VITROS ® Solutions The 10th International & 15th National Congress on Quality Improvement in Clinical Laboratories 2017. Teheran

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
VITROS ® Solutions
The 10th International & 15th National Congress on Quality Improvement in Clinical
Laboratories 2017.
Teheran
© Ortho Clinical Diagnostics 2017
Agenda
2
• Company Overview
• Daily Challenges
• VITROS® Systems
• VITROS® Technologies
• Added Values
• VITROS ® Automation Solutions

Who We AreWe are a global leader of in vitro diagnostics
serving the global clinical laboratory and
immunohematology communities.
What We Do and WhyWorldwide across hospitals, hospital networks, blood
banks and labs, our high-quality products and services
enable health care professionals to make better-informed
treatment decisions to improve and save lives.
© Ortho Clinical Diagnostics 2017 5
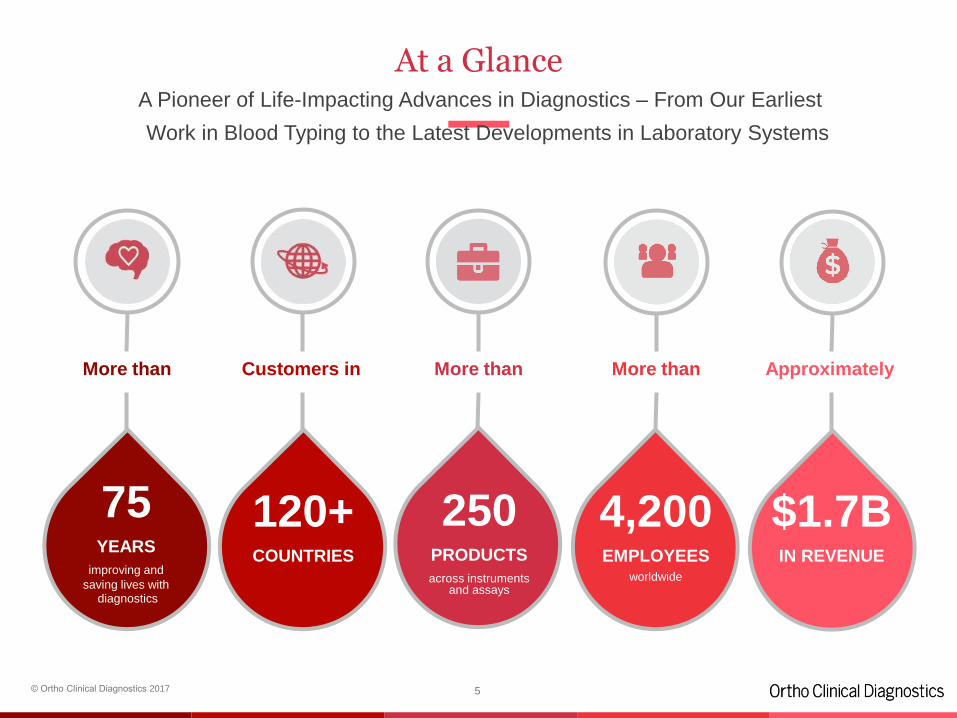
At a GlanceA Pioneer of Life-Impacting Advances in Diagnostics – From Our Earliest
Work in Blood Typing to the Latest Developments in Laboratory Systems
120+COUNTRIES
4,200EMPLOYEES
worldwide
$1.7BIN REVENUE
75YEARS
improving and
saving lives withdiagnostics
250PRODUCTS
across instruments and assays
More than Customers in More than More than Approximately
© Ortho Clinical Diagnostics 2017
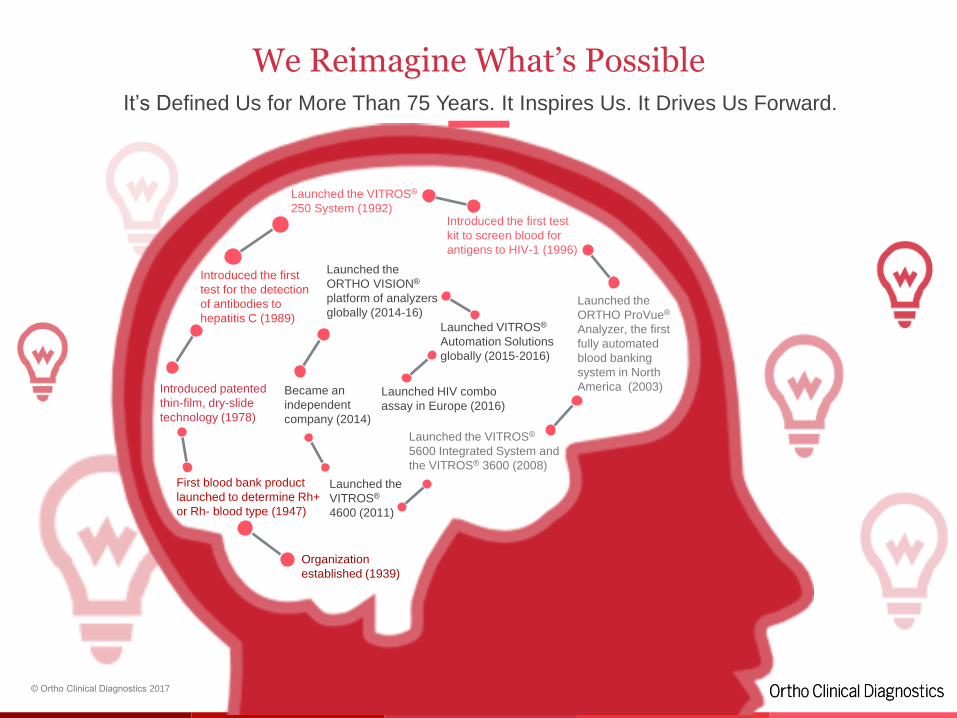
We Reimagine What’s PossibleIt’s Defined Us for More Than 75 Years. It Inspires Us. It Drives Us Forward.
6
Organization
established (1939)
First blood bank product
launched to determine Rh+
or Rh- blood type (1947)
Introduced patented
thin-film, dry-slide
technology (1978)
Introduced the first
test for the detection
of antibodies to
hepatitis C (1989)
Launched the VITROS®
250 System (1992)Introduced the first test
kit to screen blood for
antigens to HIV-1 (1996)
Launched the
ORTHO ProVue®
Analyzer, the first
fully automated
blood banking
system in North
America (2003)
Launched the VITROS®
5600 Integrated System and
the VITROS® 3600 (2008)
Launched the
VITROS®
4600 (2011)
Became an
independent
company (2014)
Launched the
ORTHO VISION®
platform of analyzers
globally (2014-16)
Launched HIV combo
assay in Europe (2016)
Launched VITROS®
Automation Solutions
globally (2015-2016)
© Ortho Clinical Diagnostics 2017 7
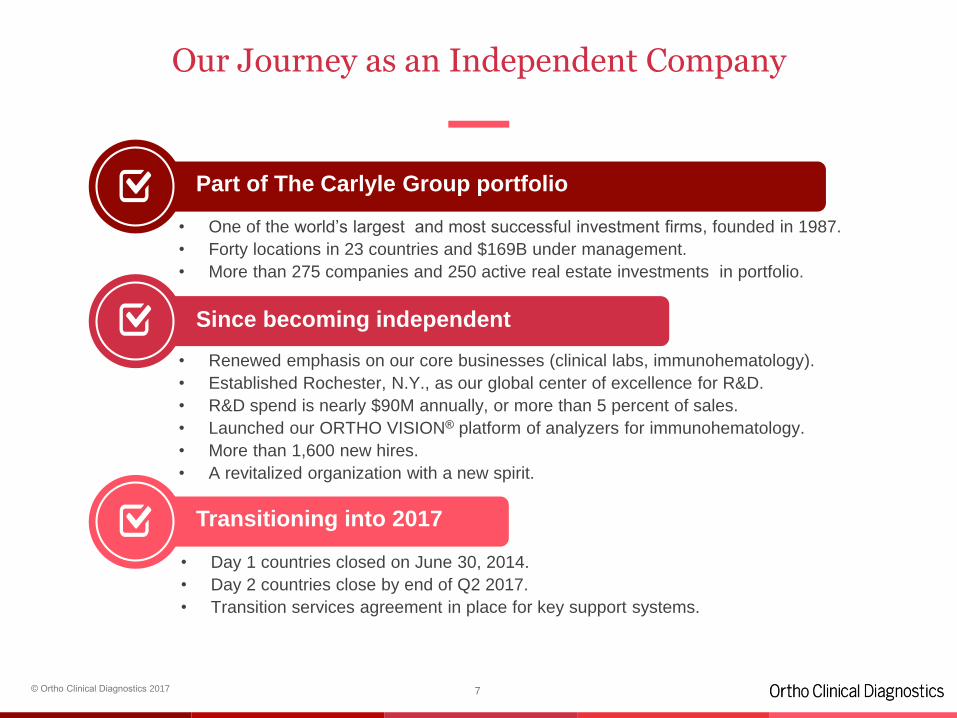
Our Journey as an Independent Company
Part of The Carlyle Group portfolio
Since becoming independent
Transitioning into 2017
• One of the world’s largest and most successful investment firms, founded in 1987.
• Forty locations in 23 countries and $169B under management.
• More than 275 companies and 250 active real estate investments in portfolio.
• Renewed emphasis on our core businesses (clinical labs, immunohematology).
• Established Rochester, N.Y., as our global center of excellence for R&D.
• R&D spend is nearly $90M annually, or more than 5 percent of sales.
• Launched our ORTHO VISION® platform of analyzers for immunohematology.
• More than 1,600 new hires.
• A revitalized organization with a new spirit.
• Day 1 countries closed on June 30, 2014.
• Day 2 countries close by end of Q2 2017.
• Transition services agreement in place for key support systems.
© Ortho Clinical Diagnostics 2017
Agenda
8
• Company Overview
• Daily Challenges
• VITROS® Systems
• VITROS® Technologies
• Summary
• VITROS® Automation Solution
© Ortho Clinical Diagnostics 2017
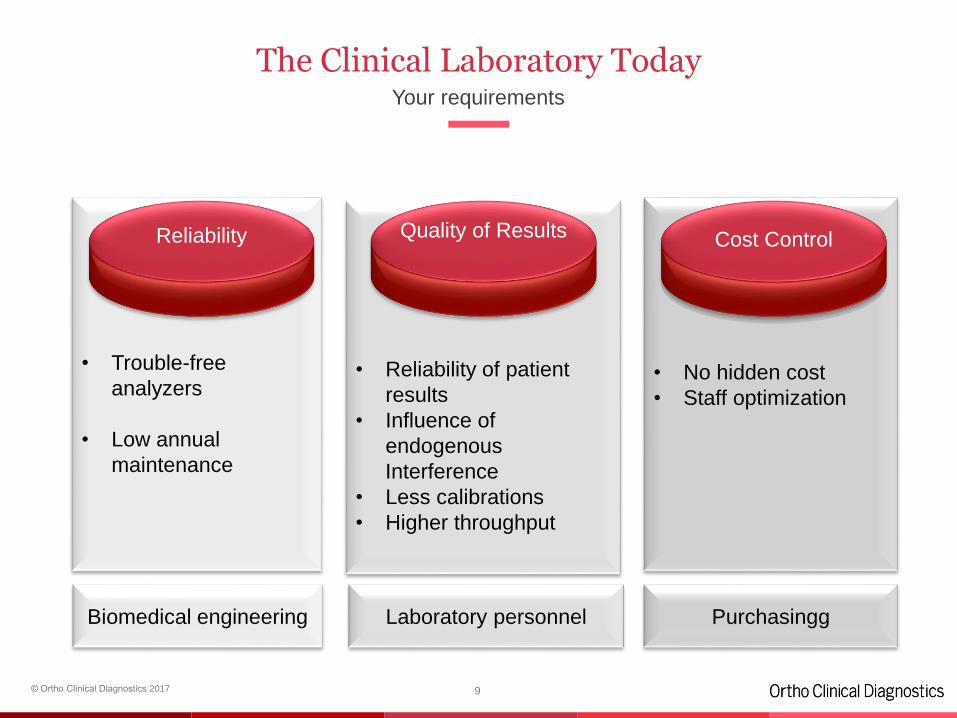
The Clinical Laboratory TodayYour requirements
• Trouble-free
analyzers
• Low annual
maintenance
• Reliability of patient
results
• Influence of
endogenous
Interference
• Less calibrations
• Higher throughput
• No hidden cost
• Staff optimization
Biomedical engineering Laboratory personnel Purchasingg
Quality of Results Cost ControlReliability
9

© Ortho Clinical Diagnostics 2017
Agenda
10
• Company Overview
• Daily Challenges
• VITROS® Systems
• VITROS® Technologies
• Summary
© Ortho Clinical Diagnostics 2017
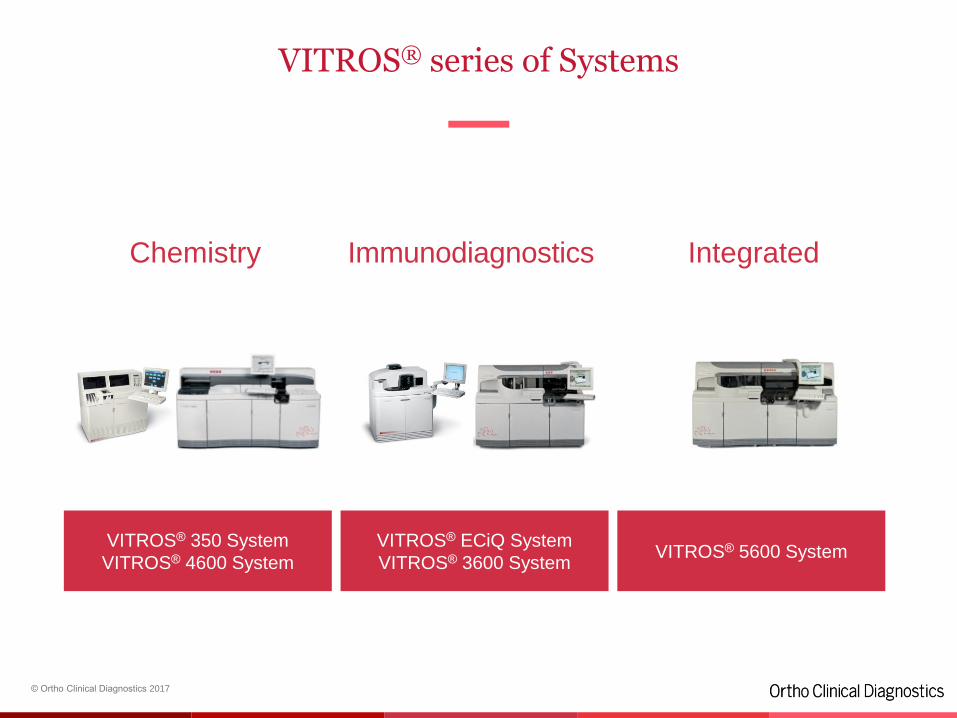
VITROS® series of Systems
11
Chemistry Immunodiagnostics Integrated
VITROS® 350 System
VITROS® 4600 System
VITROS® ECiQ System
VITROS® 3600 SystemVITROS® 5600 System
© Ortho Clinical Diagnostics 2017
Total β-hCG II
Estradiol
Progesterone
Testosterone
LH
FSH
Prolactin
Anemia
Oncology
Thyroids
Metabolic
Diabetes
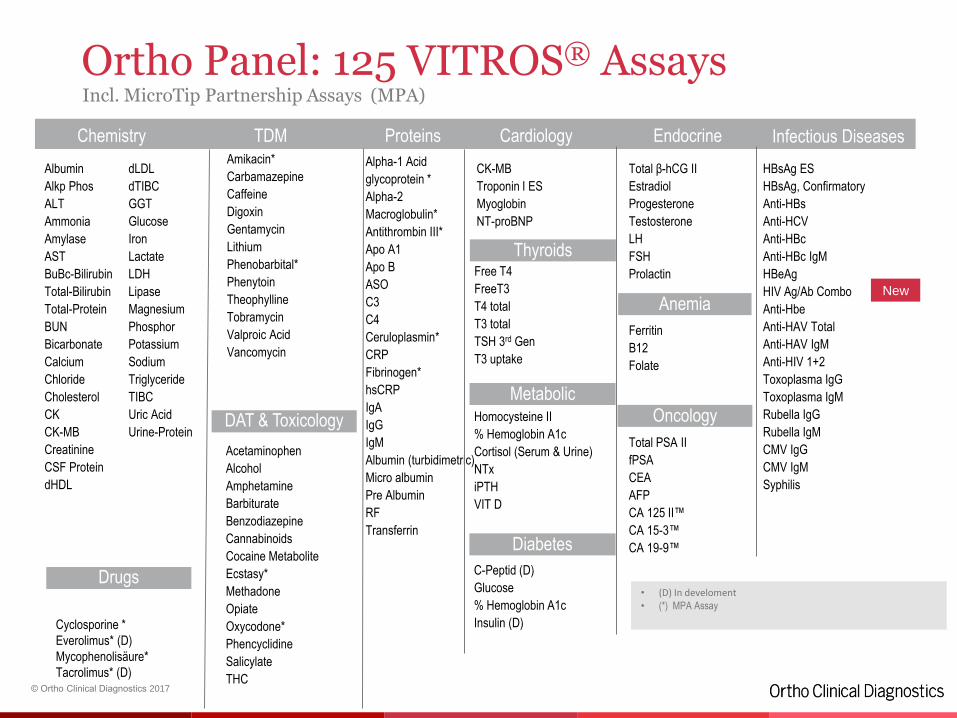
Infectious DiseasesEndocrineCardiologyProteinsTDMChemistry
DAT & Toxicology
Albumin
Alkp Phos
ALT
Ammonia
Amylase
AST
BuBc-Bilirubin
Total-Bilirubin
Total-Protein
BUN
Bicarbonate
Calcium
Chloride
Cholesterol
CK
CK-MB
Creatinine
CSF Protein
dHDL
dLDL
dTIBC
GGT
Glucose
Iron
Lactate
LDH
Lipase
Magnesium
Phosphor
Potassium
Sodium
Triglyceride
TIBC
Uric Acid
Urine-Protein
Amikacin*
Carbamazepine
Caffeine
Digoxin
Gentamycin
Lithium
Phenobarbital*
Phenytoin
Theophylline
Tobramycin
Valproic Acid
Vancomycin
Acetaminophen
Alcohol
Amphetamine
Barbiturate
Benzodiazepine
Cannabinoids
Cocaine Metabolite
Ecstasy*
Methadone
Opiate
Oxycodone*
Phencyclidine
Salicylate
THC
Alpha-1 Acid
glycoprotein *
Alpha-2
Macroglobulin*
Antithrombin III*
Apo A1
Apo B
ASO
C3
C4
Ceruloplasmin*
CRP
Fibrinogen*
hsCRP
IgA
IgG
IgM
Albumin (turbidimetric)
Micro albumin
Pre Albumin
RF
Transferrin
CK-MB
Troponin I ES
Myoglobin
NT-proBNP
Free T4
FreeT3
T4 total
T3 total
TSH 3rd Gen
T3 uptake
Homocysteine II
% Hemoglobin A1c
Cortisol (Serum & Urine)
NTx
iPTH
VIT D
C-Peptid (D)
Glucose
% Hemoglobin A1c
Insulin (D)
Total PSA II
fPSA
CEA
AFP
CA 125 II™
CA 15-3™
CA 19-9™
Ferritin
B12
Folate
HBsAg ES
HBsAg, Confirmatory
Anti-HBs
Anti-HCV
Anti-HBc
Anti-HBc IgM
HBeAg
HIV Ag/Ab Combo
Anti-Hbe
Anti-HAV Total
Anti-HAV IgM
Anti-HIV 1+2
Toxoplasma IgG
Toxoplasma IgM
Rubella IgG
Rubella IgM
CMV IgG
CMV IgM
Syphilis
Drugs
Cyclosporine *
Everolimus* (D)
Mycophenolisäure*
Tacrolimus* (D)
• (D) In develoment• (*) MPA Assay
Ortho Panel: 125 VITROS® AssaysIncl. MicroTip Partnership Assays (MPA)
New
© Ortho Clinical Diagnostics 2017
Agenda
13
• Company Overview
• Daily Challenges
• VITROS® Systems
• VITROS® Technologies
• Added Values
• VITROS® Automation Solution
The Five Enabling Technologies
14
© Ortho Clinical Diagnostics 2017
5 unique VITROS® Technologies
15
3 Assay technologies 2 Quality technologies
VITROS® MicroSlide
(or Dry slide technology) is the foundation of all
VITROS® chemistry systems.
VITROS® MicroTip
For specific proteins, TDMs and DOAs plus open
channels.
Enhanced Chemiluminescence
The critical immunoassay technology for the
VITROS® MicroWell menu, including infectious
disease
Poor sample quality, which could compromise results, is
flagged without impacting workflow by VITROS®
MicroSensor.
VITROS® Intellicheck® Technology verifies sample
integrity and reduces the risk of an incorrect result to near
zero.

