1 Name of journal: World Journal of Ophthalmology ESPS Manuscript NO: 9702 Columns: Title: Visual Outcome in Traumatic cataract in pediatric age group Short running head: Traumatic cataracts in children visual out come Authors: First Middle Last Degre Dr. Mehul A. Shah MD Dr. M. Shah MD Dr. Aarti H. Chaudhry DOMS Dr. R. Gupta DOMS Affiliations all authors: Drashti Netralaya, Dahod, Gujarat, India Address of corresponding author: Drashti Netralaya, Nr. GIDC, Chakalia Road. Dahod-389151 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
1
Name of journal: World Journal of Ophthalmology
ESPS Manuscript NO: 9702
Columns:
Title: Visual Outcome in Traumatic cataract in pediatric age
group
Short running head: Traumatic cataracts in children visual
out come
Authors:
First
Name
Middle
Name
Last
Name
Degre
eDr. Mehul A. Shah MD
Dr.
Shreya
M. Shah MD
Dr. Aarti H. Chaudhry DOMS
Dr.
Lalchand
R. Gupta DOMS
Affiliations all authors:
Drashti Netralaya, Dahod, Gujarat, India
Address of corresponding author:
Drashti Netralaya,
Nr. GIDC, Chakalia Road.
Dahod-389151
1
2
Gujarat
Ph: 00-91-2673-645364 Fax: 00-91-2673-221232
Email: [email protected]
No financial support received from any company or
institution
This study is not presented at any conference or meeting
Authors do not have any financial interest in any
aspect of this study
Author contributions:
Abstract
Objective: To review results of traumatic cataracts in
children.
Methods:
This is a retrospective cohort study .done at a tertiary eye
care center at the junction of Gujarat, Madhya Pradesh, and
Rajasthan states in central western India.
2
3
We enrolled children with specific inclusion criteria,
examined their eyes to review the co-morbidities due to
trauma, performed surgery for traumatic cataracts, and
implanted a lens, treating amblyopia if applicable. The
patients were re-examined 6 weeks postoperatively. We divided
the traumatic cataract cases into ‘open-globe’ (Group 1) and
‘closed-globe’ (Group 2) groups according to the ocular
trauma based on the Birmingham Eye Trauma Terminology System
(BETTS) and compared the determinants of visual acuity.
Result: Our cohort of 671 eyes with traumatic cataracts in
children included 544 eyes in Group 1 and 127 in Group 2. Six
weeks postoperatively, the visual acuity in the operated eye
was >6/60 in 450(82.7.%) and >/=6/12 215(39.4%) eyes in open
globe group and >20/200 in 127(81.8%) and >/=6/12 36 (28.4%)
eyes in Closed globe group (p = 0.143), and the difference
between the groups was not significant in children. Overall,
402 (39.4%) eyes gained >/=6/60 and >5/12 in 238 (35.4%)
cases. Surgical treatment caused significant difference in
3
4
visual outcome.(p=0.000) When we compared achieved visual out
come compared with ocular trauma score predicted vision.
Conclusions:
Satisfactory visual outcome can be achieved in children with
traumatic cataracts, no significant difference found amongst
open and closed globe injuries in pediatric age group
Ocular trauma score is validated tool to predict visual
outcome.
Key words: Traumatic cataract; pediatric cataract; BETTS;
OTS; Visual outcome;
Core tip: Traumatic cataract in pediatric age group may have
satisfactory visual outcome. Ocular trauma score is a
reliable predictor for visual outcome.
Introduction
Trauma is a cause of monocular blindness in the
developed world, although few studies have addressed the
problem of trauma in rural areas.(1) The etiology of ocular
injury likely differs from that in urban areas and is worthy
of investigation.(2-4) Any prevention strategy requires
knowledge of the cause of injury, which may enable more
4
5
appropriate targeting of resources toward preventing such
injuries. Both eye trauma victims and society bear a large,
potentially preventable burden, (3) as ocular injury in
children has a poor prognosis.
Ocular trauma can `cause cataracts.(1)The methods used
to evaluate the visual outcome in eyes managed for traumatic
and other cataracts are similar,(5) but the damage to other
ocular tissues due to trauma may compromise the visual gain
in eyes operated on for traumatic cataracts. Hence, the
success rates may differ between eyes with these two types of
cataract. Traumatic cataract has a poor visual outcome in
children because of amblyopia and recurrent inflammation.
The introduction of the Birmingham Eye Trauma
Terminology System (BETTS) into clinical practice
standardized the documentation of ocular trauma.(5)
Consequently, it would be interesting to study the visual
outcomes following traumatic cataract surgery and the
determinants predicting the outcome, especially in relation
to the BETTS. Visual outcomes of traumatic cataracts have
5

6
been reported in some cases.(6, 7) However, most reports
involved small samples or were case studies. Gradin et al.(7)
and Morgan et al.(8) reported series focusing on the primary
management of traumatic cataracts and perforating injuries.
In this study, we examined the visual outcomes following
cataract surgery in eyes sustaining injuries in children and
the predictors of satisfactory visual outcomes following the
management of traumatic cataracts in children. Our study was
conducted in a city located at the junction of the Indian
states of Gujarat, Madhya Pradesh, and Rajasthan.(11)
Qualified ophthalmologists at our institute provide low-cost
eye services mainly to poor people belonging to the tribal
population of 4.2 million in this area.
