29 CLINICAL DENTISTRY AND RESEARCH 2012; 36(2): 29-35 Correspondence Güliz N. Güncü, DDS, PhD Department of Periodontology, Faculty of Dentistry, Hacettepe University, 06100 Sıhhıye Ankara, Turkey Phone: +90 312 305 2237 Fax: +90 312 310 4440 E-mail: [email protected] Güliz N. Güncü, DDS, PhD Associate Professor, Department of Periodontology, Faculty of Dentistry, Hacettepe University, Ankara, Turkey H. Gencay Keçeli DDS, PhD Assistant Professor, Department of Periodontology, Faculty of Dentistry, Kırıkkale University, Kırıkkale, Turkey Esra Ercan DDS, PhD Assistant Professor, Department of Periodontology, Faculty of Dentistry, Karadeniz Technical University, Trabzon, Turkey Hasan Hatipoğlu, DDS, PhD Assistant Professor, Dental Clinic/Periodontology, Research and Training Hospital, Dumlupınar University, ,Central Campus, Kütahya, Turkey Dilek İlhan, DDS, PhD Professor, Department of Periodontology, Faculty of Dentistry, Hacettepe University, Ankara, Turkey Tolga F. Tözüm, DDS, PhD Professor, Department of Periodontology, Faculty of Dentistry, Hacettepe University, Ankara, Turkey VERTICAL AND HORIZONTAL DIMENSIONAL EVALUATION OF SUTURELESS FREE GINGIVAL GRAFTS ABSTRACT Background and Aim: Tissue adhesives can be used as an alternative to conventional sutures in periodontal surgery. The free gingival graft (FGG) is a technique used to increase the zone of keratinized gingiva. The shrinkage of FGGs is a well-known clinical phenomenon. However, to our knowledge, there is no data available regarding the dimensional changes in FGG procedure using non-suturing techniques. The aim of the present study was to evaluate the shrinkage of FGGs, either sutureless or with suturing technique, in both horizontal and vertical dimensions and to calculate the changes in the surface area of the graft at early and delayed time points. Subjects and Methods: The present study was carried out on 26 patients requiring FGG due to lack of keratinized gingiva at the buccal aspect of mandibular incisors. Patients were randomly treated by FGG using either tissue adhesive (test) or suture (control). The graft dimensions were measured and the shrinkage of the graft was calculated at baseline and at day 10, 21 and 180. Results: Significant reductions were observed in horizontal and vertical dimensions at all time-points. When compared to baseline, this difference was statistically significant during the whole study period, except in the test group at day 10. The percentage of vertical shrinkage was significantly lower in the test group at day 10 and 180 when compared to baseline. Conclusions: Present findings indicate that tissue adhesives can reduce the amount of vertical graft shrinkage that occurs following FGG procedures. Key words: Free Gingival Graft, Tissue Adhesives, Tissue Shrinkage Submitted for Publication: 01.26.2012 Accepted for Publication : 03.12.2012

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
29
CLINICAL DENTISTRY AND RESEARCH 2012; 36(2): 29-35
Correspondence
Güliz N. Güncü, DDS, PhDDepartment of Periodontology,
Faculty of Dentistry,
Hacettepe University,
06100 Sıhhıye Ankara, Turkey
Phone: +90 312 305 2237
Fax: +90 312 310 4440
E-mail: [email protected]
Güliz N. Güncü, DDS, PhD Associate Professor, Department of Periodontology,
Faculty of Dentistry, Hacettepe University,
Ankara, Turkey
H. Gencay Keçeli DDS, PhD Assistant Professor, Department of Periodontology,
Faculty of Dentistry, Kırıkkale University,
Kırıkkale, Turkey
Esra Ercan DDS, PhDAssistant Professor, Department of Periodontology,
Faculty of Dentistry, Karadeniz Technical University,
Trabzon, Turkey
Hasan Hatipoğlu, DDS, PhDAssistant Professor, Dental Clinic/Periodontology,
Research and Training Hospital,
Dumlupınar University, ,Central Campus,
Kütahya, Turkey
Dilek İlhan, DDS, PhDProfessor, Department of Periodontology,
Faculty of Dentistry, Hacettepe University,
Ankara, Turkey
Tolga F. Tözüm, DDS, PhDProfessor, Department of Periodontology,
Faculty of Dentistry, Hacettepe University,
Ankara, Turkey
VERTICAL AND HORIZONTAL DIMENSIONAL EVALUATION OF SUTURELESS FREE GINGIVAL GRAFTS
ABSTRACT
Background and Aim: Tissue adhesives can be used as an
alternative to conventional sutures in periodontal surgery.
