Oriainal Contributions Using Polymerase Chain Reaction to Human Papillomavirus in Oral and Pharyngolaryngeal Carcinomas Ignacio Alvarez Alvarez, MD, Pedro Sanchez Lazo, PhD, Sofia Ramos Gonzalez, PhD, J. Pablo Rodrigo Tapia, MD, Faustino Nudez Batalla, MD, and Carlos Suarez Nieto, MD Purpose: Increasingly, evidence has shown that human papillomavirus (HPV) plays a role in the induction of certain carcinomas. The presence of HPV sequences in 56 previously untreated oral and pharyngolaryngeal carcinomas was examined by the polymerase chain reaction (PCR). Materials and Methods: After DNA extraction, samples underwent 40 replication cycles with specific oligonucleotide primers corresponding to sequences from the E6 open-reading frame of HPV-Gb, HPV-16, and HPV-18. To determine the E6 genomic integration, positive samples were processed with specific primers for the corresponding HPV Ll genes. Genomic HPV DNA cloned into PBR 322 was used as positive control. Results: HPV E6 DNA of the 6b and 16 types was detected in 14 patients (25%). The Ll gene was not present. Conclusion: Detected HPV E6 DNA might be integrated into the cell genome in the positive cases as indicated by the absence of the Li gene-coding for the viral capside. Histological and clinical parameters, such as tumor location, degree of differentiation, stage, recurrence, and survival rates, were unrelated to the presence of HPV. Copyright o 1997 by W.B. Saunders Company. Different HPV types have been identified in human tumors of various localizations. HPV types 6b, 16, and 18 have the highest fre- quency. In the upper aerodigestive tract, malig- nant tumors have been found to contain the E6 gene from HPV type 16, and there are indica- From the Department of Otorhinolavngology, Complejo Hospitalario de Leon, Oviedo; the Department of Func- tional Biology, Facultad Medicina, Oviedo; and the Depart- ment of Otorhinolaryngology, Hospital Central de As- turias, Oviedo, Spain. Presented to the 99th Annual Meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation, New Orleans, LA, September 17-20 1995. This work was supported by a grant from the Fondo de lnvestigaciones Sanitarias de la Seguridad Social, Madrid, Spain (FIS 93/0400). Address reprint requests to lgnacio Alvarez Alvarez, MD, C/Matematico Pedrayes 22, 5”izda, 33005 Oviedo, Spain. Copyright 0 1997 by W.B. Saunders Company 0196-0709/97/l 808-0002$5.00/O tions of the implications of HPV types 6b and 18. HPV is a double-stranded DNA virus of approximately 8,000 base pairs (bp) in length, conforming seven early and two late gene open-reading frames (ORF) that code for regu- latory and structural proteins, respectively.1-3 The E6 gene appears to be integrated in the human cellular genome and probably predis- poses to the malignant transformation in the esophagus and the uterine cervix. Other early and late genes, such as E2, Ll and L2 genes, seem to be deleted in these tumors. The ab- sence of Ll has been considered confirmation of the integrated status of the EG-transforming gene in human cancers.4l5 Based in these find- ings, we have determined the E6 gene pres- ence of HPV-Gb, HPV-16, and HIV-18 in a series of oral and pharyngolaryngeal carcinomas. As a means of testing the integration state of American Journal of Otolatyngology, Vol 18, No 6 (November-December), 1997: pp 375-381 375

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Oriainal Contributions
Using Polymerase Chain Reaction to Human Papillomavirus in Oral and Pharyngolaryngeal Carcinomas
Ignacio Alvarez Alvarez, MD, Pedro Sanchez Lazo, PhD, Sofia Ramos Gonzalez, PhD, J. Pablo Rodrigo Tapia, MD, Faustino Nudez Batalla, MD, and Carlos Suarez Nieto, MD
Purpose: Increasingly, evidence has shown that human papillomavirus (HPV) plays a role in the induction of certain carcinomas. The presence of HPV sequences in 56 previously untreated oral and pharyngolaryngeal carcinomas was examined by the polymerase chain reaction (PCR). Materials and Methods: After DNA extraction, samples underwent 40 replication cycles with specific oligonucleotide primers corresponding to sequences from the E6 open-reading frame of HPV-Gb, HPV-16, and HPV-18. To determine the E6 genomic integration, positive samples were processed with specific primers for the corresponding HPV Ll genes. Genomic HPV DNA cloned into PBR 322 was used as positive control. Results: HPV E6 DNA of the 6b and 16 types was detected in 14 patients (25%). The Ll gene was not present. Conclusion: Detected HPV E6 DNA might be integrated into the cell genome in the positive cases as indicated by the absence of the Li gene-coding for the viral capside. Histological and clinical parameters, such as tumor location, degree of differentiation, stage, recurrence, and survival rates, were unrelated to the presence of HPV. Copyright o 1997 by W.B. Saunders Company.
