American Edition | March 2017 in this issue: The official journal of the American Association of Equine Practitioners, produced in partnership with BEVA. veterinary equine education From the President’s Desk: Federal challenges, new opportunities kick off 2017 The hazards associated with the use of intrauterine glass balls to suppress oestrus in mares Perinatal asphyxia syndrome

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
American Edition | March 2017
in this issue:
The official journal of the American Association of Equine Practitioners, produced in partnership with BEVA.
veterinaryequine
education
From the President’s Desk: Federal challenges, new opportunities kick off 2017
The hazards associated with the use of intrauterine glass balls to suppress oestrus in mares
Perinatal asphyxia syndrome
WHAT CAN YOUGIVE YOUR HORSETHAT ALSO GIVES YOUPEACE OF MIND?
PROTECTION.
For more information about the Arenus Colic Assurance Program visit www.arenus.com, call 866-791-3344, or speak
to your Arenus Veterinary Solutions Specialist
Up to $10,000 in coverage
Coverage for horses with PRIOR HISTORY OF COLIC*
Coverage for horses with PRIOR HISTORY OF COLIC SURGERY*
MEDICAL and SURGICAL colic coverage
Coverage while horses are TRAVELLING INTERNATIONALLY*
PURCHASING directly through Arenus or participating veterinarians and veterinary clinics for products required for coverage
Arenus’ Colic Assurance Program is the only colic insurance program to offer:
* Some restrictions and requirements may apply
c o n t e n t s
A merican Edit ion
From the President’s Desk: Federal challenges, new opportunities kick off 2017.................. III
Resolve hind suspensory and stifle problems with immersive training at AAEP’s summer 360° meeting .............................................................................................. V
Legacy gift to spur scientific discovery, welfare advancements .............................................VIII
S. WRIGHT ..........................................................................................................................119
Hindlimb lameness associated with a focal osseous metaplasia in an 18-year-old Welsh Section D mareM. GRABSKI, D. FEWS and E. BUSSCHERS ......................................................................121
The hazards associated with the use of intrauterine glass balls to suppress oestrus in maresL. H-A. MORRIS, B. S. L. FRASER, C. CANTLEY and S. WILSHER ..............................125
Diagnostic dichotomy: A question of thoracic mesotheliomaJ. MAY, D. FEWS, K. TENNANT and T. MAIR ..................................................................131
Lessons learned from a strangles outbreak on a large Standardbred farmU. CHRISTMANN and C. PINK .........................................................................................138
Causes of pleural effusions in horses resident in the UKI. JOHNS, C. MARR, A. DURHAM, T. MAIR and T. MCPARLAND ..............................144
Strangles and its complicationsA. G. BOYLE .........................................................................................................................149
Perinatal asphyxia syndromeJ. R. GOLD ...........................................................................................................................158
Nutritional management and practical feeding of the orphan foalS. J. STONEHAM, P. MORRESEY and J. OUSEY ..............................................................165
.............................................................................................................173
Cover photo by Dr. Heather Ross.
veterinaryequine
education
a)

Equine Veterinary Education is a refereed educational journal designed to keep the practicing veterinarian up to date with developments in equine medicine and surgery. Submitted case reports are accompanied by invited reviews of the subject (satellite articles) and clinical quizzes. Tutorial articles, both invited and submitted, provide in-depth coverage of issues in equine practice.
Equine Veterinary Education (American Edition ISSN 1525-8769) is published monthly by the American Association of Equine Practitioners, an international membership organization of equine veterinarians. Office of publication is 4033 Iron Works Parkway, Lexington, KY 40511. Periodicals Postage paid at Lexington, KY and additional mailing office. POSTMASTER: Send address changes to: Equine Veterinary Education, 4033 Iron Works Parkway, Lexington, KY 40511.
Communications regarding editorial matters should be addressed to: The Editor, Equine Veterinary Education, Mulberry House, 31 Market Street, Fordham, Ely, Cambridgeshire CB7 5LQ, UK. Telephone: 44 (0) 1638 720250, Fax: 44 (0) 1638 721868, Email: [email protected].
All manuscript submissions for the journal should be submitted online at http://mc.manuscriptcentral.com/eve. Full instructions and support are available on the site and a user ID and password can be obtained on the first visit. If you require assistance, click the Get Help Now link that appears at the top right of every ScholarOne Manuscripts page.
All subscription inquiries should be addressed to: Subscriptions Department, AAEP, 4033 Iron Works Parkway, Lexington, KY 40511, Telephone: (859) 233-0147, Email: [email protected]. Subscription rates: AAEP annual membership dues include $40 for a subscription to Equine Veterinary Education. Other subscriptions at $151.80. Single copies $37.50.
Canadian Subscriptions: Canada Post Corporation Number 40965005. Send change address information and blocks of undeliverable copies to IBC, 7485 Bath Road, Mississauga, ON L4T 4C1, Canada.
© World copyright by Equine Veterinary Journal Ltd 2017.
The authors, editors and publishers do not accept responsibility for any loss or damage arising from actions or decisions based or relying on information contained in this publication. Responsibility for the treatment of horses under medical or surgical care and interpretation of published material lies with the veterinarian. This is an aca-demic publication and should not be used or interpreted as a source of practical advice or instruction.
The American Association of Equine Practitioners cannot accept responsibility for the quality of products or ser-vices advertised in this journal or any claim made in relation thereto. Every reasonable precaution is taken before advertisements are accepted, but such acceptance does not imply any form of recommendation or approval.
All companies wishing to advertise in Equine Veterinary Education, American edition, must be current AAEP exhibitors. AAEP retains the right, in its sole discretion, to determine the circumstances under which an exhibitor may advertise in this journal. While all advertisers must comply with applicable legal guidelines, Compounding Pharmacies are specifically directed to limit themselves to pharmacy practices as dictated by the FDA Center for Veterinarian Medicine, Compliance Policy Guideline (www.fda.gov/ora/compliance_ref/cpg/cpgvet/cpg608-400.html). Advertising any complete or partial mimicry of drugs and dosage forms of FDA approved formulations will not be accepted. Compounding Pharmacies, or any other exhibitors/advertisers who violate this rule in any fashion, will render their advertising contract null and void.
As a private organization, the AAEP reserves the right to exclude any company from advertising in Equine Veterinary Education, American edition, for any reason. The signing and delivery of the advertising contract shall constitute an offer subject to acceptance by the AAEP. In its sole and absolute discretion, the AAEP may revoke its acceptance of the advertising contract or may terminate any contract by delivery of written notice, in which event the AAEP shall have no liability to the advertiser for damages for any other remedy.
Printed by: Cenveo Publisher Services, Lancaster Division, Lancaster, PA.
E q u i n e v e t e r i n a r y e d u c a t i o nA m e r i c a n E d i t i o n
Editor (UK) T. S. Mair, BVSc, PhD, DEIM, DESTS, DipECEIM, MRCVS
Editors (USA) N. A. White II, DVM W. D. Wilson, MRCVS
Deputy Editors Y. Elce P.R. Morresey P.A. Wilkins
Management Group D. Foley T. S. Mair N. A. White W. D. Wilson J. L. N. Wood
Management Board A. R. S. Barr P. Smith D. Foley N. A. White (US Editor) D. Mountford S. White T. S. Mair (Editor) W. D. Wilson (US Editor) S. E. Palmer J. L. N. Wood (Chairman)
American Association of
Equine Practitioners
4033 Iron Works Parkway Lexington, KY 40511
FAX (859) 233-1968EMAIL [email protected]
To access our website, go to aaep.org, select LOGIN, then enter your email and password or, for first-time visitors, enter your email as your Username and your lastname2017 as your Password.
2017 AAEP Officers
R. Reynolds Cowles, DVM, PresidentMargo Macpherson, DVM, President-ElectJeffrey T. Berk, VMD, Vice PresidentJack Easley, DVM, TreasurerKathleen Anderson, DVM, Immediate Past President
AAEP Staff
David Foley, CAE, Executive Director [email protected]
Lori Rawls, Director of Finance & Operations [email protected]
Sally J. Baker, APR, Director of Marketing & Public Relations
Keith Kleine, Director of Industry Relations [email protected]
Nick Altwies, Director of Membership [email protected]
Kevin Hinchman, Director of Information Technology [email protected]
Jodie Bingham, Foundation Development Coordinator [email protected]
Amity Brannock, Communications & Technology Coordinator [email protected]
Darcy Brumback, Student Programs Coordinator [email protected]
John Cooney, Publications Coordinator [email protected]
Megan Gray, Database Services Coordinator [email protected]
Dana Kirkland, Sponsorship & Advertising Coordinator
Bailey McCallum, EDCC Communication Manager [email protected]
Deborah Miles, CMP, Trade Show Coordinator [email protected]
Jayson Page, Office Manager [email protected]
Carey Ross, Scientific Publications Coordinator [email protected]
Pam Shook, Foundation Programs Coordinator [email protected]
Elizabeth Snellings, Member Engagement Coordinator [email protected]
Sue Stivers, Executive Assistant [email protected]
Lauren Thompson, Communications Coordinator [email protected]
Kristin Walker, Member Relations [email protected]
Elaine Young, Convention & Meetings Coordinator [email protected]
Published monthly. Deadlines are the seventh of the preceding month.Address advertising inquiries to Dana Kirkland (859) 233-0147 / [email protected]
AAEP Mission Statement: To improve the health and welfare of the horse, to further the professional development of its members, and to provide resources and leadership for the benefit of the equine industry.
Assistant Editors F. Andrews D. Archer F.T. Bain A.R.S. Barr A. Blikslager M. Bowen N. CohenV. CoudryA. Dart J.-M. Denoix T. Divers P. Dixon W. Duckett B. Dunkel S. Dyson T. Fischer D. FreemanT. Greet R. Hanson P. Harris M. Hillyer M. Holmes N. Hudson P. Johnson P.T. KhambattaJ.-P. Lavoie
S. Love M.L. MacphersonM.J. MartinelliI.G. Mayhew M. MazanC.W. McIlwraith B. McKenzieR. Moore M. OosterlinckA. Parks S. Puchalski C. Riggs H. Schott J. Schumacher S. Semevelos J. SlaterB. Sponseller C. Sweeney H. Tremaine K. WarehamS. Weese R. WellerC. Yao
Ex-officio J. Cooney

EQUINE VETERINARY EDUCATION / AE / NOVEMBER 2015 IIIEQUINE VETERINARY EDUCATION / AE / MARCH 2017 III
2017 has started with many issues facing equine practice and the equine industries we service.
As expected, the new administration in Washington, D.C., reversed or put on hold many executive and department rulings that came down at the end of the previous admin-istration. This included the USDA’s administrative ruling on soring of Walking Horses, a ruling that had the support of AAEP, AVMA, USEF, AHC and most major equine organizations.
As most are aware, the Prevent All Soring Tactics (PAST) Act has been blocked in the U.S. Senate for several years despite having the support of the majority of the House of Representatives and a near majority of the Senate. This act would authorize the USDA to hire independent inspectors to protect this great breed and prevent the abuse it has suffered at the hands of a few in the show ring. The actions by USDA would have gone around the Senate’s blockade to provide common sense protection for Walking Horses. That is now reversed and the previous state of affairs reinstated. Only the abusers are rewarded.
Let’s hope that the new administration will come to their senses and eliminate this abusive practice. Fellow AAEP member and current AVMA President Dr. Tom Meyer and
I penned an op-ed opposing this reversal that was published online in The Hill, a prominent U.S. political website. You can read our op-ed, “Don’t let horse welfare become a partisan issue,” at http://tinyurl.com/eqoped.
Changing gears, the Resort Symposium recently concluded in Grand Cayman, where 113 of your colleagues and their guests enjoyed the sand, surf and sunshine while receiving world-class CE in equine sports medicine. Many thanks to Dr. Tracy Turner who put the program together and to the speakers who did a great job. I encourage you to make plans to attend next year’s Resort Symposium in Maui.
A productive winter board of directors meeting saw devel-opment of 2017 priorities for the pillars of the strategic plan. Many other issues were also addressed, including a potential new member benefit called Vetcove, a pharma-ceutical ordering program that has been up and running for a year that would provide you, the members, with tools to seek the best pricing on many products you use daily in your practice. Complimentary access to Vetcove’s “Inner Circle” program will only be available through your AAEP membership. The Vetcove concept was approved by the board, which also beta tested the program, but final approval won’t happen until AAEP’s legal counsel has reviewed the contract. Expect to hear more about Vetcove in the near future.
In mid-February, the Continuing Education steering committee met in Lexington, Ky., to lay out the CE program for the next several years based on what you told us in the CE needs assessment survey. One thing you asked for was more small dry labs and wet labs, and I’m pleased to report that those are in the plans for future AAEP edu-cational events.
Any time you have questions or comments on any AAEP issues, do not hesitate to contact me or any of the officers or staff.
From the President’s Desk: Federal challenges, new opportunities kick off 2017
USDA
A veterinary medical officer swabs the pastern of a Tennessee Walking Horse for foreign substances. USDA regulations to strengthen enforcement of the Horse Protection Act were put on hold in January as part of a broad freeze on unpublished rules.
Dr. Reynolds Cowles
By R. Reynolds Cowles, Jr., DVM
“One thing you asked for was more small dry labs and wet labs, and I’m pleased to report that those are in the plans for future AAEP educational events.”

IV EQUINE VETERINARY EDUCATION / AE / MARCH 2017
The AAEP board of directors convened January 29 for its winter board meeting. All directors were present.
The board spent considerable time reviewing progress on strategic plan goals and developing current-year priorities for each plan goal as summarized below:
Enhancing membership valueRelaunch the Touch program with input from a member advisory group; form a millennial task force to maintain relevance to this member demographic; and finalize an agreement with comparison-based veterinary products shopping website Vetcove for the development of an exclusive AAEP member benefit. During the meeting, the board approved the “concept” of the Vetcove proposal but postponed a final vote until the contract has been fully reviewed by legal counsel and language clarifications are confirmed.
Communications/technology
efficient listserv software; and implement specific rec-ommendations from the 2016 communications assessment to facilitate sharing with members of breaking news and other time-sensitive issues.
Wellness/quality of life
features in AAEP publications; and continue to integrate as a complementary component of AAEP conferences.
Promoting the profession
using an equine veterinarian, primarily in the areas of dentistry, vaccinations and wellness exams; collab-orate with media partners and other horse owner publications; and develop additional owner education materials.
Continuing education
Committee at its mid-February meeting; however, they will likely include an increase in hands-on and other small-group interactive programming.
Following strategic plan deliberations, discussions turned to other issues pertaining to the industry or AAEP. Specific actions taken included:
American Horse Council for its proposed economic
impact study, which will be the definitive resource for legislators and other stakeholders.
USA’s request for AAEP partnership in its 2017 events. The board liked the concept but felt the need to prioritize existing resources.
relations working group. The executive director will create a proposal utilizing a different model for future consideration by the board.
The board then focused on policy issues and workgroup recommendations, taking the following actions:
Leadership Development Committee to renew the Lynda.com subscription. Instead the committee will be asked to examine alternative training methods more closely aligned with AAEP volunteer service for committee chairs and Rounds moderators.
Professional Conduct and Ethics Committee to 1) prepare a PowerPoint presentation on ethical practice in equine veterinary medicine; and 2) create a contest in which AAEP student chapters submit the best solution to an ethical situation they will likely encounter when they enter practice, with the contest winner selected by the committee.
Clinical Guidelines for Veterinarians Treating the Performance Horse presented by the Performance Horse Task Force.
submitted a proposal to conduct an Equine Welfare Summit, potentially with AVMA invited to co-host. The board did not approve this recommendation as they felt the proposal needed more specifics for it to be considered.
The meeting concluded with a few items of routine board business. The next board meeting will be held in conjunc-tion with the July Focus meetings in Lexington, Ky.
The AAEP Foundation board met in conjunction with the AAEP board meeting. Specific actions taken during the meeting included:
proposed 2017 tactics.
specialist for up to three years to assist with execution of strategic plan priorities, including fund-raising and development efforts.
research allocations with needs in the field.
AAEP board establishes 2017 priorities
By David Foley, AAEP Executive Director
David Foley
EQUINE VETERINARY EDUCATION / AE / MARCH 2017 V
Hind suspensory and stifle injuries are more common than realized, with stifle issues afflicting up to 40% of athletic horses and suspensory issues trailing only foot problems as the underlying cause of lameness in Western performance horses.
At the AAEP’s 360° Diagnosing, Imaging and Treating the Hind Suspensory and Stifle, you’ll conquer the challenges of accurately imaging these regions and staging the severity of the disease through interactive, small-group training that employs a holistic approach to identifying and resolving lameness. Building off the anatomy of both regions, you’ll refine your imaging techniques and gain a better understanding of therapeu-tics and rehabilitation methods essential to a successful athletic return of the injured horse.
Daily wet labs using cadavers and live horses will reinforce lectures and equip you to perform:
needle stick to inject all three pouches of the stifle joint
hy and ultrasound of key structures
On the final day, you will put your newly acquired skills to the test by working up unknown clinical cases on live horses. You will leave the meeting confident in your ability to implement the newly acquired knowledge and skills immediately in your practice.
This exceptional learning opportuni-ty is limited to 20 participants and is being held at Colorado State University, whose faculty has pioneered consider-able research in these areas as well as many of the diag-nostics and therapeutics used to return these horses to work. An exceptionally low student-to-instructor ratio of 1.33-to-1 provides additional opportunities to engage on outside cases during lunch and develop professional relationships at evening social events.
360° Diagnosing, Imaging and Treating the Hind Suspensory and Stifle will be held July 9-12. Early registration is strongly encouraged due to the meeting’s limited attendance. Registration will open soon at aaep.org/meetings, where you can view the syllabus and acquire additional information about the meeting.
360° Diagnosing, Imaging and Treating the Hind Suspensory and Stifle is sponsored by:
Resolve hind suspensory and stifle problems with immersive training at AAEP’s summer 360° meeting
Students and new grads: Submit a case study for chance to score convention trip
AAEP student members and recent graduates in their first year of practice or internship are invited to submit case presentations to be featured as educational resources on the AAEP website. The primary
attend the 63rd Annual Convention, Nov. 17-21, 2017, in San Antonio, Texas.
Presentations must be submitted in PowerPoint. There is no limit to the number of case studies that may be submitted; however, a primary student or first-year graduate author must be identified for each submission. Submissions will be evaluated by members of the Educational Programs Committee and
selected based on quality and educational merit. Participants are encouraged to work with mentors in the preparation and review of their submissions. Case presentation examples are available at aaep.org/case-studies.
Instructions and a case study template can be requested from Carey Ross, scientific publications coordinator, at [email protected]. Submissions are due by May 1, and winners will be announced by September 1.
VI EQUINE VETERINARY EDUCATION / AE / MARCH 2017
By Cynthia MacKenzie, DVM
The winter session of the AVMA House of Delegates (HoD) convened Jan. 12-14, 2017, in con-junction with the annual AVMA Veterinary Leadership Conference in Chicago, Ill.
For the second consecutive year, the HoD held a Veterinary Informational Forum to discuss current and emerging issues within the profession. Of particular interest to equine practitioners was the topic of telemedicine. The existing
AVMA Model Veterinary Practice Act states, “A veterinarian-client-patient relationship cannot be established solely by telephonic or other electronic means.” The AVMA has produced a report containing recommendations on telemedi-cine for potential inclusion in its Model Veterinary Practice Act. You can view and comment on the report and proposed changes at http://tinyurl.com/avmatm17. I encourage AAEP members to participate in the discussion and let your opinions be heard by visiting the website, reaching out to your state VMA representatives and your AAEP delegates.
Another item of interest involved the AVMA initiatives on the topic of wellness, which include several ongoing collab-orative efforts with veterinary colleges, allied organizations,
VMAs, corporate sponsors and the AMA; and a Veterinary Wellness Steering Committee, Well-being Coalition and LinkedIn community. More information on AVMA wellness resources can be found at avma.org/wellness.
Among resolutions considered during the meeting, the HOD amended and approved a new policy on responsible breeding of companion animals. The purpose of this policy is to support responsible breeding practices that reduce or eliminate the health and welfare concerns associated with inherited conditions, not to condemn or stigmatize specific breeds. Horses were not mentioned during the discussion as they are considered livestock per the definition of the U.S. government. A more detailed description of the policy can be found at http://tinyurl.com/resbreed.
These are just a few of the highlights from the meeting. Please don’t hesitate to contact Dr. Stuart Brown or me for additional information or clarification. As your representa-tives in the AVMA HoD, we welcome your comments and input, and we are honored to serve the AAEP in this capacity.
Dr. MacKenzie is associate director of learning and develop-ment for Merck Animal Health. She serves as AAEP delegate to the AVMA House of Delegates and is chair of the AAEP’s Welfare and Public Policy Advisory Council.
Delegate Corner: Telemedicine, wellness prominent at AVMA winter meeting
Dr. Cynthia MacKenzie
Noted sport horse practitioner assumes reins of AAEP Foundation
Dr. Rick Mitchell, co-founder in 1989 of Fairfield Equine Associates in Newtown, Conn., has been appointed chair of the Foundation Advisory Council, succeeding Dr. Jeff Berk whose three-year term expired.
As part-owner of Fairfield Equine, a sport horse practice that has served the United States Equestrian Team for over two decades, Dr. Mitchell’s specialties include equine medicine and surgery with an emphasis on lameness and imaging.
Last year marked his sixth visit to the Olympic Games as an attending veteri-narian for the U.S. Equestrian Team. Dr. Mitchell is also an accomplished rider, having won two national championships and one world championship in various disciplines.
A 1974 graduate of the Oklahoma State University College of Veterinary Medicine, Dr. Mitchell has served on the boards of multiple equine industry organizations, including a current stint as a trustee for the American Horse Council and chair of its Health and Regulatory Committee.
In addition to Dr. Mitchell’s appointment as chair, the Foundation Advisory Council recently welcomed four new members: Dr. Mark Baus, Dr. Rocky Bigbie, Dr. Elizabeth Fish and former Foundation chair Dr. Nat White.
Dr. Rick Mitchell
EQUINE VETERINARY EDUCATION / AE / NOVEMBER 2015 VIIEQUINE VETERINARY EDUCATION / AE / MARCH 2017 VII
With a strong emphasis on improved navigation and an upgrade to the Rounds listserv software, the AAEP launched a redesigned website on February 24 following beta testing by a cross-section of the membership.
The new aaep.org features unique home pages and content for both DVM and student members, as well as horse health information in the non-member section for horse owners. Although the site is new, your username and password remain the same. Once logged in, the View My Member Profile button is your portal for updating your member information, joining a Rounds discussion list, completing the Volunteer Interest Form and more.
Prominent navigation bar links offer expedited access to:
CE Meetings, including a schedule of upcoming AAEP education events.Resources, including AAEP reference documents such as guidelines, position statements and white papers.Ethics, including ethical guidelines, videos and an archive of ethics features from EVE.Wellness, including resources to assist with physical, emotional and financial health.
As with any redesign, it may take a bit of time to adjust to the new user experience. However, we think you’ll find the site offers a much-improved experience and hope it serves as a valuable resource in your daily practice.
If you have questions about the site, please contact Amity Brannock at [email protected].
Visit the new AAEP website for your membership needs
Touch Point: Use a survey to determine new services to offer your clients
AAEP market research revealed that 20% of your clients would use you more if you offered more services. This is extremely positive news for equine practice.
How do you identify the services your clients want you to provide?
sent post-visit or annually can be the tool through which you learn what your clients want.
when someone in the practice is dedicated to evaluating the responses. Online survey tools like SurveyMonkey are cost effective, tabulate the responses for you and make the process simple. The human brain trust in the practice will still need to determine what the survey data may mean for your mix of client services.
To add or not to add, that is the question. Offering a new service may require staff training, purchasing a new piece of equipment or hiring a veterinarian with the required skill set. There are simple formulas that can help you determine if the benefit in terms of revenue exceeds the cost of adding the service to your menu.
The Touch program provides the easy-to-use tools you need to survey your clients. Visit touch.aaep.org to choose from several resources:
Log in to the Touch website using the same username and password as you use for aaep.org. The Touch program is exclusively available to AAEP members.

VIII EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Legacy gift to spur scientific discovery, welfare advancements
Supporting causes that benefit the horse is essential to equine surgeon and university professor Dr.
Wayne McIlwraith and former racetrack practitioner Dr. Nancy Goodman. One such cause is the AAEP Foundation, which Dr. McIlwraith previously chaired.
By including the Foundation in their estate plan, the couple are members of the Legacy Society. They recently discussed their estate gift, which they said will benefit horse, owner and practitioner by aiding in the discovery and advancement of sci-ence-based treatments for persistent medical mysteries.
Describe the important role horses have played in your lives. Wayne: I was fascinated by horses from my early days in Oamaru, New Zealand, sneaking up to watch the occasional race meetings in our small town unbeknownst to my mother. I was taught to ride by my aunt who showed show jumpers but then didn’t really focus on horses until my internship in large animal surgery at the University of Guelph and onto the residency and Ph.D. at Purdue. I really started getting involved in the equine industry as a whole when I started doing arthroscopic surgery.
Nancy: I rode as a child. With the pressures of university studies, veterinary school and keeping ahead financially, I couldn’t afford to ride in college but team roped during veterinary school. I went to veterinary school at Colorado State University to become an equine racetrack veterinari-an and achieved that goal when I went to work for Dr. Bart Baker at Equine Medical Center after graduating in 1981. That led to a 20-year career based at Los Alamitos. I also took up riding again showing show hunters, including being Amateur Owner Hunter Champion in California two years in a row. After retirement from the racetrack, my next career has been showing and breeding horses based on our farm in Colorado.
Is there an important moment, person or special reason connected with AAEP that influenced your decision to include the AAEP Foundation in your estate plans?Nancy: We are both long-term members of AAEP and were always supportive from the time the AAEP Foundation was conceived. We became more focused when Wayne chaired the Foundation Advisory Council from 2008 to 2013. In
our various experiences with fundraising, it is certainly important that when you are doing it you also have to be participating! Including the AAEP in estate plans gives an opportunity to make a larger donation to support the ongoing work. We have always prioritized the Orthopaedic Research Center at Colorado State University as well as AAEP and ACVS in our annual donations and have continued this into our estate planning.
When you think of the AAEP Foundation, what key words or phrases come to mind?Wayne: Ensuring the welfare of the horse as well as we can. Our job as equine veterinarians is fixing horses, whether it be by individual diagnosis and optimal state-of-the-art treatment or through research answering the important questions that have still not been solved. Supportive research and recommendations based on science for current veterinarians as well as future generations will enable them to best serve their clients and the horses.
What legacy do you hope to leave through your estate gift?Wayne: A legacy for the future benefit of horses, not a personal
legacy to us. Having served on the Foundation Advisory Council for six years, I know that an accumulated corpus will be carefully used by the AAEP focusing on optimal care and education. Hopefully these actions inspire others to incorporate the AAEP Foundation into their estate planning.
If you’d like, talk about the steps, considerations or thought process that went into your planning.Wayne: Both of us appreciate what our careers as equine veterinarians have brought us in terms of pleasure, continued passion for what we do and, ultimately, a fantastic lifestyle. Much of our career successes are attributable to mentoring by equine veterinarians, great relationships all over the world with equine veterinarians and AAEP.
Nancy: Philanthropy is an important focus for us and estate planning is a critical part of life to ensure that our money goes to the worthy causes that have meant so much to us.
Drs. Nancy Goodman and Wayne McIlwraith
Interested in joining the Legacy Society?
Contact Jodie Bingham, Foundation development
EQUINE VETERINARY EDUCATION / AE / MARCH 2017 IX
Don’t let infectious diseases get the jump on you and your clients
The equine herpesvirus outbreaks that cropped up across the country this winter, including a persistent outbreak first diagnosed in December at the Fair Grounds race track in New Orleans, La., that quarantined seven of the track’s 49 barns and affected field size, handle and horse movement, reinforce the importance of real-time infectious disease updates to raise awareness and mitigate disease spread.
The Equine Disease Communication Center (EDCC), the industry-funded hub for monitoring and communicating accurate equine infectious disease information, has elevated the collection and dissemination processes so that industry stakeholders can implement proper precautions in the wake of reported outbreaks.
Through email and social media, you and your clients can be alerted of confirmed outbreaks and updates to previously reported outbreaks. Sign up through equinediseasecc.org to join the more than 2,300 individuals receiving outbreak alert emails. Outbreak information is also posted on social media. Like the EDCC on Facebook at facebook.com/EquineDiseaseCC and follow @EquineDiseaseCC on Twitter.
Visit equinediseasecc.org and click the “Sponsors” link to learn how you can make a tax-deductible contribution to support the operation of the EDCC.
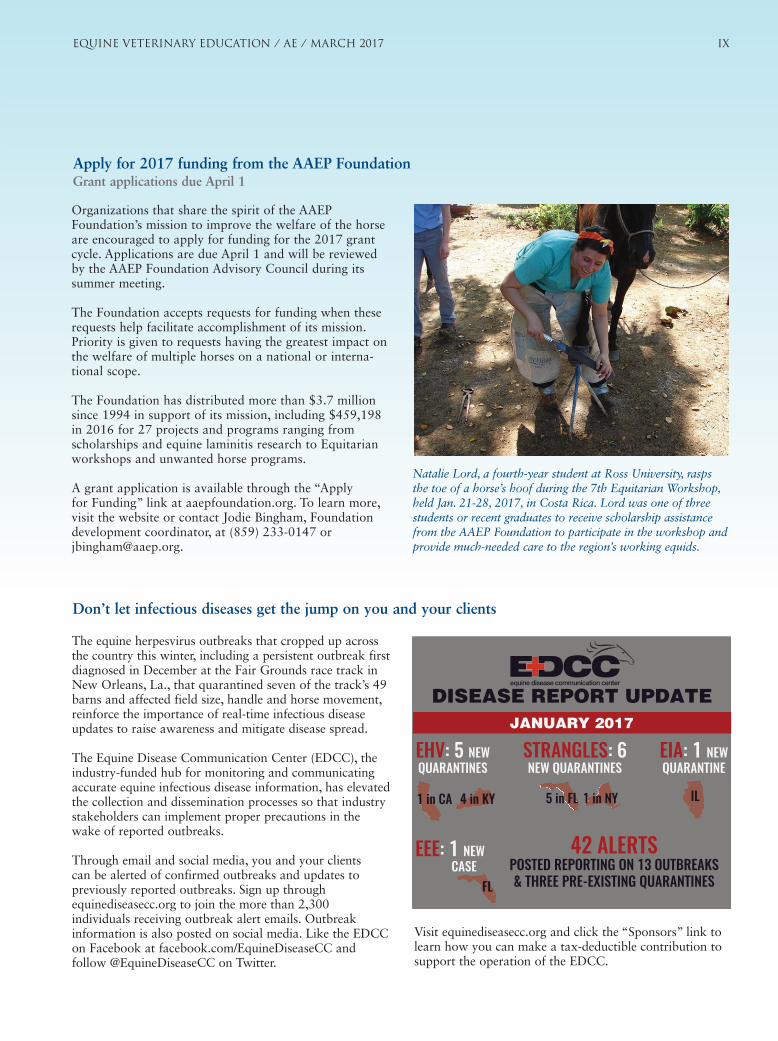
42 ALERTS POSTED REPORTING ON 13 OUTBREAKS & THREE PRE-EXISTING QUARANTINES
DISEASE REPORT UPDATEJANUARY 2017
EHV: 5 NEW QUARANTINES
4 in KY1 in CA
STRANGLES: 6 NEW QUARANTINES
5 in FL 1 in NY
EIA: 1 NEW QUARANTINE
IL
EEE: 1 NEW CASE
FL
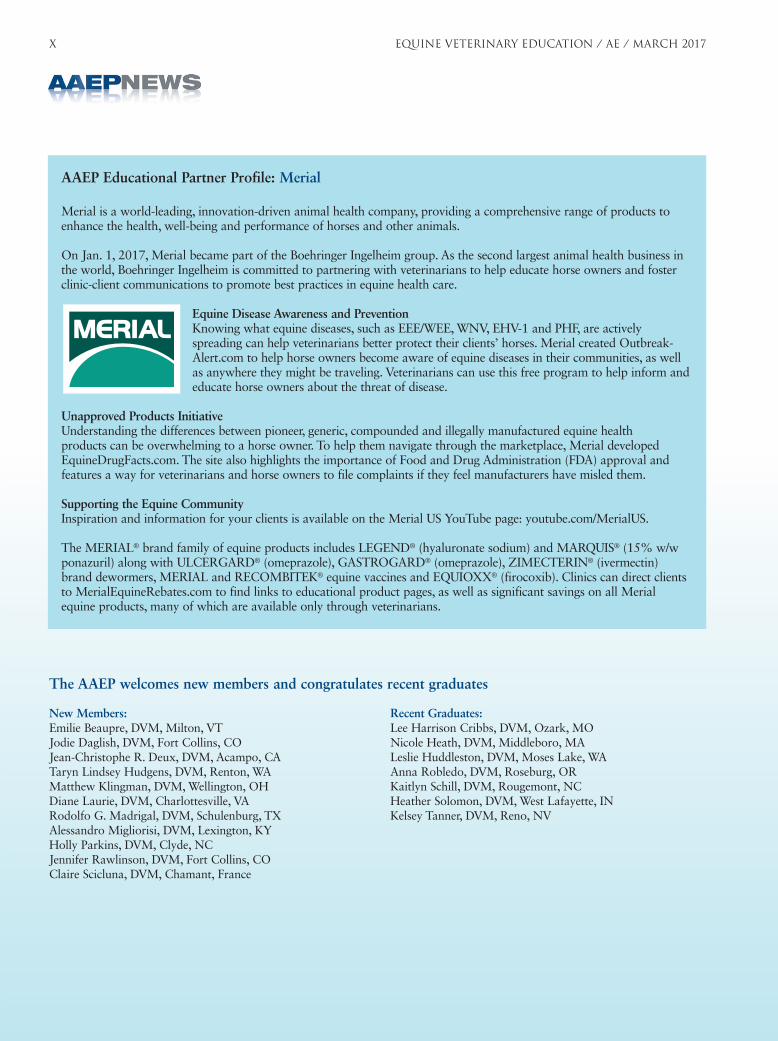
Organizations that share the spirit of the AAEP Foundation’s mission to improve the welfare of the horse are encouraged to apply for funding for the 2017 grant cycle. Applications are due April 1 and will be reviewed by the AAEP Foundation Advisory Council during its summer meeting.
The Foundation accepts requests for funding when these requests help facilitate accomplishment of its mission. Priority is given to requests having the greatest impact on the welfare of multiple horses on a national or interna-tional scope.
in 2016 for 27 projects and programs ranging from scholarships and equine laminitis research to Equitarian workshops and unwanted horse programs.
A grant application is available through the “Apply for Funding” link at aaepfoundation.org. To learn more, visit the website or contact Jodie Bingham, Foundation
Apply for 2017 funding from the AAEP Foundation Grant applications due April 1
Natalie Lord, a fourth-year student at Ross University, rasps the toe of a horse’s hoof during the 7th Equitarian Workshop, held Jan. 21-28, 2017, in Costa Rica. Lord was one of three students or recent graduates to receive scholarship assistance from the AAEP Foundation to participate in the workshop and provide much-needed care to the region’s working equids.
X EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Merial is a world-leading, innovation-driven animal health company, providing a comprehensive range of products to enhance the health, well-being and performance of horses and other animals.
On Jan. 1, 2017, Merial became part of the Boehringer Ingelheim group. As the second largest animal health business in the world, Boehringer Ingelheim is committed to partnering with veterinarians to help educate horse owners and foster clinic-client communications to promote best practices in equine health care.
Equine Disease Awareness and PreventionKnowing what equine diseases, such as EEE/WEE, WNV, EHV-1 and PHF, are actively spreading can help veterinarians better protect their clients’ horses. Merial created Outbreak-Alert.com to help horse owners become aware of equine diseases in their communities, as well as anywhere they might be traveling. Veterinarians can use this free program to help inform and educate horse owners about the threat of disease.
Unapproved Products InitiativeUnderstanding the differences between pioneer, generic, compounded and illegally manufactured equine health products can be overwhelming to a horse owner. To help them navigate through the marketplace, Merial developed EquineDrugFacts.com. The site also highlights the importance of Food and Drug Administration (FDA) approval and features a way for veterinarians and horse owners to file complaints if they feel manufacturers have misled them.
Supporting the Equine CommunityInspiration and information for your clients is available on the Merial US YouTube page: youtube.com/MerialUS.
The MERIAL® brand family of equine products includes LEGEND® (hyaluronate sodium) and MARQUIS®
ponazuril) along with ULCERGARD® (omeprazole), GASTROGARD® (omeprazole), ZIMECTERIN® (ivermectin) brand dewormers, MERIAL and RECOMBITEK® equine vaccines and EQUIOXX® (firocoxib). Clinics can direct clients to MerialEquineRebates.com to find links to educational product pages, as well as significant savings on all Merial equine products, many of which are available only through veterinarians.
AAEP Educational Partner Profile: Merial
The AAEP welcomes new members and congratulates recent graduates
New Members:Emilie Beaupre, DVM, Milton, VTJodie Daglish, DVM, Fort Collins, COJean-Christophe R. Deux, DVM, Acampo, CATaryn Lindsey Hudgens, DVM, Renton, WAMatthew Klingman, DVM, Wellington, OHDiane Laurie, DVM, Charlottesville, VARodolfo G. Madrigal, DVM, Schulenburg, TXAlessandro Migliorisi, DVM, Lexington, KYHolly Parkins, DVM, Clyde, NCJennifer Rawlinson, DVM, Fort Collins, COClaire Scicluna, DVM, Chamant, France
Recent Graduates:Lee Harrison Cribbs, DVM, Ozark, MONicole Heath, DVM, Middleboro, MALeslie Huddleston, DVM, Moses Lake, WAAnna Robledo, DVM, Roseburg, ORKaitlyn Schill, DVM, Rougemont, NCHeather Solomon, DVM, West Lafayette, INKelsey Tanner, DVM, Reno, NV

EQUINE VETERINARY EDUCATION / AE / MARCH 2017 XI
Recognize a difference maker with an AAEP award nomination
The AAEP annually honors members and others within the broader equine industry for exceptional service to the horse, profession and association. To recognize these indi-viduals, however, they first must be nominated. That’s where you come in!
The AAEP is accepting nominations until June 1 for the following awards:
AAEP Research AwardDistinguished Educator – Academic Award Distinguished Educator – Mentor Award Distinguished Service AwardGeorge Stubbs Award Sage Kester Beyond the Call AwardThe Lavin Cup (The Equine Welfare Award)
A description of each award, list of past recipients and link to the nomination form is accessible within the “About” section at aaep.org. A nomination form is also
Award recipients will be honored at the AAEP’s 63rd Annual Convention, which will be held Nov. 17–21 in San Antonio, Texas.
Dr. Dennis Brooks receives the 2016 Distinguished Educator – Academic Award from 2016 AAEP President Dr. Kathleen Anderson at the 62nd Annual Convention in Orlando, Fla.
Sunny skies and 80-degree weather blanketed the record 113 practitioners who escaped to Grand Cayman for tropical mid-winter CE at the AAEP’s 19th Annual Resort Symposium, Jan. 30–Feb. 1. Turnout was three greater than in Los Cabos, Mexico, in 2007 and Puerto Rico in 2014.
With the popular footwear choice of sandals reinforcing the relaxed nature of the meeting, attendees acquired the latest thinking in sport horse medicine during three half-day sessions devoted to neurologic and musculoskeletal disease, imaging for the sport horse, and sport horse lameness and rehabilitation. UV-protection was a welcome priority during afternoon fun in the sun, whether participating in group excursions or simply enjoying the beach or pool.
If a small, laid-back educational experience in an exotic location sounds appealing, then find your Hawaiian shirt and plan to join us Jan. 29-31, 2018, on the island of Maui for the 20th Annual Resort Symposium. Additional infor-mation about the 2018 Resort Symposium will be announced later this year.
The AAEP thanks IDEXX and Merial for their sponsorship of the 19th Annual Resort Symposium and ongoing support of equine continuing education.
Resort Symposium attendees bask in sun, sport horse medicine
Friendships were formed and renewed during the Resort Symposium’s beachfront welcome reception.

XII EQUINE VETERINARY EDUCATION / AE / MARCH 2017
AAEP Meetings and Continuing Education
For more information, contact the AAEP office at (859) 233-0147 or (800) 443-0177 or online at aaep.org.
July 9-12, 2017
360° Diagnosing, Imaging
and Treating the Hind
Suspensory and Stifle
Fort Collins, Colorado
July 16-18, 2017
Focus on Dentistry
Lexington, Kentucky
July 16-18, 2017
Focus on Colic
Lexington, Kentucky
November 17-21, 2017
63rd Annual
Convention
San Antonio, Texas
Membership Benefit
Embrace volunteer opportunities to serve the profession and industry
“One of the most important AAEP member benefits is my opportunity to volunteer as one of the voices and leaders for the health and welfare of the horse. Many of us can serve as a speaker at special events, as a mentor to an equine veterinary student or assist with one of the AAEP’s many owner education programs. Moreover, I am proud to be an AAEP member who can enhance and influence the professional development of my veterinary colleagues and aspiring veterinary students. Thank you AAEP!” —Rachel Cezar, DVM, Waldorf, Md.
Do you want to contribute to your profession in meaningful ways beyond your daily practice? If so, the AAEP wants to hear from you.
A broad and diverse network of member volunteers is critical to fulfilling the AAEP’s mission to improve the health and welfare of the horse, further the professional development of its members and provide resources and leadership for the benefit of the equine industry.
Regardless of whether your volunteer interests lie in traditional board, committee and task force assignments or in more targeted opportunities such as new member ambassador or Ask the Vet expert, a completed volunteer interest form is necessary for consideration. When volunteer positions become available, the Leadership Development Committee queries the database of potential volunteers to identify candidates who match the desired training, experience and attributes.
To complete the form and become eligible for volunteer service, just log in to aaep.org and select “View My Member Profile” to complete the Volunteer Interest Form.
Dr. Rachel Cezar
Volunteer your expertise for ‘Ask the Vet’ online forum
Do you enjoy educating owners to make more informed decisions about the health and care of their horses? If so, consider volunteering as a subject matter expert for the AAEP’s monthly Ask the Vet online forum.
Horse owners submit questions in advance related to that month’s veterinary topic. Questions are subsequently answered by the member volunteer. Each month’s Q&A is archived within the Horse Owners’ section of aaep.org to serve as an educational resource.
If you are interested in lending your veterinary expertise during May, July or September through December, please contact Dana Kirkland, sponsorship and advertising coordinator, at [email protected].
KPPvet.com
Developed by:
EVE 2017-03
More and more often you are treating patients that are overweight or challenged by metabolic disease. The clients who manage these horses are constantly struggling to meet their horses’ nutritional needs without overfeeding calories. Now you can help, with the addition of a well-balanced, low-calorie vitamin and mineral supplement. NutrientWise will fi ll in the nutritional gaps found in restricted diets.
All it takes is 2 to 4 ounces per day of NutrientWise.
• Adds required vitamins and minerals to the diets of horses that are not eating recommended levels of fortifi ed concentrates.
• Contributes essential antioxidants that counter the eff ects of oxidative stress caused by normal metabolism and exercise.
• Fills the gaps in a diet containing mostly hay, hay cubes or fi ber pellets. This is especially important when access to grass and grain are limited due to metabolic disease or weight control.
• Low in starch and sugar, this alfalfa-based pellet can be fed alone and is extremely palatable.
• Maintains adequate nutrient levels to support the healing of tissue and bones in horses that are recovering from illness or injury and are on restricted diets.
NutrientWise is available at veterinary supply distributors; sold only through licensed veterinarians.
NutrientWiseTM
Provides essential nutrients to overweight and metabolically challenged horses.
For more information, call KPP:
800-772-1988

There is
NO GENERIC ADEQUAN®
INDICATIONSFor the intramuscular treatment of non-infectious degenerative and/or traumatic joint dysfunction and associated lameness of the carpal and hock joints in horses.
IMPORTANT SAFETY INFORMATIONThere are no known contraindications to the use of intramuscular Adequan® i.m. brand Polysulfated Glycosaminoglycan in horses. Studies have not been conducted to establish safety in breeding horses. WARNING: Do not use in horses intended for human consumption. Not for use in humans. Keep this and all medications out of the reach of children. CAUTION: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
Please see Full Prescribing Information at www.adequan.com.
Adequan® and the Horse Head design are registered trademarks of Luitpold Pharmaceuticals, Inc. © Luitpold Animal Health, division of Luitpold Pharmaceuticals, Inc. 2016. AHD227 Iss. 4/2016
The ONLY FDA approved equine PSGAG for the intramuscular treatment of non-infectious degenerative joint disease (DJD) of the carpal and hock joints proven to:
• DIMINISH the destructive processes of degenerative joint disease • REVERSE the processes which result in the loss of cartilage components• IMPROVE overall joint function and associated lameness
Available for order! For more information about equine joint health and treatment with Adequan® i.m., please visit www.adequan.com.

