University of Groningen Airway inflammation in nocturnal asthma Hacken, Nicolaas Hubertus Theodorus ten IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 1998 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Hacken, N. H. T. T. (1998). Airway inflammation in nocturnal asthma. [S.n.]. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 10-02-2022

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
University of Groningen
Airway inflammation in nocturnal asthmaHacken, Nicolaas Hubertus Theodorus ten
IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite fromit. Please check the document version below.
Document VersionPublisher's PDF, also known as Version of record
Publication date:1998
Link to publication in University of Groningen/UMCG research database
Citation for published version (APA):Hacken, N. H. T. T. (1998). Airway inflammation in nocturnal asthma. [S.n.].
CopyrightOther than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of theauthor(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons).
The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license.More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne-amendment.
Take-down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons thenumber of authors shown on this cover page is limited to 10 maximum.
Download date: 10-02-2022
. AIRWAY INFLAMMATION I
IN NOCTURNAL ASTHMA
Nick ten Hacken

AIRWAY INFLAMMATION
IN NOCTURNAL ASTHMA
STELLINGEN BIJ HET PROEFSCHRIFT
AIRWAY INFLAMMATION IN NOCTURNAL ASTHMA
NICK TEN HACKEN
1. In de centrale luchtwegen neemt het aantal inflammatoire cellen 's nachts niet toe bij patienten met een hoge piekstroomvariatie (dit proefschrift).
2. lnterferon-y in het perifeer bleed van astma patienten is overdag en 's nachts gecorreleerd met belangrijke klinische variabelen als piekstroomvariatie en luchtweghyperreactiviteit voor methacholine (dit p roefsch rift).
3. De expressie van induceerbaar NO synthase (iNOS) in bronchusbiopten van personen met en zonder nachtelijk astma vertoont geen dagnacht verschil (dit proefschrift).
4. De expressie van endotheliaal NO synthase (eNOS) in bronchusbiopten van astmatici vertoont een dag-nacht verschil dat negatief gecorreleerd is met de piekstroomvariatie (dit proefschrift).
5. De endotheliale expressie van VCAM-1 in bronchusbiopten van patienten in een stabiele fase van hun astma is positief gecorreleerd met EG2 en CD25 positieve cellen in de submucosa (dit proefschrift).
6. NO in de uitademingslucht is een makkelijke niet-invasieve manier om astmapatienten met een hoger risico op nachtelijke astma op te sporen (dit proefschrift).
7. Een hoge piekstroomvariatie thuis betekent nog niet dat astmapatienten in het ziekenhuis een ernstige nachtelijke luchtwegobstructie vertonen (dit proefschrift).
8. Medische tijdschriften kunnen medische paradigma's verstevigen en de doorbraak van nieuwe inzichten blokkeren.
9. Titels van medische publicaties zijn vaak saai, soms een tikje frivool, maar zelden adembenemend verrassend.
10. Het Discours van de astmatische ontsteking is niet te vertalen door het bestuderen van ge'isoleerde in vitro gebeurtenissen.
11. Door de verplichting voorlopige arbeidscontracten na drie jaren om te zetten in definitieve, blijven voorlopige aanstellingen inderdaad voorlopig.
12. Na het nemen van een bloederig bronchusbiopt ontstaat, in tegenstelling tot een niet bloederige biopt, een sterke toename van oedeem, slijm en bronchospasme. Dit wijst op krachtige inflammatie bevorderende mediatoren in bleed.
13. Jongeren (18-45 jaar) beschikken over een lagere bloed-bronchusbarriere en/of bloed-hersenbarriere voor lidocaine dan ouderen.
•
ten Hacken, NHT Airway inflammation in nocturnal asthma Thesis Groningen - with references - with summary in Dutch. ISBN 90-367-0880-x NUGI 742
Copyright by NHT ten Hacken. All rights reserved. No part of this book may be reproduced or transmitted, in any form or by any means, without written permission from the author.
All research described in this thesis was financially supported by the Nederlands Astma Fonds (grant no. 92.28). A part of the research was supported by the Jan Kornelis de Cock Stichting and the Stichting Astmabestrijding.
The printing and presentation of this study was financially supported by:
The Nederlands Astma Fonds Stichting Astmabestrijding Groningen Institute for Drug Studies (GIDS) Astra Pharmaceutica B V Bayer BV Byk Nederland BV Boehringer lngelheim BV Glaxo Wei/come BV Merck Sharp & Dohme BV Novartis Pharma BV Ooms Allergie B V Zambon Nederland BV Zeneca Farma BV
Cover photograph: Han Jansen, schilder van Stroombeeldschilderijen.
This document was printed in the Netherlands by van Denderen BV, Groningen.
RIJKSUNIVERSITEIT GRONINGEN
AIRWAY INFLAMMATION IN NOCTURNAL ASTHMA
Proefschrift
ter verkrijging van het doctoraat in de Medische Wetenschappen
aan de Rijksuniversiteit Groningen op gezag van de Rector Magnificus
Dr. F. van der Woude · in het openbaar te verdedigen
op woensdag 1 april 1998 des namiddags te 2.45 uur
door
Nicolaas Hubertus Theodorus ten Hacken geboren op 28 oktober 1953 te Breda

Promotores: Prof. Dr. D.S. Postma Prof. Dr. W. Timens

Promotiecommissie:
Paranimfen:
Prof. Dr. H. C. Hoogsteden Prof. Dr. F.P. Nijkamp Prof. Dr. S. Poppema
Wiel de Lange Ronald Meijer
Night attack
as the fish that thrusts its jaw to water draw so I some air do seek to snare,
and I like the weanling goat upon the nipple I suck, but it is not milk so sweet I crave, but air, air so pure
clamarous rales shake my chest as I snatch up what I can, now filled in broad expanse, sated but so briefly,
I strive to move that air now vilified from inside out
the harder that I push the more it presses against my breast cramming to get free, my heart a fluttering parakeet,
my lungs two sleeping cats, in fits and spasms the air escapes where a balloon would burst
propitious gravity helps draw the air down deep, erect I sleep my craning neck unbent, more range to roam
my arms the phoenix' wings, aching to be reborn from this fire a gentler thing
so I toss the purplish sleep, gasping, rasping making noises that no human body was designed to make
each breath now leaves me breathless, the clock hands circling vultures of the night
the steaming kettle and misty bath give short relief as I rock and rale in hell, awaiting the morning sun
and the birds at dawn, to greet them with my rhonchitic song.
Harold W Horowitz, Valhalla, NY, USA (Lancet 1996; 348: 252).
CONTENTS
Chapter 1 1.1 1.2
Chapter 2.1
2.2
2.3
2.4
Chapter 3
Chapter 4
Chapter 5
Chapter 6
Chapter 7
Chapter 8
Chapter 9 9. 1 9.2 9.3 9.4
General introduction I ntroduction 1 Aims of the study 9
Quantity and morphology of bronchial biopsies taken by forceps of three different sizes 17 Differences in plastic-embedded and snap-frozen sections for CD3, CD4 and CDS immunostaining of bronchial biopsies 25 Submucosa 1 .0 x 0.1 mm in size is sufficient to count inflammatory cell numbers in human airway biopsy specimen 33 Semi-quantitative and quantitative scoring are complementary in the counting of immunostained cells in human airway-biopsies 39
Nocturnal asthma: no nocturnal increase in inflammatory cells, but more severe airway wall inflammation both day and night 47
Vascular adhesion molecules in nocturnal asthma: a possible role for VCAM-1 in ongoing airway wall inflammation 57
Nocturnal asthma: not explained by circadian variations in inducible Nitric Oxide Synthase 69
Decreased expression of eNOS at night in asthmatic subjects with large PEF variation 85
Higher levels of exhaled Nitric Oxide both at day and night in subjects with nocturnal asthma 93
Elevated serum interferon-y in atopic asthma correlates with increased airways responsiveness and circadian peak expiratory flow variation 105
Summary and Discussion Summary 117 Discussion 124 Conclusions 125 Perspectives 128
List of abbreviations
Samenvatting
Dankwoord
135
137
151

Chapter 1
General Introduction
1.1 Introduction
Nocturnal asthma Nocturnal asthma is generally described in terms of increased nocturnal airway obstruction in combination with nocturnal symptoms such as wheezing, breathlessness, chest tightness and cough (1-3). Nocturnal awakening due to dyspnea in adult asthmatic patients occurs rather frequently as shown in a large epidemiological study in England, that reported 74% of the asthmatic population had nocturnal awakening at least once a week (4). In the Netherlands, nocturnal awakening was reported at least once a week in 42% of 103 clinically stable asthmatic patients from a pulmonary outpatient clinic (5). Nocturnal symptoms occur also frequently in asthmatic children: 34% of 796 asthmatic children attending the outpatient clinic of the University Hospital Groningen reported nocturnal symptoms at least once a week (6). Noteworthy, patients with nocturnal asthma often do not present their problem spontaneously (6,7), despite the fact that disturbed sleep interferes significantly with school and work performance (8,9). The underestimation of nocturnal asthma is the more regrettable since both bronchodilator and antiinflammatory drugs have shown to improve PEF variability and nocturnal symptoms as well as daytime cognitive performance in asthmatic subjects with high levels of PEF variation (10, 11 ).
Mechanisms in nocturnal asthma Many factors, often showing a circadian rhythm, have been proposed to play a role in the occurrence of increased nocturnal airway obstruction (12). Noninflammatory factors are a.o.: gastro-esophageal reflux (13), increased cholinerg activity (14, 15), decreased adrenergic activity (16, 17), desensitization and (genetic) defects in �2-adrenergic receptors (18-20), decreased inhibitory non-adrenerg non-cholinerg (iNANC) activity (21 ), lowering of body temperature (22), temporary stopping of bronchodilators (2), decreased mucociliairy clearance (23), supine position (24), aging (25). Inflammatory factors on the other hand are a.o.: low cortisol and epinephrine levels at night (17), an allergic response after inhalation of e.g. house dust mite (26), an increased induction of inflammation at daytime (27). Intervention studies avoiding or correcting one of the above described factors indicate that many of these factors together play a role in the pathogenesis of increased nocturnal airway obstruction.
Chapter 1
Asthmatic airway inflammation It has long been recognized that patients who die from asthma attacks have grossly abnormal lungs. Post-mortem studies showed that these lungs were hyperinflated due to air trapping caused by widespread plugging of segmental and subsegmental airways. Plugs consisted of exsuded plasma proteins, mucus glycoproteins and a cellular debris of shed epithelial and inflammatory cells (28,29), indicative for severe airway wall inflammation. Thanks to the use of (induced) sputum, bronchoalveolar lavage and bronchial biopsies it is now clear that inflammation is also present, though less severe, in mild asthmatic patients. Especially the introduction of the flexible bronchoscopy has accelerated our understanding of the pathophysiology of asthma (30). Despite methodological limitations (such as sampling errors and distortion of tissues) bronchial biopsies have shown that mild asthmatic subjects suffer from an eosinophilic cell influx in the airway wall (31,32). Also epithelial shedding (33), a thickened basement membrane (34), subepithelial fibrosis (35, 36), smooth muscle hyperplasia (28) and increased numbers of epithelial glands (28) are prominent features of chronic asthmatic airway inflammation. The cellular infiltrate present in the bronchial submucosa not only consists of high numbers of activated eosinophils, but also of high numbers of activated mast cells (37), monocytes (38) and lymphocytes (39), whereas neutrophils are only scarcely present.
Cytokines in asthmatic airway inflammation Ten years ago it was reported for the first time that murine helper T-cell (Th) clones could be divided into two subsets, Th1 and Th2, based upon their pattern of specific lymphokine secretion (40). Th1 cells produce interleukin (IL)-2, interferon (IFN)-y, and lymphotoxin (or tumor necrosis factor (TNF)-B), and are involved in cell-mediated immune responses including delayed-type hypersensitivity. Th2 cells produce IL-4, -5, -6, -9, -10 and -13, and are involved in the humeral response against helminthic and parasite infections (41 ). There is now accumulating evidence that the products of Th2 lymphocytes play an important regulating role in the pathogenesis of allergic diseases including asthma (42-44). Especially the secretion of IL-4 and IL-5 are considered to be essential for the eosinophilic character of asthmatic airway inflammation (45,46). IL-4 induces an increased expression of the vascular adhesion molecule VCAM-1, important for selective recruitment of activated eosinophils into the bronchial submucosa (47,48). Moreover, IL-4 may stimulate B cells to produce lgE (49,50), which is essential for early asthmatic responses (51 ). IL-5 induces an increased proliferation, maturation and activation of eosinophils (52,53). Interestingly, the importance of the Th2 concept in human asthma has been questioned more and more in the last few years (54-56). Mast cells and eosinophils have been reported to secrete IL-4 and IL-5 as well (8,44,57). Other cytokines like IFN-y, TNF-a and IL-1 B produced by epithelial cells, mast cells
2
General Introduction
and macrophages, are also thought to be important for asthmatic airway inflammation (58-62). These cytokines are called pro-inflammatory cytokines, and they do not only lead to a higher level of proliferation, maturation, activation and recruitment of granulocytes at sites of inflammation, but are also able to induce Nitric Oxide (see later).
