108 *Correspondence and reprint requests to: David Zygun Room EG23, Foothills Medical Centre, 1403-29 Street NW, Calgary, Alberta T2N2T9. E-mail: david.zygun@ calgaryhealthregion.ca Introduction Severe traumatic brain injury (TBI) com- prises only 10% of all brain injuries (1), but contributes the greatest proportion of deaths (2,3), disabilites (2,4–6), and costs related to TBI (2,5) both in Canada (7,8) and around the Abstract Introduction: Pneumonia is an important cause of morbidity following severe traumatic brain injury (TBI). However, previous studies have been limited by inclusion of specific patient subgroups or by selection bias. The primary objective of this study was to describe the incidence, risk factors for, and outcome of ventilator-associated pneumonia in an unselected population-based cohort of patients with severe TBI. An additional goal was to define the relationship of ventilator-associated pneumonia (VAP) with nonneurological organ dysfunction. Methods: A prospective, observational cohort study was performed at Foothills Medical Centre, the sole adult tertiary-care trauma center servicing southern Alberta. All patients with severe TBI requiring ventilation for more than 48 hours between May 1, 2000 and December 30, 2002 were included. Results: A total of 60 patients (45%) acquired VAP for an incidence density of 42.7/1000 ventilator days. Patients with polytrauma were at higher risk (risk ratio 1.7, 95% confidence interval, 0.9–3.1) for development of VAP than those with isolated head injury. Development of VAP was associated with a significantly greater degree of nonneurological organ system dysfunction. Although VAP was not associated with increased hospital mortality, patients who developed VAP had a longer duration of mechanical ventilation (15 versus 8 days, p < 0.0001), longer intensive care unit (17 versus 9 days, p < 0.0001) and hospital (60 versus 28 days, p = 0.003) lengths of stay, and more often required tracheostomy (35 versus 18%, p = 0.003). Conclusions: VAP occurs frequently and is associated with significant morbidity in patients with severe TBI. Key Words: Craniocerebral trauma; pneumonia; multiple organ failure; treatment outcome; critical care. (Neurocrit. Care 2006;05:108–114) Ventilator-Associated Pneumonia in Severe Traumatic Brain Injury David A. Zygun, 1,2,5, * Danny J. Zuege, 1,3 Paul J. E. Boiteau, 1 Kevin B. Laupland, 1,3,5 Elizabeth A. Henderson, 5 John B. Kortbeek, 1,4 and Christopher J. Doig 1,3,5 Departments of 1 Critical Care Medicine, 2 Clinical Neuroscience, 3 Medicine, 4 Surgery, and Community 5 Health Sciences, University of Calgary, Calgary, Alberta, Canada world (3,6). Population-based epidemiologi- cal studies of severe TBI report a case fatality of 30–54% (9–12). In addition, complete re- covery to preinjury levels is uncommon; ap- proximately 60% of survivors have ongoing deficits in the areas of cognitive competency, Original Article Neurocritical Care Copyright © 2006 Humana Press Inc. All rights of any nature whatsoever are reserved. ISSN 1541-6933/06/5:108–114 ISSN 1556-0961 (Online) DOI: 10.1385/Neurocrit. Care 2006;05:108–114

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

108
*Correspondence and reprint requests to:
David ZygunRoom EG23, Foothills Medical Centre,1403-29 Street NW,Calgary, Alberta T2N2T9.E-mail: [email protected] Introduction
Severe traumatic brain injury (TBI) com-prises only 10% of all brain injuries (1), but contributes the greatest proportion of deaths (2,3), disabilites (2,4–6), and costs related to TBI (2,5) both in Canada (7,8) and around the
AbstractIntroduction: Pneumonia is an important cause of morbidity following severe traumatic brain injury (TBI). However, previous studies have been limited by inclusion of specific patient subgroups or by selection bias. The primary objective of this study was to describe the incidence, risk factors for, and outcome of ventilator-associated pneumonia in an unselected population-based cohort of patients with severe TBI. An additional goal was to define the relationship of ventilator-associated pneumonia (VAP) with nonneurological organ dysfunction.
Methods: A prospective, observational cohort study was performed at Foothills Medical Centre, the sole adult tertiary-care trauma center servicing southern Alberta. All patients with severe TBI requiring ventilation for more than 48 hours between May 1, 2000 and December 30, 2002 were included.
Results: A total of 60 patients (45%) acquired VAP for an incidence density of 42.7/1000 ventilator days. Patients with polytrauma were at higher risk (risk ratio 1.7, 95% confidence interval, 0.9–3.1) for development of VAP than those with isolated head injury. Development of VAP was associated with a significantly greater degree of nonneurological organ system dysfunction. Although VAP was not associated with increased hospital mortality, patients who developed VAP had a longer duration of mechanical ventilation (15 versus 8 days, p < 0.0001), longer intensive care unit (17 versus 9 days, p < 0.0001) and hospital (60 versus 28 days, p = 0.003) lengths of stay, and more often required tracheostomy (35 versus 18%, p = 0.003).
Conclusions: VAP occurs frequently and is associated with significant morbidity in patients with severe TBI.
Key Words: Craniocerebral trauma; pneumonia; multiple organ failure; treatment outcome; critical care.