Different HPV types have been identified in human tumors of various localizations. HPV types 6b, 16, and 18 have the highest fre- quency. In the upper aerodigestive tract, malig- nant tumors have been found to contain the E6 gene from HPV type 16, and there are indica-
From the Department of Otorhinolavngology, Complejo Hospitalario de Leon, Oviedo; the Department of Func- tional Biology, Facultad Medicina, Oviedo; and the Depart- ment of Otorhinolaryngology, Hospital Central de As- turias, Oviedo, Spain.
Presented to the 99th Annual Meeting of the American Academy of Otolaryngology-Head and Neck Surgery Foundation, New Orleans, LA, September 17-20 1995.
This work was supported by a grant from the Fondo de lnvestigaciones Sanitarias de la Seguridad Social, Madrid, Spain (FIS 93/0400).
Address reprint requests to lgnacio Alvarez Alvarez, MD, C/Matematico Pedrayes 22, 5”izda, 33005 Oviedo, Spain.
Copyright 0 1997 by W.B. Saunders Company 0196-0709/97/l 808-0002$5.00/O
tions of the implications of HPV types 6b and 18.
HPV is a double-stranded DNA virus of approximately 8,000 base pairs (bp) in length, conforming seven early and two late gene open-reading frames (ORF) that code for regu- latory and structural proteins, respectively.1-3
The E6 gene appears to be integrated in the human cellular genome and probably predis- poses to the malignant transformation in the esophagus and the uterine cervix. Other early and late genes, such as E2, Ll and L2 genes, seem to be deleted in these tumors. The ab- sence of Ll has been considered confirmation of the integrated status of the EG-transforming gene in human cancers.4l5 Based in these find- ings, we have determined the E6 gene pres- ence of HPV-Gb, HPV-16, and HIV-18 in a series of oral and pharyngolaryngeal carcinomas.
As a means of testing the integration state of
American Journal of Otolatyngology, Vol 18, No 6 (November-December), 1997: pp 375-381 375
376 ALVAREZ ET AL
the virus, we have determined the presence of the Ll viral gene in the HPV-positive tumors.
There are controversial reports about the prognostic significance of the presence of HPV in these tumors. Thus, some investigators have suggested differences between patients with HPV-related and -nonrelated illness concern- ing the characteristics of sex, age, tumor site, degree of differentiation, local or nodal stage, recurrence rate, and survival.6-13 Therefore, we have studied the relationship between the presence of HPV, a series of clinical findings, and tumor behavior.
MATERIALS AND METHODS
Tumor samples of 56 squamous cell carcinomas of the oral cavity, the pharynx, and the larynx were analyzed using polymerase chain reaction (PCR) to determine the presence of E6 and Ll genes of HPV-Gb, HPV-16, and HPV-18. These patients were all the surgically treated in the Hospital Central de Asturias between June 1991 and June 1993. Thirty- two (57%) of patients received postoperative radio- therapy.
At first, the E6 gene was investigated. Because the HPV Ll gene is not required for cellular oncogenic transformation and integration of the viral genome implies the loss of the nontransforming genes, the presence or absence of the Ll ORF was searched only in the positive cases.
Finally, we looked for an association between the presence of HPV DNA and the tumor site and stage, histological degree, patient’s age, local and distant recurrence, and survival.
Clinical Findings
The study group consisted of 55 men and 1 woman; the average age being 58 years (range, 38 to 78). Average duration of symptoms before diagnosis
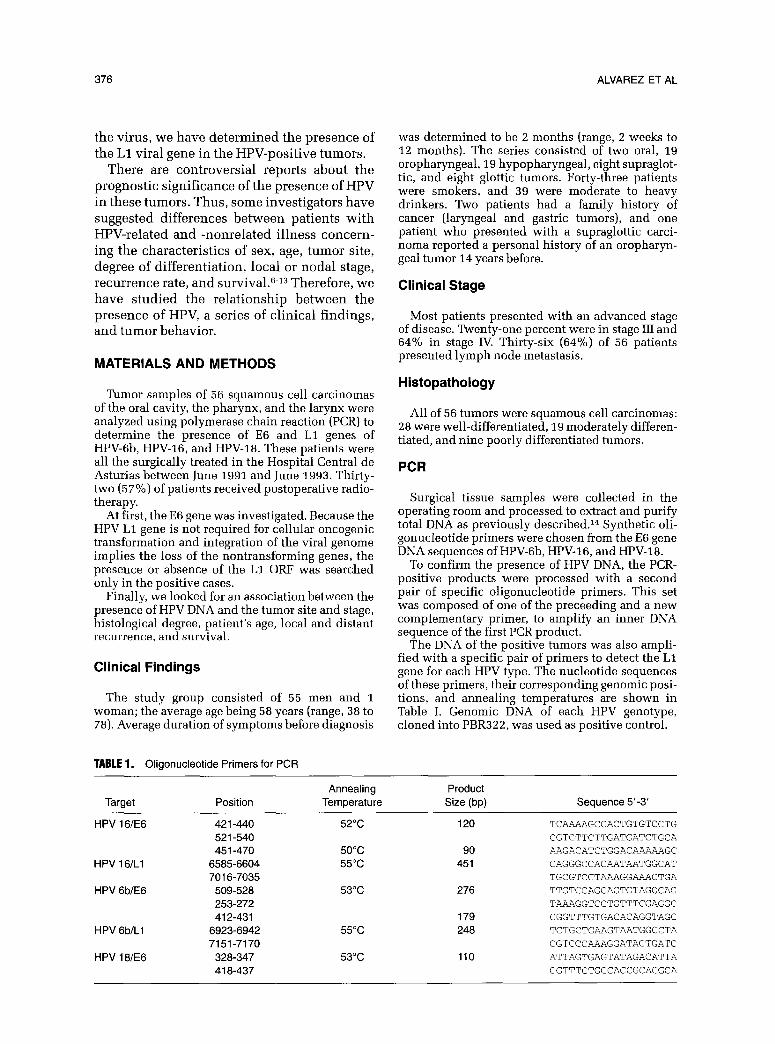
TABLE 1. Oligonucleotide Primers for PCR
was determined to be 2 months (range, 2 weeks to 12 months). The series consisted of two oral, 19 oropharyngeal, 19 hypopharyngeal, eight supraglot- tic, and eight glottic tumors. Forty-three patients were smokers, and 39 were moderate to heavy drinkers. Two patients had a family history of cancer (laryngeal and gastric tumors), and one patient who presented with a supraglottic carci- noma reported a personal history of an oropharyn- geal tumor 14 years before.
