563 Environment & Urbanization Copyright © 2011 International Institute for Environment and Development (IIED). Vol 23(2): 563–581. DOI: 10.1177/0956247811416433 www.sagepublications.com Urban governance and health care provision in Delhi STÉPHANIE TAWA LAMA-REWAL ABSTRACT This paper considers how changes in urban governance in Delhi over the last two decades have influenced the provision of health care services. It begins by describing the introduction of, or return to, elected governments for the National Capital Territory of Delhi and for the Municipal Corporation of Delhi. It then discusses public health care, which in effect serves low-income groups as most higher-income groups now use private services, and how this has changed, drawing on interviews and direct observations of elected representatives and officials at state and municipal levels, political cadres, NGOs, members of residential welfare associations and public health care users. The research focused on four municipal wards that included a middle-class area, a mixed-income area, a ward where many slum communities had been relocated and an “urban village”. The research also included an analysis of the priority given to health care issues (and what those issues are) in the Legislative Assembly and in the Municipal Health Department and Municipal Health Committee. The paper suggests that the opening by state government of new invited spaces for resident welfare associations meant that the elected members of the Legislative Assembly and of the municipal government were by-passed. It increased the influence of resident welfare associations, but these are a feature of middle-class areas whose inhabitants use private health care. It avoided contestation, as the state could decide who was invited. The role of NGOs as advocates for the urban poor also diminished, as many were drawn into becoming implementers of government programmes. In effect, this increase in participation can be seen as a new form of centralization, strengthening the position of senior bureaucrats and by-passing the elected politicians. KEYWORDS decentralization / Delhi / health care / neighbourhood associations / NGOs / participation / urban governance I. INTRODUCTION This paper considers the provision of public health care services as a case study of the changes brought about in urban governance in India in the past 20 years, with a focus on Delhi. Since the early 1990s, economic liberalization, politico–administrative decentralization and the large consensus around the desirability of “good governance” as defined by the World Bank (1) have doubtlessly transformed urban governance. Recent studies suggest that one of the characteristic features of the contemporary management of urban affairs is the multiplication of actors involved in it. (2) This evolution is particularly striking in Delhi, whose Chief Minister since 1998, Sheila Dixit, has paid special attention to governance issues. It is difficult, however, to distinguish a pattern behind the series of reforms, policies and schemes that have been announced and implemented in quick Stéphanie Tawa Lama- Rewal is a Research Fellow at the Centre d’Études de l’Inde et de l’Asie du Sud (Centre for South Asian Studies), CNRS–EHESS, Paris. Her current research interests include urban governance and local democracy in India. She recently co-edited, with Joel Ruet, Governing India’s Metropolises (Routledge, Delhi, 2009, 340 pages). Address: Centre d’Études de l’Inde et de l’Asie du Sud (CNRS–EHESS), École des Hautes Études en Sciences Sociales, Bureau 647, 190–198 avenue de France, 75244 Paris cedex 13, France; e-mail: tawalama@ ehess.fr 1. World Bank (1989), Sub- Saharan Africa: From Crisis to Sustainable Growth. A Long-term Perspective Study, Washington DC, 300 pages. 2. Baud, Isa and Joop de Wit (editors) (2008), New Forms of Urban Governance in India. Shifts, Models, Networks and Contestations, Sage, New Delhi, 402 pages; also Ruet, Joël and Stéphanie Tawa Lama-Rewal (editors) (2009), Governing India’s Metropolises, Routledge, Delhi, 315 pages. at INIST CNRS DRD on March 25, 2015 eau.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
563Environment & Urbanization Copyright © 2011 International Institute for Environment and Development (IIED).Vol 23(2): 563–581. DOI: 10.1177/0956247811416433 www.sagepublications.com
Urban governance and health care provision in Delhi
STÉPHANIE TAWA LAMA-REWAL
ABSTRACT This paper considers how changes in urban governance in Delhi over the last two decades have influenced the provision of health care services. It begins by describing the introduction of, or return to, elected governments for the National Capital Territory of Delhi and for the Municipal Corporation of Delhi. It then discusses public health care, which in effect serves low-income groups as most higher-income groups now use private services, and how this has changed, drawing on interviews and direct observations of elected representatives and officials at state and municipal levels, political cadres, NGOs, members of residential welfare associations and public health care users. The research focused on four municipal wards that included a middle-class area, a mixed-income area, a ward where many slum communities had been relocated and an “urban village”. The research also included an analysis of the priority given to health care issues (and what those issues are) in the Legislative Assembly and in the Municipal Health Department and Municipal Health Committee. The paper suggests that the opening by state government of new invited spaces for resident welfare associations meant that the elected members of the Legislative Assembly and of the municipal government were by-passed. It increased the influence of resident welfare associations, but these are a feature of middle-class areas whose inhabitants use private health care. It avoided contestation, as the state could decide who was invited. The role of NGOs as advocates for the urban poor also diminished, as many were drawn into becoming implementers of government programmes. In effect, this increase in participation can be seen as a new form of centralization, strengthening the position of senior bureaucrats and by-passing the elected politicians.
KEYWORDS decentralization / Delhi / health care / neighbourhood associations / NGOs / participation / urban governance
I. INTRODUCTION
This paper considers the provision of public health care services as a case study of the changes brought about in urban governance in India in the past 20 years, with a focus on Delhi. Since the early 1990s, economic liberalization, politico–administrative decentralization and the large consensus around the desirability of “good governance” as defined by the World Bank(1) have doubtlessly transformed urban governance. Recent studies suggest that one of the characteristic features of the contemporary management of urban affairs is the multiplication of actors involved in it.(2) This evolution is particularly striking in Delhi, whose Chief Minister since 1998, Sheila Dixit, has paid special attention to governance issues. It is difficult, however, to distinguish a pattern behind the series of reforms, policies and schemes that have been announced and implemented in quick
Stéphanie Tawa Lama-Rewal is a Research Fellow at the Centre d’Études de l’Inde et de l’Asie du Sud (Centre for South Asian Studies), CNRS–EHESS, Paris. Her current research interests include urban governance and local democracy in India. She recently co-edited, with Joel Ruet, Governing India’s Metropolises (Routledge, Delhi, 2009, 340 pages).
Address: Centre d’Études de l’Inde et de l’Asie du Sud (CNRS–EHESS), École des Hautes Études en Sciences Sociales, Bureau 647, 190–198 avenue de France, 75244 Paris cedex 13, France; e-mail: [email protected]
1. World Bank (1989), Sub-Saharan Africa: From Crisis to Sustainable Growth. A Long-term Perspective Study, Washington DC, 300 pages.
2. Baud, Isa and Joop de Wit (editors) (2008), New Forms of Urban Governance in India. Shifts, Models, Networks and Contestations, Sage, New Delhi, 402 pages; also Ruet, Joël and Stéphanie Tawa Lama-Rewal (editors) (2009), Governing India’s Metropolises, Routledge, Delhi, 315 pages.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
564
succession in the city. I will consider here the health sector as a heuristic entry point into the analysis of urban governance on two grounds: first, health care is a major social infrastructure, and its provision involves several levels of government as well as the private sector;(3) and second, health care services are usually a good analyzer of social inequalities,(4) which makes them especially relevant to question the social distribution of the costs and benefits of the “new” urban governance.
This paper will examine the period between 1991 and 2011 and will try to discern, on the basis of a variety of sources, the broad trends that characterize the evolution in the provision of public health care services in particular, and urban governance in general. It will first set the institutional context, with a brief overview of the health sector and urban governance in India’s capital city. The next section will then highlight the main changes in the public provision of health care in the past two decades. This is followed by a look, in turn, at the role of two types of intermediaries, or mediators, who have been empowered in this period, namely political intermediaries and civil society intermediaries. On the basis of these empirical data, I will then argue that the provision of health care reflects a heavy tendency to resist decentralization, a tendency that has long been characteristic of the capital city. A retrospective look at the past two decades will reveal that contrary to appearances, the concept of participation, that is both very popular and extremely ambiguous, has played a crucial role in allowing Delhi to remain, essentially, a city ruled by bureaucrats.(5)
As far as methodology is concerned, this paper is a qualitative study based on a large number of interviews with, and direct observation of, the main concerned actors: elected representatives and officials at the state and municipal levels, political party cadres, members of NGOs and resident welfare associations, doctors and public health care users.(6) I also analyzed administrative archives, such as those of Delhi’s Legislative Assembly (Vidhan Sabha) and of its municipal corporation. Finally, I used secondary sources, such as government and press reports. Interviews and direct observation were realized in 2004–2005, a period that appears in retrospect as a time when the possibilities of mediation opened up by decentralization were particularly important, before a series of initiatives led to renewed centralization.
