Benign Paroxysmal Positional Vertigo or BPPV What is it? So, what is BPPV? Let's start by defining the words we use to describe it: Benign : is not a danger to health, used to describe mild or non progressive conditions Paroxysmal : sudden onset, recurrence, or intensification of symptoms Positional : pertaining to the orientation or posture of a body part (in this case the head) Vertigo : dizziness; the feeling that the world is revolving around you or that you are spinning in place Essentially, you suddenly get dizzy because of the position, or change in position, of your head but not because of anything life threatening wrong with you. Why does it happen? Now that we know what we're talking about let's move on to why it occurs. As it so happens, your grandmother was right when she told you that you have rocks in your head. More specifically you have little crystals of calcium carbonate (the stuff lime stone is made of) in your inner ear, the medical term for them is otoconia. Those crystals are only supposed to be in two areas of the inner ear, called the utricle and saccule. Under normal conditions the otoconia help your inner ear to perceive motion in a straight line. Otoconia float in a gelatinous membrane, on top of cilia (tiny hairs), in the inner ear. When you move up, down, left, right, backward, forward or any linear movement inertia keeps the crystals from moving as quickly as the rest of your inner ear. The cilia pick up this delay in movement and send the appropriate signal to your brain to indicate which direction you are moving. With BPPV, some of the crystals have come loose from the utricle and made their way into one of the ampulla. Ampulla are located at the entrance to the three semi-circular canals. (BPPV typically affects the posterior canal.) The ampulla contain an organ that senses rotational Produced by D.B. Watkins www.dbwatkins.com Page 1 of 3 *2 *1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Benign Paroxysmal Positional Vertigoor
BPPV
What is it?So, what is BPPV? Let's start by defining the words we use to describe it:
Benign: is not a danger to health, used to describe mild or non progressive conditions
Paroxysmal: sudden onset, recurrence, or intensification of symptoms
Positional: pertaining to the orientation or posture of a body part (in this case the head)
Vertigo: dizziness; the feeling that the world is revolving around you or that you are spinning in place
Essentially, you suddenly get dizzy because of the position, or change in position, of your head but not because of anything life threatening wrong with you.
Why does it happen?Now that we know what we're talking about let's move on to why it occurs.
As it so happens, your grandmother was right when she told you that you have rocks in your head. More specifically you have little crystals of calcium carbonate (the stuff lime stone is made of) in your inner ear, the medical term for them is otoconia. Those crystals are only supposed to be in two areas of the inner ear, called the utricle and saccule. Under normal conditions the otoconia help your inner ear to perceive motion in a straight line. Otoconia float in a gelatinous membrane, on top of cilia (tiny hairs), in the inner ear. When you move up, down,left, right, backward, forward or any linear movement inertia keeps the crystals from moving as quickly as the rest of your inner ear. The cilia pick up this delay in movement and send the appropriate signal to your brain to indicate which direction you are moving.
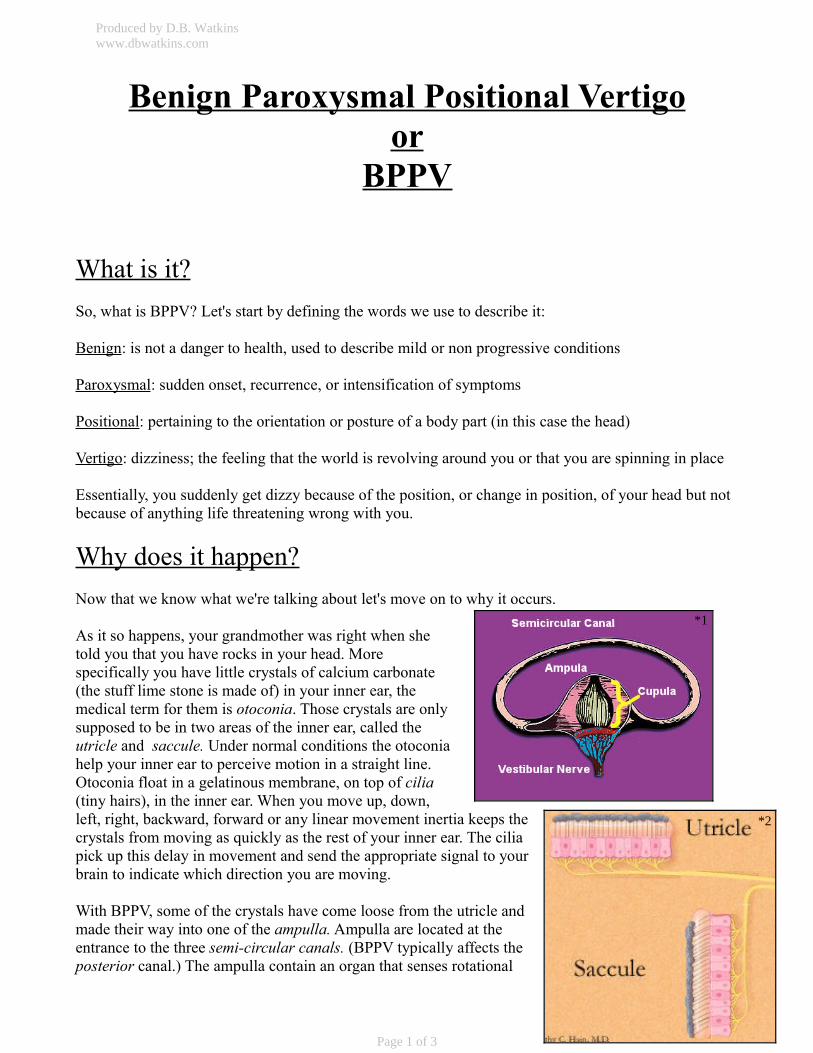
With BPPV, some of the crystals have come loose from the utricle and made their way into one of the ampulla. Ampulla are located at the entrance to the three semi-circular canals. (BPPV typically affects the posterior canal.) The ampulla contain an organ that senses rotational
Produced by D.B. Watkinswww.dbwatkins.com
Page 1 of 3
*2
*1
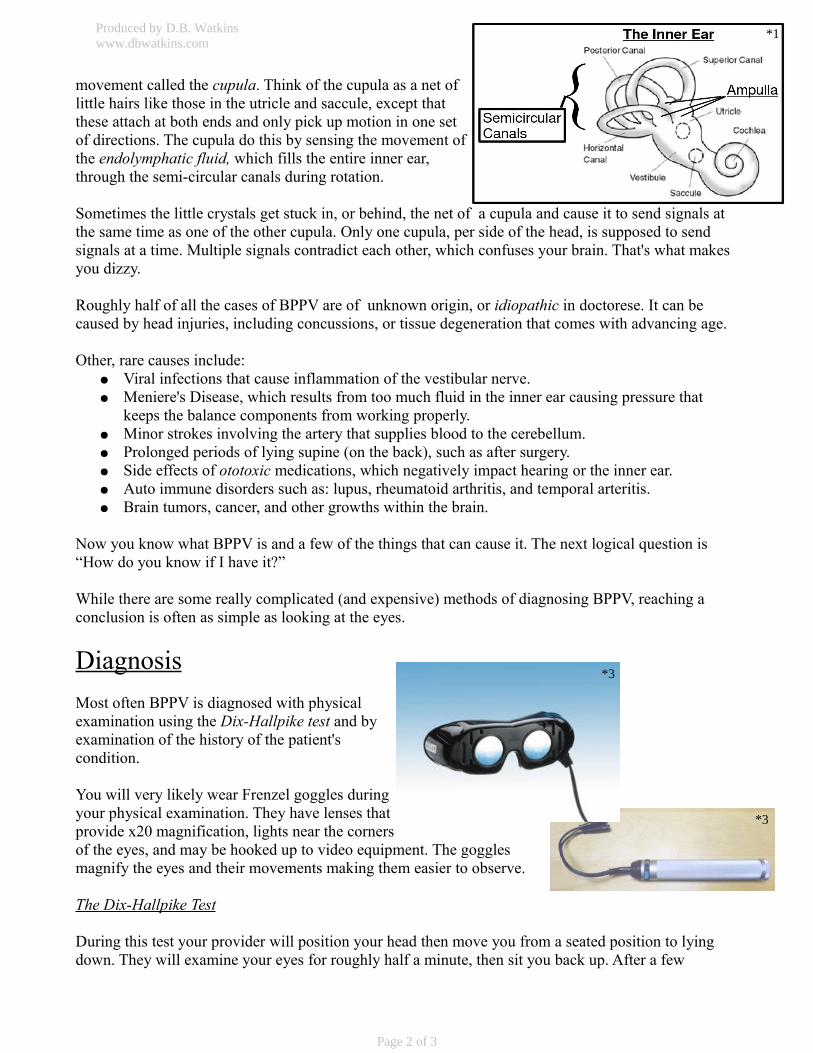
movement called the cupula. Think of the cupula as a net of little hairs like those in the utricle and saccule, except that these attach at both ends and only pick up motion in one set of directions. The cupula do this by sensing the movement of the endolymphatic fluid, which fills the entire inner ear, through the semi-circular canals during rotation.
