2/20/17 1 BASICS OF MECHANICAL VENTILATION Deborah Silverstein, DVM, DACVECC With special thanks to Drs. L. King, L. Waddell and K. Beer Garret Pachtinger, VMD, DACVECC COO, VETgirl Introduction Justine A. Lee, DVM, DACVECC, DABT CEO, VETgirl Introduction VETgirl…On-The-Run • The tech-savvy way to get online veterinary CE! • A subscription-based podcast and webinar service offering veterinary RACE-approved CE VETgirl ELITE 50-60 podcasts/year plus 30+ hours of webinars! • $199/year • 40+ hours of RACE-CE Up to 5 members: $599/year Up to 10 members: $999/year > 10 members: Ping us

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
2/20/17
1
BASICS OF MECHANICAL VENTILATION
Deborah Silverstein, DVM, DACVECC
With special thanks to Drs. L. King, L. Waddell and K. Beer
Garret Pachtinger, VMD, DACVECC
COO, VETgirl
Introduction
JustineA.Lee,DVM,DACVECC,DABTCEO,VETgirl
Introduction VETgirl…On-The-Run• The tech-savvy way to get online veterinary CE!• A subscription-based podcast and webinar service offering veterinary RACE-approved CE
VETgirl ELITE
50-60 podcasts/year plus 30+ hours of webinars!• $199/year• 40+ hours of RACE-CE
Up to 5 members: $599/year
Up to 10 members:$999/year
> 10 members:Ping us
2/20/17
2
Video Archives! New and improved video!
Download our iTunes podcasts free!
Social media and our blog! Logistics: CE Certificatesn Typeinquestionsn Emailedtoyou48hours afterthewebinarn Activeparticipation=noquizn Watchingvideolater,mustcompletequiz
n ELITEmembersonlyn Email/contactwithANYquestions

2/20/17
3
Introduction Deborah Silverstein,DVM, DACVECC
Associate ProfessorDepartment of Clinical
Studies
University of Pennsylvania School of Veterinary
Medicine
Outline• What is mechanical ventilation?• Indications
• Hypoventilation – Differentials!• Hypoxemia – Differentials!• Concern for fatigue/exhaustion
• Types and modes of ventilation• Pressure vs. volume limited• A/C, SIMV, CPAP• PEEP
• Complications• Prognosis• What is the veterinary evidence?
What is mechanical ventilation?• Using a machine to perform some or all of the work of breathing
• PPV: Positive Pressure Ventilation• Machine provides an
increase in airway pressure to move gas into the lungs
Iron Lungà negative pressure ventilation
“Mandy Jo”
• 4 yo FS American Staffordshire terrier• Found acutely paralyzed at the bottom of the stairs• No motor function x 4• Hyper-reflexive x 4• Intact pain sensation
• Respiration mainly diaphragmatic, little intercostal movement
• What are your differentials? What would you recommend to the owners?
“Mandy Jo”: Diagnostics• Suspect spinal cord injury• Myelogram shows compression at C2/C3• Impairment of respiration due to failure of impulse generation in the phrenic and intercostal nerves
2/20/17
4
“Mandy Jo”: Post-op
Dorsal laminectomy C2/C3/C4Post-op admit to ICU: No chest wall movement, cyanotic
pH 7.01PaO2 54 mmHg (FiO2 21%)
PaCO2 80 mmHgHCO3 25 mmol/L
What is your diagnosis?
Calculating the A-a gradient• Useful in determining lung function
• Is the dog just hypoventilating or is there a pulmonary parenchymal problem?
• The simplified version: • PAO2 = 150 – 1.1 x [PaCO2]• A-a gradient = PAO2 – PaO2
• Normal = 5-15 mmHg
• The REALLY simplified version: • PaO2 + PaCO2 > 120 = NORMAL A-a gradient• On room air only!
Ways to deliver oxygen “Mandy Jo” ABG following oxygen supplementation:
pH 7.003PaO2 253 mmHg (mask)
PaCO2 91 mmHgHCO3 24.2 mmol/L
What do you think now?What would you like to do?
