University of Groningen Neurophysiological signature(s) of visual hallucinations across neurological and perceptual Dauwan, Meenakshi IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2019 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Dauwan, M. (2019). Neurophysiological signature(s) of visual hallucinations across neurological and perceptual: and non-invasive treatment with physical exercise. [Groningen]: Rijksuniversiteit Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 29-08-2020

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

University of Groningen
Neurophysiological signature(s) of visual hallucinations across neurological and perceptualDauwan, Meenakshi
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:2019
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Dauwan, M. (2019). Neurophysiological signature(s) of visual hallucinations across neurological andperceptual: and non-invasive treatment with physical exercise. [Groningen]: Rijksuniversiteit Groningen.
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 29-08-2020

CHAPTER
Neuroimage Clinical, 2019; 13;22:101752
1 University of Groningen, University Medical Center Groningen, The Netherlands2 Amsterdam UMC, Vrije Universiteit, Department of Clinical Neurophysiology and MEG Center, The Netherlands 3 Brain Center Rudolf Magnus, University Medical Center Utrecht, The Netherlands 4 Department of Neurology, St. Antonius Ziekenhuis, Utrecht, The Netherlands5 Department of Neurology, Diakonessenhuis Utrecht, The Netherlands6 Department of Biological and Medical Psychology, University of Bergen, Norway
Meenakshi Dauwan1,2,3
J.I. Hoff4
E.M. Vriens5
A. Hillebrand2
C.J. Stam2*I.E. Sommer1,6*
* These authors are joint senior authors
6Aberrant resting-state
oscillatory brain activity in Parkinson’s disease patients with visual hallucinations:
An MEG source-space study

130
Chapter 6
ABSTRACT
To gain insight into possible underlying mechanism(s) of visual hallucinations (VH) in
Parkinson’s disease (PD), we explored changes in local oscillatory activity in different
frequency bands with source-space magnetoencephalography (MEG). Eyes-closed
resting-state MEG recordings were obtained from 20 PD patients with hallucinations
(Hall+) and 20 PD patients without hallucinations (Hall-), matched for age, gender
and disease severity. The Hall+ group was subdivided into 10 patients with VH only
(unimodal Hall+) and 10 patients with multimodal hallucinations (multimodal Hall+).
Subsequently, neuronal activity at source-level was reconstructed using an atlas-based
beamforming approach resulting in source-space time series for 78 cortical and 12
subcortical regions of interest in the automated anatomical labeling (AAL) atlas. Peak
frequency (PF) and relative power in six frequency bands (delta, theta, alpha1, alpha2,
beta and gamma) were compared between Hall+ and Hall-, unimodal Hall+ and Hall-,
multimodal Hall+ and Hall-, and unimodal Hall+ and multimodal Hall+ patients. PF
and relative power per frequency band did not differ between Hall+ and Hall-, and
multimodal Hall+ and Hall- patients. Compared to the Hall- group, unimodal Hall+
and lower PF (p=.011). Compared to the unimodal Hall+, multimodal Hall+ showed
showed slowing of MEG-based resting-state brain activity with an increase in theta
activity, and a concomitant decrease in beta and gamma activity, which could indicate
central cholinergic dysfunction as underlying mechanism of VH in PD. This signature
was absent in PD patients with multimodal hallucinations.

131
MEG-based resting-state brain activity in PD
1. INTRODUCTION
Visual hallucinations (VH) are the most common type of hallucinations in Parkinson’s
disease (PD) with an overall prevalence of 22% to 38% (Fénelon, 2008; Goetz et al.,
2011; Onofrj and Gilbert, 2018), followed by auditory (AH), olfactory (OH) and tactile
(TH) hallucinations, which are less common with prevalence rates of 3-22% (Fénelon,
2008), 6-16% (Fénelon, 2008; Kulick et al., 2018), and 4-7% (Goetz et al., 2011; Kulick
et al., 2018), respectively. Cognitive impairment in PD is strongly associated with
VH (Fenelon and Alves, 2010; Hepp et al., 2013; Lenka et al., 2017b). In contrast,
multimodal hallucinations in PD are not necessarily associated with a greater risk of
cognitive impairment (R Inzelberg et al., 1998; Katzen et al., 2010). Hallucinations in PD
are associated with higher caregiver burden and form a strong and independent risk
factor for nursing home placement (Aarsland et al., 2000; Fenelon and Alves, 2010).
The majority of research examining the pathophysiology of hallucinations in PD involve
studies on VH. In contrast, nonvisual hallucinations in PD, reported to accompany
VH as a second modality experience (Goetz et al., 2011), remain understudied (Kulick
et al., 2018). As such, dysfunctional activation of frontal (top-down) and posterior
(bottom-up) brain regions have been reported in PD patients with VH (Boecker et
al., 2007; Ffytche et al., 2017; Lenka et al., 2015; Nagano-Saito et al., 2004; Prell, 2018;
Ramírez-Ruiz et al., 2008; Sanchez-Castaneda et al., 2010; Stebbins et al., 2004). In
addition, multiple neurotransmitter systems have been related to hallucinations in
PD: 1) the cholinergic system, 2) the dopaminergic system, and 3) the serotonergic
system (Factor et al., 2017). First, the central cholinergic system is a modulator of the
interaction between feedback or top-down and feedforward or bottom-up processing
(Collerton et al., 2005; Friston, 2005), such that cholinergic dysfunction may increase
the uncertainty in top-down activity resulting in incorrect scene representation, and
thus hallucinations (Collerton et al., 2005; Friston, 2005). Support for this hypothesis
of impaired bottom-up (i.e. reduced activation and metabolism in the visual pathways)
and top-down (i.e. defective attentional) processing has been found in PD patients
with VH and this dysfunctional top-down and bottom-up processing has also been
associated with cognitive decline in PD (Boecker et al., 2007; Dagmar H. Hepp et al.,
6

132
Chapter 6
2017; Matsui et al., 2006; Meppelink et al., 2009; Park et al., 2013; Stebbins et al., 2004).
Second, drug-induced (mostly visual) hallucinations in PD, either or not accompanied
with delusions, have been associated with dopaminergic treatment. Dopamine agonists
have the highest risk of inducing this type of hallucinations, which are independent of
cognitive decline and reverse with adjustment of dopaminergic drug treatment (Factor
et al., 2017; Zahodne and Fernandez, 2008). Third, dysfunction of the serotonin system
has been related to hallucinations in PD. In addition, response to pimavanserin (a
5-HT2A inverse-agonist), a novel antipsychotic for PD with no effect on dopamine
receptors, underscores the role of serotonin in psychosis in PD (Factor et al., 2017;
Kianirad and Simuni, 2017). It remains unclear why some PD patients develop only
VH while others also develop hallucinations in other modalities. One hypothesis is
related to other factors such as dopaminergic medication (Goetz et al., 1998; McAuley
and Gregory, 2012). This is an interesting hypothesis, as it suggests different treatment
options for both subtypes of hallucinations. In this study, we wish to investigate the
underlying mechanisms of hallucinations in PD using magnetoencephalography (MEG).
MEG is a non-invasive technique to measure neuronal activity directly, and study
normal and pathological (oscillatory) brain activity in health and disease (Stam and
van Straaten, 2012). Activation of brain regions is often accompanied with decreases
or increases in signal power in a particular frequency band due to changes in local
synchrony in the underlying neuronal networks (Pfurtscheller and Lopes da Silva, 1999;
local cortical network interactions mainly involve oscillations above 30 Hz (i.e. gamma
band) and mediate feedforward processing, whereas long-range interactions among
distant brain regions are mediated through oscillations below 30 Hz (i.e. theta (4-8
Hz), alpha (8-13 Hz) and beta (13-30 Hz)) and facilitate integrative brain functions and
feedback attentional processing (Bastos et al., 2015; Donner and Siegel, 2011; Siegel
et al., 2012; Uhlhaas and Singer, 2013; von Stein and Sarnthein, 2000). Furthermore,
both alpha and beta oscillations are boosted by cholinergic enhancement (Bauer et al.,

133
MEG-based resting-state brain activity in PD
2012a) and play a role in feedback processes in the context of (visual) attention tasks
Lopes da Silva, 2013). In addition, the modulatory effect of acetylcholine on oscillatory
brain activity is further supported by acetylcholine antagonists that induce a so-called
‘slowing’ of oscillatory brain activity with decrease in alpha and beta activity and
increase in delta and theta activity (Bauer et al., 2012a; Simpraga et al., 2018, 2017).
Therefore, MEG may be of great value to provide an intrinsic temporal view of the
brain in relation to hallucinations.
In the present study, in order to gain insight into the pathophysiological mechanism(s)
patients with unimodal VH (unimodal Hall+) and compared this with PD patients with
multimodal hallucinations (multimodal Hall+) and PD patients without hallucinations
(Hall-). Given the predominant occurrence of VH in PD, in this study, patients were
recruited according to the criterium of presence or absence of hallucinations. After
inclusion, patients with hallucinations were divided into a subgroup with only VH and
a subgroup with multimodal hallucinations (see methods for details).
system has been associated with top-down processing and enhancement of alpha and
decrease in alpha and beta frequencies, and increase in delta and theta frequencies) of
oscillatory brain activity in PD patients who experienced only VH.
2. METHODS
2.1 Study population
Twenty PD patients with hallucinations (Hall+) and 20 without hallucinations (Hall-)
were recruited from the Understanding Hallucinations (UH) study, and included in the
Understanding Hallucinations – MEG (UH-MEG) study at the department of Clinical
Neurophysiology of the VU University Medical Center (VUmc) in Amsterdam, The
Netherlands. UH-MEG is a follow-up study of the UH study, which is an ongoing
multicenter cross-sectional study that investigates phenomenology and underlying brain
6

134
Chapter 6
mechanisms of hallucinations across different neurological, psychiatric and perceptual
³18 years, mentally competent and PD diagnosis determined by the treating neurologist,
(i.e. Hall+) or no hallucination experiences in life (i.e. Hall-). Presence of hallucinations
was assessed with the Questionnaire for Psychotic Experiences (QPE) (Sommer et al.,
complications (SCOPA-PC) (Visser et al., 2007). As part of the UH-MEG, all patients
underwent a 5-minutes eyes-closed MEG recording, followed by assessment of
hallucinations with the QPE, loneliness by De Jong-Gierveld Loneliness (DJGL) scale (de
Jong-Gierveld and Kamphuls, 1985), depression by the Beck Depression Inventory-II
(BDI-II) (Beck et al., 1996), and cognitive testing, which included the Mini-Mental State
Examination (MMSE) as a measure of global cognitive functioning (Folstein et al., 1975),
the Trail Making Test part A (TMT-A) as a measure of motor and visual processing
speed (Reitan, 1958), and the TMT part B (TMT-B) (Crowe, 1998; Oosterman et al.,
2010; Reitan, 1992) and forward condition of the Digit Span (Lindeboom and Matto,
1994) as measures of attention. A contrast score between TMT-B and TMT-A (TMTB-
A : TMT-B minus TMT-A) was calculated as a measure of attentional set-shifting (i.e.
cognitive problem in PD (Williams-Gray et al., 2008). Hall+ and Hall- patients were
matched at the group level for age, gender, educational level, disease duration (i.e. years
Hoehn and Yahr-scale (H&Y: range 0-5 with higher scores indicating more advanced
disease severity) (Goetz et al., 2004).
All participants provided written informed consent. UH and UH-MEG were approved
Declaration of Helsinki.
After assessing the phenomenology of hallucinations with the QPE, we observed a
dichotomy in the presence of type of hallucinations within the Hall+ group. Ten patients
within the Hall+ group experienced only VH, whereas ten patients experienced

135
MEG-based resting-state brain activity in PD
hallucinations in more than one modality. Therefore, we divided the Hall+ group
into subgroups (i.e. patients with only VH (unimodal Hall+, N=10) and patients with
results section for a detailed description of the phenomenology of the Hall+ patients.
2.2 MEG acquisition and preprocessing
MEG data were recorded using a 306-channel (102 magnetometers, 204 gradiometers)
whole-head MEG system (Elekta Neuromeg, Oy, Helsinki, Finland) with a sample
Hz. Five minutes of (range 262 – 400 s) eyes-closed resting-state data were recorded
with patients in supine position in the MEG-scanner inside a magnetically shielded
room (Vacuumschmelze GmbH, Hanau, Germany).
The head position relative to the MEG sensors was recorded continuously using the
as well as the outline of the patient’s scalp ( 500 points) were digitized using a 3D
digitizer (Fastrak; Polhemus, Colchester, VT, U.S.A.).
(tSSS) (Taulu and Hari, 2009; Taulu and Simola, 2006) as implemented in MaxFilter
software (Elekta Neuromeg Oy; version 2.2.15) with a sliding window of 10 seconds
and a subspace correlation limit of 0.9 was used to remove artifacts (Hillebrand
et al., 2013). The scalp surfaces of all patients were co-registered to T1-weighted
templates with 1 mm resolution, grossly matched for head-size, using a surface
matching procedure (see Supplemental Material for details). Visual inspection of the
co-registration between digitized scalp surface and the co-registered template MRI
as extracted from the co-registered template MRI was used as a volume conductor
model for source reconstruction using the beamformer approach described below.
6

136
Chapter 6
2.3 Source reconstruction using beamforming
Neuronal activity at source-level was reconstructed using an atlas-based beamforming
approach (Hillebrand et al., 2012). The automated anatomical labeling (AAL) atlas was
used to label the voxels in a patient’s co-registered surrogate MRI in 78 cortical and
12 subcortical regions of interest (ROIs) (Tzourio-Mazoyer et al., 2002). Given the
different number of voxels in each ROI, the centroid voxel (i.e. the voxel within the
ROI that is nearest, in terms of Euclidean distance, to all other points in the ROI)
was selected as representative for that ROI (Hillebrand et al., 2016). The neuronal
activity for each centroid voxel, a so-called virtual electrode (VE), was reconstructed
as the weighted sum of each MEG sensor’s time-series. The (normalized) beamformer
equivalent current dipole in the spherical head model), and the broad-band (0.5-48 Hz)
data covariance. On average, 286 s (range 262 – 394 s) of data was used to construct
the covariance matrix. See (Hillebrand et al., 2016, 2012, 2005; Hillebrand and Barnes,
2005) for a detailed description of the beamforming approach.
The beamforming approach resulted in broad band (0.5-48 Hz) time-series for each
centroid of the 90 ROIs. From these time-series 35 epochs of 4096 samples (3.2765
s) were visually selected by MD and independently evaluated on quality by one of
the senior authors (CS). Epochs without consensus were replaced by new epochs.
The selected epochs were converted to American Standard Code for Information
Interchange (ASCII) format, and loaded into BrainWave software for further analysis
(BrainWave version 0.9.152.12.5, C. J. Stam; available at http:/home.kpn.nl/stam7883/
brainwave.html).
2.4 Spectral analysis
Peak frequency (i.e. frequency with the highest power in the 4-13 Hz range, PF), and
relative power in the frequency bands delta (0.5-4 Hz), theta (4-8 Hz), alpha1 (8-10
Hz), alpha2 (10-13 Hz), beta (13-30 Hz), and gamma (30-48 Hz) were calculated as
one average value per frequency band, and for each AAL region per epoch per patient
by using the Fast Fourier Transformation. All components of the Fourier transform

137
MEG-based resting-state brain activity in PD
outside the pass band were set to zero, after which an inverse Fourier transform was
The PF and relative power values were averaged over the 35 artefact-free epochs
per patient to obtain one value per patient per frequency band and per AAL region.
2.5 Statistical analysis
Statistical analyses were performed using IBM SPSS statistics 24.0. Patient characteristics
and spectral measures were compared between the groups. Continuous data were
tested for normality using the Shapiro-Wilk test. Normally distributed variables
were compared using independent samples T-test. Data that did not follow a normal
distribution were compared using nonparametric Mann-Whitney U test. Categorical
data were compared using the chi-square test.
To explore the spatial distribution of relative power per frequency band and PF, we
compared relative power and PF of different brain regions between the subgroups
using repeated measures ANOVA with Greenhouse-Geiser correction for sphericity,
with brain regions and frequency band as the within subject factor and group as the
between subject factor, and FDR-correction for multiple comparisons. For this analysis
the following brain regions per hemisphere were tested: frontal, central, parietal,
occipital, temporal, limbic and subcortical. For frequency bands, only the bands/PF
The False Discovery Rate (FDR) approach (Benjamini and Hochberg, 1995) with
adjusted p value (i.e., q-value) of .05 was used to correct for multiple comparisons: 1)
for the main analysis where one average value per frequency band/PF was calculated,
correction was performed for the number of frequency bands and PF, 2) for the
main analysis, power/PF was further explored regionally between the groups, and
6

138
Chapter 6
Finally, Spearman correlation coefficients were calculated between each
neuropsychological test and each relative power/PF per brain region that showed
3. RESULTS
3.1 Hall+ vs. Hall- patients
3.1.1 Patient characteristics
Hall+ and Hall- patients did not differ at the group level for age, gender, educational
level, disease duration, disease severity and medication use (Table 1), which indicates
that matching was accurate. All Hall+ patients (n=20, 100%) experienced VH (Table 1).
Ten patients (n=10/20, 50%) also experienced auditory hallucinations (AH). From this
group (i.e. 10 patients with VH and AH), six patients experienced olfactory (OH) and
tactile hallucinations (TH) (n=6/20, 30%). All patients experienced recurrent complex
VH containing people, animals and inanimate objects with and without movement.
Twelve (60%) patients retained full insight, while six (30%) had partial insight into their
hallucinations and doubted the real nature of the hallucinations. Two (10%) patients
were fully convinced that their hallucinations were real (i.e. insight was absent). 80%
(n=16) of the patients had at least once interacted with their hallucinations. More than
50% of the patients also experienced minor hallucinations including visual illusions (i.e.
seeing things differently than they actually are, e.g. seeing a face in a branch of a tree),
passage hallucinations (i.e. seeing a person, animal or object passing in the peripheral
is present or nearby without being actually visible). One (5%) patient experienced
delusions in the week preceding participation in the study (Table 1).
BDI-II, and DJGL than the Hall- group (Table 1).

