Update on Addictions DC EAPA October 16, 2014 George Kolodner, M.D. Medical Director, Kolmac Clinic Clinical Professor of Psychiatry, Georgetown University and University of Maryland Schools of Medicine [email protected]

Update on Addictions DC EAPA October 16, 2014
Jan 01, 2016
Update on Addictions DC EAPA October 16, 2014. George Kolodner, M.D. Medical Director, Kolmac Clinic Clinical Professor of Psychiatry, Georgetown University and University of Maryland Schools of Medicine [email protected]. Outline. Substances - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Update on Addictions
DC EAPAOctober 16, 2014
George Kolodner, M.D.Medical Director, Kolmac ClinicClinical Professor of Psychiatry, Georgetown University and University of Maryland Schools of [email protected]

Outline
• Substances– Alcohol: 74 year prospective, longitudinal study– Cannabis: New issues for an ancient substance
If Time:• Buprenorphine update• Gambling Disorder• Basics– DSM-5– Neurobiology
Shedding Light on Alcoholism:A Unique 74 Year Prospective Study
Triumphs of Experience, George Vaillant. 2012
“The follow up is the great exposer of truth, the rock upon which fine theories are wrecked.”

Two Sets of Subjects
1. Harvard Grant Study– Orientation
• A study of health rather than disease• Selected privileged people with high level of natural ability
– Eliminated lower performers and those with known medical or psychological problems• Looked for what were the predictors of a successful life: aging well
– Extensive baseline medical and psychological data with careful follow up– 268 men, born around 1920, Harvard classes of 1939-44– 74 year follow up (1938 – 2012)– 30% lived to 90 vs. 3% of men born in 1920– Funded by
• William T Grant: interested in what made a good store manager• Tobacco industry (1954-64): looking for positive reasons that people smoke• NIAAA (1972-82): focus on understanding alcoholism
2. Inner City Cohort– 500 white male disadvantaged youth from urban Boston– Study of juvenile delinquency
Predicting Alcoholism
• Best predictors– Ability to tolerate large amounts of alcohol
without intoxication, vomiting, or hangovers– Growing up in an environment that tolerated adult
drunkenness and discouraged youth from learning safe drinking practices
• Non-predictors– Unhappy childhood, psychological instability– Psychological stability in college
Findings
• Absence of premorbid personality features– Dependent, depressed, and sociopathy – if present – came
later and were the result not the cause of alcoholism• Ambiguities for first 10 years of abusive drinking, then
issue becomes black and white– Symptoms come and go: in any given month, most alcoholics
are abstinent or asymptomatic• Problem with cross-sectional or short term prospective studies
• Course is not inexorably progressive– Progresses for first 10 years, then stays bad but does not
necessarily progress• Does not get better

Findings Continued
• Return to drinking is possible but very rare– Only for those who barely met criteria for
diagnosis– Drinking is not carefree
• Successful abstainers tended to have more severe alcoholism– Education was not a predictor– Severity of tobacco addiction was not associated
with successful abstinence

More Findings• Sustained abstinence was strongly associated with
regular AA attendance– Variables associated with AA attendance
• Severity of alcoholism, Irish ethnicity, absence of maternal neglect, warm childhood environment
• Only after 5 years of abstinence can remission from alcoholism be regarded as stable
• Alcoholics die earlier than social drinkers– Even if sober, alcoholics die earlier because of contiinued
tobacco use– Live longer only if there is “a permanent change in self-
care”

Cannabis: Ancient Use History• World wide use for 12,000 years in China, India,
and central Asia– Alcohol: 12,000 years– Opium: 5,000 years– Coca: 1,000 years
• Introduced in Western Europe 2,500 years ago• Hemp as an unusual plant, producing both:– Commercial products (paper, clothing, rope, birdseed)– A psychoactive substance• Opium poppy and coca plant: psychoactive only
History of CommercialUse in U.S.
• 1611. Grown by Jamestown settlers for fiber• 1629. Major crop in New England• 1765. Grown by George Washington at Mount
Vernon• 1800’s. Grown throughout US, centered in
Kentucky– Cannabis plantations supported by slavery
• Post Civil War. Declined due to invention of cotton gin and competition from imported hemp
Questions About Cannabis
1. Is it harmful?2. Does it have therapeutic use?3. What is a reasonable public policy for its
availability?

