VITAL SIGN ASSESSMENT SELF-REPORTED VITAL SIGN ASSESSMENT IN PHYSICAL THERAPY ______________________________________________________________________________ An Independent Research Presented to The Faculty of the Marieb College of Health and Human Services Florida Gulf Coast University In Partial Fulfillment of the Requirement for the Degree of Doctor of Physical Therapy ______________________________________________________________________________ By Clint G. Harrison 2017

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

VITAL SIGN ASSESSMENT
SELF-REPORTED VITAL SIGN ASSESSMENT
IN PHYSICAL THERAPY
______________________________________________________________________________
An Independent Research
Presented to
The Faculty of the Marieb College of Health and Human Services
Florida Gulf Coast University
In Partial Fulfillment
of the Requirement for the Degree of
Doctor of Physical Therapy
______________________________________________________________________________
By
Clint G. Harrison
2017

VITAL SIGN ASSESSMENT
APPROVAL SHEET
This Independent Research
is submitted in partial fulfillment of the requirements for
the degree of
Doctor of Physical Therapy
Clint G. Harrison
Approved: May 2017
Ellen Donald, PhD, PT
Committee Chair
Kathleen Swanick, DPT, MS, OCS
Committee Member
The final copy of this Independent Research has been examined by the signatories, and we find
that both the content and the form meet acceptable presentation standards of scholarly work in
the above mentioned discipline.
VITAL SIGN ASSESSMENT
Acknowledgements
There are so many to thank for their ongoing support of this research project & during my
continued education towards a Doctorate of Physical Therapy degree. First and foremost, I need
to thank my committee Chair, Dr. Donald, & committee member, Dr. Swanick, for the opportunity
to work on this research project and their help and guidance along the way. Important data has
been and will be used for further understanding with this area of practice in physical therapy, help
other research projects, used as a reference, and other purposes to further improve patient care in
the physical therapy profession.
Paying respects to your loved ones for their role is of the utmost importance. Each one of
these Family Members, Co-Workers, & Friends have helped me be the person I am today. I love
them all and appreciate what each has done to make my life what it is. The following are in
alphabetical order (by last name) and there are many others not specifically mentioned that have
made an amazing impact as well:
Jack Anderson, Erika Banks, Stewart Buckingham, Mary & David Chen, John & Tyler
Dam, Anne Marie Dorsa, Rashel & Dennis Dube, Angelina Ford, Dawnell Glunz, Kathy Harriman,
Ron & Sandy Harrison, Ruth & Denzel Harrison, Shelby Jones, Tylor Laflan, Dan & Emily Lavin,
Joseph Muffoletto, Betty & LaVern Nosal, John Snyder, John & Billie Walker, All of my nieces,
my nephew, aunts, uncles, cousins, friends that are my family, and anybody that has made an
influence.
I would like to thank all of the faculty, professors, clinical instructors, and every patient I
have worked with that have made a profound impact on my life and educational endeavors. To
add, multiple beautiful animals have and continue to be in my life that make lasting impressions.
I am so very thankful to have you All in my life and in my heart, God Bless!!!

VITAL SIGN ASSESSMENT 1
Table of Contents
Abstract…………………………………………………………….…………………………...….3
Introduction…………………………………………………………...………...……………….…4
Review of the Literature………………………………….…………………….……………….…5
The Vital Signs………………………………………….………...………………….…5
Vital Sign Assessment………………………………….…………………………….…6
Cardiovascular Disease…………………………………………...………………….…7
Hypertension………………………………………………………...……………….…9
Vital Sign: Blood Pressure……………………………………....……………….……10
Vital Sign: Heart Rate……….…………………………….………....………….…….11
Vital Sign: Pulse Oximetry…………………………………….…………...…………11
Physical Therapy Education and Vital Sign Assessment…………….…….…………12
American Physical Therapy Association………………………….…….……….……13
Individual State Practice Laws…….…………………………….…...……….………14
Pilot Survey…………………………………………………...………………………15
Research Questions and Hypotheses…………………………….……………………………….16
Methods………………………………………………………………………………….......……17
Research Design and Instrumentation…………………………....…………...………17
Access to Subjects and Sampling Plan……………….………….……………………18
Data Collection………………………………………………….…….………………18
Results…………………………………………………………………………………….………19
Part I-Demographic Information……………….………….……….………....………19
Part II-Practice Behaviors & Beliefs………………....……………….…….………...23
Discussion……………………………………………………….……………….……………….27
Conclusion…………………………………………………….………………………………….32
References………………………………………………………….………………….…….……34

VITAL SIGN ASSESSMENT 2
Appendices……………………………………………………….……………………….………38
A: Question 6b-Open Ended Responses, Synopsis/Report………….………….……….38
B: Question 22-Open Ended Responses, Synopsis/Report……………………………...40

VITAL SIGN ASSESSMENT 3
Abstract
Introduction. The purpose of this study was to determine how often physical therapists
(PTs) assess the vital signs of heart rate (HR), blood pressure (BP), and oxygen saturation (SpO2)
throughout the United States, and if there are key factors that may affect the assessment of these
vital signs. Review of Literature. In previous research (Peters, 2014), it was shown that there
are a variety of reasons why the assessment of vital signs is routinely used by some therapists and
not by others. Research Questions and Hypotheses. This research aimed to determine the
particular reasons why or why not HR, BP, and SpO2 are assessed, and if differences occur
between unrestricted vs. restricted direct access states. Methods. An online survey was
developed and piloted prior to distribution. All 50 physical therapy state associations and the
District of Columbia were contacted for the opportunity for their membership to participate. Of
those associations that expressed interest to participate, an email with a link was sent to that state
association once approved by the Institutional Review Board (IRB). Results. Data of 286
anonymous respondents were included in the analysis with representation from 24 states with a
distribution across most practice areas and settings. There were 60% unrestricted and 32.5%
restricted direct access practicing states. Ninety-eight percent of respondents are somewhat
confident to extremely confident with taking HR, BP, and SpO2 and 91% are able to assess these
vitals within 1-6 min. However, respondents only regularly (>75% of the time) measured vital
signs of HR 39%, BP 37%, and SpO2 30% during initial evaluations. During intervention
sessions, even less, with HR 31%, BP 26.5%, and SpO2 22%. Discussion. Various reasons were
provided for the lack of regular assessment of vital signs with patients. A statistically significant
association was noted between frequency of measurement of vital signs by participants and the
nature of the direct access in the State of licensure, with a higher frequency of measurement in
states with restricted direct access. Conclusion. Insight was gained in patterns of assessment of
vital signs as well as rationale behind therapists’ decisions to use these critical measures.
Continued research will help inform practice and maximize patient safety.

VITAL SIGN ASSESSMENT 4
Introduction
Chronic conditions and noncommunicable diseases are dominating health systems across
the globe, and physical therapists will be engaging patients in health promotion and disease
management for many years to come (Knight, Werstine, Rasmussen-Pennington, Fitzsimmons, &
Petrella, 2015). No health-related condition affects American lives more than heart disease.
According to the Center for Disease Control and Prevention, the leading cause of death in the
United States is heart disease, at a rate of 611,105 in the year 2013 (Leading Causes of Death,
2015). Pulmonary hypertension is commonly associated with, and is a major risk factor for,
coronary artery disease (Lowe et al., 2011). Hypertension is responsible for doubling all-cause
mortality, while tripling the number of stays in the hospital, as well as, morbid complications
(Lowe et al., 2011).
Physical therapists are responsible for ensuring the safety of each patient being treated,
and measuring vital signs allows clinicians to screen for undiagnosed conditions, monitor existing
conditions, and facilitate safety through prevention (Peters, 2014). Exercise interventions utilized
by PTs have the potential to be harmful if the patient is not being properly monitored (Grunig et
al., 2012). The monitoring, through assessment of vital signs to be discussed in this research
includes blood pressure (BP), heart rate (HR), and pulse oximetry (SpO2). It is recommended that
these vital signs should be utilized routinely by all practicing physical therapists in order to screen
for heart-related conditions, as well as other conditions.
This exploratory survey research gathered information on the use of these key vital sign
measurements in various physical therapy settings. Based on prior research (Peters, 2014), there
is strong suspicion currently practicing American physical therapists do not assess patients’ vital
signs regularly. This idea was evidenced in the work of J. Peters (2014), which focused on the
patterns of utilization of vital sign measures of therapists in the State of Florida. Peters found that
a majority of practicing physical therapists were not measuring vital signs during each visit

VITAL SIGN ASSESSMENT 5
because of a lack of time, or simply the perception of these measures not being important for
certain patient population (Peters, 2014).
Physical therapists have broadly become more autonomous as direct access practitioners,
and share the role of primary care professionals with other health care practitioners. With
physical therapy being a doctoring profession and having direct access to patients, it is essential
to assess vital signs for patient safety and be consistent with APTA standards of care. As part of
expanding the parameters of responsibility of physical therapy practice, this issue needs to be
studied to inform practice.
Review of the Literature
The Vital Signs
Clinical medical practitioners face patients with illness, disability, and suffering on a
daily basis (Yuen & Irwin, 2005). It is the role of a physical therapist to ascertain a patient’s
current physical condition, in addition to determining a proper PT diagnosis when seeing a new
patient. A physical therapist must first monitor the patient’s vital signs in order to achieve a
baseline report upon which to measure and compare future readings, during and after exercise.
Baseline measurements should be determined to understand whether the patient is appropriate for
exercise, and is responding appropriately to an intervention (Graham, & Clark, 2011). There are
numerous vital sign applications, found in research literature, that may be utilized in various
physical therapy settings. Included among these are the four traditional vital signs, which consist
of heart rate, blood pressure, temperature, and respiratory rate (Cretikos et al., 2008). Pulse
oximetry can be added to this fundamental list, since it has increasingly become an essential tool
in the modern practice of emergency medicine (Sinex, 1999).
The use of other standardized tests and assessments, along with vital sign administration,
can provide a better interpretation of overall health. Walking speed reflects both functional and
physiological changes, and can be a discriminating factor in determining potential for
rehabilitation, which also aids in the prediction of falls with the fear of falling (Fritz & Lusardi,

