Urinary System ANATOMY-HISTOLOGY DEPARTMENT MEDICAL FACULTY BRAWIJAYA UNIVERSITY

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Urinary System
ANATOMY-HISTOLOGY DEPARTMENT MEDICAL FACULTY BRAWIJAYA UNIVERSITY
1. Functions
2. Kidneys (ren) ◦ Positions
◦ Renal blood vessels
◦ Renal structures
3. Ureters
4. Urinary bladder (Vesica urinaria/VU)
5. Urethrae
1. Excretion: ◦ removal of organic wastes from body fluids
2. Elimination: ◦ discharge of waste products
3. Homeostatic regulation: ◦ of blood plasma volume and solute concentration

1. Ren
2. Ureter
3. Vesica urinaria
4. Urethra
Organs that excrete urine
2. Urinary Tract
►Organs that eliminate urine:
ureters (paired tubes)
urinary bladder (muscular sac)
urethra (exit tube)

Feature like soya bean; ◦ 11 X 6 X 3 cm, weight=±150 gr (♂) and ±135 gr
(♀); smooth surface (fetuslobulated);
◦ lower pole is palpable in full inspiration (thin individu)
Position: ◦ Regio abdomen posterior.
◦ Lateral columna vertebra
◦ Retroperitoneal.
◦ Between Vertebra T.XII – Vertebra L.III
◦ Ren dextra usually slightly inferior than sinistra (why?)
1. Renal projection 2. Renal relations syntopi
3. 3. Renal protection
“Dokter, pinggang saya sakit. Apakah saya terkena sakit ginjal?” Keluhan ini pasti sering disampaikan pada saat Anda di tempat praktek dokter. Tetapi apakah sakit pinggang selalu diartikan bahwa terjadi sakit ginjal? Apakah setiap penyakit ginjal akan memberikan keluhan nyeri pinggang?

Anterior: ◦ Hilum: 5cm from
midline, medial from the tip costae 9th Dex: under
transpyloricum plane
Sin: over transpyloricum plane
Posterior: ◦ Hilum: lower border of
processus spinosus vertebrae lumbalis 1st & ±5 cm from midline.

Anterior: ◦ Right kidney: Superior: gld. Suprarenal
Anterior (3/4 surface): lobus dex hepar impressio
Medial: duodenum pars descendens
Inferolateral: flexura colon dex
Inferiomedial: intestinum tenue

Anterior: ◦ Left kidney: Superior: left suprarenal
gland
Anterior-lateral: spleen
Anterior-medial: stomach
Anterior (central): pancreatic body and splenic vessels.
Inferior-lateral: left colic flexure
Inferior-medial: jejenum
Renal relations

Posterior: ◦ Superior: diaphragma
and lig. arcuata medial&lateral
◦ Inferior: Medial: M. psoas major
Intermedia: M. quadratus lumborum
Lateral: aponeurotic tendon M. transversus abdominis
◦ A/V/N subcostalis, N. iliohypogastrica, N. Ilio-inguinalis
Renal relations


1. Capsula renalis ◦ Collagen fibers covers outer surface
organ
2. capsula adiposa/perirenal fat ◦ Adipose tissue surround renal
capsule ( >>ren inferior)
3. Fascia renalis ◦ fibrous outer layer anchors kidney to
surrounding structures
4. Corpus adiposum pararenalis/pararenal fat ◦ Adipose tissue posterior to fascia
renalis

Capsula renalis
Fascia renalis (lamina
anterior & posterior
Corpus adiposum perirenalis
Corpus adiposum pararenalis
Tranversal section

Pararenal fat (corpus adiposum pararenalis): Jaringan lemak dibagian belakang fascia renalis
Coronal section


