1 VASCULAR SURGERY RESIDENCY HANDBOOK 2014-2015 Division of Vascular Surgery & Endovascular Therapy Michael E. DeBakey Department of Surgery Baylor College of Medicine Houston, Texas

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
VASCULAR SURGERY RESIDENCY HANDBOOK
2014-2015
Division of Vascular Surgery & Endovascular Therapy
Michael E. DeBakey Department of Surgery Baylor College of Medicine
Houston, Texas

2
Table of Contents
1. Program Overview
2. History of the Vascular Surgery Residency Program
3. Surgery Education Office Faculty and Staff Roster
4. Clinical Training in Vascular Surgery Residency
5. Vascular Resident Rotations
6. Conference Schedules
7. Basic Principles of Clinical Services
8. Graduate Medical Education House Staff Policies
. Recruitment & Selection of House Staff
. Eligibility & Appointment Requirements
. Responsibilities of House Staff
. Reappointment
. Program Methods for Assessment & Criteria for Promotion
. Mechanism for Remediation and/or Disciplinary Action
. Appeal of Non-Reappointment
. Adverse Action: House Staff Physicians
. Appeal of Non-Promotion
. Adverse Action
. Appeal of Probation
. Appeal of Dismissal
. Grievances & Due Processes
. Texas Medical Board Reporting
. Duty to Report
. Sexual Harassment
. Vendor Interaction Policy
. Disaster Policy
. Vacations & Leaves of Absence
. Professionalism
. Professionalism Standards & Program Expectations
. Professionalism Misconduct
9. Duty Hours & the Working Environment
. Principles
. Supervision of Residents
. Duty Hours
. Duty Hour Compliance Monitoring
. On-Call Activities
. Moonlighting
10. Stress, Fatigue, & Impairment
. Signs & Symptoms of Fatigue, Stress, or Impairment
. Resident Responsibilities
. Program Director & Associate Program Director Responsibilities
. Resources: Counseling Services for House Staff
11. Resident Responsibilities
. Duty Hours
. Conference Attendance
. Portfolios

3
. Procedure Case Logs
. Medical Records
. Certifications
. Lines of Supervision
. Evaluations
. ABSITE for Vascular Surgery Exam
. Department Holidays
. Parking
. Final Clearance Form
12. Communication
. Up-to-Date Contact Information
. Pagers
13. Travel Policy
14. Guidelines for Resident Supervision
15. Resident Research Requirements
16. Dress Code
17. Goals & Objectives of Vascular Surgery Rotation
. BSLMC
. PPH
. MEDVAMC
18. Appendix 1- Department of Surgery: Resident Travel Request Form
19. Appendix 2- Time-Off Request
20. Appendix 3- Vascular Surgery Educational Compact Learner
4
1. Program Overview
Baylor College of Medicine (BCM) has been a leader in the field of vascular surgery for the past five decades. The
standards of excellence originally established by Dr. Michael E. DeBakey and Dr. E. Stanley Crawford are still in practice
today. The Vascular Surgery Residency Program is a two-year ACGME approved program leading to eligibility for the
Certificate of Special Added Qualifications in Vascular Surgery. The program accepts two Vascular Surgery residents
each year. In order to qualify for the Residency in Vascular Surgery, a resident must have successfully completed five
years of Residency in General Surgery and be eligible for examination by the American Board of Surgery. The Vascular
Surgery Residency Program of the Michael E. DeBakey Department of Surgery at BCM is a two-year (24 months)
program. Both years are continued full accredited by the Accreditation Council for Graduate Medical Education -
Residency Review Committee (RRC) for Surgery.
The mission of the vascular surgery residency program is to provide comprehensive training in the care of vascular
patients with both open surgical and catheter-based endoluminal therapy. The residency trainees work in an environment
that emphasizes clinical excellence. This training program includes a broad clinical experience in all aspects of vascular
surgery, including but not limited to carotid occlusive disease, complex aortic aneurysm, visceral vessel disease, lower
extremity occlusive disease, dialysis access management, as well as endovascular treatment using cutting-edge devices.
The resident should perform a minimum of 250 major vascular reconstructive procedures that reflect an adequate
representation of current trends in the spectrum of surgical care of vascular diseases, which is based on the requirement by
the Accreditation Council for Graduate Medical Education (ACGME) to satisfactorily complete the vascular surgery
residency. All the case logs are entered into the ACGME website database, which should be done regularly. The program
director of BCM vascular surgery residency program will review the case logs with each vascular resident regularly.
Please review ACGME guidelines and requirements (www.acgme.org).

5
2. History of the Baylor Vascular Surgery Program
The vascular surgery program at the Baylor College of Medicine began in 1948 when Dr. Michael E. DeBakey arrived in
Houston to become the first chairman in the Department of Surgery at BCM. Also regarded as the father of modern
cardiovascular surgery, Dr. DeBakey was instrumental in creating the Veterans Affairs health care system as well as the
Houston VA Medical Center which was subsequently renamed in his honor in December 2003.
During his illustrious surgical career at Baylor, Dr. DeBakey has invented countless surgical devices and developed
innumerable surgical procedures which benefited millions of patients with cardiovascular diseases worldwide. His legacy
and contribution have resulted in a profound impact in the modern practice of vascular surgery. As an example, Dr.
DeBakey performed first carotid endarterectomy in 1959 using techniques which have become the most commonly
adopted reconstructive method in carotid surgery today.
The modern operative principle of thoracoabdominal aortic aneurysm is largely credited to the pioneering work of Dr. E.
Stanley Crawford who joined the Baylor faculty in 1954. In his ensuing 38 years of outstanding surgical career at BCM,
he became internationally known for his innovative surgical techniques in the treatment of thoracoabdominal aortic
aneurysm as well as complex aortic diseases, particularly in Marfan syndrome and aortic dissection. The legacy of
complex aortic disease management continues at Baylor today, where Dr. Joseph S. Coselli has the largest clinical
practice in thoracoabdominal aortic aneurysm in the world. Dr. Coselli continues to play an important role in the Baylor
vascular residency training program in which he provides valuable teaching experience in complex aortic operative
management to all Baylor vascular residents at the St. Luke’s Episcopal Hospital / Texas Heart Institute (SLEH/THI).
Another important Baylor surgical faculty who has provided a significant contribution in vascular surgery is Dr. Kenneth
L. Mattox. He has published extensively in articles and textbooks regarding the contemporary treatment principles of
vascular trauma. Dr. Charles H. McCollum has similarly played an important role in the Baylor vascular program. As the
director of the Methodist Hospital (TMH) vascular lab for more than 30 years, Dr. McCollum has instilled a strong
emphasis of vascular ultrasound training in the Baylor vascular residency program. His passion in surgical education is
further evidenced by his role as the program director of the Baylor general surgery residency program for more than 23
years. Additionally, he served as the program director of the Baylor vascular residency program until December 2001.
The current Division of Vascular Surgery and Endovascular Therapy at Baylor was established in December 2001. Since
then, the Baylor vascular surgery program has become a preeminent academic vascular division in the country. The
current division has a robust basic science and clinical program which include 12 clinical faculty and voluntary faculty
physicians, 2 full-time research faculty members, and 15 post-doctoral research personnel. The clinical practice of the
Baylor vascular program encompasses the Baylor Clinic, Park Plaza Hospital, SLEH/THI, Texas Children’s Hospital, and
the Michael E. DeBakey VA Medical Center (MEDVAMC). A Vascular Lab was established in 2006 in the Baylor Clinic
which provides non-invasive vascular ultrasound service in the Surgery Clinic.
Built on a heritage of over six decades of care to the patient with vascular disease, the Baylor Vascular division maintains
the tradition as envisioned by Dr. DeBakey in clinical and research excellence. The division has shifted from traditional
open surgical to minimally-invasive endovascular interventions whenever appropriate. The faculty physicians are
recognized as national leaders in training, research, and the performance of endovascular procedures.

6
3. The Surgery Education Office Faculty and Staff
The Surgery Education Office provides support for the students, residents and faculty in the Michael E. DeBakey
Department of Surgery Education Programs. The main telephone number is 713.798.6078 and the fax number is
713.798.8941.
Faculty:
Chairman Todd K. Rosengart, M.D.
713-798-1317 *Assistant Peyton Davis [email protected]
Vice Chair for Education Bradford Scott, M.D. 713-798-6078 (office) or 713-873-3941
Congenital Heart Fellowship Program Director Charles Fraser, M.D.
832-826-1929*Please contact Lesa Porterfield 832-826-5722 ([email protected])
General Surgery Residency Program Director Bradford Scott, M.D. 713-798-6078 (office) or 713-873-3941
General Surgery Residency Program Associate Program Director Eric Silberfein, M.D. 713-798-6078 (office) or 713-873-5324
Liver Transplant Fellowship Directors John Goss, M.D. and Christine O’Mahony, M.D.
832-355-1400
[email protected] and [email protected]
Pediatric Surgery Residency Program Director Mark Mazziotti, M.D.
832-822-3135
Summer DeBakey Student Program-Shayan Izaddoost, M.D., Ph.D.
713-798-6305
Surgery Critical Care Program Director Samir Awad, M.D.
713-794-7892
Thoracic Surgery Residency Program Directors Denton Cooley, M.D. and Joseph Coselli, M.D.
832-355-9910
Thoracic Surgery Residency Associate Program Director Ross Reul, M.D.
832-355-5884
UME Medical Student Programs
Core Medical Student Faculty Director
Georgia Holder-Haynes, M.D. 713-798-6078
Electives and Sub Internship Rotations Faculty Director
Bindi Naik-Mathuria, M.D. 832-822-3135
7
Vascular Surgery Residency Program Interim Program Director
Peter Lin, M.D. *effective July 1, 2014
713-798-8412
Vascular Surgery Residency Program Associate Program Director Mun Jye Poi, M.D.*Effective 7/1/2014
713-798-8412
Surgical Educator Shubha Dathatri, Ph.D. 713-798-7229
Staff:
Manager for Education, Faculty Affairs and Alumni Affairs
Holly Shilstone
713-798-6190
Academic Coordinators
Patricia Carpenter (Thoracic Surgery including Aortic Fellowship)
832-355-9936
Jaye Chambers (Vascular Surgery and Liver Surgery Transplant)
713-798-6471
Ashley Crummedyo (UME Medical Student Programs and MED Summer Program)
713.798.4163
Karen Fore (General Surgery, Pediatric Surgery and Surgical Critical Care) 713.798.5302
Denise LaGrone (General Surgery and Assists with Grand Rounds) 713.798.8629
Cathryn Linn (Plastic Surgery)
832-822-3140

