UNCORRECTED PROOF 1 Vagus nerve stimulation during rehabilitative training improves forelimb 2 strength following ischemic stroke N. Q1 Khodaparast ⁎, S.A. Hays, A.M. Sloan, D.R. Hulsey, A. Ruiz, M. Pantoja, R.L. Rennaker II, M.P. Kilgard 4 The University of Texas at Dallas, School of Behavioral Brain Sciences, 800 West Campbell Road, GR41, Richardson, TX 75080-3021, USA 5 6 abstract article info 7 Article history: 8 Received 3 July 2013 9 Revised 31 July 2013 10 Accepted 7 August 2013 11 Available online xxxx 12 13 14 15 Keywords: 16 Vagus nerve stimulation 17 Plasticity 18 Neurorehabilitation 19 Motor cortex 20 Stroke 21 Ischemia 22 Upper limb impairment is a common debilitating consequence of ischemic stroke. Physical rehabilitation after 23 stroke enhances neuroplasticity and improves limb function, but does not typically restore normal movement. 24 We have recently developed a novel method that uses vagus nerve stimulation (VNS) paired with forelimb 25 movements to drive specific, long-lasting map plasticity in rat primary motor cortex. Here we report that VNS 26 paired with rehabilitative training can enhance recovery of forelimb force generation following infarction of 27 primary motor cortex in rats. Quantitative measures of forelimb function returned to pre-lesion levels when 28 VNS was delivered during rehab training. Intensive rehab training without VNS failed to restore function back 29 to pre-lesion levels. Animals that received VNS during rehab improved twice as much as rats that received the 30 same rehabilitation without VNS. VNS delivered during physical rehabilitation represents a novel method that 31 may provide long-lasting benefits towards stroke recovery. 32 © 2013 Elsevier Inc. All rights reserved. 33 34 35 36 Introduction Q2 38 Stroke is the second most common cause of disability worldwide 39 (Leary and Saver, 2003). Ischemic stroke causes neural death due 40 to inadequate blood flow, often resulting in movement impairments 41 on the opposite side of the body (Deb et al., 2010; Lo et al., 2003). 42 Seventy-five percent of patients who survive an ischemic stroke contin- 43 ue to have significant weakness in the upper extremities even after ex- 44 tensive rehabilitative therapy (Harvey and Nudo, 2007; Kwakkel, 2009; 45 Levine and Greenwald, 2009). Impaired limb function reduces the ability 46 to perform activities of daily living, reduces the quality of life, and in- 47 creases medical costs (King, 1996; Whyte et al., 2004). The development 48 of an effective therapy to restore motor function would fulfill a large 49 unmet clinical need. 50 Physical rehabilitation after stroke drives plasticity in the form of 51 reorganization of cortical circuitry in the motor system (Johansson, 52 2000; Nudo, 2003; Rossini and Forno, 2004; Schaechter, 2004; Ward 53 and Cohen, 2004). One common rehabilitative intervention, constraint 54 induced movement therapy (CIMT) causes reorganization of the 55 motor cortex map of arm movement (Sawaki et al., 2008; Schaechter 56 et al., 2002). Additionally, new methods using virtual reality and electri- 57 cal stimulation of motor cortex may also promote increased synaptic 58 plasticity and cortical reorganization within the motor cortex (Adkins- 59 Muir and Jones, 2003; Lindenberg et al., 2012; You et al., 2005). 60 The development of additional methods to increase neural plasticity 61 may lead to improved recovery of motor function (Hallett, 2001; 62 Nudo, 2003). We have recently developed a method to induce specific 63 and long-lasting cortical map plasticity by pairing vagus nerve stimula- 64 tion (VNS) with movements or sensory stimuli in intact rats (Engineer 65 et al., 2011; Porter et al., 2011). Repeatedly delivering VNS with fore- 66 limb movements resulted in movement-specific map plasticity within 67 the primary motor cortex beyond training without VNS (Porter et al., 68 2011). We hypothesized that this enhancement in reorganization with- 69 in the motor cortex may improve recovery of function after stroke. 70 Upper limb strength is one of the best prognostic indicators for arm 71 function and chronic disability following stroke (Harris and Eng, 2007; 72 Mercier and Bourbonnais, 2004; Sunderland et al., 1989). Here, we 73 evaluated whether the delivery of VNS during rehabilitative training 74 can enhance recovery of forelimb strength in a model of ischemic stroke. 75 Rats were trained to perform an isometric force task that quantitatively 76 measures forelimb force generation (Hays et al., 2012). This task is fully 77 automated, allowing the experimenter to test several animals simulta- 78 neously and avoid the possibility of experimenter bias. Unilateral 79 injections of a peptide vasoconstrictor, endothelin-1, into primary 80 motor cortex caused an ischemic infarct and impaired function of the 81 trained forelimb (Fang et al., 2010; Gilmour et al., 2004; Hays et al., 82 2012). Rats underwent rehabilitative training for five weeks with 83 or without the delivery of VNS. No VNS was delivered on week six to 84 allow evaluation of persistent effects. VNS delivered during rehabilita- 85 tive training restored pull force generation back to pre-lesion levels, 86 whereas extensive rehabilitative training without VNS failed to restore 87 function. These findings suggest that VNS paired with physical rehabil- 88 itation may hold promise for enhancing recovery of upper extremity 89 function after stroke. Neurobiology of Disease xxx (2013) xxx–xxx ⁎ Corresponding author. Fax: +1 972 883 2491. E-mail address: [email protected] (N. Khodaparast). Available online on ScienceDirect (www.sciencedirect.com). YNBDI-03019; No. of pages: 10; 4C: 0969-9961/$ – see front matter © 2013 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.nbd.2013.08.002 Contents lists available at SciVerse ScienceDirect Neurobiology of Disease journal homepage: www.elsevier.com/locate/ynbdi Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulation during rehabilitative training improves forelimb strength following ischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.2013.08.002

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
2
3Q1
4
5
6789101112131415161718192021
35
36
37Q2
38
39
40
41
42
43
44
45
46
47
48
49
50
51
52
53
54
55
56
57
58
59
60
Neurobiology of Disease xxx (2013) xxx–xxx
YNBDI-03019; No. of pages: 10; 4C:
Contents lists available at SciVerse ScienceDirect
Neurobiology of Disease
j ourna l homepage: www.e lsev ie r .com/ locate /ynbd i
Vagus nerve stimulation during rehabilitative training improves forelimbstrength following ischemic stroke
FN. Khodaparast ⁎, S.A. Hays, A.M. Sloan, D.R. Hulsey, A. Ruiz, M. Pantoja, R.L. Rennaker II, M.P. KilgardThe University of Texas at Dallas, School of Behavioral Brain Sciences, 800 West Campbell Road, GR41, Richardson, TX 75080-3021, USA
O⁎ Corresponding author. Fax: +1 972 883 2491.E-mail address: [email protected] (N. KhAvailable online on ScienceDirect (www.sciencedire
0969-9961/$ – see front matter © 2013 Elsevier Inc. All rihttp://dx.doi.org/10.1016/j.nbd.2013.08.002
Please cite this article as: Khodaparast, N., eischemic stroke, Neurobiol. Dis. (2013), http
Oa b s t r a c t
a r t i c l e i n f o22
23
24
25
26
27
28
29
30
31
32
Article history:Received 3 July 2013Revised 31 July 2013Accepted 7 August 2013Available online xxxx
Keywords:Vagus nerve stimulationPlasticityNeurorehabilitationMotor cortexStrokeIschemia
D P
RUpper limb impairment is a common debilitating consequence of ischemic stroke. Physical rehabilitation afterstroke enhances neuroplasticity and improves limb function, but does not typically restore normal movement.We have recently developed a novel method that uses vagus nerve stimulation (VNS) paired with forelimbmovements to drive specific, long-lasting map plasticity in rat primary motor cortex. Here we report that VNSpaired with rehabilitative training can enhance recovery of forelimb force generation following infarction ofprimary motor cortex in rats. Quantitative measures of forelimb function returned to pre-lesion levels whenVNS was delivered during rehab training. Intensive rehab training without VNS failed to restore function backto pre-lesion levels. Animals that received VNS during rehab improved twice as much as rats that received thesame rehabilitation without VNS. VNS delivered during physical rehabilitation represents a novel method thatmay provide long-lasting benefits towards stroke recovery.
© 2013 Elsevier Inc. All rights reserved.
3334
E
T61
62
63
64
65
66
67
68
69
70
71
72
73
74
75
76
77
78
79
80
81
82
83
84
85
UNCO
RRECIntroduction
Stroke is the second most common cause of disability worldwide(Leary and Saver, 2003). Ischemic stroke causes neural death dueto inadequate blood flow, often resulting in movement impairmentson the opposite side of the body (Deb et al., 2010; Lo et al., 2003).Seventy-five percent of patients who survive an ischemic stroke contin-ue to have significant weakness in the upper extremities even after ex-tensive rehabilitative therapy (Harvey and Nudo, 2007; Kwakkel, 2009;Levine and Greenwald, 2009). Impaired limb function reduces the abilityto perform activities of daily living, reduces the quality of life, and in-creasesmedical costs (King, 1996;Whyte et al., 2004). The developmentof an effective therapy to restore motor function would fulfill a largeunmet clinical need.
Physical rehabilitation after stroke drives plasticity in the form ofreorganization of cortical circuitry in the motor system (Johansson,2000; Nudo, 2003; Rossini and Forno, 2004; Schaechter, 2004; Wardand Cohen, 2004). One common rehabilitative intervention, constraintinduced movement therapy (CIMT) causes reorganization of themotor cortex map of arm movement (Sawaki et al., 2008; Schaechteret al., 2002). Additionally, newmethods using virtual reality and electri-cal stimulation of motor cortex may also promote increased synapticplasticity and cortical reorganization within the motor cortex (Adkins-Muir and Jones, 2003; Lindenberg et al., 2012; You et al., 2005).The development of additional methods to increase neural plasticity
86
87
88
89odaparast).ct.com).
ghts reserved.
t al., Vagus nerve stimulation://dx.doi.org/10.1016/j.nbd.20
may lead to improved recovery of motor function (Hallett, 2001;Nudo, 2003). We have recently developed a method to induce specificand long-lasting cortical map plasticity by pairing vagus nerve stimula-tion (VNS) with movements or sensory stimuli in intact rats (Engineeret al., 2011; Porter et al., 2011). Repeatedly delivering VNS with fore-limb movements resulted in movement-specific map plasticity withinthe primary motor cortex beyond training without VNS (Porter et al.,2011).We hypothesized that this enhancement in reorganization with-in the motor cortex may improve recovery of function after stroke.
