national and regional population health managers will control 70% of the market and compete on value
Patient-centered population health organizations will replace PPO networks
Population health managers will control 70% of clinical risk

9
24© OLIVER WYMAN | CHI-HLC06101-046 24
From patient to consumer centered
2525© OLIVER WYMAN | CHI-HLC06101-046
Wave 2: Consumer engagement
I know how to livewell and be healthy –I have great resources (apps) at my disposal to inform me
I feel engagedin my health and am empowered to make informed decisions
I know what I need and how to buy it – shopping and health tools have made it easy and boosted my confidence
I use crowdsourced reviews of goods and service providers (like Yelp) to decide where I can get the best value
Competing against friends in online health challenges motivates me to live healthier – I earn great rewards that I value
I connect through social media to other “patients like me”
Consumer-driven competition is great – all the population health managers have extended office hours and most offervirtual web visits
I can surf and navigate the health system with ease and the patient-centered care models are so convenient and easy to work with
I have web-based/mobile tools so I can manage my healthcare
2626© OLIVER WYMAN | CHI-HLC06101-046
• Disease status
• Benefit status
• Episodic/point-in-Time View
Wave 2: Redefine the consumer experience by shifting the lens
• Disease status
• Benefit status
• Motivational profile
• Lifestyle factors
• Socioeconomics & life stage
• Health needs & behavioral profile
• Preferences, interests, goals
• Family situation
• Longitudinal lifetime view
Heart
patient
Whole
patient
Whole
consumer
Today’s transactional system
Wave 1 Patient-centered care
Wave 2 Consumer engagement
Consumer mindshare
Consumer loyalty
Consumer timeshare
Consumer wallet share
Consumer biodata share

10
27© OLIVER WYMAN | CHI-HLC06401-026 27
How many times a year does an average consumer visit a grocery
store?
How many consumers visit a Walmart every month in the US?
28© OLIVER WYMAN | CHI-HLC06401-026 28
Retailers have chosen to focus their investments to-date on one or more of seven potential business designs
Retailer Healthcare Business Designs
Value-based healthcare Healthcare enablement
Representative offering and early movers
Retail integrated delivery network
5
• Care delivery• Care
networks• Health
insurance / population risk
Health product marketplace
1
• Pharmacy• Optometry• Audiology• Insurance• Health &
beauty• OTC• Fresh
Population health management
4
• Care coordination
• Chronic condition management
• Frail elder programs
Wellness and lifestyle support
2
• Nutrition programs
• Health education
• Fitness games / P2P
Shopper health data and analytics
7
• Shopper purchase data sets / dashboards
• Consumer behavior analytics
Financial products & decision support
6
• Health insurance exchange
• Plan selection guidance
• HSAs• Financial
planning
Primary care delivery
3
• In-store or standalone primary care clinics
• Health kiosks• EMRs
Transactional healthcare
(emerging)
2929© Oliver Wyman
My thoughts on healthcare• Nearly everything I do affects my health• My health status directly impacts my health costs!• I need to select benefits (insurance) that fit me• There are many things I can control (nutrition, fitness)• There are some things I can’t control (genetics)• There are intrinsic and extrinsic reasons to be as
healthy as I can• I need a plan for my health, and partners to help me• I need to spend smart – and find the best value!• “Ah – Insurance means Insurance…not ‘Free’”• Out-of-pocket spending sucks!
Consumers are demanding a solution for their healthcare issues, driving them from unengaged to behaviorally and economically motivated
Things I plan for• Housing• Food • Clothing• Transportation• Fun and entertainment• Healthcare• Higher education• Retirement
Things I plan for• Housing• Food • Clothing• Transportation• Fun and
entertainment• Healthcare• Higher education• Retirement
My thoughts on healthcare• How do I get Insurance?
It’s confusing!• What’s a Healthcare exchange?• Why doesn’t it cover everything? • Should I choose a private Medicaid plan?• Where should I go for care, and how often?• Out-of-pocket spending sucks!
Healthcare today“Disconnected, unengaged,
entitled”
Healthcare tomorrow“Economically and behaviorally
aware and accountable”
11
3030© OLIVER WYMAN | CHI-HLC06101-046
Wave 2: Ultimately converging the benefits-based and consumer driven economies
Population Health Mgmt.
Health-related spend
Benefits-basedhealth
economy(B2B2C)$2.7 TN
Discretionary consumer
spend economy
(B2C)$1.4 TN
Retailers
Consumer Tech/Info
Aggregators+
Providers
Health Plans
Will incumbents reward or cover the use of consumer better living solutions?
Will consumer values shift, boosting demand for better living products and services?
3131© OLIVER WYMAN | CHI-HLC06101-046
Wave 2: Health and Lifestyle managers refine the market
Wave 2: Consumer engagement
Wave 2 predictions15% less cost, 4% trend reduction, and 15% more value
Wave 1Patient-centered care
Wave 3The science of prevention
Personalization of consumer engagement techniques and
health improvement programs is explosive as big data/analytics enable right intervention/right time/right
person applications
60% of individuals chose coverage and population health managers in free
choice retail markets
Web enables health services are broadly
available al-a-carte and through population
health managers and wellness companies
Consumer buying power increases from $0.6T to $1.2T
70% of consumers use crowd-sourced
transparency data to shop among population health managers and providers
for value
80% of chronic patients use social media to connect to
others like them for experience and support
70% of consumers use mobile
technologies to manage their health
50% of the adult population actively selects their benefit
plan coverage
90% of population managers fund member participation in
social health or gaming platforms to stay healthy and
earn rewards
3232© OLIVER WYMAN | CHI-HLC06101-046
Wave 3: Science of prevention
I understand my health and wellness profile and what I need to do to live long and well
My life advocate helps me manage my life and makes the world of health options personal and simple
I carry my personalized life plan with me in my mobile phone – It helps me make life decisions to mitigate future health risks
I feel positive about how I will live my life and how my actions contribute to longevity
Genomic diagnostic tests at the pharmacy tell me if I’m sick – the tests are automated and 100% accurate
I take medication for diseases years before they show up as symptoms
I regularly read about new cures to diseases in the news
Microsensors constantly monitor my health and detect early stages of disease –feels comforting