8
4. Clinical Training in Vascular Surgery Residency
During the academic year of 2014-2015, there will be three first-year residents at the PGY-6 level and two second-year
residents at the PGY-7 level. The rotations for first-year residents at the PGY-6 level include Michael E. DeBakey VA
Medical Center (MEDVAMC), the Baylor St. Luke’s Medical Center (BSLMC), and Park Plaza Hospital (PPH). The
second-year resident’s rotations include: Michael E. DeBakey VA Medical Center (MEDVAMC), the Baylor St. Luke’s
Medical Center (BSLMC), and Park Plaza Hospital (PPH). Clinical research is encouraged during any of these rotations.
The second-year vascular fellow rotating at the MEDVAMC vascular rotation will share calls with senior general surgery
residents covering the VA hospital only. The three remaining fellows will share calls while rotating in hospitals including
PPH, and BSLMC.
Evaluations for both the faculty members and residents are kept and maintained on E*Value in the Surgery Education
Office after every rotation. The evaluations for the residents are available for the residents to review at any time in the
Surgery Education Office and are reviewed and required by the Residency Committee. An end-of-the-year program
evaluation is to be completed by all residents on E*Value. These evaluations are reviewed by the Chairman of Surgery,
Vice Chair for Education, the Division Chief of Vascular Surgery and the Vascular Program Director.
9
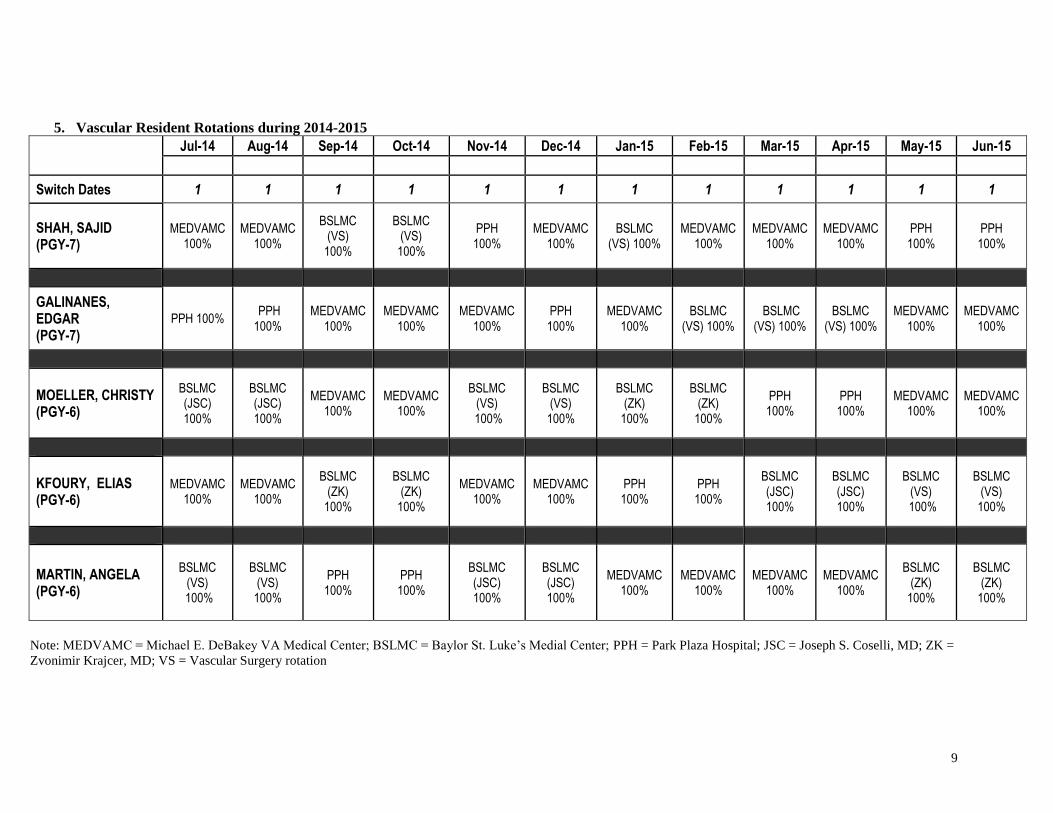
5. Vascular Resident Rotations during 2014-2015
Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
Switch Dates 1 1 1 1 1 1 1 1 1 1 1 1
SHAH, SAJID (PGY-7)
MEDVAMC 100%
MEDVAMC 100%
BSLMC (VS)
100%
BSLMC (VS)
100%
PPH 100%
MEDVAMC 100%
BSLMC (VS) 100%
MEDVAMC 100%
MEDVAMC 100%
MEDVAMC 100%
PPH 100%
PPH 100%
GALINANES, EDGAR (PGY-7)
PPH 100% PPH 100%
MEDVAMC 100%
MEDVAMC 100%
MEDVAMC 100%
PPH 100%
MEDVAMC 100%
BSLMC (VS) 100%
BSLMC (VS) 100%
BSLMC (VS) 100%
MEDVAMC 100%
MEDVAMC 100%
MOELLER, CHRISTY (PGY-6)
BSLMC (JSC) 100%
BSLMC (JSC) 100%
MEDVAMC 100%
MEDVAMC 100%
BSLMC (VS)
100%
BSLMC (VS)
100%
BSLMC (ZK)
100%
BSLMC (ZK)
100%
PPH 100%
PPH 100%
MEDVAMC 100%
MEDVAMC 100%
KFOURY, ELIAS (PGY-6)
MEDVAMC 100%
MEDVAMC 100%
BSLMC (ZK)
100%
BSLMC (ZK)
100%
MEDVAMC 100%
MEDVAMC 100%
PPH 100%
PPH 100%
BSLMC (JSC) 100%
BSLMC (JSC) 100%
BSLMC (VS)
100%
BSLMC (VS)
100%
MARTIN, ANGELA (PGY-6)
BSLMC (VS)
100%
BSLMC (VS)
100%
PPH 100%
PPH 100%
BSLMC (JSC) 100%
BSLMC (JSC) 100%
MEDVAMC 100%
MEDVAMC 100%
MEDVAMC 100%
MEDVAMC 100%
BSLMC (ZK)
100%
BSLMC (ZK)
100%
Note: MEDVAMC = Michael E. DeBakey VA Medical Center; BSLMC = Baylor St. Luke’s Medial Center; PPH = Park Plaza Hospital; JSC = Joseph S. Coselli, MD; ZK =
Zvonimir Krajcer, MD; VS = Vascular Surgery rotation

10
6. Conference Schedules
Objectives
The program has developed goals and objectives for each rotation and for the overall
training program which are provide to residents at orientation and via E*Value before the
start of each rotation. Residents progress through a structured educational environment
from total supervision to essentially independent function, although faculty members are
available to residents even after graduation for continued guidance and mentorship.
Completing our program will qualify the graduate to sit for the qualifying examination of
the American Board of Surgery.
During the surgery resident orientation program each year, all residents receive and are
expected to sign an educational compact that provides a detailed description of the
expectations that learners and educators should meet as members of our professional
educational community.
Please note that each Wednesday residents have protected time from 7:00 a.m. to
8:00 a.m. to attend Grand Rounds.
Conferences
The Department is dedicated to providing an excellent educational experience for
residents. We know that much learning occurs during clinical experiences, such as seeing
outpatients or performing surgeries. We also realize that didactic lectures and conferences
are also an integral part of increasing a resident’s knowledge base. Therefore, we have
set aside dedicated time for these lectures and conferences. Attendance at these meetings
is mandatory, and attendance is taken. The Wednesday morning conference time is
protected time, and the resident is relieved of clinical duties during this time to attend
these conferences.
Department of Surgery Grand Rounds
The Departmental Grand Rounds are scheduled each Wednesday morning, from
September to May of each academic year, with a combination of local faculty and
outstanding regional or national speakers. Topics include general, cardiothoracic,
vascular, pediatric, and plastic surgery. Attendance at Grand Rounds is required for all
surgical residents. Vascular conferences will start on Tuesday August 19, 2014.
The residents are required to attend and participate in the following conferences:
Vascular Ultrasound Conference
o Location: BSLMC, Cooley Building, basement level conference room C018
o Time: Weekly – Tuesday at 6:00am
Vascular Surgery Case Presentation
o Location: BSLMC, Cooley Building, basement level conference room C018
o Time: Weekly – Tuesday at 7:00am
Michael E. DeBakey Department of Surgery Grand Rounds
o Location: BCM 3rd
floor Auditorium N315
11
o Time: Weekly – Wednesday at 7:00am
Vascular Surgery Written/Oral Board Review
o Location: BSLMC, Cooley Building, basement level conference room C018
o Time: Weekly – Thursday at 6:00am
Vascular M&M/Journal Club
o Location: BSLMC, Cooley Building, basement level conference room C018
o Time: Bi-weekly – first and third Thursday of every month at 7:00am
Vascular Research Conference
o Location: BSLMC, Cooley Building, basement level conference room C018
o Time: Monthly – second Thursday of every month at 7:00am
Vascular Surgery Division Monthly Staff Meeting (Faculty only)
o Location: BSLMC, Cooley Building, basement level conference room C018
o Time: Monthly – fourth Thursday of every month at 7:00am
The responsibility of the Administrative Chief resident will shared by the two second year
resident in a six-month period. The fellow on the VA service will serve as the administrative
fellow. The responsibility of the Administrative Chief resident is to assign conferences (Basic
Science, Clinical Basic Science, and Journal Club), assign cases, prepare call schedules, and act
as a liaison to the vascular faculty as well at the residents. A vascular surgery residents, with the
exception of one on the Research rotation, need to forward their M&M cases to Division Chief’s
office before each M&M conference so that they can organize the list and prepare printouts for
the conference.
The weekly Vascular Case Presentation Conference involves clinical case scenarios to be
presented by vascular residents using PowerPoint presentations. One vascular resident is assigned
for the Case Presentation Conference each week. Each assigned vascular resident should have at
least 2 to 3 cases ready for presentation.
Here are some words of wisdom with regard to preparing PowerPoint case presentations: a) take
digital pictures frequently during operative procedures, b) download fluoroscopic images as soon
as a case is completed, and c) put together the PowerPoint presentation on the day when the case
is done. These tips will avoid potential procrastination of slide preparation until the last minute.
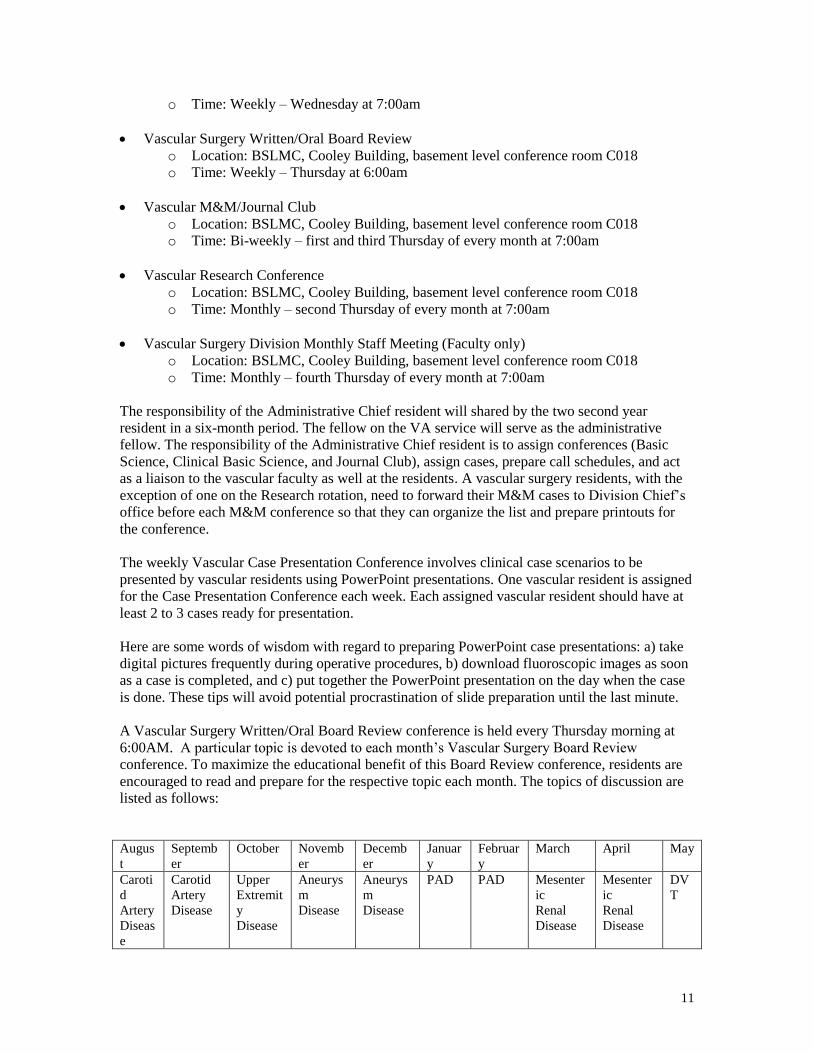
A Vascular Surgery Written/Oral Board Review conference is held every Thursday morning at
6:00AM. A particular topic is devoted to each month’s Vascular Surgery Board Review
conference. To maximize the educational benefit of this Board Review conference, residents are
encouraged to read and prepare for the respective topic each month. The topics of discussion are
listed as follows:
Augus
t
Septemb
er
October Novemb
er
Decemb
er
Januar
y
Februar
y
March April May
Caroti
d
Artery
Diseas
e
Carotid
Artery
Disease
Upper
Extremit
y
Disease
Aneurys
m
Disease
Aneurys
m
Disease
PAD PAD Mesenter
ic
Renal
Disease
Mesenter
ic
Renal
Disease
DV
T
12
All vascular surgery residents are expected to follow the following guidelines.
1. The conference starts at 7:00 am promptly and all residents are expected to arrive PRIOR
to 7:00 am. Attendance for fellows is mandatory unless out of town or operating
emergently.
2. Each fellow will be responsible for bringing at least one case in digital format and
notifying the relevant attending that it is to be presented.
3. Each case should have a brief summary of a relevant issue (literature summary, technical
tip, device description.
4. A standardized PowerPoint template will be used by all vascular surgery residents in all
conference presentations in local, regional, or national meetings.
5. All second-year residents will submit all of their PowerPoint case presentations to the
Education office prior to their graduation.
7. Basic Principles of Clinical Vascular Services
Case coverage
1. All the attendings assigned to the services should be covered
2. Cases should be prioritized. Some of the attendings have additional help ( i.e. PA’s,
postdoctoral fellows, students etc.)
3. Be aware of add-on cases
4. Dictate op note as soon as the case is finished and write the work number
5. The day is not over until the last case is done
6. Don’t leave without checking X-rays, labs etc.
7. Coverage during meetings, vacations or special cases should be assigned by the
administrative chief
8. All the beeper messages should be answered PROMPTLY
Rounds
1. Patient rounds should be done on a daily basis, regardless of type of case or post-op day,
unless a sign-off note has been written
2. ICU patients should be visited at least twice a day
3. Continuous communication with attending is emphasized
4. All incisions and wound should be checked periodically especially before discharging the
patient
5. Vital signs and labs should be checked periodically and before discharging the patient
6. You or the attending should contact as much as possible consultant physicians. This will
decrease the errors secondary to miscommunication
7. Be clear and thorough in your discharge orders (activity, shower, follow up etc) they
seem to be trivial points for us but not for the patient
13
Check Out
1. All the residents in clinical rotations should contact the resident on call to let him/her
know about patients, especially those in critical condition
2. Try to check all X-rays and labs before leaving the hospital
3. Let the resident on call know about expected patients in transfer, site of admission,
diagnosis, plans and what attending should be contacted upon arrival
Weekday Calls
1. It is divided in first call and back up call
2. It is home call
3. Call duty is from 6:00 pm to 7:00 am
4. All beeper messages should be answered promptly, the back up resident should have
his/her beeper ON and remain within hospital range
5. In all critical or questionable situations as well for transfers or new consults, the resident
on call should evaluate the cases personally
6. At the end of the shift, the resident on call should update the rest of the clinical services
residents of admissions as well as changes on their patients’ status
7. The VA fellow will take call at the VA Hospital only while on that rotation
Weekend Calls (Friday-Monday)
1. It is home call
2. Call duty is from 7:00 am to 7:00 am
3. Cases during the weekend should be covered by the resident on call
4. There will be teams of two residents (one PGY 7 and one PGY 6) to cover during the
weekend. One will be first call and the other back up. The team will round in all in-house
patients. The rest of the residents will be off.
Policy and Procedure for Time Off
To ensure that the well-being of each resident and also the facilitation of superior patient care are
maintained, a Resident Duty Hours Policy has been established and under the requirement of
ACGME compliance..
In accordance with ACGME standards, the Vascular Surgery Residency Program adheres to the
general standards relating to duty hours. Residents will work 10-12 hour days per week; with at
least one 24-hour off duty period per week, and limiting shifts to a maximum of 24 consecutive
hours. The resident will typically receive every other weekend off. Also, on-call shifts would be
no more frequent than every third night and residents would have a minimum of 10 hours off
between shifts.
With a program of this size there are clearly numerous periods when fellows will have to leave
rotations for vacation, job interviews, meetings, and personal reasons. It is clearly a matter of
courtesy, quality in patient care and efficiency in running the service to insure that the responsible
attending is made aware of planned absences from that service. The following procedures will be
instated immediately to provide for appropriate communication between fellows and the affected
service.
14
In the event of planned departures for events such as vacation, job interview, meeting, or personal
reasons, the residents must fill out “Time-Off” request to the program coordinator in the Surgery
Education office. Please also submit your request by email to a) Program Director, and b)
Program Coordinator, and c) Administrative Chief Resident. Appropriate coverage of call
schedule must be coordinated with the Administrative Chief Resident. In the case of emergency
whereby immediate departure is necessary, please contact the Program Director and
Administrative Chief Resident directly. This time off must also be documented in the duty hours
submitted to GME.
While many of you have multiple attending responsibilities, it is incumbent on us to cover as
many of the cases as are feasible. However, those fellows on the clinical vascular surgery service
should primarily provide this coverage, without pulling the fellow from the endovascular center
or the vascular laboratory. Our goal is to provide the best educational experience possible in
vascular surgery, which will likely necessitate some realignment of the services in the future.
1. Vascular Surgery will comply with resident duty hour requirements
2. Residents will not be scheduled for more than 80 hours per week, averaged over a four-
week period
3. One day in seven free of patient care responsibilities, averaged over a four-week period
4. Call no more frequently than every third night, averaged over a four-week period
5. A 24-hour limit on-call duty, with an added period of up to 6 hours for continuity and
transfer of care, educational debriefing and didactic activities; no new patients may be
accepted after 24 hours
6. A 10-hour minimum rest period will be provided between duty periods
7. When resident takes call from home and is called into the hospital, the time spent in the
hospital must be counted toward the weekly duty hour limit
Vacation Policy/Time-Off
1. Time-Off - You are allowed 21 calendar days per year (does not carry over to the next
year), three personal days (does not carry over to the next year), and 14 calendar days
paid sick time.
2. Vacation days should be scheduled one month prior to each rotation
3. If you need to change your vacation time and/or need to be off (personal, conference,
wedding, etc.), you will need to e-mail Dr. Peter Lin at [email protected] , and the Program
Coordinator of the planned absence. Please also notify the Administrative Chief resident
and the affected attending(s). Should something arise which necessitates immediate
departure, you are to notify Dr. Lin, and the Administrative Chief resident.
4. No vacation during the Annual UCLA Symposium, and the Society for Vascular Surgery
Mtg. Also, no vacation the last week of June, first two weeks of July, and the last
week of January, especially the last Friday and Saturday of January as coverage is
needed for the General Surgery ABSITE exam.
5. No two residents on the clinical services can be on vacation at the same time.
6. BCM Holidays (Labor Day, Independence Day, etc.) will be divided equally among the
five vascular surgery residents.
7. Time off is also in compliance by the American College of Surgeon and time of clinical
training.
8. Each resident’s contract period is from July 1st to June 30
th.

