1 39 th National Conference on Pediatric Health Care ©2018 March 19-22, 2018 CHICAGO Standardizing VEPTR Incision Site Documentation Roni Lynn Robinson, RN, MSN, CRNP Department of Orthopedic Surgery ©2018 Disclosures I have no relevant disclosures. ©2018 Learning Objective Gain knowledge about a novel way to assess and reduce surgical wound complications and surgical site infections (SSI) for a specific low volume, high risk surgical procedure. Vertical Expandable Prosthetic Titanium Rib VEPTR ©2018 Thoracic Insufficiency Syndrome (TIS) Inability of the thorax to support normal respiration or lung growth. ©2018 Thoracic Insufficiency Syndrome (TIS) Underlying Pathologies 1. Deformity of the spine causing distortion of the rib cage with both volume and function loss. 2. Primary thoracic dysplasia which can compromise chest volume and rib cage function. 3. Neuromuscular dysfunction causing secondary spine and chest deformity. ©2018 What Causes TIS? • CHARGE Syndrome • VACTERL • Congenital Scoliosis • Early Onset Scoliosis • Juene Syndrome • Jarcho‐Levine Syndrome • Hemihypertrophy • Charcot‐Marie‐Tooth Syndrome • Spina bifida • Muscular dystrophy • SMA • Friedreich׳s ataxia • + many more

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
39th National Conference on Pediatric Health Care
©2018
March 19-22, 2018 CHICAGO
Standardizing VEPTR Incision Site Documentation
Roni Lynn Robinson, RN, MSN, CRNPDepartment of Orthopedic Surgery
©2018
Disclosures
I have no relevant disclosures.
©2018
Learning Objective
Gain knowledge about a novel way to assess and reduce surgical wound complications and surgical site infections (SSI) for a
specific low volume, high risk surgical procedure.
Vertical ExpandableProstheticTitaniumRib
VEPTR
©2018
Thoracic Insufficiency Syndrome (TIS)Inability of the thorax to support normal
respiration or lung growth.
©2018
Thoracic Insufficiency Syndrome (TIS)
Underlying Pathologies
1. Deformity of the spine causing distortion of the rib cage with both volume and function loss.
2. Primary thoracic dysplasia which can compromise chest volume and rib cage function.
3. Neuromuscular dysfunction causing secondary spine and chest deformity.
©2018
What Causes TIS?
• CHARGE Syndrome
• VACTERL
• Congenital Scoliosis
• Early Onset Scoliosis
• Juene Syndrome
• Jarcho‐Levine Syndrome
• Hemihypertrophy
• Charcot‐Marie‐Tooth Syndrome
• Spina bifida
• Muscular dystrophy
• SMA
• Friedreich׳s ataxia
• + many more

2
©2018
VEPTR Device History
• 1989 Dr. Robert Campbell placed the 1st titanium rib in a child in Texas
• 1994 Synthes Spine Company took over production
• 2004 VEPTR approved by FDA
©2018
VEPTR Device
VEPTR expands outward to mimic the width of a typical child’s chest
Attaches to the ribs and either the ribs, pelvis or the spine.With permission, Campbell et.al; Thoracic insufficiency syndrome.Curr Probl Pediatr Health Care 2016 Mar; 46(3):72‐97.
©2018
VEPTR Device
Scoliosis
VEPTR can be used as a jack to straighten the spine & keep it straight as the patient grows.
©2018
Post VEPTR Insertion
Real life VEPTRs
©2018
Background
• Varying, nondescript documentation of incision sites in the EHR
• Difficult to capture which incision is from which surgery when there are wound concerns
– Potential to incorrectly report Surgical Site Incisions (SSI)
– Could lead to difficulty with providing optimal therapy, classification, as well as proactive identification of high risk sites
• Parents not consistently educated on incision site nomenclature when calling or coming to the ED with a wound concern
• No way of identifying specific incision sites in nursing flowsheets
©2018
Quality Improvement Project Goals
• Provide a consistent approach when communicating a VEPTR patient’s incision sites across the organization
• Standardize SSI documentation using the Center for Thoracic Insufficiency Syndrome (CTIS) Incision Site Schematic (ISS) for all skin & wound issues related to a VEPTR procedure
• Educate at least 80% of the patients/families using the ISS

