Update on Borderline Personality Disorder for Community Practitioners. Paul S. Links, MD, FRCPC Chair/Chief Department of Psychiatry, UWO

Update on Borderline Personality Disorder for Community Practitioners.
Dec 30, 2015
Update on Borderline Personality Disorder for Community Practitioners. Paul S. Links, MD, FRCPC Chair/Chief Department of Psychiatry, UWO. Disclosures. Unrestricted educational grant from Eli Lilly Canada Inc. ended in 2011, Honorarium from Lundbeck Canada. Objectives. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update on Borderline Personality Disorder for Community
Practitioners.
Paul S. Links, MD, FRCPCChair/Chief
Department of Psychiatry, UWO

Disclosures
• Unrestricted educational grant from Eli Lilly Canada Inc. ended in 2011,
• Honorarium from Lundbeck Canada.

ObjectivesAt the end of this presentation, participants willbe able to:• Describe our current knowledge related to
Borderline Personality Disorder (BPD),• Discuss the rationale for focusing on suicide
behavior rather than diagnosis,• Characterize the general principles for
psychotherapy for patients with recurrent suicide behavior.

What have we learned?
• Review of recent findings related to borderline personality disorder

Prevalence: Summary of Community Surveys
• Prevalence varied from 0.7-5.9%• Grant et al (2008) study required that
respondent endorse the requisite number of symptoms
• At least 1 of which caused social or occupational dysfunction.
• Criticized as being to broad; favored prevalence closer to 1-2%.

Comorbidity: Summary of Community Surveys
• Prevalence F=M in recent surveys,• Comorbid with anxiety, mood and substance
dependent disorders,• Most characteristic – 3 or more disorders may
be characteristic of individuals with BPD.

Consequences: Summary of Community Surveys
• BPD related to marital dysfunction, marital disruption and marital violence,
• BPD related to under and unemployment,• Mixed findings whether related to Axis II or
comorbid Axis I disorders.

Diagnosis: What have we learned?
• DSM-5 - No change to criteria• Affective criteria• Inappropriate intense anger or difficulty controlling anger—e.g., frequent displays of temper, constant anger, recurrentphysical fights• Chronic feelings of emptiness• Affective instability due to a marked reactivity of mood—e.g., intense episodic dysphoria, irritability, or anxiety usually lasting a few
hours and only rarely more than a few days

Characteristics of Affective Instability
• Based on Experience Sampling Methodology (ESM) (Nica and Links 2009)– Higher intensity of negative mood– Greater breadth of negative affect– Frequent and abrupt mood changes– Triggering by current external events –
inconclusive– Increase risk of suicide-related behaviors –
mechanism is to be clarified

Affective Instability and Suicide-Related Behavior
• Yen et al (2004) – Affective instability, identity disturbance, impulsivity predicted suicide
behaviors– Affective instability predicted attempts
• Links et al (2007)– Using Experience Sampling Methodology (ESM)– Mean negative mood intensity predicted daily self-reported suicide
ideation and modestly related to number of suicide events in past year.
• Links et al (2008)– Individuals at elevated risk for suicide behavior had high mean
negative mood intensity and high mood variability

High mood intensity and amplitude

Diagnosis in Adolescent Patients
• diagnosis can be made reliably• look for history over more than two years• similar phenomenology and developmental
history• impaired functioning, symptomatic• predictive validity still debated• early intervention in emerging BPD – Andrew
Chanen’s approach

Course: Summary of Prospective Follow-up Studies
•BPD course related to course of anxiety and mood disorders,
•Remission of BPD predicts remission of MDD,•Recurrences of MDD and predicted by no. and
types of BPD criteria,

Course: Summary of Prospective Follow-up Studies
•Absence of substance abuse/drug abuse may predict remissions in medium term (up to 6 years),
•Eating disorders independent of BPD,•Long-term course less related to comorbid Axis
I disorders.

BPD COMORBIDITY: WHICH DISORDER IS PRIMARYDisorder BPD Primary? RationaleDepression Yes Will remit if BPD does
Bipolar disorder manic not manic bipolar II
NoYes?
Unable to use BPD therapyRecurrence ↓ if BPD remitsMore research needed
Panic disorder Yes Will remit if BPD does, can precipitateBPD relapse
PTSD early onset (complex) adult onset
NoYes
Too vigilant to attach/be challengedBPD predisposes to onset, will remitif BPD does
Substance use disorder No 3-6 months sobriety makes BPD treatment feasible
Antisocial PD ? Is there 2nd gains?
Narcissistic PD Yes Will improve if BPD does
Eating disorder anorexia bulimia
No?
Unable to use BPD treatmentIs physical health stable?