VITROS® MicroWell Assay Technology
16
© Ortho Clinical Diagnostics 2017
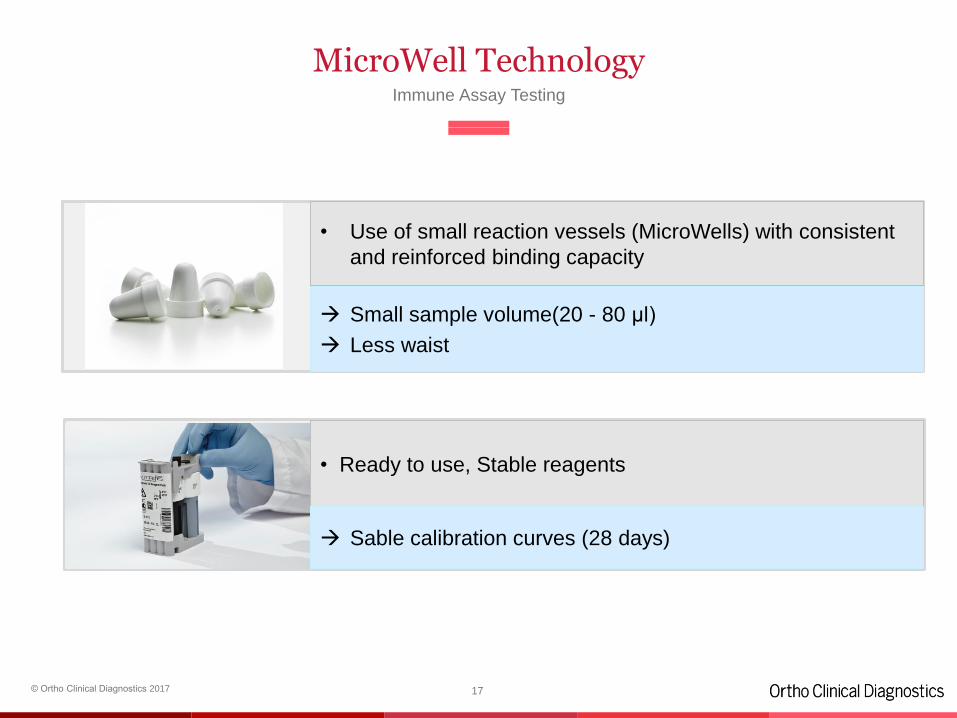
MicroWell Technology
17
• Ready to use, Stable reagents
Sable calibration curves (28 days)
• Use of small reaction vessels (MicroWells) with consistent
and reinforced binding capacity
Small sample volume(20 - 80 µl)
Less waist
Immune Assay Testing
© Ortho Clinical Diagnostics 2017
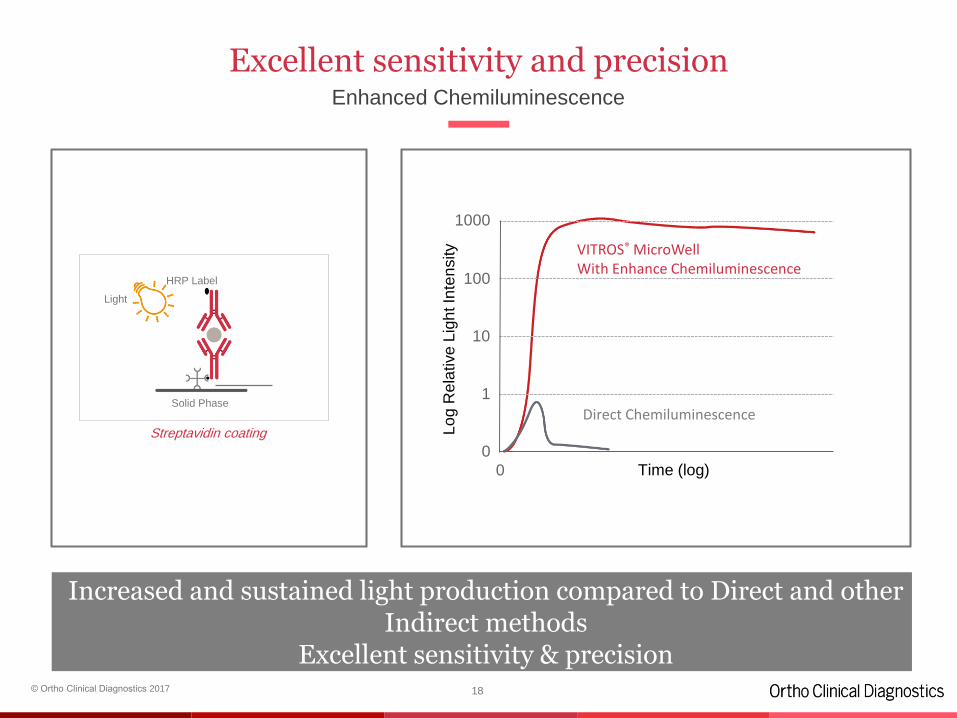
Excellent sensitivity and precisionEnhanced Chemiluminescence
18
0
1
10
100
1000
0 Time (log)
Lo
g R
ela
tive
Lig
ht In
ten
sity
Direct Chemiluminescence
VITROS® MicroWell With Enhance Chemiluminescence
Direct Chemiluminescence
Increased and sustained light production compared to Direct and other Indirect methods
Excellent sensitivity & precision
Streptavidin coating
Light
Solid Phase
HRP Label
© Ortho Clinical Diagnostics 2017
Proprietary Enhanced Chemiluminescence Detection Technology
19
• Improved Signal light output:
• Use of patented enhancer produces light output at
extremely low-analyte concentrations
• Better detection of low analyte concentrations levels
• Better performance to support medical decisions
• Excellent Sensitivity & Precision:
• More accurate results
• Ability to capture clinically significant low analyte
concentration levels
• Broad Dynamic Range:
• Less Dilutions & Repeats - Faster TAT
• Decreased Costs
© Ortho Clinical Diagnostics 2017
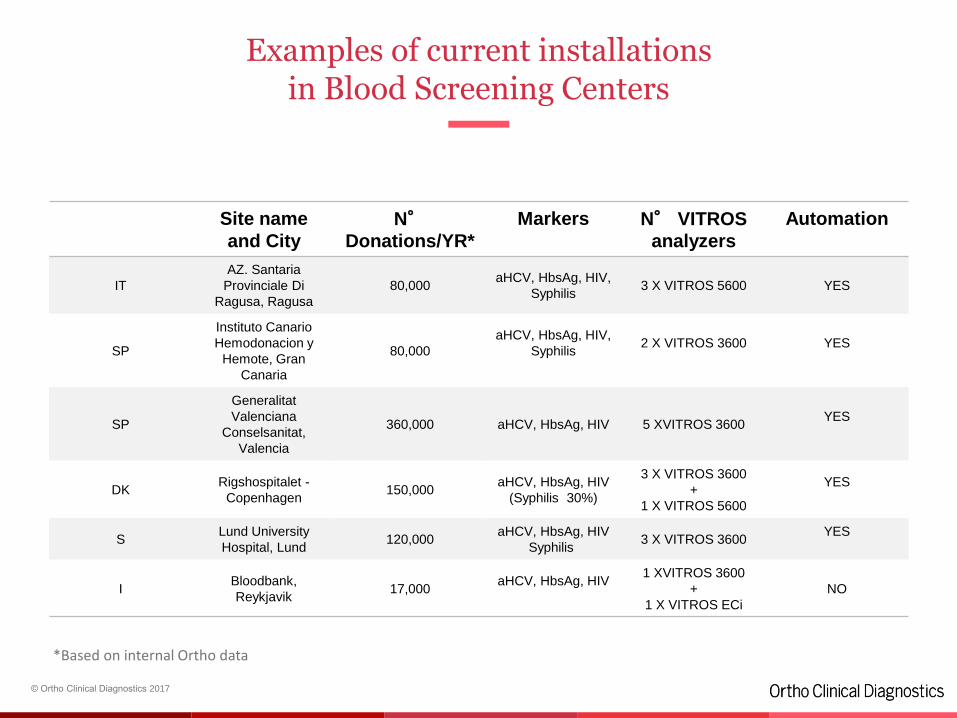
Examples of current installationsin Blood Screening Centers
Site name
and City
N°Donations/YR*
Markers N° VITROS
analyzers
Automation
IT
AZ. Santaria
Provinciale Di
Ragusa, Ragusa
80,000aHCV, HbsAg, HIV,
Syphilis3 X VITROS 5600 YES
SP
Instituto Canario
Hemodonacion y
Hemote, Gran
Canaria
80,000
aHCV, HbsAg, HIV,
Syphilis2 X VITROS 3600 YES
SP
Generalitat
Valenciana
Conselsanitat,
Valencia
360,000 aHCV, HbsAg, HIV 5 XVITROS 3600YES
DKRigshospitalet -
Copenhagen150,000
aHCV, HbsAg, HIV
(Syphilis 30%)
3 X VITROS 3600
+
1 X VITROS 5600
YES
SLund University
Hospital, Lund120,000
aHCV, HbsAg, HIV
Syphilis3 X VITROS 3600
YES
IBloodbank,
Reykjavik17,000
aHCV, HbsAg, HIV1 XVITROS 3600
+
1 X VITROS ECi
NO
*Based on internal Ortho data
HIV Combo
21
© Ortho Clinical Diagnostics 2017
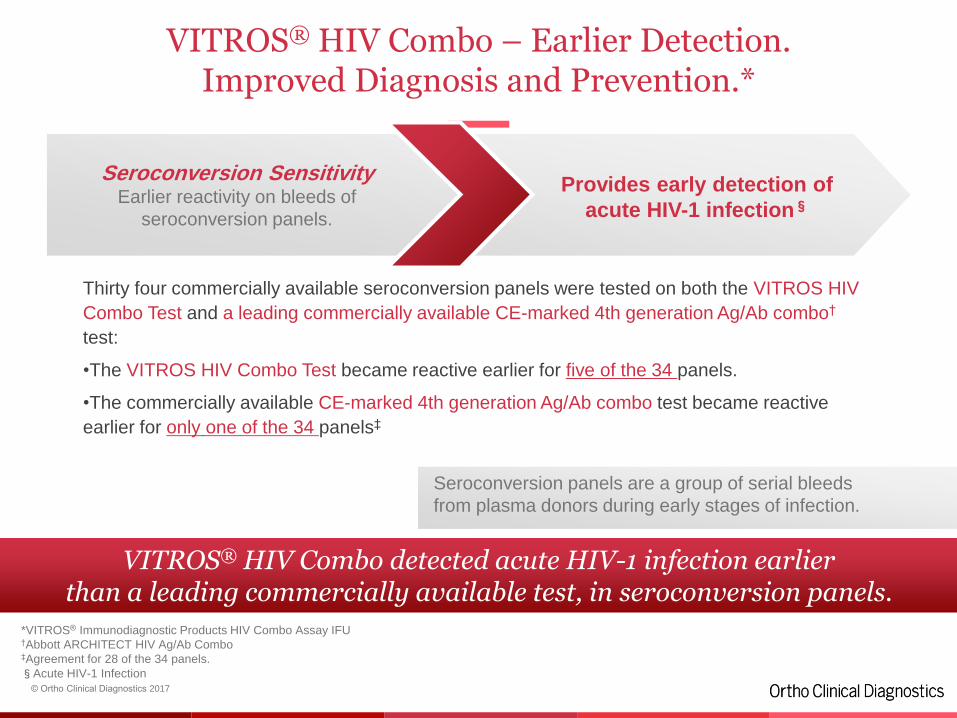
VITROS® HIV Combo – Earlier Detection. Improved Diagnosis and Prevention.*
Thirty four commercially available seroconversion panels were tested on both the VITROS HIV
Combo Test and a leading commercially available CE-marked 4th generation Ag/Ab combo†
test:
•The VITROS HIV Combo Test became reactive earlier for five of the 34 panels.
•The commercially available CE-marked 4th generation Ag/Ab combo test became reactive
earlier for only one of the 34 panels‡
22
VITROS® HIV Combo detected acute HIV-1 infection earlierthan a leading commercially available test, in seroconversion panels.
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU†Abbott ARCHITECT HIV Ag/Ab Combo‡Agreement for 28 of the 34 panels.
§Acute HIV-1 Infection
Seroconversion panels are a group of serial bleeds
from plasma donors during early stages of infection.
Seroconversion SensitivityEarlier reactivity on bleeds of
seroconversion panels.
Provides early detection of
acute HIV-1 infection§
© Ortho Clinical Diagnostics 2017
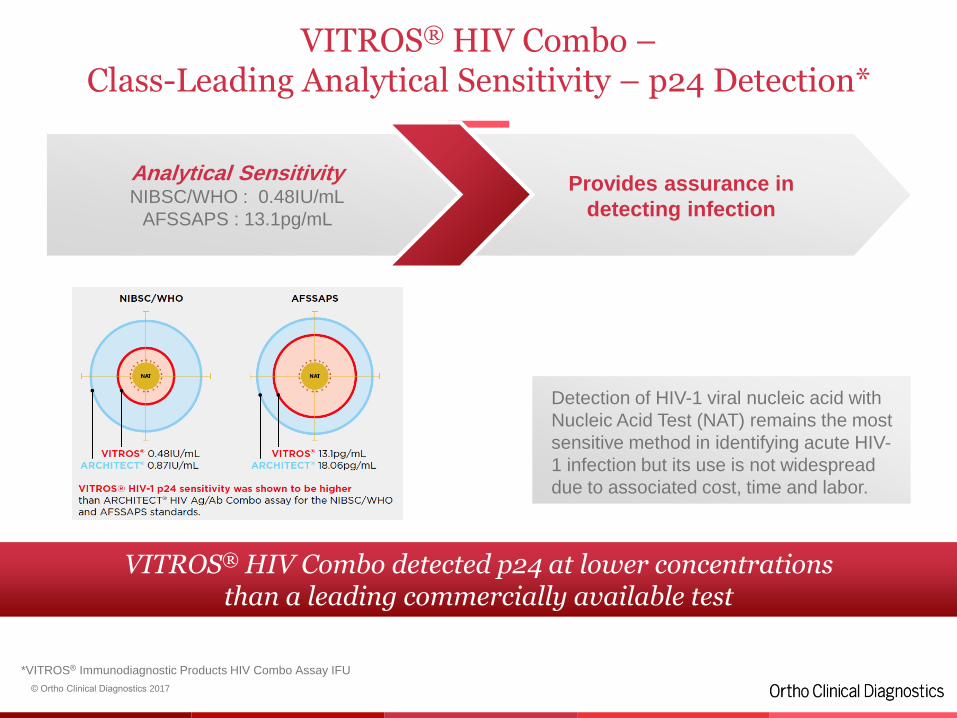
VITROS® HIV Combo –Class-Leading Analytical Sensitivity – p24 Detection*
23
VITROS® HIV Combo detected p24 at lower concentrationsthan a leading commercially available test
Detection of HIV-1 viral nucleic acid with
Nucleic Acid Test (NAT) remains the most
sensitive method in identifying acute HIV-
1 infection but its use is not widespread
due to associated cost, time and labor.
Analytical SensitivityNIBSC/WHO : 0.48IU/mL
AFSSAPS : 13.1pg/mL
Provides assurance in
detecting infection
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU
© Ortho Clinical Diagnostics 2017
VITROS® HIV Combo –Excellent Clinical Sensitivity*
• 500 samples previously determined as positive became reactive (400 for HIV-1
and 100 for HIV-2)
• 83 samples known to be infected with HIV-1 group M tested – all found to be
reactive.
24
VITROS® HIV Combo has a clinical sensitivity of 100%.
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU
Clinical Sensitivity100% (CI 99.26% - 100%)
Provides assurance in
detecting infection
© Ortho Clinical Diagnostics 2017
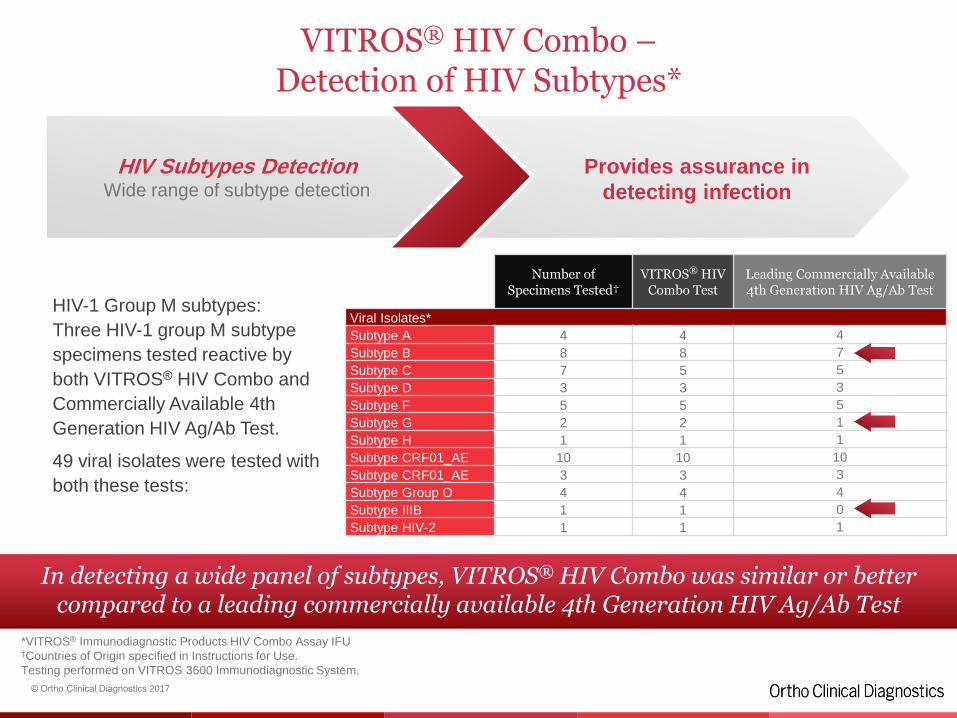
VITROS® HIV Combo –Detection of HIV Subtypes*
HIV-1 Group M subtypes:
Three HIV-1 group M subtype
specimens tested reactive by
both VITROS® HIV Combo and
Commercially Available 4th
Generation HIV Ag/Ab Test.
49 viral isolates were tested with
both these tests:
25
In detecting a wide panel of subtypes, VITROS® HIV Combo was similar or better compared to a leading commercially available 4th Generation HIV Ag/Ab Test
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU†Countries of Origin specified in Instructions for Use.
Testing performed on VITROS 3600 Immunodiagnostic System.
HIV Subtypes DetectionWide range of subtype detection
Provides assurance in
detecting infection
Number ofSpecimens Tested†
VITROS® HIV Combo Test
Leading Commercially Available 4th Generation HIV Ag/Ab Test
Viral Isolates*
Subtype A 4 4 4
Subtype B 8 8 7
Subtype C 7 5 5
Subtype D 3 3 3
Subtype F 5 5 5
Subtype G 2 2 1
Subtype H 1 1 1
Subtype CRF01_AE 10 10 10
Subtype CRF01_AE 3 3 3
Subtype Group O 4 4 4
Subtype IIIB 1 1 0
Subtype HIV-2 1 1 1
© Ortho Clinical Diagnostics 2017
VITROS® HIV Combo – Competitive Performance Uncompromised Specificity*
Testing performed at two external independent hospital laboratories.
Assay specificity assessed using 5077 blood donor samples and 607 samples from
hospitalized patients.
26
High sensitivity while maintaining specificity.
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU
Clinical Specificity99.84% (Donor Population, CI 99.69-99.93%)
100% (Clinical Population, CI 99.39-100%)
Fewer false positives to
save time, cost and labor
in repeat and
confirmatory tests
© Ortho Clinical Diagnostics 2017
VITROS® HIV Combo –Excellent Precision*
Two replicates each of 14 negative or diluted reactive patient sample pools and 5
control samples were tested on 2 separate occasions per day on at least 20
different days.
The experiment was performed using 2 reagent lots on 2 different systems on the
VITROS ECi/ECiQ, 3600 and 5600 Immunodiagnostic Systems.
27
Reliable results due to excellent precision.
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU†Clinical and Laboratory Standards Institute
PrecisionEvaluated consistent with CLSI†
document EP5
Excellent precision ensures
consistency
of test results
© Ortho Clinical Diagnostics 2017
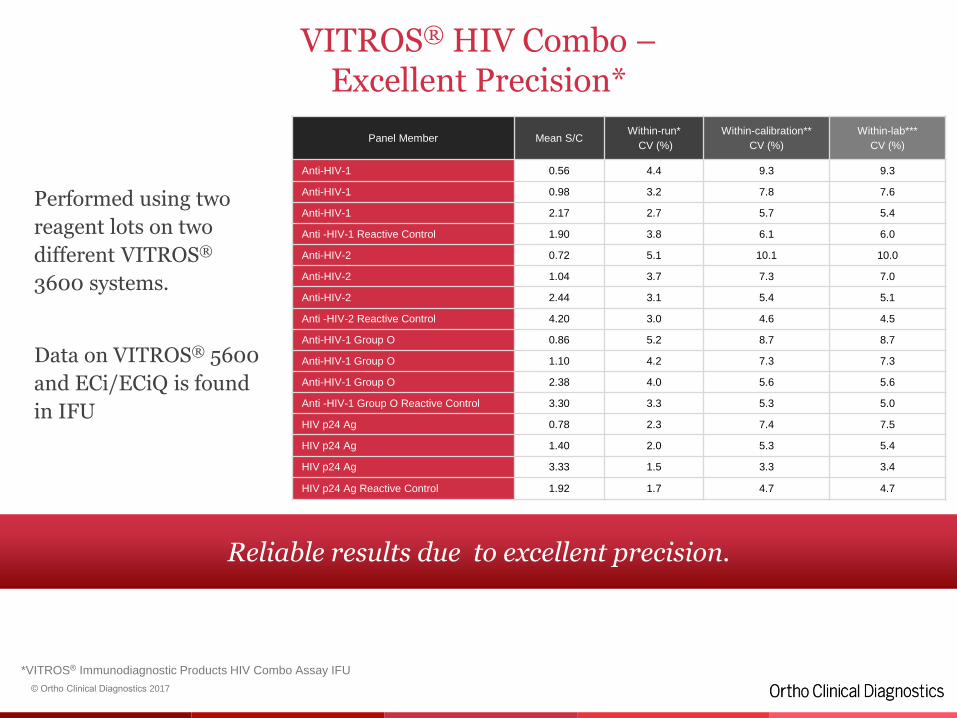
VITROS® HIV Combo –Excellent Precision*
Performed using two
reagent lots on two
different VITROS®
3600 systems.
Data on VITROS® 5600
and ECi/ECiQ is found
in IFU
28
Reliable results due to excellent precision.
*VITROS® Immunodiagnostic Products HIV Combo Assay IFU
Panel Member Mean S/CWithin-run*
CV (%)
Within-calibration**
CV (%)
Within-lab***
CV (%)
Anti-HIV-1 0.56 4.4 9.3 9.3
Anti-HIV-1 0.98 3.2 7.8 7.6
Anti-HIV-1 2.17 2.7 5.7 5.4
Anti -HIV-1 Reactive Control 1.90 3.8 6.1 6.0
Anti-HIV-2 0.72 5.1 10.1 10.0
Anti-HIV-2 1.04 3.7 7.3 7.0
Anti-HIV-2 2.44 3.1 5.4 5.1
Anti -HIV-2 Reactive Control 4.20 3.0 4.6 4.5
Anti-HIV-1 Group O 0.86 5.2 8.7 8.7
Anti-HIV-1 Group O 1.10 4.2 7.3 7.3
Anti-HIV-1 Group O 2.38 4.0 5.6 5.6
Anti -HIV-1 Group O Reactive Control 3.30 3.3 5.3 5.0
HIV p24 Ag 0.78 2.3 7.4 7.5
HIV p24 Ag 1.40 2.0 5.3 5.4
HIV p24 Ag 3.33 1.5 3.3 3.4
HIV p24 Ag Reactive Control 1.92 1.7 4.7 4.7
NT-pro BNPVideo
29
VITROS® MicroSlide Assay Technology
© Ortho Clinical Diagnostics 2017
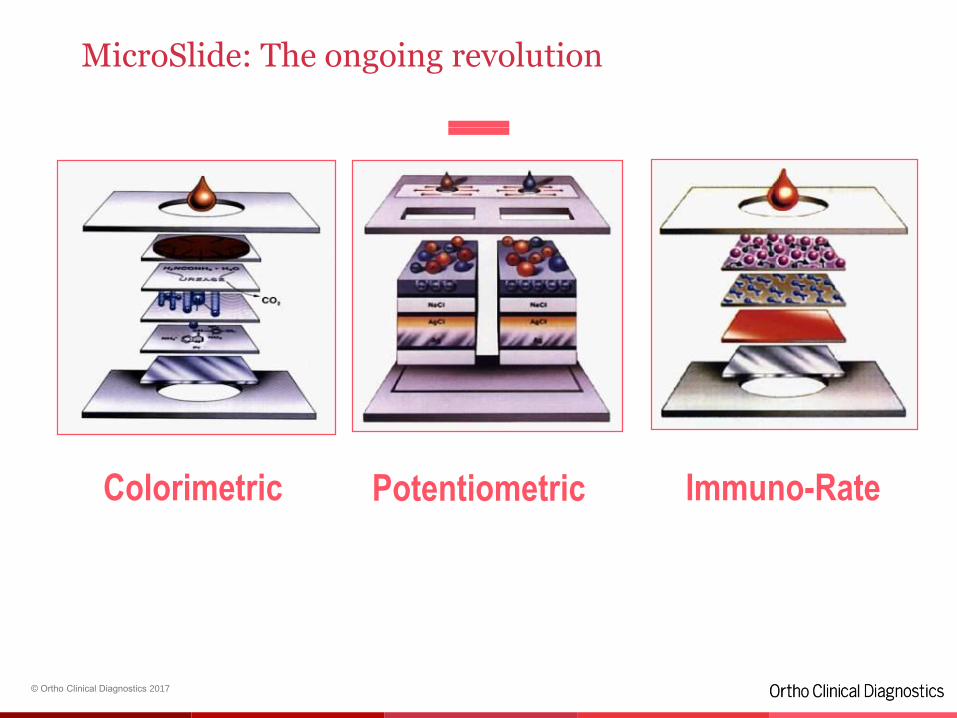
MicroSlide: The ongoing revolution
Colorimetric Potentiometric Immuno-Rate
Colorimetric MicroSlides
© Ortho Clinical Diagnostics 2017
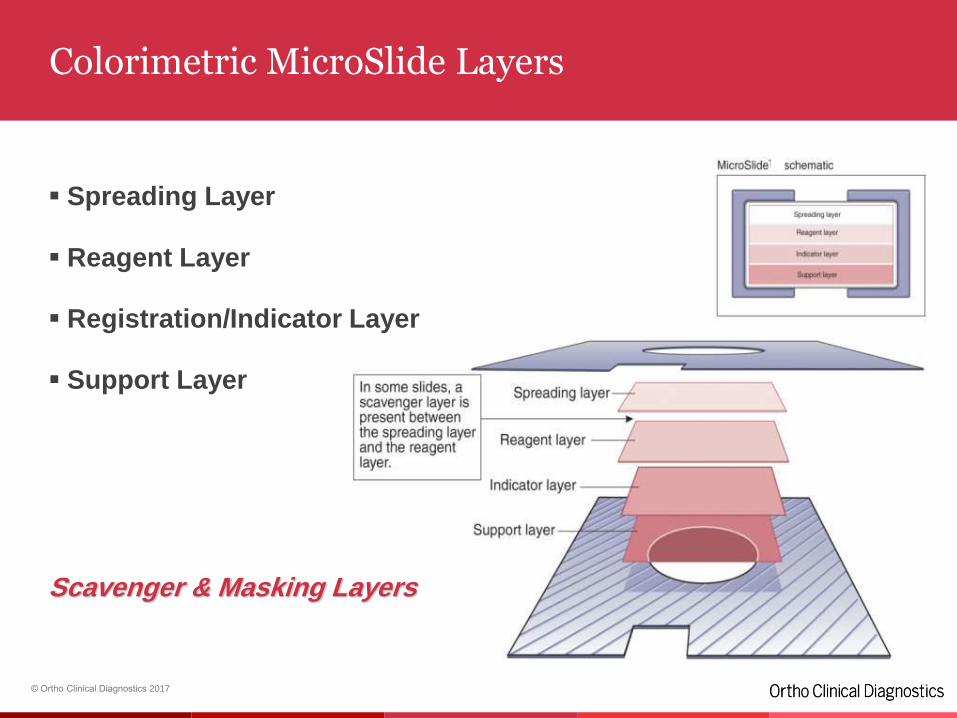
Colorimetric MicroSlide Layers
Spreading Layer
Reagent Layer
Registration/Indicator Layer
Support Layer
Scavenger & Masking Layers
© Ortho Clinical Diagnostics 2017
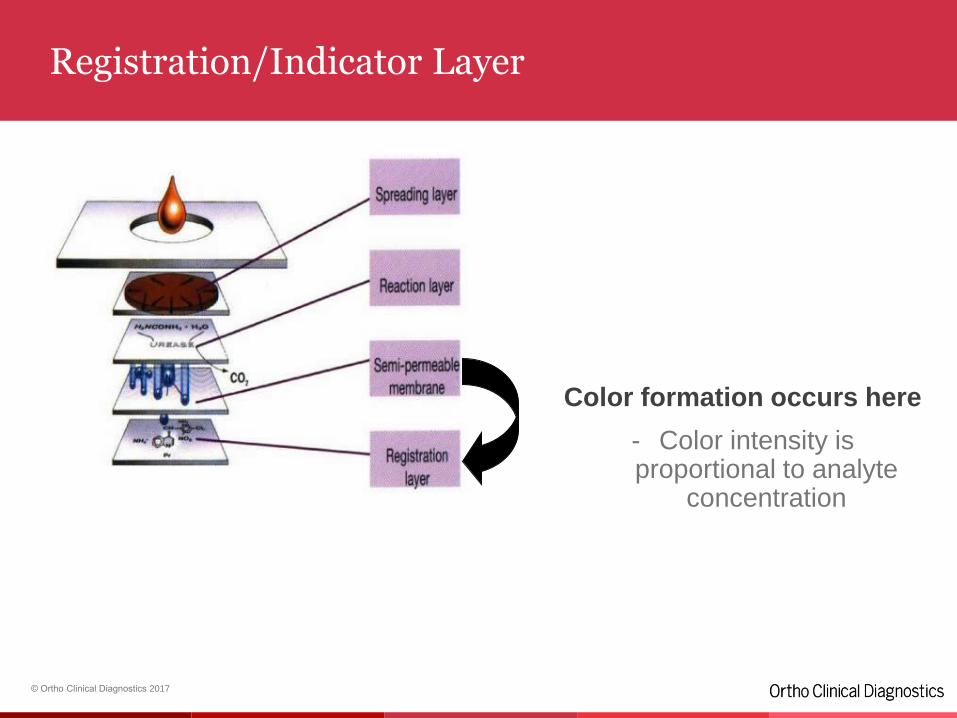
Registration/Indicator Layer
Color formation occurs here
- Color intensity is proportional to analyte
concentrationkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkk
kkkkkkkkkkkkkkkkkkkkkkkkkkkkkkk
© Ortho Clinical Diagnostics 2017
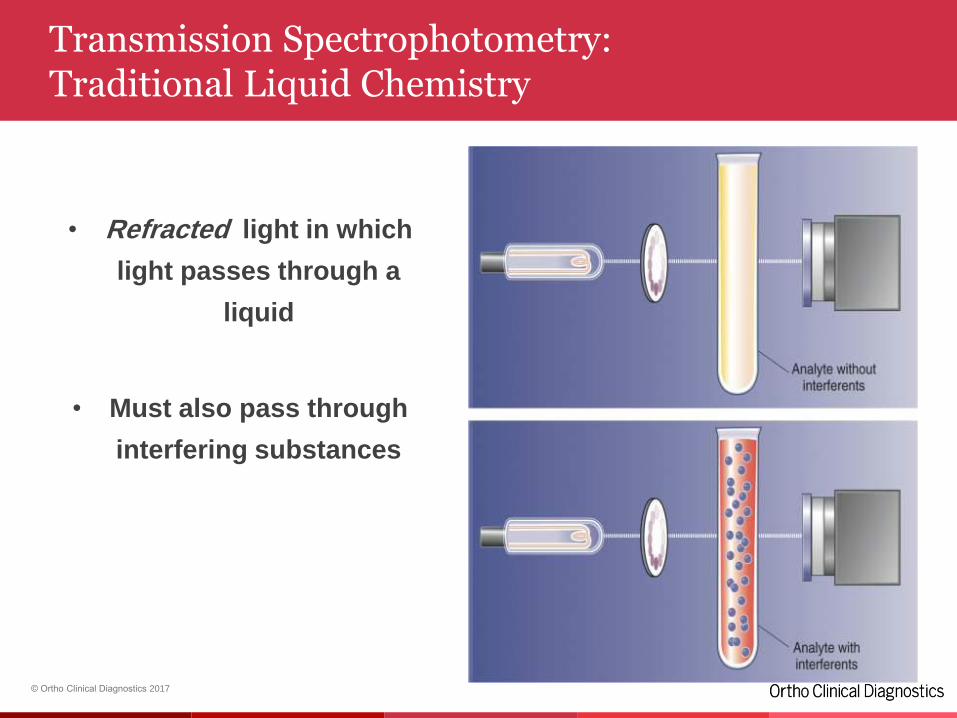
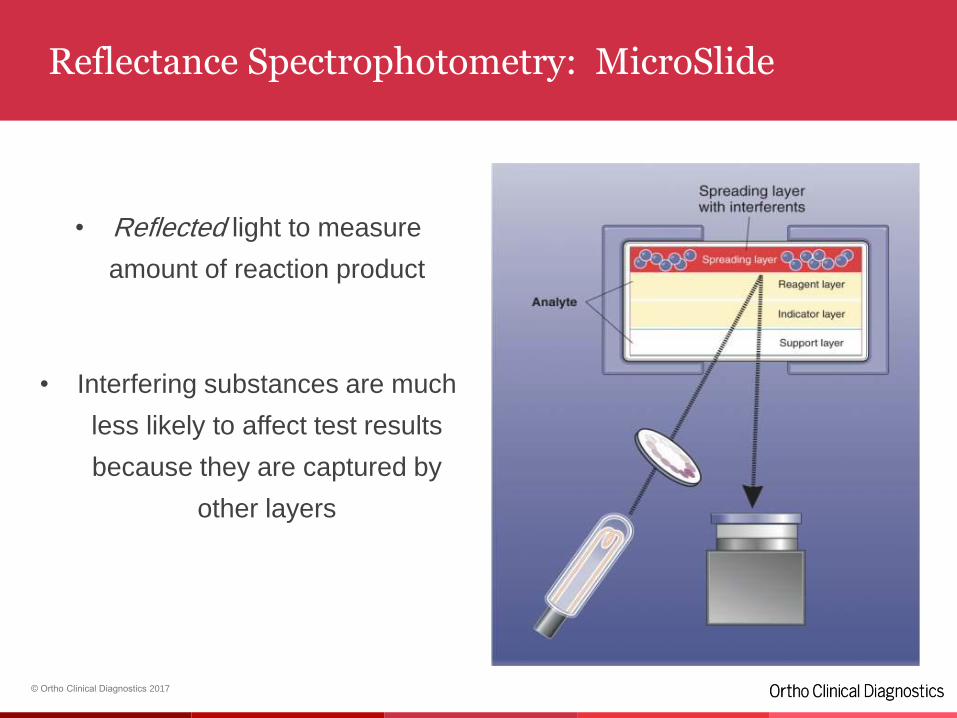
Transmission Spectrophotometry: Traditional Liquid Chemistry
• Refracted light in which
light passes through a
liquid
• Must also pass through
interfering substances
© Ortho Clinical Diagnostics 2017
Reflectance Spectrophotometry: MicroSlide
• Reflected light to measure
amount of reaction product
• Interfering substances are much
less likely to affect test results
because they are captured by
other layers
Potentiometric MicroSlidesDirect ISE
© Ortho Clinical Diagnostics 2017
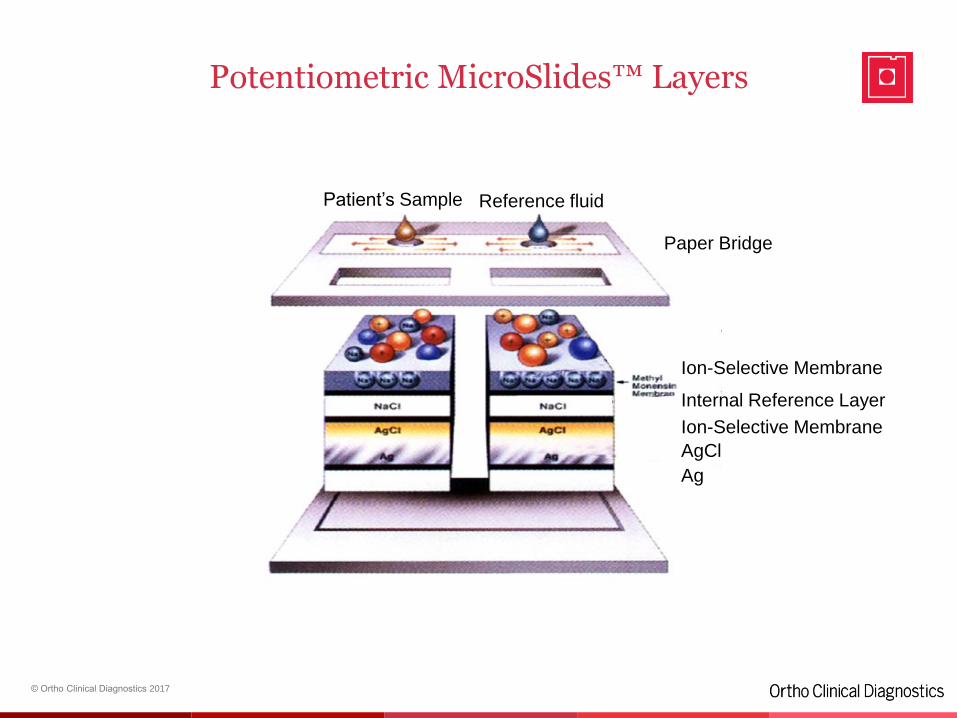
Potentiometric MicroSlides™ Layers
Patient’s Sample Reference fluid
Ion-Selective Membrane
Internal Reference Layer
Ion-Selective Membrane
AgCl
Ag
Paper Bridge
© Ortho Clinical Diagnostics 2017
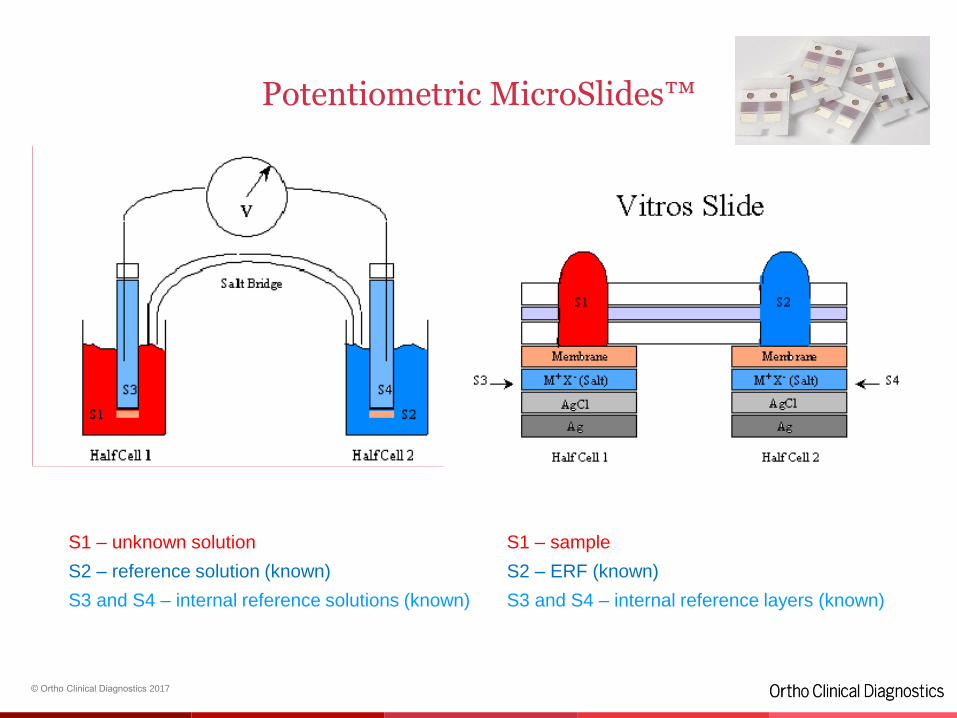
Potentiometric MicroSlides™
S1 – unknown solution
S2 – reference solution (known)
S3 and S4 – internal reference solutions (known)
S1 – sample
S2 – ERF (known)
S3 and S4 – internal reference layers (known)
© Ortho Clinical Diagnostics 2017
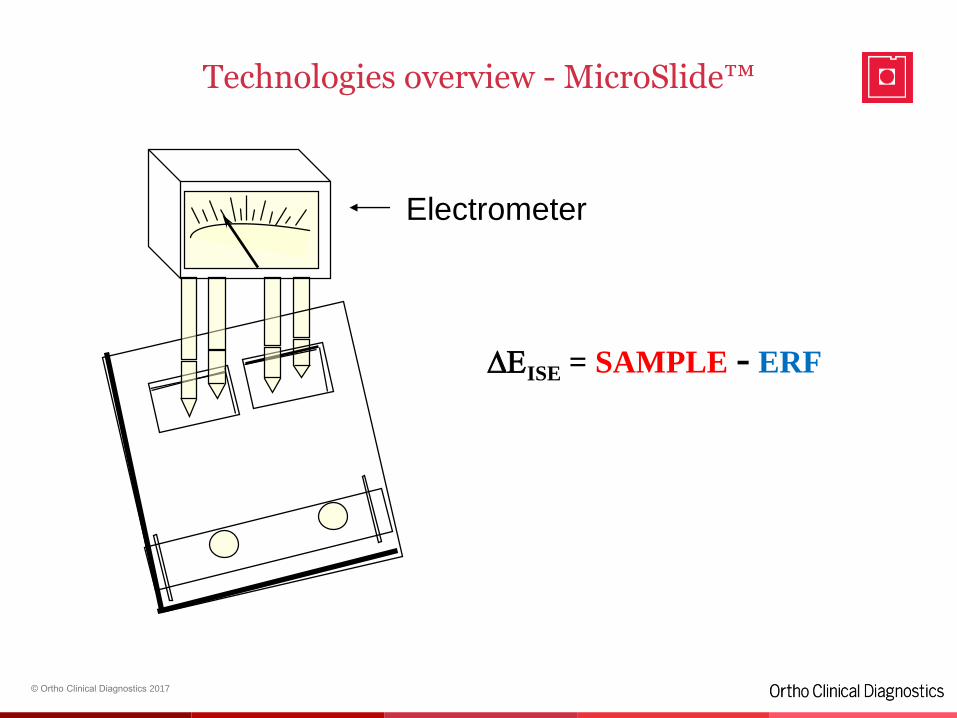
Electrometer
Technologies overview - MicroSlide™
DEISE = SAMPLE - ERF
© Ortho Clinical Diagnostics 2017
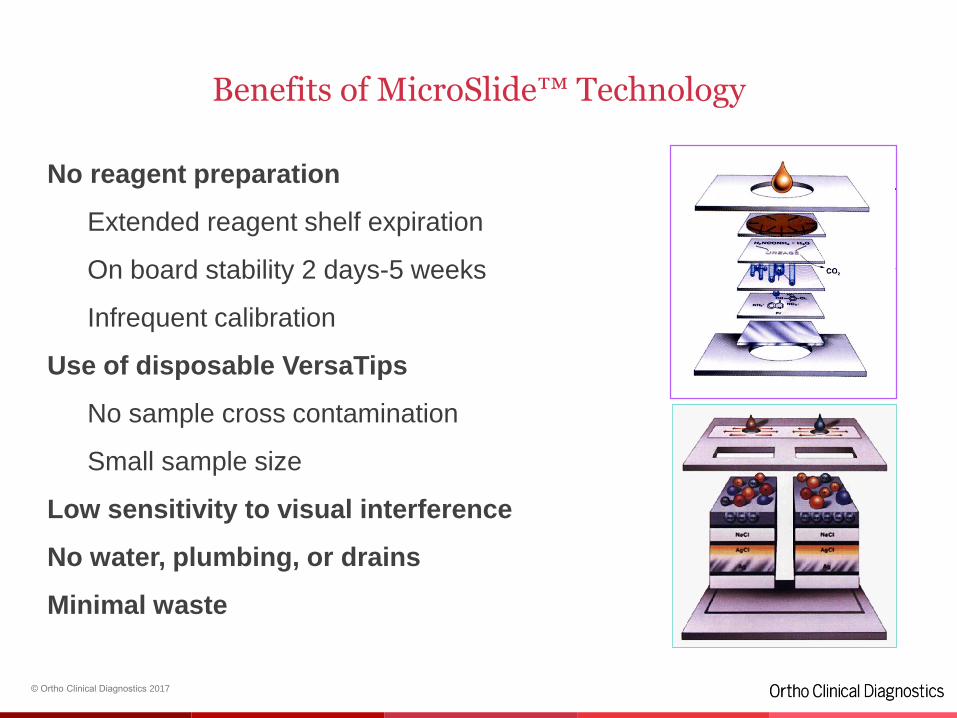
Benefits of MicroSlide™ Technology
No reagent preparation
Extended reagent shelf expiration
On board stability 2 days-5 weeks
Infrequent calibration
Use of disposable VersaTips
No sample cross contamination
Small sample size
Low sensitivity to visual interference
No water, plumbing, or drains
Minimal waste
© Ortho Clinical Diagnostics 2017
Direct vs Indirect ISE’s
• All ISE’s measure the activity of an ion
• Direct ISE’s do not dilute the sample prior to analysis
• Indirect ISE’s dilute the sample prior to analysis
The difference between direct and indirect ISE’s
is the impact of sample dilution on ion activity
© Ortho Clinical Diagnostics 2017
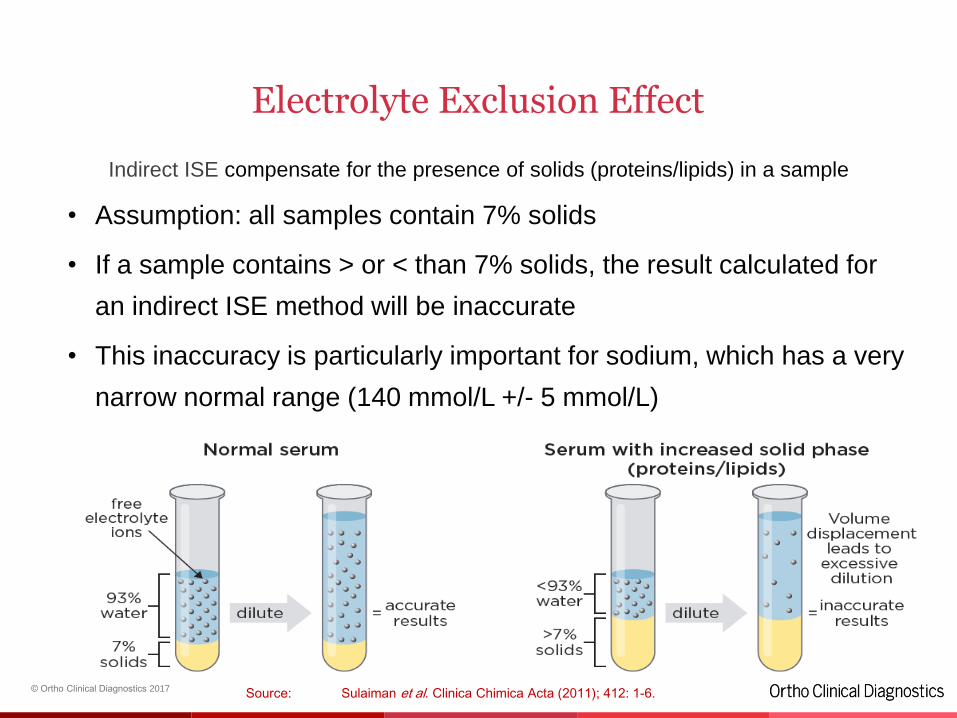
Electrolyte Exclusion Effect
Indirect ISE compensate for the presence of solids (proteins/lipids) in a sample
• Assumption: all samples contain 7% solids
• If a sample contains > or < than 7% solids, the result calculated for
an indirect ISE method will be inaccurate
• This inaccuracy is particularly important for sodium, which has a very
narrow normal range (140 mmol/L +/- 5 mmol/L)
Source: Sulaiman et al. Clinica Chimica Acta (2011); 412: 1-6.
© Ortho Clinical Diagnostics 2017
• At LOW TP levels:
the VITROS SODIUM will be LOWER THAN INDIRECT methods.
e.g. at TP of 4 g/dL (40 g/L) VITROS Na will be
LOWER by approximately 3-5 mmol/L
NOTE: The VITROS result is considered
the MORE PHYSIOLOGICALLY CORRECT RESULT.
• At NORMAL TP levels:
the VITROS SODIUM should AGREE with Indirect methods.
• At HIGH TP levels :
the VITROS SODIUM will be HIGHER THAN INDIRECT methods.
e.g. at TP of 10 g/dL (100 g/L) VITROS Na will be
HIGHER by approximately 3-5 mmol/L
NOTE: The VITROS result is considered
the MORE PHYSIOLOGICALLY CORRECT RESULT.
MicroTip Assay Technology
53
© Ortho Clinical Diagnostics 2017
VITROS® MicroTip Reagents
54
• Liquid, ready-to-use — no reagent preparation
• Integrated reagent pack design accommodates single and
dual reagents
• 36 MicroTip reagent positions = 36 MicroTip assays on board
• Refrigerated storage maximizes on system stability
• Reagent on-board stability of 7-28 days
• Conical design and level sensing minimizes dead volume
and waste
• Convenient packaging size minimizes waste
© Ortho Clinical Diagnostics 2017
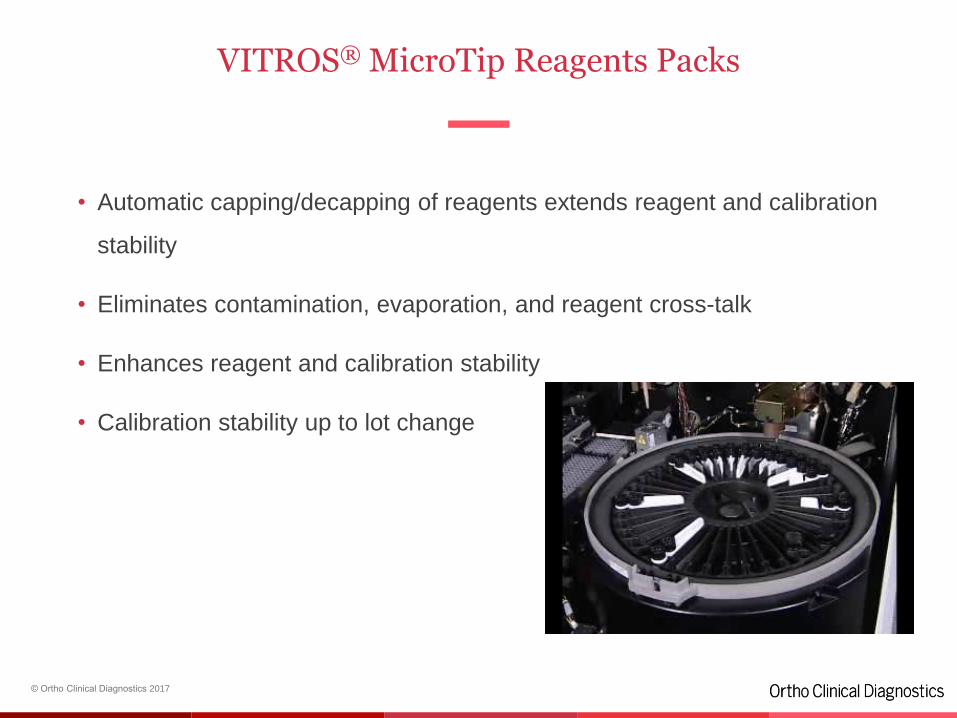
VITROS® MicroTip Reagents Packs
55
• Automatic capping/decapping of reagents extends reagent and calibration
stability
• Eliminates contamination, evaporation, and reagent cross-talk
• Enhances reagent and calibration stability
• Calibration stability up to lot change
© Ortho Clinical Diagnostics 2017
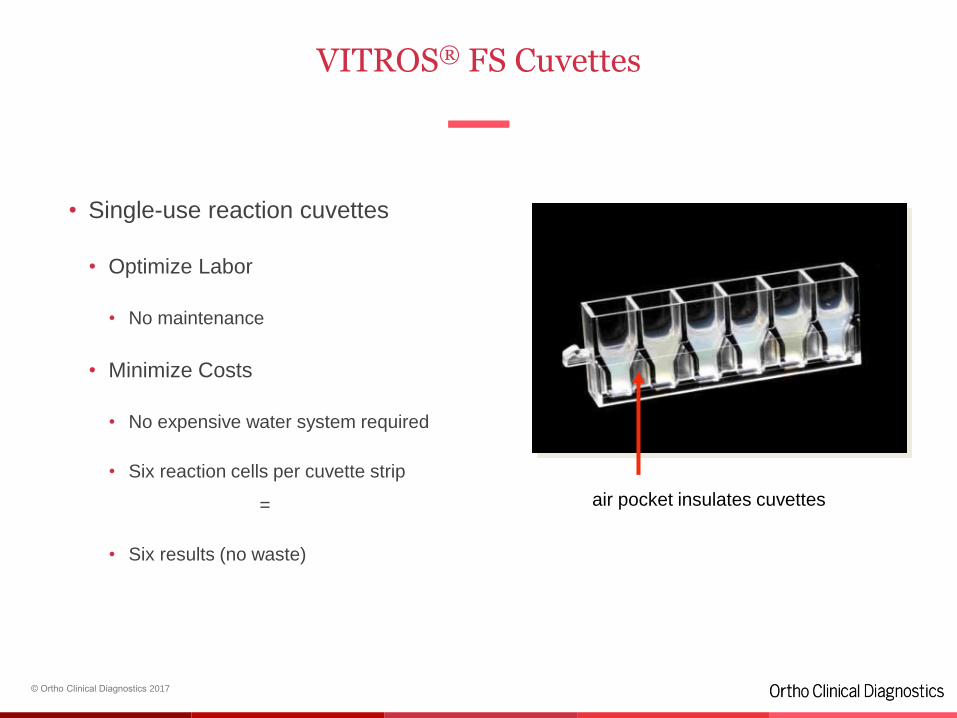
VITROS® FS Cuvettes
56
• Single-use reaction cuvettes
• Optimize Labor
• No maintenance
• Minimize Costs
• No expensive water system required
• Six reaction cells per cuvette strip
=
• Six results (no waste)
air pocket insulates cuvettes
© Ortho Clinical Diagnostics 2017
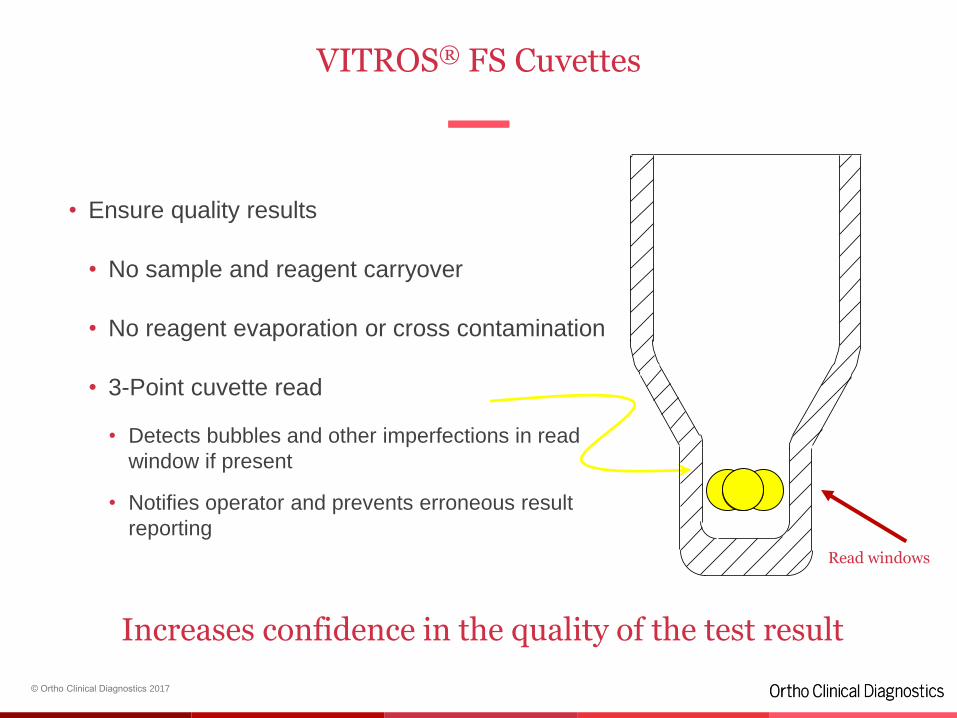
VITROS® FS Cuvettes
57
• Ensure quality results
• No sample and reagent carryover
• No reagent evaporation or cross contamination
• 3-Point cuvette read
• Detects bubbles and other imperfections in read
window if present
• Notifies operator and prevents erroneous result
reporting
Read windows
Increases confidence in the quality of the test result
© Ortho Clinical Diagnostics 2017
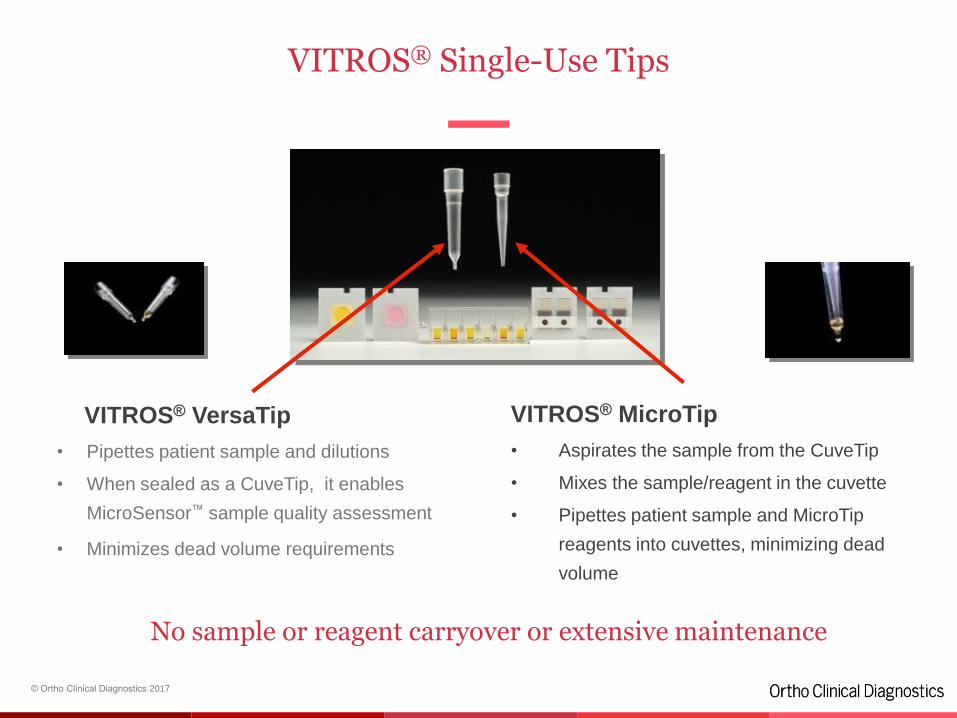
VITROS® Single-Use Tips
58
VITROS® VersaTip
• Pipettes patient sample and dilutions
• When sealed as a CuveTip, it enables
MicroSensor™ sample quality assessment
• Minimizes dead volume requirements
VITROS® MicroTip
• Aspirates the sample from the CuveTip
• Mixes the sample/reagent in the cuvette
• Pipettes patient sample and MicroTip
reagents into cuvettes, minimizing dead
volume
No sample or reagent carryover or extensive maintenance
© Ortho Clinical Diagnostics 2017
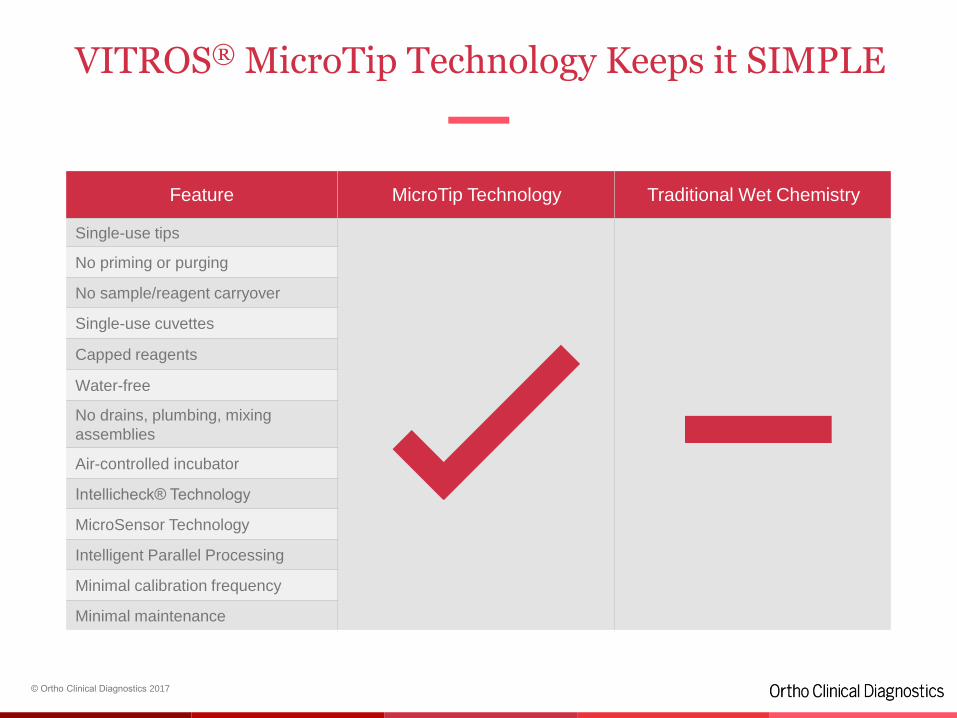
VITROS® MicroTip Technology Keeps it SIMPLE
59
Feature MicroTip Technology Traditional Wet Chemistry
Single-use tips
No priming or purging
No sample/reagent carryover
Single-use cuvettes
Capped reagents
Water-free
No drains, plumbing, mixing
assemblies
Air-controlled incubator
Intellicheck® Technology
MicroSensor Technology
Intelligent Parallel Processing
Minimal calibration frequency
Minimal maintenance
MPA-UDA MicroTip Assay
62
© Ortho Clinical Diagnostics 2017
UDA/ MPA Definitions
UDA= User Defined Assay
An assay that is run on an open channel using reagents supplied by a third party (in some
cases, reagents can also be supplied by Ortho).
The validation of the assay is the customer’s responsibility.
Ortho can suggest these solutions to customers in response to tenders, but not as a validated
solution.
MPA = Micro Tip Partnership Assay (*)
An assay that is run on an open channel using reagents validated by a third party in
collaboration with Ortho for use on the VITROS® 5,1 FS, 4600 and 5600 Integrated System
with the User Defined Assay (UDA) software using MicroTip Technology.
The reagents can be supplied by Ortho for markets where this has been agreed with the third
party.
(*) This was previously called Manufacturer Validated Assay (MVA)
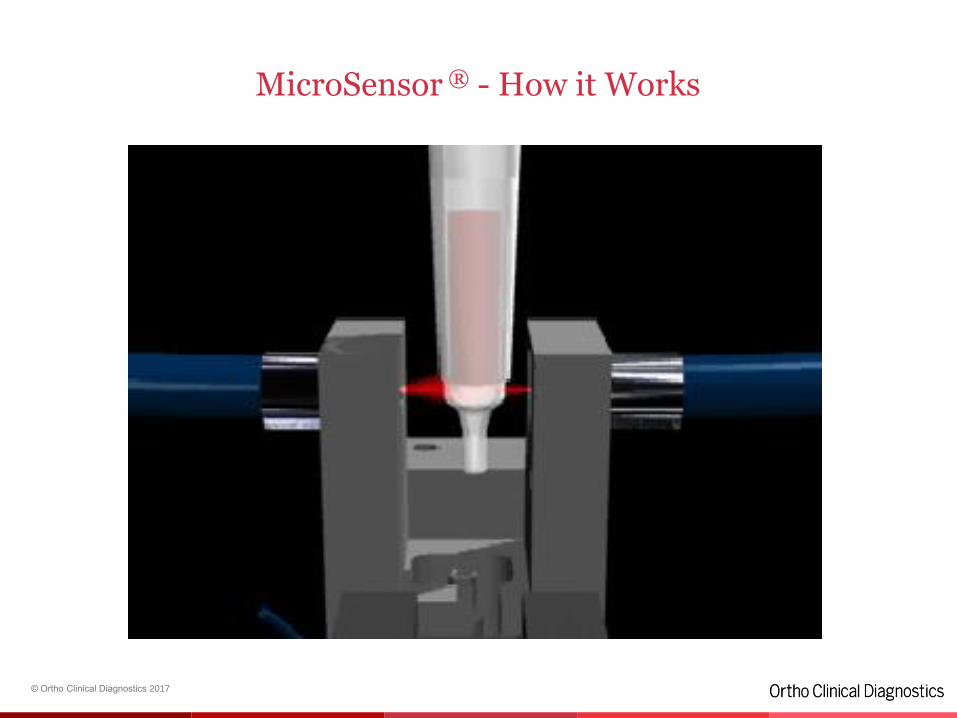
MicroSensor® Technology
© Ortho Clinical Diagnostics 2017
VITROS®
MicroSensor Technology
65
Semi Quantification and flagging of
samples for:
• Hemolysis
• Icterus
• Turbidity
© Ortho Clinical Diagnostics 2017
MicroSensor ® - How it Works
Intellicheck ® Technology
67
© Ortho Clinical Diagnostics 2017
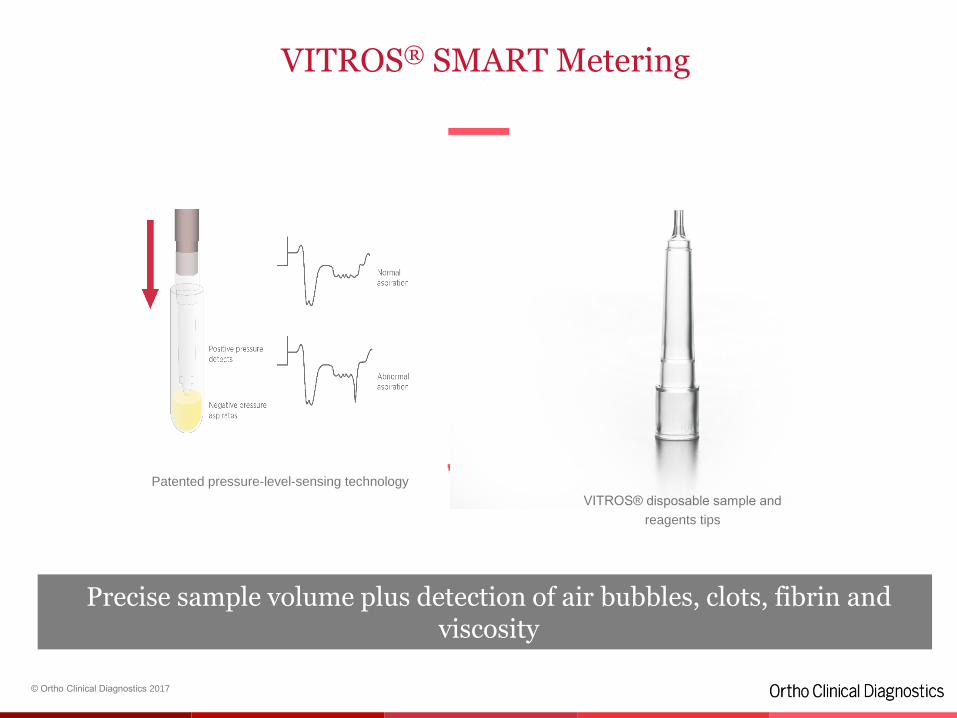
VITROS® SMART Metering
68
Precise sample volume plus detection of air bubbles, clots, fibrin and viscosity
Patented pressure-level-sensing technology
VITROS® disposable sample and
reagents tips
© Ortho Clinical Diagnostics 2017
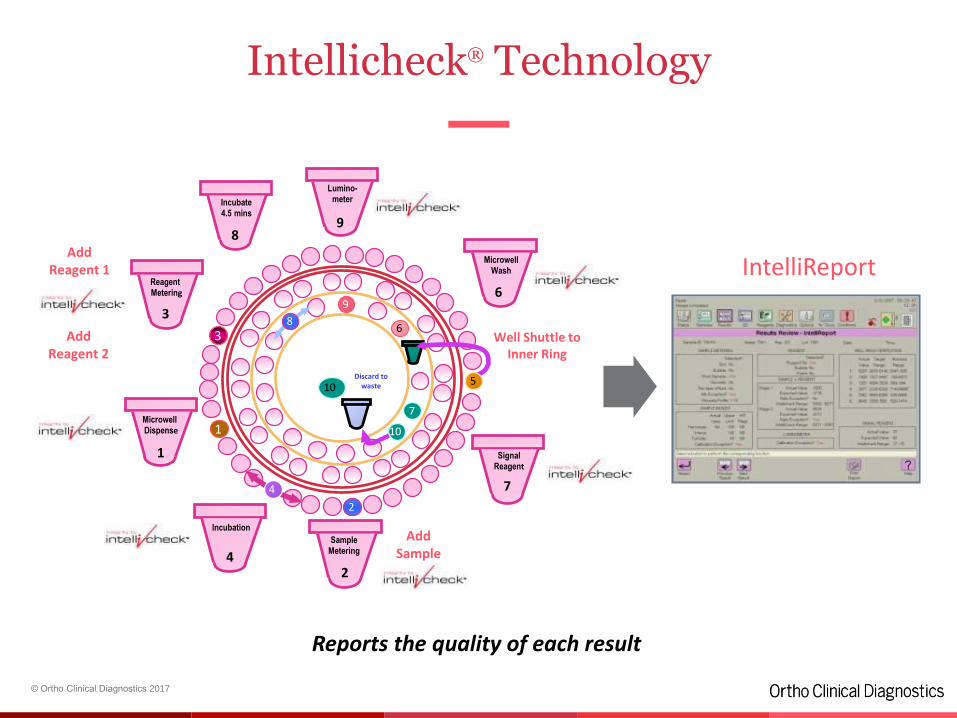
Analytical control process for each test
High Quality–Intellicheck® Technology
• Proprietary technology provides unique results integrity
– Designed to significantly reduce
analytical errors
• SMART Metering
• MicroSensor
• IntelliReport
– Integrated Process Control
– Traceability with real-time
documentation for exceptions
– Prevents reporting of results that
may be affected by exceptions
© Ortho Clinical Diagnostics 2017
6
7
9
8
IntelliReport
Intellicheck® Technology
Reports the quality of each result
Lumino-meter
9
AddReagent 2
AddReagent 1
Well Shuttle to Inner Ring
Incubation
4
Discard to waste
1
3
Microwell Dispense
1
Sample Metering
2
Reagent Metering
3
SignalReagent
7
Incubate4.5 mins
8
MicrowellWash
6
AddSample
105
10
4
2
© Ortho Clinical Diagnostics 2017
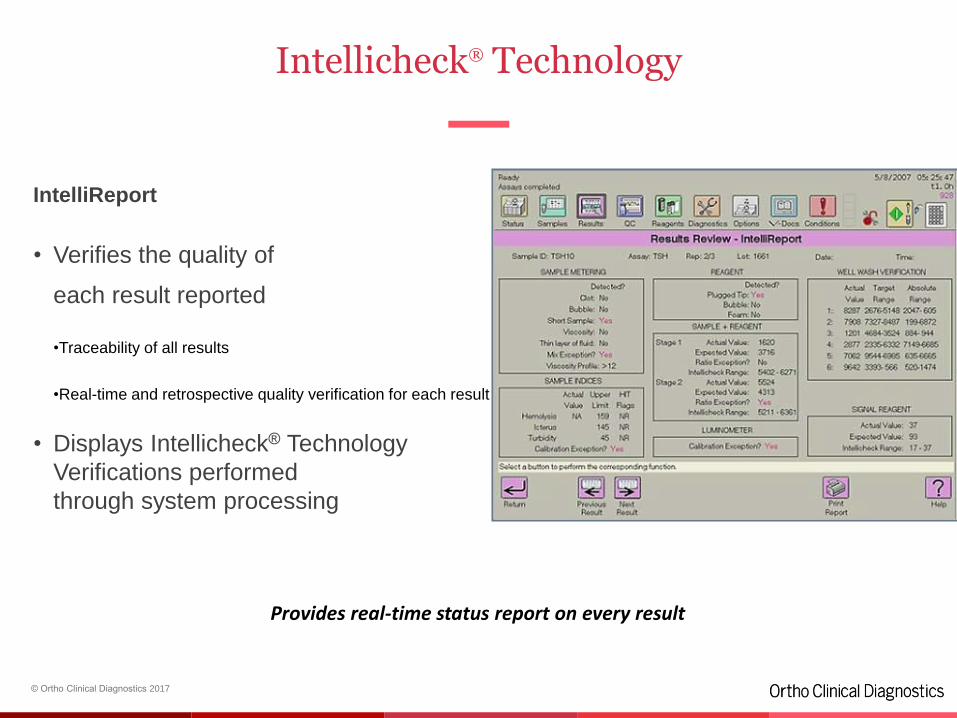
Intellicheck® Technology
IntelliReport
• Verifies the quality of
each result reported
•Traceability of all results
•Real-time and retrospective quality verification for each result
• Displays Intellicheck® Technology
Verifications performed
through system processing
Provides real-time status report on every result
© Ortho Clinical Diagnostics 2017
Agenda
72
• Company Overview
• Daily Challenges
• VITROS® Systems
• VITROS® Technologies
• Added Values
• VITROS® Automation Solution
© Ortho Clinical Diagnostics 2017
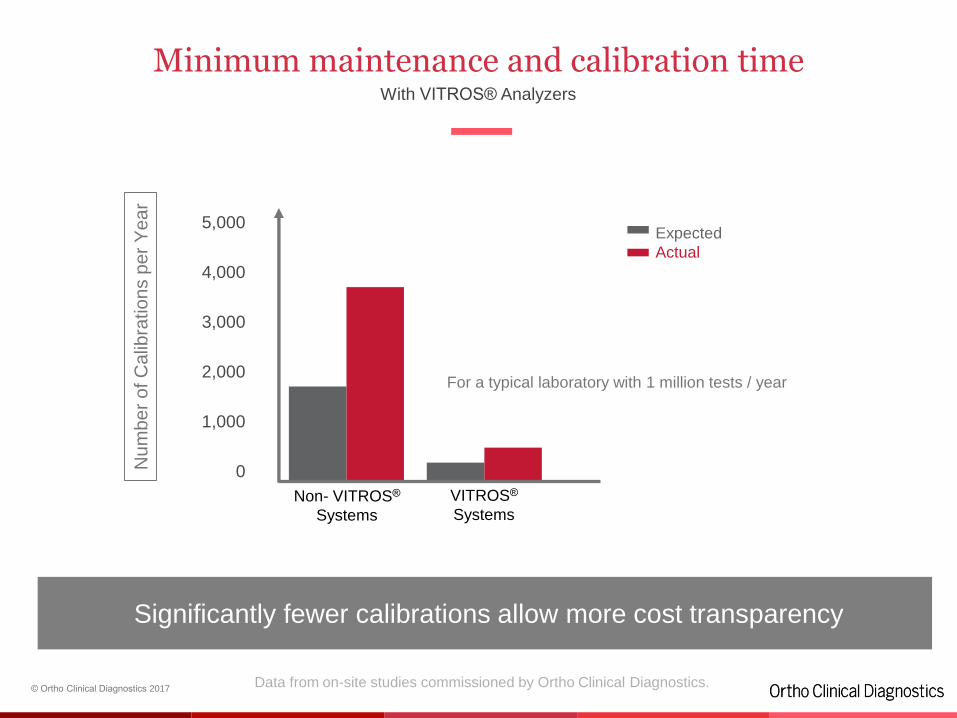
Minimum maintenance and calibration timeWith VITROS® Analyzers
73
Significantly fewer calibrations allow more cost transparency
Non- VITROS®
Systems
3,000
1,000
0
5,000
VITROS®
Systems
Nu
mb
er
of C
alib
ratio
ns p
er
Ye
ar
4,000
2,000
Expected
Actual
Data from on-site studies commissioned by Ortho Clinical Diagnostics.
For a typical laboratory with 1 million tests / year
© Ortho Clinical Diagnostics 2017
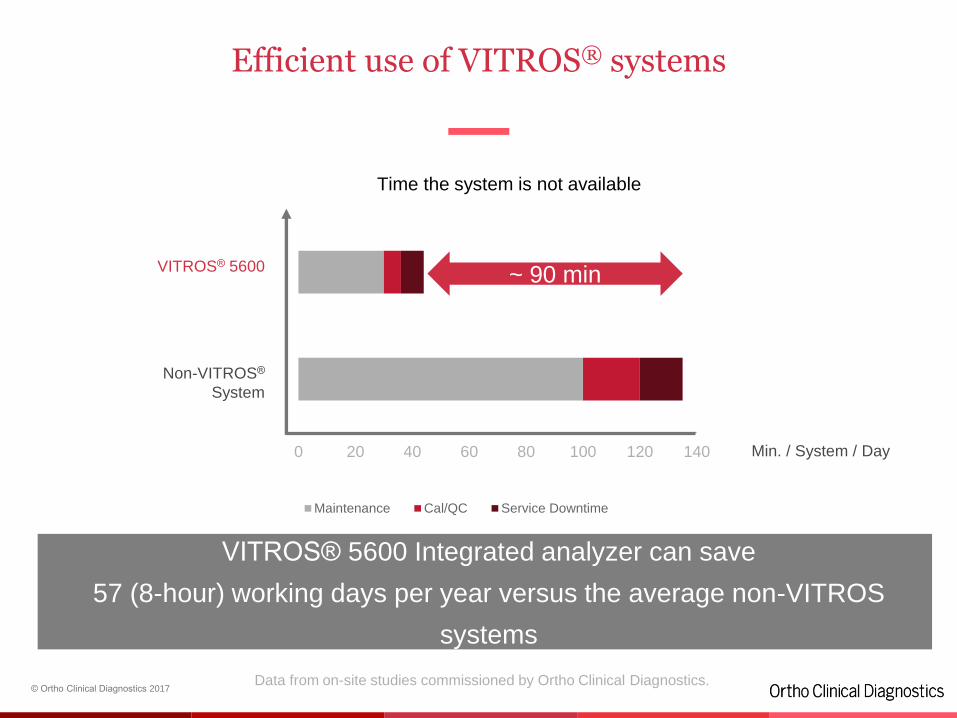
Efficient use of VITROS® systems
74
VITROS® 5600 Integrated analyzer can save
57 (8-hour) working days per year versus the average non-VITROS
systems
0 20 40 60 80 100 120 140
Maintenance Cal/QC Service Downtime
Time the system is not available
VITROS® 5600
Non-VITROS®
System
Data from on-site studies commissioned by Ortho Clinical Diagnostics.
~ 90 min
Min. / System / Day
© Ortho Clinical Diagnostics 2017
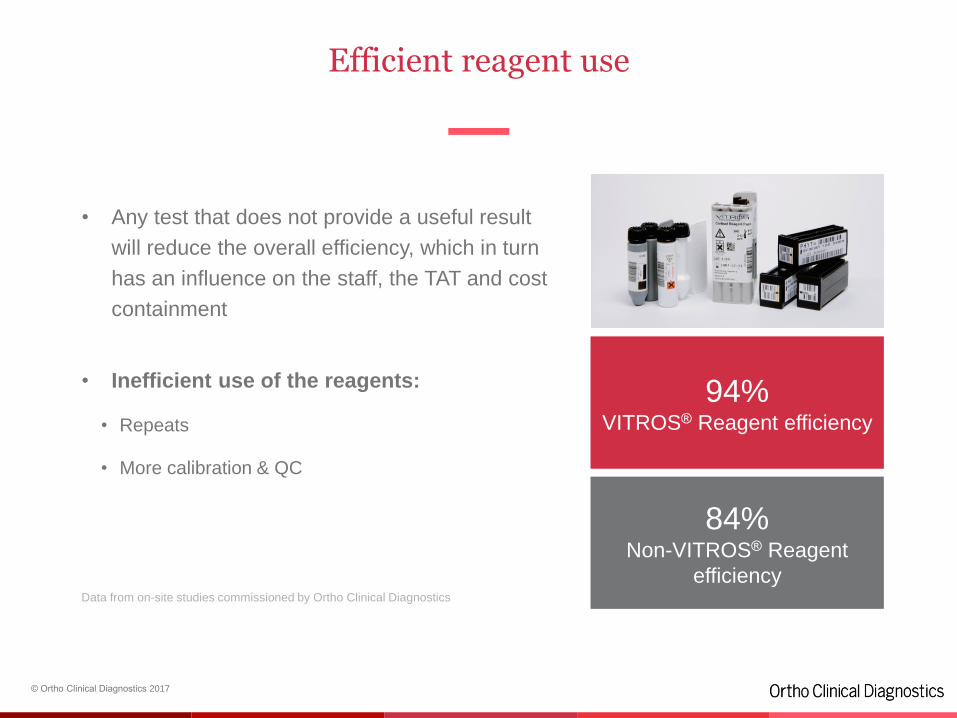
Efficient reagent use
75
• Any test that does not provide a useful result
will reduce the overall efficiency, which in turn
has an influence on the staff, the TAT and cost
containment
• Inefficient use of the reagents:
• Repeats
• More calibration & QC
94%VITROS® Reagent efficiency
84%Non-VITROS® Reagent
efficiencyData from on-site studies commissioned by Ortho Clinical Diagnostics
© Ortho Clinical Diagnostics 2017
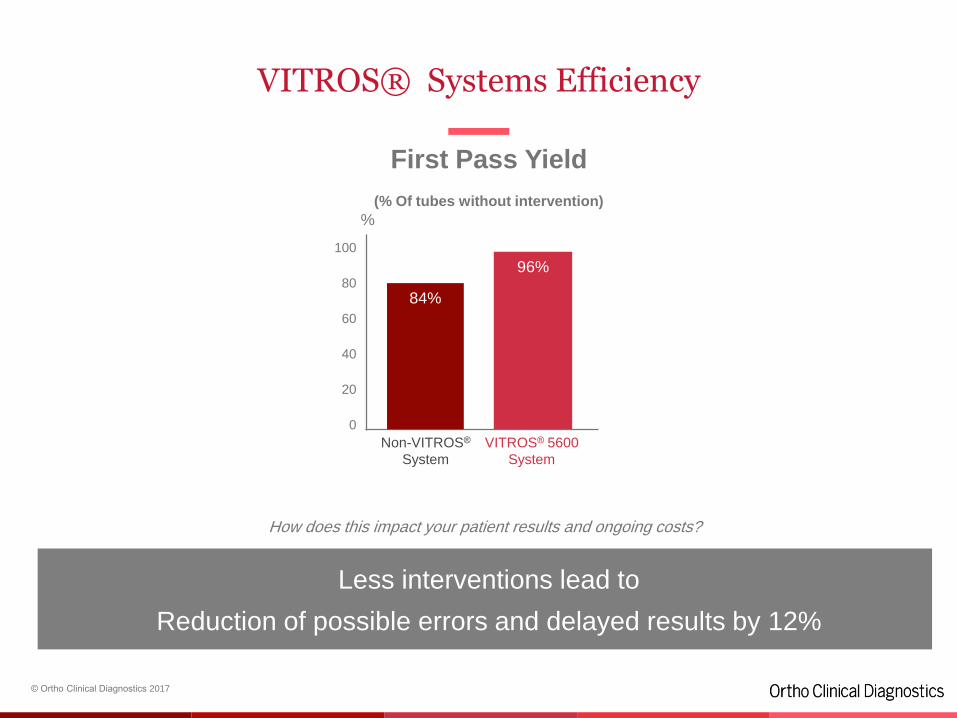
VITROS® Systems Efficiency
76
VITROS® 5600
System
Non-VITROS®
System
Less interventions lead to
Reduction of possible errors and delayed results by 12%
96%80
60
20
0
%
40
100
First Pass Yield
(% Of tubes without intervention)
84%
How does this impact your patient results and ongoing costs?
© Ortho Clinical Diagnostics 2017
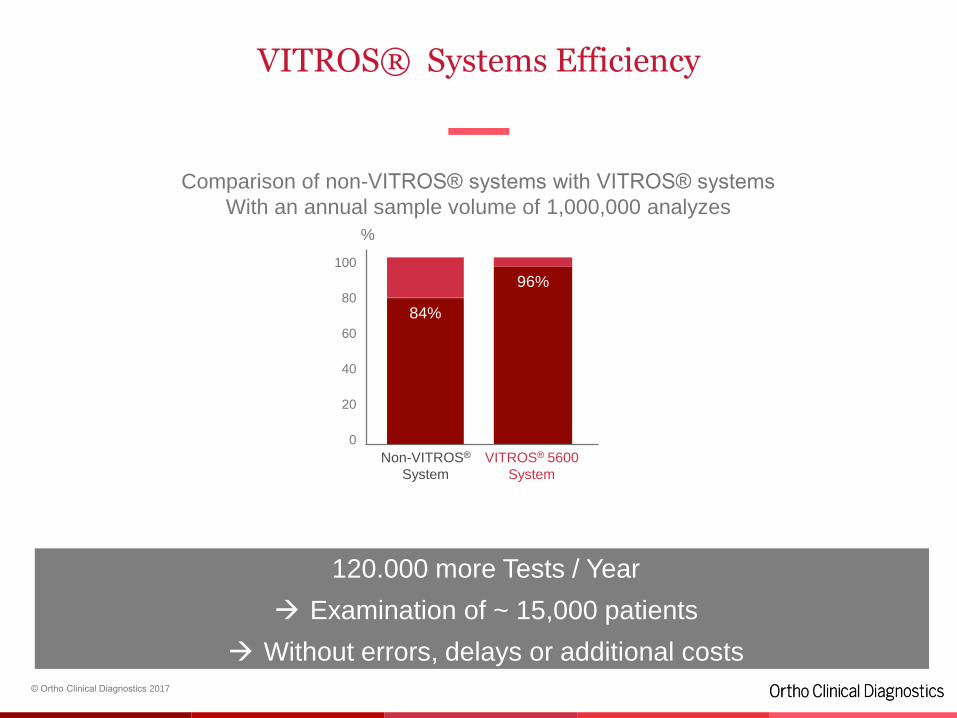
Comparison of non-VITROS® systems with VITROS® systems
With an annual sample volume of 1,000,000 analyzes
VITROS® Systems Efficiency
77
120.000 more Tests / Year
Examination of ~ 15,000 patients
Without errors, delays or additional costs
VITROS® 5600
System
Non-VITROS®
System
96%80
60
20
0
%
40
100
84%
© Ortho Clinical Diagnostics 2017
Removing water as a potential source of quality issues
78
Waterless Technology has a huge impact for the clinical laboratory
VITROS® technologies reduce the environmental impact of laboratories
• Removes water as a potential source of poor quality results
• No cost involved for water purification systems
• No resource needed for testing water quality

