SHORT COMMUNICATION Validating the Use of Wrist-Level Light Monitoring for In-Hospital Circadian Studies Anisoara C. N. Jardim, 1 Matthew D. M. Pawley, 1,2 James F. Cheeseman, 1 Mirjam J. Guesgen, 1 Christopher T. Steele, 3 and Guy R. Warman 1 1 Department of Anaesthesiology, University of Auckland, Auckland, New Zealand, 2 Institute of Information and Mathematical Sciences, Massey University, Palmerston North, New Zealand, 3 Military and Emergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, Maryland, USA This clinical methods comparison study describes the difference between light levels measured at the wrist (Actiwatch-L) and at the eye (Daysimeter) in a postoperative in-patient population. The mean difference between the two devices was less than 10 lux at light levels less than 5000 lux. Agreement between the devices was found to decrease as eye-level light exposure increased. Measurements at eye level of 5000 lux or more corresponded to a difference between the devices of greater than 100 lux. Agreement between the eye- and wrist-level light measurements also appears to be influenced by time of day. During the day, the measurement differences were on average 50 lux higher at eye level, whereas at night they were on average 50 lux lower. Although the wrist-level monitor was found to underestimate light exposure at higher light levels, it was well tolerated by participants in the clinical setting. In contrast, the eye-level monitor was cumbersome and uncomfortable for the patients to wear. This study provides light-exposure data on patients in real conditions in the clinical environment. The results show that wrist-level monitoring provides an adequate estimate of light exposure for in-hospital circadian studies. (Author correspondence: [email protected]) Keywords: Daysimeter, Actiwatch-L, Environmental monitoring/instrumentation, Hospital, Light, Circadian, Entrainment INTRODUCTION Surgery, anesthesia, and hospitalization are known to cause sleep disruption (Challet et al., 2007; Gogenur et al., 2009; Murialdo et al., 1993; Njawe, 2003; Vinzio et al., 2003; Yin et al., 2005). This sleep disruption results in part from a circadian disruption due to the absence of strong entraining light-dark cycles, character- istic of the hospital environment, and the phase-shifting effects of surgery and anesthesia. The consequences include impaired immune function, reduced mood, and delayed postoperative recovery (Arjona et al., 2006, 2008; Buijs et al., 2003; Costa e Silva, 2006; Majde et al., 2005). Light is the primary zeitgeber for the human circadian clock, and light therapy has been identified as a useful therapeutic tool to treat depression, both seasonal affec- tive disorder and nonseasonal major depression (reviewed in Terman et al., 2010). Depressed in-patients housed in bright hospital rooms have been shown to have a shorter (up to 3.7 d) stay than those housed in dimly lit rooms (Beauchemin et al., 1996; Benedetti et al., 2001). This effect is not confined to patients being treated for depression. Women hospitalized with myocardial infarc- tion also spend less time in the hospital when allocated sunnier rooms (Beauchemin et al., 1998). Such studies have led to the publication of a manual for clinicians advocating the use of light therapy to treat affective dis- orders and detailing treatment protocols (Wirz-Justice et al., 2009). Despite these data, a UK-based study of 343 828 general hospital admissions showed that the duration of hospital stay does not differ between winter and summer, which might be anticipated if light exposure is important in influencing length of stay (Diffey et al.,1988). Ambient light levels in hospitals have been measured in a number of previous studies using stationary light meters (Bullough et al., 1996; Garcia-Gonzalez et al., 2008; Glotzbach et al., 1993; Gogenur et al., 2007, 2008; Wakamura et al., 2001). All of these studies have shown the presence of dampened daily light-dark cycles with low light exposure during the day and higher levels Address correspondence to Dr. Guy Warman, Department of Anaesthesiology, Faculty of Medical and Health Sciences, The University of Auckland, Private Bag 92019, Auckland 1142, New Zealand. Tel.: + 64-9-373 7599 ext 89302; Fax: + 64-9-3737970; E-mail: g.warman@ auckland.ac.nz Submitted May 5, 2011, Returned for revision June 2, 2011, Accepted July 29, 2011 Chronobiology International, Early Online: 1–7, (2011) Copyright Informa Healthcare USA, Inc. ISSN 0742-0528 print/1525-6073 online DOI: 10.3109/07420528.2011.611603 Chronobiol Int Downloaded from informahealthcare.com by University Of Auckland on 09/27/11 For personal use only.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
S H O R T C O M M U N I C A T I O N
Validating the Use of Wrist-Level Light Monitoring for In-HospitalCircadian Studies
Anisoara C. N. Jardim,1 Matthew D. M. Pawley,1,2 James F. Cheeseman,1 Mirjam J. Guesgen,1
Christopher T. Steele,3 and Guy R. Warman1
1Department of Anaesthesiology, University of Auckland, Auckland, New Zealand, 2Institute of Information and MathematicalSciences, Massey University, Palmerston North, New Zealand, 3Military and Emergency Medicine, Uniformed Services Universityof the Health Sciences, Bethesda, Maryland, USA
This clinical methods comparison study describes the difference between light levels measured at the wrist (Actiwatch-L)and at the eye (Daysimeter) in a postoperative in-patient population. The mean difference between the two devices wasless than 10 lux at light levels less than 5000 lux. Agreement between the devices was found to decrease as eye-level lightexposure increased. Measurements at eye level of 5000 lux or more corresponded to a difference between the devices ofgreater than 100 lux. Agreement between the eye- and wrist-level light measurements also appears to be influenced bytimeof day.During theday, themeasurement differenceswereon average50 lux higher at eye level, whereas at night theywere on average 50 lux lower. Although thewrist-level monitor was found to underestimate light exposure at higher lightlevels, it was well tolerated by participants in the clinical setting. In contrast, the eye-level monitor was cumbersome anduncomfortable for the patients towear. This studyprovides light-exposure dataonpatients in real conditions in the clinicalenvironment. The results show thatwrist-level monitoring provides an adequate estimate of light exposure for in-hospitalcircadian studies. (Author correspondence: [email protected])
Keywords: Daysimeter, Actiwatch-L, Environmentalmonitoring/instrumentation, Hospital, Light, Circadian, Entrainment
INTRODUCTION
Surgery, anesthesia, and hospitalization are known tocause sleep disruption (Challet et al., 2007; Gogenuret al., 2009; Murialdo et al., 1993; Njawe, 2003; Vinzioet al., 2003; Yin et al., 2005). This sleep disruptionresults in part from a circadian disruption due to theabsence of strong entraining light-dark cycles, character-istic of the hospital environment, and the phase-shiftingeffects of surgery and anesthesia. The consequencesinclude impaired immune function, reduced mood,and delayed postoperative recovery (Arjona et al., 2006,2008; Buijs et al., 2003; Costa e Silva, 2006; Majde et al.,2005).