Patients and Methods
We obtained approval from the hospital administrators
and research committee to conduct this study and obtained the
parents’ written consent.
6
7
This was a retrospective study designed in 2002. All
traumatic cataracts in children (≤18 years old) in either eye
diagnosed and managed between January 2003 and December 2009
were enrolled in our study, and those consenting to
participate and not having other serious body injuries were
included. Their data were retrieved from the medical records
and compiled using a pretested online form.
For each patient enrolled in our study, we obtained a
detailed history including the details of the injury and
information on eye treatment and surgery performed to manage
past ocular trauma. Data for both the initial and follow-up
reports were collected using the online BETTS format of the
International Society Ocular Trauma. Details of the surgery
were also collected using a pretested online form. Ocular
trauma score was calculated.(9)
The cases of traumatic cataract were grouped as those
involving open-globe versus those involving closed-globe
injuries. The open-globe injuries were further categorized
into those with lacerations versus rupture. Lacerations of
7
8
the eyeball were subcategorized into eyes with perforating
injuries, penetrating injuries, or injuries involving an
intraocular foreign body. The closed-globe group was
subdivided into lamellar laceration and contusion.
The collected demographic details included patient
entry, residence, and activity at the time of injury, the
object causing the injury, and previous examinations and
treatments. After enrollment, all patients were examined
using a standard method. Visual acuity was checked according
to age using American Academy of Ophthalmology (AAO)
guidelines. The anterior segment was examined using a slit
lamp.
Based on lenticular opacity, the cataracts were
classified as total when an examiner did not observe clear
lens matter between the capsule and nucleus, membranous when
the capsule and organized matter were fused and formed a
membrane of varying density , a white soft cataract with a
ruptured capsule when loose cortical material was found in
the anterior chamber together with a ruptured lens capsule ,
8
9
and a rosette type cataract for a lens with a rosette pattern
of opacity . We could classify all of the cataract cases seen
with this classification. Morphology was influenced mainly by
the type, force, and object of injury and the time interval
between the injury and examination.
For a partially opaque lens, the posterior segment was
examined using indirect ophthalmoscopy and a +20 D lens. When
the optical medium was not clear, a B-scan was performed to
evaluate the posterior segment.
The surgical technique was selected according to
morphology and the condition of tissues other than the lens.
Phacoemulsification was used to operate on cataracts with
hard, large nuclei. With a lens that had either a white soft
or rosette type cataract, unimanual or bimanual aspiration
was used. Membranectomy and anterior vitrectomy, via either
an anterior or a pars plana route, were performed when the
cataract was membranous.
In all patients undergoing corneal wound repair, the
traumatic cataract was managed in a second procedure.
9

10
Recurrent inflammation was more prominent in patients who had
undergone previous surgery for trauma.(9, 10) In such cases,
when the ocular medium was hazy due to inflammation of the
anterior vitreous, we performed a capsulectomy and vitrectomy
via an anterior/pars plana route in adults.
In children younger than 2 years of age, both a
lensectomy and vitrectomy via a pars plana route were
performed, leaving the rim of the anterior capsule available
for secondary lens implantation, and the same surgical
procedures were used to manage the traumatic cataracts. Lens
implantation as part of the primary procedure was avoided in
all children younger than 2 years of age; these children were
rehabilitated with optical correction, and secondary
implantation was done after their second birthday. All
children received supportive amblyopia therapy from a
qualified pediatric orthoptist, and a pediatric
ophthalmologist treated strabismus.
All patients with injuries and without an infection were
treated with topical and systemic corticosteroids and
10
11
cycloplegics. The duration of medical treatment depended on
the degree of inflammation in the anterior and posterior
segments of the operated eye. The operated patients were re-
examined after 24 h, 3 days, and 1, 2, and 6 weeks to enable
refractive correction. Follow-up was scheduled for day 3,
weekly for 6 weeks, monthly for 3 months, and every 3 months
for 1 year.
At every follow-up examination, visual acuity was tested
according to age using the AAO guidelines. The anterior
segment was examined with a slit lamp and the posterior
segment with an indirect ophthalmoscope. Eyes with vision
better than 20/60 at the glasses appointment (6 weeks) were
defined as having a satisfactory grade of vision.
During the examination, data were entered online using a
pretested format designed by the International Society of
Ocular Trauma (initial and follow-up forms), which was
exported to a Microsoft Excel spreadsheet. The data were
audited periodically to ensure completion. We used the
Statistical Package for the Social Studies (SPSS 17) to
11
12
analyze the data. We used descriptive statistics and cross
tabulation to compare the cause and effect of different
variables. The dependent variable was vision >20/60 noted at
the follow-up 6 weeks after cataract surgery. The independent
variables were age, gender, residence, time interval between
the injury and cataract surgery, primary posterior
capsulectomy and vitrectomy procedure, and type of ocular
injury.
We have compared visual out come with predicted visual out
come and analyzed predictive value of predictive model.
