4/5/2014 1 UCSF Vascular Symposium 204 Aggressive assessment and management are the keys to healing Peter J. Pappas, M.D Professor of Surgery Chariman, Department of Surgery The Brooklyn Hospital Venous Hypertension Secondary to Reflux Leukocytes with TGF-ß 1 Granules Leukocyte Diapedesis

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

4/5/2014
1
UCSF Vascular Symposium 204
Aggressive assessment and management are the keys to
healing
Peter J. Pappas, M.DProfessor of Surgery
Chariman, Department of SurgeryThe Brooklyn Hospital
Venous Hypertension Secondary to Reflux
Leukocytes with TGF-ß1 Granules Leukocyte Diapedesis

4/5/2014
2
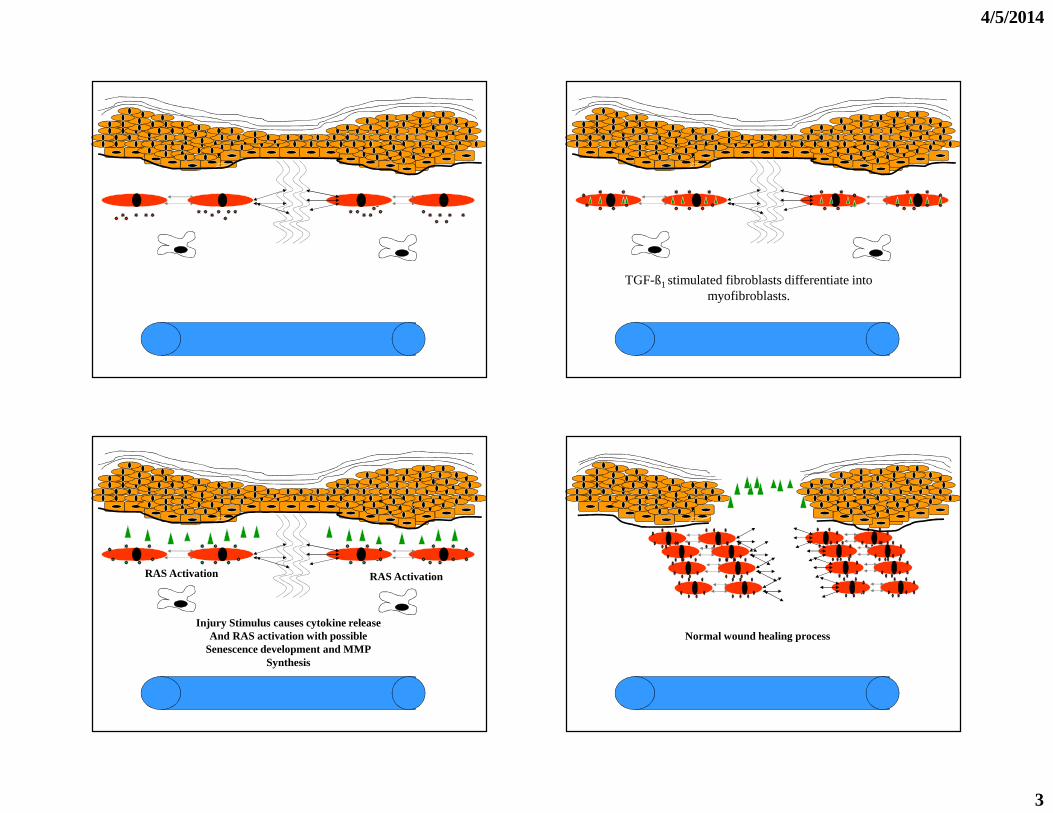
TGF-ß1 Release TGF-ß1 Release
4/5/2014
3
TGF-ß1 stimulated fibroblasts differentiate into myofibroblasts.