Light is the primary zeitgeber for the human circadianclock, and light therapy has been identified as a usefultherapeutic tool to treat depression, both seasonal affec-tive disorder and nonseasonal major depression(reviewed in Terman et al., 2010). Depressed in-patientshoused in bright hospital rooms have been shown to havea shorter (up to 3.7 d) stay than those housed in dimly litrooms (Beauchemin et al., 1996; Benedetti et al., 2001).
This effect is not confined to patients being treated fordepression. Women hospitalized with myocardial infarc-tion also spend less time in the hospital when allocatedsunnier rooms (Beauchemin et al., 1998). Such studieshave led to the publication of a manual for cliniciansadvocating the use of light therapy to treat affective dis-orders and detailing treatment protocols (Wirz-Justiceet al., 2009). Despite these data, a UK-based study of343 828 general hospital admissions showed that theduration of hospital stay does not differ between winterand summer, which might be anticipated if lightexposure is important in influencing length of stay(Diffey et al.,1988).
Ambient light levels in hospitals have been measuredin a number of previous studies using stationary lightmeters (Bullough et al., 1996; Garcia-Gonzalez et al.,2008; Glotzbach et al., 1993; Gogenur et al., 2007, 2008;Wakamura et al., 2001). All of these studies have shownthe presence of dampened daily light-dark cycles withlow light exposure during the day and higher levels
Address correspondence to Dr. Guy Warman, Department of Anaesthesiology, Faculty of Medical and Health Sciences, The Universityof Auckland, Private Bag 92019, Auckland 1142, New Zealand. Tel.: + 64-9-373 7599 ext 89302; Fax: + 64-9-3737970; E-mail: [email protected]
Submitted May 5, 2011, Returned for revision June 2, 2011, Accepted July 29, 2011
Chronobiology International, Early Online: 1–7, (2011)Copyright Informa Healthcare USA, Inc.ISSN 0742-0528 print/1525-6073 onlineDOI: 10.3109/07420528.2011.611603
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.

than normal at night. Wrist-worn light monitoringdevices are commonplace in clinical studies (Alessiet al., 2008; Ancoli-Israel et al., 2003; Berger et al., 2009;Bisgaard et al., 1999), but eye-level light monitors,which in theory provide a more accurate estimate oflight entering the eye, are less common (Grundy et al.,2009; Higgins et al., 2010; Schernhammer et al., 2001;Savides et al., 1986). The limitations of using stationarylight meters to measure light entering the eye (“entrain-ing light”) are perhaps obvious, but are noteworthy.The orientation of a stationary light meter will affect theilluminance measured. Given that almost all of the artifi-cial light sources in the hospital are ceiling lights, verticalmeasurements will always be higher than horizontalmeasurements. Theoretically, at least, similar problemsexist with the use of wrist-level measurements,given that wrist position does not reliably reflect angleof gaze.
There are no published data on the agreementbetween wrist- and eye-level light exposure in the hospi-tal setting, and there have been only two previous studiesattempting to validate the use of wrist-worn, light-moni-toring devices. The first of these (an abstract in SleepResearch in 1990) reports good overall agreement (r2 =0.93) between 24-h wrist and forehead measurementsin 10 healthy student volunteers (Cole et al., 1990), but“there are sometimes large discrepancies, since thewrist actigraph may be aimed in a very different directionfrom the forehead” (personal communication, DanKripke, 2011). The second study, which was conductedin the hospital setting, compared 24-h wrist-level lightexposure to 480 single measurements of vertical roomlight (Higgins et al., 2007). This study, however, madeno attempt to measure eye-level light exposure. Here weaimed to conduct a validation study to determine theagreement between wrist- and eye-level light monitoringin the hospital environment by simultaneously measur-ing light exposure at the wrist (Actiwatch-L) and at theeye (Daysimeter ) (Rea et al., 2008, 2011). This is essentialfor the accurate assessment of entraining light in the post-operative setting and is a first step in understanding theinfluence of hospitalization on circadian rhythms andsleep. We chose postoperative cardiac patients, as theyhave similar anesthetic treatments, surgery durations,and recovery times.
