USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM PY4 ANNUAL REPORT: OCTOBER 2016 – SEPTEMBER 2017 Signing of the MOU between the USAID/Uganda Private Health Support Program and the Laboratory Network Uganda members to launch the Labnet Franchise, July 2017 October 30, 2017 This report is made possible by the support of the American People through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of Cardno Emerging Markets USA, Ltd. and do not necessarily reflect the views of USAID or the United States Government.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM PY4 ANNUAL REPORT: OCTOBER 2016 – SEPTEMBER 2017
Signing of the MOU between the USAID/Uganda Private Health Support Program and the Laboratory Network Uganda members to launch the Labnet Franchise, July 2017
October 30, 2017
This report is made possible by the support of the American People through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of Cardno Emerging Markets USA, Ltd. and do not necessarily reflect the views of USAID or the United States Government.
USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM PY4 ANNUAL REPORT: OCTOBER 2016- SEPTEMBER 2017
Submitted by: Cardno Emerging Markets USA, Ltd. Submitted to: USAID/Uganda Contract No.: AID-617-C-13-00005
DISCLAIMER
The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016- September 2017 Page i
Table of Contents
ACRONYMS ...................................................................................................................................................... IV
EXECUTIVE SUMMARY .................................................................................................................................... 1
KEY ACHIEVEMENTS IN YEAR 4 ......................................................................................................................... 1
CHALLENGES/MITIGATION EFFORTS ................................................................................................................. 3
HIGHLIGHTS FOR NEXT QUARTER’S PLANNED ACTIVITIES ............................................................................... 4
INTERMEDIATE RESULT (IR) 1: EXPANDED AVAILABILITY OF HEALTH SERVICES BY PRIVATE SECTOR PROVIDERS ..................................................................................................................... 6
1.1. STRENGTHENED SERVICE DELIVERY IN 71 PRIVATE SECTOR FACILITIES (54 PFPS, 17 PNFPS) ... 6 1.1.1. Support delivery of comprehensive quality services ............................................................ 6
1.1.1.1. Integrate HIV Testing Services (HTS) ..................................................................................................... 6
1.1.1.2. Integrate tuberculosis (TB)/HIV services……………………………………………………………….,7 1.1.1.3. Integrate voluntary medical male circumcision (VMMC) services ....................................................... 9 1.1.1.4. Provide family planning (FP) services ................................................................................................... 10 1.1.1.5. Integrate malaria services ....................................................................................................................... 12 1.1.1.6. Strengthen reproductive, maternal newborn and child health services ............................................ 12 1.1.1.7. Integrate prevention of mother-to-child transmission (PMTCT) services ......................................... 13 1.1.1.8. Strengthen access to essential medicines, test kits and supplies ..................................................... 15 1.1.1.9. Strengthen blood safety, injection safety and health care waste management .............................. 16 1.1.1.10. Strengthen comprehensive HIV/AIDS services for children and adolescents ............................... 17 1.1.1.11. Strengthen care and treatment of identified HIV positive clients in the private sector ................. 17 1.1.1.12. Strengthen laboratory and viral load monitoring for sustained viral load testing and viral suppression ............................................................................................................................................................. 19 1.1.1.13. Strengthen nutrition assessment counselling and support (NACS) and support for nutrition through the first 1,000 days ................................................................................................................................... 20
1.1.14. Quality improvement interventions....................................................................................... 20
1.2. STRENGTHENED SYSTEMS FOR SERVICE DELIVERY IN PRIVATE SECTOR FACILITIES .............................. 22 1.2.1. Strengthen skills of health workers .............................................................................................. 22 1.2.2. Support targeted continuing medical education (CME) ............................................................ 24 1.2.3. Support innovative approaches to task sharing and task shifting ........................................... 24 1.2.4. Strengthen policies, guidelines, standard operating procedures and job aids ...................... 24 1.2.5. Strengthen health management information systems .............................................................. 25
1.2.5.1. Identify and support health management information system (HMIS) focal persons ..................... 25 1.2.5.2. Strengthen weekly option B+ reporting ................................................................................................. 25
1.2.6. Strengthen Health Systems in the faith based sector ............................................................... 26 1.2.6.1 Improve the availability of human resources to support service delivery in the faith-based health sector ........................................................................................................................................................................ 26 1.2.6.2 Strengthen health leadership and governance in the private sector .................................................. 27 1.2.6.3. Improve health financing and finance management in the private sector ........................................ 27 1.2.6.4. Improve coordination with public facilities and other stakeholders at districts and national levels .................................................................................................................................................................................. 28
1.3. STRENGTHENED SUPPORT FOR ORPHANS AND VULNERABLE CHILDREN (OVC)................................... 28 1.3.1. Support performance based grants to Faith Based and Civil society organizations ............ 28 1.3.2: Households Economic strengthening activities ........................................................................ 28
1.3.2.1. Training of caregivers in business initiation, management and follow up support .............. 28 1.3.2.2. Training of Village Saving and Loan Association Leaders on Group Dynamics and Money management skills ............................................................................................................................................... 29 1.3.2.3. Household Vulnerability assessment. .............................................................................................. 29
1.3.3. Support to Apprenticeship and Vocational Training for out of school orphans and vulnerable children .................................................................................................................................... 29 1.3.4 Support Nutrition and Food Security Interventions .................................................................... 31 1.3.5. Support provision of Formal Education services. ...................................................................... 31 1.3.6. Support provision of health, water, sanitation and housing ..................................................... 32 1.3.7. Child Protection and Legal Support services ............................................................................. 32 1.3.8. Psycho Social Support to OVC and their Households .............................................................. 33 1.3.9. Increase access to HIV/AIDS Services ....................................................................................... 33 1.3.10. Promoting Private Sector Engagement .................................................................................... 33

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016- September 2017 Page ii
1.3.11. Mainstreaming of CBOs OVC activities .................................................................................... 33 1.3.11.1. Supporting children with disabilities: ................................................................................................... 33
1.4. SUPPORT BUSINESS STRENGTHENING AND INCREASE ACCESS TO FINANCE .......................................... 34 1.4.1. Expand financial outreach through DCA banks ......................................................................... 34 1.4.2. Expand Financial Outreach through Non-DCA Banks .............................................................. 36 1.4.3. Provide technical assistance to DCA banks and borrowers (actual and potential) .............. 37 1.4.4. Supporting USAID in the identification and recommendation of a third health DCA bank partner ......................................................................................................................................................... 38 1.4.5. Provide business strengthening support .................................................................................... 39
1.5. PROGRAM TRANSITION PLAN IMPLEMENTATION ...................................................................................... 40
INTERMEDIATE RESULT (IR) 2. INCREASED AFFORDABILITY OF PRIVATE HEALTH SERVICES AND PRODUCTS ......................................................................................................................... 41
2.1. REDUCING THE PRICES OF HEALTH PRODUCTS AND SERVICES ............................................................... 41 2.1.1. Provide access to income generating opportunities for HIV/AIDS peer support groups ..... 41 2.1.2. Facilitate dialogue between MOH and private health sector to rationalize financing for health .......................................................................................................................................................... 42 2.1.3. Supporting the passage of the health financing strategy and national health insurance bill ..................................................................................................................................................................... 43 2.1.4. Exploring the possibility of a drug benefit plan as an interim step for national health insurance .................................................................................................................................................... 44
2.2. INCREASING HEALTH SERVICES AND MEDICINES PRICING TRANSPARENCY .......................................... 44 2.2.1. Conduct a pharmacy and drug shop census in Kampala to augment ongoing KCCA facility census ......................................................................................................................................................... 45 2.2.2. Conduct an Awareness Campaign on Rational Use of Medicines and Disseminate recommended EMHSL Commodity Prices ............................................................................................ 46 2.2.3. Support pooled procurement for private health providers ........................................................ 47 2.2.4. Disseminating the professional fee guidelines ........................................................................... 47
2.3. LIMITING FINANCIAL BARRIERS TO ACCESSING HEALTH SERVICES .......................................................... 48 2.3.1. Promote use of information and communication technology (ICT) in health......................... 48 2.3.2. Promoting health insurance and health savings with VSLA groups ....................................... 48 2.3.3. Document maternal health voucher program in Kiruhura district to demonstrate success of privately financed self-sustaining voucher to delivery critical health services .................................. 49
2.4. PROMOTING PREVENTATIVE CARE AMONGST WORKPLACE BASED CLIENTS AND HEALTH PROVIDERS ... 50 2.4.1. Health talks amongst private health insurers’ and health management organizations’ membership to encourage health seeking behaviour .......................................................................... 50 2.4.2. Updating and Enforcing National referral guidelines ................................................................ 50
INTERMEDIATE RESULT (IR) 3. IMPROVED QUALITY OF PRIVATE HEALTH SECTOR FACILITIES AND SERVICES ......................................................................................................................... 52
3.1. IMPLEMENT SQIS AND OTHER CONTINUOUS QUALITY IMPROVEMENT MECHANISMS .............................. 52 3.1.1. Roll out of the self-regulatory quality improvement system (SQIS) ........................................ 52 3.1.2. Link the Health as a Business (HaaB) network facilities to SQIS ........................................... 52 3.1.3. Support facility self-assessments ........................................................................................... 52 3.1.4. Maintain USAID/ASSIST continuous quality improvement (CQI) approaches and scale up to other Program activities ....................................................................................................................... 53 3.1.5. Establish a laboratory network ..................................................................................................... 53 3.1.6. Conduct DQA across all Program health areas ......................................................................... 54 3.1.7. Conduct Site service quality assessments using SIMS tool .................................................... 54
3.2. IMPLEMENT SQIS AND OTHER CONTINUOUS QUALITY IMPROVEMENT MECHANISMS .............................. 54 3.2.1. Resume updating the council acts through a performance based grant ............................... 54 3.2.2. Assist the councils to design and establish a web-based platform ......................................... 55 3.2.3. Support continuous professional development .......................................................................... 55 3.2.4. Assist Kampala City Directorate of Health Services to harmonize and field test a uniform application for facility licensure ............................................................................................................... 55 3.2.5 Assist Kampala City Directorate of Health Services and Environment to conduct a private provider census ......................................................................................................................................... 56

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016- September 2017 Page iii
3.3. ASSIST PRIVATE SECTOR REPRESENTATIVES TO PROMOTE STANDARDS OF CARE AMONG PFP
PROVIDERS ....................................................................................................................................................... 56 3.3.1. Strengthen capacity of UHF and other private sector associations to provide services valued to their members ........................................................................................................................... 56 3.3.2. Support UHF to implement strategic plan................................................................................... 56 3.3.3. Strengthen private sector engagement with MOH .................................................................... 57 3.3.4. Advance the formation of a public-private sector dialogue forum ........................................... 57
3.4. IMPLEMENT PPPHS THAT STRENGTHEN PRIVATE SECTOR CAPACITY TO DELIVER QUALITY SERVICES . 57 3.4.1. Develop the Ministry of Health PPPH Node’s capacity ............................................................ 57 3.4.2. Build support for the MOH to implement PPPs in health ......................................................... 58 3.4.3. Form a steering committee and conduct a private sector assessment .................................. 58 3.4.4. Build the MOH’s PPPH pipeline ................................................................................................... 59 3.4.5. Strengthen PPPH coordination at both the central and district level ...................................... 59
GRANTS MANAGEMENT AND PERFORMANCE ................................................................................................... 60
ANNEX 1: PHS PERFORMANCE INDICATOR TABLE, OCTOBER 2016–SEPTEMBER 2017 ........ 64
ANNEX 2: SUCCESS STORY ........................................................................................................................ 72
Table of Figures
Figure 1. HIV Yield by entry point ...................................................................................................... 6
Figure 2. HIV Testing Achievement versus Target ......................................................................... 6
Figure 3. Treatment Outcome of Patients Registered 12-15 Months Earlier ............................. 7
Figure 4. VMMC Services ................................................................................................................... 9
Figure 5. Family Planning Uptake.................................................................................................... 10
Figure 6. FP Methods and Procedures by Trainees ..................................................................... 11
Figure 7. IPT Uptake .......................................................................................................................... 12
Figure 8. Causes of Perinatal Deaths ............................................................................................. 13
Figure 9. HIV Care (Achievement versus Targets) ....................................................................... 18
Figure 10 ART: Newly initiated and Current on ART .................................................................... 18
Figure 11 Option B+ health Facility weekly reporting rates ......................................................... 26
Figure 12. Centenary DCA Utilization as % of Total Guarantee Amount as of 30 September 2017 ...................................................................................................................................................... 34
Figure 13: Ecobank DCA Utilization as a % of Total Guarantee Amount as of 30 September 2017 ...................................................................................................................................................... 35
Figure 14: Structure of the DFCU DCA .......................................................................................... 38
Figure 15: GIS map for the northern part of Nakawa sub-division, Kampala ........................... 45
Figure 16: Proposed National Referral Chain and Flow .............................................................. 50
Figure 17: OVC approved grants for the period versus funds disbursed .................................. 61
Figure 18: Care and treatment grantee approved grants versus funds disbursed .................. 62
Figure 19: PFP grantee average percentage performance for the period October - September 2017 ...................................................................................................................................................... 62
Figure 20: PFP grantee funds disbursement against budget status for the period October - September 2017 ................................................................................................................................. 63

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016- September 2017 Page iv
Acronyms
AE Adverse Event
ANC Antenatal Care
ART Antiretroviral Therapy
BDS Business Development Service
BTL Bilateral Tubal Ligation
CARDNO Cardno Emerging Markets USA, Ltd.
CD4 Cluster of Differentiation 4
CEDO Child Rights Empowerment and Development Organization
CME Continuous Medical Education
CMS Credit Management System
COP16 Country Operational Plan 2016
CSO Civil Society Organization
DCA Development Credit Authority
DFCU Development Finance Company of Uganda
DHIS2 District Health Information System 2
FGD Focus Group Discussion
FP Family Planning
HaaB Health as a Business
HBB+ Helping Babies Breathe Plus
HIPS USAID/Uganda Health Initiatives for the Private Sector Project
HIV/AIDS Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome
HMIS Health Management Information System
HRH Human Resources for Health
HSS Health Systems Strengthening
HTC HIV Testing and Counselling
ICOBI Integrated Community Based Initiatives
IDI Infectious Disease Institute
IGA Income Generating Activity
IHA Insight Health Advisors
IHSU International Health Sciences University
INH Isoniazid
IPT Isoniazid preventive therapy
IPTP Intermittent Preventive Treatment of Malaria in Pregnancy
IRCU Inter-Religious Council of Uganda
JMS Joint Medical Stores
KCCA Kampala City Council Authority
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016- September 2017 Page v
LARC/PM Long-Acting Reversible Contraception/Permanent Methods
MAUL Medical Access Uganda Limited
MCH Maternal Child Health
MEEPP Monitoring and Evaluation of the Emergency Plan Progress
MGLSD Ministry of Gender, Labor and Social Development
MOH Ministry of Health
MSH Management Sciences for Health
MSI Marie Stopes International
NACS Nutrition Assessment Counseling and Support
NDA National Drug Authority
Open MRS Open Medical Records System
OVC Orphans and Vulnerable Children
OVC MIS Orphans and Vulnerable Children Management Information System
PEPFAR President’s Emergency Plan for AIDS Relief
PFP Private for Profit
PHP Private Healthcare Provider
PHS USAID/Uganda Private Health Support Program
PLHIV People Living with HIV
PMTCT Prevention of Mother-to-Child Transmission
PNFP Private Not-For Profit
PPP Public Private Partnerships
PPPH Public Private Partnerships for Health
PPPH TWG Public Private Partnerships for Health Technical Working Group
PSA Private Sector Assessment
QA Quality Assurance
QI Quality Improvement
RDQA Routine Data Quality Assessment
SIMS Site Improvement through Monitoring Systems
SME Small and Medium-Sized Enterprises
SMC Safe Male Circumcision
SQIS Self-Regulatory Quality Improvement System
STI Sexually Transmitted Infection
TA Technical Assistance
TB Tuberculosis
TT Tetanus Toxoid
TWG Technical Working Group
UCBHCA Uganda Community Based Healthcare Association

