Our digital editions give you two unique ways to view content. The “Full Screen” option makes it easy to flip through and read each spread while the “Fit to Screen” option gives you the ability to scan thumbnails of multiple pages at once, run content searches and more. VIEW FULL SCREEN Click on the “View Full Screen” button to enlarge the digital edition to full size. All of your controls will be shown at the bottom of the page. Bottom Left • Print Page: Allows you to select specific pages or print the entire digital edition. • Fit to Window: Returns you to your original view with the navigation bar on the left. • Table of Contents: Automatically takes you to the issue’s table of contents. Bottom Right • Magnifying Glasses: Enable you to zoom in or out. • Arrows: Take you to the previous page or the next page. • Go to Page: Prompts you to enter the number of the page you want to view. • Subscribe: Takes you to a secure site where you can sign up for your FREE subscription. FIT TO WINDOW In this view, the “Fit to Window” button will be replaced with the “View Full Screen” button. You’ll also have a navigation bar on the left side of the screen. Left Navigation Bar • Pages: Features a thumbnail of every page. Click on one of the thumbnails to go directly to that page. • Bookmarks: Includes important pages that have been bookmarked. Click on one of the bookmarks to go directly to that page. • Search: Allows you to enter a word or phrase and search the digital edition for it. • How To: Offers supplementary documents with helpful tips and information. INTERACTIVE FEATURES • Ads and Advertiser Index: Click on any advertisement or any company listed in our comprehensive advertiser index to visit their website. • Table of Contents: Click on any listing in the table of contents to be take directly to the article.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Our digital editions give you two unique ways to view content. The “Full Screen” option makes it easy to flip through and read each spread while the “Fit to Screen” option gives you the ability to scan thumbnails of multiple pages at once, run content searches and more.
View Full ScreenClick on the “View Full Screen” button to enlarge the digital edition to full size. All of your controls will be shown at the bottom of the page.Bottom Left• Print Page: Allows you to select specific pages or print the entire digital edition.• Fit to Window: Returns you to your original view with the navigation bar on the left.• Table of Contents: Automatically takes you to the issue’s table of contents.
Bottom Right• Magnifying Glasses: Enable you to zoom in or out.• Arrows: Take you to the previous page or the next page.• Go to Page: Prompts you to enter the number of the page you want to view.• Subscribe: Takes you to a secure site where you can sign up for your FREE subscription.
Fit to windowIn this view, the “Fit to Window” button will be replaced with the “View Full Screen” button. You’ll also have a navigation bar on the left side of the screen.
Left Navigation Bar
• Pages: Features a thumbnail of every page. Click on one of the thumbnails to go directly to that page.
• Bookmarks: Includes important pages that have been bookmarked. Click on one of the bookmarks to go directly to that page.
• Search: Allows you to enter a word or phrase and search the digital edition for it.
• How To: Offers supplementary documents with helpful tips and information.
interactiVe FeatureS• Ads and Advertiser Index: Click on any advertisement or any company listed
in our comprehensive advertiser index to visit their website.
• Table of Contents: Click on any listing in the table of contents to be take directly to the article.

1ADVANCE for NPs & PAs • November 2011

Higher Cell Count Florajen3 contains over 15 billion living probiotic cells per capsule. Some other leading brands have as few as one billion or less.
Continuous Refrigeration Sustained potency requires refrigeration. Probiotics are living organisms. If they are on the store shelf at room temperature, the cells are being damaged and are slowly dying.
Superior Formulation Florajen3 contains three clinically proven safe bacterial strains, including essential Bifi dobacteria. Unlike many other leading brands, Florajen3 is made exclusively in the USA.
Most Affordable At $14.95 for a one month supply, Florajen3 is a far better value than other leading brands—delivering more culture at a fraction of the cost.
Our Founder and Chief Bacteriologist, David Sullivan, invites you to see for yourself how effective high potency Florajen3 can be for your patients.
©2011 American Lifeline, Inc. All rights reserved. 1011
Statements have not been evaluated by the Food and Drug Administration. This product is not medicinal and is not intended to diagnose, treat, cure or prevent any disease.
Choose a probiotic worthy of your recommendation
For over 20 years, Florajen3® has been your best choice for antibiotic side effects and digestive and vaginal health.
The Most Effective and Affordable
Probiotics AvailableProbiotics Available
Available in pharmacists’ refrigerators nationwide
High Potency Probioticswww.fl orajen.com Culture You Can Count On™
For Free Sample Packs to get your patients started, call 1-800-257-5433 or visit fl orajensamples.com!
2 November 2011 • ADVANCE for NPs & PAs

Online: www.advanceweb.com/nppa (Once on site, subscribe by clicking on the top right corner)
Phone: 800-355-1088 Or, just snap the tag to the right!
If you like this magazine and want to make sure you keep getting it, please check your
subscription label on the front cover now. You may need to officially request a subscription or
renew your subscription, EVEN IF YOU ALREADY RECEIVE THE MAGAZINE. And if you’ve
requested the magazine in the past, it might be time to renew that subscription.
Tell us you like us. Let us know our hard work is making a difference in your career.
Our magazine needs your subscription!
Contact us NOW for your FREE print and/or digital subscription!
Subscribe right now if you this
free Magazine!
3ADVANCE for NPs & PAs • November 2011

4 November 2011 • ADVANCE for NPs & PAs
Copyright 2011 by Merion Matters. All rights reserved. Reproduction in any form is forbidden without writ-ten permission of publisher. ADVANCE for NPs & PAs (ISSN 1096-6293) is published monthly by Merion Publications, Inc., 2900 Horizon Drive, Box 61556, King of Prussia, PA 19406-0956.
ADVANCE is free to certified nurse practitioners and physician assistants and students with senior status. Our company also publishes magazines and websites for audiologists, laboratory administrators, health executives, health information professionals, imaging and radiation oncology professionals, long-term care
managers and professionals, medical laboratory professionals, nurses, occupational therapy practitioners, physical therapy and rehabilitation professionals, respiratory care and sleep professionals, and speech-language pathologists.
ADVANCE is a member of the National Association for Health Care Recruitment.
Periodicals Postage Paid at Norristown, PA and additional mailing offices. Postmaster: send address changes to: ADVANCE for NPs & PAs, Circulation Department, Merion Publications, Inc., 2900 Horizon Drive, Box 61556, King of Prussia, PA 19406-0956.
ADVANCE for NPs & PAs is the official publication of the Association of Family Practice Physician Assistants.
Advertising Policy: All advertisements sent to Merion Publications Inc. for publication must comply with all applicable laws and regulations. Recruitment ads that discriminate against applicants based on sex, age, race, religion, marital status or any other protected class will not be accepted for publication. The appearance of advertisements in ADVANCE Newsmagazines is not an endorsement of the advertiser or its products or services. Merion Publications does not investigate the claims made by advertisers and is not responsible for their claims.
33 Shoulder ChondrolysisDespite advances in arthroscopic shoulder surgery, significant chal-lenges remain, including chondro-lysis. Kimberly Baird, NP, CNOR, and Kevin M. Kaplan, MD, explain presentation and management.
37 Back to the Beginning
In the late 1950s, before the first NP program and before the first PA pro-gram, Thelma Ingles, RN, and Eugene
A. Stead Jr., MD, teamed up to create the first attempt at an advanced nursing curriculum. This historical account of the program and its impact includes the first publication of excerpts from Ingles’ unpublished memoir.
November 2011 • Volume 2, Issue 11
Here&Now
25 Opioids and the Endocrine SystemDependency and abuse aren’t the only concerns associated with opioids. Long-term use is linked to endocrine alterations including hypogonadism. In this CME/CE article, William Shane Woodall, PA-C, summarizes pain management approaches that minimize endocrine dysfunction.
29 Inflammatory Arthritis and BacteriaThe treatment of inflammatory arthritis typically focuses on symptom control rather than the potential cause of the disease. Could an infectious process be the root of the problem for some patients? Sonja Huebner Wright, MSN, FNP, CEN, offers a pragmat-ic approach to assessment.
Articles20 Type 1 Diabetes and PregnancyWomen with type 1 diabetes can have healthy pregnancies, but to avoid complications, preconception planning is vital. Lauren B. Sosdorf, ARNP, MSN, PNP-BC, outlines the clinical challenges — and the need for a multidisciplinary team of healthcare providers to follow patients from preconception to delivery. (Cover image by Jeffrey Leeser/Ruth Black/iStockphoto/Thinkstock and Doris Mohr)
Columns & Departments First & Foremost . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Front & Center . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Career & Workforce. . . . . . . . . . . . . . . . . . . . . . . . . . . . 17Role & Growth. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Money & Health . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Quick Care Tips. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Calendar . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40Ad Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45Career Opportunities. . . . . . . . . . . . . . . . . . . . . . . . . . . 50Murmurs & Gallops. . . . . . . . . . . . . . . . . . . . . . . . . . . . 66
2925
®
Plea
se Recycle This Magazine

Soothe & Moisturizewith Xlear Nasal Spray
XYLITOLmade with all-natural
Xylitol is a five carbon polysacharide that occurs
naturally in virtually all fruits and vegetables.
Xylitol offers powerful oral and upper respiratory
health benefits.
Xlear (pronounced “clear”) is the only saline
nasal spray with Xylitol, clinically proven to
reduce airborne contaminants in the upper
respiratory tract while soothing and moisturizing
the sinuses and nasal passages. Great for kids
and grown-ups.
Learn more about Xylitol and its healthybenefits at xylitol.org or at r xlear.com
VISIT US AT:To order or find a location near you
www.xlear.com
Want FREE SAMPLES for the office? Call us at: 1.877.599.5327
5ADVANCE for NPs & PAs • November 2011

6 November 2011 • ADVANCE for NPs & PAs
advanceweb.com/NPPANow at
Celebrating Nurse Practitioners!Happy NP Week 2011! ADVANCE for NPs & PAs is proud to honor the
approximately 150,000 NPs who contribute so much to our healthcare
system. Read historical highlights, profiles and more in our NP Resource
Center. In this dedicated section, you’ll also find conference coverage,
salary information and an area devoted to NP students.
November 13-19
Read This Issue Online!➼ Did you know that you can read this entire issue in digital form at our website? Look for the cover image in the right upper corner of the site, then click “View Digital.”
Environmental Asthma TriggersWe are proud to partner with the Association of
Clinicians for the Underserved to present this
month’s webinar on controlling environmental
asthma triggers in at-risk populations. Join us on
Nov. 16 from 3 p.m. to 4 p.m. Eastern time for this free presentation. Space
is limited, so register now at www.advanceweb.com/NPPAwebinars.
All About SkinStay tuned for a new specialty
section of our website focused
on dermatology and aesthetics.
This section will feature a range
of articles on skin care and skin
diseases. We’ll introduce blogs
by NP and PA specialists in these
fields, as well as articles and
other information. Whether you
practice in these specialties
or just want the latest skin
news, visit the section at www.
advanceweb.com/NPPAderm.Murmurs & Gallops Memories
We’ve collected 12 months of
Murmurs & Gallops in an easily
viewed and printed package. From
myth-busting to mirth, this unique
column has served up topics that
generate great conversation. Type
“Murmurs” in our search box.
Schiff®, the maker of Move Free®, is proud to support the Arthritis Foundation’s efforts to help
people take control of arthritis. For information about arthritis, contact the Foundation at
800-568-4045 or www.arthritis.org
Move Free® Advanced starts comforting sore joints in less than 7 days.1 The clinically tested premium formula in Move Free® Advanced actually helps improve joint health.
1 Independent human clinical study (Los Angeles, 2008).
* Internet survey participants were provided with information about Move Free® Advanced. Commissioned by Schiff Nutrition, 2010.
© 2011 Schiff Nutrition Group, Inc.
THESE STATEMENTS HAVE NOT BEEN EVALUATED BY THE FOOD AND DRUG ADMINISTRATION. THESE PRODUCTS ARE NOT INTENDED TO DIAGNOSE, TREAT, CURE OR PREVENT ANY DISEASE.
FREE SAMPLES
of Move Free ® Advanced
to give to your patients.
Call 1-800-439-8040 (8-5 MST M-F) or visit
www.MoveFreeSample.com to request your samples today!
9 out of 10 Nurse Practitioners and Physician Assistants would recommend Schiff® Move Free® Advanced to their patients and colleagues
556-E1
7ADVANCE for NPs & PAs • November 2011
8 November 2011 • ADVANCE for NPs & PAs
PUbLIsheRAnn Wiest Kielinski
GeNeRAL MANAGeRW. M. “Woody” Kielinski
eDITORIAL sTAffEditor: Michelle Perron Pronsati Editor: Michael GerchufskySenior Associate Editor: Jennifer FordWeb Manager: Jennifer Montone
DesIGNVice President, Director of Creative Services: Susan Basile Design Director: Walt SaylorArt Director: Doris MohrMultimedia Director: Todd Gerber
ADVeRTIsINGDirector of Marketing Services: Christina Allmer Art Director: Chris Wofford
eVeNTsPublic Relations Director: Maria Senior Job Fair Manager: Laura SmithEvents Product Manager: Mike Connor
ADMINIsTRATIONVice President, Director of Human Resources: Jaci Nicely Vice President of Business Technology Operations: Joe RomelloInformation & Business Systems Director: Ken Nicely Circulation Manager: Maryann Kurkowski Billing Manager: Christine MarvelSubscriber Services Manager: Vikram Khambatta
MeDIA & MARkeTING OPPORTUNITIes Display Advertising Sales Director: Amy TurnquistManager of Custom Communications and Marketing Services: Shannon Coghlan ReissNational Account Executive: Shannon Ferguson Senior Account Executive: Andrea O’BrienSales Associate: Andrew Reynolds
healthcare facility AdvertisingGroup Managers: Michael Maisel, Robert Murray, Dan Stuart
Education AdvertisingSales Manager: Ed ZetoAccount Executive: Brock BamberSales Associates: Sarah Rucinski, Ashley Wayne
CUsTOM PROMOTIONsSales Manager: Mike KerrSenior Account Executives: Noel Lopez, Sue Borjeson-RomanoSales Associates: Kristen Erskine, Desirae Slaugh, Leah Stashko, Gina Willett
is published by Merion MattersPublishers of leading healthcare magazines since 1985.
how to Contact Us• for a fRee subscription: Call (800) 355-1088 or
sign up at www.advanceweb.com/NPPA
• To reach the editors: Michelle Perron Pronsati, mpronsati@
advanceweb.com or (800) 355-5627, Ext. 1221
Michael Gerchufsky, mgerchufsky@ advanceweb.com or (800) 355-5627, Ext. 1213
• To reach the senior associate editor and website editor:
Jennifer ford, [email protected] or (800) 355-5627, Ext. 1384
• To order article reprints: (800) 355-5627, Ext. 1446
• To place an advertisement (display, calendar or recruitment): (800) 355-5627, Ext. 0
ADVANCE for NPs & PAsMerion Matters • 2900 Horizon Dr.King of Prussia PA 19406
The Editor Recommends …➼ With National NP Week coming this month, and PA Week still fresh in mind, it’s a perfect time to read up on the state of both professions today from the historical and workforce perspectives. Download a free compendium of essays by healthcare workforce expert James F. Cawley, MPH, PA-C, that have appeared in ADVANCE over the last 8 years. To locate the package, enter “Cawley Collection” in the Search Articles box at www.advanceweb.com/NPPA.
First&Foremost
As we ReCOGNIze nurse practitioners’ vast contributions to Americans’ health during National NP Week, there’s no better time to reflect on how NPs have become such an indispensable healthcare force. How has something as arche-typal as a nurse — a concept that literally has been around since the dawn of human history — been improved upon so profoundly, and only in the last handful of decades?
As you’ll read in this issue’s article, “Back to the Beginning,” much of that question is answered in the as yet unpublished memoir of a remarkable nurse named Thelma Ingles. She and physician Eugene A. Stead Jr. in 1958 established a short-lived
MSN program at Duke that laid the groundwork for both the PA and NP professions. The program came 7 years before NP pioneer Loretta Ford, along with Dr. Henry K. Silver, founded the first NP program at the University of Colorado in 1965.
Here’s an intriguing snippet of Ingles’ memoir:“We came out with the idea that the nurse was qualified to do a great many things
in patient care that had not been seen as part of her role. … We even went so far as to project into the future that we were going to … [work] in the clinic as responsible individuals in care, that patients would be told to come in and see ‘the nurse.’ And she would be paid a per-visit call same as the doctor. … We saw her as having much greater input into the diagnosis and treatment and follow-up than had ever been done.”
Do you think Ingles was on to something 50-some years ago?In this issue’s “Murmurs & Gallops” column, we salute NPs with a historical time-
line of the profession. As I scoured the literature researching the piece, I whiled away hours as I came across document after fascinating document describing relatively unheralded NP accomplishments. It wasn’t easy finding many historical accounts of NPs’ development, and that led me to wonder about how much of the profession’s chronicles, like Thelma Ingles’ memoir, remain unpublished or uncataloged, with many descriptions and accounts residing only in private collections — or worse, only in the unrecorded memories and experiences of the profession’s trailblazers.
The Society for the Preservation of Physician Assistant History was founded at Duke in 2001 to foster the preservation, study and presentation of PA history and achievements. In the spirit of cooperation evinced by Ingles and Stead more than five decades ago, it’s time for a similar charge to be taken up among NPs, before so many illuminating, inspiring and instructional historical accounts are lost forever.
We at ADVANCE are honored to have even a small role in proclaiming and furthering the NP cause, and we wish happy NP Week 2011 to nurse practitioners everywhere! ■
—Michael Gerchufsky
Happy NP Week 2011!

99 Hudson Street, 12th Floor
New York, NY 100132815
Tel: 18002214904
Email: [email protected]
VISA/MasterCard
www.NPSecure.com
NPSecure®
Because Your Own Malpractice Policy Is Your Best Protection.
n Competitive Premiums
n Occurrence Policy Available In 50 States
n Portable, Seamless Protection Wherever You Work Or Volunteer
n No Conflict Of Interest In The Event Of A Claim Involving Multiple Providers
n Coverage For All Specialties IncludingHigh Risk Classes
n Employed, SelfEmployed & StudentCoverage Options
n HIPAA Coverage
n License Protection Coverage
n Defense Expenses Coverage
AdvPANP 8.10.11_AdvPA[CMF]3.16.10 8/10/11 4:50 PM Page 1
9ADVANCE for NPs & PAs • November 2011

10 November 2011 • ADVANCE for NPs & PAs
Front&CenterAAPA Names Jennifer Dorn as New CeOThe AMeRICAN ACADeMy of Physician Assistants has announced that Jennifer L. Dorn will become the organization’s chief executive officer on Oct. 31. Dorn takes the helm from interim CEO James Potter, who stepped into the position in January after the abrupt resignation of Bill Leinweber.
Dorn is now a senior fellow at the Potomac Research Group, a research firm providing Washington policy and market technical analysis to institutional investors. Before that, she had been president and CEO of the National Academy of Public Administration, a nonprofit organization dedicated to improv-ing the management of government.
“With nearly 30 years of management experience, Dorn has led multibillion dol-lar federal agencies, as well as startups and well-established nonprofit organizations,”
according to a Sept. 26 AAPA press release issued to announce the hiring. Dorn’s long resume includes four presidentially appointed senior government leadership posts: U.S. representa-tive on the Board of Directors of the World Bank, administra-tor of the Federal Transit Administration, assistant secretary
for policy at the Department of Labor, and associate deputy secretary of the Department of Transportation. She also has served as senior vice president of the American Red Cross and as president of the National Health Museum.
Dorn will be the first woman at the helm of the AAPA, at a time when the PA profession’s demographics have shifted from being nearly all men in the late 1960s and 1970s to becoming predominantly women today — in fact, 3 of 4 graduating PA students today are women. The CEO oversees all academy operations, including having fiscal oversight, and reports to the AAPA Board of Directors to develop and execute the academy’s programs and to advance the PA profession.
“Jenna is an experienced CEO with a proven track record of results. The board was impressed not only by her broad experience in national nonprofits and government, but also with her passion for our mission,” said AAPA president Robert Wooten, PA-C.
After Leinweber’s departure, a search committee chaired by Lawrence Herman, RPA-C, with assistance from execu-tive recruitment firm Spencer Stewart, recommended several candidates. The board chose Dorn unanimously.
Dorn has her work cut out for her. “We need someone to fill the (CEO) position who’s progressive and motivated for
by Jennifer ford, Michael Gerchufsky and Michelle Perron Pronsati
News for NPs & PAs
DNP Conference focuses On Healthcare PolicyNew ORLeANs — The number of DNPs is on the rise, and so is their enthusiasm. This was evident at the 4th National Doctors of Nursing Practice Conference held here in late September. Attendance was nearly four times as high as it was in the conference’s first year, maxing out at its capacity of 360 attendees. Dozens of presentations and posters were available, and attendees heard keynote presentations from nurses who hold prestigious national posts. The conference focused heavily on teaching DNP graduates how to translate their knowledge into healthcare policy changes to improve healthcare quality in the United States.
The conference keynote speaker, Diana Mason, PhD, RN, FAAN, is codirector of the Center for Health, Media and Policy at Hunter College in New York City and president-elect of the American Academy of Nursing. She emphasized teamwork in healthcare. “This is nursing’s time” to be
key agents of change in healthcare, she declared. But it’s not just about nurses. She said nurses should also partner with physician assistant groups.
Kathleen M. White, PhD, RN, NEA-BC, FAAN, senior adviser for the Health Resources and Services Administration’s National Center for Health Workforce Analysis, also called on attendees to get
involved in healthcare policy. “We are lost in translation efforts,” she said.
David O’Dell, DNP, FNP-BC, cofounder of Doctors of Nursing Practice, LLC, the host of the conference, said the organization plans to expand the event next year. The 2012 Doctors of Nursing Practice conference will be in St. Louis Sept. 19–21.
Jennifer Dorn brings decades of experience to the AAPA’s helm.
Teri Bunker, MS, FNP, past ADVANCE NP Entrepreneur of the Year winner, with her poster on practice ownership.
JEN
NIF
ER F
ORD
Cour
tesy
of th
e AA
PA

11ADVANCE for NPs & PAs • November 2011
change, and who’ll place PAs in the limelight as one of the three groups of healthcare providers in America,” AAPA then-president Patrick Killeen, PA-C, told ADVANCE after Leinweber’s departure. “The PA profession needs to continue to go forward, and as such, the academy remains committed to its strategic plan.”
Leinweber took the helm of the academy Feb. 25, 2008, and immediately declared “a new day” for the AAPA. During his tenure, the academy launched several significant initiatives, including a far-reaching strategic plan.
While stepping in as CEO, Potter retained his role as senior vice president for advocacy and government relations. An AAPA spokesperson told ADVANCE that at least in the short term, Potter will stay on in that capacity. Potter joined the AAPA in January 2010; before that, he had directed government relations and public policy at the American Speech-Language-Hearing Association and had worked for the American College of Radiology and the American Medical Association.
ACNP hosts Virtual Lobby Day to Advocate for NPs at Annual ConferenceDeNVeR — The 13th annual conference of the American College of Nurse Practitioners (ACNP) pledged to equip nurse practitioners to “shape policy and improve practice,” and it appeared to deliver just that for 1,100 conference attendees.
Many of the NPs were attending an ACNP conference for the first time, and they had their choice of dozens of posters on a variety of clinical topics. From heart failure to opioid prescribing to proton therapy targeting tumors, clinical ses-sions were available in abundance. A lively exhibit hall of more than 50 exhibitors connected NPs with universities, clinical resources and potential employers.
In addition to providing many hours of continuing education, the conference organizers encouraged political action. At the opening session, lobbyist Dave Mason reminded NPs that although he’s working hard to educate legislators about nurse practitioners and the issues that are important to the profession, “The only way I can do my job is if legislators hear from their constituents: you.”
To help accomplish that goal, ACNP hosted a Virtual Lobby Day during the conference. The organization set up phones that were directly connected to the Capitol switchboard, so that attendees could call their legislators directly and ask them for support of HR 2267/S 227,
a bill to allow NPs to order home healthcare.Also at the conference, past ACNP president Susan Apold,
RN, ANP-BC, PhD, reported on her involvement in a physician–nurse practitioner meeting to discuss the Institute of Medicine’s 2011 report on the future of nursing. During the event, the two groups addressed topic areas of disagreement. She described the meeting, which was convened by the Robert Wood Johnson
Front&Center
Dave Mason, lobbyist for nurse practitioners, asked NPs to contact legislators in support of the home health bill.
.
For over 25 years, Women’s International Pharmacy has provided quality service to practitioners and their patients in the area of bioidentical hormone therapies. Partnering with us ensures your patients of receiving the highest quality medications and customer care. We Are Your Reliable Source for information in prescribing bioidentical hormonetherapies – confidently. We have consulting pharmacists available forquestions concerning hormone-related therapies, including specific dosagesand/or formulations.
Customized Information Packet. Call us today to receive educational information along with bioidentical hormone abstracts and dosing charts for practitioners. You may also go online to www.womensinternational.com/advance to obtain information and/or request the complete information packet. Or call 800-279-5708 today to request your information packet.
When requesting this information, please mention Advance for NPs & PAs.
Custom Compounding With Our Personal Touch
Is the Compounding Pharmacy of Choice for Bioidentical Hormone Therapies!
JEN
NIF
ER F
ORD

register for this exciting event today!
www.advanceweb.com/nppa
FREE ADVANCE WEbiNAr
SPONSORED BY:
Ellen Battista, dns, anP, PnP directorPain treatment consultants of Western new yorkBuffalo, ny
F E at u R E d S p E a k E R :
Dialogues in PHN: NPs & PAs discussing a therapeutic approach for the relief of
pain of post-herpetic neuralgia Thursday, October 27 • 1:00 PM ET (10:00 AM PT)
REgistER Now!
this peer-to-peer promotional webinar uses dialogue to provide nPs and Pas with the knowledge to help recognize post-herpetic neuralgia (Phn) and to illustrate how asking specific questions may assist you in your diagnosis. in addition, the speaker will discuss a prescription treatment option for Phn.
the speaker will also be taking part in an interactive Q&a session to answer your questions regarding Phn.
YEs, i sEE AND tREAt PAtiENts witH PHN AND woulD likE to lEARN moRE ABout A PHN tREAtmENt oPtioN.
CHADDS FORD, PENNSYLVANIA 19317 2011 Endo Pharmaceuticals. All Rights Reserved. LD-01692d/Sept. 2011
www.endo.com 1-800-462-ENDO (3636)
12 November 2011 • ADVANCE for NPs & PAs
Front&Center
Foundation, as having been successful. Conclusions from the meeting were to have been published by the end of October.
“This is about patients,” Apold said of the issues that some-time divide health professions. “We needn’t be fighting, we need to be talking more.”
The 2012 ACNP Clinical Conference will take place in Toronto Oct. 3–7.
first Physician Assistant Chosen as AhRQ Medical OfficerROBERT J. McNeLLIs, MPh, PA, vice president for science and public health for the American Academy of Physician Assistants, has been appointed visiting senior scholar at the Agency for Healthcare Research and Quality (AHRQ).
McNellis will serve as a medical officer in support of the U.S. Preventive Services Task Force (USPSTF), an independent, nonfederal agency that develops and disseminates evidence-based recommendations for preventive healthcare. This is the first time a PA will serve as a medical officer at AHRQ.
McNellis will be a part of AHRQ’s Prevention and Care Management Team through October 2012. McNellis will pro-vide scientific and logistical support to the USPSTF, including oversight of systematic evidence reviews. He will also coordinate work groups that create and disseminate recommendations on a variety of health topics ranging from screening for disease to the use of hormone replacement therapy.
“This is a dream come true to be able to support the work of the task force, which I’ve loved and appreciated for so long,” McNellis said. He also noted that he supports PAs taking on roles that influence healthcare on a national level.
“There are PAs finding their way into these little niches that can influence policy, and I think that’s a really important place for PAs to be, because it magnifies our ability to affect patient care,” McNellis said.
GAPNA Celebrates 30-year Milestone At Annual ConferencewAshINGTON — Nurse practitioners who specialize in meeting the healthcare needs of older adults cel-ebrated a milestone here in mid-September, when the Gerontological Advanced Practice Nurses Association (GAPNA) held its 30th annual conference.
The nation’s capital city was an energizing setting for an event featuring a keynote address by the administrator of the Health Resources and Services
Cynthia Luther, DSN, FNP-BC, GNP-BC, of Jackson, Miss., was one of the poster presenters at the GAPNA 2011 conference.
MIC
HEL
LE P
ERRO
N P
RO
NSAT
I