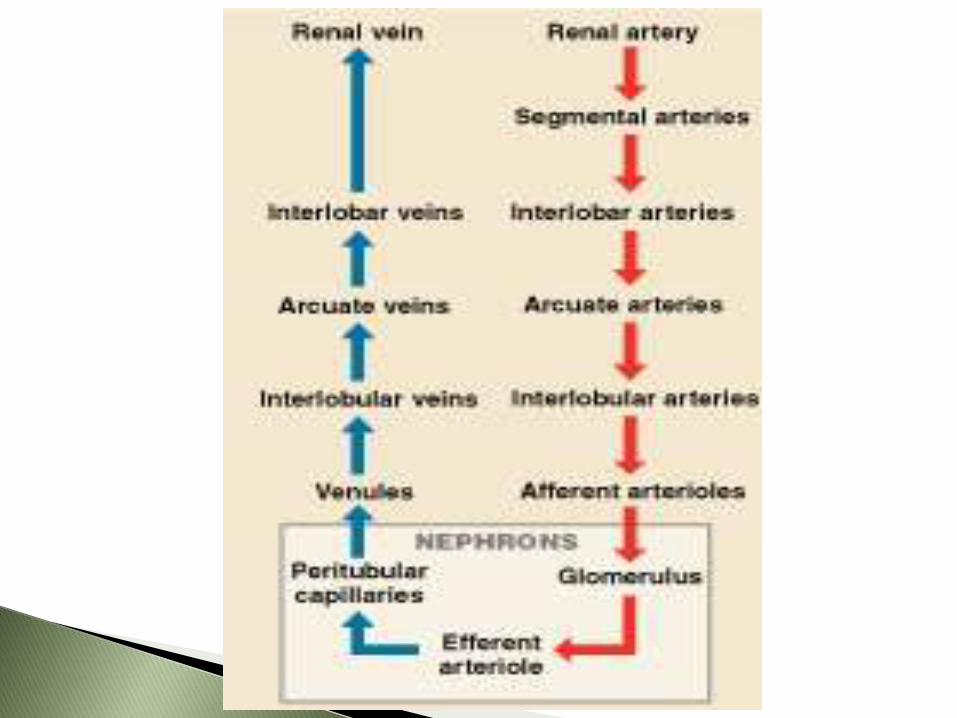
Arteri Renalis
Branch of aorta abdominalis
A. renalis gives:
◦ a. suprarenalis inferior
note: a. suprarenalis superior and media from a. phrenica inferior and aorta abdominalis
◦ Branches to the perinephric tissue, renal capsule, pelvis and proximal part of the ureter
Near the hilum a. renalis divides into divisi anterior and divisi posterior a. segmentalis

A. renalis a. segmentalis ◦ Renal vascular segmentation (by Graves 1956)
1. Apical 2. Superior (anterior) 3. Inferior 4. Middle (anterior) 5. Posterior
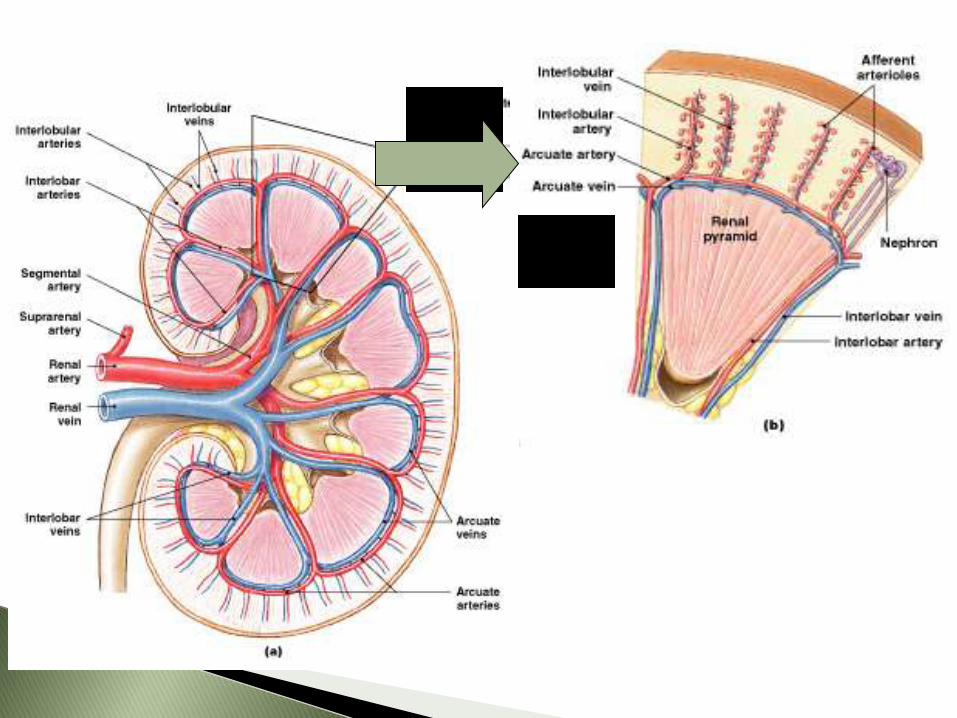
A. lobaris (one for each pyramid) divides into 2-3 a. interlobaris a. arcuata
a. interlobularis ◦ diverge radially into the cortex ◦ Some perforate surface as perforating artery
rami capsulares a. afferent a. efferent
◦ peritubular capillary plexus (around PCT & DCT in the cortical nephron)
◦ vasa recta (arteriolae rectae in the juxtamedullary nephron)
v. interlobularis