VITAL SIGN ASSESSMENT 6
2009). Prevalence of emotional distress is a screen to identify patients in need of psychosocial
support (Bultz & Johansen, 2011). Dynamometrically measured grip strength was shown to be
associated with a greater likelihood of premature mortality, the development of disability, and an
increased risk of complications or prolonged length of stay after hospitalization or surgery
(Bohannon, 2008). Health literacy as a vital sign could result from a quick screening test for
limited literacy in primary health care settings (Weiss et al., 2005). Aerobic exercise testing
allows for the manifestation of physiologic abnormalities that are not readily apparent during the
collection of resting data (Arena, Myers, & Guazzi, 2010). Finally, sleep has been referred to as a
potential vital sign since many people often sleep no more than five to six hours a night, even
though studies show that most people need between seven to eight hours (Wilson, 2005).
This research is specifically focused on three aspects of vital sign assessment. These
three are blood pressure, heart rate, and pulse oximetry. It is the position of this research that all
three applications must be given before, during, and after all exercise treatments performed by the
patient to provide best practice by the physical therapist.
Vital Sign Assessment
In general, healthcare services that utilize vital signs, will reflect the state of personal
health and aid in the detection and prevention of cardiovascular disease (Kim & Kim, 2012).
Performing vital sign assessment properly, utilizing reliable procedures/techniques, interpreting
the findings accurately, and applying appropriate clinical judgement when deciding if the patient
should proceed with treatment/exercise is of the utmost importance by PTs. In a study designed
to determine whether the taking of vital signs in a clinical setting is reproducible, two trained
technicians assessed the vital signs of 140 patients in an acute setting with medical complaints
(Edmonds et al., 2002). The results of this study showed that even among properly trained
individuals who knew they were being watched and recorded, inter-observer variability still
indicated a limited reproducibility. Whereas the heart rate assessment was a difference of 10% to
15%, and not drastically important for that clinical assessment, the diastolic and systolic blood

VITAL SIGN ASSESSMENT 7
pressure measurements were a difference of 20% to 25%. These differences in measurement
could become dangerous when they become near abnormal values (Edmonds et al., 2002).
Vital signs can be very useful predictors of mortality for patients who were admitted to
the hospital. In a retrospective study from the Wake Forest University School of Medicine
Institutional Review Board, the intent was to examine the association of critical vital signs that
occurred at any time during the hospital stay, and not just at the time of admission (Bleyer et al.,
2011). The researchers obtained 1.15 million individual vital sign determinations, and discovered
that if the patient presents with critically abnormal vital signs, it is associated with a high
mortality rate. However, early detection of these signs presented an opportunity to lower the
mortality rate (Bleyer et al., 2011).
A recent review of vital sign assessment literature showed that age of the patient may
alter the results from the analysis. The review found that in older, frailer patients, the results of
single point measurements of vital signs have less sensitivity in discovering cardiovascular
disease (Chester & Rudolph, 2010). In order to increase the sensitivity of the tests, serial vital
sign assessments should be made. However, regardless of this fact, the most important discovery
for clinical purposes is that while vital signs may change with age, the individual reference
alteration is the most important warning sign, and will require additional testing to determine the
pathological process (Chester & Rudolph 2010).
Cardiovascular Disease
According to the Center for Disease Control and Prevention, one quarter of all reported
deaths are a result from heart disease in the United States, on an annual basis. Nearly 370,000 of
the 611,105 heart related deaths, had the most common form of heart disease, which is coronary
heart disease (Heart Disease Fact Sheet, 2015). Cancer is the second leading cause at 584,881
deaths, while chronic lower respiratory diseases are listed third at a rate of 149,205 deaths. A
cerebrovascular accident (stroke) ranks fifth at 128,978 deaths after unintentional injuries and
accidents (Leading Causes of Death, 2015).

VITAL SIGN ASSESSMENT 8
There are 26.6 million adult Americans with a diagnosis of heart disease, which is 11.3%
of that population (Heart Disease, 2015). The range of major clinical heart disease conditions
include: stroke, congenital heart disease, rhythm disorders, subclinical atherosclerosis, coronary
heart disease, heart failure, valvular disease, and peripheral arterial disease (Mozaffarian et al.,
2015). As the first and fifth leading causes of death in the United States, heart disease and stroke
occur in approximately 30% of adults aged 18 years and older (Prevalence of Hypertension and
Controlled Hypertension — United States, 2007–2010, 2013).
The existence of avoidable deaths reflects poorly upon the healthcare system. Every year
the mortality rate shows a certain portion of avoidable deaths due to a lack of timely and effective
medical care. One measure of the health of Americans, deaths from treatable conditions, still does
not compare well with rates in other industrialized countries (Nolte & McKee, 2008). The
assessment of risk factors due to cardiovascular disease is crucial in the successful treatment of
cardiovascular disease resulting in patient death. In a recent study, national vital sign statistics
were analyzed from 2001 to 2010. The results showed that avoidable deaths (resulting from
ischemic or chronic rheumatic heart disease, stroke, or hypertensive disease in patients 75 years
old or less) were estimated at over 200,000 in the United States in 2010 (Schieb, 2013). The
overall death rate utilizing these parameters was generated as: 60.7 deaths per every 100,000
people, with the conclusion being that one quarter of these deaths are avoidable (Schieb, 2013).
Heart disease is the leading cause of death for both women and men in the United States,
with males being more than half of the reported deaths (Heart Disease Facts, 2014). Men suffer
coronary heart disease and heart failure more than women, while women are more susceptible to
hypertension and diabetes, suggesting that cardiovascular risk factors have a different impact on
cardiovascular events and mortality in males and females (Zhang et al., 2012). Differences hold
as well for a population advancing in age. In the last stage of lifespan, men suffer more left
ventricular systolic dysfunction and abnormally affected lipoproteins in the blood, while women
are much more susceptible to malnutrition, hyperglycemia, and arrhythmia (Zhang et al., 2012).

VITAL SIGN ASSESSMENT 9
Hypertension
A critical measure, to determine a patient’s cardiovascular health status, that a physical
therapist should assess is blood pressure. High blood pressure (hypertension), is the force of
blood pushing against the walls of the patient’s arteries, and remains at that high level for an
extended period of time (High Blood Pressure Fact Sheet, 2014). Since physical therapists now
play an important role as primary health care providers, the accurate measurement of blood
pressure is critical for making the appropriate clinical decisions (Frese et al., 2011).
Hypertension is the most common primary diagnosis in the United States, with 22% of
individuals unaware that they are hypertensive. Hypertension is also a major risk factor for renal
failure, stroke, and coronary heart disease (Frese et al., 2011).
One in every three Americans has high blood pressure, which places the physical therapy
patient at a fairly high risk of heart disease and stroke (High Blood Pressure Fact Sheet, 2014).
From the year 2011 through the year 2012, 32.5% of non-institutionalized adult Americans aged
20 and over had a diagnosis of hypertension (National Center for Health Statistics, 2015). The
total cost of high blood pressure on the United States is 46 billion dollars, which includes the
costs of health care services, missed days at work, and medication (High Blood Pressure
Frequently Asked Questions, 2015). These facts clearly show the high level of importance that
blood pressure readings have during every visit a patient has in every physical therapy setting.
The effects of respiratory and exercise training on exercise capacity was associated with a
significant improvement in quality of life. Aerobic Exercise training in patients with severe
hypertension provides beneficial psychological and physical effects, leading to an enhanced and
healthier quality of life (Mereles et al., 2006). However close monitoring must occur during this
training to provide safe care of patients.
In a recent study, it was determined that the use of taking BP was crucial over just doing
visual inspection alone or in conjunction with the patients past medical history (PMH) to
determine the accuracy of patients’ hypertensive status. Of the 68% participating patients who

VITAL SIGN ASSESSMENT 10
had a BP reading in the pre-hypertensive or hypertensive range the visual inspection and use of
PMH group would have only taken BP 9% of that time. It was concluded by the researchers that
physical therapy clinicians were unable to predict the hypertensive status with accuracy unless
they took the vital sign assessment of BP (Feldman, et al. 2016).
Vital Sign: Blood Pressure
Vital sign measurement and assessment are of great importance during the physical
therapy exam and review of symptoms for patients who present with and without
cardiopulmonary disease; for purposes of establishing a baseline status, a response to exercise,
and for future exercise prescription (Frese, Frick, & Sadowsky, 2011). Hypertension is a major
health problem and is relevant to physical therapy because relatively small reductions in blood
pressure can result in decreased risk for stroke and myocardial infarction (Taylor, Dodd, &
Damiano, 2005). In the majority of hypertensive patients, no particular cause for abnormal blood
pressure is evident (primary or essential hypertension). In contrast, in the minority of patients
with secondary hypertension a specific underlying cause is responsible for the elevated blood
pressure (Ott, Schneider, & Schmieder, 2013).
Standardizing the blood pressure measurement technique through training, is crucial
during physical therapy education and clinical practice (Frese et al., 2011). In a study at
Quinnipiac University, the physical therapy faculty received reports from their students in clinic
that the clinicians whom they work for do not follow standard protocols for routinely measuring
blood pressure with their patients. A study was conducted to assess whether there is a population
of hypertensive patients, regularly attending physical therapy sessions, that could be undiagnosed
with hypertension, or otherwise use poorly controlled antihypertensive medications (Kasinskas,
Wood, & Koch, 2011). Out of 87 patients screened for hypertension, 27 were classified as
hypertensive, and 27 were classified as pre-hypertensive (Kasinskas, Wood, & Koch, 2011). That
was almost 2/3 of those patients (62%), which again demonstrates why blood pressure screening
in the outpatient clinic is imperative.

VITAL SIGN ASSESSMENT 11
Vital Sign: Heart Rate
The average resting heart rate for most individuals is 60-80 beats per minute, while there
is typically a lower reading for physically fit people, and higher scores are found in the aged and
sedentary populations (Target Heart Rates, 2013). It is important for the physical therapist to
know the patient’s heart rate, especially when placed on an exercise program. Maximal heart rate
is one of the most commonly used values in clinical medicine and physiology, and is utilized as a
basis for prescribing exercise intensity in both rehabilitation and disease prevention programs
(Tanaka, Monahan, & Seals, 2001). Every patient is different, and every exercise program is
tailored for each individual. The physical therapist needs to dose a proper exercise regimen based
on the patient’s heart rate. It is pivotal that the physical therapist maintains knowledge of their
patient’s heart rate throughout the exercise program. Heart rate can be affected by numerous
factors, including a patient’s age, medical condition (such as fever), medications currently taking
(such as beta blockers), and their current fluid retention (Elliot & Coventry, 2012).
A survey was mailed with a 43% return rate from clinical instructors and students
working in a variety of practice settings. The purpose of the 11-item survey was to determine if
heart rate and blood pressure were taken in these practice settings (Arena, 2009). The results
showed that the clinical instructors in the outpatient setting either never or seldom assessed the
patient’s vital signs. Additionally, only 37% of clinicians believed that measuring heart rate and
blood pressure was important, while 87% of students believed it to be important (Arena, 2009).
While it is promising that the students were interested in taking vital signs, the actual practice of
the vital sign assessment is tremendously low.
Vital Sign: Pulse Oximetry
The pulse oximeter is an extremely reliable and valuable clinical tool that is easy to use
(Elliot & Coventry, 2012). The World Health Organization defines a pulse oximeter as a medical
device that monitors the level of oxygen in a patient's blood, allowing for intervention if dropped
below a safe level (Pulse oximetry, 2014). The pulse oximeter device is critical for use in

