“Updates on Emerging & Re-emerging Infectious Diseases”

“Updates on Emerging & Re-emerging Infectious Diseases”
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

“Updates on Emerging & Re-emerging Infectious Diseases”

Disease Prevention & Control Bureau, DOH
• Emerging Infections– Newly identified or previously unknown infections– New or drug-resistant infections whose incidence in
humans has increased within the past two decades or whose incidence threatens to increase in the near future
• Re-emerging Infections– Secondary to the reappearance of a previously
eliminated infection or an unexpected increase in the number of a previously known infectious disease

Disease Prevention & Control Bureau, DOH
The Global Threat of Infectious DiseasesEmerging and re-emerging diseases
Adapted from Morens, Folkers, Fauci 2004 Nature 430; 242-9

Major Factors Contributing to Emerging Infections
• Human demographics and behavior• Technology and Industry• Economic development and land use• International travel and commerce• Microbial adaptation and change• Breakdown of public health measures• Human vulnerability
Disease Prevention & Control Bureau, DOH

Major Factors Contributing to Emerging Infections
• Climate & weather• Changing ecosystems• Poverty & social inequality• War & famine• Lack of political will• Intent to harm
Disease Prevention & Control Bureau, DOH

• Surveillance and Response• Applied Research• Infrastructure and Training• Prevention and Control
Disease Prevention & Control Bureau, DOH
Prevention of Emerging Infectious Diseases Will Require Action in Each of These Areas

Surveillance and ResponseDetect, investigate, and monitor emerging
pathogens, the diseases they cause, and the factors influencing their emergence, and
respond to problems as they are identified.
Disease Prevention & Control Bureau, DOH

Applied Research
Integrate laboratory science and epidemiology to increase the
effectiveness of public health practice.
Disease Prevention & Control Bureau, DOH

Infrastructure & TrainingStrengthen public health infrastructures to support surveillance, response, and research and to implement prevention and control
programs.
Provide the public health work force with the knowledge and tools it needs.
Disease Prevention & Control Bureau, DOH

Prevention & Control
Ensure prompt implementation of prevention strategies and enhance
communication of public health information about emerging diseases.
Disease Prevention & Control Bureau, DOH

Preventing EmergingInfectious Diseases: More to Do
• Enhance communication: locally, regionally, nationally, globally
• Increase global collaboration• Share technical expertise and resources• Provide training and infrastructure support
globally• Ensure political support• Ensure judicious use of antibiotics• Vaccines for all
Disease Prevention & Control Bureau, DOH

DAGHANG SALAMAT
DR. JOANRI T. RIVERAL, FPLSDEPARTMENT OF HEALTH RO7

Middle East Respiratory Syndrome Corona Virus
( MERSCOV )

Coronaviruses
• Human CoVs first isolated in the 1960s• Six human CoVs identified to date:
– HCoV – 229E– HCoV – OC43– HCoV – NL63– HCoV – HKU1– SARS – CoV– Middle East Respiratory Syndrome Coronavirus
(MERSCoV)

Non-SARS Human CoVs
• Worldwide• Winter & spring in temperate climates• Exposure common in early childhood• Droplet, contact & indirect contact• Symptoms & viral loads high first few days of
illness• Incubation period 2-5 days

Non-SARS Human CoVs
• Most often associated with upper respiratory tract infections in children
• Pneumonia & lower tract infections in immunocompromised individuals & the elderly
• May play a role in exacerbations of underlying respiratory diseases

SARS
• 1st recognized in Nov. 2002 as sporadic cases in Guandong province, China
• Outbreak period 2002 – 2003• Hong Kong hotel contributed to spread of
virus to several countries

