US Medical Eligibility Criteria (MEC) US Selected Practice Recommendations (SPR) for Contraceptive Use Kathryn M. Curtis, PhD 2014 National Reproductive Health Conference August 5 , 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Reproductive Health

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

US Medical Eligibility Criteria (MEC)US Selected Pract ice Recommendations (SPR)
for Contracept ive UseKathryn M. Curt is, PhD
2014 National Reproduct ive Health ConferenceAugust 5, 2014
National Center for Chronic Disease Prevention and Health Promotion Division of Reproductive Health

Disclosures
Nothing to disclose

Clinical Scenario 1
• 16 year old female, healthy, nulliparous, current ly using condoms, but wants more reliable method. Which of the following opt ions are available to her?
A. IUD (copper or levonorgestrel)B. ImplantsC. DMPAD. Combined hormonal methods (pill, patch, ring)

Learning Object ives
Part icipants will be able to:
Describe the US MEC and SPR
Understand how to use the US MEC and SPR
Ident ify provider tools and training resources
Apply the guidance in specific situat ions, based on clinical scenarios
Presenter
Presentation Notes
After this presentation, participants will be able to: Describe the US Selected Practice Recommendations for Contraceptive Use or US SPR Identify the intended use of this document and the target audience for the guidance Understand how that audience can use the guidance Apply the guidance in specific clinical scenarios

Presenter
Presentation Notes
This figure provides a visual image of how QFP is related to other guidelines, such as CDC’s MEC, SPR or STD treatment guidelines. QFP complements existing guidelines in two ways. First, it integrates existing guidelines that are appropriate for use in the family planning setting, These guidelines are often used in a siloed, isolated manner and we hope that integrating them into a combined set of guidelines appropriate for the family planning setting will make them more accessible and useful to clinical providers. QFP also goes one step further, and fills gaps in existing guidelines. For example, QFP provides new recommendations about contraceptive counseling, and shows how this can be integrated with MEC and SPR. QFP also describes how to work with male clients about pregnancy prevention, and how to address the special needs of adolescent clients. Other areas in which QFP makes unique contributions are in defining the range of services that should be offered in a family planning setting, emphasizing the role of helping clients achieve as well as prevent pregnancy, describing how to provide pregnancy testing and counseling services, and highlighting the role that quality improvement can play in improving health outcomes.

Presenter
Presentation Notes
This figure provides a visual image of how QFP is related to other guidelines, such as CDC’s MEC, SPR or STD treatment guidelines. QFP complements existing guidelines in two ways. First, it integrates existing guidelines that are appropriate for use in the family planning setting, These guidelines are often used in a siloed, isolated manner and we hope that integrating them into a combined set of guidelines appropriate for the family planning setting will make them more accessible and useful to clinical providers. QFP also goes one step further, and fills gaps in existing guidelines. For example, QFP provides new recommendations about contraceptive counseling, and shows howthis can be integrated with MEC and SPR. QFP also describes how to work with male clients about pregnancy prevention, and how to address the special needs of adolescent clients. Other areas in which QFP makes unique contributions are in defining the range of services that should be offered in a family planning setting, emphasizing the role of helping clients achieve as well as prevent pregnancy, describing how to provide pregnancy testing and counseling services, and highlighting the role that quality improvement can play in improving health outcomes.

Presenter
Presentation Notes
The US Medical Eligibility Criteria for Contraceptive Use (or US MEC) was developed in 2010 by CDC and was published in the Morbidity and Mortality Weekly Report in June of 2010.

1 No restriction for the use of the contraceptive method for a woman with that condition
2Advantages of using the method generally outweigh the theoretical or proven risks
3
Theoretical or proven risks of the method usually outweigh the advantages – not usually recommended unless more appropriate methods are not available or acceptable
4Unacceptable health risk if the contraceptive method is used by a woman with that condition
US Medical Eligibility Criteria: Categories
http://www.cdc.gov/mmwr/pdf/rr/rr5904.pdf
Presenter
Presentation Notes
Each combination of a medical condition or characteristic with a contraceptive method has a recommendation for use, which is provided as a numeric classification- 1, 2, 3 or 4. A number 1 means that there is no restriction in using a particular contraceptive method for a woman with a particular condition. A number 2 means that most evidence suggests that it is generally safe for someone with the particular condition to use a particular method, and that the advantages of using the method generally outweigh the theoretical or proven risks. A number 3 means that the theoretical or proven risks of the method usually outweigh the benefits of using that method, and other methods should be considered, if possible. A number 4 means that the risk of using a particular contraceptive method for a woman with a particular medical condition is unacceptable and alternative methods should be chosen. For some conditions, the numeric classification does not entirely capture the recommendation and a clarification statement is given. Evidence summaries are also given where evidence exists. The recommendations without evidence cited are based on expert opinion from either the WHO or US expert working group meetings and selected recommendations have comment statements that generally come from those working groups.

