1 ปปปปปป ปปปปปปปปปปปป ปปปป ปปปป-ปปป 3207-755 Syllabus and teaching plan ปปปปปปปปปปปปป ปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปป ปปป ปปปปป 2 ปป. 2552, 13:00-16:00 Topic: Long-term clinical evaluation of oral rehabilitation instructors: ปปปปปปปป ปปปปปปป, ปปปปปปป ปปปปปปปปป a class of 12 students Objectives and sub-topics : The oral rehabilitation represents the integrative concept which re-establishes every segment of the dental-jaw system that is affected by edentation in different clinical forms, without eluding the induced complications and the influence of general status within the chosen therapy algorithm. ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ฟฟฟ - ฟฟฟฟฟฟฟฟ ปปปปปป ปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปป ป ป ปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป Despite the significant development of knowledge and techniques, it is still controversial to which degree the therapy solutions of oral rehabilitation approach the therapy's ideal ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปป Choosing the therapeutically solution can be made only under the impulse of external factors ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป Whether restorations are crowns, overlays, inlays, veneers or posts etc., they require good material and correct manipulating technique to the selected case. ปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปป ปปปป ปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปปป ปปปปปปปปปป Vichet Chindavanig ปปปปปปป ปปปปปปปปป 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
3207-755 Syllabus and teaching plan
ประมวลเนอหา และแผนการสอน
สมมนาทนตกรรมประดษฐชนสง เพอการฟ นฟสภาพฟนทงปาก
ศกร 2 ตค. 2552, 13:00-16:00 Topic: Long-term clinical evaluation of oral rehabilitation
instructors: ศภบรณ บรณเวช, วเชฏฐ จนดาวณค
a class of 12 students
Objectives and sub-topics:
The oral rehabilitation represents the integrative concept which re-establishes every segment of the dental-jaw system that is affected by edentation in different clinical forms, without eluding the induced complications and the influence of general status within the chosen therapy algorithm.
การบรณะระบบบดเคยวเปนการประมวลแนวคดทไดมการสรางระบบ ฟน - ขากรรไกร ขนมาใหมทงหมด ซงมนมผลมาจากการมมรปลกษณะฟนทางคลนกทแตกตางไปจากเดม ทง ๆ ทไมไดเขาใจอยางถองแทถงความซบซอนทถกกระตนขน และอทธพลของสภาวะทวไปทรวมอยกบขนตอนเชงระบบทางทฤษฎทไดคดสรรไว
Despite the significant development of knowledge and techniques, it is still controversial to which degree the therapy solutions of oral rehabilitation approach the therapy's ideal
แมวาไดมเทคนคและองคความรทมผลอยางมนยยะกตาม ระดบการแกปญหาทางคลนกยงคงเปนเรองทถกเถยงและขดแยงวา ระดบการแกปญหาใดไดเขาถงระดบเชงอดมคต
Choosing the therapeutically solution can be made only under the impulse of external factors
การเลอกรปแบบการรกษาสามารถทำาไดจากปจจยภายใตสงเราภายนอกหลายประการ
Whether restorations are crowns, overlays, inlays, veneers or posts etc., they require good material and correct manipulating technique to the selected case.
ไมวาจะเปนครอบฟน บรณะวางทบดานบนฟน หรอภายในซฟน ชนเคลอบฉาบหนา หนอเดอยฟน งานเหลานตองใชวสดคณภาพด และขนตอนการทำางานทถกตองตองานผปวยทคดสรรนน
Long-term success and failure may be divided into two categories, namely biological and physical factors.
ความสำาเรจในระยะยาว และความลมเหลว อาจจำาแนกออกเปนสองชนดทมชอเรยกวา ปจจยทางชวภาพ และปจจยทางฟสกซ
Physical factors are marginal integrity, bond strength, microleakage, retentive form, resistance form, fracture resistance etc.
ปจจยทางฟสกซประกอบดวย ความแนบสนททขอบ แรงยด การซมรวระดบจลภาค รปทรงยด รปทรงตาน แรงตานการหก เปนตน
Vichet Chindavanig วเชฏฐ จนดาวณค
1
2
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Biological factors are underlying systemic diseases and oral diseases, home-care, patient’s attitude, psychology etc.
ปจจยทางชวภาพ ไดแกโรคทางระบบทซอนอย และโรคตาง ๆ ของชองปาก การดแลทบาน ทศนคตของผปวย จตวทยา เปนตน
Full mouth rehabilitation with artificial materials, however, one important above all factors is that the occlusion must meet the physiological requirement of each specific case.
การบรณะทงปากดวยวสดสงเคราะทงหลาย ปจจยสำาคญเหนอสงอนใดคอการสบฟนนนตองเขาถงขอกำาหนดทางสรระของแตละราย
These following articles may partly answer what, how, why, where and when your intended restoration will serve patients within satisfactory time period.
บทความวชาการทงหลายเหลาน อาจใหคำาตอบไดบางสวนวา อะไร อยางไร ทไหน และเมอไร ทงานทตงใจบรณะตาง ๆ นนจะรองรบการใชงานของผปวยในหวงเวลาทเปนทพอใจ
Vichet Chindavanig
Introduction: Time 13:00-13:15 Hr Instructors
Group 1. Terminology; “attrition, erosion, abrasion, long-term”, Results of prepared tooth surface characteristic (from different dental burs) and marginal adaptation (must know), product (burs) development, selection
Time 13:15-13:40 Hr. 20 min.
Group 2. Theories and concepts of cementing; Bond strength, fracture resistance and microleakage terminology relates to dental adhesive systems (must know) up-to-date concept, present innovations (nice to know)
Time 13:40-14:00 Hr. 20 min.
Group 3. Interim restorations, long-term interim, varieties of the modification technique, material selection (must know), post length and fracture resistance, clinical techniques (must know),
Time 14:00-14:20 Hr. 20 min.
Answering questions, making conclusion and coffee break
Time 14:20 14:40 20 min.
Group 4. Luting materials (zinc phosphate, zinc polycarbocylate, glassinomer and resin cements) product development (must know), history and present innovations (nice to know)
Time 14:40-15:00 Hr. 20 min.
Group 5. Specific brand name materials; their differences (luting materials, crown structure materials, post materials), (nice to know)
Vichet Chindavanig วเชฏฐ จนดาวณค
2

3
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Time 15:00-15:20 Hr. 20 min.
Group 6. Laboratory accuracy regarding the technique, common errors, Review Critical review of some dogmas in prosthodontics Gunnar E. Carlsson (nice to know)Time 15:20-15:40 min.
Answering questions, making conclusion
Time 15:40-16:00 Hr. 15 min.
Presentation and discussion technique:
Instructor will supply number of manuscripts relating to the topic, and a CD-ROM. After the instructor introduced objectives and their importance, thereby, 6 groups of students, 2 persons of each group will precede the assigned topic to the content 15 min., following with discussion and answering to the questions among students for 3 min. (suggestion; students should form their own group and should pick a topic by chance). Students will, therefore, plan and present well-prepared PowerPoint within time limit on the date and time stated above.
Guidelines to the seminar and discussion: the whole session must answer these questions
1. Define the term “attrition, erosion, abrasion, long-term”. What can be called successful treatment?
2. What are methods and materials of choice for full mouth rehabilitation case?
3. What are accepted theories and concepts of occlusion apply to the case?
4. How could dentist improve marginal fit or adaptation of crown margin?
5. What is the nature of physics at tooth-restorative material interface?
6. Role of provisional restorations to the success.
7. Nature of failures
8. Preventive measures
9. Communicating with the dental laboratory, Laboratory techniques
10. Dogmas in prosthodontics (discussion)
Text book: Contemporary Fixed Prosthodontics. Rosential SF, land MF, Fujimoto J. The CV Mosby company
Time table
Aug 15, 09 Instructor set-up, hand-in manuscripts, CD-ROM etc., classroom activity plan
Vichet Chindavanig วเชฏฐ จนดาวณค
3

4
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Sept 25, 09 Students Hand-in PowerPoint to instructor (CD-ROM) at department office
Oct 2, 09 Class actives
File name: ประมวล แผนการสอน FMR seminar long-term oral rehab, created on Tue.12th Aug,
2009
Example topics to the conclusion
Geometry of the preparation, surface roughness and wettability, different rotary instruments had no significant influence on the wettability
Roughness of axial walls could contribute to precision of a cast restoration, tungsten carbide finishing burs
The lowest discrepancy value (19 ± 17 μm) was for tooth preparations refined with finishing burs.
Marginal fit of complete cast crowns is influenced by tooth preparation surface characteristics
Temperature rise in pulp chamber, the critical level is 5.5 degrees C
Type of bonding agent or luting cement,
To evaluate hybrid layer formation and interfacial seal, surfaces prepared with carbide bur presented less residual smear plugs (P < 0.05) than surfaces prepared with diamond burs, carbide burs leave a surface that is more conducive to bonding than diamond burs
analysis revealed no statistically significant differences in microleakage across bur types, dentin margins leaked significantly more than enamel margins for all bur types
self-etching adhesives, one-step adhesives, bond strength of self-etching adhesives applied on superficial and deep dentin
Ultrastructural characterization of tooth-biomaterial interfaces
A 12-year clinical evaluation of a three-step dentin adhesive in noncarious cervical lesions
flowable composite and compomer provided stronger dentine bond strengths and better margin sealing than the conventional glass ionomer cement
adhesives chemically bonded to amalgam such as 10-methacryloyloxydecyl dihydrogen phosphate bis-GMA resins or 4-META, 4-methacryloxyethyl trimellitate anhydride (4-META; Atta et al., 1990 )
4-META is a coupling agent which increases adhesion to enamel, composite resins (Atsuta et al., 1982 ), and dental alloys by chemically bonding to the oxidized surface of non-precious metals (Tanaka et al., 1981 ).
chemical bonding of the polycarboxylic acid in classical powder/liquid conventional glass ionomers (GI) and resin-modified glass-ionomers (RMGI) has been attributed to the excellent long-term bond strengths and clinical retention.
Self-etching adhesive systems are a new generation of materials that possess acidic methacrylates that can generate self-adhesion.
Vichet Chindavanig วเชฏฐ จนดาวณค
4
5
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
The degree of microleakage was higher on the dentin margins than on the enamel margins
Margin fit parameters and microleakage showed no strong correlations; cast crowns cemented with resin-modified glass-ionomer and resin-based luting agent had lower microleakage scores than zinc phosphate cement.
Fabrication of an interim prosthesis is an important procedure in oral rehabilitation because it aids in determining the esthetics, phonetics, and occlusal relationship of the definitive restoration. The maintenance of this prosthesis is important during treatment for protection of teeth and occlusal stability.
Considerations and steps: a series of considerations involved in managing and/or restoring the VDO and a reproducible clinical protocol aimed at improving the dentist's ability to increase the VDO while reconstructing severely worn dentition
Post length did not influence fracture resistance of crowned endodonticallly treated within a 2 mm. ferrule on healthy tooth structure.
Related Articles
Look in supplement CD-ROM
J Oral Rehabil. 2008 Jul;35(7):548-66. Links
Rehabilitation of the worn dentition.
Johansson A, Johansson AK, Omar R, Carlsson GE.
Department of Clinical Dentistry - Prosthodontics, Faculty of Medicine and Dentistry, University of Bergen, Bergen, Norway. [email protected]
The purpose of this review was to evaluate the literature on the rehabilitation of tooth wear, with some pertinent historical, epidemiological and aetiological aspects of tooth wear provided as background information. In historical skull material, extensive tooth wear, assumed to be the result of coarser diets, was found even in relatively young individuals. Such wear is seldom seen in current populations. Although many of the factors associated with extensive tooth wear in historical material are no longer present or prevalent, new risk factors have emerged. In the young individual, the literature points to a global rise in soft drink consumption as the most significant factor in the development of tooth wear through dental erosion. Among older individuals, lifestyle changes and chronic diseases that are controlled with medications that may, in turn, result in regurgitation and/or dry mouth, are possible reasons amongst others for the widespread clinical impression of an increasing prevalence of tooth wear. The aetiology of tooth wear is multifactorial and the role of bruxism is not known. Clinical controlled trials of restorative and prosthodontic approaches for the range of clinical conditions that wear can give rise to, are limited in number and quality. Equally, the striking lack of evidence regarding the long-term outcomes of treatment methods and materials calls for caution in clinical decision-making. Notwithstanding these observations, clinicians have provided and continue to provide
Vichet Chindavanig วเชฏฐ จนดาวณค
5
6
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
rehabilitative strategies for managing their patients' worn dentitions that range traditionally from extensive prosthodontics to an increasing reliance on adhesive techniques.
PMID: 18557919 [PubMed - indexed for MEDLINE]
Quintessence Int. 2003 Jun;34(6):435-46. Links
Tooth wear: attrition, erosion, and abrasion.
Litonjua LA, Andreana S, Bush PJ, Cohen RE.
Department of Periodontics and Endodontics, State University of New York at Buffalo, Buffalo, New York 14214-3008, USA. [email protected]
Attrition, erosion, and abrasion result in alterations to the tooth and manifest as tooth wear. Each classification acts through a distinct process that is associated with unique clinical characteristics. Accurate prevalence data for each classification are not available since indices do not necessarily measure one specific etiology, or the study populations may be too diverse in age and characteristics. The treatment of teeth in each classification will depend on identifying the factors associated with each etiology. Some cases may require specific restorative procedures, while others will not require treatment. A review of the literature points to the interaction of the three entities in the initiation and progression of lesions that may act synchronously or sequentially, synergistically or additively, or in conjunction with other entities to mask the true nature of tooth wear, which appears to be multifactorial.
PMID: 12859088 [PubMed - indexed for MEDLINE]
J Dent Res. 2006 Apr;85(4):306-12. Links
A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion, and abrasion.
Bartlett DW, Shah P.
Department of Prosthodontics, Guy's Tower, St. Thomas' Street, London Bridge, London SE1 9RT, UK. [email protected]
The terms 'abfraction' and 'abrasion' describe the cause of lesions found along the cervical margins of teeth. Erosion, abrasion, and attrition have all been associated with their formation. Early research suggested that the cause of the V-shaped lesion was excessive horizontal toothbrushing. Abfraction is another possible etiology and involves occlusal stress, producing cervical cracks that predispose the surface to erosion and abrasion. This article critically reviews the literature on abrasion, erosion, and abrasion, and abfraction.
Vichet Chindavanig วเชฏฐ จนดาวณค
6
7
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
The references were obtained by a MEDLINE search in March, 2005, and from this, hand searches were undertaken. From the literature, there is little evidence, apart from laboratory studies, to indicate that abfraction exists other than as a hypothetical component of cervical wear.
PMID: 16567549 [PubMed - indexed for MEDLINE]
Eur J Prosthodont Restor Dent. 2000 Dec;8(4):139-44. Links
A review of the biomechanics of abfraction.
Rees JS.
Division of Restorative Dentistry, University of Bristol Dental School, Lower Maudlin St., Bristol, BS1 2LY. [email protected]
Loss of tooth substance in the cervical region is usually attributed to abrasion or erosion. However, the role of occlusal loading is becoming increasingly prominent. It is suggested that high occlusal loads result in large stress concentrations in the cervical region of the teeth. These stresses may be high enough to cause disruption of the bonds between the hydroxyapatite crystals, eventually resulting in the loss of cervical enamel. This article reviews the available evidence to support the thesis that occlusal loading can contribute to the process of non-carious cervical tooth loss or abfraction. It also reviews the potential interactions between occlusal loading and erosion that may contribute to non-carious cervical tooth loss.
PMID: 11692996 [PubMed - indexed for MEDLINE]
Monogr Oral Sci. 2006;20:17-31. Links
Interaction between attrition, abrasion and erosion in tooth wear.
Addy M, Shellis RP.
Applied Clinical Research Group, Bristol University Dental School, Bristol, UK.
Tooth wear is the result of three processes: abrasion (wear produced by interaction between teeth and other materials), attrition (wear through tooth-tooth contact) and erosion (dissolution of hard tissue by acidic substances). A further process (abfraction) might potentiate wear by abrasion and/or erosion. Both clinical and experimental observations show that individual wear mechanisms rarely act alone but interact with each other. The most important interaction is the potentiation of abrasion by erosive damage to the dental hard tissues. This interaction seems to be the major factor in occlusal and cervical wear. The available evidence seems insufficient to establish whether abfraction is an important
Vichet Chindavanig วเชฏฐ จนดาวณค
7
8
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
contributor to tooth wear in vivo. Saliva can modulate erosive/abrasive tooth wear through formation of pellicle and by remineralisation but cannot prevent it.
PMID: 16687882 [PubMed - indexed for MEDLINE]
J Oral Rehabil. 2001 Jul;28(7):645-50. Links
Surface roughness and wettability of enamel and dentine surfaces prepared with different dental burs.
Al-Omari WM, Mitchell CA, Cunningham JL.
Jordan University of Science and Technology, Department of Restorative Dentistry, Irbid, Jordan.
The aim of dental adhesive restorations is to produce a long lasting union between the restoration and the tooth structure. This bond depends on many variables including the geometry of the preparation and the type of bonding agent or luting cement. It is therefore suggested that the topography of the tooth surface may influence the wettability and the bonding quality of adhesive systems. This study measured the surface roughness and wettability of enamel and dentine after preparation with different dental burs. The mesial and distal surfaces of 15 extracted sound human premolar teeth were prepared with a tungsten carbide crown bur, a diamond bur and a tungsten carbide finishing bur and finished in enamel or dentin, respectively. The prepared surfaces were analysed with a surface profilometer and scanning electron microscopy (SEM). The contact angle of distilled water on each of the prepared surfaces was used as the measure of wettability. The differences in average surface roughness (Ra) were significant between the rotary instrument groups, as revealed by a two-way ANOVA test. No differences were detected between enamel and dentine surfaces prepared with the same type of dental bur. The smoothest surfaces were those completed with tungsten carbide finishing burs. The diamond bur preparations were intermediate in the roughness assessment and the tungsten carbide crown burs gave the roughest surfaces. There were no significant differences in the contact angle measurements for the various groups. It was concluded that the surface roughness of enamel and dentine prepared by different rotary instruments had no significant influence on the wettability of distilled water on these surfaces.
Am J Orthod Dentofacial Orthop. 1996 Jan;109(1):57-63. Links
A scanning electron microscopy comparison of enamel polishing methods after air-rotor stripping.
Piacentini C, Sfondrini G.
Oral and Dental Research Institute, Pavia, Italy.
Vichet Chindavanig วเชฏฐ จนดาวณค
8

9
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
In the last few years, orthodontic literature has shown particular interest in the interproximal enamel reduction technique described as stripping or slenderizing. Most researchers have shown, by scanning electron microscopy (SEM) studies, the difficulties encountered while attempting to remove coarse abrasions left after stripping with the first instrument. The objective of this SEM study was to compare the different polishing methods proposed in the literature and to assess the efficiency of our own procedure. For this purpose, 48 healthy human teeth (premolars and molars) were used after removal for orthodontic or periodontal reasons. The teeth were divided into eight groups of six teeth each (two molars and four premolars), and mounted on a typodont to simulate a clinical situation. Each group underwent stripping according to one of the following techniques: 16-blade tungsten carbide bur and fine and ultrafine diamond burs; coarse diamond bur and fine and ultrafine diamond burs; coarse diamond disk and Sof-Lex disks (Dental products/3M, St. Paul, Minn.); 16-blade tungsten carbide bur and phosphoric acid on finishing strip; and 8-straight blade tungsten carbide diamond bur and Sof-Lex disks. The SEM investigations demonstrated that it is not possible to eliminate, with normal polishing and cleaning methods, the furrows left on the enamel both by the diamond burs and the diamond disks and the 16-blade tungsten carbide burs. Mechanical and chemical stripping as well did not prove to be effective. By contrast, with the use of a 8-straight blade tungsten carbide bur followed by Sof-Lex disks for polishing the enamel, it is possible to obtain well-polished surfaces that many times appear smoother than the intact or untreated enamel.
PMID: 8540483 [PubMed – indexed for MEDLINE]
J Prosthodont. 2009 Feb;18(2):145-51. Epub 2008 Nov 18. Links
Effects of tooth preparation burs and luting cement types on the marginal fit of extracoronal restorations.
Ayad MF.
Section of Restorative Dentistry, Prosthodontics, and Endodontics, College of Dentistry, University of Tanta, Egypt. [email protected]
PURPOSE: Although surface roughness of axial walls could contribute to precision of a cast restoration, it is unclear how the roughness of tooth preparation affects marginal fit of the restoration in clinical practice. The purpose of this study was to describe the morphologic features of dentin surfaces prepared by common rotary instruments of similar shapes and to determine their effects on the marginal fit for complete cast crowns. MATERIALS AND METHODS: Ninety crowns were cast for standardized complete crown tooth preparations. Diamond, tungsten carbide finishing, and crosscut carbide burs of similar shape were used (N = 30). The crowns in each group were subdivided into three groups (n = 10) for use with different luting cements: zinc phosphate cement (Fleck’s), glass ionomer cement (Ketac-Cem), and adhesive resin cement (Panavia 21). Marginal fit was measured with a light microscope in a plane parallel to the tooth surface before and after cementation between four pairs of index indentations placed at equal distances around the circumference of each
Vichet Chindavanig วเชฏฐ จนดาวณค
9

10
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
specimen. Difference among groups was tested for statistical significance with analysis of variance (ANOVA) followed by Ryan-Einot-Gabriel-Welsch Multiple Range Test (alpha= 0.05). RESULTS: Analysis of measurements disclosed a statistically significant difference for burs used to finish tooth preparations (p < 0.001); however, luting cement measurements were not significantly different (p= 0.152). Also, the interaction effect was not significantly different (p= 0.685). For zinc phosphate cement, the highest marginal discrepancy value (100 +/- 106 micron) was for tooth preparations refined with carbide burs, and the lowest discrepancy value (36 +/- 30 micron) was for tooth preparations refined with finishing burs. For glass ionomer cement, the highest marginal discrepancy value (61 +/- 47 micron) was for tooth preparations refined with carbide burs, and the lowest discrepancy value (33 +/- 40 micron) was for tooth preparations refined with finishing burs. For adhesive resin cement, the highest marginal discrepancy value (88 +/- 81 micron) was for tooth preparations refined with carbide burs, and the lowest discrepancy value (19 +/- 17 micron) was for tooth preparations refined with finishing burs. CONCLUSIONS: Marginal fit of complete cast crowns is influenced by tooth preparation surface characteristics, regardless of the type of luting agent used for cementation. Tooth preparations refined with finishing burs may favor the placement of restorations with the smallest marginal discrepancies, regardless of the type of cement used.
PMID: 19054303 [PubMed – indexed for MEDLINE]
Effects of Tooth Preparation Burs and Luting Cement Types on the Marginal Fit of Extracoronal Restorations
Mohamed F. Ayad, BDS, MScD, PhD 1
1 Assistant Professor, Section of Restorative Dentistry, Prosthodontics, and Endodontics, College of Dentistry, University of Tanta, Egypt
Correspondence Dr. Mohamed F. Ayad, PO Box 443, Tanta 31111, Egypt. E-mail: [email protected]
Presented at the 83rd annual meeting of the International Association for Dental Research, Baltimore, MD, March 9-12, 2005.
KEYWORDS
Tooth • full coverage • marginal fit • luting agent • restoration
ABSTRACTPurpose: Although surface roughness of axial walls could contribute to precision of a cast restoration, it is unclear how the roughness of tooth preparation affects marginal fit of the restoration in clinical practice. The purpose of this study was to describe the morphologic features of dentin surfaces prepared by common rotary instruments of similar shapes and to determine their effects on the marginal fit for complete cast crowns.
Materials and Methods: Ninety crowns were cast for standardized complete crown tooth preparations. Diamond, tungsten carbide finishing, and crosscut carbide burs of similar shape were used (N = 30). The crowns in each group
Vichet Chindavanig วเชฏฐ จนดาวณค
10
11
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
were subdivided into three groups (n = 10) for use with different luting cements: zinc phosphate cement (Fleck’s), glass ionomer cement (Ketac-Cem), and adhesive resin cement (Panavia 21). Marginal fit was measured with a light microscope in a plane parallel to the tooth surface before and after cementation between four pairs of index indentations placed at equal distances around the circumference of each specimen. Difference among groups was tested for statistical significance with analysis of variance (ANOVA) followed by Ryan-Einot-Gabriel-Welsch Multiple Range Test (α= 0.05).
Results: Analysis of measurements disclosed a statistically significant difference for burs used to finish tooth preparations (p < 0.001); however, luting cement measurements were not significantly different (p= 0.152). Also, the interaction effect was not significantly different (p= 0.685). For zinc phosphate cement, the highest marginal discrepancy value (100 ± 106 μm) was for tooth preparations refined with carbide burs, and the lowest discrepancy value (36 ± 30 μm) was for tooth preparations refined with finishing burs. For glass ionomer cement, the highest marginal discrepancy value (61 ± 47 μm) was for tooth preparations refined with carbide burs, and the lowest discrepancy value (33 ± 40 μm) was for tooth preparations refined with finishing burs. For adhesive resin cement, the highest marginal discrepancy value (88 ± 81 μm) was for tooth preparations refined with carbide burs, and the lowest discrepancy value (19 ± 17 μm) was for tooth preparations refined with finishing burs.
Conclusions: Marginal fit of complete cast crowns is influenced by tooth preparation surface characteristics, regardless of the type of luting agent used for cementation. Tooth preparations refined with finishing burs may favor the placement of restorations with the smallest marginal discrepancies, regardless of the type of cement used.
Accepted January 18, 2008
DIGITAL OBJECT IDENTIFIER (DOI)
J Prosthet Dent. 1997 Feb;77(2):116-21. Links
Influence of tooth surface roughness and type of cement on retention of complete cast crowns.
Ayad MF, Rosenstiel SF, Salama M.
Section of Restorative and Prosthetic Dentistry, School of Dentistry, College of Dentistry, Ohio State University, Columbus, USA.
STATEMENT OF PROBLEM: Bond strength of luting cements to dentin is a critical consideration for success of cast restorations. PURPOSE OF STUDY: This study determined the relationship between surface characteristics of teeth prepared for complete cast crowns and retention of respective cemented restorations. MATERIAL AND METHODS: Ninety artificial crowns were cast for standardized complete crown tooth preparations accomplished with the use of a milling machine on extracted human teeth. Diamond, tungsten carbide finishing, and cross-cut carbide burs of similar shape were used. The crowns in each group were randomly subdivided into three subgroups of 10 for the three luting cements selected for this study: zinc phosphate cement (Fleck’s), glass ionomer cement (Ketac-Cem), and adhesive resin cement (Panavia-EX). Retention was evaluated by measuring the tensile load required to dislodge the artificial crowns from tooth preparations with an Instron testing machine. RESULTS: Analysis of forces with parametric analysis of
Vichet Chindavanig วเชฏฐ จนดาวณค
11
12
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
variance and Tukey’s Studentized Range (HSD) disclosed a statistically significant difference for both luting cement and finishing burs (p < 0.001). A statistically significant interaction effect (p < 0.001) was also found. The greatest retention value (372.9 N) was for tooth preparations refined with carbide burs and cemented with Panavia-EX cement. However, the least retention value (201.6 N) was for tooth preparations completed with finishing burs and luted with zinc phosphate cement. CONCLUSIONS: Significant differences were found among all three cements for finishing burs. However, there was a difference only between Panavia-EX cement and the other two cements for tungsten carbide burs. For diamond rotary instruments, zinc phosphate cement was significantly different from glass ionomer and Panavia-EX cements.
PMID: 9051596 [PubMed – indexed for MEDLINE]
Angle Orthod. 2007 May;77(3):478-82. Links
Temperature rise in the pulp chamber during different stripping procedures.
Baysal A, Uysal T, Usumez S.
Department of Orthodontics, Faculty of Dentistry, Erciyes University, Kayseri, Turkey.
OBJECTIVE: To measure the temperature changes in the pulp chamber when different stripping procedures were used without any type of coolant. MATERIALS AND METHODS: Ninety intact, freshly extracted human teeth were used in this study. The teeth were separated into nine groups of 10 teeth each. Mesial and distal sides of the teeth were used separately. The stripping procedures were performed on three different tooth groups (incisor, canine, premolar) with a metal handheld stripper, perforated stripping disk, or tungsten carbide bur. A J-type thermocouple wire was positioned in the center of the pulp chamber and was connected to a data logger during application of stripping procedures. The results were analyzed by analysis of variance (ANOVA) and the Duncan test. RESULTS: Two-factor ANOVA revealed significant interaction between the stripping procedure and the tooth type (P = .000). The results of this study demonstrate that tungsten carbide burs used on mandibular incisors had the highest temperature variation (DeltaT) values, which exceeded the critical level (5.5 degrees C), and this was significantly higher than those of the other stripping procedures (DeltaT: 5.63 +/- 1.73 degrees C). On the other hand, six of the nine groups also produced temperature increases above the critical level (5.5 degrees C) for some of the specimens. CONCLUSIONS: Frictional heat is a common side effect of stripping procedures, and appropriate measures (ie, cooling application) should be taken particularly for high-speed hand-piece stripping of mandibular incisors.
PMID: 17465656 [PubMed – indexed for MEDLINE]
Dent Today. 2005 Oct;24(10):162-4, 166, 168-75. Links
Buyers’ guide to diamonds and burs. So, what’s new in burs?
Vichet Chindavanig วเชฏฐ จนดาวณค
12
13
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Freedman G.
PMID: 16277081 [PubMed – indexed for MEDLINE]
J Oral Rehabil. 2005 Nov;32(11):849-56. Links
Effect of bur type and conditioning on the surface and interface of dentine.
Barros JA, Myaki SI, Nör JE, Peters MC.
Department of Cariology, Restorative Sciences and Endodontics, University of Michigan, 1011 N. University D2361, Ann Arbor, MI 48109-1078, USA.
The purpose of this in vitro study was to evaluate the surface and resin-dentine interface characteristics of permanent tooth dentine cut with diamond or carbide burs and treated with phosphoric acid (PA) or an acidic conditioner. Labial surfaces of permanent incisors were prepared into dentine with high-speed carbide or diamond burs and divided into two halves. Phosphoric acid 36% was applied on one half and non-rinse conditioner (NRC) was applied on the other half. Ten randomly selected scanning electron microscopy (SEM) fields from each specimen (n = 15) were evaluated. Occlusal surfaces of third molars were divided in two halves for evaluation of the resin-dentine interface. The halves were randomly assigned to one of each conditioner and restored with Prime & Bond NT/Spectrum. Ten specimens were analysed by SEM to evaluate hybrid layer formation and interfacial seal. We observed that surfaces prepared with carbide bur presented less residual smear plugs (P < 0.05) than surfaces prepared with diamond burs. Surfaces conditioned with NRC, which is a smear layer modifier, presented more residual smear plugs than surfaces conditioned with PA (P < 0.05). Treatment with PA resulted in more sealed interfaces than specimens treated with NRC. Within the limitations of this study the results showed that carbide burs leave a surface that is more conducive to bonding than diamond burs.
PMID: 16202050 [PubMed – indexed for MEDLINE]
J Adhes Dent. 2004 Winter;6(4):287-91. Links
The role of cavity preparation and conditioning in the leakage of restorations.
Kihn PW, Spanganberg PA, von Fraunhofer JA.
Dental School, University of Maryland, Baltimore, MD 21201, USA.
PURPOSE: Restoration microleakage is thought to be determined by the method and location of cavity preparation, enamel etching, and dentin conditioning, as well as the restorative material. This study compared the microleakage of composite restorations placed in preparations cut with carbide and diamond burs and those treated with different bonding/conditioning agents. MATERIALS AND METHODS: Class V preparations (3 x 2 x 2
Vichet Chindavanig วเชฏฐ จนดาวณค
13

