Confidential: For Review Only Using the Clinical Research Network for psychosocial research: lessons learned from two observational studies Journal: BMJ Supportive & Palliative Care Manuscript ID: bmjspcare-2012-000410.R1 Article Type: Features Date Submitted by the Author: n/a Complete List of Authors: Wright, Penny; University of Leeds, Leeds Institute of Cancer Studies and Pathology Fenlon, Debbie; University of Southampton, Faculty of Health Sciences Jones, Helen; University of Leeds, Leeds Institute of Cancer Studies and Pathology Foster, Claire; University of Southampton, Faculty of Health Sciences Ashley, Laura; University of Leeds, Leeds Institute of Cancer Studies and Pathology Chivers Seymour, Kim; University of Southampton, Faculty of Health Sciences Velikova, Galina; University of Leeds, Leeds Institute of Cancer Studies and Pathology Okamoto, Ikumi; University of Southampton, Academic Unit of Primary Care and Population Sciences Brown, Julia; University of Leeds, Leeds Institute of Clinical Trials Research Keywords: Cancer, Methodological research, Survivorship http://mc.manuscriptcentral.com/bmjspcare BMJ Supportive & Palliative Care

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Confidential: For Review O
nly
Using the Clinical Research Network for psychosocial
research: lessons learned from two observational studies
Journal: BMJ Supportive & Palliative Care
Manuscript ID: bmjspcare-2012-000410.R1
Article Type: Features
Date Submitted by the Author: n/a
Complete List of Authors: Wright, Penny; University of Leeds, Leeds Institute of Cancer Studies and Pathology Fenlon, Debbie; University of Southampton, Faculty of Health Sciences Jones, Helen; University of Leeds, Leeds Institute of Cancer Studies and Pathology Foster, Claire; University of Southampton, Faculty of Health Sciences
Ashley, Laura; University of Leeds, Leeds Institute of Cancer Studies and Pathology Chivers Seymour, Kim; University of Southampton, Faculty of Health Sciences Velikova, Galina; University of Leeds, Leeds Institute of Cancer Studies and Pathology Okamoto, Ikumi; University of Southampton, Academic Unit of Primary Care and Population Sciences Brown, Julia; University of Leeds, Leeds Institute of Clinical Trials Research
Keywords: Cancer, Methodological research, Survivorship
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
Confidential: For Review O
nly
1
Using the Clinical Research Network for psychosocial research:
lessons learned from two observational studies
Penny Wright*1, Deborah Fenlon2, Helen Jones1, Claire Foster2, Laura Ashley1,
Kim Chivers Seymour2, Galina Velikova1, Ikumi Okamoto2 and Julia Brown3
1 Psychosocial Oncology and Clinical Practice Research Group, Leeds Institute of Cancer
Studies and Pathology, University of Leeds, Leeds, UK
2Macmillan Survivorship Research Group, Faculty of Health Sciences, University of
Southampton, Southampton, UK
3 Clinical Trials Research Unit, Leeds Institute of Clinical Trials Research, University of
Leeds, Leeds, UK
*Corresponding author
Dr Penny Wright,
Psychosocial Oncology and Clinical Practice Research Group, Level three Bexley Wing, St
James’s Institute of Oncology, St James’s University Hospital, Leeds LS9 7TF
Telephone: 00 (44) 113 2068488
Fax: 00 (44) 113 2068512
Keywords
clinical studies, patient recruitment, psychosocial, research nurses, patient accrual, clinical
research network
Word Count: 4,189
Page 1 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
2
ABSTRACT
Background
Patient recruitment to psychosocial oncology research has increased over the last 10 years
but the majority of studies have been single-site or small-scale. The National Institute for
Health Research (NIHR), Clinical Research Network (CRN) supports NIHR portfolio studies
through provision of research staff to recruit and follow-up patients, but has been little used
by psychosocial researchers. We report the experiences of two psychosocial research teams
who recently used the CRN, to undertake patient recruitment, to inform cancer researchers
of non-clinical trials of an investigational medicinal product (non-CTIMPs) of lessons learned
and to provide recommendations.
Method and outcomes
Patients were successfully recruited to two prospective observational studies: electronic
Patient-reported Outcomes from Cancer Survivors study (ePOCS; n=636) and the
ColoREctal Wellbeing study (CREW; n=1,055). ePOCS secured Comprehensive Local
Research Networks funding to appoint ePOCS-specific study research nurses. CREW
obtained research support through the NIHR Cancer Research Network. Top tips for
establishing and running studies with CRN staff are provided and suggestions given for
advancing multicentre complex non-CTIMPs.
Conclusion
Some challenges were similar to those in delivery of CTIMPs. The pros and cons of being
involved in ePOCS from the research nurse perspective are also described. Overall the
approaches used were successful.
Page 2 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
3
INTRODUCTION
The importance of psychosocial oncology has been increasingly recognised over recent
decades, leading to the Union International for Cancer Control declaring ‘distress’ the 6th
vital sign in Cancer Care 1. Despite this, psychosocial care has not become fully integrated
into routine cancer care. A number of challenges persist including how psychosocial
oncology is valued as a discipline in its own right, the costs of supportive care, and a lack of
evidence from large-scale well-designed psychosocial trials 2. In the UK cancer research has
been nurtured by the establishment of the National Cancer Research Institute (NCRI:
http://www.ncri.org.uk/ ) Clinical Studies Groups (CSGs). CSGs facilitate and prioritise
studies to address cancer diagnostic-specific questions (i.e. breast, lung) or cross-cutting
issues (i.e. palliative, psychosocial). The National Institute of Health Research (NIHR)
Cancer Research Network (http://www.ncrn.org.uk/ ), established in parallel with the NCRI,
was set up to increase the number of patients participating in high-quality clinical research
studies. The NIHR Cancer Research Network comprises 32 Local Research Networks
across England and provides an infrastructure to support study participation, including
funding for research nurses (RNs). Since 2006 their main focus has been on recruitment to
clinical trials of an investigational medicinal product (CTIMP) randomised controlled trials
(RCT). This has led to increased accrual to RCTs but not at the expense of accrual to
observational studies, may be because some observational studies provide an opportunity
for patients to enrol in RCTs at the same time 3. Timely accrual to both RCTs and
observational studies within the cancer trials portfolio has increased significantly since the
NIHR Cancer Research Network was established, rising from <5% of incidence cases in
2001 to >20% in 2010 3. Although the majority of trials within the portfolio are CTIMPs there
is interest in developing other types of interventional studies 4.The success of the NIHR
Cancer Research Network model for supporting clinical trials in England led to the
establishment of a generic Clinical Research Network (CRN) to provide infrastructure for
other clinical groups. The elements of the NIHR CRN and their inter-relationships and
Page 3 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
4
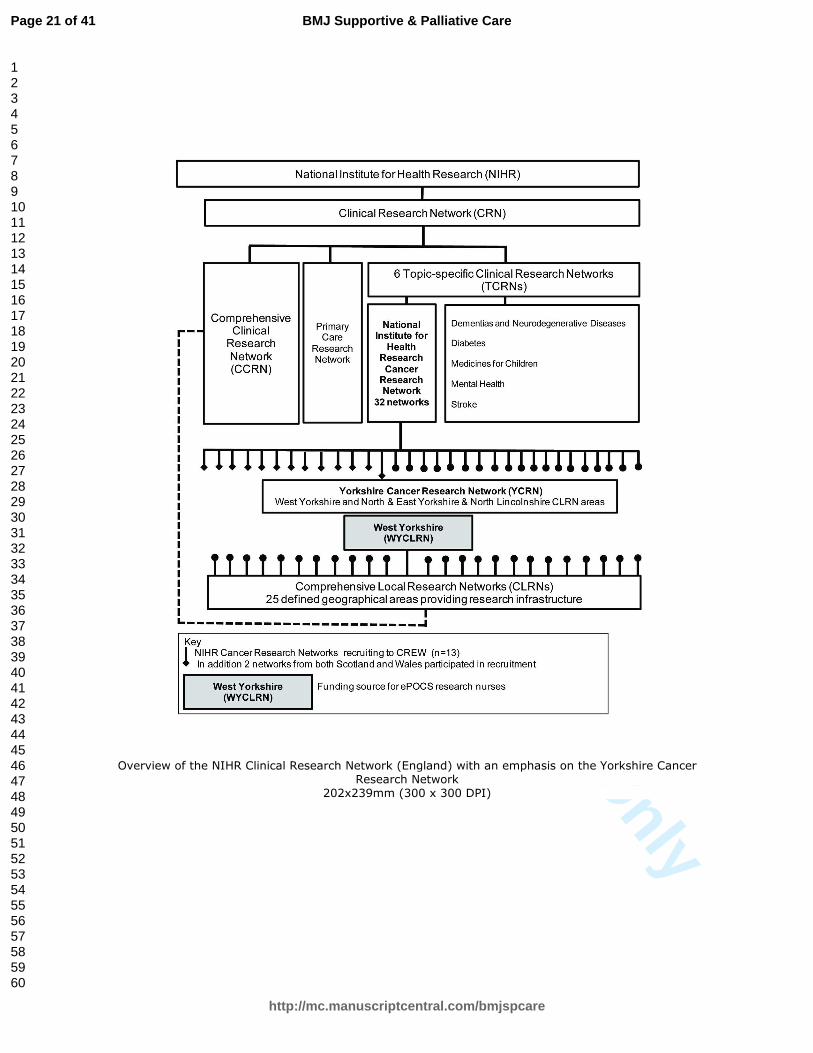
acronyms can be confusing. Figure 1 provides an overview and places the national and local
level of networks into context.