VITAL SIGN ASSESSMENT 12
intensive care, hospital settings, operating rooms, and emergency care. Pulse oximeters are also
utilized in outpatient physical therapy clinics to provide a noninvasive way to maintain the
estimated oxyhemoglobin saturation of blood in the patient’s arteries, which in turn may diagnose
hypoxemia (Mengelkoch, Martin, & Lawler, 1994). In a comprehensive Cochrane Review, five
eligible studies were discovered that showed that pulse oximetry can detect hypoxemia and other
related events (Pedersen, Møller, & Pedersen, 2003).
Pulse oximetry is now a ubiquitous and essential tool of modern medicine, and the pulse
oximeter, like any basic tool, must be used properly (McMorrow, & Mythen, 2006). To work
properly and effectively, the pulse oximeter requires adequate peripheral blood flow; for example,
anemia may provide a misreading since the patient might have a lowered potential to carry
oxygen in the blood, and the pulse oximeter could provide a misreading on the hemoglobin level
measurement (Elliot & Coventry, 2012). Pulse oximetry however, can be very useful in alerting
the physical therapist of a change in the patient’s condition.
Physical Therapy Education and Vital Sign Assessment
Physical therapy education is now at the Doctorate level in the United States and
standards of care continue to rise. Therefore, when a patient presents with undiagnosed
hypertension, and the physical therapist fails to measure vital signs, they place both their patient
and their license at considerable risk. This is not only because most patients with hypertension
are asymptomatic, but also because 50% of the American adult population has an underlying
chronic medical condition. Additionally, 66% of American adults are overweight or obese,
creating additional health risks (Graham & Clark, 2011). Aerobic capacity and the ability to
perform physical activities may be hindered by obesity, which may have implications for physical
therapists' interventions (Racette, Deusinger, & Deusinger, 2003). Consistent with the role as
autonomous practitioners, physical therapists should take a primary health care role of baseline
vital signs on every new patient and monitor vital signs during exercise (Graham & Clark, 2011).

VITAL SIGN ASSESSMENT 13
With all the education and ability to provide vital sign assessments quickly and with ease,
Physical Therapists are still showing a low frequency of taking the vital signs of their patients.
Observational research was conducted in an outpatient setting where 74 patients were seen for
either an initial evaluation, follow-up, or discharge. Only two times during the initial session, and
one time during a follow-up session, was HR and BP taken. Of these 74 patients, 19 (26%) were
diagnosed with hypertension. This lack of patient care increases the risk for the PT that a patient
will have a cardiac event in their office, while under their care (Millar et al. 2016). This study is
limited as it analyzed practice at only one location, but it still contributes to the evidence of the
lack of vital sign assessment compliance among physical therapists.
American Physical Therapy Association
The American Physical Therapy Association was founded to increase the quality of life
for patients through the advancement of physical therapist practice, education, research, and by
improving the public’s awareness and comprehension of physical therapy's role in the United
States’ health care system (About Us, 2014). As mentioned, unrestricted direct access is a prime
goal for the organization, so much so that they placed the idea firmly in their Vision 2020
strategic plan, which states:
“By 2020, physical therapy will be provided by physical therapists who are
doctors of physical therapy, recognized by consumers and other health care
professionals as the practitioners of choice to whom consumers have direct
access for the diagnosis of, interventions for, and prevention of impairments,
activity limitations, participation restrictions, and environmental barriers related
to movement, function, and health.” (Vision 2020, 2014)
Physical therapists are well-educated and licensed health care professionals who can aid
patients in reducing pain levels and improve or restore mobility, ideally without expensive
surgery and often reducing the need for long-term use of prescription medications, which can
carry heavy side effects. Physical therapists also instruct patients on ways to prevent or manage

VITAL SIGN ASSESSMENT 14
their condition so that they will achieve long-term health benefits (Who Are Physical Therapists,
2014). Physical therapists typically evaluate each patient, and then develop a plan, utilizing
techniques to treat and promote movement, the reduction of pain, the restoration of function and
mobility, and to avoid disability. They also work with patients through the development of
fitness and wellness encompassing programs, for people who are already considered healthy and
wish to enhance their active lifestyle. State licensure is a requirement for each state in which a
physical therapist practices (Who Are Physical Therapists, 2014).
According to an American Physical Therapy Association press release dated October 28,
2009, APTA President R. Scott Ward, PT, PhD, addressing the International Summit on Direct
Access and Advanced Scope of Practice, said the following:
“[W]e heard evidence from around the world that clearly demonstrates that direct
patient access to physical therapists is appropriate for all Americans. The
findings of this conference confirm that the legislation allowing patients to access
physical therapists without a referral -- legislation that currently exists in 44
states -- is worth pursuing in all states and at the federal level.” (Direct Access
Summit, 2009)
Direct access and patient self-referral specifically mean that the patient has the power and
ability to utilize physical therapy as the first choice for wellness programs and rehabilitation,
without the need of a referral from their physician (Direct Access Summit, 2009).
Individual State Practice Laws
For purposes of this research, the focus will remain solely with one aspect of healthcare;
that being the specific assessment of vital signs in all areas of physical therapy practice across the
entire United States of America. Current physical therapy practice laws are created and regulated
by each individual state. This can encompass a variety of limitations and freedoms in the ability
to practice physical therapy. All 50 states in the US have direct access to practice physical
therapy. However, the therapist is the one who is ultimately responsible for providing best

VITAL SIGN ASSESSMENT 15
practice in the screening process of patients who may have conditions that negatively impact their
response to interventions (Graham & Clark, 2011).
There are a variety of limitations within states regarding direct access. These limitations
may include the patient first obtaining a referral to see the physical therapist or that there may be
a requirement from certain states that the therapist must have spent a specific amount of time in
school, with a minimum level of education first attained by the therapist, for that patient to then
visit. There are currently 18 states with unrestricted direct access listed by the American Physical
Therapy Association, signifying that the patients in those states can have direct access to a
physical therapist, without any stipulations (American Physical Therapy Association, 2016).
Vital sign assessment is an important component of the delivery of PT services. With this
added responsibility of patients accessing PT services directly, physical therapy practice must
include the routine assessment of vital signs to ensure patient safety and to contribute to the
identification of health risks.
Pilot Survey
A pilot study was conducted by J. Peters titled Self-Reported Use of Vital Signs in the
Adult Outpatient Physical Therapy Setting (Peters, 2014). As the title indicates, he focused his
research on the assessment of vital signs in outpatient settings. The survey assessed the
frequency of HR, BP, and SpO2 measurement in the six months prior to taking the survey,
physical therapist’s beliefs about the importance of measuring vital signs, their specific reasons
for not measuring vital signs, and information pertaining to the demographics of the respondents.
He received cooperation with, and was able to place the 16 question survey on the website of the
State of Florida’s Physical Therapy Association. After 21 days of availability, data from 45
respondents was then collected and analyzed (Peters, 2014).
The outcomes reported by the study cited physical therapists’ difficulties with the
measurement of vital signs for specific reasons. For example, only 28.9% of the respondents
reported that their clinic had a policy regarding the measurement of vital signs. Additionally,
VITAL SIGN ASSESSMENT 16
66.7% reported that 81-100% of their case load over the last 6 months involved patients whose
primary problems were musculoskeletal in nature, and not related to issues deemed necessary for
the assessment of vital signs. Almost half of the respondents believed it was “extremely
important” to measure vital signs (HR n=20; BP n=21; SpO2 n=18) on patients with a
cardiovascular condition, but few believed it was “extremely important” to measure vital signs on
each patient during every visit (HR n=4, BP n=4, SpO2 n=3). The most frequently chosen
responses for not assessing vital signs were, “not important for my patient population” (40.0%;
n=18) and “lack of time” (22.2%; n=10) (Peters, 2014).
Peters’ results were able to point out the disparity between the guidelines put in place by
the American Physical Therapy Association, and actual physical therapy practice concerning the
assessment of vital signs in the State of Florida. He concluded that physical therapists are
responsible for the safety of each patient that they treat, and that it is important for vital signs to
be assessed by clinicians for undiagnosed conditions for monitoring existing conditions, and for
facilitation of safety through prevention (Peters, 2014). While Peters was able to establish a
baseline view of vital sign assessment in one state, this current research study was able to expand
his 2014 pilot study to multiple states throughout the U.S. to achieve a much more broad-based
and national view on the assessment of vital signs in all physical therapy settings.
Research Questions and Hypotheses
This survey-based research study sought to answer two research questions. The first
research question is: at what level of frequency do physical therapists assess vital signs (BP, HR,
SpO2) with their patients? The hypothesis was that physical therapists assess vital signs (BP,
HR, SpO2) at a frequency that is significantly less than every patient visit. To further consider
the role of direct access in practice, the second research question was: what is the relationship
between the frequency of physical therapists’ assessment of vital signs and the level of restriction
of patient direct access? The hypothesis was that there will be a greater frequency of assessment
of vital signs (BP, HR, SpO2) among physical therapists in states with unrestricted access than in

VITAL SIGN ASSESSMENT 17
states with restricted access. It was believed that physical therapists take on a greater primary care
role in these states and therefore have an increased responsibility to monitor patients vital signs.
Methods
Research Design and Instrumentation
A survey was designed to encompass the subject of a physical therapist’s role in patient
primary care, and attempted to illustrate a way to show the current level of importance that the
physical therapist places on the assessment of vitals in the setting they work.
This research project, using an online survey format, was an observational, non-
experimental, quantitative, & cross-sectional study. The survey evaluated participants’
demographic data, clinical practice for recording vitals (BP, HR, SpO2), why vitals may not be
taken with every patient visit, beliefs with the autonomous progression of the physical therapist
field and the importance for physical therapists to take vitals (BP, HR, SpO2) with having more
direct access to patients. The survey was web-based research tool using Check Box™ software.
There was a total of 22 questions and consisted of a combination of open-ended and multiple
choice. It took approximately 10 minutes to complete this survey. Participants remained
anonymous through the use of a numbered code assigned to the data collected that associates the
subject with the results.
The survey was fully developed after a thorough search of scholarly articles pertaining to
the purpose & research questions. Four members of the Florida Gulf Coast University Doctor of
Physical Therapy faculty, three student physical therapists, and three members of the public not
associated with the physical therapy profession, reviewed the survey for content and readability
before finalization, securing Institutional Review Board approval, and uploading to state physical
therapist association websites. Due to the survey being uploaded to the participating state
physical therapist association sites, both members and non-members for that state association
could potentially take the survey. Information was available on the website to inform subjects
about the confidentiality and security of their personal data. All the data obtained through this