14
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
mm) were cut wholly in enamel or in enamel and cementum in 100 human premolars. Twenty teeth were prepared with carbide burs and the preparations etched and conditioned with Prime&Bond NT but not restored. A second set of 20 teeth had enamel-only preparations cut with carbides (n = 10) or diamonds (n = 10), and the preparations etched, conditioned (Prime&Bond NT) and restored with Prisma TPH. The other 60 teeth were divided into 3 groups of 20 teeth each with enamel-only (n = 10) or enamel/cementum preparations (n = 10). The 3 groups of teeth were conditioned with Optibond Solo, Clearfil SE Bond or Prompt-L-Pop prior to restoration with Prisma TPH. Two mm of root was resected from all teeth, pulpal tissue removed, and insulated copper wires inserted via the root canals to contact with the pulp chamber roof before the tooth-wire interfaces and root surfaces were sealed. The teeth were immersed in 0.9% NaCl and leakage assessed over 30 d by iR drop across a resistor in series with a DC source and stainless-steel counter electrode. RESULTS: Differences (p < 0.05) in leakage were found for enamel preparations cut with carbides and diamonds, and the relationship of leakage vs time was linear. Enamel/cementum preparations showed greater leakage, and the relationship of leakage vs time was sigmoidal. Conditioned-only preparations showed the same leakage as those conditioned and restored, while preparation leakage varied with the conditioning agent. CONCLUSION: Cavity preparation location, method of cutting, and the conditioning agent markedly affect leakage behavior.
PMID: 15779313 [PubMed – indexed for MEDLINE]
Oper Dent. 2003 Nov-Dec;28(6):779-85. Links
Effect of surface roughness of cavity preparations on the microleakage of Class V resin composite restorations.
Shook LW, Turner EW, Ross J, Scarbecz M.
Department of Restorative Dentistry, University of Tennessee Health Science Center, College of Dentistry, Memphis, TN, USA. [email protected]
This study determined whether surface roughness of the internal walls of a Class V resin composite preparation, using a carbide bur, a medium-grit diamond bur and a fine-grit diamond bur, affected the degree of microleakage of the restoration. The facial and lingual surfaces of 45 non-carious extracted human molars provided 90 samples for evaluation. The specimen surfaces were assigned randomly in equal numbers to one of three groups (n = 30). Conservative Class V composite preparations were made using one of three different burs: a 330-carbide bur, a 330 fine-grit diamond bur or a 330 medium-grit diamond bur (Brasseler USA). After acid etching, PQ1 (Ultradent Products Inc) primer/bonding resin and Vitalescence (Ultradent Products Inc) were applied and cured following the manufacturers’ instructions. After minor finishing, the apices of all root surfaces were sealed with Vitrebond (3M), and the unprepared external surfaces were sealed with nail polish to within 1 mm of the restoration margins. The specimens were stored in distilled water at room temperature for 24 hours, then subjected to 1,200 thermocycles at 5 degrees C and 55 degrees C with a
Vichet Chindavanig วเชฏฐ จนดาวณค
14
15
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
30-second dwell time. After cycling, the teeth were immersed in a 5% solution of methylene blue dye for 12 hours. The molars were invested in clear acrylic casting resin, labeled, then sectioned once vertically approximately midway through the facial and lingual surfaces using a diamond coated saw blade. Microleakage was evaluated using a 10x microscope for the enamel and cementum surfaces and blindly scored by two independent examiners. In all cases, regardless of the examiner, at both the enamel and the dentin margins, the analysis revealed no statistically significant differences in microleakage across bur types. Further results show that dentin margins leaked significantly more than enamel margins for all bur types.
PMID: 14653294 [PubMed – indexed for MEDLINE]
WHY FINISH WITH DIAMOND INSTRUMENTS?
Since mounted stones are rarely perfectly round and concentric, they have a tendency to hammer the restoration, as do carbide finishing burs. This excessive vibration can dislodge the fillers from a restorative’s matrix, leaving irregularities on the surface of the restoration.
Our micron diamonds are manufactured with an extremely uniform coating of 50 Micron and 25 Micron diamond grits. This allows the instrument to cut smoothly, without causing vibration or damage to the composite or glass ionomer materials. These rotary diamond instruments should be used with minimal pressure, in a constant wiping motion, using a generous amount of water.
50 MICRON – EXTRA FINE FOR CONTOURING
Use the 50 Micron diamonds to shape and contour the final structure of your composite or glass ionomer restorations. The extra fine rotary abrasion of the 50 Micron diamond quickly cuts the restorative with minimal damage to the matrix material. Maximum Recommended Speed 50,000 RPM.
25 MICRON – ULTRA FINE FOR FINE FINISHING
Use the 25 Micron diamonds to make your final adjustments to your restoration and to smooth the surface of your composite or glass ionomer restorations. The ultra fine rotary abrasion of the 25 Micron diamond leaves the surface of your restoration very smooth, often eliminating the need for any further finishing. Maximum Recommended Speed 15,000 RPM
SS White is a recognized industry leader in the manufacture of dental burs, both carbide burs and diamond burs. Using research and advanced materials science, SS White is an innovator in new dental products, dental procedures and dental lab products.
Carbide Burs
High quality carbide burs for multiple dental procedures
SS White carbide burs are widely used for dental procedures such as dental restoration removal, pit and fissure exploration, caries removal and preparation, crown and bridge preparation, trimming and
Vichet Chindavanig วเชฏฐ จนดาวณค
15

16
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
finishing, endodontic access, bone contouring for oral surgery, and cement removal. Popular carbide bur brands include Great White, Fissurotomy and Safe End.
Carbide BursSearch by BrandEndoGroupExpress LineFissurotomyGreat White Gold SeriesGreat White UltraSS White Oral SurgerySS White Safe EndSS White Trimming & FinishingStandard Operatory Carbides
Search by Shape12 BLADE BULLET12 BLADE CONE12 BLADE EGG12 BLADE EXTRA LONG TAPER12 BLADE FLAME12 BLADE INVERTED TAPER12 BLADE NEEDLE12 BLADE ROUND12 BLADE STRAIGHT12 BLADE TAPER12 Blade Tapred Flat End30 BLADE BULLET30 BLADE EGG30 BLADE EXTRA LONG TAPER30 BLADE NEEDLE30 BLADE ROUND30 BLADE STRAIGHT30 BLADE TAPERAMALGAM PREPEggEND CUTFISSUROTOMY KITFISSUROTOMY NARROW TAPER FISSUREFISSUROTOMY NARROW TAPER FISSURE SHORT SHANKFISSUROTOMY SHALLOW TAPER FISSUREFISSUROTOMY SHALLOW TAPER FISSURE SHORT SHANKFISSUROTOMY TAPER FISSUREFISSUROTOMY TAPER FISSURE SHORT SHANKFLAT END TAPER CROSSCUT FISSURE for 44.5mm STRAIGHT HANDPIECEFLAT END TAPER CROSSCUT FISSURE for 51mm STRAIGHT HANDPIECEFLAT END TAPER CROSSCUT FISSURE for 59mm STRAIGHT HANDPIECEFLAT END TAPER CROSSCUT FISSURE for 65mm STRAIGHT HANDPIECEFLAT END TAPER CROSSCUT FISSURE STERILEGREAT WHITE ULTRA CROWN & BRIDGE PREP KITINVERTED CONELABORATORY METAL FINISHING BUR KITPEARROUNDRound End CylinderROUND END TAPER CROSSCUT FISSURE for 44.5mm STRAIGHT HANDPIECE
Vichet Chindavanig วเชฏฐ จนดาวณค
16
17
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
ROUND END TAPER CROSSCUT FISSURE for 51mm STRAIGHT HANDPIECEROUND END TAPER CROSSCUT FISSURE for 59mm STRAIGHT HANDPIECEROUND END TAPER CROSSCUT FISSURE for 65mm STRAIGHT HANDPIECEROUND END TAPER CROSSCUT FISSURE STERILEROUND for 44.5mm J-NOTCH DRILLROUND for 44.5mm STRAIGHT HANDPIECEROUND for 51mm STRAIGHT HANDPIECEROUND for 59mm STRAIGHT HANDPIECEROUND for 65mm STRAIGHT HANDPIECEROUND STERILEROUND SURGICAL LENGTHROUND SURGICAL LENGTH 2ROUND SURGICAL LENGTH 4SAFE END FINISHING BUR KITSAFE END TAPERED ROUNDSAFE SIDE CYLINDER END CUTSHORT SHANKSSTRAIGHT FISSURESTRAIGHT FISSURE ROUND ENDSTRAIGHT FISSURE SURGICAL LENGTHSTRAIGHT FLAT END CROSSCUT FISSURESTRAIGHT FLAT END CROSSCUT FISSURE for 44.5mm J-NOTCH DRILLSTRAIGHT FLAT END PLAIN FISSURESTRAIGHT ROUND END CROSSCUT FISSURESTRAIGHT ROUND END PLAIN FISSURETAPER FISSURETAPER FLAT END CROSSCUT FISSURETAPER FLAT END CROSSCUT FISSURE for 44.5mm J-NOTCH DRILLTAPER FLAT END PLAIN FISSURETAPER ROUND END CROSSCUT FISSURETAPER ROUND END CROSSCUT FISSURE for 44.5mm J-NOTCH DRILLTAPER ROUND END PLAIN FISSURETAPERED FLAT END MODIFIED EDGETapered Round ConeTAPERED ROUND ENDWHEEL
Search by ProcedureAmalgam PreparationBone Contouring and SmoothingBreaking Interproximal ContactsCaries RemovalChamfer MarginClass III Interproximal Cavity Prep on Anterior TeethComposite PreparationContouring and Finishing RestorationsCreate Retentive FormEndodontic AccessFinishing Subgingival RestorativesInitial AccessInlay/OnlayInlay/Onlay PreparationInterproximal & Subgingival FinishingInterproximal & Subgingival MarginsInterproximal AccessLab Metal FinishingLabial Surface FinishingOcclusal and Lingual Surface Finishing
Vichet Chindavanig วเชฏฐ จนดาวณค
17
18
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Occlusal MarginsPit and Fissure explorationRestoration RemovalRoot PlaningShoulder MarginThird Molar SurgeryVeneer Finishing
Composite Finishing and Trimming Burs
General Information
Vendor KOMET USA LLC
Item Composite Finishing and Trimming Burs
Other Features 5 per Pack
Shapes Available
RoundFlameFootballTaperedModified ShoulderChamfer
Shank Types Available Friction Grip
Material Indication Composite and Alloys
Trimming & Finishing Carbides
Vichet Chindavanig วเชฏฐ จนดาวณค
18
19
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
General Information
Vendor Axis Dental
Item NTI ฎ Trimming & Finishing Carbides
Other Features 5 per Pack
Shapes Available
BulletFlameBeveled CylinderParallel BevelModified Flat End CylinderFlat End TaperRoundLong FlameFlat End CylinderInterproximalCurretageFootballChristmas Tree
Shank Types Available Friction Grip
Material Indication Inquire
Product Description
NTI ฎ Trimming & Finishing Carbides feature German quality and technology, stainless steel shanks, and precision ground blades. The MW Series Trimming & Finishing Carbides are designed to provide a smooth finish on composite, amalgam, or crown & bridge restorations. The new egg and needle shapes are an ideal fit in all interproximal, buccal, lingual, and occlusal areas. Friction Grip only.
In vitro microleakage of composite restorations prepared by Er:YAG/Er,Cr:YSGG lasers and conventional drills associated with two adhesive systems.
Vichet Chindavanig วเชฏฐ จนดาวณค
19

20
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Moldes VL, Capp CI, Navarro RS, Matos AB, Youssef MN, Cassoni A.
J Adhes Dent. 2009 Jun;11(3):221-9.
PMID: 19603586 [PubMed - in process]
Related Articles
Are one-step adhesives easier to use and better performing? Multifactorial assessment of contemporary one-step self-etching adhesives.
Van Landuyt KL, Mine A, De Munck J, Jaecques S, Peumans M, Lambrechts P, Van Meerbeek B.
J Adhes Dent. 2009 Jun;11(3):175-90.
PMID: 19603581 [PubMed - in process]
Related Articles
In vitro analysis of bond strength of self-etching adhesives applied on superficial and deep dentin.
Garcia EJ, Gomes OM, Gomes JC.
Acta Odontol Latinoam. 2009;22(1):57-62.
PMID: 19601497 [PubMed - in process]
Related Articles
Ultrastructural characterization of tooth-biomaterial interfaces
prepared with broad and focused ion beams.
Coutinho E, Jarmar T, Svahn F, Neves AA, Verlinden B, Van Meerbeek B, Engqvist H.
Dent Mater. 2009 Jul 9. [Epub ahead of print]
PMID: 19596422 [PubMed - as supplied by publisher]
Related Articles
Enhancement of bonding to enamel and dentin prepared by Er,Cr:YSGG laser.
Obeidi A, McCracken MS, Liu PR, Litaker MS, Beck P, Rahemtulla F.
Lasers Surg Med. 2009 Aug;41(6):454-62.
PMID: 19588530 [PubMed - in process]
Related Articles
Fiber-reinforced onlay composite resin restoration: a case report.
Garoushi SK, Shinya A, Shinya A, Vallittu PK.
J Contemp Dent Pract. 2009 Jul 1;10(4):104-10.
Vichet Chindavanig วเชฏฐ จนดาวณค
20
21
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
PMID: 19575061 [PubMed - in process]
Related Articles Free article in PMC | at journal site
Influence of the internal conditioning of indirect restorations of resin composite in relation to microleakage using LEDs and QTH units.
Calabrez-Filho S, Calabrez VC, Reston EG, de Andrade MF, Borges LH.
Oper Dent. 2009 May-Jun;34(3):293-8.
PMID: 19544818 [PubMed - in process]
Related Articles
Shear bond strength of self-adhesive resins compared to resin cements with etch and rinse adhesives to enamel and dentin in vitro.
Lührs AK, Guhr S, Günay H, Geurtsen W.
Clin Oral Investig. 2009 May 9. [Epub ahead of print]
PMID: 19430821 [PubMed - as supplied by publisher]
Related Articles
The effect of different adhesive types and curing methods on microleakage and the marginal adaptation of composite veneers.
Maleknejad F, Moosavi H, Shahriari R, Sarabi N, Shayankhah T.
J Contemp Dent Pract. 2009 May 1;10(3):18-26.
PMID: 19430622 [PubMed - in process]
Related Articles Free article in PMC | at journal site
A 12-year clinical evaluation of a three-step dentin adhesive in noncarious cervical lesions.
Wilder AD Jr, Swift EJ Jr, Heymann HO, Ritter AV, Sturdevant JR, Bayne SC.
J Am Dent Assoc. 2009 May;140(5):526-35.
PMID: 19411519 [PubMed - in process]
Related Articles
Microleakage and scanning electron microscopy evaluation of all-in-one self-etch adhesives and their respective nanocomposites prepared by erbium:yttrium-aluminum-garnet laser and bur.
Korkmaz Y, Ozel E, Attar N, Bicer CO, Firatli E.
Lasers Med Sci. 2009 Apr 27. [Epub ahead of print]
PMID: 19396579 [PubMed - as supplied by publisher]
Related Articles
Vichet Chindavanig วเชฏฐ จนดาวณค
21

22
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Effect of operator-specific handling on tooth-composite interface and microleakage formation.
Schneider H, Busch I, Busch M, Jentsch H, Häfer M.
Oper Dent. 2009 Mar-Apr;34(2):200-10.
PMID: 19363976 [PubMed - in process]
Related Articles
Reconstruction of nonvital teeth using direct fiber-reinforced composite resin: a pilot clinical study.
Deliperi S, Bardwell DN.
J Adhes Dent. 2009 Feb;11(1):71-8.
PMID: 19343930 [PubMed - indexed for MEDLINE]
Related Articles
Fracture resistance of reattached incisor fragments with mini fibre-reinforced composite anchors.
Fennis WM, Kreulen CM, Wolke JG, Fokkinga WA, Machado C, Creugers NH.
J Dent. 2009 Jun;37(6):462-7. Epub 2009 Mar 31.
PMID: 19339099 [PubMed - in process]
Related Articles
Optimization of the concentration of photo-initiator in a one-step self-etch adhesive.
Van Landuyt KL, Cardoso MV, De Munck J, Peumans M, Mine A, Lambrechts P, Van Meerbeek B.
Dent Mater. 2009 Aug;25(8):982-8. Epub 2009 Mar 21.
PMID: 19304315 [PubMed - in process]
Related Articles
Rationale behind the design and comparative evaluation of an all-in-one self-etch model adhesive.
Kanehira M, Finger WJ, Ishihata H, Hoffmann M, Manabe A, Shimauchi H, Komatsu M.
J Dent. 2009 Jun;37(6):432-9. Epub 2009 Feb 27.
PMID: 19250732 [PubMed - in process]
Related Articles
Dent Mater. 2009 Jun;25(6):750-9. Epub 2009 Feb 23. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
22

23
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Nanohybrid vs. fine hybrid composite in Class II cavities: clinical results and margin analysis after four years.
Krämer N, Reinelt C, Richter G, Petschelt A, Frankenberger R.
Department of Pediatric Dentistry, University Medical Center Carl Gustav Carus, Technical University Dresden, Germany.
OBJECTIVES: This controlled prospective split-mouth study evaluated the clinical behavior of two different resin composites in extended Class II cavities over a period of four years. METHODS: Thirty patients received 68 direct resin composite restorations (Grandio bonded with Solobond M: n=36, Tetric Ceram bonded with Syntac: n=32) by one dentist in a private practice. All restorations were replacement fillings, 24 cavities (35%) revealed no enamel at the bottom of the proximal box, in 33 cavities (48%) the proximal enamel width was less than 0.5mm. The restorations were examined according to modified USPHS criteria at baseline, and after six months, one, two, and four years. At each recall, impressions were taken for replica preparation. Replicas of 44 select subjects were assessed for marginal quality under a stereo light microscope (SLM) at 130x and 22 replicas were assessed under a scanning electron microscope (SEM) at 200x. RESULTS: Both recall rate and survival rate were 100% after four years of clinical service. No significant difference was found between the restorative materials (p>0.05; Mann-Whitney U-test). Hypersensitivities were significantly reduced over time (p<0.05; Friedman test). A significant deterioration over time was found for the criteria marginal integrity (66% bravo after four years), tooth integrity (15% bravo), filling integrity (73% bravo) and proximal contact (p<0.05; Friedman test). SLM and SEM analysis of restoration margins revealed differences in the amount of perfect margins, in favor of Tetric Ceram (p<0.05). SIGNIFICANCES: Both materials performed satisfactorily over the four-year observation period. Due to the extension of the restorations, wear was clearly visible after four years of clinical service with 50% bravo ratings.
PMID: 19237189 [PubMed - indexed for MEDLINE]
Clin Oral Investig. 2009 Feb 19. [Epub ahead of print] Links
Marginal adaptation of three self-adhesive resin cements vs. a well-tried adhesive luting agent.
Behr M, Hansmann M, Rosentritt M, Handel G.
Department of Prosthetic Dentistry, University Hospital Regensburg, 93042, Regensburg, Germany, [email protected].
Vichet Chindavanig วเชฏฐ จนดาวณค
23
24
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
This in vitro study compared the marginal adaptation of three self-adhesive composite cements with the clinically well-tried dentin adhesive system Panavia F 2.0. A total of 32 Empress 2 all-ceramic MOD-inlays (eight in each group) were luted using the self-adhesive composite cements Maxcem, Multilink Sprint, and RelyX Unicem Clicker; Panavia F 2.0 served as a clinically well-tried control. Each luted inlay underwent long-term water storage of 90 days as well as additional mechanical and thermal loading to simulate oral service. Marginal integrity was evaluated in both dentin and enamel finishing lines using scanning electron microscopy (SEM) and dye penetration tests. Dye penetration was lowest for Panavia followed by RelyX Unicem. Maxcem and Multilink showed a considerable dye penetration of up to 60%. After aging, SEM analysis revealed a reduction of "perfect margin" areas for Multilink Sprint and RelyX Unicem in enamel and for Maxcem and Multilink in dentin. Compared with the well-tried system Panavia-which was assumed as the golden standard of adhesive luting systems-only the self-adhesive luting agent RelyX Unicem showed similar results of marginal adaptation after long-term water storage.
PMID: 19225814 [PubMed - as supplied by publisher]
Dent Mater. 2009 Jul;25(7):852-6. Epub 2009 Feb 8. Links
Polymerization contraction stress in resin-tooth bonds under hydrated and dehydrated conditions.
Hashimoto M, Nakamura K, Feilzer AJ.
Division of Biomaterials and Bioengineering, Health Sciences University of Hokkaido, School of Dentistry, 1757 Kanazawa, Ishikari-Tobetsu, Hokkaido 061-0293, Japan. [email protected]
OBJECTIVE: This study hypothesizes that, with enamel or dentin as a bonding substrate, intrinsic water affects the development of polymerization contraction stress in the bonds of self-etching adhesives during bonding. MATERIALS AND METHODS: The influence of the water content in dentin and enamel (wetness with water as control and acetone-dried specimens) on the stress development in self-etching adhesives was determined with a tensilometer. Thin layers of self-etching primer and/or adhesive resins were created between a glass plate and a flat enamel or dentin surface. RESULTS: After an initial maximum shortly after light curing for 30min, the contraction stress was decreased in the dentin (30-70%) and enamel (approximately 20%). In the acetone-dried specimens, the stress was continuously increased for 20-50%. SIGNIFICANCE: The intrinsic water content of tooth tissue influences the initial polymerization of polymers. This effect is favorable for stress relief in resin restoration but causes unwanted nanoleakage channel formation in resin-tooth bonds.
PMID: 19201458 [PubMed - in process
Vichet Chindavanig วเชฏฐ จนดาวณค
24