Sometimes the little crystals get stuck in, or behind, the net of a cupula and cause it to send signals at the same time as one of the other cupula. Only one cupula, per side of the head, is supposed to send signals at a time. Multiple signals contradict each other, which confuses your brain. That's what makes you dizzy.
Roughly half of all the cases of BPPV are of unknown origin, or idiopathic in doctorese. It can be caused by head injuries, including concussions, or tissue degeneration that comes with advancing age.
Other, rare causes include: ● Viral infections that cause inflammation of the vestibular nerve.● Meniere's Disease, which results from too much fluid in the inner ear causing pressure that
keeps the balance components from working properly.● Minor strokes involving the artery that supplies blood to the cerebellum.● Prolonged periods of lying supine (on the back), such as after surgery.● Side effects of ototoxic medications, which negatively impact hearing or the inner ear.● Auto immune disorders such as: lupus, rheumatoid arthritis, and temporal arteritis.● Brain tumors, cancer, and other growths within the brain.
Now you know what BPPV is and a few of the things that can cause it. The next logical question is “How do you know if I have it?”
While there are some really complicated (and expensive) methods of diagnosing BPPV, reaching a conclusion is often as simple as looking at the eyes.
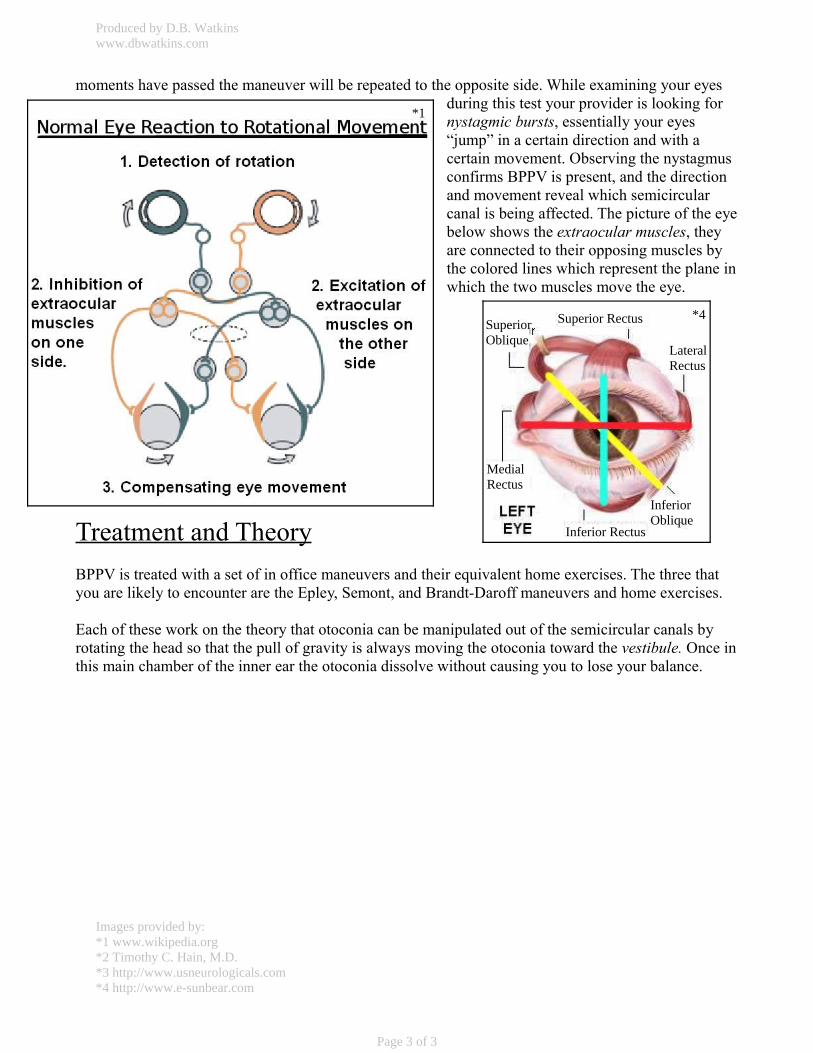
DiagnosisMost often BPPV is diagnosed with physical examination using the Dix-Hallpike test and by examination of the history of the patient's condition.
You will very likely wear Frenzel goggles during your physical examination. They have lenses that provide x20 magnification, lights near the cornersof the eyes, and may be hooked up to video equipment. The goggles magnify the eyes and their movements making them easier to observe.