MATERIALS AND METHODS
Ethics approval for this study was obtained from theMinistry of Health Northern Y Ethics Committee, andall procedures and analyses were conducted inaccordance with the ethical guidelines of the Journal(Portaluppi et al., 2010). The study was also registeredwith the Australia New Zealand Clinical Trials Registry(ACTRN 12609000180213). Twenty-one patients sched-uled for elective cardiac surgery at Auckland City Hospi-tal, Auckland, New Zealand, provided written informedconsent to participate in the observational study.
Of these, 19 wore both a wrist-worn Actiwatch-L(Philips Respironics, Eindhoven, Netherlands), whichrecords photopic illuminance in lux from 400 to 900nm, and a head-worn Daysimeter (Rensselaer Polytech-nic Institute, Troy, NY; described in Bierman et al.,2005), which records photopic illuminance in lux from400 to 700 nm with a sensor mounted at the angle ofgaze, from 1 to 6 d (24 h) postoperatively. Followingcardiac surgery, patients are transferred to the intensivecare unit (ICU). Thirty minutes after arrival in the ICU,both devices were positioned and secured to the patientsby an investigator. Once patients were stable and were nolongermechanically ventilated (usually within 24 h), theywere transferred to the cardiac ward where they spent anaverage of 3 to 7 d convalescing before being discharged.Patients wore both devices continuously from ICU ad-mission until discharge.
All artificial light sources at Auckland City Hospital arefluorescent, and all external windows are tinted andshaded. The ICU consists of a 24-bed unit (four bedsper room) with west-facing windows. Bed spaces are per-manently illuminated by individual ceiling lights. Inaddition, during the day a central room-length ceilinglight is permanently on. Patients also have access to asecond personal light source, a ceiling-light bank directlyabove the bed space. This lighting provides an averageillumination at the angle of gaze (semirecumbent)during the day of 158 lux (SE = 35 lux) and during thenight of 65 lux (SE = 19 lux). The cardiac ward is a 22-room unit (a combination of single-bed and four-bedrooms) with west-facing or internal windows. Artificiallight is provided by ceiling-light sources. Roomlights are on during the day and patients can self-selecta wall-mounted down light. Corridor lighting is onpermanently. This provides an average illumination atthe angle of gaze (semirecumbent) during the day of139 lux (SE = 20 lux) and during the night of 12 lux(SE = 3 lux).
Daysimeters and Actiwatch-Ls were calibrated using astandard 10 000-lux fluorescent light source (Pharos;Lumie, Cambridge, UK) and a Li-Cor LI-185B spectro-photometer (Li-Cor Biosciences, Lincoln, Nebraska,USA) and logged light intensity in lux every 30 s for theduration of the patients’ hospital stay. Patients werevisited between two and four times daily to confirm com-pliance and equipment position. Data were downloadedand handled with Actiwatch-L Activity and Sleep Analysis7 version 7.22 (Cambridge Neurotechnology, Cambridge,United Kingdom), DaysimeterV4 version 8.2.1 (Rensse-laer Polytechnic Institute) and analyzed using MicrosoftExcel and the statistical package R version 2.12 (R Devel-opment Core Team, 2011). Night and day were differen-tiated using local sunrise and sunset times for eachstudy day. Ten-minute averages of the lux values of thetwo devices were used to compare light measurementsbetween individual patients. Agreement between thelight measurements from the Actiwatch-L and the Daysi-meter was calculated using a modified Bland-Altman
A. C. N. Jardim et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.

procedure (Bland et al., 1999; Krouwer, 2008). Further cal-culations evaluated the difference with regards to time ofday (TOD) using a nonlinear mixed-effects model withAR1 autocorrelated error structure and a periodic spline.
RESULTS
Of the 21 subjects recruited, 19 underwent scheduledsurgery, and 12 provided sufficient data for analysis(Daysimeter download failures in six patients and studywithdrawal of one patient accounted for the difference).These patients provided data from the time they arrivedin the ICU immediately following surgery until their dis-charge from the cardiac ward. Individual subject datashowing concurrently recorded wrist- and eye-levellight data (collected from December 2008 to March2009) are displayed in Figure 1. This represents a totalof 29 subject/days of data or 86 399 light measurements.The contribution of the data of each patient to the overalldata set and the percentage of data collected from theICU and the ward are shown in Table 1. The basicdescriptive statistics for the data set are shown in Table 2.
Figure 2 shows the difference between the eye-leveland wrist-level light measurements plotted as a functionof eye-level light measurements (our gold standard). Thisincludes a locally weighted smoother to show the averagedifference as a function of the eye-level measurement.The average difference between eye-level and wrist-level light exposure is positive, indicating that levels
recorded at the eye are higher than at the wrist(Figure 2). However, this bias is low (<10 lux) whenlight levels are below 5000 lux (as indicated by theLoess smoother) as shown in Figure 2. For values of5000 lux or more, the bias increases as again shown bythe Loess smoother. However, only 286 eye-levelmeasurements of 5000 lux or greater were recorded(representing 0.3% of the data). Table 3 puts these
FIGURE 1. Concurrently measured eye-level (black) andwrist-level (gray) light exposure for 12 cardiac patients. All the patients weremon-itored from 19:00 h (except for Patient 2, who commenced monitoring at 07:00 h) and were monitored for 1–7 d. The dark shadingindicates night.