3
©2018
Incision Site Schematic
• Developed within the CTIS Safety Group
• Ability to track & monitor multiple skin incisions following a VEPTR procedure
• Ability to discern which specific SSI there are concerns about
• Allows for a standardized communication of incision sites across the board
©2018
VEPTR Post Surgery PFE
Patient Family Education: VEPTR Care Post Surgery• When can I remove my child’s dressing?• Remove your child’s secondary or cover dressing on (Date:)____• How to Care for the spine dressing• When can my child shower or take a bath?• How do I care for my child’s incision?• Signs/symptoms of infection
©2018
VEPTR Incision Diagram in EHR
Nurses are able to refer to ISS while documenting in flowsheet.
©2018
VEPTR Incision Diagram in EHR
©2018
Who will utilize the ISS?
• Ortho attending documents the specific sites in the CTIS physician survey (REDCap)
• Nursing‐newly created LDA specific to VEPTR incisions (active in EHR)– Will allow for easy identification of which sites have concerns
• Nursing & Inpatient NP’s complete PFE sheet (ISS) & educate families prior to discharge– An image of the completed ISS sheet is uploaded into the patient’s media tab
• Outpatient NP’s & coordinators utilize the ISS (media tab) to follow up with the families post operatively
• Parents use the ISS sheet provided when concerned about an incision site “PFE:VEPTR Care Post Surgery”
©2018
Quality Improvement Project Results
• A PFE was created for consistent education at discharge
• Post discharge follow up showed that 100% of families in March 2017reported receiving the VEPTR ISS & felt comfortable using it

4
©2018
Quality Improvement Project Results
• Goal: To educate 80% of patients/parents using the ISS
• As of March, 2017 92% of families had received the education
©2018
Qlikview Accessibility
©2018 ©2018
©2018 ©2018

5
©2018 ©2018

My Kid Falls ALL the Time: Common Causes of In-toeing
• Learning Objectives – Understand the 3 most common causes of in-toeing – Describe treatment for 3 the most common causes of in-toeing – Understand when to refer and when to watch
• In-toeing
– Very common – Most resolves spontaneously
Treatment for all 3:
– Reassurance – Reassurance – 2nd opinion for reassurance
• Evaluation
– Thorough H&P – Family history – Pain? – Height/Weight – LLD? – Neuro exam
• Femoral Anterversion
– Normal anterversion 15° to 20° – Increases until age 4 or 5 – Resolved by age 10-12 – “W” sitting- don’t worry about it – Surgical treatment-RARE
• Osteotomy if functionally limiting by early teen
– Physical Exam: • Hip motion
• Increased internal rotation > 70° • Decreased external rotation of < 20°
• Patella internally rotated when ambulating
• Internal Tibial Torsion – Presents at walking age – Most often bilateral – Resolves by 7 or 8 – REASSURANCE – Surgical treatment-RARE
• Derotational osteotomy
– Physical Exam • Thigh foot angle > 15°

• Increased foot progression angle • Patella faces forward, feet turn in
• Metatarsus Adductus
– “Packaging” problem • Torticollis • DDH • Excessive anterversion • Internal tibial torsion
– Treatment • Diaper change stretching • 90% resolve by 1-2 years • REASSURANCE (no special shoes) • Metatarsus Adductus
– Physical Exam:
• Normal hindfoot • Medially deviated forefoot • “C” shaped lateral border • Mild, moderate, severe
• References
– The American Academy of Orthopaedic Surgeons • https://orthoinfo.aaos.org/en/diseases--conditions/intoeing/
– Pediatric Orthopaedic Society of North America • http://orthokids.org/Condition/In-Toeing
– OrthoBullets • https://www.orthobullets.com