Upper limb strength is one of the best prognostic indicators for armfunction and chronic disability following stroke (Harris and Eng, 2007;Mercier and Bourbonnais, 2004; Sunderland et al., 1989). Here, weevaluated whether the delivery of VNS during rehabilitative trainingcan enhance recovery of forelimb strength in amodel of ischemic stroke.Rats were trained to perform an isometric force task that quantitativelymeasures forelimb force generation (Hays et al., 2012). This task is fullyautomated, allowing the experimenter to test several animals simulta-neously and avoid the possibility of experimenter bias. Unilateralinjections of a peptide vasoconstrictor, endothelin-1, into primarymotor cortex caused an ischemic infarct and impaired function of thetrained forelimb (Fang et al., 2010; Gilmour et al., 2004; Hays et al.,2012). Rats underwent rehabilitative training for five weeks withor without the delivery of VNS. No VNS was delivered on week six toallow evaluation of persistent effects. VNS delivered during rehabilita-tive training restored pull force generation back to pre-lesion levels,whereas extensive rehabilitative training without VNS failed to restorefunction. These findings suggest that VNS paired with physical rehabil-itation may hold promise for enhancing recovery of upper extremityfunction after stroke.
during rehabilitative training improves forelimb strength following13.08.002

TE
R
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
2 N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
UNCO
RREC
Materials and methods
Subjects
Nineteen adult female Sprague–Dawley rats, approximately 4 monthsold andweighing approximately 250 gwhen the experiment began,wereused in this experiment. The rats were housed in a 12:12 h reversedlight cycle environment so that behavioral testing took place during thedark cycle in order to increase daytime activity levels. Rats were fooddeprived to no less than 85% of their normal body weight during trainingasmotivation for the food pellet rewards. This studywas designed to takeinto consideration the rapid hormonal cycle of female rats. To ensure thatthedata for each ratwas collectedduring every stage of the estrus cycle allanalyses were based on the average of a week's worth of behavioral data.All handling, housing, surgical procedures, and behavioral training ofthe rats were approved by the University of Texas at Dallas InstitutionalAnimal Care and Use Committee.
Behavioral apparatus and software
The behavioral chamber consisted of an acrylic box(10 × 12 × 4.75 in.) with a slot (2.5 × 0.4 in.) located in the frontright corner of the box through which the rats could access thepull handle. The slot location restricted access such that only theright forelimb could be used to perform the task. The aluminumpull handle was centered in the slot at a height of 2.5 in. fromthe cage floor and at lateral distances varying from 0.75 in. insideto 0.75 in. outside relative to the inner wall surface of the cage,depending on the training stage. The handle was affixed to a customdesigned force transducer (Motor Pull Device, Vulintus LLC, Sachse,TX) located outside the cage. The maximum load capacity of thetransducer was 2 kg, and the typical forces generated by the ratsfell within the linear range of measurement. Forces readings weresampled at 20Hz and measured with ±1 g accuracy. Force measure-ments were calibrated with a force meter at least once per week.
Custom software was used to control the task and collect data. Amotor controller board (Motor Controller, Vulintus LLC, Sachse, TX)sampled the force transducer every 50 ms and relayed information toa custom MATLAB software which analyzed, displayed, and stored thedata. Force values and corresponding timestamps were collected ascontinuous traces for each trial to allow for the analysis of force profilesover the course of a session. If a trial was successful, the software trig-gered an automated pellet dispenser (Vulintus LLC, Sachse, TX) to delivera sucrose pellet (45 mg dustless precision pellet, BioServ, Frenchtown,NJ) to a receptacle located in the front left corner of the cage.
Isometric force task training
The isometric force task was performed as previously described.Training sessions lasted 30 min and were conducted twice daily, fivedays a week, with sessions on the same day separated by at least 2 h.During early phases of training, experimentersmanually shaped animalsby using ground sucrose pellets to encourage interaction with the han-dle. Rats pulled the handle initially located 0.75 in. inside the trainingcage to receive a sucrose reward pellet. A trial was initiated when therat generated a force of at least 10 g on the handle. After trial initiation,the force was sampled for 4 s. If the force threshold was broken withina 2 second window following the initial contact, the trial was recordedas a success and a reward pellet was delivered. If the force did not exceedthresholdwithin the 2 secondwindow, the trialwas recorded as a failureandno rewardwas given. Hit ratewas calculated based on the number ofsuccessful trials over the total number of initiated trials: Hit rate =[(total successful trials / total trials) ∗ 100]. Force on the pull handlewas sampled for 2 additional seconds following the 2 second trialwindow, regardless of the trial outcome, to capture any late attemptswhich were unrewarded. Following the 4 s of data collection there was
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
OO
F
a 50 millisecond pause before rats could initiate another trial. If rats didnot receive 50 pellets in a single day, they were given 10 g of pelletsafter daily training sessions were complete. The task was made progres-sively more difficult as rats met the criterion for number of successfultrials within a session and progressed to the next stage. As the trainingstages increased, the handle was gradually retracted to 0.75 in. outsidethe cage and the force threshold progressively increased up to 120 g.If an animal exceeded criteria for a proceeding stage, they were auto-matically advanced to the stage that matched their performance. Theprescribed position and threshold values were strictly adhered to forpre- and post-lesion measurements.
Rats were held at the pre-lesion stage until they had 10 successivesessions averaging over 85% success rate. The pre-lesion data reportedin this study is compiled from these 10 sessions. After this point, therats were given an ischemic lesion followed by seven days of recovery,after which they returned for post-lesion behavioral testing withthe same parameters as pre-lesion allowing for a direct comparison ofperformance. All rats were tested until they had 4 sessions with greaterthan 10 trials each during the post-lesion assessment. Rats then pro-ceeded to the therapy stage where VNS was delivered on each success-ful trial for 25 days (Fig. S1). Following the therapy stage, all ratsunderwent an additional two days (week 6) of rehabilitative trainingonly, to allow assessment of the persistent effects of VNS pairing.
D PUnilateral motor cortex ischemic lesion
Unilateral ischemic lesions of primarymotor cortexwere performedsimilar to a previously described method (Fang et al., 2010; Gilmouret al., 2004; Hays et al., 2012, 2013). See Supplementary Methodssection for details.
Vagus nerve cuff implantation
Following ischemic lesion, all rats were implanted with a skull-mounted two-channel connector (headcap) and a bipolar stimulatingnerve cuff constructedwith platinum-iridium leads (5–6 kΩ impedance).Implantations were performed as previously described (Engineer et al.,2011; Porter et al., 2011). See Supplementary Methods sections fordetails.
Application of VNS
Behavioral training was identical for all rats. The VNS during Rehabgroup received approximately 9000 total stimulations over 25 days(i.e., fifty 30 min sessions). VNS was delivered within 50 ms of a suc-cessful pull attempt. VNS was delivered as a 500 ms train of 15 pulsesat 30 Hz (Fig. S1). Each biphasic pulse was 0.8 mA in amplitude and100 μs in phase duration. These parameters are identical to our earlierstudies (Engineer et al., 2011; Porter et al., 2011). Previous studiesusing the same parameters employed in this study have demonstratedchanges in electroencephalographic measures and neuronal spikingsynchrony during VNS, indicating that the nerve is successfully stimu-lated (Engineer et al., 2011; Nichols et al., 2011). No stimulationwas delivered during the post-lesion assessment stage. During thefirst day of post-lesion assessment, no rats had a stimulator cable con-nected to the headcap. For both the Rehab rats and the VNS + Rehabrats, the stimulator cable was first connected during the second day ofpost-lesion assessment and was connected every day until the end ofthe fifth week of therapy. The stimulation cable for the Rehab rats wasnot connected to a stimulator. During the sixth week, the stimulatorcable was not utilized for either group. Rats were perfused and brainsremoved following the sixth week of training to quantify lesion size(see Supplementary Methods for details).
during rehabilitative training improves forelimb strength following13.08.002
207
208
209
210
211
212
213
214
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
3N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
Statistics
All data are reported as the mean ± SEM. All comparisons wereplanned in the experimental design a priori, and significant differenceswere determined using one-way ANOVA, two-way ANOVA, and t-testswhere appropriate. Statistical tests for each comparison are noted inthe text. One tailed t-tests comparing individual subject performanceafter therapy (week 6) to baseline performance (PRE) were used todetermine which rats exhibited a significant impairment after therapy.All other t-tests were two-tailed. Paired t-tests were used to comparerepeated measures over time within groups. Alpha level was set at0.05 for all comparisons. Significant differences between the Rehaband VNS + Rehab groups are noted in the figures with an asterisk.See Table S1 for statistical values for t-test comparisons.
