Update on the Diagnosis and Management of Thyroid Diseases Kristien Boelaert Reader in Endocrinology Consultant Endocrinologist University of Birmingham [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update on the Diagnosis and Management of Thyroid Diseases
Kristien BoelaertReader in Endocrinology
Consultant EndocrinologistUniversity of [email protected]

Thyroid Diseases
Hyperthyroidism
Hypothyroidism
Thyroid enlargement

Hyperthyroidism

Thyrotoxicosis: disorder of excess circulating TH Hyperthyroidism: increased synthesis and secretion of TH
Prevalence
Incidence
UK: 2%♀ and 0.2% ♂ US: 1.3%
2.1-22/100,000 ♂ 23-99/100,000 ♀
Whickham Survey Tunbridge et al. 1977 Clin Endocrinol 7: 481Golden et al. 2009, JCEM 94: 1853 Wilson et al. 2006 JCEM 91: 4809De Leo et al 2016, Lancet 388: 906 McGrogan et al. 2008, Clin Endocrinol 69: 687
Hyperthyroidism

Graves’ hyperthyroidism
Toxic nodular goitre (single or multinodular)
Thyroiditis (silent, subacute, postpartum)
Exogenous iodine
Factitious thyrotoxcosis
Drugs: amiodarone, lemtrada, immunological treatments
TSH secreting pituitary adenoma
Neonatal hyperthyroidism
Aetiology of hyperthyroidism

Most prevalent autoimmune disorder in the UK
60-80% of cases of thyrotoxicosis in UK
Pathogenetic antibodies to TSH receptor on thyroid follicular cells (Long Acting Thyroid Stimulators) Twin concordance studies: 80% genetic – 20% environmental susceptibility
Genetic regions: HLA region, CTLA4 and PTPN22 – encoding proteins involved in immune regulation
Environmental factors: infection (Yersinia enterocolitica), smoking, childbirth, stress, iodine
Brand et al. 2009, Hum Mol Genet 18: 1704 Wang et al. 2010, JCEM 95: 4012Asvold et al. 2007, Arch In Med 167: 4012 Franklyn & Boelaert 2012, Lancet 379: 1155
Graves’ Disease

System Symptoms Signs
CNS Fatigue, anxiety hyperactivity
Hair Hair loss
Eyes (GD) Soreness, grittiness Stare, lid retraction, exophthalmos, ophthalmoplegia
Thyroid Neck swelling goitre
Muscles Weakness, tremor Fine tremor, muscle wasting
Skin Heat intolerance Warm, moist skin
Cardiovascular Palpitation, SOB Tachycardia, arrhythmia
Gastro-intestinal Appetite, weight loss Weight loss
Peripheral nervous system Hyper-reflexia
Reproductive system Oligomenorrhoea, ↓ fertility
Franklyn & Boelaert 2012, Lancet 379: 1155
Clinical Presentation

Extra-thyroidal manifestations
Feature Prevalence (%)
Hyperthyroidism and diffuse goitre 95
Thyroid ophthalmopathy 50
Pretibial myxoedema 5
Acropachy 1
Thyroid eye disease without hyperthyroidism (Euthyroid Graves’ disease)
5
De Leo et al. 2016, Lancet 388: 906 Girgis 2011 Ther Adv Endocrinol Metab 2: 135

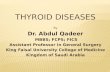
Symptoms according to age
0
10
20
30
40
50
60
18-32 y
33-44y
45-60y
over 61 y
Nu
mb
er
of
pati
en
ts (
%)
0-2 symptoms 3-4 symptoms 5 or more symptoms
P < 0.001
Boelaert et al. 2010, JCEM 95: 2715
3049 subjects with hyperthyroidism

Diagnosis of hyperthyroidismSymptoms and signs of hyperthyroidism
Serum TSH
Reduced Normal/Raised
fT4 (± fT3) Thyrotoxicosis excluded (unless RTH or TSH-oma)
Normal Raised
Subclinical hyperthyroidism
Thyrotoxicosis
• Identify extrathyroidal manifestations• Presence/character of goitre
Determine Aetiology
Franklyn & Boelaert 2012, Lancet 379: 1155

