VOLUME 23 NUMBER 3

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

VOLUME 23 NUMBER 3

VOLUME 23, NUMBER 3, 2020

Rev. Bras. Geriatr. Gerontol. 2020;23(3)
Editor / EditorRenato Peixoto Veras
Editor Associado / Associate EditorKenio Costa de Lima
Editor Executivo / Executive EditorRaquel Vieira Domingues Cordeiro
Grupo de Assessores / Editorial Advisory BoardAlexandre Kalache – Centro Internacional de Longevidade Brasil / International Longevity Centre Brazil (ILC BR). Rio de Janeiro-RJ - BrasilAnabela Mota Pinto – Universidade de Coimbra. Coimbra - PortugalAnita Liberalesso Néri – Universidade Estadual de Campinas. Campinas-SP – BrasilAnnette G. A. Leibing – Universidade Federal do Rio de Janeiro. Rio de Janeiro-RJ – BrasilAntón Alvarez – EuroEspes Biomedical Research Centre. Corunã – EspanhaCandela Bonill de las Nieves – Hospital Universitário Carlos Haya. Málaga - EspanhaCarina Berterö – Linköping University. Linköping – SuéciaCatalina Rodriguez Ponce – Universidad de Málaga. Málaga – EspanhaEliane de Abreu Soares – Universidade do Estado do Rio de Janeiro. Rio de Janeiro-RJ – BrasilEmílio H. Moriguchi – Universidade Federal do Rio Grande do Sul. Porto Alegre-RS – BrasilEmílio Jeckel Neto – Pontifícia Universidade Católica do Rio Grande do Sul. Porto Alegre-RS – BrasilEvandro S. F. Coutinho – Fundação Oswaldo Cruz. Rio de Janeiro-RJ – BrasilGuita Grin Debert – Universidade Estadual de Campinas. Campinas-SP – BrasilIvana Beatrice Mânica da Cruz – Universidade Federal de Santa Maria. Santa Maria-RS – BrasilJose F. Parodi - Universidad de San Martín de Porres de Peru. Lima – PeruLúcia Helena de Freitas Pinho França – Universidade Salgado de Oliveira. Niterói-RJ - BrasilLúcia Hisako Takase Gonçalves – Universidade Federal de Santa Catarina. Florianópolis-SC – BrasilLuiz Roberto Ramos – Universidade Federal de São Paulo. São Paulo-SP – BrasilMaria da Graça de Melo e Silva – Escola Superior de Enfermagem de Lisboa. Lisboa – PortugalMartha Pelaez – Florida International University. Miami-FL – EUAMônica de Assis – Instituto Nacional de Câncer. Rio de Janeiro-RJ – BrasilRaquel Abrantes Pêgo - Centro Interamericano de Estudios de Seguridad Social. México, D.F.Ricardo Oliveira Guerra – Universidade Federal do Rio Grande do Norte. Natal-RN – Brasil
Normalização / NormalizationMaria Luisa Lamy Mesiano SavastanoGisele de Fátima Nunes da Silva
Revista Brasileira de Geriatria e Gerontologia é continuação do título Textos sobre Envelhecimento, fundado em 1998. Tem por objetivo publicar e disseminar a produção científica no âmbito da Geriatria e Gerontologia, e contribuir para o aprofundamento das questões atinentes ao envelhecimento humano. Categorias de publicação: Artigos originais, Revisões, Relatos, Atualizações e Comunicações breves. Outras categorias podem ser avaliadas, se consideradas relevantes.
The Brazilian Journal of Geriatrics and Gerontology (BJGG) succeeds the publication Texts on Ageing, created in 1998. It aims to publish and spread the scientific production in Geriatrics and Gerontolog y and to contribute to the deepening of issues related to the human aging. Manuscripts categories: Original articles, Reviews, Case reports, Updates and Short reports. Other categories can be evaluated if considered relevant.
Colaborações / ContributionsOs manuscritos devem ser encaminhados ao Editor Executivo e seguir as “Instruções aos Autores” publicadas no site www.rbgg.com.brAll manuscripts should be sent to the Editor and should comply with the “Instructions for Authors”, published in www.rbgg.com.br
Correspondência / CorrespondenceToda correspondência deve ser encaminhada à Revista Brasileira de Geriatria e Gerontologia por meio do e-mail [email protected] correspondence should be sent to Revista Brasileira de Geriatria e Gerontologia using the email [email protected]
Revista Brasileira de Geriatria e GerontologiaUERJ/UnATI/CRDERua São Francisco Xavier, 524 – 10º andar - bloco F - Maracanã20 559-900 – Rio de Janeiro – RJ, BrasilTelefones: (21) 2334-0168 / 2334-0131 r. 229E-mail: [email protected] - [email protected]: www.scielo.br/rbggSite: www.rbgg.com.br
Indexação / IndexesSciELO – Scientific Electronic Library OnlineLILACS – Literatura Latino-Americana e do Caribe em Ciências da SaúdeLATINDEX – Sistema Regional de Información em Línea para Revistas Científicas de América Latina, el Caribe, Espana y PortugalDOAJ – Directory of Open Acess JournalsREDALYC - Red de Revistas Científicas de América Latina y el Caribe, España y PortugalFree Medical JournalsCabell s Directory of Publishing OpportunitiesThe Open Access Digital LibraryUBC Library Journals

Rev. Bras. Geriatr. Gerontol. 2020;23(3)
Contents
EDITORIALVULNERABILITIES OF THE OLDER POPULATION DURING THE CORONAVIRUS PANDEMICMauro Dias Silva Júnior
ORIGINAL ARTICLESCHRONIC PAIN IN OLDER ADULTS AND DIRECT AND INDIRECT ASSOCIATIONS WITH SOCIODEMOGRAPHIC AND HEALTH-RELATED CHARACTERISTICS: A PATH ANALYSISGraziella Ciola, Marcela Fernandes Silva, Monica Sanches Yassuda, Anita Liberalesso Neri, Flávia Silva Arbex Borim
INFLUENCE OF OBESITY ON CRITERIA FOR CLASSIFICATION OF SARCOPENIA IN OLD PEOPLEAna Paula Pillatt, Evelise Moraes Berlezi, Luana Brum de Jesus, Rodolfo Herberto Schneider, Ligia Beatriz Bento Franz
TEMPORAL TREND OF MORTALITY IN OLD PEOPLE IN CITIES IN THE STATE OF ACREThainá Souza Ribeiro, Alanderson Alves Ramalho, Suleima Pedroza Vasconcelos, Simone Perufo Opitz, Rosalina Jorge Koifman
TEMPORAL TREND OF THE INCIDENCE OF TB/HIV COINFECTION AND HIV TESTING OF THE OLD BRAZILIAN POPULATION FROM 2008 TO 2018Janderson Diego Pimenta da Silva, Rosemeiry Capriata de Souza Azevedo, Annelita Almeida Oliveira Reiners, Aenne Zandonadi Rodrigues Santana, Amanda Cristina de Souza Andrade, Ana Carolina Macri Gaspar Vendramini
KNOWLEDGE AND OVERLOAD OF THE FAMILY CARE BEFORE THE PATIENT WITH DEMENTIAJuliett Gonçalves dos Santos, Murilo Duarte da Costa Lima, Antônio Sávio Inácio, Érica Marcela Oliveira Silva, Raphael Alves da Silva, Felicialle Pereira da Silva
THE DEMANDS OF CARE AND SELF-CARE FROM THE FAMILY CAREGIVER’S OF THE ELDERLY WITH DEMENTIA PERSPECTIVEEmanuela Bezerra Torres Mattos, Jéssica Paloma Oliveira, Marcia Maria Pires Camargo Novelli
INADEQUATE KNOWLEDGE OF PRESCRIPTION DRUGS AND THEIR PREDICTORS IN VERY OLD PATIENTS AND THEIR CAREGIVERSThiago Vinicius Nadaleto Didone, Daniela Oliveira de Melo, Leonardo da Costa Lopes, Eliane Ribeiro
IMMEDIATE EFFECT OF RHYTHMIC AUDITORY STIMULATION ON THE SPATIO-TEMPORAL PARAMETERS OF GAIT IN OLD PEOPLE: A PILOT STUDYCamila Maria Mendes Nascimento, Laiza de Oliveira Lucena, Ágata Rodrigues de Lima, Jonathas Carlos de Lima, Carla Cabral dos Santos Accioly Lins, Maria das Graças Wanderley de Sales Coriolano
(GERONTO)TECHNOLOGIES OF CARE FOR OLD PEOPLE WITH ALZHEIMER’S DISEASE AND THEIR FAMILIES: CONTRIBUTION OF AWARENESS/TRAINING WORKSHOPS Silomar Ilha, Francine Casarin, Luciana de Carvalho Pires, Betânia Huppes, Claudia Zamberlan
ANALYSIS OF THE ASSOCIATION BETWEEN HAND GRIP STRENGTH AND FUNCTIONALITY IN COMMUNITY OLD PEOPLEMariana Edinger Wieczorek, Cislaine Machado de Souza, Patrícia da Silva Klahr, Luis Henrique Telles da Rosa
AESTHETICS AND HAPPINESS IN THE PERCEPTION OF OLD PEOPLE USERS OF BEAUTY PRODUCTSSabrina Fernanda Romanssini, Helenice de Moura Scortegagna, Nadir Antonio Pichler

Rev. Bras. Geriatr. Gerontol. 2020;23(3)
REVIEW ARTICLESPhysiotherapeutic interventions aimed at old people in situations of violence: a scope reviewAdriana Luna Pinto Dias, Ana Maria de Almeida, Mariana Cabral Schveitzer, Rafaella Queiroga Souto
Contents

1 of 3
Edito
rial
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200319
http://dx.doi.org/10.1590/1981-22562020023.200319
Vulnerabilities of the older population during the coronavirus pandemic
In Brazil, the current coronavirus pandemic has accounted for more than 5.5 million infections and approximately 159,000 deaths from COVID-19, the syndrome caused by the virus. The psychosocial effects, however, are equally devastating, due to their impact on the financial security of families and the mental health of the population. Every possible scenario of the pandemic has effects that reveal the insecurity of the times we are living through, such as increased reports of anxiety and the fear of leaving home to work, the significant emotional burden imposed on frontline health workers in hospitals, or even families trying to deal with the pain caused by the death or hospitalization of their loved ones. The year 2020 surely represents a watershed event in recent human history.
The vulnerabilities to which we are exposed are particularly evident in the case of the older population, who are among the most susceptible to complications from COVID-19, with 50% to 84% of those killed by the disease in Brazil included in this group. Even before the pandemic, older people were one of the population groups that suffered most from isolation, due to the social vulnerabilities imposed by a society that excludes them from family and social life. Even in pre-pandemic times, these individuals suffer the burden of isolation when the process of institutionalization is accompanied by a decline in family ties, or even when they are excluded within their own homes. In addition, older adults are particularly vulnerable due to their progressive loss of social support, with the deaths of relatives, spouses and friends, which accumulate over the years, potentially impacting their mental health problems. The death of a spouse in particular is a factor that worsens the quality of life of older adults, accelerating the decline of their mental health and often being associated with their own subsequent death. Additionally, when compared to young people, older adults have a greater tendency to touch themselves, possibly to compensate for the lack of the touch of others. Now, in view of the context of distended quarantine, and even before the possible impacts generated by the emergence of COVID-19, older adults represent the group that suffers most from the distancing needed to control the pandemic.
Studies have shown that support networks and meaningful relationships are the greatest predictors of life satisfaction and longevity, overcoming other important elements such as healthy nutrition and living habits. The importance of forming and maintaining positive social networks is not surprising when we consider the overriding pro-social characteristics of our species, and the fact that subjective well-being is positively associated with the goals of building lasting familial and loving bonds. Furthermore it is known that hormones related to feelings of pleasure and well-being are released into the bloodstream when we are touched by other people, or when we interact with a dog, for example, and even when we believe that we

2 of 3
Editorial
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200319
are in the company of another person in a non-family environment. Life’s tribulations are minimized when we have someone to rely on. It is this social support that we need, particularly in the case of older adults, who are repeatedly excluded from family and social life in our society.
Although modern Western societies do not recognize the value of older adults to the extent they should, in other societies the older population assumes an important role in social dynamics, transmitting knowledge and contributing to the health of their grandchildren, for example. Through historical alliances, older people create and maintain networks of relationships that directly and indirectly affect the daily life of their families, contributing to significant moments throughout life.
It is worrying to consider that the distancing caused by the pandemic could further aggravate the vulnerability of the older population. Since the beginning of the year, I have advocated substituting the term social distancing for physical distancing, due to the fact that technology can serve as an instrument of approximation between physically distant people. Objectively, we do not want to socially isolate people, we want to keep them physically apart to preserve their health. Social isolation can have serious emotional consequences, such as feelings of loneliness, depression and anxiety. It is not by chance that older adults are among those who most report experiencing such feelings. Using technology to bring people together can minimize the negative impacts of a lack of physical and eye to eye contact.
Times of crisis such as this can only be overcome with changes in cultural practices and values. For example, this process of change cannot occur if we do not know how to respond to the spread of the virus at an individual and collective level. With this knowledge, we can reflect and plan the changes necessary to get through the crisis in the best possible way. Thinking as a society about the world we want after the pandemic is fundamental to mitigating the negative effects of the crisis, especially on the most vulnerable groups. Perhaps the pandemic will represent an opportunity to review our choices, and to plan decision-making at individual and governmental levels that can guide such changes.
I dedicate this text to my mother-in-law, Sandra Maria Duarte Marques, victim of COVID-19, who died at the age of 70. She will be greatly missed.
Mauro Dias Silva Júnior, Doctor in Behavior Theory and Research, Adjunct Professor I and Coordinator of the Center of Psychological Studies and Care.
Universidade de Brasília, Institute of Psychology, Department of Basic Psychological Processes. Brasília, DF, Brazil
ID
REFERENCES
1. Barbosa IR, Galvão MH, de Souza T, Gomes S, Medeiros ALK. Incidence of and mortality from COVID-19 in the older Brazilian population and its relationship with contextual indicators: an ecological study. Rev Bras Geriatr Gerontol. 2020;23(1):e200171. Available from: http://dx.doi.org/10.1590/1981-22562020023.200171
2. Chan YK, Lee R. Network size, social support, and happiness in later life: a comparative study of Beijing and Hong Kong. J Happiness Stud. 2006;7:87-112.
3. Ko A, Pick C, Kwon J, Barlev M, Krems J, Varnum M, et al. Family matters: Rethinking the Psychology of Human Social Motivation. Perspect Psychol Sci. 2020:1-29. Available from: https://doi.org/10.1177/1745691619872986

3 of 3
Editorial
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200319
4. Arnot M, Brandl E, Campbell O, Chen Y, Du J, Zhang H, et al. How evolutionary behavioural sciences can help us understand behaviour in a pandemic. Evol Med Public Health. 2020:eoaa038. Available from: https://doi.org/10.1093/emph/eoaa038
5. Lee R, Ruan D, Lai G. Social structure and social support in Beijing and Hong Kong. Soc Netw. 2005;27:249-74.
6. Seitz B, Aktipis A, Buss D, Alcock J, Bloom P, Haselton H. The pandemic exposes human nature: 10 evolutionary insights. Proc Natl Acad Sci. 2020:202009787. Available from: https://doi.org/10.1073/pnas.2009787117
7. Silva Júnior MD. Por que devemos substituir o termo isolamento social por distanciamento físico? [Internet]. 2020 [cited 2020 nov. 02]. Video: 19 min. Available from: https://www.youtube.com/watch?v=67wPzoAcSjw

1 of 10
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
http://dx.doi.org/10.1590/1981-22562020023.200065
Chronic pain in older adults and direct and indirect associations with sociodemographic and health-related characteristics: a path analysis
Graziella Ciola1
Marcela Fernandes Silva1
Monica Sanches Yassuda1,2
Anita Liberalesso Neri1
Flávia Silva Arbex Borim1,3
Keywords: Chronic Pain. Self-Assessment. Health of the Elderly.
AbstractObjective: Identify the prevalence of chronic pain in individuals older than 70 years of age and identify relations between chronic pain and both sociodemographic and health-related characteristics to determine the role of chronic pain as a mediator between these variables in relation to self-rated health. Methods: A cross-sectional study was conducted with 419 individuals aged 72 years and older, between the years of 2016 and 2017. The participants were from the follow-up of the FIBRA Study, which included non-institutionalized older adults living in urban areas of the cities of Campinas and Ermelino Matarazzo in the state of São Paulo, Brazil. The mediating variable was chronic pain, which was assessed by the self-report of the presence of pain in the previous six months. The independent variables were sociodemographic characteristics, health-related behaviors, multimorbidity, depressive symptoms, insomnia and self-rated health. Direct and indirect relations were tested using path analysis. Results: A total of 57.0% of the sample reported chronic pain. The female gender, a high body mass index (BMI), multimorbidity, insomnia, and depressive symptoms were directly associated with chronic pain. Chronic pain figured as a mediator variable in the associations between self-rated health and gender, BMI, multimorbidity, and symptoms of insomnia. Conclusion: Data demonstrate a complex network of interactions between chronic pain and both sociodemographic and health-related characteristics. Such knowledge can benefit the management and care of the older adults affected with chronic pain.
1 Universidade Estadual de Campinas (Unicamp), Faculdade de Ciências Médicas, Programa de Pós-Graduação em Gerontologia. Campinas, SP, Brasil.
2 Universidade de São Paulo (USP), Escola de Artes, Ciências e Humanidades. São Paulo, SP, Brasil3 Universidade de Brasília, Departamento de Saúde Coletiva, Faculdade de Ciências da Saúde. Brasília,
DF, Brasil
Funding: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) - Nº do processo: 2972/2014; Fundação de Amparo à Pesquisa do Estado de São Paulob (FAPESP) - Nº do processo: 2016/00084-8; e Conselho Nacional de Pesquisa (CNPq) - Nº do processo 424789/2016-7. Bolsa de Mestrado da G. Ciola pela CAPES e Bolsa de Pós-doutorado de F.S.A. Borim pela FAPESP. The authors declare there are no conflicts of interest in relation to the present study.
CorrespondenceGraziella [email protected]
Received: March 6, 2020Approved: November 9, 2020
ID
ID
ID
ID
ID

2 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
INTRODUC TION
Self-rated health (SRH) is a subjective assessment measure of a comparative, evaluative nature based on personal and social criteria that reveals the impact of disease on the wellbeing of an individual. Studies report that SRH as being poor or very poor is associated with a lower socioeconomic status, physical inactivity, multimorbidity, depressive symptoms, polypharmacy, and falls in older adults1,2. SRH is considered an important measure for determining the general health of a population and is a strong predictor of negative outcomes, such as functional disability and death2-4.
Chronic pain is highly prevalent in the older population3,4 and is a determinant of self-rated health5-7. The burden of chronic pain can lead to social isolation, difficulties regarding mobility, and a reduction in quality of life, which may explain the strong association with SRH8,9. A study comparing SRH in different age groups and its association with chronic pain found that the effect of pain diminished with the increase in age and that pain had a greater influence on SRH than age per se10.
In Brazil, few studies have been published with the aim of understanding the role of chronic pain as a mediating variable in the relation between SRH and sociodemographic, psychosocial, and health-related characteristics. Observational studies on chronic pain among older people in Brazil all have a cross-sectional design and only offer data on direct associations. These studies report the prevalence of chronic pain to range from 29.3% to 73.3%, with a greater frequency in the female sex11,12.
Chronic pain can inf luence psychological, physiological, and social aspects of affected individuals. Thus, knowledge on interactions between chronic pain and both sociodemographic and health-related factors as well as the effect of these interactions on SRH could facilitate our understanding of the need for a multimodal or interdisciplinary approach to the management of chronic pain and the understanding of the complex network of interactions among different variables throughout the course of life.
Therefore, the aim of the present study was to identify the prevalence of chronic pain among individuals older than 70 years of age as well as the direct and indirect associations between chronic pain and both sociodemographic and health-related factors. A further aim was to propose an explanation for the association between chronic pain and self-rated health, highlighting potential targets of interventions, such as modifiable health-related variables, to ensure better management of chronic pain and the maintenance of health among affected older adults.
METHODS
A cross-sectional study was conducted using data from the Fragilidade em Idosos Brasileiros (FIBRA [Frailty among Older Brazilians]) study, which is a multicenter longitudinal study. All data used in the present study were from the second wave of the FIBRA study, from which the variable of interest (chronic pain) was collected.
The first wave of the FIBRA study occurred in 2008 and 2009 and involved probabilistic samples of individuals 65 years of age or older (n = 3,478) residing in seven Brazilian cities selected by convenience due to the proximity to universities with research groups in the field of aging. The seven cities were Campinas (state of São Paulo), Ermelino Matarazzo (district in the city of São Paulo), Belém (state of Pará), Parnaíba (state of Piauí), Campina Grande (state of Paraíba), Poços de Caldas (state of Minas Gerais), and Ivoti (state of Rio Grande do Sul)13. The follow-up of the FIBRA study (second wave) was conducted in 2016 and 2017 and exclusively involved the participants in the city of Campinas and district of Ermelino Matarazzo (state of São Paulo).
In the first wave, these two locations contributed 1,284 individuals 65 years of age or older (68.7% women and mean age of 72.6±5.8 years). At follow-up, 549 were located and interviewed at home (69.9% women and mean age of 72.2±5.2 years), 192 had deceased (59.9% women and mean age of 75.5±6.8), and 543 were not located (70.5% women and mean age of 72.0±5.6). Among the 549 older people with

3 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
records in the databank of the second wave, 130 were excluded due to cognitive impairment and for not answering the self-reported measures (Figure 1).
The score on the Mini Mental State Examination was considered for the selection of participants based on the cognitive criteria using the cutoff points adjusted for years of schooling established in the validation study conducted by Brucki et al.14 (17 points for illiterate individuals and those with no formal schooling, 22 points for those with one to four years of schooling, 24 points for those with five to eight years, and 26 points for those with nine or more years of schooling).
The variables of interest were chronic pain (based on the answer to the following question: Have you had any constant pain or pain that comes and goes in the last six months? [yes or no]) and self-rated health (based on the answer to the following question: Would you say your health is generally very good, good, fair, poor, or very poor?, for which the responses were dichotomized as positive SRH [very good/good] or negative SRH [fair/poor/very poor])15.
The following were independent variables: a) sociodemographic – sex (male and female, self-declared), age (measured in years from the date of birth to the date of the interview), and years of schooling (self-reported); b) physical activity – weekly frequency and daily duration of physical exercise based on answers to items selected from the adapted version of the Minnesota Leisure-time Physical Activity Questionnaire ( MLTPAQ)13,16 considered for the classification of the participants as active or inactive based on the recommendations of the American College of Sports Medicine (active =150 minutes per week of moderate activity or 120 minutes per week of vigorous activity);17 c) body mass index (BMI), calculated as body weight (kg) divided by height (m) squared (kg/m²) and using the cutoff points recommended by the Pan American Health Association18 (recorded as a continuous variable); d) morbidities – number of affirmative answers to nine dichotomous items investigating whether any physician had performed a diagnosis of heart
disease, systemic arterial hypertension, stroke, diabetes mellitus, cancer, arthritis or rheumatism, depression, lung disease, and osteoporosis (responses categorized as none/one disease and two/more diseases; e) depressive symptoms – evaluated using the 15 dichotomous items of the Geriatric Depression Scale (GDS-15) with a cutoff point of ≥ 6 points for the screening of depressive symptoms19; f ) symptoms of insomnia – evaluated using four self-report questions with a dichotomous answer (yes or no) taking the previous 12 months as reference: Does it take you a long time to fall asleep?, Do you remain awake most of the night?, Do you wake up in the middle of the night and can’t get back to sleep?, Do you sleep badly at night? An affirmative answer to at least one of these questions indicated symptoms of insomnia20.
Descriptive analyses were performed for the characterization of the sample with measures of absolute and relative frequency for categorical variables as well as mean, median, and standard deviation values for quantitative variables. Percentage distributions with respective 95% confidence intervals were calculated.
To study the relations between the variables of interest according to a previous theoretical model (Figure 2)8, structural equation analysis was used via path analysis. This type of analysis serves as an extension of the regression model and is used to determine relations among a set of variables. This resource enables an analysis of direct or indirect relations between independent and dependent variables. Straight arrows indicate a direct or indirect association, whereas elliptic arrows indicate covariance. After the adjustment of the indicators and significance tests, the final path analysis model is created, which either sustains or eliminates relations from the previous theoretical model. For the present study, the tests and acceptance values were the chi-square goodness-of-fit test > 0.05, chi-square ratio (X2/GL) <2, standardized root mean square residual (SRMR) ≤0.10, root mean square error of approximation (RMSEA) ≤0.08, comparative fit index (CFI) ≥0.90, and Tucker-Lewis index (TLI) ≥0.90.21

4 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
Figure 1. Flowchart of final sample of study based on sample of FIBRA study 2016/2017.
Figure 2. Hypothetical model of relations between chronic pain and sociodemographic variables and health conditions. São Paulo, Brazil, 2016/2017.

5 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
After the analysis of the goodness of fit of the data to the proposed paths, significance tests were performed for the path coefficients. Absolute values of t >1.96 indicate the path has a statistically significant coefficient21.
All procedures were in accordance with the ethical precepts contained in the Declaration of Helsinki as well as the ethical norms stipulated by the Brazilian Board of Health governing research involving human subjects. The FIBRA study was approved under certificate numbers 1.332.651 and 2.847.829. Process 2016/00084-8 and Conselho Nacional de Pesquisa (CNPq [National Research Council]) process 424789/2016-7. The present study received approval from the Human Research Ethics Committee of the School of Medical Sciences of the State University of Campinas (certificate number: 3258919, April 11, 2019).
RESULTS
Four hundred nineteen older adults participated in the present study. Women accounted for 70.2% of the sample and the majority (60.9%) had between one and four years of schooling. Mean age was 80.3 ± 4.75 years and mean BMI was 21.27 ± 3.78 kg/m2. A total of 74.5% of the participants were classified at inactive, 67.3% had two or more chronic diseases, 53.0% had symptoms of insomnia, and 18.8% had depressive symptoms. Regarding the variables of interest, 57.0% had chronic pain and 47.0% self-rated their health as fair/poor/very poor (Table 1).
After the third revision of the path analysis, acceptable values were obtained for all goodness-of-fit criteria (Table 2) and all path coefficients were significant ( p<0.05). In the first revision, direct
relations that did not present a significant difference in the estimate of the coefficients were excluded. In the second revision, covariances between depressive symptoms and multimorbidity as well as between depressive symptoms and insomnia were included. In the third and final revision, the bidirectional relation between chronic pain and depressive symptoms was included.
Figure 3 illustrates the results of the final path analysis. The following were the main findings for direct associations: the presence of chronic pain was associated with the female sex, a high BMI, multimorbidity, and symptoms of insomnia; negative SRH was associated with low schooling, depressive symptoms, and chronic pain. Depressive symptoms and chronic pain had a bidirectional association (Figure 3).
In the final path analysis model, chronic pain was an important mediating variable of the indirect associations between SRH and gender, BMI, multimorbidity, and symptoms of insomnia, whereas depressive symptoms constituted a mediating variable in the association between chronic pain and SRH (Figure 3).
The changes made to the final model following the prior theoretical model were the exclusion of the direct associations between age and physical activity, morbidity, insomnia, chronic pain, and SRH; between schooling and BMI, insomnia, morbidity, depressive symptoms, chronic pain, and SRH; between gender and physical activity, depressive symptoms, and BMI; between physical activity and insomnia, depressive symptoms, chronic pain, and SRH; between BMI and depressive symptoms and insomnia; between morbidity and SRH; and between insomnia and SRH.

6 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
Table 1. Characteristics of participants in study, São Paulo, Brazil, 2016/2017.
Variables n (%) 95% CI Mean (SD)Median
AgeMean (standard deviation) 80 (±4.75)Median 80SexMale 139 (29.8) 25.8 - 34.1Female 327 (70.2) 65.8 – 74.1Schooling (years of study)≥ 9 or more 50 (11.3) 8.6 - 14.55 to 8 66 (14.9) 11.8 – 18.51 to 4 277 (60.9) 56.3 – 65.4Illiterate 57 (12.9) 10.0 – 16.3Physical activityActive 119 (25.5) 19.3 - 26.9Inactive 348 (74.5) 73.3 – 80.6Body mass indexMean (standard deviation) 21.27 (±3.78)Median 21.01First quartile 18.65Third quartile 23.70Chronic diseases0 to 1 131 (32.7) 28.2 - 37.4≥ 2 270 (67.3) 62.5 - 71.7InsomniaNo 196 (47.0) 42.2 - 51.8Yes 221 (53.0) 48.1 – 57.7Depressive symptomsAbsent 311 (81.2) 76.9 - 84.8Present 72 (18.8) 15.1 – 23.0Chronic painNo 180 (43.0) 38.2 - 47.7Yes 239 (57.0) 52.2 – 61.7Self-rated healthVery good/good 222 (53.0) 48.1 - 57.7Fair/poor/very poor 197 (47.0) 42.2 – 51.8
Table 2. Goodness-of-fit measures through path analysis. São Paulo, Brazil, 2016/2017.
Goodness-of-fit criteria Initialmodel
After 1st revision
After 2nd revision
After 3rd revision
Chi-square goodness-of-fit test <0.001 <0.001 <0.022 0.079Chi-square ratio (?2/GL) <0.001 <0.001 <0.001 <0.001Tucker-Lewis index 0.818 0.675 0.818 0.902Comparative fit index 0.827 0.775 0.888 0.928Standardized root mean square residual 0.049 0.072 0.056 0.050Root mean square error of approximation 0.158 0.070 0.052 0.042

7 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
DISCUSSION
The main findings were that 57.0% of the sample reported having chronic pain, which was directly associated with sex, BMI, multimorbidity, symptoms of insomnia, and depressive symptoms. Chronic pain was also a mediating variable in the associations between SRH and sex, BMI, multimorbidity, and symptoms of insomnia.
Regarding the high prevalence of chronic pain (57.0%), a review study reported considerable variability in studies conducted in Brazil, ranging from 29.7% to 73.3%11. Among non-institutionalized older people, the prevalence ranged from 29.3% to 54.7%22,23. Van Hecke et al.5 reported that, although age is not a causal factor of chronic pain, the advance in age is an important sociodemographic factor and is associated with the increase in prevalence. Larsson et al.6 found that chronic pain was more prevalent
among individuals 85 years of age or older compared to younger elderly individuals. In the present study, the prevalence of chronic pain was higher among women than men. According to previous studies, women have a greater likelihood of developing chronic pain over time5,24,25.
BMI was directly associated with chronic pain and the latter was a mediating variable of the indirect association with SRH. Obesity can contribute to an increase in chronic pain in two ways: due to excessive load on the joints and due to the systemic proinflammatory state caused by excess weight. Moreover, pain contributes to sedentary behavior, leading to a greater likelihood of developing obesity26. The prevalence of pain is higher among obese individuals compared to those with a BMI in the ideal range27. After 12 months of follow-up, Larsson et al.6 found that gender, BMI, and pain in more than one location were associated with the persistence of pain.
Figure 3. Final model of relations between chronic pain and sociodemographic variables and health conditions according to path analysis. São Paulo, Brazil, 2016/2017.

8 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
Besides being associated with chronic diseases, excess body fat can exert a negative impact on functional capacity, psychosocial aspects, and behavioral aspects and can indirectly affect SRH1.
Multimorbidity was directly associated with chronic pain and the latter was also a mediating variable in the association between multimorbidity and SRH. In the study conducted by Xin Peng28, individuals with more morbidities had greater pain intensity measured on a numerical pain rating scale and chronic pain was a mediating variable in the associations between multimorbidity and functional disability as well as between multimorbidity and impaired physical performance28. A possible explanation for the indirect association between multimorbidity and SRH is that multimorbidity is more associated with poorer SRH when mediated by modifiable symptoms, such as pain, pain intensity, depression, somatic complaints, and restrictions to physical activity, than to chronic disease per se.
In the present study, depressive symptoms were directly associated with chronic pain. In a review study involving predominantly retrospective studies, Velly and Mohit24 found higher frequencies of depression and anxiety in patients with chronic pain, reporting a bidirectional association (greater severity of the psychological disorder related to greater pain severity). Santos et al.25 also report that the perception of pain is worse in the presence of depression and anxiety. These findings are explained by the fact that both manifestations share the same brain activations and neurotransmitters25.
Insomnia was directly associated with chronic pain and indirectly related to SRH. Sivertsen et al.29 studied different measures of sleep disorders to identify the impact on pain and found an influence on tolerance to pain. Pain can alter the signaling of dopamine, which underpins the relation between sleep and waking. However, further studies are needed to explain how sleep disorders can alter the function and release of dopamine and affect pain29. Regarding the indirect association between insomnia and SRH, Jiménez-Trujillo et al.9 state that insomnia exerts a negative impact on both the prognosis of chronic pain and SRH.
The present findings point to complex interactions between chronic pain and both sociodemographic and health-related variables, which suggests that there are numerous associated factors and the effects exert an influence on SRH. The review study by Chireh and D’Arcy10 showed direct relations between chronic pain and depression, BMI, schooling, stress, and loneliness and the authors found that, in the absence of chronic pain, individuals older than 85 years of age have a greater likelihood of rating their health as good compared to adults (45-54 years), but this probability is inverted in the presence of pain (individuals older than 85 years of age report poorer SRH). The present study draws attention to the negative impact that chronic pain exerts on SRH and shows that a poor SRH prevails in the chain of events formed by other interactions.
As limitations of the present study, selection bias should be cited, since the sample was composed of privileged survivors because institutionalized or hospitalized older people were not included, which could represent a sample with a better health status. Although observational studies involving path analysis represent a configuration of possible causal relations by means of paths21, the present study does not enable establishing causality between the variables. Thus, additional studies are needed for this type of understanding.
Further studies involving individuals 70 years of age or older are needed in Brazil, as such studies remain scarce and could offer signs, especially psychosocial signs, of resilience that differs from those found in younger cohorts10,11. Epidemiological investigations, such as cohort and intervention studies, should be conducted to understand the interactions of the causal chain of chronic pain and determine the results of interventions according to covariables, such as those cited in the present study. Moreover, pain intensity should be addressed in such studies to quantify the strength of the association according to the dose-response effect.
Chronic pain is a highly complex event affected by multiple factors that should be analyzed, especially as a mediator of negative outcomes, such as multimorbidity, functional disability, and negative SRH. This type of pain can lead to a cascade of

9 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
negative events in the older population due to the association with metabolic, psychosocial, and neurological changes as well as individual, contextual, and behavioral variables30. The strengths of the present study were the mean age of the sample (80.3 years), as few studies have been developed with this age group, which surpasses the life expectancy of the Brazilian population, and the study design both in terms of the analysis of the possible paths of chronic pain that lead to negative self-rated health as well as the age group and variables studied.
CONCLUSION
The results of the present study show the high prevalence of chronic pain in the sample (57%)
as well as the network of interactions between chronic pain and both sociodemographic and health-related characteristics. The female sex, a high BMI, multimorbidity, symptoms of insomnia, and depressive symptoms were directly associated with chronic pain, which was a mediating variable of associations between self-rated health and gender, BMI, multimorbidity, and symptoms of insomnia. The understanding of the complex interactions between chronic pain and health status can benefit the management and care of older people affected by chronic pain. Chronic pain not only exerts a negative impact on self-rated health, it is an important mediating variable in the relation between self-rated health and health conditions.
Edited by: Maria Helena Rodrigues Galvão
REFERENCES
1. Borim FSA, Barros MBA, Neri AL. Autoavaliação da saúde em idosos: pesquisa de base populacional no Município de Campinas, São Paulo, Brasil. Cad Saúde Pública. 2012;28:769-80.
2. Borim FSA, Neri AL, Francisco PMSB, Barros MBA. Dimensions of self-rated health in older adults. Rev Saúde Pública. 2014;48:714-22.
3. Wu S, Wang R, Zhao Y, Ma X, Wu M, Yan X, et al. The relationship between self-rated health and objective health status: a population-based study. BMC Public Health. 2013;13(1):1-9.
4. Falconer J, Quesnel-Vallee A. Pathway from poor self-rated health to mortality: Explanatory power of disease diagnosis. Soc Sci Med. 2017;190:227-36.
5. van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013;111(1):13-8.
6. Larsson C, Hansson EE, Sundquist K, Jakobsson U. Chronic pain in older adults: prevalence, incidence, and risk factors. Scand J Rheumatol. 2017;46(4):317-25.
7. Nutzel A, Dahlhaus A, Fuchs A, Gensichen J, Konig HH, Riedel-Heller S, et al. Self-rated health in multimorbid older general practice patients: a cross-sectional study in Germany. BMC Fam Pract. 2014;15(1): 1-9.
8. Blyth FM, Noguchi N. Chronic musculoskeletal pain and its impact on older people. Best Pract Res Clin Rheumatol. 2017;31(2):160-8.
9. Jimenez-Trujillo I, Lopez-de-Andres A, Del Barrio JL, Hernandez-Barrera V, Valero-de-Bernabe M, Jimenez-Garcia R. Gender Differences in the Prevalence and Characteristics of Pain in Spain: Report from a Population-Based Study. Pain Med. 2019;20(12):2349-59.
10. Chireh B, D’Arcy C. Pain and self-rated health among middle-aged and older Canadians: an analysis of the Canadian community health survey-healthy aging. BMC Public Health. 2018;18(1):e1006.
11. Vasconcelos FH, de Araújo GC. Prevalence of chronic pain in Brazil: a descriptive study. BrJP. 2018;1(2):176-9.
12. de Carvalho RC, Maglioni CB, Machado GB, de Araújo JE, da Silva JRT, da Silva ML. Prevalence and characteristics of chronic pain in Brazil: a national internet-based survey study. BrJP. 2018;1(4):331-8.
13. Neri AL, Yassuda MS, Araujo LF, Eulalio MC, Cabral BE, Siqueira ME, et al. Methodology and social, demographic, cognitive, and frailty profiles of community-dwelling elderly from seven Brazilian cities: the FIBRA Study. Cad Saúde Pública. 2013;29(4):778-92.
14. Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003;61(3):777-81.
15. Medeiros SM, Silva LSR, Carneiro JA, Ramos GCF, Barbosa ATF, Caldeira AP. Factors associated with negative self-rated health among non-institutionalized elderly in Montes Claros, Brazil. Ciênc Saúde Colet. 2016;21(11):3377-86.

10 of 10
Chronic pain and self-rated health in older adults: path analysis
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200065
16. Lustosa LP, Pereira DS, Dias RC, Britto RR, Parentoni AN, Pereira LSM. Translation and cultural adaptation of the Minnesota Leisure Time Activities Questionnaire in community-dwelling older people. Geriatr Gerontol Aging. 2011;5(2):57-65.
17. Nelson ME, Rejeski WJ, Blair SN, Duncan PW, Judge JO, King AC, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Circulation. 2007;116(9):1094-105.
18. Pan-american Health Organization. Multicenter survey aging, health and wellbeing in Latin América and the Caribbean (SABE): preliminary report; 2001.Washington, DC: PAHO; 2001.
19. Almeida OP, Almeida SA. Reliability of the Brazilian version of the abbreviated form of Geriatric Depression Scale (GDS) short-form. Arq Neuropsiquiatr. 1999;57(2b):421-6.
20. Pan-american Health Organization . Multicenter survey aging, health and wellbeing in Latin América and the Caribbean (SABE): preliminary report; 2001. Washington, DC: PAHO; 2004. p.905-14.
21. Acock AC. Discovering Structural Equation Modeling: Using Stata. [New York]: Stata Press; 2013.
22. dos Santos FA, de Souza JB, Antes DL, d’Orsi E. Prevalence of chronic pain and its association with the sociodemographic situation and physical activity in leisure of elderly in Florianopolis, Santa Catarina: population-based study. Rev Bras Epidemiol. 2015;18(1):234-47.
23. Lini EV, Tomicki C, Giacomazzi RB, Dellani MP, Doring M, Portella MR. Prevalence of self-referred chronic pain and intercurrences in the health of the elderly. Rev Dor. 2016;17(4):279-82.
24. Velly AM, Mohit S. Epidemiology of pain and relation to psychiatric disorders. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87(Pt B):159-67.
25. Santos KAdS, Cendoroglo MS, Santos FC. Anxiety disorder in elderly persons with chronic pain: frequency and associations. Rev Bras Geriatr Gerontol. 2017;20(1):91-8.
26. Arranz LI, Rafecas M, Alegre C. Effects of obesity on function and quality of life in chronic pain conditions. Curr Rheumatol Rep. 2014;16(1):1-9.
27. Li J, Chen J, Qin Q, Zhao D, Dong B, Ren Q, et al. Chronic pain and its association with obesity among older adults in China. Arch Gerontol Geriatr. 2018;76:12-8.
28. Peng X, Bao X, Xie Y, Zhang X, Huang J, Liu Y, et al. The mediating effect of pain on the association between multimorbidity and disability and impaired physical performance among community-dwelling older adults in southern China. Aging Clin Exp Res. 2019;32:1-8.
29. Sivertsen B, Lallukka T, Petrie KJ, Steingrimsdottir OA, Stubhaug A, Nielsen CS. Sleep and pain sensitivity in adults. Pain. 2015;156(8):1433-9.
30. Bonakdar RA. Integrative Pain Management. Med Clin North Am. 2017;101(5):987-1004.