Do Individuals with BPD Improve?
• Remissions from BPD common – 99% over 16 years follow up (Zanarini et al 2011).
• Remissions are stable; recurrence of BPD is uncommon (36% after 2-yr remission).
• BPD criteria had similar rates and levels of decline over 10 yr. follow up (Gunderson et al 2011)

Studies of Course: Clinical Implications
• Presence of substance use disorders closely associated with failure to remit.
• Improvement in BPD lessens risk of MDE; resolution of MDE little impact on BPD.

Etiology of BPD: No Single Factor
• Paris (2001) genetic vulnerability + exposure to psychological and social factors,
• Zanarini et al (2002) 50% of BPD inpatients report significant CSA,
• “Dual-brain” pathology – amygdala hyperactive + PFC insufficient inhibition.

Neuroimaging Studies of BPD
• Structural – reduced hippocampal volume; less consistent altered amygdalar volume.
• Functional – amygdalar hyperactivity with prefrontal hypoactivity.
• Inconsistency related drug exposure, comorbid disorders particularly PTSD, laboratory conditions and heterogeneity of BPD
• Next longitudinal/intervention studies.

Relationship Between Childhood Abuse (CA) and BPD
• Meta analysis “small to moderate effect” in explaining BPD (Fossati et al 1999),
• Zanarini et al (2002) 50% with significant history of childhood sexual abuse.
• Paris concludes significant etiologic role in subgroup of BPD

Relationship Between CA and BPD
• Childhood sexual abuse and emotional neglect uniquely related to deliberate self-harm (Gratz 2003)
• Not a specific causal relationship – related to substance abuse, depression and other adult outcomes.
• Gene-environment interactions.
Lack of Specificity: Gene-environment Interaction
• “One feature of a good candidate environmental risk factor is…it should not perfectly predict the disorder outcome.” (Moffitt et al 2005)
• Maltreated children with low levels of the genetic factor (monoamine oxidase A expression) more often developed conduct disorder … than children with a high levels of genetic factor (Moffitt et al 2005).

Lack of Change in Functioning
• Zanarini et al (2011) symptom and functional recovery in 60% at 16 years follow up.
• Impairment in social functioning “enduring,”• Zanarini et al (2010) vocational > social,• Functioning lacks behind symptom
improvement,• Characterizing and focusing on dysfunction
next step – Rehabilitation model

Aims of Canadian DBT Study
To evaluate the clinical effectiveness and economic impact of DBT vs a rigorous control treatment

Study DesignConditionsConditions: DBT vs. General Psychiatric : DBT vs. General Psychiatric
Management (GPM)Management (GPM)
Sample Size:Sample Size: N = 180 (90 per group) N = 180 (90 per group)
Time FrameTime Frame: 1 year treatment + 2 year follow-: 1 year treatment + 2 year follow-upup
AssessmentsAssessments: :
• Pre-treatmentPre-treatment
• Every 4 months during 1-year treatment Every 4 months during 1-year treatment phasephase
• Every 6 months during 2-year follow-upEvery 6 months during 2-year follow-up

Outcomes
Cost
• Treatment History: THI• State of Health: EuroQol-
5D• Treatment Utilization:
OHIP Database (provincial data base of health care utilization)
Clinical
• Self harm: PHI, LYPC• BPD symptoms: ZAN-BPD• Depressive symptoms: BDI • Psychopathology: SCL-90-R• Interpersonal Functioning:
IIP• Anger: STAXI• Social & Global
Functioning: SAS, GAF

Research TeamCentre for Addiction and Mental Health St. Michael’s HospitalShelley McMain, Ph.D., C. Psych. (PI) Paul Links, M.D., F.R.C.P Robert Cardish, M.D., F.R.C.P. Ian Dawe, M.D., F.R.C.P. William Gnam, M.D., F.R.C.P Adam Quastel, M.D., F.R.C.P Lorne Korman, Ph.D., C. Psych. Tim Guimond, M.D.Baycrest Centre for Geriatric Studies University Health Network
David Streiner, Ph.D., C. Psych. Larry Grupp, Ph.D(consultant)
Funded by grants from the Canadian Institutes of Health Research(Ref # 101123)