Clinical features of Graves’
Check TSH-receptor Abs: +ve in 98% of Graves’
TPO Abs reflect generalized autoimmunity (+ve in 75%)
Isotope scanning (Tc/Iodine) if TSH-RAb negative
Thyroid US: limited value
Determining the cause of hyperthyroidism
NICE guidelines 2019: Draft Recommendations

Treatment of hyperthyroidism
• Antithyroid drugs to block hormone synthesis
• Radioiodine (131I) therapy
• Surgical removal of thyroid

Carbimazole (methimazole) and propylthiouracil
In addition to β-blockers
Short-term preparation of patients for definitive treatment
Induction of remission in Graves’ disease (12-18 months)
Poor remission rates (up to 50%)
Significant side-effects
Allahabadia et al. 2000, JCEM 85: 1038 Franklyn & Boelaert 2012, Lancet 379: 1155De Leo et al 2016, Lancet 388: 906
Antithyroid drugs

Severity Carbimazole PropylthiouracilMajor side-effects (rare)
Agranulocytosis (0.2-0.5%)Cholestatic hepatitis TeratogenicityAplastic anaemia Thrombocytopaenia
Agranulocytosis (0.2-0.5%)Toxic hepatitis and fulminantliver failureANCA-positive vasculitis Aplasticanaemia Thrombocytopaenia
Common minor side-effects (1-5%)
Urticaria, rash, arthralgia, fever, transient neutropenia
Urticaria, rash, arthralgia, fever, transient neutropenia
Uncommon minorside-effects (<1%)
Nausea and vomiting, abnormalities of taste and smell, arthritis
Nausea and vomiting, abnormalities of taste and smell, arthritis
Franklyn & Boelaert (2012) Lancet 379,1155 De Leo et al 2016, Lancet 388: 906
Side-effects of antithyroid drugs

0
10
20
30
40
50
60
70
80
90
185 MBq
370 MBq
600 MBq
Ou
tco
me
acco
rdin
g to
do
se
regi
men
(%
)
Cure Hypothyroidism
***
***
***
***
**
**
1278 patients treated with 131I for hyperthyroidism
Single fixed dose of 131I
Boelaert et al. 2009, Clin End 70: 129
Outcomes following radioiodine

Cause of death Overall Whilst on Thionamide Rx
Following 131INot hypothyroid
Following 131IHypothyroid
SMR SMR P SMR P SMR P
All causesMalesFemales
1.151.261.11
1.301.361.27
0.0060.100.07
1.241.341.21
0.020.110.06
1.021.1
0.95
0.850.570.60
Comorbidity absentComorbidity present
0.951.52
1.031.68
0.84<0.001
1.091.48
0.480.002
0.811.43
0.080.01
Sinus RhythmAtrial fibrillation
1.071.59
1.181.74
0.180.006
1.171.53
0.110.02
0.921.51
0.430.08
Circulatory deaths 1.20 1.37 0.05 1.19 0.22 1.12 0.45
Boelaert et al. 2013, JCEM 98: 1869
Hyperthyroidism and mortality

Used infrequently
Pre-treatment with antithyroid drugs
Indications:
Large goitre/compression (especially if suspicion of co-existing thyroid cancer) Pregnancy (serious side-effects of drugs) Pronounced ophthalmopathy Patient preference
Franklyn & Boelaert 2012, Lancet 379: 1155 De Leo et al. 2016, Lancet 388: 906
Surgical treatment of hyperthyroidism

Clinical Case 68 y old female patient
Hypertension controlled on lisinopril
Sister had MI aged 62 years
Found to have abnormal TFT on routine testing
Asymptomatic
O/E: P76/min regular, BP 138/76 mm Hg, euthyroid, no palpable goitre/nodules
Time point TSH (mIU/L) [0.3-4.5] fT4 (pmol/L) [10-22] fT3 (pmol/L) [3.2-6.7]
3 months ago <0.02 18.2
Today <0.02 18.6 6.3

A: Thyroid US
B: TSHR-Ab
C: Radio-Isotope scan
D: 24h Holter
E: DEXA scan
F: No further tests required
Which test do you request next?

