Update Pediatric HT Guideline 2017 Nanthiya Pravitsitthikul, M.D.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update Pediatric HT Guideline 2017
Nanthiya Pravitsitthikul, M.D.
Learning Objectives
• Understand the changes in the new AAP Childhood HT Guideline
• Understand how these changes will affect the management of children and adolescents with high BP
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Rationale for the guideline
• Significant increase in interest in childhood HTN since 2004 Fourth Report
• High BP in childhood increase the risk for – Adult HT – CVD
• Even youth with HTN have evidence of accelerated vascular aging – Early heart attacks, strokes, CKD
• Detecting in children may prompt a check of the parents and other family members
Increase prevalence due
to “Obesity”
3.5% of children have
HT
10%-11% have elevated BP
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Obesity and risk of HTN in Thai Children
• 30.6% in boys • 12.8% in girls
Obesity (20.9%)
• 4.7% in boys • 3.2% in girls
HTN (3.9%)
• 5.7% for boys • 2.7% for girls Pre HTN
• OR 10.6 • 95%CI 3.75-30
Risk of HTN: Obese
children
•Cross sectional study in two public schools of 693 Thai students
•Age 8-12 yrs, Mean age 10 yrs
•Obesity BMI > P95th
Sukhonthachit P. et al, the association between obesity and blood pressure in Thai public school children, BMC Public Health 2014, 14:729

Obesity and risk of HTN worldwide
Eric L. Cheung et al, Race and obesity in adolescent hypertension. Pediatrics. 2017,139(5): e21061433
Wakako Kawarazaki et al. The role of aldosterone in obesity-
related HT, American Journal of Hypertension 29(4) April 2016

Relative Risk of sustained HTN
Eric L. Cheung et al, Race and obesity in adolescent hypertension. Pediatrics. 2017,139(5): e21061433
Rationale for the guideline
• Prior pediatric HTN guidelines were issue by the National Heart, Lungs, and Blood Institute(NHLBI)
• NHLBI ceased sponsorship of
cardiovascular guideline in 2013
• Increased emphasis on
basing new clinical practice guidelines of thorough literature reviews
NHLBI 1977
NHLBI 1987
NHLBI 1996
NHLBI 2004
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
Scope of the Guideline
• Subcommittee charged with developing an updated, evidence-based clinical practice guideline – Provide recommendations on
• Diagnosis • Evaluation • Management of Childhood HTN
– Aimed at practicing clinicians seeing patients in the OPD setting
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Major Changes from the Fourth Report
1. Rigorous evidence-based methodology 2. Revised definitions of BP categories; alignment with AHA/ACC
Guideline 3. New normative BP tables based on BP from normal-weight
children 4. Simplified screening table
5. Emphasis on use of 24-hr ambulatory BP monitoring (ABPM) to
confirm HTN diagnosis 6. Revised recommendations for performance of echocardiography 7. Lower treatment goals for primary HTN; ABPM goal for CKD
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Evidence-based Methodology
• PICOT questions developed by epidemiologist; used for literature search – Cover 2004-2015
• Review of around 15,000 papers by subcommittee members
• Generation of 30 Key Action Statements (KAS) – BRIDGE-Wiz software
• Level of evidence determination based upon AAP grading matrix*
• Patient P • Intervention • Indication I • Comparison C • Outcome O • Time T
*AAP steering committee on Quality Improvement Classifying Recommendation for clinical practice guidelines. Pediatric. 2004;114(3): 874-877

*AAP steering committee on Quality Improvement Classifying Recommendation for clinical practice guidelines. Pediatric. 2004;114(3): 874-877

