Psychopharmacology, 2021: A Master Class Beth Israel Deaconess Medical Center/Harvard Medical School CME Online Saturday April 4, 2021 USE OF STIMULANTS IN PSYCHIATRY John Ratey, MD Associate Clinical Professor of Psychiatry Harvard Medical School NO DISCLOSURES STIMULANTS IN ADULTS • USE IN ADULTS WITH ADHD • USE AS AN ADJUNCT IN DEPRESSION • USE IN BINGE-EATING DISORDER

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Psychopharmacology, 2021: A Master Class
Beth Israel Deaconess Medical Center/Harvard Medical School CME
Online
Saturday April 4, 2021
USE OF STIMULANTS IN PSYCHIATRY
John Ratey, MD
Associate Clinical Professor of Psychiatry
Harvard Medical School
NO DISCLOSURES
STIMULANTS IN ADULTS
• USE IN ADULTS WITH ADHD
• USE AS AN ADJUNCT IN DEPRESSION
• USE IN BINGE-EATING DISORDER
ADHD in Adults
• Co-morbidity- Emotional Dyscontrol primary-SUD, MDD
• Pain and Suffering- marriages, families, workplace
• Tremendous Economic Burden-loss Productivity, Ron Kessler
• Identification- General Awareness, Masked by High Performance for a time, as well as failure to thrive.
• Among adults being treated for alcohol and substance abuse, the rate of ADHD is about 25%.
Incidence of Adult ADHD
• From childhood ADHD into Adulthood is 60%.
Less Hyperactivity, more Inattentive
• Newly presenting in Adulthood is not often
recognized.
• Labeled depressed, SUD, underachiever,
mainly failure to thrive
• Children 10-11%, Adults 4.4%- with many not
reported or recognized

SYMPTOMS MISSED IN CHILDHOOD
• NOT ON FORMAL DSM SXS
• SHADOW SYNDROMES OR SUBTHRESHOLD
• DID WELL AT “APPEALING” TASKS
• INCREASING DEMAND AS WE AGE
• LOSS OF SUPPORT, I.E. COLLEGE MAJOR DX
Evaluation of the Persistence, Remission, and Emergence of Attention-Deficit/Hyperactivity Disorder in Young Adulthood.Agnew-Blais JC et al. JAMA Psychiatry. 2016 Jul 1;73(7):713-20
• Out of 2232, 247 individuals met diagnostic criteria for childhood ADHD; of these, 54 (21.9%) also met diagnostic criteria for the disorder at age 18 years. Home visits 5,10,12, mother and teacher reports
• Age 18- extensive DX interview
• Among 166 individuals with adult ADHD, 112 (67.5%) did not meet criteria for ADHD at any assessment in childhood. Individuals with late-onset ADHD showed fewer externalizing problems in childhood compared with the persistent group.

a large late-onset ADHD group with no childhood diagnosis and minimal neuropsychological
impairment, and a smaller group with persistent ADHD and associated neuropsychological
impairment. Our findings call into question the conceptualization of adult ADHD as a childhood-onset neurodevelopmental disorder
Participants were members of the Environmental Risk
(Erisk) Longitudinal Twin Study, a birth cohort of 2232
British children. The sample was drawn from a larger
birth register of twins born in England and Wales
from January 1, 1994, to December 4, 1995
TREAMENT