Results
Rats acquire skilled performance of the isometric force task
To assess forelimb function in the context of stroke, ratswere trainedto perform the isometric force task, a behavioral test that quantitativelyassesses multiple parameters of forelimb function (Hays et al., 2012).The task requires rats to reach out and grasp a handle attached to a
UNCO
RRECT
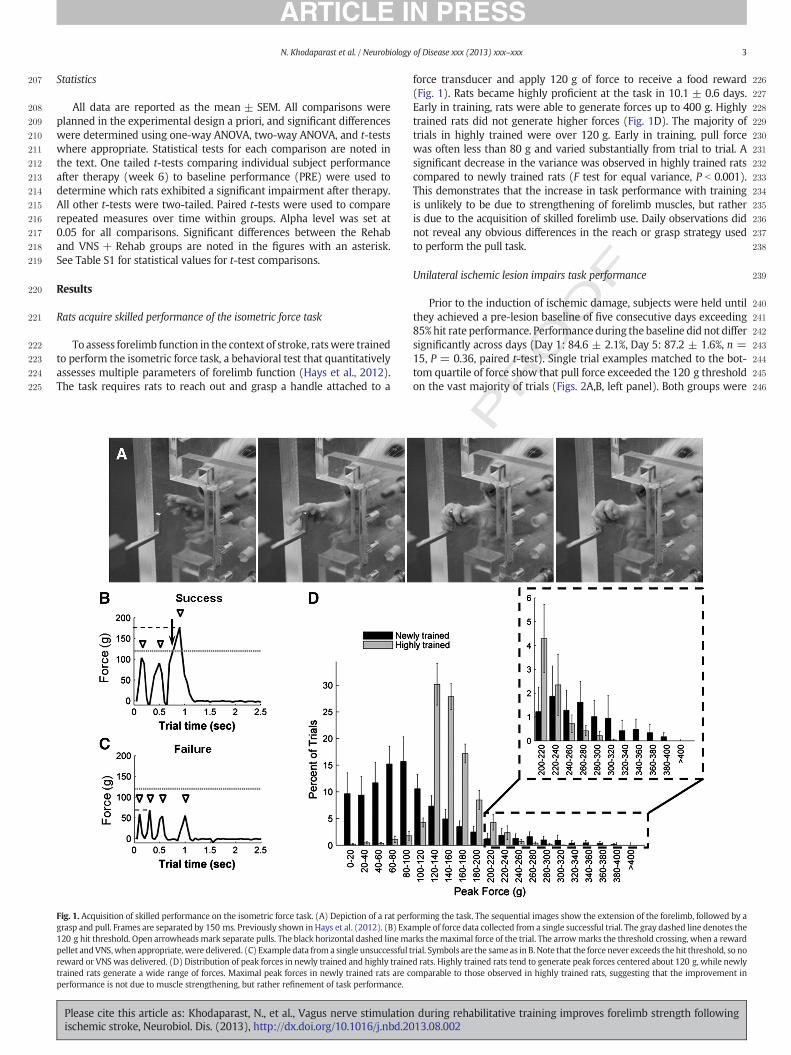
Fig. 1. Acquisition of skilled performance on the isometric force task. (A) Depiction of a rat perfgrasp and pull. Frames are separated by 150 ms. Previously shown in Hays et al. (2012). (B) Exa120 g hit threshold. Open arrowheadsmark separate pulls. The black horizontal dashed linemapellet andVNS,when appropriate,were delivered. (C) Example data from a single unsuccessful treward or VNS was delivered. (D) Distribution of peak forces in newly trained and highly trainetrained rats generate a wide range of forces. Maximal peak forces in newly trained rats are cperformance is not due to muscle strengthening, but rather refinement of task performance.
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
OO
F
force transducer and apply 120 g of force to receive a food reward(Fig. 1). Rats became highly proficient at the task in 10.1 ± 0.6 days.Early in training, rats were able to generate forces up to 400 g. Highlytrained rats did not generate higher forces (Fig. 1D). The majority oftrials in highly trained were over 120 g. Early in training, pull forcewas often less than 80 g and varied substantially from trial to trial. Asignificant decrease in the variance was observed in highly trained ratscompared to newly trained rats (F test for equal variance, P b 0.001).This demonstrates that the increase in task performance with trainingis unlikely to be due to strengthening of forelimb muscles, but ratheris due to the acquisition of skilled forelimb use. Daily observations didnot reveal any obvious differences in the reach or grasp strategy usedto perform the pull task.
Unilateral ischemic lesion impairs task performance
Prior to the induction of ischemic damage, subjects were held untilthey achieved a pre-lesion baseline of five consecutive days exceeding85%hit rate performance. Performanceduring thebaseline did not differsignificantly across days (Day 1: 84.6 ± 2.1%, Day 5: 87.2 ± 1.6%, n =15, P = 0.36, paired t-test). Single trial examples matched to the bot-tom quartile of force show that pull force exceeded the 120 g thresholdon the vast majority of trials (Figs. 2A,B, left panel). Both groups were
ED P
R
orming the task. The sequential images show the extension of the forelimb, followed by ample of force data collected from a single successful trial. The gray dashed line denotes therks themaximal force of the trial. The arrowmarks the threshold crossing, when a rewardrial. Symbols are the same as in B. Note that the force never exceeds the hit threshold, so nod rats. Highly trained rats tend to generate peak forces centered about 120 g, while newlyomparable to those observed in highly trained rats, suggesting that the improvement in
during rehabilitative training improves forelimb strength following13.08.002

CTED P
RO
OF
247
248
249
250
251
252
253
254
255
256
257
258Q3
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
Fig. 2. VNS paired with Rehab improves hit rate after ischemic lesion. (A, B) Single trial force profiles matched to the bottom quartile of force for each experimental group throughout thecourse of the experiment. The gray dashed line indicates the 120 g hit threshold. (C) Hit rate performance over the course of the experiment. VNS paired with Rehab improves recoverycompared to Rehab on most weeks. The increase in hit rate is still present at week 6, after the cessation of VNS therapy. N refers to number of rats in each group. * indicates significantdifference between Rehab and VNS + Rehab. (D) Correlation of individual subject performance prior to lesion and after the completion of therapy. Empty symbols denote a significantreduction after therapy compared to pre-lesion performance. Symbols on or above the line suggest recovery, while those below the line indicate impairment. Note the consistent recoveryin the VNS + Rehab group and the wide variability in recovery in the Rehab group.
4 N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
UNCO
RREhighly successful at the task, with no difference observed in hit rate
between groups (Fig. 2C, PRE, Rehab: 87.0 ± 0.7%; VNS + Rehab:87.7 ± 1.5%, n = 9,6, unpaired t-test, P = 0.63, also see Movie S1).
Induction of unilateral ischemic damage significantly worsenedperformance in both groups compared to pre-lesion (Fig. 2C, POST,Rehab: 37.8 ± 4.1%, paired t-test, P b 0.001; VNS + Rehab: 38.8 ± 7.5%,P b 0.001, also see Movie S2). No difference was observed betweengroups (unpaired t-test, P = 0.89). Single trial examples matched tothe bottom quartile of force after lesion illustrate the reduction in peakforce and increase in number of pulls per trial (Figs. 2A,B, center panel).
Physical rehabilitation is the most common intervention torestore motor function after stroke (Piernik-Yoder, 2013), so wesought to evaluate the effectiveness of rehabilitative training withoutVNS to improve motor outcomes. ANOVA of hit rate in this grouprevealed a significant effect (F[6,56] = 2.64, P = 0.025). Rehabilitativetrainingwithout VNS (Rehab) resulted in amodest recovery of forelimbfunction, but was unable to return performance to pre-lesion levels.Average hit ratewas significantly reduced compared to pre-lesion levelsthroughout the course of therapy (Fig. 2C, PRE vs. weeks 1–6, allP b 0.01, also see Table S1 and Movie S3). By week 6, the impairmentof hit rate had recovered 47.5 ± 15.4%. Performance of individual ratsvaried widely after therapy, ranging from a substantial impairment tofull recovery (Fig. 2D, also see Fig. S2A). 6 of 9 rats (67%) were signifi-cantly worse compared to pre-lesion performance after the therapy,suggesting that rehabilitative training without VNS is typically insuffi-cient to restore forelimb performance to pre-lesion levels.
We sought to evaluate if the addition of VNS pairedwith rehabilitativetraining enhanced recovery of forelimb function. ANOVA of hit rate
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
revealed a significant effect (F[6,35] = 11.83, P b 0.001). VNS pairedwith rehabilitative training (VNS + Rehab) fully restored forelimb per-formance to pre-lesion levels. No significant difference from pre-lesionwas observed between weeks 2 and 6 (all P N 0.05). The benefits ofVNS paired with physical rehabilitation were evident during weeksix after the cessation of VNS, suggesting a long-lasting benefit (week5 vs. week 6, within, P = 0.89). After the completion of therapy, hitrate was indistinguishable from pre-lesion performance (99.2 ± 9.6%recovery, also see Movie S4). Only 1 of 6 rats (17%) demonstrated astatistically significant impairment compared to pre-lesion performanceafter the therapy, suggesting that VNS paired with physical rehabilitationimproves recovery of forelimb function.
To determine if VNS paired with rehabilitative training confersan advantage beyond rehabilitative trainingwithout VNS, we comparedperformance across groups at each week of therapy. ANOVA of hit raterevealed a significant effect of treatment (F[1,83] = 33.21, P b 0.001)and time (F[5,83] = 3.14, P = 0.012). Post hoc comparisons demon-strated that VNS + Rehab displayed an increased hit rate comparedto Rehab on most weeks (Fig. 2C). The increase in hit rate persistedthroughout the remainder of therapy (unpaired t-test, P b 0.05 forweeks 2, 3, 5, 6). These results demonstrate that VNS paired with reha-bilitative training results in a significant increase in recovery comparedto rehabilitative training without VNS.