12
3333© OLIVER WYMAN | CHI-HLC06101-046
Pri
ce
Genomic sequencing cost curve
Time
Imp
act
Biomarker and pathway inventory
New treatment development
+ Low cost high power computing+ Big data+ Advanced analytics+ Super high speed networks+ Nano pore technology
Low cost sequencing
Advanced computing
Real economic and clinical impact
Tech platform change – PCR to sequencing
2013 20252020
$100
$1,000
$10,000
High
Low
+ =
Wave 3: Low-cost sequencing and advanced computing redefine what is possible
• $100 at home sequencing• 100% accurate diagnosis• 100% best treatment EBM• 100% personalized
3434© OLIVER WYMAN | CHI-HLC06101-046
Wave 3: Better Living organizations redefine prevention and early intervention while virtually eliminating diagnostic errors and personalizing treatments
Wave 2Consumer
engagement
Wave 1Patient-centered care
Life expectancy is 20% longer than today, with a higher
quality of life up until death
The discovery of 10,000 new biomarkers/pathways lead to more than 1,000 new predictive diagnostics and a 100 super-early stage treatments
75% of diagnosis are completed in real time through a single
sample, at home or in a convenient retail location with
100% accuracy
60% of therapeutics are focused on “prevention” and “very early stage treatment” vs. responsive
symptomatic sick care
75% of population has a life plan linked to personal genome
sequence and genomicrisk profile
Two major diseases are cured or eradicated
Wave 3The science of prevention
Wave 2 predictions15% less cost, 4% trend reduction, and 15% more value
35© OLIVER WYMAN | CHI-HLC06101-046 35
SIX BIG QUESTIONS every leader should be considering
13
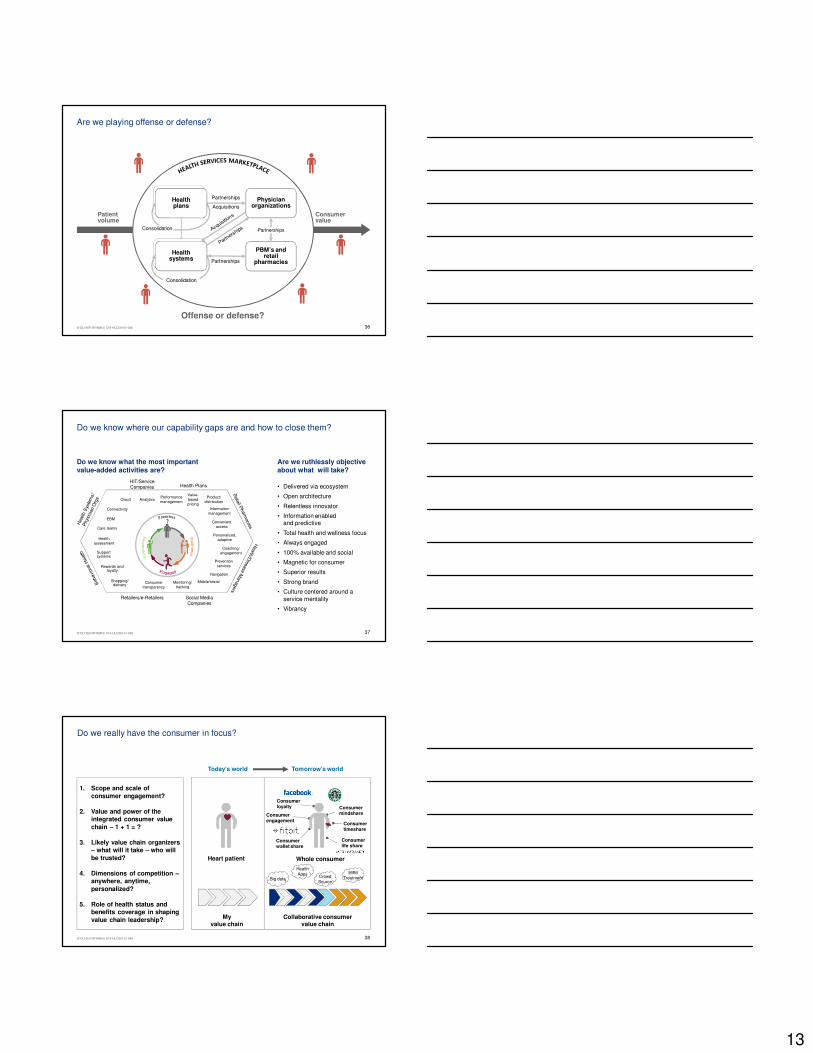
3636© OLIVER WYMAN | CHI-HLC06101-046
Patient volume
Consumer value
PBM’s and retail
pharmacies
Partnerships
Acquisitions
Partnerships
Partnerships
Healthplans
Consolidation
Healthplans
Consolidation
Healthplans
Physicianorganizations
Healthsystems
Offense or defense?
Are we playing offense or defense?
3737© OLIVER WYMAN | CHI-HLC06101-046
• Delivered via ecosystem
• Open architecture
• Relentless innovator
• Information enabled and predictive
• Total health and wellness focus
• Always engaged
• 100% available and social
• Magnetic for consumer
• Superior results
• Strong brand
• Culture centered around a service mentality
• Vibrancy
Retailers/e-Retailers Social Media Companies
HIT/Service Companies Health Plans
Healthassessment
Personalized,adaptive
Navigation
Convenientaccess
Analytics
Preventionservices
Mobile/social
Connectivity
Cloud
EBM
Monitoring/tracking
Performancemanagement
Product/distribution
Value-basedpricing
Care teams
Coaching/engagement
Shopping/delivery
Rewards andloyalty
Consumertransparency
Supportsystems
Informationmanagement
Do we know where our capability gaps are and how to close them?
Do we know what the most important value-added activities are?
Are we ruthlessly objective about what will take?
38© OLIVER WYMAN | CHI-HLC06101-046 38
Do we really have the consumer in focus?
My value chain
Collaborative consumer value chain
Heart patient
Consumer mindshare
Consumer loyalty
Consumer timeshare
Consumer engagement
Consumer wallet share
Consumer life share
Whole consumer
Today’s world Tomorrow’s world
1. Scope and scale of consumer engagement?
2. Value and power of the integrated consumer value chain – 1 + 1 = ?
3. Likely value chain organizers – what will it take – who will be trusted?
4. Dimensions of competition –anywhere, anytime, personalized?
5. Role of health status and benefits coverage in shaping value chain leadership?
Big data
Health Apps
Crowd Source
EBM Treatment

