HEALTH PSYCHOLOGY, 1982, 1 (4) 315-336 EMPIRICAL CONTRIBUTIONS Verbal Exchange Structure of Initial Medical Interviews William B. Stiles Miami University Samuel M. Putnam Departments of Medicine and Epidemiology University of North Carolina at Chapel Hill Mary Casey Jacob Department of Medicine University of North Carolina at Chapel Hill Speech acts by physicians and patients in medical interviews can be grouped into verbal exchanges, which correspond to distinct medical tasks. Speech acts, measured by a verbal response mode (VRM) coding system, were coded from transcripts of initial medical interviews by physicians with 115 female pa- tients in a hospital walk-in clinic. Factor analyses of VRM frequencies in three interview segments—the medical history, the physical examination, and the conclusion—revealed four or five verbal exchanges in each segment. Some ex- changes appeared to correspond to major medical tasks of the interview, such as (1) listening to patients' exposition and probing for specific data in the history, (2) directing patients through diagnostic procedures and inquiring about subjective reactions in the examination, and (3) giving medical informa- tion and prescribing a therapeutic regimen in the conclusion. Other exchanges appeared to serve maintenance functions, such as informative commentary on This project was supported by grant number HS 03040 from the National Center for Health Services Research, OASH. We thank the patients, physicians, and nursing staff of the North Carolina Memorial Hospital walk-in clinic for their cooperation. We also thank Dennis B. Gillings, Barbara S. Hulka, and Sherman A. James for their counsel in planning and conducting this study, and James E. Orth and Leonard G. Rorer for their comments on drafts of this article. Send reprint requests to William B. Stiles, Department of Psychology, Miami University, Oxford, Ohio 45056.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
HEALTH PSYCHOLOGY, 1982, 1 (4) 315-336
EMPIRICAL CONTRIBUTIONS
Verbal Exchange Structure ofInitial Medical Interviews
William B. StilesMiami University
Samuel M. PutnamDepartments of Medicine and EpidemiologyUniversity of North Carolina at Chapel Hill
Mary Casey JacobDepartment of Medicine
University of North Carolina at Chapel Hill
Speech acts by physicians and patients in medical interviews can be groupedinto verbal exchanges, which correspond to distinct medical tasks. Speechacts, measured by a verbal response mode (VRM) coding system, were codedfrom transcripts of initial medical interviews by physicians with 115 female pa-tients in a hospital walk-in clinic. Factor analyses of VRM frequencies in threeinterview segments—the medical history, the physical examination, and theconclusion—revealed four or five verbal exchanges in each segment. Some ex-changes appeared to correspond to major medical tasks of the interview, suchas (1) listening to patients' exposition and probing for specific data in thehistory, (2) directing patients through diagnostic procedures and inquiringabout subjective reactions in the examination, and (3) giving medical informa-tion and prescribing a therapeutic regimen in the conclusion. Other exchangesappeared to serve maintenance functions, such as informative commentary on
This project was supported by grant number HS 03040 from the National Center for HealthServices Research, OASH.
We thank the patients, physicians, and nursing staff of the North Carolina MemorialHospital walk-in clinic for their cooperation. We also thank Dennis B. Gillings, Barbara S.Hulka, and Sherman A. James for their counsel in planning and conducting this study, andJames E. Orth and Leonard G. Rorer for their comments on drafts of this article.
Send reprint requests to William B. Stiles, Department of Psychology, Miami University,Oxford, Ohio 45056.
316 STILES, PUTNAM, JACOB
examination procedures and checking the accuracy of communication. In-dexes of the extent to which a physician-patient dyad engaged in each type ofexchange were significantly correlated with patients' sociodemographiccharacteristics.
Increasing scientific interest in the medical interview attests to widespreadrecognition of its central role in primary medical care (Almy, 1980; Barsky,Kazis, Freiden, Goroll, Hatem, & Lawrence, 1980; Carroll & Monroe, 1980;DiMatteo, 1979; Francis, Korsch, & Morris, 1969; Friedman, 1979; Nar-done, Reuler, & Girard, 1980; Stone, 1979). In outpatient settings, physi-cians can make most diagnoses on the basis of the medical history alone(Hampton, Harrison, Mitchell, Pritchard, & Seymour, 1975). In the fre-quent cases where there is no organic pathology to explain the patient'sdistress, or in which disease is caused, maintained, or exacerbated by the pa-tient's behavior, the physician's social influence may be the primary or onlyintervention (Drossman, 1977-78). Even when there are organic problems,the patient's cooperation with a treatment regimen (e.g., pill taking, diet,exercise, return appointments) must be elicited via the interview. Directtherapeutic effects of the interview may speed recovery from surgery orlower the cardiovascular risk factors of blood pressure, serum glucose, andserum cholesterol (Egbert, Battit, Welch, & Bartlett, 1964; Glasunov,Dowd, Jaksic, Kesic, Ray, Steinberger, Stromberg, & Vuletic, 1973).Moreover, patients see the interview as central to their medical care, for it isthrough the interview that they can express their fears and suffering and ob-tain information or reassurance (Koos, 1955; Ort, Ford, & Liske, 1964;Reader, Pratt, & Mudd, 1957).
Because the interview is central in medical care, it deserves thoroughstudy. We have chosen to study one of the interview's many facets—the ver-bal interaction. This article offers a conceptual framework for understand-ing the verbal interaction and applies that framework to 115 initial medicalinterviews in a walk-in clinic.
Other investigators have studied verbal interaction in medical interviews(Bain, 1976; Coulthard & Ashby, 1976; Davis, 1971; Freemon, Negrete,Davis, & Korsch, 1971; Joyce, Caple, & Mason, 1969; Roter, 1977, Scott,Donnelly, Gallagher, & Hess, 1973; Smith, Polis, & Hadac, 1981; Svarstad,1976; Waitzkin & Stoeckle, 1976). However, work in this area has beenhampered by the lack of an adequate taxonomy of speech acts. Standarddesiderata for such a taxonomy include categories that are mutually ex-clusive, exhaustive, and derived from consistent classificatory principles(Holsti, 1969; Russell & Stiles, 1979). In the present study, we have used ageneral-purpose taxonomy of verbal response modes (VRMs), fully describ-
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 317
ed elsewhere (Stiles, 1978b, 1978-79, 1981) and summarized here, whichgoes farther than previous systems towards meeting these criteria.
Conceptual Framework for Verbal Encounters
Our unit of analysis is the speech act, or more precisely, the illocutionaryact (Austin, 1975; Searle, 1969; Stiles, 1981). An illocutionary act is the actperformed in making an utterance, as distinct from the content or the exter-nal effect of the utterance. For example, in uttering "When did it start hurt-ing?" one asks a question; in uttering "Your rib is cracked," one makes anassertion. Questioning and asserting are illocutionary acts. Speech actanalysis measures not what is said, but what is done when a speaker sayssomething.
Each illocutionary act has an intended recipient as well as a sender (Stiles,1981); one asks the other a question, makes an assertion to the other, and soforth. Each act can thus be considered as a microrelationship of the speakerto the other. Different categories of acts represent different kinds ofmicrorelationships. A summary of the speech acts in an encounter is thus ameasure of the participants' interpersonal relationship—of what they did toeach other in the verbal interaction.
A verbal exchange consists of particular categories of speech acts by oc-cupants of complementary roles. For example, one kind of exchange mightconsist of the physician giving instructions and the patient agreeing to com-ply; another might consist of the physician asking questions and the patientgiving information. Each speech act category, we hypothesize, has a nichein its exchange; it occurs in association with certain other categories withwhich it has functional relationships. For example, patient information-giving might be associated with physician questioning but not with physi-cian instructing or patient agreeing. Describing the verbal exchange struc-ture of an encounter thus requires a specification of what kinds of ex-changes are present and what speech act categories make up each kind of ex-change.
