Vanderbilt University Medical Center Linking Outcomes of Care to the ACGME Core Competencies: A Matrix Solution • 3:15 pm – 3:25 pm Introduction Berend Mets, MB, Ph.D., Moderator • 3:25 pm – 3:55 pm Embedding the Core Competencies Using the Matrix John Bingham Director, Center for Clinical Improvement Vanderbilt University Medical Center Nashville Tennessee • 3:55 pm – 4:10 pm Question & Answer Session • 4:10 pm – 4:40 pm Practical Examples of the Matrix Doris Quinn, Ph.D. Assistant Professor, Division of Medical Education Vanderbilt University Medical Center Nashville Tennessee • 4:10 pm – 4:55 pm Question & Answer Session

Vanderbilt University Medical Center Linking Outcomes of Care to the ACGME Core Competencies: A Matrix Solution 3:15 pm – 3:25 pmIntroduction Berend Mets,
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Vanderbilt University Medical Center
Linking Outcomes of Care to the ACGME Core
Competencies: A Matrix Solution• 3:15 pm – 3:25 pm Introduction
Berend Mets, MB, Ph.D., Moderator
• 3:25 pm – 3:55 pm Embedding the Core Competencies Using the MatrixJohn BinghamDirector, Center for Clinical ImprovementVanderbilt University Medical Center Nashville Tennessee
• 3:55 pm – 4:10 pm Question & Answer Session
• 4:10 pm – 4:40 pm Practical Examples of the MatrixDoris Quinn, Ph.D.Assistant Professor, Division of Medical EducationVanderbilt University Medical Center Nashville Tennessee
• 4:10 pm – 4:55 pm Question & Answer Session

Vanderbilt University Medical Center
Linking Outcomes of Care and the ACGME Core Competencies:
A Matrix Solution
John Bingham, MHADirector
Center for Clinical Improvement
SAAC/AAPD Annual MeetingWashington, DC
November 5, 2005
Doris Quinn, PhDAssistant Professor
Division of Medical Education

Vanderbilt University Medical Center
Objectives for today:
1. Discuss the Institute of Medicine (IOM) Aims for Improvement and the ACGME Core Competencies.
2. Describe how the Healthcare Matrix helps link outcomes of care to learning the core competencies.
3. Provide examples of how the Healthcare Matrix is used to improve education and the delivery of care.

Vanderbilt University Medical Center
1999 2001 2002 2003 2004
Emerging public
reporting of
quality
measures
“Hospital Compare”
“Kyros” Events in Healthcare:

Vanderbilt University Medical Center
Extrapolated study results imply that between 44,000-98,000 U. S. hospital patients die each year as
a result of medical errors.March 2000

Vanderbilt University Medical Center
“Five Years After To Err is Human: What Have We Learned?”
Lucian L. Leape, MD; Donald M. Berwick, MD JAMA, May 18, 2005
“If the experience of the past 5 years demonstrates anything, it is that neither strong evidence of ongoing serious harm
nor the activities, examples, and progress of a courageous minority are
sufficient to generate the national commitment needed to rapidly advance
patient safety.”
And what about today?

Vanderbilt University Medical Center
Patient Care should be:
Safe, Timely, Effective,Efficient, Equitable, Patient-
Centered(STEEEP)

Vanderbilt University Medical Center
Phase I Phase II Phase III Phase IV
7/2001 6/2002 7/2002 7/20116/2006 7/2006 6/2011 Beyond
• Improve the evaluation processes for all six of the Competencies.
• Provide aggregated resident performance data for Internal Review Process.
• Use resident performance data as the basis for improvement.
• Begin to use external quality measures to verify resident and program performance levels.
• Identify benchmark programs.
• Involve community in building knowledge about good GME.
• Define specific objectives for residents to demonstrate learning of the competencies.
• Begin integrating the teaching and learning of competencies into residents’ didactic and clinical experiences.

Vanderbilt University Medical Center
“Clinical education simply has not kept pace with or been responsive enough to:
• shifting patient demographics,• changed health system
expectations,• evolving practice requirements,• new information,• a focus on improving quality,• new technologies.”

Vanderbilt University Medical Center
– Reporting of CMS Quality Measures tied to Annual “CMS Market Basket Update”
• November 2004
– “Recommend to Congress that it adopt pay-for-performance for physicians, hospitals, and home health agencies”
• Medicare Payment Advisory Commission: March 2005
“Hospital Compare”
Emerging public
reporting of quality
measures

Vanderbilt University Medical Center
Patient Care
(Assessing it …and getting ready for physician report
cards!)
The first Core Competency:

Vanderbilt University Medical Center
Patients with
Needs
Patients with Needs
Met
What are you measuring to evaluate the quality of Anesthesia care?
How and where are these data reported?
How is the information utilized to improve:
•the education of residents?
•the quality of care provided?
Access Diagnosis Treatment Follow-upAssessment

Vanderbilt University Medical Center
Patient Care should be:
Safe, Timely, Effective,Efficient, Equitable, Patient-Centered
(STEEEP)

Vanderbilt University Medical Center
PRACTICE-BASED LEARNING AND IMPROVEMENT
(What have we learned, what will we improve)
Improvement
SYSTEM-BASED PRACTICE
(What is the Process?On whom do we depend and who depends on us)
PROFESSIONALISM(How must we act)
INTERPERSONAL AND COMMUNICATION
SKILLS(What must we say)
MEDICAL KNOWLEDGE
(What must we know)
PATIENT CARE(Overall Assessment)
Yes/No
Assessment
PATIENT-CENTERED
EQUITABLE
EFFICIENTEFFECTIVETIMELYSAFE AimsCompetencies
Healthcare Matrix: Care of Patient(s) with….

Vanderbilt University Medical Center

Vanderbilt University Medical Center
“Avoiding injuries to patients from the care
that is intended to help them”
PATIENT CARE that is…
Safe
Vanderbilt University Medical Center
PATIENT CARE that is…
Safe
•What is our Anesthesia performance for:
•% Patients with appropriate prophylactic antibiotic?
•% Cardiac Surgical Patients with controlled perioperative serum glucose (200 mg/dL)
•% Cases with documented Time Out?
•Intra- or postoperative:
•Cardiac arrest during hospitalization?
•PE during hospitalization?
•DVT during hospitalization?
•Anesthesia Complications/1000 surgeries?

Vanderbilt University Medical Center
Is Care Is Care Safe ?Safe ?VUMC Goal: Achieve lowest mortality in VUMC Goal: Achieve lowest mortality in
nationnationVUMC 2004
VUMC 2005
Observed to Expected Mortality:53 UHC AMCs with Level I Trauma
Centers

Vanderbilt University Medical Center
9 9 7 5 0 4 2 3 0 2 2 3 3 1 1 2 1 0 2 4 3 3 3 2 2 2 4 2 4 2 0 4
3 42 3
13
1 10
3 2 3 41 3 3 2 4 3
4 4 4 4 5 5 7 43
60 8 4
1828
2432
24
31 40 3330
3327 28
18 26
35 30 31 28
37 3730
4034 31
3427
40 2535
3137
4226
36
41
34
41 34
32
28
2630
56
39 30
3940
31 2147
5040
4531 42
4137
37
40
43 3640
50
1415
6
10
5
158
17
1313
10
9
712
11 14
6 13
18
14
818
1310
10 13
12
12
1116
13
14
37
0
20
40
60
80
100
120
140
Jan-
03
Feb-
03
Mar
-03
Apr-
03
May
-03
Jun-
03
Jul-0
3
Aug-
03
Sep-
03
Oct
-03
Nov
-03
Dec
-03
Jan-
04
Feb-
04
Mar
-04
Apr-
04
May
-04
Jun-
04
Jul-0
4
Aug-
04
Sep-
04
Oct
-04
Nov
-04
Dec
-04
Jan-
05
Feb-
05
Mar
-05
Apr-
05
May
-05
Jun-
05
Jul-0
5
Aug-
05
Month
Act
ual n
umbe
r of
Mor
talit
ies
0
0.2
0.4
0.6
0.8
1
1.2
O/E
Rat
e
Peds
Medicine
Surgical Science
Neurology
Other
VUMC O/E
0.85
VUMC Overall O/ E Ratio Line
(.77 for 2Q 2005)
VUMC Elevate Goal: .85
Best AMC
VUMC Observed to Expected Mortality and Actual Number of Mortalities 2003-2005

Vanderbilt University Medical Center
“Reducing waits and sometimes harmful delays for both those who receive and those who give care”
PATIENT CARE that is…
Timely
Safe