Clinical Stage
Most patients presented with an advanced stage of disease. Twenty-one percent were in stage III and 64% in stage IV. Thirty-six (64%) of 56 patients presented lymph node metastasis.
Histopathology
All of 56 tumors were squamous cell carcinomas: 28 were well-differentiated, 19 moderately differen- tiated, and nine poorly differentiated tumors.
PCR
Surgical tissue samples were collected in the operating room and processed to extract and purify total DNA as previously described.14 Synthetic oli- gonucleotide primers were chosen from the E6 gene DNA sequences of HPV-Gb, HPV-16, and HPV-18.
To confirm the presence of HPV DNA, the PCR- positive products were processed with a second pair of specific oligonucleotide primers. This set was composed of one of the preceeding and a new complementary primer, to amplify an inner DNA sequence of the first PCR product.
The DNA of the positive tumors was also ampli- fied with a specific pair of primers to detect the Ll gene for each HPV type. The nucleotide sequences of these primers, their corresponding genomic posi- tions, and annealing temperatures are shown in Table I. Genomic DNA of each HPV genotype, cloned into PBR322, was used as positive control.
Target
HPV 16/E6
HPV 16/Ll
HPV 6blE6
HPV 6b/Ll
HPV 18/E6
Position
421-440 521-540 451-470
6585-6604 7016-7035
509-528 253-272 412-431
6923-6942 7151-7170
328-347 418-437
Annealing Temperature
52°C
50°C 55°C
53°C
55°C
53°C
Product Size (bp)
120
90 451
276
179 248
110
Sequence 5’-3’
TCAAAAGCCACTGTGTCCTG
CGTGTTCTTGATGATCTGCA
AAGACATCTGGACAAAAAGC
CAGGGCCACAATAATGGCAT
TGCGTCCTAAAGGAAACTGA
TTGTCCAGCAGTGTAGGCAG
TAAAGGTCCTGTTTCGAGGC
CGGTTTGTGACACAGGTAGC
TCTGCTGAAGTAATGGCCTA
CGTCCCAAAGGATACTGATC
ATTAGTGAGTATAGACATTA
GGTTTCTGGCACCGCAGGCA
377 PCR AND HUMAN PAPILLOMAVIRUS
123 6789 121314
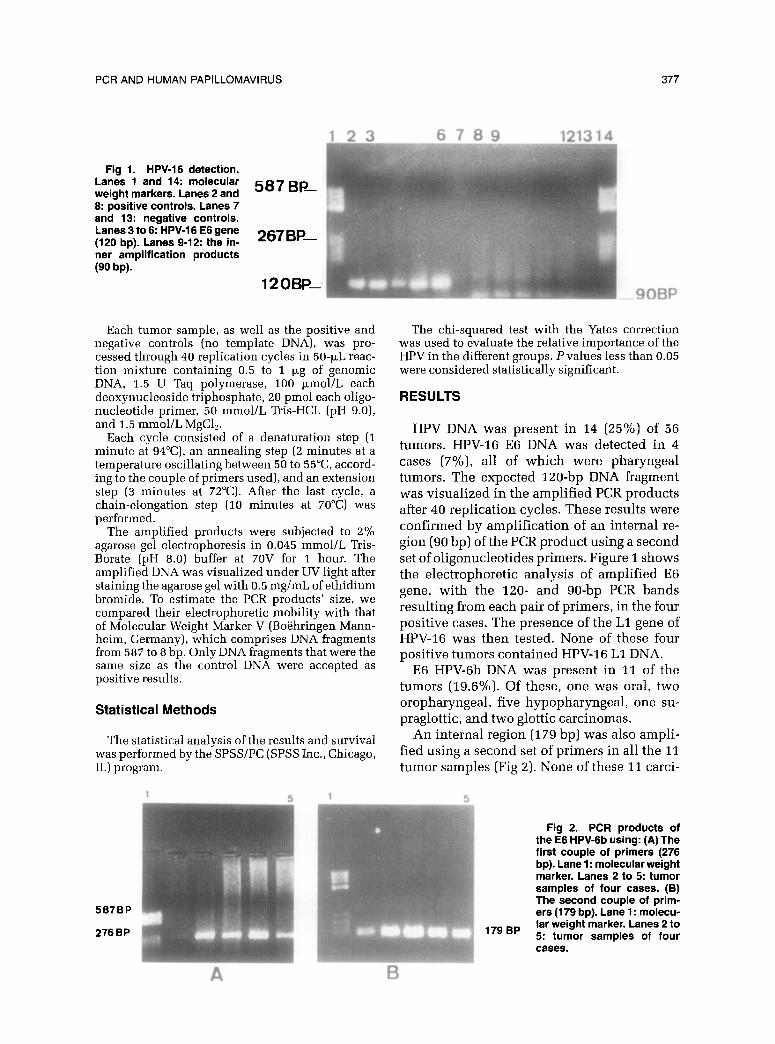
Fig 1. HPV-16 detection. Lanes 1 and 14: molecular weight markers. Lanes 2 and 587BP- 8: positive controls. Lanes 7 and 13: negative controls.