Injury Stimulus causes cytokine releaseAnd RAS activation with possible
Senescence development and MMPSynthesis
RAS Activation RAS Activation
Normal wound healing process
4/5/2014
4
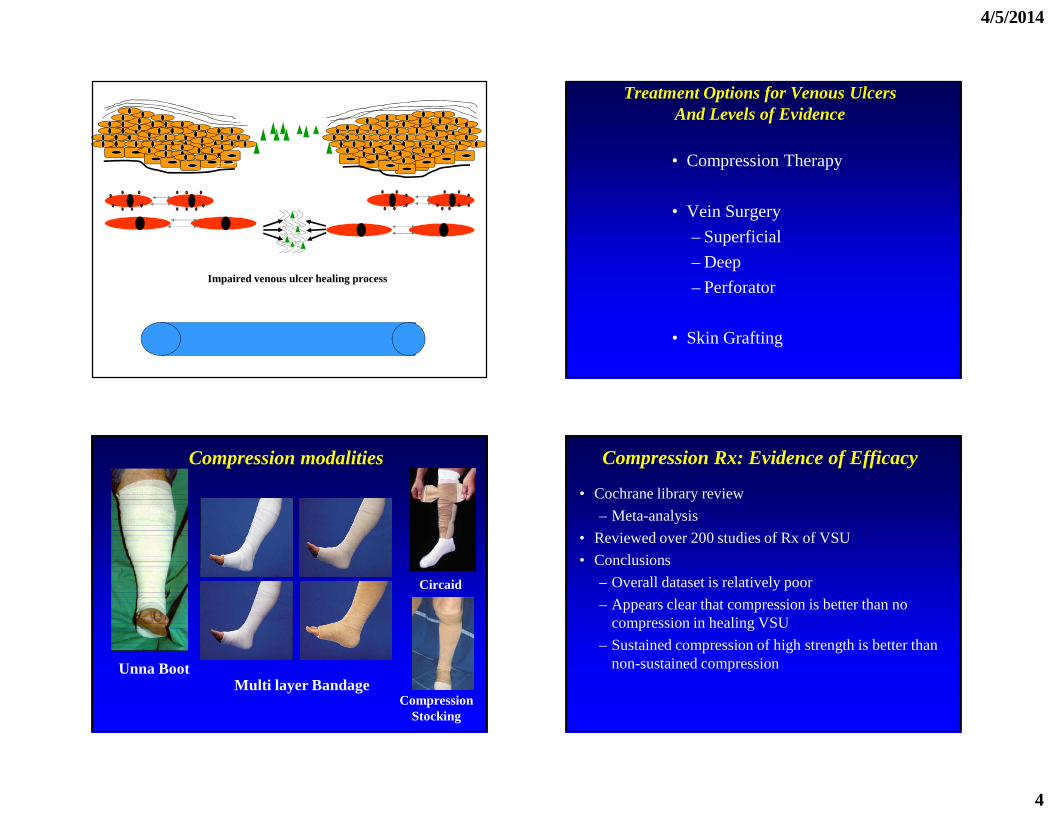
Impaired venous ulcer healing process
Treatment Options for Venous UlcersAnd Levels of Evidence
• Compression Therapy
• Vein Surgery
– Superficial
– Deep
– Perforator
• Skin Grafting
Compression modalities
Unna BootMulti layer Bandage
Circaid
CompressionStocking
Compression Rx: Evidence of Efficacy
• Cochrane library review
– Meta-analysis
• Reviewed over 200 studies of Rx of VSU
• Conclusions
– Overall dataset is relatively poor
– Appears clear that compression is better than no compression in healing VSU
– Sustained compression of high strength is better than non-sustained compression
4/5/2014
5
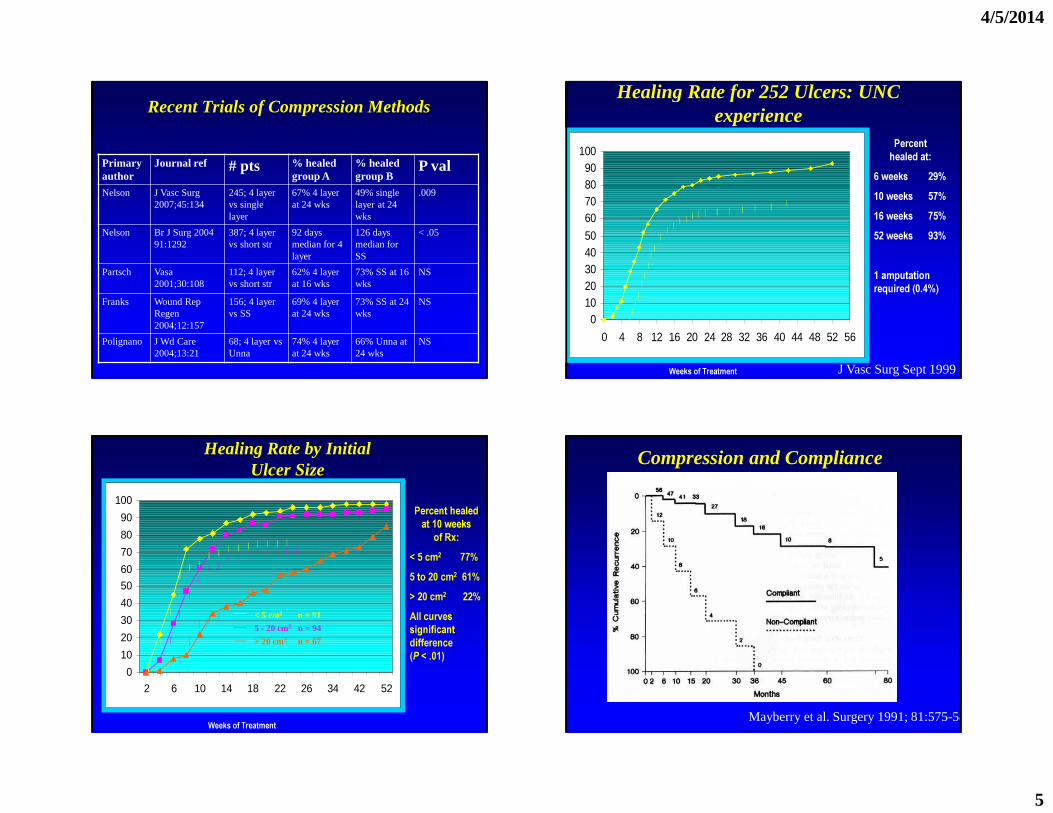
Recent Trials of Compression Methods
Primary author
Journal ref # pts % healed group A
% healed group B
P val
Nelson J Vasc Surg 2007;45:134
245; 4 layer vs single layer
67% 4 layer at 24 wks
49% single layer at 24 wks
.009
Nelson Br J Surg 2004 91:1292
387; 4 layer vs short str
92 days median for 4 layer
126 days median for SS
< .05
Partsch Vasa 2001;30:108
112; 4 layer vs short str
62% 4 layer at 16 wks
73% SS at 16 wks
NS
Franks Wound Rep Regen 2004;12:157