• Amphetamine, Methylphenidate
• Modafinil, Armodafinil
• Anti-depressants: Tricyclics, Buproprion,
Atomoxetine
• Guanfacine, Clonidine
• Anti-depressants with 5HT/NEP
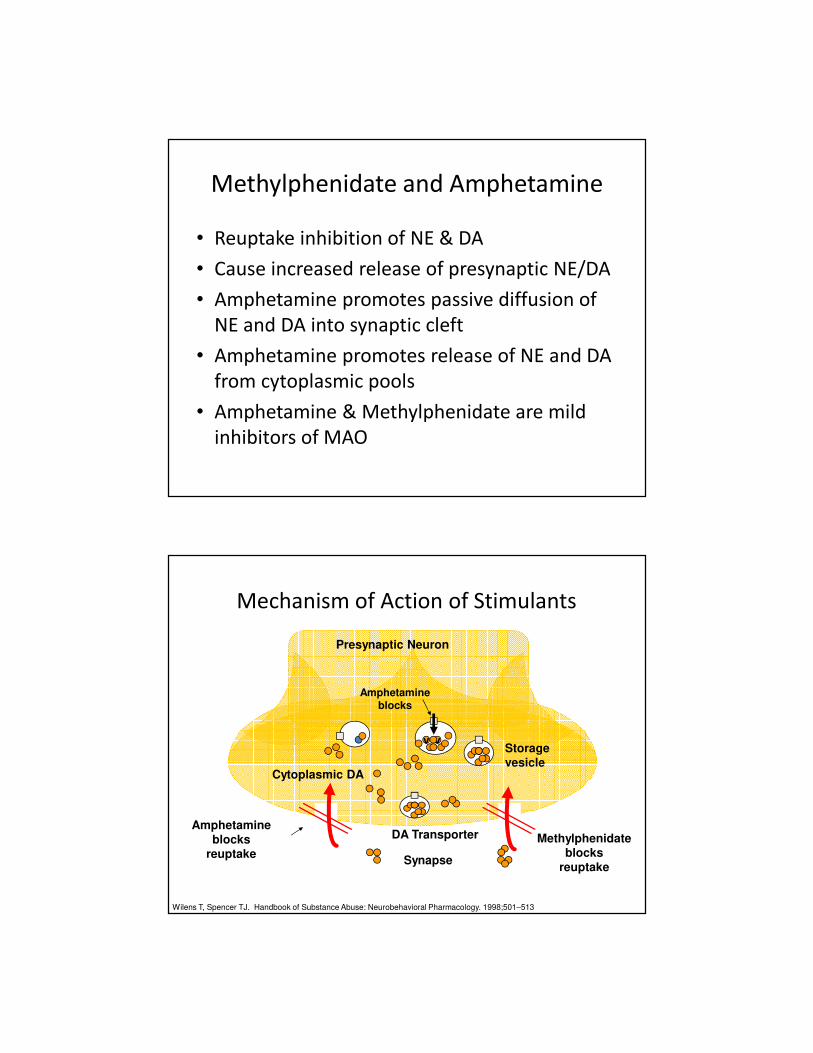
Methylphenidate and Amphetamine
• Reuptake inhibition of NE & DA
• Cause increased release of presynaptic NE/DA
• Amphetamine promotes passive diffusion of
NE and DA into synaptic cleft
• Amphetamine promotes release of NE and DA
from cytoplasmic pools
• Amphetamine & Methylphenidate are mild
inhibitors of MAO
v vStoragevesicle
DA Transporter
Cytoplasmic DA
Methylphenidate blocks
reuptake
Presynaptic Neuron
Synapse
Wilens T, Spencer TJ. Handbook of Substance Abuse: Neurobehavioral Pharmacology. 1998;501–513
Amphetamine blocks
reuptake
Amphetamine blocks
Mechanism of Action of Stimulants
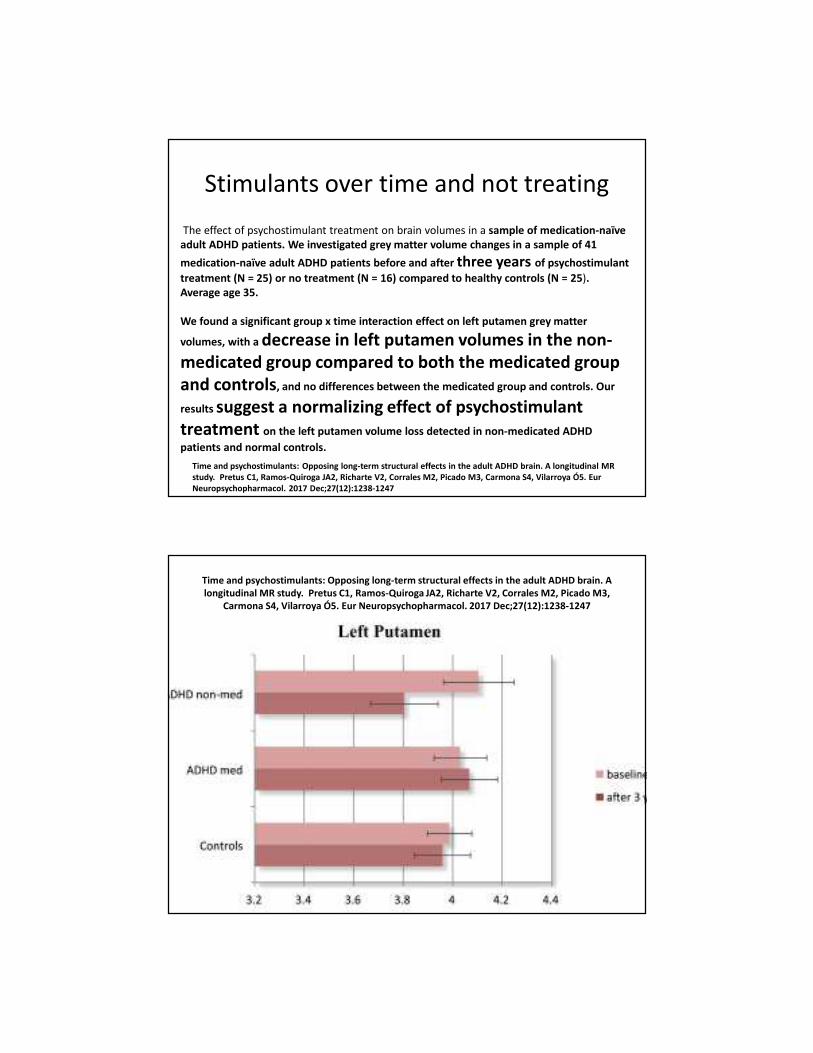
The effect of psychostimulant treatment on brain volumes in a sample of medication-naïve adult ADHD patients. We investigated grey matter volume changes in a sample of 41
medication-naïve adult ADHD patients before and after three years of psychostimulant
treatment (N = 25) or no treatment (N = 16) compared to healthy controls (N = 25). Average age 35.
We found a significant group x time interaction effect on left putamen grey matter
volumes, with a decrease in left putamen volumes in the non-medicated group compared to both the medicated group and controls, and no differences between the medicated group and controls. Our
results suggest a normalizing effect of psychostimulanttreatment on the left putamen volume loss detected in non-medicated ADHD
patients and normal controls.
Time and psychostimulants: Opposing long-term structural effects in the adult ADHD brain. A longitudinal MR study. Pretus C1, Ramos-Quiroga JA2, Richarte V2, Corrales M2, Picado M3, Carmona S4, Vilarroya Ó5. EurNeuropsychopharmacol. 2017 Dec;27(12):1238-1247
Stimulants over time and not treating
Time and psychostimulants: Opposing long-term structural effects in the adult ADHD brain. A longitudinal MR study. Pretus C1, Ramos-Quiroga JA2, Richarte V2, Corrales M2, Picado M3,
Carmona S4, Vilarroya Ó5. Eur Neuropsychopharmacol. 2017 Dec;27(12):1238-1247

Long-term Effects of Multimodal Treatment on Adult Attention-Deficit/Hyperactivity Disorder Symptoms: Follow-up Analysis of the
COMPAS Trial. JAMA Netw Open. 2019 May 3;2(5):e194980. Lam AP1 et al
• DESIGN, SETTING, AND PARTICIPANTS: GERMANY 1 YEAR TRIAL
• This observer-masked, 1.5-year follow-up of the Comparison of Methylphenidate and Psychotherapy in
Adult ADHD Study (COMPAS), a prospective, multicenter randomized clinical trial, compared cognitive
behavioral group psychotherapy (GPT) with individual clinical management (CM) and methylphenidate
(MPH) with placebo (2 × 2 factorial design). Overall, 433 adults with ADHD participated in the trial, and
256 (59.1%) participated in the follow-up assessment.