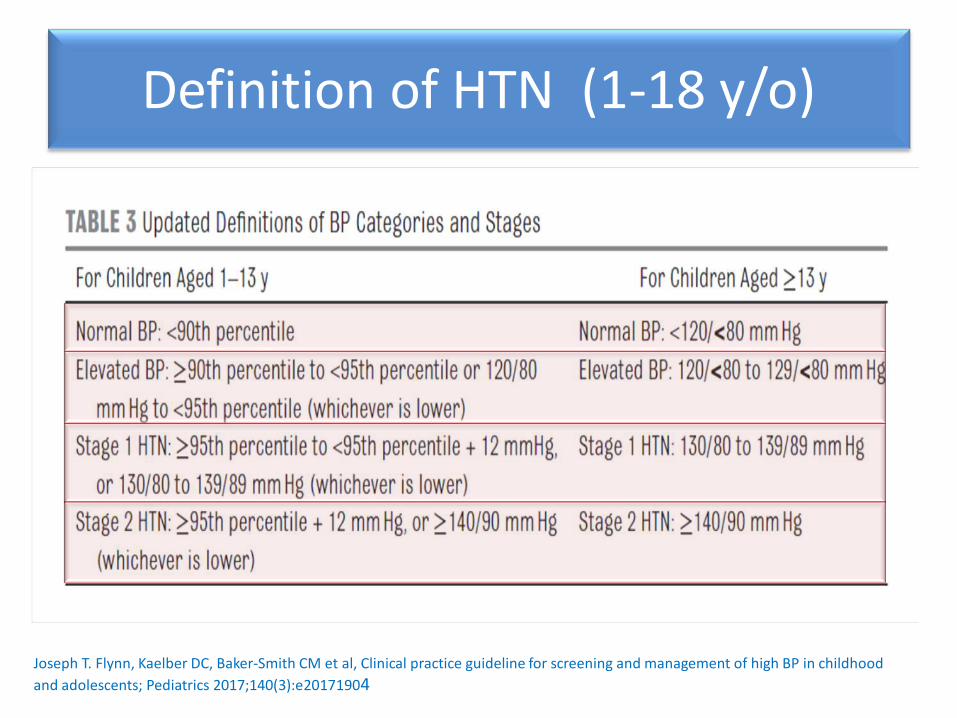
Definition of HTN (1-18 y/o)
• Lack of outcome data on BP and CV endpoints in children and adolescents
• Childhood HTN in healthy children – the approach since the 1st
NHLBI-sponsored pediatric HTN guideline (1977)
• Subcommittee maintained similar approach due to lack of new evidence
Changes in HTN categorization compared to the fourth report: •BP> P90th Elevated BP
•BP cut-points for stage1&2 HT simplified
•BP cut-points for adolescents > 13 y/o are same as in new AHA/ACC adult HTN guideline
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
Definition of HTN (1-18 y/o)
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
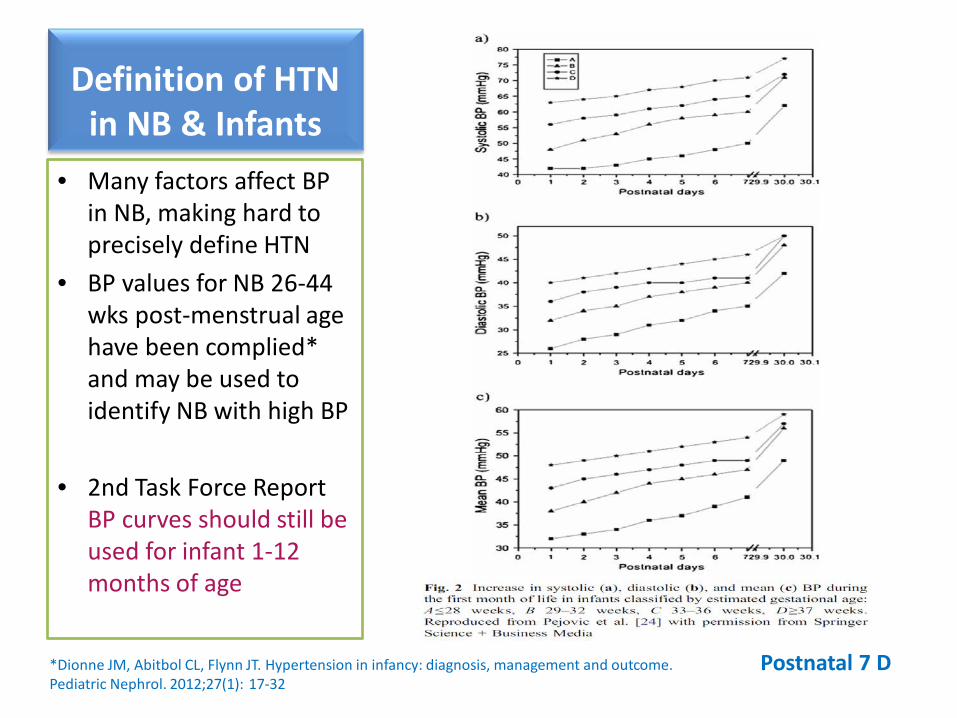
Definition of HTN in NB & Infants
• Many factors affect BP in NB, making hard to precisely define HTN
• BP values for NB 26-44 wks post-menstrual age have been complied* and may be used to identify NB with high BP