13ADVANCE for NPs & PAs • November 2011
Front&Center
OTC MULTIPURPOSEMOISTURE BARRIER
TEMPORARILY RELIEVESDISCOMFORT & ITCHING
Protects and Helps HealSkin Irritations from:
• Incontinence of Urine orFeces
• Diaper Rash• Wound Drainage• Minor Burns, Scrapes
CALL1-800-800-3405
For moreinformation
and free samples
www.calmoseptineointment.com
NP010603-0008 Calmosep.qxd 11/24/03 5:12 PM Page 1
Administration (HRSA), Mary Wakefield, PhD, RN, FAAN.
After congratulating GAPNA for its growth to 10,000 members (400 of whom attended the conference), Wakefield said, “Older adults are often the most vulnerable population, and they benefit from having healthcare professionals who are committed to excellence in practice as well as healthcare policy.
“You will take on more significance in driving our healthcare system forward,” she added.
Wakefield described the scope of the agency she heads: With its $7.8 billion budget, HRSA manages 80 programs whose overriding goal is to achieve healthy people and healthy commu-nities. Wakefield is the first nurse appointed as the administrator of HRSA. “This demonstrates President Obama’s recognition of nurses as a source of relevant expertise,” she said.
Wakefield also focused on the Patient Protection and Affordable Care Act, whose objectives she said cannot be achieved without the help of all healthcare providers. “No one professional can provide all health services to any patient. It’s everyone in …. To deliver the best care, all healthcare provid-ers need to communicate with each other and coordinate care.” Teamwork in healthcare homes will be an essential component of ensuring that all Americans have access to quality services, she said. “It’s up to you and me to write the next chapters of healthcare in America,” she concluded.
A variety of continuing education sessions were available to attendees. Highlights included a panel discussion on clinical guidelines selected for endorsement by the American Geriatrics Society, case presentations on innovative care models, and a historical look at gerontologic nurse practitioner practice.
In the exhibit hall, nearly 40 exhibitors educated attendees about their products and services, and 33 GAPNA members presented posters focused on clinical projects, research projects and clinical practice topics.
GAPNA announced that its 31st conference will be held Sept. 19–22, 2012, at Red Rock Casino Resort in Las Vegas.
NPs & PAs Share Specialty Education at Inaugural CMe/Ce ConferenceORLANDO, fLA. — As NPs and PAs work side by side in more and more clinical settings, it seems prudent that certain learning and networking activities should help foster this teamwork.
Dillehay Management Group (DMG), an association manage-ment firm based in Roswell, Ga., has done exactly that. In early September, DMG’s continuing education division held a CME/
CE conference here titled “Skin, Bones, Hearts & Private Parts,” providing specialty learning tracks focused on dermatology, orthopedics, cardiology and gynecology for both groups of healthcare providers.
Expert presenters from the NP and PA pro-fessions educated approximately 155 NPs and PAs in this kickoff event. It was so well received that DMG has planned two similar events for 2012 — with additional tracks in pediatrics and emergency medicine.
Attendees said they found the specialty track organization of the conference a valuable option for their continuing education. “I appreciated the opportunity to get more detailed information on dermatology, which is an area I’d like to grow in my practice,” said Tanya R. Hodge, ARNP, of Pensacola, Fla. DMG counts the Association of Family Practice PAs and the American College of Physicians’ Georgia chapter among the groups it manages.
ADVANCE for NPs & PAs was a sponsor of Skin, Bones, Hearts & Private Parts. ■
➼ Visit www.advanceweb.com/NPPAnews for more news and conference coverage, including photos and videos.
By the Numbers
83,466The American
Academy of Physician Assistants’ 2010
Census Report found that the number of practicing PAs
reached 83,466 — an increase of 100% over 10 years ago.
Source: Physician Assistant Census Report: Results From the 2010 AAPA Census. http://www.aapa.org/uploadedFiles/content/Common/Files/2010_Census_Report_Final.pdf
COULD YOUR PATIENTS HAVE PHN?DON’T LET YOUR PATIENTS BE AMONG THE 80% WHO ARE MISDIAGNOSED.
“I suffered for months before I wasdiagnosed with after-shingles pain. The pain was hard to describe… it was like someone stabbing or burning me all the time. Fortunately, my primary care provider remembered I had shingles… and he asked me if I could point to my pain.”Hypothetical patient for illustrational purposes only
ach year, approximately 1 million Americans will develop herpes
zoster (HZ) or shingles.1 Approximately 120,000-200,000 people
are estimated to also develop PHN each year in the United States.
The incidence rate means physician assistants and nurse practitioners
may likely see patients with HZ and who go on to develop postherpetic
neuralgia (PHN).
Unfortunately, many patients with PHN may not be diagnosed.2
Understanding PHN and its symptoms and asking patients the right
questions are important to help diagnose PHN.
POSTHERPETIC NEURALGIA
The underlying cause of HZ is infection with the varicella-zoster virus,
the same virus that causes chicken pox.3 HZ incidence among people
older than age 50 is twice that of younger people and becomes an 8-
to 10-fold increase among people older than age 60.4
PHN is severe pain that occurs in the region of the HZ cutaneous
outbreak. PHN can persist for longer than 3 months after skin lesions
have begun to heal.3 Like HZ incidence, PHN incidence increases with
age. More than 50% of patients with HZ older than age 50 will develop
PHN. The risk increases to 80% among patients with HZ older than
age 80.3
STABBING, BURNING PAIN
Patients typically describe PHN as having three components.5 Con-
stant pain can be described as deep and aching. Shooting or electric
pain can recur spontaneously. Light touches to the skin can produce
burning, tenderness, itch, sharp pain, radiating pain or an abnormal
increased sensitivity.
The multiple qualities of pain experienced by patients with PHN
may contribute to missed diagnoses. PHN pain can be intermittent
and jabbing at times and constant and burning at others. Allodynia
may be present.3
As many as 80% of patients with PHN may not be diagnosed with
PHN.2 Therefore, it is important to follow up with your patients with
HZ to determine if they are experiencing pain following resolution of
the HZ rash.
ASKING AND LISTENING
Taking a detailed history along with physical exam is critical to diag-
nosing PHN.
Asking the right questions and listening closely can increase your
chances of making the correct diagnosis.
Ask your patient if they have ever had shingles, how they describe
the pain and if they can point to it. Ask about the chronicity of the pain
and if anything makes it better or worse.
PHN can occur anywhere on the body and sometimes in more than
one area. The most common areas are the torso (chest and back),
waistline, upper arm and face.6
LIDODERM® (lidocaine patch 5%) PROVIDES LOCAL THERAPY
Alleviating pain is the primary concern for patients with PHN, and
topical anesthetics applied directly at the source of PHN pain are a
treatment option.7 One such treatment is LIDODERM® (lidocaine patch
5%). LIDODERM is the fi rst and only lidocaine-based topical medicine
approved for treatment of PHN-associated pain. It can be used alone
or with oral analgesics.8
PHN pain relief can occur with the fi rst dose of LIDODERM® (lido-
caine patch 5%). One dose of LIDODERM (up to three patches) sig-
nifi cantly reduced pain as soon as 30 minutes (P=0.0001 vs. observa-
tion).*7 Compared with placebo, LIDODERM provided signifi cant relief
at 4-12 hours (P<0.001 to P=.038).7
In a 2-week enrichment enrollment study, 84% of 32 patients re-
ported moderate-to-complete pain relief with LIDODERM, compared
with 28% of patients who received a placebo.**9
It is important to note it may take up to 2 weeks after initiating
LIDODERM therapy for patients to achieve the best outcome. Some
patients may experience an application-site reaction. These reac-
tions are typically mild and transient, resolving within a few minutes
to hours.8
INDICATION
LIDODERM is indicated for relief of pain associated with post-herpetic
neuralgia. Apply only to intact skin.
IMPORTANT SAFETY INFORMATION
• LIDODERM is contraindicated in patients with a history of sensitivity
to local anesthetics (amide type) or any product component.
• Even a used LIDODERM (lidocaine patch 5%) patch contains a
large amount of lidocaine (at least 665 mg). The potential exists for
a small child or a pet to suffer serious adverse effects from chew-
ing or ingesting a new or used LIDODERM patch, although the
risk with this formulation has not been evaluated. It is important to
store and dispose of LIDODERM out of the reach of children,
pets and others.
• Excessive dosing, such as applying LIDODERM to larger areas or
for longer than the recommended wearing time, could result in
increased absorption of lidocaine and high blood concentrations
leading to serious adverse effects.
• Avoid contact of LIDODERM with the eye. If contact occurs, immedi-
ately wash the eye with water or saline and protect it until sensation
returns. Avoid the use of external heat sources as this has not been
evaluated and may increase plasma lidocaine levels.
• Patients with severe hepatic disease are at greater risk of develop-
ing toxic blood concentrations of lidocaine, because of their inability
to metabolize lidocaine normally. LIDODERM should be used with
caution in patients receiving Class I antiarrhythmic drugs (such as
tocainide and mexiletine) since the toxic effects are additive and po-
tentially synergistic. LIDODERM should also be used with caution in
pregnant (including labor and delivery) or nursing mothers.
• Allergic reactions, although rare, can occur.
• During or immediately after LIDODERM treatment, the skin at the
site of application may develop blisters, bruising, burning sensation,
depigmentation, dermatitis, discoloration, edema, erythema, exfo-
liation, irritation, papules, petechia, pruritus, vesicles, or may be the
locus of abnormal sensation. These reactions are generally mild and
transient, resolving spontaneously within a few minutes to hours.
Other reactions may include dizziness, headache and nausea.
• When LIDODERM is used concomitantly with local anesthetic
products, the amount absorbed from all formulations must be
considered.
• Immediately discard used patches or remaining unused portions of
cut patches in household trash in a manner that prevents accidental
application or ingestion by children, pets, or others.
Please refer to the accompanying brief summary of full Pre-
scribing Information.
References:1. Weaver BA. The burden of herpes zoster and postherpetic neuralgia in the
United States. J Am Osteopath Assoc. 2007;102(suppl 1):S2-7.2. Dworkin RH, White R, O’Connor AB, et al. Healthcare costs of acute and
chronic pain associated with a diagnosis of herpes zoster. J Am Geriatr Soc. 2007;55:1168-75.
3. Cluff RS, Rowbotham MC. Pain caused by herpes zoster infection. Neurol Clin. 1998;64(4):813-32.
4. LaGuardia JL. Gilden DH. Varicella-zoster virus: a re-emerging infection. J Investig Dermatol Symp Proc. 2001;6(3):183-7.
5. Rowbotham MC. Postherpetic neuralgia. Semin Neurol. 1994;14(3):247-54.6. National Institute of Neurological Disorders and Stroke. Shingles: hope through research. National Institutes of Health Web site. http://www.ninds.nih.gov/ disorders/shingles/detail_shingles.htm?css=print. Accessed October 12, 2007.7. Rowbotham MC, Davies PS, Verkempinck C, Galer BS. Lidocaine patch: double-
blind controlled study of a new treatment method for post-herpetic neuralgia. Pain. 1996;65:39-44.
8. Lidoderm (lidocaine patch 5%) [package insert]. Chadds Ford, PA: Endo Pharmaceuticals;2010.
9. Data on fi le, DOF-LD-02, Endo Pharmaceuticals Inc.
*A randomized, double-blind, placebo-controlled, 4-way crossover trial (N=35) as-sessed safety and effi cacy of LIDODERM. Patients were allodynic with a mean age of 75 years and mean PHN duration of 48 months. Pain intensity was measured with a horizontal 100-mm Visual Analogue Scale: 0=no pain and 100=worst pain imaginable. Measurements were recorded before patch application, at 30 minutes and at hours 1, 2, 4, 6, 9 and 12. Least-squares means were used as the best unbiased estimate of the patients’ mean values.
**Demonstrated over 14 days in a post hoc analysis of a randomized, enriched-en-rollment, double-blind, placebo-controlled, crossover trial. Patients enrolled in the study had been using LIDODERM for ≥1 month (ie, enriched enrollment); mean age of 77.4 years and mean PHN duration of 7.3 years. Pain relief was measured using a 6-item verbal scale: 0 (worse), 1 (no relief), 2 (slight relief), 3 (moderate relief), 4 (a lot of relief) and 5 (complete relief). Patients exited the study if their verbal pain relief rating decreased >2 categories for any 2 consecutive days from baseline.
**Results of enriched-enrollment studies can’t be generalized to the entire population; subjects in such studies may be able to distinguish the active drug from placebo based on nontherapeutic features of the treatments.
ADVERTORIAL ADVERTORIAL
(800) 462-ENDO [3636]www.lidoderm.com
LISTEN TO YOUR PATIENTSTHE RIGHT QUESTIONS CAN HELP DIAGNOSE PHN.
How would you describe your pain?
Can you point to where the pain occurs?
How long have you felt this pain? How long does it last?
Does anything make the pain better or worse?
Have you had shingles in the past?
f
y
f
Areas most commonly affected by after-shingles painAreas most commonly affected by after-shingles pain
14 November 2011 • ADVANCE for NPs & PAs

COULD YOUR PATIENTS HAVE PHN?DON’T LET YOUR PATIENTS BE AMONG THE 80% WHO ARE MISDIAGNOSED.
“I suffered for months before I wasdiagnosed with after-shingles pain. The pain was hard to describe… it was like someone stabbing or burning me all the time. Fortunately, my primary care provider remembered I had shingles… and he asked me if I could point to my pain.”Hypothetical patient for illustrational purposes only
ach year, approximately 1 million Americans will develop herpes
zoster (HZ) or shingles.1 Approximately 120,000-200,000 people
are estimated to also develop PHN each year in the United States.
The incidence rate means physician assistants and nurse practitioners
may likely see patients with HZ and who go on to develop postherpetic
neuralgia (PHN).
Unfortunately, many patients with PHN may not be diagnosed.2
Understanding PHN and its symptoms and asking patients the right
questions are important to help diagnose PHN.
POSTHERPETIC NEURALGIA
The underlying cause of HZ is infection with the varicella-zoster virus,
the same virus that causes chicken pox.3 HZ incidence among people
older than age 50 is twice that of younger people and becomes an 8-
to 10-fold increase among people older than age 60.4
PHN is severe pain that occurs in the region of the HZ cutaneous
outbreak. PHN can persist for longer than 3 months after skin lesions
have begun to heal.3 Like HZ incidence, PHN incidence increases with
age. More than 50% of patients with HZ older than age 50 will develop
PHN. The risk increases to 80% among patients with HZ older than
age 80.3
STABBING, BURNING PAIN
Patients typically describe PHN as having three components.5 Con-
stant pain can be described as deep and aching. Shooting or electric
pain can recur spontaneously. Light touches to the skin can produce
burning, tenderness, itch, sharp pain, radiating pain or an abnormal
increased sensitivity.
The multiple qualities of pain experienced by patients with PHN
may contribute to missed diagnoses. PHN pain can be intermittent
and jabbing at times and constant and burning at others. Allodynia
may be present.3
As many as 80% of patients with PHN may not be diagnosed with
PHN.2 Therefore, it is important to follow up with your patients with
HZ to determine if they are experiencing pain following resolution of
the HZ rash.
ASKING AND LISTENING
Taking a detailed history along with physical exam is critical to diag-
nosing PHN.
Asking the right questions and listening closely can increase your
chances of making the correct diagnosis.
Ask your patient if they have ever had shingles, how they describe
the pain and if they can point to it. Ask about the chronicity of the pain
and if anything makes it better or worse.
PHN can occur anywhere on the body and sometimes in more than
one area. The most common areas are the torso (chest and back),
waistline, upper arm and face.6
LIDODERM® (lidocaine patch 5%) PROVIDES LOCAL THERAPY
Alleviating pain is the primary concern for patients with PHN, and
topical anesthetics applied directly at the source of PHN pain are a
treatment option.7 One such treatment is LIDODERM® (lidocaine patch
5%). LIDODERM is the fi rst and only lidocaine-based topical medicine
approved for treatment of PHN-associated pain. It can be used alone
or with oral analgesics.8
PHN pain relief can occur with the fi rst dose of LIDODERM® (lido-
caine patch 5%). One dose of LIDODERM (up to three patches) sig-
nifi cantly reduced pain as soon as 30 minutes (P=0.0001 vs. observa-
tion).*7 Compared with placebo, LIDODERM provided signifi cant relief
at 4-12 hours (P<0.001 to P=.038).7
In a 2-week enrichment enrollment study, 84% of 32 patients re-
ported moderate-to-complete pain relief with LIDODERM, compared
with 28% of patients who received a placebo.**9
It is important to note it may take up to 2 weeks after initiating
LIDODERM therapy for patients to achieve the best outcome. Some
patients may experience an application-site reaction. These reac-
tions are typically mild and transient, resolving within a few minutes
to hours.8
INDICATION
LIDODERM is indicated for relief of pain associated with post-herpetic
neuralgia. Apply only to intact skin.
IMPORTANT SAFETY INFORMATION
• LIDODERM is contraindicated in patients with a history of sensitivity
to local anesthetics (amide type) or any product component.
• Even a used LIDODERM (lidocaine patch 5%) patch contains a
large amount of lidocaine (at least 665 mg). The potential exists for
a small child or a pet to suffer serious adverse effects from chew-
ing or ingesting a new or used LIDODERM patch, although the
risk with this formulation has not been evaluated. It is important to
store and dispose of LIDODERM out of the reach of children,
pets and others.
• Excessive dosing, such as applying LIDODERM to larger areas or
for longer than the recommended wearing time, could result in
increased absorption of lidocaine and high blood concentrations
leading to serious adverse effects.
• Avoid contact of LIDODERM with the eye. If contact occurs, immedi-
ately wash the eye with water or saline and protect it until sensation
returns. Avoid the use of external heat sources as this has not been
evaluated and may increase plasma lidocaine levels.
• Patients with severe hepatic disease are at greater risk of develop-
ing toxic blood concentrations of lidocaine, because of their inability
to metabolize lidocaine normally. LIDODERM should be used with
caution in patients receiving Class I antiarrhythmic drugs (such as
tocainide and mexiletine) since the toxic effects are additive and po-
tentially synergistic. LIDODERM should also be used with caution in
pregnant (including labor and delivery) or nursing mothers.
• Allergic reactions, although rare, can occur.
• During or immediately after LIDODERM treatment, the skin at the
site of application may develop blisters, bruising, burning sensation,
depigmentation, dermatitis, discoloration, edema, erythema, exfo-
liation, irritation, papules, petechia, pruritus, vesicles, or may be the
locus of abnormal sensation. These reactions are generally mild and
transient, resolving spontaneously within a few minutes to hours.
Other reactions may include dizziness, headache and nausea.
• When LIDODERM is used concomitantly with local anesthetic
products, the amount absorbed from all formulations must be
considered.
• Immediately discard used patches or remaining unused portions of
cut patches in household trash in a manner that prevents accidental
application or ingestion by children, pets, or others.
Please refer to the accompanying brief summary of full Pre-
scribing Information.
References:1. Weaver BA. The burden of herpes zoster and postherpetic neuralgia in the
United States. J Am Osteopath Assoc. 2007;102(suppl 1):S2-7.2. Dworkin RH, White R, O’Connor AB, et al. Healthcare costs of acute and
chronic pain associated with a diagnosis of herpes zoster. J Am Geriatr Soc. 2007;55:1168-75.
3. Cluff RS, Rowbotham MC. Pain caused by herpes zoster infection. Neurol Clin. 1998;64(4):813-32.
4. LaGuardia JL. Gilden DH. Varicella-zoster virus: a re-emerging infection. J Investig Dermatol Symp Proc. 2001;6(3):183-7.
5. Rowbotham MC. Postherpetic neuralgia. Semin Neurol. 1994;14(3):247-54.6. National Institute of Neurological Disorders and Stroke. Shingles: hope through research. National Institutes of Health Web site. http://www.ninds.nih.gov/ disorders/shingles/detail_shingles.htm?css=print. Accessed October 12, 2007.7. Rowbotham MC, Davies PS, Verkempinck C, Galer BS. Lidocaine patch: double-
blind controlled study of a new treatment method for post-herpetic neuralgia. Pain. 1996;65:39-44.
8. Lidoderm (lidocaine patch 5%) [package insert]. Chadds Ford, PA: Endo Pharmaceuticals;2010.
9. Data on fi le, DOF-LD-02, Endo Pharmaceuticals Inc.
*A randomized, double-blind, placebo-controlled, 4-way crossover trial (N=35) as-sessed safety and effi cacy of LIDODERM. Patients were allodynic with a mean age of 75 years and mean PHN duration of 48 months. Pain intensity was measured with a horizontal 100-mm Visual Analogue Scale: 0=no pain and 100=worst pain imaginable. Measurements were recorded before patch application, at 30 minutes and at hours 1, 2, 4, 6, 9 and 12. Least-squares means were used as the best unbiased estimate of the patients’ mean values.
**Demonstrated over 14 days in a post hoc analysis of a randomized, enriched-en-rollment, double-blind, placebo-controlled, crossover trial. Patients enrolled in the study had been using LIDODERM for ≥1 month (ie, enriched enrollment); mean age of 77.4 years and mean PHN duration of 7.3 years. Pain relief was measured using a 6-item verbal scale: 0 (worse), 1 (no relief), 2 (slight relief), 3 (moderate relief), 4 (a lot of relief) and 5 (complete relief). Patients exited the study if their verbal pain relief rating decreased >2 categories for any 2 consecutive days from baseline.
**Results of enriched-enrollment studies can’t be generalized to the entire population; subjects in such studies may be able to distinguish the active drug from placebo based on nontherapeutic features of the treatments.
ADVERTORIAL ADVERTORIAL
(800) 462-ENDO [3636]www.lidoderm.com
LISTEN TO YOUR PATIENTSTHE RIGHT QUESTIONS CAN HELP DIAGNOSE PHN.
How would you describe your pain?
Can you point to where the pain occurs?
How long have you felt this pain? How long does it last?
Does anything make the pain better or worse?
Have you had shingles in the past?
f
y
f
Areas most commonly affected by after-shingles painAreas most commonly affected by after-shingles pain
www.advanceweb.com/NPPA • ADVANCE for NPs & PAs • November 2011 15www.advanceweb.com/NPPA • ADVANCE for NPs & PAs • October 2011 15www.advanceweb.com/NPPA • ADVANCE for NPs & PAs • September 2011 1515ADVANCE for NPs & PAs • November 2011

CHADDS FORD, PENNSYLVANIA 19317
LIDODERM®
is a registered trademark of Hind Health Care, Inc.
LIDODERM®
(Lidocaine Patch 5%)
Brief Summary (For full Prescribing Information refer to package insert.)INDICATIONS AND USAGELIDODERM is indicated for relief of pain associated with post-herpetic neuralgia. It should be applied only to intact skin.
CONTRAINDICATIONSLIDODERM is contraindicated in patients with a known history of sensitivity to local anesthetics of the amide type, or to any other component of the product.
WARNINGSAccidental Exposure in ChildrenEven a used LIDODERM patch contains a large amount of lidocaine (at least 665 mg). The potential exists for a small child or a pet to suffer serious adverse effects from chewing or ingesting a new or used LIDODERM patch, although the risk with this formulation has not been evaluated. It is important for patients to store and dispose of LIDODERM out of the reach of children, pets, and others. (See HANDLING AND DISPOSAL)
Excessive DosingExcessive dosing by applying LIDODERM to larger areas or for longer than the recommended wearing time could result in increased absorption of lidocaine and high blood concentrations, leading to serious adverse effects (see ADVERSE REACTIONS, Systemic Reactions). Lidocaine toxicity could be expected at lidocaine blood concentrations above 5 μg/mL. The blood concentration of lidocaine is determined by the rate of systemic absorption and elimination. Longer duration of application, application of more than the recommended number of patches, smaller patients, or impaired elimination may all contribute to increasing the blood concentration of lidocaine. With recommended dosing of LIDODERM, the average peak blood concentration is about 0.13 μg/mL, but concentrations higher than 0.25 μg/mL have been observed in some individuals.
PRECAUTIONSGeneralHepatic Disease: Patients with severe hepatic disease are at greater risk of developing toxic blood concentrations of lidocaine, because of their inability to metabolize lidocaine normally.
Allergic Reactions: Patients allergic to para aminobenzoic acid derivatives (procaine, tetracaine, benzocaine, etc.) have not shown cross sensitivity to lidocaine. However, LIDODERM should be used with caution in patients with a history of drug sensitivities, especially if the etiologic agent is uncertain.
Non-intact Skin: Application to broken or inflamed skin, although not tested, may result in higher blood concentrations of lidocaine from increased absorption. LIDODERM is only recommended for use on intact skin.
External Heat Sources: Placement of external heat sources, such as heating pads or electric blankets, over LIDODERM patches is not recommended as this has not been evaluated and may increase plasma lidocaine levels.
Eye Exposure: The contact of LIDODERM with eyes, although not studied, should be avoided based on the findings of severe eye irritation with the use of similar products in animals. If eye contact occurs, immediately wash out the eye with water or saline and protect the eye until sensation returns.
Drug InteractionsAntiarrhythmic Drugs: LIDODERM should be used with caution in patients receiving Class I antiarrhythmic drugs (such as tocainide and mexiletine) since the toxic effects are additive and potentially synergistic.
Local Anesthetics: When LIDODERM is used concomitantly with other products containing local anesthetic agents, the amount absorbed from all formulations must be considered.
Carcinogenesis, Mutagenesis, Impairment of FertilityCarcinogenesis: A minor metabolite, 2, 6-xylidine, has been found to be carcinogenic in rats. The blood concentration of this metabolite is negligible following application of LIDODERM.
Mutagenesis: Lidocaine HCl is not mutagenic in Salmonella/mammalian microsome test nor clastogenic in chromosome aberration assay with human lymphocytes and mouse micronucleus test.
Impairment of Fertility: The effect of LIDODERM on fertility has not been studied.
PregnancyTeratogenic Effects: Pregnancy Category B. LIDODERM (lidocaine patch 5%) has not been studied in pregnancy. Reproduction studies with lidocaine have been performed in rats at doses up to 30 mg/kg subcutaneously and have revealed no evidence of harm to the fetus due to lidocaine. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, LIDODERM should be used during pregnancy only if clearly needed.
Labor and DeliveryLIDODERM has not been studied in labor and delivery. Lidocaine is notcontraindicated in labor and delivery. Should LIDODERM be used concomitantly with other products containing lidocaine, total doses contributed by all formulations must be considered.
Nursing MothersLIDODERM has not been studied in nursing mothers. Lidocaine is excreted in human milk, and the milk: plasma ratio of lidocaine is 0.4. Caution should be exercised when LIDODERM is administered to a nursing woman.
Pediatric UseSafety and effectiveness in pediatric patients have not been established.
ADVERSE REACTIONSApplication Site ReactionsDuring or immediately after treatment with LIDODERM (lidocaine patch 5%), the skin at the site of application may develop blisters, bruising, burning sensation, depigmentation, dermatitis, discoloration, edema, erythema, exfoliation, irritation, papules, petechia, pruritus, vesicles, or may be the locus of abnormal sensation. These reactions are generally mild and transient, resolving spontaneously within a few minutes to hours.
Allergic ReactionsAllergic and anaphylactoid reactions associated with lidocaine, although rare, can occur. They are characterized by angioedema, bronchospasm, dermatitis, dyspnea, hypersensitivity, laryngospasm, pruritus, shock, and urticaria. If they occur, they should be managed by conventional means. The detection of sensitivity by skin testing is of doubtful value.
Other Adverse EventsDue to the nature and limitation of spontaneous reports in postmarketing surveillance, causality has not been established for additional reported adverse events including:
Asthenia, confusion, disorientation, dizziness, headache, hyperesthesia, hypoesthesia, lightheadedness, metallic taste, nausea, nervousness, pain exacerbated, paresthesia, somnolence, taste alteration, vomiting, visual disturbances such as blurred vision, flushing, tinnitus, and tremor.
Systemic (Dose-Related) ReactionsSystemic adverse reactions following appropriate use of LIDODERM are unlikely, due to the small dose absorbed (see CLINICAL PHARMACOLOGY, Pharmacokinetics). Systemic adverse effects of lidocaine are similar in nature to those observed with other amide local anesthetic agents, including CNS excitation and/or depression (light-headedness, nervousness, apprehension, euphoria, confusion, dizziness, drowsiness, tinnitus, blurred or double vision, vomiting, sensations of heat, cold, or numbness, twitching, tremors, convulsions, unconsciousness, respiratory depression, and arrest). Excitatory CNS reactions may be brief or not occur at all, in which case the first manifestation may be drowsiness merging into unconsciousness. Cardiovascular manifestations may include bradycardia, hypotension, and cardiovascular collapse leading to arrest.
OVERDOSAGELidocaine overdose from cutaneous absorption is rare, but could occur. If there is any suspicion of lidocaine overdose (see ADVERSE REACTIONS, Systemic Reactions), drug blood concentration should be checked. The management of overdose includes close monitoring, supportive care, and symptomatic treatment. Dialysis is of negligible value in the treatment of acute overdose with lidocaine.
In the absence of massive topical overdose or oral ingestion, evaluation of symptoms of toxicity should include consideration of other etiologies for the clinical effects, or overdosage from other sources of lidocaine or other local anesthetics.
The oral LD50 of lidocaine HCl is 459 (346-773) mg/kg (as the salt) in nonfasted female rats and 214 (159-324) mg/kg (as the salt) in fasted female rats,which are equivalent to roughly 4000 mg and 2000 mg, respectively, in a 60 to 70 kg man based on the equivalent surface area dosage conversion factors between species.
DOSAGE AND ADMINISTRATIONApply LIDODERM to intact skin to cover the most painful area. Apply up to three patches, only once for up to 12 hours within a 24-hour period. Patches may be cut into smaller sizes with scissors prior to removal of the release liner. (See HANDLING AND DISPOSAL) Clothing may be worn over the area of application. Smaller areas of treatment are recommended in a debilitated patient, or a patient with impaired elimination.
If irritation or a burning sensation occurs during application, remove the patch (es) and do not reapply until the irritation subsides.
When LIDODERM is used concomitantly with other products containing local anesthetic agents, the amount absorbed from all formulations must be considered.
HANDLING AND DISPOSALHands should be washed after the handling of LIDODERM, and eye contact with LIDODERM should be avoided. Do not store patch outside the sealed envelope. Apply immediately after removal from the protective envelope. Fold used patches so that the adhesive side sticks to itself and safely discard used patches or pieces of cut patches where children and pets cannot get to them. LIDODERM should be kept out of the reach of children.
Store at 25°C (77°F); excursions permitted to 15°-30°C (59°-86°F). [See USP Controlled Room Temperature].
Manufactured for:Endo Pharmaceuticals Inc.Chadds Ford, Pennsylvania 19317
LIDODERM® is a Registered Trademark of Hind Health Care, Inc.
© Endo Pharmaceuticals 2011
Rev. March 20106524-12 E1
LD-1664R/March 2010
© 2011 Endo Pharmaceuticals. All Rights Reserved. LD-0 1 /130 May 2011 www.lidoderm.com 1-800-462-ENDO (3636)
16 November 2011 • ADVANCE for NPs & PAs

17ADVANCE for NPs & PAs • November 2011
Career&Workforce
yOU DON’T hAVe to be a celebrity to have an image. Whether or not you realize it (or like it), you have an online “image,” and it is visible to anyone with Internet access. If you participate in social media or have a blog, you have an online image. Even your profession alone will churn your name and work address out in a HealthGrades (or similar) listing.
The Federal Trade Commission ruled this year that it is legal to include an online search as part of a background check. Traditional background checks have long been conducted as part of the hiring process. You sign a form grant-ing your permission, and the employer submits your name to a company that is paid to perform the check. The results of this type of background check are limited mainly to criminal records — which are all public information anyway.
An online background search differs dramatically from a traditional background check in that, theoretically, any informa-tion anywhere in the world is accessible. If the information is online, it can be found. This has the potential to reveal more than past criminal convictions.
what’s Usable? Just because it’s on the Internet doesn’t mean it is fair game in a hiring decision. Online background checks must still adhere to the rules governing traditional background checks. Information about gender, religion, race or any other pro-tected class is off-limits and cannot be used to discriminate.
All information must be gathered using ethical means. Employers or their
representatives may not pretend to be someone else in order to gain access to your information, such as creating a false account on Facebook to “friend” you.
A company that specializes in online background checks has the knowledge and skills to discover data you might not have realized was possible for anyone to access. For instance, in many states, a simple search using your address can reveal whether your home is in foreclosure or if you owe back property taxes.
The most common online background searches are less formal and might be done without your written consent or your knowledge. Quite possibly, a Google search will be performed before you are even scheduled for an interview by a curi-ous recruiter or hiring manager. Cyber snooping is common!
Conclusions DrawnWhether you like it or not, conclusions will be drawn based on your online behav-ior. If you don’t know better than to use profanity, post scantily clad pictures of yourself or brag about your outrageous alcohol intake, I cannot help you.
But what job seekers often don’t realize is that they may be inadvertently post-ing information that can hurt their job prospects. After a bad day, it’s tempting to vent workplace issues online. Ranting about long hours, bosses and coworkers may feel good at the time, but it won’t win you any admirers among employers. Nobody wants to hire a complainer.
Overactivity can also be a red flag for employers. Do you update your Facebook status frequently? If you are posting
updates during work hours, an employer might wonder about your work ethic.
Think TwiceOnline image isn’t a concern limited to job seekers. Your employer might also be checking up on you. If your boss can find you, so can patients. Resist the urge to post that interesting case or funny patient story anywhere. And don’t think that just because you don’t mention your patient by name you can’t get in trouble. More than a few NPs and PAs have lost their jobs after a patient or a friend of a patient recognized themselves in an online anecdote. And getting fired might be the least of your problems. If you vio-lated patient confidentiality, you could be in trouble with your regulating board or even land in court.
Before you delete your Facebook and Twitter accounts, realize that complete avoidance can also be a bad thing. Many benefits are associated with social media when it is used appropriately and with discretion. Employers may not want to see pictures of your tattoo, but that doesn’t mean they don’t want to see that you have a presence online.
Abstaining from online activity can make you look like a technophobe. For the healthcare provider, computer literacy is no longer optional. An active and positive online life shows an employer that you are comfortable with technology — and that’s a good thing. ■
Image alert: what do you look like online?By Renee Dahring, MSN, NP
Renee DahRing is a family nurse practitioner who practices in correctional
settings in Minnesota. She has experience as a recruiter and now conducts
workshops on resume writing and interviewing (www.nursepractitionerjobsearch.
com). Read more from Dahring in our Career Coach blog at www.advanceweb.
com/NPPAblogs.TOM
WH
ALE
N
be Careful Out There◗ Employers are
investigating the online activity of prospective and current employ-ees. If you wouldn’t say it at work, don’t say it online.
◗ Avoiding social media isn’t the best response to these personal checkups. Maintain a presence on the web, but make sure it reflects the best of you.

