Value-based Strategies for Encouraging New Development of Antimicrobial Drugs i

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
i
Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
i
AbouttheDuke-MargolisCenterforHealthPolicy
TheRobertJ.Margolis,MD,CenterforHealthPolicyatDukeUniversitybringstogetherexpertisefromtheWashington,DCpolicycommunity,DukeUniversityandDukeHealthtoaddressthemostpressingissuesinhealthpolicy.
TheCenter’smissionistoimprovehealthandthevalueofhealthcarebydevelopingandimplementingevidence-basedpolicysolutionslocally,nationally,andglobally.Formoreinformation,visithealthpolicy.duke.edu.
AuthorsGregoryW.DanielDeputyDirector,Duke-RobertJ.Margolis,MD,CenterforHealthPolicyandClinicalProfessor,FuquaSchoolofBusiness,DukeUniversity
MarkB.McClellanDirector,Duke-RobertJ.Margolis,MD,CenterforHealthPolicyandRobertJ.Margolis,MDProfessorofBusiness,MedicineandHealthPolicy,DukeUniversity
MonikaSchneider
ResearchAssociate,Duke-RobertJ.Margolis,MD,CenterforHealthPolicy,DukeUniversity
JingyuanQian
SeniorResearchAssistant,Duke-RobertJ.Margolis,MD,CenterforHealthPolicy,DukeUniversity
GabrielaLavezzariSVPBusinessDevelopment,Biocerna(formerlyResearchDirector,Duke-RobertJ.Margolis,MD,CenterforHealthPolicy,DukeUniversity)
EllendeGraffenreidDirectorofCommunications,Duke-RobertJ.Margolis,MD,CenterforHealthPolicy,DukeUniversity
AdvisoryGroupHalaAudiHead,UKAntimicrobialResistanceReviewTeam
PatrickCourneyaExecutiveVicePresident,Hospitals,QualityandCareDeliveryExcellenceChiefMedicalOfficer,MedicareAdvantage,CostandPrescriptionDrugPlans,Kaiser
EdCoxDirector,OfficeofAntimicrobialProducts,CenterforDrugEvaluationandResearch,FoodandDrugAdministration(FDA)
VanceFowlerProfessorofMedicineandinMolecularGeneticsandMicrobiologyandMemberofDukeClinicalResearchInstitute,DukeUniversitySchoolofMedicine

Value-basedStrategiesforEncouragingNewDevelopmentofAntimicrobialDrugs
ii
RobertGuidosAssociateDirectorforLegislativeAffairs,CenterforDrugEvaluationandResearch,FoodandDrugAdministration(FDA)
StephanHarbarthHead,DRIVE-ABProject,InnovativeMedicinesInitiative
AmandaJezekVicePresident,PublicPolicyandGovernmentRelations,InfectiousDiseasesSocietyofAmerica
JoeLarsenDeputyDirector(Acting),BiomedicalAdvancedResearchDevelopmentAuthority(BARDA)
RamananLaxminarayanDirector,CenterforDiseaseDynamics,Economics&Policy
ShariLingDeputyChiefMedicalOfficer,CentersforMedicareandMedicaidServices(CMS)
LynnMarksSVP,SeniorClinicalAdvisor,InfectiousDisease,GlaxoSmithKline
CliveMeanwellCEO,TheMedicinesCompany
SteveMillerSeniorVicePresidentandChiefMedicalOfficer,ExpressScripts
SumathiNambiarDirector,DivisionofAnti-InfectiveProducts,CenterforDrugEvaluationandResearch,FoodandDrugAdministration(FDA)
KevinOuttersonProfessorofLaw,BostonUniversityExecutiveDirector,CARB-X
EdmundPezallaScholarinResidence,Duke-MargolisCenterforHealthPolicy,DukeUniversityFormerVicePresident,NationalMedicalDirectorforPharmacyPolicyandStrategy,Aetna
CharleneReedCEO,FoundationtoCombatAntimicrobialResistance
JohnRexChiefStrategyOfficer,CARB-XChiefMedicalOfficer,F2G,Ltd.(formerly)SeniorVice-PresidentandChiefStrategyOfficerforInfectiousDiseases,AstraZeneca
John-ArneRottingenAssociateFellowCentreonGlobalHealthSecurity
ii

Value-basedStrategiesforEncouragingNewDevelopmentofAntimicrobialDrugs
iii
ArjunSrinivasanAssociateDirector,HealthcareAssociatedInfectionPreventionPrograms,DivisionofHealthcareQualityPromotion,CentersforDiseaseControlandPrevention(CDC)
MelissaStundickHeadofStrategicAlliances,SperoTherapeutics
EugeneSunChiefExecutiveOfficer,MelintaTherapeutics
UrsulaTheuretzbacherFounder,CentreforAnti-InfectiveAgents
BrentWallaceChiefMedicalOfficer,IntermountainHealthcare
BlakeWisePresidentandChiefOperatingOfficer,Achaogen,Inc.
Acknowledgments:TheauthorswouldliketoacknowledgethefeedbackandguidancethatwereceivedfromourAntimicrobialPaymentReformAdvisoryGroup,andtothankthemforthetimeandeffortthattheycontributedtothedevelopmentofthisproposal.ThisworkwassupportedbyfundsfromtheU.S.FoodandDrugAdministrationandfromMerck&Co.
Value-basedStrategiesforEncouragingNewDevelopmentofAntimicrobialDrugs
iv
TableofContentsExecutiveSummary..............................................................................................................................1
Overview..............................................................................................................................................3
TheProblem.........................................................................................................................................3Weakantimicrobialpipelinewithlowreturnoninvestmentrelativetopublichealthvalue...................3Reimbursementforhigh-priorityantimicrobialsdoesnotreflectpublichealthbenefit...........................4Evidenceofsuperiorityfromclinicaltrialsisnotroutinelyfeasible..........................................................4Diagnosticuncertaintylimitsappropriateuse.........................................................................................5Appropriatestewardshipmeanslowervolume........................................................................................5Fee-for-servicepaymentsfailtoencourageappropriateuse...................................................................6Consequencesofinadequatemarketreimbursementfordevelopment..................................................6
Effortstoimproveantimicrobialdevelopment.....................................................................................6Global“push”and“pull”incentives.........................................................................................................6GlobalsupportforaMarketEntryReward..............................................................................................7U.S.incentives..........................................................................................................................................8
PathforaccomplishingdelinkageintheU.S.......................................................................................10Coreprinciples........................................................................................................................................10
PriorityAntimicrobialValueandEntryAward....................................................................................12QuickAccesstoFundsthroughaMarketEntryReward.........................................................................12Transitioningtopaymentsthatsupportvalue.......................................................................................13
Implementationissues.......................................................................................................................14Determiningeligibledrugcandidates....................................................................................................14Developingevidenceforvalue-basedcontracts.....................................................................................14Financingmechanisms...........................................................................................................................15CareSettings..........................................................................................................................................16DrugsforRareInfections........................................................................................................................17TransitiontoRoutineUseofValue-BasedPaymentsforAntimicrobials................................................17
Conclusion..........................................................................................................................................17
Appendix1.U.S.NetSalesofNew-Molecule,Brand-NameAntibioticDrugsApprovedafter2000,inU.S.dollars(millions)..........................................................18
References.........................................................................................................................................19

Value-basedStrategiesforEncouragingNewDevelopmentofAntimicrobialDrugs
1
ExecutiveSummaryResistancetocurrentantimicrobialdrugsisagrowingsourceofmorbidity,mortality,andhealthcarecosts.Challengingmarketdynamicshaveledtoaweakpipelineofdrugcandidatestorespondtothesethreats.Combined,thesetwotrendsrepresentasignificantandgrowingthreattoUSandglobalhealthpreparedness.
Mostcompanieshaveexitedtheantimicrobialmarket,andthosethatremainareworkingonasmallnumberofdrugs.Lowreturnoninvestment(ROI)relativetobroadpublichealthbenefitsisamajorcontributortothesparsepipelineofdrugstargetingmultidrug-resistantorganismsthatposeseriouspublichealththreats.LowROIisdrivenlargelybyappropriateantimicrobialstewardshipprograms(ASPs)thatlimittheuseofinnovativetherapiestoappropriatepatients,availabilityofeffectiveandlow-costgenericsfortypicalinfectionsthatlimitnovelantimicrobialuse,andareimbursementsystemthatdoesnotreflectthetruepublichealthvalueofeffectivedrugsformultidrug-resistantorganisms.Inparticular,antimicrobialsforhigh-priority,resistantorganismshaveapublichealthvaluethatfarexceedsthefee-for-service(FFS)paymentforthepatientswhoactuallyhaveresistantinfections.Rather,theirvalueincludesbeingavailableforusewhennecessarytostemthespreadofresistantmicrobesbeforetheytakehold.Becauseofthesechallengingmarketconditions,awiderangeofglobalexperts(includingChathamHouse,theAMRReviewinLondon,andtheDRIVE-ABconsortiumintheE.U.)haverecommendedmuchstrongermarketentryor“pull”economicincentivestoencourageinvestmentstobringsuchantimicrobialstomarket.
However,theseapproacheshavenotyettakenhold.Thepublicinvestmentrequiredisdauntingatatimeofincreasingfiscalpressures.Moreover,bringingaproducttomarketdoesnotassureitscontinuingavailabilityandappropriateuse.Further,theU.S.healthcaresystemreliesonmultipleprivatepayersaswellaspublicfinancing,andapublicfundingapproachmightcrowdoutprivatespendinganddeliverysystems.