Unilateral ischemic lesion reduces forelimb strength
In addition to assessing hit rate performance, we sought to evaluateforelimb strength. Before ischemic lesion, peak force generated by the
during rehabilitative training improves forelimb strength following13.08.002
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
337
338
339
340
341
342
343
344
5N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
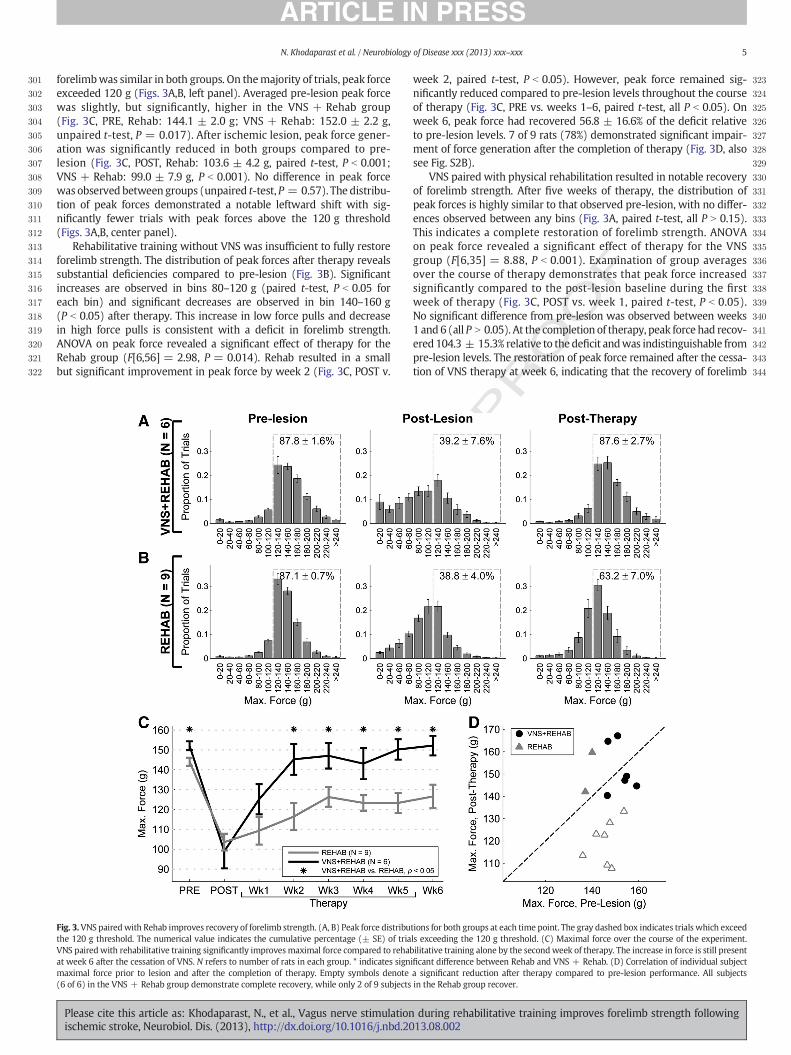
forelimbwas similar in both groups. On themajority of trials, peak forceexceeded 120 g (Figs. 3A,B, left panel). Averaged pre-lesion peak forcewas slightly, but significantly, higher in the VNS + Rehab group(Fig. 3C, PRE, Rehab: 144.1 ± 2.0 g; VNS + Rehab: 152.0 ± 2.2 g,unpaired t-test, P = 0.017). After ischemic lesion, peak force gener-ation was significantly reduced in both groups compared to pre-lesion (Fig. 3C, POST, Rehab: 103.6 ± 4.2 g, paired t-test, P b 0.001;VNS + Rehab: 99.0 ± 7.9 g, P b 0.001). No difference in peak forcewas observed between groups (unpaired t-test, P = 0.57). The distribu-tion of peak forces demonstrated a notable leftward shift with sig-nificantly fewer trials with peak forces above the 120 g threshold(Figs. 3A,B, center panel).
Rehabilitative training without VNS was insufficient to fully restoreforelimb strength. The distribution of peak forces after therapy revealssubstantial deficiencies compared to pre-lesion (Fig. 3B). Significantincreases are observed in bins 80–120 g (paired t-test, P b 0.05 foreach bin) and significant decreases are observed in bin 140–160 g(P b 0.05) after therapy. This increase in low force pulls and decreasein high force pulls is consistent with a deficit in forelimb strength.ANOVA on peak force revealed a significant effect of therapy for theRehab group (F[6,56] = 2.98, P = 0.014). Rehab resulted in a smallbut significant improvement in peak force by week 2 (Fig. 3C, POST v.
UNCO
RRECT
Fig. 3.VNS pairedwith Rehab improves recovery of forelimb strength. (A, B) Peak force distributhe 120 g threshold. The numerical value indicates the cumulative percentage (± SE) of triaVNS pairedwith rehabilitative training significantly improvesmaximal force compared to rehabat week 6 after the cessation of VNS. N refers to number of rats in each group. * indicates signmaximal force prior to lesion and after the completion of therapy. Empty symbols denote(6 of 6) in the VNS + Rehab group demonstrate complete recovery, while only 2 of 9 subjects
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
OO
F
week 2, paired t-test, P b 0.05). However, peak force remained sig-nificantly reduced compared to pre-lesion levels throughout the courseof therapy (Fig. 3C, PRE vs. weeks 1–6, paired t-test, all P b 0.05). Onweek 6, peak force had recovered 56.8 ± 16.6% of the deficit relativeto pre-lesion levels. 7 of 9 rats (78%) demonstrated significant impair-ment of force generation after the completion of therapy (Fig. 3D, alsosee Fig. S2B).
VNS paired with physical rehabilitation resulted in notable recoveryof forelimb strength. After five weeks of therapy, the distribution ofpeak forces is highly similar to that observed pre-lesion, with no differ-ences observed between any bins (Fig. 3A, paired t-test, all P N 0.15).This indicates a complete restoration of forelimb strength. ANOVAon peak force revealed a significant effect of therapy for the VNSgroup (F[6,35] = 8.88, P b 0.001). Examination of group averagesover the course of therapy demonstrates that peak force increasedsignificantly compared to the post-lesion baseline during the firstweek of therapy (Fig. 3C, POST vs. week 1, paired t-test, P b 0.05).No significant difference from pre-lesion was observed between weeks1 and 6 (all P N 0.05). At the completion of therapy, peak force had recov-ered 104.3 ± 15.3% relative to the deficit andwas indistinguishable frompre-lesion levels. The restoration of peak force remained after the cessa-tion of VNS therapy at week 6, indicating that the recovery of forelimb
ED P
R
tions for both groups at each time point. The gray dashed box indicates trials which exceedls exceeding the 120 g threshold. (C) Maximal force over the course of the experiment.ilitative training alone by the secondweek of therapy. The increase in force is still presentificant difference between Rehab and VNS + Rehab. (D) Correlation of individual subjecta significant reduction after therapy compared to pre-lesion performance. All subjectsin the Rehab group recover.
during rehabilitative training improves forelimb strength following13.08.002

T
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
366
367
368
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384Q4
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
6 N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
UNCO
RREC
function was long-lasting. None of the subjects (0 of 6) that receivedVNS + Rehab demonstrated an impairment of force generation atthe completion of therapy (Fig. 3D). These findings demonstrate thatVNS + Rehab fully restores forelimb force generation.
Consistent with the recovery observed in single subjects, averagepeak force in the VNS + Rehab group is significantly greater than theRehab group (Fig. 3C). ANOVA of peak force revealed a significant effectof treatment (F[1,83] = 47.92, P b 0.001) and time (F[5,83] = 3.74,P = 0.004). By week 2, maximal force was significantly higher inthe VNS + Rehab group. The improvement in maximal force was evi-dent throughout the remainder of therapy (unpaired t-test, P b 0.05forweeks 2–6). These results demonstrate that VNS pairedwith rehabil-itative training results in a significant increase in forelimb strength com-pared to rehabilitative training without VNS.
Intensity of training cannot account for the differences in recovery
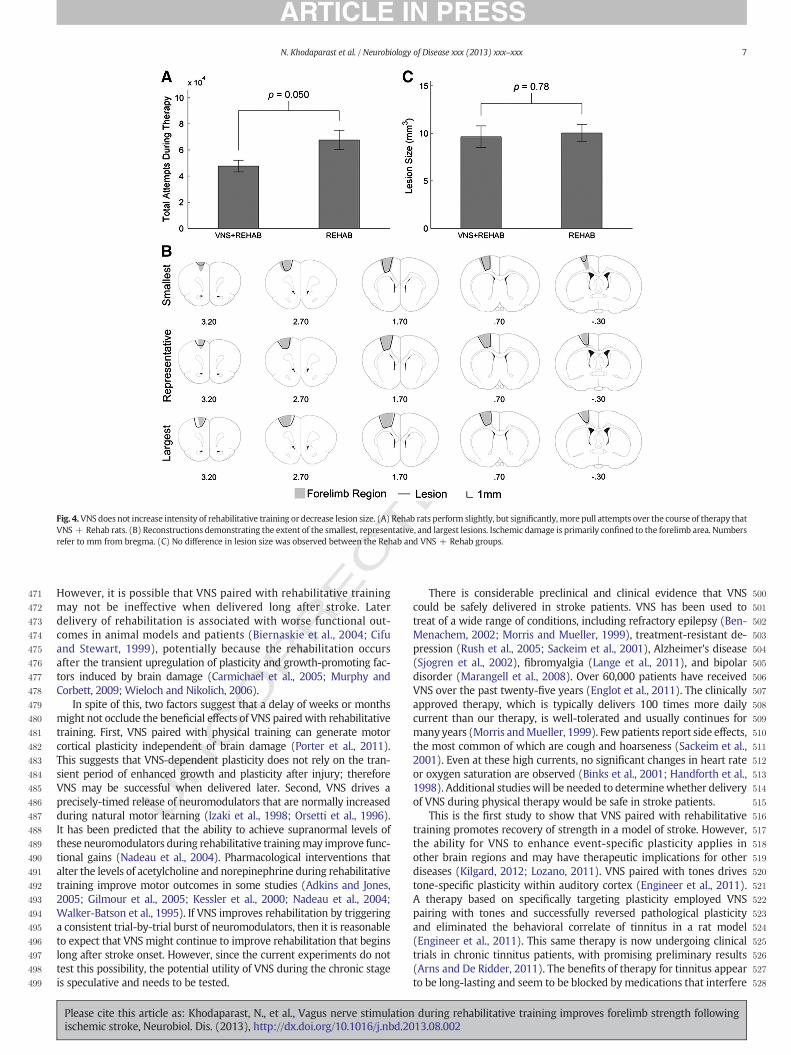
Insufficient training intensity or motivation can limit the gains fromrehabilitation (Kwakkel et al., 1999; Sivenius et al., 1985). To confirmthat the Rehab group did not perform less intensive training, we com-pared the total number of pull attempts performed over the course oftherapy. The total number of pulls during therapy is significantly higherin the Rehab group compared to the VNS + Rehab group (Fig. 4A,Rehab: 67,653 ± 7379 total attempts, VNS + Rehab: 47,656 ± 4535total attempts, unpaired t-test, P = 0.050). Because the Rehab groupperforms more repetitions but displays worse functional outcomes,the intensity of the training cannot account for the difference betweenthe groups. These findings highlight the marked benefit of VNS pairedwith rehabilitative training beyond rehabilitative training without VNS.