We hypothesize that the verbal exchange structure directly reflects an en-counter's social and task requirements. (Thus, for example the verbal ex-change structure of medical interviews should differ from that of discus-sions in college seminars or informal conversations among friends.) In par-ticular, we expect the exchanges in medical encounters to have identifiablemedical functions and to reflect the participants' social roles.
Although the structure of initial medical interviews should be the sameacross encounters—in response to common task requirements and role rela-tions—the extent of each type of exchange may vary depending on the pa-tient's personal characteristics, the presenting problem, the setting, thephysician's skill, the participants' liking for each other, and so forth. Our

318 STILES, PUTNAM, JACOB
approach to identifying verbal exchanges uses factor analysis to take advan-tage of this expected natural variation. Encounters in which one type of ex-change is common (or rare) will tend to have high (or low) frequencies of allof its constituent speech act categories. Thus, one exchange's constituentcategories should be correlated with each other across encounters, andhence should load highly on one factor, whereas constituents of other ex-changes should load on other factors.
In our framework, verbal exchanges are viewed as taking place over thecourse of an encounter, possibly intertwined with other exchanges, notnecessarily comprising discrete episodes. Although in some ex-changes—such as those consisting of questions and answers—a sequence ofacts is evident, other exchanges do not have obvious orderings. The factoranalytic approach can detect groupings of categories that do not occur infixed sequences. On the other hand, it offers no direct information onwhether the groupings do occur in sequences.1
Of course, the structure of speech acts is only one of many aspects ofmedical interaction. Future research must address the relationship of theverbal exchange structure to other levels of communication, including theinteraction's content and the nonverbally communicated affect (Cassell &Skopek, 1977; Friedman, 1979; Miller, 1974; Russell & Stiles, 1979).
Hypotheses: Functions of Verbal Exchangesin Medical Interviews
As described in major texts (Enelow & Swisher, 1972; Morgan & Engel,1969), initial medical interviews may be divided into three segments: themedical history, the physical examination, and the conclusion. Each seg-ment includes one or more major tasks, which correspond to distinct verbalexchanges, according to our hypothesis. The physician's tasks in themedical history include eliciting the patient's presenting problems and prob-ing for specific information necessary for the diagnosis; concurrently, thepatient's tasks include conveying the reasons for coming and answering thephysician's questions. Physical examination tasks include directing the pa-tient through the examination procedures and inquiring about the patient's
'Another approach to identifying verbal exchanges is by Markov analyses and cross-lag cor-relation (cf. Brent & Sykes, 1979; Gottman, 1979). This approach, which assesses the pro-bability that each category precedes or follows each other category, can detect repeated se-quences of acts, but it is less sensitive to nonsequential groupings. It is also severely limited inthe number of categories it can examine because it requires high frequencies of co-occurrencesto estimate transitional probabilities. Future research might employ a combined approach, us-ing factor analysis to identify exchanges and cross-lag correlation to explore act sequenceswithin exchanges.
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 319
reactions to them (e.g., ability to discriminate certain stimuli, bodily locusof pain). Conclusion segment tasks include giving a diagnosis and explana-tion of the patient's symptoms and prescribing a therapeutic regimen.
A previous study (Stiles, Putnam, Wolf, & James, 1979a, 1979b) foundverbal exchanges that corresponded to these major tasks. The present studywas designed to replicate and extend the previous findings. The presentstudy's larger sample (115 interviews instead of 52) allowed us to includemore of the less common modes in our factor analyses (modes used 2% ormore, instead of 5%), abiding by a rule of thumb that requires at least fiveobservations per variable in a factor analysis; this permitted a finer resolu-tion of the verbal exchange structure.
In addition to performing these task functions, we expect the interview toperform maintenance functions, that is, activity aimed at forming andmaintaining the interpersonal relationship (Bloom, 1963). The emotionalcontent of many medical encounters (pain, disability, expense, embarrass-ment) makes it essential for patient and physician to attend to each other'sfeelings and to the quality of their communication. Maintenance functionsmight appear as exchanges in which the physician gives explanations of pro-cedures or checks the accuracy of communication. Maintenance functionsmight also appear within task-oriented exchanges; for example, back-channel communication (Duncan, 1972)—brief speech acts such as "mm-hm" or "I see"—could facilitate the task-related function of gathering in-formation.
The present study also explores the relation of patient sociodemographiccharacteristics to patients' engaging in each kind of exchange with physi-cians.
METHOD
Subjects
We studied physicians' initial medical interviews with 115 patients whocame to the walk-in clinic at North Carolina Memorial Hospital betweenMarch and November of 1980.
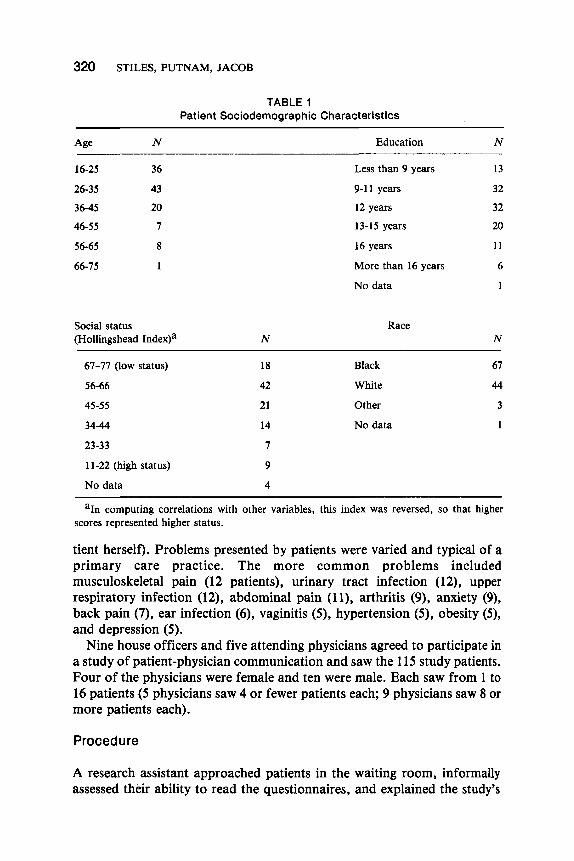
All patients were female adults who were not too ill to participate, whohad not been seen previously at the hospital for that episode of illness, whowere able to complete our written questionnaires, and who gave writtenconsent after the study's procedures had been explained to them. Frequencydistributions for patients' age, education, social status, and race are given inTable 1. Social status was measured by the Hollingshead Two-Factor index(Hollingshead & Redlich, 1958), a weighted sum of category scores for theoccupation and education of the head of household (not necessarily the pa-
3 2 0 STILES, PUTNAM, JACOB
Age
16-25
26-35
36-45
46-55
56-65
66-75
N
36
43
20
7
8
1
TABLE 1Patient Sociodemographic Characteristics
Education
Less than 9 years
9-11 years
12 years
13-15 years
16 years
More than 16 years
No data
N
13
32
32
20
11
6
1
Social status(Hollingshead Index)a
67-77 (low status)
56-66
45-55
34-44
23-33
11-22 (high status)
No data
N
18
42
21
14
7
9
4
Race
Black
White
Other
No data
N
67
44
3
1
aIn computing correlations with other variables, this index was reversed, so that higherscores represented higher status.
tient herself). Problems presented by patients were varied and typical of aprimary care practice. The more common problems includedmusculoskeletal pain (12 patients), urinary tract infection (12), upperrespiratory infection (12), abdominal pain (11), arthritis (9), anxiety (9),back pain (7), ear infection (6), vaginitis (5), hypertension (5), obesity (5),and depression (5).