TheDuke-MargolisCenterforHealthPolicyisdevelopingU.S.policyapproachesthatcouldprovidebettereconomicincentivestoantimicrobialdevelopersthatsuccessfullybringeffectivedrugstothemarket,providingasocietalbenefitthatexceedsthecostoftheincentive.Workingwithabroad-basedadvisorygroup,Duke-Margolishasdevelopedaproposalforapublicly-leveraged,value-basedpaymentmodeltoaddressthesechallengesinaU.S.context.TheCenterbaseditsworkonseveralprinciples:bepartofacomprehensivestrategy;promoteinnovation,access,andstewardship;besustainableandpredictable,leveragepublicmoneywithprivatefunds;providerapidaccesstofundsuponmarketentry;andalignwithbroadershiftsintheU.S.healthcaresystemtovalueandquality.
OurPriorityAntimicrobialValueandEntry(PAVE)Awardproposalcombinesamarketentryrewardwithpopulation-basedpaymentsfrompublicandprivatepayersthatphaseinovertime.ThemarketentryrewardprovidesfundsoverearlyyearsofmarketingafterFDAapproval.Subsequentpaymentsrelyonthedevelopertoincreaserevenuefrompopulation-basedcontractswithpayersthatarelinkedtovaluetosocietythroughinfectionprevention,availability,supportforsustainableuse,andcontinueddatacollection.Byleveragingbothpublicandprivatesupport,thePAVEAwardprovidesdeveloperswithquickaccesstoasignificantrewarduponmarketentryaswellasstrongincentivesformanufacturerstoengagewithpayersinshiftingreimbursementfromFFStopopulation-basedcontractsthatsupporthigh-value,sustainableuse.ThePAVEAward’srisk-sharingmodeldelinksROIfromvolumeusetorewardandsupportavailabilityandappropriateuseofeffectiveantimicrobials.Thismodeladdressesthefundamentalneedforpublicinvestmentindrugsthatcombatresistantbacterialinfectionsbyresolving

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
2
thecurrentconflictbetweenthedriversofROIandstrongstewardshipprograms,whilereinforcingthe“volumetovalue”shiftinhealthcarepayments,andleveraging,ratherthanreplacing,privatefinancing.Finally,themodelcancomplementandbuilduponapproachessupportedbyprivatefoundations,othercountries,andmultinationalorganizationstofurthergenerateglobalsupportforthedevelopmentofpriorityantimicrobials.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
3
OverviewIncreasingantimicrobialresistance(AMR)isaseriousandgrowingglobalpublichealththreat.IntheU.S.alone,theseinfectionsaffectmorethantwomillionpeopleannually,causeanestimated23,000deaths,andgenerateanestimatedeconomicburdenexceeding$55billion.1Ifcurrenttrendscontinue,300millionpeopleworldwideareexpectedtodieprematurelyinthenext35yearsduetoantimicrobialresistantinfections.2
InappropriateuseofexistingantimicrobialscontributestothedevelopmentofAMR.Onethirdofthe266.1millioncoursesofantibioticsdispensedtooutpatientsintheU.S.in2014wereeitherunnecessaryorinappropriate,atadirectcostofover$1billionperyear.3–5Further,theIMSInstituteforHealthcareInformaticsestimatesthatantibioticmisuseleadstomorethan$35billioninavoidablecosts.Highprescriptionratesforbroad-spectrumdrugsfurthercontributetoAMRbyincreasingtheselectivepressureonallbacteriatodevelopbroaderresistance.Unfortunately,limiteddevelopmentandadoptionofeffectiveandrapiddiagnostictoolsinclinicalpracticehinderstheuseofnarrow-spectrumantibiotics,whichtargetgroupsofbacteriamoreselectively.
In2013,theCentersforDiseaseControlandPrevention(CDC)releasedareportdetailingthemosturgentresistantbacterialthreatstopublichealth.6Additionaltypesofinfectionsarefacingadwindlingnumberoftreatmentoptions,andtheWorldHealthOrganization(WHO)independentlyidentifiedtwelveprioritybacterialpathogensthatshouldbecometheprimaryfocusofresearchanddevelopment(R&D)efforts.7AlthoughthepublichealththreatsandR&Dprioritieshavebeenidentified,thepipelineofpotentialtreatmentsislimited,highlightingtheneedforpoliciesthatprovidefinancialincentivestosupportdevelopmentandavailability.
Thispaperdescribeshowtostimulateinvestmentindevelopmentandappropriateuseofhighpriorityantimicrobialdrugs,includinganewproposalthatreflectsU.S.andglobaltrendstowardvalue-based,notvolume-basedpaymentsystems.Ourrecommendationsreflectworkguidedbyamulti-stakeholderAdvisoryGroupthatincludesrepresentativesfromprivateandpublicpayers,pharmaceuticalcompaniesofallsizes,professionalsocieties,academicresearchers,thinktanks,governmentagencies*andpatientadvocacyorganizations,aswellasthroughinteractionswithstakeholdersduringanexpertworkshopandpublicmeeting.
TheProblemWEAKANTIMICROBIALPIPELINEWITHLOWRETURNONINVESTMENTRELATIVETOPUBLICHEALTHVALUE
Avibrantandinnovativeantimicrobialdrugpipelineisneededtoaddressthegrowingpublichealththreatofresistantorganisms,yetasmallnumberofcandidatesareindevelopment.Oftheapproximately40potentialdrugsinclinicaldevelopment,onlysixteenaretargetedtoward“urgent”pathogensand,basedontypicalattritionratesacrossdrugdevelopment,onlysixofthesesixteenareexpectedtobeapprovedbetween2017and2024.8,9Incomparison,morethan170drugsfordiabetesandmorethan700forcancerareinvariousstagesofclinicaldevelopment.10,11
*e.g.,theBiomedicalAdvancedResearchandDevelopmentAuthority(BARDA),theCentersforDiseaseControlandPrevention(CDC),theNationalInstitutesofHealth(NIH),andtheU.S.FoodandDrugAdministration(FDA)

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
4
Onereasonforthelimitedpipelineistherelativelyhighcostanddifficultyofdevelopingantimicrobialsanddemonstratingtheireffectiveness.Drugdevelopmentinmanyclinicalareasisexpensiveandrisky;estimatedcostsacrossallareasrangeupto$1.2-$2.6billionfornoveldrugs,andittakesroughly8yearsformarketapprovalfrominitialINDfiling,withanoverallsuccessrateof10percent.9,12,13Butthereareotherparticularmarket-relatedchallengesthatleadtoinadequateinvestmentinantimicrobialresearchanddevelopment.
REIMBURSEMENTFORHIGH-PRIORITYANTIMICROBIALSDOESNOTREFLECTPUBLICHEALTHBENEFIT
Alongsidesubstantialdevelopmentcostsanduncertainty,thefinancialrewardsforbringingpriorityantimicrobialstomarketarelow.ProductdevelopersevaluatemarketopportunitiesbasedonNetPresentValue(NPV)analysis,whichcomparestheinvestmenttogetadrugtomarketwiththeprojectedfuturereturnsintoday’sdollars.A2014studyfromtheEasternResearchGroupcalculatedaNPVforantimicrobialdrugsintherangeof-$4.5millionto$37.4million,mainlyduetolimitedmarketrevenues.14,15Between2011and2015,themedianyearlysalesofbrand-nameantibioticswithunexpiredpatentsrangedfrom$24millionto$75million(Appendix1)*,comparedtomorethan$500millionformostbrand-nameoncologydrugsapprovedduringthesameperiod.16Amongthesixteennew,brand-nameantimicrobialsapprovedsince2000,onlyfivehavegeneratedannualsalesofmorethan$100million*.Blockbusterdrugstatusrequiresannualsalesover$1billion;antibioticsstruggletoreach10percentofthatgoal.ANPVof$200milliongenerallyhasbeenviewedasabenchmarkabovewhichcompaniesmightdeeminvestmentworthwhile,althoughthisbenchmarkmayvarybysizeandtypeofcompany.17
Incontrasttoreturnsforinnovativetherapiesfornon-communicablediseases,themarketreturnstoantimicrobialdevelopersarelowrelativetothepotentialbenefitstosocietybecausethosewhousethedrugarenottheonlybeneficiariesoftreatment.Rather,benefitsofthesedrugsaccruetothosewhoneverneedtreatment,becausetheavailabilityoftheantimicrobialpreventsthespreadoftheresistantorganism.Thepeoplewhobenefitfromavoidinginfectionsthroughavailabilityandappropriateuseofaneffectivedrugprovidenorevenueforantibioticmanufacturers.Accompaniedbystrongattentiontolimitantimicrobialusetoappropriatecases—sinceusedrivesresistance,overusedrivesresistancemorerapidly—fewindividualswilleverdevelopaseriousresistantinfection.Ideally,theavailabilityofthesehigh-prioritytreatmentswouldbeaccompaniedbystronginfectioncontrolandstewardshipprograms,tominimizetheneedfortheiruse.Fornon-communicablediseaseslikecancer,themainvalueoftreatmentislimitedtotheactualindividualswhoareatriskfororwhodevelopthedisease.
Healthcarepaymentsfocusontheindividualswhoreceivetreatment.Payersandpatientsconsiderthevalueoftreatmenttotheirindividualcases,notthebroaderbenefitsandcostsavingstotheinfectionsthatareprevented.Asaresult,especiallywhenusedappropriately,antimicrobialsforhigh-priorityinfectionsaregenerallylow-revenueproducts.
