DIAGNOSIS IN ONCOLOGY Unusual Problems in Breast Cancer and a Rare Lung Cancer Case CASE 1. CLINICAL COMPLETE RESPONSE OF BREAST CANCER METASTASES AFTER TRASTUZUMAB-BASED IMMUNOTHERAPY A 60-year-old Italian woman was diagnosed in December 1997 with undifferentiated right breast cancer infiltrating the skin. Preoperative clinical evaluation for distant metastases yielded negative results, and both pre- and postoperative serum tumor markers were in the normal range. After radical right mastectomy and axillary lymph-node dissection, her stage was pT4b, pN1bii, and she received four courses of doxorubicin and six courses of standard cyclophosphamide, methotrexate, and fluorouracil (days 1 and 8). At the end of adjuvant chemotherapy, she received local standard radiotherapy and then was placed on tamoxifen. Because of poor compliance, tamoxifen was discontinued after 3 months. In January 2000, a nodule near the scar was identified during physical examination. Pathologic examination of a fine-needle aspiration revealed local recurrence. The nodule was surgically removed, and antineoplastic chemotherapy with cyclophosphamide, epirubicin, and fluorouracil was administered for a total of three courses. In Fig 1. (A, B, C) At the beginning of immunotherapy, the erythematopapular skin relapse measured 20 20 cm. (D, E, F) After the first six courses of trastuzumab, a clinical complete regression was observed. 2215 Journal of Clinical Oncology, Vol 21, No 11 (June 1), 2003: pp 2215-2222 Downloaded from jco.ascopubs.org on February 21, 2013. For personal use only. No other uses without permission. Copyright © 2003 American Society of Clinical Oncology. All rights reserved.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DIAGNOSIS IN ONCOLOGY
Unusual Problems in Breast Cancer and a Rare LungCancer Case
CASE 1. CLINICAL COMPLETE RESPONSE OF BREAST CANCER METASTASES AFTER TRASTUZUMAB-BASEDIMMUNOTHERAPY
A 60-year-old Italian woman was diagnosed in December 1997 with undifferentiated right breast cancer infiltrating the skin.Preoperative clinical evaluation for distant metastases yielded negative results, and both pre- and postoperative serum tumor markerswere in the normal range. After radical right mastectomy and axillary lymph-node dissection, her stage was pT4b, pN1bii, and shereceived four courses of doxorubicin and six courses of standard cyclophosphamide, methotrexate, and fluorouracil (days 1 and 8).At the end of adjuvant chemotherapy, she received local standard radiotherapy and then was placed on tamoxifen. Because of poorcompliance, tamoxifen was discontinued after 3 months. In January 2000, a nodule near the scar was identified during physicalexamination. Pathologic examination of a fine-needle aspiration revealed local recurrence. The nodule was surgically removed, andantineoplastic chemotherapy with cyclophosphamide, epirubicin, and fluorouracil was administered for a total of three courses. In
Fig 1. (A, B, C) At the beginning of immunotherapy, the erythematopapular skin relapse measured 20 � 20 cm. (D, E, F) After the first six courses of trastuzumab, aclinical complete regression was observed.
2215Journal of Clinical Oncology, Vol 21, No 11 (June 1), 2003: pp 2215-2222
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.

January 2001, a new subcutaneous nodule occurred and was removed. Pathologic examination showed metastatic breast carcinoma.The patient refused chemotherapy, and 3 months later (April 2001), a new local recurrence occurred with the appearance of a largeerythematous rash (15 � 15 cm), with multiple small nodules over the right side of the chest reaching the posterior axillary line.Because of the progression of disease, she was treated with weekly vinorelbine (25 mg/m2) as a single agent. Because of localprogressive disease, this treatment was discontinued after seven courses in June 2001. Because the Hercept-test was positive (score3�/3�) by immunohistochemistry, it was decided to start immunotherapy with trastuzumab, a recombinant humanizedanti-p185HER-2 monoclonal antibody that binds with high affinity to the HER2 protein.1 Trastuzumab was administered weekly at 4 mg/kgas induction therapy and continued at 2 mg/kg, with good tolerance. At the beginning of immunotherapy, the erythematopapular skinrelapse measured 20 � 20 cm (Fig 1A, 1B, and 1C). After the first six courses of trastuzumab, a clinical complete regression was observed(Fig 1D, 1E, and 1F). The patient persists in remission almost 1 year later, still receiving trastuzumab.