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016- September 2017 Page vi
UHF Uganda Healthcare Federation
UHMG Uganda Health Marketing Group
UMA Uganda Manufacturers Association
UOMB Uganda Orthodox Medical Bureau
UPMA Uganda Private Midwives’ Association
USAID United States Agency for International Development
VMMC Voluntary Medical Male Circumcision
VSLA Village Savings and Loan Association
WAOS Web-Based HIV/AIDS Ordering and Reporting System
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 1
Executive Summary
The USAID/Uganda Private Health Support Program (PHS) is USAID’s flagship program in the private
sector in Uganda. The PHS Program leverages the private sector’s strengths while addressing
longstanding concerns about capacity, quality, and interests. Cardno Emerging Markets USA, Ltd.
(Cardno) leads this five-year program, supported by three subcontractors: Banyan Global, the Infectious
Diseases Institute (IDI), and Insight Health Advisors (IHA).
The PHS Program aims to strengthen, organize, and mobilize the private sector to provide Ugandans
with the option of obtaining high-quality health services from private providers. The goal is to improve
the credibility and cohesiveness of the private sector and expand the capacity of those providers. The
focus is to provide technical expertise, enhance quality standards, improve access to capital, support
accreditation, and provide leadership in the private sector. To achieve this, the Program has three main
intermediate results: (1) Expanded availability of health services by private providers; (2) Increased
affordability of private health services and products; and (3) Improved quality of private health sector
facilities and services.
Since August 1, 2014, PHS has expanded to support access to HIV/AIDS services through the Private
Not for Profit (PNFP) providers previously supported by USAID through the Inter- Religious Council
of Uganda (IRCU). Beginning October 1, 2016, PHS has integrated Private for Profit (PFP) sector
interventions – designed to strengthen regulatory systems, improve reporting and financing, and build
public private partnerships (PPP) – into the faith based sector, strengthening faith based sector health
systems to expand the availability of and access to quality and sustainable essential health, as well as
HIV/AIDS services. Such interventions include the adoption of self-regulatory quality improvement
standards (SQIS), access to finance initiatives like the Development Credit Authority (DCA) and
support to private sector umbrella institutions. To build a strong foundation for sustained scale-up of
integrated health and HIV/AIDS services for People Living with HIV/AIDS (PLHIV), PHS has
continued to strengthen PFP and PNFP health systems.
This report summarizes strategies and activities implemented during Program Year 4 (Quarter 4 and
Annual) while highlighting PHS achievements during the reporting period.
Key Achievements in Year 4
51,730 men received TT vaccination and were circumcised representing an achievement of 114%
of the annual target (45,448). Of those circumcised, 28,229 (55%) were within the priority age pivot
of 15-29.
94.9% (334,886/ 352,704) of the targeted individuals received HTS services of whom 3% (10,228)
were identified to be HIV positive, and of those, 8,162 individuals (80%) were linked to care.
Overall, we linked 8,162 clients to care, 150% of the annual target (5,430).
39,319 (11,494, PFP 27,825 PNFP) PLHIV were active in care (Pre-897, ART-38,422) translating
into 97.8% of PLHIV on ART. During the same time 1,318 (488 PFP, 830 PNFP) new PLHIV were
enrolled into care while 1,989 clients were initiated on ART ( 661 PFP, 1,328 PNFP). Of these 741
(254 PFP, 487 PNFP) 55.8% were male.
22,884 of 38,422 PLHIV on ART had a viral load done, with 91.5% showing virological
suppression.
39,319 (pre-ART 897, ART-38,422) HIV clients in care, 38,082 (97%) (9,768 PFP, 28,314 PNFP)
were screened for TB. Of those that were screened, 310 (0.8%) (Pre-126 & ART-184) were
diagnosed with TB and 182 (58.7%) started on anti TB treatment.
78% (19,175/24,600) of pregnant women had received at least 2 doses of Intermittent Preventive
Therapy (IPT) to prevent malaria in pregnancy.
876 (259 PFP, 617 PNFP) HIV exposed infants (HEI) received DNA PCR (1st DNA 525 (167 PFP,
358 PNFP), and 2nd DNA PCR 351 (92 PFP, 259 PNFP)). Of the samples that were sent to UNHLS,
for 1st DNA PCR, 58 % were drawn from children < two months of age (an improvement from the
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 2
previous quarter at 48.2%). Of all the returned results 14 babies were found to be positive (1st DNA
PCR 9 (1 PFP, 8 PNFP) and on 2nd DNA PCR 5 (4 PFP, 1 PNFP)) yielding a MTCT rate of 4%
across facilities. 29 health workers from 18 health facilities were trained in elimination of mother-
to-child HIV transmission course (EMTCT).
54,070 (36,273 ART clients and 17,797 non –ART clients at OPD) were assessed for nutritional
status. Of these 948 (1.8%) were malnourished with 378 newly malnourished. 430 of the total
malnourished cases received nutrition supplements and therapeutic feeds through site based
nutrition units or referral to other nutrition centres. In addition, 2,526 pregnant and lactating mothers
(8.5% HIV positive) were reached with maternal nutrition counselling and infant feeding
counseling. As a result of the counseling, 131 HIV positive exposed infants exclusively breastfed
for six months and out of those breastfed 90 (68.7%) HIV positive exposed infants breastfed up to
1 year.
Trained 245 health workers in long-term acting reversible contraceptives, and trained 17 medical
officers in permanent methods in Quarter 4.
Rolled-out the consolidated guidelines for HIV prevention and treatment in 57 (80.3%) of supported
private health facilities.
Conducted a perinatal death audit in 22 health facilities that reported a neonatal death and supported
facilities to institutionalize perinatal death review committees. In addition, mentorship and coaching
in neonatal resuscitation, partograph use and helping mothers survive techniques were integrated in
this activity.
In the PY October 2016-September 2017, the Program supported 46,572 OVC (31,898 PNFP and
14,674 PFP) from 13,993 households.
Validated and finalized the Comprehensive Health System Strengthening Needs Assessment
(HSNA) conducted in Quarter 3. At the same time PHS developed Human Resource Management
manuals for the bureaus, and modeled the Human Resource Management manuals for Hospitals
and Charters for Health units. These policies and charters will ensure the existence of codified
approaches for human resource management in Uganda’s faith based health sector/network. PHS
developed Board Governance manuals for the 4 Bureaus, and modeled the manuals for Hospitals,
Charters for Hospitals and lower health facilities. PHS developed Finance Management manuals
for the 4 Bureaus, and modeled these manuals for Hospitals and health units. A total of 69 Finance
Officers, In-Charges and members of the Management Committees of 30 Health Facilities under
UPMB and UOMB were trained in Finance Management and Internal Controls.
Finalized and completed the Uganda Private Health Sector Assessment (PSA). The PSA explores
policies supporting governance in the private health sector; health financing related to the private
health sector; human resources for health; size and scope of the private health supply chain; and
private sector delivery of key health services including HIV/AIDS, and maternal and child health.
A road map dubbed the “Private Sector Blue-print” was developed to guide public-private
interactions and discussions within the sector.
Continued to support the passage of the health financing strategy and national health insurance bill.
The Program developed an action plan for the private health insurance industry (including the
Health Management Organizations (HMO’s), to engage with the Ministry of Health (MOH) while
the proposed National Health Insurance Scheme (NHIS) is being implemented.
Provided actuarial consultancy services to select private health insurance providers and HMO’s in
Uganda to enable them to develop a health insurance product that they can market to individuals
and integrate with the proposed National Health Insurance Scheme (NHIS) once various MOH
initiatives on costing are concluded. A key outcome was an understanding of the minimum benefit
package an average Ugandan can afford in private health insurance.
Worked with the National Drug Authority (NDA) and the Kampala City Council Authority (KCCA)
to conduct the pharmacy and drug shop census (with GIS mapping) in all the five Divisions of
Kampala. Findings indicated that the number of both pharmacies and drug shops expanded
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 3
dramatically in the last six years. However, this rapid growth is a missed opportunity to increase
access to key public health services through private pharmacies and drug shops.
Provided the Washington-based USAID/DCA management office support in identifying and
recommending a third health DCA bank. Efforts have been positive and a new five-year health
DCA agreement has been concluded with DFCU Bank Limited for a US$5 million loan portfolio
guarantee, with a special focus on leasing of medical equipment.
Supported efforts to translate the Public Private Partnerships for Health (PPPH) technical working
group to a committee that doubles as a public-private sector dialogue forum. The dialogue forum
will focus on health financing and Public Private Partnerships (PPP) opportunities and create a
shared understanding of the role of the private health sector in Uganda.
Conducted a training on basic concepts on PPPH’s and on regional experiences in PPP’s for
representatives from the MOH, different social franchises, professional associations, Medical
Bureaus, and civil society organizations. The Program also continued to develop PPPH
implementation guidelines and procedures for the MOH’s PPPH Node. The Program validated the
draft MOH PPPH strategy and started on developing an Implementation Plan to operationalize the
PPPH strategy. The Program will provide technical assistance to annualize and cost the strategy.
During the year, the Program also trained 23 MOH/private sector staff as Trainers of Trainees in
PPPH.
335 facilities were enrolled in the self-regulatory quality improvement system (SQIS) platform. Out
of these, PHS supported 219 facilities to self-assess, using the online SQIS platform in 33 districts.
Health facilities can now monitor their quality improvement progress through comparing and
analyzing the different series of assessments they submit in the system. Health workers will also be
able to better prepare for pre-licensing inspections. In addition, during the year, the Program, in
partnership with the IntraHealth’s Capacity Project, printed and disseminated over 2,000 SQIS
toolkits. Health facilities can now access a toolkit from the councils at the time of registration. This
will enable facilities to understand the requirements at registration.
Held transition meetings with health facilities and incoming implementing partners (IP’s). These
meetings were attended by facility staffs, representatives of incoming IP’s, and Program staff. IPs
included IDI, Makerere University Walter Reed Program and Rakai Health Sciences Program. PHS
engaged in the transition of four OVC partners.
Reviewed and updated strategic plans for the Uganda Private Midwives’ Association (UPMA),
Uganda Community Based Healthcare Association (UCBHCA) and the Uganda Private Health
Training Institutions Association (UPHTIA). Once the strategic plans are completed, the
associations will be better positioned to fulfill their mandates and raise extra resources from
alternative sources, including donor organizations, so they can become sustainable. The Program
also provided support in legal, coordination, and logistical services to private health sector
associations. The Program 1) reviewed and improved their existing legal documents, 2) assisted
them in registering appropriately to engage in pooled procurement activities, and 3) trained their
members on pooled procurement, member recruitment, and ordering guidelines.
Faciliated formation and operation of a private-for-profit medical diagnostic laboratory network in
collaboration with the Uganda Medical Laboratory Technology Association (UMLTA). Since this
network will follow a franchise network strategy, the Program supported UMLTA adopt the Labnet
name and branding strategy with the goal of achieving a uniform, community-wide East African
identity and quality standards for qualified, independent medical laboratories.
Challenges/Mitigation Efforts
There was a frequent stock out of SMC commodities (SMC kits, anesthetics, and TT vaccines) and
cotrimoxazole. The program addressed this by carrying out internal redistribution among supported
private sector facilities and also borrowing from other implementing partners.
The supply of TB commodities to the private sector is not well streamlined for pediatric regimens
and isoniazid for prophylaxis. These commodities are distributed through National Medical Stores
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 4
(NMS) and the majority of private sector sites do not have accounts with NMS. The Program has
engaged respective, district TB logistics focal persons to design a rational approach to the supply
of TB commodities to ensure no stock outs for the private sector. Going forward in Year 5, the
Program will roll out the TB Web-based Ordering System (TWOS) in the private facilities to
improve TB logistics management.
Learned that the lack of a secondary market for medical equipment makes our partner banks
reluctant to accept such equipment as collateral, creating an obstacle to equipment financing. Crown
Healthcare is willing to work with the PHS Program to provide a buy-back guarantee for medical
equipment loans, giving the DCA banks extra assurance. However, the condition is that equipment
must be returned in reasonable condition and have been fully serviced by Crown Healthcare; the
value must be above a minimum. The Program will formalize through a memorandum of
understanding and to be signed in Quarter 1 of Year 5. The Program will also assist Crown
Healthcare in drafting partnership proposals for other interested financial institutions.
Ecobank DCA continues to underperform. The causes of the slow utilization of Ecobank DCA has
been repeatedly documented over the previous fiscal years. For administrative reasons, USAID has
decided to leave the guarantee in place, but asked the Program not to dedicate further resources to
technical assistance for Ecobank DCA at this time.
Supported efforts towards designing and approving the PPPH Node charter. However, finalization
of this work was deferred until the PPPH structure and TWG composition is aligned to the law.
Recommendations from the analysis of existing structures set out in the PPPH policy proposed an
expansion in the PPPH structure within MOH. Therefore, in order to develop a standard Node
charter it required alignment between the proposed new PPPH structure to the PPP law. This activity
is ongoing and will be concluded during the next quarter.
Out of the 335 facilities currently registered with the SQIS digital platform, 219 were self-assessed
by the end of the year. Some facilities had poor internet access, while others failed to self-assess on
their own, despite attending trainings. The Program has printed tools for facilities with limited
internet access. These same facilities will receive additional technical support to self-assess. The
Program will continue to work with an IT firm to trouble shoot the system and make it user friendly.
Highlights for Next Quarter’s Planned Activities
USAID/Uganda Private Health Support (PHS) Program is in the final phase of the project. During the
subsequent two quarters, PHS will consolidate efforts to respond to the three Intermediate Results. The
Program’s activities will focus on: finalizing key Program Year 1 through 4 interventions, consolidating
achievements, institutionalizing capacity in both public and private organizations responsible for
ensuring quality in the private health sector, transitioning interventions that have shown promise to key
private health sector associations, and disseminating various research findings and recommendations
from prior conducted studies. Key activities will be transitioned to USG IPs by March 2018 to ensure
continuity of services. Illustrative activities will include:
Support 12 facilities (3 attained, 4 scale-up aggressive, 5 scale-up saturated) in a total of seven
districts to provide comprehensive HIV/AIDS prevention, treatment, support, and care services.
Continue to provide a comprehensive Voluntary Medical Male Circumcision (VMMC) package at
five PNFP facilities in five districts (1 attained, 2 scale-up aggressive, 2 scale-up saturated).
Hold stakeholder meetings, engage the incoming IPs and health facilities to enable a seamless
transition process. Support Delivery of Comprehensive services through the Private sector
including Reproductive, Maternal Newborn and Child Health (RMNCH) Services, Family planning
(FP), Malaria and Nutrition services.
Strengthen health management information systems (MIS) and OVC MIS.
Provide grants to 42 community-based organizations (32 PNFP, 10 PFP) to support vulnerable
children along the four COP 2017 OVC thematic areas: Healthy, Stable, Safe and Schooled. While
at the same time implementing priority activities that will include: graduation of OVC households
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 5
with reduced vulnerability, and transfer of OVC Programs in scale up-districts to other PEPFAR
OVC mechanisms.
Continue technical assistances (TA) support to Centenary Bank and Ecobank for the ongoing DCAs
as well as provide TA support to DFCU Bank to utilize the new DCA. PHS will conduct a survey
to measure impact of A2F on health outcomes of DCA borrowers and develop a “How-To of a
Successful DCA in Health”, demonstrating that the DCAs have made a difference.
Provide business development services (BDS) to selected healthcare businesses and carry out an
end-line survey to measure the impact of the HaaB II BDS support on health outcomes of
participating HCBs.
Roll-out implementation of HSS activities targeting all four medical bureaus and 134 health
facilities, as informed by the HSS needs assessment findings and recommendations, and medical
bureau work plans.
Continue with efforts to develop a Drug Benefit Plan as an interim step for NHIS.
Provide TA to UHF to advocate for NHIS.
Continue to disseminate Professional fee guidelines amongst private health providers using their
respective associations.
Continue to support the formation and operation of Labnet Uganda following a franchise network
strategy.
Support Health Facilities in implementing SQIS and other continuous quality improvement
mechanisms.
Disseminate findings of the Private Sector Assessment.
Create an inventory of all PPPHs and formalize all the PPPs within the KCCA area.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 6
Intermediate Result (IR) 1: Expanded Availability of Health Services by Private Sector Providers
1.1. Strengthened Service Delivery in 71 Private Sector Facilities (54 PFPs, 17 PNFPs)
This section of the report (Task 1.1 – 1.6) details achievements from both PHP and PNFP private sector
services during the reporting period. In Year 4, the Program supported strengthening of services
delivery at all Program supported PFP and PNFP facilities. During the same time, the Program worked
to consolidate and sustain access to high impact HIV prevention and comprehensive, quality HIV and
AIDS care, support and treatment services through Program supported facilities. Key activities focused
on clinical and financial management training, access to finance, and service delivery grants for
HIV/AIDS and orphans and vulnerable children (OVC) support, as well transition and implementation.
A total of 71 facilities (54 PFPs, 17 PNFPs) and 45 OVC partners (36 PNFP, 9 PFP) received support
from the Program.
1.1.1. Support delivery of
comprehensive quality
services
The program strengthened service
delivery at all supported PHP and
PNFP health facilities in line with the
90- 90 -90 strategy for controlling the
HIV/AIDS epidemic. The PHS partner
health facilities provided
comprehensive services in HIV testing
services (HTS), Family Planning (FP),
TB, Malaria, Maternal and
Newborn/Child Health (MNCH), and
Voluntary Medical Male Circumcision
(VMMC).
1.1.1.1. Integrate HIV Testing
Services (HTS)
During the reporting period, 1,258
health workers were trained on the
revised HTS guidelines with emphasis
on key areas including test and treat,
reduced age of consent, retesting
before ART initiation, and focus on
HIV testing quality and strategies to
reach hard-to-reach and undiagnosed
populations. As a result, in Quarter 4
86,630 individuals were reached and
given same day results. Of these 2,463
were positive translating into positivity
rate of 3%. Of those found to be
positive 84% were linked into care
during the reporting period. A total of
5,924 were tested as couples of whom
389 (6.6%) were concordant positive
and 207 (3.5%) had discordant results.
50.1% individuals tested were males of
Figure 1. HIV Yield by entry point
Figure 2. HIV Testing Achievement versus Target
0.4%
2.6%
3.0%
4.0%
10.0%
24.0%
0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 30.0%
VMMC services
In patient department
Other PITC
VCT
Index client testing
TB clinic
H I V Y I E L D B Y E N T R Y P O I N T
88
17
6
17
63
52 2
64
52
8 35
27
04
79
76
6 15
60
16 2
46
98
7 33
48
86
O C T - D E C 1 6 J A N - M A R 1 7 A P R - J U N E 1 7 J U L Y - S E P T 1 7
HIV TESTING SERVICES
Target Clients rec'd HTC
Linear (Target ) Linear (Clients rec'd HTC)
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 7
whom 2.1% were identified to be living with HIV. 67.2% of the males tested were 20 years and above
with a positivity rate of 2.9%.
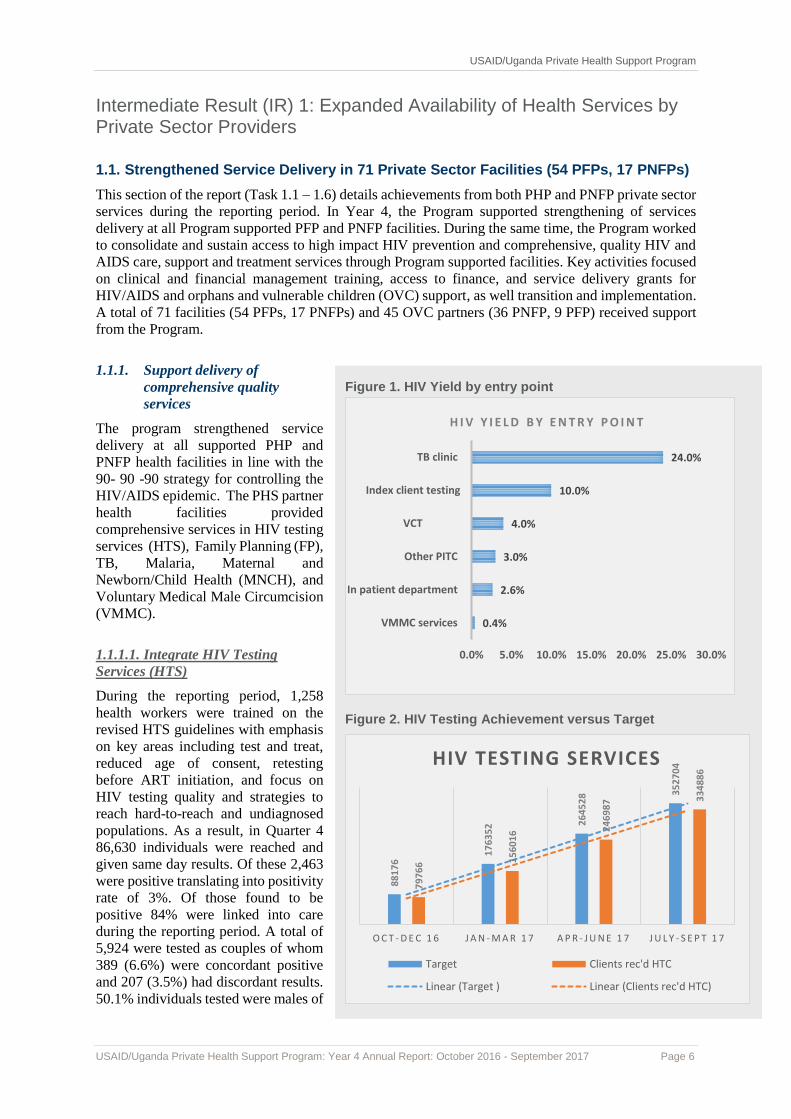
During Program Year 4, 334, 886 (94.9%) of the annual target of 352,704 individuals received HTS
services. Three percent (10,228) were identified to be HIV positive. Of those found to be HIV positive,
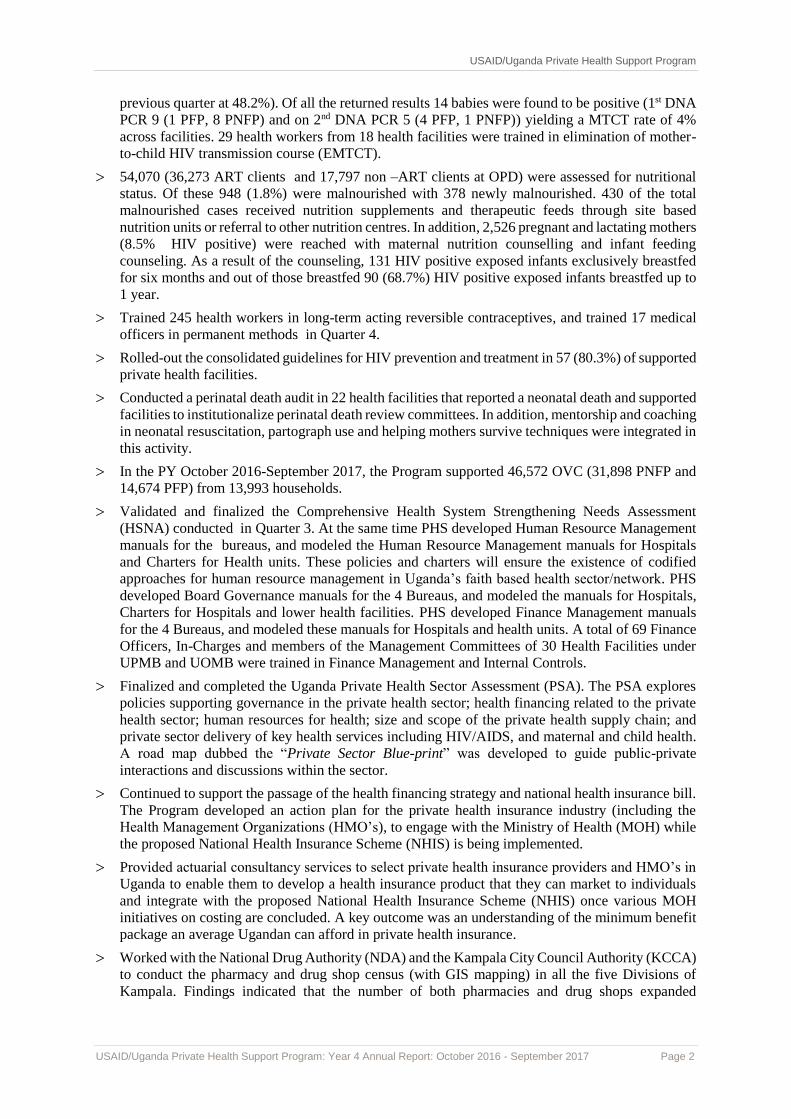
overall 8,162 (80%) were linked into care. The yield at different entry points was as follows during the
reporting period; Index client testing (10%) and TB clinic (24%). In-patient department (2.63%), VCT
(4%), VMMC services (0.4%) and other PITC (3%), see Figure 1.
By the end of Year 4, the highest yield for positives was through the TB clinic while VMMC yielded
the lowest number of positives. Going forward, boys and adolescents shall be screened and only high-
risk individuals will be tested for HIV. The program performed fairly well in providing targeted HTS
for men and this is attributed to the implementation of mixed methods to reach men such as using male
champions and opinion leaders, emphasisingthe benefits of early enrollment in care, and conducting
community health campaigns using a multi-disease approach. Other strategies included creating male
friendly HTS at facility and community level as well as prioritizing couple testing at PMTCT sites.
Although the performance on linkage rate was below the expected performance of 90%, there was
progressive improvement across the 4 quarters, (63% Quarter 1; 85% Quarter 2; 78% Quarter3; and
85% Quarter 4) and this is largely attributed to the mentorship and support of facilities on the new MOH
standard operating procedures for linkage and referral.
1.1.1.2. Integrate tuberculosis (TB)/HIV services
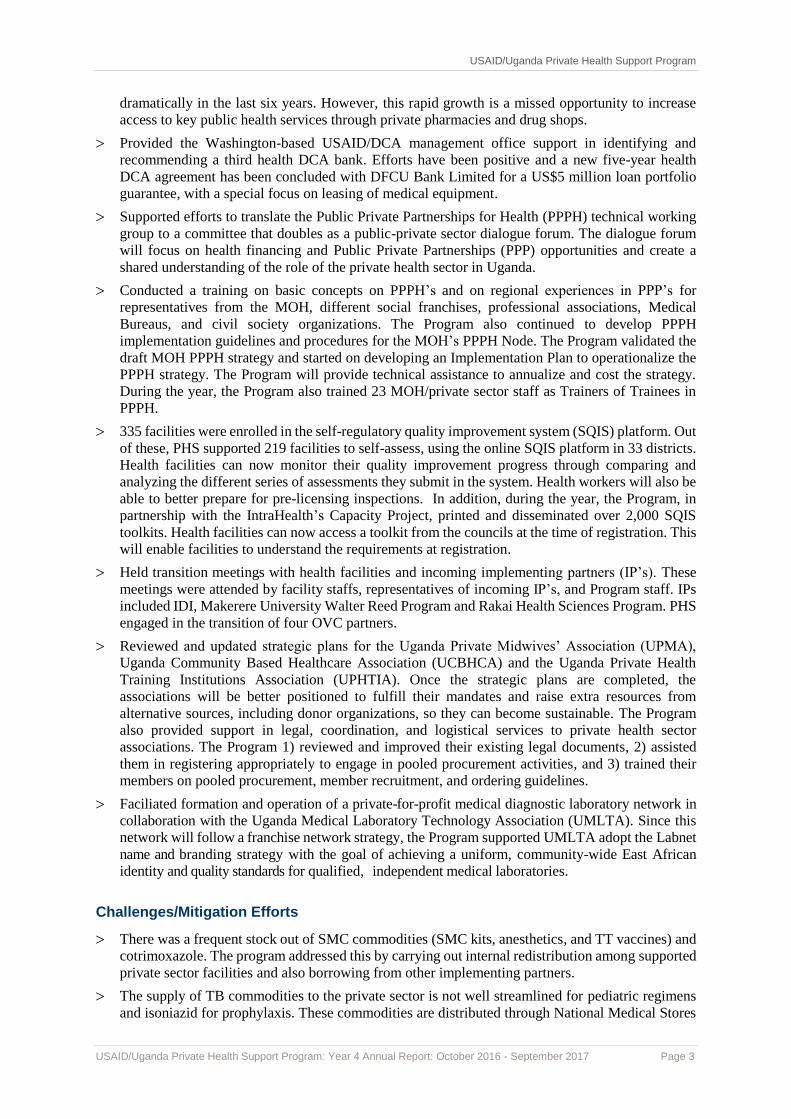
By the end of the Program Year4, out of the total 39,319 (pre-ART 897, ART 38,422) HIV clients that
were in care, 38,082 (96.9%) (9,768 PFP, 28,314 PNFP) were screened for TB. Of those that were
screened, 310 (0.8%) (Pre-ART 126 & ART 184) were diagnosed with TB. Of those that were
diagnosed with TB, 182 (58.7%) were started on TB treatment. Out of those started on treatment 180
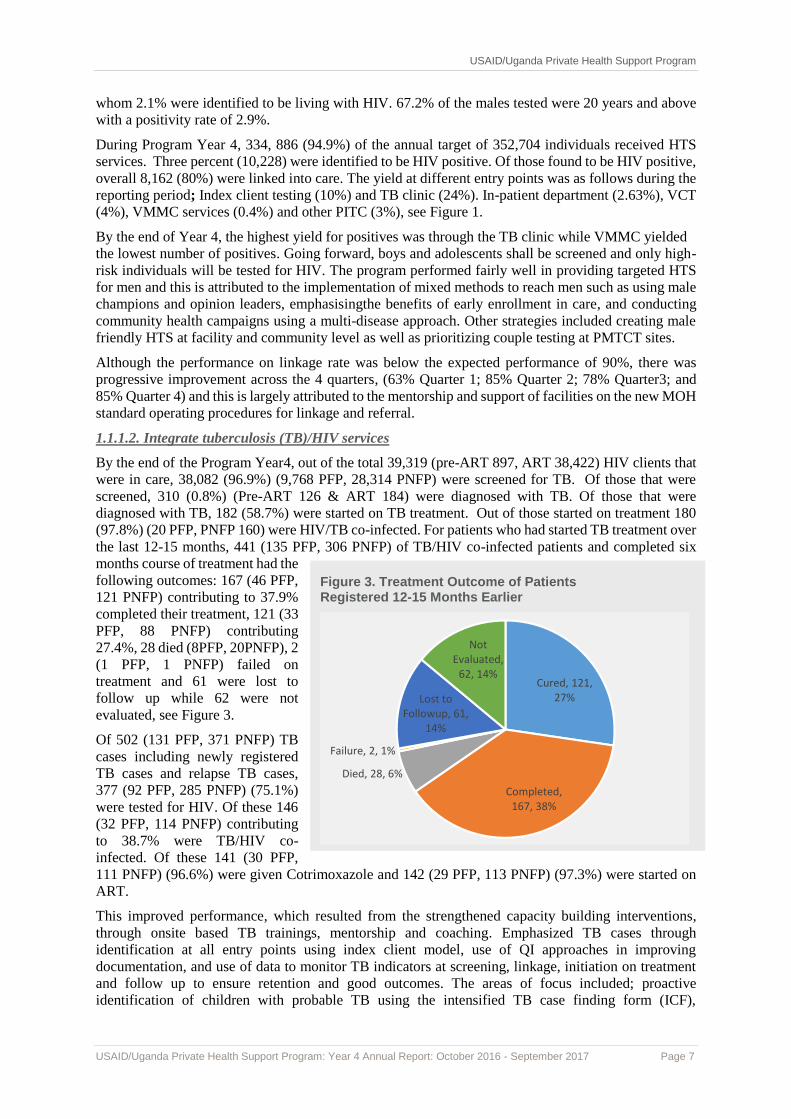
(97.8%) (20 PFP, PNFP 160) were HIV/TB co-infected. For patients who had started TB treatment over
the last 12-15 months, 441 (135 PFP, 306 PNFP) of TB/HIV co-infected patients and completed six
months course of treatment had the
following outcomes: 167 (46 PFP,
121 PNFP) contributing to 37.9%
completed their treatment, 121 (33
PFP, 88 PNFP) contributing
27.4%, 28 died (8PFP, 20PNFP), 2
(1 PFP, 1 PNFP) failed on
treatment and 61 were lost to
follow up while 62 were not
evaluated, see Figure 3.
Of 502 (131 PFP, 371 PNFP) TB
cases including newly registered
TB cases and relapse TB cases,
377 (92 PFP, 285 PNFP) (75.1%)
were tested for HIV. Of these 146
(32 PFP, 114 PNFP) contributing
to 38.7% were TB/HIV co-
infected. Of these 141 (30 PFP,
111 PNFP) (96.6%) were given Cotrimoxazole and 142 (29 PFP, 113 PNFP) (97.3%) were started on
ART.
This improved performance, which resulted from the strengthened capacity building interventions,
through onsite based TB trainings, mentorship and coaching. Emphasized TB cases through
identification at all entry points using index client model, use of QI approaches in improving
documentation, and use of data to monitor TB indicators at screening, linkage, initiation on treatment
and follow up to ensure retention and good outcomes. The areas of focus included; proactive
identification of children with probable TB using the intensified TB case finding form (ICF),
Figure 3. Treatment Outcome of Patients Registered 12-15 Months Earlier
Cured, 121, 27%
Completed, 167, 38%
Died, 28, 6%
Failure, 2, 1%
Lost to Followup, 61,
14%
Not Evaluated,
62, 14%
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 8
management of pediatric TB, use of Gene expert (indications, sample collection, packaging and
transportation and interpretation of results), infection prevention and control, HMIS support, and
facilities understanding the supply chain management for TB commodities. Engagement of District
TB/Leprosy focal persons (DTLS) improved access to anti-TB drugs and supplies and used gene Xpert
testing services through utilization of the hub system by Program supported private facilities.
Fewer cases of TB continue to be identified in the private sector due to a number of challenges
including: stock outs and inconsistency in the supply and access to Anti-TB drugs, Gene-Xpert
machines, and challenges with cartridges at the district hubs. Similarly, IPT coverage at the partner
health facilities was low due to insufficient stock of Isoniazid at the respective districts. Therefore,
children were being prioritized for IPT at most health facilities leaving out other eligible clients such as
those who completed TB treatment and newly TB diagnosed clients, which accounted for 17%
coverage.
In the Program Year 5, PHS will continue to work closely with NTLP, Regional and District TB and
Leprosy Supervisors (DTLS) to strengthen integration of TB services at all service delivery entry points.
Program will focus on the scale-up of TB intensified case finding, IPT accessibility, including capacity
building, infection prevention and control of TB and initiation of TB treatment for all confirmed cases.
All HIV positive clients will continue to be screened for TB at every ART clinic visit, and all TB
patients will be screened for HIV co-infection. They will be managed appropriately according to the
recommended guidelines. The program will support Health facilities in accessing Anti TB drugs,
including isoniazid for prophylaxis, reagents for ZN and facilitate the availability Gene-Xpert testing
for TB facilities at district hubs.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 9
1.1.1.3. Integrate voluntary medical male
circumcision (VMMC) services
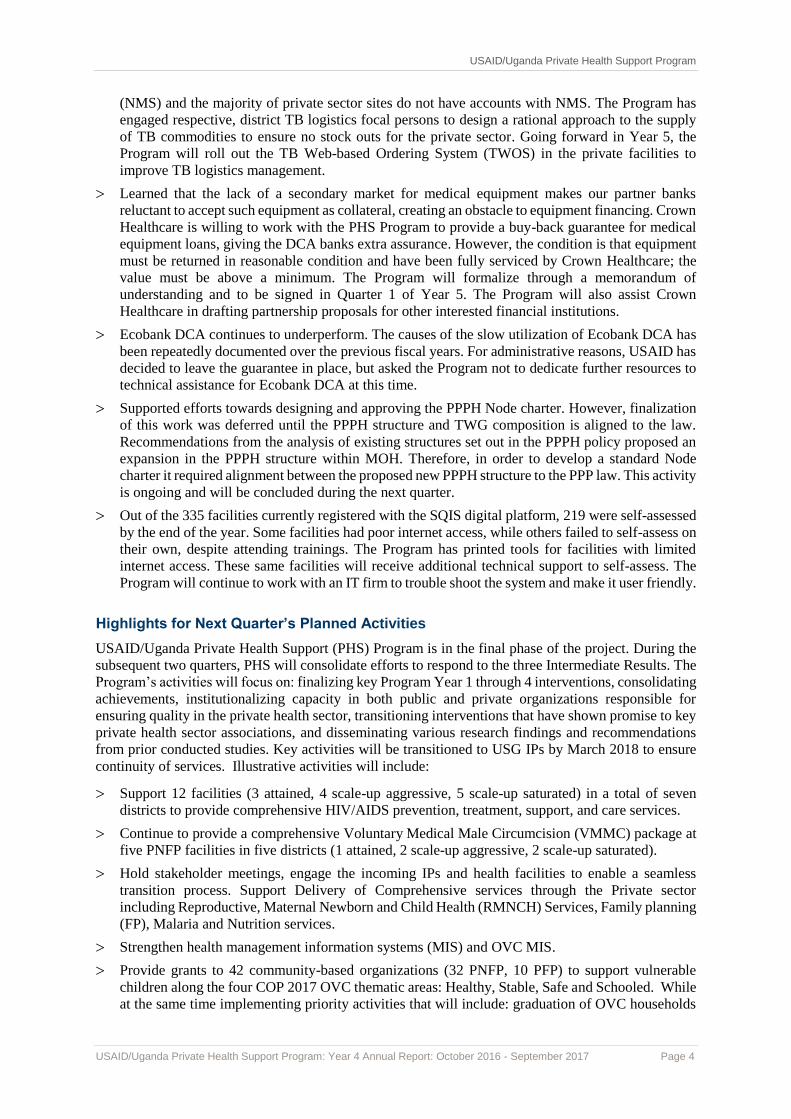
In Program Year 4, PHS supported 21
VMMC sites (11 PNFP and10 PFP) in 12
districts across the country. During the
Quarter 4, 16,525 males received TT and
were circumcised which is 151% of the
expected quarterly target (10,948). Of
these, 52% (8,616) are from the 15-29 age
group. A total of 51,730 men received TT
and were circumcised representing an
achievement of 114% of the annual target
(45,448). Of those circumcised, 28,229
(55%) were within the priority age pivot of
15-29. As part of VMMC services, HIV
testing was offered to the clients and a total
of 48,717 (96%) of males tested for HIV
and received results. Of those tested and
given results, 245 (0.5%) tested HIV
positive and were linked to care. A total of
2,308 men were not tested for HIV because
these were boys age 10-14 had low
exposure to HIV risk and when applied to
the eligibility screening tool, they were
found ineligible.
46,565 (91%) males were followed up
within 48 hours, 36,102 (71%) within 7
days, and 10,722 (21%) beyond 7 days.
The Program maintained good
performance on follow up rates especially
at 48 hours and 7 days and this was due to
intensified follow up by partner facilities.
The facilities sustained dedicated SMC
teams to conduct follow up in the
community and also emphasized to clients the benefits of returning post circumcision for review. In the
coming year, the program will continue to focus on improving performance for beyond 7 days follow
up through implementation of innovative strategies such as working with mobilisers to follow up with
clients until the completion of SMC cascade and use of phone calls.
Results from follow up indicate that 271 advance events (AEs) were encountered of which 261 were
moderate and 10 were severe and were all post-operative and managed successfully. The 10 severe
advance events were encountered at Ishaka Adventist hospital (1), Mengo hospital (3), Span Medicare
(3), Kiko HC III (1) and Kisiizi hospital (2). They comprised of excessive bleeding, identified post-
operatively and controlled during exploration, excessive hematoma that required surgical re-
exploration, anaphylaxis to local anesthetic agent, and infection that required intramuscular antibiotic
therapy. The Program will continue to support facilities to reduce adverse events (AE) through
intensified post circumcision client follow up and to manage mild AEs before they develop into
moderate AEs, and conducting regular AE audits to establish likely factors responsible for the AE
occurrences.
PHS performed well during the year surpassing Country Operational Plan 2016 (COP 16) targets. This
is attributed to Program intensifying follow up and circumcising clients that had initially received TT1
but had not returned. Other strategies implemented included reassessing and determining individualized
VMMC site capacity against performance and putting in place tailored mechanisms that enabled sites
to achieve high results. Strategies included mobilization through radio programs, peer-to-peer
Figure 4. VMMC Services
57238,302
20475
16,525
11,362 13,242
15,712
10,948
0
5000
10000
15000
20000
25000
QTR1 QTR 2 QTR 3 QTR 4NO
OF
MA
LES
CIR
CU
MC
ISED
SMC QUARTELY TARGETS AND OUTPUTS
VMMC OUTPUTS
Clients circucmcised per Qtr Quartely target
5,420
14,613
35,205
51,730
11,362
22,724
34,086
45,448
OCT-DEC 16 JAN-MAR 17 APR-JUNE 17 JULY-SEPT 17
VMMC OUTPUTS OCT 16-SEPT 2017
Clients Circumcized Total Target

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 10
mobilization especially for the older boys and using role models in the community as champions for
circumcision were employed. PHS continued to conduct continuous quality improvement approaches
and provided onsite coaching and mentorship at all private sector VMMC sites. This was coupled with
routine data validation activities and results indicate that the data reported was of good quality. Through
AIDSFree, the Program continued to work with Green Label waste management company and the SMC
waste was adequately managed.
1.1.1.4. Provide family planning (FP) services
The Program continued to support 62 facilities (47 PFP, 15 PNFP) to provide family planning (FP)
services. Through capacity building of health workers (training, mentorship, and coaching), provision
of family planning (FP) commodities and data management tools, private health facilities provided FP
services at both PNFP and PFP sites. Health workers were mentored to integrate FP into other existing
services like HIV/ART clinics, VMMC in addition to the traditional MNCH services and emphasis put
on FP, prong 2 (eMTCT) in preventing unwanted pregnancy among women living with HIV.
As a result of the above support, in Quarter 4, a total of 8,643 new acceptors (7,353 PFP, 1,290 PNFP)
accessed FP services translating into 24,695 (82.3%) new acceptors of the annual target during program
year 4. Higher number of attendance at the PFP sites points to the flexible working hours, availability
of method mix at the facilities, skilled personnel and willingness of the service providers to provide
modern methods of contraception. During the reporting period, of all new acceptors, 17.6% were
adolescents 10-19 years old, 41.0% were 20-24 years old, and 41.4% ≥ 25 years old. 7,423 (6,621 PFP,
802 PNFP) individuals returned for revisit/supply visit. Of the new acceptors, a total of 2,596 (1785
PFP, 811 PNFP) received long-acting reversible contraceptives (IUD’s and Implanon) and 105
individuals received permanent contraception (Bilateral tubal ligation) which was higher 31%
compared to 11% in the previous quarter. 80.3% (57/71) of the targeted service delivery points offered
family planning services by the end of Quarter 4. 300 (177 PFP, 123 PNFP) new users were HIV
positive. Over the year, performance verses target is as shown in the Figure 5 below.
Figure 5. Family Planning Uptake
3581
6,5885,883
86437500 7500 7500 7500
OCT-DEC 16 JAN-MAR 17 APR-JUNE 17 JULY-SEPT 17
# o
f n
ew
FP
acc
ep
tors
Time
FP uptake
New FP acceptors Total Target
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 11
In line with MOH national Implementation
Plan for LARC/PMs (2017-2020) strategic
objectives, in Quarter 4 the Program set out
to address skills gap among health workers
in providing long-term reversible
contraceptives including PPIUD. The
increase in the number of LARC and
permanent methods noted in Quarter 4, is
attributable to 10 day simulation and
practicum training in LARC and PM that
was carried out. 245 health workers were
trained from at least 46 private health
facilities. Medical Eligibility Criteria
(MEC) wheels to support health workers in
selecting the best family planning choice
based on pre-existing medical conditions
were provided to each participant.
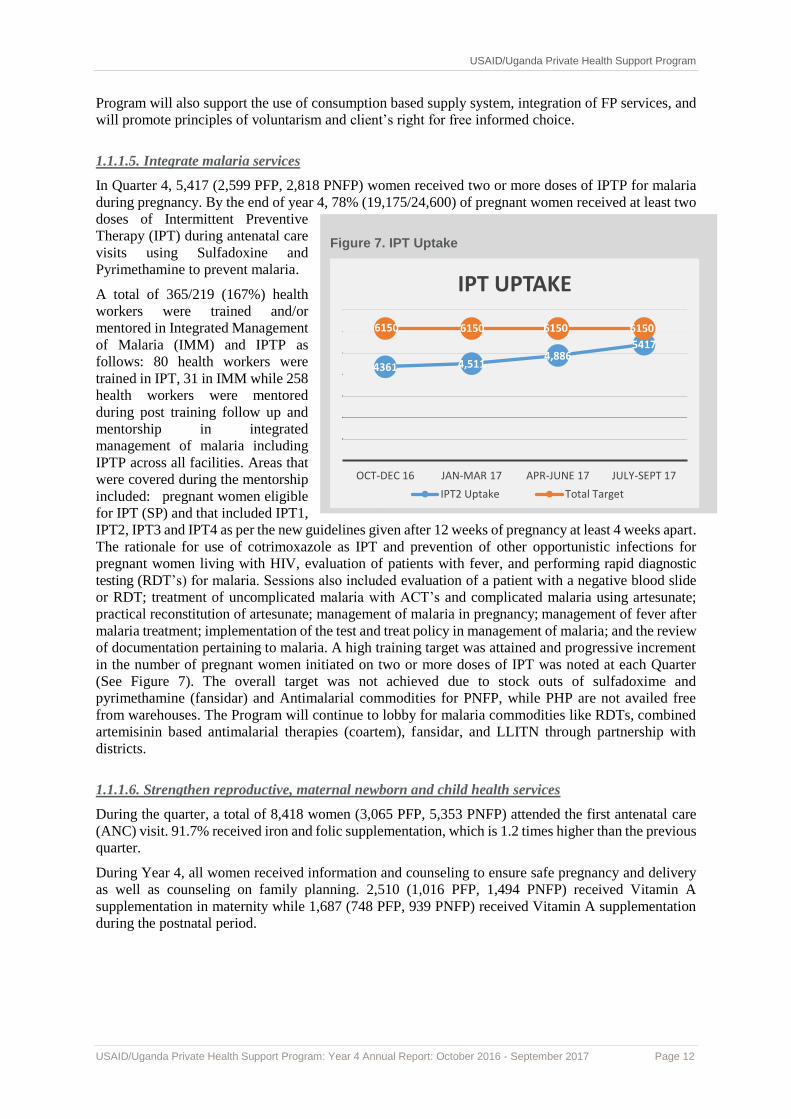
During the training, participants conducted
a total number of 1,711 procedures as a
part of the practicum. Figure 6 below
shows the number of FP methods and
procedures done by type. Participating
health facilities were provided with some
equipment for IUD insertion, implant
removal, vasectomy sets, and BTL sets,
comprehensive family planning manuals to
support service delivery, and CPDs upon
return to their facilities
Figure 6. FP Methods and Procedures by Trainees
Going forward, in order to improve access to quality of FP services, PHS will strengthen the skills of
health workers in long term/permanent methods of FP through facility based post-training follow up
and mentorship, and provision of FP commodities and supplies in partnership with UHMG. The
420
565
377
216
129
4
IUD Insertion
Implanon Insertion
Jadelle Insertion
Implant removal
IUD removal
BTL
0 100 200 300 400 500 600
Number of different FP methods and procedures done by trainees during field practicuum
Medical officers training in LARC/PM.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 12
Program will also support the use of consumption based supply system, integration of FP services, and
will promote principles of voluntarism and client’s right for free informed choice.
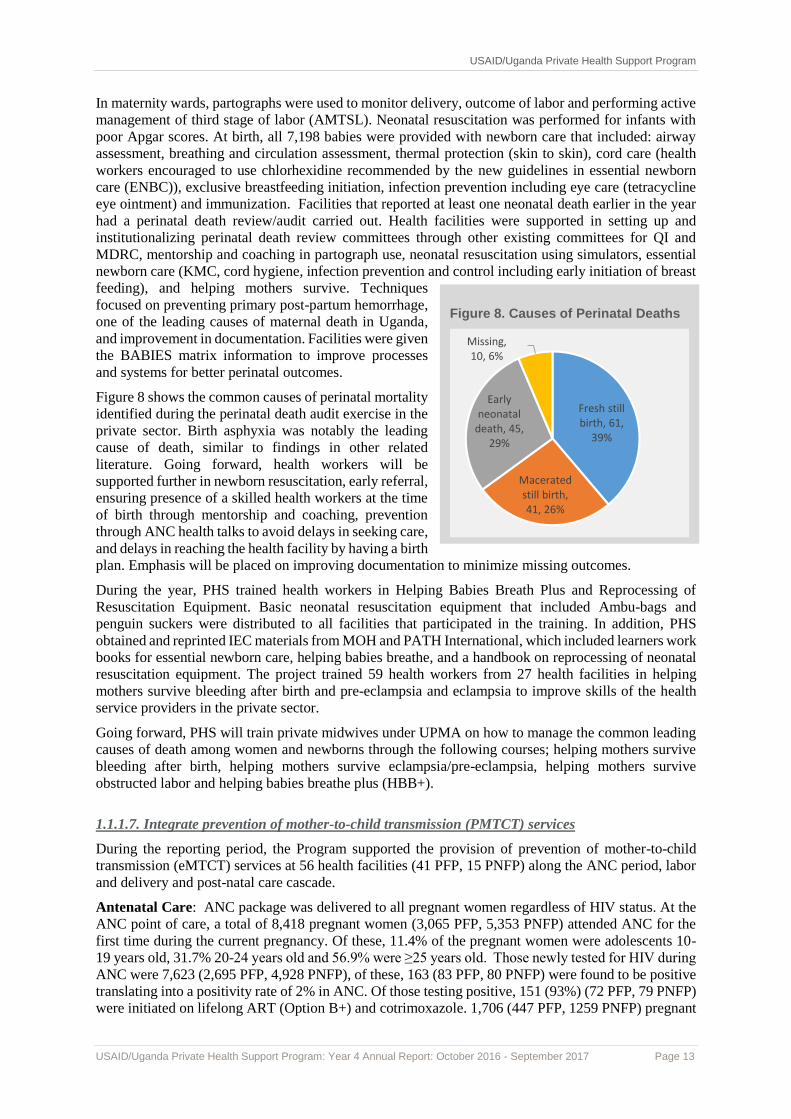
1.1.1.5. Integrate malaria services
In Quarter 4, 5,417 (2,599 PFP, 2,818 PNFP) women received two or more doses of IPTP for malaria
during pregnancy. By the end of year 4, 78% (19,175/24,600) of pregnant women received at least two
doses of Intermittent Preventive
Therapy (IPT) during antenatal care
visits using Sulfadoxine and
Pyrimethamine to prevent malaria.
A total of 365/219 (167%) health
workers were trained and/or
mentored in Integrated Management
of Malaria (IMM) and IPTP as
follows: 80 health workers were
trained in IPT, 31 in IMM while 258
health workers were mentored
during post training follow up and
mentorship in integrated
management of malaria including
IPTP across all facilities. Areas that
were covered during the mentorship
included: pregnant women eligible
for IPT (SP) and that included IPT1,
IPT2, IPT3 and IPT4 as per the new guidelines given after 12 weeks of pregnancy at least 4 weeks apart.
The rationale for use of cotrimoxazole as IPT and prevention of other opportunistic infections for
pregnant women living with HIV, evaluation of patients with fever, and performing rapid diagnostic
testing (RDT’s) for malaria. Sessions also included evaluation of a patient with a negative blood slide
or RDT; treatment of uncomplicated malaria with ACT’s and complicated malaria using artesunate;
practical reconstitution of artesunate; management of malaria in pregnancy; management of fever after
malaria treatment; implementation of the test and treat policy in management of malaria; and the review
of documentation pertaining to malaria. A high training target was attained and progressive increment
in the number of pregnant women initiated on two or more doses of IPT was noted at each Quarter
(See Figure 7). The overall target was not achieved due to stock outs of sulfadoxime and
pyrimethamine (fansidar) and Antimalarial commodities for PNFP, while PHP are not availed free
from warehouses. The Program will continue to lobby for malaria commodities like RDTs, combined
artemisinin based antimalarial therapies (coartem), fansidar, and LLITN through partnership with
districts.
1.1.1.6. Strengthen reproductive, maternal newborn and child health services
During the quarter, a total of 8,418 women (3,065 PFP, 5,353 PNFP) attended the first antenatal care
(ANC) visit. 91.7% received iron and folic supplementation, which is 1.2 times higher than the previous
quarter.
During Year 4, all women received information and counseling to ensure safe pregnancy and delivery
as well as counseling on family planning. 2,510 (1,016 PFP, 1,494 PNFP) received Vitamin A
supplementation in maternity while 1,687 (748 PFP, 939 PNFP) received Vitamin A supplementation
during the postnatal period.
Figure 7. IPT Uptake
4361 4,5114,886
5417
6150 6150 6150 6150
OCT-DEC 16 JAN-MAR 17 APR-JUNE 17 JULY-SEPT 17
IPT UPTAKE
IPT2 Uptake Total Target
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 13
In maternity wards, partographs were used to monitor delivery, outcome of labor and performing active
management of third stage of labor (AMTSL). Neonatal resuscitation was performed for infants with
poor Apgar scores. At birth, all 7,198 babies were provided with newborn care that included: airway
assessment, breathing and circulation assessment, thermal protection (skin to skin), cord care (health
workers encouraged to use chlorhexidine recommended by the new guidelines in essential newborn
care (ENBC)), exclusive breastfeeding initiation, infection prevention including eye care (tetracycline
eye ointment) and immunization. Facilities that reported at least one neonatal death earlier in the year
had a perinatal death review/audit carried out. Health facilities were supported in setting up and
institutionalizing perinatal death review committees through other existing committees for QI and
MDRC, mentorship and coaching in partograph use, neonatal resuscitation using simulators, essential
newborn care (KMC, cord hygiene, infection prevention and control including early initiation of breast
feeding), and helping mothers survive. Techniques
focused on preventing primary post-partum hemorrhage,
one of the leading causes of maternal death in Uganda,
and improvement in documentation. Facilities were given
the BABIES matrix information to improve processes
and systems for better perinatal outcomes.
Figure 8 shows the common causes of perinatal mortality
identified during the perinatal death audit exercise in the
private sector. Birth asphyxia was notably the leading
cause of death, similar to findings in other related
literature. Going forward, health workers will be
supported further in newborn resuscitation, early referral,
ensuring presence of a skilled health workers at the time
of birth through mentorship and coaching, prevention
through ANC health talks to avoid delays in seeking care,
and delays in reaching the health facility by having a birth
plan. Emphasis will be placed on improving documentation to minimize missing outcomes.
During the year, PHS trained health workers in Helping Babies Breath Plus and Reprocessing of
Resuscitation Equipment. Basic neonatal resuscitation equipment that included Ambu-bags and
penguin suckers were distributed to all facilities that participated in the training. In addition, PHS
obtained and reprinted IEC materials from MOH and PATH International, which included learners work
books for essential newborn care, helping babies breathe, and a handbook on reprocessing of neonatal
resuscitation equipment. The project trained 59 health workers from 27 health facilities in helping
mothers survive bleeding after birth and pre-eclampsia and eclampsia to improve skills of the health
service providers in the private sector.
Going forward, PHS will train private midwives under UPMA on how to manage the common leading
causes of death among women and newborns through the following courses; helping mothers survive
bleeding after birth, helping mothers survive eclampsia/pre-eclampsia, helping mothers survive
obstructed labor and helping babies breathe plus (HBB+).
1.1.1.7. Integrate prevention of mother-to-child transmission (PMTCT) services
During the reporting period, the Program supported the provision of prevention of mother-to-child
transmission (eMTCT) services at 56 health facilities (41 PFP, 15 PNFP) along the ANC period, labor
and delivery and post-natal care cascade.
Antenatal Care: ANC package was delivered to all pregnant women regardless of HIV status. At the
ANC point of care, a total of 8,418 pregnant women (3,065 PFP, 5,353 PNFP) attended ANC for the
first time during the current pregnancy. Of these, 11.4% of the pregnant women were adolescents 10-
19 years old, 31.7% 20-24 years old and 56.9% were ≥25 years old. Those newly tested for HIV during
ANC were 7,623 (2,695 PFP, 4,928 PNFP), of these, 163 (83 PFP, 80 PNFP) were found to be positive
translating into a positivity rate of 2% in ANC. Of those testing positive, 151 (93%) (72 PFP, 79 PNFP)
were initiated on lifelong ART (Option B+) and cotrimoxazole. 1,706 (447 PFP, 1259 PNFP) pregnant
Figure 8. Causes of Perinatal Deaths
Fresh still birth, 61,
39%
Macerated still birth, 41, 26%
Early neonatal
death, 45, 29%
Missing, 10, 6%