Indications for PPV
• Hypoventilation• PaCO2 > 60 mmHg
• Hypoxemia• PaO2 < 60 mmHg despite O2 supplementation
• Impending fatigue• PaCO2 increasing• PaO2 decreasing and non-responsive to increased
FiO2• “If you’re staring at your patient in the oxygen cage
and wondering if you should initiate PPV, the answer is probably yes”
• Other situations
Causes of hypoventilation• Think about it anatomically!
2/20/17
5
“Mandy Jo”The decision to ventilate
Plan: • Use the ventilator to provide
respiratory support while the spinal cord heals
Decision:• How should we do this?
“Mandy Jo”: Goals of PPV in an animal with ventilatory failure
• To increase tidal volume towards normal (Vt=10-15 ml/kg)• To improve minute ventilation to allow:
• Elimination of CO2
• Resolution of respiratory acidosis
• Resolution of distress• (Normal minute ventilation
Ve=150-250 ml/kg/min)
Modes of Ventilation
• Controlled ventilation
• Ventilator does all of the work
• Patient can trigger ventilator
• Assisted ventilation
• Patient can initiate breaths and ventilator assists
• Synchronized intermittent mandatory ventilation
• Combination of mandatory (controlled) breaths and
spontaneous breaths
Modes of Ventilation
• Pressure-controlled ventilation (PC)• Gas is delivered to a chosen airway pressure, regardless of the tidal
volume • Appropriate for animals with lung disease
• Volume-controlled ventilation (VC)• A pre-determined tidal volume is given regardless of the airway
pressure generated• Appropriate for animals with normal lungs and some with lung
disease
Trigger, Cycle and Limit Variable
• Inspiratory trigger variableà time, flow or pressure necessary to
cause the machine to start inspiration
• If the animal attempts to breathe and generates the preset negative flow or
pressure, the ventilator will synchronize or assist the breath
• Cycle variableà causes inspiration to end (flow or time)
• Limit variableà preset limits that will not terminate a breath, but
cannot be exceeded
Positive End Expiratory Pressure (PEEP)• Positive pressure applied at the end of each breath• Purpose: Recruit alveoli and hold them open for use in gas
exchange + prevent repetitive collapse and opening of the alveloi

2/20/17
6
Traditional recommendations for PPV settings
• Tidal volume 10-15 ml/kg
• RR 10-12 bpm
• Peak Inspiratory Pressure10-20 mmHg
• PEEP 0-2 cm H20
• Emphasis on maintaining adequate values for PaO2 and PaCO2
“Mandy Jo” 20kgChoosing initial ventilator settings
Pre-ventilation Initial settingsRR 68 12Vt (mls) 25 125Ve (mls/kg/min) 85 75FiO2 0.4 (mask) 0.5Pressure 7
PEEP 2PaO2 253PaCO2 91
“Mandy Jo” 20kgChoosing initial ventilator settings
Pre-ventilation Initial settingsRR 68 12Vt (mls) 25 125Ve (mls/kg/min) 85 75FiO2 0.4 (mask) 0.5Pressure 7
PEEP 2PaO2 253 136PaCO2 91 87