139
MEG-based resting-state brain activity in PD
Table 1. Patient characteristics
Hall+ (N=20) Hall- (N=20)
Age, yrs 72.15 (6.22) 70.50 (6.45)
Gender, female 7 (35.0%) 6 (30.0%)
Education level 4 (3 – 7) 7 (6 – 7)
Handedness, right 18 (90.0%) 15 (75.0%)
Disease duration, yrs 7.71 (4.35 – 12.73) 4.46 (2.75 – 9.38)
Hoehn & Yahr staging scale 3.0 (3.0 – 4.0) 3.0 (3.0 – 3.0)
LED, mg/day 882.00 (628.75 – 1188.00) 666.00 (547.25 – 1218.75) n=18
Type of hallucinations
VH 20 (100.0%)
AH 10 (50.0%)
OH 6 (30.0%)
TH 6 (30.0%)
Delusions 1 (5.0%)
BDI-II** 15.00 (10.00 – 19.75) 10.00 (5.00 – 14.75)
DJGL* 5.00 (1.00 – 6.00) 1.00 (0.00 – 4.00)
Cognition
MMSE** 26.0 (21.75 – 27.75) 28.5 (27.0 – 29.0)
Digit Span forward 8.20 (1.51) 8.85 (1.66)
TMT-A 96.47 (59.89) n=19 65.73 (58.25)
TMT-B 183.87 (113.35) n=16 121.77 (67.52) n=18
TMTB-A 101.69 (112.96) n=16 74.13 (58.16) n=18
Data are mean (SD), median (interquartile range), or n (%). Education level was assessed with the 7-item Verhage coding system for education (Verhage, 1964). Disease duration was calculated as the years diagnosed with PD at enrollment in the study. The Hoehn and Yahr staging scale was used to measure disease severity based on clinical features and functional disability. It ranges from 0-5 with higher scores indicating more advanced disease severity (Goetz et al., 2004). The total dose of dopaminergic medication (i.e. including dopaminomimetics and levodopa) was converted to a so-called levodopa equivalent dose in milligrams per day based on (Tomlinson et al., 2010). Depression was measured with the BDI-II. Loneliness was measured using the DJGL.AH: Auditory Hallucinations; BDI-II: Beck Depression Inventory-II; DJGL: De Jong Gierveld Loneliness scale; Hall+: PD patients with hallucinations; Hall-: PD patients without hallucinations; LED: Levodopa Equivalent Dose; MMSE: Mini Mental State Examination; OH: Olfactory Hallucinations; PD: Parkinson’s disease; TH: Tactile Hallucinations; TMT-A: Trail-Making Test part A; TMT-B: Trail-Making Test part B; TMTB-A: a contrast score between TMT-B and TMT-A calculated as a measure of attentional set-shifting; VH: Visual Hallucinations
6

140
Chapter 6
3.1.2 Spectral analysis
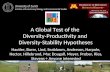
Figure 1 shows the mean power spectrum for both patient groups. The Hall+ group
showed slowing of resting state brain activity compared to Hall- group, but the groups
did not differ in relative power or PF (Table 2).
Figure 1. Average power spectra over 90 AAL regions for Parkinson’s disease patients with (Hall+: yellow) and without (Hall-: blue) hallucinations. Peak frequency (i.e. frequency with the most power in the 4-13 Hz range) is lower in Hall+ compared to Hall- patients. Filled area represents the standard error of the mean.
Table 2: Relative power per frequency band in PD patients with and without hallucinations
Hall+ (n=20) Hall- (n=20) p-value
Delta 0.262 (0.074) 0.256 (0.038) .758
Theta 0.207 (0.080) 0.183 (0.054) .285
Alpha1 0.102 (0.026) 0.104 (0.034) .833
Alpha2 0.101 (0.031) 0.098 (0.018) .758
Beta 0.257 (0.090) 0.276 (0.064) .453
Gamma 0.071 (0.019) 0.082 (0.020) .089
Peak frequency 7.97 (1.15) 8.11 (0.70) .643
Power is the relative power per frequency band (delta [0.5–4 Hz], theta [4–8 Hz], alpha1 [8–10 Hz], alpha2 [10–13 Hz], beta [13–30 Hz], and gamma [30-48 Hz]). Peak frequency is the frequency with highest power in range between 4 and 13 Hz. Hall+: Parkinson’s disease patients with hallucinations; Hall-: Parkinson’s disease patients without hallucinations

141
MEG-based resting-state brain activity in PD
3.2 Subgroup analyses
3.2.1 Patient characteristics
As described above, given the dichotomy in the presence of type of hallucinations
within the Hall+ group, namely n=10 patients with only VH and n=10 patients
with multimodal hallucinations, we performed exploratory subgroup analyses and
compared PD patients with only VH (unimodal Hall+) with PD patients with multimodal
hallucinations (multimodal Hall+), and both these subgroups separately with Hall-
Unimodal Hall+, multimodal Hall+ and Hall- patients did not differ at the group level
for age, gender, educational level, disease duration, disease severity and medication use
TMT-B, and experienced more depressive symptoms and loneliness than Hall- patients.
Multimodal Hall+ patients experienced more depressive symptoms compared to Hall-
patients (Table 3). Unimodal Hall+ and multimodal Hall+ patients did not differ on
cognition, DJGL or BDI-II (Table 3).
severe (i.e. content was more often negative) in multimodal Hall+ patients and they
also experienced more often distress from their hallucinations than unimodal Hall+
patients (Table 3).
3.2.2 Spectral analysis
Figure 2 shows the mean power spectrum for the unimodal Hall+ and multimodal Hall+
patients in relation to the Hall- group. For both relative power and PF, the unimodal
Hall+ and multimodal Hall+ group deviated in opposite direction compared to the
Hall- group (Table 4). Compared to the Hall- group, unimodal Hall+ patients showed
relative power in the beta (p=.029) and gamma (p=.007) band, and lower PF (p=.011).
The relative power per AAL region for the theta, beta and gamma frequency band,
as well as PF per AAL region, are shown in Table S1-S4. After correcting for multiple
comparisons, theta, beta, and gamma band relative power, as well as PF (Table S1-S4),
6

142
Chapter 6
power for the theta, beta and gamma frequency band, as well as the mean PF, for each
cortical ROI for both the unimodal Hall+ and Hall- patients.
Figure 2. Average power spectra over 90 AAL regions for Parkinson’s disease patients with only VH (unimodal Hall+: red), with multimodal (multimodal Hall+: green) and without (Hall-: blue) hallucinations. Peak frequency (i.e. frequency with the most power in the 4-13 Hz range) is lowest in unimodal Hall+ patients. Filled area represents the standard error of the mean. VH: Visual Hallucinations

143
MEG-based resting-state brain activity in PD
Tab
le 3
: Pat
ient
cha
ract
eris
tics
in P
arki
nson
’s di
seas
e pa
tient
s w
ith u
nim
odal
, mul
timod
al, a
nd w
ithou
t ha
lluci
natio
ns
Uni
mod
al H
all+
(N
=10)
Mul
tim
odal
Hal
l+ (
N=1
0)H
all-
(N
=20)
Age
, yrs
74.2
0 (5
.85)
70.1
0 (6
.17)
70.5
0 (6
.45)
Gen
der,
fem
ale
2 (2
0.0%
)5
(50.
0%)
6 (3
0.0%
)
Educ
atio
n le
vel
6.50
(3,
75 –
7.0
)4.
00 (
2.75
– 5
.50)
7.00
(6.0
– 7
.0)
Han
dedn
ess,
rig
ht9
(90.
0%)
9 (9
0.0%
)15
(75
.0%
)
Dis
ease
dur
atio
n, y
rs8.
13 (4
.81
– 19
.79)
6.46
(4.0
2 –
11.1
9)4.
46 (
2.75
– 9
.38)
Hoe
hn &
Yah
r st
agin
g sc
ale
3.5
(3.0
– 4
.0)
3.0
(2.3
8 –
4.0)
3.0
(3.0
– 3
.0)
LED
, mg/
day
922.
0 (5
75.2
5 –
1459
.75)
860.
0 (5
87.5
0 –
1056
.75)
666.
0 (5
47.2
5 –
1218
.75)
n=1
8
BDI-
II*§
16.0
(9.
75 –
21.
25)
14.5
0 (9
.75
– 18
.50)
10.0
(5.
0 –
14.7
5)
DJG
L*5.
0 (2
.50
– 6.
0)3.
50 (1
.0 –
6.0
)1.
00 (
0.0
– 4.
0)
Typ
e of
hal
luci
nati
ons
VH
10 (1
00.0
%)
10 (1
00.0
%)
AH
010
(100
.0%
)
OH
06
(60.
0%)
TH
06
(60.
0%)
Dis
tres
s fr
om h
allu
cina
tions
2 20
.0%
)5
(50.
0%)
Emot
iona
l val
ence
of h
allu
cina
tions
1 (1
0.0%
)4
(40.
0%)
Del
usio
ns0
1 (1
0.0%
)
6

144
Chapter 6
Tabl
e 3:
Con
tinue
d
Uni
mod
al H
all+
(N
=10)
Mul
tim
odal
Hal
l+ (
N=1
0)H
all-
(N
=20)
Cog
niti
on
MM
SE**
24.5
(16.
25 –
27.
0)27
.0 (
24.7
5 –
28.2
5)28
.5 (
27.0
– 2
9.0)
Dig
it Sp
an fo
rwar
d7.
90 (1
.97)
8.50
(0.
85)
8.85
(1.6
6)
TM
T-A
*11
8.89
(66.
10)
n=9
76.3
0 (4
8.33
)65
.73
(58.
25)
TM
T-B*
*24
2.43
(121
.84)
n=7
155.
63 (
75.0
8)12
1.77
(67.
52)
n=18
TM
TB
-A13
6.29
(138
.46)
n=7
97.8
8 (5
7.42
)74
.13
(58.
16)
n=18
Dat
a ar
e m
ean
(SD
), m
edia
n (in
terq
uart
ile r
ange
), or
n(%
).Edu
catio
n le
vel w
as a
sses
sed
with
the
7-it
em V
erha
ge c
odin
g sy
stem
for
educ
atio
n (V
erha
ge, 1
964)
. Dis
ease
du
ratio
n w
as c
alcu
late
d as
the
year
s di
agno
sed
with
PD
at e
nrol
lmen
t in
the
stud
y. T
he H
oehn
and
Yah
r st
agin
g sc
ale
was
use
d to
mea
sure
dis
ease
sev
erity
bas
ed o
n cl
inic
al
feat
ures
and
func
tiona
l dis
abili
ty. I
t ra
nges
from
0-5
with
hig
her
scor
es in
dica
ting
mor
e ad
vanc
ed d
isea
se s
ever
ity
(Goe
tz e
t al
., 20
04).
The
tot
al d
ose
of d
opam
iner
gic
med
icat
ion
(i.e.
incl
udin
g do
pam
inom
imet
ics
and
levo
dopa
) w
as c
onve
rted
to
a so
-cal
led
levo
dopa
equ
ival
ent
dose
in m
illig
ram
s pe
r da
y ba
sed
on (
Tom
linso
n et
al.,
20
10).
Dep
ress
ion
was
mea
sure
d w
ith t
he B
DI-
II. L
onel
ines
s w
as m
easu
red
usin
g th
e D
JGL.
BDI-
II: B
eck
Dep
ress
ion
Inve
ntor
y-II;
DJG
L: D
e Jo
ng G
ierv
eld
Lone
lines
s sc
ale;
Hal
l-: P
D p
atie
nts
with
out h
allu
cina
tions
; LED
: Lev
odop
a Eq
uiva
lent
Dos
e; M
MSE
: Min
i M
enta
l Sta
te E
xam
inat
ion;
Mul
timod
al H
all+
: PD
pat
ient
s w
ith m
ultim
odal
hal
luci
natio
ns; P
D: P
arki
nson
’s di
seas
e; T
MT-
A: T
rail-
Mak
ing
Test
par
t A
; TM
T-B:
Tra
il-M
akin
g Te
st p
art
B; T
MT
B-A
: a c
ontr
ast
scor
e be
twee
n T
MT-
B an
d T
MT-
A c
alcu
late
d as
a m
easu
re o
f att
entio
nal s
et-s
hift
ing;
Uni
mod
al H
all+
: PD
pat
ient
s w
ith o
nly
visu
al h
allu
cina
tions
;

145
MEG-based resting-state brain activity in PD
Tab
le 4
: Rel
ativ
e po
wer
per
freq
uenc
y ba
nd in
Par
kins
on’s
dise
ase
patie
nts
with
uni
mod
al, m
ultim
odal
, and
with
out
hallu
cina
tions
Uni
mod
al
Hal
l+ (
n=10
)M
ulti
mod
al
Hal
l+ (
n=10
)H
all-
(n=
20)
p-va
lue
Uni
mod
al H
all+
vs
. Hal
l-
p-va
lue
Mul
tim
odal
Hal
l+
vs. H
all-
p-va
lue
Uni
mod
al H
all+
vs.
M
ulti
mod
al H
all+
Del
ta0.
286
(0.0
93)
0.23
8 (0
.060
)0.
256
(0.0
38)
.296
.169
.315
The
ta0.
247
(0.0
56)
0.16
6 (0
.082
)0.
183
(0.0
54)
.005
*.2
67.0
19
Alp
ha1
0.09
5 (0
.027
)0.
109
(0.0
25)
0.10
4 (0
.034
).4
841.
000
.280
Alp
ha2
0.09
0 (0
.021
)0.
111
(0.0
36)
0.09
8 (0
.018
).3
03.3
28.2
18
Beta
0.21
9 (0
.062
)0.
295
(0.1
01)
0.27
6 (0
.064
).0
29*
.619
.063
Gam
ma
0.06
1 (0
.014
)0.
081
(0.0
19)
0.08
2 (0
.020
).0
07*
.948
.023
Peak
freq
uenc
y7.
31 (
0.88
)8.
63 (1
.01)
8.11
(0.
70)
.011
*.0
91.0
07*
Pow
er is
the
rel
ativ
e po
wer
per
fre
quen
cy b
and
(del
ta [
0.5–
4 H
z], t
heta
[4–
8 H
z], a
lpha
1 [8
–10
Hz]
, alp
ha2
[10–
13 H
z], b
eta
[13–
30 H
z], a
nd g
amm
a [3
0-48
Hz]
), av
erag
ed o
ver
all 9
0 A
AL
regi
ons.
Pea
k fr
eque
ncy
is t
he fr
eque
ncy
with
hig
hest
pow
er in
ran
ge b
etw
een
4 an
d 13
Hz,
ave
rage
d ov
er a
ll 90
AA
L re
gion
s.H
all-:
Par
kins
on’s
dise
ase
patie
nts
with
out
hallu
cina
tions
; Mul
timod
al H
all+
: Par
kins
on’s
dise
ase
patie
nts
with
mul
timod
al h
allu
cina
tions
; Uni
mod
al H
all+
: Par
kins
on’s
dise
ase
patie
nts
with
onl
y vi
sual
hal
luci
natio
ns
6

146
Chapter 6
Figure 3. Mean relative power for each region of interest (ROI) in unimodal Hall+ (left) and Hall- (right) patients displayed as a color-coded map on a parcellated template brain viewed from, in clockwise order, the left, top, right, right-midline and left-midline. Panel A: rela-tive power in the theta band. Panel B: relative power in the beta band. Panel C: relative power in the gamma band. Panel D: Peak frequency. Hot and cold colors indicate higher and
-ing subcortical regions per frequency band and for all the relative power and peak frequency values in the two groups.Hall-: Parkinson’s disease patients without hallucinations; unimodal Hall+: Parkinson’s disease patients with only visual hallucinations

147
MEG-based resting-state brain activity in PD
In the theta band, unimodal Hall+ patients showed higher relative power in 74 (82.2%)
out of 90 AAL regions compared to the Hall- group. These regions were spread across
the entire brain and included all the regions in the limbic lobes and all the subcortical
regions in both hemispheres (Table S1). In the beta band, relative power was lower in
14 (15.6%) out of 90 AAL regions in unimodal Hall+ patients. These regions were mainly
located in the parietal and occipital lobes (Table S2). In the gamma band, unimodal
Hall+ patients showed lower relative power in 47 (52.2%) out of 90 AAL regions.
These regions included mainly the frontal and limbic lobes, and subcortical regions, but
not the temporal, parietal and occipital lobes (Table S3). PF was lower in 51 (56.7%)
out of 90 AAL regions in unimodal Hall+ patients compared to Hall- patients. These
regions comprised almost the entire brain except (mainly) the frontal lobes (Table S4).
To explore whether a potential spatial pattern could be found for the AAL regions
located across the right hemisphere, and comprised the parietal, temporal, limbic and
PF included left occipital and limbic brain region, whereas in the right hemisphere, all
6

148
Chapter 6
Figure 4. unimodal Hall+ and Hall- patients, displayed as in Figure 3, for the theta (panel A), beta (panel B), and gamma (panel C) band, and for peak frequency (panel D). Red: higher relative power in unimodal Hall+ patients. Blue: lower relative power/peak frequen-cy in unimodal Hall+ patients. Gray: brain regions that did not differ between the groups.
-
and table S5 for the mean relative power/peak frequency values in the two groups. Hall-: Parkinson’s disease patients without hallucinations; unimodal Hall+: Parkinson’s disease patients with only visual hallucinations
The multimodal Hall+ and Hall- groups did not differ in relative power or PF (Table
power in the theta (p=0.19) and gamma (p=.023) frequency band and in PF (p=.007).
multimodal Hall+ patients showing higher PF than unimodal Hall+ patients (Table 4).
The relative power per AAL region for the theta and gamma band and PF are shown
in Table S7-S9.