The NIHR Cancer Research Network-NCRI CSG model for developing and delivering high-
quality large-scale trials has worked well for clinical trial evaluation of CTIMPs. Some of
these trials have either secondary quality of life outcomes as part of the main study or have
linked sub-studies with primary quality of life outcomes. In the disease site specific CSGs the
majority of members are clinicians. The trials become embedded within clinical practice
across a number of centres where patients are considered for participation at
Multidisciplinary Team (MDT) meetings by clinicians and associated RNs. Across the
country there is a network of clinicians who have duty of care for these patients, who are
research active and who contribute to accrual of portfolio CTIMPs with support mainly from
the NIHR Cancer Research Network.
The model does not work so effectively for psychosocial studies. The Psychosocial
Oncology CSG comprises a varied membership (including health psychology, social work,
nursing, clinical trials), few of whom have responsibility for clinical care. The range of studies
within the psychosocial oncology portfolio is broad, including studies of interventions from
acupuncture to cognitive-behavioural therapy, studies to develop patient decision aids, and
observational studies of patients’ quality of life, health behaviors and care experience. There
is no ready-made clinical infrastructure or experienced study recruitment network to call on
for championing multi-centre psychosocial studies. In addition, psychosocial studies may
require specialist professional input, which is not part of the standard clinical research team,
to deliver an intervention or undertake specialised interviewing or observations. As a result
although there have been some high-quality large-scale psychosocial studies 5-7, many
studies within the growing Psychosocial Oncology CSG portfolio have been single-site or
small-scale and have tended to rely on individual grant-funded appointed research
assistants, rather than using network RNs, for recruitment and follow-up of patients.
Commonly research assistants are psychology graduates looking for research experience to
aid advancement to academic doctoral studies or a clinical psychology career 8. Now there is
Page 4 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
5
an expectation that some research costs will no longer be met by some grant awarding
bodies. The recently published Department of Health AcoRD document provides the basis
for attributing the costs of health and social care research studies in three categories:
research costs (costs of activities undertaken to answer the research questions), NHS
treatment costs (costs of patient care) and NHS support costs (additional patient care costs
associated with the research)9. If a study is funded by a charity which is a member of the
Association of Medical Research Charities (AMRC) some NHS support costs will be met by
the Department of Health, via the networks, such as the identification of patients suitable to
approach for participation, obtaining consent and additional assessments. In order for the
Psychosocial Oncology CSG to consistently deliver high-quality large-scale observational
studies and trials, use of the networks for recruitment support will have to become standard
practice.
In 2010-2012 two Psychosocial Oncology CSG portfolio observational cohort studies, funded
by Macmillan Cancer Support (AMRC member) and run by University sponsored
researchers, collaborated in two different ways with the networks to support recruitment. In
the electronic Patient-reported Outcomes from Cancer Survivors (ePOCS) study the
research team applied for study specific funding for RNs to the generic West Yorkshire
Comprehensive Local Research Network (WYCLRN); in the ColoREctal Wellbeing (CREW)
study the research team asked for expressions of interest for study participation from the
NIHR Cancer Research Networks (Figure 1). Both studies were given research ethics
committee approval (ePOCS (Leeds East 10/H1306/65); CREW (Oxfordshire REC B
10/H0605/31)) and all participants provided written informed consent. We report and
compare the different approaches of ePOCS and CREW with the aim of informing non-
CTIMPs researchers of lessons learned and providing recommendations for future studies.
Figure 1 about here
Page 5 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
6
THE STUDIES
electronic Patient-reported Outcomes from Cancer Survivors (ePOCS)
http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=9403
ePOCS is a secure electronic system for collecting Patient Reported Outcome Measures
(PROMS) via the internet at multiple time-points and linking these data with patients' clinical
data transferred from the electronic patient record (EPR) to the cancer registry and
managing associated patient communications electronically 10. The ePOCS study is a
prospective observational study to test the feasibility of the ePOCS system, by running it for
two years in two NHS Trusts within the Yorkshire Cancer Network (YCN) (the cancer centre
and one cancer unit), and using the Northern and Yorkshire Cancer Registry and Information
Service 11. To test feasibility, all non-metastatic breast, colorectal and prostate cancer
patients attending the two YCN Trusts within six months post-diagnosis needed to be
considered for recruitment (estimated target n=600). Funding was obtained from the
WYCLRN to appoint RNs to be embedded within established cancer site-specific clinical
research teams to recruit expressly to ePOCS over one year. Participants were followed up
by the University of Leeds ePOCS research team.
ColoREctal Wellbeing (CREW)
http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=9374
The CREW study is a prospective observational study involving colorectal cancer patients
following primary surgery using mailed questionnaires. The aim of the study is to establish
the natural history of the recovery of health and well-being following treatment for colorectal
cancer 12. The CREW team needed to work with cancer centres across wide geographic and
socio-demographic areas which could identify, approach and recruit all study-eligible
patients to ensure best representation. To recruit a large number of patients (target n=1,000)
in one year the NIHR Cancer Research Network was approached to support study
recruitment as part of their local portfolio of studies. Sites were selected on their ability to
Page 6 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
7
recruit in a specified way and to recruit at least 2-3 participants weekly. The RNs recruiting to
CREW were established members of clinical research teams with shared responsibility for
recruitment to CREW and other CTIMPs.
Both studies
The RNs recruiting to these studies operated in much the same way as for CTIMPs in terms
of collaborating and negotiating with MDTs to identify and approach eligible patients. The
RNs informed and consented eligible patients, provided participants with written study
information, completed and returned study documentation to the ePOCS or CREW research
teams and, for the ePOCS study, entered study events onto a clinical trials database within
the EPR 13. Unlike many traditional cancer CTIMPs, the RNs consented and countersigned
the consent forms and, for CREW, in some centres were Principal Investigators. RNs were
not involved with participants after the point of study-consent. Records were kept of the
steps undertaken to encourage support for both studies, and of the outcomes of these. In
ePOCS, following recruitment completion, the RNs were interviewed by the ePOCS senior
RN to find out what it was like to work on ePOCS, how it compared with recruiting to
CTIMPS, and suggestions as to how the RN role might have been improved. Interviews
were audio-recorded and opinions collated.
PROCESSES AND OUTCOMES
How the studies were established within centres and networks
ePOCS
As ePOCS was a University of Leeds sponsored study the first task was to find managers in
each NHS trust to work with the ePOCS research team to make the application for WYCLRN
funding. Any funding approved had to be transacted through an NHS Trust and held by a
Trust budget holder. Initially, an application for responsive funding to the WYCLRN was
made on behalf of ePOCS by the Directorate Manager of non-surgical oncology in the
Page 7 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
8
Cancer Centre for three whole time equivalent (WTE) RNs for one year. Some months later,
following discussions between the WYCLRN and the cancer unit, additional funding was
requested for one further WTE RN for one year. Following funding approval there were
delays in appointing the RNs (three full-time posts; two part-time posts), with start dates
staggered over four months (Figure 2). Reasons included protracted negotiations with the
cancer centre Trust to find the staff to manage the budget, a lack of understanding by the
ePOCS research team about NHS human resources and financial systems, disjointed
communication with human resources concerning the RN appointment process and being
caught by a 4-month Trust recruitment freeze. In the cancer unit the delay in RN
appointment was due to the later application for CLRN funding. In addition, four of the five
appointed RNs were new to the role, two to the trusts and three to the tumour groups they
were recruiting, thus requiring time for induction. The delays and staggered starts meant the
recruitment period became asynchronous with the grant period and it was necessary to
negotiate a no-cost extension with the funder.
CREW
CREW put out a call to the Cancer Research Networks from the NIHR Cancer Research
Network Coordinating Centre to complete an “Expression of Interest” form.
Sites were selected according to a number of factors including: speed to achieve R&D
approval, ability to recruit good numbers, attendance at a site investigator meeting and
demonstration of close working between the clinical and research team. It was originally
planned to recruit from 24 sites, however, not all sites were able to commence recruitment
as expected or at the anticipated rate. Therefore the number of participating sites was
increased to 30 including further sites being sought from the devolved nations; 13 English, 2
Scottish and 2 Welsh cancer networks were involved.