EVIDENCEOFSUPERIORITYFROMCLINICALTRIALSISNOTROUTINELYFEASIBLE
Newantimicrobialsusuallywillnotcomewithevidencedemonstratingsuperioroutcomescomparedtostandardofcare.18Althoughnewantimicrobialswillhavepreclinicalinvitroandinvivodatashowingtheiractivityagainstbacteriathatareresistanttootherdrugs,demonstratingthismicrobiological
*Derivedfrompubliclyavailablesalesdata2010-2015

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
5
superiorityinstudiesofhumansisnotpossibleroutinely.Thelackofclinicalsuperiorityevidenceisduetobothpracticalconstraintsinantimicrobialclinicaltrialsandthedesirabilityofminimizingtherateofinfectionduetohighlyresistantbacterialstrains.Instead,mostantimicrobialshavebeen,andwillcontinuetobe,studiedusingnon-inferioritytrialdesignsinwhichthenewagentiscomparedtoanotherdrugexpectedtoalsobeactive.Ethically,thecomparisonarminatrialmustbearegimenthatrepresentswhatthetreatingphysicianthinksisthebestcourseoftreatmenttocuretheinfection.Assumingthereisaneffectiveantimicrobialdrugorregimeneffectiveagainstthebacteriaunderstudyandbecausetheoutcomeofinterestisbinary(curevsnocure),theexpectedtreatmenteffectformostnovelantimicrobialsis,atbest,acureratethatisnoworsethanusualcare.
Further,ifalargeclinicaltrialcouldbedesignedtofocusonaspecificbacteriumforwhichtherearenoeffectivetherapies,thenthatwouldindicateafailureofpoliciestopreventtheemergenceofawidespreadresistantmicrobe.Ifaccrualofsubstantialnumbersofpatientsintosuchatrialwerepossible,itwouldimplyasituationwithgrimpublichealthimplications.
Fromtheperspectiveofpayersfocusedonvalueforanindividualpatient,adesirefordemonstrationofsuperiorityisunderstandabletojustifycoverageandreimbursementofnewantimicrobialsathigherprices.Butthisperspectivedoesnotaccountforthepublichealthgoalofprovidingrobustavailabilityofantimicrobialswhentheroutinelyviablepathforregulatoryapprovalcannotbeexpectedtoproducesuchevidence.
DIAGNOSTICUNCERTAINTYLIMITSAPPROPRIATEUSE
Alackofsensitive,specific,andrapiddiagnosticsleadstochallengesbothinclinicaluseandinantibioticdevelopment.Inday-to-daypractice,acuteinfectionsrequireimmediatetreatment,butdeterminationofthespecificcauseoftheinfectionissurprisinglydifficult.Thisparadoxicalproblemarisesbecausetheorganismswhicharecommonlypartofthehealthyhumanmicrobiomeareveryoftenthesameorganismswhichcancauseinfectionandmeredetectionofapotentialpathogendoesnotmeanthatitiscausative.Asaresult,physiciansoftenoptforrelativelybroadempiricaltherapyratherthannarrow(er)therapy,andmostoftennewerandnoveltherapies,basedondiagnosticstests.Negativeresults(lackofdetectionofapathogenorlackofdetectionofresistance)areresultsthatareparticularlylikelytobeignoredifthepatienthassignificantriskfactorsforsuchinfections.
Lackofavailablerapiddiagnosticscanalsoposeachallengeinantimicrobialclinicaltrials,particularlywhenatrialseekstostudyinfectionsduetoaspecificbacterium.Ifapatientispotentiallysuitableforsuchaclinicaltrialbutthephysicianisunabletoconfirmthispromptlywithatest,thepatientmaybetreatedwithoneormoreantibioticspriortoenrollment,whichconfoundsexaminationofthetreatmenteffectsofthenewdrugunderstudy.Further,ifapatientisultimatelyfoundtonothavebeeninfectedwiththetargetorganism(withoutarapiddiagnosticthiswouldbeunknownatenrollment),butisenrolledinthetrialbecauseempiricevidencesuggeststhathemaybe,thesponsorwillhavespentadditionaltimeandmoneyfordatathatwillultimatelynotcontributetodrugapproval.Bothscenariossignificantlyincreaseinefficiency.
APPROPRIATESTEWARDSHIPMEANSLOWERVOLUME
Novelantimicrobialdrugsmustbeusedappropriatelytoslowthedevelopmentofresistance.Inhealthcaresettings,thisgoalisaccomplishedthroughASPswiththecoreelements(definedbytheCDC)ofleadershipcommitment,accountability,drugexpertise,action,tracking,reporting,andeducation.19

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
6
Stewardshipplaysacriticalpublichealthrolebyconservingnewdrugsforresistantinfections;however,thispracticealsolimitssalesvolumeandROIfornewantibiotics.Appropriatestewardshipalsomeansthatmostnovelantimicrobialshaveanarrowsetofpatientsforwhomtheymaybeclinicallyappropriate,limitinguse.IntheU.S.,theCentersforMedicareandMedicaidServices(CMS)hasmandatedstewardshipprogramsasaconditionofparticipationinMedicarefornursinghomes,andissuedaproposedruletorequirethesameconditionswithinhospitals.TheCDChassettargetstoreduceinappropriateantibioticuseintheoutpatientsettingby50percentandwithinhospitalsby20percent.Bothactionsareexcellentpublichealthmeasures,butbothaccentuatethedifficultiesofavolume-basedsalesmodelforantibiotics.Thesemeasurescanbereinforcedbyfinancialincentives:reasonablyeffectivegenericdrugsareavailableformostinfections,sothatpayersandpatientsshouldpreferthesealternativestohigh-pricednewantimicrobials.
FEE-FOR-SERVICEPAYMENTSFAILTOENCOURAGEAPPROPRIATEUSE
TheU.S.healthcaresystemreliesonFFSpayments.Thispaymentsystemisapoorfitforantimicrobialsbecausevolume-basedpaymentsarefundamentallyinconflictwithstewardshiptoavoidtheuseofvaluableantimicrobialswhennotneededtodetertheemergenceofresistance.Asanalternativetopressuresfrommanufacturers(andpotentiallypatients)toincreaseutilization,apaymentapproachthatdelinksrevenuefromvolumeofsalescouldprovidebetterincentivesforappropriateuse.InmanyareasofU.S.healthcare,theshiftfromvolume-tovalue-basedreimbursementisencouragingmoreappropriatetreatment.Butsuchpaymentmechanismshavegenerallynotbeenusedforantimicrobials.
CONSEQUENCESOFINADEQUATEMARKETREIMBURSEMENTFORDEVELOPMENT
Failureofcurrentpaymentsystemstorecognizepublichealthbenefits,pressuresforappropriatestewardship,andtheinsufficientimplementationofnewdiagnosticstoaididentificationoftherightdrugfortherightpatientattherighttimeallresultinlowrevenuesforantimicrobialdevelopers,resultinginmanycompaniesleavingtheantimicrobialspace.Remainingsmallandmediumcompaniesstrugglewithsecuringfundsfrominvestors,andlargemanufacturerswithadiversifiedpipelinestruggletojustifyinvestingR&Ddollarsinanareawithanunpredictableandlowreturncomparedtootheropportunities.Theselowrevenueshaveledmanylargerdrugdeveloperstoshifttheirdiscoveryanddevelopmenteffortstomorelucrativeareas.Forexample,AstraZenecarecentlysolditslate-stageantimicrobialportfoliotoPfizerandspunoffitsearlystageworktofocusondevelopingmedicinesinthreefocusedareas,includingoncology.20In2014,oneoftheworld’slargestprivateantibioticR&DeffortswasatCubistPharmaceuticals.AfterbeingacquiredbyMerck,thevastmajorityoftheCubistR&Deffortwasshutdown.21Ofthetop50pharmaceuticalcompanies(rankedbyglobalsales),onlyfivehaveantibioticsinclinicaldevelopment.8
EffortstoimproveantimicrobialdevelopmentGLOBAL“PUSH”AND“PULL”INCENTIVES
Toaddresstheseissues,manyglobaleffortshaveproposedeconomicincentivestostimulateandrewardinnovation,whichinclude“push”and“pull”incentives.“Push”incentivesfocusonreducingtheR&Dcostsfornewantimicrobialsbyprovidingfinancialandinfrastructuresupport.“Pull”incentivesrewardmanufacturersafteranantimicrobialentersthemarket,increasingpotentialrevenue.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
7
ChathamHouse,aLondon-basedpublicpolicyinstitute,publishedareportin2015proposingantibioticincentivesspanningtheentiredevelopmentpipeline.22Recommendedpre-clinicalandclinicaltrialpushincentivesincludepublicfundingtosupportinitialdiscoveryresearch,andtaxcredits,cashrewards,andpublic-privatepartnershipstoreduceclinicaltrialsanddevelopmentcosts,aswellasamarketentryreward(MER)thatwouldreducethemanufacturers'dependenceonsalesvolumeforROI(alsoknownas“delinkage”).
InMay2016,theReviewonAntimicrobialResistance(AMRReview),commissionedbytheU.K.PrimeMinisterandsupportedbytheWellcomeTrust,publishedadetailedproposaltocombatantimicrobialresistanceincludinganInnovationFundtosupportforearly-stagedevelopmentofantimicrobialsandalump-sumpaymentMERtodevelopersofantimicrobialsmeetingadefinedclinicalneed.23
InJune2016,DRIVE-AB,anEUinitiativecomprisedof23publicandprivatepartners,releasedapreliminaryreportdetailingfivepromisingincentivesforantimicrobialinnovation:1)grantsforearlystageresearch;2)establishinganon-profitdeveloperwhowouldmanageandfinancediscoverythroughcommercialization;3)aMERtodevelopersfollowingapprovalofanantimicrobialthatmeetscertaincriteria;4)an“annuallicensefee”todrugdevelopersforaccesstoaspecifiedvolumeofantimicrobialsaddressingunmetmedicalneeds;5)adual-pricingmodelthatchargesahigherpriceforinappropriateuse.24FinalrecommendationsfromDRIVE-ABwillbereleasedlaterintheyear.