Results
Our cohort consisted of 671 patients with traumatic
cataracts, including 544 (81.07%) eyes with open-globe ocular
injuries and 127 (18.9%) eyes with closed-globe injuries. The
patients included 496 (70.9%) males and 196 (29.2%) females.
The mean patient age was 10.53 ± 4.2 years (range 0–17)
(Table 1).
We analyzed several demographic factors, including
patient entry (p = 0.000), cases self-reported as having done
12
13
well (Table 2), socioeconomic status (79% were from lower
socioeconomic classes), and residence (95% were from rural
areas). None was significantly related to the visual acuity
six weeks. according to cross-tabulation and statistical
tests.
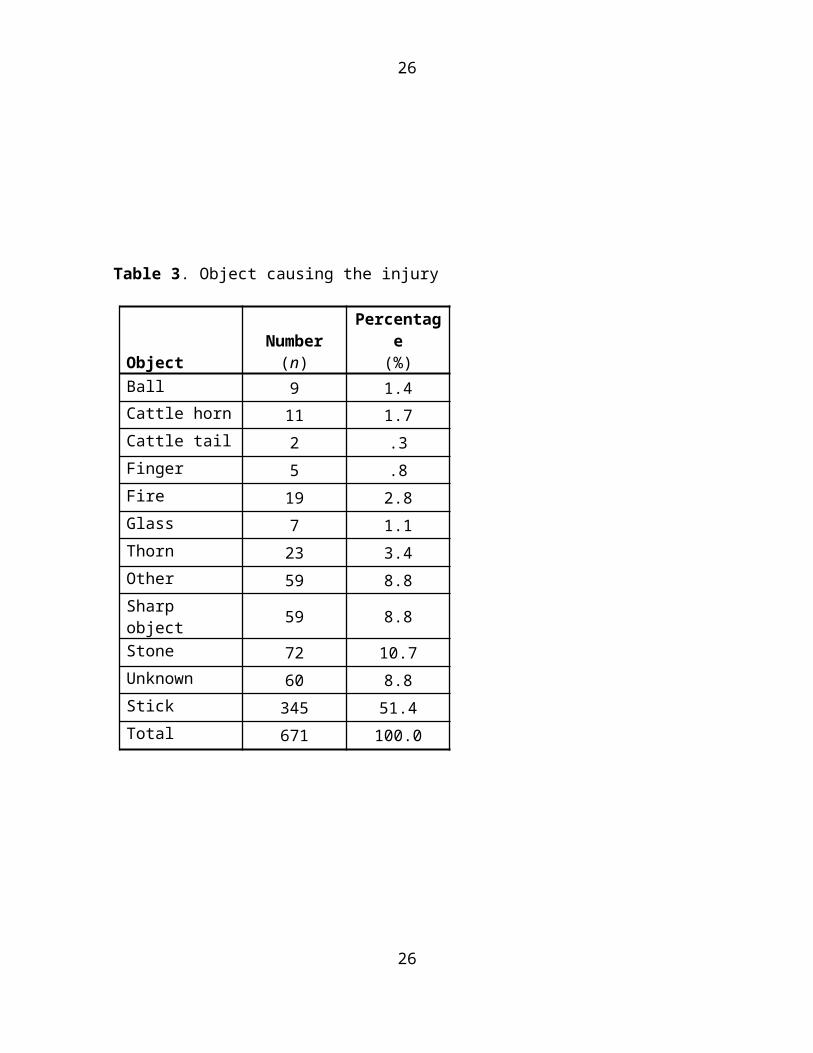
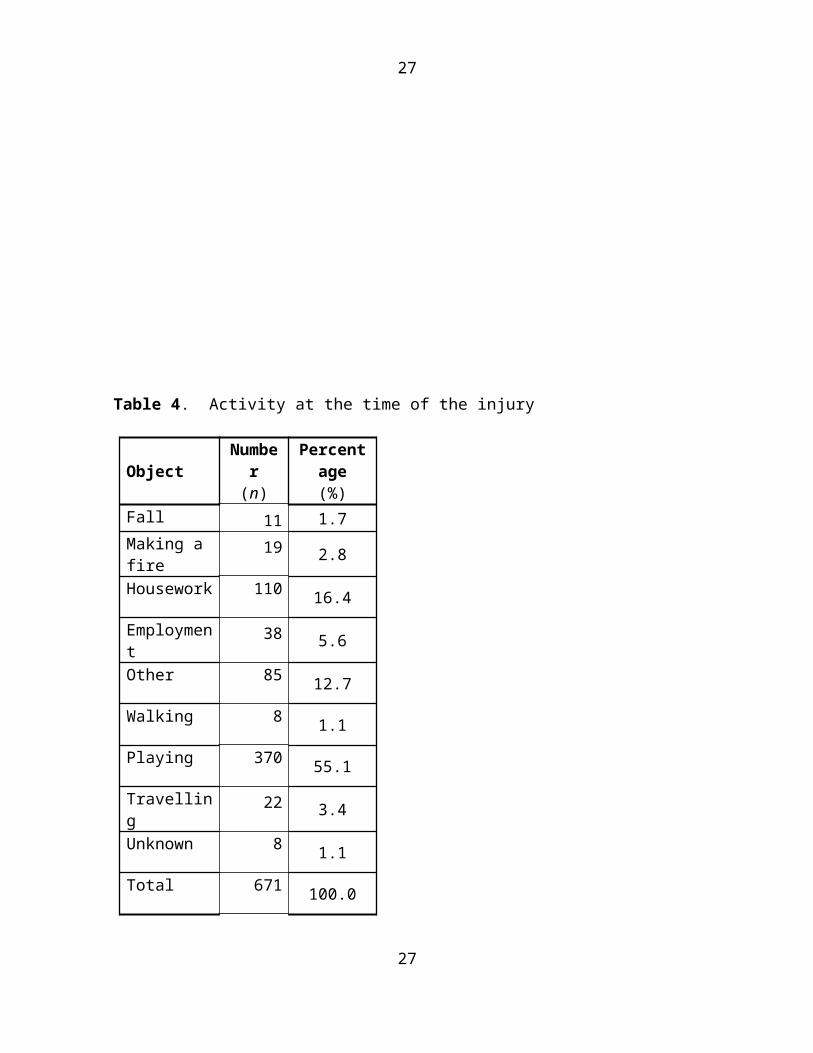
The object causing the injury ( Table 3) and the
activity at the time of the injury (p = 0.3; Table 4) were
also not significantly associated with a visual acuity at
six weeks. A stick was the most common agent of injury
(56.1%; Table 3). Better outcome was achieved in 5 years.