The Dix-Hallpike Test
During this test your provider will position your head then move you from a seated position to lying down. They will examine your eyes for roughly half a minute, then sit you back up. After a few
Produced by D.B. Watkinswww.dbwatkins.com
Page 2 of 3
*1
*3
*3
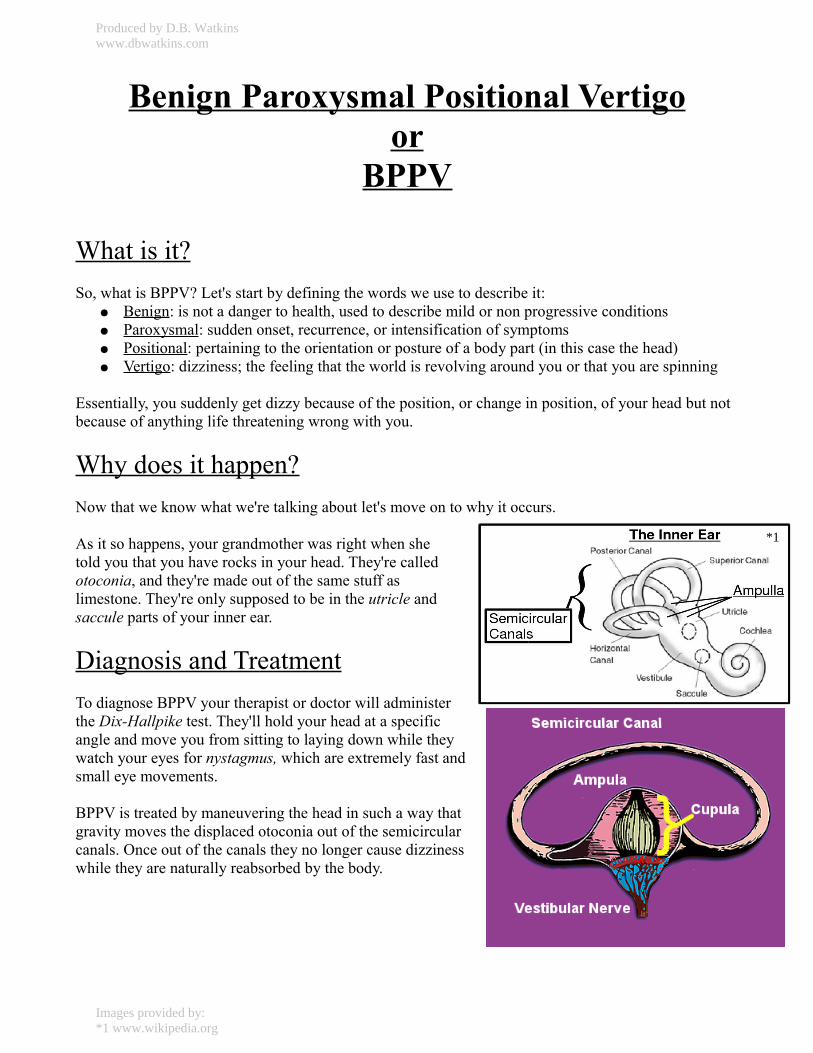
moments have passed the maneuver will be repeated to the opposite side. While examining your eyes during this test your provider is looking for nystagmic bursts, essentially your eyes “jump” in a certain direction and with a certain movement. Observing the nystagmus confirms BPPV is present, and the direction and movement reveal which semicircular canal is being affected. The picture of the eye below shows the extraocular muscles, they are connected to their opposing muscles by the colored lines which represent the plane in which the two muscles move the eye.
Treatment and TheoryBPPV is treated with a set of in office maneuvers and their equivalent home exercises. The three that you are likely to encounter are the Epley, Semont, and Brandt-Daroff maneuvers and home exercises.
Each of these work on the theory that otoconia can be manipulated out of the semicircular canals by rotating the head so that the pull of gravity is always moving the otoconia toward the vestibule. Once in this main chamber of the inner ear the otoconia dissolve without causing you to lose your balance.
Produced by D.B. Watkinswww.dbwatkins.com
Page 3 of 3
*1
*4Superior Rectus
Inferior Rectus
InferiorOblique
LateralRectus
MedialRectus
SuperiorOblique
Images provided by:*1 www.wikipedia.org*2 Timothy C. Hain, M.D.*3 http://www.usneurologicals.com*4 http://www.e-sunbear.com
Benign Paroxysmal Positional Vertigoor
BPPV
What is it?So, what is BPPV? Let's start by defining the words we use to describe it:
● Benign : is not a danger to health, used to describe mild or non progressive conditions● Paroxysmal : sudden onset, recurrence, or intensification of symptoms● Positional : pertaining to the orientation or posture of a body part (in this case the head)● Vertigo : dizziness; the feeling that the world is revolving around you or that you are spinning
Essentially, you suddenly get dizzy because of the position, or change in position, of your head but not because of anything life threatening wrong with you.
Why does it happen?Now that we know what we're talking about let's move on to why it occurs.
As it so happens, your grandmother was right when she told you that you have rocks in your head. They're called otoconia, and they're made out of the same stuff as limestone. They're only supposed to be in the utricle and saccule parts of your inner ear.
Diagnosis and TreatmentTo diagnose BPPV your therapist or doctor will administer the Dix-Hallpike test. They'll hold your head at a specific angle and move you from sitting to laying down while they watch your eyes for nystagmus, which are extremely fast and small eye movements.
BPPV is treated by maneuvering the head in such a way that gravity moves the displaced otoconia out of the semicircular canals. Once out of the canals they no longer cause dizziness while they are naturally reabsorbed by the body.
*1
Produced by D.B. Watkinswww.dbwatkins.com
Images provided by:*1 www.wikipedia.org
So, what is this whole inner ear,vestibular system thing?
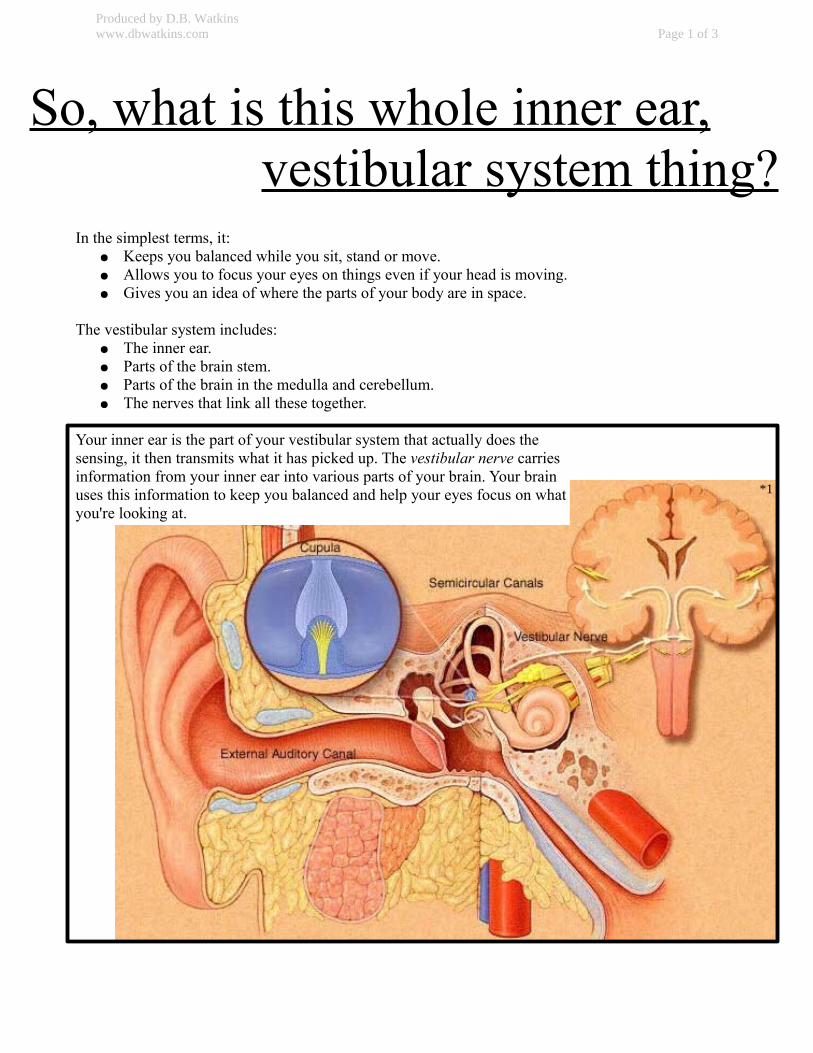
In the simplest terms, it:● Keeps you balanced while you sit, stand or move.● Allows you to focus your eyes on things even if your head is moving.● Gives you an idea of where the parts of your body are in space.