InSeptember2016,stakeholdersfromthepharmaceuticalindustryputtogetheraRoadmapforProgressonCombattingAntimicrobialResistance,whichfolloweduponthepreviousDavosDeclarationthatwassignedbyover100companiesandassociations.25Recommendationsincludedreducingtheenvironmentalimpactofantibioticproduction,encouragingappropriateuseofantibiotics,improvingaccesstoantimicrobialproducts,andgeneratingnewopportunitiesforcollaborationacrossindustryandpublicsectors,whichincludessupportforlumpsumpaymentsuponmarketentry.
TheBostonConsultingGroup(BCG)completedastudyfortheGermanGlobalUnionforAntibioticsResearchandDevelopment(GUARD)InitiativeinFebruary2017.26TworecommendationstargetedresearchanddevelopmentthroughthegenerationofTargetProductProfilestoguidedecisionsforpreclinicalresearch,andaGlobalResearchFundtobeusedtofundprojects,increasethecommunityofantibioticresearchers,andsupportinfrastructure.TwoadditionalrecommendationsincludedaGlobalDevelopmentFundtosupportclinicalresearch,andaGlobalLaunchReward,aMER,withbuiltinsustainabilitymechanismsforthecompanytopaybacktherewardovertimeandundercertainconditions.
GLOBALSUPPORTFORAMARKETENTRYREWARD
AlloftheseglobaleffortsrecommendedsomeformofaMER,whichisdesignedtopayforvitalantimicrobialdrugswithpublicfunds.TheMERprovidessubstantialadditionalrevenuestoreflectpublichealthvaluequicklyafterapproval,andremovestheneedforvolumesales,whichhelpsthedeveloperrecoupinvestments.Aformof‘delinkage’,whichremovesthe‘link’betweendevelopmentcostsandrevenues,theMERenablesuncouplingoftheROIfromthevolumeofdrugsales.DelinkagecouldbenefittheantimicrobialmarketbyremovingdependenceonsalestodriveROI,providingreimbursementandrevenueindependentofsalesvolume,removingtheneedtosethighprices,andprovidingsupportforappropriateuse.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
8
Asgenerallydescribedabove,implementationoftheMERwouldrequiretheformationofanewentitysuchasatrusttooverseetherewardandthemanagementoftheantimicrobial.Therewardwouldreplaceexistingpaymentsforantimicrobials,befundedbypublicsources,andbemanagedthroughnationalorinternationalcontractsthatwouldpreventmarketing,promotesustainableuse,andensureaccessinlow-resourcecountries.Whilefundsmaybedistributedinalumpsumoryearlypayments,currentproposalsenvisionpaymentsoverfiveyearsformeetingcertainbenchmarks.TheantimicrobialMERwouldneedtobelargeenoughforthedevelopertorecoupR&Dinvestmentsandprovideenoughrevenuetojustifyamoresubstantialcommitmenttothistherapeuticarea.Giventhesignificantpublichealthbenefitsfromthedevelopmentofpriorityantimicrobials,therecommendationshaveestimatedtheeffectivelevelofpublicpaymenttobebetween$500millionto$4billiontoachieveanNPVof$200millionforR&Dinvestmentinapriorityantimicrobial.14,23,27,28
WhiletheMERwouldprovideaclearrewardfordevelopers,thereareseveralchallengeswiththismodel.First,publicfundsaredifficulttoobtainandpotentiallysubjecttoongoingbudgetaryapproval;themoresuchfundscanleverage,notreplace,existingpaymentsources,themorelikelyaneffectiveMERcanbeimplementedandsustained.Second,manufacturershavelittletonoincentivetoremainengagedintheproductlifecycleafterreceivingtherewardunlesssomesalesvolumeincentiveremains.Finally,ifthepaymentforthisdrugwasfullydelinkedfromsalesvolume,thenproviderscouldpotentiallyaccessthedrugforfree,adisincentivetostewardship.Proposalstoaddresstheseissuesincludesettingstrictguidelinesforrewardeligibilityanddevelopingaproviderpricingsystemtoencouragestewardship.However,suchoversightwouldaddfurtheradministrativecosts,andmaynotbeeffective.
U.S.INCENTIVES
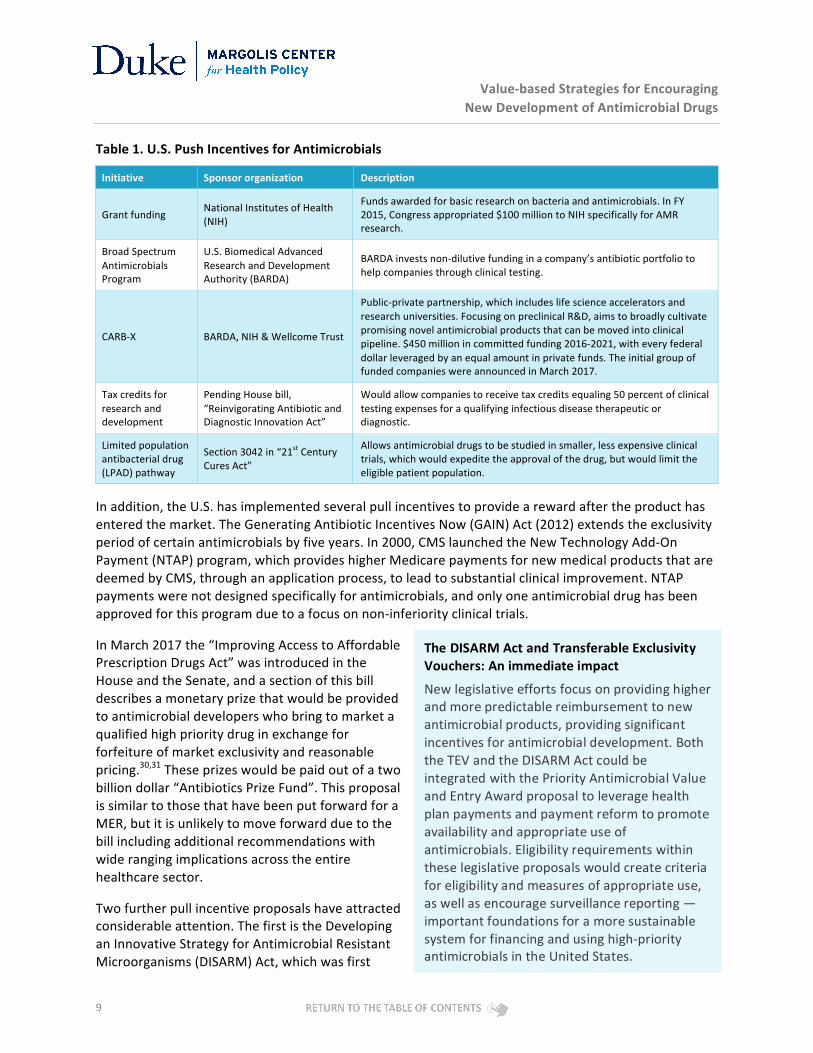
TheU.S.hasbeenleveragingpushandpullincentivestopromoteantimicrobialdevelopment.Table1summarizesthepushincentivesthathavebeenproposedorimplementedinrecentyears.TheLimitedPopulationAntibacterialDrug(LPAD)pathway,whichwasincludedinthe21stCenturyCuresAct(2016),providestheopportunityformorestreamlinedclinicaltrialsandanexpeditedapprovalprocessforantibioticsthataddressunmetmedicalneedsforlimitedpatientpopulations,butdoesnotaddresstheproblemoflimitedsalesvolumesleadingtolowexpectedROI.29
Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
9
Table1.U.S.PushIncentivesforAntimicrobials
Initiative Sponsororganization Description
Grantfunding NationalInstitutesofHealth(NIH)
Fundsawardedforbasicresearchonbacteriaandantimicrobials.InFY2015,Congressappropriated$100milliontoNIHspecificallyforAMRresearch.
BroadSpectrumAntimicrobialsProgram
U.S.BiomedicalAdvancedResearchandDevelopmentAuthority(BARDA)
BARDAinvestsnon-dilutivefundinginacompany’santibioticportfoliotohelpcompaniesthroughclinicaltesting.
CARB-X BARDA,NIH&WellcomeTrust
Public-privatepartnership,whichincludeslifescienceacceleratorsandresearchuniversities.FocusingonpreclinicalR&D,aimstobroadlycultivatepromisingnovelantimicrobialproductsthatcanbemovedintoclinicalpipeline.$450millionincommittedfunding2016-2021,witheveryfederaldollarleveragedbyanequalamountinprivatefunds.TheinitialgroupoffundedcompanieswereannouncedinMarch2017.
Taxcreditsforresearchanddevelopment
PendingHousebill,“ReinvigoratingAntibioticandDiagnosticInnovationAct”
Wouldallowcompaniestoreceivetaxcreditsequaling50percentofclinicaltestingexpensesforaqualifyinginfectiousdiseasetherapeuticordiagnostic.
Limitedpopulationantibacterialdrug(LPAD)pathway
Section3042in“21stCenturyCuresAct”
Allowsantimicrobialdrugstobestudiedinsmaller,lessexpensiveclinicaltrials,whichwouldexpeditetheapprovalofthedrug,butwouldlimittheeligiblepatientpopulation.
Inaddition,theU.S.hasimplementedseveralpullincentivestoprovidearewardaftertheproducthasenteredthemarket.TheGeneratingAntibioticIncentivesNow(GAIN)Act(2012)extendstheexclusivityperiodofcertainantimicrobialsbyfiveyears.In2000,CMSlaunchedtheNewTechnologyAdd-OnPayment(NTAP)program,whichprovideshigherMedicarepaymentsfornewmedicalproductsthataredeemedbyCMS,throughanapplicationprocess,toleadtosubstantialclinicalimprovement.NTAPpaymentswerenotdesignedspecificallyforantimicrobials,andonlyoneantimicrobialdrughasbeenapprovedforthisprogramduetoafocusonnon-inferiorityclinicaltrials.