TABLE 1. Contributions to the overall data set described bypatient, room type, and time of day
Contribution to data set (%)
Patient 1 5%Patient 2 8.33%Patient 3 5%Patient 4 3.33%Patient 5 5%Patient 6 10%Patient 7 6.67%Patient 8 8.33%Patient 9 8.33%Patient 10 11.67%Patient 11 18.33%Patient 12 10%Total
ICU 32.7%Ward 67.29%Night 52.6%Day 47.4%
Validation of Wrist Light Levels
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.
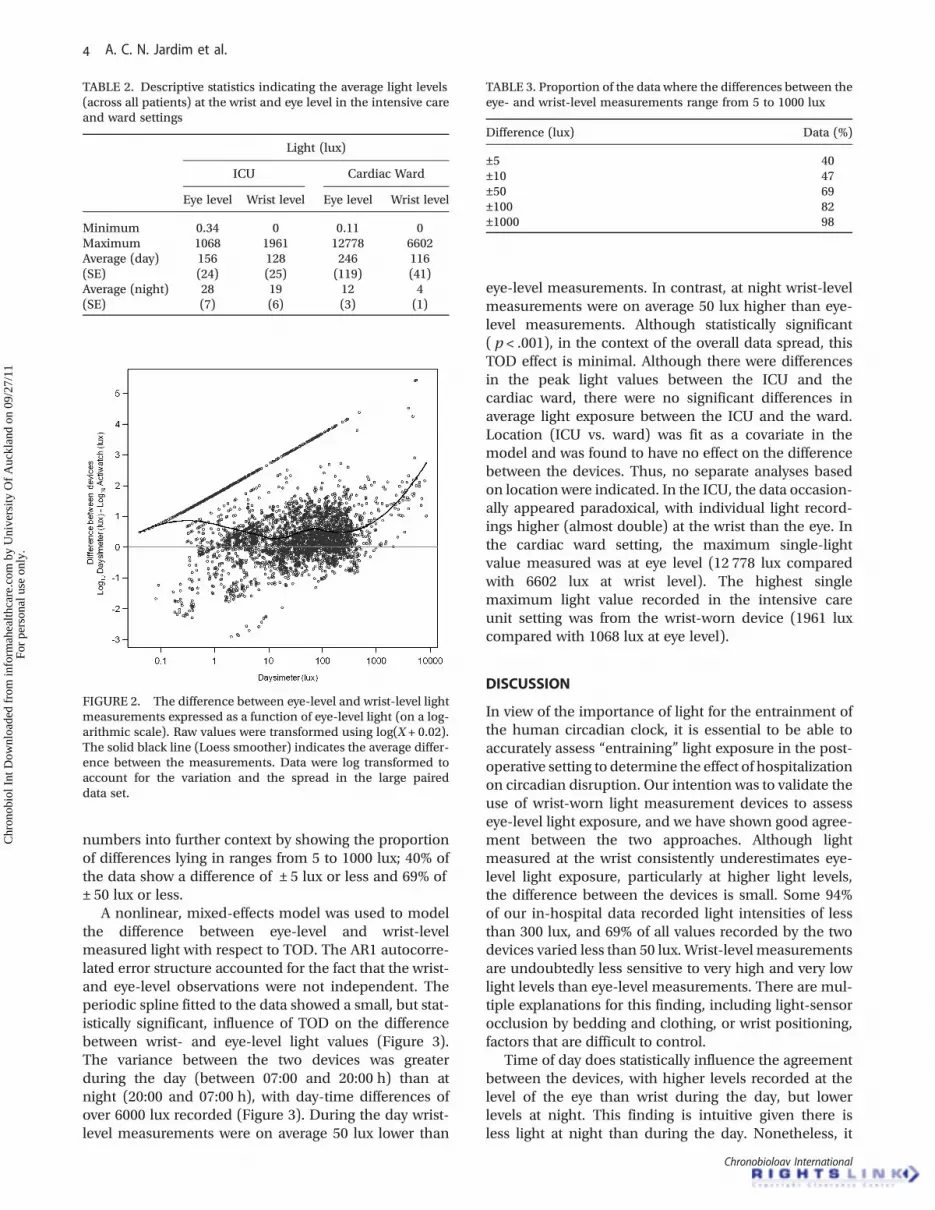
numbers into further context by showing the proportionof differences lying in ranges from 5 to 1000 lux; 40% ofthe data show a difference of ± 5 lux or less and 69% of± 50 lux or less.