II. THE CONTEXT
Economic liberalization and health sector reforms have been major determinants of the evolution of health care services in the past decades. The expansion of the private health sector dates back to the 1980s, but it reached new proportions in the 2000s as 82.5 per cent of health expenditure now goes to the private sector.(7) In that context, public health care services are used mostly by the poorest sections of society, especially primary health care services.(8)
Studies on the utilization of health services by the urban poor,(9) however, have shown that in big cities, characterized by the wide availability of private medical practitioners, even slum dwellers display a preference for the private sector despite the fact that public health care is free – at least theoretically.(10) The reasons for this have been well documented: primary health care units (whether primary health
3. I will consider only one section of the private sector here, namely civil society. The corporate (or “for profit”) private sector is obviously a major actor in the provision of health services but its role is beyond the scope of this paper.
4. Fassin, Didier (2000), Les Enjeux Politiques de la Santé. Études Sénégalaises, Équatoriennes et Françaises, Karthala, Paris, 344 pages.
5. The question of the impact of urban governance on the quality of health services is obviously a major one but it is beyond the scope of this paper.
6. I observed one House meeting of the Municipal Corporation of Delhi; one ward committee meeting; one health camp organized by the Delhi government; and one public hearing organized by an advocacy network, the Jan Swasthya Abhiyan (JSA).
7. Priya, Ritu, Alpana Sagar, Rajib Dasgupta and Sangamitra Acharya (2004), “CMP on health. Making India world class”, Economic and Political Weekly Vol 39, No 27, 3 July, pages 2971–2974.
8. Baru, Rama V (2003), “Privatization of health services. A South Asian perspective”, Economic and Political Weekly Vol 38, No 42, 18 October, pages 4433–4437.
9. Sundar, Ramamani and Abhilasha Sharma (2002), “Morbidity and utilization of health care services. A survey of urban poor in Delhi and Chennai”, Economic and Political Weekly Vol 37, No 47, 23 November, pages 4729–4740; also Yesudian, C A K (1999), “Pattern of utilization of health services”, Economic and Political Weekly Vol 34, No 5, 30 January, pages 300–304.
10. At the secondary and tertiary levels of health services, user fees are increasingly being introduced as part of the health sector reforms; see Kumar, Girish (editor) (2009), Health Sector Reforms in India, Manohar, Delhi, 269 pages.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
565
care centres or dispensaries) have a reputation for being understaffed, not adequately supplied with medical equipment and drugs, and their inconvenient opening hours translate into long queues.(11) Even though private health care is uneven in quality, it is preferred by a majority of people, including the poor, because it is perceived as being more efficient.
In Delhi, the provision of public health care services reflects the complexity that characterizes urban governance in the city: a multiplicity of agencies work in the same territory, under the responsibility of different levels of government, which translates into overlapping, inefficiency and reduced accountability. Before we turn to a description of the organization of public health care, it seems useful therefore to get a general idea of Delhi’s governance.
Delhi, being the seat of India’s central government, has long been known as a city ruled by bureaucrats. But the 1990s ushered in a democratic decentralization process that proceeded through two Constitutional amendments. In 1991, the adoption of the 69th Constitutional Amendment Act led to the creation of the National Capital Territory of Delhi. Delhi then became a quasi-state: on the one hand it now had its own Assembly and Council of Ministers; on the other hand two key areas of public action, namely land development and law and order, which normally depend on the state government, remained dependent on the national government. This exception was justified by specific security requirements linked to the fact that the Union’s government, its Parliament and its diplomatic enclaves are located in the city. In 1993, the first Delhi Legislative Assembly elections since 1956 took place, allowing 71 Members of the Legislative Assembly (MLAs) to represent Delhi’s inhabitants and elaborate policies.
One year earlier, in 1992, the 74th Constitutional Amendment Act, defining the decentralization policy in urban areas, had been adopted. It was implemented in Delhi in 1997: 134 councillors were then elected to the Municipal Corporation of Delhi (MCD), which had been superseded in 1989.
There are a number of reasons why one can consider that both MLAs and councillors, in the Delhi context, pertain to the development of local democracy, lato sensu. First, the borders of the National Capital Territory (i.e. the state) are largely co-extensive with those of the MCD (i.e. the municipality).(12) Second, Delhi’s peculiar political geography was, until 2007, further grounds for considering both MLAs and councillors as “local” representatives: in this megacity, municipal wards – i.e. the smallest electoral constituency in India’s political architecture – were characterized by their huge size.(13) Therefore the municipal and state levels of government were closer to each other than they were elsewhere in India, both geographically and statutorily: there were only two councillors for one MLA in Delhi (as opposed to 6–8 in other megacities). As a result, a strong sense of competition was perceptible between MLAs and councillors, since every councillor could virtually expect to become an MLA.
What can we expect from democratic decentralization in terms of health care services provision? The current discourse supporting decentralization, primarily carried by the World Bank and adopted, with local variations, in a majority of countries in the past two decades, argues that one of its main impacts is to make the administration more responsive to people’s needs. In the Delhi context, one may expect newly empowered local representatives to take action concerning a basic
11. Mahal, Ajay and Vivek Srivastava (2000), “People’s participation, decentralization and delivery of public sector services in India”, Working Paper Series No 71, National Council of Applied Economic Research, New Delhi; also Gangolli, Leena V, Ravi Duggal and Abhay Shukla (editors) (2005), Review of Health Care in India, CEHAT, Mumbai, 375 pages.
12. The National Capital Territory covers 1,438 square kilometres and has jurisdiction over 13.9 million people; the MCD covers 1,397 square kilometres and has jurisdiction over 13.78 million people.
13. In Delhi, until 2007, there were on average 100,000 people in each of the 134 municipal wards, and ward committees represented an average population of more than one million people; see Shah, Partha and Makarand Bakore (editors) (2006), Ward Power. Decentralized Urban Governance, Centre for Civil Society, Delhi, page 27. However, a re-delimitation of wards took place prior to municipal elections in April 2007, making the average population of the new 272 wards closer to 50,000 people – still a large figure by any standard.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
566
service that largely falls under the responsibility of state governments and municipal corporations. The fact that public health services are used mostly by the social category with the highest voting participation in local elections, i.e. slum dwellers, gives further credibility to that expectation.
However, elected representatives are not the only possible intermediaries, or mediators, between the people and public providers of health care services: civil society organizations, consisting essentially of neighbourhood associations and NGOs, have also gained a new visibility in Delhi’s urban governance.
Neighbourhood associations, known in Delhi as “resident welfare associations” (RWAs), consist of a semi-formal grouping of neighbours concerned with the maintenance of local infrastructure, and have been in existence in Delhi at least since the 1960s. In 2000, the Chief Minister, Sheila Dixit, launched the Bhagidari Scheme,(14) self-defined as a “citizen–government partnership”, which gave a new dimension to these associations. The Bhagidari Scheme, which aims to develop people’s participation in the management of local affairs, gives a new status and role to RWAs, which it calls “citizens’ groups”. We will return later to the relevance of RWAs to the provision of health care services.
Finally, in a context where the poor, supposed to be the main users of public health care, are deprived of the mobilizing capacity to demand a better quality of such services, the advocacy role played by some NGOs deserves attention. However, most NGOs active in the field of health care are actually service providers hired by the central, state or municipal administration to implement a number of schemes pertaining to public health (particularly those concerning the urban poor). We will later discuss the implications of this double role of NGOs as far as health care is concerned.
III. PUBLIC HEALTH CARE IN DELHI
Let us now look at the organization of public health care, which in Delhi depends on all three levels of government: the central (or Union) government; the government of the National Capital Territory of Delhi (or Delhi government); and the Municipal Corporation of Delhi (MCD).
At the topmost level, a major hospital such as the All-India Institute of Medical Sciences, institutions such as the Indian Council for Medical Research and dispensaries catering only to the needs of specific clients (i.e. government employees) come under the central government.
At the state level, a number of hospitals, polyclinics, dispensaries and medical colleges function under the Delhi government. That government operates through the Social Welfare Department and the Health and Family Welfare Department, whose Health Directorate coordinates the action of the different health service providers (including private providers), in order to avoid overlaps and to control the quality of services.