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 14
women were re-tested for HIV during subsequent ANC visits, of these, 57 pregnant women were found
to be positive translating into 3.3% of women testing HIV positive.
Maternity: In Quarter 4 7,198 (2,279 PFP, 4919 PNFP) deliveries were conducted across program
supported facilities. 12.7% of deliveries were to adolescents 10-19 years old, 30.0% to 20-24 years old
and 56.3% of the deliveries were to ≥25 years old. Those newly tested for HIV during labor and delivery
were 828 (310 PFP, 518 PNFP), of these, 21 (5 PFP, 16 PNFP) were found to be positive. Re-testers
were 1,773 (497 PFP, 1,276 PNFP). Of those re-testing during labor and delivery, 30 (14 PFP, 16 PNFP)
were found to be positive. A total of 51 (19 PFP, 32 PNFP) women were found to be positive during
labor and delivery and only 17 were initiated on ART. This is attributed to denial to accept results during
this period and loss to follow up upon discharge.
Postnatal Care: 8,857 women attended post-natal clinic (2,388 PFP, 6,469 PNFP). 10% of women
attending post-natal clinic were adolescents 10-19 years old, 32.5% were 20-24 years old and 57.4% of
these were ≥25 years old. Those newly diagnosed with HIV during postnatal care were 22 (2 PFP, 20
PNFP). 13 (0 PFP, 13 PNFP) tested positive on a retest. 35 tested positive, 26 were initiated on ART.
Early Infant Diagnosis: During the quarter, 876 (259 PFP, 617 PNFP) HIV exposed infants (HEI)
received DNA PCR testing using dry blood spots at Program supported facilities (1st DNA 525 (167
PFP, 358 PNFP), 2nd DNA PCR 351 (92 PFP, 259 PNFP). Through the hub system, samples are sent to
Uganda National Health Laboratory Services (UNHLS) for testing and sent back to the facilities. Of the
samples that were sent to UNHLS, for 1st DNA PCR, 58 % were drawn from children < two months of
age, an improvement from the previous quarter (48.2%). Of the samples dispatched, 61.2% were
returned to the sending facilities. During the quarter, a number of facilities reported challenges with
non-return of results up to a period of 4 months, which was reported by Kisiizi Hospital. Of all the
returned results 14 babies were found to be positive, 1st DNA PCR 9 (1 PFP, 8 PNFP) and 2nd DNA
PCR 5 (4 PFP, 1 PNFP) yielding a MTCT rate of 4% across facilities.
At 18 months of age, 264 HEI (38 PFP, 226 PNFP) had a rapid HIV confirmatory test done, 4 HEI were
found to be positive during the quarter (3 PFP, 1 PNFP) while 260 HEI were discharged with negative
results. During the reporting period, 379 HEI (78 PFP, 301 PNFP) were initiated on Cotrimoxazole,
287 (65 PFP, 222 PNFP) 75.7% of whom were initiated at less than two months of age.
In Quarter 4, 29 health workers from 18 health facilities were trained in elimination of mother-to-child
HIV transmission course (eMTCT) that covered
the following areas: chronic care, including
ART to HIV infected pregnant and lactating
women, care and treatment for HIV exposed and
infected infants and children; management of
logistics for implementation of Option B+ at the
facility; correct documentation and submission
of PMTCT Option B+ reports; and
demonstrated to participants the rationale for
HIV Exposed Infant (HEI. Conducted eMTCT
cohort monitoring, analysis, and utilization of
cohort data to enhance quality delivery of HEI
and eMTCT program. Inset is a group
discussion during eMTCT course during which
participants had a hands-on data abstraction and
cohort analysis of HEI data.
Going forward, efforts will be made to support
health workers improve on identification of HEI, and removal of samples and dispatch to UNHLS to
reduce sample rejection. The Program will also work with MOH UNHLS to improve on the TAT of
results. In line with COP17 and the 90-90-90 targets, PHS will focus to reach all pregnant and
breastfeeding women, initiate them on lifelong ART (Option B+), and improve mother baby care
retention with good outcomes.
PMTCT training for health workers

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 15
1.1.1.8. Strengthen access to essential medicines, test kits and supplies
PHS conducted logistics supportive supervision, performance assessment and mentoring of health
facility staff in 71 sites. The Program reviewed the ordering, storage, distribution and dispensing
practices at each of the facilities and reviewed electronic copies of facility ARV orders over the last two
quarters to determine their completeness, correctness of submitted information and adherence to current
guidelines when enrolling new clients. During these visits gaps in the management of commodities were
identified and together with facility personnel solutions were derived and improvement targets set.
Some of the gaps identified included: poor coordination in the supply of TT vaccines, TB and FP which
caused frequent stock outs especially of TB commodities and excess stocks especially of FP
commodities at the facilities, inappropriate storage practices, inadequate space particularly in PFP sites
and lack of skills amongst health workers for appropriate stock control and logistics management, no
use of stock books even when available and a number of sites did not have direct access to DHIS 2.
Hence, sent and scanned copies of orders to JMS inceased the probability of error and delays in
submission of orders. Strengths noted include facilities had the knowledge and skills to determine which
medicines to order using the dispensing logs, and had access to computers and connectivity.
Going forward, the Program has put in place a number of interventions including: supervision, and
performance assessment and mentoring approach to improve logistics indicators. The approach will
involve quarterly visits to assess logistics indicators with identification of gaps and challenges which
will be addressed through managerial and educational strategies. Ongoing job mentorship and coaching
will continue to be carried out to address the identified gaps. The Program procured and distributed
cabinets for 10 PFPs that were constrained by storage space. In addition, standard operating procedures
were printed and distributed to staff for future reference, while performing their logistics function.
Subsequent follow up of supported facilities will monitor progress on set indicators.
Roll out of the Web Based ARV Ordering Systems (WAOS): The program further worked with JMS to
support the acquisition of user rights and conducted on-the-job training for all staff involved in the
ordering of ARVs using the WAOS. Currently all sites have been given WAOS user rights and it is
expected that in the coming ordering cycle they will directly input their orders into DHIS 2. This will
reduce delays in entering orders into DHIS 2 and the web-based system will help highlight and correct
obvious errors in filling order forms before they are sent to the warehouse.
Streamlining TB Supply Chain Systems: The Program noted that TB medicines and supplies were the
most frequently stocked out items in the private sector. The main cause of this is the uncoordinated
ordering and supply systems which do not prioritize the private sector. The Program has continued to
advocate for a more streamlined supply system for TB medicines in the PNFP and PFP sectors. At
medicine procurement and supply chain TWG meetings, the problem of frequent stock out of TB
A before and after picture of ARVs storage at Chandaria Medical Clinic. To the left is part of the lab cupboard within the laboratory being used used to keep ARVs. To the right is the new cabinet

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 16
medicines will be addressed. There are also plans to support sites to access the TB web-based ordering
system in order to create awareness of the demand of these commodities in the private sector.
During the reporting period, PHS worked with the warehouses, Ministry of Health (NTLP, UNHLS,
ACP) to ensure a stable and constant supply of ARV’s, test kits, SMC kits and related supplies and FP
commodities medicines to minimize stock outs and reduce the risks of disrupting service delivery due
to stock outs during PHS transition process. PHS developed a warehousing and distribution system to
hold the excess stock and supplies them to the sites on a bi-monthly order and delivery schedule to
prevent expiration and pilferage.
In order to improve hygiene, Program is addressing challenges in handling waste and improving
infection prevention and control. The program procured and distributed 90 heavy duty bins and 201
hand washing stations to all sites.
1.1.1.9. Strengthen blood safety, injection safety and health care waste management
At the beginning of Year 4, the Program developed an environmental mitigation monitoring plan to
ensure safe disposal of healthcare waste in order to not negatively affect aquatic and terrestrial fauna,
flora, human health, and water sources during the delivery of integrated comprehensive health services.
By the end of the year, the Program had conducted a training of 35 health workers from 25 health
facilities in 14 districts. During this training, health workers were equipped with knowledge and skills
in healthcare waste management, sharps/injection and blood safety to improve management of
healthcare waste at Program supported health facilities. During the training, trainees developed a
healthcare waste management plan, observed safe disposal of injection/sharps, learned about blood
safety, and how to separate, transport, and dispose of waste according to the recommended guidelines.
In addition, hand washing and personal protective equipment demonstrations were conducted. As part
of integrated facility based mentorship activities, facilities will continue to be supported in
implementing their healthcare waste management plan once developed, infection and prevention
practices at the different service delivery points and implementation of 5S as a QI tool.
In addition, during the year, 31 laboratory staff and 16 laboratory/facility support staff involved in health
care waste management (Cleaners and Courier) from selected health facilities attended a five day
training in Biosafety. The overall aim for this training was to impart skills and knowledge in bio risk
and biosafety management to enable behavioural change and attitude towards health facility in risk
reduction measures and security. A facility based post training follow up and mentorship was conducted
for all health workers, reaching 102 health workers during that period.
Trainer guiding participants on how to don and doff PPE. On the right an ongoing biosafety course at Infectious Diseases Institute

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 17
1.1.1.10. Strengthen comprehensive HIV/AIDS services for children and adolescents
During the reporting period, 11,585 children <15 year were tested for HIV, 90 (0.8%) were found to be
positive and out of these 81 (90%) were linked and enrolled in care. In total 2,093 (636 PFP, 1,457
PNFP) children < 15 years are in care.
In PY4, Program in collaboration with the
MOH conducted adolescent HIV care,
treatment and trainings, reaching 76 health
workers in 36 health facilities. The
training aimed at enhancing health care
providers’ knowledge, skills, attitudes and
general competencies to provide quality
and comprehensive HIV care, treatment
and support services to adolescents living
with HIV. Healthcare providers were
trained to counsel and provide
psychosocial support, HIV care &
treatment and identify, link and refer
adolescents for comprehensive care and
support. Desk Job aids were provided,
including supported sites, to establish
adolescent friendly corners, especially in
high volume sites.
Post training follow up mentorship
and coaching were conducted for
pediatrics and Adolescent PITC at
the supported health facilities,
focusing on the strengthening
integration of adolescent services at
all entry points, identification of
HIV positive children and
adolescents and linking them to care
and treatment. Emphasis was placed
on high yield entry point testing, use
of the screening tool to identify
high-risk children particularly in
OPD, implementation of the Know
Your Child Status Days, use of the
family tracking tool to identify
positive children of index clients, providing age appropriate counselling and service delivery in friendly
settings. Adolescent index client model was emphasized to track and identify those that missed
enrollment into care. The Program supported health facilities to make use of adolescent HIV data
through analysis of viral load test data to identify challenges of unsuppressed viral load and work with
the adolescent peer groups, care takers, guardians and parents to support tracking for retention in care
and adherence to HAART to achieve viral suppression.
1.1.1.11. Strengthen care and treatment of identified HIV positive clients in the private sector
During the reporting period, a total of 39,319 (11,494 PFP 27,825 PNFP) PLHIV were active in care
(Pre-897, ART-38,422) translating into 97.8% of PLHIV on ART. Of those in care, 37,356 (9,647 PFP,
27,709 PNFP) received cotrimoxazole or dapsone for prophylaxis.
The Program enrolled 1,318 (488 PFP, 830 PNFP) new PLHIV into care. Of these 1,105 (428 PFP, 677
PNFP) (83.8%) of these received cotrimoxazole and dapsone for prophylaxis. 1,989 new clients were
initiated on ART ( 661 PFP, 1328 PNFP) with the new test and treat policy explaining the high number
HIV positive children in session at St. Francis-Buluba
Trainees' practicum at Jinja RRH Adolescent Clinic and TASO Jinja
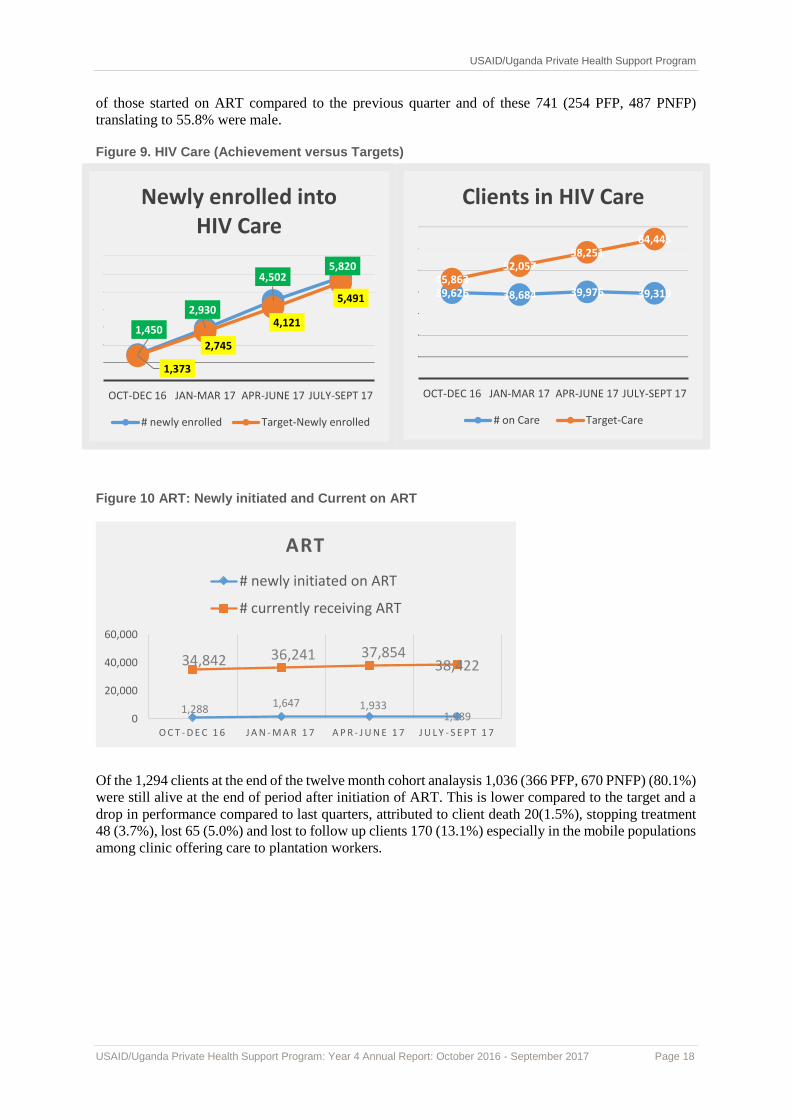
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 18
of those started on ART compared to the previous quarter and of these 741 (254 PFP, 487 PNFP)
translating to 55.8% were male.
Figure 9. HIV Care (Achievement versus Targets)
Figure 10 ART: Newly initiated and Current on ART
Of the 1,294 clients at the end of the twelve month cohort analaysis 1,036 (366 PFP, 670 PNFP) (80.1%)
were still alive at the end of period after initiation of ART. This is lower compared to the target and a
drop in performance compared to last quarters, attributed to client death 20(1.5%), stopping treatment
48 (3.7%), lost 65 (5.0%) and lost to follow up clients 170 (13.1%) especially in the mobile populations
among clinic offering care to plantation workers.
1,450
2,930
4,5025,820
1,373
2,745
4,121
5,491
OCT-DEC 16 JAN-MAR 17 APR-JUNE 17 JULY-SEPT 17
Newly enrolled into HIV Care
# newly enrolled Target-Newly enrolled
39,626 38,684 39,976 39,31945,863
52,05758,251
64,445
OCT-DEC 16 JAN-MAR 17 APR-JUNE 17 JULY-SEPT 17
Clients in HIV Care
# on Care Target-Care
1,2881,647 1,933
1,989
34,842 36,241 37,85438,422
0
20,000
40,000
60,000
O C T - D E C 1 6 J A N - M A R 1 7 A P R - J U N E 1 7 J U L Y - S E P T 1 7
ART
# newly initiated on ART
# currently receiving ART

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 19
The Program conducted onsite based rollout
trainings of the revised consolidated HIV
guideliens 2016 for HIV prevention and
treatment in the 57 (80.3%) out of 71 facilities
reaching 1,258 health workers. The health
facilities also received the job aids on
consolidated guidelines and during the training
were supported in the ordering of LPR/r pellets
for children under 3 years of age as per
guidelines.
In year 5, the Program will complete the
facilitty based trainings for remaining 14
(19.7%) facilities and will conduct follow up
assessment and mentorship in all the 71 health
facilities. Thereafter the Program will continue
to support comprehensive HIV ART follow up mentorship and coaching in 12 health facilities to ensure
all pre-ART clients are initiated on ART, viral load monitoring carried out, follow up and retention of
all clients including mother-baby pairs.
1.1.1.12. Strengthen laboratory and viral load monitoring for sustained viral load testing and viral
suppression
With support from the MOH Central Public Health Laboratory (CPHL) and in partnership with districts
through engagement and working closely with District Laboratory Focal Persons (DLFPs), all PHS
supported sites offering ART services were linked to the hub system to improve laboratory testing and
monitoring among PHLIV. Health facilities trained in viral load monitoring during year 4 have been
supported by availing viral load test kits, viral load laboratory request forms, dispatch envelopes and
supported on sample packaging and transportation through the hub system to maintain the integrity of
samples during the sample transportation process and avoid sample rejection at the hub. As a result of
the above support in Quarter 4, samples that were collected from Program supported private health
facilities had a rejection rate of 1.98%,, 5721 of clients on ART received a viral load test of whom
91.3% showed evidence viral suppression with viral copies of <1000 copies per ml. During the year,
PHS had a total of 38,422 PLHIV on ART, 22884 had a viral load done, with 91.5% had virological
suppression. Distribution by age and gender during the annual period < 15years (males 75.3%, females
80.1%) while those > 15 years had suppression rates (91.6% males, 92.1% females)
Despite progress over time, VL monitoring was affected by long turnaround time (TAT) of test results
and non-return of test results. Other limitations included failure of hub riders to pick up viral load
samples, and limited knowledge/skills of health workers in supporting non-virally suppressed clients
with intensive adherence counselling as well as facilities not ordering test kits directly from UNHLS,
which is encouraged, for purposes of sustainability. Capacity building efforts to improve on laboratory
quality service delivery have been carried out such as laboratory quality management improvement
system, laboratory logistics management, and bio risk and biosafety course for technical and support
staff aimed at reducing risk in the lab and improving efficiency.
Going forward, roll out of the revised 2016 HIV consolidated guidelines and mentorship will enable
health workers implement changes in the guidelines like test and treat strategy and intensive adherence
counselling that aim at increasing both coverage and suppression. PHS will continue working with the
districts through the DLFPs, CPHL, and avail new MOH tools like the VL suppression register, and
implement the scale up package aimed at improving coverage.
Trainees watching the LPV/r pellet video at FHRC -Kiruhura

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 20
1.1.1.13. Strengthen nutrition assessment counselling and support (NACS) and support for
nutrition through the first 1,000 days
Integrated nutritional assessment counseling and support (NACS) continued to be part of routine
services in HIVART care accorss all Program health facilities. During the reporting period, the Program
supported trainings and mentorship to strengthen integration of nutrition services in the 17 PNFP health
facilities. A total of 34 frontline health workers were trained in NACS, health facilities were supplied
with nutrition job aides, equipment for basic anthropomentric measurements like mid upper arm
circumference tapes of all age ranges, revised and updated MOH nutrition data collection and reporting
tools. Post training follow up mentorship, coaching, supporting linkage and referral of malnuourished
clients to health facilities that access ready to use therapautic feeds (RUTF) in other regional activated
and accredited RUTF sites like regional referral hospitals and district based hospitals.
Integrated nutrition mentorship and coaching as part of routine health facility techncial support
strengthened health workers knowledge and skills to routinely screen, assess, link, document and report
clients reached with nutrition services. Task shifting and multi tasking was emphasized so as to
strengthen integration of nutrition services at all entry points like OPD, YCC, MCH and TB and
HIV/ART clinics. Health facilities were supported to include QI nutrition indicators to monitor changes
in nutrition assessment, counselling and support including linkage to therapeutic feeds.
During the reporting period, a total of 54,070 (36,273 ART clients and 17,797 non –ART clients at
OPD) were assessed for nutritional status using color coded MUAC tapes and Height/Length for age
z-scores. Of these 948 ( 221 PFP, 727 PNFP) translating into 1.8% were found to be malnourished. Of
these, 132 (14%) with moderate acute malnutrition (MAM), 284 (30%) had acute malnutrition without
odema (SAM) while 39 (4%) had severe acute malnutrition with odema. The newly malnourished cases
were 378, and of these 156 ( 41.3%) were HIV positive. 430 of the total malnourished cases received
nutrition supplements and therapeutic feeds through site based nutrition units or referral to other
nutrition centres. Out of those who received thereapeatic feeds 142 ( 33%) were HIV positive. In
addition 2,526 pregnant and lactating mother were reached with maternal nutrition counseling and out
of theses 216 (8.5%) were HIV positive and 2,659 received infant feeding counselling of which 150
(5.6%) were HIV positive. During the reporting period 131 HIV exposed infants exclusively breastfed
for 6 months, 90 (68.7%) infants breastfed up to 1 year.
However, full integration of NACS services across all entry points and health facilities remained
inadequate due to lack of well caliberated weighing scales, lack of height boards and infatometer, lack
of access to thereaupeutic foods, weak referral and linkage systems to public health facilities, and lack
of affordable transport for the referred clients. Community nutrition approaches have also not been well
integrated as a way to use positive deviation in addressing malnutrition through intra-housed learning
and farming to improve household food and nutrition security.
In PY5, the Program will continue to promote task shifting and encouraging multi-tasking through
mentorship, coaching and supporting monthly CMEs to improve health workers appreciation and
understanding NACS. Use of nutrition tools and data, strengthen collaborative linkage and referral with
other nutrition centers like referral hospital and district thereapeutic hospitals and HCIVs, improving
documentation, reporting and data use will be used to improve nutrion services. For community
nutrition, the Program will to train community nutrition workers and nutrition mother mentors to
support community nutrition education, community food nutrition garden and preperation, assessment
and referral of malnuourished to nutrition center, and positive deviant homes or nutrition mother
mentors.
1.1.1.14. Quality improvement interventions
In PY4, the Program continued to conduct monthly QI mentorship and coaching to strengthen the
functionality of health facility Quality Improvement Teams (QITs) and Work Improvement teams
(WITs) in all the Program ART and VMMC sites. In coordination with USAID/ASSIST, PHS continued
to engage national, regional, and district based QI coaches to support integration and scale up of quality
improvement interventions to supported sites. In partnership with the Program, USAID ASSIST

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 21
continued to support monthly onsite VMMC QI mentorship and coaching in 9 health facilities and the
Program scaled up the best QI practices across all other 13 VMMC implementing health facilities.
However, the challenges of the national, regional and districts QI coaches not accepting the preferred
mode of support as per the USAID Local Development Partner Group schedule of allowances (2017),
the Program innovatively came up with mechanism to support continuity in strengthening the scale up
integration of QI approaches across all Program partners and health facilities. These approaches
included training Program staff and Research Assistant in QI, SQIS and SIMS and also soliciting a
competent registered consultancy firm to support the Program techncial team.
During the reporting period, the Program in collaboration with USAID/ASSIST and MOH organised
VMMC QI experience sharing and learning session for all the 21 VMMC implementing sites as a
platform for sharing implemented QI projects and showed how these change packages caused
improvement at their respective health facilities. Three health workers from each health facility VMMC
QI team participated in the learning session. During the learning sessions new updates and guidelines
on TT and VMMC implementaion packages, along with best practices were shared with partner sites.
Post learning session follow up mentorhsip, coaching, and support focused on reviewing
implementation of learned best practices, realigning change packages and QI projects, functionality
and use of data by the QIT/WIT, and health facility in general for decision making towards improving
VMMC service delivery at the respective health facilities.
In collaboration with USAID/ASSIST, the Program conducted VMMC QI baseline assessment at nine
VMMC sites to benchmark quality areas that need to be addressed. The assessment focused on
management systems, supplies, equipment, other VMMC service delivery systems, records
management, infection prevention and waste management. Based on the findings, the facilities were
given support towards improvement. Routine VMMC services assessment using the PEPFAR QI
standard tool guided improvemnet focus for specific health facility challenges. Some health facilities
have had their implementation of VMMC haulted for some time during the year due to quality gaps.
Effort was made by the Program to address and support the facilities through supportive supervison and
mentorship. By the end of the reporting period activities had resumed. Going forward, the Program will
continue to support all VMMC implementing health facilities to ensure that the set standards are
maintained and continous quality improvement interventions are in place focussing on improving the
systems and processes.
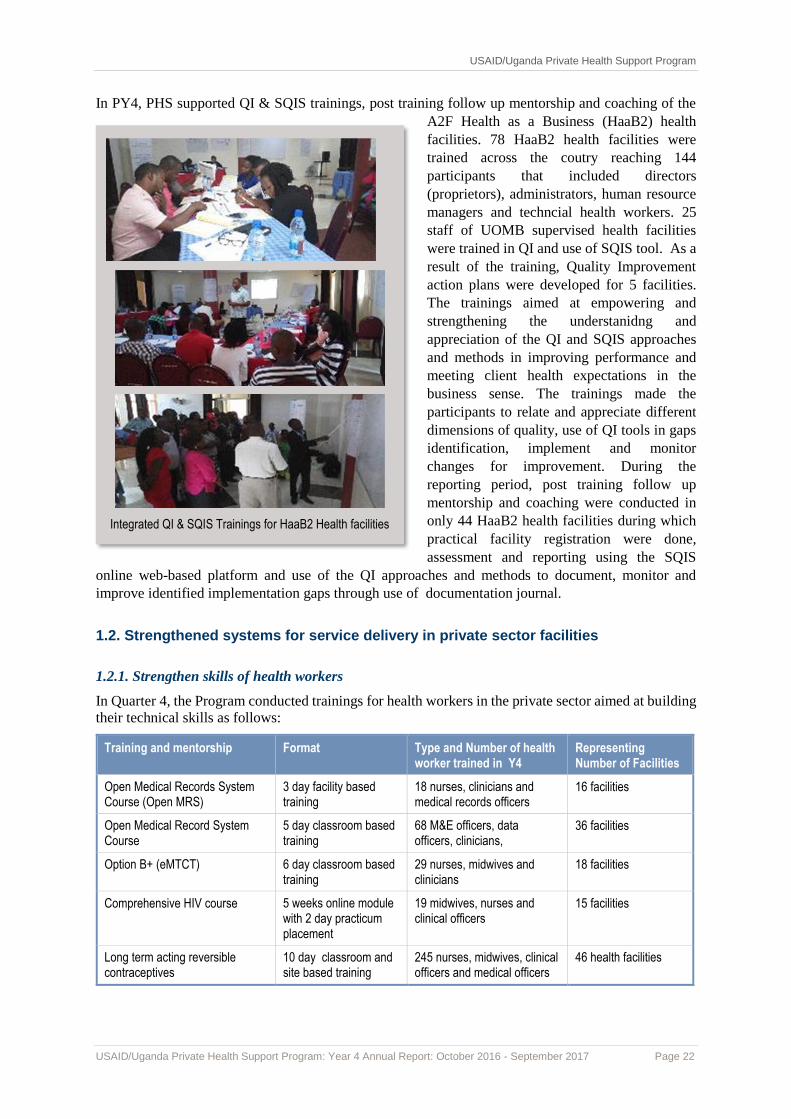
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 22
In PY4, PHS supported QI & SQIS trainings, post training follow up mentorship and coaching of the
A2F Health as a Business (HaaB2) health
facilities. 78 HaaB2 health facilities were
trained across the coutry reaching 144
participants that included directors
(proprietors), administrators, human resource
managers and techncial health workers. 25
staff of UOMB supervised health facilities
were trained in QI and use of SQIS tool. As a
result of the training, Quality Improvement
action plans were developed for 5 facilities. The trainings aimed at empowering and
strengthening the understanidng and
appreciation of the QI and SQIS approaches
and methods in improving performance and
meeting client health expectations in the
business sense. The trainings made the
participants to relate and appreciate different
dimensions of quality, use of QI tools in gaps
identification, implement and monitor
changes for improvement. During the
reporting period, post training follow up
mentorship and coaching were conducted in
only 44 HaaB2 health facilities during which
practical facility registration were done,
assessment and reporting using the SQIS
online web-based platform and use of the QI approaches and methods to document, monitor and
improve identified implementation gaps through use of documentation journal.
1.2. Strengthened systems for service delivery in private sector facilities
1.2.1. Strengthen skills of health workers
In Quarter 4, the Program conducted trainings for health workers in the private sector aimed at building
their technical skills as follows:
Training and mentorship Format Type and Number of health worker trained in Y4
Representing Number of Facilities
Open Medical Records System Course (Open MRS)
3 day facility based training
18 nurses, clinicians and medical records officers
16 facilities
Open Medical Record System Course
5 day classroom based training
68 M&E officers, data officers, clinicians,
36 facilities
Option B+ (eMTCT) 6 day classroom based training
29 nurses, midwives and clinicians
18 facilities
Comprehensive HIV course 5 weeks online module with 2 day practicum placement
19 midwives, nurses and clinical officers
15 facilities
Long term acting reversible contraceptives
10 day classroom and site based training
245 nurses, midwives, clinical officers and medical officers
46 health facilities
Integrated QI & SQIS Trainings for HaaB2 Health facilities