Example: Smoking and Contracept ive Use
Condit ion COC/P/R POP DMPA Implants Cu-IUD LNG-IUD
Smokinga. Age <35 2 1 1 1 1 1
b. A ge≥35
i. <15 cigarettes/day 3 1 1 1 1 1
II.≥15 cigarettes/day 4 1 1 1 1 1
http://www.cdc.gov/mmwr/pdf/rr/rr5904.pdf
Presenter
Presentation Notes
This is an example of the recommendations for Smoking and Contraceptive Use. Down the left side, you can see that smoking is broken into categories by age and level of smoking. Across the top are the various contraceptive methods. For CHCs (combined hormonal contraceptives) which include combined oral contraceptives, the patch and the ring, you can see that the recommendations reflect increasing safety risks with CHC use and smoking, as age and the level of smoking increases. A smoker aged <35 years generally can use CHCs (Category 2). For a smoker 35 years or older who smokes <15 cigarettes per day, however, the use of CHCs is usually not recommended unless other methods are not available or acceptable to her (Category 3). For smokers >35 years who smoke 15 or more cigarettes, the use of CHCs poses unacceptable health risks, primarily, the risk for myocardial infarction and stroke (Category 4). Safety risks vary depending on methods and conditions.

Condit ions Associated with Increased Risk for Adverse Heath Events as a Result of Unintended Pregnancy
Breast cancer Malignant liver tumors (hepatoma) and hepatocellular carcinoma of the liver
Complicated valvular heart disease Peripartum cardiomyopathyDiabetes: insulin dependent; with nephropathy/retinopathy/neuropathy or other vascular disease; or of >20 years’ duration
Schistosomiasis with fibrosis of the liver
Endometrial or ovarian cancer Severe (decompensated) cirrhosis
Epilepsy Sickle cell disease
Hypertension (systolic > 160 mm Hg or diastolic > 100 mm Hg) Solid organ transplantation within the past 2 years
History of bariatric surgery within past 2 years Stroke
HIV/AIDS Systemic lupus erythematosusIschemic heart disease Thrombogenic mutationsMalignant gestational trophoblastic disease Tuberculosis
Should consider long-acting, highly-effective contraception for these
patients
Presenter
Presentation Notes
For women with these conditions and others that may make unintended pregnancy an unacceptable health risk, long-acting highly effective contraceptive methods may be the best choice. Sole use of barrier and behavior-based methods may not be the most appropriate choice because of their relatively higher typical-use rates of failure.


US Selected Pract ice Recommendations for Contracept ive Use, 2013
Follow-up to US Medical Eligibility Criteria for Contracept ive Use, 2010 (US MEC): Recommendations for who can safely use contraception
Adapted from World Health Organizat ion (WHO) SPR
Intent: Evidence-based guidance for common, yet controversial, contracept ive management quest ions When to start Missed pills Bleeding problems Exams and tests Follow-up How to be reasonably certain that a woman is not pregnant
Presenter
Presentation Notes
The US SPR is a companion document to the US Medical Eligibility Criteria for Contraceptive Use, or US MEC, which was published in 2010. The US MEC contains recommendations for health-care providers for the safe use of contraceptive methods by women and men with various characteristics and medical conditions. These two family planning guidance documents were adapted from the World Health Organization MEC and SPR. The intention of the US SPR is to provide evidence-based recommendations for common, yet controversial contraceptive management questions, such as issues listed here.