The MCD (Delhi’s largest civic body)(15) also manages a series of hospitals, polyclinics, dispensaries, maternity and child welfare centres, mobile vans and primary health care centres. The MCD operates through its Health Department and its Slum and Jhuggi Jompri (huts) Wing, which caters to the poorest section of the population. In addition, various parastatal agencies such as the Northern Railways or the Employees of the State Insurance Corporation (ESI) also provide medical facilities
14. Bhagidari means “participation” in Hindi.
15. The other two civic bodies – the New Delhi Municipal Council and the Delhi Cantonment Board – are also health care service providers for their respective constituencies.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
567
catering to their exclusive clientele. Lastly, the voluntary sector runs a few charitable hospitals. To complicate matters, dispensaries (and hospitals to a lesser extent) provide different types of medicine: besides allopathic dispensaries, one finds ayurvedic and unani dispensaries (classified together as “Indian systems of medicine”) as well as homeopathy.
The crucial need to coordinate the work of these different agencies has been the subject of discussions and proposals since the 1990s onwards. It was decided, for instance, that the Delhi government would be in charge of all curative health care except primary health care – which would remain with the MCD, along with preventive care. But from 1999 onwards, the proposed transfer of curative functions from the MCD to the Delhi government caused recurring tensions between these two levels of government.(16)
A division of labour according to the type of medicine was also proposed: while the Delhi government would be in charge of allopathic medicine, the MCD would provide only ayurvedic and unani medicine, as well as homeopathy. However, according to senior MCD officials, this proposal was never strictly implemented.
A new coordination proposal, finalized in 2002, was more comprehensive: it planned to make the nine revenue districts of the National Capital Territory of Delhi reference units for the coordination of all medical facilities. A Chief District Medical Officer would be in charge of coordination and would check the registration of all medical practitioners, nursing homes,(17) etc.; and he would be in charge of total health planning for the concerned district.(18) In that scheme of things, all new dispensaries would offer ayurvedic and unani medicine, homeopathy and allopathy. An interesting feature of this ambitious proposal was that no presence of elected representatives was planned.
In 2007, that proposal took concrete shape as the Delhi government created a Delhi State Health Mission (modelled on the National Rural Health Mission) that was to “…function under the chairmanship of the Chief Minister...” and “…integrate the various vertical programmes implemented by the different departments of the Delhi government, MCD...” etc.(19)
One year later, the same government launched Mission Convergence, a programme meant to bring all departments dealing with social welfare together under a single-window system, through which beneficiaries could directly access schemes such as old age pensions, ration cards, etc. In 2010, this programme won two gold medals from the Commonwealth Association for Public Administration and Management (CAPAM), rewarding its contribution to good governance. However, just like the Bhagidari Scheme, Mission Convergence has been much criticized by elected representatives who resent the fact that it deprives them of their traditional role as intermediaries between the welfare departments and beneficiaries.
What can be expected from the limitation of the number and role of intermediaries between the public and public services as far as the efficiency of delivery, the quality of services and the democratic nature of governance are concerned? Looking back at interviews realized just before the launch of Mission Convergence – interviews that presented the respective perspectives of elected representatives and bureaucrats but also civil society organizations – provides a number of insights into these important questions.
My fieldwork was grounded in four municipal wards, selected with a view to provide a representative sample of the city in terms of urban
16. In 2000, four out of the seven hospitals that had been taken over by the Delhi government went back to the MCD.
17. In 2003, a survey conducted by the Health Department found 1,603 illegal nursing homes and only 400 registered ones; see Times of India, 14 March 2003.
18. Source: interview with a senior official of the Health Directorate, Delhi, November 2004.
19. Urban Health Resource Centre (2007), State of Urban Health in Delhi, UHRC/Ministry of Health and Family Welfare, New Delhi, page 31.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
568
landscape, housing pattern and socioeconomic profile of the inhabitants. Wards are too large a unit of analysis to allow a rigorous spatial comparison of the quality of health care services that are provided in different parts of the city. Yet when considered together, they suggest strong links between some types of provider,(20) some types of public, and some types of care.
The first ward is Kalkaji, in the southern, mostly residential part of the city. It is the most mixed area, and is home to a refugee colony (from the time of Partition), to an important business centre and to a series of notified slums. The private health care sector is very present in Kalkaji, while there are comparatively fewer dispensaries than elsewhere.
Proceeding anti-clock wise, we reach Seemapuri ward, across the Yamuna River, a place where many slum dwellers have been relocated in resettlement colonies. The place could very roughly be qualified as being lower-middle class, and RWAs were less prominent here than elsewhere,(21) unlike NGOs. This is where I encountered a series of NGOs catering to specific categories, such as drug addicts or HIV-infected people.
Further to the west is Jama Masjid ward, at the heart of the dense old city – a busy, commercial, congested area that is middle-middle class. NGOs were less visible here and it has a lot of dispensaries. Local RWAs repeatedly mentioned their interaction with the local MLA in matters of health care, and it was a good place to observe how patronage works.
Finally, Najafgarh ward, on the western, quasi-rural border of Delhi, is one the capital’s many “urban villages”. The presence of RWAs is very visible in Najafgarh, where both public and corporate health care providers are comparatively absent; there are few dispensaries and there was no public hospital in 2005, unlike in the other three wards.
Each of these four wards displays a specific balance between the various providers and intermediaries that I had decided to study. While state and municipal health care services are present everywhere, albeit more or less intensely and visibly, it is quite clear that RWAs are more numerous in well-off areas, while NGOs are stronger in poorer areas.
An analysis of the archives of the Delhi Legislative Assembly and the MCD, which provide a diachronic, systematic view of the content and focus of discussions concerning health issues in those two political institutions, helped to contextualize interviews. These archives do not provide verbatim quotations, but rather a lifeless rendition of the issues raised by elected representatives. Yet they are a major source of information on the process of agenda setting: whatever is being discussed is put on the agenda of the Delhi government or the MCD – even if we do not always know to what extent the agenda was translated into action.
IV. POLITICAL INTERMEDIARIES
Let us first consider the Members of the Legislative Assembly (MLAs), since they were the first “local” representatives offered to the Delhi people in the 1990s. How interested in health issues are MLAs and in what areas of the health care services are they most active? How do they influence the Delhi government’s health policy? Administrative archives provide a number of insights into these questions.
Much of the policy-making work of the MLAs is done through a series of “House committees”,(22) which are really monitoring committees; they meet once or twice a month to summon officers from the various
20. The mapping of health care realized by Chapelet and Lefebvre was extremely useful to contextualize my interviews and direct observations; see Chapelet, Pierre and Bertrand Lefebvre (2005), “Contextualizing the urban health care system. Methodology for developing a geo-database of Delhi’s health care system”, CSH Occasional Paper No 11, 135 pages.
21. The local councillor even said that she did not know of any RWA.
22. Each House committee is composed of nine MLAs and is renewed every year.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
569
departments, who will answer their queries. These committees produce reports based on information thus provided, which they eventually submit to the House. Once adopted, the resolutions contained in these reports are binding on the government. Unfortunately for researchers, the thematic classification of House committees does not correspond to the various departments, so that MLAs’ policy-making on health issues is spread among a number of committees, whose proceedings were not available.