18 November 2011 • ADVANCE for NPs & PAs
CONTINUING MeDICAL education (CME) credits and continuing education units (CEUs) for NPs are the foundation of most state health professions’ regulatory boards for licensure. Continuing educa-tion (CE) is among the primary means by which licensees demonstrate ongoing professional competence to practice.
Entire national systems of licensure, certification and demonstration of clinical proficiency are constructed around the attainment of specific types and amounts of CE.1 These systems assume that earning CE assures ongoing clinical competence. But to what degree does attaining CE pro-vide valid assurance of continued practice proficiency? Furthermore, what is the evidence that CE is effective in improving practitioner knowledge, clinical skills and, ultimately, practice outcomes?
evidence for ‘evidence-based’?“Evidence-based” has been a buzzword in health professions education for decades. We teach students evidence-based approaches to clinical decision-making and implore them to practice using critical appraisals of the literature. We demand evidence-based approaches to clinical decisions such as selecting medications and diagnostic tests.2
But apply this approach to examine the value of CE: What evidence supports CE as the optimal means of demonstrating a healthcare professional’s competence? It is pretty weak, actually — not nearly as robust as one would think or hope.
Reports point to sparse well-designed research attesting to the value of CE in improving practice competency and
patient outcomes.3,4 For example, research-ers at Johns Hopkins University systemati-cally reviewed the literature to evaluate the effectiveness of CME in improving physicians’ knowledge, attitudes, skills, behavior and clinical outcomes.4 They found that relatively few studies of CME’s effectiveness use evaluation methods with strong evidence to support reliability, and that CME’s overall effectiveness is limited by weaknesses in the evaluation methods. Nonetheless, they concluded that despite the generally low quality of evidence, most studies suggest that CME is at least somewhat effective.
More Research Is NeededThe Institute of Medicine calls for com-petency-based education and interdisci-plinary practice models for the future.5 A few advanced practice nursing specialties, such as midwifery and nurse anesthesia, have long histories of uniform accredita-tion and competency-based education. The PA profession also developed under a single accrediting body, a core curriculum and a national certification mechanism since the 1970s. The NP role, however, evolved in a more fragmented fashion, and curriculum standardization and accreditation standards followed educa-tion rather than directed it.
Licensing boards should require valid and reliable assessments of clini-cal competence to assure public safety and protect from incompetent providers. Organizations that provide CE should base their learning programs on the assessed practice needs of providers. Given that CE is the linchpin of the state licensure
system, further research into the validity of CME and CEUs is needed.
In many respects, the PA and NP pro-fessions have been progressive models of national certification systems and public accountability of competency. Our professions should closely monitor issues related to the demonstration of continued competency and participate in policy discussions on this topic. Our professions should join with physicians in support of further research on CE’s effec-tiveness, of promoting greater uniformity of CE requirements for licensing, and of developing best practices for continuing professional development and mainte-nance of clinical competence. ■
References1. Whitcomb ME. Research in medical educa-
tion: what do we know about the link between what doctors are taught and what they do? Acad Med. 2002;77(11):1067-1068.
2. Brook RH. Continuing medical education: let the guessing begin. JAMA. 2010;303(4):359-360.
3. Miller SH, et.al. Continuing medical education, professional development, and requirements for medical licensure: a white paper of the Conjoint Committee on Continuing Medical Education. J Contin Educ Health Prof. 2008;28(2):95-98.
4. Marinopolis SS, et.al. Effectiveness of continu-ing medical education. Evid Rep Technol Assess (Full Rep). 2007;(149):1-69.
5. Institute of Medicine. Health Professions Education: A Bridge to Quality. Washington, DC: National Academies Press; 2003.
Does continuing educationmake competent clinicians?By James F. Cawley, MPH, PA-C
James F. Cawley is professor and interim chair of the Department of Prevention
and Community Health in the School of Public Health and Health Services at
the George Washington University in Washington. He is the 2011 recipient of
the American Academy of Physician Assistants Eugene A. Stead Jr. Award of
Achievement. TOM
WH
ALE
N
Community-based CME Plummets➼ The number of CME providers at the state level — most of which are community hospitals — declined more than 18% between 2003 and 2010, according to the American Medical Association. These community CME providers offer more than a third of all AMA category 1 CME activities and are crucial, the AMA says, because they address clinicians’ educational and practice
needs specific to local patient populations. Among the possible reasons for the steep drop: burdensome documentation and increased fees.
Role&Growth

19ADVANCE for NPs & PAs • November 2011
Money&Health
keRMIT The fROG has never worked in healthcare, apparently. It really is easy being green. Becoming more environ-mentally aware in clinical practice can be as simple as placing a recycling bin next to the printer or swapping incandescent bulbs for compact fluorescents. But some eco-friendly (and money-saving) measures require a team effort — something NPs and PAs know a little bit about.
Get OrganizedDoes your practice or facility have a “green team”? In a larger facility, a commit-tee representing all departments, from housekeeping to the clinical staff, can brainstorm ways to reduce, recycle and reuse. In a smaller practice, the green team might be only you and a colleague.
In addition to spreading environmental enthusiasm — in this case, a good nosoco-mial infection — a green team can help a facility save money by creating operational efficiency in large and small ways. For example, one hospital installed an auto-clave system with a mechanical vacuum system instead of the typical water system. Even though the mechanical system cost $35,000 more, saving 200,000 gallons of water a month quickly paid off.
RecycleRecycling programs can save cash along with the planet. The nonprofit environ-mental organization Second Nature lists a number of model green medical centers, including New York’s Beth Israel, whose waste segregation program cut disposal costs by 60%, saving $1.5 million a year on medical waste and trash disposal; and
Albany Medical Center, whose program in its first 6 years recycled 16 million pounds of waste and saved the hospital $4 million. AMC also replaced its incinerator with a chemical distillery that converts waste into pure products that the hospital can use in its labs, saving $250,000 each year in disposal and purchasing costs.
While you might not be able to con-vince your facility to build its own dis-tillery, small changes can make a big difference. Make it easy for patients, visitors and staff to recycle everything that can be recycled. In most areas, that means at least cardboard, newspapers and magazines, copy paper, glass, cans, and plastics with recycle codes 1 and 2. Place clearly labeled recycling bins strategically throughout the facility.
While it’s true that many items in the healthcare environment can’t be safely recycled, most hospital waste is almost identical to that of any office building or hotel — mostly paper, cardboard, metal and food waste, according to the environ-mental coalition Health Care Without Harm. In fact, only 15% of the hospital waste stream is classified as “regulated” or “potentially infectious.”
Make sure your recycling program includes toner cartridges and batteries. In large facilities, recycle cooking oil from the cafeteria kitchen, xylene from the lab, mercury from the dental clinic and expired X-ray film.
Reduce and ReuseWhen it comes to conservation, no change is too small. Does your facility use com-pact fluorescent bulbs where possible? Going paperless is easier than ever thanks to electronic health records, but you can do more simply. Add a message to your emails asking recipients whether they really need to hit “print.” Have faxes sent to computers to save paper. If you must
have a hard copy, most printers are readily configured for double-sided printing.
Are carpooling and mass transit use encouraged or even rewarded? Some facili-ties designate preferred parking for drivers of hybrids and for carpoolers. Bicycle racks are an easy, cheap way to encourage less fuel use and more exercise.
Kicking a bottled water habit by refill-ing one bottle at a fountain will not only reduce your clinic’s waste stream but also save you money. If that sounds like music to your ears, consider the last line of Kermit’s “Bein’ Green”: “It’s beautiful, and I think it’s what I want to be.” ■
Going green (and saving greenbacks) in practiceBy Michael Gerchufsky
miChael geRChuFsky is
co-editor of ADVANCE for NPs
& PAs and the former editor of
its predecessor, ADVANCE for
Physician Assistants.DAV
E P
ER
ILLO
10 Ways to Cut RMWHealth Care Without Harm offers medical facilities strategies for going green, including these tips for reducing danger-ous and costly regu-
lated medical waste (RMW).
1. How much RMW is produced? Have disposal costs been analyzed?
2. Make sure containers are accessi-ble and adequate, and that clear lin-ers and red bags are used properly.
3. A central large container might be better than numerous exam room containers.
4. Are sharps disposed with RMW? Is a sharps container reuse program possible?
5. Can a cost-effective suction canis-ter treatment program render con-tents noninfectious?
6. Make sure pickup schedules are safe and efficient.
7. Confirm that signs, labels and containers match by color for each waste stream.
8. Ongoing employee education reduc-es waste, increases safety and saves money.
9. Preach the P and 3Rs: Prevent, Reduce, Reuse, Recycle
10. Less RMW = more solid waste. Less solid waste = more recycla-bles. Less purchased = less waste.
Adapted from http://www.noharm.org/lib/ downloads/waste/10_Ways_Reduce_Waste.pdf

20 November 2011 • ADVANCE for NPs & PAs
Diabetes
by Lauren M. sosdorf, ARNP, MsN, PNP-bC
lauRen m. sosDoRF is a pediatric nurse
practitioner at Tampa General Hospital in
Tampa, Fla. She has completed a disclosure
statement and reports no relationships related
to this article.
Type 1Diabetes & Pregnancy
➼ DIAbeTes IN ALL fORMs is the most common medical condition to com-plicate pregnancy.1,2 In a patient with type 1 diabetes, pregnancy is considered high risk due to fluctuations in blood glucose levels and the constant metabolic demands of the growing fetus.
Women who have type 1 diabetes at the time they become pregnant are at greater risk for maternal and fetal complications. Some of the congenital anomalies that occur in pregnancies in women with type 1 diabetes include:2
•brainandneuraltubedefects(includ-ing anencephaly)•cardiacdefects(mainlytransposition
of the great arteries and aortic stenosis)•limbanomalies•ambiguousgenitalia•genitourinarymalformations•variousmultisystemanomalysyn-
dromes.In addition to congenital anomalies,
many infants of women with diabetes experience abnormal developmental and growth rates (e.g., intrauterine growth
Planning is the best way to prevent problems
JEFF
REy L
EES
ER
/RU
TH B
LAC
K/i
STO
CK
PH
OTO
/TH
INK
STO
CK
AN
D D
OR
IS M
OH
R

21ADVANCE for NPs & PAs • November 2011
Diabetes
retardation or acceleration, respiratory system immaturity and perinatal mortal-ity).3 The literature also documents an increased risk of preterm labor, stillbirth and various pregnancy complications including preeclampsia, fetal asphyxia and the need for technical interventions during childbirth (labor induction or cesarean section).2
PathophysiologyIn diabetes, carbohydrate use is reduced and lipid and protein use are enhanced. Type 1 diabetes is caused by an abso-lute deficiency of insulin. It can result in chronic hyperglycemia, glycosuria, water and electrolyte loss, ketoacidosis and coma.4 Long-term complications include neuropathy, retinopathy, nephropathy, gen-eralized degenerative changes in large and small blood vessels, myocardial infarction, cerebrovascular accident, and increased susceptibility to infection.4
During a normal pregnancy, blood glu-cose values range between 72 mg/dL and 81 mg/dL. Women unaffected by diabetes are able to achieve this by doubling their insulin secretion from islet cells located in the pancreas. As the pregnancy con-tinues, all women (regardless of diabetes status) require higher insulin production due to increased insulin resistance. This increase in insulin resistance is a result of maternal endocrine changes includ-ing increased free cortisol levels and an increased secretion of estrogen, progester-one, human placental lactogen, and other pregnancy-related hormones.5
During pregnancy, all women experi-ence increased metabolic demand as a result of the growing fetus and placenta. The placenta causes a physiologic increase in insulin resistance throughout preg-nancy, as it works against the insulin to
supply the growing fetus with glucose and other nutrients necessary for growth. The amount of insulin resistance varies consid-erably throughout pregnancy, based on the functioning of the placenta. Insulin needs rise by about 0.8 units/kg of body weight per day in the first trimester to 1.0 units/kg per day in the second trimester and 1.2 units/kg per day in the third trimester.6 The extent of this increase in insulin resistance varies. A threefold increase in insulin requirement by the end of the third trimester has been documented in some women with diabetes.7
In pregnant women with diabetes, insu-lin acts as the primary anabolic hormone for fetal growth and development while in utero, and it can result in organomegaly and macrosomia in the infant.3 Still, insu-lin is the drug of choice for all women with type 1 diabetes during pregnancy because it cannot cross the placenta and provides more predictable blood glucose control than oral medications.8
The massive fluctuations in insulin resistance and the increase in insulin needs make the achievement of nor-moglycemia nearly impossible during pregnancy. The greater the fluctuation in blood glucose levels, the greater the risk of serious complications for both mother and baby. The higher the blood glucose levels, the more circulating glucose for the infant, which leads to an infant that is large for gestational age. When a woman with diabetes takes more insulin to try to reduce these high blood glucose levels, the excess insulin and glucose act as growth hormones for the developing fetus, again leading to an infant that is large for gestational age.
When blood glucose levels are elevated over a prolonged period, damage to the microvascular system can occur through-
out the pregnant woman’s body. Damage to microvessels also can affect the ves-sels of the placenta, leading to placental malfunction and decreased blood flow to the fetus.3 Some infants who are born to women with longstanding diabetes may therefore be born small for gesta-tional age.
An increased risk of organ malforma-tion in the fetus is also present if blood supply is decreased due to placental mal-formation early in the pregnancy. Fetal stillbirth is another potential complication in women with uncontrolled diabetes. Infants who are large for gestational age (> 4,000 g) are more likely to experience intrauterine fetal death in the last 4 to 6 weeks of gestation as a result of hyper-insulinemia, which increases the risk of respiratory distress syndrome.6
Practical ChallengesFor women with type 1 diabetes, preg-nancy can be stressful due to the difficulty associated with regulating blood glucose levels during a volatile time. Practical matters are also challenging. For example, eating the same foods 2 days in a row is not handled in the same manner by the diabetic body, making normoglycemia difficult to achieve. During pregnancy, many women feel a loss of control and become more aware of their unhealthy, high-risk bodies. As a result, many diabetic women have a higher level of emotional stress during pregnancy. They describe more anxiety, more pressure, constant worry, hostility toward the pregnancy and self-blame — all of which can make blood glucose regulation more difficult to achieve.2
NPs and PAs can assist women in work-ing through these issues. For example, insulin pumps, continuous glucose moni-
Women with type 1 diabetes at the time they become pregnant are at greater risk for maternal and fetal complications. Preconception education and prevention of unplanned pregnancy are needed.

22 November 2011 • ADVANCE for NPs & PAs
tors or similar tools provide safeguards that can help ease fears about nocturnal hypoglycemia.
ADA RecommendationsThe American Diabetes Association (ADA) Standards of Medical Care9 list four rec-ommendations for diabetic women prior to and during pregnancy:•achievementofglycosylatedhemo-
globin (A1c) levels at normal or as close to normal (< 1% above the upper limit of normal) as possible prior to conception
•educationabouttheneedfortightblood glucose control prior to concep-tion•evaluationandtreatmentforany
diabetes complications, such as diabetic retinopathy, nephropathy, neuropathy and cardiovascular disease, prior to becoming pregnant•closemonitoringbyamultidisci-
plinary team of healthcare providers during pregnancy (endocrinologist, pri-mary care provider, obstetrician, diabetes educator, dietitian, social worker and any additional specialists, as indicated).
Nutrition ManagementThe management of type 1 diabetes in pregnancy must incorporate a careful combination of diet, exercise and insulin therapy.6 Current recommendations encourage pregnant women to count carbohydrates to increase their dietary flexibility and allow them more freedom to choose their meals.6 For most diabetic women, calorie intake should increase during pregnancy by approximately 300 kcal above basal metabolic needs.6,8 Women of normal body weight should ingest 30 to 35 kcal/kg of actual weight
daily. For women who are more than 120% of desirable body weight, a decrease to 24 kcal/kg is recommended.6
For women with type 1 diabetes, a diet that includes a variety of caloric compo-nents is the most healthful. The recom-mended calorie composition during preg-nancy (and at other times) is as follows:6
•40%to50%ofcaloriesfromcomplex,high-fiber carbohydrates•20%ofcaloriesfromprotein•30%to40%ofcaloriesfromprimarily
unsaturated fats.
Between 10% and 20% of calories should be consumed at breakfast, 20% to 30% should be consumed at lunch, and 30% to 40% should be consumed at dinner.6 The remaining 30% of calories should be in the form of snacks. A pre-bedtime snack should be consumed to decrease nocturnal hypoglycemia.6,8 Ketone testing is an important aspect of care.
Preventing ComplicationsOne of the most prominent issues in diabetic pregnancy is regulation of blood glucose levels and hemoglobin A1c lev-els. As stated earlier, the ADA recom-mends that women achieve and maintain a hemoglobin A1c level as close to normal as possible (no more than 1% above the upper limit of normal) prior to becom-ing pregnant and throughout pregnancy. Most healthcare providers tell patients that a normal A1c level is 3.5% to 5.9%; therefore, diabetic women should achieve an A1c level at or below 6.9% in order to decrease their risk for severe complica-tions during pregnancy.9 Some experts recommend keeping A1c levels below 6.0% during pregnancy, but this can increase
the incidence of hypoglycemia.10
Research shows that self-monitoring of blood glucose levels has some discrepan-cies when compared with hemoglobin A1c levels. A patient who has a hemoglobin A1c level within the acceptable limits may still have capillary blood glucose level fluctuations into both hypoglycemic and hyperglycemic levels.11,12 The goal of therapy should therefore be to con-trol and limit these fluctuations and to maintain the recommended hemoglobin A1c level.
Decreasing the incidence of maternal and fetal anomalies in diabetic pregnan-cies is a primary goal of preconception counseling. The ADA9 recommends that every woman of childbearing age and ability should be counseled about preconception care and monitoring. Most congenital anomalies that occur in diabetic pregnancies develop dur-ing organogenesis, the first 42 days of pregnancy, when all major organ sys-tems are forming.9 Hyperglycemia has a teratogenic effect on the forming organs, making tight blood glucose control nec-essary to prevent malformations. Most women are not even aware that they are pregnant until they are more than 14 days into the pregnancy. As a result of this lack of knowledge, congenital anomalies are more prevalent in this population of pregnant women. The best way to decrease the occurrence of these anomalies would be to achieve and maintain optimal blood glucose readings before becoming pregnant.5
Management of PregnanciesThe single most important intervention to achieve a normal, healthy pregnancy in the presence of type 1 diabetes is edu-cation and proper planning. As in the nondiabetic population, many pregnan-cies in diabetic women are unplanned. Therefore, sex education and preconcep-tion counseling are needed for preado-lescents, adolescents and all women of reproductive age.13 Educating all women with diabetes about birth control and family planning is necessary to prevent diabetes complications during pregnancy. Prepregnancy care and education should be provided by a multidisciplinary team of healthcare providers who consider all
Diabetes
for a woman with type 1 diabetes, pregnancy can be a time of fear and frustration. Partner with patients to achieve the best possible outcomes.
Are you Current?➼ wheN wAs The LAsT time you updated your ADVANCE subscription? Check your status at www.advanceweb.com/subscribe, or snap the tag on the cover.

23ADVANCE for NPs & PAs • November 2011
areas of health maintenance.Strict monitoring and maintenance
of blood glucose levels, close medica-tion management and supplementation with folic acid are all recommended for diabetic women who are planning to conceive. In addition, women who take oral diabetes medications need to be monitored for teratogenic effects and should be switched to medications that are safer for use during pregnancy.7 It is also important for women who are anticipating pregnancy to establish a rela-tionship with a healthcare team prior to conception, in order to help ease potential fears and frustration.
The American Diabetes Association website (www.diabetes.org) provides information about diet, exercise, medi-cations and preconception counseling resources across the country. The site also contains a link to the association’s bookstore, which offers printed materials to help guide diet and exercise regimens during pregnancy.
A Balancing ActFor a woman with type 1 diabetes, preg-nancy can be a time of fear and frustra-tion. Many women feel vulnerable when dealing with blood sugar fluctuations during pregnancy.2 A healthcare pro-vider who is too strict or demanding can potentially prompt feelings of incapability in these patients.
Striking a balance between adequate blood sugar control and acknowledgement of real-life challenges can be difficult for many healthcare providers. With a thorough understanding of the clinical issues as well as the practical everyday challenges, nurse practitioners and physi-cian assistants can partner with patients to achieve the best possible outcomes.
Poor glycemic control early in pregnan-cy can influence events later in pregnancy. The best way to prevent poor glycemic control is to provide preconception edu-cation and counseling.
One study found that the incidence of major congenital malformations in women who participated in preconcep-tion care was 1.0% to 1.7% compared with 1.4% to 10.9% in women who had no preconception care.10 Preconception education and prevention of unplanned
pregnancy are the two areas that must be addressed to decrease complications associated with pregnancy in diabetic women. ■
References1. Temple RC, et al. Prepregnancy care and preg-
nancy outcomes in women with type 1 diabetes. Diabetes Care. 2006;29(8):1744-1749.
2. Berg M. Pregnancy and diabetes: how women han-dle the challenges. J Perinat Educ. 2005;14(3):23-32.
3. Persson M, et al. Obstetric and perinatal outcomes in type 1 diabetic pregnancies: a large, population-based study. Diabetes Care. 2009;32(11):2005-2009.
4. Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treat-ment. Lancet. 2001;358(9277):221-229.
5. Walkinshaw SA. Pregnancy in women with pre-existing diabetes: management issues. Semin Fetal Neonatal Med. 2005;10(4):307-315.
6. Gabbe SG, Graves CR. Management of diabetes mellitus complicating pregnancy. Obstet Gynecol. 2003;102(4):857-868.
7. Taylor R, Davison JM. Type 1 diabetes and preg-nancy. BMJ. 2007;334(7596):742-745.
8. National Institute for Health and Clinical Excellence (United Kingdom). Diabetes in pregnancy: management of diabetes and its complications from pre-conception to the postnatal period. London, England: National Institute for Health and Clinical Excellence; 2008. http://www.nice.org.uk/CG63. Accessed Oct. 11, 2011.
9. American Diabetes Association. Standards of medical care in diabetes — 2011. Diabetes Care. 2011;34(suppl 1):S11-S61.
10. Kitzmiller JL, et al. Managing preexisting dia-betes for pregnancy: summary of evidence and con-sensus recommendations for care. Diabetes Care. 2008;31(5):1060-1079.
11. Lepercq J, et al. Factors associated with preterm delivery in women with type 1 diabetes: a cohort study. Diabetes Care. 2004;27(12):2824-2828.
12. Kerssen A, et al. Do HbA1c levels and the self-monitoring of blood glucose levels adequately reflect glycaemic control during pregnancy in women with type 1 diabetes mellitus? Diabetologia. 2006;49(1):25-28.
13. Michel B, Charron-Prochownik D. Diabetes nurse educators and preconception counseling. Diabetes Educat. 2006;32(1):108-116.
U.S. Postal Service Statement of Ownership, Management and Circulation
ADVANCE for NPs & PAs, USPS Publication No. 015-957, is owned and published monthly, 12 issues per year, by Merion Publications Inc., 2900 Horizon Drive, King of Prussia, PA 19406. Ann W. Kielinski is Publisher, Michelle Perron Pronsati and Michael Gerchufsky are Editors and Managing Editors, and their address is the same as listed above. Stockholder of Merion Publications Inc. is Ann W. Kielinski, 2900 Horizon Drive, King of Prussia, PA 19406. The Total Distribution for the September 2011 issue was 109,854 news magazines mailed Regular Periodicals, with 266 office copies retained, for a net bindery run of 110,120 copies. Of the 109,854 news magazines mailed for the September 2011 issue, 55,174 were requested by the recipients, through mail subscriptions or telephone requests and 425 were sent as free complimentary copies. The Total Average Distribution for the preceding 12 issues prior to October 1, 2011 was 115,072 news magazines mailed Regular Periodicals, with an average of 263 office copies, for an average net bindery run of 115,335 copies. Of the 115,072 news magazine average for the preceding 12 months, 58,873 was the average number of copies requested by mailed subscription or telephone request and 637 was the average number of copies sent as free complimentary copies.
Diabetes
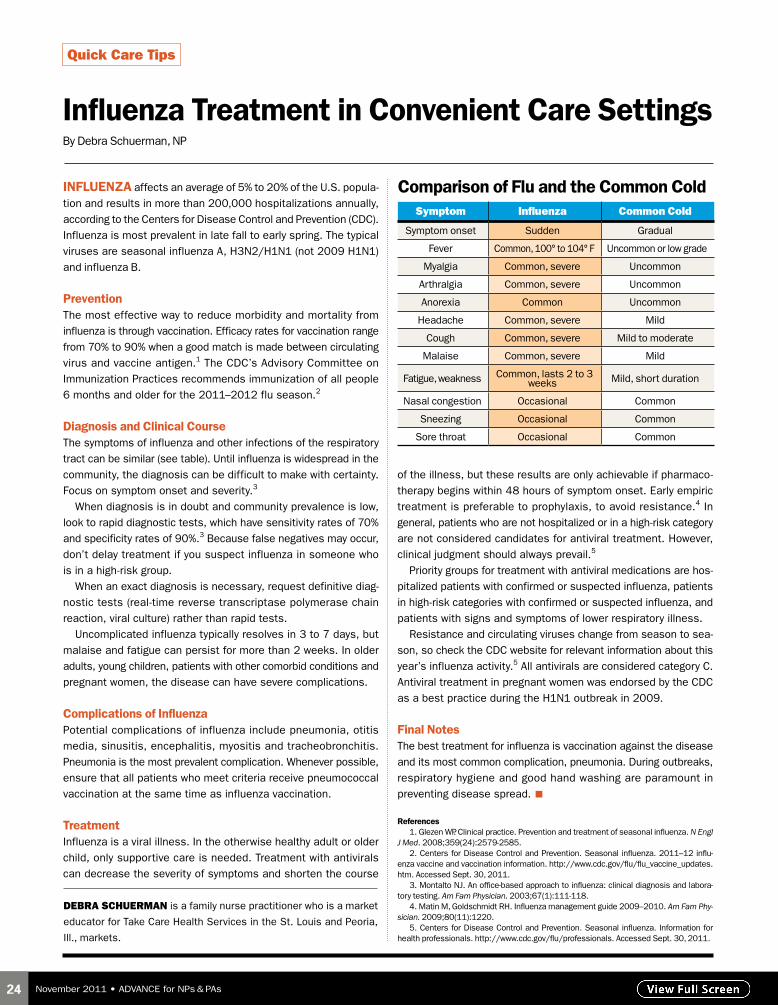
24 November 2011 • ADVANCE for NPs & PAs
INfLUeNzA affects an average of 5% to 20% of the U.S. popula-
tion and results in more than 200,000 hospitalizations annually,
according to the Centers for Disease Control and Prevention (CDC).
Influenza is most prevalent in late fall to early spring. The typical
viruses are seasonal influenza A, H3N2/H1N1 (not 2009 H1N1)
and influenza B.
PreventionThe most effective way to reduce morbidity and mortality from
influenza is through vaccination. Efficacy rates for vaccination range
from 70% to 90% when a good match is made between circulating
virus and vaccine antigen.1 The CDC’s Advisory Committee on
Immunization Practices recommends immunization of all people
6 months and older for the 2011–2012 flu season.2
Diagnosis and Clinical CourseThe symptoms of influenza and other infections of the respiratory
tract can be similar (see table). Until influenza is widespread in the
community, the diagnosis can be difficult to make with certainty.
Focus on symptom onset and severity.3
When diagnosis is in doubt and community prevalence is low,
look to rapid diagnostic tests, which have sensitivity rates of 70%
and specificity rates of 90%.3 Because false negatives may occur,
don’t delay treatment if you suspect influenza in someone who
is in a high-risk group.
When an exact diagnosis is necessary, request definitive diag-
nostic tests (real-time reverse transcriptase polymerase chain
reaction, viral culture) rather than rapid tests.
Uncomplicated influenza typically resolves in 3 to 7 days, but
malaise and fatigue can persist for more than 2 weeks. In older
adults, young children, patients with other comorbid conditions and
pregnant women, the disease can have severe complications.
Complications of InfluenzaPotential complications of influenza include pneumonia, otitis
media, sinusitis, encephalitis, myositis and tracheobronchitis.
Pneumonia is the most prevalent complication. Whenever possible,
ensure that all patients who meet criteria receive pneumococcal
vaccination at the same time as influenza vaccination.
TreatmentInfluenza is a viral illness. In the otherwise healthy adult or older
child, only supportive care is needed. Treatment with antivirals
can decrease the severity of symptoms and shorten the course
of the illness, but these results are only achievable if pharmaco-
therapy begins within 48 hours of symptom onset. Early empiric
treatment is preferable to prophylaxis, to avoid resistance.4 In
general, patients who are not hospitalized or in a high-risk category
are not considered candidates for antiviral treatment. However,
clinical judgment should always prevail.5
Priority groups for treatment with antiviral medications are hos-
pitalized patients with confirmed or suspected influenza, patients
in high-risk categories with confirmed or suspected influenza, and
patients with signs and symptoms of lower respiratory illness.
Resistance and circulating viruses change from season to sea-
son, so check the CDC website for relevant information about this
year’s influenza activity.5 All antivirals are considered category C.
Antiviral treatment in pregnant women was endorsed by the CDC
as a best practice during the H1N1 outbreak in 2009.
final NotesThe best treatment for influenza is vaccination against the disease
and its most common complication, pneumonia. During outbreaks,
respiratory hygiene and good hand washing are paramount in
preventing disease spread. ■
References1. Glezen WP. Clinical practice. Prevention and treatment of seasonal influenza. N Engl
J Med. 2008;359(24):2579-2585.2. Centers for Disease Control and Prevention. Seasonal influenza. 2011–12 influ-
enza vaccine and vaccination information. http://www.cdc.gov/flu/flu_vaccine_updates.htm. Accessed Sept. 30, 2011.
3. Montalto NJ. An office-based approach to influenza: clinical diagnosis and labora-tory testing. Am Fam Physician. 2003;67(1):111-118.
4. Matin M, Goldschmidt RH. Influenza management guide 2009–2010. Am Fam Phy-sician. 2009;80(11):1220.
5. Centers for Disease Control and Prevention. Seasonal influenza. Information for health professionals. http://www.cdc.gov/flu/professionals. Accessed Sept. 30, 2011.
Influenza Treatment in Convenient Care settingsBy Debra Schuerman, NP
Quick Care Tips
DebRa sChueRman is a family nurse practitioner who is a market
educator for Take Care Health Services in the St. Louis and Peoria,
Ill., markets.
Comparison of flu and the Common Coldsymptom influenza Common Cold
Symptom onset Sudden Gradual
Fever Common, 100° to 104° F Uncommon or low grade
Myalgia Common, severe Uncommon
Arthralgia Common, severe Uncommon
Anorexia Common Uncommon
Headache Common, severe Mild
Cough Common, severe Mild to moderate
Malaise Common, severe Mild
Fatigue, weakness Common, lasts 2 to 3 weeks Mild, short duration
Nasal congestion Occasional Common
Sneezing Occasional Common
Sore throat Occasional Common