Lesion size cannot account for the differences in recovery
We sought to determine if our stimulation parameters would conferneuroprotective effects that could reduce lesion size, and if any changescould account for differences in functional recovery. Lesion size spannedthe left caudal forelimb area through all layers of cortex (Fig. 4B, also seeFig. S5). The resulting infarct was primarily restricted to cortex, butminor white matter damage was observed in one subject in the Rehabgroup and one subject in the VNS + Rehab group. There was no differ-ence in lesion volumeobserved between groups (Fig. 4C, VNS + Rehab:9.64 ± 2.55 mm3, Rehab: 10.03 ± 2.41 mm3, n = 6,8, unpaired t-test,P = 0.78, also see Fig. S3). These findings demonstrate that the stimula-tion parameters used in this study did not confer any observableneuroprotective effects on lesion size (see Supplementary materials).
Discussion
This study tested whether delivering VNS during rehabilitativetraining could improve recovery of forelimb motor function followingcortical ischemic damage compared to rehabilitative training alone.Forelimb function was assessed using the automated isometric pull taskwith approximately 50,000 pull attempts collected per rat, resulting inunbiased data collection and high statistical power (Hays et al., 2012).Rats received rehabilitative training on an isometric force task (Hayset al., 2012) for five weeks with or without the delivery of VNS. Weeksof daily intensive rehabilitative training without VNS failed to restorepre-lesion function. Forelimb function recovered completely when briefbursts of VNS were delivered during rehabilitative training. VNS pairedwith rehabilitative training doubled recovery of hit rate performanceand forelimb strength compared to rehabilitative training without VNS.VNS did not alter the size of the lesion or increase the intensity of rehabil-itative training. The enhanced recovery facilitated by the delivery of VNSduring rehabilitative training may present an opportunity for reducingmotor impairments in stroke patients.
Stroke often results in deficits of skilled movement which persist inspite of extensive rehabilitation (Segura et al., 2006; Van Peppen et al.,
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
ED P
RO
OF
2004). Rehabilitative training is focused on improving motor functionafter stroke, which is thought to be supported by reorganization of themotor cortex (Hallett, 2001; Kleim, 2011; Nudo, 2003). Rehabilitation-induced cortical plasticity is associated with the degree of recovery inanimal models (Castro-Alamancos and Borrell, 1995; Dijkhuizen et al.,2001; Frost et al., 2003; Ramanathan et al., 2006) and in stroke patients(Calautti and Baron, 2003; Lindenberg et al., 2012). A variety of factorsthat limit neural plasticity reduce recovery following brain damage(Boyeson et al., 1992; Conner et al., 2005; Goldstein et al., 1991;McHughen et al., 2010; Siironen et al., 2007; Sweetnam et al., 2012).Because of the association of plasticity and recovery, it was reasonableto expect that enhancement of plasticity would lead to gains in func-tional recovery after stroke. Vagus nerve stimulation paired withmotor training in unlesioned animals induced robust plasticity in themotor cortex, while similar amounts of motor training without VNSdid not drive observable plasticity (Porter et al., 2011). The improve-ment of recovery observed in this study in subjects that receivedVNS during rehabilitative training is likely due to the VNS-dependentenhancement of plasticity within motor cortex. However, the cellularand molecular mechanisms that underlie VNS-dependent recoveryremain unclear.
Stimulation of the vagus nerve engages multiple neuromodulatorysystems and results in the release of acetylcholine, norepinephrine,and brain-derived neurotrophic factor (Dorr and Debonnel, 2006;Follesa et al., 2007; Groves and Brown, 2005; Hassert et al., 2004;Nichols et al., 2011; Roosevelt et al., 2006). Individually, each of theseneuromodulators is known to enhance cortical plasticity and facilitaterecovery after brain damage (Boyeson et al., 1992; Conner et al., 2005;Goldstein et al., 1991; Ramanathan et al., 2009; Schäbitz et al., 2004,2007). There is considerable evidence that these neuromodulators,particularly acetylcholine and norepinephrine, operate synergisticallyto promote plasticity (Bear and Singer, 1986; Salgado et al., 2012; Seolet al., 2007).
The ability of vagus nerve stimulation to engage these neuro-modulatory systems arises from its unique anatomy. Eighty percent ofthe vagus nerve is comprised of afferent sensory fibers that projectinto the medulla (Foley and DuBois, 1937; George et al., 2000). Thesefibers synapse bilaterally on neurons within the nucleus of the tractussolitarius, which then project to the noradrenergic locus coeruleus(LC) and the cholinergic basal forebrain (BF) (Berntson et al., 1998;George et al., 2000; Henry, 2002; Semba et al., 1988). Stimulationof the vagus nerve drives activity within both the LC and BF regionsand consequently induces release of acetylcholine and norepinephrinethroughout the cortex (Follesa et al., 2007; Nichols et al., 2011;Roosevelt et al., 2006). Both of these regions are required for the effectsof VNS in the central nervous system (Krahl et al., 1998; Nichols et al.,2011). It is not yet knownwhether the release of these neuromodulatorsis required for the robust enhancement of recovery driven by VNS.
Our results provides a proof of concept demonstration that VNSduring rehabilitative training holds promise for improving recoveryof motor function after stroke. However, translating pre-clinical strokeresearch into effective therapies for patient has proven to be difficult(Lyden and Lapchak, 2012; O'Collins et al., 2006). Many therapies re-quire delivery soon after the onset of ischemic damage, either to inhibitneuronal death or to bolster the innate transient increase in plasticityafter damage (Adams et al., 1994; Savitz, 2007). As a result, many strat-egies are less effective once chronic deficits are in place. The discrepancybetween the timing of delivery of a treatment in animal studies andhuman trials is thought to be a contributing factor the failure of manypromising preclinical therapies (Cheng et al., 2004; Gladstone et al.,2002; Kahle and Bix, 2012). In this study, VNS paired with rehabilitativetraining was effective when initiated nine days after the stroke. Theability of VNS to confer a beneficial outcome when delivered at thistime scale is an improvement over interventions that must be deliveredshortly after (i.e., typically within six hours of) stroke to be effective (Ayet al., 2009; Hiraki et al., 2012; Yenari and Hemmen, 2010; Zivin, 1998).
during rehabilitative training improves forelimb strength following13.08.002
CTED P
RO
OF
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
499
500
501
502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
Fig. 4.VNS does not increase intensity of rehabilitative training or decrease lesion size. (A) Rehab rats perform slightly, but significantly, more pull attempts over the course of therapy thatVNS + Rehab rats. (B) Reconstructions demonstrating the extent of the smallest, representative, and largest lesions. Ischemic damage is primarily confined to the forelimb area. Numbersrefer to mm from bregma. (C) No difference in lesion size was observed between the Rehab and VNS + Rehab groups.
7N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
UNCO
RREHowever, it is possible that VNS paired with rehabilitative training
may not be ineffective when delivered long after stroke. Laterdelivery of rehabilitation is associated with worse functional out-comes in animal models and patients (Biernaskie et al., 2004; Cifuand Stewart, 1999), potentially because the rehabilitation occursafter the transient upregulation of plasticity and growth-promoting fac-tors induced by brain damage (Carmichael et al., 2005; Murphy andCorbett, 2009; Wieloch and Nikolich, 2006).
In spite of this, two factors suggest that a delay of weeks or monthsmight not occlude the beneficial effects of VNS pairedwith rehabilitativetraining. First, VNS paired with physical training can generate motorcortical plasticity independent of brain damage (Porter et al., 2011).This suggests that VNS-dependent plasticity does not rely on the tran-sient period of enhanced growth and plasticity after injury; thereforeVNS may be successful when delivered later. Second, VNS drives aprecisely-timed release of neuromodulators that are normally increasedduring natural motor learning (Izaki et al., 1998; Orsetti et al., 1996).It has been predicted that the ability to achieve supranormal levels ofthese neuromodulators during rehabilitative trainingmay improve func-tional gains (Nadeau et al., 2004). Pharmacological interventions thatalter the levels of acetylcholine and norepinephrine during rehabilitativetraining improve motor outcomes in some studies (Adkins and Jones,2005; Gilmour et al., 2005; Kessler et al., 2000; Nadeau et al., 2004;Walker-Batson et al., 1995). If VNS improves rehabilitation by triggeringa consistent trial-by-trial burst of neuromodulators, then it is reasonableto expect that VNS might continue to improve rehabilitation that beginslong after stroke onset. However, since the current experiments do nottest this possibility, the potential utility of VNS during the chronic stageis speculative and needs to be tested.
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
There is considerable preclinical and clinical evidence that VNScould be safely delivered in stroke patients. VNS has been used totreat of a wide range of conditions, including refractory epilepsy (Ben-Menachem, 2002; Morris and Mueller, 1999), treatment-resistant de-pression (Rush et al., 2005; Sackeim et al., 2001), Alzheimer's disease(Sjogren et al., 2002), fibromyalgia (Lange et al., 2011), and bipolardisorder (Marangell et al., 2008). Over 60,000 patients have receivedVNS over the past twenty-five years (Englot et al., 2011). The clinicallyapproved therapy, which is typically delivers 100 times more dailycurrent than our therapy, is well-tolerated and usually continues formany years (Morris andMueller, 1999). Fewpatients report side effects,the most common of which are cough and hoarseness (Sackeim et al.,2001). Even at these high currents, no significant changes in heart rateor oxygen saturation are observed (Binks et al., 2001; Handforth et al.,1998). Additional studies will be needed to determinewhether deliveryof VNS during physical therapy would be safe in stroke patients.