Plant and Drug Names• Hemp– Oldest term, refers to the plant and its products– Defined by U.S. Customs as THC content < 0.3%
• Cannabis– Refers to both plant and drug– DSM-5: “most appropriate scientific term”
• Marijuana– Relatively new term– Refers to both plant and drug
• THC– Primary, but not only, psychoactive ingredient of plant

THC Concentrations• Standard commercial grade cannabis: leaves– Originally .5% to 5% THC, now 12%+
• Hashish: dried cannabis resin and flowers– 2% to 8% THC
• Sinsemilla: flowering tops of unfertilized female plants– 7% to 14% THC
• Hash oil: THC extracted from hashish or cannabis– 15% to 50% THC

Categories of Use
• Experimental/Recreational• Harmful• Addictive• Therapeutic

The Spectrum of Non-Medical Use• Experimental– Largest group, 40-50% of ever used report < 12 uses
• Recreational– Only in social setting without frequency or intensity– Not central in their lives
• Regular– 70+ uses in past year– Account for 90% of use– Half of them meet criteria for cannabis use disorder• Almost half of diagnosable group also have another SUD

Fluctuating Use as Intoxicant in U.S.
• Early 1900’s. Mexican immigrants• 1920’s. Jazz musicians during prohibition• 1960’s and 70’s. Use increased, peaking at 37%
in late 1970’s• 1992. Lowest use by highs school seniors (12%)• 1993 to present. Ebb and flow, increasing again
over past several years• Now the most commonly used illegal substance
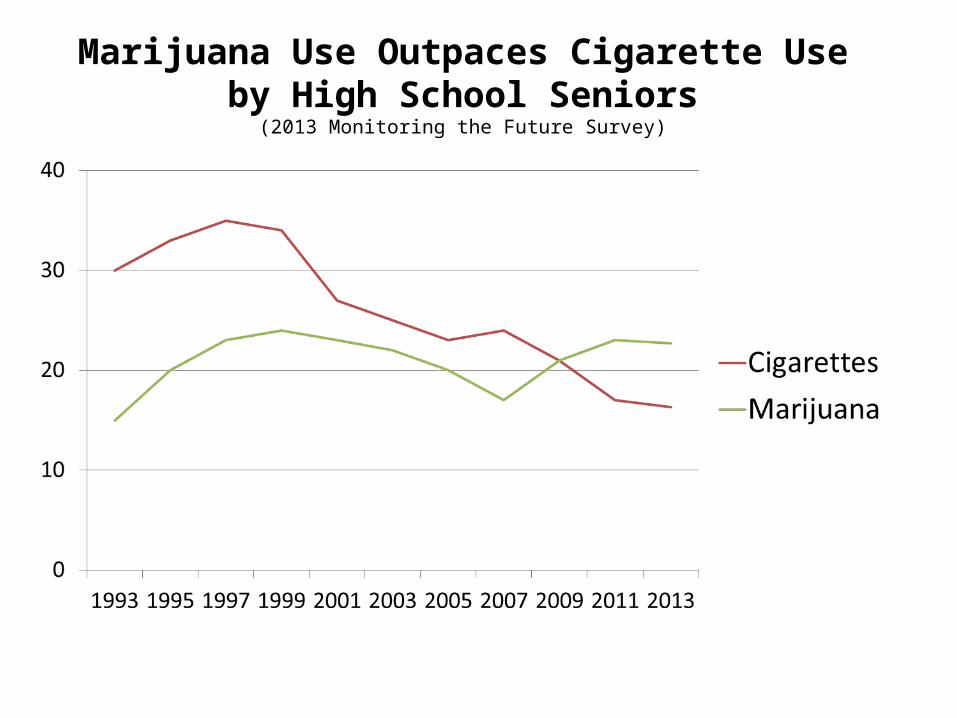
Marijuana Use Outpaces Cigarette Useby High School Seniors
(2013 Monitoring the Future Survey)