Nine house officers and five attending physicians agreed to participate ina study of patient-physician communication and saw the 115 study patients.Four of the physicians were female and ten were male. Each saw from 1 to16 patients (5 physicians saw 4 or fewer patients each; 9 physicians saw 8 ormore patients each).
Procedure
A research assistant approached patients in the waiting room, informallyassessed their ability to read the questionnaires, and explained the study's
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 321
procedures and general purpose ("a study of how doctors and patients talkwith each other"). Patients who gave written consent were taken to anotherclinic, where they were seen by one of the participating physicians. The en-tire interview was tape recorded through microphones placed unobtrusivelyin the examining room. The tape was later transcribed verbatim, omittingnames and other obvious identifying data.
On questionnaires administered before and immediately after their inter-views, and in telephone calls one week and one month later, patients gavetheir attitudes and their reactions to their medical care. Results of these in-quiries are not reported in this article.
Speech Act Coding
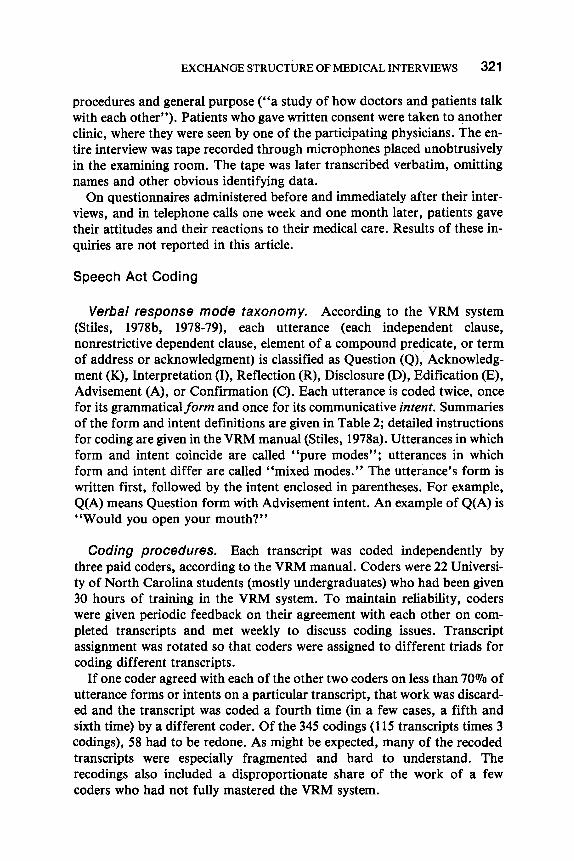
Verbal response mode taxonomy. According to the VRM system(Stiles, 1978b, 1978-79), each utterance (each independent clause,nonrestrictive dependent clause, element of a compound predicate, or termof address or acknowledgment) is classified as Question (Q), Acknowledg-ment (K), Interpretation (I), Reflection (R), Disclosure (D), Edification (E),Advisement (A), or Confirmation (C). Each utterance is coded twice, oncefor its grammatical form and once for its communicative intent. Summariesof the form and intent definitions are given in Table 2; detailed instructionsfor coding are given in the VRM manual (Stiles, 1978a). Utterances in whichform and intent coincide are called "pure modes"; utterances in whichform and intent differ are called "mixed modes." The utterance's form iswritten first, followed by the intent enclosed in parentheses. For example,Q(A) means Question form with Advisement intent. An example of Q(A) is"Would you open your mouth?"
Coding procedures. Each transcript was coded independently bythree paid coders, according to the VRM manual. Coders were 22 Universi-ty of North Carolina students (mostly undergraduates) who had been given30 hours of training in the VRM system. To maintain reliability, coderswere given periodic feedback on their agreement with each other on com-pleted transcripts and met weekly to discuss coding issues. Transcriptassignment was rotated so that coders were assigned to different triads forcoding different transcripts.
If one coder agreed with each of the other two coders on less than 70% ofutterance forms or intents on a particular transcript, that work was discard-ed and the transcript was coded a fourth time (in a few cases, a fifth andsixth time) by a different coder. Of the 345 codings (115 transcripts times 3codings), 58 had to be redone. As might be expected, many of the recodedtranscripts were especially fragmented and hard to understand. Therecodings also included a disproportionate share of the work of a fewcoders who had not fully mastered the VRM system.
322 STILES, PUTNAM, JACOB
TABLE 2Verbal Response Modes
Mode Grammatical Form Communicative Intent
Question (Q)
Acknowledgment (K)
Interpretation (I)
Reflection (R)
Disclosure (D)
Edification (E)
Advisement (A)
Confirmation (C)
Interrogative, with invertedsubject-verb order orinterrogative words.
Nonlexical or contentlessuttererances; terms of addressand salutation.
Second person ("you"), verbimplies an attribute orability of the others; termsof evaluation.
Second person; verb impliesinternal experience orvolitional action.
Declarative, first personsingular ("I") or firstperson plural ("we") whereother is not a referent.
Declarative, third person(e.g., "he" "she," "it").
Imperative; or second personwith verb of permission,prohibition, or obligation.
First person plural ("we")where referent includesother.
Requests information orguidance.
Conveys receipt of orreceptiveness to other'scommunication; simpleacceptance, salutations.
Explains or labels theother; judgments orevaluations of other'sexperience or behavior.
Puts other's experienceinto words; repetitions,restatements, clarifications.
Reveals thought, feelings,perceptions, intentions.
States objectiveinformation.
Attempts to guide behavior;suggestions, commands,permission, prohibition.
Compares speaker'sexperience with other's;agreement, disagreement,shared experience or belief.
Note. Both the form and intent of each utterance are coded. Form is written first, intent se-cond in parentheses; thus Q(A) means Question form with Advisement intent.
For the data analyses, the work of the three coders was combined into acomposite set. Codes were assigned to the form and intent of each utteranceif two of the three coders agreed; otherwise, the form or intent was coded asdisagreement. Of the 60,914 utterances coded in this study, only 1.5% ofthe forms and 3.1% of the intents were coded as disagreement. Two out ofthree coders agreed that another 3.1% of the forms and 3.0% of the intentswere unscorable, that is, incomprehensible or marked as inaudible on thetranscripts.
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 323
Each transcript was divided into three segments: medical history, physicalexamination, and conclusion.2 Two of the intereviews had no physical ex-amination.
RESULTS
Verbal Response Mode Profiles
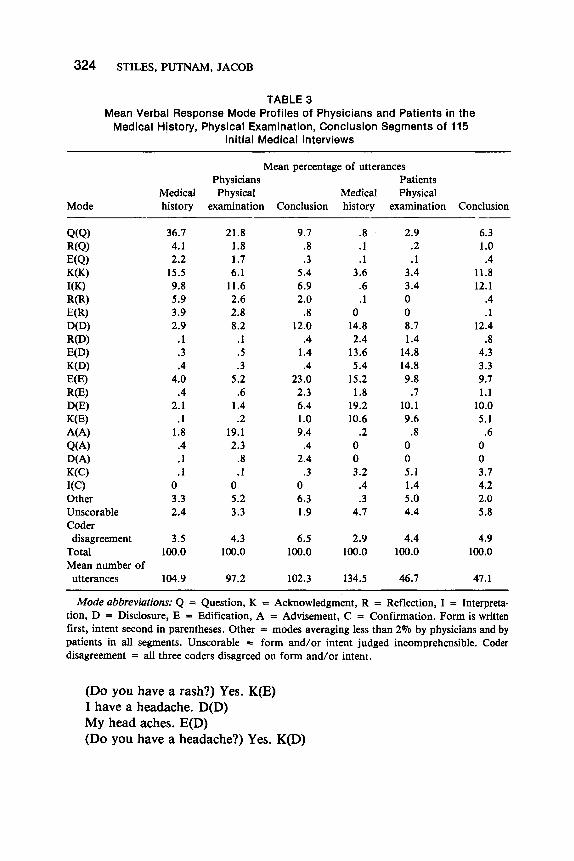
Table 3 gives the physician and patient VRM profiles, that is, the meanpercentage of utterances in each mode for each interview segment.