InMarch2017the“ImprovingAccesstoAffordablePrescriptionDrugsAct”wasintroducedintheHouseandtheSenate,andasectionofthisbilldescribesamonetaryprizethatwouldbeprovidedtoantimicrobialdeveloperswhobringtomarketaqualifiedhighprioritydruginexchangeforforfeitureofmarketexclusivityandreasonablepricing.30,31Theseprizeswouldbepaidoutofatwobilliondollar“AntibioticsPrizeFund”.ThisproposalissimilartothosethathavebeenputforwardforaMER,butitisunlikelytomoveforwardduetothebillincludingadditionalrecommendationswithwiderangingimplicationsacrosstheentirehealthcaresector.
Twofurtherpullincentiveproposalshaveattractedconsiderableattention.ThefirstistheDevelopinganInnovativeStrategyforAntimicrobialResistantMicroorganisms(DISARM)Act,whichwasfirst
TheDISARMActandTransferableExclusivityVouchers:Animmediateimpact
Newlegislativeeffortsfocusonprovidinghigherandmorepredictablereimbursementtonewantimicrobialproducts,providingsignificantincentivesforantimicrobialdevelopment.BoththeTEVandtheDISARMActcouldbeintegratedwiththePriorityAntimicrobialValueandEntryAwardproposaltoleveragehealthplanpaymentsandpaymentreformtopromoteavailabilityandappropriateuseofantimicrobials.Eligibilityrequirementswithintheselegislativeproposalswouldcreatecriteriaforeligibilityandmeasuresofappropriateuse,aswellasencouragesurveillancereporting—importantfoundationsforamoresustainablesystemforfinancingandusinghigh-priorityantimicrobialsintheUnitedStates.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
10
introducedintheHousein2015andisintendedtoallowbroaderadd-onMedicarepaymentsforinnovativeantimicrobialdrugs.WhiledrugsneedtoreceivespecificapprovalfromCMSunderNTAP,DISARMdrugsautomaticallyqualifyforadditionalpaymentsiftheytreatinfectionscausedbyqualifyingpathogens.TheseadditionalpaymentswouldeliminatethedisincentiveforhospitalstousehighpricedantimicrobialsbyoffsettingthecostoftheantimicrobialtotheMS-DRG,andthepaymentscouldpotentiallysupportbettertrackingofantimicrobialresistanceanduseofpriorityantimicrobialdrugs.However,thisincentivestilllinksrevenuetosalesvolume,potentiallycreatingincentivesforoveruse,anddoesnotrewardthepublichealthvaluefortheantimicrobialbeyondthepatientstreated.
AnotherproposedincentivethatwouldaddressthelinkageofsalesvolumeandROIisthetransferableexclusivityvoucher(TEV).32ThereareseveraladvantagestotheTEV,includingthetangiblereturntothemanufacturerandeaseofimplementation.Further,theTEVdoesnotrequiredirectgovernmentappropriations.However,theTEVischallengedbythefactthatnewrevenuescomefromraisingdrugspendinginothertherapeuticareasbydelayinggenericentry.Further,theTEVitselfdoesnotprovideanyincentiveforappropriatestewardshiporcontinuedavailabilityofthedrugoveritslifecycle.Itwouldrequirestrongadministrativeguardrailstoaddresstheseconcerns.
PathforaccomplishingdelinkageintheU.S.COREPRINCIPLES
Theglobalproposalsoutlinedabove(ChathamHouse,AMRReview,etc.)representimportantstepstopromotedevelopmentofnewantimicrobialdrugs.However,theymaybeinfeasibleforimplementationintheU.S.duetomultiplefactors,includingthelackofasinglepayersystem,limitedpublicfunds,andactivemovementfromvolumetomorepopulation-basedfinancingapproachesacrosstheU.S.healthcaresystem.Inordertoaccommodatetheseuniquefactorswhilestillaligningwithglobaleffortstocombatantimicrobialresistance,wehaveidentifiedeightcoreprinciplestoserveasafoundationforourproposal.Theseprinciples,whiledescribedinpreviousproposals,haveadditionalcomponentstoreflectuniquefactorsthataffecttheU.S.(sidebar).
Asdescribedabove,severalglobalorganizationshaveproposedtheuseofpublicfundstospurinnovation,butsoleuseofpublicfundsisnotapreferredoptionintheU.S.Instead,weproposeapartialpubliccontribution(reflectingpublicgood,populationhealthneeds,andappropriateuse)buildingoncontinuedpaymentsfrommultiplepublicandprivatepayers.Whilethesepayersserve
Coreprinciplesforantimicrobialeconomicincentives
1. Beapartofacomprehensivestrategy,whichpromotesdevelopmentacrossthelifecycleofadrug,andenablesthesuccessofbothsmallandlargedevelopers
2. Promoteandrewardinnovation3. Promoteaccess
4. Promotestewardshipsothatantibioticsaresustainableovergenerations
5. Besustainableanddependableoverthelongdrugdevelopmentcycle(atleastadecade)
6. Leveragepublicfundswithprivatepayments
7. Providedeveloperswithrapidaccesstofundsuponmarketentry
8. Supportandalignwithbroadershiftsinpaymentmodelstovalueandqualityandawayfromvolumeandintensity

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
11
distinctpopulationswithdifferentbenefitdesignsandotherfeatures,theyaregenerallymovingfromvolumetovalue-basedpaymentmodels,whichourproposalreinforcesforantimicrobials.
Theshiftfromvolume-tovalue-basedpaymentwithintheU.S.issupportedbyavarietyofmechanisms,includingAlternativePaymentModels(APMs),whichareaimedatreducingunnecessaryhealthcostswhilesustainingorimprovingthequalityofcare.Thisshiftisoftenimplementedthroughpartialorfullepisode-basedbundledpayments(e.g.,onepaymenttoallproviderstreatinganepisodeofcare),orper-patientpayments(e.g.,per-memberper-monthpaymenttoapatient’sprimaryproviders).TheAlternativePaymentModelFrameworkfromtheHealthCarePaymentLearning&ActionNetwork(HCPLAN)outlinesapathtomovefromFFStopopulation-basedpayments.33Withinthisframework,thegoalistoachievepaymentsthatarepartiallyorfullyattheepisode-orperson-levelforapopulationofpatients.
APMsareexpandingintheU.S.,andpreviousexperimentshaveprovidedevidenceofreductioninhealthcosts,especiallyincontrollingexcessspendingoninpatientcare,reducingtheaverageMedicarepaymentperepisodebytwotosixpercenteachyear.34TheMedicareAccessandCHIPReauthorizationAct(MACRA)of2015enablesphysiciansandprovidersworkingwiththemtotransitiontopaymentsbasedonqualityratherthanvolumeofcare.
Sofar,therehavebeenlimitedexamplesoftheuseofvalue-ratherthanvolume-basedpaymentsfordrugs,butsomecompanieshaveenteredintorisk-sharingagreementsbasedontheperformanceofthedrug;forexample,AmgenhasnegotiateddealswithseveralpayersfortheirPCSK9inhibitorwherepayersarereimbursedaportionofthedrugcostifagreed-uponperformancemetricsarenotmet.Therearearangeofoperationalandregulatorychallengestotheimplementationofsuchmodelsthatcomplicatetheirroutineuse,particularlyinareaslikeantimicrobialsthatcurrentlyrepresentonlyasmallpartofhealthcarepayments.Butantimicrobialsmayhavethegreatestbenefitfromashiftawayfromvolume-basedpaymentbecauseofstewardshipconcerns.Ashiftfromvolume-basedtowardper-personpaymentsforacoveredpopulation,aswellaspaymentsthatarelinkedtomeasuresofappropriateuseandcontinuedvalue,couldprovidemuchstrongerincentivesforappropriateuse—andcouldbeimplementedinamannerthatdoesnotincreaseoutlaysforpayers.Additionalpublicmarketentryrewardpayments—toreflectthepublichealthvalueoftheantimicrobial—couldreinforcethisvalue-basedpaymentstructure.Aswedescribebelow,publicsupportformarketentrylinkedtothisshiftinpaymentcouldprovideincentivesformanufacturerstoworkwithotherstakeholderstohelpovercomethebarrierstovalue-basedpaymentsforantimicrobials.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
12
PriorityAntimicrobialValueandEntryAwardToaddressthefundamentalpublichealthneedforadditionalfinancialsupportforthedevelopment,availability,andappropriateuseofhigh-priorityantimicrobialdrugswithintheU.S.healthcaresystem,weproposeapublicly-leveraged,value-basedpaymentmodel.Thismodel,calledthePriorityAntimicrobialValueandEntry(PAVE)Award,supportsandrewardsaccesstoandsustainableuseofinnovativeantimicrobialdrugs,whileprotectingthepublic’shealthfromresistantinfections.ThePAVEAwardprovidesdevelopersquickaccesstoasignificantrewarduponmarketentryofaneffectiveantimicrobial,andprovidesstrongincentivestoshiftreimbursementfrominsuranceplanstopopulation-andvalue-basedcontracts,notpaymentsbasedonvolumeofsales(Figure1).Thefollowingsectionsdescribethedetailsofthemodel,whichcombinesaversionoftheMERuponmarketentrywithsubsequentpaymentscontingentupondemonstratingincreasingrevenuefromvalue-basedcontractswithpayerslinkedtoavailability,sustainableuse,andcontinueddatacollection.