The reported incidence of chest wall recurrence after radical mastectomy or breast-conserving surgery is between 5% and 32%.2,3 In themajority of patients (80% to 90%), recurrences are multiple at the time of appearance. With standard antineoplastic therapy, clinicalcomplete regression of local relapse is rare, episodic, and short lasting. To the best of our knowledge, this is the first report of completeregression of local breast cancer recurrence induced by trastuzumab-based immunotherapy. We indicate that trastuzumab should beconsidered as a treatment option in those patients with locoregional recurrence who had a positive Hercept-test.
Giuseppe Tonini, Bruno Vincenzi, Daniele Santini, Giuseppe Avvisati, Annalisa La Cesa, and Alfonso BaldiUniversita Campus Bio-Medico, Rome, Italy; and Regina Elena Cancer Institute, Rome, Italy
Copyright © 2003 American Society of Clinical Oncology
REFERENCES
1. Baselga J, Tripathy D, Mendelsohn J, et al: Phase II study of weeklyintravenous recombinant humanized anti-p185HER2 monoclonal antibody inpatients with HER2/neu-overexpressing metastatic breast cancer. J ClinOncol 14:737-744, 1996
2. Schmoor C, Sauerbrei W, Bastert G, et al: Role of isolated locoregionalrecurrence of breast cancer: Results of four prospective studies. J Clin Oncol18:1696-1708, 2000
3. Recht A, Gray R, Davidson NE, et al: Locoregional failure 10 yearsafter mastectomy and adjuvant chemotherapy with or without tamoxifenwithout irradiation: Experience of the Eastern Cooperative Oncology Group.J Clin Oncol 17:1689-1700, 1999
DOI: 10.1200/JCO.2003.04.195
CASE 2. AGGRESSIVE FIBROMATOSIS OF THE CHEST WALL ARISING NEAR A BREAST PROSTHESIS
A 52-year-old woman with a diffuse intraductal carcinoma of the left breast underwent a radical mastectomy and immediatereconstruction with a saline-filled silicone breast implant. Seven months later, the 195-mL expander was replaced by a 240-mLimplant, and the nipple areola was reconstructed. One year later, she complained of increasing asymmetry and firmness in the leftbreast, and the implant was exchanged. However, pain in the breast and tenderness persisted. Physical examination revealed anindurated mass deeply attached to the chest wall. A blood cyst was suspected. A thoracic computed tomography scan depicted alow-density mass measuring 80 � 50 mm situated below the prosthesis (Fig 1). Biopsy specimens were obtained during surgicalremoval of the implant. Magnetic resonance imaging (T1-weighted), performed after surgery, confirmed a homogeneous massinvading three intercostal spaces (Fig 2).
Fig 1. Thoracic computed tomography scan depicting a low-density mass measur-ing 80 � 50 mm situated below the prosthesis.
2216 KHANFIR ET AL
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.

Histologic analysis of the biopsy samples disclosed aggressive fibromatosis that was confirmed by immunohistochemical tests (Fig3). The patient refused radical surgery for personal and cosmetic reasons and, therefore, received a weekly combination ofmethotrexate and vinblastine (8 weeks) followed by hormonal therapy (6 months). She experienced slow disease progression duringthis period, which necessitated radical surgery including a partial sternectomy, anterior resection of four ribs, and breastreconstruction with a de-epithelialized flap allowing immediate defect closure.