© Ortho Clinical Diagnostics 2017
Agenda
79
• Company Overview
• Daily Challenges
• VITROS® Systems
• VITROS® Technologies
• Summary
• VITROS® Automation Solution
VITROS ® Automation Solution. VAS
80
© Ortho Clinical Diagnostics 2017
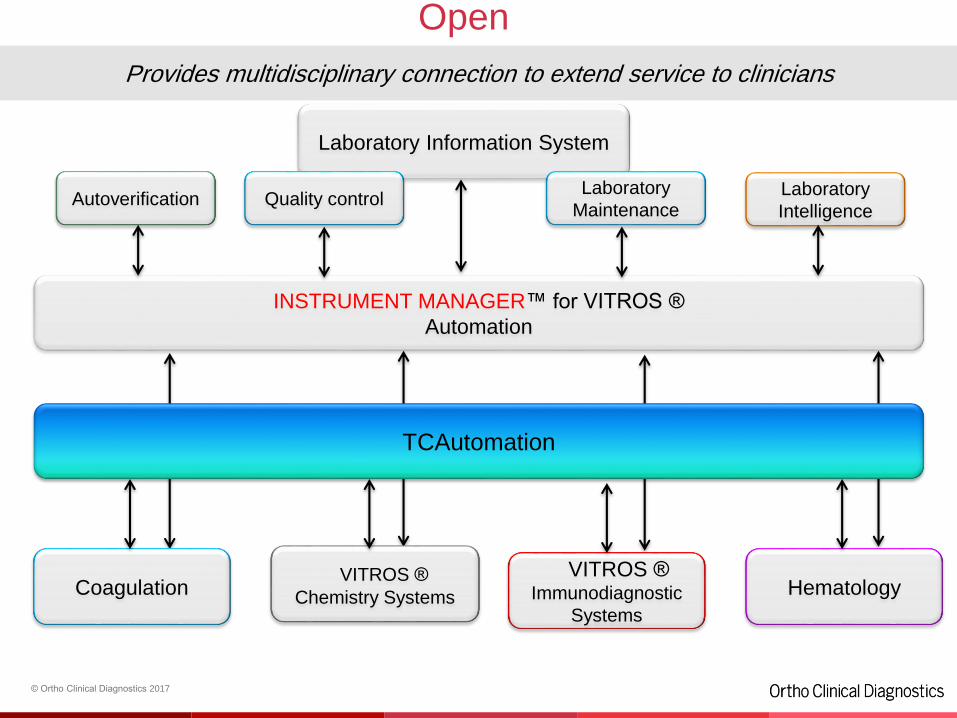
HematologyVITROS ®
Immunodiagnostic
Systems
VITROS ®
Chemistry SystemsCoagulation
Provides multidisciplinary connection to extend service to clinicians
Laboratory Information System
INSTRUMENT MANAGER™ for VITROS ®
Automation
TCAutomation
Autoverification Quality controlLaboratory
MaintenanceLaboratory
Intelligence
Open
© Ortho Clinical Diagnostics 2017
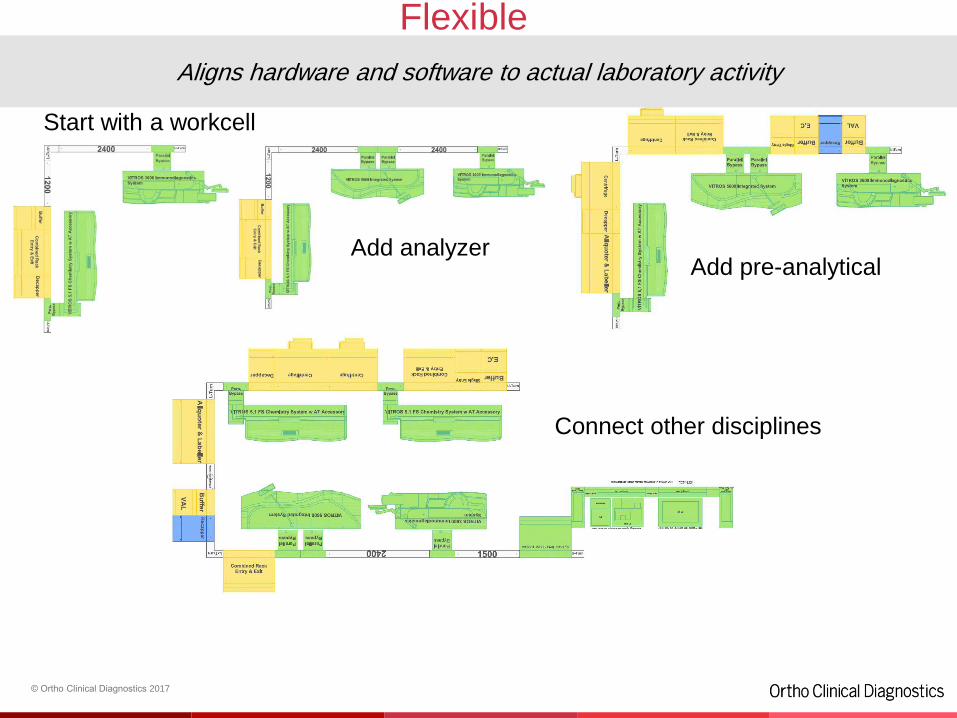
Start with a workcell
Add analyzerAdd pre-analytical
Connect other disciplines
Aligns hardware and software to actual laboratory activity
Flexible
© Ortho Clinical Diagnostics 2017
Grow at your own pace without having to completely redesign your lab
Appropriate automation
“We have relied on Ortho Clinical Diagnostics VITROS® Automation Solutions through a decade of
successful upgrades, reconfiguration and relocation. Their durability and adaptability have
proved to be crucial.” Lab Manager, Belgium.
Volume ROI
Scalable
© Ortho Clinical Diagnostics 2017
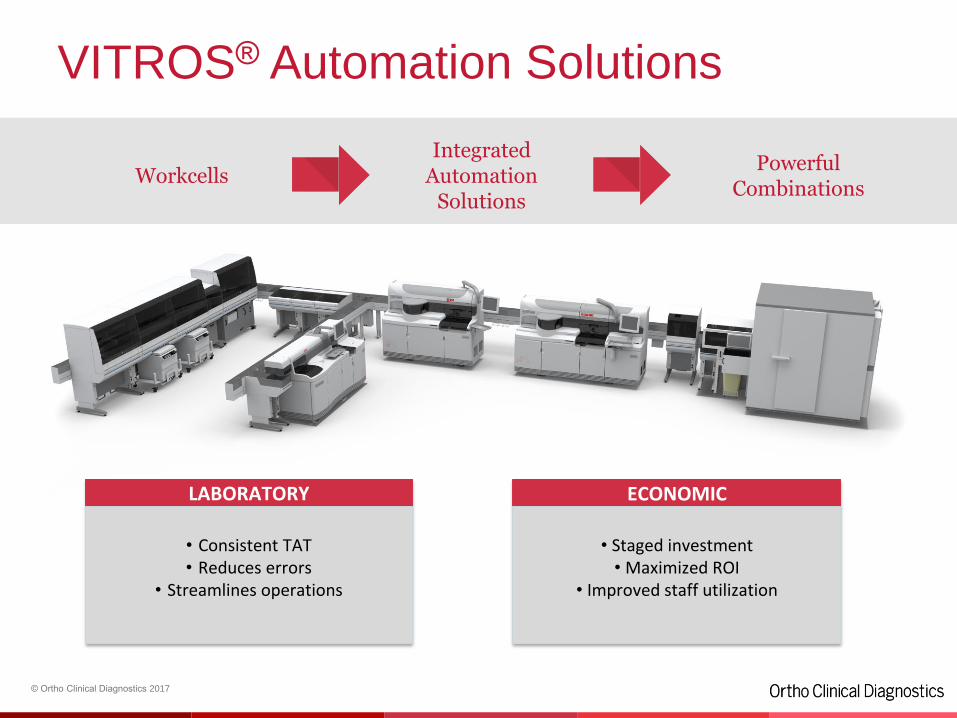
VITROS® Automation Solutions
WorkcellsIntegrated
AutomationSolutions
Powerful Combinations
LABORATORY ECONOMIC
• Consistent TAT• Reduces errors
• Streamlines operations
• Staged investment• Maximized ROI
• Improved staff utilization