QUICKACCESSTOFUNDSTHROUGHAMARKETENTRYREWARD
ThefirstcomponentofthePAVEAward,whichisbuiltupontheexistingMERmodel,includesapubliclyfinancedpullincentive,ashasbeenrecommendedbymultiplegroups.Thispublicfundingwouldreflectasocietalcontributiontoaglobalthreat.InthePAVEAward,theMERcomponentwouldbeavailableoverthefirstfewyearsuponmarketentryforaverylimitedsetofhighpriorityantimicrobialswithspecificeligibilitycriteriatogivemanufacturerscleardevelopmentgoals,andthemagnitudeoftheMERcouldincreaseifthedrugmeetsadditional,desiredcharacteristicsthatarebeneficialtolargerpublichealthneeds,suchasanovelmechanismofaction,oralavailability,ornewclassofdrug.35ThisphaseofthePAVEAwardwouldprovidedeveloperspredictablerevenue,contingentonthedrug’smarketavailability,lackofprolongedshortages,orfailuretomeettheconditionsforsupportingashifttosustainablepaymentdescribedbelow.
Figure1.OutlineofPAVEaward

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
13
TheMERwouldneedtobelargeenoughtojustifyacommitmenttoantimicrobialdevelopment,butmustalsobesustainable.WhiletheCentersupportstheconceptofasubstantialentryrewardforaproductthatmeetstheeligibilitycriteria,wefavoranapproachthatdoesn’tcompletelyrelyonthereward,toensurethatthemajorityoftherevenuefrompayersshiftstoalternativepaymentmodelsthatpromoteappropriatestewardship.FFSpaymentsforthesehigh-priorityantimicrobialsareonlyadequateifthereisahighprevalenceofhighlyresistantinfections,whichwouldbedevastatingfromthepublichealthperspective.
TRANSITIONINGTOPAYMENTSTHATSUPPORTVALUE
ThefirstcomponentofthePAVEAwarddiffersfromthetraditionalMERbyprovidingannualpayments,withthelargestportionpaidinyearone,andwithsignificantbutdecliningpaymentsthroughyearsfiveorsixasdirectpaymentsfordrugavailabilityanduserampup.Themagnitudeofthesepaymentswillvarydependingonthedrug,withthosedrugsthatrepresentahighersocietalvaluereceivinglargerpayments.
ThesecondcomponentofthePAVEAwarddirectlyincentivizesthecompanytoweanofftheMERthroughdecliningpaymentsthroughyearsfiveorsix,witheachyear’spaymentcontingentupondevelopersdemonstratinganincreasingshareoftheirrevenuefrompopulation-basedAPMslinkedtovaluetosocietythroughavailability,supportforsustainableuse,andcontinueddatacollection.ThistransitionwouldensurethatdrugsalesshifttoAPMsdelinkedfromvolume.ThespecificAPMpaymenttermsandoverallpaymentswillcontinuetobedeterminedthroughcontractnegotiationsbetweenthemanufacturerandpayers,supportedbymeasuresthatreflectvalueandstewardshipinthecoveredpopulations(Figure1).
Whilethesecontractswouldprovideapredictableandsustainablesourceofrevenueforantimicrobialdevelopers,itisimportanttoemphasizethatitwillnotresultinhigherdrugcoststopayers;rather,itcreatesincentivesandopportunitiesforthemtopaydifferently.ThesenewcontractswouldnotrequirepayerstopaymorethaninFFSmodels,butwouldstructurepaymentswithagreateremphasisonpublichealthinreturnforaccesstothedrug.Astheinfrastructureforvaluemeasurementgrows,developingthesecontractswillbeeasierandgainmorewidespreadacceptance.
Suchvalue-basedarrangementsmightinvolveapaymenttothemanufacturerforaccesstothedrugregardlessofthenumberofunitsutilized;paymentswouldbetiedtovaluetothecoveredpopulationratherthanvolumeofsales.Ifstewardshipprotocolsareinplaceandtransmissionofresistanceiscontained,lowdrugutilizationwouldbeexpected,buthavingadrugforalowprevalenceinfectionwouldbehighlyvaluable.Forexample,amanufacturermightcontractwithahealthplanona“permemberpermonth”(PMPM)basisforprovidingthedrugwhenneeded.Amanufacturermightalsoenterintoepisode-basedpaymentcontractstoprovidethedrugasneededforallhospitalizedpatientsincertainDRGs.Inbothcases,thecontractedpaymentwouldnotdependonthevolumeofthedrugactuallyused.Rather,theper-memberorper-episodepaymentwouldvarybasedonmeasuresof,forexample,appropriateuseorcontinuedeffectivenessoftheantimicrobial.Paymentsmightalsobetiedtothedevelopmentofbetterdataandevidenceonthebenefitsandrisksofthedrug,whichcouldsupportbetterpaymentcontractsinthefuture.Inthecaseofinpatientdrugsorphysician-administereddrugsforMedicarebeneficiaries,thisreformcouldbesupportedbythedevelopmentandadoptionofMedicareAPMpilotsbytheCenterforMedicareandMedicaidServicesthatcouldalignwiththeprivateAPMcontracts.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
14
ImplementationissuesDETERMININGELIGIBLEDRUGCANDIDATES
ThePAVEAwardmodelisintendedtopromotedevelopmentandsustainableuseofhigh-prioritydrugsthatcontributetothereductionofdrugresistantbacteria,andtheincentivecriteriashouldbetailoredspecificallytomeettheseneeds.TargetproductprofilescouldsetclearexpectationsofthedesireddrugcharacteristicsthatarerequiredtoqualifyforthePAVEAward,layingoutexpectedantimicrobialactivityandotherperformancestandardsforthedrug.Sucheligibilitycriteriawouldbenefitfromfurtherdevelopment,bothintheU.S.andinternationally.Near-termversionsofPAVEpaymentscouldbeawardedtodrugsthatmeetexistingcriteriarelatedtothepublichealthbenefit,suchasoralformsthatcouldbeusedmoreeasilytocontrolanoutbreakearlyoranovelmechanismofactionthatcouldplausiblysupportnewtypesofantibioticsforwhichresistancehasnotdeveloped.35TheWHOandCDClistsofferagoodstartingpointforprioritizingpathogensthatthedrugsshouldtarget.CARB-X,theleadingpublic-privatepartnershipsupportingpre-clinicalantibioticR&D,usestheseliststoprioritizeinvestments.However,asnewresistantbacteriaemerge,theeligibilitylistwillneedtoadapttothesechanges,sothecriteriawillneedtohavebuilt-inflexibilityandwillneedtobeupdatedonaperiodicbasis.
DEVELOPINGEVIDENCEFORVALUE-BASEDCONTRACTS
SuccessfulimplementationofthePAVEAwardwillrequirecooperationbetweendevelopers,payers,andproviders.Thecontractsshouldencourageshort-andlong-termsavingsfromreducedinappropriateuse,aswellasreducedinfection-relatedcosts,suchasextendedhospitalstays,treatmentcomplications,andadditionalinfections.
Asdescribedabove,demonstrationofsuperiorityduringclinicaldevelopmentcomparedtootherproductsisnearlyimpossibleandundesirableforpublichealthbecauseincreasingthenumberofpeopleforwhomthesedrugsareappropriatewouldmeanthatresistanceand/ortransmissionareincreasing.Continueddevelopmentofeffectivenessevidenceinthepost-marketsettingsisequallychallenging(thedrugwillbeusedsparinglylimitingsamplesize,highriskinfectionswithcomplicatingcomorbiditiescanleadtodeathevenwiththeuseofeffectiveantibiotics).However,continuedcollectionofdata
Public-privatepartnershipsprovideaccountabilitywhilesupportinginnovation
Public-PrivatePartnershipscandeliverresultsthataresuperiortoeithergovernmentorprivateactorsalone.CARB-Xisanewpublic-privatepartnershipprovidingpushincentivesforpre-clinicalR&Dtoaddressthethreatsofantimicrobialresistance.LaunchedonAugust1,2016,CARB-Xhasnowraised$455.5millioninfundingfromBARDA,NIAIDandtheWellcomeTrust.Thefirst11awardswereannouncedinMarch2017(http://www.carb-x.org/portfolio),andthreeoftheseinitialprojectsrepresentnewantibioticdrugclassesagainstGram-negatives,sevenhavenewmoleculartargets,fourarenon-traditionalapproaches,andalltargetCDCandWHOprioritypathogens.Theseprojectswereawardedalmost$24Minitiallyanduptoanother$24Mifmilestonesarehit.Allawardedfundsarematchedwithprivatemoney,with30-50%cost-sharing.
CARB-XwillonlyfundprojectsthroughphaseIclinicaltesting,leavingsignificantscientificandfinancialhurdlestoclearpriortoapproval.Manyofthesecompanieswillrelyonfundingfrominvestors,whichwillonlybeavailableifthereisaclearandpredictablepathtoROI.ImplementationofthePAVEAwardwouldprovideapredictablereturn,makingtheinvestmentinantimicrobialsmoreattractive.LikeCARB-X,thePAVEAwardwillsupplementpublicfundswithprivatepayers,leveragingbothtosupportinnovation.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
15
ontheuseofnovelantibiotics,outcomes(includingsafetyoutcomes),canbenefitthehealthcarecommunityinbetterunderstandingtheuseinclinicalsettingsandsupportsustainableuse.Thus,idealperformancemeasuresinthesecontractswouldbebasedonevidenceofadrug’savailability,supportforsustainableuse,andcontinueddatacollection.