Frequency of S-H and Suicide Behaviors
Treatment Phase: significant reductions in both groups (p<.001); no between group differences
2-yr Follow-up: further significant improvements in both groups (p<.0001); no between-group
differences.
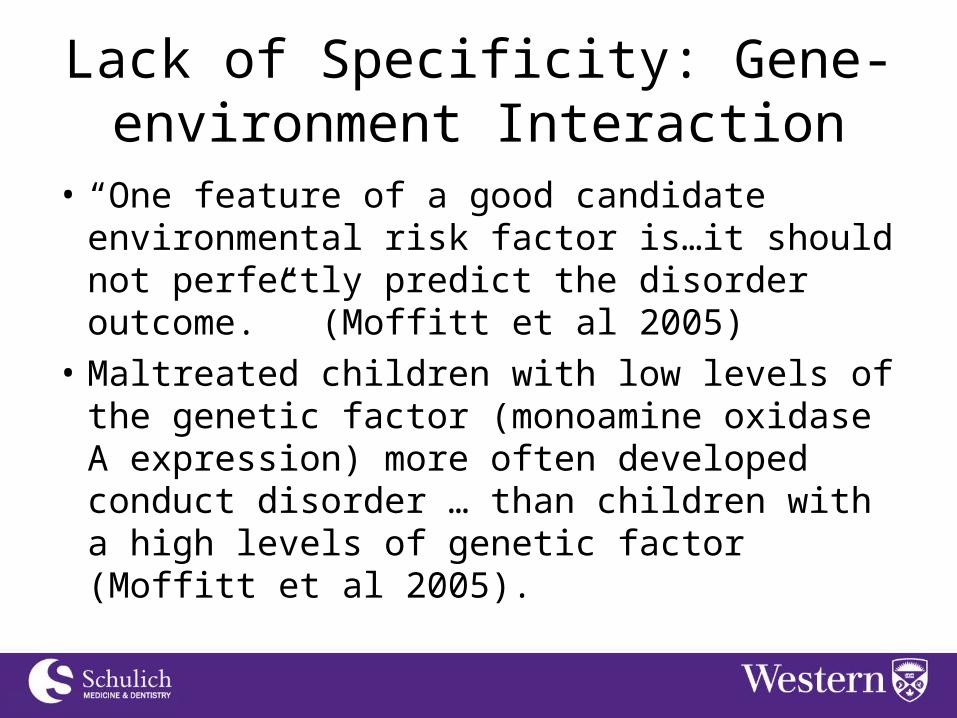
Frequency of Suicidal Frequency of Suicidal BehaviorBehavior
Frequency of Suicidal Frequency of Suicidal BehaviorBehavior Treatment
Phase: significant reductions in both groups (p<.001); no between group differences
2-yr Follow-
up: gains made during treatment were
maintained; no between-group
differences.
0.0
0.5
1.0
1.5
2.0
Suicide Number
Time(months)
Fre
quen
cy
0 4 8 12 18 24 30 36
DBT
GPM
Actual DBT
Actual GPM

Frequency of Self harm Behaviors
Frequency of Self harm Behaviors
Treatment
Phase: Significant reductions in both groups (p<.001); no between group differences
2-yr Follow-up: additional significant reductions (p<.0001); no between-group
differences.
05
1015
2025
Self-harm
Time(months)
Fre
quen
cy
0 4 8 12 18 24 30 36
DBT
GPM
Actual DBT
Actual GPM

Maximum Medical Risk of Suicidal/S-H Behaviors
Maximum Medical Risk of Suicidal/S-H Behaviors
Treatment Phase: significant decreases over time for both groups (p<.001); no between group differences
2-yr Follow-up: Gains were maintained in both groups; no between group differences
.
01
23
45
MaxMedicalRiskValue
Time(months)
Sco
re
0 4 8 12 18 24 30 36
DBT
GPM
Actual DBT
Actual GPM

Emergency Room (ER) Visits
Emergency Room (ER) Visits
Treatment Phase: time effect (p<.001) 2-yr Follow-up significant further reductions in both groups (<.0004)
Assessment Points Mixed effects model, time sig

ER Visits for Suicidal Behavior
ER Visits for Suicidal Behavior
Treatment Phase: time effect (p<.001)
2-yr Follow-up time effect (<.0002)
Assessment PointsMixed effects model, time sig

Summary
• DBT and GPM were efficacious across a broad range of outcomes over treatment phase – Suicide and self harm attempts: frequency and
medical risk– Health care utilization: emergency room use and
psych hospital days– General symptoms: Depression, anger,
interpersonal functioning, symptom distress– BPD symptoms

Summary
Two years post treatment, DBT and GPM had further improved or maintained gainsFurther improvements:Frequency of suicidal and NSSI behaviorsEmergency room visitsAnger, interpersonal functioning, symptom distress,Depression (GPM only)Overall quality of life
Maintenance of gains:Psych hospital days, BPD symptoms, lethal risk of suicidal behaviors

Shared Elements of GPM and DBT
• Manualized and adherence measured• Allegiance to approach• Focus on emotion processing deficits • Active to ensure engagement • Demonstrate empathy and validation• Provide education about BPD• Participation in supervision group required

Managing Suicide Risk by Focusing on Suicide Behavior
• Linehan (2008) “no published randomized trial has shown that interventions targeting mental disorders result in significant reductions in suicide attempts or death by suicide.”
• “treatments need to address suicidal behavior…”
• GPM addresses risk of suicide behavior (1st International Congress on Borderline Personality Disorder, Berlin, Germany, July, 2010).