Vanderbilt University Medical Center
PATIENT CARE that is…
Timely
Safe
•What is our Anesthesia performance for:
•% Patients with Anesthesia Prep Time < 15 Minutes?
•% Patients with on-time prophylactic antibiotics?
•% Patients with prophylactic antibiotics? discontinued <24 hours after surgery end time?
•% cases completed < 15% of scheduled length?
•% cases with surgical consent before day of surgery?
•Average time between cases (Gap Time)?
•Average time between “room ready” and “in room”?
Vanderbilt University Medical Center
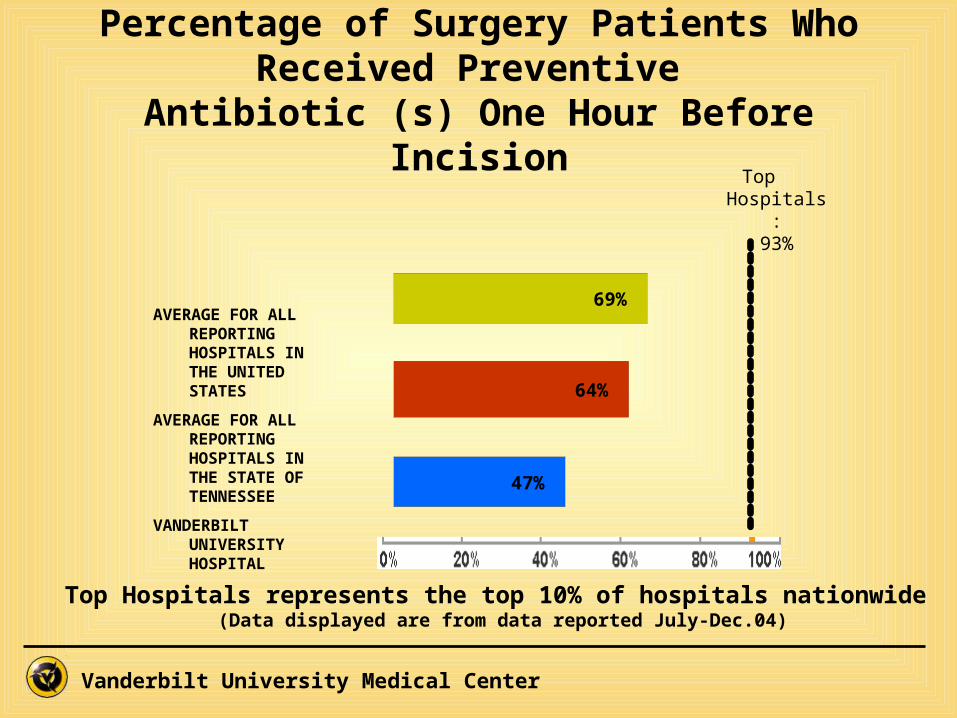
Percentage of Surgery Patients Who Received Preventive
Antibiotic (s) One Hour Before IncisionTop Hospitals:
93%
AVERAGE FOR ALL REPORTING HOSPITALS IN THE UNITED STATES
AVERAGE FOR ALL REPORTING HOSPITALS IN THE STATE OF TENNESSEE
VANDERBILT UNIVERSITY HOSPITAL
69%
64%
47%
Top Hospitals represents the top 10% of hospitals nationwide (Data displayed are from data reported July-Dec.04)

Vanderbilt University Medical Center
What is the infection rate for surgical patients (in total, by procedure, by specialty, by surgeon; by site of surgery) ?
Exceptions by procedure, by specialty, by surgeon; by site of surgery ?
Received the appropriate antibiotic?
Received prophylactic antibiotics?
Received within one hour prior to surgical incision?%
% with Infectio
n
No Yes
No
% with Infection
% with Infection
% with Infection
Yes
No Yes
Exceptions
Patients with
Needs
Patients with Needs
Met
Access Diagnosis Treatment Follow-upAssessment

Vanderbilt University Medical Center
Percentage of Surgery Patients Whose Preventive Antibiotics
are stopped Within 24 Hours After Surgery
Top Hospitals:100%
AVERAGE FOR ALL REPORTING HOSPITALS IN THE UNITED STATES
AVERAGE FOR ALL REPORTING HOSPITALS IN THE STATE OF TENNESSEE
VANDERBILT UNIVERSITY HOSPITAL
64%
58%
78%
Top Hospitals represents the top 10% of hospitals nationwide
(Data displayed are from data reported July-Dec.04)

Vanderbilt University Medical Center
“Providing services based on scientific knowledge to all who
could benefit and refraining from providing services to those not
likely to benefit”
PATIENT CARE that is…
Timely
Effective
Safe

Vanderbilt University Medical Center
PATIENT CARE that is…
Timely
Effective
Safe
•What is our Anesthesia performance for:
•% Patients that received preoperative prophylaxis for VTE?
•% non-cardiac vascular surgery patient receiving beta-blockers during perioperative period
•% Patients with CAD who received beta blockers during perioperative period?
•% Patients on a ventilator whose post op orders included elevating bed >= 30 degrees?

Vanderbilt University Medical Center

Vanderbilt University Medical Center
“Avoiding waste, including waste of equipment, supplies, ideas, and
energy”
PATIENT CARE that is…
Timely
EfficientEffective
Safe

Vanderbilt University Medical Center
PATIENT CARE that is…
Timely
EfficientEffective
Safe
•What is our Anesthesia performance (over time) for:
•Total cost per case?
•Supply cost per case?
•Supply waste per case?
•OR non-billable time delays due to Anesthesia?
•Rate of increase in revenue vs. expenses?

Vanderbilt University Medical Center
“Providing care that does not vary in quality because of personal
characteristics such as gender, ethnicity, geographic location, and
socio-economic status”
PATIENT CARE that is…
Timely
EfficientEffective
Equitable
Safe

Vanderbilt University Medical Center
Is Care Is Care Equitable?Equitable?AHRQ 2004 National Healthcare Disparities
Report Released 2/22/2005•Blacks:
• had worse access than whites for about 40% of access 40% of access measuresmeasures• received poorer quality for about 66% of quality measures66% of quality measures
•Asians:• had worse access than whites for about 33% of access 33% of access measuresmeasures• received poorer quality than whites for about 10% of quality10% of quality measuresmeasures
•Hispanics:• had worse access than non-Hispanic whites for about 90% 90% of access measuresof access measures• received lower quality of care than non-Hispanic whites for 50% of quality measures 50% of quality measures
•Poor people:• had worse access for about 80% of access measures80% of access measures than those with high incomes • received lower quality of care for about 60% of quality 60% of quality measuresmeasures

Vanderbilt University Medical Center
“Providing care that is respectful of, and responsive to:
•individual patient preferences,
•needs and values,
•and ensuring that patient values guide all clinical decisions”
PATIENT CARE that is…
Timely
EfficientEffective
Equitable
Patient Centered
Safe
Vanderbilt University Medical Center
Is Care Is Care Patient Centered?Patient Centered?HCAPS/CMS Patient Perception Surveys
Effective in 2006-Public in 2007
What are our patients’ perceptions of:
•Communications with Nurses? •Communications with Doctors?•Communications about medications?•Nursing services?•Pain management?•The hospital environment?•Adequacy of discharge information?•Our system overall?•Their willingness to recommend us?

Vanderbilt University Medical Center
“…about established and evolving biomedical, clinical, and cognate sciences, (e.g. epidemiological and social-behavior) and the application of this knowledge to
patient care”
Medical Knowledge
PATIENT CARE that is…
Timely
EfficientEffective
Equitable
Patient Centered
Safe
What must we know?
Vanderbilt University Medical Center
Medical Knowledge
Interpersonal and Communication Skills
PATIENT CARE Timely
EfficientEffective
Equitable
Patient Centered
Safe
“…that result in effective information exchange
and teaming with patients, their families, and
other health professionals.”
What must we say?

Vanderbilt University Medical Center
“…as manifested through a commitment to carrying out professional responsibilities,
adherence to ethical principles, and sensitivity to a diverse patient population.”
Medical Knowledge
Interpersonal and Communication SkillsProfessionalism
PATIENT CARE Timely
EfficientEffective
Equitable
Patient Centered
Safe
How must we behave?

Vanderbilt University Medical Center
“…as manifested by actions that demonstrate an awareness of, and responsiveness to, a
larger context and system of healthcare and the ability to effectively call on system resources to
provide care that is of optimal value.”
Medical Knowledge
Interpersonal and Communication SkillsProfessionalism
System-Based Practice
PATIENT CARE Timely
EfficientEffective
Equitable
Patient Centered
Safe
What is the Process?On whom do we depend?
Who depends on us?

Vanderbilt University Medical Center
“…involves investigation and evaluation of their own patient care, appraisal and
assimilation of scientific evidence, and improvements in
patient care.”
Medical Knowledge
Interpersonal and Communication SkillsProfessionalism
System-Based Practice
Practice-Based Learning & Improvement
PATIENT CARE Timely
EfficientEffective
Equitable
Patient Centered
Safe
What have we learned?What will we improve?

Vanderbilt University Medical Center
Patients with
Needs
Patients with Needs Met
Access Diagnosis Treatment Follow-upAssessment
Linking it all together….Linking it all together….
-Medical Knowledge
-Interpersonal and Communication Skills
-Professionalism
-Practice-Based Learning & Improvement
Timely EfficientEffective Equitable Patient CenteredSafe
-System-Based Practice
Clinicians competent in:
Patient Care that is…

Vanderbilt University Medical Center
QUESTIONS?