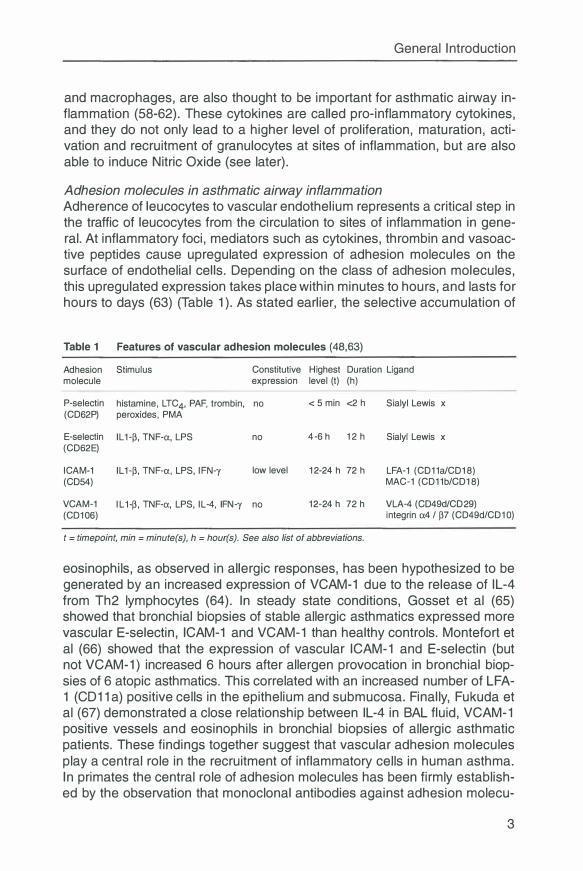
Adhesion molecules in asthmatic airway inflammation Adherence of leucocytes to vascular endothelium represents a critical step in the traffic of leucocytes from the circulation to sites of inflammation in general. At inflammatory foci, mediators such as cytokines, thrombin and vasoactive peptides cause upregulated expression of adhesion molecules on the surface of endothelial cells. Depending on the class of adhesion molecules, this upregulated expression takes place within minutes to hours, and lasts for hours to days (63) (Table 1 ). As stated earlier, the selective accumulation of
Table 1 Features of vascular adhesion molecules (48,63)
Adhesion Stimulus molecule
Constitutive Highest Duration Ligand expression level (t) (h)
P-selectin histamine, LTC4, PAF, trombin, no < 5 min <2 h Sialyl Lewis x (CD62P) peroxides, PMA
E-selectin IL 1-p, TNF-a, LPS (CD62E)
ICAM-1 (CD54)
IL 1-p, TNF-a, LPS, IFN-y
no 4-6 h 12 h Sialyl Lewis x
low level 12-24 h 72 h LFA-1 (CD11a/CD18) MAC-1 (CD11b/CD18)
VCAM-1 IL1-p, TNF-a, LPS, IL-4, IFN-y no 12-24 h 72 h VLA-4 (CD49d/CD29) (CD106 ) integrin a4 / p7 (CD49d/CD10)
t = timepoint, min = minute(s), h = hour(s). See also list of abbreviations.
eosinophils, as observed in allergic responses, has been hypothesized to be generated by an increased expression of VCAM-1 due to the release of IL-4 from Th2 lymphocytes (64). In steady state conditions, Gosset et al (65) showed that bronchial biopsies of stable allergic asthmatics expressed more vascular E-selectin, ICAM-1 and VCAM-1 than healthy controls. Montefort et al (66) showed that the expression of vascular ICAM-1 and E-selectin (but not VCAM-1) increased 6 hours after allergen provocation in bronchial biopsies of 6 atopic asthmatics. This correlated with an increased number of LFA-1 (CD11 a) positive cells in the epithelium and submucosa. Finally, Fukuda et al (67) demonstrated a close relationship between IL-4 in BAL fluid, VCAM-1 positive vessels and eosinophils in bronchial biopsies of allergic asthmatic patients. These findings together suggest that vascular adhesion molecules play a central role in the recruitment of inflammatory cells in human asthma. In primates the central role of adhesion molecules has been firmly established by the observation that monoclonal antibodies against adhesion molecu-
3

Chapter 1
les inhibited eosinophilic airway infiltration after antigen challenge (47,63,68,69). In humans, this central role still has to be confirmed in future intervention studies with monoclonal antibodies directed at cytokines.
Nitric Oxide as mediator in asthmatic airway inflammation Nitric Oxide (NO) is a highly reactive and lipophilic molecule which is important in many physiological and pathophysiological processes. The synthesis of NO takes place in many cell types and is formed by the conversion of Larginine to L-citrulline. Normally, NO is produced in low concentrations, katalysed by the constitutive enzyme Nitric Oxide Synthase (cNOS). In physiological processes, NO acts as an autocrine or paracrine hormone via the activation of adenyl guanylate cyclase and cyclic guanylate monophosphate (cGMP) (52). In inflammatory processes, the above described pro-inflammatory cytokines can upregulate another form of the enzyme, the inducible Nitric Oxide Synthase (iNOS) (70-72). Once present, iNOS induces much higher concentrations of NO, which contribute to the elimination of tumor cells and microbial agents (73). Table 2 summarizes the most important features of inducible and constitutive NO Synthase.
Table 2
Presence
Location
Stimulus
Features of constitutive and inducible NO synthase
c-NOS (type I and II)
constantly expressed (constitutively)
endothelium (eNOS), cerebrum (bNOS), neurons (NANC)(nNOS), smooth muscle
i-NOS (type Ill)
only expressed after induction
macrophages, monocytes, leucocytes, airway epithelium, endothelium
acetylcholine, histamine, leukotrienes, endotoxin, LPS, pro-inflammatory cytokines: bradykinin, ADP, ATP, VIP, PAF, substance P IFN-y, IL-1�, TNF-a
Synthesis i by Nitric Oxide, smoking corticosteroids
Dependent from calcium and calmoduline
Reaction time seconds - minutes
Reaction endurance minutes
transcription of DNA
hours
hours - days
NO production
NO effect
picomols nanomols
physiologic: neurotransmission, vasodilatation, pathophysiologic: killing of tumor cells and bronchodilatation microbial agents, cytotoxicity
See list of abbreviations.
Because pro-inflammatory cytokins are present in higher levels in asthmatic patients than in healthy controls, it can be anticipated that induction of iNOS takes place in asthma leading to the increased production of NO. Indeed, a high expression of iNOS has been demonstrated in biopsies of stable asthmatic subjects, in contrast to healthy individuals (71 ). Moreover, higher levels of NO in exhaled air have been found in asthmatics as compared to healthy
4
General Introduction
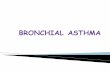
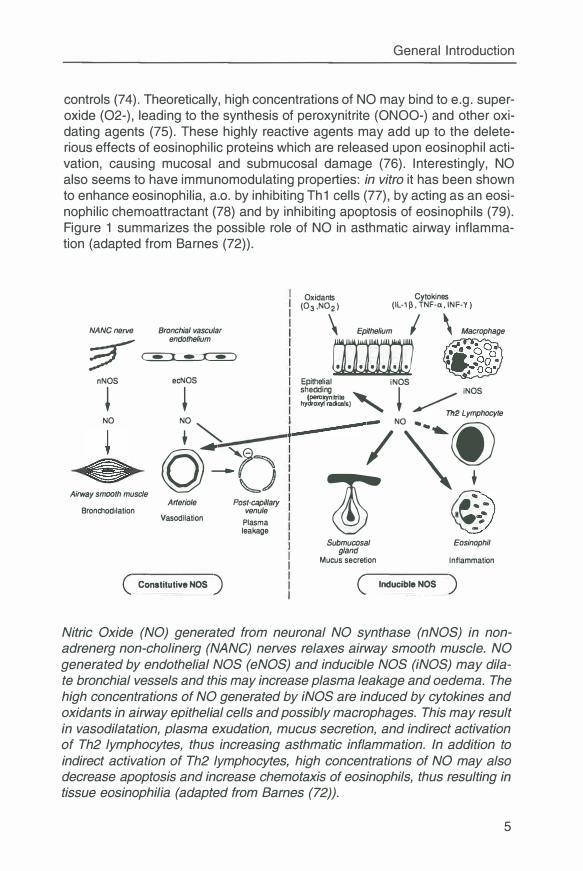
controls (74). Theoretically, high concentrations of NO may bind to e.g. superoxide (02-), leading to the synthesis of peroxynitrite (ONOO-) and other oxidating agents (75). These highly reactive agents may add up to the deleterious effects of eosinophilic proteins which are released upon eosinophil activation, causing mucosa! and submucosal damage (76). Interestingly, NO also seems to have immunomodulating properties: in vitro it has been shown to enhance eosinophilia, a.o. by inhibiting Th1 cells (77), by acting as an eosinophilic chemoattractant (78) and by inhibiting apoptosis of eosinophils (79). Figure 1 summarizes the possible role of NO in asthmatic airway inflammation (adapted from Barnes (72)).
NANC nerve Bronchial vascular
� endothelium
? � nNOS ecNOS
+ + NO NO
"' + � I
n_� y �) Airway smooth muscle
Arteriole Bronchodilation
Vasodilation
( Constitutive NOS )
Post-capillary venule
Plasma leakage
Cytokines Oxidants (03,N02) (IL-11}, TNF-a, INF-'Y)
\ Epithelium I \ Macrophage
rn Epithelial iNOS shedding
+ iNOS
( xynilrite hy�racicals)' �
Th2 Lymphocyte
�/\��, i9 .�: Submurosal
gland Mucus secretion
Eosinophil
Inflammation
( Inducible NOS )
Nitric Oxide (NO) generated from neuronal NO synthase (nNOS) in nonadrenerg non-cholinerg (NANG) nerves relaxes airway smooth muscle. NO generated by endothelial NOS (eNOS) and inducible NOS (iNOS) may dilate bronchial vessels and this may increase plasma leakage and oedema. The high concentrations of NO generated by iNOS are induced by cytokines and oxidants in airway epithelial cells and possibly macrophages. This may result in vasodilatation, plasma exudation, mucus secretion, and indirect activation of Th2 lymphocytes, thus increasing asthmatic inflammation. In addition to indirect activation of Th2 lymphocytes, high concentrations of NO may also decrease apoptosis and increase chemotaxis of eosinophils, thus resulting in tissue eosinophilia (adapted from Barnes (72)).
5
Chapter 1
NO as a marker of asthmatic airway inflammation Because NO can easily be measured in exhaled air, and because it has been shown to increase in case of airway wall inflammation, it has been put forward as a new way to monitor asthmatic airway inflammation (80). Only recently, the European Respiratory Society has published a consensus report to standardize measurements of NO (81 ). This guideline recommends to use the single breath method in adult subjects, provided that a subject is able to exhale air from the maximal level of inspiration, during 20 seconds, with a flow of 10-15 I/min, against a pressure of 5-20 cm H20. Stable asthmatic subjects not using corticosteroids were found to exhale significantly higher levels of NO than healthy subjects (74,82), whereas asthmatic subjects using inhaled corticosteroids were showing similar levels of NO as compared to healthy controls (80). In acute asthma, the exhaled NO concentration was found to be increased, which normalized after adequate therapy (83). In addition, provocation with an allergen, increased exhaled NO levels during the late asthmatic response in asthmatic subjects (84). This increase probably reflects increased airway inflammation as exhaled NO did not change after pharmacologically induced changes in airway diameter using methacholine or salbutamol (85).
Altogether, exhaled NO appears to be a promising way to monitor control of asthma, yet a few disadvantages have to be mentioned. Exhaled NO concentrations show large inter-individual variations. Consequently, this measurement is less suitable for cross sectional analyses. Further, an increase in exhaled NO is a nonspecific sign, meaning that it can not differentiate between infectious or allergic processes. Also, upper airways (nose) produce large amounts of NO (86,87) and mixing of NO from the higher and lower airways may take place during inhalation and exhalation. Finally, there is strong evidence that an important part (60-90%) of the NO production is absorbed in the alveoli (88,89). Theoretically, alveolar processes may lead to small changes in the diffusion capacity for NO, leading to important changes in exhaled NO. However, the latter has not been formally investigated.
Airway inflammation in nocturnal asthma The role of airway inflammation in nocturnal asthma has been emphasized in recent reports, and it has been suggested that it may be a key factor in inducing the nocturnal increase of airway hyperresponsiveness (90,91 ). Indirect evidence for the involvement of inflammation in nocturnal asthma is given by a study showing that increased circadian variations in airway diameter are better reflected by circadian changes in airway responsiveness induced by adenosine monophosphate (AMP) than methacholine (92). Moreover, treatment with inhaled corticosteroids has been reported to be effective in reducing nocturnal airway obstruction and nocturnal symptoms of asthma (93). Direct evidence for the involvement of inflammation in nocturnal asthma
6
General Introduction
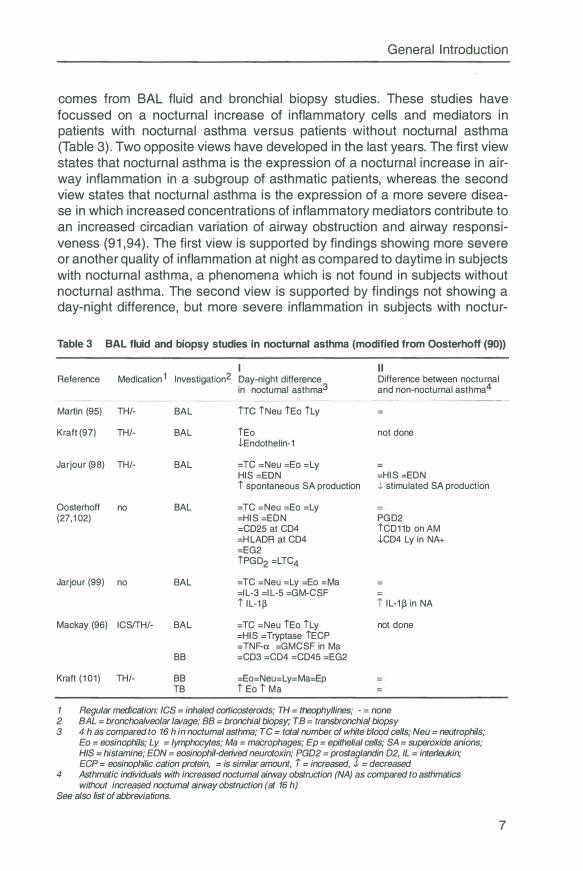
comes from BAL fluid and bronchial biopsy studies. These studies have focussed on a nocturnal increase of inflammatory cells and mediators in patients with nocturnal asthma versus patients without nocturnal asthma (Table 3). Two opposite views have developed in the last years. The first view states that nocturnal asthma is the expression of a nocturnal increase in airway inflammation in a subgroup of asthmatic patients, whereas the second view states that nocturnal asthma is the expression of a more severe disease in which increased concentrations of inflammatory mediators contribute to an increased circadian variation of airway obstruction and airway responsiveness (91,94). The first view is supported by findings showing more severe or another quality of inflammation at night as compared to daytime in subjects with nocturnal asthma, a phenomena which is not found in subjects without nocturnal asthma. The second view is supported by findings not showing a day-night difference, but more severe inflammation in subjects with noctur-
Table 3 BAL fluid and biopsy studies in nocturnal asthma (modified from Oosterhoff (90))
Reference Medication 1 lnvestigation2
Martin (95) TH/- BAL
Kraft (97) TH/- BAL
Jarjour (98) TH/- BAL
Oosterhoff no BAL (27,102)
Jarjour (99) no BAL
Mackay (96 ) ICS/ TH/- BAL
BB
Kraft (101) TH/- BB TB
Day-night difference in nocturnal asthma3
ire iNeu iEo iLy
iEo -l-Endothelin-1
= TC =Neu =Ea =Ly HIS =EON i spontaneous SA production
= TC =Neu =Ea =Ly =HIS =EDN =CD25 at CD4 =HLADR at CD4 =EG2
iPGD2 =LTC4
= TC =Neu =Ly =Ea =Ma =IL-3 =IL-5 =GM-CSF i IL-1 �
= TC =Neu iEo iLy =HIS = Tryptase iECP = TNF-a. =GMCSF in Ma =CD3 =CD4 =CD45 =EG2
=Eo=Neu=Ly=Ma=Ep i Ea i Ma
I I Difference between nocturnal and non-nocturnal asthma4
not done
=HIS =EDN J, stimulated SA production
PGD2
iCD11b on AM -l-CD4 Ly in NA+
i IL-1� in NA
not done
1 Regular medication: /CS = inhaled corticosteroids; TH = theophyllines; - = none 2 BAL = bronchoalveolar lavage; BB = bronchial biopsy; TB = transbronchia/ biopsy 3 4 h as compared to 16 h in nocturnal asthma; TC = total number of white blood cells; Neu = neutrophils;
Eo = eosinophi/s; Ly = lymphocytes; Ma = macrophages; Ep = epithelial cells; SA = superoxide anions; HIS = histamine; EON = eosinophi/-derived neurotoxin; PGD2 = prostaglandin D2, IL = interleukin; ECP = eosinophi/ic cation protein, = is similar amount, i = increased, J = decreased
4 Asthmatic individuals with increased nocturnal airway obstruction (NA) as compared to asthmatics without increased nocturnal airway obstruction (at 16 h)
See also list of abbreviations.