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 23
Training and mentorship Format Type and Number of health worker trained in Y4
Representing Number of Facilities
Permanent methods of family planning (BTL and non-scalpel vasectomy)
10 day classroom and site based training
17 medical officers 16 facilities
Quality Improvement (QI) and self-regulatory quality improvement system (SQIS)
5 day classroom based training
171 facility managers, directors, administration staff, nurses, clinicians,
35 M&E program staff plus research assistants
34 Haab2 facilities
44 facilities
Consolidated guidelines for HIV prevention and treatment in Uganda, 2016
3 day facility based training
1,258 clinical officers, nurses, midwives, medical officers, specialists, laboratory technicians /technologists, pharmacists and support staff
71 health facilities
VMMC mentorship 1 day facility based 164 nurses, medical officers, clinical officers and counsellors
15 health facilities
Bio risk and Biosafety training 5 day classroom based training
46 laboratory technicians, assistants, technologists and support staff
25 health facilities
Bio risk and Biosafety mentorship 2 day facility classroom based
102 laboratory technicians, assistants, technologists and support staff
25 health facilities
Laboratory Quality Management Improvement system mentorship
2 day facility based 48 laboratory personnel 20 health facilities
Laboratory Logistics and management
5 day classroom based 20 laboratory technicians, assistants, technologists
20 health facilities
HMIS/DHIS II mentorship 1 day facility based 95 records staff, clinicians and nurses
20 health facilities
Integrated Management of Malaria including IPTP
1 day facility based 125 nurses, midwives, clinicians, laboratory staff, pharmacy technicians and stores personnel
35 health facilities
Mentorship in perinatal audit, HBB+ and HMS, Babies matrix, HMIS 010b (integrated MNCH mentorship)
2 day facility based 145, nurses, midwives, clinicians
22 health facilities
TB/HIV co- infection management Course
5 day classroom based training
20 nurses, midwives, clinical officers and medical officers
18 facilities
HMIS/ DHIS II Course 5 day classroom based training
20 clinicians, records staff and M&E staff
20 health facilities
VMMC 10 day classroom based and site based training
45 nurses, clinicians, medical officers and counsellors
15 facilities
Nutritional Assessment Counselling and Support (NACS)
5 day classroom based training plus field practicum
34 Clinicians, nurses, midwives medical officers, counsellors
17 facilities
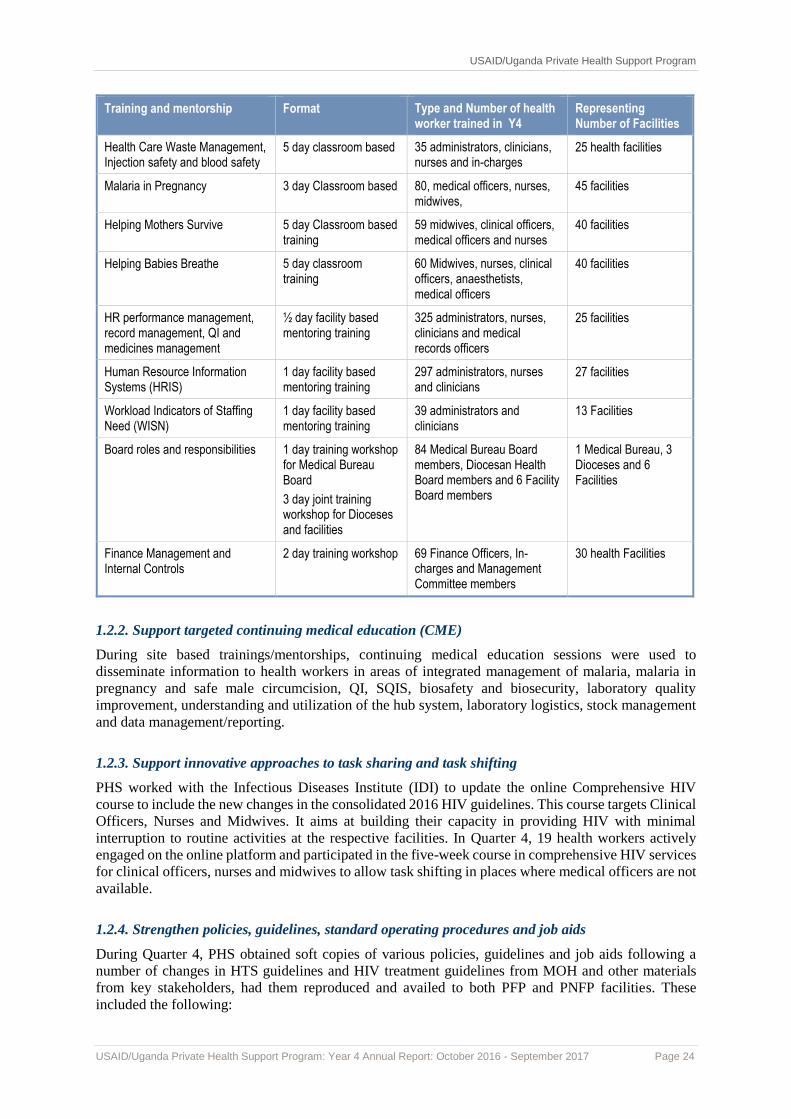
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 24
Training and mentorship Format Type and Number of health worker trained in Y4
Representing Number of Facilities
Health Care Waste Management, Injection safety and blood safety
5 day classroom based 35 administrators, clinicians, nurses and in-charges
25 health facilities
Malaria in Pregnancy 3 day Classroom based 80, medical officers, nurses, midwives,
45 facilities
Helping Mothers Survive 5 day Classroom based training
59 midwives, clinical officers, medical officers and nurses
40 facilities
Helping Babies Breathe 5 day classroom training
60 Midwives, nurses, clinical officers, anaesthetists, medical officers
40 facilities
HR performance management, record management, QI and medicines management
½ day facility based mentoring training
325 administrators, nurses, clinicians and medical records officers
25 facilities
Human Resource Information Systems (HRIS)
1 day facility based mentoring training
297 administrators, nurses and clinicians
27 facilities
Workload Indicators of Staffing Need (WISN)
1 day facility based mentoring training
39 administrators and clinicians
13 Facilities
Board roles and responsibilities 1 day training workshop for Medical Bureau Board
3 day joint training workshop for Dioceses and facilities
84 Medical Bureau Board members, Diocesan Health Board members and 6 Facility Board members
1 Medical Bureau, 3 Dioceses and 6 Facilities
Finance Management and Internal Controls
2 day training workshop 69 Finance Officers, In-charges and Management Committee members
30 health Facilities
1.2.2. Support targeted continuing medical education (CME)
During site based trainings/mentorships, continuing medical education sessions were used to
disseminate information to health workers in areas of integrated management of malaria, malaria in
pregnancy and safe male circumcision, QI, SQIS, biosafety and biosecurity, laboratory quality
improvement, understanding and utilization of the hub system, laboratory logistics, stock management
and data management/reporting.
1.2.3. Support innovative approaches to task sharing and task shifting
PHS worked with the Infectious Diseases Institute (IDI) to update the online Comprehensive HIV
course to include the new changes in the consolidated 2016 HIV guidelines. This course targets Clinical
Officers, Nurses and Midwives. It aims at building their capacity in providing HIV with minimal
interruption to routine activities at the respective facilities. In Quarter 4, 19 health workers actively
engaged on the online platform and participated in the five-week course in comprehensive HIV services
for clinical officers, nurses and midwives to allow task shifting in places where medical officers are not
available.
1.2.4. Strengthen policies, guidelines, standard operating procedures and job aids
During Quarter 4, PHS obtained soft copies of various policies, guidelines and job aids following a
number of changes in HTS guidelines and HIV treatment guidelines from MOH and other materials
from key stakeholders, had them reproduced and availed to both PFP and PNFP facilities. These
included the following:

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 25
a) HTS policy: During the reporting period, PHS liaised with the STD/AIDS Control Program
(ACP) of Ministry of Health and obtained sample copies of the HTS Policy. PHS reproduced
and disseminated these guidelines to all the PHP and PNFP facilities.
b) The Consolidated Care and Treatment Guidelines 2016: These included desk job aides and
manuals that were distributed across 71 program supported facilities.
c) LARC/permamnet methods:PHS also obtained a soft copy from MOH, Engender Health of the
Comprehensive Family Planning Manual, Post Partuum IUD Learners work book, Non- scapel
vasectomy and BTL manuals.These were printed and disseminated to all facilities to guide them
at their respective facility as resource materilas to support continuos professional development.
Other guidelines, policies and job aides printed during Program year 4 included; SQIS and SiMs
manuals, VL guidelines, HBB, ENBC and HMS job aides, pediatric TB algorithm and job aids.
1.2.5. Strengthen health management information systems
1.2.5.1. Identify and support health management information system (HMIS) focal persons
During the quarter, the Program provided onsite mentorship and technical assistance to all 71 supported
sites to ensure complete, good quality and timely submission of HMIS reports. The Program worked
with district biostatisticians and probation officers to ensure timely and accurate entry of data in the
DHIS2 and OVC MIS respectively. Health facility reporting rate in Q4 in the DHIS2 stands at 100%
for monthly reports and 97% for quarterly data. Two health facilities (Qudrah and Munobwa) still have
missing data entry screens in the DHIS2. PHS is following up with the districts and MOH resolve this
challenge. 100% of the OVC sites reported through the MGLSD OVCMIS compared to 96% in Q3.
The two sites that had moved operation to other districts were registered in the new districts and are
now reporting. The Program received and distributed needed HMIS tools to the 71 supported health
facilities. 7 sites were supported through the respective District Health Offices and Joint Medical stores
to receive access to WAOS online reporting and ordering for timely ARV and HIV test kits orders in
addition to the 22 that had received the access earlier.
During the quarter, the Program assigned research assistants to all the 71 health facilities to provide
onsite support in documentation and data management as well as general M&E support. MOUs were
signed between the Health Facility In-charges/Project Coordinators and the Program to last until end of
October 2017. The research assistants carried out brief data needs assessments and developed workplans
aimed at bridging the identified gaps. Among the activities implemented was on-site mentorship of
health workers in using HMIS tools entry of data into UgandaEMR (OpenMRS), data analysis and
utilization. All the sites were also provided with the needed HMIS tools. The 36 (51%) sites supported
in OpenMRS in previous quarters continued with data entry of backlog data while exploring reports
that can be generated by the database. Sites continue to face challenges with huge data backlogs that
may necessitate external support. The Program purchased and provided 11 computers to health
facilitates to support data management specifically in the use UgandaEMR (OpenMRS). Installation of
Open MRS was undertaken in 8 health facilities supervised by the UPMB.
Targeted technical support was provided to 34 OVC sites to improve their data management systems
including updating of their integrated registers, case management files.
1.2.5.2. Strengthen weekly option B+ reporting
The Program continued to work with the AIDS Treatment and Information Centre (ATIC) at IDI to
send weekly SMS reminders to 30 health facilities (4 for Faith based and 26 PFP sites) to submit weekly
option B+ reports. On average, the general reporting rate was 96% from 68% last quarter. Barriers to
reporting have mainly been incorrect report formats, use of unregistered numbers, change in phone
numbers, and change of facility focal persons. However, the improvement in reporting was due to the
continuous weekly reminders and monitoring of the system to ensure complete reporting. The M and E

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 26
team also provided regular onsite mentoring and support to ensure that the previously missed reports
were sent through the DHIS2 system.
Figure 11 Option B+ health Facility weekly reporting rates
1.2.6. Strengthen Health Systems in the faith based sector
During Quarter 4, the USAID/Uganda Private Health support program (PHS) implemented the
following Health System Strengthening (HSS) activities:
> Validation and Finalization of the Comprehensive HSS Needs Assessment: A total of 64
stakeholders from the Medical bureaus, Hospitals and Health Centres validated the findings of the
Health System Strengthening Needs Assessment (HSNA) conducted earlier in quarter 3. The report
will be widely disseminated to the stakeholders in first quarter of PY5.
> Integrated HSS facility visits: Integrated teams of technical advisors from Medical Bureaus and
PHS conducted Health systems support visits to health facilities in all regions of Uganda. The
purpose of the visits was to gain deeper understanding of the HSS situation in facilities, and provide
instant support appropriately. Technical advisors of Medical Bureau were supported to make
supporting supervision visits to 25 health facilities. The advisors offered on-spot mentoring to
varying capacity areas including Human resource performance management, finance/asset/medical
records management, QI and medicines management.
1.2.6.1 Improve the availability of human resources to support service delivery in the faith-based
health sector
During the quarter, PHS worked to strengthen the strategic policy frameworks of the 4 Medical bureaus
and health facilities under their respective networks. The task entailed developing Human resource
management manuals for the 4 Bureaus, and model human resource management manuals for Hospitals
and model Charters for Health units. The policies and charters will ensure the existence of codified
approaches for human resource management in Uganda’s faith based health sector/network. The human
resource manuals will be in place within the 1st quarter of PY5. Other human resource activities
implemented include:
Training of Management Committees (MCs) and staff of 27 Health Facilities under UMMB,
UOMB and UPMB in management of the Ministry of Health HRIS. The training included hands
on registration of the facility staff in the HRIS. One of the challenges to the success of the activity
was absence of computer facilities in some Health Units. PHS will work with Medical bureaus to
address gap.
Training of 15 staff and management of 5 health facilities supervised by UOMB in performance
appraisal management. A similar training will be organized for the members of the Health Unit
Management Committees in the first quarter of PY5, to strengthen their ability to supervise staff.
100 100 9785 82
100 100 97 97 97 97 100 100 97
0
50
100
150
Per
cen
tage
rep
ort
ing
rate
Option B+ Reporting rate
2 per. Mov. Avg. (Option B+ Reporting rate)

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 27
Workload Indicators of Staffing Need (WISN) human resource management tool was introduced in
13 health facilities under UMMB. The purpose of the activity was to capacitate health facility
managers with the knowledge and skill to systematically make staffing decisions to enable them
utilize their human resources well.
1.2.6.2 Strengthen health leadership and governance in the private sector
1.2.6.2.1. Strengthen health leadership and governance in the private for profit (PFP) sector
Refer to section 1.4.5. Provide business strengthening support
1.2.6.2.2 Strengthen health leadership and governance in the faith-based sector
During the quarter, PHS worked to strengthen the strategic policy frameworks of the 4 Medical bureaus and health facilities under their respective networks. The activity entailed developing Board governance
manuals for the 4 Bureaus, and model Board governance manuals for Hospitals and model Charters for
Hospitals and lower health facilities. The purpose of developing the policies and charters is to ensure
the existence of codified approaches for health governance in Uganda’s faith based health
sector/network. The governance manuals will be ready in the 1st quarter of PY5. Other governance
activities accomplished included:
Review of UOMB draft Strategic Plan 2017 – 2021: The review workshop involved 34 stakeholders
from Health Facilities, Uganda Orthodox Council and UOMB Board and staff. For the past two
years, UOMB only had a draft strategy that focused on requirements for the establishment of the
Bureau. The recognition that the Bureau had had significant transformation beyond the
establishment phase necessitated this activity. UOMB needed to refocus on strategic change in core
purpose areas. Plans are under way to develop a new strategy that will set the direction of the core
purpose components for the existence of the Bureau such as capacity strengthening of the orthodox
medical network, engagement with Government, quality assurance for the Orthodox Medical
Facilities, among others.
Induction and orientation of 11 members of the Board of UMMB in their roles, rights and
responsibilities. Board members were also supported and reviewed the implementation
performance of the Bureau Strategic Plan. Similarly, UCMB was supported to orient 73 Board
members from six different health Facilities and Diocesan Health Boards in their Terms of
Reference and contemporary Health Facility governance issues.
UCMB conducted six Health Assemblies organized by major Hospitals and Dioceses and the
Archdiocese of Kampala bringing together 501 participants representing leaders of Health
Facilities, political leaders, technical public sector officials and community leaders. The assemblies
aimed at promoting transparency, accountability to health care consumers by leaders of health
facilities in the delivery of health care.
1.2.6.3. Improve health financing and finance management in the private sector
During the quarter, PHS worked to strengthen the strategic policy frameworks of the 4 Medical bureaus
and health facilities under their respective networks. The activity entailed developing Finance
management manuals for the 4 Bureaus, and model finance management manuals for Hospitals and
model finance management manuals for health units. The purpose of developing the manuals is to
ensure the existence of codified approaches for finance management in Uganda’s faith based health
sector/network. The finance manuals will be ready in the 1st quarter of PY5. Further, a total of 69
Finance Officers, In-Charges and members of the Management Committees of 30 Health Facilities
under UPMB and UOMB were trained in Finance Management and Internal Controls. The training
aimed to improve skills and knowledge of the participants, required to improve financial management
systems at health facilities.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 28
1.2.6.4. Improve coordination with public facilities and other stakeholders at districts and national
levels
1.2.6.4.1. Strengthen Uganda Healthcare Federation (UHF)
Refer to section 3.3.2. Support UHF to implement strategic plan
1.2.6.4.2. Establish a faith based organization health coordinating mechanism
The draft concept paper for establishing a national faith-based body was shared with medical bureaus
for their input before it is shared with other stakeholders. This sharing will promote buy-in and
ownership of the process by the medical bureaus. The Program will elicit more input from other
stakeholders before a more detailed feasibility study for establishing the faith-based body is instituted.
This phase will be accomplished in the first quarter of PY5.
1.3. Strengthened support for Orphans and Vulnerable Children (OVC)
1.3.1. Support performance based grants to Faith Based and Civil society organizations
The Program provided performance based grants to OVC partners to implement support services
following the Family-Based Approach, PEPFAR/USAID/Uganda Priorities and the Ministry of Gender,
Labor and Social Development (MGLSD) objectives. Key priority activities were delivered through
implementation of a comprehensive OVC support package including: intensifying the 90-90-90
HIV/AIDS Global epidemic control strategy to ensure that OVC are Healthy, Stable, Safe and Schooled.
In the PY October 2016-September 2017, the Program supported 46,572 OVC (31,898 PNFP and
14,674 PFP) from 13,993 households. The Program supported transition of four organizations that
operated in districts of low HIV/AIDS prevalence. These included Kumi Diocese in Kumi District,
Islamic outreach Center in Bukedea District, Lango Diocese in Alebtong District and Kasana Luwero
Diocese in Nakasongola District.
1.3.2: Households Economic strengthening activities
Household Economic empowerment remained key priority intervention and central to the provision of
essential services to OVC Households. This intervention focused on enhancing capacity of OVC and
care giver to increase their incomes and assets growth through:
1.3.2.1. Training of caregivers in business initiation, management and follow up support
This training covered a total of 2,216 new OVC caregivers (535 males and 1,681 females) and equipped
them with skills on identification, initiation and management of income generation projects. Trainers
undertook tracer studies among selected caregivers to ascertain the impact of the previous trainings and
other interventions. Findings from this study revealed significant increase in incomes of caregiver
households and other vulnerable groups that benefited from the previous trainings. However the major
factors constraining growth and development of IGAs include limited access to finance, inadequate
management, technical skills and low economies of scale.
In Masanafu Child and Family Support ( MCAFS) Project and Kakira Out growers Development Fund
(KORD), the Training of Adolescent Girls and Young Women (AGYW) at risk of contracting HIV on
entrepreneurship skills like Soap making, counter book making, Pastries and baking enabled them meet
personal basic needs and reduced their exposure to unstable, exploitative sexual relationships at a tender
age. The training also empowered OVC with life skills that resulted in high self-esteem and
involvement in decision making on issues that affect their lives. A total of one Hundred and Eight (108)
Adolescent girls and young women were trained and equipped with safer health choices and decent
earning opportunities.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 29
1.3.2.2. Training of Village Saving and Loan Association Leaders on Group Dynamics and Money
management skills
A total of 3,250(906 male; 2,344 female) Group leaders from four Hundred and sixty six (466) groups
were equipped with skills to effectively manage group activities. Emphasis during the training was on
group formation and management. More time was spent on the loan disbursement procedure since all
groups are involved in saving and loaning activities. All groups were encouraged to establish loan
management committees. These committees are a prerequisite for successful management of the loan
funds since they are responsible for assessment, disbursement and recovery of the loans advanced to
members.
Follow up on Village Saving and Loan Associations (VSLAs) to offer Technical support and
mentorship in management continued throughout the year. This was jointly done by Social workers,
M&E and Program Accountants. During such follow ups, Groups were educated on basic book
keeping, records management and roles/ responsibilities of leaders. As a sustainability mechanism to
provision of services to OVC, all caregivers are encouraged to join existing groups or form new ones
where they can access loans to start/ grow family enterprises. Many caregivers are successfully running
small scale Businesses from where they are able to raise money to meet basic needs of children under
their care. ECO-AGRIC (through a private company Traidlinks) conducted trainings on market
linkages and opportunities for agricultural products. Through this 68 caregivers were supported to
market their agricultural products of maize and beans to oil companies.
1.3.2.3. Household Vulnerability assessment.
The House hold Vulnerability Assessment was conducted to determine levels of vulnerability of all the
supported caregivers with a view of graduating 70% by September 201?. Results indicated that 41.2%
of the 6,985 households assessed were ready for graduation while over half of the assessed households
were slightly vulnerable. Only 6.9% and 0.1% of the OVC households were found to be moderately and
critically vulnerable respectively. This finding implied that by assessment time, some households could
be graduated while others would be transitioned to incoming Implementing partners.
1.3.3. Support to Apprenticeship and Vocational Training for out of school orphans and vulnerable
children
During the reporting period, the Program procured and distributed start up kits to OVCs that had
completed Vocational/Apprenticeship training in the financial year 2015/2016. A total of 939 OVC
received assorted start up kits in Tailoring, Metal Fabrication, Salon and Hairdressing, shoe making and
repair, Carpentry, building and concrete practice and Baking/ confectioneries. Before the kits are
distributed, the OVC are assessed by the Directorate of Industrial training (D.I.T) to ascertain their
readiness to utilize the skills and startup kits. However trainees of Motor vehicle and cycle mechanics
did not receive their kits. These will be provided in the next quarter.
Teenage Mothers undergoing skills training in Masanafu Child and Family Support in Rubaga Division, Kampala City,
April 2017.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 30
Follow up of OVC who
were previously trained and
were provided with startup
kits was carried to ascertain
the usefulness of the Kits
received and contribution
towards reducing
Household Poverty. This
was done by Field social
workers in various CSOs.
They purposively document
the successes attained by the
OVC graduates. See
example below from
Babirye Norah aged 22
(Chain Foundation -
Sammuka Village)
An additional number of
1,857 (Male 722; Female
1,135) OVC are currently undergoing training in different trades at various training centers and are
expected to complete their training by December 2017 after which they will be assessed and provided
with startup kits.
The Program trained 260 Artisans and Vocational Instructors on the use of Apprenticeship training
manuals. The purpose of this training was to improve the Artisans and Vocational Instructors’
Pedagogical, Testing and Assessment skills. Follow up to ensure that trained instructors are putting in
practice the knowledge and skills acquired reveals that most of the Instructors are now making schemes
Some of the Apprentices who received start up kits at Chain Foundation in Mukono
Some of the OVC visited and were found to be undergoing practical lessons in different CSOs.
“My customers now know my schedule because I go to the garden in the morning and later in the day, I sit on the veranda to work on customers’ clothes. To make a new dress, I charge between 10,000 - 15,000/=. I am able to make at least 5,000 to 15,000 shillings a day. This has really transformed my life as I don’t have to beg anyone for basic necessities. I also contribute to the purchase of other essential needs in the home and pay fees to my 2 siblings. My main Challenge
Norah utilizing her sewing machine given to her as starter up kit by Chain Foundation in
Mukono
however is that some customers delay to pay me and this affects my income streams and planning”

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 31
of work and lesson plans before commencement of the training. This has greatly improved the training
and assessment of trainees before graduation and distribution of startup kits.
1.3.4 Support Nutrition and Food Security Interventions
The Program worked with NuDiets Uganda Limited to train Community Volunteers and Village Health
Teams (VHTs) on Nutrition assessment, counselling and food security. One of the key objectives of
training was to build capacity of community systems to link malnourished children to HIV care points
to assess their HIV and TB status. A total of 1,156 (760 Female, 392 Male) Community Volunteers and
VHTS were trained.
Furthermore, the Program trained a total of 3,049 OVC care givers (754 males and 2,259 females) on
food security and Nutrition. The training aimed at equipping caregivers with skills to establish kitchen
gardens, mobilize food locally, enhance their knowledge on appropriate food mix, and identify signs
for malnutrition and referral for further management. The training focused on food grouping, food
handling and preparation, identification, prevention and management of malnutrition at community
level, infant and young child feeding. Food security thematic areas focused on kitchen gardening,
modern farming Techniques, post-harvest handling, value addition, energy saving techniques, referral
and linkages with other actors. The immediate outcomes observed during the training included high
knowledge gained on how to make food mix commonly known as“ ekitoobero” using locally available
materials, establishing kitchen gardens by majority of OVC Care givers across all CSOs, water and
sanitation practices, and identification of malnutrition cases in the community.
1.3.5. Support provision of Formal Education services.
PHS continued to provide Support for the education of the most critically Vulnerable Children
(emphasis on girls). Education support in form of school fees payment and provision of scholastic
materials was made to 12,511 (Male: 5912, Female: 6,599) to ensure they were retained in school. The
Program Social Workers through contact teachers at schools ensured that regular roll calls were made
to check on the attendance and make follow up on those who were missing school.
In order to reduce the cost of providing sanitary towels to adolescent girls, a training on making of re-
usable sanitary towels was organized. A total of 1,080 girls were trained. These will train others in a
cascading way to reach as many vulnerable adolescent girls as possible. The training involved both boys
and girls to reduce stigma and increase affordability and utilization among girls.
School and Home visits were made to offer career guidance and Psycho social support to children.
During Home visits, Social workers distributed scholastic materials to OVC on a case by case basis.
This ensured improved enrollment, retention and completion of school by critically Vulnerable OVC.
Community Volunteers in Mbarara Archdiocese undertaking MUAC Exercise to identify malnourished children.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 32
1.3.6. Support provision of health, water, sanitation and housing
PHS promoted community sensitizations as a strategy to reach young people especially Adolescent
girls and young women with messages on, dangers of early/Teenage Pregnancy, Sexual and
Reproductive Health rights and responsibilities,
Gender Based Violence prevention, life skills
planning and HIV Prevention were carried out by
FBOs/ CSOs. Through these platforms
adolescents were encouraged to get tested for
HIV. A total of 25 Peer groups for both out of
school and in school were formed in Bukedi
Diocese, Family Concepts center and Agape
Nyakibaale to equip young women and
adolescent girls with the much needed life skills
to keep healthy and free of HIV infection. Social
workers continued to sensitise OVC and
caregivers during home visits and VSLA
meetings on good home hygiene standards. OVC
households were encouraged to have all the
hygiene components (e.g Pit latrine, tippy taps
for hand washing facilities and utensils drying
racks). AIDS Orphans Education Trust (AOET) Lira leveraged support from a partner to sink a borehole
was sunk at Boke Parish Adekokwoko Sub-county to increase access to safe water in the area.
1.3.7. Child Protection and Legal Support services
PHS partnered with Ministry of Gender Labour and Social Development (MGLSD) National Trainers
on Child Safeguarding to train OVC grantee staff (The Program Coordinators, Social Workers and
M&E staff) to institutionalize child safeguarding at their organizations level. A total of 88 (Male: 42,
Female 46) OVC grantee staff from 46 CSOs/ FBOs were trained. The immediate outcomes from the
training were development of child safeguarding policies and ensuring respective organizational boards
have them approved. They agreed on the roll out plan to train community volunteers and sign the code
of conduct. All OVC partners identified Focal Persons that will continuously support CSOs on child
safeguarding.
Sensitization on child rights and prevention of child abuse both at home and school were key activities
in the year. Kumi Diocese, International Needs Uganda, Family Spirit Children’s Center, South
Rwenzori Diocese, Caritas Maddo, Family Concepts Center and Bukedi Diocese handled 24 (Male 12,
Female 12)cases of child labor and re-integrated 7 (Male:2, female:5) children with their families. The
Program continued to support births registration and access to birth certificates to children from
critically vulnerable households. A total of 2182 (Male: 1073, Female 1109) OVC were supported to
get birth certificates.
Distribution of scholastic materials was done during Home and school visits.
The Social worker from Kiyinda Mityana Diocese demonstrating how to use tippy tappy to OVC at Mwera R/C in Mityana district.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 33
1.3.8. Psycho Social Support to OVC and their Households
The Program trained 1,271 teachers on provision of psychosocial Support to OVC. The trained teachers
are able to identify danger signs of Psycho-social support distress among OVC, especially those related
to HIV/AIDS, respond appropriately and where necessary engage with caregivers to find solutions. The
Program Social Workers and Community Volunteers including Religious leaders conducted home visits
to OVC households to address any emerging psychosocial issues. Agape Nyakibale, SOS Children’s
Villages, ABC, Bringing Hope to the Family, Family Concepts Center carried out Center Days where
OVC were brought together for recreational and counselling activities at school and community level.
A total of 34,678 OVC (17,534female; males 17,144) were reached with psychosocial services and
basic care services.
1.3.9. Increase access to HIV/AIDS Services
During the Year, PHS continued to focus on children in the pandemic by ensuring that all supported
OVC know their HIV status. A total of 1,257 (Male: 642, Female: 615) HIV positive OVC were
supported to access care and treatment services. During HCT outreach sessions, HIV prevention, STI
screening, information on Sexual and Reproductive Health, Gender Based Violence Prevention were
also provided in Family Concepts Center, Meeting point Kampala, AIDS Orphans Education Trust-Lira
and Bringing Hope to the Family.
1.3.10. Promoting Private Sector Engagement
A total of 15 private companies supported the implementation of OVC activities by providing cash
contributions, market linkages and seedlings for agricultural interventions among others. Below are
some of the examples during the reporting period:
Buikwe Dairy Development Cooperative Society (BDDCS) supported the buying of agriculture
farm inputs during agronomic practice training under International Needs Uganda (INUG) and
facilitated the community reflection meetings.
Kakira Sugar Limited (KSL) has also continued with the child labour awareness campaigns to
discourage child labour practices in the KORD catchment area. In addition, over 6 community
feeder roads have been graded /maintained not only for sugar cane transportation to Kakira Sugar
Factory but also to ensure easy access to other services like market centers for agriculture produce,
education and health services.
The cost share company contributions have also directly led to enrollment and retention of more
OVC in schools (30 OVC supported by DHL and 165 by Kakira Sugar Limited).
1.3.11. Mainstreaming of CBOs OVC activities
The 46 OVC grantees took part in the OVC coordination committees (DOVCCs and SOVCCs)
meetings at the sub-county and district level. The partners also took part in the evaluation of the role of
para-social workers in the implementation of the OVC project led by 4Children project.
1.3.11.1. Supporting children with disabilities:
PHS carried out two surveys in 6 organizations to identify number and challenges faced by OVC with
disabilities. The first survey identified 163 children with physical disability, visual impairment,
deafness, and mental challenges while the second survey identified 178 children with similar
disabilities. PHS innovatively utilized findings to initiate a partnership with National Referral Hospital