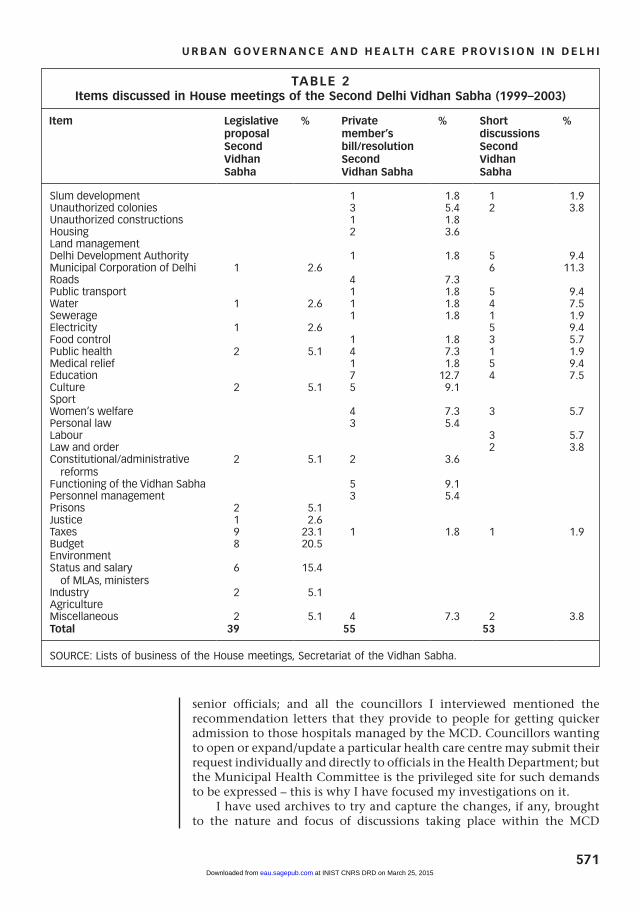
The Legislative Assembly sittings’ lists of business thus appeared to be the second best source of information. Delhi’s Legislative Assembly does not meet very often: there were 26 yearly sittings, on average, between 1993 and 1998 (the First Vidhan Sabha), and 16 yearly sittings between 1999 and 2003 (the Second Vidhan Sabha). The main purpose of sittings is, of course, for government members to answer MLAs’ queries.
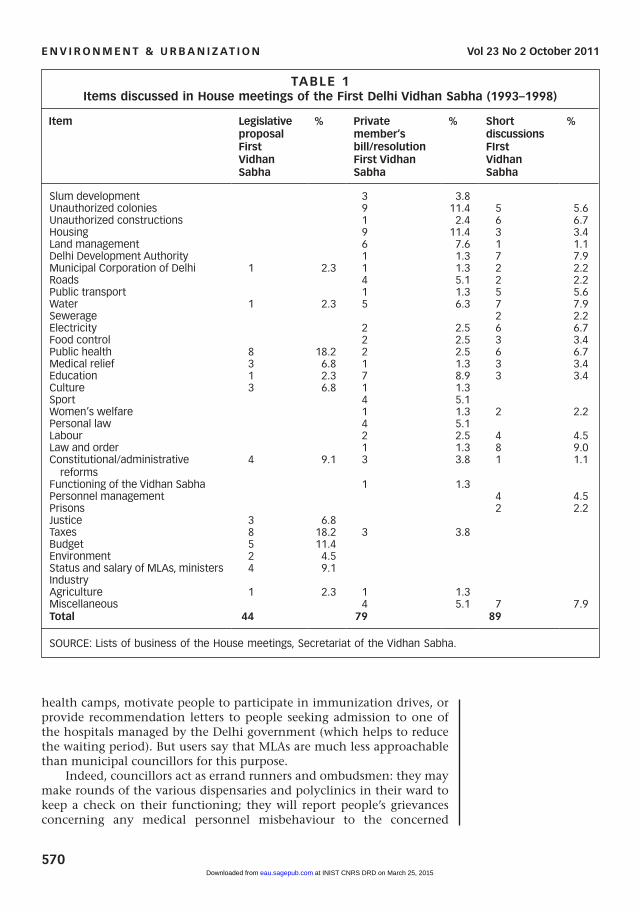
Tables 1 and 2 offer a schematic, quantified view of the nature of issues discussed in the House meetings during these two periods. They are based on an exhaustive perusal of the lists of business for each sitting (no minutes were available). The lists of business, drafted a few days prior to each House meeting, are a good indicator of the issues of concern to MLAs, which I have classified into two different categories:
• private members bills and resolutions are formal statements of interest, which may lead to legislative proposal (legislative proposals are a different category altogether, as they are put up by ministers); and
• short duration discussions (in which I have included those items raised under the “calling attention” category), which are more informal statements and usually relate to immediate problems.
Tables 1 and 2 indicate the range of issues dealt with by the Legislative Assembly, the changing priority areas (indicated by the number of interventions on a given issue), and the relative emphasis put by MLAs on various issues (as indicated by their appearance as private members bills and resolutions or in short duration discussions).(23)
As far as health care is concerned, one can first observe that it was a major object of legislative proposals in the First Vidhan Sabha. Of the 11 bills (i.e. one-quarter of the total number of bills) coming under “public health” and “medical relief”, 10 would be passed, half of which aimed to regulate private medical practice in the capital city – which might well be an answer to the growing importance of the private health care sector. In the same period, MLAs appeared to pay less attention to health issues than the government did: 10 per cent of short duration discussions were devoted to the health sector (usually to deplore the “sorry state of affairs in government hospitals”), compared to only 3.8 per cent of private members bills/resolutions. In the Second Vidhan Sabha, one finds a reverse situation: health issues were the object of only 5.1 per cent of legislative proposals but 9 per cent of private members bills/resolutions and 11.3 per cent of short discussions.
These tables inform us on MLAs’ action concerning health issues in their policy-making capacity. However, MLAs also act as errand runners for their constituents: they interact individually, and directly, with the Health Minister, with senior officials of the Health Department or even with medical staff. This interaction can take different forms. First, MLAs support the creation of health infrastructure – according to a senior official from the Health Secretariat, about 60 per cent of infrastructure provision is the result of MLA initiatives. Second, MLAs may also help organize
23. The Tables do not, however, present an exhaustive view of what is being discussed in the Legislative Assembly. I have omitted budget sessions, the presentation of reports (because the reporting mode does not provide any detail in these cases) and Motions under Rule 107, which are another way for MLAs to make a statement, but are used only exceptionally.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
570
TABLE 1Items discussed in House meetings of the First Delhi Vidhan Sabha (1993–1998)
Item Legislative proposal First Vidhan Sabha
% Private member’s bill/resolution First Vidhan Sabha
% Short discussions FIrst Vidhan Sabha
%
Slum development 3 3.8Unauthorized colonies 9 11.4 5 5.6Unauthorized constructions 1 2.4 6 6.7Housing 9 11.4 3 3.4Land management 6 7.6 1 1.1Delhi Development Authority 1 1.3 7 7.9Municipal Corporation of Delhi 1 2.3 1 1.3 2 2.2Roads 4 5.1 2 2.2Public transport 1 1.3 5 5.6Water 1 2.3 5 6.3 7 7.9Sewerage 2 2.2Electricity 2 2.5 6 6.7Food control 2 2.5 3 3.4Public health 8 18.2 2 2.5 6 6.7Medical relief 3 6.8 1 1.3 3 3.4Education 1 2.3 7 8.9 3 3.4Culture 3 6.8 1 1.3Sport 4 5.1Women’s welfare 1 1.3 2 2.2Personal law 4 5.1Labour 2 2.5 4 4.5Law and order 1 1.3 8 9.0Constitutional/administrative reforms
4 9.1 3 3.8 1 1.1
Functioning of the Vidhan Sabha 1 1.3Personnel management 4 4.5Prisons 2 2.2Justice 3 6.8Taxes 8 18.2 3 3.8Budget 5 11.4Environment 2 4.5Status and salary of MLAs, ministers 4 9.1IndustryAgriculture 1 2.3 1 1.3Miscellaneous 4 5.1 7 7.9Total 44 79 89
SOURCE: Lists of business of the House meetings, Secretariat of the Vidhan Sabha.
health camps, motivate people to participate in immunization drives, or provide recommendation letters to people seeking admission to one of the hospitals managed by the Delhi government (which helps to reduce the waiting period). But users say that MLAs are much less approachable than municipal councillors for this purpose.
Indeed, councillors act as errand runners and ombudsmen: they may make rounds of the various dispensaries and polyclinics in their ward to keep a check on their functioning; they will report people’s grievances concerning any medical personnel misbehaviour to the concerned
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
571
senior officials; and all the councillors I interviewed mentioned the recommendation letters that they provide to people for getting quicker admission to those hospitals managed by the MCD. Councillors wanting to open or expand/update a particular health care centre may submit their request individually and directly to officials in the Health Department; but the Municipal Health Committee is the privileged site for such demands to be expressed – this is why I have focused my investigations on it.