7
Chapter 1
nal asthma as compared to subjects without nocturnal asthma, both at day and night. In table 3 findings supporting the first view are presented in the column I, and findings supporting the second view in column II.
Increased airway inflammation at night in nocturnal asthma? Several findings support the hypothesis that an increased airway inflammation at night plays a role in the pathogenesis of nocturnal asthma. Responsiveness for AMP was found to be higher at night than at daytime in subjects with nocturnal asthma, in contrast to subjects without nocturnal asthma (92). The number of eosinophils and lymphocytes in BAL fluid of subjects with nocturnal asthma at night were higher than at daytime (95-97), as was ECP (96). The number of cells producing superoxide anion radicals was elevated at night in BAL fluid of subjects with nocturnal asthma (98), possibly resulting from a nocturnal increase in IL-1 � (99). This increase in IL-1 � might also be responsible for the nocturnal increase in exhaled NO as observed in mild asthmatic subjects (100). Finally, the number of eosinophils in the alveolar tissue was higher at night than at daytime in subjects with nocturnal asthma (101 ). In this last study, the number of eosinophils at night was negatively correlated with the percentage overnight fall in FEV 1 .
Opposite findings are found in other studies. The number of neutrophils, mast cells, eosinophils, (subsets of) lymphocytes, macrophages and the activation state of these cells in BAL fluid of subjects with and without nocturnal asthma did not increase at night in these studies (27,98,99, 102). Also inflammatory mediators as histamine, tryptase, prostaglandin D2, LTC4, thromboxane 82, ECP and EON in BAL fluid showed similar results at day and night (27,96, 102). Finally, the density of (activated) eosinophils, (subsets of) lymphocytes, macrophages and neutrophils in biopsies from the central airways did not differ between day and night in subjects with nocturnal asthma (96,101).
More severe airway inflammation at day and night in nocturnal asthma? Some of the studies described in the former paragraph not only indicated that subjects with nocturnal asthma have similar levels of airway inflammation at day and night (90). In addition, Oosterhoff et al showed that alveolar macrophages in BAL fluid of subjects with nocturnal asthma, obtained at 16 h, express more CD11 b than alveolar macrophages of subjects without nocturnal asthma (27). This CD11 b expression correlated positively with the circadian PEF variation (r=0.72). The authors suggested that daytime activation of macrophages predisposes for the occurrence of nocturnal asthma. Another finding of the same authors was that BAL prostaglandin D2 levels in BAL fluid of subjects with nocturnal asthma obtained at day and night were significantly higher than those of subjects without nocturnal asthma (102).
8
General Introduction
These findings led to the hypothesis that nocturnal asthma is only the reflection of a more severe and ongoing airway inflammation, with a continuous release of bronchoconstricting mediators (90,91,94). Increased circadian variations in airway obstruction in subjects with nocturnal asthma may thus be explained by normally occurring circadian variations in bronchomotor tone superimposed on chronically decreased airway diameters due to more severe airway inflammation. Another explanation is that the decrease in airway diameter at night is more pronounced because of failing counter regulating forces at night (like catecholamines and cortisol).
1 .2 Aims of the studies
Airway inflammation has been demonstrated to play an important role in the pathogenesis of asthma. In this thesis important features of airway inflammation were studied to evaluate their contribution to the manifestation of asthma, in particular nocturnal asthma. Chapter 2.1-2.4 describe some methodological problems of obtaining, processing and evaluating bronchial biopsies. Chapter 3-6 present inflammatory data obtained in studies using bronchial biopsies. Chapter 7-8 focusses on markers of inflammation in other compartments e.g. exhaled air, serum and BAL fluid.
The next questions were formulated:
1. Which biopsy forceps is superior in obtaining large and intact bronchial biopsies, acceptable for quantitative and semi-quantitative analyses ? Chapter 2. 1. Quantity and morphology of bronchial biopsies taken by forceps of three different sizes.
2. Do inflammatory cell counts in sections of fresh frozen and glycol methacrylate-embedded biopsies correspond ? Chapter 2.2. Differences in plastic-embedded and snap-frozen sections for CD3, CD4 and COB immunostaining of bronchial biopsy specimens.
3. How much tissue has to be evaluated in a section of a bronchial biopsy to produce constant cell counts ? Chapter 2. 3. Submucosa 1. O x 0. 1 mm in size is sufficient to count inflammatory cell numbers in human airway biopsy specimens.
4. Are the semi-quantitative and quantitative way of evaluating inflammatory cells in bronchial biopsies comparable ? Chapter 2.4. Semi-quantitative and quantitative scoring are complementary in the counting of immunostained cells in human airway-biopsies.
9
Chapter 1
5. Are inflammatory cell numbers at night higher than at daytime in bronchial biopsies of subjects with and without nocturnal asthma ? Chapter 3. Nocturnal asthma: no nocturnal increase in inflammatory cells, but more severe airway wall inflammation both day and night.
6. Are vascular adhesion molecules at night expressed more extensively than at daytime, and is there a relationship with increased nocturnal airway inflammation in subjects with nocturnal asthma ? Chapter 4. Vascular adhesion molecules in nocturnal asthma: a possible role for VCAM- 1 in ongoing airway wall inflammation.
7. Is expression of inducible Nitric Oxide Synthase (iNOS) upregulated at night in bronchial biopsies of subjects with nocturnal asthma ? Chapter 5. Nocturnal asthma: not explained by circadian variations in inducible Nitric Oxide Synthase.
8. Is there a change at night in the expression of endothelial Nitric Oxide Synthase (eNOS) in bronchial biopsies of subjects with and without nocturnal asthma ? Chapter 6. Decreased expression of eNOS at night in asthmatic subjects with large PEF variation.
9. Does exhaled Nitric Oxide show a circadian rhythm, inverse to the circadian rhythm in airway obstruction in subjects with nocturnal asthma? Chapter 7. Higher levels of exhaled Nitric Oxide both at day and night in subjects with nocturnal asthma.
1 0. Are the cytokines IL-4, IL-5 and interferon-y in serum and BAL fluid related to the clinical manifestation of atopic asthma ? Chapter 8. Elevated serum interferon-y in atopic asthma correlates with increased airways responsiveness and circadian peak expiratory flow variation.
References 1. Greenough A, Everett L, Pool J, Price JF. Relation between nocturnal symp
toms and changes in lung function on lying down in asthmatic children. Thorax 1991 ;46:193-6.
2. Clark T J. Diurnal rhythm of asthma. Chest 1987;91 : 137S-41 S. 3. Hetzel MR, Clark T J. Comparison of normal and asthmatic circadian rhythms
in peak expiratory flow rate. Thorax 1980;35:732-8. 4. TurnerWarwick M. Epidemiology of nocturnal asthma. Am J Med 1988;85:6-8. 5. van Keimpema ARJ , Ariaansz M, Tamminga JJ, Nauta JJP, Postmus PE.
Nocturnal awakening and morning dip of Peak expiratory flow in clinically stable asthma patients during treatment. Respiration 1997;64:29-34.
6. Meijer GG, Postma DS, Wempe JB, Gerritsen J, Knol K, van Aalderen WM.
1 0
Frequency of nocturnal symptoms in asthmatic children attending a hospital outpatient clinic. Eur Respir J 1995;8:2076-80.
General Introduction
7. Storms WW, Bodman SF, Nathan RA, Byer P. Nocturnal asthma symptoms may be more prevalent than we think. J Asthma 1994;31 :313-8.
8. Ackerman V, Marini M, Vittori E, Bellini A, Vassali G, Mattoli S. Detection of cytokines and their cell sources in bronchial biopsy specimens from asthmatic patients. Relationship to atopic status, symptoms, and level of airway hyperresponsiveness. Chest 1994; 105:687-96.
9. Fitzpatrick MF, Engleman H, Whyte KF, Deary IJ , Shapiro CMD. Morbidity in nocturnal asthma: sleep quality and daytime cognitive performance. Thorax 1991 ;46:569-73.
10. Weersink EJ, van Zomeren H, Koster GH, Postma OS. Treatment of nocturnal airway obstruction improves daytime cognitive performance in asthmatics. Am J Respir Grit Care Med 1997; 156: 1144-50.
11. Weersink EJ , Douma RR, Postma DS, Koster G. Fluticason propionate, salmeterol xinafoate, and their combination in the treatment of nocturnal asthma. Am J Respir Grit Care Med 1997; 155: 1241-6.
12. Busse WW. Pathogenesis and pathophysiology of nocturnal asthma. Am J Med 1988;85:24-9.
13. Ekstrom T, Tibbling L. Gastrooesophageal reflux and nocturnal asthma. Eur Respir J 1988;1 :636-8.
14. Morrison JF, Pearson SB. The parasympathetic nervous system and the diurnal variation of lung mechanics in asthma. Respir Med 1991 ;85:285-9.
15. Morrison JF, Pearson SB, Dean HG. Parasympathetic nervous system in nocturnal asthma. Br Med J (Clin Res Ed) 1 988;296: 1427-9.
16. Bates ME, Clayton M, Calhoun W, Jarjour N, Schrader L, Geiger KS, Sedgwick J, Swenson C, Busse W. Relationship of plasma epinephrine and circulating eosinophils to nocturnal asthma. Am J Respir Grit Care Med 1994; 149:667-72.
17. Barnes P, FitzGerald G, Brown M, Dollery C. Nocturnal asthma and changes in circulating epinephrine, histamine, and cortisol. N Engl J Med 1980;303:263-7.
18. Szefler SJ , Ando R, Cicutto LC, Surs W, Hill MR, Martin RJ . Plasma histamine, epinephrine, cortisol, and leukocyte beta-adrenergic receptors in nocturnal asthma. Clin Pharmacol Ther 1991 ;49:59-68.
19. Meurs H, Postma OS, Koster GH, Keyzer JJ, Timmermans A, Kauffman HF, De Vries K. The beta-adrenergic system of nonallergic patients with chronic airflow obstruction and early morning dyspnoea. Ann Allergy 1987;59:417-21.
20. Turki J, Pak J , Green SA, Martin RJ, Liggett SB. Genetic polymorphisms of the �2-adrenerg receptor in nocturnal and nonnocturnal asthma. J Clin Invest 1995;95: 1635-41 .
21. Mackay TW, Fitzpatrick MF, Douglas NJ. Nonadrenerg, noncholinerg nervous system and overnight airway calibre in asthmatic and normal subjects. Lancet 1991 ;338:1289
22. Chen WY, Chai H. Airway cooling and nocturnal asthma. Chest 1982;81 :675-80.
23. Martin RJ. Busse WW, Holgate ST, editors. Asthma and Rhinitis. first ed. Boston: Blackwell Scientific Publications; 1995; Chapter 108, Mechanisms of nocturnal asthma. p. 1440-52.
11
Chapter 1
24. Fitzpatrick MF, Mackay T, Walters C, Tai PC, Church MK, Holgate ST, Douglas NJ. Circulating histamine and eosinophil cationic protein levels in nocturnal asthma. Clin Sci 1 992;83:227-32.
25. Bellia V, Cuttitta G, Cibella F, Vignola AM, Crescimanno G, D'Accardi P, Catalano F, Bonsignore G. Effect of aging on peak expiratory flow variability and nocturnal exacerbations in bronchial asthma. Eur Respir J 1 997; 1 0: 1 803-8.
26. Gervais P, Reinberg A, Gervais C. Twenty fourhour rhythm in the bronchial hyperreactivity to house dust in asthmatics. J Allergy Clin lmmunol 1 977;59:207-1 3.
27. Oosterhoff Y, Hoogsteden HC, Rutgers B, Kauffman HF, Postma DS. Lymphocyte and macrophage activation in bronchoalveolar lavage fluid in nocturnal asthma. Am J Respir Grit Care Med 1 995; 1 51 :75-81 .
28. Dunnill MS. The pathology of asthma, with special references to changes in the bronchial mucosa. J Clin Pathol 1 960; 1 3:27-33.
29. Dunnill MS, Massarella GR, Anderson JA. A comparison of the quantitative anatomy of the bronchi in normal subjects and status asthmaticus in chronic bronchitis and in emphysema. Thorax 1 969;24: 1 76-9.
30. Holgate ST. The 1 992 Cournand Lecture. Asthma: past, present and future. Eur Respir J 1 993;6: 1 507-20.
31 . Laitinen LA, Laitinen A, Haahtela T. Airway mucosal inflammation even in patients with newly diagnosed asthma. Am Rev Respir Dis 1 993; 1 47:697-704.
32. Bousquet J, Chanez P, Lacoste JY, Barneon G, Ghavanian N, Enander I, Venge P, Ahlstedt S, SimonyLafontaine J, Godard P, et al. Eosinophilic inflammation in asthma. N Engl J Med 1 990;323: 1 033-9.
33. Jeffery PK, Wardlaw AJ, Nelson FC, Collins JV, Kay AB. Bronchial biopsies in asthma. An ultrastructural, quantitative study and correlation with hyperreactivity. Am Rev Respir Dis 1 989; 1 40: 1 7 45-53.
