University of Groningen The Severity of Anaphylactic and Systemic Allergic Reactions Pettersson, Maria Eleonore IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2018 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Pettersson, M. E. (2018). The Severity of Anaphylactic and Systemic Allergic Reactions. University of Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 18-12-2021

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

University of Groningen
The Severity of Anaphylactic and Systemic Allergic ReactionsPettersson, Maria Eleonore
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2018
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Pettersson, M. E. (2018). The Severity of Anaphylactic and Systemic Allergic Reactions. University ofGroningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 18-12-2021

The Severity of Anaphylactic and
Systemic Allergic Reactions
M. Eleonore Pettersson

The author gratefully acknowledges the financial contributions for the printing of this thesis:Groningen University Institute for Drug Exploration (GUIDE)University Medical Center Groningen (UMCG)University of Groningen
Lay-out and print by: ProefschriftMaken // www.proefschriftmaken.nl ISBN, printed version: 978-94-034-0558-2ISBN, electronic version: 978-94-034-0559-9Copyright © by M.E. Pettersson, 2018

The Severity of Anaphylactic and Systemic Allergic Reactions
PhD Thesis
to obtain the degree of PhD at the University of Groningen on the authority of the
Rector Magnificus Prof. E. Sterken and in accordance with
the decision by the College of Deans.
This thesis will be defended in public on
Monday 18 June 2018 at 16.15 hours
By
Maria Eleonore Pettersson
born on 16 June 1988 in Badelunda, Sweden

Supervisors Prof. A.E.J. Dubois Prof. G.H. Koppelman Assessment committee Prof. D.S. Postma Prof. A.C. Knulst Prof. G.C. Roberts

CONTENTS
Chapter 1 - General introduction 9
Chapter 2 - Is 30 minutes between doses long enough in oral food challenges? 25
Chapter 3 - Prediction of the severity of allergic reactions to foods 33
Chapter 4 - Greater severity of peanut challenge reactions using a high fat versus low fat matrix vehicle
55
Chapter 5 - Clinical reactivity to individual tree nuts and peanut differs among the sensitized pediatric population
63
Chapter 6 - Apolipoprotein B: a possible new biomarker for anaphylaxis 77
Chapter 7 - Association of STAT6 gene variants with food allergy diagnosed by double-blind placebo-controlled food challenges
85
Chapter 8 - Mastocytosis and age, but not baseline tryptase, specific IgE or total IgE, independently determine the severity of systemic reactions to yellow jacket stings.
95
Chapter 9 - Summary and general discussion 113
Appendices - Nederlandse samenvatting - Svensk sammanfattning - Biography
127129133141


ABBREVIATIONS
AF - allele frequency ApoB - apolipoprotein B BAT - basophil activation test bsT - baseline serum tryptaseCD - cumulative doseCI - confidence intervalCMA - cow’s milk allergyDBPCFC - double-blind, placebo-controlled food challengeED - eliciting doseeQTL - expression quantitative trait lociFBAT - family based association testISM - indolent systemic mastocytosisMH - methylhistamineMI - myocardial infarction MIMA - methylimidazole acetic acidOFC - oral food challengePAF - platelet-activating factorPAF-AH - platelet-activating factor, acetylhydrolasesIgE - specific immunoglobulin ESNP - single nucleotide polymorphisms SPT - skin prick testSTAT6 - signal transducer and activator of transcription 6 UMCG - University Medical Center GroningenUP - urticaria pigmentosaYJV - yellow jacket venom


CHAPTER 1
GENERAL INTRODUCTION


GENERAL INTRODUCTION 11
1When inquiring about the beliefs of the general public regarding allergies, several common misconceptions seems to exist. The word “allergy” is frequently incorrectly used as a syn-onym for all symptoms occurring after an insect sting, ingestion of a culprit food, or related to medication use. Moreover, the general public frequently confuses non-allergic food reac-tions, such as food intolerances, with food allergies, which can result in an unfounded belief that food allergy is less severe than it truly is. However, what does it really mean?
1.1 AllERgy dEfINITIONS
An abnormally strong response to a certain substance resulting in symptoms or signs, which is tolerated by the majority of the population, is known as hypersensitivity. (1)
Allergy is defined by the European Academy of Allergology and Clinical Immunology as a hypersensitivity reaction initiated by immunological mechanisms. (1) Allergy frequently arises in the first few months of life, but it can develop at any age. The term allergy is broadly used but generally includes a set of clinical symptoms elicited by immunologic mechanisms, that may be mediated by immunoglobulin and/or through cell-mediated responses. These responses are frequently mediated by Immunoglobulin E (IgE) and these individuals are generally referred to as having an IgE-mediated allergy. (1) Many allergic diseases have a chronic course, however there are ways to treat and manage them and some patients may outgrow their allergies completely, even if severe. (2)
Allergic reactions are elicited by allergens. Most allergens are glycoproteins which cause the allergic response by reacting with the immune system. Allergens may be airborne, such as grass pollen, tree pollen or mite; ingested, as in the case of food allergens; or transferred by stinging insects, for instance yellow jacket, wasp or bee. Another group of allergens are medications, with certain types of antibiotics as common elicitors. (3)
The generation of specific IgE (sIgE) after exposure to an allergen is known as sensitization. (4) However, sensitization without the development of symptoms after allergen exposure, also known as asymptomatic sensitization, is common. Thus, an sIgE mediated allergy re-quires both the development of symptoms after exposure to an allergen and the presence of sensitization. (5)
Cross-reactivity may occur when an allergen of similar structure to the original sensitizing al-lergen crosslinks with an antibody and elicits an immunologic response. For example, a birch tree pollen allergen shares structural similarities with a specific hazelnut allergen, which may lead to clinical reactivity to hazelnut in patients sensitized to birch tree pollen. (6)

12 CHAPTER 1
Atopy is defined as an individual and/or a familiar tendency to become sensitized and produce IgE antibodies in response to exposure of allergens commonly occurring in the environment. Allergic asthma, atopic dermatitis, allergic rhinoconjunctivitis, food allergy and IgE mediated anaphylaxis are examples of clinical disorders considered to fall under the definition of atopic diseases. (1)
1.2 ANAphylAxIS
Defining anaphylaxis
Anaphylaxis is defined as a “severe, life-threatening generalized or systemic hypersensitiv-ity reaction”. (1) Anaphylaxis may be mediated by sIgE but alternative mechanisms have also been suggested. (5) An anaphylactic reaction is rapid in onset, varying from minutes to a few hours, and frequently includes multiple organ systems. The skin and mucous membranes are frequently involved, with symptoms and signs such as itching, angio-edema, flushing and hives. Gastrointestinal, respiratory and cardiovascular symptoms are also common, however signs of shock is not always present, even in fatal reactions. (7) The overall fatality rate for anaphylaxis is low, under 0.001%. (8) The clinical criteria for diagnosing anaphylaxis, as defined by Sampson et al. (9), are shown in Table 1.
Table 1. The clinical criteria for diagnosing anaphylaxis, as defined by Sampson et al (9). One out of the three criteria needs to be fulfilled to receive the diagnosis of anaphylaxis.
Clinical criteria of Anaphylaxis
1. Acute onset of symptoms or signs, with involvement of:• Skin or mucosa (for example hives; generalized itch, flush or erythema; angioedema)
AND one of the following:• Reduced blood pressure (BP) or related symptoms (for example syncope)• Airway compromise(for example wheeze, bronchospasm, dyspnea, reduced peak
expiratory flow rate (PEFR))
2. Two or more of the following symptoms after exposure to a confirmed allergen for that patient:• History of severe allergic reaction• Skin or mucosa (for example hives; generalized itch, flush or erythema; angioedema)• Airway compromise (for example wheeze, bronchospasm, dyspnea, reduced PEFR)• Reduced BP or related symptoms (for example syncope)• In food allergy: gastrointestinal symptoms (for example vomiting, abdominal pain,
diarrhea )
3. Hypotension after exposure to a confirmed allergen for that patient.• Infantsandchildren:>30%dropinsystolicBPoragespecificlowsystolicBP;<70
mmHgin1month-1yearolds,<(70mmHg+(2xage))in1-10yearolds,<90mmHgin11-17yearolds.
• Adults:>30%dropinsystolicBPor<100mmHg

GENERAL INTRODUCTION 13
1Epidemiology
Anaphylaxis is frequently elicited by foods, medications or stinging insect venoms, but it could also be triggered by an unidentified cause. The distribution of the causes varies with geographic location and the age of patients. Generally, foods and drugs are the most common triggers of anaphylaxis in patients presenting to the emergency department. (8) Foods are the most common elicitor for anaphylaxis in children, while anaphylaxis caused by drugs and stinging insect venom is more common in adults. (8)
Certain external factors, so-called cofactors or augmentation factors, have also been shown to influence allergic reactions. These include the use of certain medications, in particular nonsteroidal anti-inflammatory drugs (NSAIDs); alcohol; exercise; concomitant disease; acute infection; premenstrual status in females and mast cell diseases. (10-12)
Treatment
Initial treatment of anaphylaxis consists of an intramuscular injection of adrenaline in the mid-outer thigh, and placing the patient in a supine position with the lower extremi-ties elevated. If there is respiratory distress or vomiting, a position of comfort might be preferred. If indicated, supplemental oxygen, intravenous fluid resuscitation and cardio-pulmonary resuscitation should be provided. Antihistamines, glucocorticoids and beta-2 adrenergic agonists should not be used as monotherapy or administered before treatment with adrenaline. Patients not responding to repeated dosages of adrenaline, supplemental oxygen and intravenous fluid resuscitation require intensive care treatment. (13)
Management and prevention of recurrence
Patients with previous anaphylactic reactions should be evaluated by a specialist, receive optimal treatment of additional atopic disease and be given information how to man-age and prevent recurrences. The patient should be prescribed one or more adrenaline auto-injectors, which must be carried consistently and used if anaphylaxis reoccurs. Avoid-ance of confirmed triggers and allergen specific immunotherapy should be initiated, if applicable. (13)
1.3 fOOd AllERgy
General introduction to food allergy
Food allergy has been defined as an adverse reaction to food, which is reproducible on each contact with the culprit food and mediated by an immunologic mechanism. The clinical symptoms of food allergy involves the skin, gastrointestinal, respiratory and car-

14 CHAPTER 1
diovascular tracts. (14) Reactions to foods is most commonly triggered by ingestion, but may also rarely occur after inhalation or skin contact. (13)
A thorough clinical history is vital to the diagnosis of food allergy, as it can ascertain the probability of the diagnosis, identify the potential elicitor and suggest the immunological mechanism involved. The clinical evaluation should involve associated atopic disease, such as asthma, atopic dermatitis and allergic rhinoconjunctivitis. Skin prick tests (SPT) and measurement of the level of food-specific IgE (sIgE) are first-line tests to evaluate IgE sensitization. (14) However, asymptomatic sensitization is frequent and these tests in combination with a careful clinical history frequently over-estimate the diagnosis of food allergy. (15-17) Therefore, oral food challenges (OFC) are usually required to make the diagnosis.
The double-blind, placebo controlled food challenge (DBPCFC) is the gold standard test for the diagnosis of food allergy. In this test the patient receives either the placebo or active food on two separate days in random order. The food used during the placebo and active day of the DBPCFC should be indistinguishable from each other in terms of sensory properties. (18)
In order to prevent severe reactions during the test, patients receive the food in increasing dose increments, with a set time-interval between doses. The food challenge is stopped if a clear clinical allergic reaction is observed or if the last dose is ingested without the development of a clinical reaction. Even though life-threatening reactions are rare, staff performing OFCs should be trained and equipped to treat potentially severe allergic reac-tions and anaphylaxis. (18)
The management of food allergy is divided into short-term and long-term intervention strategies. The short-term interventions are directed at the treatment of acute allergic reactions, such as injection of intra-muscular adrenaline for anaphylaxis. The long-term strategies are employed to minimize the risk of further reactions. This is achieved through patient education, dietary adjustment and prescription of adrenaline auto-injectors, if indicated. (19)
The dietary adjustment should eliminate the culprit food. Patients should be re-evaluated at regular intervals to examine whether they have developed tolerance to the food in question, as unnecessary dietary elimination impairs quality of life and extensive dietary elimination can lead to nutritional deficiencies. (19)

GENERAL INTRODUCTION 15
1Currently, there is growing interest in immune-modulating treatment options for food allergy, such as sublingual and oral immunotherapy to induce tolerance. However, these are currently not recommended outside of the research setting due to the potential for severe adverse events. (19)
Identifying patients at risk for severe reactions is important for accurate management and targeted prescription of adrenaline auto-injectors. However, accurate identification of these patients is currently not possible, which results in a great deal of uncertainty for patients, caregivers and clinicians.
Scoring of severe food allergic reactions
Various scoring systems for determination of the severity of food allergic reactions have been developed. However, currently there is no consensus among clinicians and research-ers on which scoring system to use. The use of a particular scoring system differs per center according to own preferences, research applicability and clinical experience.
Risk factors and co-factors for the severity of food allergic reactions
A correct assessment of the risk of severe food allergic reactions is important for the successful management of patients. Several risk factors have been proposed, however the impact of each factor in the development of severe reactions is unknown. Patients with previous anaphylaxis to food or severe asthma have a higher risk of severe reactions compared to other patients. (20, 21) Moreover, the age of the patients also seems to have an influence on the severity of reactions, with adolescents and young adults generally having the most severe food allergic reactions. (8)
Food allergic reactions do not seem to show a clear dose-response relationship between the ingested dose and the severity of the ensuing reaction. Threshold doses required to initiate an allergic reaction vary between patients, and do not remain stable over time in some food allergic patients. (22) In a unique study, where the food challenge procedure was allowed to continue with additional doses after the initial reaction, many, but not all patients had allergic reactions which progressed to anaphylaxis. (23) It has previously been suggested that dose sensitive patients have more severe allergic reactions, however this has not yet been shown in published research. (24-26) Thus, the precise relationship between dose and the development of severe reactions is currently unclear.
Biomarkers
There are few published studies examining biomarkers for severe food allergic reactions. Currently, there is no biomarker available which accurately can predict severe food allergic reactions in all patients.

16 CHAPTER 1
Levels of sIgE and SPT wheals to certain foods have been shown to weakly correlate with severe reactions and cut-off values have been developed to make recommendations on when oral food challenge testing is redundant. (27-29) Thus, these cut-offs are more appropriate for predicting clinical reactivity as compared to asymptomatic sensitization. However, they are not clinically useful for prediction of severe reactions in a food allergic population.
In component-resolved diagnostic tests (CRD), sIgE antibodies are measured against indi-vidual allergenic food proteins known as major allergens. This test was developed with the prospect to improve the specificity of sIgE testing. (30) The use of this technique has been broadly studied for peanut, and the allergen components Ara h 2 and Ara h 6 have been shown to be predictive markers for severe reactions to peanut. (31) However, geographi-cal differences in sensitizations patterns have been demonstrated for peanut allergy. (32) Moreover, the cut-off levels for these predictors are not applicable to the majority of the peanut allergic population and the impact of these results are controversial. (33) More large-scale studies are needed to confirm allergen components to be predictive of severe reactions for other types of food.
Currently, potential biomarkers for severe food allergic reactions such as basophil activa-tion tests (BATs), baseline serum tryptase (bsT) levels and platelet-activating factor (PAF) and/or PAF acetylhydrolase (PAF-AH) are limited to the research setting.
1.4 YEllow jackEt (VESpula SpEciES) VEnoM allERGY
General introduction to Yellow jacket venom allergy
Vespid and honeybee stings are the most prevalent insect stings in central and northern Europe. Vespula are commonly known as yellow jackets in USA and wasps in Europe. Vespula preferably build their nests in attics, underground or other similar sheltered loca-tions. Only the queens survive the winter, thus larger populations are only seen in the summer and most insect stings occur during that season. (34)
Most venom allergens are glycoproteins and the major allergens in vespid venoms are phospholipase A1 (Ves v 1), hyaluronidase (Ves v 2) and antigen 5 (Ves v 5). (35-37) Some components of the venoms have toxic effects. Generally, toxic reactions are dependent on dose, influenced by the composition of the venom, and only occur after fifty to several hundred stings. (38-40) A single vespula sting releases between 1.7 to 3.1 μg of venom. (41) The venom composition of individual allergens have many similarities, thus cross-reactivity between different species of vespids is common. (42, 43)

GENERAL INTRODUCTION 17
1Sting reactions can be classified into normal local reactions, large local reactions, systemic toxic reactions and systemic allergic reactions. Normal local sting reactions in non-allergic patients elicit symptoms of pain, erythema and mild swelling around the site of the sting. These symptoms usually fade after 24 hours, but may remain for a few days. (34) Large local reactions have been defined as a swelling larger than 10 centimeters, which persists for more than 24 hours, and rarely includes the presence of blisters. Large local reactions may last for days to weeks and involve eyes, lips or a whole limb. These reactions may also be accompanied by shivering, fever, headaches or general malaise. The pathogenesis of large local reactions is unknown. (34)
A prevalence of between 0.3 and 7.5% of systemic reactions to insect stings have been reported in Europe. (34) Venom sensitization is present in the majority of patients with previous systemic sting reactions. (44) Symptoms of the skin, gastrointestinal, cardiovas-cular and respiratory tract can occur. One of the most frequently used classifications of the severity of systemic reactions to insect stings was published by Mueller, see Table 2. (45) Symptoms usually develop within minutes after the sting, but can appear hours or rarely even days later. (46) Fatal reactions to insect stings occur, however the incidence is low, between 0.03 to 0.48 fatalities per 1.000.000 individuals a year. (47) However, between 40-85% of patients with fatal reactions to insect stings had no history of previous anaphy-lactic reactions. (48, 49)
Table 2. Classification of systemic reactions to insect stings according to Mueller. (45)
GradeI Generalized urticaria, itching, malaise and anxiety
GradeII Any of the above plus two of more of the following: angioedema, chest constriction, nausea, vomiting, diarrhea, abdominal pain, dizziness
GradeIII Any of the above plus two or more of the following: dyspnea, wheezing, stridor, dysarthria, hoarseness, weakness, confusion, feeling of impending disaster
GradeIV Any of the above plus two or more of the following: fall in blood pressure, collapse, loss of consciousness, incontinence, cyanosis.
Diagnosis and treatment of Yellow jacket venom allergy
The diagnosis of Yellow jacket venom (YJV) allergy is based on a detailed clinical history of a systemic sting reaction, in addition to clinical sensitization as shown by detection of venom specific IgE in serum and/or a positive skin test. (34) The history is highly important in making a correct diagnosis, since asymptomatic venom sensitization is frequent. (50)
All patients with a history of systemic reactions to YJV should carry adrenaline auto-injec-tors and be evaluated by an allergy specialist for the possibility of venom immunotherapy

18 CHAPTER 1
(VIT). Subcutaneous VIT is an effective treatment which reduces the risk of additional sys-temic reactions, prevents fatal reactions and improves the quality of life of patients. (34)
Risk factors for the severity of allergic reactions to Yellow jacket venom
In patients with a history of systemic sting reactions, a majority will experience a new systemic reaction after a subsequent sting. (51) The risk of developing a systemic sting re-action increases with a shorter time interval between subsequent stings. (52) Conversely, very frequent stings, more than 200 a year, seem to induce tolerance. (53, 54)
Children with a history of previous mild cutaneous reactions have been shown to have a 10% risk of recurrence of systemic reactions after an additional sting. (55) In adults this risk was 14-20% after a history of previous mild systemic reactions and 79% with a history of previous severe systemic reactions. (56, 57) Systemic sting reactions in children tend to be milder than in adults, and elderly patients generally develop more severe sting reac-tions. (58-60)
Several factors seems to be associated with severe systemic sting reactions. Cardiovascu-lar disease and treatment with beta-blockers or angiotensin-converting enzyme inhibitors have been suggested to be associated with such reactions. However reports describe conflicting results. (61) Patients diagnosed with indolent systemic mastocytosis (ISM) have clonal proliferation of abnormal mast cells and represent a particular risk group for frequent and severe anaphylactic reactions. This is likely to be caused by excessive mast cell mediator release following triggering of mast cells. (62) Moreover, patients with mas-tocytosis have been shown to have mainly severe or even fatal sting reactions in several case studies. (63, 64)
A strong relationship between reaction severity to insect venoms and elevated baseline serum tryptase (bsT) levels have been shown. The bsT level is thought to reflect the mast cell number and activity, considering that tryptase mainly is produced by mast cells. (65) Additionally, elevated bsT levels in patients without diagnosed mastocytosis have been shown to be associated with severe systemic sting reactions. (66)
1.5 aiM anD outlinE of thESiS
This thesis aims at investigating and exploring the multifactorial nature of the severity of systemic anaphylactic and allergic reactions from different perspectives. In this thesis we will explore a new possible biomarker, identify independent risk factors for the severity of systemic allergic and anaphylactic reactions and investigate the genetics of food allergy.

GENERAL INTRODUCTION 19
1Special attention will be given to examine the relationship between the eliciting dose and the severity of reaction in food allergy.
In the first part of this thesis, we will address the severity of systemic allergic reactions to foods in a pediatric population. In Chapter 2, we will look at a potential challenge in di-agnosing food allergy when using the gold standard double-blind, placebo controlled oral food challenge (DBPCFC). This chapter examines whether the DBPCFC, with a 30 minute interval between doses, is safe in patients reporting longer time-intervals between inges-tion of the suspected food and the subsequent reaction. Independent factors relevant for the prediction of the severity of food allergic reactions and the relationship between the eliciting dose and severity of reaction will be addressed in Chapter 3. This chapter also examines the influence of using different scoring systems and the impact this can have on predicting the severity outcome. In Chapter 4 we investigate whether patients receiving a high fat matrix in DBPCFCs with peanut have differences in the severity of reaction or eliciting dose, compared to when a low-fat matrix is used. The differences in frequency of clinical reactivity and severity of reaction between peanut and tree nuts is presented in Chapter 5. In Chapter 6 we will investigate the association between a new possible bio-marker, apolipoprotein B-100, and the severity of food allergic systemic reactions. Chapter 7 examines a candidate gene for the presence and severity of food allergy, by investigating STAT6 gene variants in children with food allergy diagnosed by DBPCFCs.
In the second part of this thesis we will investigate the severity of systemic allergic reac-tions to yellow jacket stings in adults. In Chapter 8 we evaluate independent clinical risk factors for the severity of systemic allergic reactions to yellow jacket stings and quantify how much of these reactions may be predicted by the identified factors.
Finally, a summary of the main results of this thesis, general discussion and future per-spectives are provided in Chapter 9.

20 CHAPTER 1
REfERENCES
1. Johansson SG, Hourihane JO, Bousquet J, Bruijnzeel-Koomen C, Dreborg S, Haahtela T et al. A revised nomenclature for allergy. An EAACI position statement from the EAACI nomenclature task force. Allergy. 2001;56:813-24.
2. Savage J, Sicherer S, Wood R. The Natural History of Food Allergy. J Allergy Clin Immunol Pract. 2016;4:196-203; quiz 204. doi: 10.1016/j.jaip.2015.11.024.
3. de Monchy JG, Demoly P, Akdis CA, Cardona V, Papadopoulos NG, Schmid-Grendelmeier P, Gayraud J. Allergology in Europe, the blueprint. Allergy 2013; 68: 1211–1218.
4. Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C et al. on behalf of the EAACI Food Allergy and Anaphylaxis Guidelines Group. EAACI Food Allergy and Ana-phylaxis Guidelines. Diagnosis and management of food allergy. Allergy 2014; 69: 1008–1025.
5. Simons FE, Frew AJ, Ansotegui IJ, Bochner BS, Golden DB, Finkelman FD et al. Risk assessment in anaphylaxis: current and future approaches. J Allergy Clin Immunol. 2007;120:S2-24.
6. Jahn-Schmid B, Radakovics A, Lüttkopf D, Scheurer S, Vieths S, Ebner C, et al. Bet v 1142-156 is the dominant T-cell epitope of the major birch pollen allergen and important for cross-reactivity with Bet v 1-related food allergens. J Allergy Clin Immunol. 2005;116:213-9.
7. Worm M, Edenharter G, Rueff F, Scherer K, Pfohler C, Mahler V et al. Symptom profile and risk factors of anaphylaxis in Central Europe. Allergy 2012;67:691–698.
8. Panesar SS, Javad S, De Silva D, Nwaru BI, Hickstein L, Muraro A et al. The epidemiology of anaphy-laxis in Europe: a systematic review. Allergy 2013;68:1353–1361.
9. Sampson HA, Muñoz-Furlong A, Campbell RL, Adkinson NF Jr, Bock SA, Branum A et al. Second symposium on the definition and management of anaphylaxis: summary report--Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol. 2006;117:391-7.
10. Hompes S, Kohli A, Nemat K, Scherer K, Lange L, Rueff F et al. Provoking allergens and treatment of anaphylaxis in children and adolescents – data from the anaphylaxis registry of German-speaking countries. Pediatr Allergy Immunol 2011;22:568–574.
11. Cardona V, Luengo O, Garriga T, Labrador-Horrillo M, Sala-Cunill A, Izquierdo A et al. Co-factor-enhanced food allergy. Allergy 2012;67:1316–1318.
12. Wimazal F, Geissler P, Shnawa P, Sperr WR, Valent P. Severe life-threatening or disabling anaphy-laxis in patients with systemic mastocytosis: a single-center experience. Int Arch Allergy Immunol 2012;157:399–405.
13. Muraro A, Roberts G, Worm M, Bilo MB, Brockow K, Fernandez Rivas M et al. Anaphylaxis: guide-lines from the European Academy of Allergy and Clinical Immunology. Allergy 2014; 69: 1026–1045.
14. Boyce JA, Assa’ad A, Burks AW, Jones SM, Sampson HA, Wood RA et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010;126:S1-58. doi: 10.1016/j.jaci.2010.10.007.
15. Niggemann B, Sielaff B, Beyer K, Binder C, Wahn U. Outcome of double-blind, placebo controlled food challenge tests in 107 children with atopic dermatitis. Clin Exp Allergy 1999;29:91–96.
16. Breuer K, Heratizadeh A, Wulf A, Baumann U, Constien A, Tetau D et al. Late eczematous reactions to food in children with atopic dermatitis. Clin Exp Allergy 2004;34:817–824. 10.

GENERAL INTRODUCTION 21
1 17. Sampson HA. Food allergy–accurately identifying clinical reactivity. Allergy 2005;60:19–24.
18. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C, Hourihane J et al. Standard-ization of food challenges in patients with immediate reactions to foods--position paper from the European Academy of Allergology and Clinical Immunology. Allergy. 2004;59:690-7.
19. Muraro A, Werfel T, Hoffmann-Sommergruber K, Roberts G, Beyer K, Bindslev-Jensen C et al. EAACI Food Allergy and Anaphylaxis Guidelines. Diagnosis and management of food allergy. Allergy 2014; 69: 1008–1025.
20. Calvani M, Cardinale F, Martelli A, Muraro A, Pucci N, Savino F et al. Risk factors for severe pediatric food anaphylaxis in Italy. Pediatr Allergy Immunol 2011;22:813–819.
21. Gonzalez-Perez A, Aponte Z, Vidaurre CF, Rodriguez LAG. Anaphylaxis epidemiology in patients with and patients without asthma: a United Kingdom database review. J Allergy Clin Immunol 2010;125:1098–1104.
22. Glaumann S, Nopp A, Johansson SG, Borres MP, Nilsson C. Oral peanut challenge identifies an al-lergy but the peanut allergen threshold sensitivity is not reproducible. PLoS One. 2013;8:e53465. doi: 10.1371/journal.pone.0053465.
23. Wainstein BK, Studdert J, Ziegler M, Ziegler JB. Prediction of anaphylaxis during peanut food chal-lenge: usefulness of the peanut skin prick test (SPT) and specific IgE level. Pediatr Allergy Immunol. 2010 Jun;21:603-11. doi: 10.1111/j.1399-3038.2010.01063.x.
24. van Erp FC, Knulst AC, Kentie PA, Pasmans SG, van der Ent CK, Meijer Y. Can we predict severe reactions during peanut challenges in children? Pediatr Allergy Immunol. 2013;24:596-602. doi: 10.1111/pai.12107.
25. Taylor SL, Moneret-Vautrin DA, Crevel RW, Sheffield D, Morisset M, Dumont P et al. Threshold dose for peanut: risk characterization based upon diagnostic oral challenge of a series of 286 peanut-allergic individuals. Food Chem Toxicol 2010;48:814–819.
26. Blumchen K, Beder A, Beschorner J, Ahrens F, Gruebl A, Hamelmann E et al. Modified oral food challenge used with sensitization biomarkers provides more real-life clinical thresholds for peanut allergy. J Allergy Clin Immunol 2014;134:390–398.
27. Cianferoni A, Garrett JP, Naimi DR, Khullar K, Spergel JM. Predictive values for food challenge-induced severe reactions: development of a simple food challenge score. Isr Med Assoc J. 2012;14:24-8.
28. Song Y, Wang J, Leung N, Wang LX, Lisann L, Sicherer SH et al. Correlations between basophil activa-tion, allergen-specific IgE with outcome and severity of oral food challenges. Ann Allergy Asthma Immunol. 2015;114:319-26. doi: 10.1016/j.anai.2015.01.006.
29. Peeters KA, Koppelman SJ, van Hoffen E, van der Tas CW, den Hartog Jager CF, Penninks AH et al. Does skin prick test reactivity to purified allergens correlate with clinical severity of peanut allergy? Clin Exp Allergy. 2007; 37:108-15.
30. van der Valk JPM, Schreurs MWJ, El Bouch R, Arends NJT, de Jong NW. Mono-sensitisation to peanut component Ara h 6: a case series of five children and literature review. Eur J Pediatr. 2016;175:1227-1234. doi: 10.1007/s00431-016-2733-7.
31. Kukkonen AK, Pelkonen AS, Makinen-Kiljunen S, Voutilainen H, Makela MJ. Ara h 2 and Ara 6 are the best predictors of severe peanut allergy: a double-blind placebo-controlled study. Allergy 2015;70:1239–1245.

22 CHAPTER 1
32. Vereda A, van Hage M, Ahlstedt S, Ibanez MD, Cuesta-Herranz J, van Odijk J et al. Peanut allergy: clinical and immunologic differences among patients from 3 different geographic regions. J Allergy Clin Immunol 2011;127:603–607.
33. Turner PJ, Baumert JL, Beyer K, Boyle RJ, Chan C-H, Clark AT et al. Can we identify patients at risk of life-threatening allergic reactions to food? Allergy 2016;71:1241-55 DOI: 10.1111/all.12924.
34. Biló BM, Rueff F, Mosbech H, Bonifazi F, Oude-Elberink JN; EAACI Interest Group on Insect Venom Hypersensitivity. Diagnosis of Hymenoptera venom allergy. Allergy. 2005;60:1339-49.
35. King TP, Spangfort MD. Structure and biology of stinging insect venom allergens. Int Arch Allergy Immunol 2000; 123:99-106.
36. Hoffman DR, Jacobson RS. Allergens in Hymenoptera venom XII: How much protein is in a sting? Ann Allergy 1984;52:276-278.
37. King TP, Kochoumian L, Joslyn A. Wasp venom proteins: phospholipase A1 and B. Arch Biochem Biophys 1984;230:1-12.
38. Watemberg N, Weizman Z, Shahak E, Aviram M, Maor E. Fatal multiple organ failure following mas-sive hornet stings. J Toxicol Clin Toxicol 1995;33:471-4.
39. Sakhuja V, Bhalla A, Pereira BJ, Kapoor MM, Bhusnurmath SR, Chugh KS. Acute renal failure follow-ing multiple hornet stings. Nephron 1988;49:319-21.
40. Kolecki P. Delayed toxic reaction following massive bee envenomation. Ann Emerg Med 1999; 33:114-6.
41. Hoffman DR, Jacobson RS. Allergens in Hymenoptera venom XII: How much protein is in a sting? Ann Allergy 1984;52:276-278.
42. Hoffman DR. Allergens in Hymenoptera venom. XXV: The amino acid sequences of antigen 5 mol-ecules and the structural basis of antigenic cross-reactivity. J Allergy Clin Immunol 1993; 92:707-16.
43. King TP, Lu G, Gonzales M, Qian N, Soldatova L. Yellow jacket venom allergens, hyaluronidase and phospholipase. Sequence similarity and antigenic cross-reactivity with hornet and wasp homologs and possible implications for clinical allergy. J Allergy Clin Immunol 1996;98:588-600.
44. Fricker M, Helbling A, Schwartz L, Müller U. Hymenoptera sting anaphylaxis and urticaria pigmen-tosa: clinical findings and results of venom immunotherapy in ten patients. J Allergy Clin Immunol 1997;100:11-5.
45. Mueller HL. Diagnosis and treatment of insect sensitivity. J Asthma Res 1966;3 :331-333.
46. Müller UR. Insect Sting Allergy 1990. Gustav Fischer, Stuttgart.
47. Antonicelli A, Bilò MB, Bonifazi F. Epidemiology of Hymenoptera allergy. Curr Opin Allergy Clin Im-munol 2002;2:1-6.
48. Mosbech H. Death caused by wasp and bee stings in Denmark 1960-1980. Allergy 1983;38:195-200.
49. Sasvari T, Müller U. Fatalities from insect stings in Switzerland 1978 to 1987. Schweiz Med Wochen-schr. 1994;124:1887-94.
50. Fernandez J, Soriano V, Mayorga L, Mayor M. Natural history of Hymenoptera venom allergy in Eastern Spain. Clin Exp Allergy. 2005;35:179-85.
51. Brown S, Wiese M, Blackman K, Heddle R. Ant venom immunotherapy: A double blind, placebo-controlled cross-over trial. Lancet 2003;361: 1001-1006.