1
39th National Conference on Pediatric Health Care
©2018
March 19-22, 2018 CHICAGO
Pediatric Fractures: A Tough Break for All
Kimberly R. Joo, DNP, APRN, CPNP‐PC, CNE©2018
Disclosures
• I have nothing to disclose.
©2018
Learning Objectives
• Define key terms
• Describing a fracture
• Review Bone Anatomy
• State the indications for an x‐ray
• Identify the different types of pediatric fractures
• Cases that require immediate referral
• Indicate cases that require follow‐up testing
• Splinting fractures
©2018
Key Terms for Fractures• Salter Harris: classification of growth plate and epiphyseal fractures
• Greenstick: incomplete fracture with angular deformity
• Buckle: compression fracture that causes the bone to bend or buckle on the damaged side
• Reduce: procedure to restore a fracture to original alignment
• Displaced: a fracture where the 2 ends of a bone are not lined up straight
• Angulated: a fracture with loss of alignment, the degree of rotation or change in bone length
• Transverse: fracture is perpendicular to the shaft
©2018
Key Terms for Fractures
• Avulsion: a fragment of bone has torn away from the main mass of bone
• Effusion: abnormal accumulation of fluid in a joint
• Open: a broken bone that penetrates the skin
• Comminuted: more than 2 fracture fragments
• Oblique: an angulated fracture line
• Segmental: comminuted fracture where a completely separate segment of bone is bordered by fracture lines
• Torus: an incomplete buckle fracture of one cortex
©2018
Key Terms for Fractures
• Spiral: multiplanar and complex fracture line
• Intra‐articular: the fracture line crosses the articular cartilage and enters the joint
• Impaction: a fracture that occurs when one bone hits an adjacent bone
• Compression: type of impaction fracture that occurs in the vertebrae, resulting in depression of the end plates
• Depression: a type of impaction fracture that occurs in the knee when the femoral condyle strikes the softer tibial plateau

2
+
Bone Anatomy
+
Growth Plate Anatomy
+
(Slideplayer.com, 2016)
©2018
Indications for Imaging
• Injury
• Pain
• Point tenderness
• Deformity
• Decreased range of motion
• Edema
• Bruising
• Pain with ambulation
• Inability to bear weight
©2018
What X‐Ray Should I Order?Anatomic Region Plain Radiograph Fracture Views
Wrist All patients: AP, lateral
Oblique: if fracture suspected, but AP and lateral are negative:
Scaphoid: if scaphoid fracture is suspected
Elbow AP, lateral, and oblique
Shoulder AP, scapular Y
Knee AP, lateral, oblique (internal or externally rotated)Sunrise (axial, tangential): patellar injury
Foot AP, lateralOblique: if fracture seen
Tibia, femur, humerus, & forearm AP, lateral
Ankle AP, lateral, and mortise
(UpToDate, 2018)
©2018
Describing a Fracture

3
©2018
Type of Fracture: Buckle (torus)
• Compression fracture
• Often at the junction between the porous metaphysis and the denser metaphysis
• Locations: distal radius, distal tibia, fibula and femur
• Stable
• Splint
• Ortho follow‐up
+
Buckle (Torus) Fracture Image
©2018
Type of Fracture: Plastic Deformation
• Bowing fracture
• Longitudinal force exceeds the bone’s ability to recoilto it’s normal position
• Microscopic fractures
• Locations: ulna, radius, and occasionally the fibula
• Self‐correcting if < 20 degrees and/or < 4 years of age
• Closed reduction or surgical intervention
+
Plastic Deformation Fracture Image
©2018
Type of Fracture: Greenstick
• Bone that is bent with a fracture line that does not extend completely through the width of the bone
• Risk for repeat fracture
• 84‐100% of forearm refractures
• Location: forearm
+Greenstick Fracture Image