(Table-5)
A comparison of the pre- and postoperative visual acuity
showed that treatment significantly improved visual acuity
(Pearson’s χ2 test, p = 0.000; ANOVA, p = 0.001; Table
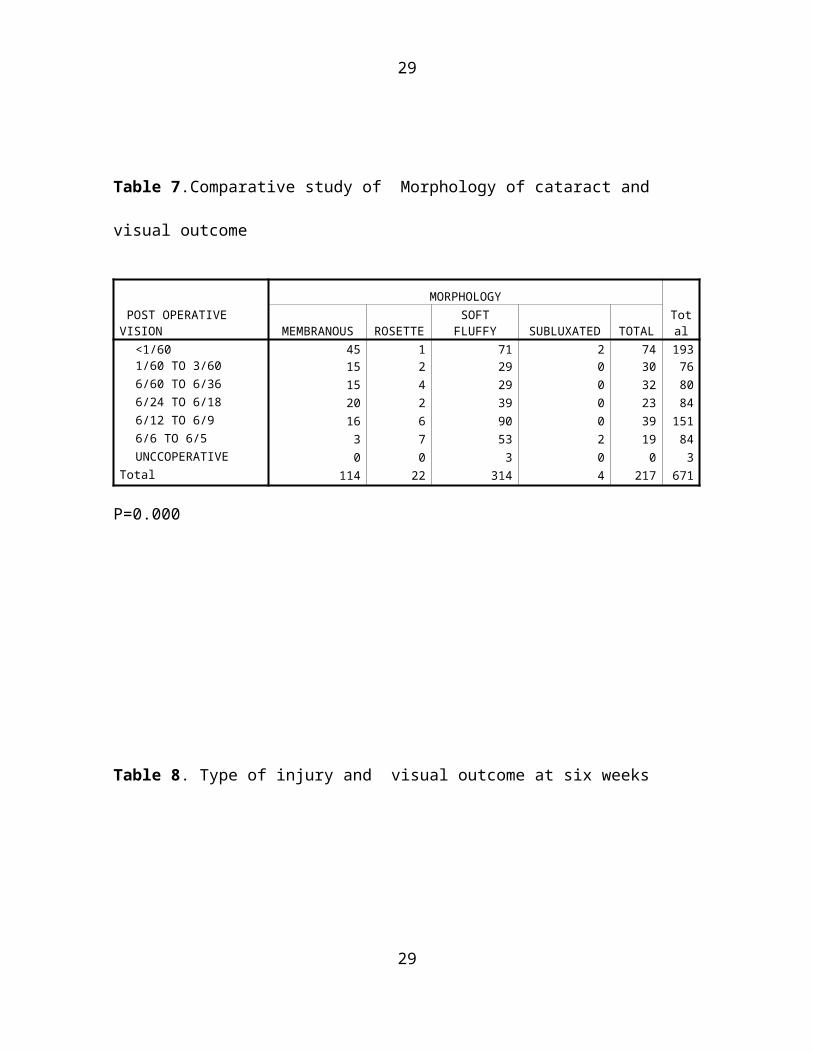
6)..Morphologically lens ruptured with soft material in
anterior chamber has done significantly better (Table-7)
Aspiration was significantly associated with improved visual
acuity (p = 0.000) and was performed using one or two ports in
48.6% of the patients in the open-globe group .
13
14
Primary posterior capsulotomy and anterior vitrectomy,
commonly performed for eyes with significant inflammation,
caused no significant improvement in the visual acuity
visual acuity at six weeks (p = 0.23).