The free gingival graft (FGG) is a technique used to increase
the zone of keratinized gingiva. The shrinkage of FGGs is a
well-known clinical phenomenon. However, to our knowledge,
there is no data available regarding the dimensional changes in
FGG procedure using non-suturing techniques. The aim of the
present study was to evaluate the shrinkage of FGGs, either
sutureless or with suturing technique, in both horizontal and
vertical dimensions and to calculate the changes in the surface
area of the graft at early and delayed time points.
Subjects and Methods: The present study was carried out
on 26 patients requiring FGG due to lack of keratinized gingiva
at the buccal aspect of mandibular incisors. Patients were
randomly treated by FGG using either tissue adhesive (test) or
suture (control). The graft dimensions were measured and the
shrinkage of the graft was calculated at baseline and at day 10,
21 and 180.
Results: Significant reductions were observed in horizontal
and vertical dimensions at all time-points. When compared to
baseline, this difference was statistically significant during the
whole study period, except in the test group at day 10. The
percentage of vertical shrinkage was significantly lower in the
test group at day 10 and 180 when compared to baseline.
Conclusions: Present findings indicate that tissue adhesives
can reduce the amount of vertical graft shrinkage that occurs
following FGG procedures.
Key words: Free Gingival Graft, Tissue Adhesives, Tissue Shrinkage
Submitted for Publication: 01.26.2012
Accepted for Publication : 03.12.2012

30
CLINICAL DENTISTRY AND RESEARCH
INTRODUCTION
Cyanoacrylates are tissue-adhesive materials that were synthesized in 1959 by Coover et al.1 The earlier methyl homologues were found to be histotoxic and thus were discontinued in clinical practice.2 N-butyl cyanoacrylate (NBC) and its isoform iso-butyl cyanoacrylate are biocompatible tissue adhesives and have good working properties like flow and fast setting, within 5-10 seconds. NBC sets by polymerization in presence of moisture and even blood, with release of heat. It is found to be bacteriostatic, and reduced postoperative pain has been observed in sites treated with NBC. It has good bonding properties and the necessary strength to hold the tissue margins together and also has hemostatic properties.3 Cyanoacrylate derivatives demonstrate many of the properties of an ideal wound closure agent. They can be used on most parts of the body and have been used in the healing of wounds ranging from 0.5 to 50 cm in length.4 These adhesives are liquid monomers that polymerize when getting in contact with the wound moisture in order to form a solid bond.5 In medical literature, successful outcomes were reported by using NBC in different operations such as the embolization and occlusion of cystic duct.6-8 Kulkarni et al.9 evaluated the healing of periodontal flaps when closed either with sutures or cyanocrylate. They reported that periodontal flaps healed by primary closure when sutured and treated with NBC. At 7 days clinically and histologically, cyanoacrylate sites presented less inflammation when compared to the sutured sites.9 Moreover, Hoexter et al.4 described a technique using cyanoacrylate by placing this agent on a transferring instrument, designed to utilize the autogenous free gingival graft without the use of sutures. The autogenous free gingival graft (FGG) is a routine technique for management of mucogingival problems. Presence of a certain width of keratinized tissue is well- demonstrated to be important in maintaining periodontal health and preventing soft tissue recession.10 The healing of the FGG primarily depends on the restoration of collateral circulation from the periosteal and connective tissue bed, while the thin blood clot promotes tensile strength and stability of the wound. Wound stability and wound contraction are important contributing factors for healing events affecting the treatment outcome.11 The dimensional changes including the contraction of the transplanted tissue may occur, especially in long-term follow-up, and as a result, expected treatment outcome including
satisfactory amount of new keratinized tissue may not be achieved.12 The vertical shrinkage of FGG is a well known clinical phenomenon that occurs mainly during healing in the first postoperative month, where 25% to 47% average shrinkage was noticed in literature.13-16 Recently, Orsini et al.10 and Hatipoglu et al.17 analyzed dimensional changes of FGG and reported average vertical shrinkages of 43.25% at 52 week and %24.8 at 24 weeks, respectively. Moreover, Hatipoglu et al.17 demonstrated significant reductions in the vertical direction in all visits, except at day 10. The sutureless graft avoids the piercing of the donor site, decreases procedure time and do not need to be removed during post-operative follow-up.4,18 Based on these properties, it can be concluded that using cyanoacrylates in FGGs, the extent of shrinkage may be reduced. To the authors’ knowledge shrinkage of FGGs, stabilized with non-suturing techniques, have not been previously studied. Therefore, the aim of the present study was to evaluate the shrinkage of FGGs, performed using either tissue adhesives or suture, in both horizontal and vertical dimensions.