149
MEG-based resting-state brain activity in PD
Further regional exploration showed that in the theta band, all but the bilateral central,
Hall+ and multimodal Hall+ group (Table S5-S6, Figure 5a). In the gamma band, relative
Figure 5. Distribution of the brain regions that showed significant difference be-tween unimodal Hall+ and multimodal Hall+ patients, displayed as in Figure 3, for the theta (panel A), and gamma (panel B) band, and for peak frequency (panel C). Red: higher relative power in unimodal Hall+ patients. Blue: lower relative power/peak fre-quency in unimodal Hall+ patients. Gray: brain regions that did not differ between the
-
groups and table S5 for the mean relative power/peak frequency values in the two groups. Multimodal Hall+: Parkinson’s disease patients with multimodal hallucinations; unimodal Hall+: Parkinson’s disease patients with only visual hallucinations
6

150
Chapter 6
Although the subgroups did not differ in use of medication (Table 3), we redid the main
analyses in the subgroups (Table 4) with medication (LED) as a covariate in order to
exclude a potential effect of medication on our results, and found that the corrected
model still showed the same effects (see Table S10).
3.2.3 Correlation with neuropsychological tests
3.2.3.1 MMSE
In the Hall- group, a negative correlation was found between relative power in the
right parietal and limbic brain region in the theta band and MMSE (Table 5). In the beta
band, MMSE was positively correlated with relative power in the right parietal brain
region (Table 5). MMSE was positively correlated with PF in all but the right occipital
the unimodal Hall+ group.
3.2.3.2 TMT-A and TMT-B
In the Hall- group, Spearman correlation showed a positive correlation between both
the TMT-A and TMT-B and relative power in all brain regions in the theta band, and
negative correlations with relative power in brain regions in the beta band (Table 5).
For PF, a negative correlation was found between all brain regions and TMT-A, whereas
band or the unimodal Hall+ group.

151
MEG-based resting-state brain activity in PD
Table 5: region and neuropsychological tests in Parkinson’s disease patients without hallucinations
Brain region Neuropsychological test N Spearman rho (r) p-value
Theta band
Right parietal MMSE 20 -0.45 .048
TMT-A 20 0.51 .023
TMT-B 18 0.53 .025
Right temporal MMSE 20 -0.44 .054
TMT-A 20 0.51 .020
TMT-B 18 0.51 .032
Right limbic MMSE 20 -0.45 .049
TMT-A 20 0.53 .016
TMT-B 18 0.47 .049
Right subcortical MMSE 20 -0.43 .062
TMT-A 20 0.55 .011
TMT-B 18 0.51 .029
Beta band
Right parietal MMSE 20 0.51 .021
TMT-A 20 -0.61 .004
TMT-B 18 -0.60 .008
Right temporal MMSE 20 0.44 .054
TMT-A 20 -0.49 .029
TMT-B 18 -0.62 .007
Gamma band
Left frontal MMSE 20 -0.01 .966
TMT-A 20 0.10 .669
TMT-B 18 0.18 .464
Right frontal MMSE 20 -0.05 .824
TMT-A 20 0.19 .433
TMT-B 18 0.20 .432
Left central MMSE 20 -0.18 .436
TMT-A 20 0.33 .160
TMT-B 18 0.14 .569
Left limbic MMSE 20 -0.05 .844
TMT-A 20 0.13 .599
TMT-B 18 0.12 .641
6

152
Chapter 6
Table 5: Continued
Brain region Neuropsychological test N Spearman rho (r) p-value
Peak frequency
Right parietal MMSE 20 0.55 .012
TMT-A 20 -0.55 .012
TMT-B 18 -0.44 .069
Left occipital MMSE 20 0.51 .023
TMT-A 20 -0.56 .010
TMT-B 18 -0.59 .011
Right occipital MMSE 20 0.41 .076
TMT-A 20 -0.47 .035
TMT-B 18 -0.50 .034
Right temporal MMSE 20 0.46 .042
TMT-A 20 -0.56 .010
TMT-B 18 -0.46 .056
Left limbic MMSE 20 0.57 .008
TMT-A 20 -0.66 .001
TMT-B 18 -0.48 .043
Right limbic MMSE 20 0.64 .002
TMT-A 20 -0.65 .002
TMT-B 18 -0.44 .068
Right subcortical MMSE 20 0.57 .009
TMT-A 20 -0.61 .005
TMT-B 18 -0.33 .184
MMSE: Mini-Mental State Examination; TMT-A: Trail-Making Test part A; TMT-B: Trail-Making Test part B
4. DISCUSSION
oscillatory brain activity in PD patients who experienced visual hallucinations, the
PD patients with and without hallucinations. However, remarkable results were found
when exploratory subgroup analyses were performed after dissecting the hallucinating
group into purely visual hallucinations (unimodal Hall+) and hallucinations also in other

153
MEG-based resting-state brain activity in PD
modalities (multimodal Hall+). Compared to patients without hallucinations, patients
with only VH showed slowing of resting-state oscillatory brain activity, with spatial
distributions characterized by an increase in theta power in all but the fronto-central
and occipital brain region in the right hemisphere, and concomitant decrease in beta
power in the right temporoparietal brain region, and decrease in gamma power in
the bilateral frontal and left limbic brain region, and lowering of PF in almost all but
the frontal brain regions. These deviations were absent in the patient group with
multimodal hallucinations compared to patients without hallucinations. Compared to
and diffuse increase in PF in all but the frontal brain regions.
Analysis of relative power/PF in relation to performance on neuropsychological tests
showed, only in patients without hallucinations, a correlation between higher theta
power and worse performance on the MMSE, better performance on MMSE and
higher beta power in the right parietal region and higher PF in all but the right occipital
brain regions. Lower theta and higher beta power were associated with a better
performance on both TMT-A and TMT-B, whereas a diffuse higher PF was associated
with a better performance on TMT-A, and higher PF in bilateral occipital and left limbic
brain region was associated with better performance on the TMT-B test.
4.2 Underlying mechanism(s) of unimodal visual and multimodal hallucinations in PD
4.2.1 Unimodal visual hallucinations
The cholinergic system is seen as a modulator of the cortical signal-to-noise ratio
(Collerton et al., 2005). Slowing in resting-state brain activity (increased power in
delta and theta frequencies and decreased power in alpha and beta frequencies) has
been associated with impaired cholinergic function (Bauer et al., 2012a; Simpraga et
al., 2018). As mentioned earlier, the central cholinergic system has been involved in
the integration of top-down attentional and bottom-up sensory processing such that
cholinergic dysfunction (results in decrease in signal-to-noise ratio) may increase the
uncertainty in top-down activity resulting in incorrect scene representation, and thus
hallucinations (Collerton et al., 2005; Friston, 2005). Indeed, impaired bottom-up (i.e.
6

154
Chapter 6
reduced activation of the visual pathways) and top-down (i.e. defective attentional)
processing, and thus cholinergic dysfunction, has frequently been reported in PD
patients who experience VH (Boecker et al., 2007; Dagmar H. Hepp et al., 2017; Matsui
et al., 2006; Meppelink et al., 2009; Park et al., 2013; Stebbins et al., 2004). Recently,
Hepp et al. proposed that impaired bottom-up visual processing in combination with
defective top-down attentional processing may underlie VH in PD (Dagmar H. Hepp
evidence that VH in PD may emerge due to central cholinergic dysfunction.
With respect to spatial distribution, compared to patients without hallucinations,
groups were located in the right hemisphere and comprised the temporoparietal brain
areas, amongst others. The right hemisphere has been shown to play a role in arousal
and attentional processes and mediate top-down attentional processing (Levy and
Wagner, 2011; Posner, 1994; Sacchet et al., 2015). The temporoparietal brain regions
form part of the ventral attentional network (VAN, also named salience network),
which is lateralized to the right hemisphere and involved in shifting attention in the
presence of salient stimuli (Corbetta et al., 2002; Vossel et al., 2014). Moreover, the
right temporoparietal brain regions have been involved in source monitoring or ‘self-
other’ distinction (i.e. discrimination between external perceptions and internally
have been reported in PD patients with VH (Barnes et al., 2003; Muller et al., 2014).
Beta band activity has been associated with long-range feedback or top-down
2000; Michalareas et al., 2016). Theta band activity has also been proposed in top-down
processing with a key inhibitory role in working memory to suppress task-irrelevant
or distracting information in situations that demand cognitive control (Klimesch,
1999; Nigbur et al., 2011). Moreover, increase in theta oscillations is observed during
lower vigilance and states of drowsiness (Strijkstra et al., 2003). In patients without
hallucinations, we found that higher power in the right temporoparietal regions

155
MEG-based resting-state brain activity in PD
in the theta band was correlated with worse performance on the tests for visual
processing speed (TMT-A) and attention (TMT-B), whereas higher power in the right
temporoparietal regions in the beta band was associated with better performance on
both tests (Table 5). These correlations were lacking in patients with only VH, which
might be due to the small sample size of the group (data available in n=9 for TMT-A
and n=7 for TMT-B). Taken together, our results provide support for alterations in
top-down attentional processing in PD patients with VH.
Gamma band activity is generated in early sensory cortices, and involved in feedforward
or bottom-up processing (Bastos et al., 2015; Herrmann et al., 2010; N Kopell et
regions between PD patients with unimodal VH and PD patients without hallucinations
suggests that there may be no alterations in bottom-up processing in PD patients with
only VH. Less straightforward is the interpretation of decreased gamma power in the
frontal brain regions in PD patients with only VH compared to PD patients without
hallucinations. Gamma oscillations are modulated by various cognitive processes such
mechanisms of the brain. Particularly, gamma oscillations are involved in working
memory storage that can be controlled by beta oscillations, such that beta rhythm
regulates the access of sensory information into working memory and controls its
maintenance (Herrmann et al., 2010; Miller et al., 2018). Hence, decreased gamma
power in the frontal brain regions might be a consequence of decreased beta power
and thus top-down processing. However, several other brain regions also showed
higher power in the theta and lower power in the gamma band, and lower PF in
patients with only VH, hence our results with respect to spatial distribution may not
pathophysiological mechanisms of VH and should be interpreted with caution. Future
work to evaluate MEG-based functional connectivity and brain network organization
may be of additional value in exploring the exact role of multiple brain regions and
networks - involved in attention and perception - in the pathophysiology of VH.
6

156
Chapter 6
Another possible explanation for slowing of resting-state brain activity in patients with
only VH as opposed to patients with multimodal hallucinations and patients without
hallucinations may be sought in the patient characteristics of the groups. Although
longer disease duration at enrollment and were slightly more cognitively impaired than
patients with multimodal hallucinations and patients without hallucinations, indicating a
slightly more advanced disease stage in patients with only VH. For decades, diffuse and
local slowing of resting state oscillatory brain activity, involving increases in theta power
and decreases in beta and gamma power, has been a consistently reported feature in
PD patients, with severity of slowing increasing with advancing disease, and predicting
risk of future dementia (Bosboom et al., 2006; Caviness et al., 2007; Fonseca et al.,
2009; Klassen et al., 2011; Neufeld et al., 1994; Olde Dubbelink et al., 2014b, 2013a;
Serizawa et al., 2008; Soikkeli et al., 1991; Stoffers et al., 2007).
4.2.2 Multimodal hallucinations
Patients with multimodal hallucinations experienced both VH and AH (with similar
prevalences) and hallucinations in other modalities but did not show more slowing
of resting-state brain activity than patients with only VH or patients without
hallucinations. Patients with multimodal hallucinations rather showed faster, although
without hallucinations, which indicates the complexity of the pathophysiology of
hallucinations in PD. In addition, given the extensive differences in spatial distribution
in the different frequency bands/PF between patients with multimodal hallucinations
A likely candidate to explain changes in spectral power in PD patients with multimodal
hallucinations may be the dopaminergic system. Research on the effect of dopaminergic
neurotransmission on resting-state oscillatory brain activity in PD is scarce.
Nonetheless, a few studies have examined the effect of exposure to dopaminergic
agents (i.e. dopaminomimetics or dopamine precursor levodopa (L-dopa)) on resting-
state brain activity in PD patients and found contradicting results (Babiloni et al., 2018;

157
MEG-based resting-state brain activity in PD
J. M. Melgari et al., 2014; Stoffers et al., 2007; Yaar and Shapiro, 1983). A previous
quantitative EEG study examined 25 PD patients on chronic L-dopa therapy and found
region (Yaar and Shapiro, 1983). In addition, Melgari et al (2014) obtained resting-state
source-space EEG recordings in 24 PD patients before and after an oral dose of L-dopa
Babiloni et al (2018), who studied resting-state EEG activity in PD patients with normal
(n=35) and impaired cognition (n=85) before and after L-dopa intake and compared
these data with EEGs from healthy individuals (n=50). Compared to the healthy
individuals, the PD groups with and without cognitive decline showed a diffuse increase
in delta power and decrease in alpha power in the posterior brain regions. In relation
to PD patients with normal cognition, cognitively impaired PD patients showed greater
increase in delta power, greater reduction in occipital alpha power with concomitant
increase in alpha power in the frontal, central and temporal brain regions (Babiloni
et al., 2018). Notably, an MEG-study by Stoffers et al in non-demented PD patients
power (Stoffers et al., 2007). Thus, there is considerable variability in the reported
relation between resting-state brain activity and dopaminergic neurotransmission,
which could be related to the demographics of the patient groups or methodological
differences between the studies.
patients with only VH, patients with multimodal hallucinations, and patients without
hallucinations (Table 3). Nonetheless, psychosis has frequently been reported as a
non-motor adverse effect of dopaminergic treatment in both early-stage and late-stage
PD (Barrett et al., 2017; Morgante et al., 2012; Ravina et al., 2007; Stowe et al., 2008).
subthalamic deep brain stimulation, which could probably be related to the reduction
dopaminergic treatment in PD may lead to psychosis, and that restoration of brain
6

158
Chapter 6
dopamine levels by drug treatment may (at least partly) restore normal patterns of
oscillatory brain activity, suggest that hyperdopaminergic neurotransmission may
underlie psychosis in PD and does not induce slowing in resting-state oscillatory brain
activity.
A highly speculative explanation for the increase in signal power in patients with
multimodal hallucinations may be sought in the decreased output from the nigrostriatal
dopaminergic system to connected brain areas. The dopamine depleted nigro-striatal-
thalamo-cortical circuit in PD may lead to reduced modulatory control on connected
cortical brain regions (J. M. Melgari et al., 2014; Rodriguez-Oroz et al., 2009). In
response, connected brain areas may lower their detection threshold for neuronal
towards incoming signals) within the connected brain regions. This hyper-excitability
without the presence of an external source; a hallucination (dependent on the
(Carter and ffytche, 2015). Dysregulation of neural circuits due to imbalance between
excitation and inhibition as a general model of hallucinations has been proposed in both
hallucinations (Jardri et al., 2016).
Alterations in serotonin neurotransmission have also been proposed in the
(Factor et al., 2017). Treatment with pimavanserin, a serotonin 2A inverse-agonist,
has been shown to alleviate psychosis in both PD patients with normal and impaired
cognitive functioning (Espay et al., 2018; Kianirad and Simuni, 2017). To date, only one
study has examined in vivo changes in serotonin receptor binding in PD with positron
emission tomography (PET) and found increased serotonin binding in the ventral
visual pathway in PD patients with VH compared to patients without hallucinations
(Ballanger et al., 2010). The use of selective serotonin reuptake inhibitors (SSRIs)
(increasing the extracellular level of serotonin) has been associated with changes in
rhythmic brain activity in the delta, theta and alpha band in prefrontal brain regions,

159
MEG-based resting-state brain activity in PD
with decreases in the delta and theta band and increases in the alpha band (Bares et al.,
were widespread throughout the brain in both patients with only VH and patients with
lower relative power in the theta band compared to both patients with only VH and
patients without hallucinations, hinting that serotonergic dysfunction may play a role
in multimodal hallucinations in PD.
provide strong support for the notion that dopaminergic or serotonergic dysfunction
may induce faster resting-state brain activity in PD patients with multimodal
hallucinations. Future studies investigating different modalities of hallucinations within
PD are needed to gain insight into other potential underlying mechanisms.
4.3 Strengths and limitations
A strength of this study is that it investigated hallucinations in PD with source-space
Second, both patients with and without hallucinations, as well as, patients with only VH
and patients with multimodal hallucinations, were carefully matched for age, gender,
educational level, disease duration, disease stage, and use of medication, which makes
This study also has limitations. First, by performing subgroup analyses we reduced the
sample size of the hallucination group, and therefore, the results should be interpreted
with caution. However, by dividing patients with hallucinations in subgroups based
group differences to the pathophysiology of VH. Second, cholinesterase inhibitors
with simultaneous decreases in low frequency power (Fogelson et al., 2003). We
observed the opposite pattern in our patients. In our study, only two patients (n=1 in
the unimodal Hall+ group and n=1 in the Hall- group) used the cholinesterase inhibitor
6

160
Chapter 6
rivastigmine. Therefore, it is unlikely that the use of cholinesterase inhibitors has
are also used to treat psychosis in PD (Wilby et al., 2017), and have been shown to
increase power in lower frequencies and decrease power in higher frequencies (Hyun
et al., 2011; Maccrimmon et al., 2012). In our study, only two patients with multimodal
hallucinations used atypical antipsychotics (n=1 clozapine, and n=1 quetiapine). As we
found decreased power in the delta and theta band, and increases in power in the alpha
and beta band in patients with multimodal hallucinations, it is unlikely that the use of
5. CONCLUSION
Source-space MEG shows distinct spectral differences between Parkinson’s disease
patients with unimodal visual hallucinations and patients without hallucinations.
Slowing of resting-state brain activity with increases in theta activity, and concomitant
decreases in beta and gamma activity indicates central cholinergic dysfunction as
underlying mechanism of visual hallucinations in Parkinson’s disease. Future work to
evaluate functional connectivity and brain network organization is needed in order to
explore the exact role of multiple brain regions and networks - involved in attention
and perception – in the pathophysiology of visual hallucinations in Parkinson’s disease.