In the history, nearly half of physicians' utterances were Question in in-tent, although some had Reflection or Edification forms.
Have you had any chest pain? Q(Q)You haven't had any chest pain? R(Q)It started bothering you on Monday? E(Q)
Physicians also gave many Acknowledgments, both as pure modes ("Mm-hm," "Yeah") and in the form of evaluative words (Interpretation forms;"Right," "Okay"), and they used Reflections, some in Edification forms.All of these modes reflect the physician's information-gathering function inthe history. In the physical examination segment, physicians began giving alarge proportion of Advisements ("Take a deep breath") and moreDisclosures of intentions, although they continued to use Questions andAcknowledgments. In the conclusion segment, physicians' most commonmode was Edification ("This is a broad spectrum antibiotic"), reflectingthis segment's information-giving function.
Complementing the physicians' information-seeking in the medicalhistory, patients used information-giving modes. Most patient utterance in-tents were Edification (objective information) or Disclosure (subjective in-formation), while most forms were Edification, Disclosure, orAcknowledgment:
My arm has a rash. E(E)I have a rash on my arm. D(E)
Segmenting followed written guidelines, which are available from the first author. Usuallythe physical examination began with a physician statement like "Please sit up on this table," or"Now I'd like to examine your chest," and ended with a statement like "You may get dressednow," or "You may step down now."
3 2 4 STILES, PUTNAM, JACOB
TABLE 3Mean Verbal Response Mode Profiles of Physicians and Patients in the
Medical History, Physical Examination, Conclusion Segments of 115Initial Medical Interviews
Mode
Q(Q)R(Q)E(Q)K(K)I(K)R(R)E(R)D(D)R(D)E(D)K(D)E(E)R(E)D(E)K(E)A(A)Q(A)D(A)K(C)I(C)OtherUnscorableCoderdisagreement
TotalMean number ofutterances
Medicalhistory
36.74.12.2
15.59.85.93.92.9
.1
.3
.44.0
.42.1
.11.8
.4
.1
.103.32.4
3.5100.0
104.9
Mean percentage of utterancesPhysiciansPhysical
examination
21.81.81.76.1
11.62.62.88.2
.1
.5
.35.2
.61.4.2
19.12.3
.8
.105.23.3
4.3100.0
97.2
Conclusior
9.7.8.3
5.46.92.0
.812.0
.41.4.4
23.02.36.41.09.4
.42.4
.306.31.9
6.5100.0
102.3
MedicalL history
.8
.1
.13.6
.6
.10
14.82.4
13.65.4
15.21.8
19.210.6
.2003.2
.4
.34.7
2.9100.0
134.5
PatientsPhysical
examination
2.9.2.1
3.43.4008.71.4
14.814.89.8
.710.19.6
.8005.11.45.04.4
4.4100.0
46.7
Conclusion
6.31.0.4
11.812.1
.4
.112.4
.84.33.39.71.1
10.05.1
.6003.74.22.05.8
4.9100.0
47.1
Mode abbreviations: Q = Question, K = Acknowledgment, R = Reflection, I = Interpreta-tion, D = Disclosure, E = Edification, A = Advisement, C = Confirmation. Form is writtenfirst, intent second in parentheses. Other = modes averaging less than 2% by physicians and bypatients in all segments. Unscorable = form and/or intent judged incomprehensible. Coderdisagreement = all three coders disagreed on form and/or intent.
(Do you have a rash?) Yes. K(E)I have a headache. D(D)My head aches. E(D)(Do you have a headache?) Yes. K(D)
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 3 2 5
Patients used a similar mix of modes in the physical examination, exceptthat there was a substantial increase in the percentage of K(D), reflectingpatients' answering "yes" or "no" to physicians' questions about subjec-tive reactions to examination procedures.
(Does it hurt when I press here?) No. K(D)
In the conclusion segment, complementing information-giving by physi-cians, patients used more Acknowledgments and Questions, indicative ofreceiving or seeking information.
The VRM profiles in Table 3 show that the patient-physician relationshipwas highly asymmetrical and that physician and patient roles changedsystematically from segment to segment, replicating previous work (Stiles etal., 1979b). Standard errors of these mean percentages are correlated withthe means and range from less than . 1 % to 2.5%, so that most of the in-tersegment differences and physician-patient differences are statisticallyhighly significant.
Verbal Exchanges
Factor analyses were conducted on the intercorrelations of physicians' andpatients' VRM frequencies in each segment. In each analysis, we includedmodes that physicians or patients used for 2°7o or more of their utterances inthat segment, and we correlated the mode frequencies (not percentages)across the 115 interviews. For example, in the history segment, 10 physicianmodes and 9 patient modes met the 2% criterion, and the intercorrelationsof the frequencies of these 19 modes were factor analyzed. As Table 3shows, the included modes accounted for 80%-90% of all utterances in eachsegment. In all three factor analyses, principal axis factors were extracteduntil eigenvalues fell below 1.0. Factor axes were then rotated to an (or-thogonal) varimax solution.
Medical history exchanges. Four factors were extracted from thehistory segment data, which account for 70.1% of the total variance. Thefirst principal factor (before rotation) accounted for 43.2% of the variance.The varimax-rotated factor matrix is presented in Table 4.
History factor 1 is a closed question exchange, with high loadings (i.e.,greater than .5) for physician modes with Question intent and for patient"yes" and "no" answers, coded K(E) or K(D). In addition, physiciansrepeated the meaning of patients' answers, coded R(R), and/oracknowledged their answers with such words as "right," "okay," or"fine," coded I(K).

326 STILES, PUTNAM, JACOB
TABLE 4Varimax Rotated Factor Matrix for History Modes
Mode
PhysicianQ(Q)R(Q)E(Q)I(K)R(R)K(K)D(D)D(E)E(E)E(R)
PatientK(E)K(D)D(D)E(D)D(E)E(E)R(D)K(K)K(C)
Factor 1"Closed question"
.75*
.80*
.62*
.63*
.60*
.33
.35
.87*
.57*
.35
.34
.38
Factor 2"Exposition"
.30
.63*
.30
.88*
.66*
.80*
.78*
.69*
.45
Factor 3"Explanation"
.76*
.82*
.86*
.46
Factor 4"Checking"
.34
.47
.32
.83*
.42
.55*
.43
.73*
Mode abbreviations: Q = Question, K = Acknowledgment, I = Interpretation, R =Reflection, D = Disclosure, E = Edification, A = Advisement, C = Confirmation. Form iswritten first followed by intent in parentheses.
Note. N = 115 interviews. Factor loadings with an absolute value less than .3 are omitted.Factor loadings of .5 or greater are marked with an asterisk (*).
History factor 2 is an exposition exchange, in which the patient told herstory3 using her own words, that is, she used Disclosure (first person) andEdification (third person) forms (rather than Acknowledgment forms suchas "yes" and "no") to convey Disclosure (subjective information) and
'Since the VRM system does not code content, inferences such as our conclusion that the ex-position factor reflects patients "telling their story" cannot rest on VRM codes alone. Con-ceivably, irrelevant comments could have been coded to the exposition modes, e.g.,"Napoleon was defeated at the battle of Waterloo" E(E). We have reviewed the transcriptsand extracted samples of utterances coded in particular modes to assess their content, and webelieve that our characterizations of the typical content of each exchange are accurate. It is animportant, if unsurprising, feature of these initial medical interviews that physicians and pa-tients stayed on topics related to the patient's health and presenting problem for the vast ma-jority of their utterances.