Page 8 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
9
Methods employed to support the recruiting centres and CRNs
ePOCS
Interest in ePOCS was generated by consultations with clinicians in the development phase
14. A detailed recruitment process map was iteratively created, and checked with the clinical
teams. As the RNs had staggered starts, their training was largely individual and undertaken
by the ePOCS senior RN. In the month before recruitment started, a half-day site
investigator meeting was held at the cancer unit to inform staff about the study background,
aims and processes (7 attendees). Two meetings were held at the cancer centre, three (11
attendees) and seven (4 attendees) months into recruitment, to review progress and share
practice. In addition to the protocol, a comprehensive study guide and copies of the
recruitment maps were provided for the RNs. Ongoing support to the RNs by the ePOCS
senior RN (and research fellow in her absence) was provided by telephone, email and
weekly visits. A log was kept of study related queries between the ePOCS team and RNs
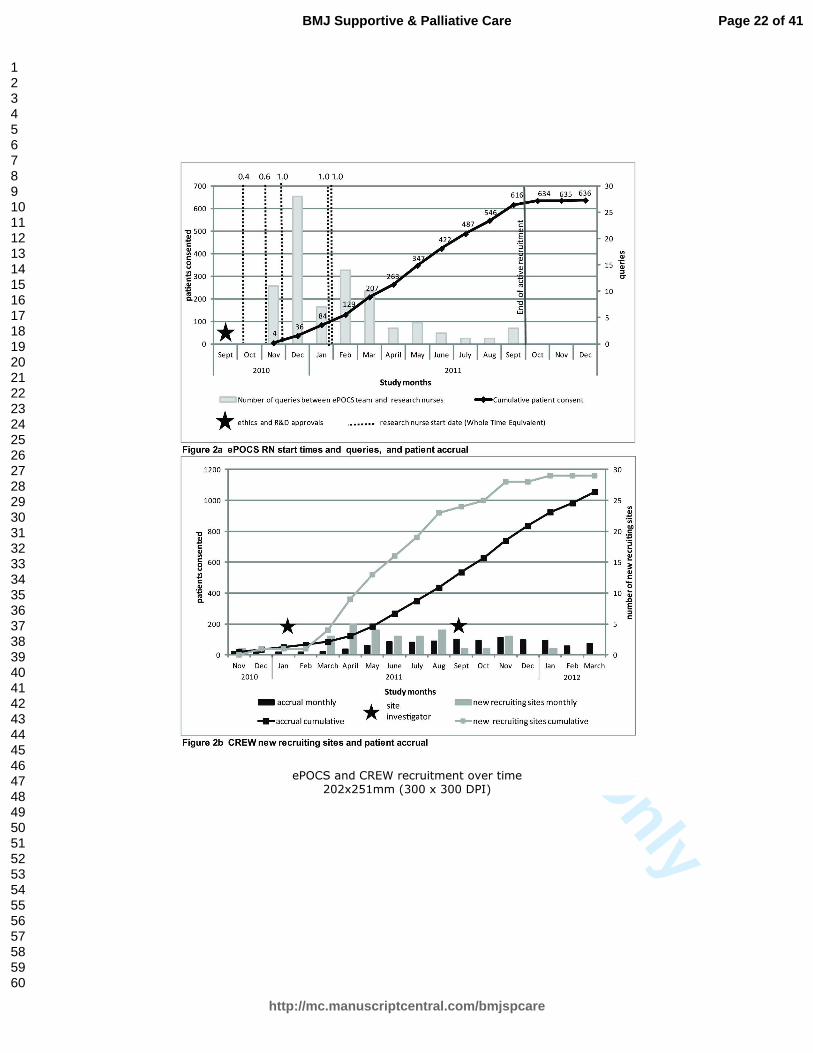
(initiated by either party). The number of RN queries was highest at the start of recruitment
and fell as the nurses became familiar with study procedures (Figure 2). Eighty-four queries
were raised in total, via phone (n=35), email (n=25) or face-to-face (n=23) (one unspecified).
Queries concerned clarification around eligibility, completion of study events on the EPR,
logistical and administrative tasks and verification of patient email addresses. The ePOCS
team sent emails to the clinical teams (and RNs) following recruitment of every fiftieth
patient, and a congratulatory email on study close. The ePOCS website
(http://www.epocs.leeds.ac.uk/) was updated about once a month with study news including
recruitment figures and information about academic presentations and publications.
CREW
Sites that joined CREW were sent instructions for recruitment and underwent a telephone
conference for study set-up. An initial CREW site investigator meeting was held in the
University of Southampton immediately prior to recruitment commencement to inform those
who would be involved in CREW recruitment about the study and for them to consider how
Page 9 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
10
to ensure they were able to approach every eligible patient in their centre (29 attendees). A
further site investigator meeting was set up after eight months to update the recruitment
staff, and for those who had not had an opportunity to attend the first meeting (21
attendees). There was a final meeting following recruitment closure in order to celebrate
reaching the accrual target (24 attendees).
All study sites were contacted at least weekly detailing data returns from each site and what
was outstanding. The CREW administrative staff had frequent email and telephone contact
with all sites. Technical queries were passed onto the study PI or clinical co-investigators.
Patient recruitment
ePOCS
Despite having planned a year to setup ePOCS, including time to apply for WYCLRN
funding and appointing RNs, the start date was slightly delayed due to the reasons outlined
above, and recruitment took time to become established in all possible clinics. It was
anticipated there would be cross-cover within the clinical research teams, such that the
ePOCS RNs would contribute to recruiting to other studies, and other RNs would help
support ePOCS. In reality, there was limited cross-cover undertaken for ePOCS by non-
ePOCS RNs. Active recruitment lasted just over ten months, two months longer than
planned, with 636 participants consenting (Figure 2).
Figure 2 about here
CREW
In order to ensure RNs undertook recruitment according to the CREW protocol, the CREW
researchers asked the teams to consider their recruitment processes and to write these into
their ‘Expression of Interest’ to participate in the study. This was also rehearsed at the site
investigator meetings. As R&D approval was protracted in some areas and there were fewer
than anticipated eligible patients in some clinics (as estimated by the sites in their expression
of interest), the overall recruitment rate was slower than expected; recruitment lasted 17
Page 10 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
11
months, 5 months longer than planned, with 1,055 participants consenting from 29 sites
across 17 cancer networks (including 66 participants from a pilot study) (Figure 2).
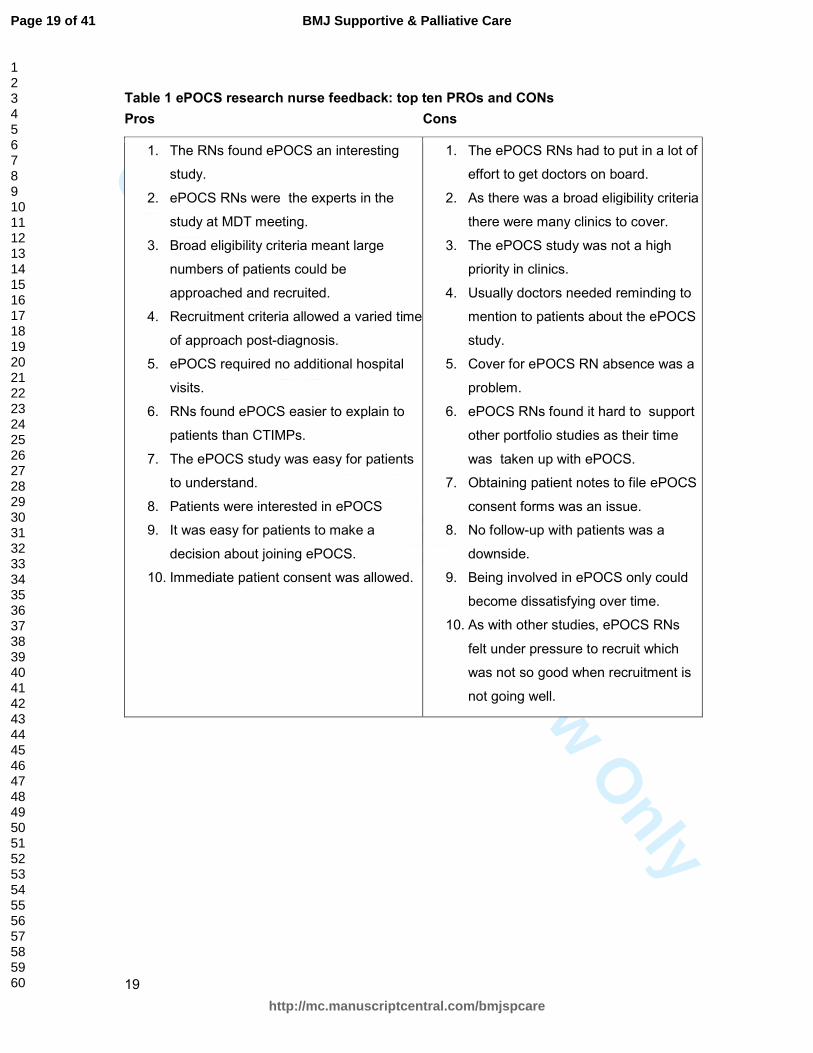
Nurse feedback (ePOCS study only)
The three full-time and one of the two part-time ePOCS RNs were interviewed at the end of
the study. In general the nurses gave positive feedback about their involvement in the
ePOCS study, although some downsides were identified (Table 1). Four out of the five
ePOCS RNs have continued to work as RNs, with one moving into the academic
psychosocial research team and the others staying in clinical research teams.
Table 1 about here
Top Tips from lessons learned
Table 2 summarises the top tips learned from these experiences, which would also apply to
CTIMPs.
Table 2 about here
DISCUSSION
Using network resources to underpin recruitment to two prospective observational
psychosocial studies was successful with both studies reaching their recruitment targets.