Highlights of recent clinically relevant papers
.Suspensory injuries in National Hunt racehorses
This cross-sectional study by A. Fairburn and colleagues in theUK aimed to investigate the prevalence of subclinicalultrasonographic abnormalities of the suspensory ligamentbranches (SLBs). It also aimed to establish cross-sectionalareas of SLBs in the National Hunt population.
The study was conducted on 62 horses at a singleNational Hunt training yard. Horses with a history of suspensoryligament injury or any abnormality detected on palpationduring veterinary examination were excluded from the study.
A standardised set of 10 images of the SLB were obtainedfor the forelimbs of each horse, anonymised images wereassessed by three clinicians. A previously reported gradingsystem was used to score each site from 0 to 3, with thehighest scores from each site being used to formulate a‘branch grade’. The cross-sectional area (CSA) at each sitewas also measured and a mean area calculated.
There was good inter-observer agreement: 58 SLBs weregraded as grade 0, 163 as grade 1 and 27 as grade 2. Of the30% of the population with a grade 2 score, all hadabnormalities at the insertion and almost all theseabnormalities were palmar-abaxial on the transverse imagesand abaxial/central-abaxial on the longitudinal images. Therewere significantly more grade 2 lesions in the medial SLBscompared to lateral SLBs, possibly related to asymmetricalloading of the medial branches.
The mean CSA of medial and lateral branches wasbetween 1.3 and 1.4 cm2 but CSA was an insensitiveindicator of subclinical injury. CSA was significantly larger inthe medial SLBs than lateral SLBs and the authors advisedcomparing CSA with the corresponding branch in thecontralateral limb to identify unilateral enlargement. Allabnormalities were classed as subclinical as no horsedeveloped SLB injury in the season following scanning.
A third of this National Hunt racehorse population hadgrade 2 ultrasonographic abnormalities of the SLB. MedialSLBs were more prone to grade 2 lesions than lateral SLBs.None of these ultrasonographic abnormalities wereassociated with clinical injury. The mean cross-sectional areaof the medial SLB was larger than the lateral SLB, hencecomparison with the contralateral limb is advised.
Peripheral neuropathy of the forelimb
The objective of this retrospective study by Anne-LaureEmond and colleagues in France was to describe the clinicalfeatures, diagnostic procedures, management, and outcomeof horses with peripheral neuropathy of a forelimb.
Records over a 4-year period were reviewed and 27horses with peripheral neuropathy of a forelimb wereidentified. Horses were grouped as having predominantlesions of a suprascapular nerve, axillary nerve, or radialnerve (alone or in association with other brachial plexusnerves) on the basis of physical examination and diagnosticimaging findings. Treatments were primarily conservative.Signalment, history, lameness characteristics, diagnosticimaging features, case management, and outcomes wereevaluated.
Predominant lesions of a suprascapular nerve (11 horses),axillary nerve (2 horses), and radial nerve (14 horses) wereidentified. Eight horses with predominant suprascapular nerveinjury and nine with injury to a radial nerve alone or inassociation with other nerves returned to their previousactivity level or intended use after mean recovery periods of9.3 and 13.3 months, respectively; two horses with apredominant axillary nerve injury had this outcome after amean 3.5-month recovery period. Ultrasonography was usefulfor evaluation of muscle atrophy and other injuries during theinitial examination (in 27 horses) and the rehabilitation period(in 7 horses).
Most horses with peripheral neuropathy of a forelimbreturned to athletic soundness following an adequate periodof rest. Horses with lesions of a radial nerve alone or inassociation with other nerves typically required longerrecovery times than did those with predominant injuries of asuprascapular nerve.
Stability and contamination of local anaesthetics
Local anaesthetics (LAs) are frequently used for diagnosticprocedures in equine veterinary practice. The objective ofthis study by D.M. Adler and colleagues in Denmark was toinvestigate the physico-chemical stability and bacterialcontamination of bupivacaine, lidocaine and mepivacaineused for lameness examinations in horses.
The LAs were stored in 12 different groups at differenttemperatures (�18°C to 70°C), light intensities and in commonveterinary field conditions for up to 16 months. The pH, presenceof bacterial contamination and concentrations of LAs andmethylparaben (a preservative present in lidocaine) weredetermined serially in both new and repeatedly punctured (RP)vials. Mepivacaine remained chemically stable. A 1.9%increase in bupivacaine concentration was evident in onegroup, whereas a 1.9–3.7% decrease was noted in six groups.Risk factors associated with a change in concentration werelight and RP vials. Lidocaine concentration decreased 6.3% inone group and increased 5.3–7.2% in two groups. Risk factors fordegradation were heat and RP vials whereas storage inpractice vehicles was a risk factor for increased concentrations.Methylparaben decreased 8.3–75.0% in seven groups, and RPvials, heat and storage in practice vehicles were risk factors fordegradation. No contamination was present in any of the LAsand pH remained stable.
The authors concluded that commercially availablesolutions of lidocaine, mepivacaine and bupivacaine storedunder common veterinary field conditions are extremelystable and sterile for extended periods. The minor changes inconcentration documented in this study are unlikely to affectanaesthetic efficacy during equine lameness examinations.When using products containing methylparaben,degradation of the preservative over time is to be expected.
Egg reappearance after anthelminitic treatment
This study by S.P. Daniels and C.J. Proudman investigatedshortened egg reappearance periods (ERP) after ivermectinor moxidectin use in horses in the UK.
© 2017 EVJ Ltd
119EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Shortened egg reappearance periods are an earlyindicator of anthelminitic resistance. This study reportedivermectin and moxidectin ERP from UK horses withpersistently positive faecal egg counts (FEC), defined aspositive FEC within the ERP of an anthelmintic post-treatment,or with FECs that remained positive after the normal ERP post-anthelmintic treatment. A selected population of UK pleasurehorses deemed at high risk of strongyle infection was studied.The earliest ERP recorded after ivermectin or moxidectin,using first positive FEC, was 5 weeks. From 16 premises wheremoxidectin was used, five had ERP ≥12 weeks using twofurther metrics. For premises where moxidectin wasadministered to only one animal (present or tested), andevaluated as one group (n = 61), ERP was ≥10 weeks. Forpremises where ivermectin was used, the ERP was ≥5 weeks.Premises with only one horse (present or tested), dosed withivermectin (n = 31), analysed as one group, demonstratedegg reappearance ≥6 weeks.
These field data suggest shortened ERPs followingmacrocyclic lactone treatment compared to previouslypublished values (8–10 and >13 weeks respectively) whenthese drugs were first marketed.
Tibial subchondral cystic lesions
This study by Alvaro Bonilla and colleagues in the USA andCanada reports on four horses with concurrent or sequentialtibial subchondral cystic lesions with medial femoral condylesubchondral cystic lesions.
Four horses with signs of chronic hindlimb lameness wereexamined; three had a history of lameness for >6 months andthe duration of lameness in one horse was unknown. On initialevaluation, grade 3 to 4 (on a scale from 1 to 5) hindlimblameness was present in all four horses. Radiography of thestifle joint of the affected limb revealed medial femoralcondyle subchondral lucencies or subchondral cystic lesions(SCLs) in all four horses, medial femorotibial osteoarthritis inthree horses, and medial tibial condyle SCLs in three horses.
Two horses were treated medically (stall rest and oralNSAID administration), and two were treated surgically withmedial femoral transcondylar lag screw placement throughthe medial femoral condyle SCLs. The two horses treatedmedically did not improve and were subjected toeuthanasia. Necropsy confirmed the presence of medialfemoral condyle and medial tibial condyle SCLs. Surgicaltreatment did not resolve the lameness in one horse with SCLsin the medial tibial condyle and medial femoral condyle, andeuthanasia was performed 150 days after surgery. In thesecond horse, a medial tibial condyle SCL was evident onradiographs obtained 3 months after surgery; however, thiswas not addressed surgically, and signs of lameness resolved11 months after surgery.
Results of this small case series suggested that SCLs in themedial tibial condyle can occur in association with SCLs ofthe medial femoral condyle, with a poor prognosis for returnto athletic function in affected horses. The authors suggestedthat further investigation is indicated.
Injuries and illness associated with transportation
This cross-sectional online survey study by B. Padalino andcolleagues in Australia and the USA aimed to provideinformation on the risk factors for illness and injury associatedwith equine transportation.
Of the 797 responses to the survey from both amateurand professional equestrians in Australia, all of whomtransported horses at least monthly, there were 214 cases ofa transport-related health problem over the previous 2 years.There was a significant association between journey time andvehicle, and transport by a commercial company. Trailersand noncommercial transporters were more commonly usedfor shorter journeys.
Ten horses died during transit (two were found dead andthe remaining eight were subjected to euthanasia due tofractures). An additional 15 horses were subjected toeuthanasia within one week of the journey, seven of whichoccurred within 24 h. Journey duration and breed wereassociated with transport-related health problems. Comparedwith Standardbreds, Thoroughbreds, Arab and Warmbloodhorses were more likely to develop illness than be injuredduring transportation.
Compared to injuries, illness including gastrointestinal andrespiratory problems, as well as death and euthanasia, weresignificantly associated with longer journey time. Respiratorydisease was the most common problem and the risk increasedwith longer journey time. Muscular problems were more likelyon an intermediate length journey than a short one. There wasno influence of journey duration on the incidence of heatstroke. Injuries were more likely to occur on shorter journeys.
This is likely to be associated with behavioural problems ormovement within the vehicle during the early part of the journey.
S. WRIGHTEVE Editorial Office
ReferencesAdler, D.M., Cornett, C., Damborg, P. and Verwilghen, D.R. (2016) The
stability and microbial contamination of bupivacaine, lidocaineand mepivacaine used for lameness diagnostics in horses. Vet. J.218, 7–12.
Bonilla, A.G., Bertone, A.L., Brokken, M.T. and Santschi, E.M. (2016)Concurrent or sequential tibial subchondral cystic lesions in 4horses with medial femoral condyle subchondral cystic lesions. J.Am. Vet. Med. Assoc. 249, 1313–1318.
Daniels, S.P. and Proudman, C.J. (2016) Shortened egg reappearanceafter ivermectin or moxidectin use in horses in the UK. Vet. J. 218, 36–39.
Emond, A.L., Bertoni, L., Seignour, M., Coudry, V. and Denoix, J.-M.(2016) Peripheral neuropathy of a forelimb in horses: 27 cases(2000–2013). J. Am. Vet. Med. Assoc. 249, 1187–1195.
Fairburn, A.J., Busschers, E. and Barr, A.R.S. (2016) Subclinicalultrasonographic abnormalities of the suspensory ligamentbranches in National Hunt racehorses. Equine Vet. J., Epub aheadof print; doi: 10.1111/evj.12639.
Padalino, B., Raidal, S.L., Hall, E., Knight, P., Celi, P., Jeffcott, L. andMuscatello, G. (2016) Risk factors in equine transport-related healthproblems: a survey of the Australian equine industry. Equine Vet. J.,Epub ahead of print; doi: 10.1111/evj.12631.
© 2017 EVJ Ltd
120 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Case Report
Hindlimb lameness associated with a focal osseous metaplasia inan 18-year-old Welsh Section D mareM. Grabski , D. Fews‡ and E. Busschers†
†Department of Clinical Veterinary Sciences, University of Bristol, Bristol, UK; and ‡Department of VeterinaryPathology, Infection and Immunity, School of Veterinary Sciences, University of Bristol, Bristol, UK.*Corresponding author email: [email protected]
Keywords: horse; osseous; metaplasia; lameness; mineralisation; calcification
SummaryThis report describes a case of chronic lameness secondaryto an extraskeletal osseous mass located in theplantaromedial aspect of the right hind pastern in a matureWelsh Section D mare. The lesion was confirmed to representmetabolically active osseous tissue in close apposition withthe adjacent plantar digital neurovascular bundle and digitalflexor tendons. Surgical resection of the mass resulted in acomplete resolution of lameness and return to previous levelof activity. Histopathological examination classified the massas a focal osseous metaplasia, which was most likely to bethe result of previous trauma causing local haemorrhage,which resulted in subsequent dystrophic mineralisation andeventually osseous metaplasia. Similar lesions have beendescribed in man, but have not been previously reported inthe horse.
Case history
An 18-year-old Welsh Section D mare (bodyweight 430 kg)used for general riding purposes was referred for nuclearscintigraphy with a history of an insidious onset right hindlimblameness of 9 months’ duration. Previous examination by thereferring veterinary surgeon did not identify any localisingclinical signs and rest had not improved the lameness.
Clinical and diagnostic imaging findings
Physical examination was within normal limits. Staticorthopaedic examination revealed a moderate effusion ofthe right femoropatellar joint, and mild effusion of bothmetatarsophalangeal joints and both hind digital flexortendon sheaths. Dynamic examination confirmed thepresence of a right hindlimb lameness which was classified asa grade 2/5 lameness when trotted in a straight line (AAEPlameness grading scale) (Keegan et al. 2010) and increasedto a grade 3/5 lameness on a soft surface circle with theaffected limb on the outside. The lameness wascharacterised by a shortened caudal phase of the stride,reduced flight arch of the foot and was exacerbated bydistal limb flexion. Clinical examination and a low 4-pointnerve block (diagnostic analgesia of the lateral and medialplantar and plantar metatarsal nerves) were performed bythe referring veterinary surgeon; however, as the results wereinconclusive, a presumptive diagnosis of upper limb lamenesswas made.
The horse was referred to University of Bristol EquineDiagnostic Centre for scintigraphic examination. Nuclear
scintigraphy of the pelvis, back and hindlimbs was performedafter i.v. administration of the radiopharmaceutical agent,technetium methylene diphosphonate (Tc99 m-MDP; 5 GBq).The images were obtained 2 h after injection of theradiopharmaceutical using static and dynamic imageacquisition modes with a gamma camera system andprocessed with motion correction software (MicasXPlus)1. Theimages showed an area of intense focal increasedradiopharmaceutical uptake (IRU) in the soft tissues of theplantaromedial aspect of the right hind pastern (Fig 1). Uponrepeat clinical examination, a focal firm subcutaneousnodule, measuring approximately 2 9 3 cm was palpated onthe plantaromedial aspect of the mid right hind pastern.Focal digital compression at this site precipitated a painfulwithdrawal response. Diagnostic analgesia of the lateral andmedial plantar digital nerves was performed with 2%mepivicaine hydrochloride (Intra-Epicaine)2 at the level of thebase of the proximal sesamoid bones, just proximal to themass. A significant improvement in the right hindlimblameness was observed after 10 min. After the nerve blockhad worn off, a medial plantar digital nerve was locallyanaesthetised which resulted in a similar improvement.
Subsequent radiographs showed a focal, well-circumscribed and somewhat mottled mineral opacity withinthe soft tissue structures of the plantaromedial aspect of the
a) b)
Fig 1: Lateral (a) and plantar (b) scintigraphic projections of theright distal limb. Intense focal IRU in the plantaromedial aspect ofthe right hind pastern (arrow). LH marker located dorsally (a) andlaterally (b).
© 2015 EVJ Ltd
121
†*
EQUINE VETERINARY EDUCATION / AE / MARCH 2017
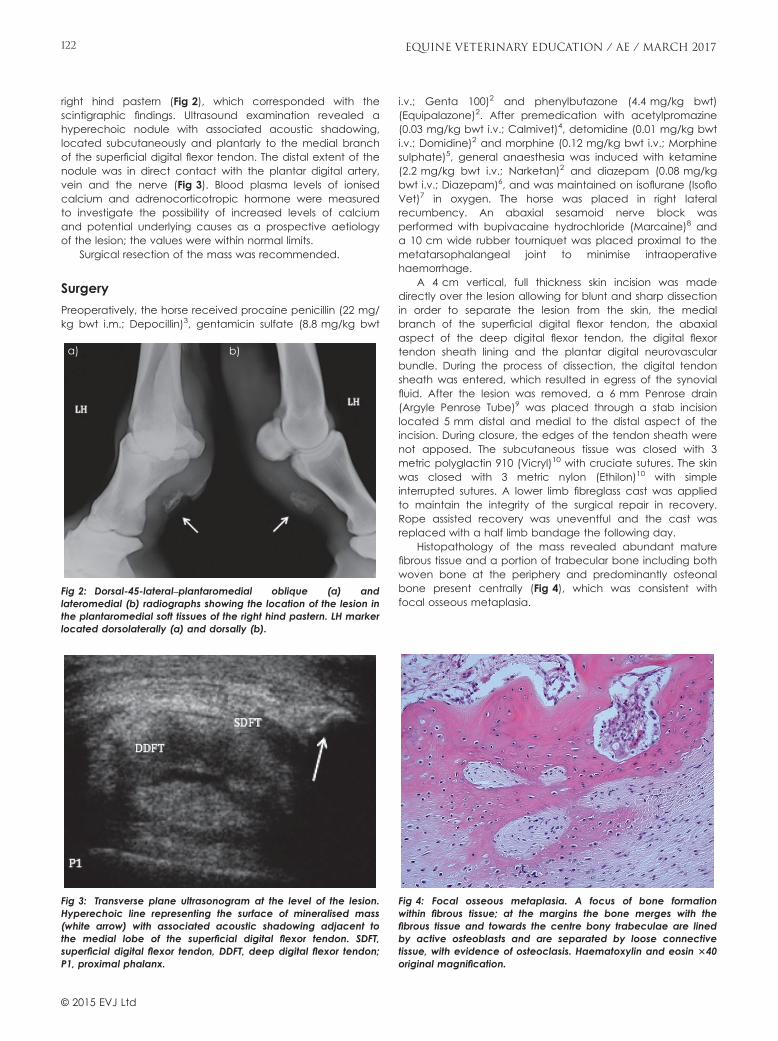
right hind pastern (Fig 2), which corresponded with thescintigraphic findings. Ultrasound examination revealed ahyperechoic nodule with associated acoustic shadowing,located subcutaneously and plantarly to the medial branchof the superficial digital flexor tendon. The distal extent of thenodule was in direct contact with the plantar digital artery,vein and the nerve (Fig 3). Blood plasma levels of ionisedcalcium and adrenocorticotropic hormone were measuredto investigate the possibility of increased levels of calciumand potential underlying causes as a prospective aetiologyof the lesion; the values were within normal limits.
Surgical resection of the mass was recommended.
Surgery
Preoperatively, the horse received procaine penicillin (22 mg/kg bwt i.m.; Depocillin)3, gentamicin sulfate (8.8 mg/kg bwt
i.v.; Genta 100)2 and phenylbutazone (4.4 mg/kg bwt)(Equipalazone)2. After premedication with acetylpromazine(0.03 mg/kg bwt i.v.; Calmivet)4, detomidine (0.01 mg/kg bwti.v.; Domidine)2 and morphine (0.12 mg/kg bwt i.v.; Morphinesulphate)5, general anaesthesia was induced with ketamine(2.2 mg/kg bwt i.v.; Narketan)2 and diazepam (0.08 mg/kgbwt i.v.; Diazepam)6, and was maintained on isoflurane (IsofloVet)7 in oxygen. The horse was placed in right lateralrecumbency. An abaxial sesamoid nerve block wasperformed with bupivacaine hydrochloride (Marcaine)8 anda 10 cm wide rubber tourniquet was placed proximal to themetatarsophalangeal joint to minimise intraoperativehaemorrhage.
A 4 cm vertical, full thickness skin incision was madedirectly over the lesion allowing for blunt and sharp dissectionin order to separate the lesion from the skin, the medialbranch of the superficial digital flexor tendon, the abaxialaspect of the deep digital flexor tendon, the digital flexortendon sheath lining and the plantar digital neurovascularbundle. During the process of dissection, the digital tendonsheath was entered, which resulted in egress of the synovialfluid. After the lesion was removed, a 6 mm Penrose drain(Argyle Penrose Tube)9 was placed through a stab incisionlocated 5 mm distal and medial to the distal aspect of theincision. During closure, the edges of the tendon sheath werenot apposed. The subcutaneous tissue was closed with 3metric polyglactin 910 (Vicryl)10 with cruciate sutures. The skinwas closed with 3 metric nylon (Ethilon)10 with simpleinterrupted sutures. A lower limb fibreglass cast was appliedto maintain the integrity of the surgical repair in recovery.Rope assisted recovery was uneventful and the cast wasreplaced with a half limb bandage the following day.
Histopathology of the mass revealed abundant maturefibrous tissue and a portion of trabecular bone including bothwoven bone at the periphery and predominantly osteonalbone present centrally (Fig 4), which was consistent withfocal osseous metaplasia.
a) b)
Fig 2: Dorsal-45-lateral–plantaromedial oblique (a) andlateromedial (b) radiographs showing the location of the lesion inthe plantaromedial soft tissues of the right hind pastern. LH markerlocated dorsolaterally (a) and dorsally (b).
Fig 3: Transverse plane ultrasonogram at the level of the lesion.Hyperechoic line representing the surface of mineralised mass(white arrow) with associated acoustic shadowing adjacent tothe medial lobe of the superficial digital flexor tendon. SDFT,superficial digital flexor tendon, DDFT, deep digital flexor tendon;P1, proximal phalanx.
Fig 4: Focal osseous metaplasia. A focus of bone formationwithin fibrous tissue; at the margins the bone merges with thefibrous tissue and towards the centre bony trabeculae are linedby active osteoblasts and are separated by loose connectivetissue, with evidence of osteoclasis. Haematoxylin and eosin 340original magnification.
© 2015 EVJ Ltd
122 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

The bandage was changed every 2–3 days for 12 days.The Penrose drain was removed after 24 h since there wasminimal discharge. The horse’s comfort was acceptable afterthe surgery although a mild shortening of the cranial phase ofthe stride in walk was noted for 72 h post operatively. Theantimicrobials were continued for 48 h and phenylbutazonefor 5 days post operatively. Prior to discharge from thehospital at 10 days after surgery 50 mg of hyaluronic acid(50 mg; HY50 Vet)2 was injected intrathecally into the digitalflexor tendon sheath. A focal compression of the medial heelbulb at the last bandage change evoked a withdrawresponse from the horse, which was consistent with preservedsensation to this aspect of the limb. A period of 6 weeks of in-hand walking exercise was recommended before gradualreturn to normal work. A telephone follow-up questionnaireafter 12 months revealed resolution of lameness with acomplete return to the previous level of activity.
Discussion
This report describes resolution of lameness after surgicalresection of an osseous mass of unknown aetiology. Chroniclameness observed in this horse was probably secondary tomechanical compression of the soft tissue structures of thedistal limb. Compression of the plantar digital nerve mayhave contributed to lameness, similar to pain associated withcompression of sensory nerves by a mineralised mass as hasbeen reported in human patients (McCarthy and Sundaram2005). Palpation of the medial aspect of the limb resulted ina strong withdrawal response suggesting that sensation in thispart of the limb was present upon initial examination. It wasnot possible to conclude whether the response to palpationwas normal or exaggerated as seen in cases of neuritis(Sommer et al. 1993). Assessment of sensory nerve pathologyhas been undertaken in clinical trials and can be performedusing nociceptive response threshold analysis (Schumacher1999), nerve conduction analysis (Bolt et al. 2004) orhistopathological examination of the nerve (Bolt et al. 2004).These tests were not performed preoperatively in this case asthey were unlikely to change the initial management of thecase or were considered too invasive. Knowledge of thesensory nerve function could be beneficial in planning thesurgical procedure since the possibility of a secondarypermanent nerve dysfunction and therefore the risk ofpersistence of the clinical signs may have warranted plantardigital neurectomy procedure. Scintigraphy was useful inlocalising the lesion, which on second examination waspalpable and painful. Thorough lameness examination,including radiographs, would likely have resulted in a moreprompt diagnosis. Due to the thick skin and feathers in thisregion, the mass was missed and a presumptive diagnosis ofupper limb lameness was made.
Scintigraphy with Tc-99 mMDP delineates calciumphosphate aggregates which can be present in 3 forms:calcium hydroxyapatite in its free form, calciumhydroxyapatite in a form of trabecular bone (Kini andNandeesh 2012) or amorphous deposits of calciumphosphate (Stoker 1999). Tc99 m-MDP is bound to calciumdeposits via the process of surface adsorption andincorporation into the crystalline structure of hydroxyapatite(Subramanian et al. 1975). This allows for the site-specificdetection of gamma rays emitted by Tc-99m. An increase inthe radiopharmaceutical uptake (IRU) on scintigraphy is,
however, nonspecific for the type of mineralisation (Stoker1999). The degree of uptake depends on the nature ofcalcium deposit and will be more intense in cases ofamorphous calcium phosphate formation with low calcium tophosphate molar ratio such as in early active soft tissueamorphous calcium deposition. It will be less intense withdeposits with higher calcium to phosphate molar ratio suchas calcium hydroxyapatite, the main inorganic component ofbone matrix and the majority of mature extraskeletal forms ofmineralisation (Stoker 1999). In cases of IRU in soft tissuesextraskeletal bone formation and nonosseous calciumdeposits can not just be differentiated based on intensity ofIRU and should be facilitated by radiographic evidence ofsome features typical of trabecular bone pattern (Stoker1999) or histopathological examination. Both were performedin this case and confirmed the diagnosis of new boneformation and not just a nonosseous calcium deposit withinthe soft tissues.
Three main forms of extraosseus calcification have beenrecognised: dystrophic, metastatic and idiopathic. Dystrophiccalcification is the most common type and is a result of localtissue necrosis. This form is not associated with systemic calciumor phosphate derangements. Examples of such lesions in horseshave been reported in the lateral digital extensor tendon(Gonzales et al. 2010), nasal conchae (Tremaine and Dixon2006) or in cases of rhabdomyolysis when muscle damageresults in intracellular calcium influx (Silberstein and Bove 1979).On occasion, as demonstrated in human patients (Kumar2013) and seen in this case, in long standing cases, a focus ofdystrophic mineralisation can undergo transformation into amature bone (osseous metaplasia).
Metastatic calcification, however, can arise in anycondition with elevated serum calcium/phosphate productand typically affects viable and not necrotic or degeneratingtissues, which are physiologically involved in hydrogen ionsecretion. At a cellular level these tissues contain morealkaline pH compartments, which facilitate precipitation ofcalcium deposits. Examples include gastric mucosa, lung,kidneys as well as systemic arteries and pulmonary veins.
Metaplastic bone formation refers to formation of non-neoplastic trabecular bone at the sites distant from theskeleton (Thompson 2007). Four factors are necessary in itspathogenesis (Kaplan et al. 2004). An inciting event, such astrauma, which often results in a haematoma formation(McCarthy and Sundaram 2005). Secondly, appropriatemolecular signalling (most commonly a protein such as bonemorphogenic protein) secreted from the cells of the injuredtissue or from inflammatory cells. Thirdly, a supply of localpluripotent mesenchymal cells. Lastly, an appropriateenvironment allowing for production of the new bone.Metaplastic bone formation must be distinguished fromheteroplasia. The latter implies anomalous primarydifferentiation of tissue and therefore is congenital in origin. Inmetaplasia alteration of tissue occurs after it has beenformed normally, implying an acquired aetiology.
Whilst there was no clinical indication for intrathecalinjection of hyaluronic acid based on the preoperativeassessment of the case, the tendon sheath was enteredduring the dissection, justifying an injection of hyaluronic acidto reduce the risk of postoperative adhesions.
Skin sensation was assessed at the last bandage changeby a focal compression of the medial heel bulb with apositive response. As resolution of the clinical signs could
© 2015 EVJ Ltd
123EQUINE VETERINARY EDUCATION / AE / MARCH 2017

have been achieved by a neurectomy due to the proximityof the nerve, this was unlikely, as the skin sensation appearedunaffected.
Late in life onset of the clinical signs, no history of previoussurgery as well as the location of the lesion, imply a possibilityof a traumatic origin in this case. Specifically, little soft tissuecoverage and the plantaromedial location of the lesionrender the site of the pathological change susceptible to anaccidental kick injury from the other limbs during normal gait.
A condition that closely resembles post traumatic newbone formation in soft tissue in human patients is myositisossificans circumpscripta where traumatic injuries in youngindividuals result in focal haematomata undergoingtransformation to mature bone, which is biologicallyindistinguishable from that of the normal skeleton (McCarthyand Sundaram 2005). Within 6 weeks, such lesions undergoprogressive mineralisation in a zonal pattern (denser at theperiphery) to transform into mature trabecular bone between6 months to a year (Mavrogenis et al. 2011). Distinctivefeatures of mature bone identified on histopathology of theexcisional biopsy presented in this report are indicative of achronic course of the condition, which is in agreement withclinical presentation and history. Although benign, similarlesions in human patients have been reported to causerestriction of movement of the nearby joint, or to undergo amalignant transformation (McCarthy and Sundaram 2005).Distinction of the histopathological nature of extraskeletalmineralisation/ossification is therefore important in the clinicalreasoning.
The history, focal localisation of this ossification in thesubcutaneous tissue, a complete resolution of lameness aftersurgical resection and histopathological examination areconsistent with a traumatic injury which caused localhaemorrhage which resulted in subsequent dystrophicmineralisation and eventually osseous metaplasia. Reports ofmalignant transformation in the human patients of similarlesions (Eckardt et al. 1981) provide further support justifyingsurgical intervention in this case. This is the first reportdescribing osseous metaplasia and associated lameness inthe horse and this differential diagnosis should be consideredif a subcutaneous ossification/calcification is identified.
Authors’ declaration of interests
No conflicts of interest have been declared.
Ethical animal research
Retrospective report of a clinical case and treatmentperformed with a high standard of clinical care.
Source of funding
This work received no specific grant from any institutional,private or commercial sector.
Authorship
Each author was directly involved in study design, studyexecution, data analysis and interpretation, preparation ofthe manuscript and its final approval.
Manufacturers' addresses1Bartec Technologies, Camberley, Surrey, UK.2Dechra Veterinary Products, Shrewsbury, Shropshire, UK.3MSD Animal Health, Milton Keynes, Buckinghamshire, UK.4V�etoquinol, Lure Cedex, France.5Martindale Pharmaceuticals, Romford, Essex, UK.6Hameln Pharmaceuticals Ltd, Gloucester, UK.7Abbot Laboratories Ltd, Maidenhead, Berkshire, UK.8Astra Zeneca, London, UK.9Covidien, Tullamore, Offaly, Ireland.10Ethicon, Livingston, UK.
ReferencesBolt, D.M., Burba, D.J., Hubert, J.D., Strain, G.M., Hosgood, G.L., Henk,
W.G. and Cho, D.-Y. (2004) Determination of functional andmorphologic changes in palmar digital nerves after nonfocusedextracorporeal shock wave treatment in horses. Am. J. Vet. Res.65, 1714-1718.
Eckardt, J.J., Ivins, J.C., Perry, H.O. and Unni, K.K. (1981) Osteosarcomaarising in heterotopic ossification of dermatomyositis: case reportand review of the literature. Cancer 48, 1256-1261.
Gonzales, L.M., Schramme, M.C., Robertson, I.D., Thrall, D.E. andRedding, R.W. (2010) MRI features of metacarpo(tarso)phalangealregion lameness in 40 horses. Vet. Radiol. Ultrasound. 51, 404-414.
Kaplan, F.S., Glaser, D.L., Hebela, N. and Shore, E.M. (2004)Heterotopic ossification. J. Am. Acad. Orthop. Surg. 12, 116-125.
Keegan, K.G., Dent, E.V., Wilson, D.A., Janicek, J., Kramer, J.,Lacarrubba, A. and Walsh, D.M. (2010) Repeatability of subjectiveevaluation of lameness in horses. Equine Vet. J. 42, 92-97.
Kini, U. and Nandeesh, B.N. (2012) Physiology of Bone Formation,Remodeling, and Metabolism. In: Radionuclide and Hybrid BoneImaging. Eds: I. Fogelman, G. Gnanasegaran and H. van der Wall,Springer Berlin Heidelberg, Berlin, Heidelberg. pp 29-57.
Kumar, V. (2013) Cell injury, cell death, and adaptations. In: RobbinsBasic Pathology, 8th edn., Eds: V. Kumar, A. Abbas and J. Aster,Saunders, Philadelphia. pp 26-29.
Mavrogenis, A.F., Soucacos, P.N. and Papagelopoulos, P.J. (2011)Heterotopic ossification revisited. Orthopedics 34, 177.
McCarthy, E.F. and Sundaram, M. (2005) Heterotopic ossification: areview. Skeletal Radiol. 34, 609-619.
Schumacher, J. (1999) Effects of analgesia of the distalinterphalangeal joint or palmar digital nerves on lameness causedby solar pain in horses. Vet. Surg. 29, 54-58.
Silberstein, E.B. and Bove, K.E. (1979) Visualization of alcohol-inducedrhab- domyolysis: a correlative radiotracer, histochemical,and electron micro- scopic study. J. Nucl. Med. 20, 127-129.
Sommer, C., Galbraith, J.A., Heckman, H.M. and Myers, R.R. (1993)Pathology of experimental compression neuropathy producinghyperesthesia. J. Neuropathol. Exp. Neurol. 52, 223-233.
Stoker, D.J. (1999) Focal and regional mineralization in the soft tissues.Curr. Orthopaed. 13, 199-211.
Subramanian, O., Blair, R.J., Kallfelz, E.A., Thomas, F.D. and McAfee,J.G. (1975) 99mTc-MDP (methylene di- phosphonate)—a superioragent for skeletal imaging. J. Nucl. Med. 16, 744-755.
Thompson, K. (2007) Bones and joints. In: Jubb, Kennedy & Palmer’sPathology of Domestic Animals, 5th edn., Ed: M.G. Maxie,Saunders, Philadelphia. pp 10-13.
Tremaine, W.H. and Dixon, P.M. (2006) A long-term study of 277 casesof equine sinonasal disease. Part 1: details of horses, historical,clinical and ancillary diagnostic findings. Equine Vet. J. 33, 274-282.
© 2015 EVJ Ltd
124 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

When we started giving American Pharoah the Healthy Weight, we just noticed an immediate difference. It kept him looking healthy and sharp during the intense Triple Crown campaign. At the end of the season, he ran against older horses in the Breeders' Cup Classic and won by 6 1/2 lengths, breaking the track record! So, all of our horses now get at least one of the Platinum formulas. Some get Osteon for their bones, especially the growing colts. Pharoah and some others get the Healthy Weight, and all of them get Platinum Equine as an overall health supplement.
American Pharoah theHealthy Weight, we justnoticed
yyan immediate
difference. It kept himlooking healthy and sharpduring the intense
y Triple
Crown campaign. At theend of the season, he ranagainst older horses inthe Breeders' Cup Classicand won by 6 1/1 2// lengths,breaking the
yy track record!
g
So, all of our horses nowget at least one of thePlatinum formulas. Someget Osteon for their bones,especially the growingcolts. Pharoah
y and some
others get the HealthyWeight, and all of them
y
get Platinum Equine as an
g g
ll l l
When we started giving American Pharoah the Healthy Weight, we just noticed an immediate difference. It kept him looking healthy and sharp during the intense Triple Crown campaign. At the end of the season, he ran against older horses in the Breeders' Cup Classic and won by 6 1/2 lengths, breaking the track record! So, all of our horses now get at least one of the Platinum formulas. Some get Osteon for their bones, especially the growing colts. Pharoah and some others get the Healthy Weight, and all of them get Platinum Equine as an overall health supplement.
To find the right Platinum Performance® solution, and to learn about the science behind the supplements,
please call us or visit our website today.
© 2016 PLATINUM PERFORMANCE, INC.
866-553-2400www.PlatinumPerformance.com
Bob Baffert, TrainerWinner of 4 Kentucky Derbies, 6 Preakness Stakes,2 Belmont Stakes, and 12 Breeders’ Cup races.Platinum Performance® Client since 2012
Bob Baffert is a sponsored endorsee and actual client.
American PharoahThe first horse to win the American “Grand Slam”:2015 Kentucky Derby, Preakness Stakes,Belmont Stakes & the Breeders’ Cup Classic
Platinum Performance® Equine supports:
Osteon®
Healthy Weight
P
O
H
• Joint Health• Hoof Health• Skin & Coat Health
• Performance & Recovery• Digestive Health• Bone & Tendon Health
• Supports Bone & Connective Tissue Health
• Provides Calories for Horses That Need to Gain Weight• Provides a Natural Source of Antioxidant, Vitamin E
this is My Platinum
THIS IS My Horse™
Bob Baffert, TrainerWinner ofr 4f Kentucky4 Derbies,y 6 Preakness Stakes
overalloverall healthhealth supplement.supplement.pp mpp m
WhenWhen wewe startedstarted givinggiving
”I recommend ColiCare for all of my patients,
and my own horses are enrolled, too!” —Marsha Severt, DVM Brown Creek Equine Hospital
SmartPak.com/ColiCare | 1-800-461-8898
ColiCare, the #1 vet-recommended colic
surgery reimbursement program† puts
you back at the center of the horse’s
wellness care and reimburses horse
owners up to $7,500 to help ease the
fi nancial burden of colic surgery.
†2016 Lebel Marketing Veterinary Market Survey

Case Report
The hazards associated with the use of intrauterine glass balls tosuppress oestrus in maresL. H-A. Morris†*, B. S. L. Fraser‡, C. Cantley§ and S. Wilsher#
†Equibreed NZ, Te Awamutu; ‡Cambridge Veterinary Services; §Hamilton Veterinary Services, New Zealand; and#The Paul Mellon Laboratory of Equine Reproduction, Newmarket, Suffolk, UK.*Corresponding author email: [email protected] Fraser’s Present address: Rainbow Equine Hospital, Old Malton, North Yorkshire, UKDr Cantley’s Present address: NZVA, Wellington 6011, New Zealand
Keywords: horse; mare; uterus; glass ball; oestrous suppression
SummaryPlacing a sterile glass ball or marble into the uterine lumenis a popular method to suppress unwanted oestrousbehaviour in mares. This is in spite of the original report ofNie et al. (2003), which detailed the lack of efficacy of thetechnique. Recent reports in the literature have described anumber of untoward problems associated with thetechnique. This paper describes two further cases, oneinvolving fragmentation of marbles in the uterine lumen anda second describing the laparoscopic removal of a marbleafter it had tracked through the endometrium and becamepedunculated between the myometrium and serosa. Theinefficiency of suppressing oestrus with glass balls, combinedwith the potential problems their placement may cause,argue strongly that this practice should be consideredunethical.
Introduction
The mare is a long day, seasonally polyoestrous animal, butalthough regular cyclicity during the breeding seasonprovides multiple mating opportunities for breeders, oestrousbehaviour is considered undesirable and disadvantageous incompeting fillies and mares by many owners and trainers.Most fillies in training, although cycling normally during thesummer months, show no outward changes in their behaviourduring the oestrous cycle.
Unwanted oestrous behaviour, aggressiveness,oversensitivity, variability in performance, refusal to moveforward (‘planting’ and rearing), bolting, bucking, kickingagainst the rider’s leg, pain and colic are all problems reportedas being associated with oestrus. However, examination ofsuch mares may reveal that they are not always in oestruswhen these problems occur and such behaviour can beassociated with dioestrus when the mare is under thedominance of progesterone (McCue 2003; Vanderwall andNie 2011). Nevertheless, there is a desire and practical need tobe able to suppress oestrous behaviour in fillies and mares inrace training and other athletic competitions using a methodthat, ideally, gives a long period of suppression which isreversible and does not lower long-term fertility.
Suppression of oestrous cyclicity can occur spontaneouslyby natural prolongation of luteal function and it is estimatedthat 5–20% of mares in any given group experience at leastone period of spontaneous prolonged dioestrus during anybreeding season (Stabenfeldt et al. 1974; Sharp 1980). Such a
situation may result from the occurrence of a late dioestrousovulation producing a corpus luteum (CL) that is insufficientlymature to respond to the cyclical release of endometrialprostaglandin (PGF2a) at the end of dioestrus, following earlyembryonic death after the release of the maternalrecognition of pregnancy (MRP) signal, or failure or inability ofa damaged or degenerate endometrium to release PGF2a atthe appropriate time, in sufficient quantities or in theappropriate pulsatile pattern to induce luteolysis (McCue andFerris 2011).
Pharmacological suppression of oestrous behaviour canbe achieved by administering one of a number of availableprogesterone or progestagens (e.g. altrenogest) althoughsuch treatment is expensive and not permitted in allcompetitive spheres. Other pharmacological andnonpharmacological methods to suppress oestrous behaviourwhich rely on extending the lifespan of the CL have alsobeen reported in the literature. These include repeatedadministration of oxytocin during the dioestrous phase of thecycle (Stout et al. 1999; Vanderwall et al. 2007), manualrupture of the conceptus between Days 16 and 22 afterovulation (Lefranc and Allen 2004), administration of humanchorionic gonadotrophin (hCG) to induce ovulation duringthe luteal phase (Hedberg et al. 2006), intrauterineadministration of a small quantity of plant oil during dioestrus(Wilsher and Allen 2011) and insertion of an inert glass orplastic ball into the uterine lumen (Nie et al. 2003; Rivera delAlamo et al. 2008).
The last method, the placing of a sterile glass ball ormarble into the uterine lumen, has proven popular due to thelow cost and relative simplicity of the protocol. However,despite the initial study reporting no detrimental effects of theglass ball on the uterus or fertility (Nie et al. 2003), recentreports in the literature have described problems associatedwith the technique. These include chronic endometritis,pyometra, fragmentation of the marble(s) within the uterinelumen, adherence of the marble or shards of it to theendometrium and chronic intermittent colic (Klabnik-Bradfordet al. 2013; Diel de Amorim et al. 2014; Freeman and Lyle2015; Turner et al. 2015). Anecdotally, it would appear thatthese are not isolated cases and here we describe twofurther cases, one involving fragmentation of marbles in theuterine lumen and a second describing the laparoscopicremoval of a marble after it had tracked through theendometrium and became pedunculated between themyometrium and serosa.
© 2016 EVJ Ltd
125EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Case 1: Fragmentation of glass marbles in theuterus
An 11-year-old Thoroughbred mare was presented forreproductive assessment in March 2015. The owner reportedthat the mare had been difficult to train when she was inoestrus. An intrauterine marble had been inserted in heruterus in an attempt to suppress this behaviour but,eventually, she was retired to stud due to her intractability;the owner assumed the marble had been expelled orremoved. Despite being mated to fertile stallions multipletimes over 5 breeding seasons the mare had failed toconceive and had a history of persistent endometritis andwas referred for further investigation.
Initial examinationsUpon presentation, the mare had a purulent vaginaldischarge. Ultrasound examination of the reproductive tractshowed the uterus to be filled with a highly echogenic fluid.Large volume saline (0.9% sodium chloride)1 lavage of theuterus was undertaken until the recovered fluid was clear. Afinal lavage was then undertaken with 1 L 0.9% sodiumchloride containing 2 g gentamicin (Gentavet 100)2 and 3 gbenzylpenicillin sodium (BenPen)3. This treatment wasrepeated 2 days later. In addition, a long acting antibiotic(6.6 mg/kg bwt ceftiofur; Excede LA)4 was administeredparentally on two occasions, 4 days apart.
Subsequent ultrasound examination of the uterusrevealed marbles in the lumen which, on initial visualisation,were difficult to discern and could easily have been mistakenfor fluid, oestrous folds or endometrial cysts (Fig 1a).
Videoendoscopic examinationSubsequent videoendoscopic examination of the uterusallowed visualisation of the marbles (Fig 1b). A total of 3marbles were present, along with numerous glass shards. Anunsuccessful attempt was made to recover the marbles bydistending and lavaging the uterine lumen with 5 L of 0.9%sterile sodium chloride. Manual recovery was thensuccessfully carried out by passing a gloved hand throughthe dilated cervix (Fig 1c). The clinician undertaking theprocedure described the fragments as ‘feeling like gravelwithin the uterine body’, although none of them could bepalpated within the endometrium.
Since it was the end of the Southern Hemisphere breedingseason the mare was not mated until the start of the followingseason (September 2015). When she was in oestrus anddisplayed a 35 mm follicle, 1500 iu hCG (Chorulon)5 wasadministered intravenously (i.v.) to induce ovulation and themare mated naturally the next day. Post-mating fluid which hadaccumulated in the uterine lumen was eliminated by theintramuscular (i.m.) administration of 20 iu oxytocin (Oxytocin V)6
2 or 3 times daily and the mare received a uterine lavage ofsaline containing antibiotics (1 L 0.9% sterile sodium chloridewith 2 g gentamicin and 3 g benzylpenicillin sodium) for2 days. She conceived to this mating and remains pregnantat around 150 days at the time of writing.
Case 2: Laparoscopic removal of a glass marble
A 6-year-old, nulliparous Thoroughbred mare was referred forremoval of a marble. The mare had been cycling normally but,
despite being mated naturally during several oestrous periodsover two seasons, had failed to conceive. The referringveterinary surgeon had palpated a hard mass, which hebelieved to be a marble, in the right uterine horn althoughexamination by two other veterinary surgeons had failed toidentify the mass, either by palpation or ultrasonography.
Initial examinationsPalpation of the reproductive tract revealed a firm,pedunculated round mass (approximately 3 cm diameter)extending from the ventral aspect of the right uterine horn,which could be visualised ultrasonographically as a structurecontaining a circular, refractory object. Videoendoscopicexamination of the uterus revealed a patent uterine lumenwith no discernible breach or abnormality of theendometrium in the right uterine horn overlying thepedunculated mass.
Laparoscopic examinationLaparoscopic evaluation of both sides of the abdomen wasundertaken. Feed was withheld for 36 h and followingpremedication with acepromazine (0.03 mg/kg bwt i.v.;Acezine 2)7, procaine penicillin (22 mg/kg bwt i.m.;Depocillin)5 and phenylbutazone (2.2 mg/kg bwt i.v.;Nabudone)8 the mare was then restrained in stocks andadministered detomidine (0.01 mg/kg bwt i.v.; Dormosedan)9
and butorphanol (0.02 mg/kg bwt i.v.; Torbugesic)9. Afterclipping, aseptic preparation and sterile draping, 20 mLlidocaine (20 mg/mL; Local)10 was infused subcutaneouslyand i.m. at 3 sites on the right side and the central site onlyon the left; 1) at the proximal border of the internalabdominal oblique muscle, halfway between the ventralaspect of tuber coxae and the last rib and 2) 5 cm dorsaland 5 cm ventral to the original portal. A 1.5 cm skin incisionwas made in the left hand side portal and the musclesseparated by blunt dissection. A 5–12 mm laparoscopictrocar (Versaport Plus 5–12 mm V2 bladed trocar)11 wasinserted after insufflation into the peritoneal cavity of CO2 toa pressure of 14 mmHg. The central portal was then createdsimilarly on the right side with the safety of preinsufflation ofthe abdomen. Under laparoscopic guidance, two furtherportals were then created dorsal and ventral to the scopeportal. The right side of the abdomen was explored and thepresumed marble identified as sitting in its semi-pedunculatedsubserosal pouch on the ventro-axial aspect of the uterinehorn equidistant between the ovary and uterine bifurcation.The uterus was grasped for stabilisation using 55 cmatraumatic forceps and the mass was confirmed to be asolid structure. Attempted incision of the overlying serosa toreflect the tissue was unsuccessful as it was firmly adhered tothe underlying structure. The scope was replaced in theventral portal and a loop created with an extra-corporealmodified Roeder knot (3.5 m polyglactin 910; Vicryl)12 placedaround the pedunculated marble. After tightening the knotthe suture was withdrawn and the portal enlarged to allowthe marble to be exteriorised (Fig 2 a,b), followed byplacement of stay sutures in the adjacent uterine horn. Theoverlying tissue was incised (Fig 2c) and, with difficulty, thetissues separated from the surface of the marble which wasgrossly pitted (Fig 2d). With the marble removed it wasapparent that it had migrated through both the mucosal andmuscle layers to sit finally in a serosal capsule covered by a
© 2016 EVJ Ltd
126 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
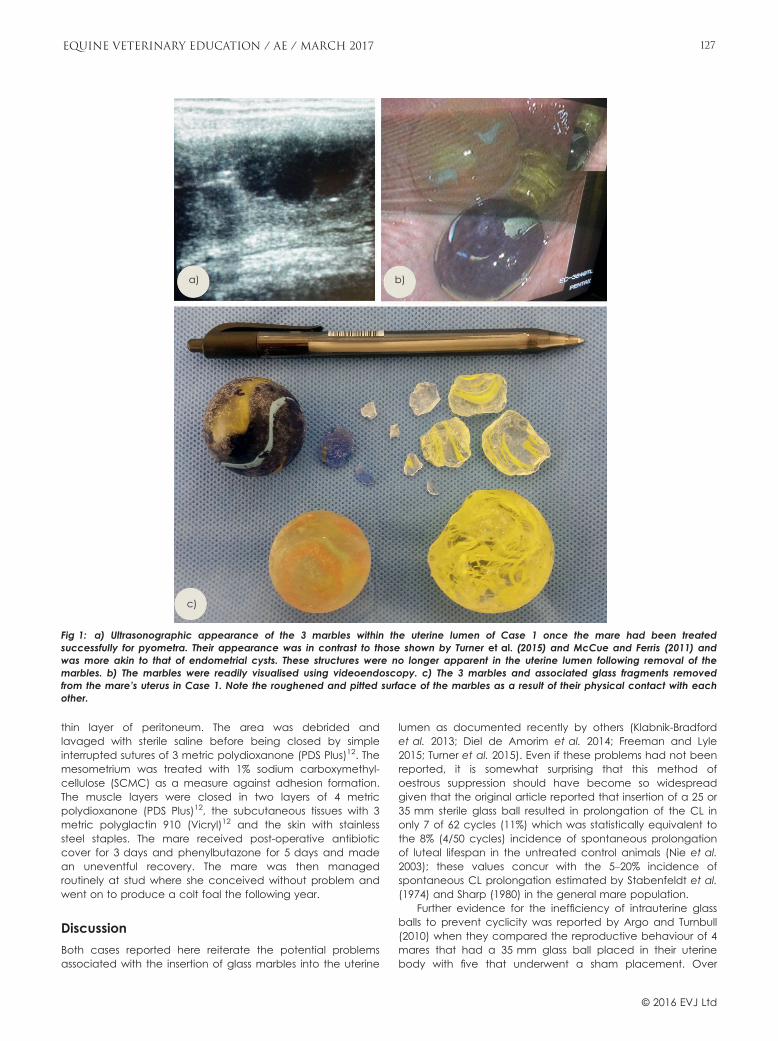
thin layer of peritoneum. The area was debrided andlavaged with sterile saline before being closed by simpleinterrupted sutures of 3 metric polydioxanone (PDS Plus)12. Themesometrium was treated with 1% sodium carboxymethyl-cellulose (SCMC) as a measure against adhesion formation.The muscle layers were closed in two layers of 4 metricpolydioxanone (PDS Plus)12, the subcutaneous tissues with 3metric polyglactin 910 (Vicryl)12 and the skin with stainlesssteel staples. The mare received post-operative antibioticcover for 3 days and phenylbutazone for 5 days and madean uneventful recovery. The mare was then managedroutinely at stud where she conceived without problem andwent on to produce a colt foal the following year.
Discussion
Both cases reported here reiterate the potential problemsassociated with the insertion of glass marbles into the uterine
lumen as documented recently by others (Klabnik-Bradfordet al. 2013; Diel de Amorim et al. 2014; Freeman and Lyle2015; Turner et al. 2015). Even if these problems had not beenreported, it is somewhat surprising that this method ofoestrous suppression should have become so widespreadgiven that the original article reported that insertion of a 25 or35 mm sterile glass ball resulted in prolongation of the CL inonly 7 of 62 cycles (11%) which was statistically equivalent tothe 8% (4/50 cycles) incidence of spontaneous prolongationof luteal lifespan in the untreated control animals (Nie et al.2003); these values concur with the 5–20% incidence ofspontaneous CL prolongation estimated by Stabenfeldt et al.(1974) and Sharp (1980) in the general mare population.
Further evidence for the inefficiency of intrauterine glassballs to prevent cyclicity was reported by Argo and Turnbull(2010) when they compared the reproductive behaviour of 4mares that had a 35 mm glass ball placed in their uterinebody with five that underwent a sham placement. Over
a)
c)
b)
Fig 1: a) Ultrasonographic appearance of the 3 marbles within the uterine lumen of Case 1 once the mare had been treatedsuccessfully for pyometra. Their appearance was in contrast to those shown by Turner et al. (2015) and McCue and Ferris (2011) andwas more akin to that of endometrial cysts. These structures were no longer apparent in the uterine lumen following removal of themarbles. b) The marbles were readily visualised using videoendoscopy. c) The 3 marbles and associated glass fragments removedfrom the mare’s uterus in Case 1. Note the roughened and pitted surface of the marbles as a result of their physical contact with eachother.
© 2016 EVJ Ltd
127EQUINE VETERINARY EDUCATION / AE / MARCH 2017