1 of 11
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
http://dx.doi.org/10.1590/1981-22562020023.200083
Influence of obesity on criteria for classification of sarcopenia in old people
Ana Paula Pillatt1 Evelise Moraes Berlezi2
Luana Brum de Jesus3
Rodolfo Herberto Schneider4
Ligia Beatriz Bento Franz2
Keywords: Sarcopenia. Obesity. Comprehensive Health Care. Health of the Elderly.
AbstractObjective: to identify the prevalence of sarcopenic obesity in old residents in the community and to analyze the relation between obesity and the sarcopenia classification criteria. Method: This is an analytical cross-sectional study linked to the project “Comprehensive Health Care for the Old People”. The assessment of sarcopenia was carried out using the criteria of the European Sarcopenia Consensus. For the classification of the old people as sarcopenic obese, we considered as likely sarcopenic, sarcopenic, or severe sarcopenic associated with a fat percentage >27% for men and >38% for women. The data were analyzed using bivariate statistics and a linear regression model. Results: from a sample of 209 community-dwelling old people, a prevalence of 23,9% of sarcopenia, 28,2% of obesity and 4,3% of sarcopenic obesity was found. Still, it can be observed that men had a higher prevalence of sarcopenia ( p=0,006) and obesity (p=0,005) than women; the obese had a lower prevalence of muscle mass loss than the non-obese old people ( p<0,001); and the obese showed an increase in muscle strength (p=0,003) and muscle mass (p<0,001) in relation to the non-obese, even when adjusted for gender, age group, multicomorbidities, and functional capacity. Conclusion: taking into account the prevalence of sarcopenic obesity in the population studied and the positive influence of obesity in the prediction of strength and muscle mass, the importance of multidimensional assessment of the old people is highlighted, in order to ascertain the real need for interventions for weight loss, with the aim of preventing strength and muscle mass loss.
1 Pontifícia Universidade Católica do Rio Grande do Sul (PUC-RS), Escola de Medicina, Programa de Pós-Graduação em Gerontologia Biomédica. Porto Alegre, RS, Brasil.
2 Universidade Regional do Noroeste do Estado do Rio Grande do Sul, Departamento de Ciências da Vida, Programa de Pós-Graduação em Atenção Integral à Saúde. Ijuí, RS, Brasil.
3 Universidade Regional do Noroeste do Estado do Rio Grande do Sul, Departamento de Ciências da Vida, Curso de Graduação em Fisioterapia. Ijuí, RS, Brasil.
4 Pontifícia Universidade Católica do Rio Grande do Sul (PUC-RS), Escola de Medicina, Programa de Pós-Graduação em Gerontologia Biomédica. Porto Alegre, RS, Brasil.
Funding: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES). Número do Edital: 88882.164931-2014-01, Código de Financiamento 001, Bolsa PROEX.The authors declare there are no conflicts of interest in relation to the present study.
CorrespondenceAna Paula [email protected]
Received: March 31, 2020Approved: November 5, 2020
ID
ID
ID
ID
ID

2 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
INTRODUC TION
Sarcopenia was previously considered a physiological alteration due to aging, but today it is classified as a disease characterized by muscle failure occurring before the aging process, with the main investigative reason being the low muscle strength 1. Measuring muscle strength is the most reliable way of measuring muscle function, and from that, it is possible to classify it as ‘probable sarcopenia’, when the old person has only low muscle strength; ‘sarcopenia’, when low muscle strength is associated with low muscle quantity or quality; and ‘severe sarcopenia’, when the old person declines in physical performance2.
Age-related changes in the musculoskeletal system and the increased prevalence of obesity currently observed in the old people reveal a new condition called sarcopenic obesity3, which is the association between sarcopenia and increased body fat4. This clinical phenotype implies a close connection between the muscle and adipose tissue and plays a central role in muscle function5. These two conditions live together, showing greater risks of mortality and worsening of disabilities such as worse physical performance, higher risk of falls, lower cognitive performance, worsening of cardiovascular diseases, and other unfavorable health conditions such as hospitalizations3. It is known that sarcopenic obesity increases the risk of mortality by 1.21 times compared to the robust old people6.
In aging, sarcopenic obesity is an important cause of frailty, disability, and loss of independence in old people4. Causal factors for sarcopenic obesity are inadequate nutrition, insulin resistance, decreased hormone concentration (GH and testosterone), inf lammation through the production of pro-inflammatory cytokines by the adipose tissue, physical inactivity, and sedentary lifestyle7. It is a consensus that weight loss is responsible for many benefits and reduced risk of complications in young or middle-aged people. In contrast, the effects on old people are still controversial8. The literature points out that there is not enough evidence to prove the association between intentional weight reduction and increased life expectancy8. Also, there is no association between overweight in old patients and
increased overall mortality9. Intentional weight loss is only recommended specifically for old people with obesity-related comorbidities such as functional limitations, metabolic syndrome, type 2 diabetes, and cardiovascular diseases8.
Given this context, the literature shows that there is no consensus on the prevalence of sarcopenic obesity in the old population10,11. Studies carried out in different regions of Brazil show the prevalence of sarcopenic obesity in old people ranging from 0.7% to 9.4%11,12,13. Also, studies suggest that further research is needed to investigate possible gender differences11, and to bring a better understanding of the influence of obesity on the health of old people as the mechanisms and clinical implications cannot be compared to those occurring in the young population8. Therefore, the objective of the present article was to identify the prevalence of sarcopenic obesity in old residents in the community and to analyze the relation between obesity and the sarcopenia classification criteria.
METHOD
The analytical cross-sectional study linked to the project “Atenção Integral à Saúde do Idoso” (comprehensive care for the health of the old people) approved by the Research Ethics Committee of Universidade Regional do Noroeste do Estado do Rio Grande do Sul under Consubstantiated Opinion No. 2,653,484. The data in the present research refer to the first evaluation carried out in the period from 2018 to 2019.
The study population consisted of individuals aged ≥60 years, both genders, users of primary care services in the urban area of a medium-sized municipality in southern Brazil. The sample calculation method, sampling technique, and selection criteria were previously described in detail14. For the sample calculation, data from the Primary Care Information System (SIAB) and the total number of old people registered in Family Health Strategies (FHS) in the urban area was used, which was 5,269 old people. Considering the population aging rate, we chose representativeness greater than 10% of the old population of the FHS. To estimate

3 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
the sample size, a tolerable sample error of 5% was defined, which defined an initial sample size of 372 old people selected by random sampling technique and stratified proportionally by FHS and by gender.
The study excluded old people who underwent a surgical procedure in less than 30 days, and those who did not have physical and/or psychological conditions to respond to the questionnaire. For this study, the individuals selected had the physical examination protocol complete to assess body composition and sarcopenia, totaling a sample of 209 old people with a minimum age of 62 and a maximum age of 93 years. The reasons for loss included recent hospitalization, deaths, change of address, and non-consent to participate in the research.
The research protocol was applied in the home space, in two stages. In the first stage, the variables of interest were collected from the responses to a structured questionnaire developed by the researchers to obtain sociodemographic data and clinical health conditions, and from tests to assess the functional capacity. Still, at this stage, instructions for carrying out physical examinations were given, and the second stage was scheduled. In the second stage, a physical examination was carried out to assess sarcopenia and measure body composition.
To assess the clinical health condition, the old people were asked to confirm the presence of comorbidit ies such as diabetes mell itus, hypercholesterolemia, systemic arterial hypertension, brain stroke, Parkinson’s disease, dementia, heart disease, kidney disease, osteoarticular diseases, and depression. For statistical purposes, the old people who presented five or more of the aforementioned conditions were classified as multicomorbidities. Also, the functional capacity of the old people was assessed using the Katz scale15 to measure dependence for basic activities of daily living (BADL), and the Lawton and Brody scale16 used to evaluate the instrumental activities of daily living (IADL). For statistical purposes, the old people who did not perform or needed help to perform at least one activity of the specific scales were classified as dependent for BADL or IADL.
Sarcopenia was assessed based on the criteria of the European Sarcopenia Consensus2 which
classifies as probable sarcopenic the old people with decreased muscle strength; as sarcopenic those with decreased muscle strength and muscle mass; and as severe sarcopenic those showing decreased muscle strength, muscle mass, and physical performance. The European Sarcopenia Consensus2 presents a wide variety of tests and techniques that can be used to characterize sarcopenia, in practice, and research. In the present study, the Handgrip Strength technique was chosen to assess the muscle strength; for muscle mass, body composition by Bioelectrical Impedance Analysis; and for physical performance, the gait speed test.
To obtain the Handgrip Strength, the dynamometry technique was used with a dynamometer (E.CLEAR, model EH101) placed on the dominant hand of the old person. The test was performed in a sitting position, with the old person’s arm adducted, the forearm flexing at an angle of 90º in relation to the arm, and the wrist in a neutral position. Three attempts were made, with a one-minute interval between them, and the mean of the values was considered. Values <27kg for men and <16kg for women17were considered low muscle strength.
The tetra polar Bioelectric Impedance analysis was performed with a portable device (RJL System Inc., model BIA101A, USA) providing resistance and reactance values with a frequency of 50 kHz and 800 μA. The criteria proposed by the equipment manual for the examination were followed, with a previous explanation to the old people regarding not exercising for a period of eight hours and not drinking alcohol for 12 hours before the examination. Also, they were asked to empty their bladder before the exam, to remain silent during the exam, not to be sweaty or urinated, and not to have a fever nor be in shock The resistance and reactance values found were used to calculate the appendicular skeletal muscle mass (ASMM) based on formula18: ASMM (kg) = -3.964 + (0.227 * normalized resistance for height) + (0.095 * body weight) + (1.384 * sex) + (0.064 * reactance). With height being expressed in centimeters, and resistance value in ohm; for gender, woman =0 and man =1. The cutoff point adopted was <20kg for men and <15kg for women19.

4 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
The anthropometric body mass and height were measured according to the criteria established by the Food and Nutritional Surveillance System (SISVAN)20. For body mass, the individuals were weighed barefoot and wearing light clothing, and oriented to remove heavy objects such as keys, belts, glasses, cell phones, and any other objects that could interfere in the weight. For height, the individual should be barefoot and with nothing in the head, in the center of the equipment, erect, with arms extended along the body, head up looking at a fixed point at eye level, head positioned on the Frankfurt plane (lower margin of the orbital opening, and the upper margin of the external auditory meatus in the same horizontal line), parallel legs, feet forming a right angle with the legs. A portable scale of brand G_Tech with a maximum capacity of 150kg was used to verify the body mass, and a pocket stadiometer brand Cescorf with a measurement range of three meters was used for height.
Gait speed was measured by the four-meter gait speed test demarcated on the ground, in which the old person walks with their usual gait pattern, and the displacement time is measured21. The gait speed test is a validated and recommended test by the European Sarcopenia Consensus due to the convenience of use and the ability to predict results related to sarcopenia2. The test was carried out in the internal or external area of the home in a place where the old person could walk four meters in a straight line with a flat surface and without obstacles. Gait speed was considered low2 with values ≤0.8m/s.
For the classification of obesity, the percentage of fat >27% for men and >38% for women was considered22. The fat percentage calculation was obtained using the formula23: Percentage of fat mass = body mass - {5,741 + {0,4551 * [(height * height) / resistance]} + (0.1405 * body weight) + (0.0573 * reactance) + (6.2467 * Gender)}, and the resistance and reactance values were obtained from the Bioelectric Impedance analysis previously mentioned. For the classification of sarcopenic obesity, the conditions of probable sarcopenic, sarcopenic, or severe sarcopenic associated with the condition of obesity were considered.
The data obtained were analyzed using the software Statistical Package for the Social Sciences (SPSS; version 22.0). For the definition of measures of descriptive and analytical statistics, normal behavior was observed by the Kolmogorov-Smirnov test. For the quantitative variables, mean and standard deviation, and the nonparametric mean comparison test for independent samples were used (Mann-Whitney test). For qualitative measures, relative and absolute frequency measures and the association test (Pearson’s chi-square test or Fisher’s exact test) were used to verify the dependence of the variables. For all cases, a 95% confidence interval (95% CI) was used. The risk probability of one group compared to the other was assessed by calculating the prevalence ratio (PR) considering increased risk values greater than 1.024. The linear regression model was used to analyze the relation between the dependent variables (muscle strength, muscle mass, and gait speed) and the independent variables (obesity, gender, age group, multicomorbidities, and functional capacity). For all tests, p<0.05 was considered statistically significant.
RESULTS
The sample consisted of 209 old people with an average age of 73.02±7.38 years. The analysis of age by sex showed that men were older (74.39±7.43 years) than women (72.25±7.27 years; p=0.038). The analysis of body composition showed that obese individuals were younger (71.10±6.83 years) than the non-obese ones (73.77±7.48 years; p=0.017). Table 1 presents the sociodemographic profile and clinical condition of obese and non-obese individuals in which the obese ones had a higher prevalence of men and multicomorbidities when compared to those non-obese.
Regarding the classification of sarcopenia, 75.6% (n=158) of the old people were robust, 13.9% (n=29) were likely to be sarcopenic, 6.2% (n=13) were diagnosed as sarcopenic, and 4.3% (n=9) as severe sarcopenic. For the purposes of statistical analysis, the old people who were probable sarcopenic, sarcopenic, or severe sarcopenic were grouped, as shown in Table 2. But the prevalence of obesity and sarcopenic obesity are presented.

5 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
Table 1. Sociodemographic profile and clinical condition of obese and non-obese old residents in the community (n=209). Ijuí-RS, 2019.
Variables Obesen (%)
Non-Obesen (%) p PR (IC 95%)
GenderMenWomen
30 (50,8)29 (49,2)
45 (30,0)105 (70,0)
0,005* 2,41 (1,30-4,48)
Civil StatusWith companionNo companion
45 (76,3)14 (23,7)
99 (66,0)51 (34,0)
0,149 1,66 (0,83-3,29)
EducationDid not attendAttended
4 (6,8)55 (93,2)
13 (8,7)137 (91,3)
0,653 1,31 (0,41-4,18)
Family Income (in minimum wage)Up to 3More than 3
53 (89,8)6 (10,2)
134 (89,3)16 (10,7)
0,916 1,06 (0,39-2,84)
Comorbidities5 or moreUp to 4
18 (30,5)41 (69,5)
25 (16,7)125 (83,3)
0,026* 2,19 (1,09-4,43)
Functional capacity - BADLDependentIndependent
14 (23,7)45 (76,3)
31 (20,7)119 (79,3)
0,628 1,19 (0,58-2,45)
Functional capacity - IADLDependentIndependent
34 (57,6)25 (42,4)
81 (54,0)69 (46,0)
0,635 1,16 (0,63-2,13)
* Pearson’s chi-square test p≤0,05; PR (IC95%) = prevalence ratio (95% confidence interval); BADL = basic activities of daily living; IADL = instrumental activities of daily living.
Table 2. Prevalence of sarcopenia, obesity, and sarcopenic obesity in old residents in the community (n=209). Ijuí-RS, 2019.
Variables n (%)SarcopeniaYesNo
50 (23,9%)159 (76,1%)
ObesityYesNo
59 (28,2%)150 (71,8%)
Sarcopenic ObesityYesNo
9 (4,3%)200 (95,7%)

6 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
Table 3 lists sarcopenia, obesity, and sarcopenic obesity with the gender of old residents in the community. It was found that men have a higher prevalence of these variables when compared to women. However, the difference was significant only for sarcopenia and obesity.
Table 4 shows the bivariate relation between obesity and the sarcopenia variables of old residents in the community. It is observed that the obese had a lower prevalence of muscle mass loss when compared to the non-obese. When comparing the means of the sarcopenia variables, the obese old people compared to the non-obese ones had greater muscle strength (27.59±10.36Kg vs. 22.43±7.18Kg; p=0.001), muscle mass (21.46±4.17 kg vs. 17.48±3.88
kg; p<0.001), but not gait speed (1.06±0.32m/s vs. 1.04±0,36m/s; p=0.719).
Table 5 shows the simple regression model adjusted by gender, age group, multicomorbidities, and functional capacity of obesity to predict muscle strength, muscle mass, and gait speed. After adjusting the model, it was noticed that obesity and male gender were significant in predicting greater muscle strength and muscle mass, whereas gender only influenced the gait speed. The age group of 80 years or more was significant in predicting lower values for the three variables analyzed, whereas multicomorbidities influenced muscle strength and gait speed and dependence for IADL only in muscle strength.
Table 3. Bivariate relation between sarcopenia, obesity, and sarcopenic obesity and sex (n=209). Ijuí-RS, 2019.
Variables Menn (%)
Womenn(%) p PR (IC 95%)
SarcopeniaYesNo
26 (34,7%)49 (65,3%)
24 (17,9%)110 (82,1%)
0,006* 2,43 (1,27-4,65)
ObesityYesNo
30 (40,0%)45 (60,0%)
29 (21,6%)105 (78,4%)
0,005* 2,41 (1,30-4,48)
Sarcopenic ObesityYesNo
5 (6,7%)70 (93,3%)
4 (3,0%)130(97,0%)
0,209 2,32 (0,60-8,92)
* Pearson’s chi-square test p≤0,05; PR (IC95%) = prevalence ratio (95% confidence interval)
Table 4. Bivariate relation between obesity and sarcopenia criteria (n=209). Ijuí-RS, 2019.
Sarcopenia Criteria Obesen (%)
Non-Obesen (%) p PR (IC 95%)
Low Muscle MassYesNo
2(3,4%)57(96,2%)
62 (41,3%)88 (58,7%)
<0,001* 0,05 (0,01-0,21)
Low Muscle StrengthYesNo
10 (16,9%)49(83,1%)
41 (27,3%)109(72,7%)
0,116 0,54 (0,25-1,17)
Low Gait SpeedYesNo
11(18,6%)48(81,4%)
35 (23,3%)115(76,7%)
0,461 0,75 (0,35-1,61)
* Fisher’s exact test p≤0,05; PR (IC95%) = prevalence ratio (95% confidence interval)

7 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
DISCUSSION
The results of the present study showed a prevalence of 23.9% of sarcopenia, 28.2% of obesity, and 4.3% of sarcopenic obesity in a sample of old residents in the community of southern Brazil. But it can be observed that men had a higher prevalence of sarcopenia and obesity than women, and obese people had a lower prevalence of muscle mass loss than eutrophic old people.
In Brazil and the world, there is evidence that obesity is increasing among the old people25,26. In Brazil, a 26% increase in obesity was observed in this population between the years 2007 and 201725, but with the associated condition of sarcopenia further epidemiological studies using the same measurement method are needed to establish better prevalence parameters. The 4.4% prevalence of sarcopenic obesity was reported in a study assessing old people from different regions of Brazil12, a data similar
to that found in our study. However, there is a variation in prevalence depending on the methods of assessing sarcopenic obesity. A comparative study presented divergent data for measurements taking into account the Body Mass Index (0.7%), the abdominal circumference (6.5%), and the percentage of fat (9.4%)11. The excess of body fat added to the reduction of lean mass due to aging can result in a Body Mass Index within the normal range. Therefore, it is not recommended that the diagnosis of sarcopenic obesity takes this assessment measure into account.
When comparing the genders, another study found a higher ratio among men aged 80 years or older (8.6%) when compared to women in the same age group (1.7%)13. In our study, a higher prevalence was found in 143% and 141% of men presenting sarcopenia and obesity, respectively, when compared to women. However, being male was the only variable that positively influenced the
Table 5. Simple and adjusted linear regression model for the criteria of sarcopenia in old residents in the community (n = 209). Ijuí-RS, 2019.
Sarcopenia Criteria Variables Simple
Regression p Adjusted Regression p
Muscle Strength (Kg)
Obesity 5,162 <0,001* 3,108 0,003*Gender 9,496 <0,001* 9,056 <0,001*Age group -6,207 <0,001* -5,046 <0,001*Multicomorbidities -2,891 0,047* -2,581 0,022*Functional disability - BADL -4,046 0,004* -0,975 0,393Functional disability - IADL -4,769 <0,001* -2,545 0,010*
Muscle Mass (Kg)
Obesity 3,974 <0,001* 2,607 <0,001*Gender 5,607 <0,001* 5,254 <0,001*Age group -1,721 0,019* -1,918 0,001*Multicomorbidities 0,402 0,590 0,163 0,767Functional disability - BADL -0,988 0,177 -0,371 0,507Functional disability - IADL -0,391 0,519 0,418 0,383
Gait Speed (m/s)
Obesity 0,021 0,693 -0,030 0,546Gender 0,117 0,021* 0,137 0,003*Age group -0,373 <0,001* -0,333 <0,001*Multicomorbidities -0,153 0,010* -0,110 0,043*Functional disability - BADL -0,179 0,002* -0,045 0,416Functional disability - IADL -0,216 <0,001* -0,090 0,056
* Linear regression model p≤0,05; Kg= kilograms; m/s= meters per second; BADL = basic activities of daily living; IADL = instrumental activities of daily living.

8 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
prediction of all criteria for sarcopenia, that is, an increase of 9.06 kg in muscle strength, 5.25 kg in muscle mass, and 0.14 m/s in gait speed, even when adjusted for obesity, age group, multicomorbidities, and functional disability. Because of this, we can suggest two hypotheses: the first related to biological differences between genders, which justifies the positive influence of males on strength and muscle mass; and the second related to the cutoff points used to classify sarcopenia and obesity, which may have influenced a higher prevalence of these conditions for men, since the cutoff points used to come from the European population and have different biopsychosocial characteristics from Brazilian old people. It should also be noted that there are no studies establishing specific cutoff points for the classification of sarcopenia in the Brazilian old population.
Our data also suggested that obese old people had a 95% lower prevalence of muscle mass loss when compared to non-obese individuals. However, this data would need to be validated with a larger sample size due to the low absolute and relative number of obese people with low muscle mass. It was also observed that the obese old people had an additional 3.11 kg of muscle strength, and 2.61 kg of muscle mass compared to the non-obese old people, even when adjusted for gender, age group, multicomorbidities, and functional disability. At first, this finding seems to be controversial, given that obesity could be a limiting factor for mobility necessary for the maintenance of the muscle mass capable of generating sufficient muscle strength to carry out the tasks of daily living. Other studies have found similar or greater muscle strength values among obese individuals when compared to their non-obese peers27,28. According to the authors, these findings have been attributed to the probable neuromuscular adaptation induced by excess body weight in the musculoskeletal structure27,28 On the other hand, when muscle strength is expressed per body mass or fat-free mass units, these differences disappeared, thus suggesting that the quality of the muscle tissue is not affected by obesity27,28.
Excess body mass represents an additional burden to the skeletal muscle structure of obese individuals, leading to possible favorable adaptations in the
muscle mass, bone mass, and muscle strength29-31. Also, the obese individuals have an altered metabolic profile compared to the non-obese ones, with higher basal insulin values, which can lead to a systemic anabolic state32. The combination of this anabolic environment and the additional overload may be responsible for the greater muscle and bone mass, as well as the higher levels of strength observed in obese individuals when compared to the non-obese ones32.
The aforement ioned studies present ing similar or even higher muscle strength values in obese individuals when compared to non-obese individuals were conducted with populations of children and adolescents29-32. Therefore, there is still a need for a more detailed investigation of what this data means for the old population since the physiological processes between these two stages of life are different. The combination of reduced muscle mass and strength has been associated with physical dependence, cognitive impairment, and increased risk of comorbidities and death in the old people33. Therefore, body weight loss strategies offered to the old population should take into account the prevention of bone and muscle loss8.
In this sense, it was evidenced that energy restriction from a low-calorie diet, regardless of being associated with physical exercise, resulted in a decrease of one-quarter of lean mass per unit of weight, and consequently worsened the conditions of sarcopenia and osteopenia 34. Another study found that individuals older than 70 years and with the lowest ratios of adipose tissue had higher mortality rates, regardless of the physical performance9. In contrast, our study also confirmed an association between obesity and multicomorbidities, which can bring many harms to the health of old people. It was noticed that obese old people have an increased prevalence of 119% of multicomorbidities when compared to non-obese old people. Also, multicomorbidity predicted 2.58Kg less of muscle strength, and 0.11m/s of gait speed, even when adjusted for gender, age group, obesity, and functional disability.
Therefore, we emphasize that interventions for intentional body weight loss in old people should be based on the basic principles of geriatrics. It is perceived the need to evaluate the benefits and harms

9 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
that these strategies can bring to the health of the old people. In this sense, it is important to have a multidimensional evaluation of the old people, and treatments with scientific evidence generated in this age group9.
Limitations of the present study include the design of the cross-sectional study which limits the conclusions and generalizations of the results, the sample number that did not reach the given probabilistic size, and the difference in age between men and women and between obese and non-obese, which may have influenced some results since men and the non-obese old people had higher means.
Also, we emphasize that the European consensus on sarcopenia2 brings dual energy absorptiometry by X-ray as the gold standard for muscle mass measurement, but this test is not yet accessible to the entire population. The consensus itself indicates the use of Bioelectric Impedance Analysis because it is an accessible and portable device, together with the equation of Sergi18 to estimate muscle mass. This equation is valid for European populations. Therefore, it is suggested that further studies be carried out to validate it in the Brazilian population. It is also worth mentioning that the data refers to the population of a single city. Therefore, the results cannot be extrapolated to the Brazilian population, since Brazil has different rates of aging,
socioeconomic, and cultural conditions among its regions. It is suggested that more research be done to compare data between the regions of Brazil.
CONCLUSION
The results of the present study showed a prevalence of 23.9% of sarcopenia, 28.2% of obesity, and 4.3% of sarcopenic obesity in the old residents in the community of southern Brazil. Also, it was observed that men had a higher prevalence ratio of sarcopenia and obesity than women. However, being male positively influenced the prediction of all variables comprising the classification criteria of sarcopenia. It was also verified that obese individuals had a lower prevalence ratio for loss of muscle mass than non-obese old people. Obesity seems to have positively influenced the prediction of strength and muscle mass.
It is concluded that obesity should be analyzed taking into account the different stages of life since the strategies for bodyweight loss in old people can cause some health harm. The importance of multidimensional evaluation of the old person is emphasized to verify the real need for body weight loss to prevent loss of muscle mass and strength.
Edited by: Daniel Gomes da Silva Machado
REFERENCES
1. Schaap LA, van Schoor NM, Lips P, Visser M. Associations of sarcopenia definitions, and their components, with the incidence of recurrent falling and fractures: the longitudinal aging study Amsterdam. J Gerontol Ser A Biol Sci Med Sci. 2018;73:1199-204.
2. Cruz-jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(6):1-10.
3. Zamboni M, Rubele S, Rossi AP. Sarcopenia and obesity. Curr Opin Clin Nutr Metab Care. 2019;22(1):13-9.
4. Cruz-jentoft AJ, Baeyens JP, Bauer JM, Boirie Y, Cederholm T, Landi F, et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39(4):412-23.
5. Tournadre A, Vial G, Capel F, Soubrier M, Boirie Y. Sarcopenia. Joint Bone Spine. 2019;86(3):309-14.
6. Zhang X, Xie X, Dou Q, Liu C, Zhang W, Yang Y, et al. Association of sarcopenic obesity with the risk of all-cause mortality among adults over a broad range of different settings: a updated meta-analysis. BMC Geriatrics. 2019;19(183):1-9.

10 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
7. Campos GC, Lopes CL, Lourenço RA. Obesidade sarcopênica e funcionalidade: Uma revisão da literatura. Rev HUPE. 2017;16(2):102-9.
8. Kim TN. Elderly Obesity: Is It Harmful or Beneficial? J Obes Metab Syndr. 2018;27(2):84-92.
9. Santos RR, Bicalho MA, Mota P, Oliveira DR, Moraes EN. Obesity in the elderly. Rev med Minas Gerais. 2013;23(1):64-73.
10. Batsis JA, Villareal DT. Sarcopenic obesity in older adults: aetiology, epidemiology and treatment strategies. Nat Rev Endocrinol. 2018;14(9):513-37.
11. Oliveira TM, Roriz AKC, Medeiros JMB, Ferreira AJF, Ramos LB. Sarcopenic obesity in community-dwelling older women, determined by different diagnostic methods. Nutr Hosp. 2019;36(6):1267-72.
12. Santos CM, Dias JMD, Samora GAR, Perracini MR, Guerra RO, Dias RC. Prevalence of obesity, sarcopenic obesity and associated factors: a FIBRA Network study. Fisioter Mov. 2017;30(Suppl 1):161-9.
13. Santos VR, Gomes IC, Bueno DR, Christofaro DG, Freitas Jr IF, Gobbo LA. Obesity, sarcopenia, sarcopenic obesity and reduced mobility in Brazilian older people aged 80 years and over. Einstein. 2017;15(4):435-40.
14. Berlezi EM, Gross CB, Pimentel JJ, Pagno AR, Fortes CK, Pillatt AP. Estudo do fenótipo de fragilidade em idosos residentes na comunidade. Ciênc Saúde Colet. 2019;24(11):4201-9.
15. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged. The index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185(12):914-9.
16. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9:179-86.
17. Dodds RM, Syddall HE, Cooper R, Benzeval M, Deary IJ, Dennison EM, et al. Grip strength across the life course: normative data from twelve British studies. PLoS ONE. 2014;9(12):e113637.
18. Sergi G, Rui M, Veronese N, Bolzetta F, Berton L, Carraro S, et al. Assessing appendicular skeletal muscle mass with bioelectrical impedance analysis in free-living Caucasian older adults. Clin Nutr. 2015;34(4):667-73.
19. Studenski SA, Peters KW, Alley DE, Cawthon PM, McLean RR, Harris TB, et al. The FNIH sarcopenia project: rationale, study description, conference recommendations, and final estimates. J. Gerontol Ser A Biol Sci Med Sci. 2014;69(5):547-58.
20. Brasil. Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. Orientações para a coleta e análise de dados antropométricos em serviços de saúde: Norma Técnica do Sistema de Vigilância Alimentar e Nutricional - SISVAN . Brasília, DF : MS; 2011. (Série G. Estatística e Informação em Saúde).
21. Maggio M, Ceda GP, Ticinesi A, de Vita F, Gelmini G, Costantino C, et al. Instrumental and Non-Instrumental Evaluation of 4-Meter Walking Speed in Older Individuals. PLoS ONE. 2016;11(4):e0153583.22. Ann N Y Acad Sci. 2000;(904):437-48.
22. Roubenoff R, Baumgartner RN, Harris TB, Dallal GE, Hannan MT, Economos CD, et al. Application of bioelectrical impedance analysis to elderly population. J Gerontol Ser A Biol Sci Med Sci. 1997;52:129-36.
23. Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3: 1-10.
24. Jonas Valente. Pesquisa de Vigilância de Fatores de Risco e Proteção de Doenças Crônicas por Inquérito Telefônico (Vigitel) 2018. Agência Brasil (Brasília) [Internet]. 2018 June 18 [cited 2019 Dec. 09]. Available from: http://agenciabrasil.ebc.com.br/saude/noticia/2018-06/obesidade-atinge-quase-um-em-cada-cinco-brasileiros-mostra-pesquisa.
25. Pesquisa de Vigilância de Fatores de Risco e Proteção de Doenças Crônicas por Inquérito Telefônico (Vigitel) 2018 Available from: <http://agenciabrasil.ebc.com.br/saude/noticia/2018-06/obesidade-atinge-quase-um-em-cada-cinco-brasileiros-mostra-pesquisa>. 2018 [cited 2019 Dec. 09].
26. Nações Unidas, Departamento de Divisão de População Econômica. Perspectivas da população mundial: a revisão de 2017, as principais conclusões e as tabelas de avanço. [sem local]: Nações Unidas; 2017. Working Paper No. ESA / P / WP / 248.
27. Zoeller RF, Ryan, ED, Gordish-Dressman H, Price TB, Seip RL, Angelopoulos TJ, et al. Allometric scaling of isometric biceps strength in adult females and the effect of body mass index. Eur J Appl Physiol. 2008;104(4):701-10.
28. Maffiuletti NA, Jubeau M, Munzinger U, Bizzini M, Agosti F, de Col A, et al. Differences in quadríceps muscle strength and fatigue between lean and obese subjects. Eur J Appl Physiol. 2007;101(1):51-9.
29. Wetzsteon RJ, Petit MA, Macdonald HM, Hughes JM, Beck TJ, McKay HA. Bone Structure and Volumetric BMD in Overweight Children: a Longitudinal Study. J Bone Miner Res. 2008;23(12):1946-53.

11 of 11
Sarcopenic obesity in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200083
30. Gracia-Marco L, Ortega FB, Jiménez-Pavón D, Rodríguez G, Castillo MJ, Vicente-Rodríguez G. Adiposity and bone health in Spanish adolescents: The HELENA study. Osteoporos Int. 2012;23(3):937-47.
31. Vanderwalle S, Taes Y, van Helvoirt M, Debode P, Herregods N, Ernst C, et al. Bone size and bone strength are increased in obese male adolescents. J Clin Endocrinol Metab. 2013;98(7):3019-28.
32. Lopes WA, Leite N, Silva LR, Moraes Jr FB, Consentino CLM, Araújo CT, et al. Influence of obesity on the upper and lower body muscular strength in adolescents Rev Bras Ativ Fis Saúde. 2013;18(6):720-9.
33. Li CI, Li TC, Lin WY, Liu CS, Hsu CC, Hsiung CA, et al. Combined association of chronic disease and low skeletal muscle mass with physical performance in the elderly in the Sarcopenia and Translational Aging Research study in Taiwan (START). BMC Geriatr. 2015;15:1-10.
34. Heymsfield SB, Gonzalez MC, Shen W, Redman L, Thomas D. Weight loss composition is one-fourth fat-free mass: a critical review and critique of this widely cited rule. Rev Obes. 2014;15(4):310-21.

1 of 14
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
http://dx.doi.org/10.1590/1981-22562020023.200018
Temporal trend of mortality in old people in cities in the state of Acre
Thainá Souza Ribeiro1
Alanderson Alves Ramalho1
Suleima Pedroza Vasconcelos1
Simone Perufo Opitz1
Rosalina Jorge Koifman1,2
Keywords: Cause of Death. Time Serie Studies. Health of the Elderly. Mortality. Information Systems.
AbstractObjective: To analyze the temporal trend of mortality in the old people population in selected municipalities in the five regional development areas in the state of Acre, Brazil. Method: Descriptive, ecological study of time series, which used data from the Mortality Information System (SIM), in which the universe of deaths occurred in old people, recorded in the cities of Acre from 1996 to 2015 was selected. Crude and age-adjusted mortality rates were calculated using the direct method and the world population as a reference. For the analysis of trends, the annual percentage change in mortality was estimated with a 95% confidence level using the Joinpoint Regression Program software. Results: The general mortality trend was decreasing in Rio Branco and with fluctuations in the other municipalities investigated. The main causes of death were diseases of the circulatory, respiratory and neoplasms. In Rio Branco, mortality rates standardized by age in diseases of the circulatory system decreased by 2.26% (p<0.001) per year and neoplasms showed an increasing and constant trend with an annual variation of 1.02% ( p=0.010). Conclusion: The study showed evidence of epidemiological, geographical and social polarization in the behavior of mortality trends. Rio Branco, the state capital, presented similar patterns to those of the developed Brazilian regions. On the other hand, the other municipalities showed considerable fluctuations in trends that may be related to the high proportion of ill-defined causes. These findings can assist in the planning of strategic actions and hypothesis suggestions for further studies.
1 Universidade Federal do Acre, Programa de Pós-Graduação em Saúde Coletiva. Rio Branco, AC, Brasil.2 Fundação Oswaldo Cruz, Escola Nacional de Saúde Pública Sergio Arouca, Departamento de Epidemiologia
e Métodos Quantitativos em Saúde. Rio de Janeiro, RJ, Brasil.
The authors declare there are no conflicts of interest in relation to the present study.No funding was received in relation to the present study.
CorrespondenceThainá Souza [email protected]
Received: February 5, 2020Approved: November 24, 2020
ID
ID
ID
ID
ID

2 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
INTRODUC TION
Population aging is a worldwide phenomenon and in Brazil it occurs in an intense and accelerated way1. This can be evidenced from the aging index (number of people aged ≥60 years for every 100 people >15 years old), which was approximately 39 in Brazil in 2010, more than the triple registered in the year 1950 with 10.22. The current demographic transition has peculiar characteristics with great social inequalities, which, consequently, reflect on a direct impact on the change of the epidemiological profile of the country, in which old people have a triple burden of diseases, with a predominance of chronic conditions, high morbidity and mortality due to acute conditions from external causes and worsening of chronic conditions1.
In the health-disease process, one of the possible final events may be death3. Mortality is an important health indicator that contains relevant information, which may reflect health conditions and the performance of health systems4. The processes of collecting, managing, storing and registering deaths in Brazil are carried out in the Mortality Information System (SIM). Through these data, health indicators are produced, which support the decisions of managers, based on the situational health panorama, through consolidated data5.
In the current epidemiological context, the transition of mortality in the country occurs in a prolonged and polarized way, with different mortality patterns between the regions of Brazil6. Even with improvements in the health system, there are still great differences between rich and poor regions, the proportion of causes of death and the age groups that compose them are differentiated between Brazilian regions, as well as the quality of vital statistics, which present scenarios more precarious in the North and Northeast7. However, despite this limitation, one should not simply discard these statistics, considering that a large part of the explanatory power of these deaths can be rescued7.
In 2017, the North region presented a proportion of 8.67% of ill-defined causes of deaths in old people8. Regarding the specific rates by defined causes, infectious and parasitic diseases had a rate
of 107.11 deaths/100,000 inhabitants, neoplasms 496.12 deaths/100,000 inhabitants, diseases of the circulatory system 1,091 deaths/100,000 inhabitants and diseases of the respiratory system 429.41 deaths/100,000 inhabitants8.
In this sense, Acre presents patterns of epidemiological polarization with distinct mortality among its five regional development areas. Population aging is present in the state and can be expressed by the additional 21 years of life for individuals who reached 60 years in 2012, close to the average number in Brazil, which was an additional 22 years8. This reinforces the growth of the old people population in the state and the importance of knowing the mortality pattern of this population, in view of the need to plan health actions that favor a decrease in the number of deaths from preventable causes and greater life expectancy.
Thus, an analysis of mortality in old people stratified by municipalities in the state of Acre is necessary, in order to obtain knowledge of the behavior of mortality according to the socioeconomic variations of each development region. Therefore, the present study aimed to analyze the temporal trend of mortality in the old people population in selected municipalities in the five regions in the state of Acre, Brazil.
METHOD
It is a descriptive, ecological and time series study. The state of Acre has 22 municipalities in five regional development regions. For this study, the most socioeconomically developed municipality in each of the five regions was selected, which had the largest population, being these: Rio Branco (Baixo Acre), Cruzeiro do Sul ( Juruá), Sena Madureira (Purus), Tarauacá (Tarauacá/Envira) and Brasileia (Alto Acre). These municipalities together represent approximately 70% of the state’s population.
According to Resolution No. 466/2012, of the National Health Council (CNS), and Law No. 12,527/2011, this study used information from the public and unrestricted access database, whose data do not have the possibility of nominal and

3 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
individual identification. Thus, it was not necessary to be evaluated by the Research Ethics Committee.
In the present study, an individual aged ≥60 years was considered an old person. Mortality data were obtained from the Informatics Department of the Unified Health System (DATASUS)9 of the Ministry of Health of Brazil, through SIM, in which the universe of deaths in old people registered in the above-mentioned municipalities was selected, in the period from 1996 to 2015. Census and inter-census population estimates, according to the age groups of 60-69 years, 70-79 years and ≥80 years, were obtained from DATASUS based on the Brazilian Institute of Geography and Statistics (IBGE).
To analyze mortality, crude mortality rates were calculated, specific for age groups and age-standardized for old people aged ≥60 years. The rates were presented for all causes and for specific ones, grouped by chapters of the 10th review of the International Classification of Disease (ICD-10), in the selected municipalities. For that, the method of proportional reallocation of ill-defined causes was carried out, which consisted of the proportional redistribution of deaths resulting from these causes in the others that resulted in deaths.
For the calculation of crude and adjusted rates, the numerator considered the number of deaths in a given period, in a given population and the denominator contemplated the sum of person time, estimated from the census or inter-census population for July 1 of the middle of the analyzed period and the municipality selected, multiplied by the number of years to which the rate referred.
Mortality rates were presented per 100,000 people/year and their standardization, relative to the population aged ≥60 years, was performed using the direct method, using the world population as the standard, proposed in 1960 and modified in 196610. This reference was adopted for making the results of this study comparable with previous studies11,12, since this is the most frequent methodology in investigations with this theme.
In order to analyze the quality of the data, calculations of the proportions of ill-defined causes
of deaths were performed. The analysis of deaths in old people by age and sex was performed only for Rio Branco due to the large number of records in the state capital, which allows a better assessment of these characteristics instead of grouping them with other municipalities, whose process could sub or overestimate some analyzes, due to the different mortality patterns between them.
To analyze the trend in mortality rates from 1996 to 2015, the Joinpoint Program version 4.5 (Statistical Research and Applications Branch, National Cancer Institute, United States) was used. This regression identifies points of statistically significant changes and the annual percentage change (Annual Percent Change - APC) of mortality rates by the statistical modeling technique, which aims to explain the relationship between two variables by means of regression lines, and the points that join these lines are called inflection or junction points. The analysis makes it possible to adjust data in a series based on the minimum number of joinpoints and tests whether the inclusion of one or more points is significant. The APC in different periods are determined by the amount of inflection points in the model13. To minimize the effect of possible autocorrelations, the fit an autocorrelated errors model based on the data option was used.
The final model selected was the one that best described the behavior of the series with APC, using the log-linear model for its calculation, based on the trend of each segment, in order to estimate the statistical significance ( p<0.05) at the 95% confidence level using the Monte Carlo permutation method13. In describing the trend, the terms “increasing” on slopes and “decreasing” on slopes were used, with a 95% confidence level and for the APC that did not show a p-value <0.05, no trend was observed.
In the municipalities of Cruzeiro do Sul, Brasileia, Sena Madureira and Tarauacá, due to the oscillation resulting from the small number of deaths, the centralized moving average of the standardized mortality rate in old people for three years was calculated in order to perform the smoothing of the time series and minimize white noise.

4 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
RESULTS
Between 1996 and 2015, there were 26,347 deaths among old people across the state of Acre, of which 20,840 (79.1%) were from residents in the cities evaluated. The municipalities of Cruzeiro do Sul, Tarauacá, Brasileia and Sena Madureira, although in 2014 they presented proportional mortality from ill-defined causes of 0.5%, 6.8%, 7.8% and 6.1%, respectively, there were moments in historical series with large random oscillations that in addition to the small volume of data, in some moments these proportions were above 50%, especially in years before 2004.
In the selected municipalities, the highest percentage of deaths was in octogenarians (39.1%), followed by those aged 70 to 79 years (33.4%) and 60 to 69 years (27.5%), being 57.8% in men, 69.7% were literate, 80.5% were non-white and 65.6% of deaths occurred in hospitals. The main causes of death were diseases of the circulatory system (29.8%), respiratory (15.0%) and neoplasms (12.9%).
In Figure 1, it can be seen that most municipalities showed changes in trends in general mortality. Rio Branco was the only one that presented a linear downward trend during the entire period studied, with an APC of -0.94%. In Cruzeiro do Sul this trend was only significant in the period from 1997 to 2004 with an APC of -3.5%. During the years 1997 to 2000, the cities of Sena Madureira and Brasileia, which have territorial limits between them, showed a similar pattern of mortality with a decline and APC of -16.55% and -9.75%, respectively; the rest of the period showed fluctuations in trends.
Table 1 shows that the mortality rate in old people due to age-related circulatory system diseases was decreasing in Rio Branco from 1996 to 2015, while neoplasms showed a substantial increase. It is worth mentioning that, except in Rio Branco,
the other municipalities showed large fluctuations in rates, as observed in Brasileia, which presented zero rates for infectious and parasitic diseases in 1996, 2012 and 2015 and for neoplasms in 1996. In Tarauacá, oscillations were of zero rate in 1996 to 1,110.12/100,000 inhabitants in 2000 and again zero rate in 2004 for neoplasms. Respiratory system diseases also had a zero rate in 2000.
Table 2 shows the trends according to the main chapters of the ICD-10 for the selected municipalities, from 1996 to 2015. It was found that in Cruzeiro do Sul, the trend of mortality from diseases of the circulatory system was also decreasing, however, this occurred in different periods (from 1997 to 2004 and from 2007 to 2014). The trend of mortality from diseases of the respiratory system in old people did not change significantly in Rio Branco. In Cruzeiro do Sul and Brasileia the trends have been increasing since 2004. The mortality rate due to infectious and parasitic diseases showed a significant reduction in Rio Branco from 1996 to 2011. Mortality rates due to neoplasms in Rio Branco and Cruzeiro do Sul have been growing and constant throughout the studied period. Sena Madureira and Tarauacá showed fluctuations in trends in mortality rates due to neoplasms, while Brasileia did not show any significant change.
In Rio Branco, a significant decline in mortality from all causes was observed in the age groups of 60-69 years and 70-79 years, while the older people showed a growing and significant trend since 2010 (Table 3). Diseases of the circulatory system showed a steadily decreasing trend only in the 70-79 age group. With regard to neoplasms, the age groups of 60-69 years and ≥80 years showed an increase in mortality over the study period. Mortality due to diseases of the respiratory system was increasing and significant only for octogenarians, ranging from 4.01% from 1996 to 2005 to 10.47% from 2009 to 2015.

5 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
*APC: Annual Percentage Change; ^ with p value <0.05.
Figure 1. Annual percentage change in general mortality rates among old people in selected municipalities in the five regional development regions of Acre, Brazil, 1996 to 2015.

6 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
Table 1. General mortality rates and by the main chapters of the ICD-10, in old people in the selected municipalities of the five regional development regions of Acre, Brazil, 1996 to 2015.
Causes by municipalities 1996 2000 2004 2008 2012 2015Rio BrancoAll causes 3963.66 3869.21 4133.18 3661.01 3636.20 3515.61Circulatory System 1578.55 1425.81 1103.91 1383.93 1078.90 1128.61Respiratory System 601.37 787.81 950.56 530.84 675.38 733.65Neoplasms 526.42 572.12 699.71 679.38 709.50 652.54Infectious and Parasitic 399.59 201.78 282.35 164.20 169.84 155.29Cruzeiro do SulAll causes 3685.76 3131.21 2262.25 3161.00 3325.42 3462.16Circulatory System 2439.74 1180.60 682.37 1204.89 1273.91 984.73Respiratory System 221.29 427.65 555.27 630.94 664.32 848.74Neoplasms 539.37 516.11 411.91 570.51 662.87 633.69Infectious and Parasitic 52.81 282.45 102.78 168.16 92.34 85.55Sena MadureiraAll causes 3103.43 1295.31 3538.43 2394.17 2904.36 3144.96Circulatory System 2052.31 637.76 2341.34 1001.16 1112.06 1394.55Respiratory System 584.24 165.90 322.90 467.21 495.43 517.77Neoplasms 233.43 223.52 149.74 398.84 507.50 501.72Infectious and Parasitic 90.65 76.75 170.49 169.55 31.06 97.13BrasileiaAll causes 1711.58 1599.67 2754.02 3053.78 3128.25 2954.09Circulatory System 391.39 120.21 966.79 1504.67 945.75 1497.66Respiratory System 391.39 653.64 274.67 217.02 826.32 516.86Neoplasms 0.00 120.21 413.82 548.64 518.22 380.72Infectious and Parasitic 0.00 378.78 271.09 132.94 0.00 0.00TarauacáAll causes 2165.07 3348.98 3983.11 2512.73 2385.26 2802.42Circulatory System 1101.07 2018.45 2178.83 1779.58 649.34 1073.49Respiratory System 329.38 0.00 340.16 90.88 281.33 434.00Neoplasms 0.00 1110.12 0.00 363.53 614.01 399.05Infectious and Parasitic 367.30 0.00 100.15 112.27 54.62 248.02

7 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
Tabl
e 2.
Ann
ual p
erce
ntag
e ch
ange
in m
orta
lity
rate
s, by
the
mai
n ch
apte
rs o
f the
ICD
-10,
in o
ld p
eopl
e in
sele
cted
mun
icipa
lities
in th
e fiv
e re
gion
al d
evelo
pmen
t re
gion
s of A
cre,
Braz
il, 1
996
to 2
015
Mun
icipa
lities
Circ
ulat
ory
syste
mRe
spira
tory
syste
mN
eopl
asm
sIn
fect
ious
and
par
asiti
cA
PC*
Perio
dp
APC
*Pe
riod
pA
PC*
Perio
dp
APC
*Pe
riod
pR
io B
ranc
o-2
.26
1996
-201
5<
0.00
10.
6019
96-2
015
0.23
01.
0219
96-2
015
0.01
0-6
.97
1996
-201
1<
0.00
1-
--
--
--
--
6.15
2011
-201
50.
450
Cruz
eiro
do
Sul
-6.2
319
97-2
004
<0.
001
0.34
1997
-200
40.
660
3.88
1997
-201
4<
0.00
113
.52
1997
-200
10.
010
9.44
2004
-200
70.
320
3.63
2004
-201
4<
0.00
1-
--
-11.4
220
01-2
004
0.43
0-3
.20
2007
-201
40.
010
--
--
--
13.6
820
04-2
007
0.40
0-
--
--
--
--
13.71
2007
-201
4<
0.00
1Se
na M
adur
eira
-16.
0319
97-2
001
<0.
001
-20.
9119
97-1
999
0.21
0-8
.96
1997
-200
8<
0.00
1-1
3.43
1997
-200
10.
040
24.95
2001
-200
40.
090
5.74
1999
-201
4<
0.00
112
.67
2008
-201
4<
0.00
13.
6320
01-2
009
0.170
-18.
0620
04-2
007
0.120
--
--
--
15.51
2009
-201
4<
0.00
14.
5120
07-2
014
0.04
0-
--
--
--
--
Bras
ileia
-12.
5819
97-2
001
0.07
0-1
8.54
1997
-200
10.1
5021
.96
1997
-199
90.
220
-23.
5019
97-2
003
<0.
001
1.19
2001
-200
40.
270
-25.
6520
01-2
004
0.37
047
.1919
99-2
000
0.07
07.1
820
03-2
009
0.36
0-
--
8.23
2004
-201
40.
020
-0.4
520
00-2
014
0.46
0-4
5.64
2009
201
20.1
70-
--
--
--
--
50.0
120
12-2
014
0.36
0Ta
raua
cá14
.23
1997
-200
3<
0.00
1-3
1.65
1997
-199
90.
200
69.0
319
97-1
999
0.190
-37.6
919
97-1
999
0.190
-8.6
020
03-2
011
<0.
001
64.8
719
99-2
002
0.110
22.9
219
99-2
005
0.01
010
.83
1999
-200
60.
010
2.90
2011
-201
40.7
00-2
3.66
2002
-200
70.
010
44.2
020
05-2
008
0.26
0-5
.1820
06-2
012
0.26
0-
--
15.8
820
07-2
014
<0.
001
0.18
2008
-201
10.
500
25.8
220
12-2
014
0.50
0*A
PC: A
nnua
l per
cent
age
chan
ge

8 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
When analyzing the behavior of mortality trends due to specific causes in the municipality of Rio Branco, it was observed that diseases of the circulatory system in both sexes showed a decreasing trend, however, in women this decline was more accentuated (Figure 2). Neoplasms in men, on the other hand, had an upward behavior throughout the analyzed period. On the other hand, women showed
Table 3. Annual percentage change in mortality rates from all causes and the main chapters of ICD-10, in old people by age group, in the municipality of Rio Branco, Acre, Brazil, 1996 to 2015.
Causes by age Annual percentage change p PeriodAll causes (years)60 to 69 -1.51 <0.001 1996-201570 to 79 -1.37 <0.001 1996-2015≥80 1.07 0.100 1996-2005≥80 -4.66 0.100 2005-2010≥80 7.99 <0.001 2010-2015Circulatory system (years) 60 to 69 -4.37 <0.001 1996-200460 to 69 4.47 0.500 2004-200860 to 69 -16.6 0.200 2008-201160 to 69 4.39 0.200 2011-201570 to 79 -2.56 <0.001 1996 -2015≥80 -0.69 0.300 1996 -2015Neoplasms (years)60 to 69 1.72 <0.001 1996-201570 to 79 -0.10 0.100 1996-2015≥80 1.55 <0.001 1996-2015Respiratory system (years)60 to 69 0.89 0.200 1996-201570 to 79 0.27 0.700 1996-2015≥80 4.01 <0.001 1996-2005≥80 -11.04 0.200 2005-2009≥80 10.47 <0.001 2009-2015
fluctuations in mortality rates without significant trends. Respiratory system diseases in men showed an increasing and constant trend in the period from 1996 to 2015. Women, in turn, showed a declining trend in the period from 2001 to 2011. Infectious and parasitic diseases among women had a reduction during the whole period analyzed, similar to men, that was until the year 2011.