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 327
Edification (objective information) intents. Physicians facilitated usingpure Acknowledgments ("mm-hm," "yeah").
History factor 3 is an explanation exchange, in which physicians gave in-formation using E(E), D(E), and D(D). These physician modes wererelatively rare in the history segment (Table 3). Patient K(K) loadedmoderately, as patients indicated receipt of the information.
History factor 4 is a checking exchange, in which physicians used Reflec-tions to check their understanding and patients responded usingAcknowledgment forms to agree or disagree, coded K(C).
Dr: So this has been bothering you all week. E(R)Pt: Yeah. K(C)
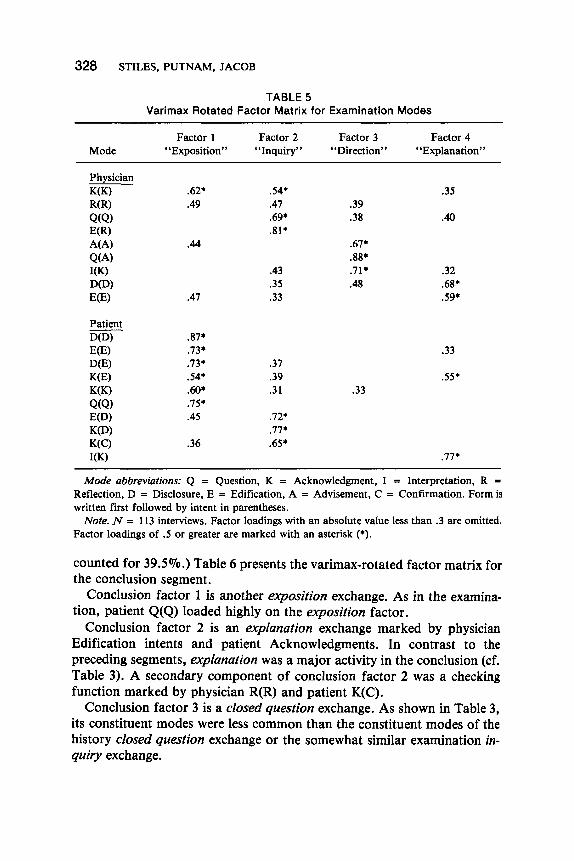
Physical examination exchanges. Four factors were extracted,which account for 74.0% of the total variance. (The unrotated first prin-cipal factor accounted for 52.7%.) Table 5 presents the varimax-rotatedfactor matrix for the physical examination.
Examination factor 1 is another exposition exchange. As in the historyexposition exchange (factor 2 in Table 4), the predominant modes suggestphysician facilitation of patients' giving information in their own words.However, the examination exposition factor's higher loading for patientK(E) and lower loading for patient E(D) suggest that it is more orientedtoward objective information and less toward subjective information. Thehigh loadings for patient Questions and Acknowledgments suggest that ac-tive information-seeking by the patient in the physical examination tendedto occur in the context of patient exposition and physician attentiveness.
Examination factor 2 is an inquiry exchange. The exchange's more com-mon constituent modes were physician Q(Q) and patient E(D) and K(D), asphysicians inquired about patients' subjective reactions to examination pro-cedures (cf. footnote 3) and patients responded by putting their subjectivereactions (Disclosure intent) into the objective forms. The loadings of theless common modes, physician E(R) and patient K(C), indicate that a secon-dary component of the inquiry exchange was checking the informationgathered, analogous to the history checking exchange (factor 4, Table 4).
Examination factor 3 is a direction exchange, in which physicians usedAdvisements to direct patients through examination procedures (cf. foot-note 3). The absence of patient modes loading highly on this factor indicatesthat the patient contribution was largely nonverbal.
Examination factor 4 is an explanation exchange, similar to the historyexplanation exchange (factor 3, Table 4).
Conclusion exchanges. Five factors were extracted, which accountfor 69.6% of the total variance. (The unrotated first principal factor ac-
328 STILES, PUTNAM, JACOB
TABLE 5Varimax Rotated Factor Matrix for Examination Modes
Mode
PhysicianK(K)R(R)Q(Q)E(R)A(A)Q(A)KK)D(D)E(E)
PatientD(D)E(E)D(E)K(E)K(K)Q(Q)E(D)K(D)K(C)I(K)
Factor 1"Exposition"
.62*
.49
.44
.47
.87*
.73*
.73*
.54*
.60*
.75*
.45
.36
Factor 2"Inquiry"
.54*
.47
.69*
.81*
.43
.35
.33
.37
.39
.31
.72*
.77*
.65*
Factor 3"Direction"
.39
.38
.67*
.88*
.71*
.48
.33
Factor 4"Explanation"
.35
.40
.32
.68*
.59*
.33
.55*
.77*
Mode abbreviations: Q = Question, K = Acknowledgment, I = Interpretation, R =Reflection, D = Disclosure, E = Edification, A = Advisement, C = Confirmation. Form iswritten first followed by intent in parentheses.
Note. N = 113 interviews. Factor loadings with an absolute value less than .3 are omitted.Factor loadings of .5 or greater are marked with an asterisk (*).
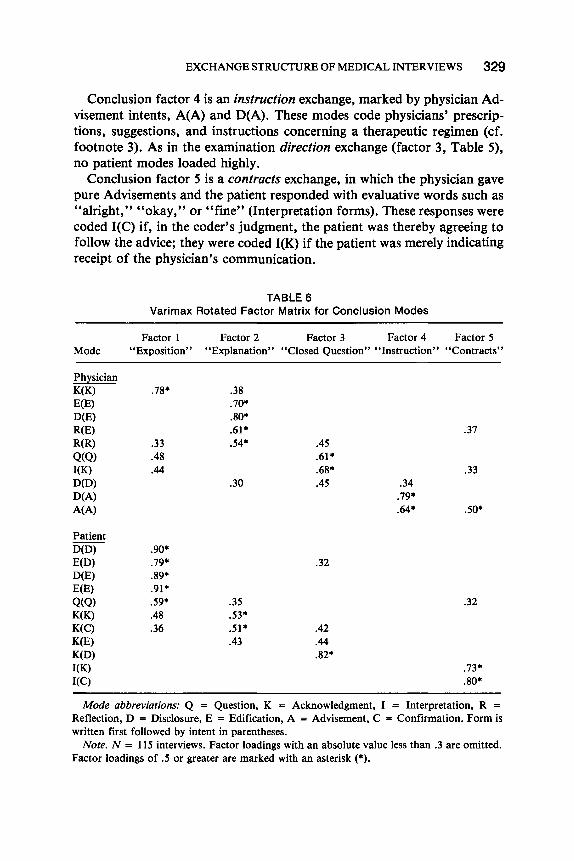
counted for 39.5%.) Table 6 presents the varimax-rotated factor matrix forthe conclusion segment.
Conclusion factor 1 is another exposition exchange. As in the examina-tion, patient Q(Q) loaded highly on the exposition factor.
Conclusion factor 2 is an explanation exchange marked by physicianEdification intents and patient Acknowledgments. In contrast to thepreceding segments, explanation was a major activity in the conclusion (cf.Table 3). A secondary component of conclusion factor 2 was a checkingfunction marked by physician R(R) and patient K(C).
Conclusion factor 3 is a closed question exchange. As shown in Table 3,its constituent modes were less common than the constituent modes of thehistory closed question exchange or the somewhat similar examination in-quiry exchange.
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 3 2 9
Conclusion factor 4 is an instruction exchange, marked by physician Ad-visement intents, A(A) and D(A). These modes code physicians' prescrip-tions, suggestions, and instructions concerning a therapeutic regimen (cf.footnote 3). As in the examination direction exchange (factor 3, Table 5),no patient modes loaded highly.