Q & A

Thank You
StripAssay® Technology for inherited diseases, genetic predispositions, pharmacogenomics and oncology diagnosticsDr. Christian OberkaninsIQC Tehran / April 23, 2017
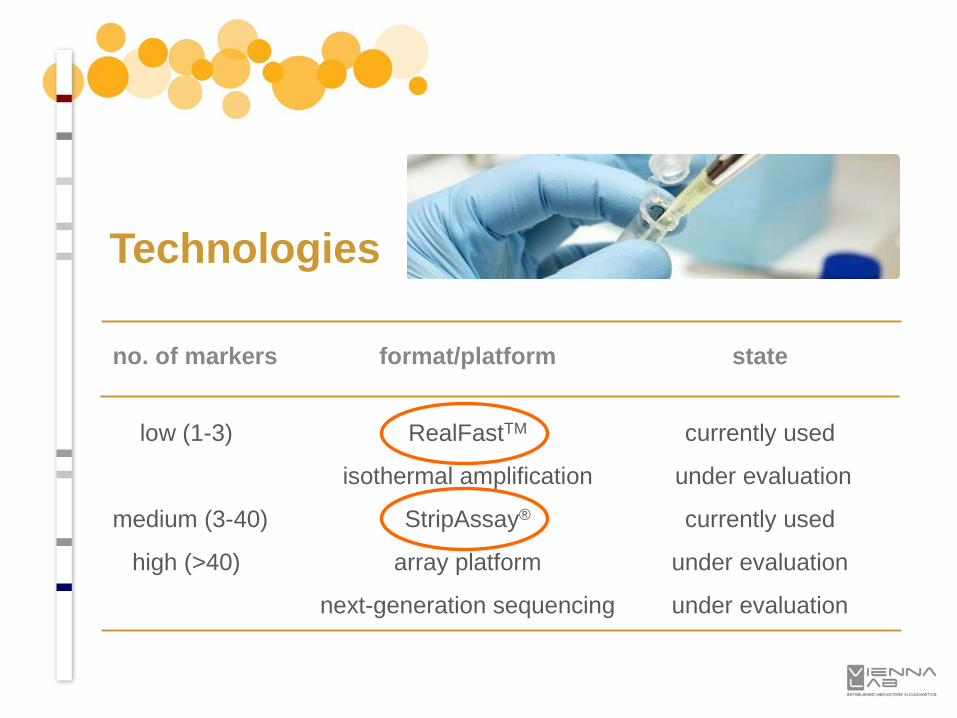
no. of markers format/platform state
low (1-3) RealFastTM currently used
isothermal amplification under evaluation
medium (3-40) StripAssay® currently used
high (>40) array platform under evaluation
next-generation sequencing under evaluation
Technologies

RealFastTM Technology
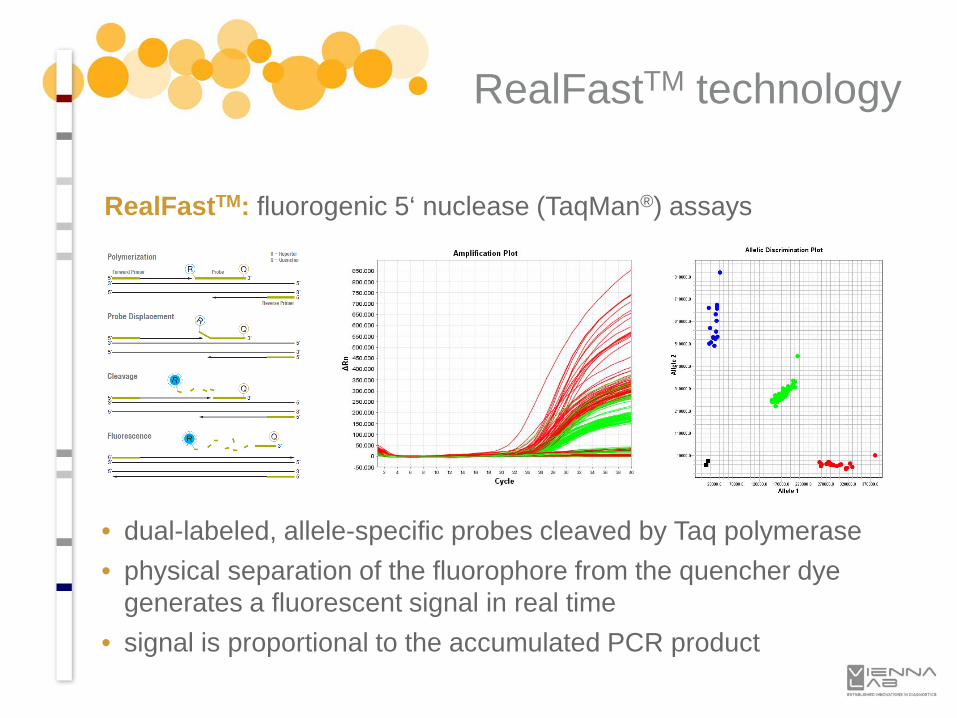
• dual-labeled, allele-specific probes cleaved by Taq polymerase• physical separation of the fluorophore from the quencher dye
generates a fluorescent signal in real time• signal is proportional to the accumulated PCR product
RealFastTM: fluorogenic 5‘ nuclease (TaqMan®) assays
RealFastTM technology
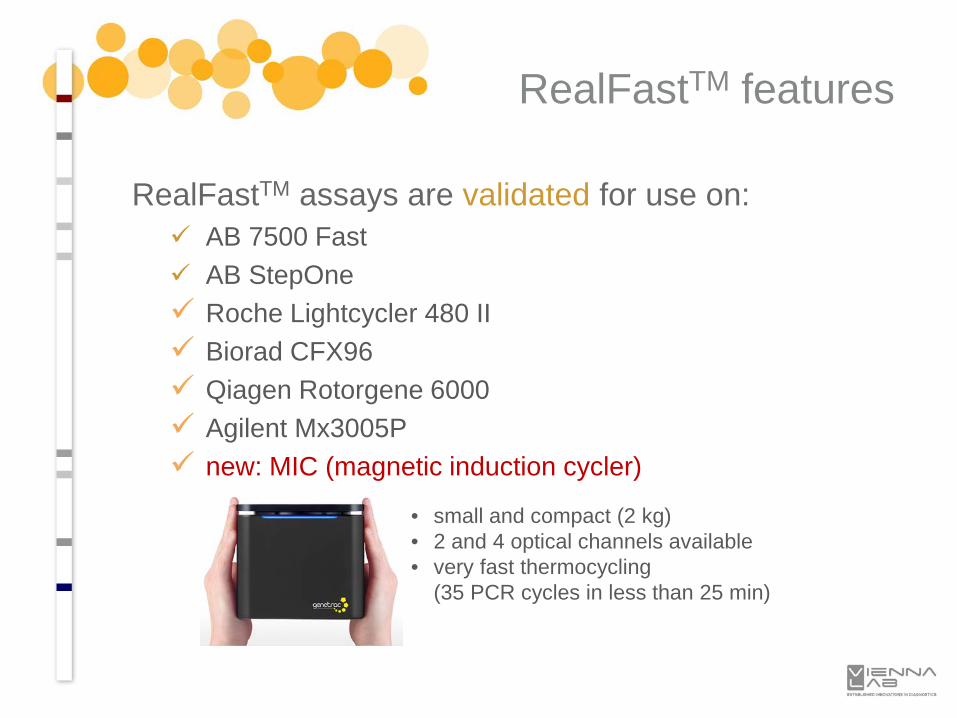
RealFastTM assays are validated for use on: AB 7500 Fast AB StepOne Roche Lightcycler 480 II Biorad CFX96 Qiagen Rotorgene 6000 Agilent Mx3005P new: MIC (magnetic induction cycler)
RealFastTM features
• small and compact (2 kg)• 2 and 4 optical channels available• very fast thermocycling
(35 PCR cycles in less than 25 min)
• Cardio-Vascular Disease (CVD):FV Leiden, Prothrombin (FII) 20210G>A, MTHFR 677C>T & 1298A>C. PAI-1 4G/5G, Beta-Fibrinogen (FGB) -455G>A, FXII 46C>T, FXIII V34L
• Coumarin anticoagulation:VKORC1 -1639G>A, CYP2C9 *2/*3
• Haemochromatosis:HFE C282Y & H63D
• Lactose intolerance:LCT -13910T>C
• HLA:HLA-B*27 (ankylosing spondylitis)HLA-B*5701 (abacavir hypersensitivity), HLA-B*1502 (carbamazepine hypersensitivity)
RealFastTM applications
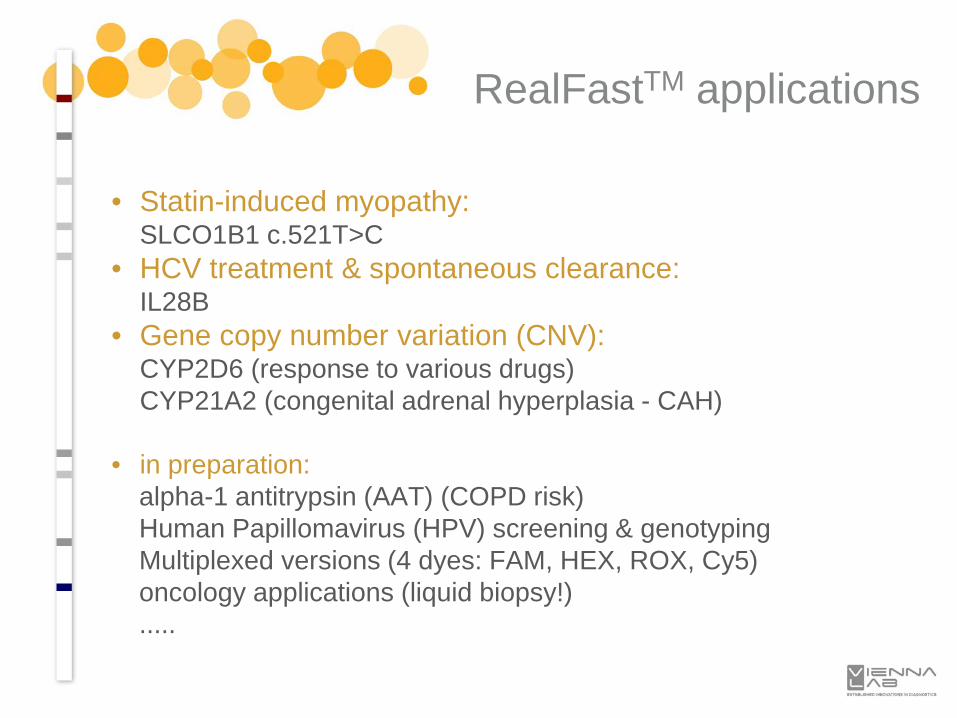
• Statin-induced myopathy:SLCO1B1 c.521T>C
• HCV treatment & spontaneous clearance:IL28B
• Gene copy number variation (CNV):CYP2D6 (response to various drugs)CYP21A2 (congenital adrenal hyperplasia - CAH)
• in preparation:alpha-1 antitrypsin (AAT) (COPD risk)Human Papillomavirus (HPV) screening & genotypingMultiplexed versions (4 dyes: FAM, HEX, ROX, Cy5)oncology applications (liquid biopsy!).....
RealFastTM applications

StripAssay® Technology

Human diagnostic assays for genotyping mutations and polymorphisms (SNPs, deletions, insertions) based on polymerase chain reaction (PCR) and reverse-hybridzation to allele-specific oligonucleotide probes immobilized on teststrips
StripAssay®
Technology
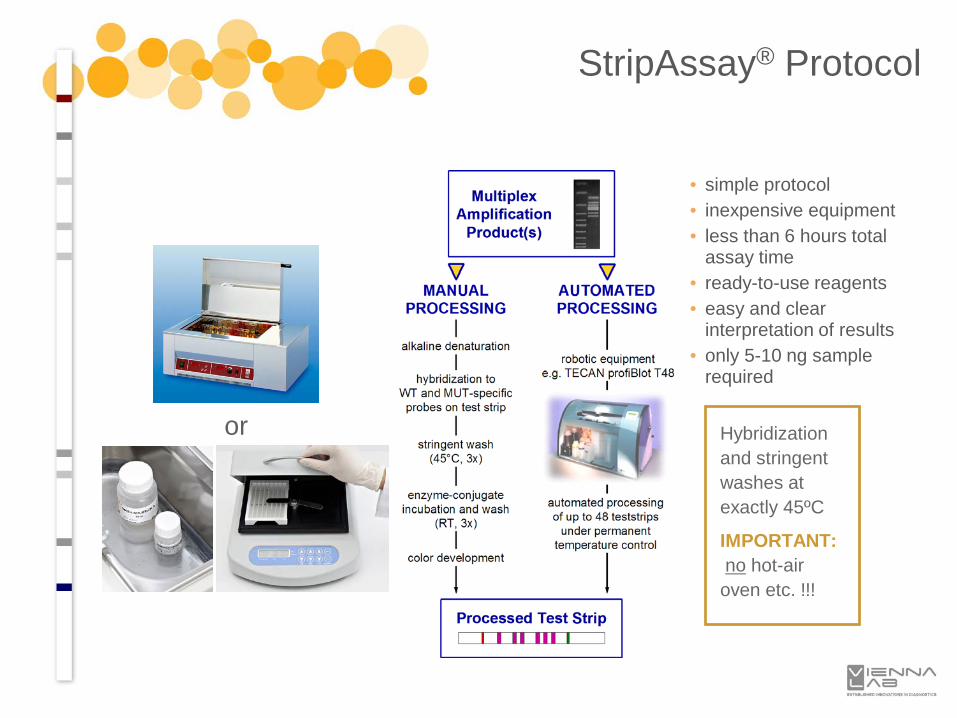
or Hybridization and stringent washes at exactly 45ºC
IMPORTANT:no hot-air oven etc. !!!
• simple protocol• inexpensive equipment• less than 6 hours total
assay time• ready-to-use reagents• easy and clear
interpretation of results• only 5-10 ng sample
required
StripAssay® Protocol