(Neurocrit. Care 2006;05:108–114)
Ventilator-Associated Pneumonia in Severe Traumatic Brain InjuryDavid A. Zygun,1,2,5,* Danny J. Zuege,1,3 Paul J. E. Boiteau,1 Kevin B. Laupland,1,3,5 Elizabeth A. Henderson,5 John B. Kortbeek,1,4 and Christopher J. Doig1,3,5
Departments of 1Critical Care Medicine, 2Clinical Neuroscience, 3Medicine, 4Surgery, and Community 5Health Sciences, University of Calgary, Calgary, Alberta, Canada
world (3,6). Population-based epidemiologi-cal studies of severe TBI report a case fatality of 30–54% (9–12). In addition, complete re-covery to preinjury levels is uncommon; ap-proximately 60% of survivors have ongoing deficits in the areas of cognitive competency,
Original Article
Neurocritical CareCopyright © 2006 Humana Press Inc.All rights of any nature whatsoever are reserved.ISSN 1541-6933/06/5:108–114 ISSN 1556-0961 (Online)DOI: 10.1385/Neurocrit. Care 2006;05:108–114
VAP in Traumatic Brain Injury 109
Neurocritical Care ! Volume 5, 2006
(population ~1.3 million). All adult patients with severe TBI who underwent mechanical ventilation for duration of greater than 48 hours from May 1, 2000 to December 30, 2002 were in-cluded. Severe TBI was defined as a TBI resulting in at least one of the following: (1) an initial resuscitated (systolic blood pressure > 90 mmHg and arterial oxygen concentration [SaO2] > 90%) Glasgow Coma Score (GCS) of 8 or less at first contact with medical services; (2) a postresuscitation GCS at presenta-tion to the trauma center of 8 or less in the absence of sedation; (3) the requirement for intracranial pressure (ICP) monitoring; or (4) the presence of clinical or radiographic herniation. The decision to use ICP monitoring followed the recommendations from the Brain Trauma Foundation (23). The herniation crite-ria required uncal or transtentorial herniation confirmed on computed tomography scan or an episode of unilateral or bi-lateral pupillary dilatation and a neurosurgeon’s or intensiv-ist’s documented diagnosis of herniation syndrome.
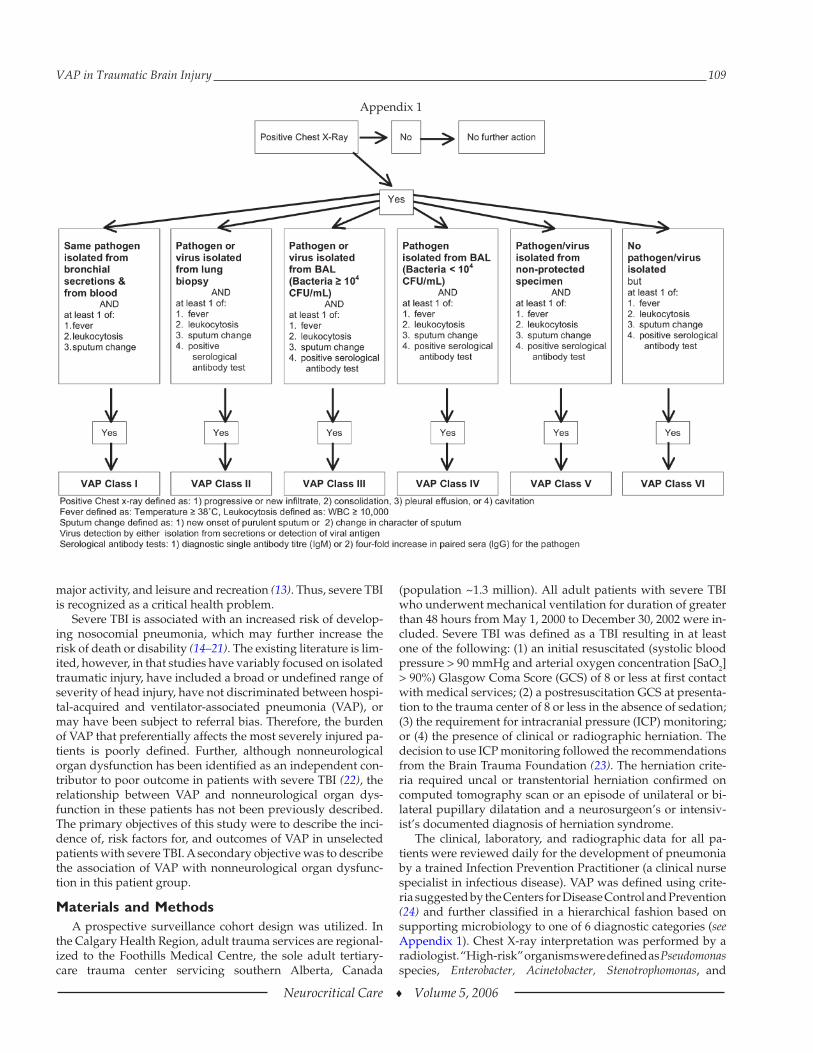
The clinical, laboratory, and radiographic data for all pa-tients were reviewed daily for the development of pneumonia by a trained Infection Prevention Practitioner (a clinical nurse specialist in infectious disease). VAP was defined using crite-ria suggested by the Centers for Disease Control and Prevention (24) and further classified in a hierarchical fashion based on supporting microbiology to one of 6 diagnostic categories (see Appendix 1). Chest X-ray interpretation was performed by a radiologist. “High-risk” organisms were defined as Pseudomonas species, Enterobacter, Acinetobacter, Stenotrophomonas, and
major activity, and leisure and recreation (13). Thus, severe TBI is recognized as a critical health problem.
