Ventricular Septal Defect in Interruption of Aortic Arch ROBERT M. FREEDOM, MD, FRCP (C), FACC HUGH H. BAIN, MB, ChB, MRCP (UK) ENRIQUE ESPLUGAS, MD RENATE DISCHE, PhD, MD RICHARD D. ROWE, MB, FRCP (Edin) Toronto, Ontario, Canada A necropsy study of 34 patients with interruption of the aortic arch was carried out to characterize more fully the ventricular septal defect and the anatomic basis of subaortic obstruction. In 21 patients (61,8 percent) the site of interruption was between the left common carotid artery and the left subclavian artery; in 13 (38.2 percent) it was distal to the left subclavian artery; no case of interruption just distal to the innominate artery was found. A ventricular septal defect was present in all but two patients, both with large aortopulmonary fenestrations. All patients had visceroatrial situs solitus and D-ventricular loop. The great arteries were normally related in 33 patients and D-transposition was found in one patient. Twenty-one patients had a ventricular septal defect involving the conal septum. Co- noventricular malalignment resulted in a typical subpulmonary ventricular defect. The malalignment was characteristically in a leftward direction, allowing for potential muscular narrowing of the left ventricular outflow tract. In some patients, the conal ventricular septal defect was charac- terized by a deficiency of the conal septum without malalignment. In 4 of the 21 patients with a ventricular septal defect involving the conal septum, the defect was immediately adjacent to the pulmonary valve. Typical infracristal membranous ventricular defects (five patients), cushion defects (3 patients) and muscular defects (3 patients), were also found. The potential for subaortic narrowing was present in some of these patients as well. No relation between position of ventricular septal defect and type of arch interruption could be discerned. The presence or absence of sub- aortic obstruction was not predictive of a specific type of interruption. Similarly, although deformity of the aortic valve was not uncommon in this series, it was not associated with any specific type of interruption. From the Departments of Paediatric Cardiology and Pathology, The Hospital for Sick Children, and the Department of Paediatrics and Pathology, The University of Toronto, Toronto, Ontario, Canada. Manuscript received July 9, 1976, revised manu- script received September 30, 1976, accepted October 6, 1976. Address for reprints: Robert M. Freedom, MD, The Hospital for Sick Children, 555 University Ave., Toronto, Ontario, Canada M5G 1X8. Interruption of the aortic arch is a rare cardiac anomaly, constituting probably less than 1 percent of all congenital heart disease. 1 In this condition, the ascending and descending portions of the aorta are not continuous, and blood flow to the descending aorta occurs through a patent ductus arteriosus. Interruption of the aortic arch rarely occurs in isolation, 2 and almost any cardiovascular malformation can coexist. 1 A ventricular septal defect is usually present. In 1971, Van Praagh et al.1 presented the anatomic findings in 10 autopsy cases of interrupted aortic arch, and suggested that a leftward shift of the crista supraventricularis, resulting in a large subpulmonary ventricular septal defect and muscular subaortic stenosis, was highly characteristic of this disorder. Before their report, little emphasis had been placed on the conal morphology in the patient with interruption of the aortic arch. 2,4 If untreated, interruption of the aortic arch is usually lethal in the neonate; the reported mean age of death is only 10 days. ~ In the past few years, reconstitution of the aortic arch has been accomplished success- 572 April 1977 The American Journal of CARDIOLOGY Volume39

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Ventricular Septal Defect in Interruption of Aortic Arch
ROBERT M. FREEDOM, MD, FRCP (C), FACC
HUGH H. BAIN, MB, ChB, MRCP (UK) ENRIQUE ESPLUGAS, MD RENATE DISCHE, PhD, MD RICHARD D. ROWE, MB, FRCP (Edin)
Toronto, Ontario, Canada
A necropsy study of 34 patients with interruption of the aortic arch was carried out to characterize more fully the ventricular septal defect and the anatomic basis of subaortic obstruction. In 21 patients (61,8 percent) the site of interruption was between the left common carotid artery and the left subclavian artery; in 13 (38.2 percent) it was distal to the left subclavian artery; no case of interruption just distal to the innominate artery was found.
A ventricular septal defect was present in all but two patients, both with large aortopulmonary fenestrations. All patients had visceroatrial situs solitus and D-ventricular loop. The great arteries were normally related in 33 patients and D-transposition was found in one patient. Twenty-one patients had a ventricular septal defect involving the conal septum. Co- noventricular malalignment resulted in a typical subpulmonary ventricular defect. The malalignment was characteristically in a leftward direction, allowing for potential muscular narrowing of the left ventricular outflow tract. In some patients, the conal ventricular septal defect was charac- terized by a deficiency of the conal septum without malalignment. In 4 of the 21 patients with a ventricular septal defect involving the conal septum, the defect was immediately adjacent to the pulmonary valve. Typical infracristal membranous ventricular defects (five patients), cushion defects (3 patients) and muscular defects (3 patients), were also found. The potential for subaortic narrowing was present in some of these patients as well.
No relation between position of ventricular septal defect and type of arch interruption could be discerned. The presence or absence of sub- aortic obstruction was not predictive of a specific type of interruption. Similarly, although deformity of the aortic valve was not uncommon in this series, it was not associated with any specific type of interruption.
From the Departments of Paediatric Cardiology and Pathology, The Hospital for Sick Children, and the Department of Paediatrics and Pathology, The University of Toronto, Toronto, Ontario, Canada. Manuscript received July 9, 1976, revised manu- script received September 30, 1976, accepted October 6, 1976.
Address for reprints: Robert M. Freedom, MD, The Hospital for Sick Children, 555 University Ave., Toronto, Ontario, Canada M5G 1X8.
Interruption of the aortic arch is a rare cardiac anomaly, constituting probably less than 1 percent of all congenital heart disease. 1 In this condition, the ascending and descending portions of the aorta are not continuous, and blood flow to the descending aorta occurs through a patent ductus arteriosus. Interruption of the aortic arch rarely occurs in isolation, 2 and almost any cardiovascular malformation can coexist. 1 A ventricular septal defect is usually present. In 1971, Van Praagh et al.1 presented the anatomic findings in 10 autopsy cases of interrupted aortic arch, and suggested that a leftward shift of the crista supraventricularis, resulting in a large subpulmonary ventricular septal defect and muscular subaortic stenosis, was highly characteristic of this disorder. Before their report, little emphasis had been placed on the conal morphology in the patient with interruption of the aortic arch. 2,4
If untreated, interruption of the aortic arch is usually lethal in the neonate; the reported mean age of death is only 10 days. ~ In the past few years, reconstitution of the aortic arch has been accomplished success-
572 April 1977 The American Journal of CARDIOLOGY Volume 39

INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
fully in the neonate, s-ll Because of the recent emphasis on pr imary surgical correct ion (when possible) of symptomat ic congenital hear t defects, in this paper we characterize more fully the spec t rum of ventr icular septal defect in respect to conal ana tomy in 34 pat ients with interrupt ion of the aortic arch, the largest number of such pat ients s tudied from any single inst i tut ion.
Definitions
Aortic arch interruptions: These are classified according to the method of Celoria and Patton 12 (types A, B and C), but we add subcategories to A and B:
Type A interruption: interruption distal to the left sub- clavian artery.
Type A1 interruption: interruption just distal to the left subclavian artery with an aberrant right subclavian artery.