TheCenterrecommendsthat,asinotherareasofhealthcareperformancemeasurement,measuresrelatedtothevalueinpracticeofapriorityantimicrobialdrugshouldbuildonmeasuresavailabletoday.Therearesomeavailablemeasuresthatcouldbeusedasastartingpoint,includingmeasuresthatwouldpertaintoongoingavailabilityandutilityaccessmeasuresandusedata,allofwhichcanhelptotrackappropriatestewardship.TheCDC’sAntimicrobialUseOptionoftheNationalHealthcareSafetyNetworkisalreadyavailabletohospitalstoreportantibioticusedataandcouldbeusedtotrackusenationally.PairingtheAntimicrobialUseoptionwithitscompanionAntimicrobialResistanceOptioncouldprovidethetypeofdatathatwouldassistinmonitoringnewantibiotics.36Asecondsetofmeasurescouldberelatedtodatacollectionandevidencedevelopment,andcouldincludeexecutionofstudiesthatbetterdefinesafetyandutilizationpatternsofanantimicrobialdrug.Specifically,thesemeasurescouldincludetheperformanceofpatientpopulationandsusceptibilitystudiesandcost-effectivenessstudiesthatestimatecoststothepayerifthedrugwerenotavailable.Finally,contractswilltakeintoconsiderationthesupplychainandavailability.
Effectivestewardshipmeasuresarecriticalforthesuccessofdevelopersunderthesecontracts.ProviderswillneedtocollaboratewithmanufacturerstodemonstrateadequateperformanceonstewardshipmeasureswithinproviderAPMs.APMcontractscanbedesignedtobalanceover-andunder-useincentives,forexample,throughacombinationofper-memberper-monthpaymentsandpaymentsforactualuse.SolongasthepaymentswereasignificantshiftawayfromFFSpayments,manufacturersandpayerscouldnegotiatemixedmodels,wheremanufacturersandpayersbothfacefinancialrisk(e.g.,apartialcapitationpayment,withsomeadjustmentsbasedonvolumeandperformance).Indeed,afurtheradvantageofthePAVEAwardmodelisthatthesamekindsofappropriateusemeasurescanbeusedbypayerstosupportaligned,value-basedpaymentsforbothmanufacturersandproviders.Thispaymentalignmentcansupportdevelopersinworkingcollaborativelywithprovidersandpatientstopromoteandensureappropriateuse,whichiscriticalforthelong-termsustainabilityoftheantimicrobialsupplyandpublichealth.
FINANCINGMECHANISMS
BoththeAMRReviewandDRIVE-ABhavesuggestedtheuseofpublicfundstofinanceMERs.Suchfundscouldcomefromgeneralgovernmentrevenues,butdedicatedfundingsourceshavealsobeenproposedtobestreflectthepublicgoodofthesedrugs.TheAMRReviewsuggesteda“payorplay”model,inwhichmanufacturersthatarenotinvestedinantimicrobialdevelopmentwouldbechargedafee.Manytherapeuticareas(includingchemotherapyandsurgery)aredependentoneffectiveantimicrobials;consequently,drugmanufacturersshouldcontributetoantimicrobialdevelopmentthroughinvestmentintheirownantimicrobialR&Dorbypayingafee.Anotherproposedfundingmechanismisataxonallantibioticuse,effectivelya“userfee”foraccesstoantibiotics.37,38Thepurposeofthistaxwouldbetonotonlygeneratefundstorewardantimicrobialdevelopment,butalsotodiscourageinappropriateuseofcurrentantimicrobialsbyincreasingthecostofuse.Theentryrewardcouldalsobefundedthroughayearlypermemberfeeforallhealthcareplans,whichwouldservetodistributethecostofdevelopmentacrosssociety.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
16
AnalternateapproachintheU.S.torelyingsolelyontaxesandfeeswouldbetorelyonthesaleoftransferableexclusivityvouchers(TEVs),eitheraloneorincombinationwithasmallertax,asdescribedabove.Insteadofbeingawardedtomanufacturerswhobringpriorityantimicrobialstothemarket,TEVscouldbeanexpedientmethodforprovidingpublicfundingforantimicrobialdevelopment.Asdescribedabove,therearesomeundueconsequencesthatcouldarisefromsuchincentives,whichcouldpotentiallybeaddressedbyestablishingguardrailstopromoteefficiency.Appropriatelimitsonthetimeand/orrevenuegeneratedbytheTEV,alongwithsufficientsupportforpatientassistanceprograms,wouldeasesomeofthenegativeimpactsofshiftingthefinancialburdenfromantimicrobialdrugstootherdiseaseareas(Table2).Additionally,thevoucherrecipientshouldbeobligatedtoprovidenoticeofwhichdrugwillbereceivingtheextensionfouryearspriortoexpirationofthatdrug’sexclusivity,whichshouldbesufficientnoticetoalleviatetheimpactongenericmanufacturers.32
Table2.Proposed“guardrails”foranantimicrobialtransferableexclusivityvoucherprogram32
Challenges Potentialsolutions
Increasescostinotherareasofhealthcare Capvoucher(invalueorduration)
Cannegativelyaffectthegenericmarket • Voucherwillonlybeawardedtonewdrugs(notapplicableforpreviouslyapproveddrugs)
• Companythatwillbeusingthevouchermustdeclarewhichdrugthevoucherwillbeusedonatleast4yearspriortoexclusivityexpiration
Doesnotencouragestewardship Linkqualityreportingrequirements(e.g.,efficacy,lengthofhospitalstay)toreceiptofvoucher
Couldbepoorlytargetedtoneededantibiotics Limiteligibilitytodrugsthatmeetcriteriasetbypublic/privatepartnershipgroup,whichwillidentifyunmetneedbasedonperiodicreviewsofinfectionrate,resistance,andthedrugpipeline
Tenyearsafterimplementationofvoucherprogram,theGAOcouldconductastudytodeterminetheeffectivenessofthevouchersandwhetherthevoucherprogramshouldcontinue
Whateverfinancingmechanismisused,publicinvestmentisneededtosupportthepublichealthbenefitsofantimicrobialdrugdevelopmentandavailabilitythatarenotcapturedwellinpaymentsforactualuseofthedrug.Whilethispublicinvestmentwouldsupportabenefittoallofsociety,givenincreasingfiscalpressures,itiscriticaltoleverageanypublicfundingtominimizethecostsoftheseeffortstothepublic.Themarketentryrewardproposedherebuildsonratherthanreplacesexistingfundingstreamsforantimicrobials,limitingtheneedforpublicfunds.
CARESETTINGS
Marketchallengesforantimicrobialdevelopmentspantheinpatientandoutpatientsettings,butmostnovelantimicrobialsunderdevelopmentandespeciallythoseintendedtotreatthemosturgentinfectionsthatwouldqualifyforthePAVEAwardwouldbeusedintheinpatientsetting.However,thePAVEAwardcouldpotentiallybeappliedovertime,ifneededtodrugsintheoutpatientsetting.Productdevelopers,payers,andprovidersareenteringintomorerisk-sharing,outcomes-basedmodelstohelpaddressproductperformanceuncertaintyandtohelpensurebettervaluefordollarsspent.FuturepaymentapproachesforantimicrobialsinthissettingcouldleverageCDCtrackingsystemsaswellasappropriateuseguidelinesthathavebeenissuedbyCDCandothergroupstoensureappropriateprescribingandstewardship.Theguidelinesandoutcomesgoverningthevalue-basedpaymentmodel

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
17
forhigh-priorityinpatientantimicrobialsmayneedadjustmentstobeapplicableintheoutpatientsetting.Butweexpectthatthesameprinciplesandapproachcanbeapplied.
DRUGSFORRAREINFECTIONS
Someantimicrobial-resistantinfectionsareextremelyrare.Newantimicrobialsthattreattheseinfectionsareunlikelytogeneratesignificantcostsforpayers—andpayersmaynotseethevalueinhavingcontractsinplacefortheiruse.Creatingvalue-basedpaymentcontracts—oranypayercontracts—maynotbeworthwhile.Inthesecaseswherenoconsequentialprivatemarketexists,aswithdrugsneededascountermeasures,aMERmightbelinkedtoappropriateaccessandcontinuedevidencedevelopment.Ofcourse,itwillgenerallybeinthemanufacturer’sinteresttoworkoutvalue-basedcontractsforpriorityantimicrobialswheneverfeasible,toprovideadditionalrevenuestreams.
TRANSITIONTOROUTINEUSEOFVALUE-BASEDPAYMENTSFORANTIMICROBIALS
Thepresentationofourmodelfocusesonthecurrentstatusoffee-for-servicepaymentsforantimicrobials,recognizingthatitmaytakeseveralyearstophaseintheuseofAPMsbasedonvaluenotvolumeofsales.Withtheincentivesandmomentumcreatedbyourproposedapproach,theaimistomakevalue-basedpaymentthenormforantimicrobialrevenues.Asthesemechanismsbecomemoreroutine,alargershareofrevenuesfromvalue-basedpaymentsshouldbeexpectedearlierafterlaunchofanewpriorityantimicrobialthatqualifiesforthemarketentrypayment.Legislationsupportingthisapproachmightevenspecifyatransitionpathtothepredominantorfulluseofvalue-basedpaymentsforantimicrobials,suchthatantimicrobialslaunchedin,forexample,2027,wouldbeexpectedtohaveahighshareofvalue-basedpaymentcontractsinplacefromlaunchonwards.
ConclusionRecognizingtheimportanceofarobustpipelineofantimicrobialdrugcandidatestomaintainingpublichealth,theproposaldescribedhereisdesignedtoprovideastrong,leveragedfinancialincentiveforpriorityantimicrobialdevelopmentwithintheU.S.ThePAVEAwardandsubsequentvalue-basedcontractswouldbuilduponpaymentstructuresthatarecurrentlyinplacetoshiftthefocusfromsalesvolumetooutcomesandappropriateuse.Thisproposalwillrequirecollaborationacrossarangeofstakeholders,allofwhomwillstandtobenefitfromtheavailabilityofeffective,high-priorityantimicrobials.Whileitmaytakeseveralyearstofullyimplementthisproposal,thePAVEAwardcouldbeginmakingamajorcontributionnowtotheglobalefforttocreateandsustainarobustpipelineofantimicrobialstoaddressurgentandgrowingpublichealthneeds.Inparticular,PAVEcouldbeintegratedwithcurrentlegislativeproposalsforTEVandDISARM,usingtheTEVasthefundingmechanismforthePAVEAwardandimplementingDISARMinawaythatsupportsthetransitiontobetterpaymentmodelsforavailabilityanduseofpriorityantimicrobialsinhospitalizedpatients.Withthegrowingthreatofantimicrobialresistance,andtheurgentneedtodevelopamoresustainablewayofassuringtheavailabilityandappropriateuseofpriorityantimicrobialsintheUnitedStates,thetimeforimplementationisnow.