t;a,n,es,;~~n;;;m~2~f~~ 267 BP- ner amplification products (90 W.
12oBE -9OBP
Each tumor sample, as well as the positive and negative controls (no template DNA), was pro- cessed through 40 replication cycles in 50-PL reac- tion mixture containing 0.5 to 1 pg of genomic DNA, 1.5 U Taq polymerase, 100 kmol/L each deoxynucleoside triphosphate, 20 pmol each oligo- nucleotide primer, 50 mmol/L Tris-HCL (pH 9.0), and 1.5 mmol/L MgCl,.
Each cycle consisted of a denaturation step (1 minute at 94”(X), an annealing step (2 minutes at a temperature oscillating between 50 to 55”C, accord- ing to the couple of primers used), and an extension step (3 minutes at 72°C). After the last cycle, a chain-elongation step (10 minutes at 70°C) was performed.
The amplified products were subjected to 2% agarose gel electrophoresis in 0.045 mmol/L Tris- Borate (pH 8.0) buffer at 70V for 1 hour. The amplified DNA was visualized under UV light after staining the agarose gel with 0.5 mg/mL of ethidium bromide. To estimate the PCR products’ size, we compared their electrophoretic mobility with that of Molecular Weight Marker V (Boehringen Mann- heim, Germany), which comprises DNA fragments from 587 to 8 bp. Only DNA fragments that were the same size as the control DNA were accepted as positive results.
Statistical Methods
The statistical analysis of the results and survival was performed by the SPSS/PC (SPSS Inc., Chicago, IL) program.
The chi-squared test with the Yates correction was used to evaluate the relative importance of the HPV in the different groups. Pvalues less than 0.05 were considered statistically significant.
RESULTS
HPV DNA was present in 14 (25%) of 56 tumors. HPV-16 E6 DNA was detected in 4 cases (7%), all of which were pharyngeal tumors. The expected 120-bp DNA fragment was visualized in the amplified PCR products after 40 replication cycles. These results were confirmed by amplification of an internal re- gion (90 bp) of the PCR product using a second set of oligonucleotides primers. Figure 1 shows the electrophoretic analysis of amplified E6 gene, with the 120- and go-bp PCR bands resulting from each pair of primers, in the four positive cases. The presence of the Ll gene of HPV-16 was then tested. None of these four positive tumors contained HPV-16 Ll DNA.
E6 HPV-6b DNA was present in 11 of the tumors (19.6%). Of these, one was oral, two oropharyngeal, five hypopharyngeal, one su- praglottic, and two glottic carcinomas.