Vanderbilt University Medical Center
“Residents live in the cracks of our health care systems and give
voice to what life is like there.”
Paul Batalden, MDDartmouth Medical School

Vanderbilt University Medical Center
Five Applications of the Matrix
I. Individual Resident Learning
II. Case Presentations
III. M & M Conference
IV. Panel of Patients for Group Learning
V. Medical Students

Vanderbilt University Medical Center
Individual LearningCase Presentation

Vanderbilt University Medical Center
IOM
ACGME
SAFETY TIMELINESSEFFECTIVE-
NESSEFFICIENCY
EQUITA-BILITY
PATIENTCENTERED-
NESS
PATIENT CARE
MEDICAL KNOWLEDGE & APPLICATION
X X
PROFESSIONALISM
INTERPERSONAL & COMMUNICATION SKILLS
SYSTEMS- & TEAMS-BASED PRACTICE
X
PRACTICE-BASED LEARNING & IMPROVEMENT(Process to Improve)
Anesthesia: One resident’s learning
Case presentation preparation before expose to the Matrix
Vanderbilt University Medical Center
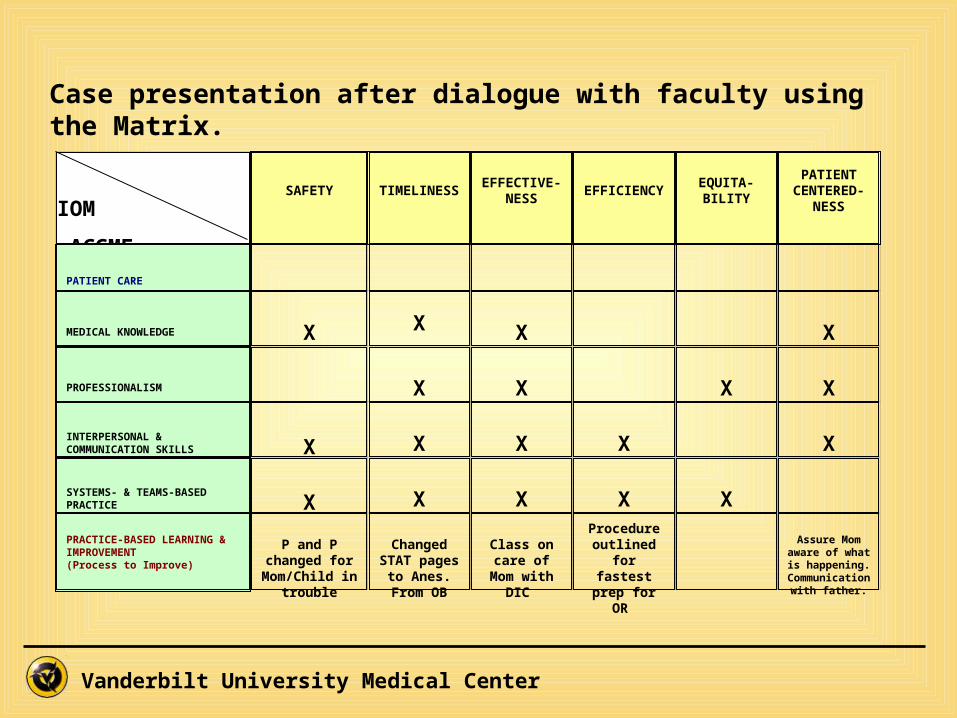
IOM
ACGME
SAFETY TIMELINESSEFFECTIVE-
NESSEFFICIENCY
EQUITA-BILITY
PATIENTCENTERED-
NESS
PATIENT CARE
MEDICAL KNOWLEDGE X X X
X
PROFESSIONALISM
X X
X X
INTERPERSONAL & COMMUNICATION SKILLS X X X X
X
SYSTEMS- & TEAMS-BASED PRACTICE X X X X X
PRACTICE-BASED LEARNING & IMPROVEMENT(Process to Improve)
P and P changed for Mom/Child in
trouble
Changed STAT pages
to Anes. From OB
Class on care of Mom
with DIC
Procedure outlined for fastest prep
for OR
Assure Mom aware of what is
happening. Communication
with father.
Case presentation after dialogue with faculty using the Matrix.

Vanderbilt University Medical Center
Patient with Pregnancy and D.I.C (Disseminated Intravascular Coagulopathy)Case Presentation
IOM ACGME
SAFE TIMELY EFFECTIVE EFFICIENT EQUITABLE PATIENT-CENTERED
Assessment of Care
PATIENT CARE(Overall
Assessment)
NOPatient
nearly died
NOLife saving
treatment was delayed for
variety of reasons
NODelays in treatment
impaired effectiveness of
therapy
NOResources (blood
products, staff time) were not utilized in an efficient manner.
NOLanguage was a
problem
NOPatient was not
adequately apprised of her own health
problems and did not participate fully in her
care decisions
MEDICAL KNOWLEDGE(What must we
know)
Priorities in hemorrhagic shock are ABC: ensure oxygen delivery, support BP, aggressive IV resuscitation, treat cause
Hemorrhagic shock is life-threatening emergency: Prompt diagnosis, recognize urgency, initiate therapy, incl. timely transport to OR. Diagnosis was made late. No urgency to treat. Delay in contacting Anesth. Inadequate assistance in transport to OR
D.I.C. in pregnancy: Physiology, diagnosis, causes, treatment. Regional v. General Anesth? Post resuscitation pulmonary edema. Hypocalcemia due to massive transfusion. Invasive monitoring indications. Pharmacology of uterotonic drugs.
Survival in postpartum hemorrhage requires aggressive IV resuscitation: always consider combining procedures (start 2nd IV while drawing blood sample for transfusion cross match).
INTERPERSONAL AND
COMMUNICATION SKILLS
(What must we say)
Safety is jeopardized unless team members are fully apprised of patient’s condition (blood loss following delivery, vital signs, plans for intervention).
Orders (blood cross match) must be prioritized and fully implemented in a timely fashion.
Effectiveness of life-saving intervention depends on effective communication between team members.
Communications of a defensive or argumentative nature are counter-productive to efficient and safe care. The focus should be patient care, with analysis of misunderstandings at a later time.
Must communicate patient’s condition and intended interventions (blood transfusion, emergency hysterectomy), and in a way that is understandable and useful to the patient, respecting patient autonomy.
PROFESSIONALISM(How must we act)
Professional duty to accompany critically ill patient to the OR, to ensure safety, and to expedite therapy.
Patient’s ethnic, socio-economic, “service patient” status should have no effect on quality of care.
Professional duty to attempt to preserve patient autonomy (make sure patient understands situation and interventions)

Vanderbilt University Medical Center
SYSTEM-BASED
PRACTICE(On whom do
we depend and who depends
on us)
System must ensure that appropriate consultants are notified when needed to ensure safety in life-threatening medical condition.
During postpartum bleeding, type & cross match must be drawn, sent, and verified promptly. Failure to do so threatens life.
Failures to draw, send, and verify cross match blood sample jeopardizes effectiveness of life-saving therapy.
Standard of care should not vary due to differences in staffing that result from time of day / night (availability of lab medicine physician, timely transport of blood samples, adequate number & expertise of obstetrics, anesthesiology, & nursing staff)
Improvement
PRACTICE-BASED
LEARNING AND
IMPROVEMENT(How must we
improve)
Policy and Procedures changed for Mother/Baby in trouble
Revise the criteria for and system of communicating urgent / emergent request for Anesthesiology consultation
Departmental Teaching Conference on management of parturient with D.I.C.
Procedure outlined for fastest prep for OR
Increased awareness of need to consider patient centeredness even in emergent or crisis situations. Communication with father / family members when appropriate and possible.
© Bingham, Quinn Vanderbilt University (Used with permission from Anesth. Dept)
Vanderbilt University Medical Center
Patient with Coronary Artery Disease
(Internal Medicine ResidentsAmbulatory Rotation)

Vanderbilt University Medical Center

Vanderbilt University Medical Center
Panel of Patients with Coronary Artery Disease
Vanderbilt University Medical Center
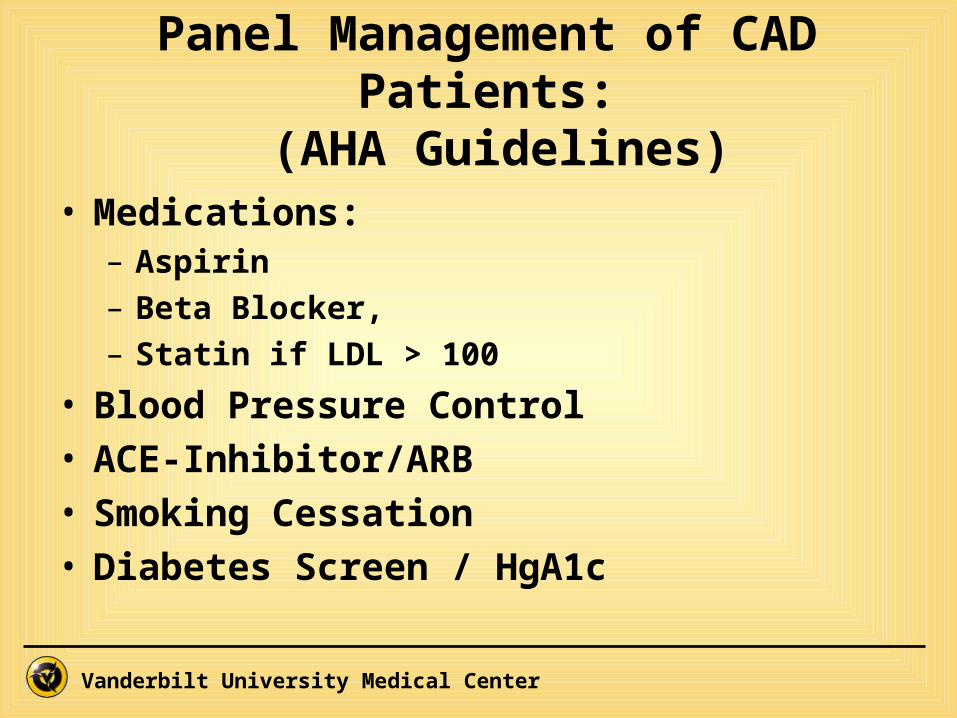
Panel Management of CAD Patients:
(AHA Guidelines)• Medications:
– Aspirin– Beta Blocker, – Statin if LDL > 100
• Blood Pressure Control• ACE-Inhibitor/ARB• Smoking Cessation• Diabetes Screen / HgA1c

Vanderbilt University Medical Center
Internal Medicine ResidentsAmbulatory Rotation

Vanderbilt University Medical Center
Practice-based learning and Improvement
(based on care of patients with CAD)
Vanderbilt University Medical Center