GENERAL INTRODUCTION 23
1 52. Pucci S, Antonicelli L, Bilò MB, Garritani MS, Bonifazi F. The short interval between two stings as a risk factor for developing hymenoptera venom allergy. Allergy 1994;49:894-6.
53. Bousquet J, Menardo JL, Aznar R, Robinet-Levy M, Francois-Bernard M. Clinical and immunologic survey in beekeepers in relation to their sensitization. J Allergy Clin Immunol. 1984;73:332-40.
54. de la Torre-Morin F, Garcia-Robaina JC, Vazquez-Moncholi C, Fierro J, Bonnet-Moreno C. Epidemiol-ogy of allergic reactions in beekeepers: a lower prevalence in subjects with more than 5 years exposure. Allergol Immunopathol (Madr) 1995; 23:127-32.
55. Schuberth KC, Lichtenstein LM, Kagey-Sobotka A, Szklo M, Kwiterovich KA, Valentine MD. Epidemio-logic study of insect allergy in children. II. Effect of accidental stings in allergic children. J Pediatr 1983;102:361-5.
56. Engel T, Heinig JH, Weeke ER. Prognosis of patients reacting with urticaria to insect sting. Results of an in-hospital sting challenge. Allergy 1988;43:289-93.
57. Reisman RE. Natural history of insect sting allergy: relationship of severity of symptoms of initial sting anaphylaxis to re-sting reactions. J Allergy Clin Immunol 1992;90:335-9.
58. Chipps BE, Valentine MD, Kagey-Sobotka A, Schuberth KC, Lichtenstein LM. Diagnosis and treat-ment of anaphylactic reactions to Hymenoptera stings in children. J Pediatr 1980;97:177-84.
59. Lockey RF, Turkeltaub PC, Baird-Warren IA, Olive CA, Olive ES, Peppe BC, Bukantz SC. The Hyme-noptera venom study I, 1979-1982: demographics and history-sting data. J Allergy Clin Immunol 1988;82:370-81.
60. Lantner R, Reisman RE. Clinical and immunologic features and subsequent course of patients with severe insect-sting anaphylaxis. J Allergy Clin Immunol. 1989;84:900-6.
61. Stoevesandt J, Hosp C, Kerstan A, Trautmann A. Hymenoptera venom immunotherapy while maintaining cardiovascular medication: safe and effective. Ann Allergy Asthma Immunol. 2015 May;114(5):411-6. doi: 10.1016/j.anai.2015.03.001.
62. Horny HP, Sotlar K, Valent P. Mastocytosis: state of the art. Pathobiology 2007;74:121-32.
63. Oude Elberink JN, de Monchy JG, Kors JW, van Doormaal JJ, Dubois AE. Fatal anaphylaxis after a yellow jacket sting, despite venom immunotherapy, in two patients with mastocytosis. J Allergy Clin Immunol. 1997;99:153-4.
64. Biedermann T, Ruëff F, Sander CA, Przybilla B. Mastocytosis associated with severe wasp sting anaphylaxis detected by elevated serum mast cell tryptase levels. Br J Dermatol 1999;14:1110-2.
65. Schwartz LB. Clinical utility of tryptase levels in systemic mastocytosis and associated hematologic disorders. Leuk Res 2001;25:553-62.
66. Haeberli G, Bronnimann M, Hunziker T, Müller U. Elevated basal serum tryptase and hymenoptera venom allergy: relation to severity of sting reactions and to safety and efficacy of venom immuno-therapy. Clin Exp Allergy 2003;33:1216-20.


CHAPTER 2
Is 30 mINUTEs bETwEEN DOsEs LONG ENOUGh IN ORAL fOOD ChALLENGEs?
M. Eleonore PetterssonBertine MJ. Flokstra- de BlokSicco van der HeideJeanet KuklerAnthony EJ. Dubois
Published in Pediatric Allergy and Immunology 2014;25:600–619.

26 CHAPTER 2
ABSTRACT
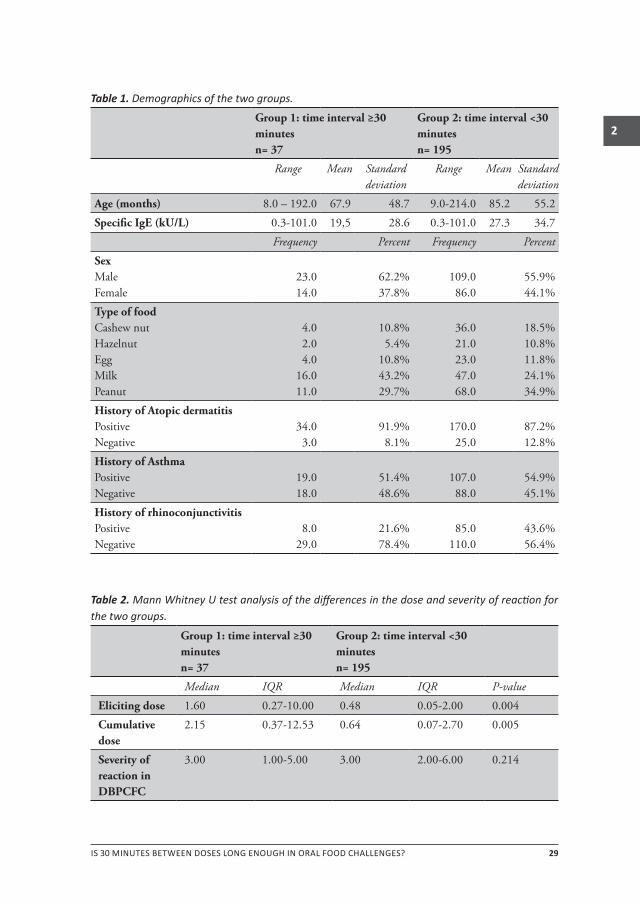
It is currently unknown whether the interval between doses in the double-blind, placebo-controlled food challenge (DBPCFC) is long enough to avoid accumulation of doses and the occurrence of potentially more severe reactions. The objective of this study was to investigate if patients who report longer time intervals (≥30 minutes) between ingestion of the allergen and the subsequent reaction, react to higher doses and have more severe reactions in the DBPCFC than patients with more rapid reactions (<30 minutes). The re-sults of this study showed that patients reporting longer time intervals between ingestion and reaction had a higher dose in the DBPCFC than those reporting more rapid reactions. (Eliciting dose: U=2531.5, P=0.004 Cumulative dose: U=2561.5, P=0.005) However, they did not experience more severe reactions (U=3149.0, P=0.214). An interval of 30 minutes between doses is thus long enough to allow for the DBPCFC to be performed safely in all patients, including those who may react to accumulated doses.

IS 30 MINUTES BETWEEN DOSES LONG ENOUGH IN ORAL FOOD CHALLENGES? 27
2
intRoDuction
To the Editor,
In clinical practice, the double-blind, placebo-controlled food challenge (DBPCFC) is consid-ered the gold standard for diagnosing food allergy (1). This test is performed with gradual increases in the dose of the culprit food at regular time intervals to reduce the adverse events. When performing the DBPCFC, an interval of 30 minutes is often used between the doses(1,2). However, it is currently unknown whether this interval is long enough to avoid reactions to accumulated doses, which might be more severe than reactions to individual doses.
The objective of this study was to investigate if an accumulation of doses in the DBPCFC occurs in patients who report longer time intervals (≥30 min) between ingestion of the culprit food and the subsequent reaction, as these patients could receive a subsequent dose before having reacted to the previous dose. This was done by dividing patients into two groups based on reaction time and comparing the eliciting dose (ED) and the cumula-tive dose (CD) as well as the severity of the challenge reaction, corrected for confounders for these outcomes. As patients with longer reaction times by history (≥30 min) might be expected to accumulate doses during challenge testing, they could have higher EDs and CDs as well as more severe reactions than those with shorter reaction times (<30 min).
METhOdS
A database analysis of positive DBPCFCs (2002–2011), performed at University Medical Center Groningen was carried out. Children were challenged as a part of routine care for sus-pected food allergy. Unstable comorbidity or unwillingness to undergo the test were the only reasons to forego challenge testing, which was the case in <2% of the individuals. No children were excluded because of a history of previous anaphylaxis. Challenges were excluded from the present analysis when multiple food challenges to the same food were performed; in which case only the first challenge to each food was included (90 cases excluded). Patients were also excluded when there was no medical history for the tested food (103 cases) or if there was incomplete data for the relevant variables (92 cases). The exclusion of patients with only subjective symptoms in the DBPCFC (28 cases) had no influence on the outcome.
Results from the five most commonly challenged foods were used for the analysis: milk, egg, peanut, hazelnut, and cashew nut. The DBPCFCs were performed according to previ-ously published procedures and protocols (2, 3). In brief, a food matrix was used to mask the suspected allergenic food. Administration of placebo and allergenic food using an

28 CHAPTER 2
incremental, ‘semi-logarithmic’ scale occurred on separate days, at least a week apart, in random order. Double blinding was maintained until 48 h after the second test day. A food challenge was considered positive when objective symptoms occurred on the allergenic food-test day but not on the placebo day (2–5).
A scoring system was used to determine the severity of the allergic reaction during the oral challenge test6. The patients’ symptoms were allocated to different categories and received a corresponding score. The categories used and their score were the following: skin (1), upper airways (3), lower airways (3), gastrointestinal (2) and cardiovascular/neurological symptoms (3). The scores of each category were summed and expressed as a severity index. The severity index ranges from 0–12 and is divided into groups. Scores from 0–2 are considered mild reactions. A score of 3–6 is regarded as a moderate reaction. The third group with scores of 7–12 is classified as severe reactions.
The statistical analysis of the data was performed using the statistics software package SPSS Statistics 17.0 for Windows. Reaction severity, ED, and CD were compared in patients with long (≥30 min) and short (<30 min) reaction times by history using the Mann–Whit-ney U-test. Possible confounders to the analysis were pre-selected through Spearman’s correlation test and multiple linear regression analysis by adopting a liberal p-value cut off (>0.2). Confounders reported in other studies were also included as well as biologi-cally plausible confounders and general demographics (age, sex). Subsequently, multiple linear regression analysis was used to assess any confounding by evaluating whether the coefficient of the association between reaction time and the outcomes changed by >10% by adding a possible confounder to the basic model. Factors tested and excluded as con-founders in the analysis were sex, age, type of allergenic food, history of asthma, history of atopic dermatitis, history of rhinoconjunctivitis, specific IgE level, and severity of the reaction following accidental ingestion by history.
RESultS
Two hundred and thirty-two cases were used for the final analysis. The age of the children ranged from 0.7 to 17.8 years, with a median of 5.8 years. Of the children, 56.9% were male and 43.1% were female. The DBPCFC were performed with peanut (34.1%), milk (27.2%), cashew nut (17.2%), egg (11.6%), and hazelnut (9.9%). For further demographics see Table 1. Patients reporting longer time intervals between ingestion and reaction (≥30 min) had a higher ED and CD in the DBPCFC than those reporting shorter time intervals between ingestion and reaction (<30 min) (Table 2). However, these patients did not have more severe reactions during the DBPCFC.
IS 30 MINUTES BETWEEN DOSES LONG ENOUGH IN ORAL FOOD CHALLENGES? 29
2
Table 1. Demographics of the two groups.
Group 1: time interval ≥30 minutesn= 37
Group 2: time interval <30 minutesn= 195
Range Mean Standard deviation
Range Mean Standard deviation
Age (months) 8.0–192.0 67.9 48.7 9.0-214.0 85.2 55.2
Specific IgE (kU/L) 0.3-101.0 19,5 28.6 0.3-101.0 27.3 34.7
Frequency Percent Frequency Percent
SexMale Female
23.014.0
62.2%37.8%
109.086.0
55.9%44.1%
Type of foodCashew nutHazelnut EggMilkPeanut
4.02.04.016.011.0
10.8%5.4%10.8%43.2%29.7%
36.021.023.047.068.0
18.5%10.8%11.8%24.1%34.9%
History of Atopic dermatitisPositive Negative
34.03.0
91.9%8.1%
170.025.0
87.2%12.8%
History of AsthmaPositive Negative
19.018.0
51.4%48.6%
107.088.0
54.9%45.1%
History of rhinoconjunctivitisPositive Negative
8.029.0
21.6%78.4%
85.0110.0
43.6%56.4%
Table 2. Mann Whitney U test analysis of the differences in the dose and severity of reaction for the two groups.
Group 1: time interval ≥30 minutesn= 37
Group 2: time interval <30 minutesn= 195
Median IQR Median IQR P-value
Eliciting dose 1.60 0.27-10.00 0.48 0.05-2.00 0.004
Cumulative dose
2.15 0.37-12.53 0.64 0.07-2.70 0.005
Severity of reaction in DBPCFC
3.00 1.00-5.00 3.00 2.00-6.00 0.214

30 CHAPTER 2
concluSion
This study has for the first time shown that patients reporting longer time intervals be-tween ingestion and allergic reaction by history (≥30 min) have higher EDs and CDs in DBPCFC compared with those with shorter time intervals (<30 min), which suggests that these patients do indeed accumulate doses in challenge procedures utilizing 30 minute intervals between dose increments. However, this did not result in more severe reactions during the DBPCFC in these patients. These results were not influenced by the possible confounding variables mentioned earlier. Thus, although some patients may accumulate and react to more than one dose of allergenic food, a dosing interval of 30 minutes is long enough to allow this test to be conducted safely in these patients.

IS 30 MINUTES BETWEEN DOSES LONG ENOUGH IN ORAL FOOD CHALLENGES? 31
2
REfERENCES
1. Sampson HA, Gerth van Wijk R, Bindslev-Jensen C, Sicherer S, Teuber SS, Burks AW et al. Standard-izing double-blind, placebo-controlled oral food challenges: American Academy of Allergy, Asthma & Immunology–European Academy of Allergy and Clinical Immunology PRACTALL consensus report. J Allergy ClinImmunol 2012: 130: 1260–74.
2. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C, Hourihane J et al. Standard-ization of food challenges in patients with immediate reactions to foods–position paper from the European Academy of Allergology and Clinical Immunology. Allergy 2004: 59: 690–7.
3. Vlieg-Boerstra BJ, Bijleveld CM, van der Heide S, Beusekamp BJ, Wolt-Plompen SA, Kukler J et al. Development and validation of challenge materials for double-blind, placebo-controlled food chal-lenges in children. J Allergy ClinImmunol 2004: 113: 341–6.
4. Vlieg-Boerstra BJ, van der Heide S, Bijleveld CM, Kukler J, Duiverman EJ, Dubois AE. Placebo reac-tions in double-blind, placebocontrolled food challenges in children. Allergy 2007: 62: 905–12.
5. Taylor SL, Hefle SL, Bindslev-Jensen C, Atkins FM, Andre C, Bruijnzeel-Koomen C et al. A consensus protocol for the determination of the threshold doses for allergenic foods: how much is too much? Clin Exp Allergy 2004: 34: 689–95.
6. van der Zee T, Dubois A, Kerkhof M, van der Heide S, Vlieg-Boerstra B. The eliciting dose of peanut in double-blind, placebocontrolled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy ClinImmunol 2011: 128: 1031–6.


CHAPTER 3
PREDICTION Of ThE sEvERITy Of ALLERGIC REACTIONs TO fOODs
M. Eleonore PetterssonGerard H. KoppelmanBertine MJ. Flokstra-de BlokBoudewijn J. KollenAnthony EJ. Dubois
Accepted – Allergy 2018

34 CHAPTER 3
ABSTRACT
Background: There is currently considerable uncertainty regarding what the predictors of the severity of diagnostic or accidental food allergic reactions are, and to what extent the severity of such reactions can be predicted.
Objective: To identify predictors for the severity of diagnostic and accidental food allergic reactions and to quantify their impact.
Methods: The study population consisted of children with a double-blind, placebo-con-trolled food challenge (DBPCFC) confirmed food allergy to milk, egg, peanut, cashew nut and/or hazelnut. The data was analyzed using multiple linear regression analysis. Missing values were imputed using multiple imputation techniques. Two scoring systems were used to determine the severity of the reactions.
Results: 734 children were included. Independent predictors for the severity of the DBP-CFC reaction were: age (B=0.04, p=0.001), skin prick test ratio (B=0.30, p<0.001), eliciting dose (B=-0.09, p<0.001), level of specific immunoglobulin E (B=0.15, p<0.001), reaction time during the DBPCFC (B=-0.01, p=0.004), and severity of accidental reaction (B=0.08, p=0.015). The total explained variance of this model was 23.5%, and the eliciting dose only contributed 4.4% to the model. Independent predictors for more severe accidental reac-tions with an explained variance of 7.3% were: age (B=0.03, p=0.014), milk as causative food (B=0.77, p<0.001), cashew as causative food (B=0.54, p<0.001), history of atopic dermatitis (B=-0.47, p=0.006), and severity of DBPCFC reaction (B=0.12, p=0.003).
Conclusions: The severity of DBPCFCs and accidental reactions to food remain largely unpredictable. Clinicians should not use the eliciting dose obtained from a graded food challenge for the purposes of making risk-related management decisions.
clinical implications
Clinicians should not assess a patient’s risk of experiencing severe reactions from the eliciting dose obtained from graded food challenges, since eliciting dose only contributes marginally to reaction severity.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 35
3
intRoDuction
Food allergic exposures vary from mild localized reactions to life-threatening anaphylaxis.(1) According to current estimates, approximately 3.1% of all children will experience a severe food allergic reaction.(2) Prediction of the severity of allergic reactions to food is a key issue for medical professionals, patients, policy makers and the food industry to be able to accurately target treatment and improve management and prevention strategies. Thus, efforts have been made to examine possible predictors of severe and/or life-threatening reactions, and recently a review has been published by Turner et al.(3) on this topic. How-ever, the previous studies used for this review have not quantified the contribution of the predictors to reaction severity and have not established them as statistically independent of one another in this regard. In addition, several studies show conflicting results,(4-15) and thus, much uncertainty still remains about the relationship between potential risk factors and the severity of reactions.
Dose has been considered to be an important factor in the development of severe re-actions,(16) although the evidence for this is scant and contradictory. A prior study has suggested that severe reactions during oral food challenges (OFC) tend to occur more frequently with increasing dose levels.(15) Moreover, in a study where the food challenge procedure was allowed to continue after initial mild symptoms, many subjects progressed to anaphylaxis with increasing dose levels.(17) In contrast, Rolinck-Werninghaus et al.(4) concluded that severe reactions may occur at any dose during oral food challenges. Ad-ditionally, patients with prior anaphylaxis to peanut do not seem to have a lower threshold dose than patients with milder reactions.(14,18,19)
It is currently unknown to what extent the severity of food allergic reactions may be predicted by a combined number of readily available clinical factors, such as age, gender, type of allergenic food, level of specific IgE (sIgE), eliciting dose (ED), previous reactions and comorbid atopic disease. Furthermore, it remains uncertain whether more severe reactions tend to occur at higher doses and whether limiting exposure would thus pref-erentially impact severe reactions accordingly. This study aimed at identifying clinically available factors predictive of the severity of reactions in DBPCFCs as well as for the most severe accidental reaction by history. Particular attention was paid to the extent to which the eliciting dose explains the severity of reactions during DBPCFCs.

36 CHAPTER 3
METhOdS
Study population
Data of all positive DBPCFCs in children (2002-2017) was extracted from the Food Chal-lenge Unit Database of our tertiary care pediatric allergy department at Beatrix Children’s Hospital, University Medical Center Groningen (UMCG). The study population consisted of children referred to our center because of suspected food allergy. No children were excluded due to a history of previous anaphylactic reactions. The medical ethics commit-tee of the UMCG deemed that formal medical ethical approval was not required for this study, since all procedures were performed as part of routine clinical care. Extraction of the data on study patients from the food challenge unit database was completed using the following inclusion criterion: a positive DBPCFC on the verum test day according to protocol. (20,21) Additionally, to allow for sufficient power for the food-specific analysis, only challenges conducted with the five most commonly challenged foods were extracted (cow’s milk, hen’s egg, peanut, hazelnut and cashew nut). In children with multiple food challenges, only the first challenge for each food was included.
Double-blind, placebo-controlled oral food challenges
The food challenges were double-blind and placebo-controlled with the suspected food and placebo administered on separate days. The food challenges were conducted accord-ing to previously published methods and protocols. (20-23) In brief, the suspected aller-genic food or placebo was hidden in a food matrix capable of masking sensory detection. (20) The dose of the allergenic food was determined using an incremental scale, specific for the food tested. The doses were given at 30 minute intervals, the dose steps used are displayed in table 1. The food challenge was considered to be positive when objective or repeated or persistent subjective allergic symptoms occurred during the verum test day but not on the placebo day. If symptoms occurring on the verum day were significantly more severe than the symptoms on the placebo day, the food challenge was deemed positive. Unblinding of the test occurred 48 hours after the second food challenge day. Information on the nature and frequency of previous food allergic reactions was obtained in addition to the general atopic history prior to the DBPCFC.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 37
3
Table 1. Dose schemes used during the DBPCFCs.
UMCG (milk, egg), mg protein
UMCG (Peanut, tree nuts), mg protein
PRACTALL, mg protein
Dose 1 1.75mg 1.75mg 1.0mg
Dose 2 3.50mg 3.50mg 3.0mg
Dose 3 14 mg 14 mg 10mg
Dose 4 70mg 70mg 30mg
Dose 5 350mg 130mg 100mg
Dose 6 1750mg 350mg 300mg
Dose7 - - 1000mg
Total 2190 mg 570 mg 1444 mg
Scoring system for the severity of reaction
A scoring system from Astier et al (24) ranging from 0-5, was used for determining the severity of reaction. The symptoms occurring during the verum day of the DBPCFC and of the most severe accidental reaction by history were used to score the severity. Patients were classified according to their most severe symptom and received the correspond-ing grade. Mild symptoms occurring at home after leaving the hospital after 2 hours of symptom-free observation after the DBPCFC on the verum day, were placed in severity grade 0. Children never having consumed the allergic food, and thus never having had an accidental reaction to the food were placed in the severity grade 0 for the accidental reaction. Since there is currently no clear consensus on the use of scoring systems for the severity of allergic reactions, an additional scoring system (25) ranging from 0-12 was used to compare the severity of allergic reactions during the food challenge and the severity of the most severe accidental reaction by history.
Measurement of food-specific igE levels
Serum samples were collected as part of the routine clinical workup for food allergy and were drawn within 6 months of the DBPCFC. The ImmunoCAP system (Thermo Fisher Scientific Inc., Phadia AB, Uppsala, Sweden) was used for determining the level of sIgE. The test was considered positive when a sIgE level of 0.35 kU/L or more was confirmed. Values of >100 kU/L received a designated value of 101 kU/L.
Skin prick tests
Skin prick tests (SPT) were performed with a sterile lancet (ALK-Abelló, Horsholm, Den-mark.) and food allergen extracts (ALK-Abelló, Horsholm, Denmark.) The size of the SPT response was calculated as a mean of the longest diameter and its perpendicular longest diameter measured at 15 minutes. In order to control for possible inter-technician vari-

38 CHAPTER 3
ability, the ratio of the size of the tested food wheal to the size of the histamine wheal was reported. Any differences in wheal size caused by the device or technician should be similar and thus minimally affect the reported ratio (26).
Statistical analysis
The statistical analysis was performed using the statistics software package IBM SPSS Statistics for Windows, version 23.0. (IBM Corp., Armonk, NY). Multiple linear regression analysis was used to study the relationship between the determinants and the severity of reactions during the DBPCFC as well as those following accidental ingestion. The stepwise backward selection method was used for constructing the prediction model. Alpha was set at 0.05. Only significant factors in the model were considered to be predictors. All assumptions of the tests were met. The determinants were pre-selected for inclusion in the analysis according to previously reported data as well as factors hypothesized to be of influence on the severity of the outcome by the authors. Dummy variables were created for the categorical variable “Type of food” with hazelnut as reference for the regression analysis. Cumulative dose (CD), ED and the level of sIgE were logarithmically transformed before being entered into the analysis in order to comply with the assumptions required for conducting linear regression.
To reduce the probability of bias that might result from excluding missing cases and performing a complete case analysis, missing data was randomly imputed using multiple imputation. A missing value analysis was performed to rule out missing not at random (MNAR) for the included variables. The missing cases for the included variables were in the range of 1-20%. The missing data were replaced using a multiple imputation procedure with a conditional specification, predictive mean matching, 20 iterations and 20 data sets. The use of 20 iterations in the multiple imputation, was based on the variable with the highest number of missing cases. The patient characteristics, severity of reaction and al-lergic features were included as predictors for the multiple imputation.
RESultS
Descriptives of study population
The initial data extraction identified 864 positive DBPCFCs. In children with multiple food challenges to the same food, only the first challenge for each type of food was included (130 cases excluded). Thus a total of 734 children with DBPCFC-confirmed food allergy were included in the final analysis. The median age of the children was 6.2 years, with a range of 0.3 to 18.2 years. The study population consisted largely of boys (59.4%). Of the participating children 87.3% had a doctors diagnosis of atopic dermatitis, 49.7% asthma

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 39
3
and 36.6% had previously been diagnosed with allergic rhinoconjunctivitis. The DBPCFCs were performed with peanut (38.7%), cow’s milk (20.4%), cashew nut (17.3%), hen’s egg (12.3%), and hazelnut (11.3%). The level of sIgE ranged from 0.01 to >100.00 kU/L, and was positive in 91.7% of the children. The median reaction time during the DBPCFC was 15.0 minutes, with an IQR of 5.0-50.0.
The interquartile range (IQR) of severity of reaction in the DBPCFC ranged from 1.0-4.0 with a median severity index of 3.0 using the scoring system by Astier et al. Additional demographics categorized according to the severity of the DBPCFC reaction are shown in table 2. The IQR of the severity of the previous accidental reaction by history ranged from 1.0-4.0 and had a median severity index of 3.0. The time interval between accidental ingestion of allergen and allergic reaction by history ranged from 0-2880 minutes in all children, with an IQR of 1.0-15.0 and a median of 5.0 minutes.
Both the CD and the ED were initially included in the analysis. However, these factors showed colinearity during multivariate analysis, thus the CD was excluded from the multi-variate analysis on the basis of the lower explained variance of the model in comparison to the model including the ED (data not shown).
Severity of reaction during DBpcfcs
Using the enter method, a significant model for prediction of the severity of reaction in the DBPCFC emerged (R2 = 0.235, P<0.001). Results from the analyses of the original data and from the pooled data following the multiple imputation procedure can be seen in table 3. After analysis with multiple linear regression, significant independent predictors for the severity of reaction during the DBPCFC were: increasing age (B=0.04, p=0.001), larger SPT ratio (B=0.30, p<0.001), a lower ED (B=-0.09, p<0.001), a higher level of sIgE (B=0.15, p<0.001), a shorter reaction time DBPCFC (B=-0.01, p=0.004), and a more se-vere previous accidental reaction (B=0.08, p=0.015). No significant relationship with the severity of reaction in the DBPCFC was found for gender; type of food; history of atopic dermatitis, asthma or allergic rhinoconjunctivitis; and family history of atopic disease. The total explained variance of this model was 23.5% of the severity of the DBPCFC reaction, and the ED only contributed 4.4% to this explained variance after inclusion in the model (adjusted R2
excluding ED=0.182, adjusted R2including ED=0.226).

40 CHAPTER 3
Tabl
e 2.
Cha
ract
eristi
cs o
f the
stud
y po
pula
tion
acco
rdin
g to
the
seve
rity
grad
e of
the
DBPC
FC re
actio
n.
Grade0
n=78
Gra
de1
n=160
Gra
de 2
n=55
Gra
de 3
n=171
Gra
de 4
n=270
Age
(yea
rs),
med
ian
(IQ
R)(5.78)2.32-11.44
4.76(2
.00-7.63)
6.24(4
.34-9.52)
5.39(3
.16-8.33)
7.99(5
.29-12.12)
Gen
der,
n (%
)
Fem
ale
32(4
1.0)
69(4
3.1)
22(4
0.0)
65(3
8.0)
110(40.7)
Mal
e46(5
9.0)
91(5
6.9)
33(6
0.0)
106(62.0)
160(59.3)
Food
, n (%
)
Cas
hew
nut
7(9.0)
19(1
1.9)
15(2
7.3)
31 (1
8.1)
55(2
0.4)
Cow
’s m
ilk
35(4
4.9)
45 (2
8.1)
7(12.7)
31 (1
8.1)
32(1
1.9)
Haz
elnut
11 (1
4.1)
17(1
0.6)
3 (5
.5)
10(5
.8)
42 (1
5.6)
Hen
’s eg
g3
(3.8
)26
(16.
3)8
(14.
5)36
(21.
1)17(6
.3)
Pean
ut22
(28.
2)53
(33.
1)22(4
0.0)
63 (3
6.8)
124(45.9)
sIgE
(kU
/L),
med
ian
(IQ
R)2.71(0
.30-23.20)
2.99(0
.96-14.08)
8.40(2
.11-40.20)
11.75(2.48-41.80)
12.10(2.83-51.10)
SPT
whe
al r
atio
, med
ian
(IQ
R)1.00(0
.00-1.55)
1.30(0
.90-1.88)
1.30(0
.90-2.00)
1.50
(1.10-2.00)
1.70(1
.30-2.20)
ED (m
g pr
otei
n), m
edia
n (I
QR)
1750.00(350.00-
1750.00)
98.00(3.50-
350.00)
139.20(2
1.00-
580.00)
70.00(14.00-350-
00)
58.00(1.75-
307.93)
CD
(mg
prot
ein)
, med
ian
(IQ
R)2189.25(577.97-
2189.25)
141.
12 (5
.25-
577.97)
226.49(3
0.80-
837.52)
89.25(19.18-
559.58)
83.52(1.75-
433.
68)
Rea
ctio
n ti
me
duri
ng th
e D
BP
CFC
(m
inut
es),
med
ian
(IQ
R)55.00(15.00-
60.00)
25.00(5.50-60.00)
12.50(5.00-
32.50)
20.0(5
.00-45.00)
15.0(5
.0-37.0)
His
tory
of a
sthm
a, n
(%)
Yes
34 (4
3.6)
70(4
3.8)
28(5
0.9)
78(4
5.6)
155(57.4)
No
41 (5
2.6)
89(5
5.6)
24 (4
3.6)
91(5
3.2)
110(40.7)

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 41
3
Tabl
e 2.
Cha
ract
eristi
cs o
f the
stud
y po
pula
tion
acco
rdin
g to
the
seve
rity
grad
e of
the
DBPC
FC re
actio
n. (c
ontin
ued)
Grade0
n=78
Gra
de1
n=160
Gra
de 2
n=55
Gra
de 3
n=171
Gra
de 4
n=270
His
tory
of a
topi
c de
rmat
itis
, n (%
)
Yes
60(7
6.9)
150(93.8)
42(7
6.4)
157(91.8)
232(85.9)
No
17(2
1.8)
9(5.6)
11(2
0.0)
13(7
.6)
36 (1
3.3)
His
tory
of r
hino
conj
unct
ivit
is, n
(%)
Yes
26 (3
3.3)
45 (2
8.1)
14 (2
5.5)
59(3
4.5)
125
(46.
3)
No
49(6
2.8)
110(68.8)
38(6
9.1)
107(62.6)
138
(51.
1)
Seve
rity
of m
ost s
ever
e ac
cide
ntal
re
acti
on, n
(%)
Gra
de 0
10(1
2.8)
34 (2
1.3)
11(2
0.0)
39(2
2.8)
48(1
7.8)
Gra
de 1
11 (1
4.1)
33(2
0.6)
6(10.9)
13(7
.6)
23(8
.50
Gra
de 2
18 (2
3.1)
30(1
8.8)
10(1
8.2)
22(1
2.9)
40(1
4.8)
Gra
de 3
13(1
6.7)
32(2
0.0)
12 (2
1.8)
40(2
3.4)
58 (2
1.5)
Gra
de 4
26 (3
3.3)
31(1
9.4)
16(2
9.1)
57(3
3.3)
101(37.4)
Abb
reviat
ions:
CD, c
umul
ative
dose;
DBP
CFC,
doub
le-bli
nd p
laceb
o con
trolle
d, foo
d cha
lleng
e; E
D, e
liciti
ng do
se; IQ
R, in
terqu
artil
e ran
ge; sI
gE, s
pecifi
c imm
unog
lobul
in E
; SPT
, ski
n pr
ick te
st.