A relatively avascular longitudinal zone along the convex renal border, because it is the border
between two areas of arterial distribution.
improved method of nephropexy using a suture.

1. Hilus renalis
2. Sinus renalis
3. Capsula renalis
4. Cortex renalis
5. Medulla renalis a. Pyramida renalis
Papilla renalis (ductus Bellini)
b. Columna renalis (columna Bertini)
6. Lobus renalis
7. Calyx minor Calyx major
8. Pelvis renalis

Fig. Renal structures
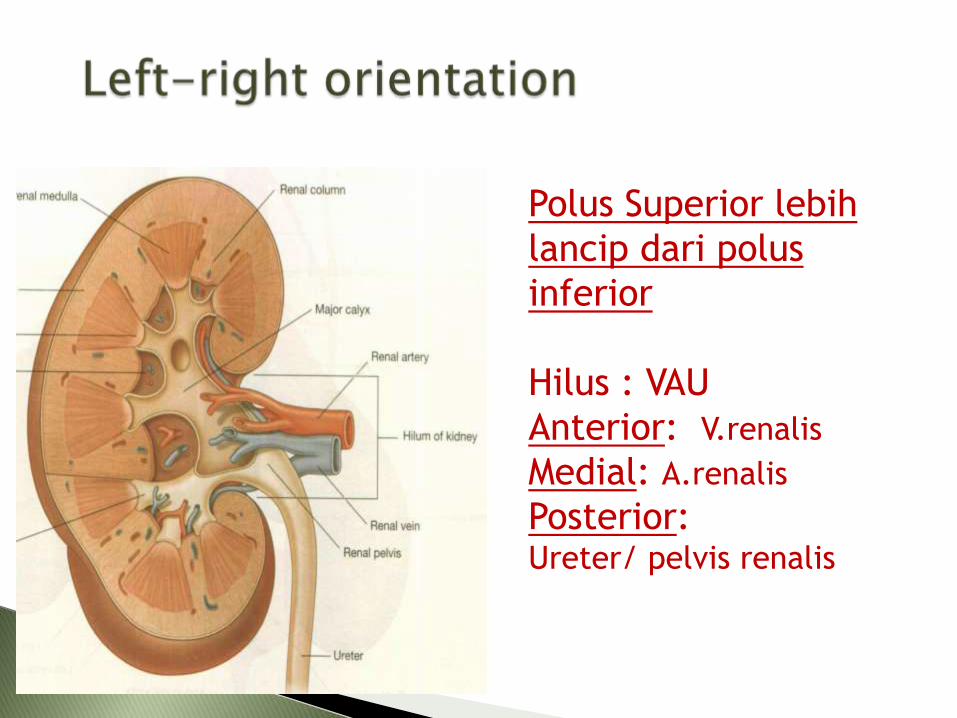
Polus Superior lebih
lancip dari polus
inferior
Hilus : VAU
Anterior: V.renalis
Medial: A.renalis
Posterior: Ureter/ pelvis renalis
Descending or excretion pyelography
Ascending or retrograde pyelography
Normal capping of the minor calyces clinically important obliterated hydronephrosis