4
©2018
Type of Fracture: Physeal (Growth Plate)
• Growth plates are susceptible to fracture
• Weak point in pediatric bones
• Tensile strength of pediatric bone is less than that of ligaments
• 21‐30% of pediatric long bone fractures
• Locations: distal radius and distal ulna
• Girls: 9‐12 years
• Boys: 12‐15 years
• 30% cause bone growth disturbance
• Once the physis closes, fractures follow adult patterns
©2018
Type of Fracture: PhysealSalter‐Harris Classification
• Type I: Disrupts the physis
• Type II: Break from the growth plate into the metaphysis
• Type III: Intraarticular‐through the epiphysis and extend across the physis
• Type IV: Cross the epiphysis, physis, and metaphysis
• Type V: Compression to the physis
+ Types of Fractures: PhysealSalter‐Harris Classification
Green = growth plate Red = fracture(UpToDate, 2018)
+Salter‐Harris Ankle Fracture Images
(Epomedicine, 2016)
+Salter‐Harris Humor
(Wordpress, 2014) ©2018
Type of Fracture:Apophyseal Avulsion
• Fibrocartilage physes instead of columnar cartilage
• Prone to overuse traction avulsions
• Osgood‐Schlatter disease: tibial tuberosity
• Sinding‐Larsen‐Johnsson syndrome: inferior pole of the patella
• Self‐limited
• Do not interfere with growth
• Adolescent athletes

5
+Apophyseal Avulsion Fracture Image
(Science Direct, 2012) (KoreamedSynapse, 2009) ©2018
Special Circumstance Fracture:Stress Fracture
• Overuse injuries• Accumulated microtrauma from repetitive strain• Small but progressive cracks in the periosteum• Adolescents• Female > males• Locations: tibia, fibula, pars interarticularis (spondylolysis) and femur
• Radiographic findings don’t present until 1‐2 weeks of symptoms
• MRI is more sensitive
©2018
Stress Fracture Sports and Sites
Sport Fracture Site
Baseball Tibia
Basketball Anterior cortex of tibia, tarsal navicular
Gymnastics Tibia, fibula
Ice Skating Distal fibula
Running Proximal tibial metaphysis, distal tibial metaphysis, fibula, tarsal navicular, midshaft of femur, distal femur, femoral neck
Soccer Patella
Swimming Proximal tibia
Volleyball Tibia
(UpToDate, 2018)
+Stress Fracture Images
©2018
Special Circumstance Fracture:Child Abuse
• Fracture in a child < 1 year• Lower extremity fracture in a non‐ambulatory child• Posterior rib fractures• Metaphyseal lesions (bucket‐handle or corner fractures)• Bilateral long bone fractures• Complex skull fractures• Spinous process fractures• Repeat fracture in an unusual location• Stage of healing that is inconsistent with injury description• Multiple fractures in various stages of healing • Mandatory reporter
+
Child Abuse Fracture Image