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 34
Orthopaedic Workshop, National Wheel Chair
Coordination Committee of Ministry of Health
and two local NGOs. A total of 51 out of 341
assessed (14.9%) have since received devices.
CWDs and family members were trained on
device use/repair. Older CWDs accessed
vocational skills training.
1.4. Support business strengthening and increase access to finance
1.4.1. Expand financial outreach through
DCA banks
The Program has continued to work with
Centenary Bank and Ecobank to increase access
to finance for the private health sector. During
year four, the following results were registered.
Centenary Bank continued to register steady growth in its DCA utilization rates. At the end of Quarter
4, utilisation of the USAID/SIDA Health DCA at Centenary Bank reached a cumulative total of UGX
6,362,000,000 (US$ 2,494,902) as illustrated in Figure 1 below. The cumulative utilization rate is 83.2%
of the total UGX 7.65 billion guarantee ceiling, with 116 loans disbursed to 84 borrowers (58 rural, 26
urban). Of these 117 loans, 71 loans (to 57 borrowers) worth UGX 3,782,500,000 (US$1,483,333) have
been fully paid off, and 45 loans (to 27 borrowers) worth UGX 2,554,500,000 (US$1,001,765) remain
outstanding. 14 new loans worth UGX 519,500,000 (US$ 203,726) were disbursed during year 4 to 3
urban borrowers and 11 rural borrowers.
Figure 12. Centenary DCA Utilization as % of Total Guarantee Amount as of 30 September 2017
In Quarter 4, four loans worth UGX 120,000,000 (US$33,333) were booked under the Centenary Bank
DCA. Two of these loans worth UGX 55,000,000 (US$15,278) were used for medical equipment
purchase, and one loan worth UGX 25,000,000 (US$6,944) went to a rural borrower to construct a
maternity wing for the clinic he operates. Most of these loans (3 out of 4) worth went to rural based
borrowers wishing to expand their clinic operations through purchase of medical equipment or
construction of new premises.
Ecobank DCA continues to underperform. The causes of the slow utilization of the Ecobank DCA have
been repeatedly documented over the previous fiscal years. For administrative reasons, USAID has
decided to leave the guarantee in place but asked us not to dedicate further resources to technical
assistance for Ecobank at this time.
At the end of Year 4, Ecobank’s utilization of the DCA had reached a cumulative total of UGX
3,120,000,000 (US$1.22 million) to four borrowers (two rural and two urban), as illustrated in Figure
83.2%
44.8%38.4%
28.8%
54.4%
10.2%
72.9%
30.1%
53.0%55.8%
10.3%5.2%10.2%1.6%
24.6%33.6%
0.8%
21.3%2.8%
Beneficiaries of wheel chairs at Karera Ecumenical Development Organization in Sheema District.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 35
2 below. This is 17.5% utilization
of the total guarantee amount of
UGX 17.85 bn. Of the four loans
placed under coverage, one loan
has been fully paid off. The
current outstanding amount is
UGX 3,057,972,543 for three
borrowers, representing 98% of
the disbursements to date. One
new loan worth US$ 500,000 was
disbursed during year 4 to one
urban borrower to draw a letter of
credit to import pharmaceutical
supplies. A waiver from USAID
was sought for this deal.
The portfolio quality of the DCA
has been mediocre, with one loan
worth UGX 1.25 billion
(US$500,000), composing 95% of
the utilized guarantee amount,
going into default. The bank has
made a claim on the DCA for the
guaranteed portion of that loan.
Figure 13: Ecobank DCA Utilization as a % of Total Guarantee Amount as of 30 September 2017
During a review of Centenary’s guaranteed health loan portfolio in FY 2017, the Program found that
contrary to the requirements of the DCA agreement, Centenary had not requested USAID’s prior written
approval for some loans which may have been used to finance pharmaceuticals. We have now addressed
this anomaly. We identified all the pharmaceuticals and sought a retroactive waiver for them from
USAID. We have now developed the following measures to avoid a repetition of this as follows:
1) We have created a checklist for the bank’s loan personnel to use in verifying qualifying borrowers
and qualifying projects which are eligible for guarantee coverage;
2) We have established a protocol for the banks for requesting prior approval from USAID on loan
requests which include financing for pharmaceuticals;
3) The protocol has been approved by USAID; and
4) The Access to Finance (A2F) Team will provide training to Centenary Bank lending personnel on
how to apply the protocol in FY 2018. It will also be put in place at the new DCA health loan
portfolio guarantee at DFCU Bank.
ALL
Bo
rro
we
rs
Ru
ral
Urb
an
Ne
w a
nd
Fir
st…
Exis
tin
g b
ank…
Fem
ale…
Mal
e o
wn
ed…
Bu
sin
ess
…
Ind
ivid
ual
/ow
…
Clin
ics
Ph
arm
acie
s/…
Med
ical
…
Equ
ipm
ent…
Den
tist
s
No
rth
East
Wes
t
Cen
tral
Loan
Pu
rpo
se-…
Loan
Pu
rpo
se-…
Loan
Pu
rpo
se-…
Loan
Pu
rpo
se-…
17.5%
7.0%
10.5%
17.3%
0.2% 0
17.5%17.5%
0.0%0.2%
10.3%
7.0%
0.0%0.0%
7.0%
0.0%0.0%
10.5%
7.0%
0.2%0.0%
10.3%
An example of how this non-DCA financing is making a positive impact is illustrated in the case of Kumi Community Clinic and Imaging Centre. This is a clinic based in Eastern Uganda serving a rural clientele. They participated in our A2F workshop, and we provided TA, linking them to suitable equipment vendors such as Crown Healthcare and Computech. With the support we gave to the clinic, they put together a financing proposal worth UGX 291 million to Centenary Bank for purchasing medical equipment. Kumi Community Clinic and Imaging Centre also made their own contribution worth UGX 80M, making the total cost of medical equipment UGX 371M. The loan was not placed under the Centenary Bank DCA guarantee because the loan repayment period is longer than the remaining life of the guarantee. The non-DCA loan has been used to purchase an X-Ray Machine,X-Ray image reader, printer, computer and ultra sound scan. Kumi Community Clinic Imaging Center's investment in this equipment has directly led to a 62.5% growth in client volume, serving 160 clients per month, along with a 100% annual growth in sales revenue. The clinic has posted an overall monthly net profit of 10,000,000 million UGX. Kumi Community Clinic and Imaging Center's growth includes an increase in the number of its employees from 7 to 16 healthcare professionals who were employed as a direct result of the acquisition of the medical machinery. This includes a radiographer, dark room attendant, a laboratory technician, two enrolled nurses, one nursing assistant and a part time medical officer.
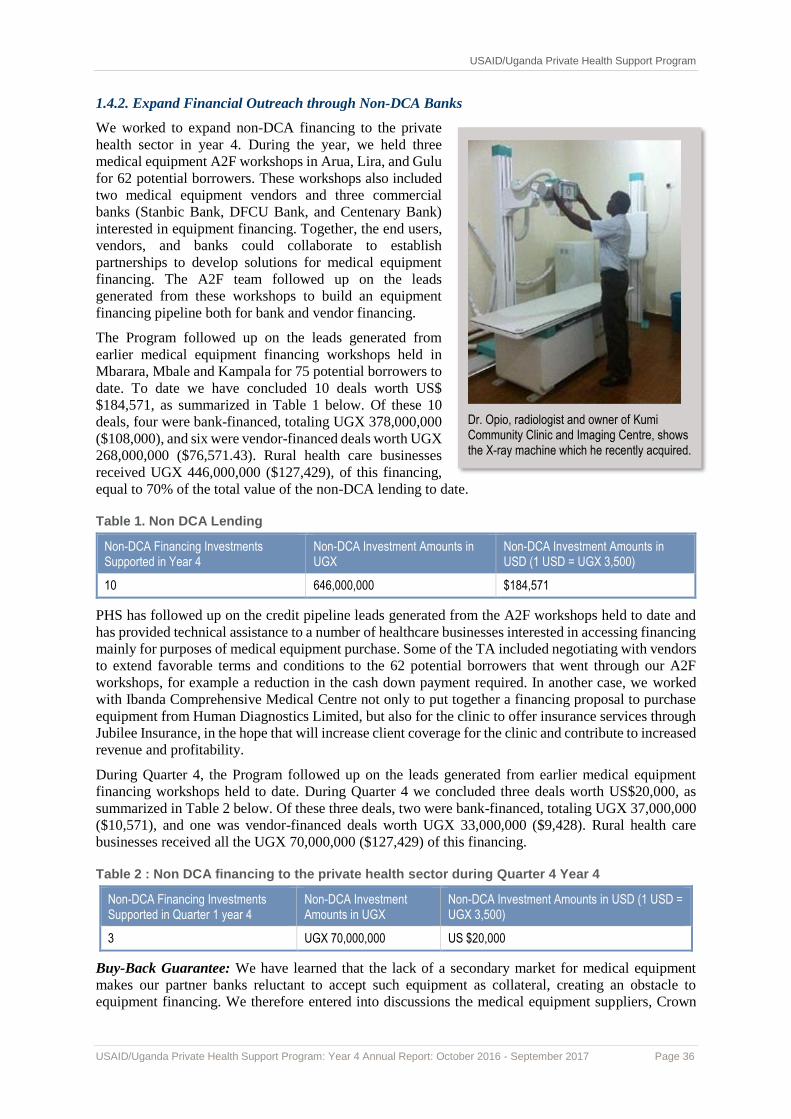
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 36
1.4.2. Expand Financial Outreach through Non-DCA Banks
We worked to expand non-DCA financing to the private
health sector in year 4. During the year, we held three
medical equipment A2F workshops in Arua, Lira, and Gulu
for 62 potential borrowers. These workshops also included
two medical equipment vendors and three commercial
banks (Stanbic Bank, DFCU Bank, and Centenary Bank)
interested in equipment financing. Together, the end users,
vendors, and banks could collaborate to establish
partnerships to develop solutions for medical equipment
financing. The A2F team followed up on the leads
generated from these workshops to build an equipment
financing pipeline both for bank and vendor financing.
The Program followed up on the leads generated from
earlier medical equipment financing workshops held in
Mbarara, Mbale and Kampala for 75 potential borrowers to
date. To date we have concluded 10 deals worth US$
$184,571, as summarized in Table 1 below. Of these 10
deals, four were bank-financed, totaling UGX 378,000,000
($108,000), and six were vendor-financed deals worth UGX
268,000,000 ($76,571.43). Rural health care businesses
received UGX 446,000,000 ($127,429), of this financing,
equal to 70% of the total value of the non-DCA lending to date.
Table 1. Non DCA Lending
Non-DCA Financing Investments Supported in Year 4
Non-DCA Investment Amounts in UGX
Non-DCA Investment Amounts in USD (1 USD = UGX 3,500)
10 646,000,000 $184,571
PHS has followed up on the credit pipeline leads generated from the A2F workshops held to date and
has provided technical assistance to a number of healthcare businesses interested in accessing financing
mainly for purposes of medical equipment purchase. Some of the TA included negotiating with vendors
to extend favorable terms and conditions to the 62 potential borrowers that went through our A2F
workshops, for example a reduction in the cash down payment required. In another case, we worked
with Ibanda Comprehensive Medical Centre not only to put together a financing proposal to purchase
equipment from Human Diagnostics Limited, but also for the clinic to offer insurance services through
Jubilee Insurance, in the hope that will increase client coverage for the clinic and contribute to increased
revenue and profitability.
During Quarter 4, the Program followed up on the leads generated from earlier medical equipment
financing workshops held to date. During Quarter 4 we concluded three deals worth US$20,000, as
summarized in Table 2 below. Of these three deals, two were bank-financed, totaling UGX 37,000,000
($10,571), and one was vendor-financed deals worth UGX 33,000,000 ($9,428). Rural health care
businesses received all the UGX 70,000,000 ($127,429) of this financing.
Table 2 : Non DCA financing to the private health sector during Quarter 4 Year 4
Non-DCA Financing Investments Supported in Quarter 1 year 4
Non-DCA Investment Amounts in UGX
Non-DCA Investment Amounts in USD (1 USD = UGX 3,500)
3 UGX 70,000,000 US $20,000
Buy-Back Guarantee: We have learned that the lack of a secondary market for medical equipment
makes our partner banks reluctant to accept such equipment as collateral, creating an obstacle to
equipment financing. We therefore entered into discussions the medical equipment suppliers, Crown
Dr. Opio, radiologist and owner of Kumi Community Clinic and Imaging Centre, shows the X-ray machine which he recently acquired.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 37
Healthcare and Sinoafrica, to see if they would be willing to establish buy-back agreements with banks
to offer assurance that if a borrower defaults on a medical equipment loan and the bank is forced to
repossess that collateral, the bank will be able to resell the equipment and recuperate the loan loss.
Although Sinoafrica has considered buy-back guarantees in the past, they are concerned about
developing a reputation for selling used equipment. Crown Health showed willingness to work with the
PHS Program to provide a buy-back guarantee for medical equipment loans, giving the DCA banks
extra assurance that if a borrower does not repay a loan, the bank could repossess the equipment and
the supplier would buy it back from the bank. Crown is willing to provide a buy-back guarantee under
certain conditions, for example equipment must be returned in reasonable condition and have been fully
serviced by Crown; the value must be above a minimum--i.e. no small items such as blood pressure
cuffs--and the maximum tenor of the buy-back period would be 36 months. The Program has therefore
started working with Crown Healthcare to put in place mechanisms for a ‘buy back’ option for
equipment purchased with financing from the Program’s DCA partner banks. This will be formalized
through a memorandum of understanding to be signed in Quarter 1 of year 5. The Program will also
assist Crown Healthcare to draft partnership proposals for other interested financial institutions.
1.4.3. Provide technical assistance to DCA banks and borrowers (actual and potential)
A corollary to the expansion of financial access of private health care businesses is the need for technical
support. We continued in this TA provider role during the year and provided the following support:
1) Met with Uganda Health Marketing Group (UHMG), whose network of approximately 270 Good
Life clinics is a potential pool of borrowers in our efforts to expand financing for the private health
sector. PHS will provide Access to Finance workshops for the Good Life clinics and provide
training of trainers to UHMG staff to build some in-house capacity for business skills training for
member providers.
2) Invited over 20 Good Life clinics under UHMG network to attend the medical equipment Access
to Finance/Leasing workshops and one of the clinics was able to acquire equipment through vendor
financing.
3) Worked with Soroti Medical Associates Nursing Home, a distressed Centenary Bank DCA
borrower, to restructure their UGX 230 million loan. The program presented the restructuring plan
to the bank, which accepted it.
4) Supported Family Health Clinic in Kiruhura in opening up a bank account with Ecobank Mbarara
Branch to commence an application for a UGX 400M to set up a diagnostic centre.
5) Gave TA support to Family Health Resource Centre to secure vendor financing from Crown
Healthcare to purchase an ultrasound scan worth UGX 60M.
6) Gave TA support to Polycare Clinic in Ntungamo for the purchase of an X-ray machine through
Sino Africa. Sino Africa carried out field visits, provided guidance and made recommendations to
the borrower regarding the structures that will house the X-ray machine by making for them the
architectural plan for the proposed structures.
7) Gave TA support to Lydda Medical Services in their UGX 60 million loan application to DFCU
Bank.
8) Brokered the linkage between Sheema Clinic in Mbarara and Crown Healthcare Care for maternity
equipment worth UGX 15 million.
9) Brokered the linkage between Case Hospital in Kampala and Sino Africa to purchase an ultrasound
scan worth UGX 120 million and a colposcopy worth UGX 30 million.
10) Brokered the linkage between Dr. Omagor Benjamin of Doctor’s Plaza-Soroti and Crown
Healthcare for laboratory equipment worth UGX 4 million.
11) Supported Mbarara Community Hospital to open up a bank account with Ecobank Mbarara Branch
to kick-start a UGX 100M loan application to construct their operating theatre and purchase
laboratory equipment.
12) Brokered the linkage between St. Martin’s Health Centre in Mbale and Crown Healthcare. We also
supported this healthcare business to open up a bank account with Stanbic Bank- Mbale Branch,

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 38
and we will assist them with a UGX 200 million loan application for purposes of purchasing medical
equipment.
During Quarter 4, PHS continued to provide technical assistance to a number of HCBs interested in
accessing financing mainly for purposes of medical equipment purchase and also expansion. These are:
> Assisted Ibanda Medical Centre to put together a loan proposal for Centenary Bank for UGX 200M
to complete construction of their clinic and to purchase an X-ray worth UGX 80 million from Sino
Africa.
> Brokered the linkage between Ibanda Comprehensive Medical Centre and Human Diagnostics
Limited a medical equipment vendor for purchase of a CBC machine worth UGX 18M (cash up
front payment); Haematology machine worth UGX 15M with an upfront cash 50% down payment
and the balance with vendor financing to be paid over a period of five months. In addition the HCB
has also been linked to Jubilee insurance and now it’s a service provider for Jubilee Insurance clients
which will help the HCB increase on its clientele and income in the long run.
> Assisted Pikwo Medical Centre in Gulu to put together a loan proposal to Centenary Bank-Gulu
Branch for UGX 17 million to complete construction of their Clinic.
> Assisted Pearl Medical Centre in Lamwo to put together a loan proposal to Centenary Bank-Kitgum
Branch for UGX 20 million to complete construction of their maternity wing.
1.4.4. Supporting USAID in the identification and recommendation of a third health DCA bank
partner
During the year, the Program gave the Washington-based USAID/DCA management office support in
identifying and recommending a third health DCA bank. This support included:
Figure 14: Structure of the DFCU DCA
Making an initial assessment of DFCU Bank’s interest in and strategy for w orking with the private
health sector. The assessment confirmed bank management’s interest in a health DCA guarantee.
Working with DFCU to determine the level of their current health lending portfolio.
Supported the Washington DCA office to carry out a risk assessment/due diligence on DFCU Bank.
The assessment was to determine the suitability of DFCU as a potential partner bank in health lending
with DCA guarantee support from USAID. The efforts have borne fruit, and a new five-year health
DCA agreement has been concluded with DFCU Bank Limited for a US$5 million loan portfolio
guarantee, with a special focus on leasing of medical equipment. USAID will provide an average 50%
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 39
guarantee on loans made by DFCU Bank to health care providers, with DFCU Bank having the option
of a variable rate guarantee coverage ranging from as low as 20% to 60% for each individual loan. The
illustration above in Figure 3 summarizes the structure of the guarantee. Under the DCA, USAID/Private
Health Support Program will be the TA provider to the bank to implement a health lending strategy to
maximize utilization. This includes assistance in better understanding the market, loan officer training,
strategy development, and pipeline development support. These skills will assist banks to better
understand the risks associated with lending to the health sector, such as low turnover and possible
delinquency. Developing loan products more tailored for the health sector will also require an improved
understanding by the banking industry of the healthcare market. Other TA offered will include:
1. Assist the bank to determine Development Indicators, Baseline Data and Utilization Targets
2. Monitor both the DCA bank and borrowers
3. Develop pipeline of health deals
4. Provide private health lending data
1.4.5. Provide business strengthening support
During the year, Phase II of the Healthcare as a Business (HaaB II) training and support activities was
launched with Makerere University College of Health Sciences as the business development services
(BDS) provider.
Working together with the BDS provider, training packages—including participant’s manual,
facilitator’s manual, power point slides, pre-test, post-test, and test key—for six modules essential for
managing growing health care businesses or large hospitals were developed and approved by the PHS
program. These modules are: Inventory Management in Your Health Care Business; Risk Management
for Your Health Care Business; Internal Controls and Audit for Your Health Care Business; Financial
Analysis for Your Health Care Business; Corporate Governance for Your Health Care Business; and
Succession Planning for Your Health Care Business.
Makerere College of Health Sciences commenced the training of managers and owners of small and
medium healthcare businesses and large Kampala hospitals, and all HaaB II workshops were delivered
as planned. Four individual business counselling visits were held during the year.
HaaB II post-training monitoring visits to the HaaB II beneficiary health care businesses sites were
made as part of the programs role of providing supervisory and oversight guidance to the project. The
feedback was very positive: HCBs found the training and business counselling very useful, as it
demystified financial information and provided skills to interpret financial statements, control
inventory, calculate and interpret financial ratios, and developed the ability to carry out trends analysis
and to make decisions based on financial statements,. The ability to make decisions using financial
statements has encouraged the smaller HCBs to be more diligent in keeping records that can enable the
preparation of financial statements.
During the year working with the program quality team and the Uganda Health Federation’s quality and
accreditation team, the SQIS and the QI training began for the HaaB II beneficiary health care
businesses.
The Program also held inception meetings with the bureaus, associations and franchise networks as part
of the strategy for ensuring that the HaaB training continues to reach a wider pool of health care
businesses even after the project closes. These meetings included Uganda Protestant Medical Bureau
(UPMB), Program for Accessible health, Communication and Education (PACE, Catholic Medical
Bureau, Uganda Private Midwives’ Association and Uganda Health Federation.
During Year 4, Quarter 4, the following achievements were made:
˃ The third and fourth business counselling sessions were held. During the third business counselling
visit, 68 small-medium health care businesses (HCBs) and 10 large hospitals were mentored with a
focus on reviewing and/or developing written internal controls, beginning trend analysis, reviewing

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 40
the status of the stock cards and remedial counseling on financial record keeping and financial
reporting. For the larger HCBs, the third visit was focused on trend and common size ratio analysis
and succession planning activities. During the fourth counselling visit, 70 small-medium health care
businesses (HCBs) and 10 large hospitals were mentored. For the small and medium HCBs, the
focus was to develop a business improvement plan, inventory control and continued review on
updating the stock cards, more trend analysis of their financial information, and colleting monthly
HMIS reports. For the large Kampala hospitals, the fourth visit was focused on developing business
improvement plans.
˃ The on-site training workshops in SQIS and QI mentoring took place during the quarter for the
HaaB II beneficiary health care businesses in the Northern, Western and part of the Eastern regions.
The health care businesses have put into place quality teams and there is visible quality
improvement even at the larger health care businesses.
˃ As part of sustainability for the HaaB activities, discussions on integrating the HaaB modules into
Makerere’s medical school curriculum began and culminated into Makerere sending a briefer
outlining the process of getting this idea off the ground and the resource implications for follow up.
Follow up meetings were held with the Head of Social Franchise, Marie Stopes Uganda, the
Executing Director of Uganda Health Federation and with the Uganda Private Midwives
Association to begin the process of institutionalizing HaaB.
˃ In our role of providing supervisory and oversight guidance to the project, HaaB II post training
monitoring visits and interviews were held with the smaller and larger health care businesses in
Kampala and Wakiso. Successes with the HaaB training continue to be registered at the health
care businesses with many health care businesses developing and implementing internal controls,
calculating financial ratios and interpreting them, updating stock cards and controlling inventory.
Some of the health care businesses have put into place quality teams and there is visible
improvement even with the larger health care businesses.
˃ As part of supporting the health care businesses in creating business linkages, the HaaB II health
care businesses were invited to participate at the Uganda Health Federation Business Event 2017
which brought together health sector players to network, share knowledge and gain experience.
1.5. Program Transition plan Implementation
During the reporting period, PHS held transition
meetings with health facilities and incoming
implementing partners (IP’s) during which the
IP’s that were expected to support the different
regions were introduced to the facilities. These
were attended by the facility staffs,
representatives of incoming IP’s, and Program
staff. Meetings have been held with IPs that
include IDI, Makerere University Walter Reed
Program and Rakai Health Sciences Program.
During these meetings, PHS discussed facility
implementation models and support, work plans,
implementation budgets for PNFP sites and asset
registers. Th e Program continued supporting all
health facilities for sustained reporting as well as
un-interrupted supply of medicines, other
supplies to avoid disruption in service delivery
and conclude planned capacity building efforts.
The Program hired a Transitions Manager to lead this process. Going forward, the Program will
continue to hold stakeholder meetings, engage the incoming IPs and health facilities to enable a
seamless transition process.
Transition meeting held at Hotel Africana. In attendance are PHS Program staff, IDI representatives, Mildmay Uganda and representatives from partner facilities from Kampala District, Wakiso District and Bunyoro region.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 41
Intermediate Result (IR) 2. Increased affordability of private health services and products
2.1. Reducing the prices of health products and services
2.1.1. Provide access to income generating opportunities for HIV/AIDS peer support groups
During the fourth quarter, the Program continued to provide access to income generating opportunities
through its performance based grant with Child Health Education and Development Foundation
(CEDO), a civil society organization. The grant promotes skills and livelihood trainings, enterprise
development, and income growth activities amongst OVC VSLA groups and HIV/AIDS peer support
groups in Wakiso, Jinja, Sheema and Rukungiri. During the first six months of the grant, the Program
conducted the following activities:
Adaption of existing training guides to tailor them for starting and improving their businesses
Selection of groups and strengthening their capacity in managing and sustaining a group enterprise
Strengthening the skills of project participants through tailor made business improvement training
sessions
Orientation of vocational institutions and local artisans on the delivery of required apprenticeship
and vocational skills
Facilitating placement of project beneficiaries to vocational centers/local artisans for non-formal
skills development to enable them to start their own enterprises
Placement of older beneficiaries 25+ years from urban centers in modern small-scale farming
Mobilization of project beneficiaries to appreciate community based health insurance
Carrying out home visits to individual member households (25 per District) to track behavioral
changes in the practice of good financial management and other recommended practices
Convening monthly progress review and coordination meetings to share notes, review progress
against set targets, and agree on actions that could ensure quality project implementation.
Table 3: Modules and number of beneficiaries trained per module
Training modules Beneficiaries Against annual target
Start and Improve your business 3,183 (53% of the overall annual target).
Participants placed for urban farming trainings 1,072 (53.6% of the annual target)
Linked to vocational centers/local artisans for non-formal skills development to enable them start own enterprises
614 (30.7% of annual target)
During Year 4, the Program developed a scope of work for a performance based grant agreement to
increase the ability of HIV/AIDS peer support groups members, VSLA group members, and their
households in Program target districts to pay for health services via various economic strengthening
initiatives. Through a competitive procurement process, the Program selected Child Rights
Empowerment and Development Organization (CEDO), to support this activity. The grantee conducted
the following initial activities in the four target districts of Jinja, Rukungiri, Sheema and Wakiso: 1)
Identified targeted beneficiaries and conducted a baseline assessment for the targeted
households/groups, 2) Conducted mapping to establish the available vocational institutions and local
artisans to offer apprenticeship training opportunities to the beneficiaries, and 3) Conducted a household
livelihoods and market assessment/survey.
2,046 out of a targeted 2,400 beneficiaries were identified and baseline information obtained to inform
benchmarks for subsequent engagements. The reason for reaching out to less than the targeted number