SUBJECTS AND METHODS
Experimental Design and Study Groups
This study was conducted on the group of patients who were referred to Department of Periodontology Hacettepe University for routine periodontal examination. Following clinical periodontal examination, 26 systemically healthy and non-smoker patients were diagnosed as lacking keratinized tissue at the buccal aspect of mandibular incisors and these patients were included in the study protocol to be treated with FGG to increase the zone of keratinized tissue. All patients were informed about the study protocol and written informed consents were obtained. Full mouth scaling and polishing was performed 4 weeks prior to the surgical treatment and patients were instructed and reinforced for routine oral hygiene procedures. After initial treatment, tension test (stretching of the lower lips) was performed to determine the width of keratinized tissue and the distance between the margin of the gingiva and the mucogingival junction was recorded to the nearest 0.5 mm using a Michigan-O-probe (23/QOW, Hu-Friedy Mfg. Inc. Chicago, IL, USA). Patients exhibiting gingival recession were excluded from the study. Patients were then randomly assigned to one of the treatment groups.

31
TiSSUE ADHESivES AnD FREE GinGivAl GRAFTS
Surgical Procedure
All surgical procedures were performed under local anesthesia (Ultracain D-S, Hoechst Marion Russel, Frankfurt/Main, and Germany). A marginal horizontal linear incision was performed at the mucogingival junction using number 15 scalpel at the recipient site. (Hu-Friedy Mfg. Inc. Chicago, IL, USA). The horizontal dimension of the recipient site was determined according to the area presenting with mucogingival stress. Split-thickness incision was extended more distally than the planned area19 and deepened to the adequate depth to prepare the appropriate recipient graft bed. Hard palate was selected as the donor site and a second surgical site was created on the palate carefully avoiding the damage of greater palatine neurovascular bundle.20 The size and thickness of the graft was measured using a Michigan-O-peridontal probe. A rectangular graft -1 mm smaller than the recipient site at the mesial, distal and apical regions and 1-2 mm in thickness- was harvested from the donor site by a partial thickness incision. In the Test Group, graft was adapted on the recipient site by pressing with sterile gauze soaked in saline in order to avoid any mobility during functional movements of the lips. NBC (Glueseal, GluStitch Inc., Delta BC, Canada) was applied to the mesial, distal and coronal borders of the graft and recipient site. After waiting 3-4 minutes, periodontal dressing was applied over the surgical area.In the Control Group, the graft was sutured to the recipient bed by 5-0 silk sliding sutures. Two or three knots of sutures were positioned between the existing intact keratinized gingiva and the transplanted tissue. Mild compress with gauze soaked in saline was applied for 5 min to adapt the graft to the recipient site. Periodontal dressing was applied over the recipient area to protect the surgical region.Antibiotics were prescribed (amoxicillin, 500 mg, four times daily) for 7 days to prevent possible postoperative infections.21,22 The periodontal dressing and/or sutures were removed 10 days after surgery. Post-surgical hemorrhage, sense alterations and pain symptoms were also recorded at 10, 21 and 180 day follow-up for both recipient and donor sites. The same clinician recorded the vertical and horizontal dimensions of the graft at 10, 21 and 180 days follow-up (Figure 1). The surface area of the transplanted tissue was calculated by multiplying the vertical and horizontal dimensions recorded. The shrinkage of the graft and the percentage of the graft area were also calculated.17
Statistical analysis
Computer software (GraphPad Instat 3.00 for Windows, Graphpad Software, San Diego, CA, USA) was used for all statistical analysis. The Mann Whitney U-test with Bonferroni correction was performed to determine the significant differences between the test and control groups. The dimensional changes within the groups between baseline and 10, 21 and 180 days were analyzed using the Wilcoxon test.