• INTERVENTIONS:
• After 1-year treatment with GPT or CM and MPH or placebo
• At follow-up, 256 of 433 randomized patients (baseline measured in 419 individuals)
participated. Of the 256 patients participating in follow-up, the observer-masked ADHD Index of Conners
Adult ADHD Rating Scale score was assessed for 251; the mean (SD) baseline age was 36.3 (10.1) years;
125 patients (49.8%) were men; and the sample was well-balanced with respect to prior randomization
(GPT and MPH: 64 of 107; GPT and placebo: 67 of 109; CM and MPH: 70 of 110; and CM and placebo: 55
of 107). At baseline, the all-group mean ADHD Index of Conners Adult ADHD Rating Scale score was 20.6,
which improved to adjusted means of 14.2 for the GPT arm and 14.7 for the CM arm at follow-up with no
significant difference between groups (difference, -0.5; 95% CI, -1.9 to 0.9; P = .48).
• CONCLUSIONS AND RELEVANCE:
• Results from COMPAS demonstrate a maintained improvement in ADHD
symptoms for adults 1.5 years after the end of a 52-week controlled
multimodal treatment period. The results indicate that MPH treatment combined with GPT or
CM provides a benefit lasting 1.5 years.
•
ADULT ADHD: Long Term Stimulant Use
• A cohort of adults diagnosed with ADHD followed-up on an average of 6 years after first evaluation. Of 168 adults, 112 (67%) who initiated medication were available for follow-up.
• Of the 112 participants assessed, 57 (51%) were still on treatment with methylphenidate (MPH) at follow-up and 55 (49%) had discontinued
• Reasons for Discontinuing: 1. lack of effect 2. elevated mood 3.lost contact with prescribing physician
• Subjects still on treatment reported increased quality of life, a higher level of functioning, and a greater understanding of their way of functioning from those being close to them compared with nonmedicated subjects.
• Participants in the current treatment group scored significantly higher on the statements, “My quality of life has improved” (P = 0.002), “My level of functioning has improved,” (P < 0.001) and “a greater understanding” (P = 0.017) as compared with those who discontinued medication
J Clin Psychopharmacol. 2018 Aug;38(4):370-375. Long-Term Tolerability and Safety of Pharmacological Treatment of Adult Attention-Deficit/Hyperactivity Disorder: A 6-Year Prospective Naturalistic Study. Edvinsson D1, Ekselius L.
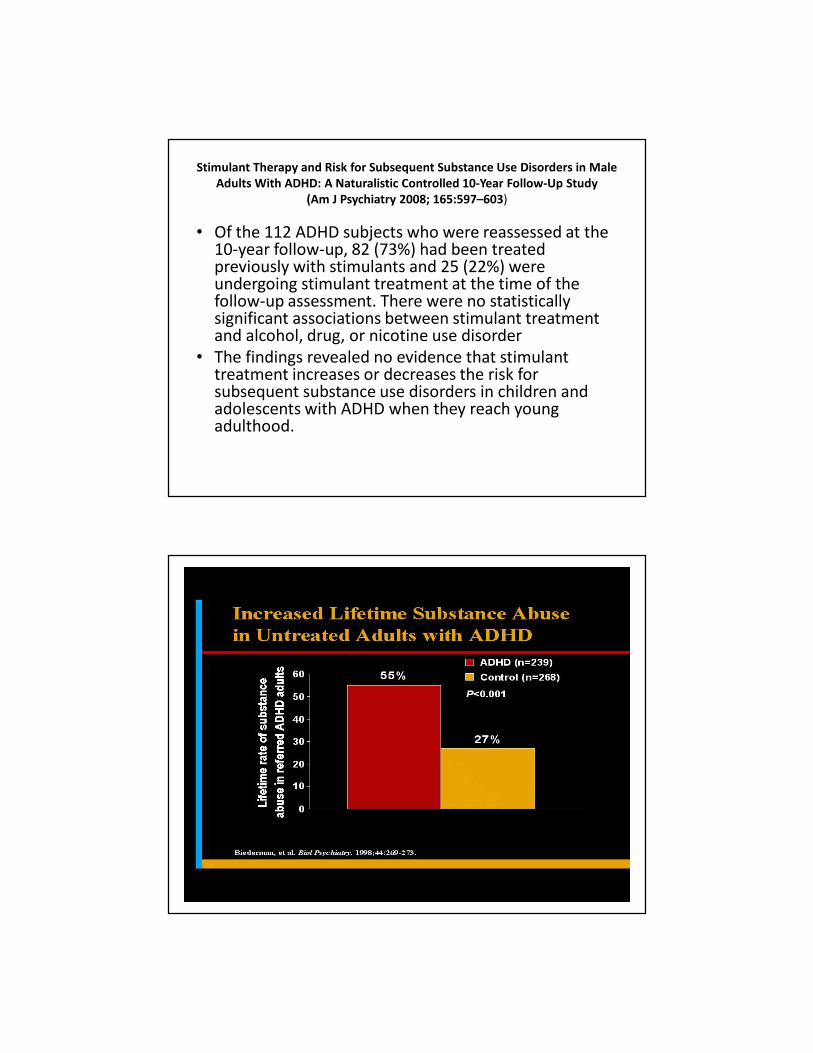
Stimulant Therapy and Risk for Subsequent Substance Use Disorders in Male Adults With ADHD: A Naturalistic Controlled 10-Year Follow-Up Study
(Am J Psychiatry 2008; 165:597–603)
• Of the 112 ADHD subjects who were reassessed at the 10-year follow-up, 82 (73%) had been treated previously with stimulants and 25 (22%) were undergoing stimulant treatment at the time of the follow-up assessment. There were no statistically significant associations between stimulant treatment and alcohol, drug, or nicotine use disorder
• The findings revealed no evidence that stimulant treatment increases or decreases the risk for subsequent substance use disorders in children and adolescents with ADHD when they reach young adulthood.