U
R
E
T
E
R

Seorang laki-laki usia 38 tahun datang dengan keluhan nyeri hebat berulang di daerah pinggang kiri dan terasa menjalar ke punggung atas. Nyeri diikuti mual dan muntah. Pada pemeriksaan didapatkan Tekanan Darah 120/85 mmHg dan nyeri tekan/ketok pinggang +.
Pemeriksaan urin menunjukkan adanya eritrosit : 15-20/lp, dan kristal +++. Pemeriksaan radiologis BNO : gambaran hydronephrosis dan batu radiopaque pada area hilus renalis

What is the most likely diagnosis?
What is the likely anatomical mechanism for this disorder?
From the sign and symptomps, what structure is likely affected?
Diagnosa : Nephrolithiasis
Nephrolithiasis is common, with a lifetime prevalence of 10% in men and 5% in women.
Most patients present with moderate to severe colic, caused by the stone entering the ureter. Stones in the proximal (upper) ureter cause pain in the flank or anterior upper abdomen. When the stone reaches the distal third of the ureter, pain is noted in the ipsilateral testicle or labia.
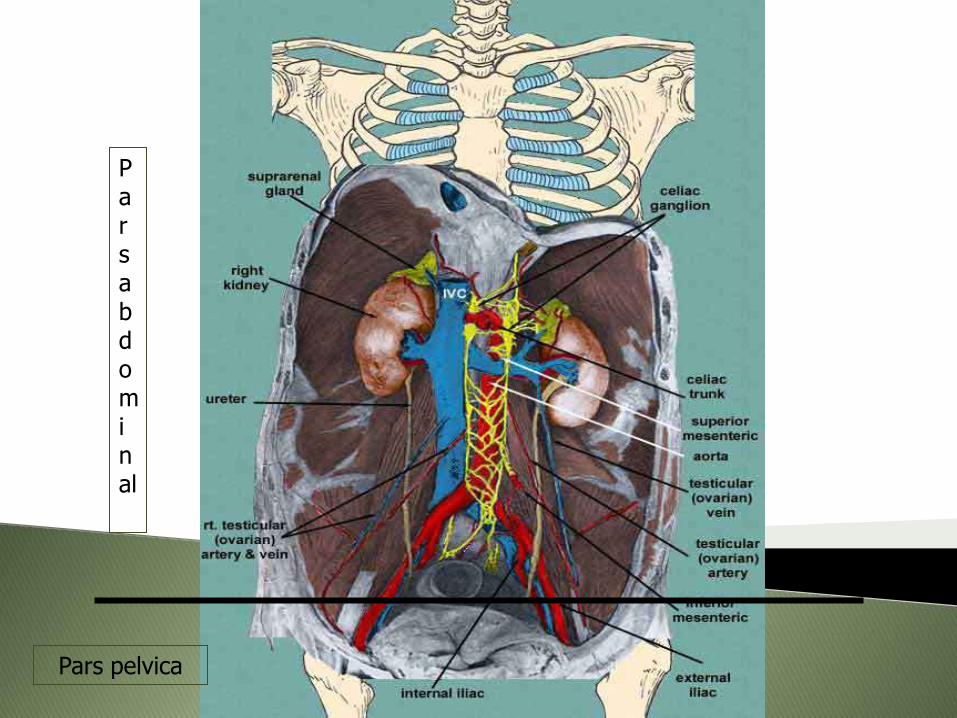
Pars abdominal
Pars pelvica

Pars abdominal ◦ Posterior to the peritoneum
◦ Medial to anterior of m. psoas major
◦ Crosses anterior n. genitofemoralis
◦ Obliquelly crossed by a/v. testicularis (ovarica)
Pars pelvica ◦ Posterolaterally on the lateral wall of pelvis minor,
along anterior border of incisura ischiadica major until spina ischiadica and turns anteromedially into fibrous adipose tissue above m. levator ani to reach base of vesica urinaria.