How to use the US MEC and SPR

How to find MEC/SPR and resources
Presenter
Presentation Notes
To access this guidance, search for CDC contraception to reach CDC’s page on Contraceptive Guidance for Healthcare Providers.

http://www.cdc.gov/reproductivehealth/UnintendedPregnancy/Contraception_Guidance.htm
Presenter
Presentation Notes
This is the introductory page, with links to both the US MEC and the US SPR. There are also badges available on the right to add to a website which will link directly to the US MEC and US SPR sites.

http://www.cdc.gov/reproductivehealth/UnintendedPregnancy/Contraception_Guidance.htm
Presenter
Presentation Notes
This is the introductory page, with links to both the US MEC and the US SPR. There are also badges available on the right to add to a website which will link directly to the US MEC and US SPR sites.

http://www.cdc.gov/reproductivehealth/UnintendedPregnancy/Contraception_Guidance.htm
Presenter
Presentation Notes
This is the introductory page, with links to both the US MEC and the US SPR. There are also badges available on the right to add to a website which will link directly to the US MEC and US SPR sites.

Hard copies E-copies

Provider Tools

Contracept ive Effect iveness Chart
Tier 1
Tier 2
Tier 3
Presenter
Presentation Notes
This figure shows currently available contraceptive methods, ranked by typical effectiveness, meaning how effective the method is at preventing pregnancy with real-world use. Incorrect or inconsistent use can impact the effectiveness of the contraceptive method. Many factors need to be considered when choosing the most appropriate contraceptive method. These include safety, effectiveness, availability and acceptability; with pregnancy prevention as a goal of contraceptive use, effectiveness is one of the most important considerations. The US MEC recommendations focus primarily on the safety of a given method for women with medical conditions or characteristics. The 1-4 recommendations generally do not take effectiveness into account. While a Category 1 recommendation means the method can be used with no restrictions in regards to safety, that method may not be the best option for that person while considering these other factors. For example, the use of spermicide in a woman with complicated valvular heart disease is category 1, meaning the use of spermicide is safe to use with her condition and will not worsen her condition. However, the use of a more effective method will reduce her risk for adverse health events as a result of unintended pregnancy.


Slide Sets
http://www.cdc.gov/reproduct ivehealth/UnintendedPregnancy/training.htm

Continuing Educat ionhttp://www.cdc.gov/mmwr/
Presenter
Presentation Notes
The continuing education activity is available via the MMWR website which can be found by searching MMWR from the CDC index Or by going directly to http://www.cdc.gov/mmwr/ Under the left panel there is a Continuing Education tab with Weekly Publications underneath; on this page are current available courses for CE There you can also find a link to http://www.cdc.gov/TCEOnline and instructions how to access the activity
CLINICAL SCENARIOS
Presenter
Presentation Notes
To demonstrate how the guidance can be used, we will now go through several clinical scenarios for which the guidance may be useful.
Clinical Scenario 1
• 16 year old female, healthy, nulliparous, current ly using condoms, but wants more reliable method. Which of the following opt ions are available to her?
A. IUD (copper or levonorgestrel)B. ImplantsC. DMPAD. Combined hormonal methods (pill, patch, ring)

Safety of IUDs for Teens IUDs and age <20: US MEC 2 IUDs and Expulsion
Evidence shows slightly increased risk of expulsion in younger women
IUDs and infert ility No evidence that IUDs cause later infertility Infertility associated with gonorrhea and chlamydia
IUDs and STIs No evidence that IUDs increase risk of STI acquisition Women with current cervicitis, chlamydial infection,
gonorrhea should not start an IUD (US MEC 4) Women with a very high individual likelihood of
exposure to chlamydial infection or gonorrhea generally should not start an IUD (US MEC 3)
Presenter
Presentation Notes
Like previously mentioned, there are various myths and misperceptions regarding IUD use in adolescents. These concerns are real and should be addressed with reassurance that evidence-based recommendations tell us that the IUD is generally safe for use in adolescents. There is concern regarding an increased risk for expulsion which has been shown in some studies and thus the recommendation for IUD in women less than 20 is a category 2. Risk of infertility has been shown to be associated with gonorrheal and chlamydial infection, not due to age. Risk of STIs is another common concern for this population and IUD use and those who are currently infected or at high risk for infection should not use or generally should not use the IUD.

