Ventricular Septal Defect in adults Dr. Mohamed Sofi MD; FRCP (London); FRCPEdin; FRCSEdin

Ventricular Septal Defect in adults Dr. Mohamed Sofi MD; FRCP (London); FRCPEdin; FRCSEdin.
Jan 17, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ventricular Septal Defect in adults
Dr. Mohamed Sofi MD; FRCP (London); FRCPEdin; FRCSEdin

• A ventricular septal defect (VSD) is a defect in the septum resulting in communication between the ventricular cavities.
• VSDs were first clinically described by Roger in 1879 ; the term maladie de Roger is still used for a small asymptomatic VSD.
• In 1898, Eisenmenger described a patient with VSD, cyanosis, and pulmonary hypertension. This combination has been termed the Eisenmenger complex.
• Morphology: 4 types– Infundibular VSD (type 1,
also referred to as supracristal, subarterial, more commomn in Asia
– Membranous – (Type 2) most common type in adults (80%)
– Inlet defects (type 3, also known as atrioventricular canal type)
– Muscular – (type 4) most common type in young children
– Complete AV septal (endocardial cushion) defects
Ventricular Septal Defect (VSD)

• Ventricular septal defect (VSD) is the most common congenital heart defect at birth, but accounts for only 10 percent of congenital heart defects in adults because many close spontaneously
• About 5 percent of patients with VSDs have chromosomal abnormalities including trisomy 13, 18, and 21 syndromes
• VSDs are of various sizes and locations, can be single or multiple an
• May be complicated in adults by subpulmonary stenosis, pulmonary hypertension, and/or aortic regurgitation
• VSDs are associated with other congenital heart defects including atrial septal defect (35 %), patent ductus arteriosus (22 %), right aortic arch (13 %), pulmonic stenosis, and more complex defects such as transposition of the great arteries and tetralogy of Fallot
• Majority of congenital VSDs in adults present as an isolated defect
VENTRICULAR SEPTAL DEFECT IN ADULTS

• VSDs affect 2-7% of live births.
• An echocardiographic study revealed a high incidence of 5-50 VSDs per 1000 newborns.
• The defects in this study were small restrictive muscular VSDs, which typically spontaneously close in the first year of life
• VSDs are the most common lesion in many chromosomal syndromes, including trisomy 13, trisomy 18, trisomy 21, and relatively rare syndromes
Sex-related demographics• VSDs are slightly more
common in female patients than in male patients (56% vs 44%).
Race-related demographics• Reports are inconclusive
regarding racial differences in the distribution of VSDs. However, the doubly committed or outlet defect occurs is most common in the Asian population. These constitute 5% of the defects in the Unites States but 30% of those reported in Japan.
Epidemiology

Pathophysiology• Defect size is often compared to aortic
annulus–Large: > 50% of annulus size–Medium: 25-50% of annulus size–Small: <25% of annulus size
• Restrictive VSD is typically small, such that a significant pressure gradient exists between the LV and RV (high velocity), with small shunt
• Moderately restrictive VSD moderate shunt • Large / non-restrictive VSD large shunt • Eisenmenger VSD irreversible pulmonary
HTN and shunt may be zero or reversed

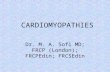
Anatomic diagram illustrates the positions of different ventricular septal defects: infundibular (1), membranous (2), inlet or canal (3), muscular or trabecular (4).Ao: aorta; LA: left atrium; LV: left ventricle; PT: pulmonary trunk; RA: right atrium; RV: right ventricle.
Types of ventricular septal defects

Echocardiographic image of a moderate ventricular septal defect in the mid-muscular part of the septum
Ventricular septal defect

Segments of the ventricular septum
Diagrammatic illustration of the various segments of the ventricular septum as viewed from the left ventricle (panel A) and along the length of interventricular septum (panel B): membranous (MS), infundibular (IS), trabecular (TS), inlet (IN), and atrioventricular (AVS) septum.

Parasternal short axis echocardiographic view with color flow Doppler demonstrating a membranous ventricular septal defect with a left-to-right shunt in proximity to the tricuspid valve (TV) (turbulent flow from LV to RV).(B) Color flow Doppler demonstrating infundibular ventricular septal defect in the right ventricular outflow tract in proximity to the pulmonary valve (PV).
Parasternal echocardiographic views of a membranous ventricular septal defect and an infundibular ventricular septal defect
Echocardiogram of infundibular VSD
TT echocardiogram showing infundibular defect with and without color flow Doppler in systole and diastole. Aortic valve prolapse is seen in early systole (A). Color flow Doppler shows left to right shunt across the VSD (B). In diastole (C), the unsupported cusp does not coapt with the other coronary cusps, resulting in aortic regurgitation (AR).

Parasternal long axis view of membranous VSD
Parasternal long axis view with Color Flow Doppler demonstrating membranous VSD (arrow) underneath the aortic valve with Color Flow Doppler demonstrating a left-to-right shunt from the left ventricular outflow tract into the right ventricle (double arrow).
Echocardiogram of inlet VSD
Apical four-chamber view demonstrating a large inlet VSD underneath the mitral and tricuspid valves.