25
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Quintessence Int. 2009 Feb;40(2):125-33. Links
Simulated fatigue resistance of composite resin versus porcelain CAD/CAM overlay restorations on endodontically treated molars.
Magne P, Knezevic A.
School of Dentistry, University of Southern California, Los Angeles, CA 90089, USA. [email protected]
OBJECTIVE: To assess the influence of material selection (porcelain versus composite resin) for overlay-type restoration of endodontically treated molars and its effect on the in vitro fatigue resistance and failure mode. METHOD AND MATERIALS: A standardized tooth preparation was applied to 30 extracted molars, including root canal treatment, 3-mm coverage of all cusps, a mesial box 1.5 mm below the cementoenamel junction (CEJ), a distal box in enamel, a glass-ionomer base, and immediately sealed dentin. Using the Cerec machine (Sirona), all teeth were restored with an overlay of standardized thickness and occlusal anatomy. Fifteen restorations were milled in the ceramic Vita MKII block (Vident) and the other 15 using the composite resin Paradigm MZ100 block (3M ESPE). The intaglio surfaces of the ceramic restorations were etched and silanated. The intaglio surfaces of the composite resin overlays were airborne-particle abraded and silanated. Preparations were airborne-particle abraded and etched before restoration insertion. All restorations were adhesively luted with an adhesive resin (Optibond FL, Kerr) and a light-curing composite resin (Filtek Z100, 3M ESPE). Cyclic isometric chewing (5 Hz) was simulated, starting with a load of 200 N (5,000 cycles), followed by stages of 400, 600, 800, 1,000, 1,200, and 1,400 N at a maximum of 30,000 cycles each. Samples were loaded until fracture or to a maximum of 185,000 cycles. RESULTS: MKII overlays fractured at a mean load of 1,147 N, and none of them withstood all 185,000 loading cycles (survival = 0%); with MZ100, the survival rate was 73%. With MKII, 40% of the fractures ended below the CEJ; with MZ100, only 25% did. CONCLUSIONS: Composite resin MZ100 increased the fatigue resistance of overlay-type restorations in endodontically treated molars when compared to porcelain MKII. The efficiency of the bond strategy (immediate dentin sealing) was demonstrated by the absence of adhesive failures.
PMID: 19169444 [PubMed - indexed for MEDLINE]
Aust Dent J. 2008 Dec;53(4):325-31. Links
Dentine bond strength and microleakage of flowable composite, compomer and glass ionomer cement.
Vichet Chindavanig วเชฏฐ จนดาวณค
25
26
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Xie H, Zhang F, Wu Y, Chen C, Liu W.
Department of Prosthodontics, Stomatology Institute of Nanjing Medical University, Nanjing, China.
BACKGROUND: To assess in vitro the dentine bond strength and microleakage of three Class V restorations viz. flowable composite, compomer and glass ionomer cement. METHODS: Eighteen dentine specimens were prepared and randomly distributed among three groups. Three kinds of restoration materials were each bonded on prepared dentine surfaces in three groups as per the manufacturers' instructions. Group Aelite: Tyrian SPE (a no-rinse, self-priming etchant) + One Step Plus (an universal dental adhesive) + Aeliteflo (a flowable composite); Group Dyract: Prime & Bond NT (a no-rinse, self-priming dental adhesive) + Dyract AP (a compomer); Group GlasIonomer: GlasIonomer Type II (a self-cured restorative glass ionomer). Fifteen dentine/restoration microtensile bond test specimens were prepared from each group and were subjected to microtensile bond strength testing. The bond interfaces were observed morphologically using a scanning electron microscope (SEM). Twenty-four cervical cavities of 4.0 mm mesiodistal length, 2.0 mm occlusogingival height and 1.5 mm depth were prepared at the cemento-enamel junction (CEJ) on both buccal and lingual surfaces of each tooth. The cavities were each filled with flowable composite (Group Aelite), compomer (Group Dyract) and glass ionomer cement (Group GlasIonomer) using the same material and methods as for the microtensile bond tests. Microleakage of each restoration was evaluated by the ratio of the length of methylene blue penetration along the tooth-restoration interface and the total length of the dentine cavity wall on the cut surface. RESULTS: One-way ANOVA and least significant difference (LSD) tests revealed statistically significant differences among the dentine bond strength for Group Aelite (28.4 MPa), Group Dyract (15.1 MPa) and Group GlasIonomer (2.5 MPa). SEM images showed intimate adaptation in the restoration/dentine interfaces of Group Aelite and Group Dyract. All of the systems tested in this study presented microleakage. However, both Group Aelite (0.808) and Group Dyract (0.863) had significantly less microleakage than Group GlasIonomer (0.964). There were no statistically significant microleakage differences between Group Aelite and Group Dyract, and no statistically significant microleakage differences between the occlusal margin and gingival margin. CONCLUSIONS: None of the systems tested in this study completely eliminated microleakage. However, both the flowable composite and compomer provided stronger dentine bond strengths and better margin sealing than the conventional glass ionomer cement. Occlusal forces exerted the same effects on microleakage of the occlusal margin and gingival margin in cervical cavities.
PMID: 19133948 [PubMed - indexed for MEDLINE]
Eur J Orthod. 2009 Apr;31(2):207-12. Epub 2008 Dec 10. Links
Shear bond strength of brackets bonded to amalgam with different intermediate resins and adhesives.
Germec D, Cakan U, Ozdemir FI, Arun T, Cakan M.
Vichet Chindavanig วเชฏฐ จนดาวณค
26
27
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Department of Orthodontics, Yeditepe University, Istanbul, Turkey. [email protected]
The aims of this study were to compare, in vitro, the shear bond strength (SBS) of stainless steel orthodontic brackets bonded to silver amalgam with the use of three different intermediate resins and two different adhesives, and to evaluate bond failure mode. Forty-five amalgam specimens were divided into three equal groups. In groups 1 and 2, the brackets were bonded with Unite (3M Unitek) using Reliance Metal Primer (RMP; Reliance Orthodontic Products) and Power Bond OLC (PB OLC; Ortho Organizers Inc.) as intermediate resins, respectively. In group 3, Resinomer and One-Step Plus (OS+; Bisco Inc.) were used. Thirty bovine teeth served as the controls to test bracket bonding to acid-etched enamel with Unite and Resinomer-OS+. After thermocycling from 10 to 50 degrees C 1000 times, all samples were tested for SBS. Bond failure sites were classified using a modified adhesive remnant index (ARI) system. Data were analyzed with one-way analysis of variance, post hoc Tukey multiple comparison and chi-square tests. The results showed that the mean SBS to amalgam surfaces were significantly lower than those to etched bovine enamel (P<0.001). There were no statistically significant differences in mean SBS between the amalgam bonding groups (P>0.05). For the ARI, significant differences were found between the amalgam- and enamel-bonding groups (P<0.001). The mean SBS of stainless steel orthodontic brackets bonded to amalgam surfaces with RMP, PB OLC, OS+ intermediate resins and Unite and Resinomer adhesives was significantly lower than to etched bovine enamel. Bond failure occurred at the amalgam-adhesive interface regardless of the adhesive system and without damage to the amalgam restoration.
PMID: 19073953 [PubMed - indexed for MEDLINE]
Dent Mater. 2009 Apr;25(4):459-66. Epub 2008 Nov 28. Links
Long-term adhesion and mechanism of bonding of a paste-liquid resin-modified glass-ionomer.
Mitra SB, Lee CY, Bui HT, Tantbirojn D, Rusin RP.
3M ESPE Dental Products, Maplewood, MN 55144, USA.
OBJECTIVES: The contribution of chemical bonding of the polycarboxylic acid in classical powder/liquid conventional glass ionomers (GI) and resin-modified glass-ionomers (RMGI) has been attributed to the excellent long-term bond strengths and clinical retention. RMGIs have been recently introduced as paste/liquid systems for convenience of clinical usage. The objective of this study was to investigate the long-term bond strengths and mechanism of adhesion of paste-liquid RMGI in order to ascertain whether similar characteristics are retained. METHODS: Long-term shear adhesion to dentin and enamel was measured on two paste-liquid RMGIs and one powder/liquid RMGI. Scanning electron microscopy (SEM),
Vichet Chindavanig วเชฏฐ จนดาวณค
27
28
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Fourier-transformed infrared spectroscopy (FTIR) and X-ray photoelectron spectroscopy (XPS) analyses were carried out on the paste-liquid RMGI Vitrebond Plus (VBP) and compared with the classical powder/liquid RMGI Vitrebond (VB). RESULTS: VBP maintains adhesion to dentin and enamel over long times; its long-term adhesive performance is equivalent to VB. FTIR data confirm that VBP exhibits the carboxylate crosslinking reaction of a true glass ionomer. SEM images show evidence of micromechanical bonding at the interface between VBP and the tooth. XPS and FTIR data show that the methacrylated copolyalkenoic acid component present in VB and VBP chemically bonds to the calcium in HAP. SIGNIFICANCE: The new paste-liquid RMGI liner, VBP, shows equivalent adhesion to its powder-liquid predecessor, VB. The adhesion mechanism was attributed to micromechanical and chemical bonding. This chemical bond is a significant factor in the excellent long-term adhesion of these materials.
PMID: 19041127 [PubMed - indexed for MEDLINE]
Braz Oral Res. 2008 Jul-Sep;22(3):198-204. Links
Bond strength of a resin cement to dentin using the resin coating technique.
dos Santos-Daroz CB, Oliveira MT, Fernando de Góes M, Nikaido T, Tagami J, Giannini M.
Department of Restorative Dentistry, Piracicaba Dental School, State University of Campinas, Piracicaba, SP, Brazil.
The aim of this study was to evaluate the bond strength of a resin cement to dentin using different adhesive systems (AS) in the presence or absence of a low-viscosity composite liner (Protect Liner F - PLF) applied over the bonded dentin. The adhesive systems selected were: AdheSE/Vivadent (AD); Clearfil Protect Bond/Kuraray (CP); One-Up Bond F/Tokuyama (OU); Single Bond/3M ESPE (SB); Tyrian SPE/One-Step Plus/Bisco (TY); Xeno III/Dentsply (XE) and Unifil Bond/GC (UN). After removing the labial and lingual enamel surfaces of bovine incisors, dentin fragments were prepared and randomly divided into 15 groups (n = 8). The dentin substrates were bonded with the AS and the PLF was applied or not before application of the resin cement (Panavia F, Kuraray). In the control group, the ED Primer (ED) and the resin cement without PLF were used. The AS, PLF and resin cement tested were used according to the manufacturers' instructions, and all treated dentin surfaces were temporized. After water storage for one week, three cylinders of resin cement were applied to each bonded dentin surface, using tygon tubing molds. The specimens were subjected to micro-shear testing and the data were statistically analyzed (two-way ANOVA, Tukey and Dunnett tests, p < 0.05). The observed mean shear bond strengths in MPa were: ED: 20.2 +/- 2.3; AD: 30.3 +/- 6.5; CP: 25.3 +/- 4.4; OU: 28.3 +/- 6.6; SB: 25.6 +/- 6.9; TY: 24.5 +/- 2.5; XE: 17.3 +/- 3.4; UN: 28.4 +/- 6.2; AD+PLF: 32.8 +/- 4.1; CP+PLF: 29.9 +/- 3.9; OU+PLF: 34.1 +/- 4.1; SB+PLF: 29.5 +/- 8.2; TY+PLF: 29.2 +/- 3.9; XE+PLF: 32.8 +/- 6.7; UN+PLF:
Vichet Chindavanig วเชฏฐ จนดาวณค
28
29
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
32.2 +/- 4.5. The bond strength of the resin cement to dentin using the tested AS was increased when the low-viscosity composite liner was applied.
PMID: 18949303 [PubMed - in process]
Oper Dent. 2008 Jul-Aug;33(4):392-9. Links
Microleakage of all-ceramic crowns using self-etching resin luting agents.
Trajtenberg CP, Caram SJ, Kiat-amnuay S.
Department of Restorative Dentistry and Biomaterials, The University of Texas Dental Branch at Houston, Houston, TX, USA. [email protected]
Self-etching adhesive systems are a new generation of materials that possess acidic methacrylates that can generate self-adhesion. There is limited data reported on the marginal leakage of ceramic restorations bonded with self-etching adhesive materials. This study assessed and compared the amount of microleakage of bonded ceramic crowns using three different types of self-etching adhesive systems with and without a die spacer. Eighteen human molars were prepared for all-ceramic IPS Empress crowns and the teeth were randomly assigned to each experimental group. The buccal side had the preparation finish line 1.5 mm below the CEJ, and the lingual finish line was 1.5 mm above the CEJ, creating margins in enamel and dentin. Two die-spacing techniques were used (three layers or no layer of die spacer). Each crown restoration was cemented with one of three self-etching resin luting agents (Panavia F 2.0, Multilink and RelyX Unicem). The specimens were thermally cycled for 1000 cycles, then immersed in a 5% methylene blue dye solution for 24 hours. The teeth were then rinsed, embedded in clear epoxy resin and sectioned. A total of 60 sections were evaluated for each type of resin luting agent using digital image analysis at 70x magnification. A novel formula, using mean percentage of microleakage, was developed by dividing the extent of dye penetration along the tooth/resin luting cement interphase and the total perimeter of the tooth crown surface. The data were analyzed using three-way analysis of variance at the 0.05 level of significance. Fisher's PLSD intervals were calculated for comparing significant means. Panavia F 2.0 showed a lower degree of microleakage than RelyX Unicem and Multilink at both the enamel and dentin margins. Interactions of the main effects (cement, margin and die spacer technique) were all highly significant (p< or =0.004). The degree of microleakage was higher on the dentin margins than on the enamel margins (p<0.0001). The degree of microleakage for the die spacer group was not significantly different from the group with no die spacer technique (p>0.1). Overall, Panavia F 2.0 showed the least microleakage, followed by RelyX Unicem and Multilink, respectively.
PMID: 18666496 [PubMed - indexed for MEDLINE]
Am J Dent. 2008 Apr;21(2):101-4. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
29
30
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Influence of oil contamination on in vitro bond strength of bonding agents to dental substrates.
Matos AB, Oliveira DC, Vieira SN, Netto NG, Powers JM.
Department of Restoratve Dentistry, Faculty of Dentistry of the University of São Paulo, São Paulo, SP, Brazil. [email protected]
PURPOSE: To evaluate the influence of cleaning procedures (pumice, anionic detergent and both procedures together) on the tensile bond strength of etch-and-rinse and self-etch adhesive systems to bovine enamel and dentin in vitro. METHODS: Eighty non-carious, bovine incisors were extracted, embedded in acrylic resin to obtain enamel/dentin specimens. Flat bonding surfaces were obtained by grinding. Groups were divided according to substrate (enamel or dentin), adhesive system [etch-and-rinse, Adper Single Bond 2 (SB) or self-etch, Clearfil Protect Bond (PB)]; and cleaning substances (pumice, anionic detergent and their combination). The teeth were randomly divided into 20 groups (n=8): G1--Enamel (E) + SB; G2--E + oil (O) + SB; G3--E + O + Pumice (P) + SB; G4--E + O + Tergentol (T) + SB; G5--E + O + P + T + SB; G6--E + PB; G7--E + O + PB; G8--E + O + P + PB; G9--E + O + T + PB; G10--E + O + P + T + PB; G11--Dentin (D) + SB; G12 D + SB + O; G13--D + SB + O + P; G14--D + SB + O + T;G15--D + SB + O + P + T; G16--D + PB; G17--D + O + PB +; G18--D + O + P + PB; G19--D + O + T + PB; G20--D + O + P + T + PB. Specimens were contaminated with handpiece oil for 5 seconds before bonding. Adhesive systems and resin composite were applied according to manufacturers' instructions. Specimens were tested in tension after 24 hours of immersion using a universal testing machine at a crosshead speed of 0.5 mm/minute. Bond strengths were analyzed with ANOVA. Failure sites were observed and recorded. RESULTS: Tensile bond strength in MPa were: G1 (23.6 +/- 0.9); G2 (17.3 +/- 2.2); G3 (20.9 +/- 0.9); G4 (20.6 +/- 0.5); G5 (18.7 +/- 2.3); G6 (23.0 +/- 1.0); G7 (21.5 +/- 2.4); G8 (19.9 +/- 1.3); G9 (22.1 +/- 1.2); G10 (19.1 +/- 1.2); G11 (18.8 +/- 1.3); G12 (15.7 +/- 2.1); G13 (17.8 +/- 3.3); G14 (15.3 +/- 2.9); G15 (15.6 +/- 1.9); G16 (14.7 +/- 2.3); G17 (5.5 +/- 0.9); G18 (19.3 +/- 1.8); G19 (15.6 +/- 1.6); G20 (20.3 +/- 3.9). Statistical analysis showed that the main factors substrate and cleaning were statistically significant, as well as the triple interaction between factors of variance. However, the factor adhesive system did not show statistical difference. Oil contamination reduced bond strengths, being less detrimental to enamel than to dentin. Etch-and-rinse (SB) and two-step self-etch (PB) systems had similar bond strengths in the presence of oil contamination. For etch-and-rinse (SB), the cleaning procedures were able to clean enamel, but dentin was better cleaned by pumice. When self-etch (PB) system was used on enamel, anionic detergent was the best cleaning substance, while on dentin the tested procedures were similarly efficient.
PMID: 18578177 [PubMed - indexed for MEDLINE]
Compend Contin Educ Dent. 2008 May;29(4):208-15; quiz 216, 218. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
30
31
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Adhesive procedures in daily practice: essential aspects.
Hilgert LA, Lopes GC, Araújo E, Baratieri LN.
Department of Operative Dentistry, Universidade Federal de Santa Catarina, Florianópolis, Brazil.
Adhesive procedures are essential to most restorative protocols used in modern dentistry. Increasing demand and constant interest in new products have stimulated dental manufacturers to produce new adhesive systems and marketing campaigns that announce fast and easy bonding. However, laboratorial and clinical studies show that, usually, ease of application of an adhesive system does not relate to its competence in creating a quality, long-term adhesive interface. This article will present relevant data from the scientific literature to help clinicians understand quality adhesion and achieve excellent results with the current adhesion systems.
PMID: 18524205 [PubMed - indexed for MEDLINE]
J Appl Oral Sci. 2008 Feb;16(1):64-9. Links
Correlation between margin fit and microleakage in complete crowns cemented with three luting agents.
Rossetti PH, do Valle AL, de Carvalho RM, De Goes MF, Pegoraro LF.
Oral Rehabilitation Program, Bauru School of Dentistry, University of São Paulo, Bauru, SP, Brazil.
Microleakage can be related to margin misfit. Also, traditional microleakage techniques are time-consuming. This study evaluated the existence of correlation between in vitro margin fit and a new microleakage technique for complete crowns cemented with 3 different luting agents. Thirty human premolars were prepared for full-coverage crowns with a convergence angle of 6 degrees, chamfer margin of 1.2 mm circumferentially, and occlusal reduction of 1.5 mm. Ni-Cr cast crowns were cemented with either zinc phosphate (ZP) (S.S. White), resin-modified glass-ionomer (RMGI) (Rely X Luting Cement) or a resin-based luting agent (RC) (Enforce). Margin fit (seating discrepancy and margin gap) was evaluated according to criteria in the literature under microscope with 0.001 mm accuracy. After thermal cycling, crowns were longitudinally sectioned and microleakage scores at tooth-cement interface were obtained and recorded at x100 magnification. Margin fit parameters were compared with the one-way ANOVA test and microleakage scores with Kruskal-Wallis and Dunn's tests (alpha=0.05). Correlation between margin fit and microleakage was analyzed with the Spearman's test (alpha=0.05). Seating discrepancy and marginal gap values ranged from 81.82 microm to 137.22 microm (p=0.117), and from 75.42 microm to 78.49 microm (p=0.940), respectively. Marginal microleakage scores were ZP=3.02, RMGI=0.35 and RC=0.12 (p<0.001), with no differences between RMGI and RC scores. The correlation coefficient values ranged from -0.27 to 0.30 (p>0.05). Conclusion: Margin fit parameters
Vichet Chindavanig วเชฏฐ จนดาวณค
31
32
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
and microleakage showed no strong correlations; cast crowns cemented with RMGI and RC had lower microleakage scores than ZP cement.
PMID: 19089292 [PubMed - indexed for MEDLINE]
J Prosthodont. 2009 Jun 10. [Epub ahead of print] Links
Esthetic Interim Acrylic Resin Prosthesis Reinforced with Metal Casting.
Verri FR, Pellizzer EP, Mazaro JV, de Almeida EO, Antenucci RM.
Professor of Dental Prostheses, Implants, and Occlusion, Adamantina School of Dentistry, Adamantina, Brazil.
Fabrication of an interim prosthesis is an important procedure in oral rehabilitation because it aids in determining the esthetics, phonetics, and occlusal relationship of the definitive restoration. The typical material (acrylic resin) used in interim prostheses commonly fails due to fractures. During extended oral rehabilitation with fixed partial prostheses, high strength interim prostheses are often required to protect hard and soft tissues, avoid dental mobility, and to allow the clinician and patient a chance to evaluate cosmetics and function before the placement of the definitive prosthesis. Furthermore, a satisfactory interim prosthesis can serve as a template for the construction of the definitive prosthesis. The maintenance of this prosthesis is important during treatment for protection of teeth and occlusal stability. Procedures to reinforce interim prostheses help to improve performance and esthetics in long-term treatment. Due to the low durability of acrylic resin in long-term use, the use of reinforcing materials, such as metal castings or spot-welded stainless steel matrix bands, is indicated in cases of extensive restoration and long-term treatment. This paper describes an easy technique for fabricating a fixed interim prosthesis using acrylic resin and a cast metallic reinforcement.
PMID: 19519710 [PubMed - as supplied by publisher]
Pract Proced Aesthet Dent. 2008 Nov-Dec;20(10):619-26. Links
Increasing vertical dimension: considerations and steps in reconstruction of the severely worn dentition.
Cutbirth ST.
Center for Aesthetic and Restorative Dentistry (CARD), Dallas, TX, USA. [email protected]
Clinicians often encounter dental patients who have lost tooth structure or demonstrate an insufficient vertical dimension of occlusion (VDO). While reconstructing the proper VDO for such patients can be challenging, the use of a systematic approach can facilitate a
Vichet Chindavanig วเชฏฐ จนดาวณค
32
33
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
successful and predictable treatment outcome. Presented herein are a series of considerations involved in managing and/or restoring the VDO and a reproducible clinical protocol aimed at improving the dentist's ability to increase the VDO while reconstructing severely worn dentition.
PMID: 19274959 [PubMed - indexed for MEDLINE]
J Am Dent Assoc. 2009 May;140(5):526-35. Links
A 12-year clinical evaluation of a three-step dentin adhesive in noncarious cervical lesions.
Wilder AD Jr, Swift EJ Jr, Heymann HO, Ritter AV, Sturdevant JR, Bayne SC.
Department of Operative Dentistry, School of Dentistry, University of North Carolina, 439 Brauer Hall, Chapel Hill, N.C. 27599-7450, USA. [email protected]
BACKGROUND: The authors conducted a study to evaluate the clinical performance of a dual-cured, three-step dentin adhesive (OptiBond Dual Cure, Kerr, a subsidiary of Sybron Dental Specialties, Orange, Calif.; no longer on the market) at 12 years. METHODS: The authors restored 100 noncarious cervical lesions without use of macromechanical retention or enamel bevels. In one-half of the lesions (group A), the authors etched only the enamel; in the other half (group B), they etched both enamel and dentin. After etching, they applied a light-cured primer and dual-cured adhesive to enamel and dentin in both groups. They restored the preparations with a resin-based composite. They performed direct evaluations by using modified U.S. Public Health Service criteria at insertion (baseline) and at one year and 12 years after insertion. RESULTS: The 12-year retention rates were 93 percent in group A and 84 percent in group B, for an overall retention rate of 89 percent. Except for marginal discoloration in both groups and retention in group B, the restorations in both groups had Alfa ratings of 88 percent or greater in all of the direct clinical evaluation categories. CONCLUSIONS: The 12-year clinical performance, including retention rate, of a dual-cured dental adhesive was excellent and was not affected by dentin acid-etching. CLINICAL IMPLICATIONS: This clinical study provides additional evidence for the long-term durability of a three-step etch-and-rinse adhesive in non-carious cervical lesions.
PMID: 19411519 [PubMed - indexed for MEDLINE]
Rev Med Chir Soc Med Nat Iasi. 2008 Apr-Jun;112(2):507-11. Links
Oral rehabilitation between reality and paradigm.
Forna NC.
Department of Removable Prosthesis, School of Dental Medicine, "Gr.T. Popa" University of Medicine and Pharmacy Iaşi.
Vichet Chindavanig วเชฏฐ จนดาวณค
33
34
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
The oral rehabilitation represents the integrative concept which re-establishes every segment of the dental-jaw system that is affected by edentation in different clinical forms, without eluding the induced complications and the influence of general status within the chosen therapy algorithm. Despite the significant development of knowledge and techniques, it is still controversial to which degree the therapy solutions of oral rehabilitation approach the therapy's ideal, and also the way in which particular aspects of the prosthetic treatment, the general status and socioeconomic criterion influence the clinical result. The implant-prosthetic therapy represents the state of art in modern treatment of edentulous patients, starting from the simplest cases and ending up with complex situations. However the problem of choosing the best treatment option remains, the patient being confused between several possibilities and numerous limits. In the best of cases, the patient understands, accepts and can afford the adequate treatment option. In other cases, choosing the therapeutically solution can be made only under the impulse of external factors. In critical situations, the patient's fear, disbelief, the restrained economic possibilities exclude the ideal solution and compromise the long-term success of the treatment. Several complex cases that were treated accordingly to the ideal option, using complex integrated algorithms, support the idea that future economic development and improved education should surpass present obstacles, the reality becoming a paradigm.
PMID: 19295028 [PubMed - indexed for MEDLINE]
algorithm An algorithm is a special series of instruction that are carried out in a particular order, for example as part of a computer program. Vichet C
Odontology. 2009 Jan;97(1):8-17. Epub 2009 Jan 29. Links
Dental occlusion: modern concepts and their application in implant prosthodontics.
Carlsson GE.
Department of Prosthetic Dentistry, The Sahlgrenska Academy, University of Gothenburg, Box 450, SE 405 30, Göteborg, Sweden. [email protected]
The aim of this article was to review the literature on various aspects of occlusion related to implant prosthodontics, using PubMed and the Cochrane library. Even if the number of studies on implants and prosthodontics is very large, no randomized controlled trials or Cochrane reviews were found on the possible influence of occlusal design or characteristics of occlusion on treatment outcome. Therefore, studies and articles of a lower evidence level were accepted as the main part of the review. The widely spread opinion that implants are superior to natural teeth was refuted by two recent consensus conferences, which concluded that the long-term outcome of implant restorations is not better than that of natural teeth. No controlled studies on the optimal features of a harmonious natural and/or restored occlusion, including implant prostheses, were found. Nor was there any evidence that more sophisticated methods in jaw registration, e.g., using face-bows and adjustable
Vichet Chindavanig วเชฏฐ จนดาวณค
34