“Mandy Jo” 20kgChoosing initial ventilator settings
Initial settings New settingsRR 12Vt 125Ve 75FiO2 0.5Pressure 7
PEEP 2PaO2 136PaCO2 87
“Mandy Jo” 20kgChoosing initial ventilator settings
Initial settings New settingsRR 12 15Vt 125 210Ve 75 158FiO2 0.5 0.3Pressure 7 12
PEEP 2 2PaO2 136PaCO2 87
“Mandy Jo” 20kgChoosing initial ventilator settings
Initial settings New settingsRR 12 15Vt 125 210Ve 75 158FiO2 0.5 0.3Pressure 7 12
PEEP 2 2PaO2 136 123PaCO2 87 42
2/20/17
7
Airway management in ventilator patients
• Low pressure high volume endotracheal tubes
• Heated humidifiers always added to circuit
• Suction airway secretions as needed• Maintain sterile airway as much as possible
• Immunosuppression and invasive airway tubes increase risk of ventilator acquired pneumonia
“Mandy Jo”
•Volume limited ventilation
•Tracheostomy tube
•Nutritional support
The benefits of tracheostomy Modes of Ventilation
Synchronized intermittent mandatory ventilation (SIMV)
• Ventilator is set to deliver a minimum desired number of breaths per minute
• Patient can breathe spontaneously between ventilator breaths• Some work of breathing is assumed by the patient• Useful for weaning, preventing muscle atrophy
“Mandy Jo”: Progression
• Gradual improvement in
respiratory muscle activity
• Weaned from ventilator after 5
days
• Walking after 4 weeks
Ventilator outcomes in dogs with cervical spinal cord injury (Beal MW, et al. JAVMA 2001)
Objectives• Describe ventilator management, clinical course, and outcome in dogs with ventilatory failure secondary to cervical spinal cord disease or injury
• Identify risk factors for perioperative ventilation in surgically managed cases of cervical spinal cord disease/injury

2/20/17
8
Results
• 268 dogs with cervical spinal cord surgeries• 13 required perioperative PPV• 4.9% incidence in surgical patients• 1 non-surgical cervical injury included (FCE?)
• No significant relationship between the need for perioperative PPV and• Breed• Age• Underlying disease process
Results: Outcome
• 10 of 14 dogs weaned from ventilator (71%)
• 4/14 euthanized• Multiple organ failure (n=2)• No improvement in ventilation after 10 days (n=1)• Owner elected euthanasia (n=1)
ResultsDuration of ventilation• Mean (n=14) = 4.5 days• Mean (survivors) = 4.5 days • Range = (0.4-13 days)
Neurologic outcome in survivors• 9/10 dogs were ambulatory with bladder and bowel function• 1/10 non-ambulatory• Mean time to return to function = 53.4 days (n=7)
“Sasha”• 30 kg FS Golden Retriever • Hit by car 1 hour prior to presentation• Heart rate 200 bpm, weak pulses and pale mucous membranes
• Distended abdomen, possible fluid wave• Respiration rate 48 bpm, significantly increased respiratory effort
• Diffuse crackles on lung auscultation
• PCV 34% TS 4.2 g/dl