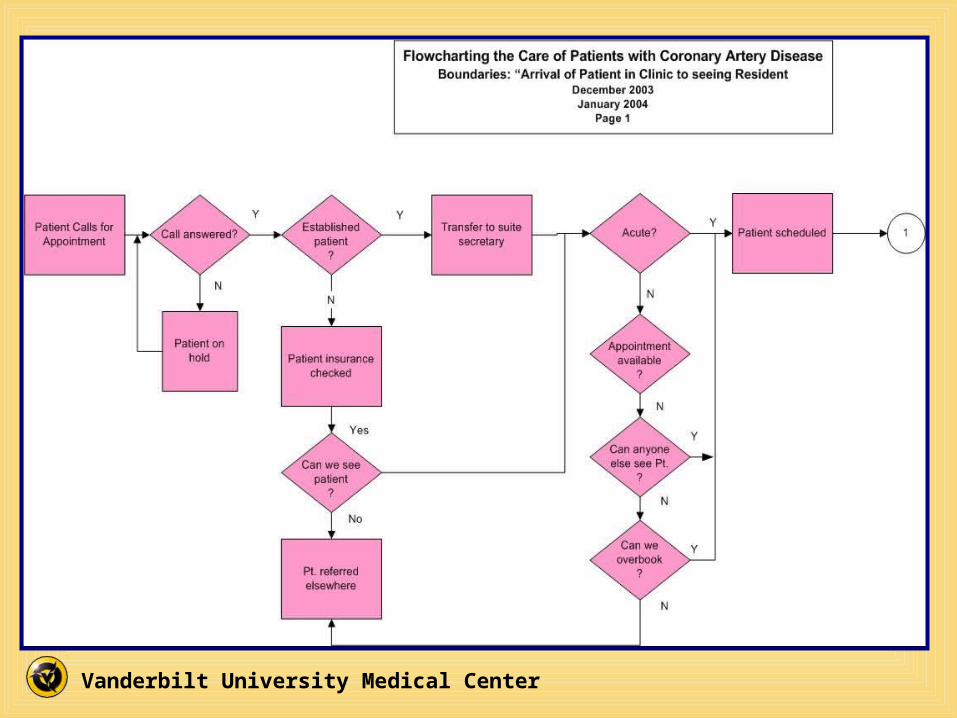
Vanderbilt University Medical Center
NewPatient.
?
Follow-upon CADPatient
Y
2
Y
Physical Exam
Wait time for testsresults
Location ofpatients while they
wait
All patients mayhave long list ofcomplaints. MD
has to see pt in 15minutes
N
Patient with CADInternal Medicine Residents
February, 04April, 04 (class 3)May, 04 (class 4)
Page 3
Seen at VUMCbefore
?
Acute visit?
Get as muchinformationas possible
Focused/Directed
H&P
Get pt.Information
fromStarPanel
Review ofsystemsapproach
-Meds-EBM-etc
N
Previous info notavailable. Can wehave pt fill in infoin waiting room?
Problem list shouldinclude what hasbeen tried and
failed (with meds)
Explain computerissues with pt (esp
problem list) sothey don’t feel
ignored
N
Location ofcomputer and notbeing able to look
at patient
Othercomplaints to be
addressed?
Does MD havetime to address
all issues?
Address only acutecomplaint and
reschedule for otherissues if needed
Get updatedhistory includingall risk factors
Review: VS
Medication listProblem list
Y
N
N
Could we have timefor visit match whatneeds to be done?
Especially for pts withChronic diseases
Physician in room withPatient
SynthesizeInformation
Information sharedwith patient
Formulate Plan(confer withAttending as
needed)
NeedHospitalization
?
Y
Different Process
Patient Education(or other
preventive healthissues)
N
3

Vanderbilt University Medical Center
Delays in Patient Care
NURSING &TECH INFO
PRE-VISIT INFORMATIONFROM PATIENTS
PROBLEM LIST& MEDS
ROOMUTILIZATION
MEDICINERESIDENT CLASS
04/01/045/21/04
STAR PANELPATIENTVISIT ISSUES
DOCUMENTATIONOF NEW PTS.
ROOMENVIRONMENT
LATEARRIVALSTESTS
Not using pt waiting timeto capture info
Obtaining outside records
Test from OSH (Imaging,Labs, Vaccinations, etc.
Pt needs to bring meds orlist of meds to confirm
Previous infonot available
Room turnover is an issue.Other rooms are not ready togo or there are pts in waiting rmw/ no tech to bring them back
Variation in whether ornot vitals are even done
Variation in time it takes eachnurse to check in a pt
Room for pt to wait whileMD sees next pt
Location of pts while they wait
Nurse write down medsor put on problem listwhen doing intakeassessment
Time lost: time spent w/tech in room should notexceed 2 - 3 min.
If no available problemlist, a hard copy of lastStar note in chart or doorto review last times visit
Current Med list/Previous Med list
Problem list should includewhat has been tried &failed (meds)
Meds I don’t like - why?
Most important problem/issue today (SMIP - singlemost important problem!)
Start Labs (MP, CBC w/ diff,Lipid profile, HgAIC, EKG)
Allergies (true)
StarPanelnote organization
StarPanel tutorials to showthe ins & outs of new toolsin StarPanel
Window popup w/ age, gender-specific standard of careguidelines for ICD-9 code or dx
StarPanel too slow, alwayspops up w/ wrong pt
OPOC too slow, takes toomuch time to get pt out ofroom (the only room we have!)
Search engine for Meds!
List of formulary meds forthat pt’s ins. Available in apopup/menu, also timeliness
Log into system - slow!!
Location of computer -not being able to see pt
Explain computerissues to pt (i.e.problem list) so theydon’t feel ignored
Communicating w/referring physician/pt: typeletter or call
Proper followup: interventions,referrals, tests, teaching
Benefits of each medicineby class; “your Dr has startedyou on a B Blocker because…"“this medicine will help with…"
6th grade level educationalmaterials for Dx (i.e. highcholesterol: diet/nutrition, quitsmoking, etc)
Documentation hold-up ofencounters, particularlynew pts
Documentation: typingnew pt note
Having to type noteson new pts
Typing new ptnotes too slow
Wait time for testresults too long
No definition for pt appointmenttime (check-in, vitals, to room, tosee Dr?)
Parking for patients
No-show patients
No pt in room when ready to see pt
Confusion about who does whatin clinic (tech/nurse/secretary)
Check-in takes too long
Redundant info (tech gets cc)we redo this
Vital signs are optional
Too many formsto fill out for tests
Paper charts were designed by?- not easily useful to physicians
SCHEDULING
Staff: Decision chartregarding what to dowith late arrivals
Pt scheduled for f/u apptwith another appt previously scheduled, ends up as noshow for one
All residents in clinic have ptsscheduled at same time
Except for new pts & femalephysical, all appts are samelength of time (20 mins)
Multiple pts scheduled atsame time for physician
Appointment template isnever right!
Scheduler will not allow foralternate ways to schedulepts
Resident workrooms arepoorly configured andpoorly furnished
Malfunctioning diagnosticequipment
Too few rooms for 4residents
Residents all waitingfor preceptor at sametime, major holdup inschedule
Insufficient room space
One location for labs to be drawn & vitalstaken by nurse for all pts, creates roadblock

Vanderbilt University Medical Center
Improvements From Medicine Residents:
Pat Covington RN, Manager
EMR: We can now text message across departments. Use of pt waiting time: Have Kiosk in exam room to fill in review of systems. Questionnaires being sent to pts ahead of time. Those with email get questionnaire and can return via email. Availability of techs: Modified schedule of techs to improve service. Residents’ schedules were also changed to better utilize staff. Patient visit survey and phone calls will now be done after visit. Patient Letter revised: “Bring old records, come 15 minutes before appt.”

Vanderbilt University Medical Center
Transforming M&M Conferences
into
Practice-based Learning and Improvement

Vanderbilt University Medical Center
Care of Child with Hyperleukocytosis M&M 3/25/04 (Peds Hem/Onc)
IOM ACGME
SAFE1 TIMELY
2 EFFECTIVE
3 EFFICIENT
4 EQUITABLE
5 PATIENT -CENTERED
6
Assessment
I.PATIENT CARE 7
Mostly yes
(Toxicity of chemo needed better monitoring)
Yes
Yes (but variation
exists) WBC dropped from
324K to 37K by midnight
Yes
Yes
Yes
Family told of possible Dx within 2
hours of ED visit.
II. A MEDICAL
KNOWLEDGE 8 (What must I know)
-Hypercalcemia led to hypotension. -Respiratory distress secondary to fluid overload and atelectasis required intubation Complications of Leukopheresis was discussed.
Full dose Chemotherapy started quickly
Management of Hyperleukocytosis: was major discussion for M&M conference.
Discussed lack of benefit and increase cost of cranial irradiation
How to tell family bad news (lecture at VU). Pediatrics Oncologists have a lot of experience and are very family centered. Family was well informed of likely dx and plan of action.
II. B PROFESSIONALIS M 9
(How must I act)
PCP referred child to ED for evaluation very quickly (from community 40 miles away).
Feedback to PCP was done as soon as a concern was voiced.
Some physician variation noted at VU for treatment. Can we standardize with pathway?
Able to talk to family and PCP in professional and evidenced -based manner.
II. C INTERPERSONAL AND
COMMUNICATION SKILLS 10
(What must I say)
Experienced physicians and researchers communicated well.
Hand -offs were smooth and well executed.
Pare nts felt comfortable providing inform consent by 7 PM the same day.
II. D SYSTEM -BASED
PRACTICE11
(On whom do I depend
and who depends on me)
Toxicity was an issue and the team needed to do a better job of recording what was happening.
Quick response by VCH to PCP. hyperleukocytosis 5 hours to Dx 8 hours to start of Tx
Discussed issue of dialysis for treatment. Consulted nephrology and PICU. Dialysis nurse notified early and circuit primed.
Lab results were done quickly from ED. Team worked well to have treatment begin quickly with good results within 10 hours
ED good communication with House Officer. Social worker met with family to explain what was happening.
Improvement
III. PRACTICE -BASED
LEARNING AND IMPROVEMENT
12
(How can I improve)
Be s ure everyone knows the toxicity and complications and document.
Create pathway for hyperleukocytosis to decrease variation
© 2004 Bingham, Quinn Vanderbilt University