• 2nd Task Force Report BP curves should still be used for infant 1-12 months of age
*Dionne JM, Abitbol CL, Flynn JT. Hypertension in infancy: diagnosis, management and outcome. Pediatric Nephrol. 2012;27(1): 17-32
Postnatal 7 D
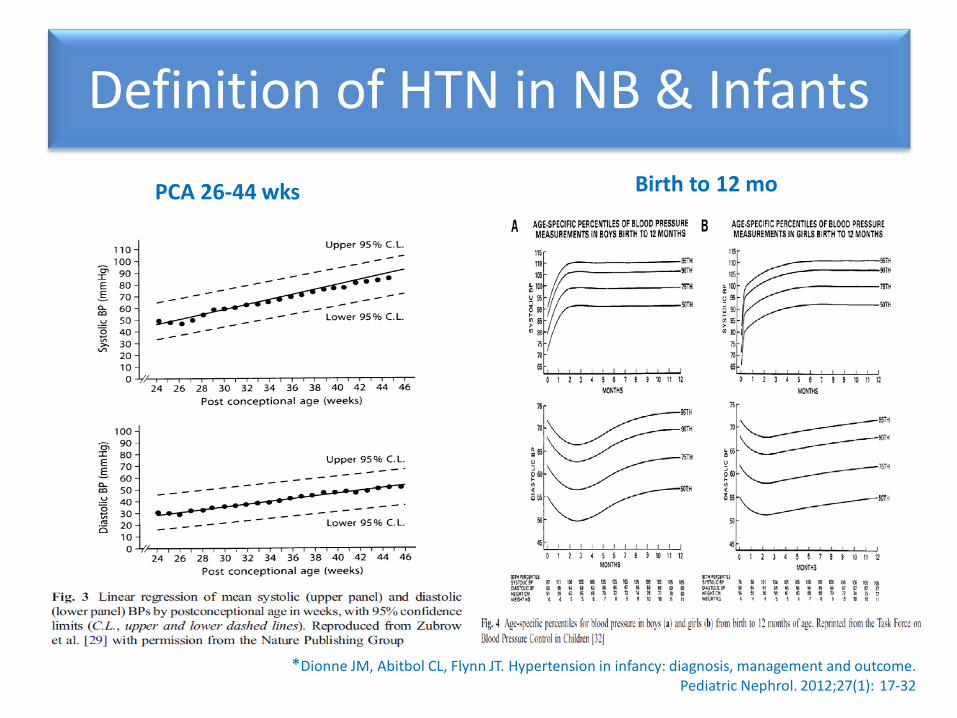
Definition of HTN in NB & Infants
*Dionne JM, Abitbol CL, Flynn JT. Hypertension in infancy: diagnosis, management and outcome. Pediatric Nephrol. 2012;27(1): 17-32
PCA 26-44 wks Birth to 12 mo
New Normative BP Tables
• The 4th Report tables generated from BP values in 70,000 healthy children – Many children had overweight or obesity – Inclusion of these children likely biased normative
BP value upward
• New normative BP tables commissioned for this clinical practice guideline, based only on BP reaching from 50,000 normal-age children
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