35
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
articulators, compared with simpler methods, will yield better clinical prosthodontic results. This article discusses, among other things, concepts of occlusion of implant-supported restorations, occlusal material, cantilevers, and occlusal risk factors. Within the limitations of the review, it was concluded that many factors can influence implant failure and peri-implant bone loss but that little is known of the relative importance of such factors. Most probably, however, occlusal factors and details of occlusion are in general of minor importance for the outcome of implant restorations. Occlusion can be managed successfully by using simple methods for jaw registration and different occlusal concepts.
PMID: 19184293 [PubMed - indexed for MEDLINE]
refute If you refute something such as a theory or argument, you prove that it is wrong; a formal word. EG… The argument cannot be refuted at the moment... Vichet C
Dent Today. 2008 Dec;27(12):80, 82-3. Links
Long-term composite provisionalization: the conversion.
Goldstein MB.
International Academy of Dento-Facial Esthetics. [email protected]
PMID: 19133637 [PubMed - indexed for MEDLINE]
J Dent. 2009 Feb;37(2):115-21. Epub 2008 Dec 17. Links
Long-term survival of endodontically treated, maxillary anterior teeth restored with either tapered or parallel-sided glass-fiber posts and full-ceramic crown coverage.
Signore A, Benedicenti S, Kaitsas V, Barone M, Angiero F, Ravera G.
Department of Biophysics, Medicine and Dentistry, University of Genoa, Largo Rosanna Benzi 10, 16132 Genoa, Italy. [email protected]
OBJECTIVES: This retrospective study investigated the clinical effectiveness over up to 8 years of parallel-sided and of tapered glass-fiber posts, in combination with either hybrid composite or dual-cure composite resin core material, in endodontically treated, maxillary anterior teeth covered with full-ceramic crowns. METHODS: The study population comprised 192 patients and 526 endodontically treated teeth, with various degrees of hard-tissue loss, restored by the post-and-core technique. Four groups were defined based on post shape and core build-up materials, and within each group post-and-core restorations were assigned randomly with respect to root morphology. Inclusion criteria were symptom-free endodontic therapy, root-canal treatment with a minimum apical seal of 4mm, application of rubber dam, need for post-and-core complex because of coronal tooth loss, and tooth with at least one residual coronal wall. Survival rate of the post-and-core restorations was
Vichet Chindavanig วเชฏฐ จนดาวณค
35

36
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
determined using Kaplan-Meier statistical analysis. RESULTS: The restorations were examined clinically and radiologically; mean observation period was 5.3 years. The overall survival rate of glass-fiber post-and-core restorations was 98.5%. The survival rate for parallel-sided posts was 98.6% and for tapered posts was 96.8%. Survival rates for core build-up materials were 100% for dual-cure composite and 96.8% for hybrid light-cure composite. CONCLUSIONS: For both glass-fiber post designs and for both core build-up materials, clinical performance was satisfactory. Survival was higher for teeth retaining four and three coronal walls.
PMID: 19091452 [PubMed - indexed for MEDLINE]
J Adhes Dent. 2008 Oct;10(5):393-8. Links
Leucite-reinforced glass ceramic inlays and onlays after 12 years.
Frankenberger R, Taschner M, Garcia-Godoy F, Petschelt A, Krämer N.
Dental Clinic 1, Operative Dentistry and Periodontology, University Medical Center, University of Erlangen-Nuremberg, Germany. [email protected]
PURPOSE: This controlled clinical trial aimed to evaluate IPS Empress inlays and onlays over 12 years. The null hypothesis was that different luting resins would have no influence on clinical outcome. MATERIALS AND METHODS: In the course of a prospective clinical long-term trial, 96 ceramic inlays and onlays were placed in 34 patients using one adhesive (Syntac) and four different luting composites (Tetric, Variolink Low, Variolink Ultra, Dual Cement). Recalls were carried out by two calibrated investigators using modified USPHS codes and criteria at baseline, 1, 2, 4, 6, 8, and 12 years. RESULTS: Fifteen of the 96 restorations had to be replaced (failure rate 16%; Kaplan-Meier); 12 of them suffered bulk fractures. After twelve years of clinical service, significantly more bulk fractures were found when light-curing composite was used for luting (p < 0.05). Fractures were noticed between 3 and 4 years of clinical service and later after 11 to 12 years; aside from those times, no single fracture occurred. Secondary caries was not observed. CONCLUSION: IPS Empress inlays and onlays exhibited satisfactory clinical outcomes over a 12-year clinical period. Restorations luted with dual-cured resin composites revealed significantly fewer bulk fractures.
PMID: 19058686 [PubMed - indexed for MEDLINE]
J Can Dent Assoc. 2002 Apr;68(4):233-7. Links
Comment in:
Evid Based Dent. 2004;5(3):73.
Longevity and clinical performance of IPS-Empress ceramic restorations--a literature review.
Vichet Chindavanig วเชฏฐ จนดาวณค
36
37
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
El-Mowafy O, Brochu JF.
Discipline of Restorative Dentistry, Department of Clinical Dental Sciences, Faculty of Dentistry, University of Toronto, Toronto, Ontario, Canada. [email protected]
A literature review of longevity and clinical performance of IPS-Empress restorations is presented. A MEDLINE search was conducted in fall 2000. Selection criteria were set so as to identify suitable clinical trials that were published in full and that had lasted more than 2 years. A total of 6 clinical trials on the performance of IPS-Empress inlays and onlays and a total of 3 clinical trials on the performance of IPS-Empress crowns were identified. Survival rates for IPS-Empress inlays and onlays ranged from 96% at 4.5 years to 91% at 7 years; most failures were due to bulk fracture. IPS-Empress crowns had a survival rate ranging from 92% to 99% at 3 to 3.5 years; crown failure was also mainly due to fracture. Dentists should inform their patients about these survival rates when offering such treatment. The use of IPS-Empress crowns in the posterior of the mouth is not recommended until the results of more long-term clinical trials are available.
PMID: 12626277 [PubMed - indexed for MEDLINE]
Oper Dent. 2008 Sep-Oct;33(5):484-7. Links
Long-term survival of Cerec restorations: a 10-year study.
Zimmer S, Göhlich O, Rüttermann S, Lang H, Raab WH, Barthel CR.
Dept of Operative and Preventive Dentistry, Witten, Germany. [email protected]
This clinical retrospective study assessed the longevity of CAD-CAM ceramic restorations (Cerec) inserted into the cavities of 95 patients in a private practice in Berlin, Germany. Three hundred and eight ceramic restorations were inserted into cavities in the posterior teeth of 95 patients between 1992 and 1994. One operator placed all restorations in a single sitting. Seventy-four patients, including 226 restorations, returned to the practice for a final examination at the end of 10 years. Reasons for non-attendance include relocation (15), death (2) and personal reasons (4). Again, all examinations were performed by a single examiner, however, not the same dentist who initially treated the patients. Out of the 226 restorations, 39 had been inserted in Class I cavities and 187 in Class II cavities (84 two-surfaces, 103 three or more surfaces). In the latter group, one cusp was replaced in 20 cases and two cusps in three cases. All the restorations were fabricated using Cerec 1 (46 Dicor, 180 Vita Mark II) and cemented adhesively with Vita Cerec Duo Cement in combination with Syntac Classic under a rubber dam. Kaplan-Meier survival analysis was calculated under the following failure-criteria: (1) secondary decay, (2) any kind of loss of the restoration, (3) fracture of the restoration, (4) tooth fracture and (5) marginal gap reaching dentin or base material. For statistical analysis, SPSS 12.0 was used. The survival rate was 94.7% (12 failures) after five years and 85.7% (23 failures) after 10 years. The
Vichet Chindavanig วเชฏฐ จนดาวณค
37
38
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
results of the current study show that the survival rate of Cerec 1 restorations, as applied in this study, are comparable with the survival rates of cast gold restorations.
PMID: 18833853 [PubMed - indexed for MEDLINE]
J Adhes Dent. 2001 Spring;3(1):45-64. Links
Longevity of restorations in posterior teeth and reasons for failure.
Hickel R, Manhart J.
Department of Restorative Dentistry and Periodontology, Ludwig Maximilians University, Munich, Germany. [email protected]
PURPOSE: This article compiles a survey on the longevity of restorations in stress-bearing posterior cavities and assesses possible reasons for failure. MATERIALS AND METHODS: The dental literature predominantly of the last decade was reviewed for longitudinal, controlled clinical studies and retrospective cross-sectional studies of posterior restorations. Only studies investigating the clinical performance of restorations in permanent teeth were included. Longevity and annual failure rates of amalgam, direct composite restorations, glass ionomers and derivative products, composite and ceramic inlays, and cast gold restorations were determined for Class I and II cavities. RESULTS: Annual failure rates in posterior stress-bearing restorations are: 0% to 7% for amalgam restorations, 0% to 9% for direct composites, 1.4% to 14.4% for glass ionomers and derivatives, 0% to 11.8% for composite inlays, 0% to 7.5% for ceramic restorations, 0% to 4.4% for CAD/CAM ceramic restorations, and 0% to 5.9% for cast gold inlays and onlays. CONCLUSION: Longevity of dental restorations is dependent upon many different factors that are related to materials, the patient, and the dentist. The principal reasons for failure were secondary caries, fracture, marginal deficiencies, wear, and postoperative sensitivity. A distinction must be made between factors causing early failures and those that are responsible for restoration loss after several years of service.
PMID: 11317384 [PubMed - indexed for MEDLINE]
Clin Implant Dent Relat Res. 2008 Sep 9. [Epub ahead of print] Links
Stability of Prototype Two-Piece Zirconia and Titanium Implants after Artificial Aging: An In Vitro Pilot Study.
Kohal RJ, Finke HC, Klaus G.
Department of Prosthodontics, Albert-Ludwigs-University, Hugstetter Strasse 55; 79106 Freiburg, Germany.
Vichet Chindavanig วเชฏฐ จนดาวณค
38
39
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Background: Zirconia oral implants are a new topic in implant dentistry. So far, no data are available on the biomechanical behavior of two-piece zirconia implants. Therefore, the purpose of this pilot investigation was to test in vitro the fracture strength of two-piece cylindrical zirconia implants after aging in a chewing simulator. Materials and Methods: This laboratory in vitro investigation comprised three different treatment groups. Each group consisted of 16 specimens. In group 1, two-piece zirconia implants were restored with zirconia crowns (zirconia copings veneered with Triceram(R); Esprident, Ispringen, Germany), and in group 2 zirconia implants received Empress(R) 2 single crowns (Ivoclar Vivadent AG, Schaan, Liechtenstein). The implants, including the abutments, in the two zirconia groups were identical. In group 3, similar titanium implants were reconstructed with porcelain-fused-to-metal crowns. Eight samples of each group were submitted to artificial aging with a long-term load test in the artificial mouth (chewing simulator). Subsequently, all not artificially aged samples and all artificially aged samples that survived the long-term loading of each group were submitted to a fracture strength test in a universal testing machine. For the pairwise comparisons in the different test groups with or without artificial loading and between the different groups at a given artificial loading condition, the Wilcoxon rank-sum test for independent samples was used. The significance level was set at 5%. Results: One sample of group 1 (veneer fracture), none of group 2, and six samples of group 3 (implant abutment screw fractures) failed while exposed to the artificial mouth. The values for the fracture strength after artificial loading with 1.2 million cycles for group 1 were between 45 and 377 N (mean: 275.7 N), in group 2 between 240 and 314 N (mean: 280.7 N), and in the titanium group between 45 and 582 N (mean: 165.7 N). The fracture strength results without artificial load for group 1 amounted to between 270 and 393 N (mean: 325.1 N), for group 2 between 235 and 321 N (mean: 281.8 N), and between 474 and 765 N (mean: 595.2 N) for the titanium group. The failure mode during the fracture testing in the zirconia implant groups was a fracture of the implant head and a bending/fracture of the abutment screw in the titanium group. Conclusions: Within the limits of this pilot investigation, the biomechanical stability of all tested prototype implant groups seems to be - compared with the possibly exerted occlusal forces - borderline for clinical use. A high number of failures occurred already during the artificial loading in the titanium group at the abutment screw level. The zirconia implant groups showed irreparable implant head fractures at relatively low fracture loads. Therefore, the clinical use of the presented prototype implants has to be questioned.
PMID: 18783418 [PubMed - as supplied by publisher]
J Dent Res. 2008 Sep;87(9):829-33. Links
In vitro performance of nano-heterogeneous dentin adhesive.
Ye Q, Park JG, Topp E, Wang Y, Misra A, Spencer P.
Bioengineering Research Center, University of Kansas, 1530 W. 15th Street, Lawrence, KS 66045, USA.
Vichet Chindavanig วเชฏฐ จนดาวณค
39

40
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Water is ubiquitous in the mouths of healthy individuals and routinely interferes with efforts to bond restorations to dental tissues. Our previous studies using tapping-mode atomic force microscopy (TMAFM) have shown that nanophase separation is a general feature of cross-linked polymethacrylates photocured in the presence of water. To explore the relationship between nanophase separation in dentin adhesives and their long-term mechanical properties, we evaluated model adhesives after 3 months of aqueous storage. The degree of contrast in the TMAFM phase image depended on the formulations used, ranging from 'not observable' to 'very strong'. Correspondingly, the mechanical properties of these model adhesives varied from 'minimal change' to 'significant depreciation'. The results support the hypothesis that a high degree of heterogeneity at the nano-scale is associated with poor mechanical durability in these model adhesives.
PMID: 18719208 [PubMed - indexed for MEDLINE]
PMCID: PMC2599950
Eur J Prosthodont Restor Dent. 2008 Jun;16(2):81-4. Links
A long term study on residual monomer release from denture materials.
Zissis A, Yannikakis S, Polyzois G, Harrison A.
The aim of this long term study was to investigate the release of residual monomer from different denture materials, throughout a 38 months time period after curing and storage in water Specimens made of four denture base resins (three heat polymerizing, one auto polymerizing) and one hard liner were subjected to residual monomer determination using gas liquid chromatography. The residual monomer estimation carried out on three occasions: one week, 12 months and 38 months after curing. The data obtained were analyzed using two-way Anova followed by Scheffe's test for post hoc multiple comparisons at alpha=0.05. Heat polymerized denture base acrylic resins showed less residual monomer than auto polymerized ones (p<0.001) and released no statistically significant amounts of monomer (p>0.05), during the 38 months storage time period. Auto polymerized denture materials, which had higher residual monomer content, released statistically significant amounts of monomer (p<0.001) during the first twelve months storage, but not during the last twenty six months period (p>0.05). Heat polymerized denture base acrylic resins released insignificant amounts of residual monomer during the storage period, whereas both the auto polymerized denture base resin and the hard liner released significant amounts of residual monomer during the initial storage time period but insignificant ones during the remainder of the storage period.
J Prosthet Dent. 2002 Sep;88(3):297-301. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
40
41
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Comment in:
Evid Based Dent. 2004;5(2):45.
Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restoration.
Mannocci F, Bertelli E, Sherriff M, Watson TF, Ford TR.
Department of Restorative Dentistry, University of Siena, Siena, Italy. [email protected]
STATEMENT OF PROBLEM: Little information exists regarding the outcome of crown build-ups on endodontically treated teeth restored with metal-ceramic crowns or with only a direct-placed composite. PURPOSE: The aim of this study was to evaluate the clinical success rate of endodontically treated premolars restored with fiber posts and direct composite restorations and compare that treatment with a similar treatment of full-coverage with metal-ceramic crowns. MATERIAL AND METHODS: Subjects included in this study had one maxillary or mandibular premolar for which endodontic treatment and crown build up was indicated and met specific inclusion/exclusion criteria. Only premolars with Class II carious lesions and preserved cusp structure were included. Subjects were randomly assigned to 1 of the following 2 experimental groups: (1) teeth endodontically treated and restored with adhesive techniques and composite or (2) teeth endodontically treated, restored with adhesive techniques and composite, and then restored with full-coverage metal-ceramic crowns. Sixty teeth were included in the first group and 57 in the second. All restorations were performed by one operator. Causes of failure were categorized as root fracture, post fracture, post decementation, clinical and/or radiographic evidence of marginal gap between tooth and restoration, and clinical and/or radiographic evidence of secondary caries contiguous with restoration margins. Subjects were examined for the listed clinical and radiographic causes of failure by 2 calibrated examiners at intervals of 1, 2, and 3 years. Exact 95% confidence intervals for the difference between the 2 experimental groups were calculated. RESULTS: At the 1-year recall, no failures were reported. The only failure modes observed at 2 and 3 years were decementations of posts and clinical and/or radiographic evidence of marginal gap between tooth and restoration. There was no difference in the failure frequencies of the 2 groups (95% confidence interval, -17.5 to 12.6). There was no difference between the number of failures caused by post decementations and the presence of marginal gaps observed in the 2 groups (95% confidence intervals, -9.7 to 16.2 and -17.8 to 9.27). CONCLUSION: Within the limitations of this study, the results upheld the research hypothesis that the clinical success rates of endodontically treated premolars restored with fiber posts and direct composite restorations after 3 years of service were equivalent to a similar treatment of full coverage with metal-ceramic crowns.
PMID: 12426500 [PubMed - indexed for MEDLINE]
J Contemp Dent Pract. 2008 May 1;9(4):92-8. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
41
42
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Clinical diagnosis and oral rehabilitation of a patient with amelogenesis imperfecta: a case report.
Sholapurkar AA, Joseph RM, Varghese JM, Neelagiri K, Acharya SR, Hegde V, Pai KM, Bhat M.
Department of Oral Medicine & Radiology, Manipal College of Dental Sciences, Manipal, Karnataka, India. [email protected]
AIM: This clinical report describes the oral rehabilitation of a young female patient diagnosed with the hypocalcified, autosomal recessive type of Amelogenesis imperfecta (AI). A brief discussion on diagnosis of AI is also included. BACKGROUND: AI has been defined as a group of hereditary enamel defects not associated with evidence of systemic disease. It can be characterized by enamel hypoplasia and/or hypomaturation or hypocalcification of the existing teeth. Restoration for patients with this condition should be oriented toward the functional and esthetic rehabilitation and the protection of these teeth. REPORT: A 31-year-old female patient presented with concerns including extreme sensitivity; dissatisfaction with size, shape, and shade of teeth; and poor masticatory efficiency. She was very conscious about the appearance of her teeth and reported that her primary dentition was affected in the same manner. The specific objectives of this treatment were to eliminate tooth sensitivity, enhance esthetics, and restore masticatory function. Treatment included crown lengthening procedures and placement of anterior and posterior metal-ceramic crowns. A 12-month follow-up with clinical and radiographic examinations revealed no evidence of any untoward effects of the treatment on the restored teeth or their supporting structures. SUMMARY: Management of a patient with AI is a challenge for the clinician. The treatment options vary considerably depending on several factors such as the age of the patient, socio-economic status, periodontal condition, loss of tooth structure, severity of the disorder, and, most importantly, the patient's cooperation. The clinician has to consider the long-term prognosis of the treatment outcome. This clinical report describes the fabrication of metal ceramic and all metal crowns for the restoration of severely worn teeth in a patient with AI which requires meticulous maintenance of oral hygiene and patient co-operation.
PMID: 18473032 [PubMed - indexed for MEDLINE]
J Prosthet Dent. 2006 Jan;95(1):10-3. Links
Oral rehabilitation of a young adult with hypoplastic amelogenesis imperfecta: a clinical report.
Robinson FG, Haubenreich JE.
University of Kentucky, College of Dentistry, Lexington, 40536, USA. [email protected]
Vichet Chindavanig วเชฏฐ จนดาวณค
42

43
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
This clinical report describes the oral rehabilitation of a young adult patient diagnosed with hypoplastic amelogenesis imperfecta. The specific objectives of this treatment were to eliminate tooth sensitivity while enhancing esthetics and restoring masticatory function. Treatment included removal of several teeth, lengthening of the maxillary and mandibular clinical crowns, and placement of anterior and posterior metal-ceramic fixed partial dentures. The 2-year recall examination revealed no pathology associated with the rehabilitation, and the patient's esthetic and functional expectations were satisfied.
PMID: 16399268 [PubMed - indexed for MEDLINE]
[What prosthodontic therapy should we select for periodontally compromised patients? Part 1: Review of the literature focusing on implant therapy for periodontally compromised patients]
[Article in Japanese]
Kanno T, Nakamura K, Hayashi E, Kimura K, Hirooka H, Kimura K.
Division of Fixed Prosthodontics, Department of Restorative Dentistry, Tohoku University Graduate School of Dentistry. [email protected]
PURPOSE: From a large number of experimental and clinical studies, it has been suggested that dental implant therapy has good prognosis for totally and partially edentulous patients. However, it is unclear whether we can use the implants for periodontally compromised patients. The aim of the present study was is to consider scientific evidence on implant treatment for periodontitis-susceptible subjects with partially edentulous dentate. STUDY SELECTION: Clinical studies that documented survival rates or success rates of implant therapy for periodontally compromised patients were selected and reviewed. RESULTS: Most of the 22 reports that were reviewed suggested good survival or success rate of implant therapy in short-term or medium-term clinical results. CONCLUSION: Although there were only a few long-term follow up studies, it was indicated that individuals who had susceptibility to periodontal disease can be treated successfully with the implants. In all reports, treatment for infection was done before implants installation, and the importance of regular maintenance after the installation has been emphasized. From this literature review, it was advocated that periodontally compromised patients could be treated successfully with the implants. However, implant therapy should be reconsidered if oral infection cannot be satisfactorily controlled.
PMID: 18467782 [PubMed - indexed for MEDLINE]
Int J Prosthodont. 2008 Jan-Feb;21(1):75-85. Links
Long-term results of short-span versus long-span fixed dental prostheses: an up to 20-year retrospective study.
De Backer H, Van Maele G, De Moor N, Van den Berghe L.
Vichet Chindavanig วเชฏฐ จนดาวณค
43

44
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Centre for Special Care, PaeCaMed Research, Unit of Gnathology and Temporomandibular Disorders, Dental School, Faculty of Medicine and Health Sciences, Ghent University, Belgium. [email protected]
PURPOSE: This study of short-span fixed dental prostheses (Ss-FDPs) versus long-span FDPs (Ls-FDPs) evaluated the long-term efficacy and determined the frequencies and causes of failures. MATERIALS AND METHODS: A total of 236 Ss-FDPs and 86 Ls-FDPs made in an undergraduate university clinic for 149 and 70 patients, respectively, were evaluated over a 20-year period. Kaplan-Meier analysis with a 95% confidence interval was used to estimate the survival probability. Failures of the FDPs were divided into irreversible (loss of FDPs or finish line involvement) or reversible (FDPs and abutments intact after conservative treatment) complications and into biologic and technical/patient-related failures. RESULTS: The overall survival estimations for Ss-FDPs (70.8%; 95% Cl: 63%-79%) and Ls-FDPs (52.8%; 36%-70%) at year 20, were statistically significantly different (P = .030). There was no statistically significant difference (P = .126) for the survival estimations for Ss-FDPs (60.4%; 48%-73%) versus Ls-FDPs (59.0%; 44%-74%) at year 19 in the root-canal treated (RCT) group. For the Ss-FDPs group there was a statistically significant difference (P = .009) between the vital (82.4%; 73%-92%) and RCT (60.4%; 49%-73%) groups at year 20. The reason for failure in the Ss-FDP group was of biologic origin in 55.6% to 66.7% of cases, but for the Ls-FDP group the failures were of technical origin in 56.0% to 84.0% of cases. CONCLUSION: The survival of Ss-FDPs and Ls-FDPs over a 20-year period was favorable. The overall survival estimation for Ss-FDPs was statistically significantly better than for Ls-FDPs at year 20. The use of an RCT abutment becomes more significant in fixed prosthetic restorations with 4 or more units. Occurrence of a previously reversible complication is a predictive factor for an irreversible complication later on. A reversible complication within the first 2 years for an Ss-FDP will lead to an irreversible complication.
PMID: 18350953 [PubMed - indexed for MEDLINE]
Dent Mater. 2009 Jun;25(6):820-7. Epub 2009 Mar 31. Links
Five-year survival of 3-unit fiber-reinforced composite fixed partial dentures in the anterior area.
van Heumen CC, van Dijken JW, Tanner J, Pikaar R, Lassila LV, Creugers NH, Vallittu PK, Kreulen CM.
Department of Oral Function and Prosthetic Dentistry, College of Dental Science, University Medical Centre Nijmegen, Netherlands. [email protected]
OBJECTIVES: The purpose of this clinical study was to evaluate the long-term outcome of 3-unit anterior fixed partial dentures (FPDs) made of fiber-reinforced resin composite (FRC), and to identify design factors influencing the survival rate. METHODS: 52 patients (26 females, 26 males) received 60 indirectly made FRC FPDs, using pre-impregnated unidirectional glass fibers, requiring manual wetting, as framework material. FPDs were
Vichet Chindavanig วเชฏฐ จนดาวณค
44