Drunk and Drugged Driving• Alcohol effects are greater with complex tasks
that require conscious control• Cannabis effects are greater with automatic
driving functions• Cannabis users are more aware of being
impaired and tend to use various behavioral strategies to compensate for impairmentsAdding alcohol eliminates the ability to use these
strategies effectively, resulting in impairments at doses that would be insignificant if either substances were used alone

Delayed Effects of Acute Use
• Airline pilots in flight simulator, 24 hours after single cannabis cigarette– Decreased performance– No awareness of lowered functioning

Negative Effects of Heavy Cannabis Use, Starting Before Age 18
• Cognitive deficits, with decreases in:– IQ (8 points, no recovery, prospective study)– Attention (poor recovery)– Memory– Processing speed– Reasoning skill
• Anxiety and insomnia: short term improvement but long term exacerbation

Possible Secondary Problems
• Psychosis– Association is clear, but cause and effect not
documented• Cancer– Increased likelihood of lung and head and neck
cancer

Addiction PotentialAn Institute of Medicine study found addiction rates for marijuana were far lower than those for other substances.
Source: Institute of Medicine, 1999

The Dilemma of the Cannabis Addict
• General lay community– Cannabis is used without problem by peers– Non-addictiveness is confidently argued
• Addiction recovery community– Not always taken seriously by members of 12 Step
groups• Creation of Marijuana Anonymous
Cannabis Use Disorder
• Treated with abstinence based approach just as with other substance use disorders– Importance of quantitative urine testing to track
falling levels• Can take one month to reach zero
• Non addictive use can complicate treatment of other substance use disorders

Cannabis Withdrawal Syndrome• New diagnostic category in DSM-5• Symptoms usually mild– Irritability, anxiety, insomnia, disturbing dreams,
decreased appetite, restlessness, depressed mood• Time course– Onset 24 to 72 hours, peak within first week,
duration 1 to 2 weeks• Sleep difficulties may last more than 30 days
• Usually manageable with mild medication– Research: positive response to dronabinol

Discovery ofEndocannabinoid System
• Cannabinoids: all endogenous ligands of the cannabinoid receptor and synthetic analogues
• 1965: THC isolated• 1988: Cannabinoid receptors identified• 1992: Endogenous ligands found


Synthetic Cannabinoids: Recreational
• 1988. Initially synthesized for legitimate research on endocannabinoid system– Full agonists: 100 times more potent than THC (a
partial agonist)• More sympathomimetic effects and hallucinations
• Internet appropriation by recreational users– “Spice,” “K2”– Chemical alterations to evade illegality
• 2012. Synthetic Drug Abuse Prevention Act• 2013. 30% decrease in use by teenagers (MTF)

Synthetic Cannabinoids: Recreational (Continued)
• Acute toxicity– Nausea and vomiting precipitate treatment seeking.
Also hypertension and tachycardia– Anxiety, agitation, psychosis– Supportive management. No antidote
• Withdrawal syndrome– Tachycardia, agitation– No defined withdrawal management protocol
Early History of Medicinal Use
• 2700 BC. Medicinal use first documented• 1850 to 1942. Listed in US Pharmacopoeia as
fluid extracts (not raw plant for inhalation) marketed by major pharmaceutical companies
• Widely used in 19th and early 20th Centuries• Included in major medical testbooks– 1898. William Osler : “probably the most
satisfactory remedy” for migraine headaches

Multiple Ingredients
• Contains 60 cannabinoids, most nonpsychoactive• Tetrahydrocannibinol (THC): major psychoactive
cannabinoid in cannabis plant• Cannabidiol (CBD): non-psychoactive– Has anti-seizure properties (Dravet’s Syndrome)– May counteract some psychoactive effects of THC
• THC/CBD ratio varies by plant– Influenced by goal of grower

Parallel Systems“Medical” Marijuana
Pharmaceutical Cannabinoids
Form Raw plant Synthesized or extracted by FDA standards
Route Smoked Oral (capsule or spray)
PhysicianRole Recommend Prescribe
SourceIndependent growers and dispensaries
Pharmaceutical companies and pharmacies