42 CHAPTER 3
Table 3. Independent predictors for the severity of the DBPCFC reaction (Astier).
Predictor Original dataN=544
R2=0.235
Imputed data – pooledN=734
B 95% CI p-value B 95% CI p-value
Age 0.06 0.04to0.09
<.001 0.04 0.02to0.06
.001
SPT 0.33 0.18to0.47
<.001 0.30 0.17to0.43
<.001
ED* -0.07 -0.13to-0.02
.007 -0.09 -0.14to-0.04
<.001
sIgE* 0.17 0.09to0.27
<.001 0.15 0.07to0.24
<.001
Reaction time DBPCFC -0.004 -0.01to0.00
.037 -0.005 -0.01to-0.00
.004
Severity of Accidental reaction
0.10 0.03to0.17
.005 0.08 0.02to0.06
.015
Abbreviations: CI, confidence interval; DBPCFC, double-blind, placebo controlled, food challenge; sIgE, specific im-munoglobulin E; R2, explained variance. *Backtransformed values.
Severity of accidental reactions
A significant model was also found for predicting the severity of reactions following ac-cidental ingestion (R2= 0.073, P<0.001). Results from the analysis of the original data and from the pooled multiple imputation can be seen in table 4. Significant independent pre-dictors for more severe reactions were: increasing age (B=0.03, p=0.014), milk as causative food (B=0.77, p<0.001), cashew as causative food (B=0.54, p<0.001), a negative history of atopic dermatitis (B=-0.47, p=0.006), and a more severe DBPCFC reaction (B=0.12, p=0.003). Thus, children with a history of atopic dermatitis generally had less severe accidental reactions. Having uncontrolled asthma, defined as having daily symptoms; a clinical history of asthma; or allergic rhinoconjunctivitis were not predictive of the severity of the accidental reaction. Moreover, age of onset of food allergy; time interval between ingestion and reaction; and a family history of atopic disease were not predictive of the severity of the accidental reaction (data not shown).

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 43
3
Table 4. Predictors for the severity of the most severe, accidental reaction by history (Astier), dis-playing significant independent factors.
Predictor Original dataN=727
R2=0.073
Imputed data – pooledN=734
B 95% CI p-value B 95% CI p-value
Age 0.03 0.01to0.06
.016 0.03 0.01to0.06
.014
Milk 0.77 0.47to1.06
<.001 0.77 0.48to1.06
<.001
Cashew 0.58 0.29to0.87
<.001 0.54 0.40to0.69
<.001
History of Atopic dermatitis
-0.48 -0.81to-0.15
.005 -0.47 -0.80to-0.14
.006
Severity of DBPCFC reaction
0.12 0.04to0.19
.003 0.12 0.04to0.19
.003
Abbreviations: CI, confidence interval; DBPCFC, double-blind, placebo controlled, food challenge; R2, explained vari-ance.
Sub-group analysis for the severity of reaction per type of food
To examine possible differences between the types of food, the data was analyzed sepa-rately for each type of food, see table 5 and table 6. This analysis showed that there was a large difference in the ability to predict the severity of cow’s milk DBPCFCs compared to peanut DBPCFCs. The severity of cow’s milk DBPCFCs was independently predicted by a higher level of sIgE level, a larger SPT ratio and a family history of atopic dermatitis with an explained variance of 27.0%. In contrast, the model for prediction of the severity of peanut DBPCFC reactions had an explained variance of only 10.9% and was independently predicted by: a history of rhinoconjunctivitis, a shorter reaction time during the DBPCFC, a lower ED, and a higher level of sIgE. A positive family history of asthma (mother) was protective of more severe DBPCFC reactions to peanut.

44 CHAPTER 3
Tabl
e 5.
Pre
dicti
on o
f the
seve
rity
of D
BPCF
C re
actio
n (A
stier
) per
type
of f
ood.
Orig
inal
dat
aIm
pute
d an
alys
is -
pool
ed
Food
Pred
ictor
NB
95%
CI
p-va
lue
NB
95%
CI
p-va
lue
Cas
hew
R2 =0.1
49
Age
125
0.07
0.01to
0.12
.018
127
0.07
0.01to
0.12
.016
Seve
rity
of a
ccid
enta
l rea
ctio
n0.17
0.03to
0.32
.019
0.17
0.03to
0.31
.017
Fam
ily h
istor
y of
asth
ma
(fath
er)
-1.08
-1.71to-0
.45
.001
-1.06
-1.68to-0
.44
.001
Cow
’s m
ilk
R2 =0.2
70
sIgE
*130
0.18
-0.03to0.44
.091
150
0.26
0.04to
0.52
.017
SPT
0.72
0.32to
1.13
.001
0.66
0.25to
1.07
.002
Fam
ily h
istor
y of
ato
pic
derm
atiti
s (m
othe
r)0.47
0.01to
0.93
.045
0.46
0.03to
0.89
.036
Haz
elnu
t
R2 =0.1
95
ED*
77-0.26
-0.45to-0
.09
.002
83-0.30
-0.50to-0
.14
<.001
Fam
ily h
istor
y of
ato
pic
derm
atiti
s (fa
ther
)-0.98
-1.75to-0
.22
.012
-0.98
-1.74to-0
.23
.010
Fam
ily h
istor
y of
asth
ma
(fath
er)
1.03
0.04to
2.02
.041
1.15
0.13to
2.16
.027
Hen
’s Eg
g
R2 =0.1
28
SPT
770.46
0.06to
0.87
.025
900.44
0.07to
0.81
.020
Fam
ily h
istor
y of
food
alle
rgy
(mot
her)
-0.95
-1.86to-0
.05
.040
-0.91
-1.72to-0
.10
.028
Pean
ut
R2 =0.109
Hist
ory
of R
hino
conj
unct
iviti
s23
40.33
0.01to
0.65
.045
284
0.31
0.003to0.62
.048
Reactio
ntim
eDBP
CFC
-0.004
-0.01to0.001
.124
-0.01
-0.01to0.00
.035
ED*
-0.10
-0.20to-0
.02
.021
-0.18
-0.28to-0
.09
<.001
sIgE
*0.19
0.06to
0.33
.004
0.12
0.001to0.26
.048
Fam
ily h
istor
y of
asth
ma
(mot
her)
-0.43
-0.85to-0
.01
.045
-0.41
-0.81to-0
.02
.042
Abb
reviat
ions:
CI, c
onfid
ence
inter
val;
DBP
CFC,
doub
le-bli
nd, p
laceb
o con
trolle
d, foo
d cha
lleng
e; E
D, e
liciti
ng do
se; s
IgE
, spe
cific i
mmun
oglob
ulin
E; R
2 , exp
laine
d var
iance;
SPT
, ski
n pr
ick te
st. *
Back
trans
forme
d va
lues.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 45
3
Tabl
e 6.
Pre
dicti
on o
f the
seve
rity
of a
ccid
enta
l rea
ction
s (As
tier)
per
type
of f
ood.
Orig
inal
dat
aIm
pute
d an
alys
is -
pool
ed
Food
Pred
ictor
NB
95%
CI
p-va
lue
NB
95%
CI
p-va
lue
Cas
hew
Non
e 127
--
--
--
-
Cow
’s m
ilk
R2 =0.0
63
Age
137
0.04
-0.01to0.10
.120
150
0.06
0.01to
0.11
.033
SPT
0.33
0.07to
0.60
.014
0.30
0.03to
0.57
.032
Haz
elnu
tN
one
83-
--
--
--
Hen
’s Eg
gN
one
90-
--
--
--
Pean
ut
R2 =0.0
50
Hist
ory
of R
hino
conj
unct
iviti
s278
-0.42
-0.82to-0
.02
.041
284
-0.43
-0.84to-0
.03
.034
Age
(yea
rs)
0.09
0.04to
0.14
<.001
0.08
0.04to
0.13
<.001
Abb
reviat
ions:
CI, c
onfid
ence
inter
val;
R2 , exp
laine
d va
rianc
e; SP
T, sk
in p
rick
test.

46 CHAPTER 3
The severity of accidental reactions to cow’s milk were predicted by an increasing age and higher ratio of the SPT. A positive history of rhinoconjunctivitis was protective for the severity of accidental reactions to peanut, while increasing age was predictive of more severe reactions. For the accidental reaction, no predictive factors for the severity of reac-tion per type of food could be determined for cashew, hazelnut and hen’s egg.
Sensitivity analysis scoring systems
The analysis was repeated by using the scoring system from van der Zee et al. to com-pare the results with the scoring system from Astier et al. Independent predictors for the severity of the DBPCFC reaction were: a higher SPT ratio (B=0.31, p<0.006), a higher ED (B=0.09, p=0.026), a higher level of sIgE (B=0.31, p<0.001), a more severe accidental reaction (B=0.07, p=0.003), a history of rhinoconjunctivitis (B=0.35, p=0.034) and cashew as causative food (B=0.71, p=0.002). The total explained variance of this model was 10.5%, and the ED only contributed 2.0% to the model.
Independent predictors for the severity of accidental reactions with an explained variance of 5.7% were: increasing age (B=0.06, p=0.041), milk as causative food (B=1.37, p<0.001), cashew as causative food (B=1.41, p<0.001), a lower reaction time for the accidental reac-tion (B=-0.002, p=0.005), and a higher level of sIgE (B=0.32, p=0.004).
DiScuSSion
Prediction of the severity of reactions is important to be able to accurately target the management of food allergic reactions, for example, with the prescription of epinephrine auto-injectors. However, with the risk factors identified in our study we were only able to predict 23.5% of the severity of reactions during DBPCFC and 7.3% of the severity of the most severe accidental reaction by history. Moreover, the results of this study show that the ED only contributes 4.4% to the variance of the severity of DBPCFC reactions, and are in agreement with most of the previously published work on predictive factors for severe reactions. Here we add to those previous results and show to what degree eliciting dose and other factors independently contribute to the severity of DBPCFC reactions.
The result of this study also substantiates the statement by Turner et al.(3) that dose sensitivity and severity of reaction should be considered as different entities in the risk as-sessment of food allergic reactions. Therefore, our findings indicate that clinicians should not make decisions regarding prescription of epinephrine auto-injectors or give advice about the level of stringency of allergen avoidance based on the eliciting dose obtained from graded food challenges, since eliciting dose only contributes marginally to reaction

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 47
3
severity. The ED as obtained from the DBPCFC was not predictive of the severity of the accidental reaction. This shows that, although previous studies have shown that the ED relates to the frequency of accidental reactions(19, 27), it does not have a large impact on the severity of accidental reactions. From a public health perspective, limiting dose exposure is one of the few measures possible in efforts to control severe allergic reactions. However, our results suggest that the impact of dose limitation as a public health measure is unlikely to reduce severe reactions significantly more than milder ones.
The assessment of the severity of the food allergic reaction is a matter of debate. We show that our results are quite consistent when two different scoring systems are used. The dif-ference in these two scoring systems is to be found in the severe end of the range, which is reached more quickly as symptoms increase with the Astier scoring system than with that of van der Zee. Factors related to severity which have a distribution similar to the severity scores generated by one or the other of these scoring systems will give differences in their ability to predict the outcome. This may even give conflicting results within the same data set, as was the case in our study, where a lower ED was seen to predict greater severity using the scoring system of Astier, but a lower severity using that of van der Zee. This underlines the need for analyses using different scoring systems to identify factors which are sensitive to the scoring system used. Conversely, such an approach may also identify factors which are not sensitive to such differences, hence reflecting the robustness of such factors. Our current data showed that higher SPT ratio, a higher level of sIgE and a more severe accidental reaction were in the latter category and thus were independent predic-tors of the severity of challenge reactions for both scoring systems. For the severity of the accidental reaction, independent predictors for both scoring systems were: increasing age, and reactions to milk and cashew.
The severity of cow’s milk DBPCFC reactions could be predicted by the level of sIgE, SPT ratio and a family history of atopic dermatitis with an explained variance of 27.0%. This is higher than for the whole combined group (23.5%) and for the peanut DBPCFC reactions (5.3%). This result suggests that different factors might be more relevant for predicting the severity of reaction for each type of food, including factors which are currently unknown.
Age has previously been examined as a predictor for the severity of reactions. Adolescents and young adults have a higher risk of severe OFC- and accidental reactions than younger children.(28, 29) The results of the current study also confirm increasing age as a predictor for the severity of DBPCFC reactions and for accidental reactions in a pediatric population.
Our data shows no significant difference in the severity of DBPCFC reactions by type of food. This could be due to that the severity of DBPCFC reactions are deliberately kept at a

48 CHAPTER 3
minimum, and thus could show less difference in severity by type of food. Moreover, there is currently very limited data on individual allergen protein concentrations as compared to whole food protein thresholds. It is possible that differences in severity between different types of foods could become more apparent if data on individual allergen protein con-centrations eliciting clinical reactions in sensitized patients were used in the comparison. However, our data also shows that for our population, accidental reactions to cashew and milk are generally more severe than reactions to hazelnut independent of age, sIgE level, and severity of the DBPCFC reaction. These results are partly in agreement with Johnson et al.(30), who have previously reported cashew and peanut anaphylaxis to be more severe than anaphylaxis to hazelnut in a pediatric population. However, in our population accidental reactions to peanut were not more severe than those to hazelnut. A possible explanation for this could be that many of the previously published studies have not cor-rected for other factors, such as age, possibly confounding the relationship between type of food and severity of reaction.
The inverse relationship between the length of the time interval between ingestion of the allergen and the onset of the reaction with the severity of reaction is a phenomenon often thought to be important in clinical practice. In other words, severe reactions tend to occur quickly. Our data thus confirms, for the first time, that more severe DBPCFC reactions tend to be rapid in onset.
The role of the level of sIgE in the severity of reactions is not clear. Various studies have shown that the level of sensitization (sIgE and SPT) and previous severe accidental re-actions are predictive of more severe food challenge reactions.(4, 6, 7, 11, 17, 29, 31, 32) However, other studies present conflicting results.(10, 33) Our results show that the contribution of the level of sIgE and SPT to the severity of reactions is present, but small and therefore, based on our results, as well as previous studies, we conclude that SPT and the level of sIgE is not particularly useful on its own in clinical practice for predicting more severe reactions in individual patients. Therefore the use of absolute values with cut offs would be very unlikely to reveal any useful cut off values for clinical practice.
Our data show that previous more severe accidental reactions are weakly predictive of the severity of oral food challenge reactions and vice versa. Even though this effect is small, and not particularly useful in clinical practice, this suggests that individual patients may have a certain, to date unidentified, intrinsic severity component.
Asthma has been proposed to be a risk factor for severe reactions.(9) However, our re-sults show that asthma is not a significant predictor for the severity of reaction during DBPCFC after correcting for age. Additionally, no relationship between asthma and the

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 49
3
severity of accidental reactions was found. This could be due to that asthma is generally well controlled during the food challenges in our center and that it therefore contributes very little to the severity of reactions. Furthermore, as has been pointed out by others,(3) although asthma is common in patients with fatal or near fatal reactions, the vast majority of asthmatic, food allergic patients will never experience such reactions. Thus, asthma does not seem to independently be a strong predictor for the severity of reactions.
Our data show that more severe reactions during DBPCFCs tend to occur more frequently at lower dose levels using the scoring system by Astier et al. However, this effect was weak and severe reactions were not limited to low doses. The analysis per type of food showed that ED is a predictor for the severity of reaction for peanut and hazelnut, but not for milk, cashew or egg. For the latter three foods the contribution of ED to the severity of reaction could be much smaller than for peanut and hazelnut, and therefore, it is possible that this potential effect was not shown. This is an argument for further studies with larger groups.
The weak association between the eliciting dose and the severity of the DBPCFC reaction has been proposed to be at least partly due to inter-patient variability of the accumulation of doses during the DBPCFC,(34) which could confound the relationship between the elicit-ing dose and the severity of reactions during oral food challenges on the population level. Blumchen et al.(19) have previously shown that most of the study population reacted at a time interval greater than the standard dose interval of 30 minutes in a modified oral food challenge procedure. In this modified oral food challenge, doses were given with a 2-hour interval. This suggests that some patients do indeed accumulate doses during oral food challenges. However, no relationship between the severity of clinical reactions during the OFC with the ED could be shown by Blumchen et al. This is surprising, since the relationship between the ED and the severity of symptoms would be expected to be stronger during the modified OFC, due to the longer dose interval, compared to a standard food challenge procedure. The Blumchen study therefore suggests that the limited effect of the ED on the severity of the DBPCFC reaction in the current study is probably not due to accumulation of doses in some patients.
There are several strengths of this study; firstly, the diagnosis of food allergy was con-firmed by DBPCFCs, and children with a history of previous anaphylaxis were included in the analysis. More importantly, this study gives statistically underpinned evidence for the identified factors, independently of the other determinants. Some of the factors have, for the first time, been shown to be independent predictors for the severity of reactions, and the quantification of these factors is important to be able to allow for an accurate assess-ment of the risk of developing such reactions. Nonetheless, there are some limitations that should be considered in interpretation of the results of this study. Firstly, the gener-

50 CHAPTER 3
alizability of the conclusions needs to be externally validated in other studies using this prediction model in other settings. Because of the protocol used, graded food challenges may influence the ED and severity of reaction, and these parameters may therefore differ from those relevant to single exposures, such as occurs in accidental reactions. Moreover, severe reactions can be halted by prompt treatment and may therefore be more difficult to predict because treatment modifies the outcome independently of severity. It is a reasonable to conclude that this occurs during the food challenge setting, where patients are observed at all times and treated relatively quickly.
In conclusion, the severity of reactions during DBPCFCs and accidental reactions to foods are determined by numerous factors, most of which currently seem to be unknown. Thus, the severity of food allergic reactions remain largely unpredictable. The use of different severity scoring systems may give different or even contradictory results depending on the distribution of the data in a particular population. Sensitivity analysis may reveal the robustness of the conclusions based on the data in this regard. Interestingly, the severity of milk DBPCFC reactions may be predicted to a greater extent than the severity of peanut DBPCFC reactions. Although the severity of DBPCFC reactions are associated with a lower eliciting dose, the small size of this effect suggests that the impact of dose limitation as a public health measure is unlikely to reduce severe reactions more than milder ones. Fi-nally, clinicians should not use the eliciting dose obtained from a graded food challenge for the purposes of making risk-related management decisions such as the need for stringent avoidance of allergenic foods or the prescription of self-injectable epinephrine. Studies us-ing methodology more comparable to real-life situations than the DBPCFC are required to further examine the influence of dose on the severity of reactions. Single dose challenges could be used for examining this relationship in future research.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 51
3
REfERENCES
1. Sampson HA. Anaphylaxis and emergency treatment. Pediatrics 2003; 111:1601–8.
2. Gupta RS, Springston EE, Warrier MR, Smith B, Kumar R, Pongracic J et al. The Prevalence, Severity, and Distribution of Childhood Food Allergy in the United States. Pediatrics 2011;128:e9–e17. doi: 10.1542/peds.2011-0204.
3. Turner PJ, Baumert JL, Beyer K, Boyle RJ, Chan CH, Clark AT et al. Can we identify patients at risk of life-threatening allergic reactions to food? Allergy 2016;71:1241-55. doi: 10.1111/all.12924
4. Rolinck-Werninghaus C, Niggemann B, Grabenhenrich L, Wahn U, Beyer K. Outcome of oral food challenges in children in relation to symptom-eliciting allergen dose and allergen-specific IgE. Al-lergy. 2012; 67:951-7. doi: 10.1111/j.1398-9995.2012.02838.x.
5. Perry TT, Matsui EC, Conover-Walker MK, Wood RA. Risk of oral food challenges. J Allergy Clin Im-munol. 2004; 114:1164-8.
6. Neuman-Sunshine DL, Eckman JA, Keet CA, Matsui EC, Peng RD, Lenehan PJ, Wood RA. The natural history of persistent peanut allergy. Ann Allergy Asthma Immunol. 2012; 108:326-331. doi: 10.1016/j.anai.2011.11.010.
7. Benhamou AH, Zamora SA, Eigenmann PA. Correlation between specific immunoglobulin E levels and the severity of reactions in egg allergic patients. Pediatr Allergy Immunol. 2008;19:173-9. doi: 10.1111/j.1399-3038.2007.00602.x.
8. Sampson HA, Ho DG. Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents. J Allergy Clin Immunol. 1997;100:444-51.
9. Calvani M, Cardinale F, Martelli A, Muraro A, Pucci N, Savino F et al. Risk factors for severe pediatric food anaphylaxis in Italy. Pediatr Allergy Immunol. 2011;22:813-9. doi: 10.1111/j.1399-3038.2011.01200.x.
10. Flinterman AE, Pasmans SG, Hoekstra MO, Meijer Y, van Hoffen E, Knol EF et al. Determination of no-observed-adverse-effect levels and eliciting doses in a representative group of peanut-sensitized children. J Allergy Clin Immunol. 2006 Feb;117(2):448-54.
11. Hourihane JO, Grimshaw KE, Lewis SA, Briggs RA, Trewin JB, King RM et al. Does severity of low-dose, double-blind, placebo-controlled food challenges reflect severity of allergic reactions to peanut in the community? Clin Exp Allergy. 2005;35:1227-33.
12. Sicherer SH, Morrow EH, Sampson HA. Dose-response in double-blind, placebo-controlled oral food challenges in children with atopic dermatitis. J Allergy Clin Immunol. 2000;105:582-6.
13. Santos AF, Du Toit G, Douiri A, Radulovic S, Stephens A, Turcanu V et al. Distinct parameters of the basophil activation test reflect the severity and threshold of allergic reactions to peanut. J Allergy Clin Immunol. 2015;135:179-86. doi: 10.1016/j.jaci.2014.09.001.
14. van Erp FC, Knulst AC, Kentie PA, Pasmans SG, van der Ent CK, Meijer Y. Can we predict severe reactions during peanut challenges in children? Pediatr Allergy Immunol. 2013;24:596-602. doi: 10.1111/pai.12107.
15. Zhu J, Pouillot R, Kwegyir-Afful EK, Luccioli S, Gendel SM. A retrospective analysis of allergic reaction severities and minimal eliciting doses for peanut, milk, egg, and soy oral food challenges. Food Chem Toxicol. 2015 Jun;80:92-100. doi: 10.1016/j.fct.2015.02.023.

52 CHAPTER 3
16. Ballmer-Weber BK, Fernandez-Rivas M, Beyer K, Defernez M, Sperrin M, Mackie AR et al. How much is too much? Threshold dose distributions for 5 food allergens. J Allergy Clin Immunol. 2015;135:964-71. doi: 10.1016/j.jaci.2014.10.047.
17. Wainstein BK, Studdert J, Ziegler M, Ziegler JB. Prediction of anaphylaxis during peanut food chal-lenge: usefulness of the peanut skin prick test (SPT) and specific IgE level. Pediatr Allergy Immunol. 2010 Jun;21:603-11. doi: 10.1111/j.1399-3038.2010.01063.x.
18. Taylor SL, Moneret-Vautrin DA, Crevel RW, Sheffield D, Morisset M, Dumont P et al. Threshold dose for peanut: risk characterization based upon diagnostic oral challenge of a series of 286 peanut-allergic individuals. Food Chem Toxicol 2010;48:814–819.
19. Blumchen K, Beder A, Beschorner J, Ahrens F, Gruebl A, Hamelmann E et al. Modified oral food challenge used with sensitization biomarkers provides more real-life clinical thresholds for peanut allergy. J Allergy Clin Immunol 2014;134:390–398.
20. Vlieg-Boerstra BJ, Bijleveld CM, van der Heide S, Beusekamp BJ, Wolt-Plompen SA, Kukler J, et al. Development and validation of challenge materials for doubleblind, placebo-controlled food chal-lenges in children. J Allergy Clin Immunol 2004;113:341-6.
21. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C, Hourihane J, et al. Standard-ization of food challenges in patients with immediate reactions to foods—position paper from the European Academy of Allergology and Clinical Immunology. Allergy 2004;59:690-7.
22. Vlieg-Boerstra BJ, van der Heide S, Bijleveld CM, Kukler J, Duiverman EJ, Dubois AE. Placebo reac-tions in double-blind, placebo-controlled food challenges in children. Allergy 2007;62:905-12.
23. Taylor SL, Hefle SL, Bindslev-Jensen C, Atkins FM, Andre C, Bruijnzeel-Koomen C, et al. A consensus protocol for the determination of the threshold doses for allergenic foods: how much is too much? Clin Exp Allergy 2004;34:689-95.
24. Astier C, Morisset M, Roitel O, Codreanu F, Jacquenet S, Franck P et al. Predictive value of skin prick tests using recombinant allergens for diagnosis of peanut allergy. J Allergy Clin Immunol. 2006;118:250-6.
25. van der Zee T, Dubois AEJ, Kerkhof M, van der Heide S, Vlieg-Boerstra B. The eliciting dose of peanut in double-blind, placebo-controlled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy Clin Immunol 2011;128:1031-6.
26. Knight AK, Shreffler WG, Sampson HA, Sicherer SH, Noone S, Mofidi S et al. Skin prick test to egg white provides additional diagnostic utility to serum egg white-specific IgE antibody concentration in children. J Allergy Clin Immunol. 2006;117:842-7.
27. Baumert JL, Taylor SL, Koppelman SJ. Quantitative Assessment of the Safety Benefits Associated with Increasing Clinical Peanut Thresholds Through Immunotherapy. J Allergy Clin Immunol Pract. 2017 Jun 29. [Epub ahead of print] doi: 10.1016/j.jaip.2017.05.006.
28. Worm M, Edenharter G, Rueff F, Scherer K, Pfohler C, Mahler V, Treudler R, Lang R, Nemat K, Koehli A, Niggemann B, Hompes S. Symptom profile and risk factors of anaphylaxis in Central Europe. Allergy 2012; 67: 691-698.
29. Cianferoni A, Garrett JP, Naimi DR, Khullar K, Spergel JM. Predictive values for food challenge-induced severe reactions: development of a simple food challenge score. Isr Med Assoc J. 2012;14:24-8.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 53
3
30. Johnson J, Malinovschi A, Alving K, Lidholm J, Borres MP, Nordvall L. Ten-year review reveals chang-ing trends and severity of allergic reactions to nuts and other foods. Acta Paediatr. 2014;103:862-7. doi: 10.1111/apa.12687.
31. Song Y, Wang J, Leung N, Wang LX, Lisann L, Sicherer SH et al. Correlations between basophil activa-tion, allergen-specific IgE with outcome and severity of oral food challenges. Ann Allergy Asthma Immunol. 2015;114:319-26. doi: 10.1016/j.anai.2015.01.006.
32. Peeters KA, Koppelman SJ, van Hoffen E, van der Tas CW, den Hartog Jager CF, Penninks AH et al. Does skin prick test reactivity to purified allergens correlate with clinical severity of peanut allergy? Clin Exp Allergy. 2007; 37:108-15.
33. Sampson HA, Ho DG. Relationship between food-specific IgE concentrations and the risk of positive food challenges in children and adolescents. J Allergy Clin Immunol. 1997;100:444-51.
34. Turner PJ, Wainstein BK. Crossing the threshold: can outcome data from food challenges be used to predict risk of anaphylaxis in the community? Allergy. 2017;72:9-12. doi: 10.1111/all.12997.


CHAPTER 4
GREATER sEvERITy Of PEANUT ChALLENGE REACTIONs UsING A hIGh fAT vERsUs LOw fAT mATRIx vEhICLE
M. Eleonore PetterssonGerard H. KoppelmanAfke MM. SchinsC. Doriene van GinkelBertine MJ. Flokstra-de BlokBoudewijn J. KollenAnthony EJ. Dubois
Conditionally accepted – Clinical and Experimental Allergy 2018

56 CHAPTER 4
ABSTRACT
Previous studies have suggested that the properties of the food matrix may influence the clinical response to a particular allergenic food. The aim of this study was to examine the difference between the severity of reactions and eliciting doses, resulting from DBPCFCs with peanut, by using two different recipes differing in fat content. 210 children with posi-tive DBPCFCs to peanut were included. Children challenged with peanut in the high fat matrix had more severe reactions during the DBPCFC (B=0.77, 95%CI: 0.06-1.49, p-value= 0.03), compared to children challenged with peanut in the low fat matrix. However, there was no significant difference in eliciting dose (B=-9.60, 95%CI: -51.11-31.91, p-value= 0.65). This result supports the role of the food matrix as a factor which may enhance the severity of reactions. It also raises the possibility that unintentional matrix effects during oral immunotherapy with peanut could elicit adverse events during such treatment.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 57
4
intRoDuction
Food allergy is a potentially life-threatening disease with a detrimental effect on the qual-ity of life of caregivers and children.(1) Although many different types of food have been identified as potential elicitors of allergic reactions, only a small number of these foods cause the majority of reactions.(2)
Food consists of a complex mixture of nutrient and non-nutrient components and their molecular interactions which are known as the food matrix. Individual matrix components, or the matrix as a whole, may interact with a food allergen and may influence the clinical response to that allergen.(3) However, data on this role of the food matrix in the clinical allergic response is scarce.
Establishing the influence of the food matrix is important because allergens are not in-gested in a pure state. The main influences of the food matrix on an allergic reaction are considered to be caused by changes in allergen bioavailability and release, digestibility and consequent interactions with the immune system.(3) The fat content of the food matrix has previously been shown to have an impact on this bioavailability of the allergenic pro-tein in vitro for peanuts.(4) Thus, the food matrix could influence the uptake of allergens from food, and as a consequence confound the relationship between exposure to these allergens and the resultant clinical reaction.
A case series of double-blind, placebo-controlled food challenges (DBPCFC) with four peanut allergic patients by Grimshaw et al., suggested that a lower fat content of the peanut matrix reduced the amount of peanut required to elicit a reaction in three of the four subjects. These three subjects also had more severe symptoms in the food challenge using a high fat peanut matrix.(5) However, due to the small number of subjects, only a descriptive evaluation of the results was possible and thus no definite conclusions could be drawn from this study.
So far, the current evidence suggests that the qualities of the food matrix plays an impor-tant role in eliciting the allergic reaction. However, to the best of the authors’ knowledge, no previous study has shown an association between the fat content of a matrix and the clinical allergic response. A previous study from our center with hen’s egg challenges failed to find such an association.(6) The aim of this study was to examine possible matrix effects of a high and low fat content food matrix during DBPCFCs with peanut by comparing the severity of reactions and eliciting doses.