Not Just Substances
• Gaming, Gambling - Technology• All things internet: facebook, porn, DraftKings
• Extreme Sports
• Sex
• Shopping
• Risk taking behavior
• Smart Phone
• Exercise
• Food – Obesity and Binge Eating Disorder
• Among adults being treated for alcohol and substance abuse, the rate of ADHD is about 25%.
International Consensus Statement on Screening, Diagnosis and Treatment of Substance Use Disorder Patients with Comorbid Attention
Deficit/Hyperactivity Disorder. Eur Addict Res. 2018;24(1):43-51. Crunelle CL1,2, et
al
• Simultaneous and integrated treatment of ADHD and SUD, using a combination of pharmaco- and psychotherapy, is recommended. Long-acting methylphenidate, extended-release amphetamines, and atomoxetine with up-titration to higher dosages may be considered in patients unresponsive to standard doses.
They compared the Multimodal Treatment Study of ADHD (MTA)
study subjects with ADHD (n = 579) to a local normative comparison group (LNCG, n = 289) at 4 different assessment points: 6, 8, 12, and 14 years of follow-ups.
CONCLUSION: Individuals with ADHD do not appear to be at significantly greater risk for developing BD, but do show higher rates of BD symptoms, especially non-specific manic (NSM). The greater linkage of irritability to NSM than to pathognomonic manic suggests caution when making BD diagnoses based on irritability alone as one of 2 (A-level) symptoms for BD diagnosis, particularly in view of its frequent presentation with other psychopathologies.
Risk for emerging bipolar disorder, variants, and symptoms in children with attention deficit hyperactivity disorder, now grown up.Elmaadawi AZ1, Jensen PS1, Arnold LE1, Molina BS1, Hechtman L1, Abikoff HB1, Hinshaw SP1, Newcorn JH1, Greenhill LL1, Swanson JM1, Galanter CA1.
World J Psychiatry. 2015 Dec 22;5(4):412-24.
To determine the prevalence of bipolar disorder (BD) and sub-threshold symptoms in children with attention deficit hyperactivity disorder (ADHD) through 14 years' follow-up, when participants were between 21-24 years
old.
Which stimulant to use ?
• Importantly, the neurobiological substrates that mediate behaviors
associated with ADHD share commonalities to some extent with those
involved in various comorbid disorders
• Genetic studies have also identified shared genetic risk factors between
ADHD and associated comorbid disorders
• However, there is no conclusive clinical evidence supporting a prospective choice for an AMP-based agent over an MPH based agent (or vice versa) based on the mechanisms of action of these drug classes
• In the words of Paul Wender, the grandfather of ADHD treatment: Some drugs work in some people, at some dose, some of the time.
The pharmacology of amphetamine and methylphenidate: Relevance to the neurobiology of attention-
deficit/hyperactivity disorder and other psychiatric comorbidities. Neurosci Biobehav Rev. 2018 Apr;87:255-270.
Faraone SV1
Tricyclics for ADHD
• Desipramine in adults w/68% positive responses (Wilens et al 1996, n = 41)
• Desipramine w/comorbid tic d/o in children & adolescents (Spencer et al 2002 n = 41); 71% of pts w/ADHD responded positively; 30% decrease in tics, 42% decrease in ADHD symptoms
• Desipramine statistically better than clonidine for ADHD with comorbid tourettes in children and adolescents; neither exacerbated tics (Singer et al 1995 n = 34)
• Tricyclic antidepressants - third-line treatment for attention deficit hyperactivity disorder in school-aged children.Bell G, Efron D.J Paediatr Child Health. 2015 Dec;51(12):1232-4
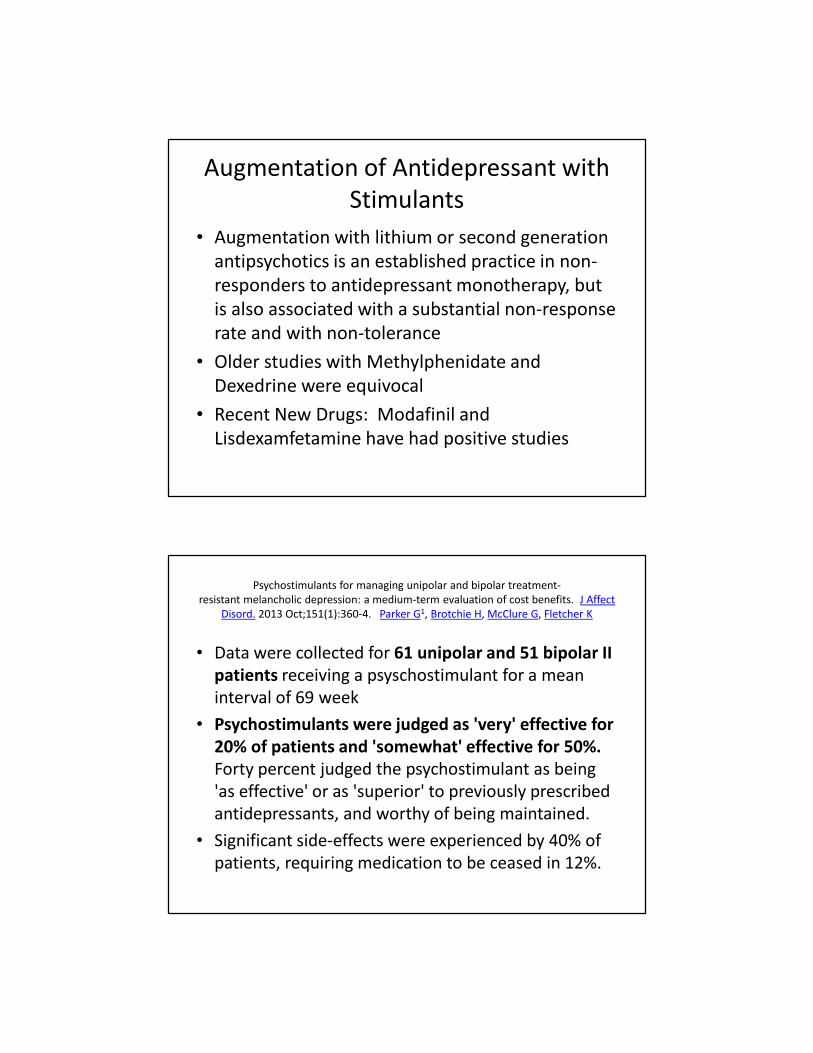
Modafinil is Not a Phenylethylamine
AmphetamineC C N
H
H
C H 3
H
H
H
Methylphenidate
C C N
C
H H
O
O
C H 3
H
ModafinilC
H
S C