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 42
was that the survey teams had to go to the
respective district authorities for introductory
letters during a time when the responsible
officers/authorities were participating in
workshops to develop district budgets for FY
2017. This slowed down progress of the activity.
However, four district-based-mapping exercises
were undertaken to ascertain availability of
vocational and apprenticeship opportunities and
their capacities. To facilitate placement and
apprenticeship opportunities in small and micro-
scale industries, 40 partners (including NGOs,
vocational centers and artisans) were identified
to do so in each of the three mapped districts. An
average of 10 institutions per district was
selected after the capacity assessment for each institution. A database which profiles the baseline
information for the targeted beneficiaries was put in place. 1,367 of the direct project beneficiaries (57%
of the target) were oriented on the market-driven vocational and livelihoods skills they would wish to
take based on the market survey findings. Below is a table summarizing key opportunities identified
during the district based mapping.
Table 4: Key opportunities identified within each district
SHEEMA RUKUNGIRI JINJA WAKISO
› Banana bulking with emphasis on formation of collection centers and business links with large markets ( especially Kampala)
› Growing urbanization with need for support services especially in places with lower supplies of foods such as vegetables
› A linear network of roads with connectivity to the town and markets.
› Rice growing and trading especially in Bwambara sub- county
› Matoke growing and trading in Bunganga and Nyakishenyi sub-counties
› Irish, maize, beans and ground nuts growing especially in Nyakishenyi
› Support services such as saloons & catering services
› Value addition and bi product use on milk ghee making, ice cream among others
› A strong factory base thus available employment and business potential for skilled beneficiaries
› Contemporary farming in areas like rabbits rearing, poultry among others
› The district is intertwined with a strong road network connecting it to the wider Nansana, Matugga, Kawempe and Kampala market
› Urban farming including vegetable growing, rabbits rearing, poultry among others
› Trade and commerce
2.1.2. Facilitate dialogue between MOH and private health sector to rationalize financing for
health
During Year 4, the Program worked with the Uganda Healthcare Federation (UHF) to get health
financing on the MOH’s agenda. The Program approached the Ministry of Health, particularly the
Planning Department, and identified which tasks from the National Health Financing Strategy agenda
were most appropriate to engage MOH with. The purpose was to assist UHF ensure that the private
sector is included in MOH’s upcoming Performance Based Financing initiatives since the PNFP’s had
been included while the private healthcare providers (PHP’s) had not. After a series of consultative
meetings between UHF and the MOH, UHF was able to get MOH to have PHP’s participate in its World
Bank supported results based financing initiatives such as the vouchers for pregnant mothers.
CEDO team during the capacity assessment visit to the artisan to offer training in modern small-scale farming.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 43
2.1.3. Supporting the passage of the health financing strategy and national health insurance bill
During the fourth quarter, the Program worked with UHF to review the Management Sciences for
Health (MSH) terms of reference on costing the national health insurance. The Program supported UHF
to review the MSH terms of reference on costing the national health insurance package of services. The
Program found that policy considerations had not been made in the TOR’s and worked with MSH to
include policy advocacy on best practices from other successful African health insurance programs.
During Year 4, the Program provided actuarial consultancy services to select private health insurance
providers and health management organizations (HMO’s) in Uganda to enable them to enroll more
members and develop a health insurance product that they can market to individuals and integrate with
the proposed national health insurance scheme (NHIS) once various MOH initiatives on costing are
concluded. For each participating company that provided sufficient information, individual actuarial
reports were provided. These reports included an overall business overview; relevant trends in
experience and profitability, claims reserving; premium and pricing adequacy; adequacy of reinsurance
arrangements; asset and liability management; and solvency and capital requirements for each.
The Program further developed an action plan for the private health insurance industry (including the
HMO’s), to engage with the MOH as the proposed National Health Insurance Scheme is implemented.
A major finding of this study was that a minimum benefit package for an average Ugandan who can
afford private health insurance is as summarized in Table 5 below:
Table 5: Health Insurance Benefit Package (Annual limits)
Benefit Package A. Limit for a shared family benefit B. Limit for an individual benefit
Outpatient excluding Dental and Optical
UGX 1.5M per family (USD 420) UGX 500,000 per person (USD 140)
Outpatient Co-pay amount per visit
UGX 5,000 (USD 2) UGX 5,000 (USD 2)
Inpatient Cover with standard exclusions
UGX 5M per family
(USD 1,400)
UGX 3M per person (USD 835)
Chronic Limit within Inpatient 40% 40%
Maternity Limit within inpatient UGX 1M per family (USD 280) UGX 1M (USD 280)
The recommended pricing based on statistics provided by the participants of this study was as follows.
The pricing was based on the type of private health facility that would be providing the package, i.e.
whether it was an insurance company or an HMO which owns its own hospital facilities, and on whether
it was an individual or shared benefits/family plan being purchased.
Table 6: Proposed Pricing for the individual benefit package (Annual premiums)
Proposed Pricing for the individual benefit package
Private Health Insurers (UGX)
Health Management Organizations (UGX)
Private Health Insurers (USD)
Health Management Organizations (USD)
Outpatient Premium 105,762 114,107 30 32
Inpatient Premium 47,256 45,944 13 13
Maternity Premium 487,482 422,964 135 117
Total Premium 640,500 583,015 $179 $162
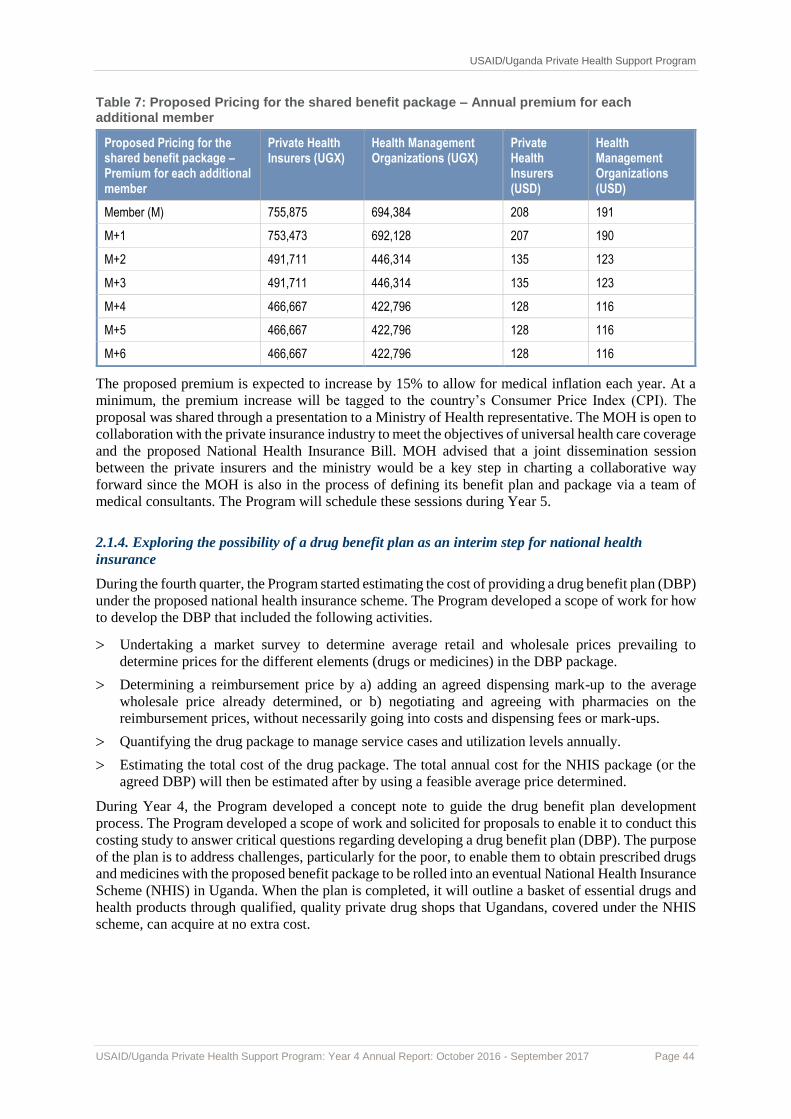
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 44
Table 7: Proposed Pricing for the shared benefit package – Annual premium for each additional member
Proposed Pricing for the shared benefit package – Premium for each additional member
Private Health Insurers (UGX)
Health Management Organizations (UGX)
Private Health Insurers (USD)
Health Management Organizations (USD)
Member (M) 755,875 694,384 208 191
M+1 753,473 692,128 207 190
M+2 491,711 446,314 135 123
M+3 491,711 446,314 135 123
M+4 466,667 422,796 128 116
M+5 466,667 422,796 128 116
M+6 466,667 422,796 128 116
The proposed premium is expected to increase by 15% to allow for medical inflation each year. At a
minimum, the premium increase will be tagged to the country’s Consumer Price Index (CPI). The
proposal was shared through a presentation to a Ministry of Health representative. The MOH is open to
collaboration with the private insurance industry to meet the objectives of universal health care coverage
and the proposed National Health Insurance Bill. MOH advised that a joint dissemination session
between the private insurers and the ministry would be a key step in charting a collaborative way
forward since the MOH is also in the process of defining its benefit plan and package via a team of
medical consultants. The Program will schedule these sessions during Year 5.
2.1.4. Exploring the possibility of a drug benefit plan as an interim step for national health
insurance
During the fourth quarter, the Program started estimating the cost of providing a drug benefit plan (DBP)
under the proposed national health insurance scheme. The Program developed a scope of work for how
to develop the DBP that included the following activities.
Undertaking a market survey to determine average retail and wholesale prices prevailing to
determine prices for the different elements (drugs or medicines) in the DBP package.
Determining a reimbursement price by a) adding an agreed dispensing mark-up to the average
wholesale price already determined, or b) negotiating and agreeing with pharmacies on the
reimbursement prices, without necessarily going into costs and dispensing fees or mark-ups.
Quantifying the drug package to manage service cases and utilization levels annually.
Estimating the total cost of the drug package. The total annual cost for the NHIS package (or the
agreed DBP) will then be estimated after by using a feasible average price determined.
During Year 4, the Program developed a concept note to guide the drug benefit plan development
process. The Program developed a scope of work and solicited for proposals to enable it to conduct this
costing study to answer critical questions regarding developing a drug benefit plan (DBP). The purpose
of the plan is to address challenges, particularly for the poor, to enable them to obtain prescribed drugs
and medicines with the proposed benefit package to be rolled into an eventual National Health Insurance
Scheme (NHIS) in Uganda. When the plan is completed, it will outline a basket of essential drugs and
health products through qualified, quality private drug shops that Ugandans, covered under the NHIS
scheme, can acquire at no extra cost.
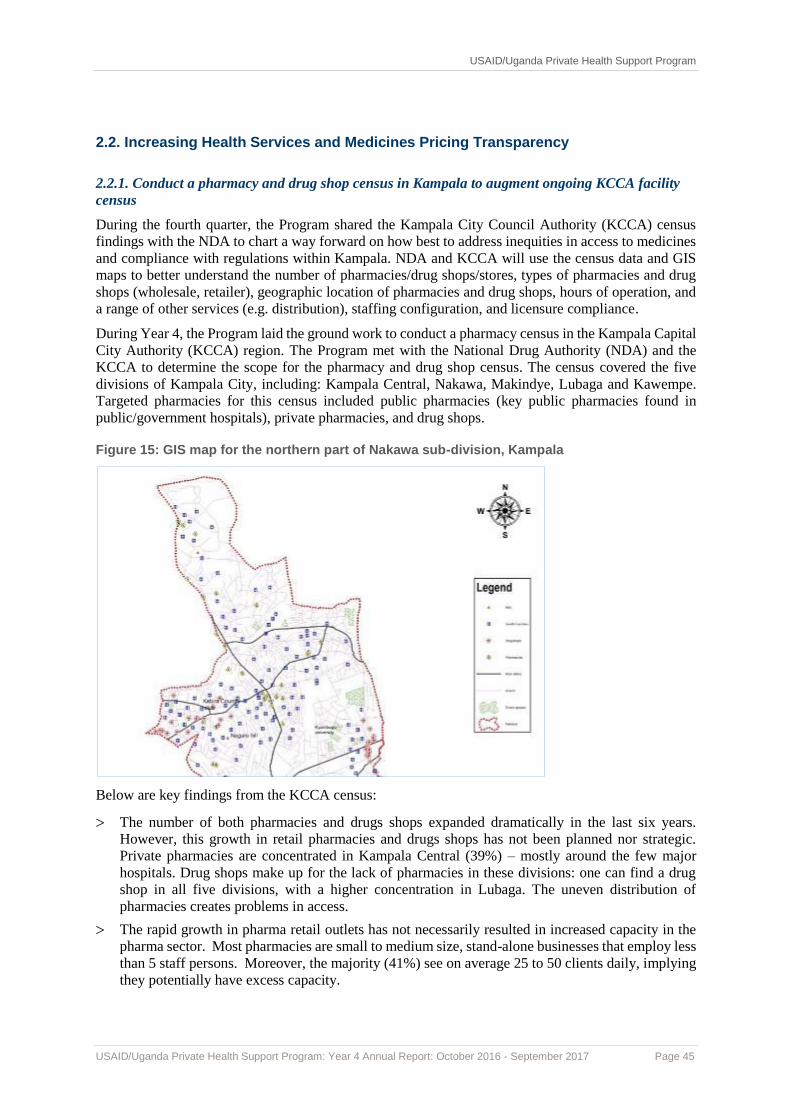
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 45
2.2. Increasing Health Services and Medicines Pricing Transparency
2.2.1. Conduct a pharmacy and drug shop census in Kampala to augment ongoing KCCA facility
census
During the fourth quarter, the Program shared the Kampala City Council Authority (KCCA) census
findings with the NDA to chart a way forward on how best to address inequities in access to medicines
and compliance with regulations within Kampala. NDA and KCCA will use the census data and GIS
maps to better understand the number of pharmacies/drug shops/stores, types of pharmacies and drug
shops (wholesale, retailer), geographic location of pharmacies and drug shops, hours of operation, and
a range of other services (e.g. distribution), staffing configuration, and licensure compliance.
During Year 4, the Program laid the ground work to conduct a pharmacy census in the Kampala Capital
City Authority (KCCA) region. The Program met with the National Drug Authority (NDA) and the
KCCA to determine the scope for the pharmacy and drug shop census. The census covered the five
divisions of Kampala City, including: Kampala Central, Nakawa, Makindye, Lubaga and Kawempe.
Targeted pharmacies for this census included public pharmacies (key public pharmacies found in
public/government hospitals), private pharmacies, and drug shops.
Figure 15: GIS map for the northern part of Nakawa sub-division, Kampala
Below are key findings from the KCCA census:
The number of both pharmacies and drugs shops expanded dramatically in the last six years.
However, this growth in retail pharmacies and drugs shops has not been planned nor strategic.
Private pharmacies are concentrated in Kampala Central (39%) – mostly around the few major
hospitals. Drug shops make up for the lack of pharmacies in these divisions: one can find a drug
shop in all five divisions, with a higher concentration in Lubaga. The uneven distribution of
pharmacies creates problems in access.
The rapid growth in pharma retail outlets has not necessarily resulted in increased capacity in the
pharma sector. Most pharmacies are small to medium size, stand-alone businesses that employ less
than 5 staff persons. Moreover, the majority (41%) see on average 25 to 50 clients daily, implying
they potentially have excess capacity.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 46
The rapid growth is a missed opportunity to increase access to key public health services through
private pharmacies and drugs shops. The data showed that more than half (53%) the drug shops
offer family planning methods, probably because the majority of drug shop owners are retired MOH
nurses trained in FP counselling. But a very small percentage offered basic health services.
Compliance with regulations among private pharmacies and drug shops is uneven. Although, a
relatively large number of pharmacies and drug shops are registered (83% and 97%, respectively),
most facility licenses are not valid and were expired. Possible explanations for the alarming number
of invalid facility licenses include: i) few facilities being aware of recent changes in NDA
regulations, and ii) many facilities waiting to register in the new year to avoid paying full licensing
fees for a partial year. Moreover, drugs shops dispensed drugs that were not part of their scope.
In addition to the non-compliance issues, the several gaps in the systems supporting pharmacies
and drug shops. The facility census highlights the acute shortage in human resource in the pharma
sector. Of the facilities contacted, only 46% had a full-time pharmacist while 24% had a pharmacy
technician/ dispenser. Most facilities rely on health cadres – clinical officer, registered nurse or
midwife – who are not trained in good prescribing practices to dispense medicines.
2.2.2. Conduct an Awareness Campaign on Rational Use of Medicines and Disseminate
recommended EMHSL Commodity Prices
During the fourth quarter, the Program concluded its nine-month campaign on promoting the rational
use of medicines and disseminating recommended retail prices for essential medicines. The Program
assessed the success of the campaign throughout retail medicine outlets in Mukono, Jinja, and Kamuli
districts. Key results of its assessment showed that in all three districts, the proportion of respondents
who reported that private drug providers clearly provide information on use of medicines increased
slightly, from 71% to 73%. Mukono and Jinja registered marked increases, from 62% to 93% and from
56% to 71%, respectively. The proportion of respondents who agree that medicines envelops are clearly
marked with the name of medicine, dose and duration of treatment increased slightly, from 60% to 66%
on average. The largest increase was registered in Mukono,
from 55% to 86%.
The proportion of respondents who report that private health
providers consider their ability to pay when they decide which
medicines to sell increased markedly from 21% to 37%.
Likewise, the proportion that reported that medicines costs in
private drug outlets in their area are affordable increased
marginally from 18% to 20%, on average. The highest
proportion was registered in Jinja, at 37%, from 25%.
However, the proportion of respondents who report that the
quality of services delivered by private health care providers
in their neighborhood is good increased significantly, from
46% to 65%, overall. Mukono district registered the biggest
increase, from just 34% in the baseline survey, to 97% in the
end line survey. The results further show that the community
practices in seeking quality services improved. For instance,
the proportion of the respondents who reported that they only
went to a licensed health facility such as an RMO to get their
medicines more than doubled, from 33% to 72%.
During Year 4, the Program achieved a reduction in essential
medicines sold by RMOs in particular areas. The Program
monitored trends in medicine prices in the three target districts to track price trends. An assessment
conducted in July in Jinja district revealed that 15 PHPs were selling ACTs between UGX 3500 - 4500
and only four facilities namely, Mwinike drug shop in Buwenge town council, Calvary drug shop in
Wanyange subcounty, and Nabweteme drug shop and Erunasser drug shop in Mafubira sub-county
were selling ACTs in the range of UGX 5000 - 6000. The tracking of medicine prices enabled the
HEPS staff member Mr. J.B. Luyima and Mr. Julius Mayengo of the NDA during a radio talk show on Radio Simba

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 47
Program to engage the district drug inspector (DDI) Jinja on the issue of Mafubira having higher-than-
average prices for medicines. He noted it was because they were facing high licensing charges from the
town council.
The Program therefore engaged members of RMO associations and the subcounty local governments
over the issue of high trading license fees. The DDI and private health sector association members
proceeded to engage subcounty leaders in Kisozi, Balawoli and Nawanyago on the problem of high
licensing fees which were being transferred to health consumers through higher medicine prices. In
these specific sub-counties, it has been agreed that PHPs will be assessed according to the value of the
businesses effective 2017/18 financial year.
2.2.3. Support pooled procurement for private health providers
During the fourth quarter, the Program worked with Joint Medical Stores (JMS) to provide pooled
procurement services to four private health sector associations and one district based private health
sector association. The Program provided legal, coordination and logistical support services to the
Uganda Healthcare Federation (UHF), Uganda Private Midwives Association (UPMA), Uganda Private
Health Training Institution Association (UPHTIA), Uganda Community Based Health Care Association
(UBHCA), and Mukono District Private Health Sector Association. Specific activities provided
included training in pooled procurement methods, and legal reviews of the associations’ registrations
so they can engage in pooled procurement services. This work is ongoing and will continue into
Program Year 5.
During Year 4, the Program provided legal, coordination and logistical services to private health sector
associations. Specific activities the Program conducted for the private health sector associations
included 1) Reviewing and improving existing legal documents, 2) Assisting private sector associations
to register appropriately so they can engage in pooled procurement activities, and 3) Training
association members on pooled procurement, member recruitment and ordering guidelines.
2.2.4. Disseminating the professional fee guidelines
During the fourth quarter, as agreed during prior engagements with the Uganda Medical Association,
the Program scheduled eight professional fee guidelines dissemination meetings with the Uganda
Medical Association members in the four geographical regions of Uganda (Eastern, Western, Northern
and Central regions). During these
meetings, the Program will
facilitate adoption of the guidelines
within the private health sector by
sharing them with the respective
district based regulatory
institutions, holding consultative
meetings with all the medical
professional associations’
representatives in the districts, and
undertaking the necessary
consultative meetings with the
Uganda Medical and Dental
Practitioners Council to gazette the
fees.
During Year 4, the Program
finalized its work with the Uganda
Medical Association (UMA) and
the Uganda Medical and Dental
Practitioners Council (UMDPC) to develop professional fee guidelines for the private health sector. The
Program held planning meetings with the Uganda Medical Association (UMA), the Uganda Dental
“Medical Council Sets Doctors’ Fees” article in the Daily Monitor. January 9, 2017
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 48
Association (UDA), and the Uganda Private Medical Practitioners Association (UPMPA) to develop a
way forward on how to disseminate the final guidelines. The stakeholders agreed that a bigger meeting
be held with all UMA, UDA, and UPMPA individual members to solicit their input and
recommendations on how best to disseminate the guidelines. UMA had raised concerns that some of its
members were opposed to the dissemination of the professional fee guidelines because of
misinformation that the fees had already been gazetted by the regulatory councils. As a result, the
Program organized a consultative meeting with all stakeholders at which UMA members unanimously
agreed to conduct stakeholder consultations to review the updated guidelines before proceeding with
the regional disseminations. These disseminations will continue into Year 5.
2.3. Limiting financial barriers to accessing health services
2.3.1. Promote use of information and communication technology (ICT) in health
During the quarter, the Program signed MOU’s with six high volume sites to take on e-health students
from institutions with information and communication technologies (ICT) programs. However, the ICT
institution with which the Program signed an MOU, International Health Sciences University (IHSU),
did not have any graduate students ready for placement by the end of the reporting period. According
to IHSU, the first batch of graduating students will be ready for placement in January 2018.
During Year 4, facilitated the process of working towards improving the quality of health data and
information services in five private health facilities by signing an MOU with IHSU. The purpose of the
MOU was to develop e-health solutions, support data systems management processes, and provide
recommendations on how developed solutions could be adopted, scaled up, and institutionalized by
Program health facilities. The Program therefore identified six high volume facilities to benefit from
this initiative. The facilities were Family Health Resource Centre in Kiruhura district, Engari
Community Health Centre in Kiruhura district, Mayanja Memorial Hospital in Mbarara district, Ishaka
Adventist Hospital in Ishaka district, St. Francis Buluba Hospital in Mayuge district, and Meeting Point
Kampala in Kampala district.
2.3.2. Promoting health insurance and health savings with VSLA groups
During the fourth quarter, the Program worked with Integrated Community Based Initiatives (ICOBI)
through a performance based grant to promote and provide community health insurance (CHI) to 1,350
households (with up to 7,227 beneficiaries) in the rural and peri urban communities of Sheema,
Rukungiri, Jinja and Wakiso districts. During the quarter the Program specifically:
42 additional community health volunteers were identified in the four target districts to boost
mobilization of groups and households to be enrolled in the project.
Five additional health facilities were mapped and assessed.
Financial Savings groups’ leaders were mobilized and trained on saving for health concepts as well
as accessing health care under a health Plan.
Over 600 district and sub county leaders were mobilized and sensitized on the community health
insurance.
During Year 4, the first enrolment of clients on community health insurance was initiated in the four
target districts of Sheema, Rukungiri, Jinja, and Wakiso. Identity cards were distributed to all the
enrolled members. Five MOU’s were signed with five different private health providers after
negotiations and sensitizations on how community health insurance is conducted. By the end of the first
12-month phase of the performance based grant, a total of UGX 35.8 million shillings had been
collected for health savings amongst the five private health facilities.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 49
2.3.3. Document maternal health voucher program in Kiruhura district to demonstrate success of
privately financed self-sustaining voucher to delivery critical health services
During the fourth quarter, the Program completed the process of documenting the maternal health
voucher program at Family Health Resource Center, Kiruhura. The Program found the following
structure on the FHRC model:
The voucher cards with health services were designed, printed, marketed and purchased by women
who in turn used them to access health services from the FHRC or from the two outreach posts of
Rwetamu and Biguri.
The voucher card entitled the holder the four visits of antenatal care, STI screening, delivery,
postnatal care and Family Planning, specific tests such as; hemoglobin , TB, HIV and syphilis
screening. For other persons who were screened for STIs and other infections, treatment costs would
be subsidized so they would end up paying 60% of the cost.
Most respondents learnt about the FHRC voucher scheme through the FHRC health workers while
the smallest category learnt about it through VHTs who were by design supposed to sell and inform
the masses about the voucher scheme.
The Program found that the FHRC voucher scheme contributed immensely to the improvement of
health seeking behaviors among the women of Kiruhura district. Below are the RH/FP related outcomes
realized under the FHRC voucher scheme for mothers. The program came up with the following
recommendations for scaling up a similar approach:
There is need to link the innovative voucher scheme to the strategic health financing plan in the
country to increase its strategic importance.
Beneficiary awareness is crucial for the voucher system to succeed. The voucher benefits should be
made universally known to all voucher clients. Increasing awareness of program benefits among
target populations is thus necessary for demand creation. Awareness among women on subsidized
services and financial benefits covered by voucher requires expanding demand creation channels at
the community level.
There is need to link the marketing power of the other voucher schemes provided in the private
sector using social franchise umbrella CSOs. Because the funding is low especially for startup,
continuation will require working in combination with a social franchise which are becoming much
more interested in the voucher approach.
The treatment or referral emergency transport for the services purchased by the voucher need to be
offered.
VHTs’ roles of distribution and marketing the voucher has to be accentuated where there are
intentions of scaling up because the current assessment revealed that they fell short in the
highlighted areas.
Documentation of processes and activities at the facilities is crucial so monitoring and eventual
impact measurement can be made easy and smooth.
The voucher scheme could target populations with preferences for private sector providers.
The voucher scheme could target private health facilities.
Create space for claims processing and fraud control and let different entities manage the different
processes: not all by the same manager.
Setting up a voucher scheme monitoring system to facilitate documentation, claims processing, and
fraud control is essential. r
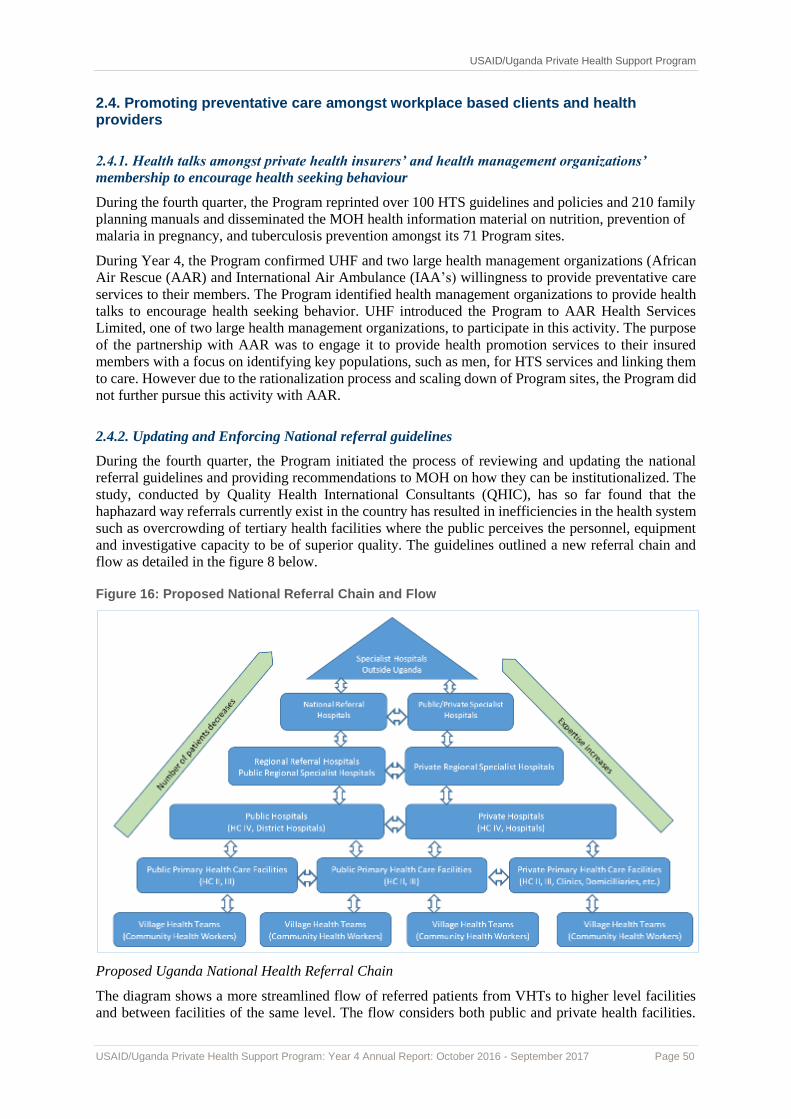
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 50
2.4. Promoting preventative care amongst workplace based clients and health providers
2.4.1. Health talks amongst private health insurers’ and health management organizations’
membership to encourage health seeking behaviour
During the fourth quarter, the Program reprinted over 100 HTS guidelines and policies and 210 family
planning manuals and disseminated the MOH health information material on nutrition, prevention of
malaria in pregnancy, and tuberculosis prevention amongst its 71 Program sites.
During Year 4, the Program confirmed UHF and two large health management organizations (African
Air Rescue (AAR) and International Air Ambulance (IAA’s) willingness to provide preventative care
services to their members. The Program identified health management organizations to provide health
talks to encourage health seeking behavior. UHF introduced the Program to AAR Health Services
Limited, one of two large health management organizations, to participate in this activity. The purpose
of the partnership with AAR was to engage it to provide health promotion services to their insured
members with a focus on identifying key populations, such as men, for HTS services and linking them
to care. However due to the rationalization process and scaling down of Program sites, the Program did
not further pursue this activity with AAR.
2.4.2. Updating and Enforcing National referral guidelines
During the fourth quarter, the Program initiated the process of reviewing and updating the national
referral guidelines and providing recommendations to MOH on how they can be institutionalized. The
study, conducted by Quality Health International Consultants (QHIC), has so far found that the
haphazard way referrals currently exist in the country has resulted in inefficiencies in the health system
such as overcrowding of tertiary health facilities where the public perceives the personnel, equipment
and investigative capacity to be of superior quality. The guidelines outlined a new referral chain and
flow as detailed in the figure 8 below.
Figure 16: Proposed National Referral Chain and Flow
Proposed Uganda National Health Referral Chain
The diagram shows a more streamlined flow of referred patients from VHTs to higher level facilities
and between facilities of the same level. The flow considers both public and private health facilities.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 51
The referral chain also depicts a pyramid-like structure of the facilities denoting the existence of far
more abundant lower level primary health care (PHC) facilities than tertiary level hospitals and a
corresponding expectation that fewer patients and clients should be seeking care at tertiary facilities
where there are fewer but higher trained personnel. With the expected implementation of the National
Health Insurance Scheme soon, the PHC facilities will be made gatekeeper facilities for the scheme.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 52
Intermediate Result (IR) 3. Improved quality of private health sector facilities and services
3.1. Implement SQIS and other continuous quality improvement mechanisms
3.1.1. Roll out of the self-regulatory quality improvement system (SQIS)
During the fourth quarter, the Program enrolled up to 41 health facilities on the online SQIS from over
20 districts. Wakiso district had the highest number of facilities (38).
During Year 4, a total of 335 facilities were enrolled onto the SQIS platform. Out of these, 219 facilities
were supported to self-assess on the online SQIS platform in 33 districts. Health facilities can now
monitor their quality improvement progress through comparing and analyzing the different series of
assessments they submit in the system. Health workers will also be able to prepare better for pre-
licensing inspections. Also, during the year, the Program, in partnership with the Intrahealth Capacity
Project, printed and disseminated over 2,000 SQIS tool kits. Health facilities can now access a tool kit
from the councils at the time of registration. This will enable facilities to understand the requirements
at registration.
3.1.2. Link the Health as a Business (HaaB) network facilities to SQIS
During the fourth quarter, the Program supported five-day integrated Quality Improvement (QI) and
SQIS trainings, follow up mentorships, and coaching of the
Program facilities engaged in the access to finance initiatives.
During Year 4, 78 HaaB-participating health facilities were
trained across the country reaching 144 participants. These
included facility directors (proprietors), administrators,
human resource managers and technical health workers. The
trainings aimed at providing the skills and knowledge to effect
appreciation of quality improvement approaches and
application of the SQIS tool to assess and improve health
service delivery in the private health sector. The trainings also
aimed at empowering and strengthening an understanding and
appreciation of the QI and SQIS approaches and methods in
improving performance and meeting client health
expectations. The trainings helped the participants appreciate
different dimensions of quality and the use of QI tools in gaps
identification. Also during Year 4, post training follow-up
mentorship and coaching were conducted in 44 HaaB health
facilities. Sites were taken through the practical facility
registration, assessment and reporting using the SQIS online
web-based platform and the use of the QI approaches and
methods to document, monitor and improve identified
implementation gaps in their documentation journals.
3.1.3. Support facility self-assessments
During the quarter, the Program supported 41 facilities to conduct self-assessments. Overall, during the
year, a total of 219 facilities in 33 districts were supported to self-assess on the online SQIS platform.
Assessed health facilities can now monitor their quality improvement progress by comparing and
Integrated QI & SQIS Trainings for HaaB2 Health facilities
QI&SQIS onsite follow up mentorship –taking health workers through the online
web-based platform
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 53
analyzing the different series of assessments they submit in the system. Health workers are also better
able to prepare for pre-licensing inspections.
During Year 4, the Program in partnership with the Intrahealth Capacity Project, printed and
disseminated over 2,000 SQIS tool kits to private health facilities and the medical regulatory
professional councils. Health facilities can now access a tool kit from the councils at the time of
registration to enable them understand their requirements at registration time. .
3.1.4. Maintain USAID/ASSIST continuous quality improvement (CQI) approaches and scale up to
other Program activities
During Year 4, the Program in collaboration with the USAID/ASSIST project scaled up quality
improvement approaches through trainings, mentorship and coaching to all partner health facilities.
Over 95% of the Program health facilities have QI teams. During the next quarter, the Program will
focus on cementing the institutionalization of QI principles and methods using best practices and lesson
learnt by engagement of the facility’s management. The purpose will be to strengthen the support and
sustainability of CQI activities in all sites through managers’ orientation to conduct Monthly QI
mentorship and coaching, sharing and learning sessions, technical specific performance review
meetings to monitor KPIs, and harvesting meetings to document best practices packages of tested QI
changes in the private sector.
3.1.5. Establish a laboratory network
During the fourth quarter, the Program continued with the process of supporting the formation and
operation of a private for-profit medical diagnostic laboratory network from amongst members of the
Uganda Medical Laboratory Technology Association (UMLTA). Since this network will follow a
franchise network strategy, the Program supported UMLTA adopt the Labnet name and branding
strategy with a goal of achieving a uniform East African Community-wide identity for qualified
independent medical laboratories.
Since Labnet is a for-profit commercial organization owned and operated by its members, the Program
supported the organization to develop a shareholding structure with Labnet members in the majority.
Minority shares were set aside for the possibility of financial investors taking an equity stake. The
Program also achieved the following during the quarter:
Drafted Memorandum and Articles of Association (Memarts) after which a meeting between the
lawyer and representatives of the interim board of Labnet Uganda was successfully held to discuss
formation, governance and registration issues prior to company registration. The following issues
were clarified in the meeting; process for allotment of shares, price per share, shareholding
structure, process of appointing a board and for how long the board will serve;
Procured a branding company to develop branding guidelines including a logo for Labnet Uganda;
Finalized the company registration process and the registration certificate will be ready by next
month; and
Completed the first round of reviews of the Standard Operating Procedures (Quality standards) for
Labnet
During Year 4, the Program conducted a training on market based approaches that covered the basic
concepts of the Making Markets Work for the Poor (M4P) approaches. This training was attended by 30
people from amongst the Program’s partners including those in the laboratory sector. The Ugandan
laboratory network draws upon experiences in Kenya where the Association of Kenya Medical
Laboratory Scientific Officers (AKMLSO) launched the Labnet network in 2015, which currently has
90 members. Labnet offers consumers of all income levels a clearly identifiable place to obtain accurate
diagnostic tests at an affordable price, with opportunities for standardizing quality, lowering prices,
mitigating competition from unregulated informal market players, and overall better health outcomes
for patients.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 54
3.1.6. Conduct DQA across all Program health areas
Five OVC sites (Alqudus, Nankyama Foundation and Karera Ecumenical Development Organization,
Kakira Out-growers Rural Development (KORD) and International Needs Network (INN)) were visited
by MGLSD, MEEPP and the Program team for an external Data Quality Assessment & Improvement
(DQAI) exercise. The draft reports indicate strengths in the M and E structure, systems and availability
of tools. However there was limited understanding of the OVC indicators and data utilization. These
areas of improvement have been planned for the next quarter.
During the quarter, the program continued to carryout safe male circumcision (SMC) data validation
and provided on-site support in reporting. Results from validation reports indicate that all the data
verified was within the + or -3% variation and therefore no significant errors reported in VMMC data.
The program continued to put emphasis on men aged 15 – 29 years through age specific mobilization,
VMMC sensitization in Secondary Schools and use of circumcision champions.
3.1.7. Conduct Site service quality assessments using SIMS tool
The Program trained 40 frontline health workers from high volume ART and VMMC health facilities
in the use of Site Improvement Monitoring System (SIMS) to support SIMS tools application in data
collection, assessment, monitoring and remedial action for improvement. During the reporting period,
the Program conducted SIMS assessment at 25 PHP sites in quarter 1 and at 40 high volume health
facilities including VMMC implementing sites in Quarter 4. The findings were summarised in a
dashbaords that were shared with each individual health facility. The findings revealed challenges
across all health facilities in the areas of patient tracking, lack of policy guidelines on gender, patient
charter and stigma & discrimination, limited or no services for key populations, limited adolescent
services and weak laboratory systems, especially quality testing, monitoring and quality assuarance
more evidently in low volume PHPs health facilities. These challenges were addressed in subsquent
quarters 2 and 3, and the findings in the Quarter 4 assessment revealed significant performance
improvement in all technical areas though little was being done in relation to supporting services for
key populations. The Program dessiminated and oriented health workers on patient’s charter, guidelines
on stigma & discrimination, trained health workers in adolescent HIV care guidelines and distributed
job aids, in addition to supporting gender integration in health programming and service delivery.
3.2. Implement SQIS and other continuous quality improvement mechanisms
3.2.1. Resume updating the council acts through a performance based grant
During the fourth quarter, the Program conducted a
stakeholder consultation on drafting of regulations for the
Uganda Medical and Dental Practitioners’ Council, Allied
Health Professionals’ Council and Uganda Nurses and
Midwives’ Council Acts. Through the consultation, it was
agreed that regulations be drafted for both the old and
amended Acts as the processes of passing these bills by
Parliament may be longer than anticipated. The Program
also consulted the Law Reform Commission and Ministry
of Justice on the progress of the Bills and drafting of
regulations. The Program lobbied members of parliament
through their Parliamentary Forum on Quality of Health
Services in Uganda for support of the Bills when tabled
before parliament. The Program identified two champions:
Hon. Herbert Kinobere, Chair of the Parliamentary forum
on quality of health services and Hon. Michael Bukenya,
Chairman Parliamentary Committee on Health.
HF QI implemented Project sharing
Guided QI learning sessions