VITAL SIGN ASSESSMENT 18
study was stored on a flash drive and stored under lock and key in the committee chair’s office on
Florida Gulf Coast University campus for the 3-year required period in compliance with the
Institutional Review Board. After this time period the flash drive will be destroyed.
Access to Subjects and Sampling Plan
The online survey was utilized that allowed respondents to fill out the survey
anonymously. All 50 physical therapy state associations and the District of Columbia were
contacted via phone giving them the opportunity for their members to participate. Of those that
responded back, an additional email was sent with the Online Survey Consent form with details
about the study, and the need for each Association to send a response email stating that state
association’s willingness to participate.
Once IRB approval was obtained, the researcher contacted each association via phone the
email was sent with the survey link. It was also discussed that the state association could decide
how to disperse the online survey link. Follow up contacts were made with each participating
association after 2-4 weeks, via phone and email, to request a second distribution of the survey
link to increase the response rate.
Response rates were monitored throughout the study to ensure that any technical errors
were perceived and resolved. Participants were given full disclosure of the nature and purpose of
the study through an informed consent letter that was part of the online survey. Participation was
voluntary and anonymous, with the submission of the survey implied informed consent.
Data Collection
An approximate 6-week window was given for each association to participate, with the
overall the availability from May-November 2016. The total number of states that expressed
willingness to participate totaled 29, these included: Alabama, Arizona, Arkansas, California,
Connecticut, Delaware, Florida, Hawaii, Illinois, Iowa, Kentucky, Maine, Maryland,
Massachusetts, Montana, Nebraska, Nevada, New Hampshire, New Jersey, New York, North
Dakota, North Carolina, North Dakota, Oklahoma, Pennsylvania, Rhode Island, Vermont,

VITAL SIGN ASSESSMENT 19
Washington, & West Virginia. The District of Columbia physical therapy association expressed
willingness to participate as well.
Results
Part I-Demographic Information
Once data collection was ended, there were 286 participating respondents to the online
survey. Of the 29 states and District of Columbia that participated in this research project, 22 of
those states had at least 1 response. An additional 2 states were represented although the
associations of that state did not participate. In total, the respondents to this survey represented
24 states. Table 1 represents the states with the highest number of respondents.
Table 1
Respondents Primary Practicing State
State Frequency (%) of the Respondents
California 29 10.14
Florida 20 7.00
Iowa 103 36.01
New York 16 5.60
Nebraska 14 4.90
North Dakota 37 12.94
West Virginia 21 7.34
Other States 46 16.07
Total 286 100
Respondents were asked for their practice area and more than one answer was allowed.
Table 2 shows the most common practice areas chosen by the respondents. While
orthopedic/musculoskeletal and geriatrics represented the majority of areas in which respondents
practiced, the data represented all categories of practice.

VITAL SIGN ASSESSMENT 20
Table 2
Respondents Areas of Practice
Area of Practice Frequency (%) of Respondents
Orthopedics/Musculoskeletal 179 62.59
Geriatrics 123 43.01
Adult Neurological Rehab 63 22.03
Cardiovascular & Pulmonary 46 16.08
Sports Physical Therapy 31 10.84
Other 91 (N/A)
The following table shows the patient populations with which the respondents provided
care. Again, respondents were provided the opportunity to respond to all patient populations
currently in their caseload. Table 3 includes the most common patient populations that were
reported. Once again, the respondents represented a broad spectrum of the patients commonly
seen in physical therapy practice.
Table 3
Patient Population Type
Patient Population Type Frequency % of Respondents
Musculoskeletal 165 61.12
Neurological 52 19.92
Cardiovascular 18 8.65
Pulmonary 14 7.41
Metabolic 9 5.36
Integumentary 3 1.89
Lymphatic 0 0

VITAL SIGN ASSESSMENT 21
The current practice settings of responding PTs are found in the table below. Respondents
were able to choose more than one practice setting if applicable. These settings represent the most
common areas in which physical therapy is practiced throughout the US.
Table 4
Current Practice Setting
Practice Setting Frequency (%) of Respondents
Hospital Based Outpatient 87 30.42
Physical Therapy Owned 76 26.57
Acute Care Hospital 66 23.08
Home Care Agency 39 13.64
Skilled Nursing Facility 28 9.8
Other 51 17.83
Respondents were asked about the payor mix for their caseload in the past 6 months for
Medicare, other insurance, and private pay. The majority of respondents described their payor as
being made up of Medicare and other insurance, with 61% reporting that 1-25% of their patients
were private pay.
Respondents were asked if there was a policy regarding measurement/recording of vital
signs in the setting they work. Of the 285 that answered this question, 223 respondents (78.25%)
said ‘No’ and 62 respondents said ‘Yes’ (21.75%). For those that responded ‘Yes’, they were
given the opportunity to explain in more detail. Appendix A discusses the open-ended responses
and categorizes certain commonalities between the respondents.
Responses to the participants initial/entry level of PT degree is shown in the table below,
with a representative mix of Bachelor, Master, and DPT educated therapists.
VITAL SIGN ASSESSMENT 22
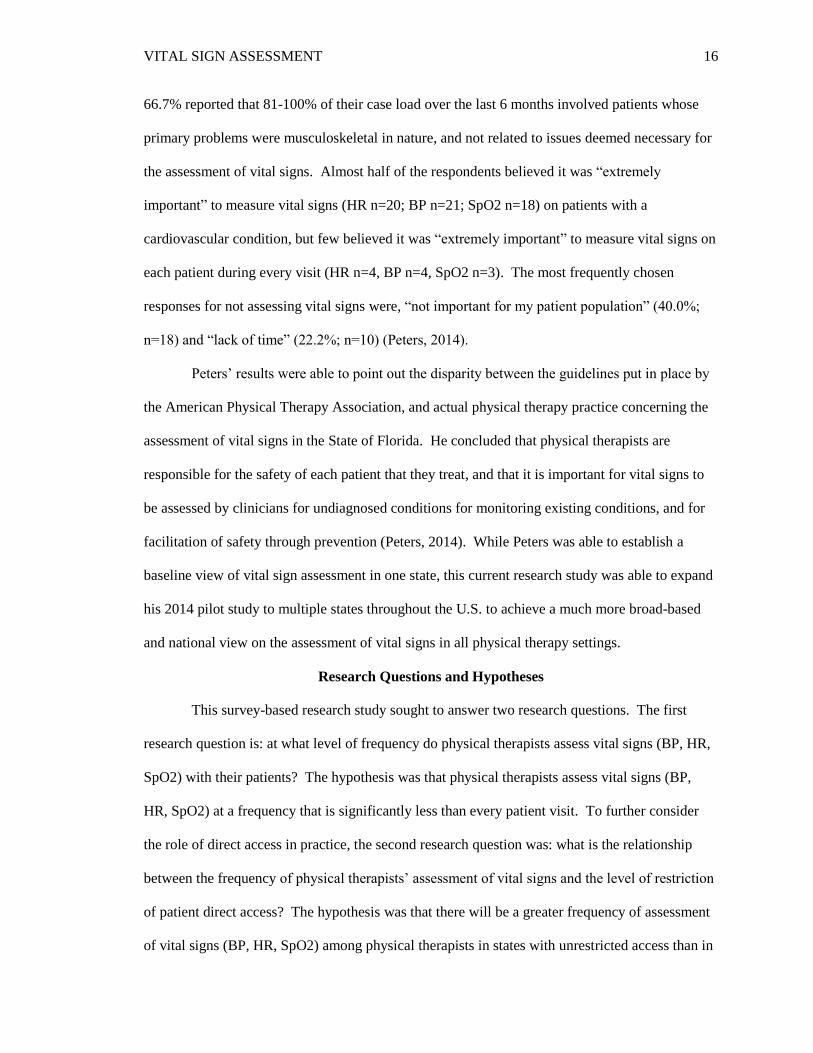
Table 5
Entry Level Physical Therapy Degree
Degree Frequency Percentage of respondents
Certificate 27 9.44
Bachelors 73 25.52
Masters 80 27.97
DPT 106 37.06
Total 286 100
When asked for the highest-level degree earned, better than half of the respondents
indicated that they earned a DPT (Table 6). A total of 257 (90.81%) respondents answered ‘No’
and 26 (9.19%) answered ‘Yes’ if they had completed a residency and/or fellowship.
There were 213 (74.74%) respondents that answered ‘No’ and 72 (25.26%) answer ‘Yes’
if they had an American Board of Physical Therapy Specialty certification (ABPTS).
Table 6
Highest Degree Earned
Degree Frequency Percentage of respondents
Bachelors 39 13.78
Masters 59 20.85
Doctorate (Clinical/DPT) 156 55.12
Post-Professional doctorate 17 6.01
PhD/DSc 12 4.24
Total 283 100
Forty-seven percent of respondents were licensed for 0-15 years with 34% reporting
licensure for 16-30 years. The remaining 20% were licensed for over 30 years. Of the 286

VITAL SIGN ASSESSMENT 23
respondents, 14 (4.90%) said ‘No’ & 272 (95.10%) said ‘Yes’ with being members of the
American Physical Therapy Association. Of those that said ‘Yes’, the length of membership
distribution was consistent with the length of licensure across the sample.
Part II-Practice Behaviors and Beliefs
This section of the survey asked the respondents specific questions about practice
behaviors and beliefs with the key vital signs this research focused on (HR, BP, and SpO2).
Also, respondents were asked questions regarding direct access in their state, Medicare and
assessing vital signs, and an open-ended question for additional comments.
The following results in this section answers the first research question ‘at what level of
frequency do physical therapists assess vital signs (HR, BP, and SpO2) with their patients’?
The first survey question in this section asked how often in the past 6 months have
respondents measured HR, BP, and SpO2 during the initial evaluation. The following table
shows the frequency of respondents assessing these vitals greater than 50% of the time during the
initial evaluation.
Table 7
Initial Evaluation: Respondents Reporting that they Assess HR, BP, and/or SpO2 greater than
50% of the time
Vital Sign Frequency Percentage of Respondents
Heart Rate 119 44.57
Blood Pressure 113 42.33
SpO2 93 34.97
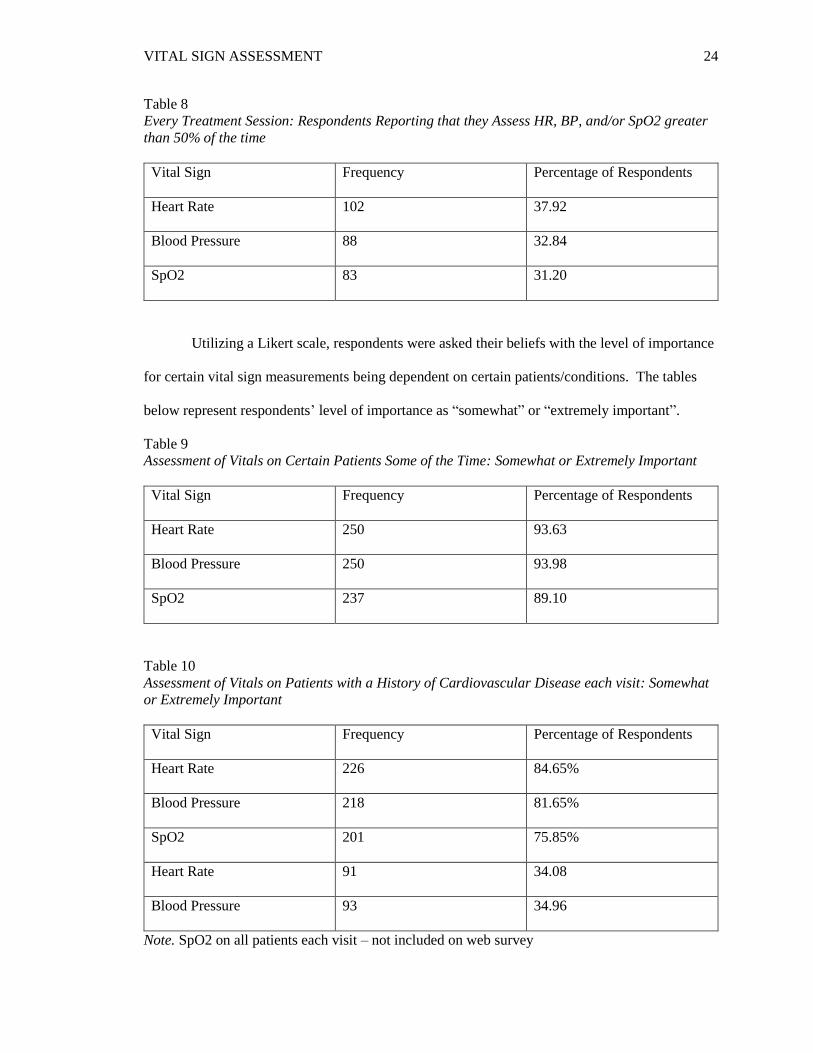
Respondents were asked how often in the past 6 months have they taken BP, HR, and
SpO2 during treatment sessions. The following table shows the frequency of respondents
assessing these vitals greater than 50% of the time during their treatment sessions.
VITAL SIGN ASSESSMENT 24
Table 8
Every Treatment Session: Respondents Reporting that they Assess HR, BP, and/or SpO2 greater
than 50% of the time
Vital Sign Frequency Percentage of Respondents
Heart Rate 102 37.92
Blood Pressure 88 32.84
SpO2 83 31.20
Utilizing a Likert scale, respondents were asked their beliefs with the level of importance
for certain vital sign measurements being dependent on certain patients/conditions. The tables
below represent respondents’ level of importance as “somewhat” or “extremely important”.
Table 9
Assessment of Vitals on Certain Patients Some of the Time: Somewhat or Extremely Important
Vital Sign Frequency Percentage of Respondents
Heart Rate 250 93.63
Blood Pressure 250 93.98
SpO2 237 89.10
Table 10
Assessment of Vitals on Patients with a History of Cardiovascular Disease each visit: Somewhat
or Extremely Important
Vital Sign Frequency Percentage of Respondents
Heart Rate 226 84.65%
Blood Pressure 218 81.65%
SpO2 201 75.85%
Heart Rate 91 34.08
Blood Pressure 93 34.96
Note. SpO2 on all patients each visit – not included on web survey