161
MEG-based resting-state brain activity in PD
SUPPLEMENTAL MATERIAL
Methods
Co-registration
The scalp surfaces of all patients were co-registered to a T1-weighted MNI template
with 1 mm resolution using a surface matching procedure. For this, the T1-weighted
average structural MNI template from the SPM toolbox was used (Douw et al., 2018).
This matching was repeated with templates of different sizes (i.e. very small, small,
medium, and large). The small, medium and large templates had been created from
77 MRIs from the Amsterdam Dementia Cohort (ADC) (Van Der Flier et al., 2014),
MRIs. The subjects were split in quartiles based on the size of the ellipsoid (= the length
of the ellipsoid-axis pointing in the y-direction, i.e. roughly through the nose). The
1st
the other 2 quartiles for the medium template (N=39). The MRIs were aligned using
DARTEL toolbox in SPM and averaged. Lastly, 9 MRIs from people with very small
heads were selected from the ADC and aligned to create a very small template. The
a surrogate MRI for that patient.
Normalization MEG spectra
power value over all epochs and all subject. Subsequently, the curves for each epoch
and each subject were divided by this maximum value. Finally, the mean and standard
6

162
Chapter 6
Results
Table S1: Relative power per AAL region in the theta band in Parkinson’s disease patients with unimodal hallucinations and patients without hallucinations
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
1 Gyrus rectus L 0.211 (0.046) 0.167 (0.045) .021
2 Olfactory cortex L 0.241 (0.054) 0.183 (0.051) .007
3 Superior frontal gyrus, orbital part L 0.201 (0.051) 0.162 (0.037) .023
4 Superior frontal gyrus, medial orbital part L 0.206 (0.052) 0.161 (0.036) .009
5 Middle frontal gyrus, orbital part L 0.189 (0.055) 0.161 (0.041) .132
6 Inferior frontal gyrus, orbital part L 0.206 (0.051) 0.170 (0.050) .077
7 Superior frontal gyrus L, dorsolateral 0.208 (0.044) 0.170 (0.038) .020
8 Middle frontal gyrus L 0.206 (0.057) 0.167 (0.040) .039
9 Inferior frontal gyrus, opercular part L 0.212 (0.062) 0.166 (0.052) .045
10 Inferior frontal gyrus, triangular part L 0.206 (0.059) 0.162 (0.044) .027
11 Superior frontal gyrus, medial part L 0.222 (0.047) 0.171 (0.039) .004
12 Supplementary motor area L 0.211 (0.052) 0.170 (0.036) .016
13 Paracentral lobule L 0.181 (0.054) 0.166 (0.037) .364
14 Precentral gyrus L 0.195 (0.060) 0.160 (0.037) .059
15 Rolandic operculum L 0.245 (0.065) 0.177 (0.061) .009
16 Postcentral gyrus L 0.194 (0.065) 0.155 (0.047) .070
17 Superior parietal gyrus L 0.232 (0.063) 0.178 (0.061) .031
18 Inferior parietal gyri L 0.232 (0.067) 0.170 (0.060) .015
19 Supramarginal gyrus L 0.245 (0.069) 0.181 (0.084) .041
20 Angular gyrus L 0.285 (0.081) 0.202 (0.098) .027
21 Precuneus L 0.250 (0.064) 0.187 (0.063) .017
22 Superior occipital gyrus L 0.281 (0.078) 0.202 (0.080) .016
23 Middle occipital gyrus L 0.297 (0.802) 0.222 (0.106) .059
24 Inferior occipital gyrus L 0.302 (0.094) 0.247 (0.098) .154
0.291 (0.077) 0.216 (0.077) .018
26 Cuneus L 0.284 (0.078) 0.201 (0.073) .008
27 Lingual gyrus L 0.306 (0.083) 0.227 (0.082) .019
28 Fusiform gyrus L 0.308 (0.087) 0.235 (0.099) .058
29 Heschl gyrus L 0.271 (0.072) 0.190 (0.076) .009
30 Superior temporal gyrus L 0.263 (0.073) 0.185 (0.074) .012
31 Middle temporal gyrus L 0.290 (0.095) 0.202 (0.099) .027
32 Inferior temporal gyrus L 0.281 (0.081) 0.210 (0.085) .036
33 Temporal pole: superior temporal gyrus L 0.236 (0.061) 0.183 (0.058) .029
34 Temporal pole: middle temporal gyrus L 0.234 (0.054) 0.187 (0.057) .038

163
MEG-based resting-state brain activity in PD
Table S1: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
35 Parahippocampal gyrus L 0.282 (0.071) 0.206 (0.067) .007
36 Anterior cingulate and paracingulate gyri L 0.238 (0.056) 0.176 (0.046) .003
37 Median cingulate and paracingulate gyri L 0.240 (0.059) 0.184 (0.048) .009
38 Posterior cingulate gyrus L 0.269 (0.060) 0.196 (0.060) .004
39 Insula L 0.239 (0.061) 0.176 (0.050) .006
40 Gyrus rectus R 0.210 (0.045) 0.164 (0.039) .007
41 Olfactory cortex R 0.239 (0.053) 0.181 (0.049) .006
42 Superior frontal gyrus, orbital part R 0.196 (0.045) 0.157 (0.032) .011
43 Superior frontal gyrus, medial orbital part R 0.204 (0.048) 0.159 (0.032) .005
44 Middle frontal gyrus, orbital part R 0.184 (0.060) 0.152 (0.029) .133
45 Inferior frontal gyrus, orbital part R 0.200 (0.057) 0.164 (0.046) .076
46 Superior frontal gyrus R, dorsolateral 0.206 (0.045) 0.165 (0.038) .013
47 Middle frontal gyrus R 0.195 (0.048) 0.156 (0.039) .023
48 Inferior frontal gyrus, opercular part R 0.200 (0.045) 0.155 (0.042) .014
49 Inferior frontal gyrus, triangular part R 0.204 (0.056) 0.148 (0.038) .004
50 Superior frontal gyrus, medial part R 0.216 (0.049) 0.164 (0.036) .003
51 Supplementary motor area R 0.201 (0.046) 0.166 (0.038) .036
52 Paracentral lobule R 0.186 (0.055) 0.159 (0.036) .111
53 Precentral gyrus R 0.195 (0.036) 0.158 (0.051) .048
54 Rolandic operculum R 0.259 (0.066) 0.172 (0.079) .005
55 Postcentral gyrus R 0.213 (0.054) 0.156 (0.059) .016
56 Superior parietal gyrus R 0.251 (0.067) 0.172 (0.055) .002
57 Inferior parietal gyri R 0.264 (0.086) 0.171 (0.072) .004
58 Supramarginal gyrus R 0.283 (0.080) 0.167 (0.074) .000
59 Angular gyrus R 0.298 (0.090) 0.189 (0.087) .003
60 Precuneus R 0.283 (0.083) 0.191 (0.063) .002
61 Superior occipital gyrus R 0.291 (0.076) 0.202 (0.082) .007
62 Middle occipital gyrus R 0.313 (0.093) 0.218 (0.089) .011
63 Inferior occipital gyrus R 0.294 (0.081) 0.220 (0.084) .030
0.297 (0.079) 0.213 (0.079) .011
65 Cuneus R 0.291 (0.076) 0.196 (0.067) .002
66 Lingual gyrus R 0.300 (0.077) 0.217 (0.079) .011
67 Fusiform gyrus R 0.287 (0.078) 0.222 (0.087) .056
68 Heschl gyrus R 0.292 (0.071) 0.180 (0.082) .001
69 Superior temporal gyrus R 0.305 (0.092) 0.177 (0.082) .001
70 Middle temporal gyrus R 0.315 (0.109) 0.200 (0.097) .006
6

164
Chapter 6
Table S1: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
71 Inferior temporal gyrus R 0.271 (0.075) 0.199 (0.093) .044
72 Temporal pole: superior temporal gyrus R 0.230 (0.056) 0.177 (0.063) .031
73 Temporal pole: middle temporal gyrus R 0.230 (0.055) 0.168 (0.057) .008
74 Parahippocampal gyrus R 0.274 (0.070) 0.196 (0.064) .005
75 Anterior cingulate and paracingulate gyri R 0.229 (0.057) 0.173 (0.042) .005
76 Median cingulate and paracingulate gyri R 0.229 (0.054) 0.177 (0.046) .010
77 Posterior cingulate gyrus R 0.281 (0.067) 0.193 (0.057) .001
78 Insula R 0.244 (0.068) 0.176 (0.058) .008
79 Hippocampus L 0.282 (0.067) 0.214 (0.078) .026
80 Hippocampus R 0.287 (0.071) 0.196 (0.073) .003
81 Amygdala L 0.262 (0.069) 0.199 (0.064) .019
82 Amygdala R 0.259 (0.064) 0.192 (0.063) .011
83 Caudate nucleus L 0.241 (0.052) 0.186 (0.052) .012
84 Caudate nucleus R 0.247 (0.052) 0.181 (0.048) .002
85 Lenticular nucleus, putamen L 0.248 (0.060) 0.189 (0.058) .014
86 Lenticular nucleus, putamen R 0.250 (0.064) 0.182 (0.051) .003
87 Lenticular nucleus, pallidum L 0.264 (0.067) 0.201 (0.066) .021
88 Lenticular nucleus, pallidum R 0.256 (0.063) 0.188 (0.053) .004
89 Thalamus L 0.251 (0.057) 0.197 (0.060) .024
90 Thalamus R 0.261 (0.053) 0.190 (0.058) .003
Parkinson’s disease patients without hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations

165
MEG-based resting-state brain activity in PD
Table S2: Relative power per AAL region in the beta band in Parkinson’s disease patients with unimodal hallucinations and patients without hallucinations
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
1 Gyrus rectus L 0.213 (0.056) 0.253 (0.054) .069
2 Olfactory cortex L 0.210 (0.058) 0.256 (0.063) .061
3 Superior frontal gyrus, orbital part L 0.231 (0.056) 0.262 (0.049) .126
4 Superior frontal gyrus, medial orbital part L 0.223 (0.051) 0.264 (0.041) .025
5 Middle frontal gyrus, orbital part L 0.233 (0.059) 0.264 (0.056) .169
6 Inferior frontal gyrus, orbital part L 0.231 (0.078) 0.262 (0.050) .193
7 Superior frontal gyrus L, dorsolateral 0.270 (0.071) 0.294 (0.051) .307
8 Middle frontal gyrus L 0.279 (0.089) 0.300 (0.064) .452
9 Inferior frontal gyrus, opercular part L 0.294 (0.102) 0.319 (0.062) .411
10 Inferior frontal gyrus, triangular part L 0.277 (0.100) 0.300 (0.061) .437
11 Superior frontal gyrus, medial part L 0.237 (0.069) 0.273 (0.046) .101
12 Supplementary motor area L 0.281 (0.077) 0.310 (0.056) .248
13 Paracentral lobule L 0.311 (0.064) 0.310 (0.056) .946
14 Precentral gyrus L 0.329 (0.099) 0.341 (0.062) .667
15 Rolandic operculum L 0.256 (0.080) 0.304 (0.064) .085
16 Postcentral gyrus L 0.308 (0.077) 0.352 (0.065) .117
17 Superior parietal gyrus L 0.224 (0.058) 0.305 (0.089) .006
18 Inferior parietal gyri L 0.241 (0.069) 0.329 (0.095) .015
19 Supramarginal gyrus L 0.238 (0.066) 0.316 (0.096) .028
20 Angular gyrus L 0.173 (0.070) 0.276 (0.112) .013
21 Precuneus L 0.210 (0.054) 0.292 (0.085) .003
22 Superior occipital gyrus L 0.152 (0.043) 0.242 (0.102) .002
23 Middle occipital gyrus L 0.144 (0.056) 0.239 (0.114) .005
24 Inferior occipital gyrus L 0.143 (0.059) 0.210 (0.103) .067
0.138 (0.039) 0.218 (0.089) .002
26 Cuneus L 0.137 (0.036) 0.233 (0.090) .000
27 Lingual gyrus L 0.145 (0.047) 0.219 (0.096) .030
28 Fusiform gyrus L 0.156 (0.060) 0.232 (0.096) .029
29 Heschl gyrus L 0.224 (0.068) 0.295 (0.089) .037
30 Superior temporal gyrus L 0.213 (0.075) 0.289 (0.084) .023
31 Middle temporal gyrus L 0.180 (0.069) 0.260 (0.100) .032
32 Inferior temporal gyrus L 0.178 (0.065) 0.244 (0.087) .043
33 Temporal pole: superior temporal gyrus L 0.219 (0.069) 0.263 (0.056) .065
34 Temporal pole: middle temporal gyrus L 0.204 (0.054) 0.247 (0.052) .040
35 Parahippocampal gyrus L 0.190 (0.070) 0.247 (0.074) .057
6

166
Chapter 6
Table S2: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
36 Anterior cingulate and paracingulate gyri L 0.230 (0.077) 0.274 (0.055) .087
37 Median cingulate and paracingulate gyri L 0.266 (0.071) 0.300 (0.064) .197
38 Posterior cingulate gyrus L 0.211 (0.060) 0.279 (0.079) .023
39 Insula L 0.258 (0.087) 0.303 (0.068) .132
40 Gyrus rectus R 0.212 (0.057) 0.251 (0.057) .086
41 Olfactory cortex R 0.210 (0.062) 0.259 (0.063) .053
42 Superior frontal gyrus, orbital part R 0.223 (0.065) 0.255 (0.053) .159
43 Superior frontal gyrus, medial orbital part R 0.224 (0.064) 0.257 (0.048) .117
44 Middle frontal gyrus, orbital part R 0.225 (0.055) 0.257 (0.046) .099
45 Inferior frontal gyrus, orbital part R 0.238 (0.082) 0.267 (0.053) .338
46 Superior frontal gyrus R, dorsolateral 0.280 (0.080) 0.304 (0.054) .337
47 Middle frontal gyrus R 0.300 (0.107) 0.317 (0.066) .662
48 Inferior frontal gyrus, opercular part R 0.296 (0.107) 0.326 (0.074) .434
49 Inferior frontal gyrus, triangular part R 0.272 (0.099) 0.307 (0.066) .253
50 Superior frontal gyrus, medial part R 0.243 (0.076) 0.272 (0.044) .293
51 Supplementary motor area R 0.292 (0.079) 0.319 (0.064) .323
52 Paracentral lobule R 0.314 (0.084) 0.319 (0.064) .849
53 Precentral gyrus R 0.314 (0.094) 0.346 (0.070) .291
54 Rolandic operculum R 0.232 (0.063) 0.305 (0.078) .017
55 Postcentral gyrus R 0.271 (0.073) 0.364 (0.097) .013
56 Superior parietal gyrus R 0.216 (0.054) 0.299 (0.080) .006
57 Inferior parietal gyri R 0.191 (0.063) 0.309 (0.103) .001
58 Supramarginal gyrus R 0.207 (0.081) 0.322 (0.107) .006
59 Angular gyrus R 0.156 (0.053) 0.271 (0.107) .000
60 Precuneus R 0.195 (0.060) 0.276 (0.082) .010
61 Superior occipital gyrus R 0.154 (0.054) 0.248 (0.102) .002
62 Middle occipital gyrus R 0.135 (0.051) 0.236 (0.105) .001
63 Inferior occipital gyrus R 0.146 (0.058) 0.220 (0.089) .024
0.141 (0.051) 0.216 (0.090) .023
65 Cuneus R 0.148 (0.050) 0.231 (0.088) .003
66 Lingual gyrus R 0.139 (0.054) 0.223 (0.095) .016
67 Fusiform gyrus R 0.157 (0.060) 0.232 (0.094) .030
68 Heschl gyrus R 0.200 (0.061) 0.286 (0.088) .010
69 Superior temporal gyrus R 0.175 (0.061) 0.273 (0.100) .009
70 Middle temporal gyrus R 0.153 (0.057) 0.254 (0.103) .007
71 Inferior temporal gyrus R 0.171 (0.053) 0.243 (0.089) .026
72 Temporal pole: superior temporal gyrus R 0.221 (0.064) 0.262 (0.066) .123