Guangdong
Province, ChinaA
A
Hotel MHong Kong
B
J
H
Hospital 2
Hong Kong A
H
J
B
4 other Hong Kong
Hospitals
CD
E
Hospital 3 Hong Kong
Hospital 1 HK
Hospital 4 Hong Kong 2 family
members
C D E
34 HCWs
HCW
B Germany
Bangkok
Singapore
United States
I
IL§
M§
Vietnam
K † Ireland
K †
37 HCWs
HCW
0 HCWs
28 HCWs
156 close
contacts of HCWs
and patients
FG †
Canada
G †
F
4 family
members
10 HCWs
37 close contacts
99 HCWs (includes 17
medical students)
4 HCWs*
3 HCWs
HCW
HCW
2 family
members
Unknown number
close contacts
2 close contacts
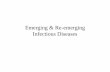
* Health-care workers; † All guests except G and K stayed on the 9th floor of the hotel. Guest G stayed on the 14th floor, and Guest K stayed on the 11th floor; § Guests L and M (spouses) were not at Hotel M during the same time as index Guest A but were at the hotel during the same times as Guests G, H, and I, who were ill during this period.
Chain of transmission among guests at Hotel M—Hong Kong, 2003
Data as of 3/28/03

SARS
• Incubation period 2-10 days• Droplet transmission
– Aerosol spread– Fomites– Fecal – respiratory transmission at an apartment
complex in Hong Kong• Transmission most likely during 2nd week of
illness• Super spreading events

Middle East Respiratory Syndrome Corona Virus
• 1st identified in September 2012• Cases retrospectively identified as early as
March 2012• Different from other coronaviruses in humans,
including SARS• Most similar to coronaviruses found in bats

MERS-CoV
• Several studies have identified MERS-CoV in high proportion of camels– Likely reservoir
• Identical gene segment found in one bat• Mode of transmission is unclear
– Respiratory?– Foodborne?– Few primary cases with direct camel contact

MERS-CoV• Range of presentation
– 62% severe respiratory illness– 5% mild symptoms– 21% asymptomatic
• Data from early cases– High mortality– Lower respiratory tract illness, fever
• Data from more recent cases– Lower mortality– Higher proportion with upper respiratory tract illness
• No vaccine, no specific treatment

MERS-CoV
• Most people who got infected with MERS-CoV developed severe acute respiratory illness with symptoms of fever, cough, and shortness of breath
• Common symptoms are acute, serious respiratory illness with fever, cough, shortness of breath and breathing difficulties

MERS-CoV
• Case demographics– Males > Females– Median age 49 years (9 months – 94 years)
• Incubation period 2 – 14 days• Infection period
– Under investigation– Not believed to be contagious before onset

MERS-CoV
• 75% identified as ‘secondary’– Mostly healthcare workers (19% of all cases)– Many with no or minor symptoms
• Many clusters identified– Healthcare– Household (estimated 1.3% secondary attack rate)
• No sustained human to human transmission

MERS-CoV
• MERS-CoV has been shown to spread between people who are in close contact*
• Transmission from infected patients to healthcare personnel has also been observed
• Clusters of cases in several countries are being investigate
*Close contact is defined as a) any person who provided care for the patient, including a healthcare worker or family member, or had similarly close physical contact; or b) any person who stayed at the same place (e.g. lived with, visited) as the patient while the patient was ill.

MERS-CoV
• Treatment is largely supportive and should be based on the patient’s clinical condition
• Medical care is supportive and to help relieve symptoms
• Currently, there is no available vaccine against MERSCoV

MERS-CoV
• Infection Control– Healthcare settings
• Contact, droplet & airborne isolation– Fit-tested N95 or higher level respirators– Gowns, gloves & eye protection– Negative – pressure airborne infection isolation
• Surgical mask when out of room
– Home• Precautions for ill persons, care givers & close contacts
• Self-monitor if asymptomatic

MERS-CoV
• Critical to prevent the possible spread of MERS-CoV in health care facilities
• Health-care facilities that provide for patients suspected or confirmed to be infected with MERS-CoV infection should take appropriate measures to decrease the risk of transmission of the virus from an infected patient to other patients, health-care workers and visitors
• Health-care workers should be educated, trained and refreshed with skills on infection prevention and control