58 CHAPTER 4
METhOdS
All positive peanut DBPCFCs performed at the Beatrix’s Children’s Hospital in the Univer-sity Medical Center Groningen between 2002-2014 were included. Food challenges were excluded if they were performed with any other than the two most frequently used recipes (11 cases excluded). In children with repeated DBPCFCs, only the first test was included (37 cases excluded). 14 cases were excluded because the challenge recipe was not specified.
DBPCFCs were performed as part of routine clinical care and according to previously pub-lished protocols.(7-10) Briefly, the peanut and placebo was concealed in a food matrix. The recipes used were peanut in cookies and peanut in gingerbread, with a fat content of 23.9% and 5.9% respectively. The contents of the recipes are shown in table 1. The recipe used in the DBPCFC was based on the patient’s own preference. The placebo and active days were randomized and took place on two separate days. The code was broken 48 hours after the second food challenge day. The food challenge was deemed positive when objective and/or repeated subjective allergic symptoms were observed on the active day. In addition, the food challenge was considered to be positive if symptoms occurring on the placebo day were considerably less severe than the symptoms occurring on the active day.
Table 1. The contents of the peanut recipes used during DBPCFCs.
Peanut in gingerbread (5.9% fat) Peanut in cookie (23.9 % fat)
Self-rising flour 40g Cane sugar 25g
Rice milk 35g Dairy-free margarine 20g
Caster sugar 29g Whole wheat flour 14g
Peanut flour (defatted) 8g Flour 14g
Dairy-free margarine 5g Coconut 10g
Cinnamon, coriander, nutmeg, cloves, ginger, cardamom Wheat germs 5g
Peanut flour (defatted) 2g
Total 117g Total 90g
The severity of reaction during the DBPCFC was determined using the scoring system by van der Zee et al,(11) with a severity index ranging from 0 to 12. A second scoring system, published by Astier et al.(12) was used for sensitivity analysis. The influence of the matrix on the severity of the challenge reaction and eliciting dose was analyzed by linear regression analysis, with correction for possible confounders. A variable was considered a confounder when it changed the beta coefficient by more than 10%. The alpha significance level was set at 0.05. The level of sIgE was logarithmically transformed to normalize the residuals.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 59
4
RESultS
210 peanut allergic children were included in the analysis. Of these patients, 69 children ingested peanut in gingerbread, and 141 children ingested peanut in cookie during the active day of the DBPCFC. The included children were predominately boys (57.6%) and had a median age of 7.4 years with an interquartile range of 5.2-12.0 years. A substantial proportion of the children suffered from additional atopic disease; 90.5% had a history of atopic dermatitis, 42.9% had a history of allergic rhinoconjunctivitis and 63.3% had a his-tory of asthma. The median level of peanut specific IgE was 15.4 kU/L with an interquartile range of 3.9-60.8 kU/L. For further demographics according to the recipe used see table 2.
Table 2. Differences in demographics according to the recipe used.
Recipe used
n=210
Peanut in gingerbread (5.9% fat)
n=69
Peanut in cookie (23.9 % fat)
n=141
Age,median(IQR) 8.4 (5.2-12.8) 7.3(5.3-11.9)
Gender,n(%) Male:37(53.6)Female: 32 (46.4)
Male:84(59.6)Female:57(40.4)
Asthma,n(%) 35.0(50.7) 98.0(69.5)
Atopicdermatitis,n(%) 62.0(89.9) 128.0(90.8)
Allergicrhinoconjunctivitis,n(%) 32.0(46.4) 71.0(50.4)
LevelofpeanutsIgE,median(IQR) 13.6 (5.1-43.2) 15.6(3.2-89.3)
Elicitingdose,median(IQR) 70.0(3.5-350.0) 70.0(14.0-350.0)
ReactiontimeDBPCFC,median(IQR) 15.0(5.5-40.0) 15.0(5.0-42.0)
SeverityofDBPCFCreaction,median(IQR) 3.0(3.0-5.0) 4.0(3.0-6.0)
Severityofaccidentalreactionbyhistory,median(IQR) 2.0(0.5-4.0) 2.0(0.0-6.0)
All assumptions of the linear regression analysis were met when using the scoring system by van der Zee et al. However, when using the scoring system by Astier et al, the as-sumption of normally distributed residuals was not fulfilled. Thus, the final analysis was performed using the scoring system by van der Zee et al only.
Linear regression analysis showed that children challenged with the high fat recipe, peanut in cookies, had more severe reactions during the DBPCFC (B=0.77, 95%CI: 0.06-1.49, p-value= 0.03), compared to children challenged with the low fat recipe, peanut in gingerbread. However, there was no significant difference in the eliciting dose for the high and low fat recipes (B=-9.60, 95%CI: -51.11-31.91, p-value= 0.65). These results were not confounded by age, gender, level of sIgE, severity of the most severe previous accidental

60 CHAPTER 4
reaction by history, eliciting dose, reaction time during the DBPCFC, history of atopic dermatitis, asthma or allergic rhinoconjunctivitis.
DiScuSSion
The results of this study shows that children receiving peanut in a high fat matrix during an oral food challenge have more severe reactions compared to children undergoing this test with a low fat matrix. This supports the role of the food matrix as a factor which may enhance the severity of both diagnostic challenge reactions as well as accidental reactions.
Our results showed no statistically significant difference in eliciting dose between the high and low fat recipes. Unfortunately, the case study by Grimshaw et al(5) could not statistically verify their results, due to their low number of participants, and therefore no meaningful comparison with this study can be made.
In a previous study by Libbers et al,(6) no matrix effect was shown for two different matrices used during DBPCFC with hen’s egg. This suggests that matrix effects differ per type of allergenic food. Thus, further studies are required to investigate matrix effects in other types of food allergy. Libbers et al. suggested a possible explanation for differences in matrix effect, between peanut and hen’s egg, to be the fat content of the allergenic food itself. Thus, the inherent difference in fat content between peanut and hen’s egg may influence to what extent components of the allergenic food may dissolve in the food matrix in question and may therefore affect the rate of allergen release and bioavailability to the immune system.6
Basophils have emerged as possible influential contributors to the immune response in allergic reactions to food. Recently, certain parameters of the basophil activation test (BAT) was shown to reflect specific features of the allergic reaction.(13,14) The basophil reactivity, or proportion of activated basophils, was associated with severity of allergic reaction to peanuts. Moreover, the basophil sensitivity was associated with the eliciting dose during the oral food challenge. This, and the results of the current study, may suggest that a high fat matrix could affect the proportion of basophils being activated in the im-mune response to an allergen, but is not likely to influence the basophil sensitivity.
A possible limitation of this study is that the two recipes used differed in other ways than the fat content. Moreover, the low fat recipe had a higher concentration of peanut per gram of food matrix. However, children receiving the high fat matrix still had more severe reactions, thus this does not seem to significantly have influenced the outcome.

PREDICTION OF THE SEVERITY OF ALLERGIC REACTIONS TO FOODS 61
4
Moreover, to be able to draw conclusions on causality between a high fat matrix and the severity of reaction, a prospective study examining the effects of the food matrix on the clinical reaction is warranted. Nevertheless, the two groups were well matched in terms of important clinical and immunological characteristics.
In conclusion, this study shows a matrix effect for peanut, seen in differences in the sever-ity of reactions in oral food challenges. Consequently, to be able to compare the results of oral food challenges in different patient groups or from different centers, the develop-ment of standardized food challenge materials may be necessary. Moreover, matrix effects could possibly influence accidental reactions to peanut and adverse events during peanut immunotherapy. This may be important from a regulatory perspective as well as for the food industry.

62 CHAPTER 4
REfERENCES
1. Goossens NJ, Flokstra-de Blok BM, van der Meulen GN, Botjes E, Burgerhof HG,et al. Food al-lergy knowledge of parents - is ignorance bliss? Pediatr Allergy Immunol. 2013 Sep;24:567-73. doi: 10.1111/pai.12099.
2. NIAID-Sponsored Expert Panel, Boyce JA, Assa’ad A, Burks AW, Jones SM et al. Guidelines for the diagnosis and management of food allergy in the United States: report of the NIAID-sponsored expert panel. J Allergy Clin Immunol. 2010 Dec;126:S1-58. doi: 10.1016/j.jaci.2010.10.007.
3. McClain S, Bowman C, Fernández-Rivas M, Ladics GS, Ree Rv. Allergic sensitization: food- and protein-related factors. Clin Transl Allergy. 2014 Apr;4:11. doi: 10.1186/2045-7022-4-11.
4. van Odijk J, Ahlstedt S, Bengtsson U, Borres MP, Hulthén L. Double-blind placebo-controlled chal-lenges for peanut allergy the efficiency of blinding procedures and the allergenic activity of peanut availability in the recipes. Allergy. 2005 May;60:602-5.
5. Grimshaw KE, King RM, Nordlee JA, Hefle SL, Warner JO et al. Presentation of allergen in different food preparations affects the nature of the allergic reaction--a case series. Clin Exp Allergy. 2003 Nov;33:1581-5.
6. Libbers L, Flokstra-de Blok BM, Vlieg-Boerstra BJ, van der Heide S, van der Meulen GN et al. No matrix effect in double-blind, placebo-controlled egg challenges in egg allergic children. Clin Exp Allergy. 2013 Sep;43:1067-70. doi: 10.1111/cea.12164
7. Vlieg-Boerstra BJ, Bijleveld CM, van der Heide S, Beusekamp BJ, Wolt-Plompen SA et al. Develop-ment and validation of challenge materials for double-blind, placebo-controlled food challenges in children. J Allergy Clin Immunol. 2004 Feb;113:341-6.
8. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C et al. Standardization of food challenges in patients with immediate reactions to foods--position paper from the European Academy of Allergology and Clinical Immunology. Allergy. 2004 Jul;59:690-7.
9. Vlieg-Boerstra BJ, van der Heide S, Bijleveld CM, Kukler J, Duiverman EJ et al. Placebo reactions in double-blind, placebo-controlled food challenges in children. Allergy. 2007 Aug;62:905-12.
10. Taylor SL, Hefle SL, Bindslev-Jensen C, Atkins FM, Andre C et al. A consensus protocol for the deter-mination of the threshold doses for allergenic foods: how much is too much? Clin Exp Allergy. 2004 May;34:689-95.
11. van der Zee T, Dubois A, Kerkhof M, van der Heide S, Vlieg-Boerstra B. The eliciting dose of peanut in double-blind, placebo-controlled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy Clin Immunol. 2011 Nov;128:1031-6. doi:10.1016/j.jaci.2011.07.050.
12. Astier C, Morisset M, Roitel O, Codreanu F, Jacquenet S et al. Predictive value of skin prick tests using recombinant allergens for diagnosis of peanut allergy. J Allergy Clin Immunol. 2006 Jul;118:250-6.
13. Santos AF, Du Toit G, Douiri A, Radulovic S, Stephens A et al. Distinct parameters of the basophil activation test reflect the severity and threshold of allergic reactions to peanut. J Allergy Clin Im-munol. 2015;135(1):179–86.
14. Song Y, Wang J, Leung N, Wang LX, Lisann L, et al. Correlations between basophil activation, allergen-specific IgE with outcome and severity of oral food challenges. Ann Allergy Asthma Im-munol. 2015;114(4):319–26.

CHAPTER 5
CLINICAL REACTIvITy TO INDIvIDUAL TREE NUTs AND PEANUT DIffERs AmONG ThE sENsITIzED PEDIATRIC POPULATION
Anne E. RichterM. Eleonore Pettersson Annemarie Oomkes-Pilon Boudewijn J. Kollen Bertine MJ. Flokstra-de Blok Anthony EJ. Dubois
Manuscript in preparation

64 CHAPTER 5
ABSTRACT
Background: Although peanuts and tree nuts are allergens considered capable of eliciting severe reactions, little is known about the relative potency of different tree nuts compared to peanut and to each other. Our objective was therefore to investigate differences in the frequency and severity of diagnostic and accidental allergic reactions to tree nuts and peanut in children undergoing double-blind placebo-controlled food challenges (DB-PCFCs).
Methods: 710 DBPCFCs performed mainly for peanut, cashew, hazelnut, walnut and al-mond were retrospectively analyzed using logistic and linear regression. Frequency of clinical reactivity was derived from the proportion of positive DBPCFCs. Severity of acci-dental and challenge reactions was scored according to van der Zee et al. The relationships were adjusted for confounders.
Results: Compared to peanut , allergic reactivity as ascertained by DBPCFC was significantly less frequent for hazelnut and almond (adjusted OR=0.55, p=0.02 and OR=0.06, p=0.02, respectively) and sensitization was more frequently asymptomatic. In contrast, chal-lenges with cashew and walnut more frequently resulted in a positive reaction (adjusted OR=2.44, p=0.01 and OR=2.18 p=0.03, respectively) than did those with peanut. While no differences in DBPCFC reaction severity were found, cashew was the only tree nut associated with more severe accidental reactions than peanut (adjusted B=1.23, p=0.01).
Conclusions: The frequency of true clinical reactivity differs significantly between patients sensitized to peanut and tree nuts. The DBPCFC is especially important for the confirma-tion of hazelnut and almond allergy due to common asymptomatic sensitization. Cashew nut should be prioritized for improving measures that reduce the risk of accidental exposure.

CLINICAL REACTIVITY TO INDIVIDUAL TREE NUTS AND PEANUT DIFFERS AMONG THE SENSITIZED PEDIATRIC POPULATION 65
5
intRoDuction
Peanut and tree nuts are among the most common allergenic foods consumed by the pediatric population. In the USA these nuts are reported to cause allergy in about 1-2% of children (1, 2). Furthermore, they are responsible for about 90% of deaths due to food allergic reactions, with peanut accounting for over two thirds of these fatalities (3, 4). Exposure is often unintentional as cross-contamination during industrial processing of these foods is common (5).
There are several methods in common use to diagnose food allergies. Skin prick tests (SPT) and specific IgE (sIgE) determinations are commonly used, but positive test do not necessarily imply clinical reactivity (6-9). Clinical history and open food challenges may be unreliable due to subjectivity of symptoms, a lack of relation between the described symptoms and the food in question, and a higher likelihood of false-positivity (10, 11). Currently, the gold standard is the double-blind, placebo-controlled food challenge (DBP-CFC) (12, 13). Despite the high reliability of such tests, large studies on the true frequency of clinical peanut and tree nut allergy determined by DBPCFCs are scarce. In terms of frequency and severity, tree nut allergies are less well characterized than peanut allergy. Specifically, a comparison of odds for true clinical reactivity as opposed to asymptomatic sensitization comparing peanut and specific tree nuts to each other has not been per-formed. Such a comparative characterization, however, may be useful not only for clinical decision making but also for labeling of processed foods (14). The aim of this study was thus to investigate differences in frequency and, secondarily, severity of clinical allergy to peanut and tree nuts and to rank these foods according to these differences.
METhOdS
Study population
This retrospective cross-sectional study included pediatric patients suspected of allergy to peanut and/or tree nuts, and who had undergone DBPCFCs in the Food Challenge Unit of the University Medical Center of Groningen (UMCG) between 2002 and 2013. The data collected included patient characteristics such as age, sex, sIgE levels, previous reaction history, atopic comorbidities and atopic family history as well as details of the DBPCFC such as the type of nut tested, symptoms and eliciting dose (defined as the last dose of protein ingested and evoking an allergic reaction during the active food day of a positive DBPCFC). The sIgE levels were measured using the ImmunoCAP assay (Thermo Fisher Scientific, Uppsala, Sweden). Levels below 0.35 kU/l were considered negative. Data on previous reactions was based on reaction histories routinely determined before the challenge. For this parents were asked

66 CHAPTER 5
about previous symptoms upon consumption of the suspected food, the amount ingested, and the time interval between consumption and onset of symptoms.
All DBPCFCs were performed because of clinical suspicion of food allergy. For inclusion, the results of the DBPCFC needed to be conclusive, data had to be complete and the ImmunoCAP test and the food challenge had to be no longer than six months apart. In patients who had undergone multiple DBPCFCs with the same food, only the first chal-lenge was included.
The institutional medical ethics committee deemed that ethical approval was not required as all tests were carried out as part of routine care and patients were informed about the use of their medical records for research.
dBpCfCs
DBPCFCs were performed according to the guidelines proposed by the European Academy of Allergy and Clinical Immunology and later modified PRACTALL Guidelines (12, 15). Verum and placebo were given on separate days using a 6 to 8 step incremental scale, in which the food was ingested in stepwise increasing quantities until the final dose was reached or symp-toms occurred. Objective symptoms (urticaria, angioedema, worsening eczema, vomiting, diarrhea, rhinoconjunctivitis, wheezing, coughing, and hypotonicity) or repeated subjective symptoms (itching, oral allergy, abdominal pain, nausea, difficulty breathing or swallowing, and dizziness) were considered when comparing the verum and placebo days according to a previously established protocol for determining test positivity (16).
Scoring system for reaction severity
Reaction severity was determined as previously described (17). The severity scores for the previous accidental reaction and the immediate challenge reaction were based on the type of organ system affected and ranged from 1 to 12. Upper airway, lower airway, or cardiovascular/neurological symptoms were considered most severe and each of these organ systems scored 3 if involved, the presence of gastrointestinal symptoms scored 2, and the presence of cutaneous symptoms scored 1. The sum of scores for each involved organ system resulted in the final severity score.
Statistical analysis
The frequency of clinical reactivity was studied using univariate and multiple logistic regression analysis with the DBPCFC outcome as the binomial variable (positive/nega-tive). To address the sub-questions concerning differences in severity of both previous accidental and DBPCFC reactions, univariate and multiple linear regression analyses were used, and by using the severity score as the outcome variable.

CLINICAL REACTIVITY TO INDIVIDUAL TREE NUTS AND PEANUT DIFFERS AMONG THE SENSITIZED PEDIATRIC POPULATION 67
5
Factors that changed the regression coefficients of three nuts by 10% or more were treated as confounding variables and included into the regression models. Variables taken into consideration were age, sex, sIgE level, being allergic to more than one type of food included in the analysis, the presence and/or severity of a previous accidental reaction, atopic comor-bidity (rhinoconjunctivitis, eczema, and asthma), an atopic family history, and, for positive food challenges, the eliciting dose and the severity of the DBPCFC reaction.
The analysis was performed using the statistical program SPSS, version 20.0 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered to be significant. Due to multiple testing concerning our primary analysis on the frequency of clinical reactivity, the Benjamini–Hochberg’s step-up procedure was used to control the false discovery rate (18). When applicable, adjusted p-values are reported. The assumptions for logistic and linear regres-sion were fulfilled. When required, variables were logarithmically transformed in order to normalize the distribution of the residuals. In such cases, the back-transformed coef-ficients and confidence intervals are reported.
RESultS
Study population
Of 872 food challenges performed to diagnose allergy to peanut or tree nut in children, 30 cases were excluded due to an inconclusive challenge outcome, 12 cases on the basis of incomplete data, and 66 cases in which the sIgE testing and food challenge were more than six months apart. Furthermore, 54 challenges were excluded as they represented the second or third challenge performed with the same food in the same patient. A total of 710 DBPCFCs were thus included in the analysis.
The majority of patients were challenged with peanut (n=391), followed by hazelnut (n=136), cashew nut (n=104), walnut (n=49), and almond (n=20). Less frequently tested were macadamia nut (n=3), pistachio (n=5), pecan nut (n=1), and Brazil nut (n=1). The 710 challenges were performed in a total of 532 patients, of whom 382 were challenged with only one type of nut , 107 were challenged with two types of nuts, and 24 were challenged with three nuts or more.
The population age ranged from 10 months to 18 years of age, and 58.7% of challenges were performed in male patients. Atopic comorbidities were common, with 86.2% having a medical history of eczema, 55.2% asthma, and 47% with allergic rhinoconjunctivitis. In 82% of cases a family history of atopy was noted.

68 CHAPTER 5
Sixty-six percent of cases had a history of previous reactions to the type of nut tested, for the remainder it was their first exposure. Fifty-six percent of all challenges were positive, including both DBPCFCs with immediate and late home reactions. This number was slightly higher for those with a positive reaction history (63.4%). For all types of nuts tested, a history of a previous reaction occurred more often than a positive food challenge outcome. Out of 605 cases with sIgE levels ≥ 0.35 kU/l, 62% were found to be DBPCFC posi-tive, while this percentage was lower for those sensitized but without a positive reaction history (44.8%). Of the 105 cases with sIgE levels <0.35 kU/l 18.1% had a positive DBPCFC outcome. Reactions to placebo were only observed in 6.2% of cases and more than two thirds of these cases also had a reaction on the verum day. The characteristics of the study population per nut are described in Table 1.
Table 1. Characteristics of the study population per nut.
Peanut Hazelnut Cashew nut
Walnut Almond
Number of cases 391 136 104 49 20
Sex, females/males 144/247 59/77 47/57 29/20 8/12
Age (years), median [IQR] 6.8[4.9-11.8]
7.6[5.6-12.0]
8.3[5.2-11.7]
8.7[6.7-11.6]
9.1[6.2-11.0]
sIgE level > 0.35 kU/l, % (n)
86.4 (338) 89.7(122) 83.7(87) 75.5(37) 65.0(13)
PR history, % (n) 64.2 (251) 51.5(70) 86.5(90) 71.4(35) 55.0(11)
PR severity score, median [IQR]
3[2-6] 3[2-6] 4[2-6] 3[2-6] 2[1-5]
History of eczema, % (n) 88.2 (345) 88.2(120) 79.8(83) 77.6(38) 95.0(19)
History of rhinoconjunctivitis, % (n)
46.3 (181) 51.5(70) 50.0(52) 34.7(17) 55.0(11)
History of asthma 59.8(234) 58.1(79) 43.3 (45) 30.6(15) 70.0(14)
Atopic family history, % (n)
85.4 (334) 75.7(103) 78.8(82) 81.6(40) 80.0(16)
Positive DBPCFC, % (n)
56.0(219) 47.1(64) 72.1(75) 67.3(33) 5.0(1)
Positive DBPCFC and sensitized, % (n)
62.1(210) 50.0(61) 81.6(71) 81.1(30) 7.7(1)
Eliciting dose (mg), median [IQR]
6.0[70.0-194.0]
14.0[2.0-155.0]
14.0[2.0-70.0]
15.0[3.0-315.0]
285.0[285.0-285.0]
DBPCFC severity score, median [IQR]
3[2-5] 3[2-5] 3[2-5] 3[2-4] 3
IQR, interquartile range; PR, previous reaction.

CLINICAL REACTIVITY TO INDIVIDUAL TREE NUTS AND PEANUT DIFFERS AMONG THE SENSITIZED PEDIATRIC POPULATION 69
5
Figure 1 shows the types of organ system affected during DBPCFCs with peanut and the most commonly encountered tree nuts. Cashew and peanut were the only foods associ-ated with cardiovascular symptoms (1.4% and 0.5%, respectively). Severe cardiovascular or airway symptoms were not seen for any of the tested foods. Lower airway symptoms occurred relatively frequently upon ingestion of walnut (21.9%). Oral allergy symptoms were seen in about 20.9% of peanut challenges, 26.0% of cashew challenges, 30.5% of hazelnut challenges, and 25.0% of challenges with walnut. Concerning data on less fre-quently challenged nuts, 1 out of the 3 DBPCFCs with macadamia nut was positive and resulted in cutaneous symptoms. Pistachio elicited a (gastrointestinal) reaction in 1 out of the 5 challenges. DBPCFCs performed for pecan nut and Brazil nut were negative in all cases. Challenges with almond only resulted in one positive food challenge, with upper airway symptoms.
Figure 1: Involvement of organ systems upon DBPCFCs with peanut and tree nuts.
frequency of allergy confirmed by DBpcfc
Both patients who were sIgE positive and those who were sIgE negative to the challenged nut, were included in the analysis (n=710). Adjusted for sIgE levels and the severity of

70 CHAPTER 5
previous accidental reactions, DBPCFCs with cashew nut or walnut were more than twice as likely to elicit a positive reaction compared to peanut (adjusted OR=2.44 and 2.18, respectively). In contrast, challenges with almond were only 0.06 times as likely to result in a positive test result compared to challenges performed with peanut, and challenges with hazelnut were about half as likely to result in a positive reaction (Table 2a).
A sub-analysis with the exclusion of non-sensitized patients resulted in a total of 605 DBPCFCs. For hazelnut, almond and other nuts, adjusted logistic regression including only sensitized patients resulted in odds ratios and p-values similar to those resulting from inclusion of both sIgE positive and sIgE negative patients (Table 2b). Odds ratios for cashew and walnut increased to 3.18 and 3.33, respectively.
By only including patients with a previous accidental reaction to the type of nut tested (n=472), and adjusting for sIgE levels and previous reaction severity, the odds for a positive reaction upon ingestion of almond or cashew nut remained significantly different from the odds for peanut (OR=0.10 and OR=3.74, respectively). For hazelnut, however, the odds for eliciting a positive DBPCFC did not differ significantly from the odds of peanut eliciting a positive DBPCFC (Table 2c).
Table 2. Odds ratios for a positive DBPCFC outcome – comparing individual tree nuts to peanut.
Unadjusted Adjusted*
OR [95% CI] p-value OR [95% CI] p-value
a. Including sensitized and non-sensitized patients; n(peanut)=391
Almond (n=20) 0.04[0.01-0.31] 0.010BH 0.06[0.01-0.50] 0.018BH
Cashew nut (n=104) 2.03[1.27-3.26] 0.010BH 2.44[1.48-4.03] 0.010BH
Hazelnut (n=136) 0.70[0.47-1.03] 0.090BH 0.55[0.35-0.86] 0.018BH
Walnut (n=49) 1.62[0.86-3.04] 0.113BH 2.18[1.14-4.18] 0.032BH
Other nuts (n=10)† 0.20[0.04-0.94] 0.059BH 0.26[0.05-1.27] 0.107BH
b. Including sensitized patients only; n(peanut)=338
Almond (n=13) 0.05[0.01-0.40] 0.004 0.07[0.01-0.54] 0.011
Cashew nut (n=87) 2.71[1.51-4.86] 0.001 3.18[1.72-7.97] <0.001
Hazelnut (n=122) 0.61[0.40-0.93] 0.020 0.48[0.30-0.77] 0.002
Walnut (n=37) 2.61[1.12-6.12] 0.027 3.33[1.39-7.97] 0.007
Other nuts (n=8) † 0.20[0.04-1.02] 0.053 0.27[0.05-1.43] 0.123
c. Including only patients with a previous accidental reaction; n(peanut)=256
Almond (n=11) 0.07[0.01-0.52] 0.010 0.10[0.01-0.88] 0.037
Cashew nut (n=90) 2.28[1.32-3.98] 0.004 3.74[2.06-6.77] <0.001
Hazelnut (n=72) 1.39[0.80-2.42] 0.247 1.21[0.65-2.25] 0.555

CLINICAL REACTIVITY TO INDIVIDUAL TREE NUTS AND PEANUT DIFFERS AMONG THE SENSITIZED PEDIATRIC POPULATION 71
5
Walnut (n=35) 1.25[0.60-2.62] 0.557 2.00[0.92-4.35] 0.081
Other nuts (n=8) † 0.09[0.01-0.77] 0.027 0.18[0.02-1.51] 0.113
BH Benjamini-Hochberg adjusted p-value. *adjusted for sIgE levels and the severity of previous accidental reactions. †Other nuts include Brazil nut, macadamia nut, pecan nut, and pistachio. OR, odds ratio; CI, confidence interval.
Severity of allergic reactions during DBpcfc
In the analysis of the clinical reaction severity 373 positive DBPCFCs were included. No significant differences in severity were found for peanut and tree nuts in terms of type and degree of reaction, whether unadjusted or adjusted for possible confounders (Table 3a). The use of a different scoring system, developed by Astier et al. (19), did not change these results.
Severity of previous accidental reactions reported by history
Analysis of the severity of previous accidental reactions to the challenged nuts included 464 cases, for which severity scores were calculated. Accidental reactions to cashew were found to be significantly more severe than accidental reactions to peanut (adjusted and back-transformed B=1.23). This result was also shown by using the Astier scoring system. The severities of accidental reactions to hazelnut, walnut, and almond were not statisti-cally different from those reported for peanut (Table 3b).
Table 3. Differences in allergic reaction severity – comparing individual tree nuts to peanut.
Unadjusted Adjusted*
B [95% CI] p-value B [95% CI] p-value
a. Immediate DBPCFC reaction severity; n(peanut)=206
Cashew (n=73) 1.02[0.91-1.14] 0.777 1.06[0.93-1.20] 0.370
Hazelnut (n=59) 0.95[0.85-1.08] 0.437 0.95[0.85-1.08] 0.467
Walnut (n=32) 1.05[0.90-1.24] 0.514 1.11[0.95-1.31] 0.193
Other nuts (n=3) † 0.68[0.41-1.11] 0.122 0.78[0.47-1.28] 0.327
b. Severity of previous accidental reactions; n( peanut)=250
Almond (n=11) 0.81[0.50-1.33] 0.408 0.85[0.51-1.41] 0.535
Cashew (n=90) 1.18[1.03-1.34] 0.014 1.23[1.08-1.41] 0.002
Hazelnut (n=70) 0.98[0.85-1.13] 0.780 0.96[0.84-1.11] 0.620
Walnut (n=35) 1.00[0.82-1.21] 0.981 1.05[0.87-1.27] 0.630
Other nuts (n=8) † 1.11[0.76-1.62] 0.593 1.21[0.81-1.80] 0.355
*adjusted for sIgE levels, the presence of a previous reaction (only a.), a history of eczema (only b.), age (only b), and the eliciting dose (only a). †Other nuts include almond (only in a), macadamia nut, pistachio, Brazil nut (only in b), and pecan nut (only in b). B, regression coefficient; CI, confidence interval. This table reports back-transformed regression coefficients and confidence intervals.

72 CHAPTER 5
DiScuSSion
This study provides a head-to-head comparison of the frequency and severity of double-blind challenge-proven clinical allergy between different kinds of tree nuts and peanut. In children suspected of having nut allergies, we demonstrated that the odds of a positive challenge reaction to that nut were more than twice as high for cashew and walnut than for peanut. Under the same circumstances almond and hazelnut showed significantly lower odds of eliciting an allergic reaction compared to peanut. Among our study population, sub-analysis further demonstrated asymptomatic sensitization to hazelnut and almond to be significantly more frequent than asymptomatic sensitization to peanut. Sensitization to cashew and walnut, in contrast, was significantly less frequently asymptomatic than sensitization to peanut. We were not able to demonstrate any significant difference in severity of DBPCFC reactions between peanut and tree nuts. However, based on reaction history, cashew causes more severe reactions than peanut upon accidental ingestion.
The differences in frequency of clinical reactions found between peanut, hazelnut and almond are in contrast with the results of Ludman et al. who could not demonstrate a significant difference in the probability of a positive challenge between these foods (8). However, it is not clear whether they based their results on DBPCFCs or open challenges, and their study included only 98 patients, none of whom had ever previously consumed the food tested. The differences observed in our study may largely be explained by a high frequency of asymptomatic sensitization for hazelnut and almond as sub-analysis sug-gests. The relatively high frequency of asymptomatic sensitization observed in patients challenged with hazelnut may be explained by cross-reactivity with pollen, which is usually more common in older children and adults (20). Flinterman et al., however, found more than 80% of children older than 3.5 years living in birch-endemic areas to be sensitized to the hazelnut protein Cor a 1, a homologue of Bet v 1 (21). Therefore, cross-reactivity with birch pollen may indeed be quite common in our hazelnut study population as well, despite the median age of only 7.63 years. This relatively high level of cross-sensitization could increase the level of suspicion for hazelnut allergy and may result in the inclusion of more children with doubtful histories and positive sIgE levels in the hazelnut group than in the peanut group. This hypothesis is also supported by the fact that the difference in clinical reactivity between hazelnut and peanut is much less and almost negligible when only children with previous reactions are included. The study by Flinterman et al. shows that children without previous allergic reactions or with only oral allergy symptoms upon DBPCFCs with hazelnut may be significantly more frequently sensitized to only Bet v 1 homologues than children with objective symptoms (21). The cross-reactivity between almond and Bet v 1 homologues may similarly be responsible for the relatively high rate of asymptomatic sensitization seen with almond (22).