Safety of DMPA for Teens
DMPA and age <18: US MEC 2 DMPA and Bone mineral density Small amounts of BMD lost using DMPA BMD regained after discontinuation Unclear how BMD relates to fracture risk in adolescents No evidence that DMPA increases fracture in
adolescents DMPA and Obesity Obese adolescents who use DMPA may be more likely
to gain weight than non-obese DMPA users and obese users of other methods
Presenter
Presentation Notes
There has also been a lot of concern regarding use of DMPA in adolescents, specifically regarding loss of bone mineral density and weight gain. There is no evidence that DMPA use increases fracture risk in adolescents and it is unclear how bone mineral density measures are associated with future fractures in adolescents. We do know that bone mineral density is lost in small amounts during DMPA use in women, including adolescents. And we also know that the bone mineral density is regained after discontinuation. As for obesity, obese adolescents using DMPA may be more likely to gain weight compared to non-obese users and obese users of other methods. Thus, DMPA is a category 2 opposed to a category 1 for women <18 years old.

Clinical Scenario 1• 16 year old female, healthy, nulliparous, current ly using
condoms, but wants more reliable method. What opt ions are available to her?
A. IUD (copper or levonorgestrel) (US MEC 2)B. Implants (US MEC 1)C. DMPA (US MEC 2)D. Combined hormonal methods (pill, patch, ring)
(US MEC 1)
ALL OF THE ABOVE! Plus…
Encourage cont inued condom use for dual protect ion

Clinical scenario 2:When to start a contracept ive method
24 y.o. female comes to office desiring contracept ion and wants to start pills
Q: When can she start?

When to start a contracept ive method Barriers to start ing Filling a prescription Starting during menses Coming back for a second (or more) visit
Start ing when woman requests contracept ion (“Quick start ” ) May reduce time woman is at risk for pregnancy May reduce barriers to starting
Presenter
Presentation Notes
There are several barriers to initiating contraception which increases the time a woman is at risk for unintended pregnancy. Some examples of these barriers are the need to fill a prescription, to wait for next menses to start the method or to come back for another visit. Quick start is the start of a contraceptive method when a woman requests it rather than waiting. Quick start may reduce the time a woman is at risk for pregnancy and may reduce barriers to starting a method.

Evidence for Risk of Pregnancy
Two types of risk:
Risk of already being pregnant Risk that woman already pregnant
with “Quick start” of CHCs low Risk of becoming pregnant Risk of pregnancy with “Quick start” of
CHCs low
Brahmi, Contraception, 2013.
Presenter
Presentation Notes
Providers may have concerns that a woman may already be pregnant and therefore may not want to start her on contraception right away. A recent systematic review shows that the risk of pregnancy with Quick Start of combined hormonal contraceptives is low and that the risk that a woman is already pregnant using the Quick Start method is also low.

Other findings
Start ing CHCs on different days of the cycle does not affect bleeding changes or other side effects
“Quick start ” may increase cont inuat ion of combined oral contracept ives (COCs) and patch in the short term; this difference disappears over t ime
Brahmi, Contraception, 2013.
Presenter
Presentation Notes
Another concern may be that starting CHCs on days of the cycle not consistent with menses may cause irregular bleeding; however studies from the same systematic review have shown that starting on different days of the cycle does not affect bleeding changes or other side effects. Quick start may increase short term continuation of both COCs and the patch, however this difference disappeared over time in studies comparing quick start to other initiation.

Exposure in early pregnancy
No increased risk for adverse outcomes (congenital anomalies, neonatal death, infant death) among infants exposed in utero to COCs
Bracken, Obstet Gynecol. 1990;76:552-7.
Presenter
Presentation Notes
Another concern is risk of fetal exposure to hormonal contraception in early pregnancy. In several studies examining fetal exposure to COCs, there has been no increased risk for adverse outcomes among infants.

Need for back-up contracept ion
Later start days are associated with greater follicular act ivity, but not ovulat ion, through day 5 (implicat ions for back up)
Brahmi, Contraception, 2013.
Presenter
Presentation Notes
Providers may also be concerned for how long a woman will have to wait until her method is effective if she does not start her method with menses. The US SPR also provides evidence-based guidance on the need for back-up contraception or need to abstain from sexual intercourse for each method initiation. For CHCs, starting on later days in the cycle is associated with greater follicular activity through day 5, but not including ovulation.