15
8. Graduate Medical Education House Staff Policies:
Please see the following Baylor College of Medicine website
http://intranet.bcm.edu/index.cfm?fuseaction=Policies.Policies&area=25 for complete and up to
date information about GME policies and procedures.
BCM Policies and Procedures
Graduate Medical Education
GME Leadership
25.1.1 - Administrative Structure, GMEC, Designated Institutional Official
Recruitment and Selection of House Staff;
Eligibility & Appointment Requirements
Hiring: House Staff Physicians
25.2.1 - Financial Support for House Staff Physicians
25.2.2 - Recruitment
25.2.3 - Requirements for Appointment
25.2.4 - Responsibilities of House Staff Physicians
25.2.5 - Selection of House Staff Physicians
The Program follows the Baylor College of Medicine Graduate Medical Education policies 25.2.2
and 25.2.5 regarding “Recruitment” and “Selection of House Staff.”
Recruitment
It is the policy of Baylor College of Medicine that recruitment into all graduate medical education
programs at this institution follow the guidelines of fair practice established by the National
Residency Matching Program (NRMP). This includes supplying all applicants who interview
with a sample copy of the house staff physician contract. All applicants will be treated equally.
No discrimination based on gender, age, nationality, ethnicity, religious background or sexual
preference will be tolerated.
Selection of House Staff Physicians
Selection of house staff physicians shall not be influenced by race, gender, age, religion, color,
national origin, disability, veteran status, or sexual orientation, but shall be based upon such
factors as preparedness, ability, aptitude, academic credentials, communication skills, motivation,
and integrity.
The selection of General Surgery Residents is via the NRMP Match (through ERAS). A Resident
Selection Committee is led by the Program Director and Associate Program Director to assist
them in the selection process of qualified applicants for training in General Surgery at Baylor
College of Medicine.
16
1. Applicants are eligible for appointment with one of the following qualifications:
a. Graduates of medical schools in the United States and Canada accredited by the
LCME.
b. Graduates of colleges of osteopathic medicine in the United States accredited by
the American Osteopathic Association.
c. Graduates of medical schools outside the United States and Canada who meet
one of the following qualifications:
i. Have received a valid certificate from the ECFMG.
ii. Have a full and unrestricted license to practice medicine in a U.S.
licensing jurisdiction.
d. Graduates of medical schools outside the United States who have completed a
Fifth Pathway program provided by an LCME-accredited medical school.
2. The resident applicant must apply through ERAS and the NRMP (Match) for General
Surgery.
3. The resident applicant’s application is reviewed by the Program Director and Associate
Program Director and/or their designees.
4. The resident applicant is interviewed by at least two faculty members.
5. The Program Director and Associate Program Director, with the assistance of the
Resident Selection Committee, establish the rank order of applicants for the General
Surgery Match.
6. The Program Director and Associate Program Director provide the selected applicants
with a contract for one year of training at the PGY1 level (first year of General Surgery).
7. The applicant must qualify for a Texas Educational Permit or have an active Texas
license to practice medicine.
The goal of the Resident Selection Committee is to select and match the best-qualified applicants
for the program based on factors as outlined above.
Responsibilities of House Staff:
Responsibilities and Policies: House Staff Physicians
25.3.1 - Change in Specialty or Program While Under Contract
25.3.2 - Committee Assignments
25.3.3 - Communication
25.3.4 - Disaster Response
25.3.5 - Duty Hours Policy
25.3.6 - Evaluations
25.3.7 - Grievance Procedure and Due Process
25.3.8 - Insurance / Benefits
25.3.9 - Leaves of Absence and Vacation
25.3.10 - Medical Records - Affiliated Hospitals
25.3.11 - Medical Records - BCM Owned Patient Care Facilities
25.3.12 - Moonlighting Policy
25.3.13 - Physician-Patient Relationships
25.3.14 - Prohibition of Restrictive Covenants
25.3.15 - Sexual Harassment Policy
25.3.16 - Vendor Interactions Policy
House staff physicians shall abide by BCM’s drug-free workplace policy. This policy can be
found on the BCM intranet website under “Employee Relations Substance Abuse” at
http://intranet.bcm.edu/?fuseaction=home.showpage&tmp=hr/employeerelations/subabuse.

17
Reappointment
Program Methods for Assessment & Criteria for Promotion
The Surgery Education Office and the Program Director and Associate Program Director review
the evaluations from each rotation. Problem areas are discussed further with the Surgery
Education Committee that meets approximately every two months. Problems noted are
considered and corrective actions are discussed.
Annual promotions are made contingent on satisfactory performance within the core
competencies and are decided upon by the Surgery Education Committee each January.
The following performance assessment approaches are used by the General Surgery Residency
Program to determine residents’ eligibility for advancement from one rotation to the next and
from one year/level of training to the next, as well as completion of the program and graduation:
Core competency evaluations completed by supervising faculty for each rotation,
Evaluations completed by medical students,
Self-assessment evaluations,
Direct and indirect supervision and evaluation by the Program Director and Associate
Program Director,
Semi-annual evaluations by Program Director and Associate Program Director,
National in-service examination results, and
Documented attendance at conferences.
Mechanism for Remediation and/or Disciplinary Action
Failure of a resident to meet any one of the criteria for advancement will result in the following
steps to be taken by the Program:
The Program Director and Associate Program Director will counsel the resident
regarding performance deficiency(ies), revisit the goals and objectives of the rotations
and expectations of the program, and review the resident’s overall performance in the
training program.
The Program Director and Associate Program Director will provide information to the
Surgery Education Committee for the Committee to convene and discuss the resident’s
performance and to make recommendations and plans for remedial action in writing to
the Program Director and Associate Program Director. The recommendations of the
Surgery Education Committee are based on the severity of the deficiencies and on a
majority vote (two-thirds) of the committee.
The Program Director and Associate Program Director will meet with the resident again
and provide a letter to the resident outlining the recommendations and plans for remedial
action for acknowledgment and dated signature. If the resident is not available, the letter
will be sent by certified mail (return receipt requested) to the resident’s address on file.
The Program Director and Associate Program Director will present outcomes of remedial
plans and overall performance of the resident to the Surgery Education Committee on a
monthly basis.
Appeal of Non-Reappointment

18
Please refer to the BCM intranet website as follows for detailed information regarding appeal of
non-appointment:
http://intranet.bcm.edu/index.cfm?fuseaction=Policies.Policies&area=25&expand=5
Responsibilities and Policies: Programs
25.4.1 - Completion of Training
25.4.2 - Reappointment and Promotion
25.4.3 - Record Retention
25.4.4 - Residency Closure / Reduction
Adverse Actions: House Staff Physicians
25.5.1 - Administrative Notice / Leave
25.5.2 - Adverse Actions
25.5.3 - Appeal of Adverse Actions
25.5.21 - Conduct of Adverse Actions Hearings
The Program bases the policy regarding non-reappointment on the Baylor College of Medicine
Graduate Medical Education policy 25.4.2 governing “Appeal of Non-Reappointment.”
Appeal of Non-Promotion
In the event that the Surgery Education Committee determines that a resident is not progressing
as expected, remediation (non-promotion) may be required. Remediation will be considered for
any resident that fails to achieve proficiency in any one of the six ACGME core competencies.
Residents may seek appeal of non-promotion using the Graduate Medical Education policy
“Appeal of Non-Promotion.”
Adverse Action
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.5.2 governing “Adverse Action.”
Appeal of Probation
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.5.2 governing “Appeal of Probation.”
Appeal of Dismissal
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.5.21 governing “Appeal of Dismissal.”
Grievances and Due Process
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.3.7 governing “House Staff Grievance Procedures and Due Process.”
Texas Medical Board Reporting

19
Duty to Report
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
governing “Texas Medical Board Reporting” as outlined by the Texas State Board of Medical
Examiners (www.tsbme.org).
Sexual Harassment
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.3.15 governing “Sexual Harassment.” It is the policy of Baylor College of Medicine to
provide a work environment free from sexual harassment. Any house staff physician who wishes
to report an incident of sexual harassment should contact the Director of the Office of Graduate
Medical Education (GME) (713-798-3356), the Office of Employee Relations (713-798-4346), or
a member of the BCM Committee on Prevention of Sexual Harassment.
Vendor Interaction Policy
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.3.16 governing “Vendor Interaction.”
Disaster Policy
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.3.4 governing “Disaster Response.”
Vacations and Leaves of Absence
The following are Department-specific guidelines for vacations and leaves of absence. For
additional information regarding College-wide policies, please refer to Graduate Medical
Education policy 25.3.9 on “Leaves of Absence and Vacation” via the BCM intranet.
Residents must properly complete their duty hours in compliance with any and all leaves.
Reports of duty hours will be maintained in the Surgery Education Office and must reflect any
time off including any type of leave and not limited to the following: vacation, sick,
maternity/paternity leave, etc. as noted below.
Vacation: Fourteen calendar days of vacation per year are allowed for Level I house staff
physicians (if weekends are not part of the normal work week for a house staff physician, then ten
working days are allowed). Twenty-one calendar days of vacation per year are allowed for Level
II and higher house staff (or fifteen working days if weekends are not part of the normal work
week for a house staff physician). Vacation must be taken in the year earned and may not be
carried over to subsequent years. House staff physicians will not be paid for any unused vacation.
Vacation shall not be used to shorten a house staff physician’s length of training program. The
Graduate Medical Education program shall make a good faith effort to meet house staff
physicians’ requests for vacations and shall not assign vacations arbitrarily. However, the GME
program shall have the final say in assignment of vacations and has the responsibility to assign
vacations in such a way as not to impair patient care. All vacations shall be in blocks of seven
calendar days unless both the GME program and the house staff physician agree otherwise. In
the situation of five or less vacation days contiguous with a weekend off, the weekend shall count
as vacation unless both the GME program and the house staff physician agree otherwise.