Severe TBI is associated with an increased risk of develop-ing nosocomial pneumonia, which may further increase the risk of death or disability (14–21). The existing literature is lim-ited, however, in that studies have variably focused on isolated traumatic injury, have included a broad or undefined range of severity of head injury, have not discriminated between hospi-tal-acquired and ventilator-associated pneumonia (VAP), or may have been subject to referral bias. Therefore, the burden of VAP that preferentially affects the most severely injured pa-tients is poorly defined. Further, although nonneurological organ dysfunction has been identified as an independent con-tributor to poor outcome in patients with severe TBI (22), the relationship between VAP and nonneurological organ dys-function in these patients has not been previously described. The primary objectives of this study were to describe the inci-dence of, risk factors for, and outcomes of VAP in unselected patients with severe TBI. A secondary objective was to describe the association of VAP with nonneurological organ dysfunc-tion in this patient group.
Materials and MethodsA prospective surveillance cohort design was utilized. In
the Calgary Health Region, adult trauma services are regional-ized to the Foothills Medical Centre, the sole adult tertiary-care trauma center servicing southern Alberta, Canada
Appendix 1

110 Zygun et al.
Neurocritical Care ! Volume 5, 2006
Staphylococcus aureus. Survival status and dichotomized Glasgow outcome (<4, !4) score was determined at the time of hospital discharge. The Sequential Organ Failure Assessment (SOFA, Appendix 2) score was collected daily based on the rec-ommendations in the original publication (25). We have previ-ously described our regional collection of data on these patients (26). The study was approved by the local Institutional Review Board.
Statistical AnalysisDescriptive statistics and boxplots were used to analyze
each variable separately. Analyses of continuous, normally distributed variables within and between groups were under-taken using the appropriate Student’s t-test. Nonnormally dis-tributed continuous variables were analyzed using the Mann Whitney U test. Categorical variables were analyzed using Fisher’s exact test. A P-value of less than 0.05 was considered significant. All statistical tests were two-sided. Consistent with National Nosocomial Infections Surveillance program meth-odology, the incidence rate of VAP was expressed as the num-ber of VAPs per 1000 ventilator days. To quantify the degree of nonneurological organ dysfunction, the modified maximum SOFA score, which is defined as the sum of the most abnormal nonneurological multiple organ dysfunction component scores obtained by each patient during intensive care unit (ICU) man-agement, was calculated. Multivariable logistic regression analysis was performed to determine the independent contri-bution of VAP and nonneurological organ dysfunction to the prediction of hospital mortality. Model fit was assessed using the Hosmer Lemeshow goodness of fit test and discrimination was assessed using the area under the receiver operating char-acteristic curve.
ResultsA total of 134 patients with severe TBI underwent mechani-
cal ventilation for greater than 48 hours during the study pe-riod. The characteristics of these patients are presented in Table 1. Of these, 60 patients (45%) were diagnosed with VAP during their hospitalization (incidence density 42.7/1000 ven-tilator days). No patient was diagnosed with more than one VAP. The VAP diagnostic category (Appendix 1) distribution was as follows: category I, one patient (2%); category II, no pa-tients; category III, 26 patients (43%); category IV, 13 patients (22%); category V, seven patients (12%); and category VI, 13 patients (22%). VAP was diagnosed on median (interquartile range [IQR]) day 5 (3.5, 6) of ICU admission. A total of 78% of patients diagnosed with VAP had positive microbiology (VAP diagnostic categories I–V). Therefore, the incidence of culture-positive VAP was 33.4/1000 ventilator days. Of the 47 patients diagnosed with culture positive VAP, 29 patients (62%) had monomicrobial VAP and 18 patients (38%) had polymicrobial VAP. The microbiological results are presented in Table 2. An analysis of factors and outcomes associated with VAP is pre-sented in Table 3. The only admission variable significantly as-sociated with the development of VAP was the Injury Severity Score. Patients with isolated head injury (maximum abbrevi-ated injury scores for chest, abdomen, and pelvis/extremities "1) were at lower risk for the development of VAP than those with associated polytrauma (30.4/1000 ventilator days versus
Table 1 Patient Characteristics
Number of patients 134Age [mean (range)] 38 (16, 90)Male (%) 78Smokers (%) 13Injury Severity Score (mean ± SD) 34 ± 11ICU admission APACHE II (mean ± SD) 18 ± 6Postresuscitation GCS [median (IQR)] 5 (3,7)Proportion of patients with: AIS chest ! 3 AIS abdomen ! 3 AIS extremities/pelvis ! 3
0.460.130.28
Proportion of patients with isolated severe traumatic brain injurya
0.38
Mechanical ventilation days [median (IQR)] 8 (5, 13)ICU length of stay [median (IQR)] 9 (7,15)Hospital length of stay [median (IQR)] 28 (9, 81)Glasgow Outcome Score 4 or 5 (%) 27Hospital mortality (%) 28
SD, standard deviation; ICU, intensive care unit; APACHE II, Acute Physiology and Chronic Health Evaluation; GCS, Glasgow coma score; IQR, interquartile range; AIS, abbreviated injury scale.
aIsolated severe traumatic brain injury was defined as having AIS scores “1 for chest, abdomen, and pelvis/extremities.