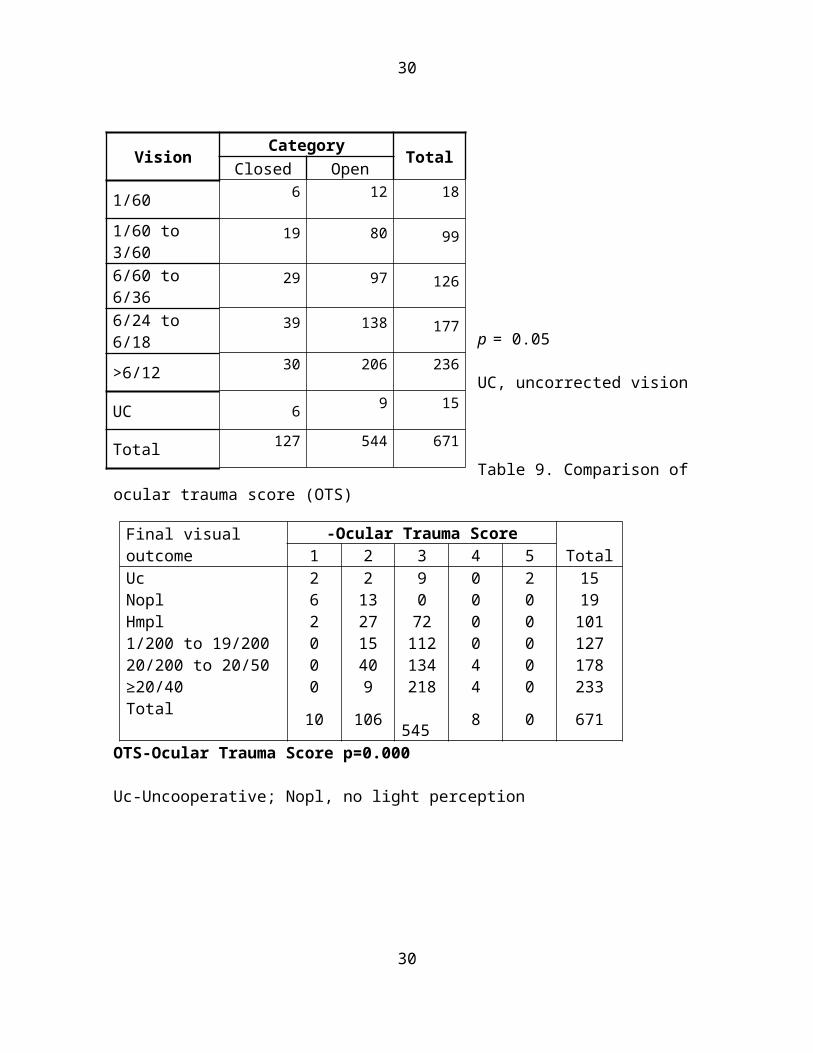
We also compared these variables in the open-globe and
closed-globe (Tables 8) according to BETTS.
Six weeks postoperatively, the visual acuity in the operated
eye was >6/60 in 450(82.7.%) and >/=6/12 215(39.4%) eyes in
open globe group and >20/200 in 127(81.8%) and >/=6/12 36
(28.4%) eyes in Closed globe group (p = 0.143), and the
difference between the groups was not significant in
children. Overall, 402 (39.4%) eyes gained >/=6/60 and >5/12
in 238 (35.4%) cases. Surgical treatment caused significant
difference in visual outcome.(p=0.000)
We implanted an intraocular lens in 82% of the cases,
90% of which was Poly methyl meth acrylate and 10% acrylic,
5 IOL subluxated or dislocated, Poly methyl meth acrylate
lenses used for secondary implant and 30% of the cases
underwent more than one operative procedure. Of the children,
14

15
30% reported within the first 24 hours of the injury. Time
interval between injury and intervention did not make
significant difference in outcome at six weeks .( p=0.172)
Follow up ranged between 45 days to 1076 days with mean
follow up 71.8 days. Three cases developed secondary
glaucoma.
The final visual outcomes according to the OTS
predictions in children with traumatic cataracts are
presented in Table 9,10 (P = 0.265, 0.22, 0.22, 0.172).
(Figure-1,2,3,4,)
Discussion
Visual gain following surgery for traumatic cataracts is
a complex problem. Electrophysiological (10) and radio-
imaging (11-13) investigations are important tools for
assessing the co-morbidities associated with an opaque lens.
Our study examined patients with open- and closed-globe
injuries who developed traumatic cataracts. A satisfactory
grade of vision following the management of traumatic
15
16
cataracts was significantly more frequent in the eyes with
open-globe injuries (Tables 6 and 7).
Various authors have reported different results in
children with traumatic cataracts: Shah et al.[4] reported
20/60 or better in 56% of their cases; Kumar [13] reported
6/18 or better in 50%; Staffieri, (14) 6/12 or better in 35%;
Bekibele, (15) 6/18 or better in 35.6%; Gradin, (7)20/60 or
better in 64.7% Brar,(17) 0.2 or better in 62%; Cheema, (18)
6/18 in more than 68% of their cases; Karim, (19) 0.2 or
better in 62%; Krishnamachary, (13) 20/60 or better in 74%;
Knight-Nanan, (20) 20/60 or better in 64%; Bienfait, (21) 0.7
in 27%; and Anwar (22) reported 20/40 or better in 73% of
their cases.
Using a polymethyl methacrylate (PMMA) lens, Verma (23)
reported a visual outcome similar to that found in our study.