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
18
Appendix1.U.S.NetSalesofNew-Molecule,Brand-NameAntibioticDrugsApprovedafter2000,inU.S.dollars(millions)
BrandName MoleculeName Owner ApprovalYear
SALES
2011 2012 2013 2014 2015
Avycaz ceftazidime/avibactam Allergen 2015 Productnotyetlaunched 35.8
Sivextro tedizolidphosphate Merck 2014 Productnotyetlaunched 2.4 37
Dalvance dalbavancin Allergen 2014 Productnotyetlaunched 14.6 20.3
Orbactiv oritavancin MedicinesCo. 2014 Productnotyetlaunched 0.8 9.1
Dificid fidaxomicin Merck 2011 24.4 74.4 51.6 47.7 39.8
Teflaro Ceftarolinefosamil Allergen 2010 2.7 22.4 44 70.3 118.5
Vibativ Telavancin Theravance 2009 10.0 0.0 0.0 4.4 9.4
Doribax Doripenem J&J(divested) 2007 Marketinganddevelopmenthaltedin2010
Tygacil Tigecycline Pfizer 2005 148 152 150 112 110
Ketek Telithromycin Sanofi(divested) 2004 Offthemarket
Cubicin Daptomycin Merck 2003 698.8 809.2 908 977 1127
Factive Gemifloxacin Vansen(Divested) 2003 6.3 0.36 -0.12 Divestedthedrugin2012.
Spectracef Cefditorenpivoxil Vansen(Divested) 2001 8.1 0.33 -0.72 Divestedthe
drugin2012.
Invanz Ertapenem Merck 2001 406 445 488 529 569
Zyvox Linezolid Pfizer 2000 640 665 688 680 457.8

Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
19
References1. CentersforDiseasesControlandPrevention.AntibioticResistanceThreatsintheUnitedStates,2013.114
(2013).
2. AntimicrobialResistance:Tacklingacrisisforthehealthandwealthofnations.(TheReviewonAntimicrobialResistance,2014).
3. GetSmartAboutAntibiotics|MeasuringOutpatientPrescribing|CDC.Availableat:http://www.cdc.gov/getsmart/community/programs-measurement/measuring-antibiotic-prescribing.html.(Accessed:29thNovember2016)
4. Fleming-Dutra,K.E.etal.PrevalenceofInappropriateAntibioticPrescriptionsAmongUSAmbulatoryCareVisits,2010-2011.JAMA315,1864(2016).
5. AvoidableCostsinU.S.Healthcare.62(IMSInstituteforHealthcareInformatics,2013).
6. AntibioticResistantThreatsintheUnitedStates,2013.(U.S.DepartmentofHealthandHumanServices,CentersforDiseaseControlandPrevention,2013).
7. WHOpublisheslistofbacteriaforwhichnewantibioticsareurgentlyneeded.(2017).Availableat:http://www.who.int/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/.(Accessed:1stMarch2017)
8. Shore,C.TrackingthePipelineofAntibioticsinDevelopment.Availableat:http://bit.ly/1x8YgVA.(Accessed:5thJanuary2017)
9. Hay,M.,Thomas,D.W.,Craighead,J.L.,Economides,C.&Rosenthal,J.Clinicaldevelopmentsuccessratesforinvestigationaldrugs.Nat.Biotechnol.32,40–51(2014).
10. MedicinesinDevelopmentforDiabetes-AReportonDiabetesandRelatedConditions.4(PharmaceuticalResearchandManufacturersofAmerica,2016).
11. MedicinesinDevelopmentforCancer.4(PharmaceuticalResearchandManufacturersofAmerica,2015).
12. DiMasi,J.A.,Grabowski,H.G.&Hansen,R.W.Innovationinthepharmaceuticalindustry:NewestimatesofR&Dcosts.J.HealthEcon.47,20–33(2016).
13. OfficeoftheAssistantSecretaryforPlanningandEvaluation(ASPE).PrescriptionDrugs:Innovation,Spending,andPatientAccess.(2016).
14. AylinSertkaya,JohnEyraud,AnnaBirkenbach,CalvinFranz,NyssaAckerley,ValerieOverton,KevinOutterson.AnalyticalFrameworkforExaminingtheValueofAntibacterialProducts.(OfficeoftheAssistantSecretaryforPlanningandEvaluation,2014).
15. InfectiousDiseasesSocietyofAmerica.NoNewDrugstoCombatAntimicrobialResistantBugs.IDSAAntimicrobialResistanceInfographics2016(2016).Availableat:https://www.idsociety.org/uploadedFiles/IDSA/Policy_and_Advocacy/Current_Topics_and_Issues/Advancing_Product_Research_and_Development/Bad_Bugs_No_Drugs/Press_Releases/IDSA%20Antibiotic%20Incentives%20Infographic%202016%20Final.pdf.
16. MurrayAitken,MichaelKleinrock,KimPennente,JenniferLyle,DeannaNass,LaurenCaskey.MedicinesUseandSpendingintheU.S.AReviewof2015andOutlookto2020.(IMSInstituteforHealthcareInformatics,2016).
17. Towse,A.&Sharma,P.IncentivesforR&DforNewAntimicrobialDrugs.Int.J.Econ.Bus.18,331–350(2011).
Value-basedStrategiesforEncouraging NewDevelopmentofAntimicrobialDrugs
20
18. Rex,J.H.etal.ProgressintheFightAgainstMultidrug-ResistantBacteria2005–2016:ModernNoninferiorityTrialDesignsEnableAntibioticDevelopmentinAdvanceofEpidemicBacterialResistance.Clin.Infect.Dis.(2017).doi:10.1093/cid/cix246
19. CoreElementsofHospitalAntibioticStewardshipPrograms.(2017).Availableat:https://www.cdc.gov/getsmart/healthcare/implementation/core-elements.html.(Accessed:20thMarch2017)
20. AstraZenecatosellsmallmoleculeantibioticsbusinesstoPfizer.(2016).
21. DamianGarde.Merckdumps120Cubistresearchersafterits$9.5Bmerger.FierceBiotech(2015).Availableat:http://www.fiercebiotech.com/r-d/merck-dumps-120-cubist-researchers-after-its-9-5b-merger.
22. ChathamHouseWorkingGrouponNewAntibioticBusinessModels.TowardsaNewGlobalBusinessModelforAntibiotics.(ChathamHouse).
23. O’Neill,J.TacklingDrug-ResistantInfectionsGlobally:FinalReportandRecommendations.(TheReviewonAntimicrobialResistance,2016).
24. Incentivestostimulateantibioticinnovation:ThepreliminaryfindingsofDRIVE-AB.(DRIVE-AB,2016).
25. IndustryRoadmapforProgressonCombattingAntimicrobialResistance-September2016.(2016).
26. SelmaSternetal.BreakingthroughtheWall-ACallforConcertedActiononAntibioticsResearchandDevelopment.84(BostonConsultingGroupfortheGermanFederalMinistryofHealth,2017).
27. NicholasBagley&KevinOutterson.WeWillMissAntibioticsWhenThey’reGone.TheNewYorkTimes(2017).
28. JimenaS.Ferraro,AdrianTowse&JorgeMestre-Ferrandiz.IncentivesforNewDrugstoTackleAnti-MicrobialResistance.(TheOfficeofHealthEconomics,2017).
29. TheU.S.HouseofRepresentatives,21stCenturyCuresAct.
30. Sen.AlFranken.ImprovingAccessToAffordablePrescriptionDrugsAct.(2017).
31. Rep.JaniceSchakowsky.ImprovingAccesstoAffordablePrescriptionDrugsAct.(2017).
32. Outterson,K.&McDonnell,A.FundingAntibioticInnovationWithVouchers:RecommendationsOnHowToStrengthenAFlawedIncentivePolicy.HealthAff.(Millwood)35,784–790(2016).
33. AlternativePaymentModelFrameworkandProgressTracking(APMFPT)WorkGroup.AlternativePaymentModel(APM)Framework.(2016).
34. Cromwell,J.,Dayhoff,D.A.&Thoumaian,A.H.CostsavingsandphysicianresponsestoglobalbundledpaymentsforMedicareheartbypasssurgery.HealthCareFinanc.Rev.19,41–57(1997).
35. Rex,J.H.&Outterson,K.Antibioticreimbursementinamodeldelinkedfromsales:abenchmark-basedworldwideapproach.LancetInfect.Dis.16,500–505(2016).
36. AntimicrobialUseandResistance(AUR)Module.(2017).
37. Hollis,A.&Ahmed,Z.PreservingAntibiotics,Rationally.N.Engl.J.Med.369,2474–2476(2013).
38. InfectiousDiseasesSocietyofAmerica(IDSA).CombatingAntimicrobialResistance:PolicyRecommendationstoSaveLives.Clin.Infect.Dis.52,S397–S428(2011).
Related Documents







![Creating Value Successful Business Strategies[1]](https://static.cupdf.com/doc/110x72/5439d65aafaf9fbe2e8b5413/creating-value-successful-business-strategies1.jpg)