MERS-CoV
• It is not always possible to identify patients with MERS-CoV early because some have mild or no symptoms at all!!!– It is important that health-care workers apply
standard precautions consistently with all patients – regardless of their diagnosis – in all work practices all the time

MERS-CoV
• Droplet precautions should be added to the standard precautions when providing care to all patients with symptoms of acute respiratory infection
• Contact precautions and eye protection should be added when caring for probable or confirmed cases of MERS-CoV infection
• Airborne precautions should be applied when performing aerosol generating procedures





“Updates on Emerging & Re-emerging Infectious Diseases”WELCOME BACK..
EMERGING AND RE-EMERGING INFECTION

Disease Prevention & Control Bureau, DOH
• Emerging Infections– Newly identified or previously unknown infections– New or drug-resistant infections whose incidence in
humans has increased within the past two decades or whose incidence threatens to increase in the near future
• Re-emerging Infections– Secondary to the reappearance of a previously
eliminated infection or an unexpected increase in the number of a previously known infectious disease

Disease Prevention & Control Bureau, DOH
The Global Threat of Infectious DiseasesEmerging and re-emerging diseases
Adapted from Morens, Folkers, Fauci 2004 Nature 430; 242-9

EBOLA VIRUS

Updates on the Ebola Virus Disease Outbreak in West Africa

What is Ebola Virus Disease?
• A severe, infectious, often fatal disease in humans and non-human primates (monkeys, gorillas and chimpanzees) caused by infection with Ebola virus.
• EVD is very infectious, kills in a short time but can be prevented.
• The Ebola virus can cause severe viral hemorrhagic fever outbreaks in humans with a case fatality rate of up to 90% (25-90%).

What is Ebola Virus Disease?
• Belongs to family of RNA viruses - Filoviridae• Five identified subtypes of Ebola virus:
– Ebola – Zaire– Ebola – Sudan– Ebola – Ivory Coast– Ebola – Bundibugyo– Ebola - Reston

What is Ebola Virus Disease?
• Incubation period ranges from 2 to 21 days
• Onset of illness is abrupt
• Ebola Hemorrhagic Fever (EHF) is a severe acute viral illness often characterized by the sudden onset of fever, headache, intense weakness, joint and muscle pain, headache and sore throat.
• This is followed by vomiting, diarrhea, stomach pain, rash, impaired kidney and liver function, and in some cases, both internal and external bleeding.
• A rash, red eyes, hiccups and bleeding from body openings may be seen in some patients.




Transmission
• Infections with Ebola virus are acute• Transmitted in several ways
– Direct contact with the blood and/or secretions of an infected person
– Through contact with objects, such as needles, that have been contaminated with infected secretions

Risk of TransmissionRisk Level Type of Contact
Very low or No recognized risk
Casual contact with a feverish, ambulant, self-caring patientEg. Sharing a sitting area or public transportation; receptionist tasks
Low risk Close face to face contact with with a feverish, ambulant patient.Eg. Physical examination, measuring temperature & blood pressure
Moderate risk Close face to face contact without appropriate personal protective equipment (including eye protection) with a patient who is coughing or vomiting, has nosebleeds or who has diarrhea
High risk Percutaneous, needle stick or mucosal exposure to virus-contaminated blood, bodily fluids, tissues or laboratory specimens in severely ill or known positive patients

What is Ebola Virus Disease?
• Laboratory findings of low counts of white blood cells and platelets as well as elevated liver enzymes
• EVD can only be diagnosed definitively in the laboratory by a number of different tests:
Enzyme-linked immunosorbent assay (ELISA) Antigen detection tests Serum neutralization test Reverse transcriptase polymerase chain reaction
(RT-PCR) assay Virus isolation by cell culture

WHO Update on the Situation ofEbola Virus Disease in West Africa
(as of July 31, 2104)According to WHO, the outbreak of Ebola in West Africa is the largest in history in terms of the number of cases, deaths and geographic spread.
Since March 2014, when Guinea reported its first cases of EVD to the WHO, the cases have spread to its capital city and to its neighboring countries of Liberia and Sierra Leone, after being initially confined to a rural area Guinea. On July 25, Nigeria reported its first probable case and death.
As of July 31, 2014, the number of cases in the four affected West African countries has so far reached 1323, which includes 729 deaths. The over-all case fatality rate is at 55%.