The process of engaging the research networks and NHS trusts in these recruitment
initiatives was, on occasion, complicated, time-consuming and frustrating for all concerned,
but with perseverance and goodwill from individual champions positive outcomes were
achieved. Using traditional psychosocial recruitment methods, with grant funded RAs, would
have been financially prohibitive for a national multicentre study and impractical, not only
due to the pragmatic and logistical difficulties of finding employers to recruit, and of inducting
new staff, but also due to the difficulty of promoting a psychosocial study, not linked with an
existing randomised CTIMP clinical trial, led by a non-clinical RA in a busy clinical
environment. The feedback from the ePOCS RNs was on the whole positive. The lessons
Page 11 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
12
learned from ePOCS and CREW should help non-clinically based academic researchers
wishing to undertake psychosocial research in the NHS.
Common to many studies, recruitment took a while to become established and gain
momentum. For the ePOCS study this related in the main to the ePOCS team not being
experienced in navigating NHS human resources systems, NHS processes slowing RN
appointments and, as this was a new scenario for the RNs, a ‘learning’ period was required.
As psychosocial researchers become more experienced and familiar with NHS systems, and
build relationships with NHS colleagues, some of these challenges will be overcome in future
collaborations. Having adequate support from relevant local organisations (R&D, CLRN,
trusts and clinical teams) is key for good representative recruitment. Although in principle
these organisations support all portfolio-adopted studies, non-clinical studies may be seen
as less important than clinical studies. This can lead to a recruitment bias where
psychosocial studies may only have access to patients not involved in clinical trials. In the
ePOCS study this was not a problem as it was accepted by all parties that patients could be
approached about ePOCS even if they were involved in clinical trials. This was more difficult
for the CREW study where in some sites recruitment was squeezed due to competing trials.
To eliminate this problem, where possible, the CREW team chose sites without competing
studies. Uptake of psychosocial studies may be further challenged when the chief and
principal investigators are not embedded in clinical services and are not therefore party to
the traditional medical model of clinical colleagues supporting each other’s studies.
Again, similar to many CTIMPs, one main delay in recruitment to the CREW study was
obtaining R&D approvals. Although research governance application and approval
processes have improved over the last ten years, problems with R&D approvals continue to
cause delays in many studies 15 16. Despite these initial challenges, accrual targets were
met; an important contributory factor may have been the careful attention to planning and
trial management as advocated in one multicentre ovarian cancer screening trial 17.
The RNs who undertook recruitment were part of established clinical research teams whose
main research activities related to cancer CTIMPs, as described by the UK Clinical Research
Page 12 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
13
Collaboration 18. The classical role of the RN has been defined as covering five main
activities: clinical practice, care coordination and continuity, study management, human
subject protection and contributing to science, with the most important of these reported by
RNs as being clinical practice and care coordination and continuity 19. In ePOCS and CREW,
clinical practice and care coordination and continuity were not part of the RN role. In the
long-term, if RNs were restricted to involvement with simple consenting for non-
interventional studies only, job satisfaction may be compromised, as highlighted in the
ePOCS RN feedback. The CREW approach may provide a more sustainable model, by
providing RNs with a mixed workload and delivering high recruitment figures which reflect
well on the clinical teams and networks. This may have wider benefits by raising awareness
of psychosocial studies at MDT/clinic level within a portfolio of classic medical interventions.
The CREW approach has been effective in the highest recruiting psychosocial portfolio study
to date: the multinational Computerised Adaptive Testing for EORTC-QLQ-C30 (CAT) study
(UKCRN ID 5256). Between April 2010 and March 2011 NIHR CRN RNs recruited 1,603
participants to CAT across the UK (personal communication K. Poole, 2012). CAT has wide
eligibility criteria and requires a single administration of one questionnaire (personal
communication T. Young, 2012). CAT, CREW and ePOCS are all simple observational
studies where no new skills were required for the RNs. ePOCS, CREW and the CAT study
described earlier, accounted for 57% of participants recruited to the Psychosocial Oncology
CSG portfolio between April 2011 and March 2012. It may be a much more difficult task if
there is a need to train RNs in new skills (e.g. for psychosocial intervention studies).
Other recruitment models have also been shown to be successful. In the Northern Cancer
Research Network, Clinical Trial Officer roles have been developed resulting in increased
recruitment to network adopted studies 20. In Southampton, the Macmillan research team
has appointed a Macmillan-funded trials coordinator to support their portfolio studies by
working within the research team to raise awareness of the processes and clinical realities
impacting on non-clinical research.
Page 13 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
14
Other challenges to psychosocial research may arise as NIHR/Government funders adhere
strictly to AcoRD documents and insist on classifying many of the psychosocial researchers'
tasks as NHS support costs (to be paid for by CLRN and done by RNs in general). As
demonstrated in ePOCS, there is considerable administrative burden in study set-up and
appointing, training and supporting RNs. The appointment of research staff (financially
supported by the funders) is even more important for these studies and possibly requires
more senior researchers with longer contracts. The balance between research and NHS
support staff is different for psychosocial studies and should be recognised by researchers
and funders. In Leeds, following closure of ePOCS, other WYCLRN funded RNs have been
appointed to work within the university psychosocial oncology research group rather than
within clinical research teams. This approach may be particularly useful for more complex
randomised intervention studies which may involve patient tracking, interviewing, delivering
interventions and/or audio-recording consultations. Nurses will bring experience and
knowledge of communicating with patients and carers, and of the patient experience and
treatment pathways, as well as familiarity with medical terminology and the clinical
environment. The psychosocial oncology research team can provide research training and
ongoing support and supervision to RNs appointed in this way. This may help to promote
RNs knowledge of research and thus in some cases nurture their transition from RNs to
individuals pursuing their own research career 18. The disadvantage of this approach is the
partial separation from clinical teams and resultant research governance issues concerning
screening and recruiting patients for trial participation which may require application to the
Care Quality Commission National Information Governance Committee (formally National
Information and Governance Board for Health and Social Care). It also generates problems
with running multicentre psychosocial studies if the RNs are trained and based for more
complex psychosocial studies in one centre only. In addition there may be repercussions for
staff. RNs who have taken on more complex leadership roles in non-traditional clinical trials
have reported challenges with isolation, role conflict, limited co-operation from clinical staff
and difficulties maintaining motivation 21. Appointing RNs rather than research assistants to
Page 14 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
15
undertake these roles may also undermine opportunities to nurture future academic leads
from psychology and behavioural sciences, who offer an important different perspective from
clinical colleagues, and who in the past have significantly contributed to psychosocial cancer
research.
Quality of life sub-studies in large trials have been very successful in increasing
understanding of patient reported outcomes following specific treatments. However, this
approach is not suitable for many studies where the primary question addresses
psychosocial issues or complex interventions in more depth and in a wider population.
Independent purely psychosocial studies will need to be designed to investigate these
questions. Using the networks to support more complex multi-centred psychosocial
oncology intervention trials will require considerable effort and new ways of working. One
way of taking this forward may be to encourage networks active in psychosocial oncology
recruitment to identify a staff member to act as a network expert with the remit to encourage
development and support of the psychosocial portfolio and liaise with the NCRI Psychosocial
Oncology CSG. There are ten networks which have participated in five or more psychosocial
studies (personal communication K. Poole, 2012). Another way will be for members of the
Psychosocial Oncology CSG to learn from ours and others experiences, work more
collaboratively across the Psychosocial Oncology CSG, with site-specific CSGs and with
clinical partners, harness the resources of the networks and gradually build expertise across
selected networks. By using these approaches psychosocial oncology research in the UK
may increase the numbers of large complex multi-centre intervention studies.
The ePOCS and CREW studies have demonstrated that hard work and collaborative
working to harness network resources to support psychosocial studies does result in positive
outcomes. Many challenges experienced were similar to those found in CTIMPs. To achieve
parity with CTIMPs in front line clinical research, psychosocial researchers will have to
continue investing time and effort to promote the importance and value of psychosocial
Page 15 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
16
research to clinical colleagues, train network RNs to undertake more complex tasks and
deliver well-designed clinical trials with demonstrable patient benefits.
Acknowledgements
We thank all the patients, staff and the research nurses who supported these studies. We
are grateful to Karen Poole and Teresa Young, Mount Vernon Cancer Centre, UK for
providing us with personal communications and to Karen Poole, National Institute for Health
Research Cancer Research Network (NCRN), and Eileen Loucaides, NCRI Clinical Studies
Groups Secretariat, for their feedback on this article.
Funding
This research was funded by Macmillan Cancer Support. They had no involvement in the
study design; in the collection, analysis and interpretation data; in the writing of the report;
and in the decision to submit the paper for publication.
Licence for Publication
The Corresponding Author has the right to grant on behalf of all authors and does grant on
behalf of all authors, an exclusive licence (or non exclusive for government employees) on a
worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be
published in BMJ Supportive and Palliative Care and any other BMJPGL products and
sublicences such use and exploit all subsidiary rights, as set out in our licence
(http://group.bmj.com/products/journals/instructions-for-authors/licence-forms).
Competing Interest
Competing Interest: None declared.
REFERENCES
1. Holland J, Watson M, Dunn J. The IPOS New International Standard of Quality Cancer
Care: integrating the psychosocial domain into routine care. Psychooncology 2011;20:677-
80.
Page 16 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
17
2. Bultz BD, Johansen C. Screening for Distress, the 6th Vital Sign: where are we, and
where are we going? Psychooncology 2011;20:569-71.
3. Cameron D, Stead M, Lester N, et al. Research-intensive cancer care in the NHS in the
UK. Ann Oncol 2011;22:29-35.
4. Stead M, Cameron D, Lester N, et al. Strengthening clinical cancer research in the United
Kingdom. Br J Cancer 2011;104:1529-34.