9 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
*APC: Annual Percentage Change; ^ with p value <0.05.
Figure 2. Annual percentage change in mortality rates by the main chapters of the ICD-10 for all causes, in old people by sex, in the municipality of Rio Branco, AC, Brazil, 1996 to 2015.

10 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
DISCUSSION
This investigation analyzed the temporal trend of mortality in the old people population in selected municipalities in the five regional development areas in the state of Acre, Brazil. As a main result, it can be seen that the general mortality trend was decreasing in Rio Branco, while in the other municipalities there were oscillations. The main causes of mortality were diseases of the circulatory and respiratory systems and neoplasms.
The study identified a higher proportion of deaths in long-lived old people, with a result similar to others performed in different regions of Brazil14-18. Similar to other studies, deaths were more frequent in men14,16,19. One of the hypotheses is that women, generally attend health services20,21, perform more prevention practices such as reducing the consumption of salt and fatty diet, less alcohol and smoking20 and culturally experience a greater practice of self-care when compared to men, and since their pre-adolescence they are encouraged to perform gynecological and preventive exams22. In addition, occupational injuries and traffic accidents are also more frequent in men23. It is worth mentioning the low demand of men for primary care, making them more vulnerable to some diseases and when they finally access services, there is no time for effective treatment of the disease, which can cause greater male morbidity and mortality24.
In Rio Branco, the mortality rate from all causes showed a decreasing and constant trend over the study period (APC=-0.94%) and (APC=-1.37%) for the age group from 70 to 79 years old. A study carried out in this municipality, which analyzed the trend of mortality from all causes in the period from 1980 to 2012 when assessing by age group, the trends are also similar in terms of their declining behavior in individuals aged 70 to 79 years with a decrease in -1.3%12, similar to that found in this investigation. Other studies also showed similar results, such as the one carried out in Recife, PE, Brazil, which assessed mortality in old people from 1996 to 2007 and showed a decreasing trend of -0.86% per year16. This decreasing and significant trend may be a reflection of better health conditions in the old people population25, with more favorable
quality of care and the effectiveness of care provided in primary care, as observed in a study carried out in Florianópolis, SC, Brazil, in the period from 2008 to 201511. In contrast, the municipalities of Sena Madureira, Brasileia and Tarauacá showed a non-constant trend and, when assessing the evolution of the periods analyzed, most of the time they showed a significant increase in mortality rates in old people. This may be the result of regional inequalities inherent to social unevenness, especially with regard to greater difficulty in accessing health services by the less favored population6.
The results showed the presence of geographic polarization in Acre, characterized by the difference in mortality rates between the municipalities of different regions of development, since Rio Branco is a more developed city, with greater socioeconomic power in the state and greater availability of health services for old people, reflected a mortality pattern typical of developed regions, while municipalities such as Tarauacá, Sena Madureira and Brasileia showed remarkable fluctuations in mortality rates
The mortality trend due to diseases of the circulatory system was decreasing and constant in Rio Branco throughout the studied period, with an annual reduction of -2.26%. In Recife-PE, Brazil in the period from 1996 to 2007, the reduction in mortality due to diseases of the circulatory system presented a greater magnitude with a decreasing trend of -5.13% per year16. In Rio Grande do Sul, Brazil, the mortality rate for this cause per 1,000 inhabitants also decreased from 19.34 in 1996 to 17.15 in 200414.
Mortality rates due to neoplasia in Rio Branco and Cruzeiro do Sul showed an increasing and linear trend throughout the study period. In a nationwide study by Lima-Costa et al.26, there was also a significant increase in the mortality rate from neoplasms, which went from 549.5/100,000 inhabitants in 1980 to 652.3/100,000 inhabitants in the 2000s. Neoplasms play an important role in changing the profile of Brazilian public health and several factors contribute to the increase in mortality from neoplasms in Brazil, such as: increased life expectancy, changes in lifestyle with greater exposure to environmental factors and to carcinogenic agents, improvements in cancer

11 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
diagnosis services and advances in the quality of death records27. On the other hand, mortality from neoplasms in the municipalities of Sena Madureira, Brasileia and Tarauacá showed an irregular trend. Such behavior may be due to the fluctuation of data and the quality of records, due to the high proportion of ill-defined causes.
The mortality rates due to diseases of the respiratory system in Cruzeiro do Sul and Brasileia showed an increasing trend in the period from 2004 to 2014, similar to the behavior observed in the state of Mato Grosso, Brazil, in the period from 1986 to 200615. It is noteworthy that the pollutants produced by fires can influence the health of old people and be transported over large areas from the areas of origin28. According to the National Institute for Space Research in Brazil, in 2005, Acre had the largest number of active fires ever recorded29. The points detected by satellites showed high numbers of fires in Brasileia, a city bordering Bolivia and the municipality of Cruzeiro do Sul presented increasing fires in the western limit of the border with the state of Amazonas30. These facts may corroborate the upward behavior of mortality from respiratory diseases in these municipalities from 2004 onwards.
Mortality from infectious and parasitic diseases declined in the capital Rio Branco, as well as in another capital Recife-PE, Brazil, which showed a reduction of -34.4% when compared to the rates of 1996 and 200716. However, despite the decline it is noteworthy that in these capitals there is epidemiological polarization, as they simultaneously present high mortality rates due to chronic-degenerative diseases and infectious and parasitic diseases, whose mortality is still high when compared to developed countries6.
The comparative analysis of mortality by sex and by age group was carried out only in the state capital, Rio Branco, due to a better record of the declaration of deaths that occurred. Individuals aged ≥80 years have health aspects that are different from other old people, due to a series of factors such as higher frequency of chronic diseases and comorbidities, greater social vulnerability and reduced functional capacity31. Mortality in octogenarians showed an increasing trend due to neoplasms throughout the analyzed period and due to diseases of the
respiratory system in the periods 1996-2005 and 2009-2015. Older people have a lower immune response, decreased diaphragmatic muscle tone and less effective cough reflex, in addition to remaining largely confined to bed, which may favor increased mortality from this cause, notably in this age group32.
Although mortality from circulatory and infectious and parasitic diseases are declining in both sexes, this has occurred more intensely in women. Bearing in mind that men have a lower life expectancy and higher mortality, resulting in higher male mortality in all age groups, including old people. Similarly, an ecological study in Araraquara-SP, Brazil, which assessed mortality from 2006 to 2011 also identified a greater reduction in mortality from diseases of the circulatory system in women when compared to men, in the period from 2006 to 2008, with a statistically significant difference between the rates33. Corroborating this hypothesis, the presence of biological determinants, such as the higher concentration of coronary atherosclerotic complications inherent to males, results in a higher mortality from diseases of the circulatory system, in addition to the cultural and social determinants of less access to health services23.
Mortality due to neoplasms and diseases of the respiratory system was increasing in men, while in women, no significant trends were detected. The high male mortality from neoplasms was also present in a descriptive study carried out in Florianópolis-SC, Brazil, in 2007, which, when comparing mortality in old people between genders, observed a higher rate in men, mainly due to lung cancer34.
Regarding the limitations of the study, we can mention the high proportion of deaths from ill-defined causes, demanding caution in the interpretation of results. The redistribution of ill-defined causes between defined causes (except external causes) was applied in order to minimize this limitation. However, the high proportion of ill-defined causes is a reality of the inadequate filling in of death certificates, which reflects in a problem in the data quality of the Mortality Information System. The high proportions of ill-defined causes, especially in old people, were higher in 2013 in the North (11.1%), specifically in the states of Acre (9.5%),

12 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
Amazonas (17.9%), Amapá (12.6%), in addition to states in other regions such as Bahia with (15.7%)35.
Despite these limitations, one of the strengths of this study is the analysis of trends in general and specific mortality rates in old people in municipalities in each state’s regional development, which represent about 70% of the old people in Acre, which may make it possible to monitor and evaluate health services, as well as assist in planning for public health actions. In addition to the analysis by chapter of the ICD-10, for Rio Branco the rates were analyzed specific by sex and age group. This assessment allows us to suggest more hypotheses according to the behavior of mortality in these two variables. Another highlight is the methodology used, as there was an approach to mortality rates adjusted by the world population (which allows comparison with other studies that used this methodology) and with correction of ill-defined causes.
CONCLUSION
The results of this study demonstrated the presence of epidemiological, geographical and social polarization with the trend of decreasing
general mortality in Rio Branco, while the other municipalities showed oscillations. The main causes of mortality in old people were diseases of the circulatory, respiratory and neoplasms, thus presenting results similar to those in developed Brazilian regions.
Such results may contribute to the discussion of the current epidemiological picture through the evaluation of the mortality indicator, highlighting the basic causes of deaths in old people, according to the main municipalities of each regional development in the state, identifying the main variations in health conditions that can assist in the planning of strategic actions, resource allocation and suggestion of hypotheses for further studies in other locations.
ACKNOWLEDGEMENTS
We thank the teachers of the Postgraduate Program in Collective Health at the Federal University of Acre, Gina Torres Rego Monteiro and Maria Fernanda de Sousa Oliveira Borges for their contributions in the final review of the manuscript.
Edited by: Daniel Gomes da Silva Machado
REFERENCES
1. Brasil. Ministério da Saúde. Saúde da pessoa idosa: prevenção e promoção à saúde integral [Internet]. MS; 2019 [cited 2020 Feb.08]. Available from: https://saude.gov.br/saude-de-a-z/saude-da-pessoa-idosa.
2. Duarte Miranda GM, Gouveia Mendes AC, da Silva ALA. O envelhecimento populacional brasileiro: desafios e consequências sociais atuais e futuras. Rev Bras Geriatr Gerontol. 2016;19(3):507-19. Available from: https://doi.org/10.1590/1809-98232016019.150140
3. Leavell H, Clark E. Medicina preventiva. Rio de Janeiro: McGraw-Hill do Brasil; 1976.
4. Organização Pan-Americana da Saúde. Indicadores básicos para a saúde no Brasil: conceitos e aplicações. 2ª ed. Brasília, DF: OPAS; 2008.
5. de Morais RM, Costa AL. Uma avaliação do Sistema de Informações sobre Mortalidade. Saúde Debate. 2017;41(esp):101-17. Available from: http://dx.doi.org/10.1590/0103-11042017s09 .
6. de Araújo JD. Polarização epidemiológica no Brasil. Epidemiol. Serv Saúde. 2012;21(4):533-8. Available from: http://dx.doi.org/10.5123/S1679-49742012000400002 .
7. Paes NA. A geografia da mortalidade por causas dos idosos no Brasil. In: Anais da ABEP [Internet]. [Sem local]: ABEP; 2016 [cited 2020 Sep. 11]. p. 1-22. Available from: http://abep.org.br/~abeporgb/publicacoes/index.php/anais/article/viewFile/1007/972 .
8. Sistema de Indicadores de Saúde e Acompanhamento de Políticas do Idoso [Internet]. Rio de Janeiro: Fundação Oswaldo Cruz; 2020 [cited 2020 Feb. 08]. Available from: https://sisapidoso.icict.fiocruz.br/.
9. DATASUS: Departamento de Informática do Sistema Único de Saúde [Internet]. Brasília, DF: Ministério da Saúde; 2020 [cited 2020 Feb. 08]. Available from: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/obt10uf.def .

13 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
10. Doll R, Muir CS, Waterhouse JAH. Cancer Incidence in Five Continents: Volume 2 [Internet]. Heidelberg: Springer Berlin Heidelberg; 1970 [cited 2018 Feb. 18]. Available from: http://public.eblib.com/choice/publicfullrecord.aspx?p=3098316 .
11. Rodrigues MM, Alvarez AM, Rauch KC. Trends in hospitalization and mortality for ambulatory care sensitive conditions among older adults. Rev Bras Epidemiol. 2019;22:1-11. Available from: https://www.scielo.br/pdf/rbepid/v22/1980-5497-rbepid-22-e190010
12. Bezerra PCL, Monteiro GTR. Trends in overall mortality and from diseases of the circulatory system in elderly individuals in Rio Branco, Acre, 1980-2012. Rev Bras Geriatr Gerontol. 2018;21(2):143-54. Available from: https://doi.org/10.1590/1981-22562018021.170128
13. Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335-51. Available from: https://doi.org/10.1002/(SICI)1097-0258(20000215)19:3
14. Rosa LHT, Rossato DD, Bombardelli CL, Sturmer G, da Rosa PV. Estudo da mortalidade em população idosa de municípios do Rio Grande do Sul no período de 1996 a 2004. Rev Bras Geriatr Gerontol. 2010;13(1):111-9. Available from: https://doi.org/10.1590/S1809-98232010000100012
15. Carmo CN, de Souza SH, Jacobson LSV, Mourão DS, Ignotti E. Mortalidade por doenças cardiorrespiratórias em idosos no estado de Mato Grosso, 1986 a 2006. Rev Saúde PúblIca. 2010;44(6):1-10. Available from: https://doi.org/10.1590/S0034-89102010005000043 .
16. Silva VL, Albuquerque MFPM, Cesse EAP, Luna CF. Perfil de mortalidade do idoso: análise da evolução temporal em uma capital do Nordeste brasileiro de 1996 a 2007. Rev Bras Geriatr Gerontol. 2012;15(3):433-41. Available from: https://doi.org/10.1590/S1809-98232012000300005
17. Borim FSA, Francisco PMSB, Neri AL. Sociodemographic and health factors associated with mortality in community-dwelling elderly. Rev Saúde Pública. 2017;51:42:1-10. Available from: https://doi.org/10.1590/s1518-8787.2017051006708 .
18. Pereira BR, Jesus IMO, Martins MMF. Perfil sociodemográfico da mortalidade da população idosa no nordeste brasileiro. Rev Atenção à Saúde. 2020:18(64):1-9. Available from: https://doi.org/10.13037/ras.vol18n64.6273.
19. Gomes MMF, Turra CM, Fígoli MGB, Duarte YA, Lebrão ML. Associação entre mortalidade e estado marital: uma análise para idosos residentes no Município de São Paulo, Brasil, Estudo SABE, 2000 e 2006. Cad Saúde Pública. 2013;29(3):566-78. Available from: http://dx.doi.org/10.1590/S0102-311X2013000300014
20. Guibu IA, de Moraes JC, Guerra Jr AA, Costa EA, Acurcio FA, Costa KS, et al. Características principais dos usuários dos serviços de atenção primária à saúde no Brasil. Rev Saúde Pública. 2017;51:1-13. Available from: https://doi.org/10.11606/S1518-8787.2017051007070
21. Malta DC, Bernal RTI, Lima MG, de Araújo SSC, da Silva MMA, Freitas MIF, et al. Noncommunicable diseases and the use of health services: analysis of the National Health Survey in Brazil. Rev Saúde Pública. 2017;51(suppl 1):1-9. Available from: http://dx.doi.org/10.1590/s1518-8787.2017051000090
22. Botton A, Cúnico SD, Strey MN. Diferenças de gênero no acesso aos serviços de saúde: problematizações necessárias. Mudanças Psicol Saúde. 2017;25(1):67-72. Available from: https://www.metodista.br/revistas/revistas-metodista/index.php/MUD/article/view/7009/5608 .
23. Laurenti R, Jorge MHPM, Gotlieb SLD. Perfil epidemiológico da morbi-mortalidade masculina. Ciênc Saúde Colet. 2005:10(1):35-46. Available from: http://dx.doi.org/10.1590/S1413-81232005000100010 .
24. Souza GST. Adesão dos homens às práticas preventivas. REVISE. 2019;2:141-52. Available from: https://doi.org/10.46635/revise.v0iDossiê%20de.1414
25. Ishii S, Ogawa S, Akishita M. The state of health in older adults in Japan: trends in disability, chronic medical conditions and mortality. PLoS ONE. 2015;10(10):e0139639. Available from: https://doi.org/10.1371/journal.pone.0139639
26. Lima-Costa MF, Peixoto SV, Giatti L. Tendências da mortalidade entre idosos brasileiros (1980-2000). Epidemiol Serv Saúde. 2004;13(4):217-28. Available from: http://dx.doi.org/10.5123/S1679-49742004000400004
27. Brasil. Ministério da Saúde. ABC do câncer: abordagens básicas para o controle do câncer [Internet]. 6ª ed. Rio de Janeiro: INCA; 2020 [cited 2020 Sept. 20]. Available from: https://www.inca.gov.br/sites/ufu.sti.inca.local/files/media/document/livro-abc-5-edicao .
28. de Andrade Filho VS, Artaxo Netto PE, Hacon SS, do Carmo CN. Distribuição espacial de queimadas e mortalidade em idosos em região da Amazônia Brasileira, 2001 – 2012. Ciênc Saúde Colet. 2017;22(1):245-53. Available from: http://dx.doi.org/10.1590/1413-81232017221.09622015

14 of 14
Temporal trend of mortality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200018
29. Brasil. Ministério da Ciência, Tecnologia, Inovações e Comunicações. Instituto de Nacional de Pesquisas Espaciais. Programa Queimadas [Internet]. Brasília, DF: IMPE; 2020 [cited 2020 Jan. 20]. Available from: http://queimadas.dgi.inpe.br/queimadas/portal-static/estatisticas_estados.
30. Miranda EE, Moraes AVC, Oshiro OT. Queimadas. Embrapa Monit por Satél-Artigo Divulg. na Mídia INFOTECA-E. 2006 [cited 2018 Feb. 04]. Available from: https://docplayer.com.br/77536879-Queimadas-na-amazonia-brasileira-em-2005-evaristo-eduardo-de-miranda-1-adriana-vieira-de-camargo-de-moraes-2-osvaldo-tadatomo-oshiro-3.html.
31. Lourenço TM, Lenardt MH, Kletemberg DF, Seima MD, Tallmann AEC, Neu DKM. Functional capacity in elderly longevity: an integrative review. Rev Gaúcha Enferm. 2012;33(2):176-85. Available from: https://doi.org/10.1590/S1983-14472012000200025
32. de Oliveira TC, Medeiros WR, de Lima KC. Diferenciais de mortalidade por causas nas faixas etárias limítrofes de idosos. Rev Bras Geriatr Gerontol. 2015;18(1):85-94. Available from: http://dx.doi.org/10.1590/1809-9823.2015.14203 .
33. Telarolli Jr R, Loffredo LCM. Mortalidade de idosos em município do Sudeste brasileiro de 2006 a 2011. Ciênc Saúde Colet. 2014;19(3):975-84. Available from: https://doi.org/10.1590/1413-81232014193.10482012
34. Virtuoso JF, Balbé GP, Mazo GZ, Pereira MGS, dos Santos FS. Morbidity and mortality of the elderly population in Florianopolis city: a comparative study between men and women. Rev Bras Geriatr Gerontol. 2010;13(2):215-23. Available from: https://doi.org/10.1590/S1809-98232010000200006
35. Martins Jr DF, Felzemburg RDM, Dias AB, Costa TM, Santos PNP. Trends in mortality from ill-defined causes among the elderly in Brazil, 1979-2013: ecological study. São Paulo Med J. 2016;134(5):437-45. Available from: https://doi.org/10.1590/1516-3180.2016.0070010616

1 of 9
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
http://dx.doi.org/10.1590/1981-22562020023.200215
Temporal trend of the incidence of TB/HIV coinfection and HIV testing of the old Brazilian population from 2008 to 2018
Janderson Diego Pimenta da Silva1
Rosemeiry Capriata de Souza Azevedo1
Annelita Almeida Oliveira Reiners1
Aenne Zandonadi Rodrigues Santana1
Amanda Cristina de Souza Andrade2
Ana Carolina Macri Gaspar Vendramini1
Keywords: Coinfection. Tuberculosis. HIV. Time Series Studies. Heath of the Elderly.
AbstractObjective: Analyze the temporal trend of the incidence of TB/HIV coinfection and the ratio of HIV testing in the Brazilian old population and its regions from 2008 to 2018. Method: Ecological, time-series study carried out with all new cases of old people with TB/HIV coinfection. The data were extracted from SINAN-TB and analyzed using the Prais-Winstenmethod. Results: In the temporal analysis of the incidence, Brazil showed a stable trend (VPA 2.1), and regarding the regions: Southeast, decreasing trend (VPA -2.15); Northeast and North, increasing trends (VPA 9.92; VPA 10.18, respectively); and South and Midwest, stable trends (VPA 0.17; VPA 4.81, respectively). In Brazil and its regions, the ratio of HIV testing showed growing trends: Brazil (VPA 12.82), North (VPA 20.46), Northeast (VPA 17.85), Southeast (VPA 10.29), South (VPA 7.11), and Midwest (VPA 6.10). Of the 3213 new cases of TB/HIV coinfection reported during the study period, most (68.66%) were male, 78.74% in the age group from 60 to 69. As for the clinical form, the majority (72.70%) was of the pulmonary type. Conclusion: Given the magnitude and implications of TB/HIV coinfection in the old population for health care services, these findings may support health professionals and managers in adopting effective measures to control these diseases.
1 Universidade Federal de Mato Grosso, Faculdade de Enfermagem, Programa de Pós-Graduação em Enfermagem. Cuiabá, MT, Brasil.
2 Universidade Federal de Mato Grosso, Instituto de Saúde Coletiva, Programa de Pós-Graduação em Saúde Coletiva. Cuiabá, MT, Brasil.
Funding: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES). Nº do processo: 88882.459096. Bolsa de Mestrado.The authors declare there are no conflicts of interest in relation to the present study.
CorrespondenceJanderson Diego Pimenta da Silva [email protected]
Received: July 17, 2020Approved: November 06, 2020
ID
ID
ID
ID
ID
ID

2 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
INTRODUC TION
Tuberculosis (TB)/HIV coinfection has been a major challenge for global health. In 2017, among the 10 million people with TB in the world, 9% had TB/HIV coinfection1. In Brazil, the percentage of new coinfection cases varied from 11.5% in 2009 to 12.4% in 2014, and in 2017 it was 11.4% being the 19th position in the ranking of the 30 countries with high TB / HIV coinfection load2.
The TB/HIV association causes complications of the clinical condition and treatment such as mental confusion, hepatotoxicity, and nephrotoxicity, as well as drug resistance3. Also, it causes modification of both infections, which impacts the sexual, work, social, and behavioral lives of people living with HIV (PVHIV)4.
Studies on TB/HIV coinfection show that the disease is more frequent in adults5.6, and temporal trend studies conducted with the general population show an increase in prevalence, incidence, and mortality in the age group of 60 years and over7.8. In Brazil, there was an increase in the incidence of TB/HIV coinfection in this population from 0.32/100,000 inhabitants in 2002 to 0.99/100,000 inhabitants in 2012, with a total variation of 209.38%7, as well as increased mortality8.
TB/HIV coinfection in the old population is the result of increased HIV3 and vulnerability to TB. Older people living with HIV are more susceptible not only because of the disease9 but also due to the alterations inherent to aging10.
In the old population, TB/HIV coinfection is worrying since TB increases the possibility of association with other chronic diseases and unfavorable events11, and HIV promotes increased comorbidity and frailty in old people12. Besides, the economic burden of TB/HIV coinfection is high due to the increased demand for the health system13.
The knowledge of TB/HIV coinfection by temporal distribution allows identifying the magnitude of the disease. In Brazil, the literature has so far investigated this outcome through secondary data considering the general population and focusing on the mortality and incidence of this coinfection7.8. In the international context, a study
focusing only on incidence was carried out in the Xinjiang Province, China14.
Considering the magnitude of TB/HIV coinfection, the increasing frequency of this disease in older people, population aging, and the ratio that TB/HIV coinfection can achieve in this population, the objective of the present study was to analyze the temporal trend of TB/HIV coinfection, and the ratio of HIV testing in the old population of Brazil and its regions from 2008 to 2018.
METHOD
This is a population-based, ecological, time-series study carried out in Brazil and its geographic regions from 2008 to 2018. All new cases of TB/HIV coinfection in the age group of 60 years or over were included.
TB/HIV coinfection was defined as new TB cases (comprising new, unknown, and post-mortem cases) covering all forms and types of diagnosis whose status of the HIV variable was “positive”15. A new case includes any patient who has never been treated for TB or has been for up to 30 days; unknown are those identified at the time of or after death, considering the individuals when the possibilities for investigating previous entries and post-death are exhausted16.
Data on the annual incidence of TB/HIV coinfection were obtained from the Notifiable Diseases Information System (SINAN-TB) on Tuberculosis available on the website of the SUS Department of Informatics (DATASUS). Population data were obtained through intercensus estimates made available by the Brazilian Institute of Geography and Statistics (IBGE) available at DATASUS.
The sociodemographic variables investigated in the study were gender (male, age group - 60 to 69 years, 70 to 79 years, 80 years and over), period in years (2008, 2009, 2010, 2011, 2012, 2013, 2014, 2015, 2016, 2017 and 2018), and regions (North, Northeast, Southeast, South, and Midwest). The clinical variables were clinical form (pulmonary, extrapulmonary, pulmonary + extrapulmonary), and use of antiretroviral (ignored/white, yes, no).

3 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
The data were organized in a database with the aid of the program Excel and analyzed with the statistical program Stata version 12.0. Absolute and relative frequencies were used for the descriptive analysis from 2008 to 2018.
Incidence rates of TB/HIV coinfection were calculated per 100,000 inhabitants. Subsequently, the incidence rates adjusted by age were directly standardized using as reference the Brazilian population from intercensus projections (2000 - 2030) available in DATASUS, to nullify the effect of the unequal demographic distribution of the population. The testing ratio was obtained by dividing the number of positive, negative, and ongoing cases of the HIV variable by the total number of new TB cases, by year of study and geographic region.
The regression of Prais-Winsten 17was used to calculate the annual percentage change (APC). The increasing, decreasing, and stable trends were expressed as APC with the respective confidence intervals (95%). An increasing trend was considered when the APC was positive, negative decreasing, and stable when there was no significant difference between its value and the zero number (p < 0.05):
APC=[-1+10b1]*100%
CI95%=[-1+10b1min.]*100%; [-1+10b1max]*100%
RESULTS
In Brazi l , 3,213 new cases of TB/HIV coinfection were reported in the elderly population
from 2008 to 2018. Table 1 shows the number and percentage of new cases and the trend in the incidence rates of TB/HIV coinfection in Brazil and its regions. Although the Southeast region had a higher ratio of cases (TB/HIV) (41.70%), it was the region with one of the lowest rates (1.17/100,000 inhabitants), and a decreasing trend of TB/HIV coinfection (APC -2,15%). The northern region had the highest average rate of TB/HIV coinfection (2.50/100,000 inhabitants), and an increasing trend (APC 10.18%), as well as the Northeast region (APC 9.92%).
In some regions, long confidence intervals are observed due to the lower case records in these regions. The historical series of the incidence rates of TB/HIV coinfection in Brazil and its geographic regions is shown in Figure 1.
Table 2 shows the characterization by gender, age group, clinical form, and antiretroviral. Most of the cases were male aged between 60 and 69 years old and clinical form of pulmonary type. Less than 40% of antiretroviral information has been completed.
Table 3 shows the percentage and trend of cases tested for HIV. The trend in the testing ratio increased both in Brazil and in its regions, and a higher APC was observed in the North and Northeast regions, which showed lower testing ratios of 55.95% and 54.36%, respectively.
Figure 2 shows the representation of the historical series of HIV testing ratios in Brazil and its geographic regions.
Table 1. Number and percentage of new cases in the old population, average coefficient per 100,000 inhabitants, and the trend in the incidence rates of TB/HIV coinfection in Brazil and its geographic regions. 2008 – 2018.
Region Cases Average coefficient* APC** 95% CI*** InterpretationN (%)
North 318 (9.90) 2.50 10.18 1.09 - 20.08 IncreasingNortheast 758 (23.59) 1.28 9.92 1.11 - 19.50 IncreasingSoutheast 1.340 (41.70) 1.17 - 2.15 - 4.14 - -0.12 DecreasingSouth 648 (20.17) 1.60 0.17 - 7.36 - 8.32 StableCentral-West 149 (4.64) 0.96 4.81 - 4.39 - 14.91 StableBrazil 3.213 (100.00) 1.32 2.10 - 0.24 - 4.52 Stable
*Standardized taxes for the population of Brazil; **Annual percentage variation; ***Confidence Interval of APC.

4 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
Figure 1. Historical series of standardized incidence rates of TB/HIV coinfection in old people in Brazil and its geographic regions. 2008 – 2018.
Table 2. Distribution of new cases of TB/HIV coinfection by sociodemographic and clinical variables in the old population in Brazil and its geographic regions. 2008 – 2018.
Variables North Northeast Southeast South Central-West BrazilGender n* %** n* %** n* %** n* %** n* %** n* %**Male 211 66.35 561 74.01 911 67.99 421 64.97 102 68.46 2206 68.66Female 107 33.65 197 25.99 429 32.01 227 35.03 47 31.54 1007 31.34Age group (years)60 – 69 231 72.64 563 74.27 1078 80.45 540 83.33 118 79.19 2530 78.7470 – 79 69 21.70 148 19.53 231 17.24 93 14.35 26 17.45 567 17.6580 and over 18 5.66 47 6.20 31 2.31 15 2.31 5 3.36 116 3.61Clinical formPulmonary 238 74.84 622 82.06 961 71.72 401 61.88 114 76.51 2336 72.70Extrapulmonary 56 17.61 103 13.59 275 20.52 177 27.31 24 16.11 635 19.80Pulmonary+Extrapulmonary
24 7.55 33 4.35 103 7.69 70 10.80 11 7.38 241 7.50
AntiretroviralIgnored/Blank 234 73.58 561 74.01 1010 75.37 395 60.96 100 67.11 2300 71.59Yes 60 18.87 132 17.41 216 16.12 168 25.93 41 27.52 617 19.20No 24 7.55 65 8.58 114 8.51 85 13.12 8 5.37 296 9.21
*Absolute frequency; **Relative frequency; Source: SINAN.

5 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
DISCUSSION
The present study allowed to know the profile and the time trend of TB/HIV coinfection in the Brazilian old population, as well as the HIV testing. These findings enable the development of strategies to control these outcomes, reduce morbidity and mortality in this population, as well as contribute to the maintenance of sexuality and healthy aging.
The stable trend of TB/HIV coinfection in the old population found in Brazil in the period studied
Figure 2. Historical series of the HIV testing ratio in the old people in Brazil and its geographic regions. 2008 – 2018.
is a different finding from that found in the study by Gaspar et al.7 evaluating the progression of TB and TB/HIV coinfection in Brazil in the period from 2002 to 2012 with the general population. During the period under analysis, the trend of this condition was increasing in all age groups, including those aged 60 and over.
The trend towards the stability of TB/HIV coinfection may be due to the combined treatment (therapy for TB and HIV) that was more effective in reducing TB/HIV coinfection by proposing a
Table 3. Number and percentage of tests carried out in the old population, average coefficient, and trend in the HIV testing ratio in Brazil and its geographic regions. 2008 – 2018.
Region Cases Average coefficient* APC** 95% CI*** InterpretationN (%)
North 6.905 (9.55) 55.93 20.46 11.42; 30.23 IncreasingNortheast 19.105 (26.41) 54.36 17.85 12.59; 23.35 IncreasingSoutheast 32.223 (44.55) 70.26 10.29 7.39; 13.27 IncreasingSouth 10.362 (14.32) 75.93 7.11 3.50; 10.85 IncreasingCentral-West 3.736 (5.17) 61.57 6.10 2.25; 10.09 IncreasingBrazil 72.331 (100.00) 63.89 12.82 9.01; 16.75 Increasing
*Average testing rates; **Annual percentage variation; ***APC confidence interval.

6 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
deterministic model for the transmission of the coinfection including the use of both treatments as ideal control strategies18.
The difference in time trend among the Brazilian regions analyzed in the present study was coincident with the findings of the study by Gaspar et al.7 in which there was growth in the North, Northeast, and Central-West regions, whereas the South did not present significant differences, and differently from other regions in the Southeast region there was a reduction in rates.
In the present study, both the growing trend of TB/HIV coinfection observed in the North and Northeast regions and the decreasing trend of cases in the Southeast region may be related to health, education, and income indicators in these regions19. Brazil is a large country with distinct regional characteristics, in particular regarding social and economic characteristics.
The regional difference in terms of trends in the incidence of TB/HIV coinfection may be related to the quality of health care services resulting from socioeconomic inequalities that in turn influence the control of TB/HIV coinfection. A study analyzing the epidemiological aspects of co-infection in Northeastern Brazil showed that the region is an important endemic area for TB/HIV coinfection. Furthermore, the low percentage of cure, high percentage of non-adherence, occurrence of severe forms of extrapulmonary TB, and high lethality rate reflect the challenge to control TB/HIV coinfection in the Northeast region20.
Another research a imed to ver ify the epidemiological aspects of TB/HIV coinfection in the state of Mato Grosso do Sul, and its association with the HDI showed that the cases of coinfection were associated with the HDI in areas with a higher population density, showing the need to adopt specific strategies21.
An integrative review analyzed the relation between TB and social inequalities and showed that age, income, education, professional training, poverty, unemployment, access to health care services, and basic sanitation are factors that can interfere in the
control of the disease22. Therefore, socioeconomic vulnerabilities can determine unfavorable results in the treatment of TB/HIV coinfection.
On the other hand, a study analyzing the quality and management of care for TB/HIV coinfection in the state of São Paulo showed that in the municipalities where quality was satisfactory there was a low ratio of TB/HIV coinfection, and a low AIDS incidence rate. In the municipalities where quality was unsatisfactory, there was a high ratio of TB/HIV coinfection, and a high AIDS incidence rate23.
The higher frequency of TB/HIV coinfection in males is a similar finding to that found in another study carried out with a population aged 20 to 60 years or more in Brazil24. It seems likely that these results are because men are more likely to deny their vulnerability to diseases and exempt themselves from responsibility for self-care25. Regarding vulnerability to HIV, the old population cannot understand they are at risk of having the disease. Therefore, they usually do not use condoms during sexual intercourse26.
Regarding age group, the incidence of TB/HIV coinfection in the younger age group is a result corroborated by studies analyzing the trend in the incidence and mortality of TB/HIV coinfection7,8 in the general population. Both found higher rates in the younger old population. When compared to previous generations, people in this age group are more sexually free, and they are generally single or divorced, have more casual relationships27, and do not use condoms28 which makes them more vulnerable to HIV and consequently to TB.
The predominance of the clinical pulmonary form of TB is probably because this form is the most frequent one and the main infectious source for the disease spread29. Its incidence is similar to that found in the general population5.6.
Comparing the percentage of those making use or not of antiretroviral therapy (ART), most of them are being treated. This is probably due to the early treatment of PLHIV with active TB to reduce mortality3. The importance of using ART

7 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
in co-infected people has been emphasized in some studies. A study in Ethiopia showed that ART had a protective effect against TB30. Similarly, a Chinese study found that not using ART was a risk factor for TB31. Other studies have shown that late-onset of ART32 or not doing it33 were risk factors for mortality in cases of coinfection.
The significant absence of national records regarding the use of antiretroviral drugs is a result that draws attention. This high percentage may be because the records regarding ART were included in SINAN only from the year 2014, and in the State of São Paulo only in the second half of 2016. Underreporting also contributes to the incompleteness of data, reflecting the result of organizational and structural problems on epidemiological surveillance systems, such as lack of notification by health professionals, late notification, manual or bureaucratic systems, extensive or inadequate forms requiring more time to complete, and notification of only a few diseases depending on the severity34, which reinforces the need to improve data on coinfection.
The time trend of HIV testing in the old population with increasing TB in Brazil and all its regions is a relevant result. This increase in the testing ratio possibly results from the recommendation of testing all people with active TB for HIV, for which the use of the rapid HIV test is recommended since 20153. WHO data show that of the 4.3 million TB cases reported in the general population in 2018, 64% were tested for HIV, representing a 27-fold increase in the number of people with TB tested for HIV when compared to 20049.
The early diagnosis of HIV in old people does not reduce the incidence of the disease, but promotes the timely onset of treatment with ART, and contributes to the improvement of health conditions and reduction of mortality35.
The trends observed regionally must be analyzed with caution due to the inequalities of the data record in SINAN-TB, since the increased trends may reflect more an improvement in the quality of the information system than an increase in incidence.
Although the present study allows knowing the movement of measures of interest in health - in this case, TB/HIV coinfection -, it has some limitations. The population is old, therefore their results may be subject to survival bias. Other limitations were the use of secondary data from SINAN-TB and IBGE, the operational difficulties of this system such as underreporting, incorrect, incomplete, and duplicate filling of the variables, which can interfere in the interpretation of the data. Therefore, we recommend the linkage between databases and the HIV/AIDS Notifiable Diseases Information System (SINAN-Aids), Tuberculosis Mortality Information System (SIM-TB), and the HIV/AIDS Mortality Information System (SIM-AIDS) to improve data analysis in future studies.
Further studies on aging, sexuality, and prevention of TB/HIV coinfection in older people should be developed. Follow-up studies are recommended to analyze the impact of TB/HIV coinfection in the old population, as well as intervention research to control these diseases in this population.
CONCLUSION
The incidence of TB/HIV coinfection showed a stable trend in Brazil. However, it was decreasing in the Southeast, and increasing in the North and Northeast. The occurrence of an increasing trend in the HIV testing ratio in Brazil and its regions is emphasized.
Given the magnitude and implications of TB/HIV coinfection in the old population for health care services, these findings may support health professionals and managers in adopting effective measures to control these diseases.
As the population ages, new challenges in the health care sector appear. Therefore, the epidemiological knowledge and the behavior of these diseases over time allow to outline strategies aimed at the prevention and control of these diseases in this population, contributing to healthy aging.
Edited by: Yan Nogueira Leite de Freitas

8 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
REFERENCES
1. Programa Conjunto das Nações Unidas sobre HIV/AIDS (UNAIDS) [Internet]. Genebra: UNAIDS; 2018 [cited 2019 July 02]. Estatísticas globais sobre HIV; [2 telas]. Available from: https://unaids.org.br/estatisticas/.
2. Brasil. Ministério da Saúde. Boletim Epidemiológico: Panorama epidemiológico da coinfecção TB-HIV no Brasil 2019 [Internet]. Brasília, DF: MS; 2019 [cited 2020 Feb. 02]. Available from: http://www.aids.gov.br/pt-br/pub/2019/boletim-epidemiologico-tb-hiv-2019.
3. Brasil. Ministério da Saúde. Manual Técnico para o Diagnóstico da infecção pelo HIV em adultos e crianças [Internet]. Brasília, DF: MS; 2018 [cited 2020 Feb. 02]. Available from: http://www.aids.gov.br/pt-br/node/57787.
4. Lemos LA, Feijão AR, Gir E, Galvão MTG. Aspectos da qualidade de vida de pacientes com coinfecção HIV/tuberculose. Acta Paul Enferm. 2012;25(1):41-47. Available from: http://dx.doi.org/10.1590/S0103-21002012000800007.
5. Oliveira LB, Costa CRB, Queiroz AAFLN, Araújo TME, Sousa kAA, Reis RK. Epidemiological analysis of tuberculosis/HIV coinfection. Cogitare Enferm. 2018;23(1):1-10. Available from: http://dx.doi.org/10.5380/ce.v23i1.51016.
6. Tshitenge S, Ogunbanjo GA, Citeya A. A mortality review of tuberculosis and HIV co-infected patients in Mahalapye, Botswana: does cotrimoxazole preventive therapy and/or antiretroviral therapy protect against death? Afr J Prim Health Care Fam Med. 2018;10(1):1-5. Available from: https://doi.org/10.4102/phcfm.v10i1.1765.
7. Gaspar RS, Nunes N, Nunes M, Rodrigues VP. Temporal analysis of reported cases of tuberculosis and of tuberculosis-HIV co-infection in Brazil between 2002 and 2012. J Bras Pneumol. 2016;42(6):416-22. Available from: http://dx.doi.org/10.1590/S1806-37562016000000054.
8. Lima MS, Martins-Melo FR, Heukelbach J, Alencar CH, Boigny RN, Ramos Jr AN. Mortality related to tuberculosis-HIV/AIDS co-infection in Brazil, 2000-2011: epidemiological patterns and time trends. Cad Saúde Pública. 2016;32(10):1-11. Available from: http://dx.doi.org/10.1590/0102-311X00026715.
9. Organização Mundial da Saúde. Global tuberculosis report [Internet]. Genebra: OMS; 2019 [cited 2019 July 02]. Available from: https://www.who.int/tb/publications/global_report/en/.
10. Vendramini SHF, Villa TCS, Gonzales RIC, Monroe AA. Tuberculose no idoso: análise do conceito. Rev Latinoam Enferm. 2003;11(1):96-103. Available from: http://dx.doi.org/10.1590/S0104-11692003000100014.
11. Rocha MS, Oliveira GP, Aguiar FP, Saraceni V, Pinheiro RS. Do que morrem os pacientes com tuberculose: causas múltiplas de morte de uma coorte de casos notificados e uma proposta de investigação de causas presumíveis. Cad Saúde Pública. 2015;31(4):709-21. Available from: http://dx.doi.org/10.1590/0102-311X00101214.
12. Calvo M, Martinez E. Update on metabolic issues in HIV patients. Curr Opin HIV AIDS. 2014;9(4):332-9. Available from: https://doi.org/10.1097/COH.0000000000000075.
13. Siqueira-Filha NT, Albuquerque MFM, Rodrigues LC, Legood R, Santos AC. Economic burden of HIV and TB/HIV coinfection in a middle-income country: a costing analysis alongside a pragmatic clinical trial in Brazil. Sex Transm Infect. 2018;94(6):1-10. Available from: https://doi.org/10.1136/sextrans-2017-053277.
14. Wang W, Wei-Sheng Z, Ahan A, Ci Y, Wei-Wen Z, Ming-Qin C. The characteristics of TB epidemic and TB/HIV co-infection epidemic: A 2007-2013 retrospective study in Urumqi, Xinjiang Province, China. Plos ONE. 2016;11(10):1-12. Available from: https://doi.org/10.1371/journal.pone.0164947.
15. Brasil. Ministério da Saúde. Boletim Epidemiológico, Coinfecção TB-HIV no Brasil: panorama epidemiológico e atividades colaborativas. Brasília, DF: MS; 2017 [cited 2019 July 02]. Available from: http://www.aids.gov.br/pt-br/pub/2017/coinfeccao-tb-hiv-no-brasil-panorama-epidemiologico-e-atividades-colaborativas-2017.
16. Brasil. Ministério da Saúde. Sistema de informação de agravos de notificação dicionário de dados – SINAN net – versão 5.0 [Internet]. Brasília, DF: MS; 2014 [cited 2020 Nov. 04]. Available from: http://siteantigo.suvisa.ba.gov.br/sites/default/files/sinan/arquivos/2016/09/26/dic_dados.html.
17. Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saúde. 2015;24(3):565-76. Available from: http://dx.doi.org/10.5123/S1679-49742015000300024.
18. Fatmawati, Tasman H. An Optimal Treatment Control of TB-HIV Coinfection. Hindawi. 2016:1-11. Available from: http://dx.doi.org/10.1155/2016/8261208.