Implementation Problems of Medical Marijuana
• Qualifying medical conditions– California: loosely regulated = de facto
recreational legalization• Dosing and purity• Relationship with physician

Pharmaceutical: Synthetic
• dronabinol (“Marinol”)– Approved by FDA, 1985– Oral capsule, synthetic THC isomer, Schedule III– Anorexia from AIDS– Anti-emetic for cancer chemotherapy when other
medications have failed
• nabilone (“Cesamet”)– Oral capsule, analogue of dronabinol, Schedule II– Anti-emetic for cancer chemotherapy when other
medications have failed

Pharmaceutical: Plant Derived
• Sativex (Not in USA)– THC/CBD/other cannabinoids. Schedule IV in UK– Oromucosal spray– Approved: spasticity from multiple sclerosis,
cancer pain, neuropathic pain• Epidiolex (Orphan Drug Status from FDA, pre-IND)– Purified CBD– Liquid– Anti-seizure for Dravet’s syndrome

Therapeutic Applications• Antiemetic: good evidence• Appetite stimulation: good evidence• Anticonvulsant: noted for 70 years• Spasticity: MS and spinal cord injury• Analgesia: dysphoria and intoxication– Acute: In combination with opioids– Chronic: No tolerance, unlike opioids
• Glaucoma: Reduces pressure, but impractical

Alternatives to Current Status• Decriminalize– Treat possession of small amounts as a civil
offence or misdemeanor instead of a felony• Manage offenses with fines instead of incarceration
– Intent: discourage use, prohibit distribution– Does not appear to increase teen use
• Legalize for recreational use– Regulate and tax like alcohol– Intent: eliminate black market, collect taxes– Opens door for commercial marketing
• Legalize for medical use (“medical marijuana”)

Successful “Il-legalization” Campaign by Harry Anslinger
• State laws prohibiting use (1933-37)• Marijuana Tax Act (1937)– Adopted despite AMA opposition
• Removed from U.S. Pharmacopeia (1942)• Included in UN Convention (1961)• Classified as Schedule 1 by DEA in Controlled
Drug Substances Act (1970)

Schedule I Criteria
1. High potential for abuse2. No currently accepted medical use in
treatment in the United States3. Lack of accepted safety for use under medical
supervision

Research Obstacles
• Access– Only one source– 5 levels of approval (more than any other drug)• Include NIDA, FDA, DEA
– Focus on harm rather than benefit• Quality– THC concentration increasing but not yet at street
levels– CBD concentration an issue
Unsuccessful Attemptsto Reduce Restrictions
• Appointment of high level, prestigious commission to study the issue– 1970. President Nixon
• Recommendation for decriminalization– 1972. Nixon Commission report– 1977. President Carter message to Congress

Polarization
• Pushback from law enforcement, government officials, politicians citing:– Gateway hypothesis– Equivalent danger as other drugs
• Change proponents deny any danger• Transition from a rational, evidence-based
process to an emotional one that can degenerate to disrespectful

President Nixon to Bob Haldeman
"You know, it's a funny thing, every one of the bastards that are out for legalizing marijuana is Jewish. What the Christ is the matter with the Jews, Bob? What is the matter with them? I suppose it’s because most of them are psychiatrists.“
Nixon Tapes, 1971

2013: Recent Drug Czar
“Science clearly demonstrates that marijuana is not a benign substance. It hampers academic performance. It impairs driving. It impacts productivity. And for some to say that it is less dangerous than other substances is a ridiculous statement.”
• Gil Kerlikowske

Stalemate
• Minimal change – Decriminalized in 11 states after 1972 Commission
report • Social tension from increased covert use
despite active law enforcement– 1970’s peak use: Broad demographic included
medical students and lawyers

A New Era
• 1996. Trend of liberalization began with approval of medical marijuana in California– Currently, 37 states plus D.C. have liberalized laws,
affecting 76% of U.S. population• Increasing support for legalization– Now favored by 54% vs. 12% in 1969 (Pew Research)– Already legalized in Colorado and Washington state– 10/5/14 NY Times editorial endorses current
legalization ballot initiatives in DC, Alaska, Oregon