VITAL SIGN ASSESSMENT 25
The most common reasons respondents expressed they did not take vital signs is in the
table below with frequency and percentage of the total responses.
Table 11
Most Common reasons for Physical Therapists to not assess vitals
Reason Frequency Percentage of Respondents
Not Important for My Patient
Population
104 41.77
Lack of Time 75 30.12
Vitals are measured by other
staff members at my clinic
67 26.91
Equipment not available 38 15.26
Other 63 (N/A)
The amount of time respondents expressed it took them to assess vitals is shown in the
table below, with frequency and percentage of the total responses.
Table 12
Average Time to Assess Vitals: HR, BP, & SpO2
Average Time Frequency Percentage of respondents
1-3 minutes 153 56.88
4-6 minutes 111 41.26
7-9 minutes 3 1.12
9+ minutes 2 <1
Total responses 269 100
Of the 265 respondents that answered the question regarding if they would recommend a
patient’s vitals be taken more often if there was someone else that could assess them, 112
VITAL SIGN ASSESSMENT 26
(42.26%) said ‘No’ & 153 (57.74%) said ‘Yes’. Of the 268 respondents that answered the
question about living in a restricted or unrestricted state, 161 (60.07%) said they lived in an
‘unrestricted’ state, 87 (32.46%) said they lived in a ‘restricted’ state, and 20 (7.46%) said they
were ‘unsure’. For respondents who reported ‘unsure’, data was coded using reported state of
practice to record level of restriction of direct access for the respondent.
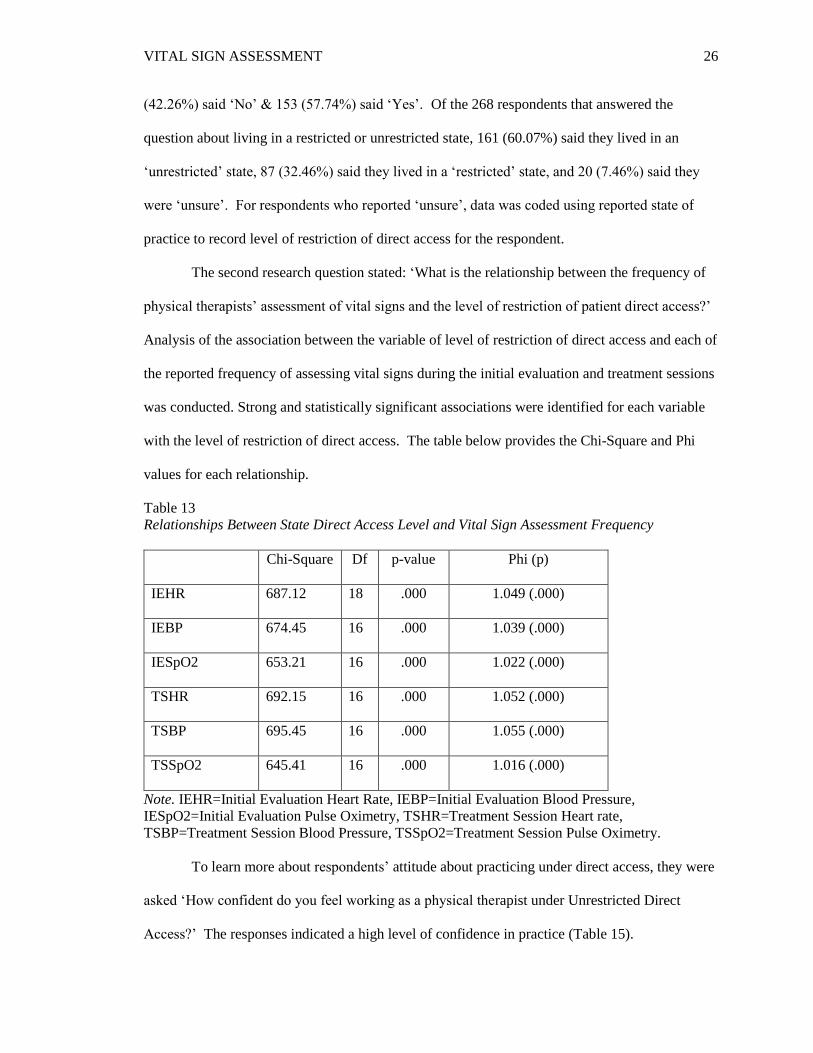
The second research question stated: ‘What is the relationship between the frequency of
physical therapists’ assessment of vital signs and the level of restriction of patient direct access?’
Analysis of the association between the variable of level of restriction of direct access and each of
the reported frequency of assessing vital signs during the initial evaluation and treatment sessions
was conducted. Strong and statistically significant associations were identified for each variable
with the level of restriction of direct access. The table below provides the Chi-Square and Phi
values for each relationship.
Table 13
Relationships Between State Direct Access Level and Vital Sign Assessment Frequency
Chi-Square Df p-value Phi (p)
IEHR 687.12 18 .000 1.049 (.000)
IEBP 674.45 16 .000 1.039 (.000)
IESpO2 653.21 16 .000 1.022 (.000)
TSHR 692.15 16 .000 1.052 (.000)
TSBP 695.45 16 .000 1.055 (.000)
TSSpO2 645.41 16 .000 1.016 (.000)
Note. IEHR=Initial Evaluation Heart Rate, IEBP=Initial Evaluation Blood Pressure,
IESpO2=Initial Evaluation Pulse Oximetry, TSHR=Treatment Session Heart rate,
TSBP=Treatment Session Blood Pressure, TSSpO2=Treatment Session Pulse Oximetry.
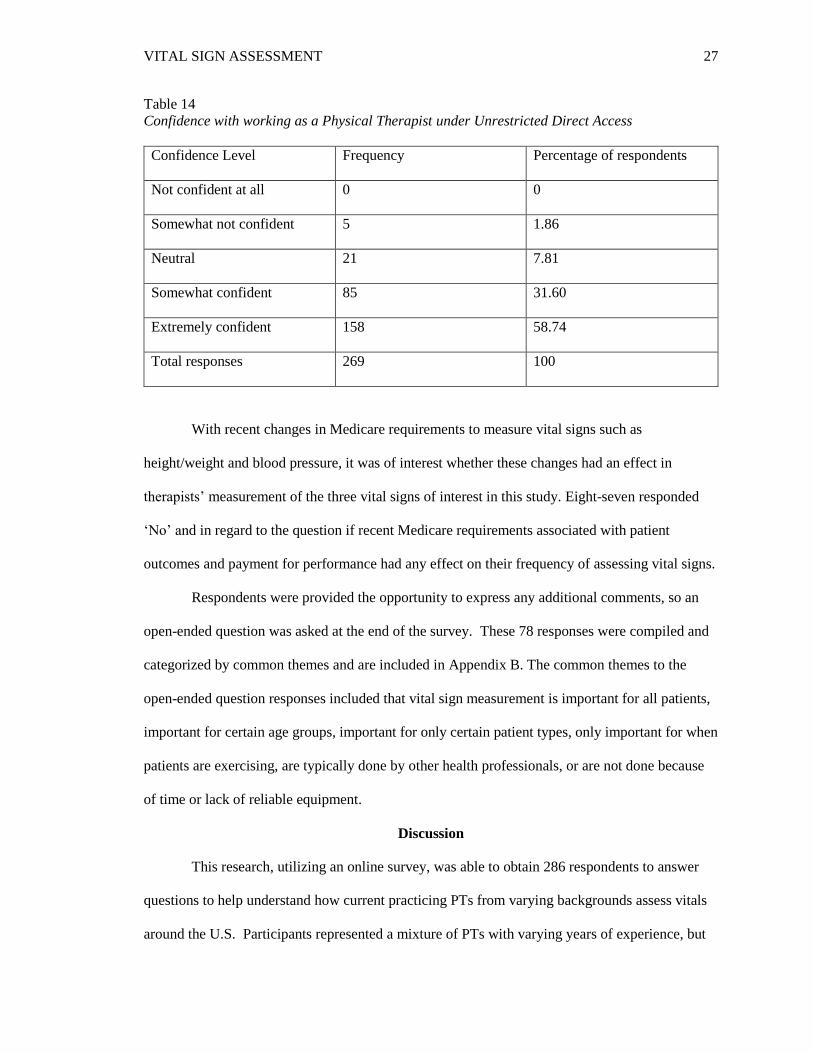
To learn more about respondents’ attitude about practicing under direct access, they were
asked ‘How confident do you feel working as a physical therapist under Unrestricted Direct
Access?’ The responses indicated a high level of confidence in practice (Table 15).
VITAL SIGN ASSESSMENT 27
Table 14
Confidence with working as a Physical Therapist under Unrestricted Direct Access
Confidence Level Frequency Percentage of respondents
Not confident at all 0 0
Somewhat not confident 5 1.86
Neutral 21 7.81
Somewhat confident 85 31.60
Extremely confident 158 58.74
Total responses 269 100
With recent changes in Medicare requirements to measure vital signs such as
height/weight and blood pressure, it was of interest whether these changes had an effect in
therapists’ measurement of the three vital signs of interest in this study. Eight-seven responded
‘No’ and in regard to the question if recent Medicare requirements associated with patient
outcomes and payment for performance had any effect on their frequency of assessing vital signs.
Respondents were provided the opportunity to express any additional comments, so an
open-ended question was asked at the end of the survey. These 78 responses were compiled and
categorized by common themes and are included in Appendix B. The common themes to the
open-ended question responses included that vital sign measurement is important for all patients,
important for certain age groups, important for only certain patient types, only important for when
patients are exercising, are typically done by other health professionals, or are not done because
of time or lack of reliable equipment.
Discussion
This research, utilizing an online survey, was able to obtain 286 respondents to answer
questions to help understand how current practicing PTs from varying backgrounds assess vitals
around the U.S. Participants represented a mixture of PTs with varying years of experience, but