45
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
surface (n=48) or hybrid (n=12) retained and mainly located in the upper jaw. Hybrid FPDs had a combination of retainers; i.e. crown at one and surface retention at the other abutment tooth. Surface FPDs were either purely adhesively retained (n=29) or with additional mechanical retention (n=19). Follow-up period was at minimum 5 years, with check-ups every 1-2 years. Six operators were involved, in three centers in the Netherlands, Finland and Sweden. Survival rates, including repairable defects of FPDs, and success rates were determined. RESULTS: Kaplan-Meier survival rate at 5 years was 64% (SE 7%). For the level of success, values were 45% (SE 7%) and the estimated median survival time 58 (SE 10.1) months. For surface FPDs, additional mechanical retention did not improve survival significantly. There was a trend towards better survival of surface FPDs over hybrid FPDs, but differences were not significant. Main failure modes were fracture of the FPD and delamination of veneering composite. SIGNIFICANCE: A success rate of 45% and a survival rate of 64% after 5 years was found. Fracture of the framework and delamination are the most prevalent failure modes, especially for surface FPDs.
PMID: 19339043 [PubMed - indexed for MEDLINE]
J Adhes Dent. 2008 Aug;10(4):301-6. Links
Long-term clinical performance of resin-bonded fixed partial dentures with retentive preparation geometry in anterior and posterior areas.
Aggstaller H, Beuer F, Edelhoff D, Rammelsberg P, Gernet W.
Department of Prosthodontics, Ludwig Maximilians University, Munich, Germany. [email protected]
PURPOSE: The aim of this prospective clinical evaluation was to show the long-term clinical behavior of resin-bonded fixed partial dentures (RBFPD) with a retentive, minimally invasive preparation design. MATERIALS AND METHODS: Since 1985, 232 RBFPDs with a retentive preparation design were placed under controlled clinical conditions. In 2005 and 2006, 84 fixed partial dentures could be re-evaluated. Using Kaplan-Meier analysis, the survival rate was determined. The probability of survival was calculated with several risk factors: location (anterior/posterior, maxilla/mandible), metal alloy of the framework (titanium/CoCr), number of pontics, and number of supporting teeth. RESULTS: A total of 12 failures was observed and resulted in a survival rate of 77% after 10 years. However, only 4 catastrophic failures occurred. In such cases, the restoration was lost, or could not be re-bonded or repaired (survival rate 88% after 10 years). RBFPDs made of a titanium alloy exhibited a statistically significantly higher survival rate than RBFPDs made of a nonprecious CoCr alloy in terms of all failures. Only slight but not statistically significant differences between the covariates maxilla, mandible, anterior/posterior region, number of pontics, and number of abutment teeth were observed. CONCLUSION: Within the limitations of this study, RBFPDs seem to be a reliable restorative alternative to conventional short-span fixed dental prostheses.
PMID: 18792701 [PubMed - indexed for MEDLINE]
Vichet Chindavanig วเชฏฐ จนดาวณค
45
46
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Eur J Prosthodont Restor Dent. 2008 Mar;16(1):2-9. Links
An update on resin-bonded bridges.
Barber MW, Preston AJ.
School of Clinical Dentistry, University of Sheffield, Sheffield. [email protected]
Since the introduction of the 'Rochette' bridge in the 1970s the resin-bonded bridge has undergone a number of developments to become a commonly used technique for replacement of a missing tooth, especially in a minimally restored dentition. One of the major advantages of the resin-bonded bridge is that it requires less tooth preparation than conventional bridgework, with some authorities advising no preparation at all. Some reports have suggested poor long-term success rates, however, if used in appropriate clinical situations, this treatment modality can be extremely successful. The aim of this paper is to review the literature relating to resin-bonded bridges and suggest recommendations for clinicalpractice concerning the provision of resin-bonded bridges.
PMID: 18468318 [PubMed - indexed for MEDLINE]
J Clin Dent. 2008;19(1):37-41. Links
Clinical evaluation of a visible light-cured indirect composite for long-term provisionalization.
Ewoldsen N, Sundar V, Bennett W, Kanya K, Magyar K.
Dentsply Prosthetics, York, PA, USA.
OBJECTIVE: To clinically evaluate a visible light-cured (VLC) resin composite system for long-term provisional and esthetic diagnostic restorations, fabricated using indirect techniques. METHODS: One-hundred and nine teeth were restored in 31 patients. Preoperational impressions were used to create VLC resin composite restorations (Radica) using indirect techniques. Restorations were relined as necessary and placed using various provisional cements at a follow-up appointment, subsequent to preparation of the teeth. Both fabricating laboratory technicians and placing dentists rated the restorations for acceptability in esthetics, marginal fit, occlusion, and functionality in various stages of provisionalization. RESULTS: All restorations (100%) were rated acceptable for esthetics prior to relining. After relining, a majority (93-100%) of restorations were rated acceptable in esthetic and functional criteria. At the placement of the permanent restoration, a majority (96-100%) of restorations were rated acceptable in esthetic and functional criteria. Terms of service ranged from two to seventy-six days. CONCLUSION: In combination with in vitro results, the clinical performance of the Radica VLC system for provisionalization and esthetic diagnostic restorations was judged to be acceptable. The system offers esthetics that are superior to conventional provisional restorations, and should be a valuable option to practitioners considering longer-term provisionalization in complex cases.
Vichet Chindavanig วเชฏฐ จนดาวณค
46
47
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
PMID: 18500159 [PubMed - indexed for MEDLINE]
Curr Opin Cosmet Dent. 1997;4:16-21. Links
Long-term esthetic provisional restorations in dentistry.
Lodding DW.
The role of interim dental restorations used for indirect restorative and prosthodontic procedures has changed dramatically in the past several years. These restorations are no longer regarded as temporary restorations but rather as provisional restorations with distinct functions and purposes. Provisional restorations have become a vital diagnostic and assessment tool to evaluate function color, shape, contour, occlusion, periodontal response, implant healing, and overall esthetics. An accurate fit and margination is essential to insure and maintain pulpal health of the tooth. With increased demands being placed on provisional restorations, new materials and techniques are being developed and some existing protocols are being refined to accomplish the desired goals. Provisional restorations are often in the oral environment for several months, requiring a well-fabricated and stable restoration. This review is designed to report on current materials, techniques, and concepts in fabricating and maintaining long-term esthetic provisionals.
PMID: 9663045 [PubMed - indexed for MEDLINE]
Clin Oral Implants Res. 2007 Jun;18 Suppl 3:193-204. Links
Erratum in:
Clin Oral Implants Res. 2008 Mar;19(3):326-8.
Comment in:
Clin Oral Implants Res. 2007 Jun;18 Suppl 3:257-61.
To what extent does the longevity of fixed dental prostheses depend on the function of the cement? Working Group 4 materials: cementation.
Edelhoff D, Ozcan M.
Department of Prosthodontics, Ludwig-Maximilians-University, Munich, Germany. [email protected]
AIMS/BACKGROUND: The objective of this review was to define the impact of cementation mode on the longevity of different types of single tooth restorations and fixed dental prostheses (FDP). METHODS: Literature search by PubMed as the major database was used utilizing the terms namely, adhesive techniques, all-ceramic crowns, cast-metal, cement, cementation, ceramic inlays, gold inlays, metal-ceramic, non-bonded fixed-partial-dentures,
Vichet Chindavanig วเชฏฐ จนดาวณค
47

48
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
porcelain veneers, resin-bonded fixed-partial-dentures, porcelain-fused-to-metal, and implant-supported-restorations together with manual search of non-indexed literature. Cementation of root canal posts and cores were excluded. Due to lack of randomized prospective clinical studies in some fields of cementation, recommendations had to be based on lower evidence level (Centre of Evidence Based Medicine, Oxford) for special applications of current cements. RESULTS: One-hundred-and-twenty-five articles were selected for the review. The primary function of the cementation is to establish reliable retention, a durable seal of the space between the tooth and the restoration, and to provide adequate optical properties. The various types of cements used in dentistry could be mainly divided into two groups: Water-based cements and polymerizing cements. Water-based cements exhibited satisfying long-term clinical performance associated with cast metal (inlays, onlays, partial crowns) as well as single unit metal-ceramic FDPs and multiple unit FDPs with macroretentive preparation designs and adequate marginal fit. Early short-term clinical results with high-strength all-ceramic restorations luted with water-based cements are also promising. Current polymerizing cements cover almost all fields of water-based cements and in addition to that they are mainly indicated for non-retentive restorations. They are able to seal the tooth completely creating hybrid layer formation. Furthermore, adhesive capabilities of polymerizing cements allowed for bonded restorations, promoting at the same time the preservation of dental tissues.
PMID: 17594382 [PubMed - indexed for MEDLINE]
J Adhes Dent. 2002 Spring;4(1):7-22. Links
Are adhesive technologies needed to support ceramics? An assessment of the current evidence.
Burke FJ, Fleming GJ, Nathanson D, Marquis PM.
University of Birmingham School of Dentistry, UK. [email protected]
Despite large variations in the reported fracture strengths of dispersion strengthened, glass infiltrated, castable, pressable and machinable ceramics utilised for the construction of all-ceramic crowns, the annual clinical failure rate reported for these materials in the dental literature is remarkably consistent at ca 3%. These results emphasise that there may be little correlation between the average fracture strength and resultant clinical performance. Consequently, if ceramics are to be used for dental applications, then clearly more detailed information on the statistical variations in strength combined with the influence of cementation media are required. The effect of adhesive technology has been examined in laboratory and clinical studies. The laboratory studies focused on the effect of cement lute on crown performance, whilst surface degradation and strengthening effects with different systems were examined utilising conventional materials science techniques. Clinical studies focused on the failure rates of conventionally luted and adhesively luted crowns and inlays. There would appear to be evidence from clinical studies that crowns luted with a resin cement and with the placement procedure incorporating a dentine bonding stage have
Vichet Chindavanig วเชฏฐ จนดาวณค
48
49
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
enhanced rates of survival. It is therefore concluded that the available research strongly suggests that the use of resin as a luting material for ceramic restorations is indicated, given the research from three differing sources - laboratory fracture studies comparing restorations luted with resin vs other materials, clinical studies, and laboratory studies examining the surface sealing/strengthening effect of resin on ceramic. Laboratory studies also confirm the enhanced resistance to fracture of crowns cemented with an adhesive procedure.
PMID: 12071631 [PubMed - indexed for MEDLINE]
Int J Prosthodont. 2003 Sep-Oct;16(5):538-42. Links
The influence of different cements on the fracture resistance and marginal adaptation of all-ceramic and fiber-reinforced crowns.
Behr M, Rosentritt M, Mangelkramer M, Handel G.
Department of Prosthodontics, Faculty of Medicine, University of Regensburg, Germany. [email protected]
PURPOSE: This in vitro study investigated the marginal adaptation and fracture resistance of heat-pressed glass-ceramic and fiber-reinforced composite molar crowns luted with resin, resin-modified glass-ionomer, or zinc-oxide-eugenol-free cements. MATERIALS AND METHODS: A total of 24 heat-pressed all-ceramic and 24 glass fiber-reinforced composite crowns were constructed and cemented using the above-mentioned luting agents (eight crowns per cement). The restorations were thermocycled and mechanically stressed, and fracture resistance was determined. Marginal adaptation was evaluated before and after stress application using semiquantitative analysis in a scanning electron microscope. RESULTS: All-ceramic and fiber-reinforced composite crowns reached the highest fracture resistance after stress application in combination with the resin cement. When luted with resin-modified glass-ionomer or zinc-oxide-eugenol-free cements, the fracture resistance of all-ceramics decreased significantly, while the fiber-reinforced composite crowns maintained their fracture resistance level; the lowest values were found for zinc-oxide-eugenol-free cements. The marginal adaptation remained unchanged after stress for all-ceramics and fiber-reinforced composite restorations if they were luted with resin cements. Luting with resin-modified glass-ionomers significantly deteriorated the marginal adaptation after stress application, with the exception of the crown-cement interface of all-ceramics. CONCLUSION: The highest fracture resistance and marginal adaptation were found for all-ceramic and glass fiber-reinforced composite molar crowns if they were luted with resin cement.
PMID: 14651242 [PubMed - indexed for MEDLINE]
J Dent. 2001 Mar;29(3):187-96. Links
Comparison of three types of fiber-reinforced composite molar crowns on their fracture resistance and marginal adaptation.
Behr M, Rosentritt M, Latzel D, Kreisler T.
Vichet Chindavanig วเชฏฐ จนดาวณค
49

50
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Department of Prosthetic Dentistry, University of Regensburg, 93053, Regensburg, Germany. [email protected]
Three types of fiber-reinforced composite (FRC) molar crowns were tested on their fracture resistance and marginal adaptation under simulated oral stress conditions. Two glass fiber systems, one processed with a vacuum/pressure system, the other by manual fiber adaptation, and a polyethylene fiber system were evaluated. Every group consisted of 12 crowns.All crowns were luted adhesively on human molars and exposed to thermal cycling and mechanical loading (TCML: 6000 x 5 degrees C/55 degrees C; 1.2 x 10(6) x 50N; 1.66Hz). The marginal adaptation was evaluated through dye-penetration and analyzed semi-quantitatively with a scanning electron microscope. The fracture resistance was measured using a Zwick universal testing machine.The highest fracture resistance was observed on the glass-fiber systems (FibreKor/Sculpture 1875N +/- 596; Vectris/Targis 1726+/-542), though statistically, the polyethylene system (belleGlass/Connect 1388+/-620) was not significantly weaker. All systems exceeded the fracture resistance required to withstand the maximum masticatory forces expected in the molar region. The marginal adaptation generally had a tendency towards larger gaps after TCML. The crown/composite-cement bond deteriorated significantly after TCML with the manual fiber adaptation and the polyethylene fiber system. The cement/tooth bond strength depended on which composite-cement/dentin-adhesive system was used. CONCLUSION: The fracture resistance of molar crowns made of glass-fiber reinforced composite was higher than those of polyethylene fiber-reinforced composite crowns. However, there was no statistically significant difference. The marginal adaptation seems to depend on the fiber systems and composite-cement/dentin adhesive system used.
PMID: 11306160 [PubMed - indexed for MEDLINE]
Proc Inst Mech Eng H. 2005 Jul;219(4):245-55. Links
Engineering properties and performance of dental crowns.
Mitchell CA, Orr JF.
Division of Restorative Dentistry, School of Dentistry, Queen's University Belfast, Grosvenor Road, Belfast BT12 6BA, UK. [email protected]
Dental crowns are used to replace damaged natural crowns of teeth and are fixed to prepared teeth with luting cements, which should provide an adhesive bond to the tooth structure giving reliable retention and minimal microleakage. Mechanical testing of crowns in vitro gives failure load distributions that are well described by Weibull models, comparing probabilities of survival and reliability. Fatigue testing of crowns is time consuming, but regression analysis to interpolate functions through data points quoting probability limits or applying Weibull analysis is achievable. A complementary approach is to conduct materials tests with appropriate interfacial geometries. Luting cements are used in thin layers of 40-150 microm. Contraction during polymerization is restrained by adhesion to substrates,
Vichet Chindavanig วเชฏฐ จนดาวณค
50

51
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
allowing little relaxation of stresses. Conventional and resin-modified glass ionomer cements create thin zones of interaction with dentine and fail cohesively. The chevron notch short rod technique has been used to measure fracture toughness and rank cements. A development of this method, using chevron notch short bar specimens, permitted fracture toughness to be determined for luting cement--dentine substrate interfaces. Representative fracture experiments need to be developed to apply mixed mode conditions. The basic challenge to predict long-term performance from short-term laboratory tests remains.
PMID: 16050215 [PubMed - indexed for MEDLINE]
Int J Prosthodont. 2006 Mar-Apr;19(2):143-53. Links
A 20-year retrospective survival study of fixed partial dentures.
De Backer H, Van Maele G, De Moor N, Van den Berghe L, De Boever J.
Centre for Special Care, PaeCaMed Research, Unit of Gnathology and Temporomandibular Disorders, Dental School, Faculty of Medicine and Health Sciences, Ghent University, Belgium. [email protected]
PURPOSE: This study of fixed partial dentures (FPDs) evaluated the long-term efficacy and determined frequencies and causes of failures. MATERIALS AND METHODS: A total of 322 FPDs in 193 patients, fabricated at an undergraduate university clinic, were evaluated over a 20-year period. All patients were invited to participate in a supportive maintenance program. Failures of the FPDs were divided into irreversible complications (loss of FPD/abutment) and reversible complications (FPD intact after conservative treatment) and into biologic and technical/patient-related failures. RESULTS: The Kaplan-Meier survival rate after 20 years was 66.2%. Statistically significant differences in survival rates were found between FPDs without post-and-core abutment teeth as compared to FPDs with at least one post-and-core abutment tooth (P = .002) and for vital abutments versus post-and-core abutments (P = .001), but significant differences were not found between restorations in the maxilla and mandible (P = .27). Caries and loss of retention were the main reasons for failure and accounted for 61% of the failures. CONCLUSION: The survival of FPDs by undergraduate students at a university clinic during a 20-year period was comparable to the results published by university departments or general practitioners. Occurrence of a previously reversible complication is a predictive factor for an irreversible complication later on. A reversible complication within the first 2 years will probably lead to an early irreversible complication.
PMID: 16602362 [PubMed - indexed for MEDLINE]
J Dent Res. 2006 Mar;85(3):277-81. Links
Fracture surface analysis of clinically failed fixed partial dentures.
Vichet Chindavanig วเชฏฐ จนดาวณค
51
52
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Taskonak B, Mecholsky JJ Jr, Anusavice KJ.
Department of Restorative Dentistry, Division of Dental Biomaterials, Indiana University, School of Dentistry, 1121 W. Michigan St., Indianapolis, IN 46202, USA. [email protected]
Ceramic systems have limited long-term fracture resistance, especially when they are used in posterior areas or for fixed partial dentures. The objective of this study was to determine the site of crack initiation and the causes of fracture of clinically failed ceramic fixed partial dentures. Six Empress 2 lithia-disilicate (Li(2)O x 2SiO(2))-based veneered bridges and 7 experimental lithia-disilicate-based non-veneered ceramic bridges were retrieved and analyzed. Fractography and fracture mechanics methods were used to estimate the stresses at failure in 6 bridges (50%) whose fracture initiated from the occlusal surface of the connectors. Fracture of 1 non-veneered bridge (8%) initiated within the gingival surface of the connector. Three veneered bridges fractured within the veneer layers. Failure stresses of the all-core fixed partial dentures ranged from 107 to 161 MPa. Failure stresses of the veneered fixed partial dentures ranged from 19 to 68 MPa. We conclude that fracture initiation sites are controlled primarily by contact damage.
PMID: 16498078 [PubMed - indexed for MEDLINE]
PMCID: PMC2242727
Int J Prosthodont. 2005 Nov-Dec;18(6):489-96. Links
A systematic review of the scientific documentation of fixed partial dentures made from fiber-reinforced polymer to replace missing teeth.
Jokstad A, Gökçe M, Hjortsjö C.
Faculty of Dentistry, Department of Prosthetic Dentistry and Oral Function, Institute of Clinical Dentistry, University of Oslo, Oslo, Norway. [email protected]
PURPOSE: Many restorative systems have become commercially available that are based on fiber-reinforced polymers (FRP) for production of fixed partial dentures. However, the clinical documentation of their use has not been systematically reviewed and critically appraised. This systematic review aimed to identify the scientific documentation of all commercially available products within this material group. MATERIALS AND METHODS: MEDLINE was searched for all clinical and laboratory studies on FRP, and papers were browsed to identify product names. Moreover, the Internet was searched to find manufacturers of FRP products. Also, several large trade exhibitions were visited to identify products and manufacturers. All papers that included any data from a clinical setting of an identifiable product were critically appraised. Each product was categorized according to the scientific clinical documentation of their intended clinical use. RESULTS: Eleven commercial products were identified. The scientific clinical documentation of these products varied markedly, but was generally poor. No randomized controlled trials have been carried out on FRPs versus, eg, conventional treatments, nor are any long-term cohort studies available. None of the products demonstrate good evidence for usage as a technical solution to permanently replace lost
Vichet Chindavanig วเชฏฐ จนดาวณค
52
53
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
teeth. CONCLUSION: The use of FRP for fixed partial dentures must still be regarded as experimental.
PMID: 16335168 [PubMed - indexed for MEDLINE]
Int J Prosthodont. 2005 Sep-Oct;18(5):371-6. Links
Long-span, fixed-movable, resin-bonded fixed partial dentures: a retrospective, preliminary clinical investigation.
Botelho MG, Dyson JE.
Prince Philip Dental Hospital, University of Hong Kong, 34 Hospital Rd, Sai Ying Pun, Hong Kong, SAR China. [email protected]
PURPOSE: Long-span, resin-bonded fixed partial dentures (FPDs) have been associated with higher debonding rates than short-span prostheses. The use of modified nonrigid connectors that allow movement between the abutments in long-span resin-bonded prostheses may reduce harmful interabutment forces that stress the metal framework and resin-bonded interface. This preliminary investigation aimed to evaluate the longevity of long-span resin-bonded FPDs of 4 or more units with a modified nonrigid connector and increased extension of the retainer framework around the major abutment. MATERIALS AND METHODS: Thirty-eight patients attended a clinical examination; each had been provided with 1 or more resin-bonded FPD of 4 or more units (43 prostheses). For each patient, the following data were recorded: gender, age, cementation date, and endodontic treatment, if performed. Data regarding the occurrence of any debondings and patient expectations were also recorded. RESULTS: The mean service life for the 43 prostheses was 46.9 months (SD 22.0), with a range of 12 days to 87 months. Three prostheses had debonded, resulting in a clinical retention rate of 92.2%. CONCLUSION: Long-span resin-bonded FPDs incorporating nonrigid connectors that allow independent movement between the major and minor retainer, combined with increased framework extension on the major abutment, appear successful in the short term. Further research is required to determine their long-term efficacy.
PMID: 16220800 [PubMed - indexed for MEDLINE]
Long-term clinical evaluation of fixed dentures--two to fifteen years after insertion.
Hubálková H, Charvát J, Dostálová T, Linetskiy I.
Department of Stomatology of the First Faculty of Medicine, Charles University in Prague, Czech Republic. [email protected]
Fixed denture durability is characterized as a period of time for which a dental appliance satisfies functional and esthetic requirements. First of all, its durability is based on the properties of materials it is made of, and depends, at the same time, on the characteristics
Vichet Chindavanig วเชฏฐ จนดาวณค
53
54
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
of biological environment, in which the denture is placed. The purpose of this study was a long-term monitoring of changes taking place in the fixed dental constructions during their application in the oral cavity. These changes were to be evaluated for different types of materials used for fixed dentures manufacturing, namely metal alloys, ceramics, and plastics. A set of 454 full crowns from 134 patients divided in 6 clinical studies was examined and both qualitative and quantitative changes evaluated after 2 and 8 to 15 years after cementation. Clinical assessment adopted the United States Public Health Service System criteria. Alloys of precious metals veneered with ceramics are considered the optimal method of choice for both high precision of execution and consideration of future changes brought on by the use of the dentures.
PMID: 16007909 [PubMed - indexed for MEDLINE]
Dent Update. 2008 Oct;35(8):551-2, 555-8. Links
Techniques for restoring worn anterior teeth with direct composite resin.
Robinson S, Nixon PJ, Gahan MJ, Chan MF.
Leeds Dental Institute, Leeds, UK.
Toothwear is increasing in prevalence. Traditional treatment methods for moderate or advanced toothwear, such as indirect restorations and crown lengthening surgery, are invasive and destructive of remaining tissues. The 'Dahl technique' has been used to obtain space for anterior restorations and has been modified such that direct composite restorations are placed at increased occlusal vertical dimension. These restorations have proved durable and aesthetic, protect tooth structure and posterior occlusal contact is predictably re-established. The authors describe and compare two techniques using composite resin to treat localized anterior toothwear in a general practice setting. Clinical Relevance: Toothwear is a significant clinical problem and general dental practitioners and specialists alike must be familiar with the available conservative treatment options.
PMID: 19055092 [PubMed - indexed for MEDLINE]
Dent Update. 2004 Oct;31(8):442-4, 446-7. Links
Reviewing the concept of Dahl.
Saha S, Summerwill AJ.
Department of Restorative Dentistry, Birmingham Dental Hospital.
Toothwear may have a multifactorial aetiology but is often localized to the upper anterior teeth. This is normally accompanied by a loss of interocclusal space. This paper aims to outline the management of localized anterior toothwear. It discusses several options
Vichet Chindavanig วเชฏฐ จนดาวณค
54
55
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
available to create space for anterior restoration, with particular reference to the use of the 'Dahl' technique. Dahl described a non-invasive technique to create increased interocclusal space. The increased space eliminates the need for further occlusal reduction during crown preparation which is ideal in the worn dentition. This paper illustrates and describes the clinical applications of Dahl's original technique.
PMID: 15554048 [PubMed - indexed for MEDLINE]
Eur J Prosthodont Restor Dent. 1997 Dec;5(4):175-80. Links
Fixed prostheses in the treatment of tooth wear.
Briggs P, Bishop K.
King's Dental Institute, London, UK.
The restorative implications of tooth wear are often complicated by the age of the patient, the destructive nature and aesthetic compromise of conventional fixed restorations and the lack of inter-occlusal space. This paper focuses on the fixed prosthetic treatment options for such patients and the utilisation of fixed restorations to create inter-occlusal space.
PMID: 9680876 [PubMed - indexed for MEDLINE]
Dent Update. 2001 Apr;28(3):118-23. Links
A question of space: options for the restorative management of worn teeth.
Dyer K, Ibbetson R, Grey N.
Edinburgh Dental Institute.
The prevalence of tooth surface loss has increased in recent years. The essence of management is an effective preventive regime; however, in many instances restoration may also be necessary. A number of strategies is available for creating sufficient space to enable restoration and several techniques for restoration known. This article reviews the significance of the vertical dimension of occlusion and describes the restorative management of a patient affected by severe tooth wear.
PMID: 11819971 [PubMed - indexed for MEDLINE]
Am J Orthod Dentofacial Orthop. 2009 Jun;135(6):696.e1-8; discussion 696-7. Links
An engineering analysis of dental occlusion principles.
Vichet Chindavanig วเชฏฐ จนดาวณค
55
56
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Katona TR.
Department of Orthodontics and Oral Facial Genetics, School of Dentistry, Indiana University, Indianapolis, IN 46202-5186, USA. [email protected]
INTRODUCTION: The purpose of this study was to develop an analytical model of contacting teeth, based on principles of basic engineering statics. The model would be used to demonstrate the interactions between occlusal contacts and tooth loading (forces and moments) and to critique occlusion-related dogma. METHODS: Free-body diagrams were drawn to depict 2 teeth in occlusal contact. In combination with the concept of the center of resistance, the governing equilibrium equations were derived and used to solve for the forces and moments on the teeth and to investigate the influences of tripod and cusp-fossa occlusal schemes. RESULTS: With a specific load on a tooth, it was demonstrated that the load on the opposing tooth and the concomitant occlusal scheme dictated crown-crown contact forces that can be computed. CONCLUSIONS: This engineering analysis suggests flaws in widely held notions about the mechanics of occlusion. Loading that is generally considered clinically desirable is certain to produce undesirable loading on the opposing tooth. The complex relationships between the loads on teeth and crown-crown occlusal contacts make it virtually impossible to control tooth loading with occlusal equilibration. For computational and conceptual reasons, it is essential to consider the center of resistance.
PMID: 19524821 [PubMed - in process]
J Oral Rehabil. 2009 Jun;36(6):435-41. Epub 2009 May 5. Links
Effect of non-working occlusal contacts on vertical condyle position.
Seedorf H, Weitendorf H, Scholz A, Kirsch I, Heydecke G.
Department of Prosthetic Dentistry, University Medical Center Hamburg-Eppendorf, Hamburg, Germany. [email protected]
The presence of non-working occlusal contacts is often considered harmful for the temporomandibular joint. Thus, the purpose of this study was to investigate the effect of non-working occlusal contacts on the condylar position during submaximal and maximal clenching. The study comprised 22 healthy subjects having a canine-guided occlusion. None of them had a third molar and none of them had a missing tooth or showed tooth mobility. All subjects clenched on (i) the canine, (ii) the canine while a stiff bite registration material was positioned between the second premolar and the first molar on the non-working side. The clenching level was controlled by surface electromyography of the masseter muscle. During clenching, the vertical and horizontal condylar position was predicted using six degrees of freedom ultrasonic motion analyser. Clenching on the canine caused a cranial movement of the non-working side condyle. This movement was reduced by 0.6-0.9 mm when the subjects clenched while the artificial non-working side contacts were in place. These results indicate that the contacts on the non-working side may be able to prevent upward joint movement.
PMID: 19422437 [PubMed - in process]
Vichet Chindavanig วเชฏฐ จนดาวณค
56
57
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
J Prosthodont Res. 2009 Jan;53(1):3-10. Epub 2008 Oct 7. Links
Critical review of some dogmas in prosthodontics.
Carlsson GE.
Department of Prosthetic Dentistry, The Sahlgrenska Academy, University of Gothenburg, Box 450, SE 405 30 Göteborg, Sweden. [email protected]
PURPOSE: In prosthodontics like in other dental disciplines there are many clinical procedures that lack support of good evidence, which means that the effect is unknown, and even worse, we do not know if they do more good than harm. It is the aim of this paper to review current evidence for selected procedures based on a scrutiny of the prosthodontic literature. STUDY SELECTION: A MEDLINE/PubMed search was conducted for articles on the selected items with a focus on best available evidence. RESULTS: Many "old truths" regarding prosthodontic interventions can be called dogmas, opinions based more on belief than scientific evidence. There is, for example, lack of evidence to support the opinion that a face-bow is necessary in the fabrication of prostheses, and many theories related to occlusion are not evidence-based. Some such dogmas in various areas of the discipline are exemplified and discussed in the article. CONCLUSION: A scrutiny of the prosthodontic literature indicates that many common clinical procedures lack scientific support. In the era of evidence-based dentistry, ineffective interventions should be eliminated and decisions should be made on best available evidence.
PMID: 19318064 [PubMed - in process]
Publications relating to occlusal rehabilitation Vichet Chindavanig
J Craniofac Surg. 2009 Jun 19. [Epub ahead of print] Links
Fabrication of an Auricular Prosthesis Using Computed Tomography and Rapid Prototyping Technique.
Karayazgan-Saracoglu B, Gunay Y, Atay A.
From the *Department of Prosthodontics, Faculty of Dentistry, Baskent University; and daggerGATA Military Training Hospital, Dental Clinic, Istanbul, Turkey.
This article describes the use of computed tomography and rapid prototyping method to produce a wax pattern of a missing ear. Computed tomographic scans were obtained from the patient, and a three-dimensional digital image was produced using a computer-aided design software. Then, the image of the present ear was extracted, and its mirror image was obtained with the software. The pattern of the inverted three-dimensional cast was produced using a rapid prototyping machine. The
Vichet Chindavanig วเชฏฐ จนดาวณค
57