Table 2 Microbiological Results
Organism category Number of isolates (%)
Staphylococus aueus 20 (31)Hemophilus influenzae 18 (28)Escherichia coli 4 (6)Enterobacter species 4 (6)Acinetobacter species 3 (5)Other Gram negatives 10 (15)Other Gram positives 5 (8)Candida species 1 (2)
50.8/1000 ventilator days, risk ratio [RR] 1.7, 95% confidence interval [CI], 0.9–3.1). VAP was not associated with hospital mortality. However, patients who developed VAP had a sig-nificantly longer duration of mechanical ventilation, longer ICU and hospital length of stay, and more often required tracheostomy.
We could not demonstrate an association between hospital mortality and a specific microbiological result. A trend toward increased mortality was identified for patients with a “high-risk” organism (RR 2.1, 95% CI 0.8–5.5, p = 0.1). For patients with VAP, diagnostic category (Appendix 1) was not signifi-cantly associated with hospital mortality, ICU length of stay, ventilator days, or hospital length of stay. Development of late VAP (>4 days) was not associated with an increased risk of hospital mortality when compared to patients who developed VAP within 4 days (p = 0.8). The proportion of patients with a “high-risk” organism did not differ between those patients who developed early VAP ("4 days) and those who developed VAP late (>4 days) (0.52 versus 0.45, p = 0.8). Dichotomized
VAP in Traumatic Brain Injury 111
Neurocritical Care ! Volume 5, 2006
Glasgow outcome score, which was available for 84 patients, was not associated with VAP.
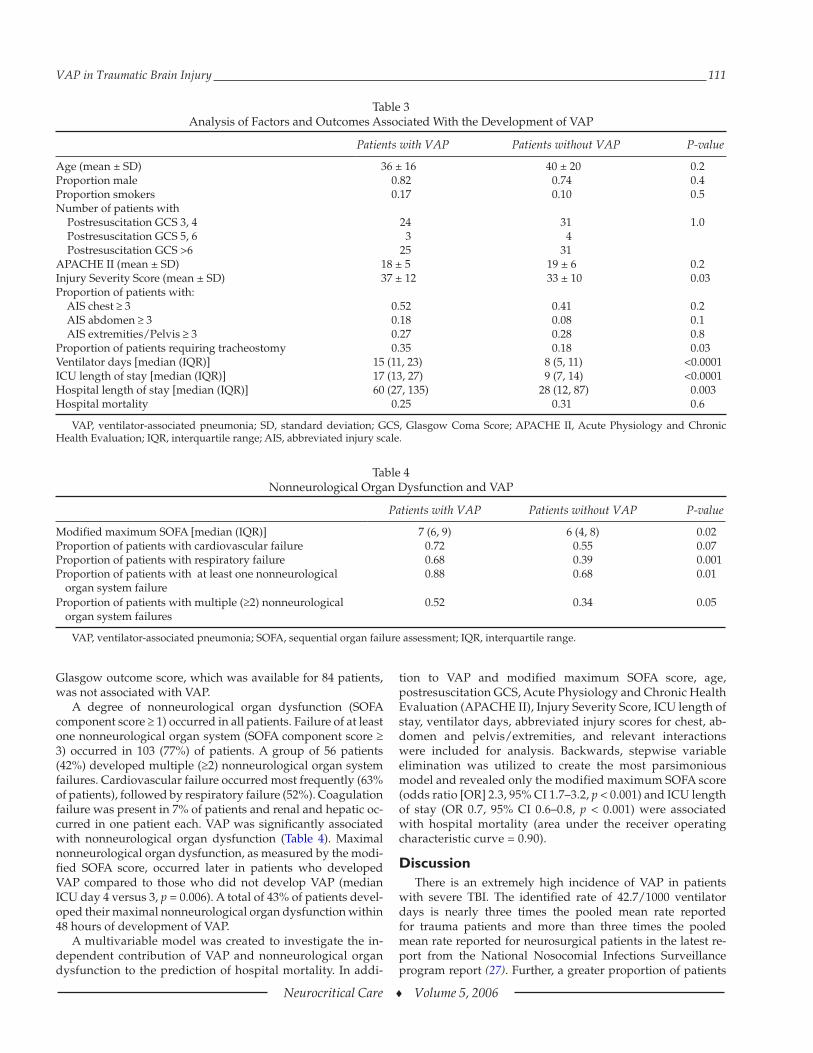
A degree of nonneurological organ dysfunction (SOFA component score ! 1) occurred in all patients. Failure of at least one nonneurological organ system (SOFA component score ! 3) occurred in 103 (77%) of patients. A group of 56 patients (42%) developed multiple (!2) nonneurological organ system failures. Cardiovascular failure occurred most frequently (63% of patients), followed by respiratory failure (52%). Coagulation failure was present in 7% of patients and renal and hepatic oc-curred in one patient each. VAP was significantly associated with nonneurological organ dysfunction (Table 4). Maximal nonneurological organ dysfunction, as measured by the modi-fied SOFA score, occurred later in patients who developed VAP compared to those who did not develop VAP (median ICU day 4 versus 3, p = 0.006). A total of 43% of patients devel-oped their maximal nonneurological organ dysfunction within 48 hours of development of VAP.