I have used archives to try and capture the changes, if any, brought to the nature and focus of discussions taking place within the MCD
TABLE 2Items discussed in House meetings of the Second Delhi Vidhan Sabha (1999–2003)
Item Legislative proposal Second Vidhan Sabha
% Private member’s bill/resolution Second Vidhan Sabha
% Short discussions Second Vidhan Sabha
%
Slum development 1 1.8 1 1.9Unauthorized colonies 3 5.4 2 3.8Unauthorized constructions 1 1.8Housing 2 3.6Land managementDelhi Development Authority 1 1.8 5 9.4Municipal Corporation of Delhi 1 2.6 6 11.3Roads 4 7.3Public transport 1 1.8 5 9.4Water 1 2.6 1 1.8 4 7.5Sewerage 1 1.8 1 1.9Electricity 1 2.6 5 9.4Food control 1 1.8 3 5.7Public health 2 5.1 4 7.3 1 1.9Medical relief 1 1.8 5 9.4Education 7 12.7 4 7.5Culture 2 5.1 5 9.1SportWomen’s welfare 4 7.3 3 5.7Personal law 3 5.4Labour 3 5.7Law and order 2 3.8Constitutional/administrative reforms
2 5.1 2 3.6
Functioning of the Vidhan Sabha 5 9.1Personnel management 3 5.4Prisons 2 5.1Justice 1 2.6Taxes 9 23.1 1 1.8 1 1.9Budget 8 20.5EnvironmentStatus and salary of MLAs, ministers
6 15.4
Industry 2 5.1AgricultureMiscellaneous 2 5.1 4 7.3 2 3.8Total 39 55 53
SOURCE: Lists of business of the House meetings, Secretariat of the Vidhan Sabha.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
572
committee in charge of health care by the implementation of the 74th Constitutional Amendment Act in 1997 – that is, essentially by the new presence of elected representatives after eight years of supersession. The MCD’s deliberative wing is organized into a series of thematic “municipal committees” composed of 10–20 councillors selected for one year by their respective parties, which mirrors the executive wing’s organization into “municipal departments”. The MCD’s Medical Relief and Public Health Committee, like other municipal committees, meets about once a month to discuss a number of issues. Its role consists of examining recommendations expressed by the executive wing and in making new recommendations.
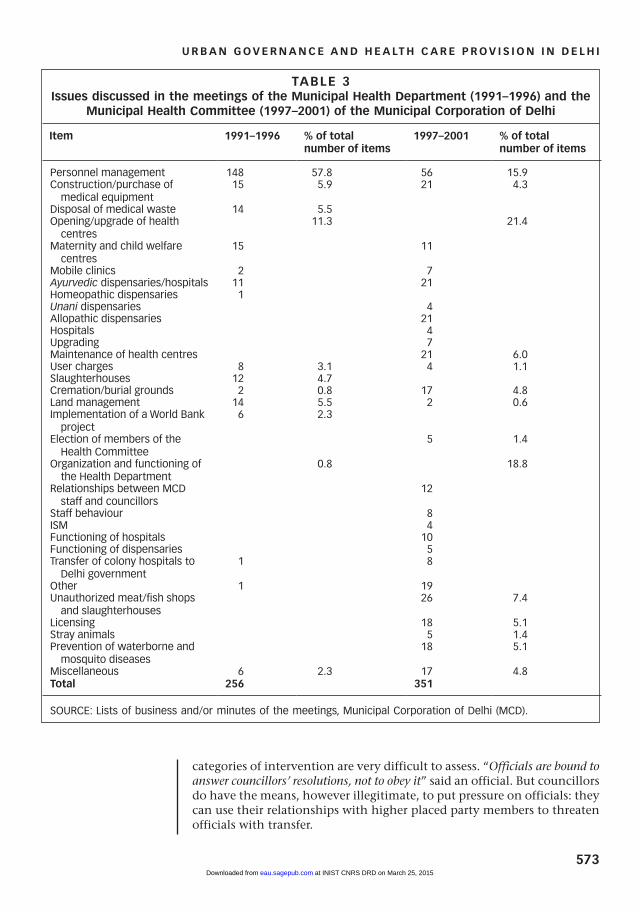
Table 3 offers a schematic, quantified view of these discussions, but it cannot be compared with Tables 1 and 2 – whose equivalent would have been an index of those issues discussed in the monthly House meetings of the MCD. Table 3 does not provide an exhaustive view of discussions relating to health issues in the MCD, since those can also take place both within ward committee meetings and House meetings. It is based on two types of sources: the lists of business of the Municipal Health Department prior to 1997, and both the lists of business and the minutes of the meetings of the Municipal Health Committee after 1997. These two types of document are essentially similar since minutes do not contain any verbatim quotations but only show what part of the list of business, i.e. the meeting’s agenda, was actually dealt with.
Table 3 compares two periods of five years each: 1991–1996(24) (when the MCD was a purely administrative civic body) and 1997–2001 (when the MCD became a politico–administrative institution of local self-government as a result of the implementation of the 74th Constitutional Amendment Act). It shows, first, that many more items were discussed after 1997, i.e. after the election of the first batch of councillors. Second, a clear contrast appears in the focus of discussions in these two periods: “personnel management” was the object of 57.8 per cent of officials’ discussions but only of 15.9 per cent of councillors’ discussions.(25) Councillors’ discussions really focused on the opening or upkeep of various types of health care centres (21.4 per cent as opposed to 11.3 per cent of discussions before 1997), and to a lesser extent on their maintenance (6 per cent). These figures suggest that councillors, on the one hand, are keen to create new health care infrastructure and, on the other hand, confirm that they do monitor the functioning of existing structures.
Another interesting point is the importance of discussions focusing on the functioning and organization of the Municipal Health Department (18.8 per cent); councillors regularly questioned the status quo – particularly the relationships between the executive and the legislative wings.
Table 3 does not indicate to what extent the issues being discussed have been translated into action. However, items mentioned prior to 1997 are more likely to have been followed by action since they were already in the administrative process. After 1997, items appear via different types of intervention: either a collective resolution or a request by the Municipal Health Committee as such (usually addressed to the MCD administrative and/or medical staff)(26) or some individual councillor’s resolution or councillors’ observations. The actual consequences of these different
24. Instead of 1992–1996, because no archives were available for the year 1992.
25. In 2004, the total staff of the MCD numbered 150,000 employees.
26. Many administrative posts in the Health Department are occupied by medical doctors.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
573
categories of intervention are very difficult to assess. “Officials are bound to answer councillors’ resolutions, not to obey it” said an official. But councillors do have the means, however illegitimate, to put pressure on officials: they can use their relationships with higher placed party members to threaten officials with transfer.
TABLE 3Issues discussed in the meetings of the Municipal Health Department (1991–1996) and the
Municipal Health Committee (1997–2001) of the Municipal Corporation of Delhi
Item 1991–1996 % of total number of items
1997–2001 % of total number of items
Personnel management 148 57.8 56 15.9Construction/purchase of medical equipment
15 5.9 21 4.3
Disposal of medical waste 14 5.5Opening/upgrade of health centres
11.3 21.4
Maternity and child welfare centres
15 11
Mobile clinics 2 7Ayurvedic dispensaries/hospitals 11 21 Homeopathic dispensaries 1Unani dispensaries 4Allopathic dispensaries 21 Hospitals 4Upgrading 7Maintenance of health centres 21 6.0User charges 8 3.1 4 1.1Slaughterhouses 12 4.7Cremation/burial grounds 2 0.8 17 4.8Land management 14 5.5 2 0.6Implementation of a World Bank project
6 2.3
Election of members of the Health Committee
5 1.4
Organization and functioning of the Health Department
0.8 18.8
Relationships between MCD staff and councillors
12
Staff behaviour 8ISM 4Functioning of hospitals 10Functioning of dispensaries 5Transfer of colony hospitals to Delhi government
1 8
Other 1 19Unauthorized meat/fish shops and slaughterhouses
26 7.4
Licensing 18 5.1Stray animals 5 1.4Prevention of waterborne and mosquito diseases
18 5.1
Miscellaneous 6 2.3 17 4.8Total 256 351
SOURCE: Lists of business and/or minutes of the meetings, Municipal Corporation of Delhi (MCD).
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
574
a. The conflictual relationship between elected representatives and officials
On the whole, a constant tension is perceptible between councillors and MCD officials,(27) whether administrators or doctors. Despite their lifeless character, the archives reveal that councillors struggle to assert their authority, to define their role in an organization that did function (albeit differently) without them; they constantly demand information, they often suggest coordination mechanisms.