9 of 9
The trend of TB/HIV coinfection in the old Brazilian population
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200215
19. Programa das Nações Unidas para o Desenvolvimento -PNUD. Desenvolvimento humano nas macrorregiões brasileiras [Internet]. Brasília: IPEA; 2016 [cited 2020 Feb. 02]. Available from: http://www.ipea.gov.br/portal/images/stories/PDFs/livros/livros/20160331_livro-idhm.pdf.
20. Barbosa IR, Costa ICC. Estudo epidemiológico da coinfecção tuberculose-HIV no Nordeste do Brasil. Rev Patol Trop. 2014;43(1):27-38. Available from: https://doi.org/10.5216/rpt.v43i1.29369.
21. Baldan SS, Ferraudo AS, Andrade M. Características clínico-epidemiológicas da coinfecção por tuberculose e HIV e sua relação com o Índice de Desenvolvimento Humano no estado do Mato Grosso do Sul, Brasil. Rev Pan-Amaz Saúde. 2017 [cited 2020 Oct. 27];8(3):59-67. Available from: http://dx.doi.org/10.5123/s2176-62232017000300007.
22. Bertolozzi MR, Takahashi RF, França FOS, Hino P. A ocorrência da tuberculose e sua relação com as desigualdades sociais: estudo de revisão Integrativa na Base PubMed. Esc Anna Nery. 2020;24(1):1-9. Available from: http://dx.doi.org/10.1590/2177-9465-ean-2018-0367.
23. Campoy LT, Arakawa T, Andrade RLP, Ruffino-Netto A, Monroe AA, Arcêncio RA. Qualidade e gestão da atenção à coinfecção tuberculose e HIV no estado de São Paulo. Texto & Contexto Enferm. 2019;28: e20180166. Available from: https://doi.org/10.1590/1980-265x-tce-2018-0166.
24. Bastos SH, Taminato M, Fernandes H, Figueiredo TMRM, Nichiata LYI, Hino P. Perfil sociodemográfico e de saúde da coinfecção TB / HIV no Brasil: uma revisão sistemática. Rev Bras Enferm. 2019;72(5):1458-65. Available from: http://dx.doi.org/10.1590/0034-7167-2018-0285.
25. Cortez MB, Trindade ZA, Menandro MCS. Racionalidade e sofrimento: homens e práticas de autocuidado em saúde. Psicol Saúde Doenças. 2017;18(2):556-66. Available from: http://dx.doi.org/10.15309/17psd180222.
26. Brito NMI, Andrade SSC, Silva FMC, Fernandes MRCC, Brito KKG, Oliveira SHS. Idosos, infecções sexualmente transmissíveis e aids: conhecimentos e percepção de risco. ABCS Health Sci. 2016;41(3):140-5. Available from: http://dx.doi.org/10.7322/abcshs.v41i3.902.
27. Brasil. Centro Internacional de Longevidade (CIL-BRASIL). Envelhecimento ativo: um marco político em resposta à revolução da longevidade [Internet]. Rio de Janeiro: CIL-BRASIL; 2015 [cited 2019 July. 02]. Available from: http://ilcbrazil.org/portugues/wp-content/uploads/sites/4/2015/12/Envelhecimento-Ativo-Um-Marco-Pol%C3%ADtico-ILC-Brasil_web.pdf .
28. Aguiar RB, Leal MCC, Marques APO, Torres KMS, Tavares MTDB. Idosos vivendo com HIV: comportamento e conhecimento sobre sexualidade: Revisão integrativa. Ciênc Saúde Colet. 2018. Available from: http://www.cienciaesaudecoletiva.com.br/artigos/idosos-vivendo-com-hiv-comportamento-e-conhecimento-sobre-sexualidade-revisao-integrativa/16889?id=16889.
29. Brasil. Ministério da Saúde. Guia de Vigilância em Saúde [Internet]. Brasília, DF: MS; 2019 [cited 2019 July 02]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/guia_vigilancia_saude_3ed.pdf.
30. Alemu YM, Awoke W, Wilder-Smith A. Determinants for tuberculosis in HIV-infected adults in Northwest Ethiopia: multicentre case-control Study. BMJ Open. 2016;4:1-7. Available from: http://dx.doi.org/10.1136/bmjopen-2015-009058.
31. Zhezhe C, Lin M, Nie S, Lan R. Risk factors associated with Tuberculosis (TB) among people living with HIV/AIDS: a pairmatched case-control study in Guangxi, China. Plos ONE. 2017;12(3):1-12. Available from: https://doi.org/10.1371/journal.pone.0173976.
32. Yong-Jia J, Liang PP, Shen JY, Sun JJ, Yang JY, Chen J, et al. Risk factors affecting the mortality of HIV-infected patients with pulmonary tuberculosis in the cART era: a retrospective cohort study in China. Infect Dis Poverty. 2018;7(1):1-10. Available from: https://doi.org/10.1186/s40249-018-0405-8.
33. Silva DI, Ceccato MGB, Silveira MR, Miranda SS, Gomes RM, Haddad JPA, et al. Predictors of mortality among individuals with tuberculosis and human immunodeficiency virus coinfection at a reference center in southeastern Brazil: A retrospective cohort study. J Young Pharm. 2018;10(4):476-80. Available from: https://doi.org/10.5530/jyp.2018.10.103.
34. Melo MAS, Coleta MFD, Coleta JAD, Bezerra JCB, Castro AM, Melo ALS, et al. Percepção dos profissionais de saúde sobre os fatores associados à subnotificação no Sistema Nacional de Agravos de Notificação. Rev Adm Saúde. 2018;18(71):1-17. Available from: http://dx.doi.org/10.23973/ras.71.104.
35. Alencar RA, Ciosak SI. O diagnóstico tardio e as vulnerabilidades dos idosos vivendo com HIV/aids. Rev Esc Enferm USP. 2014;49(2):229-35. Available from: http://dx.doi.org/10.1590/S0080-623420150000200007.

1 of 9
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
http://dx.doi.org/10.1590/1981-22562020023.200189
The demands of care and self-care from the family caregiver’s of the elderly with dementia perspective
Emanuela Bezerra Torres Mattos1
Jéssica Paloma Oliveira2
Marcia Maria Pires Camargo Novelli3
Keywords: Aging. Dementia. Caregiver. Occupational Therapy.
AbstractObjective: Aimed to know the personal demands of family caregivers through conducted roundtables. Method: In 2017, two groups were conducted with 6 roundtables each with the following guiding questions: 1) “Who am I? Who do I take care of?”; 2) “What is dementia for me?”; 3) “What is my role in the daily care activities of the person with dementia?”; 4) “What are my thoughts or emotions that are triggered by caring?” 5) “Can I see something positive in this caring experience?”; and 6) “How do I care or could take care of myself?”. Inclusion criteria were: to be a caregiver of the elderly with dementia, to have been doing this role for at least 6 months, and to be available and willing to participate in the meetings. The roundtables took place every fortnight with an hour and a half minutes of duration each, with an occupational therapist as facilitator. All the roundtables were recorded, transcribed, and analyzed through the thematic content analysis. Results: Fifteen family caregivers participated. From the analysis, nine thematic categories emerged: self-perception of physical and emotional impairment; the search for support; caregiver overload and stress; what I learned from this experience; the mixture of feelings; the losses; valuing the simple aspects of daily life; I already take care of myself; and I need to take care of myself. Conclusion: the identification of these personal demands of family caregivers of elderly people with dementia can raise awareness and make health professionals aware of the importance of considering these aspects in proposing interventions focused on caregivers.
1 Universidade Federal de São Paulo, Departamento Saúde Educação e Sociedade. São Paulo, SP, Brasil.2 Universidade Federal de São Paulo, Curso de Terapia Ocupacional. São Paulo, SP, Brasil.3 Universidade Federal de São Paulo, Programa de Pós Graduação de Ciências do Movimento Humano e
Reabilitação. São Paulo, SP, Brasil.
Funding: Programa Institucional de Bolsas de Iniciação Científica / Conselho Nacional de Desenvolvimento Científico e Tecnológico (PIBIC/CNPq). Bolsa de Iniciação Científica.The authors declare there are no conflicts of interest in relation to the present study.
CorrespondenceEmanuela Bezerra Torres [email protected]
Received: August 8, 2020Approved: November 16, 2020
ID
ID
ID

2 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
INTRODUC TION
Currently, 47 million people worldwide live with dementia. Approximately 70% of them reside in the community. Most people living with dementia in the community require assistance to perform their Basic Activities of Daily Living (BADL’s) such as eating, dressing and cleaning, and to perform the Instrumental Activities of Daily Living (IADL’s) that involve financial control and administration of medication, among other activities, as well as the need for help and/or support for rest, sleep and leisure activities1.
Care in dementia has been provided mainly by families, represented in the figure of a main family caregiver¹. Studies have pointed out the negative impacts on the exercise of care regarding changes in the lifestyle, financial and health problems of the caregiver2-5. However, more recent research has identified positive aspects related to the role of caring (e.g., personal growth, approximation of broken relationships), which can minimize caregiver burden and stress6,7.
This care represents a great burden on the caregiver due to its progressive nature, its long duration, and the absence of disease-modifying treatments. In addition, dealing with the decline in cognitive and functional skills of the person with dementia, offering physical and emotional support, administering medication, dealing with symptoms, with personality changes and with the loss of communication, among other aspects, ends up compromising physical and emotional health, quality of life and well-being of the caregiver.
Many interventions, including occupational therapies, are aimed at family caregivers with a focus on orientation in relation to managing daily activities, handling behavioral changes, and dealing with the the burden of care. Dizazzo-Miller et al.8 point out that support groups and educational programs are as essential for caregivers as medications are for people with dementia. Nevertheless, a review study with the objective of knowing interventions proposed to caregivers shows that there are few actions that work on the personal aspects of caregivers themselves9.
Thus, it is essential to know the care and self-care demands of family caregivers of elderly people with dementia, through their perspectives, shared on roundtables.
METHOD
The present research is a pilot and was developed from the realization of two groups with 6 roundtables each, with the main objective of identifying the personal demands for care and self-care of family caregivers of people with dementia.
The study is in accordance with Resolution No. 466/2012 and Resolution No. 510/2016. It was submitted to the Ethics Committee in Research with Human Beings at Federal University of São Paulo (UNIFESP) and divulged on social media in the Baixada Santista region only after approval. The registration of the family caregivers was done by digital means through a disclosed e-mail. The registrants were contacted and invited to participate in the roundtables at a previously scheduled date and place. All participants were informed about the ethical principles and objectives of the research and asked to sign the informed consent form (ICF).
To reach a larger number of relatives, two groups of family caregivers were conducted in the year 2017 (April to June and September to November). The inclusion criteria of caregivers were: to have been exercising the role of family caregiver for at least six months; to be a caregiver of the elderly with dementia; to be interested and willing to participate in the meetings. The exclusion criteria were: being a professional caregiver, not being willing to be present at two or more meetings.
To guarantee the ethical principle of secrecy and non-identification, all caregivers were identified with the abbreviation of the acronym caregiver (C) followed by the ordinal number (1-15).
Morin10 points out that “the roundtables, from the point of view of complexity, connect seemingly separate issues, so that the parts and the whole are captured as facets of the same object, which is in itself

3 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
complex and contradictory, hard and utopian: the social conditions and the reality to be (re)constructed “. Each roundtable had an open-ended question that guided the discussions. In each group, six roundtables were held with a fortnightly frequency between each of the meetings, lasting one and a half hours each, facilitated by two occupational therapists, one of them being the responsible researcher and the other being a scientific initiation scholarship student (PIBIC-CNPq).
The guiding questions were: 1) “Who am I? Who do I take care of?”; 2) “What is dementia for me?”; 3) “What is my role in the daily care activities of the person with dementia?”; 4) “What are my thoughts or emotions that are triggered by caring?”; 5) “Can I see something positive in this caring experience?”; and lastly 6) “How do I take care or could I take care of myself?”.
All the roundtables were recorded, transcribed, and subsequently analyzed through the thematic content analysis proposed by Minayo11. This method presupposes the comprehensive reading of the selected material for the impregnation of the speech, the exploration of the material in order to reach from the “revealed” to the “veiled” and the elaboration of an interpretative synthesis articulating central themes. The meetings were conducted by the responsible occupational therapist. The statements were transcribed by the collaborator and later analyzed by the two of them. In the process, each of the therapists qualified the transcriptions in units of meaning. Then, a consensual analysis of these units was carried out, from which nine thematic categories emerged and which will be discussed in the following results.
RESULTS AND DISCUSSION
Eight family caregivers participated in the first group. Six (75%) were women and two were (25%) men. In the second group, seven (100%) were women. The average age of the participants was 66 years old, ranging from 49 to 88 years old, while 13 (86.66%) family caregivers were over 60 years old. The most common degree of kinship was that of spouse in
eight (53.33%) of the participants, followed by six (40%) offspring and one (6.66%) sisters. Regarding the diagnosis, 14 (93.33%) reported that their relative had dementia from Alzheimer’s disease. From the previous explanation about the disease phases as well as the main signs and symptoms of the respective phases, the caregivers identified that seven (46.66%) of their family members were in the moderate phase, four (26.66%) in the initial phase and four (26.66%) in the advanced phase.
The thematic categories discussed below emerged from the collected reports.
In the first roundtable, the facilitator presented the group’s objectives and participation rules. Henceforth, asked the following question: “Who am I? Who do take care of?”, allowing space for each caregiver to present themselves by highlighting the name, degree of kinship with those they cared for and other information deemed important. From the analysis of the caregivers’ reports collected, two categories were identified:
1ª) Self-perception of physical and emotional impairment
There is an abundance of literature based on stress coping paradigms, because of the scientific evidence that family caregivers of people with dementia experience stress, overload, depression, and a variety of changes in physical health as a response to their role as caregiver. Duggleby et al.12 point out that among the changes in physical health are the decrease in immune system response and increase in risk of cardiovascular disease, hypertension, and insomnia.
C9 (Sister) points out, “I don’t think she is depressed, but I am.” Researchers examined the differences between depression and anticipatory grief in caregivers and observed that the symptoms of separation anxiety or anxiety in general are part of the experience of bereavement, but not of depression13. Anticipatory grief (AG) refers to the process of experiencing as phases of mourning (postmortem)

4 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
before the concrete loss of a significant person14. The cognitive focus of depression is on the negative interpretation of self and the world, while in AG the focus is on the experience of loss15. Such aspects deserve the gaze of health professionals regarding the specific demands of this care.
2ª) The search for support
Study by Grigorovich et al. identifies that family caregivers, despite searching for information about the disease, largely on the internet, recognize as essential the participation in support groups for the exchange of experiences and guidelines for daily care, as well as for sharing services available in the community, sometimes not well publicized and accessed15.
“All I have difficulty with, I seek to understand, because when I understand, I begin to accept”. C10 (Daughter).
This statement suggests that the possibility of seeking information, participating in discussions and sharing experiences can be strategies used to assist in the elaboration of the diagnosis and in the developments involved in each stage of the disease. A study carried out with 226 pairs of family caregivers and their elderly relatives with dementia identified 505 unmet needs of these family caregivers. Of these 226 family caregivers, 171 (75.7%) had at least one unmet need. These unmet needs were grouped into 17 categories, 19% of which were related to support groups. This study also points out that factors such as the low level of education and the advanced age of the family caregiver, as well as being the spouse of the elderly person with dementia and the greater degree of functional impairment of this person, as the disease progresses, are associated with higher levels of unmet needs9.
The second roundtable aimed at answering the question: “What is dementia for me?”. Each of the participants spoke about their perceptions and impressions regarding the disease. The third and fourth category emerged in this encounter:
3ª) Caregiver burden and stress
Alzheimer’s disease significantly changes the daily lives of families and, especially, the caregiver’s. Because it is a chronic and progressive disease that lasts for many years, it carries great emotional and socioeconomic repercussion, besides the physical, emotional, and social demands. Au et al. point out that such aspects may have negative long-term effects on the family caregiver who will carry out a greater number of care tasks besides the need to devote more hours as the disease progresses16.
“Almost two and a half years ago, my life completely changed! I do not do what I like to do anymore”. C8 (Wife).
“There are times when I totally lose my temper. I sleep very little because I get caught up all the time thinking about the situation we are in. I sleep 2 to 3 hours per night”. C12 (Wife).
The care provided to elderly people with dementia becomes very complex, as the family finds themselves involved in feelings that are difficult to manage, which end up imposing a certain isolation on self-care activities, which can affect emotional systems, generate deprivation and changes in the lifestyle in order to include the new needs of their relative.
4ª) What I learned from this experience
Some studies have pointed out the perception of positive aspects related to the experience of caring for dementia. An integrative review developed by Doris, Sheung-Tak and Jungfang identified four central themes that were grouped into personal performance, feelings of reciprocity, greater family cohesion and life purpose. Such findings corroborate with some statements identified in our groups17.
“My husband has always been a man who did everything. I’ve never had any responsibilities. Suddenly I found myself in a situation where I had to take over everything and take care of him. Now I am able to give him the quality of life that he deserves. With patience, I was able to learn things I never thought I would”. C5 (Wife).

5 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
Peacock et al. in their study identified that wives tended to feel that care was a natural continuation of the marital relationship18, just as C12 (Wife) puts it: “I think I have an obligation to care of him because we are married. We grew old together, so I have to take care of him”. In each one of the reports described, it was possible to identify the recognition of situations in which caregivers mention positive aspects related to care, but that, perhaps, the number of negative situations routinely lived did not allow them to reflect on this matter before the participation in the group19.
The objective of the third roundtable was to identify, based on the reports, the difficulties of the caregivers in relation to the demands on the basic activities of daily life of their relatives. Thus, when asked the question, “What is my role in the daily care activities of the person with dementia?” The caregivers’ reports have more broadly emphasized the emotions and feelings that come with the activities of care rather than the activities themselves. The fifth category emerged:
5ª) The mixture of feelings
Feelings such as sadness, regret, guilt, emotional pain, anxiety, loneliness and anger are related to anticipatory grief, which is defined as a reaction to the perception of loss, and tends to be a primary reaction to the care of a person with dementia.
While C13 (Wife) realizes that she is isolating herself from her previously performed activities and says: “I need to worry less because it makes me sad. Every time you look at yourself, you become dissatisfied with your attitudes and your isolation”, C15 (Wife) feels limited in the sense that she has lost her freedom and says, “I feel angry and stuck on some occasions. I feel a certain limitation.”
Still in the face of perceived loss, in the report of C4 (Wife), the loss of relationship and intimacy in relation to her husband and his social role is clear when she says: “I feel very alone. I also feel great sadness, because before he was sick, I had someone to share my problems with, I had my husband.”
Studies relate the grief experienced by the caregiver to multiple losses throughout the disease. Research on grief in caregivers has identified that, among the multiple losses that are experienced throughout the illness, are the loss of socialization, intimacy, communication, roles, and relationships22-25.
The fourth roundtable had as a guiding question: “What are my thoughts or emotions that are triggered by caring?” and gave rise to the following category:
6ª) The losses
The emotional and psychological suffering experienced by family caregivers has challenged the paradigm of overload and stress by recognizing AG as a critical component of this experience. This recognition emerged in an attempt to understand what family caregivers experience during the care trajectory. In the context of dementia, the AG can extend for many years while family members witness the deterioration in the affected person’s cognitive, social and physical functioning, as well as experience losses in relation to the past, present and future27.
The following statements are from three family caregivers (spouses) in which we can identify aspects related to anticipatory grief respectively, in relation to the present and future losses:
“When I l ie down to sleep, I think about everything. The situation I am in, what I am going through, what will happen...”. C12 (Wife).
“I’m very whiny. I’m afraid. I wonder what is going to happen from now on and I am very worried about the future”. C4 (Wife).
“I think I’m afraid and I do not even know to what extent. I’ve been distressed because sometimes I’m worrying by anticipation!”. C11 (Wife).
Sanders et al. based on the principles of Bowlby’s Theory of Attachment, says that grief occurs naturally in these caregivers because the bonds or feelings of attachment they had with their family member before the start of cognitive decline become tense as memory loss and cognitive impairment progress.

6 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
The stronger the attachment, whether it is physical, psychological or emotional, between the caregiver and the person with dementia, the stronger the feelings of grief and loss will be28.
Marwit and Meuser point out:
“The anticipatory grief of family caregivers in the context of dementia is more like true grief than the anticipatory grief experienced by caregivers of people with other terminal illnesses” (p.202)27.
These researchers also sought to differentiate the grief experienced by caregivers based on the relationship status they have with the elderly with dementia and stage of the disease. They also examined the anticipatory mourning experienced by adult spouses and offspring at each stage of the disease (initial, intermediate, and advanced). The results showed that the anticipated mourning experienced by the spouse increased as the disease progressed, corroborating the above-mentioned reports29.
We began the fifth roundtable addressing the simple aspects of daily life that should be valued. We present the video: “Who, me?”30 scored by Fernando Aguzzoli. Next, we opened spaces for the caregivers to reflect on the question: “Can I see something positive in this caring experience?”. With the analysis of the reports, the seventh thematic category was identified:
7ª) Appreciation of the simple aspects of everyday life
Qualitative research conducted with family caregivers of elderly people with dementia aimed to understand the nature of caregivers’ daily occupations about well-being. The results showed that the centrality of occupations in daily life represents for family caregivers a way to monitor the well-being of their family members through some indicators such as: expressions of affection, humor, pleasure and success in performing IADL’s31.
In fact, these indicators were present in the reports of some caregivers in our roundtables. C5
(Wife) described a well-being situation in the face of her husband showing affection:
“(...) I asked him (husband) if he wanted to lie down. That was when he turned to me and gave the impression that he recognized me, recognized my voice. I turned to the chair where he was sitting and he gave me a smile... I got up to him, gave him a hug and took him to the room, where I said, “I’m glad you’re going to sleep now,” and you know what he said to me? “I know you!”. Then he put his hand on my face. It had been a long time since he had said anything of that sort”.
The sixth and final roundtable aimed to identify and reflect on the activities dedicated to taking care of oneself. With the trigger question: “How do I take care or can I take care of myself?” the last two categories discussed below emerged:
8ª) I already take care of myself
A study on the use of family caregivers’ time brought the classification of Chapin’s activities into two groups defined as mandatory and/or discriminatory activities. While in the former, the caregiver has a greater degree of restriction of choice because the activities are related to the basic necessities of survival of themselves and of who receives their care, in the discriminatory, the caregiver is more open to the options of activities that involve social interaction inside and outside the family, religious activities, reading, TV, listening to the radio, recreation, relaxation and rest. Factors such as age, education, income, marital status, socioeconomic status, cognition and the environment itself may interfere with the choice, flow and investment in certain groups of activities32.
In this last roundtable group, it was fundamental to reflect on all the themes developed during our meetings in a way that could bring aspects marked from the experience in the roundtables. Some caregivers have reported to be already dedicating some time from their routines to activities that bring pleasure and satisfaction.

7 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
C2 (Spouse) identifies the significant activities already inserted in her daily life when speaking:
“I go hiking every day and take care of my diet. When I find the time, I do crossword puzzles. Sometimes I use my computer, search the internet, and play games. I visit my children whenever it is possible... Sometimes I think, “If she is (wife) sick I have a problem, but if I also get sick, I’m going to have two problems”.
C12 (Wife) uses her hand skill as a way to relax: “I really like doing crafts and sewing. That’s how I get distracted.”. On the other hand, C5 (Wife), to relax, prefers to leave the environment in which she lives and dedicates care to her husband and points out: “I try to do everything I can to not feel bad. I go out, I go to the cinema, most of the time, alone”.
9ª) I need to take care of myself
Although a large part of the activities carried out by the caregivers are related to caring for the other to the detriment of self-care, the groups facilitated awareness and reflection on the importance of (re) inserting significant moments previously abandoned in the daily life.
C6 (Daughter) recognized:
“To take care of myself I do not need to go to the hairdresser, I do not have to buy expensive clothes, I just need some time for myself. And I have not had that time; time to travel, to meet new people, different places... freedom that I do not have.”
The loss of freedom and social contact to the detriment of the accumulation of functions aimed at the care of the other was pointed out as one of the forms of detachment from this look to itself.
C5 (Wife) concluded:
“It’s time to take care of myself. Go back to doing my physical activities and walks. My joys will give me strength to continue to look after him and always be able to offer and say that I love what I do!”.
Carvalho draws attention to the importance of organizing the day-to-day care of these family caregivers to ensure that they carry out meaningful activities sufficient to meet their interests, without competing with caregiving activities. Thus, the physical and psychological well-being of the caregivers can increase, benefiting not only them, but also those who receive their care33.
A study developed with the objective of helping family caregivers to reach their personal goals, through telephone intervention, using the cognitive-behavioral therapy method, identified, as results, three central themes. They are:
• Problem solving (Managing behavior changes, increasing time for your own needs and activities, getting more support with care);
• Cognitive dysfunctions (Reducing the permanent concerns that something might happen to your relative with dementia when you are not around; learning to deal with feelings of guilt by doing pleasant things without the relative; enjoying life more and seeing things in a more positive manner; managing the feeling of guilt when delegating care tasks; reducing the perfectionist standard of care);
• Emotional Regulation (Learning to deal with changes in one’s life and increasing the acceptance of the disease; feeling calmer when dealing with behavioral symptoms; learning to accept and deal with feelings of loss; talking about what it feels like to have emotional relief; dealing with the fear of the future and the death of their family member)34.
Despite the results of the aforementioned study corroborating the findings of this study, it is important to emphasize the need for an expanded look, which needs to be more personalized to family caregivers. Still, it is worth pointing out some limiting aspects were encountered: the number of groups evaluated was reduced because it is a pilot study; it would be necessary to understand and adapt these thematic categories for other groups in different social, economic, cultural contexts, as well as to different regions from the country.

8 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
CONCLUSION
Sensitizing and making family caregivers aware of the need of self-care is an important strategy to facilitate the elaboration of negative aspects arising from the care of others, promoting the expansion of their gaze to the positive perspective of care and valuing simple actions inserted in this daily life.
It is important to consider that, currently, most services and health professionals focus their gaze and their intervention proposals on the care of elderly people with dementia based on the guidelines restricted to this care, with a focus on caregiver overload.
This proposal for differentiated intervention is already described in the international literature, but it is little explored Brazilian literature9,34,35. Proposing actions that broaden this view to the care and self-care demands of family caregivers in dementia, in their perspective, can be a more effective approach, as it would allow a space for reception to the central emotional issues involved, which compromise the quality of care, life and well-being of these caregivers.
Edited by: Yan Nogueira Leite de Freitas
REFERENCES
1. Cheng ST. Dementia caregiver burden: a research update and critical analysis. Curr Psychiatry Rep. 2017;19(9):1-8.
2. Roberts E, Struckmeyer KM. The impact of respite programming on caregiver resilience in dementia care: a qualitative examination of family caregiver perspectives. Inquiry. 2018;55:1-9.
3. Brodaty H, Donkin M. Family caregivers of people with dementia. Dialog Clin Neurosc. 2009;11(2):217-28.
4. White CL, Overbaugh KJ, Pickering CEZ, Piernik-Yoder B, James D, Patel DI, et al. Advancing care for family caregivers of persons with dementia through caregiver and community partnerships. Res Involv Engagem. 2018;4(1):1-2. Available from: https://doi.org.10.1186/s40900-018-0084-4
5. Frias CE, Garcia-Pascual M, Montoro M, Ribas N, Risco E, Zabalegue A. Effectiveness of a psychoeducational intervention for caregivers of people with dementia with regard to burden, anxiety and depression: a systematic review. J Adv Nurs. 2020;76(3):787-802.
6. Carbonneau H, Chantal C, Desrosiers J. Development of a conceptual framework of positive aspects of caregiving in dementia. Dementia. 2010;9(3):327-53.
7. Han A. Interventions for attitudes and empathy toward people with dementia and positive aspects of caregiving: a systematic review and meta-analysis. Res Aging. 2020;42(2):72-82.
8. Dizazzo-Muller R, Samuel PS, Barnas JM, Welker KM. Addressing everyday challenges: feasibility of a family caregiver training program for people with dementia. Am J Occup Ther. 2014;68(2):212-20.
9. Zwingmann I, Michalowsky B, Esser A, Kaczynski A, Monsees J, Keller A, et al. Identifying unmet needs of family dementia caregivers: results of the baseline assessment of a cluster-randomized controlled intervention trial. J Alzheimers Dis. 2019;67:527-39. Available from: https://doi.org/10.3233/JAD-180244 .
10. Morin E. Introdução ao pensamento complexo. Lisboa: Piaget; 2003.
11. Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. Hucitec: São Paulo; 2015.
12. Hinton L, Tran D, Nguyen TN, Janis Ho J, Gitlin L. Interventions to support family caregivers of people living with dementia in high, middle and low income countries in Asia: a scoping. BMJ Global Health. 2019;4:1-9.
13. Boelen PA, van Den Bout F. Complicated grief, depression, and anxiety as distinct post loss syndromes. a confirmatory factor analysis study. Am J Psychiatry. 2005;162(11):2175-77.
14. Cheung DSK, Ho KHM, Cheung TF, Lam SC, Tse MMY. Anticipatory grief of spousal and adult children caregivers of people with dementia. BMC Palliat Care. 2018;17(124):1-10.
15. Raphael B, Minkov C, Dobson M. Manual de investigação do luto: Consequências, enfrentamento e cuidados. Am Psychol Assoc. 2001;(1):587- 612.
16. Grigorovich A, Rittenberg N, Dick T, McCann A, Abbott A, Kmielauskas, et al. Roles and coping strategies of sons caring for a parent with dementia. Am J Occup Ther 2016;70(1):1-9. Available from: https://doi.org/10.5014/ajot.2016.017715

9 of 9
The demands of care and self-care: perspective of the caregiver
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200189
17. Van Wijngaarden E, van der Wedden H, Henning Z, Komen R, The AM. Entangled in uncertainty: the experience of living with dementia from the perspective of family caregivers. PLos ONE. 2018;13(6):1-10.
18. Doris SFY, Sheung-Tak C, Jungfang W. Unravelling positive aspects of caregiving in dementia: an integrative review of research literature. Int J Nurs Stud. 2018;79:1-26.
19. Peacock S, Forbes D, Markle-Reid M, Hawranik P, Morgan D, Jansen L, et al. The positive aspects of the caregiving journey with dementia: using a strengths-based perspective to reveal opportunities. J Appl Gerontol. 2010;29(5):640-59. Available from: https//:doi.org/10.1177/0733464809341471
20. Shuchter SR, Zisook S, Stroebe MS, Stroebe W, Hansson RO. Handbook of bereavement: Theory, research, and intervention. New York: Cambridge Press; 1993.
21. Worden JW. Grief counseling and grief therapy: a handbook for the mental health practitioner. New York: Springer Publishers; 2002.
22. Wilson S, Toye C, Aoun S, Slatyer S, Moyle W, Beattie E. Effectiveness of Psychosocial Interventions in Reducing Grief Experienced by Family Carers of People With Dementia: a Systematic Review. JBI Database System Rev Implement Rep 2017; 15(3):1-10.
23. Arruda EH, Paun O. Dementia caregiver grief and bereavement: an integrative review. West J Nurs Res. 2017;39(6):825-51.
24. Sanders S, Corley CS. Are they grieving? A qualitative analysis examining grief in caregivers of individuals with Alzheimer’s disease. Soc Work Health Care. 2003;37:35-53.
25. Liew TM, Tai BC, Yap P, Choon-Huat G. Comparing the Effects of Grief and Burden on Caregiver Depression in Dementia Caregiving: a Longitudinal Path Analysis over 2.5 Years. J Am Med Dir Assoc. 2019;20:977-86.
26. Williams C, Moretta B. Systematic understanding of loss and grief related to Alzheimer’s disease. In: Doka KJ, Davidson J. Living with grief when illness is prolonged. Systematic understanding of loss and grief related to Alzheimer’s disease. Washington: Hospice Foundation of America; 1997. p. 119-32.
27. Marwit SJ, Meuser TM. Development of a short form inventory to assess grief in caregivers of dementia patients. Death Stud. 2005;29(3):191-205.
28. Sanders S, Ott CH, Kelber ST, Noonan P. The experience of high levels of grief in caregivers of persons with Alzheimer’s disease and related dementia. Death Stud. 2008;32:495-523.
29. Gibson K, Peacock S, Bayly M. Qualitative exploration of emotional and social changes from diagnosis to bereavement for spousal caregivers of persons with dementia. BMJ Open. 2019;9(9):1-10.
30. Aguzzoli F. Quem, eu? Fortaleza: TEDx; 2014. Vídeo: 17 min. Available from: https://youtu.be/xb8vDxNhuJI .
31. Hasselkus BR, Murray BJ. Everyday occupation, well-being, and identity: The experience of caregivers in families with dementia. Am J Occup Ther. 2007;61(1):9-20.
32. Chapin FS. Human activity in the city. Toronto: John Wiley 1974.
33. Carvalho EB, Neri AL. Padrões de uso do tempo em cuidadores familiares de idosos com demências. Revista Brasileira de Geriatria e Gerontologia, 2019; 22(1): e180143.
34. Wilz G, Weise L, Reiter C, Reder M, Machmer A, Soellner R. Intervention Helps Family Caregivers of People with Dementia Attain Own TherapyGoals. American Journal of Alzheimer’s Disease & Other Dementias, 2018; 33(5): 301-308.
35. van Wijngaarden E, van der Wedden H, Henning Z, Komen R. Entangled in uncertainty: The experience of living with dementia from the perspective of family caregivers. PLoS ONE, 2018; 13(6):e0198034.

1 of 10
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
http://dx.doi.org/10.1590/1981-22562020023.200193
Inadequate knowledge of prescription drugs and their predictors in very old patients and their caregivers
Thiago Vinicius Nadaleto Didone1
Daniela Oliveira de Melo2
Leonardo da Costa Lopes3
Eliane Ribeiro4
Keywords: Aged, 80 And Over. Caregivers. Patient Education as Topic. Patient Medication Knowledge. Surveys and Questionnaires.
AbstractObjective: Identify predictors of inadequate knowledge about the medication prescribed to very old outpatients and their caregivers. Method: The knowledge on the medication prescribed for 80 patients aged 80 years and over was assessed using a validated questionnaire to interview patients or their caregivers (when patients had communication difficulties, dementia, or any need for care to help them take the medication). Two hierarchical logistic regression models assessed the association between inadequate knowledge of the medication and sociodemographic and drug variables. Results: Thirty-nine (48.8%) respondents were caregivers. Inadequate knowledge was found in 81.5% (404/496) of medication prescribed. Route of Administration, Dose, Frequency, and Duration of Treatment were the aspects of greatest knowledge, whereas Adverse Effects, Precautions, Interactions, and Contraindications were the least known ones. In the first model, inadequate knowledge was associated to the level of education from complete elementary school to incomplete high school (Odds Ratio (OR): 0.12; p=0.018), from high school to incomplete higher education (OR: 0.12; p<0.001), complete higher education (OR: 0.13; p<0.001), agents acting on the renin-angiotensin system (RAS) (OR: 0.30; p=0.001), diuretics (OR: 0.31; p=0.013) and antithrombotic (OR: 12.59; p=0.027). In the second model, the predictors were caregivers (OR: 0.17; p<0.001), agents working in the RAS (OR: 0.33; p=0.002), diuretics (OR: 0.35; p=0.024) and antithrombotic (OR: 12.57;
1 Universidade Federal de São Paulo, Escola Paulista de Medicina, Departamento de Oncologia Clínica e Experimental, Programa de Pós-Graduação em Medicina (Hematologia e Oncologia). São Paulo, SP, Brasil.
2 Universidade Federal de São Paulo, Instituto de Ciências Ambientais, Químicas e Farmacêuticas, Departamento de Ciências Farmacêuticas. Diadema, SP, Brasil.
3 Universidade de São Paulo, Hospital Universitário, Departamento de Clínica Médica. São Paulo, SP, Brasil.
4 Universidade de São Paulo, Faculdade de Ciências Farmacêuticas, Departamento de Farmácia e Hospital Universitário da Universidade de São Paulo. São Paulo, SP, Brasil.
Funding: Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) e Ministério da Ciência e Tecnologia (MCT). Nº do processo: 135839/2012-2. Bolsa de Mestrado.The authors declare there are no conflicts of interest in relation to the present study.
CorrespondenceThiago Vinicius Nadaleto [email protected]
Received: June 22, 2020Approved: November 3, 2020
ID
ID
ID
ID

2 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
INTRODUC TION
The stratum of very old people (i.e., 80 years and over)1 has grown and will grow dramatically in Brazil2 where 94.3% of very old people use at least one medication in the long term, and 19.5% use at least five3.
There is evidence that the older the individual, the less they know about medications4-6. As an example, polymedicated Dutch patients in primary care aged 80 and over were 53% more likely to incorrectly remember the prescription for at least one medication prescribed compared to their younger peers (60-69 years)6. Also, knowledge about medication among old people is insufficient4,6-9, which can lead to non-adherence to medication7,10 and negative clinical implications such as inadequate anticoagulation control5 and visits to the emergency service11. A cross-sectional study carried out with 348 patients aged 75 years illustrates this relation: while only 21% of them knew about the consequences of omitting a medication or dose prescribed, those who knew them were 1.8 times more likely to follow the pharmacotherapy prescribed, and 2.3 times more likely to follow the daily dose prescribed7. Also, patients well informed about the possible side effects of the medications being used can seek care to manage them before they become intractable and engage in preventive health behaviors12.
Although knowledge of medication is important for their appropriate use, there is still no consensus on how to measure it, especially regarding the aspects investigated, and the method for classifying responses and calculating scores. For example, depending on the method, individuals are asked to name a range from one (e.g., indication13) to 1114 aspects of knowledge on medication. Also, few studies have evaluated its predictors or exclusive knowledge of the medication used by old people. Age, gender, education, income, family arrangement, cognitive functionality, and the number of medications used
are some of the independent predictors that have already been identified among old people6,12,13.
To date, Brazilian studies investigating the knowledge on medication have applied questionnaires with no validity nor reliability evaluated. Also, they did not demonstrate the predictive factors for this outcome, which are necessary for the clinical practice for the early identification of patients at greater risk for insufficient knowledge, as well as for the adequate design of educational interventions capable of contributing in this context. Therefore, the present study aimed to assess the knowledge of the medication prescribed and to identify their predictors in very old outpatients and their caregivers.
METHOD
This cross-sectional study was carried out at the geriatric outpatient clinic of Hospital Universitário da Universidade de São Paulo in São Paulo (SP), Brazil, which provides geriatric care to individuals aged 80 years and over with at least one of the following conditions: dementia, Parkinson’s disease, use of five or more medications, two or more falls in the previous year, functional decline, and use of walking aid. The patients treated at this outpatient clinic from March/2013 to February/2014 (N=251) were considered eligible. The geriatrician referred patients to a pharmaceutical appointment after their initial appointment, and the researcher responsible for the study (pharmacist) invited the patient to participate. Those who wanted to be interviewed and who took at least one medication were included. However, the caregivers were interviewed instead of the patients when they had communication difficulties (i.e., aphonia, dysarthria, or aphasia), dementia, or needed the care to help them use the medication. In this case, we made sure that the caregiver was responsible for managing the patient’s medication. There were no exclusion criteria.
p=0.026). Conclusion: Most of the medication prescribed for very old people is not very well known. Also, advice on drug information should be more intensive to patients than to their caregivers, with a focus on safety information and targeted at antithrombotics.

3 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
The decision not to interview the patient was made along with the geriatrician responsible for following them at the outpatient clinic and upon the medical diagnosis of aphasia and/or dementia, and/or the caregiver’s report of being their current responsible for assisting the patient in taking the medication.
Information about the medication prescribed was collected from each patient’s medical record based on the most recent prescription. The medications were identified according to the second level of the Anatomical Therapeutic Chemical (ATC)15 code. The complexity of a patient’s pharmacotherapy was measured by the Medication Regimen Complexity Index (MRCI) cross-culturally adapted to Brazilian Portuguese16. This tool is divided into sections A (dosage forms), B (dose frequency), and C (additional instructions such as the specific time of taking). Each section is scored based on the analysis of the patient’s prescription, and the index is the sum of the scores of each section16.
The sociodemographic data and that on the knowledge on medication were collected in a face-to-face interview with the patient or their caregiver conducted by the researcher responsible for the study (pharmacist). The monthly income was expressed in minimum wages (MW) of 678 Brazilian reais in 2013, and 724 Brazilian reais in 2014.
A Spanish questionnaire with 11 questions was used, and cross-culturally adapted to Brazilian Portuguese17 to know about each of the medications listed in the most recent geriatrician prescription. Each question assesses one of the following aspects of interest regarding the use of medications: indication, dose, frequency, duration of treatment, Route of Administration, precautions, Adverse Effects, contraindications, effectiveness, interactions, and conservation18. The participants’ answers were classified as correct (2 points), incomplete (1 point), unknown (0), or incorrect (-1 point)14 according to their degree of agreement with the database UpToDate 19. Two pharmacist clinicians rated the responses independently. If necessary, a third one was consulted. In the end, the knowledge on medication was numerically represented by the weighted average of the grades and grouped into four categories: none
(0), insufficient (0.60 to 1.26), sufficient (1.27 to 1.60), and excellent ( 1.61 to 2.00)14. The questions have one of four possible weights: 1.20 (questions 2 to 5), 1.10 (questions 1 and 9), 0.85 (questions 6, 7, 8 and 10), or 0.60 (question 11)14.
To facilitate the interpretation of the results, knowledge on medication was recategorized into a dichotomous variable: inadequate knowledge on medication (categories ‘none’ and ‘insufficient’ combined), and adequate (categories ‘sufficient’ and ‘excellent’ combined). Income, number of medications prescribed, and MRCI were categorized into tertiles.
Categorical and numerical variables were described as absolute and relative counts and medians with interquartile ranges, respectively. Bivariate and multivariate hierarchical logistic regression models were calculated to predict inadequate knowledge of medication (reference category: adequate knowledge of medication) from the knowledge information collected for all medications prescribed. The fixed effects were the following variables: age of the respondent, monthly income, education (without education to incomplete elementary school, complete elementary school to incomplete high school, complete high school to incomplete higher education, complete higher education), type of respondent (patient, caregiver), number of medications (<5, 5-6, ≥7), MRCI (<12.0, 12.0-18.9, ≥19.0), duration of medication use (first time, not the first time), prescription by generic name (no, yes), and the following ATCC (non-user, user): C09, B01, N06, A10, and C03. Only the five most prevalent second-level ATCCs were considered. The only random effect was to the intercept.
All variables with significance in the bivariate analysis entered the multivariate model in a single block. Pairs of variables were checked for associations using the chi-square and Kruskal-Wallis tests before carrying out the multivariate analyzes to avoid collinearity. Of the two variables, only that significantly associated with greater clinical and conceptual relevance was included in the multivariate analysis. A p-value <0.050 (two-tailed) was considered statistically significant.
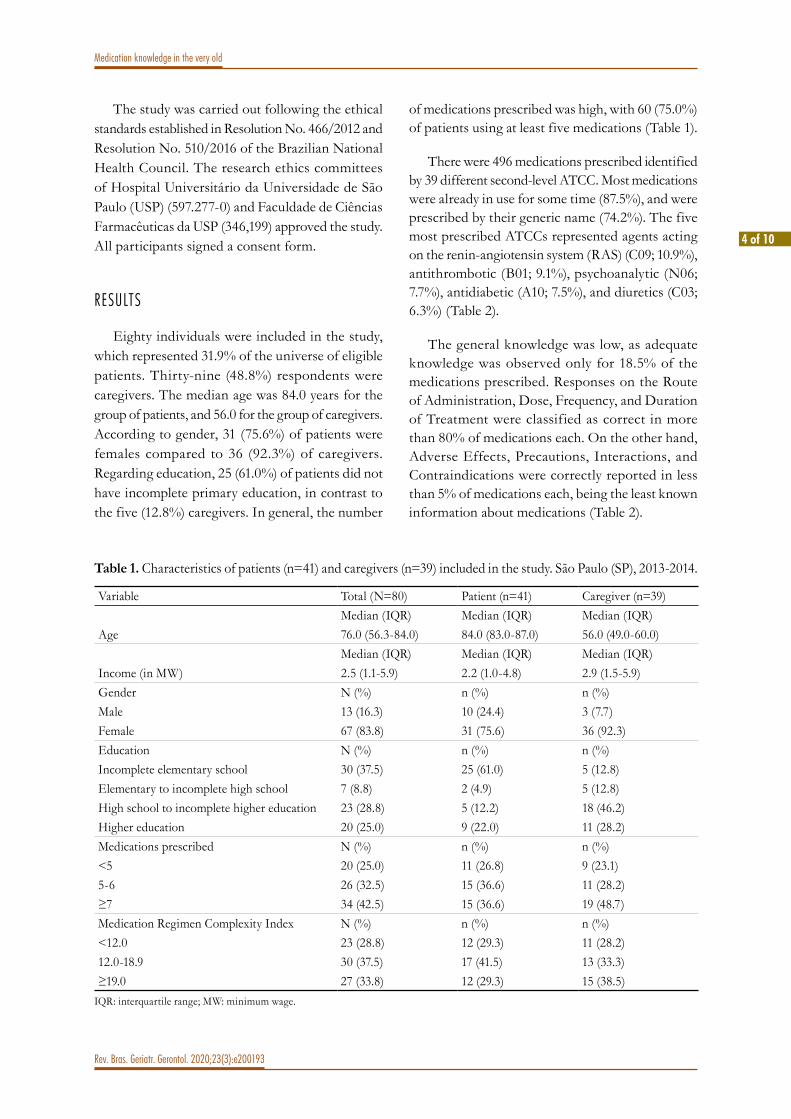
4 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
The study was carried out following the ethical standards established in Resolution No. 466/2012 and Resolution No. 510/2016 of the Brazilian National Health Council. The research ethics committees of Hospital Universitário da Universidade de São Paulo (USP) (597.277-0) and Faculdade de Ciências Farmacêuticas da USP (346,199) approved the study. All participants signed a consent form.
RESULTS
Eighty individuals were included in the study, which represented 31.9% of the universe of eligible patients. Thirty-nine (48.8%) respondents were caregivers. The median age was 84.0 years for the group of patients, and 56.0 for the group of caregivers. According to gender, 31 (75.6%) of patients were females compared to 36 (92.3%) of caregivers. Regarding education, 25 (61.0%) of patients did not have incomplete primary education, in contrast to the five (12.8%) caregivers. In general, the number
of medications prescribed was high, with 60 (75.0%) of patients using at least five medications (Table 1).
There were 496 medications prescribed identified by 39 different second-level ATCC. Most medications were already in use for some time (87.5%), and were prescribed by their generic name (74.2%). The five most prescribed ATCCs represented agents acting on the renin-angiotensin system (RAS) (C09; 10.9%), antithrombotic (B01; 9.1%), psychoanalytic (N06; 7.7%), antidiabetic (A10; 7.5%), and diuretics (C03; 6.3%) (Table 2).
The general knowledge was low, as adequate knowledge was observed only for 18.5% of the medications prescribed. Responses on the Route of Administration, Dose, Frequency, and Duration of Treatment were classified as correct in more than 80% of medications each. On the other hand, Adverse Effects, Precautions, Interactions, and Contraindications were correctly reported in less than 5% of medications each, being the least known information about medications (Table 2).
Table 1. Characteristics of patients (n=41) and caregivers (n=39) included in the study. São Paulo (SP), 2013-2014.
Variable Total (N=80) Patient (n=41) Caregiver (n=39)Median (IQR) Median (IQR) Median (IQR)
Age 76.0 (56.3-84.0) 84.0 (83.0-87.0) 56.0 (49.0-60.0)Median (IQR) Median (IQR) Median (IQR)
Income (in MW) 2.5 (1.1-5.9) 2.2 (1.0-4.8) 2.9 (1.5-5.9)Gender N (%) n (%) n (%)Male 13 (16.3) 10 (24.4) 3 (7.7)Female 67 (83.8) 31 (75.6) 36 (92.3)Education N (%) n (%) n (%)Incomplete elementary school 30 (37.5) 25 (61.0) 5 (12.8)Elementary to incomplete high school 7 (8.8) 2 (4.9) 5 (12.8)High school to incomplete higher education 23 (28.8) 5 (12.2) 18 (46.2)Higher education 20 (25.0) 9 (22.0) 11 (28.2)Medications prescribed N (%) n (%) n (%)<5 20 (25.0) 11 (26.8) 9 (23.1)5-6 26 (32.5) 15 (36.6) 11 (28.2)≥7 34 (42.5) 15 (36.6) 19 (48.7)Medication Regimen Complexity Index N (%) n (%) n (%)<12.0 23 (28.8) 12 (29.3) 11 (28.2)12.0-18.9 30 (37.5) 17 (41.5) 13 (33.3)≥19.0 27 (33.8) 12 (29.3) 15 (38.5)
IQR: interquartile range; MW: minimum wage.