25ADVANCE for NPs & PAs • November 2011
➼ OVeR The LAsT DeCADe, the management of chronic painful condi-tions, especially with opioid medications, has received much-needed and much-deserved attention.
The use of opioids for noncancer pain is increasing in the United States.1 The Drug Enforcement Agency estimates that between 360 million and 400 million pre-scriptions for opioid pain relievers were sold in 2005 alone.2 Thus, prescribers of opioid medications should have a full understanding of their long-term effects in addition to the more prominent issues of dependence and abuse.
For example, a significant body of evi-dence suggests that long-term opioid use can be associated with a decline in endocrine function; however, a number of studies suggests that this connection has not been explored and discussed thoroughly enough within the healthcare community.3,4
In recent years, researchers have begun to build studies and review information about the relationship between long-term opioid use and endocrine dysfunction. Whether opioids are ingested for medi-cal purposes or as drugs of abuse, their long-term use reportedly has been linked to hypogonadism, adrenal dysfunction, reduced bone mineral density and growth hormone abnormalities.
Opioid medications are used in a wide variety of chronic pain syndromes such as osteoarthritis, neuropathic pain and chronic low back pain. Synthetic and semi-synthetic derivations of the opium poppy plant can reduce pain by binding to specific receptors in the brain and spinal cord, thereby limiting the pain signal to the brain. Among the most common side effects of opioids are drowsiness, constipation and dependence.
HypogonadismRecent research has shed new light on the negative endocrine effects of long-term opioid therapy, either for chronic pain syndromes or as illicit drug use. Several studies in humans and in animal subjects have found evidence that opioids induce hypogonadism by suppressing the hypothalamic–pituitary–gonadal axis.5
william shane wooDall is a physician assistant at Select Medical Clinic in North Miami
Beach, Fla. He has completed a disclosure statement and reports no relationships related to
this article. The ADVANCE for NPs & PAs CME coordinator, John McGinnity, MS, PA-C, discloses
receiving honoraria from Boehringer Ingelheim.SC
OTT
DER
By
CME/CE: Endocrinology
Opioids & the Endocrine SystemLong-term opioid analgesia can lead to hypogonadism and other endocrine dysfunction
by william shane woodall, PA-C
Learning objectives1. Discuss the evidence linking long-term opioid use and endocrine dysfunction.
2. Describe the signs and symptoms of hypogonadism in men and women.
3. Review the effect of long-term opioids on endocrine system function.
4. Summarize the treatment of patients with chronic pain and opioid-induced endocrine dysfunction.
➤

26 November 2011 • ADVANCE for NPs & PAs
A review of these studies conducted over the last several years suggests that opioids induce hypogonadism by suppressing the secretion of the gonadotropin-releasing hormones — luteinizing hormone (LH) and follicle-stimulating hormone (FSH) — by the hypothalamus. The gonadotropins stimulate the production of androgen hormones by the gonads and adrenal glands.
Hypogonadism is a relatively common endocrine disorder, and it is diagnosed by clinical signs and symptoms and cor-relating laboratory studies. In men and women alike, complaints of sexual dys-function, depression and decreased body hair can be among the symptoms in an initial presentation of hypogonadism. Men might complain of gynecomastia and decreased testicle size; women are more likely to have complaints of missed menstrual periods and infertility.
Physical signs in both sexes can include increased body fat with a decrease in lean muscle mass, and osteopenia confirmed by bone density screening. Decreases in bone mineral density can lead to osteo-porosis, increase the risk of fractures
and prolong healing time. Low levels of testosterone in particular are associated with heart disease, increased cholesterol levels and decreased insulin sensitivity.
Tests of plasma levels of testosterone, estrogen, FSH and LH can be ordered in conjunction with the patient history and physical examination. Table 1 sum-marizes the normal reference ranges for these hormones.
Clinical EvidenceIn a cross-sectional study conducted in Canada, researchers studied the effects of long-term oral opioid use on the gonadal status and bone mineral density of men and women with chronic pain not relat-ed to cancer. Participants were treated with oral opioids for at least 1 year. The authors reported that, based on labora-tory measurements of hormone levels at baseline and again after at least 1 year, the prevalence of hypogonadism was considerably higher among the men, at 75%, compared with the women, of whom 21% had oligomenorrhea or amenorrhea indicating hypogonadism.6 Moreover, osteopenia was confirmed in 50% of the
men, while women were reported to have had bone loss at 21%.
Studies using animal models have reported similar findings. Researchers investigated the result of several widely used opioid medications to determine their effects on levels of plasma testos-terone and estradiol and levels of brain testosterone in male rats.7 The animals were injected subcutaneously with con-centrations of morphine, fentanyl, trama-dol, buprenorphine or saline for control. At 4 hours and again at 24 hours after opioid administration, blood samples were collected to measure testosterone and estradiol levels. The rats studied at 4 hours had a decrease in testosterone com-pared with controls, with the exception of rats treated with tramadol. Estradiol levels at 4 hours were decreased in the rats injected with morphine, tramadol or buprenorphine. Brain levels of tes-tosterone were dramatically reduced at 4 hours compared with controls. The study further investigated the magnitude and time-course of the effects of the opioids, and the authors concluded that commonly prescribed opioids had negatively affected
CME/CE: Endocrinology
Table 1
hormone Reference Ranges
hormone adult men adult women
Testosterone, total, serum (ng/dL)
249–836 (20–49 y) 8–48 (20–49 y)
193–740 (> 49 y) 3–41 (> 49 y)
estradiol, sensitive, serum (pg/mL)
3–70 9–175 (follicular phase)
107–281 (ovulation phase)
44–196 (luteal phase)
0–91 (with oral contraceptives)
42–289 (postmenopausal, treated)
0–19 (postmenopausal, untreated)
follicle-stimulating hormone, serum (mIU/mL)
1.5–12.4 3.5–12.5 (follicular phase)
4.7–21.5 (ovulation phase)
1.7–7.7 (luteal phase)
25.8–134.8 (postmenopausal)
Luteinizing hormone, serum (mIU/mL)
1.7–8.6 2.4–12.6 (follicular phase)
14.0–95.6 (ovulation phase)
1.0–11.4 (luteal phase)
7.7–58.5 (postmenopausal)
Source: Laboratory Corporation of America. Test menu. https://www.labcorp.com/wps/portal/provider/testmenu. Accessed Oct. 6, 2011.

27ADVANCE for NPs & PAs • November 2011
sex hormones in the brain and blood of laboratory rats.
In a study of HIV-positive participants, Cooper and colleagues found that opioid use added to the complicated metabolic and endocrine abnormalities associ-ated with HIV.8 The authors mentioned additional problems with glucose and lipid metabolism resulting from opioid use. Each of the studies concluded that opioids induced suppression of sex hor-mones and gonadotropins (FSH and LH) in men and women.
Other studies that include assessments of opioid-induced endocrinopathies have produced similar results, with study par-ticipants including men with and without chronic pain from cancer, HIV-positive male heroin users, and men and women with a variety of health statuses.8-11 Based on these studies, men appear to be gen-erally more affected by opioid-related endocrinologic disturbances, particu-larly suppression of sex hormones and gonadotropins, than women.
TreatmentWhen a patient is diagnosed with opi-oid-induced hypogonadism, among the therapeutic options are nonopioid pain management, opioid rotation and/or hormone replacement therapy when appropriate.
Testosterone replacement generally is recommended for men with a con-firmed hypogonadism diagnosis. In addi-tion to its indication for hypogonadism, replacing testosterone in men may pro-mote cardiovascular health by reducing inflammatory factors, creating healthier cholesterol levels and improving insulin sensitivity.12 Note that men older than 50 should be screened for prostate cancer before testosterone therapy is initiated, since certain prostate cancer types are androgen-dependent.
The preferred delivery of testosterone is a once-daily gel applied to the skin of the shoulders, upper arms or abdo-men. Weekly or biweekly intramuscu-
lar injections of testosterone cypionate or testosterone enanthate are another option. These oil-based preparations are usually injected in the gluteal muscles. Transdermal testosterone patches are commercially available; however, applica-tion site reactions have been reported.13 Table 2 summarizes testosterone delivery systems.
Estrogen replacement for opioid-induced hypogonadism in women is gen-erally recommended. Levels of estrogen, testosterone and gonadotropin should be obtained before a hypogonadism diagno-sis is confirmed in a woman.
Multiple delivery systems of estrogen are available for women, including pills, injections and patches. Where indicated, women younger than 40 may be treated with human chorionic gonadotropin (hCG) to stimulate the production of FSH and LH, important hormones in the induction of ovulation and fertility. Note, however, that the use of hCG may produce multiple births, and it should be prescribed and used with caution.
Understand the RisksIn an era with an emphasis on proper pain control and the escalating use of opioid pain medications,1,2 it is important for healthcare providers and their patients to be aware of the risks and benefits of long-term opioid use.
Opioids carry a well documented and often discussed risk of abuse and depen-dency, and research has demonstrated a connection between long-term opioid use and a negative effect on the endo-
crine system. A better understanding and awareness of these effects can help clinicians across multiple specialties better manage chronic pain and avoid the possible complications of long-term opioid use. ■
References1. Rhodin A, et al. Opioid endocrinopathy: a clinical
problem in patients with chronic pain and long-term oral opioid treatment. Clin J Pain. 2010;26(5):374-380.
2. U.S. Justice Department. DEA Congressional Testimony: Statement of Joseph T. Rannazzisi, Deputy Assistant Administrator, Office of Diversion Control, Drug Enforcement Administration, regard-ing “Electronic Prescribing of Controlled Substances: Addressing Health Care and Law Enforcement Priorities,” before the Senate Judiciary Committee. Dec. 4, 2007. http://www.usdoj.gov/dea/pubs/cngrtest/ct120407p.html. Accessed Sept. 16, 2011.
3. Katz N, Mazer NA The impact of opioids on the endocrine system. Clin J Pain. 2009;25(2):170-175.
4. Chapman CR, et al. Opioid pharmacotherapy for chronic non-cancer pain in the United States: a research guideline for developing an evidence-base. J Pain. 2010;11(9):807-829.
5. Aloisi AM, et al. Endocrine consequences of opioid therapy. Psychoneuroendocrinology. 2009;34(suppl 1):S162-S168.
6. Fraser LA, et al. Oral opioids for chronic non-cancer pain: higher prevalence of hypogonadism in men than in women. Exp Clin Endocrinol Diabetes. 2009;117(1):38-43.
7. Ceccarelli I, et al. Single opioid administration modifies gonadal steroids in both the CNS and plasma of male rats. Neuroscience. 2006;140(3):929-937.
8. Cooper OB, et al. Opiate drug use: a potential contributor to the endocrine and metabolic complica-tions in human immunodeficiency virus disease. Clin Infect Dis. 2003;37(suppl 2):S132-S136.
9. Wisniewski AB, et al. Hypothalamic-pituitary-gonadal function in men and women using heroin and cocaine, stratified by HIV status. Gend Med. 2007;4(1):35-44.
10. Elliott JA, et al. The endocrine effects of long-term oral opioid therapy: a case report and review of the literature. J Opioid Manag. 2011;7(2):145-154.
11. Merza Z. Chronic use of opioids and the endocrine system. Horm Metab Res. 2010;42(9):621-626.
12. Feeley RJ, et al. Testosterone in men’s health: a new role for an old hormone. J Mens Health. 2009;6(3):169-176.
13. Lakshman KM, Basaria S. Safety and efficacy of testosterone gel in the treatment of male hypogonad-ism. Clin Interv Aging. 2009;4:397-412.
CME/CE: Endocrinology
Table 2
Testosterone Delivery Systems
Transdermal 1% testosterone gel 5–10 g applied each morning
Intramuscular injections
Testosterone cypionate 100–200 mg weekly or biweekly
Testosterone enanthate 100–400 mg weekly to monthly
Transdermal patches, 1 or 2 patches (5–10 mg) applied daily
Subcutaneous pellet implants
26 pellets implanted every 3–6 months
A significant body of evidence suggests that long-term opioid use can be associated with a decline in endocrine function. This connection has not been explored and discussed thoroughly enough by the healthcare community.

28 November 2011 • ADVANCE for NPs & PAs
CME/CE: Endocrinology
Registrant Information (Please Print)
Subscriber No. (see mailing label) ____ ____ ____ ____ ____ ____ ____ ____ ____
Required for Florida NPs: License No. ___________________________________________
E-mail Address ______________________________________________________________
Name ______________________________________________________________________
Address ❏ Work ❏ Home ___________________________________________________
City ____________________________________ State ______ Zip Code _______________
Phone No. ❏ Work ❏ Home _________________________________________________
Payment: $10❏ For PAs: Check Payable to Wayne State University
❏ For NPs: Check Payable to Merion Matters
❏ For PAs or NPs: Credit Card No. ________________________ Exp. Date___________
Cardholder Name ________________________________________________________
Signature _______________________________________________________________
❏ American Express ❏ Visa ❏ MasterCard ❏ Discover
statement of CompletionI attest to having completed the CME/CE activity.
Signature _____________________________________________ Date _________________
Profession ❏ Nurse Practitioner ❏ Physician Assistant
Questions1. which one of the following is not among the conditions linked to long-term opioid use?a. Hypogonadismb. Hypergonadismc. Adrenal dysfunctiond. Reduced bone mineral density
2. which one of the following lists the most common side effects of opioids?a. Sexual dysfunction, depression and decreased body hairb. Heart disease, increased cholesterol levels and decreased insulin sensitivityc. Drowsiness, constipation and dependenced. Osteoarthritis, neuropathic pain and chronic low back pain
3. studies in humans and in animals suggest that opioids induce hypogonadism by suppressing ________.a. the hypothalamic–pituitary–gonadal axisb. the hypothalamic–pituitary–adrenal axisc. the renal–angiotensin–aldosterone axisd. the hypothalamic–pituitary–thyroid axis.
4. A test for which one of the following is not typically ordered when hypogonadism is suspected?a. testosteroneb. estrogenc. follicle-stimulating hormoned. fasting glucose
5. Results of one cross-sectional study of long-term oral opioid use on patients’ gonadal status and bone mineral density showed that:a. Hypogonadism and osteopenia were both more prevalent in women.b. Hypogonadism and osteopenia were both more prevalent in men.c. Hypogonadism and osteopenia were equally as prevalent in men and women.d. Hypogonadism was more prevalent in men, while osteopenia was more prevalent in women.
6. which of the following are not among the therapeutic options for a patient with opioid-induced hypogonadism?a. Non-opioid pain managementb. Opioid rotationc. Hormone replacement therapyd. Synthetic opioid medications
7. In addition to its indication for hypogonadism, replacing testosterone in men has
been reported to promote cardiovascular health by reducing inflammatory factors, creating healthier cholesterol levels and improving insulin sensitivity.a. Trueb. False
8. which of the following testosterone delivery methods is associated with reports of application site reactions?a. Topical testosterone gelsb. Intramuscular testosterone cypionate injectionsc. Intramuscular testosterone enanthate injectionsd. Transdermal patches
9. Levels of estrogen, testosterone and gonadotropin should be obtained before a hypogonadism diagnosis is confirmed in a woman.a. Trueb. False
10. women younger than 40 may be treated with ____ in order to stimulate the production of fsh and Lh.a. oral contraceptivesb. human chorionic gonadotropinc. testosteroned. estrogen
Evaluation1. The content was appropriate for my needs.a. strongly disagreeb. disagreec. neutrald. agreee. strongly agree
2. The educational objectives were achieved.a. strongly disagreeb. disagreec. neutrald. agreee. strongly agree
3. The information provided was practical and can be applied to my professional needs.a. strongly disagreeb. disagreec. neutrald. agreee. strongly agree
4. The information in the article was fair, balanced, free of commercial bias and supported by scientific evidence.a. strongly disagreeb. disagreec. neutrald. agreee. strongly agree
Opioids & the endocrine system • NPPA15Registration & Answer formThis activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of Wayne State University School of Medicine and ADVANCE for NPs & PAs. The Wayne State University School of Medicine is accredited by the ACCME to provide continuing medical education for physicians.
The Wayne State University School of Medicine designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit(s).™ Physicians should only claim credit commensurate with the extent of their participation in the activity.
This activity also is approved for 2 CE contact hours. The issuer of CE contact hours is Merion Publications (a division of Merion Matters), which is approved as a provider of continuing education in nursing by three agencies. For details on CE provider numbers, visit the CE Test Center on our website, www.advanceweb.com/NPPA.
for PAs:To obtain CME credit, send the completed answer form and registrant information to Wayne State University School of Medicine, Attn PA, University Health Center 9A, 4201 Saint Antoine St., Detroit, MI 48201. Include a check for $10 payable to Wayne State University. Or fax the completed form and credit card information to (313) 577-7554. For online payment, visit http://www.med.wayne.edu/cme/calendarReg.html. Test takers who earn a passing score will receive a CME certificate by mail, or if paying online can receive an online transcript once registered at http://www.med.wayne.edu/cme/calendarTran.html. For questions about CME, call Wayne State University at (313) 577-1453. This CME form must be postmarked or received within 6 months of the last day of the month of this issue of ADVANCE.
for NPs:To obtain CE contact hours, take this test online at www.advanceweb.com/NPPA and receive instant test results and a printable CE certificate upon passage. Or fax the completed form and credit card information to (610) 278-1426. Or send the completed answer form and registrant information to Merion Matters CE Program for NPs, 2900 Horizon Dr., King of Prussia, PA 19406. Include a check for $10 payable to Merion Matters. This activity is eligible for CE credit for 2 calendar years after publication.
Test NPPA15 A B C D
1.
2.
3.
4.
5.
A B C D
6.
7.
8.
9.
10.
Evaluation A B C D E
1.
2.
3.
4.
Opioids & the Endocrine System November 2011

29ADVANCE for NPs & PAs • November 2011
Rheumatology
➼ INfLAMMATORy ARThRITIs can have disabling effects on otherwise healthy adults and children. In both primary care and specialty settings, NPs and PAs may face challenges when selecting effective treatments for patients experiencing the sequelae of inflammatory arthritis.
Inflammatory arthritis is characterized by inflammation of tissues surrounding the joints. Connective tissue diseases, crystal deposition diseases, infectious arthritis and spon-dyloarthropathies are examples of inflammatory arthritis. Osteoarthritis does not fall into the category of inflammatory arthritis because it is a degenerative disease.
Current treatment for inflammatory arthritis focuses on alleviating symptoms rather than targeting the cause of the condition. This approach primarily employs anti-inflammatory medications for first-line treatment. For severe cases, immu-nomodulatory drugs are used.
For decades, researchers have examined and debated the possibility of an infectious cause for inflammatory arthritis. A notable body of research has identified Mycoplasma as a possible causative organism for many cases of inflammatory arthritis. This article outlines these findings and discusses their implications for practice.
Inflammatory ArthritisThe category of inflammatory arthritis encompasses several types of arthritis, including rheumatoid and psoriatic arthritis. These forms of arthritis have an etiology that is not thoroughly understood, but each type is thought to involve autoimmune processes.1,2
Rheumatoid arthritis is characterized by variable levels of joint inflammation, usually occurring bilaterally in peripheral joints. Symptoms range from mild intermittent stiffness, swelling and discomfort to severe and debilitating joint dam-age.1 The cause of rheumatoid arthritis is unknown, but a proposed theory is that it involves an immune system reaction to infection in patients who are genetically predisposed to this response.1 Polyclonal immunoglobulin and autoantibody rheumatoid factor are produced within the synovial tissue,
sonJa huebneR wRighT is a family nurse practitioner at The Valley
Clinic in Ellensburg, Wash. She has completed a disclosure statement
and reports no relationships related to this article.TOM
WH
ALE
N
leading to local formation of immune complexes.1 Antibodies to the components of synovial tissue may also contribute to inflammation.1
In patients with rheumatoid arthritis, the synovium contains secreted products of activated lymphocytes, macrophages and fibroblasts. The local production of these cytokines and chemokines appears to account for many of the pathologic and clinical manifestations of rheumatoid arthritis.1
In comparison, psoriatic arthritis occurs only in patients with psoriasis. It is a diagnosis based on exclusion of other arthritis etiologies and the presence of psoriatic skin lesions. Erythrocyte sedimentation rate and C-reactive protein are often elevated in psoriatic arthritis, but these are nonspecific findings.2
Interestingly, the inflamed synovium evident in psori-atic arthritis resembles that seen in rheumatoid arthritis.2 Many rheumatology experts believe that psoriatic arthritis is immune-mediated because the synovium in affected patients shows infiltration with T cells, B cells, macrophages and NK receptor-expressing cells. Also evident is upregulation of leukocyte homing receptors.2 These features suggest a shared etiology of autoimmune-related inflammation in psoriatic and rheumatoid arthritis.
Research About PathogenesisIn 2000, Johnson and colleagues conducted a landmark study that investigated a suspected association between Mycoplasma fermentans and rheumatoid arthritis; this possible association
Inflammatory ArthritisDon’t overlook a possible infectious process by sonja huebner wright, MsN, fNP, CeN

30 November 2011 • ADVANCE for NPs & PAs
had been discussed for several decades.3 The researchers used polymerase chain reaction (PCR) techniques to identify pathogens in the synovial fluid of patients with inflammatory arthritis. Of the 26 study participants with rheumatoid arthritis, 23 (88%) had M fermentans in their synovial fluid. Although M fermen-tans was not identified in three patients with rheumatoid arthritis, two of these patients had “clinically quiescent disease” at the time of study.
Outside the participants with rheu-matoid arthritis, 8 patients had other arthritis conditions including reactive arthritis, pauciarticular juvenile chronic arthritis, gout, ankylosing spondylitis and psoriatic arthritis. In this group of patients with other forms of inflammatory arthritis, 7 of 8 (88%) had M fermentans in their synovial fluid. Ten participants had osteoarthritis, and M fermentans was not detected in any of them.
The researchers concluded that due to the frequency with which Mycoplasma was found in the synovial fluid of patients with inflammatory arthritis, these bac-teria were likely playing a role in the pathology of these diseases.3
An earlier study (1996) by Schaeverbeke and colleagues had also sought to isolate M fermentans from synovial fluid in patients with rheumatoid arthritis. In this study, researchers detected M fer-mentans in the joints of 21% of patients with rheumatoid arthritis, 20% of patients with psoriatic arthritis and 13% of patients with unclassified arthritis.4 Although the authors concluded that Mycoplasma was likely associated with rheumatic disease, they acknowledged that the exact explanation for and consequence of this organism in synovial fluid was not understood. Johnson and colleagues
mentioned the Schaeverbeke study in their article and attributed the lower detection of Mycoplasma organisms to decreased sensitivity of PCR assays at that time.3
Given existing research, M fermentans appears to be associated with inflam-matory arthritis. But is it involved in the pathogenesis of the diseases in this category? An experimental study by Rivera and colleagues, published in 2002, explored this question. The researchers injected two strains of M fermentans (P 140 and PG 18) into the knees of 14 rabbits.5 They injected one strain of M fermentans (P 140) in the trachea of 14 other rabbits to investigate the ability of M fermentans to reach the joints of these animals and produce arthritis.
The researchers found that M fer-mentans produced acute arthritis in the rabbits, and that the P 140 strain was associated with a more rapid and severe onset of arthritis compared with the PG 18 strain. Joints other than those inoculated directly with the Mycoplasma strains also developed arthritis, as did the joints of the rabbits inoculated with Mycoplasma via the trachea.
A study by Kawahito and colleagues, published in 2008, further investigated the role of M fermentans as a patho-gen by making the connection between Mycoplasma glycolipids, the known anti-gens of Mycoplasma, and rheumatoid arthritis symptoms.6 Researchers found the glycolipid antigen of Mycoplasma, GGPL-III, in the synovial fluid of 38.1% of patients with rheumatoid arthritis. They detected none in the synovial fluid of patients with osteoarthritis or in the synovial fluid of patients who were unaf-fected by arthritis.
The authors concluded that glycolipids
from M fermentans may play a role in initiating and perpetuating the synovitis of rheumatoid arthritis.6
Although the intricacies of the Mycoplasma–arthritis connection are not fully understood, what we do know about Mycoplasma, its effect on the immune system and its pathogenic role in arthritis is compelling.
Additional research would further clarify this, but considerable evidence of the connection between Mycoplasma and inflammatory arthritis exists — enough to warrant consideration of this pathology when treating arthritis.
Research About TreatmentIn the 1990s, several studies evaluated the effects of antibiotic therapy on inflam-matory arthritis, particularly rheumatoid arthritis.7 The results showed signifi-cant improvement in arthritis symptoms and associated laboratory results among patients who received oral minocycline compared with patients who were treated with placebo.7
In a large double-blind, placebo-controlled trial, Tilley and colleagues examined the safety and efficacy of mino-cycline in the treatment of rheumatoid arthritis.8 Study participants were 219 adults with active rheumatoid arthri-tis in six clinical centers in the United States. After 48 weeks, the group who had received minocycline 200 mg daily demonstrated more improvement in joint swelling and tenderness than did patients in the placebo group. Patients who received minocycline treatment had improved hematocrits, erythrocyte sedimentation rates, platelet counts and IgM rheumatoid factor levels. And at 48 weeks, more patients in the minocycline group had laboratory values within nor-mal ranges. The frequency of reported side effects was similar in both groups, and no serious toxicity occurred.8
Other research has investigated the use of doxycycline 100 mg twice daily
Rheumatology
Infectious etiologies for inflammatory arthritis should be examined with further research. we owe it to patients to provide the best treatment possible for this disabling group of conditions.
More Arthritis Articles➼ ReAD AbOUT all types of arthritis at our website. In the Search Articles box at www.advanceweb.com/NPPA, enter “arthritis.”