34. Jeffery PK, Godfrey RW, Adelroth E, Nelson F, Rogers A, Johansson SA. Effects of treatment on airway inflammation and thickening of basement membrane reticular collagen in asthma. A quantitative light and electron microscopic study. Am Rev Respir Dis 1 992; 1 45:890-9.
35. Roche WR, Beasley R, Williams JH, Holgate ST. Subepithelial fibrosis in the bronchi of asthmatics. Lancet 1 989; 1 :520-4.
36. Wilson JW, Li X. The measurement of reticular basement membrane and submucosal collagen in the asthmatic airway. Clin Exp Allergy 1 997;27:361 -71 .
37. Pesci A, Foresi A, Bertorelli G, Chetta A, Olivieri D. Histochemical characteristics and degranulation of mast cells in epithelium and lamina propria of bronchial biopsies from asthmatic and normal subjects. Am Rev Respir Dis 1 993; 1 47:684-9.
38. Poston RN, Chanez P, Lacoste JY, Litchfield T, Lee TH, Bousquet J. lmmunohistochemical characterization of the cellular infiltration in asthmatic bronchi. Am Rev Respir Dis 1 992; 1 45:91 8-21 .
39. Azzawi M, Bradley B, Jeffery PK, Frew AJ, Wardlaw AJ, Knowles G, Assoufi B, Collins JV, Durham S, Kay AB. Identification of activated T lymphocytes and eosinophils in bronchial biopsies in stable atopic asthma. Am Rev Respir Dis 1 990; 1 42: 1 407-1 3.
12
General Introduction
40. Mosmann TR, Cherwinski HM, Bond MW, Giedlin MA, Coffman RL. Two types of murine helper T cell clone. Definition according to the profiles of lymphokine activities and secreted proteins. J /mmuno/ 1986; 136:2348-57.
41. Mosmann TR, Sad S. The expanding universe of T cell subsets: Th1, Th2 and more. lmmunol Today 1996;17:138-46.
42. Robinson OS, Durham SR, Kay AB. Cytokines in asthma. Thorax 1993;48:845-53.
43. Robinson OS, Hamid Q, Y ing S, Tsicopoulos A, Barkans J , Bentley AM, Corrigan C, Durham SR, Kay AB. Predominant TH2 like bronchoalveolar T lymphocyte population in atopic asthma. N Engl J Med 1992;326:298-304.
44. Y ing S, Durham SR, Corrigan CJ, Hamid Q, Kay AB. Phenotype of cells expressing mRNA for TH2 type (interleukin 4 and interleukin 5) and TH1 type (interleukin-2 and interferon-gamma) cytokines in bronchoalveolar lavage and bronchial biopsies from atopic asthmatic and normal control subjects. Am J Respir Cell Mo/ Biol 1995;12:477-87.
45. Ricci M. IL-4: a key cytokine in atopy. Clin Exp Allergy 1994;24:801-12. 46. Walker C, Bauer W, Braun RK, Menz G, Braun P, Schwarz F, Hansel TT,
Villiger B. Activated T cells and cytokines in bronchoalveolar lavages from patients with various lung diseases associated with eosinophilia. Am J
Respir Grit Care Med 1994; 150:1038-48. 47. Smith CH, Barker JN, Lee TH. Adhesion molecules in allergic inflammation.
Am Rev Respir Dis 1993; 148:S75-8. 48. Montefort S, Holgate ST, Howarth PH. Leucocyte endothelial adhesion mole
cules and their role in bronchial asthma and allergic rhinitis. Eur Respir J
1993;6: 1044-54. 49. Geha RS. Regulation of lgE synthesis in humans. J Allergy Clin lmmuno/
1992;90: 143-50. 50. Lebman DA, Coffman RL. lnterleukin-4 causes isotype switching to lgE in T
cell stimulated clonal B cell cultures. J Exp Med 1988; 168:853-85. 51. De Monchy JGR, Kaufman HF, De Vries K. lgE gemedieerde allergie voor
inhalatie allergenen. Pharmaceutisch Weekblad 1988;123:249-54. 52. Ohnishi T, Kita H, Weiler D, Sur S, Sedgwick JB, Calhoun WJ, Busse WW,
Abrams JS, Gleich GJ. IL-5 is the predominant eosinophilactive cytokine in the antigen induced pulmonary late phase reaction. Am Rev Respir Dis 1993;147:901-7.
53. Gleich GJ , Adolphson CR, Leiferman KM. The biology of the eosinophilic leucocyte. Annu Rev Med 1993;44:85-101.
54. Kelso A. Th1 and Th2 subsets: paradigms lost ? Immunology Today 1995 ;16 55. Hessel EM, Van Oosterhout AJ , Van Ark I, Van Esch B , Hofman G, Van
Loveren H, Savelkoul HF, Nijkamp FP. Development of airway hyperresponsiveness is dependent of interferon-gamma and independent of eosinophil infiltration. Am J Respir Cell Mo/ Bio/ 1997;16:325-34.
56. Krug N, Madden J, Redington AE, Lackie P, Djukanovic R , Schauer U, Holgate ST, Frew AJ , Howarth PH. T cell cytokine profile evaluated at the single cell level in BAL and blood in allergic asthma. Am J Respir Cell Mo/ Bio/ 1996;14:319-26.
13
Chapter 1
57. Bradding P, Roberts JA, Britten KM, Montefort S, Djukanovic R, Mueller R, Heusser CH, Howarth PH, Holgate ST. lnterleukin-4, -5, and -6 and tumor necrosis factor alpha in normal and asthmatic airways: evidence for the human mast cell as a source of these cytokines. Am J Respir Cell Mo/ Biol 1994; 10:471-80.
58. Kips JC, Tavernier JH, Joos GF, Peleman RA, Pauwels RA. Review. The potential role of tumor necrosis factor-a in asthma. Clin Exp Allergy 1993;23: 247-50.
59. Shah A, Church MK, Holgate ST. Tumour necrosis factor-alpha: a potential mediator of asthma. Clin Exp Allergy 1995;25: 1038-44.
60. Barnes PJ. Cytokines as mediators of chronic asthma. Am J Respir Grit Care Med 1994; 150:S42-9.
61. Tsukagoshi H, Sakamoto T, Xu W, Barnes PJ , Chung KF. Effect of interleukin 1 beta on airway hyperresponsiveness and inflammation in sensitized and nonsensitized Brown-Norway rats. J Allergy Clin /mmuno/ 1994;93:464-9.
62. Thomas PS, Yates DH, Barnes PJ. Tumor necrosis factor alpha increases airway responsiveness and sputum neutrophilia in normal human subjects. Am J Respir Grit Care Med 1995; 152:76-80.
63. Gundel RH, Wegner CD, Letts LG. Busse WW, Holgate ST, editors. Asthma and rhinitis. First ed. Boston: Blackwell Scientific Publications; 1995; Chapter 58, Leucocyte endothelial adhesion. p. 752-63.
64. Kay AB. T lymphocytes and their products in atopic allergy and asthma. Int Arch Allergy Appl lmmunol 1991 ;94:189-93.
65. Gosset P, TillieLeblond I, Janin A, Marquette CH, Gopin MC, Wallaert B, Tonne! AB. Expression of E-selectin, ICAM-1 and VCAM-1 on bronchial biopsies from allergic and nonallergic asthmatic patients. Int Arch Allergy /mmunol 1995; 106:69-77.
66. Montefort S, Gratziou C, Goulding D, Polosa R, Haskard DO, Howarth PH, Holgate ST, Carroll MP. Bronchial biopsy evidence for leukocyte infiltration and upregulation of leukocyte endothelial cell adhesion molecules 6 hours after local allergen challenge of sensitized asthmatic airways. J Clin Invest 1994;93: 1411-21.
67. Fukuda T, Fukushima Y, Numao T, Ando N, Arima M, Nakajima H, Sagara H, Adachi T, Motojima S, Makino S. Role of interleukin-4 and vascular cell adhesion molecule-1 in selective eosinophil migration into the airways in allergic asthma. Am J Respir Cell Mo/ Biol 1996; 14:84-94.
68. Wegner CD, Rothlein R, Gundel RH. Adhesion molecules in the pathogenesis of asthma. Agents Actions Suppl 1991 ;34:529-44.
69. Wegner CD, Gundel RH, Reilly P, Haynes N, Letts LG, Rothlein R. l ntercellular adhesion molecule-1 (ICAM-1) in the pathogenesis of asthma. Science 1990;247:456-9.
70. Barnes PJ, Liew FY. Nitric oxide and asthmatic inflammation. lmmunol Today 1995; 16: 128-30.
71. Hamid Q, Springall DR, RiverosMoreno V, Chanez P, Howarth PR, Bousquet J , Godard P, Holgate S, Polak JM. Induction of nitric oxide synthase in asthma. Lancet 1993;342: 1510-3.
72. Barnes PJ. NO or no NO in asthma ? Thorax 1996;51 :218-20. 73. Lyons CR. The role of nitric oxide in inflammation. Advances in Immunology
1995;60:323-71.
14
General I ntroduction
74. Persson MG, Zetterstrom 0, Agrenius V, lhre E , Gustafsson LE. Single breath nitric oxide measurements in asthmatic patients and smokers. Lancet 1 994;343: 1 46-7.
75. Beckman JS, Koppenol WH. Nitric oxide, superoxide, and peroxynitrite: the good, the bad, and ugly. Am J Physiol 1 996;271 :C1 424-37.
76. Sadeghi Hashjin G, Folkerts G, Henricks PA, Verheyen AK, van der Linde HJ, Van Ark I , Coene A, Nijkamp FP. Peroxynitrite induces airway hyperresponsiveness in guinea pigs in vitro and in vivo. Am J Respir Grit Care Med 1 996; 1 53: 1 697-701 .
77. Taylor Robinson AW, Liew FY, Severn A, Xu D, Mcsorley SJ, Garside P, Padron J, Phillips RS. Regulation of the immune response by nitric oxide differentially produced by T helper type 1 and T helper type 2 cells. Eur J
/mmuno/ 1 994;24:980-4. 78. Ferreira HHA, Medeiros MV, Lima CSP, Flores CA, Sannomiya P, Antunes
E, De Nucci G. Inhibition of eosinophil chemotaxis by chronic blockade of nitric oxide biosynthesis. Eur J Pharmacol 1 996;31 0:201 -7.
79. Beauvais F, Michel L, Dubertret L. The nitric oxide donors, azide and hydroxylamine, inhibit the programmed cell death of cytokine deprived human eosinophils. FEBS Lett 1 995;361 :229-32.
80. Kharitonov SA, Yates D, Robbins RA, LoganSinclair R, Shinebourne EA, Barnes PJ. Increased nitric oxide in exhaled air of asthmatic patients. Lancet 1 994;343: 1 33-5.
81 . Kharitonov SA, Alving K, Barnes PJ. ERS Task Force Report. Exhaled and nasal nitric oxide measurements: recommendations. Eur Respir J
1 997; 1 0: 1 683-93. 82. Alving K, Weitzberg E, Lundberg JM. Increased amount of nitric oxide in
exhaled air of asthmatics. Eur Respir J 1 993;6: 1 368-70. 83. Massaro AF, Gaston B, Kita D, Fanta C, Stamler JS, Drazen JM. Expired
nitric oxide levels during treatment of acute asthma. Am J Respir Grit Care Med 1 995; 1 52:800-3.
84. Kharitonov SA, O'Connor BJ, Evans DJ, Barnes PJ. Allergen induced late asthmatic reactions are associated with elevation of exhaled nitric oxide. Am J Respir Grit Care Med 1 995; 1 51 : 1 894-9.
85. Garnier P, Fajac I , Dessanges JF, Dall'Ava Santucci J, Lockhart A, Dinh Xuan AT. Exhaled nitric oxide during acute changes of airways calibre in asthma. Eur Respir J 1 996;9: 1 1 34-8.
86. Furukawa K, Harrison DG, Saleh D, Shennib H, Chagnon FP, Giaid A. Expression of nitric oxide synthase in the human nasal mucosa. Am J Respir Grit Care Med 1 996; 1 53:847-50.
87. Kimberly B, Nejadnik B, Giraud GD, Holden WE. Nasal contribution to exhaled nitric oxide at rest and during breath holding in humans. Am J Respir Grit Care Med 1 996; 1 53:829-36.
88. Gerlach H, Rossaint R, Pappert D, Knorr M, Falke KJ. Autoinhalation of nitric oxide after endogenous synthesis in nasopharynx [see comments] . Lancet 1 994;343:51 8-9.
89. Hyde RW, Geigel EJ, Olszowka AJ, Krasney JA, Forster II RE, Utell M , Frampton MW. Determination of production of nitric oxide by lower airways of humans theory. J Appl Physiol 1 997;82: 1 290-7.
90. Oosterhoff Y, Timens W, Postma DS. The role of airway inflammation in the pathophysiology of nocturnal asthma. C/in Exp Allergy 1 995;25:91 5-21 .
1 5
Chapter 1
91 . Postma OS, Oosterhoff Y, van Aalderen WM, Kauffman HF, Wempe JB, KoNter GH. I nflammation in nocturnal asthma? Am J Respir Grit Care Med 1994; 150:S83-6.
92. Oosterhoff Y, Keeter GH, de Monchy JGR, Postma DS. Circadian variation in airway responsiveness to metacholine, and AMP in atopic asthmatic subjects. Am Rev Respir Dis 1 993;147:512-7.
93. Wempe JB, Tammeling EP, Postma DS, Auffarth B, Teengs JP, Keeter GH. Effects of budesonide and bambuterol on circadian variation of airway responsiveness and nocturnal symptoms of asthma. J Allergy Clin lmmunol 1992;90:349-57.
94. Weersink EJ, Postma DS. Nocturnal asthma: not a separate disease entity. Respir Med 1994;88:483-91.
95. Martin RJ, Cicutto LC, Smith HR, Ballard RD, Szefler SJ. Airways inflammation in nocturnal asthma. Am Rev Respir Dis 1991; 143:351-7.
96. Mackay TW, Wallace WAH, Howie SEM, Brown PH, Greening AP, Church MK, Douglas NJ. Role of inflammation in nocturnal asthma. Thorax 1994;49:257-62.
97. Kraft M, Beam WR, Wenzel SE, Zamora MR, O'Brien RF, Martin RJ. Blood and bronchoalveolar lavage endothelin1 levels in nocturnal asthma. Am J Respir Grit Care Med 1994; 149:946-52.
98. Jarjour NN, Busse WW, Calhoun WJ . Enhanced production of oxygen radicals in nocturnal asthma. Am Rev Respir Dis 1992; 146:905-11 .