Fibromatosis is a benign neoplasm derived from fibrous tissue that arises in musculoaponeurotic structures from the supportingconnective tissue.1 The tumors occur most frequently in the musculature of the anterior abdominal wall. Musculoaponeuroticfibromatosis, extra-abdominal desmoid aggressive fibromatosis, and low-grade sarcoma are the variety of terms used to describe thislesion. Heredity, hormones, trauma, and a previous surgical incision have been indicated as etiologic factors. Cytogeneticabnormalities consistent with clonality have also been reported.2 In this case, however, karyotype analysis did not reveal anychromosomal abnormality. A review of the literature indicated that aggressive fibromatosis arising near a breast prosthesis is a rareevent, with only sporadic cases occurring. Such cases have indeed been documented after surgical placement of saline-filled implantsand silicone gel–filled implants, all of which were in a silicone pouch.3-6 Tumor may arise from the fibrous capsule developingaround the implant.3,4 Radical surgery is the treatment of choice for fibromatosis, but recurrence is common despite adequate,free-tumor margins. External-beam irradiation or brachytherapy may be helpful in the management of these neoplasms, in particularfor recurrence and positive margins at excision.7
Fig 2. Magnetic resonance image (T1-weighted) of a homogeneous massinvading three intercostal spaces. Fig 3. Aggressive fibromatosis confirmed by immunohistochemical tests.
2217DIAGNOSIS IN ONCOLOGY
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.

Tumor regression has been reported in advanced inoperable fibromatosis with conventional chemotherapy, such as vincristine,dactinomycin, and cyclophosphamide, or more recently, with a weekly schedule of vinblastine and methotrexate.8 Hormonal therapywith tamoxifen could be an alternative treatment option in estrogen receptor–positive fibromatosis.9
Kaouthar Khanfir, Jean-Marc Guinebretiere, Daniel Vanel, Lise Barreau-Pouhaer, Sylvie Bonvalot, and Axel Le CesneInstitut Gustave Roussy
Villejuif, FranceCopyright © 2003 American Society of Clinical Oncology
REFERENCES
1. Enzinger FM, Weiss SW: Soft tissue tumors. St Louis, MO, CVMosby, 1983, pp 53-71
2. Bridge JA, Sreekantaiah C, Mouron B, et al: Clonal chromosomalabnormalities in desmoid tumors: Implications for histopathogenesis. Cancer69:430-436, 1992
3. Schiller VL, Arndt R, Brenner R: Aggressive fibromatosis of the chestassociated with a silicone breast implant. Chest 108:1466-1468, 1995
4. Jewet ST, Mead JH: Extra-abdominal desmoid tumor arising from acapsule around a silicone breast implant. Plast Reconstr Surg 63:577-579,1979
5. Schuh ME, Radford DM: Desmoid tumor of the breast followingaugmentation mammoplasty. Plast Reconstr Surg 93:603-605, 1994
6. Rosen PP, Ernsberger D: Mammary fibromatosis: A benign spindle-cell tumor with significant risk for local recurrence. Cancer 63:1363-1369, 1989
7. Ballo MT, Zagars GK, Pollack A, et al: Desmoid tumor: Prognosticfactors and outcome after surgery, radiation therapy, or combined surgeryand radiation therapy. J Clin Oncol 17:158-167, 1999
8. Azzarelli A, Gronchi A, Bertulli R, et al: Low dose chemotherapy withmethotrexate and vinblastine for patients with advanced aggressive fibroma-tosis. Cancer 92:1259-1264, 2001
9. Kinzbrunner B, Ritter S, Domingo J, et al: Remission of rapidlygrowing desmoid tumors after tamoxifen therapy. Cancer 52:2201-2204,1983
DOI: 10.1200/JCO.2003.04.189
CASE 3. SIMULTANEOUS AND SYNCHRONOUS BILATERAL INFLAMMATORY BREAST CANCER
A 69-year-old woman with no family history of malignancy presented with a 3-week onset of progressive dyspnea andsimultaneous bilateral breast swelling. On physical examination, both breasts were symmetrically enlarged, indurated, warm,erythematous, and had a peau d’orange appearance with inverted nipples (Fig 1). There was no discrete mass in either breastor regional lymphadenopathy. Mammography showed diffuse increased density bilaterally with extensive edema andmicrocalcification only in the central portion of the left breast. Computed tomography of the chest revealed diffusely thickenedmammary skin, soft tissue edema both in the breasts and in the subcutaneous tissues surrounding the entire anterior chest wall,bilateral axillary adenopathy, and bilateral pleural effusions (Fig 2). Bilateral breast biopsies revealed infiltrating ductalcarcinoma with extensive involvement of dermal lymphatics (Figs 3A and 3B). Immunochemistry showed that the lesions wereestrogen and progesterone receptor–positive with overexpression of HER-2/neu. Pleural fluid cytology on the left breast
Fig 1. Patient presenting with bilateral inflammatory breast cancer.