Conclusion factor 5 is a contracts exchange, in which the physician gavepure Advisements and the patient responded with evaluative words such as"alright," "okay," or "fine" (Interpretation forms). These responses werecoded I(C) if, in the coder's judgment, the patient was thereby agreeing tofollow the advice; they were coded I(K) if the patient was merely indicatingreceipt of the physician's communication.
TABLE 6Varimax Rotated Factor Matrix for Conclusion Modes
Mode
PhysicianK(K)E(E)D(E)R(E)R(R)
Q(Q)I(K)D(D)D(A)A(A)
PatientD(D)E(D)D(E)E(E)
Q(Q)K(K)K(C)K(E)K(D)I(K)I(C)
Factor 1"Exposition"
.78*
.33
.48
.44
.90*
.79*
.89*
.91*
.59*
.48
.36
Factor 2"Explanation"
.38
.70*
.80*
.61*
.54*
.30
.35
.53*
.51*
.43
Factor 3"Closed Question"
.45
.61*
.68*
.45
.32
.42
.44
.82*
Factor 4"Instruction"
.34.79*.64*
Factor 5' 'Contracts''
.37
.33
.50*
.32
.73*
.80*
Mode abbreviations: Q = Question, K = Acknowledgment, I = Interpretation, R =Reflection, D = Disclosure, E = Edification, A = Advisement, C = Confirmation. Form iswritten first followed by intent in parentheses.
Note. N = 115 interviews. Factor loadings with an absolute value less than .3 are omitted.Factor loadings of .5 or greater are marked with an asterisk (*).
330 STILES, PUTNAM, JACOB
Correlations of Exchange Indexes withPatient Characteristics
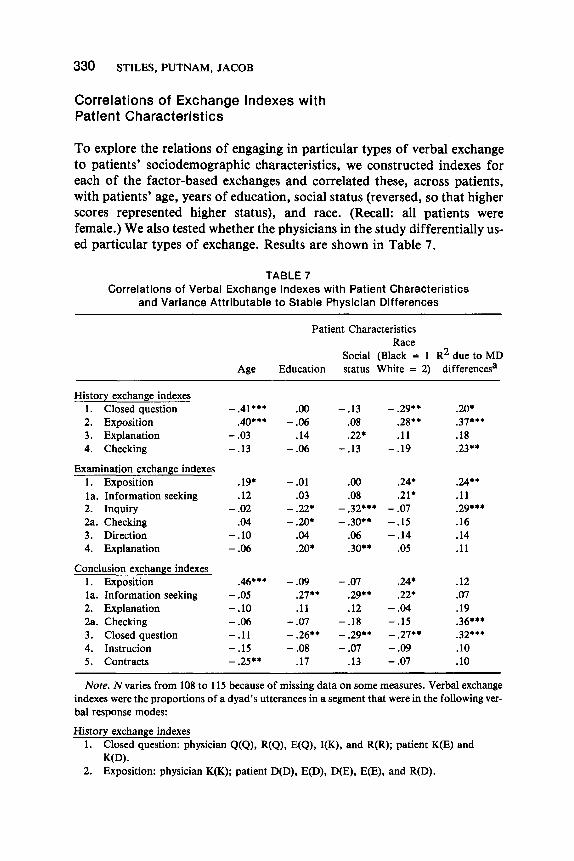
To explore the relations of engaging in particular types of verbal exchangeto patients' sociodemographic characteristics, we constructed indexes foreach of the factor-based exchanges and correlated these, across patients,with patients' age, years of education, social status (reversed, so that higherscores represented higher status), and race. (Recall: all patients werefemale.) We also tested whether the physicians in the study differentially us-ed particular types of exchange. Results are shown in Table 7.
TABLE 7Correlations of Verbal Exchange Indexes with Patient Characteristics
and Variance Attributable to Stable Physician Differences
History exchange indexes1. Closed question2. Exposition3. Explanation4. Checking
Examination exchange indexes1. Expositionla. Information seeking2. Inquiry2a. Checking3. Direction4. Explanation
Conclusion exchange indexes1. Expositionla. Information seeking2. Explanation2a. Checking3. Closed question4. Instrucion5. Contracts
Age
-.41***.40**•
-.03-.13
.19*
.12-.02
.04-.10-.06
.46***-.05-.10-.06-.11-.15-.25**
Patient Characteristics
Education
.00-.06
.14-.06
-.01.03
-.22*-.20*
.04
.20*
-.09.27**.11
-.07- .26**-.08
.17
Socialstatus
-.13.08.22*
-.13
.00
.08-.32***- .30**
.06
.30**
-.07.29**.12
-.18- .29**-.07
.13
Race(Black = 1White = 2)
- .29**.28**.11
-.19
.24*
.21*-.07-.15-.14
.05
.24*
.22*-.04-.15- .27**-.09-.07
R2 due to MDdifferencesa
.20*
.37***
.18
.23**
.24**
.11
.29***
.16
.14
.11
.12
.07
.19
.36***
.32***
.10
.10
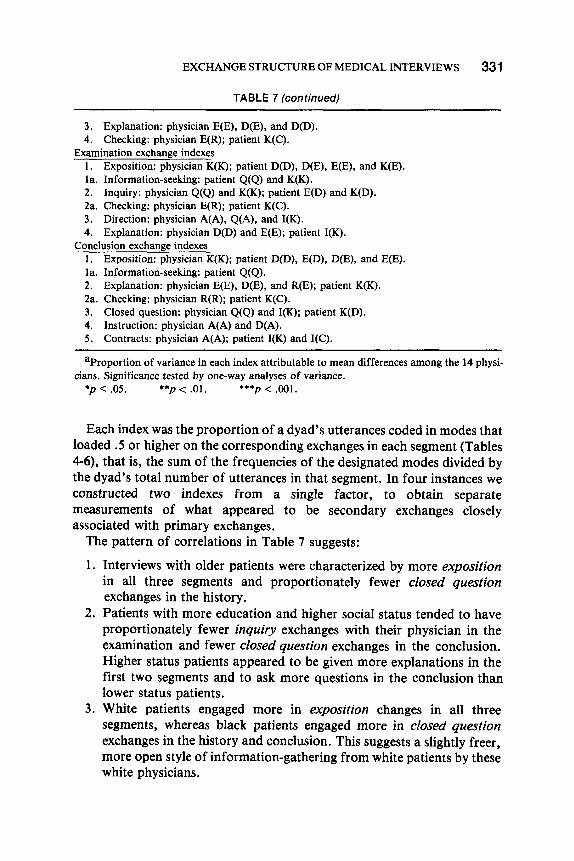
Note. N varies from 108 to 115 because of missing data on some measures. Verbal exchangeindexes were the proportions of a dyad's utterances in a segment that were in the following ver-bal response modes:
History exchange indexes1. Closed question: physician Q(Q), R(Q), E(Q), I(K), and R(R); patient K(E) and
K(D).2. Exposition: physician K(K); patient D(D), E(D), D(E), E(E), and R(D).
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 331
TABLE 7 (continued)
3. Explanation: physician E(E), D(E), and D(D).4. Checking: physician E(R); patient K(C).
Examination exchange indexes1. Exposition: physician K(K); patient D(D), D(E), E(E), and K(E).la. Information-seeking: patient Q(Q) and K(K).2. Inquiry: physician Q(Q) and K(K); patient E(D) and K(D).2a. Checking: physician E(R); patient K(C).3. Direction: physician A(A), Q(A), and I(K).4. Explanation: physician D(D) and E(E); patient I(K).
Conclusion exchange indexes1. Exposition: physician K(K); patient D(D), E(D), D(E), and E(E).la. Information-seeking: patient Q(Q).2. Explanation: physician E(E), D(E), and R(E); patient K(K).2a. Checking: physician R(R); patient K(C).3. Closed question: physician Q(Q) and I(K); patient K(D).4. Instruction: physician A(A) and D(A).5. Contracts: physician A(A); patient I(K) and I(C).
aProportion of variance in each index attributable to mean differences among the 14 physi-cians. Significance tested by one-way analyses of variance.