99. Jarjour NN, Busse WW. Cytokines in bronchoalveolar lavage fluid of patients with nocturnal asthma. Am J Respir Grit Care Med 1995; 152: 1 474-7.
1 00. Kharitonov SA, O'Connor BJ, Barnes PJ . Circadian variation in exhaled and nasal nitric oxide in normal and mild asthmatic subjects. Am J Respir Grit Care Med 1997; 155:A825
1 01. Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolar tissue inflammation in asthma. Am J Respir Grit Care Med 1 996; 154: 1505-10.
102. Oosterhoff Y, Kauffman HF, Rutgers B, Zijlstra FJ , Koeter G, Postma DS.
1 6
I nflammatory cell number and mediators in bronchoalveolar lavage fluid and peripheral blood in asthmatic subjects with increased nocturnal airways narrowing. J Allergy Clin lmmunol 1995;96:219-29.
Chapter 2.1
Quantity and morphology of bronchial biopsy specimens taken by forceps of three different sizes
Roel Aleva, Jan Kraan, Mieke Smith, Nick ten Hacken, Dirkje Postma, Wim Timens
Chest 1998; 113:182-185
Abstract
In recent years fiberoptic bronchoscopy has been introduced successfully in the research of bronchial asthma. Bronchial biopsies obtained by this procedure are small and an optimal biopsy technique is necessary to obtain highquality tissue samples, as sufficient length of intact basement membrane and sufficient depth of submucosal tissue are required. We compared size and qualitative aspects of bronchial biopsy specimens from non-asthmatic subjects, obtained by forceps of three different sizes, types F B-19C, FB-21 C and FB-35C (Olympus, Tokyo, Japan).We conclude from this study that the hypothesis that the bigger the biopsy forceps, the larger the biopsy specimen and the better the quality of the tissue does not hold. Bronchial biopsy specimens obtained with forceps type FB-35C and FB21-C were equal in size, but the FB-35C biopsies showed more damage and crush artifacts, whereas biopsy specimens obtained with forceps type FB-21 C had more intact basement membrane, more submucosal depth and well-preserved morphology.
Introduction
Fiberoptic bronchoscopy is at present a routine diagnostic procedure in pulmonary diseases. In recent years this procedure has been introduced in the research of pathophysiological mechanisms of bronchial asthma (1,2). It appears to be a safe procedure, even in patients with bronchial obstructive disease (3). With the forceps generally used, the biopsy specimens have a diameter of approximately 2 mm (4,5). The diagnostic utility of these tissue samples is limited by their small size, which may result in several technical problems. First, there is a low yield of sections per biopsy specimen. Second, the mechanical damage of the biopsy specimen by the forceps used causes difficulties in interpretation of the anatomical structure of the bronchial mucosa and the histopathological changes. Finally, epithelium and epithelial basement membrane are not always present and examination of the submucosa is hampered if there is no recognisable basement membrane (BM). The aim of this study is to compare biopsies of bronchial mucosa taken with three
17
Chapter 2.1
types of biopsy forceps. We compared both the size of the biopsy specimen, the morphologic appearance, and the extent of mechanical damage.
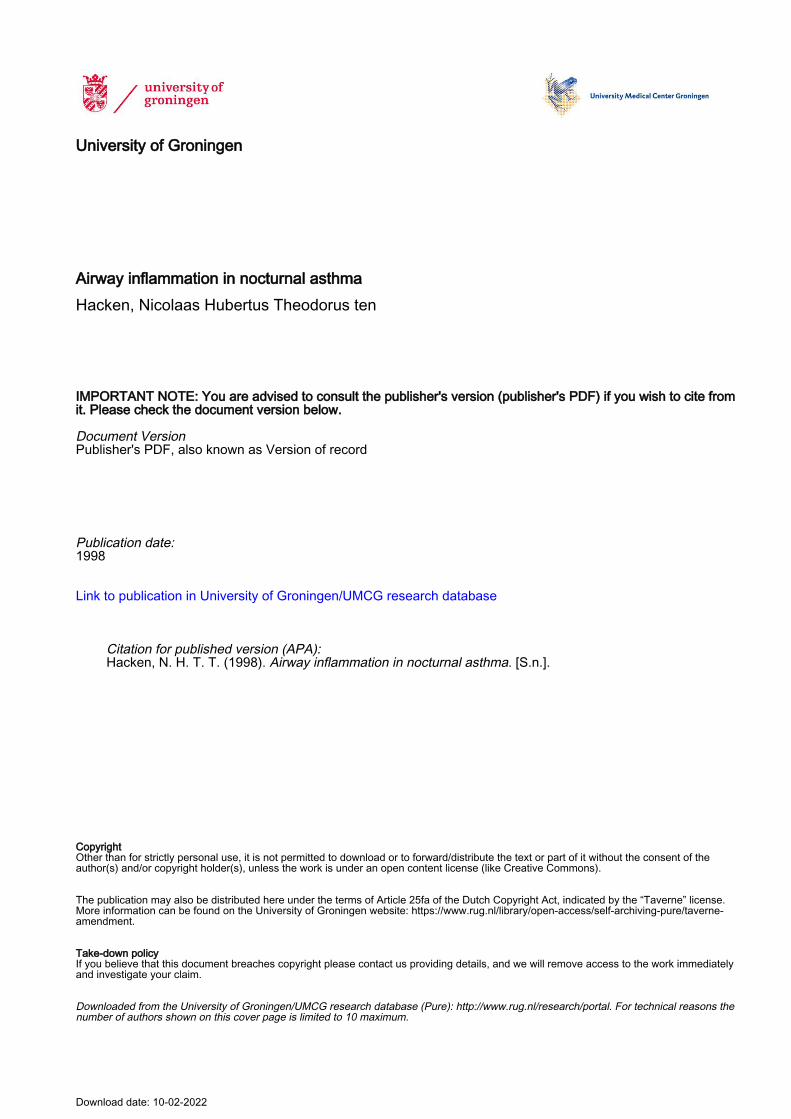
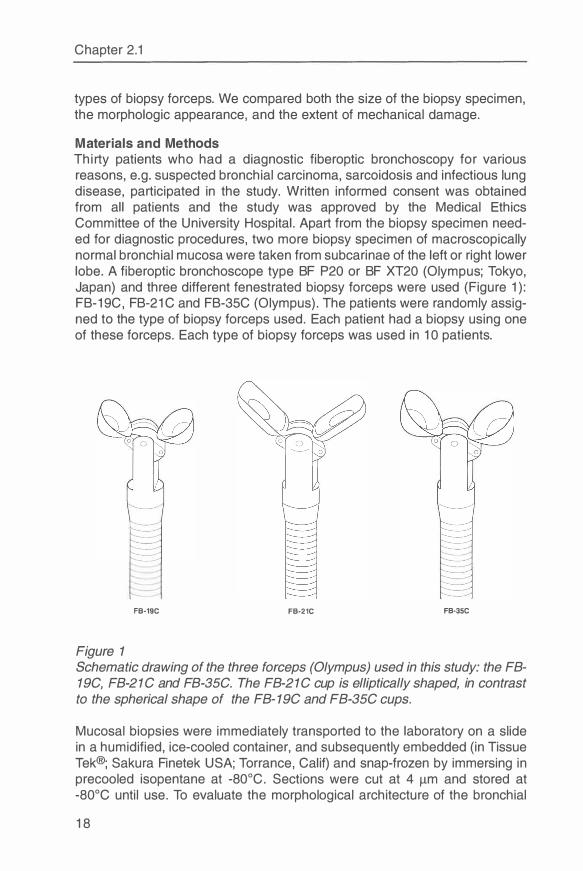
Materials and Methods Thirty patients who had a diagnostic fiberoptic bronchoscopy for various reasons, e.g. suspected bronchial carcinoma, sarcoidosis and infectious lung disease, participated in the study. Written informed consent was obtained from all patients and the study was approved by the Medical Ethics Committee of the University Hospital. Apart from the biopsy specimen needed for diagnostic procedures, two more biopsy specimen of macroscopically normal bronchial mucosa were taken from subcarinae of the left or right lower lobe. A fiberoptic bronchoscope type BF P20 or BF XT20 (Olympus; Tokyo, Japan) and three different fenestrated biopsy forceps were used (Figure 1 ): F B-19C, FB-21 C and FB-35C (Olympus). The patients were randomly assigned to the type of biopsy forceps used. Each patient had a biopsy using one of these forceps. Each type of biopsy forceps was used in 10 patients.
FB-19C FB-21C FB-35C
Figure 1 Schematic drawing of the three forceps (Olympus) used in this study: the FB-19C, FB-21 C and FB-35C. The FB-21C cup is elliptically shaped, in contrast to the spherical shape of the FB- 19C and FB-35C cups.
Mucosa! biopsies were immediately transported to the laboratory on a slide in a humidified, ice-cooled container, and subsequently embedded (in Tissue Tek®; Sakura Finetek USA; Torrance, Calif) and snap-frozen by immersing in precooled isopentane at -80°C. Sections were cut at 4 µm and stored at -80°C until use. To evaluate the morphological architecture of the bronchial
18
Forceps of three different sizes
tissue, the sections were stained in intervals of 50 µm with Mayer's hematoxylin-eosin. The largest section of a series of 20 serial sections was selected for size estimation. Size of the tissue was estimated using an eyepiece graticule (double square lattice with cross-points each 100 µm at 80 x magnification), counting the number of points covering morphologically intact tissue (6). Morphology was assessed by the aspect of the epithelium, the BM, and the intactness of the submucosa. Crush artifacts and disruption of tissue are defined as any disruption of tissue leading to inaccurate determination of cell counts per area. These were considered relevant when causing > 10 % false increase or decrease of tissue area in which cell counting is to be performed (false increase in surface area is observed in case of edema and diffuse disruption, whereas crush artifacts are mainly responsible for false decrease of real biopsy area). The biopsy specimens were assessed in a blinded fashion. The MannWhitney U test was used to compare between the three groups the number of grid crossings covering morphologically intact tissue. The x2 test was used to compare the intactness of the submucosa and the integrity of the epithelium. Statistical analysis was performed with a statistical package (SPSS/PC+ v 4.0.1 ; SPSS/PC Inc. ; Chicago); p values <0.05 were considered statistically significant.
Results Biopsy specimens from 5 patients could not be evaluated. They contained only mucus or blood without tissue (two with forceps type FB19C, two with FB35C); biopsy specimens of another patient could not be used due to technical artifacts (FB19C). Thus bronchial biopsies of 25 patients were available for evaluation.
The biopsy specimens taken with the FB-35C and FB-21 C forceps were equal in size, and the biopsy specimens taken with the FB-19C were the smallest, when measured by the number of grid crossings. The difference in size between the FB-21 C and F B-19C biopsy specimens was significant (p<0.05, table 1 ). In the biopsy specimens taken with the FB-21 C forceps, the epithelium had the best preserved morphology; the biopsy specimens taken with the F B-19C and FB-35C showed damage of the epithelium in a larger proportion of the tissue sections (Figures 2 and 3).
The submucosal layer in the biopsy specimens taken with the FB-35C forceps was relatively superficial (Table 1 ), which means that less than 100 µm of submucosa beneath the BM was available for evaluation. All sections taken with FB-21 C forceps showed submucosa with intact morphological architecture. The depth of the submucosal layer in the biopsy specimens obtained with the forceps FB-21 C was larger than in the sections of the biop-
19
Chapter 2.1
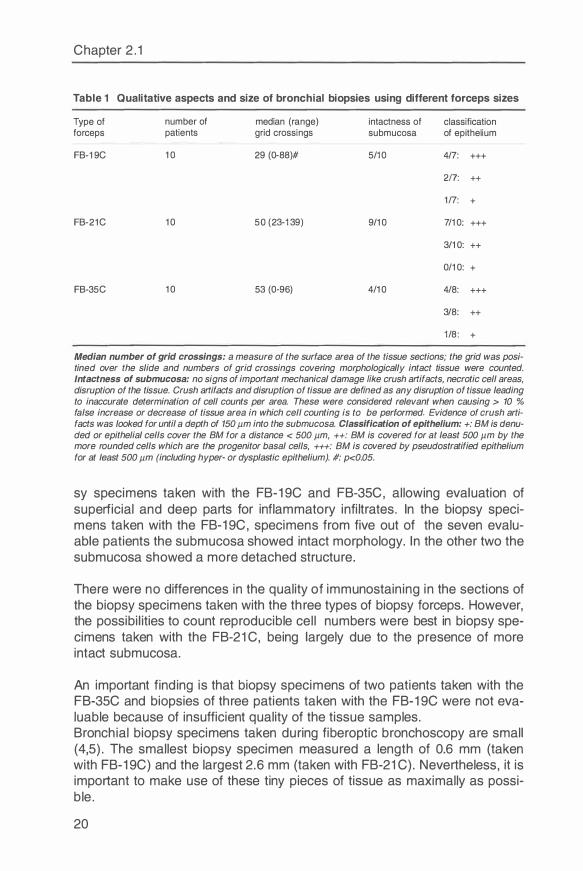
Table 1 Qualitative aspects and size of bronchial biopsies using different forceps sizes
Type of number of median (range) intactness of classification forceps patients grid crossings submucosa of epithelium
FB-1 9C 10 29 (0-88)# 5/10 4/7 : +++
217: ++
1/7 : +
FB-21C 10 50 (23-1 39) 9/10 7/10: +++
3/10: ++
0/10: +
FB-35C 10 53 (0-96) 4/10 4/8: +++
3/8: ++
1 /8: +
Median number of grid crossings: a measure of the surface area of the tissue sections; the grid was positined over the slide and numbers of grid crossings covering morphologically intact tissue were counted. Intactness of submucosa: no signs of important mechanical damage like crush artifacts, necrotic cell areas, disruption of the tissue. Crush artifacts and disruption of tissue are defined as any disruption of tissue leading to inaccurate determination of cell counts per area. These were considered relevant when causing > 10 % false increase or decrease of tissue area in which cell counting is to be performed. Evidence of crush artifacts was looked for until a depth of 150 µm into the submucosa. Classification of epithelium: +: BM is denuded or epithelial cells cover the BM for a distance < 500 µm, ++: BM is covered for at least 500 µm by the more rounded cells which are the progenitor basal cells, +++: BM is covered by pseudostratified epithelium for at least 500 µm (including hyper- or dysplastic epithelium). #: p<0.05.
sy specimens taken with the FB-19C and FB-35C, allowing evaluation of superficial and deep parts for inflammatory infiltrates. In the biopsy specimens taken with the FB-19C, specimens from five out of the seven evaluable patients the submucosa showed intact morphology. In the other two the submucosa showed a more detached structure.