5 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
Table 2. Characteristics and knowledge of the medications prescribed according to the type of respondent. São Paulo (SP), 2013-2014.
Variable Total (N=496)N (%)
Patient (n=261)n (%)
Caregiver (n=235)n (%)
Duration of medication useFirst time 62 (12.5) 23 (8.8) 39 (16.6)Not the first time 434 (87.5) 238 (91.2) 196 (83.4)Prescription by generic nameNo 128 (25.8) 71 (27.2) 57 (24.3)Yes 368 (74.2) 190 (72.8) 178 (75.7)ATCC C09 (agents acting at RAS)Non-user 442 (89.1) 233 (89.3) 209 (88.9)User 54 (10.9) 28 (10.7) 26 (11.1)ATCC B01 (antithrombotic)Non-user 451 (90.9) 237 (90.8) 214 (91.1)User 45 (9.1) 24 (9.2) 21 (8.9)ATCC N06 (psychoanalytic)Non user 458 (92.3) 252 (96.6) 206 (87.7)User 38 (7.7) 9 (3.4) 29 (12.3)ATCC A10 (antidiabetics)Non user 459 (92.5) 238 (91.2) 221 (94.0)User 37 (7.5) 23 (8.8) 14 (6.0)ATCC C03 (diuretics)Non-user 465 (93.8) 244 (93.5) 221 (94.0)User 31 (6.3) 17 (6.5) 14 (6.0)Knowledge of medicationsNone 284 (57.3) 178 (68.2) 106 (45.1)Insufficient 120 (24.2) 63 (24.1) 57 (24.3)Sufficient 89 (17.9) 20 (7.7) 69 (29.4)Excellent 3 (0.6) 0 3 (1.3)Questions about the knowledge of medications classified as correctRoute of Administration 424 (85.5) 211 (80.8) 213 (90.6)Dose 417 (84.1) 200 (76.6) 217 (92.3)Frequency 415 (83.7) 200 (76.6) 215 (91.5)Duration of Treatment 402 (81.0) 191 (73.2) 211 (89.8)Indication 242 (48.8) 102 (39.1) 140 (59.6)Effectiveness 191 (38.5) 72 (27.6) 119 (50.6)Storage 56 (11.3) 1 (0.4) 55 (23.4)Adverse Effects 23 (4.6) 3 (1.1) 20 (8.5)Precautions 10 (2.0) 2 (0.8) 8 (3.4)Interactions 5 (1.0) 1 (0.4) 4 (1.7)Contraindications 3 (0.6) 1 (0.4) 2 (0.9)
RAS: renin-angiotensin system.

6 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
The regression models were made considering all the medications prescribed (N=496). Significant associations were observed in the bivariate models only for age, education, type of respondent, ATCC C09, ATCC B01, and ATCC C03. As age was associated with education ( p<0.001) and the type of respondent (p<0.001), it was not included in the multivariate regression analyzes. Also, as education was associated with the type of respondent (p<0.001), two multivariate models were calculated - one including the aforementioned ATCCs and education as independent variables, and the other including the same ATCCs and the type of respondent (Table 3).
Table 3 shows the two multivariate models predicting inadequate knowledge of medications at the medication level. In both models, the odds ratio (OR) of having inadequate knowledge on medications decreased significantly for elementary to incomplete high school, high school to incomplete higher education, complete higher education, caregivers, RAS agents, and diuretics. On the other hand, the OR of having inadequate knowledge of medications increased significantly for antithrombotics in both models.
Table 3. Bi and multivariate hierarchical logistic regression models predicting inadequate knowledge of medication (N=496). São Paulo (SP), 2013-2014.
PredictorInadequate knowledge of medicationsOR * (95% CI) p OR** (95% CI) p OR*** (95% CI) p
GenderFemale 1Male 0.79 (0.24-2.59) 0.702Age of the respondent 1.05 (1.03-1.08) <0.001Monthly income 1.00 (0.94-1.07) 0.972EducationIncomplete elementary school
1 1
Elementary to incomplete high school
0.16 (0.03-0.86) 0.033 0.12 (0.02-0.69) 0.018
High school to incomplete higher education
0.14 (0.05-0.40) <0.001 0.12 (0.04-0.35) <0.001
Higher education 0.16 (0.05-0.46) 0.001 0.13 (0.04-0.39) <0.001RespondentPatient 1 1Caregiver 0.18 (0.08-0.42) <0.001 0.17 (0.07-0.40) <0.001Number of medications<5 15-6 1.82 (0.61-5.41) 0.279≥7 1.87 (0.66-5.28) 0.235Medication Regimen Complexity Index<12,0 112,0-18,9 1.30 (0.46-3.66) 0.619≥19,0 1.52 (0.54-4.32) 0.431Duration of medication useFirst time 1Not the first time 0.71 (0.33-1.52) 0.374
to be continued

7 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
PredictorInadequate knowledge of medicationsOR * (95% CI) p OR** (95% CI) p OR*** (95% CI) p
Prescription by generic nameNo 1Yes 0.74 (0.43-1.27) 0.275ATCC C09 (agents acting at RAS)Non-user 1 1 1User 0.33 (0.19-0.59) <0.001 0.30 (0.15-0.61) 0.001 0.33 (0.17-0.66) 0.002ATCC B01 (antithrombotic)Non-user 1 1 1User 15.00 (1.71-131.24) 0.015 12.59 (1.34-118.00) 0.027 12.57 (1.35-117.04) 0.026ATCC C03 (diuretics)Non-user 1 1 1User 0.39 (0.18-0.88) 0.024 0.31 (0.12-0.78) 0.013 0.35 (0.14-0.87) 0.024ATCC N06 (psychoanalytic)Non-user 1User 1.20 (0.63-2.29) 0.574ATCC A10 (antidiabetics)Non-user 1User 0.52 (0.23-1.17) 0.111
CI: confidence interval; OR: odds ratio; RAS: renin-angiotensin system; *Not adjusted; **Adjusted: multivariate model including education and codes C09, B01, and C03; ***Adjusted: multivariate model including respondent and codes C09, B01, and C03.
Continuation of Table 3
DISCUSSION
The Brazilian Portuguese questionnaire applied in the present study was used in Spain14,20 and Portugal21 to assess the knowledge of patients over 18 years who attend community pharmacies to obtain one or more medications dispensed. None was the most prevalent category identified in 65.7%14, 68.2%20, and 82.5%21 of patients, which matches our results. This shows the general deficiency in the knowledge of pharmacological treatment found in many other studies carried out with adults and/or old people, community residents, or outpatients from different countries and using different methods4-9,22-24.
We found that information on the use and action of medications was the most widely known aspect of pharmacotherapy, whereas information on medication safety was the least known. These findings are consistent with the results of studies carried out in other countries, both with individuals
over 18 years14,21,24 and old individuals5,7-9,12. A probable explanation would be that health professionals tend to discuss with patients more about the use than the possible problems associated with medication (e.g., side effects) because they consider only the former as their professional responsibility25. As an example, in a sample of 412 old patients from two public outpatient clinics in Hong Kong, 72.2% were instructed about administration, 73.0% were not informed about the side effects of the medication prescribed during the appointment, prescription, or discharge12.
It is believed that the group of caregivers had greater knowledge on medications, not only because they were younger and more educated, but also because of their experience in dealing with the difficulties in administering the medicines. They must know enough about the prescription to adapt the times of medication intake to the care routine and manage dose adjustments26. Besides, they feel responsible for monitoring side and toxic effects since

8 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
their patients may no longer be able to recognize and report them26.
Education was negatively associated with inadequate knowledge of medicat ion. This association was found in other old populations8,12. Although intuitive, this association is complex, and there may be stronger predictors of knowledge on medication than formal education. For example, two studies carried out with old patients living in the community did not show education as a significant and independent predictor of their knowledge on medication6,13.
It is believed that the chances of having inadequate knowledge were lower for the agents acting in the RAS and for diuretics because patients generally seek and know the main information about them. A qualitative study carried out with hypertensive patients showed that although they did not know the name of the antihypertensive medication they used, they were aware it helped control blood pressure. Also, they often sought to learn more about antihypertensive medications through the mainstream media and the education of health professionals23.
Antithrombotics were positively associated with inadequate knowledge, showing that our sample had less knowledge about these medications. Likewise, among 122 patients seen at an anticoagulation clinic in Hong Kong, half did not remember the effect of warfarin on the body, and about 70% were unaware of the possible complications resulting from the overdose of this medication5. The lack of safety information about antithrombotic agents can lead to serious consequences. For example, users of apixaban with little knowledge of possible drug interactions affecting the risk of bleeding were 85% more likely to regularly use over-the-counter medications with potentially serious interactions with apixaban (e.g., acetylsalicylic acid and St. John’s wort - hypericum perforatum) compared to those with more knowledge22.
Considering that old people may be exposed to clinical complications of pharmacotherapy due to their inadequate knowledge of medication, a joint effort including the multi-professional health team, government agents, and the pharmaceutical industry is necessary to create patient-centered educational
programs. A study of 150 patients with chronic conditions showed that knowledge of medication was positively associated with patient satisfaction in having their doubts cleared by physicians10. In this sense, health professionals should regularly discuss with patients aspects of concern about the use of medicines (i.e., the process of use, the therapeutic objective, safety, and storage), and meet their needs by providing sufficient verbal and written information to ensure the proper use of medication.
One of the strengths of the present study was the use of a validated and reliable questionnaire. Still, it was the first time this tool was used to assess the knowledge of medication used exclusively by old people. The inclusion of caregivers was another positive point because as the old people living in the community get older, their need for a caregiver increases. Assessing the knowledge of caregivers rather than the patients is a reasonable comparison to the real world, as they may be responsible for administering medication to patients. Also, the literature about the knowledge on medication of caregivers of old people is scarce. Most studies are carried out with pediatric patients, and they assess the knowledge of the patient’s clinical condition. Finally, the use of a hierarchical regression model enabled the characteristics of all medications prescribed to be evaluated as independent variables.
Some limitations of the present study must be mentioned. First, the sampling procedure excluded patients unwilling to participate (e.g., patients with gait disorders and caregivers late for work), which could have added some selection bias. Secondly, the inclusion of medications used for the first time may have underestimated the knowledge. Thirdly, no common predictors of inadequate knowledge on medication such as the number of medications were found, probably due to our limited sample size. Fourth, as caregivers were more educated than patients, it is questionable whether inadequate knowledge was associated with education or the caregiver’s own condition. Nevertheless, the heterogeneity of the sample comprised of both patients and caregivers may have been a confounding factor, although one of the multivariate models included the respondent as an independent variable. Fifth, only one researcher

9 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
was responsible for applying the questionnaire, which did not have a previous calibration study and allowed for information bias. However, this is the same researcher responsible for the cross-cultural adaptation of the questionnaire to Brazilian Portuguese17, thus they deeply knew its method of application and score. Sixth, despite the absence of a previous sample size calculation, the authors used a convenience sample representing 31.9% of eligible individuals. Future studies should be carried out with larger and more homogeneous samples to evaluate the strategies to improve knowledge of medication with controlled studies.
CONCLUSION
The vast majority of drugs prescribed for very old outpatients were little known. Adverse Effects, Precautions, Interactions, and Contraindications were aspects of less knowledge of medication. Education,
the type of respondent, medications acting in the RAS, and diuretics were negatively associated with inadequate knowledge on medication; antithrombotic agents were positively associated with it.
Geriatricians, gerontologists, and other professionals who care for very old people should unquestionably advise them about the information on medicat ions, especial ly those who take antithrombotic agents (e.g., warfarin, enoxaparin, platelet aggregation inhibitors, factor Xa inhibitors) and who do not depend on caregivers to help them take their medication. Also, education should focus on improving patient and caregiver knowledge on safety aspects of medication use such as side effects, precautions and warnings, interactions, and contraindications. Clinical care services should be organized to provide reliable written and verbal information on medication to patients.
Edited by: Ana Carolina Lima Cavaletti
REFERENCES
1. Eendebak R; World Health Organization. World Report on Ageing and Health. Luxembourg: WHO; 2015.
2. Instituto Brasileiro de Geografia e Estatística [Internet]. Rio de Janeiro: IBGE; [1995]-. Projeção da população do Brasil e das Unidades da Federação [Internet]. 2020 [cited 2020 Fev. 13]; [2 screens]. Available from: https://www.ibge.gov.br/apps/populacao/projecao/.
3. Ramos LR, Tavares NU, Bertoldi AD, Farias MR, Oliveira MA, Luiza VL, et al. Polypharmacy and polymorbidity in older adults in Brazil: a public health challenge. Rev Saúde Pública. 2016;50(suppl 2):1-9.
4. Hartholt KA, Val JJ, Looman CW, Petrovic M, Schakel A, van der Cammen TJ. Better drug knowledge with fewer drugs, both in the young and the old. Acta Clin Belg. 2011;66(5):367-70.
5. Tang EO, Lai CS, Lee KK, Wong RS, Cheng G, Chan TY. Relationship between patients’ warfarin knowledge and anticoagulation control. Ann Pharmacother. 2003;37(1):34-9.
6. Bosch-Lenders D, Maessen DW, Stoffers HE, Knottnerus JA, Winkens B, van den Akker M. Factors associated with appropriate knowledge of the indications for prescribed drugs among community-dwelling older patients with polypharmacy. Age Ageing. 2016;45(3):402-8.
7. Barat I, Andreasen F, Damsgaard EM. Drug therapy in the elderly: what doctors believe and patients actually do. Br J Clin Pharmacol. 2001;51(6):615-22.
8. Si P, Koob KN, Poonb D, Chew L. Knowledge of prescription medications among cancer patients aged 65 years and above. J Geriatr Oncol. 2012;3(2):120-30.
9. Pinto IVL, Reis AMM, Almeida-Brasil CC, da Silveira MR, Lima MG, Ceccato MGB. An evaluation of elderly people’s understanding of pharmacotherapy among those treated in the Primary Healthcare System in Belo Horizonte, Brazil. Ciênc Saúde Colet. 2016;21(11):3469-81.
10. Burge S, White D, Bajorek E, Bazaldua O, Trevino J, Albright T, et al. Correlates of medication knowledge and adherence: findings from the residency research network of South Texas. Fam Med. 2005;37(10):712-8.

10 of 10
Medication knowledge in the very old
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200193
11. Hope CJ, Wu J, Tu W, Young J, Murray MD. Association of medication adherence, knowledge, and skills with emergency department visits by adults 50 years or older with congestive heart failure. Am J Health Syst Pharm. 2004;61(19):2043-9.
12. Chan FW, Wong FY, So WY, Kung K, Wong CK. How much do elders with chronic conditions know about their medications? BMC Geriatr. 2013;13:1-10.
13. Guénette L, Moisan J. Elderly people’s knowledge of the purpose of their medicines. Am J Geriatr Pharmacother. 2011;9(1):49-57.
14. Romero-Sanchez J, Garcia-Cardenas V, Abaurre R, Martínez-Martínez F, Garcia-Delgado P. Prevalence and predictors of inadequate patient medication knowledge. J Eval Clin Pract. 2016;22(5):808-15.
15. World Health Organization.Collaborating Centre for Drug Statistics Methodology [Internet]. International language for drug utilization research. Oslo: WHO; 2020 [cited 2020 Feb 13]; [2 screens]. Available from: https://www.whocc.no.
16. Melchiors AC, Correr CJ, Fernández-Llimos F. Translation and Validation into Portuguese Language of the Medication Regimen Complexity Index. Arq Bras Cardiol. 2007;89(4):191-6.
17. Didone TVN, García-Delgado P, Melo DO, Romano-Lieber NS, Martínez- Martínez F, Ribeiro E. Validação do questionário “Conocimiento del Paciente sobre sus Medicamentos” (CPM-ES-ES). Ciênc Saúde Colet. 2019;24(9):3539-50.
18. Delgado PG, Garralda MAG, Parejo MIB, Lozano FF, Martínez FM. Validation of a questionnaire to assess patient knowledge of their medicines. Aten Primaria. 2009;41(12):661-9.
19. UpToDate [Internet]. [place unknown]: Wolters Kluwer; 2020 [cited 2020 Feb. 13]. Available from: https://www.uptodate.com/home
20. Abaurre-Labrador R, Maurandi-Guillén MD, García-
Delgado P, Moullin JC, Martínez-Martínez F, García-Corpas JP. Effectiveness of a protocolized dispensing service in community pharmacy for improving patient medication knowledge. Int J Clin Pharm. 2016;38(5):1057-62.
21. Rubio JS, García-Delgado P, Iglésias-Ferreira P, Mateus-Santos H, Martínez-Martínez F. Measurement of patients’ knowledge of their medication in community pharmacies in Portugal. Ciênc Saúde Colet. 2015;20(1):219-28.
22. Tarn DM, Barrientos M, Wang AY, Ramaprasad A, Fang MC, Schwartz JB. Prevalence and Knowledge of Potential Interactions Between Over-the-Counter Products and Apixaban. J Am Geriatr Soc. 2020;68(1):155-62.
23. Tan CS, Hassali MA, Neoh CF, Saleem F. A qualitative exploration of hypertensive patients’ perception towards quality use of medication and hypertension management at the community level. Pharm Pract. 2017;15(4):1-10.
24. Dresch AP, Amador TA, Heineck I. Conhecimento dos pacientes sobre medicamentos prescritos por odontólogos no sul do Brasil. Ciênc Saúde Colet. 2016;21(2):475-84.
25. Auyeung V, Patel G, McRobbie D, Weinman J, Davies G. Information about medicines to cardiac in-patients: patient satisfaction alongside the role perceptions and practices of doctors, nurses and pharmacists. Patient Educ Couns. 2011;83(3):360-6.
26. Travis SS, Bethea LS, Winn P. Medication administration hassles reported by family caregivers of dependent elderly persons. J Gerontol Ser A Biol Sci Med Sci. 2000;55(7):412-7.

1 of 10
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
http://dx.doi.org/10.1590/1981-22562020023.200121
Immediate effect of rhythmic auditory stimulation on the spatio-temporal parameters of gait in old people: a pilot study
Camila Maria Mendes Nascimento1
Laiza de Oliveira Lucena1
Ágata Rodrigues de Lima2
Jonathas Carlos de Lima3
Carla Cabral dos Santos Accioly Lins4
Maria das Graças Wanderley de Sales Coriolano4
Keywords: Health of the Elderly. Gait. Acoustic stimulation. Music.
AbstractObjectives: Evaluate the immediate effect of rhythmic auditory stimulation (RAS) with music on the spatio-temporal parameters of gait in sedentary old people and analyze possible interactions with episodes of falls. Methods: Pilot intervention study with sedentary old people (n= 15), age ≥60 years, both sexes, independent in gait. Additionally, participants were divided into two groups, fallers (n= 5) and non-fallers (n= 10), based on the history of falls in the last year. The evaluation of the spatio-temporal parameters of the gait was performed using the 10-meter walk test performed with free walking (T0), repeated with RAS with music (T1), and without RAS again (T2). For data analysis, repeated measures ANOVA and two-way ANOVA were used for comparison between groups, with Tukey’s post hoc. The effect size of the intervention was also calculated. Results: There was a significant reduction in time and number of steps and an increase in walking speed ( p<0.0001; with great effect) between moments T0-T1 and T0-T2. Both the faller and non-fallers groups showed a significant reduction in time and number of steps (p<0.0001) and an increase in speed (p<0.0001), but only in the cadence variable was there an effect of the group and of time and group interaction. Conclusion: There was an immediate positive effect of the use of RAS on the space-time parameters of gait in sedentary old people, with a greater effect on the cadence of non-falling old people.
1 Universidade Federal de Pernambuco, Centro de Ciências da Saúde, Programa de Pós-Graduação em Gerontologia. Recife, PE, Brasil.
2 Centro Universitário Maurício de Nassau (Uninassau/João Pessoa). João Pessoa, PB, Brasil.3 Hospital Regional Belarmino Correia, Projeto Saúde do Idoso. Goiana, PE, Brasil.4 Universidade Federal de Pernambuco, Centro de Ciências da Saúde, Departamento de Anatomia. Recife,
PE, Brasil.
Funding: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Código de Financiamento 001 e Programa Institucional de Apoio a Produção Científica na UFPE (PROAP-CAPES). The authors declare there are no conflicts of interest in relation to the present study
CorrespondenceCamila Maria Mendes [email protected] Received: April 29, 2020
Approved: November 17, 2020
ID
ID
ID
ID
ID
ID

2 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
INTRODUC TION
Due to the demographic transition, Brazil has an increasingly aging population with the prospect of reaching the mark of 41 million old people in the year 20301. Accompanying this growth, concerns about the difficulties that affect this age group also increase2. The limitation of physical independence is one of the greatest fears during the aging process, being one of the factors that can make old people more and more dependent1-3. Decreased agility, altered muscle strength, decreased functional capacity, changes in gait and loss of balance are factors that can contribute to mobility problems4.
Changes in mobility are manifested in the form of instability when walking, difficulty in sitting and getting up from a chair, among others, closely related to changes in gait that are easily identified in the old people population5. The reduction in gait speed, the decrease in stride length and the reduction of cadence, can occur in pathological conditions or in physiological changes related to aging6,7, increasing the risk of adverse mobility results, including falls8,9.
It is estimated that about a third of the old people fall at least once a year. The annual fall rate is between 28-35% in the population over 65 years old and this prevalence increases among old people 70 years old or more to 32-42%10. Studies on fall profiles show that the decline in gait speed is proportional to the increase in age, in which individuals aged 70 years or more have significant reductions in gait speed when compared to individuals aged 40 to 59 years old7,11. Deficit and gait disorders are important factors to be studied for the prevention of falls and their consequences12. With this, it is perceived the need for effective strategies in prevention, in the control of health problems, rehabilitation measures and incentive to active participation in improving health so that it is possible to add quality to additional years of life13.
A form of gait therapy for old people that has been recently implemented is training with rhythmic auditory stimulation (RAS), presenting itself as an area of emerging interest that is still underestimated in this population. RAS uses rhythmic techniques, such as hand clapping, musical beat and metronome
as auditory cues that synchronize auditory-motor responses and have been used mostly as a strategy in the rehabilitation of gait disorders14-17. However, the effects of external rhythmic cues on specific gait parameters in sedentary old people, as well as their relationship with episodes of falls, are not yet clear and deserve further investigation. Therefore, this study aimed to evaluate the immediate effect of RAS with music on the spatio-temporal parameters of gait in sedentary old people and to analyze possible interactions with episodes of falls.
METHODS
This is a pilot intervention study (immediate effect), carried out between August and December 2019, with participants from the Health of the Old People Project at the Hospital Regional Belarmino Correia (PSI/HRBC), Goiana, Pernambuco (PE), Brazil. The Health of the Old People Project was implemented in 2017 as an initiative that aims to monitor the aging process through health actions aimed at improving the quality of life, given the need for specialized care aimed at this population. The project’s activities aim to prevent injuries and promote the health of old people through multidisciplinary care.
The base population registered with the PSI/HRBC in 2018, was composed of 300 participants according to the medical file sector. The selection of subjects and the verification of eligibility for the study was carried out in the geriatric consultations that take place once a week at the clinic. The sample was selected for convenience. Twenty old people were interviewed, among whom, five were excluded for not meeting the eligibility criteria. Thus, 15 old people were included in the data analysis (5% of the base population) and later divided into two groups, fallers (n=5) and non-fallers (n=10).
Old men and women, aged ≥60 years, physically inactive, with the ability to move independently, without medical contraindications for walking, with the ability to understand instructions and active participation in tasks, were included, considering the scores of Mini Mental State Examination (MMSE) corresponding to their level of education18,19.

3 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
Exclusion criteria were: old people who had neurological diseases, orthopedic, rheumatic and/or vascular pathologies that led to moderate or severe functional restriction in one or both lower limbs, with a history of fracture in the last year, labyrinthitis and/or uncontrolled or severe vestibulopathy, hypertension and/or uncontrolled heart disease. Also excluded were old people with visual impairment that led to moderate or severe functional restriction, such as deafness or with moderate or severe difficulty in listening to music. Other disorders of the external ear that were seen in the routine of the consultation with the service’s geriatrician were also considered.
Participants were instructed on their collaboration in the research and study objectives, as well as the risks and benefits, issuing their formal consent by signing the Informed Consent Form. All stages of the study followed the guidelines of the resolutions of the National Health Council No. 466 of 2012 that govern research involving human beings. The project was approved by the Human Research Ethics Committee of the Federal University of Pernambuco (CAAE: 17868719.5.0000.5208).
Initially, information on age, sex, education, fear of falling (with the possibility of answering yes or no) and the history of falls in the last year were collected, which was used to divide the old people into two groups, fallers and non-fallers.
To assess the level of physical activity, it was asked if the old person had practiced any type of physical exercise and/or sport in the last three months and how often. Old people who answered ‘no’ were considered physically inactive. After this stage, the participants were sent to the outpatient corridors to carry out the analysis of the spatio-temporal parameters of the gait, using the 10-meter walk test (10mwt).
The 10mwt is an instrument used for kinetic and kinematic analysis of gait that consists of walking during a 10-meter (m) course, which initial 2m is for acceleration, 6m for walking at normal speed and 2 m for deceleration. The patient was instructed to walk on a flat surface, in a straight line and at a comfortable pace. The test has good reproducibility and reliability (Intraclass Correlation Coefficient =0.86, with an
average difference of −0.03±0.16 m/s and the 95% Bland and Altman agreement limits for the mean difference were −0,33 to 0.27) 20, in addition to being a simple measure, of quick execution and with a prognostic factor of the risk of falls in old patients.
For the analysis of the variables of time and number of steps, the central 6 meters were considered, in which the components of acceleration and deceleration of the gait were discounted. The evaluator used a 1/100s digital stopwatch (Poker Ergo Digital, REF 08089-2018®, Montenegro, RS, Brazil), to get the walk time for the volunteers. The number of steps was counted during the test and a camera was positioned to assist in confirming the capture of the number of steps. The cadence, expressed in steps / second, was calculated by dividing the total number of steps (P) by the time (T) in seconds, spent on the route. Multiplying by 60 [C=P/Tx60] was performed to select the song whose frequency is expressed in beats per minute (bpm). The speed was calculated by dividing the total distance (D) by the time (T) spent in seconds to complete the route and multiplied by 60 [V= D/T x 60]21.
Participants performed an initial take of the 10mwt to familiarize themselves with the test and knowledge of the route. After this phase, the steps of the experiment were carried out. Sequentially, the old people performed the 10mwt without stimulation to measure the variables (T0 - without RAS). Then they performed the same test with rhythmic auditory stimulation with music, in which the same variables were measured (T1 - with RAS). Finally, they performed the 10mwt without stimulation (T2 - without RAS). In each 10mwt outlet, three measurements were made sequentially, namely: T0 (T01, T02 and T03), T1 (T11, T12 and T13) and T2 (T21, T22 and T23), the final result of each outlet being obtained through the arithmetic mean of the three measurements at each moment.
The tests were carried out in a single meeting, successively, with a resting time of 1 minute between the measurements of the space-time parameters of the gait, so that there was a return to the initial condition of the test. If necessary, the rest time could be increased. However, no old person presented this need and all were able to carry out the nine

4 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
measurements, taking an average of 20 minutes between the explanation and the tests.
The RAS used was composed of musical tracks with a marked and constant rhythm provided by the ParkinSONS® app using a smartphone, Android operating system. The app was developed by the research group Pró-Parkinson (Registration with the National Institute of Intellectual Property - INPI, nº BR512020001451-8) and is in the process of commercialization. The comfortable cadence obtained in the 10mwt was used as a parameter for selecting the RAS for stage T1. The comfortable cadence was increased by 10% to obtain the training cadence, enabling the selection of music for the RAS. The regional musical rhythms provided by the app present the frequencies 70 bpm, 80 bpm, 90 bpm, 100 bpm, 110 bpm and 120 bpm, which can be selected individually for each participant. The sound intensity offered was approximately 75 dB HL (decibel hearing level), a level above that perceived by old people with mild to moderate peripheral hearing loss, verified by audiometry, which is around 30 to 70dB HL22. Connected supra-aural headsets were used simultaneously by the old person and therapist to guarantee the performance of the test in the selected training cadence. In addition, a check was made to listen to the music and understand the test before it was performed.
The RAS provides patients with a temporal orientation that facilitates the regulation of their movements during walking. This is because the auditory and motor systems have rich connectivity at various cortical, subcortical and spinal levels. The auditory system - a fast, accurate and temporal information processor - projects itself into motor structures in the brain, creating a connection between the rhythmic signal and the motor response23. Therefore, it is recommended the early incorporation of rhythmic auditory cues with time variations of ± 10% in relation to the preferred cadence to improve gait performance. With the RAS customized for the individual’s cadence, the speed that can be achieved is respected and, at the same time, it encourages and encourages the improvement of their gait pattern15,17,23.
The data were tabulated in a Microsoft Excel spreadsheet and compiled using descriptive statistics and processed using the Statistical Package for the Social Science software version 20.0 (SPSS Inc, Chicago, IL, USA). The normality of the data was confirmed through the Shapiro-Wilk test. To evaluate the differences between the measures for the total sample, an ANOVA of repeated measures was used. The two-way ANOVA with repeated measures was used to compare the outcome variables considering the group (fallers vs. non-fallers) and time (T0, T1 and T2) as comparison factors followed by the Mauchly sphericity test and if necessary Greenhouse-Geisser correction was applied. In both analyzes, Tukey’s post hoc was used to spot differences and considered p <0.05. The size of the immediate effect of RAS with music on the spatio-temporal parameters of gait was also calculated using the Hedges test (g), with its values classified as: insignificant (<0.19); small (0.20-0.49); medium (0.50-0.79); large (0.80-1.29) and very large (>1.30)24.
RESULTS
Sociodemographic data, study time and the survey on falls are shown in Table 1. The average age was 71.3 ± 6.45 years, with a minimum age of 65 and a maximum of 83 years. In the sample, 33% of the old people reported having suffered a fall episode in the last year and 73% expressed the fear of falling, whether they were fallers or not.
The results regarding the effect of the RAS effect with music on the spatio-temporal parameters of the gait of the old people were presented in Figure 1 and the analysis of the effect size in Table 2. There was a significant reduction in the walking time in the 10mwt (ANOVA. P<0.0001). The post hoc indicated that the time to perform the gait on the 10mwt reduced significantly between moments T0 and T1 (-0.85sec), with a large effect size (g=1.07), and this effect was maintained in T2. Regarding the number of steps, there was a significant reduction (ANOVA. P<0.0001). In the post hoc test, significant reductions were observed between T0-T1 and between T0-T2, with a large effect (g=1.03

5 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
and g=1.02, respectively). In the speed parameter, ANOVA indicated a significant increase (p<0.0001). The post hoc indicated a significant increase in speed between T0-T1 with the maintenance of this large
effect (g=1.05) in T2. As for cadence, it was possible to verify a significant increase (ANOVA. P=0.026*). The post hoc indicated a significant increase between T0 and T2 with large effect size (g=0.97).
Table 1. Characterization of the sample of users of the Health for the Old Person Project(n=15). Goiana, PE, 2019.
Characteristics Median (sd)Age 71.3 ± 6.45Years of education 3.67 ± 3.92 Sex n (%)FemaleMale
7 (46.7)8 (53.3)
Survey on falls Yes n (%) No n (%)Falling episode (faller) 5 (33) 10 (67)Fear of Falling 11 (73) 4 (27)
sd = standard deviation
Repeated measures ANOVA with Tukey’s post hoc; T0: initial walk test as an evaluation parameter without Rhythmic Auditory Stimulation; T1: walk test using Rhythmic Auditory Stimulation and T2: final walk test as a reevaluation parameter without Rhythmic Auditory Stimulation.
Figure 1. Repercussion of the immediate effect of rhythmic auditory stimulation with music on the spatio-temporal parameters of gait in old people (n=15). Goiana, PE, 2019.

6 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
Table 2. Size analysis of the immediate effect of rhythmic auditory stimulation with music on the spatio-temporal parameters of gait in old people (n=15). Goiana, PE, 2019.
Space-timegait parameter
g of Hedges 95% CI Effect Size Classification
Time T0 vs T1 g= 1.07T0 vs T2 g= 1.07T1 vs T2 g= 0
[0.31 - 1.81][0.31 - 1.81][-0.70 - 0.70]
LargeLargeInsignificant
Steps T0 vs T1 g= 1.03T0 vs T2 g= 1.02T1 vs T2 g= -0.06
[0.28 - 1.77][0.27 - 1.76][-0.76 - 0.64]
LargeLargeInsignificant
Cadence T0 vs T1 g= -0.63T0 vs T2 g= -0.64T1 vs T2 g= -1.07
[-1.34 - 0.09][-1.35 - 0.08][-0.80 - 0.60]
MediumMediumLarge
Speed T0 vs T1 g= -1.05T0 vs T2 g= -0.97T1 vs T2 g= 0.10
[-1.79 - -0.30][-1.71 - -0.23][-0.54 - 0.85]
LargeLargeInsignificant
CI: confidence interval; T0: initial walk test as an evaluation parameter without Rhythmic Auditory Stimulation; T1: walk test using Rhythmic Auditory Stimulation and T2: final walk test as a reevaluation parameter without Rhythmic Auditory Stimulation.
Table 3 presents the results of the repercussion of the RAS on the spatio-temporal parameters of gait in the falling and non-falling groups. In both groups, there was a significant reduction in time [F(2,26)=21.00; p<0.0001] and number of steps [F(2,26)=24.23; p<0.0001] and increase in speed [F(2,26)=17.68; p<0.0001], no effect of group or interaction (ps> 0.05).
On the cadence variable, there was an effect of the group [F(1-13)= 5.36; p=0.037], indicating a
significantly higher cadence in the non-falling group. In addition, there was an effect of the time x group interaction [F(2,26)=4.66; p=0.018], where the post hoc pointed out that the cadence increased only in the non-falling group between T0 and T1 (p=0.024) and between T0 and T2 (p=0.004) (Table 3). The Mauchly test indicated that the sphericity of the cadence data was not violated (X2=4.83; p=0.089), and it was not necessary to apply Greenhouse-Geisser correction.
Table 3. Repercussion of the immediate effect of rhythmic auditory stimulation with music on the spatio-temporal parameters of gait in the falling (n=5) and non-falling (n=10) groups. Goiana, PE, 2019.
Variables Condition T0 T1 T2 p-value T p-value G p-value TxGTime Fallers
Non-fallers6.57 ± 0.256.16 ± 0.81
6.02 ± 0.255.17 ± 0.89
5.95 ± 0.625.36 ± 0.81
<0.0001ª 0.119 0.260
Steps Fallers Non-fallers
11.67 ± 0.5311.00 ± 0.97
10.53 ± 0.779.97 ± 1.23
10.47 ± 0.8410.10 ± 1.11
<0.0001ª 0.316 0.692
Cadence Fallers Non-fallers
1.78 ± 0.091.80 ± 0.12
1.75 ± 0.131.94 ± 0.14*
1.74 ± 0.121.98 ± 0.20**
0.146 0.037 0.018
Speed Fallers Non-fallers
0.91 ± 0.040.99 ± 0.13
1.00 ±0.041.19 ± 0.18
1.02 ± 0.121.14 ± 0.16*
<0.0001ª 0.084 0.100
Two-way ANOVA with Tukey’s post hoc, followed by the Mauchly test; aeffect of time, indicating a reduction in the time and steps parameters and an increase in the gait speed parameter in both groups. *effect of the group, indicating an increase in cadence between moments T0 and T1* and T0 and T2** only in the non-falling group; T0: initial walk test as an evaluation parameter without Rhythmic Auditory Stimulation; T1: walk test using Rhythmic Auditory Stimulation and T2: final walk test as a reevaluation parameter without Rhythmic Auditory Stimulation; T = effect of time; G = group effect; TxG = interaction between group and time effects.

7 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
DISCUSSION
The present study investigated the immediate effect of RAS with music on the spatio-temporal parameters of gait in sedentary old people. The results show a significant reduction in the time and number of steps and an increase in the speed and cadence of the gait when the old people perform the route using the RAS resource with music (T0 vs T1). The effect tended to remain when the route was taken again without the use of the resource (T0 vs T2), which may indicate that the RAS with music had an immediate positive effect on the spatio-temporal parameters of the gait of these old people.
It is known that gait speed is an important indicator for its ability to predict adverse events such as loss of independence, increased disability, functional limitations, falls, hospitalizations and death. Physiological aging is responsible for a 1.2% reduction in gait speed annually25. One of the most affected systems is the neuromuscular with the loss of alpha motor neurons in the spinal cord, with the deterioration of their axons and consequent attenuation in the recruitment of motor units, resulting in limitations in the functioning of these systems, impacting the performance and speed of gait in old people26.
A key concept of RAS is auditory-motor synchronization through the spinal reticulum. As a neurophysiological explanation, the activation of the motor areas of the brain using stimuli with rhythm can increase the excitability of spinal motor neurons, reducing the substantial time for the muscles to respond to a motor command, improving muscle activation and control of movements influencing the speed improvement21,27.
The study by Wilson et al.28 suggests a clinically significant difference> 0.05m/s, which was obtained during the comparison of gait speed between different tests. The average speed increase of 0.17m/s (T0 vs T1) and 0.14m/s (T1 vs T2) was higher than the one considered clinically significant, also verified by other authors in studies with RAS21,29.
The reduction in time, the increase in cadence and speed in walking, observed in this study reflect
a qualitatively better gait29. These parameters showed a significant improvement indicating that the natural rhythmic movements of the gait can be corrected through synchronization processes and external attention promoted by RAS30. During the aging process, the gait ceases to be carried out automatically, with greater compensatory executive control. With the use of auditory stimulus, the neuromuscular system can perform the action with less conscious control and allowing for smoother movements, which can result in improved gait31,32.
The results also showed that the spatio-temporal parameters of gait in old people were positively influenced with the use of the auditory stimulus, with an improvement that remains even without the auditory stimulus (T2). It is possible to observe a possible motor learning provided by RAS, promoting an indicative of immediate effect that remained after the test was carried out without the presence of the stimulus that may be related to the somatosensory system. The somatosensory system of the motorways is also responsible for the coordination and perception of the body and environmental status that are essential for movement control. The use of rhythmic-sound beat excites the auditory-motor pathways to create a quick connection leading to a temporal synchronization between the sensory input and motor output mechanisms, reconfiguring this system through neuroplasticity16,33. Thus, it promotes an increase in rhythmic awareness, allowing to increase concentration, attention and the ability to perceive both the direction of movement and the speed of the movements performed, reflecting in the improvement of gait parameters34.
Another hypothesis to be considered to explain the findings is the old person’s learning curve in the face of repetitions at each moment of the test that would be independent of the RAS offer. However, two arguments can refute this hypothesis. First, it would be expected, in this case, to observe significant differences between all moments (T0 vs T1; T1 vs T2 and T0 vs T2) demonstrating the learning related to progressive improvement in performance with the increase of repetitions, which did not occur. The second point concerns the modulation of the gait rhythm provided by the RAS at T1,

8 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
where the old people were offered a stimulus with an increase of 10% in their comfortable walking cadence, which favored the performance during the offer (T1 moment) and its maintenance (moment T2). However, the absence of a control group and other studies in the literature does not allow us to completely exclude the effect of time (repetition/learning), making this finding to be interpreted with caution.
A review study showed that changes in space-time parameters improve gait variability, which is important in preventing falls. The gait variability found in the old people population has been associated with an increased risk of falling and thus, the greater rhythmicity that is promoted by the RAS has been shown to reduce the variability in the musculoskeletal activation patterns, thus allowing acceleration of joint movements, reducing the time of gait and increasing speed15.
Both in the fallers group and in the non-fallers group, a significant reduction in time and number of steps was observed, as well as an increase in walking speed when the old people perform the route using the RAS with music (T0 vs T1). The effect was maintained when the route was taken again without the use of the resource (T0 vs T2) which indicates that the RAS with music promoted an immediate positive effect on these parameters regardless of the history of falls. However, when comparing the groups, we observed that the non-fallers group performed significantly better than the fallers group in all the gait parameters analyzed, pointing to the possibility that the history of falls also influences the benefits obtained with interventions like this. The absence of comparison with other variables that could explain or interfere in this relationship leads us to be cautious in the interpretation of these results, which should be analyzed in future studies.
All old people who are fallers in the sample reported the fear of falling. Some authors report that the fear of falling has a negative effect on the gait of old people, with estimates of the frequency of falls
varying between 29% and 77%35. Hadjistavropoulos et al.35 presented a model representing strong associations between fear of falling and reduced balance, impairing gait performance in old people. Only one study investigated the effect of using RAS to prevent falls, this being in the population with Parkinson’s disease17. The results indicated that gait training with RAS reduced the number of falls and modified gait kinematics in falling individuals with Parkinson’s disease (with an increase in gait speed and stride length).
The use of the RAS strategy showed good viability, low cost, easy application and encouraging results regarding the immediate effect in this sample. However, it is worth mentioning that an uncontrolled pilot study limits the generalization of results that must be interpreted with caution. We recommend conducting clinical trials that can investigate the effect of using this strategy on gait and the possible repercussions on the daily activities of sedentary old people.
We emphasize that the theme is new and relevant, and similar studies with the use of RAS in the sedentary old population are not found in the national literature. We also consider that the strategy has potential for use in other areas besides physical therapy in the context of intervention in rhythmic functional activities.
CONCLUSION
This pilot study points to an immediate positive effect of the use of rhythmic auditory stimulation on the space-time gait parameters of sedentary old people, especially gait speed, which is an important indicator for predicting adverse events such as falls and changes in functionality. There was a better performance in the parameters of time, speed and gait cadence of non-faller old people submitted to RAS. However, clinical trials are needed to investigate the effects of this strategy on healthy aging.
Edited by: Daniel Gomes da Silva Machado

9 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
REFERENCES
1. Miranda GMD, Mendes ACG, Silva ALA. O envelhecimento populacional brasileiro: desafios e consequências sociais atuais e futuras. Rev Bras Geriatr Gerontol. 2016;19(3):507-19. Available from: 90/1809-98232016019.15014https://doi.org/10.150 .
2. Abdala RP, Barbieri Jr W, Bueno Jr CR, Gomes MM. Padrão de marcha, prevalência de quedas e medo de cair em idosas ativas e sedentárias. Rev Bras Med Esporte. 2017;23(1):26-30. Available from: http://dx.doi.org/10.1590/1517-869220172301155494 .
3. Aboutorabi A, Arazpour M, Bahramizadeh M, Hutchins SW, Fadayevatan R. The effect of aging on gait parameters in able-bodied older subjects: a literature review. Aging Clin Exp Res. 2015;28(3):393-405. Available from: http://doi.org/10.1007/s40520-015-0420-6 .
4. Monteiro D, Silva LP, Sá PO, Oliveira ALR, Coriolano MGWS, LINS OG. Prática mental após fisioterapia mantém mobilidade funcional de pessoas com doença de Parkinson. Fisioter Pesqui. 2018;25(1):65-73. Available from: https://doi.org/10.1590/1809-2950/17192425012018 .
5. Camara FM, Gerez AG, Miranda MLJ, Velardi M. Capacidade funcional do idoso: formas de avaliação e tendências. Acta Fisiatr. 2008;15(4):249-56. Available from: http://www.revistas.usp.br/actafisiatrica/article/view/103005/101285 .
6. Novaes RD, Miranda AS, Dourado VZ. Usual gait speed assessment in middle-aged and elderly Brazilian subjects. Rev Bras Fisioter. 2011;15(2):117-22. Available from: https://doi.org/10.1590/S1413-35552011000200006 .
7. Santos IR, Carvalho RC, Lima KBSP, Silva SC, Ferreira AS, Vasconcelos NN, et al. Análise dos parâmetros da marcha e do equilíbrio dos idosos após exercícios aeróbicos e terapêuticos. Arq Ciênc Saúde UNIPAR. 2016;20(1):19-23. Available from: https://doi.org/10.25110/arqsaude.v20i1.2016.5778 .
8. Clark DJ. Automaticity of walking: functional significance, mechanisms, measurement and rehabilitation strategies. Front Hum Neurosci. 2015;9(246):1-13. Available from: https://doi.org/10.3389/fnhum.2015.00246 .
9. Conradsson D, Halvarssona A. The effects of dual-task balance training on gait in older women with osteoporosis: a randomized controlled trial. Gait Posture. 2019;68:562-68. Available from: https://doi.org/10.1016/j.gaitpost.2019.01.005 .
10. Silveira MB, Saldanha RP, Leite JCC, Silva TOF, Silva T, Filippin LI. Construção e validade de conteúdo de um instrumento para avaliação de quedas em idosos. Einstein. 2018;16(2):1-8. Available from: https://doi.org/10.1590/s1679-45082018ao4154 .
11. Na’emani F, Zali ME, Sohrabi Z, Fayaz-Bakhsh A. Prevalence of risk factors for falls among the elderly receiving care at home. Salmand: Iran J of Ageing. 2019,13(5):638-51. Available from:: http://dx.doi.org/10.32598/SIJA.13.Special-Issue.638 .
12. Ferreira LMBM, Javier Jerez-Roig J, Andrade FLJP, Oliveira NPD, Araújo JRT, Lima KCL. Prevalência de quedas e avaliação da mobilidade em idosos institucionalizados. Rev Bras Geriatr Gerontol. 2016;19(6):995-1003. Available from: https://doi.org/10.1590/1981-22562016019.160034 .
13. Veras RP, Oliveira M. Envelhecer no Brasil: a construção de um modelo de cuidado. Ciênc Saúde Colet. 2018;23(6):1929-36. Available from: https://doi.org/10.1590/1413-81232018236.04722018 .
14. Luessi F, Mueller LK, Breimhorst M, Vogt T. Influence of visual cues on gait in Parkinson’s disease during tredmill walking at multiples velocities. J Neurol Sci. 2012;314(1-2):78-82. Available from: https://doi.org/10.1016/j.jns.2011.10.027 .
15. Ghai S, Ghai I, Effenberg AO. Effect of Rhythmic Auditory Cueing on Aging Gait: a Systematic Review and Meta-Analysis. Aging Dis. 2018;9(5):901-23. Available from: https://doi.org/10.14336/AD.2017.1031 .
16. Vitorio R, Stuart , Gobbi LTB, Rochester L, Alcock L, Pantall A. Reduced gait variability and enhanced brain activity in older adults with auditory cues: a functional near-infrared spectroscopy study. Neurorehabil Neural Repair. 2018;32(11):976-87. Available from: https://doi.org/10.1177/1545968318805159 .
17. Thaut MH, Rice RR, Braun Janzen T, Hurt-Thaut CP, McIntosh GC. Rhythmic auditory stimulation for reduction of falls in Parkinson’s disease: a randomized controlled study. Clin Rehabil. 2019;33(1):34-43. Available from: https://doi.org/10.1177/0269215518788615 .
18. Folstein MF, Folstein SE, Mchugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189-98. Available from: https://doi.org/10.1016/0022-3956(75)90026-6 .