5. Fallowfield L, Jenkins V, Farewell V, et al. Efficacy of a Cancer Research UK
communication skills training model for oncologists: a randomised controlled trial. Lancet
2002; 359: 650-656.
6. Velikova G, Booth L, Smith AB, et al. Measuring quality of life in routine oncology
practice improves communication and patient well-being: A randomized controlled trial. J Clin
Oncol 2004, 22: 714-724.
7. Armes J, Crowe M, Colbourne L, et al. Patients' supportive care needs beyond the end of
cancer treatment: a prospective, longitudinal survey. J Clin Oncol 2009 27: 6172-6179.
8. British Psychological Society. Becoming a clinical psychologist. 2012; Available from:
http://www.bps.org.uk/careers-education-training/how-become-psychologist/types-
psychologists/becoming-clinical-psychologis . (Accessed 31st October 2012).
9. Department of Health Research and Development Directorate. Attributing the costs of
health and social care Research & Development (AcoRD). Department of Health. London:
Crown, 2012.
10. Ashley L, Jones H, Thomas J, et al. Integrating cancer survivors' experiences into UK
cancer registries: design and development of the ePOCS system (electronic Patient-reported
Outcomes from Cancer Survivors). Br J Cancer 2011;105(S1):S74-S81.
11. Ashley L, Jones H, Forman D, et al. Feasibility test of a UK-scalable electronic system
for regular collection of patient-reported outcome measures and linkage with clinical cancer
registry data: The electronic Patient-reported Outcomes from Cancer Survivors (ePOCS)
system. BMC Med Inform Decis Mak 2011;11:66.
Page 17 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
18
12. Fenlon D, Richardson A, Addington-Hall J, et al. A cohort study of the recovery of health
and wellbeing following colorectal cancer (CREW study): protocol paper. BMC Health Serv
Res 2012;12:90.
13. Newsham AC, Johnston C, Hall G, et al. Development of an advanced database for
clinical trials integrated with an electronic patient record system. Comput Biol Med
2011;41:575-86.
14. Ashley L, Jones H, Velikova G, et al. Cancer patients’ and clinicians’ opinions on the
best time in secondary care to approach patients for recruitment to longitudinal
questionnaire-based research. Support Care Cancer: 2012;20:3365-3372.
15. Chester P, Khunti K. Approval times for a multi-centre diabetes study in UK primary
care. Diabet Med. 2012;29:554-55.
16. Fudge N, Redfern J, Wolfe C, et al. Streamlined research governance: are we there yet?
BMJ. 2010;341.
17. Menon U, Gentry-Maharaj A, Ryan A, et al. Recruitment to multicentre trials—lessons
from UKCTOCS: descriptive study. BMJ 2008;337.
18. UKCRC Subcommittee for Nurses in Clinical Research (Workforce). Developing the
best research professionals - Qualified graduate nurses: recommendations for preparing and
supporting clinical academic nurses of the future. London, 2007.
19. Bevans M, Hastings C, Wehrlen L, et al. Defining Clinical Research Nursing Practice:
Results of a Role Delineation Study. CTS-Clin. Transl. Sci. 2011;4:421-27.
20. Cox K, Avis M, Wilson E, et al. An evaluation of the introduction of Clinical Trial Officer
roles into the cancer clinical trial setting in the UK. European Journal of Cancer Care
2005;14:448-56.
21. Spilsbury K, Petherick E, Cullum N, et al. The role and potential contribution of clinical
research nurses to clinical trials. Journal of Clinical Nursing 2008;17:549-57.
Page 18 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
19
Table 1 ePOCS research nurse feedback: top ten PROs and CONs
Pros Cons
1. The RNs found ePOCS an interesting
study.
2. ePOCS RNs were the experts in the
study at MDT meeting.
3. Broad eligibility criteria meant large
numbers of patients could be
approached and recruited.
4. Recruitment criteria allowed a varied time
of approach post-diagnosis.
5. ePOCS required no additional hospital
visits.
6. RNs found ePOCS easier to explain to
patients than CTIMPs.
7. The ePOCS study was easy for patients
to understand.
8. Patients were interested in ePOCS
9. It was easy for patients to make a
decision about joining ePOCS.
10. Immediate patient consent was allowed.
1. The ePOCS RNs had to put in a lot of
effort to get doctors on board.
2. As there was a broad eligibility criteria
there were many clinics to cover.
3. The ePOCS study was not a high
priority in clinics.
4. Usually doctors needed reminding to
mention to patients about the ePOCS
study.
5. Cover for ePOCS RN absence was a
problem.
6. ePOCS RNs found it hard to support
other portfolio studies as their time
was taken up with ePOCS.
7. Obtaining patient notes to file ePOCS
consent forms was an issue.
8. No follow-up with patients was a
downside.
9. Being involved in ePOCS only could
become dissatisfying over time.
10. As with other studies, ePOCS RNs
felt under pressure to recruit which
was not so good when recruitment is
not going well.
Page 19 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
20
Table 2 Top tips for using the Clinical Research Network to support patient recruitment to psychosocial cancer research
1. Allow more time than you expect for study set-up.
2. Find local NHS and network champions (clinical and management) with whom to
collaborate.
3. For a multi-centre study consider the challenges of ensuring your study is included
into the local portfolio of a network and appropriately supported by clinical
research network staff.
4. If conducting a multi-centre study liaise with national coordinating centre to
discuss feasibility and deliverability to develop achievable milestones.
5. For limited site studies consider whether it would be more efficient to seek
dedicated clinical research staff (either from existing establishments or through
applying for time-limited funding through NIHR Comprehensive Local Research
Networks).
6. Work closely with local R&D managers and invite them to site investigator
meetings where possible.
7. Give as much information as possible in advance so that local teams can make
realistic assessments of what is achievable, especially for UK-wide trials.
8. Provide clear and comprehensive resources for the RNs for their own use, and for
them to educate clinical and MDT colleagues.
9. Be flexible to accommodate local variation; one size does not fit all. Work with
local RNs and clinical teams to establish best recruitment methods for specific
clinical practices.
10. Invest time in training RNs to undertake recruitment, especially if they are new to
post.
11. Respond quickly to RN queries and ensure you have senior research team
members available to answer complex questions.
12. Create good relationships with clinical staff by developing open communication
using a variety of methods (email, fax, face-to-face meetings, phone, website).
13. Regularly provide feedback on local and overall recruitment to networks, clinical
teams and RNs. Arrange study events/workshops for recruiting teams. Celebrate
success.
14. Keep the funder up to date with progress and challenges.
15. Thank all involved and acknowledge them in presentations and publications.
Page 20 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
Overview of the NIHR Clinical Research Network (England) with an emphasis on the Yorkshire Cancer Research Network
202x239mm (300 x 300 DPI)
Page 21 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
ePOCS and CREW recruitment over time
202x251mm (300 x 300 DPI)
Page 22 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
1
Using the Clinical Research Network for psychosocial research:
lessons learned from two observational studies
Penny Wright*1, Deborah Fenlon2, Helen Jones1, Claire Foster2, Laura Ashley1,
Kim Chivers Seymour2, Galina Velikova1, Ikumi Okamoto2 and Julia Brown3
1 Psychosocial Oncology and Clinical Practice Research Group, Leeds Institute of Cancer
Studies and Pathology, University of Leeds, Leeds, UK
2Macmillan Survivorship Research Group, Faculty of Health Sciences, University of
Southampton, Southampton, UK
3 Clinical Trials Research Unit, Leeds Institute of Clinical Trials Research, University of
Leeds, Leeds, UK
*Corresponding author
Dr Penny Wright,
Psychosocial Oncology and Clinical Practice Research Group, Level three Bexley Wing, St
James’s Institute of Oncology, St James’s University Hospital, Leeds LS9 7TF
Telephone: 00 (44) 113 2068488
Fax: 00 (44) 113 2068512
Keywords
clinical studies, patient recruitment, psychosocial, research nurses, patient accrual, clinical
research network
Word Count: 4,078
Page 23 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
2
ABSTRACT
Background
Patient recruitment to psychosocial oncology research has increased over the last 10 years
but the majority of studies have been single-site or small-scale. The National Institute for
Health Research (NIHR), Clinical Research Network (CRN) supports NIHR portfolio studies
through provision of research staff to recruit and follow-up patients, but has been little used
by psychosocial researchers. We report the experiences of two psychosocial research teams
who recently used the CRN, to undertake patient recruitment, to inform cancer researchers
of non-clinical trials of an investigational medicinal product (non-CTIMPs) of lessons learned
and to provide recommendations.
Method and outcomes
Patients were successfully recruited to two prospective observational studies: electronic
Patient-reported Outcomes from Cancer Survivors study (ePOCS; n=636) and the
ColoREctal Wellbeing study (CREW; n=1,055). ePOCS secured Comprehensive Local
Research Networks funding to appoint ePOCS-specific study research nurses. CREW
obtained research support through the NIHR Cancer Research Network. Top tips for
establishing and running studies with CRN staff are provided and suggestions given for
advancing multicentre complex non-CTIMPs.
Conclusion
Some challenges were similar to those in delivery of CTIMPs. The pros and cons of being
involved in ePOCS from the research nurse perspective are also described. Overall the
approaches used were successful.