Shifting Political Winds
• Newest driver has been concern about racial inequality in enforcement of laws– 2014. Maryland Governor O’Malley
• Obama administration has withheld enforcement of Federal law in states with liberalized laws– Could be reversed by a new administration

Medical Marijuana in DC• 2010. Bill passed– Limited to 5 qualifying conditions
• 2013. First dispensaries opened• 2014 changes in qualifying conditions– May: list expanded– July: list (quietly) eliminated
• Oral tinctures and topical salves added• October, 2014: 1,300 patients registered

DC Medical Marijuana Process
1. Doctor meets with patient and recommends medical marijuana
2. Patient fills out application, which is confirmed by the doctor– Forms available at http://doh.dc.gov/mmp
3. Application is approved by DC DOH and patient is given a registration card
4. Patient obtains marijuana from dispensary
Arguments For and Against“Medical” Marijuana
• FOR: People are suffering from medical conditions that respond to smoked marijuana and no other medication, including dronabinol.
• AGAINST: Marijuana is a complex substance that is taken via a high potency route of administration. It should therefore be subjected to the same quality standards and dosing studies as any other pharmaceutical and be commercially prepared and regulated by the FDA.

Some Unresolved Issues
• How to deal with drugged driving?• Restricting commercial advertising aimed at
under aged users?• Quality control of cannabis products?
Questions About Cannabis1. Is it harmful?– Not usually, but it can be
2. Does it have therapeutic use?– Yes, but rarely dramatic– Most studies are anecdotal
3. What is reasonable public policy?– Reduce barriers to research and pharmaceutical
development– Stay tuned

Buprenorphine: Recent Issues
• Improved clinical results when patients stay on buprenorphine longer
• Residual resistances within the addiction field– 28 day residential treatment centers and Narcotics
Anonymous– Diminishing: Hazelden has patients remain on
buprenorphine beyond withdrawal• New generic and brand formulations available• Some diversion, primarily of “mono” form

Gambling Disorder
• Clinical and neurobiological similarities to substance use disorders have led to increased acceptance as an addiction– DSM-5: moved gambling from Impulse Disorder to
Addiction section• Limited availability of treatment programs• Growth of Gamblers Anonymous and Gam-
Anon

DSM-5 Terminology Changes
• Alcohol Use Disorder, Opioid Use Disorder, etc.– Instead of “Alcohol Abuse” or “Alcohol
Dependence”• Uses 11 criteria from DSM-IV– “Mild” if 2 to 3 criteria are met– “Moderate” if 4 to 5– “Severe” if 6 or more
Neurobiology Summary
1. Genetic differences allow CNS exposure to larger doses of addictive substances– Endogenous systems are hijacked or altered– Many neurotransmitters are involved, dopamine is
key
2. Because of “brain neuroplasticity,” the heavy use of the substances:Enhances limbic system (reward, fear, and stress)Suppresses cortical areas (reason, inhibitory control)

All Drugs of Abuse Increase Dopamine Release in Nucleus Accumbens
• Older understanding: “pleasure chemical”– Triggered by• Natural rewards: food, sex, social interactions• All drugs of abuse
• Discovery: release is also increased by stress

Drugs, Neurotransmitters, and Reward

Dopamine Release:Newer Understanding
• Initially, signals a “prediction error”– Discrepancy between expectation and experience (“I
didn’t expect that.”)• With reward repetition, mediates conditioning– Decreased release with actual reward– Increased release from a predictor of reward
• Addicts, when told that drug will be given, can successfully inhibit craving– Inhibit nucleus accumbens, activate PFC– Cannot do this once substance is taken

Dopamine (D2) Receptors
• Find low levels of D2 receptors in addiction to all substances– Creates vulnerability but does not equate to addiction
• Some normals have low levels D2 but no addiction• Can alter alcohol intake in rats by manipulating D2 levels
• Past: thought vulnerability to addiction caused by sensitivity of DA system
• Now: think that continued use is driven by insensitivity– Can no longer feel reward, but cannot stop
Thank you
Related Documents