*p < .05. **p < .01. ***p < .001.
Each index was the proportion of a dyad's utterances coded in modes thatloaded .5 or higher on the corresponding exchanges in each segment (Tables4-6), that is, the sum of the frequencies of the designated modes divided bythe dyad's total number of utterances in that segment. In four instances weconstructed two indexes from a single factor, to obtain separatemeasurements of what appeared to be secondary exchanges closelyassociated with primary exchanges.
The pattern of correlations in Table 7 suggests:
1. Interviews with older patients were characterized by more expositionin all three segments and proportionately fewer closed questionexchanges in the history.
2. Patients with more education and higher social status tended to haveproportionately fewer inquiry exchanges with their physician in theexamination and fewer closed question exchanges in the conclusion.Higher status patients appeared to be given more explanations in thefirst two segments and to ask more questions in the conclusion thanlower status patients.
3. White patients engaged more in exposition changes in all threesegments, whereas black patients engaged more in closed questionexchanges in the history and conclusion. This suggests a slightly freer,more open style of information-gathering from white patients by thesewhite physicians.
332 STILES, PUTNAM, JACOB
Patient age was negatively correlated (-.39, p < .001) with education,but was not significantly correlated with the social status index (-.16) orrace (.15). Education and social status were highly correlated with eachother (.77, p < .001). White patients had higher status than black patients(.29, p < .01; correlation based on black = 1, white = 2), but race wasnot significantly related to education (.16).
The last column of Table 7 shows that physicians did use systematicallydifferent interviewing styles, but these differences accounted for at mostabout one-third of the variance of any exchange index. The stylistic dif-ferences appeared larger for the information-gathering exchanges (exposi-tion, closed question, inquiry, checking) than for the information-giving ex-changes. Patients' sociodemographic characteristics did not differ signifi-cantly across physicians.
We also computed correlations (not shown) based on the frequencies(rather than the proportions) of the designated modes. (The length of theseinterviews was highly variable, ranging from 159 utterances to 1,885 ut-terances.) Although the general trends were similar in both analyses, resultswere clearer using the proportion-based indexes.
DISCUSSION
The verbal exchanges identified in this study clearly reflect the primarymedical tasks within each interview segment, as hypothesized. The historytask of eliciting and facilitating patients' expression of their problems cor-responds to the history exposition exchange (factor 2, Table 4). The historytask of probing for specific information corresponds to the history closedquestion exchange (factor 1, Table 4). The examination task of directing pa-tients through diagnostic procedures corresponds to the examination direc-tion exchange (factor 3, Table 5). The examination task of inquiring aboutpatients' subjective reactions to these procedures corresponds to the ex-amination inquiry exchange (factor 2, Table 5). The conclusion task of ex-plaining the patient's illness and treatment corresponds to the conclusionexplanation exchange (factor 2, Table 6). And the conclusion task ofprescribing a therapeutic regimen corresponds to the conclusion instructionand contracts exchanges (factors 4 and 5, Table 6).
These results replicate and extend those of the earlier study (Stiles et al.,1979a). Four of the previous study's exchanges reappeared unchanged,history exposition, history closed question, examination exposition, andconclusion exposition. Two previous large factors appeared split intosmaller, related exchanges; a single physical examination exchange ap-peared split into the inquiry and direction exchanges and a single conclusionfeedback exchange appeared split into explanation, instruction, and con-
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 3 3 3
tracts exchanges. The splits clearly represent a finer resolution of task-oriented functions, made possible by the inclusion of more of the less com-mon modes.
The present study also identified several new exchanges, composed of lesscommon modes, that appear to us to serve maintenance functions, that is,facilitating communication, providing emotional support, and strengthen-ing the relationship. The explanation exchanges in the history and examina-tion segments (factor 3, Table 4 and factor 4, Table 5) reflect physicians'giving an informative commentary on the interview and diagnostic pro-cedures. Giving information can demystify potentially frightening or in-trusive procedures or lines of inquiry and can contribute to patientautonomy in the realm of health (Rodin & Janis, 1979; Waitzkin &Stoeckle, 1976). The history checking exchange (factor 4, Table 4) and thesecondary checking functions associated with examination inquiry exchange(factor 2, Table 5) and the conclusion explanation exchange (factor 2, Table6) reflect physicians' making certain that they understand patients'thoughts, by repeating them and having them confirmed (or disconfirmed)by the patients. In addition to improving the accuracy of the patient-physician communication, checking may contribute to patients' feelingunderstood and supported by their physicians.
Exposition exchanges appeared in all three segments, and in each theycomprised a large proportion of all utterances (especially patient utterances;see Table 3). In them, patients conveyed both objective information(Edification intents) and subjective information (Disclosure intents) in theirown words (i.e., in Disclosure and Edification forms—declarativesentences—rather than in Acknowledgment forms which convey informa-tion by yes/no answers to the physician's closed questions), while physi-cians facilitated with back-channel communications such as "mm-hm" and"yeah," coded K(K). Probably this sort of exchange serves both task andmaintenance functions. Physicians can use exposition exchanges both togather detailed information (task) and to show interest in the patient's con-cerns (maintenance). Patients can use exposition exchanges for transmittingdata they believe to be relevant (task) and for catharsis, expression of con-cerns, and showing trust in their physician (maintenance).
In the examination and the conclusion, patient Q(Q) was associated withthe exposition exchanges. Perhaps patients can seek information more com-fortably in an atmosphere of physician attentiveness, after they have"warmed up" by talking about their problems in their own words. Becausepatients' use of questions may have major implications for medical treat-ment decisions (Fisher, in press), this finding may be important for healtheducation efforts. Roter (1977) found that when patients were given ten-minute preinterview sessions aimed at formulating questions and encourag-ing question-asking, they asked more questions in the interview and were
334 STILES, PUTNAM, JACOB
more likely to return for scheduled appointments; however, their interviewswere characterized by more negative affect, and they reported less satisfac-tion with their encounters, as compared with controls. Perhaps the negativi-ty and dissatisfaction were related to taking patient Questions out of their"ecological niche" in exposition exchanges and forcing them into a separateexchange. The educators rehearsed question-asking with patients and en-couraged patients to write down their questions, in effect suggesting aseparation of question-asking from other exchanges. Our results suggestthat patient question-asking might be facilitated more comfortably by in-creasing the proportion of exposition exchanges.
The correlations of exchange indexes with patient characteristics (Table7) show that different patients received systematically different kinds of in-terviews. Some of the differences may reflect systematic adaptations to dif-fering patient needs. Others may reflect wider social role relationships; ex-changes that could give patients greater freedom and respect, that is, exposi-tion and explanation, as opposed to closed question or inquiry, tended to bemore common among patients who were older, more educated, higherstatus, and white—characteristics associated with greater social power inour culture.
The verbal exchange structure offers an analytic framework for medicalinterviews. By itself, it is not a complete characterization; other kinds of in-formation are needed to put flesh on the exchange structure skeleton, as il-lustrated by our informal use of content in describing some of the exchangeswe found. The framework may permit investigators to ask more soph-isticated questions about other interview aspects, such as what was the con-tent of the examination inquiry exchanges (were the probes appropriate andcomplete for the presenting problem?), what affect was displayed in the ex-planation exchanges (did giving information seem to reduce the patient'sanxiety?), or what was the sequence and timing of speech acts within the ex-position exchanges (are some patterns of back-channel responding morefacilitative than others?). We have come to believe that no one kind of inter-view is "best" in any general way, and that a basic scientific understandingof human interaction processes—to which we hope our framework can con-tribute—is prerequisite to prescribing particular interviews for particularpatients.