What would I do?
B: TSHR-Ab

Subclinical hyperthyroidism - Epidemiology Below normal serum thyrotropin – fT4 and fT3 within population reference
range
Prevalence 0.3-12% depending on iodine status
Mild/Grade 1: TSH = 0.1-0.4 mIU/L (~75%)
Severe/Grade 2: TSH < 0.1 mIU/L
Exogenous (~ 20% of patients on L-T4) or endogenous
Endogenous: causes similar to overt hyperthyroidism
T3 normal or high normal in endogenous Shyper
? Disparate long term consequences endogenous vs exogenous SHyper
Biondi & Cooper. NEJM 2018, 378: 2411

Boelaert. 2013 Nat Rev Endocrinol, 9: 194
? Only present in individuals with co-morbidities
Increased risk of incident atrial fibrillation
? Higher risk of AF with more TSH suppression
Absolute risks increase with age
Cardiovascular effects of SHyper

22212019181716151413121110
12
11
10
9
8
7
6
5
4
3
2
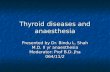
serum free T4 concentration (pmol/L)
Pre
vale
nce
of A
F(%
)
Gammage et al. 2007 Arch Int Med, 167: 928
5860 patients aged > 65 years
AF and fT4 in reference range

19 Cohort studies, N = 79,368 participants
Yang et al. 2018 J Bone Miner Metab, 36: 209
Shyper and fracture risk

Factor TSH < 0.1 mIU/L TSH 0.1-0.5 mIU/L
Age ≥ 65y Yes Consider treatment
Age < 65 y with co-morbiditiesCardiac Risk Factors/Heart DiseaseOsteoporosisMenopausalHyperthyroid symptoms
YesYesYesYes
Consider treatmentConsider treatment
NoConsider treatment
Age < 65 y asymptomatic Consider treatment Observe
Treatment Guidelines
Biondi et al. 2015 ETA guidelines on subclinical hyperthyroidism, Eur Thyroid J 4: 14
Ross et al. 2016 ATA Guidelines, Thyroid 26 : 1343-1421

Hypothyroidism

Prevalence 40/1000 females
Prevalence increases with age
Aetiology:
Autoimmune – Hashimoto’s thyroiditis (TPO and Tgantibodies - genetic predisposition)
After treatment for hyperthyroidism
Subacute/silent thyroiditis
Iodine deficiency
Congenital (thyroid agenesis/enzyme defects)
Hypothyroidism

Symptoms and signs of hypothyroidism
Cardiovascular
Bradycardia
Heart failure
Pericardial effusion
Gastrointestinal
Weight gain
Constipation
Skin
Myxoedema
Vitiligo
Neurological
Depression
Psychosis
Carpal tunnel syndrome

Treatment of hypothyroidism
2014: 3rd most prescribed medication in UK
29 million tablets of levothyroxine prescribed
Most common endocrine condition
Goal of therapy is to restore patients to euthyroid state and to normalise serum T4 and TSH concentrations

Ongoing symptoms despite replacement
Approximately 10% of people on T4 have continuing symptoms
Screen for associated auto-immune disorders
T3 or T3+T4 combination treatment not recommended
“Natural thyroid” – Armour not endorsed by national/international professional societies
Identification of subgroup with common deiodinase 2 gene variation - ? Benefit from T3+T4
Jonklaas et al. ATA guidelines 2014 Thyroid, 24: 1670
Okosieme et al. BTA guidelines 2016 Clin Endo, 84: 799
Dayan C et al 2018 Thyroid research, 11:1Panicker et al. 2009 JCEM, 94: 1623

Clinical Case 71 y old woman
Fatigue and mild depression and MI 4 years ago
PMH: Hypertension (Lisinopril)
FHx: sister with hypothyroidism
O/E: Wt = 159 lb (72 kg); BMI = 26.4 kg/m2; no palpable thyroid enlargement
Normal FBC, renal function, Ca and ESR
TPO Abs: 276 IU/ml [<35]
Time point TSH (mIU/L) [0.4-4.5] fT4 pmol/L [10-22]
3 months ago 6.9 18.0
Today 6.8 18.0

What is the best management plan?
A: Start levothyroxine 50 mcg daily
B: Start levothyroxine 112 mcg (1.6 mcg/kg)
C: Repeat TFT after 6 months
D: Re-check anti TPOAbs and start levothyroxine if higher than before
E: Discharge patient