The vestibular system includes:● The inner ear.● Parts of the brain stem.● Parts of the brain in the medulla and cerebellum.● The nerves that link all these together.
Your inner ear is the part of your vestibular system that actually does the sensing, it then transmits what it has picked up. The vestibular nerve carries information from your inner ear into various parts of your brain. Your brain uses this information to keep you balanced and help your eyes focus on what you're looking at.
Produced by D.B. Watkinswww.dbwatkins.com Page 1 of 3
*1
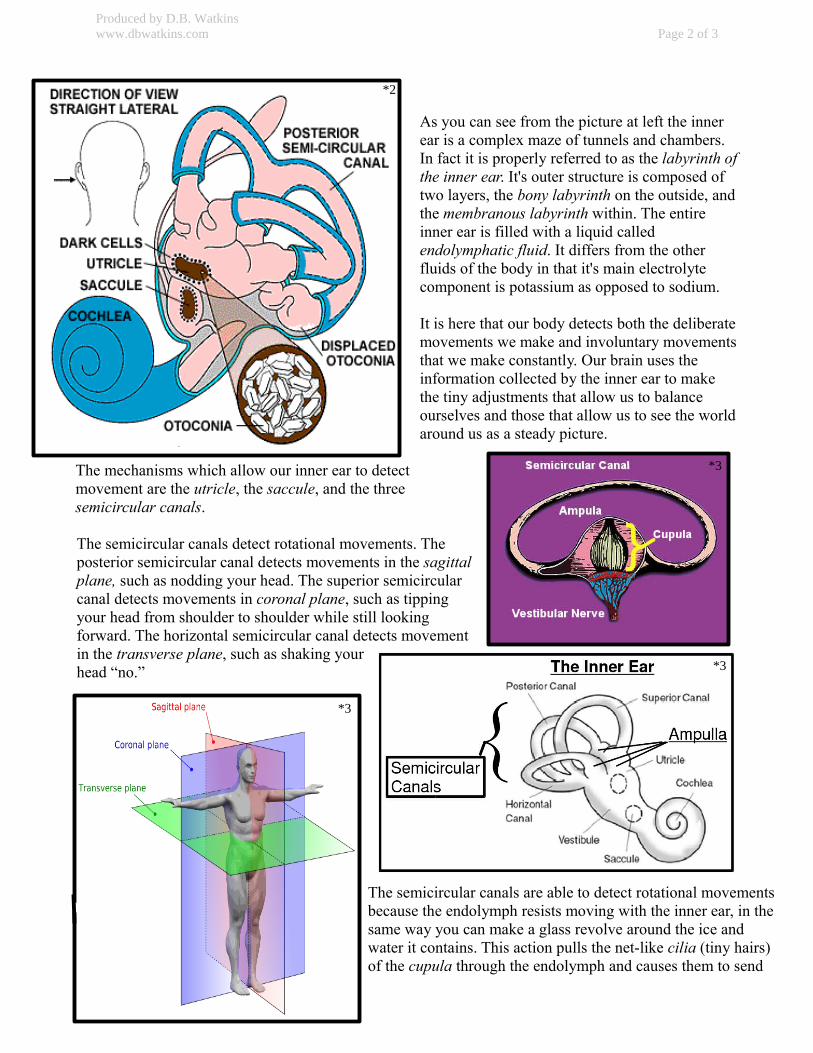
As you can see from the picture at left the inner ear is a complex maze of tunnels and chambers. In fact it is properly referred to as the labyrinth of the inner ear. It's outer structure is composed of two layers, the bony labyrinth on the outside, and the membranous labyrinth within. The entire inner ear is filled with a liquid called endolymphatic fluid. It differs from the other fluids of the body in that it's main electrolyte component is potassium as opposed to sodium.
It is here that our body detects both the deliberate movements we make and involuntary movements that we make constantly. Our brain uses the information collected by the inner ear to make the tiny adjustments that allow us to balance ourselves and those that allow us to see the world around us as a steady picture.
The mechanisms which allow our inner ear to detect movement are the utricle, the saccule, and the three semicircular canals.
The semicircular canals detect rotational movements. The posterior semicircular canal detects movements in the sagittal plane, such as nodding your head. The superior semicircular canal detects movements in coronal plane, such as tipping your head from shoulder to shoulder while still looking forward. The horizontal semicircular canal detects movementin the transverse plane, such as shaking your head “no.”
The semicircular canals are able to detect rotational movements because the endolymph resists moving with the inner ear, in the same way you can make a glass revolve around the ice and water it contains. This action pulls the net-like cilia (tiny hairs) of the cupula through the endolymph and causes them to send
Produced by D.B. Watkinswww.dbwatkins.com Page 2 of 3
*2
*3
*3
*3
either an excite signal or no signal (which the brain interprets to mean inhibit) through the vestibular nerve.
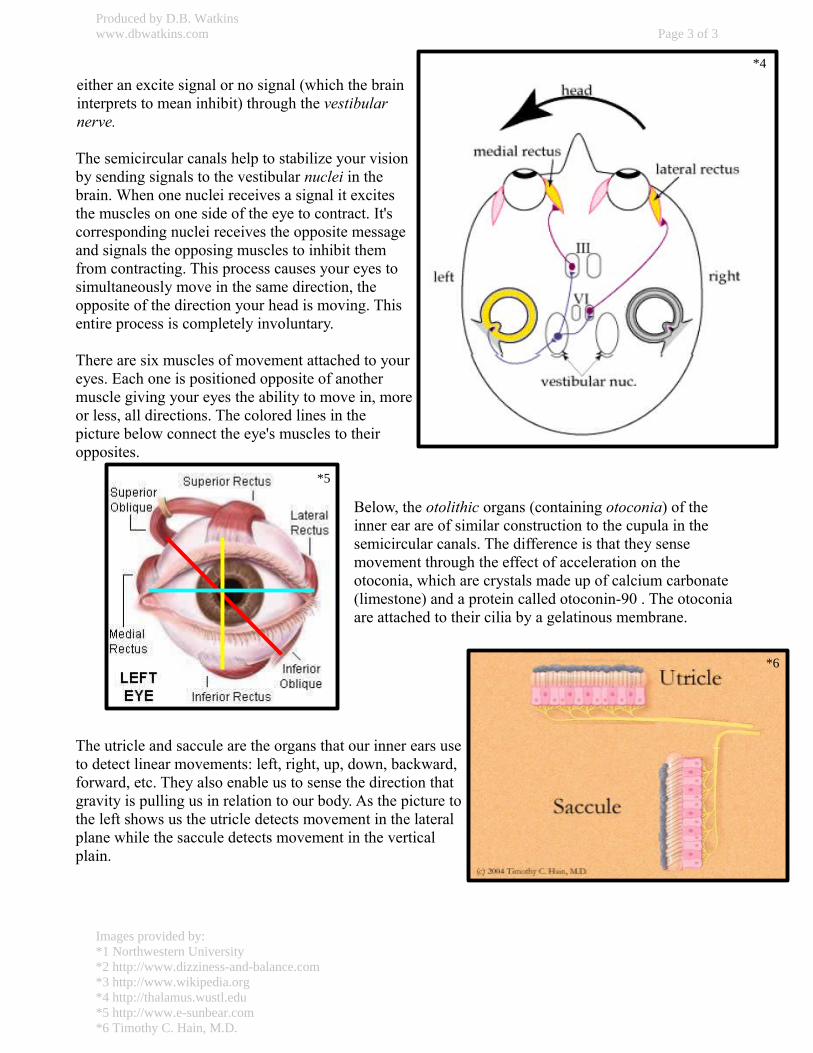
The semicircular canals help to stabilize your vision by sending signals to the vestibular nuclei in the brain. When one nuclei receives a signal it excites the muscles on one side of the eye to contract. It's corresponding nuclei receives the opposite message and signals the opposing muscles to inhibit them from contracting. This process causes your eyes to simultaneously move in the same direction, the opposite of the direction your head is moving. This entire process is completely involuntary.