20
Personal Leave: Up to three calendar days per year are provided to all house staff physicians for
personal or family problems with the prior approval of the Program Director and Associate
Program Director or their designees. Personal days may not be appended to vacation except in
situations of urgent problems and with the approval of the Program Director and Associate
Program Director. Personal days are reserved for urgent and unexpected absences. They do not
accrue and may only be used in the academic year in which they are earned.
Educational Leave: Attendance at professional meetings as part of the educational activity of the
house staff physician will not be considered leave, unless otherwise determined by the Program
Director and Associate Program Director or their designees.
Military Leave: House staff physicians with U.S. military obligations are allowed up to 14
calendar days of unpaid military leave per year. House staff physicians whose military
obligations exceed 14 days are required to request an unpaid leave of absence. House staff
physicians called to active duty will have a residency slot when they are released from such duty,
pursuant to federal law.
Jury Duty: Paid leave will be provided for jury duty as required by law.
Family and Medical Leave Act (FMLA): A house staff physician may be eligible for job
protection under the federal Family and Medical Leave Act (FMLA) for his/her own serious
medical condition or that of a spouse, child, or parent. Other qualifying events are the birth of a
child or the house staff physician’s adoption or foster placement of a child. Job protection under
this law is a maximum of 12 weeks within a 12-month period. All requests for leave under this
law must be reported to the Offices of GME and Human Resources. Final approval shall be made
by the Human Resources Regulatory Compliance Office and the Program Director and Associate
Program Director or their designees.
In order to be eligible for FMLA, a house staff physician must have been employed by BCM for
at least 12 months (does not have to be consecutive) and have worked at least 1,250 hours during
the last 12 months prior to the start date of the leave. Absences due to illness, whether the house
staff physician’s or a family member’s, must be verified by a statement from the treating
physician. A statement is required from the court system or the involved social services agency
to confirm the foster placement or adoption of a child; a birth certificate, alone, is also acceptable
when adopting.
A house staff physician taking leave under FMLA for his/her own health condition must first use
accrued sick leave, and if necessary, may take any available paid vacation and personal leave.
Accrued vacation and paid personal leave may be taken for other types of qualifying absences.
Paid sick leave may be used only for the house staff physician’s own illness. When all paid leave
has been used, the house staff physician should contact the BCM Human Resources Department –
Benefits Center to arrange for continuation of insurance and payment of premiums during the
remaining period of authorized unpaid leave.
Further information on the Family and Medical Leave Act (FMLA) can be found on the BCM
Human Resources – Regulatory Compliance website or by calling 713/798-3114, or emailing
Unpaid Leave of Absence: A house staff physician may request and take unpaid leave of
absence for up to 12 months for personal or family problems with the approval of the Program
21
Director and Associate Program Director or their designees. Additionally, enrollment with at
least half-time status in a degree program at an institution of higher education that is related to the
house staff physician’s medical career is an acceptable reason for requesting and being approved
for leave of absence. A letter stating the purpose of the leave, arrangements made for completing
the GME program, and the mechanism for payment of medical, dental, term life, accident death
and dismemberment, and long-term disability insurance premiums and the psychiatric counseling
service benefit shall be signed by the Program Director, the Associate Program Director, and the
house staff physician with a copy kept on file in the Office of GME. If all or any part of this
leave of absence is due to illness or injury, the GME Program Director and Associate Program
Director shall require a physician’s statement. Leave under the federal Family and Medical
Leave Act may be granted in accordance with the guidelines set forth in this policy.
Sick Leave: House staff physicians are entitled to up to 14 calendar days paid sick leave per year.
Unused sick days will be carried forward and be available to the house staff physicians in each
subsequent academic year.
Sick leave may only be taken for the house staff physician’s own actual illness or bona fide
health-related issues, such as a doctor’s visit or a diagnostic or therapeutic procedure. Sick leave
may not be used as personal leave or for non-illness or non-health related issues.
In the event a house staff physician suffers from work-related illness or injury and uses all
accumulated sick leave before s/he is able to return to work, additional pay will be granted to
supplement any benefits available under workers’ compensation to bring the house staff
physician’s gross pay up to his/her current stipend level until disability insurance payments begin.
Injuries or illness will be considered work-related only when a workers’ compensation claim is
filed and approved.
Pay for non-work-related illness or injury will be limited to the house staff physician’s accrued,
but unused, sick leave. Short term disability insurance is available for purchase during Open
Enrollment and may be the only source of income for an extended illness or injury until long term
disability begins.
A treating physician’s statement, from a non-house staff physician, is necessary if the illness or
injury extends beyond three (3) consecutive calendar days. In addition, to return to work, a
statement is required from the treating physician that stipulates that the involved house staff
physician is fit to return to duty. The Senior Associate Dean for Graduate Medical Education
shall resolve any disputes regarding the house staff physician’s fitness for duty (e.g.,
disagreements between the house staff physician, Program Director and Associate Program
Director, or director of the OHP).
A house staff physician may be eligible to take sick leave under the federal Family and Medical
Leave Act.
Maternity / Paternity Leave: A house staff physician may be eligible to take maternity /
paternity leave under the federal Family and Medical Leave Act.
Makeup: It is important to understand the American Board of Surgery requirements and policies
regarding any leave. The Program Director and Associate Program Director will assist house
staff physicians in understanding certifying Board requirements for their respective programs.
Time missed for any reasons beyond that permitted by the relevant certifying Board must be
made up. All time required to be made up for GME program completion will be paid.

22
When total (cumulative) time lost for any reason exceeds that permitted by the appropriate
certifying Board, the house staff physician’s promotion to the next level of training will be
delayed by an amount equal to the time that needs to be made up. This delay supersedes any
existing letter of appointment regarding dates, year of appointment, and stipend, but does not
negate the reappointment.
For more detailed information regarding leave policy according to the American Board of
Surgery, please refer to the ABS webpage (http://www.absurgery.org/default.jsp?policygsleave).
Professionalism
The expectations and standards of professionalism that are mandated by the General Surgery
Residency Program, and their significance and implications with regard to residents’ compliance
with such standards and expectations are outlined below.
Professionalism Standards & Program Expectations
Exercise a high level of ethics, honesty and integrity in all aspects of interpersonal
relationships and patient care.
Highly professional and responsive behavior to the needs of the patient, medical professionals
and the community.
Interpersonal communication that adheres to professional courtesy and mutual respect among
residents at all levels.
Mature professional behavior: Avoidance of negativism such as gossip, stereotyping,
hostility, defamation, slander, inappropriate comments, argumentative behavior, anger and
undermining of colleagues, the Program and the organization.
Commitment to serving as a role model for resident colleagues, students, staff and
subordinates regardless of level of training.
Willingness to engage in conflict resolution with colleagues in a courteous and timely
manner.
Full commitment to sustaining work team relationships through cooperation and
collaboration with resident colleagues and other team members.
Exercise of high leadership and moral skills.
Full commitment to protect and advance the Program reputation individually and as a
member of a team.
Compliance with administrative responsibilities including call schedules, responsiveness to
pages with courtesy and professionalism, and timely response to requests for evaluations of
program and faculty.
Full compliance with the policies, rules, and regulations of the Program, Baylor College of
Medicine, and the affiliated institutions.
Professionalism Misconduct
Substandard conduct or any occurrence of professional misconduct or deviation from the
standards described above by a resident at any level will result in the following:
Immediate counseling with resident(s) involved.
Immediate investigation and disciplinary action(s), the outcome of which may be:
o Documentation of such professional misconduct in the resident’s permanent record and
reporting to state licensing agencies and the American Board of Surgery of failure to
comply with professional conduct standards of the Program;

23
o Failure to reappoint and renew contract in the Program;
o Repeat rotation(s) or year(s) of training;
o Failure to graduate in the scheduled year with reporting of such to the Board in the
professional conduct category;
o Immediate dismissal from the Program.
9. Duty Hours and the Working Environment
The Program adheres to the Baylor College of Medicine Graduate Medical Education policy
25.3.5 governing “Duty Hours.”
Baylor College of Medicine requires all graduate medical education programs to be in
compliance with the Accreditation Council for Graduate Medical Education (ACGME) duty
hours requirements, as stipulated in the Institutional, Common and Specialty-Specific Program
Requirements. Each program must have its own duty hours policy. Every BCM house staff
physician must log his/her duty hours on E*Value in a regular and timely manner. Failure to log
duty hours as expected may be viewed as a failure in professionalism, and may result in a house
staff physician being suspended from duty without pay until the logging responsibility is
completed. Program compliance with duty hours requirements and policies will be monitored
through E*Value, annual program evaluations, and the internal review process. All house staff
physicians are expected to limit their program and program-related moonlighting activities to the
maximum number of hours allowed by ACGME policy. Any disputes or other issues related to
compliance should be referred to the Senior Associate Dean for Graduate Medical Education.
BCM house staff physicians may use GME’s online anonymous form to report concerns about
duty hours compliance or may report such concerns to the GMEC Ombudsman.
The BCM GMEC does not permit programs to request an expansion or extension of duty hours
beyond the standard ACGME requirements.
Principles
1. The Michael E. DeBakey Department of Surgery General Surgery Residency Program is
committed to and responsible for promoting patient safety and resident well-being and to
providing a supportive educational environment.
2. The learning objectives of the program are not to be compromised by excessive reliance on
residents to fulfill service obligations.
3. Didactic and clinical education have priority in the allotment of the resident’s time and
energy.
4. Duty hours assignments recognize that faculty and residents collectively have responsibility
for the safety and welfare of patients.
Supervision of Residents
1. The attending physician has both an ethical and a legal responsibility for the overall care of
the individual patient and for the supervision of the resident involved in the care of that
patient.
2. Although senior residents require less direction than junior residents, even the most senior
resident must be supervised. The program should establish a chain of command that
emphasizes graded authority and increasing responsibility as experience is gained.
24
3. The attending surgeon who is ultimately responsible for the patient’s care should make
judgments on this delegation of responsibility; such judgments shall be based on the
attending surgeon’s direct observation and knowledge of each resident’s skills and ability.
4. A fellow may not supervise chief residents.
Duty Hours
1. Duty hours are defined as all clinical and academic activities related to the residency
program, i.e., patient care (both inpatient and outpatient), administrative duties related to
patient care, the provision for transfer of patient care, time spent in-house during call
activities, and scheduled academic activities such as conferences. Duty hours do not include
reading and preparation time spent away from the duty site.
2. Duty hours must be limited to 80 hours per week, averaged over a four-week period,
inclusive of all in-house activities.
3. Residents must be provided with 1 day in 7 free from all educational and clinical
responsibilities, averaged over a 4-week period, inclusive of call. One day is defined as one
continuous 24-hour period free from all clinical, educational, and administrative activities.
4. Adequate time for rest and personal activities must be provided. This should consist of a 10-
hour time period between all daily work hours and after in-house call.
Duty Hours Compliance Monitoring
The Program Director and Associate Program Director and faculty will monitor compliance with
duty hour policies by monitoring call and duty schedules, direct observation of the residents,
interviews/discussions with the residents, and review of residents’ evaluations of rotations.
Residents are instructed to notify the Program Director and Associate Program Director if they or
other residents are requested or pressured to work in excess of duty hour limitations. The
Program Director and Associate Program Director maintain an open-door policy so that any
resident with a concern can seek immediate redress. If problems are suspected, the Program
Director and Associate Program Director will gather duty hour data to clarify and to resolve the
problem (BCM Policy 25.3.5).
25
On Call Activities
The objective of on-call activities is to provide residents with continuity of patient care
experiences throughout a 24-hour period. In-house call is defined as those duty hours beyond the
normal workday when residents are required to be immediately available in the assigned
institution.
1. In-house call must occur no more frequently than every third night, averaged over a four-
week period.
2. Continuous on-site duty, including in-house call, must not exceed 24 consecutive hours.
Residents may remain on duty for up to six additional hours to participate in didactic
activities, transfer care of patients, conduct outpatient clinics, and maintain continuity of
medical and surgical care as defined in Specialty and Subspecialty Program Requirements.
3. No new patients may be accepted after 24 hours of continuous duty. A new patient is
defined as any patient for whom the surgery service or department has not previously
provided care. The resident should evaluate the patient before surgery.
4. At-home call (pager call) is defined as call taken from outside the assigned institution.
a) The frequency of at-home call is not subject to the every third night limitation, or 24+6
limitation. However, at-home call must not be so frequent as to preclude rest and
reasonable personal time for each resident.
b) Residents taking at-home call must be provided with one day in seven completely free
from all educational and clinical responsibilities, averaged over a four-week period.
c) When residents are called into the hospital from home, the hours they spend in-house
are counted toward the 80-hour limit.
Moonlighting
Because residency education is a full-time endeavor and duty-hours regulations must be adhered
to, it is the policy of the General Surgery Residency Program that moonlighting is not allowed
(BCM Policy 25.3.12).
10. Stress, Fatigue and Impairment
The Program Director and Associate Program Director and faculty realize that residency training
is a time of high stress. They will make every effort to monitor residents on their rotations for
signs of stress, fatigue, and impairment. The resident can assist on his/her own behalf by
adhering to duty-hour mandates and by communicating problems with his/her senior level
resident, faculty, or the Program Director and Associate Program Director. The program strives
to ensure that an environment conducive to communicating problems exists. It is the
responsibility of the entire department and program to be aware of signs and symptoms of these
problems.
In situations of stress, fatigue, or impairment, the faculty or resident may approach the Program
Director and Associate Program Director, or the Program Director and Associate Program
Director may themselves call a meeting with the resident. The problem will be discussed, and the
Program Director and Associate Program Director will make recommendations for resolving the
problem. Such recommendations may include use of services within Baylor College of Medicine
such as the Employee Assistance Program, or referral to a counselor or psychiatrist.