There were no differences in the quality of immunostaining in the sections of the biopsy specimens taken with the three types of biopsy forceps. However, the possibilities to count reproducible cell numbers were best in biopsy specimens taken with the FB-21 C, being largely due to the presence of more intact submucosa.
An important finding is that biopsy specimens of two patients taken with the F B-35C and biopsies of three patients taken with the FB-19C were not evaluable because of insufficient quality of the tissue samples. Bronchial biopsy specimens taken during fiberoptic bronchoscopy are small (4,5). The smallest biopsy specimen measured a length of 0.6 mm (taken with FB-19C) and the largest 2.6 mm (taken with FB-21 C). Nevertheless, it is important to make use of these tiny pieces of tissue as maximally as possible.
20
Forceps of three different sizes
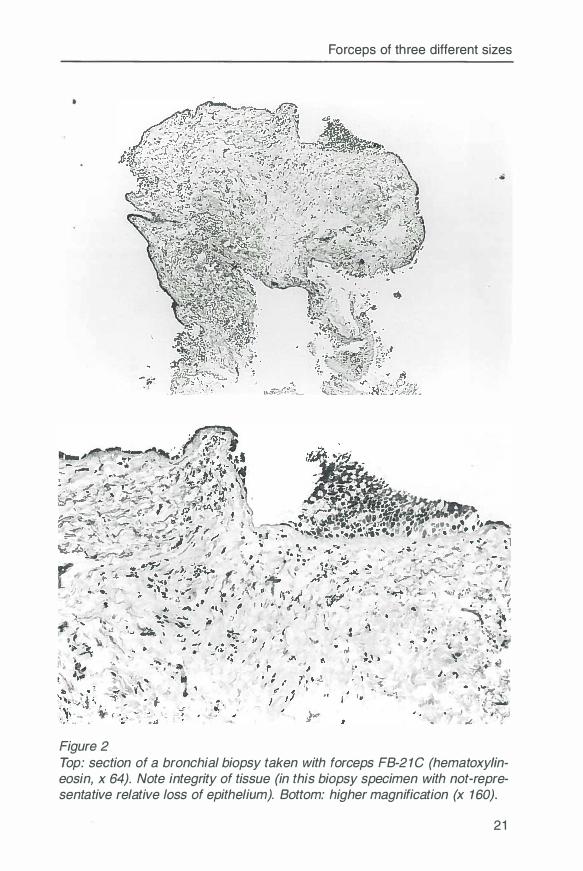
Figure 2 Top: section of a bronchial biopsy taken with forceps FB-21C (hematoxylineosin, x 64). Note integrity of tissue (in this biopsy specimen with not-representative relative loss of epithelium). Bottom: higher magnification (x 160).
21
Chapter 2.1
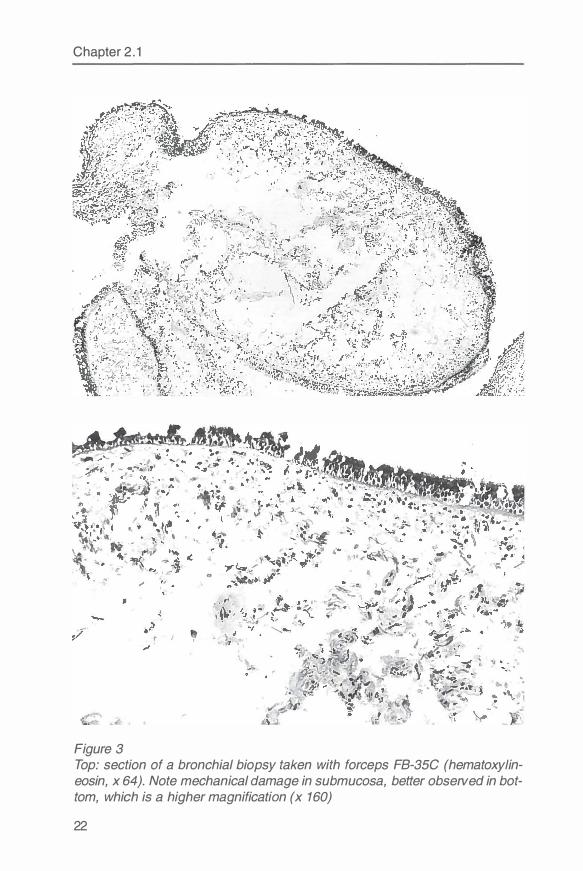
Figure 3 Top: section of a bronchial biopsy taken with forceps FB-35C (hematoxylineosin, x 64). Note mechanical damage in submucosa, better observed in bottom, which is a higher magnification (x 160)
22
Forceps of three different sizes
Discussion Our study shows that the hypothesis that the bigger the biopsy forceps, the larger the biopsy specimen and the better the quality of the tissue, holds only partially. The FB-19C forceps is the smallest and so are the biopsy specimens taken with it . The jaws of the forceps FB-35C were much larger than the jaws of the other forceps types. It was, however, often difficult to place the FB-35C in the right position on the subcarina of the basal segments. When the forceps were closed the jaws probably made a scraping movement. This may be the reason that the tissue sections taken with the FB-35C were not the largest, and showed crush artifacts in four of the eight patients. Tissue sections of the biopsy specimens taken with the FB-21 C were more oval-formed given its ell iptically formed jaws. The oval form of the tissue biopsy specimens had the advantage that morphology of epithelium and submucosa were more intact at the long side, compared with the more rounded form of the tissue sections taken with forceps FB-19C or FB-35C.
Earlier studies evaluated the forceps size in transbronchial biopsies (7,8). One study showed that larger forceps did increase the number of alveoli and the diagnostic yield (8). The largest biopsy forceps used in that study (FB-20C) is comparable with the FB-21 C that we used. The other study showed that transbronchial biopsy specimens taken with smaller forceps (FB-19C and FB-20C) give a greater diagnostic yield than biopsy specimens taken with the greater FB-15C alligator forceps.
To our knowledge our study is the first to compare different biopsy forceps sizes with respect to the yield and quality of bronchial tissue. This is an important issue because at one hand the possibility to study pathology of pulmonary disease in large detail has been increased greatly by the availability of advanced (immuno-)histopathology. However, the possibility to perform these techniques is limited by the size and quality of tissue samples that can be obtained.
We conclude that bronchial biopsy specimens taken with forceps FB-21 C are similar in size to biopsy specimens taken with the FB-35C, but show a better quality and morphology. It is important that larger and more detailed studies will be conducted to confirm these results and to establish the method of taking biopsies with the best yield for studying the pathology of airway inflammation.
References 1. Lundgren R. Scanning electron microscopic studies of bronchial mucosa
before and during treatment with beclomethasonedipropionate inhalations. Scan J Respir Dis 1977; 101 : 179S-87S.
2. Beasley R, Roche WR, Roberts JA, Holgate ST. Cellular events in the bronchi in mild asthma and after bronchial provocation. Am Rev Respir Dis 1 989; 139:806-17.
23
3. Djukanovic R, Wilson JW, Lai CKW, Holgate ST, Howarth PH. The safety aspects of fiberoptic bronchoscopy, bronchoalveolar lavage, and endobronchial biopsy in asthma. Am Rev Respir Dis 1991 ; 143:772-7.
4. Jeffery PK, Wardlaw AJ, Nelson FC, Collins JV, Kay AB. Bronchial biopsies in asthma. An ultrastructural, quantitative study and correlation with hyperreactivity. Am Rev Respir Dis 1989; 140: 17 45-53.
5. Azzawi M, Bradley BL, Jeffery PK, et al. I dentification of activated T lymphocytes and eosinophils in bronchial biopsies in stable atopic asthma. Am Rev Respir Dis 1990;142: 1407-13.
6. Baak JPA, Oort J. Practical morphometry: In: Baak J PA, Oort J. A manuel of morphometry in diagnostic pathology pp. 159-81. Springe�-Verlag Berlin 1983.
7. Smith LS, Seaquist M, Schillaci RF. Comparison of forceps used for transbronchial lung biopsy: bigger may not be better. Chest 1985;87:57 4-6.
8. Laube DI , Johnson JE, Wiener D, Anders GT, Blanton HM, Hayes JA. The effect of forceps size on the adequacy of specimens obtained by transbronchial biopsy. Am Rev Respir Dis 1993; 148:1411-3.
24
Chapter 2.2
Differences in plastic-embedded and snap-frozen sections for CD3, CD4 and CDS immunostaining of bronchial biopsy specimens
Nick ten Hacken, Roel Aleva, Bea Rutgers, Jan Kraan, Harry van Goor, Dirkje Postma, Wim Timens
Modern Pathology 1 997; 1 0: 1 043-1 046
Abstract Today, the quantification of inflammatory cells in human airway biopsies might be facilitated by better morphologic resolution provided by special resin (plastic-)-embedding techniques. The present study compares the numbers of CD3-, CD4- and CDS-positive cells in glycolmethacrylate-embedded versus snap-frozen biopsy specimens of normal bronchial mucosa in 1 0 patients with various pulmonary diseases. In general, larger numbers of CD3-,CD4-and CDS-positive cells were counted in snap-frozen specimens than in plastic-embedded ones. Loss of antigenic properties during storage of plasticembedded tissue (blocks) might have contributed to the weak correlation between both methods. An additional study showed that the number of CD3-, CD4- and CDS-positive cells decreased significantly within a few months after embedding in glycolmethacrylate. Therefore, we recommend processing glycolmethacrylate-embedded specimens as soon as possible. For standard evaluation of established inflammatory cell parameters such as CD3, CD4, CDS, and EG2, frozen tissue is preferable because of the ease of the method and its reliable cell counting. Because glycolmethacrylate-embedded tissue shows superior morphologic resolution, under strict rules this method seems attractive for the study, in particular, of cell-cell and cell-matrix relationships.
Introduction The quantitative examination of leucocyte antigens in biopsy specimens obtained from human airways is an essential tool for studying the pathophysiology of asthma. It is complicated by several morphologic changes resulting from mechanical, physical, and chemical influences linked with the biopsy procedure and tissue processing. Snap-freezing of biopsy specimens does not lead to chemical alterations of membrane-bound glycoproteins, so it offers optimal conditions for immunohistochemical investigation. Strong temperature shifts, however, and sectioning of snap-frozen specimens can result
25

Chapter 2.2
in volume changes and artifacts, thereby introducing errors in cell counting. Special resin (plastic)-embedding techniques are attractive in combining optimal morphologic resolution with supposedly a small loss of antigenicity (1-4). In addition, cel l counting and semi-quantitative scoring have been succcesfully performed in a variety of studies that used plastic-embedded sections (5-6). Embedding in plastic, however, might result in ongoing polymerization, which, in theory, decreased the availability of antigenic determinants.
Because of the immunomodulating role of T lymphocytes in asthma, we were interested in a reliable quantification method for these cel ls in bronchial biopsies. To date, there is no literature available that discusses the specific advantages and disadvantages of the above mentioned methods of tissue treatment. The first part of the present study compares the numbers of CD3-, CD4- and CDS-positive cel ls in glycolmethacrylate (GMA)-embedded versus snap-frozen biopsy specimens. The second part of this study addresses the preseNation of antigenic properties during storage of specimens in GMA.
Materials and Methods
Comparative study Bronchial tissue was obtained from 1 O patients undergoing a diagnostic bronchoscopy for various reasons e.g., suspected bronchial carcinoma, sarcoidosis, and infectious lung disease. The study was approved by the Medical Ethics Committee of the University Hospital of Groningen, and all of patients gave their written informed consent. Two additional biopsy specimens of normal mucosa were taken from the subcarinae of the left or right lower lobe using a fenestrated forceps (FB-21 C; Olympus, Tokyo, Japan). The first biopsy was placed in Tissue-Tek (Sakura, Tokyo, Japan), snap-frozen by immersion in isopentane (-80°C) and stored at -80°C. F rozen sections 4 µm thick were cut and stored at -20°c until use. The second specimen was fixed for 30 min at -40°C in 2% paraformaldehyde in phosphate-buffered saline (PBS), washed overnight in PBS containing 6% sucrose, dehydrated in 100% aceton for 15 min at -40°C, and then infiltrated in Technovit 8100 solution A (Kulzer, Wernheim, Germany) for 3 hours at -40°C. After infiltration, the tissue was embedded in a 30 to1 mixture of Technovit 8100 solution A and solution B, respectively. Polymerization was accomplished overnight on crushed ice at -40°C. Paraffin was poured around the block holders to prevent inhibition of the polymerization by oxygen. Sections 2 µm thick were cut on a Reichert-Jung (Leica, Rijswijk, The Netherlands) supercut plasti� microtome using tungsten carbide knives, and stored at -20°C until use. Before they were immunostained, the plastic sections were dried for 1 hour at 37°C and pre-treated with 0.005% trypsin in 0.1 M Tris buffer (pH 7.8 with 0.1 % CaCl2) for 5-30 minutes at 37°C. lmmunostaining for CD3, CD4 and CD8 was performed with Leu-4, Leu-3a (Becton-Dickinson, San Jose, CA) and T8 Moabs (our laboratory), using an immunoperoxidase streptavidin-biotin method
26

Plastic-embedded versus snap-frozen sections
(DAKO, Glostrup, Denmark) with hematoxylin as counterstain. To evaluate the bronchial architecture, additional sections were stained with Mayer's hematoxylin and eosin. Sections were examined using a lightmicroscope at a magnification of 400 x. Positive cells were counted using an eyepiece graticule (cross-points each 25 µm at a 400 x magnification), in representative sections in a 100 µm deep area below the intact basement membrane (BM), with a cumulative length of 1000 µm. Cell counts were expressed as the number of positive cells per mm of BM. Selection of representative sections was based on the integrity of bronchial tissue, the thickness of submucosa (> 100 µm) and the absence of smooth muscle cells or glandular epithelium. Statistical analysis was performed with SPSS/PC+ v. 5.0 statistical package (SPSS, Chicago, IL). Correlations between the two methods were calculated using Spearman's Rank Test. P values less than 0.05 were considered statistically significant. Agreements between the two methods are graphically presented (Figure 2) according the method of Bland and Altman (7).
Antigen preservation study During the study, it seemed that plastic sections stored for a longer period of time were characterized by lower cell counts. Therefore, plastic-embedded and frozen sections of 5 patients were immunostained again after 5 to 15 months. The plastic-embedded sections showed lower cell counts, whereas the frozen sections showed cell counts similar to the original cell counts. To study in a more systematical way the time-dependent loss of antigenic properties, we used plastic blocks of embedded biopsies of another study (unpublished data). From this study we selected specimens from five patients with and five without respiratory symptoms and hyperresponsiveness. The techniques of taking, storing, processing and examining the specimens were the same as described above. All tasks were performed by the same investigators. The plastic blocks, however, were not stored for longer than 1 month, and additional sections were cut each month.