There are six muscles of movement attached to your eyes. Each one is positioned opposite of another muscle giving your eyes the ability to move in, more or less, all directions. The colored lines in the picture below connect the eye's muscles to their opposites.
Below, the otolithic organs (containing otoconia) of the inner ear are of similar construction to the cupula in the semicircular canals. The difference is that they sense movement through the effect of acceleration on the otoconia, which are crystals made up of calcium carbonate (limestone) and a protein called otoconin-90 . The otoconia are attached to their cilia by a gelatinous membrane.
The utricle and saccule are the organs that our inner ears use to detect linear movements: left, right, up, down, backward, forward, etc. They also enable us to sense the direction that gravity is pulling us in relation to our body. As the picture to the left shows us the utricle detects movement in the lateral plane while the saccule detects movement in the vertical plain.
Produced by D.B. Watkinswww.dbwatkins.com Page 3 of 3
Images provided by:*1 Northwestern University*2 http://www.dizziness-and-balance.com*3 http://www.wikipedia.org*4 http://thalamus.wustl.edu*5 http://www.e-sunbear.com*6 Timothy C. Hain, M.D.
*6
*4
*5
So, what is this whole inner ear,vestibular system thing?
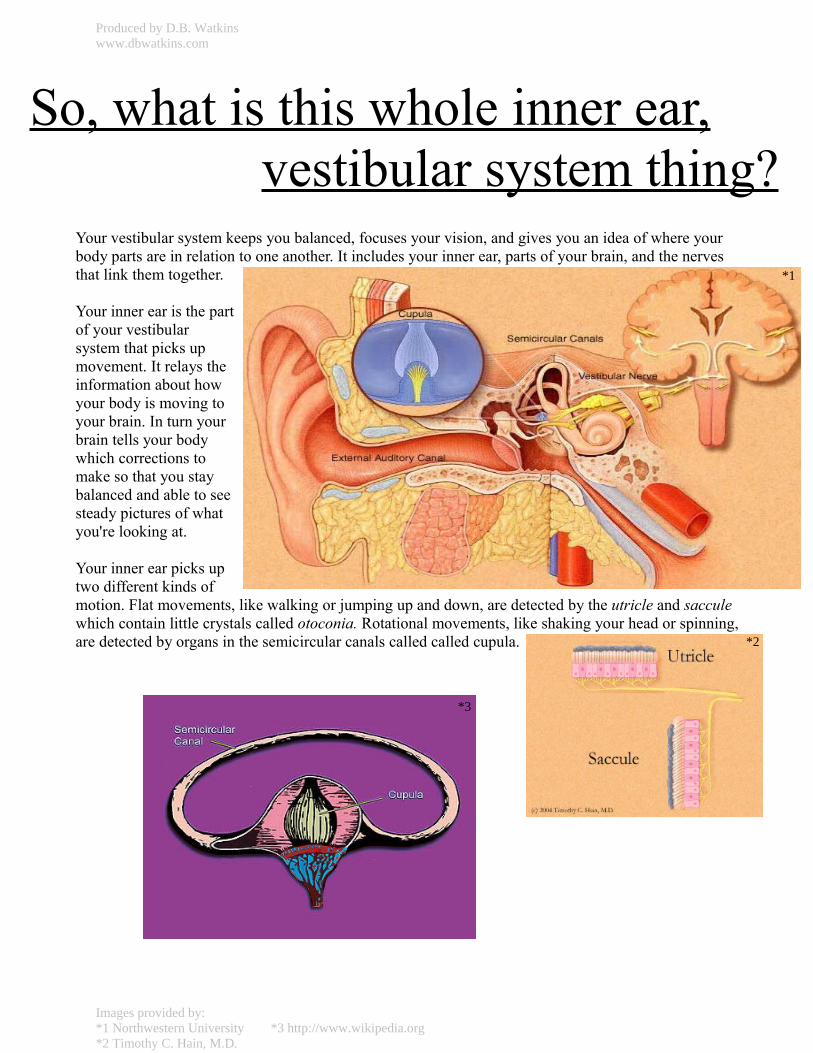
Your vestibular system keeps you balanced, focuses your vision, and gives you an idea of where your body parts are in relation to one another. It includes your inner ear, parts of your brain, and the nerves that link them together.
Your inner ear is the part of your vestibular system that picks up movement. It relays the information about how your body is moving to your brain. In turn your brain tells your body which corrections to make so that you stay balanced and able to see steady pictures of what you're looking at.
Your inner ear picks up two different kinds ofmotion. Flat movements, like walking or jumping up and down, are detected by the utricle and saccule which contain little crystals called otoconia. Rotational movements, like shaking your head or spinning, are detected by organs in the semicircular canals called called cupula.
*1
*2
*3
Produced by D.B. Watkinswww.dbwatkins.com
Images provided by:*1 Northwestern University *3 http://www.wikipedia.org*2 Timothy C. Hain, M.D.