26
Signs & Symptoms of Stress, Fatigue, or Impairment
Signs and symptoms or fatigue, stress, or impairment include some of the following:
Recent changes in behavior, including irritability, mood swings, inappropriate behavior, a
breakdown in logical thought, trembling, slurred speech
Irresponsibility, such as failure to respond to calls, late arrivals at rounds or call, rounding at
irregular times, neglect of patients, incomplete charting, unexplained absences
Inaccurate or inappropriate orders or prescriptions
Insistence on personally administering patients’ analgesics or other mood-altering
medications rather than allowing nursing staff to carry out orders
Poor concentration or poor memory, such as failure to remember facts about current and/or
recent individual patients
Depression
Evidence of use or possession of alcohol or other drugs while on duty; intoxication at social
events
Anger, denial, or defensiveness when approached about an issue
Unkempt appearance and/or poor hygiene
Complaints by staff or patients
Unexplained accidents or injuries to self
Noticeable dependency on alcohol or drugs to relieve stress
Isolation from friends and peers
Financial or legal problems
Loss of interest in professional activities or social/community affairs
Attending Clinician & Supervising Resident Responsibilities
1. In the interest of patient and resident safety, the recognition that a resident is demonstrating
evidence of excess fatigue and/or stress requires the attending or supervising resident consider
immediate release of the resident from any further patient care responsibilities.
2. The attending clinician or supervising resident should privately discuss his/her opinion with
the resident, attempt to identify the reason for excess fatigue and/or stress, and estimate the
amount of rest that will be required to alleviate the situation.
3. The attending clinician should attempt to notify the chief/supervising resident on-call and/or
the Program Director and Associate Program Director of the decision to release the resident
from further patient care responsibilities at that time.
4. If excess fatigue is the issue, the attending clinician must advise the resident to rest for a
period that is adequate to relieve the fatigue before operating a motorized vehicle. This may
mean that the resident should go first to the on-call room for a sleep interval no less than 30
minutes. The resident may also be advised to consider calling someone to provide
transportation home.
5. If stress is the issue, the attending, upon privately counseling the resident, may opt to take
immediate action to alleviate the stress. If, in the opinion of the attending, the resident stress
has the potential to negatively affect patient safety, the attending must immediately release the
resident from further patient care responsibilities at that time. In the event of a decision to
release the resident from further patient care activity, notification of program administrative
personnel shall include the chief/supervising resident of the service, Program Director, and
Associate Program Director.
6. A resident who has been released from further immediate patient care because of excess
fatigue and/or stress cannot appeal the decision to the responding attending.
7. A resident who has been released from patient care cannot resume patient care duties without
permission of the Program Director and/or Associate Program Director.

27
Resident Responsibilities
1. Residents who perceive that they are manifesting signs of excess fatigue and/or stress have the
professional responsibility to immediately notify the attending clinician, the chief resident, the
Program Director, and/or Associate Program Director without fear of reprisal.
2. Residents recognizing signs of fatigue and/or stress in fellow residents should report their
observations and concerns immediately to the attending physician, the chief resident, the
Program Director, and/or Associate Program Director.
Program Director & Associate Program Director Responsibilities
1. Following removal of a resident from duty, the Program Director and Associate Program
Director will determine the need for an immediate adjustment in duty assignments for
remaining residents in the program.
2. The Program Director and Associate Program Director will review the resident’s call
schedules, work hours, extent of patient care responsibilities, any known personal problems,
and stresses contributing to these issues for the resident.
3. The Program Director and Associate Program Director will notify the Director of the rotation
in question to discuss methods to reduce resident fatigue.
4. In matters of resident stress, the Program Director and Associate Program Director will meet
with the resident personally. If counseling by the Program Director and Associate Program
Director is judged to be insufficient, the resident will be referred to appropriate professionals
for counseling.
Resources: Counseling Services for House Staff
Baylor College of Medicine, along with the Graduate Medical Education office, is committed to
providing safe, effective, timely, and respectful medical care while fostering an environment that
promotes practitioner health. Medical and graduate training programs are rewarding and exciting,
but they can also be stressful. The most common reasons for seeking counseling include
relationship difficulties, anxiety and depression. For confidential services from the House Staff
Physician Psychiatric Counseling Service, residents should call 713.798.4881 to schedule an
appointment. This number may also be used in case of emergencies. This counseling services
program serves medical students, graduate students, residents, physician assistants, nurse
anesthetist students and clinical fellows as well as their spouses and significant others.
Services Offered Individual Counseling
Premarital Counseling
Marital or Relationship Counseling
Psychopharmacology
Services are provided at no cost for up to 12 sessions and are provided by members of the faculty
in the Department of Psychiatry and Behavioral Sciences. All provided services abide by the
strictest rules of confidentiality. The service does not issue any report to administrative
personnel within your department or any others of Baylor College of Medicine.
How Will I Know I Need the House Staff Psychiatric Counseling Service?
Work Problems
o I keep thinking I’ve chosen the wrong profession.
o My work is suffering.

28
o I feel pulled in too many directions.
o My relationship with my colleagues is strained.
Depression/Anxiety
o I’m depressed much of the time.
o I’m anxious much of the time.
o I feel angry much of the time.
o I’m drinking more.
o I think I have an eating disorder.
Relationship Problems
o I am having serious doubts about my marriage or relationship.
o My partner tells me I’m retreating.
o I don’t like going home.
o My relationship gives me little pleasure.
11. Resident Responsibilities
The following document outlines various administrative responsibilities of all General Surgery
residents. Compliance with the following is mandatory. Non-compliance will weigh heavily on
assessment of the resident’s achievement in the Professionalism core competency.
FULL COMPLIANCE WITH DUTY HOUR REGULATIONS AS REQUIRED BY
THE ACGME MUST BE FOLLOWED, AND NO EXCEPTIONS WILL BE
TOLERATED.
Duty Hours
The ACMGE requires us to restrict duty hours to 80 hours per week. This rule applies to hours
dedicated to clinical activities within the hospital. The 80-hour rule does not apply to time spent
reading outside the hospital(s) or at-home call. Residents are charged with the self-reporting of
all violations on this system. Please refer to “Duty Hours and the Work Environment” policy in
the section above titled “Duty Hours and the Working Environment” for further information and
explanation of duty hours restrictions.
Our program takes this requirement very seriously and monitors work hours on a regular basis.
Recording of duty hours is ideally done on a daily basis in E*Value. Residents must record their
hours daily (not just for the week), and the record should reflect actual hours worked.
Conference Attendance
All General Surgery residents (categorical surgery and preliminary residents) are required to
attend at least 75% of the mandatory conferences in order to be eligible for promotion into the
next year. Residents will be considered absent if they are more than fifteen (15) minutes late to
any conference session.
Portfolios
The residents’ portfolios are maintained in the Surgery Education Office. Any lectures (even
five-minute case presentations), M&M presentations, case reports, letters of appreciation, special
29
projects, publications, research reports, abstracts, etc. should be placed in the portfolio. This
needs to be done frequently and as academic/research work is completed and/or presented.
Procedure Case Logs
As every resident knows, hospital privileges are earned by experience. These experiences must
be recorded to prove that they have been completed. Accuracy is a necessity. Notably, if the
experience is not recorded, it will not be considered to have been completed. Additionally, case
log reports are reviewed regularly by the ACGME Surgery Resident Review Committee (RRC).
These reviews require detailed records of resident experience in the program. Accurate case log
statistics are critical to our successful continued accreditation.
The ACGME created the Resident Case Log System to allow residents to enter surgical and
clinical case data. Cases should be entered on a weekly basis. Procedures may be entered on a
hand-held computer or other device with internet access. The Surgery Education Office will
provide residents with their individual login and password.
All residents are required to enter cases in this system on a daily basis upon completion of the
case – no exceptions.
The Program Coordinators and Program Director and Associate Program Director review reports
monthly to ensure that data entry is occurring in a timely manner.
If a resident is not in compliance upon review on a monthly basis, the resident will receive a
warning and resolution expected immediately. If not compliance at the end of the month
upon review, the resident will be placed on academic probation. If the resident continues to
be non-compliant in maintaining their operative data after warning and academic
probation, the Program Director will review with the Vice Chair and Chairman to
recommend further disciplinary action which includes dismissal from the program.
Medical Records
Residents are required to maintain up-to-date medical records in order to remain in compliance
with their contract. Delinquent records are reported to the Program Director and Associate
Program Director for follow up. Operative reports must be dictated by the responsible resident at
the time of surgery.
Certifications
All residents are required to maintain Advanced Cardiac Life Support (ACLS) status. One must
be re-certified every two years. A copy of up-to-date cards must be kept on file in the resident’s
folder as proof of certification. If the cards are current, re-certification courses are available that
require much less time commitment. If the cards have expired, one must repeat the entire course
including lectures. Courses are available throughout the year at facilities in the Texas Medical
Center.
Lines of Supervision
The Vascular Surgery Program is a hierarchical program. When multiple levels of residents are
working together as a team on a given service, it is expected that the senior level resident on the
service will be ultimately responsible for the efficient conduct of the service. This will include

30
assignment of duties to junior residents as appropriate. The senior level resident will also be
responsible for communicating with the assigned attending. The junior residents on the service
are expected to perform the duties assigned by the senior level resident and to report
appropriately to the senior level resident. The attending physician is ultimately responsible for
oversight of resident activities. In all cases, there is a designated attending physician who is
readily available for resident consultation and oversight as defined by regulatory agencies that
account for the hospital(s) and department policies. For further information regarding lines of
supervision, please refer to “Guidelines for Resident Supervision.”
Teaching is an essential component of this residency program at all levels. The following is
expected of residents in this program:
1. Residents at all levels will be responsible for the supervision and instruction of medical
students.
2. Senior residents will be responsible for the supervision and instruction of junior residents.
3. Chief residents will be responsible for the supervision and instruction of all other residents and
medical students.
4. Attendings will be responsible for the supervision and instruction of all residents in the
program and medical students rotating through the program-affiliated institutions.
Evaluations
1. Each resident will be assessed for competence in the six required core competencies as
defined by the ACGME. Evaluation of the resident’s performance will occur at the end of
each rotation using E*Value. These evaluations are available for review by the program and
the resident via E*Value, and will be placed in the resident’s file in the Surgery Education
Office (BCM Policy 25.3.6).
2. If at any time a resident’s performance is judged to be detrimental to the care of the
patient(s), action will be taken immediately to assure safety of the patient(s). A face-to-face
meeting with the resident and the attending staff from the individual institution will be
mandatory for any resident receiving an unsatisfactory (rating of 1 or 2) grade after
completion of the rotation. Residents will have a chance to voice their opinions and provide
a response to the grade at this time, as well as at a later meeting with the Program Director
and Associate Program Director if they so choose.
3. Each resident will be given the opportunity to complete a formal written evaluation of the
appropriate attending surgeon via E*Value, addressing the provision of clinical supervision
(e.g. availability, responsiveness, depth of interaction and knowledge gained). The
evaluations will be reviewed by the Program Director and Associate Program Director and
integrated into discussions with the clinical faculty. Evaluations will be completed at the
end of the resident’s rotation. The Program Director and Associate Program Director will
strive to create an atmosphere that ensures residents are comfortable completing evaluations
of attending faculty.
4. Semi-Annual Evaluations: The Program Director and Associate Program Director for the
General Surgery Residency Program will meet personally with each resident semi-annually.
These meetings will be documented in the resident’s cumulative record. Meetings between
the Program Director / Associate Program Director and an individual resident may be more
frequent in the event of specific and repeated problems or complaints against that resident.
5. Residents who are placed on probation will be notified as per the guidelines set forth by the
Graduate Medical Education Committee of Baylor College of Medicine.
31
Department Holidays
Residents are required to work and take call during the holidays as dictated by the rotation
schedule and the call schedule.
Parking
Residents are responsible for payment of parking fees. Parking at the Michael E. DeBakey
Veterans Affairs Medical Center is free. Texas Medical Center garage parking is rotation-
dependent and is arranged by the GME Office at the College. Parking in the Texas Medical
Center garages is deducted from the residents’ payroll checks.
Final Clearance Form
Graduating residents and those leaving the program (preliminary residents) must check out with
the Surgery Education Office and the Office of Graduate Medical Education to receive a diploma
or certificate. All items specified on the departmental clearance form as well as the GME
clearance form must be completed in order for the resident to receive a diploma.
12. Communication
Good communication is essential to the smooth operation of any organization and is especially
critical where patient care is involved. This section discusses communication policies that must
be followed both in and out of the clinical setting (BCM Policy 25.3.3).
Up-to-Date Contact Information
It is critical that we have your most up-to-date contact information, especially in the case of
emergency. Please communicate any changes in address, phone number, emergency contact
information, etc. to the Surgery Education Office immediately.
Pagers
Baylor College of Medicine issues pagers to residents to be used over the course of the training
program. It is considered the preferred method of immediate contact for patient care and
administrative needs. Rotation-specific pagers are required at some institutions. Pagers must be
carried at all times.
Baylor College of Medicine establishes free e-mail accounts for all residents upon entry into the
program. This account is to be used for the duration of the residency program. An address will
be assigned along with a changeable password.
Residents are required to check their email daily and respond in a timely and
appropriate manner, as email is used as a standard means to communicate information
within the department.
32
13. Travel Policy
Education Office Travel
In order to encourage legitimate research and academic efforts, the department will pay for travel
for residents to present at surgical meetings. However, to insure that the money is spent fairly and
appropriately, the department has instituted a policy concerning resident travel policy.
Which residents
are eligible for
travel
reimbursement?
All residents in the Department of Surgery, including preliminary and non-
designated preliminary residents who are first author on an oral presentation at an
approved meeting (listed in Approved Meetings section) within the continental
United States or Canada. Reimbursement for travel for poster presentations will be
limited to one trip per resident per year. If the resident is able to obtain funding
from another source for additional poster presentations, they will be given
permission to attend the meeting, but the department will not pay their expenses.
Reimbursement for expenses will be provided by the Department of Surgery up to
$1000.00.
Senior residents will be given permission to attend one approved meeting during
their PGY-4 or chief year. The expenses for this meeting will be reimbursed up to
$1000.00 if the resident has met their research publication submission requirement
(see below). Residents who have not met the research requirement will be given
permission to attend an approved meeting, but will not be eligible for travel
reimbursement.
All categorical general surgery residents are expected to submit three manuscripts
to peer reviewed journals before the start of their chief year. The submission
requirement is being phased in based on a given resident’s level of training as of
July 2013. Current PGY-1 residents are expected to submit three manuscripts,
current PGY-2 residents are expected to submit two manuscripts, and current PGY-
3 and PGY-4 residents are expected to submit one manuscript. Please see the
Resident Research Requirements section for additional details.