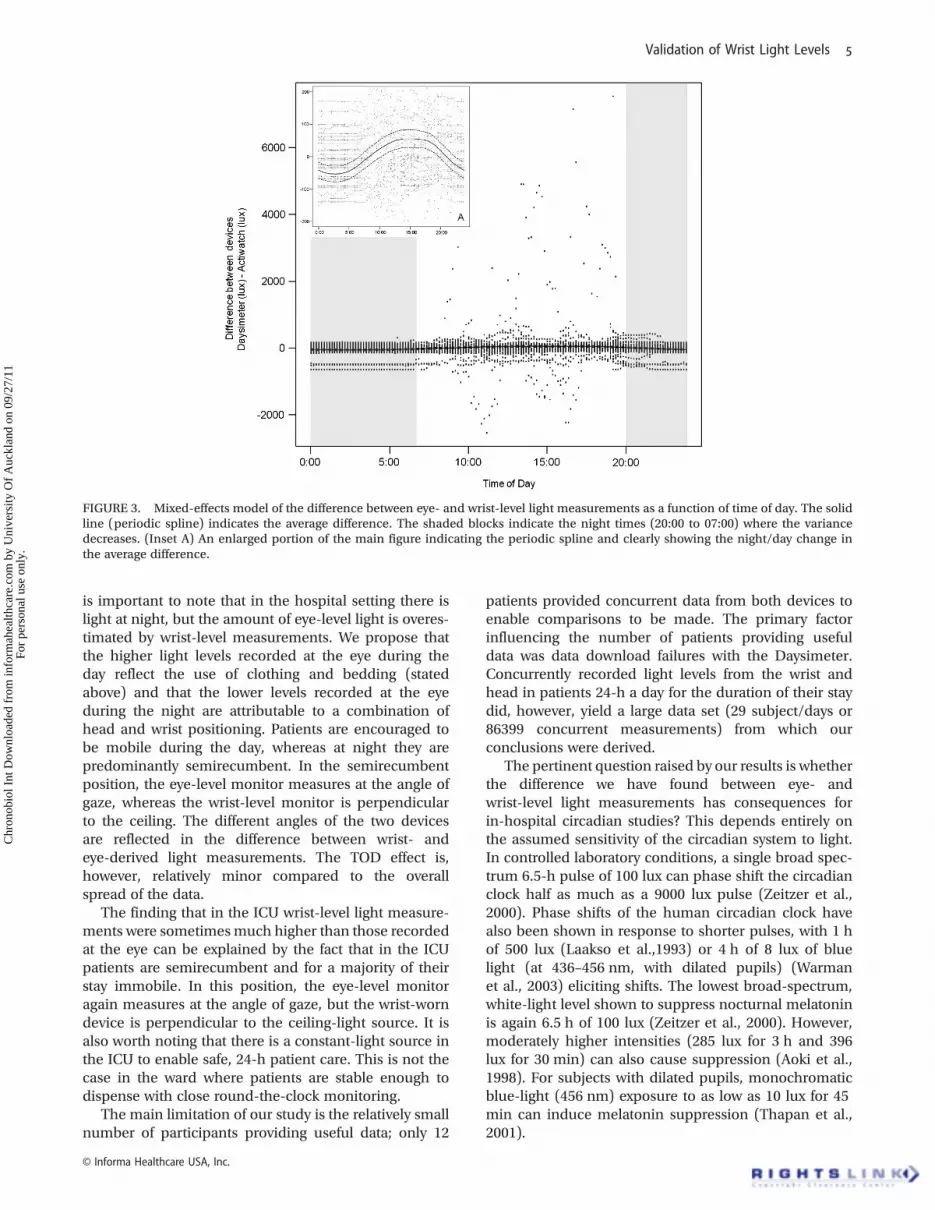
A nonlinear, mixed-effects model was used to modelthe difference between eye-level and wrist-levelmeasured light with respect to TOD. The AR1 autocorre-lated error structure accounted for the fact that the wrist-and eye-level observations were not independent. Theperiodic spline fitted to the data showed a small, but stat-istically significant, influence of TOD on the differencebetween wrist- and eye-level light values (Figure 3).The variance between the two devices was greaterduring the day (between 07:00 and 20:00 h) than atnight (20:00 and 07:00 h), with day-time differences ofover 6000 lux recorded (Figure 3). During the day wrist-level measurements were on average 50 lux lower than
eye-level measurements. In contrast, at night wrist-levelmeasurements were on average 50 lux higher than eye-level measurements. Although statistically significant( p < .001), in the context of the overall data spread, thisTOD effect is minimal. Although there were differencesin the peak light values between the ICU and thecardiac ward, there were no significant differences inaverage light exposure between the ICU and the ward.Location (ICU vs. ward) was fit as a covariate in themodel and was found to have no effect on the differencebetween the devices. Thus, no separate analyses basedon location were indicated. In the ICU, the data occasion-ally appeared paradoxical, with individual light record-ings higher (almost double) at the wrist than the eye. Inthe cardiac ward setting, the maximum single-lightvalue measured was at eye level (12 778 lux comparedwith 6602 lux at wrist level). The highest singlemaximum light value recorded in the intensive careunit setting was from the wrist-worn device (1961 luxcompared with 1068 lux at eye level).