Fig 2. Computed tomography of patient showing diffusely thickened mammaryskin, soft tissue edema both in the breasts and in the subcutaneous tissuessurrounding the entire anterior chest wall, bilateral axillary adenopathy, andbilateral pleural effusions.
2218 AGRAWAL ET AL
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.

revealed adenocarcinoma. Skeletal scintigraphy was positive for metastases. Computed tomography of the abdomen and pelvis,upper endoscopy, and colonoscopy were all normal.
The term bilateral breast cancer implies that, in a patient with a known unilateral breast cancer, a malignancy is detectedin the contralateral breast. In a comprehensive review, 836 (3.7%) of 25,563 breast cancers were bilateral, with one third beingsynchronous and two thirds being metachronous.1 The reported incidence of bilateral breast cancer varies according to thelength of follow-up and method of diagnosis. Bilateral primary breast cancers described as synchronous or metachronous arearbitrary regarding designation of time and have no biologic significance. There is no correlation of bilateral breast cancer withtumor size, histologic differentiation, hormonal receptor status, or the number of lymph nodes involved. There are, however,a few true risk factors, including age at the time of initial breast cancer diagnosis, family history, genetic mutation,multicentricity, and pathologically infiltrating lobular carcinoma. Inflammatory breast cancer (IBC) is the reported diagnosisin 1% to 3% of patients with newly identified invasive breast cancer. There is no consistent histologic type of breast carcinomaassociated with this entity. The histologic type ranges from infiltrating ductal to medullary. The carcinoma series ofHaagensen,2 which studied 40 patients, included 19 (47%) with the large-cell undifferentiated-type carcinoma. The diagnosisof IBC is based on the clinical presentation, defined by the American Joint Committee on Cancer staging manual as “diffusebrawny induration of the skin of the breast with an erysipeloid edge, usually without underlying palpable mass.” The skin overthe breast is warm and thickened, with an orange peel appearance. The classic histologic finding in IBC on biopsy of affectedskin is dermal lymphatic invasion by tumor cells. However, dermal lymphatic invasion is not a necessary criterion for thediagnosis of IBC. IBC is diagnosed by clinical presentation. Affected patients may present with clinical signs only withoutdermal lymphatic invasion, or with dermal lymphatic involvement without clinical signs, or with both clinical signs and dermallymphatic invasion. Our patient had both the clinical and the pathologic findings of IBC.
Metastatic tumors to the breast appear as relatively small, superficially located, poorly defined, irregular nodules withoutcalcification on mammography and ultrasonography. However, when the lesion is diffuse, the appearance is indistinguishable fromthat of IBC. Two cases of breast metastasis from signet ring cell gastric cancer3,4 and three case reports of metastasis from primaryovarian carcinoma mimicking bilateral IBC have been published.5-7 In our patient, such possibilities were excluded based on history,physical examination, and histologic and radiologic findings.
A patient like ours, who presents with simultaneous and synchronous primary IBC, is exceedingly rare. Similar cases reported inthe literature include that of a male patient presenting with bilateral inflammatory medullary breast carcinoma8 and a female patientwith bilateral IBC who was treated with chemotherapy, radiation, and bilateral mastectomy.9
Bharat L. Agrawal, Amaresh R. Nath, Thomas P. Glynn, Jr, David Velazco, and Richard F. Garnett, JrCancer and Blood Disease Center and Reid Hospital and Health Care Services
Richmond, INCopyright © 2003 American Society of Clinical Oncology
REFERENCES
1. Wanebo HJ, Senofsky GM, Fechner RE, et al: Bilateral breast cancer:Risk reduction of contralateral biopsy. Ann Surg 201:667-677, 1985
2. Haagensen CD: Diseases of the Breast. Philadelphia, PA, WB Saun-ders, 1986, pp 808-814
Fig 3. (A, B) Bilateral breast biopsies revealing infiltrating ductal carcinoma with extensive involvement of dermal lymphatics.