58
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
cast was duplicated in wax of identical dimensions and shape of the opposing ear, and the auricular prosthesis was fabricated with traditional methods.
PMID: 19553846 [PubMed - as supplied by publisher]
J Prosthodont. 2009 Jun 10. [Epub ahead of print] Links
Esthetic Interim Acrylic Resin Prosthesis Reinforced with Metal Casting.
Verri FR, Pellizzer EP, Mazaro JV, de Almeida EO, Antenucci RM.
Professor of Dental Prostheses, Implants, and Occlusion, Adamantina School of Dentistry, Adamantina, Brazil.
Fabrication of an interim prosthesis is an important procedure in oral rehabilitation because it aids in determining the esthetics, phonetics, and occlusal relationship of the definitive restoration. The typical material (acrylic resin) used in interim prostheses commonly fails due to fractures. During extended oral rehabilitation with fixed partial prostheses, high strength interim prostheses are often required to protect hard and soft tissues, avoid dental mobility, and to allow the clinician and patient a chance to evaluate cosmetics and function before the placement of the definitive prosthesis. Furthermore, a satisfactory interim prosthesis can serve as a template for the construction of the definitive prosthesis. The maintenance of this prosthesis is important during treatment for protection of teeth and occlusal stability. Procedures to reinforce interim prostheses help to improve performance and esthetics in long-term treatment. Due to the low durability of acrylic resin in long-term use, the use of reinforcing materials, such as metal castings or spot-welded stainless steel matrix bands, is indicated in cases of extensive restoration and long-term treatment. This paper describes an easy technique for fabricating a fixed interim prosthesis using acrylic resin and a cast metallic reinforcement.
PMID: 19519710 [PubMed - as supplied by publisher]
J Oral Rehabil. 2009 Feb;36(2):102-9. Links
A novel statistical model for mandibular helical axis analysis.
Hayashi K, Reich B, DeLong R, Lee SP, Mizoguchi I.
Department of Orthodontics and Dentofacial Orthopedics, School of Dentistry, Health Sciences University of Hokkaido, Ishikari-Tobetsu, Hokkaido, Japan. [email protected]
The purpose of this study was to establish a new statistical method for the analysis of noisy mandibular helical axis parameters, especially the position vector of the finite helical axis (FHA). The subjects were children with anterior cross-bite who had received orthodontic treatment. Maximum mouth-opening was measured by means of an opto-electronic motion analysis system. These movements were compared with similar movement in the same group after treatment of their anterior cross-bite. Each curve of FHA position vectors was modelled as a spline function with random coefficients. To determine the optimal number of knots, two criteria were used: deviance information criteria (DIC) and mean
Vichet Chindavanig วเชฏฐ จนดาวณค
58
59
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
squared prediction error (MSE). We were interested in estimating a typical curve for a population. Self-modelling regression (SEMOR) was extended to three dimensions to model groups of three-dimensional curves. Each curve was modelled as a spline function using nine knots. Population average curves were created using SEMOR. This study provided detailed information about jaw movement for comparing cross-bite to normal occlusion by calculating the population mean curves of the position vector of the FHA. Our results suggested that the two population mean curves for the position vector of the FHA were significantly different in the closing phase. The combination of a spline function with random coefficients and SEMOR extended to three dimensions can be used not only for FHA analysis but also for the analysis of other jaw movements.
PMID: 19522894 [PubMed - in process]
N Y State Dent J. 2009 Jan;75(1):39-43. Links
Rationale and technique for achieving occlusal harmony.
Kimmel SS.
For a patient to function normally with natural or restored dentition, the occlusal contacts should be in harmony with the musculature and the temporomandibular joint. Many times, this harmonious relationship is altered by restorative treatment, periodontal disease or tooth loss. If the adaptive capacity of the patient is less than the forces placed upon the tooth or restoration, failure in one form or another often results. This article presents a rational method the dentist can use to recognize and understand the markings made with articulating paper so that harmonious contacts can be detected and contacts that disturb occlusal harmony eliminated.
PMID: 19280827 [PubMed - indexed for MEDLINE]
Pract Proced Aesthet Dent. 2008 Nov-Dec;20(10):619-26. Links
Increasing vertical dimension: considerations and steps in reconstruction of the severely worn dentition.
Cutbirth ST.
Center for Aesthetic and Restorative Dentistry (CARD), Dallas, TX, USA. [email protected]
Clinicians often encounter dental patients who have lost tooth structure or demonstrate an insufficient vertical dimension of occlusion (VDO). While reconstructing the proper VDO for such patients can be challenging, the use of a systematic approach can facilitate a successful and predictable treatment outcome. Presented herein are a series of considerations involved in managing and/or restoring the VDO and a reproducible clinical protocol aimed at improving the dentist's ability to increase the VDO while reconstructing severely worn dentition.
PMID: 19274959 [PubMed - indexed for MEDLINE]
Vichet Chindavanig วเชฏฐ จนดาวณค
59
60
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Int J Periodontics Restorative Dent. 1998 Feb;18(1):46-57. Links
Restoration of the severely worn dentition using a systematized approach for a predictable prognosis.
Stewart B.
Pankey Institute, Key Biscayne, Florida, USA. [email protected]
Dental literature supports the concept that vertical dimension of occlusion is normally not lost in severely worn dentition, and the bite should generally not be opened to facilitate dental reconstruction. However, restoration of a periodontally sound but severely worn dentition, at existing vertical dimension, frequently presents unique challenges in patient management, diagnosis, treatment planning, and restorative methodology. This report reviews and demonstrates an integrated and planned approach to this complex treatment situation that can lead to a favorable and predictable prognosis. The approach also allows a practitioner free use of various techniques if certain goals of occlusion are followed.
PMID: 9558556 [PubMed - indexed for MEDLINE]
Pract Proced Aesthet Dent. 2008 Nov-Dec;20(10):619-26. Links
Increasing vertical dimension: considerations and steps in reconstruction of the severely worn dentition.
Cutbirth ST.
Center for Aesthetic and Restorative Dentistry (CARD), Dallas, TX, USA. [email protected]
Clinicians often encounter dental patients who have lost tooth structure or demonstrate an insufficient vertical dimension of occlusion (VDO). While reconstructing the proper VDO for such patients can be challenging, the use of a systematic approach can facilitate a successful and predictable treatment outcome. Presented herein are a series of considerations involved in managing and/or restoring the VDO and a reproducible clinical protocol aimed at improving the dentist's ability to increase the VDO while reconstructing severely worn dentition.
PMID: 19274959 [PubMed - indexed for MEDLINE]
J Prosthodont. 2007 Jul-Aug;16(4):277-81. Epub 2007 Jun 9. Links
The use of a diagnostic matrix in the management of the severely worn dentition.
Doan PD, Goldstein GR.
The Jonathan and Maxine Ferencz Advanced Education Program in Prosthodontics, New York University College of Dentistry, New York, NY, USA. [email protected]
Vichet Chindavanig วเชฏฐ จนดาวณค
60
61
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
The management of the interim phase of a complete oral rehabilitation in patients with severely worn dentition is often challenging due to loss of occlusal vertical dimension, loss of tooth structure, uneven wear of teeth creating an uneven plane of occlusion, and para-functional habits. This paper will demonstrate how a clear thermo-forming matrix fabricated from the diagnostic wax-up can be used as a guide to facilitate treatment.
PMID: 17559528 [PubMed - indexed for MEDLINE]
Pract Proced Aesthet Dent. 2008 Nov-Dec;20(10):619-26. Links
Increasing vertical dimension: considerations and steps in reconstruction of the severely worn dentition.
Cutbirth ST.
Center for Aesthetic and Restorative Dentistry (CARD), Dallas, TX, USA. [email protected]
Clinicians often encounter dental patients who have lost tooth structure or demonstrate an insufficient vertical dimension of occlusion (VDO). While reconstructing the proper VDO for such patients can be challenging, the use of a systematic approach can facilitate a successful and predictable treatment outcome. Presented herein are a series of considerations involved in managing and/or restoring the VDO and a reproducible clinical protocol aimed at improving the dentist's ability to increase the VDO while reconstructing severely worn dentition.
PMID: 19274959 [PubMed - indexed for MEDLINE]
Gen Dent. 2003 Jan-Feb;51(1):70-4; quiz 75-6. Links
Erratum in:
Gen Dent. 2003 Mar-Apr;51-2.
Rehabilitating a patient with bruxism-associated tooth tissue loss: a literature review and case report.
Yip KH, Chow TW, Chu FC.
Faculty of Dentistry, University of Hong Kong, China.
Tooth tissue loss from bruxism has been demonstrated to be associated with various dental problems such as tooth sensitivity, excessive reduction of clinical crown height, and possible changes of occlusal relationship. A literature search revealed a number of treatment modalities, with an emphasis on prevention and rehabilitation with adhesive techniques. Rehabilitating a patient with bruxism-associated tooth tissue loss to an acceptable standard of oral health is clinically demanding and requires careful diagnosis and proper treatment planning. This article describes the management of excessive tooth tissue loss in a 43-year-old woman with a history of bruxism. The occlusal vertical dimension of the patient was re-established with the use of an acrylic maxillary occlusal splint,
Vichet Chindavanig วเชฏฐ จนดาวณค
61
62
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
followed by resin composite build-up. Full-mouth oral rehabilitation ultimately involved constructing multiple porcelain veneers, adhesive gold onlays, ceramo-metal crowns, and fixed partial dentures.
PMID: 15061339 [PubMed - indexed for MEDLINE]
Pract Proced Aesthet Dent. 2008 Mar;20(2):81-7; quiz 88, 121. Links
A systematic approach to full-mouth reconstruction of the severely worn dentition.
Lerner J.
Aesthetic and functional restoration of the severely worn dentition represents a significant clinical challenge. One of the most demanding aspects of such cases involves the development of sufficient restorative space, while simultaneously fulfilling aesthetic, occlusal, and functional parameters essential to long-term success. When evaluating and diagnosing a patient with severely worn dentition, emphasis must be placed on the occlusal prematurities preventing condylar seating into the centric relation position. Success in maintaining severe wear cases depends on the development of proper anterior guidance to allow for posterior disclusion within the patient's envelope of function.
PMID: 18478894 [PubMed - indexed for MEDLINE]
Eur J Dent. 2009 Jan;3(1):75-80. Links
The use of zirconium and feldspathic porcelain in the management of the severely worn dentition: a case report.
Malkoc MA, Sevimay M, Yaprak E.
Research Assistant, Selcuk University, Faculty of Dentistry, Department of Prosthodontics, Konya, Turkey.
The management of the interim phase of a complete oral rehabilitation in patients with severely worn dentition is often challenging due to the loss of occlusal vertical dimension, loss of tooth structure, uneven wear of teeth creating an uneven plane of occlusion, and parafunctional habits. This case report describes the management of excessive tooth tissue loss in a 45 year old woman with a history of bruxism, esthetical complaints in anterior teeth, and impaired dental function due to reduced tooth height. The patient used occlusal splint for a month and than resection of the alveolar bone was performed on the vestibular sides of the maxillary anterior teeth, except the interdental alveolar crest. Maxillary anterior teeth were restored with zirconia porcelain. Feldspathic porcelain was chosen to restore remaining teeth in both jaws; the patient also was given an occlusion guard to protect the restoration against future bruxism. Regardless of the cause of occlusal instability, it is important that the restorative dentist should be able to recognize its signs such as tooth hypermobility, tooth wear, periodontal breakdown, occlusal dimpling, stress fractures,
Vichet Chindavanig วเชฏฐ จนดาวณค
62
63
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
exostosis, muscle enlargement, and loss of posterior disclusion. When restoring the worn dentition, the clinician should bear in mind the five P's: proper planning prevents poor performance.
PMID: 19262736 [PubMed - in process]
PMCID: PMC2647964
J Esthet Restor Dent. 2008;20(4):251-63; discussion 264-5. Links
Utilization of multiple restorative materials in full-mouth rehabilitation: a clinical report.
Nam J, Raigrodski AJ, Heindl H.
Graduate Prosthodontics, Department of Restorative Dentistry, School of Dentistry, University of Washington, Seattle, WA, USA.
Many different restorative materials are currently available for use in modern dentistry. Clinicians and dental technicians should be able to choose the most suitable materials for each patient based on research, anecdotal evidence, clinical experience, as well as patient's expectations and desires. The purpose of this article is to share the challenges presented in full-mouth rehabilitation and to describe the considerations in selecting three different restorative materials to achieve a successful restoration in terms of biomechanics, function, and esthetics. CLINICAL SIGNIFICANCE: Interdisciplinary treatment planning, knowledge of available restorative materials, sequencing treatment modalities, and adequate communication between all parties involved are key to a successful treatment outcome when pursuing full-mouth restorative rehabilitation.
PMID: 18767998 [PubMed - indexed for MEDLINE]
Gen Dent. 2007 Sep-Oct;55(5):426-8. Links
Tooth preparation design for anterior abutments of resin-bonded fixed partial dentures: a technical report.
Shimizu H, Takahashi Y.
Department of Oral Rehabilitation, Fukuoka Dental College, Japan.
One challenged associated with the placement of maxillary resin-bonded fixed partial dentures (RBFPDs) that include anterior abutments is creating an effective preparation design to ensure mechanical retention of the dentures and anterior-guided occlusion. This article presents a methodical preparation design for anterior abutments of RBFPDs. One innovative feature involves extending the reduction to part of the occlusal wear facets. This
Vichet Chindavanig วเชฏฐ จนดาวณค
63
64
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
design makes it possible to preserve the patient's innate occlusal function and to hold the retainer firmly by means of applied occlusal force.
PMID: 17899720 [PubMed - indexed for MEDLINE]
Gerodontology. 2007 Jun;24(2):105-10. Links
Electromyographic evaluation of masseter and anterior temporalis muscles in rest position of edentulous patients with temporomandibular disorders, before and after using complete dentures with sliding plates.
Zuccolotto MC, Vitti M, Nóbilo KA, Regalo SC, Siéssere S, Bataglion C.
Discipline of Complete Denture Prosthetics and Occlusion, School of Dentistry, University of Ribeirão Preto (UNAERP), Brazil.
OBJECTIVES: This study was performed with the purpose of investigating electromyographic (EMG) activity of the anterior temporalis and masseter muscles in edentulous individuals with temporomandibular disorder (TMD), before and after using sliding plates on complete dentures in the mandibular rest position. BACKGROUND: Edentulous patients may present TMD, which is characterised by pain in temporomandibular joints, masticatory and neck muscles, uncoordinated and limited mandible movements, joint sounds and an altered occlusal relationship. It is imperative to offer treatment in order to re-establish stomatognathic system structures before submitting the individual to any definitive restorative treatment. MATERIALS AND METHODS: The patients were edentulous for at least 10 years. EMG recordings were made before the insertion of the dentures (0 months) and also after using the sliding plates at the fourth month, 9th month and 12th month, using computerised electromyography K6-I/ EMG Light Channel Surface. EMG evaluations of the muscles were performed under the following clinical conditions: rest position with dentures (R1), rest position without dentures (R2), rest position with dentures post-activity (chewing) (R3), rest position without dentures post-activity (chewing) (R4). RESULTS: All patients obtained remission of muscular fatigue and reduced pain in stomatognathic system structures. Temporalis muscle showed significant increase in EMG activity compared with initial values (p < 0.01). Masseter muscles showed significantly lower mean values (p < 0.01) compared with initial values. CONCLUSION: The sliding plates allowed the process of neuromuscular deprogramming, contributing to muscular balance of the masticatory system, and are therefore indicated to be used before the fabrication of definitive complete dentures in patients with TMD.
PMID: 17518958 [PubMed - indexed for MEDLINE]
N Y State Dent J. 2006 Apr-May;72(3):32-5. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
64

65
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Maxillary and mandibular overlay removable partial dentures for restoration of worn teeth. A three-year follow-up.
Almog DM, Ganddini MR.
Department of Oral Diagnostic Sciences, University of Buffalo School of Dental Medicine, USA.
This clinical report describes the fabrication and a three-year follow-up of maxillary and mandibular cast overlay removable partial dentures for the restoration of severely worn dentition with accompanying loss of vertical dimension of occlusion. The frameworks supported porcelain veneers for esthetics, and metal occlusal surfaces for strength and durability.
PMID: 16774170 [PubMed - indexed for MEDLINE]
Int J Orofacial Myology. 2008 Nov;34:5-14. Links
Republished from:
Int J Orofacial Myology. 2005 Nov;31:5-14.
A retrospective and prospective view of orofacial myology.
Mason RM.
Department of Communication Sciences and Disorders, University of North Carolina-Greensboro, USA. [email protected]
Orofacial myofunctional disorders include specific conditions or behaviors that can have a negative impact on oral postures and functions. Historically, interest has focused on behaviors in the horizontal plane, highlighted by tongue thrusting. Currently, the scope of practice also includes tongue forward posturing, lip incompetence, open mouth rest posture, thumb and finger sucking, bruxism, and biting habits involving lips, fingers, tongue and cheeks. The common denominator for myofunctional conditions is a change in the inter-dental arch vertical rest posture dimension, the dental freeway space. The purposes of myofunctional therapy include normalizing the freeway space dimension by eliminating noxious habits or postures related to freeway space change. Improving cosmesis with a lips-together rest posture is also an important treatment goal. The clinical significance of the freeway space is explained in terms of the dental consequences of differential eruption patterns that can develop from postural modification of the freeway space. When the freeway space is opened for extended periods beyond the normal range, the tongue can act as a functional appliance and contribute to the development of anterior open bite or a Class II malocclusion. A clinical procedure is proposed for evaluating the freeway space dimension and incorporating the information into treatment planning and evaluation of treatment success. While dentistry/orthodontics has a primary focus on dental occlusion, or teeth-
Vichet Chindavanig วเชฏฐ จนดาวณค
65
66
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
together relationships, orofacial myologists focus on teeth-apart behaviors and postures that can lead to, or have already resulted in malocclusion.
PMID: 19545087 [PubMed]
Clin Oral Investig. 2009 Jun 18. [Epub ahead of print] Links
Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea.
Aarab G, Lobbezoo F, Hamburger HL, Naeije M.
Department of Oral Function, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and VU University Amsterdam, Louwesweg 1, 1066 EA, Amsterdam, The Netherlands, [email protected].
The aim of the study was to assess the influence of four mandibular protrusion positions, at a constant vertical dimension, on obstructive sleep apnea (OSA). Seventeen OSA patients (49.2 +/- 8.5 years) received an adjustable mandibular advancement device (MAD). The patients underwent four polysomnographic recordings with their MAD in situ at, in random order, 0%, 25%, 50%, and 75% of the maximum protrusion. The mean apnea-hypopnea index (AHI) values of the patients differed significantly between the protrusion positions (P < 0.000). The 25% protrusion position resulted in a significant reduction of the AHI with respect to the 0% position, while in the 50% and 75% positions, even lower AHI values were found. The number of side effects was larger starting at the 50% protrusion position. We therefore recommend coming to a weighted compromise between efficacy and side effects by starting a MAD treatment in the 50% protrusion position.
PMID: 19536571 [PubMed - as supplied by publisher
Am J Orthod Dentofacial Orthop. 2009 Apr;135(4):438-41. Links
Glenoid fossa position in Class III malocclusion associated with mandibular protrusion.
Innocenti C, Giuntini V, Defraia E, Baccetti T.
Department of Orthodontics, University of Florence, Florence, Italy.
INTRODUCTION: Our aim in this study was to investigate the position of the glenoid fossa in subjects with Class III malocclusion associated with mandibular protrusion to better clarify the role of this craniofacial component in Class III skeletal disharmony. METHODS: A sample of 30 subjects, aged 8 years +/- 6 months, with skeletal and dental Class III malocclusion associated with mandibular protrusion, normal skeletal vertical relationships, and normal mandibular dimensions, was compared with a control group of 33 subjects with skeletal and
Vichet Chindavanig วเชฏฐ จนดาวณค
66
67
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
dental Class I relationships. The comparisons between the Class III group and the control group on the cephalometric measures for the assessment of glenoid fossa position were performed with the Mann-Whitney U test at P <0.05. RESULTS: Subjects with Class III malocclusion had a significantly more mesial position of the glenoid fossa, when compared with the control group as measured with 3 parameters. CONCLUSIONS: An anterior position of the glenoid fossa is a possible diagnostic anatomic feature of Class III malocclusion associated with mandibular protrusion. An effective measurement to evaluate glenoid fossa position in craniofacial relationships is the cephalometric distance from the glenoid fossa to the frontomaxillary-nasal suture.
PMID: 19361728 [PubMed - indexed for MEDLINE
Quintessence Int. 2008 Oct;39(9):727-32. Links
Evaluation of vertical accuracy of interocclusal recording materials.
Ghazal M, Ludwig K, Habil RN, Kern M.
Department of Prosthodontics, Propaedeutics, and Dental Materials, School of Dentistry, Christian-Albrechts University at Kiel, Kiel, Germany.
OBJECTIVE: To evaluate 4 interocclusal recording materials for their ability to reproduce accurately interocclusal relationships after a storage time of 1 or 48 hours. METHOD AND MATERIALS: A custom-made metal apparatus was used to simulate the maxilla and mandible. The vertical discrepancies were measured by a precision dial gauge. Eight inter-occlusal records were made in each of the following groups: (G1) Futar D (polyvinyl siloxane; Kettenbach), (G2) Ramitec (polyether; 3M ESPE), (G3) LuxaBite (composite resin based on bisacryl; DMG), (G4) Aluwax (aluminum wax; Aluwax Dental Products), (G5) LuxaBite corrected with LuxaBite, and (G6) LuxaBite corrected with Aluwax. The vertical discrepancies were measured after storage of the records for 1 and 48 hours at room temperature and repositioning of the records in the metal apparatus. Data were statistically analyzed using 1-way analysis of variance followed by the Games-Howell test (P < or = .05). RESULTS: After storage times of 1 and 48 hours, respectively, the mean vertical discrepancies (microm) for G1 (23/33) and G2 (25/30) were statistically significantly lower than for G3 (431/745) and G4 (110/151) (P < .05) but higher than for G5 (8/16) and G6 (7/17). There was no statistically significant difference between G1 and G2 or between G5 and G6 for either measurement. CONCLUSION: These vertical discrepancies increased after a storage time of 48 hours. However, correction of the LuxaBite records with LuxaBite or Aluwax showed significantly lower vertical discrepancies than all other materials. Clinically, the vertical discrepancies the corrected records caused could be insignificant.
PMID: 19093044 [PubMed - indexed for MEDLINE]
Dent Update. 2008 Oct;35(8):551-2, 555-8. Links
Vichet Chindavanig วเชฏฐ จนดาวณค
67
68
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Techniques for restoring worn anterior teeth with direct composite resin.
Robinson S, Nixon PJ, Gahan MJ, Chan MF.
Leeds Dental Institute, Leeds, UK.
Toothwear is increasing in prevalence. Traditional treatment methods for moderate or advanced toothwear, such as indirect restorations and crown lengthening surgery, are invasive and destructive of remaining tissues. The 'Dahl technique' has been used to obtain space for anterior restorations and has been modified such that direct composite restorations are placed at increased occlusal vertical dimension. These restorations have proved durable and aesthetic, protect tooth structure and posterior occlusal contact is predictably re-established. The authors describe and compare two techniques using composite resin to treat localized anterior toothwear in a general practice setting. Clinical Relevance: Toothwear is a significant clinical problem and general dental practitioners and specialists alike must be familiar with the available conservative treatment options.
PMID: 19055092 [PubMed - indexed for MEDLINE]
J Prosthet Dent. 2008 Oct;100(4):320-2. Links
Simple technique to transfer occlusal vertical dimension and articulate a definitive implant cast for a full arch implant prosthesis.
Papaspyridakos P, Lal K.
Division of Prosthodontics, Columbia University College of Dental Medicine, New York, NY 10032, USA.
PMID: 18922262 [PubMed - indexed for MEDLINE]
J Prosthodont. 2009 Jan;18(1):64-70. Links
Fixed rehabilitation of an ACP PDI class III patient with amelogenesis imperfecta.
Sadighpour L, Geramipanah F, Nikzad S.
Department of Prosthodontics, School of Dentistry, Medical Science, Tehran University, Tehran, Iran.
This clinical report describes the oral rehabilitation of a 19-year-old woman diagnosed with hypoplastic-type amelogenesis imperfecta (AI). She presented with discolored and mutilated teeth, missing teeth, anterior open bite, and posterior short crowns. She was classified as an American College of Prosthodontists Prosthodontic Diagnostic Index (ACP PDI) class III patient. The aim of treatment was to restore esthetics and improve masticatory function.
Vichet Chindavanig วเชฏฐ จนดาวณค
68
69
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
The patient's esthetic and functional expectations were successfully attained with porcelain laminate veneers and all-ceramic and metal-ceramic restorations after extensive crown lengthening. The patient was regularly recalled during the postoperative period. Loss of retention of one all-ceramic crown and minimal recession of the gingiva of one laminate veneer were noted at 4-year recall.
PMID: 18798781 [PubMed - indexed for MEDLINE
Dentomaxillofac Radiol. 2008 Jul;37(5):293-9. Links
Comparison of transcranial radiograph and magnetic resonance imaging in the evaluation of mandibular condyle position.
Menezes AV, de Almeida SM, Bóscolo FN, Haiter-Neto F, Ambrosano GM, Manzi FR.
Oral Radiology, School of Dentistry of Piracicaba - UNICAMP, Brazil. [email protected]
OBJECTIVES: Several image modalities have been used to assess the condylar position in the glenoid fossa. However, despite the development of more advanced techniques for imaging the temporomandibular joint (TMJ), the transcranial projection remains widely used in dentistry. The purpose of this study was to compare the condylar position in transcranial radiography (TRANS) with MRI. METHODS: 70 matched pairs of TMJs (35 patients) who had undergone TRANS and MRI were evaluated. The TRANS scans were compared with the lateral, central and medial MRI scans, and the condylar position was assessed in the closed and open mouth position according to subjective and objective methods. The sensitivity, specificity and accuracy values were calculated for each group and Bowker's test was used to analyse the data. RESULTS: There was no statistical significance between TRANS and MRI (P > 0.05). However, even though there were similar mean values between them, the comparison with the lateral image showed higher values, which might be due to TRANS representing the lateral one-third of the condyle. CONCLUSIONS: It can be concluded that TRANS seems to be an acceptable method and its applicability as an adjunctive method in the condylar position should not be rejected.
PMID: 18606752 [PubMed - indexed for MEDLINE]
Oper Dent. 2008 May-Jun;33(3):332-7. Links
Esthetic restorative materials and opposing enamel wear.
Olivera AB, Marques MM.
Departamento de Dentistica, Universidade de São Paulo, São Paulo, SP, Brazil.
Vichet Chindavanig วเชฏฐ จนดาวณค
69