Results
Comparative study Qualitative examination showed that the integrity of bronchial tissue was better preserved in plastic-embedded than in snap-frozen specimens (Figure 1 ). When large cell numbers were present, positive cells could easily be distinguished from each other in plastic sections, but not in frozen ones. On the other hand, positive cells in plastic did not stain as intensively as did frozen sections.
Quantitative examination revealed larger numbers of CD3-, CD4-, and CDSpositive cells in frozen tissue sections. The mean (SEM) CD3-, CD4- and CDS-positive cell numbers in fresh frozen sections were 70.6 (11.2), 48.5 (13.7) and 46.8 (9.0) cells per mm BM, respectively. The mean (SEM) CD3-,
27
Chapter 2.2
• I
t,, •
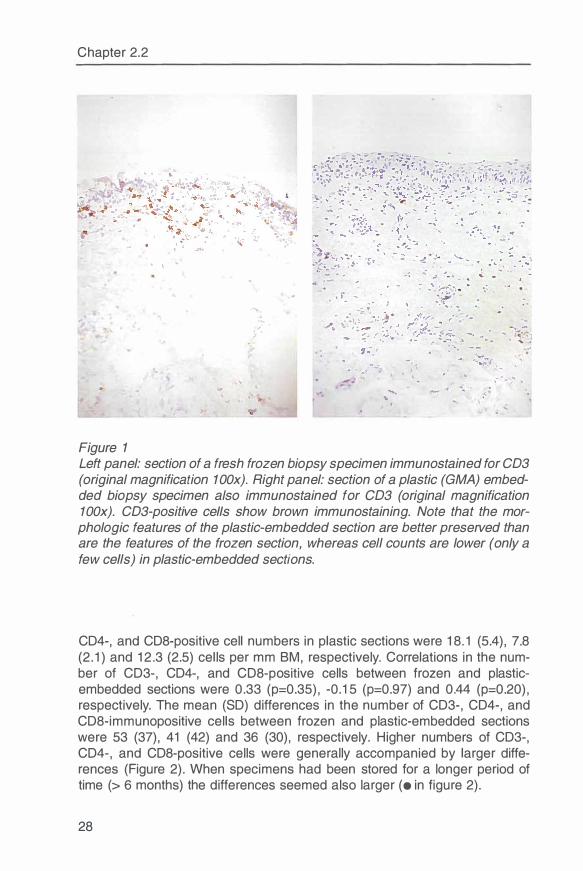
Figure 1
...... .. ,· .
i .
...... ,.
Left panel: section of a fresh frozen biopsy specimen immunostained for CD3 (original magnification 1 00x). Right panel: section of a plastic (GMA) embedded biopsy specimen also immunostained for CD3 (original magnification 1 00x). CD3-positive cells show brown immunostaining. Note that the morphologic features of the plastic-embedded section are better preserved than are the features of the frozen section, whereas cell counts are lower (only a few cells) in plastic-embedded sections.
CD4-, and CDS-positive cell numbers in plastic sections were 18.1 (5.4), 7.8 (2.1) and 12.3 (2.5) cells per mm BM, respectively. Correlations in the number of CD3-, CD4-, and CDS-positive cells between frozen and plasticembedded sections were 0.33 (p=0.35), -0.15 (p=0.97) and 0.44 (p=0.20), respectively. The mean (SD) differences in the number of CD3-, CD4-, and CD8-immunopositive cells between frozen and plastic-embedded sections were 53 (37), 41 (42) and 36 (30), respectively. Higher numbers of CD3-, CD4-, and CDS-positive cells were generally accompanied by larger differences (Figure 2). When specimens had been stored for a longer period of time (> 6 months) the differences seemed also larger (• in figure 2).
28
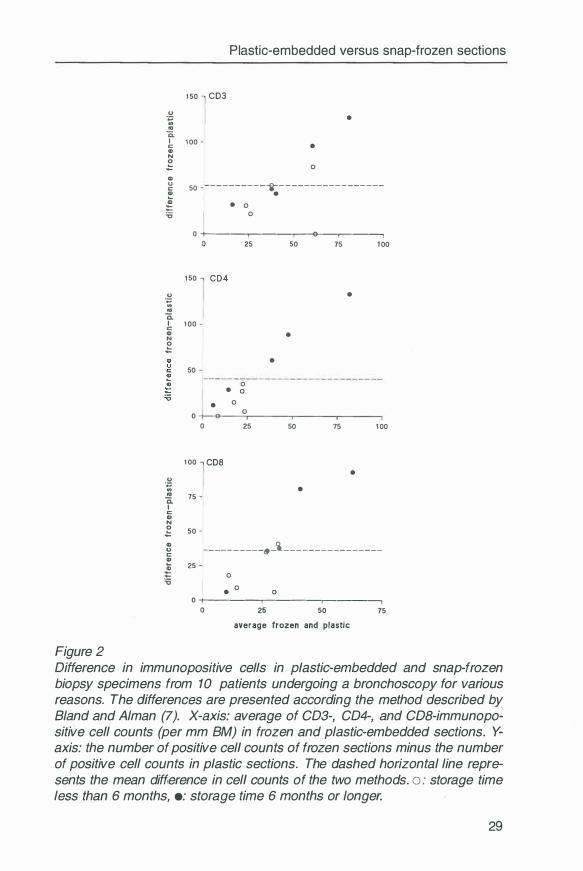
Figure 2
Plastic-embedded versus snap-frozen sections
u
-� ca
1 50 CD3
1:: 1 00 CD N
,g CD
•
• 0
g 50 ---------"j-- - ---------------
� . � • 0 'o 0
0 +-----.-----.------e--.-------,
u
·�
ci.
1 50 CD4
I 1 00 CD
,g 50
25
0 • 0
u -� ca
ci. 1:: G> N
0
1 00
75
,g 50
• 0 0
0 25
CD8
50 75 1 00
•
•
•
50 75 1 00
• •
CD u C
---------�-i _______________ _ � 25
0
• 0
0
0 +----.-------�--�
0 25 50 75
average frozen and plastic
Difference in immunopositive cells in plastic-embedded and snap-frozen biopsy specimens from 1 O patients undergoing a bronchoscopy for various reasons. The differences are presented according the method described by Bland and Alman (7). X-axis: average of CD3-, CD4-, and CDB-immunopositive cell counts (per mm BM) in frozen and plastic-embedded sections. Yaxis: the number of positive cell counts of frozen sections minus the number of positive cell counts in plastic sections. The dashed horizontal line represents the mean difference in cell counts of the two methods. o : storage time less than 6 months, •: storage time 6 months or longer.
29
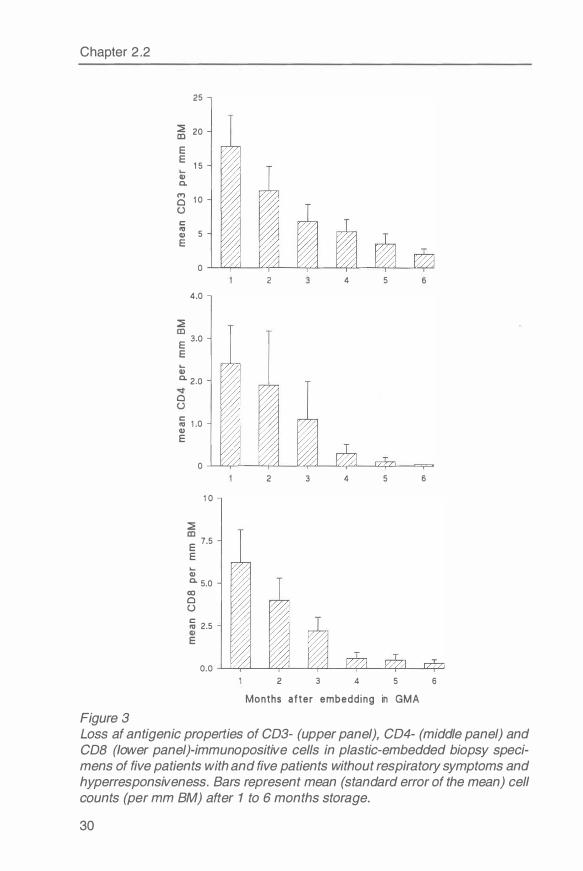
Chapter 2.2
25
� 20
E E
1 5 Cl> a.
(T') 1 0 0
C 11:1 5 Cl> E
0 2 4 5
4.0
� E 3.0
E ... Cl> a. 2.0
0
� 1 .0 Cl> E
0 2 3 4 5
1 0
� E
7.5
E
Q) a. 5.0
00 0
{.)
� 2.5
E
0.0 2 3 4 5
Months af ter embedd ing in GMA
Figure 3
6
6
6
Loss af antigenic properties of CD3- (upper panel), CD4- (middle panel) and COB (lower panel)-immunopositive cells in plastic-embedded biopsy specimens of five patients with and five patients without respiratory symptoms and hyperresponsiveness. Bars represent mean (standard error of the mean) cell counts (per mm BM) after 1 to 6 months storage.
30

Plastic-embedded versus snap-frozen sections
Antigen preservation study Figure 3 illustrates month to month loss of antigenic properties for CD3, CD4 and CD8 monoclonal antibodies during storage of plastic-embedded specimens.
Discussion The present study shows that cell counts in plastic-embedded and snap-frozen specimens give rise to rather large differences in the numbers of CD3-, CD4-, and CDS-positive cells. Several reasons might explain the lower cell numbers found in plastic sections. First, the thin layer (5 nm) of trypsin treated plastic sections (2 µm) contains approximately 30% fewer cells and cellcaps than did the frozen sections (4 µm) because of the Holmes effect (8). Second, cells that were potentially immunopositive contained in these trypsin-treated plastic sections a lower number of antigenic determinants (per cell) than did frozen sections. This truncation effect (8) underlies the observation that immunopositive cells in plastic sections more frequently are below the level of visual detection. Third, trypsin treatment might not remove all cross links and therefore might not uncover all antigenic determinants. We found, according to the principles of Bland and Altman (7), that the absolute difference in cell numbers between the snap-frozen and plastic-embedded technique is not constant but rather increases with higher cell counts, a phenomenon that might partially be explained by the Holmes effect, and not by truncation.
While looking for other explanations for the large differences in cell counts, we discovered that a longer period of storage (>6 months) was accompanied by larger differences in cell counts. An additional study was undertaken to investigate the time-dependent loss of antigenic properties in plastic-embedded specimens. The second study showed an important loss of antigenicity for all three cell types, occurring even within a few months. In theory, this loss is the result of ongoing polymerization and cross-linking of antigenic determinants. This finding stresses the importance of immediate processing and staining of specimens after embedding in GMA. This might often conflict, however, with the principle of many studies, which is to stain all of their specimens at one point in time, to avoid variations caused by intrinsic differences in the staining method.
We conclude that quantitative evaluation of bronchial biopsies for CD3-, CD4-, and CDS-positive cells in plastic have a poor agreement with counts of positive cells in frozen tissue. The loss of antigenic properties during storage of plastic blocks might have played an important role in this finding, and therefore, we recommend quick processing and immunostaining of specimens. Because plastic leaves the normal bronchial architecture intact (Figure 1 ), this method is very attractive for qualitative studies of cell-cell and cell-matrix
31
Chapter 2.2
relationships. Nevertheless, it should be used with caution in quantitative studies, because antigenic expression often might be below the level of visual detection.
References 1. Van Goar H, Harms G, Gerrits PO, Kroese FG, Poppema S, Grand J.
lmmunohistochemical antigen demonstration in plastic-embedded lymphoid tissue. J Histochem Cytochem 1988;36: 115-20.
2. Beckstead J H, Sternberg PE, Mcever RP, Shuman MA, Bainton DF. lmmunohistochemical localization of membrane and a-granule proteins in human megakaryocytes: application to plastic-embedded bone marrow specimens. Blood 1986;67:285-93.
3. Casey TT, Cousar JB, Collins RD. A simplified plastic embedding and immunohistologic technique for immunophenotypic analysis of human haematopoietic and lymphoid tissues. Am J Patho/ 1988;131 : 183-99.
4. Bradding P, Roberts JA, Britten KM, Montefort S, Djukanovic R, Mueller R, Heusser CH, Howarth PH, Holgate ST. lnterleukin-4, -5, and -6 and tumor necrosis factor-alpha in normal and asthmatic airways: evidence for the human mast cell as a source of these cytokines. Am J Resp Cell Mo/ Biol 1992; 10:471-80.
5. Van Goar H, van der Horst MLC, Fidler V, Grand J. Glomerular macrophage modulation affects mesangial expansion in the rat after renal ablation. Laboratory Investigation 1992;66:564-71.
6. Brouwer L, Huitema MG, Mulder AHL, Heerenga P, van Goar H, Cohen Tervaert JW, Weening JJ, Kallenberg CAG. Neutrophil activation in vitro and in vivo in Wegener's granulomatosis. Kidney Int 1994;45: 1120-31.
7. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307-10.
8. Weibel ER. Stereologica/ methods. San Francisco: Academic Press; 1980:128-9.
32

Chapter 2.3
Submucosa 1 .0 x 0.1 mm in size is sufficient to count inflammatory cell numbers in human airway biopsy specimens
Nick ten Hacken, Roel Aleva, Ytske Oosterhoff, Mieke Smith, Jan Kraan, Dirkje Postma, Wim Timens
In press (Modern Pathology)
Abstract
Counting of inflammatory cells in human airway biopsy specimens is difficult because immunopositive cells are present in varying density in lung tissue. The goal of our study was to assess the minimum amount of tissue that is necessary for the counting of constant cell numbers. In bronchial biopsy specimens from 5 healthy controls and 5 patients with asthma, we evaluated 20 successive areas of submucosa 0.1 x 0.1 mm in size. We recorded positive and negative changes of more than 10% in the counted numbers of CD4-, CDB-, and EG2-positive cells. We demonstrated that tissue 1.0 x 0.1 mm in size, along 1-mm basement membrane, is sufficient to obtain constant cell numbers.