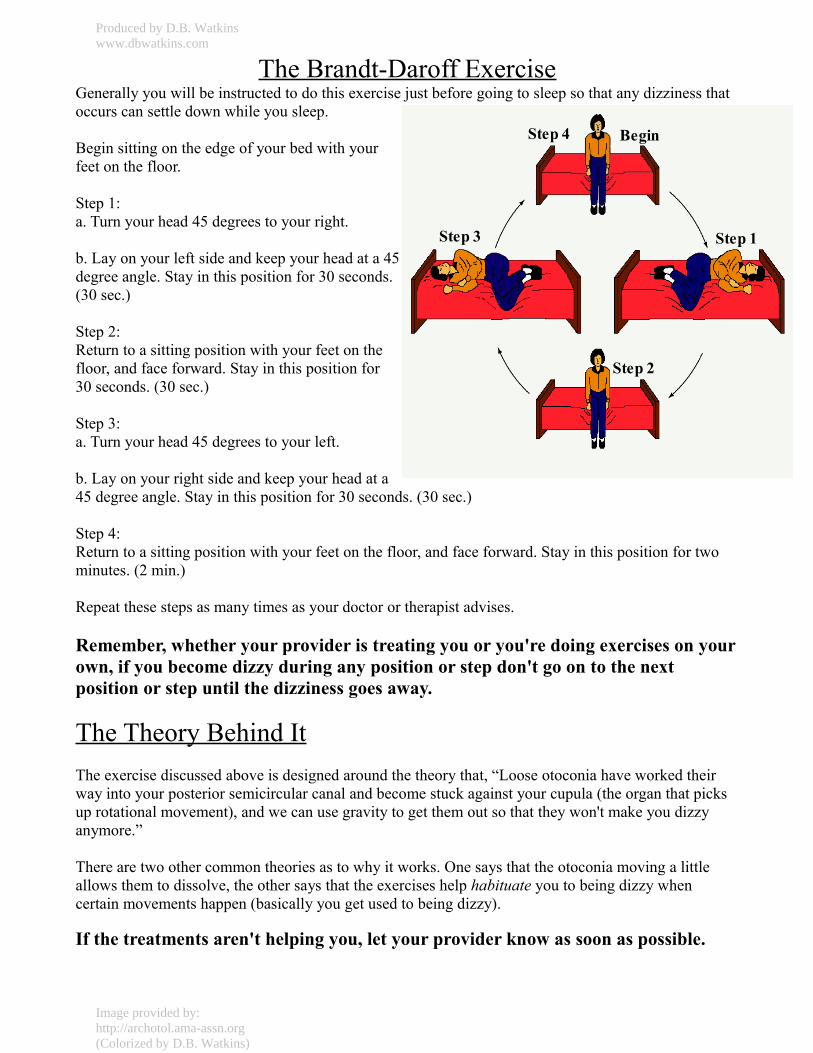
The Brandt-Daroff ExerciseGenerally you will be instructed to do this exercise just before going to sleep so that any dizziness that occurs can settle down while you sleep.
Begin sitting on the edge of your bed with your feet on the floor.
Step 1:a. Turn your head 45 degrees to your right.
b. Lay on your left side and keep your head at a 45 degree angle. Stay in this position for 30 seconds. (30 sec.)
Step 2:Return to a sitting position with your feet on the floor, and face forward. Stay in this position for 30 seconds. (30 sec.)
Step 3:a. Turn your head 45 degrees to your left.
b. Lay on your right side and keep your head at a45 degree angle. Stay in this position for 30 seconds. (30 sec.)
Step 4:Return to a sitting position with your feet on the floor, and face forward. Stay in this position for two minutes. (2 min.)
Repeat these steps as many times as your doctor or therapist advises.
Remember, whether your provider is treating you or you're doing exercises on your own, if you become dizzy during any position or step don't go on to the next position or step until the dizziness goes away.
The Theory Behind ItThe exercise discussed above is designed around the theory that, “Loose otoconia have worked their way into your posterior semicircular canal and become stuck against your cupula (the organ that picks up rotational movement), and we can use gravity to get them out so that they won't make you dizzy anymore.”
There are two other common theories as to why it works. One says that the otoconia moving a little allows them to dissolve, the other says that the exercises help habituate you to being dizzy when certain movements happen (basically you get used to being dizzy).
If the treatments aren't helping you, let your provider know as soon as possible.
Step 1
Step 2
Step 3
Step 4 Begin
Produced by D.B. Watkinswww.dbwatkins.com
Image provided by:http://archotol.ama-assn.org(Colorized by D.B. Watkins)
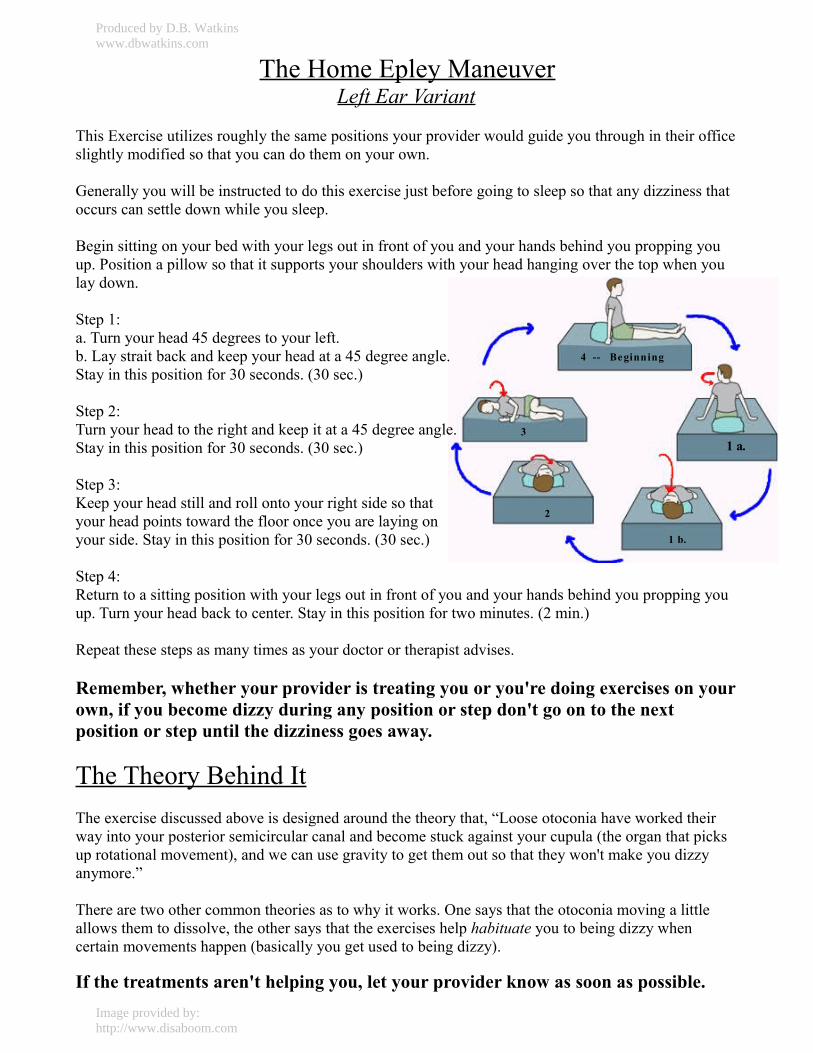
The Home Epley ManeuverLeft Ear Variant
This Exercise utilizes roughly the same positions your provider would guide you through in their office slightly modified so that you can do them on your own.
Generally you will be instructed to do this exercise just before going to sleep so that any dizziness that occurs can settle down while you sleep.
Begin sitting on your bed with your legs out in front of you and your hands behind you propping you up. Position a pillow so that it supports your shoulders with your head hanging over the top when you lay down.
Step 1:a. Turn your head 45 degrees to your left.b. Lay strait back and keep your head at a 45 degree angle. Stay in this position for 30 seconds. (30 sec.)
Step 2:Turn your head to the right and keep it at a 45 degree angle. Stay in this position for 30 seconds. (30 sec.)
Step 3:Keep your head still and roll onto your right side so that your head points toward the floor once you are laying on your side. Stay in this position for 30 seconds. (30 sec.)