167
MEG-based resting-state brain activity in PD
Table S2: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
73 Temporal pole: middle temporal gyrus R 0.210 (0.056) 0.244 (0.059) .141
74 Parahippocampal gyrus R 0.177 (0.061) 0.240 (0.075) .029
75 Anterior cingulate and paracingulate gyri R 0.236 (0.080) 0.276 (0.058) .131
76 Median cingulate and paracingulate gyri R 0.277 (0.079) 0.311 (0.075) .250
77 Posterior cingulate gyrus R 0.201 (0.064) 0.272 (0.082) .024
78 Insula R 0.248 (0.093) 0.287 (0.074) .227
79 Hippocampus L 0.192 (0.072) 0.256 (0.083) .048
80 Hippocampus R 0.182 (0.067) 0.252 (0.080) .024
81 Amygdala L 0.212 (0.062) 0.261 (0.067) .065
82 Amygdala R 0.203 (0.076) 0.254 (0.069) .077
83 Caudate nucleus L 0.239 (0.082) 0.278 (0.062) .157
84 Caudate nucleus R 0.236 (0.080) 0.290 (0.064) .058
85 Lenticular nucleus, putamen L 0.244 (0.081) 0.291 (0.069) .111
86 Lenticular nucleus, putamen R 0.243 (0.088) 0.292 (0.068) .108
87 Lenticular nucleus, pallidum L 0.227 (0.078) 0.277 (0.072) .095
88 Lenticular nucleus, pallidum R 0.234 (0.085) 0.287 (0.068) .076
89 Thalamus L 0.233 (0.071) 0.284 (0.077) .092
90 Thalamus R 0.230 (0.072) 0.281 (0.073) .080
Hall-: Parkinson’s disease patients without hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations
6

168
Chapter 6
Table S3: Relative power per AAL region in the gamma band in Parkinson’s disease patients with unimodal hallucinations and patients without hallucinations
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
1 Gyrus rectus L 0.073 (0.017) 0.091 (0.023) .036
2 Olfactory cortex L 0.054 (0.013) 0.075 (0.017) .002
3 Superior frontal gyrus, orbital part L 0.088 (0.016) 0.108 (0.028) .045
4 Superior frontal gyrus, medial orbital part L 0.088 (0.018) 0.112 (0.026) .013
5 Middle frontal gyrus, orbital part L 0.090 (0.019) 0.116 (0.032) .029
6 Inferior frontal gyrus, orbital part L 0.070 (0.017) 0.100 (0.029) .006
7 Superior frontal gyrus L, dorsolateral 0.090 (0.021) 0.116 (0.024) .007
8 Middle frontal gyrus L 0.087 (0.031) 0.113 (0.024) .017
9 Inferior frontal gyrus, opercular part L 0.068 (0.026) 0.108 (0.045) .016
10 Inferior frontal gyrus, triangular part L 0.077 (0.032) 0.111 (0.030) .008
11 Superior frontal gyrus, medial part L 0.085 (0.024) 0.113 (0.024) .007
12 Supplementary motor area L 0.078 (0.021) 0.103 (0.020) .004
13 Paracentral lobule L 0.083 (0.021) 0.101 (0.019) .024
14 Precentral gyrus L 0.066 (0.020) 0.108 (0.026) .001
15 Rolandic operculum L 0.046 (0.014) 0.080 (0.029) .001
16 Postcentral gyrus L 0.057 (0.020) 0.086 (0.023) .002
17 Superior parietal gyrus L 0.077 (0.024) 0.087 (0.021) .210
18 Inferior parietal gyri L 0.060 (0.019) 0.074 (0.019) .064
19 Supramarginal gyrus L 0.053 (0.019) 0.071 (0.027) .067
20 Angular gyrus L 0.045 (0.012) 0.060 (0.017) .018
21 Precuneus L 0.065 (0.022) 0.080 (0.021) .081
22 Superior occipital gyrus L 0.055 (0.015) 0.063 (0.019) .298
23 Middle occipital gyrus L 0.045 (0.017) 0.054 (0.019) .248
24 Inferior occipital gyrus L 0.046 (0.019) 0.049 (0.024) .765
0.043 (0.011) 0.049 (0.017) .284
26 Cuneus L 0.046 (0.014) 0.060 (0.017) .033
27 Lingual gyrus L 0.043 (0.013) 0.048 (0.019) .428
28 Fusiform gyrus L 0.041 (0.014) 0.054 (0.018) .058
29 Heschl gyrus L 0.043 (0.013) 0.065 (0.019) .003
30 Superior temporal gyrus L 0.049 (0.033) 0.070 (0.025) .064
31 Middle temporal gyrus L 0.043 (0.018) 0.066 (0.041) .113
32 Inferior temporal gyrus L 0.055 (0.017) 0.072 (0.035) .147
33 Temporal pole: superior temporal gyrus L 0.063 (0.018) 0.093 (0.035) .016
34 Temporal pole: middle temporal gyrus L 0.069 (0.019) 0.096 (0.031) .017
35 Parahippocampal gyrus L 0.051 (0.013) 0.071 (0.029) .017

169
MEG-based resting-state brain activity in PD
Table S3: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
36 Anterior cingulate and paracingulate gyri L 0.070 (0.023) 0.094 (0.017) .003
37 Median cingulate and paracingulate gyri L 0.057 (0.020) 0.074 (0.017) .025
38 Posterior cingulate gyrus L 0.050 (0.017) 0.061 (0.018) .116
39 Insula L 0.059 (0.022) 0.092 (0.037) .015
40 Gyrus rectus R 0.071 (0.017) 0.087 (0.021) .043
41 Olfactory cortex R 0.055 (0.014) 0.074 (0.020) .011
42 Superior frontal gyrus, orbital part R 0.082 (0.016) 0.102 (0.022) .014
43 Superior frontal gyrus, medial orbital part R 0.083 (0.020) 0.108 (0.027) .014
44 Middle frontal gyrus, orbital part R 0.088 (0.020) 0.111 (0.028) .026
45 Inferior frontal gyrus, orbital part R 0.075 (0.017) 0.104 (0.038) .028
46 Superior frontal gyrus R, dorsolateral 0.087 (0.022) 0.111 (0.025) .014
47 Middle frontal gyrus R 0.084 (0.024) 0.113 (0.030) .011
48 Inferior frontal gyrus, opercular part R 0.063 (0.020) 0.102 (0.044) .013
49 Inferior frontal gyrus, triangular part R 0.075 (0.021) 0.116 (0.052) .025
50 Superior frontal gyrus, medial part R 0.089 (0.023) 0.114 (0.025) .013
51 Supplementary motor area R 0.082 (0.018) 0.102 (0.019) .012
52 Paracentral lobule R 0.078 (0.023) 0.102 (0.020) .007
53 Precentral gyrus R 0.065 (0.019) 0.095 (0.028) .005
54 Rolandic operculum R 0.051 (0.017) 0.090 (0.067) .084
55 Postcentral gyrus R 0.062 (0.028) 0.080 (0.024) .071
56 Superior parietal gyrus R 0.072 (0.028) 0.087 (0.029) .188
57 Inferior parietal gyri R 0.053 (0.018) 0.071 (0.022) .031
58 Supramarginal gyrus R 0.051 (0.021) 0.071 (0.026) .046
59 Angular gyrus R 0.050 (0.016) 0.063 (0.021) .097
60 Precuneus R 0.059 (0.023) 0.073 (0.022) .130
61 Superior occipital gyrus R 0.052 (0.013) 0.061 (0.021) .241
62 Middle occipital gyrus R 0.046 (0.014) 0.059 (0.024) .130
63 Inferior occipital gyrus R 0.056 (0.018) 0.064 (0.029) .465
0.041 (0.013) 0.048 (0.021) .372
65 Cuneus R 0.050 (0.018) 0.055 (0.017) .500
66 Lingual gyrus R 0.039 (0.013) 0.050 (0.022) .132
67 Fusiform gyrus R 0.049 (0.019) 0.060 (0.023) .187
68 Heschl gyrus R 0.043 (0.013) 0.073 (0.054) .088
69 Superior temporal gyrus R 0.046 (0.015) 0.076 (0.058) .123
70 Middle temporal gyrus R 0.045 (0.017) 0.069 (0.033) .037
71 Inferior temporal gyrus R 0.060 (0.014) 0.081 (0.033) .057
72 Temporal pole: superior temporal gyrus R 0.072 (0.018) 0.092 (0.026) .021
6

170
Chapter 6
Table S3: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
73 Temporal pole: middle temporal gyrus R 0.076 (0.012) 0.097 (0.027) .007
74 Parahippocampal gyrus R 0.051 (0.014) 0.072 (0.024) .006
75 Anterior cingulate and paracingulate gyri R 0.072 (0.023) 0.095 (0.020) .007
76 Median cingulate and paracingulate gyri R 0.058 (0.018) 0.077 (0.019) .014
77 Posterior cingulate gyrus R 0.046 (0.015) 0.061 (0.018) .039
78 Insula R 0.059 (0.017) 0.089 (0.045) .059
79 Hippocampus L 0.046 (0.016) 0.063 (0.018) .025
80 Hippocampus R 0.048 (0.018) 0.072 (0.030) .026
81 Amygdala L 0.056 (0.016) 0.074 (0.026) .043
82 Amygdala R 0.056 (0.012) 0.074 (0.025) .012
83 Caudate nucleus L 0.056 (0.019) 0.077 (0.019) .007
84 Caudate nucleus R 0.055 (0.018) 0.078 (0.018) .003
85 Lenticular nucleus, putamen L 0.056 (0.020) 0.081 (0.028) .017
86 Lenticular nucleus, putamen R 0.055 (0.014) 0.079 (0.028) .005
87 Lenticular nucleus, pallidum L 0.052 (0.018) 0.073 (0.025) .027
88 Lenticular nucleus, pallidum R 0.053 (0.015) 0.075 (0.023) .006
89 Thalamus L 0.052 (0.018) 0.068 (0.020) .041
90 Thalamus R 0.049 (0.014) 0.068 (0.022) .008
Hall-: Parkinson’s disease patients without hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations

171
MEG-based resting-state brain activity in PD
Table S4: Peak frequency per AAL region in Parkinson’s disease patients with unimodal hallucinations and patients without hallucinations
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
1 Gyrus rectus L 7.06 (0.85) 7.76 (0.72) .026
2 Olfactory cortex L 7.27 (0.95) 8.06 (0.69) .015
3 Superior frontal gyrus, orbital part L 7.06 (0.87) 7.48 (0.68) .156
4 Superior frontal gyrus, medial orbital part L 6.81 (0.81) 7.29 (0.73) .107
5 Middle frontal gyrus, orbital part L 6.85 (0.96) 7.37 (0.88) .148
6 Inferior frontal gyrus, orbital part L 7.15 (1.06) 7.75 (0.72) .077
7 Superior frontal gyrus L, dorsolateral 7.03 (0.95) 7.22 (0.73) .563
8 Middle frontal gyrus L 7.17 (1.06) 7.29 (0.71) .721
9 Inferior frontal gyrus, opercular part L 7.55 (1.08) 7.83 (0.85) .446
10 Inferior frontal gyrus, triangular part L 7.35 (0.99) 7.83 (0.83) .169
11 Superior frontal gyrus, medial part L 6.84 (0.82) 7.26 (0.77) .181
12 Supplementary motor area L 7.36 (1.12) 7.41 (0.85) .896
13 Paracentral lobule L 7.96 (1.28) 7.64 (0.87) .423
14 Precentral gyrus L 8.21 (1.53) 7.75 (0.75) .388
15 Rolandic operculum L 7.70 (0.94) 8.31 (0.79) .072
16 Postcentral gyrus L 8.56 (1.13) 8.27 (0.92) .446
17 Superior parietal gyrus L 7.49 (1.03) 8.25 (0.91) .050
18 Inferior parietal gyri L 7.98 (1.18) 8.56 (0.89) .144
19 Supramarginal gyrus L 7.86 (0.10) 8.59 (0.79) .036
20 Angular gyrus L 7.51 (1.06) 8.50 (0.91) .012
21 Precuneus L 7.24 (0.95) 8.41 (0.99) .004
22 Superior occipital gyrus L 7.15 (1.07) 8.56 (0.97) .001
23 Middle occipital gyrus L 7.20 (1.03) 8.49 (1.11) .005
24 Inferior occipital gyrus L 7.12 (0.93) 8.24 (1.08) .010
7.24 (1.11) 8.57 (0.99) .002
26 Cuneus L 7.31 (1.14) 8.52 (0.91) .004
27 Lingual gyrus L 7.20 (1.06) 8.42 (0.97) .004
28 Fusiform gyrus L 7.10 (0.99) 8.44 (1.07) .003
29 Heschl gyrus L 7.61 (1.03) 8.52 (0.89) .018
30 Superior temporal gyrus L 7.49 (1.04) 8.60 (0.89) .005
31 Middle temporal gyrus L 7.70 (1.25) 8.66 (0.90) .023
32 Inferior temporal gyrus L 7.41 (0.97) 8.44 (0.96) .010
33 Temporal pole: superior temporal gyrus L 7.37 (1.00) 8.21 (0.67) .011
34 Temporal pole: middle temporal gyrus L 7.05 (0.73) 8.09 (0.74) .001
35 Parahippocampal gyrus L 7.34 (1.12) 8.24 (0.91) .025
6

172
Chapter 6
Table S4: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
36 Anterior cingulate and paracingulate gyri L 7.05 (0.97) 7.43 (0.88) .284
37 Median cingulate and paracingulate gyri L 7.47 (0.89) 8.02 (0.77) .089
38 Posterior cingulate gyrus L 7.43 (0.97) 8.48 (0.79) .004
39 Insula L 7.47 (0.95) 8.14 (0.81) .056
40 Gyrus rectus R 7.19 (0.86) 7.69 (0.85) .143
41 Olfactory cortex R 7.22 (0.87) 8.01 (0.84) .023
42 Superior frontal gyrus, orbital part R 7.00 (0.91) 7.46 (0.83) .177
43 Superior frontal gyrus, medial orbital part R 6.77 (0.85) 7.35 (0.88) .098
44 Middle frontal gyrus, orbital part R 7.07 (0.79) 7.28 (0.82) .519
45 Inferior frontal gyrus, orbital part R 7.35 (0.78) 7.63 (0.79) .384
46 Superior frontal gyrus R, dorsolateral 7.25 (1.42) 7.34 (0.82) .814
47 Middle frontal gyrus R 7.20 (1.21) 7.27 (0.96) .857
48 Inferior frontal gyrus, opercular part R 7.70 (1.04) 7.90 (0.81) .563
49 Inferior frontal gyrus, triangular part R 7.30 (0.73) 7.82 (0.91) .132
50 Superior frontal gyrus, medial part R 6.88 (0.76) 7.23 (0.82) .279
51 Supplementary motor area R 7.60 (1.17) 7.59 (0.88) .979
52 Paracentral lobule R 7.83 (1.14) 7.96 (0.92) .751
53 Precentral gyrus R 7.90 (1.07) 8.14 (0.93) .523
54 Rolandic operculum R 7.45 (1.03) 8.46 (0.85) .008
55 Postcentral gyrus R 8.08 (1.13) 8.58 (1.08) .248
56 Superior parietal gyrus R 7.23 (0.89) 8.26 (0.94) .007
57 Inferior parietal gyri R 7.67 (1.36) 8.71 (1.00) .024
58 Supramarginal gyrus R 7.45 (1.06) 8.63 (0.87) .003
59 Angular gyrus R 7.14 (1.11) 8.64 (1.02) .001
60 Precuneus R 7.30 (0.89) 8.33 (0.96) .009
61 Superior occipital gyrus R 6.98 (1.03) 8.42 (1.06) .001
62 Middle occipital gyrus R 6.88 (1.01) 8.37 (1.01) .001
63 Inferior occipital gyrus R 6.86 (1.06) 8.29 (1.06) .002
7.12 (1.13) 8.53 (1.00) .002
65 Cuneus R 7.02 (1.05) 8.60 (1.02) .000
66 Lingual gyrus R 6.98 (1.07) 8.47 (1.02) .001
67 Fusiform gyrus R 7.06 (0.95) 8.42 (1.06) .002
68 Heschl gyrus R 7.37 (0.92) 8.74 (0.91) .001
69 Superior temporal gyrus R 7.42 (1.03) 8.78 (0.97) .001
70 Middle temporal gyrus R 7.10 (0.95) 8.66 (1.03) .000
71 Inferior temporal gyrus R 7.16 (1.04) 8.58 (0.94) .001
72 Temporal pole: superior temporal gyrus R 7.02 (0.76) 8.29 (0.85) .000