O
H
H
CO
N H 2

Modafinil Demonstrates Highly Selective CNS Activity
in Animal Studies
AH = anterior hypothalamusCA = caudate
Modafinil MethylphenidateAmphetamine
Modafinil is thought to work selectively in areas of the brain (e.g., anterior
hypothalamus), believed to regulate normal wakefulness
Also binds weakly to Dopamine/Norepinephrine Transporter
Hypocretins or Orexins

Published Modafinil Studies
• A randomized, double-blind and placebo-controlled trial of modafinil in children and
adolescents with attention deficit and hyperactivity disorder. Kahbazi et al, 2009
• Modafinil improves symptoms of attention-deficit/hyperactivity disorder across
subtypes in children and adolescents. Biederman et al, 2008
• Modafinil as a treatment for Attention-Deficit/Hyperactivity Disorder in children and
adolescents: a double blind, randomized clinical trial. Amiri et al, 2008
• Efficacy and safety of modafinil film-coated tablets in children and adolescents with or
without prior stimulant treatment for attention-deficit/hyperactivity disorder: pooled
analysis of 3 randomized, double-blind, placebo-controlled studies. Wigal et al, 2006
• A comparison of once-daily and divided doses of modafinil in children with attention-
deficit/hyperactivity disorder: a randomized, double-blind, and placebo-controlled
study. Biederman et al, 2006
• Modafinil contains both the S- and R-enantiomers of modafinil, while armodafinil only contains the R-modafinil enantiomer
Modafinil Almost FDA approved
• 2006- made it to the final meeting FDA
• One case of Stevens Johnson syndrome
• This came against a backdrop of increased safety concerns about drugs already used to treat ADHD and the SSRIs being linked to suicide. Suicide worry 2004, black box warning 2006
• HELPS particularly with decision-making, planning and fluid intelligence. The more complex the task, the more that modafinilhelped

Conclusions
• Medications are extremely useful in treating Adult ADHD
• Stimulant Medications are the Gold Standard and have few side effects. Use of two different ones!
• Buproprion, Atomoxetine, are useful alternatives to Stimulants
• Clonidine and Guanfacine XR can be useful. Rejection Sensitive Dysphoria
• Tricyclics are also useful but may have worrisome side effects
• Don’t forget Modafinil
ADJUNCT STIMULANT
USE IN DEPRESSION
Augmentation of Antidepressant with
Stimulants
• Augmentation with lithium or second generation
antipsychotics is an established practice in non-
responders to antidepressant monotherapy, but
is also associated with a substantial non-response
rate and with non-tolerance
• Older studies with Methylphenidate and
Dexedrine were equivocal
• Recent New Drugs: Modafinil and
Lisdexamfetamine have had positive studies
Psychostimulants for managing unipolar and bipolar treatment-
resistant melancholic depression: a medium-term evaluation of cost benefits. J Affect
Disord. 2013 Oct;151(1):360-4. Parker G1, Brotchie H, McClure G, Fletcher K
• Data were collected for 61 unipolar and 51 bipolar II patients receiving a psyschostimulant for a mean
interval of 69 week
• Psychostimulants were judged as 'very' effective for 20% of patients and 'somewhat' effective for 50%. Forty percent judged the psychostimulant as being
'as effective' or as 'superior' to previously prescribed
antidepressants, and worthy of being maintained.
• Significant side-effects were experienced by 40% of
patients, requiring medication to be ceased in 12%.

Efficacy and tolerability of lisdexamfetamine as an antidepressant augmentation strategy: A meta-analysis of randomized controlled trials. J Affect Disord. 2018 Jan 15;226:294-300 Giacobbe P1, Rakita
U2, Lam R3, Milev R4, Kennedy SH5, McIntyre RS5.