This is the first study to show that VNS paired with rehabilitativetraining promotes recovery of strength in a model of stroke. However,the ability for VNS to enhance event-specific plasticity applies inother brain regions and may have therapeutic implications for otherdiseases (Kilgard, 2012; Lozano, 2011). VNS paired with tones drivestone-specific plasticity within auditory cortex (Engineer et al., 2011).A therapy based on specifically targeting plasticity employed VNSpairing with tones and successfully reversed pathological plasticityand eliminated the behavioral correlate of tinnitus in a rat model(Engineer et al., 2011). This same therapy is now undergoing clinicaltrials in chronic tinnitus patients, with promising preliminary results(Arns and De Ridder, 2011). The benefits of therapy for tinnitus appearto be long-lasting and seem to be blocked bymedications that interfere
during rehabilitative training improves forelimb strength following13.08.002
T
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547
548
549
550
551
552
553Q6
554
555
556
557
558
559
560
561
562
563
564
565
566
567
568
569
570
571
572
573574575576577578579580581582
583584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614615616617618619620621622623624625626627628629630631632633634635636637638639640641642643644645646647648649650651652653654655656657658659660661662663664665666667668
8 N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
UNCO
RREC
with acetylcholine and norepinephrine, providing further mechanisticsupport of a neuromodulatory basis of VNS-directed plasticity. In addi-tion to tinnitus and stroke, targeted plasticity represents a potential toolfor other neurological disorders, including aphasia, apraxia, dystonia,and pain (Lozano, 2011).
Conclusion/implications
This study provides a proof of concept demonstration that stimula-tion of the vagus nerve paired with rehabilitative training can improverecovery of forelimb function in a rat model of stroke. VNS deliveredduring rehabilitative training fully restored forelimb force generationto pre-lesion levels. A similar amount of rehabilitative training withoutVNS was insufficient to restore performance. These results suggestthat VNS paired with physical rehabilitation is a potentially viable newtherapy for enhancing recovery of motor function after stroke.
Supplementary data to this article can be found online at http://dx.doi.org/10.1016/j.nbd.2013.08.002.
Funding
This work was supported by MicroTransponder, Inc.
Author contributions
N.K., S.A.H., andM.P.K. wrote themanuscript. N.K., M.P.K., R.L.R., andA.M.S. designed the study. N.K., S.A.H., D.R.H., A.R., and M.P. performedbehavioral testing. N.K., S.A.H., and A.M.S. analyzed the data. A.M.S.and R.L.R. provided software and hardware support. All authors discussedthe results and provided comments on the manuscript.
Uncited references
Atkinson and Santer, 1999Black-Schaffer and Winston, 2004Boyke et al., 2008Carey et al., 2002Dick et al., 1995Gallo, 2006Müller-Dahlhaus et al., 2008O'Donnell et al., 2010Pascual-Leone et al., 2011Paxinos and Watson, 2007Roger et al., 2012Sawaki et al., 2003Seidler, 2007Soltanpour and Santer, 1996
Acknowledgments
We would like to T. Fayyaz, N. Alam, F. Naqvi, D. Cao, R. Babu, R.Gattamaraju, V. Konduru, S. Burghul, and R. Joseph for help withbehavioral training.
References
Adams, H.P., Brott, T.G., Crowell, R.M., Furlan, A.J., Gomez, C.R., Grotta, J., Helgason, C.M.,Marler, J.R., Woolson, R.F., Zivin, J.A., 1994. Guidelines for themanagement of patientswith acute ischemic stroke. A statement for healthcare professionals from a specialwritinggroupof the Stroke Council, AmericanHeart Association. Stroke 25, 1901–1914.
Adkins, D.L., Jones, T.A., 2005. D-Amphetamine enhances skilled reaching after ischemiccortical lesions in rats. Neurosci. Lett. 380, 214–218.
Adkins-Muir, D., Jones, T., 2003. Cortical electrical stimulation combined with rehabilitativetraining: enhanced functional recovery and dendritic plasticity following focal corticalischemia in rats. Neurol. Res. 25 (8), 780–788.
Arns, M., De Ridder, D., 2011. Neurofeedback 2.0? J. Neurother. 15, 91–93.
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
ED P
RO
OF
Atkinson, C.J., Santer, R.M., 1999. Quantitative studies on myelinated and unmyelinatednerve fibres in the interatrial septal region of aged rat hearts. J. Auton. Nerv. Syst. 77,172–176.
Ay, I., Lu, J., Ay, H., Gregory Sorensen, A., 2009. Vagus nerve stimulation reduces infarctsize in rat focal cerebral ischemia. Neurosci. Lett. 459, 147–151.
Bear, M.F., Singer, W., 1986. Modulation of Visual Cortical Plasticity by Acetylcholineand Noradrenaline.
Ben-Menachem, E., 2002. Vagus-nerve stimulation for the treatment of epilepsy.Lancet Neurol. 1, 477–482.
Berntson, G.G., Sarter, M., Cacioppo, J.T., 1998. Anxiety and cardiovascular reactivity:the basal forebrain cholinergic link. Behav. Brain Res. 94, 225–248.
Biernaskie, J., Chernenko, G., Corbett, D., 2004. Efficacy of rehabilitative experiencedeclines with time after focal ischemic brain injury. J. Neurosci. 24, 1245–1254.
Binks, A., Paydarfar, D., Schachter, S., Guz, A., Banzett, R., 2001. High strength stimulation ofthe vagus nerve in awake humans: a lack of cardiorespiratory effects. Respir. Physiol.127, 125–133.
Black-Schaffer, R.M., Winston, C., 2004. Age and functional outcome after stroke. Top.Stroke Rehabil. 11, 23–32.
Boyeson, M.G., Callister, T.R., Cavazos, J.E., 1992. Biochemical and behavioral effects of asensorimotor cortex injury in rats pretreated with the noradrenergic neurotoxinDSP-4. Behav. Neurosci. 106, 964.
Boyke, J., Driemeyer, J., Gaser, C., Büchel, C., May, A., 2008. Training-induced brain struc-ture changes in the elderly. J. Neurosci. 28, 7031–7035.
Calautti, C., Baron, J., 2003. Functional neuroimaging studies of motor recovery afterstroke in adults a review. Stroke 34, 1553–1566.
Carey, J.R., Kimberley, T.J., Lewis, S.M., Auerbach, E.J., Dorsey, L., Rundquist, P., Ugurbil, K.,2002. Analysis of fMRI and finger tracking training in subjects with chronic stroke.Brain 125, 773–788.
Carmichael, S.T., Archibeque, I., Luke, L., Nolan, T., Momiy, J., Li, S., 2005. Growth-associatedgene expression after stroke: evidence for a growth-promoting region in peri-infarctcortex. Exp. Neurol. 193, 291–311.
Castro-Alamancos, M., Borrell, J., 1995. Functional recovery of forelimb response capacityafter forelimb primary motor cortex damage in the rat is due to the reorganization ofadjacent areas of cortex. Neuroscience 68, 793–805.
Cheng, Y.D., Al-Khoury, L., Zivin, J.A., 2004. Neuroprotection for ischemic stroke: twodecades of success and failure. NeuroRx 1, 36–45.
Cifu, D.X., Stewart, D.G., 1999. Factors affecting functional outcome after stroke: a criticalreview of rehabilitation interventions. Arch. Phys. Med. Rehabil. 80, S35–S39.
Conner, J.M., Chiba, A.A., Tuszynski, M.H., 2005. The basal forebrain cholinergic system isessential for cortical plasticity and functional recovery following brain injury. Neuron46, 173–179.
Deb, P., Sharma, S., Hassan, K., 2010. Pathophysiologic mechanisms of acute ischemicstroke: an overviewwith emphasis on therapeutic significance beyond thrombolysis.Pathophysiology 17, 197–218.
Dick, M.B., Nielson, K.A., Beth, R.E., Shankle, W.R., Cotman, C.W., 1995. Acquisition and long-term retention of a fine motor skill in Alzheimers-disease. Brain Cogn. 29, 294–306.
Dijkhuizen, R.M., Ren, J., Mandeville, J.B., Wu, O., Ozdag, F.M., Moskowitz, M.A., Rosen, B.R.,Finklestein, S.P., 2001. Functional magnetic resonance imaging of reorganization inrat brain after stroke. Proc. Natl. Acad. Sci. 98, 12766–12771.
Dorr, A.E., Debonnel, G., 2006. Effect of vagus nerve stimulation on serotonergic andnoradrenergic transmission. J. Pharmacol. Exp. Ther. 318, 890–898.
Engineer, N.D., Riley, J.R., Seale, J.D., Vrana, W.A., Shetake, J.A., Sudanagunta, S.P., Borland,M.S., Kilgard, M.P., 2011. Reversing pathological neural activity using targeted plasticity.Nature 470, 101–104.
Englot, D.J., Chang, E.F., Auguste, K.I., 2011. Vagus nerve stimulation for epilepsy: a meta-analysis of efficacy and predictors of response: a review. J. Neurosurg. 115, 1248–1255.
Fang, P., Barbay, S., Plautz, E.J., Hoover, E., Strittmatter, S.M., Nudo, R.J., 2010. Combinationof NEP 1–40 treatment and motor training enhances behavioral recovery after a focalcortical infarct in rats. Stroke 41, 544–549.
Foley, J.O., DuBois, F.S., 1937. Quantitative studies of the vagus nerve in the cat. I. The ratioof sensory to motor fibers. J. Comp. Neurol. 67, 49–67.
Follesa, P., Biggio, F., Gorini, G., Caria, S., Talani, G., Dazzi, L., Puligheddu, M., Marrosu, F.,Biggio, G., 2007. Vagus nerve stimulation increases norepinephrine concentrationand the gene expression of BDNF and bFGF in the rat brain. Brain Res. 1179, 28–34.