GET EXCLUSIVE CONTENT DELIVERED RIGHT TO YOUR INBOX EACH WEEK
ADVANCE HAS A HELPFUL SOLUTION TO FIT YOUR HECTIC SCHEDULE.
Once a week, we’ll send you an email highlighting the latest
imaging and radiation oncology developments, including:
• Timely industry news updates
• Featured articles you won’t fi nd in print
• Stimulating blog entries
• Exclusive multimedia
• Contests and surveys
SIGN UP TODAYVisit www.advanceweb.com/NPPA. Just enter your name, email address and zip code halfway down the right side of the page. It’s that simple!
Sign up for our FREE weekly e-newsletter and we’ll bring the news to you.
advance FOR
31ADVANCE for NPs & PAs • November 2011

32 November 2011 • ADVANCE for NPs & PAs
for rheumatoid arthritis. Two placebo-controlled studies per-formed in the late 1990s documented benefit in the treatment groups after 26 weeks.9
A significant study by O’Dell and colleagues, published in 1999, examined the long-term effects of treating rheumatoid arthritis with minocycline.10 The study followed up with 46 patients who had participated in a double-blind study of twice-daily dosing of 100 mg of minocycline 4 years prior. After the initial study, all patients had been returned to conventional treatments for rheumatoid arthritis. O’Dell and colleagues discovered that 40% of the patients who had received the minocycline treatment 4 years earlier had rheumatoid arthritis that was in remission — without the use of steroid therapy or disease-modifying anti-rheumatic drugs (DMARDs). The same was true in less than 0.6% of patients who had been in the placebo group.
The authors concluded that if patients with early rheumatoid arthritis are treated with minocycline, the need for conven-tional therapy may be reduced and remissions may be more frequent.10 This research suggests that antibiotic therapy may be considered in the treatment of patients with inflammatory arthritis, along with NSAIDs and disease-modifying drugs.
Current PracticeCurrent recommended therapies for rheumatoid and psoriatic arthritis do not include antibiotics and emphasize NSAIDs,
intra-articular glucocorticoid injections, DMARDs (including sulfasalazine, leflunomide, methotrexate and cyclosporine) and tumor necrosis factor inhibitors.11,12 Prescribing practices occur in that general order, based on disease severity.11,12
Given the improvements documented in rheumatoid arthri-tis patients treated with minocycline therapy compared with placebo, it is reasonable to ask why this therapy is not more widely used for inflammatory arthritis.
PCR analysis of synovial fluid could be conducted beforehand to confirm the presence of Mycoplasma. If research to date is considered insufficient to recommend a trial of antibiotics, further research should be conducted. If antibiotic therapy targeting Mycoplasma has a high likelihood of success, it merits consideration.
Application in Clinical SettingsAlthough research has identified Mycoplasma in cases of inflammatory arthritis and some studies show significant improvement in arthritis symptoms with antibiotic therapy, this approach to the treatment of inflammatory arthritis has not been incorporated into general guidelines for treatment.
Nurse practitioners and physician assistants should be aware of published research that has linked Mycoplasma with inflam-matory arthritis, as well as successes in treating inflammatory arthritis with antibiotic therapy. When treating a patient affected by inflammatory arthritis, consider PCR testing of synovial fluid to rule out Mycoplasma infection. And with or without this confirmatory test, consider the potential risks and benefits of a trial of antibiotic therapy in each clinical scenario. However, limited information is available about the dosing and duration of antibiotic therapy for Mycoplasma-associated arthritis.
Infectious etiologies for inflammatory arthritis should be examined with further research. We owe it to patients to provide the best treatment possible for this disabling group of conditions. ■
References1. Lipsky PE. Rheumatoid arthritis. In: Fauci AS, et al, eds. Harrison’s Principles
of Internal Medicine. 17th ed. New York, NY: McGraw-Hill; 2008: 2083-2091.2. Taurog JD. The spondylarthritides. In: Fauci AS, et al, eds. Harrison’s Principles
of Internal Medicine. 17th ed. New York, NY: McGraw-Hill; 2008: 2109-2118.3. Johnson S, et al. Identification of Mycoplasma fermentans in synovial fluid
samples from arthritis patients with inflammatory disease. J Clin Microbiol. 2000;38(1):90-93.
4. Schaeverbeke T, et al. Mycoplasma fermentans, but not M penetrans, detected by PCR assays in synovium from patients with rheumatoid arthritis and other rheumatic disorders. J Clin Pathol. 1996;49(10):824-828.
5. Rivera A, et al. Experimental arthritis induced by a clinical Mycoplasma fermentans isolate. BMC Musculoskelet Disord. 2002;3(3):15.
6. Kawahito Y, et al. Mycoplasma fermentans glycolipid-antigen as a pathogen of rheumatoid arthritis. Biochem Biophys Res Commun. 2008;369(2):561-566.
7. Vojdani A. Scientific reality versus hypothesis about mycoplasma. Biomed Ther. 1998;16(4):277-279.
8. Tilley BC, et al. Minocycline in rheumatoid arthritis. A 48-week, double-blind, placebo-controlled trial. MIRA Trial Group. Ann Intern Med. 1995;122(2):81-89.
9. Yanick P Jr. Mycoplasma: its hidden role in rheumatoid arthritis and other clinical syndromes. Townsend Letter for Doctors & Patients. May 2002:40-42.
10. O’Dell JR, et al. Treatment of early seropositive rheumatoid arthritis with minocycline: four-year followup of a double-blind, placebo-controlled trial. Arthritis Rheum. 1999;42(8):1691-1695.
11. Ritchlin CT, et al. Treatment recommendations for psoriatic arthritis. Ann Rheum Dis. 2009;68(9):1387-1394.
12. Saag KG, et al. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59(6):762-784.
Rheumatology
FREE WEBINARSFROM ADVANCE
■ Environmental Asthma Triggers: Primary Care TipsWednesday, Nov. 16 • 3:00 - 4:00 PM ET
Improve the quality of comprehensive asthma care by incorporating culturally and linguisti-cally appropriate education on environmental asthma trigger management consistent with the 2007 NAEPP guidelines.
About the Speakers: Lois Wessel, RN, CFNP (R) is the associatedirector for programs at the Association of Clinicians for theUnderserved (ACU). Wessel has developed and delivered trainingmodules for community-based clinics in the areas of asthma education, prevention of early childhood caries, health literacy, medication management for patients with limited English pro-fi ciency (LEP) and use of medical interpreters. Anna M. Gard, FNP-BC (L) is a certifi ed family nurse practitioner and a team clinician for the VNA Community Health Services Children’sClinic, a nurse managed health center, and a participant in the Pennsylvania Chronic Care Initiative.
NOVEMBER 2011
SIGN UP ONLINE FOR THESE FREE EVENTS! www.advanceweb.com/NPPA

33ADVANCE for NPs & PAs • November 2011
Orthopedics
➼ shOULDeR PAIN is a common musculoskeletal complaint.1 Among younger patients, shoulder pain often results from athletic activities. Excessive, repetitive overhead motions such as those in tennis, swimming, weightlifting and pitching can produce injury to the shoul-der.2 The most common shoulder injuries
are instability, impingement and rotator cuff tears.2 Many of these conditions are serious enough to warrant surgery.
Shoulder arthroscopy is a common surgical approach used when noninvasive treatment modalities don’t sufficiently reduce pain.3 Within the category of arthroscopic shoulder surgery, the pro-
kimbeRly baiRD is a family nurse practitioner and certified perioperative nurse who practices
at Jacksonville Pediatric Associates in Jacksonville, Fla. kevin m. kaplan is an orthopedic
surgeon who specializes in sports medicine and advanced arthroscopy at Jacksonville Orthopaedic
Institute in Jacksonville.
JEFF
REy L
EES
ER
Shoulder Chondrolysis This rare complication has been linked with postop pain management
by kimberly baird, fNP-bC, MsN, CNOR, and kevin M. kaplan, MD
cedures are numerous. These surgical interventions have inherent risks but offer potential significant benefits to the patient. A rare but potentially devastat-ing complication of arthroscopic surgery within the glenohumeral joint, especially in young athletes, is chondrolysis.
AnatomyThe shoulder is a complex structure com-posed of three bones and four articula-tions: the clavicle, scapula and humerus bones and the acromioclavicular, ster-noclavicular, scapulothoracic and gle-nohumeral joints.4
The glenohumeral joint is an articula-tion between the humeral head and the shallow curvature between the lateral thickening of the scapula (the glenoid).3 The concave and convex surfaces provide stability when muscle forces compress the joint during movement and at rest. Although the joint assimilates a ball-and-socket movement, only one-third of the humeral head is covered by the glenoid during rotation or movement.3
Articular cartilage is the dense con-nective tissue that covers the articulating surfaces of synovial joints.5 As a conse-quence of normal motion and degradation, the appearance of cartilage can change over time. Its thickness varies depend-ing on the function and biomechanics of the joint.
Articular cartilage lacks a blood sup-ply, lymphatic system and nerves.5 It is composed of a solid matrix and water.5 Chondrocytes are part of the solid matrix, along with collagen and proteoglycans. Proteoglycans are the protein core and are connected with chains of repeating disaccharide units of chondroitin, gly-cosaminoglycan subunits and hyaluronic acid. The proteoglycans are important in fluid transport and hydration. Collagen helps provide support for the stresses generated by an articulation.5 A synovial joint is formed by two opposing articular surfaces, each covered by articular carti-lage. The joint is enclosed within a capsule that contains synovial fluid.6
Chondrocytes represent a relatively small percentage of the articular car-tilage, and they produce extracellular material, proteoglycans and collagen. ➤

34 November 2011 • ADVANCE for NPs & PAs
Orthopedics
Table 1
NsAID Treatment for shoulder Chondrolysis, Osteoarthritis and Inflammatory Processes20
DRUG DOSAGE (> 14 years old) CONTRAINDICATIONs
Ibuprofen 200–800 mg every 6–8 hours as needed. Max 3,200 mg/24 hours. Use lowest effective dose for the shortest duration. Take with food.
Hypersensitivity to drug, class or components; CABG surgery; perioperative pain; pregnancy 3rd trimester, if taken with ASA, COX-2 inhibitors, thiazide, ACE inhibitors, beta-blockers, acetaminophen or ARBs. Caution in presence of CAD, HTN, HF, dehydration, PUD, history of GI bleed, coagulopathy, chronic alcohol abuse, smoker, hepatic impairment, renal impairment, asthma, prolonged use
Acetaminophen 325–650 mg every 4–6 hours, not to exceed 4 g/day. Use lowest effective dose for the shortest duration. Take with food.
Hypersensitivity to drug, class or components, chronic alcohol use, hepatic impairment, renal impairment (long-term use) G6PD deficiency, PKU
Celecoxib 50, 100, 200 mg; 200 mg by mouth once daily or 100 mg by mouth twice daily. Start at 50% of lowest dose if poor CyP2C9 metabolizer. Use lowest effective dose for shortest duration.
Same as ibuprofen plus: sulfonamides, poor CyP2C9 metabolizer, JRA
Diclofenac sodium 25, 50, 75 mg; 75 mg twice daily or max 150 mg/day. Use lowest effective dose for the shortest duration. Take with food.
Same as ibuprofen plus: corticosteroid use, anticoagulant use
Etodolac 200, 300 mg; 300 mg by mouth three times daily for 7–14 days. Use lowest effective dose for the shortest duration.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
Indomethacin 25, 50 mg; 25–50 mg by mouth three times daily; max 200 mg/day. Use lowest effective dose for the shortest duration. Take with food.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
ketoprofen 50, 75, or 200 ER; 75 mg by mouth three times daily or 50 mg by mouth four times daily or 200 ER by mouth once daily; max 300 mg/day or 200 mg/day ER. Use lowest effective dose for the shortest duration. Take with food.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
Meclofenamate 50, 100 mg; 50–100 mg by mouth twice or three times daily; max 400 mg/day. Use lowest effective dose for the shortest duration. Take with food.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
Nabumetone 500, 750 mg; 1,000–2,000 mg by mouth per day divided once daily or twice daily; max 2,000 mg/day for 7–14 days. Use lowest effective dose for the shortest duration.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
Naproxen sodium 220, 275, 550 mg; 275–550 mg by mouth every 12 hours; max 1,375 mg/day acute; 1,100 mg/day chronic. Use lowest effective dose for the shortest duration.
Same as ibuprofen plus: sodium restriction, smoking habit changes, debilitated patients, elderly patients
Oxaprozin 600 mg; 1,200 mg by mouth once daily; max 1,800 mg/day. Use lowest effective dose for the shortest duration.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
Piroxicam 10, 20 mg; 20 mg by mouth once daily; max 20 mg/day. May divide dose twice daily. Use lowest effective dose for the shortest duration.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics
Sulindac 150, 200 mg; 150–200 mg by mouth twice daily; max 400 mg/day. Use lowest effective dose for the shortest duration. Take with food.
Same as ibuprofen plus: corticosteroid use, anticoagulant use, concurrent diuretics, SLE, mixed connective tissue disease, history of renal lithiasis
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; ASA, acetylsalicylic acid; CABG, coronary artery bypass graft; CAD, coronary artery disease; COX-2, cyclo-oxygenase-2; ER, extended release; G6PD, glucose-6-phosphate dehydrogenase; HF, heart failure; HTN, hypertension; JRA, juvenile rheumatoid arthritis; PKU, phenylketonuria; PUD, peptic ulcer disease; SLE, systemic lupus erythematosus.
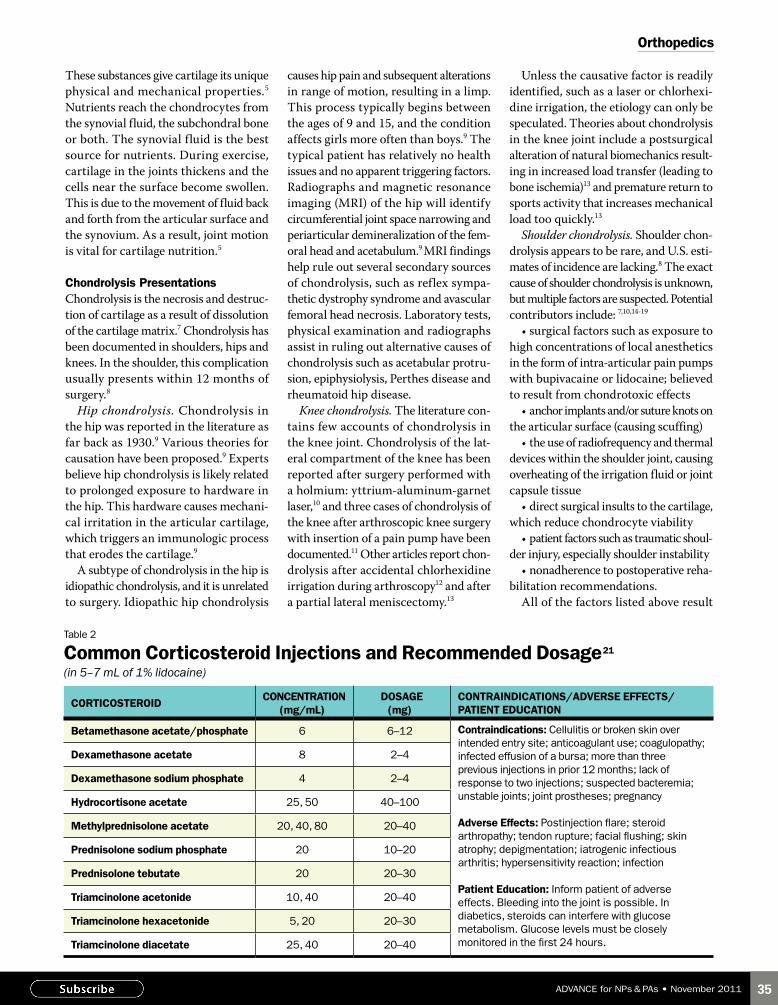
35ADVANCE for NPs & PAs • November 2011
These substances give cartilage its unique physical and mechanical properties.5 Nutrients reach the chondrocytes from the synovial fluid, the subchondral bone or both. The synovial fluid is the best source for nutrients. During exercise, cartilage in the joints thickens and the cells near the surface become swollen. This is due to the movement of fluid back and forth from the articular surface and the synovium. As a result, joint motion is vital for cartilage nutrition.5
Chondrolysis PresentationsChondrolysis is the necrosis and destruc-tion of cartilage as a result of dissolution of the cartilage matrix.7 Chondrolysis has been documented in shoulders, hips and knees. In the shoulder, this complication usually presents within 12 months of surgery.8
Hip chondrolysis. Chondrolysis in the hip was reported in the literature as far back as 1930.9 Various theories for causation have been proposed.9 Experts believe hip chondrolysis is likely related to prolonged exposure to hardware in the hip. This hardware causes mechani-cal irritation in the articular cartilage, which triggers an immunologic process that erodes the cartilage.9
A subtype of chondrolysis in the hip is idiopathic chondrolysis, and it is unrelated to surgery. Idiopathic hip chondrolysis
causes hip pain and subsequent alterations in range of motion, resulting in a limp. This process typically begins between the ages of 9 and 15, and the condition affects girls more often than boys.9 The typical patient has relatively no health issues and no apparent triggering factors. Radiographs and magnetic resonance imaging (MRI) of the hip will identify circumferential joint space narrowing and periarticular demineralization of the fem-oral head and acetabulum.9 MRI findings help rule out several secondary sources of chondrolysis, such as reflex sympa-thetic dystrophy syndrome and avascular femoral head necrosis. Laboratory tests, physical examination and radiographs assist in ruling out alternative causes of chondrolysis such as acetabular protru-sion, epiphysiolysis, Perthes disease and rheumatoid hip disease.
Knee chondrolysis. The literature con-tains few accounts of chondrolysis in the knee joint. Chondrolysis of the lat-eral compartment of the knee has been reported after surgery performed with a holmium: yttrium-aluminum-garnet laser,10 and three cases of chondrolysis of the knee after arthroscopic knee surgery with insertion of a pain pump have been documented.11 Other articles report chon-drolysis after accidental chlorhexidine irrigation during arthroscopy12 and after a partial lateral meniscectomy.13
Unless the causative factor is readily identified, such as a laser or chlorhexi-dine irrigation, the etiology can only be speculated. Theories about chondrolysis in the knee joint include a postsurgical alteration of natural biomechanics result-ing in increased load transfer (leading to bone ischemia)13 and premature return to sports activity that increases mechanical load too quickly.13
Shoulder chondrolysis. Shoulder chon-drolysis appears to be rare, and U.S. esti-mates of incidence are lacking.8 The exact cause of shoulder chondrolysis is unknown, but multiple factors are suspected. Potential contributors include: 7,10,14-19
•surgicalfactorssuchasexposuretohigh concentrations of local anesthetics in the form of intra-articular pain pumps with bupivacaine or lidocaine; believed to result from chondrotoxic effects•anchorimplantsand/orsutureknotson
the articular surface (causing scuffing)•theuseofradiofrequencyandthermal
devices within the shoulder joint, causing overheating of the irrigation fluid or joint capsule tissue •directsurgicalinsultstothecartilage,
which reduce chondrocyte viability •patientfactorssuchastraumaticshoul-
der injury, especially shoulder instability •nonadherencetopostoperativereha-
bilitation recommendations.All of the factors listed above result
Orthopedics
Table 2
Common Corticosteroid Injections and Recommended Dosage21
(in 5–7 mL of 1% lidocaine)
CORTICOsTeROIDCONCeNTRATION
(mg/mL)DOSAGE
(mg)CONTRAINDICATIONs/ADVeRse effeCTs/ PATIeNT eDUCATION
Betamethasone acetate/phosphate 6 6–12 Contraindications: Cellulitis or broken skin over intended entry site; anticoagulant use; coagulopathy; infected effusion of a bursa; more than three previous injections in prior 12 months; lack of response to two injections; suspected bacteremia; unstable joints; joint prostheses; pregnancy
Adverse effects: Postinjection flare; steroid arthropathy; tendon rupture; facial flushing; skin atrophy; depigmentation; iatrogenic infectious arthritis; hypersensitivity reaction; infection
Patient Education: Inform patient of adverse effects. Bleeding into the joint is possible. In diabetics, steroids can interfere with glucose metabolism. Glucose levels must be closely monitored in the first 24 hours.
Dexamethasone acetate 8 2–4
Dexamethasone sodium phosphate 4 2–4
Hydrocortisone acetate 25, 50 40–100
Methylprednisolone acetate 20, 40, 80 20–40
Prednisolone sodium phosphate 20 10–20
Prednisolone tebutate 20 20–30
Triamcinolone acetonide 10, 40 20–40
Triamcinolone hexacetonide 5, 20 20–30
Triamcinolone diacetate 25, 40 20–40

36 November 2011 • ADVANCE for NPs & PAs
in the destruction of chondrocytes and dissolution of the cartilage matrix within the glenohumeral joint space.
Clinical EvaluationWhen a patient presents with complaints of new onset pain, crepitus and stiffness in the shoulder within 3 to 12 months of arthroscopic shoulder surgery, a complete history and physical are required.8,10,15-17 A family history of early arthritis, known arthritic or other joint conditions, colla-gen disorders, traumatic shoulder injuries, instability or recurrent dislocation can potentially contribute to the formation of chondrolysis.7 In a patient whose primary complaint is new onset pain after surgery, it is crucial to rule out postoperative infection.
Patient demographics that can con-tribute to chondrolysis include young age (mean age 27.9 years), active lifestyle, participation in sports that require over-head motion (volleyball, baseball, softball, swimming), and shoulder conditions such as instability, impingement and superior labrum anterior posterior lesion.7,10,16,20
The symptoms of chondrolysis after arthroscopic surgery of the shoulder can include:8,10,15
•suddenincreasedpainafterpostsur-gical improvement•painoutofproportiontoexpec-
tations, both at rest and with motion (pain intensity usually increases with motion)•painthatthepatientcharacterizes
as different from the original pain com-plaint•insomepatients,crepitus,catching,
popping or locking and decreased active motion due to pain•insomepatients,decreasedrangeof
motion compared with previous visits
•glenohumeraljointspacenarrowingon radiographs and/or MRI.
When a patient presents with shoulder pain, collect a thorough history of the complaint.4 Gather information about the surrounding anatomy, including the neck, elbow, chest, cervical spine and related nerves.
The physical exam should consist of inspection, palpation and passive and active range-of-motion exercises — spe-cifically forward elevation, external rota-tion with elbow at the side, internal rota-tion, and internal rotation at 90 degrees of forward flexion.8,10,15,16,18 The goal is to rule out adhesive capsulitis or frozen shoulder, new onset instability, new labral tears and new rotator cuff tears. Taking a careful and thorough history and physi-cal that includes new symptoms, ruling out recent trauma and comparing new radiographs or MRI scans with previous studies can assist in ruling out these conditions. A careful physical also can rule out referred pain from gallbladder disease, referred pain from the neck, and possible myocardial infarction.
Diagnosis and TreatmentThe diagnosis of chondrolysis can be difficult because symptoms begin to appear when patients are starting or are within the active phase of rehabilitation. Many patients are initially told that their symptoms are due to excess activity too soon after surgery.8
A true anteroposterior radiograph is mandatory, and a full trauma radiographic study should be conducted.16 Compare original preoperative and postopera-tive films to establish the degree of joint changes. Order MRI scans to investigate any suspicion of joint changes, since these can provide detailed information about
the cartilage. If infection is suspected, blood work and nuclear imaging stud-ies can be helpful in conjunction with arthroscopic culture and lavage.8
Once shoulder chondrolysis has been diagnosed, treatment should be tailored based on symptoms, severity and age.10,21 In primary care, recommend conservative management until orthopedic special-ist evaluation can be performed.8,10,16 Conservative treatment includes gentle range-of-motion exercises, activity modi-fication and NSAIDs (Table 1). Treat patients at increased risk for gastrointes-tinal complications with a cyclo-oxyge-nase-2 (COX-2) NSAID such as diclofenac sodium or celecoxib.19,21,22 Some patients respond to intra-articular corticosteroids, but the duration of pain control usually is short term (Table 2).8,21,23
OutcomesTreatment options for shoulder chon-drolysis are determined case by case. In the typical scenario, the orthopedic specialist repeats diagnostic arthroscopy for debridement and to rule out infection or other factors. This is often followed by steroid injection and conservative and palliative treatments,10 possibly including NSAIDs, gentle range-of-motion exercises and, in some cases, narcotic medications. In extreme cases or when conservative and palliative treatment is ineffective, a surgeon may perform hemiarthroplasty or humeral resurfacing with meniscal grafting or other biologic agents.24
The lack of a recommended treatment regimen for shoulder chondrolysis con-tributes to poor long-term outcomes. Although some patients improve after hemiarthroplasty, hemiarthroplasty with biologic glenoid resurfacing, total shoulder arthroplasty or continued nonsurgical treatment,17,21,24 the majority continue to experience stiffness, decreased range of motion and pain even after further surgical intervention.8,15-21
In the young patient whose functional
Orthopedics
The diagnosis of chondrolysis can be difficult because symptoms begin to appear when patients are starting or are in rehabilitation. Many patients are told their symptoms are due to excess activity too soon after surgery.
Interested in specializing in Orthopedics?➼ READ AbOUT ONe NP’s path from intensive care and emergency department trauma to specialist in spinal health. http://nurse-practitioners-and-physician-assistants.advanceweb.com/Archives/Article-Archives/NPs-in-Orthopedics.aspx
Continued on page 42
37ADVANCE for NPs & PAs • November 2011
Professional Issues
➼ ThROUGh DeCADes of role confusion and conflict among nurse practitioners, clinical nurse specialists and physician assistants, little attention has been given to their mutual ante-cedent, a short-lived (1958–1962) master of science in nursing program established at Duke University in Durham, N.C.
Under the leadership of Thelma Ingles, RN, and Eugene A. Stead Jr., MD, a groundbreaking plan to educate a new type of healthcare provider briefly became reality. Prior to this Duke program, MSN degrees had been awarded only in the func-tional areas of education, supervision or administration, or in the specialized areas of anesthesia and psychiatric nursing.1,2 Ingles and Stead designed a unique curriculum to expand the scope of nursing practice to include skills such as taking a patient history and performing a physical examination.3 This MSN program laid the groundwork for the PA profession and helped pave the way for the NP and CNS roles.
Thelma InglesThelma Ingles was born in Redfield, S.D., in 1909. She earned a bachelor of arts in English literature from UCLA in 1931, followed by a diploma in nursing from Massachusetts General Hospital in 1935 and a master of arts in English literature from Western Reserve University in 1941.
She ultimately decided to focus her career on nursing, so she did postgraduate studies in clinical nursing at Duke University and in public health nursing and sociology at the University of California at Berkeley. Her early academic appoint-ments included the Boston Nursery for Blind Babies (1936), the University of Virginia (1941–1945) and Admiral Bristol Hospital in Istanbul (1945–1948). In 1949, Ingles accepted a position as professor of medical surgical nursing at Duke University School of Nursing.3
The LandscapeSeveral critical events set the stage for Duke’s advanced prac-tice nursing attempt. Before World War II, 3-year hospital-based nursing schools served as the primary source of nursing education. Physicians often owned small private hospitals
and created nursing schools to ensure a supply of inexpensive labor. The physicians taught the courses, and what they taught largely depended on the type of patients being treated in the hospital. In response to this haphazard approach to teaching, early nursing leaders formed the National League for Nursing Education (renamed the National League for Nursing [NLN] in 1952). One of the first goals of this organization was for nurses to create, teach and evaluate nursing school curricula.4
Advances in pharmacology, medicine and surgery increased the quantity and quality of services healthcare agencies offered after the war. To accommodate this ability, Congress passed the Hill-Burton Act in 1946, which funded hospital expansion and construction across the nation and provided a funding
phoebe polliTT is an assistant professor of nursing at Appalachian
State University in Boone, N.C. kaRen Reesman is an associate
professor of nursing at Appalachian State University. The authors have
completed disclosure statements and report no relationships related
to this article.All p
hoto
s co
urte
sy D
uke
Uni
vers
ity M
edic
al C
ente
r Ar
chiv
es
Back to the BeginningThe PA and NP professions each got a nudge from an MSN program at Duke
by Phoebe Pollitt, PhD, RN, and karen Reesman, PhD, RN, NeA-bC
Thelma Ingles, RN, in partnership with the eventual founder of the PA profession, made the first effort at an advanced practice nursing role.
38 November 2011 • ADVANCE for NPs & PAs
Professional Issues
mechanism for indigent care. The addi-tional beds, coupled with the variety of services hospitals could offer, led to an increased number of hospitalizations. Concurrently, health insurance coverage grew so more people were able to receive new inpatient services.5
In the 1950s, experts predicted an impending shortage of physicians at a time when more people were seeking healthcare. Additional healthcare profes-sionals were needed.4,6
In the background, the nursing pro-fession underwent tremendous change. Baccalaureate programs grew in number and influence. Two-year associate degree nursing programs flourished. The role of licensed practical and vocational nurses expanded, and soon nursing assistants appeared on the scene. The roles, respon-sibilities and interrelationships of these healthcare workers were hotly debated. Nurses had yet to reach consensus on educational preparation and the best way to use nursing staff with varying creden-tials and years of schooling. Academic accrediting organizations and state boards of nursing had their hands full managing the changes in nursing education and practice.7 Against this already confusing backdrop, Ingles and Stead introduced yet another type of nurse.
A Pivotal Conversation All of these factors contrib-uted to a pivotal conversation between Ingles and Stead in 1957. As a professor of medical surgical nursing, Ingles interacted with Duke physicians and medi-cal school faculty on a regular basis.3 Stead was chairman of the Department of Medicine at Duke and had served in the same capacity at Emory University in Atlanta during World War II.
Stead became convinced that much of the routine hospital care, then provided by physi-cians, could be taught to and performed by a new type of healthcare provider. Stead ini-tially envisioned teaching nurses to fill this new role. These nurses would expand healthcare to many underserved people cost-effi-
ciently.8 During a meeting in the spring of 1957 attended by both Ingles and Stead, the topic of advanced nursing practice came up. Ingles had planned a sabbatical for the 1957–1958 academic year, with a goal of increasing her clinical compe-tence. Stead and Ingles agreed that Ingles would spend her sabbatical year studying under Stead, learning more about the care of medical and surgical patients through collaboration with physicians,
laboratory and imaging staff and others to improve patient outcomes.9 Many of Stead’s colleagues were unsure what to make of a nurse in an expanded role. In her unpublished memoir, Ingles9 wrote of this time:
“[W]hen I was studying neurology, for example … making rounds with Dr. Conkle, who was chairman of that division, he didn’t exactly know how to treat me. When I would ask him some questions, he would say ‘I don’t think that has anything to do with the nursing realm.’ I’d say ‘It has something to do with the nursing realm because this nurse wants to know it.’”
At the end of that year, Ingles9 wrote this about the experience:
“I had learned a tremendous amount about clinical medicine. … I felt that this year that I had with Dr. Stead was such a superb year that we ought to replicate it with a group of students and give them the same thing. Obviously, Dr. Stead could not continue year after year to take one nurse, and that would have little effect. But maybe we could have a group. So we began to talk about setting up a master’s program in nursing ….”
Collaboration ContinuesIngles and Stead continued to collaborate. They secured a 5-year, $250,000 grant (a
sizable sum for that time) from the Rockefeller Foundation to develop the first nursing clini-cal specialist program at the master’s level.8,9
The 1-year program included 12 hours a week of classroom instruction in theory, 3 hours a week of research and 30 hours a week in clinical rotations. Duke’s Department of Medicine physi-cians contributed many lectures and assisted with classes, par-ticularly the advanced medical surgical nursing course.10
Students spent 6 weeks in four required clinical areas: respira-tory, neurology, cardiology and gastroenterology. After com-pleting those areas, students could choose any other two areas (such as obstetrics, pediatrics or psychiatry) or repeat areas. In the seminar in teaching course,
Ingles’s colleague, Eugene A. Stead Jr., MD
Duke was home to an early plan for a new healthcare provider.