156; 4 layer vs SS
69% 4 layer at 24 wks
73% SS at 24 wks
NS
Polignano J Wd Care 2004;13:21
68; 4 layer vs Unna
74% 4 layer at 24 wks
66% Unna at 24 wks
NS
Percent healed at:
6 weeks 29%10 weeks 57%16 weeks 75%52 weeks 93%
1 amputation required (0.4%)
Weeks of Treatment
01020304050
60708090
100
0 4 8 12 16 20 24 28 32 36 40 44 48 52 56
Healing Rate for 252 Ulcers: UNC experience
J Vasc Surg Sept 1999
Weeks of Treatment
Percent healed at 10 weeks
of Rx:< 5 cm2 77%5 to 20 cm2 61%> 20 cm2 22% All curves significant difference (P < .01)
0
10
20
30
40
50
60
70
80
90
100
2 6 10 14 18 22 26 34 42 52
< 5 cm2 n = 91
5 - 20 cm2 n = 94
> 20 cm2 n = 67
Healing Rate by Initial Ulcer Size
Compression and Compliance
Mayberry et al. Surgery 1991; 81:575-581.

4/5/2014
6
Wrong Diagnosis: Venous Mimics
• Basal or squamous cell carcinoma.
• Rheumatoid, lupus, scleroderma and other collagen vascular disorders.
• Tuberculosis and syphilis.
• Pyoderma gangrenosum.
• AIDS.
• Arteriovenous malformations.
• Cryoglobulinemia and macroglobulinemia.
• Burns and insect bites.
Level of Evidence for Venous Ulcer SurgeryVersus Compression
Summation Data for Studies Prior to 2000
Howard et al. The role of superficial venous surgery in the management ofVenous ulcers: A systematic review. Eur J Vasc Endovasc Surg. 2008;36: 458-465.