A multivariable model was created to investigate the in-dependent contribution of VAP and nonneurological organ dysfunction to the prediction of hospital mortality. In addi-
tion to VAP and modified maximum SOFA score, age, postresuscitation GCS, Acute Physiology and Chronic Health Evaluation (APACHE II), Injury Severity Score, ICU length of stay, ventilator days, abbreviated injury scores for chest, ab-domen and pelvis/extremities, and relevant interactions were included for analysis. Backwards, stepwise variable elimination was utilized to create the most parsimonious model and revealed only the modified maximum SOFA score (odds ratio [OR] 2.3, 95% CI 1.7–3.2, p < 0.001) and ICU length of stay (OR 0.7, 95% CI 0.6–0.8, p < 0.001) were associated with hospital mortality (area under the receiver operating characteristic curve = 0.90).
DiscussionThere is an extremely high incidence of VAP in patients
with severe TBI. The identified rate of 42.7/1000 ventilator days is nearly three times the pooled mean rate reported for trauma patients and more than three times the pooled mean rate reported for neurosurgical patients in the latest re-port from the National Nosocomial Infections Surveillance program report (27). Further, a greater proportion of patients
Table 4 Nonneurological Organ Dysfunction and VAP
Patients with VAP Patients without VAP P-value
Modified maximum SOFA [median (IQR)] 7 (6, 9) 6 (4, 8) 0.02Proportion of patients with cardiovascular failure 0.72 0.55 0.07Proportion of patients with respiratory failure 0.68 0.39 0.001Proportion of patients with at least one nonneurological
organ system failure0.88 0.68 0.01
Proportion of patients with multiple (!2) nonneurological organ system failures
0.52 0.34 0.05
VAP, ventilator-associated pneumonia; SOFA, sequential organ failure assessment; IQR, interquartile range.
Table 3 Analysis of Factors and Outcomes Associated With the Development of VAP
Patients with VAP Patients without VAP P-value
Age (mean ± SD) 36 ± 16 40 ± 20 0.2Proportion male 0.82 0.74 0.4Proportion smokers 0.17 0.10 0.5Number of patients with Postresuscitation GCS 3, 4 Postresuscitation GCS 5, 6 Postresuscitation GCS >6
243
25
314
31
1.0
APACHE II (mean ± SD) 18 ± 5 19 ± 6 0.2Injury Severity Score (mean ± SD) 37 ± 12 33 ± 10 0.03Proportion of patients with: AIS chest ǃ 3 AIS abdomen ǃ 3 AIS extremities/Pelvis ǃ 3
0.520.180.27
0.410.080.28
0.20.10.8
Proportion of patients requiring tracheostomy 0.35 0.18 0.03Ventilator days [median (IQR)] 15 (11, 23) 8 (5, 11) <0.0001ICU length of stay [median (IQR)] 17 (13, 27) 9 (7, 14) <0.0001Hospital length of stay [median (IQR)] 60 (27, 135) 28 (12, 87) 0.003Hospital mortality 0.25 0.31 0.6
VAP, ventilator-associated pneumonia; SD, standard deviation; GCS, Glasgow Coma Score; APACHE II, Acute Physiology and Chronic Health Evaluation; IQR, interquartile range; AIS, abbreviated injury scale.

112 Zygun et al.
Neurocritical Care ! Volume 5, 2006
in this study developed VAP than those in large cohort stud-ies of patients with general trauma (28,29) or patients with subarachnoid hemorrhage (30,31). Patients with severe TBI may represent a specific subgroup of patients with an inher-ently higher risk of VAP and a specific target population for studies examining the prevention, diagnosis, or treatment of VAP.
Unique to our study, we addressed the issue of certainty of diagnosis with a six-level categorization. The incidence of VAP in our report would decrease by approximately 25% if the di-agnosis required positive microbiology (VAP diagnostic cate-gories I–V). Furthermore, if the diagnosis was restricted to only VAP diagnostic categories I, II, and III, the incidence would fall to 19.2 per 1000 ventilator days and more closely re-semble the National Nosocomial Infections Surveillance pro-gram rates. Although VAP diagnostic criteria that rely on stringent microbiological criteria are likely to be more specific, sensitivity will be lost with their use. Given that the recovery of organisms is dependent on the choice of sampling method and timing in relationship to antibiotic administration, we felt the diagnosis must include clinical and microbiological crite-ria. This was particularly important in this group of patients in which invasive diagnostic techniques may have been contrain-dicated because of poor intracranial compliance (32). It is im-portant to note that marked discrepancies with National Nosocomial Infections Surveillance program rates have been reported in other conditions (33).