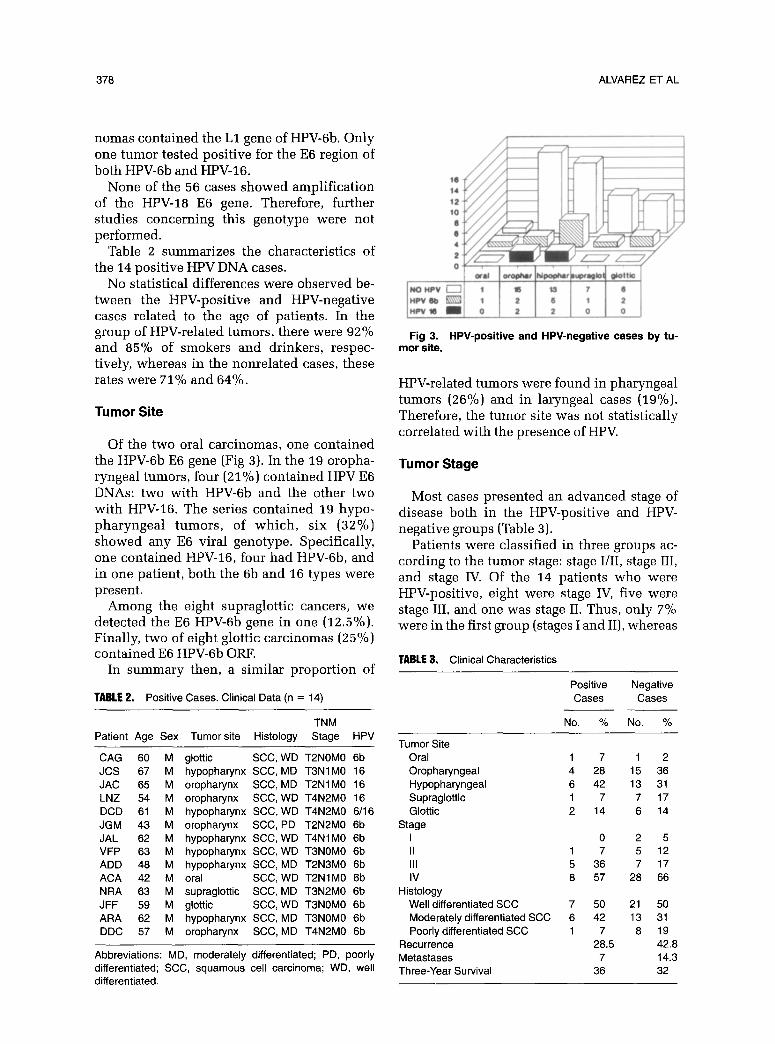
An internal region (179 bp) was also ampli- fied using a second set of primers in all the 11 tumor samples (Fig 2). None of these 11 carci-
376 ALVAREZ ET AL
nomas contained the Ll gene of HPV-6b. Only one tumor tested positive for the E6 region of both HPV-6b and HPV-16.
None of the 56 cases showed amplification of the HPV-18 E6 gene. Therefore, further studies concerning this genotype were not performed.
Table 2 summarizes the characteristics of the 14 positive HPV DNA cases.
No statistical differences were observed be- tween the HPV-positive and HPV-negative cases related to the age of patients. In the group of HPV-related tumors, there were 92% and 85% of smokers and drinkers, respec- tively, whereas in the nonrelated cases, these rates were 71% and 64%.
Tumor Site
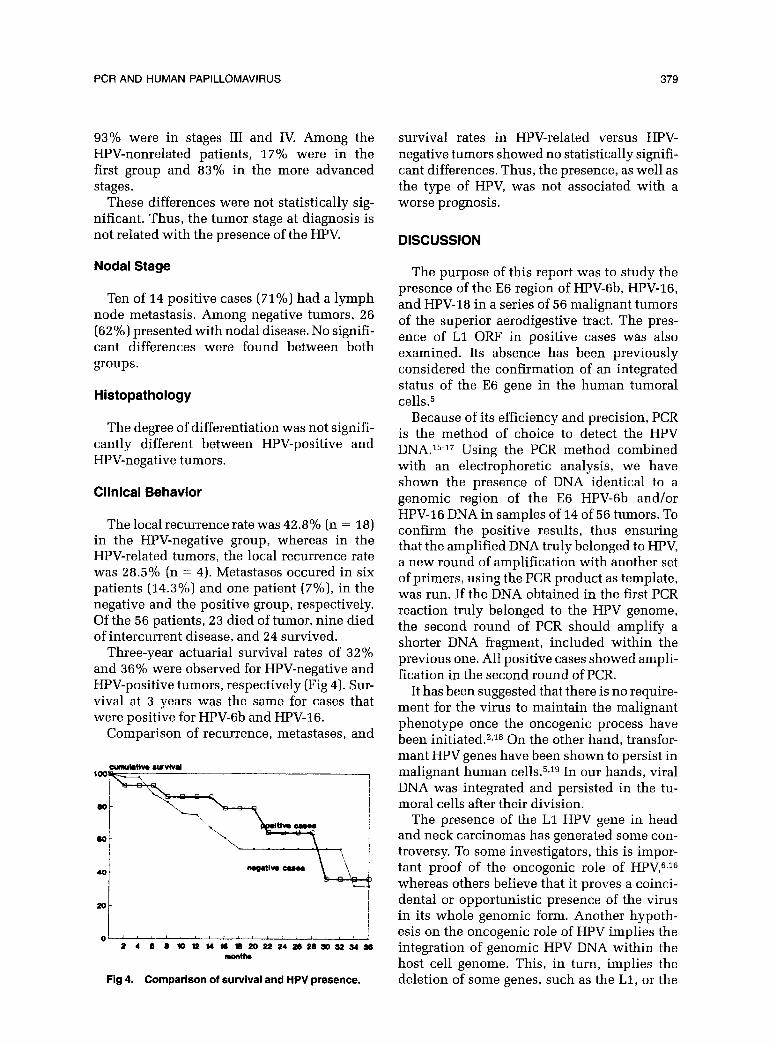
Of the two oral carcinomas, one contained the HPV-6b E6 gene (Fig 3). In the 19 oropha- ryngeal tumors, four (21%) contained HPV E6 DNAs: two with HPV-6b and the other two with HPV-16. The series contained 19 hypo- pharyngeal tumors, of which, six (32%) showed any E6 viral genotype. Specifically, one contained HPV-16, four had HPV-Gb, and in one patient, both the 6b and 16 types were present.