CLINICAL REACTIVITY TO INDIVIDUAL TREE NUTS AND PEANUT DIFFERS AMONG THE SENSITIZED PEDIATRIC POPULATION 73
5
Sub-analysis showed no lower frequency of clinical allergy for cashew and walnut when including only sensitized patients. In fact, sensitization to cashew and walnut even in-creased the odds of true clinical allergy to these nuts, while non-sensitization seemed to have the opposite effect (data not shown). Van der Valk et al. have recently reported a high rate (76.5%) of DBPCFC reactivity in a population sensitized to cashew nut (23), comparable to that observed in our group (81.6%). Sensitization is therefore likely to be an important predictor of allergy to cashew and walnut. Moreover, sensitization to peanut and especially cashew and walnut is less commonly reported to be associated with cross-reactivity to pollen, possibly because primary sensitization to these tree nuts and peanut seems to be acquired through the gastrointestinal rather than through the respiratory tract (24, 25). This partially theoretical construct (illustrated in table 4) is suggested by our findings, since we observed clinical reactivity to cashew, walnut (and less so to peanut) to be more frequent than to hazelnut and almond, while the opposite is true for asymptom-atic sensitization.
Table 4. Ranking tree nuts and peanut according to true clinical allergy, asymptomatic sensitiza-tion, cross-reactivity, and severity of the allergic reaction.
Type of nut DBPCFCpositivity
Asymptomaticsensitization
Cross-reactivity with pollen*
Accidental reaction severity
Hazelnut/almond - ++ ++ +
Peanut + + + +
Cashew/walnut ++ - - ++/+
*Based on literature (19-21, 23, 24)
With respect to the severity of allergy, we found cardiovascular reactions only to occur with the ingestion of peanut and cashew. This observation is in accordance with the lit-erature, which shows peanut and cashew to be associated with the most severe allergic reactions in children (25, 26). However, cardiovascular reactions were rare and linear regression was not able to confirm significant differences in the severity of DBPCFC reac-tion based on the type of organ system affected. In fact, differences with peanut could not be established for any of the tested tree nuts in terms of challenge severity. Blom et al. identified no significant differences in threshold dose distribution curves between peanut, cashew and hazelnut, although peanut and cashew seemed to give reactions within a smaller dose range (27). Their results are in agreement with ours, since the eliciting doses of the different nuts and peanut are not significantly different from each other in our study. However, whether eliciting doses correlate with severity of allergic reactions to foods is controversial (28).

74 CHAPTER 5
Furthermore, comparing differences in the severity of allergic reactions based on DBPCFCs may be of limited value since in DBPCFCs the clinical reactions are kept as mild as possible without completing dosing after the onset of symptoms, whereas accidental reactions with initial exposure to higher doses may become much more severe (12, 29). Indeed, analysis of the severity of previous accidental reactions showed reactions to cashew to be significantly more severe than accidental reactions to peanut. This finding is in accordance with other studies proposing cashew to be associated with more severe reactions than peanut based on patient reports (9, 30).
Our study was limited to the most common tree nuts encountered in our region. As sample sizes for almond, pistachio, macadamia, pecan, and Brazil nut were modest, in-ferences about the frequency and severity of allergy to these types of nuts need to be interpreted with caution. Further studies including more patients for these types of nuts are required. Additionally, larger studies on age-related sensitization profiles for peanut and tree nuts using component testing are needed to complement the knowledge gained from this study. Another limitation is that data on SPTs were not available for this study. Sensitization based on SPTs may deviate from sensitization based on positive sIgE levels. Therefore a part of the group determined as sIgE negative in the analysis, could indeed show sensitization if additionally tested with SPT. Our data may not be applicable to adults, particularly in those whose peanut allergy begins in adulthood, which may show a closer relation with cross-reactivity to pollen than in children (31). Finally, our data was derived from a tertiary care center in Nothern Europe and may differ from other populations or geographic areas.
In conclusion, this study gives a differentiated overview of the frequency and severity of clinical allergy in children to individual tree nuts in relation to peanut using a uniform test procedure including the DBPCFC, which minimizes the risk of overdiagnosis inher-ent when relying on histories, open challenges, and sIgE (32). Our results show that the frequency of true clinical allergy in sensitized individuals is lowest for hazelnut and almond and highest for cashew and walnut, probably because of differences in the frequency of cross-reactivity with birch-pollen. This fact emphasizes the special need for DBPCFCs as confirmation of hazelnut or almond allergy. Secondly, we found that there is no significant difference in the severity of challenge reactions between tree nuts and peanut, probably because reactions during DBPCFCs tend to be milder than accidental reactions. While this finding confirms the safety of DBPCFCs, it also demonstrates the limited value of DBPCFCs for studying the severity of allergic reactions. However, based on reaction history, cashew elicited significantly more severe accidental reactions than peanut. Cashew nut should thus be considered a priority in preventive initiatives which aim to reduce the risk of ac-cidental exposure, including labeling of prepared food products.

CLINICAL REACTIVITY TO INDIVIDUAL TREE NUTS AND PEANUT DIFFERS AMONG THE SENSITIZED PEDIATRIC POPULATION 75
5
REfERENCES
1. Sicherer SH, Sampson HA. Food allergy: Epidemiology, pathogenesis, diagnosis, and treatment. J Allergy Clin Immunol. 2014;133(2):291,307; quiz 308.
2. Skripak JM, Wood RA. Peanut and tree nut allergy in childhood. Pediatr Allergy Immunol. 2008;19(4):368-73.
3. Bock SA, Munoz-Furlong A, Sampson HA. Fatalities due to anaphylactic reactions to foods. J Allergy Clin Immunol. 2001;107(1):191-3.
4. Bock SA, Munoz-Furlong A, Sampson HA. Further fatalities caused by anaphylactic reactions to food, 2001-2006. J Allergy Clin Immunol. 2007;119(4):1016-8.
5. Zurzolo GA, Mathai ML, Koplin JJ, Allen KJ. Hidden allergens in foods and implications for labelling and clinical care of food allergic patients. Curr Allergy Asthma Rep. 2012 Aug;12(4):292-6.
6. Clark A, Ewan P. Interpretation of tests for nut allergy in one thousand patients, in relation to allergy or tolerance. Clinical & Experimental Allergy. 2003;33(8):1041-5.
7. Osborne NJ, Koplin JJ, Martin PE, Gurrin LC, Lowe AJ, Matheson MC, et al. Prevalence of challenge-proven IgE-mediated food allergy using population-based sampling and predetermined challenge criteria in infants. J Allergy Clin Immunol. 2011;127(3):668,676. e2.
8. Ludman S, Ballabeni P, Eigenmann PA, Wassenberg J. Predicting positive food challenges in children sensitised to peanuts/tree nuts. Pediatric Allergy and Immunology. 2013;24(3):276-81.
9. Maloney JM, Rudengren M, Ahlstedt S, Bock S, Sampson HA. The use of serum-specific IgE measurements for the diagnosis of peanut, tree nut, and seed allergy. J Allergy Clin Immunol. 2008;122(1):145-51.
10. Lieberman JA, Cox AL, Vitale M, Sampson HA. Outcomes of office-based, open food challenges in the management of food allergy. J Allergy Clin Immunol. 2011;128(5):1120-2.
11. Sampson HA. Food allergy. Part 2: Diagnosis and management. Journal of Allergy and Clinical Im-munology. 1999;103(6):981-9.
12. Bindslev-Jensen C, Ballmer-Weber BK, Bengtsson U, Blanco C, Ebner C, Hourihane J, et al. Standard-ization of food challenges in patients with immediate reactions to foods--position paper from the European Academy of Allergology and Clinical Immunology. Allergy. 2004;59(7):690-7.
13. Sampson HA. Update on food allergy. J Allergy Clin Immunol. 2004;113(5):805,19; quiz 820.
14. Houben G, Burney P, Chan CH, Crevel R, Dubois A, Faludi R et al. Prioritisation of allergenic foods with respect to public health relevance: Report from an ILSI Europe Food Allergy Task Force Expert Group. Food Chem Toxicol. 2016;89:8-18. doi: 10.1016/j.fct.2015.12.028.
15. Sampson HA, Gerth van Wijk R, Bindslev-Jensen C, Sicherer S, Teuber SS, Burks A, et al. Standard-izing double-blind, placebo-controlled oral food challenges: American Academy of Allergy, Asthma & Immunology–European Academy of Allergy and Clinical Immunology PRACTALL consensus report. J Allergy Clin Immunol. 2012;130(6):1260-74.
16. Vlieg-Boerstra BJ, van der Heide S, Bijleveld CM, Kukler J, Duiverman EJ, Dubois AE. Placebo reac-tions in double-blind, placebo-controlled food challenges in children. Allergy. 2007;62(8):905-12.
17. van der Zee T, Dubois A, Kerkhof M, van der Heide S, Vlieg-Boerstra B. The eliciting dose of peanut in double-blind, placebo-controlled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy Clin Immunol. 2011;128(5):1031-6.

76 CHAPTER 5
18. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. Journal of the royal statistical society.Series B (Methodological). 1995:289-300.
19. Astier C, Morisset M, Roitel O, Codreanu F, Jacquenet S, Franck P, et al. Predictive value of skin prick tests using recombinant allergens for diagnosis of peanut allergy. J Allergy Clin Immunol. 2006;118(1):250-6.
20. Masthoff LJ, van Hoffen E, de Reus A, Boonacker CW, Bruijnzeel-Koomen CA, Pasmans SG, et al. Ha-zelnut allergy differs between children and adults in frequency of severity, aetiology and relevance of diagnostic parameters. Clin Exp Allergy. 2014;44(12):1539-45.
21. Flinterman AE, Akkerdaas JH, den Hartog Jager CF, Rigby NM, Fernandez-Rivas M, Hoekstra MO, et al. Lipid transfer protein-linked hazelnut allergy in children from a non-Mediterranean birch-endemic area. J Allergy Clin Immunol. 2008;121(2):423,428.e2.
22. Costa J, Mafra I, Carrapatoso I, Oliveira MB. Almond allergens: molecular characterization, detec-tion, and clinical relevance. J Agric Food Chem. 2012;60(6):1337-49.
23. van der Valk JP, Gerth van Wijk R, Dubois AE, de Groot H, Reitsma M, Vlieg-Boerstra B, et al. Mul-ticentre Double-Blind Placebo-Controlled Food Challenge Study in Children Sensitised to Cashew Nut. PLoS One. 2016;11(3):e0151055.
24. Mittag D, Akkerdaas J, Ballmer-Weber BK, Vogel L, Wensing M, Becker W, et al. Ara h 8, a Bet v 1–homologous allergen from peanut, is a major allergen in patients with combined birch pollen and peanut allergy. J Allergy Clin Immunol. 2004;114(6):1410-7.
25. van der Valk JP, Dubois AE, Gerth van Wijk R, Wichers HJ, de Jong NW. Systematic review on cashew nut allergy. Allergy. 2014;69(6):692-8.
26. Johnson J, Malinovschi A, Alving K, Lidholm J, Borres MP, Nordvall L. Ten-year review reveals chang-ing trends and severity of allergic reactions to nuts and other foods. Acta Paediatr. 2014;103(8):862-7.
27. Blom WM, Vlieg-Boerstra BJ, Kruizinga AG, van der Heide S, Houben GF, Dubois AE. Threshold dose distributions for 5 major allergenic foods in children. J Allergy Clin Immunol. 2013;131(1):172-9.
28. Turner PJ, Baumert JL, Beyer K, Boyle RJ, Chan C-H, Clark AT et al. Can we identify patients at risk of life-threatening allergic reactions to food? Allergy. 2016;71:1241-55. doi: 10.1111/all.12924.
29. Luccioli S. Food allergy guidelines and assessing allergic reaction risks: a regulatory perspective. Curr Opin Allergy Clin Immunol. 2012;12(3):323-30.
30. Clark AT, Anagnostou K, Ewan PW. Cashew nut causes more severe reactions than peanut: case-matched comparison in 141 children. Allergy. 2007;62(8):913-6.
31. Namork E, Stensby BA. Peanut sensitization pattern in Norwegian children and adults with specific IgE to peanut show age related differences. Allergy Asthma Clin Immunol. 2015;11:32,015-0095-8. eCollection 2015.
32. Kattan JD, Sicherer SH. Optimizing the diagnosis of food allergy. Immunol Allergy Clin North Am.
2015;35(1):61-76.

CHAPTER 6
APOLIPOPROTEIN b: A POssIbLE NEw bIOmARkER fOR ANAPhyLAxIs
M. Eleonore PetterssonGerard H. KoppelmanBertine MJ. Flokstra-de BlokC. Doriene van GinkelCaroline RoozendaalAnneke C. Muller-KoboldBoudewijn J. KollenAnthony EJ. Dubois
Published in Annals of Allergy Asthma and Immunology 2017;118: 505-523


APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 79
6
intRoDuction
There are few published studies describing biochemical markers that correlate with the severity of anaphylactic reactions during oral food challenges or accidental reactions to foods. Identifying patients with increased risk of severe reactions is a priority within the field of anaphylaxis. Previous studies have examined laboratory markers such as specific immunoglobulin E (IgE; to allergenic foods or components thereof), parameters of the basophil activation test, and platelet-activating factor (PAF).
It has been shown that PAF takes part in various inflammatory events and plays a key role in the life-threatening events that cause anaphylaxis (1,2). PAF has been shown to be more closely correlated to the severity of anaphylactic reactions than histamine or tryptase in humans (3,4). PAF mediates reactions causing increased vascular permeability, hypoten-sion, and bronchoconstriction (5,6).
Anaphylactic responses are influenced by PAF acetylhydrolase (PAF-AH), which catalyzes the degradation of PAF to its inactive products. PAF-AH in plasma is probably produced by cells from hematopoietic lineage cells (7) Relative deficiency of PAF-AH has been shown to lead to an increased risk of life-threatening anaphylaxis (3). In other words, high levels of PAF-AH before an anaphylactic reaction will limit the production of PAF during the ongoing reaction and thus limit the severity of that reaction. However, the exact mechanism of this pathway is unknown.
In human plasma, PAF-AH circulates in complexes with low- and high-density lipoproteins, and the main protein component of low-density lipoprotein particles is apolipoprotein B-100 (ApoB). A recent study of a pediatric population allergic to peanuts showed a strong correlation between PAF-AH activity and the concentration of the more stable ApoB (8). Because of inactivation of PAF by PAF-AH, these data suggest a relation between the sever-ity of allergic reactions and the plasma concentration of ApoB. Thus, the objective of this study was to examine serum ApoB as a possible biomarker for the occurrence and severity of anaphylactic reactions to foods.
METhOdS
Data and serum samples were collected from the food challenge unit data and serum bank at the University Medical Center Groningen (UMCG; 2002-2014). Serum was collected before the double-blinded, placebo-controlled food challenge (DBPCFC). The study popula-tion consisted of children referred to the UMCG for a clinical suspicion of food allergy. No

80 CHAPTER 6
patients were excluded for a history of severe allergic reactions. Patient data were collected by history and laboratory analysis was performed as part of routine clinical care. Assenting children underwent a DBPCFC with the suspected food using previously described materials, methods, and protocols (9). The medical ethics committee of the UMCG deemed that formal medical ethical approval was not required for this study. Cases without a matching available serum sample or having missing variables necessary for the analysis were excluded. However, children with an unknown history of asthma, atopic dermatitis, or rhinoconjunctivitis were included in the analysis, and the inclusion of this patient group did not influence the results.
A symptom-based scoring system was used to determine the severity of the most severe accidental reaction as obtained from the history and the severity of the DBPCFC reaction as observed during the challenge test, as previously described (10). Briefly, the allergic symptoms received a score corresponding to the involved organ system. Skin symptoms were given a score of 1, upper airway symptoms (eyes, nose, and throat) were given a score of 3, lower airway symptoms (lungs) were given a score of 3, gastrointestinal symptoms were given a score of 2, and cardiovascular and/or neurological symptoms were given a score of 3. The scores of the involved organ systems were added together and the total severity score was calculated (range 0-12). Scores of 0 to 2 were considered mild allergic reactions, scores of 3 to 6 were considered moderate allergic reactions, and scores of 7 to 12 were considered severe allergic reactions.
The concentration of ApoB in the serum samples was determined by nephelometry. Linear regression analysis was used to examine the association between the concentration of ApoB and the severity of the DBPCFC reaction and the severity of the previous most severe accidental allergic reaction by history. Logistic regression analysis was used to study the relation between the concentration of ApoB and the food challenge outcome. A factor was considered a confounder when it changed the B coefficient of the effect of ApoB on the severity of anaphylactic reactions by at least 10%. For all tests, a 2-tailed significance level of a P value less than 0.05 was used.
RESultS
Eight hundred thirty-seven cases were included in the final analysis. The study popula-tion consisted of children with a median age of 5.8 years (interquartile range 3.6-10.4), of which 62.7% were boys. A history of asthma was reported in 52.0% of children. Most of the study population had atopic dermatitis (88.4%) and 41.5% had rhinoconjunctivitis. Specific IgE was measured in all subjects and was positive in 82.1% of the children included (Table 1 presents additional patient characteristics).

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 81
6
Table 1. Characteristics of the study population. Patient characteristic Frequency (Percent)Subjects 837 (100%)Girls 312 (37.3%)Boys 525 (62.7%)FoodPeanut 244 (29.2%)Cow’s milk 233 (27.8%)Egg 111 (13.3%)Hazelnut 84 (10.0%)Cashew nut 82 (9.8%)Soy milk 30 (3.6%)Walnut 19 (2.3%)Almond 15 (1.8%)Wheat 14 (1.7%)Pistachio 2 (0.2%)Beef 1 (0.1%)Lupine seed 1 (0.1%)Sesame seed 1 (0.1%)History of atopic dermatitisa
Yes 740 (88.4 %)No 93 (11.1%)History of asthmaa
Yes 435 (52.0 %)No 393 (47.0 %)History of rhinoconjunctivitisa
Yes 347 (41.5 %)No 468 (55.9 %)Food challenge outcomePositive 466 (55.7 %)Negative 371 (44.3 %)
N (range) IQR (median)Apolipoprotein B (g/l) 837 (0.24-1.31) 0.53-0.77 (0.65)Age (months) 837 (6.00-215.00) 43.00-124.50 (70.00)Specific IgE (kU/l) 837 (0.10-101.00) 0.56-16.80 (3.31)Severity of accidental reaction 837 (0-12) 0.00-5.00 (3.00)Severity of DBPCFC reactionb 466 (1-9) 2.00-5.00 (3.00)Eliciting dose (mg protein)b 466 (0.58-1925.00) 14.00-350.00 (70.00)
Abbreviations: DBPCFC, double-blinded, placebo-controlled food challenge; IgE, immunoglobulin E; IQR, interquar-tile range. aMissing data not shown. bSeverity of DBPCFC reaction and eliciting dose only available for positive food challenge outcomes.

82 CHAPTER 6
The severity of the accidental reaction by history was inversely associated with the con-centration of ApoB (B=-0.09, 95% confidence interval [CI]: -2.53 to -0.33, P=0.011). This relation was not confounded by age, sex, type of food, level of specific IgE, eliciting dose, history of asthma, atopic dermatitis, and rhinoconjunctivitis. This significant association also was seen in the subgroup of patients with a positive history but a negative food chal-lenge outcome (B=-0.15, 95% CI:-3.75 to -0.66, P=0.005) but, remarkably, not for children with a positive history and a positive food challenge outcome (B=-0.05, 95% CI:-2.24 to 0.72, P=0.313).
The concentration of ApoB was not associated with the food challenge outcome (adjusted odds ratio= 0.90, 95% CI: 0.41 to 1.98, P=0.790) or the severity of the DBPCFC reaction (B =-0.01, 95% CI:-1.17 to 1.02, P=0.894). All association models used for the analysis met the assumptions of the test. To examine whether the outliers (the 10 cases outside the CI) had an effect on the outcome, the data were reanalyzed with these cases excluded. However, this analysis showed no difference in the results, and the inverse association between ApoB and the severity of the accidental reaction remained unchanged (data not shown).
DiScuSSion
This study has, for the first time, shown an association between ApoB and the severity of the accidental reaction in children with suspected food allergy. The results of this study suggest that ApoB might be a biomarker for the severity of anaphylactic reactions, prob-ably by virtue of its association with the less stable PAF-AH.
The finding that this marker is associated with severity of anaphylaxis in patients with negative food challenge outcomes is surprising but could be due to the fact that the sever-ity of reactions to foods are governed to a larger extent by other factors such as type and dose of the ingested food, making the relation with ApoB more tenuous. A second conclusion suggested by this finding is that most patients with a negative food challenge outcome indeed experienced an anaphylactic event in the past. In view of the natural history of patients with negative food challenge outcomes, this finding suggests that such anaphylactic events do not seem to have an obvious allergic cause and do not tend to recur.
The association between ApoB and the severity of the accidental reaction is in agree-ment with the previous findings concerning the role of PAF and PAF-AH in anaphylactic reactions. In contrast to PAF-AH, ApoB can be accurately determined from stored frozen serum samples and is more stable, convenient, and inexpensive to measure. Although

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 83
6
measurement of ApoB explains only a relatively small part of the anaphylactic risk, serum samples obtained closer to the time of the anaphylactic reaction and from patients with other forms of anaphylaxis might be more informative. Further studies on this topic are indicated to evaluate this biomarker in food-induced anaphylaxis and other types of ana-phylaxis.
acknowledgments
The authors thank Neomi S. Grotenboer of the Department of Pediatric Pulmonology and Pediatric Allergology at the UMCG for aliquoting the serum samples for analysis.

84 CHAPTER 6
REfERENCES
1. Ogawa Y, Grant JA. Mediators of anaphylaxis. Immunol Allergy Clin North Am. 2007;27:249e260. vii.
2. Brown SG, Stone SF, Fatovich DM, Burrows SA, Holdgate A, Celenza A et al. Anaphylaxis: clinical patterns, mediator release, and severity. J Allergy Clin Immunol. 2013;132:1141e1149.e5.
3. Vadas P, Gold M, Perelman B, Liss GM, Lack G, Blyth T et al. Platelet-activating factor, PAF acetylhy-drolase, and severe anaphylaxis. N Engl J Med. 2008;358:28e35.
4. Vadas P, Perelman B, Liss G. Platelet-activating factor, histamine, and tryptase levels in human anaphylaxis. J Allergy Clin Immunol. 2013;131:144e149.
5. Yost CC, Weyrich AS, Zimmerman GA. The platelet activating factor (PAF) signaling cascade in systemic inflammatory responses. Biochimie. 2010;92: 692e697.
6. Miwa M, Miyake T, Yamanaka T, Sugatani J, Suzuki Y, Sakata S et al. Characterization of serum plateletactivating factor (PAF) acetylhydrolase: correlation between deficiency of serum PAF acetyl-hydrolase and respiratory symptoms. J Clin Invest. 1988;82:1983e1991.
7. Asano K, Okamoto S, Fukunaga K, Shiomi T, Mori T, Iwata M et al. Cellular source(s) of plateletacti-vating-factor acetylhydrolase activity in plasma. Biochem Biophys Res Commun. 1999;261:511e514.
8. Perelman B, Adil A, Vadas P. Relationship between platelet activating factor acetylhydrolase ac-tivity and apolipoprotein B levels in patients with peanut allergy. Allergy Asthma Clin Immunol. 2014;10:20.
9. Vlieg-Boerstra BJ, Bijleveld CM, van der Heide S, Beusekamp BJ, Wolt-Plompen SA, Kukler J et al. Development and validation of challenge materials for double-blind, placebo controlled food chal-lenges in children. J Allergy Clin Immunol. 2004;113:341e346.
10. van der Zee T, Dubois AEJ, Kerkhof M, van der Heide S, Vlieg-Boerstra B. The eliciting dose of peanut in double-blind, placebo-controlled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy Clin Immunol. 2011;128:1031.

CHAPTER 7
AssOCIATION Of STAT6 GENE vARIANTs wITh fOOD ALLERGy DIAGNOsED by DOUbLE-bLIND PLACEbO-CONTROLLED fOOD ChALLENGEs
C. Doriene van GinkelM. Eleonore PetterssonAnthony EJ. DuboisGerard H. Koppelman
Accepted– Allergy 2018

86 CHAPTER 7
ABSTRACT
This study describes the role of two STAT6 gene variants in food allergy using data of patients and their parents who underwent double-blind placebo-controlled food chal-lenges (DBPCFCs). After quality control, 369 trios were analyzed including 262 children (71.0%) with food allergy. Associations were tested by the family based association test (FBAT). The A alleles of both SNPs were associated with food allergy (p=0.036 and p=0.013 for rs324015 and rs1059513, respectively). Furthermore, these A alleles were associated with peanut allergy, higher sIgE levels to both peanut and cow’s milk, more severe symp-toms and higher eliciting doses during peanut and cow’s milk DBPCFCs (all p<0.05). In silico analysis indicates that the identified risk variants increase STAT6 expression which stimulates the differentiation of CD4+ T cells to the Th2 subset. In conclusion, STAT6 vari-ants may be involved in the pathophysiology of food allergy and their role seems to be independent of the allergenic food.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 87
7
intRoDuction
Multiple studies have provided evidence that food allergy is partly genetically determined (1). One potentially important but less well studied gene in this context is signal transducer and activator of transcription 6 (STAT6), which stimulates the differentiation of naive CD4+ T cells to the Th2 subset (2). Two SNPs within STAT6 have been reported to be associated with IgE concentrations and sensitization to foods (3–7), a history of nut allergy (8) and persistence of cow’s milk allergy (CMA) (9). These last studies were based on a history of nut allergy or open food challenges for cow’s milk allergy, both known to have high false-positive rates. Therefore, we used the double-blind placebo-controlled food challenge (DBPCFC), the gold standard, to investigate the genetics of food allergy.
This study aims to investigate the association of two selected SNPs in STAT6, rs324015 and rs1059513, with food allergy defined by any positive DBPCFC. In two subgroups of children who had a DBPCFC for the two most frequently tested allergenic foods (peanut or cow’s milk) we studied the association with 1) peanut and CMA 2) peanut or cow’s milk-specific IgE (sIgE); 3) the dose sensitivity to the tested food and 4) the severity of the food allergic reaction during the DBPCFC.
METhOdS
The GENEVA cohort included 421 trios (parents and child) in which the child had a DBPCFC as part of regular tertiary paediatric allergy care because of a history consistent with an IgE mediated reaction after ingestion of a food. A subgroup of the GENEVA cohort was described previously (10,11). Recruitment took place at the University Medical Center Groningen from 2005 onwards. This study was ethically approved (METc 2004-146) and written informed (parental) consent was obtained.
All DBPCFCs with positive or negative results were included. The DBPCFCs were performed as previously described (12) and sIgE for foods tested in DBPCFC was measured by CAP-FEIA (ImmunoDiagnostics, Uppsala, Sweden). A severity score was calculated based on symptoms registered on the active day of positive DBPCFCs ranging from 0-12 with 1 point for skin symptoms, 2 points for gastrointestinal symptoms and 3 points for upper airway, lower airway and/or cardiovascular/neurological symptoms (13). The eliciting dose was defined as the last dose in milligrams of protein of the allergenic food ingested by the patient on the active day of a positive DBPCFC.

88 CHAPTER 7
The two SNPs were selected because they have previously been shown to be associated with sensitisation to food or a history of food allergy(3-8). DNA was extracted from buccal swabs, saliva (Oragene Saliva Self-Collection Kits (OG-575 DNA-Genotek, Ottawa, Canada) or EDTA blood (DNA investigator kit, QIAGEN, Venlo, the Netherlands). Genotyping was performed by competitive allele-specific PCR by LGC Genomics (LGC, Teddington, UK).
Associations were tested by the family based association test (FBAT 2.0.4 using the addi-tive model (14)) which is robust to population stratification and tests for Mendelian errors. The FBAT is based on the transmission disequilibrium test which compares the alleles transmitted to affected offspring with the expected distribution of alleles among offspring. We did not apply correction for multiple testing since this data reflects a validation of previously identified associations. However, we tested in a two-tailed approach since lit-erature reported conflicting direction of effects. Linkage disequilibrium (LD) between the studied variants was calculated using Haploview 4.2 (15). Trios were excluded when 1) the outcome of the DBPCFC was inconclusive (n=18); 2) ≥2 Mendelian errors were detected (n=6) or 3) when one of the members of the trio had a call rate ≤50% (n=28, the latter two criteria included data of previously published gene variants (10,11)).
The functional consequences and LD patterns were checked in the Finnish and British population using 1000 genomes phase 3 via ensembl.org (16) (r2 threshold 0.8). Expression quantitative trait loci (eQTL) characteristics were studied by genenetwork.nl/bloodeqtl-browser (17) and expression and genomic annotation was studied in the online Haploreg (18) and GTEx project (19) databases.
RESultS
Of the 369 children, 14.1% of the DNA was extracted from blood. Call rates and HWE p-values were 98.9% and 0.57 for rs324015, and 98.2% and 0.94 for rs1059513, respectively. Allele frequencies (AF) of both risk alleles were concordant with literature (AF of minor allele A of rs324015=0.26 with reported AF=0.31(8), 0.24-0.29(20); AF of major allele A of rs1059513 with reported AF=0.91(3), 0.93-0.92(20)). The two SNPS were independent (R2=0.03, D’=1.00) (15).
Of all children, 262 (71.0%) had at least one positive DBPCFC and were thereby defined as hav-ing food allergy. Baseline characteristics are shown in table 1 and genetic association results with a p<0.10 are shown in table 2. The A alleles of both SNPs were significantly associated with being allergic to at least one food. In the subgroup of 205 children tested for peanut, both A alleles were associated with peanut allergy, higher sIgE levels to peanut and more severe symptoms and greater eliciting doses during the peanut DBPCFC. In the subgroup of

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 89
7
117 children tested for CMA, the A allele of rs324015 was significantly associated with higher sIgE levels to cow’s milk and the A allele of rs1059513 was significantly associated with more severe symptoms and greater eliciting doses during the cow’s milk DBPCFC.
Table 1. Descriptive statistics of the study population.DBPCFC confirmed food allergy71.0%(n=262)
DBPCFC confirmed tolerant29.0%(n=107)
Total (n=369)
Male,%(n) 57.1(149) 61.1 (66) 58.3 (215)Number of foods tested in DBPCFC, median, range1 2, 1-5 1, 1-4 1, 1-5Any Positive DBPCFC*%(n/ntested)Peanut 75.8(122/161) (0/44) 59.5(122/205)Cow’s milk 78.0(64/82) (0/35) 54.7(64/117)Hen’s egg 62.9(44/70) (0/20) 48.9(44/90)Hazelnut 56.5(39/69) (0/6) 52.0(39/75)Cashew 93.0(53/57) (0/7) 82.8 (53/64)Walnut 87.0(20/23) (0/6) 69.0(20/29)Soy 34.8 (8/23) (0/3) 30.8(8/26)Almond 9.1(1/11) (0/2) 7.7(1/13)Wheat (0/4) (0/2) 0(0/6)Lupine seed (0/3) (0/2) 0(0/5)Pistachio (0/1) (0/2) 0(0/3)Sesame seed 100(2/2) 100(2/2)Pine nut 100(2/2) 100(2/2)Macadamia nut (0/1) (0/1) 0(0/2)Brazilnut 100(1/1) 100(1/1)Atopic comorbidities%(n/ntested)Atopic dermatitis 89.5(230/257) 83.7(87/104) 87.8(317/361Asthma 58.5 (151/258) 48.5(50/103) 55.7(201/361)Rhinoconjunctivitis 50.2(127/253) 32.0(32/100) 45.0(159/353)sIgE*(KU/l)median,range1 (n)Peanut 6.5,0.0-101.0(162) 2.0,0.3-66.5(43) 5.1,0.0-101.0(205)Cow’s milk 5.2,0.0-101.0(83) 0.3,0.0-19.7(34) 1.9,0.0-101.0(117)Severity of reaction*mean,SD(n)Peanut 3.7,2.3(113)Cow’s milk 3.5, 2.3 (61)Eliciting dose*(mgprotein)median,range1 (n)Peanut 69.9,0.6-725.0(109)Cow’s milk 1750.0,1.8-1750.0(58)
DBPCFC, double-blind placebo-controlled food challenge; FA, food allergy; SD, standard deviation; IQR, interquartile range. *When children had a DBPCFC for multiple foods, they are listed for each food-specific variable. 1Variables which were defined as not normally distributed after visual inspection of the Q-Q plot are presented by median and interquartile range.