Although the proportion of patients who developed VAP in this study (45%) is slightly higher than the rates reported by Bronchard (15) (41.3%), Piek (21) (40.6%), Hsieh (18) (41%), and Berrouane (14) (26.2%), important methodological differ-ences exist. Studies by Bronchard and Berrouane included a range of severity of TBI and may have included a group of pa-tients at lower risk for VAP. Vitaz and colleagues found a com-
paratively lower 33% incidence of pneumonia in a study of patients with moderate head injury (34). Furthermore, their results may have been subject to referral bias compared to our study sample, which was inclusive of all patients with severe TBI in southern Alberta. Hsieh studied only patients with iso-lated head injury, and the study by Piek did not differentiate hospital-acquired pneumonia from VAP and utilized a liberal definition of pneumonia (21).
Consistent with previous studies (15,17,18), the develop-ment of VAP was associated with significant morbidity. The burden associated with VAP included increased length of me-chanical ventilation, increased ICU and hospital lengths of stay, and increased requirement for tracheostomy. These re-sults, if proven to be causally related in subsequent work, and the estimated attributable cost of $11,897 (35) would define VAP as a critical health issue both to the patient with severe TBI and the health care system charged with their care.
Patients who developed VAP experienced more nonneuro-logical organ dysfunction than those who did not develop VAP. In addition to the recently identified association with poor outcome following severe TBI (36), MOD has been shown to be a major determinant of poor physical health at 6-month follow-up of ICU survivors (37). However, the majority of pa-tients developed maximal nonneurological organ dysfunction more than 48 hours from the diagnosis of VAP. This suggests that although VAP likely contributes to the development of nonneurological organ dysfunction, it is not the sole mecha-nism responsible.
It is important to note the observed VAP rate occurred after the implementation of a regional, multidisciplinary VAP pre-vention program. This program standardized diagnostic algo-rithms and significantly revised regional policy according to evidence-based recommendations for the prevention of VAP. These revisions included many of the interventions suggested
Appendix 2 Sequential Organ Failure Assessment (SOFA) Score
Organ Score
System 0 1 2 3 4
RespiratoryPaO2/FiO2 >400 "400 "300 "200 "100RenalCreatinine (µmol/L) "110 110–170 171–299 300–440
Urine output "500 mL/day
>440Urine output
< 200 mL/dayHepaticBilirubin (µmol/L) "20 20–32 33–101 102–204 >204CardiovascularHypotension
No hypotension MAP < 70 mmHg Dopamine " 5a,Dobutamine (any dose)
Dopamine > 5a or epinephrine "0.1a or norepinephrine "0.1a
Dopamine > 15a or epinephrine > 0.1a or norepinephrine > 0.1a
HematologicalPlatelet count >150 "150 "100 "50 "20Neurological Glasgow Coma Score 15 13–14 10–12 6–9 <6
MAP, mean arterial pressure.a adrenergic agents administered for at least 1 hour (doses given are in µg/[kg • minute])

VAP in Traumatic Brain Injury 113
Neurocritical Care ! Volume 5, 2006
recently by Kollef (38). Although noncompliance with such evidence-based recommendations has been identified as a important issue (39), one must consider that nonpharmacolog-ical interventions may not make a significant impact on VAP rates in these high-risk patients. Early tracheal colonization has been identified as a risk factor for the development of pneumonia in patients with TBI (40,41). Sirvent studied the prophylactic intravenous cefuroxime after intubation in pa-tients with structural coma and found benefit compared to controls in terms of ICU and hospital stay (42). Although early exposure to short-term antibiotics may be protective against initial tracheal colonization, such use has also been associated with an increased risk for subsequent colonization with Gram-negative enteric bacilli and Pseudomonas species (40). Thus, the impact of systemic prophylactic antibiotic in patients with se-vere TBI for the prevention of VAP has not been fully eluci-dated. An alternative to systemic antibiotics is pathogen-targeted topical eradication. In this study and others, S. aureus is a lead-ing cause of pneumonia in patients with severe TBI, and nasal carriage of this pathogen is a risk factor for development of pneumonia (15,43). Although topical therapy with mupirocin is highly effective for eradication of nasal carriage, it has not yet been shown to reduce rates of infection (44). This study identifies polytrauma patients with severe TBI as an extremely high-risk subgroup that potentially could benefit from topical eradication.
The use of prospective surveillance and inclusion of con-secutive patients with severe TBI in a defined region was uti-lized to minimize systematic error. However, our study has limitations that warrant discussion. Significant morbidity was found to be associated with the development of VAP. It is important to note a causal relationship cannot be assumed from these data. It is likely that days of mechanical ventila-tion, ICU length of stay, requirement for tracheostomy, and hospital length of stay are determined by a number of factors in addition to VAP including concomitant injury, requirement for surgery, ICU complications, and clinician preference. We were unable to demonstrate an association of VAP with mor-tality. The possibility exists that this study was underpowered to detect a true difference in mortality rates. To our knowl-edge, only one study in head injury has described an asso-ciation of VAP with mortality. In this study of 734 patients from the Trauma Coma Data Bank (21), pulmonary infection was identified as an independent predictor of poor outcome following severe TBI but employed a somewhat liberal definition of pneumonia (the presence of infiltrate on chest X-ray and a positive sputum on Gram stain or culture). Furthermore, hospital-acquired pneumonia and VAP were not differentiated.