several oestrous cycles no differences occurred between thetwo groups in the interovulatory interval, ovarian activity,endometrial oedema, levels of oestradiol, progesterone,testosterone or luteinising hormone in peripheral blood or,perhaps most importantly, sexual behaviour. Likewise, in thetwo cases reported here, both mares had continued to cycledespite the presence of uterine marble(s).
The belief persists among some veterinary surgeons,trainers and mare owners that insertion of a marble into theuterine lumen will prevent unwanted oestrus-associatedbehaviour despite the lack of scientific evidence in supportof such a claim. Indeed, 60% of the owners of mares whichhad a 35 mm glass ball placed in their uteri reported animprovement in their animal’s performance for at least a year(Argo and Turnbull 2010). Such divergence from reality isbelieved to be due, in part, to a ‘placebo effect’ (Nie et al.2003; Katila 2015).
The demonstrated cyclicity of many mares in thepresence of an intrauterine marble and the frequent lack ofa full or accurate reproductive history of mares, particularlywhen they change ownership, argues that any routinereproductive examination of a mare should include a checkfor such intrauterine foreign objects. However, visualising aglass ball within the uterus is not always easy, especially inmares that accumulate intrauterine fluid or present withpyometra (Katila 2015). Endometrial oedema can also makedetection difficult and this may be exaggerated byunderlying endometritis, which can be associated withretained intrauterine objects (Daels and Hughes 1995; Nie
et al. 2003; Diel de Amorim et al. 2014). Careful transrectalpalpation, combined with ultrasonography, is moreproductive than ultrasound alone in detecting intrauterinemarbles in the uterine lumen (Freeman and Lyle 2015).Videoendoscopic hysteroscopy is perhaps the most accuratemethod to locate marbles within the uterine lumen, but this isunlikely to be undertaken as a routine procedure.
The difficulty of detecting marbles placed in the uterus isillustrated in the two cases reported here. In Case 1 themarbles had not been detected over five consecutivebreeding seasons. The mare was referred to a specialist clinicand the marbles identified ultrasonographically after thepyometra had resolved. In Case 2, the marble was detectedby careful palpation and ultrasonography, but its locationoutside the uterine lumen made this challenging. However,even in the absence of fluid or migration to an unexpectedlocation, an intrauterine marble may still be missed ormistaken for a conceptus, endometrial folds or endometrialcysts. Hence, it is essential that stud veterinary surgeonsshould, regardless of the apparent history of a marepresented to them for examination, keep in mind that anintrauterine marble(s) may be present.
Multiple marbles were present in Case 1 and it is likelythat the second and then the third marble were inserted intothe mare’s uterus when she returned to oestrus following theplacement of previous marbles under the assumption thatthey had been expelled. The presence of multiple marbles inthe uterine lumen has been previously reported (Vanderwall2013; Diel de Amorim et al. 2014; Turner et al. 2015) and, as in
a)
c) d)
b)
Fig 2: a and b) Exteriorisation of the semi-pedunculated marble in its subserosal pouch. c) Incision of the overlying tissue to reveal themarble. d) The grossly pitted marble; note the small pieces of tissue still adherent to its surface (38 mm hypodermic needle for scale).
© 2016 EVJ Ltd
128 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

the present Case 1, these were pitted on their surface or hadfragmented into shards while in the uterine lumen. Althoughveterinary surgeons have reported pitting of a singleintrauterine marble, physical abrasion between two or moremarbles during uterine contractions, peristalsis of the intestinesin contact with the uterus and/or physical movement of thewhole animal may increase the propensity for them tofracture. The difficulty of removing all fragments of glassleaves the potential for the creation of a nidus for infection orinflammation and the possibility of a glass shard penetratingthe endometrium or conceptus, all potentially impairing thefertility of the mare.
In Case 2 the marble did not fracture but it migratedintact through the endometrium and myometrium tobecome encapsulated in the uterine serosa. No evidence ofa fistula was seen during videoendoscopic examination ofthe uterine lumen or when the pedunculated marble wasremoved laparoscopically. Numerous reports exist of themigration of contraceptive intrauterine devices (IUDs), placedin the uteri of women, to sites outside of the uterine lumen,including the broad ligament, omentum, sigmoid colon,rectum and bladder. While many such cases wereasymptomatic, others had serious consequences, includingdamage to internal organs, abscess formation and peritonitis(Jatti et al. 2007; Vilallonga et al. 2010). Likewise, surgicalswabs left in patients have been shown to migrate throughthe body (Silva et al. 2001; Guner et al. 2012; Rafie et al.2013), most likely as a result of an inflammatory reactionaround the foreign body forming an eroding abscess.Contractility or peristaltic movements of the affected organ,or those surrounding it, allow the foreign body to moveforward leaving a fistula in its wake, which eventually heals toform a fibrotic scar at the site of migration(Wattanasirichaigoon 1996; Dhillon and Park 2002). Tworeported cases that support such a hypothesis are of surgicalswabs left in the abdomen having migrated into the lumen ofthe intestines without any visible opening in the intestinal wall(Silva et al. 2001; Rafie et al. 2013).
In Case 2, it is likely that migration of the marble fromthe uterine lumen to the serosa of the uterus occurred bya similar mechanism. Initially, the glass marble would haveadhered to the lumenal epithelium of the endometrium, aspreviously mentioned as a potential sequela of theirplacement in the uterine lumen (Diel de Amorim et al.2014). In addition, other authors have reported on therelative lack of movement of intrauterine devices (Riveradel Alamo et al. 2008) which would potentially contributeto their adherence to the lumenal epithelium of theendometrium. Although, Rivera del Alamo et al. (2008)found no difference in inflammation between control maresand those with intrauterine devices they did identifyneutrophils around the IUD which they surmised wasindicative of localised inflammation. Hence, in Case 2,localised inflammation around the marble may haveeroded the underlying endometrium and allowed thepassage of the foreign object to the myometrium and ontothe serosa. During both videoendoscopic and laparoscopicexaminations no fistula or tract was observed, as with theaforementioned cases of migration of a surgical swabthrough the gut wall (Silva et al. 2001; Rafie et al. 2013). It isplausible that the inability of the mare to conceive prior toremoval of the marble may have been due to mating at atime when the fistula or tract was still patent or a nidus for
inflammation or infection remained at the site. It could beargued that since the mare had an apparently normaluterus apart from the displaced marble, the laparoscopicremoval of the marble was not warranted. However, giventhat the marble had already migrated through theendometrium and myometrium it could well, in time, havemigrated further into the peritoneal cavity with potentiallydisastrous consequences.
In conclusion, there are mounting anecdotal andpublished reports of the potential adverse sequelaeassociated with placing glass balls in the uterine lumen ofcycling mares (Vanderwall 2012, 2013; Klabnik-Bradfordet al. 2013; Diel de Amorim et al. 2014; Freeman and Lyle2015; Turner et al. 2015). This, coupled with the inefficiencyof the technique to prevent oestrous behaviour, indicatesthat the practice of placing marbles in the uteri of maresto suppress oestrous behaviour should be consideredunethical and tantamount to quackery. Armed with currentknowledge, veterinary surgeons should educate mareowners as to the reasons why this technique should bediscontinued.
Authors’ declaration of interests
No conflicts of interest have been declared.
Ethical animal research
Ethical review and approval is not required for this casereport.
Source of funding
None.
Authorship
L. H-A. Morris, C. Cantley and B. Fraser undertook the clinicalwork for the case studies. S. Wilsher and B. Fraser wrote themanuscript. S. Wilsher prepared the manuscript. All authorsedited and approved the final draft of the manuscript.
Manufacturers' addresses1Baxter Healthcare Pty Ltd, Toongabbie, New South Wales, Australia.2Bayer New Zealand Ltd, Auckland, New Zealand.3CLS Limited, Melbourne, Victoria, Australia.4Pfizer NZ Ltd, Auckland, New Zealand.5MSD Animal Health Ltd, Wellington, New Zealand.6Phoenix Pharm, Auckland, New Zealand.7Ethical Agents Veterinary Marketing Ltd, Auckland, New Zealand.8Ethical Agents, Manukau, New Zealand.9Zoetis New Zealand Ltd, Auckland, New Zealand.10Virbac New Zealand Ltd, Hamilton, New Zealand.11Covidien NZ Ltd, Auckland, New Zealand.12Ethicon Inc., Somerville, New Jersey, USA.
ReferencesArgo, C.M. and Turnbull, E.B. (2010) The effect of intra-uterine devices
on the reproductive physiology and behaviour of pony mares. Vet.J. 186, 39-46.
Daels, P.F. and Hughes, J.P. (1995) Fertility control using intrauterinedevices: an alternative for population control in wild horses.Theriogenology 44, 629-639.
© 2016 EVJ Ltd
129EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Dhillon, J.S. and Park, A. (2002) Transmural migration of a retainedlaparotomy sponge. Am. Surg. 68, 603-605.
Diel de Amorim, M., Chenier, T. and Manning, S. (2014) Complicationsrelated to the use of intrauterine glass marbles in mares. Proc. Am.Ass. Equine Practnrs. 60, 317.
Freeman, C.E. and Lyle, S.K. (2015) Chronic intermittent colic in amare attributed to uterine marbles. Equine Vet. Educ. 27,469-473.
Guner, A., Hos, G., Kahraman, I. and Kece, C. (2012) Transabdominalmigration of retained surgical sponge. Case Rep. Med. 2012.Article ID 249859. doi:10.1155/2012/249859.
Hedberg, Y., Dalin, A.M., Santesson, M. and Kindahl, H. (2006) Apreliminary study on the induction of dioestrous ovulation in themare – a possible method for inducing prolonged luteal phase.Acta Vet. Scand. 48, 12.
Jatti, J., James, S. and James, M.C. (2007) Peritoneal abscess resultingfrom a translocated copper intrauterine device. J. Fam. Plann.Reprod. Health Care 33, 57-58.
Katila, T. (2015) Techniques to supress oestrus in mares. Equine Vet.Educ. 27, 344-345.
Klabnik-Bradford, J., Ferrer, M.S., Blevins, C. and Beard, L. (2013)Marble-induced pyometra in an Appaloosa mare. Clin.Theriogenol. 5, 410.
Lefranc, A.-C. and Allen, W.R. (2004) Non-pharmacologicalsuppression of oestrus in the mare. Equine Vet. J. 36, 183-185.
McCue, P.M. (2003) Estrus suppression in performance horses. J.Equine. Vet. Sci. 23, 342-344.
McCue, P.M. and Ferris, R.A. (2011) The abnormal estrus cycle. In:Equine Reproduction, 2nd edn., Eds: A.O. McKinnon, E.L. Squires,W. Vaala and D.D. Varner, Wiley-Blackwell, Chichester, UK. pp1754-1768.
Nie, G.J., Johnson, K.E., Braden, T.D. and Wenzel, J.G.W. (2003) Use ofan intrauterine glass ball protocol to extend luteal function inmares. J. Equine. Vet. Sci. 23, 266-273.
Rafie, B.A., AbuHamdan, O.J. and Trengganu, N.S. (2013) Intraluminalmigration of retained surgical sponge as a cause of intestinalobstruction. J. Surg. Case Rep. 2013, pii: rjt032. doi: 10.1093/jscr/rjt032.
Rivera del Alamo, M.M., Reilas, T., Kindahl, H. and Katila, T. (2008)Mechanisms behind intrauterine device-induced luteal persistencein mares. Anim. Reprod. Sci. 107, 94-106.
Sharp, D.C. (1980) Factors associated with the maternal recognition ofpregnancy in the mare. Vet. Clin. North Am. Large Anim. Pract. 2,277-290.
Silva, C.S., Caetano, M.R., Silva, E.A., Falco, L. and Murta, E.F. (2001)Complete migration of retained surgical sponge into ileum withoutsign of open intestinal wall. Arch. Gynecol. Obstet. 265, 103-104.
Stabenfeldt, G.H., Hughes, J.P., Evans, J.W. and Neely, D.P. (1974)Spontaneous prolongation of luteal activity in the mare. EquineVet. J. 6, 158-163.
Stout, T.A.E., Lamming, G.E. and Allen, W.R. (1999) Oxytocin prolongsluteal function in cyclic mares. J. Reprod. Fertil. 116, 315-320.
Turner, R.M., Vanderwall, D.K. and Stawicki, R. (2015) Complicationsassociated with the presence of two intrauterine glass balls foroestrus suppression in a mare. Equine Vet. Educ. 27, 340-343.
Vanderwall, D.K. (2012) Suppression of oestrus in mares. In:Proceedings of the 51st British Equine Veterinary AssociationCongress, Birmingham, UK. p 201.
Vanderwall, D.K. (2013) Prolonging function of the corpus luteum tosuppress estrus in mares. Proc. Am. Ass. Equine Practnrs. 59, 342-349.
Vanderwall, D.K. and Nie, G.J. (2011) Estrus suppression. In: EquineReproduction, 2nd edn., Eds: A.O. McKinnon, E.L. Squires, W. Vaalaand D.D. Varner. Wiley-Blackwell, Chichester, UK. pp 1845-1853.
Vanderwall, D.K., Rasmussen, D.M. and Woods, G.L. (2007) Use ofexogenous oxytocin to block luteolysis in mare: a plausible methodof long-term suppression of estrus. Proc. Am. Ass. Equine Practnrs.53, 578-579.
Vilallonga, R., Rodriguez, N., Vilchez, M. and Armengol, M. (2010)Translocation of an intrauterine contraceptive device: incidentalfinding in the rectosigmoid colon. Obstet. Gynecol. Int. 2010,Article ID: 404160. doi:10.1155/2010/404160.
Wattanasirichaigoon, S. (1996) Transmural migration of a retainedsurgical sponge into the intestinal lumen: an experimental study. J.Med. Ass. Thai. 79, 415-422.
Wilsher, S. and Allen, W.R. (2011) Intrauterine administration of plantoils inhibits luteolysis in the mare. Equine Vet. J. 43, 99-105.
© 2016 EVJ Ltd
130 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
CAUTION: Federal law restricts this drug to use by or on the order of a licensed veterinarian.
EQUIOXX® (firocoxib) is indicated for the control of pain and inflammation associated with osteoarthritis in horses. Firocoxib belongs to the coxib class of non-narcotic, non-steroidal anti-inflammatory drugs (NSAID).
CONTRAINDICATIONS: Horses with hypersensitivity to firocoxib should not receive EQUIOXX.
WARNINGS: EQUIOXX is for use in horses only. Do not use in horses intended for human consumption. Do not use in humans. Store EQUIOXX Tablets out of the reach of dogs, children, and other pets in a secured location in order to prevent accidental ingestion or overdose. Consult a physician in case of accidental human exposure.
Horses should undergo a thorough history and physical examination before initiation of NSAID therapy. Appropriate laboratory tests should be conducted to establish hematological and serum biochemical baseline data before and periodically during administration of any NSAID. NSAIDs may inhibit the prostaglandins that maintain normal homeostatic function. Such anti-prostaglandin effects may result in clinically significant disease in patients with underlying or pre-existing disease that has not been previously diagnosed.
Treatment with EQUIOXX should be terminated if signs such as inappetance, colic, abnormal feces, or lethargy are observed. As a class, cyclooxygenase inhibitory NSAIDs may be associated with gastrointestinal, renal, and hepatic toxicity. Sensitivity to drug-associated adverse events varies with the individual patient. Horses that have experienced adverse reactions from one NSAID may experience adverse reactions from another NSAID. Patients at greatest risk for adverse events are those that are dehydrated, on diuretic therapy, or those with existing renal, cardiovascular, and/or hepatic dysfunction. The majority of patients with drug-related adverse reactions recover when the signs are recognized, drug administration is stopped, and veterinary care is initiated.
Concurrent administration of potentially nephrotoxic drugs should be carefully approached or avoided. Since many NSAIDs possess the potential to produce gastrointestinal ulcerations and/or gastrointestinal perforation, concomitant use of EQUIOXX with other anti-inflammatory drugs, such as NSAIDs or corticosteroids, should be avoided. The concomitant use of protein bound drugs with EQUIOXX has not been studied in horses. The influence of concomitant drugs that may inhibit the metabolism of EQUIOXX has not been evaluated. Drug compatibility should be monitored in patients requiring adjunctive therapy.
The safe use of EQUIOXX in horses less than one year of age, horses used for breeding, or in pregnant or lactating mares has not been evaluated. Consider appropriate washout times when switching from one NSAID to another NSAID or corticosteroid.
The Safety Data Sheet (SDS) contains more detailed occupational safety information. For technical assistance, to request an SDS, or to report suspected adverse events call 1-877-217-3543. For additional information about adverse event reporting for animal drugs, contact FDA at 1-888-FDA-VETS, or http://www.fda.gov/AnimalVeterinary.
Rev 10/2016
Merial is now part of Boehringer Ingelheim.
®EQUIOXX is a registered trademark of Merial.©2017 Merial, Inc., Duluth, GA. All rights reserved. EQUIEQX1607 (1/17)
IMPORTANT SAFETY INFORMATION: As with any prescription medication, prior to use, a veterinarian should perform a physical examination and review the horse’s medical history. A veterinarian should advise horse owners to observe for signs of potential drug toxicity. As a class, nonsteroidal anti-inflammatory drugs may be associated with gastrointestinal, hepatic and renal toxicity. Use with other NSAIDs, corticosteroids or nephrotoxic medication should be avoided. EQUIOXX has not been tested in horses less than 1 year of age or in breeding horses, or pregnant or lactating mares. For additional information, please refer to the prescribing information or visit www.equioxx.com.
1Data on file at Merial, Safety Study, PR&D 0144901.2 Doucet MY, Bertone AL, et al. Comparison of efficacy and safety of paste formulations of firocoxib and phenylbutazone in horses with naturally occurring osteoarthritis. J Am Vet Med Assoc. 2008;232(1):91-97.
3EQUIOXX product labels and FOI summaries and supplements.4Data on file at Merial, Clinical Experience Report PHN 471, PR&D 0030701.
Because managing OA pain
shouldn’t cause more pain.
EQUIOXX delivers efficacy with an exceptional safety profile.
EQUIOXX.com
When you do the research, you’ll find EQUIOXX is the right choice for treating osteoarthritis pain and
inflammation for your clients.
• First and Only – EQUIOXX – the first and only coxib NSAID for horses – spares COX-1
while inhibiting COX-21*
• More Effective – In a study, EQUIOXX was rated as effective or more effective than phenylbutazone, including
improvement in pain on manipulation, range of motion, joint circumference and overall improvement scores2
• Safety – EQUIOXX has been tested on more horses in safety studies than any other NSAID;3,4
at the recommended dose, most horses had no side effects
• Convenient – One dose controls pain up to 24 hours which can also aid in compliance
*Clinical relevance has not been determined.
Time to put your old NSAID out to pasture. See how
EQUIOXX can make a difference for your clients.wwwww
EQUIOXX.com
Available in three formulations to fit in and out of competition needs: Injection, Paste and Tablet.

EUROPEAN EDUCATIONAL OFFERINGS
ENGLAND
Bell Equine 3 Day Module April 6-8 Open to All
Veterinarians Proximal Forelimb: Shoulder,
Elbow, & Antebrachium
ITALY Cascina Gufa 3 Day Module
July 6-8 Open to All Veterinarians Neck & Back
THE NETHERLANDS
Sporthorse Medical Diagnostic Centre 3 Day Module
September 8-10 Open to All Veterinarians
Foot & Pastern
FRANCE Grosbois 3 Day Module
October 19-21 Open to All Veterinarians
Fetlock, Metacarpus, & Carpus
NORTH AMERICAN EDUCATIONAL OFFERINGS
CALIFORNIA
Peninsula Equine Medical Center
3 Day Module Open to All Veterinarians
May 4-6 Distal Hindlimb & Proximal
Suspensory Ligament ISELP Certification Exam-May 6
CANADA Kleider Veterinary Services Vancouver British Columbia
3 Day Module September 29-October 1 Open to All Veterinarians
Pelvis
MISSOURI Homestead Veterinary Hospital 1-Day Hands On Talk & Wet Lab
October 7 –Open to All Veterinarians
The Stifle
2716 Landmark School Road * The Plains * Virginia 20198 * USA * 540-687-4663 * www.iselp.org
Visit www.iselp.org for Registration Information A. Kent Allen, DVM, Vice President & Executive Director, ISELP Certified

Case Report
Diagnostic dichotomy: A question of thoracic mesotheliomaJ. May†,*1, D. Fews‡, K. Tennant§ and T. Mair†
†Bell Equine Veterinary Clinic, Mereworth, Maidstone, Kent, UK; ‡Veterinary Pathology, School of Veterinary Science,Bristol, UK and §Diagnostic Laboratories, Langford Veterinary Services, Langford House, Langford, Bristol, UK.*Corresponding author email: [email protected] Present address: Department of Veterinary Clinical Services, The Hong Kong Jockey Club, 1/F Central ComplexBuilding, Sha Tin Racecourse, New Territories, Hong Kong
Keywords: horse; diagnostic; mesothelioma; thoracic; neoplasia
SummaryA 12-year-old Irish Sport Horse gelding was presented with atwo-day history of acute onset dyspnoea, pyrexia,tachycardia and ventral sternal oedema. A pleural effusionwas identified, and thoracocentesis yielded a haemorrhagicmodified transudate. Cytological examination of the fluidshowed numerous red blood cells with smaller numbers oflarge nucleated cells that exhibited mild anisocytosis andanisokaryosis. Thoracoscopy identified adhesions betweenthe visceral and dorsal parietal pleura, haemorrhagic effusionventrally and haemorrhagic soft tissue plaques scattered overthe diaphragm and mediastinum; biopsies of tissue on thecaudal mediastinum were obtained. Histopathologicalexamination of the biopsies identified inflammation, with asuspicion of underlying neoplasia; adenocarcinoma,haemangiosarcoma or mesothelioma were considered mostlikely, but could not be confirmed on the basis of theseexaminations. The horse was euthanased, and mesotheliomawas diagnosed following post mortem examination. This casedemonstrates some of the difficulties associated with theaccurate premortem diagnosis of mesothelioma.
Introduction
Malignant mesothelioma (mesothelioma) is a rare neoplasmthat has been reported in people, horses, cats (Heerkenset al. 2011) and dogs (Stevens et al. 2014). It arises from thesingle layer of mesothelial cells that line the peritoneal,pleural or pericardial cavities. Only a limited number of casereports of equine mesothelioma have been published (Straubet al. 1974; Kramer et al. 1976; Ricketts and Peace 1976;Carnine et al. 1977; Kolbl 1979; Wallace et al. 1987;Colbourne et al. 1992; Mair et al. 1992; Harps et al. 1996; Fryet al. 2003; Stoica et al. 2004). In man, this neoplasm isstrongly associated with asbestos exposure (Brenner et al.1982); however, there is little clinical evidence for this inanimals, although one author associated airborne fibres withmesothelioma in 6 urban-dwelling dogs (Harbison andGodleski 1983).
Mesothelioma and other types of thoracic neoplasmscan present a diagnostic challenge for equine cliniciansbecause the clinical signs are nonspecific. They includedepression, inappetence, weight loss and pyrexia (Mair andBrown 1993; Davis and Rush 2013). Coughing, dyspnoea andpulmonary haemorrhage may also occur, dependent onthe location and extent of the tumour (Mair et al. 2004),and voluminous cavity effusions are often present (Kramer
et al. 1976; Mair and Brown 1993; Davis and Rush 2013).Cytological analysis of effusions and histopathologicalevaluation of representative tissue biopsies are used to makea diagnosis. However, difficulty in reaching a definitivediagnosis can arise due to problems in differentiatingbetween reactive and neoplastic mesothelial cells incytological and histopathological preparations (Kramer et al.1976; Mair et al. 2004; Addis and Roche 2009; Davis and Rush2013) and, as such, only 3 case reports describe antemortem diagnosis of mesothelioma in horses (Kramer et al.1976; Mair et al. 1992; Fry et al. 2003). The rapid progressionof the disease and the grave prognosis associated withmesothelioma mean that euthanasia often precedesaccurate diagnosis.
The purpose of this case report is to describe thepresentation and diagnostic pathway of thoracicmesothelioma in a horse, and to illustrate some of thecomplexities of establishing a definitive premortem diagnosis,even when tissue biopsies are obtained.
Case history
A 12-year-old Irish Sport Horse gelding, used for eventing,was presented with a 2-day history of acute onsetdyspnoea, pyrexia (39.2°C) and tachycardia (52 beats/min).A transient improvement in clinical signs had been seenfollowing administration of atropine1, phenylbutazone2 anddexamethasone3 by the referring veterinarian. After 24 h thepyrexia had resolved, but the horse had developed a soft,frequent cough and increasing tachycardia (72 beats/min).Flunixin meglumine4, furosemide4 and clenbuterol3 wereadministered, and the horse was subsequently hospitalised forfurther evaluation.
Clinical findings
On clinical examination, the horse was quiet, but alertand responsive. Abnormal findings included tachycardia(80 beats/min) and tachypnoea (30 breaths/min), withsevere inspiratory and expiratory dyspnoea. A plaque ofsubcutaneous, ventral sternal oedema was present. Mucousmembranes were mildly cyanotic. On cardiothoracicauscultation, the lung sounds were inaudible in the ventral halfof the thorax bilaterally, the heart sounds were muffled, andthere was distant radiation of the cardiac beat. These clinicalfindings were considered to be consistent with bilateral pleuraleffusion.
© 2016 EVJ Ltd
131EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Haematology and serum biochemical analyses revealedlymphopenia (lymphocytes 1.00 9 109/l, reference range [rr]1.5–4 9 109/l), mildly elevated haematocrit (49.5%, rr 30–47%),azotaemia (blood urea 9.5 mmol/l, rr 2.8–7.3 mmol/l),hyperfibrinogenaemia (plasma fibrinogen 11.3 g/l, rr 1–4 g/l)and elevated serum amyloid A concentration (3680 mg/l, rr<20 mg/l). Venous blood gas analysis indicated respiratoryalkalosis with secondary metabolic alkalosis (pH 7.33; PCO2
56.4 mmHg; PO2 21.1 mmHg; cHCO3� 29.8 mmol/l).
Thoracic ultrasonography, performed with a 5 MHzcurvilinear probe, revealed a bilateral pleural effusion, andatelectasis of the ventral lung lobes; the pleural fluid had ahyperechoic and swirling appearance consistent with ahaemorrhagic effusion. There was no pericardial effusion.Transabdominal ultrasonography and rectal palpation wereunremarkable. Airway endoscopy revealed moderatemucosal swelling of the carina and a small volume ofhaemorrhagic fluid in the bronchial tree.
Thoracocentesis, performed on the right side of the chest,yielded a frothy haemorrhagic modified transudate (totalnucleated cell count 1.1 9 109/l; total protein 20 g/l,haematocrit 1.2%; Fig 1). On cytological examination, therewas a background of high numbers of erythrocytes and lownumbers of nucleated cells, which exhibited criteria thatraised the suspicion for carcinoma or very reactivemesothelial cells. Many of the latter were large cells, 5–10times an erythrocyte in diameter, and exhibited mildanisocytosis and anisokaryosis. They had a moderate to veryhigh nuclear to cytoplasmic ratio. The nuclei were round andthe nuclear chromatin was lacy to coarse. Occasionalexamples contained 1–4 indistinct nucleoli with variable sizeand shape. The cytoplasm was moderately basophilic andcontained high numbers of variably sized vacuoles that wereoccasionally displacing the nucleus. Vacuoles were alsofrequently seen inside the nuclei. Low numbers ofmacrophages were noted; these showed markedvacuolation and rare erythrophagocytosis. Low numbers ofnondegenerate neutrophils were also present (Fig 2),probably due to the presence of blood.
Following drainage of the pleural effusion, standingthoracic radiographs revealed an interstitial pulmonarypattern in the dorsal lung fields with an abnormal soft tissueopacity ventrally. The remaining pleural fluid opacityobscured the ventral lung fields (Fig 3).
Treatment
Initial stabilisation was achieved by draining approximately35 litres of pleural fluid from the right side of the chest, whichwas performed slowly to minimise possible cardiovasculareffects; this resulted in resolution of the dyspnoea andimprovement of the mucous membrane colour. Intravenousfurosemide4 (1 mg/kg bwt) and tranexamic acid5 (4.5 mg/kgbwt) were administered, as well as antimicrobial therapy,(benzylpenicillin sodium4, 10 Mega/500 kg bwt i.v.; procainebenzylpenicillin4, 17 mg/kg bwt i.m. b.i.d.; gentamicin2,6.6 mg/kg bwt i.v. s.i.d.). Over the next 12 h the pleural fluidvolume increased again (as demonstrated by thoracicultrasonography), and the horse’s dyspnoea recurred. He alsodeveloped mild diarrhoea, and treatment with isotoniccrystalloid fluids (Hartmann’s solution2; 3 ml/kg bwt/h i.v.) anddi-tri-octahedral smectite6 (240 cm3 per os) wascommenced.
Thoracoscopy (Vachon and Fischer 1998) was performedunder standing sedation and local anaesthesia(Supplementary Item 1). The horse was restrained in stocksand administered flunixin meglumine4 (1.1 mg/kg bwt) i.v.and morphine sulphate7 (0.1 mg/kg bwt) i.v. A single bolus ofdetomidine hydrochloride8 (10 lg/kg bwt) i.v. wasadministered, followed by continuous rate infusion (0.8 mg/kgbwt/min), as previously described by Peroni et al. (2001). Thepleural effusion was drained using a chest drain (36 French)9
placed in the right eighth intercostal space. Thorascopicexamination of the left side identified adhesions (Fig 3)between the visceral and dorsal parietal pleura,haemorrhagic effusion ventrally and haemorrhagic soft tissueplaques (Fig 4) scattered over the diaphragm andmediastinum, from which biopsies at the caudal mediastinumwere obtained. The left hemithorax had a comparableappearance to the right, and further biopsies were obtained.
Fig 1: Gross appearance of the pleural effusion obtained bythoracocentesis, which yielded a frothy, haemorrhagic modifiedtransudate.
Fig 2: Pleural fluid cytology. Modified Wright’s stain. Three largeabnormal cells and a single neutrophil. The nuclei containrounded nucleoli (arrowhead) 3100 oil immersion lens.
© 2016 EVJ Ltd
132 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
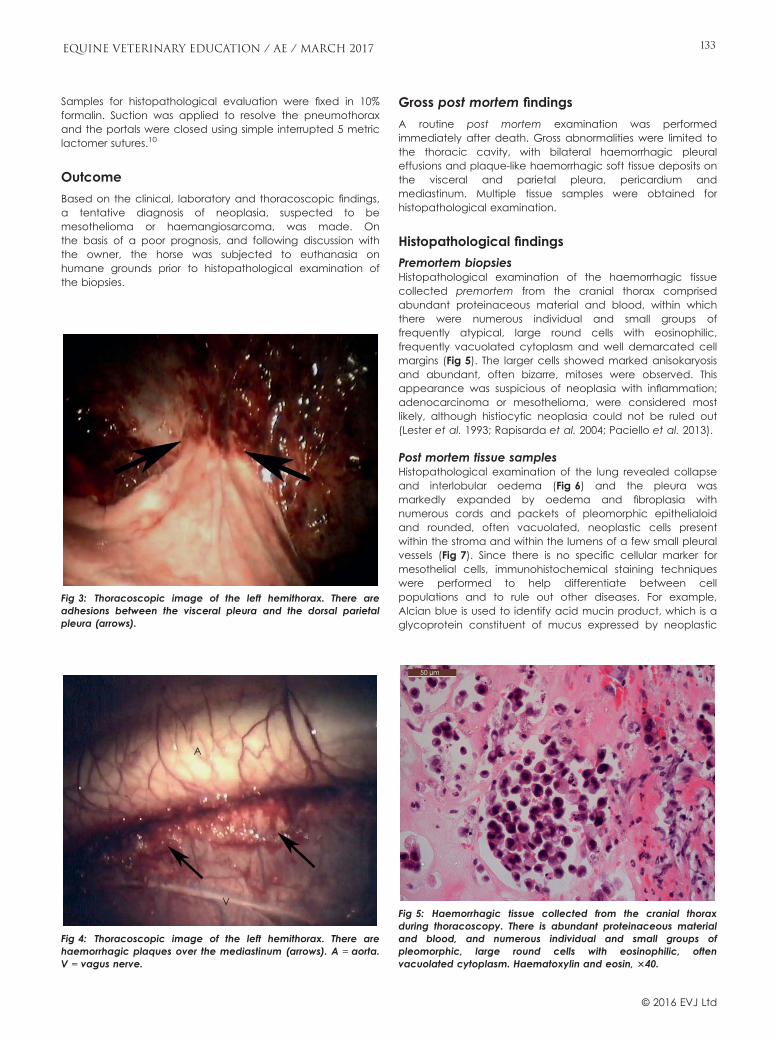
Samples for histopathological evaluation were fixed in 10%formalin. Suction was applied to resolve the pneumothoraxand the portals were closed using simple interrupted 5 metriclactomer sutures.10
Outcome
Based on the clinical, laboratory and thoracoscopic findings,a tentative diagnosis of neoplasia, suspected to bemesothelioma or haemangiosarcoma, was made. Onthe basis of a poor prognosis, and following discussion withthe owner, the horse was subjected to euthanasia onhumane grounds prior to histopathological examination ofthe biopsies.
Gross post mortem findings
A routine post mortem examination was performedimmediately after death. Gross abnormalities were limited tothe thoracic cavity, with bilateral haemorrhagic pleuraleffusions and plaque-like haemorrhagic soft tissue deposits onthe visceral and parietal pleura, pericardium andmediastinum. Multiple tissue samples were obtained forhistopathological examination.
Histopathological findings
Premortem biopsiesHistopathological examination of the haemorrhagic tissuecollected premortem from the cranial thorax comprisedabundant proteinaceous material and blood, within whichthere were numerous individual and small groups offrequently atypical, large round cells with eosinophilic,frequently vacuolated cytoplasm and well demarcated cellmargins (Fig 5). The larger cells showed marked anisokaryosisand abundant, often bizarre, mitoses were observed. Thisappearance was suspicious of neoplasia with inflammation;adenocarcinoma or mesothelioma, were considered mostlikely, although histiocytic neoplasia could not be ruled out(Lester et al. 1993; Rapisarda et al. 2004; Paciello et al. 2013).
Post mortem tissue samplesHistopathological examination of the lung revealed collapseand interlobular oedema (Fig 6) and the pleura wasmarkedly expanded by oedema and fibroplasia withnumerous cords and packets of pleomorphic epithelialoidand rounded, often vacuolated, neoplastic cells presentwithin the stroma and within the lumens of a few small pleuralvessels (Fig 7). Since there is no specific cellular marker formesothelial cells, immunohistochemical staining techniqueswere performed to help differentiate between cellpopulations and to rule out other diseases. For example,Alcian blue is used to identify acid mucin product, which is aglycoprotein constituent of mucus expressed by neoplastic
A
V
Fig 4: Thoracoscopic image of the left hemithorax. There arehaemorrhagic plaques over the mediastinum (arrows). A = aorta.V = vagus nerve.
Fig 3: Thoracoscopic image of the left hemithorax. There areadhesions between the visceral pleura and the dorsal parietalpleura (arrows).
50 μm
Fig 5: Haemorrhagic tissue collected from the cranial thoraxduring thoracoscopy. There is abundant proteinaceous materialand blood, and numerous individual and small groups ofpleomorphic, large round cells with eosinophilic, oftenvacuolated cytoplasm. Haematoxylin and eosin, 340.
© 2016 EVJ Ltd
133EQUINE VETERINARY EDUCATION / AE / MARCH 2017