Eckstein (24) and Zou(25) reported that primary intraocular
lens implantation is important for a better visual outcome,
similar to our results. Also similar to our results, Vajpayee
16

17
(26) and Gupta (27) reported primary insertion of an
intraocular lens with posterior capsule rupture.
Shah (28) reported that a better visual outcome was
achieved when intervention was done between 5 and 30 days in
adults with traumatic cataracts. As in our study, Rumelt (29)
found no significant difference between primary and secondary
implantation.
Staffieri (15) performed primary implantation in 62% of
cases versus 82% in our study. Kumar (14) and Verma (23)
advocated primary posterior capsulotomy and vitrectomy for a
better outcome; our results concurred.
We are not aware of any study that has compared the
visual outcome visual acuity at six weeks in children between
two groups classified using BETTS. Shah et al.(30) reported a
comparison between open- and closed-globe injuries in general
population. We are also not aware of another large series of
successfully treated traumatic cataracts in children.
In our study, final visual outcomes were achieved
according to the OTS 31 prediction in children with traumatic
17
18
cataracts. Although similar findings have been reported by
other 32,33,34, our study presents one of the largest reported
databases following cases of pediatric traumatic cataracts
classified according to BETTS. Despite the long time delay
between injury and treatment in many of the cases in our
study, the OTS was still relevant.
Lesniak and Bauza 32 reported no significant differences
between the final visual acuities and the visual acuities
predicted by OTS in children. Sharma 33 proposed that the OTS
calculated at the initial examination may be of prognostic
value in children with penetrating eye injuries. However,
Unver 34 suggested that OTS calculations may have limited
value as predictors of visual outcome in a pediatric
population. Lima-Gomez Hans and Unver 35 reported estimates
for a 6-month visual prognosis, but some of the variables
required evaluation by an ophthalmologist. Using the OTS,
98.9% of the eyes in the general population could be graded
in a trauma room. Knyazer 36 reported the prognostic value of
the OTS in zone-3 open globe injuries, and Man 37 claimed
18
19
equal prognostic effectiveness of both the OTS and CART in
the general population.
Conclusions:
Satisfactory visual outcome can be achieved in children with
traumatic cataracts, no significant difference found amongst
open and closed globe injuries in pediatric age group.
COMMENTS
Bibliography:
1. Khatry SK, Lewis AE, Schein OD, Thapa MD, Pradhan EK,Katz J, The epidemiology of ocular trauma in ruralNepal. Br J Ophthalmol.2004; 88:456-60.
2. Abraham DI, Vitale SI, West SI, Isseme I (1999) Epidemiology of eye injuries in rural Tanzania. Ophthalmic Epidemiol.1999;6:85-94
3. D. Virgil Alfaro, Eric P. Jablon, Monica Rodriguez Fontal, Simon J. Villalba, Robert E.Morris, Michael Grossman, Enrique Roig-Melo Fishing-related ocular trauma. American Journal of Ophthalmology.2005;139: 488-492
4. Shah M, Shah S, Khandekar R.(2008) Ocular injuries and
19
20
visual status before and after Their management in thetribal areas of Western India-A historical cohort studyGrafes Arch Clin Exp Ophthalmol. 2008;246:191–197.
5. Kuhn F, Morris R, Witherspoon CD, Mester V, TheBirmingham Eye Trauma Terminology system (BETT). J FrOphtalmol.2004; 27:206-10.
6. Zhang Y, Zhang J, Shi S. (1998) Determination ofposterior lens capsule status in traumatic cataract withB-Ultrasonography. Zhonghua Yan Ke Za Zhi.1998;34:298-299.
7. Gradin D, Yorston D. Intraocular lens implantation fortraumatic cataract in children in East Africa. JCataract Refract Surg.2001; 27:2017-25.
8. Morgan KS. Cataract surgery and intraocular lensimplantation in children. Curr Opin Ophthalmol.1993;4:54-60.
9. American Society of Ocular Trauma. Ocular trauma Score(OTS) http://www.asotonline.org/ots.html visited on10/12/2008.
10. Behbehani AM, Lotfy N, Ezzdean H, Albader S, Kamel
M, Abul N. open eye injuries in the pediatric population
in Kuwait. Med Princ Pract.2002;11:183
11. Segev Y, Goldstein M, Lazar M, Reider-Groswasser I
CT appearance of a traumatic cataract. AJNR Am J
Neuroradiol.1995;16:1174-1175.
20
21
12. McWhae JA, Crichton AC, Rinke M Ultrasound
Biomicroscopy for the assessment of zonules after ocular
trauma. Ophthalmology. 2003;110:1340-1343.
13. Krishnamachary M, Rathi V, Gupta S Management oftraumatic cataract in children. J Cataract RefractSurg.1997; 23:681-7.
14. Kumar, S., A. Panda, et al. Safety of primary intraocular lens insertion in unilateral childhood traumatic cataract. JNMA J Nepal Med Assoc 2008;47: 179-85.
15. Staffieri, S. E., J. B. Ruddle, et al. "Rock, paperand scissors? Traumatic paediatric cataract in Victoria 1992-2006." Clin Experiment Ophthalmol 38: 237-41.