Vanderbilt University Medical Center

Vanderbilt University Medical Center
System Based Practice
(What is the process? On
whom do I depend? Who depends on
me?)
The Team did not always know what was going on. Hand-offs were not well managed
All steps of the process of care were not known (including who was key in each step) therefore delays occurred.
Plan of care should have been shared with all (Pharmacy, surgeons, residents, support services to make system work for pt rahter than hinder care.
Needless variation among clinicians is a problem and caused inefficiency of care.
Team should advocate for pt in a complex system. Care was not coordinated and integrated. Expectations and comfort of pt were not known and addressed.
Improvement
PRACTICE-BASED
LEARNING AND
IMPROVEMENT(How must we
improve)
Residents need to know principles of flowcharting and RCA to address these issues.
Anesthesia residents should take the lead in getting the team to discuss pain mgmt and changes needed while pt still in our system.
Team could share talk of lit review for this complex pt. Run chart of pain scale could be one metric to determine results of care.
Patient and family should be included in improvement and monitoring of his own care. Feedback to be sought and used for further improvement.
Information Technology
© Bingham, Quinn Vanderbilt University (Used with permission from Anesth. Dept)
Vanderbilt University Medical Center
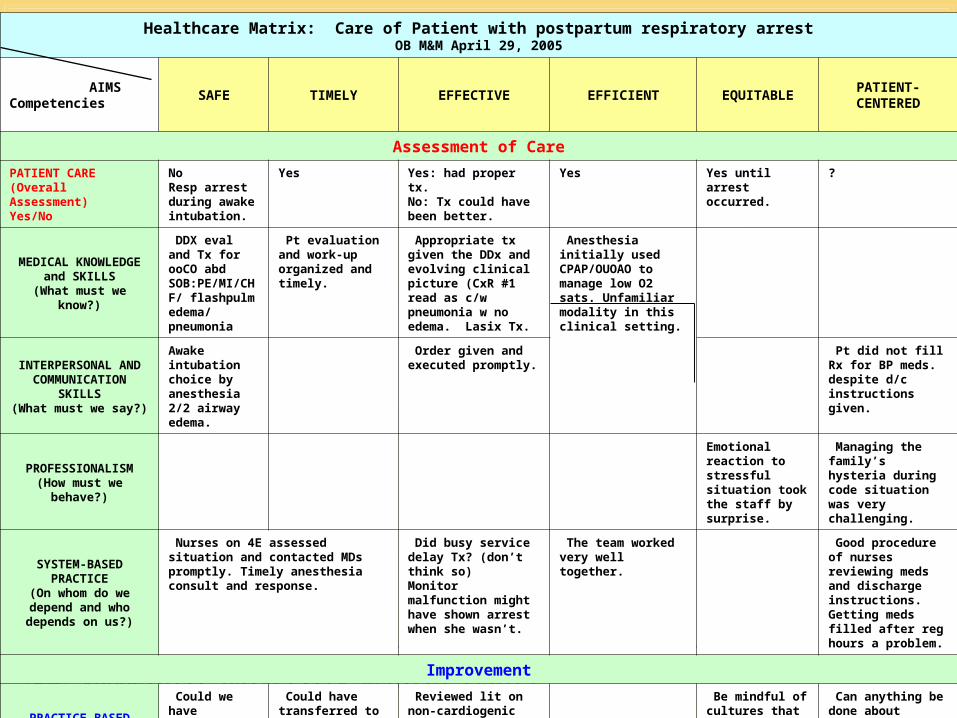
Healthcare Matrix: Care of Patient with postpartum respiratory arrestOB M&M April 29, 2005
AIMS Competencies
SAFE TIMELY EFFECTIVE EFFICIENT EQUITABLEPATIENT-
CENTERED
Assessment of Care
PATIENT CARE(Overall Assessment)Yes/No
NoResp arrest during awake intubation.
Yes Yes: had proper tx.No: Tx could have been better.
Yes Yes until arrest occurred.
?
MEDICAL KNOWLEDGE and SKILLS
(What must we know?)
DDX eval and Tx for ooCO abd SOB:PE/MI/CHF/ flashpulm edema/ pneumonia
Pt evaluation and work-up organized and timely.
Appropriate tx given the DDx and evolving clinical picture (CxR #1 read as c/w pneumonia w no edema. Lasix Tx.
Anesthesia initially used CPAP/OUOAO to manage low O2 sats. Unfamiliar modality in this clinical setting.
INTERPERSONAL AND COMMUNICATION
SKILLS(What must we say?)
Awake intubation choice by anesthesia 2/2 airway edema.
Order given and executed promptly.
Pt did not fill Rx for BP meds. despite d/c instructions given.
PROFESSIONALISM(How must we behave?)
Emotional reaction to stressful situation took the staff by surprise.
Managing the family’s hysteria during code situation was very challenging.
SYSTEM-BASED PRACTICE
(On whom do we depend and who depends on us?)
Nurses on 4E assessed situation and contacted MDs promptly. Timely anesthesia consult and response.
Did busy service delay Tx? (don’t think so)Monitor malfunction might have shown arrest when she wasn’t.
The team worked very well together.
Good procedure of nurses reviewing meds and discharge instructions. Getting meds filled after reg hours a problem.
Improvement
PRACTICE-BASED LEARNING AND IMPROVEMENT
(What have we learned? What will we improve?)
Could we have prevented the resp arrest? C. Osmotic pressures need to be done.
Could have transferred to L&D faster.
Reviewed lit on non-cardiogenic Pulm Edema.Need to be more aggressive with Lasix.
Be mindful of cultures that tend to react more physically and emotionally to stressful events.
Can anything be done about getting a few doses of meds for pts being discharged at odd times?
© 2004 Bingham, Quinn Vanderbilt University All rights reserved.
Vanderbilt University Medical Center
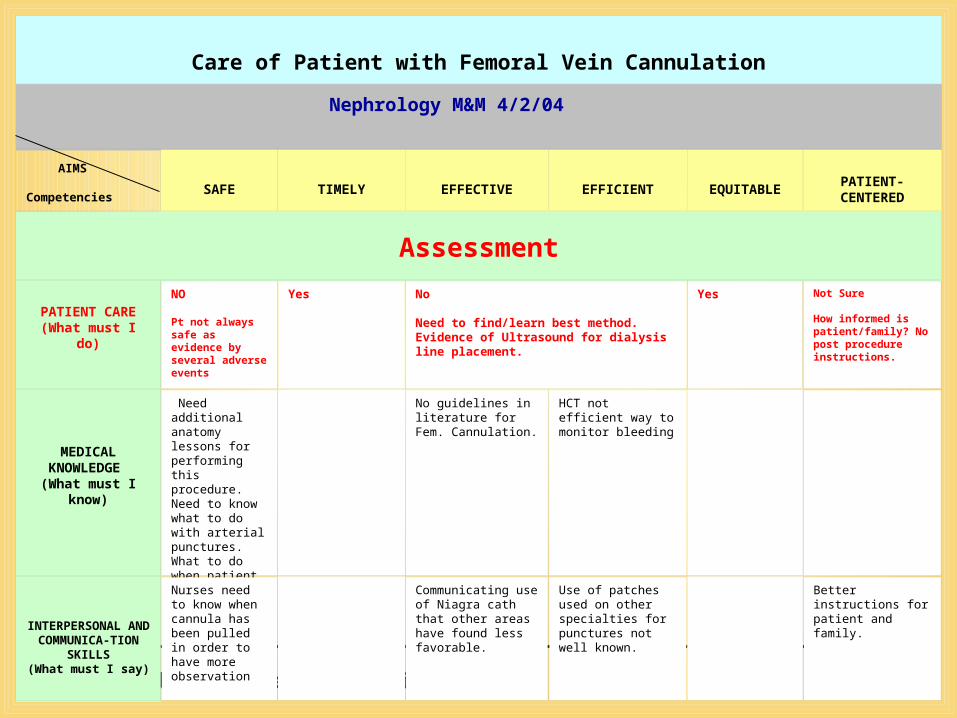
Care of Patient with Femoral Vein Cannulation
AIMS
Competencies
SAFE TIMELY EFFECTIVE EFFICIENT EQUITABLEPATIENT-
CENTERED
Assessment
PATIENT CARE(What must I
do)
NO
Pt not always safe as evidence by several adverse events
Yes No
Need to find/learn best method.Evidence of Ultrasound for dialysis line placement.
Yes Not Sure
How informed is patient/family? No post procedure instructions.
MEDICAL KNOWLEDGE (What must I
know)
Need additional anatomy lessons for performing this procedure. Need to know what to do with arterial punctures. What to do when patient cannot be still?
No guidelines in literature for Fem. Cannulation.
HCT not efficient way to monitor bleeding
INTERPERSONAL AND
COMMUNICA-TION SKILLS
(What must I say)
Nurses need to know when cannula has been pulled in order to have more observation
Communicating use of Niagra cath that other areas have found less favorable.
Use of patches used on other specialties for punctures not well known.
Better instructions for patient and family.
Nephrology M&M 4/2/04
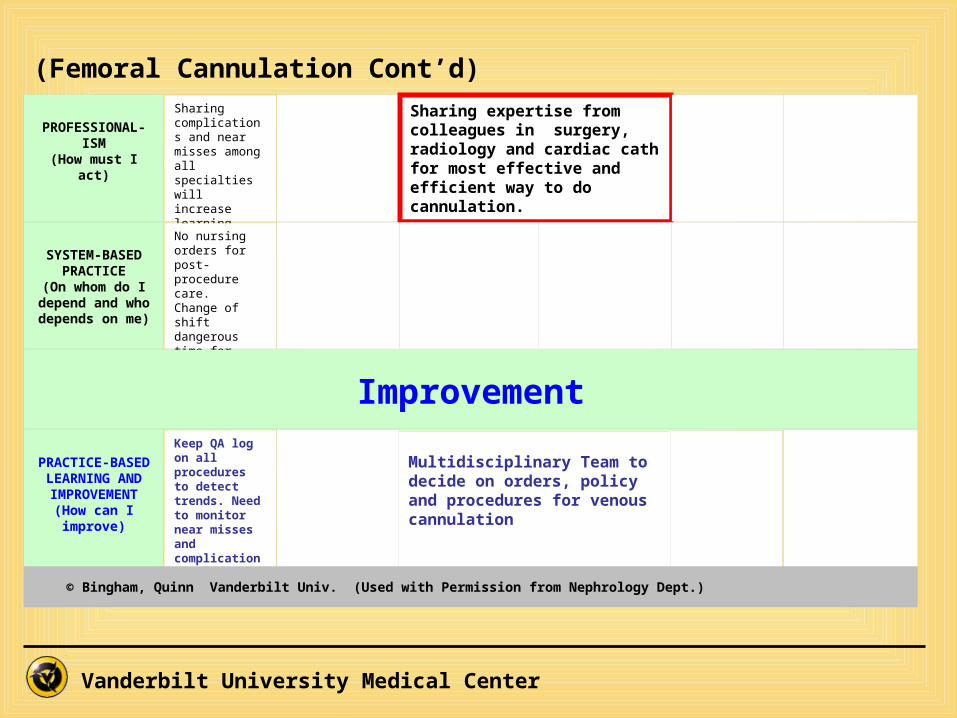
Vanderbilt University Medical Center
PROFESSIONAL-ISM
(How must I act)
Sharing complications and near misses among all specialties will increase learning.
Sharing expertise from colleagues in surgery, radiology and cardiac cath for most effective and efficient way to do cannulation.
SYSTEM-BASED PRACTICE
(On whom do I depend and
who depends on me)
No nursing orders for post-procedure care. Change of shift dangerous time for patients.
Improvement
PRACTICE-BASED
LEARNING AND IMPROVEMENT
(How can I improve)
Keep QA log on all procedures to detect trends. Need to monitor near misses and complications to learn.
Multidisciplinary Team to decide on orders, policy and procedures for venous cannulation.
© Bingham, Quinn Vanderbilt Univ. (Used with Permission from Nephrology Dept.)
(Femoral Cannulation Cont’d)
Multidisciplinary Team to decide on orders, policy and procedures for venous cannulation