Type B interruption: interruption distal to the left common carotid artery.
Type B1 interruption: interruption distal to the left com- mon carotid artery with an aberrant right subclavian ar- tery.
Type C interruption: interruption distal to the innominate artery.
Conal structures: Because there are considerable differ- ences regarding the terminology of conal structures,~,~:~- ~ we will be using the definition of terms as suggested by Anderson and Becker and their associates. 16,17
1. Conal septum: This represents the embryonic septum between the aortic and pulmonary conuses. It can be consid- ered to possess two components: (a) that portion between the aortic and pulmonary valves, forming part of the ventricular septum; (b) the segment extending from this septal compo- nent to the parietal wall of the right ventricle and forming an integral part of the crista supraventricularis. Septal defects in the conal septum are termed conal or infundibular.
2. Crista supraventricularis: Becker et al. 17 use this term to describe a structure in the normal heart. As such, it is considered to be that muscle mass that separates the pulmo- nary valve from the tricuspid valve.
3. Trabecula septomarginalis: This describes the septal trabecula that extends from beneath the pulmonary valve toward the ventricular apex and continues as the moderator band. The trabecula septomarginalis has anterior and pos- terior limbs at its superior extent. The septal part of the conal septum is inserted between these limbs in the normal heart.
Case Material
The computer files of the Cardiac Records Division of The Hospital for Sick Children, Toronto, were reviewed for the
T A B L E I
Type and Incidence of Aortic Arch Interruption*
T y p e Number % o f To ta l
A 12 35 .3 } 38.2 A~ 1 2.9 B 18 5 2 . 9 } 61.7 B~ 3 8.8 C 0 0
To ta l 34 100
* Proved at necropsy at The Hospi ta l f o r Sick Chi ldren• This s tudy excludes pat ients w i t h arch atresia ( that is, those w i t h a f ib rous strand connecting the ascending and descending aor ta) .
diagnosis of interruption of the aortic arch. In 50 recorded cases, with this diagnosis, 34 necropsy specimens from our cardiac registry were available for study. Of the 34 patients, 22 were male and 12 female; their median age of death was 8 days (range less than 1 day to 10 years).
Results
Types of aortic arch interruption (Table I): In 21 of 34 pat ients (61.8 percent) , the aorta had type B in- terrupt ion, with an aber ran t right subclavian ar tery in 3. Thi r teen patients had aortic arch interruption distal to the left subclavian ar tery (type A, 38.2 percent), with only one pat ient having an aberrant r ight subclavian artery. Ty p e C in ter rupt ion (distal to the innominate artery) was not found.
All pat ients had visceroatrial situs solitus and a D- ventr icular loop. The great arteries were normally re- lated in 33 of the 34 patients. One pat ient had D- t ransposi t ion of the great arteries, ventr icular septal defect and type B in ter rupt ion of the aortic arch. Two of the 34 pat ients (5.9 percent) each with a type B in- terrupt ion, had type I t runcus arteriosus. Of the 31 re- maining patients, 12 had type A interruption, including one with an aberrant right subclavian artery, and 19 had type B interruption, including 3 with an aberrant right subclavian artery.
Ventricular septal defect (Table II): All but two pat ients (93.8 percent) had a defect of the ventr icular septum; the remaining two had a large aort icopulmo- nary fenestrat ion (Fig. 1). The ventr icular defect in- volved the conal septum in 21 patients, and in 7 of these, the membranous septum was also involved. In 14 pa- tients, the conal defect resulted from malal ignment (and, hence, lack of fusion) between the c.onal septum and anter ior and posterior limbs of the t rabecula sep- tomarginalis (Fig. 2 to 4). This malal ignment of the conal septum was characterist ical ly in a leftward di- rection, allowing actual or potential narrowing of the left ventr icular outflow tract, above the level of the yen- tricular septal defect (Fig. 2B). Fur thermore , the mal- alignment of the conal septum usually resulted in a large subpulmonary ventricular septal defect (from the right ventr icular aspect) and subaortic defect (from the left ventr icular aspect) (Fig. 2 to 4). Although the majori ty of conal defects resulted from conoventr icular mal-
T A B L E II
Correlation of Ventricular Septal Defect With Type of Aortic Arch Interruption
Type o f In te r rup t ion
Posit ion o f VSD Tota l A A~ B B~ C
Conal 14 4 8 2 Conal and membranous 7 1 " i " 4 1 Membranous 5 1 . . . 4 . . Cushion type or A-V 3 2 . . . 1 . .
canal Muscular 3 3 . . . . . . . Intact vent r icu la r septum 2 . . . . . . 2 . .
. ° .
A-V = a t r ioven t r i cu la r ; VSD = vent r icu lar septal defect .
April 1977 The American Journal of CARDIOLOGY Volume 39 573
INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
P
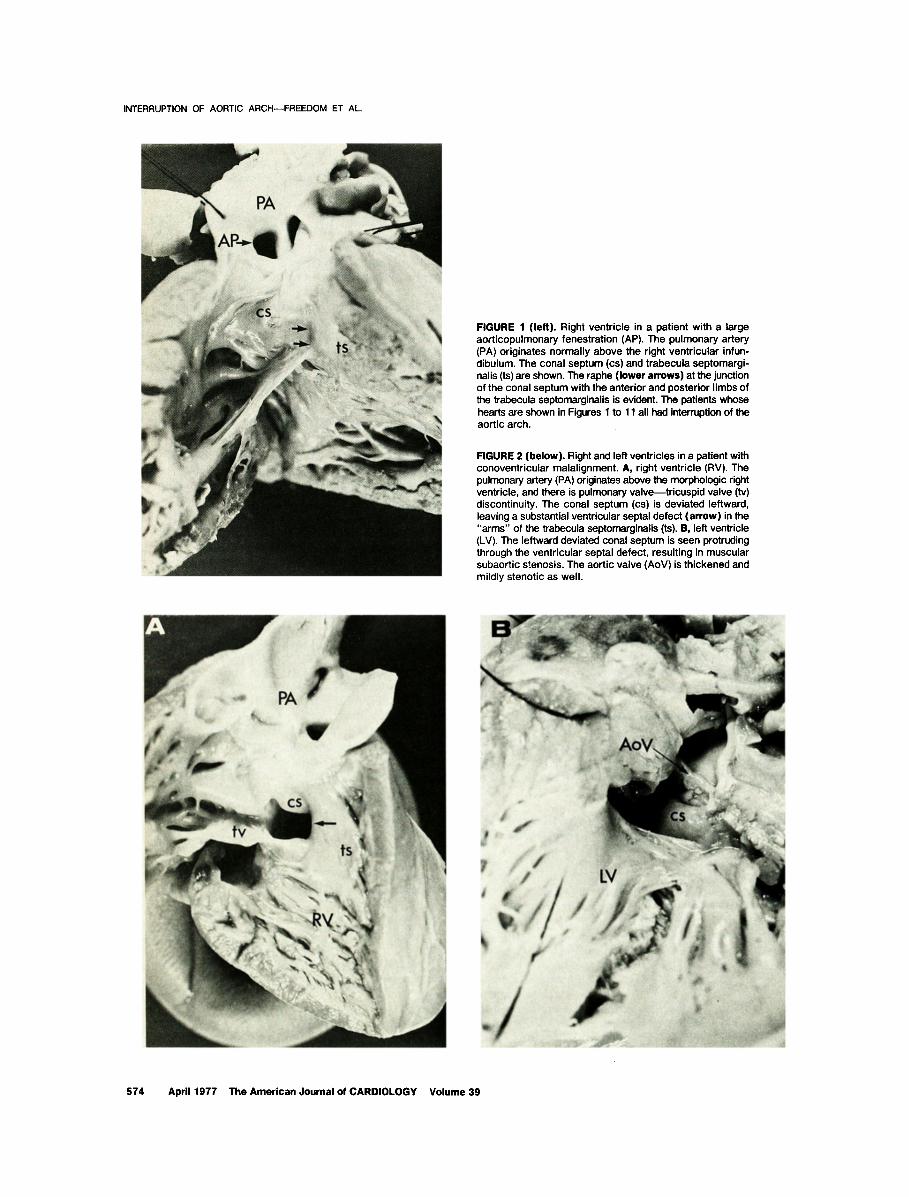
FIGURE 1 (left). Right ventricle in a patient with a large aorticopulmonary fenestration (AP). The pulmonary artery (PA) originates normally above the right ventricular infun- dibulum. The conal septum (cs) and trabecula septomargi- nalis (ts) are shown. The raphe (lower arrows) at the junction of the conal septum with the anterior and posterior limbs of the trabecula septomarginalis is evident. The patients whose hearts are shown in Figures 1 to 11 all had interruption of the aortic arch.