RESULTS
Healing at the donor and recipient sites was uneventful in both study groups. Twelve patients (10 females and 2 males, were treated with FGG using tissue adhesive and 14 patients (8 females and 6 males) were treated with FGG using sutures in the control group. The dimensions of the graft in both horizontal and vertical directions were recorded at baseline, 10, 21, and 180 days for both groups. The dimensional changes and shrinkage of FGGs during the follow-up period are presented in Table 1 and Table 2, respectively.None of the subjects in either of the study groups presented with any complications such as clinical paresthesia, bleeding
Figure 1. a. Preoperative view of the recipient area. Lack of keratinized gingiva is observed.b. Postoperative view of the area at day 180. Vertical and horizontal dimensions were shown in a schematic way. Note the color difference between graft and recipient area.

32
CLINICAL DENTISTRY AND RESEARCH
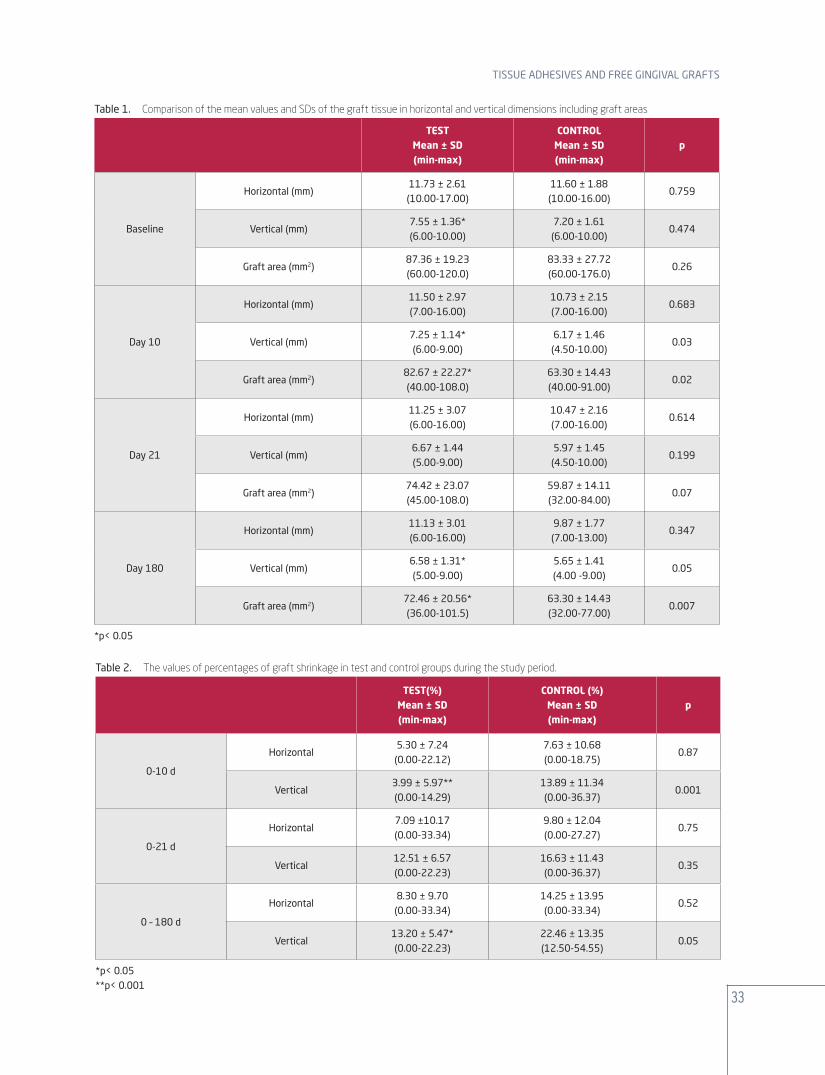
or pain during the 6 month follow-up. When the dimensional changes of the grafts were analyzed, reductions in horizontal and vertical dimensions were detected at all time-points regardless of the treatment procedure. This difference was statistically significant during the whole study period, except at day 10 for the test group. Calculated graft area also significantly decreased during the follow-up period compared to baseline for both groups (p<0.05) (Table 1).When horizontal dimensions and graft area were concerned, no statistically significant differences were detected between the groups at baseline (Table 1). However, at day 10 and 180, vertical graft dimensions and graft area values were significantly higher in the test group (p<0.05) (Table 1). Percentage of vertical shrinkage was significantly lower in the test group at day 10 (p=0.001) and 180 (p=0.05) when compared to baseline (Table 2.)Additionally, three different tissue biotypes were detected according to the thickness of the graft (thick, normal, thin) in both test and control groups. The thin biotype was the most frequent type in the present study group (58.3% and 57.4% in test and control groups respectively). No statistically significant differences were detected between the test and the control groups in terms of the thickness of FGG (p>0.05)
DISCUSSION
The present study was carried out to evaluate the amount of shrinkage of FGGs performed with sutures or tissue adhesives. Although all values were found to be lower in the test group, statistically significant differences were only noted at day 10 and 180 for vertical shrinkage measurements. This difference may be due to the properties of tissue adhesives. Tissue adhesives were reported to be superior in immediate hemostasis, controlling of bleeding rapidly, less time consuming, easier to apply, decreased procedure time and having the not need to be removed during post operative follow-up.23 In the test group, FGG surgeries were performed successfully without using sutures, thus avoiding the unnecessarily piercing of the grafts4 and not disrupting the circulation from the periosteal and connective tissue bed. Kulkarni et al.9 evaluated the healing of flaps stabilized with cyanoacrylates and reported less inflammation histologically when compared with sutured sites. Giray et al.24 compared and evaluated the clinical and electron microscopic results of mucosal incisions stabilized with cyanoacrylates and silk sutures. Epithelization was reported to be better for the sites treated with tissue adhesive at