16. Bekibele, C. O. and O. Fasina Visual outcome of traumatic cataract surgery in Ibadan, Nigeria. Niger J Clin Pract 2008; 11: 372-5.
17. Brar, G. S., J. Ram, et al. Postoperative complications and visual results in uniocular pediatric traumatic cataract. Ophthalmic Surg Lasers 2001;32: 233-8
18. Cheema, R. A. and A. D. Lukaris . "Visual recovery in unilateral traumatic pediatric cataracts treated withposterior chamber intraocular lens and anterior vitrectomy in Pakistan." Int Ophthalmol 1999;23: 85-9.
19. Karim, A., A. Laghmari, et al. Therapeutic and prognostic problems of traumatic cataracts. Apropos of 45 cases J Fr Ophtalmol 1998;21: 112-7.
20. Knight-Nanan, D., M. O'Keefe, et al. Outcome and 21
22
complications of intraocular lenses in children with cataract. J Cataract Refract Surg1996; 22: 730-6.
21. Bienfait, M. F., J. H. Pameijer, et al. Intraocularlens implantation in children with unilateral traumatic cataract. Int Ophthalmol 1990;14: 271-6.
22. Anwar, M., J. H. Bleik, et al. Posterior chamber lens implantation for primary repair of corneal lacerations and traumatic cataracts in children. J Pediatr Ophthalmol Strabismus 1994;31: 157-61.
23. Verma, N., J. Ram, et al. Outcome of in-the-bag implanted square-edge polymethyl methacrylate intraocular lenses with and without primary posterior capsulotomy in pediatric traumatic cataract. Indian J Ophthalmol 59: 347-51.
24. .Eckstein, M., P. Vijayalakshmi, et al. (1998). "Use of intraocular lenses in children with traumatic cataract in south India." Br J Ophthalmol 1998; 82: 911-5.
25. Zou, Y., W. Yang, et al.Primary posterior chamber intraocular lens implantation in traumatic cataract withposterior capsule breaks. Yan Ke Xue Bao 1995;11: 140-2.
26. Vajpayee, R. B., S. K. Angra, et al. Pre-existing posterior capsule breaks from perforating ocular injuries. J Cataract Refract Surg 1994;20: 291-4.
27. Gupta, A. K., A. K. Grover, et al. Traumatic cataract surgery with intraocular lens implantation in children. J Pediatr Ophthalmol Strabismus1992; 29: 73-8.
22

23
28. Shah MA, Shah SM, Shah SB, Patel UA. Effect of interval between time of injury and timing of intervention on final visual outcome in cases of traumatic cataract.Eur J Ophthalmol. 2011 Mar 24. pii:338AC21D-E9FB-42DF-9C28-6FDE61928C9D. doi: 10.5301/EJO.2011.6482. [Epub ahead of print]
29. Rumelt, S. and U. Rehany The influence of surgery and intraocular lens implantation timing on visual outcome in traumatic cataract Graefes Arch Clin Exp Ophthalmol 248(9): 1293-7.
30. Shah MA, Shah SM, Shah SB, Patel CG, Patel UA, Appleware A, Gupta A. Comparative study of final visual outcome between open- and closed-globe injuries following surgical treatment of traumatic cataract. Graefes Arch Clin Exp Ophthalmol. 2011 Jul 7. [Epub ahead of print]
31. Kuhn, F., R. Maisiak, The Ocular Trauma Score (OTS)." Ophthalmol Clin North Am 2001;15(2): 163-5
32. Lesniak, S. P., A. Bauza,Twelve-Year Review of Pediatric Traumatic Open Globe Injuries in an Urban U.S.Population." J Pediatr Ophthalmol Strabismus: 1-7.
33. Sharma, H. E., N. Sharma, Comment on a new ocular trauma score in pediatric penetrating eye injuries." Eye(Lond) 25(9): 1240.
34. Unver, Y. B., N. Acar.Visual predictive value of the ocular trauma score in children." Br J Ophthalmol 2008; 92(8): 1122-4.
35. Lima-Gomez, V., D. M. Blanco-Hernandez, et al. "Ocular trauma score at the initial evaluation of oculartrauma." Cir Cir 78(3): 209-13.
23
24
36. Knyazer, B., J. Levy.Prognostic factors in posterior open globe injuries (zone-III injuries)." ClinExperiment Ophthalmol 2008;36(9): 836-41.