6
©2018
Special Circumstance Fracture:Pathologic Fracture
• Fracture in a bone that is weakened by an underlying abnormality
• Bone tumors
• Rickets
• McCune‐Albright syndrome
• Juvenile osteoporosis
• Chronic renal insufficiency
• Osteogenesis imperfecta
• Osteopetrosis
• Location: proximal femur and humerus
+Pathologic Fracture Image
(Radiopaedia, 2018)
©2018
Special Circumstance Fracture:Repeat Fractures
• 1 in 1,000
• 5‐13% of forearm fractures
• Risk:
– Incomplete bony union
– Residual angulation
– Early cast removal
– Radial or ulnar diaphyseal fracture
– Greenstick fracture
©2018
Immediate Referral
• Open fractures
• Deformed/angulated fractures
• Rotated fractures
• Displaced fractures
• Fractures with dislocations
• Joint/articular surface involvement
• Any fracture with neurovascular compromise
• Consult orthopedics whenever you have a question
©2018
Immobilization Guidelines
1. Document vascular, sensory, and motor function before and after immobilization. Immobilize above and below the site of injury, generally in a position of function.
2. Immediate consultation with orthopedics for all findings on previous slide.
3. Consult orthopedics whenever you have a question. If you consult an attending physician, follow‐up with that physician.
4. With any fracture (except torus), the fracture could progress (even in a cast).
5. True buckle/torus fractures should not demonstrate completion of fracture through volar cortex and should not have angulation.
©2018
Immobilization Guidelines
6. Elbows: for children < 6 years, consider obtaining comparative lateral film of contralateral elbow; for condyle fractures, consider obtaining oblique view to more clearly delineate amount of displacement.
7. Any displacement at a growth plate should prompt a consult to ortho.
8. Ensure good after‐care instructions, pain control, and specify follow‐up (ortho or PCP and timing).
9. These guidelines are very generalized. Care must be taken to alter treatment according to individualized patient situation.
7
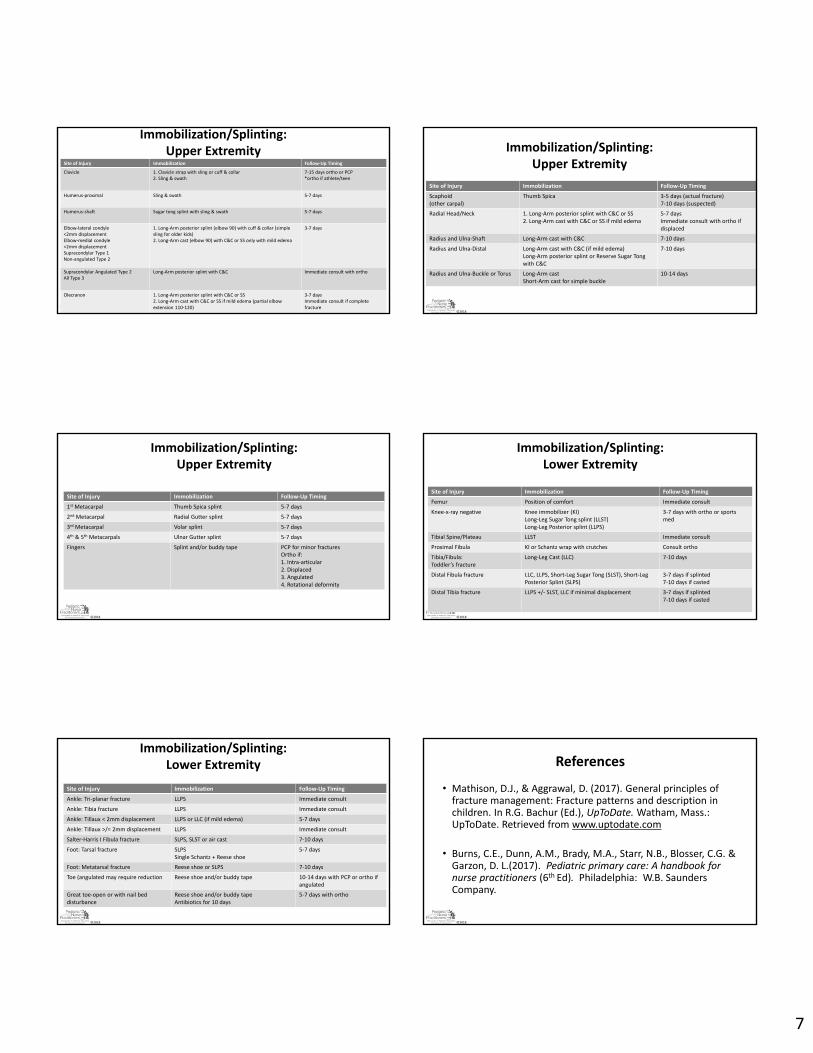
©2018
Immobilization/Splinting:Upper Extremity
Site of Injury Immobilization Follow‐Up Timing
Clavicle 1. Clavicle strap with sling or cuff & collar2. Sling & swath
7‐15 days ortho or PCP*ortho if athlete/teen
Humerus‐proximal Sling & swath 5‐7 days
Humerus‐shaft Sugar tong splint with sling & swath 5‐7 days
Elbow‐lateral condyle<2mm displacementElbow‐medial condyle<2mm displacementSupracondylar Type 1Non‐angulated Type 2
1. Long‐Arm posterior splint (elbow 90) with cuff & collar (simple sling for older kids)2. Long‐Arm cast (elbow 90) with C&C or SS only with mild edema
3‐7 days
Supracondylar Angulated Type 2 All Type 3
Long‐Arm posterior splint with C&C Immediate consult with ortho
Olecranon 1. Long‐Arm posterior splint with C&C or SS2. Long‐Arm cast with C&C or SS if mild edema (partial elbow extension 110‐120)