day 3 and 7.24 Similiarly, in the present study less shrinkage was observed in tissue adhesive group. This difference may be due to the occurrence of less inflammation and rapid epithelization. However, histological analysis is needed to determine the healing process in tissue adhesive stabilized FGGs. The shrinkage of FGGs is a well known clinical phenomenon that occurs during the wound healing in the first postoperative month.20,25 Different clinical studies presented a broad range of shrinkage percentages between 12% and 48%.20,26,27 It has been suggested that shrinkage occurs during the first year after surgery and the width of the keratinized tissue remains stable thereafter. The percentage of shrinkage in vertical direction were 3.99%, 12.51%, 13.20% in the test group and 13.89%, 16.63%, 22.46% in control group at days 10, 21 and 180, respectively. The present vertical shrinkage data is in accordance with the literature. Hatipoglu et al.17 evaluated the vertical and horizontal dimensions of FGG at mandibular incisor region at days 10, 21 and 180 and reported 3.6%, 5.8% and 10.2% horizontal graft shrinkage percentages. In the test group 5.30%, 7.09%, 8.30% and in the control group 7.63%, 9.80%, 14.25% shrinkage in horizontal direction were noticed in the present study at days 10, 21 and 180, respectively. Statistically significant reductions in the horizontal and vertical dimensions were detected at all time-points for both groups, except in the test group at day 10. The possible explanation for the higher extent of the shrinkage of FGGs performed in the present study may be the higher percentage of patients presenting with thin tissue biotypes (%57.14 in test and 58% in control group) when compared to the previous study group conducted by Hatipoğlu et al.17 (40%). Tissue thickness might be related to the dimensional changes both in horizontal and vertical directions. Three different tissue biotypes were described (thick, normal, thin) in the literature and Claffey and Shanley28 reported increased tendency of gingival recession for thin tissue biotypes. In the present study, although there were statistically no differences between the test and the control group in terms of tissue biotypes, differences in graft shrinkage and dimensions were detected. Further studies including different gingival biotypes are needed to determine the distinct impact of tissue biotype on graft shrinkage. In the present study, the graft area and shrinkage values are calculated based on the two dimensional measurements
33
TiSSUE ADHESivES AnD FREE GinGivAl GRAFTS
Table 1. Comparison of the mean values and SDs of the graft tissue in horizontal and vertical dimensions including graft areas
TESTMean ± SD(min-max)