Randomized Clinical Trials For Venous Ulcer Surgery

4/5/2014
7
C5-6 Disease - The ESCHAR Trial Barwell JR, Lancet 2004
• Prospective randomized trial
– High ligation, stripping, phlebectomy and
Compression versus
– Multilayer compression bandaging
• 500 patients with CEAP 5 and 6 disease
– Isolated superficial reflux - 300 (60%)
– Mixed superficial / deep reflux - 200 (40%)
• Endpoints
– 24 week ulcer healing
– 12 month ulcer recurrence
Barwell et al. Eschar Trial.Lancet 2004; 363: 1854-1859
ESCHAR Trial - Ulcer Healing Barwell JR, Lancet 2004
• 24 week ulcer healing - 65% in both groups
0%10%20%30%40%50%60%70%80%90%
100%
0 3 6 9 12
Months
% H
eale
d
SurgeryCompression
ESCHAR Trial - Ulcer Recurrence Barwell JR, Lancet 2004
• 12 month freedom from recurrence (p < 0.0001)– Surgery + Compression -
12%– Compression alone
- 28%
• Four year freedom fromRecurrence (p<0.01)– Surgery + compression
31%– Compression alone
56%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0 3 6 9 12
Months
Fre
edo
m f
rom
Rec
urre
nce
Surgery
Compression
4/5/2014
8
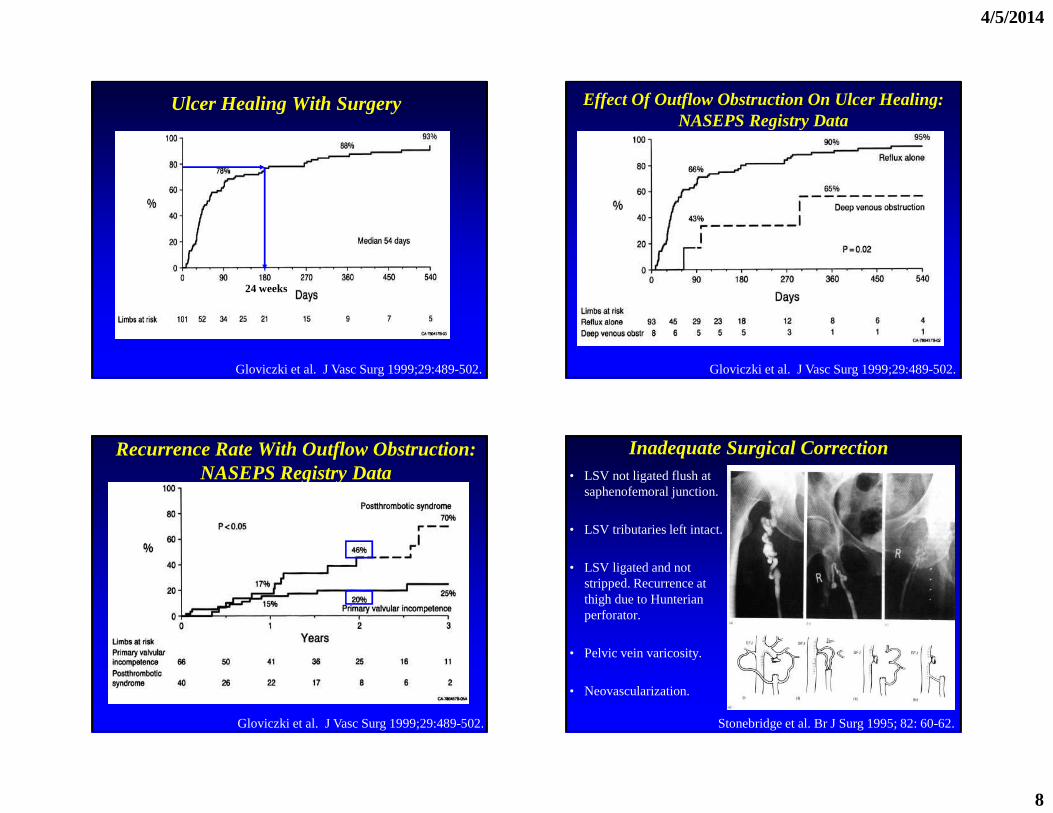
Ulcer Healing With Surgery
24 weeks
Gloviczki et al. J Vasc Surg 1999;29:489-502.
Effect Of Outflow Obstruction On Ulcer Healing:NASEPS Registry Data
Gloviczki et al. J Vasc Surg 1999;29:489-502.
Recurrence Rate With Outflow Obstruction:NASEPS Registry Data
Gloviczki et al. J Vasc Surg 1999;29:489-502.
Inadequate Surgical Correction• LSV not ligated flush at
saphenofemoral junction.