Actions taken by the Philippine Government
The Philippines has many OFWs in the three affected countries, including a Filipino contingent of UN Peacekeepers
Inter-Agency Task Force has convened to share information & discuss preparations & response to potential arrival of OFWs & foreign nationals from West Africa:• DFA, DOLE, DOH, DILG, PNP, DOTC, Bureau of
Immigration

Inter-Agency Coordination
DFA raised Alert Level 2 for the three initially affected countries:• a deployment ban on newly
hired OFWs to these countries is now in effect
DOLE provided info that recruitment agencies have been notified by employers in West Africa of repatriation of 20 OFWs from Sierra Leone.
DOH is monitoring these OFWs for 30 days after their departure from their points of origin.

Recommendations to Prevent Spread of EVD
The following recommendations were jointly developed by the DOH, DFA and DOLE:
1. Careful coordination of the repatriation of OFWs from EVD-affected countries should be done:
a. OFWs should coordinate with their recruitment agencies in assessing the risk of the spread of the epidemic in their places of deployment.
b. Proper coordination of Philippine labor officials (DOLE, POEA, OWWA) should be undertaken in the possible repatriation with the DFA and the Bureau of Immigration.
c. Any returning symptomatic Filipino (those who have fever, headache, intense weakness, joint and muscle pains and sore throat) should seek clearance with the local health authorities from the country of employment before being allowed to embark.

Recommendations (cont)
2. The Bureau of Immigration (BI) will also forward data on recent travel history to the affected countries of non-repatriated OFWs and foreigners to the DOH Bureau of Quarantine (BOQ).
3. The repatriation of Filipino U.N. Peacekeepers will be coordinated by DND & PNP to monitor arrival of any enlisted personnel: Coordination with DFA & BI on info on travel & health status
while in EVD affected country, including possible exposure to cases while in place of assignment & any initial management provided to them

Recommendations (cont)
4. Upon the arrival of repatriated OFWs or foreign nationals who had recent travel to the three affected countries of Guinea, Liberia, Sierra Leone and possibly Nigeria, the BOQ will undertake the following:
a. Health checklist should be distributed to passengers from all incoming flights to the Philippines.
b. Determine the status of returning Filipinos upon arrival and refer symptomatic cases to the appropriate health facilities for clinical care (Research Institute for Tropical Medicine, San Lazaro Hospital or Lung Center of the Philippines)
c. Passengers from affected areas will be provided a notification card to facilitate consultation and laboratory testing should they manifest any symptom.
d. Coordinate with DOLE on other possible repatriation activities from other manpower agencies in the affected countries.

Recommendations (cont)
5. Once asymptomatic individuals are cleared by BOQ, they will be closely monitored daily by Heath Emergency Management Staff (HEMS) up to 30 days from potential exposure (i.e. date of departure from point of origin).
6. Once an individual is found to be symptomatic after their arrival, HEMS will coordinate with National Epidemiology Center (NEC) & health officials of CHDs & local government units to facilitate pick-up of patients by the DOH and brought to the appropriate hospital and managed accordingly. The NEC will organize possible contact tracing for possible exposed
individuals and conduct the necessary epidemiologic investigation in coordination with HEMS.
7. National Center for Disease Prevention and Control (NCDPC) will provide policy and program support as well as technical assistance to the other DOH agencies involved.

The single biggest threat to man’s continued dominance on the planet is the virus.
• Joshua Lederburg, Ph D Nobel laureate



DAGHANG SALAMAT
DR. JOANRI T. RIVERAL, FPLSDEPARTMENT OF HEALTH RO7
Related Documents