DISCUSSION
In view of the importance of light for the entrainment ofthe human circadian clock, it is essential to be able toaccurately assess “entraining” light exposure in the post-operative setting to determine the effect of hospitalizationon circadian disruption. Our intention was to validate theuse of wrist-worn light measurement devices to assesseye-level light exposure, and we have shown good agree-ment between the two approaches. Although lightmeasured at the wrist consistently underestimates eye-level light exposure, particularly at higher light levels,the difference between the devices is small. Some 94%of our in-hospital data recorded light intensities of lessthan 300 lux, and 69% of all values recorded by the twodevices varied less than 50 lux. Wrist-level measurementsare undoubtedly less sensitive to very high and very lowlight levels than eye-level measurements. There are mul-tiple explanations for this finding, including light-sensorocclusion by bedding and clothing, or wrist positioning,factors that are difficult to control.
Time of day does statistically influence the agreementbetween the devices, with higher levels recorded at thelevel of the eye than wrist during the day, but lowerlevels at night. This finding is intuitive given there isless light at night than during the day. Nonetheless, it
TABLE 2. Descriptive statistics indicating the average light levels(across all patients) at the wrist and eye level in the intensive careand ward settings
Light (lux)
ICU Cardiac Ward
Eye level Wrist level Eye level Wrist level
Minimum 0.34 0 0.11 0Maximum 1068 1961 12778 6602Average (day) 156 128 246 116(SE) (24) (25) (119) (41)Average (night) 28 19 12 4(SE) (7) (6) (3) (1)
FIGURE 2. The difference between eye-level and wrist-level lightmeasurements expressed as a function of eye-level light (on a log-arithmic scale). Raw values were transformed using log(X + 0.02).The solid black line (Loess smoother) indicates the average differ-ence between the measurements. Data were log transformed toaccount for the variation and the spread in the large paireddata set.
TABLE 3. Proportion of the data where the differences between theeye- and wrist-level measurements range from 5 to 1000 lux
Difference (lux) Data (%)
±5 40±10 47±50 69±100 82±1000 98
A. C. N. Jardim et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.
is important to note that in the hospital setting there islight at night, but the amount of eye-level light is overes-timated by wrist-level measurements. We propose thatthe higher light levels recorded at the eye during theday reflect the use of clothing and bedding (statedabove) and that the lower levels recorded at the eyeduring the night are attributable to a combination ofhead and wrist positioning. Patients are encouraged tobe mobile during the day, whereas at night they arepredominantly semirecumbent. In the semirecumbentposition, the eye-level monitor measures at the angle ofgaze, whereas the wrist-level monitor is perpendicularto the ceiling. The different angles of the two devicesare reflected in the difference between wrist- andeye-derived light measurements. The TOD effect is,however, relatively minor compared to the overallspread of the data.
The finding that in the ICU wrist-level light measure-ments were sometimesmuch higher than those recordedat the eye can be explained by the fact that in the ICUpatients are semirecumbent and for a majority of theirstay immobile. In this position, the eye-level monitoragain measures at the angle of gaze, but the wrist-worndevice is perpendicular to the ceiling-light source. It isalso worth noting that there is a constant-light source inthe ICU to enable safe, 24-h patient care. This is not thecase in the ward where patients are stable enough todispense with close round-the-clock monitoring.
The main limitation of our study is the relatively smallnumber of participants providing useful data; only 12
patients provided concurrent data from both devices toenable comparisons to be made. The primary factorinfluencing the number of patients providing usefuldata was data download failures with the Daysimeter.Concurrently recorded light levels from the wrist andhead in patients 24-h a day for the duration of their staydid, however, yield a large data set (29 subject/days or86399 concurrent measurements) from which ourconclusions were derived.
The pertinent question raised by our results is whetherthe difference we have found between eye- andwrist-level light measurements has consequences forin-hospital circadian studies? This depends entirely onthe assumed sensitivity of the circadian system to light.In controlled laboratory conditions, a single broad spec-trum 6.5-h pulse of 100 lux can phase shift the circadianclock half as much as a 9000 lux pulse (Zeitzer et al.,2000). Phase shifts of the human circadian clock havealso been shown in response to shorter pulses, with 1 hof 500 lux (Laakso et al.,1993) or 4 h of 8 lux of bluelight (at 436–456 nm, with dilated pupils) (Warmanet al., 2003) eliciting shifts. The lowest broad-spectrum,white-light level shown to suppress nocturnal melatoninis again 6.5 h of 100 lux (Zeitzer et al., 2000). However,moderately higher intensities (285 lux for 3 h and 396lux for 30 min) can also cause suppression (Aoki et al.,1998). For subjects with dilated pupils, monochromaticblue-light (456 nm) exposure to as low as 10 lux for 45min can induce melatonin suppression (Thapan et al.,2001).
FIGURE 3. Mixed-effects model of the difference between eye- and wrist-level light measurements as a function of time of day. The solidline (periodic spline) indicates the average difference. The shaded blocks indicate the night times (20:00 to 07:00) where the variancedecreases. (Inset A) An enlarged portion of the main figure indicating the periodic spline and clearly showing the night/day change inthe average difference.
Validation of Wrist Light Levels
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.

Practically, measuring eye-level light exposure withthe equipment described here is problematic. Patientcompliance is already a challenge, as patients are bur-dened by a large number of clinical monitoring devicesduring their postoperative stay. In addition, the eye-level device used in this study is impractical and wasfound to be technically unreliable. The development ofsmaller and less invasive personal light meters wouldfurther facilitate the accurate measurement of eye-levellight exposure in the clinical setting. However, for thepurposes of in-hospital ambulatory circadian studies,this may not proffer any great advantage over wrist-monitoring devices. Given that the light sources in ourhospital are exclusively fluorescent, and that 94% of theall of the data recorded were less than 300 lux, unlessthe circadian system is proven to be more sensitive tolight than has been reported previously, a difference of50 lux between the wrist- and eye-level measurementsmay have little relevance.