Lies along the tips of proc.transversus
Crosses in front of art.sacroiliaca
Swings out to the spina ischiadica
Passes medial to the VU
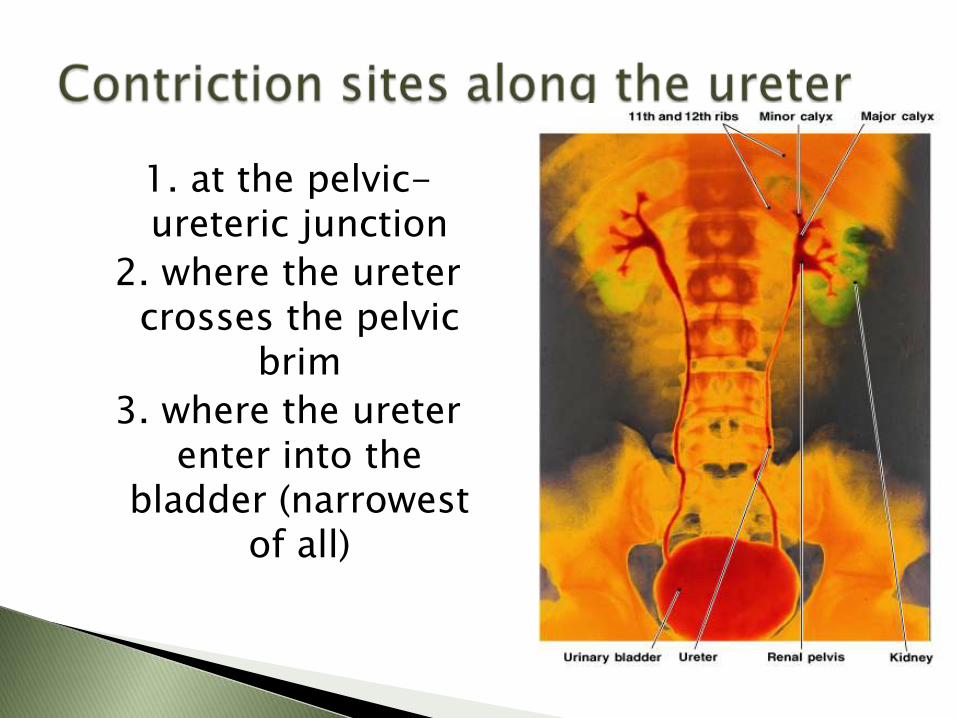
1. at the pelvic-ureteric junction
2. where the ureter crosses the pelvic
brim
3. where the ureter enter into the
bladder (narrowest of all)

NOTE:
Male ureter: ◦ Crossed
anterosuperiorly from lateral to medial by ductus deferens
◦ Anterior to the upper pole of vesicula seminalis
Begin at renal pelvis
Sweep along ureter
Force urine toward urinary bladder
Every 30 seconds
Blood supply ◦ A. renalis, aorta, a. iliaca communis, a. vesicalis
Nerve supply ◦ T11 to L2 segments of the spinal cord via the plexus
renalis, hypogastrica, and pelvica
◦ excessive distension and spasm of the ureter caused by calculus; spasmodic; mainly innervated by T11-L2 branch: N. iliohypogastrica; N. ilioinguinalis; N. genitofemoralis, the pain may be spread from the loin to the groin and scrotum and labium majus to proximal anterior of thigh.