• Cochrane review show little data of stimulant help• Lisdexamfetamine more gradual and better tolerated
• At least it was well tolerated
• Meta-analysis of 971 pts, in 3 studies; half LDX, half placebo
• Failed to demonstrate superiority except in one study
• Focused on residual executive function and fatigue
• Superior clinical effects would be seen with add-on LDX if its use was restricted to those with a profile of residual fatigue and cognitive symptoms, which are known to be preferentially targeted by psychostimulants.
Stimulants for depression: On the up and up?Aust N Z J Psychiatry. 2016 Mar;50(3):203-7 .Maihi et al.
• The use of traditional psychostimulants (methylphenidate and dexamphetamine) and
stimulant-like drugs (modafinil and armodafinil) for the treatment of depression is a growing
concern given the lack of research evidence supporting their effectiveness.
• Clinically, the rapid amelioration of depressive symptoms with traditional psychostimulants is
often dramatic but short-lived, and this suggests that they likely operate via different
mechanisms to conventional antidepressants.
• More importantly, there is little evidence from randomised controlled trials supporting their efficacy in treating depression, although modafinil has been shown to be effective in reducing prominent depressive symptoms, such as fatigue.
• Research is urgently required to clarify psychostimulants' mechanisms of action and to
evaluate their long-term benefits and risks in the treatment of major and bipolar depression.
• Until then they should only be prescribed if absolutely necessary, and even then their prescription should be facilitatory and time limited unless it is for investigational purposes.

Citalopram, methylphenidate, or their combination in geriatric depression: a randomized, double-blind, placebo-controlled trial.
Am J Psychiatry. 2015 Jun;172(6):561-9. Lavretsky H1, Reinlieb M1, St
Cyr N1, Siddarth P1, Ercoli LM1, Senturk D1.
• This was a 16-week, double-blind, three-arm, parallel-design study comparing the combination of methylphenidate and citalopram and either drug plus placebo. mean age of 69 years, and all had a diagnosis of major depressive disorder.
• The authors found that the combination treatment accelerated response and increased the remission rate, and the differences were statistically significant and clinically meaningful. Although cognition improved with treatment, there were no significant differences between treatments.
• Methylphenidate was started at 2.5 mg twice a day, and the dosage was increased by 2.5 mg twice a day every 4 days. The mean final dosage was 16 mg/day
• Amid recent reports of the rapid antidepressant effects of intravenous ketamine, early reports of rapid effects of stimulants in depression are all but forgotten
Low incidence of “Switch” in Bipolar
Depression• A review of the use of stimulants and stimulant
alternatives in treating bipolar depression and major depressive disorder. Corp SA1, Gitlin MJ, Altshuler LL. J Clin Psychiatry. 2014 Sep;75(9):1010-8. .
• Four completed RCTs suggested that modafinil/armodafinilwere beneficial as treatment adjuncts for unipolar and bipolar depression, with very low rates of mood switch in bipolar depression. One study was stopped prematurely due to safety concerns of increased suicidality.
• Modafinil and armodafinil are recommended treatment adjuncts for refractory unipolar and bipolar depression.
. Modafinil augmentation therapy in unipolar and bipolar depression: a systematicreview and meta-analysis of randomized controlled trials.
J Clin Psychiatry. 2013 Nov;74(11):1101-7
Goss AJ1, Kaser M, Costafreda SG, Sahakian BJ, Fu CH.
Residual symptoms include a persistent low mood and neurovegetative symptoms such as
fatigue.
• Double-blind, randomized, placebo-controlled clinical trials of adjunctive treatment with
modafinil or armodafinil of standard treatment for depressive episodes in MDD and bipolar
depression were selected.
• Data from 6 RCTs, with a total of 910 patients with MDD or bipolar depression, consisting of 4
MDD RCTs (n = 568) and 2 bipolar depression RCTs (n = 342) were analyzed. The meta-
analysis revealed significant effects of modafinil on improvements in overall depression scores (point estimate = -0.35; 95% CI, -0.61 to -0.10) and remission rates (odds ratio = 1.61;
95% CI, 1.04 to 2.49).
• The treatment effects were evident in both MDD and bipolar depression, with no difference
between disorders.
• Modafinil showed a significant positive effect on fatigue symptoms (95% CI, -0.42 to -0.05).
The adverse events were no different from placebo.
• Modafinil is an effective augmentation strategy for acute depressive episodes, including for symptoms of fatigue, in both unipolar and bipolar disorders.
DSM 5 Criteria for Binge Eating Disorder
• A. Recurrent episodes of binge eating (same as bulimia nervosa)
B. Binge eating episodes are associated with three (or more) of the
following
1. Eating much more rapidly than normal.
2. Eating until feeling uncomfortably full.
3. Eating large amounts of food when not feeling physically
hungry.
4. Eating alone because of embarrassment.
5. Feeling disgusted with oneself, depressed, or very guilty
after overeating.
C. Marked distress regarding binge eating is present.
D. At least once a week for 3 months.
E. The binge eating is not associated with the recurrent use of
inappropriate compensatory behavior.

1/3 of Binge eating disorder patients met criteria for ADHD
BMC Psychiatry. 2017 Jan 17;17(1):19.. Svedlund NE1,2, Norring C3,4, Ginsberg Y3,5, von Hausswolff-Juhlin Y3,4.
Symptoms of Attention Deficit Hyperactivity Disorder (ADHD) among adult eating disorder patients.METHODS: In total 1165 adults with an eating disorder were assessed with a battery of standardized instruments, for measuring
inter alia ADHD screening, demographic variables, eating disorder symptoms and psychiatric comorbidity
RESULTS: Almost one third (31.3 %) of the patients scored above the screening cut off indicating a possible ADHD
CONCLUSIONS: There is a high frequency of ADHD symptoms in patients with binge eating/purging eating disorders The finding that the frequency of ADHD symptoms in anorexia nervosa with binge eating/purging is as high as in
bulimia nervosa highlights the need also for this group.