Step 4:Return to a sitting position with your legs out in front of you and your hands behind you propping you up. Turn your head back to center. Stay in this position for two minutes. (2 min.)
Repeat these steps as many times as your doctor or therapist advises.
Remember, whether your provider is treating you or you're doing exercises on your own, if you become dizzy during any position or step don't go on to the next position or step until the dizziness goes away.
The Theory Behind ItThe exercise discussed above is designed around the theory that, “Loose otoconia have worked their way into your posterior semicircular canal and become stuck against your cupula (the organ that picks up rotational movement), and we can use gravity to get them out so that they won't make you dizzy anymore.”
There are two other common theories as to why it works. One says that the otoconia moving a little allows them to dissolve, the other says that the exercises help habituate you to being dizzy when certain movements happen (basically you get used to being dizzy).
If the treatments aren't helping you, let your provider know as soon as possible.
31 a.
1 b.
2
4 -- Beginning
Produced by D.B. Watkinswww.dbwatkins.com
Image provided by:http://www.disaboom.com
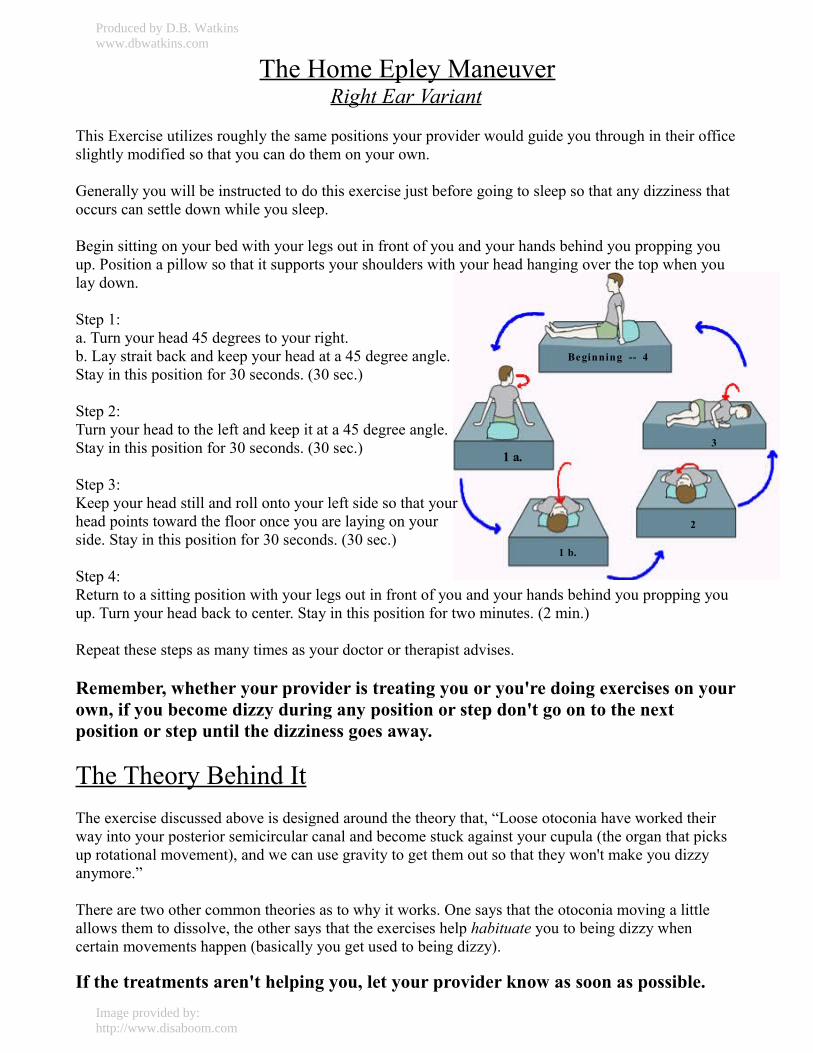
The Home Epley ManeuverRight Ear Variant
This Exercise utilizes roughly the same positions your provider would guide you through in their office slightly modified so that you can do them on your own.
Generally you will be instructed to do this exercise just before going to sleep so that any dizziness that occurs can settle down while you sleep.
Begin sitting on your bed with your legs out in front of you and your hands behind you propping you up. Position a pillow so that it supports your shoulders with your head hanging over the top when you lay down.
Step 1:a. Turn your head 45 degrees to your right.b. Lay strait back and keep your head at a 45 degree angle. Stay in this position for 30 seconds. (30 sec.)
Step 2:Turn your head to the left and keep it at a 45 degree angle. Stay in this position for 30 seconds. (30 sec.)
Step 3:Keep your head still and roll onto your left side so that your head points toward the floor once you are laying on your side. Stay in this position for 30 seconds. (30 sec.)
Step 4:Return to a sitting position with your legs out in front of you and your hands behind you propping you up. Turn your head back to center. Stay in this position for two minutes. (2 min.)
Repeat these steps as many times as your doctor or therapist advises.
Remember, whether your provider is treating you or you're doing exercises on your own, if you become dizzy during any position or step don't go on to the next position or step until the dizziness goes away.
The Theory Behind ItThe exercise discussed above is designed around the theory that, “Loose otoconia have worked their way into your posterior semicircular canal and become stuck against your cupula (the organ that picks up rotational movement), and we can use gravity to get them out so that they won't make you dizzy anymore.”
There are two other common theories as to why it works. One says that the otoconia moving a little allows them to dissolve, the other says that the exercises help habituate you to being dizzy when certain movements happen (basically you get used to being dizzy).
If the treatments aren't helping you, let your provider know as soon as possible.
31 a.
1 b.
2
Beginning -- 4
Produced by D.B. Watkinswww.dbwatkins.com
Image provided by:http://www.disaboom.com
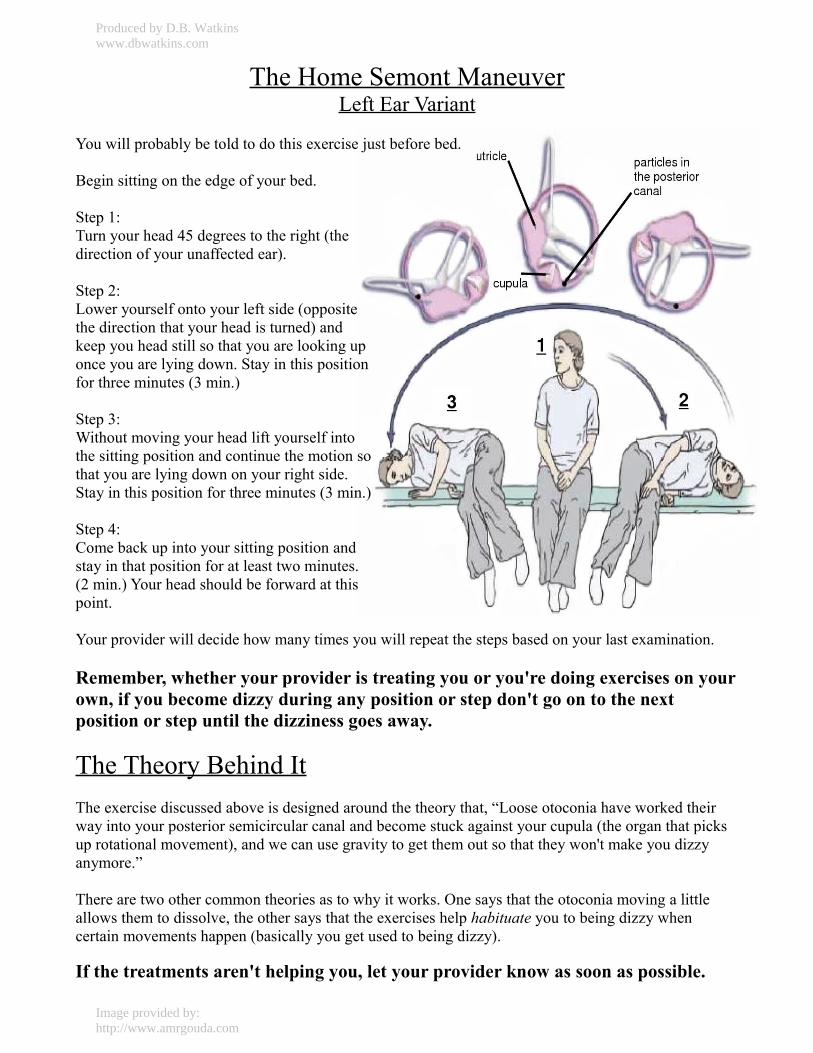
The Home Semont ManeuverLeft Ear Variant
You will probably be told to do this exercise just before bed.