90 CHAPTER 7
Of both SNPs, only rs1059513 is in LD with another variant, rs3024971 (R2=1.0) (16). Both genotyped SNPs are localized in the 3’ untranslated region of STAT6 (16), compatible with a role in post-transcriptional gene expression by influencing polyadenylation, translation efficiency and stability of mRNA(21). Locations of both rs324015 and rs3024971 are char-acterized by enhancer histone marks in multiple tissues (18) which influence the acces-sibility to the transcriptional machinery and can be modified by environmental exposures (22). Both genotyped SNPs and rs3024971 are listed in the eQTL browser as CIS-eQTLs for STAT6 in peripheral blood in which the A alleles increase expression of STAT6 (rs324015 minor allele A: Z-score 49.74, p=9.91E-198 and rs1059513 major allele A: Z-score 16.12, p=1.83E-58, rs3024971 major allele A: Z-score=15.93, p=4.03E-57) (17). Furthermore, rs324015 is described as a single-tissue eQTL in oesophageal mucosa (effect size 0.20 for the A allele, p=3.8E-7) and STAT6 is highly expressed in whole blood, skin and small intestines (19).
Table 2. The Family Based Association Test (FBAT) results with a p<0.10.
Trait #fam Z P Risk (ref )
Rs324015
Food allergy DBPCFCconfirmedfoodallergy 221 2.097 0.036 A(g)
Peanut allergy DBPCFCconfirmedpeanutallergy 122 2.365 0.018 A(g)
sIgE 89 2.063 0.039 A(g)
Severity 64 2.131 0.033 A(g)
ED 54 2.558 0.011 A(g)
Cow’s milk allergy
DBPCFCconfirmedcow’smilkallergy 72 1.781 0.075 A(g)
sIgE 58 2.812 0.005 A(g)
Severity 43 1.693 0.090 A(g)
Rs1059513
Food allergy DBPCFCconfirmedfoodallergy 103 2.488 0.013 A(g)
Peanut allergy DBPCFCconfirmedpeanutallergy 60 2.412 0.016 A(g)
sIgE 41 2.195 0.028 A(g)
Severity 31 2.265 0.024 A(g)
ED 29 2.168 0.030 A(g)
Cow’s milk allergy
Severity 18 2.428 0.015 A(g)
ED 15 2.261 0.024 A(g)
Associations of significance are shown in bold. DBPCFC = double-blind placebo-controlled food challenge, sIgE= specific IgE, log transformed to improve distribution (LN(sIgE+1)), ED= Eliciting Dose, log transformed to improve distribution (LN(ED+1)), #fam= numbers of informative families, Z= Z-score, P= p-value, Risk(ref) = risk allele (reference allele).

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 91
7
DiScuSSion
We show for the first time that both A alleles of rs324015 and rs1059513 are associated with food allergy and peanut allergy as diagnosed by DBPCFCs, IgE sensitisation to peanut and cow’s milk, as well as more severe allergic reactions. We therefore conclude that STAT6 genetic polymorphisms may be involved in the pathophysiology of food allergy and their role seems to be independent of the causal allergenic food.
In previous studies, the A allele of rs1059513 was described as a risk variant, associated with asthma (23), atopic dermatitis (24), higher IgE levels (3,7) and sensitisation to com-mon food and inhalant allergens (5). The A allele of rs324015 was previously associated with an increased risk for atopic asthma in a meta-analysis (25) and with eosinophilia in local inflammatory sites (4). In contrast, this A allele was also described as the protec-tive allele for nut allergy in 300 British subjects (8). Interestingly, a gene-gene interaction between the A allele of rs324015 and GT dinucleotide repeat polymorphisms in STAT6 exon 1 was reported to influence the risk of any allergic disease in 168 Japanese subjects (26). Such a gene-gene interaction could explain these conflicting results or they might be due to an as yet unidentified gene-environment interaction, similar to that previously described for CD14 (27). Such a gene-environment interaction is likely to be mediated by epigenetic modifications (22). The functional consequences of the A allele of rs324015 as presented in this paper lends further credence to its role as a risk variant for food allergy.
We show in peanut and cow’s milk allergic cases associations between the A alleles of rs1059513 and rs324015 and a greater eliciting dose. This implies that these A alleles are associated with lower clinical sensitivity (allergic reaction at higher allergen dosages) and that peanut allergic subjects carrying these alleles are at lower risk for allergic reactions. Interestingly, a higher eliciting dose was previously associated with earlier resolution of peanut/tree nut allergy and CMA (28). Therefore our results are consistent with another report describing the association between the A genotype in rs324015 and an earlier age of developing tolerance for CMA (9). However, the A allele is the risk variant for having food allergy and is associated with more severe food allergy. This confirms recent insights regarding the independence of severity and dose sensitivity in food allergy (29). Here we add to these observations and show that clinical reaction severity and dose sensitivity may be under genetic control by a pleotropic effect of STAT6.
Other STAT6 SNPs, which are independent from the 2 SNPs reported here (i.e. rs167769, rs1059513 and rs12368672), have been associated with other allergy related phenotypes such as total IgE, atopic dermatitis, and eosinophilic esophagitis) (6, 30-32), yet prior evi-dence on their association with IgE-mediated food allergy was lacking. Therefore, these

92 CHAPTER 7
SNPs were not included in our study, as our aim was to replicate and validate SNPs with prior evidence for food allergy. We therefore cannot exclude that these other SNPs may also be involved in (food) allergy and IgE production.
The A alleles of both SNPs are risk variants for food allergy and these A alleles are associ-ated with higher expression of STAT6 in several tissues (17,19). By inducing expression of GATA-3, STAT6 enhances expression of the Th2 cytokine genes IL-4, IL-5 and IL-13 which stimulates differentiation of naïve CD4+ T cells to the Th2 subset (2,22). These cytokines subsequently activate mast cells, macrophages and eosinophils to promote allergic re-sponses. In activated B cells, STAT6 promotes immunoglobulin class switching to IgE and expression of antigen presenting cell surface molecules (2). To summarize, STAT6 genetic polymorphisms may be involved in the pathophysiology of food allergy and their role seems to be independent of the causal allergenic food.
acknowledgements
We gratefully acknowledge the cooperation of the children and parents who have partici-pated in the GENEVA study.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 93
7
REfERENCES
1. Hong X, Tsai H-J, Wang X. Genetics of Food allergy. Curr Opin Pediatr. 2009;21(6):770–6.
2. Potaczek DP, Kabesch M. Current concepts of IgE regulation and impact of genetic determinants. Clin Exp Allergy. 2012;42(6):852–71.
3. Granada M, Wilk JB, Tuzova M, Strachan DP, Weidinger S, Albrecht E, et al. A genome-wide as-sociation study of plasma total IgE concentrations in the Framingham Heart Study. J Allergy Clin Immunol. 2012;129(3):840–845.e21.
4. Negoro T, Orihara K, Irahara T, Nishiyama H, Hagiwara K, Nishida R, et al. Influence of SNPs in cytokine-related genes on the severity of food allergy and atopic eczema in children. Pediatr Allergy Immunol. 2006;17(8):583–90.
5. Bønnelykke K, Matheson MC, Pers TH, Granell R, Strachan DP, Alves AC, et al. Meta-analysis of genome-wide association studies identifies ten loci influencing allergic sensitization. Nat Genet. 2013;45(8):902–6.
6. Pino-Yanes M, Cignoux CR, Galanter JM, Levin AM, Campbell CD, Eng C, et al. Genome-wide Associa-tion Study and Admixture Mapping Reveal New Loci Associated with Total IgE Levels in Latinos. J Allergy Clin Immunol. 2015;25(3):1–30.
7. Sharma V, Michel S, Gaertner V, Franke A, Vogelberg C, Von Berg A, et al. Fine-mapping of IgE-associated loci 1q23, 5q31, and 12q13 using 1000 Genomes Project data. Allergy Eur J Allergy Clin Immunol. 2014;69(8):1077–84.
8. Amoli MM, Hand S, Hajeer a H, Jones KP, Rolf S, Sting C, et al. Polymorphism in the STAT6 gene encodes risk for nut allergy. Genes Immun. 2002;3(4):220–4.
9. Yavuz ST, Buyuktiryaki B, Sahiner UM, Birben E, Tuncer A, Yakarisik S, et al. Factors that predict the clinical reactivity and tolerance in children with cow ’ s milk allergy. Ann Allergy, Asthma Immunol. 2013;110(4):284–9.
10. van Ginkel CD, Flokstra-de Blok BMJ, Kollen BJ, Kukler J, Koppelman GH, Dubois AEJ. Loss-of-function variants of the filaggrin gene are associated with clinical reactivity to foods. Allergy. 2015;70(4):461–4.
11. Asai Y, Eslami A, Ginkel CD van, Akhabir L, Wan M, Ellis G, et al. Genome-wide association study and meta-analysis in multiple populations identifies new loci for peanut allergy and establishes c11orf30/EMSY as a genetic risk factor for food allergy. J Allergy Clin Immunol. 2017
12. Vlieg-boerstra BJ, Bijleveld CMA, Heide S Van Der, Beusekamp BJ, Wolt-plompen SAA, Kukler J, et al. Development and validation of challenge materials for double-blind , placebo- controlled food challenges in children. J Allergy Clin Immunol. 2004;113(2):341–6.
13. van der Zee T, Dubois A, Kerkhof M, van der Heide S, Vlieg-Boerstra B. The eliciting dose of peanut in double-blind, placebo-controlled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy Clin Immunol. 2011;128(5):1031–6.
14. Laird N, Horvath S, Xu X. Implementing a unified approach to family based tests of association. Genet Epidemiol. 2000;19(Suppl 1):s36–42.
15. Barrett JC, Fry B, Maller J, Daly MJ. Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics. 2005;21(2):263–5.

94 CHAPTER 7
16. Aken BL, Ayling S, Barrell D, Clarke L, Curwen V, Fairley S, et al. The Ensembl gene annotation system. Database. 2016;2016:1–19.
17. Westra H-J, Peters MJ, Esko T, Yaghootkar H, Schurmann C, Kettunen J, et al. Systematic identification of trans eQTLs as putative drivers of known disease associations. Nat Genet. 2013;45(10):1238–43.
18. Ward LD, Kellis M. HaploReg : a resource for exploring chromatin states , conservation , and regula-tory motif alterations within sets of genetically linked variants. Nucleic Acids Res. 2012;40(D1):930–4.
19. Lonsdale J, Thomas J, Salvatore M, Phillips R, Lo E, Shad S, et al. The Genotype-Tissue Expression (GTEx) project. Nat Genet. 2013;45(6):580–5.
20. Sherry ST. dbSNP: the NCBI database of genetic variation. Nucleic Acids Res. 2001;29(1):308–11.
21. Mayr C. Evolution and Biological Roles of Alternative 3’UTRs. Trends Cell Biol. 2016;26(3):227–37.
22. Potaczek DP, Harb H, Michel S, Alhamwe BA, Renz H, Tost J. Epigenetics and allergy: from basic mechanisms to clinical applications. Epigenomics. 2017;9:539–71.
23. Moffatt MF, Phil D, Gut IG, Demenais F, Strachan DP, Bouzigon E, et al. A Large-Scale, Consortium-Based Genomewide Association Study of Asthma. N Engl J Med. 2010;363(13): 1211–21.
24. Paternoster L, Standl M, Chen C-M, Ramasamy A, Bønnelykke K, Duijts L, et al. Meta-analysis of genome-wide association studies identifies three new risk loci for atopic dermatitis. Nat Genet. 2011;44(2):187–92.
25. Qian X, Gao Y, Ye X, Lu M. Association of STAT6 variants with asthma risk : A systematic review and meta-analysis. Hum Immunol. 2014;75(8):847–53.
26. Tamura K, Suzuki M, Arakawa H, Tokuyama K, Morikawa A. Linkage and Association Studies of STAT6 Gene Polymorphisms and Allergic Diseases. Int Arch Allergy Immunol. 2003;131:33–8.
27. Simpson A, John SL, Jury F, Niven R, Woodcock A, Ollier WER, et al. Endotoxin exposure, CD14, and allergic disease: an interaction between genes and the environment. Am J Respir Crit Care Med. 2006;174(4):386–92.
28. Wainstein BK, Saad RA. Repeat oral food challenges in peanut and tree nut allergic children with a history of mild/moderate reactions. Asia Pac Allergy. 2015;5(3):170.
29. Turner PJ, Baumert JL, Beyer K, Boyle RJ, Chan CH, Clark AT, et al. Can we identify patients at risk of life-threatening allergic reactions to food? Allergy Eur J Allergy Clin Immunol. 2016;71(9):1241–55.
30. Sleiman PMA, Wang M-L, Cianferoni A, Aceves S, Gonsalves N, Nadeau K, et al. GWAS identifies four novel eosinophilic esophagitis loci. Nat Commun. 2014;5:5593.
31. Levin AM, Mathias RA, Huang L, Roth LA, Daley D, Myers RA, et al. A meta-analysis of genome-wide association studies for serum total IgE in diverse study populations. J Allergy Clin Immunol. 2013;131(4):1176–84.
32. Weidinger S, Gieger C, Rodriguez E, Baurecht H, Mempel M, Klopp N, et al. Genome-wide scan on to-tal serum IgE levels identifies FCER1A as novel susceptibility locus. PLoS Genet. 2008;4(8):e1000166.

CHAPTER 8
mAsTOCyTOsIs AND AGE, bUT NOT bAsELINE TRyPTAsE, sPECIfIC IGE OR TOTAL IGE, INDEPENDENTLy DETERmINE ThE sEvERITy Of sysTEmIC REACTIONs TO yELLOw jACkET sTINGs.
M. Eleonore Pettersson*Byrthe JPR. Vos*Boudewijn J. Kollen,Suzanne ArendsJoanne NG. Oude ElberinkAnthony EJ. Dubois*These authors contributed equally to this work
Conditionally accepted – Clinical and Experimental Allergy 2018

96 CHAPTER 8
ABSTRACT
Background: Although entities such as mastocytosis, elevated basal tryptase values and cardiovascular disease are considered to increase the risk of severe reactions to hyme-noptera stings, it is largely unknown to what extent these factors independently predict reaction severity and thus how much clinicians may rely on them to risk stratify venom allergic patients.
Objective: To determine independent clinical risk factors for systemic reaction severity to yellow jacket stings in untreated patients, with and without indolent systemic mastocyto-sis (ISM).
Methods: All patients visiting our center between 2009 and 2015 because of a systemic reaction to a yellow jacket sting and subsequently receiving a diagnosis of yellow jacket venom allergy were included. All patients were screened for mastocytosis. Systemic reac-tions were classified according to Mueller. The statistical analysis was performed using linear regression.
Results: Independent predictors for the severity grade were ISM (β= 0.415, P<0.001) and older age (β= 0.219, P<0.001), but not baseline serum tryptase (bsT) (β=0.177, P=0.054), cardiovascular event (β=0.111, P=0.054), cardiovascular risk score (β=0.017, P=0.881), level of total IgE (β=-0.042, P=0.473) or level of sIgE (β=0.044, P=0.541). This prediction model explained 23.0% of the variance of the severity grade (N=253, P<0.001).
Conclusions: ISM and age should be considered in the risk assessment of severe reactions to yellow jacket stings. BsT cannot predict the reaction severity independently of the diagnosis of ISM, but it is useful in diagnosis and screening for ISM. However, the severity of reactions to yellow jacket stings remains for the greatest part unpredictable.
clinical implications
Although several factors increase the risk of severe reactions to yellow jacket stings, these can only predict the severity of a reaction to a small extent. Thus, clinicians should not strongly rely on these factors to risk stratify venom allergic patients.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 97
8
intRoDuction
Several patient characteristics have previously been shown to be associated with severe systemic sting reactions. Systemic reactions can present at any age although they occur less often, and are mostly mild in children. In contrast, individuals above 65 years of age are at risk for more severe reactions.(1, 2) Remarkably, there is no association between the risk of, or severity of systemic reactions and having an atopic constitution or having experienced anaphylaxis from other causes. Moreover, high levels of total IgE (>250 kU/L) do not seem to increase risk and might even be protective.(3-5)
Although it is plausible that patients with pre-existing respiratory and cardiovascular disease are prone to have more severe reactions, reports are contradictory.(6, 7) This also applies to beta-blocker and ACE-inhibitor use, which theoretically could lead to more severe and protracted anaphylaxis due to beta-adrenergic blockade and imbalances in the renin-angiotensin system. However, this effect has not consistently been found clinically.(7-10)
There is a strong relationship between reaction severity to insect venoms and elevated baseline serum tryptase (bsT) levels. BsT is thought to reflect the mast cell burden (mast cell number and activity) as tryptase is predominantly produced by mast cells.(11) Approximately 10% of the Hymenoptera venom allergic population has an elevated bsT level, consisting of enzymatically inactive α- and β-protryptase that is spontaneously secreted by mast cells without stimulation.(10, 12) Even a small increase in this level seems to be associated with more frequent and severe systemic reactions, although this result was not adjusted for mastocytosis.(10)
Patients with indolent systemic mastocytosis (ISM) suffer from a clonal proliferation of abnormal mast cells and represent a particular risk group for frequent and severe anaphy-lactic reactions, which probably relates to excessive mediator release following triggering of mast cells.(13)
It has previously been shown that platelet-activating factor (PAF), is closely correlated to the severity of anaphylactic reactions.(14, 15) PAF triggers hypotension, bronchoconstric-tion and vascular permeability.(16, 17) The catalyzation of the degradation of PAF is initi-ated by PAF acetylhydrolase (PAF-AH), and a lower level of of PAF-AH has been shown to increase the risk of life-threatening anaphylaxis.(18) PAF-AH circulates in complexes with low- and high-density lipoproteins in human plasma, and the main protein component of low-density lipoprotein particles is apolipoprotein B-100 (ApoB). A strong correlation between the activity of PAF-AH and the concentration of the more stable ApoB has previ-ously been shown.(19) Thus, this suggests an association between the severity of allergic reactions and the plasma concentration of ApoB.

98 CHAPTER 8
Although entities such as mastocytosis and elevated basal tryptase are known to increase the risk of severe reactions to hymenoptera stings, it is largely unknown to what extent these factors predict reaction severity and thus how much clinicians may rely on them to risk stratify venom allergic patients. Moreover, it is currently not clear if tryptase and ISM are predictors of the reaction severity independently of each other. Thus, the purpose of this study was to determine independent clinical risk factors for the severity of systemic reactions to yellow jacket stings in untreated patients, with and without ISM.
METhOdS
Subjects
Study design and population. All patients visiting the department of Allergology in our ter-tiary care clinic between 2009 and 2015 because of a systemic reaction to a yellow jacket sting, and who after clinical evaluation received a diagnosis of yellow jacket venom (YJV) allergy, were included in the analysis. The diagnosis of YJV allergy followed international guidelines and was based on the patient’s history and YJV-specific (s)IgE ≥0.35 KUA/L or a positive intracutaneous skin test (mean wheal diameter ≥5 mm at a concentration of ≤1 µg/mL).(20) Systemic reactions were classified according to Mueller, (21) with separation of grade IV reactions into severe (a) and very severe (b), as previously described.(22) The severity grade was determined by the severity of the systemic sting reaction immediately preceding the biochemical and immunological serum sampling, from now on referred to as the index sting. The local medical ethics committee deemed that official medical ethical approval was not required.
Exclusion criteria. Patients who visited our clinic after more than 3 years since the last sting reaction were excluded, because the determinants (e.g. sIgE and bsT) in serum and urine may not be representative of the moment of the sting.(23, 24) Included patients were not treated with venom immunotherapy (VIT) before the index sting.
Clinical and biochemical data collection. All information was gathered from medical charts regarding the severity of systemic reactions and demographic data, including cardiovascu-lar risk factors (hypertension, hypercholesterolemia, left ventricular hypertrophy, diabetes mellitus) and cardiovascular events (myocardial infarction (MI) or stroke) and antihyper-tensive medication use at the time of the index sting. All serum and urine samples were taken at the first patient visit. The time interval between the index sting and sample col-lection was at least two weeks, circumventing a potential interference of the index allergic reaction on the bsT level.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 99
8
Cardiovascular risk score. A modified version of the scoring system from Pocock et al.(25) was used to determine the cardiovascular risk profile of patients. This scoring system indi-cates the risk of death due to cardiovascular disease and gives weighed scores to sex, age, hypertension, hypercholesterolemia, a history of MI or stroke, left ventricular hypertrophy, and diabetes. Each factor received a corresponding weighed score while antihypertensive treatment reduced the score (Table 1). All of the individual scores for each factor were summed, and the total score ranged from 0-50.
Table 1. Cardiovascular risk score.
Female
Risk factor Addition to risk score Risk score
Age (years) 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74
0 +5 +9 +14 +18 +23 +27 +32
No Yes
Systolicbloodpressure>140mm Hg
0 +3
Totalcholesterol>6.5mmol/l 0 +1
History of myocardial infarction 0 +8
History of stroke 0 +8
Left ventricular hypertrophy 0 +3
Diabetes 0 +9
Total risk score*
Male
Risk factor Addition to risk score Risk score
Male gender +12
Age (years) 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74
0 +4 +7 +11 +14 +18 +22 +25
No Yes
Systolicbloodpressure>140mm Hg
0 +3
Totalcholesterol>6.5mmol/l 0 +4
History of myocardial infarction 0 +8
History of stroke 0 +8
Left ventricular hypertrophy 0 +3
Diabetes 0 +2
Total risk score*
*If antihypertensive drugs are taken, the risk score is reduced by 2 points. Table modified from Pocock et al.9 Values beginning with + indicate extra points added to the score.

100 CHAPTER 8
Diagnostic procedures
Serum analytes. YJV-sIgE and total IgE was measured using the ImmunoCAP system (Ther-mo Fisher Scientific Inc., Phadia AB, Uppsala, Sweden). ApoB levels were determined in the same stored samples by means of immunonephelometry on the BNII System (Siemens Healthcare GmbH, Erlangen, Germany). BsT levels were determined with the B12 assay using ImmunoCAP Tryptase reagents and the Phadia 250 analysis device (Thermo Fisher Scientific Inc., Phadia AB, Uppsala, Sweden). The inter-assay analytical coefficient of varia-tion in our laboratory is 5.8%. BsT concentrations >10 µg/L were checked and corrected for heterophilic antibodies.
Urine analytes. Urine samples for MH and MIMA determination were collected in contain-ers with a small amount of chlorhexidine. Values consistent with mastocytosis were re-evaluated, collecting new samples after an overnight fast and discarding the first morning voiding. Subjects were asked to refrain from histamine-rich foods and drinks for 24 hours before urine collection. Levels of MH and MIMA were determined by an isotope-dilution mass fragmentographic method.(26, 27) The inter-assay analytical coefficient of variation in our laboratory is 6.8% for MH and 4.2% for MIMA.
Mastocytosis screening. The diagnosis of ISM was established according to the World Health Organization (WHO) criteria.(28) All patients were screened for mastocytosis by serum bsT measurement, clinical history and skin inspection for clinical lesions compatible with urticaria pigmentosa (UP). All patients with UP underwent bone marrow examina-tions, irrespective of the bsT concentration. Patients without UP underwent bone marrow examinations when the bsT concentration was >10 µg/L. Bone marrow examinations were also performed when the bsT concentration was <10 µg/L and if the urinary meth-ylhistamine (MH) concentration was ≥176 and/or a methylimidazole acetic acid (MIMA) concentration of ≥2.0.(29) Patients with clinical suspicion of ISM that did not undergo bone marrow examinations for exclusion or confirmation of this diagnosis were classified as possible mastocytosis, because systemic mastocytosis cannot be ruled out.(29)
Bone marrow examinations. Bone marrow examinations were performed as previously described.(30) Briefly, bone marrow biopsies were taken from the iliac crest and examined for the presence of multifocal clusters or cohesive aggregates/infiltrates of >15 mast cells and for spindle-shaped, immature mast cells and for mast cells with atypical morphology by tryptase and CD117 staining. Mast cell immunophenotyping was performed by analyz-ing CD45-positive/bright CD117-positive mast cells for expression of CD2 and CD25 by flow cytometry. The presence of the KIT D816V mutation was examined in RNA of bone marrow aspirates.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 101
8
Statistical methods
Statistical analysis was performed with IBM Statistics 22.0 (SPSS, Armonk, NY). P values <0.05 were considered statistically significant. The variables included in the analysis were pre-selected according to previously published data in addition to variables hypothesized to be of influence on the outcome by the authors.
Predictor analysis for reaction severity was performed by using multivariate linear regres-sion with a conditional stepwise backward selection procedure (P<0.05). Only variables which had a P value of ≤0.20 in univariate analysis were included. Only statistically signifi-cant factors were included in the model. The variables time interval between index sting and serum sampling, level of MH, MIMA, bsT, YJV-sIgE and total IgE were logarithmically transformed. Back-transformed values were reported. All assumptions for conducting this statistical analysis were met.
RESultS
characteristics of the whole patient cohort
Between 2009 and 2015, 294 patients visited our clinic because of a YJV allergy of which 42 (14.3%) were ultimately diagnosed with ISM. After applying the pre-defined selection criteria, 270 patients were included in the analysis. The diagnosis of ISM was excluded in 211 patients. Two patients without clinical suspicion of ISM, in whom MH and MIMA determinations had not been done and with bsT levels of 3.2 and 4.1 µg/L were included in this non-mastocytosis group, since none of the patients without clinical suspicion of ISM and a bsT <5.0 µg/L had an elevated MH or MIMA. An overview of the patient selection procedure according to the diagnosis or exclusion of ISM is provided in Figure 1.
In the total study population, the mean patient age was 51.9 ±13.8 years and the majority of patients were male (52.6%). More than half of the patients had a severe or very severe reaction to the index sting (58.5%). Of all patients with a very severe reaction, 41.1% had a confirmed diagnosis of ISM. Some patients had known concomitant cardiovascular risk factors such as hypertension (21.9%), hypercholesterolemia (5.9%), left ventricular hypertrophy (1.1%), diabetes (7.4%) or had experienced cardiovascular events (7.0%). Some were taking antihypertensive medication at the time of the index sting for instance ACE-inhibitors (10.7%), beta-blockers (12.2%), or any antihypertensive drug (25.2%). The median time between the index sting and sampling of serum and urine was 4.8 months (2.3-8.5). The median YJV-sIgE was 4.3 kUA/L (1.2-12.7), median total IgE 61.0 kUA/L (29.3-136.0), median bsT 5.6 µg/L (4.2-8.2), and the mean ApoB g/L 1.10 ±0.31. Further patient

102 CHAPTER 8
characteristics according to the severity grade are shown in Table 2. The results of the univariate analysis is shown in Table 3.
Figure 1. Flowchart of the patient selection procedure according to the status of indolent systemic mastocytosis.
Abbreviations: ISM, indolent systemic mastocytosis; MH, methylhistamine; MIMA, Methylimidazole acetic acid; SR, severity grade; UP, Urticaria pigmentosa; YJV, yellow jacket venom.*MH and MIMA missing in two cases.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 103
8
Tabl
e 2.
Clin
ical
and
bio
chem
ical
cha
ract
eristi
cs o
f sub
ject
s with
a h
istor
y of
syst
emic
reac
tions
to y
ello
w ja
cket
sting
s acc
ordi
ng to
seve
rity
grad
e.
SRgradeI
SRgradeII
SRgradeIII
SRgradeIV
aSR
gradeIV
b
Num
ber
1741
5468
90Ag
e at
stin
g (y
ears
)50.9±12.7
49.1±15.0
45.6±11.8
53.6±13.4
56.0±13.5
Male,n(%
)8(47.1)
20(4
8.8)
29(5
3.7)
35 (5
1.5)
50(5
5.6)
ISM,n
(%)
0(0)
0(0)
0(0)
5(7.4)
37(4
1.1)
Non
-ISM
,n(%
)14
(6.6
)36(1
7.1)
52 (2
4.6)
57(2
7.0)
52 (2
4.6)
Hypertension,n(%
)6
(35.
3)6
(14.
6)9(16.7)
17(2
5.0)
21 (2
3.3)
Hypercholesterolemia,n
(%)
0(0)
3(7.3)
2(3.7)
4(5.9)
7(7.8)
Myocardialinfarctionorstroke,n
(%)
0(0)
2(4.9)
2(3.7)
6 (8
.8)
9(10.0)
Leftventricularhypertro
phy,n(%
)0(0)
0(0)
1(1.9)
0(0)
2 (2
.2)
Diabetesm
ellitus,n
(%)
1(5.9)
3(7.3)
3 (5
.6)
4(5.9)
9(10.0)
ACE-inhibitoru
se,n
(%)
1(5.9)
4(9.8)
2(3.7)
10(1
4.7)
12 (1
3.3)
Beta-blockeruse,n
(%)
3(17.6)
3(7.3)
4(7.4)
10(1
4.7)
13 (1
4.4)
Anyantih
ypertensivemedicationuse,n(%
)4
(23.
5)9(22.0)
9(16.7)
19(2
7.9)
27(3
0.0)
Cardiovascularrisk
(score0-50)
19.3±11.0
19.0±10.2
15.6±10.3
21.4±12.2
23.7±10.6
Tim
e in
terv
al b
etw
een
inde
x sti
ng a
nd
seru
m sa
mpl
ing
(mon
ths)
4.1(2.3-7.3)
6.9(3.0-9.2)
4.3(2.3-6.9)
4.6
(2.3
-11.
6)5.3(2.1-8.7)
YJV-sIgE
(kUA/L)
8.23(2
.00-25.15)
4.09(1
.65-11.96)
4.97(1
.53-10.53)
4.62(1
.46-17.68)
2.52(0
.81-7.67)
TotalIgE
(kUA/L)
100.00
(43.95-128.00)
67.80
(32.50-154.50)
66.2
5
(33.75-123.25)
88.9
(38.60-158.00)
49.95
(19.78-109.25)
BsT(μ
g/L)
4.62(3
.05-5.68)
5.23
(3.4
3-6.
25)
4.76(3
.65-6.32)
5.47(4
.24-8.08)
8.03(5
.28-18.80)
MH(μ
mol/m
olcreatinine)
83.00
(59.50-119.00)
97.00
(71.00-113.00)
92.50
(72.00-120.25)
102.00
(78.00-143.00)
115.00
(83.50-184.00)
MIM
A(m
mol/m
olcreatinine)
1.50(1
.13-2.18)
1.40(1
.28-2.10)
1.40(1
.23-1.75)
2.50(1
.70-3.40)
2.50(1
.70-3.43)
ApoB
(g/L)
1.04±0.36
1.05±0.28
1.10±0.29
1.15±0.34
1.10±0.30
Dat
a is
prese
nted
as m
eans
with
stan
dard
dev
iation
s, me
dian
with
inter
quar
tile r
anges
and
freq
uenc
ies w
ith p
ercen
tages
. Abb
reviat
ions:
Apo
B, A
polip
opro
tein
B; B
sT, b
aseli
ne se
rum
trypt
ase;
ISM
, ind
olent
syste
mic m
astoc
ytosis
; MH
, meth
ylhist
amin
e; M
IMA
, meth
ylimi
dazo
le ac
etic a
cid; S
R; sy
stemi
c rea
ction
; YJV
; yell
ow ja
cket
venom
.

104 CHAPTER 8
Table 3. Selection of variables for the prediction model of the severity grade based on univariate analysis.
N B 95%CI P-value
Age (years) 270 0.019 0.009-0.030 <0.001
Malegender* 270 0.119 -0.183-0.421 0.439
DiagnosisorexclusionofISM 253 1.421 1.047-1.795 <0.001
DiagnosisorexclusionofUrticariaPigmentosa 270 1.227 0.585-1.870 <0.001
Historyofrespiratorydisease* 270 -0.034 -0.479-0.410 0.880
HistoryofMI/Stroke 270 0.556 -0.031-1.143 0.063
Cardiovascularrisk(score0-50) 270 0.022 0.009-0.035 0.001
Beta-blockeruse* 270 0.202 -0.259-0.663 0.388
ACE-inhibitor use 270 0.364 -0.122-0.850 0.142
Any antihypertensive medication use 270 0.244 -0.103-0.591 0.167
YJV-sIgE(kUA/L)# 268 -0.113 -0.261-0.018 0.093
TotalIgE(kUA/L)# 268 -1.201 -1.366-1.054 0.006
sIgE-totalIgEratio#* 267 0.005 -1.113-1.124 0.929
BsT(μg/L)# 270 1.113 0.718-1.599 <0.001
MH(μmol/molcreatinine)# 268 2.075 1.543-2.790 <0.001
MIMA(mmol/molcreatinine)# 88 1.892 0.568-4.339 0.001
ApoB(g/L)* 250 0.305 -0.198-0.809 0.234
Time interval between index sting and serum sampling(months)#*
2700.046 -0.164-0.274 0.652
Abbreviations: ApoB, Apolipoprotein B; B, regression coefficient; BsT, baseline serum tryptase; CI, confidence interval; ISM, indolent systemic mastocytosis; MH, methylhistamine; MIMA, methylimidazole acetic acid; SR; systemic reac-tion; YJV; yellow jacket venom. *The variable was not tested in multivariate regression analysis because of a P value > 0.20 in univariate regression analysis. #Backtransformed values.
Risk factors for severe systemic reactions to a Yj field sting
In the population where the diagnosis of ISM was established or excluded (N=253), sig-nificant independent predictors for the severity grade were ISM (β= 0.415, P<0.001) and age (β= 0.219, P<0.001). This prediction model could explain 23.0% of the variance of the severity grade, see Table 4. Factors not found to independently predict the reaction sever-ity were bsT (β=0.177, P=0.054), history of MI or stroke (β=0.111, P=0.054), cardiovascular risk score (β=0.017, P=0.881), ACE-inhibitor use (β=0.029, P=0.643), any antihyperten-sive medication use (β=0.007, P=0.920), UP (β=-0.014, P=0.842), level of MH (β=0.071, P=0.318), level of total IgE (β=-0.042, P=0.473) or level of sIgE (β=0.044, P=0.541).