VITAL SIGN ASSESSMENT 28
almost half of the respondents have worked as a PT for 0-15 years of experience. Almost all the
respondents to the survey reported being APTA members with varying years of membership and
more than half of the respondents have been members between 0-15 years.
Twenty-two state associations demonstrated interest in participating in the distribution of
the survey. Not all states were willing/able to participate for various reasons or researcher was
not able to get a hold of a representative after multiple attempts. There was skewed
representation for the states that did participate. The 7 states with the most frequency of
respondents represented 83.92% of total responses.
Respondents represented a variety of practice settings and patient types with the majority
working in outpatient settings with musculoskeletal and geriatric patient populations. This is
consistent with the previous study by Peters (2014) and may be representative of the distribution
of physical therapists within practice. It is less clear if there are differences in the behaviors and
beliefs of therapists in other practice settings and with other populations as they were less
represented in the sample.
The data indicates a lack of policy for vital sign assessment in the clinical facilities
represented in the sample. Policy for vital sign assessment was reported to be none for greater
than ¾ of the respondents showing a lack of focus on this aspect of patient care in many physical
therapy settings. This seems to show a similar pattern as the pilot study on vital sign assessment
in outpatient PT settings, by Josh Peters (2014) for the state of Florida, where policy for vital
signs is <30% according to responses. This present study does not seem to show a
comprehensive understanding of vital sign policy across all practice settings, due to the outpatient
setting being the most represented in the sample.
Most of the respondents were highly educated, with the initial degree being at the
graduate level for almost two-thirds of them (either masters or doctorate), and an even greater
number earning a clinical or academic doctorate as their highest degree. Most responders to the
survey did not express having a specialty certification (ABPTS) or that they completed a

VITAL SIGN ASSESSMENT 29
residency or fellowship. Of those that do hold a specialty certification most have either an
orthopedic or geriatric ABPTS. There seems to be a pattern of similarity with the majority who
responded with having a specialty ABPTS and the majority of respondents reporting their area of
practice being in orthopedics/musculoskeletal and/or geriatrics. The respondents with geriatric
ABPTS demonstrated higher support in taking HR, BP, and SpO2, as they reported they would
with over half of their patient population during initial evaluations. Therapists with an orthopedic
ABPTS reported they were of lesser support of taking HR, BP, and SpO2, as they reported they
would not assess these vitals with over half of their patient population during the initial
evaluation. This may be due to the PT respondents reasoning regarding their patient population
they work with and feelings about this. The most common reasons that geriatric specialty
certified respondents expressed for why vitals are not measured was that either their patient was
young and medically stable or that others measure the vital signs already at other medical visits.
Orthopedic specialty certified respondents expressed that it was not important for their patient
population and approximately one-third expressed a lack of time. The results are similar and
appear to support the pattern of results found in the pilot study by Peters (2014). Although other
areas of practice may have differing reasons for why vital signs are not assessed, these data
provide insight into the similar reasons of why a PT may or may not take vitals.
Data were able to address the research questions for this study. The hypothesis for the
first research question is supported with the current research. Results indicate that vital sign
assessment of BP, HR, and SpO2 occur at a frequency significantly less than every patient visit.
The results for assessment of SpO2 for initial patient visit and following treatments were less than
for HR and BP. A technical error did not allow for the collection of data on frequency of SpO2
measurement during regular treatment sessions. Most respondents expressed that they did not feel
that taking vital signs of HR and BP for all patients all the time was important. More expressed
that it was important to take vital signs of HR, BP, and SpO2 during initial evaluation than for
every treatment visit, but even taking vitals at initial evaluation occurred less than half the time

VITAL SIGN ASSESSMENT 30
for the respondents’ patient caseloads in the past 6 months. Again, HR and BP was measured
more than SpO2. There was similarity in that a majority of the respondents do feel that taking
vitals of BP, HR, and SpO2 are important for some patients some of the time and for patients with
cardiovascular known diseases, supporting Peters (2014) findings.
As mentioned earlier, many respondents who participated in this online survey, reported
that assessing vitals was dependent on their patient population, which was the top reason for why
these vital signs are not taken. Also, lack of time or others are taking the vital signs were
frequent reasons to why HR, BP, and/or SpO2 are not taken. It is important to highlight that
asked about the time it would take to assess vitals, over half of the therapists said it would take
one to three minutes to assess and almost all said it would take between one and six minutes. It
appears that almost all respondents would take less time than one billable unit, which is eight
minutes (Jannenga, 2016), to assess vitals.
Secondly, this research attempted to investigate the relationship between state direct
access to physical therapy and the frequency of measurement of vital signs. The data did not
support the hypothesis for research question two. The hypothesis was that there will be a greater
frequency of assessment of vital signs (BP, HR, SpO2) among physical therapists in states with
unrestricted access than in states with restricted access. There was statistically significant
relationship between the variables of level of direct access and frequency of measuring vital
signs, with a greater frequency of respondents in restricted direct access states measuring HR, BP,
and SpO2 than therapists in unrestricted direct access states during both initial evaluations and
during treatment sessions. Additionally, there was close to two-times more respondents that live
in unrestricted vs. restricted states according to the survey results. Due to a smaller sample size
of under 300, generalization of these results and conclusions are limited. Future research is
necessary to get a firm understanding of vital sign assessment with unrestricted and restricted
states.

VITAL SIGN ASSESSMENT 31
Lastly, Medicare reimbursement was the greatest for the respondents to this survey
followed by other insurance providers. Very few providers had private pay in their payor mix. A
majority of the responding PTs do not feel that Medicare requirements associated with patient
outcomes and payment for performance are affecting their frequency of assessing vital signs. It
will be important to continue to monitor how reimbursement shapes the practice of physical
therapist in these health monitoring measures.
When asked if the responding PTs would have their patients’ vitals assessed more often if
there was a qualified person to assess them, there were mixed feelings about this with ~15% more
saying ‘yes’ than ‘no’.
This study gathered further information regarding the thoughts, feelings, and practice of
vital sign assessment through the inclusion of an open-ended question. Of the 78 respondents that
remarked to this question, certain trends were noted. The most frequent responses, as discussed
in the results, were: Vital sign assessment is important for all patients; vital sign assessment is
important but limited by time/equipment and/or availability/reliable supply issues; vital sign
assessment is important especially for cardio/pulmonary compromised patients; and vital sign
assessment is important for certain patients (e.g., past medical history/symptoms). One can see
the diversity in the comments but also the cohesiveness. All of these responses attest that vital
signs are important, but the difference lies with which patients and how often. Although most
PTs do not feel assessing vitals is important every patient visit, many PTs do. As patients in all
practice settings continue to have more comorbidities, there may be a shift in PTs practice of the
measurement of these vital signs.
There are a few limitations to this study. First, by using an internet-based survey, not
everyone is willing to take a survey online, with some people being more comfortable with other
methods (e.g., paper or phone surveys). Second, distribution of the survey was reliant on state
physical therapy associations. Most of the physical therapists obtaining the online survey were
likely to be members of that association. Not all of the state associations were willing to

VITAL SIGN ASSESSMENT 32
participate, some expressing that it would be too much to take on every research project from
around the country so they only take projects from within the state. Some of the states did not
respond which decreased the geographic representation of the survey results. Also, each state
association participating was allowed to disperse the survey as they saw fit. State associations
were provided a variety of methods: email blast, placing on the website, to sending it out in a
news-letter. It is not fully known how each state dispersed the survey and how many times they
dispersed the survey. This may have had an effect on the number of responses from each state.
Obtaining input from physical therapists not associated with state association would have been
difficult to achieve due to the privacy of contact information for licensed physical therapists.
Continued analysis of the data obtained in this research project will be important to
determine the various relationships that may exist. Further data collection in states and practice
areas that are underrepresented may improve the understanding of the practice of vital sign
assessment across all areas of practice. Due to many respondents utilizing other methods of vital
sign assessment, having research focused on different vital sign assessment (e.g., BMI, pain,
temperature, RR) or in combination with the vitals researched in this project would be beneficial.
The responses from the open-ended questions may inform further research. Many
therapists expressed that an older population would require vital sign assessment more than a
younger population. Future research that specifically focuses on vital sign assessment among the
older adult population would be beneficial to determine how often vital signs are assessed in this
higher risk population, and how many negative medical events are lessened by detection of
cardiac pathologies.
Conclusion
Vital sign assessment among many health care providers allows the practitioner to
develop an initial plan of action for patient care and identify serious health issues in patients.
These measures are quick, easy, and objective methods to determine a patient’s general health
status. Physical therapists are well educated to both measure and interpret the findings of these

VITAL SIGN ASSESSMENT 33
measures within their role as primary care providers. This research provides a better
understanding of vital sign assessment among physical therapists in various regions around the
U.S. Further research will continue to add to the understanding of practice.
Assessing vitals is not just pertinent for patient care that treatment session, but may
provide valuable insight on that patient’s current status, which may be known or unknown.
Physical therapists being primary health care providers need to be part of the health care team in
identifying signs of pathology in patients. Physical Therapists are able to provide valuable
information regarding vital sign assessment that will inform physicians, nurses, rehabilitation
specialists, and other health care providers. Increasing the comprehensiveness of patient care and
communication between health care providers benefits both patients and the health care system.
As mentioned previously, cardiovascular disease is the number one cause of death among
people in the United States. Vital sign assessment utilizing HR, BP, and SpO2 may show warning
signs that could save a persons’ life. This practice is not just for the immediate treatment session,
but could also be a key indicator for some complication that may warrant a referral or
communication with that patient’s physician’s office. As many respondents in this survey
mentioned, by assessing vitals, some of their patients’ lives were saved because they contacted
that patient’s physician about an abnormality with their patients’ vitals.
It can be questioned if are vital sign assessments should just be taken at one treatment
session or is this a measure that should be regularly assessed for rapid detection of underlying
pathology. These measures, once done regularly, were not reported to be difficult or time
consuming to assess, based on survey results. Once part of routine practice, these objective
measures can provide insight for each patient’s cardiovascular health and prevention of further
health events.