FIGURE 2 (below). Right and left ventricles in a patient with conoventricular malalignment. A, right ventricle (RV). The pulmonary artery (PA) originates above the morphologic right ventricle, and there is pulmonary valve--tricuspid valve (tv) discontinuity. The conal septum (cs) is deviated leftward, leaving a substantial ventricular septal defect (arrow) in the "arms" of the trabecula septomarginalis (ts). B, left ventricle (LV). The leftward deviated conal septum is seen protruding through the ventricular septal defect, resulting in muscular subaortic stenosis. The aortic valve (AoV) is thickened and mildly stenotic as well.
-1
574 April 1977 The American Journal of CARDIOLOGY Volume 39
INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
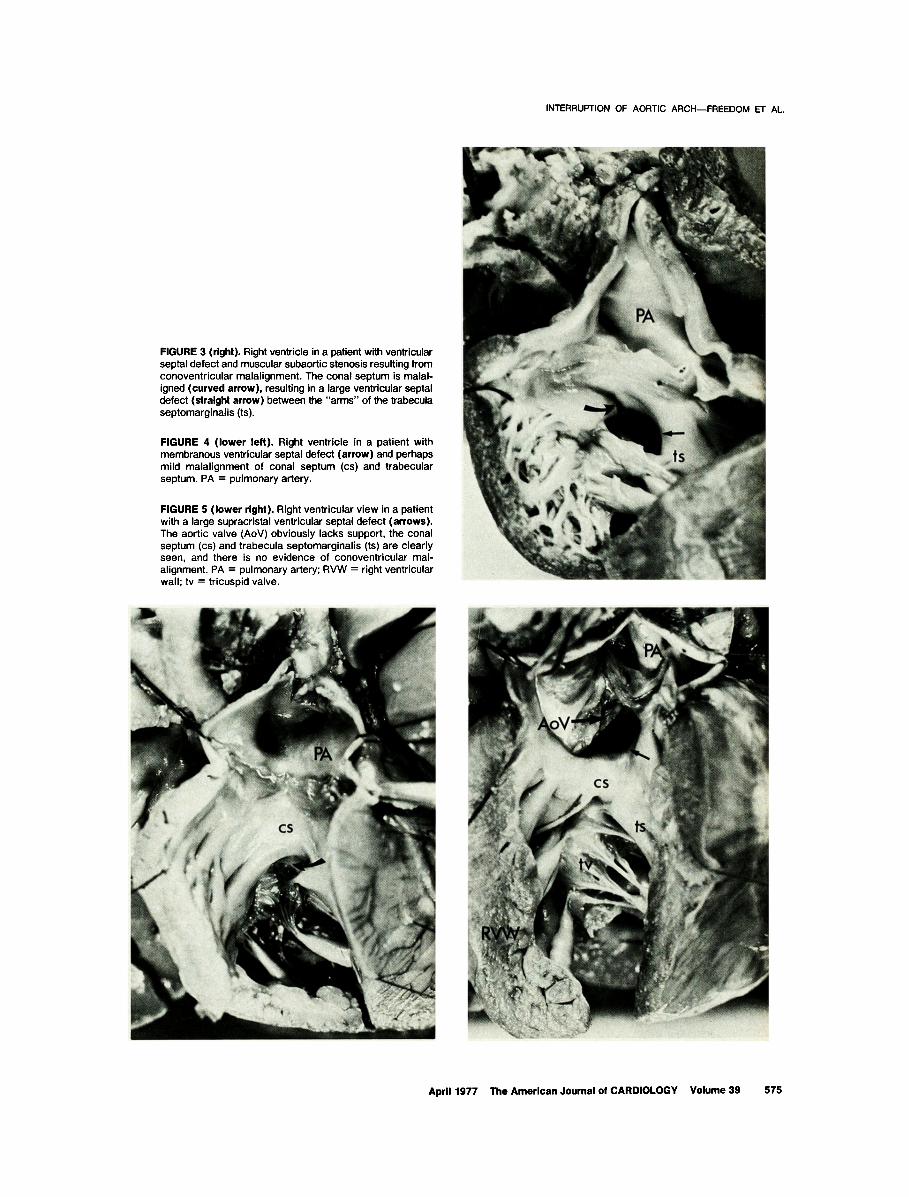
FIGURE 3 (right). Right ventricle in a patient with ventricular septal defect and muscular subaortic stenosis resulting from conoventricular malalignment. The conal septum is malal- igned (curved arrow), resulting in a large ventricular septal defect (straight arrow) between the "arms" of the trabecula septomarginalis (ts).
FIGURE 4 ( lower left). Right ventricle in a patient with membranous ventricular septal defect (arrow) and perhaps mild malalignment of conal septum (cs) and trabecular septum. PA = pulmonary artery.
FIGURE 5 ( lower right). Right ventricular view in a patient with a large supracristal ventricular septal defect (arrows). The aortic valve (AoV) obviously lacks support, the conal septum (cs) and trabecula septomarginalis (ts) are clearly seen, and there is no evidence of conoventricular mal- alignment. PA = pulmonary artery; RVW = right ventricular wall; tv = tricuspid valve.