mesothelial cells. In this case it was found within thecytoplasm of many of the neoplastic cells (Fig 8).
Sections of the lung and of the haemorrhagic tissue in thecranial thorax were stained for vimentin, cytokeratin andMAC 387. Vimentin is a cytoskeletal protein expressed bymesenchymal cells, and cytokeratin is a keratin-containingprotein expressed by epithelial tissue. They are nonspecificimmunohistochemical markers known to be co-expressed bymesothelial cells (Dobromylskyj et al. 2011). Anti-macrophagemonoclonal antibody (MAC 387) is used to detectmonocytes. Within the section collected from the lung,neoplastic cells within some aggregates showed weak tooccasionally moderate cytoplasmic staining for vimentin;however, the neoplastic cells within some aggregatesshowed weak to moderate cytoplasmic staining forcytokeratin; the vacuolated cells generally failed to stain,and, within some aggregates, the majority of the cells failed
to stain for cytokeratin. Staining for MAC 387 was negativewithin the neoplastic cells. Approximately 50% of the roundcells within the haemorrhagic tissue collected from thecranial thorax stained strongly positive for vimentin and asimilar number showed weak to moderate cytoplasmicstaining for cytokeratin. Less than 50% of the round cellsstained positively for MAC 387 and generally the large,vacuolated cells failed to stain.
Within the section of lung lobe, neoplastic cells werepresent within the pleura, including within pleural lymphatics.Differential diagnoses included mesothelioma or metastasesof a carcinoma. The cells were epithelioid, and staining withAlcian blue was positive within the neoplastic cells. It wastherefore considered most likely that the neoplastic tissuerepresented a mesothelioma, and presumed that neoplasticmesothelial cells must also be present within thehaemorrhagic pleural effusion. Immunohistochemical stainingof the neoplastic cells for vimentin, cytokeratin and MAC 387was, however, inconclusive, which may suggest that the cellswere poorly differentiated.
The histopathological appearance of the haemorrhagictissue collected post mortem was similar to that collected atsurgery and, in addition, staining with Alcian blue identifiedthe presence of acid mucin product within the cytoplasm ofmany of the cells.
Discussion
Pleural effusion in the mature horse is most commonlyassociated with either infectious or neoplastic processes. Inaddition, Echinococcus equinus is reported to be endemic inGreat Britain, and several other European countries (Blutkeet al. 2010), so hydatid cysts should also be considered as adifferential diagnosis for the presence of a proteinaceouspleural effusion. Management of horses with pleural effusion istherefore reliant upon being able to distinguish betweenthese causes. Cytological examination of pleural fluid is theusual way of establishing this in clinical cases. However,definitive diagnosis can be confounded by the similarcytological characteristics of reactive mesothelial cells andneoplastic cells. In particular, it may be difficult to
500 μm
Fig 6: Lung. Thickened pleura (top), showing multiple infiltratesand aggregates of darkly basophilic cells (centre), withcollapsed and congested lung parenchyma (below).Haematoxylin and eosin, original magnification 320.
50 μm
Fig 7: Pleura. Islands of pleomorphic epithelialoid and rounded,occasionally vacuolated, neoplastic cells within the pleuralstroma and within the lumen of a small pleural vessel.Haematoxylin and eosin, original magnification 340.
50 μm
Fig 8: Pleura. Several cells within an island of neoplastic cellscontain Alcian blue positive acid mucins within the cytoplasm.Alcian blue, original magnification 340.
© 2016 EVJ Ltd
134 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
distinguish between reactive mesothelial cells and neoplasticcells associated with malignant mesothelioma andadenocarcinoma (Kramer et al. 1976; Addis and Roche2009). The most consistently reported features of pleural fluidcytology in equine mesothelioma cases include pleomorphicmesothelial cells forming sheets or clumps, with multiplenuclei, anisokaryosis and mitotic figures; histologicalexamination of tissue samples shows fibrous pleural stromawith reactive mesothelium, granulation tissue, necrotic fociand clumps of pleomorphic cells (Kramer et al. 1976; Mairet al. 1992; Mair and Brown 1993; Fry et al. 2003; Stoica et al.2004; Dobromylskyj et al. 2011). Unfortunately, cellularchanges or neoplastic cells may not always be observed ineffusions (Kramer et al. 1976; Stoica et al. 2004). In thecurrent case, the nondiagnostic findings may have been dueto poor exfoliation of malignant cells and variablecellular preservation in the samples. An admixed cellularpopulation was reported in an equine case of peritonealmesothelioma, including reactive fibroblasts, adipocytes,neutrophils, lymphocytes and plasma cells, and necrosis andhaemorrhage (Dobromylskyj et al. 2011), demonstrating thata combination of neoplastic and concomitant inflammatorypathology should not be unexpected in this disease.
Pleural biopsies have generally been considered to bediagnostic for equine mesothelioma (Davis and Rush 2013);however, distinguishing mesothelioma from other types ofepithelial and connective tissue tumours, and from someinflammatory diseases, is also recognised as a problem inman (Addis and Roche 2009). Examination of tissue samplesobtained post mortem in the current case showed evidenceof neoplasia, most consistent with mesothelioma; this was notappreciated on examination of the premortem biopsies orthe cytological examination of the pleural fluid. Although thisfailure to diagnose mesothelioma premortem had no effecton the ultimate outcome in this case, clinicians should beaware of these difficulties when managing suspectedthoracic neoplasia cases.
Immunohistochemistry (vimentin, cytokeratin and MAC387) and histochemistry (Alcian blue and oil red O to identifylipid) are adjunct methods to diagnosis; these stains can beused to identify mesothelial cells in equine tissue samples(Dobromylskyj et al. 2011). Markers that distinguish reactivefrom neoplastic mesothelial cells are not yet established inthe veterinary species; however, mesothelial cells would beexpected to show varying degrees of staining for vimentin,cytokeratin (Dobromylskyj et al. 2011) and Alcian blue, butnegatively stain for MAC 387. In the present case, in a sectionof lung parenchyma, the stromal, endothelial and surfacemesothelial cells stained positively for vimentin but theneoplastic cells failed to stain. In the same tissue, staining forMAC 387 was positive within alveolar macrophages butnegative within the neoplastic cells. Within a haemorrhagicblood clot collected from the cranial thorax, 50% ofabnormal round cells stained positively with vimentin, and<50% of the round cells stained positively for MAC 387; <50%also stained positively with Alcian blue. In human medicine, awide panel of immunohistochemical markers are availablefor subtyping mesotheliomas; for example, calretinin hasbeen reported to be a specific and sensitiveimmunohistochemical marker of epitheloid-typemesotheliomas (Cury et al. 2000), and is expressed in bothreactive and neoplastic mesothelium (Doglioni et al. 1996).
Calretinin has also been used in an equine case to distinguishdiffuse malignant metastatic mesothelioma fromadenocarcinoma (Stoica et al. 2004) but it cannotdifferentiate reactive from malignant mesothelial cells.
Biopsy size is also an important aspect to consider in thediagnosis of malignant mesothelioma. One human study,comparing the accuracy of pleural biopsy techniques,illustrated a dramatic difference in diagnostic outcome inrelation to biopsy size (Attanoos and Gibbs 2008). Theirdata showed that specimens >10 mm enabled a diagnosisto be made in 75% of cases, whereas a biopsy size<10 mm only provided a diagnosis in 8% of cases. Themost reliable diagnostic criteria for human malignantmesothelioma is stromal invasion (Attanoos and Gibbs2008), which demonstrates the importance of obtainingadequate depth of tissue for analysis. The results of boththe cytological examination of pleural fluid and thehistopathological examination of thoracoscopic biopsies inthe present case demonstrate that characteristics ofneoplastic and reactive change can appear identical, andthat they may, in fact, have been present concurrently inthese specimens.
A prompt diagnosis is important to prevent prolongationof suffering and to limit the financial impact of treatment. Inthis case, the clinical picture, including age, clinical signs, alarge volume pleural effusion and thorascopic findings, wasstrongly suggestive of neoplasia. The owner’s decision toperform euthanasia prior to the availability of thehistopathology results of the biopsies was influenced by thepoor prognosis based on the clinical presentation, andthe cytological appearance of the pleural fluid and thethoracoscopic findings. These procedures raised the suspicionof carcinoma as well as the possibility of very reactivechanges. The long-term prognosis for future athleticism wasconsidered to be poor – unlike the situation in septicpleuropneumonia and pleuritis where the prognosis isgenerally favourable in horses receiving prompt andaggressive treatment in the absence of complicatedsequelae (Smith 1997; Raphel and Beech 1982; Byars andBecht 1991; Seltzer and Byars 1996). It has previously beensuggested that in the UK more (approximately 60%) cases ofpleural effusion in horses are associated with neoplasia,unlike in North America, where the majority of such casesare the result of pleuropneumonia (Mair 1987). Thepresence of a serosanguinous or haemorrhagic pleuraleffusion, such as was present in this case, should beconsidered as particularly suspicious of neoplasia (Mair et al.1985; Davis and Rush 2013). Although lymphoma andhaemangiosarcoma are more common forms of thoracicneoplasia, mesothelioma should also be considered as adifferential diagnosis.
In conclusion, this case illustrates some of the difficultiesthat may arise in the diagnosis of thoracic neoplasia in horses.Although the clinical signs shown by the horse and the grossappearance of the pleural effusion were considered to behighly suspicious of thoracic neoplasia, a specific diagnosiswas not confirmed premortem, even following thoracoscopyand histopathological examination of pleural biopsies.
Authors’ declaration of interests
No conflicts of interest have been declared.
© 2016 EVJ Ltd
135EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Ethical animal research
This is a single case report. No ethical review was required.Consent from the owner to publish the case report wasobtained.
Source of funding
None.
Antimicrobial stewardship policy
No horse were given quinolone, extended spectrum beta-lactam antimicrobials or macrolides. This study does not aimto investigate any of the above pharmaceuticals.
Authorship
J. May contributed to data analysis and interpretation, andpreparation of the manuscript. D. Fews, K. Tennant and T.Mair contributed to data analysis and interpretation,preparation of the manuscript, editing of the manuscript, andgave their final approval.
Manufacturers' addresses1Animalcare, Nether Poppleton, York, UK.2Dechra Veterinary Products, Shrewsbury, Shropshire, UK.3Boehringer Ingelheim, Bracknell, Berkshire, UK.4MSD Animal Health, Walton, Buckinghamshire, UK.5Pfizer (Pharmacia and Upjohn Company), New York, USA.6Platinum Performance, Buellton, California, USA.7Elanco Animal Health, Basingstoke, Hampshire, UK.8Wockhardt UK Limited, Wrexham, UK.9Smiths Medical, Ashford, Kent, UK.10Covidien plc, Dublin, Ireland.
ReferencesAddis, B. and Roche, H. (2009) Problems in mesothelioma diagnosis.
Histopathology 54, 55-68.
Attanoos, R.L. and Gibbs, A.R. (2008) The comparative accuracy ofdifferent pleural biopsy techniques in the diagnosis of malignantmesothelioma. Histopathology 53, 340-344.
Blutke, A., Hamel, D., H€uttner, M., Gehlen, H., Romig, T., Pfister, K. andHermanns, W. (2010) Cystic echinococcosis due to Echinococcusequinus in a horse from Southern Germany. J. Vet. Diagn. Invest.22, 458-462.
Brenner, J., Sordillo, P.P., Magill, G.B. and Golbey, R.B. (1982)Malignant mesothelioma of the pleura: review of 123 patients.Cancer 49, 2431-2435.
Byars, T.D. and Becht, J.L. (1991) Pleuropneumonia. Vet. Clin. N. Am.Equine Pract. 7, 63-78.
Carnine, B.L., Schneider, G., Cook, J.E. and Leipold, H.W.(1977) Pericardial mesothelioma in a horse. Vet. Pathol. 14, 513-515.
Colbourne, C.M., Bolton, J.R., Mills, J.N., Whitaker, D., Yovich, J.V. andHowell, J.M. (1992) Mesothelioma in horses. Aust. Vet. J. 69, 275-278.
Cury, P.M., Butcher, D.N., Fisher, C., Corrin, B. and Nicholson, A.G. (2000)Value of the mesothelium-associated antibodies thrombomodulin,cytokeratin 5/6, calretinin, and CD44H in distinguishing epithelioidpleural mesothelioma from adenocarcinoma metastatic to thepleura. Mod. Pathol. 13, 107-112.
Davis, E.G. and Rush, B.R. (2013) Diagnostic challenges: equinethoracic neoplasia. Equine Vet. Educ. 25, 96-107.
Dobromylskyj, M.J., Copas, V., Durham, A., Hughes, T.K. and Patterson-Kane, J.C. (2011) Disseminated lipid-rich peritoneal mesotheliomain a horse. J. Vet. Diagn. Invest. 23, 615-618.
Doglioni, C., Dei Tos, A.P., Laurino, L., Luzzolino, P., Chiarelli, C., Celio,M.R. and Viale, G. (1996) Calretinin: a novel immunocytochemicalmarker for mesothelioma. Am. J. Surg. Pathol. 20, 1037-1046.
Fry, M.M., Magdesian, K.G., Judy, C.E., Pusterla, N., Vidal, J.D.,Pesavento, R.A. and Zinkl, J.G. (2003) Antemortem diagnosis ofequine mesothelioma by pleural biopsy. Equine Vet. J. 35, 723-727.
Harbison, M.L. and Godleski, J.J. (1983) Malignant mesothelioma inurban dogs. Vet. Pathol. 20, 531-540.
Harps, O., Brumhard, J., Bartmann, C.P. and Hinrichs, U. (1996) Ascitesas a result of peritoneal mesotheliomas in a horse. Tierarztl. Prax.24, 270-274.
Heerkens, T.M., Smith, J.D., Fox, L. and Hostetter, J.M. (2011) Peritonealfibrosarcomatous mesothelioma in a cat. J. Vet. Diagn. Invest. 23,593-597.
Kolbl, S. (1979) Pleuramesothelion also Todesurache bei einem Pferd.Wien. Tierarztl. Mschr. 1, 22-25.
Kramer, J.W., Nickels, F.A. and Bell, T. (1976) Cytology of diffusemesothelioma in the thorax of a horse. Equine Vet. J. 8, 81-83.
Lester, G.D., Alleman, A.R., Raskin, R.E. and Mays, M.B. (1993)Malignant histiocytosis in an Arabian filly. Equine Vet. J. 25, 471-473.
Mair, T.S. (1987) Pleural effusions in the horse. In: The VeterinaryAnnual, 27th edn., Eds: C.S. Grunsell, F.W. Hill and M.E. Raw,Scientechnica, Bristol. pp 139-146.
Mair, T.S. and Brown, P.J. (1993) Clinical and pathologicalfeatures of thoracic neoplasia in the horse. Equine Vet. J. 25,220-223.
Mair, T.S., Lane, J.G. and Lucke, V.M. (1985) Clinicopathologicalfeatures of lymphosarcoma involving the thoracic cavity in thehorse. Equine Vet. J. 17, 428-433.
Mair, T.S., Hillyer, M.H. and Brown, P.J. (1992) Mesothelioma of thepleural cavity in a horse: diagnostic features. Equine Vet. Educ. 4,59-61.
Mair, T.S., Rush, B.R. and Tucker, R.L. (2004) Clinical and diagnosticfeatures of thoracic neoplasia in the horse. Equine Vet. Educ. 16,30-36.
Paciello, O., Passantino, G., Costagliola, A., Papparella, S. and Perillo,A. (2013) Histiocytic sarcoma of the nasal cavity in a horse. Res.Vet. Sci. 94, 648-650.
Peroni, J.F., Horner, N.T., Robinson, N.E. and Stick, J.A. (2001) Equinethoracoscopy: normal anatomy and surgical technique. EquineVet. J. 33, 231-237.
Raphel, C.F. and Beech, J. (1982) Pleuritis secondary to pneumoniaor lung abscessation in 90 horses. J. Am. Vet. Med. Ass. 181, 808-810.
Rapisarda, G., Marino, F., Ferrara, G., Gioffr�e, F. and Galofaro, V.(2004) Benign fibrous histiocytoma of prepuce in the mule. Reprod.Dom. Anim. 39, 61-63.
Ricketts, S.W. and Peace, C.K. (1976) A case of peritonealmesothelioma in a Thoroughbred mare. Equine Vet. J. 8, 78-80.
Seltzer, K.L. and Byars, T.D. (1996) Prognosis for return to racing afterrecovery from infectious pleuropneumonia in thoroughbredracehorses: 70 cases (1984–1989). J. Am. Vet. Med. Ass. 208, 1300-1301.
Smith, B.P. (1977) Pleuritis and pleural effusion in the horse: a study of37 cases. J. Am. Vet. Med. Ass. 170, 208-211.
Stevens, B.J., Montgomery, S.A., Phillips, K.L., Wester, M.W. andJennings, S.H. (2014) Pathology in practice. Malignantmesothelioma in a dog. J. Am. Vet. Med. Ass. 245, 57-59.
Stoica, G., Cohen, N., Mendes, O. and Kim, H.-T. (2004) Use ofimmunohistochemical marker calretinin in the diagnosis of adiffuse malignant metastatic mesothelioma in an equine. J. Vet.Diagn. Invest. 16, 240-243.
© 2016 EVJ Ltd
136 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Continued on page 143


Case Report
Lessons learned from a strangles outbreak on a large StandardbredfarmU. Christmann†* and C. Pink‡
†Department of Population Health Sciences, Virginia-Maryland Regional College of Veterinary Medicine, VirginiaTech and University of Maryland, Blacksburg, USA; and ‡Private Practitioner, Hanover, Pennsylvania, USA.*Corresponding author email: [email protected] Christmann’s Present address: Lincoln Memorial University, College of Veterinary Medicine, DeBusk VeterinaryTeaching Centre, Ewing, Virginia, USA
Keywords: horse; strangles; Streptococcus equi subspecies equi; equine respiratory disease; outbreak
SummaryStreptococcus equi subspecies (ssp.) equi infection(strangles) remains one of the most frequently diagnosed andcostly infectious diseases of horses. Large breeding herds,where a disease outbreak competes for personnel andfinancial resources needed for foaling management, presenta special challenge for equine practitioners. A 15-monthoutbreak involving 62 clinical cases of strangles occurred ona large Standardbred breeding farm (average population of1400 horses). Sixteen asymptomatic horses were found to bePCR (polymerase chain reaction)-positive for S. equi ssp.equi. During the outbreak, serological samples from 48clinically normal horses were found to be seropositive for S.equi ssp. equi, confirming herd-wide exposure. After severalclinical cases of strangles had been diagnosed, an intranasalS. equi ssp. equi vaccine was administered to clinicallynormal horses (n = 558) considered to be at risk of exposure.Strangles complications included 7 fatalities (none invaccinated horses) and 6 cases of purpura haemorrhagica (4in vaccinated horses). Midway through the outbreak,injectable, sustained release ceftiofur crystalline free acid(CCFA), given as an initial dose followed by a second dose4 days later, was used exclusively for systemic antimicrobialtreatment of clinically affected and PCR-positive horses. Thisantimicrobial regimen coincided with a reduction in diseaseincidence and eventual resolution of the outbreak. Twohorses with persistent guttural pouch infection wereendoscopically confirmed as carrier horses. The herd historydemonstrated that a strangles outbreak will often result inasymptomatic carrier horses and that identification andtreatment of these horses are necessary to eliminate long-term sources of infection. Ceftiofur crystalline free acid wasfound to be a suitable antimicrobial due to its activity againstS. equi ssp. equi and the efficiencies associated with twiceparenteral dosing during a 10-day treatment period.Occurrence of purpura in 4 vaccinated horses suggests thatvaccination should be reserved for healthy seronegativehorses and avoided during an active outbreak.
Introduction
The extensive literature related to Streptococcus equi ssp.equi infection (strangles) in horses includes an AmericanCollege of Veterinary Internal Medicine (ACVIM) ConsensusStatement considered to be the principal guidelinedocument for managing the disease (Sweeney et al. 2005).
Despite availability of evidence-based guidelines andwidespread clinical experience with strangles, there isconsiderable debate about the risks and benefits ofvaccination and antimicrobial treatment to prevent andcontrol outbreaks of the disease. Whether vaccination cancause or exacerbate clinical signs in exposed horses andwhether antimicrobial treatment can impair the host immuneresponse are questions yet to be resolved (Ainsworth andHackett 2004; Sweeney et al. 2005). What is not in dispute isthat strangles remains one of the most frequently diagnosedand serious infectious diseases of horses (Gross et al. 2000;Holland et al. 2006). Strangles has a number of potentiallyserious complications such as purpura haemorrhagica,metastatic abscessation, myositis and death due toasphyxiation or euthanasia (Sweeney et al. 2005; Boyle 2011).The fact that strangles may cause persistent infection inasymptomatic carrier horses ensures that a subpopulation ofchronically infected animals will continue to harbour S. equissp. equi (Newton et al. 1997; Chanter et al. 2000; Davidsonet al. 2008). Strangles is considered to be a reportabledisease in certain US states (i.e. Maine, Massachusetts,Kentucky, Georgia, Florida) but not in others (i.e.Pennsylvania, Virginia, New York, New Hampshire).
Most equine practitioners encounter strangles inindividual animals or small groups of horses. The dynamics ofclinical strangles are usually described in terms of a relativelysmall number of cases from individual or multiple herds (Jorm1990; Mumford et al. 1998; Gross et al. 2000; Holland et al.2006); outbreaks in large numbers of animals in a single herdhave not been extensively reported. The S. equi ssp. equioutbreak described in this report is noteworthy for severalreasons: the large numbers of clinical cases of strangles onone farm, the role of carrier horses in maintaining herdinfection over a 15-month period, the effect of antimicrobialtreatment with agents not available at the time of thepublication of the ACVIM Consensus Statement and theoccurrence of disease complications in a population ofseropositive horses, some of which were recently vaccinated.Large breeding herds, where managing a strangles outbreakcompetes with foaling management, represent a specialchallenge for the equine practitioner, not least because ofthe potential for sizeable economic loss. The authors offerseveral recommendations (‘lessons learned’) for controllingstrangles under these conditions where resources must beallocated and leveraged to minimise the impact of adisease outbreak.
© 2015 EVJ Ltd
138 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
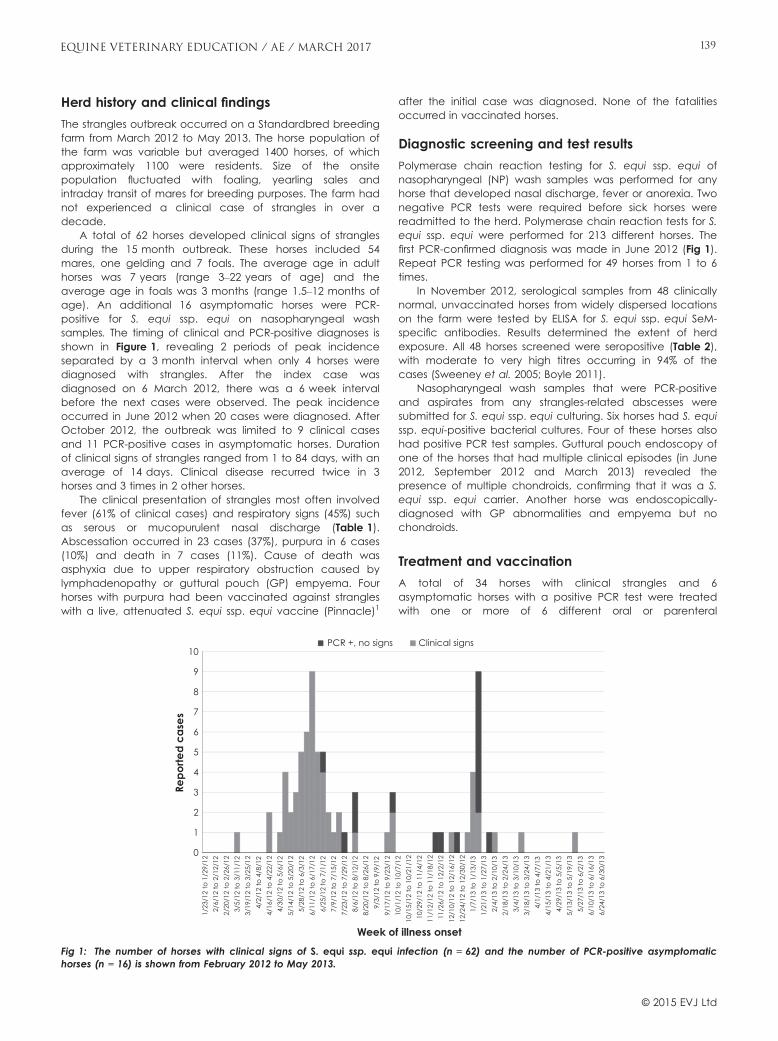
Herd history and clinical findings
The strangles outbreak occurred on a Standardbred breedingfarm from March 2012 to May 2013. The horse population ofthe farm was variable but averaged 1400 horses, of whichapproximately 1100 were residents. Size of the onsitepopulation fluctuated with foaling, yearling sales andintraday transit of mares for breeding purposes. The farm hadnot experienced a clinical case of strangles in over adecade.
A total of 62 horses developed clinical signs of stranglesduring the 15 month outbreak. These horses included 54mares, one gelding and 7 foals. The average age in adulthorses was 7 years (range 3–22 years of age) and theaverage age in foals was 3 months (range 1.5–12 months ofage). An additional 16 asymptomatic horses were PCR-positive for S. equi ssp. equi on nasopharyngeal washsamples. The timing of clinical and PCR-positive diagnoses isshown in Figure 1, revealing 2 periods of peak incidenceseparated by a 3 month interval when only 4 horses werediagnosed with strangles. After the index case wasdiagnosed on 6 March 2012, there was a 6 week intervalbefore the next cases were observed. The peak incidenceoccurred in June 2012 when 20 cases were diagnosed. AfterOctober 2012, the outbreak was limited to 9 clinical casesand 11 PCR-positive cases in asymptomatic horses. Durationof clinical signs of strangles ranged from 1 to 84 days, with anaverage of 14 days. Clinical disease recurred twice in 3horses and 3 times in 2 other horses.
The clinical presentation of strangles most often involvedfever (61% of clinical cases) and respiratory signs (45%) suchas serous or mucopurulent nasal discharge (Table 1).Abscessation occurred in 23 cases (37%), purpura in 6 cases(10%) and death in 7 cases (11%). Cause of death wasasphyxia due to upper respiratory obstruction caused bylymphadenopathy or guttural pouch (GP) empyema. Fourhorses with purpura had been vaccinated against strangleswith a live, attenuated S. equi ssp. equi vaccine (Pinnacle)1
after the initial case was diagnosed. None of the fatalitiesoccurred in vaccinated horses.
Diagnostic screening and test results
Polymerase chain reaction testing for S. equi ssp. equi ofnasopharyngeal (NP) wash samples was performed for anyhorse that developed nasal discharge, fever or anorexia. Twonegative PCR tests were required before sick horses werereadmitted to the herd. Polymerase chain reaction tests for S.equi ssp. equi were performed for 213 different horses. Thefirst PCR-confirmed diagnosis was made in June 2012 (Fig 1).Repeat PCR testing was performed for 49 horses from 1 to 6times.
In November 2012, serological samples from 48 clinicallynormal, unvaccinated horses from widely dispersed locationson the farm were tested by ELISA for S. equi ssp. equi SeM-specific antibodies. Results determined the extent of herdexposure. All 48 horses screened were seropositive (Table 2),with moderate to very high titres occurring in 94% of thecases (Sweeney et al. 2005; Boyle 2011).
Nasopharyngeal wash samples that were PCR-positiveand aspirates from any strangles-related abscesses weresubmitted for S. equi ssp. equi culturing. Six horses had S. equissp. equi-positive bacterial cultures. Four of these horses alsohad positive PCR test samples. Guttural pouch endoscopy ofone of the horses that had multiple clinical episodes (in June2012, September 2012 and March 2013) revealed thepresence of multiple chondroids, confirming that it was a S.equi ssp. equi carrier. Another horse was endoscopically-diagnosed with GP abnormalities and empyema but nochondroids.
Treatment and vaccination
A total of 34 horses with clinical strangles and 6asymptomatic horses with a positive PCR test were treatedwith one or more of 6 different oral or parenteral
0
1
2
3
4
5
6
7
8
9
10
1/23
/12
to 1
/29/
122/
6/12
to 2
/12/
122/
20/1
2 to
2/2
6/12
3/5/
12 to
3/1
1/12
3/19
/12
to 3
/25/
124/
2/12
to 4
/8/1
24/
16/1
2 to
4/2
2/12
4/30
/12
to 5
/6/1
25/
14/1
2 to
5/2
0/12
5/28
/12
to 6
/3/1
26/
11/1
2 to
6/1
7/12
6/25
/12
to 7
/1/1
27/
9/12
to 7
/15/
127/
23/1
2 to
7/2
9/12
8/6/
12 to
8/1
2/12
8/20
/12
to 8
/26/
129/
3/12
to 9
/9/1
29/
17/1
2 to
9/2
3/12
10/1
/12
to 1
0/7/
1210
/15/
12 to
10/
21/1
210
/29/
12 to
11/
4/12
11/1
2/12
to 1
1/18
/12
11/2
6/12
to 1
2/2/
1212
/10/
12 to
12/
16/1
212
/24/
12 to
12/
30/1
21/
7/13
to 1
/13/
131/
21/1
3 to
1/2
7/13
2/4/
13 to
2/1
0/13
2/18
/13
to 2
/24/
133/
4/13
to 3
/10/
133/
18/1
3 to
3/2
4/13
4/1/
13 to
4/7
/13
4/15
/13
to 4
/21/
134/
29/1
3 to
5/5
/13
5/13
/13
to 5
/19/
135/
27/1
3 to
6/2
/13
6/10
/13
to 6
/16/
136/
24/1
3 to
6/3
0/13
Repo
rted
case
s
Week of illness onset
PCR +, no signs Clinical signs
Fig 1: The number of horses with clinical signs of S. equi ssp. equi infection (n = 62) and the number of PCR-positive asymptomatichorses (n = 16) is shown from February 2012 to May 2013.
© 2015 EVJ Ltd
139EQUINE VETERINARY EDUCATION / AE / MARCH 2017

antimicrobials for varying periods (Table 3). Some horses weretreated with more than one antimicrobial. Horses that hadfever, nasal discharge or ruptured submandibular or otherabscesses were treated with antimicrobials and anti-inflammatory agents. Injectable sustained release ceftiofurcrystalline free acid (CCFA, Excede)1 and procaine penicillinG (PPG) were the 2 most commonly used antimicrobials. Oraldoxycycline was given to some horses (n = 8) either that didnot respond to PPG or to avoid local reactions to injectableantimicrobials. Metronidazole and gentamicin were given to2 horses that developed diarrhoea in addition to clinical signsof strangles. Because of the extended duration of effect andthe fewer number of doses required for a complete course oftreatment, sustained release CCFA was used exclusivelyduring the second phase of the outbreak beginning inSeptember 2012. The mean number of treatment days was2.5 days for CCFA and 5.2 days for PPG. Normal probabilityplots showed that the observed duration of clinical signs forhorses treated with ceftiofur vs. PPG and/or doxycycline wasskewed. Subsequently, the outcomes were summarised asmedians (range). The median duration of symptoms for horsesthat received ceftiofur was compared with the medianduration of symptoms for horses that received PGG/Doxyusing the Wilcoxon rank sum test. Statistical significance wasset to P<0.05. All analyses were performed using statisticalsoftware (SAS version 9.4)2. The 5 day median duration ofclinical signs in horses receiving CCFA was shorter comparedwith the 12 day median duration of clinical signs in horsestreated with PPG and/or doxycycline (P = 0.036).
Guttural pouch lavage was performed in 2 mares withendoscopic confirmation of GP chondroids or empyema.Chondroids were removed endoscopically by snare in onehorse. Both horses were treated by GP infusion with penicillin(PPG or potassium penicilline gel) and parenteral treatmentwith CCFA. Post treatment PCR analysis of GP fluids fromthese horses were negative for S. equi ssp. equi. Tracheotomywas attempted in 2 horses that developed acute severeupper respiratory distress. However, the procedure wasperformed late in the disease course and both horsessubsequently died. Horses with purpura haemorrhagica weretreated with dexamethasone.
Because strangles had not been recently diagnosed onthe farm, S. equi ssp. equi vaccination was not practised priorto the outbreak. After the onset of the outbreak, 558 mares,foals, yearlings and stallions considered to be at risk ofexposure were vaccinated intranasally with the live,attenuated S. equi ssp. equi vaccine according to labelrecommendations.
Biosecurity measures
Pre-outbreak biosecurity measures were limited by the size ofthe farm and circumstances. Prior to the outbreak, arrivingmares were only briefly quarantined and admitted withoutprior vaccination or PCR screening for S. equi ssp. equi.During the summer when the outbreak was occurring, manyof the horses lived on pastures rather than returning to stallsat night, making regular temperature checks and earlyrecognition of clinical signs difficult. Biosecurity measures wereintensified once clinical strangles was identified in the herd.Interventions included quarantines for new horses (horseswere kept in a field remote from the main farm for 2 weeksand had to have a negative nasopharyngeal wash PCR testprior to their introduction to the herd), strict isolation of sickand convalescent horses pending negative PCR results,enhanced environmental sanitation (disinfection of waterersand objects in contact with affected horses), use ofprotective clothing and boots by personnel and controlledmovement of horses and handlers. The demands of breeding,foaling and yearling sales that are part of a large breedingoperation unavoidably diverted personnel resources frombiosecurity. However, the basic biosecurity measures thatwere implemented or reinforced, prioritised according to thehorse’s risk and clinical status were considered an importantfactor in curtailing the outbreak.
Discussion
The 62 clinical cases and 16 PCR-positive horses probablyunderstated the true incidence of disease on the farm. Therisk of strangles increases dramatically when the broodmarepopulation exceeds 100 (Jorm 1990) and an outbreak ofteninvolves far more infected but asymptomatic horses than thenumber of animals showing clinical signs. During an extendedinfectious respiratory outbreak such as occurred in this herd, itshould be assumed that all horses on the premises willeventually be exposed.
Six horses, including 4 vaccinates, developed purpura, ahypersensitivity reaction sometimes associated with S. equissp. equi vaccination (Pusterla et al. 2003; Sweeney et al.2005). A cause and effect relationship between vaccinationand purpura has not been demonstrated and the type of
TABLE 1: Incidence of S. equi ssp. equi-associated sequelae inhorses with strangles (n = 62)
Clinical sign in order of frequency No. cases (%)*
Fever 38 (61)Respiratory 28 (45)Abscesses and site 23 (37)Submandibular 13Guttural pouch 4Mandible 2Coronary band 1Retropharyngeal 1Udder 1Unspecified site 1
Death 7 (11)Lymphadenopathy 6 (10)Purpura 6 (10)
* Some horses developed more than one strangles-related clinicalsign.
TABLE 2: Distribution of Streptococcus equi ssp. equi titres inserologically tested asymptomatic horses (n = 48)
Titre No. horses Interpretation
<200 0 Negative200–400 3 Weak positive800–1600 29 Moderate positive3200–6400 14 High positive12,800–16,000 2 Very high positiveTotal 48
© 2015 EVJ Ltd
140 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
vaccine antigen may play a role in the occurrence of thiscomplication (Ainsworth 2010). Some epidemiological dataindicate that the prevalence of purpura is quite low (0.2cases per 10,000 doses) in horses given the intra-nasal S. equissp. equi vaccine used in this herd (Timoney 1999). TheACVIM guidelines nevertheless caution that vaccinationduring an active outbreak should be limited to horses with noknown contact with infected or exposed horses to avoid postvaccination reactions (Sweeney et al. 2005). One of thelessons learned was that it would be wise to err on the side ofcaution and avoid vaccination in the face of an activeoutbreak. Conversely, a herd with widespread low ornegative S. equi ssp. equi titres and no known or suspectedexposure, would be a suitable candidate for a selectivevaccination programme. Discretion should be exercised ininterpreting serological data in clinically normal horses. Thetime required for S. equi ssp. equi seroconversion and decayof convalescent titres varies considerably. Moreover, a recentEuropean study found that a SeM-based ELISA had asensitivity of 89.9% but a specificity of only 77.0% comparedwith a sensitivity of 99.3% and specificity of 99.3% achievedwhen using an ELISA test based on the detection of 2 S. equispecific antigens (Robinson et al. 2013). Strategies foridentifying seropositivity in clinically normal horses mayinclude evaluation of paired samples in an adequatenumber of horses and combining different serological assaysto optimise sensitivity and specificity. It should be noted thatserological status may be affected by a horse’s vaccinationhistory since a serological response to vaccination isindistinguishable from that occurring after natural exposure.Seven horses affected during the outbreak died, including 2horses on which a tracheotomy was performed. Thesefindings underscore the importance of performingpreventative tracheotomies to avoid asphyxiation in horsesthat develop respiratory distress due to severelymphadenopathy or lymph node abscessation (Sweeneyet al. 1987).
Various antimicrobial regimens were employed to treatcases of clinical strangles (Table 3). Parenteral PPG hashistorically been used as the drug of choice for systemic
treatment of acute-phase strangles (Sweeney et al. 2005;Boyle 2011). Procaine penicillin G has the disadvantage of atwice-daily dosing schedule, a frequency that in somecircumstances may contribute to compliance shortfalls. Theaverage treatment duration for PPG during the outbreak was5.2 days, well short of the 7 to 10 days that generally ensurecase resolution when a time-dependent antimicrobial is used(Holland et al. 2006; Boyle 2011). In the case of oraldoxycycline given b.i.d., some horses were treated for as longas 42 days, representing a considerable resourcecommitment. Although the veterinary medical staffadministered all medications and were careful to avoidmissed doses, human medical data across a variety oftherapeutic regimens consistently show that compliancedeclines substantially as dosage frequency increases,particularly when administered by nonclinical personnel(Claxton et al. 2001; Saini et al. 2009; Coleman et al. 2012).
Sustained release CCFA, the only extended durationcephalosporin approved for equine use, was given twiceparentally over a 10 day dosing interval, with the seconddose given 4 days after the initial dose as labelled. This 2dose regimen reduced the burden of labour needed forlong-term treatment, particularly in comparison to PPG ordoxycycline. The exclusive use of sustained release CCFAduring the second half of the outbreak coincided with adeclining incidence of clinical cases (Fig 1) even before thecarrier horses were identified. This suggests that sustainedrelease CCFA, combined with enhanced biosecuritymeasures and improved immunity, played an important rolein the cessation of the outbreak because of its efficacyagainst the target organism, compliance improvements orboth.
Ceftiofur crystalline free acid has demonstrated consistentactivity against S. equi ssp. equi, making it a viablealternative to PPG for parenteral antimicrobial treatment ofstrangles (Salmon et al. 1996; Weese et al. 2008). Treatmentguidelines published subsequently to the ACVIM ConsensusStatement list penicillin, ceftiofur and trimethoprim-sulfadiazine as the first, second and third choices,respectively, for treatment of strangles caused by S. equi ssp.
TABLE 3: Treatment regimens used in clinical cases of strangles
Treatment regimenTherapeutic agent and usage frequency
Antimicrobial treatmentAntimicrobial agent AZI-RIF CCFA DOX GEN MET PPGNo. horses 2 26 8 2 2 15Mean No. treatment days (range) 12 (1–15) 2.5 (1–6) 26.9 (20–42) 5 (1–9) 2.5 (1–4) 5.2 (1–11)
Anti-inflammatory treatmentAnti-inflammatory agent BAN DEX KET PBZNo. horses 23 6 1 1Mean No. doses (range) 2.7 (1–11) 7.5 (1–10) 1 17
Fluid therapyNo. horses 4
Guttural pouch lavageAntimicrobial agent PPGNo. horses 2Mean No. doses (range) 3 (2–4)
AZI/RIF = azithromycin/rifampin (10 mg/kg bwt per os s.i.d. and 5 mg/kg bwt per os b.i.d.); BAN = banamine (1.1 mg/kg bwt i.v., s.i.d.);CCFA = ceftiofur crystalline free acid (6.6 mg/kg bwt i.m. every 4 days); DEX = dexamethasone (0.05 mg/kg bwt i.v., s.i.d.); DOX =doxycycline (10 mg/kg per os b.i.d.); GEN = gentamicin (6.6 mg/kg bwt i.v., s.i.d.); KET = ketofen (2.2 mg/kg bwt i.v., s.i.d.); MET =metronidiazole (10 mg/kg per os b.i.d.); PBZ = phenylbutazone (2 mg/kg bwt per os s.i.d.); PPG = procaine penicillin G (20,000 iu/kg bwti.m., b.i.d.).
© 2015 EVJ Ltd
141EQUINE VETERINARY EDUCATION / AE / MARCH 2017

equi (Weese et al. 2008). Compared with PPG, ceftiofur has abroader spectrum of activity against both Gram-positive andGram-negative bacteria including beta-lactamase producingstrains. Because the narrower spectrum of PPG makes it amore ‘targeted’ antimicrobial compared with CCFA, its usewould be consistent with judicious use guidelines in caseswhere PPG has confirmed efficacy against the causativeorganism. However, one of the reasons that stranglescontinues to be a problem 60 years after the introduction ofPPG is the failure of this antimicrobial formulation to maintaintherapeutic blood levels for an appropriate period of timedue to compliance shortfalls, often because of the horse’sresistance to repeated injections. Trimethoprim-sulfadiazinemay be used but is easily inactivated by purulent material.Because of the treatment response and less frequent dosingrequired, sustained release CCFA proved to be the preferredantimicrobial during the outbreak, with PPG held in reserve asa second option.
Identifying and effectively treating the S. equi ssp. equicarrier horse cannot be overestimated in terms of itsimportance in controlling the outbreak. At least half of allstrangles outbreaks produce at least one asymptomaticcarrier horse (Newton et al. 2000) and up to 10% of the horsesmay become carriers (Sweeney et al. 2005). Clinically normal,convalescent horses can shed S. equi ssp. equi for aminimum of 2–6 weeks, whereas long-term intermittentshedding occurs in cases where chronic GP infection ispresent (Sweeney et al. 2005; Holland et al. 2006).
The relatively high prevalence of asymptomatic carrierhorses following a strangles outbreak tends to refute theviewpoint that uncomplicated strangles is a self-resolvingdisease requiring no active intervention (Sweeney et al. 2005;Boyle 2011). Convalescent horses, even when asymptomatic,should be evaluated by multiple NP lavages or ideally bydirect endoscopic assessment of the GP associated withcollection of a GP lavage sample. This method permits oneto endoscopically detect GP abnormalities such asempyema and chondroids (Sweeney et al. 2005; Boyle 2011)and to test for presence or absence of infection. Culturing ofGP fluid used to be considered the diagnostic gold standardfor strangles. However, obtaining culture results is more timeconsuming and this test is less sensitive than more recentlydeveloped triplex qPCR tests (Webb et al. 2013; Waller 2014).In fact, triplex qPCR has replaced culture as the newdiagnostic gold standard. Either qPCR, commerciallyavailable in the UK but not in the US or real-time PCR,available in both markets, is a more sensitive diagnosticoption than culturing for S. equi ssp. equi. Of note, PCRtesting or culturing of NP swabs may be negative and fail todetect GP carriage of S. equi ssp. equi (Timoney 1999).
Among the lessons learned in the aftermath of theoutbreak, several were considered to be paramount.Following a strangles outbreak, it should be assumed thatsome asymptomatic horses are infected and that at leastone horse will be a chronic S. equi ssp. equi carrier.Identification of persistent carrier horses is necessary toeliminate long-term sources of infection in the herd and is themost important diagnostic challenge associated with astrangles outbreak. Sustained release CCFA was found to bea suitable choice for antimicrobial treatment due to itsconsistent activity against S. equi ssp. equi and theefficiencies realised from parenteral administration twiceduring a 10 day period. This treatment is particularly
recommended for horses with early clinical signs of strangles(i.e. fever, anorexia with minimal submandibular lymph nodeswelling) from a herd with at least one confirmed case of S.equi spp. equi and horses with strangles complications suchas enlarged retropharyngeal lymph nodes causing dyspnoeaor dysphagia. Horses treated during the early phase of thedisease should ideally be isolated from horses with overtclinical signs as they may be susceptible to reinfection due toa lack of protective immune response (Sweeney et al. 2005).Vaccination should be reserved for healthy, serologicallynegative horses at low risk of immediate exposure to S. equissp. equi. Although there is a high probability of S. equi ssp.equi exposure in large herds, these control procedures willhelp minimise the impact of disease and avoid long-termconsequences of a strangles outbreak. Particularly in largeherds, electronic record keeping would be a valuable, timesaving resource for monitoring sick horses and the diagnostictesting status of all horses on the premises.
A central reality of the strangles outbreak was thedisparity between the personnel resources needed for thebreeding farm’s primary mission of breeding and foaling vs.disease control. The 62 cases of clinical strangles occurredduring the same period as >350 foalings, illustrating the needto allocate the majority of personnel resources to foaling vs.disease management. These circumstances precluded orcompromised close monitoring of horses that would bepossible in a small herd. Two interventions helpedcompensate for these staffing limitations and were successfulin ending the outbreak: use of appropriate antimicrobialtherapy in the form of sustained release CCFA andidentification and effective treatment of carrier horses.
Authors’ declaration of interests
No conflicts of interest have been declared.
Ethical animal research
Ethical review is not applicable for this case report.
Source of funding
Zoetis, Florham Park, New Jersey, USA.
Acknowledgements
The authors acknowledge the contributions of M. Dana ofScientific Communications Services, LLC in the writing andediting of the manuscript. Appreciation is expressed to A.Boyle of the School of Veterinary Medicine, University ofPennsylvania for providing diagnostic testing services. Theauthors also thank S. Werre from the Laboratory for StudyDesign and Statistical Analysis, Virginia-Maryland RegionalCollege of Veterinary Medicine, Blacksburg, Virginia, for hishelp with statistical analysis of data.
Authorship
C. Pink observed and treated the cases described in thestudy and provided all the data described in the study. U.Christmann analysed and interpreted the data and preparedthe manuscript together with C. Pink. Both authors approvedthe final version of the manuscript.
© 2015 EVJ Ltd
142 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Antimicrobial stewardship
Ceftiofur, a 3rd generation cephalosporin was used duringthe outbreak. It was chosen as an antimicrobial because itallowed longer treatment intervals and improved treatmentcompliance.
Manufacturers’ addresses1Zoetis, Florham Park, New Jersey, USA.2Cary, North Carolina, USA.
ReferencesAinsworth, D.M. (2010) Caught in the middle of a strangles outbreak
- review of the diagnostic and management procedures. Proc.Am. Ass. Equine Practnrs - Focus meeting. Salt Lake City, UT.Focus Upper Lower Respiratory Dis. pp 49-53.
Ainsworth, D.M. and Hackett, R.P. (2004) Disorders of the respiratorysystem. In: Equine Internal Medicine, 2nd edn., Eds: Reed, S.M.,Bayly, W.M. and Sellon, D.C. W.B. Saunders, St. Louis. pp 289-353.
Boyle, A. (2011) Streptococcus equi subspecies equi infection(strangles) in horses. Comp. Cont. Educ. Pract. Vet. 33, E1-E7.
Chanter, N., Talbot, N.C., Newton, J.R., Hewson, D. and Verheyen, K.(2000) Streptococcus equi with truncated M-proteins isolated fromoutwardly healthy horses. Microbiol. 146, 1361-1369.
Claxton, A.J., Cramer, J. and Pierce, C. (2001) A systematic review ofthe associations between dose regimens and medicationcompliance. Clin. Ther. 23, 1296-1310.
Coleman, C.I., Roberts, M.S., Sobieraj, D.M., Lee, S., Alam, T. andKaur, R. (2012) Effect of dosing frequency on chroniccardiovascular disease medication adherence. Curr. Med. Res.Opin. 28, 669-680.
Davidson, A., Traub-Dargatz, J.L., Magnuson, R., Hill, A., Irwin, V.,Newton, R., Waller, A., Smith, K., Callan, R.J., Meehan, M., Owen, P.and Salman, M. (2008) Lack of correlation between antibody titersto fibrinogen-binding protein of Streptococcus equi and persistentcarriers of strangles. J. Vet. Diagn. Invest. 20, 457-462.
Gross, D.K., Morley, P.A., Traub-Dargatz, J., Wagner, B.A. and Garber,L.P. (2000) A national estimate of acute infectious upperrespiratory disease (IURD) and risk factors associated with infectionfor horses in the United States during 1998-1999. Proc. Am. Ass.Equine Practnrs. 46, 274-276.
Holland, R.E., Harris, D.G. and Monge, A. (2006) How to controlstrangles infections on the endemic farm. Proc. Am. Ass. EquinePractnrs. 52, 78-80.
Jorm, L.R. (1990) Strangles in horse studs: incidence, risk factors andeffect of vaccination. Aust. Vet. J. 67, 436-439.
Mumford, E.L., Traub-Dargatz, J.L., Salman, M.D., Collins, J.K., Getzy,D.M. and Carman, J. (1998) Monitoring and detection of acute viralrespiratory disease in horses. J. Am. Vet. Med. Ass. 213, 385-390.
Newton, J.R., Wood, J.L., Dunn, K.A., DeBrauwere, M.N. and Chanter,N. (1997) Naturally occurring persistent and asymptomaticinfection of the guttural pouches of horses with Streptococcusequi. Vet. Rec. 140, 84-90.
Newton, J.R., Verheyen, K., Talbot, N.C., Timoney, J.F., Wood, J.L.,Lakhanim, K.H. and Chanter, N. (2000) Control of stranglesoutbreaks by isolation of guttural pouch carriers identified usingPCR and culture of Streptococcus equi. Equine Vet. J. 32, 515-526.
Pusterla, N., Watson, J.L., Affolter, V.K., Magdesian, K.G., Wilson, W.D.and Carlson, G.P. (2003) Purpura haemorrhagica in 53 horses. Vet.Rec. 153, 118-121.
Robinson, C., Steward, K.F., Potts, N., Barker, C., Hammond, T., Pierce,K., Gunnarsson, E., Svansson, V., Slater, J., Newton, J.R. and Waller,A.S. (2013) Combining two serological assays optimises sensitivityand specificity for the identification of Streptococcus equi subsp.equi exposure. Vet. J. 197, 188-191.
Saini, S.D., Schoenfeld, P., Kaulback, K. and Dubinsky, M.C. (2009)Effect of medication dosing frequency on adherence in chronicdiseases. Am. J. Managed Care 15, e22-e33.
Salmon, S.A., Watts, J.L. and Yancey, R.J. Jr (1996) In vitro activity ofceftiofur and its primary metabolite, desfuroylceftiofur, againstorganisms of veterinary importance. J. Vet. Diagn. Invest. 8, 332-336.
Sweeney, C.R., Whitlock, R.H., Meirs, D.A., Whitehead, S.C. andBarningham, S.O. (1987) Complications associated withStreptococcus equi infection on a horse farm. J. Am. Vet. Med.Ass. 191, 1446-1448.
Sweeney, C.R., Timoney, J.F., Newtonm, J.R. and Hines, M.T. (2005)Streptococcus equi infections in horses: guidelines for treatment,control and prevention of strangles. J. Vet. Intern. Med. 18, 123-124.
Timoney, J.F. (1999) Equine strangles: 1999. Proc. Am. Ass. EquinePractnrs. 45, 31-37.
Waller, A.S. (2014) New Perspectives for the diagnosis, control,treatment, and prevention of strangles in horses. Vet. Clin. N. Am.:Equine Pract. 30, 591-607.
Webb, K., Barker, C., Harrison, T., Heather, Z., Steward, K.F., Robinson, J.,Newton, J.R. and Waller, A.S. (2013) Detection of Streptococcus equisubspecies equi using a triplex qPCR assay. Vet. J. 195, 300-304.
Weese, J.S., Baptiste, K.E., Baverud, V. and Toutain, P.-L. (2008)Guidelines for antimicrobial use in horses. In: Guide to AntibacterialUse in Animals, Eds: L. Guardabassi, L.B. Jensen and H. KruseBlackwell Publishing, Oxford, UK. pp 161-182.
© 2015 EVJ Ltd
143EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Continue page 136d from
Straub, R., von Tscharner, C., Pauli, B., Lazary, S. and Schatzmann, U.(1974) Pleural mesothelioma in a horse. Schweizer Archiv.Tierheilkunde 116, 207-211.
Vachon, A.M. and Fischer, A.T. (1998) Thoracoscopy in the horse:diagnostic and therapeutic indications in 28 cases. Equine Vet. J.30, 467-475.
Wallace, S.S., Jayo, M.J., Maddux, J.M., DeBowes, R.M., Brandt, G.W.and Leipold, H.W. (1987) Mesothelioma in a horse. Comp. Cont.Ed. Pract. Vet. 9, 210-216.
Supporting information
Additional Supporting Information may be found in the onlineversion of this article at the publisher’s website:
Supplementary Item 1: Video of mesothelioma biopsy.