Moreover, the well-known contrast between the respective styles of expression of bureaucrats and politicians is striking in the MCD archives: while bureaucrats base their demands on previous administrative decisions or norms, politicians always give pride of place to “people’s demands, needs or wishes” – usually a very vague notion.(28) Both types of demand always refer to the same set of criteria, i.e. population density and distance to the nearest medical facility, but councillors also display a wish to make available a variety of medicines – i.e. Indian systems of medicine and homeopathy, beside allopathy – to their constituents. Lastly, targets are usually specified in the pre-1997 archives, which often mention jhuggi jhompri (hut) dwellers, mothers and children or school children, while councillors merely mention “poor people” or “the weaker section”.(29)
These contrasts find a more violent echo in interviews with officials, both in the Delhi government and in the MCD, who express mostly negative feelings about the impact of elected representatives. When interviewed about the changes brought about in their own work by the presence of councillors from 1997 onwards, most MCD officials mention a necessary evil: “It was easier before 1997” one of them simply said. “For the officer it’s easier to work without the local representative; but for the general public it makes things simpler: they won’t hesitate to go to the councillor’s house, while they will hesitate to go and meet the official”, a Deputy Commissioner said.
First, officials frequently display a certain contempt towards what they perceive as elected representatives’ incompetence: “The Health Committee is supposed to formulate the guidelines of the [MCD health] policy, and the Health Department is supposed to work in collaboration with them to implement their decisions; but rarely do they make policy on their own” said a senior official from the Health Department.
They criticize politicians’ obsession with their re-election; both MLAs and councillors are accused of focusing on opening new facilities for the sake of visibility.(30) “Each MLA wants a dispensary in his locality, for electoral and other benefits; they will say that they want health at people’s doorstep” said a Health Department official.
More generally, officials complain of the demagogical approach of elected representatives. According to a deputy health officer (MCD):
“Councillors have no good perception of preventive health… They want the government to provide everything. Pulse polio programmes are popular with them; they always go for any formal gathering. But when perceptions have to be changed (for instance, to fight mosquito breeding) we receive hardly any support from them, they accuse us of chalaning [giving fines to] people.”
They also complain of councillors’ limited perspective: “Councillors’ perception is limited to their ward; they lack in planning capacity for the larger area” said another deputy health officer.
27. Baud and Nainan observe the same phenomenon in Mumbai; see Baud, Isa and Navtej Nainan (2008), “‘Negotiated spaces’ for representation in Mumbai: ward committees, advanced locality management and the politics of middle-class activism”, Environment and Urbanization Vol 20, No 2, October, page 493.
28. The reference to people’s demands appears only once in the pre-1997 archives and concerns the need to open a homeopathic dispensary in a locality.
29. However, councillors also occasionally display gender concerns. For instance, a lady representative demanded that women be given priority in the recruitment for a technician’s post devoted to examining mostly female patients; this might be a consequence of the fact that the Health Committee is roughly made up of half male and half female councillors.
30. Corruption, which is notorious in the relationship between political authorities and builders, might well be another reason for the strong interest of elected representatives in physical infrastructure.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
575
Observing ward committee meetings, however, sheds a different light on this argument. I saw two different types of relationship, depending on the decentralization level in the MCD, with noticeable contrasting attitudes adopted by officials and councillors towards each other during House meetings and ward committee meetings. In the former, the Commissioner (i.e. the head of the executive wing), sits side by side with the Mayor (i.e. the head of the deliberative wing) and faces the House in a chairing position. While councillors present their requests they are literally obliged to look up to him, and he in turn answers, while looking down on them.
On the other hand, in ward committee meetings the dozen councillors face zone level officials representing all MCD departments around a table, and the session is chaired by the ward committee chairperson (elected from among the ward’s councillors). Here, councillors take officials to task regarding specific issues, and the nature of discussions reveals that they have a precise knowledge of local problems concerning civic amenities. “Area officials(31) know that I’m very strict and don’t tolerate administrative neglect; if no action is taken, I charge them in ward committee meetings” said a woman councillor. “At the zone level, we usually don’t counterstand [oppose] councillors” said a deputy health officer.
These two types of meeting differ in their solemnity, their visibility (journalists usually attend only House meetings), the level of officials facing councillors and, of course, the issues and the budget at stake. Ward committee meetings allow councillors to display the minute attention they pay to civic amenities and their maintenance, but no planning activity is conducted at that level and discretionary spending powers are limited to Rs 500,000.
Another negative feeling that is often mentioned is that of resentment: “Your tenure is normally for two to three years, but you get transferred as soon as a politician wants you to be” said an official in the Health Department. “In the planning process, the political factor dominates: an influential person can get a dispensary open even if it is not required” added another official. Yet unlike administrative officials, doctors mostly seem to think that the presence of elected representatives is beneficial:
“The councillor comes and visits my primary health centre regularly, to see that everything and everybody is working. We can tell him about our problems, for instance when a water pump is out of order he can use his own fund or get the department to repair it… Corruption is there, but some work is also there” said the medical officer in South Delhi.
“The councillor makes it easier to get things done; she conveys requests to the relevant departments; whereas the MLA is rarely seen” said a medical officer in charge of an MCD dispensary.
Lastly, councillors, when interviewed about their actions in terms of health issues, hardly mentioned the role of officials. This fact, in addition to the clear contrast between the perceptions of the medical and administrative MCD staff, suggests that the conflicting relations between elected representatives and officials mostly result from the latter’s frustration at having to deal with politicians, in a city where bureaucrats have long been very powerful.
31. That is, officials at the zonal or ward committee level.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
576
V. CIVIL SOCIETY INTERMEDIARIES
Two types of civil society organization have been given an official role in the delivery of health care in Delhi, namely the resident welfare associations (RWAs) and the NGOs.
Thanks to the Bhagidari Scheme, the RWAs now enjoy official status provided they follow (at least on paper(32)) a series of rules (such as selecting their representatives through a secret ballot election held every three years), which entitles two of their representatives to become card-holding members of the Chief Minister’s “Team Delhi”. RWAs are also given an official role, namely representing the inhabitants of a given area when dealing with the administration – be it the MCD, the police or the parastatal agencies in charge of urban services – on a range of subjects, from monitoring maintenance works to managing community halls.The Bhagidari Scheme projects itself as a tool for making the administration more transparent and accountable: it provides RWAs with information about public works to be conducted and about the personal details of the officials in charge, which gives them the power to “keep officials on their toes”, as several officials said.
As far as health care is concerned, RWAs are considered by the municipal administration as a major channel of communication, particularly useful for its public health mission. RWAs are certainly a key instrument of communication between local people and the MCD; they both inform the administration about local needs, for instance in terms of anti-mosquito measures, and also convey public health recommendations from the administration to the people. Their role is quite formal in this regard; in each of the 12 MCD zones (each zone encompassed a dozen wards prior to the 2007 re-delimitation), the MCD zonal health officer (and sometimes the Deputy Commissioner) holds monthly meetings with RWAs in order to exchange information regarding public health issues.
However, “...the major demands of RWAs are for curative health services: better medicines, a greater availability of doctors and drugs” said a deputy health officer. In this regard, one might be surprised by the fact that RWAs do not use their mobilizing power to demand better health services. Considering that the Bhagidari Scheme gives RWAs some means to demand that public services be of a certain quality, one might expect them to mobilize their members on the important issue of health services. But the mobilizing capacity of RWAs, revealed in the past two years by their interventions against the method to calculate house tax and against the raise in electricity tariffs – interventions that embarrassed the MCD and the Delhi government, respectively – has not so far applied to health issues. One likely explanation for this is that RWAs are essentially a feature of middle-class colonies – whether planned or unauthorized – whose inhabitants would rather use private health care services. When I asked a South Delhi RWA representative whether his association had put any pressure on the local councillor concerning the dilapidated state of the local dispensary, he replied: “We are not concerned with that dispensary, we don’t use it, only the servants go there.”
RWAs however do play a role in the provision of health care services, for instance through the organization of an informal ambulance service or the setting up of a health camp in their locality. But these local initiatives can hardly qualify as public health care: they rely on a series of private resources and are directed at a very specific set of beneficiaries – usually the colony’s inhabitants.
32. Interviews with RWA representatives reveal that many different realities co-exist behind this common appellation. RWAs are sometimes formed through co-option rather than election, and they raise resources in a variety of ways that are more or less transparent.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
577
As far as NGOs are concerned, their dependency on the administration to get paid contracts is not conducive, a priori, to their playing an advocacy role. Yet, some keep a check on health issues, build cases and actually get legislative action, as the Centre for Science and Environment did, for example, in fighting air pollution in Delhi.