CONTROLMean ± SD(min-max)
p
Baseline
Horizontal (mm)11.73 ± 2.61(10.00-17.00)
11.60 ± 1.88(10.00-16.00)
0.759
vertical (mm)7.55 ± 1.36*(6.00-10.00)
7.20 ± 1.61(6.00-10.00)
0.474
Graft area (mm2)87.36 ± 19.23(60.00-120.0)
83.33 ± 27.72(60.00-176.0)
0.26
Day 10
Horizontal (mm)11.50 ± 2.97(7.00-16.00)
10.73 ± 2.15(7.00-16.00)
0.683
vertical (mm)7.25 ± 1.14*(6.00-9.00)
6.17 ± 1.46(4.50-10.00)
0.03
Graft area (mm2)82.67 ± 22.27*(40.00-108.0)
63.30 ± 14.43(40.00-91.00)
0.02
Day 21
Horizontal (mm)11.25 ± 3.07(6.00-16.00)
10.47 ± 2.16(7.00-16.00)
0.614
vertical (mm)6.67 ± 1.44(5.00-9.00)
5.97 ± 1.45(4.50-10.00)
0.199
Graft area (mm2)74.42 ± 23.07(45.00-108.0)
59.87 ± 14.11(32.00-84.00)
0.07
Day 180
Horizontal (mm)11.13 ± 3.01(6.00-16.00)
9.87 ± 1.77(7.00-13.00)
0.347
vertical (mm)6.58 ± 1.31*(5.00-9.00)
5.65 ± 1.41(4.00 -9.00)
0.05
Graft area (mm2)72.46 ± 20.56*(36.00-101.5)
63.30 ± 14.43(32.00-77.00)
0.007
*p< 0.05
Table 2. The values of percentages of graft shrinkage in test and control groups during the study period.
TEST(%) Mean ± SD(min-max)
CONTROL (%)Mean ± SD(min-max)
p
0-10 d
Horizontal5.30 ± 7.24(0.00-22.12)
7.63 ± 10.68(0.00-18.75)
0.87
vertical3.99 ± 5.97**(0.00-14.29)
13.89 ± 11.34(0.00-36.37)
0.001
0-21 d
Horizontal7.09 ±10.17(0.00-33.34)
9.80 ± 12.04(0.00-27.27)
0.75
vertical12.51 ± 6.57(0.00-22.23)
16.63 ± 11.43(0.00-36.37)
0.35
0 – 180 d
Horizontal8.30 ± 9.70(0.00-33.34)
14.25 ± 13.95(0.00-33.34)
0.52
vertical13.20 ± 5.47*(0.00-22.23)
22.46 ± 13.35(12.50-54.55)
0.05
*p< 0.05**p< 0.001
34
CLINICAL DENTISTRY AND RESEARCH
which avoids evaluating the effect of thickness of the graft on dimensional changes. Thus, using 3D photogrammetric methods taking the thickness values in account for calculating the area of the grafts may be beneficial for evaluating the dimensional changes more precisely.
CONCLUSION
In conclusion, results of the present study suggest that stabilization of FGGs with tissue adhesives may result in less graft shrinkage when compared with suturing techniques. Further clinical and histological studies, performed in larger study groups may further clarify the impact of tissue adhesives on healing and dimensional stability of FGGs.
REFERENCES
1. Levin MP. Periodontal suture materials and surgical dressings. Dent Clin North Am 1980; 24: 767-781.
2. Greer RO, Jr. Studies concerning the hsitotoxicity of isobutyl-2-cyanoacrylate tissue adhesive when employed as an oral hemostat. Oral Surg Oral Med Oral Pathol 1975; 40: 659-669.
3. Xu X, Lau K, Taira BR, Singer AJ. The current management of skin tears. Am J Emerg Med 2009; 27: 729-733.
4. Hoexter DL. The sutureless free gingival graft. J Periodontol. 1979; 50: 75-78.
5. Hochberg J, Meyer KM, Marion MD. Suture choice and other methods of skin closure. Surg Clin North Am 2009; 89: 627-641.
6. Pollak JS, White RI Jr. The use of cyanoacrylate adhesives in peripheral embolization. J Vasc Interv Radiol 2001; 12: 907-913.
7. Matsumoto T, Yamagami T, Kato T, Hirota T, Yoshimatsu R, Nishimura T. Transcatheter arterial embolisation of a ruptured pseudoaneurysm of the lingual artery with n-butyl cyanoacrylate. Br J Radiol 2007; 80: 54-57.