US SPRWhen to start a contracept ive method
Contracept ive Method
When to start, if provider is reasonably certain
woman is not pregnant
Back-up needed
LNGIUD Any time If > 7 days of cycle, use back-up method or abstain for 7 days
Copper IUD Any time Not needed
Implant (etonogestrel) Any time If > 5 days of cycle, use back-up
method or abstain for 7 days
Injectable Any time If > 7 days of cycle, use back-up method or abstain for 7 days
CHC Any time If > 5 days of cycle, use back-up method or abstain for 7 days
Progest in-Only Pills (POPs) Any time If > 5 days of cycle, use back-up
method or abstain for 2 days
Presenter
Presentation Notes
Thus the recommendation for initiation of CHCs is to use backup or abstain from intercourse for 7 days if the method is initiated greater than 5 days from the start of last menstrual period. The US SPR also provides guidance both within the document and summarized in a user-friendly chart to guide providers on how to counsel patients on backup needs for all methods. As you can see from this chart, all methods of contraception can be started at any time, if the provider is reasonably certain the woman is not pregnant. This ensures she is not pregnant at the time of initiation. To ensure that she not get pregnant once the method is started, she should use appropriate backup for the recommended time period to prevent a new unintended pregnancy.

Guidance for Special Considerat ions
Amenorrheic
Postpartum Breastfeeding Not breastfeeding
Postabort ion
Switching from another contracept ive method
Presenter
Presentation Notes
For women in other situations who may not have a last menstrual cycle to refer to, guidance on how to initiate methods is also provided. These situations refer to women who are amenorrheic, postpartum, postabortion or are switching from another method.

Clinical scenario 2: When to start a contracept ive method ?
24 y.o. female comes to office desiring contracept ion and wants to start pills Q: When can she start? A:
• Anytime, if reasonably certain she is not pregnant.
• If it has been more than 5 days since menstrual bleeding started, she will need to abstain from sex or use additional contraceptive protection for the next 7 days
Presenter
Presentation Notes
To answer this question, the recommendation for pills and for all methods is a woman can start a method anytime, if a provider can be reasonably certain she is not pregnant. If it has been more than 5 days since menstrual bleeding started, she will need to abstain from sex or use additional contraception for the next 7 days after starting her combined pills.

Clinical scenario 3: How to be reasonably certain that a
woman is not pregnant
24 y.o. female comes to office desiring contracept ion and wants to start pills
Q: How can you be reasonably certain she is not pregnant?
Presenter
Presentation Notes
So how can you be reasonably certain she is not pregnant?

Evidence: Pregnancy test limitat ions Pregnancy detect ion rates can vary based
on sensit ivity of test and t iming with respect to missed menses
Pregnancy test not able to detect pregnancy result ing from recent intercourse
Pregnancy test may remain posit ive several weeks after pregnancy ends
Cervinski, Clin Chem Lab Med. 2010;48:935-42.Cole LA, Expert Rev Mol Diagn. 2009;9:721-47.Wilcox, JAMA. 2001;286:1759-61.Korhonen, Clin Chem. 1997;43:2155-63.Reyes, Am J Obstet Gynecol. 1985;153:486-9.Steier, Obstet Gynecol. 1984;64:391-4.`
Presenter
Presentation Notes
Some providers may question whether or not they should do a pregnancy test to rule out pregnancy and may also question if a pregnancy test is enough. The evidence shows that pregnancy testing does have limitations. Pregnancy detection rates vary depending on the sensitivity of the test and the timing of testing with respect to missed menses, last intercourse or last pregnancy. False negatives may occur with recent intercourse while false positives may occur after recent pregnancy.