The Jan Swasthya Abhiyan (JSA), self-defined as “a coalition of the networks of voluntary organizations and people’s movements involved in health care delivery and health care policy”, has been organizing a national campaign for the past ten years demanding that access to basic health care be given the status of a constitutional right. In this Right to Health Care Campaign, the JSA organizes public hearings on the denial of the right to health care in different regions and on different scales (they can involve lay people or community representatives). The demand to recognize access to health care as a basic human right is legally justified in the JSA’s manifesto by reference to the Alma Ata Declaration, signed by India at the end of the WHO conference held in the town of Alma Ata in Kazakhstan in 1978, which took the pledge of achieving “health for all by the year 2000”.(33)
However, most NGOs involved in the health sector act as service providers. They often provide curative health services to the most precarious populations, for instance through their involvement in immunization programmes, in the tuberculosis control programme,(34) in the mobile health scheme of the Delhi government, or in health camps, which can be organized by the Delhi government, by the MCD or even by a group of RWAs.
VI. COORDINATION, CONVERGENCE, CENTRALIZATION
In retrospect, the early 2000s appeared to be a time of exceptional proliferation of intermediaries in the delivery of public health care as a result of the creation of the National Capital Territory of Delhi, along with the democratic revival of the MCD and the implementation of the Bhagidari Scheme, all of which took place between 1993 and 2000. Before we examine the changes brought about by Mission Convergence at the end of that decade, it is worth looking beyond the apparent fragmentation of the delivery of health services, and to the various mechanisms and opportunities for coordination that could connect MLAs, councillors, RWAs and NGOs with each other.
As far as the relationship between MLAs and councillors is concerned, coordination seemed quite rare. Institutionally, 15 MLAs are nominated each year by the Assembly Speaker to be members of the MCD – but without voting rights. Individually, collaboration between MLAs and councillors catering to the same territory appears to be the exception: “If they belong to different parties, they will clash at the party level; if they belong to the same party, they will clash at the individual level” as a knowledgeable observer put it.
What about relationships between the respective officials of the Delhi government and the MCD? The only systematic form of coordination between the State Health Department and the Municipal Health Department was devoted to preventing waterborne and mosquito-driven diseases on a seasonal basis: from March until November, the State Health Department would call a weekly meeting with the Municipal Health
33. The JSA is part of a global People’s Health Movement, born from an assembly of representatives from 93 countries who met in Dhaka in December 2000, calling to renew that pledge.
34. The increasing role of NGOs is linked to the fact that a number of national health programmes are actually supported by international funding agencies, who tend to trust NGOs more than local bureaucracies to implement such programmes.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
578
Officer, the Health Secretary, the Health Directorate, as well as officials from the MCD Sanitation Department and representatives of the Delhi Water Board in order to monitor the development of these diseases.(35)
There were also established coordination mechanisms between RWAs and both the MCD and Delhi government officials (which pre-dated the Bhagidari Scheme). RWAs participated in monthly meetings with the (MCD) deputy health officer at the ward committee level, and they also had monthly meetings with the District Commissioner, which testifies to their established role as a communication channel between the administration and the people.
The relationship between RWAs and councillors generally seemed to be good, even though it remained informal: “Since 1997, we have a representative close at hand; he is more approachable to us, more accessible; before, we used to approach the MLA… We approach whoever can be of help, depending on the case; most of time it is the councillor” said a South Delhi RWA representative.
Lastly, there seemed to be little relationship between NGOs and elected representatives, or between NGOs and RWAs; but NGOs regularly interacted with officials, insofar as the administration outsources part of health care services provision to them.
Yet through my interviews, I came across a number of piecemeal initiatives characterized by the informal collaboration between officials, elected representatives, RWAs, NGOs and doctors (including from the private sector). I was told, for instance, of a RWA that financed the rehabilitation of a municipal community hall and obtained the services of a private doctor (with the help of the local MLA) to function as a part-time homeopathic dispensary – on the condition that access be limited to the colony’s senior citizens only. Most often, these collaborations would take the form of health camps, which always involve the cooperation of several of the actors observed so far: the state or municipal administration (who may provide the venue, medical personnel and social workers to mobilize local people); elected representatives (who will rely on party workers to mobilize people); RWAs (who may provide the venue, mobilize local private doctors and local people); and NGOs (who will assist in running the camps).
Typically, health camps are public initiatives in poor areas and semi-private initiatives in middle-class areas. They may be the modus operandi of a public health scheme – such as the Stree Shakti programme of the Delhi government(36) – or they may be the result of ad hoc initiatives launched by RWAs or by councillors in middle-class localities, where they are not so much a substitute for basic health care as a sign of the growing concern for one’s health; in that case, they will usually offer preventive health care services – measuring blood sugar or cholesterol levels, for instance. Health camps offer health services as a form of patronage.(37) Beyond the variety of actors usually involved in their organization, health camps always appear to be the product of a benevolent patron – whether the Chief Minister, the local MLA, the local councillor or the local RWA – who duly visits the camp when it is most crowded. The patron then designates its clients more or less implicitly through the targeted beneficiaries: the local RWA members, the area’s voters, etc.
Looking at Mission Convergence in this context highlights some of its implicit objectives and offers elements for a critical evaluation. The Mission Convergence programme projects itself as an effort towards
35. The Trans-Yamuna Development Board is an exception, as it includes MLAs and councillors as well as senior officials from both the Delhi government and the MCD.
36. I attended a camp organized by the Delhi government within the framework of the Stree Shakti programme. This aimed to offer health services to women and children living in areas deprived of basic health infrastructure through monthly health camps held in each of the nine revenue districts of the National Capital Territory. I interviewed a random sample of 12 attendees at the camp and most interviews pointed to the crucial importance of a minimum of “rootedness” to have access to the intermediaries mentioned above. First – and this confirms existing studies – the majority of interviewees, even though they were obviously poor people (most of them were recent migrants), said that they usually preferred to use private medical facilities because they found it was not much more expensive (they complained that in dispensaries they would be asked to pay a registration fee anyway) and they provided better quality drugs. Moreover, they said that staff from the dispensaries would ask them to provide a ration card, which they didn’t have, being essentially precarious people. When I asked them about their relationship with councillors or RWAs, they said that as new immigrants they weren’t registered on the electoral rolls and did not know the councillor. They also explained that there were no RWAs in their area.
37. Tawa Lama-Rewal, Stéphanie (2009), “Local democracy and access to health services in Delhi: preliminary remarks”, in Alain Vaguet (editor), Indian Health Landscapes under Globalization, Manohar, Delhi, pages 351–370.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
579
rationalizing and simplifying access to welfare and therefore making welfare services more efficient. While the end is doubtlessly worthwhile, the means need to be looked at critically. As far as health care is concerned, Mission Convergence breaks with the situation that prevailed in the early 2000s on three main points: it gives a greater role to NGOs (and to RWAs to a lesser extent); it relies a lot on health camps; and it does not offer any role to elected representatives, whether MLAs or councillors.
In that latter respect, Mission Convergence really appears to be in line with one of the implicit, but very real objectives of the Bhagidari Scheme, namely to encourage direct interaction between residents and the administration, and therefore to bypass elected representatives.(38) Already in 2005, interviews suggested that the Bhagidari Scheme was altering the relationship between residents and their local representative: “Since we are part of the Bhagidari programme, we don’t go to the MLA or councillor any more [in case of health problems], we talk directly to the medical superintendent, who talks to other officials” said a representative from an East Delhi RWA. More generally, the modus operandi of Mission Convergence seems to exclude intermediaries very effectively. On the one hand, those whom I called “political intermediaries” have no place at all in the scheme. On the other hand, “civil society intermediaries” are co-opted, since NGOs are now strongly integrated into the delivery process. Mission Convergence proceeds through district resource centres, to be run by “district nodal NGOs”, whose task is to coordinate the action of departments concerned with social welfare, health, education, women and children, labour and urban development.(39) Such functioning suggests a new interpretation of the public–private partnership model, which so far has translated, as far as the non-profit private sector is concerned, into outsourcing a part of some programmes or sometimes entire programmes to NGOs. NGOs thus seem to have moved from a peripheral to a more central position: that of coordinating agents.