Begin sitting on the edge of your bed.
Step 1:Turn your head 45 degrees to the right (the direction of your unaffected ear).
Step 2:Lower yourself onto your left side (opposite the direction that your head is turned) and keep you head still so that you are looking up once you are lying down. Stay in this position for three minutes (3 min.)
Step 3:Without moving your head lift yourself into the sitting position and continue the motion so that you are lying down on your right side. Stay in this position for three minutes (3 min.)
Step 4:Come back up into your sitting position and stay in that position for at least two minutes. (2 min.) Your head should be forward at this point.
Your provider will decide how many times you will repeat the steps based on your last examination.
Remember, whether your provider is treating you or you're doing exercises on your own, if you become dizzy during any position or step don't go on to the next position or step until the dizziness goes away.
The Theory Behind ItThe exercise discussed above is designed around the theory that, “Loose otoconia have worked their way into your posterior semicircular canal and become stuck against your cupula (the organ that picks up rotational movement), and we can use gravity to get them out so that they won't make you dizzy anymore.”
There are two other common theories as to why it works. One says that the otoconia moving a little allows them to dissolve, the other says that the exercises help habituate you to being dizzy when certain movements happen (basically you get used to being dizzy).
If the treatments aren't helping you, let your provider know as soon as possible.
Produced by D.B. Watkinswww.dbwatkins.com
Image provided by:http://www.amrgouda.com
The Home Semont ManeuverRight Ear Variant
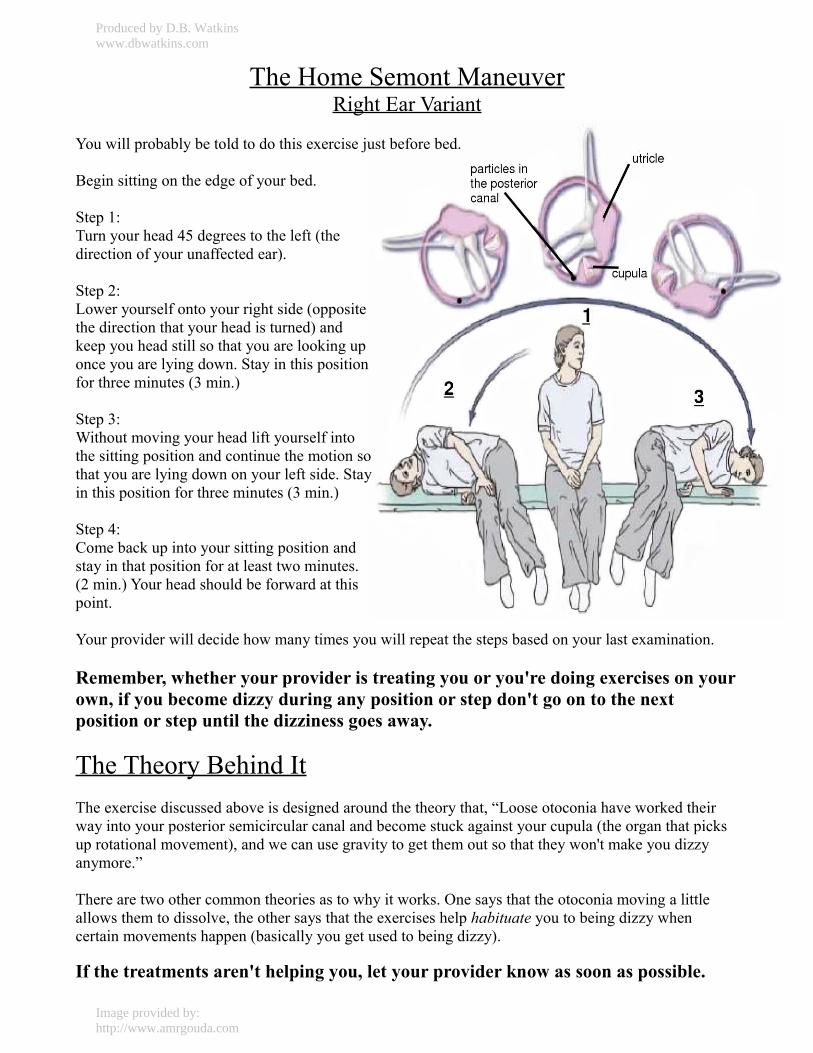
You will probably be told to do this exercise just before bed.
Begin sitting on the edge of your bed.
Step 1:Turn your head 45 degrees to the left (the direction of your unaffected ear).
Step 2:Lower yourself onto your right side (opposite the direction that your head is turned) and keep you head still so that you are looking up once you are lying down. Stay in this position for three minutes (3 min.)
Step 3:Without moving your head lift yourself into the sitting position and continue the motion so that you are lying down on your left side. Stay in this position for three minutes (3 min.)
Step 4:Come back up into your sitting position and stay in that position for at least two minutes. (2 min.) Your head should be forward at this point.
Your provider will decide how many times you will repeat the steps based on your last examination.
Remember, whether your provider is treating you or you're doing exercises on your own, if you become dizzy during any position or step don't go on to the next position or step until the dizziness goes away.
The Theory Behind ItThe exercise discussed above is designed around the theory that, “Loose otoconia have worked their way into your posterior semicircular canal and become stuck against your cupula (the organ that picks up rotational movement), and we can use gravity to get them out so that they won't make you dizzy anymore.”
There are two other common theories as to why it works. One says that the otoconia moving a little allows them to dissolve, the other says that the exercises help habituate you to being dizzy when certain movements happen (basically you get used to being dizzy).
If the treatments aren't helping you, let your provider know as soon as possible.
Produced by D.B. Watkinswww.dbwatkins.com
Image provided by:http://www.amrgouda.com
Related Documents