New Normative BP Tables
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

New Normative BP Tables
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
Elevated BP
Stage 1 HT
Stage 2 HT
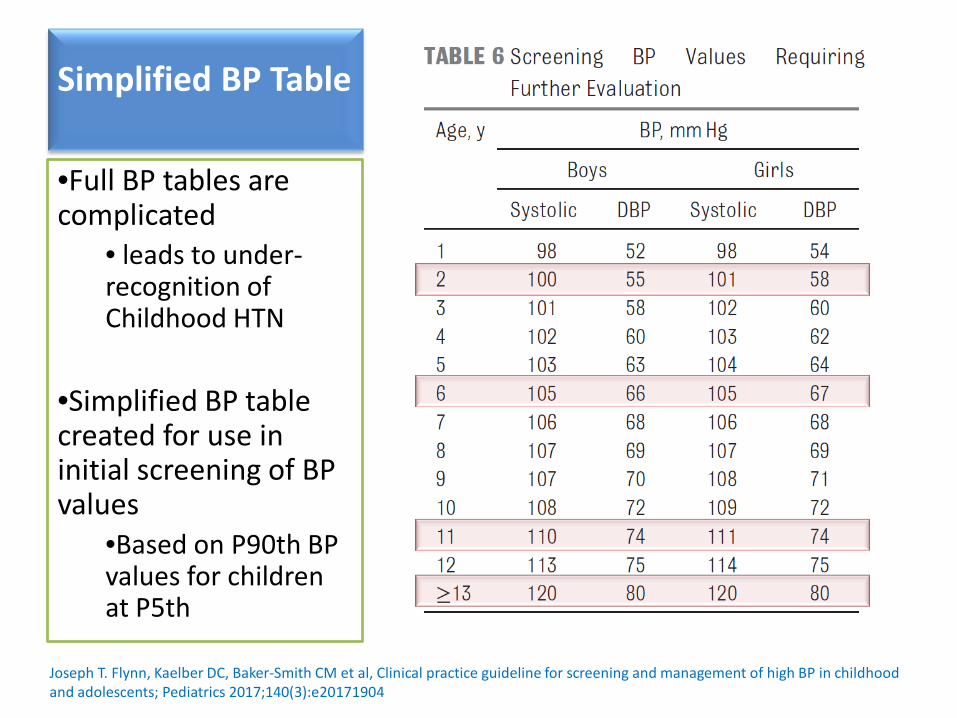
Simplified BP Table •Full BP tables are complicated
• leads to under-recognition of Childhood HTN
•Simplified BP table created for use in initial screening of BP values
•Based on P90th BP values for children at P5th
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Appropriate bladder cuff
Mid-arm circumference Bladder cuff
Width > 40% of MAC Length > 80-100% of MAC Width to length ratio > 1:2
The 4th report on the diagnosis, evaluation and treatment of high BP in children and adolescents; NHBPEP working group. Pediatrics. Vol. 114 No. 2, August 2004