Vesica urinaria (VU)

Empty: tetrahedral / pyramid in shape ◦ Apex: anterior, connected by urachus to the umbilicus.
◦ Basis/fundus (posterior surface):
Male: related to the rectum separated by recessus rectovesical
Female: related to the anterior wall of vagina & cervix of uterus separated by recessus vesicouterine
◦ Superior surface: covered by peritoneum
◦ Inferolateral surface: separated by the adipose retropubic pad from pubis and lig. puboprostatic/pubovesical.
Fills: ovoid ◦ above umbilicus
► Is a triangular area bounded by:
► openings of ureters (ostium ureteris dex-sin)
Crista inter-ureterica
► entrance to urethra (ostium urethrae internum)
► Consist of smooth muscle
► M. trigonum superficialis and profundus
► Acts as a funnel:
channels urine from bladder into urethra

Lies at apex of trigone: ◦ at most inferior point in urinary bladder

Is the region surrounding urethral opening
Contains a musculus sphincter urethrae interna (sphincter vesicae- Smooth muscle of sphincter provide involuntary control of urine discharge)
Blood supply of VU
A. vesicalis superior & inferior
Nerve supply of VU
Plexus vesicalis:
T10-L2 sympathetic
S2-S4 parasympathetic

►Male urethrae
►Female urethrae
Extends from neck of urinary bladder
To the exterior of the body
The Male Urethra
►Extends from neck of urinary bladder
►To tip of penis (18–20 cm)
3. Spongy urethra/penile urethra (pars spongiosa):
◦ extends from urogenital diaphragm
◦ to external urethral orifice (ostium urethrae externum)
◦ Epithel: stratified squamous
3 Parts of the Male Urethra
1. Prostatic urethra (pars prostatica):
passes through center of prostate gland
Epithel: transitional
2. Membranous urethra (pars membranacea):
short segment that penetrates the
urogenital diaphragm
Epithel: pseudo-stratified columnar / stratified columnar

Pars membranacea Pars prostatica
Pars spongiosa

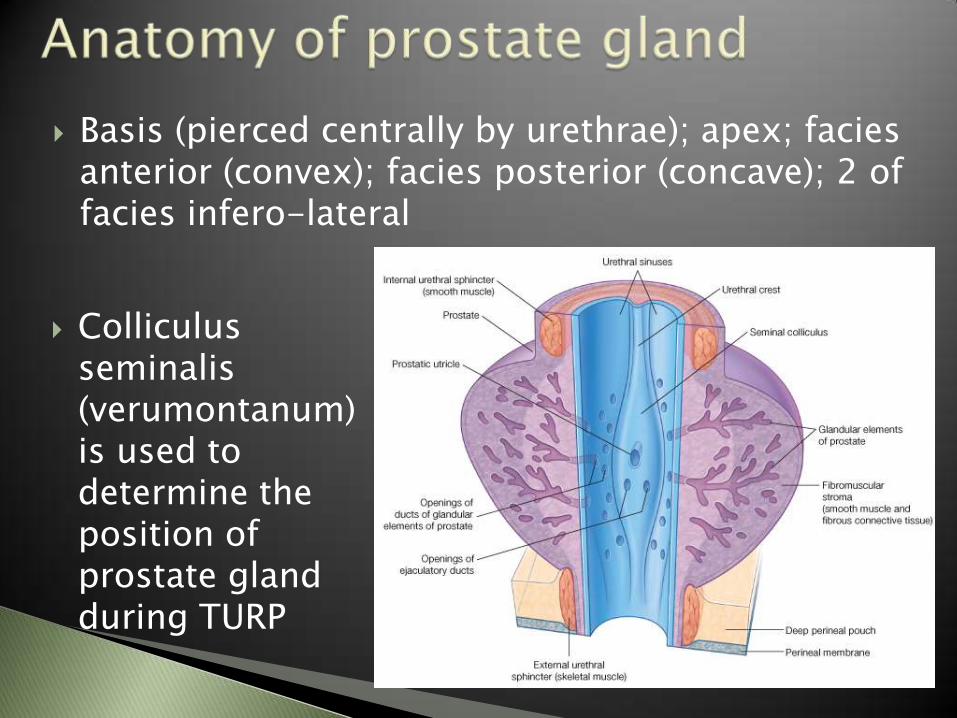
Basis (pierced centrally by urethrae); apex; facies anterior (convex); facies posterior (concave); 2 of facies infero-lateral
Colliculus
seminalis (verumontanum) is used to determine the position of prostate gland during TURP