ConclusionsPatients with severe TBI, especially those with associated
polytrauma, are at very high risk for the development of VAP. In these patients, VAP is associated with significant morbidity including a longer duration of mechanical ventilation, longer ICU and hospital length of stay, more frequent tracheostomy, and a greater severity of nonneurological organ dysfunction. Further studies are needed to evaluate preventative strategies in this group of patients.
AcknowledgmentsThe authors would like to thank the Infection Control
Practioners of the Calgary Health Region for their assistance with the provision of the surveillance data. Funding, in part, was provided by the Health Research Fund from the Alberta Heritage Foundation for Medical Research. The Alberta Heritage Foundation for Medical Research had no part in study design, writing of the manuscript, or the decision to submit the manuscript for publication. No financial or other potential conflicts of interest exist.
References 1. Mosenthal AC, Lavery RF, Addis M, et al. Isolated traumatic
brain injury: age is an independent predictor of mortality and early outcome. J Trauma 2002;52:907–911.
2. McGarry LJ, Thompson D, Millham FH, et al. Outcomes and costs of acute treatment of traumatic brain injury. J Trauma 2002;53:1152–1159.
3. Adekoya N, Thurman DJ, White DD, Webb KW. Surveillance for traumatic brain injury deaths--United States, 1989-1998. MMWR Surveill Summ 2002;51:1–14.
4. Bulger EM, Nathens AB, Rivara FP, Moore M, MacKenzie EJ, Jurkovich GJ. Management of severe head injury: institutional variations in care and effect on outcome. Crit Care Med 2002;30:1870–1876.
5. MacKenzie EJ, Siegel JH, Shapiro S, Moody M, Smith RT. Func-tional recovery and medical costs of trauma: an analysis by type and severity of injury. J Trauma 1988;28:281–297.
6. Masson F, Vecsey J, Salmi LR, Dartigues JF, Erny P, Maurette P. Disability and handicap 5 years after a head injury: a population-based study. J Clin Epidemiol 1997;50:595–601.
7. Snow WG, Macartney-Filgate MS, Schwartz ML, Klonoff PS, Ridgley BA. Demographic and medical characteristics of adult head injuries in a Canadian setting. Can J Surg 1988;31:191–194.
8. Wong PP, Dornan J, Schentag CT, Ip R, Keating M. Statistical pro-file of traumatic brain injury: a Canadian rehabilitation popula-tion. Brain Inj 1993;7:283–294.
9. Zygun DA, Laupland KB, Hader WJ, et al. Population based study of severe traumatic brain injury in a large Canadian health region. Can J Neurol Sci 2005;32:87–92.
10. Kraus JF, Black MA, Hessol N, et al. The incidence of acute brain injury and serious impairment in a defined population. Am J Epi-demiol 1984;119:186–201.
11. Masson F, Thicoipe M, Aye P, et al. Epidemiology of severe brain injuries: a prospective population-based study. J Trauma 2001;51:481–489.
12. Tiret L, Hausherr E, Thicoipe M, et al. The epidemiology of head trauma in Aquitaine (France), 1986: a community-based study of hospital admissions and deaths. Int J Epidemiol 1990;19:133–140.
13. Dikmen SS, Machamer JE, Powell JM, Temkin NR. Outcome 3 to 5 years after moderate to severe traumatic brain injury. Arch Phys Med Rehabil 2003;84:1449–1457.
14. Berrouane Y, Daudenthun I, Riegel B, et al. Early onset pneumo-nia in neurosurgical intensive care unit patients. J Hosp Infect 1998;40:275–280.
15. Bronchard R, Albaladejo P, Brezac G, et al. Early onset pneumo-nia: risk factors and consequences in head trauma patients. Anesthesiology 2004;100:234–239.
16. Cazzadori A, Di Perri G, Vento S, et al. Aetiology of pneumonia following isolated closed head injury. Respir Med 1997;91:193–199.
17. Leone M, Bourgoin A, Giuly E, et al. Influence on outcome of ventilator-associated pneumonia in multiple trauma patients with head trauma treated with selected digestive decontamina-tion. Crit Care Med 2002;30:1741–1746.
114 Zygun et al.
Neurocritical Care ! Volume 5, 2006
18. Hsieh AH, Bishop MJ, Kubilis PS, Newell DW, Pierson DJ. Pneu-monia following closed head injury. Am Rev Respir Dis 1992;146:290–294.
19. Rodriguez JL, Gibbons KJ, Bitzer LG, Dechert RE, Steinberg SM, Flint LM. Pneumonia: incidence, risk factors, and outcome in in-jured patients. J Trauma 1991;31:907–912; discussion 912–914.
20. Rello J, Ausina V, Ricart M, Puzo C, Net A, Prats G. Nosocomial pneumonia in critically ill comatose patients: need for a differen-tial therapeutic approach. Eur Respir J 1992;5:1249–1253.
21. Piek J, Chesnut RM, Marshall LF, et al. Extracranial complica-tions of severe head injury. J Neurosurg 1992;77:901–907.