33
Which meetings
are eligible?
Meetings which are eligible for reimbursement are listed on the Departmental list
of approved meetings. Residents wishing to attend meetings not on the
departmental list may appeal to the Education Committee for funding.
You will be given permission to leave the day before your presentation and stay the
night after your presentation. Permission to stay additional days will be at the
discretion of the Program Director.
How to get
reimbursed
In order to obtain permission to attend the meeting and be reimbursed, the
following must occur.
Please note: There will be NO exceptions to these rules.
1. Any submitted abstract must be sent to the Surgery Education Office within
one week of submission. The easiest way to handle this is to make sure you
submit your abstract to the Surgery Education Office at the same time you
submit it to the meeting.
2. The Surgery Education Office must be notified of any abstract accepted within
a week of receipt. At the same time a signed request for travel form must be
submitted. Travel forms are available via the Surgery Education Office.
Again, the easiest way to handle this is to fax or email a copy of your
acceptance letter to the Surgery Education Office the day you receive it and
follow it within seven days with the request for travel form.
a. All expenses during the trip, including the hotel, will be paid for by the
resident. Temporary loans are available through the Surgery Education
office if needed and will be given at the discretion of the Program
Director.
b. No reimbursement for expenses will be made without receipts. Baylor
College of Medicine requires a copy of your hotel invoice (showing a
$0 balance) and your airfare invoice, credit card statement, and/or
cancelled checks for any payments made on this trip, as well as a copy
of the front cover of the program brochure (listing conference name,
location, and dates) as supporting documentation for reimbursements.
c. Expenses eligible for reimbursement include
1. shuttle service to and from airport
2. Room charges, taxes
3. Meals (see below for specific guidelines)
4. Airport parking (Remote only)
5. Airfare
6. Internet access in the room
d. The following will are NOT reimbursable expenses
1. In room movies
2. Taxis to and from the airport (if shuttles are available)
3. Mini-bar expenses
4. Entertainment expenses (other than meals), including
alcoholic beverages
5. Car rental (unless pre-approved by the Program Director)
6. Terminal airport parking
7. Office expenses at the meeting (printing posters, handouts,
etc.)

34
3. Residents will be reimbursed for meals using the same guidelines as Baylor
College of Medicine faculty (see below):
a. For trips within the United States, travelers are required to provide
meal receipts not to exceed $55 per day including tip.
b. Tips may not exceed 20% of the cost of the meal.
c. For travel beginning after 3:00 p.m., the maximum meal allowance is
½ the regular daily maximum.
d. Meals will not be reimbursed when attending a local (within a 50-mile
radius of the Texas Medical Center) conference or seminar or when
claiming local travel.
e. Itemized receipts are required for all meal reimbursements.
Approved Meetings Meetings that are eligible for reimbursement are listed below. Residents wishing to attend a meeting that is not on this list may appeal to the Education Committee for approval and potential funding. Academic Surgery, General Surgery and Regional Surgical Societies: Academic Surgical Congress American College of Surgeons Association for Surgical Education/Surgical Education Week Association of VA Surgeons Central Surgical Society Michael E. DeBakey International Surgical Society South Texas Chapter, American College of Surgeons Southern Surgical Association Southwestern Surgical Congress Texas Surgical Society Western Surgical Association Cardiothoracic Surgery: American Association for Thoracic Surgery American College of Cardiology American College of Chest Physicians American Heart Association International Society for Minimally Invasive Cardiothoracic Surgery Society of Thoracic Surgeons Southern Thoracic Surgical Association Western Thoracic Surgical Association GI, Endocrine Surgery, Surgical Oncology and Transplantation: American Association of Endocrine Surgeons American Cancer Society American Society for Gastrointestinal Endoscopic Surgery American Society of Clinical Oncology (including GI and breast symposia) American Society of Colon and Rectal Surgeons American Transplant Congress Americas Hepato-Pancreato-Biliary Association Digestive Disease Week International Society of Geriatric Oncology (SIOG) Society for Surgery of the Alimentary Tract Society of American Gastrointestinal and Endoscopic Surgeons Society of Surgical Oncology
35
Pediatric Surgery: American Academy of Pediatrics - Surgical Section American Pediatric Surgical Association American Society of Parenteral and Enteral Nutrition Pacific Pediatric Surgical Association Texas Society of Pediatric Surgeons Trauma, Acute Care Surgery and Critical Care: American Trauma Society American Association for the Surgery of Trauma Eastern Association for the Surgery of Trauma Society for Academic Emergency Medicine Society of Critical Care Medicine Surgical Infection Society Western Trauma Society Vascular Surgery: Arteriosclerosis, Thrombosis and Vascular Biology Vascular and Endovascular Surgery Society Society for Clinical Vascular Surgery Southern Association for Vascular Surgery Vascular Annual Meeting (Society for Vascular Surgery)
14. Guidelines for Resident Supervision
The purpose of this section of the handbook is to outline the policy and procedure requirements
for supervision of postgraduate residents within the Department of Surgery.
Definition of Attending Physician
Each patient will be under the direct care of an attending physician, and this will be clearly noted
on the patient’s admission card and paperwork. Residents work under the direct supervision of
the attending physicians. Attending physician refers to those surgeons who staff the teaching
service at each of the affiliated hospitals. Each surgeon must be Board eligible/certified in
vascular surgery or an appropriate subspecialty, and must show interest in participating in the
education of residents. Furthermore, surgeons on the teaching service must exhibit regular
contribution to the education of the residents to maintain their status on the teaching service.
Lines of Supervision
The attending physician is ultimately responsible for the care of all patients on his/her service.
Residents participate in this care under the direction of the attending. The attending physician
controls resident participation through observation and direction, or consultation, and by
imparting specific skills and knowledge to the resident. Attending supervision may be direct
(person-to-person) supervision or through discussion, for example by telephone. At all times
there will be an appropriately privileged attending surgeon immediately available to the resident
or by telephone and able to be present within a reasonable period of time, if needed. The
attending surgeons are responsible to assure continuity of care provided to patients.
It is recognized that other attending physicians may, at times, be delegated responsibility for the
care of a patient and provide supervision instead of, or in addition to, the assigned attending
surgeon. Within the scope of the training program, all residents, without exception, will function

36
under the supervision of attending surgeons. A responsible attending must be immediately
available to the resident in person or by telephone and able to be present within a reasonable
period of time, if needed. Each service will publish, and make available, “call schedules”
indicating the responsible staff practitioner(s) to be contacted.
Graduated Responsibility in Resident Training
The surgery residency program is structured to encourage and permit residents to assume
increasing levels of responsibility commensurate with their individual progress in experience,
skill, knowledge, and judgment throughout the course of their training. Each facility must adhere
to current accreditation requirements as set forth by Baylor College of Medicine for all matter
pertaining to the training program including the level of supervision provided. The requirements
of the American Board of Surgery and the ACGME will be incorporated into training programs to
ensure that each successful program graduate will be eligible to sit for a certifying examination.
Roles & Responsibilities:
The Department Chair, Program Director, & Associate Program Director
The Department Chair, Program Director, and Associate Program Director are responsible
for implementation of and compliance with the requirements of the American Board of Surgery
and the ACGME.
Roles & Responsibilities: The Attending Surgeon
The Attending Surgeon is responsible for, and must be familiar with, the care provided to the
patient as exemplified by the following:
1. Direct the care of the patient and provide the appropriate level of supervision based on the
nature of the patient’s condition, the likelihood of major changes in the management plan,
the complexity of care, and the experience and judgment of the resident being supervised.
Documentation of this supervision will be via progress notes, or countersignature of or
reflected within the resident’s progress note at a frequency appropriate to the patient’s
condition. In all cases where the provision of supervision is reflected within the resident’s
progress note, the note shall include the name of the attending surgeon with whom the case
was discussed and the nature of that discussion.
2. Meet the patient early in the course of care (for inpatients, within 24 hours of admission) and
document, in a progress note, concurrence with the resident’s initial diagnoses and treatment
plan. At a minimum, the progress note must state such concurrence and be properly signed
and dated. If a patient is admitted during the weekend or holiday for non-emergent care, a
senior resident may evaluate the patient and discuss the patient’s circumstances via
telephone with an appropriate attending surgeon. This discussion will be documented in the
patient record. An attending physician will then see the patient within 24 hours, since there
will always be an attending making rounds with the surgical team (residents and students) on
weekends and holidays.
3. Participate in attending rounds. Participation in bedside rounds does not require that the
attending surgeon see every patient in person each day. It does require physical presence of
the attending in the facility for sufficient time to provide appropriate supervision of
residents. A variety of face-to-face interactions such as chart rounds, x-ray review sessions,
pre-operative reviews, and informal patient discussions fulfill this requirement.
37
4. Assure that all technically complex diagnostic and therapeutic procedures which carry a
significant risk to the patient are:
a) Medically indicated,
b) Fully explained to the patient,
c) Properly executed,
d) Correctly interpreted, and
e) Evaluated for appropriateness, effectiveness, and required follow up.
Evidence of this assurance will be documented in the patient’s record via the progress
note(s), or through countersignature of the resident’s progress note(s).
5. Assure that discharge, or transfer, of the patient from an integrated or affiliated hospital or
clinic is appropriate based on the specific circumstances of the patient’s diagnoses and
treatment. The patient will be provided appropriate information regarding prescribed
therapeutic regimen, including specifics on physical activity, medications, diet, functional
status, and follow-up plans. At a minimum, evidence of this assurance will be documented
by countersignature of the hospital discharge summary or clinic discharge note.
6. Assure that residents are given the opportunity to contribute to discussions in committees
where decisions being made affect their activities. Facilities are encouraged, to the extent
practicable, to include resident representation on committees such as Medical Records,
Quality Assurance, Utilization Review, Infection Control, Surgical Case Review, and
Pharmacy and Therapeutics.
Graduated Levels of Responsibility
1. Residents, as part of their training program, may be given progressive responsibility for the
care of their patients. A senior level resident may act as a teaching assistant to less
experienced residents. Assignment of the level of responsibility must be commensurate with
the resident’s acquisition of knowledge and development of judgment and skill, and
consistent with the requirements of the accrediting body.
2. Based on the attending surgeon’s assessment of a resident’s knowledge, skill, experience and
judgment, the resident may be assigned graduated levels of responsibility to:
a) Perform procedures or conduct activities without a supervisor present; and/or
b) Act as a teaching assistant to less experienced residents.
3. The determination of a resident’s ability to accept responsibility for performing procedures
or activities without a supervisor present and/or act as a teaching assistant will be based on
evidence of the resident’s clinical experience, judgment, knowledge, and technical skill.
Such evidence may be obtained from evaluations by attending surgeons or the Program
Director and Associate Program Director, and/or other clinical practice information.
When a resident is acting as teaching assistant, the staff practitioner remains responsible for the
quality of care of the patient, providing supervision and meeting medical record documentation
requirements as defined previously.
Supervision of Residents Performing Invasive Procedures or
Surgical Operations