Among the eight supraglottic cancers, we detected the E6 HPV-6b gene in one (12.5%). Finally, two of eight glottic carcinomas (25%) contained E6 HPV-6b ORF.
In summary then, a similar proportion of
TABLE 2. Positive Cases. Clinical Data (n = 14)
TNM Patient Age Sex Tumor site Histology Stage HPV
CAG 60 M glottic SCC, WD T2NOMO 6b JCS 67 M hypopharynx SCC, MD T3NlMO 16 JAC 65 M oropharynx SCC, MD T2NlMO 16 LNZ 54 M oropharynx SCC, WD T4N2MO 16 DCD 61 M hypopharynx SCC, WD T4N2MO 6/16 JGM 43 M oropharynx SCC, PD T2N2MO 6b JAL 62 M hypopharynx SCC, WD T4NlMO 6b VFP 63 M hypopharynx SCC, WD TBNOMO 6b ADD 48 M hypopharynx SCC, MD T2N3MO 6b ACA 42 M oral SCC, WD T2NlMO 6b NRA 63 M supraglottic SCC, MD T3N2MO 6b JFF 59 M glottic SCC, WD T3NOMO 6b ARA 62 M hypopharynx SCC, MD T3NOMO 6b DDC 57 M oropharynx SCC, MD T4N2MO 6b
Abbreviations: MD, moderately differentiated; PD, poorly differentiated; SCC, squamous cell carcinoma; WD, well differentiated.
Fig 3. HPV-positive and HPV-negative cases by tu- mor site.
HPV-related tumors were found in pharyngeal tumors (26%) and in laryngeal cases (19%). Therefore, the tumor site was not statistically correlated with the presence of HPV.
Tumor Stage
Most cases presented an advanced stage of disease both in the HPV-positive and HPV- negative groups (Table 3).
Patients were classified in three groups ac- cording to the tumor stage: stage I/II, stage III, and stage IV. Of the 14 patients who were HPV-positive, eight were stage IV, five were stage III, and one was stage II. Thus, only 7% were in the first group (stages I and II), whereas
TABLE 3. Clinical Characteristics
Positive Negative Cases Cases
No. % No. %
Tumor Site Oral Oropharyngeal Hypopharyngeal Supraglottic Glottic
Stage I II Ill IV
Histology Well differentiated SCC Moderately differentiated SCC Poorly differentiated SCC
Recurrence Metastases Three-Year Survival
1 7 1 2 4 28 15 36 6 42 13 31 1 7 7 17 2 14 6 14
0 25 1 7 5 12 5 36 7 17 8 57 28 66
7 50 21 50 6 42 13 31 1 7 8 19
28.5 42.8 7 14.3
36 32
PCR AND HUMAN PAPILLOMAVIRUS 379
93% were in stages III and IV. Among the HPV-nonrelated patients, 17% were in the first group and 83% in the more advanced stages.
These differences were not statistically sig- nificant. Thus, the tumor stage at diagnosis is not related with the presence of the HPV.
survival rates in HPV-related versus HPV- negative tumors showed no statistically signifi- cant differences. Thus, the presence, as well as the type of HPV, was not associated with a worse prognosis.
DISCUSSION
Nodal Stage The purpose of this report was to study the presence of the E6 region of HPV-Gb, HPV-16, and HPV-18 in a series of 56 malignant tumors of the superior aerodigestive tract. The pres- ence of Ll ORF in positive cases was also examined. Its absence has been previously considered the confirmation of an integrated status of the E6 gene in the human tumoral cells.5
Ten of 14 positive cases (71%) had a lymph node metastasis. Among negative tumors, 26 (62%) presented with nodal disease. No signifi- cant differences were found between both groups.
Histopathology
The degree of differentiation was not signifi- cantly different between HPV-positive and HPV-negative tumors.
Clinical Behavior
The local recurrence rate was 42.8% (n = 18) in the HPV-negative group, whereas in the HPV-related tumors, the local recurrence rate was 28.5% (n = 4). Metastases occured in six patients (14.3%) and one patient (7%), in the negative and the positive group, respectively. Of the 56 patients, 23 died of tumor, nine died of intercurrent disease, and 24 survived.
Three-year actuarial survival rates of 32% and 36% were observed for HPV-negative and HPV-positive tumors, respectively (Fig 4). Sur- vival at 3 years was the same for cases that were positive for HPV-6b and HPV-16.