“Sasha”:Thoracic radiographs at admission
Pulmonary contusion• Hemorrhage from multiple capillaries into the pulmonary
parenchyma and alveoli
• Can progress over 12-24 hours following initial trauma• Ongoing hemorrhage• Pulmonary edema following fluid therapy
• Respiratory distress often worsens before it improves
2/20/17
9
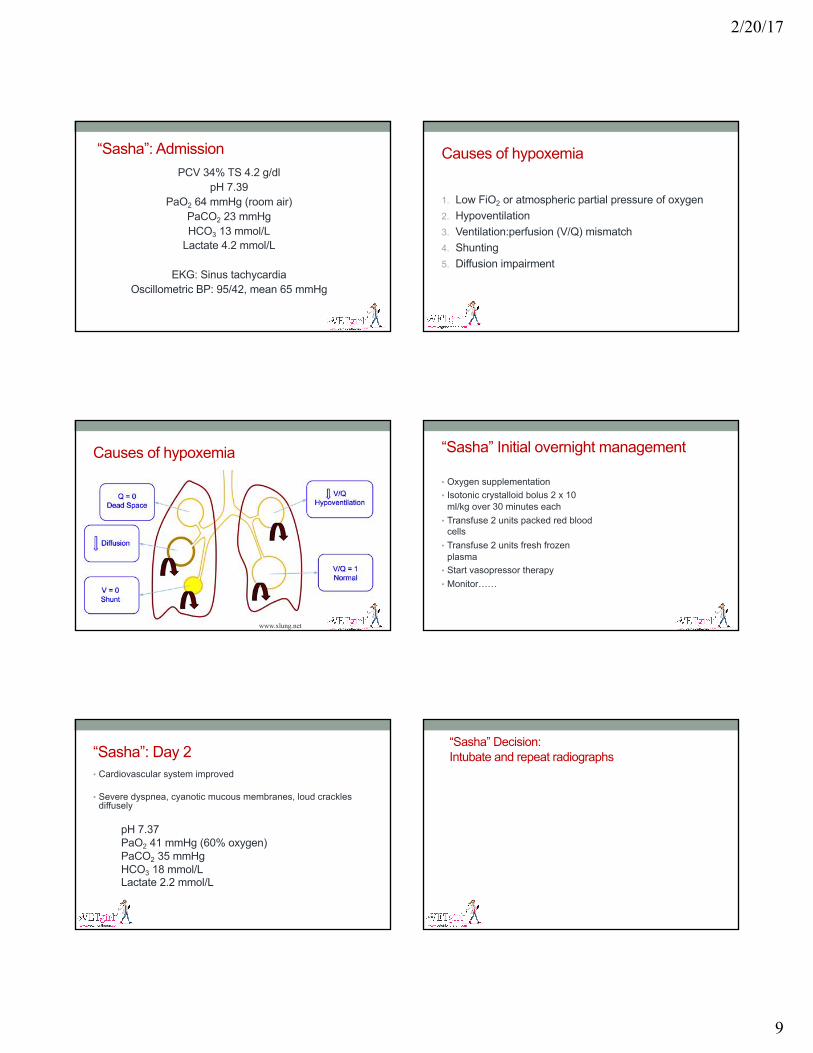
“Sasha”: AdmissionPCV 34% TS 4.2 g/dl
pH 7.39PaO2 64 mmHg (room air)
PaCO2 23 mmHgHCO3 13 mmol/L
Lactate 4.2 mmol/L
EKG: Sinus tachycardiaOscillometric BP: 95/42, mean 65 mmHg
Causes of hypoxemia
1. Low FiO2 or atmospheric partial pressure of oxygen2. Hypoventilation3. Ventilation:perfusion (V/Q) mismatch4. Shunting5. Diffusion impairment
Causes of hypoxemia
www.xlung.net
“Sasha” Initial overnight management
• Oxygen supplementation• Isotonic crystalloid bolus 2 x 10
ml/kg over 30 minutes each• Transfuse 2 units packed red blood
cells• Transfuse 2 units fresh frozen
plasma• Start vasopressor therapy• Monitor……
“Sasha”: Day 2• Cardiovascular system improved
• Severe dyspnea, cyanotic mucous membranes, loud crackles diffusely
pH 7.37PaO2 41 mmHg (60% oxygen)PaCO2 35 mmHgHCO3 18 mmol/LLactate 2.2 mmol/L
“Sasha” Decision: Intubate and repeat radiographs

2/20/17
10
“Sasha”The decision to ventilate
Plan: • Use the ventilator to provide respiratory support while the lung parenchyma heals
Decision:• How should we do this?
“Sasha”: Goals of PPV for patients with failure of pulmonary gas exchange
• To improve tidal volume • To improve gas exchange by opening
recruitable alveoli• To minimize the energy expenditure
associated with increased work of breathing • To resolve respiratory distress• To minimize ventilator-induced lung injury by
avoiding high airway distending pressures
Long term anesthesia in ventilator patients
• Anesthesia is needed to facilitate maintenance of the endotracheal tube
• Injectable anesthetics and sedatives usually given by CRI• Opioids• Benzodiazepines• Ketamine• Dexmedetomidine• Propofol• Alfaxalone
• Neuromuscular blockade if needed
Barotrauma and volutrauma in abnormal lungs
• Normal tidal volumes may • Over-distend compliant alveoli• Produce high airway pressures
• Some alveoli and terminal bronchioles may be collapsed at end expiration and expanded during inspiration: termed “recruitable”
• Cyclical expansion and collapse of recruitable alveoli may result in shear stress in these and adjacent alveoli
Problems with PPV in abnormal lungs
• Over-distension → alveolar epithelial and capillary endothelial injury in previously normal alveoli
• High airway pressures may contribute to barotrauma, resulting in:• Interstitial emphysema• Pneumomediastinum• Pneumoperitoneum• Subcutaneous emphysema• Pneumothorax
Pneumothorax in ventilated animals: What do our studies show?