10 of 10
Rhythmic auditory stimulation and gait parameters
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200121
19. Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini exame do estado mental no Brasil. Arq Neuropsiquiatr. 2003;61(3):777-81. Available from: https://doi.org/10.1590/S0004-282X2003000500014 .
20. Adell E, Wehmhörner S, Rydwik E. The Test-Retest Reliability of 10 Meters Maximal Walking Speed in Older People Living in a Residential Care Unit. J Geriatr Phys Ther. 2013;36(2):74-7. Available from: https://doi.org/10.1519/JPT.0b013e318264b8ed .
21. Matsumoto L, Magalhães G, Antunes GL, Torriani-Pasin C. Efeitos do estímulo acústico rítmico na marcha de pacientes com Doença de Parkinson. Rev Neurocienc. 2014;22(3):404-9. Available from: https://doi.org/10.34024/rnc.2014.v22.8075 .
22. Koohi N, Vickers DA, Utoomprurkporn N, Werring DJ, Bamiou DE. A Hearing Screening Protocol for Stroke Patients: An Exploratory Study. Front Neurol. 2019;10(842):1-8.Available from: https://doi.org/10.3389/fneur.2019.00842 .
23. Hove MJ, Keller PE. Impaired movement timing in neurological disorders: rehabilitation and treatment strategies. Ann N Y Acad Sci. 2015;1337(1):111-7. Available from: https://doi.org/10.1111/nyas.12615 .
24. Silva VM, Arruda ASF, Silva LSV, Pontes Junior FL, Cachioni M, Melo RC. Efetividade de uma intervenção múltipla para a prevenção de quedas em idosos participantes de uma Universidade Aberta à Terceira Idade. Rev Bras Geriatr Gerontol. 2019;22(2):1-13. Available from: http://dx.doi.org/10.1590/1981-22562019022.190032 .
25. Perera S, Patel KV, Rosano C, Rubin SM, Satterfield S, Harris T, et al. Gait Speed Predicts Incident Disability: a Pooled Analysis. J Gerontol Ser A Biol Sci Med Sci. 2016;71(1):63-71. Available from: https://doi.org/10.1093/gerona/glv126 .
26. Leite LEA, Resende TL, Nogueira GM, da Cruz IBM, Schneider RH, Gottlieb MGV. Envelhecimento, estresse oxidativo e sarcopenia: uma abordagem sistêmica. Rev Bras Geriatr Gerontol. 2012; 15(2):365-80. Available from: https://doi.org/10.1590/S1809-98232012000200018.
27. Koshimori Y, Thaut MH. Future perspectives on neural mechanisms underlying rhythm and music based neurorehabilitation in Parkinson’s disease. Ageing Res Rev. 2018;47:133-9. Available from: https://doi.org/10.1016/j.arr.2018.07.001 .
28. Wilson CM, Kostsuca SR, Boura JA. Utilization of a 5-Meter Walk Test in Evaluating Self-selected Gait Speed during Preoperative Screening of Patients Scheduled for Cardiac Surgery. Cardiopulm Phys Ther J. 2013;24(3):36-43. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3751713/pdf/cptj0024-0036.pdf .
29. Rizzo JR, Raghavan P, McCrery JR, Oh-Park M, Verghese J. Effects of emotionally charged auditory stimulation on gait performance in the elderly: a preliminary study. Arch Phys Med Rehabil. 2015;96(4):690-6. Available from: https://doi.org/10.1016/j.apmr.2014.12.004 .
30. Sejdić E, Fu Y, Pak A, Fairley JA, Chau T. The effects of rhythmic sensory cues on the temporal dynamics of human gait. PLoS ONE. 2012;7(8):1-7. Available from: https://doi.org/10.1371/journal.pone.0043104 .
31. Shahraki M, Sohrabi M, Taheri Torbati HR, Nikkhah K, NaeimiKia M. Effect of rhythmic auditory stimulation on gait kinematic parameters of patients with multiple sclerosis. J Med Life. 2017;10(1):33-7. Available from: https://www.ncbi.nlm.nih.gov/pubmed/28255373 .
32. Huijben B, van Schooten KS, van Dieën JH, Pijnappels M. The effect of walking speed on quality of gait in older adults. Gait Posture. 2018; 65:112-16. Available from: https://doi.org/10.1016/j.gaitpost.2018.07.004 .
33. Yu L, Zhang Q, Hu C, Huang Q, Ye M, Li D. Effects of different frequencies of rhythmic auditory cueing on the stride length, cadence, and gait speed in healthy young females. J Phys Ther Sci. 2015;27(2):485-7.Available from: https://doi.org/10.1589/jpts.27.485 .
34. Dalla Bella S, Dotov D, Bardy B, de Cock VC. Individualization of music-based rhythmic auditory cueing in Parkinson’s disease. Ann N Y Acad Sci. 2018;1423:1-10. Available from: https://doi.org/10.1111/nyas.13859 .
35. Hadjistavropoulos T, Delbaere K, Fitzgerald TD. Reconceptualizing the role of fear of falling and balance confidence in fall risk. J Aging Health. 2011;23(1):3-23. Available from: https://doi.org/10.1177/0898264310378039 .

1 of 10
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
http://dx.doi.org/10.1590/1981-22562020023.200129
(Geronto)Technologies of care for old people with Alzheimer’s disease and their families: contribution of awareness/training workshops
Silomar Ilha1
Francine Casarin2
Luciana de Carvalho Pires2
Betânia Huppes2
Claudia Zamberlan3
Keywords: Health of the Elderly. Alzheimer disease. Family. Technology. Health Personnel.
AbstractObjective: To describe (geronto)technologies of care for old people with Alzheimer’s disease and their families, from awareness/training workshops. Methods: Strategic action research, developed with 12 nursing, physiotherapy, dentistry and occupational therapy students from a University of Rio Grande do Sul, Brazil. The data collected from September to December 2019, through semi-structured interview, after awareness-raising workshops on care (geronto) technologies for old people and their families, were subjected to textual discursive analysis. Results: They allowed the description of (geronto)technology in the form of a product: identification plates for objects and rooms; products for organizing medication; Identification badge; support bars, rounders, non-slip mats and various adaptations; bath calendar; Games, books and manual activities. And, in the form of process/knowledge/strategies: dialogue, memories and negotiations; accompanying the old people and advising neighbors on Alzheimer’s disease; and, division of responsibilities. Conclusion: The awareness/training workshops contributed to the knowledge of students from different training centers and showed potential to contribute to the care of old people with Alzheimer’s disease and their families, through suggested (geronto)technologies.
1 Universidade Franciscana, Curso de Enfermagem, Pós-Graduação em Ciências da Saúde e da Vida. Santa Maria, RS, Brasil.
2 Universidade Franciscana, Curso de Enfermagem. Santa Maria, RS, Brasil.3 Universidade Franciscana, Curso de Enfermagem, Pós-Graduação em Saúde Materno Infantil. Santa
Maria, RS, Brasil. There was no funding for the execution of this work.The authors declare that there is no conflict in the conception of this work.
CorrespondenceSilomar [email protected]
Received: June 05, 2020Approved: November 04, 2020
ID
ID
ID
ID
ID

2 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
INTRODUC TION
The aging process makes the human being more susceptible to chronic diseases of progressive character, as is the case of Alzheimer’s disease (AD), which is responsible for approximately 50 to 75% of dementias in several countries1. In Brazil, it is estimated that one million people are affected by AD; however, there is still not much data regarding its incidence in the country2.
Due to its neurodegenerative characteristic, AD compromises the physical, mental and social integrity of the old person, triggering, over time, a situation of dependence that requires everything from helping with Activities of Daily Living (ADLs), to comprehensive and complex care, performed, in most cases, by a family member at home3. This situation sometimes leads to the need for professional assistance.
The nurse is the professional responsible for leading and systematizing the care process for people in the different scenarios in which they find themselves. However, it is not feasible for a single professional to be able to develop care in the context of AD, in an expanded and consistent way with individual/collective needs4. In this sense, it is necessary for health professionals to dialogue and, together, to develop expanded care plans, which should focus on the old person and family members/caregivers, with a view to assisting them in minimizing the emotional changes resulting from of the care process3.
Public policies, in the context of the health of old people, recommend the use of creative strategies that favor communication between professional, subject and group5. Thus, some professionals, teaching and health institutions have invested efforts in the context of Gerontology, in the understanding and use of gerontotechnological possibilities6.
Among these, there is the use of complex (geronto) care-educational technologies, comprised of products, processes, strategies, services and/or knowledge, with the care-educational purpose of old people and their family members/caregivers, as a result of a complex collective construction/
experience that values the relationships, interactions and feedback of those involved, through inter-multi-trans-meta-disciplinary knowledge7.
Thus, it is evident that (geronto)technology is sometimes not a product, but the result of work that involves a set of actions that aim at health care6. They are characterized as important tools for the development of the care model, as they enhance care skills, both for the old person, as well as for the family member and/or caregiver. And they assist in promoting effective strategies for maintaining and improving health care for old people8.
In this context, interventions that aim to train future health professionals to use (geronto)technologies are necessary in order to assist in the daily care of old people with AD. However, as important as carrying out an intervention is to assess its contribution to the identification of (geronto)technologies, a fact that justifies the need and relevance of this research. It is also justified, anchored in that described by the Ministry of Health (MH), which points out issues related to the health of old people, as well as technologies, as research priorities in Brazil9.
In view of the above, the question arises: What (geronto) care technologies can be thought of to assist in the daily care of old people with Alzheimer’s disease? In an attempt to answer the question, the objective was to describe (geronto) care technologies for old people with Alzheimer’s disease and their families, from awareness/training workshops.
METHOD
It is a strategic action-research10, held with students from the last semester of Nursing, Physiotherapy, Dentistry and Occupational Therapy at a university, in the State of Rio Grande do Sul (RS), Brazil. Participants were randomly selected from the call list, made available by the professor, at which point the invitation was made to five students from each course.
Academics from the last semester were selected, as they had already taken the disciplines that deal with

3 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
the theme of aging in their undergraduate course, in addition to having already experienced different realities offered during their training process. As inclusion criteria, the following were established: being an academic in one of the aforementioned health courses; being in the last semester of the course and have already taken the subjects related to gerontology, geriatrics or equivalent. Students on medical leave, maternity leave or academic exchanges on the date of the draw were excluded. Up to the end of the study, 12 academics formed the corpus of this research.
In September 2019, the participants underwent an individual semi-structured interview (moment 1), in a university classroom, conducted by the questions: Have you heard/read anything about (geronto)technologies? Have you ever used some kind of (geronto)technolog y? This moment allowed the identification of knowledge gaps and, therefore, aroused the need for intervention.
Thus, in November 2019, participants underwent the intervention, in the form of workshops (moment 2), with a view to raising awareness and training on issues related to (geronto) care technologies, in the context of old people with AD and their families. The workshops were held from a conversation circle, in a university classroom, and lasted an average of one and a half hours. The activity was coordinated by one of the five researchers, who is a nurse with a specialization in Gerontology.
The workshops started with welcoming participants and thanking them for participating in the research; then, each participant was introduced, so that the group could get to know each other. In sequence, the researchers talked to the participants, explaining aspects related to aging and about the (geronto) care technologies, expanding some points and deepening others, as they perceived the need or were requested by the participants. To aid in the activities, audiovisual material was used and students were encouraged to verbalize experiences they had experienced during the training process.
After the awareness and training workshops, semi-structured interviews with each participant were held again in November and December
2019 (moment 3). Initially, the questions used in the interview (moment 1) were resumed, in order to identify whether the knowledge gaps had been overcome or whether other moments of awareness and training should be programmed. From the understanding that the students had been sensitized, the question was asked: What (geronto)technologies can be adopted by family members/caregivers to assist them in their daily care for the old person?
The interviews (moment 1 and moment 3) were recorded with an MP3 player and transcribed in full, mechanographically, by the researchers, with the aid of the Microsoft Word program (version 16.31). The data were processed using the discursive textual analysis technique, organized from a recursive sequence of three components: unitarization, establishment of relationships and communication11. Initially, the researchers examined the texts in depth, forming the central category, from the identification of (geronto)technologies suggested by the academics. It was unified in two base units; in the first unit, all (geronto)technologies were grouped into product form; in the second, in the form of process/knowledge and/or strategies.
Afterwards, a new reading was made from the central category and the base units, seeking to establish relationships between them, that is, each report inserted in the base units was read in detail, when they were separated into different units, according to the purpose of using the (geronto)technology. Finally, we proceeded to the last stage of the analysis method, by the communication process between the (geronto)technologies in the form of product and the (geronto)technologies in the form of process/knowledge/strategy, according to the need to which they were directed, resulting in the categories11.
Ethical and legal precepts were considered, according to Resolution 466/12 of MH12. The Project was approved by the Research Ethics Committee under Opinion nº 3.368.520 and CAAE: 14430619.5.0000.5306. The anonymity of the participants was maintained, identifying them by the letter A (academic) followed by a number (A1, A2 ... A12).

4 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
RESULTS
Of the 12 survey participants, 11 were female and one male, aged between 20 and 37 years. Of these, four were studying nursing; five, dentistry; two, occupational therapy; and one, physical therapy. The analyzed data allowed the construction of a central
category: (geronto) care technologies for old people with Alzheimer’s disease and their families. It was unified in two basic units: (geronto) technology in the form of a product; (geronto) technologies in the form of Process/Knowledge/Strategy (PKS). Such units generated nine categories, as shown in Figure 1.
(Geronto)Technology in the form of identif ication plates for objects and rooms
One of the (geronto) technologies, in the form of a product, suggested by academics in the health field, deals with signs for the identification of objects and furniture in the home of the old person with AD.
“[...] we can also identify the parts of the house, bathroom, kitchen, with signs [...]” (A4)
“[...] rooms can be identified with signs to facilitate for the old person [...]” (A6)
“Signs can be placed inside the house reminding the name of the object and rooms of the house [...]” (A7)
“Place signs in the house to make it easier to know the parts and objects [...]; organize the environment to avoid falls; to indicate, with small signs, where the plates, cutlery are; make reminders of the tasks that the old person has to do, organize their routine” (A9).
Figure 1. Demonstrative scheme of the central category, base units and categories.
Source: Authors, 2020.

5 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
(Geronto)Technology in the form of products for organizing medication
Strategies to assist the old person and their family in the organization of medicines were also signaled by academics as (geronto)technologies in the form of a product. It is a matter of separating them, by schedule or shift, in devices such as small pots. Also, number the pills on the blister pack, so that the number assigned on top of the pill label represents the day on which it should be ingested/administered.
“Using the medication organization box, too, the numbering can be placed on the medication pack itself, on top of each pill, representing the day to be taken, to know what medicine they took, always trying to make them more independent [...]” (A2)
“Separate the medication according to the shift to be taken, it can be in jars, or writing on the cards [...]” (A7)
“Separate the medicines by shift, in jars, and use reminders; always try to include the old person in the activities carried out” (A9).
“[...] the medicine storage box according to the shift: morning, afternoon and night, can be used [...]” (A11)
(Geronto)Technology in the form of identif ication badge
Another (geronto)technology in the form of a product, suggested by academics, concerns the making of a badge with data about the old person, such as the name, the information that the person lives with AD, as well as the telephone number of a family member/caregiver .
“[...] embroider on some coat that the old person usually wears their name, the information that they have Alzheimer’s and the phone number of a family member/caregiver” (A4).
“An identification badge can be made for the old person, embroidering on their clothes that they have Alzheimer’s, the name of the old person and the caregiver’s phone number” (A9).
(Geronto)Technologies: support bars, rounders, non-slip mats and various adaptations
Support bars, rounders for furniture corners, non-slip mats and various adaptations, such as cutlery, furniture height and toilet seat, were also (geronto)technologies suggested by the academics from health courses.
“Adapting the height of the furniture with lifting devices that can be placed on the feet of beds, sofas, chairs and other furniture, adaptations in their corners to round them [...]” (A1)
“[...] putting on handles in the bathroom, the support bars placed in the bathroom and the use of a wheelchair [...]” (A2)
“[...] in the bathroom, placing non-slip mats, support bars, keeping the furniture at an easily accessible height and with rounded corners” (A4).
“Putting on a handrail, removing carpet, protecting all corners to avoid getting hurt, putting on a raised toilet seat in the toilet bowl, as they no longer have so much balance [...] adapted cutlery, remove the rugs to reduce the risk of falling [...]” (A7)
“[...] raising the height of the furniture, removing objects from the floor that may cause the old person to fall, such as carpets [...]” (A9)
“[...] bars on the wall to help with balance and locomotion” (A11).
(Geronto) Product technology in the form of a bathing schedule
Another (geronto)technology in the form of a suggested product refers to the use of a device called the bathing schedule. It is the materialization of a strategy used to negotiate body hygiene for the old person.
“Always try to negotiate with the old person with Alzheimer’s, such as the bathing schedule [...]” (A3)
“Always be stimulating, the bathing schedule, as was said in the training. As he supported Internacional, she created a table on the wall,

6 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
the day he took a shower it was Internacional’s goal, the day he didn’t take it, it was Grêmio’s goal. In this way, try to adapt to what the old person likes, as this will be a stimulus and will avoid discussions; one should never try to contradict the old person [...]” (A10)
“The bathing schedule and negotiations must be implemented [...]” (A11)
(Geronto) Cognitive stimulation technologies: games, books and manual activities
For academics participating in this research, the (geronto) used in product form are relevant, with the purpose of cognitive stimulation of old people. Among these, memory games, such as crosswords, books and manual activities, such as knitting, stood out.
“[...] stimulating memory with memory games [...] performing activities such as crosswords, when still not in a more advanced stage” (A1).
“[...] always stimulating them with books, tours [...]” (A2)
“[...] offering reading materials, or knitting needles to make them feel important and useful [...]” (A4)
“[...] it is also good to continue stimulating these old people with memory games” (A6).
“[...] always working with the old person’s cognitive, with activities that they liked to do before, or even memory game [...]” (A9)
“Activities that stimulate thinking, memory, such as games” (A12).
Dialogue, memories and negotiations: (geronto) PKS technologies for cognitive stimulation
(Geronto)Technologies for the cognit ive stimulation of the old person were also suggested in the form of process/knowledge and strategy, such as dialogue, stimulation of memories and negotiations. In addition, patience, the need to maintain autonomy and independence for ADLs and Instrumental
Activities of Daily Living (IADLs), such as cooking, brushing teeth and performing body hygiene alone.
“[...] try to talk to the person with Alzheimer’s as much as possible, bring current information, even more if they were people who liked to get information, news” (A1).
“[...] try to never upset the person, if the old person does not feel at home, take a walk with them, until they feel they have arrived home, be very patient, answer as many times as necessary [...]” (A4)
“[...] try to maintain their autonomy and independence, such as cooking, brushing teeth, bathing alone, always with a lot of dialogue and with the supervision of the caregiver” (A9).
“[...] talk a lot with the old person and bring memories to make them as comfortable as possible [...]. The caregiver should never contradict or say that the old person with Alzheimer’s disease is wrong, as they [old person] will be agitated; the caregiver must always adapt to their reality” (A11).
Accompany the old person and advise neighbors about AD: (geronto) PKS care-educational technology
The monitoring of the old person to go out on the street, without, however, them noticing being accompanied due to their illness, was suggested as (geronto)technology in the form of process/knowledge/strategy. The orientation of neighbors about AD and the request that they communicate to the family member/caregiver if they see the old person alone on the street was also suggested by academics, as (geronto) educational-care technology in the form of PKS.
“[...] when the old person goes out on the street, go behind them, discreetly, or find an excuse to accompany them [...]” (A2)
“Always find a way to accompany them when they leave the house, warn all neighbors about the old person having Alzheimer’s, explain about the disease and guide them to, when they suspect or find them lost, call the family member [...]” (A4)

7 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
Division of responsibilit ies: (geronto) PKS technology for family members/caregivers
Another (geronto)technology in the form of process/knowledge/strategy suggested refers to the division of responsibilities, alternation of care, in addition to time off for the family member/caregiver, which denotes the understanding of care for the caregiver by the academics of Health area.
“[...] alternate care with another person at least once a week, so that the family caregiver can rest one day, as it is a very exhausting job [...]” (A3)
“It is also necessary to share the responsibilities with the family, not only overburden anyone [...]” (A4)
“[...] it is always good to leave a day off for the caregiver because, as they will be constantly with the old person, they will be exhausted. So, with at least one day off, the risk of getting sick will already decrease” (A10).
DISCUSSION
The awareness and training workshop developed in this research, enabled the identification of (geronto) technologies divided into two groups: in the form of product and the process/knowledge/strategy. The (geronto)technologies in the form of a product are characterized by equipment, machines and the materialization of care strategies. In the form of process/knowledge/strategy, there are the various tools, not materialized, used to care for the old people6.
One of the (geronto) technologies in the form of products suggested by academics refers to the use of signs to identify objects and furniture in the old person’s home. Such (geronto)technologies have a potential impact on the health of the old person with AD, especially in the initial phase, in which language difficulties, recent memory loss and the ability to recognize places occur13.
Corroborating the data of the present research, a study developed in a municipality in the north of Ceará (CE), described that the adaptation of
the physical environment helps in maintaining the autonomy and independence of the old person with AD. Therefore, it highlights, among the (geronto)technologies aimed at the home, the signs for the identification of the rooms of the house14.
The academics suggested the organization of the medication, by means of jars, separating it by morning, afternoon and night, as well as numbering the pills on the pack, so that the number assigned on top of the pill label represents the day on which it must be ingested/administered. These (geronto)technologies are relevant in the three stages of AD, with an emphasis on the moderate or intermediate phase, characterized by increasing memory loss and the beginning of language changes, reasoning and motor difficulties, which leads to the need for constant care. And in the advanced phase, when the old person with AD has bed restriction, mutism, retention and or intestinal/urinary incontinence14.
In these phases, the number of medications tends to increase due to the manifestations of the disease. Thus, the organization of medication is necessary for the care of the old person. However, the success in the use of (geronto)technologies will be greater if they are developed/used according to the needs of each old person, assisting family members/caregivers in the administration of medications6.
The badge containing the name of the old person, the information that they live with AD, as well as the phone number of a family member/caregiver was also suggested by the academics, as (geronto)technology in the form of a product. Similar data was evidenced in a research that aimed to identify the gerontechnologies developed/used by family members/caregivers as care strategies for the old person/family with AD6. In the research in question, family members developed an identification badge or bracelet for the old person, with the family’s telephone contact. Thus, if the old person left home and did not remember the way to return, people could help them, through the information of the badge/bracelet6.
Support bars, rounders for furniture corners, non-slip rugs and various adaptations in cutlery, at the height of furniture and in the toilet seat were also (geronto) technologies suggested by academics

8 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
in health courses. Similar data was evidenced in a study that aimed to know challenges and care technologies developed by family members/caregivers of patients with AD15.
By its nature, it is understood that the badge, the support bars, as well as the other (geronto)technologies used with the objective of physical security of the old person have a greater impact on the intermediate stage of AD, since the old person still maintains autonomy and independence, but already has a marked limitation. Thus, it is possible that they leave home and get lost along the way due to cognitive decline, as well as suffering physical injuries resulting from functional impairment.
Also due to cognitive impairment, it is common for old people with AD, in the intermediate stage of the disease, to refuse to bathe or argue that they have already done so4. In this regard, the academics suggested as (geronto)technology, in the form of a product, the use of a device called the bathing schedule. This (geronto)technology was presented, for the first time, by Brazilian nurses and has the potential to assist in the old person’s acceptance of body hygiene, reducing irritability, in addition to reducing the burden on family members/caregivers16. The schedule can serve as an explanation for the construction of other forms of (geronto)technologies, according to the preferences of each person16.
Still on the cognitive aspect, the academics suggested (geronto) technologies for the purpose of cognitive stimulation of old people. Among the products suggested for this purpose, memory games stood out; crosswords; books and manual activities, such as knitting. A study carried out with 31 old people, with a focus on promoting active and healthy aging, showed that the use of cognitive gerontechnologies is positive and they act as tools that facilitate nursing care for the old person17.
For cognitive stimulation, (geronto)technologies in the form of process/knowledge/strategies were also referred to, of which dialogue, stimulation of memories and negotiations with the old person stood out. A study that aimed to know the challenges and technologies of care developed by caregivers of people with AD describes that dialogue and the
stimulation of memories from the past are important tools for the attempt to maintain cognition for a longer time, aiming at prolonging integration and social connection of the old person15.
It is suggested that these (geronto)technologies be employed from the initial stage of the disease, as it is understood that the greater the cognitive stimulation of the old person, the greater the preservation of cognition or the slowing of neuronal degradation. Cognitive performance involves mental functioning, including perception, attention, memory, reasoning, decision making, problem solving and formation of complex structures of knowledge18, which suffer a considerable decline in the intermediate stage of AD.
With regard to the safety of the old person, the academics suggested that they be monitored when they go out on the street, without, however, them realizing that they are being monitored due to their illness. In addition, they signaled the need for guidance for neighbors about AD and the request that they communicate to the family member/caregiver, if they see the old person alone on the street. These data were also evidenced in other research4,6.
This (geronto)technology in the form of PKS has a considerable impact on the health of the old person with AD. It should be noted that the more autonomy and independence the old person has, the longer their functionality will be preserved. Functional capacity can be defined as the ability to perform ADLs, which are divided into basic activities of daily living (BADLs), which include the ability to perform personal hygiene, sphincter control and feeding; and instrumental activities of daily living (IADLs), comprised of the ability to prepare a meal, perform housework, care for finances, correspondence and administering the medication themselves19.
Thus, there is a close relationship between functional and cognitive capacity, as well as the level of autonomy and independence with the health of the old person, and it is necessary to encourage such capacities for a longer period of time in people with AD. For that, the (geronto)technologies in the form of product and PKS demonstrate their practical applicability in this context.

9 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
Regarding the family member/caregiver, the academics suggested the need to share the responsibilities, the alternation of care and the time off for the caregiver, which denotes the understanding of care for the caregiver by academics from the health area. This data corroborates with the study that describes that the daily care of an old person with AD produces emotional, psychological and financial stress, due to the high demand for care time that the old person derives from the loss of cognitive functions, pointing out the need for support and care for family members/caregivers20-21.
This research had limitations, of which the scarcity of bibliographies on technologies related to the theme of AD in old people and families stands out. From the results obtained, the contribution of this research to the teaching and practice of gerontology and geriatrics in health courses is evident, since it helped in the teaching process during the training of professionals from different centers, which will possibly have an impact on care for old people/families.
CONCLUSION
The study made it possible to describe suggestions for (geronto) care technologies for old people with Alzheimer’s disease and their families, based on awareness and training workshops. They were divided into two groups: that of (geronto)technologies in the form of a product; and process/knowledge/strategy.
In the form of process/knowledge/strategy, dialogue, stimulation of memories and negotiations with the old person are found mainly; the monitoring of the old person when going out on the street, without them realizing that they are being monitored due to their illness; and the orientation of neighbors about Alzheimer’s disease. These (geronto)technologies can be used in patients with dementia in the early and intermediate stages, since in these stages, old people still have the ability to remember past events and have cognitive and motor conditions for walking.
The division of responsibilities, alternation of care and time off for the caregiver were also evidenced in this research as (geronto) technologies in the form of process/knowledge/strategy. They are important in all stages of Alzheimer’s disease, especially in the advanced stage, when the demands for care become constant and more exhausting for caregivers.
In the form of a product, the identification signs of objects and rooms are grouped; the identification badge; support bars, rounders, non-slip mats; the bathing schedule; games, books and manual activities for cognitive stimulation of old people. Such (geronto) technologies can be used especially in the initial and intermediate stages of the disease. Devices such as pots for organizing medications have a greater contribution in the moderate and severe stages, moments when the old person no longer administer their medication regimen alone. Various adaptations, such as devices for raising the height of the bed and the toilet, are (geronto)technologies with the greatest contribution in the advanced stage of the disease, when the old person is restricted to the bed or with marked motor limitation.
It was possible to observe that the (geronto)technological models of the strategies adopted in this study can be incorporated into the day-to-day care of patients with dementia, as long as they are previously evaluated regarding their evolutionary phase. It is understood, in this context, that the (geronto)technologies suggested by academics can directly contribute to care, making it possible to improve the daily lives of old people and family members/caregivers.
It is suggested that research be developed, in different scenarios, in order to assist in the production of knowledge about aging, Alzheimer’s disease and in the strengthening and expansion of (geronto) care technologies.
Edited by: Ana Carolina Lima Cavaletti

10 of 10
(Geronto)Technologies of care for old people and families
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200129
REFERENCES
1. Warmling AMF, Santos SMA, Mello ALSF. Home-based oral healthcare strategies of elderly people with Alzheimer’s disease. Rev Bras Geriatr Gerontol. 2016;19(5):851-60. Available from: https://doi.org/10.1590/1809-98232016019.160026 .
2. de Falco A, Cukierman DS, Hauser-Davis RA, Rey NA. Doença de Alzheimer: hipóteses etiológicas e perspectivas de tratamento. Quim Nova. 2016;39(1):63-80. Available from: http://dx.doi.org/10.5935/0100-4042.20150152 .
3. Manzini CSS, Vale FSC. Emotional disorders evidenced by family caregivers of older people with Alzheimer’s disease. Dement Neuropsychol. 2020;14(1):56-61. Available from: https://doi.org/10.1590/1980-57642020dn14-010009
4. Ilha S, Backes DS, Santos SSC, Gautério-Abreu DP, Silva BT, Pelzer MT. Alzheimer’s disease in elderly/family: Difficulties experienced and care strategies. Esc Anna Nery. 2016;20(1):138-46. Available from: https://doi.org/10.5935/1414-8145.20160019 .
5. Brasil. Portaria nº 2.528 de 19 de outubro de 2006. Aprova a Política Nacional de Saúde da Pessoa Idosa. Saúde Legis. 2006. Available from: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2006/prt2528_19_10_2006.html
6. Ilha S, Santos SSC, Backes DS, Barros EJL, Pelzer MT, Gautério-Abreu DP. Gerontechnologies used by families/caregivers of elderly people with Alzheimers: contribution to complex care. Texto Contexto Enferm. 2018;27(4):e5210017. Available from: http://dx.doi.org/10.1590/0104-07072018005210017
7. Ilha S, Santos SSC, Backes DS, Barros EJL, Pelzer MT, Oliveira AMN. Educational and care-related (geronto) technology in Alzheimer’s disease and in supporting the elderly/family: perspective of teachers and students. Esc Anna Nery Rev. 2017;21(2):e20170039. Available from: https://doi.org/10.5935/1414-8145.20170039
8. Carleto DG, Santana CS. Relações intergeracionais mediadas pelas tecnologias digitais. Rev Kairós. 2017;20(1):73-91. Available from: https://doi.org/10.23925/2176-901X.2017v20ilp73-91
9. Brasil. Ministério da Saúde, Secretaria de Ciência, Tecnologia e Insumos Estratégicos, Departamento de Ciência e Tecnologia. Agenda nacional de prioridades de pesquisa em saúde [Internet]. Brasília, DF:MS; 2018 [acesso 20 março 2020]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/agenda_prioridades_pesquisa_ms.pdf
10. Franco MAS. Pedagogia da pesquisa-ação. Educ Pesqui. 2005;31(3):483-502. Available from: : http://www.scielo.br/pdf/ep/v31n3/a11v31n3.pdf .
11. Moraes R, Galiazzi MC. Análise textual discursiva. 2ª ed. Ijuí: Editora Unijuí; 2011.
12. Brasil. Resolução nº 466, de 12 de dezembro de 2012. Aprova Diretrizes e normas regulamentadoras de pesquisa em seres humanos. Diário Oficial da União, nº 12. 13 jun. 2013. Seção 1. p. 59.
13. Vizzachi BA, Daspett C, Cruz MGS, Horta ALM. Family dynamics in face of Alzheimer’s in one of its members. Rev Esc Enferm USP. 2015;49(6):933-8. Available from: http://dx.doi.org/10.1590/S0080-623420150000600008
14. Goyanna NF, Freitas CASL, Brito MCC, Netto JJM, Gomes DF. Elderly with alzheimer’s disease: how they live and notice the attention in the health strategy of the family. Rev Pesqui. 2017;9(2):379-86. Available from: https://doi.org/10.9789/2175-5361.2017.v9i2.379-386
15. Vizzachi BA, Daspett C, Cruz MGS, Horta ALM. Family dynamics in face of Alzheimer’s in one of its members. Rev Esc Enferm USP. 2015;49(6):933-8. Available from: : http://dx.doi.org/10.1590/S0080-623420150000600008.
16. Schmidt MS, Locks MOH, Hammerschmidt KSA, Fernandez DLR, Tristão FR, Girondi JBR. Challenges and technologies of care developed by caregivers of patients with Alzheimer’s disease. Rev Bras Geriatr Gerontol. 2018;21(5):601-9. Available from: https://doi.org/10.1590/1981-22562018021.180039 .
17. Ilha S, Santos SSC, Backes DS. AMICA: (Geronto)Tecnologia cuidativo-educacional complexa no contexto da Doença de Alzheimer. Curitiba: CRV; 2017.
18. Plympio PCAP, Alvim NAT. Board games: gerotechnology in nursing care practice. Rev Bras Enferm [Internet]. 2018;71(suppl 2):818-26. Available from: https://doi.org/10.1590/0034-7167-2017-0365
19. de Moraes EM, de Moraes FL, Lima SDPP. Características biológicas e psicológicas do envelhecimento. Rev Med Minas Gerais. 2010;20(1):67-73. Available from: http://www.observatorionacionaldoidoso.fiocruz.br/biblioteca/_artigos/197.pdf
20. Moraes EN, Moraes FL. Coleção Guia de Bolso em Geriatria e Gerontologia: Avaliação multidimensional do Idoso. 5ª ed. Belo Horizonte: Folium; 2016.
21. Carraro PFH, Magalhães CMC, Carvalho PD. Qualidade de vida de cuidadores de idosos com diagnóstico de Alzheimer e o emprego de acupuntura: revisão de Literatura. Mudanças Psicol Saúde. 2016;24(2):65-70. Available from: http://dx.doi.org/10.15603/2176-1019/mud.v24n2p65-70

1 of 8
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
http://dx.doi.org/10.1590/1981-22562020023.200214
Analysis of the association between hand grip strength and functionality in community old people
Mariana Edinger Wieczorek1
Cislaine Machado de Souza1
Patrícia da Silva Klahr1
Luis Henrique Telles da Rosa1
Keywords: Elderly Population. Muscle Strength. Muscle strength dynamometer. Physical Functional Performance. Walk test.
AbstractObjective: To analyze the association between hand grip strength (HGS) and physical ability tests by healthy, non-institutionalized old people. Method: This is a cross-sectional research. The sample comprised 36 old people (66.69±4.84 years), and they all responded two questionaires, one containing a cognitive assessment and another to assess the level of physical activity, in addition to sociodemographic data and health conditions. The HGS was measured using the JAMAR hydraulic dynamometer, and the six-minute walk test (6MWT) and the Timed Up and Go (TUG) test were carried out to assess the submaximal cardiorespiratory capacity during displacement and body mobility. Results: The Pearson coefficient allowed to verify the weak and significant association between the HGS and the 6MWT (p=0.05) and TUG (p=0.027) variables. Conclusion: The HGS showed a weak but significant correlation with the physical ability tests. Therefore, it can be used when contextualized with other variables to assess the functionality in old people in the community.
1 Universidade Federal de Ciências da Saúde de Porto Alegre, Departamento de Fisioterapia, Programa de Pós-Graduação em Ciências da Reabilitação. Porto Alegre, RS, Brasil.
The authors declare there are no conflicts of interest in relation to the present study.No funding was received in relation to the present study.
CorrespondenceMariana Edinger [email protected]
Received: July 22, 2020Approved: November 19, 2020
ID
ID
ID
ID

2 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
INTRODUC TION
The aging process is naturally followed by several multifactorial and progressive changes. Among these, there are not only physiological and metabolic transformations, but also structural and functional ones. The declines resulting from the aging process as well as the dysfunctions and diseases prevalent in this age group can compromise the functionality, independence and quality of life of the old people1-4.
The loss of muscle mass and consequently muscle strength and power is the main responsible for the deterioration in mobility and functionality of the aging individual2-4. Old people have decreased muscle strength due to muscular, neurological, endocrine or environmental mechanisms2,5. The decline in strength and mobility of the old person interferes with the performance of essential activities for functional performance, such as walking, sitting, standing up, climbing stairs, among others1,4.
The hand grip strength (HGS) has been used as a general indicator of muscle strength and power in clinical practice6,7. In addition, the assessment of HGS is used as an indicator of global strength8,9
and functionality7,8. However, not all studies have been able to demonstrate the existence of significant correlations between HGS and physical capacity10,11. There are several ways to assess the physical capacity of old people, often by inference, as it is known that the worse the health status, the greater the negative impact on mobility, the ability to carry out a submaximal task, and the independence of the old person12-15.
Muscle groups that are essential to support body weight such as trunk and lower limb stabilizing muscles are usually used to perform functional tests11-13. Performance is due to the ability to generate strength in a given test time (slow contraction fibers type I), whereas the HGS assesses the peak muscle strength of the upper groups (fast contraction fibers type II) that are less resistant to fatigue12,13. In general, physical ability tests involve tasks requiring postural, mobility, and displacement transfer11,13,14,16.
There are still gaps in the relation between HGS and the functionality of the old person10,11. There are physiological factors related to the aging
process concomitant to reduced strength and motor control, such as proprioceptive alterations in the sensory receptors, neuromuscular and vestibular function, and visual acuity, which directly affect mobility, gait performance, and postural control15,16. The applicability of HGS as a unique indicator for assessing the physical capacity in people over 60 years old is questionable. The present study aimed to analyze the correlation between HGS and the physical ability tests in healthy old people in the community.
METHOD
This is an observational study with a cross-sectional design approved by the Research Ethics Committee of Universidade Federal de Ciências da Saúde de Porto Alegre under the protocol number 2,137,840/2017. The present study integrates a larger research on the subject of functionality of old people developed at the institution by the Study Group in Rehabilitation (GEReab).
The sample was calculated using the WinPepi software havig the study by Merchant, et al. 201615 as a reference, considering a standard deviation of 5.93kg for hand grip strength, and adopting an acceptable difference of 2kg; confidence level of 95%, and significance level set at 5% (p≤0.05). Therefore, the number of old people should be at least 37.
The individuals were recruited by social media (Facebook and Instagram), and local publicity actions with flyer distribution (distributed in parks in the city of Porto Alegre, RS, Brazil) and billboards (in the surroundings of the most central area of the City, close to the University). Individuals aged 60 years or over were included. Healthy individuals who had autonomy and independence, and with controlled chronic diseases and physical symptoms were considered for the inclusion criteria17. Old people in the postoperative period of any nature, with physical or mental diseases or deficits characterizing a process of pathological aging that prevented the tests were excluded.
The sociodemographic and clinical variables of interest were gender, age, weight and height, body mass index, education, health problems, medication

3 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
use, occupational and social activities, and physical exercise. The Mini Mental State Examination (MMSE)18 was applied for to assess the cognition of the old people, with the following cutoff points being used: 18 points for illiterates, 21 for those with education between one and three years, 24 for individuals between four and seven years of formal education, and 26 for people with more than seven years of education. To assess the level of physical activity, the International Physical Activity Questionnaire (IPAQ)19, short form, was applied. This version presents seven questions whose information estimates the time spent per week in different domains of physical activity, such as work, means of transportation, domestic activities, recreation, sport or leisure, and time spent sitting. The final classification determines individuals as sedentary, irregularly active, active, and very active20.
To ensure the quality of the assessment protocol, the researchers responsible for data collection were properly trained. Both the initial interview and the protocol for test application to the individuals included in the research took place at the Physical Therapy Laboratory of Universidade Federal de Ciências da Saúde de Porto Alegre from January 2018 to July 2019. The hand grip strength test and functional tests were applied on the same day. The individuals participating in the research were informed about the procedures and signed the Informed Consent Form (ICF).
Hand grip strength (HGS)
A JAMAR portable hydraulic dynamometer21 was used to measure the hand grip strength. The individual was measured sitting on a chair with a backrest and no armrests. The shoulder of the limb tested was adducted and in neutral rotation, elbow flexed at 90 degrees, forearm in neutral position, and wrist between 0 and 30 degrees of extension and between 0 to 15 degrees of ulnar deviation6,21,22.
There was a demonstration of how the test should be performed for the participants to be familiarized with the equipment, then there was a simulation. During the test, there was encouragement by standardized verbal commands. Participants were instructed to contract to the maximum using their dominant
hand6,22. They were measured three times, and the best performance among the three attempts was the reference6,22. There was a rest interval of 30 seconds after each attempt21.22. Some factors can hinder the establishment of normative values of HGS, among which can be mentioned gender, age, dominance, time of assessment, body position, and anthropometric characteristics6,21,22.
Six-minute walk test (6MWT)
It measures the maximum distance covered in the 6-minute period, and is commonly used to assess submaximal cardiorespiratory capacity during activities requiring displacement14. The test was applied as recommended by the American Thoracic Society23; briefly: the subjects were instructed to walk from side to side in a 30-meter long hall for a period of 6 minutes, being instructed to walk as fast as possible, but without running. Before starting the test, blood pressure (BP), peripheral oxygen saturation (SpO2), Borg scale, heart rate (HR), and respiratory rate (RR) were measured. The variables were measured again after the end of the test. The evaluator walked throughout the test a little behind the individual who was monitored throughout the period by the oximeter. During the test, all participants were verbally encouraged in a pre-established manner every one minute. Anyone feeling tired could slow down the pace or even stop, if necessary, but the timer was not stopped during rest. After 6 minutes, the individual was instructed to stop, and the distance traveled on the last lap was measured.
Timed Up and Go (TUG) Test
It indicates the functional mobil ity, the performance of which is related to the gait, postural and direction changes during the walk, being evaluated throughout the time spent on the test13,14. For the test, a chair with a backrest was positioned, and the individual was asked to get up from the chair without hand support, cover a distance of 3 meters, turn around, and return to sit on the chair again. During the test, the timer was started when the participant got up from the

4 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
chair, and interrupted when their back toutched the backrest. TUG time was measured in seconds (s). Each participant could practice beforewards to become familiar with the task24.
Quantitative variables were expressed as mean ± standard deviation. Initially, the Shapiro-Wilk test was carried out to verify the normality of the data, which was confirmed (p>0.05). The descriptions of the qualitative variables were expressed in absolute and relative frequencies. Pearson’s correlation coefficient was used to verify the correlation between the HGS and the 6MWT and TUG physical ability
tests. To compare the other variables of the tests, the Student’s t test was used for dependent samples. The level of significance adopted was p≤0.05.
RESULTS
Table 1 lists the characteristics of the sample studied. All survey participants declared to be retired or pensioners; of these, 21 (58.33%) reported having another occupation, and 3 (8.33%) informal work. The 26 (72.22%) old people participating in social activities reported having mostly religious commitments and participation in craft groups.
Table 1. Characterization of the sample of 36 healthy old people. Porto Alegre, RS, 2019.
Quantitative variables Mean and SD±Age (years) 66,69 (± 4,84)Height (m) 1,6 (± 0,08)Weight (kg) 76,85 (± 14,4)BMI (Kg/m2) 29,9 (± 5,26)
Years of education 15,21 (± 3,7)MMSE 24 (± 9)Qualitative variables n (%)GenderFemale 30 (83,33)Male 6 (16,67)ActivitiesOccupation 21 (58,33)Informal employment 3 (8,33)Social activities 26 (72,22)Leisure activities 9 (25,00)Physical exerciseTakes walks 7 (19,44)Lifts weight 1 (2,78)IPAQ classificationVery Active 2 (5,55)Active 3 (8,33)Irregularly active A 10 (27,78)Irregularly active B 17 (47,22)Sedentary 4 (11,11)
Many quantitative variables were expressed as Mean = mean and SD = standard deviation. Qualitative variables expressed in n = absolute frequency and % = relative frequency. BMI = Body Mass Index; MMSE = Mini Mental State Examination; IPAQ = International Physical Activity Questionnaire.