Vanderbilt University Medical Center
ACTION PLAN

Vanderbilt University Medical Center
Medical Students(Neurology Clerkship)

Vanderbilt University Medical Center
Healthcare Matrix: Care of Patient with stroke - occlusion of the ICA of unknown origin.
AIMS Competencies
SAFE TIMELY EFFECTIVE EFFICIENT EQUITABLEPATIENT-
CENTERED
Assessment of Care
I.PATIENT CARE
(Overall Assessment)Yes/No
Yes No Yes Yes, from VUMC,
No for placement.
Yes from VUMC
No b/c of insurance issues
Yes – patient was informed and incorporated in decision making process
II. AMEDICAL
KNOWLEDGE(What must we know)
Yes. Everyone on the stroke service was on top of the latest in knowledge.
Yes. Yes. Yes. Yes.
II. BINTERPERSONAL AND
COMMUNICATION SKILLS
(What must we say)
Yes. Communication between neuro and surgery was clear. Attendings and residents were in contact
Yes – phone calls and meetings were used when things couldn’t wait for note in chart
Yes and no – comm. Between medical teams was great. Ins issues led to placement problems though
Yes yes Yes – always kept in mind patients perspective
II. CPROFESSIONALISM(How must we act)
Yes There was no breakdown in safety due to pro problems
Yes – there were never any delays in doing anything for the pt in terms of pro
Yes Yes
Yes and no – pt was on service for a while,– but not really treated much better than others
Yes –
II. DSYSTEM-BASED
PRACTICE(On whom do we depend and who depends on us)
Yes – patient was monitored and kept in system
Yes and no – no delays in providing emergent care, but getting rehab was hard.
Yes No– consultants used appropriately. Problem was not in Vanderbilt system, but in insurance system
Yes Yes – all resources were used according to pts own goals for rehab
Improvement
III.PRACTICE-BASED
LEARNING AND IMPROVEMENT
(What have we learned and what do we
improve)
Patient safety was maintained at all times. We still don’t know what caused stroke after surgery though.
Rehab placement took too long – everyone worked hard, but maybe could have worked harder
Care was administered effectively within limits – not much treatment for strokes like this yet
A lot of energy and time was used ineffectively trying to place him
Everyone worked hard for him because he was there so long and trying hard to rehab. not more than everyone else
Pt was very involved in his own care and course and his wishes were always respected.

Vanderbilt University Medical Center

Vanderbilt University Medical Center
Practice-based Learning and Improvement
Tools and Methods

Vanderbilt University Medical Center
What are we trying to accomplish?- AIM -
What are we trying to accomplish?- AIM -
How will we know that a change is an improvement?- Data Over Time –
(Tools: Run Charts, Control Charts)
How will we know that a change is an improvement?- Data Over Time –
(Tools: Run Charts, Control Charts)
What changes can we make that will result in an improvement?- Process Analysis –
(Tools: Flowchart, Cause & Effect Diagram, Pareto Chart, etc.)
What changes can we make that will result in an improvement?- Process Analysis –
(Tools: Flowchart, Cause & Effect Diagram, Pareto Chart, etc.)
IMPROVEMENT MODEL
Planthe
Improvement
Studythe
Results
Dothe
Improvement
Act
Act to keep changeor Abandon and try
another change
PDSA Cycle—Small rapid cycles of change
P
A D
S
Vanderbilt University Medical Center
Operating Room Team
AIM:Reduce “Start Time” Delays in O.R.
©VUMC2001

Vanderbilt University Medical Center
Run Chart of DelaysOR Delays in Start Time
0
15
30
45
60
75
90
105
120
1 3 5 7 9 11 13 15 17 19 21 23 25
Patients
Tim
e
©VUMC2001

Vanderbilt University Medical Center
Process Flowchart
©VUMC2001
Nursing evaluation
done?
Surgery H&P done?
Yes Surgical consent signed?
Yes Anesthesia evaluation
done?
Yes Risk & medicolegal
issues addressed?
YesNeed pre-op lines in holding?
Yes OR ready?
Yes
Perform nursing
evaluation weight
No
Perform H&P
No
Obtain signed consent
No
Perform evaluation:H&P
Indicated tests:labsECGCXR
No
Cancel Surgery
No
Place indicated lines
No
Wait
No

Vanderbilt University Medical Center
Cause and Effect Diagram
©VUMC2001
OR StartTime
Delays
PEOPLE PROCEDURES
EQUIPMENT POLICY
Surgeon Late
Anesthesia latePatientcomplications
Consultationnot done
Consult notesnot in chart
No pre-opeducation
Meds notgiven
Tests notdone
H&P not done
Nursing evaluation not done
Anesthesia evaluationnot done
Test resultsnot in chart
Doublebooked
Instrumentsnot ready
Not available
Medical record missing
Instruments notavailable
No patientconsent
Noauthorization
Registrationnot complete
No pre-op check list

Vanderbilt University Medical Center
Pareto Chart
42.37
59.32
72.88
83.05
89.8394.92
100
A B C D E F G
11.80
0.00
23.60
35.40
47.20
59.00
PARETO CHART
0.00 # of errorsCum Freq
Cum
. Fr
eq.
©VUMC2001

Vanderbilt University Medical Center
New Aim (Based on Data)
To reduce the number of preoperative tests performed so that only those which are important to the medical mgmt of adult surgical pt during pre-op period are ordered.
©VUMC2001

Vanderbilt University Medical Center
How Will We Know a Change Is an Improvement?
Measurement:
Percentage Excess Tests Per Specialty
Based Upon Agreed Upon Guidelines
©VUMC2001
Vanderbilt University Medical Center
What Changes Can We Make?
Develop disease and surgical proceduraltesting guidelines for:
-laboratory testing, -electrocardiography
-chest radiography
in adult surgical patients
©VUMC2001

Vanderbilt University Medical Center©VUMC2001

Vanderbilt University Medical Center
Preoperative Testing Variation Rates by Service
25
464
38
310
7 28 53
330
108 94
951 51
157120 12
19
323940
545555596162636667
86
0
100
200
300
400
500
600
700
800
900
1000O
ncol
ogy
Ort
ho
Ora
l/Max
il
Gen
eral
Tra
uma
Ren
al/T
x
Gyn
-Onc Oto
Neu
ro
Gyn
ecol
ogy
Hep
atob
il/T
x
CT
Sur
g
Vas
cula
r
Pla
stic
s
Uro
logy
Surgical Service
Ad
dit
ion
al T
esti
ng
Rat
e (%
)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Nu
mb
er o
f P
atie
nts
# Patients
% Excess Tests
©VUMC2001