70
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
This in vitro study compared the effects of a gold alloy (Degulor M), four dental ceramics (IPS Empress, IPS Empress 2, Duceram Plus, Duceram LFC) and a laboratory-processed composite (Targis) on the wear of human enamel. The amount of wear of the enamel (dental cusps) and restorative materials (disks) were tested in water at 37 degrees C under standard load (20 N), with a chewing rate of 1.3 Hz and was determined after 150,000 and 300,000 cycles. Before the test, the average surface roughness of the restorative materials was analyzed using the Ra parameter. The results of this study indicate that Targis caused enamel wear similar to Degulor M and resulted in significantly less wear than all the ceramics tested. IPS Empress provoked the greatest amount of enamel wear and Degulor M caused less vertical dimension loss. Targis could be an appropriate alternative material to ceramic, because it is esthetic and produces opposing enamel wear comparable to gold alloy.
PMID: 18505225 [PubMed - indexed for MEDLINE]
J Appl Oral Sci. 2008 Feb;16(1):64-9. Links
Correlation between margin fit and microleakage in complete crowns cemented with three luting agents.
Rossetti PH, do Valle AL, de Carvalho RM, De Goes MF, Pegoraro LF.
Oral Rehabilitation Program, Bauru School of Dentistry, University of São Paulo, Bauru, SP, Brazil.
Microleakage can be related to margin misfit. Also, traditional microleakage techniques are time-consuming. This study evaluated the existence of correlation between in vitro margin fit and a new microleakage technique for complete crowns cemented with 3 different luting agents. Thirty human premolars were prepared for full-coverage crowns with a convergence angle of 6 degrees, chamfer margin of 1.2 mm circumferentially, and occlusal reduction of 1.5 mm. Ni-Cr cast crowns were cemented with either zinc phosphate (ZP) (S.S. White), resin-modified glass-ionomer (RMGI) (Rely X Luting Cement) or a resin-based luting agent (RC) (Enforce). Margin fit (seating discrepancy and margin gap) was evaluated according to criteria in the literature under microscope with 0.001 mm accuracy. After thermal cycling, crowns were longitudinally sectioned and microleakage scores at tooth-cement interface were obtained and recorded at x100 magnification. Margin fit parameters were compared with the one-way ANOVA test and microleakage scores with Kruskal-Wallis and Dunn's tests (alpha=0.05). Correlation between margin fit and microleakage was analyzed with the Spearman's test (alpha=0.05). Seating discrepancy and marginal gap values ranged from 81.82 microm to 137.22 microm (p=0.117), and from 75.42 microm to 78.49 microm (p=0.940), respectively. Marginal microleakage scores were ZP=3.02, RMGI=0.35 and RC=0.12 (p<0.001), with no differences between RMGI and RC scores. The correlation coefficient values ranged from -0.27 to 0.30 (p>0.05). Conclusion: Margin fit parameters and microleakage showed no strong correlations; cast crowns cemented with RMGI and RC had lower microleakage scores than ZP cement.
Vichet Chindavanig วเชฏฐ จนดาวณค
70
71
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
PMID: 19089292 [PubMed - indexed for MEDLINE]
Journal of Prosthodontic ResearchVolume 53, Issue 1, January 2009, Pages 3-10
ReviewCritical review of some dogmas in prosthodontics
Gunnar E. Carlsson , a,
aDepartment of Prosthetic Dentistry, The Sahlgrenska Academy, University of Gothenburg, Box 450, SE 405 30 Göteborg, Sweden
Received 27 April 2008;
accepted 2 June 2008.
Available online 7 October 2008.
Abstract
Purpose
In prosthodontics like in other dental disciplines there are many clinical procedures that lack support of good evidence, which means that the effect is unknown, and even worse, we do not know if they do more good than harm. It is the aim of this paper to review current evidence for selected procedures based on a scrutiny of the prosthodontic literature.
Study selection
A MEDLINE/PubMed search was conducted for articles on the selected items with a focus on best available evidence.
Results
Many “old truths” regarding prosthodontic interventions can be called dogmas, opinions based more on belief than scientific evidence. There is, for example, lack of evidence to support the opinion that a face-bow is necessary in the fabrication of prostheses, and many theories related to occlusion are not evidence-based. Some such dogmas in various areas of the discipline are exemplified and discussed in the article.
Conclusion
A scrutiny of the prosthodontic literature indicates that many common clinical procedures lack scientific support. In the era of evidence-based dentistry, ineffective interventions should be eliminated and decisions should be made on best available evidence.
Vichet Chindavanig วเชฏฐ จนดาวณค
71
72
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Keywords: Complete dentures; Dental occlusion; Evidence-based care; Jaw registration; Oral implants
Article Outline
1. Introduction
2. Materials and methods
3. Evidence-based care
4. Review of some dogmas regarding complete denture fabrication
4.1. Quality of dentures and patient satisfaction
4.2. Psychological factors
4.3. Jaw relation records
4.4. Occlusion
4.5. Impressions
5. Loss of teeth and the health of the masticatory system
6. Oral implants will solve all problems
6.1. Prosthetic complications
6.2. Implant failure
7. Dogmas related to temporomandibular disorders
7.1. The role of occlusion in TMD etiology
7.2. Occlusal splints/intraoral appliances
8. Discussion
References
1. Introduction
A dogma is defined as a belief or opinion held to be true. On closer scrutiny, many such dogmas lack evidence to be
valid but are still cherished with implicit faith. A well-known historical example of the risk of questioning dogmas is
what happened to Galileo Galilei, when he disavowed that earth was the centre of the universe, the article of faith at
that time. In 1632 the Church in Rome forced him to abjure this theory and sentenced him to life imprisonment, later
on mitigated to lifelong house arrest. In 1992, 360 years later, the Pope declared the Galileo case closed. Errors had
been made …
To question dogmas may still be risky, e.g. in most religions, in non-democratic societies, in political parties, and even in the scientific community if you are a researcher who presents results that do not fit into existing paradigms. A paradigm, i.e. opinions that members within a scientific branch share, may lead to considerable restriction of one’s
Vichet Chindavanig วเชฏฐ จนดาวณค
72
73
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
field of view, and attempts of a paradigm shift usually generate great resistance [1]. Such an attitude to new findings may have devastating consequences for scientific development as has been expressed by a famous scientist: “It is what we think we know that prevents us from learning more” (Albert Einstein, 1879–1955). Another citation of relevance when discussing old dogmas is: “Science is not to solve the extreme questions. Science is to gradually terminate preconceived opinions” (Niels Bohr, 1885–1962). The following statement should always be considered by clinicians both in medicine and dentistry: “Half of what you are taught as medical students will in 10 years have been shown to be wrong, and the trouble is none of your teachers knows which half” (Sidney Burwell, 1893–1956). It can be argued that the period is even shorter today, perhaps only five years.
To critically inspect current opinions of clinical methods is an essential part in the development of evidence-based care. It is the aim of this paper to review current evidence for some selected clinical procedures in prosthodontics based on a scrutiny of the literature.
2. Materials and methods
MEDLINE/PubMed searches were conducted for articles on selected aspects of clinical prosthodontic procedures with a focus on best available evidence. Since the prosthodontic literature is abundant (78,430 hits in PubMed; April 21, 2008) the review was limited to studies of the highest possible level of evidence (Table 1). If publications of the highest levels, i.e. clinical randomized controlled trials (RCT) and systematic reviews of RCTs, were not available, other studies were considered. The selected areas included various aspects of complete denture fabrication, jaw registration methods, tooth loss and the health of the masticatory system, the role of oral implants in prosthodontic treatment, and the role of occlusion in temporomandibular disorders (TMDs). Because of space limitations, the review is condensed and focused on specific aspects of the selected areas.
Table 1.
Grading of evidence in the literature
Level Type of evidence
Ia Evidence from systematic reviews of RCT
Ib Evidence from at least one RCT
IIa Evidence from at least one controlled study without randomization
IIb Evidence from at least one well-designed quasi-experimental study
IIIEvidence from non-experimental descriptive studies, such as comparative, correlation, cohort, and case-control studies
IV Evidence from expert committee reports, consensus conferences, and opinions or
Vichet Chindavanig วเชฏฐ จนดาวณค
73

74
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
Level Type of evidence
clinical experience of recognized authorities
Full-size table
3. Evidence-based care
It has been demonstrated that only a minor part of all methods that are routinely used in clinical dentistry has strong scientific support. It is hardly any comfort for dentists that the situation is similar in medical care [2]. Investigations of high quality are required for valid comparisons between different methods, materials, and medications. It is well established that among various study designs, the RCTs give the strongest evidence, which is reflected in the hierarchy of scientific strength (Table 1). RCTs can easily be done in comparisons of various drugs, but they are difficult to conduct in restorative dentistry and almost impossible for extensive treatments such as oral rehabilitation. Thus, no RCT seems to have been performed to compare clinical results of conventional fixed prostheses on teeth and implant-supported reconstructions for replacement of lost teeth. An extensive study of the prosthodontic literature up to the end of 2000 identified 90 RCTs, but the critical authors maintained that only a small part of them was presented in accordance with current requirements of reporting scientific studies, which made the interpretation of the results difficult [3].
It can be concluded that only a minor part of all questions in clinical prosthodontics can be answered with strong evidence. The situation is similar in other dental disciplines as well as in the medical fields [4].
4. Review of some dogmas regarding complete denture fabrication
4.1. Quality of dentures and patient satisfaction
Textbooks and undergraduate teaching have strongly emphasized that the best way to achieve a successful outcome of complete denture treatment is to strictly follow the traditional prosthodontic rules for optimal quality. Over the years, however, several studies have demonstrated that there is often poor correlation between a dentist’s assessment of denture quality and a patient’s satisfaction with the treatment [5], [6] and [7]. The majority of complete denture wearers are satisfied with their dentures, irrespective of denture quality, and some 10–20% are dissatisfied even if the dentures are constructed according to the best known prosthodontic rules [8]. In a study of 500 complete denture wearers, a close correlation was found between patient and dentist appreciation when the dentures were rated as poor, but little or no correspondence when dentists and patients rated the dentures highly [9]. This can explain why we sometimes have patients who complain about the dentures when we assess the quality as excellent.
It is a common clinical opinion that there is a relationship between the qualities of the anatomical conditions (e.g. height of residual ridges, characteristics of mucosal tissues, etc.) and the outcome of the denture treatment. However, several studies have failed to show strong correlations between such factors and patient satisfaction with the dentures [6], [7], [10] and [11]. One of these studies concluded that clinicians’ assessments of the quality of denture-supporting tissues are poor predictors of patient satisfaction with mandibular prostheses [7].
The rationale of relining and replacing poorly fitting dentures is to improve denture quality, and most patients experience an improvement, but all are not satisfied. This underlines the often poor correlation between denture quality and patient satisfaction [12] and [13]. It must also be remembered that bite force and masticatory performance tend to diminish rather than increase for a substantial time period after delivery of new dentures [14] and [15]. There
Vichet Chindavanig วเชฏฐ จนดาวณค
74

75
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
is also no certain evidence that making better complete dentures will change the dietary selection or improve the quality of diet in edentulous subjects [16] and [17]. Studies that also included comparison with implant-supported prostheses, found improved chewing ability, but no dietary changes after treatment [18], [19] and [20]. All these studies concluded that, in the absence of tailored dietary advice, successful rehabilitation, including improved chewing capacity, does not necessarily result in a satisfactory diet.
4.2. Psychological factors
The lack of strong evidence for an association between anatomical and technical prerequisites of a successful treatment with complete dentures should be balanced with the fact that psychological factors and the patient’s – and the dentist’s – personality are of great importance for the outcome of treatment [21]. Several studies have demonstrated that dentists’ and patients’ interpersonal appraisals of each other were most significant factors, accounting for patients’ evaluation of treatment outcome [22] and [23]. Reviews of the literature on this topic have suggested that the creation of a good relationship with the patient seems to be more important than a technically perfect denture construction for achieving patient satisfaction [24], [25] and [26].
4.3. Jaw relation records
Practically all textbooks in prosthodontics have described a face-bow record as necessary for orienting the casts to the articulator for all types of prosthetic work. It is generally suggested that the more sophisticated and complex methods that are used, the better the results that will be achieved. This belief was refuted with respect to fabrication of complete dentures in a classical longitudinal series of RCTs initiated in 1969 [27]. The studies compared 64 edentulous patients randomly allocated to two treatment groups: one complex technique involving, among other things, hinge-axis location for a face-bow transfer to an advanced articulator, the other using a simple technique without face-bow and with an arbitrary mounting in a simple articulator. No significant differences in outcome between the two patient groups could be established in the short- or long-term follow-ups over 20 years, either in the professional or patient evaluations of dentures and clinical results [28]. In spite of the strong evidence that this series of well conducted studies provided, the belief in the necessity to use face-bows continued in most prosthodontic literature and teaching well into the new millennium [29] and [30]. Among many general practitioners, the value of the face-bow has been questioned and in Scandinavia practically all dentists abandoned the use of face-bows long ago, not only for complete denture fabrication, but also in other types of prosthodontic work. Already in 1991, the Scandinavian Society for Prosthetic Dentistry (SSPD) presented a consensus publication stating that a face-bow is not necessary and recommended simple methods in jaw recording for all types of prosthodontic work. Average mounting in the articulator is sufficient and easy to perform. The message was based on the fact that there was no published evidence that the use of a face-bow will lead to better clinical end results than when not using a face-bow, nor has any such evidence appeared since then [29]. There are no studies that contradict the opinion that an average setting of the articulator is satisfactory, for example, 30° for the sagittal and 15° for the lateral condylar path inclination.
Now more studies are appearing corroborating that mounting in the articulator with or without face-bow gives similar clinical results [31], [32], [33] and [34]. One of these studies comparing the traditional and a simplified technique in producing complete dentures concluded, “the quality of complete dentures does not suffer when manufacturing techniques are simplified to save time and materials. Dental educators should consider these findings when redesigning prosthodontic training programs” [33]. This suggestion also fits in well with the concept of Appropriatech: “To provide treatment for the many, cost-effective conventional treatment is required, but with adequate quality control” [35].
4.4. Occlusion
The concept that complete dentures need balanced occlusion to create stability has been so dominant in textbooks that it deserves to be characterized as a dogma. However, the statement has been questioned since balance is often lost during chewing. Studies have also demonstrated that the balanced occlusion existing at delivery of the dentures is often lost within a relatively short time, without patients complaining about it [36] and [37].
Some gnathologically oriented dentists have maintained, without being believed by most prosthodontists, that complete dentures with canine-guided occlusion can function well. A controlled study compared balanced occlusion and canine guidance in a group of complete denture wearers. The patients assessed canine-guided dentures to be
Vichet Chindavanig วเชฏฐ จนดาวณค
75

76
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
significantly more satisfying in aesthetic appearance, mandibular denture retention, and chewing ability [38]. Available evidence thus indicates that complete dentures can function successfully without a balanced occlusion. This is thus an example of another “old truth” that needs to be modified.
Other factors related to complete denture occlusion, such as occlusal pattern, form, material, and arrangement of the artificial teeth have been the focus of heated discussions during many decades, but there is a lack of well-controlled studies. A Cochrane Review on occlusal schemes identified more than 1000 titles, but only one study that fully met the inclusion criteria of scientific quality [39]. This study compared lingualized teeth with cusps with zero-degree teeth. It was concluded that there was weak evidence for recommending teeth with cusps since significantly more of the patients preferred them compared to cuspless teeth. One more study can now be added to the mentioned one, a recent RCT compared three types of posterior occlusal forms for complete dentures. Lingualized and anatomic occlusal forms were perceived to be significantly superior in terms of chewing ability, when compared with zero-degree posterior occlusal surfaces [40].
An extensive review of the literature on complete denture occlusion concluded, “Despite its biomechanical importance, occlusion, as well as the technical quality of the denture, plays only a minor role in determining success or failure of a denture treatment. A number of psychosocial factors are likely to be more important than prosthodontic factors for a positive outcome” [24].
4.5. Impressions
Most textbooks advocate a two-stage procedure: (1) preliminary impression, often with an irreversible hydrocolloid (alginate) in a stock tray; and (2) final impression in a custom tray usually made of acrylic resin. There are many materials for the final impression, such as gypsum, zinc oxide and eugenol (ZOE) paste, polysulfide rubber, polyether, polyvinyl siloxane, and alginate.
Preferences vary much among dentists. However, there is no evidence that one technique or material produces better long-term results than another. Among hundreds of articles on impression materials and methods, only two controlled studies were found. The first one compared fluid wax and polysulfide rubber for mandibular complete denture impression and demonstrated that there was no difference in adjustment of the dentures up to one year after delivery [41]. The other controlled study compared three materials for the final impression in 11 patients. It was found that ZOE was the least favored material, and the authors concluded that care should be exercised when selecting impression materials when constructing mandibular complete dentures [42].
Without strong evidence for recommending a specific impression material and technique it is of interest to know the normal practice for complete dentures among general practitioners. A survey in a region in the UK revealed that practically all responding dentists used alginates for primary impressions. Also for the secondary impression irreversible hydrocolloid was mentioned as an option by 94%, ZOE paste by 29%, and polyvinyl siloxane by 13% (more than one material could be mentioned). Laboratory special trays were used by 75% for the final impression [43]. In North American dental schools 98% used custom trays with border molding for final impressions, but with variation regarding materials used [44]. There does not seem to be any evidence of better clinical long-term results with dentures made with than without boulder molding [45].
Many general practitioners use a single alginate impression as the definitive impression for the construction of complete dentures, which conflicts with the teaching in practically all dental schools. It is, therefore, of interest that a RCT found neither patient assessed nor dentist evaluated differences between dentures fabricated according to a traditional or a simplified method. The simple technique used alginate in a standard tray for the definitive impression, whereas the traditional technique included an individual tray with border molding and polyether for the final impression [33]. Although impression materials differ in many aspects and a variety of techniques exist in taking the impressions, there is no evidence to conclude that the clinical long-term outcome of dentures fabricated using varying materials and methods would differ significantly. These and other aspects of variation in methods and techniques are discussed in a review of an evidence base for complete dentures [45].
5. Loss of teeth and the health of the masticatory system
For a long time, it was stated so frequently in prosthodontic textbooks and dental school education that it stood out as a dogma: teeth that are lost must be replaced if the health of the masticatory system is to be maintained. Some
Vichet Chindavanig วเชฏฐ จนดาวณค
76
77
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
clinicians dared to questioned this dogma, e.g. the American prosthodontist De Van, who already in 1951, when discussing indications for removable partial dentures (RPDs), wrote: “Many times it is much better to preserve what is left instead of replacing what has been lost” [46]. Half a century later, the international prosthodontic community seems to agree with this statement on RPDs [47]. However, it was the Dutch prosthodontist Käyser who started an unyielding campaign against the dogma when, in 1981, he published his opinions on the shortened dental arch (SDA) [48]. His message was that there is sufficient adaptive capacity in subjects with SDA when at least four occlusal units are left. His and his successor’s research groups have conducted a series of clinical cross-sectional and longitudinal studies on SDA. The results have convincingly demonstrated that most people can manage well with a reduced number of teeth without severe negative consequences, either as assessed by the patients themselves or according to professional clinical examination of the function of the masticatory system. The conclusion has been that earlier presumptions of the negative sequelae of loss of teeth were exaggerated. An extensive review of the literature on SDA could not identify any systematic clinical studies from other centres refuting the main results of the Dutch group [49].
The SDA concept was first received with skepticism, and those who believed in the necessity of a complete dentition considered it heretical. However, the SDA concept has gradually met increased acceptance [50] and [51]. The WHO guidelines published in 1992 provided strong support by suggesting that the SDA concept was a possible clinical alternative in situations when economy and service resources are limited [52]. Shortened dental arches comprising anterior and premolar teeth fulfill in general the requirements of a functional dentition. This statement is of great importance for the large number of people in the world that lack possibilities to pay for extensive and high-cost dental care. Even in the wealthiest countries, substantial parts of the population do not have economical means to ask for complete prosthodontic treatment when affected by tooth losses [35]. Patients’ needs and demands vary much and should be individually assessed, but the SDA concept deserves to be included in the treatment planning process. In complex treatment plans, the SDA approach offers alternatives of less treatment that is also less complicated, time-consuming, and expensive. The SDA concept has significantly influenced prosthodontic thinking in the past few decades and received well-deserved attention. However, with ongoing global changes, e.g. in dental health and economy, the SDA concept requires continuing research and discussion [49].
A healthy, complete natural dentition is of course an ideal worth aiming at whenever feasible. From the literature it can be concluded, however, that the earlier professional belief in full reconstitution of reduced dental arches per se as a prerequisite for optimal oral health and function lacks compelling scientific support [51]. A concept that has recently received increasing attention is that perceived oral health is not related only to the level of oral function, but also to psychological factors. A Japanese study examined the relationship between missing occlusal units and oral health-related quality of life (OHRQoL) in patients with SDA [53]. The results suggested that missing occlusal units were related to impairment of OHRQoL in subjects with SDA. Quality of life aspects certainly deserve to be more studied in various areas of prosthodontics.
6. Oral implants will solve all problems
Oral implants have revolutionized the treatment of edentulous and partially edentulous patients. Within a few decades after the introduction of osseointegrated implants [54], previously unforeseen possibilities have been developed to help patients suffering of functional and psychological problems with conventional removable dentures. The successful results of implant treatment have been followed by an explosive development of new materials and methods including a great variety of brands of implant designs, most of which, more or less, resemble the original titanium screw implant. The rapidly growing implant market has created what by many is considered a dogma: implants can solve all problems related to tooth loss. This is of course not true. The greatest obstacle is economic. Up to now probably less than 1% of edentulous people in the world have received implant treatment. Neither will the great majority of the world’s edentulous individuals be able to afford such treatment in the foreseeable future. There are also other obstacles. An interesting study in Canada showed that more than one third (36%) of edentulous subjects declined implant treatment despite it being offered free of charge [55]. The reasons for the refusal varied, but the most common was that the complete dentures functioned well, and many people fear the surgical operation and the subsequent treatment. Other studies have also reported fairly high proportions of individuals who say that they would never consider receiving dental implants [56] and [57].
The recommendations expressed above all by implant manufacturers to extract teeth and replace them with implants have been contradicted by recent systematic reviews that have concluded that the survival rate of teeth are higher than that of implants. This was true also for compromised, but successfully treated and maintained, teeth [58] and [59].
Vichet Chindavanig วเชฏฐ จนดาวณค
77