Page 24 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
3
INTRODUCTION
The importance of psychosocial oncology has been increasingly recognised over recent
decades, leading to the Union International for Cancer Control declaring ‘distress’ the 6th
vital sign in Cancer Care 1. Despite this, psychosocial care has not become fully integrated
into routine cancer care. A number of challenges persist including how psychosocial
oncology is valued as a discipline in its own right, the costs of supportive care, and a lack of
evidence from large-scale well-designed psychosocial trials 2. In the UK cancer research has
been nurtured by the establishment of the National Cancer Research Institute (NCRI:
http://www.ncri.org.uk/ ) Clinical Studies Groups (CSGs). CSGs facilitate and prioritise
studies to address cancer diagnostic-specific questions (i.e. breast, lung) or cross-cutting
issues (i.e. palliative, psychosocial). The National Institute of Health Research (NIHR)
Cancer Research Network (http://www.ncrn.org.uk/ ), established in parallel with the NCRI,
was set up to increase the number of patients participating in high-quality clinical research
studies. The NIHR Cancer Research Network comprises 32 Local Research Networks
across England and provides an infrastructure to support study participation, including
funding for research nurses (RNs). Since 2006 their main focus has been on recruitment to
clinical trials of an investigational medicinal product (CTIMP) randomised controlled trials
(RCT). This has led to increased accrual to RCTs but not at the expense of accrual to
observational studies, may be because some observational studies provide an opportunity
for patients to enrol in RCTs at the same time 3. Timely accrual to both randomised
controlled trials (RCTs) and observational studies within the cancer trials portfolio has
increased significantly since the NIHR Cancer Research Network was established, rising
from <5% of incidence cases in 2001 to >20% in 2010 3. Although the majority of trials
within the portfolio are clinical trials of an investigational medicinal product (CTIMPs) there is
interest in developing other types of interventional studies 4.The success of the NIHR Cancer
Research Network model for supporting clinical trials in England led to the establishment of
a generic Clinical Research Network (CRN) to provide infrastructure for other clinical groups.
Page 25 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
4
The elements of the NIHR CRN and their inter-relationships and acronyms can be confusing.
Figure 1 provides an overview and places the national and local level of networks into
context.
The NIHR Cancer Research Network-NCRI CSG model for developing and delivering high-
quality large-scale trials has worked well for clinical trial evaluation of CTIMPs. Some of
these trials have either secondary quality of life outcomes as part of the main study or have
linked sub-studies with primary quality of life outcomes. In the disease site specific CSGs the
majority of members are clinicians. The trials become embedded within clinical practice
across a number of centres where patients are considered for participation at
Multidisciplinary Team (MDT) meetings by clinicians and associated RNs. Across the
country there is a network of clinicians who have duty of care for these patients, who are
research active and who contribute to accrual of portfolio CTIMPs with support mainly from
the NIHR Cancer Research Network.
The model does not work so effectively for psychosocial studies. The Psychosocial
Oncology CSG comprises a varied membership (including health psychology, social work,
nursing, clinical trials), few of whom have responsibility for clinical care. The range of studies
within the psychosocial oncology portfolio is broad, including studies of interventions from
acupuncture to cognitive-behavioural therapy, studies to develop patient decision aids, and
observational studies of patients’ quality of life, health behaviors and care experience. There
is no ready-made clinical infrastructure or experienced study recruitment network to call on
for championing multi-centre psychosocial studies. In addition, psychosocial studies may
require specialist professional input, which is not part of the standard clinical research team,
to deliver an intervention or undertake specialised interviewing or observations. As a result
although there have been some high-quality large-scale psychosocial studies 5-7, many
studies within the growing Psychosocial Oncology CSG portfolio have been single-site or
small-scale and have tended to rely on individual grant-funded appointed research
assistants, rather than using network RNs, for recruitment and follow-up of patients.
Commonly research assistants are psychology graduates looking for research experience to
Page 26 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
5
aid advancement to academic doctoral studies or a clinical psychology career 58. Now there
is an expectation that some research costs will no longer be met by some grant awarding
bodies. The recently published Department of Health AcoRD document provides the basis
for attributing the costs of health and social care research studies in three categories:
research costs (costs of activities undertaken to answer the research questions), NHS
treatment costs (costs of patient care) and NHS support costs (additional patient care costs
associated with the research) 69. If a study is funded by a charity which is a member of the
Association of Medical Research Charities (AMRC) some NHS support costs will be met by
the Department of Health, via the networks, such as the identification of patients suitable to
approach for participation, obtaining consent and additional assessments. In order for the
Psychosocial Oncology CSG to consistently deliver high-quality large-scale observational
studies and trials, use of the networks for recruitment support will have to become standard
practice.
In 2010-2012 two Psychosocial Oncology CSG portfolio observational cohort studies, funded
by Macmillan Cancer Support (AMRC member) and run by University sponsored
researchers, collaborated in two different ways with the networks to support recruitment. In
the electronic Patient-reported Outcomes from Cancer Survivors (ePOCS) study the
research team applied for study specific funding for RNs to the generic West Yorkshire
Comprehensive Local Research Network (WYCLRN); in the ColoREctal Wellbeing (CREW)
study the research team asked for expressions of interest for study participation from the
NIHR Cancer Research Networks (Figure 1). Both studies were given research ethics
committee approval (ePOCS (Leeds East 10/H1306/65); CREW (Oxfordshire REC B
10/H0605/31)) and all participants provided written informed consent. We report and
compare the different approaches of ePOCS and CREW with the aim of informing non-
CTIMPs researchers of lessons learned and providing recommendations for future studies.
Figure 1 about here
Page 27 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
6
THE STUDIES
electronic Patient-reported Outcomes from Cancer Survivors (ePOCS)
http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=9403
ePOCS is a secure electronic system for collecting Patient Reported Outcome Measures
(PROMS) via the internet at multiple time-points and linking these data with patients' clinical
data transferred from the electronic patient record (EPR) to the cancer registry and
managing associated patient communications electronically 710. The ePOCS study is a
prospective observational study to test the feasibility of the ePOCS system, by running it for
two years in two NHS Trusts within the Yorkshire Cancer Network (YCN) (the cancer centre
and one cancer unit), and using the Northern and Yorkshire Cancer Registry and Information
Service 811. To test feasibility, all non-metastatic breast, colorectal and prostate cancer
patients attending the two YCN Trusts within six months post-diagnosis needed to be
considered for recruitment (estimated target n=600). Funding was obtained from the
WYCLRN to appoint RNs to be embedded within established cancer site-specific clinical
research teams to recruit expressly to ePOCS over one year. Participants were followed up
by the University of Leeds ePOCS research team.
ColoREctal Wellbeing (CREW)
http://public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=9374
The CREW study is a prospective observational study involving colorectal cancer patients
following primary surgery using mailed questionnaires. The aim of the study is to establish
the natural history of the recovery of health and well-being following treatment for colorectal
cancer 912. The CREW team needed to work with cancer centres across wide geographic
and socio-demographic areas which could identify, approach and recruit all study-eligible
patients to ensure best representation. To recruit a large number of patients (target n=1,000)
in one year the NIHR Cancer Research Network was approached to support study
recruitment as part of their local portfolio of studies. Sites were selected on their ability to
Page 28 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
7
recruit in a specified way and to recruit at least 2-3 participants weekly. The RNs recruiting to
CREW were established members of clinical research teams with shared responsibility for
recruitment to CREW and other CTIMPs.
Both studies
The RNs recruiting to these studies operated in much the same way as for CTIMPs in terms
of collaborating and negotiating with MDTs to identify and approach eligible patients. The
RNs informed and consented eligible patients, provided participants with written study
information, completed and returned study documentation to the ePOCS or CREW research
teams and, for the ePOCS study, entered study events onto a clinical trials database within
the EPR 1013. Unlike many traditional cancer CTIMPs, the RNs consented and countersigned
the consent forms and, for CREW, in some centres were Principal Investigators. RNs were
not involved with participants after the point of study-consent. Records were kept of the
steps undertaken to encourage support for both studies, and of the outcomes of these. In
ePOCS, following recruitment completion, the RNs were interviewed by the ePOCS senior
RN to find out what it was like to work on ePOCS, how it compared with recruiting to
CTIMPS, and suggestions as to how the RN role might have been improved. Interviews
were audio-recorded and opinions collated.
PROCESSES AND OUTCOMES
How the studies were established within centres and networks
ePOCS
As ePOCS was a University of Leeds sponsored study the first task was to find managers in
each NHS trust to work with the ePOCS research team to make the application for WYCLRN
funding. Any funding approved had to be transacted through an NHS Trust and held by a
Trust budget holder. Initially, an application for responsive funding to the WYCLRN was
made on behalf of ePOCS by the Directorate Manager of non-surgical oncology in the
Page 29 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
8
Cancer Centre for three whole time equivalent (WTE) RNs for one year. Some months later,
following discussions between the WYCLRN and the cancer unit, additional funding was
requested for one further WTE RN for one year. Following funding approval there were
delays in appointing the RNs (three full-time posts; two part-time posts), with start dates
staggered over four months (Figure 2). Reasons included protracted negotiations with the
cancer centre Trust to find the staff to manage the budget, a lack of understanding by the
ePOCS research team about NHS human resources and financial systems, disjointed
communication with human resources concerning the RN appointment process and being
caught by a 4-month Trust recruitment freeze. In the cancer unit the delay in RN
appointment was due to the later application for CLRN funding. In addition, four of the five
appointed RNs were new to the role, two to the trusts and three to the tumour groups they
were recruiting, thus requiring time for induction. The delays and staggered starts meant the
recruitment period became asynchronous with the grant period and it was necessary to
negotiate a no-cost extension with the funder.