BP Measurement Frequency
• Unclear what age is optimal to begin routine BP measurement
• Data suggest that prevention and intervention efforts should begin early
• New guideline does not change recommendation to begin BP measurement at age 3
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
Now, only annual measurement is recommended unless risk factors are present

KAS1: BP measurement frequency
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
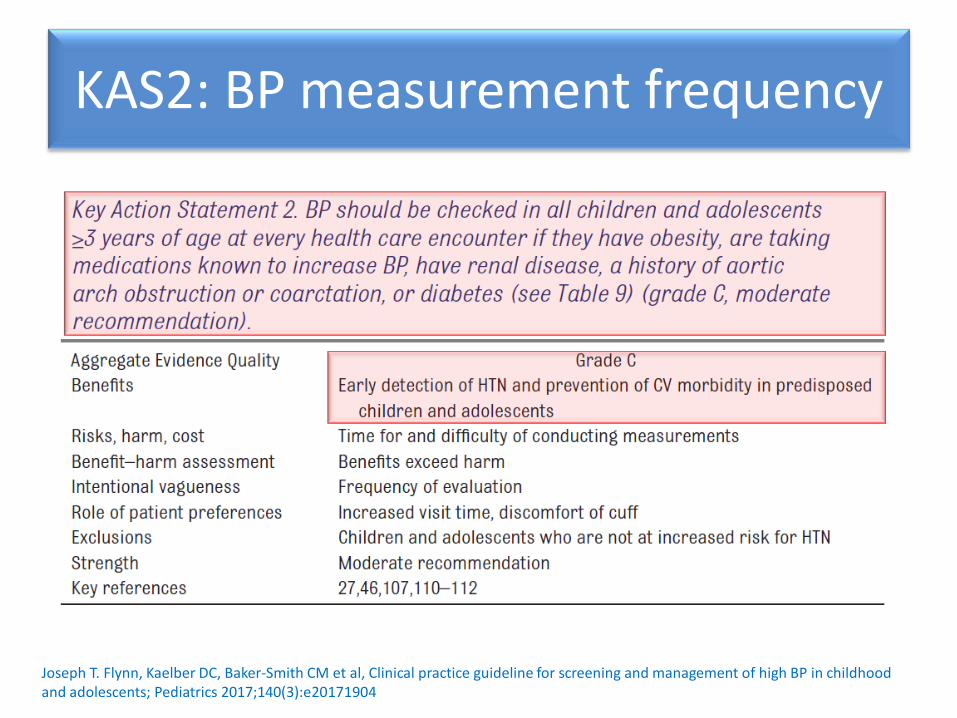
KAS2: BP measurement frequency
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