for 48 teststrips: Roboblot or ProfiBlot T48 or BeeBlot
Hybridization + Stringent Washes + Color Development fully automated under controlled temperature on one instrument
for 20/30 teststrips: Dynablot Heat or Autoblot 3000H or B20
StripAssay® Protocol
Optional: Automated processing of teststrips
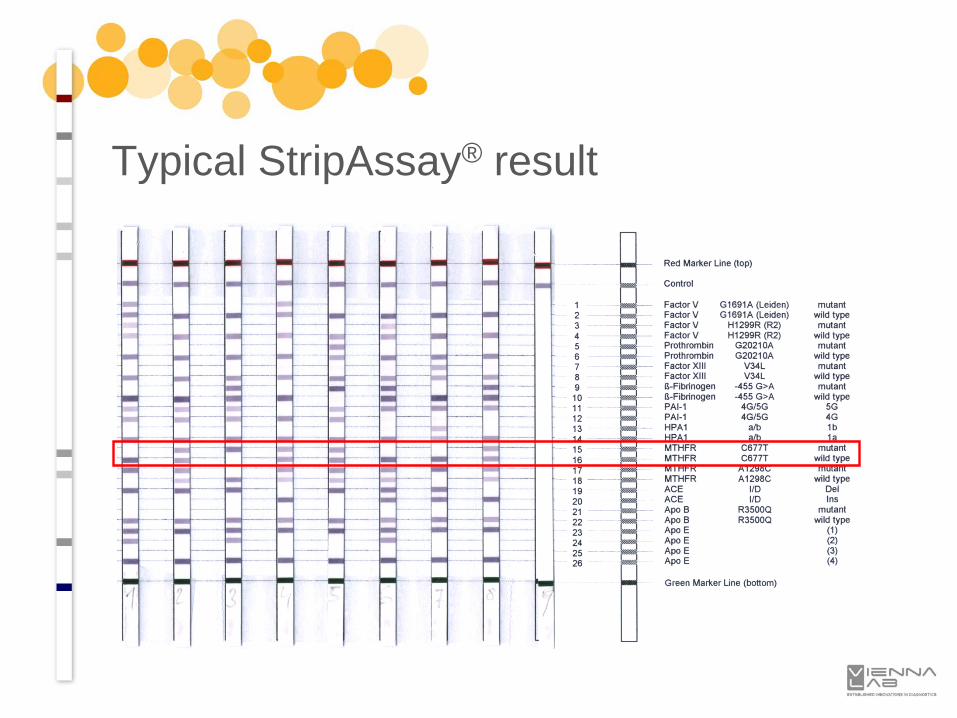
Typical StripAssay® result
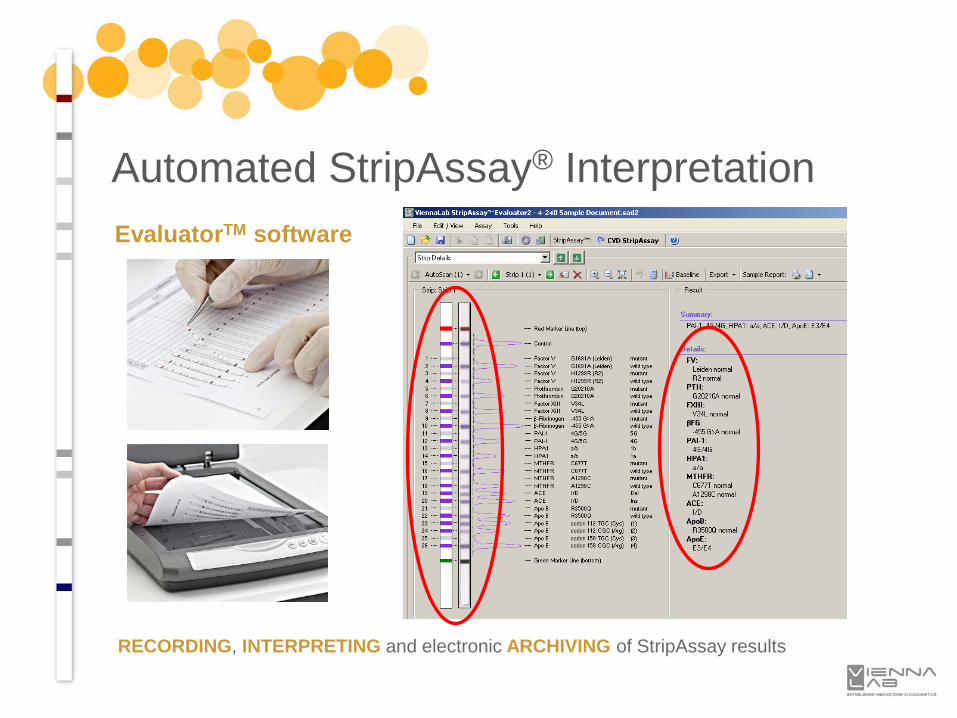
EvaluatorTM software
RECORDING, INTERPRETING and electronic ARCHIVING of StripAssay results
Automated StripAssay® Interpretation
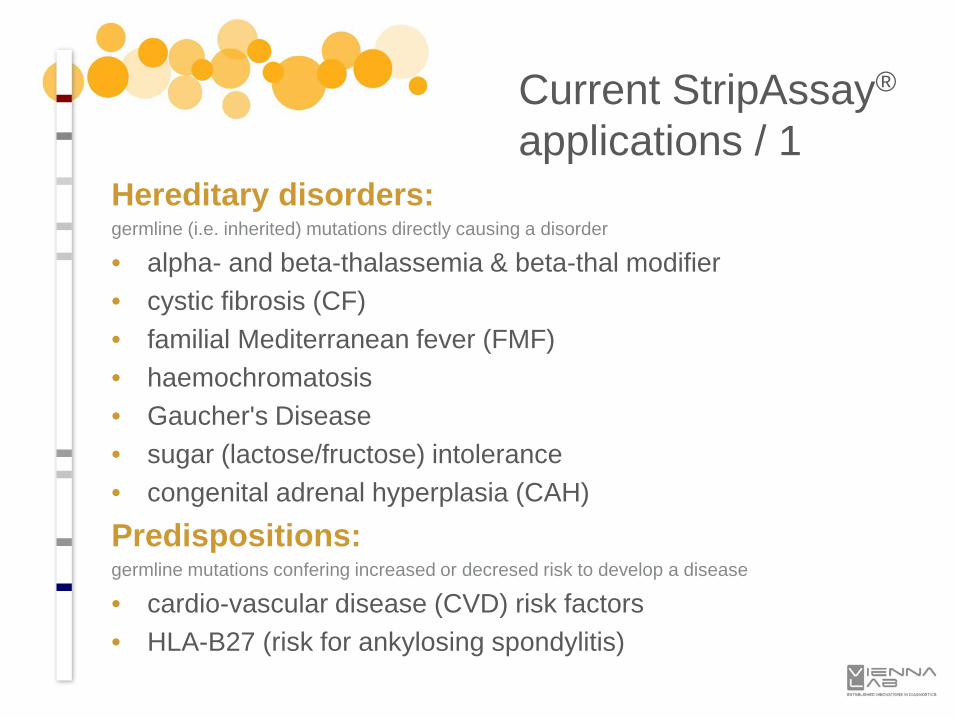
Hereditary disorders:germline (i.e. inherited) mutations directly causing a disorder
• alpha- and beta-thalassemia & beta-thal modifier• cystic fibrosis (CF)• familial Mediterranean fever (FMF)• haemochromatosis• Gaucher's Disease• sugar (lactose/fructose) intolerance• congenital adrenal hyperplasia (CAH)
Predispositions:germline mutations confering increased or decresed risk to develop a disease
• cardio-vascular disease (CVD) risk factors• HLA-B27 (risk for ankylosing spondylitis)
Current StripAssay®
applications / 1
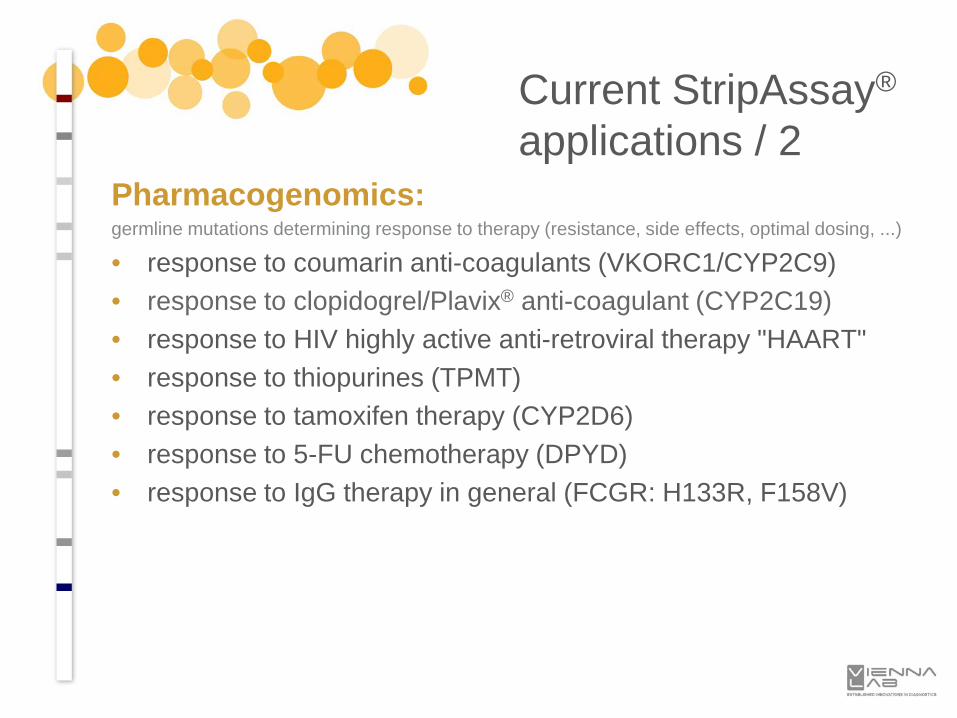
Pharmacogenomics:germline mutations determining response to therapy (resistance, side effects, optimal dosing, ...)
• response to coumarin anti-coagulants (VKORC1/CYP2C9)• response to clopidogrel/Plavix® anti-coagulant (CYP2C19)• response to HIV highly active anti-retroviral therapy "HAART"• response to thiopurines (TPMT)• response to tamoxifen therapy (CYP2D6)• response to 5-FU chemotherapy (DPYD)• response to IgG therapy in general (FCGR: H133R, F158V)
Current StripAssay®
applications / 2
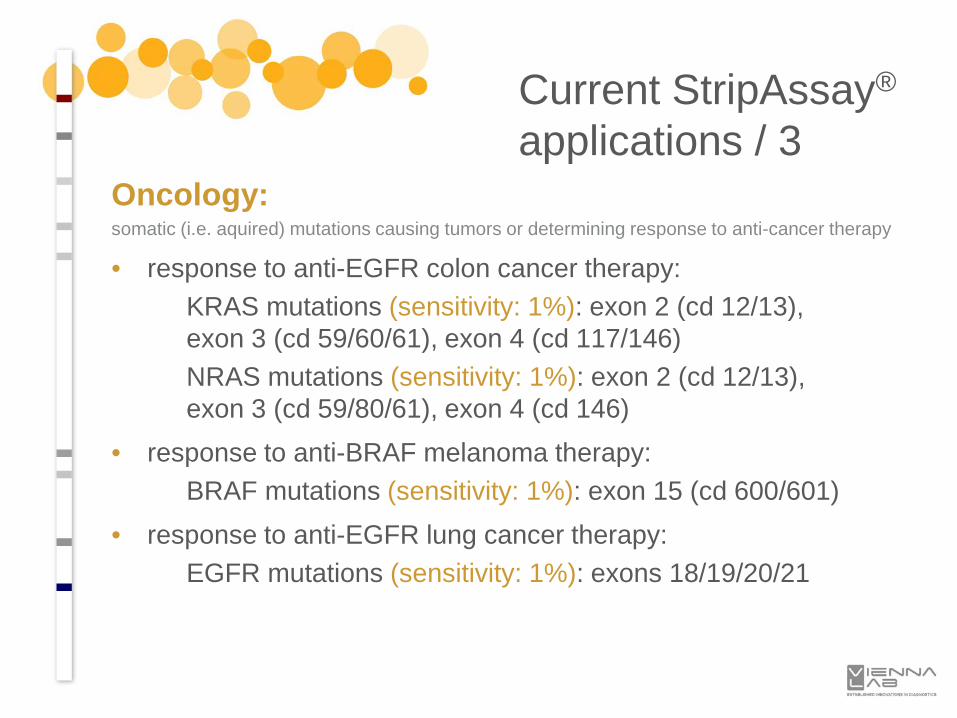
Oncology:somatic (i.e. aquired) mutations causing tumors or determining response to anti-cancer therapy
• response to anti-EGFR colon cancer therapy:KRAS mutations (sensitivity: 1%): exon 2 (cd 12/13), exon 3 (cd 59/60/61), exon 4 (cd 117/146)NRAS mutations (sensitivity: 1%): exon 2 (cd 12/13), exon 3 (cd 59/80/61), exon 4 (cd 146)
• response to anti-BRAF melanoma therapy:BRAF mutations (sensitivity: 1%): exon 15 (cd 600/601)
• response to anti-EGFR lung cancer therapy:EGFR mutations (sensitivity: 1%): exons 18/19/20/21
Current StripAssay®
applications / 3
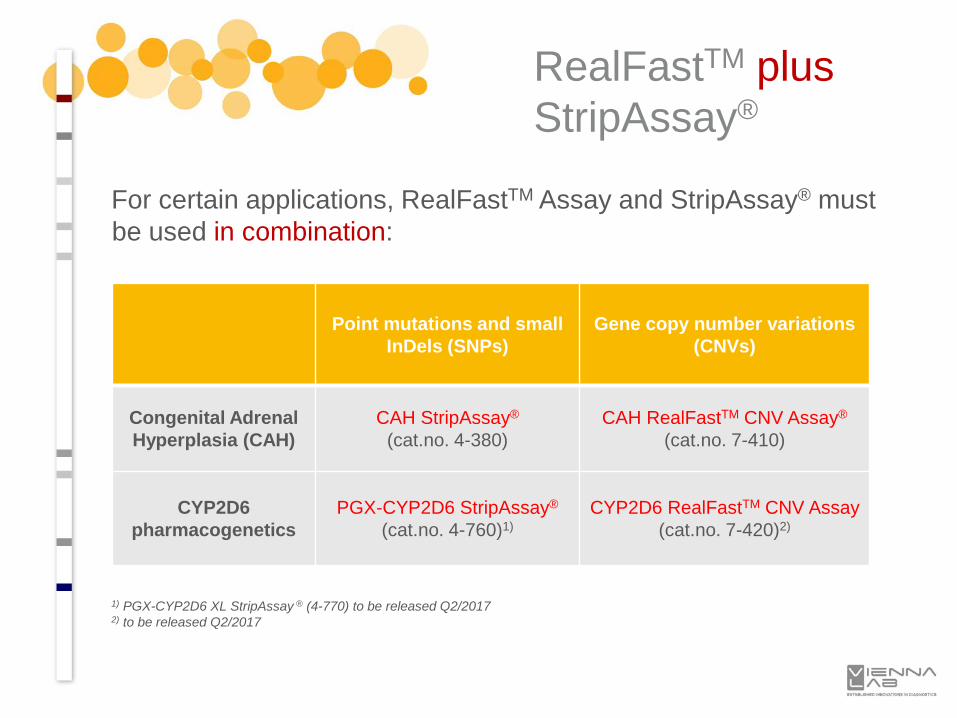
RealFastTM plusStripAssay®
For certain applications, RealFastTM Assay and StripAssay® must be used in combination:
1) PGX-CYP2D6 XL StripAssay ® (4-770) to be released Q2/20172) to be released Q2/2017
Point mutations and small InDels (SNPs)
Gene copy number variations (CNVs)
Congenital Adrenal Hyperplasia (CAH)
CAH StripAssay®
(cat.no. 4-380)CAH RealFastTM CNV Assay®
(cat.no. 7-410)
CYP2D6pharmacogenetics
PGX-CYP2D6 StripAssay®
(cat.no. 4-760)1)CYP2D6 RealFastTM CNV Assay
(cat.no. 7-420)2)
StripAssay® Applications for Human Genetics and Pharmacogenomics
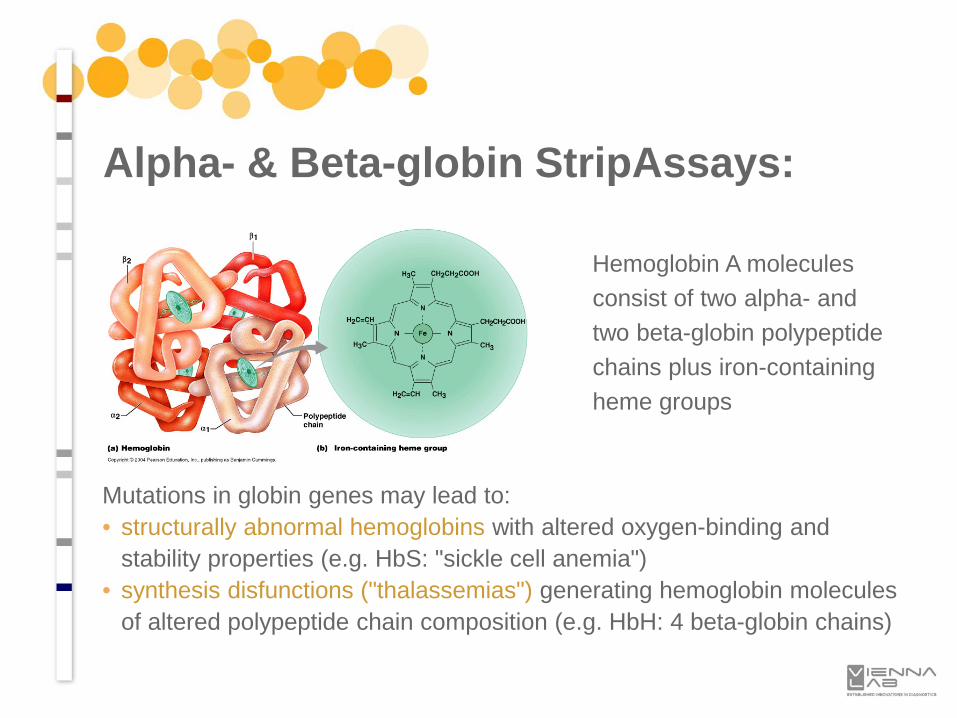
Hemoglobin A molecules consist of two alpha- and two beta-globin polypeptide chains plus iron-containing heme groups
Alpha- & Beta-globin StripAssays:
Mutations in globin genes may lead to:• structurally abnormal hemoglobins with altered oxygen-binding and
stability properties (e.g. HbS: "sickle cell anemia")• synthesis disfunctions ("thalassemias") generating hemoglobin molecules
of altered polypeptide chain composition (e.g. HbH: 4 beta-globin chains)
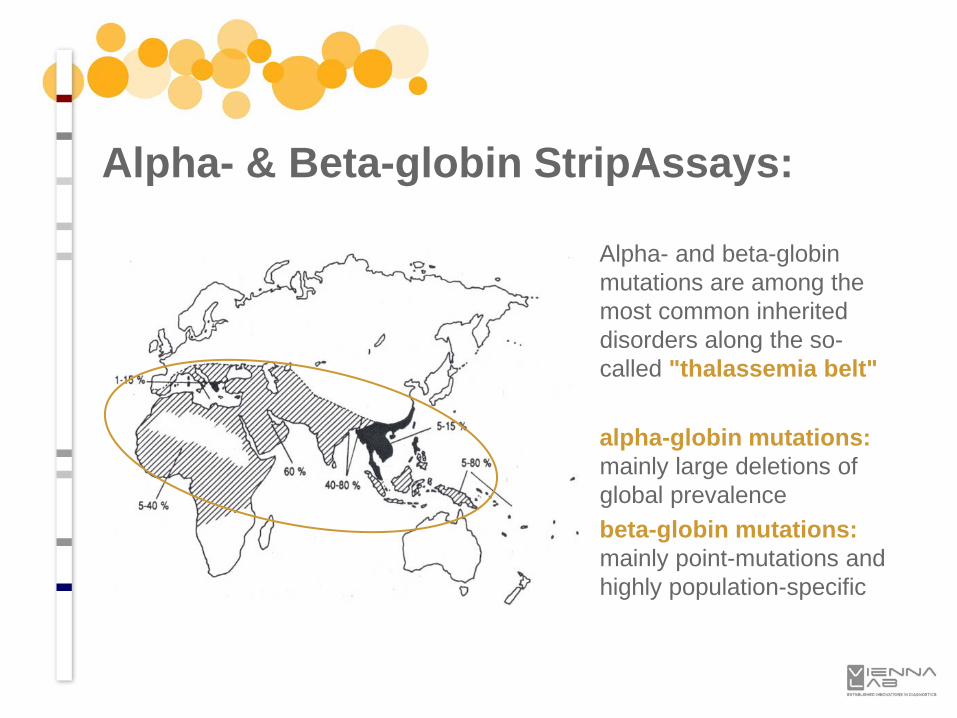
Alpha- and beta-globin mutations are among the most common inherited disorders along the so-called "thalassemia belt"
alpha-globin mutations: mainly large deletions of global prevalencebeta-globin mutations: mainly point-mutations and highly population-specific
Alpha- & Beta-globin StripAssays:
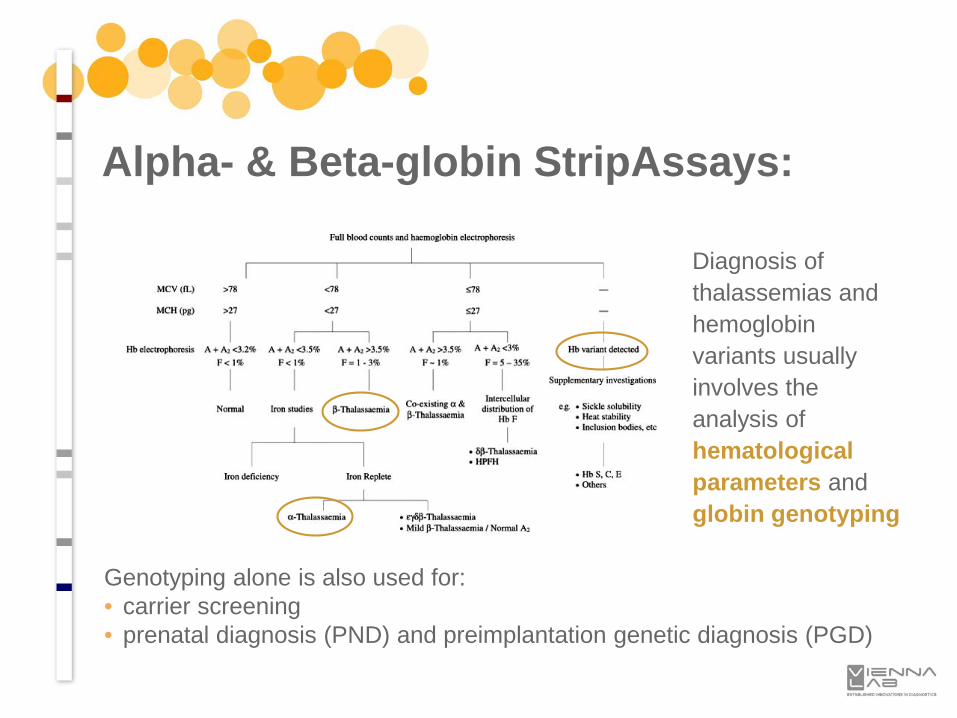
Diagnosis of thalassemias and hemoglobin variants usually involves the analysis of hematological parameters and globin genotyping
Alpha- & Beta-globin StripAssays:
Genotyping alone is also used for:• carrier screening• prenatal diagnosis (PND) and preimplantation genetic diagnosis (PGD)
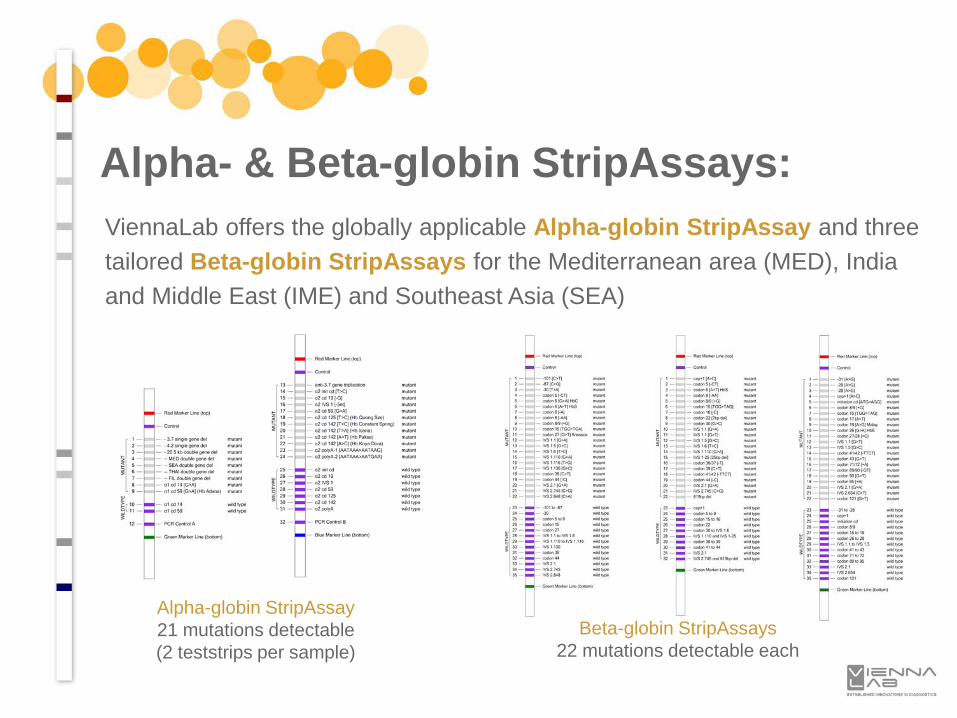
ViennaLab offers the globally applicable Alpha-globin StripAssay and three tailored Beta-globin StripAssays for the Mediterranean area (MED), India and Middle East (IME) and Southeast Asia (SEA)
Alpha- & Beta-globin StripAssays:
Alpha-globin StripAssay21 mutations detectable(2 teststrips per sample)
Beta-globin StripAssays22 mutations detectable each
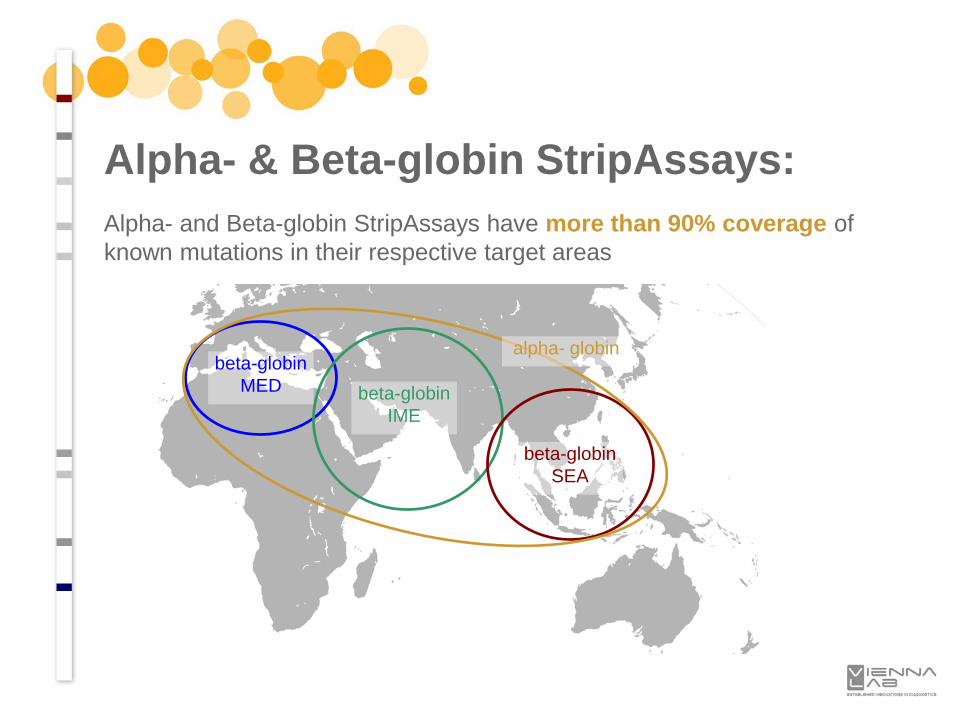
Alpha- and Beta-globin StripAssays have more than 90% coverage of known mutations in their respective target areas
Alpha- & Beta-globin StripAssays:
beta-globinMED beta-globin
IME
beta-globinSEA
alpha- globin
• beta-thalassemia phenotypes are variable, ranging from the severe transfusion-dependent thalassemia (thal) major to the mild form of thalassemia (thal) intermedia
• thal major patients have severe anemia and usually require medical attention within the first two years of life; without treatment, affected children have severely compromised growth and development and shortened life expectancy
• thal intermedia patients present later in life, have milder anemiaand never or only rarely require blood transfusion; occasionally thal intermedia patients are completely asymptomatic until adult life with only mild anemia
Beta-thal Modifier StripAssay:
• phenotypical variability is mainly associated with the type of beta-globin mutation, the coinheritance of alpha-thalassemia and the ability for persistent production of fetal haemoglobin (HbF) in adult life
• quantitative trait loci (QTL) known to account for HbF variability comprise single nucleotide polymorphisms (SNPs) in the: gamma-globin gene promoter (HBG2): rs7482144
("XmnI"; g.-158 C>T) BCL11A gene: rs1427407 and rs10189857 HBS1L-MYB intergenic region: rs28384513 and rs9399137
Beta-thal Modifier StripAssay:
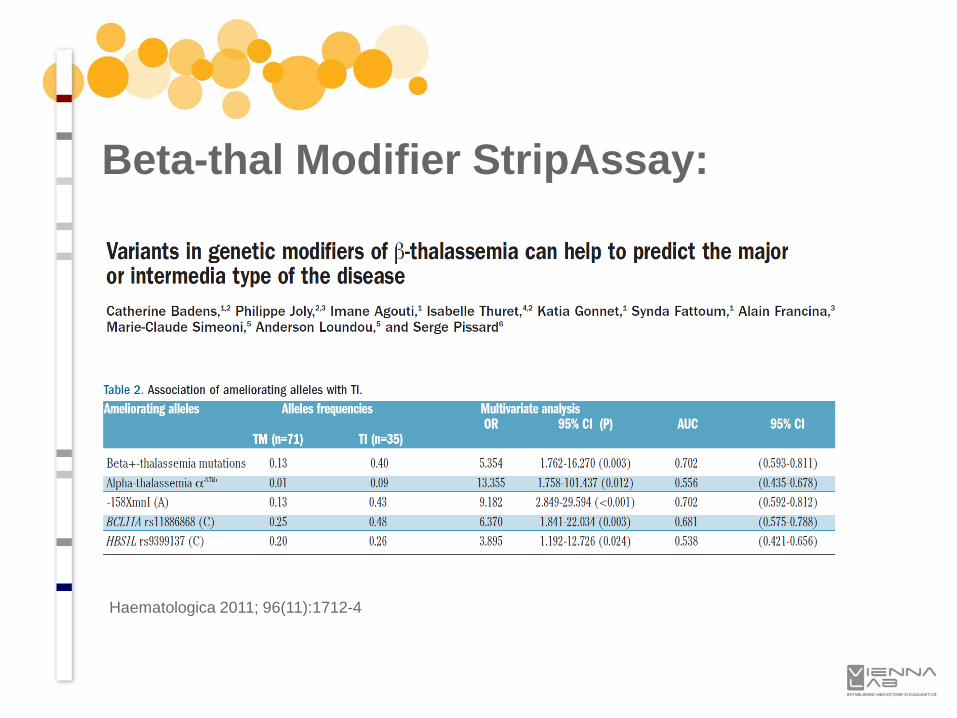
Haematologica 2011; 96(11):1712-4
Beta-thal Modifier StripAssay:
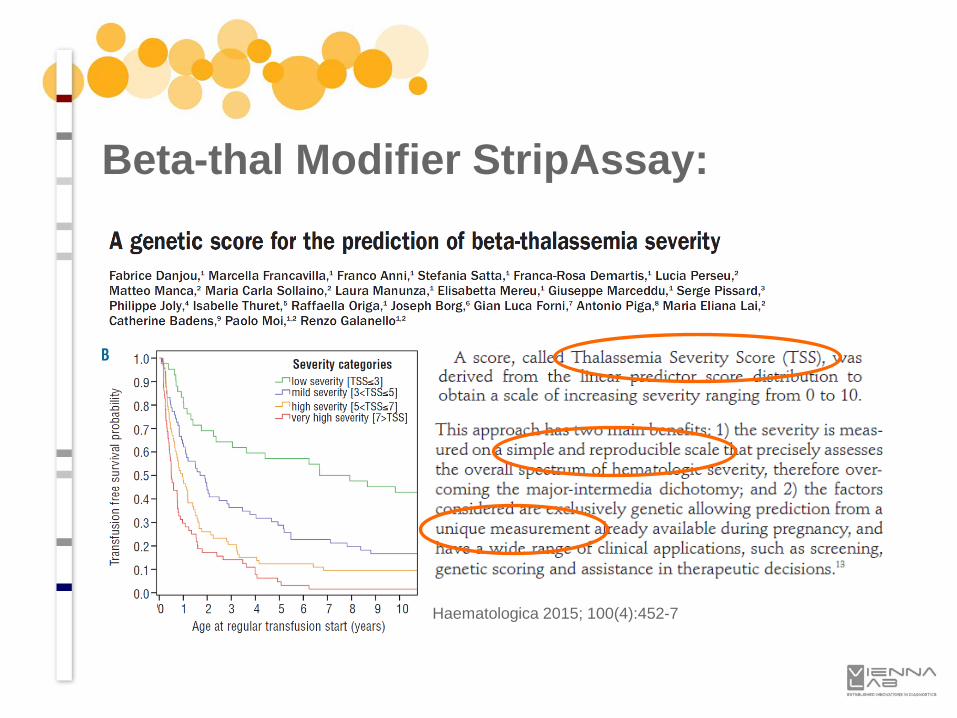
Beta-thal Modifier StripAssay:
Haematologica 2015; 100(4):452-7
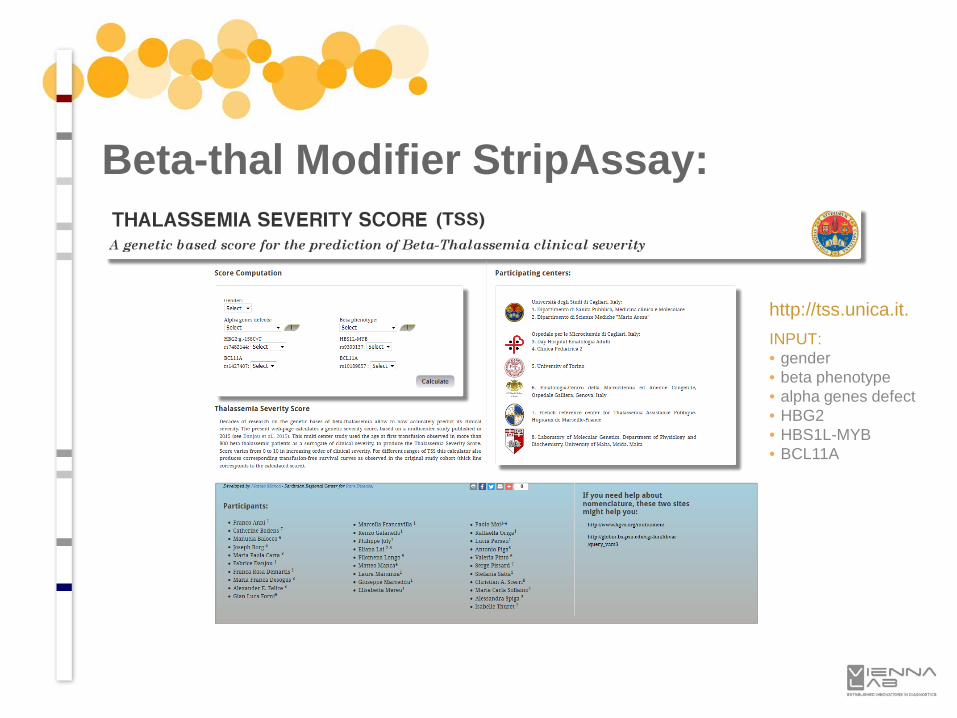
Beta-thal Modifier StripAssay:
http://tss.unica.it.INPUT:• gender• beta phenotype• alpha genes defect• HBG2• HBS1L-MYB• BCL11A
Beta-thal Modifier StripAssay:
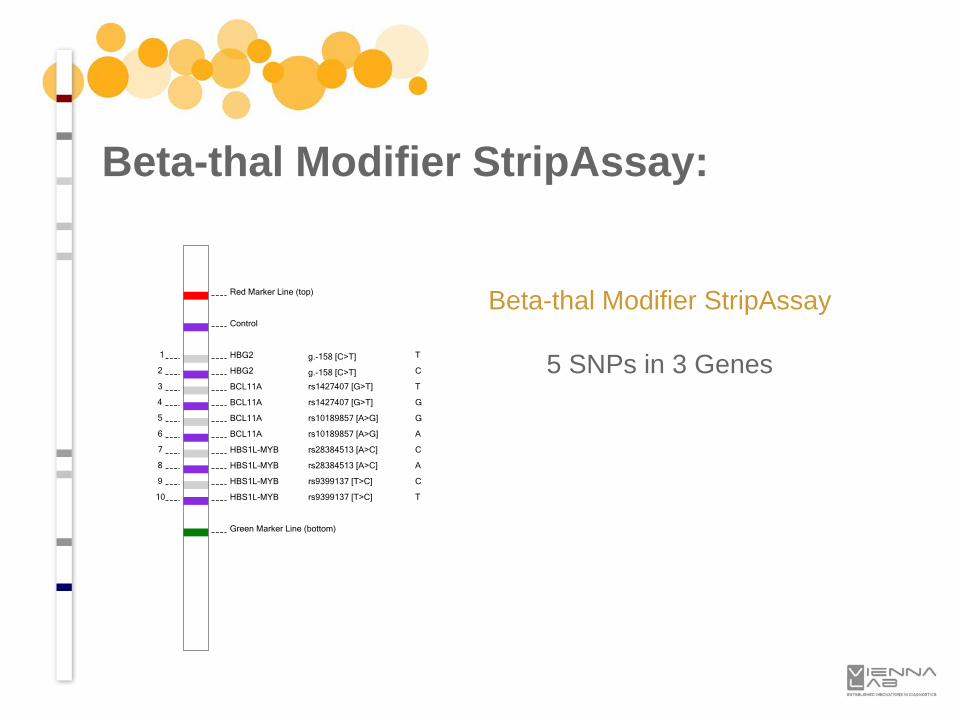
Red Marker Line (top)
Control
1 HBG2 g.-158 [C>T] T
2 HBG2 g.-158 [C>T] C
3 BCL11A rs1427407 [G>T] T
4 BCL11A rs1427407 [G>T] G
5 BCL11A rs10189857 [A>G] G
6 BCL11A rs10189857 [A>G] A
7 HBS1L-MYB rs28384513 [A>C] C
8 HBS1L-MYB rs28384513 [A>C] A
9 HBS1L-MYB rs9399137 [T>C] C
10 HBS1L-MYB rs9399137 [T>C] T
Green Marker Line (bottom)
Beta-thal Modifier StripAssay
5 SNPs in 3 Genes
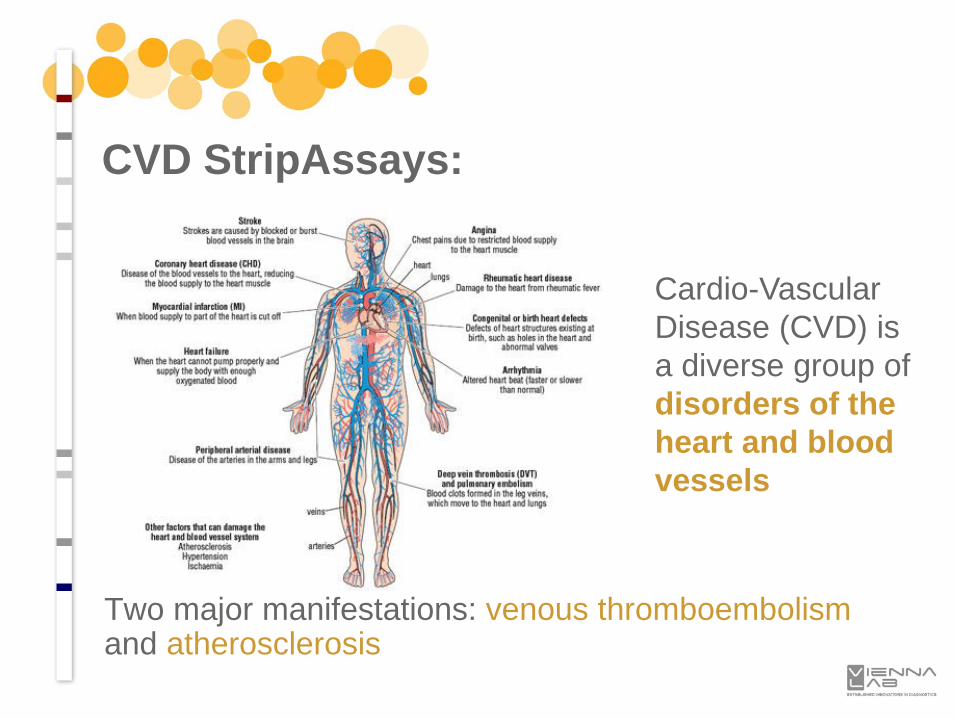
CVD StripAssays:
Cardio-Vascular Disease (CVD) is a diverse group of disorders of the heart and blood vessels
Two major manifestations: venous thromboembolismand atherosclerosis
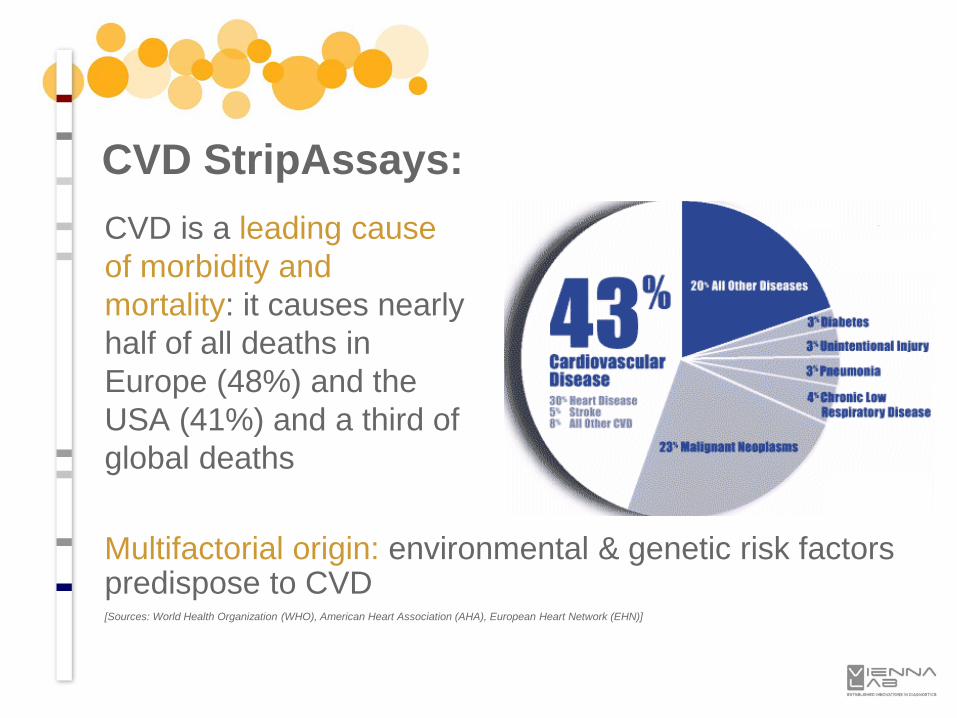
CVD StripAssays:CVD is a leading cause of morbidity and mortality: it causes nearly half of all deaths in Europe (48%) and the USA (41%) and a third of global deaths
Multifactorial origin: environmental & genetic risk factors predispose to CVD[Sources: World Health Organization (WHO), American Heart Association (AHA), European Heart Network (EHN)]