5 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
Table 2. Results of the Hand grip strength and Physical ability tests. Porto Alegre, RS, 2019.
Tests Mean and SD±
Hand grip strength (kgf) 30,22 (± 8,36)
Six-minute Walk Test (m) 455,17 (± 90,41)
Timed Up and Go (s) 6,89 (± 1,6)
Mean = arithmetic mean, and SD = standard deviation.
The results for the tests are shown in Table 2. All old people participating in the survey were able to complete the physical ability tests without interruption. Table 3 shows the variables analyzed in the 6MWT pre and post test, and the scores show that there was an adequate response to exercise.
Table 4 shows the correlation between the HGS and the results of the 6MWT (distance covered in meters) and in the TUG (travel time in seconds). The results of Pearson’s coefficient revealed the existence of a weak but significant correlation between HGS and functionality measured in the physical ability tests.
Table 3. Variables of the 6-minute walk test in the pre and post test moments. Porto Alegre, RS, 2019.
Variables Pre-testMean and SD±
Post-testMean and SD± *p
SpO2 (%) 97 (± 1,84) 97,68 (± 1,20) 0,010Heart rate (bpm) 77,15 (± 10,68) 82,5 (± 10,62) 0,004SBP (mmHg) 131,88 (± 16,71) 140,35 (± 19,79) 0,003DBP (mmHg) 77,5 (± 9,77) 82,18 (± 10,01) 0,003RF (irpm) 17,5 (± 2,69) 20,56 (± 3,26) 0,000
SpO2 = Oxygen saturation; HR = heart rate; SBP = systolic blood pressure; DBP = diastolic blood pressure; RF = respiratory frequency; *Student’s t test for paired samples; p= level of significance.
Table 4. Correlation between hand grip strength and physical ability tests in 36 old people. Porto Alegre, RS, 2019.
Pearson's Correlation TestHand grip strengthr p
Six-minute Walk Test 0,324 0,05Timed Up and Go -0,385 0,027
r = Pearson’s correlation; p = level of significance.
DISCUSSION
By analyzing the results of the present study, we can see that the HGS measure can be associated with the functional physical capacity of the old person in the community. Other studies have already shown positive associations between HGS and functional tasks. In their study, Geraldes et al.10 show a moderate correlation between HGS and performance in motor tasks. This association proved to be stronger with
the set of tests than with each one taken in isolation. This result is probably due to the study also presents function tests with fine motor skills such as taking and putting the key in a lock and taking and replacing a lamp in a nozzle, in addition to the physical ability tests such as TUG and the gait speed test, which also require some skills and strength of the upper limb.
Similarly, Oliveira et al.7 showed in their study that the HGS serves as an indicator of functionality

6 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
related to ADL’s and IADL’s. The results were obtained with the use of the Barthel Index and the Lawton and Brody Scale, which classify the activities carried out by the old people according to a score. Many of the motor activities present on the scales such as feeding, locomotion, personal hygiene, administration of social, economic and self-care functions are verified by means of interviews or simple tests of functional performance within the usual environment where the old person lives.
In scientific research and clinical practice, HGS and leg extension strength (isokinetic dynamometer) seem to be adequate for the global tracking of muscle weakness in the old people16,25. However, there is a differential decline in the motor units between static and dynamic muscle fibers, and asymmetric loss of muscle trophism with muscular atrophy of the lower limb exceeding the upper limb11,26. In addition, some conditions prevalent in the old people such as pain complaints, biomechanical alterations, neuropathies, deformities, among others, can also influence the results obtained with dynamometry11.
Felicio, et al.11 observed that the HGS did not show any correlation between the variables assessed by the isokinetic dynamometer - considered the gold standard - in assessing muscle strength, showing that HGS should not be used indiscriminately since other factors must also be taken into account regarding the use of HGS as a representative measure of functionality.
On the other hand, in the study by Alonso et al.16, the lowest HGS was correlated with the worst performance of mobility and dynamic postural balance in the TUG, and significantly correlated with muscle strength in the lower limbs, suggesting that the HGS could be used as a substitute indicator of global muscle strength for screening among older women.
Muscle strength is not the only determinant decline in functionality. According to the World report on aging and health, 201527, functionality is also characterized by intrinsic factors refering to the physical and mental characteristics that the individual develops during the course of their life, and this is influenced in turn by extrinsic factors determined by the context of life in which the old person is inserted,
and built through personal relationships, attitudes, values, systems, and health and social policies reflecting as positive or negative factors in their functionality.
Regarding the characteristics of the sample, only 3 (8.33%) old people were classified as physically active, and 2 (5.55%) as very active. According to Lenardt et al. 28, men and women over 60 with a lower level of physical activity also have less muscle mass, and consequently a higher prevalence of physical disability. In this sense, Martin et al.29 argue that physical inactivity can contribute to the functional loss of the old people due to the physiological alteration of muscle mass and strength, thus decreasing the physical performance and fitness.
The present study with healthy old people compared to cutoff points already established in the literature showed that the mean values of HGS 30.22 Kgf (±8.36) and physical ability tests 6MWT 455.17m (±90.41) and TUG 6.89s (±1.6) were considered relatively high for this population30-32. This is probably due to the significant number of old people in the study participating in social activities - 26 (72.22%) - and having some occupation - 21 (58.33%) -, which can indirectly predict greater physical capacity, thus increasing the HGS and test performance. Exercising in a systematic way contributes positively to higher levels of HGS30,33 and physical fitness28.29. However, an active behavior in other domains and activities, even if not structured but performed spontaneously during the day especially at leisure, can positively influence in the same way33.
Exploring a tool of easy and quick applicability by health professionals for tracking the functionality of the old person is relevant. The present study excelled for its methodological rigor, quality of description, and application of the tests, as well as the selection and inclusion criteria in the research and collection of information to characterize the sample. However, a possible limitation must be considered: the fact that women correspond to almost the entire sample. This confirms the Brazilian demographic pattern in which the absolute number of women over 60 years old is greater than that of men34. HGS values are significantly higher among men, whereas the decline over the years does not occur homogeneously between genders, being greater in men than in

7 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
women35. Thus, studies with more homogeneous samples and stratification by gender are suggested.
CONCLUSION
The hand grip strength presented a weak but significant correlation with the physical ability tests.
Therefore, it may be one of the factors to contribute to the outcome of functionality, but it should be used with caution to assess functionality in old people in the community. In view of the biopsychosocial context involving these individuals, the measure can be used when contextualized with other variables.
Edited by: Yan Nogueira Leite de Freitas
REFERENCES
1. Vieira MCA, Souza CF, Câmara SMA, Matos GSR, Moreira MA, Maciel ACC. Relação entre força de preensão manual e força de membro inferior em mulheres de meia idade: um estudo transversal. Rev Bras Ativ Fis Saúde. 2015;20(5):467-75.
2. Araújo MLM, Fló CM, Muchale SM. Efeitos dos exercícios resistidos sobre o equilíbrio e a funcionalidade de idosos saudáveis: artigo de atualização. Fisioter Pesqui. 2010;17(3):277-83.
3. Mazo GZ, Liposcki DB, Ananda C, Prevê D. Condições de saúde, incidência de quedas e nível de atividade física dos idosos. Rev Bras Fisioter. 2007;11(6):437-42.
4. Mendonça CS, Moura SKMSF, Lopes DT. Benefícios do treinamento de força para idosos: revisão bibliográfica. Rev Campo Saber. 2018;4(1):74-87.
5. Martinez BP, Camelier FWR, Camelier AA. Sarcopenia em idosos: um estudo de revisão. Rev Pesqui Fisioter. 2014;4(1):62-70.
6. Dias JA, Ovando AC, Külkamp W, Junior NGB. Força de preensão palmar: métodos de avaliação e fatores que influenciam a medida. Rev Bras Cineantropom Desempenho Hum. 2010;12(3):209-16.
7. Oliveira EN, Santos KT, Reis LA. Força de preensão manual como indicador de funcionalidade em idosos. Rev Pesqui Fisioter. 2017;7(3):384-92.
8. Mattioli RA, Cavalli AS, Ribeiro JAB, Silva MC. Associação entre força de preensão manual e atividade física em idosos hipertensos. Rev Bras Geriatr Gerontol. 2015;18(4):881-91.
9. Santos LB, Vilela ABA, Santos CA, Lessa RS, Rocha SV. Sensibilidade e especificidade da força de preensão manual como discriminador de risco para multimorbidades em idosos. Cad Saúde Colet. 2018;26(2):146-52.
10. Geraldes AAR, Oliveira ARM, Albuquerque RB, Carvalho JM, Farinatti PTV. A Força de Preensão Manual é Boa Preditora Do Desempenho Funcional de Idosos Frágeis: um Estudo Correlacional Múltiplo. Rev Bras Med Esporte 2008;14(1):12-6.
11. Felicio DC, Pereira DS, Assumpção AM, Jesus-Moraleida FR, Queiroz BZ, Silva JP, et al. Poor correlation between handgrip strength and isokinetic performance of knee flexor and extensor muscles in community-dwelling elderly women. Geriatr Gerontol Int. 2014;14:185-9.
12. Santos PHG, Pereira JE, Soares WN, Colato H. Potência muscular e sua relação com a autonomia funcional de idosos participante de programas sociais de um município da Amazônia Legal. Rev Bras Prescriç Fisiol Exerc. 2018;12(75):488-95.
13. Wamsera EL, Valderramas SR, Paula JA, Schieferdecker MEM, Amarante TP, Pinotti F, et al. Melhor desempenho no teste timed up and go está associado a melhor desempenho funcional em idosas da comunidade. Geriatr Gerontol Aging 2015;9(4):138-43.
14. Pedrosa R, Holanda G. Correlação entre os testes da caminhada, marcha estacionária e TUG em hipertensas idosas. Rev Bras Fisioter. 2009;13(3):252-6.
15. Merchant RA, Banerji S, Singh G, Chew E, Poh CL, Tapawan SC, et al. Is Trunk Posture in Walking a Better Marker than Gait Speed in Predicting Decline in Function and Subsequent Frailty? J Am Med Dir Assoc. 2016;17(1):65-70.
16. Alonso AC, Ribeiro SM, Luna NMS, Peterson MD, Bocalini DS, Serra MM, et al. Association between handgrip strength, balance, and knee flexion/extension strength in older adults. PLoS One. 2018;13(6):e0198185.

8 of 8
Association between hand grip strength and functionality in old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200214
17. Valer DB, Bierhals CCBK, Aires M, Paskulin LMG. O significado de envelhecimento saudável para pessoas idosas vinculadas a grupos educativos. Rev Bras Geriatr Geronto.l 2015;18(4):809-19.
18. Melo DM, Barbosa AJG. O uso do Mini-Exame do Estado Mental em pesquisas com idosos no Brasil: uma revisão sistemática. Ciênc Saúde Colet. 2015;20(12):3865-76.
19. Matsudo S, Araujo T, Matsudo V, Andrade D, Andrade E, Oliveira LC, et al. Questionário internacional de atividade física (IPAQ): estudo de validade e reprodutibilidade no Brasil. Rev Bras Ativ Fis Saúde. 2001;6(2):5-18.
20. Kolchraiber FC, Rocha JS, César DJ, Monteiro OO, Frederico GA, Gamba MA. Nível de atividade física em pessoas com diabetes mellitus tipo 2. Rev Cuid. 2018;9(2):2105-16.
21. Reis MM, Arantes PMM. Medida da força de preensão manual - validade e confiabilidade do dinamômetro saehan. Fisioter Pesqui. 2011;18(2):176-81.
22. Figueiredo IM, Sampaio RF, Mancini MC, Silva FCM, Souza MAP. Teste de força de preensão utilizando o dinamômetro Jamar. Acta Fisiatr. 2007;14(2):104-10.
23. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166:111-7.
24. Bennell K, Dobson F, Hinman R. Measures of physical performance assessments. Arthritis Rheumatol. 2011;63(11):350-70.
25. Riviati N, Setiati S, Laksmi PW, Abdullah M. Factors Related with Handgrip Strength in Elderly Patients. Indones J Intern Med. 2017;49(3):215-9.
26. Mitchell WK, Williams J, Atherton P, Larvin M, Lund J, Narici M. Sarcopenia, Dynapenia, and the Impact of Advancing Age on Human Skeletal Muscle Size and Strength; a Quantitative Review. Front Physiol. 2012;3:260.
27. World Health Organization. World report on ageing and health [Internet]. Geneva: WHO. Available from: https://apps.who.int/iris/handle/10665/186463
28. Lenardt MH, Binotto MA, Carneiro NHK, Cechinel C, Betiolli SE, Lourenço TM. Força de preensão manual e atividade física em idosos fragilizados. Rev Esc Enferm. 2016;50(1):88-94.
29. Martin FG, Nebuloni CC, Najas MS. Correlação entre estado nutricional e força de preensão palmar em idosos. Rev Bras Geriatr Gerontol. 2012;15(3):493-504.
30. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2). Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2018;1-16.
31. Britto RR, Sousa LAP. Teste de caminhada de seis minutos uma normatização brasileira. Fisioter Mov.2006;19(4):49-54.
32. Rodrigues RAS, Teodózio MM, Espinosa MM, Fett WCR, Melo CD, Fett CA. Timed up and go test and self-perceived health in elderly: population-based study. Rev Bras Cineantropom Desempenho Hum. 2018;20(3):247-57.
33. Lima TR, Silva DAS, Kovaleski DF, González-Chica DA. Associação da força muscular com fatores sociodemográficos e estilo de vida em adultos e idosos jovens no Sul do Brasil. Ciênc Saúde Colet. 2018;23(11):3811-20.
34. Sousa NFS, Lima MG, Cesar CLG, Barros MBA. Envelhecimento ativo: prevalência e diferenças de gênero e idade em estudo de base populacional. Cad Saúde Pública. 2018;34(11):e00173317.
35. Wearing J, Konings P, Stokes M, Bruin ED. Handgrip strength in old and oldest old Swiss adults: a cross-sectional study. BMC Geriatr. 2018;18:266.

1 of 9
Origi
nal A
rticles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
http://dx.doi.org/10.1590/1981-22562020023.200028
Aesthetics and happiness in the perception of old people users of beauty products
Sabrina Fernanda Romanssini1
Helenice de Moura Scortegagna1
Nadir Antonio Pichler1
Keywords: Women. Aesthetics. Happiness. Health of the Elderly.
Abstract Objective: To identify the relationship between aesthetics and happiness in the perception of old people users of beauty products. Method: This is an exploratory and descriptive research, of qualitative nature, through a semi-structured interview, with 21 women aged ≥60 years. The information was synthesized according to the thematic content analysis of Bardin. Results: The participants mentioned that there are connections between aesthetics and happiness, conceiving them as inner beauty, generating subjective well-being, because they are linked to the goods of the soul, character, love, respect for others, reciprocity, humility, ethics, joy and dialogue, way of being and acting, in contemplating nature, in relationships trust and coexistence with others and belief in God and the care of the spirit, of the mind. They considered interior beauty more significant than the exterior, which is focused on the body, facial, and capillary aesthetics, but without aesthetic exaggerations, since the care of body image with exterior aesthetics is a way, a means, of social insertion and search for more lasting happiness. Conclusion: a balance between inner and outer beauty is necessary to achieve happiness, but with a preponderance of the aesthetics of existence, of the inner aesthetics, which generates more happiness because it is based on self-knowledge, self-control, autonomy, personal and social fulfillment.
1 Universidade de Passo Fundo, Programa de Pós-graduação em Envelhecimento Humano. Passo Fundo, RS, Brasil.
The authors declare there are no conflicts of interest in relation to the present study.No funding was received in relation to the present study.
CorrespondenceHelenice de Moura [email protected]
Received: February 3, 2020Approved: November 20, 2020
ID
ID
ID

2 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
INTRODUC TION
The aging process is characterized by the dimensions of heterogeneity, multifactoriality and multi-causality, also part of the body experience and self-recognition, the perception of self-esteem, beauty and happiness, especially when considering that the bodily transformations, coming with aging, may deviate from the standards of aesthetics in force in society1,2. For Japiassú and Marcondes3, aesthetics is one of the areas of philosophy, which had its definition coined by Alexander Von Baumgarten, in the 18th century, to designate the study of sensation, the science of beauty, taste and subjective world, pleasant to the senses, for the purpose of elaboration of an ontology of the beautiful. Of Greek origin, aisthesis, it is a term that means the individual’s ability to receive sensitive impressions from the objects that surround him, judge its appearances and perceive how the five senses are affected by the impressions4.
According to Ferreira5, from the 20th to the 21st century, new ethical and aesthetic issues, linked to the human body, were developed from biotechnology, such as the search for aesthetic surgeries and the “eugenics” of beauty, placing public health in front of ethical issues involving aesthetics, which comprises beauty. In the last century, attitudes towards beauty and aging, as a synonym for happiness, have undergone radical changes, in which there is an exacerbated concern with the physical appearance of people, especially women5.
The job market demanded an appreciation of appearance, which required subjects to invest more in their bodies, resulting in “a world of competition in which beauty helps to conquer and maintain spaces, at the price of eternal vigilance and strict sovereignty of oneself” (p.193)5. Beauty has always been based on contemporary customs, with the influence of current aesthetic standards1. However, in this scenario, the aging process, often associated with negative images, can generate dissatisfaction in the way people perceive themselves throughout this process2. Thus, investigating the stage of old age refers to understanding old people in their entirety, as it involves multi and interdisciplinary issues of a biopsychosocial nature, since the meaning of the
changes that occur with aging depends on the act, think, question, interpret of each person2,4,6-8.
In the last decades, care for body aesthetics has become synonymous with happiness and the human body has been elevated to the category of true cultural, symbolic, social and economic capital9,10. But, after all, what does happiness consist of? For ancient and medieval thinkers, such as Socrates, Plato, Aristotle, Seneca, Saint Augustine and Thomas Aquinas, happiness is the supreme good of man. It is what people most crave in life and the search for external goods, such as money, material goods, fame, the cult of the body, aesthetic beauty, etc., produce a simple, apparent happiness, because these goods are means, instrument, path, possibility11,12. What generates more happiness are the inner goods, of the soul, such as knowledge, self-knowledge, self-control, autonomy, personal, social and political fulfillment11,12.
A study developed by Sumngern et al.13 comes close to this conception of happiness structured in the goods of the soul. They demonstrated that the old people who did not need to work in order to survive, nor were they focused on the search for external goods and excessive care for their body, considered themselves happier than those who had these concerns13.
Currently, many attributes are given to happiness. For Ferry12, the dimension of happiness has a complex nature. It is an existential project that can be carried out continuously12. In summary, the most recent empirical research, when defining happiness, including with old people, associates this concept with self-care, satisfaction with life, pleasure, contentment, health, physical, psychological and spiritual well-being and not only the search for money and external goods12-16. It is synonymous with quality of life, social insertion, freedom of choice, autonomy, healthy aging, intelligence, knowledge, functional capacity, love, emancipation, creativity, admiration, acting, wisdom, family relationships, friendships, connection with nature and a god12-16.
Aesthetic perception is relative and subjective, particular to each individual, but influenced by each person’s worldview. Adequate appearance,

3 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
satisfaction with self-image and the relentless pursuit of aesthetics have become essential requirements for obtaining quality of life and the pursuit of happiness, as they are linked with the way of perceiving yourself in relation to society2,17.
The use of techniques, aesthetic procedures and cosmetic products for the quality and longevity of old people is growing. And old people enter this market and seek these treatments18. A study carried out in France in 2013 showed that a woman is at the height of her beauty at the age of thirty; 92% said that it is possible to age “beautifully”, to be well aesthetically at 70 and 50% of them used cosmetic procedures19.
There are already several studies on the possible relationships between aesthetics and happiness or satisfaction with life1,2,6,8-10,16, which signal that old people recognize the beauty standards of society and seek to achieve them, through self-care, body image, self-esteem and self-confidence with the use of beauty products. This attitude generates empowerment, healthy aesthetics and physical, psychological and social balance, because the appreciation of the body has become a cultural and economic capital, a business card. It is also identified the need to advance in studies involving old people and the relationships of existential aesthetics. In this sense, considering that our focus is to establish a more specific relationship between aesthetics and happiness, this study aimed to identify the relationships between aesthetics and happiness in the perception of old people users of beauty products.
METHOD
This is an exploratory and descriptive, qualitative study, carried out in 2019, with old women. The inclusion criteria were: being old (age ≥60 years) and being a user of beauty products. The justification for this criterion is the understanding that there has been an increasing demand for services that include aesthetics by the old people segment of the population, especially for the female audience. In this sense, this study, linked to the research line biopsychosocial aspects of human aging, is aligned with a larger study that investigates beauty, self-image and aesthetic resources, part of the research project
Reasons for happiness in longevity, developed in the stricto sensu program in Human Aging, approved by the University’s Ethics Committee, with opinion no. 898,152.
The choice of participants was made in the format of a non-probabilistic sample. Twenty-one old women participated in the interview, who attended a social group, and who accepted to participate voluntarily. The number of participants was determined using the method of gradual theoretical sampling, in which subjects were included in the sample, until it was finalized by theoretical saturation of the topic to be investigated20. All participants signed the Free and Informed Consent Form, in compliance with Resolution 466 of December 12, 2012, of the National Health Council. In this sense, the extracts of the statements of the participants are identified with the letter P of the participant, and the Arabic numbering corresponds to the order in which the interviews were conducted.
The research was carried out through a semi-structured interview, lasting 30 minutes. The guiding questions of the interviews were designed in order to meet the objective of the study that aims at the relationship between aesthetics and happiness: What do you mean by beauty and aesthetics? Do beauty and aesthetics make you happier? What brings you the most happiness in this life? In order to hold the meetings, prior contact was made with the participants, through a visit to the coexistence group, to present the study, its purpose and invitation, upon acceptance, the interviews were scheduled on the date, time and place of the participants’ preference. The option for the location was a room in the living group itself. The record of the meetings was done through an audio recorder, and the interviews were transcribed in full later, with the guarantee of being deleted at the end of the study.
The qualitative information was submitted to Bardin’s thematic content analysis21 by a pair of specialists, who also participated in the data collection, with special attention to categorize, collate and seek agreements until reaching 100% agreement between the examiners. Thematic content analysis followed the stages of pre-analysis, content exploration and interpretation, followed by inference.

4 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
The pre-analysis consisted of the construction of the corpus, through a fluctuating reading of all the information obtained, in order to apprehend the initial ideas, paying attention to the similarities and contrasts. Then, the exploration of the content and interpretation, based on readings and re-readings of the material, sought to define the units of meaning, which were separated graphically, one in each line of a spreadsheet built for this purpose, constituting the corpus, which would be submitted, by inference, the condensation and prominence of the information for analysis, considering the completeness, representativeness, relevance and homogeneity, in the progressive refinement of the thematic categories, based on semantic criteria, which allowed to abstract and interpret what is relevant, according to the research objective.
RESULTS E DISCUSSIONS
The participants were between 60 and 68 years old. Most were married (75%) and all were retired, with monthly income of one to three minimum wages. From what emerged from the participants’ speeches, it was possible to build three categories: aesthetics as inner beauty, aesthetics as exterior beauty and family and friends as a synonym for happiness and beauty.
Aesthetics as inner beauty
The participants associated aesthetics with intrinsic dimensions, understood as the inner beauty, which is expressed by psychic well-being, love, character, reciprocity, humility, respect for others, ethics, kindness, solidarity, joy, dialogue. These virtues are manifested in the extrinsic qualities of the body, in attitudes, in the way of being and acting, as attested by the statements below:
“It is no use to be beautiful on the outside and ugly on the inside. Beauty is in the person’s heart and goodness” (P 21).
“It is the beauty inside [...], but it shows on the outside. People’s attitude of helping others” (P 16).
“It means being beautiful inside [...]. It is a set [...]. Stimulation inside and out, how to be nice, dear, friend, kind” (P 17).
“Beauty comes from within [...]. Aesthetics does not influence [...]. To see how a person is doing, look inside” (P 5).
“Beauty is to be happy [...], to greet people, to talk (P 14).
“Beauty is something inside [...]. If this one is fine, the exterior will also be fine” (P 20).
For Alves et al.,22 the aesthetic beauty of an old person is in conduct, behavior, the ability to accept the other, respect, the search for health, attention and care. A survey conducted by Albarello et al.,23 with the objective of knowing the relationship between the perception of beauty and aesthetic care, with 20 rural women in the post-menopause, demonstrated that the participants did not consider the corporal beauty standards as significant and were cautious in the use of aesthetic and cosmetic products.
The participants mentioned that inner beauty is also manifested in the person through contemplation and contact with nature, in the cultivation of gardens, in relationships of loyalty, trust and sharing in coexistence with others, in the belief in a god, in the institution and in religious rites:
“Beauty is contemplating nature, cultivating flowers, garden, plants” (P 14).
“Of course, the person has to look well, too [...], with God in the first place. He is everything [...]. Exterior aesthetics are important, but not the main” (P 3).
“Beauty is receiving the risen Jesus, going to church, taking communion [...]. Nature, the sun [...], the natural and inner beauty of the world with whom we live” (P 19).
“Beauty is nature [...]. Live and let other people live [...]. One has to be the first beauty - the heart and kindness” (P 10).

5 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
“Beauty is the people who help each other [...]. Inner beauty is the most important [...]. Outwardly beauty deceives. Being a good person and a person of God” (P 15).
“The beauty inside is the best [...]. The person becomes special [...]. Nature is also beautiful: the birds singing, the trees” (P9).
According to Fin, Portella and Scortegagna1, many old women conceive and resort to the foundations of the religious and Christian tradition to justify inner beauty. In this cultural imaginary, the inner dimension, connected to “the sensations of the sublime, the wonderful and the divine”, is valued more than body aesthetics.
According to Brito et al.24, aesthetics is a reflection around the beautiful, which encompasses the branch of aesthetic properties, the sensitive, linked to the act of feeling, imagining and art, which comprises creation, imitation, inspiration, artistic, cultural and religious value. The beautiful pleases, rejoices and achieves the sensation of pleasure provided by beauty, related to the senses. However, the experience of the beautiful is not only the sensation that causes pleasure, but the conception and apprehension that people realize through sensation. But it depends on people’s interest in relating and seeking a deeper view with objects, such as contemplating nature, religious objects and images, a flower and garden cultivation, where the pleasure felt does not come from colors, but of the action in which the eyes and the mind perceive the figure and the fixation of the eyes on everything that catches the eye.
Among the aspects of aesthetics as interior beauty highlighted in the statements above, two of them, the contemplation of God and nature, are considered in the Western philosophical tradition as promoters of happiness, because they are related to the state of mind to which man aspires, for the which both material and spiritual goods are needed11,12. God is identified as the supreme and sublime principle, a pure act, that is, without movement, immobile, eternal, source of true happiness for the human, fragile and contingent creature12. Nature, on the other hand, is valued for its aesthetic, sensitive dimension,
pleasant to the senses and the mind, as a carrier of the ontology of the beautiful3.
Aesthetics as ex terior beauty
The participants, in addition to considering the inner beauty as a preponderant to be happy and have satisfaction in life, said that the outer beauty, with the care of body, facial and hair aesthetics is also significant and can be appreciated as a means, a balance between body and soul, intrinsic beauty, care for spirit, mind:
“Get dressed, cut your hair, get your nails done” (P 19).
“Beauty is high self-esteem [...]. In the person who gets dressed, the inner beauty is the most important [...]. Being okay with myself, I’ll be okay with everyone” (P 22).
“Dress up well, hair, lips, dress well, do makeup [...]. You need to be satisfied, in a good mood” (P 12).
“Beauty is beautiful skin, beautiful hair [...]. Is to be well dressed” (P 6).
“Beauty is to be well, beautiful, with skin, eyebrows, eyes [...]. But it is not worth being beautiful on the outside and without content [...] The inner beauty is part of 99% of the beauty of a woman” (P 7).
“Beauty is getting dressed [...]. Being happy [...]. Giving good energy, being beautiful, positive, staying with a good mind, having friends [...]. Being with brushed hair and makeup” (P 21).
For Valentim, Falcão and Campos25, there is a new construction of the corporal beauty of women in the 21st century, in which they start to have the function no longer of production, but of body-consumer. Therefore, self-care becomes essential, as it increases the person’s quality of life, self-esteem, confidence and security. For Ehlinger-Martin et al.6, the level of awareness of cosmetic procedures is high and has been included in medical and psychological

6 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
consultations. In a study with a thousand French women, these authors6 observed that, with advancing age, there is a disparity between internal and external age, which leads to tension and dissatisfaction with appearance, especially facial, which increases with time and results in regular use of anti-aging products in 40% of women over 45 years of age. However, in a historical-philosophical approach focused on happiness, Sant’Ana-Loos et al.7, evaluated the need to rescue the idea that life can be beautiful at any time, which depends, significantly, on the posture of who lives it.
However, according to Copatti et al.2, aesthetic beauty or appearance is related to positive body self-image, which consequently has a favorable effect on self-esteem, which can influence also positive behaviors and attitudes. Therefore, according to the way old people perceive and value their own body, they feel more optimistic and become more sociable2.
In the search for satisfaction with body image, the search for invasive treatments, such as plastic surgery, botulinum toxin and permanent makeup, as well as cosmetic procedures (facial, capillary and body), have been growing, often in an abusive way, which can lead, in some cases, to emotional and psychological suffering for not meeting social expectations1. In this sense, more incentive programs are suggested to promote the health of old people that involve, in addition to caring for diseases and their stakeholders, self-care with beauty as a strategy for valuing self-esteem6,8,17,25.
Family and friends as a synonym of happiness and beauty
In relation to what provides the most motivation to live and exist, the participants highlighted that the greatest beauty of their lives is in living with the family as a promoter of inner well-being and happiness. The family was considered to be a pillar, something irreplaceable, essential, a carrier of meaning for life:
“When I receive the family (son-in-law, grandchildren, daughter-in-law) and go to mass [...]. This keeps me standing [...] and is a reason to live” (P 2).
“Being with the family [...]. That’s something money can’t buy” (P 15).
“Loving people, family” (P 20).
“To be with the family, to receive the visit of the grandchildren and to see the children well. That makes me happy” (P 6).
“Peace with the family [...]. Believing in God is everything” (P 21).
“The family” (P 16).
According to Rocha et al.26, the family is constituted as a social support network, a hierarchical group of people who maintain reciprocal bonds of affection, tenderness, compassion and balance, of protection and care, especially for old people. Joia and Ruiz27 developed a qualitative research with 30 old people in the city of Barreiras (BA), Brazil, in order to understand the factors associated with life satisfaction. They demonstrated that the construction of affections among the family has a strong association of satisfaction and happiness with life27. The old people who did not live with family members, were identified with higher levels of stress and little motivation to live and face existential vicissitudes27. In another study, by Araújo, Castro and Santos28, with the objective of understanding the social representations of family for the old people who participated and did not participate in social groups, with 60 participants, identified that the family, even with conflicting relationships, is a provider of happiness, autonomy, security, care, support and social representation and integrity.
Happiness was also associated with the beauty of friendship, through living with friends, carrying out projects, leisure, helping others, participating in religious life, in the search for peace and tranquility, as attested by the statements below:
“Being healthy, [...] leisure, dancing, partying, being useful, being able to help” (P 14).
“Help the Church! [...], then the others, people” (P 13).
“To serve God, Jesus [...]. Help, have peace” (P 20).

7 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
“To serve God, Jesus [...]. Love people, family [...]. Help, have peace” (P 7).
“Beauty is the understanding that comes with a set that adds up [...]. Conquering inner and outer beauty, well-being is also achieved: taking care of yourself, eating right, being at ease with life and yourself, helping others, traveling and contemplating God and nature” (P 3).
Relating to friends and being sociable makes the individual feel loved, esteemed, cared for, valued and welcomed. It makes the old person belong to common and mutual relationships and obligations22. According to a study by Nguyen et al.29, with 837 old people of African descent, in order to examine the impact of informal social support from family and friends on the development of well-being, it demonstrated that the beauty of subjective interactions are promoters of satisfaction with life, happiness and self-esteem.
Regarding the benefits of religiosity in the lives of old people, a literature review study by Agli, Bailly and Ferrand30 suggested that spirituality and religion have a positive effect to delay cognitive decline and help people use coping strategies in the face of the disease and to have a better quality of life.
For Foucault31, when a citizen manages to develop and improve his way of being, taking care of himself, including in the physical and aesthetic sense, extolling autonomy, freedom and coexistence with others, he becomes the creator of his beauty and makes his life a work of art, molding itself, called the aesthetics of existence. Thus, there is a relationship between aesthetics and happiness, because taking care of oneself requires valuing both the inner beauty, the values and virtues of the soul, and the outer beauty, linked to body, hair and facial aesthetics. As participant 16 of our survey pointed out, “happiness is being well, encouraging, loving, motivating [...]. It is a set [...]. It is necessary to balance and have good feelings”.
The study by Jung and Moon32 also demonstrated that there is a relationship between aesthetics and happiness. Old people with high self-esteem, with inner beauty, were more motivated to seek aesthetic products and services and this relationship promotes
successful aging32. A study carried out with old women participating in a social group, which aimed to describe and explore the care and the impact of aesthetic appearance on the social perception of these old women, identified in the participants’ perceptions that body care is related to body, facial and capillary aesthetics, and are generators of self-esteem, satisfaction, happiness, freedom, psychological well-being and social well-being33. They were also conceived as effective means of family, social and professional integration, motivating them to face the existential vicissitudes33.
This study, as well as its potential in expanding knowledge by exploring the ways of perceiving, feeling and taking care of the body by the old people segment of the population, has limitations in the sample, in terms of its definition, considering that it was not random, its size, which does not allow generalizations, and its characterization, which did not identify the religious orientation and body mass distribution of the participants, as well as the fact that it was carried out with old women who use beauty products, which may have different relations with the aesthetic aspects compared to those who do not use such products. In this sense, it is suggested to improve the methodology in future studies, and to further explore the complementary relationships between aesthetics and happiness, relating them to research with other old people and in other settings.
CONCLUSION
According to the objective of the research, to identify the relationship between aesthetics and happiness in the perception of old people users of beauty products, the participants reported that there is a connection between the themes, because aesthetics as inner beauty is linked to intrinsic dimensions, to the subjective well-being, to the goods of the soul, to character, love and respect for others, reciprocity, humility, ethics, to the bonds of solidarity, joy and dialogue, to the way of being and acting. Still, beauty was identified with contemplation of nature, in the relationships of trust and coexistence with others and belief in God, in the care of the spirit, of the mind. They considered the interior beauty more significant than the exterior, focused

8 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
on body, facial and capillary aesthetics, but without aesthetic exaggerations.
Furthermore, for the participants, happiness is connected to inner beauty. What brings more happiness in their lives is the coexistence with family, friends, the execution of personal, social and religious projects and the search for peace and tranquility. Finally, a balance between inner and outer
beauty is necessary to achieve happiness, but with a preponderance of the aesthetics of existence, of the inner aesthetics, capable of promoting knowledge and self-care, self-knowledge, wisdom. The care of body image with external aesthetics is a way, a means, an instrument of social insertion and the search for a more lasting happiness.
Edited by: Daniel Gomes da Silva Machado
REFERENCES
1. Fin TC, Portella MR, Scortegagna SA. Old age and physical beauty among elderly women: a conversation between women. Rev Bras Geriatr Gerontol. 2017;20(1):74-84.
2. Copatti SL, Kuczmainski AG, Ferretti F, Sá CAD. Imagem corporal e autoestima em idosos: uma revisão integrativa da literatura. Estud Interdiscipl Envelhec. 2017;22(3):47-62.
3. Japiassú H, Marcondes D. Dicionário Básico de Filosofia. 3ª. ed. Rio de Janeiro: Jorge Zahar; 2001.
4. Leite PSC. Contribuições dos estudos marxianos para a estética: reflexões sobre a sociedade contemporânea. Filosof Educ. 2015;7(1):33-62.
5. Ferreira FR. Corpo feminino e beleza no século XX. Rev Alceu. 2010;11(21):186-201.
6. Ehlinger-Martin A, Cohen-Letessier A, Taïeb M, Azoulay E, Crest D. Women’s attitudes to beauty, aging, and the place of cosmetic procedures: insights from the QUEST Observatory. J Cosme Dermatol. 2016;15(1):89-94.
7. Sant’Ana-Loos RS, Loos-Sant’Ana H, Lima DMMF, Bueno PAR. A condução do bem viver na velhice: um ensaio sobre ética, felicidade e morte. Psicol Argum. 2016;34(85):89-103.
8. Oliveira EFS, Mercadante EF, Pôrto EF. Percepção de homens e mulheres maiores de 50 anos sobre a estética do envelhecimento. LifeStyle J. 2016;2(2):83-98.
9. Goldenberg M. A bela velhice. São Paulo: Editora Record; 2014.
10. Kowalski JP, Schemes C, Saraiva JIS, Magalhães Ml. Mulheres idosas: percepções sobre beleza e envelhecimento. Rev Temas Mujeres. 2017;13:76-97.
11. Aristóteles. Ética a Nicômacos. Kury MG, trad. 3. ed. Brasília, DF: Editora Universidade de Brasília; 2001.
12. Ferry L. Sete maneiras de ser feliz: Como viver de forma plena. Melo JAD, trad. Rio de Janeiro: Objetiva; 2018.
13. Sumngern C, Azeredo Z, Subgranon R, Sungvorawongphana N, Matos E. Happiness among the elderly in communities: a study in senior clubs of Chonburi Province, Thailand. Japan J Nurs Sci. 2010;7:47-54.
14. Ergin I, Mandiracioglu A. Demographic and socioeconomic inequalities for self-rated health and happiness in elderly: the situation for Turkey regarding World Values Survey between 1990 and 2013. Arch Gerontol Geriatr. 2015;61(2):224-30
15. Connors S, Khamitov M, Moroz S. Time, money, and happiness: does putting a price on time affect our ability to smell the roses? J Exp Soc Psychol. 2016;67:60-4.
16. Lobos G, Lapo MC, Schnettler B. In the choice between health and money, health comes first: an analysis of happiness among rural Chilean elderly. Cad Saúde Pública. 2016;32(5):1-12.
17. Pradeep GC, Tiraphat S, Chompikul J. Factors associated with quality of life among the elderly in Baglung District, Nepal. J. Public Health. 2017;15(3):51-64.
18. Dos Santos ACS, Silva AH, Araújo CS, Moreira MG. Comportamento de compra de cosméticos na melhor idade: diferenças ou similaridades entre os gêneros? Int J Bus Mark. 2018;3(2):88-97.
19. Pereira JAC, Formiga N. Comportamento de consumo na sociedade pós-moderna e sua influência na terceira idade. Psicologia. pt. 2019;2(1):1-15.
20. Fontanella BJB, Luchesi BM, Saidel MGB, Ricas J, Turato ER, Melo DG. Amostragem em pesquisas qualitativas: proposta de procedimentos para constatar saturação teórica. Cad Saúde Pública. 2011;27(2):389-94.

9 of 9
Aesthetics and old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200028
21. Bardin L. Análise de Conteúdo. 4ª. ed. Pinheiro LA, trad. São Paulo: Edições 70; 2016.
22. Alves BS, Ferreira ZAB, Ferreira JB, Pinheiro LMG. A relação entre autoestima e aspectos psicoemocionais em idosos de grupo de convivência. Integrart. 2019;4(1):111-31.
23. Albarello M, Winkelmann E, Fontela P, Schneider J, Berlezi E. Percepção de beleza e cuidados estéticos em mulheres rurais pós-menopausa residentes em um município do interior do Rio Grande do Sul. Rev Bras Ciênc Envelhec Hum. 2016;13(1):35-47.
24. Brito DE, Kyonayra QMNT, Figueroa OPD, Tôrres CE. Percepção da imagem corporal e fatores associados em idosos residentes em município do nordeste brasileiro: um estudo populacional. Ciênc Saúde Coletiva. 2014;24(2):451-60.
25. Valentim PP, Falcão RPGF, Campos RD. O corpo nos estudos de consumo: uma revisão bibliográfica sobre o tema. Consum Behav Rev. 2017;1(Special Edition):32-48.
26. Rocha RC, Côrtes MCJW, Dias EC, Gontijo ED. Veiled and revealed violence against the elderly in Minas Gerais, Brazil: analysis of complaints and notifications. Saúde Debate. 2018;42(4):81-94.
27. Joia LC, Ruiz T. Satisfação com a Vida na Percepção dos Idosos. Rev Kairós. 2013;16(6):79-102.
28. Araújo LF, Castro JLC, Santos JVL. A família e sua relação com o idoso: Um estudo de representações sociais. Psicol Pesqui. 2018;12(2):14-23.
29. Nguyen AW, Chatters LM, Taylor RJ, Mouzon DM. Social support from family and friends and subjective well-being of older african americans. J Happiness Stud. 2016;17:959-79.
30. Agli O, Bailly N, Ferrand C. Spirituality and religion in older adults with dementia: a systematic review. Int Psychogeriatr. 2015;27(5):715-25.
31. Foucault M. História da sexualidade 3: O cuidado de si. Albuquerque MTC, trad. 9ª. ed. Rio de Janeiro: Graal; 2009.
32. Jung MH, Moon JS. A Study on the effect of beauty service of the elderly on successful ageing: Focused on Mediated Effect of Self-esteem.J Asian Finan Econ Bus. 2018;5(4):213-23.
33. de Mello M, Scortegagna HM, Pichler NA. Cuidados e o impacto da aparência estética na percepção social de um grupo de mulheres idosas. Rev Bras Geriatr Gerontol. 2020;23(2): e190271.