Vanderbilt University Medical Center
System-Based Practiceat the
Organization Level
Vanderbilt University Medical Center
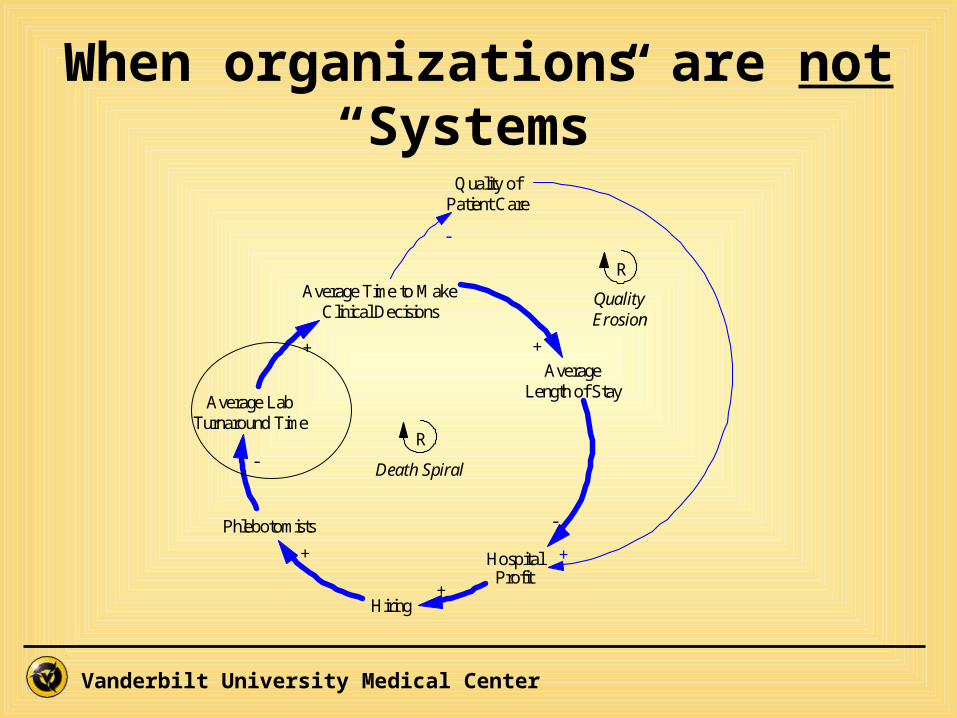
When organizations are not “Systems”
Average LabTurnaround Time
Average Time to MakeClinical Decisions
AverageLength of Stay
HospitalProfit
Phlebotomists
+ +
-
-
R
Hiring
+
+
Quality ofPatient Care
-
+
R
Death Spiral
QualityErosion
Vanderbilt University Medical Center
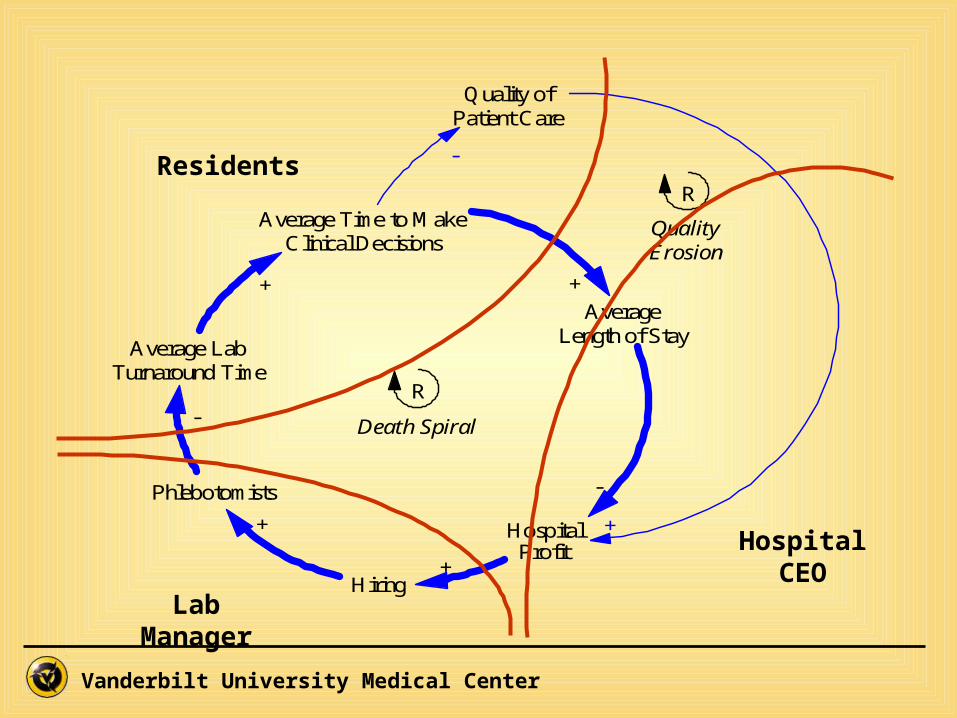
Average LabTurnaround Time
Average Time to MakeClinical Decisions
AverageLength of Stay
HospitalProfit
Phlebotomists
+ +
-
-
R
Hiring
+
+
Quality ofPatient Care
-
+
R
Death Spiral
QualityErosion
Lab Manager
Residents
Hospital CEO

Vanderbilt University Medical Center
History Physical Exam Labs Tests Consults Etc.
DiagnosisCare of Patient(Matrix)
Using the Matrix
Vanderbilt University Medical Center
“Closing the Loop”
• Start with diagnosis as basis for assessment
• Identify issues of care related to Aims and Competencies
• Identify lessons learned and improvement needed
• Complete action plan for improvements with accountabilities and timeline

Vanderbilt University Medical Center
Upcoming Matrix Enhancements

Vanderbilt University Medical Center © 2004 Bingham, Quinn Vanderbilt University
PRACTICE-BASED LEARNING AND IMPROVEMENT
(What have we learned, what will we improve)
Improvement
SYSTEM-BASED PRACTICE
(What is the Process?On whom do we depend and who depends on us)
PROFESSIONALISM(How must we act)
INTERPERSONAL AND COMMUNICATION
SKILLS(What must we say)
MEDICAL
KNOWLEDGE(What must we know)
PATIENT CARE(Overall Assessment)
Yes/No
Assessment
PATIENT-CENTERED
EQUITABLE
EFFICIENTEFFECTIVETIMELYSAFE AimsCompetencies
Healthcare Matrix: Care of Patient(s) with Stroke
An Oracle Database is being built that will collect
data from each cell and allow analysis and reports
to be generated by:
InstitutionDepartmentDiagnosisIOM Aim
Competency

Vanderbilt University Medical Center
positiveLung Cancer with Brain Mets
Team took the time to know the patient and her desire for treatment.Medical Knowledge
Patient-Centered2
TranslatorsnegativeHydrocephalus
This patient spoke Spanish. Skilled interpreters were not available. Medical students and family were used often as interpreters which was not ideal.
Interpersonal Communication skillsEquitable12
EBMnegativeCeliac Sprue
Repeated imaging and brain biopsies were unnecessary. Reduce switching of primary neurologists to avoid repeat testing.System-basedEfficient18
Care PlanimprovementStroke
We could have taken the time to do a better initial H&P to better discern what his condition was like at initial presentation to compare it to discharge condition
Practice-Based Learning & ImprovementEffective4
Teamworknegative
Pregnancy IntracerebralHemorrhage
Delays in communication increased the time it took to get an initial head CT and begin treatment.
Interpersonal Communication skillsTimely19
EBMpositiveStroke
Decisions were made based on accepted algorithms and consensus within the team.ProfessionalismSafe3
Secondary Code
Primary Code (positive, negative,
improvement)Diagnosis ContentCompetenciesAimsStudent ID
Excel Spreadsheet for Matrix Analysis
Vanderbilt University Medical Center
Matrix as “Front Door” to Data and Education

Vanderbilt University Medical Center © 2004 Bingham, Quinn Vanderbilt University
PRACTICE-BASED LEARNING AND IMPROVEMENT
(What have we learned, what will we improve)
Improvement
Process Flowcharts
SYSTEM-BASED PRACTICE
(What is the Process?On whom do we depend and who depends on us)
PROFESSIONALISM(How must we act)
INTERPERSONAL AND COMMUNICATION
SKILLS(What must we say)
Evidence basedOrder sets
MEDICAL
KNOWLEDGE(What must we know)
Pt and family satisfaction data
Outcomes by race, gender, SES
Cost per discharge
Outcomes data
Time Studies
FMEA
EventsPATIENT CARE
(Overall Assessment)Yes/No
Assessment
PATIENT-CENTERED
EQUITABLE
EFFICIENTEFFECTIVETIMELYSAFE AimsCompetencies
Healthcare Matrix: Care of Patient(s) with Stroke
Data linked directly to cells
in the Matrix
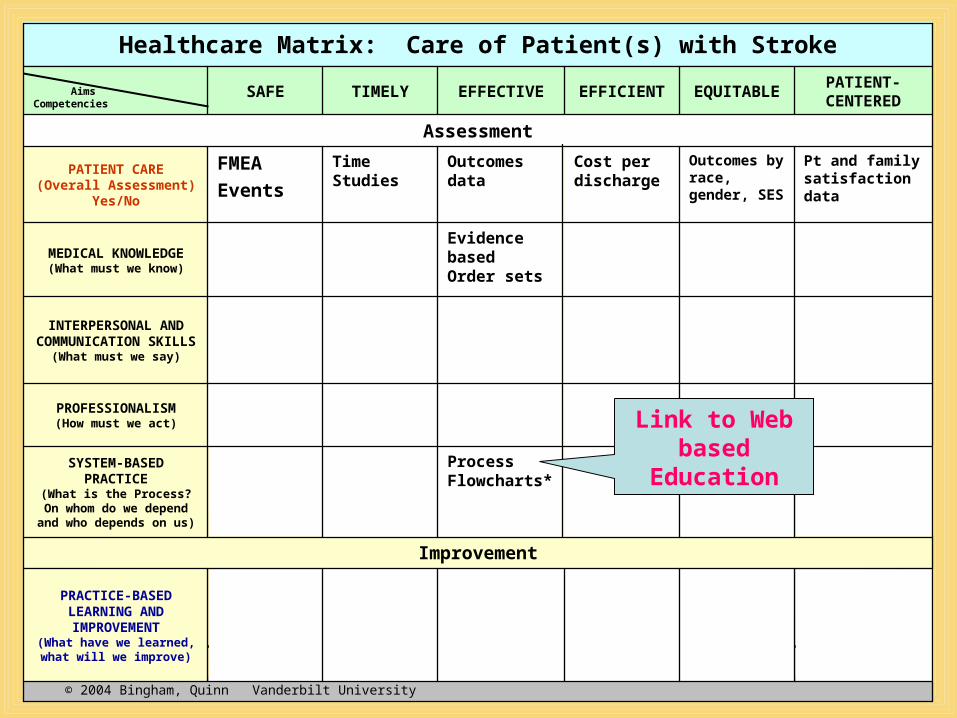
Vanderbilt University Medical Center © 2004 Bingham, Quinn Vanderbilt University
PRACTICE-BASED LEARNING AND IMPROVEMENT
(What have we learned, what will we improve)
Improvement
Process Flowcharts*
SYSTEM-BASED PRACTICE
(What is the Process?On whom do we depend and who depends on us)
PROFESSIONALISM(How must we act)
INTERPERSONAL AND COMMUNICATION
SKILLS(What must we say)
Evidence basedOrder sets
MEDICAL
KNOWLEDGE(What must we know)
Pt and family satisfaction data
Outcomes by race, gender, SES
Cost per discharge
Outcomes data
Time Studies
FMEA
EventsPATIENT CARE
(Overall Assessment)Yes/No
Assessment
PATIENT-CENTERED
EQUITABLE
EFFICIENTEFFECTIVETIMELYSAFE AimsCompetencies
Healthcare Matrix: Care of Patient(s) with Stroke
Link to Web based
Education
Vanderbilt University Medical Center
How to Flowchart a Process
• On-line web site for Improvement education
http://mot.vuse.vanderbilt.edu/mt322
(Dr. Quinn’s current course being redesigned for managers and physicians)