14
39© OLIVER WYMAN | CHI-HLC06101-046 39
Are we prepared to play in a multi-chain world?
From To
Solo-sport orientation Ecosystem-based
Wholesale Retail
Sickness Total health & wellness
Reactive Predictive/preventative
Body part or diagnostic code Whole person
Physical Virtual/anywhere/real-time
Transactional Relational
One-size-fits-all Personalized
Opaque Transparent
Individual/expert Crowd
My value chain Collaborative consumer value chain
Big data
Health Apps
Crowd Source
EBM Treatment
40© OLIVER WYMAN | CHI-HLC06101-046 40
Health retailers and e-retailers
Tech, consumer goods and services
Providers
Health plans
Have we really considered the compete or converge question?
Extra-industry players
Race to capitalize on higher value consumer relationships
Traditional healthcare players
Consumer mindshare
Consumer loyalty
Consumer timeshare
Consumer wallet share
Consumer biodata share
4141© OLIVER WYMAN | CHI-HLC06101-046
• Is the cost of inaction on the rise?
• Is there an inflection point where we can’t catch up to the leaders of the pack?
• If one of these models entered our markets, could we respond?
Are we moving fast enough?
The leader advantage is expanding, fueled by new technology, capital markets, and hare earned lessons
Today-player questions
Today’s Volume Players
Org
an
iza
tio
na
l s
op
his
tic
ati
on
Value creation
2nd Generation Leaders
1st Generation Leaders

15
42© OLIVER WYMAN | CHI-HLC06101-046 42
Volume to Value Post-Test• When is the estimated tipping point to value based insurance coverage?
– A. 2020
– B. 2017
– C. 2025
• What is the potential reduction in hospital admissions with value-based care?
– A. 10%
– B. 20%
– C. 30%
• What % of patients drive 45% of the cost?
– A. 10%
– B. 15%
– C. 5%
• What is the potential range of savings for these patients?
– A. 15%
– B. 25%
– C 35%
Related Documents