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 55
During Year 4, the Program established contact with the First Parliamentary Council for refinement of
the Bills prior to presentation to the Minister of Health. The Program engaged the Members of
Parliament for buy-in and identification of champions for the Amendment Bills.
3.2.2. Assist the councils to design and establish a web-based platform
During the fourth quarter, the Program facilitated trainings to equip IT staff from the respective
Councils with the web-based platform. The health professional’s registration and licensing workflow
was illustrated end-to-end for the IT staff. Also, a staff capacity assessment was undertaken and skills
divulged to the Council staff with knowledge to manage the common digital platform. By the end of
the quarter, all questions relating to the system were answered, such as: how to operationalize the
platform; where the platform should be hosted; how to sensitize the health professionals, and; what
should the platform be called. The system will be hosted via cloud and was named “The e-Health
Licensing Platform”. It is now live and available at the following URL – www.e-health.med.ug. Further
trainings of the Council staff will be done after SQIS integration.
During Year 4, the Program conducted a technical review of the web-based platform. The purpose of
the review was to streamline and harmonize all the Council’s systems so they could register, certify and
license all HRH personnel and private sector facilities. The review revealed that challenges still existed
that had slowed down the process of harmonization and streamlining of council policies and procedures
for a variety of reasons - most important among them - the Councils’ reluctance to abandon their current
practices. The Program also engaged the National Information and Technology Authority (NITA),
Ministry of Health, and each of the three councils to conduct a systems analysis. Necessary changes to
simplify, streamline and unify all Councils online procedures were incorporated. All the necessary
changes will be completed by end of October and the system re-instated and hosted on Cloud at the
same time.
3.2.3. Support continuous professional
development
During the fourth quarter, the Program printed
1,000 copies of continuous professional
development (CPD) guidelines and also provided
technical assistance to the National CPD steering
Committee to advocate for and disseminate CPD
guidelines for health professionals. The CPD
module was incorporated into the e-health licensing
platform and was illustrated to all three councils.
During Year 4, the Program revitalized the National
CPD Steering Committee which had been dormant
for many years. All three council CPD guidelines were updated and approved by each Council. The
guidelines will be useful to all medical practitioners to reflect on how their learning and development
improves the quality of care they provide to patients. Fulfillment of minimum CPD requirements will
bring about improved quality of care in the health system by ensuring that every practitioner continually
updates their knowledge and skills in their respective fields.
3.2.4. Assist Kampala City Directorate of Health Services to harmonize and field test a uniform
application for facility licensure
During Year 4, a technical review of the web-based licensure system revealed that there were still some
challenges that had slowed down the process of harmonizing and streamlining the council policies and
procedures. The key challenge was the councils’ reluctance to abandon their current licensing practices.
As a result, the current web-based version had “digitized” each Council’s old, isolated and inefficient
ways of registration and licensing instead of having one uniform application. This will be addressed
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 56
during Year 5 to make the system less siloed and more unified by engaging each of the Councils and
having them agree on similar indicators and attributes that do not need to be duplicated in the system.
3.2.5 Assist Kampala City Directorate of Health Services and Environment to conduct a private
provider census
During the fourth quarter, the Program in partnership with KCCA, disseminated the health facility
census findings to multiple stakeholders. Some of the fora at which KCCA disseminated these findings
included presentations during the National QI conference and the Parliamentary forum on QI task force
meeting. KCCA is currently using this data to monitor health service provision and distribution within
the Kampala region. The Program also started upon the process of designing and populating an
inventory of existing public-private partnerships (PPP’s) in health within the KCCA region.
During Year 4, the Program completed the private provider census within the Kampala region. One of
the key census recommendations was for the professional councils to use the KCCA facility census data
to improve upon the council web based platform especially the master sheet which has all facilities in
KCCA. These additions will make the web-based system more efficient as opposed to manually
inserting facility numbers. KCCA also reviewed and analyzed the facility census and service delivery
data to identify opportunities to strengthen referral between public and private sectors.
3.3. Assist private sector representatives to promote standards of care among PFP providers
3.3.1. Strengthen capacity of UHF and other private sector associations to provide services valued
to their members
During the fourth quarter, the Program supported the review of the draft five year strategic plans
developed by the Uganda Private Midwives’ Association (UPMA), Uganda Community Based
Healthcare Association (UCBHCA) and the Uganda Private Health Training Institutions Association
(UPHTIA). Once the strategic plans are completed, the associations will be better placed to fulfil their
mandates and raise extra resources from alternative sources, including donor organizations, so they can
become sustainable.
During Year 4, the Program provided support in legal, coordination and logistical services to private
health sector associations. These included the Uganda Healthcare Federation (UHF), Uganda Private
Midwives Association (UPMA), Uganda Private Health Training Institution Association (UPHTIA),
Uganda Community Based Health Care Association (UBHCA) and Mukono District Private sector
association. When this support is concluded in Year 5, the associations will have up-to-date
constitutions and all required legal documentation for them to provide more services of value to their
members such as pooled procurement.
3.3.2. Support UHF to implement strategic plan
During the fourth quarter, the Program supported UHF to write a financial proposal to the World Bank
totaling US $100,000. The purpose of the proposal was to win a grant to support UHF enroll and conduct
a self-assessment of 100 Uganda Private Midwives Association health facilities on the SQIS online
version. UHF will then verify the self-assessment reports and support the facilities to address the gaps.
Currently UHF is in final phases of signing this contract.
During Year 4, the Program supported UHF to achieve two objectives that are in the UHF Strategic
Plan (2016 - 2021). These were 1) Making UHF financially self-sustaining by financing 50% of
operational costs independently and, 2) Establishing UHF health sector working relationships. The
Program achieved the first objective by helping UHF write two proposals to the World Bank and to
Merck for Mothers which brought the UHF income for the year to a total of over UGX 700 Million. For
the second objective, the Program supported UHF to represent the private sector in the MOH TB
coordination committee and the MOH Quality Assurance and Inspection Department Committee.
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 57
3.3.3. Strengthen private sector engagement with MOH
During the fourth quarter, the Program facilitated a UHF member engagement event where all UHF
members and representatives from MOH got together to share insights and perspectives as they
reviewed UHF’s purpose and its role as a private sector voice. This meeting agreed on the future
organizational and strategic direction of UHF. The Program also sponsored six PHPs to attend the 3rd
National Quality Improvement Conference where the Program and UHF submitted and presented two
abstracts: one on the KCCA facility/provider census and the other on SQIS. In addition, UHF co-
organized the 3rd Members of Parliament Quality Improvement Forum symposium on September 28th
at Collin Hotel, Mukono. Finally, UHF represented the private sector during the 23rd Joint Review
Mission, where Program efforts to improve QI in the private sector through SQIS were recognized.
These engagements provided UHF an opportunity to ably represent and voice private sector
perspectives on the various health sector issues.
During Year 4, in order to build closer working relations with the public sector, UHF co-chaired three
MOH PPPH technical working group (TWG) meetings, attended the NHIS Taskforce meetings and
three (3) HPAC meetings. UHF also took part in and co-organized the Members of Parliament Quality
Improvement Forums meeting held on April 28th- 29th at Ridar Hotel. These interactions enabled
stronger leverage for lobbying and advocacy activities with key stakeholders that take part in these
meetings. UHF also spearheaded the formation of a stakeholder group to support the NHIS and Patients
Responsibility Bills which are crucial in achieving Universal Health Coverage in Uganda.
3.3.4. Advance the formation of a public-private sector dialogue forum
During the fourth quarter, the Program supported UHF to translate the PPPH technical working group
to a committee that doubles as a public-private sector dialogue forum. UHF is now co-chair of the new
PPPH TWG and ensures that the PPPH TWG meets at least once per month. The dialogue forum will
focus on health financing and PPP opportunities and create a shared understanding of the role of the
private health sector in Uganda. It will share ideas, demonstrate the private sector’s role in contributing
to sustainable development, offer recommendations to government from the private sector, and inspire
new public-private partnerships to overcome systemic challenges in Uganda.
During Year 4, the Program continued its efforts towards supporting the recently revived public-private
sector dialogue forum. The Program supported three PPPH TWG meetings and used these meetings to
promote the public-private sector dialogue agenda. Specifically, the Program
Identified five critical private sector stakeholders to form the core of the PPD forum. These were
UHF (who are now the co-chair of the TWG), Uganda Health Marketing Group (UHMG), Health
Partners Uganda, Uganda National Health Consumers Organization (UNHCO), and PACE Uganda.
Convened above mentioned key private sector stakeholders to determine the terms of engagement
of the PPD forum. These terms include regular monthly meetings, stakeholder involvement in
developing meeting agendas, and distribution of signed minutes amongst all stakeholders.
Presented the the draft implementation plan of the PPPH and costing of the PPPH five-year strategic
plan to PPPH TWG members.
3.4. Implement PPPHs that strengthen private sector capacity to deliver quality services
3.4.1. Develop the Ministry of Health PPPH Node’s capacity
During Year 4, the Program conducted a training on basic concepts on PPP’s in health (PPPH) and on
regional experiences in PPP’s. Participants included representatives from different social franchises,
professional associations, medical bureaus, and civil society organizations. The Program also supported
efforts towards designing and approving the PPPH Node charter. Finalization of this work was deferred
until when the PPPH structure and TWG composition is aligned to the law. This decision was because
the recommendations of the analysis of the existing structures set out in the PPPH policy proposed an
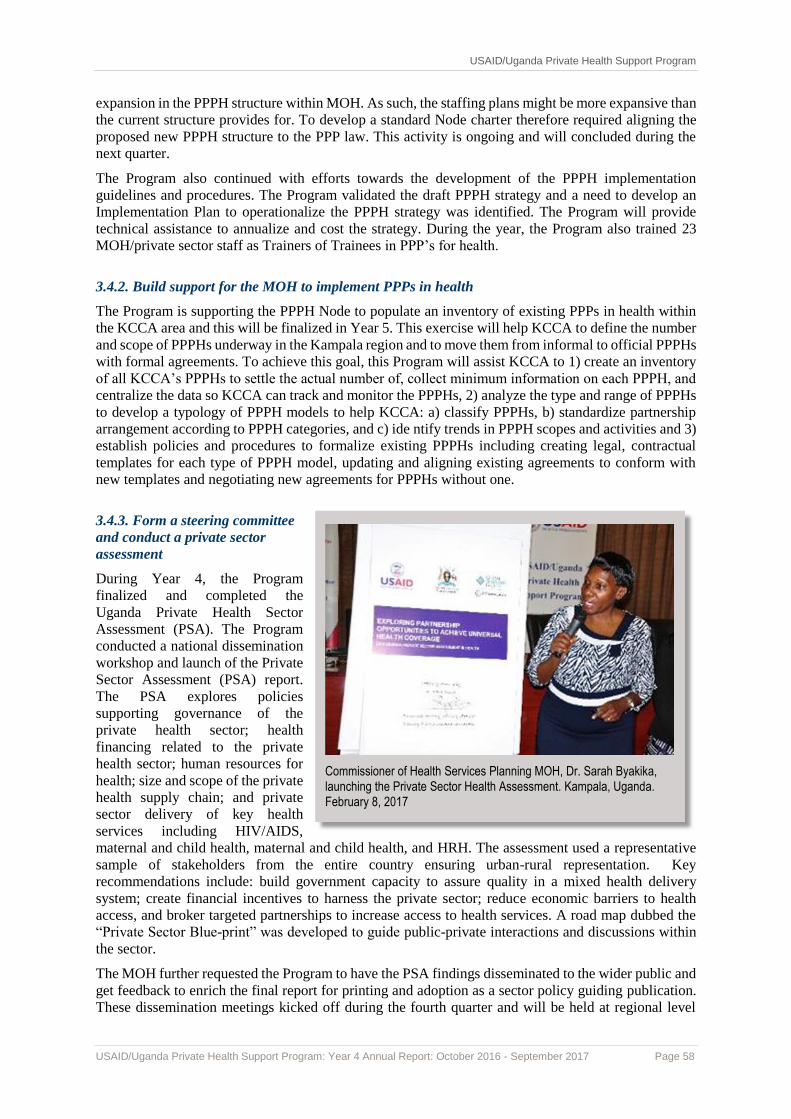
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 58
expansion in the PPPH structure within MOH. As such, the staffing plans might be more expansive than
the current structure provides for. To develop a standard Node charter therefore required aligning the
proposed new PPPH structure to the PPP law. This activity is ongoing and will concluded during the
next quarter.
The Program also continued with efforts towards the development of the PPPH implementation
guidelines and procedures. The Program validated the draft PPPH strategy and a need to develop an
Implementation Plan to operationalize the PPPH strategy was identified. The Program will provide
technical assistance to annualize and cost the strategy. During the year, the Program also trained 23
MOH/private sector staff as Trainers of Trainees in PPP’s for health.
3.4.2. Build support for the MOH to implement PPPs in health
The Program is supporting the PPPH Node to populate an inventory of existing PPPs in health within
the KCCA area and this will be finalized in Year 5. This exercise will help KCCA to define the number
and scope of PPPHs underway in the Kampala region and to move them from informal to official PPPHs
with formal agreements. To achieve this goal, this Program will assist KCCA to 1) create an inventory
of all KCCA’s PPPHs to settle the actual number of, collect minimum information on each PPPH, and
centralize the data so KCCA can track and monitor the PPPHs, 2) analyze the type and range of PPPHs
to develop a typology of PPPH models to help KCCA: a) classify PPPHs, b) standardize partnership
arrangement according to PPPH categories, and c) ide ntify trends in PPPH scopes and activities and 3)
establish policies and procedures to formalize existing PPPHs including creating legal, contractual
templates for each type of PPPH model, updating and aligning existing agreements to conform with
new templates and negotiating new agreements for PPPHs without one.
3.4.3. Form a steering committee
and conduct a private sector
assessment
During Year 4, the Program
finalized and completed the
Uganda Private Health Sector
Assessment (PSA). The Program
conducted a national dissemination
workshop and launch of the Private
Sector Assessment (PSA) report.
The PSA explores policies
supporting governance of the
private health sector; health
financing related to the private
health sector; human resources for
health; size and scope of the private
health supply chain; and private
sector delivery of key health
services including HIV/AIDS,
maternal and child health, maternal and child health, and HRH. The assessment used a representative
sample of stakeholders from the entire country ensuring urban-rural representation. Key
recommendations include: build government capacity to assure quality in a mixed health delivery
system; create financial incentives to harness the private sector; reduce economic barriers to health
access, and broker targeted partnerships to increase access to health services. A road map dubbed the
“Private Sector Blue-print” was developed to guide public-private interactions and discussions within
the sector.
The MOH further requested the Program to have the PSA findings disseminated to the wider public and
get feedback to enrich the final report for printing and adoption as a sector policy guiding publication.
These dissemination meetings kicked off during the fourth quarter and will be held at regional level
Commissioner of Health Services Planning MOH, Dr. Sarah Byakika, launching the Private Sector Health Assessment. Kampala, Uganda. February 8, 2017

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 59
targeting the Central, Western, Northern and Eastern regions - inviting 10 districts per region and at
least three representatives per district. Thereafter the PPPH Node will incorporate the feedback and
produce the final report during the next quarter.
3.4.4. Build the MOH’s PPPH pipeline
During the Year, this activity was accomplished. Please refer to activity 3.4.2 above for more details.
3.4.5. Strengthen PPPH coordination at both the central and district level
During the Year, the Program accomplished the following regarding PPPH coordination.
MOH PPPH Node organization chart/linkages at the central level, in and out of the health ministry
were developed and shared with the MOH for approval.
Designed a PPPH Node charter, a staffing plan and individual work plans and shared these with the
MOH
Completed a report on the PPPH implementation guidelines which was submitted to the MOH
PPPH Node office. The draft guidelines places focus in nine areas with the aim of reducing the
operational nature of the previously developed guidelines especially for the TCMP (Traditional and
Complimentary Medicine practitioners). The draft report was reviewed at a stakeholders’ validation
meeting in August.
Developed the terms of reference (TORs) for the development of the operating systems and
procedures for the PPPH implementation guidelines. The development of the operations manual is
awaiting approval of the implementation guidelines since it would rely on the content within them.
Developed costed activities along the four strategic areas of the 5-year PPPH Strategic Plan. The
draft plan, estimated to cost US $5 million over the five years of the PPPH Strategy, is pending a
stakeholders’ validation meeting.
The Program held two quarterly debriefing
meetings with at which it shared information on
the progress of the PPPH project. At the MOH
senior management committee meeting, the MOH
team was briefed about the overall progress of the
Program’s grant to UNACOH. In addition, the
meeting was briefed about the progress of
development of a 5-year PPPH Strategic Plan and
the development of the costed implementation
plan to operationalize the strategy. The meeting
was also briefed about the studies so far
conducted, including the “Review of the proposed
composition and TORs of the PPPH TWG” which
the SMC were informed would have an impact on
the staffing structure of the PPPH Node in the
MOH. The SMC meeting appreciated the briefing
on the PPPH project, and recommended that a
summary of key issues on the project should be
shared in the meeting of the Health Policy
Advisory Committee (HPAC). The SMC also
commended USAID for the support towards upscaling of the profiling of the Public Private
partnerships.
A cross-section of members attending the PPPH TWG meeting in Kampala. In the TWG meeting, UNACOH had the opportunity to share the draft report of the development of the combined implementation guidelines, for members to critique.
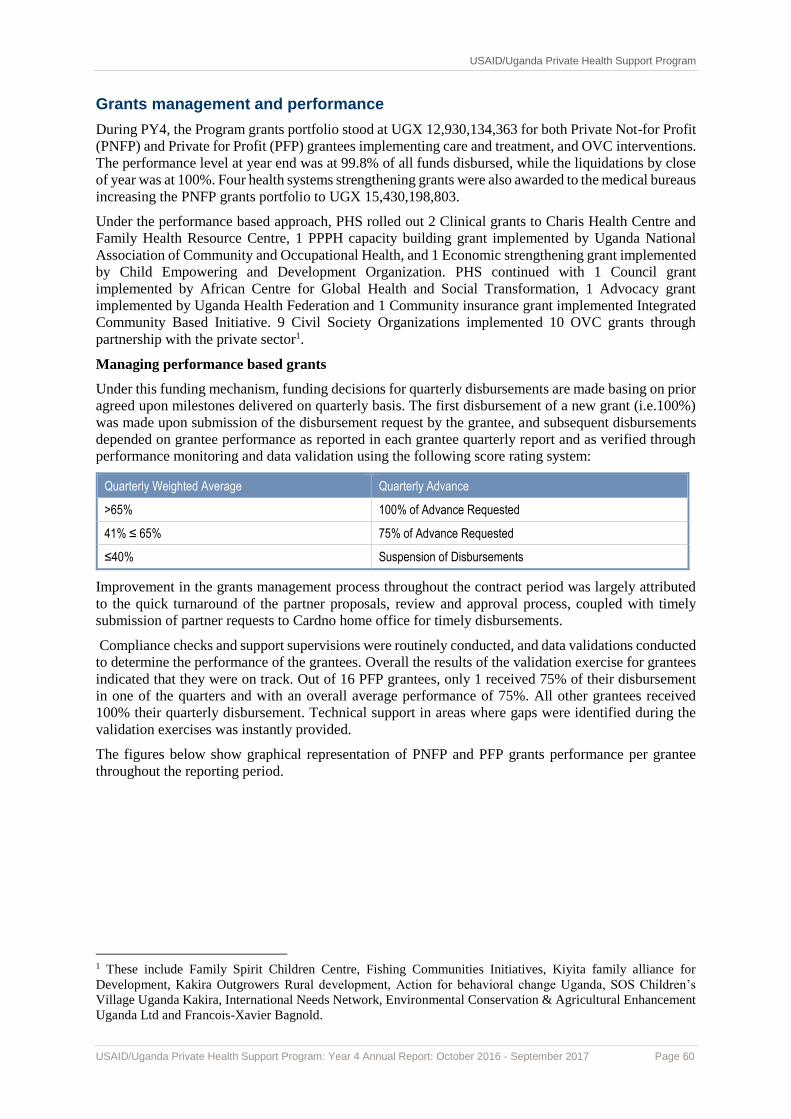
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 60
Grants management and performance
During PY4, the Program grants portfolio stood at UGX 12,930,134,363 for both Private Not-for Profit
(PNFP) and Private for Profit (PFP) grantees implementing care and treatment, and OVC interventions.
The performance level at year end was at 99.8% of all funds disbursed, while the liquidations by close
of year was at 100%. Four health systems strengthening grants were also awarded to the medical bureaus
increasing the PNFP grants portfolio to UGX 15,430,198,803.
Under the performance based approach, PHS rolled out 2 Clinical grants to Charis Health Centre and
Family Health Resource Centre, 1 PPPH capacity building grant implemented by Uganda National
Association of Community and Occupational Health, and 1 Economic strengthening grant implemented
by Child Empowering and Development Organization. PHS continued with 1 Council grant
implemented by African Centre for Global Health and Social Transformation, 1 Advocacy grant
implemented by Uganda Health Federation and 1 Community insurance grant implemented Integrated
Community Based Initiative. 9 Civil Society Organizations implemented 10 OVC grants through
partnership with the private sector1.
Managing performance based grants
Under this funding mechanism, funding decisions for quarterly disbursements are made basing on prior
agreed upon milestones delivered on quarterly basis. The first disbursement of a new grant (i.e.100%)
was made upon submission of the disbursement request by the grantee, and subsequent disbursements
depended on grantee performance as reported in each grantee quarterly report and as verified through
performance monitoring and data validation using the following score rating system:
Quarterly Weighted Average Quarterly Advance
>65% 100% of Advance Requested
41% ≤ 65% 75% of Advance Requested
≤40% Suspension of Disbursements
Improvement in the grants management process throughout the contract period was largely attributed
to the quick turnaround of the partner proposals, review and approval process, coupled with timely
submission of partner requests to Cardno home office for timely disbursements.
Compliance checks and support supervisions were routinely conducted, and data validations conducted
to determine the performance of the grantees. Overall the results of the validation exercise for grantees
indicated that they were on track. Out of 16 PFP grantees, only 1 received 75% of their disbursement
in one of the quarters and with an overall average performance of 75%. All other grantees received
100% their quarterly disbursement. Technical support in areas where gaps were identified during the
validation exercises was instantly provided.
The figures below show graphical representation of PNFP and PFP grants performance per grantee
throughout the reporting period.
1 These include Family Spirit Children Centre, Fishing Communities Initiatives, Kiyita family alliance for
Development, Kakira Outgrowers Rural development, Action for behavioral change Uganda, SOS Children’s
Village Uganda Kakira, International Needs Network, Environmental Conservation & Agricultural Enhancement
Uganda Ltd and Francois-Xavier Bagnold.
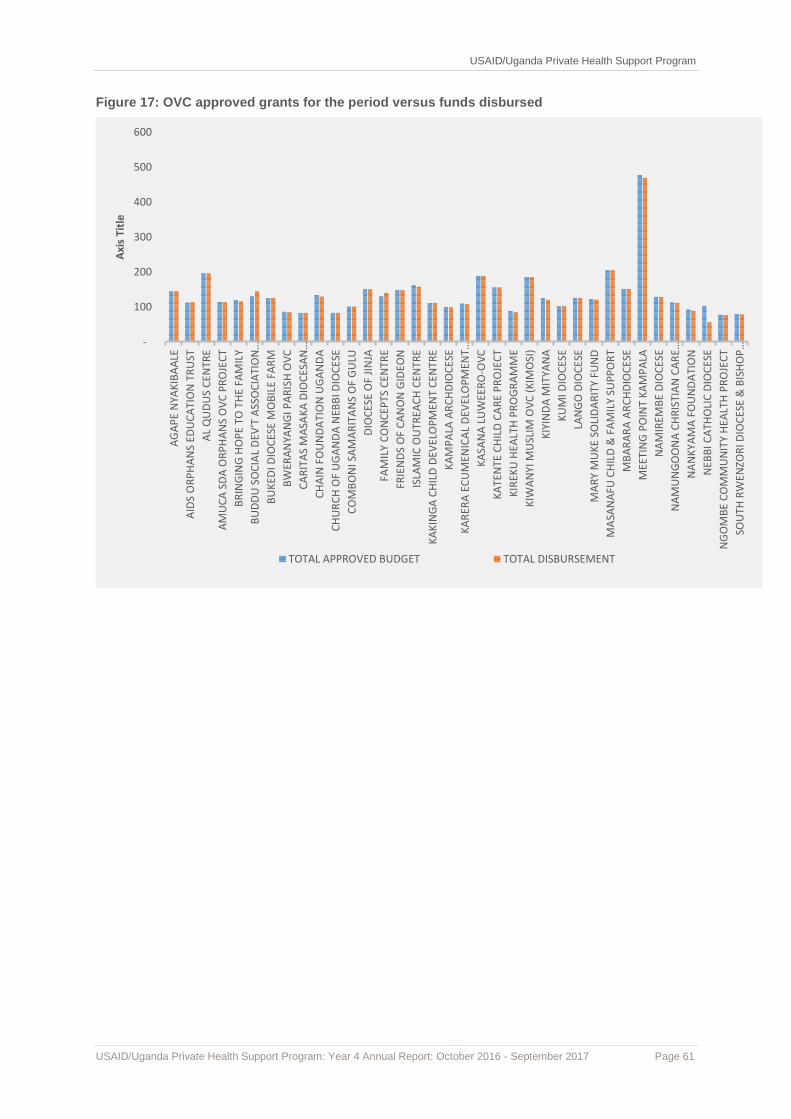
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 61
Figure 17: OVC approved grants for the period versus funds disbursed
-
100
200
300
400
500
600
AG
AP
E N
YAK
IBA
ALE
AID
S O
RP
HA
NS
EDU
CA
TIO
N T
RU
ST
AL
QU
DU
S C
ENTR
E
AM
UC
A S
DA
OR
PH
AN
S O
VC
PR
OJE
CT
BR
ING
ING
HO
PE
TO T
HE
FAM
ILY
BU
DD
U S
OC
IAL
DEV
'T A
SSO
CIA
TIO
N…
BU
KED
I DIO
CES
E M
OB
ILE
FAR
M
BW
ERA
NYA
NG
I PA
RIS
H O
VC
CA
RIT
AS
MA
SAK
A D
IOC
ESA
N…
CH
AIN
FO
UN
DA
TIO
N U
GA
ND
A
CH
UR
CH
OF
UG
AN
DA
NEB
BI D
IOC
ESE
CO
MB
ON
I SA
MA
RIT
AN
S O
F G
ULU
DIO
CES
E O
F JI
NJA
FAM
ILY
CO
NC
EPTS
CEN
TRE
FRIE
ND
S O
F C
AN
ON
GID
EON
ISLA
MIC
OU
TREA
CH
CEN
TRE
KA
KIN
GA
CH
ILD
DEV
ELO
PM
ENT
CEN
TRE
KA
MP
ALA
AR
CH
DIO
CES
E
KA
RER
A E
CU
MEN
ICA
L D
EVEL
OP
MEN
T…
KA
SAN
A L
UW
EER
O-O
VC
KA
TEN
TE C
HIL
D C
AR
E P
RO
JEC
T
KIR
EKU
HEA
LTH
PR
OG
RA
MM
E
KIW
AN
YI M
USL
IM O
VC
(K
IMO
SI)
KIY
IND
A M
ITYA
NA
KU
MI D
IOC
ESE
LAN
GO
DIO
CES
E
MA
RY
MU
KE
SOLI
DA
RIT
Y FU
ND
MA
SAN
AFU
CH
ILD
& F
AM
ILY
SUP
PO
RT
MB
AR
AR
A A
RC
HD
IOC
ESE
MEE
TIN
G P
OIN
T K
AM
PA
LA
NA
MIR
EMB
E D
IOC
ESE
NA
MU
NG
OO
NA
CH
RIS
TIA
N C
AR
E…
NA
NK
YAM
A F
OU
ND
ATI
ON
NEB
BI C
ATH
OLI
C D
IOC
ESE
NG
OM
BE
CO
MM
UN
ITY
HEA
LTH
PR
OJE
CT
SOU
TH R
WEN
ZOR
I DIO
CES
E &
BIS
HO
P…
Axi
s Ti
tle
TOTAL APPROVED BUDGET TOTAL DISBURSEMENT
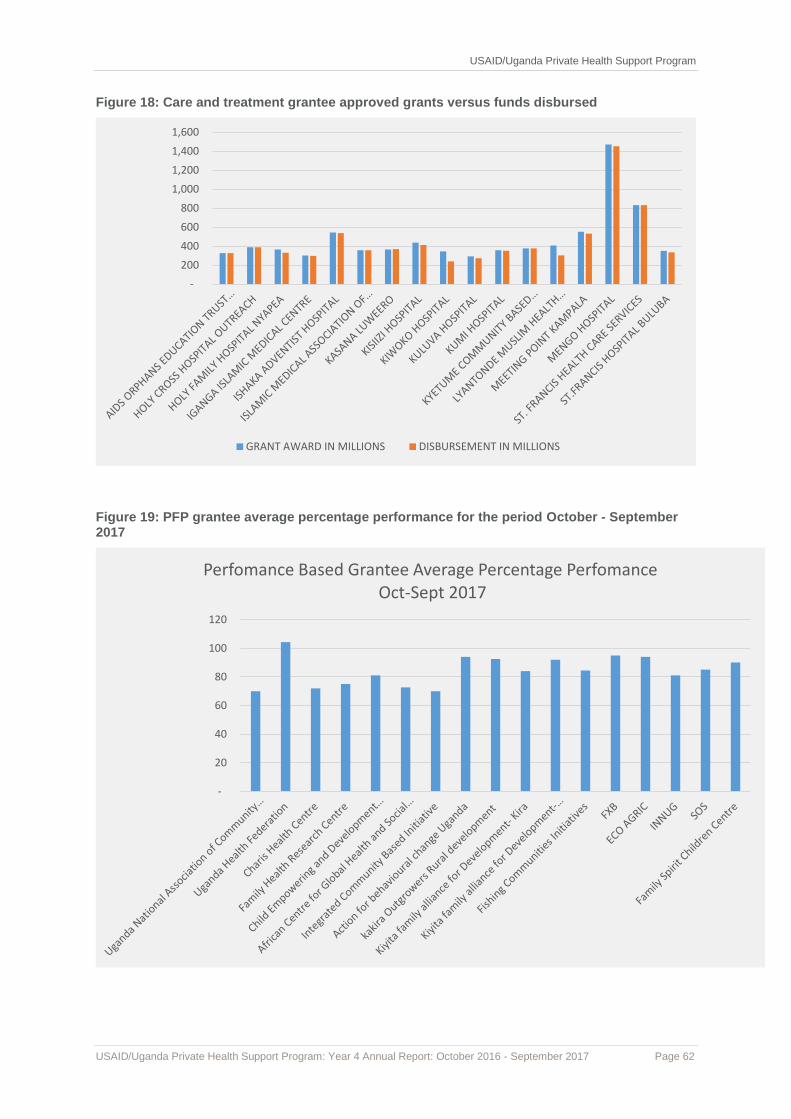
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 62
Figure 18: Care and treatment grantee approved grants versus funds disbursed
Figure 19: PFP grantee average percentage performance for the period October - September 2017
-
200
400
600
800
1,000
1,200
1,400
1,600
GRANT AWARD IN MILLIONS DISBURSEMENT IN MILLIONS
-
20
40
60
80
100
120
Perfomance Based Grantee Average Percentage PerfomanceOct-Sept 2017
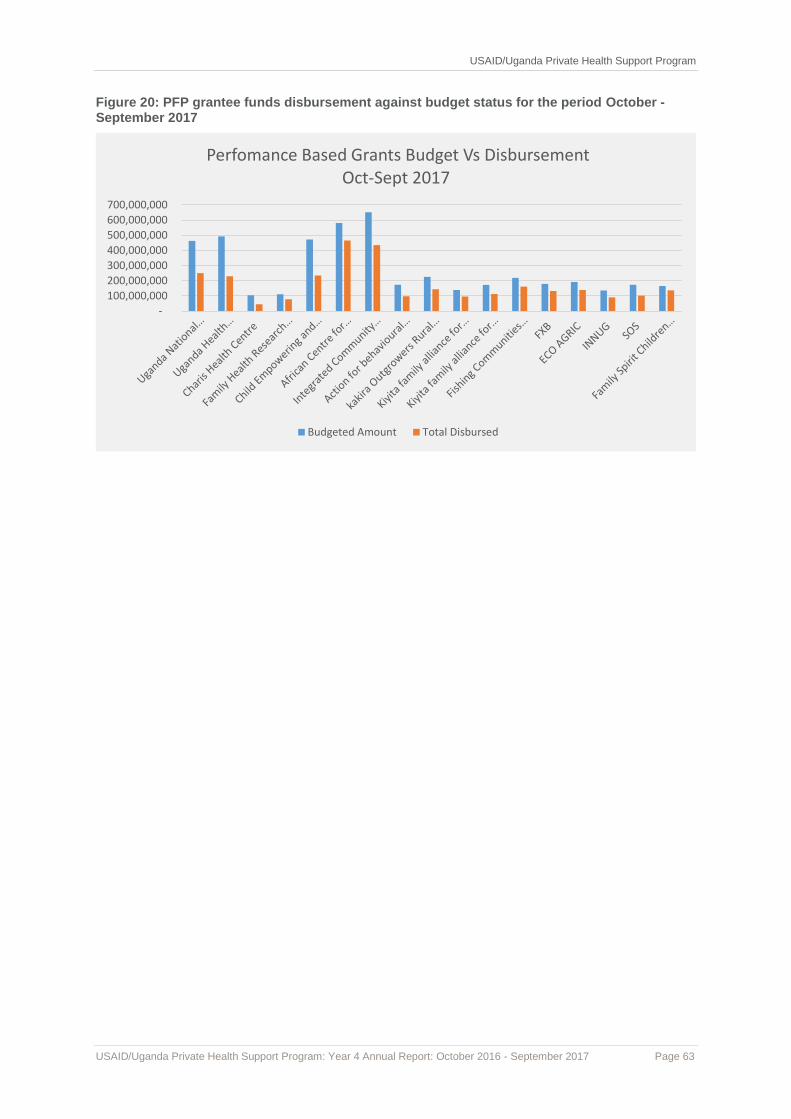
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 63
Figure 20: PFP grantee funds disbursement against budget status for the period October - September 2017
-
100,000,000
200,000,000
300,000,000
400,000,000
500,000,000
600,000,000
700,000,000
Perfomance Based Grants Budget Vs Disbursement Oct-Sept 2017
Budgeted Amount Total Disbursed