39ADVANCE for NPs & PAs • November 2011
Professional Issues
students were often in charge of teaching other MSN students and were expected to explain the pathophysiology of the disease, discuss the disease process, and describe and demonstrate the nursing care the patient needed.
Ingles9 described the intent of the new program in a prophetic statement:
“[W]e came out with the idea that the nurse was qualified to do a great many things in patient care that had not been seen as part of her role. … We even went so far as to project into the future that we were going to have our graduates in the master’s program working in the clinic as responsible individuals in care, that patients would be told to come in and see ‘the nurse.’ And she would be paid a per-visit call same as the doctor. We thought that this was particularly relevant to patients with chronic disease. We saw her as having much greater input into the diagnosis and treatment and follow-up than had ever been done in the past. But we knew that we had to move slowly ….”
In another entry, she wrote:9
“One of the things I told the students right from the inception was we are pre-paring you for a job that doesn’t exist because there are no jobs in hospitals for the clinical nurse practitioner. This was a new kind of role. But we have to prepare people before we can set up the role so that we have people who know what the role should be.”
The MSN program began with five students in 1958.9 When Ingles and the nursing department sought NLN accredi-tation, however, they were denied on the grounds that the program lacked struc-ture and contained more medicine than nursing. The NLN also criticized the use of physicians as instructors.6,11 In addition, Ingles9 said that the NLN indicated she did not have the credentials necessary to teach in an MSN program, since her highest level of education in nursing was the diploma. To remedy the situa-tion and comply with NLN guidelines, Ingles took a year off from teaching to earn additional credits at UC Berkeley.
While she was in California, the Duke nursing department again tried to obtain accreditation for the MSN program and again was denied.9,11 In fact, the ANA and NLN did not embrace advanced clinical nursing practice until the 1970s.12,13
Another Door OpensWithout accreditation, the Duke MSN program could not attract students and closed in 1962. Stead was still enthusi-astic about the idea of creating a new healthcare professional to perform many of the routine functions usually done by physicians, but he veered from using nurs-es to using military corpsmen. In 1965, he admitted and taught the first class of physician assistants at Duke University Medical Center. Stead is credited with founding the PA profession, and his birth-day, Oct. 6, is National PA Day.
Also in 1965, nurse Loretta Ford and physician Henry Silver began the first pediatric nurse practitioner program, at the University of Colorado. Within 9 years, more than 1,000 nurses were practicing as NPs.10 This program began as a certificate program, as did most early NP programs, thus bypassing the need for accreditation.12 The NLN did not accredit the first MSN programs for NPs and CNSs until more than a decade after the Duke program’s inception.
Thelma’s LegacyThelma Ingles left Duke in 1961 and joined the Rockefeller Foundation as a nurse con-sultant. For 20 years, she traveled around the globe on behalf of nursing. She worked to improve nursing education everywhere she went. In Cali, Colombia, for instance, she established bachelor’s and master’s programs in nursing. As a consultant to the World Health Organization, she vis-ited nursing schools in places as diverse
as Finland, India, Thailand, Russia and England. In addition, she worked with Project HOPE, the Peace Corps and the Robert Wood Johnson Foundation. Ingles died in 1983.
Ingles’ belief that the care of patients was more important than the growth and prestige of the nursing profession never wavered.9 The story of Thelma Ingles and the first master’s-level nurse clinician program teaches us to be more open to new ideas, to be willing to try new experi-ences, and to support each other in our efforts to improve our profession. ■
References1. Mick DJ, Ackerman MH. Deconstructing the myth
of the advanced practice blended role: support for role divergence. Heart Lung. 2002;31(6):393-398.
2. Morrison JD. Evolution of the perioperative clinical nurse specialist role. AORN J. 2000;72(2):227-232.
3. Biographies. Thelma M. Ingles, RN, MA (1909–1983). Physician Assistant History Center. http://www.pahx.org/inglesBio.htm. Accessed Oct. 5, 2011.
4. Kalisch PA, Kalisch BJ. American Nursing: A History. 4th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2003.
5. Williams CA. The history of public and com-munity health and nursing. In: Stanhope M, Lancaster J, eds. Foundations of Nursing in the Community: Community-Oriented Practice. 3rd ed. St. Louis, MO: Mosby; 2010:15-31.
6. Holt N. “Confusion’s Masterpiece”: the develop-ment of the physician assistant profession. Bull Hist Med. 1998;72(2):246-278.
7. Hughes EC, et al. This company called nurses. In: Twenty Thousand Nurses Tell Their Story: A Report on Studies of Nursing Functions Sponsored by the American Nurses Association. Philadelphia, PA: Lippincott; 1958:19-41.
8. Laszlo J, Neelon FA. The Doctors’ Doctor: A Biography of Eugene A. Stead, Jr. MD. Durham, NC: Carolina Academic Press; 2006.
9. Ingles TM, Haradon S. Care from the heart. 2007. (Unpublished manuscript written by Ingles and edited by her niece, Susan Haradon.)
10. Wilson D. Nurse practitioners: the early years (1965-1974). Nurse Pract. 1994;19(12):26-35.
11. Fisher DW, Horowitz S. The physician’s assis-tant: profile of a new health profession. In: Bliss AA, Cohen EH, eds. The New Health Professionals: Nurse Practitioners and Physician Assistants. Germantown, MD: Aspen Systems Corp; 1977: 40-54.
12. Fairman J. The AMA and ANA under siege. In: Making Room in the Clinic: Nurse Practitioners and the Evolution of Modern Health Care. New Brunswick, NJ: Rutgers University Press; 2008: 114-133.
13. Fulton JS. Evolution of clinical nurse specialist role and practice in the United States. In: Fulton JS, et al, eds. Foundations of Clinical Nurse Specialist Practice. New York, NY: Springer Publishing; 2009: 3-13.
The Lessons of history➼ LeARN MORe about the formation and development of the NP and PA professions at our website. Visit www.advanceweb.com/NPPA and select the NP Resource Center or the PA Resource Center.
we came out with the idea that the nurse was qualified to do a great many things in patient care that had not been seen as part of her role.’
‘

40 November 2011 • ADVANCE for NPs & PAs
Calendar
We now proudly offer the
C O L L E G E O F N U R S I N G
Doctor of Nursing Practice (DNP)
umassd.edu/nursing/academic_programs/phd/
(for nurses who already have the MS degree in Nursing)
Please contact: Dr. Gail RussellGraduate Program Director508.999.8251 [email protected]
Starts Summer 2012
Part-time program
500 hours of practicum with emphasis
on health systems change
only 28-30 post MS credits for degree
Distance Education
Medical AestheticsOnline Courses
Cosmetic Nurse Concepts introduces these exciting online
courses for RNs and NPs. Learn the basics of the exciting
world of medical aesthetics and earn up to 14 nursing contact
hours. Explore topics such as the aging process, botulinum
toxin, dermal fillers, lasers, chemical peels, legal issues and
much more! Take these courses from the comforts of your
home! Contact: http://cosmeticnurseconcepts.litmos.com/
online-courses to register or obtain more information.
LEARN to inject BOTOX and DERMAL FILLERS
through award-winning, comprehensive
instructional DVDs.
BOOST your INCOME! FREE Catalog.
Aesthetic VideoSource800-414-2434
www.videoshelf.com
Oct 20 ................ Philaelphia(NE), PA
Oct 21 .....................Atlantic City, NJ
Oct 25 ........................Rochester, NY
Nov 16 ..............................Edison, NJ
Dec 1 ..........................New York City
Dec 2 ............. Plainview, Long Island
Stethoscope Skills!Improve your physical assessment skills!
One day class covers Heart, Breath, & Abdominal Sounds. Everything you need to know about the sounds you hear!
Choose from these locations:
9am-4:30pm each day. Approved 6 CEUsFee $79 • Group & Student Discounts Available
Call 800-227-3372 • www.stethoscopeskills.com
SAVE YOURMONEY
SUbScRibE TODAY! iT’S EASY!call 800-355-1088 or visit www.advanceweb.com
print & digital subscriptions are both FREE

41ADVANCE for NPs & PAs • November 2011
Calendar
1-800-462-1944 | Hamden / North Haven, Connecticut
TAKE GREAT CARE OF OTHERS AND YOUR CAREERWITH OUR NEW DOCTOR OF NURSING PRACTICE PROGRAM.
The Quinnipiac Advantage: • Rigorous and focused educational goals • Superb clinical affiliations• Immersion and residency experiences• International health option• Portfolio capstone project
Advance your career with our new DNP program. Designed to challenge and excite you, this degree will prepare you to become a leader in health care. Taught at our new health science facility, students benefit from advanced technology and a convenient class schedule. Learn more, e-mail [email protected] or visit www.quinnipiac.edu/gradnursing.
Tracks include: • Adult Nurse Practitioner • Family Nurse Practitioner • Women’s Health Nurse Practitioner • Post Master’s Care of the Individual • Post Master’s Care of Populations
A P E A’s Adult & Family NP Review Courses2011-2012 Sites
Indianapolis, IN Nov 7-9Los Angeles, CA Dec 4-6Knoxville, TN Jan 6-8Lafayette, LA Jan 13-15Memphis, TN Jan 19-21Norfolk, VA Jan 26-28Phoenix, AZ Mar 8-10Winston-Salem Mar 15-17Shreveport, LA Mar 22-24Houston, TX Mar 30-Apr 1
Visit our website for additional course sites
99% Passing RateWe’ll come to your university!Call us for more information
Can’t come to us?APEA’s On-line Review Course
Web video and multimedia presentations!
We guarantee you’ll pass oryour next course is FREE!
No bones about it... a 99% pass rate! Weʼve consistently demonstrated a first-attempt pass rate of 99% on both national certification exams for 11 years!
Earn 17.25 Contact hours (includes 9.0 pharm hours)Entertaining. Engaging. Energetic speaker!More than exam prep. It's PRACTICE prep.
Advanced Practice Education Associates800-899-4502 (tel) 337-981-0509 (fax) 103 Darwin Cir. . Lafayette, LA 70508
Visit our website: www.apea.com Or e-mail us: [email protected]
VISIT OUR ON-LINE TESTING CENTER @ www.apea.comSharpen your skills and test your readiness for the certification exam.
Identify your strengths and weaknesses with our diagnostic tool!
NEW! CE CENTERVIEW streaming video and multimedia presentations! Earn contact hours
on your schedule

THE COLLEGE OF MEDICINE, USAT MONTSERRAT
www.usat-montserrat.org • http://usatpga.webs.com
Become a part of the Fastest Growing Health Care Professionals (HCP) to MD program in AmericasThe University of Science Arts & Technology, Montserrat is inviting applicants for the PA to MD and NP to MD transition program. Consists of a 12 month medical basic science transition program designed to prepare for USMLE Steps I & II, followed by supervised clinical training in the USA or abroad. Qualifi ed applicants may also earn a degree in Osteopathic or Natural Medicine or a graduate degree in a related area simultaneous to their MD program.
Transition Program for HCPs (PA, RN, NP, DNP or similar) to MD / DO/ MBBS and/or DNP • All programs are 1.5 to 4 years in duration depending on pre-qualifi cations
• Affordable Tuition, experienced Faculty, many Locations in USA
• Maximum transfer credit for prior studies; Graduate programs available
• US Clinical training; IMED/FAIMER Listed For ease of US Licensure and Residency
• VA GI Bill Approved, Fully Accredited in the USA [AAHEA]
Toll Free: 866-596-9577 Tel: 727-252-6210 • 727-388-2687 • Fax: 664-491-5362
Email: [email protected]
UNIVERSITY OF SCIENCE ARTS & TECHNOLOGY, MONTSERRATPO Box 506, South Mayfi eld Estate Drive, Olveston, Montserrat
Tel: 664-491-5364 • Toll Free 866-596-9577 Email: [email protected]
Set Your Sails for Montserrat, the "Emerald Isle of the Caribbean"
42 November 2011 • ADVANCE for NPs & PAs
Shoulder ChondrolysisContinued from page 36
shoulder demands are significant, prosthetic glenohumeral arthroplasty is not typically recommended. Newer implants are being developed to improve the possibility of normal motion and function.8,10 Early identification of shoulder chondrolysis and timely referral to an orthopedic specialist are essential to achieving the best possible outcomes. ■
References1. American Academy of Orthopaedic Surgeons.
Orthopaedic fast facts. http://orthoinfo.aaos.org/topic.cfm?topic=A00130. Accessed Sept. 30, 2011.
2. American Academy of Orthopaedic Surgeons. Common shoulder injuries. http://orthoinfo.aaos.org/topic.cfm?topic=A00327. Accessed Sept. 30, 2011.
3. Cole BJ, Katolik LI. Shoulder. In: Miller MD, et al, eds. Review of Sports Medicine and Arthroscopy. 2nd ed. Philadelphia, PA: Saunders; 2002:142-218.
4. Miller MD, Sekiya JK. Shoulder history, physical examination, and imaging. In: Miller MD, Sekiya JK, eds. Sports Medicine: Core Knowledge in Orthopaedics. Philadelphia, PA: Mosby/Elsevier; 2006:252-327.
5. Roth V, et al. Biophysical and electromechanical properties of articular cartilage. In: Simmons DJ, Kunin AS, eds. Skeletal Research: An Experimental Approach. New York, NY: Academic Press; 1979:301-341.
6. Cailliet R. Shoulder Pain. 3rd ed. Philadelphia, PA: FA Davis; 1991.
7. Solomon DJ, et al. Glenohumeral chondrolysis after arthroscopy: a systematic review of potential contributors and causal pathways. Arthroscopy. 2009;25(11):1329-1342.
8. Bailie DS, Ellenbecker TS. Severe chondrolysis after shoulder arthroscopy: a case series. J Shoulder Elbow Surg. 2009;18(5):742-747.
9. Mounach A, et al. Idiopathic chondrolysis of the hip. Joint Bone Spine. 2007;74(6):656-658.
10. Petty DH, et al. Glenohumeral chondrolysis after shoulder arthroscopy: case reports and review of the literature. Am J Sports Med. 2004;32(2):509-515.
11. Fester EW, Noyes FR. Postoperative chondrolysis of the knee: 3 case reports and a review of the literature. Am J Sports Med. 2009;37(9):1848-1854.
12. Douw CM, et al. Clinical and pathological changes in the knee after accidental chlorhexidine irrigation during arthroscopy. Case reports and review of the literature. J Bone Joint Surg. 1998;80(3):437-440.
13. Ishida K, et al. Rapid chondrolysis after arthroscopic partial lateral meniscectomy in athletes: a case report. Knee Surg Sports Traumatol Arthrosc. 2006;14(12):1266-1269.
14. Chu CR, et al. The in vitro effects of bupivacaine on articular chondrocytes. J Bone Joint Surg Br. 2008;90(6):814-820.
15. Hansen BP, et al. Postarthroscopic glenohumeral chondrolysis. Am J Sports Med. 2007;35(10):1628-1634.
16. Greis PE, et al. Bilateral shoulder chondrolysis fol-lowing arthroscopy. A report of two cases. J Bone Joint Surg Am. 2008;90(6):1338-1344.
17. Saltzman M, et al. Postsurgical chondrolysis of the shoulder. Orthopedics. 2009;32(3):215.
18. McNickle AG, et al. Postsurgical glenohumeral arthritis in young adults. Am J Sports Med. 2009;37(9):1784-1791.
19. Rapley JH, et al. Glenohumeral chondrolysis after shoulder arthroscopy associated with continuous bupiva-caine infusion. Arthroscopy. 2009;25(12):1367-1373.
20. Rey J II, et al. Postarthroscopic chondrolysis of the glenohumeral joint. Semin Arthroplasty. 2009;20(2):98-103.
21. McCarron JA. Shoulder arthritis and the young patient. Curr Orthop Pract. 2009;20(4):382-387.
22. Drugs used in treating inflammatory processes. In: Woo TM, Wynne AL, eds. Pharmacotherapeutics for Nurse Practitioner Prescribers. 3rd ed. Philadelphia, PA: FA Davis; 2011:745-781.
23. Pfenninger JL. Joint and soft tissue aspiration and injection (arthrocentesis). In: Pfenninger JL, Fowler GC, eds. Procedures for Primary Care. 3rd ed. St Louis, MO: Mosby/Elsevier; 2010:1303-1321.
Calendar

CONTINUING EDUCATION SEMINARSClinical Pharmacology Boston, MA .......................... March 26-31, 2012Nashville, TN ....................... October 15-20, 2012
Pharmacology UpdateMt Snow, VT ........................ January 12-13, 2012Maui, HI ................................ February 16-17, 2012Rome, Italy ........................... March 14-15, 2012
Advanced PathophysiologyAtlanta, GA .......................... April 23-28, 2012
Speaker SchoolNorth Andover, MA ........... April 4-5, 2012
Wound RepairAtlanta, GA .......................... April 26, 2012Chicago, IL ........................... September 18, 2012
NOW AVAILABLE! Dr. Fitzgerald’s Review CDs
Content is revised extensively each year to reflect changes in national treatment guidelines, immunization
NP CERTIFICATION REVIEWCourse locations and dates.
Family and AdultSacramento, CA ..................Huntsville, AL ......................North Andover, MA ........... January 3-5, 2012Atlanta, GA .......................... January 6-8, 2012Chicago, IL ........................... January 6-8, 2012
.................... January 7-9, 2012Oakland, CA ......................... January 13-15, 2012Cleveland, OH ..................... January 20-22, 2012Manhattan, NY ................... January 31-Feb. 2, 2012Minneapolis, MN ............... February 25-27, 2012Charlotte, NC ....................... March 7-9, 2012
Pediatric
Acute CareChicago, IL ...............................May 2-4, 2012
..............................May 18-20, 2012
GeriatricManhattan, NY ................... June 8-9, 2012
Women’s Health
HOME STUDY CEPrescriber Lecture Series
guidelines and advances in treatment therapy
NP Expert Skills Series
assessment courses
SPEAKER SERVICES
MORE THAN 60 HOME STUDY COURSES TO EARN CE CREDITS
Expert Exam: Practical Orthopedics — Knee
knee problems commonly seen in the primary care setting. Video and seminar notes, 2.4 contact hours.
NEW DATES AND LOCATIONS!
Call 800.927.5380 or visit
our website to place your order or enroll, mention promotion code
103 and receive the SPECIAL ADVANCE FOR NPS
DISCOUNT.
“How did you prepare to pass your NP certification exam?”
“I called Fitzgerald. Their comprehensive exam prep and up-to-date continuing education programs helped me
get certified, and they keep me current clinically.”
43ADVANCE for NPs & PAs • November 2011

44 November 2011 • ADVANCE for NPs & PAs
Calendar
ONLINE HITECH Trainingin 6 months or less!
Certificate Options:• Practice Workflow and Information Management Redesign Specialist• Clinician/Practitioner Consultant• Implementation Manager• Technical and Implementation Support Specialist DUAL certificate• Trainer
ONC grant award # 90CC078/01 (region D)
Classes Start Often! - 6 month online training - Tuition reimbursement available - 50,000 qualified workers needed - Crosstraining Healthcare & IT professionals
Only $40020 AHIMA CEU CreditsOptimal Training for
Your Staff
(432) 685-6891 • www.midland.edu/hitt/hitech.phpFunding for this publication and any other related publications and/or printed materials and oral presentation, is provided by the of ce of National Coordinator,
Department of Health and Human Services support, under grant number 90CC0078. Said grant was issued under the authority of the American Recovery and Reinvestment Act, 2009 (P.I. 111-5), Title XIII
InternationallyAccredited
Oceania University of Medicine has earned accreditationfrom the Philippine Accrediting Association for Schools,Colleges and Universities, one of only 20 internationalmedical school accrediting agencies recognized by theUS Department of Education.
Isn’t it time to take the next step? Earn an MD degreefrom an accredited medical school. Now accepting applications.
OUM
-IntA
ccre
d121
0
OCEANIA UNIVERSITY OF MEDICINEFor more information, visit www.oceaniamed.org or call toll free 877-463-6686.
Everything You Need...
Log onto advanceweb.com today!
Just a click away.
This is an abbreviated version of our guidelines.
Click the Resources tab at www.advanceweb.
com/NPPA for a more detailed version.
➼ ADVANCE for NPs & PAs considers clinical
manuscripts written by nurse practitioners,
physician assistants and other members
of the healthcare team. We also consider
manuscripts by NP and PA students.
Our editorial advisory board of NPs and
PAs performs blinded review of all submis-
sions.
At the top of the article document, list
author name, credentials, workplace name
and city, email address, postal mailing
address and daytime phone number. Disclose
any financial or other support received from
a medical writing firm or healthcare-related
business.
List and format all references according to
the American Medical Association Manual of
Style. Save tables and figures in separate
word processing documents. Provide the
citation for the original source for table and
figure content, if applicable.
Suggest a title, which the editors will use
as a guide in writing the headline. Include
subheadings throughout the article to
improve readability.
Obtain copyright permission for reproducing
or adapting any previously published mate-
rial that you have included with the article.
Label all tables, illustrations and diagnostic
images to provide appropriate credit to the
owner or creator. Provide captions describing
what is depicted.
All submissions are edited for clarity, style
and conciseness. Articles should emphasize
how NPs and PAs can use the information
in daily practice. The final version of the
article will be emailed to the author prior to
publication. After an article is accepted for
publication, authors transfer first-time North
American publishing rights to ADVANCE for
NPs & PAs and the websites of its publisher,
Merion Matters.
Email submissions to ONE of the journal’s
editors:
Michelle Perron Pronsati at mpronsati@
advanceweb.com or Michael Gerchufsky at
ADVANCE for NPs & PAs
Guidelines for Contributors

45ADVANCE for NPs & PAs • November 2011
At www.advanceweb.com/NPPA, our searchable online Resource Directory allows you to access information about companies and products, as well as submit
requests for additional details. Find the Resource Directory under the Products tab on the homepage.
support the Companies who support your Profession
The companies listed in this advertiser index support the NP and PA professions by advertising in ADVANCE for NPs & PAs. Their support keeps our peer-reviewed
journal coming to you free of charge. Please contact these advertisers or visit their websites to learn more about their products or services.
Advertiser Index
NP
PA
11
/1
1
ADVERTISER PHONE # OR WEB ADDRESS PG # ADVERTISER PHONE # OR WEB ADDRESS PG #
Advanced Practice Education Associates www.apea.com 41
American Lifeline www.florajen.com 2
Calmoseptine www.calmoseptineointment.com 13
Chamberlain Medical Resources, Inc. www.CMR4CME.com 40, 42
CM&F Group, Inc. www.NPSecure.com 9
Contemporary Forums www.contemporaryforums.com 45
Endo Pharmaceuticals www.lidoderm.com 14–16
Endo Pharmaceuticals www.advanceweb.com/nppa 12
Fitzgerald Health Education Associates www.fhea.com 43
Merion Matters www.advancehealthcareshop.com 46–49
Merion Matters www.advancecustompromotions.com 67
Midland College www.midland.edu/hitt/hitech.php 44
New York State Department of Health TalkToYourPatients.org 31
NIPRO Diagnostics accuracyontarget.com 68
Oceania University of Medicine www.oceaniamed.org 44
Quinnipiac University www.quinnipiac.edu/gradnursing 41
Schiff Nutrition Group www.MoveFreeSample.com 7
UMass Dartmouth umassd.edu/nursing/academic_programs/phd/ 40
University of Science, Arts & Technology www.usat-montserrat.org 42
Women’s International Pharmacy www.womensinternational.com 11
Xlear, Inc. www.xlear.com 5
Calendar
Live & Online CE Conferences . . .Over 250,000 healthcare professionals have attended our nationalConferences and readily attest to the quality, attention to detail andprofessional enrichment provided.
CE ConferencesPresenting a wide variety of accredited National Conferences, including:
To view a complete list of our conferences visit our website...Phone: (800) 377-7707, Email: [email protected]
www.ContemporaryForums.comMake Contemporary Forums your rst choice for continuing education - Register Today!!
• Brain Injuries• Case Management• Critical Care• Emerging Technologies• Family Practice
• Neonatal• Obesity• Obstetrics• Legal Nurse• Pediatrics
••Pharmacology• Primary Care• Psychiatric• Nursing Education• Women’s Health
2011 ConferencesContraceptive Technology: Quest for Excellence Atlanta, GA November 3-5Become A Professional Legal Nurse Consultant Las Vegas, NV November 6-7Pharmacology for Advanced Practice Clinicians Las Vegas, NV November 7-13AACN Progressive Care Pathways Las Vegas, NV November 9-12The Fetus & Newborn: State-of-the-Art Care Las Vegas, NV November 9-12Developmental Interventions In Neonatal Care Las Vegas, NV November 13-16
2012 ConferencesElsevier/Mosby’s Faculty Development Institute Las Vegas, NV January 2-4Contraceptive Technology San Francisco, CA March 7-10 The Young Child With Special Needs Las Vegas, NV March 21-24The National Conference of Neonatal Nursing Orlando, FL March 21-24Contraceptive Technology Boston, MA March 28-31A Slice of AACN NTI Las Vegas, NV April 9-13Obstetric Nursing Las Vegas, NV April 15-18Psychiatric Nursing Philadelphia, PA April 18-21Pediatric Nursing: Care of the Hospitalized Child Boston, MA May 2-5Psychiatric Nursing Las Vegas, NV May 16-19Advances in Health Care for Women Over 40 Las Vegas, NV May 17-19Adolescent Health Care San Francisco, CA May 31-June 2Neonatal Pharmacology Washington, DC June 6-9International Nurse Education Conference (NetNep) Baltimore, MD June 17-20Perinatal Dilemmas Jackson Hole, WY July 15-18Hot Topics in Primary Care Jackson Hole, WY July 29-August 1
Online CE LibraryAccess over 2,500 hours of Conference Presentations Onlineincluding CE Credit!

Get in the loop – click the BLOG icon on our home page.
Join our email list online for special offers
Connect with us at facebook.com/ShopAdvance
Follow us on Twitter.com/ShopAdvance
� Women’s Soft Shell Jacket*Personalizable. #19006 $59.99 S-XL; $62.99 2XL
BLACK
NAVY
BLACK
TRUE RED LIGHT BLUE
PALE PINK
BLACK
WHITE
Men's style also available
� Unisex Half-Zip Wind Shirt*Personalizable. #14788 $35.99 XS-XL; $38.99 2XL-4XL
�
� �
� Women’s Johnny Collar Polo Shirt*Personalizable. #19409 $15.99 S-XL; $18.99 2XL
���
�
*Additional charge for personalization.
new! new!
� Women’s ¾-Sleeve Blouse*Personalizable. #17874 $35.99 XS-XL; $38.99 2XL-4XL
PURPLE/WHITE
TRUE ROYAL/ WHITE
MAROON/WHITE
BLACK/WHITE
TRUE NAVY/GOLD
It’s Time to Celebrate
Nurse Practitioner Week with our exclusive embroidered apparel & accessories
that are perfect for outfi tting your entire team!
� Men’s & Women’s Textured Soft-Shell Jackets*Personalizable. #17825 Men’s#17836 Women’s$65.99 XS-XL; $68.99 2XL-4XL
CAFÉ
INSIGNIA BLUE STONE
BLACK
NPPA1143_C01-C02.indd 1 9/20/11 2:45:39 PM
46 November 2011 • ADVANCE for NPs & PAs

Get in the loop – click the BLOG icon on our home page.
Join our email list online for special offers
Connect with us at facebook.com/ShopAdvance
Follow us on Twitter.com/ShopAdvance
� Women’s Soft Shell Jacket*Personalizable. #19006 $59.99 S-XL; $62.99 2XL
BLACK
NAVY
BLACK
TRUE RED LIGHT BLUE
PALE PINK
BLACK
WHITE
Men's style also available
� Unisex Half-Zip Wind Shirt*Personalizable. #14788 $35.99 XS-XL; $38.99 2XL-4XL
�
� �
� Women’s Johnny Collar Polo Shirt*Personalizable. #19409 $15.99 S-XL; $18.99 2XL
���
�
*Additional charge for personalization.
new! new!
� Women’s ¾-Sleeve Blouse*Personalizable. #17874 $35.99 XS-XL; $38.99 2XL-4XL
PURPLE/WHITE
TRUE ROYAL/ WHITE
MAROON/WHITE
BLACK/WHITE
TRUE NAVY/GOLD
It’s Time to Celebrate
Nurse Practitioner Week with our exclusive embroidered apparel & accessories
that are perfect for outfi tting your entire team!
� Men’s & Women’s Textured Soft-Shell Jackets*Personalizable. #17825 Men’s#17836 Women’s$65.99 XS-XL; $68.99 2XL-4XL
CAFÉ
INSIGNIA BLUE STONE
BLACK
NPPA1143_C01-C02.indd 1 9/20/11 2:45:39 PM
1-877-405-9978 • advancehealthcareshop.com Turn the page for more great products from ADVANCE!
� Canvas Messenger Bag*16" x 11½" x 4¾". Personalizable.NP or Nurse Practioner. #14306$27.99
JAVA
DENIM
FLAMINGO
KHAKI GREEN
BLACK
PUTTY
Personalizeinitials on strap
� Poster18" x 24". #14397$16.99
� Pocket JotterBusiness card slots, pen loop and notepad.#15400$4.99
� Clock/Picture Frame4" x 6" x ¾". #15402$8.99
� Ceramic Mugs*15 oz. Personalizable.#15401 Nurse
Practitioner#14631 Pediatric
Nurse Practitioner
$9.99 ea.
� Lapel Pin1" x 1". #02330$4.99
� Stickers2". Set of 3 sheets.#14396$3.99
� Carabiner PenBlack ink.#02380$1.99
� Business Card Case3½" x 2½".#15399$9.99
personalize
set of 60 stickers
�
�
�
�
�
�
*Additional charge for personalization.
$9.9
�� L1" x 1$4.9
�
�
NPPA1143_C01-C02.indd 2 9/20/11 2:51:02 PM
47ADVANCE for NPs & PAs • November 2011

Be in the know & get exclusive offers:
Get in the loop – click the BLOG icon on our home page.
Join our email list online for special offers
Connect with us at facebook.com/ShopAdvance
Follow us on Twitter.com/ShopAdvance
Inside Pocket
� Women’s 36½" Traditional “iPad®” Lab Coat*65% polyester / 35% cotton with two oversized interior pockets for an iPad®, two lower pockets, chest pocket, mesh ID pocket and three-button closure. Personalizable. Classic fi t #19155$34.99 2-20 and 40-42
42
� Unisex 30" Consultation iCoat*65% polyester / 35% cotton with soil release, two oversized front patch iPad® pockets, two concealed patch and interior pockets, left chest pocket with pen divider and three-button closure. Personalizable. Classic fi t #15645$32.99 XXS-XL; $35.99 2XL-5XL
� Men’s 37" “iPad®” Lab Coat*65% polyester / 35% cotton with two oversized interior pockets for an iPad®, two lower pockets, chest pocket, mesh ID pocket and four-button closure. Personalizable. Classic fi t #19150$34.99 32-52
52
from XXS up to
5XL
� Women’s 30" Contrast Stitch Lab Coat*65% polyester / 35% cotton with contrast stitching, two front and side pockets (not made to hold iPad®) and button front closure. Personalizable. Slim fi t Black or White. #04933$29.99 S-XL Contrast
Stitching*Additional charge for personalization.
available inwhite withblack
stitching
Children’s3-Pocket Lab Coat*
Personalizable.#09139
$18.99 2-12/14
More Children’s Lab Coats,
Scrubs &Accessories
availableonline!
� � �
�
Our newest lab coats with oversized pockets for iPads®!
NPPA1143_C03-C04.indd 1 9/20/11 3:08:22 PM
48 November 2011 • ADVANCE for NPs & PAs