US SPR
Presenter
Presentation Notes
The US SPR provides highly accurate criteria, shown here, that a provider can review with a patient. If a woman has no signs or symptoms of pregnancy and meets any one of the criteria, a provider can be reasonably certain that she is not pregnant. Criteria include… (READ LIST)

Evidence on Pregnancy Checklist (PC)Study, year, country
# Women Posit ive preg test
Sensit ivity of PC
Specificity of PC
PPV of PC
NPV of PC
Stanback,1999, Kenya
1852 1% 64% 89% 6% 99%
Stanback, 2006, Kenya
1852(without signs/sx)
1% 55% 90% 6% 99%
Stanback, 2008, Nicaragua
263 1% 100% 60% 3% 100%
Torpey,2010, Africa 535 HIV+ 4% 90.9% 38.7% 6% 99%
Stanback, Lancet, 1999;354:566.Stanback, J Fam Plann Reprod Health Care, 2006;32:27.Stanback, Rev Panam Salud Publica, 2008;23:116.Torpey, BMC Public Health, 2010;10:249.
Presenter
Presentation Notes
Several studies have been conducted comparing the negative predictive value of this criteria with a pregnancy test. These studies all showed a negative predictive value of 99% or 100%. This means of the 100 who had a negative result according to the pregnancy checklist, 99 to 100 of them were not pregnant according to a pregnancy test. This indicates that this pregnancy checklist criteria can be used to accurately rule out pregnancy and safely start contraception. Currently there are no published studies in the US but there is no reason to think it would be any different than the situations in these studies.

Clinical scenario 3: How to be reasonably certain that a
woman is not pregnant
24 y.o. female comes to office desiring contracept ion and wants to start pills
Q: How can you be reasonably certain she is not pregnant?
A: If she has no signs or symptoms of pregnancy and fulfills one of criteria, a provider can be reasonably certain that the woman is not pregnant.
Presenter
Presentation Notes
The recommendation therefore states that if a woman has no signs or symptoms of pregnancy and fulfills one of the criteria, a provider can be reasonably certain that the woman is not pregnant. Routine pregnancy testing for every woman is not necessary.

Clinical scenario 4: Exams and tests
24 y.o. female comes to office desiring contracept ion and wants to start pills
Q: Do you need to do any exams or tests before she starts?
Presenter
Presentation Notes
Are there other tests to consider or exams that need to be done before providing her with pills?

US SPRExams and tests prior to init iat ion
Unnecessary tests may be barrier to start ing Women (adolescents) may not be comfortable with pelvic exam Coming back for a second (or more) visit to receive test results
Recommendat ions address exams and tests needed prior to init iat ion Class A = essential and mandatory
Class B = contributes substantially to safe and effective use, but implementation may be considered within the public health and/or service context
Class C = does not contribute substantially to safe and effective use of the contraceptive method
Presenter
Presentation Notes
This question addresses other barriers to initiating contraception A pelvic exam itself may be a barrier to women getting contraception, especially adolescents, if they are not willing to participate in the exam Waiting for test results may be another barrier that delays contraceptive use The US SPR provides recommendations that address exams and tests needed prior to starting a woman on a method These recommendations are categorized into 3 classes: Class A are essential and mandatory for a given method Class B exams and tests contribute substantially to safe and effective use, but implementation may be considered within the public health and/or service context Finally, Class C does not contribute substantially to safe and effective use of the method