38
1. Diagnostic or therapeutic invasive procedures or surgical operations, with significant risk to
patients, require a high level of expertise in their performance and interpretation. Such
procedures may be performed only by residents who possess the required knowledge, skill
and judgment to perform these procedures under the appropriate level of supervision by staff
physicians. Attending surgeons will be responsible for authorizing the performance of such
invasive procedures or surgical operations. The name of the attending surgeon performing
and/or directing the performance of a procedure should appear on the informed consent
form.
2. During the performance of such procedures or operations, an attending surgeon will provide
an appropriate level of supervision. Determination of this level of supervision is generally
left to the discretion of the attending surgeon and is a function of the experience and
competence of the resident, and of the complexity of the specific case.
3. Attending surgeons will provide appropriate supervision for the evaluation of patients, the
scheduling of cases, and the assignment of priority, pre-operative preparations, and the
operative/procedural and post-operative care of patients.
Emergency Situations
An emergency is defined as a situation where immediate care is necessary to preserve the life of
or prevent serious impairment of the health of a patient. In such situations, any resident, assisted
by medical center personnel, shall be permitted to do everything possible to save the life of a
patient or to save a patient from serious harm. The appropriate attending surgeon will be
contacted and apprised of the situation as soon as possible. The resident will document the nature
of this discussion in the patient’s record.
15. Resident Research Requirements
Although not all surgeons need to be trained to be independent researchers, understanding the
basics of research is a core competency for all practicing surgeons. Therefore, our training
program has developed a program to provide opportunities for residents to learn the fundamentals
of research. Additionally, the department will provide mentorship and resources to optimize
resident participation in research projects. For example, junior residents will be matched with
research resident mentors and guided in selecting faculty mentors. Further, residents will have
access to a core of departmental experts in education, clinical study design and analysis, and
scientific writing.
The manuscripts should be original research articles, review articles, or case reports, and should
be submitted to established academic journals. Residents may be the first author or a co-author, as
appropriate; manuscripts should comply with standard guidelines for authorship
(http://www.icmje.org/ethical_1author.html). Submissions falling outside of these parameters will
need to be approved by the Vice Chair for Research to qualify toward the overall requirement.
During the semi-annual review with the Program Director, residents will review their research
productivity.
Residents are required to submit a copy of all abstracts, manuscript submissions, presentations
(PowerPoint slides or poster) to the Program Director and the Vice Chair for Research. All
resident research activities will be compiled by the Vice Chair for Research and will be submitted
to the Chair and the Education committee as an annual report.
16. Dress Code
39
It is important that proper and professional personal appearance is maintained at all times since
each vascular surgery resident represents the Baylor vascular surgery program. Dress codes are
standard in most business-related environments and promote an organization’s public
image, encourage a productive work environment, and ensure compliance with health and safety
standards.
The following apply to all institutions where vascular surgery residents may be working.
White coats will be clean: blood stains, coffee stains, dirt, tears, etc are not acceptable.
Scrubs must be changed before leaving the OR area if splattered with blood (check
bottom of pants).
Denim jeans (standard Levis, etc.) are never acceptable unless in an emergency.
Shoes cannot be blood spattered: get dark OR shoes or wear shoe covers. We suggest
keeping a second or separate pair of shoes in the call room or in a locker for when not in
the OR.
When we have dinners with visiting Professors, a shirt and tie is required for men and
business attire for women (skirt, dress, or pants suit; no midriff tops that show skin and
no excessively short skirts).
A well-groomed, appearance is always important and appropriate. Our competence may be
judged by how well we can take care of ourselves. Remember, how we appear is very important
in how you are perceived- by both us and everyone else you interact with.
40
17. Goals and Objectives of Vascular Surgery Rotation (BSLMC)
VASCULAR SURGERY ROTATION – BAYLOR ST. LUKE’S MEDICAL CENTER
(BSLMC)
Duration 6 months (PGY-6), 3 months (PGY-7)
Supervising Faculty Peter Lin, MD
Location BSLMC
Level of Resident PGY-6, PGY-7
Goals:
Following completion of vascular surgery training on clinical services, the vascular surgery
resident is expected to have achieved a broad base of knowledge and skills concerning the
preoperative, operative, and postoperative care of the general vascular surgery patients with aortic
pathologies. The resident is to be competent and knowledgeable in the indications and the
technical skills to carry out the procedures requiring traditional open and catheter-based
technology.
Objectives:
To learn the principles of the radiation physics and apply this knowledge to the use of
protection and exposure during angiographic examinations.
To be able to perform angiographic examinations and learn basic (PGY6) and advanced
(PGY7) catheter and guide- wired techniques.
To learn the indications for any complications of the angiographic procedures enabling them
to order appropriate procedures.
To acquire proficiency in the operative management of complex endovascular operations,
including peripheral and carotid angioplasty (including the use of neuroprotection),
mechanical thrombectomy, atherectomy and to be familiar with the various types of
angioplasty and stent devices and to be able to apply them in an appropriate indicated clinical
situations.
To participate either as an assistant or surgeon in thoracic and abdominal endovascular
procedures.
To attend regular scheduled conferences and present selected topics demonstrating
knowledge of various endovascular procedures.
Patient Care
Round with the assigned general surgery residents on the ICU and floor (endovascular)
patients
Communicate after rounds with the attendings(s)
Round on ICU patients
Admit vascular patients for the attending
Communicate immediately any changes in vascular patient status with the attending(s)
Sign out any major issues pending labs/ major tests to on-call intern
View all imaging studies
Ensure weekend coverage and sign out

41
Participates in all aspects of patient care, pre-op, post-op, surgical procedures, endovascular
cases, and clinic
Non-invasive vascular laboratory:
Understand the role and relevance of noninvasive vascular testing in the diagnosis and
treatment of vascular disease
Review of Doppler and ultrasound technology
Hands on performance of arterial and venous studies
Interpretation of results of arterial and venous vascular studies
Weekly practical and didactic conference with case presentations
Preparation for taking the RVT examination
Differentiate between normal and abnormal Duplex and physiologic test findings
Relate examination findings to the underlying anatomic/physiologic and hemodynamic
changes attributable to vascular disease
Use recommended interpretation criteria, understanding the varying strengths and limitations
of each test modality
Understand the important elements of composing and generating formal preliminary and final
reports
Understand the importance of Quality Assurance in the Vascular Laboratory
Duplex procedure guidance
Understand the role of Duplex imaging in guiding access to the arterial and venous system.
Utilize ultrasound for guiding catheter positioning during radiofrequency or laser ablation of
the saphenous vein.
Medical Knowledge
Demonstrate established and evolving medical knowledge in anatomy, physiology, and
pathology and a wide variety of vascular diseases, including arterial, venous and lymphatic
systems.
Requirements include a level of proficiency approved by the Association of Program
Directors in Vascular Surgery and two national vascular societies (Journal of Vascular
Surgery 29:177-186, 1999). Completion of this RRC requirement will be supervised by the
vascular surgical faculty.
Interpersonal and Communication Skills
Apply interpersonal skills in a team environment composed of peers, nurses, students, staff
and supervising faculty; listen and communicate effectively with patients and families
Professionalism
Practice with high standards of ethical principles in clinical care, patient confidentiality
Demonstrate progressively mature behavior and leadership skills; accept constructive
criticism
Respond to the needs of the patient and the medical and professional community
Practice-Based Learning and Improvement
Demonstrate practice-based learning, especially in basic and advanced endovascular surgical
procedures, emergency procedures and perioperative care of the vascular surgery patient;
demonstrate commitment to improving patient care
42
Systems-Base Learning
Apply knowledge to practice cost effective quality patient care
Understand the various health care systems and their relationship to managed care in a
hospital setting
Scholarly Activity
Engage in discussion and participate in case presentations at educational conferences
Supervisory Lines of Responsibility
All vascular surgery patient evaluations are discussed with an attending before clinical care
decisions are made. In addition, the house staff and fellows perform open and endovascular
surgery cases under the direct supervision of an attending.

43
Goals and Objectives of Vascular Surgery Rotation (PPH)
VASCULAR SURGERY ROTATION – PARK PLAZA HOSPITAL (PPH)
Duration 2 months (PGY-6), 3 months (PGY-7)
Supervising Faculty Peter Lin, MD
Location PPH
Level of Residents PGY-6 & PGY-7
Goals:
Following completion of vascular surgery training on clinical services, the vascular surgery
resident is expected to have achieved a broad base of knowledge and skills concerning the
preoperative, operative, and postoperative care of the general vascular surgery patients. The
resident is to be competent and knowledgeable in the indications and the technical skills to carry
out the procedures requiring traditional open and catheter-based technology.
Objectives:
To learn the principles of the radiation physics and apply this knowledge to the use of
protection and exposure during angiographic examinations.
To be able to perform angiographic examinations and learn basic (PGY6) and advanced
(PGY7) catheter and guide- wired techniques.
To learn the indications for any complications of the angiographic procedures enabling them
to order appropriate procedures.
To acquire proficiency in the operative management of complex endovascular operations,
including peripheral and carotid angioplasty (including the use of neuroprotection),
mechanical thrombectomy, atherectomy and to be familiar with the various types of
angioplasty and stent devices and to be able to apply them in an appropriate indicated clinical
situations.
To participate either as an assistant or surgeon in thoracic and abdominal endovascular
procedures.
To attend regular scheduled conferences and present selected topics demonstrating
knowledge of various endovascular procedures.
Patient Care
Round with the assigned general surgery residents on the ICU and floor (endovascular)
patients
Communicate after rounds with the attendings(s)
Round on ICU patients
Admit vascular patients for the attending
Communicate immediately any changes in vascular patient status with the attending(s)
Sign out any major issues pending labs/ major tests to on-call intern
View all imaging studies
Ensure weekend coverage and sign out
Participates in all aspects of patient care, pre-op, post-op, surgical procedures, endovascular
cases, and clinic
Non-invasive vascular laboratory:
44
Understand the role and relevance of noninvasive vascular testing in the diagnosis and
treatment of vascular disease
Review of Doppler and ultrasound technology
Hands on performance of arterial and venous studies
Interpretation of results of arterial and venous vascular studies
Weekly practical and didactic conference with case presentations
Preparation for taking the RVT examination
Differentiate between normal and abnormal Duplex and physiologic test findings
Relate examination findings to the underlying anatomic/physiologic and hemodynamic
changes attributable to vascular disease
Use recommended interpretation criteria, understanding the varying strengths and limitations
of each test modality
Understand the important elements of composing and generating formal preliminary and final
reports
Understand the importance of Quality Assurance in the Vascular Laboratory
Duplex procedure guidance
Understand the role of Duplex imaging in guiding access to the arterial and venous system.
Utilize ultrasound for guiding catheter positioning during radiofrequency or laser ablation of
the saphenous vein.
Medical Knowledge
Demonstrate established and evolving medical knowledge in anatomy, physiology, and
pathology and a wide variety of vascular diseases, including arterial, venous and lymphatic
systems.
Requirements include a level of proficiency approved by the Association of Program
Directors in Vascular Surgery and two national vascular societies (Journal of Vascular
Surgery 29:177-186, 1999). Completion of this RRC requirement will be supervised by the
vascular surgical faculty.
Interpersonal and Communication Skills
Apply interpersonal skills in a team environment composed of peers, nurses, students, staff
and supervising faculty; listen and communicate effectively with patients and families
Professionalism
Practice with high standards of ethical principles in clinical care, patient confidentiality
Demonstrate progressively mature behavior and leadership skills; accept constructive
criticism
Respond to the needs of the patient and the medical and professional community
Practice-Based Learning and Improvement
Demonstrate practice-based learning, especially in basic and advanced endovascular surgical
procedures, emergency procedures and perioperative care of the vascular surgery patient;
demonstrate commitment to improving patient care
Systems-Base Learning
Apply knowledge to practice cost effective quality patient care
Understand the various health care systems and their relationship to managed care in a
hospital setting

45
Scholarly Activity
Engage in discussion and participate in case presentations at educational conferences
Supervisory Lines of Responsibility
All vascular surgery patient evaluations are discussed with an attending before clinical care
decisions are made. In addition, the house staff and fellows perform open and endovascular
surgery cases under the direct supervision of an attending.