■ Shop and Order Online – 24 hours a day, 7 days a week at advancehealthcareshop.com
■ Order by Phone – 1-877-405-9978 – Live operators available 7 days a week to assist you in completing your order
■ Download a printable order form – Missing the order form? Go to advanceweb.com/NPPAorderform
■ Order by Fax or Mail – Send your completed printable order form with payment to: Fax: 1-610-278-1424 or Mail to: ADVANCE Healthcare Shop Order Department 3100 Horizon Drive, King of Prussia, PA 19406, USA
Four Easy Ways To Order
1-877-405-9978 • advancehealthcareshop.com
More than 4,500 different products for over 75 medical and allied
healthcare specialties
Catalog Code: NPPA-1143Prices and offers valid through 11/20/11
20% OFF
any order $50 or more!Use promo code NPPAEVT822
now through 11/20/11. Limit one promo code per order. Cannot be combined with other
codes. Not available on clearance items, ADC Digital Pulse Oximeter (#13221), UltraScope (#11840) or Littmann stethoscopes.
new!new!
#19454 Holiday Angel #14244 Lab Coat31⁄2" x 3"
• Round porcelain ornaments are 2¾" in diameter with a metallic gold hanging string and come packaged in an organza gift bag for only $6.99 each.
• Customize these ADVANCE exclusive ornaments with up to two lines of personalization for only $1!
• Create memorable gifts for friends, family, co-workers, organizationsand groups.
Personalize our ornamentsfor anyone on your list!
#19455 Holiday Snowman
new!new!
#19466 Reindeer
Chooseup to 12 characters
Chooseup to 18
characters
NPPA1143_C03-C04.indd 2 9/20/11 3:11:27 PM
Be in the know & get exclusive offers:
Get in the loop – click the BLOG icon on our home page.
Join our email list online for special offers
Connect with us at facebook.com/ShopAdvance
Follow us on Twitter.com/ShopAdvance
Inside Pocket
� Women’s 36½" Traditional “iPad®” Lab Coat*65% polyester / 35% cotton with two oversized interior pockets for an iPad®, two lower pockets, chest pocket, mesh ID pocket and three-button closure. Personalizable. Classic fi t #19155$34.99 2-20 and 40-42
42
� Unisex 30" Consultation iCoat*65% polyester / 35% cotton with soil release, two oversized front patch iPad® pockets, two concealed patch and interior pockets, left chest pocket with pen divider and three-button closure. Personalizable. Classic fi t #15645$32.99 XXS-XL; $35.99 2XL-5XL
� Men’s 37" “iPad®” Lab Coat*65% polyester / 35% cotton with two oversized interior pockets for an iPad®, two lower pockets, chest pocket, mesh ID pocket and four-button closure. Personalizable. Classic fi t #19150$34.99 32-52
52
from XXS up to
5XL
� Women’s 30" Contrast Stitch Lab Coat*65% polyester / 35% cotton with contrast stitching, two front and side pockets (not made to hold iPad®) and button front closure. Personalizable. Slim fi t Black or White. #04933$29.99 S-XL Contrast
Stitching*Additional charge for personalization.
available inwhite withblack
stitching
Children’s3-Pocket Lab Coat*
Personalizable.#09139
$18.99 2-12/14
More Children’s Lab Coats,
Scrubs &Accessories
availableonline!
� � �
�
Our newest lab coats with oversized pockets for iPads®!
NPPA1143_C03-C04.indd 1 9/20/11 3:08:22 PM
49ADVANCE for NPs & PAs • November 2011
50 November 2011 • ADVANCE for NPs & PAs
Massachusetts, Connecticut, New HampshireC
aree
r O
ppor
tuni
ties Looking for a new career
opportunity?
Each month, the ADVANCE for NPs & PAs Opportunities Section presents the latest job openings from across the country. For convenience, listings are arranged by region, with state headings to further guide your search. These positions are also posted and updated daily at the “Jobs” tab at our website, www.advanceweb.com/NPPA.
Sign up or renew your fRee subscription at thewebsite or by calling (800) 355-1088.
To place an ad in this section,call ADVANCE at
(800) 355-JObs (5627).
Regional Directory:
New England. . . . . . . . . . . . . . . . . . . . 50
Middle Atlantic . . . . . . . . . . . . . . . . . . 54
Upper South Atlantic . . . . . . . . . . . . . . 58
Lower South Atlantic . . . . . . . . . . . . . . 61
East South Central . . . . . . . . . . . . . . . 61
East North Central. . . . . . . . . . . . . . . . 61
Southwest . . . . . . . . . . . . . . . . . . . . . 62
West North Central . . . . . . . . . . . . . . . 63
West South Central . . . . . . . . . . . . . . . 63
Mountain . . . . . . . . . . . . . . . . . . . . . . 63
Pacific . . . . . . . . . . . . . . . . . . . . . . . . 64
National . . . . . . . . . . . . . . . . . . . . . . . 65
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
We have exciting positions for Physician Assistants with Orthopedic Surgery, Plastic Surgery, Hematology/Oncology or OTL/Communication experience.When clinicians from around the world ask how pedi-atric care will look in ten, twenty or thirty years, they turn to Children’s Hospital Boston. Oft en, they’ll fi nd tomorrow’s treatments fi nding their fi rst successes right here, right now.We off er a highly competitive benefi ts program providing fl exibility and choice to meet the needs of our diverse workforce and their families.
For details please visit our website at www.childrenshospital.jobs and refer to
AutoReqld# 24235BR (Ortho) 25582BR (Plastic) 25450BR (HemOnc) 25840BR (OTC/COMM)
Nurse Practitioners & Physician Assistants
life works here.
We are an equal opportunity employer.
One Medical Center Drive • Lebanon, NH • 03756
Qualified candidates will have completedan accredited nurse practitioner orphysician assistant program and be eligiblefor NH licensure. Academic preparation at aMasters level is preferred.
Nurse Practitioners:• General Internal Medicine• Gastroenterology/Hepatology• Palliative Care• Orthopaedics• Neurology
Physician Assistants:• General Internal Medicine• Orthopaedics• Neurology
Please apply online at:www.Dartmouth-Hitchcock.org
MIDDLESEX CARDIOLOGYMiddletown, CT
has a Full-Time opening for a PA or APRN
Experience in Cardiology preferred. Must possess a Bachelor of Science
Degree from accredited PA program and/or Masters Degree in Nursing with degree and current licensure as a Nurse
Practitioner. Forward CV/Resume to [email protected]
LOG ON TODAY TOADVANCEWEB.COM
THE NUMBER ONE ONLINE RESOURCE FOR CLINICAL INFORMATION AND CAREER DEVELOPMENT.
SIGN UP FOR YOUR FREE E-NEWSLETTER AT WWW.ADVANCEWEB.COM
Rhode Island, Connecticut
51ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
We provide high-quality healthcare to veteransresiding in Rhode Island and southeastern
Massachusetts. Our staff consists of over 900 dedi-cated professional, technical and support personnel.
With the excitement of urban living and the tranquilityof rural living, our location in Rhode Island offers the
best of both worlds, not to mention 400 miles of windingcoastline. Bring your career to an environment that is both
professionally and personally rewarding!
ProvidenceVA Medical Center
Nurse PractitionersMSN from an NLNAC/CCNE accredited college with current ANCCor other nationally recognized certification as an Adult, Family orGerontological Nurse Practitioner. Minimum of 2-3 years of progressiveexperience as an RN. Active, current, full and unrestricted AdvancedPractice Nurse license with prescriptive privileges in Rhode Island.
• Orthopedics – Full Time: Recent experience in caring fororthopedic patients in an outpatient setting preferred
• Dermatology – Full Time: Recent experience in caring fordermatology patients in an office/clinic setting required.
Benefits package includes 5 weeks of vacation, up to 5% matching on401(k) type plan, free on-site parking, and a competitive salary scale.
Apply online at www.usajobs.gov or send resumeto [email protected]. citizens only. An Equal Opportunity Employer
LOOKING FOR THE LARGEST LISTING OF DEGREE,
CERTIFICATION AND CE
PROGRAMS?
YOU’RE IN THE RIGHT PLACE.
Connecticut
52 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
Provide optimum patient care in an urgent care setting.BA or BS degree and graduate from an approved
Physician Assistant or Associate program accreditedby the AMA council on medical education required.
PA certification by the National Commission on Certificationof Physician Assistants and CT PA licensure required.1 - 3 years’ experience with ER or urgent care required.
Please use the online application at
www.stmh.organd click on Career Portal
PHYSICIAN ASSISTANTS
Full-time or per diem
WATERBURY, CT
design • marketing • websites • recruitment • broadcast • socialmedia
GG
gustinadvertising115 Dean Ave, Suite 100, Franklin, MA 02038 ■ Tel 888.541.1238 ■ Fax 508.541.8006 ■ www.gustinadvertising.com
Gustinadvertising © ALL RIGHTS RESERVED. This material is developed by, and is the property of, Gustinadvertising and is to be used only in connectionwith services rendered by Gustinadvertising. It is not to be copied, reproduced, published, exhibited or otherwise used without the express written consentof Gustinadvertising.
We are an Equal EmploymentOpportunity Employer M/F/D/V
www.ynhhcareers .org Careers for Life®New Haven, CT
Realize your full potential.
When U.S. News & World Report recently named Yale-New Haven Hospital as one of the nation’s leading medical centers, it confirmed what we already knew: our team does extraordinary work. We are proud of our
dedicated nurses and congratulate them on earning the American Nurses Credentialing Center’s distinguished Magnet® recognition.
Located on the Connecticut shore, Yale-New Haven Hospital is a 966-bed tertiary care facility with an international reputation for advanced care and leading-edge research. For more information, please call us toll-free at (866) 811-7797 or visit us online at: www.ynhhcareers.org. EOE
Cardiology
Cystic Fibrosis/Interstitial Lung Disease
Emergency Medicine (Guilford site)
Inpatient GYN/GYN Oncology
Neurosurgery
Newborn ICU
Pediatric ED
Surgical ICU
Surgical Subspecialties
Thoracic Surgery
Trauma
Wound Care
YCAAD/Asthma
Sign-on bonus, temporary housing and relocation stipend available for select mid-level positions
Our service expansion has created many new opportunities for mid-level Physician Assistants & Nurse Practitioners!
DON’T MISS A SINGLE FREE ISSUE OFADVANCE
SUBSCRIBE TODAY800.355.1088
JOB OPENINGS – SENT DIRECTLY TO YOUR E-MAILSIGN UP TODAY AT WWW.ADVANCEWEB.COM

Connecticut
53ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
As a member of our Cardiac Surgery practice you will first assist in coronary bypass surgery, valve surgery and heart transplantation. Experience with endoscopic and radial artery harvesting preferred: will train suitable candidate. Week-end on call coverage once a month. Current CT PA license is required.
Hartford Specialists is a multi-specialty surgical group with practices in 13 specialties that include: Transplant Surgery, Surgical Oncology, Orthopedic Surgery, Cardiac Surgery, and Neurosurgery. We provide surgical services at convenient locations throughout Central Connecticut.
Join a team of medical professionals dedicated in providing excellent clinical performance and exceptional patient service.
HARTFORD SPECIALISTS / HARTFORD HEALTHCARE
Exciting opportunity available for a FT Experienced Cardiac Surgery Physician Assistant.
Hartford Specialists is a member of Hartford HealthCare Corporation, affiliated with Hartford Hospital, the cornerstone of Connecticut’s finest full-spectrum health care system.
Hartford Specialists offers a competitive salary, medical and dental benefits, 401(k) savings and retirement plan, flexible spending accounts, life insurance, and paid vacation, sick and holiday time.
Central Connecticut offers all the great aspects of New England, easy access to Boston and New York, without the traffic and hassle of a large urban center. It is also one of the best places to raise a family with numerous recreation activities and top ranking public and private educational opportunities.
To submit your resume online please visit us at:www.harthosp.org/careers/search/HCAPC
Email [email protected] for more information or questions.
Hartford Specialists is an equal
opportunity employer who believes
diversity brings out the best in everyone!
EEO/M/F/D/V
WE MAKE IT EASY TO DO YOUR RESUME WITH RESUME BUILDER!
FIND IT AT
RENEW YOUR FREE SUBSCRIPTION TODAY! CALL 800.355.1088
• From the publishers of ADVANCE Newsmagazines• Custom gifts, giveaways & promotional products
• Exclusive healthcare designs you won't fi nd anywhere else• Free design, copy & creative services
• Staff gifts & event giveaways for every budget
advancecustompromotions.com
Call: 1-877-776-6680

Rhode Island, Connecticut, New York
54 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
Excellent opportunity for an experienced PA to work with busy 6 MD, 4 PA orthopedic group
in NW CT. Responsibilities include assisting in surgery, inpatient and outpatient care.
Competitive salary and benefits. Must be NCCPA certified and hold or be eligible for CT licensure.
Please fax resume to 860.482.4316 attention PA Dept
or e-mail ksi [email protected]
FAMILY or PEDIATRIC NURSE PRACTITIONERS
Full-Time and Part-Time Opportunities
The Providence Community Health Centers Inc., (PCHC), the largest state-wide network of com-munity health centers in inner-city Providence, provides primary care to 36,000+ patients. Our services include Family Practice, Pediatric, Internal Medicine, OB/GYN, allergy/asthma, dermatology, nutrition, reproductive health and WIC.
PCHC seeks experienced Certi ed Family and/or Pe-diatric Nurse Practitioners (Spanish is a plus) for our centers. As a National Health Service Core Approved Site, school loan repayment may be possible.
Quali cations include: Licensed Registered Nurse with a Bachelors of Science, Certi ed Family Nurse Practitioner and/or Pediatric Nursing Practitioner with 3-5 years experience.
To learn more about these exciting positions, please forward your resume to:
Diana Christian Senior Human Resources Generalist
Fax: 401-444-0469 or e-mail: [email protected]
“Connecting Communities to Quality Care”
Nurse PractitionerFull-time positions available to provide health services to clients of Child and Family Agencys School-Based Health Centers in New London and Norwich.
Excellent benefi ts and a Great Incentive Plan available for staff. $2000 Hiring Incentive
Compensation is currently being offered and will be paid after the successful completion of
six months employment.
Benefi t package includes fi fteen vacation days, twelve sick days; eleven paid holidays, fi ve family leave days, and medical dental insurance. AA/EOE. For information regarding Child and Family Agency, please visit our website at www.cfapress.org.
Per-diem candidates also accepted.
Sites are National Health Service Corp approved.
Interested applicants should send resume, references and salary requirements to:
Child and Family Agency, 255 Hempstead Street New London, CT 06320
or e-mail resume to [email protected].
APPLY INSTANTLY TO OPENINGS USING
RESUME BUILDERGO TO WWW.ADVANCEWEB.COM
RENEW YOUR FREE ADVANCE SUBCRIPTION TODAY!CALL 800-355-1088
advancecustompromotions.com
Custom gifts giveaways and promotional products.
1- 87 7 - 7 7 6 - 6 6 8 0
The choice is easy. The promise is sincere.
Brookhaven Memorial Hospital Medical CenterHR Dept, 101 Hospital Road, Patchogue, NY 11772
Visit us at www.brookhavenhospital.org
shore of Long Island has immediate openings. Interested in
we welcome you to join our team!
PHYSICIAN ASSISTANTS Trauma/Surgical/House* NEW $6,000 INCENTIVE BONUS for F/T Exp’d PAs
Surgical/House/Trauma
acute inpatient care including vascular, neuro and ortho with minimum 2 years recent
NCCPA, BLS and ACLS certification; ATLS preferred.
Pennsylvania, New York, New Jersey
55ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
SM
SM
SM
Nurse Practitioner Opportunities
Lancaster General Health has a variety of CRNP opportunities available.
Positions include:
• Psychiatry - full-time; psychiatric NP preferred; will consider FNP• Pediatrics - full-time; pediatric NP required• Urgent Care - part-time; FNP or PA required• Family Medicine - part-time; FNP required• Retail - full and part-time; FNP required
Benefi ts package is available, including the ability to purchase Medical/Dental insurance, paid malpractice insurance and more.
For further information andconfi dential consideration, send resume/CV to Beth A. Calabria at [email protected] Fax 717-544-1902 Visit our website at www.lancastergeneral.org
Nurse Practitioner/Physician Assistant
FT/PT for busy Family Practice in Bergen County, NJ. New Grads Welcome.E-mail resumé to [email protected]
or Fax: 201-368-9618
Nurse PractitionerPart-time, 17.5 hours/wk, Non-Exempt
Mental Health Recovery ServicesNew Hempstead, NY (TECH Building)Master’s degree req’d, 4 years exp.,
or equiv. combinationMust have Certifi cate and current registration to
practice as a Nurse Practitioner in New York State.
Contact info [email protected] (see www.Jawonio.org for full desc.)
Mount Sinai has long been one of the world’s most respected institutions, with outstanding nurses known for their excellence in patient care delivery. We are also recognized for our collaborative environment - where nurses can reach their maximum potential as clinical leaders, working alongside all members of the health care team who are second to none. In 2004, our nurses made Mount Sinai the fi rst full-service hospital in Manhattan to achieve Magnet status. In 2009, they earned us re-designation. And in 2011, the exemplary quality of their patient care has contributed to Mount Sinai being ranked 16th in the nation on U.S.News and World Report’s Honor Roll of “Best Hospitals.”
These are some of the things that make Mount Sinai exceptional. These are some of the things that make for great nursing careers.
NURSE PRACTITIONERS Exceptional opportunities are available for experienced Nurse Practitioners to join our team of professionals delivering specialty care. A Master’s degree in nursing and an NYS certifi cation as an NP required. Must have related clinical experience.
• Cancer Centers - Head & Neck & BMT• Surgery
• Diabetes Education • Cardiac Cath Lab
UPCOMING EVENTS
Online: www.mountsinai.org/nursing Call: (212) 241-9061/(866) SinaiRN (outside NYC)
Fax: (212) 860-6631
3 E A S Y WAY S T O A P P LY
EOE
E xceptional
Where
is the Norm.
2011 Mount SinaiNurse Practitioner Symposium
Friday, November 4, 2011
Registration: 7am – 8amConference: 8am – 5:45pm
New York Academy of Medicine1216 5th Ave (at 103rd St)
To register, please visitwww.mountsinaiheartnp.org
AdvanceJob Fair
Tuesday, October 25, 2011
9:30am - 2:30pmJacob K. Javits Convention Center
Visit us at Booth #102
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.
Call: 1-877-776-6680Visit: advancecustompromotions.com
• From the publishers of ADVANCE Newsmagazines
• Custom gifts, giveaways & promotional products
• Exclusive healthcare designs you won't fi nd anywhere else
• Free design, copy & creative services
• Staff gifts & event giveaways for every budget
THEY ALL WANT TO HIRE YOU. MEET THEM AT AN ADVANCE JOB FAIR & CAREER EVENTS
WWWADVANCEWEB.COM/JOBFAIRSATTEND AN ADVANCE JOB FAIR & CAREER EVENT CALL 800.546.4987

New York, Pennsylvania, New Jersey
56 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
Orthopedic Hospital • Bensalem, PA Nurse Practitioner
Utilization Review RN Case Manager• Minimum of 8 years experience
in Orthopedic setting• Competitive salary and benefi ts
For more information, visitwww.rothmanspecialtyhospital.com
E-mail resume to: [email protected] line: Nurse Practitioner or UR Case Mgr • EOE
NeonatalNurse Practitioner
Southern, NJ (Philadelphia Suburbs)
Virtua Health System seeks a Neonatal Intensive Care Nurse Practitioner to join 8 other Neonatal Nurse Practitioners and 8 Neonatologists in a hospital employed practice. State-of-the-art Level III NICU, 46 private beds, large obstetrics service (8000 deliveries system wide) with excellent MFM support, a caring and collegial staff, and an outstanding location will afford you a great deal of professional and personal satisfaction.
Very competitive salary and full bene ts are offered. MSN as well as NCC certi cation required.
You will nd outstanding schools, affordable homes, the culture and nightlife of Philadelphia (less than 30 minutes into Center City), as well as many of the coun-trys nest restaurants, intriguing historical sites, fantastic shopping districts, exciting sports teams, captivating music venues, beautiful theater productions, and world-class museums.
Contact Ken Sammut at 888-372-9415 E-mail: [email protected] or visit
www.cejkasearch.com ID#138631WB
One Career. Endless Opportunities.W W W . C H O P . E D U / C A R E E R S
We are an equal opportunity employer.
At The Children’s Hospital of Philadelphia, our nursescontribute to a renowned nursing team that delivers pediatriccare centered on evidence-based research, so they can achievethe best possible outcomes for our patients and their families.Re-designated as a Magnet® institution in November, 2008,the CHOP Department of Nursing gives our professionals theindependence to participate in individual research programsat the bedside, along with the tools and environment to ensurean unmatched career.
We currently have opportunities for new and experienced
Acute Care Pediatric Nurse Practitioners
For more information or to apply please contact Jessica McElroy at 267-426-5787 or [email protected].
CHOP Nursing: Leaders and Partners at All Levels
The Children’s Hospital of Philadelphia is rankedas one of America’s besthospitals for children by
U.S. News & World Reportand Parents Magazine.
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.
NORTH COUNTRY EMERGENCY MEDICINE CONSULTANTS, PC, is recruiting a Physician Assistant to join our current group of 9 Physicians, 5 Physician Assistants, and 2 Nurse Practitioners. NC EMC, PC contracts with Samaritan Medical Center to staff the Emer-gency Department which has an annual volume of 50,000 patients. PAs, working closely with MDs, staff the ED in both the Urgent Care and Triage areas. SMC recently opened a new ED 11/10 which has in-ED radiology, CT scan, ED Ultrasound and point of care testing. The compensation package is approximately $120,000 PLUS benefi ts for approximately 140 hours/month. A RVU-based productivity bonus is rewarded quarterly. Upstate New York is an outdoor enthusiast’s para-dise with 4-season recreation in the world famous Thousand Islands, Lake Ontario and Adirondack regions. Montreal, Toronto, and NYC are a short drive away and Syracuse International Airport is within 1 hour drive. If this opportunity interests you, and you have a minimum 3 years Emergency Medicine/Urgent Care experience, please send your CV and cover letter to:
Dr. Maja Lundborg-Gray, MD, FAAEM, FACEPPresident, North Country Emergency Medicine Consultants, PCSamaritan Medical CenterDepartment of Emergency Medicine830 Washington StreetWatertown, NY 13601Or e-mail to: [email protected]
New Jersey, Pennsylvania
57ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
NURSE PRACTITIONERS (FNP)Easton, Allentown, Quakertown,Reading, Lebanon, Palmerton, Tamaqua, Pottsville, PA areas
and Delaware
We will Educate and Train for Dermatology
Excellent Salary & Benefi ts,Vacation, Incentives, &
Time off for CMEs.
Call 732.814.0769 • Fax 732.244.2804E-mail: [email protected]
JERSEY REHAB, P.A.
PHYSICIAN ASSISTANTNURSE PRACTITIONER
Pain Management, Physical Medicine & Rehab practice, with multiple offi ces in Northern New Jersey and New York City, is seeking Full-time/Part-time PAs and NPs to join our team of professionals. Must have a NJ and/or NY license. We offer a competitive salary and benefi ts including 401k.
Call 973-652-3676E-mail [email protected]
Private physician owned and operated group currentlyrecruiting PA/NPs at the following New Jersey locations:
• Essex County - Academic hospital with an annual volume of 30k. Shifts are 12 hours, no overnights.
• Middlesex County - Community teaching hospital with an annual volume of 45k. Shifts are 12 and 8 hours.
• Mercer County - Community hospital with an annual volume of 30k. Shifts are 12 hours, no overnights.
LEAD POSITION ALSO AVAILABLE
We require a minimum of one (1) year of Emergency Department experience. We offer a highly com-petitve salary, CME stipend, medical malpractice and comprehensive benefi ts.
Forward CV to [email protected]
The Division of Trauma Surgery and Critical Care at The Reading Hospital and Medical Center (TRHMC) is seeking Nurse Practitioners and Physician Assistants to add to its trauma practice of 5 full-time, fellowship-trained trauma surgeons, Philadelphia College of Osteopathic Medicine surgical residents, and 7 Advanced Practitioners. TRHMC is a Level II trauma center with approximately 3,000 trauma contacts/year and is a member of the University of Pennsylvania Trauma Network. As a Trauma AP, you will participate in providing primary management of injured patients through all phases of care, including the initial trauma resuscitation, OR, ICU, general care floor and outpatient clinic. Additionally, the service participates in elective and acute care surgery.
You’ll play a central role in a high-volume and diverse inpatient and outpatient clinical practice, as well as maintain responsibilities in the Division’s Performance Improvement Program. Clinical continuity, consultation, communication and compliance with evidence-based medicine are the hallmarks of this exciting and unique position. Opportunities for professional growth and development are available through research, lecturing, publications and involvement with divisional and hospital projects and committees. Critical care experience and experience as an ACNP or PA is preferred. Candidates must also be board-certified/eligible as a CRNP or PA-C. The positions are full-time, 4 days a week and average 40 hours per week with no call responsibility. We are located within an hour of Philadelphia and Allentown. Competitive salary and benefits package included.
For more information, please contact:
Ken NicholsManager, Medical Staff RecruitmentThe Reading Hospital and Medical CenterOffice: 610-898-5640 Efax: [email protected]
Trauma Advanced PractitionerWest Reading, PA
Involvement from Initial Resuscitation through Outpatient Care
REACHING
BE
YO
ND
EOE
{ ADVANCE }NOBODY DOES IT BETTER THAN THE BEST
WWW.ADVANCEWEB.COM SUBSCRIBE ONLINE! WWW.ADVANCEWEB.COM
UPDATING YOUR RESUME IS THE FIRST STEP TO
A NEW CAREER!
GET STARTED AT www.advanceweb.com
FIND A NEW JOB ATwww.advanceweb.com
www.cfghealthsystems.com EOE
If you’d like to hear about great opportunities that you may not have thought of, speak to Nancy. She can tell you about the rewards of careers in correctional and outpatient nursing, answer your questions while you tour a facility, and tell you about the opportunities for professional growth and advancement.
PSYCHIATRIC NPsFull-Time and Part-Time at Outpatient
Facilities and Child Partial Day Programs and Hospital Consults Throughout NJ.
Current NJ RN / NP and DEA licenses required. Corrections and/or Outpatient experience a plus.
ALSO SEEKING:CLINCAL DIRECTOR
of Child/Adolescent Inpatient Unit.
APNsChild/Adolescent experience.
Key openings in Southern & Northern NJ.Sign-on and referral bonuses.
We offer excellent compensation. Full-Time employees enjoy a generous benefi ts package.
Call or send resume:
Nancy DeLapo, Director of Staff Development
Phone 856-797-4761 [email protected]
Fax 856-797-4798
Learn About Nursing’s Best Kept Secrets...Let’s Speak. –Nancy

New Jersey, Maryland, New York
58 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
Apply online: www.sjhealthcare.net
Equal opportunity employer.
Nurse PractitionerPer Diem, Days 16 hours/week
IMPACT ProgramVineland, NJ
The IMPACT Program (Innovative Model for Preschool and Community Teaming), a collaboration between South Jersey Healthcare and two local school districts, provides an array of programs designed to improve the health and well-being of young people and their families. NP will provide acute and episodic healthcare, including preventative health education to an adolescent population, to students at the Vineland High School through the Vineland School Based Youth Services Program. Will also provide education for pregnant and parenting teens.
Requirements:
active NJ license in good standing.
adolescents.
Visiting Physician Services is looking for an
NPor PA to care for elderly homebound
patients in Middlesex County, NJ. Full and part-time
positions are available.
Please fax CV to
732-571-1156
EOE
NURSE PRACTITIONERSAll NP positions require Master’s Degree, NYS NP licensewith ANCC/AANP certification as an Adult or Family NP,and AHA BLS & ACLS. All positions are 8 hour shifts.
• Cardiology - FT, EveningsPrevious Cardiology experience preferred.
• Electrophysiology - FT, Days M-FRequires electrophysiology experience.
• Palliative & Geriatric - FT, Days M-FHospice or Palliative Care experience preferred.
PHYSICIAN ASSISTANTSAll PA positions require NYS PA license with NCCPA certi-fication, and AHA BLS & ACLS. Experience and/or skills inarea of practice is preferred.
• Surgical Operating RoomFT, Days & Evenings (8 hour shifts)
• OrthopedicsPD, Nights, Saturday (12 hour shift)
APPLY ONLINE: www.SouthNassau.org
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.
APPLY FOR THE JOB YOU’VE BEEN WAITING FOR WITHRESUME BUILDER!
Visitwww.advanceweb.com
RENEW YOUR FREE SUBSCRIPTION TO
REVIVE YOUR CAREER.CALL 800.355.1088
in Westminster, Maryland
OB/GYN CARROLL HEALTH GROUPPhysician PracticePerform basic gynecologic evaluation, management services, pre & post-natal care, weekdays from 9am-5pm with occasional Saturday mornings. No hospital or ER call required but after hours “telephone on call” can be expected at least 2 days/week. CNRP with at least 1 year of OB/GYN experience and active Maryland license preferred. To apply, please email resume to: [email protected]
EOE. Smoke & Drug Free Campus.
Superior Commitment. Exceptional Careers.
NURSE PRACTITIONERS
Behavioral Health Hospital SettingLooking for a unique and shared practice model? You’ll find it at Carroll Hospital Center, where you’ll work alongside 3 experienced psychiatrists in ambulatory care, inpatient or outpatient rehabilitation. MSN with ACNP and 2-4 years experience with adult/adolescent population required. Apply online at: carrollhospitalcenter.org
It’s all right here

Maryland, Delaware
59ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
Neurocritical Care Advanced Practice NurseChristiana Hospital
Christiana Care Health System is one of the country’s largest health care providers. A major teaching hospital serving more than 600,000 patients yearly through 1, 100 patient beds in two hospitals, it was recently awarded Magnet status for excellence in nursing by the American Nurses Credentialing Center (ANCC).
Christiana Hospital is recruiting for a Neurocritical Care Advanced Practice Nurse. The selected candidate will collaborate with the medi-cal care team to perform direct medical management through utili-zation of approved protocols and procedures as well as appropriate medical consultation for neurocritical care patients. Patients with vari-ous neurological and neurosurgical issues are admitted to the Neuro-science Critical Care Unit including but not limited to non-traumatic SAH/aneurysms/AVM, ischemic stokes, traumatic head bleeds, brain masses/tumors, traumatic spinal cord injuries, non-traumatic spinal cord problems, Aronld-Chiari Malformations and myasthenia gravis. Additionally, various brain pressure and brain tissue oxygen devices are inserted at the bedside in the critical care unit. Unique to this unit is that it will be led by an all Nurse Practitioner group.
Requirements: Master’s degree in nursing with an eligibility for APN licensure in Delaware as a Nurse Practitioner or Clinical Nurse Specialist. The candidate must have or be eligible to obtain prescrip-tive authority. At least 3 years experience as an RN in adult and/or pediatric neurosurgical/neurocritical care/trauma/surgical critical care or emergency nursing is required; critical care experience preferred.
Apply online at http://careers.christianacare.org/Or send your resume to [email protected]
ummc n u r s i n g . c om
Today,I am part of something bigger than myself.
Whether you are a newly graduated Nurse Practitioner or a seasoned professional, no other NP career can offer you the challenges – or the prestige – of a UMMC career. Here, talented Nurse Practitioners like you enjoy the kind of collaboration, resources and support from an organization that can truly maximize your impact. Opportunities are available for Nurse Practitioners in a number of specialty areas, including:
Acute Care Emergency ServicesBariatric Surgery
GYN OncologyLung TransplantNeuroCare ICU
Neurology ClinicNeuroSurgery Service
OncologySurgical Intermediate Care
Transplant Surgery
Advancing the practice of nursing, every day. That’s our commitment at UMMC. Join us, and be a part of the excitement. We offer generous relocation assistance, a healthy work/life balance and a dynamic location in vibrant downtown Baltimore.Apply online today.
UMMC is proud to support an environment of diversity and encourages inquiry from all applicants. EOE
Joe, CRNPOrthopaedic Trauma
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.
WITH JUST ONE NAME TO REMEMBER,
SEARCHING FOR INFORMATION ON THE
WEB JUST GOT EASIER!
Visit www.bayviewjobs.org for more information and to apply today!
EOE/AA, M/F/D/V
At Johns Hopkins Bayview Medical Center you can be assured of a career filled with exploration, growth and variety, featuring the latest technology and opportunities for advancement. As an academic medical center, we believe that your career should be full of stimulating experiences and continued exploration.
We invite you to see for yourself what’s special about a career at Johns Hopkins Bayview Medical Center.
We currently have full-time, part-time and PRN opportunities for Physician Assistants and Nurse Practitioners in the Hospitalist service and Neuroscience department.
If helping people is your calling...