April 1977 The American Journal of CARDIOLOGY Volume 39 575
INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
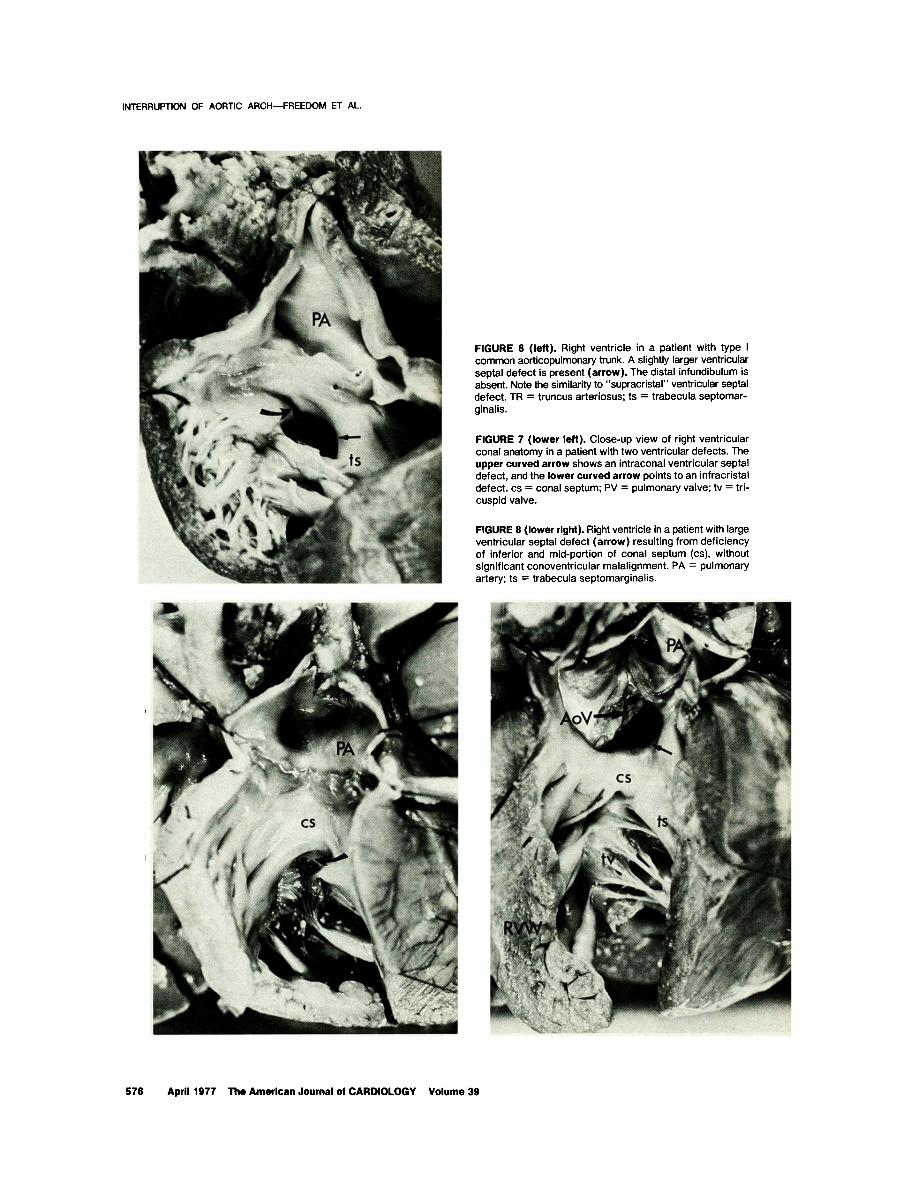
FIGURE 6 (left). Right ventricle in a patient with type I common aorticopulmonary trunk. A slightly larger ventricular septal defect is present (arrow). The distal infundibulum is absent. Note the similarity to "supracristal" ventricular septal defect. TR = truncus arteriosus; ts = trabecula septomar- ginalis.
FIGURE 7 (lower left). Close-up v iew of right ventricular conal anatomy in a patient with two ventricular defects. The upper curved arrow shows an intraconal ventricular septal defect, and the lower curved arrow points to an infracristal defect, cs = conal septum; PV = pulmonary valve; tv = tri- cuspid valve.
FIGURE 8 (lower right). Right ventricle in a patient with large ventricular septal defect (ar row) resulting from deficiency of inferior and mid-portion of conal septum (cs), without significant conoventricular malalignment. PA = pulmonary artery; ts = trabecula septomarginalis.
!_
576 April 1977 The American Journal of CARDIOLOGY Volume 39

INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
alignment, this was not invariably so. In four patients, the ventricular septal defect could be characterized as "supracristal" (actually intraconal, involving the most cephalad portion of the conal septum), lying immedi- ately adjacent to the left and right pulmonary cusps and separated from the membranous ventricular septum by various amounts of conal septum (Fig. 5). In both pa- tients with interruption of the aortic arch and common aorticopulmonary trunk, the septal defect was indis- tinguishable from that observed in isolated truncus arteriosus (Fig. 6 to 9). The conal ventricular septal defect was not restrictive, and a muscular "subtruncal" stenosis was not seen in these two patients. Thus, in 14 (67 percent) of 21 patients with a ventricular defect involving a conal structure, the defect resulted from conoventricular malalignment; in the two patients with truncus arteriosus, there was virtual absence of the conal septum and parietal conus with absence of the truncal septum; and in four patients (19 percent), the defects were intraconal and immediately adjacent to the pul- monary valve ("supracristal" type). In some patients, the defect involved the inferior or mid-portion of the conal septum, but there was no associated conoventri- cular malalignment (Fig. 7 and 8).
A typical infracristal membranous ventricular septal defect was present in five patients (14.7 percent) (Fig. 9A and 10). Two patients had an atrioventricular (A-V) communis defect (Fig. 11), and one patient with D- transposition had a ventricular septal defect in the "canal" position. Three patients had a large muscular ventricular communication. Common or single ventricle was not identified in any patient.
Subaor t ic obs t ruc t ion (Table III): The anatomic potential for subaortic obstruction is most evident in patients with a ventricular septal defect resulting from conoventricular malalignment (Table III). In our study, the anatomic potential for subaortic obstruction was based on (1) unequivocal anatomic narrowing of the systemic outflow tract when compared with that of a matched normal subject, or (2) documentation of a pressure gradient of at least 10 mm Hg across the sys- temic outflow tract. Using these criteria, we probably excluded some patients with mild subaortic obstruction. These patients have a large subpulmonary (conal) ventricular septal defect and a leftward deviated conal septum. Thirteen of 21 patients with a ventricular septal defect of the conoventricular malalignment type had anatomic evidence of subaortic obstruction resulting from the abnormally positioned conal septum. This group included patients whose defect resulted from isolated conoventricular malalignment and those who had associated contiguous membranous defects. Pa- tients with an isolated membranous, muscular cushion type defect may also exhibit subaortic obstruction, usually related to mitral valve abnormality of deposits of accessory endocardial cushion tissue, or both {Fig. 9B).
The aortic valve was tricuspid in 22 patients and was grossly deformed and stenotic in only 1 of these (Table IV). A bicuspid aortic valve was evident in 10 patients, and was stenotic in 3 of these. Both truncal valves were
tricuspid and the free valve margins were mildly thickened. Truncal valve stenosis was not present in either patient. There was clearly the potential for aortic valve prolapse in the patient with high, intraconal ventricular defect.
There was no obvious relation between the position of the ventricular septal defect and the type of aortic interruption (Table III) in our small study group, and the presence or absence of subaortic obstruction did not predispose to any specific type of interruption.
Significant underdevelopment of the left ventricle was found in only one patient who had a very small conal defect, partly occluded by both mitral and tri- cuspid valve tissue, and severe subaortic obstruction.