The natural history of isolated ventricular VSDs depends on the type, size of defect, and associated hemodynamic abnormalities
• Spontaneous closure — Spontaneous closure occurs in 40 to 60 % of individuals with VSDs, during early childhood
• Spontaneous closure occurring between the ages of 17 and 45 years was observed in 10 percent of 188 adults with VSD followed for a mean of 13 years
• Endocarditis — Endocarditis risk persists in those with unrepaired VSD with an incidence of 22 to 24 per 10,000 patient years. The risk of endocarditis is higher in those with unrepaired VSD compared to those who have undergone repair
• Arrhythmias — Arrhythmias including atrial and ventricular PMB and tachycardias have been observed in adult patients with VSD. The incidence of VT and sudden death in natural history studies of VSDs are 5.7 and 4.0 percent, respectively
• Heart failure — Heart failure due to chronic volume overload of the left ventricle occurs in medium or large VSDs
• Left-sided heart failure can develop in the setting of significant aortic regurgitation in association with a residual infundibular or membranous VSD.
Natural History

• Patients with an isolated small restrictive defect with small left to right shunt (often referred to as “maladie de Roger”) generally remain asymptomatic in adulthood, but aortic regurgitation may develop and there is a low risk of endocarditis.
• Patients with moderate sized VSDs may remain asymptomatic or develop symptoms of mild heart failure in childhood.
• Heart failure usually resolves with medical therapy and with time as the child grows and the VSD gets smaller in absolute and/or relative terms.
• The following scenarios may occur with large VSDs:
• Have early large left to right shunting with development of heart failure during infancy.
• In rare cases, Eisenmenger syndrome occurs sometime during late childhood to early adulthood. The right to left shunt causes cyanosis.
CLINICAL MANIFESTATIONS

Dyspnea and fatigue in patients with VSDs result from:
• Progressive left ventricular overload due to the VSD
• significant aortic regurgitation,
• Pulmonary hypertension (PHTN)
• Double chambered right ventricle (DCRV).
• Syncope is a rare symptom in patients with VSD
• Patients with VSDs may also present with arrhythmias or sudden death
Physical examination:• Patients may also present
with a change in the murmur due to:
• Development of DCRV, PHTN, or aortic regurgitation.
• Membranous VSD may close spontaneously via adherence of the septal leaflet of the tricuspid valve, which forms an aneurysm of the membranous septum
• Septal aneurysm may cause a new midsystolic click and may lead to syncope due to RV outflow obstruction.
CLINICAL MANIFESTATIONS

Exams and TestsListening with a stethoscope usually reveals a heart
murmur. The loudness of the murmur is related to the size of the defect and amount of blood crossing the defect.
Tests may include:• Chest x-ray -- looks to see if there is a large heart with
fluid in the lungs• ECG -- shows signs of an enlarged left ventricle• Echocardiogram -- used to make a definite diagnosis • MRI of the heart -- used to find out how much blood
is getting to the lungs• Cardiac catheterization (rarely needed, unless
there are concerns of high blood pressure in the lungs)

Parasternal echocardiographic views of a membranous ventricular septal defect and an infundibular ventricular septal defect
(A) Parasternal short axis echocardiographic view with color flow Doppler demonstrating a membranous ventricular septal defect with a left-to-right shunt in proximity to the tricuspid valve (TV) (turbulent flow from LV to RV).(B) Color flow Doppler demonstrating infundibular ventricular septal defect in the right ventricular outflow tract in proximity to the pulmonary valve (PV).

Treatment• Small VSD: no treatment may be needed. But closely
monitored to make sure that the hole eventually closes properly and signs of heart failure do not occur.
• Large VSD: who have symptoms related to heart failure may need medicine to control the symptoms and surgery to close the hole. Medications may include digoxin and diuretics.
• If symptoms continue, even with medication, surgery to close the defect with a patch is needed.
• Some VSDs can be closed with a special device during a cardiac catheterization, which avoids the need for surgery, but only certain types of defects can successfully be treated this way.
• Having surgery for a VSD with no symptoms is controversial.

Indications for closure of a VSD in an adult are include:
• Closure of a VSD is indicated when there is a clinical evidence of left ventricular volume overload.
• Closure of a VSD is indicated when the patient has a history of infective endocarditis.
• Closure of a VSD is reasonable when there is net left to right shunting with pulmonary artery pressure less than two thirds of systemic pressure and pulmonary vascular resistance is less than two-thirds of systemic vascular resistance.
• Closure of a VSD is reasonable when there is net left to right shunting in the presence of left ventricular systolic or diastolic dysfunction or failure.
• Closure of a VSD is not recommended in patients with severe irreversible pulmonary artery hypertension
INDICATIONS FOR INTERVENTION
Related Documents