37. Man, C. Y. and D. Steel "Visual outcome after open globe injury: a comparison of two prognostic models--theOcular Trauma Score and the Classification and Regression Tree." Eye (Lond) 24
24

25
Table 1 Age and sex distribution
SEX Tot
alF M0 to 2 6 7 13
3 to 5 27 52 79
6 to 10 74 17
9 253
11 to18 88 23
8 326
Total 195
476 671
Table 2. Patient entry and visual outcome at six weeks
Vision Entry Total Self ORD<1/60 19 0 191/60 to 3/60 68 30 986/60 to 6/36 74 53 1276/24 to 6/18 125 55 180>6/12 to 6/9 178 53 231Un cooperative 11 5 16Total 475 196 671
p = 0.000ORD, [Out reach department]
25
26
Table 3. Object causing the injury
ObjectNumber(n)
Percentage(%)
Ball 9 1.4Cattle horn 11 1.7Cattle tail 2 .3Finger 5 .8Fire 19 2.8Glass 7 1.1Thorn 23 3.4Other 59 8.8Sharp object 59 8.8
Stone 72 10.7Unknown 60 8.8Stick 345 51.4Total 671 100.0
26
27
Table 4. Activity at the time of the injury
ObjectNumber(n)
Percentage(%)
Fall 11 1.7Making a fire
19 2.8
Housework 110 16.4
Employment
38 5.6
Other 85 12.7
Walking 8 1.1
Playing 370 55.1
Travelling
22 3.4
Unknown 8 1.1
Total 671 100.0
27

28
Table 5. Age and visual outcome at six weeks
POST OPERATIVE VISION
Age categoriesTotal
0to2
3to5
6 to10
11 to18
<1/60 2 32 76 83 193 1/60 TO 3/60 1 3 37 35 76 6/60 TO 6/36 7 25 29 19 80 6/24 TO 6/18 1 8 35 40 84 6/12 TO 6/9 1 8 53 89 151 6/6 TO 6/5 1 2 21 60 84 UNCCOPERATIVE 0 1 2 0 3Total 13 79 253 326 671
P=0.000
Table 6. Pre-treat and post-treatment vision comparison
POST OPERATIVE VISION
PRE OPERATIVE VISIONTotal
<1/60
1/60 TO3/60
6/60 TO6/36
6/24 TO6/18
6/12TO 6/9 UNCCOPERATIVE
<1/60 182 4 6 0 1 0 1931/60 TO 3/60 70 5 1 0 0 0 766/60 TO 6/36 55 8 15 1 0 1 806/24 TO 6/18 71 10 2 1 0 0 846/12 TO 6/9 125 17 7 1 1 0 1516/6 TO 6/5 64 10 6 4 0 0 84UNCCOPERATIVE 2 0 0 0 0 1 3
Total 569 54 37 7 2 2 671
P=0.000
28
29
Table 7.Comparative study of Morphology of cataract and
visual outcome
POST OPERATIVE VISION
MORPHOLOGYTotalMEMBRANOUS ROSETTE
SOFTFLUFFY SUBLUXATED TOTAL
<1/60 45 1 71 2 74 1931/60 TO 3/60 15 2 29 0 30 766/60 TO 6/36 15 4 29 0 32 806/24 TO 6/18 20 2 39 0 23 846/12 TO 6/9 16 6 90 0 39 1516/6 TO 6/5 3 7 53 2 19 84UNCCOPERATIVE 0 0 3 0 0 3
Total 114 22 314 4 217 671
P=0.000
Table 8. Type of injury and visual outcome at six weeks
29
30
p = 0.05
UC, uncorrected vision
Table 9. Comparison of ocular trauma score (OTS)
Final visual outcome
-Ocular Trauma ScoreTotal1 2 3 4 5
Uc 2 2 9 0 2 15Nopl 6 13 0 0 0 19Hmpl 2 27 72 0 0 1011/200 to 19/200 0 15 112 0 0 12720/200 to 20/50 0 40 134 4 0 178≥20/40 0 9 218 4 0 233Total 10 106
545 8 0 671
OTS-Ocular Trauma Score p=0.000
Uc-Uncooperative; Nopl, no light perception
30
Vision Category TotalClosed Open1/60 6 12 18
1/60 to 3/60
19 80 99
6/60 to 6/36
29 97 126
6/24 to 6/18
39 138 177
>6/12 30 206 236
UC 6 9 15
Total 127 544 671

31
Table 10. Comparison of final visual outcome according to
ocular trauma score (OTS)
Table 10. Comparison of final visual outcome according to ocular trauma score (OTS)
OTS-1 OTS-2 OTS-3 OTS-4VisionCategory
Achieved
FinalVisualAcuity
OTSPredictedFinalVisualAcuity
Achieved
FinalVisualAcuity
OTSPredictedFinalVisualAcuity
Achieved
FinalVisualAcuity
OTSPredictedFinalVisualAcuity
Achieved
FinalVisualAcuity
OTSPredictedFinalVisualAcuity
Nopl
75 73 12 16 0 2 0 1lphm
25 17 25 26 13.5 11 0 21/200to19/200
0 7 14 14 21.3 15 0 220/200to
20/500 2 38 38 24.5 28 50 21
>/=20/40 0 1 00 4 40.5 44 50 74P value P = 0.265 P = 0.220 P = 0.220 P = 0.172
Values are percentage of cases. Nopl, no light perception
Legends:
Figure Legends
31

32
Fig. 1: Comparison between OTS and achieved results in OTS-1
score category.
Fig. 2: Comparison between OTS and achieved results in OTS-2
score category.
Fig. 3: Comparison between OTS and achieved results in OTS-3
score category.
Fig. 4: Comparison between OTS and achieved results in OTS-4
score category.
The English in this document has been checked by at least two
professional editors, both native speakers of English. For a
certificate, please see:
http://www.textcheck.com/certificate/4e2LWD
32

33
figure 1
33
34
figure 2
figure 3
34

35
Figure 4
35
Related Documents