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 105
8
Table 4. Prediction models for the severity grade in the whole study group, and for only those with a definite diagnosis (either confirmed ISM or those without clinical suspicion of ISM).
Study population Predictor B 95%CI P-value
N=268, ISM excluded.
R2=0.221 Age 0.016 0.005-0.026 0.003
HistoryofMI/Stroke 0.546 0.004-1.087 0.048
BsT# 0.793 0.409-1.282 <0.001
MH# 1.477 1.067-2.046 0.019
N=253, ISM included.
R2=0.230 Age 0.020 0.010-0.030 <0.001
ISM 1.380 1.016-1.744 <0.001
Abbreviations: ApoB, Apolipoprotein B; B, regression coefficient; BsT, baseline serum tryptase; CI, confidence interval; ISM, indolent systemic mastocytosis; MH, methylhistamine; MIMA, methylimidazole acetic acid; R2, explained vari-ance; SR, systemic reaction; YJV, yellow jacket venom. #Backtransformed values.
In the total study population, also including patients for whom the diagnosis of ISM was in-conclusive (N=17), ISM was not included in the prediction model. Significant independent predictors for the severity grade were age (β= 0.173, P=0.003), bsT (β= 0.365, P <0.001), level of MH (β= 1.165, P=0.019) and history of MI or stroke (β= 0.111, P=0.048). This prediction model explained 22.1% of the variance of the severity grade. MIMA was only tested in a sub-group with available data (N=88), but it was not found to be a significant independent predictor for the severity grade (B=-0.374, P=0.384).
In linear regression analysis, there was no collinearity between the bsT concentration and ISM (data not shown). The analysis of a potential interaction between the level of bsT in patients with and without ISM was not significant (P=0.106 for the tryptase/ISM interac-tion term in the model).
Additionally, in patients not suspected of systemic mastocytosis with bsT levels within the normal range (<10.0μg/L; n=206), the association with the severity grade in univari-ate analysis (B=0.950, 95%CI=0.184-2.212, P=0.009) disappeared when corrected for age (B=0.597, 95%CI=-0.034-1.635, P=0.067). Thus, the level of bsT did not independently predict the severity grade in non-ISM patients with bsT levels within the normal range, since this effect was abrogated by including age in the model.

106 CHAPTER 8
DiScuSSion
With the identified clinical risk factors, we are able to predict only 23.0% of the severity grade of systemic reactions to yellow jacket stings. Independent risk factors for severe sting reactions were diagnosis of ISM and older age. ISM was shown to be the largest independent risk factor for predicting reaction severity. This result confirms ISM to be the most important clinical risk factor for reaction severity to YJV.
In the study group where the diagnosis or exclusion of ISM was inconclusive, older age, a higher bsT level, a higher MH level and a history of cardiovascular events were shown to be independent predictors of reaction severity. However, the level of bsT, MH level and history of cardiovascular events are likely to represent ISM, since these factors were not significant predictors when ISM was included in the model.
Strikingly, we found that bsT level within the normal range (<10.0μg/L) does not predict reaction severity in patients without ISM, after adjusting for age. This is in contrast to a previous study(10), in which, however, ISM was not taken into account. Thus, bsT seems to merely be an indicator of ISM and increasing age, and it is not an independent de-terminant of reaction severity. Notably, the bsT level have previously been shown to be inappropriately elevated in older and overweight patients.(30)
No role for beta-blockers or ACE-inhibitors could be found in predicting the severity of reaction, in line with a recent review article.(31) Similarly, the level of MIMA was not shown to be an independent predictor in a sub-group analysis. This result is not likely to be caused by a lack of power, since the level of MIMA was shown to be a significant factor in the univariate analysis.
Total IgE was not an independent predictor for the severity grade after adjusting for ISM. It has previously been suggested that patients with stinging insect allergy and high levels of total IgE generally have milder systemic reactions, whereas patients with low levels of total IgE generally have more severe systemic reactions.(5) However, a more recent study correcting for additional factors, such as age and level of baseline serum tryptase, no such relationship for vespula venom allergy was found.(32) Thus, an increased level of total IgE could possibly be linked to an unknown diagnosis of ISM or increasing age, which is probably why total IgE is not an independent predictor of reaction severity. It has previously been shown that the presence of venom sIgE is significantly associated with a history of systemic reactions to Hymenoptera stings. However, the level of venom sIgE was not related to severity.(33) This is in agreement with our results.
APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 107
8
In contrast to a previous study, which showed a relationship between the severity grade and the level of PAF-AH, (34) we could not show a relationship between the severity grade and ApoB. However, this previous study did not take ISM into account. Moreover, PAF and PAF-AH have previously been shown to be linked to cardiovascular disease.(35) Thus the influence of PAF and/or PAF-AH on the severity of reaction could be difficult to demon-strate in a population with pre-existing cardiovascular disease.
According to a previous study, it is possible that some patients classified as being in the non-ISM group, without UP and without an increased level of bsT, may nevertheless have unidentified ISM.(36) However, this previous study used a higher bsT cut-off value (11.4 ng/ml), had a highly selected study population and only included patients with severe systemic reactions. In addition, this previous study did not determine levels of MH and/or MIMA. Moreover, a previous study from our own center (29) showed that the risk of ISM is very low in patients without UP and a bsT below 10 µg/l.
To date, the majority of factors determining the severity of reaction remains unknown. This could be explained by the fact that systemic reactions to stinging insects take place under specific individual circumstances, with varying augmenting factors present for each occurrence. Furthermore, the clinical outcome of a severe reaction could be influenced by prompt treatment with an adrenaline auto-injector.
A possible limitation of this study is that the data was collected from patient charts, which could have led to an underestimation of minor risk factors such as hypertension and hypercholesterolemia due to the registration method. However, serious cardiovascular events were not predictive of the reaction severity when including ISM in the model. A larger impact on reaction severity by minor cardiovascular risk factors, as compared to serious cardiovascular events is improbable. Thus, it is unlikely that minor cardiovascular risk factors would be associated with reaction severity if another data collection method was used.
The strengths of this study were the determination of the diagnosis of ISM with the gold standard bone marrow biopsy, that tryptase was determined in all subjects and that many probable factors were included in the model. The inclusion of a comprehensive number of factors is important for accurate interpretation of the impact of individual factors on the reaction severity.
In conclusion, the majority of factors determining reaction severity to YJV remains un-known. ISM is the most important determinant of severe systemic reactions to yellow jacket stings. Serum baseline tryptase is not an independent predictor of the reaction

108 CHAPTER 8
severity, but merely reflects the impact of ISM. Thus, ISM and age are the most important known independent factors in the risk assessment of severe reactions to yellow jacket stings.
acknowledgements
The authors thank P.M. Kluin of the Department of pathology for critically revising the bone marrow biopsies, and A.B. Mulder of the Department of laboratory medicine for immunophenotyping and C-KIT mutation analysis.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 109
8
REfERENCES
1. Chipps BE, Valentine MD, Kagey-Sobotka A, et al. Diagnosis and treatment of anaphylactic reactions to Hymenoptera stings in children. J Pediatr 1980;97:177-84.
2. Bilò MB. Anaphylaxis caused by Hymenoptera stings: from epidemiology to treatment. Allergy 2011;66 Suppl 95:35-7.
3. Settipane GA, Newstead GJ, Boyd GK. Frequency of Hymenoptera allergy in an atopic and normal population. J Allergy Clin Immunol 1972;50:146-50.
4. Solley GO. Stinging and biting insect allergy: an Australian experience. Ann Allergy Asthma Immunol 2004;93:532-7.
5. Sturm GJ, Heinemann A, Schuster C, et al. Influence of total IgE levels on the severity of sting reactions in Hymenoptera venom allergy. Allergy 2007;62:884-9.
6. Mueller UR. Cardiovascular disease and anaphylaxis. Curr Opin Allergy Clin Immunol 2007;7:337-41.
7. Stoevesandt J, Hain J, Kerstan A, et al. Over- and underestimated parameters in severe Hymenop-tera venom-induced anaphylaxis: cardiovascular medication and absence of urticaria/angioedema. J Allergy Clin Immunol 2012;130:698,704.e1.
8. Toogood JH. Beta-blocker therapy and the risk of anaphylaxis. CMAJ 1987;136:929-33.
9. Stumpf JL, Shehab N, Patel AC. Safety of Angiotensin-converting enzyme inhibitors in patients with insect venom allergies. Ann Pharmacother 2006;40:699-703.
10. Ruëff F, Przybilla B, Bilò MB, et al. Predictors of severe systemic anaphylactic reactions in patients with Hymenoptera venom allergy: importance of baseline serum tryptase-a study of the European Academy of Allergology and Clinical Immunology Interest Group on Insect Venom Hypersensitivity. J Allergy Clin Immunol 2009;124:1047-54.
11. Schwartz LB. Clinical utility of tryptase levels in systemic mastocytosis and associated hematologic disorders. Leuk Res 2001;25:553-62.
12. Bonadonna P, Perbellini O, Passalacqua G, et al. Clonal mast cell disorders in patients with sys-temic reactions to Hymenoptera stings and increased serum tryptase levels. J Allergy Clin Immunol 2009;123:680-6.
13. Horny HP, Sotlar K, Valent P. Mastocytosis: state of the art. Pathobiology 2007;74:121-32.
14. Ogawa Y, Grant JA. Mediators of anaphylaxis. Immunol Allergy Clin North Am. 2007;27:249e260.
15. Brown SG, Stone SF, Fatovich DM, et al. Anaphylaxis: clinical patterns, mediator release, and sever-ity. J Allergy Clin Immunol. 2013;132:1141e1149.e5.
16. Yost CC, Weyrich AS, Zimmerman GA. The platelet activating factor (PAF) signaling cascade in systemic inflammatory responses. Biochimie. 2010;92:692e697.
17. Miwa M, Miyake T, Yamanaka T, et al. Characterization of serum plateletactivating factor (PAF) acetylhydrolase: correlation between deficiency of serum PAF acetylhydrolase and respiratory symptoms. J Clin Invest. 1988;82:1983e1991.
18. Vadas P, Gold M, Perelman B, et al. Platelet-activating factor, PAF acetylhydrolase, and severe anaphylaxis. N Engl J Med. 2008;358:28e35.

110 CHAPTER 8
19. Perelman B, Adil A, Vadas P. Relationship between platelet activating factor acetylhydrolase ac-tivity and apolipoprotein B levels in patients with peanut allergy. Allergy Asthma Clin Immunol. 2014;10:20.
20. Golden DB, Moffitt J, Nicklas RA, et al. Stinging insect hypersensitivity: a practice parameter update 2011. J Allergy Clin Immunol 2011;127:852-4.
21. Müller HL. Diagnosis and treatment of insect sensitivity. J Asthma Res 1966;3:331-3.
22. Vos BJPR, van Anrooij B, van Doormaal JJ, Dubois AEJ, Oude Elberink JNG. Fatal Anaphylaxis to Yellow Jacket Stings in Mastocytosis: Options for Identification and Treatment of At-Risk Patients. J Allergy Clin Immunol Pract. 2017;5:1264-1271. doi: 10.1016/j.jaip.2017.03.019.
23. Golden DB. Insect sting anaphylaxis. Immunol Allergy Clin North Am 2007;27:261,72, vii.
24. Alvarez-Twose I, Zanotti R, Gonzalez-de-Olano D, et al. Nonaggressive systemic mastocytosis (SM) without skin lesions associated with insect-induced anaphylaxis shows unique features versus other indolent SM. J Allergy Clin Immunol 2014;133:520-8.
25. Pocock SJ, McCormack V, Gueyffier F, et al. A score for predicting risk of death from cardiovascular disease in adults with raised blood pressure, based on individual patient data from randomised controlled trials. BMJ 2001;323:75-81.
26. Keyzer JJ, Wolthers BG, Breukelman H, et al. Determination of N tau-methylhistamine in urine by gas chromatography using nitrogen-phosphorus detection. J Chromatogr 1983;275:261-9.
27. Keyzer JJ, Wolthers BG, Breukelman H, et al. Determination of N tau-methylimidazoleacetic acid (a histamine metabolite) in urine by gas chromatography using nitrogen-phosphorus detection. Clin Chim Acta 1982;121:379-87.
28. Valent P, Akin C, Escribano L, et al. Standards and standardization in mastocytosis: consensus statements on diagnostics, treatment recommendations and response criteria. Eur J Clin Invest 2007;37:435-53.
29. van Doormaal JJ, van der Veer E, van Voorst Vader PC, et al. Tryptase and histamine metabolites as diagnostic indicators of indolent systemic mastocytosis without skin lesions. Allergy 2012;67:683-90.
30. Vos BJ, van der Veer E, van Voorst Vader PC, et al. Diminished reliability of tryptase as risk indicator of mastocytosis in older overweight subjects. J Allergy Clin Immunol 2015;135:792-8.
31. Sturm GJ, Varga EM, Roberts G, Mosbech H, Bilò MB, Akdis CA et al. EAACI Guidelines on Allergen Immunotherapy: Hymenoptera venom allergy. Allergy. 2017 Jul 27. doi: 10.1111/all.13262. [Epub ahead of print]
32. Blum S, Gunzinger A, Muller UR, Helbling A. Influence of total and specific IgE, serum tryptase, and age on severity of allergic reactions to Hymenoptera stings. Allergy 2011; 66: 222–228.)
33. Bilo BM, Rueff F, Mosbech H, Bonifazi F, Oude-Elberink JN, the EAACI Interest Group on Insect Venom Hypersensitivity. Diagnosis of Hymenoptera venom allergy. Allergy 2005;60:1339–1349.).
34. Pravettoni V, Piantanida M, Primavesi L, Forti S, Pastorello EA. Basal platelet-activating factor acetyl-hydrolase: prognostic marker of severe Hymenoptera venom anaphylaxis. J Allergy Clin Immunol. 2014 Apr;133(4):1218-20. doi: 10.1016/j.jaci.2013.10.033.)
35. Triggiani M, Montagni M, Parente R, Ridolo E. Anaphylaxis and cardiovascular diseases: a dangerous liaison. Curr Opin Allergy Clin Immunol. 2014;14:309-15. doi: 10.1097/ACI.0000000000000071.

APOLIPOPROTEIN B: A POSSIBLE NEW BIOMARKER FOR ANAPHYLAXIS 111
8
36. Zanotti R, Lombardo C, Passalacqua G, Caimmi C, Bonifacio M, De Matteis G et al. Clonal mast cell disorders in patients with severe Hymenoptera venom allergy and normal serum tryptase levels. J Allergy Clin Immunol. 2015;136:135-9. doi: 10.1016/j.jaci.2014.11.035.


CHAPTER 9
sUmmARy AND GENERAL DIsCUssION


SUMMARY AND GENERAL DISCUSSION 115
9
This thesis provides an overview of a number of biochemical, genetic and clinical factors influencing the severity of systemic allergic and anaphylactic reactions. Special attention was given to the relationship between the eliciting dose and the severity of reaction in food allergy. In this chapter, we provide a summary and general discussion of the main results of our research, with future perspectives.
SuMMaRY of paRt i: thE SEVERitY of SYStEMic anaphYlactic anD AllERgIC REACTIONS IN pEdIATRIC fOOd AllERgy
chapter 2 - is 30 minutes between doses long enough in oral food challenges?
The objective of the study in chapter 2 was to investigate whether an interval of 30 min-utes between doses in the DBPCFC is long enough for patients reporting time intervals of ≥30 minutes between ingestion of the culprit food and the subsequent reaction. These patients could receive a subsequent dose before having reacted to the previous dose and thus react to accumulated doses, which might be more severe than reactions to individual doses.
Patients were divided into two groups based on their reaction time, with comparison of the eliciting dose (ED), cumulative dose (CD) and the severity of the challenge reaction. This analysis showed that patients reporting time intervals of ≥30 minutes between inges-tion and reaction had higher EDs and CDs in the DBPCFC, than those reporting shorter time intervals between ingestion and reaction (<30 min). However, these patients did not have more severe reactions. This suggests that these patients do indeed accumulate doses in oral food challenges with 30 minute intervals between dose increments.
In conclusion, although some patients may accumulate and react to more than one dose during the DBPCFC, a dosing interval of 30 minutes is long enough to allow for this test to be conducted safely in these patients.
chapter 3 - prediction of the severity of allergic reactions to foods
The aim of this study was to identify independent predictors for the severity of diagnostic and accidental food allergic reactions. An additional objective was to quantify the impact of these factors and to investigate whether more severe reactions tended to occur at higher doses. The analysis was performed by using two different scoring systems for the reaction severity.

116 CHAPTER 9
The results of this study showed that the severity of reactions during DBPCFCs and ac-cidental reactions to foods are determined by numerous factors. However, the severity of food allergic reactions remains largely unpredictable.
The results also showed that the use of different severity scoring systems may give differ-ent or even contradictory results depending on the distribution of the data in a particular population. Although the severity of DBPCFC reactions are associated with a lower elicit-ing dose, the small size of this effect suggests that the impact of dose limitation as a public health measure is unlikely to reduce severe reactions more than milder ones. Finally, clinicians should not use the eliciting dose obtained from a graded food challenge to as-sess the need for stringent avoidance of allergenic foods or prescription of self-injectable epinephrine.
chapter 4 - Greater severity of peanut challenge reactions using a high fat versus low fat matrix vehicle
In chapter 4, we examined possible matrix effects of a high fat and low fat content food matrix during DBPCFCs with peanut, by comparing the severity of reactions and eliciting doses.
The results of this study showed that children challenged with peanut in the high fat ma-trix had more severe reactions during the DBPCFC, compared to children challenged with peanut in the low fat matrix. However, there was no significant difference in eliciting dose.
In conclusion, this supports the role of the food matrix as a factor which may increase the severity of reactions. This result could have implications for the safety of oral food challenges and peanut immunotherapy.
chapter 5 - clinical reactivity to individual tree nuts and peanut differs among the sensitized pediatric population
The aim of the study in chapter 5 was to investigate whether there are any differences in the frequency and severity of accidental and DBPCFC reactions between tree nuts and peanut in children.
This showed that true clinical reactivity to hazelnut and almond was less frequent com-pared to peanut. Moreover, sensitization was more frequently asymptomatic for hazelnut and almond when compared to peanut. However, true clinical reactivity for cashew and walnut was more frequent than for peanut. No difference in the severity of the DBPCFC reaction between the different types of nuts was found. However, accidental reactions to cashew were more severe than those for peanut.

SUMMARY AND GENERAL DISCUSSION 117
9
In conclusion, the frequency of true clinical reactivity differs between patients sensitized to peanut and tree nuts. The DBPCFC is especially important for the confirmation of ha-zelnut and almond allergy due to common asymptomatic sensitization. Finally, cashew nut allergy should be prioritized for the development of measures to prevent severe ac-cidental reactions.
chapter 6 - apolipoprotein B: a possible new biomarker for anaphylaxis
The objective of this study was to examine the serum level of apolipoprotein B-100 as a potential biomarker for the occurrence and severity of anaphylactic reactions to foods. A more severe accidental reaction was associated with a lower serum level of apolipopro-tein B. The level of apolipoprotein B was not associated with the food challenge outcome or the severity of the DBPCFC reaction.
This suggests that the level of apolipoprotein B might be a biomarker for the severity of anaphylactic reactions, probably through its association with the less stable platelet-activating factor acetyl hydrolase. The serum level of apolipoprotein B only explains a relatively small part of the reaction severity, however serum samples collected closer in time to the reaction or from other types of anaphylactic reactions may be more informa-tive.
chapter 7 - association of Stat6 gene variants with food allergy diagnosed by double-blind placebo-controlled food challenges
The study in chapter 7 describes the role of two STAT6 gene variants in food allergic chil-dren diagnosed by double-blind placebo-controlled food challenges. This was performed by investigating the association of two selected single nucleotide polymorphisms (SNPs) in the STAT6 gene, rs324015 and rs1059513, with the level of sIgE, eliciting dose and the severity of the reaction during the DBPCFC.
The results showed that there is an association between a greater eliciting dose and the A alleles of rs1059513 in children allergic to peanut and cow’s milk. There was also an as-sociation with the A allele of rs324015 in peanut allergic children. This suggest that these A alleles are associated with a less dose sensitive phenotype, and that allergic subjects carrying these alleles are probably at lower risk for the occurrence of accidental allergic reactions. However, these A alleles were also associated with more severe DBPCFC reac-tions. This suggests that the severity of reaction and dose sensitivity should be considered as independent entities in food allergy, with separate genetic control.
In conclusion, STAT6 genetic polymorphisms are involved in the pathophysiology of food allergy and their role seems to be independent of the culprit food.

118 CHAPTER 9
SuMMaRY of paRt ii: thE SEVERitY of SYStEMic anaphYlactic anD allERGic REactionS in aDultS with YEllow jackEt VEnoM allERGY
chapter 8 - Mastocytosis and age, but not baseline tryptase, specific igE or total igE, independently determine the severity of systemic reactions to yellow jacket stings.
The purpose of this study was to determine independent clinical risk factors for systemic reaction severity to yellow jacket stings in untreated patients, with and without indolent systemic mastocytosis (ISM). An additional aim was to quantify the impact of these factors.
The results showed that ISM and older age were independent predictors for the severity grade, but not baseline serum tryptase (bsT) level , specific IgE, total IgE or a history of serious cardiovascular event. This prediction model explained 23.0% of the variance of the severity grade. Thus, ISM and older age should be considered in the risk assessment of severe yellow jacket sting reactions. BsT does not predict the reaction severity indepen-dently of the diagnosis of ISM. However it is useful for diagnosing and screening for ISM. In conclusion, the severity of reactions to yellow jacket stings remains for the greatest part unpredictable.
GEnERal DiScuSSion
the relationship between dose and severity of reactions
The relationship between the dose and the severity of reaction is complex. The concept of threshold dose illustrates this complex relationship. The threshold dose has been defined as the lowest dose which elicits an allergic reaction in an individual patient. (1) Ingestion of a dose below this amount will not elicit an allergic response. This phenomenon is shown during oral food challenges, since not all allergic patients react to the first dose. How-ever, this concept has been further extrapolated to the notion that a larger dose above a subject’s individual threshold will cause a more severe reaction, even though there is no direct evidence for this. (2) In this section we will look more closely into the relationship between the severity of reaction and dose.
The threshold dose is a theoretical concept and therefore it cannot be determined clini-cally. An estimation of the threshold dose in clinical practice is the eliciting dose as deter-mined during diagnostic graded oral food challenges. The eliciting dose is thus probably slightly higher than the theoretical threshold dose, but it can identify highly dose sensitive patients as well as patients who react to large doses during the DBPCFC. (1)

SUMMARY AND GENERAL DISCUSSION 119
9
the eliciting dose and severity of reaction during DBpcfc reactions
There are several difficulties with examining the relationship between the eliciting dose and severity of reaction during oral food challenges. One of these difficulties is the stepwise administration of doses. Patients reporting longer time intervals between ingestion of the culprit food and the allergic reaction, compared to the time interval between doses, could receive a subsequent dose before having reacted to the previous dose and thus react to accumulated doses. This was examined in the study in chapter 2, which showed that these patients indeed had higher EDs and CDs, however they did not have more severe reac-tions. Thus, even though these patients received a higher dose in the DBPCFC, they did not have more severe reactions. Moreover, the stepwise administration of doses during oral food challenges have previously been shown to induce a short-lived desensitization effect in some patients, and could thus result in a transient oral tolerance to the tested food. (3) However, this effect was no longer present when the total cumulative dose ingested during the food challenge was given as one dose the next day.
Another challenge in examining the relationship between the severity of reaction and dose is the influence of the food matrix. Not only could the food matrix influence the digestion and the amount of allergen absorbed, but it could also have an impact on the immunological response to the specific allergen. (4) In chapter 4 this matrix effect was examined for peanut by using a high fat and a low fat food matrix during the DBPCFC. However, a previous study from our center showed no such effect for DBPCFC with hen’s egg. (5) Thus, matrix effects may differ for different types of food.
The severity of reaction during DBPCFCs are generally milder than accidental reactions.(chapter 3) This is probably due to that oral food challenges take place in a controlled environment and augmentation factors must be minimized and the patient stable before commencement of the test. However, relatively severe reactions do occur during oral food challenges, in spite of the previously mentioned reasons, and even though an incremental dosing scheme is being used.
accidental reactions, dose sensitivity and ingested dose
The relationship between the ingested dose and the severity of the accidental reaction is also difficult to study. Clinicians must rely on the ingested dose reported by patients, which is inexact and may be affected by recall bias. In addition, to be able to determine the difference between the ingested dose and the level of dose sensitivity, the eliciting dose for that patient must be known. Thus, in a research setting, using the eliciting dose is more reliable than estimations of the ingested dose. (2) The eliciting dose did not predict the severity of the accidental reaction.(chapter 3) This suggests that dose sensitivity does not have a large impact on the severity of accidental reactions.

120 CHAPTER 9
A recent study of single dose oral food challenges, which is more similar to accidental exposures than incremental oral food challenges, showed surprisingly mild reactions during the single low-dose oral food challenges. (6) In another study, where the oral food challenge procedure was allowed to continue with additional doses after an initial mild reaction, 62% of patients had allergic reactions which progressed to anaphylaxis with increasing doses. However, the eliciting dose did not predict anaphylaxis. (7) Thus, the concept that a larger dose above a subject’s individual threshold will cause a more severe reaction for all patients, seems to be too simplistic.
a theory for explaining the relationship between the severity of reaction and dose
The weak relationship between the eliciting dose and the severity of the DBPCFC reaction,(chapter 3) could theoretically be explained by differences in the slope and/or shift of dose-response curves in individual patients. These curves could possibly shift and reshape by the influence of augmentation factors, development of tolerance and other factors associated with the severity of reaction and eliciting dose. An example of factors previously shown to influence the threshold dose during oral peanut immunotherapy is lack of sleep, exercise and acute infections. (8) Furthermore, factors previously shown to be associated with a lower eliciting dose in children are increasing age, higher specific IgE level, and the absence of atopic dermatitis. (9) These factors were also shown to be predictive of the severity of accidental and/or DBPCFC reactions in chapter 3. Below we will explore the relationship between an increasing dose and the severity of reaction in four individual, hypothetical subjects.
In Figure 1 and Figure 2 the dose-response relationship for 4 subjects are shown, when ad-ditional doses are given after the initial response. Severity of reaction is graded as: mild= 1, moderate= 2, and severe= 3. In Figure 1, subject 1 reacts to the second dose and a severe reaction is provoked after dose 5 has been ingested. In subject 2, a reaction is seen after the 4th dose, however after all doses have been given the maximum reaction severity is a moderate reaction. Thus a severe reaction could not be triggered in this subject.
In Figure 2, subject 3 reacts to the 2nd dose given and the severity of reaction gradually in-creases with each additional dose given, until the final dose, where the maximal response is reached. For subject 4 however, the initial reaction is instantly the most possible severe reaction at dose 7. Thus for subject 3, having a lower dose sensitivity compared to subject 4, but an equal maximum response, there is a clear dose-response relationship since the slope is less steep than the curve of subject 4.

SUMMARY AND GENERAL DISCUSSION 121
9
Figure 1. Dose-response relationship in subject 1 & 2 when additional doses are given after the initial response.
In Figure 2, subject 3 reacts to the 2nd dose given and the severity of reaction gradually increases with each additional dose given, until the final dose, where the maximal response is reached. For subject 4 however, the initial reaction is instantly the most possible severe reaction at dose 7. Thus for subject 3, having a lower dose sensitivity compared to subject 4, but an equal maximum response, there is a clear dose-response relationship since the slope is less steep than the curve of subject 4.
0
1
2
3
Dose 1Dose 2Dose 3Dose 4Dose 5Dose 6Dose 7Dose 8
Seve
rity
of re
actio
n (0
-3)
Subject 1
Subject 2
Figure 1. Dose-response relationship in subject 1 & 2 when additional doses are given after the initial response.
Figure 2. Dose-response relationship in subject 3 & 4 when additional doses are given after the initial response.
These figures illustrate that it is not possible to trigger a severe reaction all subjects, (subject 2) when additional doses are given. (7) It also shows that for some subjects the initial response is the most severe possible outcome (subject 4), while for others there is a clear dose-response relationship (subject 1-3). Previous studies have shown that the severity of reaction is associated with the basophil reactivity and that the eliciting dose is associated with the basophil sensitivity in the basophil activation test. (10, 11)
A possible explanation for why it is not possible to trigger a severe reaction in certain subjects when additional doses are given could be that these subjects have a reduced amount of reactive basophils. As a result, a severe reaction cannot be elicited because of a ceiling effect of the basophil activation and/or another immunological process. In addition, it is possible that the slope of the curve, could represent a function of the basophil activity and basophil sensitivity. Knowing the slope of the dose-response curve in individual patients, could be important for risk management. Thus it might be possible in the future to identify patients who show a dose-
0
1
2
3
Dose1
Dose2
Dose3
Dose4
Dose5
Dose6
Dose7
Dose8
Seve
rity
of re
actio
n (0
-3)
Subject 3
Subject 4
Figure 2. Dose-response relationship in subject 3 & 4 when additional doses are given after the initial response.
These figures illustrate that it is not possible to trigger a severe reaction all subjects, (sub-ject 2) when additional doses are given. (7) It also shows that for some subjects the initial response is the most severe possible outcome (subject 4), while for others there is a clear

122 CHAPTER 9
dose-response relationship (subject 1-3). Previous studies have shown that the severity of reaction is associated with the basophil reactivity and that the eliciting dose is associated with the basophil sensitivity in the basophil activation test. (10, 11)
A possible explanation for why it is not possible to trigger a severe reaction in certain sub-jects when additional doses are given could be that these subjects have a reduced amount of reactive basophils. As a result, a severe reaction cannot be elicited because of a ceiling effect of the basophil activation and/or another immunological process. In addition, it is possible that the slope of the curve, could represent a function of the basophil activity and basophil sensitivity. Knowing the slope of the dose-response curve in individual patients, could be important for risk management. Thus it might be possible in the future to identify patients who show a dose-response relationship by basophil activation assays. In addition, it might also be possible to identify patients who will not develop a severe reaction, such as subject 2, with this test.
Genetics in food allergy, the severity of reaction and eliciting dose
In chapter 7 we examined the role of two STAT6 gene variants in food allergic children diagnosed by DBPCFCs. Interestingly, the results showed an association between the A alleles of rs1059513 in children allergic to peanut and cow’s milk. There was also an as-sociation with the A allele of rs324015 in peanut allergic children. This suggests that these A alleles are associated with a less dose sensitive phenotype, and that allergic subjects carrying these A alleles are thus probably at lower risk for the occurrence food allergic reactions. (chapter 7) Furthermore, in a previous study, a higher eliciting dose was associ-ated with an earlier resolution of milk, peanut and tree nut allergy. (12) Thus, our results are in line with another study which describes an association between the A genotype in rs324015 and a younger age of developing tolerance in cow’s milk allergy. (13)
However, both A alleles were also shown to be the risk allele for having food allergy and more severe DBPCFC reactions. (chapter 7) This result confirms recent insights into the in-dependence of clinical reaction severity and dose sensitivity in food allergy. (2, 7, 14) Here we add to these observations and show that clinical reaction severity and dose sensitivity may be under genetic control by a pleiotropic effect of STAT6. (chapter 7)
conclusion on the relationship between the eliciting dose and severity of reaction
Even though there seems to be a weak relationship between the eliciting dose and the severity of DBPCFC reactions, this association is not clinically useful. (chapter 3) Moreover, the results of this thesis shows clearly that the eliciting dose and the severity of reaction should be considered as separate factors in food allergy.(chapter 2-5 and 7)

SUMMARY AND GENERAL DISCUSSION 123
9
apolipoprotein B as a possible biomarker for the severity of anaphylactic reactions
Apolipoprotein B had a significant association with the severity of the accidental reaction in children suspected of food allergy. (chapter 6) However, apolipoprotein B was not a significant predictor for the severity of the yellow jacket venom sting reaction in an adult population. (chapter 8) This could be explained by the high rate of cardiovascular disease in the adult population as compared to the pediatric one. Apolipoprotein B does not only seem to be related to anaphylactic reactions (chapter 6), but it also has a strong con-nection to cardiovascular disease. (15) In our pediatric population this relationship was inverse, thus a higher level of apolipoprotein B was associated with less severe accidental reactions. However, an increasing level of apolipoprotein B is associated with several cardiovascular diseases and low levels may even be protective. (15) This could explain why apolipoprotein B was not a significant predictor for the reaction severity in yellow jacket venom allergy in adults.
current challenges and future perspectives in predicting the severity of anaphylactic and systemic allergic reactions
There are several challenges when aiming to predict the severity of anaphylactic and systemic allergic reactions. The multifactorial nature makes it difficult to predict and to identify all independent factors. (Chapter 3, 8) In addition, it has previously been shown that there is noteworthy inter-investigator variability in the interpretation of food allergic clinical symptoms. (16) The implementation of a widely accepted definition and clinical guidelines for diagnosing severe reactions could help to improve this issue. These will need to be applicable to diagnostic allergic reactions and to accidental reactions.
The use of different scoring systems for severe reactions can lead to unexpected differ-ences in the results. An example of this was shown in chapter 3, where the direction of the association between the eliciting dose and severity of the DBPCFC reaction depended on the scoring system used. Therefore, the development of a unified scoring system for severe reactions would make the definition of severe reactions more clear and make the results of research easier to interpret and compare in systematic reviews.
In conclusion, the severity of anaphylactic and systemic allergic reactions is multifactorial and difficult to predict. Thus, the majority of factors determining the severity of anaphy-lactic and systemic allergic reaction remain unknown. New factors need to be identified to allow for accurate prediction of these severe reactions.