173
MEG-based resting-state brain activity in PD
Table S4: Continued
AAL region Unimodal Hall+ (n=10)
Hall- (n=20) p-value
73 Temporal pole: middle temporal gyrus R 7.08 (0.94) 8.07 (0.69) .003
74 Parahippocampal gyrus R 7.23 (1.08) 8.18 (0.89) .016
75 Anterior cingulate and paracingulate gyri R 7.01 (0.88) 7.44 (0.78) .182
76 Median cingulate and paracingulate gyri R 7.67 (1.15) 8.07 (0.93) .310
77 Posterior cingulate gyrus R 7.42 (1.03) 8.48 (0.76) .004
78 Insula R 7.27 (1.03) 8.19 (0.85) .014
79 Hippocampus L 7.22 (0.90) 8.31 (0.84) .003
80 Hippocampus R 7.19 (0.86) 8.49 (0.86) .001
81 Amygdala L 7.30 (1.02) 8.24 (0.74) .007
82 Amygdala R 7.22 (1.16) 8.20 (0.87) .015
83 Caudate nucleus L 7.33 (0.98) 7.98 (0.79) .058
84 Caudate nucleus R 7.12 (0.96) 7.93 (0.74) .016
85 Lenticular nucleus, putamen L 7.40 (0.85) 8.08 (0.83) .046
86 Lenticular nucleus, putamen R 7.12 (1.05) 8.23 (0.75) .002
87 Lenticular nucleus, pallidum L 7.43 (0.87) 8.10 (0.81) .048
88 Lenticular nucleus, pallidum R 7.11 (1.03) 8.21 (0.66) .001
89 Thalamus L 7.32 (1.00) 8.17 (0.87) .023
90 Thalamus R 7.36 (0.92) 8.41 (0.88) .005
Hall-: Parkinson’s disease patients without hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations
6

174
Chapter 6
Tab
le S
5: M
ean
rela
tive
pow
er/p
eak
freq
uenc
y pe
r br
ain
regi
on
Hal
l- (
N=2
0)U
nim
odal
Hal
l+ (
N=1
0)M
ulti
mod
al H
all+
(N
=10)
Reg
ion
per
freq
uenc
y ba
ndM
ean
SD
Mea
nS
DM
ean
SD
Fron
tal L
eft
thet
a.1
67.0
38.2
08.0
47.1
49.0
58
Fron
tal L
eft
beta
.282
.048
.253
.068
.314
.096
Fron
tal L
eft
gam
ma
.105
.022
.079
.019
.106
.019
Fron
tal L
eft
PF7.
55.6
587.
19.8
698.
023
.794
Fron
tal R
ight
the
ta.1
61.0
35.2
03.0
45.1
48.0
61
Fron
tal R
ight
bet
a.2
85.0
50.2
56.0
74.3
11.1
03
Fron
tal R
ight
gam
ma
.104
.023
.078
.017
.104
.016
Fron
tal R
ight
PF
7.58
.741
7.26
.813
8.12
1.8
25
Cen
tral
Lef
t th
eta
.164
.045
.211
.060
.150
.088
Cen
tral
Lef
t be
ta.3
32.0
59.2
98.0
82.3
67.1
37
Cen
tral
Lef
t ga
mm
a.0
89.0
24.0
56.0
17.0
87.0
31
Cen
tral
Lef
t PF
8.11
.724
8.16
1.10
78.
79.9
32
Cen
tral
Rig
ht t
heta
.162
.061
.222
.048
0.1
51.0
93
Cen
tral
Rig
ht b
eta
.338
.075
.272
.073
.368
.123
Cen
tral
Rig
ht g
amm
a.0
88.0
35.0
59.0
19.0
84.0
23
Cen
tral
Rig
ht P
F8.
39.8
417.
811.
006
9.16
1.04
4
Pari
etal
Lef
t th
eta
.184
.068
.249
.064
.168
.112
Pari
etal
Lef
t be
ta.3
04.0
92.2
17.0
61.3
18.1
36
Pari
etal
Lef
t ga
mm
a.0
75.0
17.0
60.0
17.0
71.0
22
Pari
etal
Lef
t PF
8.46
.778
7.61
.991
9.09
1.26
1

175
MEG-based resting-state brain activity in PD
Tabl
e S5
: Con
tinue
d
Hal
l- (
N=2
0)U
nim
odal
Hal
l+ (
N=1
0)M
ulti
mod
al H
all+
(N
=10)
Reg
ion
per
freq
uenc
y ba
ndM
ean
SD
Mea
nS
DM
ean
SD
Pari
etal
Rig
ht t
heta
.178
.067
.276
.077
.166
.104
Pari
etal
Rig
ht b
eta
.295
.093
.193
.060
.313
.128
Pari
etal
Rig
ht g
amm
a.0
73.0
21.0
57.0
19.0
69.0
187
Pari
etal
Rig
ht P
F8.
51.8
907.
361.
004
9.12
1.28
6
Occ
ipita
l Lef
t th
eta
.221
.085
.296
.078
.190
.103
Occ
ipit
al L
eft
beta
.228
.097
.145
.047
.234
.094
Occ
ipita
l Lef
t ga
mm
a.0
54.0
17.0
46.0
13.0
50.0
12
Occ
ipita
l Lef
t PF
8.46
.941
7.19
1.01
88.
931.
30
Occ
ipit
al R
ight
the
ta.2
12.0
79.2
96.0
77.1
91.0
98
Occ
ipit
al R
ight
bet
a.2
29.0
93.1
46.0
53.2
28.0
87
Occ
ipita
l Rig
ht g
amm
a.0
57.0
20.0
48.0
13.0
54.0
16
Occ
ipita
l Rig
ht P
F8.
44.9
766.
981.
015
8.85
1.32
2
Tem
pora
l Lef
t th
eta
.197
.082
.276
.078
.178
.101
Tem
pora
l Lef
t be
ta.2
72.0
86.1
99.0
68.2
85.1
00
Tem
pora
l Lef
t ga
mm
a.0
68.0
27.0
47.0
19.0
70.0
34
Tem
pora
l Lef
t PF
8.55
.872
7.55
1.03
28.
981.
223
Tem
pora
l Rig
ht t
heta
.189
.086
.300
.084
.187
.104
Tem
pora
l Rig
ht b
eta
.264
.093
.175
.055
.259
.088
Tem
pora
l Rig
ht g
amm
a.0
75.0
43.0
48.0
11.0
68.0
30
Tem
pora
l Rig
ht P
F8.
69.9
237.
26.9
588.
921.
259
6

176
Chapter 6
Tabl
e S5
: Con
tinue
d
Hal
l- (
N=2
0)U
nim
odal
Hal
l+ (
N=1
0)M
ulti
mod
al H
all+
(N
=10)
Reg
ion
per
freq
uenc
y ba
ndM
ean
SD
Mea
nS
DM
ean
SD
Lim
bic
Left
the
ta.1
92.0
55.2
55.0
55.1
73.0
80
Lim
bic
Left
bet
a.2
66.0
61.2
16.0
63.2
82.0
98
Lim
bic
Left
gam
ma
.079
.021
.058
.015
.076
.022
Lim
bic
Left
PF
8.11
.670
7.27
.886
8.67
1.00
8
Lim
bic
Rig
ht t
heta
.183
.054
.252
.055
.167
.079
Lim
bic
Rig
ht b
eta
.265
.064
.215
.063
.285
.098
Lim
bic
Rig
ht g
amm
a.0
81.0
20.0
61.0
12.0
82.0
28
Lim
bic
Rig
ht P
F8.
15.7
167.
23.8
508.
641.
022
Subc
ortic
al L
eft
thet
a.1
94.0
58.2
53.0
58.1
69.0
87
Subc
ortic
al L
eft
beta
.278
.067
.231
.073
.307
.112
Subc
ortic
al L
eft
gam
ma
.075
.022
.054
.016
.078
.031
Subc
ortic
al L
eft
PF8.
11.7
457.
35.9
138.
711.
057
Subc
ortic
al R
ight
the
ta.1
87.0
53.2
55.0
57.1
72.0
88
Subc
ortic
al R
ight
bet
a.2
81.0
66.2
29.0
78.3
01.11
0
Subc
ortic
al R
ight
gam
ma
.075
.022
.054
.014
.077
.028
Subc
ortic
al R
ight
PF
8.19
.726
7.18
.989
8.72
1.15
6
Hal
l-: P
arki
nson
’s di
seas
e pa
tient
s w
ithou
t hal
luci
natio
ns; M
ultim
odal
Hal
l+: P
arki
nson
’s di
seas
e pa
tient
s w
ith m
ultim
odal
hal
luci
natio
ns; P
F: p
eak
freq
uenc
y; S
D: s
tand
ard
devi
atio
n; U
nim
odal
Hal
l+: P
arki
nson
’s di
seas
e pa
tient
s w
ith o
nly
visu
al h
allu
cina
tions

177
MEG-based resting-state brain activity in PD
Tab
le S
6: R
esul
ts r
egio
n by
freq
uenc
y ba
nd b
y gr
oup
anal
ysis
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Fron
tal l
eft
The
taC
ontr
olU
nim
odal
-.040
.018
.028
-.076
-.005
mul
timod
al.0
18.0
18.3
19-.0
18.0
54
Uni
mod
alm
ultim
odal
.058
.020
.007
.017
.100
Beta
Con
trol
Uni
mod
al.0
29.0
26.2
75-.0
24.0
82
mul
timod
al-.0
32.0
26.2
28-.0
85.0
21
Uni
mod
alm
ultim
odal
-.061
.030
.051
-.122
.000
Gam
ma
Con
trol
Uni
mod
al.0
26.0
08.0
03.0
09.0
42
mul
timod
al-.0
01.0
08.9
44-.0
17.0
16
Uni
mod
alm
ultim
odal
-.026
.009
.008
-.045
-.007
Peak
freq
uenc
yC
ontr
olU
nim
odal
.364
.290
.217
-.223
.951
mul
timod
al-.4
71.2
90.11
2-1
.058
.116
Uni
mod
alm
ultim
odal
-.835
.335
.017
-1.5
13-.1
57
Fron
tal r
ight
The
taC
ontr
olU
nim
odal
-.042
.017
.019
-.078
-.007
mul
timod
al.0
12.0
17.4
80-.0
23.0
48
Uni
mod
alm
ultim
odal
.055
.020
.009
.014
.095
Beta
Con
trol
Uni
mod
al.0
29.0
28.3
00-.0
27.0
86
mul
timod
al-.0
26.0
28.3
56-.0
83.0
30
Uni
mod
alm
ultim
odal
-.055
.032
.094
-.121
.010
6

178
Chapter 6
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Gam
ma
Con
trol
Uni
mod
al.0
26.0
08.0
02.0
10.0
42
mul
timod
al-.0
01.0
08.9
45-.0
16.0
15
Uni
mod
alm
ultim
odal
-.026
.009
.006
-.045
-.008
Peak
freq
uenc
yC
ontr
olU
nim
odal
.319
.302
.298
-.293
.931
mul
timod
al-.5
42.3
02.0
81-1
.154
.071
Uni
mod
alm
ultim
odal
-.861
.349
.018
-1.5
67-.1
54
Cen
tral
left
The
taC
ontr
olU
nim
odal
-.047
.024
.056
-.096
.001
mul
timod
al.0
13.0
24.5
77-.0
35.0
62
Uni
mod
alm
ultim
odal
.061
.028
.034
.005
.117
Beta
Con
trol
Uni
mod
al.0
35.0
35.3
21-.0
35.1
05
mul
timod
al-.0
34.0
35.3
29-.1
04.0
36
Uni
mod
alm
ultim
odal
-.069
.040
.093
-.150
.012
Gam
ma
Con
trol
Uni
mod
al.0
33.0
10.0
01.0
14.0
52
mul
timod
al.0
02.0
10.8
61-.0
18.0
21
Uni
mod
alm
ultim
odal
-.031
.011
.007
-.053
-.009
Peak
freq
uenc
yC
ontr
olU
nim
odal
-.050
.342
.885
-.742
.643
mul
timod
al-.6
80.3
42.0
54-1
.373
.012
Uni
mod
alm
ultim
odal
-.631
.395
.118
-1.4
30.1
69

179
MEG-based resting-state brain activity in PD
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Cen
tral
rig
htT
heta
Con
trol
Uni
mod
al-.0
60.0
26.0
27-.1
14-.0
07
mul
timod
al.0
11.0
26.6
73-.0
42.0
64
Uni
mod
alm
ultim
odal
.072
.030
.023
.010
.133
Beta
Con
trol
Uni
mod
al.0
66.0
34.0
63-.0
04.1
36
mul
timod
al-.0
29.0
34.4
02-.0
99.0
41
Uni
mod
alm
ultim
odal
-.095
.040
.022
-.176
-.015
Gam
ma
Con
trol
Uni
mod
al.0
29.0
11.0
14.0
06.0
52
mul
timod
al.0
04.0
11.7
18-.0
19.0
27
Uni
mod
alm
ultim
odal
-.025
.013
.064
-.051
.002
Peak
freq
uenc
yC
ontr
olU
nim
odal
.584
.362
.115
-.150
1.31
8
mul
timod
al-.7
68.3
62.0
41-1
.502
-.034
Uni
mod
alm
ultim
odal
-1.3
52.4
18.0
03-2
.200
-.505
Pari
etal
left
The
taC
ontr
olU
nim
odal
-.066
.031
.041
-.128
-.003
mul
timod
al.0
15.0
31.6
25-.0
48.0
78
Uni
mod
alm
ultim
odal
.081
.036
.030
.008
.153
Beta
Con
trol
Uni
mod
al.0
87.0
38.0
29.0
09.1
64
mul
timod
al-.0
14.0
38.7
13-.0
92.0
63
Uni
mod
alm
ultim
odal
-.101
.044
.028
-.190
-.011
6

180
Chapter 6
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Gam
ma
Con
trol
Uni
mod
al.0
15.0
07.0
50-2
.862
E-06
.029
mul
timod
al.0
04.0
07.5
87-.0
11.0
19
Uni
mod
alm
ultim
odal
-.011
.008
.209
-.028
.006
Peak
freq
uenc
yC
ontr
olU
nim
odal
.846
.375
.030
.087
1.60
6
mul
timod
al-.6
29.3
75.1
02-1
.388
.130
Uni
mod
alm
ultim
odal
-1.4
75.4
33.0
02-2
.352
-.598
Pari
etal
rig
htT
heta
Con
trol
Uni
mod
al-.0
98.0
31.0
03-.1
60-.0
35
mul
timod
al.0
12.0
31.6
92-.0
50.0
75
Uni
mod
alm
ultim
odal
.110
.036
.004
.037
.182
Beta
Con
trol
Uni
mod
al.1
03.0
37.0
09.0
27.1
78
mul
timod
al-.0
17.0
37.6
46-.0
93.0
58
Uni
mod
alm
ultim
odal
-.120
.043
.009
-.207
-.032
Gam
ma
Con
trol
Uni
mod
al.0
16.0
08.0
48.0
00.0
32
mul
timod
al.0
04.0
08.6
29-.0
12.0
20
Uni
mod
alm
ultim
odal
-.012
.009
.186
-.030
.006
Peak
freq
uenc
yC
ontr
olU
nim
odal
1.15
5.3
98.0
06.3
491.
961
mul
timod
al-.6
13.3
98.1
32-1
.419
.193
Uni
mod
alm
ultim
odal
-1.7
68.4
59.0
00-2
.698
-.837

181
MEG-based resting-state brain activity in PD
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Occ
ipita
l lef
tT
heta
Con
trol
Uni
mod
al-.0
74.0
34.0
37-.1
44-.0
05
mul
timod
al.0
31.0
34.3
71-.0
38.1
01
Uni
mod
alm
ultim
odal
.105
.040
.011
.025
.186
Beta
Con
trol
Uni
mod
al.0
83.0
34.0
18.0
15.1
50
mul
timod
al-.0
07.0
34.8
38-.0
75.0
61
Uni
mod
alm
ultim
odal
-.089
.039
.026
-.168
-.011
Gam
ma
Con
trol
Uni
mod
al.0
08.0
06.1
68-.0
04.0
20
mul
timod
al.0
04.0
06.4
76-.0
08.0
16
Uni
mod
alm
ultim
odal
-.004
.007
.556
-.018
.010
Peak
freq
uenc
yC
ontr
olU
nim
odal
1.27
3.4
10.0
04.4
432.
103
mul
timod
al-.4
72.4
10.2
56-1
.302
.358
Uni
mod
alm
ultim
odal
-1.7
45.4
73.0
01-2
.704
-.787
Occ
ipita
l rig
htT
heta
Con
trol
Uni
mod
al-.0
83.0
32.0
14-.1
49-.0
18
mul
timod
al.0
22.0
32.5
02-.0
43.0
87
Uni
mod
alm
ultim
odal
.105
.037
.008
.030
.181
Beta
Con
trol
Uni
mod
al.0
84.0
32.0
13.0
18.1
49
mul
timod
al.0
01.0
32.9
71-.0
64.0
66
Uni
mod
alm
ultim
odal
-.082
.037
.033
-.158
-.007
6