VITAL SIGN ASSESSMENT 34
References
About Us. (2014). About Us. Retrieved July 5, 2014, from http://www.apta.org/AboutUs/
American Physical Therapy Association. (2016). Levels of Patient Access to Physical Therapist
Services in the States. Retrieved April 2nd, 2017, from
http://www.apta.org/uploadedFiles/APTAorg/Advocacy/State/Issues/Direct_Access/Dire
ctAccessbyState.pdf
Arena, R., Myers, J., & Guazzi, M. (2010). The future of aerobic exercise testing in clinical
practice: Is it the ultimate vital sign?. Future Cardiology, 6(3), 325-342.
Arena, S.K. (2009). Self-reported frequency and importance of measuring heart rate and blood
pressure at physical therapy clinical sites: a descriptive study. Cardiopulmonary Physical
Therapy Journal, 20(4), 26-27.
Bleyer, A. J., Vidya, S., Russell, G. B., Jones, C. M., Sujata, L., Daeihagh, P., et al. (2011).
Longitudinal analysis of one million vital signs in patients in an academic medical center.
Resuscitation, 82(11), 1387-1392.
Bohannon, R. W. (2008). Hand‐Grip Dynamometry Predicts Future Outcomes in Aging Adults.
Journal of Geriatric Physical Therapy, 31(1), 3-10.
Bultz, B. D., & Johansen, C. (2011). Screening for distress, the 6th vital sign: where are we, and
where are we going?. Psycho‐Oncology, 20(6), 569-571.
Chester, J. G., & Rudolph, J. L. (2010). Vital signs in older patients: age-related changes.
Journal of the American Medical Directors Association, 12(5), 337-343.
Cretikos, M. A., Bellomo, R., Hillman, K., Chen, J., Finfer, S., & Flabouris, A. (2008).
Respiratory rate: the neglected vital sign. Medical Journal of Australia, 188(11), 657-
659.
Direct Access Summit. (2009). Direct Access Summit. October 22nd-24th, 2009. Retrieved July
5, 2014, from http://www.directaccesssummit.com/apta-press-release.pdf
Edmonds, Z. V., Mower, W. R., Lovato, L. M., & Lomeli, R. (2002). The reliability of vital sign
measurements. Annals of Emergency Medicine, 39(3), 233-237.
Elliot, M., & Coventry, A. (2012). Critical care: the eight vital signs of patient monitoring.
British Journal of Nursing, 21(10), 621-625.
Feldman, K., Householder, M., Hale, S., Jackson, A., McKinney, D., & McVey, L. (2016).
Physical Therapists’ Ability to Predict Hypertensive Status Based on Visual Observation
With and Without Past Medical History. Cardiopulmonary Physical Therapy Journal,
27(2), 49-54.
Frese, E. M., Frick, A., & Sadowsky, H. (2011). Blood pressure measurement guidelines for
physical therapists. Cardiopulmonary Physical Therapy Journal, 22(2), 5-12.

VITAL SIGN ASSESSMENT 35
Fritz, S., & Lusardi, M. (2009). White Paper: “Walking speed: the sixth vital sign”. Journal of
Geriatric Physical Therapy, 32(2), 2-5.
Graham, C., & Clark, D. (2011). Podcast: Pump Up The Cuff: The Importance of
Monitoring Vital Signs. Retrieved March 20, 2015, from http://www.apta.org/Podcast/
2011/8/11/VitalSigns/
Grunig, E., Lichtblau, M., Ehlken, N., Ghofrani, H., Reichenberger, F., Staehler, G., et al. (2012).
Safety and efficacy of exercise training in various forms of pulmonary hypertension.
European Respiratory Journal, 40(1), 84-92.
Heart Disease. (2015). Centers for Disease Control and Prevention. Retrieved March 15, 2015,
from http://www.cdc.gov/nchs/fastats/heart-disease.htm
Heart Disease Fact Sheet. (2015). Centers for Disease Control and Prevention. Retrieved March
19, 2015, from http://www.cdc.gov/ dhdsp/data_ statistics/
fact_sheets/fs_heart_disease.htm
Heart Disease Facts. (2014). Centers for Disease Control and Prevention. Retrieved
July 5, 2014, from http://www.cdc.gov/heartdisease/facts.htm
High Blood Pressure Fact Sheet. (2014). Centers for Disease Control and Prevention.
Retrieved July 6, 2014, from http://www.cdc.gov/dhdsp/data_statistics/fact_sheets
/fs_bloodpressure.htm
High Blood Pressure Frequently Asked Questions. (2015). Centers for Disease Control and
Prevention. Retrieved March 20, 2015, from http://www.cdc.gov/bloodpressure/faqs.htm
Kasinskas, C., Wood, R., & Koch, M.L. (2011). Blood pressure monitoring in outpatient
physical therapy clinics: should it be performed routinely?. Cardiopulmonary Physical
Therapy Journal. 22(4), 31-32.
Jannenga, H. (2016). Physical Therapists’ Guide to the 8-Minute Rule. WebPT. Retrieved April
1st, 2017, from https://www.webpt.com/8-minute-rule
Kim, T., & Kim, H. (2012). A healthcare system as a service in the context of vital signs:
Proposing a framework for realizing a model. Computers & Mathematics with
Applications, 64(5), 1324-1332.
Knight, E., Werstine, R.J., Rasmussen-Pennington, D.M., Fitzsimmons, D., & Petrella, R.J.
(2015). Physical Therapy 2.0: leveraging social media to engage patients in rehabilitation
and health promotion. Physical Therapy, 95(3), 389-396.
Leading Causes of Death. (2015). Retrieved March 15, 2015, from http://www.cdc.gov/nchs/
fastats/leading-causes-of-death.htm
Lowe, B., Therrien, J., Ionescu-Ittu, R., Pilote, L., Martucci, G., & Marelli, A. (2011). Diagnosis
of Pulmonary Hypertension in the Congenital Heart Disease Adult Population. Journal of
the American College of Cardiology, 58(5), 538-546.
VITAL SIGN ASSESSMENT 36
McMorrow, R. C., & Mythen, M. G. (2006). Pulse oximetry. Current Opinion in Critical Care,
12(3), 269-271.
Mengelkoch, L.J., Martin, D., & Lawler, J.A. (1994). Review of the principles of pulse oximetry
and accuracy of pulse oximeter estimates during exercise. Physical Therapy, 74(1), 40-
49.
Mereles, D., Ehlken, N., Kreuscher, S., Ghofrani, S., Hoeper, M. M., Halank, M., et al. (2006).
Exercise and respiratory training improve exercise capacity and quality of life in patients
with severe chronic pulmonary hypertension. Circulation, 114(14), 1482-1489.
Millar, L.A., Village, D., King, T., McKenzie, G., Lee, J., & Lopez, C. (2016). Heart Rate and
Blood Pressure Assessment by Physical Therapists in the Outpatient Setting-An
Observational Study. Cardiopulmonary Physical Therapy Journal, 27(3), 90-95.
Mozaffarian, D., Benjamin, E. J., Go, A. S., Arnett, D. K., Blaha, M. J., Cushman, M., et al.
(2015). Executive Summary: Heart Disease and Stroke Statistics-2015-Updated A Report
From the American Heart Association. Circulation, 131(4), 434-441.
National Center for Health Statistics. (2015). Health, United States, 2014: With Special Feature
on Adults Aged 55–64. Hyattsville, MD. Obtained from:
www.cdc.gov/nchs/data/hus/hus14.pdf#215
Nolte, E., & McKee, C. M. (2008). Measuring the health of nations: updating an earlier analysis.
Health Affairs, 27(1), 58-71.
Ott, C., Schneider, M. P., & Schmieder, R. E. (2013). Ruling out secondary causes of
hypertension. Euro Intervention: Journal of Euro PCR in Collaboration with the Working
Group on Interventional Cardiology of the European Society of Cardiology, 9(R), R21-
28.
Pedersen, T., Møller, A. M., & Pedersen, B. D. (2003). Pulse oximetry for perioperative
monitoring: systematic review of randomized, controlled trials. Anesthesia &
Analgesia, 96(2), 426-431.
Peters, J. J. (2014). Self-Reported Use of Vital Signs in the Adult Outpatient Physical Therapy
Setting. Retrieved March 20th, 2015, from
http://fgcu.digital.flvc.org/islandora/search/Peters?type=edismax&collection=fgcu%3Aet
d
Prevalence of Hypertension and Controlled Hypertension — United States, 2007–2010. (2013).
Retrieved March 16, 2015, from http://www.cdc.gov/Mmwr/preview/mmwrhtml/su6203
a24.htm
Pulse oximetry. (2014). World Health Organization. Retrieved July 6, 2014, from
http://www.who.int/patientsafety/safesurgery/pulse_oximetry/en/
Racette, S. B., Deusinger, S. S., & Deusinger, R. H. (2003). Obesity: overview of prevalence,
etiology, and treatment. Physical Therapy, 83(3), 276-288.

VITAL SIGN ASSESSMENT 37
Schieb, L. J. (2013). Vital signs: avoidable deaths from heart disease, stroke, and hypertensive
disease-United States, 2001-2010. MMWR. Morbidity and Mortality Weekly Report,
62(35), 721-727.
Sinex, J. E. (1999). Pulse oximetry: Principles and limitations. American Journal of Emergency
Medicine, 17(1), 59-66.
Tanaka, H., Monahan, K. D., & Seals, D. R. (2001). Age-predicted maximal heart rate revisited.
Journal of the American College of Cardiology, 37(1), 153-156.
Target Heart Rates. (2013). Target Heart Rates. Retrieved July 5, 2014, from http://www.heart.
org/HEARTORG/GettingHealthy/PhysicalActivity/Target-Heart-Rates_UCM_
434341_Article.jsp
Taylor, N. F., Dodd, K. J., & Damiano, D. L. (2005). Progressive resistance exercise in physical
therapy: a summary of systematic reviews. Physical Therapy, 85(11), 1208-1223.
Vision 2020. (2014). Vision 2020. Retrieved July 5, 2014, from http://www.apta.org/Vision
2020/
Weiss, B. D., Mays, M. Z., Martz, W., Castro, K. M., DeWalt, D. A., Pignone, M. P., et al.
(2005). Quick assessment of literacy in primary care: the newest vital sign. The
Annals of Family Medicine, 3(6), 514-522.
Wilson, J. F. (2005). Is sleep the new vital sign?. Annals of Internal Medicine, 142(10), 877-880.
Who Are Physical Therapists?. (2013). Who Are Physical Therapists?. Retrieved July 5, 2014,
from http://www.apta.org/AboutPTs/
Yuen, T. S., & Irwin, M. G. (2005). The 'fifth vital sign'. Hong Kong Medical Journal, 11(3),
145-146.
Zhang, Y., Agnoletti, D., Iaria, P., Protogerou, A. D., Safar, M. E., Xu, Y., et al. (2012). Gender
difference in cardiovascular risk factors in the elderly with cardiovascular disease in the
last stage of lifespan: The PROTEGER study. International Journal of Cardiology,
155(1), 144-148.