• King et al. JAVMA 1994
• Pneumothorax developed in 12 animals (29%) during PPV
• Mean PIP in pneumothorax dogs: 36.9 � 13.1 cm H2O
• Mean PIP in those without pneumothorax: 23 � 7.7 cm H2OP < 0.05
2/20/17
11
Pneumothorax in ventilated animals: What do our studies show?
• Lee et al. JAVMA 2005• Pneumothorax developed during PPV in 15/53 cats (28%)
• Pneumothorax developed in:• PIP > 25 cm H2O: 7 of 16 cats • PIP < 25 cm H2O: 8 of 20 cats • No statistical significance
Pneumothorax in ventilated animals: What do our studies show?
Hopper et al. JAVMA 2007• Pneumothorax developed during PPV in 10/148 animals (7%)
• No variables tested were associated with development of pneumothorax
Rutter et al. JVECC 2011Dogs with LMN disease• Pneumothorax in 10/14 dogs
Hoareau et al. JVECC 2011Brachycephalics• Pneumothorax in 0/15 dogs
More problems with PPV
• High FiO2 values may exacerbate inflammation and oxidative injury
• Placement of an endotracheal or tracheostomy tube bypasses host defenses in already immunocompromized patients
• Hemodynamic compromise
Inflammation associated with PPV in diseased lungs
Pro-inflammatory cytokines produced as a result of:• over-distension• shear stress• infection• oxidative injury (high FiO2)
• Cause progression of lung disease• May be released into the circulation and contribute to or cause SIRS and multiple organ failure
What about ALI/ARDS? • Life-threatening complications of critical illness
• Inflammation and changes in the alveolar-capillary membrane lead to pulmonary edema → alveolar flooding with protein-rich fluid and loss of lung volume
• ALI: acute lung injury• ARDS: acute respiratory distress syndrome
• Diagnosed based on clinical signs and findings!
Diagnosing ALI/ARDS1. Acute onset (< 72 hours) of tachypnea and labored breathing2. Known risk factors3. Evidence of pulmonary capillary leak without increased
pulmonary capillary pressurea. Bilateral pulmonary infiltrates on radiographs or CTb. High protein fluid in conducting airways
4. Evidence of inefficient gas exchangea. P:F < 300 for ALI, < 200 for ARDSb. Increased A-a gradient
5. Evidence of diffuse pulmonary inflammation
2/20/17
12
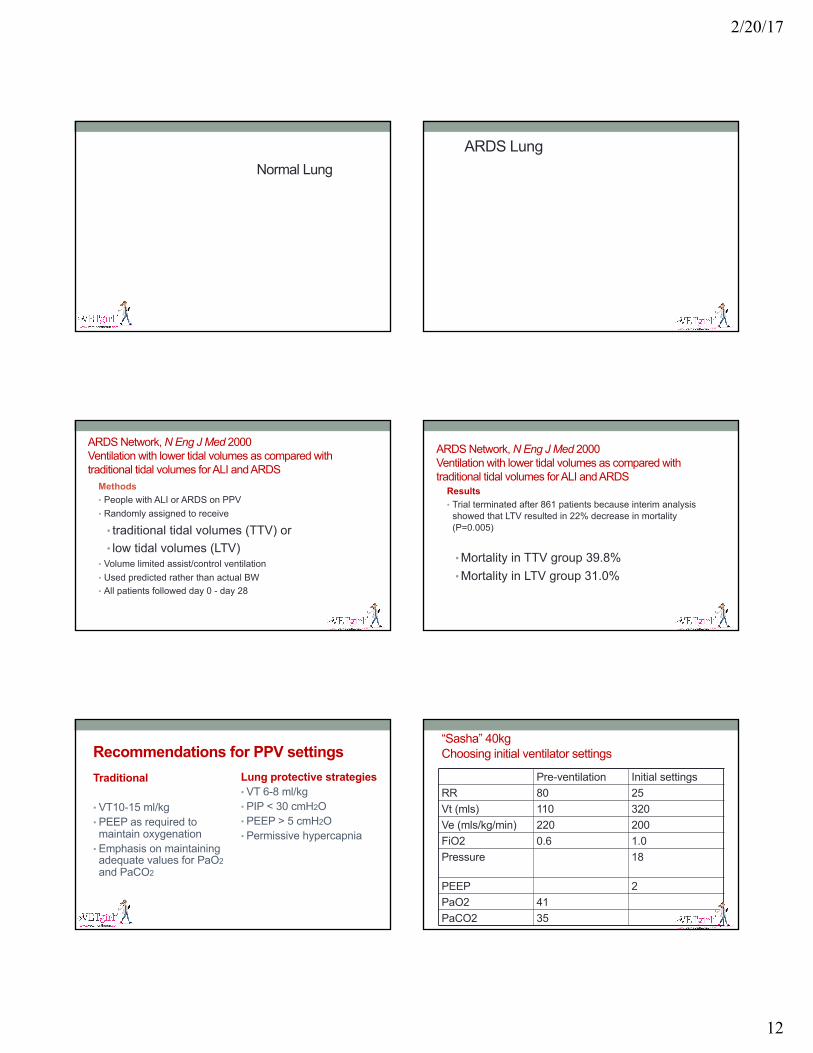
Normal LungARDS Lung
ARDS Network, N Eng J Med 2000Ventilation with lower tidal volumes as compared with traditional tidal volumes for ALI and ARDS
Methods• People with ALI or ARDS on PPV• Randomly assigned to receive
• traditional tidal volumes (TTV) or • low tidal volumes (LTV)
• Volume limited assist/control ventilation• Used predicted rather than actual BW• All patients followed day 0 - day 28