Original Article
Causes of pleural effusions in horses resident in the UKI. Johns†*, C. Marr‡, A. Durham§, T. Mair# and T. McParland†
†Equine Referral Hospital, Royal Veterinary College, North Mymms, Hertfordshire; ‡Rossdales Equine Hospital andDiagnostic Centre, Exning, Newmarket, Suffolk; §Liphook Equine Hospital, Forest Mere, Liphook, Hampshire; and#Bell Equine Veterinary Clinic, Mereworth, Maidstone, Kent, UK.*Corresponding author email: [email protected]
Keywords: horse; equine; pneumonia; cancer
SummaryPleural effusions (PE) reportedly occur most commonlysecondary to bacterial pneumonia with neoplastic effusionscontributing a minority of cases. The majority of reportsoriginate from the USA and Australia, where long distancetransport of horses, a recognised risk factor, may occur morefrequently than in the UK. Anecdotally, a greater proportion ofhorses with PE are diagnosed with neoplasia in the UK thanhas been reported. The aim of this retrospective study was todescribe the causes of PE in horses in the UK, and to identifymarkers that can help differentiate between septic andneoplastic causes of PE. Medical records from 4 equinehospitals in the UK were searched for horses diagnosed withPE. Information recorded included case background,admission physical examination and biochemical findings,and characteristics of the effusion (volume, cell count, totalprotein [TP] concentration). A total of 69 horses were identified,with 26 (38%) diagnosed with a neoplastic effusion. Theremainder were categorised as septic, including 14/43(32.5%) that had a history of international transport. Horses withseptic effusions were significantly younger (8 vs. 13 years;P = 0.001) and had significantly smaller volumes of pleuralfluid drained at admission (9.8 l vs. 32.2 l; P<0.001). Horses withseptic PE had a significantly higher rectal temperature (38.6°Cvs. 38.2°C; P = 0.03), fibrinogen concentration (7.8 g/l vs.5.3 g/l; P = 0.01) and serum amyloid A concentration(230 mg/l vs. 59 mg/l; P = 0.02) than those with neoplasticeffusions. Significantly higher pleural fluid cell count and TPconcentration were identified in horses with septic PE(63.9 3 109/l vs. 8.6 3 109/l; P<0.001; 57.5 g/l vs. 35.9 g/l;P = 0.04). These results suggest that in the UK, neoplasticeffusions account for a greater proportion of PE thanpreviously reported. A large volume of PE in an older horsewith a low cell count and relatively low TP concentrationshould increase the index of suspicion of neoplasia.
Introduction
Themajority of cases of pleural effusion reported in the scientificliterature describe horses with septic pleuropneumonia,resulting from extension of bacterial infection of the lungs intothe pleural cavity, and most of these studies originate from theUSA or Australia (Smith 1977; Raphel and Beech 1982; Sweeney1992; Collins et al. 1994; Austin et al. 1995; Racklyeft et al. 2000;Arroyo et al. 2015). In the UK, however, a greater proportionof pleural effusion cases seem to be caused by neoplasia,although the evidence to support this is scarce (Mair et al.2004; Mair 2012). Early determination of the cause of apleural effusion is paramount, so that prompt and
appropriate treatment can be instigated in cases amenableto treatment, or euthanasia be performed in cases with ahopeless prognosis. The aim of this study was thus todetermine whether horses identified with pleural effusion andresident in the UK are more frequently diagnosed withneoplasia than has been reported in previous studies, and todetermine whether factors present at admission could beused to increase the index of suspicion for a neoplasticpleural effusion.
Methods
Records of horses presented to 4 equine referral hospitals in theUK between 2000 and 2014 were searched for horses in whicha pleural effusion had been diagnosed. The cause of theeffusion was then categorised as either neoplastic, septic or‘other’ based on information in the medical records includinghistory, analysis of pleural fluid and tracheal washcharacteristics, ultrasonographic and radiographic findings,and post mortem results as applicable. A history of travel priorto the development of clinical signs was recorded, as wasadmission clinical and clinicopathological data, andoutcome. Outcome was recorded as survival to discharge.Clinical data recorded included case history, admission heartrate, respiratory rate and rectal temperature, clinical signs andduration of those signs prior to admission, and volume ofpleural fluid drained at admission. Clinicopathologicaldata included admission packed cell volume, total plasmaprotein concentration, serum amyloid A and fibrinogenconcentrations, pleural fluid nucleated cell count (NCC) andtotal protein concentration, results of cytological examinationof pleural fluid, and bacterial culture results of tracheal washsamples, pleural fluid or both. When a sample was obtainedfrom both sides of the thorax, the mean protein and nucleatedcell count was used for statistical comparisons. Normality ofcontinuous data was assessed utilising the Kolmogorov–Smirnov statistic, and differences between categoriescompared as appropriate. No cases of pleural effusion due to‘other’ reasons were identified and thus differences betweenseptic and neoplastic pleural effusions were compared usingeither the independent t test or the Mann Whitney U test. For alltests, the null hypothesis was rejected when P<0.05.
Results
A total of 69 horses with pleural effusions was identified. Notall data were available for all horses. The horses ranged inage from 1–28 years (n = 56; median 10.5 years, interquartilerange 10 years) and included a variety of breeds, with the
© 2016 EVJ Ltd
144 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
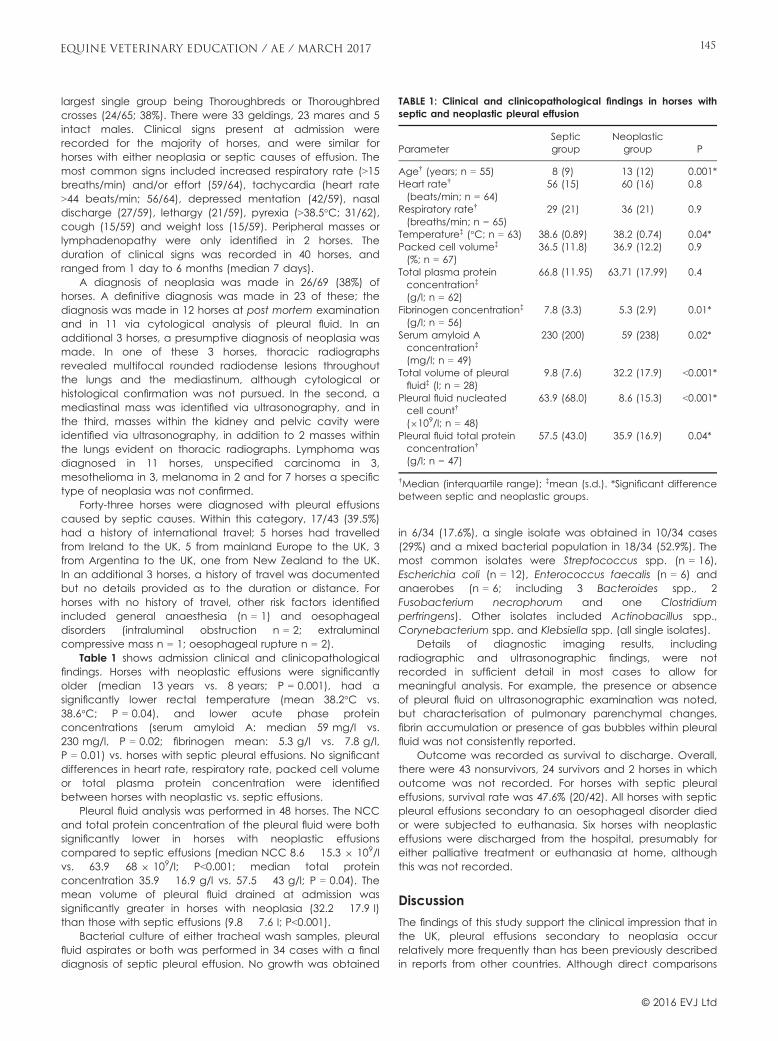
largest single group being Thoroughbreds or Thoroughbredcrosses (24/65; 38%). There were 33 geldings, 23 mares and 5intact males. Clinical signs present at admission wererecorded for the majority of horses, and were similar forhorses with either neoplasia or septic causes of effusion. Themost common signs included increased respiratory rate (>15breaths/min) and/or effort (59/64), tachycardia (heart rate>44 beats/min; 56/64), depressed mentation (42/59), nasaldischarge (27/59), lethargy (21/59), pyrexia (>38.5°C; 31/62),cough (15/59) and weight loss (15/59). Peripheral masses orlymphadenopathy were only identified in 2 horses. Theduration of clinical signs was recorded in 40 horses, andranged from 1 day to 6 months (median 7 days).
A diagnosis of neoplasia was made in 26/69 (38%) ofhorses. A definitive diagnosis was made in 23 of these; thediagnosis was made in 12 horses at post mortem examinationand in 11 via cytological analysis of pleural fluid. In anadditional 3 horses, a presumptive diagnosis of neoplasia wasmade. In one of these 3 horses, thoracic radiographsrevealed multifocal rounded radiodense lesions throughoutthe lungs and the mediastinum, although cytological orhistological confirmation was not pursued. In the second, amediastinal mass was identified via ultrasonography, and inthe third, masses within the kidney and pelvic cavity wereidentified via ultrasonography, in addition to 2 masses withinthe lungs evident on thoracic radiographs. Lymphoma wasdiagnosed in 11 horses, unspecified carcinoma in 3,mesothelioma in 3, melanoma in 2 and for 7 horses a specifictype of neoplasia was not confirmed.
Forty-three horses were diagnosed with pleural effusionscaused by septic causes. Within this category, 17/43 (39.5%)had a history of international travel; 5 horses had travelledfrom Ireland to the UK, 5 from mainland Europe to the UK, 3from Argentina to the UK, one from New Zealand to the UK.In an additional 3 horses, a history of travel was documentedbut no details provided as to the duration or distance. Forhorses with no history of travel, other risk factors identifiedincluded general anaesthesia (n = 1) and oesophagealdisorders (intraluminal obstruction n = 2; extraluminalcompressive mass n = 1; oesophageal rupture n = 2).
Table 1 shows admission clinical and clinicopathologicalfindings. Horses with neoplastic effusions were significantlyolder (median 13 years vs. 8 years; P = 0.001), had asignificantly lower rectal temperature (mean 38.2°C vs.38.6°C; P = 0.04), and lower acute phase proteinconcentrations (serum amyloid A: median 59 mg/l vs.230 mg/l, P = 0.02; fibrinogen mean: 5.3 g/l vs. 7.8 g/l,P = 0.01) vs. horses with septic pleural effusions. No significantdifferences in heart rate, respiratory rate, packed cell volumeor total plasma protein concentration were identifiedbetween horses with neoplastic vs. septic effusions.
Pleural fluid analysis was performed in 48 horses. The NCCand total protein concentration of the pleural fluid were bothsignificantly lower in horses with neoplastic effusionscompared to septic effusions (median NCC 8.6 � 15.3 9 109/lvs. 63.9 � 68 9 109/l; P<0.001; median total proteinconcentration 35.9 � 16.9 g/l vs. 57.5 � 43 g/l; P = 0.04). Themean volume of pleural fluid drained at admission wassignificantly greater in horses with neoplasia (32.2 � 17.9 l)than those with septic effusions (9.8 � 7.6 l; P<0.001).
Bacterial culture of either tracheal wash samples, pleuralfluid aspirates or both was performed in 34 cases with a finaldiagnosis of septic pleural effusion. No growth was obtained
in 6/34 (17.6%), a single isolate was obtained in 10/34 cases(29%) and a mixed bacterial population in 18/34 (52.9%). Themost common isolates were Streptococcus spp. (n = 16),Escherichia coli (n = 12), Enterococcus faecalis (n = 6) andanaerobes (n = 6; including 3 Bacteroides spp., 2Fusobacterium necrophorum and one Clostridiumperfringens). Other isolates included Actinobacillus spp.,Corynebacterium spp. and Klebsiella spp. (all single isolates).
Details of diagnostic imaging results, includingradiographic and ultrasonographic findings, were notrecorded in sufficient detail in most cases to allow formeaningful analysis. For example, the presence or absenceof pleural fluid on ultrasonographic examination was noted,but characterisation of pulmonary parenchymal changes,fibrin accumulation or presence of gas bubbles within pleuralfluid was not consistently reported.
Outcome was recorded as survival to discharge. Overall,there were 43 nonsurvivors, 24 survivors and 2 horses in whichoutcome was not recorded. For horses with septic pleuraleffusions, survival rate was 47.6% (20/42). All horses with septicpleural effusions secondary to an oesophageal disorder diedor were subjected to euthanasia. Six horses with neoplasticeffusions were discharged from the hospital, presumably foreither palliative treatment or euthanasia at home, althoughthis was not recorded.
Discussion
The findings of this study support the clinical impression that inthe UK, pleural effusions secondary to neoplasia occurrelatively more frequently than has been previously describedin reports from other countries. Although direct comparisons
TABLE 1: Clinical and clinicopathological findings in horses withseptic and neoplastic pleural effusion
ParameterSepticgroup
Neoplasticgroup P
Age† (years; n = 55) 8 (9) 13 (12) 0.001*Heart rate†
(beats/min; n = 64)56 (15) 60 (16) 0.8
Respiratory rate†
(breaths/min; n = 65)29 (21) 36 (21) 0.9
Temperature‡ (°C; n = 63) 38.6 (0.89) 38.2 (0.74) 0.04*Packed cell volume‡
(%; n = 67)36.5 (11.8) 36.9 (12.2) 0.9
Total plasma proteinconcentration‡
(g/l; n = 62)
66.8 (11.95) 63.71 (17.99) 0.4
Fibrinogen concentration‡
(g/l; n = 56)7.8 (3.3) 5.3 (2.9) 0.01*
Serum amyloid Aconcentration‡
(mg/l; n = 49)
230 (200) 59 (238) 0.02*
Total volume of pleuralfluid‡ (l; n = 28)
9.8 (7.6) 32.2 (17.9) <0.001*
Pleural fluid nucleatedcell count†
(9109/l; n = 48)
63.9 (68.0) 8.6 (15.3) <0.001*
Pleural fluid total proteinconcentration†
(g/l; n = 47)
57.5 (43.0) 35.9 (16.9) 0.04*
†Median (interquartile range); ‡mean (s.d.). *Significant differencebetween septic and neoplastic groups.
© 2016 EVJ Ltd
145EQUINE VETERINARY EDUCATION / AE / MARCH 2017

are difficult due to differing study designs, one similar studyfrom the USA reported neoplasia as a cause of pleural effusionin only 11% of 37 horses (Smith 1977). A second study, alsofrom the USA, identified 32/122 (26%) of horses with effusioncaused by ‘noninfectious’ causes, although these were notfurther categorised (Raphel and Beech 1982). Long distancetransport is a recognised risk factor for the development ofpleuropneumonia and septic pleural effusion (Raphel andBeech 1982; Austin et al. 1995). Head elevation duringtransportation minimises a horse’s ability to clear lowerrespiratory tract (LRT) secretions and inhaled bacteria (Nortonet al. 2013). Combined with the physiological stress associatedwith travelling, the defence mechanisms of the LRT such asmucociliary transport, pulmonary alveolar macrophages andneutrophils can become overwhelmed (Oikawa et al. 1995;Smith et al. 1996; Norton et al. 2013). Establishment of infectionwithin the lungs results in increased capillary permeability ofthe inflamed lung and visceral pleura, resulting in theaccumulation of a sterile transudate within the pleural cavity.Bacteria from the infected lung rapidly invade the pleuralspace, resulting in the accumulation of a large volume of fluidpacked with inflammatory cells, cellular debris and bacteria(Oikawa et al. 1995; Reuss and Gigu�ere 2015). Most studiesdefine long distance transport as over 500 miles, and, as such, itis possible that the relatively short distances that horses travelwithin the UK, as compared to countries such as the USA andAustralia, may contribute to the lower proportion of septicpleural effusions. Interestingly, in the current study, 40.5% ofhorses with septic pleural effusions had a history of long distancetravel (in 14/17, known international transport) in comparison to24.4% reported by Raphel and Beech (1982). Thus, longdistance transport is a consistent risk factor for the developmentof pleuropneumonia, regardless of geographic location.
In this study, horses with neoplasia were significantly olderthan those with septic pleural effusions. Horses withpleuropneumonia are typically young, with mean ages of3.6 years and 2.5 years in 2 studies (Collins et al. 1994; Arroyoet al. 2015). Presumably, this is associated with an increasedlikelihood for younger horses to be transported long distancesfor competitive reasons, or to undertake high intensityexercise. In the current study, horses with septic pleuraleffusions were older than in other reports with a median ageof 8 years, suggesting that age in itself may not be a specificrisk factor, more that factors that increase the risk ofdeveloping septic pleural effusions are more likely to occur inyounger horses. Whilst horses with neoplasia were older thanthose with septic pleural effusions in the current study,neoplasia can affect any age of horse (Taintor and Schleis2011). Lymphoma is typically identified in horses aged 4–10 years, with a mean age of 7 years in one study (Mair et al.1985; Taintor and Schleis 2011). As such, although there was astatistically significant difference between the age of bothgroups, young age in itself should not be relied on to rule outneoplasia as a cause of pleural effusion.
Consistent with previous reports, neoplasia in this studywas associated with large volume accumulation of pleuralfluid, with up to 55 l drained in several horses (Fig 1) (Mairet al. 1985, 2004). The development of such large volumeeffusions is presumed to occur due to decreased lymphaticdrainage, especially when mediastinal masses are present,and/or to increased fluid production, when the neoplasmaffects the pleural surfaces (DeHeer et al. 2002; Mair et al.2004). In most horses with neoplasia in the current report, the
pleural fluid was described as a modified transudate, with arelatively low NCC and moderately increased total proteinconcentration. As would be expected, both the NCC andthe total protein concentration were significantly higher inhorses with septic causes of pleural effusion.
A definitive diagnosis of neoplasia can be made ifcytological evaluation of the fluid identifies neoplastic cellsor if masses are accessible for biopsy (Figs 2 and 3)(Sweeney and Gillette 1989; Mair et al. 2004). Lymphoma isbelieved commonly to result in exfoliation of neoplastic cellsinto the pleural fluid and in 2 reports up to 40% of caseswere diagnosed ante mortem via cytological analysis ofpleural fluid (Mair et al. 2004; Lee et al. 2013). Similarly, in thecurrent study, a diagnosis of neoplasia was made in 38% ofhorses via cytological examination of pleural fluid. As has
Fig 1: Large volume effusion drained from the pleural cavity of ahorse with lymphoma.
100 μm
Fig 2: Histopathology from a lymph node obtained at postmortem examination in a horse with lymphoma. Sheets ofimmature and mitotically active lymphomatous cells are notedthroughout the section.
© 2016 EVJ Ltd
146 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
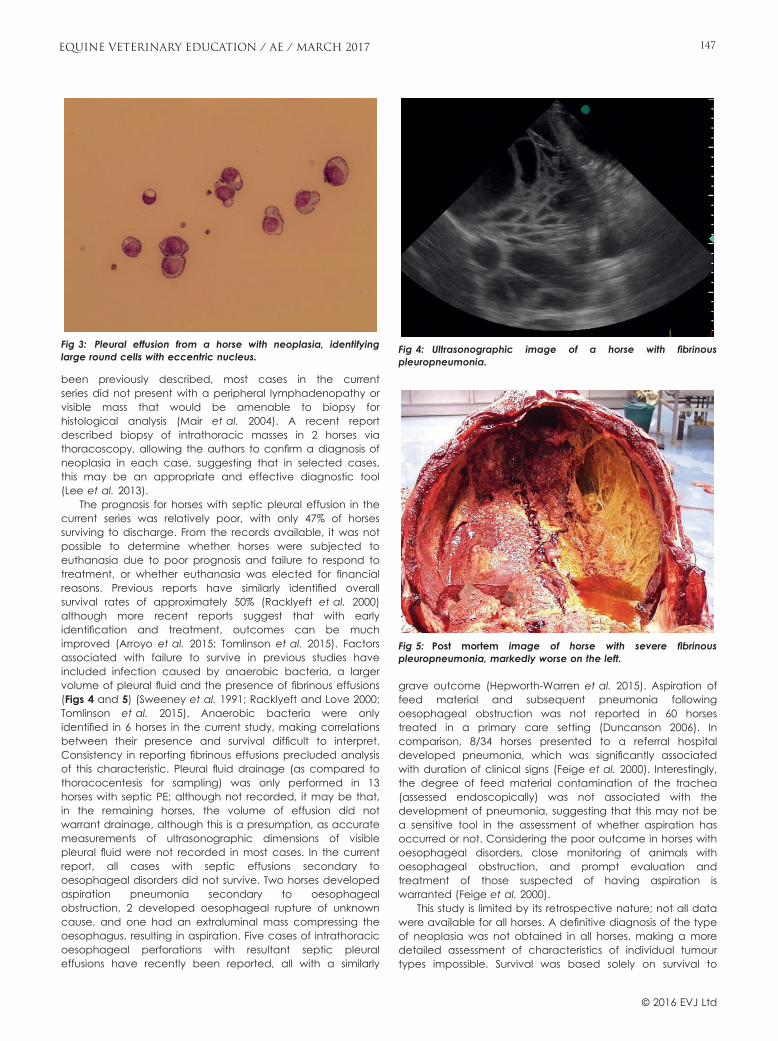
been previously described, most cases in the currentseries did not present with a peripheral lymphadenopathy orvisible mass that would be amenable to biopsy forhistological analysis (Mair et al. 2004). A recent reportdescribed biopsy of intrathoracic masses in 2 horses viathoracoscopy, allowing the authors to confirm a diagnosis ofneoplasia in each case, suggesting that in selected cases,this may be an appropriate and effective diagnostic tool(Lee et al. 2013).
The prognosis for horses with septic pleural effusion in thecurrent series was relatively poor, with only 47% of horsessurviving to discharge. From the records available, it was notpossible to determine whether horses were subjected toeuthanasia due to poor prognosis and failure to respond totreatment, or whether euthanasia was elected for financialreasons. Previous reports have similarly identified overallsurvival rates of approximately 50% (Racklyeft et al. 2000)although more recent reports suggest that with earlyidentification and treatment, outcomes can be muchimproved (Arroyo et al. 2015; Tomlinson et al. 2015). Factorsassociated with failure to survive in previous studies haveincluded infection caused by anaerobic bacteria, a largervolume of pleural fluid and the presence of fibrinous effusions(Figs 4 and 5) (Sweeney et al. 1991; Racklyeft and Love 2000;Tomlinson et al. 2015). Anaerobic bacteria were onlyidentified in 6 horses in the current study, making correlationsbetween their presence and survival difficult to interpret.Consistency in reporting fibrinous effusions precluded analysisof this characteristic. Pleural fluid drainage (as compared tothoracocentesis for sampling) was only performed in 13horses with septic PE; although not recorded, it may be that,in the remaining horses, the volume of effusion did notwarrant drainage, although this is a presumption, as accuratemeasurements of ultrasonographic dimensions of visiblepleural fluid were not recorded in most cases. In the currentreport, all cases with septic effusions secondary tooesophageal disorders did not survive. Two horses developedaspiration pneumonia secondary to oesophagealobstruction, 2 developed oesophageal rupture of unknowncause, and one had an extraluminal mass compressing theoesophagus, resulting in aspiration. Five cases of intrathoracicoesophageal perforations with resultant septic pleuraleffusions have recently been reported, all with a similarly
grave outcome (Hepworth-Warren et al. 2015). Aspiration offeed material and subsequent pneumonia followingoesophageal obstruction was not reported in 60 horsestreated in a primary care setting (Duncanson 2006). Incomparison, 8/34 horses presented to a referral hospitaldeveloped pneumonia, which was significantly associatedwith duration of clinical signs (Feige et al. 2000). Interestingly,the degree of feed material contamination of the trachea(assessed endoscopically) was not associated with thedevelopment of pneumonia, suggesting that this may not bea sensitive tool in the assessment of whether aspiration hasoccurred or not. Considering the poor outcome in horses withoesophageal disorders, close monitoring of animals withoesophageal obstruction, and prompt evaluation andtreatment of those suspected of having aspiration iswarranted (Feige et al. 2000).
This study is limited by its retrospective nature; not all datawere available for all horses. A definitive diagnosis of the typeof neoplasia was not obtained in all horses, making a moredetailed assessment of characteristics of individual tumourtypes impossible. Survival was based solely on survival to
Fig 3: Pleural effusion from a horse with neoplasia, identifyinglarge round cells with eccentric nucleus.
Fig 4: Ultrasonographic image of a horse with fibrinouspleuropneumonia.
Fig 5: Post mortem image of horse with severe fibrinouspleuropneumonia, markedly worse on the left.
© 2016 EVJ Ltd
147EQUINE VETERINARY EDUCATION / AE / MARCH 2017

hospital discharge, which is likely to have skewed the data asseveral horses with neoplasia were classified as survivors dueto the fact that they went home, presumably for euthanasiaor palliative therapy. Although successful treatment ofthoracic neoplasia has been reported, the prognosis is stillconsidered hopeless (Mair et al. 2004; Saulez et al. 2004).
Pleural effusions can develop for a number of reasons, thetwo most common being pleuropneumonia (septic) andneoplasia. In this study, horses with septic pleural effusions wereyounger than those with neoplasia, had significantly higheracute phase protein concentrations at admission, and had asmaller volume of pleural effusion with a higher NCC and totalprotein concentration. Of the 26 horses with confirmed orsuspected neoplasia, the diagnosis was confirmed at postmortem examination in 12 horses, although in some cases ahigh index of suspicion existed without confirmation viacytological analysis of pleural fluid or lymph node aspirate. In 11horses, a diagnosis was made ante mortem using cytologicalanalysis of pleural fluid, and, in 3 horses, masses evident onultrasound or radiography were consistent with neoplasia butcytological confirmation was not pursued. This information maybe helpful in making a prompt diagnosis when the clinician ispresented with a horse with pleural effusion.
Authors’ declaration of interests
No conflicts of interest have been declared.
Ethical animal research
This was a retrospective study utilising clinical cases that doesnot require institutional ethical approval. Client confidentialityhas been maintained and no horses can be individuallyidentified based on either written descriptions or images.
Source of funding
None.
Acknowledgements
Miss Kate English and Dr Ken Smith for providing images ofcytology and histopathology. Dr Claire Wylie for assisting withadditional data acquisition.
Authorship
I. Johns and T. McParland were involved in all aspects of thestudy. The remaining authors were involved in dataacquisition, manuscript preparation and final approval of themanuscript.
ReferencesArroyo, M., Slovis, N. and Moore, G. (2015) Septic pleuropneumonia in
97 horses. In: Proceedings of the American College of VeterinaryInternal Medicine Annual Forum, Indianapolis.
Austin, S.M., Foreman, J.H. and Hungerford, L.L. (1995) Case–controlstudy of risk factors for the development of pleuropneumonia inhorses. J. Am. Vet. Med. Ass. 207, 325-328.
Collins, M.B., Hodgson, D.R. and Hutchins, D.R. (1994) Pleural effusionassociated with acute and chronic pleuropneumonia and pleuritis
secondary to thoracic wounds in horses: 43 cases (1982–1992). J.Am. Vet. Med. Ass. 205, 1753-1758.
DeHeer, H.L., Parry, B.W. and Grindem, C.B. (2002) Pleural fluid. In:Diagnostic Cytology and Hematology of the Horse, Eds: R.L.Cowell and R.D. Tyler, Mosby Inc., St Louis. pp 107-126.
Duncanson, G.R. (2006) Equine oesophageal obstruction: a long termstudy of 60 cases. Equine Vet. Educ. 18, 262-265.
Feige, K., Schwarzwald, C., F€urst, A. and Kaser-Hotz, B. (2000)Esophageal obstruction in horses: a retrospective study of 34cases. Can. Vet. J. 41, 207-210.
Hepworth-Warren, K.L., Wilgenbusch, C.M., Wong, D.M., Fales-William,A.J., Wiechert, S.A. and Sponseller, B.A. (2015) Intrathoracicoesophageal perforation and secondary pleuropneumonia: fivecases. Equine Vet. Educ. 27, 283-290.
Lee, W.L., Tennent-Brown, B.S., Barton, M.H., Almy, F.S., Uhl, E.W.,Howerth, E.W., Reis, J.L., Linnenkohl, W.L. and Peroni, J.F. (2013) Twohorses with thoracic lymphoma diagnosed using thoracoscopicbiopsy. Equine Vet. Educ. 25, 79-83.
Mair, T. (2012) Pleural effusions and pleuropneumonia. In: Proceedingsof the 51st British Equine Veterinary Association Congress,Birmingham.
Mair, T.S., Lane, J.G. and Lucke, V.M. (1985) Clinicopathologicalfeatures of lymphosarcoma involving the thoracic cavity in thehorse. Equine Vet. J. 17, 428-433.
Mair, T.S., Rush, B.R. and Tucker, R.L. (2004) Clinical and diagnosticfeatures of thoracic neoplasia in the horse. Equine Vet. Educ. 16,30-36.
Norton, J.L., Jackson, K., Chen, J.W., Boston, R. and Nolen-Walston,R.D. (2013) Effect of clenbuteral on tracheal mucociliary transportin horses undergoing simulated long-distance transportation. J.Vet. Intern. Med. 27, 1523-1527.
Oikawa, M., Takagi, S., Anzai, R., Yoshikawa, H. and Yoshikawa, T.(1995) Pathology of equine respiratory disease occurring inassociation with transport. J. Comp. Pathol. 113, 29-43.
Racklyeft, D.J. and Love, D.N. (2000) Bacterial infection of the lowerrespiratory tract in 34 horses. Aust. Vet. J. 78, 549-559.
Racklyeft, D.J., Raidal, S. and Love, D. (2000) Towards anunderstanding of equine pleuropneumonia; factors relevant forcontrol. Aust. Vet. J. 78, 334-338.
Raphel, C.F. and Beech, J. (1982) Pleuritis secondary to pneumoniaor lung abscessation in 90 horses. J. Am. Vet. Med. Ass. 181, 808-810.
Reuss, S.M. and Gigu�ere, S. (2015) Update on bacterial pneumoniaand pleuropneumonia in the adult horse. Vet. Clin. N. Am.: EquinePract. 31, 105-120.
Saulez, M.N., Schlipf, J.W., Cebra, C.K., McDonough, S.P. and Bird, K.E.(2004) Use of chemotherapy for treatment of a mixed-cell thoraciclymphoma in a horse. J. Am. Vet. Med. Ass. 224, 733-738.
Smith, B.P. (1977) Pleuritis and pleural effusion in the horse: a study of37 cases. J. Am. Vet. Med. Ass. 170, 208-211.
Smith, B.L., Jones, J.H., Hornof, W.J., Miles, J.A., Longworth, K.E. andWillits, N.H. (1996) Effects of road transport on indices of stress inhorses. Equine Vet. J. 28, 446-454.
Sweeney, C.R. (1992) Causes of pleural effusion in the horse. EquineVet. Educ. 4, 75-77.
Sweeney, C.R. and Gillette, D.M. (1989) Thoracic neoplasia in equids:35 cases (1967–1987). J. Am. Vet. Med. Ass. 195, 374-377.
Sweeney, C.R., Holcombe, S.J., Barningham, S.C. and Beech, J. (1991)Aerobic and anaerobic bacterial isolates from horses withpneumonia or pleuropneumonia and antimicrobial susceptibilitypatterns of the aerobes. J. Am. Vet. Med. Ass. 198, 839-842.
Taintor, J. and Schleis, S. (2011) Equine lymphoma. Equine Vet. Educ.23, 205-213.
Tomlinson, J.E., Reef, V.B., Boston, R.C. and Johnson, A.J. (2015) Theassociation of fibrinous pleural effusion with survival andcomplications in horses with pleuropneumonia (2002–2012): 74cases. J. Vet. Intern. Med. 29, 1410-1417.
© 2016 EVJ Ltd
148 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Review Article
Strangles and its complicationsA. G. Boyle
Department of Clinical Studies, University of Pennsylvania, New Bolton Center, USA.Corresponding author email: [email protected]
Keywords: horse; strangles; Streptococcus equi; guttural pouch empyema; purpura haemorrhagica
SummaryStrangles, caused by the Gram-positive bacteria Strepto-coccus equi subspecies equi (S. equi), is a highly contagiousupper respiratory infection in horses. The infection istransmitted by inhalation or direct contact with mucopurulentdischarge from an infected animal, resulting in fever,depression, and submandibular and retropharyngeal lymphnode enlargement that can lead to respiratory distress.Complications include secondary cellulitis at externalabscessation sites, guttural pouch empyema and itspersistence into the carrier state, purpura haemorrhagica,metastatic abscessation, emergency tracheostomies andrarely secondary S. equi pneumonia or myositis. Control ofoutbreaks requires strict isolation protocols and hygienemeasures. Detection methods of the index case and carrierstate are constantly being refined to assist in the identificationand prevention of disease perpetuation.
Introduction
Strangles is a worldwide, contagious acute upper respiratoryinfection in horses, resulting in high morbidity but low mortality(Sweeney et al. 1989, 2005; Duffee et al. 2015). It is areportable disease in many countries and some states in theUnited States. Strangles is caused by the Gram-positive cocciStreptococcus equi subspecies equi (S. equi). The infection ischaracterised by fever, lethargy, purulent nasal dischargeand regional lymph node abscessation. Highly concentratedand transient populations are at greater risk of contractingthe disease (Sweeney et al. 1989, 2005).
Pathophysiology
Streptococcus equi is inhaled or ingested after direct contactwith mucopurulent discharge from infected horses orcontaminated equipment. The bacterium attaches to thecrypts and epithelium of the lingual and palatine tonsils withthe assistance of the fibronectin binding surface proteins,SeM and SEQ2190. The organism does not colonise themucosal surface but penetrates into deeper tissue and entersthe mandibular and pharyngeal lymph nodes. The hyaluronicacid capsule and surface proteins allow the bacterium toavoid phagocytosis by neutrophils. Clinical signs develop 3–14 days after exposure (Lannergard et al. 2005; Sweeneyet al. 2005; Robinson et al. 2013).
Clinical signs
The severity of clinical signs of strangles can vary dependingon the previous exposure of the individual horse. The firstclinical sign of classical strangles disease is usually acute
onset fever (often >103°F [39.4°C]) which may be missed bycaretakers if the horse continues to eat. It is then followed bylethargy, depression, bilateral mucopurulent discharge,lymphadenopathy and abscessation most commonly of theretropharyngeal and mandibular lymph nodes (Figs 1 and 2).Early cases may only show sensitivity on palpation of theretropharyngeal area without obvious swelling. Occasionally,the parotid and cranial cervical lymph nodes are affectedand have been misidentified as foreign bodies or trauma.Streptococcus equi abscessation can occur at the site of anysubcutaneous lymph node and have been seen in unusuallocations such as ventral to the eye with S. equi positivepurulent drainage from the medial canthus (Fig 3).Secondary cellulitis of the surrounding tissues can developafter drainage occurs if proper hygiene is not maintained.Clinical signs are more severe in immunologically naive(1–5 years of age), geriatric (older than 20 years) andimmunocompromised horses, whereas mature horses withsome immunity often have a milder version of the diseasecalled ‘atypical’ or ‘catarrhal’ strangles. These horses canpresent with only nasal discharge and small abscesses (if any)and rapid resolution of disease. Strangles is often overlookedas a differential by veterinarians and owners in these cases,representing a significant biosecurity risk for they shed virulentS. equi that can produce significant disease in the na€ıvepopulation (Sweeney et al. 1989, 2005).
Transmission and immunity
Shedding of S. equi begins 2–3 days after onset of feverproviding a window during which febrile horses can besegregated, but also a period of false negatives whenperforming diagnostic tests. In most cases, shedding persists fora minimum of 2–3 weeks but often as long as 6 weeks(Sweeney et al. 2005). If organisms are harboured in theguttural pouches, horses can shed S. equi for months or years.These outwardly healthy horses (S. equi carriers) that still shedorganisms are the source of infection when introduced into anew population of horses (Newton et al. 1997a,b, 2000;Verheyen et al. 2000). Transmission occurs through nose-to-nose contact and fomites. Organism could be cultured offsurfaces in an environmental field setting experiment for only3 days (Weese et al. 2009), but moist environments (e.g. waterbuckets) are known to allow the organism to persist forextended periods (Sweeney et al. 2005).
A total of 75% of horses that have been infected withS. equi and have not been treated with antimicrobialsdevelop waning immunity for approximately 5 years (Todd1910). Foals of mares that have recovered from strangles areusually protected by maternal antibodies until weaning(Hamlen et al. 1994; Sweeney et al. 2005).
© 2016 EVJ Ltd
149EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Complications
Guttural pouch disease and persistent carriersRetropharyngeal lymph node enlargement can result innarrowing of the pharynx, whether or not external swelling ofthe retropharyngeal area is visible. This results in respiratorystridor/stertor, dysphagia and neck extension. Horses maydevelop respiratory distress requiring emergencytracheotomy. Upper airway endoscopy often reveals anarrowed pharynx due to axial deviation of the gutturalpouches and enlarged retropharyngeal lymph nodes arevisible, bulging through the respiratory mucosa on the floor ofthe guttural pouch. Empyema results when the
retropharyngeal lymph nodes drain into the guttural poucheson the floor of the medial compartment. On endoscopicexamination, drainage from the opening of the gutturalpouch with difficult entry is highly suggestive of gutturalpouch empyema, but certainly not a requirement for thepresence of S. equi. Dysphagia is the most commonneurological sign in horses with strangles and may besecondary to pharyngeal pain, swelling, or cranial nerveinflammation secondary to guttural pouch disease. Aspirationpneumonia due to S. equi has been seen in horses withsevere dysphagia secondary to strangles. Horses with gutturalpouch empyema can develop into persistent asymptomaticcarriers of S. equi. Inspissated pus (chondroids) can developin the guttural pouch (Fig 4) while the horse has a normaloutward appearance. The guttural pouch can be grosslynormal and still carry S. equi in a microscopic biofilm andtherefore microbiological conformation of the absence ofS. equi is required to rule out the horse being a carrier.Prevalence of carrier status after an outbreak can be as high
Fig 1: Nasal discharge in a horse with strangles.
Fig 2: Enlarged submandibular lymph node in a foal withstrangles. Image courtesy Dr S. Berkowitz, Unionville, Pennsylvania,USA.
Fig 3: Streptococcus equi positive purulent ocular discharge.Image courtesy Dr E. Koch, Wolfeboro, New Hampshire, USA.
Fig 4: Chondroids in an open guttural pouch at necropsy. Imagecourtesy Dr J. Engiles, Kennett Square, Pennsylvania, USA.
© 2016 EVJ Ltd
150 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
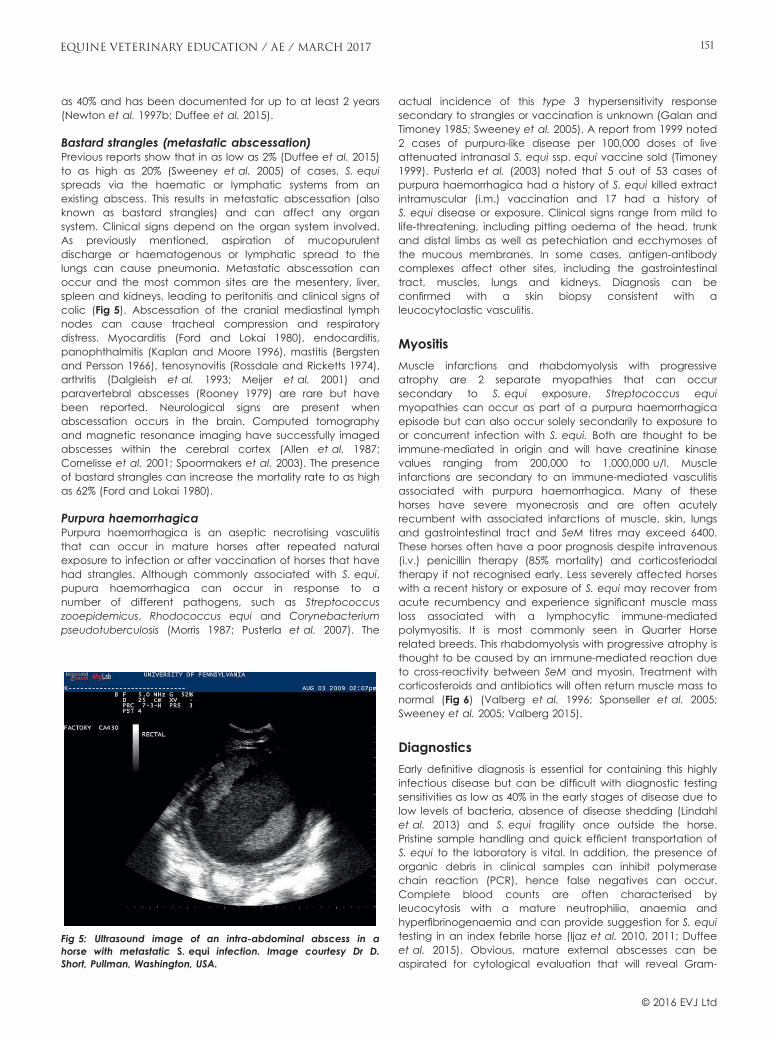
as 40% and has been documented for up to at least 2 years(Newton et al. 1997b; Duffee et al. 2015).
Bastard strangles (metastatic abscessation)Previous reports show that in as low as 2% (Duffee et al. 2015)to as high as 20% (Sweeney et al. 2005) of cases, S. equispreads via the haematic or lymphatic systems from anexisting abscess. This results in metastatic abscessation (alsoknown as bastard strangles) and can affect any organsystem. Clinical signs depend on the organ system involved.As previously mentioned, aspiration of mucopurulentdischarge or haematogenous or lymphatic spread to thelungs can cause pneumonia. Metastatic abscessation canoccur and the most common sites are the mesentery, liver,spleen and kidneys, leading to peritonitis and clinical signs ofcolic (Fig 5). Abscessation of the cranial mediastinal lymphnodes can cause tracheal compression and respiratorydistress. Myocarditis (Ford and Lokai 1980), endocarditis,panophthalmitis (Kaplan and Moore 1996), mastitis (Bergstenand Persson 1966), tenosynovitis (Rossdale and Ricketts 1974),arthritis (Dalgleish et al. 1993; Meijer et al. 2001) andparavertebral abscesses (Rooney 1979) are rare but havebeen reported. Neurological signs are present whenabscessation occurs in the brain. Computed tomographyand magnetic resonance imaging have successfully imagedabscesses within the cerebral cortex (Allen et al. 1987;Cornelisse et al. 2001; Spoormakers et al. 2003). The presenceof bastard strangles can increase the mortality rate to as highas 62% (Ford and Lokai 1980).
Purpura haemorrhagicaPurpura haemorrhagica is an aseptic necrotising vasculitisthat can occur in mature horses after repeated naturalexposure to infection or after vaccination of horses that havehad strangles. Although commonly associated with S. equi,pupura haemorrhagica can occur in response to anumber of different pathogens, such as Streptococcuszooepidemicus, Rhodococcus equi and Corynebacteriumpseudotuberculosis (Morris 1987; Pusterla et al. 2007). The
actual incidence of this type 3 hypersensitivity responsesecondary to strangles or vaccination is unknown (Galan andTimoney 1985; Sweeney et al. 2005). A report from 1999 noted2 cases of purpura-like disease per 100,000 doses of liveattenuated intranasal S. equi ssp. equi vaccine sold (Timoney1999). Pusterla et al. (2003) noted that 5 out of 53 cases ofpurpura haemorrhagica had a history of S. equi killed extractintramuscular (i.m.) vaccination and 17 had a history ofS. equi disease or exposure. Clinical signs range from mild tolife-threatening, including pitting oedema of the head, trunkand distal limbs as well as petechiation and ecchymoses ofthe mucous membranes. In some cases, antigen-antibodycomplexes affect other sites, including the gastrointestinaltract, muscles, lungs and kidneys. Diagnosis can beconfirmed with a skin biopsy consistent with aleucocytoclastic vasculitis.
Myositis
Muscle infarctions and rhabdomyolysis with progressiveatrophy are 2 separate myopathies that can occursecondary to S. equi exposure. Streptococcus equimyopathies can occur as part of a purpura haemorrhagicaepisode but can also occur solely secondarily to exposure toor concurrent infection with S. equi. Both are thought to beimmune-mediated in origin and will have creatinine kinasevalues ranging from 200,000 to 1,000,000 u/l. Muscleinfarctions are secondary to an immune-mediated vasculitisassociated with purpura haemorrhagica. Many of thesehorses have severe myonecrosis and are often acutelyrecumbent with associated infarctions of muscle, skin, lungsand gastrointestinal tract and SeM titres may exceed 6400.These horses often have a poor prognosis despite intravenous(i.v.) penicillin therapy (85% mortality) and corticosteriodaltherapy if not recognised early. Less severely affected horseswith a recent history or exposure of S. equi may recover fromacute recumbency and experience significant muscle massloss associated with a lymphocytic immune-mediatedpolymyositis. It is most commonly seen in Quarter Horserelated breeds. This rhabdomyolysis with progressive atrophy isthought to be caused by an immune-mediated reaction dueto cross-reactivity between SeM and myosin. Treatment withcorticosteroids and antibiotics will often return muscle mass tonormal (Fig 6) (Valberg et al. 1996; Sponseller et al. 2005;Sweeney et al. 2005; Valberg 2015).
Diagnostics
Early definitive diagnosis is essential for containing this highlyinfectious disease but can be difficult with diagnostic testingsensitivities as low as 40% in the early stages of disease due tolow levels of bacteria, absence of disease shedding (Lindahlet al. 2013) and S. equi fragility once outside the horse.Pristine sample handling and quick efficient transportation ofS. equi to the laboratory is vital. In addition, the presence oforganic debris in clinical samples can inhibit polymerasechain reaction (PCR), hence false negatives can occur.Complete blood counts are often characterised byleucocytosis with a mature neutrophilia, anaemia andhyperfibrinogenaemia and can provide suggestion for S. equitesting in an index febrile horse (Ijaz et al. 2010, 2011; Duffeeet al. 2015). Obvious, mature external abscesses can beaspirated for cytological evaluation that will reveal Gram-
Fig 5: Ultrasound image of an intra-abdominal abscess in ahorse with metastatic S. equi infection. Image courtesy Dr D.Short, Pullman, Washington, USA.
© 2016 EVJ Ltd
151EQUINE VETERINARY EDUCATION / AE / MARCH 2017

positive extracellular cocci in long chains to confirm a beta-haemolytic infection, but not confirm S. equi. Diagnosis viaculture or PCR can be obtained from aspirates of matureabscesses, nasopharyngeal washes (Fig 7), or guttural pouchwashes (Sweeney et al. 2005; Holland et al. 2006). Swabs ofthe rostral nasal passage have poor sensitivity unless theanimal has obvious nasal discharge (Lindahl et al. 2013).Nasopharyngeal swabs (via an unguarded uterine cultureswab) have been commonly used, but nasopharyngealwashes have been found to be more sensitive presumablydue to the larger surface area of respiratory epithelium
sampled (Lindahl et al. 2013; Boyle et al. 2015). Historically,S. equi bacterial culture was considered the gold standardfor diagnosis, but has been shown repeatedly to have poorsensitivity when dealing with low levels of infection (earlydisease stages or carriers). Polymerase chain reaction for thedetection of DNA has been shown to be more sensitive,although more expensive, while supplying same day or nextday results (Boyle et al. 2012a,b, 2015, 2016; Lindahl et al.2013; Webb et al. 2013). Detection of early cases of stranglescan be improved by multiple samples taken from the samehorse on the same day (Lindahl et al. 2013). The triplex PCR(Webb et al. 2013) is considered the gold standard for PCRstrangles diagnosis due to its increased sensitivity andspecificity by looking for 3 different superantigens on the SeMgene. This is currently not available in the United States, butthe SeeI PCR (Baverud et al. 2007) is still much more sensitivethan the culture (Boyle et al. 2012a,b, 2015, 2016 Lindahlet al. 2013). The combination of PCR and culture will furtherincrease the sensitivity of S. equi recovery and thiscombination should be the diagnostic test of choice fornasopharyngeal washes and guttural pouch lavages. Manylaboratories already offer this combination for the same priceas the PCR alone, but may not advertise that they areproviding both services. Polymerase chain reaction negativebut culture positive samples (PCR false negatives) arepossible (Grønbaek et al. 2006). It is argued that PCR falsepositives occur due to the detection of ‘dead DNA’,although others argue that dead S. equi bacteria cannotadhere to the respiratory mucosal surfaces and would not bepresent in the horse. The mucociliary clearance in thenasopharynx is highly efficient at removing particles includingDNA. In addition, clinical evidence of disease transmission hasoccurred from horses with PCR positive, culture negativeguttural pouch washes to a na€ıve population, supporting thatthis bacteria was alive and infectious, just below of the limitof detection for the S. equi bacterial culture (Waller 2014).
Carriers can appear outwardly healthy but harbour S. equiin their guttural pouches. Definitive determination of carrierstatus requires endoscopic examination of the gutturalpouches as well as the combination of PCR testing andculture of guttural pouch fluid (Newton et al. 1997a,b;Verheyen et al. 2000; Sweeney et al. 2005; Waller 2014; Boyleet al. 2015, 2016). Cases of metastatic abscessation may becharacterised by anaemia of chronic disease. Rectalexamination, abdominal ultrasonography and rectalultrasonography of cases suspected of having metastaticabscessation often reveal an intra-abdominal mass. Chemistryprofiles reflect abnormalities indicative of the body systemaffected in bastard strangles and purpura haemorrhagica.The latter disease often produces an abnormal coagulationprofile (Sweeney et al. 2005; Pusterla et al. 2007).
Two types of serological tests are currently available. Oneinvolves the use of an ELISA to detect the surface proteinSeM and is available in the United States. This test has beenuseful for detecting recent (4–6 weeks), but not currentinfection; identifying horses that may be predisposed to, ordiagnosed with, purpura haemorrhagica and diagnosingS. equi metastatic abscessation (titres often ≥12,800)(Sweeney et al. 2005). It has been shown that the SeM ELISAis not associated with the identification of carrier horses(Davidson et al. 2008). A more recently developedserological test available in the UK evaluates for 2 surfaceproteins; SEQ2190 and SeM. This test detects animals that
Fig 6: Bilateral semimembranosus and semitendinosus muscleatrophy secondary to S. equi associated immune-mediatedpolymyositis.
Fig 7: Nasopharyngeal wash sampling performed for S. equidiagnostics. Briefly, the horse is sedated and a uterine pipettepunctured from the outside to the inside of a rectal sleeve. Therectal sleeve is placed over the horse’s nose and the pipettepassed up the ventral meatus to the level of the pharynx at whichtime 50 ml sterile saline is infused. The rectal sleeve then catchesthe nasopharyngeal lavage sample via gravity flow.
© 2016 EVJ Ltd
152 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