ACKNOWLEDGMENTS
This work was funded by a University of Auckland StaffResearch Award to G.R.W. and an equipment grantfrom the Maurice and Phyllis Paykel Trust. A.C.N.J.received a University of Auckland Doctoral Scholarship.M.J.G. received a University of Auckland summer stu-dentship stipend. We are grateful for the participationof the clinical staff from the Cardiovascular IntensiveCare Unit and Cardiovascular Ward 42 at Auckland CityHospital, Auckland District Health Board, New Zealand.We are grateful to Professor Dan Kripke for sharing infor-mation regarding his work on this topic.
Declaration of Interest: The authors report no knownconflicts of interest. The authors alone are responsiblefor the content and writing of the paper.
REFERENCES
Alessi CA, Martin JL, Webber AP, Alam T, Littner MR, Harker JO,Josephson KR. (2008). More daytime sleeping predicts less func-tional recovery among older people undergoing inpatient post-acute rehabilitation. Sleep 31:1291–1300.
Ancoli-Israel S, Cole R, Alessi C, Chambers M, Moorcroft W, Pollak CP.(2003). The role of actigraphy in the study of sleep and circadianrhythms. Sleep 26:342–392.
Aoki H, Yamada N, Ozeki Y, Yamane H, Kato N. (1998). Minimum lightintensity required to suppress nocturnal melatonin concentrationin human saliva. Neurosci. Lett. 252:91–94.
Arjona A, Sarkar DK. (2006). The circadian gene mPer2 regulates thedaily rhythm of IFN-gamma. J. Interferon Cytokine Res. 26:645–649.
Arjona A, Sarkar DK. (2008). Are circadian rhythms the code of hypo-thalamic-immune communication? Insights from natural killercells. Neurochem. Res. 33:708–718.
Beauchemin KM,Hays P. (1996). Sunny hospital rooms expedite recov-ery from severe and refractory depressions. J. Affect. Disord.40:49–51.
Beauchemin KM, Hays P. (1998). Dying in the dark: sunshine, genderand outcomes in myocardial infarction. J. R. Soc. Med. 91:352–354.
Benedetti F, Colombo C, Barbini B, Campori E, Smeraldi E. (2001).Morning sunlight reduces length of hospitalization in bipolardepression. J. Affect. Disord. 62:221–223.
Berger AM, Wielgus K, Hertzog M, Fischer P, Farr L. (2009). Patterns ofcircadian activity rhythms and their relationships with fatigue andanxiety/depression in women treated with breast cancer adjuvantchemotherapy. Support Care Cancer 18:105–114.
Bierman A, Klein T, Rea MS. (2005). The Daysimeter: a device formeasuring optical radiation as a stimulus for the circadiansystem. Measure. Sci. Technol. 16:2292–2299.
Bisgaard T, Kjaersgaard M, Bernhard A, Kehlet H, Rosenberg J. (1999).Computerized monitoring of physical activity and sleep in post-operative abdominal surgery patients. J. Clin. Monit. Comput.15:1–8.
Bland JM, Altman DG. (1999). Measuring agreement in method com-parison studies. Stat. Methods Med. Res. 8:135–160.
Buijs RM, van Eden CG, Goncharuk VD, Kalsbeek A. (2003). The bio-logical clock tunes the organs of the body: timing by hormones andthe autonomic nervous system. J. Endocrinol. 177:17–26.
Bullough J, Rea MS, Stevens RG. (1996). Light and magnetic fields in aneonatal intensive care unit. Bioelectromagnetics 17:396–405.
Challet E, Gourmelen S, Pevet P, Oberling P, Pain L. (2007). Reciprocalrelationships between general (Propofol) anesthesia and circadiantime in rats. Neuropsychopharmacology 32:728–735.
Cole R, Kripke D, Gruen W, Nava J. (1990). Ambulatory monitoring oflight exposure: comparison of measurements at forehead and wrist[abstract]. Sleep Res. 19:364.
Costa e Silva JA. (2006). Sleep disorders in psychiatry. Metabolism 55:S40–S44.
Diffey BL, Storey A. (1988). Light and length of stay in hospital[abstract]. J. R. Soc. Med. 81:643
Garcia-Gonzalez MJ, Dominguez-Rodriguez A, Abreu-Gonzalez P.(2008). Light-dark variations in neopterin serum levels in patientswith ST-segment elevation acute coronary syndrome undergoingprimary angioplasty. Rev. Esp. Cardiol. 61:1280–1286.
Glotzbach SF, Rowlett EA, Edgar DM, Moffat RJ, Ariagno RL. (1993).Light variability in the modern neonatal nursery: chronobiologicissues. Med. Hypotheses 41:217–224.
Gogenur I, Ocak U, Altunpinar O, Middleton B, Skene DJ, Rosenberg J.(2007). Disturbances inmelatonin, cortisol and core body tempera-ture rhythms after major surgery. World J Surg. 31:290–298.