KAS2: BP measurement frequency • BP should be checked in all
children and adolescents > 3 y/o at every health care encounter if they have
o Obesity o Taking medication known to
increase BP* o Have renal disease o History of Aortic arch
obstruction or coarctation o Diabetes
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
KAS2: BP measurement frequency
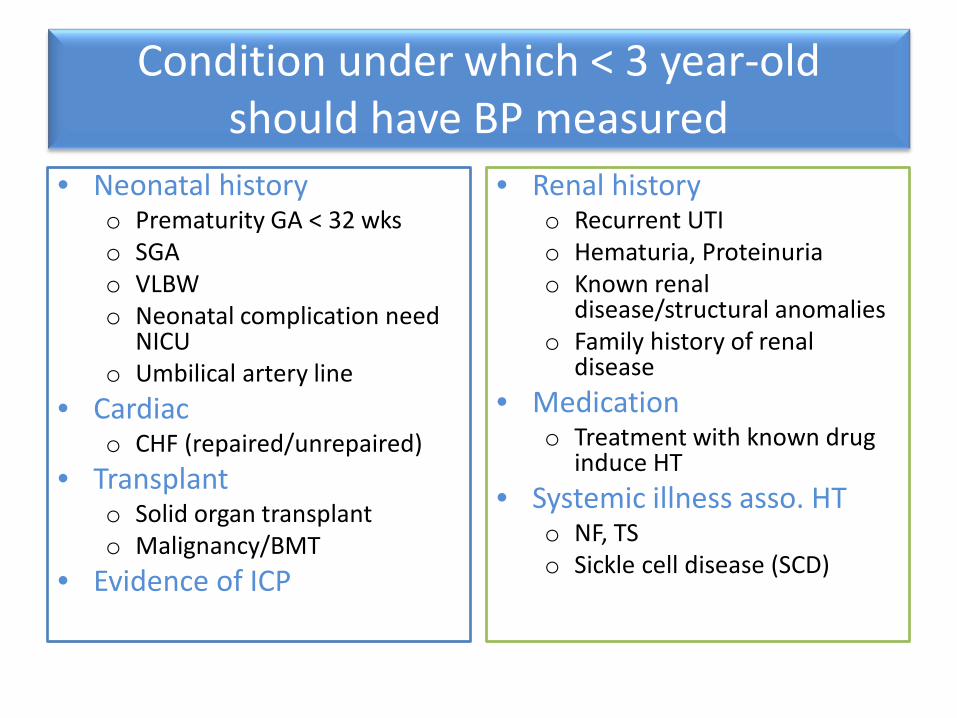
Condition under which < 3 year-old should have BP measured
• Neonatal history o Prematurity GA < 32 wks o SGA o VLBW o Neonatal complication need
NICU o Umbilical artery line
• Cardiac o CHF (repaired/unrepaired)
• Transplant o Solid organ transplant o Malignancy/BMT
• Evidence of ICP
• Renal history o Recurrent UTI o Hematuria, Proteinuria o Known renal
disease/structural anomalies o Family history of renal
disease • Medication
o Treatment with known drug induce HT
• Systemic illness asso. HT o NF, TS o Sickle cell disease (SCD)

Repeat high BP measurements
• BP in childhood may vary considerably between visits and even during the same visit
• Many potential etiologies for isolated elevated BP in children and adolescents
• Therefore, the clinician should;
– Repeat high BP reading at a visit – Obtain multiple measurements over time before
diagnosing HTN
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

KAS3: Diagnosis of HTN
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
Seat child correctly and measure BP by
Auscultation or by Using oscillometric device
Is Percentile > P90th?
Remeasure BP twice and average these 2
Repeat Ausculatory?
Remeasure BP twice by using auscultatory
technique; average these 2
Classify BP

Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Patient evaluation and management
• ABPM is done to confirm HTN before initiating diagnostic evaluation
• Treatment may be initiated by primary care provider or subspecialty
If the patient is •symptomatic or
•BP is > 30 mmHg above the P95th •OR > 180/120 mmHg in adolescents
sent to the ED!
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

KAS5: Oscillometric vs Auscultatory
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
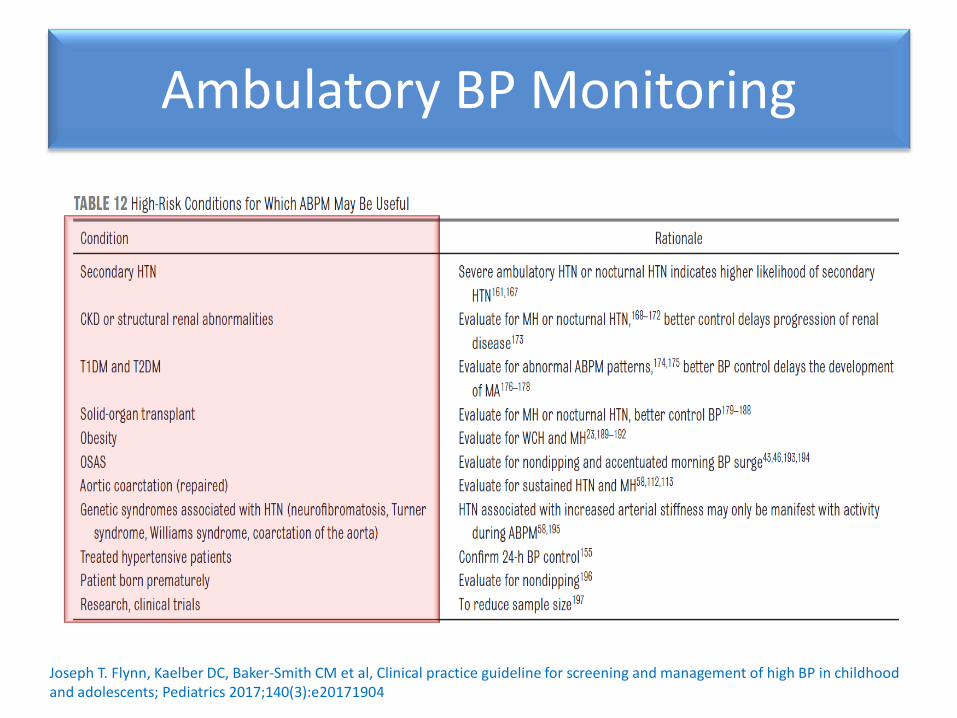
Ambulatory BP Monitoring
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
• Should be performed for confirmation of HTN in children and adolescents with office BP measurement in – Elevated BP for > 1 yr OR – Stage 1 HTN over 3 clinic visits
• High risk condition patients (table12) – Reveal masked HTN in high risk group
• Exclude white coat HTN
Ambulatory BP Monitoring
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