Discussion
Distortion of conal anatomy is responsible for a wide spectrum of congenital heart defects, is In our study, we demonstrated that defects of the conal septum are common in patients with interruption of the aortic arch, occurring in 21 of 34 patients. Conoventricular mal- alignment, as Van Praagh et al.1 observed, is responsible for the presence of a large subpulmonary ventricular septal defect and for the anatomic basis of the subaortic obstruction often evident in these patients. Conal maldevelopment in some of these patients is manifested as absence of the conal septum in its inferior, middle or superior portion. These defects can be considered in- tracristal and are not invariably characterized by co- noventricular malalignment. Indeed, the raphe at the line of insertion of the conal septum with the anterior and posterior limbs of the trabecula septomarginalis has been preserved in these patients. In the patient with conoventricular malalignment, this bulbar raphe is not evident, and the ventricular communication lies "in the arms" of the trabecula septomarginalis.
Fac tors de te rmin ing type of ven t r i eu la r septal defect: conoven t r i cu la r development and align- ment . There are considerable variations in the ap- pearance of the conal ventricular septal defect, and this is related in part, to its embryogenesis. Goor et al. 14,19 presented a classification of ventricular septal defect based on developmental characteristics of the septum. In their classification, the infundibular ventricular septal defect represents a significant category of defect, and was found in 33 of 112 isolated defects. They sug- gested that the common denominator anatomically for the infundibular ventricular septal defect is the in- volvement of the crista supraventricularis from the right ventricular aspect, the anterior margin of such defects is placed anteriorly to the so-called infundibulo-ven- tricular line. What Goor et al. characterized as infun- dibular ventricular septal defect encompasses what we and others term conal ventricular septal defect. Ven- tricular defects of the infundibular or conal type have at least four subtypes: (1) ventricular septal defect of the membranous septum cutting into the adjacent in- ferior aspect of the conal septum; (2) mid-conal ven- tricular septal defect; (3) "supracristal" ventricular septal defect, lying adjacent to the left and right pul-
Ai)rll 1977 The American Journal of CARDIOLOGY Volume 39 577
INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
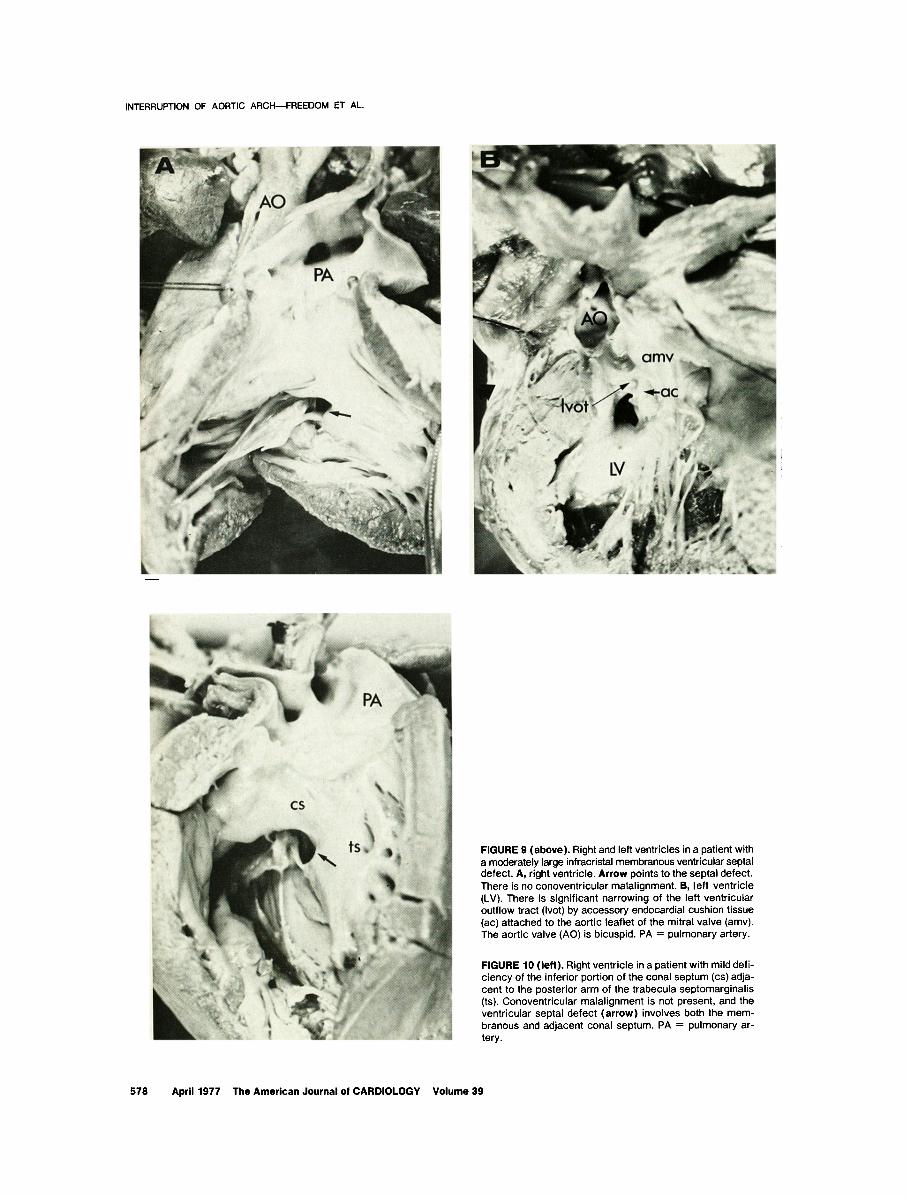
FIGURE 9 (above). Right and left ventricles in a patient with a moderately large infracristal membranous ventricular septal defect. A, right ventricle. Arrow points to the septai defect. There is no conoventricular malalignment. B, left ventricle (LV). There is significant narrowing of the left ventricular outflow tract (Ivot) by accessory endocardial cushion tissue (ac) attached to the aortic leaflet of the mitral valve (amv). The aortic valve (AO) is bicuspid. PA = pulmonary artery.
FIGURE 10 (left). Right ventricle in a patient with mild defi- ciency of the inferior portion of the conal septum (cs) adja- cent to the posterior arm of the trabecula septomarginalis (ts). Conoventricular malalignment is not present, and the ventricular septal defect (arrow) involves both the mem- branous and adjacent oonal septum. PA = pulmonary ar- tery.
578 April 1977 The American Journal of CARDIOLOGY Volume 39

INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
FIGURE 11. Left ventricle in a patient with complete common A-V canal. The left ventricular (LV) outflow tract is not appreciably narrowed. The aort ic valve (AO) is tricuspid•
monary cusps; and (4) ventricular septal defect char- acterized by complete absence of the conal septum. Indeed, the ventricular defects observed in the present study encompass this spectrum of conal defect.
It is difficult to ascertain the incidence of conal versus nonconal ventricular septal defect because relatively little attention has been focused on this finding in the patient with interruption of the aortic arch. Ventricular septal defect was very common in our patients but can be absent. Eight (80 percent) of 10 patients with aortic arch interruption studied by Van Praagh et al. I had muscular subaortic stenosis, a finding that suggests the presence of a conal ventricular septal defect in these patients. Of 32 patients with ventricular septal defect in our study, the conal septum was involved in 21 (66 percent). Immagoulou et al. 2° stated that muscular subaortic stenosis above the ventricular septal defect was present in 6 of their 18 necropsy cases (33 percent). In these three series involving 64 patients, 35 probably had involvement of the conal septum (incidence rate 55 percent).