VITAL SIGN ASSESSMENT 38
Appendices
Appendix (A): Question 6b-Open Ended Responses, Synopsis/Report
In total, question 6b (Please Describe the Policy) received 52 responses of the total 285
responses to Question 6a. Question 6a (Does your clinic have a policy regarding the
measurement/recording of vital signs? Yes or No) had 62 responses that marked ‘Yes’. This
survey only allowed a participant to respond to 6b if they marked ‘Yes’ for 6a.
Most of the responses expressed vital sign assessment was done, mandatory, highly
expected, should do, etc. Since this research study did not get actual organization policy
documents, the complete understanding is not going to be fully understood. It still gives valuable
information to how the PT profession is currently regarding vital sign assessment, for example,
out of the 285 that responded to Question 6a, 21.75% of the respondents marked ‘Yes’ that their
organization had a policy on vital sign assignment. The participants that marked ‘No’
represented 78.25% of the respondents; there are multiple reasons why a respondent marked
‘No’, further research would need to be conducted to determine these specifics.
The researchers grouped the 52 responses into the following categories, based off of the
survey participants’ responses to question 6b:
• Are required to take ‘Vitals’ during the evaluation and during proceeding treatment
sessions: 22
• Required during evaluations but at their discretion for subsequent patient treatments:
12
• Evaluations and treatments of patients were at the therapists’
discretion/recommended by organization but not mandatory: 5
• Vitals are required to take for all company pre-work screens, but at therapist
discretion for other patients based on PMHx and symptoms: 2
• Had to report the ‘pain’ vital sign only: 1

VITAL SIGN ASSESSMENT 39
Appendix (A): Question 6b-Open Ended Responses, Synopsis/Report (continued)
• Acute Care Patients needed vitals to be monitored: 1
• Computer Updates: 1
• Pre-employment vital sign assessment tests: 1
• All Medicare patients’ vitals are to be taken at evaluation and at PT discretion during
treatments & all non-Medicare is at PT discretion during evaluation and during
treatments but encouraged: 1
• All Medicare patients’ height and weight are recorded for BMI but they do not take
HR or BP: 1
It was difficult to determine which vital signs, specifically, the respondents to this survey
are required, expected, highly encouraged, recommended, deemed appropriate, etc. at their
organization of employment. A few mentioned specifics, but not enough to where clarifying
would gain any realistic understanding, as a whole, for this research project, in regard to vital sign
assessment. Health care providers know that vital signs encompass multiple items used to assess a
patient’s health status. Each vital sign helps the health care provider, and for the purpose of this
research project, the Physical Therapist health care provider to determine pathological conditions
of their patients or lack there-of. The survey respondents, whom did not clarify in their responses,
may have been referring to this research projects focus of the three vital signs BP, HR, and SpO2,
but the researchers are not assuming that, since the respondents did not specify!

VITAL SIGN ASSESSMENT 40
Appendix (B): Question 22-Open Ended Responses, Synopsis/Report
Of the 78 relevant responses (not reporting respondents saying, N/A, No, or other
responses similar) the researchers found that 19 of the 62 respondents (31.1%) that answered
‘Yes’ to question 6a (Does your clinic have a policy regarding the measurement/recording of vital
signs?), made it to the end of the survey and responded to question 22. The remaining 59
respondents to question 22 marked ‘no’ to question 6a. There were 206 participants that marked
‘no’ to question 6a, so 28.6% of those respondents made additional comments to this question.
The responses obtained for this question have been categorized based off the
interpretation of what the participating responders shared. Some shared one thought others shared
multiple thoughts. A person that shared multiple thoughts will be included in all the categories
that they shared in their response. Below are frequency of responders and categories of this open-
ended question’s responses set up by the researchers:
• Vital sign assessment is important for All patients: 17
• Vital sign assessment is important but time/equipment availability/reliable supplies
issues: 12
• Vital sign assessment is important especially for cardio/pulmonary compromised
patients: 11
• Vital sign assessment is important for certain patients (e.g., Past Medical History,
Symptoms): 10
• Vital sign assessment is important for certain age groups (e.g., older vs. younger
population): 8
• Vital sign important due to Physical Therapists being active/exercising patients: 8
• Vital sign assessment in certain settings are not as important unless signs/symptoms
due to other staff (e.g., nurses) and/or machines take them: 7
• Vital sign assessment depends on the setting a Physical Therapist works: 5

VITAL SIGN ASSESSMENT 41
Appendix (B): Question 22-Open Ended Responses, Synopsis/Report (continued)
• Educators & clinicians should teach the importance of vital sign assessment more: 4
• Vital sign assessment in OP settings is lacking: 4
• Physical Therapists under-utilize this aspect of care: 3
• Vital sign assessment important at least during the initial evaluation of a patient: 3
• Vital sign assessment is important as it could find an abnormality that could help a
patient’s quality of life/save their life: 2
• Important with helping Physicians with patient care: 2
• Important to educate patients to self-assess their own vitals as well: 2
• If I had a PT tech I would do it more regularly: 2
• Only response was that they take Rate of Perceived Exertion: 1
• Vital sign assessment is bothersome to certain patients: 1
• Importance of vital sign assessment and justifying services/progress made: 1
• Respondents expressed that in addition to the one’s mentioned in the study the
following are also important:
o Temperature (Temp): 1
o Temp & Pain: 1
o Temp and Respiratory Rate (RR): 1
o Walking Speed & Weight for certain patients (e.g. Congestive Heart Failure): 1
o RR & pedal pulses: 1
o Bruits & Cardiac/Lung sounds when appropriate: 1
• Should be done regularly but am an older clinician and feel that other older clinicians
would be less likely to as well: 1
• Physical Therapy is a Doctoring Profession: 1

VITAL SIGN ASSESSMENT 42
Appendix (B): Question 22-Open Ended Responses, Synopsis/Report (continued)
• Measure Vitals with Rest & Activity as well as assist Medical Doctor with diagnosis
and medicine changes that make significant improvement in patients’ lives: 1
• Patients are unable to see the physician as regularly, Physical Therapists are their
more regular line of health care: 1
• Specifically mentioned that Blood Pressure and Heart Rate as Important: 1
• Need Physician approval for SpO2: 1
• Physical therapists should be able to assess SpO2 without physician approval as some
non-respiratory patients whose O2 saturation may drop need that type of assessment:
1
• Important of All practice settings: 1
• Imperative for unrestricted direct access: 1
• Use of subjective vital sign assessment more (e.g., facial features, breathing patterns):
1
• Do not rely on heart rate as much as RPE due to many patients taking beta-blockers:
1
• Should be more consistent with taking vitals on patients: 1
• Uncertainty with what to do if the numbers of a patient’s vitals are bad, do I send
them home or monitor them: 1
• May not bring in axillary equipment for vital sign assessment in a patient’s room
with infection control issues: 1
• Vital sign assessment is in a Physical Therapists scope of practice, if we do not do it
then we are essentially giving up that part of our practice: 1
• Others do it so I don’t have to: 1

VITAL SIGN ASSESSMENT 43
Appendix (B): Question 22-Open Ended Responses, Synopsis/Report (continued)
• Work in a program with patients who have chronic illnesses so I take them regularly:
1
• Document what the machines or nurse document as this facility has policies that
certain machines be utilized to take vitals, but these are limited (3 machines per 25
patients): 1
• As physical therapist professionals, we should be able to make up our own minds
when vital sign assessment should be taken with patients: 1
• Important to assess vitals due to what physical therapists do to the lungs, heart, and
oxygen consumption, plus need to be confident with vital sign assessment: 1
• The leaders in the settings that physical therapists work need to have the vital sign
assessment tools readily available: 1
• Need to review vital sign assessment skills: 1
• Needed cleared guidelines for all physical therapists on vital sign assessment: 1
• More physical therapists should take vitals more often: 1
• Recent APTA or Cardiology Association guidelines, not sure which, say that it is safe
to work with patients that have a Blood Pressure that is higher than I am comfortable
with: 1
In addition to the above responses to vital sign assessment certain responders made other
remarks about vital sign assessment, physical therapy practice, and patient care. These remarks,
show variances in practice patterns, shed insight to other issues/concerns that may need to be
addressed with further research to help improve physical therapists’ autonomy, practice setting,
and/or patient care:

VITAL SIGN ASSESSMENT 44
Appendix (B): Question 22-Open Ended Responses, Synopsis/Report (continued)
“The pay for performance and value based purchasing system essentially discriminates
against those really ill or physically challenged. That is providers will be financially
penalized for not making good outcomes and so have negative reason to accept and service those
individuals.”
“I unfortunately just had to terminate a DPT student on final affiliation for multiple
reasons, lack of monitoring vital sign responses to treatment & interventions being one of them.”
“Vital signs…can be very helpful for getting patients with cardiovascular and pulmonary
histories more visits (in outpatient) or an increased length of stay (inpatient).”
“Although my state…has restricted DA, I am a hospital-based PT and we are still bound
by a decades-old regulation called Title 22, which requires us to have Dr. Diagnosis and signed
plan of care. So, essentially in my setting, I cannot yet practice DA.”
“It is dangerous to not measure vital signs in each patient.”
“Physical therapists are part of the Professional Continuum of Care needed for providing
and achieving optimal patient care.”
“It is an essential part of good practice. In diabetic patients, I also ask for recent blood
glucose readings or ask the patient to test before exercise.”
“With a non-verbal population it is more than necessary to be able to constantly be
‘reading’ and being sensitive to physical cues via clinical observation, including but not limited to
the following: energy level fatigue…respiratory rate…respiratory pattern use of diaphragm, use
of accessory muscles, changes in lips, skin, fingers.”
“What about PTs reconciling meds like beta blockers? That is equally important as well.”
“Should be done but not sure some of the old dogs…me included will change willingly.”
“Temperature and respiration should be included. In direct access/primary care you will
encounter patients with infections that have Msk referral.”
“Find that many times the wrong size cuff is used or done to quickly to obtain accurate
information.”
“I see lots of young athletes. I do not regularly take a BP on these patients. When I see
older adults, I ALWAYS take BP.”
“Typical patient is a 0-3 year old child in a home or an older school child…training
parents/school staff on activities. Typically this does not warrant vital sign assessment. I do have
one baby with some heart issues and parents and I both watch vital signs closely.”
Related Documents