What would I do?
A: Start levothyroxine 50 mcg daily

Subclinical Hypothyroidism - Epidemiology
Raised serum thyrotropin – fT4 within population reference range
Incidence 3-15%
Mild: Normal reference range < TSH < 10 mIU/L (75% of patients)
Severe: TSH > 10 mIU/L
Exogenous (~ 20% of patients on L-T4) or endogenous
Risk of progression 2-6%
Increased risk in: Women Higher serum TSH Higher levels of thyroid auto-antibodies Low-normal fT4
R Peeters 2017 NEJM, 376: 2556

SHypo - Progression
Normalisation of thyrotropin in 46% when TSH <7.0 mIU/L
Higher rates of progression with higher TSH and positive TPO
Meyerovitch et al. Arch Intern Med 2007, 167: 1533
Somwaru et al. 2012 JCEM , 97: 1962
Huber et al. 2002 Clin Endo, 87: 3221

Upper serum TSH concentrations
Surks and Hollowell 2007 JCEM, 92: 4575
Age and physiological changes to TSH

SHypo - Symptoms
Colorado Health Fair Study
Range: asymptomatic-multitude of symptoms
Canaris et al. Arch Intern Med 2000, 160: 526
Fewer symptoms in older people
? Better physical function if SHypo
Simonsick et al. Arch Intern Med 2009, 169: 2591Bano et al. Sci Rep 2016, 6: 38912

SHypo – CHD events and mortality
Rodondi et al. JAMA 2010, 304: 1365

SHypo – Effect of treatment on symptoms
TRUST-trial
737 adults aged ≥ 65 years
TSH: 4.6-19.9 IU/L
Randomised to receive levothyroxine or placebo with dose adjustment
No difference in Hypothyroid Symptom or Tiredness Score
No difference in secondary outcomes (BMI, BP, handgrip strength, waist circumference)
Stott et al. NEJM 2017, 376: 2534
Relatively mild Shypo
27% of subjects had no hypothyroid symptoms at baseline

SHypo – Treatment Guidelines Repeat TFT and check TPOAbs
Annual TFT if TPOAb positive
R Peeters. NEJM 2017, 376: 2556; Pearce S et al. ETA Guidelines Eur Thyroid J 2013, 2: 215Garber et al. ATA Guidelines Thyroid 2012, 22: 1200; Jonklaas et al. ATA Guidelines Thyroid2014, 24: 1670
TSH < 10 mIU/L TSH ≥ 10 mIU/L
7 ≤ TSH > 10 mIU/L4.5 < TSH > 7 mIU/L ≤ 70y > 70y
Treatment not recommended
Consider 6 month levothyroxine trial if
symptoms
Repeat TFT after 6 monthsTSH nl: discharge
TSH < 10: as aboveTSH ≥ 10 treat if < 70 y
Treatment recommended,
especially if symptoms, TPOAb
pos, cardiac risk factors
Consider 6 month levothyroxine trial if
symptoms regardless of age, or <70, cardiac risk factors,
TPOAb pos
Treatment not recommended
Treatment not recommended
Consider 6 month levothyroxine trial if
symptoms regardless of age, or TPOAb pos, or low
fT4 rising TSH
Repeat TFT after 6 monthsTSH nl: discharge
TSH < 10: as indicated on leftTSH ≥ 10 as above

Thyroid enlargement

Thyroid nodules: epidemiology
Definition: “Discrete lesions within the thyroid gland, radiologically distinct from surrounding parenchyma”
May be discovered on palpation, imaging, incidentally Most common in women (4:1) and in older populations Increased in areas of low iodine intake
Cooper DS et al. 2009 Revised ATA Guidelines Thyroid 2009, 19: 1167-1214Popoveniuc & Jonklaas Med Clin North Am 2012, 96: 329-349

Significance of thyroid nodules
May cause thyroid dysfunction
May cause compression
Need to exclude thyroid cancer
Prevalence of malignancy is 4 – 6.5%
Independent of nodule size
Malignancy risk in incidentalomas remains controversial
Risk of PET-positive thyroid nodule: 27%