Managing Suicide Risk by Focusing on Suicide Behavior
• Prospective study of BPD and recently discharged patients,
• Consistent with risk factors in high risk settings:– Not diagnosis– Recent attempts– Number of attempts– Medical lethality of attempts.

Managing Suicide Risk by Focusing on Suicide Behavior
• Are suicide and disorders the result of common or separate causal chains?
• Mishara – Suicide caused by consequences of having a mental disorder
• Could psychotherapy management focus on suicide behavior across disorders?

Common Elements for the Psychotherapy Management of BPD
• Francesca Schiavone & Dr. Paul LinksChild Abuse & Neglect (in press)
• Review of previous expert reviews• Experience from DBT vs GPM comparison.

Coherent Treatment Model
• Well structured and clearly focused approach increases therapist confidence
• Patient is not blamed for their difficulties• General Psychiatric Management : Disrupted
Attachment/Emotional Dysregulation -> Self Injurious Behavior

Active Therapeutic Stance
• Must addressed the need for an active therapeutic stance – several aspects:– Attention to treatment framework– Therapist emotionally and mentally engages with
patient– Creation of a strong attachment relationship
between therapist and patient

Balance between Validation and Change
• Change-oriented interventions can seem aversive and invalidating.
• Validation “[affirms] existing thoughts, feelings or behaviors of the patient” (Weinburg et al, 2010)
• Balancing the two builds rapport and helps the patient to tolerate change

Fostering Self-Agency
• Self-Agency: the sense that that the environment is altered by and responsive to the individual’s actions and intentions.
• A “co constructive relational process” between therapist and patient restores a sense of self agency (Knox, 2011)
• Therapy allows the patient to experience expressing self-agency without being rejected

Connecting Actions and Feelings
• Psychoeducation on emotional dysregulation and self injurious behavior
• Patient is encouraged to objectively observe and recognize emotions and identify early warning signs of self injurious behavior

Differentiating Lethal and Non Lethal Self Injurious Behavior
• Patients will have some degree of chronic ideation
• Focus on situations which create acute-on-chronic risk (risk assessment)
• Detailed safety planning

Developing a safety plan:Adapted from Stanley B; Brown GK. Safety planning intervention: A brief intervention to mitigate suicide risk. Cognitive and Behavioral
Practice. 2012:19: 256-264
• Develop when patient not in crisis,• Complete all the steps as shown in video
– Step 1: Warning signs:Warnings signs that are proximal triggers to crisis events– Step 2: Coping using distraction or soothing strategies– Step 3: Social situations and/or people that can help distract me:– Step 4: People who I can ask for help (note if a person is unhelpful when you are in crisis)– Step 5: Professionals or agencies I can contact during a crisis:– Making the environment safer:
• Plan is meant to be modified and revised over time,• The plan should be shared with significant others and other care providers
(primary care physician).
• *
Therapist Access to Supervision
• Patients who self injure can be especially challenging to work with
• Therapists may experience strong negative countertransference
• Supervision increases treatment coherence while reducing therapist stress

Treating BPD in Clinical PracticeA. Bateman AJP June 2012
• Improved prognosis over last 2 decades,• General treatment of TAU improved or less
harmful,• Examples:
– DBT vs TFP vs Supportive psychotherapy (Clarkin et al)
– CAT vs good clinical care (Chanen et al)– MBT vs structured clinical management (Bateman
& Fonagy)

Treating BPD in Clinical PracticeShared characteristics:•Structured for common problems,•Encourage activity and self-agency for patients,•Focus on emotion processing,•Model of pathology,•Active stance by therapist.

Common Strategies in Treatment of Suicidality (Weinberg et al 2010)
Evaluation of 5 treatment manuals (DBT, MBT, TFP, SFT, CBT).
• Importance of treatment framework• Agreed-upon strategy to manage suicide crises• Attention to affect• Active therapist• Exploratory interventions such as clarification,
confrontation, exploration, behavioral analysis• Change-oriented interventions.

Group for Advancement of Psychiatry: Psychotherapy Committee
• Developing consensus statement on factors to improve psychotherapy outcomes for suicidal patients.
• Similar factors identified.

Future Directions
• Extend research to treatment of suicidal behaviour outside of BPD,
• Test if common elements effective.

Future Directions
• To foster dissemination develop “Good Psychiatric Management” as a “basic” treatment for BPD – Gunderson,
• Reference from AP Press in preparation,
Future Directions
Bateman calls for study regarding BPD:– Mechanisms of change– Moderators of outcome– Attention to functional impairment
Related Documents