46
Goals and Objectives of Vascular Surgery Rotation (MEDVAMC)
VASCULAR SURGERY ROTATION – MICHAEL E. DEBAKEY VA MEDICAL CENTER
(MEDVAMC)
Duration 4 months (PGY 6), 6 months (PGY 7)
Supervising Faculty Panos Kougias, MD
Location MEDVAMC
Level of Residents PGY-6 & PGY-7
Goals:
Following completion of vascular surgery training on clinical services at the VAMC, the vascular
surgery resident is expected to have achieved a broad base of knowledge and skills concerning
the preoperative, operative, and postoperative care of the general vascular surgery patient. The
resident is to be competent and knowledgeable in the indications and the technical skills to carry
out the procedures requiring basic and advanced catheter-based technology.
Objectives:
To learn the principles of the radiation physics and apply this knowledge to the use of
protection and exposure during angiographic examinations.
To be able to perform angiographic examinations and learn basic (PGY6) and advanced
(PGY7) catheter and guide- wired techniques.
To learn the indications for any complications of the angiographic procedures enabling them
to order appropriate procedures.
To acquire proficiency in the operative management of complex endovascular operations,
including peripheral and carotid angioplasty (including the use of neuroprotection),
mechanical thrombectomy, atherectomy and to be familiar with the various types of
angioplasty and stent devices and to be able to apply them in an appropriate indicated clinical
situations.
To participate either as an assistant or surgeon in thoracic and abdominal endovascular
procedures.
To attend regular scheduled conferences and present selected topics demonstrating
knowledge of various endovascular procedures.
Patient Care
Round with the assigned general surgery residents on the ICU and floor (endovascular)
patients
Communicate after rounds with the attendings(s)
Round on ICU patients
Admit vascular patients for the attending
Communicate immediately any changes in vascular patient status with the attending(s)
Sign out any major issues pending labs/ major tests to on-call intern
View all imaging studies
Ensure weekend coverage and sign out

47
Participates in all aspects of patient care, pre-op, post-op, surgical procedures, endovascular
cases, and clinic
Non-invasive vascular laboratory:
Understand the role and relevance of noninvasive vascular testing in the diagnosis and
treatment of vascular disease
Review of Doppler and ultrasound technology
Hands on performance of arterial and venous studies
Interpretation of results of arterial and venous vascular studies
Weekly practical and didactic conference with case presentations
Preparation for taking the RVT examination
Differentiate between normal and abnormal Duplex and physiologic test findings
Relate examination findings to the underlying anatomic/physiologic and hemodynamic
changes attributable to vascular disease
Use recommended interpretation criteria, understanding the varying strengths and limitations
of each test modality
Understand the important elements of composing and generating formal preliminary and final
reports
Understand the importance of Quality Assurance in the Vascular Laboratory
Duplex procedure guidance
Understand the role of Duplex imaging in guiding access to the arterial and venous system.
Utilize ultrasound for guiding catheter positioning during radiofrequency or laser ablation of
the saphenous vein.
Medical Knowledge
Demonstrate established and evolving medical knowledge in anatomy, physiology, and
pathology and a wide variety of vascular diseases, including arterial, venous and lymphatic
systems.
Requirements include a level of proficiency approved by the Association of Program
Directors in Vascular Surgery and two national vascular societies (Journal of Vascular
Surgery 29:177-186, 1999). Completion of this RRC requirement will be supervised by the
vascular surgical faculty.
Interpersonal and Communication Skills
Apply interpersonal skills in a team environment composed of peers, nurses, students, staff
and supervising faculty; listen and communicate effectively with patients and families
Professionalism
Practice with high standards of ethical principles in clinical care, patient confidentiality
Demonstrate progressively mature behavior and leadership skills; accept constructive
criticism
Respond to the needs of the patient and the medical and professional community
Practice-Based Learning and Improvement
Demonstrate practice-based learning, especially in basic and advanced endovascular surgical
procedures, emergency procedures and
perioperative care of the vascular surgery patient; demonstrate commitment to improving
patient care

48
Systems-Base Learning
Apply knowledge to practice cost effective quality patient care
Understand the various health care systems and their relationship to managed care in a
hospital setting
Scholarly Activity
Engage in discussion and participate in case presentations at educational conferences
Supervisory Lines of Responsibility
All vascular surgery patient evaluations are discussed with an attending before clinical care
decisions are made. In addition, the house staff and fellows perform open and endovascular
surgery cases under the direct supervision of an attending.
49
Appendix 1 - Department of Surgery - Resident Travel Request Form
This form must be competed and approved by the Surgery Education Office prior to any
travel arrangements being made. Once the travel request is approved, the Chief of
General Surgery at the hospital where the resident will be assigned during the time of the
meeting, will be provided a copy of this approved form.
Name of traveler:
_____________________________________________________________________________
Name of event:
_____________________________________________________________________________
City/State: ______________________________________________________________
Date(s) of event:
_____________________________________________________________________________
Date(s) of travel:
_____________________________________________________________________________
I have read the Department of Surgery Resident Travel Policy and agree with the conditions.
____________________________________________________________________________________
Resident Signature Date
The above travel request is approved.
___________________________________________________________________________________
Approver Signature (Program Director) Date
Travel Expense Estimate (To Be Completed by Traveler):
Airfare:
Hotel:
Registration:
Meals:
Parking:
Shuttle:
Misc (Please explain):
Total:

50
Appendix 2 - Time-Off Request Form
Time-Off Request Form
Use this form to request time off or change schedule
All time-off request forms are to be submitted one month before the rotation.
Please complete and return to the Vascular Surgery Program Coordinator
You will be notified of approval or disapproval.
Name
Institution
Date submitted
Date(s) requesting off
Reason for time off X
Requestor’s signature
Office Use Only
Approved Disapproved
X
Faculty Signature
51
Appendix 3 – Educational Compact Michael E. DeBakey Department of
Surgery Compact between Teachers, Learners, and Educational Staff
Learners pursuing a professional career at Baylor assume responsibility to develop in-depth knowledge,
acquire and apply special skills, and demonstrate professionalism. Teachers guide and educate learners, and
model appropriate attitudes, interpersonal skills and
professional behaviors. Core educational staff members support both learners and teachers. This Compact serves
both as a pledge and a
reminder to teachers, learners, and educational staff that moral, ethical, and professional behavior by all BCM
personnel is essential to the basic principles of this institution.
Guiding Principles of the Educational
Compact
Duty All participants in the education mission have the duty to sustain a learning
environment
conducive to maintaining the knowledge, attitudes, and skills necessary for
providing contemporary standards of professional behavior.
Integrity All education participants/parties will behave in a manner
that reflects individual and institutional commitment to
intellectual and moral excellence.
Respect Fundamental to the ethic of professions is respect for every individual. Mutual respect between learners, as newer members of the profession, and their teachers, as experienced professionals, is essential for nurturing that ethic. In addition to individual respect, all educational parties must respect and follow established professional policies.
As a teacher, I pledge to: • Maintain currency in my professional knowledge and skills • Ensure excellence of the educational curriculum • Be a model of professionalism in all of my interactions with faculty, learners, patients, colleagues, and staff • Respect all faculty, learners, patients, colleagues, and staff as individuals, without
regard to gender, age, race, national origin, religion, or sexual orientation; and oppose observed disrespect or bias
• Nurture learner commitment to achieve personal, family, and professional balance
• Recognize and acknowledge expressions of professional attitudes and behaviors as well as the achievement of quantifiable academic excellence
• Respond vigorously to unprofessional behavior and indications of abuse or exploitation of faculty, learners, patients, colleagues, or staff
• Create a safe environment inwhich individuals can communicate any concern about breaches of this compact • Accept responsibility for instilling these attributes in learners and faculty for whom I have responsibility

52
As a learner, Ipledge to: • Acquire the knowledge, skills, attitudes, and behaviors necessary to fulfill all established educational objectives • Embody the professional virtues of integrity, empathy, altruism,
compassion, respect, honesty, courage, and trustworthiness • Respect as individuals, without regard to gender, race, national origin, religion, or
sexual orientation, all patients, peers, faculty, and staff • Uphold the highest professional standards and conduct myself accordingly in all
interactions with patients, peers, faculty, and staff • Assist my fellow learners in meeting their professional obligations, while
fulfilling my own obligations as a professional • Help create a safe environment in which individuals can communicate any concern about breaches of this compact
As an educational staff member, I pledge to: • Maintain currency in my professional knowledge and skills • Help ensure excellence of the educational curriculum • Embody professionalism in all of my interactions with faculty, learners, patients, colleagues, and staff • Respect all faculty, learners, patients, colleagues, and staff as individuals, without
regard, to gender, age, race, national origin, religion, or sexual orientation; and oppose observed disrespect or bias
• Help create a safe environment inwhich faculty, learners, and staff can work and can communicate any concern about breaches of this compact
We gratefully acknowledge the inspiration for this Compact provided by Jordan J. Cohen, M.D., President of the Association of American Medical Colleges through his "Compact between Faculty and Learners," published November 4, 2001.
53
Michael E. DeBakey Department of Surgery Vascular Surgery Residency Program Graduate Medical Trainee Guidelines
RESIDENT NAME:
Please initial on each line and sign the last page.
The term of my employment is for one year, from 7/1/2014 through 6/30/2015.
I understand that I am expected to maintain the highest ethical and moral character at all times.
I will be responsible for my professional work to the Program Director.
I will check and read my BCM e-mail daily with the understanding
that there may be important communications that need my attention.
I agree to stay current in procedural and administrative tasks, particularly
completing medical records in a timely manner, submitting QA and M&M
documentation, and maintaining up-to-date health assessments as these are
a reflection of my professionalism as a physician.
I agree to complete medical records and all documentation requested by
all program-affiliated hospitals promptly and in accordance with the policies
and recommendations of the program.
I will be responsible for developing a personal program of self-study and
professional growth, and I will seek the assistance and supervision of the
teaching staff of the Michael E. DeBakey Department of Surgery and its
affiliated hospitals in meeting these goals and expectations.
I have read and understand the Overall Competency-Based Goals and
Objectives for the Vascular Surgery
Residency Program.
I will read the competency-based goals and objectives pertinent to each
clinical rotation at the start of each rotation and review these objectives as well
as expectations and responsibilities with the Rotation Director.
I will participate fully in the clinical and educational activities of the Residency
Program and affiliated hospitals, and especially in those relating to quality
management, patient care review activities, and the appropriate use of
resources.
I will round twice daily on all inpatients with members of the surgical team of
which I am a part.
54
I will attend, and actively and meaningfully participate in the mandatory
weekly Conferences and other teaching conferences, including Surgical Grand
Rounds, all of which are intended to benefit my education. I commit to
attending and signing in to at least 75% of each conference’s session for the
academic year, understanding that bona fide vacation or active on-call
responsibilities are the sole reasons excusing participation from these activities.
I will complete the weekly reading and study assignments pertinent to the
Curriculum Didactic
Conferences and to the cases presented at the weekly M&M Conference which I attend.
I will (co-)facilitate the Resident Curriculum Didactic Conferences under
the guidance of attending faculty moderators as assigned.
I understand that unexcused absences from Surgical Grand Rounds, M&M, and
Conferences, and from other teaching conferences and activities will adversely
affect my promotion through the program.
I understand that I may be subject to weekly testing, coincident with my core
curriculum reading assignments. My performance on these examinations will
demonstrate my commitment to learning and to becoming a competent surgeon.
I understand the research and scholarly expectations that I must meet over the
course of residency training, specifically that I must submit manuscripts to
peer-reviewed journals as outlined by the travel and research policy of the
Department.
I will assume an appropriate level of responsibility for teaching and
supervising other residents and medical students.
I understand that I must have a passing score on the V S ITE for Vascular
Surgery. I understand that I will be placed on remediation and/or academic
warning. The Program Director and core educational faculty will discuss
strategies for a remediation plan to help improve my scores and performance.
I understand that I must be ACLS o r /and ATLS certified of the academic
year listed above and remain current in my certification status thereafter.
I understand that it is my responsibility to ensure that my pager is operable
at all times, and that I must respond appropriately and in a timely manner to
my pages.
I understand that my surgical rotations may take place at any of the
hospitals affiliated with the residency program, or at other defined
55
hospitals, at the discretion of the Program Director, as they provide
comprehensive educational experiences deemed consistent with the educational
mission of the Program.
Commensurate with my level of training and advancement, I will
participate in safe, compassionate, and effective patient care under general
supervision as determined by the Program Director.
I will be prepared to participate in the operating room by having a
thorough knowledge of the patient’s history, of the pathophysiology of the
disease, and of technical aspects of the procedure.
I will keep my operative log up to date.
[https://www.acgme.org/ResidentDataCollectionNet/ACGME/
ResidentCaseLogs/Login.aspx]
I will endeavor to develop an understanding of ethical, socioeconomic, and
medical/legal issues affecting medical care and practice, as well as to utilize
review measures in the provision of patient care.
I understand that I am expected to deal with patients and their families as if they
were my own.
I understand that I must accept and deal with authority appropriately.
I understand that I must demonstrate genuine dependability, good clinical
judgment, and the ability to interact in a professional manner with attending
staff, nursing staff, mid-level and ancillary medical practitioners, as well as with
fellows, resident colleagues, and students.
I understand that I must use all my vacation time in the current academic year
as vacation time is not carried over to the following academic year. I
understand also that the American Board of Surgery considers vacation time to
be a part of my training.
I will not participate in any medical practice or employment other than that
pursuant to my agreement with the Baylor College of Medicine and the Michael
E. DeBakey Department of Surgery except in case of emergency or while on
vacation. If I choose to do so, I must seek permission from the Program
Director and I must purchase separate malpractice liability insurance. I
understand that moonlighting is not permitted while I am enrolled in the Baylor
College of Medicine General Surgery Residency Training Program.
I will notify the Program Director if I receive a summons, complaint,
subpoena, or court paper of any kind relating to my activities in connection
with the Department, the affiliated hospitals, and the residency program.

56
I have read and understand the ACGME/ TSBME duty hour regulations. I will
adhere to these regulations and will record my hours worked on a weekly basis.
I have been advised that the policies and procedures affecting the Michael E.
DeBakey Department of Surgery residents are available in the GME Office, the
Surgical Education Administration Office, and on E*Value [https://www.e-
value.net/].
Vascular Resident Signature Date Vascular Resident Name [PRINTED]
Peter Lin, MD Date
Program Director
I acknowledge that I have received the Vascular Surgery Residency Handbook electronically
and have been made aware of the educational expectations I must meet, as described during
the Michael E. DeBakey Department of Surgery’s annual orientation. By signing below, I
agree to abide by the policies of Baylor College of Medicine and the Michael E. DeBakey
Department of Surgery and commit to making my best effort to meet the educational
standards of the College and Department.
Vascular Resident Signature Date
Related Documents