have seroconverted within 2 weeks of infection and can bea preliminary screening for persistently infected animals(Robinson et al. 2013). Seropositive horses can be identifiedprior to arrival on a new farm or during quarantine. Gutturalpouch endoscopy and PCR and culture combination on thelavage is then performed to identify S. equi carriers.Unfortunately, if the horse was previously vaccinated, thesource of the antibody response measured on theseserological tests cannot be determined (Waller 2014).
Treatment
The goal of treating strangles is to control transmission andeliminate infection while providing future immunity to thedisease. Uncomplicated cases of strangles are often left torun their course with supportive care, providing immunity thatwanes over time. Isolation in a clean, dry stall and moist,palatable food should be available. Nonsteriodal anti-inflammatories should be used judiciously to decreaseswelling and promote eating. Hot compresses or topical 20%ichthammol can be used to accelerate maturation ofabscessation. Mature external abscesses should be lanced toallow drainage, followed by daily lavage of open abscessesusing 3–5% povidone iodine solution. This expedites resolutionof abscessation as well as alleviation of compression ofsurrounding structures, such as the pharynx.
The use of antimicrobials for treating strangles iscontroversial. The preferred antimicrobial is penicillin (procainepenicillin [22,000 to 44,000 iu/kg bwt i.m. q. 12 h] or aqueouspotassium or sodium benzyl penicillin [22,000 to 44,000 iu/kgbwt i.v. q. 6 h]). Although often susceptible in vitro totrimethoprim sulfa, repeated failures in vivo have occurred(Verheyen et al. 2000). For horses that are refractory to twicedaily i.m. injections, ceftiofur crystalline free acid (Excede)1 is auseful option, although it provides more broad spectrumcoverage than clinically needed. Chloramphenicol has beena useful oral option in horses in the need for extendedtreatments.
A short course (3–5 days) of penicillin has been effectiveduring the acute phase of fever and depression to preventabscessation, but these animals will not potentially developimmunity and are at risk of infection as soon as antibiotics arediscontinued. Antibiotics are not recommended in horses withexternal abscesses as the treatment will prolong theirmaturation and resolution. Systemic antibiotics are indicatedif these horses are concurrently anorexic, persistently febriledespite antipyretics, at risk of respiratory obstruction, orappear otherwise systemically affected. If rupture into theguttural pouch has occurred and aspiration of themucopurulent discharge is possible, an extended course(10 days) of systemic penicillin is also warranted to preventaspiration pneumonia and aid in the resolution of gutturalpouch empyema. It has been argued that antimicrobial useafter abscess development may lead to metastasis based onthe theory that protein synthesis by the organism is changedby antimicrobial treatment and that a decreasedimmunogen level results in a suboptimal immune response.There are no experimental or clinical data to support such anoccurrence, but treated horses are at high risk of infectionafter antibiotic discontinuation (Ramey 2007). There are alsoreports of outbreaks in which no antimicrobials were usedand the incidence of complications was high (Sweeney et al.1989; Spoormakers et al. 2003). Horses with complications
such as purpura or metastatic abscessation definitely requirethe use of systemic antimicrobials for extended periods, thelatter often requiring months of treatment. In cases withcomplications such as S. equi internal abdominal abscesses,the mean duration of treatment was 2 months in one study(Pusterla et al. 2007). Cases of purpura haemorrhagica alsorequire the use of systemic corticosteroids (dexamethasone0.1–0.2 mg/kg bwt i.v. or i.m. q. 12–24 h; prednisolone 0.5–1 mg/kg bwt per os q. 24 h) for an average of 3 weeks toreduce systemic vasculitis (Pusterla et al. 2003).
Treatment of carriers can vary depending on thesituation. Many carriers identified at the end of an outbreakvia active screening require only a topical gelatin/penicillinmixture (Sweeney et al. 2005) infused into the gutturalpouches once free of visual empyema. Elimination of gutturalpouch empyema requires repeated lavage (intensity variesdepending on the severity) via polyethylene tubing throughan endoscope, via a chambers catheter, or indwellingcatheters into the guttural pouch (Fig 8) (Newton et al.1997b). A total of 20% acetylcysteine in buffered salinesolution (Bentz et al. 1996) have been added to lavages withsuccess (although not always immediate). Long-standingcarriers often have chondroids which are particularly difficultto remove, often requiring manual removal with endoscopicequipment such as a memory helical polyp retrieval basket(Fig 9) or surgical removal. Successful elimination of S. equi inthese carriers requires local treatment of the guttural pouchwith a gelatin/penicillin mixture after removal of the materialwithin the guttural pouch (Fig 10). Repeated local treatmentwith concurrent systemic penicillin treatment for 10 days isnecessary for refractory cases (Freeman 1980; Newton et al.1997a).
Fig 8: Embryo transfer catheter placed in the right guttural pouchof a horse with S. equi empyema.
© 2016 EVJ Ltd
153EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Methods of outbreak control
Most outbreaks are thought to originate from introduction ofan infected horse to a na€ıve population. All new horsesshould be isolated for 3 weeks and monitored for any signs ofdisease, including fever (>38.5°C or 101.3°F), or suddenincrease in normally recorded biphasic temperatures. If cost isnot prohibitive, horses should be screened for S. equi viaguttural pouch endoscopy and lavage PCR and culturecombination. If the animal is not previously vaccinated forS. equi and is located in a country that provides access toserology developed in the UK testing for both the SEQ2190and SeM genes, screening can be implemented as previouslydescribed in the section on serology (Robinson et al. 2013).
Once an outbreak has occurred, twice daily monitoring ofrectal temperatures of all horses on the farm is essential tocontain the outbreak. Because febrile horses do not sheddisease for the initial 2 days, immediate identification offebrile horses enables caretakers to isolate these horsesbefore shedding occurs. Animals should be isolated based onthe following categories: infected, contacts, recovered (butnot yet tested for carrier status), recovered (and testednegative) and clean (unaffected). If any systemic antibioticshave been used at any time in the course of disease, theseanimals should not be reintroduced into an untested group ofhorses. All movement of horses to and from the farm shouldbe stopped until they are determined to be noninfectious. Allequipment (e.g. pitchforks, buckets, grooming tools) shouldalso be segregated. Personnel handling infected horsesshould wear barrier precautions (i.e. gowns, gloves, plasticshoe covers) and, ideally, should not handle noninfectedhorses or should handle infected horses last. Water bucketsshould be disinfected daily. Facilities and equipment shouldbe cleaned first to remove all organic material and thendisinfected with phenols, iodophors, chlorhexidinecompounds, bleach, or steam cleaned (Newton et al. 2000;Sweeney et al. 2005). Surfaces and equipment must beallowed to dry thoroughly. Ideally, paddocks that holdinfected horses should be rested for at least 2 weeks.Recovery of the organism was not possible after 3 days onwooden fencing in 3 different outdoor environmentalconditions using the less sensitive bacterial culture (Weeseet al. 2009), but has been recovered for as long as 40–60 days on glass and wood, respectively in laboratory settings(Jorm 1992). If nasal discharge persists for longer than2 weeks, guttural pouch endoscopy should be performed atthat time. Since horses are known to typically shed S. equi for2–3 weeks (and sometimes up to 6 weeks) (Sweeney et al.2005), waiting a minimum of 4 weeks after the resolution ofclinical signs has been recommended prior to performingguttural pouch endoscopy and testing. Guttural pouchlavage PCR and culture combination should be performedon the cases and their contacts to screen for carriers. Onecould argue that it is not practically and financially feasibleto wait that long in an equine business operation so a costanalysis needs to be performed to determine whether earlierscreening (which could result in treatment of more positives)outweighs waiting. A minimum recommended time to startguttural pouch screening is 2 weeks after the resolution ofclinical signs. Going straight into the guttural pouchesprovides increased efficiency (both time and monetary) andsensitivity over 3 nasopharyngeal washes 3 weeks apartfollowed by guttural pouch endoscopy of the positives(Fig 11) (Boyle et al. 2015). If the outbreak is located in acountry in which the combined SeM and SEQ2190 serology isoffered and the horses have no history of vaccination, thenthis serology can be used to identify seropositives in thecontact population that need to scoped (Robinson et al.2013; Waller 2014). Eradication of this disease will not bepossible until carriers are eliminated.
Vaccination
A systemic extract vaccine (Strepvax II)2 is available in theUnited States that is administered i.m. Historically, i.m.vaccines have tended to cause injection site reactions andare therefore not administered routinely. An intranasal
Fig 9: Helical polyp retrieval basket passed through a flexibleendoscope in the guttural pouch of a horse with S. equichondroids.
Fig 10: Infusion of penicillin antibiotic into the guttural pouchthrough tubing placed in the instrument channel of the flexibleendoscope in a S. equi carrier.
© 2016 EVJ Ltd
154 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
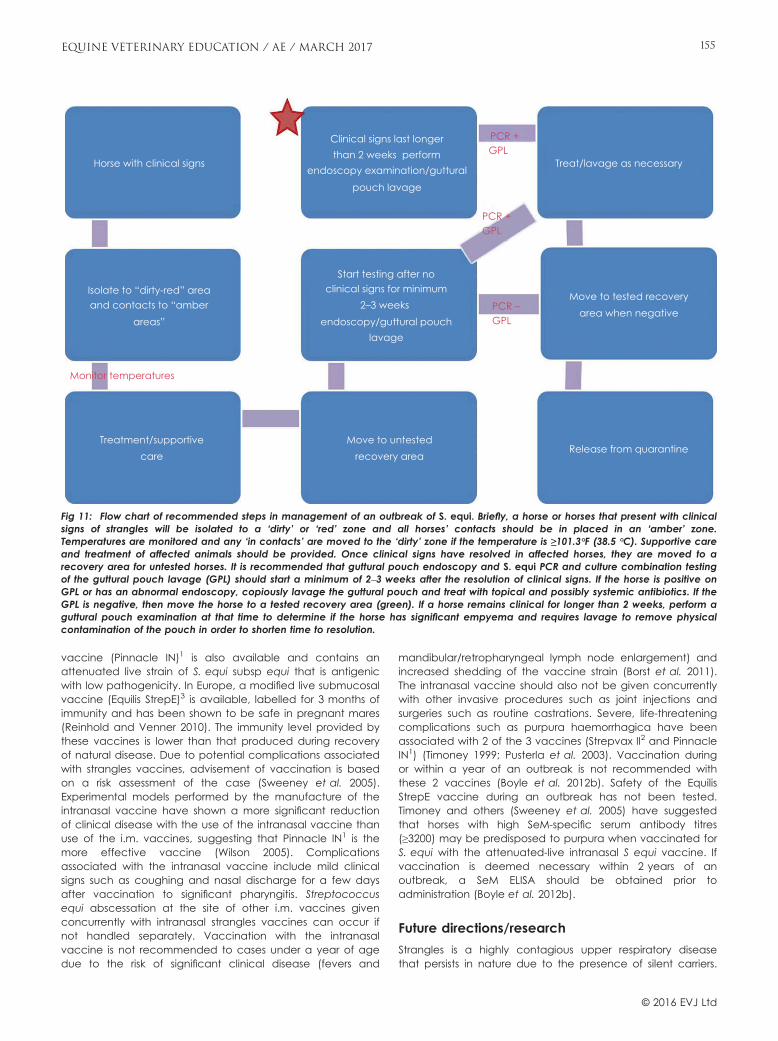
vaccine (Pinnacle IN)1 is also available and contains anattenuated live strain of S. equi subsp equi that is antigenicwith low pathogenicity. In Europe, a modified live submucosalvaccine (Equilis StrepE)3 is available, labelled for 3 months ofimmunity and has been shown to be safe in pregnant mares(Reinhold and Venner 2010). The immunity level provided bythese vaccines is lower than that produced during recoveryof natural disease. Due to potential complications associatedwith strangles vaccines, advisement of vaccination is basedon a risk assessment of the case (Sweeney et al. 2005).Experimental models performed by the manufacture of theintranasal vaccine have shown a more significant reductionof clinical disease with the use of the intranasal vaccine thanuse of the i.m. vaccines, suggesting that Pinnacle IN1 is themore effective vaccine (Wilson 2005). Complicationsassociated with the intranasal vaccine include mild clinicalsigns such as coughing and nasal discharge for a few daysafter vaccination to significant pharyngitis. Streptococcusequi abscessation at the site of other i.m. vaccines givenconcurrently with intranasal strangles vaccines can occur ifnot handled separately. Vaccination with the intranasalvaccine is not recommended to cases under a year of agedue to the risk of significant clinical disease (fevers and
mandibular/retropharyngeal lymph node enlargement) andincreased shedding of the vaccine strain (Borst et al. 2011).The intranasal vaccine should also not be given concurrentlywith other invasive procedures such as joint injections andsurgeries such as routine castrations. Severe, life-threateningcomplications such as purpura haemorrhagica have beenassociated with 2 of the 3 vaccines (Strepvax II2 and PinnacleIN1) (Timoney 1999; Pusterla et al. 2003). Vaccination duringor within a year of an outbreak is not recommended withthese 2 vaccines (Boyle et al. 2012b). Safety of the EquilisStrepE vaccine during an outbreak has not been tested.Timoney and others (Sweeney et al. 2005) have suggestedthat horses with high SeM-specific serum antibody titres(≥3200) may be predisposed to purpura when vaccinated forS. equi with the attenuated-live intranasal S equi vaccine. Ifvaccination is deemed necessary within 2 years of anoutbreak, a SeM ELISA should be obtained prior toadministration (Boyle et al. 2012b).
Future directions/research
Strangles is a highly contagious upper respiratory diseasethat persists in nature due to the presence of silent carriers.
Horse with clinical signs
Isolate to “dirty-red” areaand contacts to “amber
areas”
Treatment/supportivecare
Clinical signs last longerthan 2 weeks perform
endoscopy examination/gutturalpouch lavage
Start testing after no
Treat/lavage as necessary
Move to tested recoveryarea when negative
Release from quarantine
clinical signs for minimum2–3 weeks
endoscopy/guttural pouchlavage
Move to untestedrecovery area
Monitor temperatures
PCR +GPL
GPLPCR +
GPLPCR –
Fig 11: Flow chart of recommended steps in management of an outbreak of S. equi. Briefly, a horse or horses that present with clinicalsigns of strangles will be isolated to a ‘dirty’ or ‘red’ zone and all horses’ contacts should be in placed in an ‘amber’ zone.Temperatures are monitored and any ‘in contacts’ are moved to the ‘dirty’ zone if the temperature is ≥101.3°F (38.5 °C). Supportive careand treatment of affected animals should be provided. Once clinical signs have resolved in affected horses, they are moved to arecovery area for untested horses. It is recommended that guttural pouch endoscopy and S. equi PCR and culture combination testingof the guttural pouch lavage (GPL) should start a minimum of 2–3 weeks after the resolution of clinical signs. If the horse is positive onGPL or has an abnormal endoscopy, copiously lavage the guttural pouch and treat with topical and possibly systemic antibiotics. If theGPL is negative, then move the horse to a tested recovery area (green). If a horse remains clinical for longer than 2 weeks, perform aguttural pouch examination at that time to determine if the horse has significant empyema and requires lavage to remove physicalcontamination of the pouch in order to shorten time to resolution.
© 2016 EVJ Ltd
155EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Improved diagnostics are needed to detect infectionearlier, more conveniently and at less cost. Stall-sidedetection would accelerate identification of affectedhorses, which in turn would lead to faster quarantineprotocols and less spread of disease. Loop-mediatedisothermal amplification (LAMP) technology can identifyDNA without the use of heat cycling and has beeninvestigated for the detection of S. equi (North et al. 2012;Boyle et al. 2015). Researchers are also working to improvevaccination for S. equi (Rodrigues et al. 2012; Waller 2014;Robinson et al. 2015).
Author’s declaration of interests
No conflicts of interest have been declared.
Ethical animal research
Ethical review not applicable for this review article.
Source of funding
This article received no funding.
Manufacturers' addresses1Zoetis, New Jersey, USA.2Boehringer Ingelheim Pharmaceuticals Inc, Ridgefield, Connecticut,USA.3MSD Animal Health, Walton, Milton Keynes, Bucks, UK.
ReferencesAllen, J.R., Barbee, D.D., Boulton, C.R., Major, M.D., Crisman, M.V. and
Murnane, R.D. (1987) Brain abscess in a horse: diagnosis bycomputed tomography and successful surgical treatment. EquineVet. J. 19, 552-555.
Baverud, V., Johansson, S.K. and Aspan, A. (2007) Real-time PCR fordetection and differentiation of Streptococcus equi subsp. equiand Streptococcus equi subsp. zooepidemicus. Vet. Microbiol. 124,219-229.
Bentz, B. G., Dowd, A. L. and Freeman, D. E. (1996) Treatment ofguttural pouch empyema with acetylcysteine irrigation. EquinePract. 18, 33-35.
Bergsten, G. and Persson, S. (1966) Studies on the ECG in horses withacute strangles. In: Proceedings of the 1st InternationalConference Equine Infectious Diseases, Ed: J.T. Bryans, University ofKentucky, Lexington, USA. pp 76-81.
Borst, L.B., Patterson, S.K., Lanka, S., Barger, A.M., Fredrickson, R.L. andMaddox, C.W. (2011) Evaluation of a commercially availablemodified-live Streptococcus equi subsp equi vaccine in ponies.Am. J. Vet. Res. 72, 1130-1138.
Boyle, A.G., Boston, R.C., O’Shea, K., Young, S. and Rankin, S.C.(2012a) Optimization of an in vitro assay to detect Streptococcusequi subsp. equi. Vet. Microbiol. 159, 406-410.
Boyle, A.G., Smith, M.A. and Boston, R.C. (2012b) Risk factors for highserum SeM titers after natural outbreaks of Streptococcus equiequi in horses. J. Equine. Vet. Sci. 32, S19.
Boyle, A.G., Stefanovski, D. and Rankin, S.C. (2015) Determiningoptimal sampling site for Streptococcus equi subsp equi carriersusing a loop-mediated isothermal pcr assay. ACVIM ForumResearch Reports Program. J. Vet. Intern. MedEd. 29, 1278.
Boyle, A.G., Rankin, S.C., Duffee, L.R., Boston, R.C. and Wheeler-Aceto,H. (2016) S. equi detection polymerase chain reaction assay forequine nasopharyngeal and guttural pouch wash samples. J. Vet.Intern. Med. 30, 276-281.
Cornelisse, C.J., Schott, H.C. II, Lowrie, C.T. and Rosenstein, D.S. (2001)Successful treatment of intracranial abscesses in 2 horses. J. Vet.Intern. Med. 15, 494-500.
Davidson, A., Traub-Dargatz, J.L., Magnuson, R., Hill, A., Irwin, V.,Newton, R., Waller, A., Smith, K., Callan, R.J., Meehan, M., Owen, P.and Salman, M. (2008) Lack of correlation between antibody titersto fibrinogen-binding protein of Streptococcus equi and persistentcarriers of strangles. J. Vet. Diagn. Invest. 20, 457-462.
Duffee, L.R., Stefanovski, D., Boston, R.C. and Boyle, A.G. (2015)Predictor variables for and complications associated withStreptococcus equi subs equi infection in horses. J. Am. Vet. Med.Ass. 247, 1161-1168.
Ford, J. and Lokai, M.D. (1980) Complications of Streptococcus equiinfection. Equine Pract. 4, 41-44.
Freeman, D.E. (1980) Diagnosis and treatment of diseases of theguttural pouch (part 2). Comp. Cont. Educ. Pract. Vet. 2, S25-S31.
Galan, J.E. and Timoney, J.F. (1985) Immune complexes in purpurahemorrhagica of the horse contain IgA and M antigen ofStreptococcus equi. J. Immunol. 135, 3134-3137.
Grønbaek, L.M., Angen, O., Vigre, H. and Olsen, S.N. (2006) Evaluationof a nested PCR test and bacterial culture of swabs from the nasalpassages and from abscesses in relation to diagnosis ofStreptococcus equi infection (strangles). Equine Vet. J. 38, 59-63.
Hamlen, H.J., Timoney, J.F. and Bell, R.J. (1994) Epidemiologic andimmunologic characteristics of Streptococcus equi infection infoals. J. Am. Vet. Med. Ass. 204, 768-775.
Holland, R.E., Harris, D.G. and Monge, A. (2006) How to controlstrangles infections on the endemic farm. Proc. Am. Ass. EquinePractnrs. 52, 78-80.
Ijaz, M., Khan, M.S., Khan, M.A., Avais, M., Maqbool, A., Ali, M.M. andShahzad, W. (2010) Prevalence and serum protein values ofstrangles (Streptococcus equi) affected mules at Remount Depot,Sargodha (Pakistan). Equine Vet. Educ. 22, 196-198.
Ijaz, M., Khan, M.S., Khan, M.A., Avais, M., Ali, M.M. and Saleem, M.H.(2011) Molecular identification and haematological values ofstrangles (Streptococcus equi) affected mules in Pakistan. PakistanJ. Zool. 43, 587-592.
Jorm, L.R. (1992) Laboratory studies on the survival of Streptococcusequi subspecies equi on surfaces. In: Proceedings of EquineInfectious Disease VI, Eds: W. Plowright, P.D. Rossdale and J.F.Wade, R & W Publications Ltd, Newmarket, UK. pp 39-43.
Kaplan, N.A. and Moore, B.R. (1996) Streptococcus equi endocarditis,meningitis and panophthalmitis in a mature horse. Equine Vet.Educ. 8, 313-316.
Lannergard, J., Flock, M., Johansson, S., Flock, J.I. and Guss, B. (2005)Studies of fibronectin binding proteins of Streptococcus equi.Infect. Immun. 73, 7243-7251.
Lindahl, S., Baverud, V., Egenvall, A., Asp�an, A. and Pringle, J. (2013)Comparison of sampling sites and laboratory diagnostic tests forS. equi subsp. equi in horses from confirmed strangles outbreaks. J.Vet. Intern. Med. 27, 542-547.
Meijer, M.C., van Weeren, P.R. and Rijkenhiuizen, A.B.M. (2001)Streptococcus equi in the fetlock joint of a mature horse. EquineVet. Educ. 13, 72-74.
Morris, D.D. (1987) Cutaneous vasculitis in horses: 19 cases (1978–1985).J. Am. Vet. Med. Ass. 191, 460-464.
Newton, J.R., Wood, J.L.N. and Chanter, N. (1997a) Strangles: longterm carriage of Streptococcus equi in horses. Equine Vet. Educ. 9,98-102.
Newton, J.R., Wood, J.N., Dunn, K.A., DeBrauwere, M.N. and Chanter,N. (1997b) Naturally occurring persistent and asymptomaticinfection of the guttural pouches of horses with Streptococcusequi. Vet. Rec. 140, 84-90.
Newton, J.R., Verheyen, K., Talbot, N.C., Timoney, J.F., Wood, J.L.,Lakhani, K.H. and Chanter, N. (2000) Control of strangles outbreaksby isolation of guttural pouch carriers identified using PCR andculture of Streptococcus equi. Equine Vet. J. 32, 515-526.
© 2016 EVJ Ltd
156 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Clients can save on their next purchase. MAX.merial.com
Some diagnoses you have to face head-on.
MARQUIS® (15% w/w ponazuril) Antiprotozoal Oral Paste
IMPORTANT SAFETY INFORMATION: The safe use of MARQUIS in horses used for breeding purposes, during pregnancy, or in lactating mares, has not been evaluated. In animal safety studies, loose feces, sporadic inappetence, lost weight, and moderate edema in the uterine epithelium were observed.
‰MARQUIS is a registered trademark, and ™MAX, Merial Awards Xpress is a trademark, of Merial. ©2016 Merial, Inc., Duluth, GA. All rights reserved. EQUIOMQ1506-B (04/16)
fregnancy,afetyndd.Awards Xpress isights reserved.
Equine Protozoal Myeloencephalitis (EPM) is an expert in deception and your clients may at first confuse it with other issues, such as lameness. Only stopping the parasite responsible can stop EPM from causing further damage to the horse’s brain and CNS. Time matters. The sooner EPM is detected and diagnosed, the better the chance for recovery.
That’s why you need a tube of MARQUIS on every truck to initiate treatment immediately. MARQUIS is a powerful anti-protozoal.
Only MARQUIS offers a 3X loading dose protocol that allows it to reach steady state in 24 to 48 hours.*,1
*Clinical relevance has not been determined.
The signs can be subtle. The treatment should be aggressive.
1 MARQUIS Freedom of Information Summary and Supplement and product label.
North, S.E., Das, P., Wakeley, P.R. and Sawyer, J. (2012) Developmentof a rapid isothermal assay to detect the causative agent ofstrangles. J. Equine. Vet. Sci. 32, S54-S55.
Pusterla, N., Watson, J.L., Affolter, V.K., Magdesian, K.G., Wilson, W.D.and Carlson, G.P. (2003) Purpura haemorrhagica in 53 horses. Vet.Rec. 153, 118-121.
Pusterla, N., Whitcomb, M.B. and Wilson, W.D. (2007) Internalabdominal abscesses caused by Streptococcus equi subspeciesequi in 10 horses in California between 1989 and 2004. Vet. Rec.160, 589-592.
Ramey, D. (2007) Does early antibiotic use in horses with ‘strangles’cause metastatic Streptococcus equi bacterial infections? EquineVet. Educ. 19, 14-15.
Reinhold, B. and Venner, M. (2010) Safety of multiple submucosalinoculations of a live attenuated strangles vaccine in pregnantmares. Equine Vet. Educ. 22, 40-42.
Robinson, C., Steward, K., Potts, N., Barker, C., Hammond, T., Pierce, K.,Gunnarsson, E., Svansson, V., Slater, J., Newton, J.R. and Waller, A.(2013) Combining two serological assays optimizes sensitivity andspecificity for the identification of Streptococcus equi subsp equiexposure. Vet. J. 197, 188-191.
Robinson, C., Heather, Z., Slater, J., Potts, N., Steward, K.F., Maskell,D.J., Fontaine, M.C., Lee, J.J., Smith, K. and Waller, A.S. (2015)Vaccination with a live multi-gene deletion strain protects horsesagainst virulent challenge with Streptococcus equi. Vaccine 33,1160-1167.
Rodrigues, M.A., Figueiredo, L., Padrela, L., Cadete, A., Tiago, J.,Matos, H.A., Gomes de Azevedo, E., Florindo, H.F., Gonc�alves, L.M.and Almeida, A.J. (2012) Development of a novel mucosalvaccine against strangles by supercritical enhanced atomizationspray-drying of Streptococcus equi extracts and evaluation in amouse model. Eur. J. Pharm. Biopharm. 2, 392-400.
Rooney, J.R. (1979) Sequelae of strangles. Mod. Vet. Pract. 60,463-464.
Rossdale, P.D. and Ricketts, S.W. (1974) The Practice of Equine StudMedicine, Williams & Wilkins Co., Baltimore. pp 328-330.
Sponseller, B.T., Valberg, S.J., Tennent-Brown, B.S., Foreman, J.H.,Kumar, P. and Timoney, J.F. (2005) Severe acute rhabdomyolysisassociated with Streptococcus equi infection in four horses. J. Am.Vet. Med. Ass. 227, 1800.
Spoormakers, T.J., Ensink, J.M. and Goehring, L.S. (2003) Brainabscesses as a metastatic manifestation of strangles:
symptomatology and the use of magnetic resonance imaging asa diagnostic aid. Equine Vet. J. 35, 146-151.
Sweeney, C.R., Benson, C.E., Whitlock, R.H., Meirs, D.A., Barningham,S.O., Whitehead, S.C. and Cohen, D. (1989) Description of anepizootic and persistence of Streptococcus equi infections inhorses. J. Am. Vet. Med. Ass. 9, 1281-1286.
Sweeney, C.R., Timoney, J.F., Newton, J.R. and Hines, M.T. (2005)Streptococcus equi infections in horses: guidelines for treatment,control, and prevention of strangles. J. Vet. Intern. Med. 19, 123-134.
Timoney, J.F. (1999) Equine strangles. Proc. Am. Ass. Equine Practnrs.45, 31-37.
Todd, A.G. (1910) Strangles. J. Comp. Path. Thera. 23, 212-229.
Valberg, S.J. (2015) Rhabdomyolysis associated with Streptococcusequi. In: Large Animal Internal Medicine, 5th edn., Ed: B.P. Smith,Elsevier Mosby, St. Louis, Missouri. pp 1288-1289.
Valberg, S.J., Bullock, P., Hogetvedt, W., Ames, T., Hayden, D. W., andOtt, K. (1996) Myopathies associated with Streptococcus equiinfections in horses. Proc. Am. Ass. Equine Practnrs. 42, 292-293.
Verheyen, K., Newton, J.R., Talbot, N.C., de Brauwere, M.N. andChanter, N. (2000) Elimination of guttural pouch infection andinflammation in asymptomatic carriers of Streptococcus equi.Equine Vet. J. 32, 527-532.
Waller, A.S. (2014) New perspectives for the diagnosis, control,treatment, and prevention of strangles in horses. Vet. Clin. N. Am.:Equine Pract. 30, 591-607.
Webb, K., Barker, C., Harrison, T., Heather, Z., Steward, K.F., Robinson,C., Newton, J.R. and Waller, A.S. (2013) Detection ofStreptococcus equi subspecies equi using a triplex qPCR assay.Vet. J. 195, 300-304.
Weese, J.S., Jarlot, C. and Morley, P.S. (2009) Survival of Streptococcusequi on surfaces in an outdoor environment. Can. Vet. J. 50,968-970.
Wilson, J. H. (2005) Vaccine efficacy and controversies. Proc. Am. Ass.Equine Practnrs. 51, 409-420.
Supporting information
Additional Supporting Information may be found in the onlineversion of this article at the publisher’s website:
Supplementary Item 1: Video of guttural pouch empyema.
© 2016 EVJ Ltd
157EQUINE VETERINARY EDUCATION / AE / MARCH 2017
MARQUIS®
(15% w/w ponazuril)Antiprotozoal Oral Paste
Caution: Federal (U.S.A.) law restricts this drug to use by or on the order of a licensed veterinarian.
For The Treatment Of Equine Protozoal Myeloencephalitis (EPM) In Horses
For Oral Use OnlyBRIEF SUMMARYBefore using MARQUIS, please consult the product insert, a summary of which follows:
INDICATIONSMARQUIS (ponazuril) is indicated for the treatment of equine protozoal myeloencephalitis (EPM) caused by Sarcocystis neurona.
WARNINGSFor use in animals only. Not for use in horses intended for food. Not for human use. Keep out of reach of children.
PRECAUTIONSPrior to treatment, a complete neurologic exam should be completed by a veterinarian. In most instances, ataxia due to EPM is asymmetrical and affects the hind limbs. Clinicians should recognize that clearance of the parasite by ponazuril may not completely resolve the clinical signs attributed to the natural progression of the disease.
The prognosis for animals treated for EPM may be dependent upon the severity of disease and the duration of the infection prior to treatment. The safe use of MARQUIS (ponazuril) in horses used for breeding purposes, during pregnancy, or in lactating mares, has not been evaluated. The safety of MARQUIS (ponazuril) with concomitant therapies in horses has not been evaluated.
ADVERSE REACTIONSIn the field study, eight animals were noted to have unusual daily observations. Two horses exhibited blisters on the nose and mouth, three animals showed skin reactions for up to 18 days, one animal had loose stools, one had a mild colic on one day and one animal had a seizure while on medication. The association of these reactions to treatment was not established.
ANIMAL SAFETY SUMMARYMARQUIS (ponazuril) was administered to 24 adult horses (12 males and 12 females) in a target animal safety study. Three groups of 8 horses each received 0, 10 or 30 mg/kg (water as control, 2X and 6X for a 5 mg/kg [2.27 mg/lb] dose). Horses were dosed after feeding. One half of each group was treated for 28 days and the other half for 56 days followed by necropsy upon termination of treatment. There were several instances of loose feces in all animals in the study irrespective of treatment, sporadic inappetence and one horse at 10 mg/kg (2X) lost weight while on test. Loose feces were treatment related. Histopathological findings included moderate edema in the uterine epithelium of three of the four females in the 6X group (two treated for 28 days and one for 56 days).
For customer care or to obtain product information, including a Material Safety Data Sheet, call 1-888-637-4251 Option 2, then press 1.
®MARQUIS is a registered trademark of Merial.
©2016 Merial, Inc., Duluth, GA. All rights reserved.

Review Article
Perinatal asphyxia syndromeJ. R. Gold
Department of Clinical Sciences, Washington State University, Pullman, USA.Corresponding author email: [email protected]
Keywords: horse; asphyxia; hypoxia; neonatal maladjustment
SummaryHypoxic ischaemic encephalopathy (HIE) has beendescribed in foals for over 80 years. This condition has adiversity of names including ‘dummy foals’, ‘wanderers’,‘barkers’, neonatal encephalopathy, neonatal maladjustmentsyndrome (NMS) and perinatal asphyxia syndrome (PAS). Thelatter descriptive terms are all encompassing for a syndromethat has varying degrees of multi-systemic effects rather thanjust neurological disease. While foals with PAS are commonlyreported in the literature, the aetiology and underlyingpathophysiology are still very poorly understood, with amajority of the information extrapolated from human andanimal models. Currently, no antemortem test exists anddiagnosis is made based on the history of the mare and foalas well as reliance on clinical signs. Recent studies haveshown that neuroactive pregnanes may play a key role inthe syndrome; however, further research is needed toclarify these findings. Another investigation comparedneurobiomarkers for brain injury in both sick and normalneonatal foals. The mainstay of therapy for PAS is supportivetreatment. Specific therapies such as antioxidants andneuroprotectants are used by some clinicians but littlescientific evidence exists that proves the therapeuticprotocols implemented improve overall outcome. Preventionof PAS in foals revolves around the health of the mareincluding, but not limited to, the prevention of placentitis orother illnesses and observation and/or intervention duringparturition when necessary. More research is necessary tofully comprehend this syndrome, its diagnosis and treatmentoptions.
Introduction
Reynolds (1930) first described hypoxic ischaemicencephalopathy (HIE) as an alteration in behaviour ofneonatal Thoroughbreds. Symptoms noted included seizures,central blindness, loss of suckle and loss of affinity for the dam(Vaala 1999). In 1968, Rossdale described the condition as‘neonatal maladjustment syndrome’ (NMS), which pertainedto foals with behavioural dysfunction and disruption of normaladaptive responses needed for survival (Rossdale 1972;Rossdale and Leadon 1975). Hypoxic ischaemic damage tothe brain was thought to be the cause of NMS.
Over the next 25 years, neurological dysfunction wasconsidered to be the hallmark clinical sign of this syndrome.Pathological findings associated with this syndrome identifieda variety of central nervous system (CNS) lesions whichincluded subdural, epidural subarachnoid, parenchymal andnerve root haemorrhage of the brain and spinal cord(Rossdale and Leadon 1975). Central nervous systemoedema and necrosis were also noted as well as hepatic
and renal lesions (Rossdale and Leadon 1975; Clement 1985).Survival rate for foals at this time was about 50% (Clement1985; Vaala 1994).
It has become evident over the last 15–20 years that manyfoals with HIE experience varying degrees of multi-systemiceffects due to hypoxia rather than just neurological disease.Thus, perinatal asphyxia syndrome (PAS) has become a betterdescriptive term because it recognises cardiopulmonary,endocrine, gastrointestinal and renal abnormalities, along withthe neurological and behavioural disturbances that canoccur in these foals (Vaala 2009). The incidence of PAS isreported to be 1–2% of all foals born (Bernard et al. 1995).
In contrast to neonatal foals, HIE or neonatalencephalopathy in man affects 3.8 of every 1000 live infantbirths (Badawi et al. 1998; Cowan et al. 2003; Kurinczuk et al.2010) worldwide. About 60% of infants with HIE die and 25%of survivors are left with a significant neurological disability(Ballet 2010). The most significant lasting disability in infants isthe development of cerebral palsy (Vannucci and Hagberg2004). Cerebral palsy is defined as multiple disorders of thedeveloping fetal or infant brain affecting movement, postureand muscle disorders (Rosenbaum et al. 2007). Cerebral palsyaffects 3.6 per 1000 human infant births in the United States(Yeargin-Allsopp et al. 2008). Severely affected foals tend todie similarly to their human counterparts but the long-termprognosis for foals is generally much better than for man. Thereason for the disparity in survival and clinical signs betweenfoals and man is likely multifaceted. Foals are precocious andtherefore brain development is further advanced than inhuman infants, thus hypoxia/ischaemic events may notmanifest in a similar fashion.
Pathophysiology
The pathophysiology of HIE, brain damage simply stated,occurs due to a decrease in cerebral blood flow andoxygenation which leads to a cascade of deleteriousphysiological and biochemical events during the ante-, peri-or post partum period. Multiple different factors maycontribute to the clinical signs associated with HIE. It isimportant to understand that HIE is a specific category ofneonatal encephalopathy and not all cases are caused byhypoxic ischaemia (Dickey et al. 2011).
Evidence exists in human infants that inflammatorymediators may play an important role in the cascade ofevents leading to neonatal brain injury (Badawi et al. 1998;Shalak et al. 2002). Therefore, especially with mares which areill during pregnancy or have placentitis (a known risk factorfor neurological deficits in foals), it is plausible but notconfirmed that a fetal inflammatory response may play a rolein the development of PAS in foals (Vaala 1999).
© 2015 EVJ Ltd
158 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
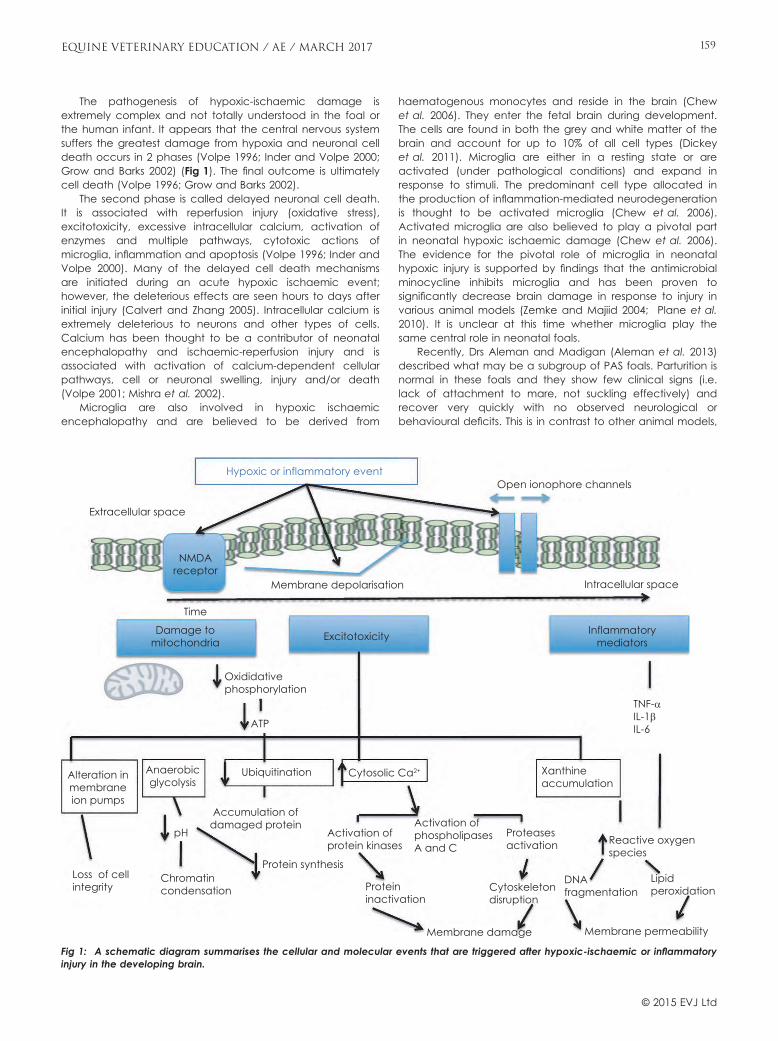
The pathogenesis of hypoxic-ischaemic damage isextremely complex and not totally understood in the foal orthe human infant. It appears that the central nervous systemsuffers the greatest damage from hypoxia and neuronal celldeath occurs in 2 phases (Volpe 1996; Inder and Volpe 2000;Grow and Barks 2002) (Fig 1). The final outcome is ultimatelycell death (Volpe 1996; Grow and Barks 2002).
The second phase is called delayed neuronal cell death.It is associated with reperfusion injury (oxidative stress),excitotoxicity, excessive intracellular calcium, activation ofenzymes and multiple pathways, cytotoxic actions ofmicroglia, inflammation and apoptosis (Volpe 1996; Inder andVolpe 2000). Many of the delayed cell death mechanismsare initiated during an acute hypoxic ischaemic event;however, the deleterious effects are seen hours to days afterinitial injury (Calvert and Zhang 2005). Intracellular calcium isextremely deleterious to neurons and other types of cells.Calcium has been thought to be a contributor of neonatalencephalopathy and ischaemic-reperfusion injury and isassociated with activation of calcium-dependent cellularpathways, cell or neuronal swelling, injury and/or death(Volpe 2001; Mishra et al. 2002).
Microglia are also involved in hypoxic ischaemicencephalopathy and are believed to be derived from
haematogenous monocytes and reside in the brain (Chewet al. 2006). They enter the fetal brain during development.The cells are found in both the grey and white matter of thebrain and account for up to 10% of all cell types (Dickeyet al. 2011). Microglia are either in a resting state or areactivated (under pathological conditions) and expand inresponse to stimuli. The predominant cell type allocated inthe production of inflammation-mediated neurodegenerationis thought to be activated microglia (Chew et al. 2006).Activated microglia are also believed to play a pivotal partin neonatal hypoxic ischaemic damage (Chew et al. 2006).The evidence for the pivotal role of microglia in neonatalhypoxic injury is supported by findings that the antimicrobialminocycline inhibits microglia and has been proven tosignificantly decrease brain damage in response to injury invarious animal models (Zemke and Majiid 2004; Plane et al.2010). It is unclear at this time whether microglia play thesame central role in neonatal foals.
Recently, Drs Aleman and Madigan (Aleman et al. 2013)described what may be a subgroup of PAS foals. Parturition isnormal in these foals and they show few clinical signs (i.e.lack of attachment to mare, not suckling effectively) andrecover very quickly with no observed neurological orbehavioural deficits. This is in contrast to other animal models,
Hypoxic or inflammatory event
Extracellular space
NMDAreceptor
Membrane depolarisation Intracellular space
Open ionophore channels
Time
Damage tomitochondria Excitotoxicity Inflammatory
mediators
Oxididativephosphorylation
Xanthineaccumulation
TNF-αIL-1βIL-6ATP
Alteration inmembraneion pumps
Anaerobicglycolysis
Ubiquitination
pH
Accumulation ofdamaged protein
Protein synthesis
Protein inactivation
Proteasesactivation
Cytoskeletondisruption
Membrane damage Membrane permeability
DNAfragmentation
Lipidperoxidation
Reactive oxygenspecies
Activation ofprotein kinases
Cytosolic Ca2+
Activation ofphospholipasesA and C
Chromatincondensation
Loss of cellintegrity
Fig 1: A schematic diagram summarises the cellular and molecular events that are triggered after hypoxic-ischaemic or inflammatoryinjury in the developing brain.
© 2015 EVJ Ltd
159EQUINE VETERINARY EDUCATION / AE / MARCH 2017
some human neonatal hypoxic encephalopathy cases andother PAS foals require a significant amount of time devotedto recovery and long-term neurological deficits are noted.Therefore, not all foals suffering from PAS may have a hypoxicevent but have other factors contributing to their behaviouralabnormalities.
Several other publications (Holtan et al. 1991; Houghtonet al. 1991; Rossdale et al. 1995) have shown that neonatalfoals have high concentrations of pregnanes at parturitionwhich decrease rapidly over the first 48 h of life (Holtan et al.1991; Houghton et al. 1991; Rossdale et al. 1995; Alemanet al. 2013). Increased concentrations of pregnanes and acorrelation between decreasing concentrations and clinicalrecovery have been previously reported (Holtan et al. 1991;Houghton et al. 1991; Rossdale et al. 1995; Aleman et al.2013). The elevated pregnanes may be responsible for someof the behavioural modifications seen in foals with PAS. Theexact reason why plasma pregnane values are increased inthese foals remains unexplained at this time but may have todo with persistence of in utero signals of being quiet andnonambulatory (Aleman et al. 2013).
Consequently, it is likely that multiple factors (e.g.pregnanes, hypoxia, inflammatory mediators) contribute toPAS in foals and for numerous reasons it is important not tolabel all neurologically abnormal foals as having perinatalasphyxia. As an alternative, each foal should be individuallyevaluated by obtaining a good history and performing athorough diagnostic work-up.
Risk factors
Numerous different influences can lead ultimately to hypoxiaand the abnormalities noted in PAS foals. Maternal diseasescan cause hypotension or decreased tissue perfusion such asrespiratory disease, endotoxaemia, haemorrhage/anaemia,surgery or caesarean delivery (Galvin and Collins 2004).Pathology of the placenta impairs uteroplacentaloxygenation/perfusion such as with placentitis (bacterial,fungal, endophyte), chronic uteroplacental separation, whichleads to chronic hypoxia in the fetus, or acute/prematureuteroplacental separation (Galvin and Collins 2004).Placentitis and other maternal diseases may causeinflammation as well as leading to the clinical signs seen infoals (LeBlanc et al. 2002, 2004, 2013; Cummin et al. 2008).Problems that may lead to hypoxia in the fetus/foal may betwinning, congenital abnormalities, dystocia, meconiumaspiration, umbilical cord compression, sepsis, prematurityand dysmaturity (Galvin and Collins 2004). Twin fetuses leadto reduced areas of placentation available for perfusion toeach individual fetus and tend to predispose the mare todystocia and its associated complications (Galvin and Collins2004). Therefore, multiple different factors (maternal, fetal orboth) may contribute to the development of PAS in foals.
Clinical signs
Foals with PAS have a variety of clinical signs; generalisedweakness, lack of interest in the dam, lack of suckle reflex,inability to lie down, recumbency and seizures (Rossdale1972; Rossdale and Leadon 1975). Manifestations in otherbody systems may also be seen such as ileus, enterocolitis,decreased cardiac output or decreased renal output(Mackay 2005). Abnormalities of one organ system may
prevail over others or all systems may be involved dependingupon the degree of hypoxia (Galvin and Collins 2004;Mackay 2005).
Due to the continuum of clinical signs possible in foalswith PAS, they have also been characterised into two groups.Category 1 foals are born with normal mentation anddevelop clinical signs within the first 48 h (Galvin and Collins2004; Mackay 2005). Category 2 foals typically have riskfactors associated with PAS and are abnormal at birth(Galvin and Collins 2004; Mackay 2005). Typically prognosisfor Category 1 foals is excellent for survival (Vaala 1999;Mackay 2005) and for Category 2 foals there is a tendencytowards a lower survival rate because abnormalities areusually worse and foals deteriorate within the first 48 h of life(Vaala 1999; Mackay 2005). However, due to theimprovement of neonatal care, survival for both categories offoals is likely increased from previously reported data.
Human infants with HIE are also broken down intodifferent groups. Their categories depend upon the lengthand severity of disease. For example, an infant with mildhypoxic ischaemic encephalopathy may have slightlyincreased muscle tone and deep tendon reflexes may bebrisk for the first few day of life (Zanelli 2014). These infantsalso have behavioural abnormalities such as poor feeding,irritability or excess crying or sleepiness (Zanelli 2014). Thisdegree of HIE typically resolves in less than 24 h (Zanelli 2014)and clinical signs worsen depending on the degree of HIE.Many of these infants also have multi-organ dysfunction.
Paediatricians depend upon history, clinical signs, bloodgases and APGAR scores in human neonates to assess theextent of hypoxic injury. An APGAR score has been modifiedfor neonatal foals and this scoring system, along with bloodgases and a detailed history of the dam, may help withdiagnosis and prognosis for neonatal foals.
Diagnosis
Diagnosis of PAS in foals thus far is very limited. Many of theclinical signs seen in foals can occur with other diseases suchas neonatal sepsis, hypoglycaemia and prematurity.Therefore, PAS can be the only problem in the neonatal foal orcan be complicated by other conditions. Haematology andbiochemistry profile, blood culture, arterial blood gases andIgG concentrations can help identify failure of passive transferof maternal antibodies and other clinical problems such assepsis or issues with other body systems. The diagnosis of PAStypically relies on an accurate history and identification ofneurological deficits while excluding other causes of centralnervous system problems such as congenital malformation,infectious, metabolic or developmental conditions. At thistime, no clinicopathological findings have been specific forPAS; however, Bernard et al. (1995) found that 32% of foalswith PAS had an increase in serum creatinine concentrationsand 61% an increase in creatine kinase concentrations(Bernard et al. 1995). Furthermore, increases in serumcreatinine (>309.4 lmol/l) and/or low blood glucoseconcentrations before suckling (<1.94–2.5 mmol/l) have beenassociated with placental insufficiency and an increase in PAS(Vaala 1999). A study by Chaney et al. (2010) found that 20/28 foals with elevated creatinine had clinical signs suggestiveof PAS. Abnormalities such as hyperlactaemia, hypoxaemia,hypercapnoea, acidosis and hypocalcaemia have all beennoted in foals with PAS; however, these laboratory
© 2015 EVJ Ltd
160 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