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 64
Annex 1: PHS Performance Indicator Table, October 2016–September 2017
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
IR1: Expanded availability of health services by program supported private service providers
Continuing to scale up high impact HIV prevention services
HIV Testing Services (HTS)
Indicator 1: Number of individuals receiving HIV Testing and Counseling (HTC) services for HIV and received their test results
352,704 79,766 76,250 92,240 86,630 334,886 94.9%
(147,022 PFP, 189,864 PNFP) Good performance at 95% of the annual target. This was as a result of site based mentorship, improved mobilization, conducting community HTC outreaches and availability of HTC kits and supplies.
Indicator 2: Total Number of Individuals Testing HIV Positive
12,536 2,328 2,645 2,792 2,463 10,228 81.6%
(4,127 PFP, 6,101 PNFP) Good performance at 81.6% of the annual target though positivity is below the national prevalence of 6.2%. Facility staff have been supported to provide Targeted HTS at high yield entry points and focus on priority and key community groups. This is likely to increase the positive yield in the next quarters.
Indicator 3: Total Number of Positives Linked into Care
5,430 1,799 2,107 2,180 2,076 8,162 150.3%
3,250, PFP, 4,912 PNFP). Linked 84.3% of the positives identified during the last quarter. Achieved 150.3% of the annual target of 5,430. Mentorship and support on use of the National Standard Operating Procedures for Linkage and Referral will continue to improve on linkage and enrollment into care.
Prevention of Mother To Child Transmission (PMTCT)
Indicator 4: Percentage of pregnant women with known HIV status
95% 97% 94.6% 100% 98% 97.3% 102.4% Good performance at 102.4% of the annual target. Support to continue being provided to staff implement the changes in the HTS guidelines for mothers attending ANC.
Indicator 5: Percentage of HIV-positive pregnant women who received antiretrovirals to reduce risk of mother-to-child-transmission (MTCT) during pregnancy and delivery
98% 72% 98.7% 95% 91% 91.3% 93.2%
Good performance at 93.2% of the annual target of 98% of HIV-positive pregnant women receiving antiretroviral to reduce risk of mother-to-child-transmission (MTCT). The staff are doing intensified follow up for missed opportunities in maternity.
Indicator 6: Percentage of infants born to HIV-positive pregnant women who were started on Cotrimoxazole (CTX) prophylaxis within two months of birth
80% 70% 91% 52.0% 89% 68.9% 86% Some of the infants born are yet to make 6 weeks when CTX is initiated.
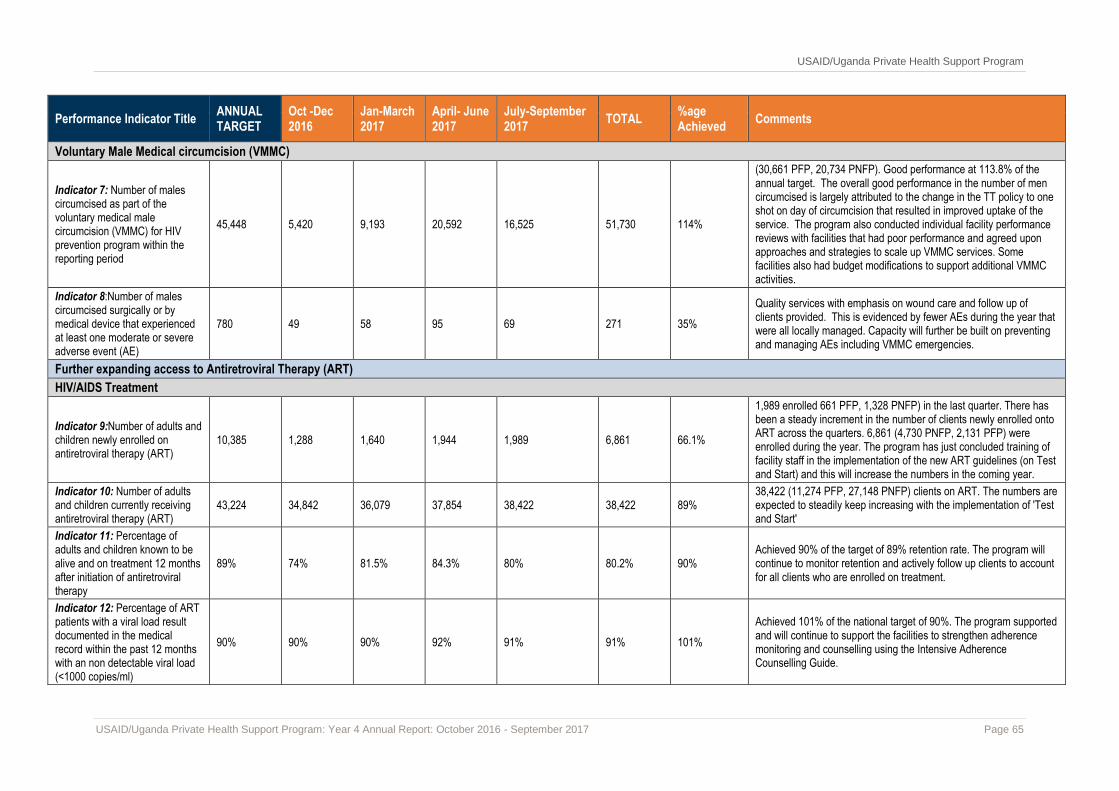
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 65
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
Voluntary Male Medical circumcision (VMMC)
Indicator 7: Number of males circumcised as part of the voluntary medical male circumcision (VMMC) for HIV prevention program within the reporting period
45,448 5,420 9,193 20,592 16,525 51,730 114%
(30,661 PFP, 20,734 PNFP). Good performance at 113.8% of the annual target. The overall good performance in the number of men circumcised is largely attributed to the change in the TT policy to one shot on day of circumcision that resulted in improved uptake of the service. The program also conducted individual facility performance reviews with facilities that had poor performance and agreed upon approaches and strategies to scale up VMMC services. Some facilities also had budget modifications to support additional VMMC activities.
Indicator 8:Number of males circumcised surgically or by medical device that experienced at least one moderate or severe adverse event (AE)
780 49 58 95 69 271 35%
Quality services with emphasis on wound care and follow up of clients provided. This is evidenced by fewer AEs during the year that were all locally managed. Capacity will further be built on preventing and managing AEs including VMMC emergencies.
Further expanding access to Antiretroviral Therapy (ART)
HIV/AIDS Treatment
Indicator 9:Number of adults and children newly enrolled on antiretroviral therapy (ART)
10,385 1,288 1,640 1,944 1,989 6,861 66.1%
1,989 enrolled 661 PFP, 1,328 PNFP) in the last quarter. There has been a steady increment in the number of clients newly enrolled onto ART across the quarters. 6,861 (4,730 PNFP, 2,131 PFP) were enrolled during the year. The program has just concluded training of facility staff in the implementation of the new ART guidelines (on Test and Start) and this will increase the numbers in the coming year.
Indicator 10: Number of adults and children currently receiving antiretroviral therapy (ART)
43,224 34,842 36,079 37,854 38,422 38,422 89% 38,422 (11,274 PFP, 27,148 PNFP) clients on ART. The numbers are expected to steadily keep increasing with the implementation of 'Test and Start'
Indicator 11: Percentage of adults and children known to be alive and on treatment 12 months after initiation of antiretroviral therapy
89% 74% 81.5% 84.3% 80% 80.2% 90% Achieved 90% of the target of 89% retention rate. The program will continue to monitor retention and actively follow up clients to account for all clients who are enrolled on treatment.
Indicator 12: Percentage of ART patients with a viral load result documented in the medical record within the past 12 months with an non detectable viral load (<1000 copies/ml)
90% 90% 90% 92% 91% 91% 101%
Achieved 101% of the national target of 90%. The program supported and will continue to support the facilities to strengthen adherence monitoring and counselling using the Intensive Adherence Counselling Guide.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 66
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
Sustained care and support
Clinical Care
Indicator 13: Number of HIV-positive adults and children newly enrolled in clinical care during the reporting period who received at least one of the following at enrollment: clinical assessment (WHO staging) OR CD4 count OR viral load
5,491 1,450 1,478 1,572 1,318 5,818 106.0% Achieved 106% of the annual target. The program will continue to support utilization of linkage and referral SOPs with an emphasis on active follow-up and linkage.
Indicator 14: Number of HIV-positive adults and children who received at least one of the following during the reporting period: clinical assessment (WHO staging) OR CD4 count OR viral load
64,445 39,626 38,520 39,976 39,319 39,319 61.0% 11,494 PFP, 27,825 PNFP) Numbers in care are expected to increase at most of the sites following the implementation of 'Test and Start'.
Tuberculosis (TB)/HIV
Indicator 15: Percentage of registered new and relapse TB cases with documented HIV status
90% 80% 68.9% 92.7% 80% 78.7% 87% Performance expected to improve with continued guidance in TB/HIV documentation provided to Facility TB staff
Indicator 16: Percentage of HIV-positive new and relapsed registered TB cases on ART during TB treatment
100% 93% 91.3% 96.4% 97% 97.3% 97% Support provided during the quarter for TB/HIV implementation improved service implementation.
Indicator 17: Percentage of PLHIV newly enrolled in HIV clinical care who start isoniazid preventative therapy (IPT)
30% 8.3% 1.7% 5.8% 7.6% 7.8% 26% Few authorized IPT implementing facilities under PHS and in the country because of limited quantities/stock. The current stock can't meet the demand from eligible clients in the country.
Indicator 18: TB treatment outcomes among registered new and relapsed TB cases who are HIV-positive
100% 73% 71.2% 72.8% 68% 71.4% 71.4%
Treatment success rates stagnated at around 71% during the year. The program will continue supporting facilities to follow up all clients, conduct outcome evaluations and improve documentation using QI approach.
Indicator 19: Percentage of PLHIV in HIV clinical care who were
90% 88% 88.6% 94.8% 97% 97% 108% Mentorship and support for TB screening and documentation will continue to be provided to further improve performance.
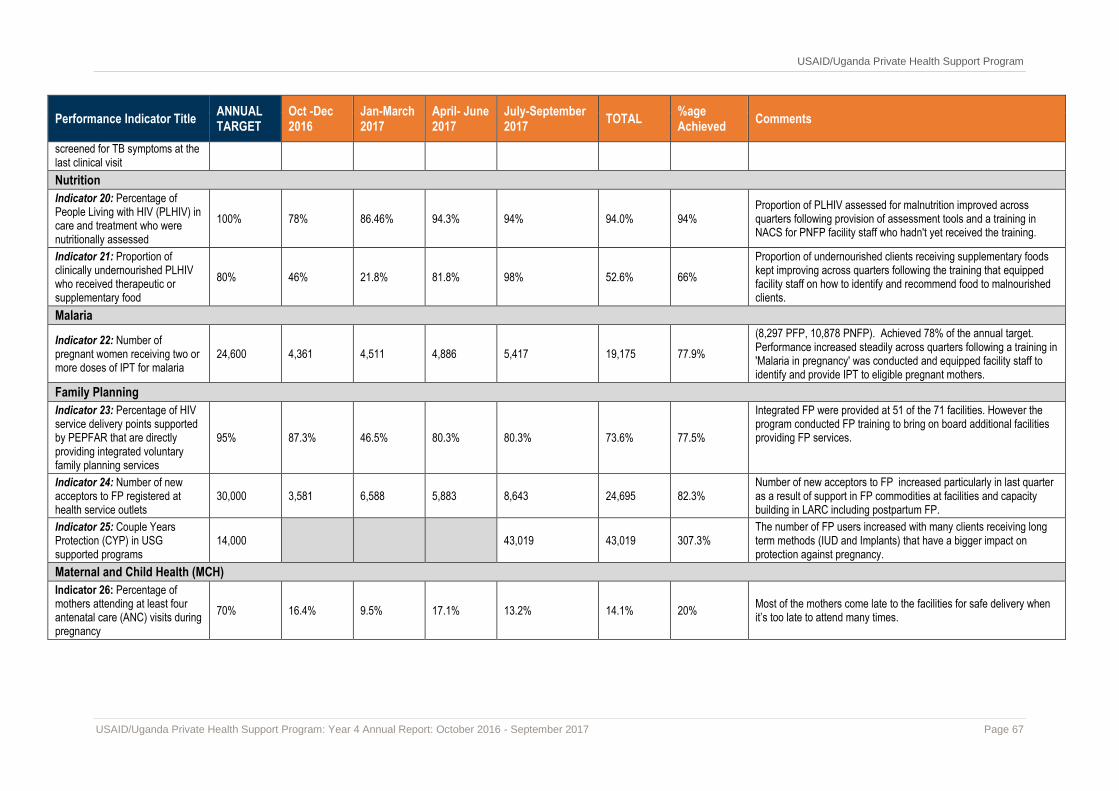
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 67
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
screened for TB symptoms at the last clinical visit
Nutrition
Indicator 20: Percentage of People Living with HIV (PLHIV) in care and treatment who were nutritionally assessed
100% 78% 86.46% 94.3% 94% 94.0% 94% Proportion of PLHIV assessed for malnutrition improved across quarters following provision of assessment tools and a training in NACS for PNFP facility staff who hadn't yet received the training.
Indicator 21: Proportion of clinically undernourished PLHIV who received therapeutic or supplementary food
80% 46% 21.8% 81.8% 98% 52.6% 66%
Proportion of undernourished clients receiving supplementary foods kept improving across quarters following the training that equipped facility staff on how to identify and recommend food to malnourished clients.
Malaria
Indicator 22: Number of pregnant women receiving two or more doses of IPT for malaria
24,600 4,361 4,511 4,886 5,417 19,175 77.9%
(8,297 PFP, 10,878 PNFP). Achieved 78% of the annual target. Performance increased steadily across quarters following a training in 'Malaria in pregnancy' was conducted and equipped facility staff to identify and provide IPT to eligible pregnant mothers.
Family Planning
Indicator 23: Percentage of HIV service delivery points supported by PEPFAR that are directly providing integrated voluntary family planning services
95% 87.3% 46.5% 80.3% 80.3% 73.6% 77.5%
Integrated FP were provided at 51 of the 71 facilities. However the program conducted FP training to bring on board additional facilities providing FP services.
Indicator 24: Number of new acceptors to FP registered at health service outlets
30,000 3,581 6,588 5,883 8,643 24,695 82.3% Number of new acceptors to FP increased particularly in last quarter as a result of support in FP commodities at facilities and capacity building in LARC including postpartum FP.
Indicator 25: Couple Years Protection (CYP) in USG supported programs
14,000 43,019 43,019 307.3% The number of FP users increased with many clients receiving long term methods (IUD and Implants) that have a bigger impact on protection against pregnancy.
Maternal and Child Health (MCH)
Indicator 26: Percentage of mothers attending at least four antenatal care (ANC) visits during pregnancy
70% 16.4% 9.5% 17.1% 13.2% 14.1% 20% Most of the mothers come late to the facilities for safe delivery when it’s too late to attend many times.
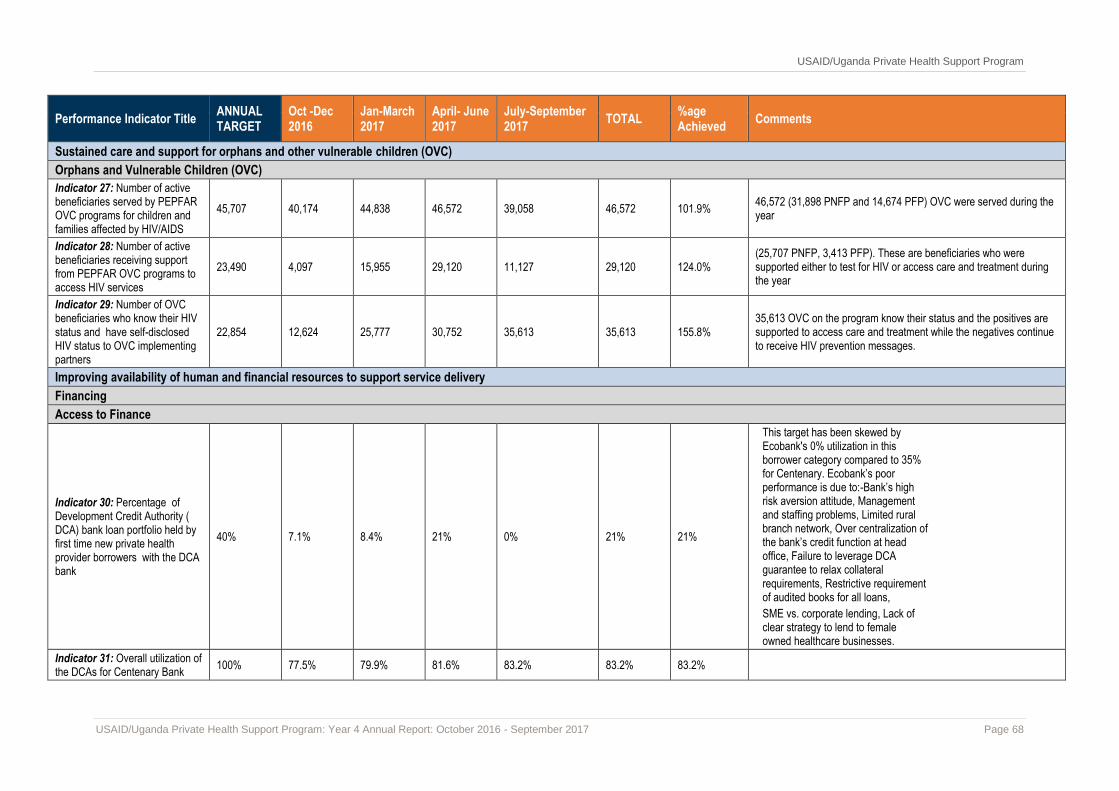
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 68
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
Sustained care and support for orphans and other vulnerable children (OVC)
Orphans and Vulnerable Children (OVC)
Indicator 27: Number of active beneficiaries served by PEPFAR OVC programs for children and families affected by HIV/AIDS
45,707 40,174 44,838 46,572 39,058 46,572 101.9% 46,572 (31,898 PNFP and 14,674 PFP) OVC were served during the year
Indicator 28: Number of active beneficiaries receiving support from PEPFAR OVC programs to access HIV services
23,490 4,097 15,955 29,120 11,127 29,120 124.0% (25,707 PNFP, 3,413 PFP). These are beneficiaries who were supported either to test for HIV or access care and treatment during the year
Indicator 29: Number of OVC beneficiaries who know their HIV status and have self-disclosed HIV status to OVC implementing partners
22,854 12,624 25,777 30,752 35,613 35,613 155.8% 35,613 OVC on the program know their status and the positives are supported to access care and treatment while the negatives continue to receive HIV prevention messages.
Improving availability of human and financial resources to support service delivery
Financing
Access to Finance
Indicator 30: Percentage of Development Credit Authority ( DCA) bank loan portfolio held by first time new private health provider borrowers with the DCA bank
40% 7.1% 8.4% 21% 0% 21% 21%
This target has been skewed by Ecobank's 0% utilization in this borrower category compared to 35% for Centenary. Ecobank’s poor performance is due to:-Bank’s high risk aversion attitude, Management and staffing problems, Limited rural branch network, Over centralization of the bank’s credit function at head office, Failure to leverage DCA guarantee to relax collateral requirements, Restrictive requirement of audited books for all loans,
SME vs. corporate lending, Lack of clear strategy to lend to female owned healthcare businesses.
Indicator 31: Overall utilization of the DCAs for Centenary Bank
100% 77.5% 79.9% 81.6% 83.2% 83.2% 83.2%

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 69
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
Indicator 32: Overall utilization of the DCAs for Ecobank
40% 14.5% 17.5% 17.5% 17.5% 17.5% 43.7%
Indicator 33: Number of relationships established with banks (DCA & non DCA)
16 4 4 0
3
11 69%
Indicator 34: Percentage of successful loan applications from rural private health providers outside the central region with both DCA banks
58% 49.5% 48.6% 43.9% 36% 44.5% 76.7%
IR2: Increased affordability of private health services and products
Indicator 35: Reduction in sales price of essential health medicines, services, and commodities
6% 10% 10% 166.7%
During Year 4, the Program continued to monitor trends in medicine prices in target districts to track price trends. Following an awareness campaign on rational use of medicines and disseminating essential medicines prices, a July assessment in one of the target districts (Jinja) revealed that 15 PHPs were selling ACTs between UGX 3500 - 4500 and only four facilities were still selling ACTs in the range of UGX 5000 – 6000.
Considered the most conservative difference from the figures above i.e. [(5,000 – 4,500) / 5,000] X 100%
Indicator 36: Number of groups (such as VSLAs) in which new health service products are implemented
120 0 0 0 70 70 58.3%
During Year 4, the Program targeted 120 VSLA groups in four districts (Jinja, Wakiso, Sheema and Rukungiri) to implement health service products. By the end of the year, 70 VSLA groups had endorsed policies for saving for health and were enrolled in community health insurance products within their respective communities.
Indicator 37: Number of partnership agreements established with private sector pharmaceutical firms/franchises
2 0 0 0 2 2 100%
Signed an MOU with Joint Medical Stores to promote health savings and Nilkanth Group of Pharmacies.
Improved governance and management of services
Governance
Indicator 38: Number of health facilities with functional health facility boards and committees
22 17 17 77.3% 17 health facilities have functional health facility boards and committees (that meet regularly and document their proceedings)
Indicator 39: Number of private health facilities that have
22 19 19 86.4% 19 facilities out of the targeted 22 have strong involvement of communities and patients in their planning and provision of health

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 70
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
participation of patients and communities in activity implementation
services. This is mainly through the suggestions boxes, community health days and use of VHTs for community mobilization and health promotion.
Indicator 40: Number of health facilities with properly functioning accounting systems
22 19 19 86.4% 19 facilities out of the targeted 22 have functioning accounting systems and have been efficiently and effectively managing grants given to them.
Management
Indicator 41: Percentage of private health facilities reporting on time in the DHIS2
80% 98.6% 98.6% 100% 100% 100.0% 125%
All the health facilities are reporting timely in the DHIS2. However two sites lack entry screens for Care and Treatment data (HMIS 106a). We have engaged the MOH to activate them to enable complete reporting.
Indicator 42: Proportion of private health facilities generating strategic information and using it for planning, organization and management of health services within their facilities
80% 77.3% 100% 100% 100% 100% 125.0% All the 22 targeted facilities are using the information to inform targets during planning and when ordering for supplies.
Indicator 43: Number of private health facilities with the capacity in use of information and communications technology (ICT) for improved monitoring, evaluation and decision making
22 0 0 17 22 100% 100% All the 22 targeted facilities have computer for data management and are supported to analyze data and generate information to use for planning and decision making.
Coordination
Indicator 44: Number of private health facilities that formally participate in district planning, or decision-making or other activities
22 17 17 77.3% Most of the targeted facilities work well with the district structures and participate in all the key health related events including performance reviews, data cleaning meetings.
Indicator 45: Existence of a functional faith-based health body serving as a platform for better health advocacy, resource mobilization and stakeholder engagement
1 0 0 0.0%
Draft concept paper was shared with medical bureaus for their input before it is shared with other stakeholders. This is to promote buy-in and ownership of the process by the medical bureaus. The Program will elicit more input from other stakeholders in the first quarter of PY5.
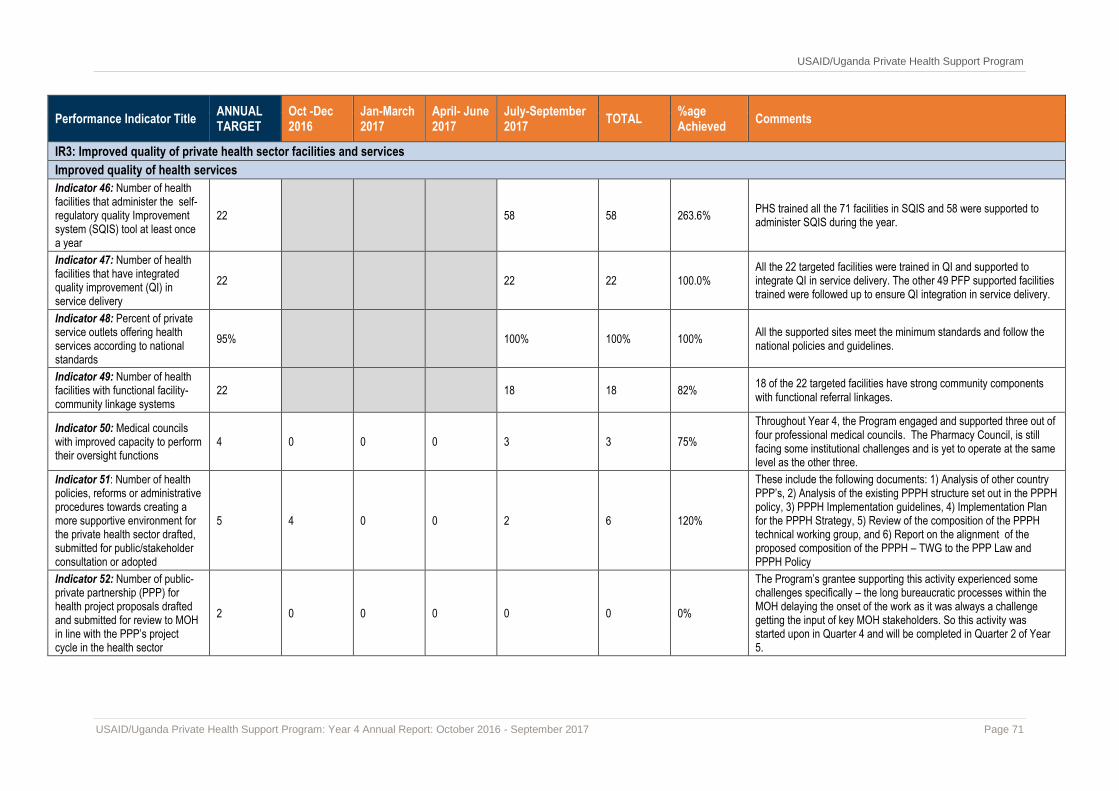
USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 71
Performance Indicator Title ANNUAL TARGET
Oct -Dec 2016
Jan-March 2017
April- June 2017
July-September 2017
TOTAL %age Achieved
Comments
IR3: Improved quality of private health sector facilities and services
Improved quality of health services
Indicator 46: Number of health facilities that administer the self-regulatory quality Improvement system (SQIS) tool at least once a year
22 58 58 263.6% PHS trained all the 71 facilities in SQIS and 58 were supported to administer SQIS during the year.
Indicator 47: Number of health facilities that have integrated quality improvement (QI) in service delivery
22 22 22 100.0% All the 22 targeted facilities were trained in QI and supported to integrate QI in service delivery. The other 49 PFP supported facilities trained were followed up to ensure QI integration in service delivery.
Indicator 48: Percent of private service outlets offering health services according to national standards
95% 100% 100% 100% All the supported sites meet the minimum standards and follow the national policies and guidelines.
Indicator 49: Number of health facilities with functional facility-community linkage systems
22 18 18 82% 18 of the 22 targeted facilities have strong community components with functional referral linkages.
Indicator 50: Medical councils with improved capacity to perform their oversight functions
4 0 0 0 3 3 75%
Throughout Year 4, the Program engaged and supported three out of four professional medical councils. The Pharmacy Council, is still facing some institutional challenges and is yet to operate at the same level as the other three.
Indicator 51: Number of health policies, reforms or administrative procedures towards creating a more supportive environment for the private health sector drafted, submitted for public/stakeholder consultation or adopted
5 4 0 0 2 6 120%
These include the following documents: 1) Analysis of other country PPP’s, 2) Analysis of the existing PPPH structure set out in the PPPH policy, 3) PPPH Implementation guidelines, 4) Implementation Plan for the PPPH Strategy, 5) Review of the composition of the PPPH technical working group, and 6) Report on the alignment of the proposed composition of the PPPH – TWG to the PPP Law and PPPH Policy
Indicator 52: Number of public-private partnership (PPP) for health project proposals drafted and submitted for review to MOH in line with the PPP’s project cycle in the health sector
2 0 0 0 0 0 0%
The Program’s grantee supporting this activity experienced some challenges specifically – the long bureaucratic processes within the MOH delaying the onset of the work as it was always a challenge getting the input of key MOH stakeholders. So this activity was started upon in Quarter 4 and will be completed in Quarter 2 of Year 5.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 72
Annex 2: Success Story
Improving Business at Pikwo Medical Centre in Gulu
Ph
oto
s b
y C
yn
thia
Aye
za
A small laboratory at one of the main branches of Pikwo Medical Centre in Gulu district.
By supporting the growth of viable and sustainable business opportunities for private providers, USAID’s Uganda Private Health Support Program helps fuel the overall expansion of the healthcare industry.
The BDS team provides training to private for profit (PFP) and private not for profit (PNFP) providers to strengthen business management skills. This helps health facilities operate more efficiently and gives them the tools to obtain financing and thereby to grow and improve services
Kenneth Odong’s employees, below (on the next page), at the counter of his facility.
The USAID/Uganda Private Health Support Program is taking a
variety of approaches to expand the availability of services,
increase their affordability, and improve quality in the private
sector. An important component of this is strengthening private
health businesses by expanding access to financing (A2F) and
providing business development services (BDS). At least half of
Uganda’s health care needs are met by the private health care
sector through private-for-profit (PFP) health facilities which are
particularly popular for their accessibility, medicines availability,
shorter waiting times, and higher perceived quality of service.
In Gulu district, Kenneth Odong, the proprietor of Pikwo medical
Center says that the population is large enough to keep several
health facilities in business. His health facility has been in operation
since July 2011.
“We are in Kanyagoga in Badege division of the four divisions in
Gulu. It is one of the more heavily populated areas on Gulu.
However, we are surrounded by many health facilities i.e. two
hospitals as well as IMC and the regional referral hospital. But
being a private facility gives us advantages that larger facilities
cannot provide e.g. faster and more friendly service, as well as
nearly no queues to deal with for patients. We started smaller than
we are right now but by 2013, we had expanded to our current size,
and we offer a range of services, including a laboratory with over
20 different tests, general consultation, investigations, and
comprehensive family planning – long and short term,” – Kenneth
Odong, Pikwo Medical Centre (August 2017)
Despite the advantages that these private health facilities offer to
the populations they serve, they face many of the same constraints
in accessing financing as do other small businesses in Uganda.
When it comes to supply, financial institutions see a much higher
perceived risk in lending to them. USAID and SIDA’s
Development Credit Authority (DCA) reduces that risk by
providing technical assistance to the DCA partner banks and
working with non-DCA banks to develop pipelines of loan deals
with the private health sector. The Program is working with
Centenary Bank, Ecobank and DFCU bank.
In 2016, Kenneth Odong secured a loan worth US $4,000 from
Centenary Bank to increase the capacity of his health facility. With
the loan, he was able to open up a second unit 15 km away from his
facility. This new unit now serves an average of 10 – 15 people per
day.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 74
“When we went for training in Lira, the Program staff spoke to us
about what we could do to access financial support. As soon as I
returned to Gulu, I began to visualise how I could move on from
where I was and how I could access the financial support. The
Program linked me to the Credit Manager of Centenary Rural
Development Bank. Within a short time, we were able to get the
support. While busy with this process, I also began looking for a
new location for a second facility that could house a maternity
section.” – Kenneth Odong, Proprietor of Pikwo Medical Centre,
(August 2017)
Beyond linking Health Care Businesses (HCBs) to financial
institutions, the Program also provides critical training for facility
owners in order for them to effectively and efficiently run their
health facilities. Most HCBs have poor business practices due to
lack of skilled managers. Mr. Odong has benefited from the
program by expanding his services, improved his accountability,
and financial systems, and was able to earn additional income.

USAID/Uganda Private Health Support Program
USAID/Uganda Private Health Support Program: Year 4 Annual Report: October 2016 - September 2017 Page 1
Related Documents







![USAID/UGANDA ENVIRONMENTAL THREATS AND … ETOA Final Report[1].… · USAID/UGANDA ENVIRONMENTAL THREATS ... KCCL Kasese Cobalt Corporation Limited ... PERSUAP Pesticide Evaluation](https://static.cupdf.com/doc/110x72/5aff49377f8b9a944d9035b1/usaiduganda-environmental-threats-and-etoa-final-report1usaiduganda.jpg)