182
Chapter 6
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Gam
ma
Con
trol
Uni
mod
al.0
09.0
07.1
90-.0
05.0
23
mul
timod
al.0
03.0
07.6
75-.0
11.0
17
Uni
mod
alm
ultim
odal
-.006
.008
.434
-.022
.010
Peak
freq
uenc
yC
ontr
olU
nim
odal
1.45
9.4
18.0
01.6
122.
306
mul
timod
al-.4
12.4
18.3
31-1
.259
.435
Uni
mod
alm
ultim
odal
-1.8
71.4
83.0
00-2
.849
-.893
Tem
pora
l lef
tT
heta
Con
trol
Uni
mod
al-.0
80.0
33.0
22-.1
47-.0
12
mul
timod
al.0
19.0
33.5
79-.0
49.0
86
Uni
mod
alm
ultim
odal
.098
.038
.015
.020
.176
Beta
Con
trol
Uni
mod
al.0
73.0
33.0
35.0
05.1
40
mul
timod
al-.0
13.0
33.7
03-.0
80.0
55
Uni
mod
alm
ultim
odal
-.086
.038
.032
-.164
-.008
Gam
ma
Con
trol
Uni
mod
al.0
21.0
11.0
58-.0
01.0
42
mul
timod
al-.0
02.0
11.8
25-.0
24.0
19
Uni
mod
alm
ultim
odal
-.023
.012
.067
-.048
.002
Peak
freq
uenc
yC
ontr
olU
nim
odal
.999
.390
.015
.210
1.78
9
mul
timod
al-.4
28.3
90.2
79-1
.218
.362
Uni
mod
alm
ultim
odal
-1.4
27.4
50.0
03-2
.339
-.515

183
MEG-based resting-state brain activity in PD
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Te
mp
or
al
righ
tT
heta
Con
trol
Uni
mod
al-.1
07.0
35.0
04-.1
78-.0
36
mul
timod
al.0
01.0
35.9
68-.0
70.0
72
Uni
mod
alm
ultim
odal
.108
.041
.011
.026
.190
Beta
Con
trol
Uni
mod
al.0
89.0
33.0
09.0
23.1
55
mul
timod
al.0
05.0
33.8
77-.0
61.0
71
Uni
mod
alm
ultim
odal
-.084
.038
.031
-.160
-.008
Gam
ma
Con
trol
Uni
mod
al.0
27.0
13.0
55-.0
01.0
54
mul
timod
al.0
07.0
13.5
87-.0
20.0
35
Uni
mod
alm
ultim
odal
-.019
.015
.221
-.051
.012
Peak
freq
uenc
yC
ontr
olU
nim
odal
1.42
7.3
96.0
01.6
242.
229
mul
timod
al-.2
34.3
96.5
59-1
.036
.569
Uni
mod
alm
ultim
odal
-1.6
60.4
57.0
01-2
.587
-.733
Lim
bic
left
The
taC
ontr
olU
nim
odal
-.062
.024
.014
-.111
-.013
mul
timod
al.0
19.0
24.4
26-.0
29.0
68
Uni
mod
alm
ultim
odal
.082
.028
.006
.025
.138
Beta
Con
trol
Uni
mod
al.0
51.0
28.0
77-.0
06.1
07
mul
timod
al-.0
16.0
28.5
72-.0
72.0
41
Uni
mod
alm
ultim
odal
-.067
.032
.046
-.132
-.001
6

184
Chapter 6
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Gam
ma
Con
trol
Uni
mod
al.0
21.0
08.0
11.0
05.0
36
mul
timod
al.0
02.0
08.7
69-.0
13.0
18
Uni
mod
alm
ultim
odal
-.018
.009
.045
-.036
.000
Peak
freq
uenc
yC
ontr
olU
nim
odal
.838
.317
.012
.196
1.47
9
mul
timod
al-.5
60.3
17.0
85-1
.202
.081
Uni
mod
alm
ultim
odal
-1.3
98.3
66.0
00-2
.139
-.657
Lim
bic
righ
tT
heta
Con
trol
Uni
mod
al-.0
69.0
24.0
06-.1
17-.0
21
mul
timod
al.0
16.0
24.5
06-.0
32.0
64
Uni
mod
alm
ultim
odal
.085
.027
.004
.029
.140
Beta
Con
trol
Uni
mod
al.0
50.0
28.0
85-.0
07.1
08
mul
timod
al-.0
19.0
28.5
02-.0
77.0
38
Uni
mod
alm
ultim
odal
-.070
.033
.041
-.136
-.003
Gam
ma
Con
trol
Uni
mod
al.0
20.0
08.0
16.0
04.0
37
mul
timod
al-.0
01.0
08.9
05-.0
17.0
15
Uni
mod
alm
ultim
odal
-.021
.009
.027
-.040
-.003
Peak
freq
uenc
yC
ontr
olU
nim
odal
.914
.323
.007
.261
1.56
8
mul
timod
al-.4
98.3
23.1
31-1
.151
.156
Uni
mod
alm
ultim
odal
-1.4
12.3
72.0
01-2
.167
-.658

185
MEG-based resting-state brain activity in PD
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Sub
cort
ical
le
ftT
heta
Con
trol
Uni
mod
al-.0
59.0
26.0
28-.1
11-.0
07
mul
timod
al.0
25.0
26.3
33-.0
27.0
77
Uni
mod
alm
ultim
odal
.084
.030
.007
.024
.144
Beta
Con
trol
Uni
mod
al.0
47.0
32.1
46-.0
17.11
1
mul
timod
al-.0
29.0
32.3
65-.0
93.0
35
Uni
mod
alm
ultim
odal
-.076
.036
.044
-.150
-.002
Gam
ma
Con
trol
Uni
mod
al.0
20.0
09.0
31.0
02.0
39
mul
timod
al-.0
03.0
09.7
42-.0
22.0
15
Uni
mod
alm
ultim
odal
-.023
.011
.032
-.045
-.002
Peak
freq
uenc
yC
ontr
olU
nim
odal
.759
.338
.031
.075
1.44
3
mul
timod
al-.5
99.3
38.0
84-1
.283
.085
Uni
mod
alm
ultim
odal
-1.3
58.3
90.0
01-2
.148
-.568
Sub
cort
ical
ri
ght
The
taC
ontr
olU
nim
odal
-.068
.025
.009
-.119
-.018
mul
timod
al.0
14.0
25.5
76-.0
37.0
65
Uni
mod
alm
ultim
odal
.082
.029
.007
.024
.141
Beta
Con
trol
Uni
mod
al.0
51.0
32.11
4-.0
13.11
6
mul
timod
al-.0
20.0
32.5
35-.0
84.0
44
6

186
Chapter 6
Tabl
e S6
: Con
tinue
d
mea
n di
ffer
ence
Reg
ion
Freq
uenc
y ba
ndG
roup
Gro
upM
ean
diff
eren
ceS
Ep-
valu
eL
ower
bou
ndU
pper
bou
nd
Uni
mod
alm
ultim
odal
-.071
.037
.059
-.145
.003
Gam
ma
Con
trol
Uni
mod
al.0
21.0
08.0
18.0
04.0
38
mul
timod
al-.0
03.0
08.7
65-.0
20.0
15
Uni
mod
alm
ultim
odal
-.024
.010
.021
-.043
-.004
Peak
freq
uenc
yC
ontr
olU
nim
odal
1.00
8.3
54.0
07.2
921.
724
mul
timod
al-.5
22.3
54.1
48-1
.239
.194
Uni
mod
alm
ultim
odal
-1.5
30.4
08.0
01-2
.358
-.703
Con
trol
: Par
kins
on’s
dise
ase
patie
nts
with
out
hallu
cina
tions
; Mul
timod
al H
all+
: Par
kins
on’s
dise
ase
patie
nts
with
mul
timod
al h
allu
cina
tions
; SE:
sta
ndar
d er
ror;
U
nim
odal
Hal
l+: P
arki
nson
’s di
seas
e pa
tient
s w
ith o
nly
visu
al h
allu
cina
tions

187
MEG-based resting-state brain activity in PD
Table S7: Relative power per AAL region in the theta band in Parkinson’s disease patients with unimodal and multimodal hallucinations
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
1 Gyrus rectus L 0.211 (0.046) 0.151 (0.061) .029
2 Olfactory cortex L 0.241 (0.054) 0.159 (0.074) .015
3 Superior frontal gyrus, orbital part L 0.201 (0.051) 0.147 (0.054) .035
4 Superior frontal gyrus, medial orbital part L 0.206 (0.052) 0.145 (0.043) .007
5 Middle frontal gyrus, orbital part L 0.189 (0.055) 0.141 (0.053) .143
6 Inferior frontal gyrus, orbital part L 0.206 (0.051) 0.149 (0.064) .023
7 Superior frontal gyrus L, dorsolateral 0.208 (0.044) 0.149 (0.052) .007
8 Middle frontal gyrus L 0.206 (0.057) 0.144 (0.056) .035
9 Inferior frontal gyrus, opercular part L 0.212 (0.062) 0.149 (0.073) .075
10 Inferior frontal gyrus, triangular part L 0.206 (0.059) 0.140 (0.052) .019
11 Superior frontal gyrus, medial part L 0.222 (0.047) 0.155 (0.047) .009
12 Supplementary motor area L 0.211 (0.052) 0.161 (0.071) .075
13 Paracentral lobule L 0.181 (0.054) 0.152 (0.077) .123
14 Precentral gyrus L 0.195 (0.060) 0.150 (0.078) .089
15 Rolandic operculum L 0.245 (0.065) 0.152 (0.093) .029
16 Postcentral gyrus L 0.194 (0.065) 0.149 (0.094) .043
17 Superior parietal gyrus L 0.232 (0.063) 0.163 (0.104) .029
18 Inferior parietal gyri L 0.232 (0.067) 0.161 (0.121) .052
19 Supramarginal gyrus L 0.247 (0.069) 0.168 (0.116) .035
20 Angular gyrus L 0.285 (0.081) 0.183 (0.123) .029
21 Precuneus L 0.250 (0.064) 0.167 (0.100) .029
22 Superior occipital gyrus L 0.281 (0.078) 0.181 (0.114) .023
23 Middle occipital gyrus L 0.297 (0.080) 0.194 (0.114) .029
24 Inferior occipital gyrus L 0.302 (0.094) 0.201 (0.092) .043
0.291 (0.077) 0.178 (0.095) .009
26 Cuneus L 0.284 (0.078) 0.180 (0.112) .019
27 Lingual gyrus L 0.306 (0.083) 0.181 (0.088) .007
28 Fusiform gyrus L 0.308 (0.087) 0.219 (0.121) .089
29 Heschl gyrus L 0.271 (0.072) 0.158 (0.089) .009
30 Superior temporal gyrus L 0.263 (0.073) 0.163 (0.090) .029
31 Middle temporal gyrus L 0.290 (0.095) 0.196 (0.123) .052
32 Inferior temporal gyrus L 0.281 (0.081) 0.196 (0.112) .052
33 Temporal pole: superior temporal gyrus L 0.236 (0.061) 0.167 (0.081) .063
34 Temporal pole: middle temporal gyrus L 0.234 (0.054) 0.159 (0.070) .019
35 Parahippocampal gyrus L 0.282 (0.071) 0.196 (0.100) .063
6

188
Chapter 6
Table S7: Continued
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
36 Anterior cingulate and paracingulate gyri L 0.238 (0.056) 0.156 (0.054) .004
37 Median cingulate and paracingulate gyri L 0.240 (0.059) 0.169 (0.088) .023
38 Posterior cingulate gyrus L 0.269 (0.060) 0.172 (0.093) .029
39 Insula L 0.239 (0.061) 0.158 (0.085) .043
40 Gyrus rectus R 0.210 (0.045) 0.152 (0.060) .015
41 Olfactory cortex R 0.239 (0.053) 0.163 (0.072) .019
42 Superior frontal gyrus, orbital part R 0.196 (0.045) 0.142 (0.048) .019
43 Superior frontal gyrus, medial orbital part R 0.204 (0.048) 0.142 (0.048) .004
44 Middle frontal gyrus, orbital part R 0.184 (0.060) 0.136 (0.042) .075
45 Inferior frontal gyrus, orbital part R 0.200 (0.057) 0.148 (0.058) .089
46 Superior frontal gyrus R, dorsolateral 0.206 (0.045) 0.147 (0.062) .029
47 Middle frontal gyrus R 0.195 (0.048) 0.148 (0.069) .063
48 Inferior frontal gyrus, opercular part R 0.200 (0.049) 0.149 (0.082) .063
49 Inferior frontal gyrus, triangular part R 0.204 (0.056) 0.150 (0.073) .063
50 Superior frontal gyrus, medial part R 0.216 (0.049) 0.144 (0.043) .003
51 Supplementary motor area R 0.201 (0.046) 0.155 (0.074) .035
52 Paracentral lobule R 0.186 (0.055) 0.152 (0.081) .052
53 Precentral gyrus R 0.195 (0.036) 0.149 (0.088) .015
54 Rolandic operculum R 0.259 (0.066) 0.159 (0.096) .011
55 Postcentral gyrus R 0.213 (0.054) 0.144 (0.096) .011
56 Superior parietal gyrus R 0.251 (0.067) 0.160 (0.102) .015
57 Inferior parietal gyri R 0.264 (0.086) 0.154 (0.102) .015
58 Supramarginal gyrus R 0.283 (0.080) 0.169 (0.126) .011
59 Angular gyrus R 0.298 (0.090) 0.181 (0.105) .029
60 Precuneus R 0.283 (0.083) 0.164 (0.094) .007
61 Superior occipital gyrus R 0.291 (0.076) 0.184 (0.095) .015
62 Middle occipital gyrus R 0.313 (0.093) 0.208 (0.105) .029
63 Inferior occipital gyrus R 0.294 (0.081) 0.196 (0.096) .019
0.297 (0.079) 0.183 (0.099) .015
65 Cuneus R 0.291 (0.076) 0.172 (0.101) .009
66 Lingual gyrus R 0.300 (0.077) 0.189 (0.101) .019
67 Fusiform gyrus R 0.287 (0.078) 0.204 (0.104) .063
68 Heschl gyrus R 0.292 (0.071) 0.179 (0.109) .011
69 Superior temporal gyrus R 0.305 (0.092) 0.175 (0.105) .009
70 Middle temporal gyrus R 0.315 (0.109) 0.206 (0.121) .023
71 Inferior temporal gyrus R 0.271 (0.075) 0.190 (0.089) .052
72 Temporal pole: superior temporal gyrus R 0.230 (0.056) 0.161 (0.085) .043

189
MEG-based resting-state brain activity in PD
Table S7: Continued
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
73 Temporal pole: middle temporal gyrus R 0.230 (0.055) 0.155 (0.066) .009
74 Parahippocampal gyrus R 0.274 (0.070) 0.184 (0.093) .029
75 Anterior cingulate and paracingulate gyri R 0.229 (0.057) 0.150 (0.054) .007
76 Median cingulate and paracingulate gyri R 0.229 (0.054) 0.164 (0.085) .019
77 Posterior cingulate gyrus R 0.281 (0.067) 0.170 (0.089) .007
78 Insula R 0.244 (0.068) 0.162 (0.086) .029
79 Hippocampus L 0.282 (0.067) 0.191 (0.099) .075
80 Hippocampus R 0.287 (0.071) 0.183 (0.097) .035
81 Amygdala L 0.262 (0.069) 0.184 (0.094) .063
82 Amygdala R 0.259 (0.064) 0.175 (0.086) .043
83 Caudate nucleus L 0.241 (0.052) 0.159 (0.075) .019
84 Caudate nucleus R 0.247 (0.052) 0.164 (0.076) .015
85 Lenticular nucleus, putamen L 0.248 (0.060) 0.163 (0.087) .019
86 Lenticular nucleus, putamen R 0.250 (0.064) 0.169 (0.090) .043
87 Lenticular nucleus, pallidum L 0.264 (0.067) 0.168 (0.089) .015
88 Lenticular nucleus, pallidum R 0.256 (0.063) 0.171 (0.089) .023
89 Thalamus L 0.251 (0.057) 0.171 (0.105) .019
90 Thalamus R 0.261 (0.053) 0.183 (0.105) .035
Multimodal Hall+: Parkinson’s disease patients with multimodal hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations
6