8. Ganguly EK, Najarian KE, Vecchio JA, Moses PL. Endoscopic occlusion of cystic duct using N-butyl cyanoacrylate for postoperative bile leakage. Dig Endosc 2010; 22: 348-350.
9. Kulkarni S, Dodwad V, Chava V. Healing of periodontal flaps when closed with silk sutures and N-butyl cyanoacrylate: a clinical and histological study. Indian J Dent Res 2007; 18: 72-77.
10. Orsini M, Orsini G, Benlloch D, Aranda JJ, Lazaro P, Sanz M. Esthetic and dimensional evaluation of free connective tissue grafts in prosthetically treated patients: a 1-year clinical study. J Periodontol 2004; 75: 470-477.
11. Bouchard P, Malet J, Borghetti A. Decision-making in aesthetics: root coverage revisited. Periodontol 2000 2001; 27: 97-120.
12. Donoff RB. Biological basis for vestibuloplasty procedures. J Oral Surg 1976; 34: 890-896.
13. Sullivan HC, Atkins JH. Free autogenous gingival grafts. I. Principles of successful grafting. Periodontics 1968; 6: 121-129.
14. Soehren SE, Allen AL, Cutright DE, Seibert JS. Clinical and histologic studies of donor tissues utilized tissues utilized for free grafts of masticatory mucosa. J Periodontol 1973; 44: 727-741.
15. Egli U, Vollmer WH, Rateitschak KH. Follow-up studies of free gingival grafts. J Clin Periodontol 1975; 2: 98-104.
16. Rateitschak KH, Egli U, Fringeli G. Recession: A 4-year longitudinal study after free gingival grafts. J Clin Periodontol 1979; 6: 158-164.
17. Hatipoglu H, Keceli HG, Guncu GN, Sengun D, Tozum TF. Vertical and horizontal dimensional evaluation of free gingival grafts in the anterior mandible: a case report series. Clin Oral Investig 2007; 11: 107-113.
18. Grisdale J. The use of cyanoacrylates in periodontal therapy. J Can Dent Assoc 1998; 64: 632-633.
19. Mormann W, Schaer F, Firestone AR. The relationship between success of free gingival grafts and transplant thickness. Revascularization and shrinkage--a one year clinical study. J Periodontol 1981; 52: 74-80.
20. Reiser GM, Bruno JF, Mahan PE, Larkin LH. The subepithelial connective tissue graft palatal donor site: anatomic considerations for surgeons. Int J Periodontics Restorative Dent 1996; 16: 130-137.
21. de Queiroz Cortes A, Sallum AW, Casati MZ, Nociti FH, Jr., Sallum EA. A two-year prospective study of coronally positioned flap with or without acellular dermal matrix graft. J Clin Periodontol 2006; 33: 683-689.
22. Wang HL, Greenwell H. Surgical periodontal therapy. Periodontol 2000 2001;25:89-99.
23. Perez M, Fernandez I, Marquez D, Bretana RM. Use of N-butyl-2-cyanoacrylate in oral surgery: biological and clinical evaluation. Artif Organs 2000; 24: 241-243.
24. Giray CB, Atasever A, Durgun B, Araz K. Clinical and electron microscope comparison of silk sutures and n-butyl-2-cyanoacrylate in human mucosa. Aust Dent J 1997; 42: 255-258.
25. Ericsson I, Lindhe J. Recession in sites with inadequate width of the keratinized gingiva. An experimental study in the dog. J Clin Periodontol 1984; 11: 95-103.
26. Matter J, Cimasoni G. Creeping attachment after free gingival grafts. J Periodontol 1976; 47: 574-579.
35
TiSSUE ADHESivES AnD FREE GinGivAl GRAFTS
27. Stetler KJ, Bissada NF. Significance of the width of keratinized gingiva on the periodontal status of teeth with submarginal restorations. J Periodontol 1987; 58: 696-700.
28. Claffey N, Shanley D. Relationship of gingival thickness and bleeding to loss of probing attachment in shallow sites following nonsurgical periodontal therapy. J Clin Periodontol 1986; 13: 654-657.
Related Documents