ARDS Network, N Eng J Med 2000Ventilation with lower tidal volumes as compared with traditional tidal volumes for ALI and ARDS
Results• Trial terminated after 861 patients because interim analysis
showed that LTV resulted in 22% decrease in mortality (P=0.005)
• Mortality in TTV group 39.8%• Mortality in LTV group 31.0%
Recommendations for PPV settingsTraditional
• VT10-15 ml/kg• PEEP as required to maintain oxygenation
• Emphasis on maintaining adequate values for PaO2and PaCO2
Lung protective strategies• VT 6-8 ml/kg • PIP < 30 cmH2O• PEEP > 5 cmH2O• Permissive hypercapnia
“Sasha” 40kgChoosing initial ventilator settings
Pre-ventilation Initial settingsRR 80 25Vt (mls) 110 320Ve (mls/kg/min) 220 200FiO2 0.6 1.0Pressure 18
PEEP 2PaO2 41PaCO2 35

2/20/17
13
“Sasha” 40kgChoosing initial ventilator settings
Pre-ventilation Initial settingsRR 80 25Vt (mls) 110 320Ve (mls/kg/min) 220 200FiO2 0.6 1.0Pressure 18
PEEP 2PaO2 41 75PaCO2 35 39
Positive End Expiratory Pressure (PEEP)• Improves oxygenation in the hypoxemic patient• Positive airway pressure prevents complete exhalation, resulting in• Increased FRC• Increased alveolar recruitment• Prevention of early airway closure• Improved oxygenation on lower FiO2
• But…..• Decreases venous return• Increases airway pressures
“Sasha” 40kgChoosing initial ventilator settings
Initial settings New settingsRR 25 25Vt (mls) 320 320Ve (mls/kg/min) 200 200FiO2 1.0 1.0Pressure 18 23
PEEP 2 5PaO2 75PaCO2 39
“Sasha” 40kgChoosing initial ventilator settings
Initial settings New settingsRR 25 25Vt (mls) 320 320Ve (mls/kg/min) 200 200FiO2 1.0 1.0Pressure 18 23
PEEP 2 5PaO2 75 183PaCO2 39 41
“Sasha” 40kgChoosing initial ventilator settings
New settings #1 New settings #2RR 25 25Vt (mls) 320 320Ve (mls/kg/min) 200 200FiO2 1.0 1.0Pressure 23 26
PEEP 5 8PaO2 183PaCO2 41
“Sasha” 40kgChoosing initial ventilator settings
New settings #1 New settings #2RR 25 25Vt (mls) 320 320Ve (mls/kg/min) 200 200FiO2 1.0 1.0Pressure 23 26
PEEP 5 8PaO2 183 257PaCO2 41 40

2/20/17
14
“Sasha” 40kgChoosing initial ventilator settings
New settings #2 New settings #3RR 25 25Vt (mls) 320 320Ve (mls/kg/min) 200 200FiO2 1.0 0.5Pressure 26 26
PEEP 8 8PaO2 257PaCO2 40
“Sasha” 40kgChoosing initial ventilator settings
New settings #2 New settings #3RR 25 25Vt (mls) 320 320Ve (mls/kg/min) 200 200FiO2 1.0 0.5Pressure 26 26
PEEP 8 8PaO2 257 95PaCO2 40 41
“Sasha” day 4
• Progressive improvement in lung function over 48 hours
• Weaned from ventilator day 4
• Discharged from hospital day 7
When to Wean?• General guidelines:
• Improvement in primary disease process
• ABG (or SpO2 and PvCO2) WNL and
• FiO2 ≤40% and