190
Chapter 6
Table S8: Relative power per AAL region in the gamma band in Parkinson’s disease patients with unimodal and multimodal hallucinations
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
1 Gyrus rectus L 0.073 (0.017) 0.092 (0.021) .043
2 Olfactory cortex L 0.054 (0.013) 0.071 (0.019) .052
3 Superior frontal gyrus, orbital part L 0.088 (0.016) 0.115 (0.020) .004
4 Superior frontal gyrus, medial orbital part L 0.088 (0.018) 0.117 (0.020) .003
5 Middle frontal gyrus, orbital part L 0.090 (0.019) 0.124 (0.021) .004
6 Inferior frontal gyrus, orbital part L 0.070 (0.017) 0.100 (0.026) .011
7 Superior frontal gyrus L, dorsolateral 0.090 (0.021) 0.115 (0.021) .023
8 Middle frontal gyrus L 0.087 (0.031) 0.114 (0.022) .043
9 Inferior frontal gyrus, opercular part L 0.068 (0.026) 0.107 (0.044) .023
10 Inferior frontal gyrus, triangular part L 0.077 (0.032) 0.109 (0.026) .015
11 Superior frontal gyrus, medial part L 0.085 (0.024) 0.114 (0.015) .007
12 Supplementary motor area L 0.078 (0.021) 0.098 (0.020) .075
13 Paracentral lobule L 0.083 (0.021) 0.097 (0.022) .165
14 Precentral gyrus L 0.066 (0.020) 0.090 (0.021) .029
15 Rolandic operculum L 0.046 (0.014) 0.095 (0.070) .011
16 Postcentral gyrus L 0.057 (0.020) 0.077 (0.022) .029
17 Superior parietal gyrus L 0.077 (0.024) 0.080 (0.027) .739
18 Inferior parietal gyri L 0.060 (0.019) 0.066 (0.026) .529
19 Supramarginal gyrus L 0.053 (0.019) 0.076 (0.036) .165
20 Angular gyrus L 0.045 (0.012) 0.059 (0.018) .105
21 Precuneus L 0.065 (0.022) 0.072 (0.025) .436
22 Superior occipital gyrus L 0.055 (0.015) 0.059 (0.015) .684
23 Middle occipital gyrus L 0.045 (0.017) 0.048 (0.016) .796
24 Inferior occipital gyrus L 0.046 (0.019) 0.047 (0.011) .971
0.043 (0.011) 0.044 (0.017) .796
26 Cuneus L 0.046 (0.014) 0.055 (0.018) .280
27 Lingual gyrus L 0.043 (0.013) 0.047 (0.015) .529
28 Fusiform gyrus L 0.041 (0.014) 0.048 (0.011) .393
29 Heschl gyrus L 0.043 (0.013) 0.075 (0.048) .035
30 Superior temporal gyrus L 0.049 (0.033) 0.076 (0.047) .105
31 Middle temporal gyrus L 0.043 (0.018) 0.064 (0.026) .035
32 Inferior temporal gyrus L 0.054 (0.017) 0.067 (0.018) .143
33 Temporal pole: superior temporal gyrus L 0.063 (0.018) 0.093 (0.036) .023
34 Temporal pole: middle temporal gyrus L 0.069 (0.019) 0.094 (0.032) .019
35 Parahippocampal gyrus L 0.051 (0.013) 0.065 (0.031) .481

191
MEG-based resting-state brain activity in PD
Table S8: Continued
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
36 Anterior cingulate and paracingulate gyri L 0.070 (0.023) 0.094 (0.015) .019
37 Median cingulate and paracingulate gyri L 0.057 (0.021) 0.071 (0.016) .089
38 Posterior cingulate gyrus L 0.050 (0.017) 0.055 (0.019) .529
39 Insula L 0.059 (0.022) 0.095 (0.044) .023
40 Gyrus rectus R 0.071 (0.017) 0.092 (0.022) .023
41 Olfactory cortex R 0.055 (0.014) 0.075 (0.019) .015
42 Superior frontal gyrus, orbital part R 0.082 (0.016) 0.110 (0.024) .003
43 Superior frontal gyrus, medial orbital part R 0.083 (0.020) 0.114 (0.026) .007
44 Middle frontal gyrus, orbital part R 0.088 (0.020) 0.114 (0.021) .015
45 Inferior frontal gyrus, orbital part R 0.075 (0.017) 0.102 (0.016) .001
46 Superior frontal gyrus R, dorsolateral 0.087 (0.022) 0.109 (0.018) .089
47 Middle frontal gyrus R 0.084 (0.024) 0.113 (0.022) .023
48 Inferior frontal gyrus, opercular part R 0.063 (0.020) 0.101 (0.035) .005
49 Inferior frontal gyrus, triangular part R 0.075 (0.021) 0.106 (0.022) .009
50 Superior frontal gyrus, medial part R 0.089 (0.023) 0.118 (0.017) .004
51 Supplementary motor area R 0.082 (0.018) 0.100 (0.017) .035
52 Paracentral lobule R 0.078 (0.023) 0.101 (0.025) .052
53 Precentral gyrus R 0.065 (0.019) 0.091 (0.020) .009
54 Rolandic operculum R 0.051 (0.017) 0.087 (0.036) .019
55 Postcentral gyrus R 0.062 (0.028) 0.075 (0.021) .280
56 Superior parietal gyrus R 0.072 (0.028) 0.079 (0.024) .529
57 Inferior parietal gyri R 0.053 (0.018) 0.065 (0.018) .089
58 Supramarginal gyrus R 0.051 (0.021) 0.074 (0.026) .075
59 Angular gyrus R 0.050 (0.016) 0.061 (0.016) .105
60 Precuneus R 0.059 (0.023) 0.068 (0.022) .529
61 Superior occipital gyrus R 0.052 (0.013) 0.061 (0.014) .247
62 Middle occipital gyrus R 0.046 (0.014) 0.053 (0.014) .579
63 Inferior occipital gyrus R 0.056 (0.018) 0.056 (0.024) .912
0.041 (0.013) 0.046 (0.017) .631
65 Cuneus R 0.050 (0.018) 0.055 (0.016) .739
66 Lingual gyrus R 0.039 (0.013) 0.048 (0.018) .280
67 Fusiform gyrus R 0.049 (0.019) 0.058 (0.024) .481
68 Heschl gyrus R 0.043 (0.013) 0.064 (0.036) .105
69 Superior temporal gyrus R 0.046 (0.015) 0.070 (0.036) .063
70 Middle temporal gyrus R 0.045 (0.017) 0.062 (0.030) .165
71 Inferior temporal gyrus R 0.060 (0.014) 0.073 (0.023) .247
72 Temporal pole: superior temporal gyrus R 0.072 (0.018) 0.101 (0.042) .190
6

192
Chapter 6
Table S8: Continued
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
73 Temporal pole: middle temporal gyrus R 0.076 (0.012) 0.101 (0.045) .280
74 Parahippocampal gyrus R 0.051 (0.014) 0.070 (0.036) .280
75 Anterior cingulate and paracingulate gyri R 0.072 (0.023) 0.097 (0.016) .015
76 Median cingulate and paracingulate gyri R 0.058 (0.018) 0.080 (0.022) .029
77 Posterior cingulate gyrus R 0.046 (0.015) 0.056 (0.023) .190
78 Insula R 0.059 (0.017) 0.089 (0.033) .063
79 Hippocampus L 0.046 (0.016) 0.062 (0.030) .218
80 Hippocampus R 0.048 (0.018) 0.067 (0.033) .218
81 Amygdala L 0.055 (0.016) 0.080 (0.045) .190
82 Amygdala R 0.056 (0.013) 0.082 (0.043) .190
83 Caudate nucleus L 0.056 (0.019) 0.074 (0.015) .035
84 Caudate nucleus R 0.055 (0.018) 0.075 (0.016) .029
85 Lenticular nucleus, putamen L 0.056 (0.020) 0.084 (0.031) .019
86 Lenticular nucleus, putamen R 0.055 (0.014) 0.080 (0.027) .035
87 Lenticular nucleus, pallidum L 0.052 (0.018) 0.078 (0.033) .035
88 Lenticular nucleus, pallidum R 0.053 (0.015) 0.079 (0.032) .035
89 Thalamus L 0.052 (0.018) 0.072 (0.035) .143
90 Thalamus R 0.049 (0.014) 0.070 (0.030) .165
AAL regions between unimodal Hall+ and multimodal Hall+ groups after FDR-correction for multiple comparisons)Multimodal Hall+: Parkinson’s disease patients with multimodal hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations

193
MEG-based resting-state brain activity in PD
Table S9: Peak frequency per AAL region in Parkinson’s disease patients with unimodal and multimodal hallucinations
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
1 Gyrus rectus L 7.06 (0.85) 8.24 (1.12) .015
2 Olfactory cortex L 7.27 (0.95) 8.81 (1.16) .007
3 Superior frontal gyrus, orbital part L 7.06 (0.87) 7.83 (0.95) .052
4 Superior frontal gyrus, medial orbital part L 6.81 (0.81) 7.72 (0.68) .015
5 Middle frontal gyrus, orbital part L 6.85 (0.96) 7.69 (1.04) .075
6 Inferior frontal gyrus, orbital part L 7.15 (1.06) 8.32 (0.92) .029
7 Superior frontal gyrus L, dorsolateral 7.03 (0.95) 7.56 (0.84) .247
8 Middle frontal gyrus L 7.17 (1.06) 7.64 (0.69) .247
9 Inferior frontal gyrus, opercular part L 7.55 (1.08) 8.32 (0.85) .123
10 Inferior frontal gyrus, triangular part L 7.35 (0.99) 8.01 (0.99) .123
11 Superior frontal gyrus, medial part L 6.84 (0.82) 7.61 (0.61) .043
12 Supplementary motor area L 7.36 (1.12) 7.96 (0.76) .190
13 Paracentral lobule L 7.96 (1.28) 8.58 (1.13) .247
14 Precentral gyrus L 8.21 (1.53) 8.50 (1.01) .436
15 Rolandic operculum L 7.70 (0.94) 8.88 (0.97) .035
16 Postcentral gyrus L 8.56 (1.13) 8.98 (1.07) .529
17 Superior parietal gyrus L 7.49 (1.03) 9.07 (1.14) .007
18 Inferior parietal gyri L 7.98 (1.18) 9.19 (1.31) .063
19 Supramarginal gyrus L 7.86 (1.00) 9.01 (1.17) .015
20 Angular gyrus L 7.51 (1.06) 9.05 (1.36) .019
21 Precuneus L 7.24 (0.95) 9.13 (1.49) .007
22 Superior occipital gyrus L 7.15 (1.07) 8.96 (1.51) .009
23 Middle occipital gyrus L 7.20 (1.03) 8.91 (1.21) .005
24 Inferior occipital gyrus L 7.12 (0.93) 8.78 (1.31) .009
7.24 (1.11) 8.04 (1.34) .004
26 Cuneus L 7.31 (1.14) 9.01 (1.43) .015
27 Lingual gyrus L 7.20 (1.06) 8.99 (1.25) .007
28 Fusiform gyrus L 7.10 (0.99) 8.84 (1.29) .009
29 Heschl gyrus L 7.61 (1.03) 9.19 (1.16) .023
30 Superior temporal gyrus L 7.49 (1.04) 8.94 (1.22) .029
31 Middle temporal gyrus L 7.70 (1.25) 8.95 (1.34) .089
32 Inferior temporal gyrus L 7.41 (0.97) 8.85 (1.31) .019
33 Temporal pole: superior temporal gyrus L 7.37 (1.00) 8.46 (0.95) .043
34 Temporal pole: middle temporal gyrus L 7.05 (0.73) 8.54 (0.99) .004
35 Parahippocampal gyrus L 7.34 (1.12) 8.79 (1.24) .043
6

194
Chapter 6
Table S9: Continued
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
36 Anterior cingulate and paracingulate gyri L 7.05 (0.97) 8.35 (0.84) .009
37 Median cingulate and paracingulate gyri L 7.47 (0.89) 8.76 (1.08) .003
38 Posterior cingulate gyrus L 7.43 (0.97) 0.12 (1.27) .005
39 Insula L 7.47 (0.95) 8.53 (0.83) .029
40 Gyrus rectus R 7.19 (0.86) 8.25 (0.98) .019
41 Olfactory cortex R 7.22 (0.87) 8.71 (1.19) .011
42 Superior frontal gyrus, orbital part R 7.00 (0.91) 7.89 (0.92) .043
43 Superior frontal gyrus, medial orbital part R 6.77 (0.85) 7.80 (0.85) .011
44 Middle frontal gyrus, orbital part R 7.07 (0.79) 7.79 (0.89) .063
45 Inferior frontal gyrus, orbital part R 7.35 (0.78) 8.29 (1.07) .029
46 Superior frontal gyrus R, dorsolateral 7.25 (1.42) 7.83 (0.75) .123
47 Middle frontal gyrus R 7.20 (1.21) 7.91 (0.75) .089
48 Inferior frontal gyrus, opercular part R 7.70 (1.04) 8.74 (1.12) .052
49 Inferior frontal gyrus, triangular part R 7.30 (0.73) 8.11 (0.91) .035
50 Superior frontal gyrus, medial part R 6.88 (0.76) 7.74 (0.69) .023
51 Supplementary motor area R 7.60 (1.17) 8.08 (0.82) .123
52 Paracentral lobule R 7.83 (1.14) 8.44 (1.15) .436
53 Precentral gyrus R 7.90 (1.07) 9.08 (1.09) .035
54 Rolandic operculum R 7.45 (1.03) 9.11 (1.17) .005
55 Postcentral gyrus R 8.08 (1.13) 9.30 (1.15) .029
56 Superior parietal gyrus R 7.23 (0.89) 8.95 (1.45) .009
57 Inferior parietal gyri R 7.67 (1.36) 9.45 (1.43) .009
58 Supramarginal gyrus R 7.45 (1.06) 9.10 (1.28) .009
59 Angular gyrus R 7.14 (1.11) 9.00 (1.28) .005
60 Precuneus R 7.30 (0.89) 9.12 (1.26) .004
61 Superior occipital gyrus R 7.98 (1.03) 8.88 (1.50) .009
62 Middle occipital gyrus R 6.88 (1.01) 8.69 (1.21) .004
63 Inferior occipital gyrus R 6.86 (1.06) 8.76 (1.35) .004
7.12 (1.13) 9.00 (1.35) .009
65 Cuneus R 7.02 (1.05) 9.06 (1.42) .007
66 Lingual gyrus R 6.98 (1.07) 8.88 (1.37) .004
67 Fusiform gyrus R 7.06 (0.95) 8.71 (1.32) .009
68 Heschl gyrus R 7.37 (0.92) 9.02 (1.10) .004
69 Superior temporal gyrus R 7.42 (1.03) 9.10 (1.19) .007
70 Middle temporal gyrus R 7.10 (0.95) 8.77 (1.38) .015
71 Inferior temporal gyrus R 7.16 (1.04) 8.80 (1.42) .015
72 Temporal pole: superior temporal gyrus R 7.02 (0.76) 8.62 (1.04) .003

195
MEG-based resting-state brain activity in PD
Table S9: Continued
AAL region Unimodal Hall+ (N=10)
Multimodal Hall+ (N=10)
p-value
73 Temporal pole: middle temporal gyrus R 7.08 (0.94) 8.62 (0.99) .005
74 Parahippocampal gyrus R 7.23 (1.08) 8.70 (1.28) .011
75 Anterior cingulate and paracingulate gyri R 7.01 (0.88) 8.23 (0.90) .007
76 Median cingulate and paracingulate gyri R 7.67 (1.15) 8.63 (1.00) .063
77 Posterior cingulate gyrus R 7.42 (1.03) 9.04 (1.17) .007
78 Insula R 7.27 (1.03) 8.99 (1.20) .004
79 Hippocampus L 7.22 (0.90) 8.68 (1.20) .015
80 Hippocampus R 7.19 (0.86) 8.67 (1.21) .009
81 Amygdala L 7.30 (1.02) 8.72 (1.16) .019
82 Amygdala R 7.22 (1.16) 8.71 (1.27) .019
83 Caudate nucleus L 7.33 (0.98) 8.51 (1.06) .019
84 Caudate nucleus R 7.12 (0.96) 8.54 (1.10) .007
85 Lenticular nucleus, putamen L 7.40 (0.85) 8.72 (0.93) .007
86 Lenticular nucleus, putamen R 7.12 (1.05) 8.80 (1.31) .009
87 Lenticular nucleus, pallidum L 7.43 (0.87) 8.73 (1.01) .019
88 Lenticular nucleus, pallidum R 7.11 (1.03) 8.78 (1.15) .005
89 Thalamus L 7.32 (1.00) 8.89 (1.27) .015
90 Thalamus R 7.36 (0.92) 8.75 (1.11) .011
Multimodal Hall+: Parkinson’s disease patients with multimodal hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations
6

196
Chapter 6
Table S10: Relative power per frequency band and peak frequency, corrected for medication, in Parkinson’s disease patients with unimodal, multimodal, and without hallucinations
Unimodal Hall+vs. Hall-
Multimodal Hall+vs. Hall-
Unimodal Hall+ vs. Multimodal Hall+
Delta F(7,19)=1.37, p=.254 F(7,19)=1.71, p=.203 F(7,11)=1.85, p=.191
Theta F(7,19)=7.77, p=.010 F(7,19)=0.60, p=.448 F(7,11)=5.48, p=.032
Alpha1 F(7,19)=0.22, p=.640 F(7,19)=0.52, p=.480 F(7,11)=1.55, p=.230
Alpha2 F(7,19)=1.16, p=.291 F(7,19)=3.35, p=.079 F(7,11)=3.03, p=.100
Beta F(7,19)=4.68, p=.040 F(7,19)=0.36, p=.555 F(7,11)=2.93, p=.105
Gamma F(7,19)=7.92, p=.009 F(7,19)=0.01, p=.935 F(7,11)=5.82, p=.027
Peak frequency F(7,19)=6.56, p=.017 F(7,19)=3.56, p=.071 F(7,11)=8.77, p=.009
Power is the relative power per frequency band (delta [0.5–4 Hz], theta [4–8 Hz], alpha1 [8–10 Hz], alpha2 [10–13 Hz], beta [13–30 Hz], and gamma [30-48 Hz]), averaged over all 90 AAL regions. Peak frequency is the frequency with highest power in range between 4 and 13 Hz, averaged over all 90 AAL regions.Hall-: Parkinson’s disease patients without hallucinations; Multimodal Hall+: Parkinson’s disease patients with multimodal hallucinations; Unimodal Hall+: Parkinson’s disease patients with only visual hallucinations

197
MEG-based resting-state brain activity in PD
6

Related Documents