Ventricular septal defect in tetralogy of Fal lo t versus aortic arch interruption: The ventricular septal defect in tetralogy of Fallot and that in inter- ruption of the aortic arch are caused by conoventricular malalignment. Van Praagh et al. 21 have suggested that
TABLE II I
Correlation of Position of Ventricular Septal Defect and Subaortic Obstruction*
Subaortic Obstruction
Position of VSD Number no, %
Conal 14 9 64.2 Conal and membranous 7 4 57.1 Membranous 5 2 40 "Cushion" type 2 1 50 Muscular 3 1 33 Other . . . . . . . . .
* Excluding the patient w i th D-transposition of the great arteries.
the essence of tetralogy of Fallot resides in subpulmo- nary conal underdevelopment and in failure of the subpulmonary conus to be carried in a posterior, inferior and rightward direction. This is thought to result in a subpulmonary infundibulum that is too small in all di- rections. Furthermore, the conoventricular malalign- ment results in a defect posterior to the conus and in the limbs of the trabecula septomarginalis.
Rosenquist et al. 22 suggested that tetralogy of Fallot comprises a spectrum of anomalies in which a variable portion of the conal septum remains in its usual posi- tion, forming the inferior and posterior margins of the ventricular septal defect. The remainder of the conal septum is deviated anteriorly, partitioning off a stenotic outflow tract and forming the anterior border of the ventricular septal defect. Becker et al., 17 in their mor- phometric and geometric study of tetralogy of Fallot, concluded that lack of conal inversion and conal mal- septation are the morphogenetic mechanisms respon- sible for tetralogy of Fallot. Despite various interpre- tations of the embryologic events, disturbances of conal growth, maturation and geometry are obviously implicit to the pathogenesis of Fallot's tetralogy. Similarly, in the patient with interruption of the aortic arch, conal ventricular septal defect and subaortic stenosis, dis- turbances of conoventricular development and align- ment result in these features. Furthermore, the leftward deviation of the conal septum may interfere with ade- quate antegrade flow of blood through the left ventric- ular outflow tract during the critical embryonic stages
T A B L E I V
M o r p h o l o g i c Features of Aort ic Valve and Type of Interruption of Aort ic A r c h *
Type of Aort ic Arch Interrupt ion
Aort ic Valve A A I B BI C
1. Tricuspid, normal ly formed 9 1 9 2 2. Tricuspid, stenotic 1 . . . . . 3. Bicuspid, not stenotic 1 . . . "6 ' 4. Bicuspid, stenotic 1 . . . 1 " i
• . •
* Excluding the two patients wi th common aort icopulmonary trunk.
April 1977 The American Journal of CARDIOLOGY Volume 39 579

INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
in the morphogenesis of the aortic arch and may be re- sponsible for the frequent associations with severe anomalies of the aortic arch. 1,23
Yentricular septal defec t in t r un cus a r t e r iosus versus aor t ic a r ch in te r rupt ion : The ventricular septal defect in common aorticopulmonary trunk (truncus arteriosus) results from conal maldevelopment, and superficially there is a resemblance between the ventricular septal defect in truncus arteriosus and in- terrupted aortic arch. Van Praagh and Van Praagh 24 suggested that the ventricular septal defect in truncus arteriosus results from virtual absence of the distal pulmonary infundibulum (conus), with the ventricular septal defect lying between the anterior and posterior limbs of the septal band (trabecula septomarginalis). Recently, Rosenquist et al. 25 called attention to a spectrum of conal and truncal septal defects in patients with truncus arteriosus, and mentioned patients with small or diminutive conal septal defects. Angelini and Leachman 26 have described the spectrum of truncoco- nal septal defects and proposed a classification based on the degree of absence of the truncoconal septum. 26 It is of interest that the two patients with truncus ar- teriosus and interruption of the aortic arch in our study both had conal defects typical of truncus, not Of aortic arch interruption (Fig. 8 to 10). To our knowledge, truncus arteriosus has not been complicated by a "subtruncal" stenosis, although a restrictive conal ventricular septal defect would result in obstruction to flow from both ventricles into the truncus.
Single or common ventr ic le: This was not an as- sociated cardiovascular malformation in our study, al- though this association has been sporadically docu- mented. 1 In the compilation by Van Praagh et al. of patients with aortic arch interruption through October 1969, 4 of 184 cases (2 percent) had single ventricle. This association was not observed in the 20 patients de- scribed by Immagoulou et al. 2° However, Collins et al. 9 recently reported that 3 of 29 patients (10 percent) with interruption of the aortic arch had single ventricle. 9 In necropsy and angiocardiographic reviews of patients with single or common ventricle culled from six series of patients, 27-32 aortic arch interruption was noted in 2 of 261 patients (although Van Praagh et al.32 recorded 3 patients with aortic arch atresia among 60 patients with single or common ventricle).
Subaor t i c obs t ruc t i on - - su rg i ca l implications: Subaortic obstruction, or at least the anatomic potential for subaortic obstruction, is noted commonly in the patient with interruption of the aortic arch. Van Praagh et al. 2 attributed this anatomic substrate to a charac- teristic leftward shift of the crista supraventricularis which results in a muscular subaortic stenosis. 1 Sub- aortic obstruction in these patients is not invariably the result of conoventricular malalignment. Accessory en- docardial cushion tissue or anomalous mitral attach- ment may also result in subaortic narrowing. 33,34
Recently, Moulaert and Oppenheimer-Dekker 35 de- scribed the anterolateral muscle bundle of the left ventricle. This bundle, which is found between the left coronary aortic semilunar cusp and the anterior leaflet of the mitral valve, was reported to be present in ap-
proximately 40 percent of normal hearts. This tissue is thought to be derived embryologically from the left extremity of the bulboatrioventricular flange. These authors comment that when a ventricular septal defect is present it is frequently associated with severe anomalies of the aortic arch, including interruption, atresia, coarctation and tubular hypoplasia. Both co- noventricular malalignment and the anterolateral muscle bundle of the left ventricle may result in ana- tomic subaortic stenosis.
It is difficult to state with any precision the incidence of subaortic stenosis in patients with interruption of the aortic arch. Fifty percent in the present series had an- atomic evidence of a potential for left ventricular out- flow tract narrowing. Moller and Edwards 36 reported that 8 of 105 patients (8 percent) with interruption of the aortic arch had subaortic stenosis. In a recent clin- ical and pathologic study of interruption of the aortic arch, 2° muscular subaortic stenosis above the ventric- ular septal defect was found in 6 of 18 necropsy cases (33 percent). It is our impression that at least 25 to 30 per- cent of patients, possibly more in symptomatic neo- nates, might be anticipated to have subaortic obstruc- tion. According to Tyson et al. 6 when there is evidence of ventriculoaortic obstruction, thoughts of arch re- construction in the neonate should be abandoned, and pulmonary arterial banding should be employed. It is possible, however, that pulmonary arterial banding might aggravate and intensify the subaortic obstruction in at least some of these patients. Freed et al. 37,3s doc- umented the development of subaortic obstruction after pulmonary arterial banding for ventricular septal defect and suggested that a leftward deviated conal septum that hypertrophied in response to the banding might be responsible for this complication. There is not enough experience with the surgical management of patients with arch interruption and subaortic obstruction to provide firm guidelines. It is possible that this subaortic muscular obstruction, in some of these patients, could be surgically approached through the ventricular septal defect.