REFERENCES
Almy, T. P. The healing bond: Doctor and patient in an era of scientific medicine. AmericanJournal of Gastroenterology, 1980, 73, 403-407.
Austin, J. L. How to do things with words (2nd ed.). Oxford: Clarendon Press, 1975.Bain, D. J. G. Doctor-patient communication in general practice consultations. Medical
Education, 1976, 10, 125-131.
EXCHANGE STRUCTURE OF MEDICAL INTERVIEWS 335
Barsky, A. J., Kazis, L. E., Freiden, R. B., Goroll, A. H., Hatem, C. J., & Lawrence, R. S.Evaluating the interview in primary care medicine. Social Science & Medicine, 1980,14A, 653-658.
Bloom, S. W. The doctor and his patient: A sociological interpretation. New York: Russell-Sage Foundation, 1963.
Brent, E. E., & Sykes, R. E. A mathematical model of symbolic interaction between policeand suspects. Behavioral Science, 1979, 24, 388-402.
Carroll, J., & Monroe, J. Clinical interviewing in the health profession: A review of empiricalresearch. Evaluation of Health Professions, 1980, 3, 21-45.
Cassell, E. J., & Skopek, L. Language as a tool in medicine: Methodology and theoreticalframework. Journal of Medical Education, 1977, 52, 197-203.
Coulthard, M., & Ashby, M. A linguistic description of doctor-patient interviews. In M.Wadsworth & D. Robinson (Eds.), Studies in everyday medical life. London: MartinRobertson & Co., 1976.
Davis, M. Variations in patients' compliance with doctors' orders: Medical practice anddoctor-patient interaction. Psychiatry in Medicine, 1971, 2, 31-54.
DiMatteo, M. R. A social-psychological analysis of physician-patient rapport: Toward ascience of the art of medicine. Journal of Social Issues, 1979, 35, 12-33.
Drossman, D. A. Can the primary care physician be better trained in the psychosocialdimensions of patient care? International Journal of Psychiatry in Medicine, 1977-78,8, 169-184.
Duncan, S., Jr. Some signals and rules for taking turns in conversations. Journal of Per-sonality and Social Psychology, 1972, 23, 283-292.
Egbert, L. D., Battit, G. E., Welch, C. E., & Bartlett, M. K. Reduction of postoperativepain by encouragement and instruction of patients. New England Journal of Medicine,1964, 270, 825-827.
Enelow, A. J., & Swisher, S. N. Interviewing and patient care. New York: Oxford UniversityPress, 1972.
Fisher, S. The negotiation of treatment decisions in doctor/patient communication.Language in Society, in press.
Francis, V., Korsch, B. M., & Morris, M. J. Gaps in doctor-patient communication:Patients' response to medical advice. New England Journal of Medicine, 1969, 280,535-540.
Freemon, B., Negrete, V. F., Davis, M., & Korsch, B. M. Gaps in doctor-patient communica-tion: Doctor-patient interaction analysis. Pediatric Research, 1971, 5, 298-311.
Friedman, H. S. Nonverbal communication between patients and medical practitioners.Journal of Social Issues, 1979, 35, 82-99.
Glasunov, I. S., Dowd, J. E., Jaksic, Z., Kesic, B., Ray, D., Steinberger, C , Stromberg,J., & Vuletic, S. Repetitive health examinations as an intervention measure. Bulletin ofthe World Health Organization, 1973, 49, 423-432.
Gottman, J. M. Marital interaction: Experimental investigations. New York: AcademicPress, 1979.
Hampton, J. R., Harrison, M. J. G., Mitchell, J. R. A., Pritchard, J. S., & Seymour, C.Relative contribution of history taking, physical examination, and laboratory investigationto diagnosis and management of medical outpatients. British Medical Journal, 1975, 2,486-489.
Hollingshead, A. B., & Redlich, F. C. Social class and mental illness: A community study.New York: Wiley, 1958.
Holsti, O. R. Content analysis for the social sciences and the humanities. Reading, Mass.:Addison-Wesley, 1969.
Joyce, C. R. B., Caple, G., Mason, M., Reynolds, E., & Mathews, J. A. Quantitative studyof doctor-patient communication. Quarterly Journal of Medicine, 1969, 38, 183-194.
336 STILES, PUTNAM, JACOB
Koos, E. L. "Metropolis"—What city people think of their medical services. AmericanJournal of Public Health, 1955,45, 1551-1557.
Miller, G. A. Psychology, language, and levels of communication. In A. Silverstein (Ed.),Human communication: Theoretical explorations. New York: John Wiley, 1974.
Morgan, W. L., & Engel, G. L. The clinical approach to the patient. Philadelphia: W. B.Saunders Co., 1969.
Nardone, D. A., Reuler, J. B., & Girard, D. E. Teaching history-taking: Where are we?Yale Journal of Biology and Medicine, 1980, 53, 233-250.
Ort, R. S., Ford, A., & Liske, R. The doctor-patient relationship as described by physiciansand medical students. Journal of Health and Human Behavior, 1964, 5, 25-34.
Reader, G. G., Pratt, L., & Mudd, M. C. What patients expect from their doctors. ModernHospital, 1957, 89{\), 88-94.
Rodin, J., & Janis, I. L. The social power of health-care practitioners as agents of change.Journal of Social Issues, 1979, 35, 60-81.
Roter, D. L. Patient participation in the patient-provider interaction: The effects of patientquestion asking on quality of interaction, satisfaction, and compliance. Health EducationMonographs, 1977, 5, 281-315.
Russell, R. L., & Stiles, W. B. Categories for classifying language in psychotherapy.Psychological Bulletin, 1979, 86, 404-419.
Scott, N., Donnelly, M., Gallagher, R., & Hess, J. Interaction analysis as a method forassessing skill in relating to patients: Studies on validity. British Journal of MedicalEducation, 1973, 7, 174-178.
Searle, J. R. Speech acts: An essay in the philosophy of language. Cambridge: CambridgeUniversity Press, 1969.
Smith, C. K., Polis, E., & Hadac, R. R. Characteristics of the initial medical interviewassociated with patient satisfaction and understanding. Journal of Family Practice, 1981,12, 283-288.
Stiles, W. B. Manual for a taxonomy of verbal response modes. Chapel Hill: Institute forResearch in Social Science, University of North Carolina at Chapel Hill, 1978. (a)
Stiles, W. B. Verbal response modes and dimensions of interpersonal roles: A method ofdiscourse analysis. Journal of Personality and Social Psychology, 1978, 36, 693-703. (b)
Stiles, W. B. Discourse analysis and the doctor-patient relationship. International Journalof Psychiatry in Medicine, 1978-79, 9, 263-274.
Stiles, W. B. Classification of intersubjective illocutionary acts. Language in Society,1981, 10, 227-249.
Stiles, W. B., Putnam, S. M., Wolf, M. H., & James, S. A. Interaction exchange structureand patient satisfaction with medical interviews. Medical Care, 1979, 17, 667-681. (a)
Stiles, W. B., Putnam, S. M., Wolf, M. H., & James, S. A. Verbal response mode profilesof patients and physicians in medical screening interviews. Journal of Medical Education,1979, 54, 81-89. (b)
Stone, G. C. Patient compliance and the role of the expert. Journal of Social Issues, 1979,35, 34-59.
Svarstad, B. L. Physician-patient communication and patient conformity with medical advice.In D. Mechanic (Ed.), The growth of bureaucratic medicine: An inquiry into the dynamicsof patient behavior and the organization of medical care. New York: John Wiley & Sons,1976.
Waitzkin, H., & Stoeckle, J. D. Information control and the micropolitics of health care:Summary of an ongoing research project. Social Science and Medicine, 1976,10A, 263-276.
Related Documents