• RR ≤20 bpm with normal TV
• PEEP <4 cm H20
• Cardiovascular stability
Outcomes in dogs ventilated to treat pulmonary contusion following trauma
Campbell VL, et al. JAVMA 2000Objectives• To assess pulmonary function, ventilator management and
outcome in dogs that required PPV for acute pulmonary contusion following trauma (10 cases): 1994-1998
Results: Patient population
• 10 dogs eligible for study• 8 female, 2 male• Type of trauma
Hit by car (n=8)Dragged by car (n=1)Fell from deck (n=1)
• Mean body weight = 19.2 +/- 16 kgRange 5-50 kg
2/20/17
15
Results: OutcomeGroup A• Survival to discharge (n=3)• Improved lung function but died in hospital (n=2)Group B• Died or euthanized because of progressive lung dysfunction
(n=5)
Published outcomes:Dogs and cats ventilated to manage Pulmonary Gas Exchange FailurePenn data (King and Hendricks)• 20 patients 1990-1992: 4 survived (20%)• JAVMA 1994, 204 (7): 1045-1051Davis data (Drellich)• 45 patients over 7 years: 9 survived (20%), 5 discharged alive (11%)• VCNA 2002, 32: 1087-1100Penn data – Cats only (Lee)• 5 cats out of 36 survived (14%)• JAVMA 2005; 226(6):924-31.Davis data (Hopper)• 73 patients: 26 weaned and 16 survived to discharge (22%)• JAVMA 2007; 230: 64-75
ConclusionPositive pressure ventilation can be used for short-term support of respiratory function in small animal patients
QUESTIONS?
This material is copyrighted by VETgirl, LLC. None of the materials provided may be used, reproduced or transmitted, in whole or in part, in any form or by any means, electronic or otherwise, including photocopying, recording or the use of any information storage and retrieval system, without the consent of VETgirl,
LLC. Unless expressly stated otherwise, the findings, interpretations and conclusions expressed do not necessarily represent the views of VETgirl, LLC. Medical information here should be references by the practitioner prior to use. Under no circumstances shall VETgirl, LLC. be liable for any loss, damage, liability or expense
incrred or suffered that is claimed to have resulted from the use of the information provided including, without limitation, any fault, error, omission, interruption or delay with respect thereto. If you have any questions regarding the information provided, please contact [email protected]
Related Documents










![INDEX []...Social networking sites (e.g. Facebook, MySpace, Bebo, Friendster, LinkedIn) Video and photo sharing sites (e.g. Flickr, YouTube) Video podcasts Wikis Any other websites](https://static.cupdf.com/doc/110x72/5f91f83682c1cc51a3503d2f/index-social-networking-sites-eg-facebook-myspace-bebo-friendster.jpg)