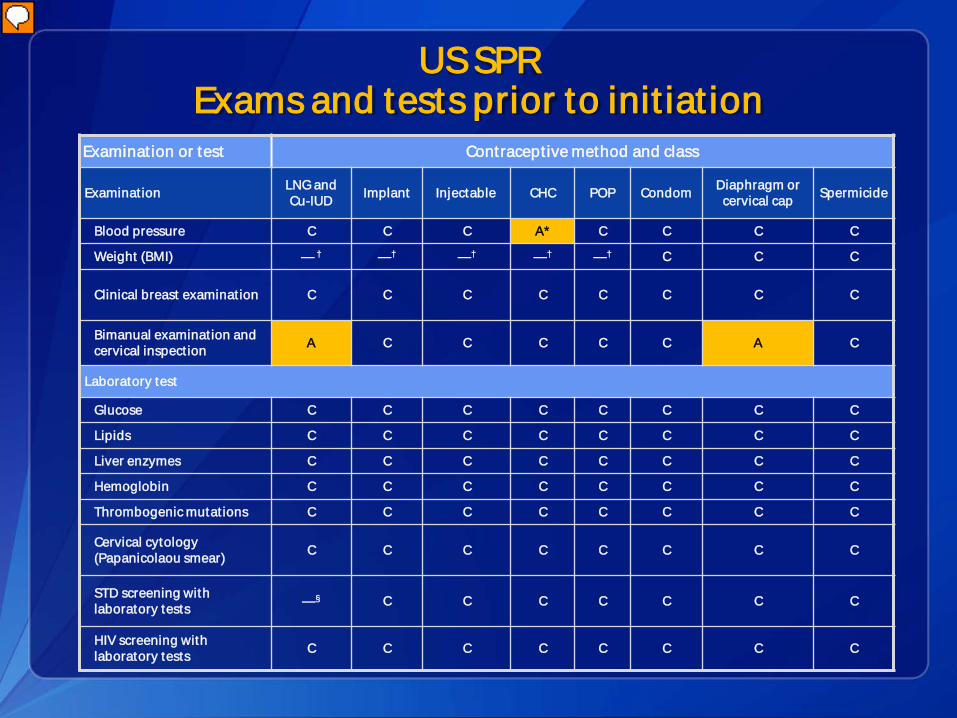
US SPR Exams and tests prior to init iat ion
Examination or test Contraceptive method and class
Examinat ion LNG and Cu-IUD Implant Injectable CHC POP Condom Diaphragm or
cervical cap Spermicide
Blood pressure C C C A* C C C C
Weight (BMI) — † —† —† —† —† C C C
Clinical breast examinat ion C C C C C C C C
Bimanual examinat ion and cervical inspect ion A C C C C C A C
Laboratory test
Glucose C C C C C C C C
Lipids C C C C C C C C
Liver enzymes C C C C C C C C
Hemoglobin C C C C C C C C
Thrombogenic mutat ions C C C C C C C C
Cervical cytology (Papanicolaou smear) C C C C C C C C
STD screening with laboratory tests —§ C C C C C C C
HIV screening with laboratory tests C C C C C C C C
Presenter
Presentation Notes
This slide replicates the summary chart in the US SPR for all contraceptive methods and commonly performed screening exams and tests
US SPR Exams and tests prior to init iat ion
Examination or test Contraceptive method and class
Examinat ion LNG and Cu-IUD Implant Injectable CHC POP Condom Diaphragm or
cervical cap Spermicide
Blood pressure C C C A* C C C C
Weight (BMI) — † —† —† —† —† C C C
Clinical breast examinat ion C C C C C C C C
Bimanual examinat ion and cervical inspect ion A C C C C C A C
Laboratory test
Glucose C C C C C C C C
Lipids C C C C C C C C
Liver enzymes C C C C C C C C
Hemoglobin C C C C C C C C
Thrombogenic mutat ions C C C C C C C C
Cervical cytology (Papanicolaou smear) C C C C C C C C
STD screening with laboratory tests —§ C C C C C C C
HIV screening with laboratory tests C C C C C C C C
Presenter
Presentation Notes
This slide replicates the summary chart in the US SPR for all contraceptive methods and commonly performed screening exams and tests

US SPR Exams and tests prior to init iat ion
Examination or test Contraceptive method and class
Examinat ion LNG and Cu-IUD Implant Injectable CHC POP Condom Diaphragm or
cervical cap Spermicide
Blood pressure C C C A* C C C C
Weight (BMI) — † —† —† —† —† C C C
Clinical breast examinat ion C C C C C C C C
Bimanual examinat ion and cervical inspect ion A C C C C C A C
Laboratory test
Glucose C C C C C C C C
Lipids C C C C C C C C
Liver enzymes C C C C C C C C
Hemoglobin C C C C C C C C
Thrombogenic mutat ions C C C C C C C C
Cervical cytology (Papanicolaou smear) C C C C C C C C
STD screening with laboratory tests —§ C C C C C C C
HIV screening with laboratory tests C C C C C C C C
Presenter
Presentation Notes
There are also the categories highlighted here which address body weight for hormonal methods and IUDs, as well as STD screening prior to IUD placement For CHC initiation, the recommendation for checking weight is “Obese women generally can use combined hormonal contraceptives (U.S. MEC); therefore, screening for obesity is not necessary for the safe initiation of combined hormonal contraceptives. However, measuring weight and calculating BMI at baseline might be helpful for monitoring any changes and counseling women who might be concerned about weight change perceived to be associated with their contraceptive method .” For IUD use, the US SPR recommendation states that most women do not require additional STD screening at the time of IUD insertion if they have already been screened according to CDC’s STD Treatment Guidelines Those who have not be screened can be screened at time of IUD placement and insertion should not be delayed for test results unless at a very high individual likelihood of STD exposure