A randomized comparison of long acting methylphenidate and cognitive behavioral therapy in the treatment of binge eating disorder. Psychiatry Res. 2019 Jan
17;273:467-474. Quilty LC1, Allen TA2, Davis C3, Knyahnytska Y4, Kaplan AS4.
• Dopamine neurotransmission has been associated with dysregulated eating, and pharmaceutical agents targeting the dopamine system are associated with decreased binge eating and weigh
• Female outpatients with BED were randomized to receive methylphenidate (n = 22) or CBT (n = 27) for 12 weeks.
• Results showed that both treatments had a significant impact on primary and secondary outcomes.
• Methylphenidate and CBT were associated with decreases in subjective and objective binge episodes; methylphenidate was associated with greater decreases in BMI.
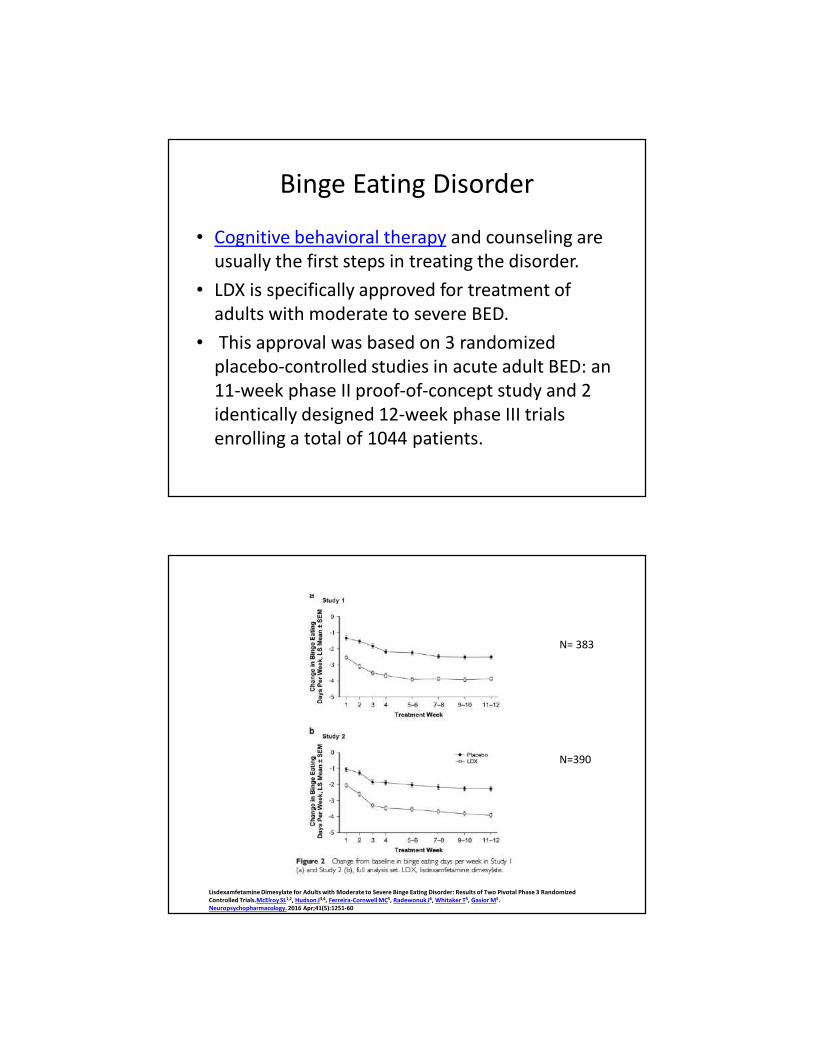
Binge Eating Disorder
• Cognitive behavioral therapy and counseling are
usually the first steps in treating the disorder.
• LDX is specifically approved for treatment of
adults with moderate to severe BED.
• This approval was based on 3 randomized
placebo-controlled studies in acute adult BED: an
11-week phase II proof-of-concept study and 2
identically designed 12-week phase III trials
enrolling a total of 1044 patients.
Lisdexamfetamine Dimesylate for Adults with Moderate to Severe Binge Eating Disorder: Results of Two Pivotal Phase 3 Randomized Controlled Trials.McElroy SL1,2, Hudson J3,4, Ferreira-Cornwell MC5, Radewonuk J6, Whitaker T5, Gasior M5. Neuropsychopharmacology. 2016 Apr;41(5):1251-60
N= 383
N=390

IMPORTANCE: Binge-eating disorder (BED), a public health problem associated with psychopathological symptoms
and obesity and possibly with metabolic syndrome, lacks approved pharmacotherapies.
.
INTERVENTIONS: Lisdexamfetamine dimesylate at dosages of 30, 50, or 70 mg/d or placebo were provided to study
participants (1:1:1:1). Dosages were titrated across 3 weeks and maintained for 8 weeks. We followed
up participants for a mean (SD) of 7 (2) days after the last dose.
CONCLUSIONS AND RELEVANCE: The 50- and 70-mg/d treatment groups demonstrated efficacy compared with the placebo group in decreased BE days, BE cessation, and global improvement. The safety profile was generally consistent with previous findings in adults with attention-deficit/hyperactivity disorder.
Efficacy and safety of lisdexamfetamine for treatment of adults with moderate to severe binge-eating disorder: a randomized clinical trial. McElroy SL1, Hudson JI2,
Mitchell JE3, Wilfley D4, Ferreira-Cornwell MC5, Gao J5, Wang J6, Whitaker T5, Jonas J7,
Gasior M5. JAMA Psychiatry. 2015 Mar;72(3):235-46..
