VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007 Risk assessment for VTE Dr Roopen Arya

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Risk assessment for VTE
Dr Roopen Arya

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
VERITY & VTE risk
• VERITY risk factor data
• VERITY thromboprophylaxis data
• Thrombosis prevention in the NHS
• Risk assessment & risk scores
• The way forward

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
VERITY and thromboprophylaxis
• Most cases present after discharge
• Data highlight risk in medical and surgical patients
• Variation in thromboprophylaxis

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Thrombosis prevention in the NHS
• House of Common Health Committee
Report March 2005
• Government response July 2005
• CMO publishes Independent Expert
Working Group report April 2007
• NICE guidance re: surgical patients April
2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Health Committee: Key themes
• Awareness• National guidelines• NICE guidelines (2007)• Education• Implementation
Risk assessmentThrombosis CommitteesThrombosis Teams

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Government response to Health Committee report July 2005
• CMO communication re: existing guidance
• Independent VTE experts working group:review evidence & guidelinesframework for implementation
make recommendations to CMO
• Discuss with NICE a separate clinical guideline covering patients excluded from the scope of current guidance.
• CMO to write to relevant bodies involved in medical education regarding necessary changes in curricula..

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Independent VTE Expert Group
• Quickly assess available guidance• Consider use of mechanical devices and
clarify the role of aspirin• Consider VTE awareness and education• Better monitoring systems to improve data on
VTE outcome and mortality• Make recommendations regarding
implementation of thrombosis prevention

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
CMO Recommendations April 2007• CMO communication: published VTE Expert Working
Group’s guidance in full
1.1. Systems, processes and knowledge base
Documented mandatory risk assessment (all hospitalised patients)
VTE risk assessment embedded in CNST
Improved public/professional understanding of VTE (communication, information, education)

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
CMO Recommendations April 2007
1.1. Systems, processes and knowledge base (cont)
VTE demo sites (strategy, educational material, develop national risk assessment strategy, advice)
Core Standards from DOH to ensure compliance with risk assessment
HCC monitors standards
Evaluate impact on patient: systematic approach to ensure compliance, communication strategy, better outcome measures, raise awareness)

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
CMO Recommendations April 2007CMO Recommendations April 20072. Thromboprophylaxis Strategy (Medical)
All medical patients considered for thrombo-prophylaxis as part of mandatory risk assessment Particularly > 4 days in hospital, Reduced mobility Heart failure, Resp failure, Acute infection, Inflammatory illness,
Cancer
Regimen: UFH/LMWH(preferred) Aspirin not recommended Mechanical not recommended (no current evidence)

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
CMO Recommendations April 2007
2. Thromboprophylaxis Strategy (Surgical)
• All high risk surgical/orthopaedic patients managed according to NICE guidance
• Intermediate risk surgical: mandatory risk assessment
– GCS+heparin– Not aspirin
• Low risk surgical: early mobilisation only

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
NICE clinical guideline 46: VTEKey priorities for implementation
• Risk assessment• Patient information• Thigh-length graduated compression / anti-
embolism stockings• Patients shown to wear them correctly• Intermittent pneumatic compression or foot
impulse devices may be used as alternatives or in addition to AES.

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
NICE clinical guideline 46: VTEKey priorities for implementation
• In addition to mechanical prophylaxis, patient at increased risk of VTE because they have individual risk factors and patients having orthopaedic surgery should be offered LMWH.
• Fondaparinux, within its licensed indications, may be used as an alternative.
• LMWH or fondaparinux continued for 4 weeks after hip fracture surgery.
• Suitability of regional anaesthesia considered.• Early mobilisation after surgery.

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Risk Assessment & Clinical Governance
• The highest ranking safety practice was the appropriate use of prophylaxis to prevent VTE in patients at risk.AHRQ “Making Health Safer: A Critical Analysis of Patient Safety Practices” 2001
• We recommend that every hospital develop a formal strategy that addresses prevention of thromboembolic complications. This should generally be in the form of a written thromboprophylaxis policy especially for high risk groups.ACCP guidelines “ Prevention of VTE” 2004

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Risk Assessment & Clinical Governance
Identifying at-risk patientIdentifying at-risk patient
Counselling at-risk Counselling at-risk patientpatient
PrescribingPrescribingthromboprophylaxisthromboprophylaxis

1
0
2
3
Lowrisk
Increasedrisk
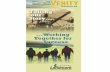
Lutz L et al. Med Welt 2002;53:231–4
0 1 2 3
Class of predisposing risk Dehydration Polycythaemia or thrombocytosis Varicosis VTE in family HRT Obesity
Thrombophilia History of VTE Active malignancy or 3 risks from category 1 2 risks from category 2
No basic risk Age 65 years Pregnancy Oral contraception Nephrotic syndrome Myeloproliferative syndrome 2 risks from category 1
0 1 2 3
Ischaemic stroke with paralysis Acute decompensation of COPD with ventilation
MI Heart failure NYHA III + IV Acute decompensation of COPD without ventilation Sepsis Infection/acute inflammatory disease: bed rest
Infection/acute inflammatory disease: non-strict bed rest Central venous lines or port system
No acute risk 0
1
2
3
COPD: chronic obstructive pulmonary diseaseHRT: hormone replacement therapy
Individual Risk Assessmentfor Internal Medicine Patients
Class of exposing risk

KCH guidelines for medical thromboprophylaxis

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Venous thromboembolism risk score
Kucher, N. et al. N Engl J Med 2005;352:969-977

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Risk score for VTE
Kucher, N. et al. N Engl J Med 2005;352:969-977
Clinical Feature Score
Active cancer (treatment ongoing or within 6 months or palliative) 3
Personal history of VTE 3
Thrombophilia 3
Recent major surgery 2
Advanced age (≥ 75 years) 1
Obesity (BMI >29) 1
Bed rest 1
Hormonal therapy (OCP/HRT) 1

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Risk score for VTE
• The computer program alerted physicians to the increased risk for VTE and more than doubled the rate of prophylaxis (14.5% to 33.5%)
• Overall rate of VTE at 90 days was reduced by 41%
Kucher, N. et al. N Engl J Med 2005;352:969-977

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
Risk score analysis using VERITY
• Retrospective analysis of risk score in VERITY population aiming to validate this as a decision aid to enable use of thromboprophylaxis.
• Risk score applied to complete population (VTE +ve and VTE –ve patients)
• Examine risk factor profiles in our patients and reveal existing levels of thromboprophylaxis.

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007

VERITY (Venous Thromboembolism Registry) Fourth Annual Report 2007
The way forward
• Implementation of VTE Expert working group & NICE guidance
• National: Implementation working groupDevelop a national risk assessment toolProvide leadership
• Local: thrombosis committeeslocal guidelines100% risk assessment
• Role of VERITY
Related Documents