Gogenur I, Wildschiotz G, Rosenberg J. (2008). Circadian distributionof sleep phases after major abdominal surgery. Br. J. Anaesth.100:45–49.
Gogenur I, Bisgaard T, Burgdorf S, van Someren E, Rosenberg J. (2009).Disturbances in the circadian pattern of activity and sleep after la-paroscopic versus open abdominal surgery. Surg. Endosc.23:1026–1031.
Grundy A, SanchezM, RichardsonH, Tranmer J., BorugianM, GrahamCH, Aronson KJ. (2009). Light intensity exposure, sleep duration,physical activity, and biomarkers of melatonn among rotatingshift nurses. Chronobiol. Int. 26:1443–1461.
Higgins PA, Winkelman C, Lipson AR, Guo SE, Rodgers J. (2007). Lightmeasurement in the hospital: a comparison of two methods. Res.Nurs. Health 30:120–128.
Higgins PA, Hornick TR, Figueiro MG. (2010). Rest-activity and lightexposure patterns in the home setting: a methodological casestudy. Am. J. Alzheimers Dis. Other Demen. 25:353–361.
Krouwer JS. (2008).Why Bland-Altman plots should use X, not (Y+X)/2when X is a reference method. Stat. Med. 27:778–780.
Laakso ML, Hatonen T, Stenberg D, Alila A, Smith S. (1993). One-hourexposure to moderate illuminance (500 lux) shifts the human mel-atonin rhythm. J. Pineal Res. 15:21–26.
Majde JA, Krueger JM. (2005). Links between the innate immunesystem and sleep. J. Allergy Clin. Immunol. 116:1188–1198.
Murialdo G, Costelli P, Fonzi S, Parodi C, Torre F, Cenacchi T, Polleri A.(1993). Circadian secretion of melatonin and thyrotropin in hospi-talized aged patients. Aging (Milano) 5:39–46.
A. C. N. Jardim et al.
Chronobiology International
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.

Njawe P. (2003). Sleep and rest in patients undergoing cardiac surgery.Nurs. Stand. 18:33–37.
Portaluppi F, Smolensky MH, Touitou Y. (2010). Ethics and methodsfor biological rhythm research on animals and human beings.Chronobiol Int. 27:1911–1929.
ReaMS, BiermanA, FigueiroMG, Bullough JD. (2008). A new approachto understanding the impact of circadian disruption on humanhealth. J. Circadian Rhythms 6:7.
Rea MS, Brons JA, Figueiro MG. (2011). Measurements of light at night(LAN) for a sample of female school teachers. Chronobiol. Int. Inpress. doi.10.3109/07420528.2011.602198
RDC Team. (2011). R: a language and environment for statistical com-puting. Vienna: R Foundation for Statistical Computing. 3-900051-07-0. http://www.R-project.org/;.
Savides TJ, Messin S, Senger C, Kripke DF. (1986). Natural lightexposure of young adults. Physiol. Behav. 38:571–574.
Schernhammer ES, Laden F, Speizer FE, Willett WC, Hunter DJ,Kawachi I, Colditz GA. (2001). Rotating night shifts and risk ofbreast cancer in women participating in the nurses’ health study.J. Natl. Cancer Inst. 93:1563–1568.
Terman M, Terman JS. (2010). Light therapy. In Krieger M, Roth T,Dement W (eds.). Principles and practice of sleep medicine. 5thed. Philadelphia: Elsevier, pp. 1682–1695.
Thapan K, Arendt J, Skene DJ. (2001). An action spectrum formelatoninsuppression: evidence for a novel non-rod, non-cone photoreceptorsystem in humans. J. Physiol. 535:261–267.
Vinzio S, Ruellan A, Perrin AE, Schlienger JL, Goichot B. (2003). Acti-graphic assessment of the circadian rest-activity rhythm inelderly patients hospitalized in an acute care unit. PsychiatryClin. Neurosci. 57:53–58.
Wakamura T, Tokura H. (2001). Influence of bright light duringdaytime on sleep parameters in hospitalized elderly patients.J. Physiol. Anthropol. Appl. Hum. Sci. 20:345–351.
Warman VL, Dijk DJ, Warman GR, Arendt J, Skene DJ. (2003). Phaseadvancing human circadian rhythms with short wavelength light.Neurosci. Lett. 342:37–40.
Wirz-Justice A, Benedetti F, Berger M, Lam RW, Martiny K, Terman M,Wu JC. (2005). Chronotherapeutics (light and wake therapy) inaffective disorders. Psychol. Med. 35:939–944.
Yin YQ, Luo AL, Guo XY, Li LH, Ren HZ, Ye TH, Huang YG. (2005).[Perioperative cortisol circadian secretion and neuropsychologicalstates in patients undergoing coronary artery bypass graftingsurgery]. Zhonghua Wai Ke Za Zhi 43:463–467. [Chinese]
Zeitzer JM, Dijk DJ, Kronauer R, Brown E, Czeisler C. (2000). Sensitivityof the human circadian pacemaker to nocturnal light: melatoninphase resetting and suppression. J. Physiol. 526(Pt 3):695–702.
Validation of Wrist Light Levels
© Informa Healthcare USA, Inc.
Chr
onob
iol I
nt D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
Of
Auc
klan
d on
09/
27/1
1Fo
r pe
rson
al u
se o
nly.
Related Documents