Vanderbilt University Medical Center
On Transformation:“And one should bear in mind that there is nothing more difficult to execute, nor more dubious of success, nor more dangerous
to administer than to introduce a new system of things; for he who introduces it
has all those who profit from the old system as his enemies, and he has only lukewarm allies in all those who might
profit from the new system.”Machiavelli

Vanderbilt University Medical Center
Healthcare Matrix Summary Points:
• Is a framework for integrating competencies into existing educational activities
• Provides a new mental model for Clinicians
analyzing patient care
• Facilitates use of “resident performance data as the basis for improvement”
• Encourages use of “external quality measures to verify resident and program performance levels”

Vanderbilt University Medical Center
Thank You!

Vanderbilt University Medical Center
Implementation of Healthcare Matrix
Vanderbilt University Medical Center
Internal Review QuestionnaireCore Competencies
1. How does your program provide education that develops patient care practice that is
compassionate, appropriate and effective?
How effective is that training?
1Not
effective
2Somewhat effective
3Moderately
Effective
4Effective
5Very
effective

Vanderbilt University Medical Center
ImplementationInternal Review Process:
– Analyze responses to competency questionnaire and discuss with program director; suggest improvements if needed
– Provide information on competencies and use of Matrix
– Offer to assist in the integration of competencies in M&M and case conferences, etc.

Vanderbilt University Medical Center
Implementation• Introduction to Matrix: Program Director or
Dept. Chairs invite us to do lecture or Grand Rounds to introduce competencies and Matrix.
• Using the Matrix: – Attend M&M or case conferences as
observers – Note the discussion on a blank Matrix
showing which cells/competencies were discussed and which were omitted
– Send Matrix to program director and discuss next steps

Vanderbilt University Medical Center
Implementation• Residents and the Matrix:
– Residents fill in Matrix on their own – Best to let them struggle a little with the
competencies as they think about care of their patient
– Get someone (coach) to review Matrix with them – If the situation/case is difficult, Dept Chair,
Program Director and mentors may assist with filling out Matrix and presentation
• Helpful hint: – Find a “coach” to help residents. At the outset,
we work with the residents and faculty. Then Chief residents or interested faculty take the lead. Sometimes nurses can be coaches such as in Psychiatry at VU.

Vanderbilt University Medical Center
Phase I Phase II Phase III Phase IV
7/2001 6/2002 7/2002 7/20116/2006 7/2006 6/2011 Beyond
• Improve the evaluation processes for all six of the Competencies.
• Provide aggregated resident performance data for Internal Review Process.
• Use resident performance data as the basis for improvement.
• Begin to use external quality measures to verify resident and program performance levels.
• Identify benchmark programs.
• Involve community in building knowledge about good GME.
• Define specific objectives for residents to demonstrate learning of the competencies.
• Begin integrating the teaching and learning of competencies into residents’ didactic and clinical experiences.

Vanderbilt University Medical Center
Research Agenda to Validate Matrix
(Based on Kirkpatrick, Evaluation of Training, 1994)
• Does the Matrix provide a useful framework for teaching and evaluating the performance of clinicians around the competencies?
• Phase I of ACGME : – Define objectives for learning– Begin integrating the teaching and learning
of competencies into didactic and clinical educational experiences
Vanderbilt University Medical Center
Research Agenda to Validate Matrix
• What are we learning about the care (columns) and education (rows) from completed matrices?
• Phase II of ACGME: – Improve the evaluation processes for all
six of the Competencies– Provide aggregated resident performance
data for Internal Review Process

Vanderbilt University Medical Center
• Are the behaviors of clinicians changing based on their completion of practice-based learning and improvement?
• Phase III of ACGME:– Use resident performance data as the
basis for improvement– Begin to use external quality measures to verify
resident and program performance levels
Research Agenda to Validate Matrix

Vanderbilt University Medical Center
• Are the processes and outcomes of care improving?
• Phase III of ACGME:– Begin to link clinical quality indicators
and patient surveys with education
• Phase IV of ACGME: – Adapt and adopt generalizable
information about emerging models of excellence. Involve community building knowledge about good GME.
Research Agenda to Validate Matrix

Vanderbilt University Medical Center
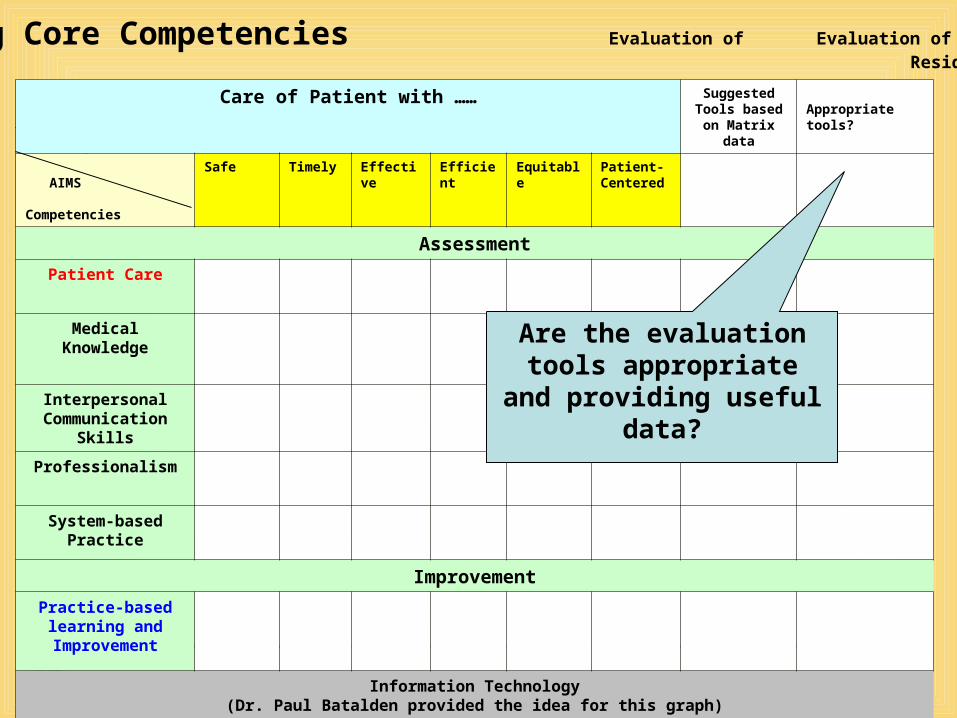
Learning Core Competencies Evaluation of Evaluation of Residents (2006) Tools (2011)
Care of Patient with …… Suggested Tools based on Matrix
data
Appropriate tools?
AIMS
Competencies
Safe Timely Effective
Efficient
Equitable
Patient-Centered
Assessment
Patient Care
MedicalKnowledge
Interpersonal Communication
Skills
Professionalism
System-based Practice
Improvement
Practice-based learning and Improvement
Information Technology(Dr. Paul Batalden provided the idea for this graph)
Based on matrices for a dept or diagnosis,
which evaluation tools best fit the
need?
Vanderbilt University Medical Center
Care of Patient with …… Suggested Tools based on Matrix
data
Appropriate tools?
AIMS
Competencies
Safe Timely Effective
Efficient
Equitable
Patient-Centered
Assessment
Patient Care
MedicalKnowledge
Interpersonal Communication
Skills
Professionalism
System-based Practice
Improvement
Practice-based learning and Improvement
Information Technology(Dr. Paul Batalden provided the idea for this graph)
Are the evaluation tools appropriate and
providing useful data?
Learning Core Competencies Evaluation of Evaluation of Residents (2006) Tools (2011)
Related Documents