Hypoplas t ic lef t ventr ic le: Gross underdevelop- ment of the left ventricle occurred only once in our se- ries. Collins et al., 1° summarizing the experience of the New England regional infant cardiac program, stated that 8 of 29 patients had hypoplasia of the left heart chambers 9. None of the 10 cases personally studied by Van Praagh 1 were characterized as having a grossly underdeveloped left heart, and this was not mentiond in the study of Immagoulou et al. 2° Angiocardiogra- phically, and at necropsy, the morphologic left ventricle appears relatively small when compared with the usu- ally significantly hypertrophied and dilated morpho- logic right ventricle. It has been our experience based on our large necropsy series, on selective left ventricu- lograms in nearly 50 patients with interruption of the aortic arch, and on diagnostic ultrasonic studies in 10 patients that left ventricular dimensions are usually normal when compared with the normal values of Rowlatt et al. 39
The aortic valve was bicuspid in 10 of our 34 patients, and in 5 of the 10 cases studied by Van Praagh et al)
580 April 1977 The American Journal of CARDIOLOGY Volume 39

INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
Clinical Implications and Speculations 1. In the patient with interruption of the aortic arch,
one must be cognizant of the frequency of conal ven- tricular septal defect and conal-ventricular malalign- ment, the latter resulting in the anatomic potential for subaortic narrowing. It is therefore desirable to obtain a pressure recording across the left ventricular outflow tract. Selective left ventricular angiocardiograms should demonstrate both the high conal position of the van- tricular septal defect and the subaortic narrowing.
2. In some patients with ventricular septal defect secondary to conoventricular malalignment, although the leftward deviated conal septum may encroach on the left ventricular outflow tract, no pressure gradient can be demonstrated across the aortic valve at cardiac catheterization. Partial correction with reconstitution of the aortic arch and pulmonary arterial banding may set the stage for acquired subaortic obstruction after banding for the ventricular septal defect. 38,39 In these patients, it was suggested that an abnormally deviated conal septum becomes hypertrophied in response to the pulmonary arterial band, thus narrowing the left ven- tricular outflow tract. These observations indicate that aggressive at tempt at total repair using the technique of profound hypothermia may help to avoid certain difficulties.
3. Gross underdevelopment of the left ventricle oc- curred only once and was associated with a restrictive ventricular septal defect.
4. Although aortic valve abnormalities were not un- common, severe aortic valve stenosis was unusual. Recognition of aortic valve stenosis in the patient with interruption of the aortic arch requires pressure re- cordings across the aortic valve and retrograde aortog- raphy.
5. The patient with muscular and "cushion" ven- tricular septal defects may have left ventricular outflow tract obstruction. The patient with A-V communis and interruption of the aortic arch undoubtably has a se- verely distorted mitral valve (or common A-V valve), and both the valve leaflet and accessory endocardial cushion tissue conjointly narrow the left ventricular outflow tract. This combination of defects may prove inoperable. Mechanisms for subaortic obstruction in the patient with muscular ventricular septal defect include muscular, fibrous and cushion tissue deposits.
6. Interruption of the aortic arch is distinctly rare in the patient with situs inversus totalis, L-ventricular loop, the heterotaxy syndrome or the syndrome of jux- taposition of the atrial appendages.
7. When interruption of the aortic arch occurs in double outlet right ventricle with L-transposition of the great arteries, there must be gross underexpansion of the subaortic conus.
8. Aorticopulmonary fenestration occurs rarely with interruption of the aortic arch. 1,2°,4° The ventricular septum is usually intact, but the aorticopulmonary septum is virtually absent.
9. The patient who survives surgical reconstitution of the aortic arch and palliative pulmonary arterial banding (leaving the ventricular septal defect open) is at risk for the development of aortic regurgitation. An important pathogenetic mechanism for aortic valve prolapse and subsequent regurgitation is lack of ana- tomic support for the aortic valve structure. 41-44 Ob- viously, the patient with a conal ventricular septal de- fect, especially with an immediate subpulmonary ven- tricular septal defect, lacks sufficient support for the right coronary sinus and anulus and is predisposed to aortic regurgitation. Although aortic regurgitation secondary to a prolapse mechanism is uncommon in the first year of life, it is conceivable that the timing and severity of aortic runoff will be aggravated by restenosis at the site of arch reconstruction. 45,48 One might therefore conclude that total primary repair of the arch and ventricular septal defect would present these complications.
10. Interruption of the aortic arch rarely occurs as an isolated anomaly, and almost any cardiovascular mal- formation can be coexistent. As Van Praagh et al. 1 stated, interruption of the aortic arch is indicative of a significant intracardiac anomaly. Moulaert et al. 47 re- cently presented evidence in a small group of patients that certain ventricular defects may influence prenatal patterns of intracardiac flow, potentially resulting in reduced aortic flow and predisposing to anomalies of the aortic arch. Although our study expands the observa- tions of both Van Praagh and Moulaert and their col- leagues, it defines a considerably wider anatomic spectrum of ventricular septal defect than that pre- viously reported. Indeed, our observations suggest that at least in some patients (particularly those with an isolated membranous or muscular ventricular defect, typical truncal ventricular defect or intact ventricular septum), there is no obvious intracardiac anomaly that predisposes to a reduced aortic flow.
Acknowledgment We acknowledge the photographic assistance of Mr. Mi-
chael Starr, and the secretarial assistance of Miss Kathy Forde.
References 1. Van Praagh R, Bernard WF, Rosenthal A, et ah Interrupted aortic
arch: surgical treatment. Am J Cardiol 27:200-211, 1971 2. Dische MR, Tsai M, Baltaxe HI: Solitary interruption of the arch
of the aorta. Clinicopathologic review of eight cases. Am J Cardiol 35:271-277, 1975
3. Becu LM, Tauxe WN, DuShane JW, et al: A complex of congenital cardiac anomalies: Ventricular septal defect, biventricular origin of the pulmonary trunk, and subaortic stenosis. Am Heart J 50: 901-911, 1955
4. Neufeld HN, Ongley PA, Swan HJC, et ah Biventricular origin of the pulmonary trunk with subaortic stenosis shown above the ventricular septal defect. Am Heart J 61:189-198, 1961
5. Trusler GA, Izukawa T: Interrupted aortic arch and ventricular septal defect. Direct repair through a median sternotomy incision in a 13 day old infant. J Thorac Cardiovasc Surg 69: 126-131, 1975
6. Barrett-Boyes BG, Nicholls 17, Brandt PWT, el al: Aortic arch interruption associated with patent ductus arteriosus, ventricular
April 1977 The American Journal of CARDIOLOGY Volume 39 581
INTERRUPTION OF AORTIC ARCH--FREEDOM ET AL.
septal defect, and total anomalous pulmonary venous return. J Thorac Cardiovasc Surg 63:367-372, 1972
7. Tyson KRT, Harris LC, Nghlem QX: Repair of aortic arch inter- ruption in the neonate. Surgery 67:1006-1010, 1970
8. Flshman NH, Bronstein MH, Berman W Jr, et ah Surgical man- agement of severe aortic coarctation and interrupted aortic arch in neonates. J Thorac Cardiovasc Surg 71:35-48, 1976
9. Tawes RI Jr, Panagopoulos P, Aberdeen E, et ah Aortic arch atresia and interruption of the aortic arch. Experiences in 11 cases of operation. J Thorac Cardiovasc Surg 58:492-501, 1969
10. Collins RL, Dick M, ParlsI-Buckley L, et al: Surgical management of interrupted aortic arch (abstr). Am J Cardiol 35:128,1975
11. Allard J, Poirer N, Dobell ARC: Interrupted aortic arch: factors influencing post-operative prognosis (abstr). Canadian Cardiovasc Society, Montreal, 1975 (Abstr.).