Environmental risk factors:• tobacco smoke• physical inactivity• overweight and obesity• alcohol and drug abuse• stress• .....
CVD StripAssays:Inherited risk factors:• mutated blood coagulation factors• mutated lipoproteins• mutated regulators of blood pressure• mutated regulators of homocysteine• mutated regulators of inflammation• .....
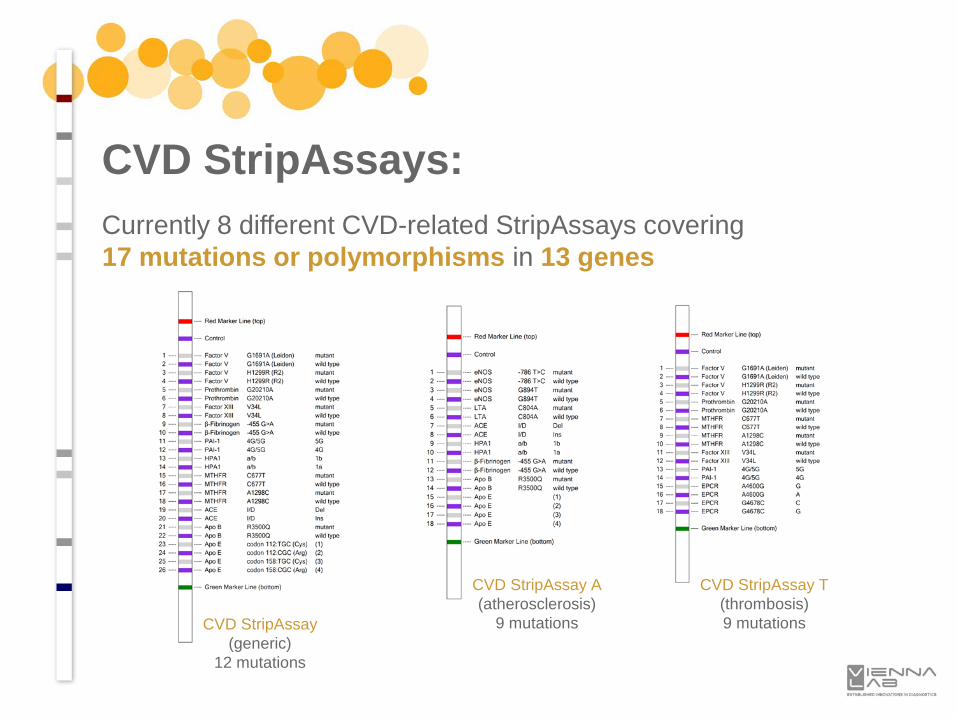
Currently 8 different CVD-related StripAssays covering 17 mutations or polymorphisms in 13 genes
CVD StripAssays:
CVD StripAssay(generic)
12 mutations
CVD StripAssay A(atherosclerosis)
9 mutations
CVD StripAssay T(thrombosis)9 mutations
CVD: Pregnancy complications"Vienna recurrent pregnancy loss study"genetic CVD risk factors were compared between patients with a history of RPL and a matched control group using CVD StripAssays
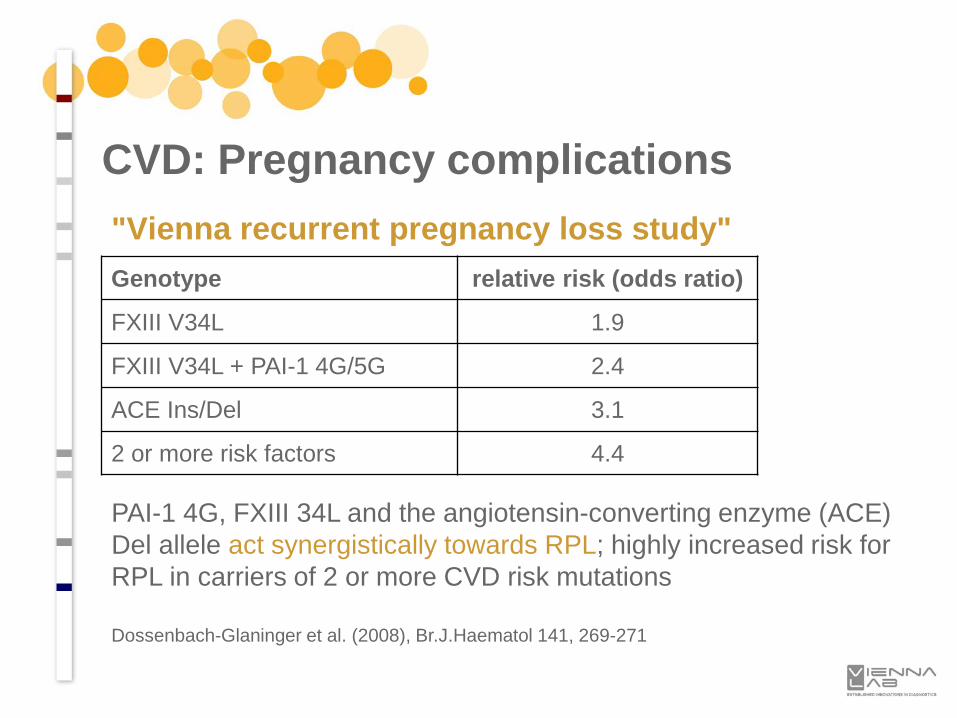
CVD: Pregnancy complications"Vienna recurrent pregnancy loss study"
PAI-1 4G, FXIII 34L and the angiotensin-converting enzyme (ACE) Del allele act synergistically towards RPL; highly increased risk for RPL in carriers of 2 or more CVD risk mutations
Dossenbach-Glaninger et al. (2008), Br.J.Haematol 141, 269-271
Genotype relative risk (odds ratio)
FXIII V34L 1.9
FXIII V34L + PAI-1 4G/5G 2.4
ACE Ins/Del 3.1
2 or more risk factors 4.4
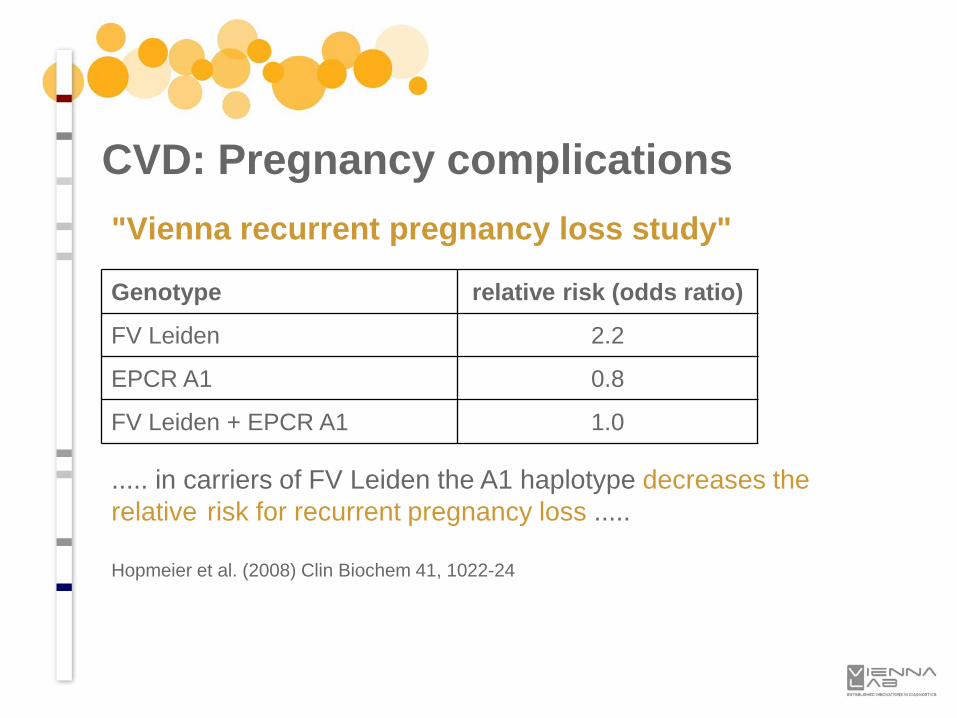
CVD: Pregnancy complications"Vienna recurrent pregnancy loss study"
Genotype relative risk (odds ratio)
FV Leiden 2.2
EPCR A1 0.8
FV Leiden + EPCR A1 1.0
..... in carriers of FV Leiden the A1 haplotype decreases the relative risk for recurrent pregnancy loss .....
Hopmeier et al. (2008) Clin Biochem 41, 1022-24
Cystic Fibrosis (CF) is the most common life-limiting genetic disorder (incidence approx. 1:3,000 live births in Caucasians)
CF is caused by mutations in the Cystic Fibrosis Transmembrane Conductance Regulator (CFTR) gene
Newborn screening programs based on immunoreactive trypsinogen (IRT), sweat cloride and genetic testing are widely in place
CF StripAssay:
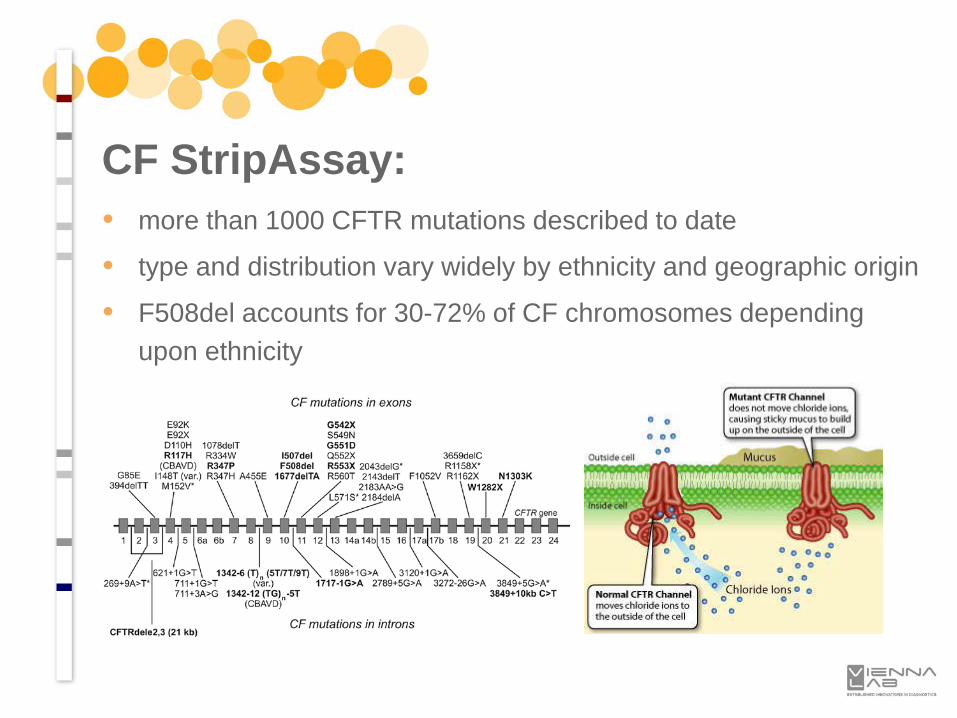
• more than 1000 CFTR mutations described to date
• type and distribution vary widely by ethnicity and geographic origin
• F508del accounts for 30-72% of CF chromosomes depending upon ethnicity
CF StripAssay:
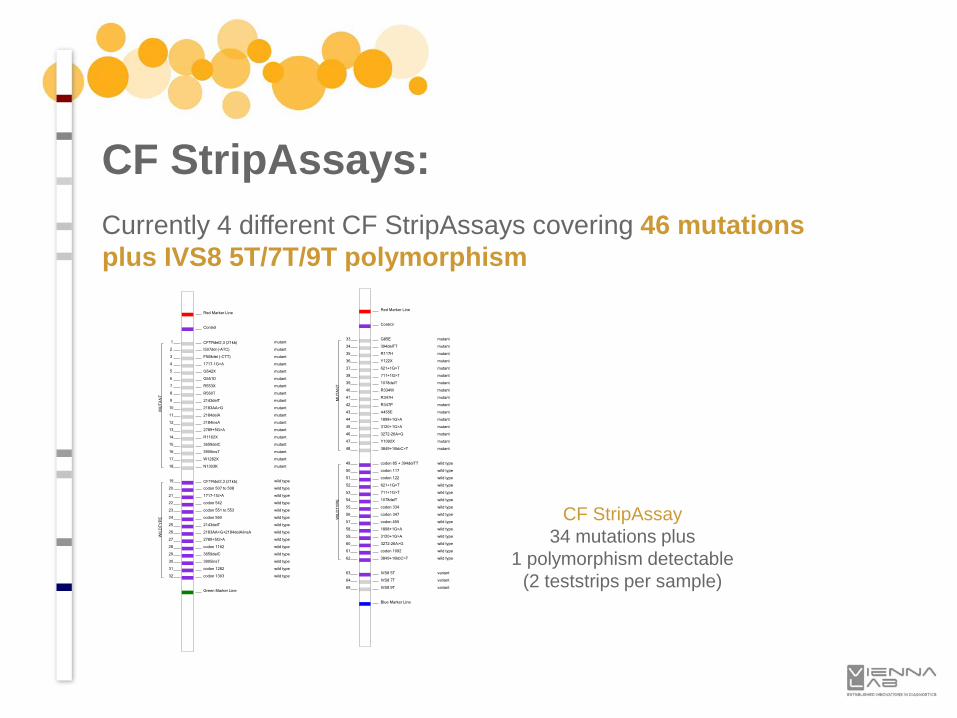
Currently 4 different CF StripAssays covering 46 mutations plus IVS8 5T/7T/9T polymorphism
CF StripAssays:
Red Marker Line
Control
1 CFTRdel2,3 (21kb) mutant
2 I507del (-ATC) mutant
3 F508del (-CTT) mutant
4 1717-1G>A mutant
5 G542X mutant
6 G551D mutant
7 R553X mutant
8 R560T mutant
9 2143delT mutant
10 2183AA>G mutant
11 2184delA mutant
12 2184insA mutant
13 2789+5G>A mutant
14 R1162X mutant
15 3659delC mutant
16 3905insT mutant
17 W1282X mutant
18 N1303K mutant
19 CFTRdel2,3 (21kb) wild type
20 codon 507 to 508 wild type
21 1717-1G>A wild type
22 codon 542 wild type
23 codon 551 to 553 wild type
24 codon 560 wild type
25 2143delT wild type
26 2183AA>G+2184delA/insA wild type
27 2789+5G>A wild type
28 codon 1162 wild type
29 3659delC wild type
30 3905insT wild type
31 codon 1282 wild type
32 codon 1303 wild type
Green Marker Line
MU
TA
NT
WIL
DT
YP
E
Red Marker Line
Control
33 G85E mutant
34 394delTT mutant
35 R117H mutant
36 Y122X mutant
37 621+1G>T mutant
38 711+1G>T mutant
39 1078delT mutant
40 R334W mutant
41 R347H mutant
42 R347P mutant
43 A455E mutant
44 1898+1G>A mutant
45 3120+1G>A mutant
46 3272-26A>G mutant
47 Y1092X mutant
48 3849+10kbC>T mutant
49 codon 85 + 394delTT wild type
50 codon 117 wild type
51 codon 122 wild type
52 621+1G>T wild type
53 711+1G>T wild type
54 1078delT wild type
55 codon 334 wild type
56 codon 347 wild type
57 codon 455 wild type
58 1898+1G>A wild type
59 3120+1G>A wild type
60 3272-26A>G wild type
61 codon 1092 wild type
62 3849+10kbC>T wild type
63 IVS8 5T variant
64 IVS8 7T variant
65 IVS8 9T variant
Blue Marker Line
MU
TA
NT
WIL
DT
YP
E
CF StripAssay34 mutations plus
1 polymorphism detectable(2 teststrips per sample)
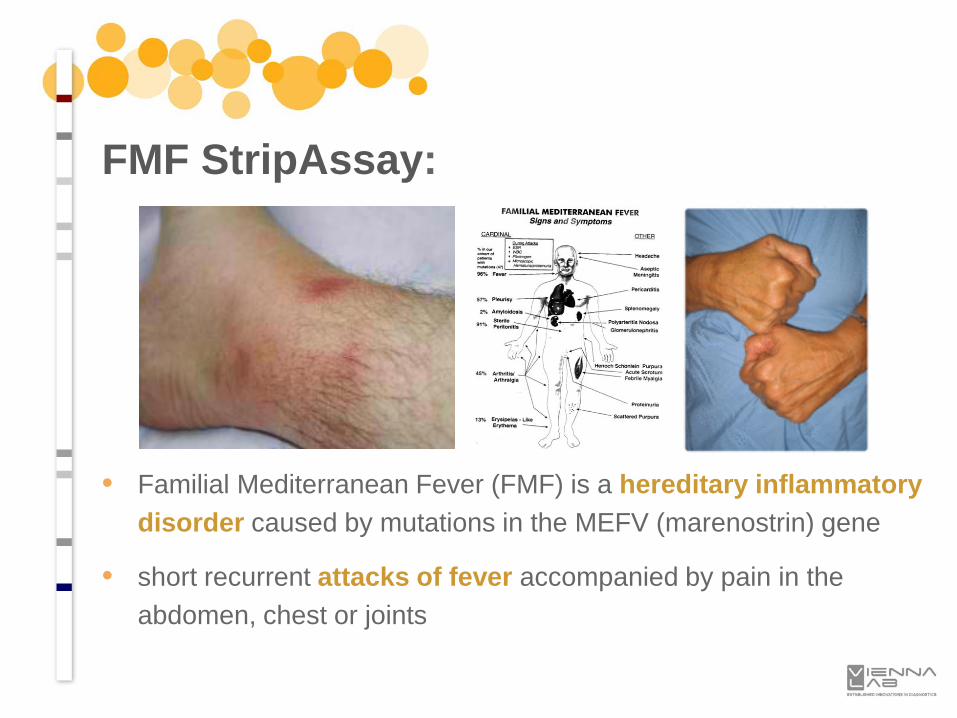
• Familial Mediterranean Fever (FMF) is a hereditary inflammatory disorder caused by mutations in the MEFV (marenostrin) gene
• short recurrent attacks of fever accompanied by pain in the abdomen, chest or joints
FMF StripAssay:
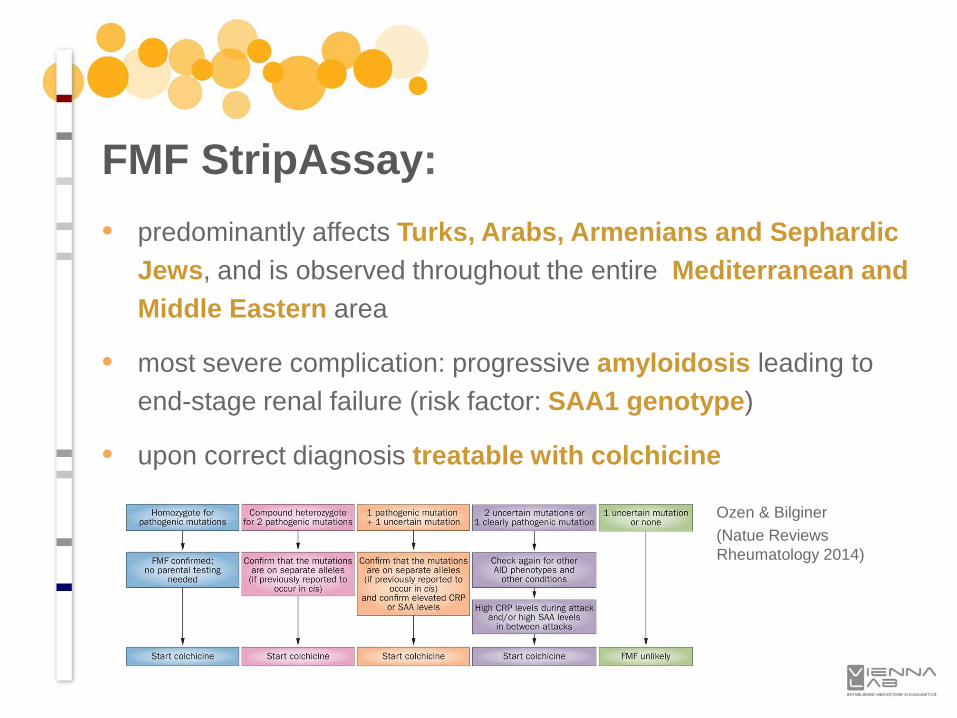
• predominantly affects Turks, Arabs, Armenians and Sephardic Jews, and is observed throughout the entire Mediterranean and Middle Eastern area
• most severe complication: progressive amyloidosis leading to end-stage renal failure (risk factor: SAA1 genotype)
• upon correct diagnosis treatable with colchicine
FMF StripAssay:
Ozen & Bilginer(Natue Reviews Rheumatology 2014)
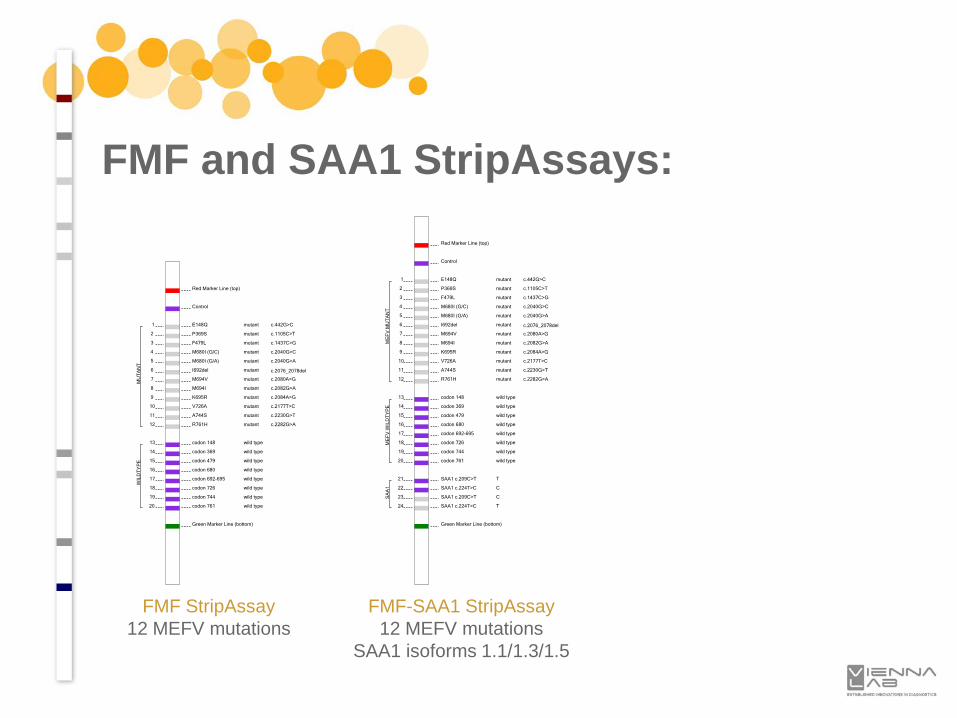
FMF and SAA1 StripAssays:
FMF StripAssay12 MEFV mutations
Red Marker Line (top)
Control
1 E148Q mutant c.442G>C
2 P369S mutant c.1105C>T
3 F479L mutant c.1437C>G
4 M680I (G/C) mutant c.2040G>C
5 M680I (G/A) mutant c.2040G>A
6 I692del mutant c.2076_2078del
7 M694V mutant c.2080A>G
8 M694I mutant c.2082G>A
9 K695R mutant c.2084A>G
10 V726A mutant c.2177T>C
11 A744S mutant c.2230G>T
12 R761H mutant c.2282G>A
13 codon 148 wild type
14 codon 369 wild type
15 codon 479 wild type
16 codon 680 wild type
17 codon 692-695 wild type
18 codon 726 wild type
19 codon 744 wild type
20 codon 761 wild type
Green Marker Line (bottom)
MU
TA
NT
WIL
DT
YP
E
Red Marker Line (top)
Control
1 E148Q mutant c.442G>C
2 P369S mutant c.1105C>T
3 F479L mutant c.1437C>G
4 M680I (G/C) mutant c.2040G>C
5 M680I (G/A) mutant c.2040G>A
6 I692del mutant c.2076_2078del
7 M694V mutant c.2080A>G
8 M694I mutant c.2082G>A
9 K695R mutant c.2084A>G
10 V726A mutant c.2177T>C
11 A744S mutant c.2230G>T
12 R761H mutant c.2282G>A
13 codon 148 wild type
14 codon 369 wild type
15 codon 479 wild type
16 codon 680 wild type
17 codon 692-695 wild type
18 codon 726 wild type
19 codon 744 wild type
20 codon 761 wild type
21 SAA1 c.209C>T T
22 SAA1 c.224T>C C
23 SAA1 c.209C>T C
24 SAA1 c.224T>C T
Green Marker Line (bottom)
ME
FV
MU
TA
NT
ME
FV
WIL
DT
YP
ES
AA
1
FMF-SAA1 StripAssay12 MEFV mutations
SAA1 isoforms 1.1/1.3/1.5
• Congenital adrenal hyperplasia (CAH) comprises inborn errors in the synthesis of adrenal corticoid hormones
• average incidence approx. 1:15,000 births worldwide
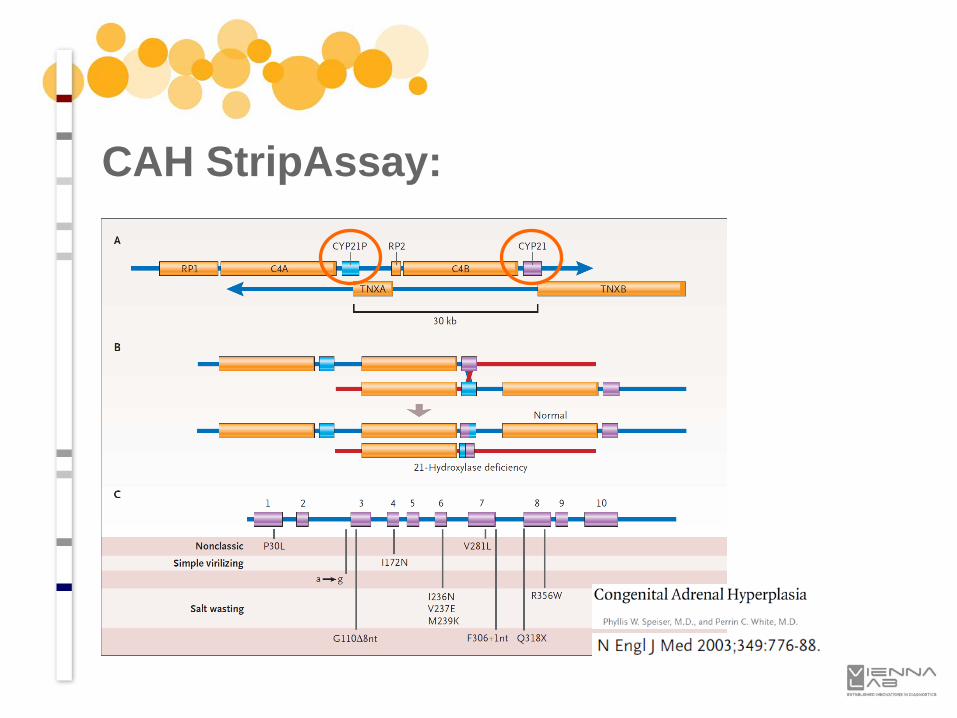
• more than 90% of cases arise from mutations in the CYP21A2 gene
• severe forms cause life-threatening salt-wasting crisis - treatable!
• newborn screening programs based on 17-hydroxyprogesterone (17-OHP) levels have been introduced, but have a high false positive recall rate
• concurrent genetic testing saves costs and efforts for repeated testing and minimizes emotional stress for parents
CAH StripAssay:
CAH StripAssay:
CAH StripAssay:
Red Marker Line (top)
Control
1 P30L c.89C>T
2 I2 splice c.290-13A/C>G
3 Del 8 bp E3 c.329_336del GAGACTAC
4 I172N c.515T>A
5 Cluster E6 c.707T>A,c.710T>A,c.716T>A
6 V281L c.841G>T
7 L307 frameshift c.920_921insT
8 Q318X c.952C>T
9 R356W c.1066C>T
10 P453S c.1357C>T
11 R483P c.1448G>C
12 codon 30
13 I2
14 E3
15 codon 172
16 E6
17 codon 281
18 codon 307
19 codon 318
20 codon 356
21 codon 453
22 codon 483
Green Marker Line (bottom)
MU
TA
NT
WIL
DT
YP
E
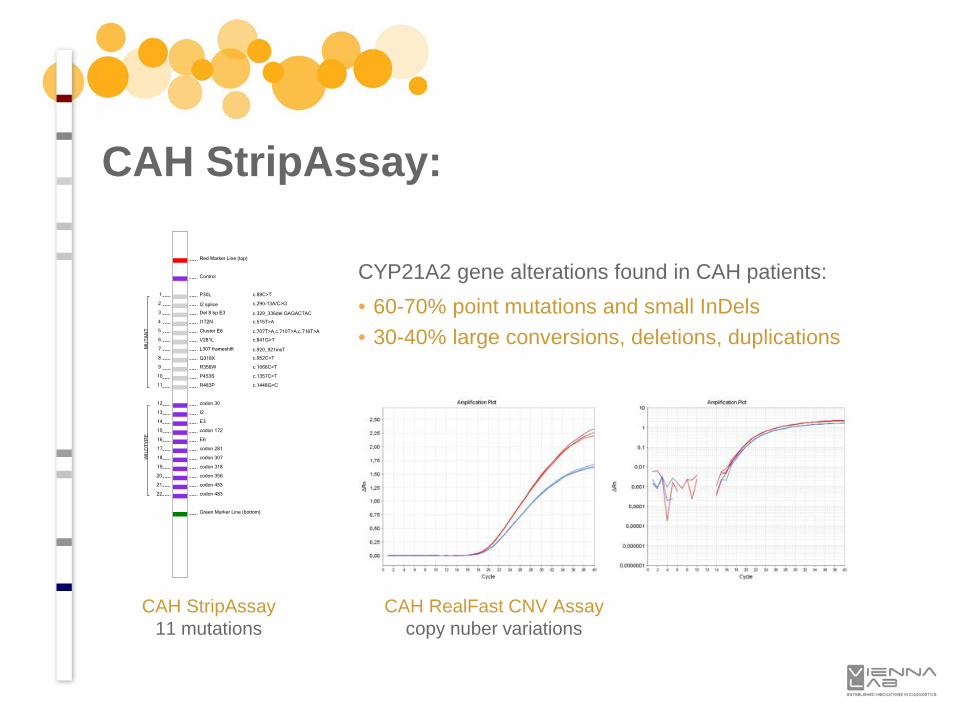
CAH StripAssay11 mutations
CAH RealFast CNV Assaycopy nuber variations
CYP21A2 gene alterations found in CAH patients:• 60-70% point mutations and small InDels• 30-40% large conversions, deletions, duplications
• Coumarin derivatives (e.g. warfarin, phenprocoumon) are the most widespread oral anticoagulant drugs for the prevention and treatment of thromboembolic disorders.
• Coumarins have a narrow therapeutic range and a wide inter-individual variability in dose requirement.
• delays in achieving a stable maintenance dose and adverse eventsare frequently encountered during the initial phase of therapy(overdosing -> bleeding; underdosing -> insufficient anticoagulation).
• known parameters influencing coumarin doserequirement include age, sex, body size andweight, co-medication and genetic factors.
PGX-Thrombo StripAssay:
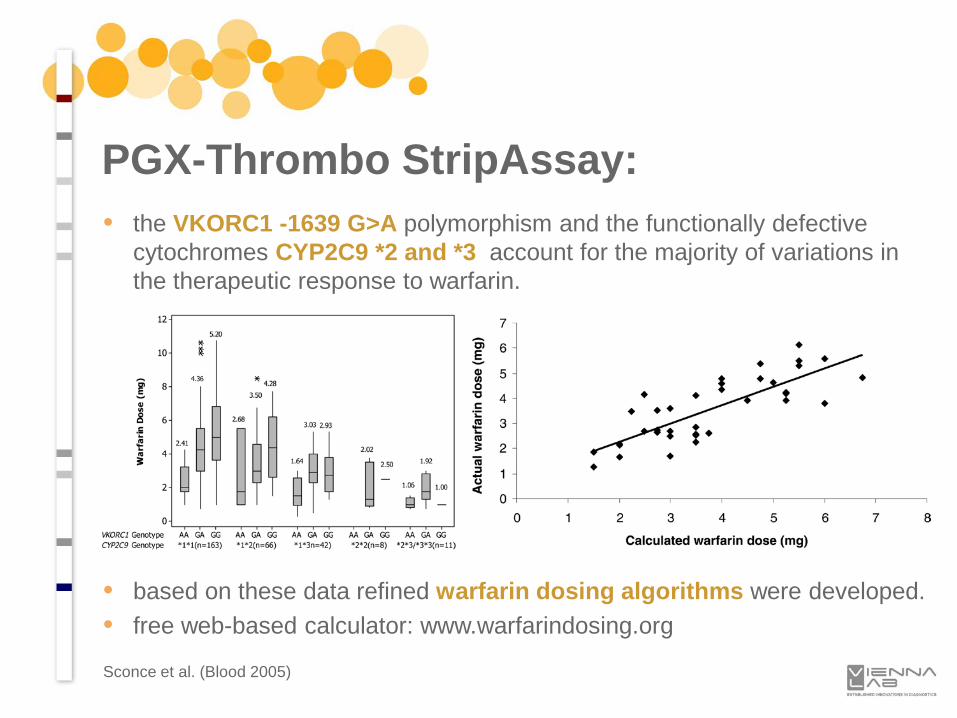
• the VKORC1 -1639 G>A polymorphism and the functionally defective cytochromes CYP2C9 *2 and *3 account for the majority of variations in the therapeutic response to warfarin.
• based on these data refined warfarin dosing algorithms were developed.• free web-based calculator: www.warfarindosing.org
PGX-Thrombo StripAssay:
Sconce et al. (Blood 2005)
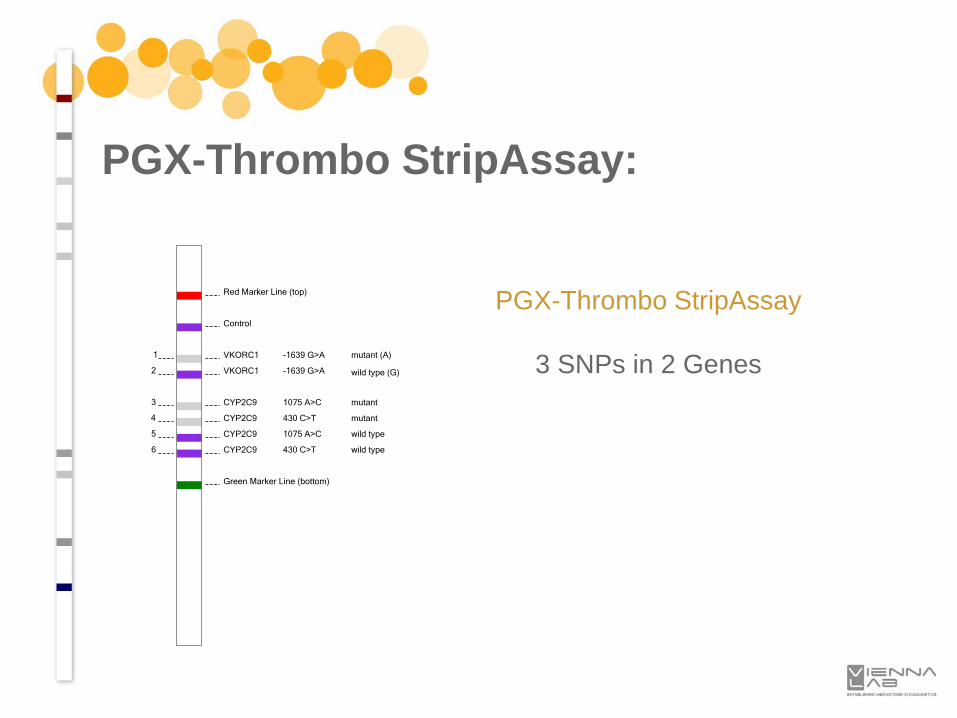
PGX-Thrombo StripAssay
3 SNPs in 2 Genes
PGX-Thrombo StripAssay:
Red Marker Line (top)
Control
1 VKORC1 -1639 G>A mutant (A)
2 VKORC1 -1639 G>A wild type (G)
3 CYP2C9 1075 A>C mutant
4 CYP2C9 430 C>T mutant
5 CYP2C9 1075 A>C wild type
6 CYP2C9 430 C>T wild type
Green Marker Line (bottom)
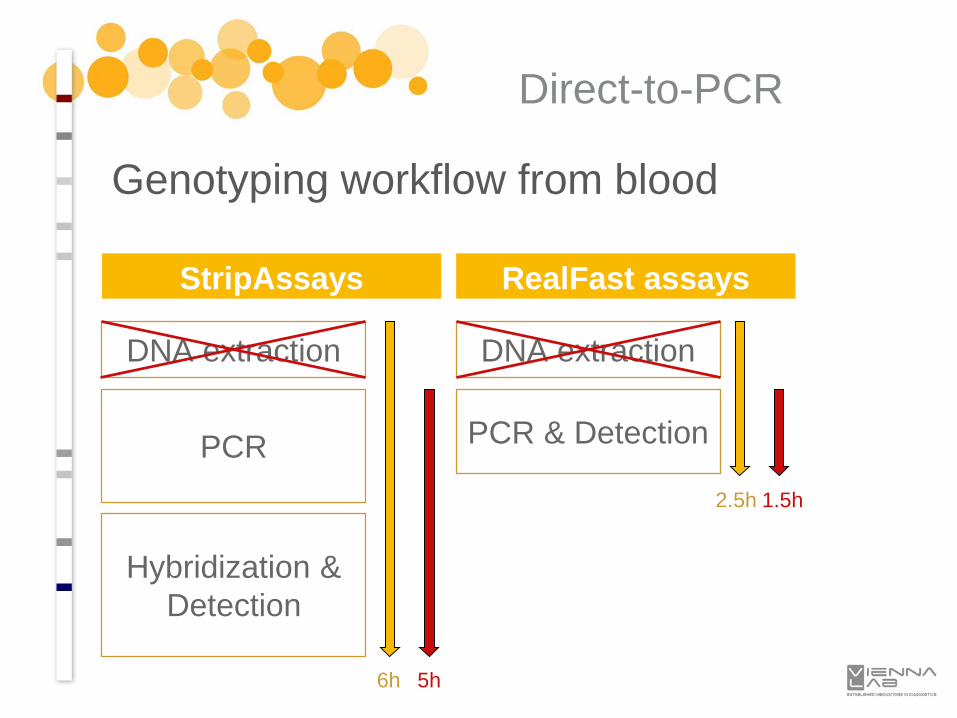
Genotyping workflow from blood
StripAssays
DNA extraction
RealFast assays
DNA extraction
PCR PCR & Detection
Hybridization & Detection
6h
2.5h
5h
1.5h
Direct-to-PCR
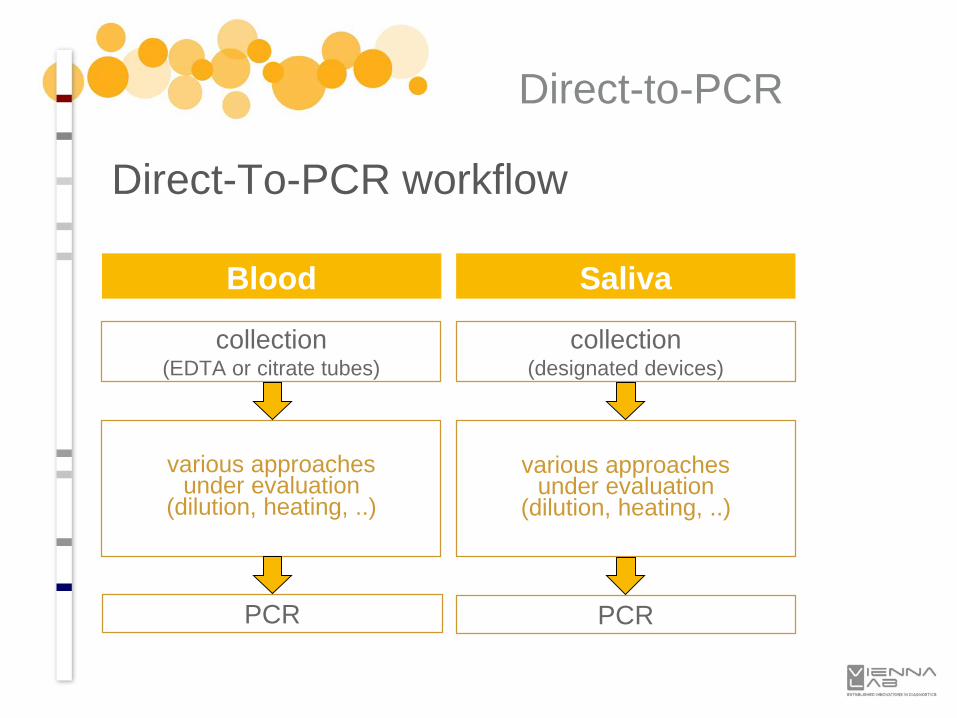
Direct-To-PCR workflow
Blood
collection(EDTA or citrate tubes)
Saliva
collection(designated devices)
various approachesunder evaluation
(dilution, heating, ..)
various approachesunder evaluation
(dilution, heating, ..)
PCR PCR
Direct-to-PCR
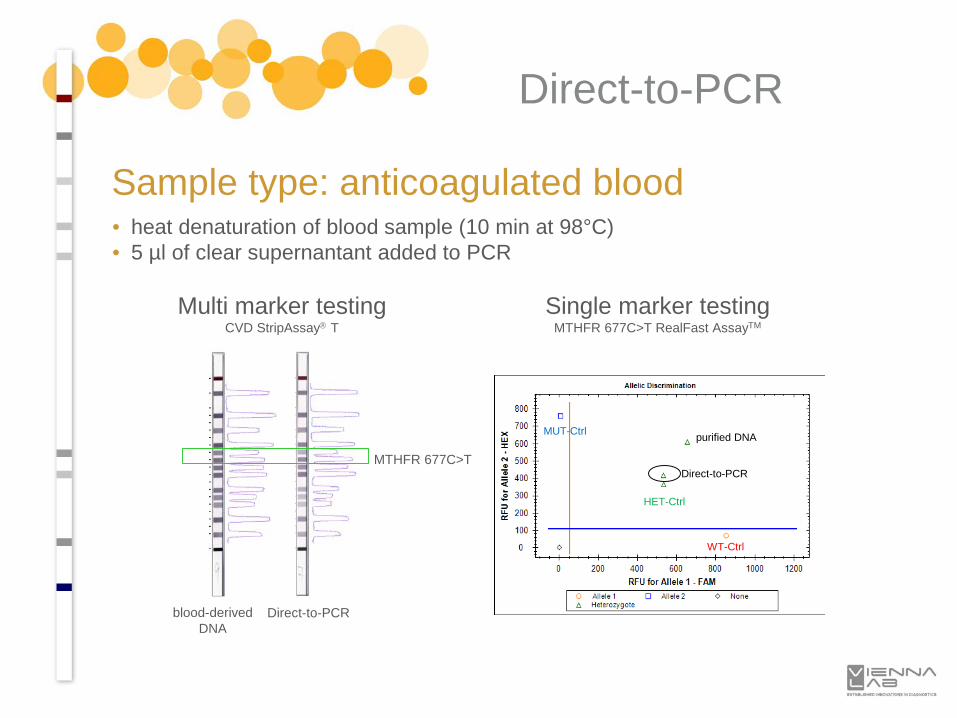
Multi marker testingCVD StripAssay T
blood-derivedDNA DNA
Direct-to-PCRDNA
Single marker testingMTHFR 677C>T RealFast AssayTM
MUT-Ctrl
WT-Ctrl
HET-Ctrl
Direct-to-PCR
purified DNA
• heat denaturation of blood sample (10 min at 98°C)• 5 µl of clear supernantant added to PCR
MTHFR 677C>T
Direct-to-PCR
Sample type: anticoagulated blood
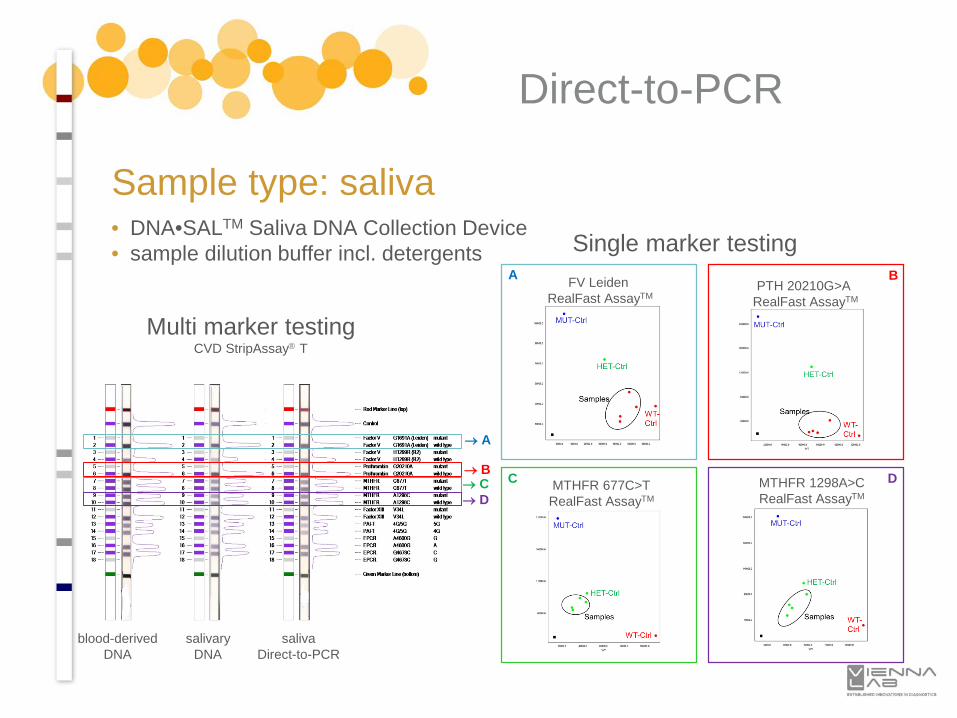
Multi marker testingCVD StripAssay T
→ B
→ A
→ C→ D
blood-derivedDNA DNA
salivaryDNA
salivaDirect-to-PCR
Single marker testingFV Leiden
RealFast AssayTMPTH 20210G>A
RealFast AssayTM
MTHFR 677C>TRealFast AssayTM
MTHFR 1298A>CRealFast AssayTM
A B
C D
Direct-to-PCR
Sample type: saliva• DNA•SALTM Saliva DNA Collection Device• sample dilution buffer incl. detergents