22. Zygun DA, Kortbeek JB, Fick GH, Laupland KB, Doig CJ. Non-neurologic organ dysfunction in severe traumatic brain injury. Crit Care Med 2005;33:654–660.
23. The Brain Trauma Foundation. The American Association of Neurological Surgeons. The Joint Section on Neurotrauma and Critical Care. Indications for intracranial pressure monitoring. J Neurotrauma 2000;17:479–491.
24. Emori TG, Culver DH, Horan TC, et al. National nosocomial in-fections surveillance system (NNIS): description of surveillance methods. Am J Infect Control 1991;19:19–35.
25. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis- Related Prob-lems of the European Society of Intensive Care Medicine. Inten-sive Care Med 1996;22:707–710.
26. Doig CJ, Zygun DA, Fick GH, et al. Study of clinical course of or-gan dysfunction in intensive care. Crit Care Med 2004;32:384–390.
27. National Nosocomial Infections Surveillance (NNIS) System Re-port, data summary from January 1992 through June 2003, issued August 2003. Am J Infect Control 2003;31:481–498.
28. Tejada Artigas A, Bello Dronda S, Chacon Valles E, et al. Risk fac-tors for nosocomial pneumonia in critically ill trauma patients. Crit Care Med 2001;29:304–309.
29. Mostafa G, Huynh T, Sing RF, Miles WS, Norton HJ, Thomason MH. Gender-related outcomes in trauma. J Trauma 2002;53:430–434; discussion 434–435.
30. Wartenberg KE, Schmidt JM, Claassen J, et al. Impact of medical complications on outcome after subarachnoid hemorrhage. Crit Care Med 2006;34:617–623; quiz 624.
31. Friedman JA, Pichelmann MA, Piepgras DG, et al. Pulmonary complications of aneurysmal subarachnoid hemorrhage. Neuro-surgery 2003;52:1025–1031; discussion 1031–1032.
32. Kerwin AJ, Croce MA, Timmons SD, Maxwell RA, Malhotra AK, Fabian TC. Effects of fiberoptic bronchoscopy on intracranial
pressure in patients with brain injury: a prospective clinical study. J Trauma 2000;48:878–882; discussion 882–883.
33. Eggimann P, Hugonnet S, Sax H, Touveneau S, Chevrolet JC, Pittet D. Ventilator-associated pneumonia: caveats for bench-marking. Intensive Care Med 2003;29:2086–2089.
34. Vitaz TW, Jenks J, Raque GH, Shields CB. Outcome following moderate traumatic brain injury. Surg Neurol 2003;60:285–291; discussion 291.
35. Warren DK, Shukla SJ, Olsen MA, et al. Outcome and attributable cost of ventilator-associated pneumonia among intensive care unit patients in a suburban medical center. Crit Care Med 2003;31:1312–1317.
36. Zygun DA, Kortbeek JB, Fick GH, Laupland KB, Doig CJ. Non-neurological organ dysfunction in severe traumatic brain injury. Crit Care Med 2005;in press:
37. Wehler M, Geise A, Hadzionerovic D, et al. Health-related qual-ity of life of patients with multiple organ dysfunction: individual changes and comparison with normative population. Crit Care Med 2003;31:1094–1101.
38. Kollef MH. The prevention of ventilator-associated pneumonia. N Engl J Med 1999;340:627–634.
39. Rello J, Lorente C, Bodi M, Diaz E, Ricart M, Kollef MH. Why do physicians not follow evidence-based guidelines for preventing ventilator-associated pneumonia?: a survey based on the opin-ions of an international panel of intensivists. Chest 2002;122:656–661.
40. Ewig S, Torres A, El-Ebiary M, et al. Bacterial colonization pat-terns in mechanically ventilated patients with traumatic and medical head injury. Incidence, risk factors, and association with ventilator-associated pneumonia. Am J Respir Crit Care Med 1999;159:188–198.
41. Sirvent JM, Torres A, Vidaur L, Armengol J, de Batlle J, Bonet A. Tracheal colonisation within 24 h of intubation in patients with head trauma: risk factor for developing early-onset ventilator-as-sociated pneumonia. Intensive Care Med 2000;26:1369–1372.
42. Sirvent JM, Torres A, El-Ebiary M, Castro P, de Batlle J, Bonet A. Protective effect of intravenously administered cefuroxime against nosocomial pneumonia in patients with structural coma. Am J Respir Crit Care Med 1997;155:1729–1734.
43. Campbell W, Hendrix E, Schwalbe R, Fattom A, Edelman R. Head-injured patients who are nasal carriers of Staphylococcus aureus are at high risk for Staphylococcus aureus pneumonia. Crit Care Med 1999;27:798–801.
44. Laupland KB, Conly JM. Treatment of Staphylococcus aureus colo-nization and prophylaxis for infection with topical intranasal mu-pirocin: an evidence-based review. Clin Infect Dis 2003;37:933–938.
Related Documents

![Ventilator Associated Pneumonia Treatment[1]](https://static.cupdf.com/doc/110x72/577d23921a28ab4e1e9a2bfc/ventilator-associated-pneumonia-treatment1.jpg)