CREW
CREW put out a call to the Cancer Research Networks from the NIHR Cancer Research
Network Coordinating Centre to complete an “Expression of Interest” form.
Sites were selected according to a number of factors including: speed to achieve R&D
approval, ability to recruit good numbers, attendance at a site investigator meeting and
demonstration of close working between the clinical and research team. It was originally
planned to recruit from 24 sites, however, not all sites were able to commence recruitment
as expected or at the anticipated rate. Therefore the number of participating sites was
increased to 30 including further sites being sought from the devolved nations; 13 English, 2
Scottish and 2 Welsh cancer networks were involved.
Page 30 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
9
Methods employed to support the recruiting centres and CRNs
ePOCS
Interest in ePOCS was generated by consultations with clinicians in the development phase
1114. A detailed recruitment process map was iteratively created, and checked with the
clinical teams. As the RNs had staggered starts, their training was largely individual and
undertaken by the ePOCS senior RN. In the month before recruitment started, a half-day site
investigator meeting was held at the cancer unit to inform staff about the study background,
aims and processes (7 attendees). Two meetings were held at the cancer centre, three (11
attendees) and seven (4 attendees) months into recruitment, to review progress and share
practice. In addition to the protocol, a comprehensive study guide and copies of the
recruitment maps were provided for the RNs. Ongoing support to the RNs by the ePOCS
senior RN (and research fellow in her absence) was provided by telephone, email and
weekly visits. A log was kept of study related queries between the ePOCS team and RNs
(initiated by either party). The number of RN queries was highest at the start of recruitment
and fell as the nurses became familiar with study procedures (Figure 2). Eighty-four queries
were raised in total, via phone (n=35), email (n=25) or face-to-face (n=23) (one unspecified).
Queries concerned clarification around eligibility, completion of study events on the EPR,
logistical and administrative tasks and verification of patient email addresses. The ePOCS
team sent emails to the clinical teams (and RNs) following recruitment of every fiftieth
patient, and a congratulatory email on study close. The ePOCS website
(http://www.epocs.leeds.ac.uk/) was updated about once a month with study news including
recruitment figures and information about academic presentations and publications.
CREW
Sites that joined CREW were sent instructions for recruitment and underwent a telephone
conference for study set-up. An initial CREW site investigator meeting was held in the
University of Southampton immediately prior to recruitment commencement to inform those
who would be involved in CREW recruitment about the study and for them to consider how
Page 31 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
10
to ensure they were able to approach every eligible patient in their centre (29 attendees). A
further site investigator meeting was set up after eight months to update the recruitment
staff, and for those who had not had an opportunity to attend the first meeting (21
attendees). There was a final meeting following recruitment closure in order to celebrate
reaching the accrual target (24 attendees).
All study sites were contacted at least weekly detailing data returns from each site and what
was outstanding. The CREW administrative staff had frequent email and telephone contact
with all sites. Technical queries were passed onto the study PI or clinical co-investigators.
Patient recruitment
ePOCS
Despite having planned a year to setup ePOCS, including time to apply for WYCLRN
funding and appointing RNs, the start date was slightly delayed due to the reasons outlined
above, and recruitment took time to become established in all possible clinics. It was
anticipated there would be cross-cover within the clinical research teams, such that the
ePOCS RNs would contribute to recruiting to other studies, and other RNs would help
support ePOCS. In reality, there was limited cross-cover undertaken for ePOCS by non-
ePOCS RNs. Active recruitment lasted just over ten months, two months longer than
planned, with 636 participants consenting (Figure 2).
Figure 2 about here
CREW
In order to ensure RNs undertook recruitment according to the CREW protocol, the CREW
researchers asked the teams to consider their recruitment processes and to write these into
their ‘Expression of Interest’ to participate in the study. This was also rehearsed at the site
investigator meetings. As R&D approval was protracted in some areas and there were fewer
than anticipated eligible patients in some clinics (as estimated by the sites in their expression
of interest), the overall recruitment rate was slower than expected; recruitment lasted 17
Page 32 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
11
months, 5 months longer than planned, with 1,055 participants consenting from 29 sites
across 17 cancer networks (including 66 participants from a pilot study) (Figure 2).
Nurse feedback (ePOCS study only)
The three full-time and one of the two part-time ePOCS RNs were interviewed at the end of
the study. In general the nurses gave positive feedback about their involvement in the
ePOCS study, although some downsides were identified (Table 1). Four out of the five
ePOCS RNs have continued to work as RNs with one moving into the academic
psychosocial research team and the others staying in clinical research teams.
Table 1 about here
Top Tips from lessons learned
Table 2 summarises the top tips learned from these experiences, which would also apply to
CTIMPs.
Table 2 about here
DISCUSSION
Using network resources to underpin recruitment to two prospective observational
psychosocial studies was successful with both studies reaching their recruitment targets.
The process of engaging the research networks and NHS trusts in these recruitment
initiatives was, on occasion, complicated, time-consuming and frustrating for all concerned,
but with perseverance and goodwill from individual champions positive outcomes were
achieved. Using traditional psychosocial recruitment methods, with grant funded RAs, would
have been financially prohibitive for a national multicentre study and impractical, not only
due to the pragmatic and logistical difficulties of finding employers to recruit, and of inducting
new staff, but also due to the difficulty of promoting the a psychosocial studies study, not
Page 33 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
12
linked with an existing randomised CTIMP clinical trial, led by a non-clinical RA in a busy
clinical environment. alongside clinical trials. The feedback from the ePOCS RNs was on
the whole positive. The lessons learned from ePOCS and CREW should help non-clinically
based academic researchers wishing to undertake psychosocial research in the NHS.
Common to many studies, recruitment took a while to become established and gain
momentum. For the ePOCS study this related in the main to the ePOCS team not being
experienced in navigating NHS human resources systems, NHS processes slowing RN
appointments and, as this was a new scenario for the RNs, a ‘learning’ period was required.
As psychosocial researchers become more experienced and familiar with NHS systems, and
build relationships with NHS colleagues, some of these challenges will be overcome in future
collaborations. Having adequate support from relevant local organisations (R&D, CLRN,
trusts and clinical teams) is key for good representative recruitment. Although in principle
these organisations support all portfolio-adopted studies, non-clinical studies may be seen
as less important than clinical studies. This can lead to a recruitment bias where
psychosocial studies may only have access to patients not involved in clinical trials. In the
ePOCS study this was not a problem as it was accepted by all parties that patients could be
approached about ePOCS even if they were involved in clinical trials. This was more difficult
for the CREW study where in some sites recruitment was squeezed due to competing trials.
To eliminate this problem, where possible, the CREW team chose sites without competing
studies. Uptake of psychosocial studies may be further challenged when the chief and
principal investigators are not embedded in clinical services and are not therefore party to
the traditional medical model of clinical colleagues supporting each other’s studies.
Again, similar to many CTIMPs, one main delay in recruitment to the CREW study was
obtaining R&D approvals. Although research governance application and approval
processes have improved over the last ten years, problems with R&D approvals continue to
cause delays in many studies 12 1315 16. Despite these initial challenges, accrual targets were
met; an important contributory factor may have been the careful attention to planning and
trial management as advocated in one multicentre ovarian cancer screening trial 1417.
Page 34 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
13
The RNs who undertook recruitment were part of established clinical research teams whose
main research activities related to cancer CTIMPs, as described by the UK Clinical Research
Collaboration 1518. The classical role of the RN has been defined as covering five main
activities: clinical practice, care coordination and continuity, study management, human
subject protection and contributing to science, with the most important of these reported by
RNs as being clinical practice and care coordination and continuity 1619. In ePOCS and
CREW, clinical practice and care coordination and continuity were not part of the RN role. In
the long-term, if RNs were restricted to involvement with simple consenting for non-
interventional studies only, job satisfaction may be compromised, as highlighted in the
ePOCS RN feedback. The CREW approach may provide a more sustainable model, by
providing RNs with a mixed workload and delivering high recruitment figures which reflect
well on the clinical teams and networks. This may have wider benefits by raising awareness
of psychosocial studies at MDT/clinic level within a portfolio of classic medical interventions.
The CREW approach has been effective in the highest recruiting psychosocial portfolio study
to date: the multinational Computerised Adaptive Testing for EORTC-QLQ-C30 (CAT) study
(UKCRN ID 5256). Between April 2010 and March 2011 NIHR CRN RNs recruited 1,603
participants to CAT across the UK (personal communication K. Poole, 2012). CAT has wide
eligibility criteria and requires a single administration of one questionnaire (personal
communication T. Young, 2012). CAT, CREW and ePOCS are all simple observational
studies where no new skills were required for the RNs. ePOCS, CREW and the CAT study
described earlier, accounted for 57% of participants recruited to the Psychosocial Oncology
CSG portfolio between April 2011 and March 2012. It may be a much more difficult task if
there is a need to train RNs in new skills (e.g. for psychosocial intervention studies).