.
This study evaluated the efficacy, tolerability, and safety of armodafinil in the treatment
of binge eating disorder (BED). Sixty participants with BED were randomized to receive
armodafinil (150-250 mg/day) (N = 30) or placebo (N = 30) in a 10-week,
In the primary longitudinal analysis, armodafinil and placebo produced similar rates of
improvement in binge eating day frequency (the primary outcome measure); however, armodafinil was associated with a statistically significantly higher rate of decrease in binge eating episode frequency.
In the secondary baseline-to-endpoint analyses, armodafinil was associated with
statistically significant reductions in obsessive-compulsive features of binge eating and
BMI. The mean (SD) armodafinil daily dose at endpoint evaluation was 216.7 (43.9) mg.
There were no serious adverse events
Armodafinil in binge eating disorder: a randomized, placebo-controlled trial.
McElroy SL1, Guerdjikova AI, Mori N, Blom TJ, Williams S, Casuto LS, Keck PE Jr. Int Clin
Psychopharmacol. 2015 Jul;30(4):209-15

BED Medication
• LDX dosed at 50 mg or 70 mg(but not 30 mg) significantly reduced binge-eating symptoms, obsessive-compulsive features of binge eating, and other measures of EDs psychopathology
• Armodafinil was associated with a statistically significantly higher rate of decrease in binge eating episode frequency.
• Armodafinil was associated with statistically significant reductions in obsessive-compulsive features of binge eating and BMI
Armodafinil in binge eating disorder: a randomized, placebo-controlled trial.McElroy SL, Guerdjikova AI, Mori N, Blom TJ, Williams S, Casuto
LS, Keck PE Jr. Int Clin Psychopharmacol. 2015 Jul;30(4):209-15
USING PHENTERMINE-TOPIRAMATE EXTENDED RELEASE
Qsmiya
• Phentermine was first introduced in 1959, and became part of the drug combination fen-phen that was withdrawn from the market in 1997 due to the fenfluramine component damaging people's heart
valves. In 2012 a different combination drug, (Qysmia) phentermine/topiramate was approved in the US.
• Phentermine– topiramate (phentermine 3.75mg–topiramate 23mg extended-release) was given daily in the morning for 14 days.
• Thereafter, the dose was increased to phentermine 7.5mg–topiramate 46mg daily and maintained during the treatment period.
• Phentermine-topiramate treatment was associated with significant reductions in weight, body mass index, binge-eating episode frequency, and measures of global clinical severity, eating disorder psychopathology, and obsessive-compulsive symptoms
Combination Phentermine-Topiramate Extended Release for the Treatment of Binge Eating Disorder: An Open-Label,
Prospective Study. Guerdjikova AI, Williams S, Blom TJ, Mori N, McElroy SL. Innov Clin Neurosci. 2018 Jun 1;15(5-6):17-21

FIGURE 1. Cumulative mean weight (kg) change and weekly binge episodes over 12 weeks of phentermine–topiramate treatment
Combination Phentermine-Topiramate Extended Release for the Treatment of Binge Eating Disorder: An Open-Label, Prospective Study.
Guerdjikova AI, Williams S, Blom TJ, Mori N, McElroy SL. Innov Clin Neurosci. 2018 Jun 1;15(5-6):17-21
A randomized, placebo-controlled crossover trial of phentermine-topiramate ER in patients with binge-eating disorder and bulimia nervosa. Safer DL1, Adler S1, Dalai SS1, Bentley JP2, Toyama H3, Pajarito S1,
Najarian T4. Int J Eat Disord. 2020 Feb;53(2):266-277.
OBJECTIVE:, this trial aimed to evaluate PHEN/TPM-ERs efficacy and safety in a crossover RCT for patients
with binge-eating disorder (BED) or bulimia nervosa (BN).
Participants were randomized to 12-weeks PHEN/TPM-ER (3.75 mg/23 mg-15 mg/92 mg) or placebo
followed by 2-weeks drug washout, then 12-week crossover. Demographics, vitals, eating disorder behaviors,
mood, and side effects were measured. Primary outcome was objective binge-eating (OBE) days/4-weeks;
secondary outcomes included binge abstinence. Mixed-effect models estimated treatment effects, with fixed
effects adjusting for treatment, study period, and diagnosis.
RESULTS:
The 22 adults (BED = 18, BN = 4) were female (96%), Caucasian (55%), aged 42.9 (SD = 10.1) years with body
mass index = 31.1 (SD = 6.2) kg/m2 . Baseline OBE days/4-weeks decreased from 16.2 (SD = 7.8) to 4.2 (SD =
8.4) after PHEN/TPM-ER versus 13.2 (SD = 9.1) after placebo (p < .0001), with abstinence rates = 63.6% on
PHEN/TPM-ER versus 9.1% on placebo (p < .0001). Weight changes = -5.8 kg on PHEN/ TPM-ER versus +0.4
kg on placebo. Drop-out = 2 (9%) on PHEN/TPM-ER and 2 (9%) on placebo, with few side effects. Vital sign
changes with PHEN/TPM-ER were minimal and similar to placebo. Responses were not significantly different
for BED versus BN.
DISCUSSION:
This first RCT to evaluate the efficacy and safety of PHEN/TPM-ER for BED/BN found this drug combination
significantly more effective at reducing binge eating than placebo and well tolerated. However, with only
four participants with BN.

Take aways
• When to use stimulants
• Worrying about Addictions
• In Adult ADHD, using multiple stimulants
• The antidepressant-like stimulants
• Modafinil, armodafinil
• Refractory Depression
• Binge Eating Disorder
Related Documents