2219DIAGNOSIS IN ONCOLOGY
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.

3. Briest S, Horn LC, Haupt R, et al: Metastasizing signet ring carcinomaof the stomach-mimicking bilateral inflammatory breast cancer. GynecolOncol 74:491-494, 1999
4. Cavazzini G, Colpani F, Cantore M, et al: Breast metastasis fromgastric signet ring cell carcinoma, mimicking inflammatory carcinoma.Tumori 79:450-453, 1993
5. Krishnan EU, Phillips AK, Randell A, et al: Bilateral metastaticinflammatory carcinoma in the breast from primary ovarian cancer. ObstetGynecol 55:s94-s96, 1980 (suppl 3)
6. Ozguroglu M, Ersavasti G, Ilvan S, et al: Bilateral inflammatory breastmetastases of epithelial ovarian cancer. Am J Clin Oncol 22:408-410, 1999
7. Oksuzoglu B, Guler N, Kose F: Bilateral inflammatory breast involvementas the first site of relapse of ovarian carcinoma. Am J Clin Oncol 24:211, 2001
8. Jeelani G, Beg MA, Hussain A, et al: Simultaneous bilateral inflam-matory medullary carcinoma of male breast. Int Surg 62:147-148, 1977
9. Nakagawa H, Kikuhara M, Sato M, et al: A case report of inflammatorybreast cancer effectively treated with cis-platinum. Gan To Kagaku Ryoho14:2767-2770, 1987
DOI: 10.1200/JCO.2003.11.105
CASE 4. PRIMARY LYMPHOEPITHELIOMA-LIKE CARCINOMA OF THE LUNG
A 65-year-old Chinese woman was referred for evaluation of pulmonary and pleural nodules found on a chest x-ray when she initiallypresented with pneumonia. A subsequent computed tomography (CT) scan of the chest revealed a peripheral 2 � 3–cm lung massin the superior segment of the left lower lobe (Fig 1A), a 1 � 2–cm lingular nodule, and a 1 � 2.5–cm left-sided nodular pleuralthickening (Fig 2A). These corresponded to sites of marked uptake on positron emission tomography scan (Figs 1B and 2B). Therewere also other areas of thickening in the anterior and posterior chest walls. Her past medical history was remarkable for ductalcarcinoma-in-situ of the right breast, which was treated with lumpectomy and radiation 3 years before this presentation withoutevidence of recurrence. She also had hypothyroidism and hypercholesterolemia, which were well controlled. She immigratedat the age of 10 years from Canton, China, to the United States and denied tobacco use, regular alcohol use, or any known toxinexposures. She described a dry, nonproductive cough and occasional dysphagia. Her physical examination and routinelaboratory results were unremarkable.