78
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
6.1. Prosthetic complications
The spread opinion that implant treatment is more secure than conventional fixed prostheses is not in accordance with current literature. Several longitudinal studies have demonstrated that complications after implant treatment are common and repair and remaking of the reconstructions can be both time-consuming and costly [60]. In the absence of RCTs comparing long-term results of conventional fixed prostheses and implant-supported reconstructions, systematic reviews have shown that the incidence of technical complications was higher for implant-supported than for tooth-supported reconstructions [61]. Dentists should observe these results and the patients must be informed before the start of the treatment.
6.2. Implant failure
Loss of implants after loading is rare, especially in the mandible [62]. Sometimes a failure occurs and the reason is often difficult to establish. Occlusal conditions and overloading have often been proposed as the most important cause of late failures, sometimes with such an emphasis that it has been looked upon as a dogma by many people. Evidence for this opinion has been demonstrated only in a single animal study, whereas it has been difficult to prove an association between overload and implant failure in human studies. A consensus conference in 2006 concluded, “Although it has been postulated from clinical studies that occlusal forces have been associated with a loss of oral implants, a causative relationship has never been convincingly demonstrated” [63]. At present, it thus seems that the dogma of an association between occlusal forces and implant failure, regarding the biological effects, should be abandoned. On the other hand, it is clear that heavy occlusal load may have negative effects on the implant supra-construction, e.g. fractures of components [64].
Oral implants offer fantastic possibilities to treat patients who have lost teeth, but they cannot solve all therapeutic problems. There are many reasons to further develop conventional prosthodontics because in the foreseeable future tooth-borne crowns and fixed dental prostheses as well as removable dentures will continue to be the most common treatment alternatives in general practice.
7. Dogmas related to temporomandibular disorders
The literature on TMDs has over the years exhibited a great number of controversial opinions, which has created much confusion, especially regarding diagnosis and treatment of TMDs. Already the numerous names given to the disorders during the past decades indicate different views on the etiology, which naturally have had influence on the management of the patients. For long, TMD patients were managed in prosthodontic clinics in many countries with a focus on occlusal etiology. During the past few decades special TMD clinics have appeared in many places and the focus has changed to psychological factors and pain physiology [65] and [66]. This review will be limited to two controversial areas, the role of occlusion and occlusal splints.
7.1. The role of occlusion in TMD etiology
Occlusal disturbances were for long believed to be the dominant cause of TMDs. It is no exaggeration to say that for many clinicians the close relationship between TMDs and occlusion was a dogma. Elimination of so-called occlusal interferences with various types of occlusal therapy such as occlusal adjustment was taught in dental schools and became a common treatment modality for TMD in general practice. TMD patients often get better after occlusal adjustment, which strengthens the dentist’s belief in an association between occlusal disturbances and TMDs. Only when RCTs were introduced in the TMD field was it revealed that other therapies without effects on occlusion provided equally good or better results. Systematic literature reviews have demonstrated that the association between occlusal factors and TMDs is weak and consequently there is seldom an indication for irreversible occlusal therapy in TMD patients [67], [68], [69] and [70]. Simple treatments including brief information, counseling/reassurance, analgesic medication for pain relief, and jaw exercises will help the majority of patients with TMD [65] and [66]. A recent Japanese study on TMD patients comparing the treatment outcome between two clinics, one focusing on occlusal therapy and splints, the other on patient education and physiotherapy, found better results for the latter [71]. A systematic review compared simple versus multimodal therapy in TMD patients [72]. It was concluded that patients without major psychological symptoms do not require more than simple therapy, such as brief information, self-care instructions, home remedies, and over-the-counter drugs.
Vichet Chindavanig วเชฏฐ จนดาวณค
78
79
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
7.2. Occlusal splints/intraoral appliances
Many dentists have had difficulties to abandon the opinion of a close relationship between occlusal disturbances and TMDs as it was earlier taught in most dental schools. The good treatment outcome of occlusal splints is often put forward as an argument that the occlusion is etiologically important. The name of the most common splint, the stabilization appliance, suggests that an improvement of the occlusion should explain the treatment effect. However, there are other possible mechanisms (Table 2). An anterior bite plate with occlusal contacts only on the incisors and canines has proven to be as effective as a stabilization splint. And to many a surprising result: a so-called placebo splint that only covers the palate without touching the occlusion is largely as effective as an occlusal splint [73]. It has been proposed that occlusal splints are temporary means like crutches in orthopedic treatment, and the outcome can be explained as effects of, for example, placebo, the time factor, and the fluctuation of the complaints [74]. In spite of the more critical attitude toward the traditional explanations of the efficacy, there is currently close to consensus among TMD experts that an occlusal splint provides an efficient treatment in the management of TMD patients. However, the mechanism of action is not clear, and the effect is probably not at all, or only to a small extent, influenced by the occlusion. A consequence would be to call these devices intraoral appliances rather than occlusal splints.
Table 2.
Proposed mechanisms explaining the treatment effect of intraoral appliances (besides the possible influence on the occlusion)
Mechanisms discussed in the literature
Occlusal disengagement
Neurophysiologic effects on the masticatory system
Change of vertical dimension
Change of caput–fossa relation
Cognitive awareness of harmful behavior (e.g. parafunctions)
Stress absorber/reduced load on masticatory system components
Placebo effect
Vichet Chindavanig วเชฏฐ จนดาวณค
79
80
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
8. Discussion
Many “old truths” in prosthodontics and occlusion can be characterized as dogmas based more on belief than science. Some such dogmas have been exemplified in the article but many more exist as demonstrated in a recently published extensive review [75]. The focus has been on the fabrication of complete dentures, but it is easy to find corresponding lack of strict scientific support in other areas of prosthodontics. In fact, only a minor part of all opinions that governs the activities in clinical dentistry – as well as in medicine – is based on strong evidence. Without good evidence it is unnecessarily difficult and uncertain to make clinical decisions. There is, therefore, need for more research with systematic and controlled studies to be able to answer the many remaining controversial questions and improve the quality and security of clinical care. Biological, psychological, economical, and quality-of-life aspects should be incorporated in the research besides clinical comparisons between different therapies. The scarcity of RCTs and difficulty in conducting such trials will necessitate the evaluation of studies on lower evidence levels (Table 1) to draw any relevant conclusions. Systematic reviews of available literature have been shown to provide valuable guidelines for clinicians in decision-making [76], [77] and [78]. Clinical practice should be based on the best possible evidence and include the clinical experience and expertise of the therapeutic team as well as the patients’ wishes and preferences. In the longer perspective, many of today’s “truths” will be questioned, and dogmas that lack strong evidence will be abandoned. The prosthodontic community should take an active part in this process.
References
[1] T.S. Kuhn, The structure of scientific revolutions (2nd ed.), University of Chicago Press, Chicago (1970).
[2] P. Sjögren and A. Halling, Quality of reporting randomised clinical trials in dental and medical research, Br Dent J
192 (2002), pp. 100–103. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (12)
[3] A. Jokstad, M. Esposito, P. Coulthard and H.V. Worthington, The reporting of randomised controlled trials in
prosthodontics, Int J Prosthodont 15 (2002), pp. 230–242. View Record in Scopus | Cited By in Scopus (15)
[4] P. Sjögren, Randomised clinical trials and evidence-based general dentistry 865, Linköping University Medical
Dissertations, Linköping, Sweden (2004).
[5] A. Langer, J. Michman and I. Seifert, Factors influencing satisfaction with complete dentures in geriatric patients, J
Prosthet Dent 11 (1961), pp. 1019–1024.
[6] C. de Baat, A.A. van Aken, J. Mulder and W. Kalk, Prosthetic condition” and patients’ judgment of complete
dentures, J Prosthet Dent 78 (1997), pp. 472–478. Article | PDF (770 K) | View Record in Scopus | Cited By in
Scopus (14)
[7] G. Heydecke, E. Klemetti, M.A. Awad, J.P. Lund and J.S. Feine, Relationship between prosthodontic evaluation
and patient ratings of mandibular conventional and implant prostheses, Int J Prosthodont 16 (2003), pp. 307–312.
View Record in Scopus | Cited By in Scopus (20)
[8] E. Berg, Acceptance of full dentures, Rev Int Dent J 43 (Suppl. 1) (1993), pp. 299–306. View Record in Scopus |
Cited By in Scopus (26)
[9] M.R. Fenlon and M. Sherriff, Investigation of new complete denture quality and patients’ satisfaction with and use
of dentures after two years, J Dent 32 (2004), pp. 327–333. Article | PDF (171 K) | View Record in Scopus | Cited
By in Scopus (6)
Vichet Chindavanig วเชฏฐ จนดาวณค
80

81
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
[10] G.E. Carlsson, A. Otterland and A. Wennström, Patient factors in appreciation of complete dentures, J Prosthet
Dent 17 (1967), pp. 322–328. Abstract | PDF (473 K) | View Record in Scopus | Cited By in Scopus (38)
[11] A. Wolff, A. Gadre, A. Begleiter, D. Moskona and H. Cardash, Correlation between patient satisfaction with
complete dentures and denture quality, oral condition, and flow rate of submandibular/sublingual salivary glands, Int J
Prosthodont 16 (2003), pp. 45–48. View Record in Scopus | Cited By in Scopus (14)
[12] N.R. Garrett, K.K. Kapur and P. Perez, Effects of improvements of poorly fitting dentures and new dentures on
patient satisfaction, J Prosthet Dent 76 (1996), pp. 403–413. Article | PDF (1340 K) | View Record in Scopus |
Cited By in Scopus (28)
[13] M.K. Peltola, A.M. Raustia and M.A. Salonen, Effect of complete denture renewal on oral health—a survey of 42
patients, J Oral Rehabil 24 (1997), pp. 419–425. View Record in Scopus | Cited By in Scopus (11)
[14] N.R. Garrett, P. Perez, C. Elbert and K.K. Kapur, Effects of improvements of poorly fitting dentures and new
dentures on masticatory performance, J Prosthet Dent 75 (1996), pp. 269–275. Article | PDF (893 K) | View
Record in Scopus | Cited By in Scopus (29)
[15] F. Müller, M.R. Heath and R. Ott, Maximum bite force after the replacement of complete dentures,
Gerodontology 18 (2001), pp. 58–62. View Record in Scopus | Cited By in Scopus (6)
[16] H.S. Gunne and A.K. Wall, The effect of new complete dentures on mastication and dietary intake, Acta Odontol
Scand 43 (1985), pp. 257–268. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (42)
[17] R.S. Shinkai, J.P. Hatch, J.D. Rugh, S. Sakai, C.C. Mobley and M.J. Saunders, Dietary intake in edentulous
subjects with good and poor quality complete dentures, J Prosthet Dent 87 (2002), pp. 490–498. Abstract | PDF
(190 K) | View Record in Scopus | Cited By in Scopus (13)
[18] B. Sandström and L.W. Lindquist, The effect of different prosthetic restorations on the dietary selection in
edentulous patients. A longitudinal study of patients initially treated with optimal complete dentures and finally with
tissue-integrated prostheses, Acta Odontol Scand 45 (1987), pp. 423–428. Full Text via CrossRef | View Record in
Scopus | Cited By in Scopus (25)
[19] F. Allen and A. McMillan, Food selection and perceptions of chewing ability following provision of implant and
conventional prostheses in complete denture wearers, Clin Oral Implants Res 13 (2002), pp. 320–326. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (19)
[20] J.S. Ellis, J.M. Thomason, N.J. Jepson, F. Nohl, D.G. Smith and P.F. Allen, A randomized-controlled trial of food
choices made by edentulous adults, Clin Oral Implants Res 19 (2008), pp. 356–361. Full Text via CrossRef | View
Record in Scopus | Cited By in Scopus (1)
[21] M.R. Fenlon, M. Sherriff and J.T. Newton, The influence of personality on patients’ satisfaction with existing and
new complete dentures, J Dent 35 (2007), pp. 744–748. Article | PDF (309 K) | View Record in Scopus | Cited By
in Scopus (3)
Vichet Chindavanig วเชฏฐ จนดาวณค
81
82
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
[22] F. al Quran, T. Clifford, C. Cooper and P.J. Lamey, Influence of psychological factors on the acceptance of
complete dentures, Gerodontology 18 (2001), pp. 35–40. View Record in Scopus | Cited By in Scopus (12)
[23] S.M. Auerbach, A.R. Penberthy and D.J. Kiesler, Opportunity for control, interpersonal impacts, and adjustment
to a long-term invasive health care procedure, J Behav Med 27 (2004), pp. 11–29. Full Text via CrossRef | View
Record in Scopus | Cited By in Scopus (9)
[24] S. Palla, Occlusal considerations in complete dentures. In: C. McNeill, Editor, Science and practice of occlusion,
Quintessence, Chicago (1997), pp. 457–467.
[25] G.E. Carlsson, Clinical morbidity and sequelae of treatment with complete dentures, J Prosthet Dent 79 (1998),
pp. 17–23. Article | PDF (126 K) | View Record in Scopus | Cited By in Scopus (37)
[26] H.M. Landesman, Building rapport: the art of communication in the management of the edentulous predicament.
In: G.A. Zarb and C.L. Bolender, Editors, Prosthodontic treatment for edentulous patients (12th ed.), Mosby, St. Louis
(2004), pp. 177–189.
[27] J.C. Hickey, D. Henderson and R. Straus, Patient response to variations in denture technique. I. Design of a
study, J Prosthet Dent 22 (1969), pp. 158–170. Abstract | PDF (1010 K) | View Record in Scopus | Cited By in
Scopus (4)
[28] C.W. Ellinger, R.C. Wesley, B.J. Abadi and T.M. Armentrout, Patient response to variations in denture technique.
Part VII: twenty-year patient status, J Prosthet Dent 62 (1989), pp. 45–48. Abstract | PDF (690 K) | View Record
in Scopus | Cited By in Scopus (5)
[29] T. Tangerud and G.E. Carlsson, Jaw registration and occlusal morphology. In: S. Karlsson, K. Nilner and B.L.
Dahl, Editors, A textbook of fixed prosthodontics. The Scandinavian approach, Gothia, Stockholm (2000), pp. 209–
230.
[30] B. Rashedi and V.C. Petropoulos, Preclinical complete dentures curriculum survey, J Prosthodont 12 (2003), pp.
37–46. View Record in Scopus | Cited By in Scopus (5)
[31] S.P. Shodadai, J.C. Turp, T. Gerds and J.R. Strub, Is there a benefit of using an arbitrary facebow for the
fabrication of a stabilization appliance?, Int J Prosthodont 14 (2001), pp. 517–522. View Record in Scopus | Cited By
in Scopus (5)
[32] D.F.F. Nascimento, R.B.L. Patto, L. Marchini and V.P.P. Cunha, Double-blind study for evaluation of complete
dentures made by two techniques with and without face-bow, Braz J Oral Sci 3 (2004), pp. 439–445.
[33] Y. Kawai, H. Murakami, B. Shariati, E. Klemetti, J.V. Blomfield and L. Billette et al., Do traditional techniques
produce better conventional dentures than simplified techniques?, J Dent 33 (2005), pp. 659–668. Article | PDF
(121 K) | View Record in Scopus | Cited By in Scopus (5)
Vichet Chindavanig วเชฏฐ จนดาวณค
82
83
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
[34] G. Heydecke, A.S. Akkad, M. Wolewitz, M. Vogeler, J.C. Türp and J.R. Strub, Patient ratings of chewing ability
from a randomised crossover trial: lingualised vs. first premolar/canine-guided occlusion for complete dentures,
Gerodontology 24 (2007), pp. 77–86. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (1)
[35] P. Owen, Appropriatech: prosthodontics for the many, not just for the few, Int J Prosthodont 17 (2004), pp. 261–
262. View Record in Scopus | Cited By in Scopus (10)
[36] B. Bergman, G.E. Carlsson and B. Hedegård, A longitudinal two-year study of a number of full denture cases,
Acta Odontol Scand 22 (1964), pp. 3–26. Full Text via CrossRef
[37] K.H. Utz, Studies of changes in occlusion after the insertion of complete dentures (part II), J Oral Rehabil 24
(1997), pp. 376–384. View Record in Scopus | Cited By in Scopus (6)
[38] I. Peroz, A. Leuenberg, I. Haustein and K.P. Lange, Comparison between balanced occlusion and canine
guidance in complete denture wearers—a clinical, randomized trial, Quintessence Int 34 (2003), pp. 607–612. View
Record in Scopus | Cited By in Scopus (7)
[39] A.F. Sutton, A.M. Glenny and J.F. McCord, Interventions for replacing missing teeth: denture chewing surface
designs in edentulous people, Cochrane Database Syst Rev (1) (2005), p. CD004941. View Record in Scopus | Cited
By in Scopus (1)
[40] A.F. Sutton, H.V. Worthington and J.F. McCord, RCT comparing posterior occlusal forms for complete dentures,
J Dent Res 86 (2007), pp. 651–655. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (3)
[41] D.N. Firtell and J.H. Koumjian, Mandibular complete denture impressions with fluid wax or polysulfide rubber: a
comparative study, J Prosthet Dent 67 (1992), pp. 801–804. Abstract | PDF (670 K) | View Record in Scopus |
Cited By in Scopus (5)
[42] J.F. McCord, L.M. McNally, P.W. Smith and N.J. Grey, Does the nature of the definitive impression material
influence the outcome of (mandibular) complete dentures?, Eur J Prosthodont Restor Dent 13 (2005), pp. 105–108.
View Record in Scopus | Cited By in Scopus (2)
[43] T.P. Hyde and J.F. McCord, Survey of prosthodontic impression procedures for complete dentures in general
dental practice in the United Kingdom, J Prosthet Dent 81 (1999), pp. 295–299. Article | PDF (122 K) | View
Record in Scopus | Cited By in Scopus (9)
[44] V.C. Petropoulos and B. Rashedi, Current concepts and techniques in complete denture final impression
procedures, J Prosthodont 12 (2003), pp. 280–287. View Record in Scopus | Cited By in Scopus (3)
[45] G.E. Carlsson, Facts and fallacies: an evidence base for complete dentures, Dent Update 33 (2006), pp. 134–
142. View Record in Scopus | Cited By in Scopus (5)
[46] M.M. De Van, Physical, biological and psychological factors to be considered in the construction of dentures, J
Am Dent Assoc 42 (1951), pp. 290–293.
Vichet Chindavanig วเชฏฐ จนดาวณค
83
84
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
[47] B. Wöstmann, E. Budtz-Jorgensen, N. Jepson, E. Mushimoto, S. Palmqvist and A. Sofou et al., Indications for
removable partial dentures: a literature review, Int J Prosthodont 18 (2005), pp. 139–145. View Record in Scopus |
Cited By in Scopus (16)
[48] A.F. Käyser, Shortened dental arches and oral function, J Oral Rehabil 8 (1981), pp. 457–462. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (108)
[49] T. Kanno and G.E. Carlsson, A review of the shortened dental arch concept focusing on the work by the
Käyser/Nijmegen group, J Oral Rehabil 33 (2006), pp. 850–862. Full Text via CrossRef | View Record in Scopus |
Cited By in Scopus (13)
[50] In: N.D. Mohl, G.A. Zarb, G.E. Carlsson and J.D. Rugh, Editors, A textbook of occlusion, Quintessence Publ,
Chicago (1988).
[51] G.E. Carlsson and R. Omar, Trends in prosthodontics, Med Princ Pract 15 (2006), pp. 167–179. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (5)
[52] World Health Organization. Recent Advances in Oral Health. WHO Technical Report Series. Geneva: WHO
1992; 826:16–7.
[53] K. Baba, Y. Igarashi, A. Nishiyama, M.T. John, Y. Akagawa and K. Ikebe et al., The relationship between missing
occlusal units and oral health-related quality of life in patients with shortened dental arches, Int J Prosthodont 21
(2008), pp. 72–74. View Record in Scopus | Cited By in Scopus (2)
[54] P.-I. Brånemark, Osseointegration and its experimental background, J Prosthet Dent 50 (1983), pp. 399–410.
Abstract | PDF (7175 K) | View Record in Scopus | Cited By in Scopus (301)
[55] J.N. Walton and M.I. MacEntee, Choosing or refusing oral implants: a prospective study of edentulous volunteers
for a clinical trial, Int J Prosthodont 18 (2005), pp. 483–488. View Record in Scopus | Cited By in Scopus (9)
[56] F. Müller, G. Wahl and K. Fuhr, Age-related satisfaction with complete dentures, desire for improvement and
attitudes to implant treatment, Gerodontology 11 (1994), pp. 7–12. Full Text via CrossRef | View Record in Scopus |
Cited By in Scopus (13)
[57] P.F. Allen, J.M. Thomason, N.J. Jepson, F. Nohl, D.G. Smith and J. Ellis, A randomized controlled trial of
implant-retained mandibular overdentures, J Dent Res 85 (2006), pp. 547–551. Full Text via CrossRef | View Record
in Scopus | Cited By in Scopus (10)
[58] N.P. Lang and F. Müller, Epidemiology and oral function associated with tooth loss and prosthetic dental
restorations. Consensus report of Working Group I, Clin Oral Impl Res 18 (Suppl. 3) (2007), pp. 46–49. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (2)
[59] C. Tomasi, J.L. Wennström and T. Berglundh, Longevity of teeth and implants—a systematic review, J Oral
Rehabil 35 (Suppl. 1) (2008), pp. 23–32. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (6)
Vichet Chindavanig วเชฏฐ จนดาวณค
84
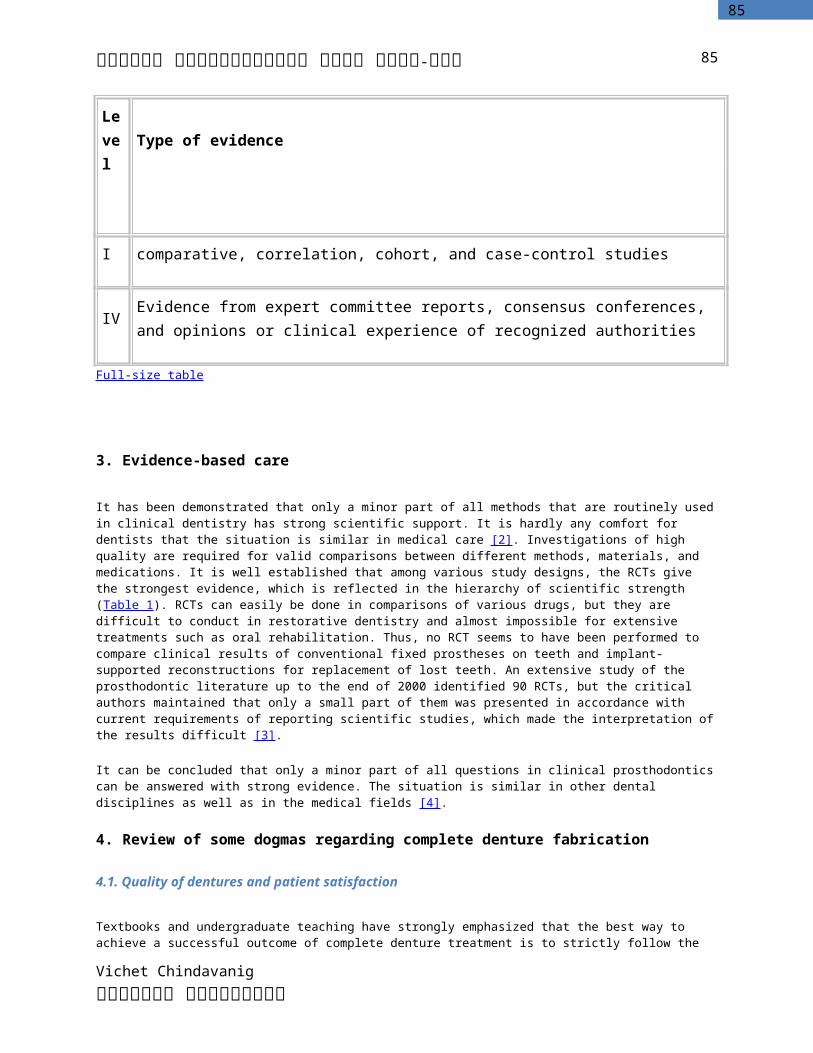
85
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
[60] T. Berglundh, L. Persson and B. Klinge, A systematic review of the incidence of biological and technical
complications in implant dentistry reported in prospective longitudinal studies of at least 5 years, J Clin Periodontol 29 (Suppl. 3) (2002), pp. 197–212. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (115)
[61] B.E. Pjetursson, U. Brägger, N.P. Lang and M. Zwahlen, Comparison of survival and complication rates of tooth-
supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs), Clin Oral Impl Res
18 (Suppl. 3) (2007), pp. 97–113. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (18)
[62] J.-A. Ekelund, L.W. Lindquist, G.E. Carlsson and T. Jemt, Implant treatment in the edentulous mandible: a
prospective study on Brånemark system implants over more than 20 years, Int J Prosthodont 16 (2003), pp. 602–608.
View Record in Scopus | Cited By in Scopus (55)
[63] J.A. Hobkirk and H.W.A. Wiscott, Biomechanical aspects of oral implants. Consensus report of Working Group I,
Clin Oral Impl Res 17 (Suppl. 2) (2006), pp. 52–54. Full Text via CrossRef | View Record in Scopus | Cited By in
Scopus (9)
[64] M.S. Schwartz, Mechanical complications of dental implants, Clin Oral Impl Res 11 (2000), pp. 156–158.
[65] G.E. Carlsson and T. Magnusson, Management of temporomandibular disorders in the general dental practice,
Quintessence, Chicago (1999).
[66] In: D.M. Laskin, C.S. Greene and W.L. Hylander, Editors, Temporomandibular disorders. An evidence-based
approach to diagnosis and treatment, Quintessence, Chicago (2006).
[67] J.A. De Boever, G.E. Carlsson and I.J. Klineberg, Need for occlusal therapy and prosthodontic treatment in the
management of temporomandibular disorders. Part I. Occlusal interferences and occlusal adjustment, J Oral Rehabil
27 (2000), pp. 367–379. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (40)
[68] J.A. De Boever, G.E. Carlsson and I.J. Klineberg, Need for occlusal therapy and prosthodontic treatment in the
management of temporomandibular disorders. Part II Tooth loss and prosthodontic treatment, J Oral Rehabil 27
(2000), pp. 647–659. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (15)
[69] H. Forssell and E. Kalso, Application of principles of evidence-based medicine to occlusal treatment for
temporomandibular disorders: are there lessons to be learned?, J Orofac Pain 18 (2004), pp. 9–22. View Record in
Scopus | Cited By in Scopus (40)
[70] C.S. Stohler, Management of dental occlusion. In: D.M. Laskin, C.S. Greene and W.L. Hylander, Editors,
Temporomandibular disorders. An evidence-based approach to diagnosis and treatment, Quintessence, Chicago
(2006), pp. 403–411.
[71] M. Funato, R. Kataoka, R. Furuya, N. Narita, K. Kino and Y. Abe et al., Comparison of the clinical features of
TMD patients and their treatment outcomes between prosthodontic and TMD clinics, Prosthodont Res Pract 6 (2007),
pp. 188–193. Full Text via CrossRef
[72] J.C. Türp, A. Jokstad, E. Motschall, H.J. Schindler, I. Windecker-Gétaz and D.A. Ettlin, Is there a superiority of
multimodal as opposed to simple therapy in patients with temporomandibular disorders? A qualitative systematic
Vichet Chindavanig วเชฏฐ จนดาวณค
85
86
ประมวล และแผนการสอน วชา ๓๒๐๗-๗๕๕
review of the literature, Clin Oral Impl Res 18 (Suppl. 3) (2007), pp. 138–150. Full Text via CrossRef | View Record
in Scopus | Cited By in Scopus (4)
[73] J.C. Türp, F. Komine and A. Hugger, Efficacy of stabilization splints for the management of patients with
masticatory muscle pain: a qualitative systematic review, Clin Oral Invest 8 (2004), pp. 179–195. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (17)
[74] T.T. Dao and G.J. Lavigne, Oral splints: the crutches for temporomandibular disorders and bruxism?, Crit Rev
Oral Biol Med 9 (1998), pp. 345–361. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (75)
[75] C.L. Harwood, The evidence base for current practices in prosthodontics, Eur J Prosthodont Rest Dent 16
(2008), pp. 24–34. View Record in Scopus | Cited By in Scopus (3)
[76] K. Gotfredsen, G.E. Carlsson, A. Jokstad, K. Arvidson Fyrberg, M. Berge and B. Bergendal et al., Implants
and/or teeth: consensus statements and recommendations, J Oral Rehabil 35 (Suppl. 1) (2008), pp. 2–8. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (3)
[77] M. Lulic, U. Brägger, N.P. Lang, M. Zwahlen and G.E. Salvi, Ante’s (1926) law revisited: a systematic review on
survival rates and complications of fixed dental prostheses (FDPs) on severely reduced periodontal tissue support,
Clin Oral Impl Res 18 (Suppl. 3) (2007), pp. 63–72. Full Text via CrossRef | View Record in Scopus | Cited By in
Scopus (7)
[78] B.E. Pjetursson and N.P. Lang, Prosthetic planning on the basis of scientific evidence, J Oral Rehabil 35 (Suppl.
1) (2008), pp. 72–79. Full Text via CrossRef | View Record in Scopus | Cited By in Scopus (7)
Tel.: +46 31 786 3191; fax: +46 31 786 3193.
Vichet Chindavanig วเชฏฐ จนดาวณค
86
Related Documents