1 of 15
Revie
w Art
icles
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
http://dx.doi.org/10.1590/1981-22562020023.200100
Physiotherapeutic interventions aimed at old people in situations of violence: a scope review
Adriana Luna Pinto Dias1
Ana Maria de Almeida2
Mariana Cabral Schveitzer3
Rafaella Queiroga Souto4
Keywords: Helth of the Elderly. Violence. Elder Abuse. Delivery of Health Care. Physical Therapy Specialty.
AbstractObjective: Identify physical therapy interventions aimed at old people in situations of violence. Method: This is a scope review, in which the following databases/libraries/search engines and gray literature were accessed: VHL, PubMed, Web of Science, Scopus, CINAHL, PEDro, BDTD, OpenGrey, OpenThesis, RCAAP, CAPES Thesis and Dissertation Portal, DART-Europe E-theses Portal and Theses Canada Portal. The searches used the descriptors and keywords, which were combined using the Boolean operators OR and AND: Fisioterapeutas, Fisioterapia, “Physical Therapists”, Physiotherapy, “Physical Therapy”, “Physical Therapy Specialty”, “Physical Therapy Modalities”, Rehabilitation, Reabilitação, “Elder Abuse”, “Maus-tratos ao Idoso”, “Physical Abuse”, “Elder Neglect”, “Aged Abuse” e “Elder Mistreatment”. Results: Of the 601 records found, 46 were excluded because they were duplicated, and 555 were selected to read the respective titles and abstracts. 548 publications were excluded because they did not meet the inclusion criteria, and 7 papers were pre-selected. Through the Snowballing strategy, one was identified, resulting in a final result of 8 studies. Conclusion: Physical therapy interventions aimed at old people in situations of violence include: health education, measures of caregiver stress, community resources, screening/triage, evaluation, identification, therapeutic/rehabilitation plan and reporting. In view of the findings, it is observed that, despite the lack of knowledge on this topic, the physiotherapist plays an essential role in the conduct of cases of violence against old people.
1 Universidade Federal da Paraíba, Programa de Mestrado Profissional em Gerontologia. João Pessoa, PB, Brasil.
2 Universidade Federal da Paraíba, Programa de Pós-Graduação em Enfermagem. João Pessoa, PB, Brasil.3 Universidade Federal de São Paulo, Escola Paulista de Medicina, Departamento de Medicina Preventiva.
São Paulo, SP, Brasil.4 Universidade Federal da Paraíba, Departamento de Enfermagem em Saúde Coletiva, Programa de
Mestrado Profissional em Gerontologia; Programa de Pós-Graduação em Enfermagem. João Pessoa, PB, Brasil.
Funding: Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). Edital Universal: 28/2018. Nº do processo: 424604-2018-3. The authors declare there are no conflicts of interest in relation to the present study.
CorrespondenceRafaella Queiroga [email protected]
Received: April 15, 2020Approved: November 9, 2020
ID
ID
ID
ID

2 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
INTRODUC TION
Violence against old people (VAOP) is a growing international phenomenon. No society is immune from the occurrence of this disease, representing an important public health problem and of global interest, especially in the last decades1.
The nature of VAOP can manifest itself in different ways: physical, psychological, sexual, financial, abandonment and neglect. Whatever the type of aggression, it represents a violation of human rights, which can result in psychological distress, depression, suicidal thoughts, increased use of health services, pain, physical injuries, trauma or early death1-3.
Studies point to physical, psychological violence and negligence as the most frequently identified occurrences4,5. However, many old people do not report violence due to ignorance of their rights, fear of the consequences or fear of negatively affecting their relationships and family integrity6.
The following are pointed out as risk factors for VAOP: advanced age, female gender, low family support, unfavorable socioeconomic context, depressive mood, social isolation, caregiver stress, disrespectful intergenerational relationships, cognitive impairment and physical, psychological, financial and functional dependencies of old people1,7,8.
As it is a phenomenon l itt le recognized and denounced, coping with VAOP requires a multidisciplinary approach. Health professionals have a significant responsibility in this situation, since they maintain contact with victims in health services and homes, and can trigger effective protection and coping mechanisms9,10.
In this sense, the National Health Policy for the Old Person (PNSPI)11 establishes that every health professional must promote the quality of life of the old person, through the establishment of actions that involve everything from primary care to rehabilitation. In addition, the National Policy for the Reduction of Accident and Violence Morbimortality (PNRMAV)12 highlights the role of the rehabilitation of sequelae and disabilities arising from violence,
providing conditions for their social and family reintegration and favoring the achievement of the individual’s independence within a new situation.
The physiotherapist is a professional who works in the prevention of injuries, health promotion and rehabilitation of the old person, establishing a continuous bond with this population, and often integrating into their family environment, where the aggressors are most commonly found10,13. Thus, this professional is able to intervene in the entire context of VAOP: from the prevention and screening of cases to the rehabilitation of functional sequelae resulting from situations of violence experienced by many old people.
Despite this, the literature on this topic is scarce and the official documents are not clear in relation to the management of cases of VAOP by the physiotherapist. It is therefore important to carry out a scope review on publications related to interventions carried out by physical therapists with old people in situations of violence, as a way of examining the extent and nature of evidence on this topic, in order to support the practice of the professionals who deal with this population and favor the decision-making process. Therefore, the objective of the present study is to identify physical therapy interventions aimed at old people in situations of violence.
METHOD
This is a scope review. These studies aim to synthesize and disseminate the results of studies; map concepts that support a given area of knowledge, pointing out the main sources and types of evidence available; and identify gaps in the literature14.
In order to improve the writing of the manuscript, this review followed the PRISMA Extension for Scoping Reviews (PRISMA-ScR)15. However, this study does not have a registered and/or accessible review protocol. The databases/libraries/search engines accessed were: Virtual Health Library (VHL); PubMed; Web of Science; Scopus; Cumulative Index to Nursing and Allied Health Literature (CINAHL); and Physiotherapy Evidence Database (PEDro).

3 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
Gray literature research and unpublished studies included: Digital Base of Theses and Dissertations (BDTD), OpenGrey, OpenThesis, Portugal Open Access Scientific Repositories (RCAAP), CAPES Thesis and Dissertation Portal, DART-Europe E-theses Portal and Theses Canada Portal (Aurora and Voilà catalogs). The Snowballing search strategy was also carried out, by reading all references of the articles selected in this review16.
The methodological path was based on the PCC strategy - acronym for Population (P), Concept (C) and Context (C)14 – considering P (physical therapist), C (physical therapy interventions in the face of violence) and C (old people in situations of violence). Thus, the following guiding question was established: what are the physical therapy
interventions aimed at old people in situations of violence?
From each strategy item, keywords and descriptors were found in the MeSH (Medical Subject Headings) and DeCS (Health Sciences Descriptors): Fisioterapeutas, Fisioterapia, “Physical Therapists”, Physiotherapy, “Physical Therapy”, “Physical Therapy Specialty”, “Physical Therapy Modalities”, Rehabilitation, Reabilitação, “Elder Abuse”, “Maus-tratos ao Idoso”, “Physical Abuse”, “Elder Neglect”, “Aged Abuse” e “Elder Mistreatment”.
These descriptors and keywords were combined using the Boolean operators OR and AND, and applied to databases/libraries/search engines and gray literature, as shown in Chart 1.
Chart 1. Search strategies used in databases/libraries/search engines and gray literature, included in the scope review of physical therapy interventions aimed at old people in situations of violence. João Pessoa, PB, 2019.
Databases/ Libraries/ Search engines/Gray Literature
Search Strategies
VHL(BIREME)
(tw:( fisioterapeutas OR fisioterapia OR "Physical Therapists")) AND (tw:("maus-tratos ao idoso" OR "elder abuse"))
PubMed Central: PMC((“Physical Therapists” OR “Physical Therapy Specialty” OR “Physical Therapy Modalities” OR Rehabilitation OR “Physical therapy” OR “Physiotherapy”)) AND (“Elder abuse” OR “Physical abuse” OR “Elder neglect” OR “Aged abuse” OR “Elder mistreatment”)
Web of Science:Coleção Principal
(“Physical Therapists” OR “Physical Therapy Specialty” OR “Physical Therapy Modalities” OR Rehabilitation OR “Physical therapy” OR “Physiotherapy”) AND (“elder abuse” OR “Physical abuse” OR “Elder neglect” OR “Aged abuse” OR “Elder mistreatment”)
Scopus(Elsevier)
((Physical Therapists OR Physical Therapy Specialty OR Physical Therapy Modalities OR Rehabilitation OR Physical therapy OR Physiotherapy) AND (Elder abuse OR Aged abuse))
CINAHL (EBSCO) (“physical therapists” OR “physical therapy” OR rehabilitation OR “physical therapists specialty”) AND (“elder abuse” OR “aged abuse” OR “elder neglect”)
PEDro Simple search: “Elder abuse”, “Aged abuse”, “Physical abuse”, “Elder Neglect”, “Elder mistreatment”
BDTD Fisioterapeutas OR fisioterapia OR reabilitação AND “maus-tratos ao idoso”
OpenGrey ((“physical therapists” OR “physical therapy” OR rehabilitation) AND (“elder neglect” OR “physical abuse” OR “elder abuse” OR “aged abuse”))
OpenThesis ("physical therapists" OR "Physical therapy" OR rehabilitation) AND ("elder abuse" OR "aged abuse" OR "elder neglect")
RCAAP fisioterapia OR "physical therapists" AND "elder abuse" OR "maus-tratos ao idoso"CAPES Thesis and Dissertation Portal fisioterapeutas OR fisioterapia OR reabilitação AND “maus-tratos ao idoso”
DART ("physical therapists" OR "Physical therapy" OR rehabilitation) AND ("elder abuse" OR "aged abuse" OR "elder neglect")
Theses Canada Portal(Aurora and Voilà)
("physical therapists" OR "physical therapy" OR rehabilitation OR "physical therapist modalities") AND ("elder abuse" OR "aged abuse" OR "elder neglect" OR "physical abuse")

4 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
Studies that met the eligibility criteria were included: quantitative, qualitative studies, with mixed methods and gray literature (texts by specialists, dissertations and theses, editorial texts, among others); in English, Portuguese, French or Spanish; that were accessible and/or available in full (full texts), in electronic or printed media; that approached physical therapists working with old people in situations of violence; and that described any physiotherapy intervention recognized and/or implemented by professionals in the face of old people in situations of violence.
There was no delimitation as to the period of publication of the studies, due to the small number of publications on this topic. The search and selection of studies were carried out by two researchers, independently, from September to November 2019. The selection took place in two stages: an initial screening, considering only the reading of the titles and abstracts, from which studies were selected to read the full texts; and a second stage, when the eligibility criteria were applied after a complete reading of the texts. Disagreeing cases were resolved through a third researcher.
Data extraction took place using an instrument developed by the reviewers, which included: country of study; year and magazine of publication; type and objective(s) of the study; education of the main author; professional category(ies) addressed; and physical therapy interventions recognized and/or implemented by professionals in the face of old people in situations of violence.
The analysis of the quality of the articles and the level of scientific evidence were not used as a criterion for the exclusion of articles, therefore they were not carried out, since this type of review aims to identify the available production on the investigated subject14.
RESULTS
Crossed between the descriptors in the databases/libraries/search engines, 135 articles were found, two in the VHL, 71 in the Web of Science, 24 in the Scopus, 36 in the CINAHL, two in the PEDro and no article in the PubMed. In the gray literature, 466 productions were identified, of which one in BDTD, five in OpenGrey, 85 in OpenThesis, 22 in the CAPES Theses and Dissertations Portal, 188 in RCAAP, 165 in the Theses Canada Portal, with no material rescued at DART-Europe E-theses Portal.
Of the 601 records found, 46 were excluded because they were duplicated, and 555 were selected to read the respective titles and abstracts. After analyzing them, 548 publications were excluded because they did not meet the inclusion criteria: 13 were published in languages different from those established in the criteria; two were not accessible in full; and 533 did not address physiotherapists working at VAOP and/or did not describe any physical therapy intervention directed at old people in situations of violence.
At the end of this phase, 7 studies were pre-selected to be read in full, a study rescued by the Snowballing strategy17, resulting ultimately in 8 studies included17-24. The result of the search and selection can be seen in Figure 1.

5 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
Figure 1. Flowchart of search and selection of studies on physical therapy interventions aimed at old people in situations of violence. João Pessoa, PB, 2019.
Source: Adapted from PRISMA-ScR15.
All studies (n=8) came from the United States, produced between 1982 and 2005, in magazines in the area of Physiotherapy (n=3), Geriatric Physiotherapy (n=2), Physiotherapy and Geriatric Occupational Therapy (n=2), and Geriatrics (n=1).
With regard to the education of the main authors, half (n=4) of the studies had a Physiotherapist as the main author; one study by an Occupational Therapist; one written by Social Worker; and in two studies it was not possible to identify this information. Regarding the methodological characterist ics, one article was identif ied as descriptive quantitative, five ref lective studies and two editorials.
Considering the professional categories covered, six studies presented the Physiotherapist as the only professional approached, while one included both the Physiotherapist and the Occupational Therapist. The last study (n=1) portrayed other professionals such as Doctor, Nurse, Social Worker, in addition to Occupational Therapist and Physiotherapist. These data, as well as the objectives of the studies, can be seen in Chart 2.
Chart 3 shows the description of the physical therapy intervent ions recogn ized and/or implemented by the physical therapists directed to the old person in a situation of violence, for each study included in this review.

6 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
Chart 2. Description of studies included in the scope review of physical therapy interventions aimed at old people in situations of violence. João Pessoa, PB, 2019.
Author(s), Year/Type of study
Main Author Formation
Professional category(ies)
addressedStudy objective(s)
Dalton, 200518/ Editorial Not identified Physiotherapist
Discuss child violence, by the intimate partner and old people, examining the multiple ways that physical therapists and their assistants can recognize and provide care to the victims of such violence.
Saliga et al., 200419/
Quantitative Descriptive
Physiotherapist Physiotherapist
Determine the extent of knowledge of Physiotherapists in an urban Michigan segment, in three areas of violence management against old people: signs/symptoms of physical violence; mandatory state reporting laws; and professionals' knowledge about institutional reporting protocols. In addition to investigating whether the participants had already suspected or reported a case of violence against old people.
Little, 200217/ Reflection
Physiotherapist Physiotherapist
Assist physiotherapists to recognize signs and symptoms of violence against old people; show prevalence and provide guidelines for determining this type of violence; and recommend interventions in suspected cases.
Camaratta et al., 200020/ Reflection
Physiotherapist Physiotherapist
Provide a protocol for physical therapists who face possible violence against old people; provide information on signs and symptoms, laws governing complaints and an approach to intervention and documentation in these cases of violence.
Foose, 199921/ Editorial Not identified Physiotherapist Share experiences of physical therapists' interventions
in cases of violence against old people.
Holland et al., 198722/ Reflection
Occupational Therapist
Physiotherapistand Occupational
Therapist
Review the literature on violence against old people and describe the potential role of the Physiotherapist and Occupational Therapist in their detection, treatment and prevention.
Mildenberger e Wessman, 198623/
ReflectionPhysiotherapist Physiotherapist
Provide physiotherapists with recognition of violence against old people, intervention procedures, prevention points and available community resources.
Tomita, 198224/ Reflection Social Worker
Occupational Therapist, Social Worker, Nurse,Physician and
Physiotherapist
Describe a protocol for an integrated response by health professionals in the problem of violence against old people.

7 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
Chart 3. Physiotherapeutic interventions recognized and/or implemented by physiotherapists targeting old people in situations of violence, identified in the studies included in the scope review. João Pessoa, PB, 2019.
Author(s), Year Physiotherapeutic interventions recognized and/or implemented by physical therapists aimed at old people in situations of violence
Dalton, 200518
Routine screening and triage (incorporate into the evaluation protocol); Observation of the patient's behavior (nervousness and tendency to distance themselves from others; non-adherence to the treatment program) and family members (impatience and unreasonable expectations on the part of family members); Documentation (history of multiple fractures, contusions, bruises or unusual skin injuries), using body maps; Report to the supervising physiotherapist; Guidelines (where to get advice, shelter and assistance from professionals); Provision of informative material to the patient; Complaint in accordance with current state law.
Saliga et al., 200419
Observations/behaviors identified by professionals as potential sources of violence: malnutrition, wound healing, behavior changes, untreated injuries, inconsistent wound sites, caregiver refusal to leave the old person alone during visits, unilateral contusion, difficulty for the old person to walk/sit without evidence of musculoskeletal disease, family/caregiver who answer questions and do not allow decision making by the old person; poor hygiene with the use of inappropriate clothing. Knowledge of local laws; contact with a social worker or supervisor when faced with a case of violence; and complaint.
Little, 200217
Identification: warning signs and indicators of physical abuse (multiple fractures/injuries at various stages of healing, contusions grouped in a regular pattern, bilateral bruises, groin injuries, dental fractures, injuries around the face and neck, glove and sock-shaped burns, irregular hair loss); emotional (confusion and disorientation, fear of strangers and the environment, depression or anger, ambivalence about the caregiver, hesitation of the patient to speak in the presence of the caregiver, low self-esteem, yearning for attention); financial (unexplained loss of social security, anxiety and lack of knowledge about financial status, lack of payment for contracted services, lost belongings); and negligence (deterioration of health, dehydration or malnutrition, dirt and excessive odor on clothes/body, absent auxiliary devices, inappropriate clothing for environmental conditions, unexplained apathy or fatigue, over/under-medication causing sedation). Assessment: interview with questions about security; observation of the patient's general condition, behavior and care; caregiver-patient interaction; neuro-musculoskeletal review (including fractures) and functional activities; geriatric scales. Interventions: documentation (description of injuries, use of body model and photos) and report to the authorities; educating the patient about his/her protection (staying active, sociable and informed about financial, legal and protection obligations for old people); functional independence plan (through therapeutic exercises and functional activities).
Camaratta et al., 200020
Screening and triage incorporated into the care routine, involving direct questions away from family members/caregivers and observation of general signs of violence (frequent unexplained crying, anxiety, tremors, irritability, abuse of alcohol or prescription drugs, fear or suspicion of certain people in the residence); physical violence (bruises, black eyes, rope marks, open wounds, cuts, punctures, burns, fractures, broken glasses, laboratory findings of over/under-dosage medications, untreated injuries and in various stages of centralized healing - head, neck, breasts, abdomen, back and genitals); negligence (dehydration, malnutrition, untreated bed sores and poor hygiene). In all American states (with the exception of six of them), there are laws that require health professionals to report cases of violence against old people. Assessment including complaints, financial status, social support, emotional stress, observation of patient-family/caregiver interaction and physical examination to provide evidence. Intervention involving a specific security plan, education and validation of patient rights. Documentation, containing a record with body graphic, descriptions and photos of injuries.
to be continued

8 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
Continuation of Chart 3
Author(s), Year Physiotherapeutic interventions recognized and/or implemented by physical therapists aimed at old people in situations of violence
Foose, 199921
Recognition of the signs of violence, understanding its origins, referring to social services and reporting. Differentiation between real violence and the result of an accident/illness. Assessment of the need to indicate institutionalization in the absence of a family support network and/or caregiver. Screening for: physical/biomechanical problems; physical evidence of violence (contusions, hand-shaped bruises, head/neck injuries, dislocations, open wounds, broken glasses); signs of neglect (malnutrition, dehydration, poor care, multiple contractures and decubitus ulcers); inappropriate emotional interactions (aggressive behavior); social well-being. Assessment of the caregiver's physical, cognitive and social capacity to provide assistance to old person; need for additional assistance in care; and ways to relieve caregiver stress. Caregiver education regarding patient safe positioning/transfers, hygiene care, skin inspection and health-disease process. Ensuring fitness for the old person through exercise, making them less vulnerable, as part of the Conditioning against Crime Program.
Holland et al., 198722
Detection of violence during assessment and treatment. More direct intervention consists of the rehabilitation of adaptive self-care skills (decreasing the old person's dependence), as well as information on energy conservation and the recommendation of auxiliary devices; in addition to helping the old person to rescue old leisure interests, identifying new areas of potential skills in domestic tasks, strengthening the family unit and increasing their self-esteem. Intervention in the family and caregiver structure, providing information on available community support resources (transportation and recreation services for old people, friendly visitors and geriatric daycare centers), alleviating the day-to-day responsibilities of caregivers. Community education on violence against old people.
Mildenberger e Wessman,
198623
Recognition of warning signs for violence: physical (bruises on the chest, shoulders, back, arms or legs; cigarette burns; rope/chain marks resulting from physical restrictions; lacerations on the face; head injuries, absence of hair or scalp hemorrhage); psychological (behavior changes, being scared or upset, avoiding talking about the family); interruption of physical therapy treatment; family prevents the old person from remaining alone during visits; financial (the old person reports loss of money or valuables); negligence (physical deterioration, malnutrition, weight loss, neglected or broken teeth, broken glasses, poor hygiene, repeatedly used clothing); violation of rights (caregivers impose unrealistic restrictions on decision making by the old person, on physical mobilizations and opportunities for socialization). Interventions include family counseling and specific training for dependent old people caregivers; use of community support services (day care, home nursing service, accessible transport, financial assistance - allowing caregiver stress relief), social and health education. In suspected cases, the action will depend on the type of abuse and physical danger to the old person. If it threatens life, professionals must know local protection agencies to report.
Tomita, 198224
Functional assessment: assess activities of daily living (ability to self-care and prepare meals, use transport, shopping) and walking condition; observation of trauma or bruising, consistent with the patient's condition of dependence. Request a description of a typical day and your expectations about yourself and your caregiver. Physical examination: if there is an injury resulting from an accident, document the circumstances and record in sketches and graphics of the upper body and extremities; examine effects of over/under-medication, nutrition, hygiene and personal care. Assessment of burns, physical injuries to the head, bruises (bilaterally on the arm, clusters on the upper body), presence of bruises and injuries at different stages of resolution, fractures, falls, contractures, poor muscle tone and evidence of physical restriction; walking condition (if disabled it may suggest sexual aggression). Observation if the bruises presented on a hospital admission disappear during hospitalization (in this case, suspecting violence). Interview with the caregiver: age and sources of income of the caregiver, responsibilities inside and outside the home, expectations of the caregiver in relation to the patient and their difficulties experienced in caring for the old person; assessment of the caregiver's ability to withstand the stress of care and the support systems available to the caregiver. Educational plan: self-care education for the patient; inform the caregiver about the aging process. Therapeutic plan: instruction in self-care techniques to reduce dependence on caregivers; helping the patient with alternative arrangements, changing his life situation (using day centers, congregating housing or nursing homes).

9 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
It is observed that physical therapy interventions aimed at the old person in situations of violence involved: health education, measures on caregiver stress, community resources, screening/triage, evaluation, identification, therapeutic/rehabilitation plan and reporting.
Educational interventions involved the education of the old person, the caregiver and the community/society. The most reported, in half of the studies, were those aimed at the old people population: guidance on places of shelter, protection, counseling and assistance from professionals; provision of educational material; activities to prevent violence, maintain activities and socialize; providing information on legal and protection provisions for old people; rights and self-care education17,18,20,24.
In three of the studies, educational activities with the caregiver were described as follows: specific training for the caregiver of dependent old people, including safe positioning/transfers, hygiene care and skin inspection; and information to the caregiver about the aging and health-disease processes21,23,24. Community education was also an intervention reported in two of the studies22,23.
The assessment of caregiver stress was an intervention addressed in four studies, which reinforce the assessment of support systems available to families, the difficulties experienced in caring for old people and the caregiver’s ability to withstand the stress of care. These studies report that the physiotherapist can suggest ways to reduce caregiver stress and burden, providing information on community support services21-24.
Community resources were described in three papers. Among these resources, we can mention: friendly visitors, geriatric daycare, transportation and recreation services for old people, and financial aid22-24.
Regarding screening/triage, three studies reported the importance of tracking potential sources of violence, and this strategy can be incorporated into the assessment protocol and the routine of care18-20.
The general assessment included observation of the patient, family and patient-caregiver interaction. In seven studies, the general signs of VAOP, which
may also indicate probable psychological violence, were: confusion; disorientation; fear of strangers and the environment; frequent unexplained crying; sudden changes in behavior; depression; low self-esteem; longing for attention; nervousness; rage; aggressiveness; non-adherence to the physical therapy treatment program; tendency to isolation; fear or suspicion of certain people at home; ambivalence of feeling towards the caregiver; and hesitation to talk about the caregiver17-21,23,24.
The importance of assessing family behavior has been reported in three studies, and included as signs: family impatience; refusal to leave the old person alone; family members answering questions instead of the old person; not allowing the old person to make decisions; and unreasonable expectations on the part of the family, such as wanting the old person to walk, when they no longer want that goal17,18,23.
In four studies, there were reports of the observation of signs and symptoms of neglect against old people, listed as: poor care or deteriorating health; malnutrition; dehydration; poor body hygiene; neglected teeth; use of dirty and/or inappropriate clothing for the climate; absent auxiliary devices; unexplained apathy or fatigue; over/under-medication, with possible sedation; multiple contractures or pressure ulcers17,20,21,23.
Half of the studies (n=4) recommended documenting unusual skin injuries, contusions, bruises, fractures and injuries resulting from accidents. This documentation takes place through the description of the lesions, recording on maps/body models and photographs17,18,20,24.
Assessment of the neuro-musculoskeletal system and/or functional assessment has been reported in two studies. Functional assessment should involve activities of daily living (self-care skills, preparing meals, using transport, shopping) and observing whether the occurrence of trauma is consistent with the patient’s condition of dependence17,24. In one study, there is a report of the need to screen for physical and biomechanical disorders21.
The identification of cases, reported in seven of the studies, can be done during the evaluation and/or physical therapy, by recognizing the following

10 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
warning signs: injuries to the face, head and neck; irregular hair loss; broken glasses; dental fractures; cuts; perforations; burns, which may be in glove and sock shape; inconsistent sites of unusual skin wounds or injuries; grouped bruises or contusions, in a regular or central pattern (head, neck, breasts, abdomen, back and genitalia/groin); bruises/injuries/fractures at different stages of resolution; falls; bad muscle tone; and evidence of physical restraint (rope/chain marks)17-21,23,24.
In four studies, interventions that make up a therapeutic and rehabilitation plan were described: therapeutic exercises to maintain functional independence and good shape; rehabilitation of functional activities and self-care skills; in addition to energy conservation measures and recommendations for auxiliary devices17,21,22,24.
Finally, the complaint was an intervention reported in six articles17-21,23. Complaints are mandatory according to current local legislation. In two studies, the physiotherapist’s report to his supervisor or a social worker was included as an intervention prior to the complaint18,19.
DISCUSSION
Many countries have endeavored to strengthen policies to protect and support old people in situations of violence, yet the United States stands out for the development of programs that are being implemented to provide victims with multidisciplinary social and health support25. This reality portrays the origin of the studies included in this review, in which the unanimity of North American studies with this theme is observed.
The first publication about VAOP, approached by physiotherapists, took place in 198623. After this production, a few reflective texts were produced in an incipient attempt to debate the role of the physiotherapist in this area.
In 2011, Aveiro et al.13 contributed to the discussion about the participation of the physiotherapist in health promotion, disease prevention and recovery of the main health problems of old people, including VAOP. Only in 2020, a case study was published
reporting physical therapy interventions performed on an institutionalized old person, victim of urban violence26. Thus, the scarcity of publications reflects the timid involvement of physiotherapists in this context, suggesting misunderstanding and/or ignorance of this problem on the part of these professionals.
The Secretariat for Human Rights of the Republic of Brazil (SDHRB)2 recommends that health professionals specialize and act in all types of VAOP. However, the physiotherapists who identify these situations understand them as a matter of psychological management and/or social assistance, not perceiving themselves as protagonists of relevant interventions in these situations. Ribeiro and Barter27 evidenced this distance, reporting that physical therapists did not consider themselves responsible for listening, support, care and guidance to old people with a history of violence. On the contrary, these professionals assumed that they should only act on physical injuries and transfer the responsibility for the situation of violence to other professionals (such as psychologists and social workers).
Reinforcing this perception, this study also evaluated, as a distant practice, the consolidation of the safety net for cases of old people victims of violence. The professionals considered the rehabilitation services as an isolated, discontinuous and punctual action, demonstrating the lack of engagement in this issue.27.
Regarding educational interventions, the literature recognizes that the best way to prevent VAOP is knowledge. Many old people are unaware of their rights or do not even recognize themselves as victims, nor their ways of prevention and defense in these situations28,29.
In addition, some studies also report that the role of caregiver is often assumed by family members, often unprepared, causing care to occur in an intuitive and mistaken way, which can cause situations of neglect30. Therefore, many cases of VAOP could be avoided with educational interventions aimed at family members and caregivers.
SDHRB2 highlights the importance of producing awareness campaigns on aging and valuing old people,

11 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
aimed at the entire Brazilian society. For Hirst et al.31, education is a fundamental preventive strategy, so public awareness campaigns and educational initiatives are essential to avoid situations of violence for old people. In this way, education is a powerful tool for preventing this violence and physiotherapists can contribute with necessary clarifications for old people, family/caregivers and community.
Measures focused on caregiver stress were also reported, as this condition acts as a risk factor for situations of violence32. Caregivers are predisposed to stress, mental fatigue, difficulty concentrating, memory loss, apathy, emotional indifference, anxiety attacks and depression33.
Pillemer et al.1 affirm that the potential for the beginning of violence can be reduced by interventions to support the caregiver, as well as Lopes et al.30 describe factors related to VAOP: absence of formal and informal support, and of public policies or support for families providing care.
Caregiver interventions are therefore a promising approach to prevention, and it is also necessary to assess the support systems available to caregivers. SDHRB2 highlights the need to support families with social facilities such as: Community Centers, Day Centers, Collective Residences and Support Services for Family Caregivers. It is worth mentioning that these community environments favor new relational dynamics and strengthening the autonomy and protagonism of the old person, favoring their access to protection networks and services34.
It is known that the caregiver burden increases the greater the functional dependence of the old person30. Furthermore, studies have linked impairment of functional capacity to the risk of violence, as well as signs of violence in this population35-37. Maia et al.38 they also reported that the old person who suffers some type of violence is in a situation of functional dependence. That is, old people who need assistance for activities of daily living can trigger stressful situations in the caregiver and increase the chance of suffering some type of violence.
In this scenario, the physiotherapist is committed to the universality and comprehensiveness of
care, with interventions aimed at the functional independence of the old person, promoting relief from the caregiver’s stress and thereby preventing situations of violence. Thus, these interventions consist of preventive actions against violence, as well as contributing to improving the quality of life of the old person, their family and caregiver.
To detect abuse situations early, it is necessary to recognize the warning signs of all types of violence, which includes general signs in the behavior of the old person, as well as visible physical signs. The warning signs described in this article corroborate literary findings from other reviews, guidelines and government publications39-41.
The physiotherapist, having a focus on physical interventions, can pay attention to physical signs of violence. However, due to the physiotherapist-patient relationship that develops during therapy, this professional must be aware of psychological, behavioral changes and the old person-family/caregiver interact ion, which may indicate psychological violence. Thus, through a situation of violence, the old person may present changes in the emotional state29,39,41, that corroborate the general signs and likely psychological violence presented in this review.
PNSPI11 establishes that management instruments must be implemented to face the difficulties faced by the old person, and one of these instruments includes functional assessment. From it, depending on the functional condition of that person, actions will be established such as: rehabilitation for the recovery of maximum functional autonomy, prevention of functional decline and/or recovery of health.
Thus, it is pertinent to use therapeutic exercises aimed at the rehabilitation of functional activities, making it possible to promote quality of life for the old person and to act in the prevention of situations of violence.
Among these exercises, st rength and multicomponents (strength training combined with balance, aerobic and stretching exercises) stand out as good strategies to improve functionality in old people42.

12 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
In addition, the combination of individual and collective physical therapy interventions aimed at assisting old people who are victims of violence can improve cognitive, social, physical-functional capacities and quality of life in general.26.
Some studies have already shown optimistic results with the inclusion of rehabilitation services for old people, victims of violence. Physiotherapists showed positive results acting in the rehabilitation of patients, such as the resumption of locomotion, guidance to families, return to the community and social reintegration27.
The resumption of locomotion and social reintegration can be favored by the use of assistive walking devices, as well as other Assist ive Technologies (AT), such as prostheses and orthoses. The assessment, prescription, adequacy and training of AT are strategies used to minimize motor dysfunction and reduced mobility, allowing greater autonomy, delaying or rehabilitating functional disabilities, and thus improving the quality of life of old people43.
Regarding complaints, in Brazil, the Old People Statute44 warns of the obligation of public and private services to report suspected or confirmed cases of VAOP to the competent authorities, and establishes as an administrative infraction the lack of this communication by the health professional.
In the ethical sphere, physiotherapists are responsible for the Code of Ethics and Deontology of the Federal Council of Physiotherapy and Occupational Therapy, which establishes that “the physiotherapist must communicate to the immediate head of the institution in which he works or to the competent authority, a fact that he is aware of, typified as a crime, misdemeanor or ethical infraction”45.
Thus, it appears that the notification of the situation of violence is compulsory to the physiotherapist, and its communication to the immediate boss is an intervention based on ethical conduct, making its omission an administrative infraction.
However, Oliveira et al.9 describe that the main difficulty pointed out by professionals in communicating VAOP cases is the failure to recognize
this situation. Professionals admit that better training is necessary in order to identify and prevent this health issue46. In the study by Saliga et al.19, physiotherapists reported lack of training/information about VAOP, reinforcing the conception of this professional’s distance from the problem in question.
The present study has limitations inherent to scope reviews, as it includes several studies, not being concerned with the quality or level of evidence. In addition, this review mostly identified reflective and editorial texts, published more than 15 years ago, demonstrating the scientific fragility with which this content has been approached.
In addition, most studies emphasized the identification of signs and symptoms, and the assessment of the old person in the context of violence, to the detriment of more specific concrete physiotherapeutic interventions. Furthermore, in some studies, different professional categories were addressed, covering interventions common to other professionals, limiting the recognition of the physiotherapist’s actions.
CONCLUSION
This review provided a summary of the physical therapy interventions aimed at the old person in situations of violence, which involved: health education, measures of caregiver stress, community resources, screening/triage, assessment, identification, therapeutic plan/rehabilitation and reporting.
These interventions are in line with health policies aimed at the old person, including the National Policy for the Old Person, the Statute for the Old Person, the National Health Policy for the Old Person and the National Policy for Reducing Morbidity and Mortality from Accidents and Violence. These policies converge so that health care for old people is guaranteed at different levels of care, protecting them from any type of violence.
Despite this, the scarcity of updated observational and experimental studies, published on this topic, was identified. Thus, it is observed that some questions still need to be answered: how is the physiotherapist

13 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
REFERENCES
1. Pillemer K, Burnes D, Riffin C, Lachs MS. Elder Abuse: Global Situation, Risk Factors, and Prevention Strategies. Gerontologist. 2016;56(S2):194-205.
2. Brasil. Secretaria de Direitos Humanos da Presidência da República. Manual de Enfrentamento à Violência contra a Pessoa Idosa: É possível prevenir. É necessário superar [Internet]. Brasília, DF: Secretaria de Direitos Humanos; 2014 [cited 2019 Nov. 09]. Available from: https://www.gov.br/mdh/pt-br/sdh/noticias/2014/junho/ ManualdeEnfrentamentoViolnciacontraaPessoaIdosa.pdf/view
3. Yunus RM, Hairi NN, Yuen CW. Consequences of Elder Abuse and Neglect: A Systematic Review of Observational Studies. Trauma Violence Abuse. 2019;20(2):197-213.
4. Hohendorff JV, Paz AP, Freitas CPP, Lawrenz P, Habigzang LF. Caracterização da violência contra idosos a partir de casos notificados por profissionais da saúde. Rev SPAGESP. 2018;19(2):64-80.
5. Garbin CAS, Joaquim RC, Rovida TAS, Garbin AJI. Idosos vítimas de maus-tratos: cinco anos de análise documental. Rev Bras Geriatr Gerontol. 2016;19(1):87-94.
6. Adib M, Esmaeili M, Zakerimoghadam M, Nayeri ND. Barriers to help-seeking for elder abuse: A qualitative study of older adults. Geriatr Nurs. 2019;40(6):565-71.
7. Alves CS, Serrão C. Fatores de risco para a ocorrência de violência contra a pessoa idosa: revisão sistemática. PAJAR. 2018;6(2):58-71.
8. Paiva MM, Tavares MS. Violência física e psicológica contra idosos: prevalência e fatores associados. Rev Bras Enferm. 2015;68(6):1035-41
9. Oliveira BG, Freire IV, Assis CS, Sena ELS, Boery RNSO, Yarid SD. Responsabilidade dos profissionais de saúde na notificação dos casos de violência. Rev bioét. 2018;26(3):403-11.
10. Lopes LGF, Leal MCC, Souza EF, Silva SZR, Guimarães NNA, Silva LSR. Violência contra a pessoa idosa. Rev Enferm UFPE on line. 2018;12(9):2257-68.
11. Brasil. Portaria nº 2.528, de 19 de outubro de 2006. Aprova a Política Nacional de Saúde da Pessoa Idosa. Diário Oficial da União. 20 out. 2006.
12. Brasil. Portaria nº 737, de 16 de maio de 2001. Aprova a Política Nacional de Redução da Morbimortalidade por Acidentes e Violências. Diário Oficial da União. 18 maio 2001.
13. Aveiro MC, Aciole GG, Driusso P, Oishi J. Perspectivas da participação do fisioterapeuta no Programa Saúde da Família na atenção à saúde do idoso. Ciênc Saúde Colet. 2011;16(S1):1467-78.
acting in situations of violence against old people (VAOP)? What would be the specific actions of the physical therapist in these situations? Which actions are multiprofessional? How effective are these interventions in this problem? How should the protocol for physiotherapeutic assistance be faced with VAOP?
Considering that many important actions in coping with VAOP, mainly at the levels of prevention and promotion, are shared with other health professionals, it is suggested that future reviews be carried out that include interdisciplinary approaches aimed at this problem, enabling the identification of updated studies and portray proven interventions.
On the other hand, physiotherapists contribute with specific and significant actions for this
problem, especially with regard to the therapeutic and rehabilitation plan, and which constitute the differential of these professionals in the context of VAOP, needing to be disseminated among researchers and professionals of the practice.
Based on this and future reviews, it is suggested to conduct methodological research for the elaboration and validation of care protocols, both specific to the physiotherapist and multiprofessional. These protocols could support a qualified professional practice with a focus on comprehensive care for old people who are victims of violence, contributing to the implementation of existing public health policies and improving the quality of life and health of this population.
Edited by: Maria Helena Rodrigues Galvão

14 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
14. Peters MDJ, Godfrey C, McInerney P, Munn Z, Tricco AC, Khalil, H. Scoping Reviews. In: Aromataris E, Munn Z, Editors. JBI Manual for Evidence Synthesis [Internet]. 2020 [cited 2020 Apr.05]. Chapter 11. Available from: https://reviewersmanual.joannabriggs.org/
15. Tricco AC, Lillie E, Zarin W, O’Brien KK, Colquhoun H, Levac D, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018;169(7):467-73.
16. Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. BMJ. 2005;331(5):1064-65.
17. Little CD. What every Physical Therapist should know about Elder Abuse. Gerinotes. 2002;9(4):5-9.
18. Dalton A. Family Violence: Recognizing the Signs, Offering Help. PT Magazine. 2005;13(1):34-40.
19. Saliga S, Adamowicz C, Logue A, Smith K. Physical Therapist’s Knowledge of physical elder abuse: signs, symptoms, laws, and facility protocols. J Geriatr Phys Ther. 2004;27(1):5-12.
20. Camaratta F, Fenstermaker J, Hoffman AJ, Kolongowski M, Tecklin JS. Elder Abuse and the Physical Therapist. Issues Aging. 2000;23(1):9-12.
21. Foose D. Elder Abuse: Stepping in and Stopping It. PT Magazine. 1999;7(1):56-62.
22. Holland LR, Kasraian KR, Leonardelli CA. Elder Abuse: an analysis of the current problem and the potential role of the rehabilitation professional. Phys Occup Ther Geriatr. 1987;5(3):41-50.
23. Mildenberger C, Wessman HC. Abuse and neglect of elderly persons by family members: a special communication. Phys Ther. 1986;66(4):537-9.
24. Tomita SK. Detection and treatment of elderly abuse and neglect: a protocol for health care professionals. Phys Occup Ther Geriatr. 1982;2(2):37-51.
25. Bobitt J, Carter J, Kuhne J. Advancing National Policy on Elder Abuse. Public Policy Aging Rep. 2018;28(3):85-9.
26. Neto EM, Rocha DS, Silva EA, Silva MB. Intervenção Fisioterapêutica em Idoso institucionalizado vítima de violência urbana: estudo de caso. J Ciênc Biomed Saúde. 2020;5(3):58-60.
27. Ribeiro AP, Barter EACP. Atendimento de reabilitação à pessoa idosa vítima de acidentes e violência em distintas regiões do Brasil. Ciênc Saúde Colet. 2010;15(6):2729-40.
28. Colussi EL, Kuyawa A, de Marchi ACB, Pichler NA. Percepções de idosos sobre envelhecimento e violência nas relações intrafamiliares. Rev Bras Geriatr Gerontol. 2019;22(4):e190034.
29. São Paulo. Instituto de Assistência Médica ao Servidor Público. Manual de Segurança e Direitos da Pessoa Idosa [Internet]. São Paulo: CEDEP; 2013 [cited 2019 Nov. 09]. Available from: http://www.iamspe.sp.gov.br/wp-content/uploads/2017/01/manual-segurana-direitos-pessoa-idosa.pdf
30. Lopes EDS, Ferreira AG, Pires CG, Moraes MCS, D´Elboux MJ. Maus-tratos a idosos no Brasil: uma revisão integrativa. Rev Bras Geriatr Gerontol. 2018;21(5):652-62.
31. Hirst SP, Penney T, McNeill S, Boscart VM, Podnieks E, Sinha SK. Best-Practice guideline on the prevention of abuse and neglect of older adults. Can J Aging. 2016;35(2):242-60.
32. Lino VTS, Rodrigues NCP, Lima IS, Athie S, Souza ER. Prevalência e fatores associados ao abuso de cuidadores contra idosos dependentes: a face oculta da violência familiar. Ciênc Saúde Colet. 2019;24(1):87-96.
33. Souza LR, Hanus JS, Libera LBD, Silva VM, Mangilli EM, Simões PW, et al. Sobrecarga no cuidado, estresse e impacto na qualidade de vida de cuidadores domiciliares assistidos na atenção básica. Cad Saúde Colet. 2015;23(2):140-9.
34. Moura LBA, Noronha VMAS, Vieira ABD, Faustino AM. Percepções de qualidade de vida e as experiências de violências em idosos. Rev Enferm UFPE on line. 2018;12(8):2146-53.
35. Dias VF, Araújo LSLR, Cândido ASC, Lopes AOS, Pinheiro LMG, Reis LA. Dados sociodemográficos, condições de saúde e sinais de violência contra idosos longevos. Rev Saúde Colet. 2019;9:186-92.
36. Oliveira BS, Dias VF, Reis LA. Relação entre capacidade funcional e sinais de violência e maus tratos em idosos longevos. Fisioter Brasil. 2015;16(1):32-7.
37. Santos MAB, Moreira RS, Faccio PF, Gomes GC, Silva VL. Fatores associados à violência contra o idoso: uma revisão sistemática da literatura. Ciênc Saúde Colet. 2020;25(6):2153-75.
38. Maia PHS, Ferreira EF, Melo EM, Vargas AMD. A ocorrência da violência em idosos e seus fatores associados. Rev Bras Enferm. 2019;72(Suppl 2):64-70.
39. Borda LMF, Porto SH, Martínez VB, Ramírez RAH. Maltrato a las personas mayores: una revisión narrativa. Univ Med. 2019;60(4):1-16.

15 of 15
Physiotherapy in violence against old people
Rev. Bras. Geriatr. Gerontol. 2020;23(3):e200100
40. Elder Abuse Task Force of Santa Clara County. Elder Abuse: Guidelines for Professional Assessment and Reporting: Identification, Assessment, Reporting, Prevention, Resources [Internet]. California: EATF; 2019 [cited 2019 Dec. 18]. Available from: https://www.sccgov.org/sites/da/prosecution/DistrictAttorneyDepartments/Documents/Elder%20Abuse%20%E2%80%93%E2%80%93%20Guidelines%20For%20Professional%20Assessment%20and%20Reporting%20%28April%202019%29.pdf
41. Rio Grande do Sul. Secretaria de Estado da Saúde. Enfrentamento da Violência contra Pessoa Idosa na Saúde: Orientações para Gestores e Profissionais de Saúde [Internet]. Porto Alegre; Secretaria de Estado da Saúde do Rio Grande do Sul. 2016 [cited 2019 Nov. 15]. Available from: https://saude.rs.gov.br/upload/arquivos/201705/ 22152615-cartilha-enfrentamento-da-violencia-contra-pessoa-idosa.pdf
42. Lemos ECWM, Guadagnin EC, Mota CB. Influência do treinamento de força e do treinamento multicomponente na funcionalidade de idosos: revisão sistemática e metanálise. Rev Bras Cineantropom Desempenho Hum. 2020;22:e60707.
43. Lustosa LP, Andrade MAP, Araújo MRN, Bonolo PF, Campos TVO, Araújo VL. Uso terapêutico de tecnologias assistivas: direitos das pessoas com deficiência e habilidade física e motora. Belo Horizonte: Nescon; 2015.
44. Brasil. Lei nº 10.741, de 1º de Outubro de 2003. Dispõe sobre o Estatuto do Idoso e dá outras providências. Diário Oficial da União. 3 out. 2003.
45. Conselho Federal de Fisioterapia e Terapia Ocupacional. Resolução nº 424 de 08 de Julho de 2013. Estabelece o Código de Ética e Deontologia da Fisioterapia. Diário Oficial da União. 01 ago 2013.
46. Mazzotti MC, Scarcella E, D’Antone E, Fersini F, Salsi G, Ingravallo F, et al. Italian healthcare professionals’ attitude and barriers to mandatory reporting of elder abuse: an exploratory study. J Forensic Leg Med. 2019;63:26-30.

Related Documents