BP patterns by office BP and ABPM
Ambulatory
BP
Office BP
Normal BP Normal Normal
Sustained HTN
Elevated Elevated
White coat HTN
Normal Elevated
Marked HTN Elevated Normal
Courtesy of Professor Joseph T. Flynn; 2017 AAP guideline in childhood hypertension
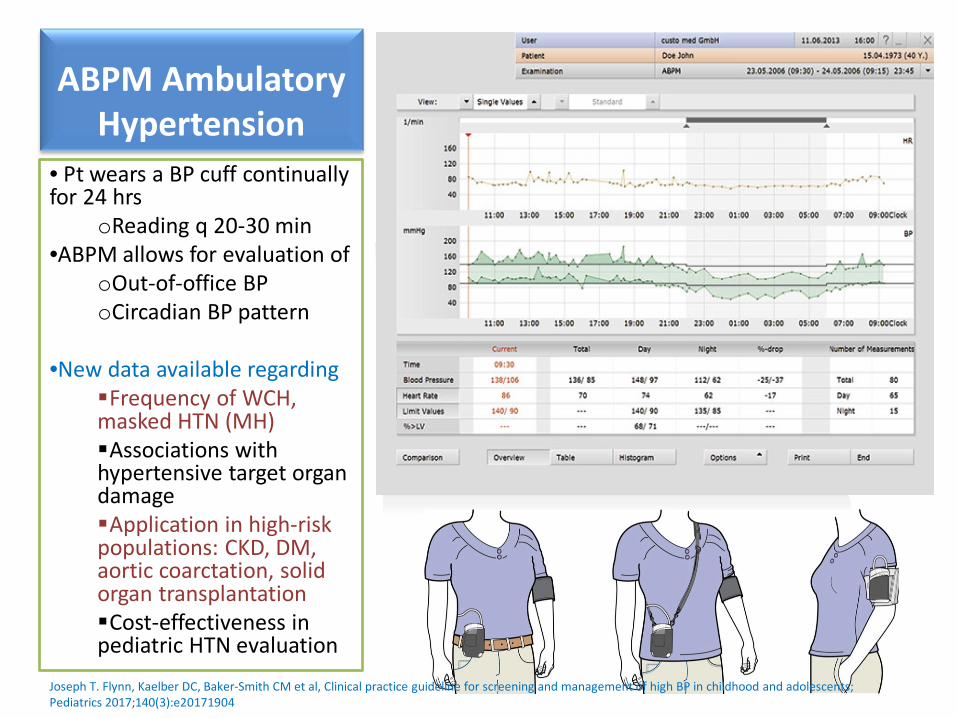
• Pt wears a BP cuff continually for 24 hrs
oReading q 20-30 min •ABPM allows for evaluation of
oOut-of-office BP oCircadian BP pattern
•New data available regarding Frequency of WCH, masked HTN (MH) Associations with hypertensive target organ damage Application in high-risk populations: CKD, DM, aortic coarctation, solid organ transplantation Cost-effectiveness in pediatric HTN evaluation
ABPM Ambulatory Hypertension
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
LVH and Echocardiography
• Prevalence of LVH 30-40% in childhood HTN
• LVH increase CV risk independently of BP and BMI
• 2004 Fourth Report
recommended obtaining echo. At time of dx of HTN
• If LVH present, indication to start anti-HTN medications
•Revise definition of abnormal LV mass:
• > 51g/m2.7; or • > 115 g/BSA in boys, • > 95 g/BSA in girls
•LVH is not a treatment target of antihypertensive therapy •Frequent/repeated echocardiography in the presence of LVH or abnormal LV function is encourages
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Causes of pediatric Hypertension
11%
65%
11% 10% 3%
Children evaluated at the tertiary pediatric HTN clinic for
elevated BP
Normotension
HT
WCH
PreHT
Dx pending
3(1%) 4(3%)
9(6%) 2(1%)
1(1%)
21(13%)
19(13%)
53(34%)
32(20%)
12(8%)
Causes of secondary HTN in a tertiary pediatric HTN clinic
Autoimmune
Cardiac
Endocrine
GI
Hematology
Medication
Neurology
Renal
Respiratory
Sleep-disorderedbreathing
Essential HT 43%
Secondary HT 57%