3‐7 daysImmediate consult if complete fracture
©2018
Immobilization/Splinting:Upper Extremity
Site of Injury Immobilization Follow‐Up Timing
Scaphoid(other carpal)
Thumb Spica 3‐5 days (actual fracture)7‐10 days (suspected)
Radial Head/Neck 1. Long‐Arm posterior splint with C&C or SS2. Long‐Arm cast with C&C or SS if mild edema
5‐7 days Immediate consult with ortho if displaced
Radius and Ulna‐Shaft Long‐Arm cast with C&C 7‐10 days
Radius and Ulna‐Distal Long‐Arm cast with C&C (if mild edema)Long‐Arm posterior splint or Reserve Sugar Tong with C&C
7‐10 days
Radius and Ulna‐Buckle or Torus Long‐Arm castShort‐Arm cast for simple buckle
10‐14 days
©2018
Immobilization/Splinting:Upper Extremity
Site of Injury Immobilization Follow‐Up Timing
1st Metacarpal Thumb Spica splint 5‐7 days
2nd Metacarpal Radial Gutter splint 5‐7 days
3rd Metacarpal Volar splint 5‐7 days
4th & 5th Metacarpals Ulnar Gutter splint 5‐7 days
Fingers Splint and/or buddy tape PCP for minor fracturesOrtho if:1. Intra‐articular2. Displaced3. Angulated4. Rotational deformity
©2018
Immobilization/Splinting:Lower Extremity
Site of Injury Immobilization Follow‐Up Timing
Femur Position of comfort Immediate consult
Knee‐x‐ray negative Knee immobilizer (KI)Long‐Leg Sugar Tong splint (LLST)Long‐Leg Posterior splint (LLPS)
3‐7 days with ortho or sports med
Tibial Spine/Plateau LLST Immediate consult
Proximal Fibula KI or Schantz wrap with crutches Consult ortho
Tibia/Fibula:Toddler’s fracture
Long‐Leg Cast (LLC) 7‐10 days
Distal Fibula fracture LLC, LLPS, Short‐Leg Sugar Tong (SLST), Short‐Leg Posterior Splint (SLPS)
3‐7 days if splinted7‐10 days if casted
Distal Tibia fracture LLPS +/‐ SLST, LLC if minimal displacement 3‐7 days if splinted7‐10 days if casted
©2018
Immobilization/Splinting:Lower Extremity
Site of Injury Immobilization Follow‐Up Timing
Ankle: Tri‐planar fracture LLPS Immediate consult
Ankle: Tibia fracture LLPS Immediate consult
Ankle: Tillaux < 2mm displacement LLPS or LLC (if mild edema) 5‐7 days
Ankle: Tillaux >/= 2mm displacement LLPS Immediate consult
Salter‐Harris I Fibula fracture SLPS, SLST or air cast 7‐10 days
Foot: Tarsal fracture SLPSSingle Schantz + Reese shoe
5‐7 days
Foot: Metatarsal fracture Reese shoe or SLPS 7‐10 days
Toe (angulated may require reduction Reese shoe and/or buddy tape 10‐14 days with PCP or ortho if angulated
Great toe‐open or with nail bed disturbance
Reese shoe and/or buddy tapeAntibiotics for 10 days
5‐7 days with ortho
©2018
References
• Mathison, D.J., & Aggrawal, D. (2017). General principles of fracture management: Fracture patterns and description in children. In R.G. Bachur (Ed.), UpToDate. Watham, Mass.: UpToDate. Retrieved from www.uptodate.com
• Burns, C.E., Dunn, A.M., Brady, M.A., Starr, N.B., Blosser, C.G. & Garzon, D. L.(2017). Pediatric primary care: A handbook for nurse practitioners (6th Ed). Philadelphia: W.B. Saunders Company.
Related Documents