1. The transitional/mucosal zone (5%)
◦ Where BPH occurs
2. The central/submucosal zone (25%)
◦ Contains ductus ejaculatorius
◦ <<<diseases (rare)
3. The peripheral zone (60-70%)
◦ >>>glands
◦ The most of zone where prostate ca/carcinoma form
4. The anterior zone
◦ >>>fibromuscular
◦ glandular (-)

Is very short (3–5 cm)
Extends from bladder to vestibule
External urethral orifice (ostium urethrae externum) is near anterior wall of vagina
Epithel: transitional stratified-squamous


In both sexes: ◦ is a circular band of skeletal muscle
◦ where urethra passes through urogenital diaphragm
Acts as a valve
Is under voluntary control: ◦ via perineal branch of pudendal nerve
Has resting muscle tone
Voluntarily relaxation permits micturition
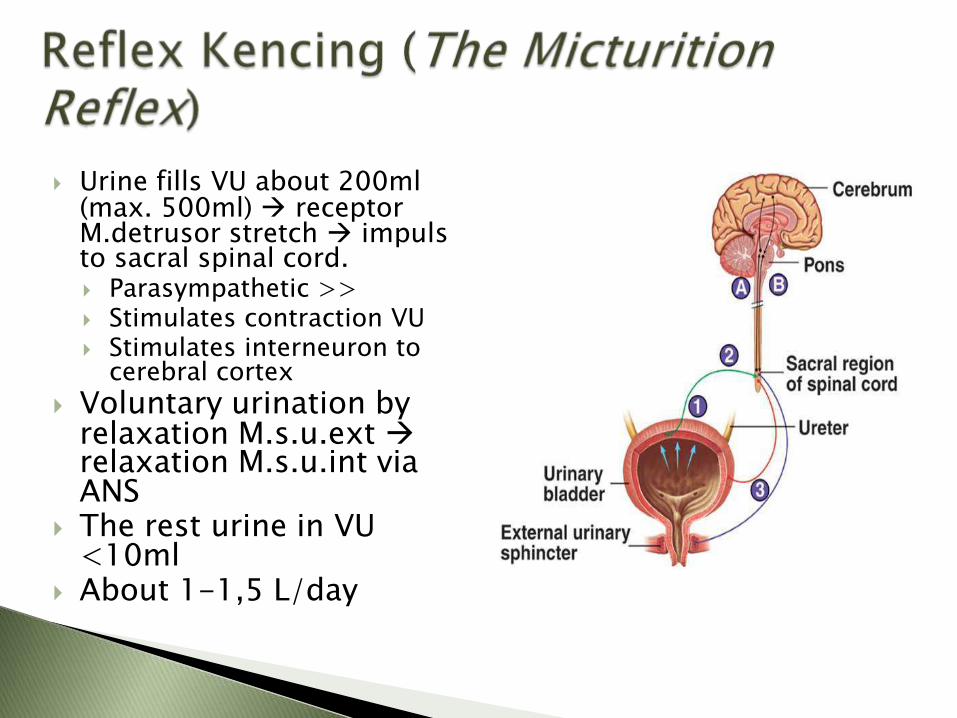
Urine fills VU about 200ml (max. 500ml) receptor M.detrusor stretch impuls to sacral spinal cord. Parasympathetic >> Stimulates contraction VU Stimulates interneuron to
cerebral cortex
Voluntary urination by relaxation M.s.u.ext relaxation M.s.u.int via ANS
The rest urine in VU <10ml
About 1-1,5 L/day

Less of voluntary control
<< corticospinal junction
Incontinence is the lack of ability to control urination voluntary.

Decline number of functional nephron Reduction in glomerular filtration Reduced sensitivity to ADH ◦ Less reabsorption of water and sodium ions;
frequent urination
Problem with micturition reflex ◦ << sphincter muscles tone incontinence ◦ Ability to control micturition is often lost after
stroke, Alzheimer, CNS problem.
◦ BPH urinary retention in male.

Belajar yang
rajin yaa…
Miaw
…
Related Documents