Clinical scenario 4: Exams and tests
24 y.o. female comes to office desiring contracept ion and wants to start pills
Q: Do you need to do any exams or tests before she starts?
A: Blood pressure measurement essential
Presenter
Presentation Notes
Thus the recommendation is that blood pressure measurement should be obtained and evaluated before a woman starts combined hormonal contraceptives, including pills

Pelvic Exam before Init iat ing Hormonal Contracept ion
Is not necessary before start ing hormonal contracept ion
Ident ify women who should not use hormonals? Conditions which are U.S. MEC categories 3 or 4 for use of
hormonals: breast cancer, hypertension, heart disease, vascular disease, smoking and age >35, migraine with aura, liver disease
Not detected by pelvic exam
Ident ify gynecologic condit ions Fibroids, ovarian masses, ovarian cancer, endometriosis U.S. MEC categories 1 or 2 for use of hormonals
Tepper Contraception 2013
Presenter
Presentation Notes
Pelvic examination is not necessary before initiation of combined hormonal contraceptives because it does not facilitate detection of conditions for which hormonal contraceptives would be unsafe Women with certain conditions such as current breast cancer, severe hypertension or vascular disease, heart disease, migraine headaches with aura, and certain liver diseases, as well as women aged ≥35 years who smoke ≥15 cigarettes per day, should not use or generally should not use combined hormonal contraceptives (US MEC recommendations); However, none of these conditions are likely to be detected by pelvic examination A systematic review examined two case-control studies comparing delayed and immediate pelvic examination before initiation of oral contraceptives or DMPA No differences in risk factors for cervical neoplasia, incidence of STDs, incidence of abnormal Papanicolaou smears, or incidence of abnormal wet mounts were found

US MEC: Take Home Messages
Most women can safely use most contracept ive methods
Certain medical condit ions can increase risk for adverse events with unintended pregnancy
Women, men, and couples should be informed of full range of methods

US SPR: Take Home Messages Most women can start most methods anyt ime
Few, if any, exams or tests are needed
Routine follow-up generally not required
Many circumstances call for considerat ion of emergency contracept ion use
Regular contracept ion should be started after EC
Presenter
Presentation Notes
Most women can start most methods of contraception anytime (including on the day of the visit), as long as the provider is reasonably certain that the woman is not pregnant. Few, if any, examinations or tests are needed before starting a contraceptive method. Bleeding problems are a major reason for contraceptive discontinuation; recommendations on anticipatory counseling before starting a method and management of bleeding problems are provided. Women should be advised to return at any time to discuss side effects or other problems, if they want to change the method being used, and when it is time to remove or replace the contraceptive method. Otherwise, routine follow-up is generally not required. Many options for emergency contraception are available, including the copper-IUD and different formulations of pills, and there are many circumstances tor which EC use should be considered. Regular contraception should be started after emergency contraceptive use.

Adolescents: Take Home Messages
Adolescents are eligible to use all methods of contracept ion
Long-act ing, reversible contracept ion (LARCs) may be part icularly suitable for many adolescents
Dual protect ion should be encouraged for adolescents
Presenter
Presentation Notes
Rates of adolescent pregnancy in the US are decreasing, but remain high. Adolescents who are at risk of unintended pregnancy need access to highly effective contraceptive methods. Adolescents are eligible to use all methods of contraception. There is no contraceptive method that an adolescent cannot use based on age alone. Long-acting, reversible contraception (LARCs) including IUDs and implants may be particularly suitable for many adolescents. Dual protection should be encouraged for adolescents.

Resources CDC evidence-based family planning
guidance documents: http://www.cdc.gov/reproductivehealth/unintendedpregnancy/USMEC.htmhttp://www.cdc.gov/reproductivehealth/unintendedpregnancy/USSPR.htm Sign up to receive alerts!
Presenter
Presentation Notes
All of this US SPR information, as well as tools and aides for contraceptive guidance can be found at the listed website. You can also sign up for email alerts to be up to date with any new guidance updates or new tools released from CDC. The WHO family planning website is also listed to access WHO family planning guidance.
Related Documents