Comparison of recurrence, metastases, and
Because of its efficiency and precision, PCR is the method of choice to detect the HPV DNA.15-17 Using the PCR method combined with an electrophoretic analysis, we have shown the presence of DNA -identical to a genomic region of the E6 HPV-6b and/or HPV-16 DNA in samples of 14 of 56 tumors. To confirm the positive results, thus ensuring that the amplified DNA truly belonged to HPV, a new round of amplification with another set of primers, using the PCR product as template, was run. If the DNA obtained in the first PCR reaction truly belonged to the HPV genome, the second round of PCR should amplify a shorter DNA fragment, included within the previous one. All positive cases showed ampli- fication in the second round of PCR.
Fig 4. Comparison of survival and HPV presence.
It has been suggested that there is no require- ment for the virus to maintain the malignant phenotype once the oncogenic process have been initiated.2J8 On the other hand, transfor- mant HPV genes have been shown to persist in malignant human cells.5Jg In our hands, viral DNA was integrated and persisted in the tu- moral cells after their division.
The presence of the Ll HPV gene in head and neck carcinomas has generated some con- troversy. To some investigators, this is impor- tant proof of the oncogenic role of HPV,“J6 whereas others believe that it proves a coinci- dental or opportunistic presence of the virus in its whole genomic form. Another hypoth- esis on the oncogenic role of HPV implies the integration of genomic HPV DNA within the host cell genome. This, in turn, implies the deletion of some genes, such as the Ll, or the

380
selective replication of the transformant early genes, such as E6 in humans and E7 in ro- dents.5J0 It is worth noting that integration may be increased by radiation therapy or carcinogens3
The retained HPV E6 gene, in addition to some other factors such as immunosupres- sion, infection, radiations or chemical agents, should induce a sequence of molecular events, activating cellular oncogenes or blocking the regulatory effect of some tumor supressor genes. HPV may act via different molecular mechanisms, in cooperation with the activa- tion of some oncogenes, as occurs in other instances.2*J-2
To demonstrate the genomic integration of the E6 gene of HPV types 6b and 16 (HPV-18 was not detected), we processed the cases that tested positive by PCR with specific primers for the Ll ORF. None of these showed the expected PCR product corresponding to the Ll gene. In this regard, it is interesting that the only case (not included in this series) in which we found the Ll sequence corresponded to a verrucous carcinoma in which the presence of viral particles might be expected because of its special degree of differentiation and keratini- zation.
Contrary to the findings of some investiga- tors,6z7 but in accordance with others,23 recur- rence rate and survival were not influenced by the presence of the HPV. No significant differ- ences between HPV-positive and HPV-nega- tive tumors were observed concerning the degree of differentiation, as reported by a majority of authors,6,8*g and yet contradicted by others.Z4
The presence of HPV was neither related to the local and nodal stage, or to the patients’ age or sex, or tumor site, as shown in other reports.“s1°-13 Similar to what has been previ- ously described, 3~11~12,21 HPV was present in 25% of the pharyngolaryngeal carcinomas in our study. However, this study documents the finding of a significantly higher global fre- quency of HPV-6b. HPV-16 represented only 29% of the positive cases, whereas in other studies, it was the most frequent HPV type.13J5
It is also interesting that HPV-16 was selec- tively detected in pharyngeal carcinomas, whereas HPV-6b showed a homogeneous dis- tribution in tumors with different localization.
HPV-6b has been considered a “low-risk”
ALVAREZ ET AL
genotype, at least in the anogenital area.20,26 In the head and neck, however, this HPV type appears strongly related to the malignant tu- mors.
As for HPV-18, it was found in some studies in the pharynx and larynx. In the oral cavity, where it was more frequently detected, the average of positive cases reached 10%.13J5
Our study indicates that HPV-6b and HPV-16 might play a role in the induction of upper aerodigestive tract tumors, based on the hy- pothesis of the retention of the early genomic region in the tumor cells, whereas late genes are deleted. Our results indicate that the major- ity of cases (75%) were not related to the virus. This suggests that other molecular events may be involved in the ethiopathogenesis of head and neck tumors.
CONCLUSION
In agreement with previous studies, we found the rate of HPV-positive tumor cases to be 25%. The HPV-6b represented 78.5% of positive cases. Only one case simultaneously showed the 6b and 16 types. HPV-16 was exclusively detected in pharyngeal carcinomas. No positive cases were found for HPV-18. E6 ORF was retained by the tumors whereas the Ll was deleted, suggesting that the integration of viral genome into the host cell DNA may contribute to the oncogenic pro- cess. The tumor site, degree of differentiation, stage, recurrence, and survival were inde- pendent of the HPV presence. From the present results, it is suggested that HPV plays an oncogenic role in only a minority of cases in the head and neck, thus implying that other oncogenic factors should be implicated.
ACKNOWLEDGMENT
We are greateful to Dr Pedro A. Lazo, from Instituto Carlos III (Madrid) for providing us with the HPV plasmids.