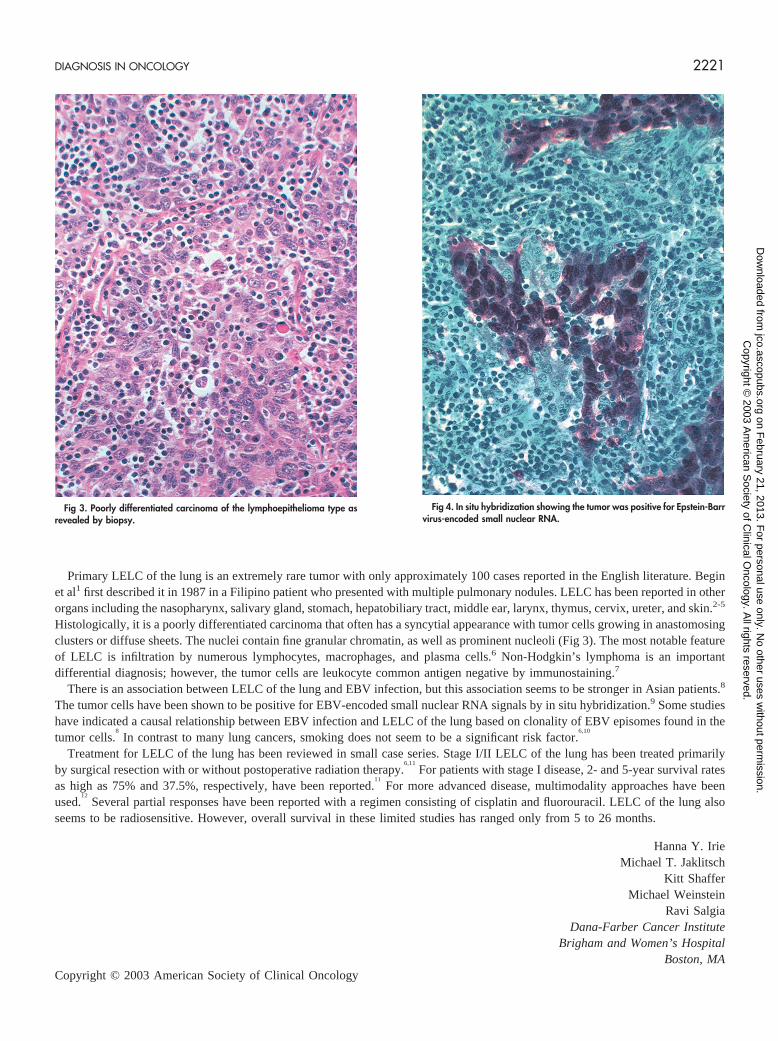
After an initial nondiagnostic CT-guided transthoracic needle biopsy, the patient underwent a thoracoscopic wedge excision of thetwo dominant nodules in the left lung. Intraoperatively, a pleural plaque overlying one of the nodules was also biopsied. Thepathology of one of the nodules and the pleural plaque revealed poorly differentiated carcinoma of the lymphoepithelioma type (Fig3). Immunoperoxidase stains were positive for cytokeratin but negative for estrogen receptor, gross cystic disease fluid protein(GCDFP), and thyroid transcription factor-1 (TTF-1), making primary lung or metastatic breast cancer unlikely. The tumor was alsofocally positive for Epstein-Barr virus (EBV)-encoded small nuclear RNA by in situ hybridization (Fig 4). Given the diagnosis, thepatient also underwent an ear, nose, and throat evaluation that did not reveal a primary nasopharyngeal carcinoma. Therefore, thistumor was classified as primary lymphoepithelioma-like carcinoma (LELC) of the lung.
Fig 1. (A) A computed tomography scan of the chest showing a 2 � 3-cmlung mass in the superior segment of the lower left lobe. (B) A positronemission tomography scan showing corresponding site of marked uptake.
Fig 2. (A) A computed tomography scan showing a 1 � 2-cm lung mass and a1 � 2.5-cm left-sided nodular pleural thickening. (B) A positron emission tomog-raphy scan showing corresponding sites of marked uptake.
2220 IRIE ET AL
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.
Primary LELC of the lung is an extremely rare tumor with only approximately 100 cases reported in the English literature. Beginet al1 first described it in 1987 in a Filipino patient who presented with multiple pulmonary nodules. LELC has been reported in otherorgans including the nasopharynx, salivary gland, stomach, hepatobiliary tract, middle ear, larynx, thymus, cervix, ureter, and skin.2-5
Histologically, it is a poorly differentiated carcinoma that often has a syncytial appearance with tumor cells growing in anastomosingclusters or diffuse sheets. The nuclei contain fine granular chromatin, as well as prominent nucleoli (Fig 3). The most notable featureof LELC is infiltration by numerous lymphocytes, macrophages, and plasma cells.6 Non-Hodgkin’s lymphoma is an importantdifferential diagnosis; however, the tumor cells are leukocyte common antigen negative by immunostaining.7
There is an association between LELC of the lung and EBV infection, but this association seems to be stronger in Asian patients.8
The tumor cells have been shown to be positive for EBV-encoded small nuclear RNA signals by in situ hybridization.9 Some studieshave indicated a causal relationship between EBV infection and LELC of the lung based on clonality of EBV episomes found in thetumor cells.