Rao G. et al, Diagnosis, epidemiology and management of HT in children. Pediatrics 2016;138(2):e20153616
Monasha Gupta-Malhotra et al, Essential HT vs. secondary HT among children. American Journal of Hypertension 28(1), Jan 2015
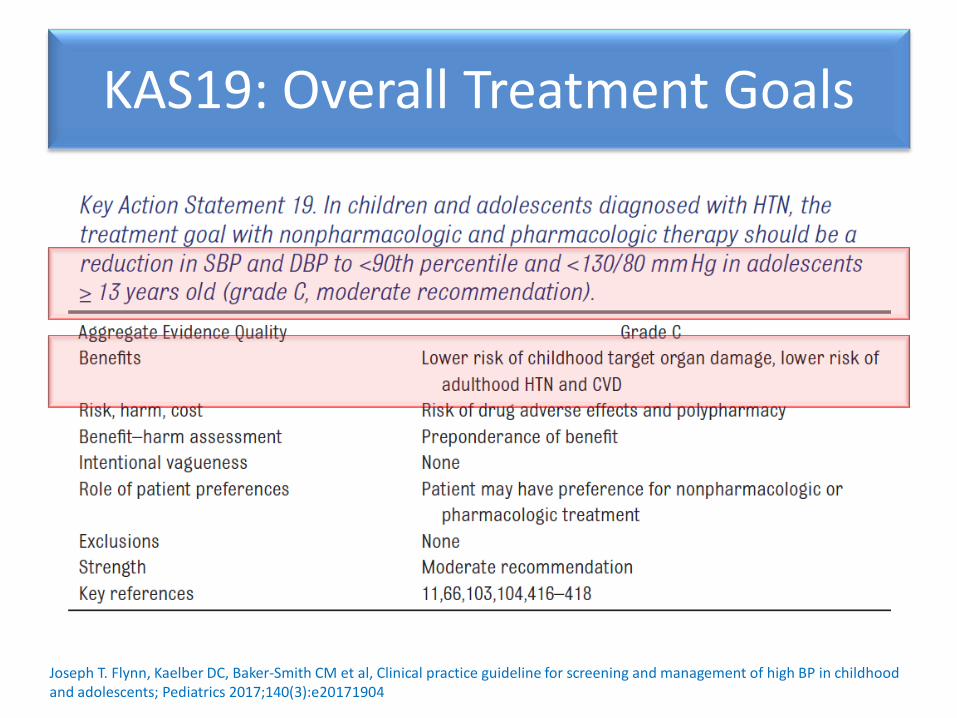
KAS19: Overall Treatment Goals
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
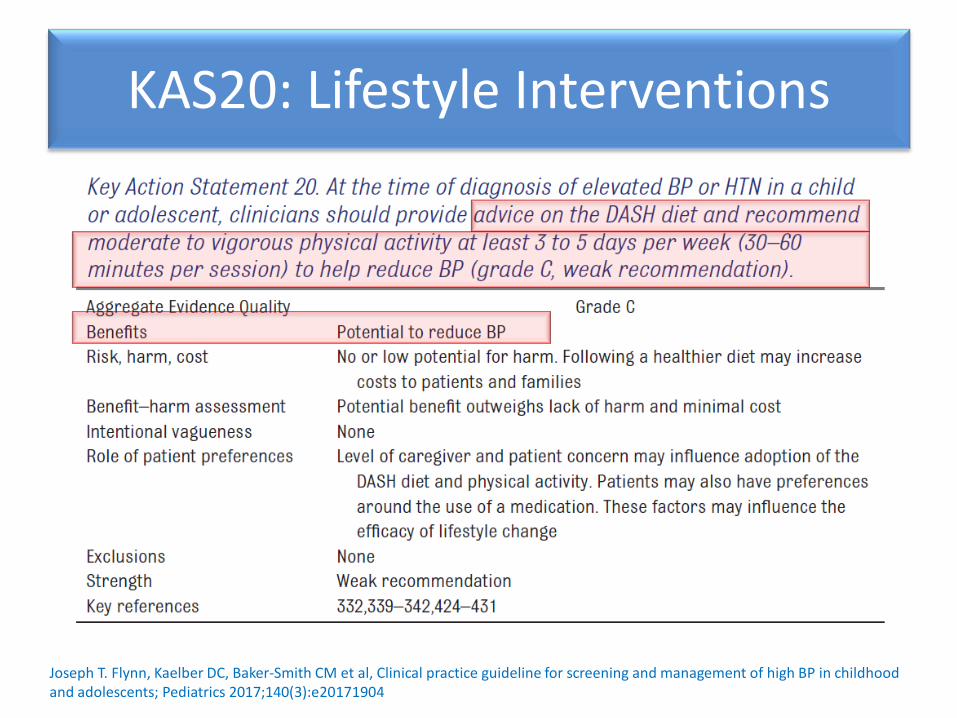
KAS20: Lifestyle Interventions
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
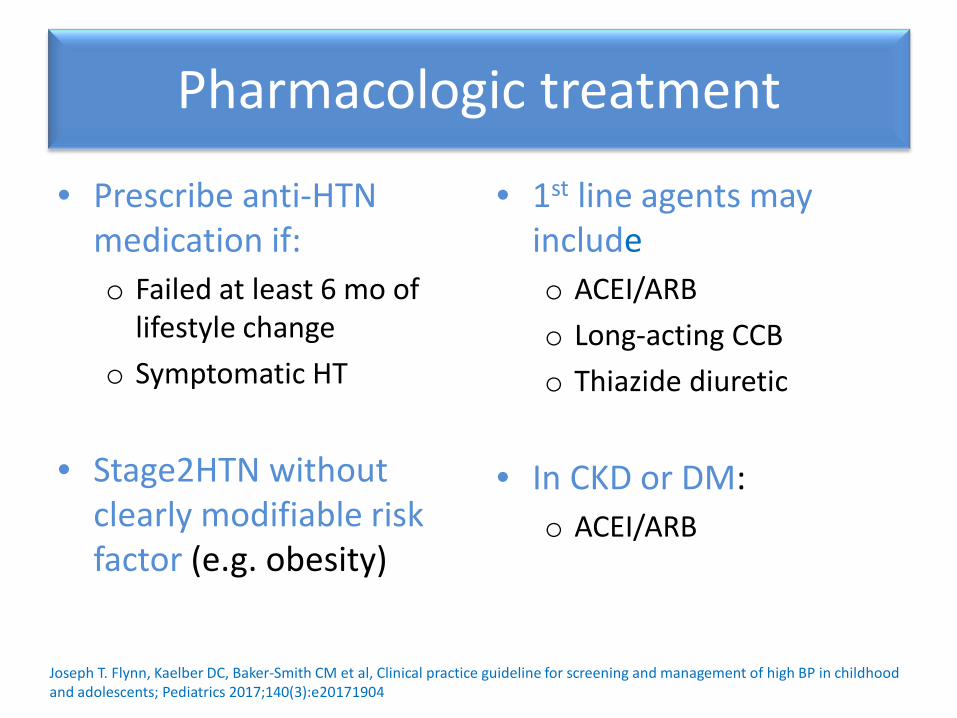
Pharmacologic treatment
• Prescribe anti-HTN medication if: o Failed at least 6 mo of
lifestyle change o Symptomatic HT
• Stage2HTN without clearly modifiable risk factor (e.g. obesity)
• 1st line agents may include o ACEI/ARB o Long-acting CCB o Thiazide diuretic
• In CKD or DM: o ACEI/ARB
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

KAS23: CKD
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

KAS26: DM
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

Major Points
• Changes in HTN categorization • Revised BP tables and screening table • ABPM to confirm HTN diagnosis and for
special populations • Lower treatment goals and emphasis on BP
reduction, no LVH
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904
Implication for practice
• Review manual BP measurement with your staff and ensure that appropriate equipment is available in your office
• Post new simplified BP table and have more detailed BP table available for consultation
• Develop process for performing/obtaining 24-hr
ABPM • Familiarize yourself with indication for and
approaches to treatment of HTN
Joseph T. Flynn, Kaelber DC, Baker-Smith CM et al, Clinical practice guideline for screening and management of high BP in childhood and adolescents; Pediatrics 2017;140(3):e20171904

THANK YOU FOR YOUR ATTENTION
Related Documents