Frost, S., Barbay, S., Friel, K., Plautz, E., Nudo, R., 2003. Reorganization of remotecortical regions after ischemic brain injury: a potential substrate for strokerecovery. J. Neurophysiol. 89, 3205–3214.
Gallo, B.V., 2006. Epilepsy, surgery, and the elderly. Epilepsy Res. 68, 83–86.George, M.S., Sackeim, H.A., Rush, A.J., Marangell, L.B., Nahas, Z., Husain, M.M., Lisanby, S.,
Burt, T., Goldman, J., Ballenger, J.C., 2000. Vagus nerve stimulation: a new tool forbrain research and therapy. Biol. Psychiatry 47, 287–295.
Gilmour, G., Iversen, S.D., O'Neill, M.F., Bannerman, D.M., 2004. The effects of intracorticalendothelin-1 injections on skilled forelimb use: implications for modelling recoveryof function after stroke. Behav. Brain Res. 150, 171–183.
Gilmour, G., Iversen, S.D., O'Neill, M.F., O'Neill, M.J., Ward, M.A., Bannerman, D.M., 2005.Amphetamine promotes task-dependent recovery following focal cortical ischaemiclesions in the rat. Behav. Brain Res. 165, 98–109.
Gladstone, D.J., Black, S.E., Hakim, A.M., 2002. Toward wisdom from failure lessonsfrom neuroprotective stroke trials and new therapeutic directions. Stroke 33,2123–2136.
Goldstein, L.B., Coviello, A., Miller, G.D., Davis, J.N., 1991. Norepinephrine depletionimpairs motor recovery following sensorimotor cortex injury in the rat. Restor. Neurol.Neurosci. 3, 41–47.
Groves, D.A., Brown, V.J., 2005. Vagal nerve stimulation: a review of its applications andpotential mechanisms that mediate its clinical effects. Neurosci. Biobehav. Rev. 29,493–500.
during rehabilitative training improves forelimb strength following13.08.002
T
669670671672673674675676677678679680681Q7682683684Q8685686687688689Q9690691692693694695696697698699Q10700701702703704705706707708709710711712713714715716717718719720721722723724725726727728729730731732733734735Q11736737738739740741742743744745746747748749750751752753754
755756757758759760761762763764765Q12766767768769770771772773774775776777778779780781782783784785786787788789790791792793794795796797798799800801802803804805806807808809810811812813814815816817818819820821822823824825826827828829830831832833834835836837838839840
9N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
UNCO
RREC
Hallett, M., 2001. Plasticity of the human motor cortex and recovery from stroke. BrainRes. Rev. 36, 169–174.
Handforth, A., DeGiorgio, C., Schachter, S., Uthman, B., Naritoku, D., Tecoma, E., Henry, T.,Collins, S., Vaughn, B., Gilmartin, R., 1998. Vagus nerve stimulation therapy for partial-onset seizures: a randomized active-control trial. Neurology 51, 48–55.
Harris, J.E., Eng, J.J., 2007. Paretic upper-limb strength best explains arm activity in peoplewith stroke. Phys. Ther. 87, 88–97.
Harvey, R.L., Nudo, R.J., 2007. Cortical brain stimulation: a potential therapeutic agentfor upper limb motor recovery following stroke. Top. Stroke Rehabil. 14, 54–67.
Hassert, D., Miyashita, T., Williams, C., 2004. The effects of peripheral vagal nerve stimu-lation at a memory-modulating intensity on norepinephrine output in the basolateralamygdala. Behav. Neurosci. 118, 79.
Hays, S.A., Khodaparast, N., Sloan, A.M., Hulsey, D.R., Pantoja, M., Ruiz, A.D., Kilgard, M.P.,Rennaker II, R.L., 2012. The isometric pull task: a novel automated method forquantifying forelimb force generation in rats. J. Neurosci. Methods.
Hays, S.A., Khodaparast, N., Sloan, A.M., Fayyaz, T., Hulsey, D.R., Ruiz, A.D., Pantoja, M.,Kilgard, M.P., Rennaker II, R.L., 2013. The bradykinesia assessment task: an automatedmethod to measure forelimb speed in rodents. J. Neurosci. Methods.
Henry, T.R., 2002. Therapeutic mechanisms of vagus nerve stimulation. Neurology 59,S3–S14.
Hiraki, T., Baker, W., Greenberg, J.H., 2012. Effect of vagus nerve stimulation duringtransient focal cerebral ischemia on chronic outcome in rats. J. Neurosci. Res.
Izaki, Y., Hori, K., Nomura, M., 1998. Dopamine and acetylcholine elevation on lever-pressacquisition in rat prefrontal cortex. Neurosci. Lett. 258, 33–36.
Johansson, B.B., 2000. Brain plasticity and stroke rehabilitation. The Willis lecture. Stroke31, 223–230.
Kahle, M.P., Bix, G.J., 2012. Successfully climbing the “STAIRs”: surmounting failed trans-lation of experimental ischemic stroke treatments. Stroke Res. Treat. 2012.
Kessler, J., Thiel, A., Karbe, H., Heiss, W., 2000. Piracetam improves activated blood flowand facilitates rehabilitation of poststroke aphasic patients. Stroke 31, 2112–2116.
Kilgard, M.P., 2012. Harnessing plasticity to understand learning and treat disease.Trends Neurosci.
King, R.B., 1996. Quality of life after stroke. Stroke 27, 1467–1472.Kleim, J.A., 2011. Neural plasticity and neurorehabilitation: teaching the new brain old
tricks. J. Commun. Disord. 44, 521–528.Krahl, S.E., Clark, K.B., Smith, D.C., Browning, R.A., 1998. Locus coeruleus lesions suppress
the seizure‐attenuating effects of vagus nerve stimulation. Epilepsia 39, 709–714.Kwakkel, G., 2009. Towards integrative neurorehabilitation science. Physiother. Res. Int.
14, 137–146.Kwakkel, G., Wagenaar, R.C., Twisk, J.W., Lankhorst, G.J., Koetsier, J.C., 1999. Intensity
of leg and arm training after primary middle-cerebral-artery stroke: a randomisedtrial. Lancet 354, 191–196.
Lange, G., Janal, M.N., Maniker, A., FitzGibbons, J., Fobler, M., Cook, D., Natelson, B.H., 2011.Safety and efficacy of vagus nerve stimulation in fibromyalgia: a phase I/II proof ofconcept trial. Pain Med. 12, 1406–1413.
Leary, M.C., Saver, J.L., 2003. Annual incidence of first silent stroke in the United States:a preliminary estimate. Cerebrovasc. Dis. 16, 280–285.
Levine, J., Greenwald, B.D., 2009. Fatigue in Parkinson disease, stroke, and traumatic braininjury. Phys. Med. Rehabil. Clin. N. Am. 20, 347–361.
Lindenberg, R., Zhu, L.L., Schlaug, G., 2012. Combined central and peripheral stimulationto facilitate motor recovery after stroke: the effect of number of sessions on outcome.Neurorehabil. Neural Repair 26, 479–483.
Lo, E.H., Dalkara, T., Moskowitz, M.A., 2003. Mechanisms, challenges and opportunities instroke. Nat. Rev. Neurosci. 4, 399–414.
Lozano, A.M., 2011. Harnessing plasticity to reset dysfunctional neurons. N. Engl. J. Med.364, 1367–1368.
Lyden, P., Lapchak, P., 2012. Sisyphus and translational stroke research. Sci. Transl. Med. 4(156ps20-156ps20).
Marangell, L.B., Suppes, T., Zboyan, H.A., Prashad, S.J., Fischer, G., Snow, D., Sureddi, S.,ALLEN, J.C., 2008. A 1-year pilot study of vagus nerve stimulation in treatment-resistant rapid-cycling bipolar disorder. J. Clin. Psychiatry 69, 183–189.
McHughen, S.A., Rodriguez, P.F., Kleim, J.A., Kleim, E.D., Crespo, L.M., Procaccio, V., Cramer,S.C., 2010. BDNF val66met polymorphism influences motor system function in thehuman brain. Cereb. Cortex 20, 1254–1262.
Mercier, C., Bourbonnais, D., 2004. Relative shoulder flexor and handgrip strength is relatedto upper limb function after stroke. Clin. Rehabil. 18, 215–221.
Morris, G.L., Mueller, W.M., 1999. Long-term treatment with vagus nerve stimulation inpatients with refractory epilepsy. Neurology 53, 1731–1735.
Müller-Dahlhaus, J.F.M., Orekhov, Y., Liu, Y., Ziemann, U., 2008. Interindividual variabilityand age-dependency of motor cortical plasticity induced by paired associative stimu-lation. Exp. Brain Res. 187, 467–475.
Murphy, T.H., Corbett, D., 2009. Plasticity during stroke recovery: from synapse to behaviour.Nat. Rev. Neurosci. 10, 861–872.
Nadeau, S.E., Behrman, A.L., Davis, S.E., Reid, K., Wu, S., Stidham, B., Helms, K., Rothi, L.G.,2004. Donepezil as an adjuvant to constraint-induced therapy for upper-limbdysfunction after stroke: an exploratory randomized clinical trial. J. Rehabil. Res. Dev.41, 525–534.
Nichols, J., Nichols, A., Smirnakis, S., Engineer, N., Kilgard,M., Atzori, M., 2011. Vagus nervestimulation modulates cortical synchrony and excitability through the activation ofmuscarinic receptors. Neuroscience 189, 207–214.
Nudo, R.J., 2003. Functional and structural plasticity in motor cortex: implications forstroke recovery. Phys. Med. Rehabil. Clin. N. Am. 14, S57.
O'Collins, V.E., Macleod, M.R., Donnan, G.A., Horky, L.L., van der Worp, Bart H., Howells,D.W., 2006. 1,026 experimental treatments in acute stroke. Ann. Neurol. 59, 467–477.