8
In contrast to many lung cancers, smoking does not seem to be a significant risk factor.6,10
Treatment for LELC of the lung has been reviewed in small case series. Stage I/II LELC of the lung has been treated primarilyby surgical resection with or without postoperative radiation therapy.
6,11
For patients with stage I disease, 2- and 5-year survival ratesas high as 75% and 37.5%, respectively, have been reported.
11
For more advanced disease, multimodality approaches have beenused.
12
Several partial responses have been reported with a regimen consisting of cisplatin and fluorouracil. LELC of the lung alsoseems to be radiosensitive. However, overall survival in these limited studies has ranged only from 5 to 26 months.
Hanna Y. IrieMichael T. Jaklitsch
Kitt ShafferMichael Weinstein
Ravi SalgiaDana-Farber Cancer Institute
Brigham and Women’s HospitalBoston, MA
Copyright © 2003 American Society of Clinical Oncology
Fig 3. Poorly differentiated carcinoma of the lymphoepithelioma type asrevealed by biopsy.
Fig 4. In situ hybridization showing the tumor was positive for Epstein-Barrvirus-encoded small nuclear RNA.
2221DIAGNOSIS IN ONCOLOGY
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.

REFERENCES
1. Begin LR, Eskandari J, Joncas J, et al: Epstein-Barr virus relatedlymphoepithelioma-like carcinoma of lung. J Surg Oncol 36:280-283, 1987
2. Tsai CC, Chen CL, Hsu HC: Expression of Epstein-Barr virus incarcinomas of major salivary glands: A strong association with lymphoepi-thelioma-like carcinoma. Hum Pathol 27:258-262, 1996
3. Vortmeyer AO, Kingman DW, Fenton RG, et al: Hepatobiliarylymphoepithelioma-like carcinoma associated with Epstein-Barr virus. Am JClin Pathol 109:90-95, 1998
4. Leung SY, Yuen ST, Ho CM, et al: Presence of Epstein-Barr virus inlymphoepithelioma-like carcinoma of the middle ear. J Clin Pathol 51:602-605, 1998
5. Tseng CJ, Pao CC, Tseng LH, et al: Lymphoepithelioma-like carci-noma of the uterine cervix: Association with Epstein-Barr virus and humanpapillomavirus. Cancer 80:91-97, 1997
6. Chan JK, Hui PK, Tsang WY, et al: Primary lymphoepithelioma-likecarcinoma of the lung: A clinicopathologic study of 11 cases. Cancer 74:413-422, 1995
7. Butler AE, Colby TV, Weiss L, et al: Lymphoepithelioma-like carci-noma of the lung. Am J Surg Pathol 13:632-639, 1989
8. Anagnostopoulos I, Hummel M: Epstein-Barr virus in tumors. Histo-pathology 29:297-315, 1996
9. Weiss LM, Movahed LA, Butler AE, et al: Analysis of lympho-epithelioma and lymphoepithelioma-like carcinomas for Epstein Barrviral genomes by in situ hybridization. Am J Surg Pathol 13:625-631,1989
10. Frank MW, Shields TW, Joob AW, et al: Lymphoepithelioma-likecarcinoma of the lung. Ann Thorac Surg 64:1162-1164, 1997
11. Han A-J, Xiong M, Gu Y-Y, et al: Lymphoepithelioma-like carci-noma of the lung with a better prognosis. Am J Clin Pathol 115:841-850,2001
12. Chan ATC, Teo PML, Lam KC, et al: Multimodality treatment ofprimary lymphoepithelioma-like carcinoma of the lung. Cancer 83:925-929,1998
DOI: 10.1200/JCO.2003.09.088
2222 IRIE ET AL
Dow
nloaded from jco.ascopubs.org on F
ebruary 21, 2013. For personal use only. N
o other uses without perm
ission.C
opyright © 2003 A
merican S
ociety of Clinical O
ncology. All rights reserved.
Related Documents