abnormalities also arise from other neonatal foal diseases(Vaala 1994; Furr 1996; Borchers et al. 2012).
A study by Ringger et al. (2011) showed the potential foruse of neurobiomarkers; ubiquitin C-terminal hydrolase (UCHL-1) and phosphorylated axonal forms of neurofilament H (PNF-H) as an aid in the antemortem diagnosis of PAS in neonatalfoals. The study found that UCHL-1 was significantly better atdiagnosis of neonatal encephalopathy then PNF-H with asensitivity of UCHL-1 of 70% and specificity of 94% (Ringgeret al. 2011). Although promising, the study only included afew cases and measurement of neurobiomarkers are notreadily available at this time.
The study by Aleman et al. (2013) of elevated pregnanesin PAS foals is also promising as stated earlier. However, morework is needed to clarify the role of pregnanes and themeasurement of these concentrations is also not readilyavailable at present.
In human infants, magnetic resonance imaging (MRI)tends to be the modality of choice for diagnosis of HIE. Theconventional T1- and T2-weighted sequences provide veryaccurate anatomical detail; however, when injury to thebrain occurs, these type sequences may remain normal forseveral days (Volpe 2001). Therefore, the diffusion-weightedimaging (DWI) appears to be better at early detection ofperinatal brain ischaemia (Chau et al. 2009).
Despite the increased use of MRI in equine patients, onlyone previous study has been performed which looked at thenormal neonatal foal (Chaffin et al. 1997). Another projectdescribed MRI findings of 12 neurological horses, one ofwhich was a 2-day-old foal with a high suspicion of PAS.However, this foal had severe hydrocephalus not PAS (Ferrellet al. 2002). With the larger magnets in MRI andimprovements in CT imaging techniques, perhaps more canbe gleaned from MRI and/or CT in the equine neonate.
Ambulatory electroencephalograpy (aEEG) is a modalityused for continuous monitoring of electrical activity ofcritically ill human neonates (Volpe 2001). Another diagnosticmodality which is not utilised in neonatal foals iselectroencephalography (EEG). In a recent study by Tothet al. (2012), the authors looked at neonatal consciousnesswhere they utilised EEG without sedation to study the effectof squeeze-induced somnolence. Although used for othertypes of research, EEG has not been used to identify seizuresin foals with PAS.
Ambulatory electroencephalography has be shown to besensitive for early prediction of outcome of HIE newborninfants (Hellstr€om-Westas et al. 2006). Because aEEG providesconstant appraisal of cerebral function, it can showelectrographic seizure activity when no obvious clinical signsare present. Thus the aEEG may provide evidence thatfurther injury to the brain may occur despite no clinical signsof seizures.
One study has looked at using aEEG in ambulatory horses(Wingberg et al. 2013) and Aleman et al. (2006) has utilisedEEG for research on juvenile epilepsy in Arabian foals but nostudies have been performed in PAS foals. Seizures in neonatalfoals vary from very subtle such as lip smacking or mildstretching to the severity of grand mal seizures. A question thatremains is whether foals, like human infants, have suspectedseizures or abnormal movements shows seizure activity with noclinical notable seizures. An aEEG might answer the abovequestion and increase our understanding of seizure patternand the potential response to treatment. However, this
modality would not be available to all practitioners and abilityto perform it is limited to those with the equipment and whounderstand the reading. Accurate determination of seizureactivity is important because neonatal seizures caused bybirth asphyxia in the human infant are associated with a worseneurodevelopmental outcome regardless of the severity ofhypoxic ischaemic brain injury (Glass et al. 2009).
Treatment
For neonatal foals and infants alike, therapy for neonatalencephalopathy tends to be supportive care and the varioustherapies instituted depend upon the multiple organ systemsinvolved. Typical treatments revolve around maintenance ofglucose, oxygen supplementation, maintenance of bloodpressure and seizure control as well as a variety ofantioxidants and neuroprotectants.
It is important to be aware that, although many therapiesexist for neonatal foals with PAS, use of these therapiesremains entirely hypothetical. No specific information existsregarding the outcome of foals treated with the variety oftherapies implemented. Most therapies are adjunct tosupportive care and do not harm the foal per se but whetherthey actually help is unknown.
Treatment for human infants like those of equine neonatalfoals is supportive care, as well as the use of hypothermia.Hypothermia has been documented as a protectivemechanism in multiple medical circumstances such as organtransplants, cardiopulmonary bypass, spinal cord injury andneonatal hypoxic ischaemia (Tang and Yenari 2010). Themechanism of action of hypothermia appears to not just slowmetabolism but potentially has an effect on cell death andcell survival pathways which leads to inhibition of inflammationand apoptosis (Globus et al. 1995; Tang and Yenari 2010).Human infants with HIE are now treated with hypothermia asthe major treatment modality. It involves reducing the normalbody temperature to 33°C within 6 h of delivery which is thencontinued for a total of 72 h. The infant is then graduallyrewarmed to normal body temperature over 12 h. The goal isto decrease the temperature of the susceptible deep brainstructures to 32–34°C. Multiple studies show that hypothermiadecreases the risk of the combined outcome of mortality andmoderate to severe neurodevelopmental disability in infantsand children (Jacobs et al. 2007; Gressans et al. 2008).However, hypothermia does not provide complete protectionand is not successful in the most severely effected neonates,although in combination with other therapies remains themost promising (Cilio and Ferriero 2010).
Little data exists on the use of hypothermia in neonatalfoals and several studies have shown neonatal foals actuallyhave a worse prognosis if hypothermic (Furr et al. 1997;Rohrback et al. 2006). However, the foals in these studieswere hypothermic due to disease and were not hypothermicfor therapeutic reasons. Thus, therapeutic hypothermia shouldnot be ruled out as a possible treatment and furtherinvestigation into this topic is warranted. Other treatmentmodalities that may merit study in foals are melatonin anddesferrioxamine. Research in animal models of HIE have usedmelatonin and desferroxamine which were found to bebeneficial as free radical scavengers (Palmer et al. 1994;Shadid et al. 1998; Sun et al. 2004; Welin et al. 2007; Carloniet al. 2008; McPherson and Juul 2008; Hutton et al. 2009;Elmahdy et al. 2010; Fan et al. 2010; Wong et al. 2011).
© 2015 EVJ Ltd
161EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Hyperbaric oxygen therapy has been studied in rat models ofHIE and has been shown to reduce apoptosis, promoteneuronal stem cells, enhance oxygen radical scavengers andincrease oxygen delivery to the brain (Calvert and Zhang2007; Wang et al. 2008; Feng et al. 2013). In human infants,hyperbaric oxygen has been shown to increase superoxidedismutase; decreased levels of malondialdehyde and nitricoxide which lead to improved neurological assessment (Zhouet al. 2008). A study by Slovis (2006) in neonatal foals with PASalso had positive outcomes.
Prevention
Although risk factors for the development of PAS have beenidentified in foals, preventative measures need to revolvearound the health of the mare.
Placentitis prevention and treatment, decreasinginflammatory mediators if the mare is ill during pregnancyand observation of foaling and assistance when needed, arethe goals of prevention. Preventive measures for the foalrevolve around recognition of distress and initiatingappropriate therapy (e.g. respiratory support orcardiopulmonary resuscitation).
As stated earlier in treatment methods, neurosteroids mayalso become a preventative treatment for neonatal foals.Research has recently shown that the brain is able to formneurosteroids which have a protective role and may possiblyprevent neonatal encephalopathy (Hirst et al. 2008; Tsutsui2008). High allopregnanolone levels cause suppression of theCNS and sleep-like behaviour in utero (Hirst et al. 2008).However, after birth, neurosteroid concentrations decreaseand this may increase the susceptibility of neonates to braininjury (Hirst et al. 2008). Therefore, neurosteroids may have aprotective effect on the fetal brain from hypoxic inducedinjury, necessitating its potential usage as a preventivetherapy. Further research is needed to examine the possibilities.
Conclusion
Although PAS is thought to be the most common disorderseen in neonatal foals, the understanding of this syndromeremains unclear. Ample scientific publications exist on humanneonatal encephalopathy; however, limited literature existson neonatal foals with PAS. Therefore most of our knowledgeof the pathophysiology, risk factors, treatment and preventionrevolve around studies in man.
Maintaining the health of the mare, recognising equineneonatal distress, treatment of multiple body systems, alongwith supportive care are the key to successful managementof PAS.
Author’s declaration of interests
No conflicts of interest have been declared.
Acknowledgements
Special thanks to Drs C. Cable, A. Forbes and C. Ziegler.
ReferencesAleman, M., Gray, L.C., Williams, D.C., Holliday, T.A., Madigan, J.E.,
LeCouteur, R.A. and Magdesian, K.G. (2006) Juvenile idiopathic
epilepsy in Egyptian Arabian foals: 22 cases (1985–2005). J. Vet.Intern. Med. 20, 1443-1449.
Aleman, M., Pickles, K.J., Conley, A.J., Stanley, S., Haggett, E., Toth, B.and Madigan, J.E. (2013) Abnormal plasma neuroactiveprogestagen derivatives in ill, neonatal foals presented to theneonatal intensive care unit. Equine Vet. J. 45, 661-665.
Badawi, N., Kurinczuk, J.J., Keogh, J.M., Allesandri, L.M., O’Sullivan, F.,Burton, P.R., Pemberton, P.J. and Stanley, F.J. (1998) Intrapartumrisk factors for newborn encephalopathy: the Western Australiancase-control study. Br. Med. J. 317, 1554-1558.
Ballet, D.E. (2010) Cooling for newborns with hypoxic ischemicencephalopathy: RHL commentary: The WHO Reproductive HealthLibrary. World Health Organization, Geneva. http://apps.who.int/rhl/newborn/cd00331_ballotde_com/en/
Bernard, W.V., Reimer, J.M. and Cudd, T. (1995) Historical factors,clinicopathologic findings, clinical features, and outcome of equineneonates presenting with or developing signs of central nervoussystem disease. Proc. Am. Assoc. Equine Practnrs. 41, 221-224.
Borchers, A., Wilkens, P.A., Marsh, P.M., Axon, J.E., Read, J.,Castagenetti, C., Patealeon, L., Clark, C., Qura, L., Belgrave, R.,Trachsel, D., Levy, M., Bedenice, D., Saulez, M.N. and Boston, R.C.(2012) Association of admission L-lactate concentration inhospitalised equine neonates with presenting complaint,periparturient events, clinical diagnosis and outcome: a prospectivemulticentre study. Equine Vet. J. 44, Suppl. 41, 57-63.
Calvert, J.W. and Zhang, J.H. (2005) Pathophysiology of an hypoxic-ischaemic insult during the neonatal perinatal period. NeurologicRes. 27, 246-260.
Calvert, J.W. and Zhang, J.H. (2007) Oxygen treatment restores energystatus following experimental neonatal hypoxic-ischemia. Pediatr.Crit. Care Med. 8, 165-173.
Carloni, S., Perrone, S., Buonoccore, G., Longini, M. and Badluini, W.(2008) Melatonin protects from the long-term consequences ofneonatal hypoxic-ischaemic brain injury in rats. J. Pineal Res. 44,157-164.
Chaffin, M.K., Walker, M.A., McArthur, N.H., Perris, E.E. and Matthews,N.S. (1997) Magnetic resonance imaging of the brain of normalneonatal foals. Vet. Radiol. Ultrasound. 38, 102-111.
Chaney, K.P., Holcombe, S.J., Schott, H.C. 2nd and Barr, B.S. (2010)Spurious hypercreatininemia: 28 neonatal foals (2000-2008). J. Vet.Emerg. Crit. Care 20, 244-249.
Chau, V., Poskitt, K.J. and Miller, S.P. (2009) Advanced neuroimagingtechniques for the term newborn with encephalopathy. Pediatr.Neurol. 40, 181-188.
Chew, L.J., Takanohashi, A. and Bell, M. (2006) Microglia andinflammation: impact on the development of brain injuries. Ment.Retard. Dev. Disabil. Res. Rev. 12, 105-112.
Cilio, M.R. and Ferriero, D.M. (2010) Synergistic neuroprotective therapieswith hypothermia. Semin. Fetal Neonatal. Med. 15, 293-298.
Clement, S.F. (1985) Behavioral alterations and neonatalmaladjustment syndrome in the foal. Proc. Am. Assoc. EquinePractnrs. 31, 145-148.
Cowan, F., Rutherford, M., Groenendaal, F., Eken, P., Mercuri, E.,Bydder, G.M., Meiners, L.C., Dubowitz, L.M. and de Vries, L.S. (2003)Origin and timing of brain lesions in term infants with neonatalencephalopathy. Lancet 361, 736-742.
Cummin, S., Carrington, C., Fitzpatrick, E. and Duggan, V. (2008)Ascending placentitis in the mare-a review. Irish Vet. J. 5, 307-313.
Dickey, E.J., Long, S.N. and Hunt, R.W. (2011) Hypoxic ischaemicencephalopathy-what can we learn from humans? J. Vet. Intern.Med. 25, 1231-1240.
Elmahdy, H., El-Mashad, A.R., El-Bahrawy, H., El-Gohary, T., El-Barbary,A. and Aly, H. (2010) Recombinant erythropoiten in asphyxianeonatorum: pilot trail. Pediatrics 125, 1135-1142.
Fan, X., Kavelaars, A., Helinen, C.J., Groenendaal, F. and van Bel, F.(2010) Pharmacological neuroprotection after perinatal hypoxic-ischaemic brain injury. Curr. Neuropharm. 8, 324-334.
Feng, Z., Liu, J. and Ju, R.R. (2013) Hyperbaric oxygen treatmentpromotes neural stem cell proliferation in the subventricular zone
© 2015 EVJ Ltd
162 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
of neonatal rats with hypoxic-ischaemic brain damage. NeuralRegen. Res. 8, 1220-1227.
Ferrell, E.A., Gavin, P.R., Tucker, R.L., Sellon, D.C. and Hines, M.T. (2002)Magnetic resonance for evaluation of neurologic disease in 12horses. Vet. Radiol. Ultrasound. 43, 510-516.
Furr, M. (1996) Perinatal asphyxia in foals. Comp. Cont. Educ. Pract.Vet. 18, 1342-1351.
Furr, M., Tinker, M.K. and Edens, L. (1997) Prognosis for neonatal foals inan intensive care unit. J. Vet. Intern. Med. 11, 183-188.
Galvin, N. and Collins, D. (2004) Perinatal asphyxia syndrome in thefoal: review and a case report. Irish Vet. J. 57, 707-714.
Glass, H.C., Glidden, D., Jeremy, R.J., Barkovich, A.J., Ferriero, D.M.and Miller, S.P. (2009) Clinical Neonatal Seizures are independentlyassociated with outcome in infants at risk for hypoxic-ischaemicbrain injury. J. Pediatr. 155, 318-323.
Globus, M.Y., Alonso, O., Deitrich, W.D., Busto, R. and Ginsberg, M.D.(1995) Glutamate release and free radical production followingbrain injury: effects of posttraumatic hypothermia. Neurochem. 65,1704-1711.
Gressans, P., Dingley, J., Plaisant, F., Porter, H., Schwendimann, L.,Verney, C., Tooley, J. and Thoresen, M. (2008) Analysis of neuronal,glial, endothelial, axonal and apoptotic markers followingmoderate therapeutic hypothermia and anesthesia in thedeveloping piglet brain. Brain Pathol. 18, 10-20.
Grow, J. and Barks, J.D.E. (2002) Pathogenesis of hypoxic-ischemiccerebral injury in the term infant: current concepts. Clin. Perinatal29, 585-602.
Hellstr€om-Westas, L., Ros�en, I., deVries, L.S. and Greisen, G. (2006)Amplitude-integrated EEG classifications and interpretation inpreterm and term infants. Neo. Review 7, e76-e87.
Hirst, J.J., Palliser, H.K., Yates, D.M., Yawno, T. and Walker, D.W. (2008)Neurosteroids in the fetus and neonate: potential protective role incompromised pregnancies. Neurochem. Int. 52, 602-610.
Holtan, D.W., Houghton, E., Silver, M., Fowden, A.I., Ousey, J. andRossdale, P.D. (1991) Plasma progestagens in the mare, fetus andnewborn foal. J. Reprod. Fertil. Suppl. 44, 517-528.
Houghton, E., Holtan, D., Grainger, L., Voller, B.E., Rossdale, P.D. andOusey, J.C. (1991) Plasma progestagen concentrations in thenormal and dysmature newborn foal. J. Reprod. Fertil. Suppl. 44,609-617.
Hutton, L.C., Abbass, M., Dickinson, H., Ireland, Z. and Walker, D.W.(2009) Neuroprotective properties of melatonin in a model of birthasphyxia in the spiny mice (Acomys cahirinus). Dev. Neurosci. 31,437-451.
Inder, T.E. and Volpe, J.J. (2000) Mechanisms of perinatal brain injury.Seminn. Neonatal. 5, 3-16.
Jacobs, S.E., Hunt, R., Tarnow-Mordi, W.O., Inder, T.E. and Davis, P.G.(2007) Cooling for newborns with hypoxic ischaemicencephalopathy. Cochrane Database of Systemic Reviews 4,Article no: CD003311. DOI:10.1002/14561858.CD003311.pub2.
Kurinczuk, J.J., White-Koning, M. and Badawi, J. (2010) Epidemiology ofneonatal encephalopathy and hypoxic-ischaemicencephalopathy. Early Human Dev. 86, 329-338.
LeBlanc, M.M., Giguere, S., Brauer, K., Paccamonti, D.L., Horohov,D.W., Lester, G.D., O’Donnell, L.J., Sheerin, B.R., Pablo, L. andRodgerson, D.H. (2002) Premature delivery and ascendingplacentitis is associated with increased expression of placentalcytokines and allantoic fluid prostaglandin expression E2 and F2.Theriogenol. 58, 841-844.
LeBlanc, M.M., Macpherson, M. and Sheerin, P. (2004) Ascendingplacentitis: what we know about pathophysiology, diagnosis andtreatment. Proc. Am. Assoc. Equine Practnrs 50, 127-143.
LeBlanc, M.M., Giguere, S., Lester, G.D., Brauer, K. and Paccamonti,D.L. (2013) Relationship between infection, inflammation andpremature parturition in mares with placentitis. Equine Vet. J. 44,Suppl. 41, 8-14.
Mackay, R.J. (2005) Neurologic disorders of neonatal foals. Vet. Clin.Equine. 21, 387-406.
McPherson, R.J. and Juul, S.E. (2008) Recent trends in erythropoietin-tin-induced brain protection in neonatal hypoxia-ischaemia ratmodel. J. Cereb. Blood Flow Metabol. 24, 259-278.
Mishra, O.P., Zanelli, S., Ohnishi, S.T. and Delivoria-Papadopoulos, M.(2002) Hypoxic-induced generation of nitric oxide free radicals incerebral cortex of newborn guinea pigs. Neurochem. Res. 25,1559-1565.
Palmer, C., Roberts, R.L. and Bero, C. (1994) Deferoxamineposttreatment reduces ischaemic brain injury in neonatal rats.Stroke 25, 1039-1045.
Plane, J.M., Shen, Y., Pleasure, D.E. and Deng, W. (2010) Prospects forMinocycline neuroprotection. Arch. Neurol. 67, 1442-1448.
Reynolds, E.B. (1930) Clinical notes on some conditions met within themare following parturition and in the newly born foal. Vet. Rec. 10,277.
Ringger, N.C., Giguere, S., Morresey, P.R., Yang, C. and Shaw, G.(2011) Biomarkers of brain injury in foals with hypoxic-ischemicencephalopathy. J. Vet. Intern. Med. 25, 132-137.
Rohrback, B.W., Buchanan, B.R., Drake, J.M., Andrews, F.M., Bain, F.T.,Byars, D.T., Bernard, W.V., Furr, M.O., Paradis, M.R., Lawler, J.,Gigu�ere, S. and Dunkel, B. (2006) Multivariable model to estimatethe probability of discharge in hospitalized foals that are 7 days ofage or less. J. Am. Vet. Med. Assoc. 228, 1748-1756.
Rosenbaum, P., Paneth, N., Leviton, A., Goldstein, M., Bax, M.,Damiano, D., Dan, B. and Jacobsson, B. (2007) A report: thedefinition and classification of cerebral palsy April 2006. Dev. Med.Child Neurol. Suppl. 49, 480.
Rossdale, P.D. (1972) Modern concepts of neonatal disease in foals.Equine Vet. J. 4, 117.
Rossdale, P.D. and Leadon, D.P. (1975) Equine neonatal disease: areview. J. Reprod. Fertil. 23, 658-661.
Rossdale, P.D., Ousey, J.C., McGladdery, A.J., Prandi, S., Holdstock, N.,Grainger, L. and Houghton, E. (1995) A retrospective study ofincreased plasma progestagen concentrations in compromisedneonatal foals. Reprod. Fertil. Dev. 7, 567-575.
Shadid, M., Buonocore, G., Groenendaal, F., Moison, R., Ferrali, M.,Berger, H.M. and van Bel, F. (1998) Effect of deferoxamine andallopurinol on non-protein-bound iron concentrations in plasmaand cortical brain tissue of newborn lambs following hypoxiaischaemia. Neurosci. Lett. 22, 5-8.
Shalak, L.F., Laptook, A.R., Jafri, H.S., Ramilo, O. and Perlman, J.M.(2002) Clincal chorioamnionitis, elevated cytokines, and braininjury in term infants. Pediatrics 110, 673-680.
Slovis, N. (2006) Hyperbaric oxygen therapy in horses. Proc. A.C.V.I.M.pp 150-152.
Sun, Y., Zhou, C., Polk, P., Nanda, A. and Zhang, J.H. (2004) Mechanismsof erythropoietin-induced brain protection in neonatal-ischaemiarat model. J. Cereb. Blood Flow Metab. 24, 259-270.
Tang, X.N. and Yenari, M.A. (2010) Hypothermia as a cytoprotectivestrategy in ischaemic tissue injury. Ageing Res. Rev. 9, 61-68.
Toth, B., Aleman, M., Brosnan, R.J., Dickinson, P.J., Conley, A.J.,Stanley, S.D., Nogradi, N., Williams, C.D. and Madigan, J.E. (2012)Evaluation of squeeze-induced somnolence in neonatal foals. Am.J. Vet. Res. 73, 1882-1890.
Tsutsui, K. (2008) Neurosteroids in the Purkinje cell: biosynthesis, modeof action and functional significance. Mol. Neurobiol. 37, 116-125.
Vaala, W.E. (1994) Peripartum asphyxia. Vet. Clin. North Am. EquinePract. 10, 187-218.
Vaala, W.E. (1999) Peripartum asphyxia syndrome in foals. Proc. Am.Assoc. Equine Practnrs. 45, 247-253.
Vaala, W.E. (2009) Perinatal asphyxia syndrome in foals compendium.Compendium Equine: Continuing Educ. Veterinarians. 4, 134-140.
Vannucci, S.J. and Hagberg, H. (2004) Review Hypoxic-ischaemia inthe immature brain. J. Expt. Biol. 207, 3149-3154.
Volpe, J. (1996) Hypoxic-ischaemic encephalopathy: Biochemicaland physiological aspects. In: Neurology of the Newborn, Ed: J.Volpe, Saunders, Philadelphia. pp 211-259.
© 2015 EVJ Ltd
163EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Volpe, J.J. (2001) Perinatal brain injury: from pathogenesis toneuroprotection. Ment Retard Dev Disabil Res Rev. 7, 56-64.
Wang, X.L., Zhao, Y.J., Yang, Y.J., Xie, M. and Yu, X.H. (2008)Therapeutic window of hyperbaric oxygen therapy for hypoxicischaemic brain damage in new born rats. Brain Res. 10, 87-94.
Welin, A.K., Svedin, P., Lapatto, R., Sultan, B., Hagberg, H., Gressens, P.,Kjellmer, I. and Mallard, C. (2007) Melatonin reduces inflammationand cell death in white matter in the mid-gestation fetal umbilicalcord occlusion. Pediatr. Res. 61, 153-158.
Wingberg, I.D., van der Ree, M. and van Someren, P. (2013) Theapplicability of ambulatory electroencephalography (AEEG) inhealthy horses and horses with abnormal behavior or clinical signsof epilepsy. Vet. Q 33, 121-131.
Wong, D.M., Wilkens, P.A., Bain, F.T. and Brockus, C.W. (2011) Neonatalencephalopathy in foals. Comp. Cont. Educ. Pract. Vet. 9, E1-E9.
Yeargin-Allsopp, M., Van Naarden, K., Doernberg, N.S., Benedict, R.E.,Kirby, R.S. and Durkin, M.S. (2008) Prevalence of cerebral palsy in 8-year-old children in three areas of the United States in 2002: amultisite collaboration. Pediatrics 121, 537-554.
Zanelli, S.A. (2014) Hypoxic ischaemic encephalopathy. Emedicine.Medscape.com/article/973501-overview.
Zemke, D. and Majiid, A. (2004) The potential of minocycline forneuroprotection in human neurologic disease. Clin.Neuropharmacol. 102, 9936-9941.
Zhou, B.Y., Lu, G.J., Huang, Y.Q., Ye, Z.Z. and Han, Y.K. (2008)Hyperbaric oxygen therapy under different pressures on neonatalhypoxic ischemic encephalopathy. Zhongguo Dan Dai Er Ke ZaZhi. 10, 133-135.
© 2015 EVJ Ltd
164 EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Basic Arthroscopic Surgery course teaches the basic principles of equine arthroscopy in the carpus and dorsal fetlock joint including instrumentation and basic techniques, diagnostic arthroscopy of the carpus and fetlock joints; arthroscopic surgery of the carpus for osteochondral chip fragment removal and arthroscopic surgery of the dorsal compartment of the fetlock joint for proximal P1 chips, villonodular synovitis and OCD. Registration Fee: $850
Advanced Arthroscopic Surgery includes four laboratories to give optimal practical information on how to do advanced arthroscopy and with particular emphasis on approaches for internal fixation of fractures in the carpus and fetlock, new arthroscopic techniques in the femoropatellar and femorotibial joints, advanced arthroscopic surgery of the hock and important tenoscopic surgical techniques as well as bursoscopy. Registration Fee: $1,250.00
Basic & Advanced Equine Arthroscopic Surgery Registration Fee: $1,450.00 (combined) Other Courses offered: Diagnostic Stifle Course: Ultrasound & Standing Arthroscopy—July , 201
Basic Equine Arthroscopic Surgery - July 2 , 201
Advanced Equine Arthroscopic Surgery - July 2 -2 , 201
Enrollment is limited. Register Early! You must enroll prior to the course date. Online registration is available as well as registration by phone or fax. Please check individual course registration instructions. http://www.cvmbs.colostate.edu/ce/arthroscop

Review Article
Nutritional management and practical feeding of the orphan foalS. J. Stoneham†*, P. Morresey‡ and J. Ousey§
†Cheshire Equine Clinic, Tattenhall, Cheshire, UK; ‡Rood and Riddle Equine Hospital, Lexington, Kentucky, USA;and §Beaufort Cottage Stables, Rossdale and Partners, Newmarket, Suffolk, UK.*Corresponding author email: [email protected]
Keywords: horse; foal; nutrition; orphan; growth
SummaryFoals are dependent on a milk-based diet for the first 3–4 months of life. If they are orphaned during this period theyrequire appropriate nutritional and behavioural managementto allow them to develop into sound, well-grown horses andponies with well established normal behavioural patterns. Inorder to meet these needs it is necessary to understand themetabolic requirements of the foal and the composition ofmares’ milk. Usually managing these foals requires short-term,emergency feeding of the foal while a long-term option issought. Long-term options include use of a foster mare,induction of lactation in a parous, barren mare or handrearing with suitable equine company. It is important tomonitor growth and development of these foals to ensure thatover the long term their nutritional needs are being met toallow normal growth and development.
Introduction
A foal may become orphaned at any time prior to normalweaning age around 5–6 months, foals younger than 3–4 months require special nutritional management due to theirreliance on a milk based diet.
Compared to mature horses, young foals are poorlyadapted to cope with periods of nutritional deficit. Energystores are minimal when compared to the neonates of otherspecies (Fowden et al. 1990). Glycogen stores in the neonate,contained in liver and muscle, are only sufficient to maintainnormal body temperature for less than 1 h (Ousey et al.1992).
Foals consume a considerable amount of milk – between20 and 25% of bodyweight/day (Oftedal et al. 1983; Martinet al. 1992).
Over the first 2–3 months, digestion is principally smallintestinal with lactase being the main hydrolytic enzyme(Roberts 1975). A recent study (Faubladier et al. 2013)showed the establishment of bacterial carbohydratedegrading capacity by age 2 months. However, it wassuggested that it was not comparable to the adult in thepreweaning period. Over the first 3–4 months, maltase andamylase are the predominant hydrolytic enzymes (Roberts1975) and the foal becomes increasingly reliant on hindgutfermentation. Before the establishment of cellulolytic andfibrinolytic bacteria at age about 2 months, foals are poorlyadapted to a herbivorous diet (Faubladier et al. 2013). As aresult, management of orphan foals younger than 3 monthsrequires special consideration, to enable them to continue togrow and develop in a similar way to foals reared on theirdams.
Understanding the orphan foal’s nutritionalrequirements
Metabolic considerationsUnderstanding the foals’ metabolic requirements is importantin order to calculate the nutritional needs of healthy orphanfoals. The metabolic energy demands of neonatal foals arehigh compared to adult horses and, therefore, their milkintakes need to be high to satisfy this energy demand. Mares’milk provides the foal with all its energy and nutrition duringthe first few weeks post partum and it remains the primarynutrient source until weaning (Martin et al. 1992; Grace et al.1999). To calculate the milk energy requirements of orphanfoals, in simple terms their gross energy (GE) intakes mustexceed energy lost through processes of ingestion anddigestion, energy expended on metabolism, activity andthermoregulation, in order for net energy to be retained forreplenishment of energy stores and growth of the foal (Fig 1).Mean GE intakes in healthy 2- to 7-day-old Thoroughbred (TB)foals sucking from their dams are 29.7–32.8 MJ/day or 544–593 kJ/kg bwt (Ousey et al. 1996). This equates to drinkingbetween 11.6 and 13.5 l milk/day or 23% bwt as milk, and iscomparable to previously published values (20 to 27% foalbwt) for TB and Quarter Horse foals aged <2 weeks (Gibbset al. 1982; Oftedal et al. 1983; Martin et al. 1992). Mares’ milkis digested very efficiently in healthy neonatal foals and only2–4% GE is lost via digestive processes (Table 1). Thiscompares with about 37% digestible losses in adult horses fedconcentrate feeds (Pagan and Hintz 1986). When raisingorphan foals, the aim is to provide similar milk volumes andGE intakes as mare nursed foals in order that growth ratesmay be maintained within the normal range. RecommendedGE intakes for healthy neonatal foals on artificial feedingregimes are about 500–630 kJ/kg bwt (Vaala 2011). Mares’milk replacers have a similar energy density to mares’ milk ona dry matter basis (about 21 MJ/kg dry mass). When dilutedaccording to manufacturer’s recommendations, the GE (3.1–3.8 MJ/l) and dry matter content (11–20%) may be higherthan that of mares’ milk (GE = 2.4 MJ/l, dry matter = 10–12%)(Naylor and Bell 1985; Ousey 2003; Buechner-Maxwell 2005).Therefore it may be necessary to dilute formula feeds furtherbut increase intake to satisfy the foal’s energy and nutritionaldemands. Initially orphan foals may be reluctant to acceptformula feed or milk from other species e.g. goats’ milk, butusually fluid and GE intakes comparable to those of marenursed foals are achieved within 2–4 days (Table 1).Measured GE intakes for orphan pony foals fed milk replacerfrom birth were below those of mare nursed foals (Table 1) onDay 2 post partum, although fluid intakes were comparable(mean � s.e.m.: 5.9 � 0.2 and 5.4 � 0.4 l/day). There is some
© 2016 EVJ Ltd
165EQUINE VETERINARY EDUCATION / AE / MARCH 2017
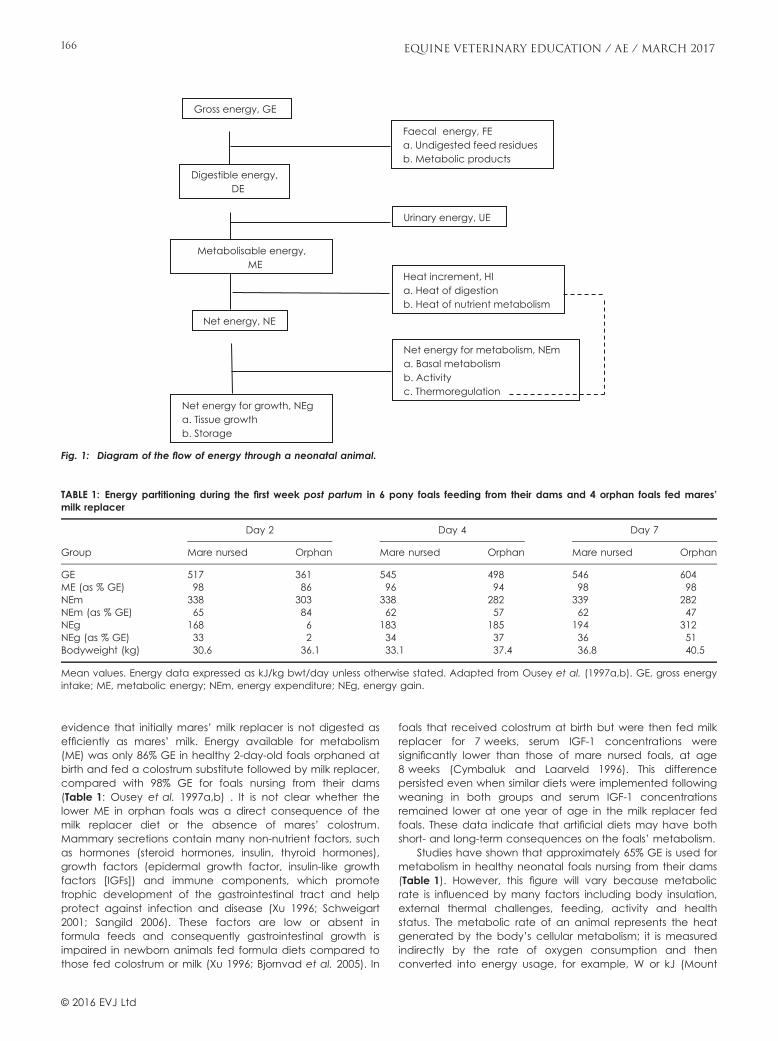
evidence that initially mares’ milk replacer is not digested asefficiently as mares’ milk. Energy available for metabolism(ME) was only 86% GE in healthy 2-day-old foals orphaned atbirth and fed a colostrum substitute followed by milk replacer,compared with 98% GE for foals nursing from their dams(Table 1: Ousey et al. 1997a,b) . It is not clear whether thelower ME in orphan foals was a direct consequence of themilk replacer diet or the absence of mares’ colostrum.Mammary secretions contain many non-nutrient factors, suchas hormones (steroid hormones, insulin, thyroid hormones),growth factors (epidermal growth factor, insulin-like growthfactors [IGFs]) and immune components, which promotetrophic development of the gastrointestinal tract and helpprotect against infection and disease (Xu 1996; Schweigart2001; Sangild 2006). These factors are low or absent informula feeds and consequently gastrointestinal growth isimpaired in newborn animals fed formula diets compared tothose fed colostrum or milk (Xu 1996; Bjornvad et al. 2005). In
foals that received colostrum at birth but were then fed milkreplacer for 7 weeks, serum IGF-1 concentrations weresignificantly lower than those of mare nursed foals, at age8 weeks (Cymbaluk and Laarveld 1996). This differencepersisted even when similar diets were implemented followingweaning in both groups and serum IGF-1 concentrationsremained lower at one year of age in the milk replacer fedfoals. These data indicate that artificial diets may have bothshort- and long-term consequences on the foals’ metabolism.
Studies have shown that approximately 65% GE is used formetabolism in healthy neonatal foals nursing from their dams(Table 1). However, this figure will vary because metabolicrate is influenced by many factors including body insulation,external thermal challenges, feeding, activity and healthstatus. The metabolic rate of an animal represents the heatgenerated by the body’s cellular metabolism; it is measuredindirectly by the rate of oxygen consumption and thenconverted into energy usage, for example, W or kJ (Mount
Gross energy, GE
Digestible energy, DE
Metabolisable energy, ME
Net energy, NE
Net energy for growth, NEga. Tissue growthb. Storage
Faecal energy, FEa. Undigested feed residuesb. Metabolic products
Urinary energy, UE
Net energy for metabolism, NEma. Basal metabolismb. Activityc. Thermoregulation
Heat increment, HIa. Heat of digestionb. Heat of nutrient metabolism
Fig. 1: Diagram of the flow of energy through a neonatal animal.
TABLE 1: Energy partitioning during the first week post partum in 6 pony foals feeding from their dams and 4 orphan foals fed mares’milk replacer
Group
Day 2 Day 4 Day 7
Mare nursed Orphan Mare nursed Orphan Mare nursed Orphan
GE 517 361 545 498 546 604ME (as % GE) 98 86 96 94 98 98NEm 338 303 338 282 339 282NEm (as % GE) 65 84 62 57 62 47NEg 168 6 183 185 194 312NEg (as % GE) 33 2 34 37 36 51Bodyweight (kg) 30.6 36.1 33.1 37.4 36.8 40.5
Mean values. Energy data expressed as kJ/kg bwt/day unless otherwise stated. Adapted from Ousey et al. (1997a,b). GE, gross energyintake; ME, metabolic energy; NEm, energy expenditure; NEg, energy gain.
© 2016 EVJ Ltd
166 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

1979). Because the metabolic rate varies under differentconditions, it should be defined clearly. Basal metabolic ratein adults (i.e. metabolic heat produced at rest [recumbent]under neutral thermal conditions and >18 h after the lastfeed) cannot be obtained under field conditions whereresting metabolic rates are usually recorded (i.e. partially fed,quiet [recumbent or standing] at prevailing ambienttemperatures). In neonatal foals that feed several times everyhour, resting metabolic rates are rarely measured in theunfed state. Compared to adults, neonatal animals havehigher resting metabolic rates per kg bodyweight becausethey have a larger body surface area to volume ratio andless body insulation which means they are less tolerant ofextremes in the thermal environment (Mount 1979). Theaverage metabolic rate of standing TB and pony foals agedone day under nonthermoneutral conditions is about 153 and105 W/m2, respectively (Ousey et al. 1991). These valuesdecrease by about a third to 110 and 70 W/m2, respectively,when they are recumbent in thermoneutral conditions.Average metabolic rates measured over 8 h in healthyorphan pony foals were lower (109–114 W/m2) than those ofpony foals raised with their dams (128–134 W/m2) during thefirst week post partum (Ousey et al. 1997a,b). Thesedifferences could not be explained by air temperature oractivity but the feeding interval was longer in the orphanfoals (2–3 h). After feeding heat production increases byabout 10% associated with the processes of ingestion anddigestion of food (termed heat increment of feeding, Fig 1);therefore, mare-nursed foals feeding frequently from theirdams tend to have higher metabolic rates. Infrequentfeeding causing lower metabolic rates, and improveddigestive efficiency in older orphan foals, means their rates ofenergy storage were greater compared with those of marenursed foals (Table 1). If sustained, this would result in greaterenergy storage and growth in the orphan foals. However,most long-term nutritional studies have reported comparablegrowth rates between formula-fed, and mare nursed, foals(Knight and Tyznik 1985; King and Nequin 1989; Cymbaluket al. 1993).
The thermal environment has a substantial impact onmetabolic rate. Metabolic rate rises as air temperaturesdecline below the lower critical temperature (Mount 1979).The metabolic rates in neonatal pony foals exposed to airtemperatures of 5°C are double those measured at airtemperatures above 20°C. Calculated lower criticaltemperature is higher for pony compared to TB foals (20°C vs.10°C, respectively) because pony foals have a lower restingmetabolic rate and, therefore, are less cold tolerant than TBfoals (Ousey et al. 1991). Consequently milk intakes will needto increase in pony foals at air temperatures <20°C to meettheir metabolic energy expenditure whereas the sameresponse will only occur in TB foals when air temperatures arebelow 10°C. The main mechanism of increased heatproduction in foals is shivering thermogenesis. In contrast,neonates of many other species generate heat viauncoupling protein in brown adipose tissue (nonshiveringthermogenesis) but foals appear to have little or no brownadipose tissue (Symmonds et al. 1995; M.E. Symmonds andJ.C. Ousey, unpublished observations). The ability to increasetheir metabolic rate in the cold is influenced by the foal’sbody insulation, i.e. thickness of subcutaneous fat andthickness of their hair coat, which varies between individualfoals. Estimates for nonstructural body fat range from 1–3%,
which, for a well-nourished foal, would provide sufficientenergy to last >24 h (Meyer and Ahlswede 1976). Thereforehealthy orphan foals can maintain their metabolic ratesunder normal conditions for several hours even in theabsence of feeding. However, body energy stores are likelyto be depleted in foals with low birth weights or those thathave been challenged in utero. Moreover, birth hypoxia orplacental insufficiency inhibits heat production in newbornanimals (Eales et al. 1982; Mellor 1993). Foals suffering withhypoxic ischaemic encephalopathy, sepsis or prematurityhave low metabolic rates compared with healthy foals andfrequently cannot maintain their body temperature evenwhen provided with additional warmth and insulation (Ouseyet al. 1997a,b; Jose-Cunilleras et al. 2012). The effects of thethermal environment on metabolic rate have not beenspecifically investigated in healthy orphan foals fed milkreplacer. However, Cymbaluk (1990) reported that MErequirements in 7-month-old weanling colts were 32% greaterin cold winter conditions (mean �5°C) than those of coltsmaintained at a warmer +10°C.
Activity level (time spent standing, sleeping, exercising,udder seeking) clearly increases metabolic rate andnutritional demands. It is difficult to measure oxygenconsumption in mobile foals and, therefore, metaboliccalculations must be based on measurements collected fromfoals when standing and recumbent. Many factors affectenergy metabolism and utilisation of nutrients in young foalsand more work is needed to monitor the short- and long-termeffects of formula diets on the endocrine and metabolicresponses of growing orphan foals.
Mares’ milk is best?
Mares’ milk provides the best nutrition for the young foalbecause its composition is unique compared to milk fromother domestic animals.
Mare’s milk compositionMare’s milk is significantly lower in fat when compared withthat of other species. This fat is dispersed throughout theliquid and organised in globules approximately 3 lm indiameter (Kharitonova 1978). These globules are complexmultilayered structures consisting of proteins, phospholipidsand glycoproteins (Solaroli et al. 1993). Triglyceride levels arelower than in cow’s milk (approximately 80% vs. 98%respectively) (Pastukhova and Gerbeda 1981; Doreau andBoulot 1989). Mare’s milk contains higher levels of free fattyacids (Pastukhova and Gerbeda 1981) and phospholipids(Kharitonova 1978). Shorter chain fatty acids (less than C16)are higher in mare’s milk, which is similar to ruminants butdiffers from other monogastric species, probably due todiffering dietary substrates (herbivorous) in the horse (Linzellet al. 1972). Some longer chain (C18) fatty acids, such asstearic acid, are relatively low, whereas those derived fromforages, such as linoleic and linolenic acids, are relativelyhigh (Doreau and Boulot 1989). Unsaturated fatty acidcontent is higher in mare’s milk than cow’s milk offering anutritional advantage (Solaroli et al. 1993).
Protein makeup differs substantially from cow’s milk(Csap�o-Kiss et al. 1995), although total crude proteinpercentage is similar to both cow’s and goat’s milk. Withrespect to cow’s milk, the whey protein fraction is almostdouble at around 40%. Casein quantity, however, is
© 2016 EVJ Ltd
167EQUINE VETERINARY EDUCATION / AE / MARCH 2017

approximately half that of cow’s milk, with a different make-up consisting of a higher percentage of b-casein. Micellesare also considerably larger in the mare than the cow. Whilestudies have detected differences between breeds withrespect to protein levels, including whey and casein fractions,the effects of dietary influences on results have not beendetermined (Martuzzi and Doreau 2006).
The predominant carbohydrate is lactose, which is muchhigher than that found in cow’s milk (Doreau and Boulot1989). However, overall energy content is lower than cow’smilk. Other sugars present include very low levels of glucoseand galactose. Lactose content of milk varies throughoutlactation, and is almost uniformly found to increase withincreasing duration of lactation (Doreau and Boulot 1989;Doreau et al. 1990).
Mineral and ash content are low in mare’s milk. Totalsolids, mineral and ash concentrations peak during the firstweek of lactation, then steadily decline (Schryver et al. 1986).Other equids (donkeys) do not necessarily follow this patternand are unaffected by dietary trace elementsupplementation (Fantuz et al. 2013). The concentration andratio between the elements in mare milk during ongoinglactation is continually changing and determination of theaverage mineral content of milk for comparative purposes istherefore impossible. Little difference has been foundbetween the milk of various breeds of horses, with only ashcontent being lower in the draught breeds when comparedwith light breeds (Linton 1937).
In addition to being nutritive, the ingestion of milk hasconsiderable beneficial effects in many species. Local gutprotectants, cytokines, soluble microbial receptors andantibacterial enzymes are present in milk (Hanson andKorotkova 2002). Lysozyme is one compound known to havenonspecific but bacteriostatic effects within the gut(Goldman 1993). Lactoferrin is also present, albeit in lowquantities (Solaroli et al. 1993). Enteral feeding also hasdevelopmentally beneficial effects in other species and,while not proven in the foal, growth factors in milk promotehealthy development of digestive organs and intestinalmucosa (Lucas et al. 1986). Mare’s milk has been shown tocontain IGF-1, which stimulates enteral development(Cymbaluk and Laarveld 1996).
Donkey milk is grossly similar in composition to mares’ milk,with the exception of increased lysozyme content andcomposition of whey proteins (Salimei et al. 2004).
Practical management of the orphan foal
When looking at the options for an orphan foal it isimportant to consider both the foal’s nutritional requirementsand its welfare. Development of normal behaviouralpatterns are vital if the foal is to mature into a ‘happyathlete’. Hand-reared foals with inadequate equinecompany can develop into mature horses with poor socialskills. Some horses may develop dangerous and abnormalbehaviour towards humans (S.J. Stoneham, unpublishedobservation; Diehl 2015). This can make them unsuitable fortheir intended use.
It is also important not to overlook their exerciserequirements. It is well recognised that adequate exerciseover the first few months of life are vital for the developmentof a healthy, durable musculoskeletal system (Kurvers et al.2006; Lepeule et al. 2013). Complete recommendations on
appropriate behavioural and exercise requirements arebeyond the scope of this article.
Meeting the foal’s short-term requirementsWhen dealing with an orphaned newborn foal it essential toensure that it has received 0.5–2 l of good quality colostrumin the first 4 h post partum. The quantity required is dictatedby bodyweight of the foal and IgG concentration of thecolostrum. Colostral quality should be assessed using arefractometer or colostrometer.
In the short-term (first 2–3 days), orphan foals can bebucket or bowl fed mare milk replacer while a suitable long-term option is sought. In an emergency, either goat’s milk orcow’s semi-skimmed milk with the addition of 20 g/l dextrosecan be used. Foals usually require some patient training todrink from a bucket or feed scoop, but the authors considersthis preferable to bottle feeding, which can increasehumanisation and, if operator technique is poor or the foalhas any degree of pharyngeal dysfunction, aspirationpneumonia can develop.
To meet energy requirements, the newborn foal sucklesthe mare up to 7 times per hour within the first week of life,decreasing to approximately once per hour at age 6 months(Carson and Wood-Gush 1983). This is an impracticalschedule at which to feed an orphan neonatal foal;therefore trade-offs must be made with respect to frequencyand amount (see Table 2).
Long-term solutionsUse of foster mareIn most situations, in foals younger than 2–3 months, the useof a suitable foster mare best meets the nutritional and socialneeds of an orphan foal. This may be a mare that has losther foal or a ‘professional’ foster mare.
It is important to consider the following when selecting apotential foster mare:• Temperament – the mare should have previously
successfully reared a foal, be calm and easy to handlewith good maternal behaviour.
• Disease risk – care must be taken to evaluate the risk ofinfectious diseases such as equine herpesvirus-1 andstrangles
• Stage of lactation – ideally it should match the age of thefoal; however, this is not insurmountable and the use ofcreep feed for the foal will help when a mare in latelactation is used for a neonatal foal.
Fostering is labour intensive and may take several days;however, in the long term, it is cost effective. Techniques arewell described (Kelly 1999; Stoneham 2013).
Induction of lactation and fostering with a multiparous barrenmare
TABLE 2: Example of short term feeding schedule for a healthy50 kg newborn orphan foal. (Ousey et al. 1996)
Age Frequency of feeding Volume of mares milk (l/day)
1–2 days Hourly 8–123–7 days 2 hourly 11.5–13.5
If milk replacer is used, dilution needs to be calculated based onmanufacturer’s recommended daily dry weight of milk powder.
© 2016 EVJ Ltd
168 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