StripAssay® Applications for Oncology
Prognostic biomarker:
Indicates the likely course of the diseasein an untreated individual.
Predictive biomarker:
Identifies subpopulations of patients whoare most likely to respond to a given therapy.
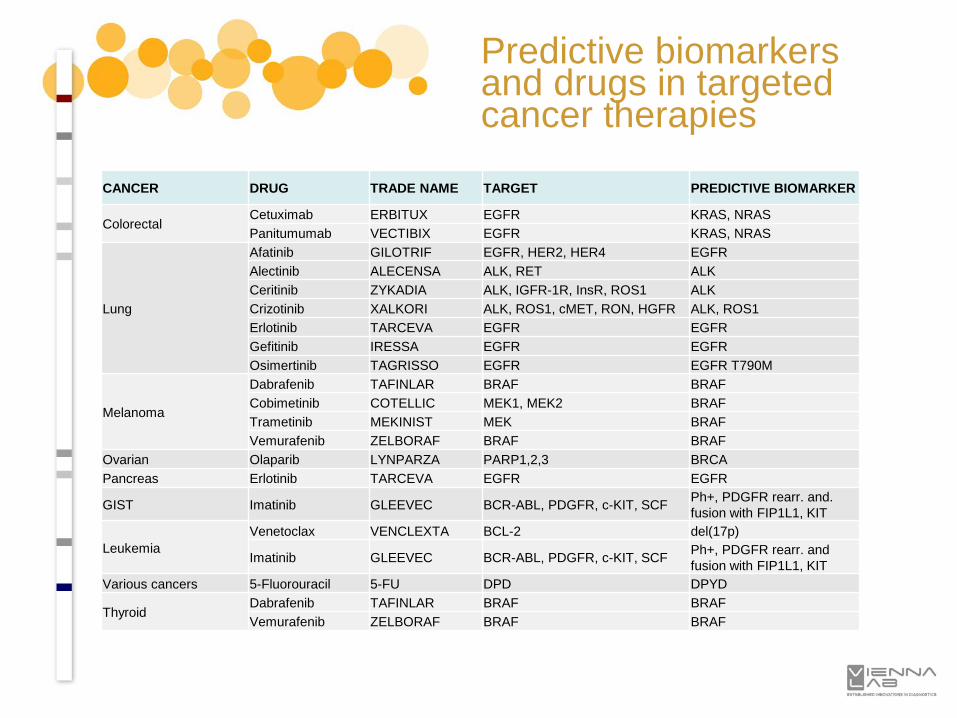
CANCER DRUG TRADE NAME TARGET PREDICTIVE BIOMARKER
ColorectalCetuximab ERBITUX EGFR KRAS, NRASPanitumumab VECTIBIX EGFR KRAS, NRAS
Lung
Afatinib GILOTRIF EGFR, HER2, HER4 EGFRAlectinib ALECENSA ALK, RET ALKCeritinib ZYKADIA ALK, IGFR-1R, InsR, ROS1 ALK Crizotinib XALKORI ALK, ROS1, cMET, RON, HGFR ALK, ROS1Erlotinib TARCEVA EGFR EGFRGefitinib IRESSA EGFR EGFROsimertinib TAGRISSO EGFR EGFR T790M
Melanoma
Dabrafenib TAFINLAR BRAF BRAFCobimetinib COTELLIC MEK1, MEK2 BRAFTrametinib MEKINIST MEK BRAFVemurafenib ZELBORAF BRAF BRAF
Ovarian Olaparib LYNPARZA PARP1,2,3 BRCAPancreas Erlotinib TARCEVA EGFR EGFR
GIST Imatinib GLEEVEC BCR-ABL, PDGFR, c-KIT, SCF Ph+, PDGFR rearr. and. fusion with FIP1L1, KIT
LeukemiaVenetoclax VENCLEXTA BCL-2 del(17p)
Imatinib GLEEVEC BCR-ABL, PDGFR, c-KIT, SCF Ph+, PDGFR rearr. and fusion with FIP1L1, KIT
Various cancers 5-Fluorouracil 5-FU DPD DPYD
ThyroidDabrafenib TAFINLAR BRAF BRAFVemurafenib ZELBORAF BRAF BRAF
Predictive biomarkers and drugs in targeted cancer therapies
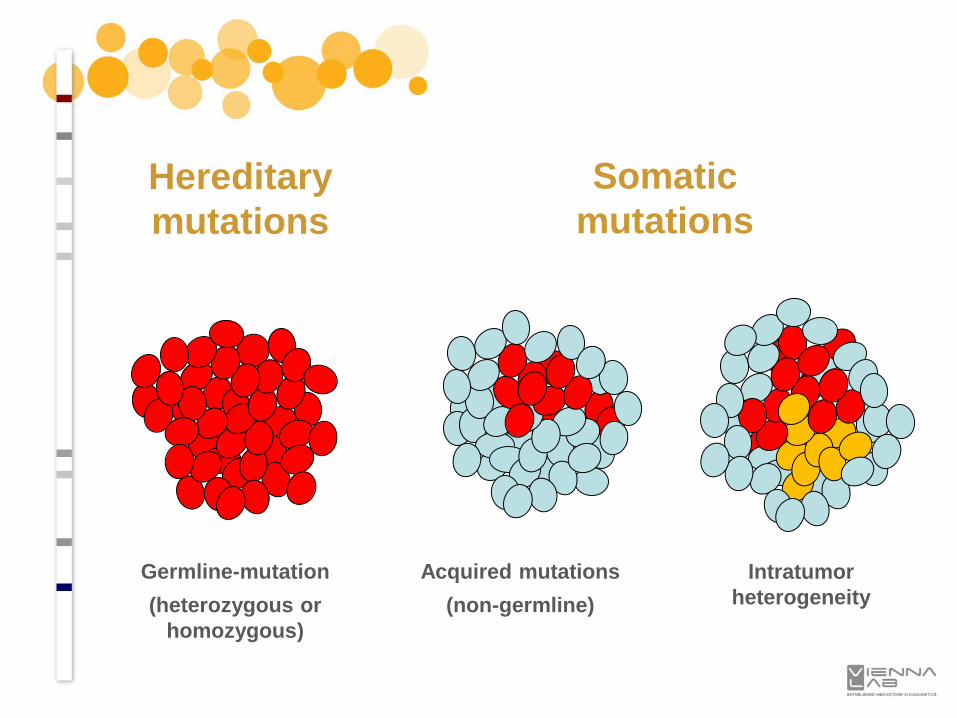
Somaticmutations
Hereditarymutations
Germline-mutation(heterozygous or
homozygous)
Acquired mutations(non-germline)
Intratumor heterogeneity
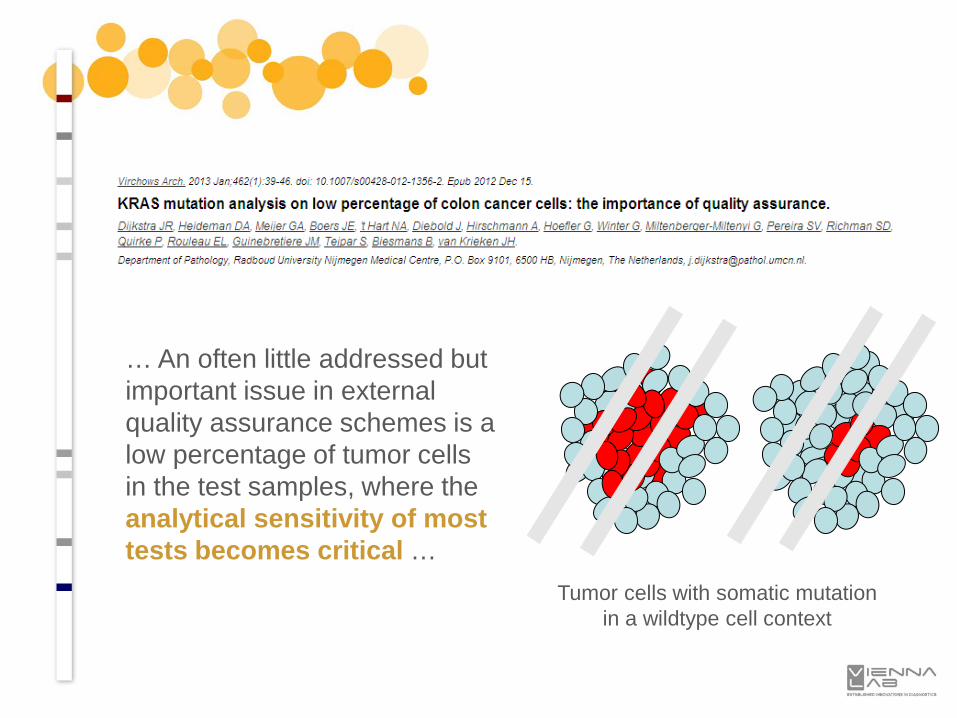
… An often little addressed but important issue in external quality assurance schemes is a low percentage of tumor cells in the test samples, where the analytical sensitivity of most tests becomes critical …
Tumor cells with somatic mutationin a wildtype cell context
… although traditional Sanger sequencing detects all clinically important KRAS mutations, its sensitivity is too low to be used in routine clinical tests (mutant alleles must be present in at least 30-40% of cells for reproducible detection) …
… if a mutation is identified, the affected codon and the specific change should be reported. This is an important aspect of the report because recommendations for treatment eligibility are continuously evolving …
... One can imagine that a perfect approach would be the combination of manual microdissection (under the microscope) with high-sensitivity (1% mutation in a 99% wild-type background limit of detection)methods for KRAS mutation testing.
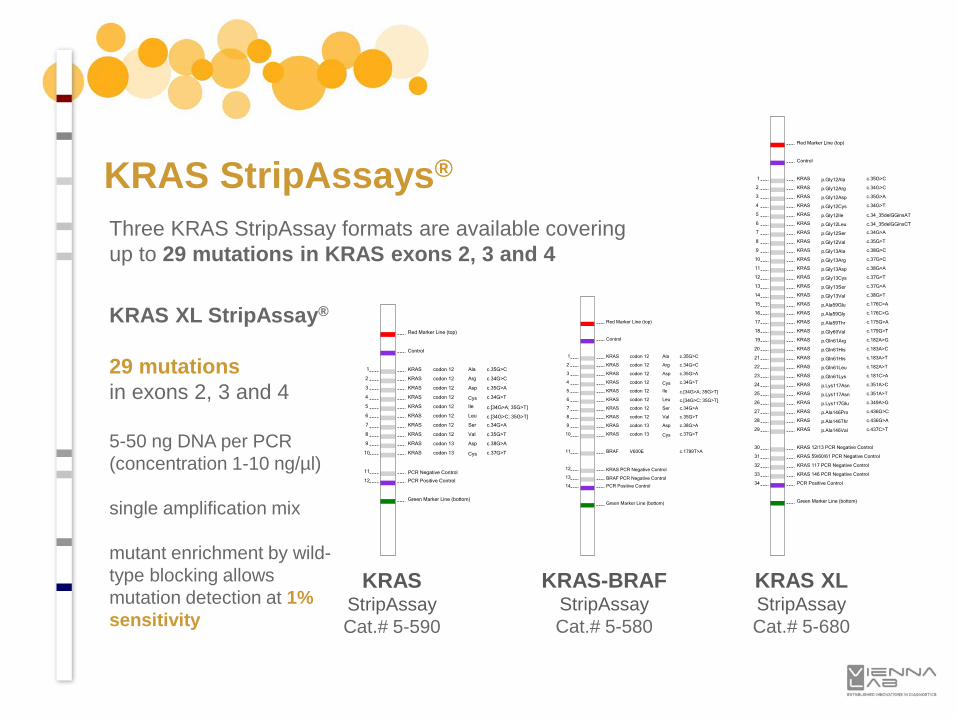
Three KRAS StripAssay formats are available coveringup to 29 mutations in KRAS exons 2, 3 and 4
KRASStripAssayCat.# 5-590
Red Marker Line (top)
Control
1 KRAS p.Gly12Ala c.35G>C
2 KRAS p.Gly12Arg c.34G>C
3 KRAS p.Gly12Asp c.35G>A
4 KRAS p.Gly12Cys c.34G>T
5 KRAS p.Gly12Ile c.34_35delGGinsAT
6 KRAS p.Gly12Leu c.34_35delGGinsCT
7 KRAS p.Gly12Ser c.34G>A
8 KRAS p.Gly12Val c.35G>T
9 KRAS p.Gly13Ala c.38G>C
10 KRAS p.Gly13Arg c.37G>C
11 KRAS p.Gly13Asp c.38G>A
12 KRAS p.Gly13Cys c.37G>T
13 KRAS p.Gly13Ser c.37G>A
14 KRAS p.Gly13Val c.38G>T
15 KRAS p.Ala59Glu c.176C>A
16 KRAS p.Ala59Gly c.176C>G
17 KRAS p.Ala59Thr c.175G>A
18 KRAS p.Gly60Val c.179G>T
19 KRAS p.Gln61Arg c.182A>G
20 KRAS p.Gln61His c.183A>C
21 KRAS p.Gln61His c.183A>T
22 KRAS p.Gln61Leu c.182A>T
23 KRAS p.Gln61Lys c.181C>A
24 KRAS p.Lys117Asn c.351A>C
25 KRAS p.Lys117Asn c.351A>T
26 KRAS p.Lys117Glu c.349A>G
27 KRAS p.Ala146Pro c.436G>C
28 KRAS p.Ala146Thr c.436G>A
29 KRAS p.Ala146Val c.437C>T
30 KRAS 12/13 PCR Negative Control
31 KRAS 59/60/61 PCR Negative Control
32 KRAS 117 PCR Negative Control
33 KRAS 146 PCR Negative Control
34 PCR Positive Control
Green Marker Line (bottom)
Red Marker Line (top)
Control
1 KRAS codon 12 Ala c.35G>C
2 KRAS codon 12 Arg c.34G>C
3 KRAS codon 12 Asp c.35G>A
4 KRAS codon 12 Cys c.34G>T
5 KRAS codon 12 Ile c.[34G>A; 35G>T]
6 KRAS codon 12 Leu c.[34G>C; 35G>T]
7 KRAS codon 12 Ser c.34G>A
8 KRAS codon 12 Val c.35G>T
9 KRAS codon 13 Asp c.38G>A
10 KRAS codon 13 Cys c.37G>T
11 PCR Negative Control
12 PCR Positive Control
Green Marker Line (bottom)
Red Marker Line (top)
Control
1 KRAS codon 12 Ala c.35G>C
2 KRAS codon 12 Arg c.34G>C
3 KRAS codon 12 Asp c.35G>A
4 KRAS codon 12 Cys c.34G>T
5 KRAS codon 12 Ile c.[34G>A; 35G>T]
6 KRAS codon 12 Leu c.[34G>C; 35G>T]
7 KRAS codon 12 Ser c.34G>A
8 KRAS codon 12 Val c.35G>T
9 KRAS codon 13 Asp c.38G>A
10 KRAS codon 13 Cys c.37G>T
11 BRAF V600E
c.1799T>A
12 KRAS PCR Negative Control
13 BRAF PCR Negative Control
14 PCR Positive Control
Green Marker Line (bottom)
KRAS-BRAFStripAssayCat.# 5-580
KRAS XLStripAssayCat.# 5-680
KRAS StripAssays®
KRAS XL StripAssay®
29 mutationsin exons 2, 3 and 4
5-50 ng DNA per PCR(concentration 1-10 ng/µl)
single amplification mix
mutant enrichment by wild-type blocking allows mutation detection at 1% sensitivity
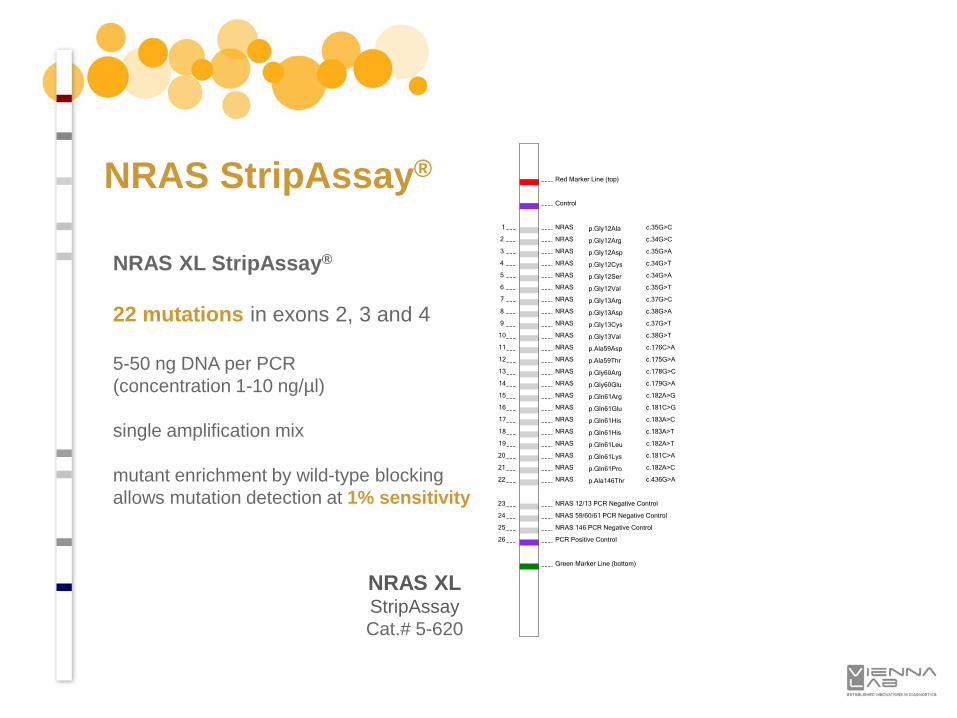
NRAS XL StripAssay®
22 mutations in exons 2, 3 and 4
5-50 ng DNA per PCR(concentration 1-10 ng/µl)
single amplification mix
mutant enrichment by wild-type blocking allows mutation detection at 1% sensitivity
NRAS StripAssay®Red Marker Line (top)
Control
1 NRAS p.Gly12Ala c.35G>C
2 NRAS p.Gly12Arg c.34G>C
3 NRAS p.Gly12Asp c.35G>A
4 NRAS p.Gly12Cys c.34G>T
5 NRAS p.Gly12Ser c.34G>A
6 NRAS p.Gly12Val c.35G>T
7 NRAS p.Gly13Arg c.37G>C
8 NRAS p.Gly13Asp c.38G>A
9 NRAS p.Gly13Cys c.37G>T
10 NRAS p.Gly13Val c.38G>T
11 NRAS p.Ala59Asp c.176C>A
12 NRAS p.Ala59Thr c.175G>A
13 NRAS p.Gly60Arg c.178G>C
14 NRAS p.Gly60Glu c.179G>A
15 NRAS p.Gln61Arg c.182A>G
16 NRAS p.Gln61Glu c.181C>G
17 NRAS p.Gln61His c.183A>C
18 NRAS p.Gln61His c.183A>T
19 NRAS p.Gln61Leu c.182A>T
20 NRAS p.Gln61Lys c.181C>A
21 NRAS p.Gln61Pro c.182A>C
22 NRAS p.Ala146Thr c.436G>A
23 NRAS 12/13 PCR Negative Control
24 NRAS 59/60/61 PCR Negative Control
25 NRAS 146 PCR Negative Control
26 PCR Positive Control
Green Marker Line (bottom)
NRAS XLStripAssayCat.# 5-620
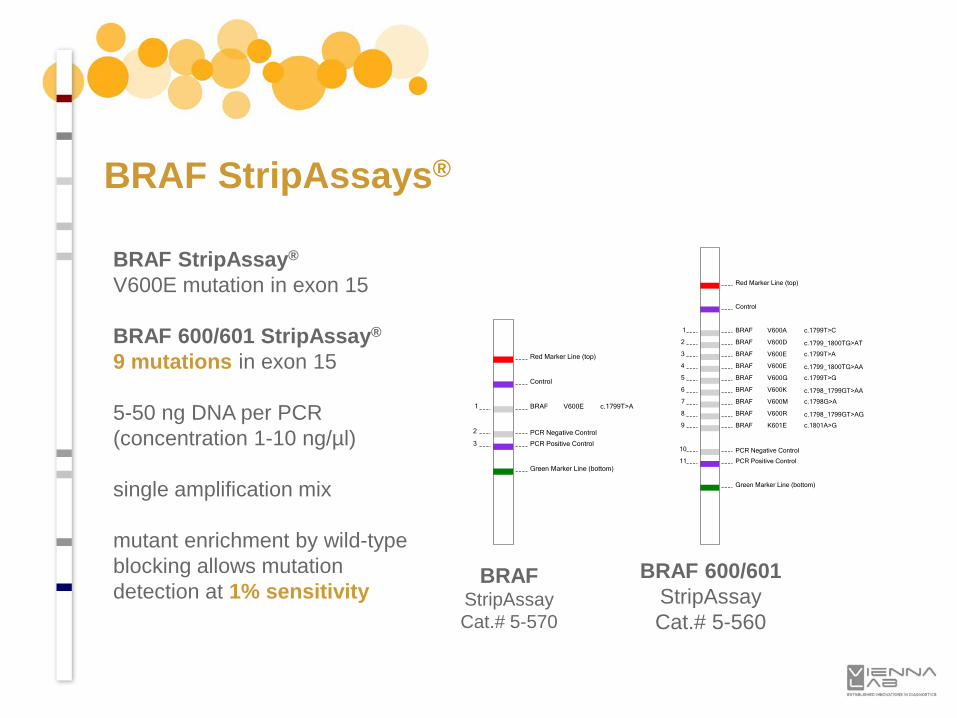
Red Marker Line (top)
Control
1 BRAF V600A c.1799T>C
2 BRAF V600D c.1799_1800TG>AT
3 BRAF V600E c.1799T>A
4 BRAF V600E c.1799_1800TG>AA
5 BRAF V600G c.1799T>G
6 BRAF V600K c.1798_1799GT>AA
7 BRAF V600M c.1798G>A
8 BRAF V600R c.1798_1799GT>AG
9 BRAF K601E c.1801A>G
10 PCR Negative Control
11 PCR Positive Control
Green Marker Line (bottom)
BRAF StripAssay®
V600E mutation in exon 15
BRAF 600/601 StripAssay®
9 mutations in exon 15
5-50 ng DNA per PCR(concentration 1-10 ng/µl)
single amplification mix
mutant enrichment by wild-type blocking allows mutation detection at 1% sensitivity
Red Marker Line (top)
Control
1 BRAF V600E c.1799T>A
2 PCR Negative Control
3 PCR Positive Control
Green Marker Line (bottom)
BRAFStripAssayCat.# 5-570
BRAF 600/601StripAssayCat.# 5-560
BRAF StripAssays®
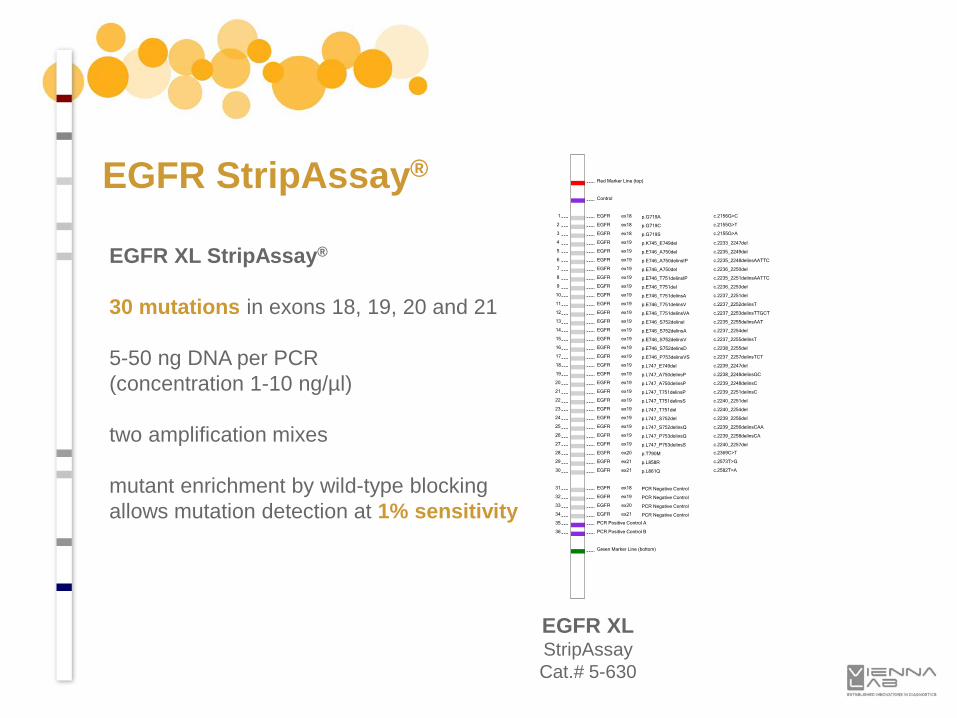
EGFR StripAssay®
EGFR XL StripAssay®
30 mutations in exons 18, 19, 20 and 21
5-50 ng DNA per PCR(concentration 1-10 ng/µl)
two amplification mixes
mutant enrichment by wild-type blocking allows mutation detection at 1% sensitivity
Red Marker Line (top)
Control
1 EGFR ex18 p.G719A c.2156G>C
2 EGFR ex18 p.G719C c.2155G>T
3 EGFR ex18 p.G719S c.2155G>A
4 EGFR ex19 p.K745_E749del c.2233_2247del
5 EGFR ex19 p.E746_A750del c.2235_2249del
6 EGFR ex19 p.E746_A750delinsIP c.2235_2248delinsAATTC
7 EGFR ex19 p.E746_A750del c.2236_2250del
8 EGFR ex19 p.E746_T751delinsIP c.2235_2251delinsAATTC
9 EGFR ex19 p.E746_T751del c.2236_2253del
10 EGFR ex19 p.E746_T751delinsA c.2237_2251del
11 EGFR ex19 p.E746_T751delinsV c.2237_2252delinsT
12 EGFR ex19 p.E746_T751delinsVA c.2237_2253delinsTTGCT
13 EGFR ex19 p.E746_S752delinsI c.2235_2255delinsAAT
14 EGFR ex19 p.E746_S752delinsA c.2237_2254del
15 EGFR ex19 p.E746_S752delinsV c.2237_2255delinsT
16 EGFR ex19 p.E746_S752delinsD c.2238_2255del
17 EGFR ex19 p.E746_P753delinsVS c.2237_2257delinsTCT
18 EGFR ex19 p.L747_E749del c.2239_2247del
19 EGFR ex19 p.L747_A750delinsP c.2238_2248delinsGC
20 EGFR ex19 p.L747_A750delinsP c.2239_2248delinsC
21 EGFR ex19 p.L747_T751delinsP c.2239_2251delinsC
22 EGFR ex19 p.L747_T751delinsS c.2240_2251del
23 EGFR ex19 p.L747_T751del c.2240_2254del
24 EGFR ex19 p.L747_S752del c.2239_2256del
25 EGFR ex19 p.L747_S752delinsQ c.2239_2256delinsCAA
26 EGFR ex19 p.L747_P753delinsQ c.2239_2258delinsCA
27 EGFR ex19 p.L747_P753delinsS c.2240_2257del
28 EGFR ex20 p.T790M c.2369C>T
29 EGFR ex21 p.L858R c.2573T>G
30 EGFR ex21 p.L861Q c.2582T>A
31 EGFR ex18 PCR Negative Control
32 EGFR ex19 PCR Negative Control
33 EGFR ex20 PCR Negative Control
34 EGFR ex21 PCR Negative Control
35 PCR Positive Control A
36 PCR Positive Control B
Green Marker Line (bottom)
EGFR XLStripAssayCat.# 5-630
o Quality of neutral-buffered formalin solution:formalin degradation products impair nucleic acid quality
o Fix tissue as quickly as possible after surgical removal
o Fixation time between 14-24 hours:penetration approx. 1 mm / hour
o To improve DNA quality avoid tissue staining:high pH and heavy metal ions may affect DNA integrity
o Use 5-10 µm thick sections for DNA extraction:discard the first 2-3 sections if the surface was exposed to air
References: Qiagen “Unlocking your FFPE archive” and “QIAamp DNA FFPE Tissue Handbook”.
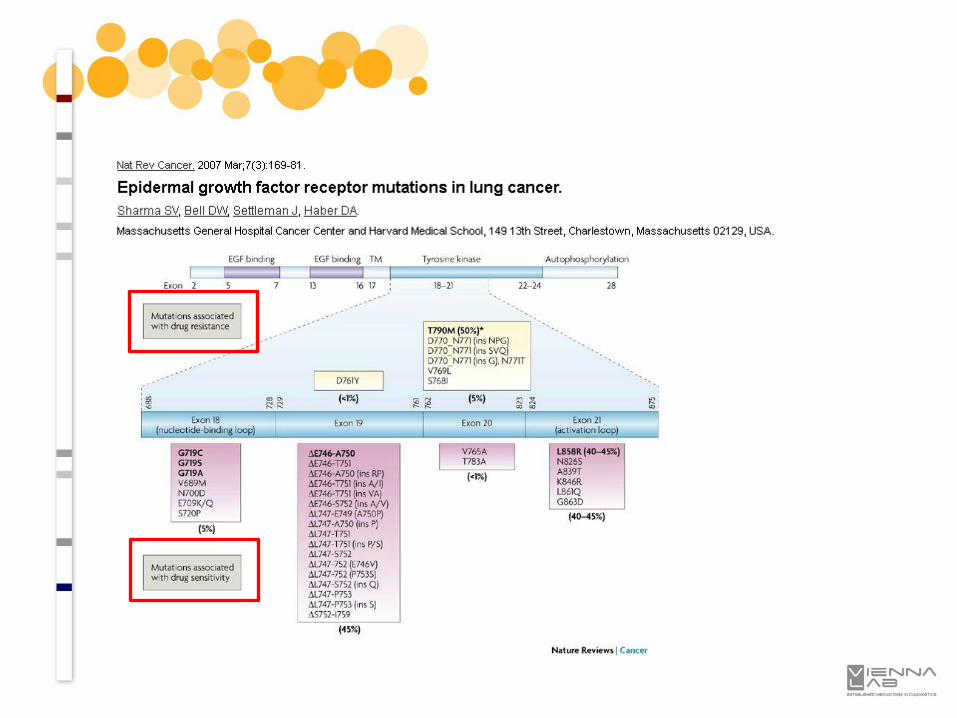
Mutation detection in DNA from formalin-fixed paraffin-embedded (FFPE) tissue
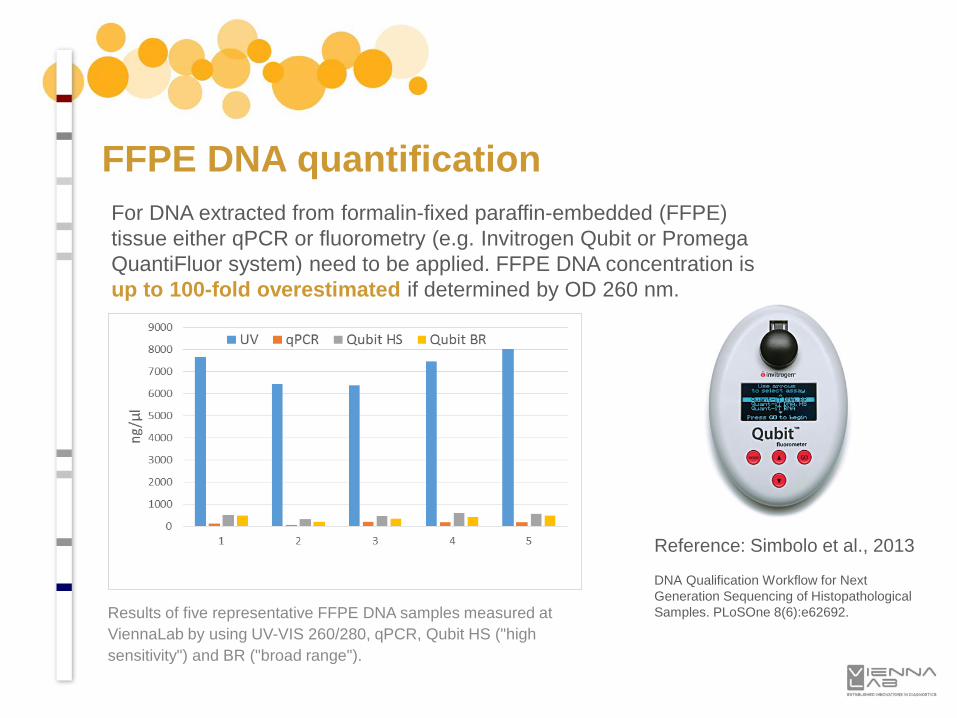
For DNA extracted from formalin-fixed paraffin-embedded (FFPE) tissue either qPCR or fluorometry (e.g. Invitrogen Qubit or Promega QuantiFluor system) need to be applied. FFPE DNA concentration is up to 100-fold overestimated if determined by OD 260 nm.
Results of five representative FFPE DNA samples measured at ViennaLab by using UV-VIS 260/280, qPCR, Qubit HS ("high sensitivity") and BR ("broad range").
Reference: Simbolo et al., 2013
DNA Qualification Workflow for Next Generation Sequencing of HistopathologicalSamples. PLoSOne 8(6):e62692.
FFPE DNA quantification
BRAF1 2
3 4
(A) (B)
Sample I
1 2 3 4
- + BSA
- + BSASample II
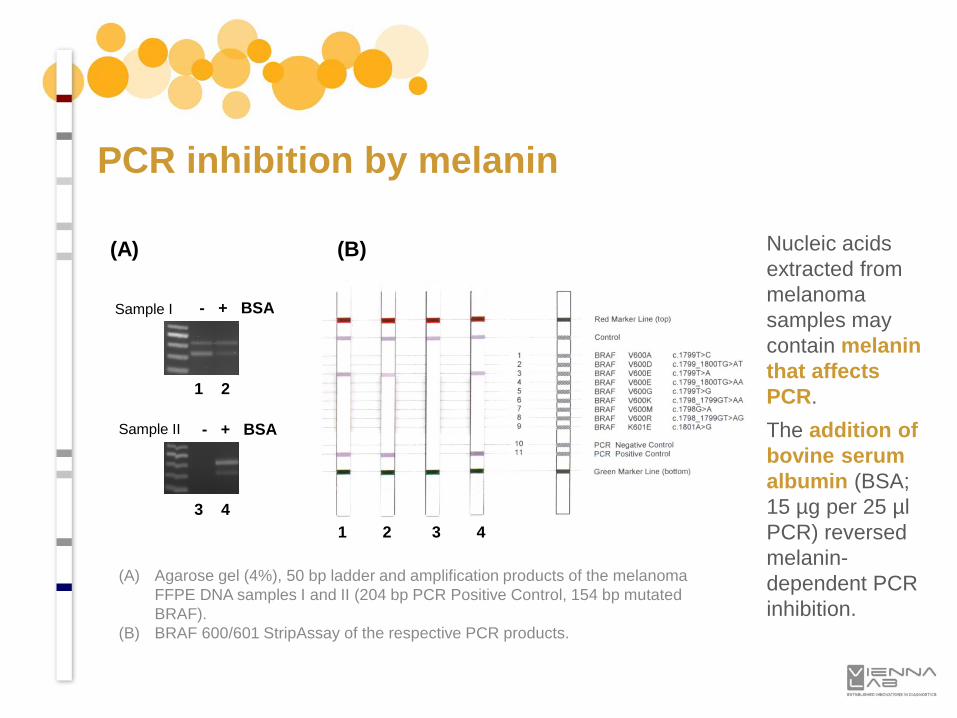
PCR inhibition by melanin
(A) Agarose gel (4%), 50 bp ladder and amplification products of the melanoma FFPE DNA samples I and II (204 bp PCR Positive Control, 154 bp mutated BRAF).
(B) BRAF 600/601 StripAssay of the respective PCR products.
Nucleic acids extracted from melanoma samples may contain melanin that affects PCR. The addition of bovine serum albumin (BSA; 15 µg per 25 µl PCR) reversed melanin-dependent PCR inhibition.
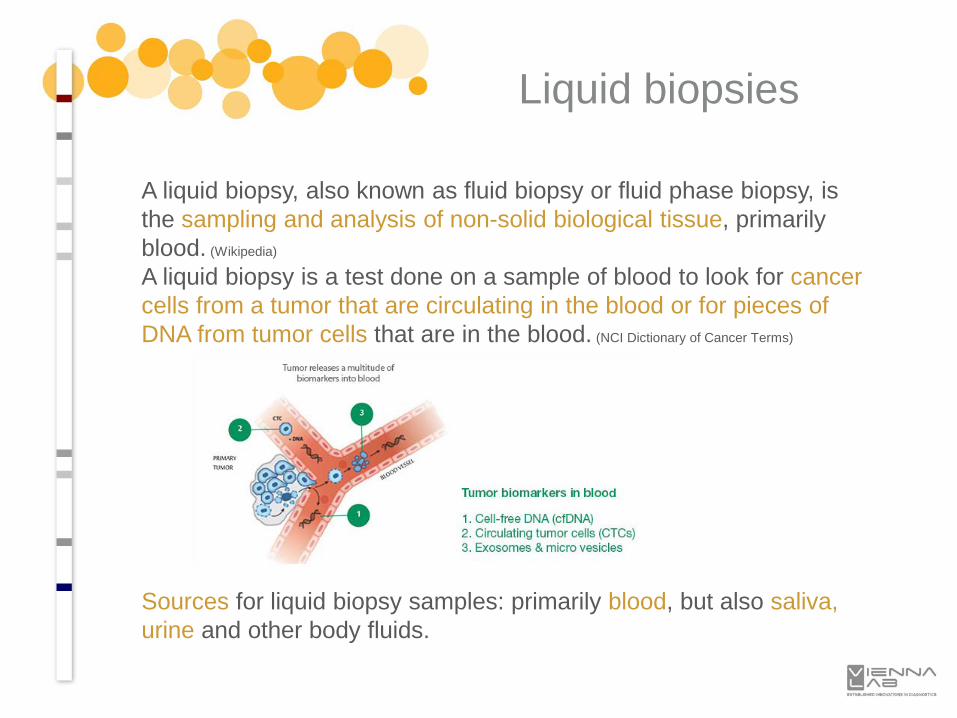
A liquid biopsy, also known as fluid biopsy or fluid phase biopsy, is the sampling and analysis of non-solid biological tissue, primarily blood. (Wikipedia)
A liquid biopsy is a test done on a sample of blood to look for cancer cells from a tumor that are circulating in the blood or for pieces of DNA from tumor cells that are in the blood. (NCI Dictionary of Cancer Terms)
Liquid biopsies
Sources for liquid biopsy samples: primarily blood, but also saliva, urine and other body fluids.
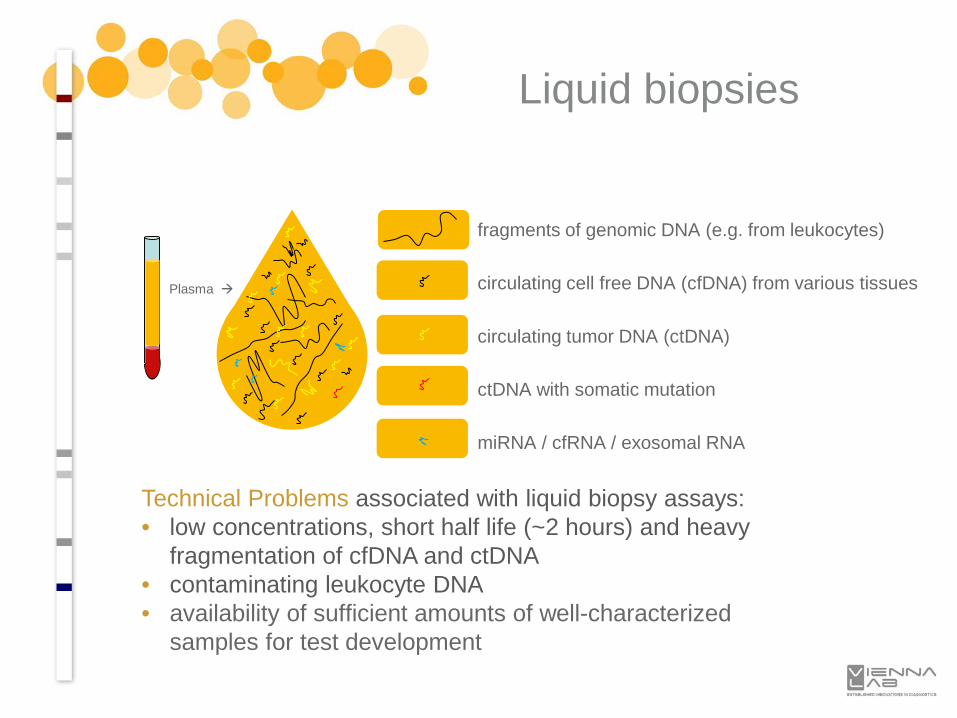
Plasma
fragments of genomic DNA (e.g. from leukocytes)
circulating cell free DNA (cfDNA) from various tissues
circulating tumor DNA (ctDNA)
ctDNA with somatic mutation
miRNA / cfRNA / exosomal RNA
Liquid biopsies
Technical Problems associated with liquid biopsy assays:• low concentrations, short half life (~2 hours) and heavy
fragmentation of cfDNA and ctDNA• contaminating leukocyte DNA• availability of sufficient amounts of well-characterized
samples for test development
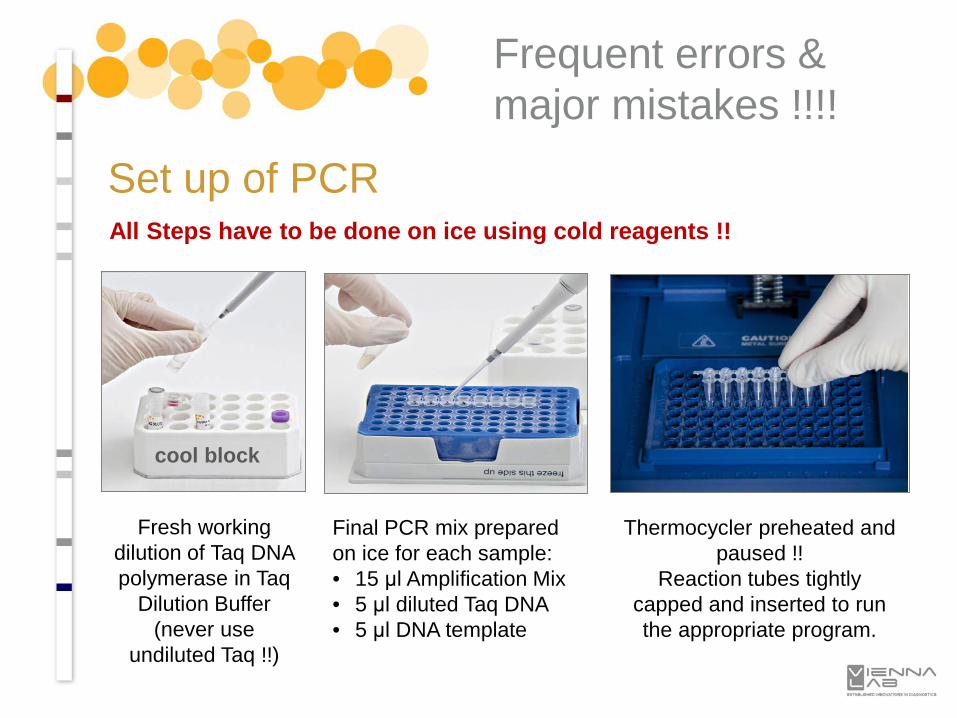
Set up of PCRAll Steps have to be done on ice using cold reagents !!
Frequent errors & major mistakes !!!!
cool block
Fresh working dilution of Taq DNA polymerase in Taq
Dilution Buffer(never use
undiluted Taq !!)
Final PCR mix prepared on ice for each sample:• 15 μl Amplification Mix• 5 μl diluted Taq DNA• 5 μl DNA template
Thermocycler preheated and paused !!
Reaction tubes tightly capped and inserted to run the appropriate program.
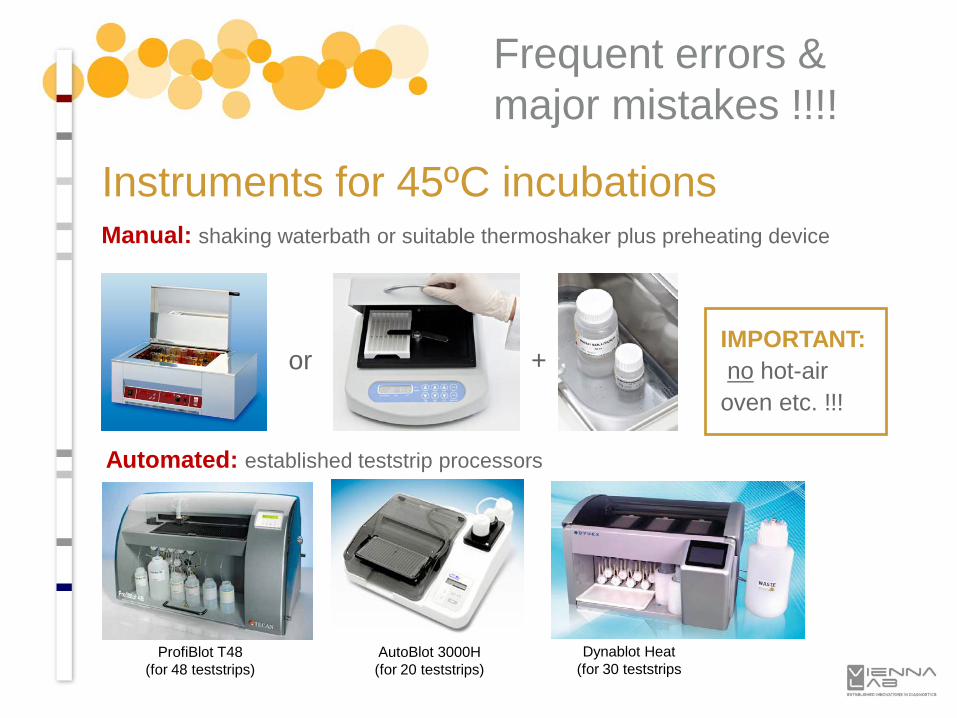
Instruments for 45ºC incubationsManual: shaking waterbath or suitable thermoshaker plus preheating device
Automated: established teststrip processors
IMPORTANT:no hot-air
oven etc. !!!
+
ProfiBlot T48(for 48 teststrips)
AutoBlot 3000H(for 20 teststrips)
Dynablot Heat(for 30 teststrips
or
Frequent errors & major mistakes !!!!
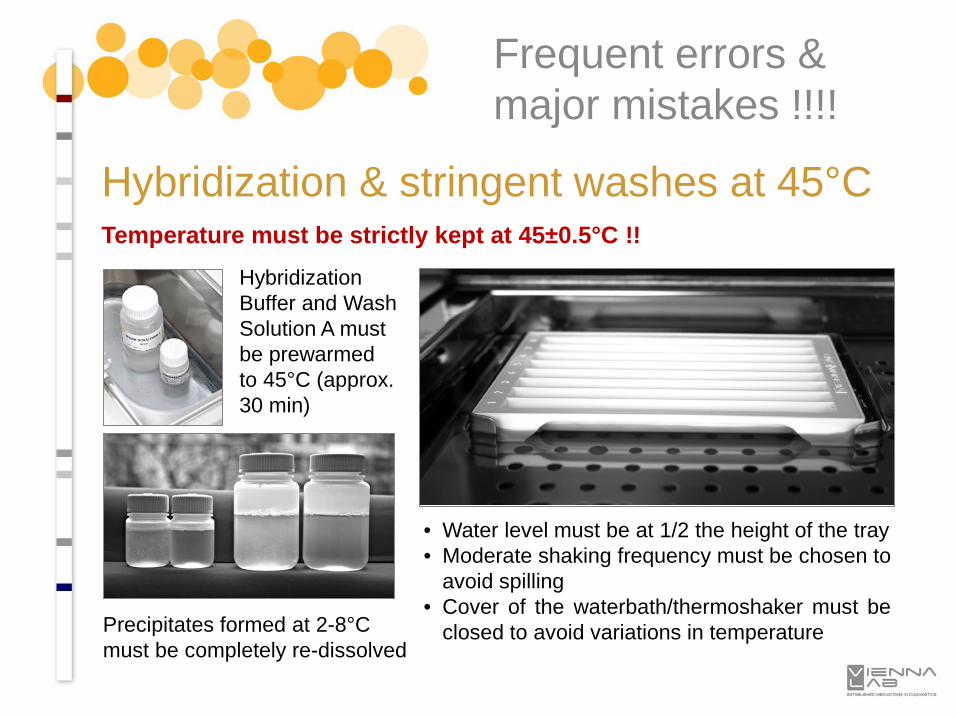
Hybridization & stringent washes at 45°CTemperature must be strictly kept at 45±0.5°C !!
Frequent errors & major mistakes !!!!
Hybridization Buffer and Wash Solution A must be prewarmed to 45°C (approx. 30 min)
Precipitates formed at 2-8°C must be completely re-dissolved
• Water level must be at 1/2 the height of the tray• Moderate shaking frequency must be chosen to
avoid spilling• Cover of the waterbath/thermoshaker must be
closed to avoid variations in temperature