124 CHAPTER 9
REfERENCES
1. Taylor SL, Hefle SL, Bindslev-Jensen C, Bock SA, Burks AW Jr, Christie L et al. Factors affecting the determination of threshold doses for allergenic foods: how much is too much? J Allergy Clin Im-munol. 2002;109:24-30.
2. Turner PJ, Baumert JL, Beyer K, Boyle RJ, Chan C-H, Clark AT et al. Can we identify patients at risk of life-threatening allergic reactions to food? Allergy. 2016;71:1241-55. doi: 10.1111/all.12924.
3. Niggemann B, Lange L, Finger A, Ziegert M, Müller V, Beyer K. Accurate oral food challenge requires a cumulative dose on a subsequent day. J Allergy Clin Immunol. 2012;130:261-3. doi: 10.1016/j.jaci.2012.03.021.
4. McClain S, Bowman C, Fernández-Rivas M, Ladics GS, Ree Rv. Allergic sensitization: food- and protein-related factors. Clin Transl Allergy. 2014;4:11. doi: 10.1186/2045-7022-4-11.
5. Libbers L, Flokstra-de Blok BM, Vlieg-Boerstra BJ, van der Heide S, van der Meulen GN et al. No matrix effect in double-blind, placebo-controlled egg challenges in egg allergic children. Clin Exp Allergy. 2013 Sep;43:1067-70. doi: 10.1111/cea.12164
6. Hourihane JO, Allen KJ, Shreffler WG, Dunngalvin G, Nordlee JA, Zurzolo GA et al. Peanut Al-lergen Threshold Study (PATS): Novel single-dose oral food challenge study to validate eliciting doses in children with peanut allergy. J Allergy Clin Immunol. 2017;139:1583-1590. doi:10.1016/j.jaci.2017.01.030.).
7. Wainstein BK, Studdert J, Ziegler M, Ziegler JB. Prediction of anaphylaxis during peanut food chal-lenge: usefulness of the peanut skin prick test (SPT) and specific IgE level. Pediatr Allergy Immunol. 2010;21:603-11. doi: 10.1111/j.1399-3038.2010.01063.x.
8. Anagnostou K, Clark A, King Y, Islam S, Deighton J, Ewan P. Efficacy and safety of high-dose peanut oral immunotherapy with factors predicting outcome. Clin Exp Allergy. 2011;41:1273-81. doi: 10.1111/j.1365-2222.2011.03699.x.
9. van der Zee T, Dubois A, Kerkhof M, van der Heide S, Vlieg-Boerstra B . The eliciting dose of peanut in double-blind, placebo-controlled food challenges decreases with increasing age and specific IgE level in children and young adults. J Allergy Clin Immunol. 2011;128:1031-6. doi:10.1016/j.jaci.2011.07.050.
10. Santos AF, Du Toit G, Douiri A, Radulovic S, Stephens A, Turcanu V et al. Distinct parameters of the basophil activation test reflect the severity and threshold of allergic reactions to peanut. Allergy Clin Immunol. 2015;135:179-86. doi: 10.1016/j.jaci.2014.09.001.
11. Song Y, Wang J, Leung N, Wang LX, Lisann L, et al. Correlations between basophil activation, allergen-specific IgE with outcome and severity of oral food challenges. Ann Allergy Asthma Im-munol. 2015;114:319–26.
12. Elizur A, Rajuan N, Goldberg MR, Leshno M, Cohen A, Katz Y. Natural course and risk factors for persistence of IgE-mediated cow’s milk allergy. J Pediatr. 2012;161:482-487.e1. doi: 10.1016/j.jpeds.2012.02.028.
13. Yavuz ST, Buyuktiryaki B, Sahiner UM, Birben E, Tuncer A, Yakarisik S, Karabulut E, Kalayci O, Sacke-sen C. Factors that predict the clinical reactivity and tolerance in children with cow’s milk allergy. Ann Allergy Asthma Immunol. 2013;110:284-9. doi: 10.1016/j.anai.2013.01.018.

SUMMARY AND GENERAL DISCUSSION 125
9
14. Rolinck-Werninghaus C, Niggemann B, Grabenhenrich L, Wahn U, Beyer K. Outcome of oral food challenges in children in relation to symptom-eliciting allergen dose and allergen-specific IgE. Al-lergy Eur. J. Allergy Clin. Immunol. 2012;6:951–957.
15. Benn M. Apolipoprotein B levels, APOB alleles, and risk of ischemic cardiovascular disease in the general population, a review. Atherosclerosis. 2009;206:17-30. doi: 10.1016/j.atherosclero-sis.2009.01.004.
16. van Erp FC, Knulst AC, Meijer Y, Gabriele C, van der Ent CK. Standardized food challenges are subject to variability in interpretation of clinical symptoms. Clin Transl Allergy. 2014;4:43. doi: 10.1186/s13601-014-0043-6.


APPENDICEs


APPENDICES 129
A
NEdERlANdSE SAMENVATTINg
Dit proefschrift geeft een overzicht van een aantal biochemische, genetische en klinische factoren die van invloed zijn op de ernst van systemische allergische en anafylactische reacties. Specifieke focus werd besteed aan de relatie tussen de ingenomen dosis voed-sel en de ernst van de reactie bij voedselallergie. In dit hoofdstuk presenteren wij een samenvatting van de onderzoeksresultaten en de implicaties hiervan.
Samenvatting van Deel i: de ernst van systemische anafylactische en allergische reacties bij kinderen met voedselallergie
Hoofdstuk 2 De studie in hoofdstuk 2 evalueert of een interval van 30 minuten tussen de doses in de dubbelblinde, placebo gecontroleerde voedsel provocatietest (DBPCVP) lang genoeg is voor patiënten die tijdsintervallen van ≥30 minuten rapporteren tussen de inname van het allergene voedingsmiddel en de daaropvolgende reactie. Deze patiënten zouden theore-tisch een volgende dosis kunnen krijgen voordat zij hebben gereageerd op de vorige dosis en daardoor reageren op geaccumuleerde doses, die mogelijk ernstigere reacties geven dan reacties op individuele doses.
Patiënten werden in twee groepen verdeeld op basis van hun reactietijd, met een ver-gelijking van de eliciting dosis (ED), de cumulatieve dosis (CD) en de ernst van de reactie tijdens de DBPCVP. De ED is de laatste ingenomen dosis voedsel tijdens de DBPCVP welke leidt tot een reactie. De resultaten lieten zien dat patiënten met een tijdsinterval van ≥30 minuten tussen de inname en de reactie een hogere ED en CD in de DBPCVP hebben dan degenen met een kortere tijdsinterval tussen inname en reactie (<30 min). Deze patiënten hebben echter geen ernstigere reacties. Dit doet vermoeden dat deze patiënten inderdaad doses accumuleren tijdens orale, getrapte voedselprovocaties met intervallen van 30 minuten tussen de doseringen. Concluderend, een dosisinterval van 30 minuten is lang genoeg om deze test veilig uit te voeren ondanks dat sommige patiënten tijdens de DBPCVP doseringen kunnen accumuleren, en op meer dan één dosis kunnen reageren.
Hoofdstuk 3 Het doel van deze studie was om onafhankelijke voorspellers te identificeren voor de ernst van diagnostische en accidentele voedselallergische reacties. Een bijkomend doel was om de invloed van deze factoren te kwantificeren en om te onderzoeken of ernstige reacties vaker voorkomen bij hogere doseringen. De analyse werd uitgevoerd met twee verschil-lende scoring systemen voor de ernst van de reactie.

130 APPENDICES
De resultaten van deze studie lieten zien dat de ernst van reacties tijdens DBPCVPs en accidentele reacties op voedingsmiddelen worden bepaald door talrijke factoren. De ernst van voedselallergische reacties blijft echter grotendeels onvoorspelbaar.
De resultaten toonden ook aan dat het gebruik van verschillende scoring systemen voor de ernst van de reactie verschillende of zelfs tegenstrijdige resultaten kan opleveren, afhankelijk van de distributie van de data in een bepaalde populatie. Hoewel de ernst van reacties tijdens DBPCVPs geassocieerd is met een lagere ED, doet de beperkte relatie tus-sen deze factoren vermoeden dat dosisbeperking als maatregel voor de volksgezondheid waarschijnlijk geen merkbaar effect heeft om ernstige reacties te voorkomen. Ten slotte moeten zorgverleners de ED niet gebruiken om de noodzaak van een strikte vermijding van allergene voedingsmiddelen of adrenaline auto-injectoren in te schatten.
Hoofdstuk 4 In hoofdstuk 4 exploreren wij mogelijke matrixeffecten van voedselmatrices met een hoog- en laag vetgehalte die gebruikt worden tijdens DBPCVPs met pinda, door de ED en de ernst van de reacties te vergelijken. Dit onderzoek liet zien dat kinderen die tijdens de DBPCVP met pinda de matrix met een hogere vetgehalte kreeg, ernstiger reacties hadden tijdens de voedselprovocatietest, in vergelijking met kinderen die de matrix met een laag vetgehalte kreeg. Er was echter geen significant verschil in de ED.
Concluderend, de voedselmatrix wordt hier als een factor die de ernst van reacties kan veranderen bevestigd. Dit resultaat kan gevolgen hebben voor de veiligheid van orale voedselprovocaties en immunotherapie met pinda.
Hoofdstuk 5Het doel van het onderzoek in hoofdstuk 5 was om te onderzoeken of er verschillen zijn in de frequentie en ernst van accidentele reacties en reacties tijdens DBPCVPs tussen boom-noten en pinda’s bij kinderen. Dit liet zien dat echte klinische reactiviteit voor hazelnoot en amandel minder frequent was in vergelijking met pinda’s. Bovendien was sensibilisatie vaker asymptomatisch voor hazelnoot en amandel in vergelijking met pinda. De werkelijke klinische reactiviteit voor cashewnoot en walnoot was echter frequenter dan voor pinda. Er werd geen verschil in de ernst van de DBPCVP-reactie tussen de verschillende soorten noten gevonden. Accidentele reacties tegen cashewnoot waren echter ernstiger dan die voor pinda.
Concluderend, de frequentie van echte klinische reactiviteit verschilt tussen patiënten die gesensibiliseerd zijn voor pinda’s en boomnoten. De DBPCVP is vooral belangrijk voor de bevestiging van hazelnoot- en amandelallergie als gevolg van frequente asymptomatische

APPENDICES 131
A
sensibilisatie. Allergie tegen cashewnoten moet geprioriteerd worden voor het ontwik-kelen van nieuwe maatregelen om ernstige accidentele reacties te voorkomen.
Hoofdstuk 6Het doel van deze studie was om het serumniveau van apolipoproteïne B-100 te onder-zoeken als een potentiële biomarker voor het optreden van en de ernst van anafylactische reacties op voedingsmiddelen. Een ernstigere accidentele reactie was geassocieerd met een lagere serumspiegel van apolipoproteïne B. Het niveau van apolipoproteïne B was niet geassocieerd met de uitkomst van de voedselprovocatie of de ernst van de DBPCVP-reactie.
Dit suggereert dat apolipoproteïne B een biomarker kan zijn voor de ernst van anafy-lactische reacties, waarschijnlijk door de associatie met de minder stabiele bloedplaatjes activerende factor acetylhydrolase. Het serumniveau van apolipoproteïne B verklaart slechts een relatief klein deel van de ernst van de reactie, maar serummonsters die korter voor of na de reactie zijn verzameld of bij andere soorten anafylactische reacties zouden meer informatief kunnen zijn.
Hoofdstuk 7De studie in hoofdstuk 7 beschrijft de rol van twee STAT6-genvarianten bij voedselaller-gische kinderen gediagnosticeerd met DBPCVPs. De associatie van twee geselecteerde enkel-nucleotide polymorfismen (SNPs) in het STAT6-gen, rs324015 en rs1059513, met het niveau van sIgE, ED en de ernst van de reactie tijdens de DBPCFC werden onderzocht.
De resultaten lieten zien dat er een verband is tussen een hogere ED en de A-allelen van rs1059513 bij kinderen die allergisch zijn voor pinda’s en koemelk. Er was ook een verband met het A-allel van rs324015 bij pinda-allergische kinderen. Dit suggereert dat deze A-allelen geassocieerd zijn met een minder dosisgevoelig fenotype en dat allergische personen die deze allelen dragen waarschijnlijk een lager risico hebben voor het optreden van accidentele allergische reacties. Deze A-allelen werden echter ook geassocieerd met meer ernstige DBPCVP-reacties. Dit suggereert dat de ernst van de reactie en de dosis-gevoeligheid als onafhankelijke factoren in voedselallergie moeten worden beschouwd, genetische controle van STAT6. Concluderend, STAT6 genetische polymorfismen zijn mo-gelijk betrokken bij de pathofysiologie van voedselallergie en hun rol lijkt onafhankelijk te zijn van het allergene voedingsmiddel.

132 APPENDICES
Samenvatting van Deel ii: de ernst van systemische anafylactische en allergische reacties in volwassenen met wespenallergie
Hoofdstuk 8 Het doel van deze studie was om onafhankelijke klinische risicofactoren te bepalen voor de ernst van de systemische reactie op wespensteken bij onbehandelde patiënten, met en zonder indolente systemische mastocytose (ISM). Een bijkomend doel was om de impact van deze factoren te kwantificeren.
De resultaten lieten zien dat ISM en oudere leeftijd onafhankelijke voorspellers waren voor de ernst van de reactie, maar dit geldt niet voor basaal serum tryptase (bsT), specifiek IgE, totaal IgE of een voorgeschiedenis van myocard infarct of beroerte. Deze statistische model verklaarde 23,0% van de variantie van de ernst van de reactie. Dus, ISM en oudere leeftijd moeten meegenomen worden in de risicobeoordeling van ernstige wespenreac-ties. BsT voorspelt niet de ernst van de reactie onafhankelijk van de diagnose van ISM. BsT is echter geschikt voor het diagnosticeren en screenen van ISM. Concluderend, de ernst van reacties op wespensteken blijft voor het grootste deel onvoorspelbaar.
conclusies
De relatie tussen de ED en de ernst van DBPCVP-reacties is niet geschikt voor klinische besluitvorming, hoewel er een zwakke relatie lijkt te bestaan. (hoofdstuk 3) De ED en de ernst van de reactie moeten als afzonderlijke factoren bij voedselallergie worden be-schouwd (hoofdstuk 2-5 en 7).
De ernst van anafylactische en systemische allergische reacties is multifactorieel bepaald en moeilijk te voorspellen. De meerderheid van de factoren die de ernst van anafylactische en systemische allergische reacties bepalen, blijft dus onbekend. Om een nauwkeurigere voorspelling van deze ernstige reacties mogelijk te maken moeten nieuwe factoren wor-den geïdentificeerd.

APPENDICES 133
A
SVENSK SAMMANfATTNINg
Denna avhandling ger en översikt över ett antal biokemiska, genetiska och kliniska fakto-rer som påverkar svårighetsgraden av systemiska allergiska och anafylaktiska reaktioner. Särskild tonvikt har lagts vid förhållandet mellan mängden allergen och reaktionens svå-righetsgrad vid matallergi. I detta kapitel sammanfattar vi resultaten av vår forskning och dess innebörd.
Sammanfattning av del i: svårighetsgraden av systemiska anafylaktiska och allergiska reaktioner vid matallergi hos barn
Kapitel 2 Syftet med studien i kapitel 2 var att undersöka huruvida ett intervall på 30 minuter mellan doserna i dubbelblinda placebokontrollerade matprovokationer (DBPKMP) är tillräckligt långa för patienter som rapporterar tidsintervall på ≥30 minuter mellan intag av livsmedlet och den efterföljande allergiska reaktionen. Dessa patienter skulle kunna få en efterföljan-de dos innan de hunnit reagera på föregående dos och sådeles reagera på ackumulerade doser, vilket kan ge en svårare reaktion än de reaktioner som sker på enskilda doser.
Patienterna delades upp i två grupper baserat på deras reaktionstid, med jämförelse av framkallande dos (eliciting dose, ED), kumulativ dos (KD) och svårighetsgraden av reaktio-nen under DBPKMP. ED är den sista dosen av livsmedlet som intas under den DBPKMP och som leder till en allergisk reaktion. Denna analys visade att patienter som rapporterade tidsintervall på ≥30 minuter mellan intag och reaktion hade en högre ED och KD i DBPKMP än de som rapporterade kortare tidsintervall mellan intag och reaktion (<30 minuter). Men dessa patienter hade inte svårare reaktioner. Detta tyder på att dessa patienter ackumule-rar doser i orala matprovakationer med 30 minuters mellanrum mellan dosintervallerna. Sammanfattningsvis, även om vissa patienter kan ackumulera och reagera på mer än en dos under DBPKMP, är ett doseringsintervall på 30 minuter tillräckligt långt för att detta test ska kunna utföras säkert på dessa patienter.
Kapitel 3 Syftet med denna studie var att identifiera oberoende prediktorer för svårighetsgraden av diagnostiska och oförutsedda matallergiska reaktioner. Ett ytterligare syfte var att kvantifi-era effekterna av dessa faktorer och undersöka om mer allvarliga reaktioner tenderade att inträffa vid högre doser. Analysen utfördes genom att använda två olika kategoriserings-system för att definiera reaktionssvårigheten.

134 APPENDICES
Resultaten av studien visade att svårighetsgraden av reaktioner under DBPKMP och oförutsedda matallergiska reaktioner beror på ett flertal faktorer. Svårighetsgraden av matallergiska reaktioner förblir emellertid i stor utsträckning oförutsägbar. Resultaten visade även att användningen av olika kategoriseringssystem för reaktionssvårigheten kan ge olika eller till och med motsägelsefulla resultat beroende på fördelningen av datan i en viss population. Även om svårighetsgraden av reaktioner under DBPKMP är förknippad med en lägre ED, så antyder den lilla effekten av denna faktor att inflytandet av dosbe-gränsning som en folkhälsoåtgärd sannolikt inte minskar svåra reaktioner mer än milda reaktioner. Slutligen bör läkare inte använda den ED som erhålls från en matprovokation för att bedöma behovet av en strikt elimination av allergiframkallande livsmedel, eller recept på adrenalinpenna.
Kapitel 4 I kapitel 4 undersöktes inflytandet av livsmedlet som den allergiska beståndsdelen befin-ner sig i vid matallergi, genom att jämföra svårighetsgraden av reaktioner och ED mel-lan ett recept med hög fetthalt och ett med låg fetthalt under DBPKMP med jordnötter. Resultaten av denna studie visade att barn under matprovokationer med jordnötter i det feta receptet hade mer allvarliga reaktioner under DBPKMP, jämfört med barn som fick jordnötter i receptet med låg fetthalt. Det fanns emellertid ingen signifikant skillnad i ED.
Sammanfattningsvis, så stöder detta att sammansättningen av livsmedlet kan öka svårig-hetsgraden av allergiska reaktioner. Detta resultat kan få konsekvenser för utförandet av orala matprovokationer och immunterapi med jordnötter.
Kapitel 5Syftet med studien i kapitel 5 var att undersöka om det finns skillnader i frekvensen och svårighetsgraden av oförutsedda matallergiska reaktioner och reaktioner under DBPKMP mellan trädnötter och jordnötter hos barn. Detta visade att klinisk reaktivitet under DBP-KMP mot hasselnöt och mandel var mindre frekvent jämfört med för jordnötter. Vidare var sensibilisering oftare asymptomatisk för hasselnöt och mandel jämfört med för jordnötter. Klinisk reaktivitet under DBPKMP för cashewnöt och valnöt var emellertid vanligare än för jordnötter. Det påvisades ingen skillnad i svårighetsgrad av reaktionen under DBPKMP för de olika typerna av nötter. Oförutsedda reaktioner mot cashewnöt var dock svårare än för jordnötter.
Sammanfattningsvis, frekvensen av klinisk reaktivitet under DBPKMP skiljer sig mellan patienter som är sensibiliserade för jordnötter och trädnötter. Utförandet av DBPKMP är särskilt viktigt för bekräfta diagnosen av hasselnöt- och mandelallergi på grund av frekvent asymptomatisk sensibilisering. Slutligen bör cashewnötallergi prioriteras för att utveckla

APPENDICES 135
A
förebyggandeåtgärder med syfte att undvika allvarliga oförutsedda matallergiska reaktio-ner.
Kapitel 6 Syftet med denna studie var att undersöka serumnivån av apolipoprotein B-100 som en potentiell biomarkör för förekomsten och svårighetsgraden av anafylaktiska reaktioner på livsmedel. En allvarligare oförutsedd matallergisk reaktion var förknippad med en lägre se-rumnivå av apolipoprotein B. Nivån av apolipoprotein B var inte associerat med resultatet av matprovokationen eller svårighetsgraden av reaktionen under DBPKMP.
Detta tyder på att nivån av apolipoprotein B kan vara en biomarkör för svårighetsgraden av anafylaktiska reaktioner, förmodligen genom dess association med den mindre stabila blodplättsaktiverande faktorn acetylhydrolas. Serumnivån av apolipoprotein B förklarar bara en relativt liten del av svårighetsgraden av reaktionen, men serumprover som tas närmare i tiden till reaktionen eller från andra typer av anafylaktiska reaktioner kan vara mer bidragande.
Kapitel 7 Studien i kapitel 7 beskriver rollen av två STAT6-genvarianter hos matallergiska barn diag-nostiserade av DBPKMP. Detta utfördes genom att undersöka associeringen av två enkla nukleotidpolymorfismer (SNP) i STAT6-genen, rs324015 och rs1059513, med nivån av sIgE, ED och svårighetsgraden av reaktionen under DBPKMP.
Resultaten visade att det finns en koppling mellan en högre ED och A-allelen av rs1059513 hos barn som är allergiska mot jordnötter och komjölk. Det fanns också en association med A-allelen av rs324015 hos jordnötsallergiska barn. Vilket tyder på att dessa A-alleler är förknippade med en mindre doskänslig fenotyp, och att allergiska personer som bär dessa alleler sannolikt löper lägre risk att drabbas av oförutsedda matallergiska reaktioner. Dessa A-alleler var dock också förknippade med svårare reaktioner under DBPKMP. Detta tyder på att svårighetsgraden av reaktionen och doskänsligheten bör betraktas som oberoende enheter i matallergi, med genetisk kontroll av STAT6. Sammanfattningsvis, STAT6 genetiska polymorfismer är troligen involverade i patofysiologin av matallergi och deras roll verkar vara oberoende av vilken typ av mat det beträffar.

136 APPENDICES
Sammanfattning av del ii: svårighetsgraden av systemiska anafylaktiska och allergiska reaktioner vid getingallergi hos vuxna
Kapitel 8 Syftet med denna studie var att bestämma oberoende kliniska riskfaktorer för systemisk reaktionssvårighet hos obehandlade patienter med getingallergi, med och utan indolent systemisk mastocytos (ISM). Ett sekundärt syfte var att kvantifiera effekterna av dessa faktorer.
Resultaten visade att ISM och högre ålder var oberoende prediktorer för svårighetsgraden, men inte basal serum tryptas (bsT) nivå, allergenspecifikt IgE, totalt IgE eller en tidigare myokard infakt eller stroke. Denna prediktionsmodell förklarade 23,0% av variansen av svårighetsgraden. Således bör ISM och högre ålder övervägas i riskbedömningen av svåra allergiska reaktioner mot getingstick. BsT förutsäger inte svårighetsgraden av reaktionen oberoende av diagnosen ISM. BsT är dock användbart för att identifiera och diagnosera ISM. Sammanfattningsvis, svårighetsgraden av allergiska reaktioner mot getingstick förblir till en stor del oförutsägbar.
SlutsatserÄven om det verkar finnas en svag relation mellan ED och svårighetsgraden av reaktioner under DBPKMP, är denna association inte kliniskt användbar. (kapitel 3) Resultatet av denna avhandling visar dessutom tydligt att ED och svårighetsgraden av reaktionen bör ses som separata faktorer inom matallergi. (kapitel 2-5 och 7)
Sammanfattningsvis är svårighetsgraden av anafylaktiska och systemiska allergiska reak-tioner multifaktoriell och svår att förutsäga. Således förblir majoriteten av faktorer som påverkar svårighetsgraden av anafylaktiska och systemiska allergiska reaktioner okända. Nya faktorer måste identifieras för att möjliggöra en korrekt prediktion av dessa svåra reaktioner.

APPENDICES 137
A
ACKNOWlEdgEMENTS
The last few years of research have certainly had its ups and downs and I know that I would not have been able to finalize this thesis without the help of a number of people. Therefore, I would like to thank everyone who has helped me in the process of making this thesis. I would like to particularly acknowledge the help of the following people:
Firstly, I would like to thank all of the patients, children and parents for their participation, commitment and dedication in the Palisade trial. Even though this clinical trial did not make it into my thesis in the end, it was probably the most challenging part of my PhD. I deeply appreciated getting to know you during the trial. I wish you all the best in the future!
My first promoter Prof. A.E.J. Dubois. Dear Ewoud, this thesis would not have been pos-sible without you. Thank you for triggering my interest in research, challenging me, steer-ing me in the right direction and all of your good advice regarding research, career and life. You are a great inspiration and I have learnt a lot from you. Through thick and thin, I could always count on you. I am very grateful for having you as my promoter. Dear Joyce, thank you for being such a warm, considerate person and for organizing the Christmas drinks for us every year. I will always remember them fondly.
My second promoter, Prof. G.H. Koppelman. Dear Gerard, your genuine interest, knowl-edge and diligence makes you a great researcher. I have always valued your advice and opinion greatly. Even with your busy schedule and numerous responsibilities, you always took the time to thoroughly discuss my projects. Your input improved the quality of the studies greatly. I feel very lucky you wanted to become my promoter.
I would also like to thank the members of the assessment committee, Prof. D.S. Postma, Prof. G.C. Roberts and Prof. A.C. Knulst, for their time and effort in the assessment of this thesis.
The nurses at the food challenge unit. Dear Anneke Dijkstra and Annemarie Oomkes-Pilon, I really enjoyed working with the two of you during the Palisade trial. Anneke, thank you for your unconditional support and that you always go above and beyond for your patients. Thank you Annemarie, for being so caring and for sharing your great knowledge of the oral food challenges. Also thank you Stefanie, for your positive energy in the food challenge unit, always with a smile on your face!
138 APPENDICES
I would also like to especially mention and thank a number of people for their collabora-tion during the Palisade trial: Dr. Aline Sprikkelman, Dr. Hanneke Oude-Elberink, Maria Heuving, Egbert Horst, Berta Beusekamp, Kirsten Weerstand, Jannie Ijbema, Gregory Deira, Iryna Monastyrska-Pen and the representatives of Aimmune Therapeutics.
Medical students, Faisal Bakhsh, Anne Richter and Afke Schins, thank you for all of your hard work during the different research projects. I wish you all the best with your future careers!
My fellow PhD-roommates in the Triade building of the University Medical Center Gron-ingen, Dorien, Nicole, Anke and Erik. Thank you for all the laughs, coffee breaks and for experiencing the successes and challenges of our PhDs together! It would certainly have been less fun without you!
I would also like to thank all of the co-authors for their contribution to this thesis. A special thanks to Boudewijn Kollen for your help with the statistics. Also a special thanks to Byrthe Vos, my former MD-PhD colleague, for a great time together during our shared project. I wish you all the best with your future career in plastic surgery!
I would also like to thank Ruben’s family, my unofficial in-laws, for their support and help with this thesis. Thank you for including me in your family. A special thanks to Jan-Peter and Jeanette for their help with the Dutch summary and brainstorming regarding the cover of my thesis.
My paranymphs, Ulla Al Saad and Nathalie Rynler. Dear Ulla, I had the pleasure of meeting you almost 9 years ago during the selection day for medicine in Groningen. Together we took on all of the challenges of moving to a new country, adapting to the Dutch culture and the medical studies. I cannot imagine a better friend to have gone through this with! Even though we do not see each other as frequently anymore, with you living in Amsterdam, our special connection remains every time we see each other. Dear Nathalie, my older sister and role model. Growing up we were frequently told how alike we were, mostly to your disapproval and to my appreciation. To this day, I could still not be prouder of having you as my sister. I am very thankful and honored that you and Ulla want to stand by my side during my thesis defense.
Alexander, my dear brother. Thank you for your help with the Swedish summary for this thesis, for your thoughtfulness, for teaching me new things and for not only being my brother, but a great friend. Mamma & pappa, thank you for your love, unconditional sup-port and for always being there for me. I am incredibly grateful to be your daughter.

APPENDICES 139
A
My Ruben, thank you for supporting and putting up with me during the more difficult periods of making this thesis. A lot has happened since we met six years ago. I am looking forward to exploring the new adventures life brings us in the future!


APPENDICES 141
A
BIOgRAphy
Maria Eleonore Pettersson was born on the 16th of June 1988 in the local parish of Badelunda, in the city of Västerås, Sweden. She grew up in Västerås with her parents, older sister and younger brother. In 2007, she graduated from upper secondary school after completing the Natural Science program at Rudbeckianska Gymnasiet in Västerås, where she received a scholarship for excellent study results. After graduation Eleonore moved to London, United Kingdom for one year where she worked as an aupair. The fol-lowing year she moved back to Sweden, where she worked in home care with children with developmental disorders. During this year she applied for admission to the English taught International Bachelor of Medicine with a global health profile in Groningen, the Netherlands. After having participated in the decentralized selection procedure, she was admitted.
In September 2009 Eleonore moved to Groningen to begin her medical studies. During the first three years in Groningen she participated in the extracurricular activities of the Junior Scientific Masterclass and took several Dutch courses at the university language center. In 2011, she completed a research project for her bachelor thesis at the Department of Pe-diatric Pulmonology and Allergology at the University Medical Center Groningen (UMCG) under the supervision of Prof. Dubois. In 2012 she graduated from the International Bachelor of Medicine, where she was a graduation speaker. In the same year she passed the state examination in Dutch at University level and a medical Dutch course. In October 2012 she started the Master of Medicine in Dutch with clinical internships in Groningen, Emmen, Hoogeveen, Assen and Västerås. In 2014 she began a second research internship under the supervision of Prof. Dubois for her Master thesis.
In 2015 she was admitted to the MD/PhD program and graduated from the her medical studies. During the MD/PhD program Eleonore followed courses, supervised students and presented her research at several international congresses. In addition, during this period she was the study coordinator and sub-investigator of an international multicenter clinical trial of oral peanut immunotherapy at the department of Internal Medicine and depart-ment of Pediatric Pulmonology and Allergology in the UMCG.
Related Documents