• LSV tributaries left intact.
• LSV ligated and not stripped. Recurrence at thigh due to Hunterian perforator.
• Pelvic vein varicosity.
• Neovascularization.
Stonebridge et al. Br J Surg 1995; 82: 60-62.

4/5/2014
9
Calf Muscle Pump Dysfunction
• Always consider calf muscle pump dysfunction in patients with venous ulcer and no evidence of reflux on duplex examination.
• Important cause of pump dysfunction is poor ankle range of motion.
• Role of physical therapy?
Back et al. J Vasc Surg, 1995;22:519-523.
Clinical Trials Data For Varicose Veins, Not Ulcer Healing: Stripping and compression versus Endovenous
Technologies
CEAP Class 2 and 3 Disease:Primary Varicose Veins
History of Venous Surgery
• Trendelenburg (1890) GSV ligation upper/mid 1/3
• Homans (1916) - Flush Saphenofemoral ligation
• Mayo (1906) - Extraluminal stripper
• Babcock (1907) - Rigid intraluminal stripper
• Myers (1947) - Flexible intraluminal stripper
• 2006 - Endovenous Ablation (Laser / RF)

4/5/2014
10
Mechanism of Action
Randomized Controlled Trials
• RF versus SurgeryRautio 2002Lurie 2005Hinchcliff 2006Stötter 2006
• Laser versus Surgeryde Medeiros 2005Rasmussen 2007Kalteis 2008Ogawa 2008Darwood 2008
• RF versus LaserMorrison 2005Almeida 2008Goode 2008
• Varisolve Foam vs Surgery/ScleroWright 2006
* Foam sclero combined with sapheno-femoral ligation vs surgeryBountouroglou 2006,
2008
Stripping vs Endovenous RF AblationLurie et al, J Vasc Surg 2003
Eur J Vasc Endovasc Surg 2005
• Prospective, multicenter randomized trial
Stripping
n = 36
RF Ablation
n = 44
p
Ablation @ 1 wk 100% 90.5%
Ablation @ 2 yrs 100% 92%
Return to nl activity 3.89 days 1.15 days .02
Return to work 12.4 days 4.7 days < .05
Global QOL @ 1 wk + 3.7 - 9.2 .001
Global QOL @ 4 mo NS

4/5/2014
11
Evolves TrialVenous Clinical Severity Scores
Eur J Vasc Endovasc Surg 2005
Global Quality of Life Scores
Eur J Vasc Endovasc Surg 2005
QoL scores: Immediate and Long-Term
Eur J Vasc Endovasc Surg 2005
4/5/2014
12
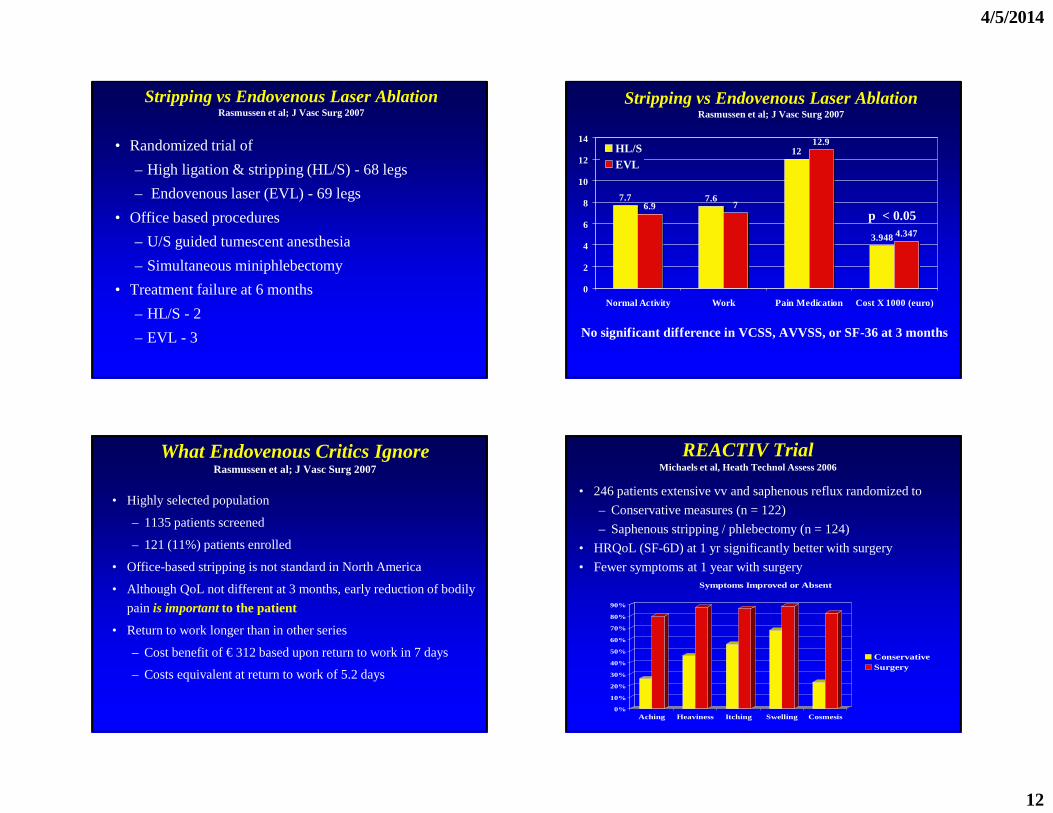
Stripping vs Endovenous Laser AblationRasmussen et al; J Vasc Surg 2007
• Randomized trial of
– High ligation & stripping (HL/S) - 68 legs
– Endovenous laser (EVL) - 69 legs
• Office based procedures
– U/S guided tumescent anesthesia
– Simultaneous miniphlebectomy
• Treatment failure at 6 months
– HL/S - 2
– EVL - 3
Stripping vs Endovenous Laser AblationRasmussen et al; J Vasc Surg 2007