Features suggestive of malignancy
History Examination Imaging
Family Hx of MEN, MTC, PTC Firm nodule Suspicious US features
History of head and neck irradiation
Nodule fixed to adjacent structures
Lymphadenopathy
History of Hodgkin and non-Hodgkin lymphoma
Growth of nodules, especially during therapy to suppress TSH
Age < 20 Abnormal cervical lymph nodes
Age > 70 Vocal cord paralysis
Male gender
Symptoms of compression: hoarseness, dysphagia, dyspnoea, cough, dysphonia
Popoveniuc & Jonklaas Med Clin North Am 2012, 96: 329-349Hegedus 2004 NEJM;351:1764-1771

UK Thyroid Cancer Incidence
Cancer Research UK, 2013
< 1% of all cancers
Incidence in UK = 3.2 per 100,000
Male:female = 1:3 (1:13 in Japan)
2013: 3,241 new cases – 373 deaths

52 y old male patient
Hx of increasing lower back and neck pain
PMH: Hypertension
FHx: Mother: hypothyroidism
Sister: ca colon aged 58 y
Rx: Bendroflumethazide
O/E: P 72/’ BP 132/68
- Normal systems examination
- Reduced neck movement due to pain
MRI neck
Clinical Case

Neck MRI
Neck examination: palpable 1 x 1.5 cm R sided thyroid nodule, thyroid gland not enlarged, no abnormal neck nodes
TSH: 4.2 mU/l

What would you do next?
A: Reassure patient
B: Check serum thyroglobulin
C: Request thyroid ultrasound
D: Request thyroid isotope scan
E: Check serum calcitonin

C: Request thyroid ultrasound
What would I do?

Clinical Case
Neck examination: palpable 1 x 1.5 cm R sided thyroid nodule, thyroid gland not enlarged
TSH: 4.2 mIU/l

Thyroid ultrasonography
Extremely sensitive for diagnosis of thyroid nodules
Specific for thyroid ca diagnosis (papillary)
Aids decision making to select nodules for FNA
Increases yield of diagnostic FNA
Patients with possible thyroid cancer should undergo ultrasonographicevaluation of neck by experienced operator
British Thyroid Association, RCP 2014 Revised guidelines for the management of thyroid cancerClin Endo (2014) 81: 1-122

Ultrasound features
Benign nodule Malignant nodule: Papillary/medullary
Follicular lesion
Spongiform/honeycomb Solid and hypoechoic Hyperechoic/homogeneous/halo benign
Purely cystic Irregular margin Hypoechogencity/loss of halo suspicious
Egg shell calcification Intranodular vasularity
Iso/hyper echoic (hypoechoichalo)
Absence of halo
Peripheral vascularity Taller than wide
Microcalcifications
British Thyroid Association, RCP 2014 Revised guidelines for the management of thyroid cancerClin Endo (2014) 81: 1-122

Scoring system:U1-U5
U1: NormalU2: BenignU3: IndeterminateU4: SuspiciousU5: Malignant
British Thyroid Association, RCP 2014 Revised guidelines for the management of thyroid cancerClin Endo (2014) 81: 1-122

THY classification
Classification Cytology Action
Thy 1 Non-diagnostic US +/- repeat FNA
Thy 2 Non-neoplastic Correlate with clinical and US findings
Thy 3a Neoplasm possible (atypical features)
Further US +/- FNAMDT discussion if Thy3a on repeat sample
Thy 3f Follicular neoplasm Diagnostic hemi-thyroidectomy
Thy 4 Suspicious of malignancy Diagnostic hemi-thyroidectomy
Thy 5 Diagnostic of malignancy Therapy appropriate to tumour type: usually surgery
British Thyroid Association, RCP 2014 Revised guidelines for the management of thyroid cancerClin Endo (2014) 81: 1-122

Take home messages
Treatment of overt hyperthyroidism is to block/ablate thyroid gland (drugs – 131-I)
Treatment of subclinical hyperthyroidism in selected patients considering patients’ age and long term risk
Treatment of overt hypothyroidism with levothyroxine monotherapy
Consider treatment of subclinical hypothyroidism based on degree of TSH rise and risk
Management of thyroid nodules based on combination of clinical suspicion, US and cytology
Related Documents