12. Celoria GC, Patton RB: Congenital absence of the aortic arch. Am Heart J 58:407-413, 1959
13. Thiene G, Razzolini R, Dalla-Volta S: Aortopulmonary relationship, arterio-ventricular alignment, and ventricular septal defects in complete transposition of the great arteries. Eur J Cardiol 4:13-24, 1976
14. Goor DA, Edwards JE, LIIlehel CW: The development of the in- terventricular septum of the human heart. Correlative morpho- genetic study. Chest 58:453-467, 1970
15. Jimlnez MQ, MarUnez VP: Uncommon conal pathology in com- plete dextrotransposition of the great arteries with ventricular septal defect. Chest 66:411-417, 1974
16. Anderson RH, Wilkinson JL, Arnold R, et ah Morphogenesis of bulboventricular malformations. I. Consideration of embryogenesis in the normal heart. Br Heart J 36:242-255, 1974
17. Becket AE, Connor M, Anderson RH: Tetralogy of Fallot: a mor- phometric and geometric study. Am J Cardiol 35: 402-412, 1975
18. Van Praagh R: Conotruncal malformations. In, Heart Disease in Infancy: Diagnosis, and Surgical Treatment. (Barratt-Boyes BG, Neutze J, Harris FA, ed). London, Churchill Livingstone, 1973, p 141
19. Goor DA, LIIlehei CW, Rees R, et al: Isolated ventricular septal defects. Development basis for various types and presentation of classification. Chest 58: 468-482, 1970
20. Immagoulou A, Anderson RC, Moiler JH: Interruption of the aortic arch: clinical features in 20 patients. Chest 61: 276-282, 1972
21. Van Praagh R, Van Praagh S, Nebesar RA, et ah Tetralogy of Fallot: underdevelopment of the pulmonary infundibulum and its sequelae. Am J Cardiol 26:25-33, 1970
22. Rosenquist GC, Sweeny LJ, Stemple DR, et al.: Ventricular septal defect in tetralogy of Fallot. Am J Cardiol 31:749-754, 1973
23. Rudolph AM, Heymann MA, Spltznas U: Hemodynamic consid- erations in the development of narrowing of the aorta. Am J Cardiol 30:514-525, 1972
24. Van Praagh R, Van Praagh S: The anatomy of common aortico- pulmonary trunk (truncus arteriosus communis) and its embryologic implications. Am J Cardiol 16:406-425, 1965
25. Rosenquisl GC, Bharatl S, McAIIIster HA, et al: Truncus arterjosus communis: truncal valve anomalies associated with small conal or truncal septal defects. Am J Cardiol 37:410-412, 1976
26. Angelini P, Leachman RD: Trunco-conal septal defects. An ana- tomic and embryologic study of common truncus and related malformations. Eur J Cardiol 2:11-22, 1974
27. Marln-Garcla J, Tandon R, Moiler JH, et al.: Common (single) ventricle with normally related great vessels. Circulation 49: 565-573, 1974
28. Marin-Garcla J, Tandon R, Moiler JH, et al.: Single ventricle with transposition. Circulation 49:994-1004, 1974
29. Lev M, Liberthson RR, Klrkpatrick JR, et al.: Single (primitive) ventricle. Circulation 39:577-591, 1969
30. Kozuka T, Sato K, FuJlno M, et al.: Roentgenographic diagnosis of single ventricle. Am J Roentgenol 119:512-523, 1973
31. Macartney FJ, Partridge JB, Scott O, el al.: Common or single ventricle. An angiocardiographic and hemodynamic study of 42 patients. Circulation 53:543-554, 1976
32. Van Praagh R, Ongley PA, Swan HJC: Anatomic types of single or common ventricle in man: Morphologic and geometric aspects of 60 necropsied cases. Am J Cardiol 13:367-386, 1964
33. Sellers RD, Ullehel CW, Edwards JE: Subaortic stenosis caused by anomalies of the atrioventricular valves. J Thorac Cardiovasc Surg 48:289-302, 1964
34. MacLean LD, Culllgan JA, Kane DJ: Subaortic stenosis due to accessory tissue on the mitral valve. J Thorac Cardiovasc Surg 45:382-388, 1963
35. Moulaert AJ, Oppenhelmer-Dekker A: Anterolateral muscle bundle of the left ventricle, bulboventricular flange and subaortic stenosis. Am J Cardiol 37:78-81, 1976
36. Moiler JH, Edwards JE: Interruption of the aortic arch. Anatomic patterns and associated cardiac malformations. Am J Roentgenol 95:557-572, 1965
37. Freed M, Freedom R, Rossnthal A, el al: Development of subaortic stenosis after pulmonary artery banding (abstr). Circulation 46: Supp111:11o35, 1972
38. Freed M, Rosenthal A, Plauth WH Jr, et al: Development of sub- aortic stenosis after pulmonary artery banding. Circulation 47, 48: Suppl Ilhlll-7-111-10, 1973
39. Rowlatt UF, Rlmoldl HJA, Lev M: The quantitative anatomy of the normal child's heart. Pediatr Clin North Am 10:499-588, 1963
40. Todd EP, Nicoloff DM, Utley JR, et ah Aorticopulmonary septal defect: anatomical and surgical considerations (abstr). Circulation 52:Suppl Ihll-100, 1975
41. Van Praagh R, McNamara JJ: Anatomic types of ventricular septal defects with aortic insufficiency. Am Heart J 75:604-621, 1968
42. Tatsuno K, Konno S, Sakaklbara S: Ventricular septal defect with aortic insufficiency. Angiocardiographic aspects and a new clas- sification. Am Heart J 85:13-21, 1973
43. Tatsuno K, Konno S, Ando M, et al: Pathogenetic mechanisms of prolapsing aortic valve and aortic regurgitation associated with ventricular septal defect. Anatomical, angiographic and surgical considerations. Circulation 48:1028-1037, 1973
44. Steinfeld L, Dimich I, Park SC, et al.: Clinical diagnosis of isolated subpulmonic (supracristal) ventricular septal defect. Am J Cardiol 30:19-24, 1972
45. Nadas AS, Thilenlus OG, LaFarge LG, et ah Ventricular septal defect with aortic regurgitation. Medical and pathologic aspects. Circulation 29:862-873, 1964
46. Somerville J, Brandao A, Ross DN: Aortic regurgitation with ventricular septal defect. Circulation 41:317-330, 1970
47. Moulaert AJ, Brains CC, Oppenheimer-Dekker A: Anomalies of the aortic arch and ventricular septal defects. Circulation 53: 1011-1015, 1976
582 April 1977 The American Journal of CARDIOLOGY Volume 39
Related Documents








![Comunicación interventricular [Ventricular Septal Defect]](https://static.cupdf.com/doc/110x72/559262691a28ab33128b4573/comunicacion-interventricular-ventricular-septal-defect.jpg)