7.7 7.6
12
3.948
6.9 7
12.9
4.347
0
2
4
6
8
10
12
14
Normal Activity Work Pain Medication Cost X 1000 (euro)
HL/SEVL
No significant difference in VCSS, AVVSS, or SF-36 at 3 months
p < 0.05
What Endovenous Critics IgnoreRasmussen et al; J Vasc Surg 2007
• Highly selected population
– 1135 patients screened
– 121 (11%) patients enrolled
• Office-based stripping is not standard in North America
• Although QoL not different at 3 months, early reduction of bodily
pain is important to the patient
• Return to work longer than in other series
– Cost benefit of € 312 based upon return to work in 7 days
– Costs equivalent at return to work of 5.2 days
REACTIV TrialMichaels et al, Heath Technol Assess 2006
• 246 patients extensive vv and saphenous reflux randomized to
– Conservative measures (n = 122)
– Saphenous stripping / phlebectomy (n = 124)
• HRQoL (SF-6D) at 1 yr significantly better with surgery
• Fewer symptoms at 1 year with surgery
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Aching Heaviness Itching Swelling Cosmesis
Symptoms Improved or Absent
ConservativeSurgery

4/5/2014
13
The Economics of Venous Ablation
4.7
12.4
7 7.6
20
14
4
17
8.9
11.5
0
2
4
6
8
10
12
14
16
18
20
Ret
urn
to
Wo
rk (
Day
s)
Lurie Rasmussen Kalteis Darwood WeightedAverage
EndovenousStripping
• Return to work variable with• Healthcare system• Social expectations• Adjunct procedures (high ligation, phlebectomy)
Cost-Effectiveness of SurgeryRatcliffe et al; Br J Surg 2006
• Randomized trial of conservative tx vs surgery
• 24 mo cost effectiveness of £4682 per QALY gained
• Below NHS threshold of £20,000 per QALY
Conservative Surgery Mean Difference
Mean NHS Cost £344.53 £733.10 £388.57
AUC SF-6D 1.42 1.50 0.083
ICER * £4682
* Incremental cost effectiveness ratio
Results of Valvular Repair Techniques
Kistner, Surgical Management of Venous Disease, ed Raju, Villavicencio, 1997
Combined Arterial And Venous Insufficiency
• Treiman et al. studied patients with combined arterial and venous disease*.– Group 1:
• Patent arterial graft, venous stripping for superficial reflux, no DVT.
• 95% of ulcers healed
– Group 2: • Patent arterial graft, superficial and deep venous
reflux, no DVT.• Four ulcers healed, three remained unhealed.
Treiman et al. J Vasc Surg 2001;33:1158-1164.

4/5/2014
14
Combined Arterial And Venous Insufficiency
• Group 3: Patent arterial graft and prior proximal DVT.