Virginia, Delaware, Maryland
60 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
Consider the rewards of a career at Harbor Hospital. We are a proud member of MedStar Health and winner of the prestigious Delmarva Excellence Award for 6 years! Join our team as a:
NURSE PRACTITIONER MANAGER
(Occupational Health)
Must be a graduate from an NP program approved by the MD Board of Nurses, have 2 years’
experience and certifi cation as an Adult/Family NP.
Learn more and apply online at:
www.harborhospital.org
Refl ect on a better future.
EOE
Precious moments happen every day
At Bon Secours, you don’t have to choosebetween life and work.
We invite you to become a part of the excitement as we continue to build a great environment — all in a place that adds quality to your life. Visit us at bonsecoursnursing.com.
BON SECOURS VIRGINIA HEALTH SYSTEM
all year ‘round.
EOE
It’s not about summertime’s hot, sunny weather. It’s not about bathing suits or tans. There’s a feeling you get from being near the beach. Locals in Lewes, Delaware know it.
People who’ve moved here wonder how they ever lived without it.
Find out for yourself why it’s better at Beebe Medical Center.
Neonatal Nurse PractitionerRequires current DE APN licensure and CPR certification and two-four years expe-rience at a Neonatal Inpatient care practice. Prefer experience in Neonatal, Pediat-rics, GYN and Family Medicine. Prefer 12 months previous experience as staff nurse. Experience in urgent care, women’s health (GYN only) and pediatrics (especially well baby care) preferred.
Nurse Practitioner–Wound CareRequires Graduate of a Nationally Certified and Accredited Physician Assistant or Nurse Practitioner Program. Current Delaware Licensure required. Experience as a Nurse Practitioner in an outpatient setting preferred. CWOCN certification preferred.
Please see our website, www.beebemed.org for fullposition descriptions and to apply online.
Beebe Medical Center, 424 Savannah Rd., Lewes, DE 19958. Phone: 302-645-3336. Email: [email protected].
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.

North Carolina, Georgia, Tennessee, Illinois, Ohio, Michigan
61ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRAL
EAST NORTH CENTRAL
EAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRAL
INTERNATIONAL
INTERNATIONAL
INTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
EAST NORTH CENTRAL
EAST NORTH CENTRAL
EAST NORTH CENTRAL
EAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRAL
INTERNATIONAL
INTERNATIONAL
INTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
Nurse Practitioner/Physician Assistant
Traverse Heart and Vascular is a single specialty, 18-member practice that is fully integrated with Munson Medical Center. We currently have a full-time Nurse Practitioner or Physician Assistant opportunity to care for patients in the inpatient and outpatient setting. Cardiology experience highly preferred. Duties include: implementing patient manage-ment plans, and records progress notes. Also prescribes pharmacologic and other therapeutic treatment for the benefi t of patient health, including post-procedure wound care.
Munson Medical Center’s reputation for the highest qualitycare is represented by repeated national recognition as follows: #1 in the nation for medical excellence in coro-nary bypass surgery in the 2011 Care Chex Hospital Quality ratings; Top 50 Cardiovascular Hospital in 2011 by Thomason Reuters; Top 100 Hospital 13 times and Top 100 Hospital for Cardiovascular Services four years in a row. Munson Medical Center is a 391-bed tertiary care facility located in Northwestern Lower Michigan. For more information or to apply online visit munsonhealthcare.org or call 800-713-3206 ext. 1
Raleigh Adult Medicine is seeking a full-time PA/NP. Minimum of 1 year of clinical experience required preferably in a family or internal medicine environment. We have an excellent benefi ts package.
Apply by e-mail: [email protected]
JOB OPPORTUNITYDo you have a passion for quality healthcare?
Do you want to contribute to healthier women and families and stronger, sustainable communities?Sign-on bonus available up to $2,500.
Planned Parenthood of Northeast Ohio is seeking energetic, motivated mid-level clinicians to fi ll openings at our Lorain, Cleveland, Akron, and Canton health centers.
PPNEO encourages clients to take control of their lives and health and promotes prevention by offering top-quality family planning and reproductive health care services to nearly 60,000 clients at 16 health centers in 21 North-east Ohio counties. Our services are designed to help people make lifelong informed choices that focus on responsibility and prevention of unintended pregnancies, sexually transmitted infections and reproductive cancers. PPNEO offers a generous and comprehensive benefi t package including:
• Paid Time Off (PTO) policy of 19 PTO days annually for new full-time employees• Medical, dental, vision, voluntary short-term disability, fl exible spending account (FSA), employer paid Life and AD&D insurance and LTD• 401K to include employer match after 1 year of service• Reimbursement of fees to be used for dues/CEUs/CMEs/licensure
Position SummaryThe Clinician acts as part of the medical services team providing reproduc-tive health care and patient care including history review, health education, physical exam, counseling, diagnosis and treatment.In addition to the above responsibilities, the Charge Clinician is responsible for the medical oversight of the health center. The Charge Clinician works in partnership with the Health Center Manager as a leadership team to provide quality patient care and customer service.
Position RequirementsPosition requires education commensurate with Ohio statute licensure re-quirements for practice capacity (NP, CNM). Must have current Ohio nursing license, COA and CTP or be eligible for CTP-externship. 2-3 years of practice experience in women’s health is preferred.To apply, please visit our website at www.ppneo.org and click the PP-NEO Jobs link to view and apply to all of our active job postings.
Planned Parenthood is an equal opportunity employer and we believe that a multicultural perspective is an essential element of a 21st Century organization.
Lakeshore Mental Health Institute in Knoxville, TN has a full-time position open for a Nurse Practitioner.
Lakeshore Mental Health Institute is a 24 / 7 hospital with two inpatient programs. Both the Acute and Extended Care Programs serve individuals
with severe and persistent mental illnesses.
Minimum Qualifi cations: Education and experience: from an accredited college or university with a masters degree in a nursing clinical specialty area with preparation in spe-cialized practitioner skills and possession of a Certifi cate of Fitness from the Tennessee Board of Nursing specializing in psychiatric care.
Special Qualifi cations:Licensed or eligible for licensure as a registered Nurse and an Advance Prac-tice Nursing license in the State of TN and current national certifi cation or eligible for national certifi cation in the appropriate nursing specialty area. Licensure as a Registered Nurse in the State of TN and national certifi cation in the appropriate nursing specialty area are required within a reasonable time after employment. Possession of a Certifi cation of Fitness from the Tennessee Board of Nursing is also required within a reasonable time after employment. Adult Psychiatric Certifi cation preferred.
Contact Bert Simpson, MD, Clinical Director, today to discuss this unique opportunity at (865) 583-8768. Come enjoy your work and enjoy your life. Pre-employment drug testing required. The State of TN is an Equal Opportunity, Equal Access, Affi rmative Action Employer.
Physician AssistantPinehurst, NCSandhills Emergency Physicians, PA has immediate openings for Physician Assistants with prior Urgent Care/ED experience. 65k ED visits/year and growing with excellent bene ts and salary. Great place to live-2 hrs. from NC Coast 4 hrs from NC mountains.
Please contact Jonathan Brower, MD E-mail resume to [email protected]
website www.sandhillsep.com
Physician Assistant/Family Nurse PractitionerFull-time Position - Glenwood Avenue Location.Raleigh Orthopaedic seeks a North Carolina licensed Physician Assistant or Family Nurse Practitioner to join our mid-level provider team immediately. This is an outpatient clinic setting alternating work week schedules of 8 AM to 6 PM for clinic and 1 PM to 9 PM for After Hours Clinic. Position supports regular daytime clinic as well as marketing responsibilities for the growth and development of the After Hours Clinic. Compensation includes incentivized pay as well as shift differential for After Hours Clinic between the hours of 6 and 9 PM. Orthopaedic experience required.
Submit resume and cover letter to [email protected]
Shepherd Center, located in Atlanta, GA, is aworld-renowned, nonprofit hospital specializingin medical treatment, research and rehabilitationfor peoplewith spinal cord or brain injury.Shepherdcurrently has a full-time opportunity availablefor a Mid-Level Provider to support our Physiciansinour Inpatientprograms. RequiresGeorgiaLicensedPhysician Assistant or Nurse Practitioner. Rehabexperience preferred. Apply or learn more aboutShepherd Center at shepherd.org
EOE
Mid-LevelProvider
Nurse Practitioner(NP, FNP, ANP or WHNP)For a Family Practice Clinic
in Arlington Heights IL.Some local travel to locations in Western
or NW Suburbs may be required.(Main Base Arlington Heights IL).
Please send resumes to [email protected]
OR fax to 847-398-4585.Please include code NP103
with all submissions.
DON’T LET YOUR FREE ADVANCE SUBSCRIPTION EXPIRE!CALL 800.355.1088
UPDATING YOUR RESUME IS THE FIRST STEP TO A NEW CAREER!
GET STARTED AT WWW.ADVANCEWEB.COM
FOR JOB OPPORTUNITES THROUGHOUT THE NATION!WWW.ADVANCEWEB.COM

Illinois, New Mexico
62 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
Nurse Practitioner OpportunitiesOutpatient Full-Time/ Part-Time
New retail quick care clinic in the Lakeview area of Chicago with
opportunity for continuity care and rotation to immediate care clinics.
CNP with strong customer service skills.Experience/training in family medicine,
urgent care, ER or retail health. FT & PT openings.
Competitive benefi t/salary package.
Send inquiries to:
Phone: [email protected]
Very Interesting opportunity for 2 to 3 Exceptional NPs or PAs to build an After Hours Clinic based on a very busy private practice in Barrington, IL. Unique opportunity to see a variety of patients while enjoying the satisfaction of continuity of care with an existing practice. Be the fi rst to claim your own PT hours schedule. Evenings and weekends. We also have additional PT & FT private Family Practice and Internal Medicine Opportunities. Additional opening for a FT Surgical PA to join busy Premier Ortho Practice. Responsibilities include; surgical assist in OR, hospital rounds, and some call.Explore these outstanding opportunities to join a health system that serves one of the fastest growing counties in the Midwest. We are located only forty-fi ve minutes from all that downtown Chicago has to offer, maintaining our status as “one of the top ten communities for families” ranked by national magazines.Qualifi ed candidates will become a part of our highly reputable team of providers and join us as we continue toward our goal of becoming one of the best community hospitals in the nation. Sherman hospital, our brand new 255-all private bed facility features a 15 acre geothermal lake that heats and cools the hospital and saves us over $ 1 Million per year in resources! The award winning lake is one of the largest in the world and just one of the reasons Sherman is leading the way to a cleaner, brighter future.
Call Kathy Walters at 224-783-6270 to schedule a phoneinterview with the Recruiter, Cheryl Vanderlaan or E-mail CV directly to [email protected]
EOE
WE MAKE IT EASY TO DO YOUR RESUME WITH RESUME BUILDER
FIND IT AT WWW.ADVANCEWEB.COM
THOUSANDS OF JOB OPPORTUNITIES ONWWW.ADVANCEWEB.COM
UNMH is the only teaching hospital with the only Level 1 Trauma Center in NM. In addition to being the state’s only Stroke Certified Center, we are also the first in NM to be designated as a Pathway to Excellence Organization, recognized by Consumer
Reports as one of the nation’s Top 3 Hospitals for conservative care, cited by Nursing Professionals magazine among the 2009 Top 100Hospitals to Work For, and honored by Working Mother magazine as one of the 6 Best Companies for Hourly Workers. We were just ranked
#16 in Training Magazine’s Top 125 Training Organizations – a true testament to our emphasis on continuing education. We are also currently pursuing MAGNET status.
Come, be part of our extraordinary team. We have openings in the following areas:
Nurse Practitioners/Physician Assistants
CulturalImagine yourself in picturesque Albuquerque, NM enjoying all the lifestyle amenities you can name.
A promising career in the Land of Enchantment...What could be better?
You wear so many hats so well...We take our hats off to you.
• Nurse Practitioners/Physician Assistants• Advanced Practice Psych Nurses
To learn more and to apply online, visit:
http://hospitals.unm.edu/jobs/ and refer to the corresponding REQ #’s
Advanced Practice Psych Nurses• Psychiatry (Req # 11134506) • MHC – Continuing Care Clinic (Req # 11224074)
• Outpatient Psych (Req #s 11291888, 11277962)
At UNMH everything is attainable. Nothing is out of reach.
• Infectious Disease (Req # 11244134)• Hematology – Oncology (Req # 11263439)• CT Surgery – Floors & Clinic (Req # 11203481)• Pediatric Urology – Inpatient & possible OR (Req # 11270278)
• Emergency Department (Req # 11203488) • ENT Surgery – Inpatient & Clinic (Req # 11203459)• Surgical Services – Evening/Night Shifts (Req # 11270256) • Vascular Surgery – Inpatient & Clinic (Req # 11270252)
EOE
Kansas, Texas, Idaho
63ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
Senior PsychCare provides evaluations, psychiatric management and mental health services to nursing home residents throughout the
state of Texas. NP or PA with Geriatric or Psychiatric experience preferred but willing to train. TX license, PT/FT available, EMR, fl exible schedules (no nights or weekends). Dallas, San Antonio, Austin, Houston.
[email protected] or fax 713-627-7302
Southwest Idaho OpportunitiesNURSE PRACTITIONERS
• Urgent Care • Glycemic Management • Urgent Care Float
We offer competitive compensation, outstanding bene ts including CME stipend, paid education leave and malpractice insurance. Plus, you’ll enjoy the con dence that comes with knowing you’re working with an outstanding team of physicians, surgeons and specialists in a collegial, supportive environment.
MSN, NP/PA certi cation required, plus current DEA and Idaho Board of Pharmacy controlled substance license.
To learn more about the difference that is Saint Alphonsus and how you can make a critical difference for your patients, please contact:
Sylvia Chariton, Physician RecruiterPhone: (208) 367-3074 or (800) 309-5388
FAX: (208) 367-7964E-mail: [email protected]
www.saintalphonsus.orghttp://www.saintalphonsus.org/careers-video.html
MBS Integrated Care, a division of Harden Healthcare, provides Nurse Practitioners in the long-term care and home health setting. We are a growing company with opportunities available across Texas. We are cur-rently seeking the following:
Nursing Home Providers:Corpus Christi,
Fort Worth, Fredericksburg, Killeen, Round Rock, San Angelo, San Antonio,
Temple and Waco
House Call Providers in Austin, Georgetown,
(Full-time and Part-time Available)If you are interested in a great opportunity with
an expanding organization please contact:
Tracy Shultz, Recruiter at [email protected]
or by phone at 1-866-607-2722.Feel free to visit our website to learn more:
www.mbsintegratedcare.com
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.
D O N ’ T M I S S A S I N G L E I S S U E —RENEW YOUR FREE SUBSCRIPTION TODAY!
• From the publishers of ADVANCE Newsmagazines
• Custom gifts, giveaways & promotional products
• Exclusive healthcare designs you won't fi nd anywhere else
• Free design, copy & creative services
• Staff gifts & event giveaways for every budget
Call: 1-877-776-6680Visit: advancecustompromotions.com
ATTEND FREE CE SESSIONS AT ADVANCE JOB FAIR & CAREER EVENTS AT WWW.ADVANCEWEB.COM/JOBFAIRS
Scott County Hospital Provider Extender Opportunity
PA or ARNP: Practice in a beautiful spacious 69,000 square foot Replacement Hospital opening May 2012. Join a pro-gressive organization and work with 4 family practice physicians, 1 PA, in provider-based Rural Health Clinic and CAH Hospital. Call coverage is 1:4. Total compen-sation including benefi ts will exceed $100,000.
Send resumes or inquiries to: Karma Huck, COO,
Scott County Hospital, 310 East Third Street, Scott City, Kansas 67871
620-872-7711 or [email protected]

Alaska, California, Oregon
64 November 2011 • ADVANCE for NPs & PAs
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
PeaceHealthSacred Heart Medical CenterPeaceHealth Medical Group
Located in the lush Willamette Valley between the rugged Paci c Coast and the magni cent Cascade Mountains, Eugene, Oregon is a welcoming blend of cutting-edge culture and breathtaking wilderness. Guided by our mission and values, PeaceHealth provides evidence-based and compassionate healthcare in the Paci c Northwest.
PeaceHealth Medical Group is seeking experienced, board certi ed Nurse Practitioners to join our group.
We have opportunities in:Retail Clinic • Cardiology NP/PA
Internal Medicine • Hospitalist NPNeurohospitalist NP and Family Medicine
Urgent Care NPPsychiatric NPSleep NP/PA
If you are looking for a career that engages your heart as well as your mind, we encourage you to consider PeaceHealth.
Please visit our website at www.peacehealth.org.Contact Denise Etchison at 541-222-2529 or e-mail at
[email protected] for more information or to apply.
NURSE PRACTITIONER OPPORTUNITIES
HealthCare Partners Medical Group is a multi-specialty medical group that is recognized for its quality of care and high rates of patient satisfaction. HealthCare Partners has over 3,500 employees, including 500+ primary care and specialty physicians, caring for more than 500,000 patients throughout Los Angeles County and Northern Orange County. HCP operates 40 medical clinics, five urgent care centers, two medical spas, and an ambulatory surgery center. If you’re looking to make a difference with a large, financially stable, well recognized, privately-owned Medical Group, HealthCare Partners is the employer for you! As part of our continued growth, we are currently seeking outgoing Nurse Practitioners and Physician Assistants to join our team.
In this role, you will have the opportunity to provide care and support to variety of patients and work in a multi-disciplinary office practice while achieving the work/life balance you’ve been looking for!! HealthCare Partners offers competitive salaries and a wide range of benefits to our full and part-time employees including medical, dental and vision insurance, 401(k), continuing education, tuition reimbursement, free Basic Life and AD&D, free long term disability coverage, a generous holiday schedule, paid time off and more.
live | work | relax
Voted one of the "Best Places to Work in LA - 2011"
Beautiful Southern Oregon - Grants PassSeeking an experienced certifi ed FNP for an in-house acute care department. The practice will include some primary care. Guaranteed salary and generous benefi ts. No call requirements. Financially healthy multi-specialty group serving southern Oregon for over 58 years. Visit our website at www.grantspassclinic.com. Contact Susan Sartain by e-mail at [email protected] or by telephone at 541-472-5505.
Orthopaedic PASeeking an experienced Ortho PA.
Includes clinic, surgical & some trauma. Call required.
888-890-8301, ext. 1907-228-8324 (fax)
Bridging the NP and PA Knowledge Gap‘The two professions suffer from huge holes in understanding what, where, why and how they each exist. It’s in the eye of the beholder how much the dif-ferences matter.’
—Roderick S. Hooker, PhD, MBA, PA,in the September 2010
issue of ADVANCE.
President Obama Proclaims PA WeekOn PA Day on Oct. 6, 2010, President Barack Obama proclaimed October 6–12 as National Physician Assistant Week. It marked the first time this cel-ebration had been recognized by presi-dential proclamation.
NPs & PAs Have Prescribing PowerConsidering that about 3.9 billion pre-scriptions were written in the United States in 2009, NPs and PAs pull their prescribing weight. Given that there are an estimated 773,800 active physicians, NPs and PAs together write roughly 23% of all prescriptions while accounting for 21% of prescribers.
Job Market Competition‘In most areas of the country, the sup-ply of NPs and PAs is greater than the demand. For every job posted, record numbers of applicants apply.’
—Renee Dahring, MSN, NP,in the September 2010
issue of ADVANCE.
How Many NPs?There are 158,348 U.S. nurse practitio-ners, according to the Health Resources and Services Administration’s recently published quadrennial study of the U.S. nursing population.
NPs, PAs and the Healthcare Home‘NP and PA organizations are monitoring implementation of healthcare homes carefully, seeking to ensure that language permits NPs and PAs to be leaders.’
—Editor Michelle Pronsati in the December 2010 issue of ADVANCE.
Celebrating NPs & PAs‘Despite that you and your colleagues still are relatively small in number, you are loud in voice, and you have made and will continue to make an enormous impact on health care in America. Countless millions of patients who’d have otherwise gone untreated will con-tinue to be able to access healthcare because of the dedicated work of you and your colleagues. In the case of the NP–PA team, the whole is much greater than the sum of its parts.’
—Editor Michael Gerchufsky in the December 2010 issue of ADVANCE.
Mideast Gets Its 1st PA ProgramThe Kingdom of Saudi Arabia initiated its inaugural physician assistant class of 27 students at the Prince Sultan Military College of Health Sciences in the Eastern Province capital of Dhahran this past autumn.
FIND THOUSANDS OF JOBS ONWWW.ADVANCEWEB.COM
RENEW YOUR FREE SUBSCRIPTION TO REVIVE YOUR CAREER
We’re not your typical corporate health care organization, and if you went into medicine with a passion to help improve the healthcare of the patients in need, we have several fulfi lling career opportunities.• Outpatient Services Manager• Clinicians (NPs & PAs) Orange & San Bernardino Counties• Health Center Director• Director of Patient SafetyWe offer highly competitive pay and benefi ts and a dynamic and independent work place. Plus, you’ll go home each night knowing you’ve made a positive and lasting difference in the lives of your patients.
To Apply, please contact Rachel Rodriguez, [email protected]
700 S. Tustin St., Orange, CA 92866 714-633-6373 x179 • fax: 714-633-1443
Providing world class reproductive health services to men and women is not
just our practice...it’s our mission!

National
65ADVANCE for NPs & PAs • November 2011
Car
eer
Opp
ortu
nities
EAST NORTH CENTRAL
EAST NORTH CENTRALEAST NORTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALEAST SOUTH CENTRALFACULTYFACULTYFACULTYINTERNATIONALINTERNATIONALINTERNATIONALLOWER SOUTH ATLANTICLOWER SOUTH ATLANTICLOWER SOUTH ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MIDDLE ATLANTIC
MOUNTAIN
MOUNTAINMOUNTAIN
NATIONAL
NATIONALNATIONAL
NEW ENGLAND
NEW ENGLAND
NEW ENGLAND
PACIFIC
PACIFIC
PACIFIC
SOUTHWEST
SOUTHWESTSOUTHWESTUPPER SOUTH ATLANTIC
UPPER SOUTH ATLANTICUPPER SOUTH ATLANTIC
WEST NORTH CENTRAL
WEST NORTH CENTRALWEST NORTH CENTRALWEST SOUTH CENTRAL
WEST SOUTH CENTRALWEST SOUTH CENTRAL
Emergency Medical Associates (EMA) Join a democratic group which is nationally recognized for delivering high quality care, innovation, unparalleled support (i.e. scribes) and exceptional patient satisfaction for over 30 years! Work in a culture that is committed to life-work balance.
EMA NP’s and PA’s enjoy excellent compensation, comprehensive benefi ts (Full Health, 401k match, Profi t Sharing, PTO & Professional Expenses) and career growth.
Contact: Dan Rizzo 877-692-4665 x1048
Career Positions Available for Nurse Practitioners
and Physician Assistants in New Jersey, New York and North Carolina.
The Sign of Excellence in Emergency Medicine ®DON’T MISS A SINGLE FREE ISSUE OFADVANCE
SUBSCRIBE TODAY800.355.1088
1-877-776-6680advancecustompromot ions.comTHE BEST JOB FAIR & CAREER EVENT
WWW.ADVANCEWEB.COM/JOBFAIRS

1960
1958
1974
1989
1966
1970
1980
1990
2000
2010
1993
66
Murmurs&Gallops
Nurse Practitioners: A TimelinewhILe NP fIRsTs aren’t always easily identifiable due to differences in definitions, there’s no debate that from a first graduating class
of one in 1966 has emerged a vibrant and vital profession. Happy National Nurse Practitioner Week 2011! —Michael Gerchufsky
Sou
rces
incl
ude
the
Amer
ican
Aca
dem
y of
NPs
; the
Am
eric
an C
olle
ge o
f NPs
; the
Hea
lth R
esou
rces
Ser
vice
s Ad
min
istr
atio
n; th
e IC
N In
tern
atio
nal N
P/AP
N
Net
wor
k; th
e Lo
uisi
ana
Asso
ciat
ion
of N
Ps; U
nite
d AP
RN
s of
Geo
rgia
; The
Doc
tor o
f Nur
sing
Pra
ctic
e an
d Cl
inic
al N
urse
Lea
der,
edite
d by
Joy
ce J
. Fitz
patr
ick
and
Mer
edith
Wal
lace
(Spr
inge
r Pub
lishi
ng, 2
009); N
urse
Pra
ctiti
oner
Edu
catio
n in
the
Uni
ted
Sta
tes:
A S
ucce
ss S
tory
, by
Joyc
e Pu
lcin
i and
Mar
y W
agne
r (Cl
in E
xcel
l N
urse
Pra
ct. 2
002;6
[2]:51-5
6); a
nd N
urse
Pra
ctiti
oner
s: T
he E
arly
yea
rs (1
965-1
974),
by D
ebor
a W
ilson
(Nur
se P
ract
. 1994;1
9[1
2]:26-3
5).
TOM
WH
ALE
N
1965 Loretta C. Ford, RN, EdD, and Henry K. Silver, MD, begin the first pediatric NP program at the University of Colorado.
1958 Thelma M. Ingles, RN, and Eugene A. Stead Jr., MD, establish a short-lived MSN program at Duke, laying the groundwork for the PA profession and the NP role.
1973 The National Association of Pediatric NPs is established.
2008
Susan G. Stearly, MS, is the first to receive an NP certificate from the Colorado program. Each year thereafter, graduating classes grew, with 3 in the second, 5 in the third and 7 in the fourth.
The first issue of ADVANCE for Nurse Practitioners is published.
The National NP Coalition is born at the first NP Leadership Summit.
1980 The National Organization of NP Faculties, the National Association of NPs in Reproductive Health, and NP Associates for Continuing Education are founded.
1985 The American Academy of NPs and the National Alliance of NPs are founded.
1991 The first NPs enter practice in the United Kingdom. Today, NPs practice internationally in Australia, Bahrain, Canada, England, Ireland, Scotland, South Africa and beyond.
1976 250 NPs attend the first National NP Symposium in Denver.
1979 The first professional clinical doctorate in nursing (ND) program is begun at Case Western Reserve University.
The first national meeting of NP educators is held.
The first AANP national conference is held in Philadelphia with 158 attendees.
1994 The NNPC is renamed the American College of NPs.
1994 NPs are granted Medicare provider status.
1994 A New England Journal of Medicine article concludes that the primary care provided by NPs “is equivalent or superior to that provided by physicians.”
1996 In Louisiana, an amended Nurse Practice Act explicitly including the NP role goes into effect on Jan. 1. NPs now can practice everywhere in the United States.
1999 ACNP hosts its first national clinical conference in Nashville.
2001 The National Organization of NP Faculties establishes a task force to examine NP educational issues, including the DNP.
2004 The American Association of Colleges of Nursing calls for the DNP to become the terminal degree by 2015.
2004 National NP Week, held annually in November, is recognized by Congress.
2006 Georgia’s governor signs a law allowing NPs to sign prescriptions. NPs now prescribe in every state.
2010 ADVANCE for Nurse Practitioners and ADVANCE for Physician Assistants unite to form ADVANCE for NPs & PAs.
A work group of major nursing and APRN organizations issues the Consensus Model for APRN Regulation: Licensure, Accreditation, Certification & Education.
2011 As many as 150,000 U.S. NPs are in practice.
2011 About 9,500 new NPs graduate from nearly 350 programs.
November 2011 • ADVANCE for NPs & PAs

Deliver a double dose of good wishes and brand exposure with
“No one has made ordering promo items as fun as you!”Cathy KiserAsheville Radiology Associates
“Great quality and best of all, unsurpassed customer service and attention to detail.” Susan SmithSales & Marketing ManagerHQ, Inc.
“ADVANCE took care of everything for me, from the design of the product to shipping the fi nished item to my destination – and with excellent customer service!”Lydia OstermeierMSN, RN, CHCR PresidentNational Association for Health Care Recruitment
Executive GiftsRecognize your most loyal clients with a high-end custom gift. Order as few as 12 pieces for many of these custom luxury items. • Desktop accessories • Premium gift sets • Padfolios &
briefcases
Staff RecognitionReward top employees with economical gifts. Add your corporate brand or custom message for that personal touch.• Bags & Totes• Drinkware• Frames & keepsakes
AwardsCelebrate your corporate accomplishments in style. Laser engrave employee names & their achievements.• Crystal awards• Wooden plaques• Custom
engraving
Corporate Gifts & Promotions
“I fi nd their selection of items to be humongous. It’s bigger than even what you see online. Their prices are great, too.” Lisa Ambrose Montclair State University
Save $50on your
holiday order!*Call 1-877-776-6680 for
more details.
cessoriesft sets
1- 877-776-6680advancecustompromotions.com
*Applies to orders of $500 or more. Offer is limited to one per order. Offer cannot be applied to previous or pending orders and cannot be combined with any other offer. Discounts not valid on taxes, shipping or set-up fees. Use code CPHOL50 when ordering. Offer ends 12/15/2011.
154716_holiday-ad.indd 1 9/15/11 2:45:15 PM
67ADVANCE for NPs & PAs • November 2011

68 November 2011 • ADVANCE for NPs & PAs
Related Documents











![Window Sox Cataloguetcag.com.au/documents/Window Sox Catalogue[2].pdf · 2015. 3. 13. · SHEVRON WINDOW SOX - Complete Catalogue Make and Model Date of Manufacture Custom Fit Part](https://static.cupdf.com/doc/110x72/6123fcf7ead757623703a91a/window-sox-sox-catalogue2pdf-2015-3-13-shevron-window-sox-complete-catalogue.jpg)