VII. CONCLUSIONS
Looking back at the provision of health care services in the mid-2000s highlights a great fragmentation: that period saw the multiplication of the channels usable by people to express their grievances. State and municipal officials had to interact on a regular basis with MLAs, councillors, RWAs and (to a lesser extent) NGOs. This proliferation of mediators was the result of a series of governance reforms aiming at decentralization (with the creation of the National Capital Territory of Delhi and the democratic revival of the MCD) but also at participation (with the Bhagidari Scheme that empowers RWAs). The “good governance” discourse suggests that decentralization and participation go hand in hand, as both are supposed to promote a better responsiveness of decision makers to local specificities. However, as shown here, these two types of reform do not necessarily converge. In Delhi, decentralization established two new, local levels of representation, embodied by the MLA and the councillor, while the participatory scheme promoted direct interaction between residents and the administration. In other words, while decentralization established local mediators, participation developed an unmediated relationship between residents and the municipal and state governments. The confrontation of a series of data collected in the mid-2000s with today’s
38. For an analysis of the neo-populist dimension of the Bhagidari Scheme, see Tawa Lama-Rewal, Stéphanie (forthcoming), “Participation as a support to neo-populism? The case of the Bhagidari Scheme”, in Karen Coelho, Lalitha Kamath and M Vijayabaskar (editors), Participolis, Consent and Contention in Neoliberal Urban Governance, Routledge, Delhi, pages 198–212.
39. Source: http://southasia.oneworld.net/weekend/on-a-mission-to-empower-the-urban-poor.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from

E N V I R O N M E N T & U R B A N I Z AT I O N Vol 23 No 2 October 2011
580
situation suggests that the great movement towards decentralization that marked the late 1990s has evolved, 10 years later, towards a new form of centralization (aiming, as before, at concentrating responsibilities in the hands of high levels bureaucrats), a U-turn that was made possible by the great use, in the political discourse, of the conveniently ambiguous notion of participation.
Mission Convergence makes the contradiction between decentralization and participation quite obvious. In the name of efficiency, this programme has aimed to limit the role of intermediaries between the administration and residents: while political intermediaries have been made irrelevant, civil society intermediaries have been integrated into the delivery process.
Making elected representatives irrelevant as ombudsmen and patrons amounts to limiting their role in the implementation of policies; this might encourage them to focus on their role as policy makers, which would certainly go a long way to improving the quality of local government. However, studies on health care in India repeatedly underline that a crucial, but much ignored, aspect of the problem is the performance of medical personnel.(40) In this regard, the conflictual relationship between elected representatives and officials suggests that the presence of councillors can keep a check on possible officials’ misbehaviour – something that NGOs, who do not have the same legitimacy and access to power, cannot do.
Mission Convergence, in keeping with the Bhagidari Scheme, claims to rely on the participation of the beneficiaries of welfare services. It effectively creates new “invited spaces”.(41) This is a trend characteristic of contemporary urban governance in India.(42) Increasingly, citizens are invited to participate in the elaboration, or more frequently in the implementation, of public action; but the fact that only the state can decide who is invited, and what they are really invited for, means that such invited spaces of participation are not likely to promote contestation.
The participation of NGOs and RWAs has been redefined, from a role of mediation to one of consultation. The fact that such consultation is now in-built in the delivery process can be seen both as a sign that it is being taken more seriously and that any possibility of collective action is pre-empted.
A major challenge to Mission Convergence being able to achieve its goal of providing health care services to all is precisely the fact that it has drastically reduced the contestation capacities of the two types of mediators who catered to the poor: the large co-optation of NGOs in the programme makes it even more difficult for those NGOs that specialize in advocacy to raise resources; while the exclusion of councillors from the programme ignores the fact that they are the preferred recourse of the urban poor.(43)
40. See, for instance, reference 13, Shah and Bakore (editors) (2006).
41. Cornwall, A (2002), “Locating citizen participation”, IDS Bulletin Vol 33, No 2, pages 49–58. The latest initiative in the framework of the Bhagidari Scheme is the creation, announced in January 2011, of 24 Rogi Kalyan Samitis (RKSs) (patient welfare committees). These were first experimented with in Madhya Pradesh in the mid-1990s as a model of hospital management based on community participation (see http://siteresources.worldbank.org/INTINDIA/Resources/rks.pdf). In the Delhi context, RKSs are groups composed of the local MLA (as chairman) and official and non-official members (although the total number cannot exceed 11), who receive a small subsidy from the government (Rs 500,000 in 2011) to monitor the functioning of government hospitals. RKSs are meant to “ensure community participation” in monitoring the functioning of health care facilities, but their role is an advisory one.
42. See reference 27.
43. This is also the case in Mumbai, as shown by Baud and Nainan (2008), see reference 27, page 495.
REFERENCES
Baru, Rama V (2003), “Privatization of health services. A South Asian perspective”, Economic and Political Weekly Vol 38, No 42, 18 October, pages 4433–4437.
Baud, Isa and Joop de Wit (editors) (2008), New Forms of Urban Governance in India. Shifts, Models, Networks and Contestations, Sage, New Delhi, 402 pages.
Baud, Isa and Navtej Nainan (2008), “‘Negotiated spaces’ for representation in Mumbai: ward committees, advanced locality management and the politics of middle-class activism”, Environment and Urbanization Vol 20, No 2, October, pages 483–499.
Chapelet, Pierre and Bertrand Lefebvre (2005), “Contextualizing the urban health care system.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
U R B A N G O V E R N A N C E A N D H E A LT H C A R E P R O V I S I O N I N D E L H I
581
Methodology for developing a geo-database of Delhi’s health care system”, CSH Occasional Paper No 11, 135 pages.
Cornwall, A (2002), “Locating citizen participation”, IDS Bulletin Vol 33, No 2, pages 49–58.
Fassin, Didier (2000), Les Enjeux Politiques de la Santé. Études Sénégalaises, Équatoriennes et Françaises, Karthala, Paris, 344 pages.
Gangolli, Leena V, Ravi Duggal and Abhay Shukla (editors) (2005), Review of Health Care in India, CEHAT, Mumbai, 375 pages.
http://southasia.oneworld.net/weekend/on-a-mission-to-empower-the-urban-poor.
http://siteresources.worldbank.org/INTINDIA/Resources/rks.pdf).
Kumar, Girish (editor) (2009), Health Sector Reforms in India, Manohar, Delhi, 269 pages.
Mahal, Ajay and Vivek Srivastava (2000), “People’s par-ticipation, decentralization and delivery of public sector services in India”, Working Paper Series No 71, National Council of Applied Economic Research, New Delhi.
Priya, Ritu, Alpana Sagar, Rajib Dasgupta and Sangamitra Acharya (2004), “CMP on health. Making India world class”, Economic and Political Weekly Vol 39, No 27, 3 July, pages 2971–2974.
Ruet, Joël and Stéphanie Tawa Lama-Rewal (editors) (2009), Governing India’s Metropolises, Routledge, Delhi, 315 pages.
Shah, Partha and Makarand Bakore (editors) (2006), Ward Power. Decentralized Urban Governance, Centre for Civil Society, Delhi, 232 pages.
Sundar, Ramamani and Abhilasha Sharma (2002), “Morbidity and utilization of health care services. A survey of urban poor in Delhi and Chennai”, Economic and Political Weekly Vol 37, No 47, 23 November, pages 4729–4740.
Times of India, 14 March 2003.Tawa Lama-Rewal, Stéphanie (2009), “Local democracy
and access to health services in Delhi: preliminary remarks”, in Alain Vaguet (editor), Indian Health Landscapes under Globalization, Manohar, Delhi, pages 351–370.
Tawa Lama-Rewal, Stéphanie (forthcoming) “Participation as a support to neo-populism? The case of the Bhagidari Scheme”, in Karen Coelho, Lalitha Kamath and M Vijayabaskar (editors), Participolis, Consent and Contention in Neoliberal Urban Governance, Routledge, Delhi, pages 198–212.
Urban Health Resource Centre (2007), State of Urban Health in Delhi, UHRC/Ministry of Health and Family Welfare, New Delhi.
World Bank (1989), Sub-Saharan Africa: From Crisis to Sustainable Growth. A Long-term Perspective Study, Washington DC, 300 pages.
Yesudian, C A K (1999), “Pattern of utilization of health services”, Economic and Political Weekly Vol 34, No 5, 30 January, pages 300–304.
at INIST CNRS DRD on March 25, 2015eau.sagepub.comDownloaded from
Related Documents