– 41% healed their ulcers, 36% remained unhealed and 13% required BKA.
• Group 4: Occluded arterial grafts
– 0% ulcer healing.
Future Directions
Bioengineered Skin Bioengineered Skin
4/5/2014
15
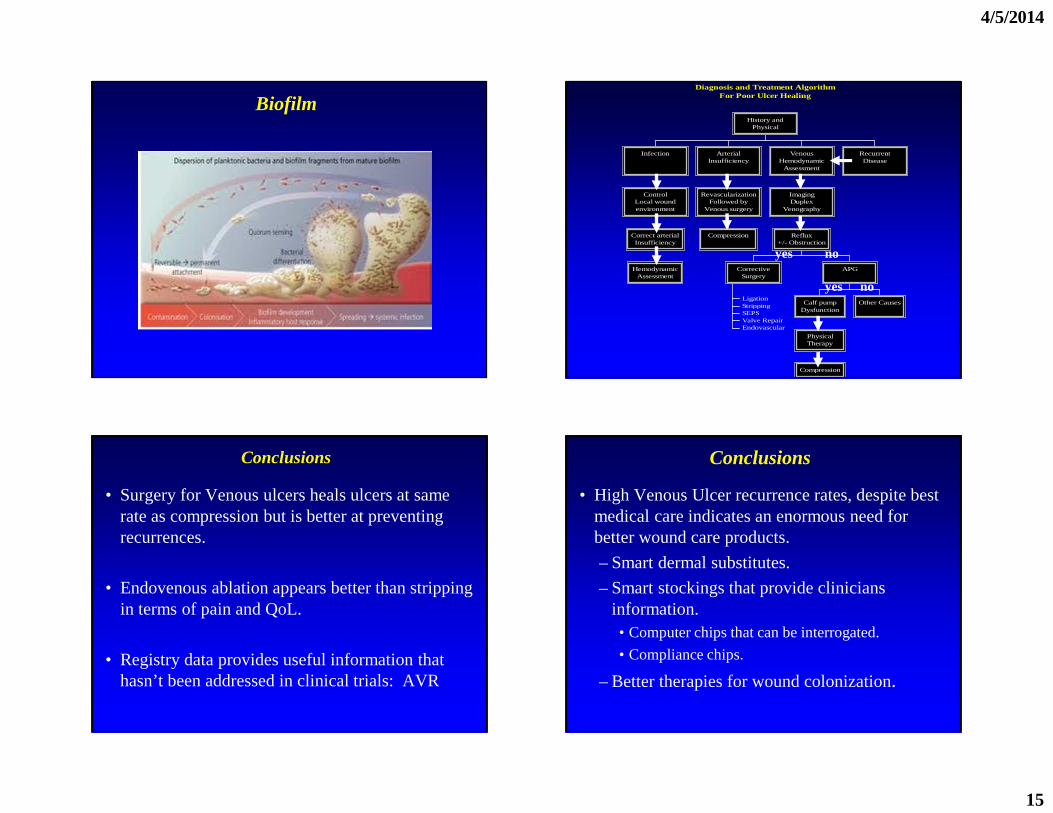
BiofilmDiagnosis and Treatment Algorithm
For Poor Ulcer Healing
HemodynamicAssessment
Correct arterialInsufficiency
ControlLocal woundenvironment
Infection
Compression
RevascularizationFollowed by
Venous surgery
ArterialInsufficiency
LigationStrippingSEPSValve RepairEndovascular
CorrectiveSurgery
Compression
PhysicalTherapy
Calf pumpDysfunction
Other Causes
APG
Reflux+/- Obstruction
ImagingDuplex
Venography
VenousHemodynamic
Assessment
RecurrentDisease
History andPhysical
yes no
yes no
Conclusions
• Surgery for Venous ulcers heals ulcers at same rate as compression but is better at preventing recurrences.
• Endovenous ablation appears better than stripping in terms of pain and QoL.
• Registry data provides useful information that hasn’t been addressed in clinical trials: AVR
Conclusions
• High Venous Ulcer recurrence rates, despite best medical care indicates an enormous need for better wound care products.
– Smart dermal substitutes.
– Smart stockings that provide clinicians information.• Computer chips that can be interrogated.
• Compliance chips.
– Better therapies for wound colonization.
Related Documents