Other recruitment models have also been shown to be successful. In the Northern Cancer
Research Network, Clinical Trial Officer roles have been developed resulting in increased
recruitment to network adopted studies 1720. In Southampton, the Macmillan research team
has appointed a Macmillan-funded trials coordinator to support their portfolio studies by
Page 35 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
14
working within the research team to raise awareness of the processes and clinical realities
impacting on non-clinical research.
Other challenges to psychosocial research may arise as NIHR/Government funders adhere
strictly to AcoRD documents and insist on classifying many of the psychosocial researchers'
tasks as NHS support costs (to be paid for by CLRN and done by RNs in general). As
demonstrated in ePOCS, there is considerable administrative burden in study set-up and
appointing, training and supporting RNs. The appointment of research staff (financially
supported by the funders) is even more important for these studies and possibly requires
more senior researchers with longer contracts. The balance between research and NHS
support staff is different for psychosocial studies and should be recognised by researchers
and funders. In Leeds, following closure of ePOCS, other WYCLRN funded RNs have been
appointed to work within the university psychosocial oncology research group rather than
within clinical research teams. This approach may be particularly useful for more complex
randomised intervention studies which may involve patient tracking, interviewing, delivering
interventions and/or audio-recording consultations. Nurses will bring experience and
knowledge of communicating with patients and carers, and of the patient experience and
treatment pathways, as well as familiarity with medical terminology and the clinical
environment. The psychosocial oncology research team can provide research training and
ongoing support and supervision to RNs appointed in this way. This may help to promote
RNs knowledge of research and thus in some cases nurture their transition from RNs to
individuals pursuing their own research career 1518. The disadvantage of this approach is the
partial separation from clinical teams and resultant research governance issues concerning
screening and recruiting patients for trial participation which may require application to the
Care Quality Commission National Information Governance Committee (formally National
Information and Governance Board for Health and Social Care). It also generates problems
with running multicentre psychosocial studies if the RNs are trained and based for more
complex psychosocial studies in one centre only. In addition there may be repercussions for
staff. RNs who have taken on more complex leadership roles in non-traditional clinical trials
Page 36 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
15
have reported challenges with isolation, role conflict, limited co-operation from clinical staff
and difficulties maintaining motivation 1821. Appointing RNs rather than research assistants to
undertake these roles may also undermine opportunities to nurture future academic leads
from psychology and behavioural sciences, who offer an important different perspective from
clinical colleagues, and who in the past have significantly contributed to psychosocial cancer
research.
Quality of life sub-studies in large trials have been very successful in increasing
understanding of patient reported outcomes following specific treatments. However, this
approach is not suitable for many studies where the primary question addresses
psychosocial issues or complex interventions in more depth and in a wider population.
Independent purely psychosocial studies will need to be designed to investigate these
questions. Using the networks to support more complex multi-centred psychosocial
oncology intervention trials will require considerable effort and new ways of working. One
way of taking this forward may be to encourage networks active in psychosocial oncology
recruitment to identify a staff member to act as a network expert with the remit to encourage
development and support of the psychosocial portfolio and liaise with the NCRI Psychosocial
Oncology CSG. There are ten networks which have participated in five or more psychosocial
studies (personal communication K. Poole, 2012). Another way will be for members of the
Psychosocial Oncology CSG to learn from ours and others experiences, work more
collaboratively across the Psychosocial Oncology CSG, with site-specific CSGs and with
clinical partners, harness the resources of the networks and gradually build expertise across
selected networks. By using these approaches psychosocial oncology research in the UK
may increase the numbers of large complex multi-centre intervention studies.
The ePOCS and CREW studies have demonstrated that hard work and collaborative
working to harness network resources to support psychosocial studies does result in positive
outcomes. Many challenges experienced were similar to those found in CTIMPs. To achieve
parity with CTIMPs in front line clinical research, psychosocial researchers will have to
Page 37 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
16
continue investing time and effort to promote the importance and value of psychosocial
research to clinical colleagues, train network RNs to undertake more complex tasks and
deliver well-designed clinical trials with demonstrable patient benefits.
Acknowledgements
We thank all the patients, staff, the research nurses and the research networks who
supported these studies We are grateful to Karen Poole and Teresa Young, Mount Vernon
Cancer Centre, UK for providing us with personal communications and to Karen Poole,
National Institute for Health Research Cancer Research Network (NCRN), and Eileen
Loucaides, NCRI Clinical Studies Groups Secretariat, for their feedback on this article.
Funding
This research was funded by Macmillan Cancer Support. They had no involvement in the
study design; in the collection, analysis and interpretation data; in the writing of the report;
and in the decision to submit the paper for publication.
Licence for Publication
The Corresponding Author has the right to grant on behalf of all authors and does grant on
behalf of all authors, an exclusive licence (or non exclusive for government employees) on a
worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be
published in BMJ Supportive and Palliative Care and any other BMJPGL products and
sublicences such use and exploit all subsidiary rights, as set out in our licence
(http://group.bmj.com/products/journals/instructions-for-authors/licence-forms).
Competing Interest
Competing Interest: None declared.
Competing interests
None.
Page 38 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
17
REFERENCES
1. Holland J, Watson M, Dunn J. The IPOS New International Standard of Quality Cancer
Care: integrating the psychosocial domain into routine care. Psychooncology 2011;20:677-
80.
2. Bultz BD, Johansen C. Screening for Distress, the 6th Vital Sign: where are we, and
where are we going? Psychooncology 2011;20:569-71.
3. Cameron D, Stead M, Lester N, et al. Research-intensive cancer care in the NHS in the
UK. Ann Oncol 2011;22:29-35.
4. Stead M, Cameron D, Lester N, et al. Strengthening clinical cancer research in the United
Kingdom. Br J Cancer 2011;104:1529-34.
5. Fallowfield L, Jenkins V, Farewell V, et al. Efficacy of a Cancer Research UK
communication skills training model for oncologists: a randomised controlled trial. Lancet
2002; 359: 650-656.
6. Velikova G, Booth L, Smith AB, et al. Measuring quality of life in routine oncology
practice improves communication and patient well-being: A randomized controlled trial. J Clin
Oncol 2004, 22: 714-724.
7. Armes J, Crowe M, Colbourne L, et al. Patients' supportive care needs beyond the end of
cancer treatment: a prospective, longitudinal survey. J Clin Oncol 2009 27: 6172-6179.
58. British Psychological Society. Becoming a clinical psychologist. 2012; Available from:
http://www.bps.org.uk/careers-education-training/how-become-psychologist/types-
psychologists/becoming-clinical-psychologis . (Accessed 31st October 2012).
69. Department of Health Research and Development Directorate. Attributing the costs
of health and social care Research & Development (AcoRD). Department of Health. London:
Crown, 2012.
Page 39 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
18
710. Ashley L, Jones H, Thomas J, et al. Integrating cancer survivors' experiences into UK
cancer registries: design and development of the ePOCS system (electronic Patient-reported
Outcomes from Cancer Survivors). Br J Cancer 2011;105(S1):S74-S81.
811. Ashley L, Jones H, Forman D, et al. Feasibility test of a UK-scalable electronic system
for regular collection of patient-reported outcome measures and linkage with clinical cancer
registry data: The electronic Patient-reported Outcomes from Cancer Survivors (ePOCS)
system. BMC Med Inform Decis Mak 2011;11:66.
912. Fenlon D, Richardson A, Addington-Hall J, et al. A cohort study of the recovery of
health and wellbeing following colorectal cancer (CREW study): protocol paper. BMC Health
Serv Res 2012;12:90.
1013. Newsham AC, Johnston C, Hall G, et al. Development of an advanced database for
clinical trials integrated with an electronic patient record system. Comput Biol Med
2011;41:575-86.
1114. Ashley L, Jones H, Velikova G, et al. Cancer patients’ and clinicians’ opinions on the
best time in secondary care to approach patients for recruitment to longitudinal
questionnaire-based research. Support Care Cancer: 2012;20:3365-3372.
1215. Chester P, Khunti K. Approval times for a multi-centre diabetes study in UK primary
care. Diabet Med. 2012;29:554-55.
1316. Fudge N, Redfern J, Wolfe C, et al. Streamlined research governance: are we there
yet? BMJ. 2010;341.
1417. Menon U, Gentry-Maharaj A, Ryan A, et al. Recruitment to multicentre trials—lessons
from UKCTOCS: descriptive study. BMJ 2008;337.
1518. UKCRC Subcommittee for Nurses in Clinical Research (Workforce). Developing
the best research professionals - Qualified graduate nurses: recommendations for preparing
and supporting clinical academic nurses of the future. London, 2007.
1619. Bevans M, Hastings C, Wehrlen L, et al. Defining Clinical Research Nursing Practice:
Results of a Role Delineation Study. CTS-Clin. Transl. Sci. 2011;4:421-27.
Page 40 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
19
1720. Cox K, Avis M, Wilson E, et al. An evaluation of the introduction of Clinical Trial
Officer roles into the cancer clinical trial setting in the UK. European Journal of Cancer Care
2005;14:448-56.
1821. Spilsbury K, Petherick E, Cullum N, et al. The role and potential contribution of
clinical research nurses to clinical trials. Journal of Clinical Nursing 2008;17:549-57.
Page 41 of 41
http://mc.manuscriptcentral.com/bmjspcare
BMJ Supportive & Palliative Care
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Related Documents