REFERENCES
1. De Villiers EM: Heterogeneity of the human papillo- mavirus group. J Virol63:4898-4903, 1991
2. Spalholz BA, Howley PM: Papillomavirus-host cell interactions. Adv Virol Oncol8:27-53,1989
PCR AND HUMAN PAPILLOMAVIRUS 381
3. Steimberg BM: Human papillomaviruses and upper airway oncogenesis. Am J Otolaryngol 11:370-374,199O
4. Choo KB, Pan CH, Han SH: Integration of human papillomavirus type 16 into cellular DNA of cervical carcinoma: Preferential deletion of the E2 gene and invari- able retention of the long control region and the E6/E7 open reading frames. Virology 161:259-261,1987
5. Toh Y, Kuwano H, Tanaka S, et al: Detection of human papillomavirus DNA in esophageal carcinoma in Japan by polymerase chain reaction. Cancer 70:2234- 2238,1992
6. Clayman GL, Stewart M, Weber RS, et al: Human papillomavirus in laryngeal and hypopharyngeal carcino- mas. Arch Otolaryngol Head Neck Surg 120:743-748,1994
7. Furihata M, Ohtsuki Y, Ogoshi S, et al: Prognostic significance of human papillomavirus genomes (type-16,- 18) and aberrant expression of p53 protein in human esophageal cancer. Int J Cancer 54:226-30, 1993
8. Hoshikawa T, Nakajima T, Uhara H, et al: Detection of human papillomavirus DNA in laryngeal squamous cell carcinomas by polymerase chain reaction. Laryngoscope 100:647-650,199O
9. Kiyabu M, Shibata D, Arnheim N, et al: Detection of human papillomavirus in formalin-fixed invasise squa- mous carcinomas using the polvmerase chain reaction. Am J Surg Path01 13:22?-224, i989
10. Kulski TK, Demeter T. Mutavdzic S, et al: Survev of histologic specimens of human cancer for human papillo- mavirus types 6/11/16/18 by filter in situ hybridization. Am J Clin Path01 94:566-570,199O
11. Niedobitek G, Pitteroff S, Herbst H, et al: Detection of human papillomavirus type 16 DNA in carcinomas of the palatine tonsil. J Clin Path01 43:918-921,199O
12. Brandsma J, Abramson AL: Association of papillo- mavirus with cancers of the head and neck. Arch Otolaryn- go1 Head Neck Surg 115:621-625, 1989
13. Tyan YS, Liu ST, Ong WR, et al: Detection of Epstein-Barr virus and human papillomavirus in head and neck tumors. J Clin Microbial 31:53-56,1993
14. Sambrook J, Fritsch ET, Maniatis T (eds): in Molecu- lar Cloning: A Laboratory Manual (ed 2). Cold Spring Harbor Laboratory Press, 1989, pp 14-14
15. Young LS, Bevan IS, Johnson MA, et al: The poly-
merase chain reaction: A new epidemiological tool for investigating cervical human papillomavirus infection. Br Med J 298:14-18,1989
16. Kasperbauer JL, O’Halloran GL, Espy MJ, et al: Polymerase chain reaction (PCR) identification of human papillomavirus (HPV) DNA in verrucous carcinomas of the larynx. Laryngoscope 103:416-420,1993
17. Shibata D, Fu YS, Gupta JW, et al: Detection of human papillomavirus in normal and dysplastic tissue by the polymerase chain reaction. Lab Invest 59:555-559, 1988
18. Saveria Campo M, Jarrett WF: Papillomaviruses and disease. Adv Virol Oncol8:215-243,1989
19. Phelps WC, Yee CL, Miinger K, et al: The human papillomavirus type 16 E7 gene encodes transactivation and transformation functions similar to those of adenovi- rus ElA. Cell 53:539-547,1988
20. Miinger K, Werness B, Dyson N, et al: Complex formation of human papillomavirus E7 proteins with the retinoblastoma tumor suppressor gene product. EMBO J 8:4099-4105,1989
21. Anwar K, Nakakuki K, Naiki H, et al: Ras gene mutations and HPV infection are common in human laryngeal carcinoma. Int J Cancer 53:22-28, 1993
22. Ireland CM: Activated N-ras oncogenes in human neuroblastoma. Cancer Res 49:5530-5533,1989
23. Lee NK, Ye W, Chen J, et al: P53, retinoblastoma and human papillomavirus in squamous cell carcinoma and adjacent normal mucosa of the upper aerodigestive tract. Arch Otolaryngol Head Neck Surg 119:1125-1131,1993
24. Ishibashi T, Matsushima S, Tsunokawa Y, et al: Human papillomavirus DNA in squamous cell carcinoma of the upper aerodigestive tract. Arch Otolaryngol Head Neck Surg 116:294-298, 1990
25. Watts SL, Brewer EE, Fry TL, et al: Human papillo- mavirus DNA types in squamous cell carcinomas of the head and neck. Oral Surg Oral Med Oral Path01 71:701- 707,1991
26. Gissmann L, Wolnik L, Ikenberg H, et al: Human papillomavirus types 6 and 11 DNA sequences in genital and laryngeal papillomas and in some cervical cancers. Proc Nat1 Acad Sci USA 80:560-563, 1983
Related Documents