Selected StripAssay® Reports
Alpha-globin StripAssay
Beta-globin StripAssay
Beta-globin StripAssay
Beta-thal Modifier StripAssay
Haemochromatosis StripAssay
Haemochromatosis StripAssay
CAH StripAssay
CVD StripAssay
CVD StripAssay
FMF StripAssay
FMF StripAssay
FMF StripAssay
FMF StripAssay
FMF StripAssay
Gaucher Disease StripAssay
Sugar Intolerance StripAssay
PGX-Thrombo StripAssay
KRAS StripAssay
BRAF StripAssay
KRAS-BRAF StripAssay
EGFR StripAssay

Selected Iranian StripAssay® Reports
Alpha-globin StripAssay
Alpha-globin StripAssay
Alpha-globin StripAssay
Alpha-globin StripAssay
Alpha-globin StripAssay
Alpha-globin StripAssay
Alpha-globin StripAssay
Alpha-globin StripAssay
Beta-globin StripAssay
"... samples were screened for a panel of 22 relatively common β-globin mutations using an assay based on polymerase chain reaction (PCR) and reverse-hybridization to oligonucleotide arrays immobilized on test strips ... a single amplification and hybridization step, allowing even very small amounts of DNA (e.g. prenatal samples) to be rapidly and comprehensively typed."
Beta-globin StripAssay
FMF StripAssay
"In this regard, the FMF StripAssay demonstrated to be a reliable and cost-effective first-line screening tool ... a very suitable strategy for population-based FMF genotyping in Iran.."
J Genet 2016; 95(3):667-74
FMF StripAssay
FMF StripAssay
CF StripAssay
"In Iran, complete genetic information is currently lacking to implement solid population-based CFTR screening programs that could enable adequate carrier detection of either typical or atypical CF patients or their family members. For national policies of CF prevention, it is acceptable to include only the most frequent mutations present in the population, which allows a 90% detection rate."
Thank you !Dr. Christian [email protected]: +43 1 8120156 40
Related Documents