O'Donnell, M.J., Xavier, D., Liu, L., Zhang, H., Chin, S.L., Rao-Melacini, P., Rangarajan, S.,Islam, S., Pais, P., McQueen, M.J., 2010. Risk factors for ischaemic and intracerebral
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
ED P
RO
OF
haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case–controlstudy. Lancet 376, 112–123.
Orsetti, M., Casamenti, F., Pepeu, G., 1996. Enhanced acetylcholine release in thehippocampus and cortex during acquisition of an operant behavior. Brain Res.724, 89–96.
Pascual-Leone, A., Freitas, C., Oberman, L., Horvath, J.C., Halko, M., Eldaief, M., Bashir, S.,Vernet, M., Shafi, M., Westover, B., 2011. Characterizing brain cortical plasticityand network dynamics across the age-span in health and disease with TMS-EEGand TMS-fMRI. Brain Topogr. 24, 302–315.
Paxinos, G., Watson, C., 2007. The Rat Brain in Stereotaxic Coordinates. Academic Press.Porter, B.A., Khodaparast, N., Fayyaz, T., Cheung, R.J., Ahmed, S.S., Vrana,W.A., Rennaker II,
R.L., Kilgard, M.P., 2011. Repeatedly pairing vagus nerve stimulationwith amovementreorganizes primary motor cortex. Cereb. Cortex.
Ramanathan, D., Conner, J.M., Tuszynski, M.H., 2006. A form of motor cortical plasticitythat correlates with recovery of function after brain injury. Proc. Natl. Acad. Sci.103, 11370–11375.
Ramanathan, D., Tuszynski, M.H., Conner, J.M., 2009. The basal forebrain cholinergicsystem is required specifically for behaviorally mediated cortical map plasticity.J. Neurosci. 29, 5992–6000.
Roger, V.L., Go, A.S., Lloyd-Jones, D.M., Benjamin, E.J., Berry, J.D., Borden, W.B.,Bravata, D.M., Dai, S., Ford, E.S., Fox, C.S., 2012. Heart disease and strokestatistics—2012 update. A report from the American Heart Association. Circulation125, e2–e220.
Roosevelt, R.W., Smith, D.C., Clough, R.W., Jensen, R.A., Browning, R.A., 2006. Increasedextracellular concentrations of norepinephrine in cortex and hippocampus followingvagus nerve stimulation in the rat. Brain Res. 1119, 124–132.
Rossini, P.M., Forno, G.D., 2004. Neuronal post-stroke plasticity in the adult. Restor. Neurol.Neurosci. 22, 193–206.
Rush, A.J., Sackeim, H.A., Marangell, L.B., George, M.S., Brannan, S.K., Davis, S.M., Lavori, P.,Howland, R., Kling, M.A., Rittberg, B., 2005. Effects of 12 months of Vagus NerveStimulation in Treatment-resistant Depression: A Naturalistic Study.
Sackeim, H.A., Rush, A.J., George, M.S., Marangell, L.B., Husain, M.M., Nahas, Z., Johnson,C.R., Seidman, S., Giller, C., Haines, S., 2001. Vagus nerve stimulation (VNS™)for treatment-resistant depression: efficacy, side effects, and predictors of outcome.Neuropsychopharmacology 25, 713–728.
Salgado, H., Köhr, G., Treviño, M., 2012. Noradrenergic ‘tone’ determines dichotomouscontrol of cortical spike-timing-dependent plasticity. Sci. Rep. 2.
Savitz, S.I., 2007. A critical appraisal of the NXY-059 neuroprotection studies for acutestroke: a need for more rigorous testing of neuroprotective agents in animal modelsof stroke. Exp. Neurol. 205, 20–25.
Sawaki, L., Yaseen, Z., Kopylev, L., Cohen, L.G., 2003. Age‐dependent changes in the abilityto encode a novel elementary motor memory. Ann. Neurol. 53, 521–524.
Sawaki, L., Butler, A.J., Leng, X., Wassenaar, P.A., Mohammad, Y.M., Blanton, S., Sathian, K.,Nichols-Larsen, D.S., Wolf, S.L., Good, D.C., 2008. Constraint-induced movementtherapy results in increased motor map area in subjects 3 to 9 months after stroke.Neurorehabil. Neural Repair 22, 505–513.
Schäbitz, W., Berger, C., Kollmar, R., Seitz, M., Tanay, E., Kiessling, M., Schwab, S., Sommer,C., 2004. Effect of brain-derived neurotrophic factor treatment and forced arm use onfunctional motor recovery after small cortical ischemia. Stroke 35, 992–997.
Schäbitz, W., Steigleder, T., Cooper-Kuhn, C.M., Schwab, S., Sommer, C., Schneider, A.,Kuhn, H.G., 2007. Intravenous brain-derived neurotrophic factor enhances poststrokesensorimotor recovery and stimulates neurogenesis. Stroke 38, 2165–2172.
Schaechter, J.D., 2004. Motor rehabilitation and brain plasticity after hemiparetic stroke.Prog. Neurobiol. 73, 61.
Schaechter, J.D., Kraft, E., Hilliard, T.S., Dijkhuizen, R.M., Benner, T., Finklestein, S.P., Rosen,B.R., Cramer, S.C., 2002. Motor recovery and cortical reorganization after constraint-induced movement therapy in stroke patients: a preliminary study. Neurorehabil.Neural Repair 16, 326–338.
Segura, A.P.C., Fontes, S.V., Fukujima, M.M., de Andrade Matas, S.L., 2006. The impactevaluation of physical therapy on the quality of life of cerebrovascular stroke patients.Int. J. Rehabil. Res. 29, 243–246.
Seidler, R.D., 2007. Older adults can learn to learn newmotor skills. Behav. Brain Res. 183,118–122.
Semba, K., Reiner, P., McGeer, E., Fibiger, H., 1988. Brainstem afferents to themagnocellular basal forebrain studied by axonal transport, immunohistochemistry,and electrophysiology in the rat. J. Comp. Neurol. 267, 433–453.
Seol, G.H., Ziburkus, J., Huang, S.Y., Song, L., Kim, I.T., Takamiya, K., Huganir, R.L., Lee, H.K.,Kirkwood, A., 2007. Neuromodulators control the polarity of spike-timing-dependentsynaptic plasticity. Neuron 55, 919–929.
Siironen, J., Juvela, S., Kanarek, K., Vilkki, J., Hernesniemi, J., Lappalainen, J., 2007.The Met allele of the BDNF Val66Met polymorphism predicts poor outcome amongsurvivors of aneurysmal subarachnoid hemorrhage. Stroke 38, 2858–2860.
Sivenius, J., Pyörälä, K., Heinonen, O., Salonen, J., Riekkinen, P., 1985. The significance ofintensity of rehabilitation of stroke—a controlled trial. Stroke 16, 928–931.
Sjogren, M.J.C., Hellstrom, P.T.O., Jonsson, M.A.G., Runnerstam, M., Silander, H.C.,Ben-Menachem, E., 2002. Cognition-enhancing effect of vagus nerve stimula-tion in patients with Alzheimer's disease: a pilot study. J. Clin. Psychiatry 63,972–980.
Soltanpour, N., Santer, R.M., 1996. Preservation of the cervical vagus nerve in aged rats:morphometric and enzyme histochemical evidence. J. Auton. Nerv. Syst. 60, 93–101.
Sunderland, A., Tinson, D., Bradley, L., Hewer, R.L., 1989. Arm function after stroke.An evaluation of grip strength as a measure of recovery and a prognostic indicator.J. Neurol. Neurosurg. Psychiatry 52, 1267–1272.
Sweetnam, D., Holmes, A., Tennant, K.A., Zamani, A., Walle, M., Jones, P., Wong, C., Brown,C.E., 2012. Diabetes impairs cortical plasticity and functional recovery followingischemic stroke. J. Neurosci. 32, 5132–5143.
during rehabilitative training improves forelimb strength following13.08.002

841842843844845846847848849850
851852853854855856857858859860
861
10 N. Khodaparast et al. / Neurobiology of Disease xxx (2013) xxx–xxx
Van Peppen, R.P., Kwakkel, G., Wood-Dauphinee, S., Hendriks, H.J., Van der Wees, Ph.J.,Dekker, J., 2004. The impact of physical therapy on functional outcomes after stroke:what's the evidence? Clin. Rehabil. 18, 833–862.
Walker-Batson, D., Smith, P., Curtis, S., Unwin, H., Greenlee, R., 1995. Amphetamine pairedwith physical therapy accelerates motor recovery after stroke: further evidence. Stroke26, 2254–2259.
Ward, N.S., Cohen, L.G., 2004. Mechanisms underlying recovery of motor function afterstroke. Arch. Neurol. 61, 1844.
Whyte, E.M., Mulsant, B.H., Vanderbilt, J., Dodge, H.H., Ganguli, M., 2004. Depression afterstroke: a prospective epidemiological study. J. Am. Geriatr. Soc. 52, 774–778.
UNCO
RRECT
Please cite this article as: Khodaparast, N., et al., Vagus nerve stimulationischemic stroke, Neurobiol. Dis. (2013), http://dx.doi.org/10.1016/j.nbd.20
Wieloch, T., Nikolich, K., 2006. Mechanisms of neural plasticity following brain injury.Curr. Opin. Neurobiol. 16, 258–264.
Yenari, M.A., Hemmen, T.M., 2010. Therapeutic hypothermia for brain ischemia: wherehave we come and where do we go? Stroke 41, S72–S74.
You, S.H., Jang, S.H., Kim, Y., Hallett, M., Ahn, S.H., Kwon, Y., Kim, J.H., Lee, M.Y.,2005. Virtual reality-induced cortical reorganization and associated locomotorrecovery in chronic stroke an experimenter-blind randomized study. Stroke 36,1166–1171.
Zivin, J.A., 1998. Factors determining the therapeutic window for stroke. Neurology 50,599–603.
ED P
RO
OF
during rehabilitative training improves forelimb strength following13.08.002
Related Documents