This technique, described by Daels et al. (2002), Steiner(2006), Daels (2014) and Korosue et al. (2012), is whenlactation is induced pharmacologically in a nonparturientmare. It has also been described in barren jennies(Quartuccio et al. 2015). Dopamine-D2 antagonists(domoperidone or sulpiride) are used to increaseendogenous prolactin secretion in parous, cycling barrenmares. Several techniques are described, and the availabilityof drugs will limit their use in some countries.
The following techniques have been used successfully bythe authors:• 1.1–2.2 mg/kg bwt domperidine per os q. 12 h, 10 mg
oestrogen i.m. q. 24 h and 150 mg progesterone i.m. q.24 h; this is continued until there is adequate milk supply.No milking may be necessary using this method (P.Morresey, unpublished observation).
• 5 mg dinoprost (for 500–600 kg mare) i.m. on Day 1followed by domperidone (1.1 mg/kg) twice daily; thisregime has been used with some success without milking(S.J. Stoneham, unpublished observation); however, milkingseveral times daily after 5–7 days treatment has beendescribed with this technique (Daels et al. 2002). Maresthat do not accept milking are usually not suitablecandidates. By Day 7, mares should be producing >3 l/dayand are ready for adoption. Domperidone is continued forno more than 7 days after adoption.
In the first few days, it is usually necessary to providesupplementary milk for the foal. Not all mares will produceadequate quantities of milk to rear a foal but can be used incombination with supplementation with a bucket and creepfeed. The authors consider this preferable to hand rearing asit meets the foal’s social needs as it can be managed in amore normal way and avoids the behavioural problemsassociated with hand rearing.
It is considered that mares that have raised several foals,exhibit good maternal behaviour and are gentle and calmare the best candidates. They should be healthy and in goodbody condition with a normal udder (Daels 2014). Atechnique for the use of prostaglandin F2a to inducematernal behaviour at the time of adoption is also described(Daels 2014) and has been used successfully by one of theauthors (P.J.S.).
This method is useful when a suitable foster mare is notavailable; however, it takes about 7 days to prepare themare during which time the foal’s needs must be met.
Hand rearingAlthough bucket reared foals grow satisfactorily it is harder tomeet their normal behavioural needs. Horses are very social,herd animals. Young foals develop a close bond with thedam over the first 2 weeks and, after 7–8 weeks, spendincreasing amounts of time with other equine companions,especially other foals in the group (McGreevy 2004).
Unless orphan foals are reared with equine company,they are likely to develop behavioural problems. Williams(1974) reported that orphan foals reared without equinecompany fail to respond to social signals from other horseslater in life and may show evidence of mal-imprinting. Theyalso can become over familiar with their handlers, failing torespect human personal space and can fail to move awayfrom the tactile stimuli as they must to become safe andresponsive working animals later in life (McGreevy 2004).
Providing continuous equine company, such as a docileolder pony will help an orphan foal to develop normalbehavioural patterns towards both other horses and humans.
What to feedThe ideal foal milk replacer would be nutritionally completeand compatible with the differing needs of the equineneonate compared to other large animal species. It wouldbe cost effective, suffer minimal degradation during storage,mix easily and once reconstituted avoid spoilage over theperiod offered. Importantly, it would be uniform betweenbatches as dietary inconsistencies are a major cause ofdiarrhoea. It would provide a similar energy, protein, andmineral density to mare’s milk when reconstituted at its finaldilution prior to feeding.
There is no commercially available milk replacer or milkfrom another species that can match the composition ofmare milk (Table 2). In the UK, mare milk replacers arerelatively expensive; when considering the cost of the optionsthis should be taken into consideration (Table 3).
The use of other species milk, chiefly goat or cow, canprovide acceptable nutrition if the differences (describedabove) are compensated for. To approximate mare’s milk,2% fat cow’s milk with 20 g of dextrose per litre can be used.Goat’s milk is highly palatable to foals and can also be useddespite differences in constituents; however, it benefits from asimilar addition of dextrose (Wilson 1988). Donkey milk is verysimilar to mare’s milk (Salimei et al. 2004); however, it is veryexpensive from commercial sources.
How to feedIt is important to maintain high standards of hygiene in thepreparation and storage of milk or milk replacer products. Allutensils and feeding buckets must be kept clean and unusedreplacer stored in a fridge between feeds.
Ousey (2003) recommends that, for the first 2 days postpartum, newborn foals are fed hourly, then every 2 h over thenext 12 days. The interval and volume per feed can beincreased gradually after this. Total dry weight of replacershould be fed in line with manufacturer’s recommendations;it may be appropriate for the first few days to increase thedilution of replacer as the foal adjusts to the new diet. Thetotal intake required in a 24 h period is calculated and thendivided into the appropriate number of feeds.
A less demanding technique is to offer the foal a regularamount in a bucket placed in an accessible location. This isusually accepted rapidly, although training for a few daysmay be needed. Up to 25% of bodyweight of milk replacerdiluted to 10% divided into 3–5 feedings daily was reported toallow appropriate growth rates with minimal occurrence ofdiarrhoea (King and Nequin 1989). This is generally consideredappropriate for older foals that are already consumingforage and creep feed.
While foals will mirror mare behaviour by attempting toeat solids, the gastrointestinal tract, particularly the largecolon, is initially unable to digest roughage and time isneeded for adaptation of the microbial population to enablethe foal to be supported as a herbivore.
However, to provide an environment more attune to thatof a mare-reared foal, provision of high quality leafy hay andcreep feed suitable for foals younger than 3 months to themilk replacer-fed foal is of great benefit. They should alsohave free access to a clean water source and forage from
© 2016 EVJ Ltd
169EQUINE VETERINARY EDUCATION / AE / MARCH 2017
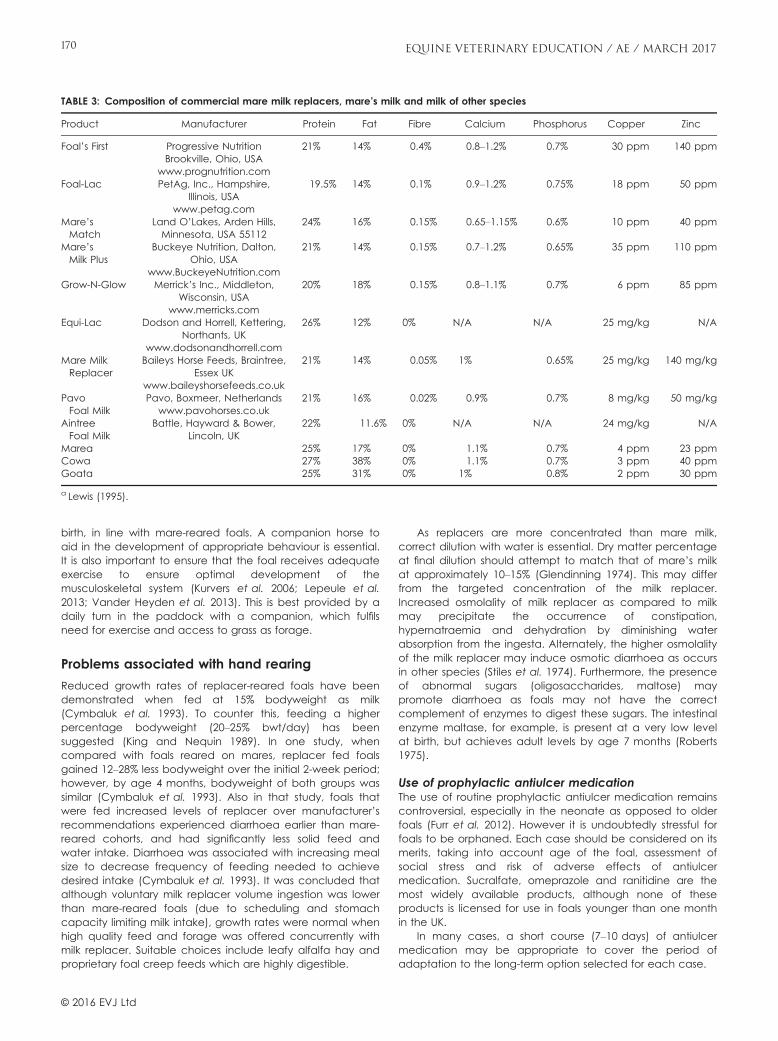
birth, in line with mare-reared foals. A companion horse toaid in the development of appropriate behaviour is essential.It is also important to ensure that the foal receives adequateexercise to ensure optimal development of themusculoskeletal system (Kurvers et al. 2006; Lepeule et al.2013; Vander Heyden et al. 2013). This is best provided by adaily turn in the paddock with a companion, which fulfilsneed for exercise and access to grass as forage.
Problems associated with hand rearing
Reduced growth rates of replacer-reared foals have beendemonstrated when fed at 15% bodyweight as milk(Cymbaluk et al. 1993). To counter this, feeding a higherpercentage bodyweight (20–25% bwt/day) has beensuggested (King and Nequin 1989). In one study, whencompared with foals reared on mares, replacer fed foalsgained 12–28% less bodyweight over the initial 2-week period;however, by age 4 months, bodyweight of both groups wassimilar (Cymbaluk et al. 1993). Also in that study, foals thatwere fed increased levels of replacer over manufacturer’srecommendations experienced diarrhoea earlier than mare-reared cohorts, and had significantly less solid feed andwater intake. Diarrhoea was associated with increasing mealsize to decrease frequency of feeding needed to achievedesired intake (Cymbaluk et al. 1993). It was concluded thatalthough voluntary milk replacer volume ingestion was lowerthan mare-reared foals (due to scheduling and stomachcapacity limiting milk intake), growth rates were normal whenhigh quality feed and forage was offered concurrently withmilk replacer. Suitable choices include leafy alfalfa hay andproprietary foal creep feeds which are highly digestible.
As replacers are more concentrated than mare milk,correct dilution with water is essential. Dry matter percentageat final dilution should attempt to match that of mare’s milkat approximately 10–15% (Glendinning 1974). This may differfrom the targeted concentration of the milk replacer.Increased osmolality of milk replacer as compared to milkmay precipitate the occurrence of constipation,hypernatraemia and dehydration by diminishing waterabsorption from the ingesta. Alternately, the higher osmolalityof the milk replacer may induce osmotic diarrhoea as occursin other species (Stiles et al. 1974). Furthermore, the presenceof abnormal sugars (oligosaccharides, maltose) maypromote diarrhoea as foals may not have the correctcomplement of enzymes to digest these sugars. The intestinalenzyme maltase, for example, is present at a very low levelat birth, but achieves adult levels by age 7 months (Roberts1975).
Use of prophylactic antiulcer medicationThe use of routine prophylactic antiulcer medication remainscontroversial, especially in the neonate as opposed to olderfoals (Furr et al. 2012). However it is undoubtedly stressful forfoals to be orphaned. Each case should be considered on itsmerits, taking into account age of the foal, assessment ofsocial stress and risk of adverse effects of antiulcermedication. Sucralfate, omeprazole and ranitidine are themost widely available products, although none of theseproducts is licensed for use in foals younger than one monthin the UK.
In many cases, a short course (7–10 days) of antiulcermedication may be appropriate to cover the period ofadaptation to the long-term option selected for each case.
TABLE 3: Composition of commercial mare milk replacers, mare’s milk and milk of other species
Product Manufacturer Protein Fat Fibre Calcium Phosphorus Copper Zinc
Foal’s First Progressive NutritionBrookville, Ohio, USA
www.prognutrition.com
21% 14% 0.4% 0.8–1.2% 0.7% 30 ppm 140 ppm
Foal-Lac PetAg, Inc., Hampshire,Illinois, USA
www.petag.com
19.5% 14% 0.1% 0.9–1.2% 0.75% 18 ppm 50 ppm
Mare’sMatch
Land O’Lakes, Arden Hills,Minnesota, USA 55112
24% 16% 0.15% 0.65–1.15% 0.6% 10 ppm 40 ppm
Mare’sMilk Plus
Buckeye Nutrition, Dalton,Ohio, USA
www.BuckeyeNutrition.com
21% 14% 0.15% 0.7–1.2% 0.65% 35 ppm 110 ppm
Grow-N-Glow Merrick’s Inc., Middleton,Wisconsin, USA
www.merricks.com
20% 18% 0.15% 0.8–1.1% 0.7% 6 ppm 85 ppm
Equi-Lac Dodson and Horrell, Kettering,Northants, UK
www.dodsonandhorrell.com
26% 12% 0% N/A N/A 25 mg/kg N/A
Mare MilkReplacer
Baileys Horse Feeds, Braintree,Essex UK
www.baileyshorsefeeds.co.uk
21% 14% 0.05% 1% 0.65% 25 mg/kg 140 mg/kg
PavoFoal Milk
Pavo, Boxmeer, Netherlandswww.pavohorses.co.uk
21% 16% 0.02% 0.9% 0.7% 8 mg/kg 50 mg/kg
AintreeFoal Milk
Battle, Hayward & Bower,Lincoln, UK
22% 11.6% 0% N/A N/A 24 mg/kg N/A
Marea 25% 17% 0% 1.1% 0.7% 4 ppm 23 ppmCowa 27% 38% 0% 1.1% 0.7% 3 ppm 40 ppmGoata 25% 31% 0% 1% 0.8% 2 ppm 30 ppm
a Lewis (1995).
© 2016 EVJ Ltd
170 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Use of probiotics in neonatal foalsHistorically, probiotics have been widely used in clinicalpractice in foals without any evidence for their safety orefficacy. It has been assumed that even if they areineffective they are likely to be harmless. A recentrandomised placebo controlled blinded field trial (Schosteret al. 2015) investigated the effect of probiotics onprevention of diarrhoea and shedding of Clostridium difficleand Clostridium perfringens in neonatal foals and reported anincreased incidence of diarrhoea and no difference inshedding of C. difficle or C. perfringens in foals givenprobiotics for first 3 weeks of life as opposed to the controlgroup. This confirms results of an earlier study (Weese andRousseau 2005) in which neonatal foals were given probioticsfor a week, the incidence of diarrhoea and diarrhoearequiring veterinary attention was higher in the probioticgroup as opposed to the control group.
These studies indicate that the use of probiotics inneonatal foals cannot be considered harmless, as bothstudies report increased incidence of diarrhoea anddiarrhoea associated with clinical abnormalities in the groupsof foals fed probiotics as opposed to control foals.
The use of probiotics in neonatal foals cannot beadvised in the absence of safety and efficacy data aboutthe specific product (Schoster et al. 2015). The use ofmannose oligosaccharide supplementation of mares as apreventative for neonatal foal diarrhoea has been reported(Ott 2002).
Care should be exercised, however, as the use of somebacterial probiotics with favourable in vivo activity has led toincreased incidence of diarrhoea in some cases (Weese andRousseau 2005).
Lactose intoleranceLactase is present in the brush border of the cells situated atthe tips of the intestinal villi. Detectable in the fetus, maximallevels are present at birth (Roberts 1975). A steady declinethen occurs beginning at age 4 months (Roberts 1975).Lactase is essential for the digestion of the milk sugar lactose,the primary source of energy in milk. While primary deficiencyhas been reported (Roberts et al. 2008), deficiency usuallyarises secondary to mucosal damage secondary to theaction of infectious agents such as rotavirus and Clostridiumspp. (Weese et al. 1999). An osmotic diarrhoea and intestinalbacterial overgrowth exacerbating the existing digestivedysfunction results. Supplementation of foal with suspectedlactase deficiency is indicated with clinical suspicion. Asuitable dose rate is 120 units of lactase per kg bwt q. 4–8 h(Magdesian 2005).
Monitoring growth and development
It is important to monitor growth and development oforphaned foals carefully and regularly. To ensure adequatenutritional intake, fortnightly weighing, body condition scoringusing the scoring system described by Henneke et al. (1983)of the foal is helpful. Weigh scales are considered preferablewhen determining foal weights as weigh tapes and adultweight equations have only been validated for adults notgrowing foals. However, in the absence of scales they mayprovide a relative guide to weight change. During the firstmonth of life, an average daily weight gain for aThoroughbred foal was 1.5–1.7 kg/day (Pagan et al. 1996,
2009). Growth rates should be compared to availablestandard for sex and breed. It is generally considered that amoderate, consistent growth rate is most appropriate; Staniar(2013) reviews this in detail. Variations from the standardshould be addressed. Excessive growth rates and weight gainin the first month can increase the risks of a foal developingjuvenile osteochondral conditions (Van Weeren and Denoix2013).
Conclusion
Orphan foals are an emergency occurrence in equinepractice. It is important to understand the requirements forhealthy growth and development to be able to give the bestpossible care and advice to clients on rearing theseindividuals to be behaviourally normal, sound athletes.
The milk of the mare is superbly designed to meet theneeds of the developing foal. The unique qualities of maremilk when compared to many other domestic species makessubstitution a challenge. While the mammary gland volume iscomparatively small, the needs of the foal are met by a highfrequency of suckling, making human provision of adequatenutrition for the orphan foal a significant commitment oflabour and time.
Where possible, fostering an orphan foal on to a nursemare provides the most elegant solution. However, nursemares require a considerable financial commitment, theymay not be available in a timely fashion, andpharmacological induction of lactation and acceptance inthe barren mare requires time. Where hand rearing isrequired, the rapid growth and exacting dietary requirementsof the neonate necessitate adequate planning and athorough commitment to the process for a considerable timeuntil weaning is possible.
Vets have a key role in providing management ofimmediate age-appropriate nutritional needs of the foal andadvice on a long-term solution that fulfils the foal’s longerterm nutritional and behavioural needs and monitoringgrowth and development.
Authors’ declaration of interests
No conflicts of interest have been declared.
Ethical animal research
Ethical review not applicable for this review article.
Source of funding
None.
Authorship
All three authors were involved in preparation of themanuscript and have approved the final draft. S. Stonehamwas the lead author.
ReferencesBjornvad, C.R., Schmidt, M., Peteresen, Y.M., Jensen, S.K., Offenberg,
H.O., Elniff, J. and Sangild, P.T. (2005) Preterm birth makes theimmature intestine sensitive to feeding and induced intestinalatrophy. Am. J. Physiol. Regul. Intergr. Comp. Physiol. 289, R1212-R1222.
© 2016 EVJ Ltd
171EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Buechner-Maxwell, V. (2005) Nutritional support for neonatal foals. Vet.Clin. N. Am.: Equine Pract. 21, 487-510.
Carson, K. and Wood-Gush, D.G.M. (1983) Behaviour of Thoroughbredfoals during nursing. Equine Vet. J. 15, 257-262.
Csap�o-Kiss, Z., Stefler, J., Martin, T.G., Makray, S. and Csap�o, J. (1995)Composition of mares’ colostrum and milk. Protein content, aminoacid composition and contents of macro and micro-elements. Int.Dairy J. 5, 403-415.
Cymbaluk, N.F. (1990) Cold housing effects on growth and nutrientdemand of young horses. J. Anim. Sci. 68, 3152-3162.
Cymbaluk, N.F. and Laarveld, B. (1996) The ontogeny of seruminsulin-like growth factor-1 concentration in foals: effects of damparity, diet, and age at weaning. Domest. Anim. Endocrinol. 13,197-209.
Cymbaluk, N.F., Smart, M.E., Bristol, F.M. and Pouteaux, V.A. (1993)Importance of milk replacer intake and composition in rearingyoung foals. Can. Vet. J. 34, 479-486.
Daels, P. (2014) Induction of lactation and adoption of an orphanfoal. Proceedings of the Rossdales Foal Care Course, WhorlPublishing, Newmarket.
Daels, P.F., Duchamp, G. and Porter, D. (2002) Induction of lactationand adoption of foals by non-parturient mares. Proc. Am. Ass.Equine Practnrs. 48, 68-71.
Diehl, N. (2015) Orphan foal behaviour. http://www.thehorse.com/articles/35579/orphan-foal-behavior
Doreau, M. and Boulot, S. (1989) Recent knowledge on mare milkproduction: a review. Livest. Prod. Sci. 22, 213-235.
Doreau, M., Boulot, S., Barlet, J.P. and Patureau-Mirand, P. (1990) Yieldand composition of milk from lactating mares: effect of lactationstage and individual differences. J. Dairy Res. 57, 449-454.
Eales, F.A., Gilmour, J.S., Barlow, R.M. and Small, J. (1982) Causes ofhypothermia in 89 lambs. Vet. Rec. 6, 118-120.
Fantuz, F., Ferraro, S., Todini, L., Mariani, P., Piloni, R. and Salimei, E.(2013) Essential trace elements in milk and blood serum oflactating donkeys as affected by lactation stage anddietary supplementation with trace elements. Animal 7, 1893-1899.
Faubladier, C., Julliand, V., Danel, J. and Phillppeau, C. (2013)Bacterial carbohydrate – degrading capacity in foal faeces:changes from birth to preweaning and the impact of maternalsupplementation with fermented feed products. Br. J. Nutr. 110,1040-1052.
Fowden, A.L., Mundy, L., Ousey, J.C., McGladdery, A. and Silver, M.(1990) Tissue glycogen and glucose 6-phosphatase levels in fetaland newborn foals. J. Reprod. Fertil. Suppl. 44, 537-542.
Furr, M., Cohen, N.D., Axon, J.E., Sanchez, L.C., Pantaleon, L., Haggett,E., Campbell, R. and Tennent-Brown, B. (2012) Treatment withhistamine type 2 receptor antagonists and omeprazole increasethe risk of diarrhoea in neonatal fosals treated in intensive careunits. Equine Vet. J. 44, Suppl. 41, 80-86.
Gibbs, P.G., Potter, G.D., Blake, R.W. and McMullan, W.C. (1982) Milkproduction of quarter horse mares during 150 days of lactation. J.Anim. Sci. 54, 496-499.
Glendinning, S.A. (1974) A system of rearing foals on an automaticcalf feeding machine. Equine Vet. J. 6, 12-16.
Goldman, A.S. (1993) The immune system of human milk:antimicrobial, antiinflammatory and immunomodulating properties.Pediatr. Infect. Dis. J. 12, 664-672.
Grace, N.D., Pearce, S.G., Firth, E.C. and Fennessy, P.F. (1999)Concentrations of macro- and micro-elements in the milk ofpasture-fed thoroughbred mares. Aust. Vet. J. 77, 177-180.
Hanson, L.�A. and Korotkova, M. (2002) The role of breastfeedingin prevention of neonatal infection. Semin. Neonatol. 7,275-281.
Henneke, D.R., Potter, G.D., Kreider, J.L. and Yeates, B.F. (1983)Relationship between condition score, physical measurements andbody fat percentage in mares. Equine Vet. J. 15, 371-372.
Jose-Cunilleras, E., Viu, J., Corradini, I., Armengou, L., Cesarini, C. andMonreal, L. (2012) Energy expenditure of critically ill foals. EquineVet. J. 44, Suppl. 41, 48-51.
Kelly, A.J. (1999) Practical tips on fostering. In: Proc. BEVA SpecialistDays on Behaviour and Nutrition.
Kharitonova, I. (1978) Fatty acids and phospholipids in mare’s milk.Konevodstvo Konnyi Sport 12, 24.
King, S.S. and Nequin, L.G. (1989) An artificial rearing method toproduce optimm growth in orphaned foals. J. Equine. Vet. Sci. 9,319-322.
Knight, D.A. and Tyznik, W.J. (1985) The effect of artificial rearing onthe growth of foals. J. Anim. Sci. 60, 1-5.
Korosue, K., Murase, H., Sato, F., Ishimaru, M., Harada, T., Watanabe,G., Taya, K. and Nambo, Y. (2012) Successful induction of lactationin a barren Thoroughbred mare: growth of a foal raised oninduced lactation and the corresponding maternal hormoneprofiles. J. Vet. Med. Sci. 74, 995-1002.
Kurvers, C.M., van Weeren, P.R., Rogers, C.W. and Van Dierendonch,M.C. (2006) Quantification of spontaneous locomotion activity infoals kept in pastures under various management conditions. Am.J. Vet. Res. 67, 1212-1217.
Lewis, L.D. (1995) Chapter 15 growing horse feeding and care. In:Equine Clinical Nutrition: Feeding and Care, Ed: L.D. Lewis, Williams& Wilkins, Baltimore. p 345.
Lepeule, J., Bareille, N., Roberts, C., Valette, J.P., Jacquet, S., Blanchard,G., Denoix, J.M. and Seegers, H. (2013) Association of growth,feeding practices and exercise conditions with the severity of theosteoarticular status of limbs in French foals. Vet. J. 197, 52-57.
Linton, R.G. (1937) The composition of mare’s milk. II. The variation incomposition during lactation. III. The influence of intra-mammarypressure on the composition of milk with special reference to themare and cow. J. Dairy Res. 8, 143-172.
Linzell, J.L., Annison, E.F., Bickerstaffe, R. and Jeffcott, L.B. (1972)Mammary and whole-body metabolism of glucose, acetate andplamitate in the lactating horse. Proc. Nutr. Soc. 31, 72A-73A.
Lucas, A., Bloom, S.R. and Aynsley-Green, A. (1986) Gut hormones and‘minimal enteral feeding’. Acta Paediatr. 75, 719-723.
Magdesian, K.G. (2005) Neonatal foal diarrhea. Vet. Clin. N. Am.:Equine Pract. 21, 295-312.
Martin, R.G., McMeniman, N.P. and Dowsett, K.F. (1992) Milk andwater intakes of foals sucking grazing mares. Equine Vet. J. 24,295-299.
Martuzzi, F. and Doreau, M. (2006) Mare milk composition: recentfindings about protein fractions and mineral content. ThirdEuropean Workshop in Equine Nutrition, Campobasso, Italy.Nutrition and feeding of the broodmare 120, 65-76.
McGreevy, P. (2004) Learning: Equine Behaviour, Saunders Elsevier,Philadelphia.
Mellor, D.J. (1993) Some aspects of perinatal maturation andadaptation. Equine Vet. J. 25, Suppl. 14, 17-22.
Meyer, H. and Ahlswede, L. (1976) Uber das intrauterine wachstumund die korperzusammentragender stuten. Ubersicht. Tierernahr. 4,263-292.
Mount, L.E. (1979) Adaptation to Thermal Environment: Man and hisProductive Animals, 1st edn., E. Arnold Ltd, London.
Naylor, J.M. and Bell, R. (1985) Raising the orphan foal. Vet. Clin. N.Am.: Equine Pract. 1, 169-178.
Oftedal, O.T., Hintz, H.F. and Schryver, H.F. (1983) Lactation in thehorse: milk composition and intake by foals. J. Nutr. 113, 2096-2106.
Ott, E.A. (2002) Use of mannose oligosaccharides in diets of maresand their suckling foals. Nutritional Biotechnology in the Feed andFood industries. In: Proceedings of the 18th Annual Symposium.Nottingham University Press, Nottingham, UK. pp 367–371.
Ousey, J.C. (2003) Feeding the foal in health and disease. Equine Vet.Educ. Manual 6, 50-54.
© 2016 EVJ Ltd
172 EQUINE VETERINARY EDUCATION / AE / MARCH 2017

Ousey, J.C., McArthur, A.J. and Rossdale, P.D. (1991) Metabolicchanges in thoroughbred and pony foals during the first 24 h postpartum. J. Reprod. Fertil. Suppl. 44, 561-570.
Ousey, J.C., McArthur, A.J., Murgatroyd, P.R., Stewart, J.H. andRossdale, P.D. (1992) Thermoregulation and total body insulation inthe neonatal foal. J. Therm. Biol. 17, 1-10.
Ousey, J.C., Holdstock, N., Rossdale, P.D. and McArthur, A.J. (1996)How much energy do sick neonatal foals require compared withhealthy foals? Pferdeheilkunde 12, 231-237.
Ousey, J.C., McArthur, A.J. and Rossdale, P.D. (1997a)Thermoregulation in sick foals aged less than one week. Vet. J.153, 185-196.
Ousey, J.C., Prandi, S., Zimmer, J., Holdstock, N. and Rossdale, P.D.(1997b) Effects of various feeding regimens on the energy balanceof equine neonates. Am. J. Vet. Res. 58, 1243-1251.
Pagan, J.D. and Hintz, H.F. (1986) Equine energetics: I. Relationshipbetween body weight and energy requirements in horses. J. Anim.Sci. 63, 815-821.
Pagan, J.D., Jackson, S.G. and Caddel, S. (1996) A summary ofgrowth rates of thoroughbreds in Kentucky. Pferdeheilkunde 12,285-289.
Pagan, J.D., Brown-Douglas, C.G. and Caddel, S. (2009) Body weightand condition of Kentucky Thoroughbred mares and their foals asinfluenced by month of foaling, season, and gender. In: Advancesin Equine Nutrition IV, Ed: J.D. Pagan, Nottingham University Press,Nottingham. pp 137-145.
Pastukhova, Z.M. and Gerbeda, V.V. (1981) [Comparative lipidcomposition of mare’s milk and a koumiss mixture prepared withcow’s milk]. Vopr. Pitan. 1, 34-36.
Quartuccio, M., Cristarella, S., Medica, P., Rizzo, M., Cravana, C. andFabio, E. (2015) Assessment of prolactin and quantitative milkproduction after induction of lactation in Barren Jennies (Equusasinus): a pilot study. J. Equine Vet. Sci. 35, 679-685.
Roberts, M.C. (1975) The development and distribution of mucosalenzymes in the small intestine of the fetus and young foal. J.Reprod. Fertil. Suppl. 23, 717-723.
Roberts, V.L.H., Knottenbelt, D.C., Williams, A. and McKane, S.A. (2008)Suspected primary lactose intolerance in neonatal foals. EquineVet. Educ. 20, 249-251.
Salimei, E., Fantuz, F., Coppola, R., Chiofalo, B., Polidori, P. andVarisco, G. (2004) Composition and characteristics of ass’s milk.Anim. Res. 53, 67-78.
Sangild, P.T. (2006) Gut responses to enteral nutrition in preterm infantsand animals. Exp. Biol. Med. 231, 1695-1711.
Schoster, A., Staempfli, H.R., Abrahams, M., Jalali, M., Weese, J.S. andGuardabassi, L. (2015) Effect of a probiotic on prevention ofdiarrhoea and Clostridium difficle and Clostridium perfringensshedding in foals. J. Vet. Intern. Med. 29, 925-931.
Schryver, H.F., Oftedal, O.T., Williams, J., Soderholm, L.V. and Hintz, H.F.(1986) Lactation in the horse: the mineral composition of maremilk. J. Nutr. 116, 2142-2147.
Schweigart, F.J. (2001) Milk more than a nutrient: hormones, growthfactors and bioactive factors. Pferdeheilkunde 18, 665-668.
Solaroli, G., Pagliarini, E. and Peri, C. (1993) Composition andnutritional quality of mare’s milk. Ital. J. Food Sci. 5, 3-10.
Staniar, W. (2013) Feeding the growing horse. In: Equine Applied andClinical Nutrition, Ed: R.J. Geor, P.A. Harris and M. Coenen,Saunders Elsevier, Philadelphia. pp 243-260.
Steiner, J.V. (2006) How to induce lactation in non-pregnant mares.Proc. Am. Ass. Equine Practnrs. 52, 259-260.
Stiles, R.P., Grieve, D.G., Butler, D.G. and Willoughby, R.A. (1974)Effects of fluid intake level and dry matter concentration of theincidence of scours in milk replacer-fed-calves. Can. J. Anim. Sci.54, 73-78.
Stoneham, S.J. (2013) Feeding orphan and sick foals. In: EquineApplied and Clinical Nutrition, Eds: R.J. Geor, P.A. Harris and M.Coenen, Saunders Elsevier, Philadelphia. pp 618-627.
Symmonds, M.E., Bird, J.A., Clarke, L., Gate, J.J. and Lomax, M.A.(1995) Nutrition, temperature and homeostasis during perinataldevelopment. Exp. Physiol. 80, 907-940.
Vaala, W.E. (2011) Enteral and parenteral nutrition for the neonatalfoal. In: Equine Reproduction, 2nd edn., Eds: A.O. McKinnon, E.L.Squires, W.E. Vaala and D.D. Varner, Wiley-Blackwell, Philadelphia.pp 263-279.
Van Weeren, P.R. and Denoix, J.M. (2013) The Normandy field studyon Juvenile Osteochondral conditions: conclusions regardingthe influence of genetics, environmental conditions andmanagement, and the effect on performance. Vet. J. 197, 90-95.
Vander Heyden, L., Lejeune, J.P., Caudron, I., Detilleux, J., Sandersen,C., Chavatte, P., Paris, J., Deli�ege, B. and Serteyn, D. (2013)Association of breeding conditions with prevalence ofosteochondrosis in foals. Vet. Rec. 172, 68.
Weese, J.S. and Rousseau, J. (2005) Evaluation of Lactobacilluspentosus WE7 for the prevention of diarrhoea in neonatal foals. J.Am. Vet. Med. Ass. 226, 2031-2034.
Weese, J.S., Parsons, D.A. and Staempfli, H.R. (1999) Association ofClostridium difficile with enterocolitis and lactose intolerance in afoal. J. Am. Vet. Med. Ass. 214, 229-232, 205.
Williams, M. (1974) Effect of artificial rearing on social behaviour offoals. Equine Vet. J. 6, 17-18.
Wilson, J.H. (1988) Feeding considerations for neonatal foals. Proc. Am.Ass. Equine Practnrs. 34, 823-829.
Xu, R.J. (1996) Development of the newborn GI tract and its relationto colostrum/milk intake: a review. Reprod. Fertil. Dev. 8, 35-48.
© 2016 EVJ Ltd
173EQUINE VETERINARY EDUCATION / AE / MARCH 2017
Advertisers’ Index AAEP CE …....….…………….........Cover 4 Luitpold Animal Health ……..XIV Arenus …..………………………….Cover 2 Merial ………………….…….130A, 156B Colorado State University …………. 164 Platinum Performance.……….124A Hallmarq ……………………………156A SmartPak ……………………..124B ISELP …………………….…………130B Vetel Diagnostics …………….137 Kentucky Performance Products ……XIII Zoetis …………………………174, Cover 3
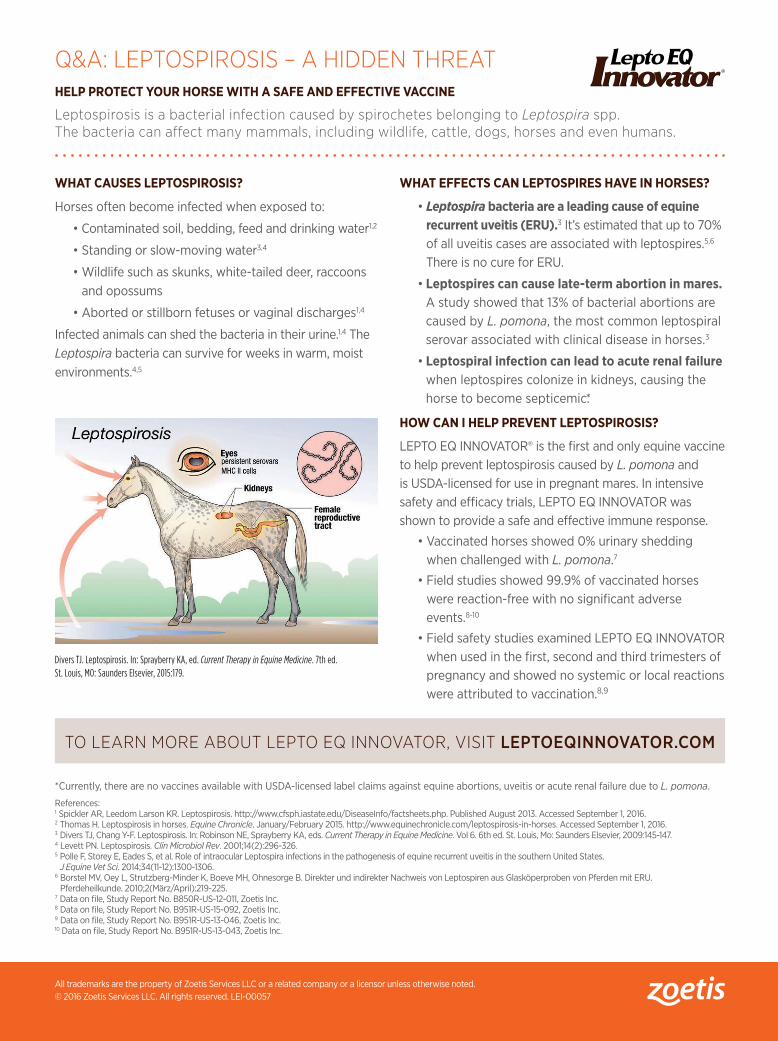
Q&A: LEPTOSPIROSIS – A HIDDEN THREATHELP PROTECT YOUR HORSE WITH A SAFE AND EFFECTIVE VACCINE
Leptospirosis is a bacterial infection caused by spirochetes belonging to Leptospira spp. The bacteria can affect many mammals, including wildlife, cattle, dogs, horses and even humans.
WHAT CAUSES LEPTOSPIROSIS?
Horses often become infected when exposed to:
• Contaminated soil, bedding, feed and drinking water1,2
• Standing or slow-moving water3,4
• Wildlife such as skunks, white-tailed deer, raccoons and opossums
• Aborted or stillborn fetuses or vaginal discharges1,4
Infected animals can shed the bacteria in their urine.1,4 The Leptospira bacteria can survive for weeks in warm, moist environments.4,5
WHAT EFFECTS CAN LEPTOSPIRES HAVE IN HORSES?
• Leptospira bacteria are a leading cause of equine recurrent uveitis (ERU).3 It’s estimated that up to 70% of all uveitis cases are associated with leptospires.5,6 There is no cure for ERU.
• Leptospires can cause late-term abortion in mares. A study showed that 13% of bacterial abortions are caused by L. pomona, the most common leptospiral serovar associated with clinical disease in horses.3
• Leptospiral infection can lead to acute renal failure when leptospires colonize in kidneys, causing the horse to become septicemic.*
HOW CAN I HELP PREVENT LEPTOSPIROSIS?
LEPTO EQ INNOVATOR® is the first and only equine vaccine to help prevent leptospirosis caused by L. pomona and is USDA-licensed for use in pregnant mares. In intensive safety and efficacy trials, LEPTO EQ INNOVATOR was shown to provide a safe and effective immune response.
• Vaccinated horses showed 0% urinary shedding when challenged with L. pomona.7
• Field studies showed 99.9% of vaccinated horses were reaction-free with no significant adverse events.8-10
• Field safety studies examined LEPTO EQ INNOVATOR when used in the first, second and third trimesters of pregnancy and showed no systemic or local reactions were attributed to vaccination.8,9
Divers TJ. Leptospirosis. In: Sprayberry KA, ed. Current Therapy in Equine Medicine. 7th ed. St. Louis, MO: Saunders Elsevier, 2015:179.
All trademarks are the property of Zoetis Services LLC or a related company or a licensor unless otherwise noted. © 2016 Zoetis Services LLC. All rights reserved. LEI-00057
*Currently, there are no vaccines available with USDA-licensed label claims against equine abortions, uveitis or acute renal failure due to L. pomona.
References:1 Spickler AR, Leedom Larson KR. Leptospirosis. http://www.cfsph.iastate.edu/DiseaseInfo/factsheets.php. Published August 2013. Accessed September 1, 2016.2 Thomas H. Leptospirosis in horses. Equine Chronicle. January/February 2015. http://www.equinechronicle.com/leptospirosis-in-horses. Accessed September 1, 2016.3 Divers TJ, Chang Y-F. Leptospirosis. In: Robinson NE, Sprayberry KA, eds. Current Therapy in Equine Medicine. Vol 6. 6th ed. St. Louis, Mo: Saunders Elsevier, 2009:145-147.4 Levett PN. Leptospirosis. Clin Microbiol Rev. 2001;14(2):296-326.5 Polle F, Storey E, Eades S, et al. Role of intraocular Leptospira infections in the pathogenesis of equine recurrent uveitis in the southern United States.
J Equine Vet Sci. 2014;34(11-12):1300-1306.6 Borstel MV, Oey L, Strutzberg-Minder K, Boeve MH, Ohnesorge B. Direkter und indirekter Nachweis von Leptospiren aus Glasköperproben von Pferden mit ERU.
Pferdeheilkunde. 2010;2(März/April):219-225.7 Data on file, Study Report No. B850R-US-12-011, Zoetis Inc.8 Data on file, Study Report No. B951R-US-15-092, Zoetis Inc.9 Data on file, Study Report No. B951R-US-13-046, Zoetis Inc.10 Data on file, Study Report No. B951R-US-13-043, Zoetis Inc.
TO LEARN MORE ABOUT LEPTO EQ INNOVATOR, VISIT LEPTOEQINNOVATOR.COM

KEEP YOUR HORSE IN THE PICTURE.
Leptospira interrogans serovar Pomona (L. pomona) can cause devastating problems for your horse. LEPTO EQ INNOVATOR® is the first vaccine developed specifically for horses to help prevent leptospirosis caused by L. pomona. It helps prevent infections of the blood caused by L. pomona, which could, but has not been demonstrated to, help reduce the potential risk of equine recurrent uveitis, abortion and acute renal failure caused by L. pomona.* Intensive safety and efficacy trials have demonstrated LEPTO EQ INNOVATOR safely helps prevent L. pomona infections with 0% urinary shedding.1-4 Field safety trials have shown the vaccine is 99.9% reaction free.2-4 To learn more, visit LEPTOEQINNOVATOR.COM.
*Currently, there are no vaccines available with USDA-licensed label claims against equine abortions, uveitis or acute renal failure due to L. pomona.
1 Data on file, Study Report No. B850R-US-12-011, Zoetis Inc.2 Data on file, Study Report No. B951R-US-13-043, Zoetis Inc.3 Data on file, Study Report No. B951R-US-13-046, Zoetis Inc.4 Data on file, Study Report No. B951R-US-15-092, Zoetis Inc.
All trademarks are the property of Zoetis Services LLC or a related company or licensor unless otherwise noted. © 2016 Zoetis Services LLC. All rights reserved. LEI-00053
Now USDA-licensed for use in all trimesters of pregnancy.
The AAEP provides practical CE in multiple learning formats for professional growth and practice
success. AAEP CE connects you with relevant take-home knowledge; new diagnostics and treat-
ments; innovative practice solutions; recognized experts; and colleagues old and new. When
considering your CE options in 2017, make plans to be part of the AAEP herd!
July 9-12 July 15-18 July 16-18
July 16-18 November 17-21
Diagnosing, Imaging
and Treating the Hind
Suspensory and Stifle
63rd
annual
convention
San Antonio, Texas
Heard about AAEP CE for 2017?
For more information, visit www.aaep.org.
Lexington, KentuckyFort Collins, Colorado
DENTISTRY
COLIC
STUDENTS
Sponsored by Sponsored by
Lexington, Kentucky
Sponsored by
Lexington, Kentucky
Sponsored by
Related Documents