Introduction
The study of inflammatory cells in biopsy specimens from human airways has become very important in understanding the pathophysiology of asthma (1-2). Most reports present their data in quantitative cell numbers, but there is no standard method of quantifying and expressing results (3). Only recently, did the European Respiratory Society begin to standardize the pathologic methods of assessing airway inflammation (personal communication, Dr. M. Saetta, Padova, Italy). One of the problems is that immunopositive cells are present in varying density within a biopsy specimen. This problem is even more pronounced in fresh frozen biopsy specimen, with relatively less preserved morphologic features. It has been suggested that counting subsequent areas until the mean cell count remains constant might be used to obtain reliable results (4). Because this method is very labor intensive, we tried to assess the optimal area of cell counting necessary to obtain constant cell numbers per unit of tissue.
33
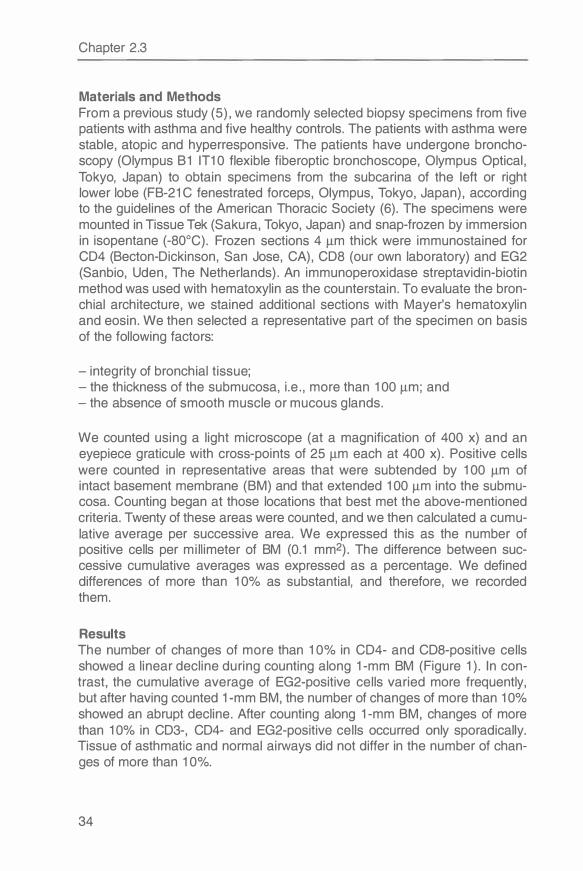
Chapter 2.3
Materials and Methods From a previous study (5), we randomly selected biopsy specimens from five patients with asthma and five healthy controls. The patients with asthma were stable, atopic and hyperresponsive. The patients have undergone bronchoscopy (Olympus B1 IT10 flexible fiberoptic bronchoscope, Olympus Optical, Tokyo, Japan) to obtain specimens from the subcarina of the left or right lower lobe (FB-21 C fenestrated forceps, Olympus, Tokyo, Japan), according to the guidelines of the American Thoracic Society (6). The specimens were mounted in Tissue Tek (Sakura, Tokyo, Japan) and snap-frozen by immersion in isopentane (-80°C). Frozen sections 4 µm thick were immunostained for CD4 (Becton-Dickinson, San Jose, CA), CD8 (our own laboratory) and EG2 (Sanbio, Uden, The Netherlands). An immunoperoxidase streptavidin-biotin method was used with hematoxylin as the counterstain. To evaluate the bronchial architecture, we stained additional sections with Mayer's hematoxylin and eosin. We then selected a representative part of the specimen on basis of the following factors:
- integrity of bronchial tissue; - the thickness of the submucosa, i.e., more than 100 µm; and - the absence of smooth muscle or mucous glands.
We counted using a light microscope (at a magnification of 400 x) and an eyepiece graticule with cross-points of 25 µm each at 400 x). Positive cells were counted in representative areas that were subtended by 100 µm of intact basement membrane (BM) and that extended 100 µm into the submucosa. Counting began at those locations that best met the above-mentioned criteria. Twenty of these areas were counted, and we then calculated a cumulative average per successive area. We expressed this as the number of positive cells per millimeter of BM (0.1 mm2). The difference between successive cumulative averages was expressed as a percentage. We defined differences of more than 10% as substantial, and therefore, we recorded them.
Results The number of changes of more than 10% in CD4- and CDS-positive cells showed a linear decline during counting along 1-mm BM (Figure 1 ). In contrast, the cumulative average of EG2-positive cells varied more frequently, but after having counted 1-mm BM, the number of changes of more than 10% showed an abrupt decline. After counting along 1-mm BM, changes of more than 10% in CD3-, CD4- and EG2-positive cells occurred only sporadically. Tissue of asthmatic and normal airways did not differ in the number of changes of more than 10%.
34
Figure 1
1 0
8 A en
:g, 6 C: CV .r. 0
0 4 ... Q)
E 2
::, C:
A en
1 0
8
:g, 6 C: CV
.r. 0
0 4 ... Q)
E 2 ::, C:
A en
1 0
8
:g, 6 C: CV
.r. 0
0 4
Q) E 2
::, C:
0.0 0.5
0.0 0.5
0.0 0.5
1 .0
1 .0
1 .0
mm BM
Optimum area of cell counting
1 .5 2.0
1 .5 2.0
1 .5 2.0
Changes of more than 10% in the number of CD4-, COB- and EG2-positive cells after counting 20 successive 0. 1 x 0. 1 -mm areas of submucosa in biopsy specimens from 5 healthy controls and 5 patients with asthma.
35
Chapter 2.3
Discussion After counting immunopositive cells along 1-mm of BM in 10 successive areas 0.1 x 0.1 mm in size, changes in cell number of more than 10% occurred only sporadically, indicating constant cell numbers. This might not apply, however, when cell counts are low, because the sporadic presence of even one cell might have a substantial effect on cell numbers in that case (as can be seen for EG2 staining). Moreover, we examined biopsy specimens from stable asthmatics and healthy controls, that showed relatively little inflammation of the bronchial submucosa.
Figures 1 shows that after counting cells along 1-mm BM, changes in cell number of more than 10% still occurred regularly. Theoretically, this variation might be caused by any of the following factors:
- the disruption or compression of the tissue, resulting in volume changes; - the presence of smooth muscle, mucous glands and distended vessels; - inhomogeneous or aspecific staining of the tissue; or - the irregular distribution of immunopositive cells.
After obtaining our results, we re-examined those specimens that showed a change in cell number of more than 10% after counting 1-mm BM. We found that volume artifacts and the presence of smooth muscle and glands were responsible for these rather large variations. Furthermore, re-examination made clear that local accumulations of inflammatory cells in the submucosa were present in our asthmatic patients. These cell clusters, however, had no important effect on cell numbers after the cumulative counting of 1 O successive 0.1 x 0.1-mm areas.
On the basis of our analysis, we conclude that the cumulative counting of 10 0.1 x 0.1-mm areas along intact 1-mm BM is sufficient to obtain constant cell numbers (per area), provided that a proper selection of a representative part of the biopsy has been made. The optimum amount depends on many factors, and should be established before counting large series of sections.
Acknowledgment The authors thank Dr. Ewoud Dubois for his correction of their English grammar.
References 1 . Holgate ST, Wilson JR, Howard PH. New insights into airway inflammation
by endobronchial biopsy. Am Rev Respir Dis 1 992; 1 45(Suppl) :S2-S6. 2 . Holgate ST. Asthma: past, present and future. Eur Respir J 1 993; 1 0: 1 507-
20. 3. Haahtela T, Laitinen A. Laitinen LA. Using biopsies in the monitoring of in
flammation in asthmatic patients. Allergy 1 993;48:65-9.
36
Optimum area of cell counting
4. Weibel ER. Sampling of tissue. In : Stereological methods, first ed Vol 1. Weibel ER. London, Academic Press, 1979;63-100.
5. Oosterhoff Y, Hoogsteden HC, Rutgers B, Kauffman HF, Postma OS. Lymphocyte and macrophage activation in bronchoalveolar lavage fluid in nocturnal asthma. Am J Respir Grit Care Med 1995; 151 : 75-81.
6. NHLBI Workshop summaries. Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis 1985; 132: 180-82.
37

Chapter 2.4
Semi-quantitative and quantitative scoring are complementary in the determination of immunostained cells in human airway biopsies
Nick ten Hacken, Roel Aleva, Ytske Oosterhoff, Mieke Smith, Jan Kraan, Dirkje Postma, Wim Timens
Submitted
Abstract The study of inflammatory cells in human airway biopsies has become very important in our understanding of asthmatic airway disease. Density of inflammatory cells in airway biopsies can be determined by quantitative or semi-quantitative methods. The aim of this study was to determine whether the results of these two methods are corresponding. Moreover, we tried to determine which method discriminates best between biopsies of asthmatic and healthy subjects. Fresh frozen airway biopsies of 7 asthmatic and 7 healthy subjects were immunostained for CD3, CD4, COB, CD25 and EG2 antigen. Density of inflammatory cells was examined in a quantitative and semiquantitative way. This study demonstrated that both methods were correlating in the density of CD4-, CDS-, and EG2- immunopostive cells (rho 0.73, 0.73, 0.85 respectively). The quantitative method showed a higher density of CDS- and CD25-positive cells in biopsies of asthmatic subjects as compared to healthy subjects (p<0.05), whereas the semi-quantitative method showed a relatively higher density of CD3- and CD4-positive cells. We conclude that, dependent on the cell antigen to be counted, the two methods may correspond in estimating the density of immunostained cells, but there are also important differences. The semi-quantitative method enables inclusion of deeper and larger parts of the biopsy, and seems to be more useful when high cell numbers are present. In addition, an advantage of this method is that biopsies of lower morphological quality do not have to be discarded. The quantitative method as generally used includes only the superficial layers and is restricted to a small part of the biopsy. This method seems to be more useful when low cell numbers are present. Depending on the aim of a study a choice can be made for one or both methods of cell counting.
Introduction The study of inflammatory cells in human airway biopsies has become very important in our understanding of asthmatic airway disease (1-2). Recently
39

Chapter 2.4
the European Respiratory Society (ERS) has started a Task Force to standardize the histopathological methods of assessing airways inflammation in bronchial biopsies of asthma and COPD patients (personal communication Dr. Marina Saetta, Padova, Italy). One of the questions to be solved is how to determine the density of inflammatory cells in sections of bronchial biopsies (3). The two ways to obtain information on cell density, with quantitative or semi-quantitative methods, are both complicated by several factors. Disruption or compression of the bronchial tissue during biopsy and further processing may lead to volume-changes and thus counting errors. The presence of smooth muscle, glands and vessels may contribute to an underestimation of inflammatory cells. Moreover, non-specific and inhomogeneous staining patterns may result in false high or low cell counts. Finally, a high density of immunostained cells makes that individual cells are sometimes difficult to discern. We feel that the choice to evaluate inflammatory cells in bronchial biopsies either quantitatively or semi-quantitatively, should take into account the specific advantages and disadvantages of the two methods in relation to the above described factors.
Quantitative examination of inflammatory cells is usually performed in a small part of the biopsy, generally the superficial layers of the submucosa (4-8). Selection of this part is based on the integrity of the tissue and the absence of smooth muscle and glandular structures. Sometimes it is very difficult to find an area in the bronchial submucosa that complies with all these qualifications, and than selection can be biased. Thus, the quantitative way of determining inflammatory cell density has the risk of insufficient selection of a representative part of the biopsy. On the other hand, the quantitative method has the advantage that detection of (small) differences in cell numbers is possible in a wide range, not being dependent on attribution to categories.
Semi-quantitative examination of inflammatory cells is performed in larger parts of the biopsy, also taking the deeper layers of the submucosa into account. This method is not limited by restrictions with respect to intactness of surface area or presence of smooth muscle, glands etc. Semi-quantitative scoring leads to ranking of inflammatory cell density into categories. Small differences in cell numbers especially with low cell density will easily fall into one category, and often will not be detected.
In the present study we investigated whether the quantitative and semi-quantitatieve method correspond in estimating the density of inflammatory cells in airway biopsies of asthmatic and healthy subjects. Moreover we investigated which method discriminates best between asthmatic and healthy subjects, with attention to specific advantages and disadvantages of each method.
40
Semi-quantitative versus quantitative
Materials and Methods Seven healthy volunteers were selected on basis of absence of atopy and airway hyperresponsiveness. The 7 atopic asthmatics that were selected were stable and showed the next median (range) lungfunction variables: FEV 1 % predicted: 92 (80-100) %, PC20 methacholine: 0.66 (0.36-1.68) mg/ml and mean circadian PEF variation : 13 (6-44) %. Fiberoptic bronchoscopy was performed according to the guidelines of the American Thoracic Society (9), by use of an Olympus B1 IT10 flexible fiberoptic bronchoscope (Olympus Optical, Tokyo, Japan). Biopsies of normal appearing mucosa were taken from the subcarinae of the left or right lower lobe using a fenestrated forceps (FB-21 C, Olympus, Tokyo, Japan).
The biopsies were snap-frozen in OCT (Sakura, Tokyu, Japan) by immersing in isopentane (-80°C) and stored at -80°C. Four µm thick frozen sections were cut and stored at -20°C until use. lmmunostaining for CD3, CD4, CD25, CDS and EG2 was performed with Leu-4, Leu-3a, IL2 receptor (BectonDickinson, San Jose, CA), CDS moabs (own laboratory) and EG2 (Sanbio, Uden, The Netherlands) respectively, using an immunoperoxidase streptavidin-biotin method, with haematoxylin as counterstain. In order to evaluate the bronchial architecture serial sections were stained with Mayer's haematoxylin and eosin.
Quantitative counting was performed independently from the semi-quantitative evaluation, also in a blinded fashion, using a lightmicroscope at a magnification of 400 x. Positive cells were counted using an eyepiece graticule (cross-points each 25 µm at 400 x magnification), in representative sections at a depth of 100 µm beneath the intact basal membrane with a cumulative length of 1000 µm. Selection of representative sections was based on integrity of bronchial tissue, thickness of submucosa (> 100 µm) and absence of smooth muscle or glandular epithelium. Cell numbers were expressed as cells per millimeter basement membrane (mm BM).
Semi-quantitative examination was performed by one of the investigators in a blinded fashion using a lightmicroscope at a 200x magnification. Sections were considered to be representative if the basement membrane had a continuous length of at least 200 µm and the submucosa was at least 100 µm in depth. The density of immunopositive cells was estimated directly underneath the basement membrane and throughout the available submucosa. Categories were defined for each immunostained cell type separately. These categories were based on the relative differences of cell density between the 14 biopsies, and ranged from no stained cells (value 0) to many stained cells (value 3). At least four sections per subject per immunostaining were analyzed in this way. The semi-quantitative value was calculated by taking the average score of these sections.
41
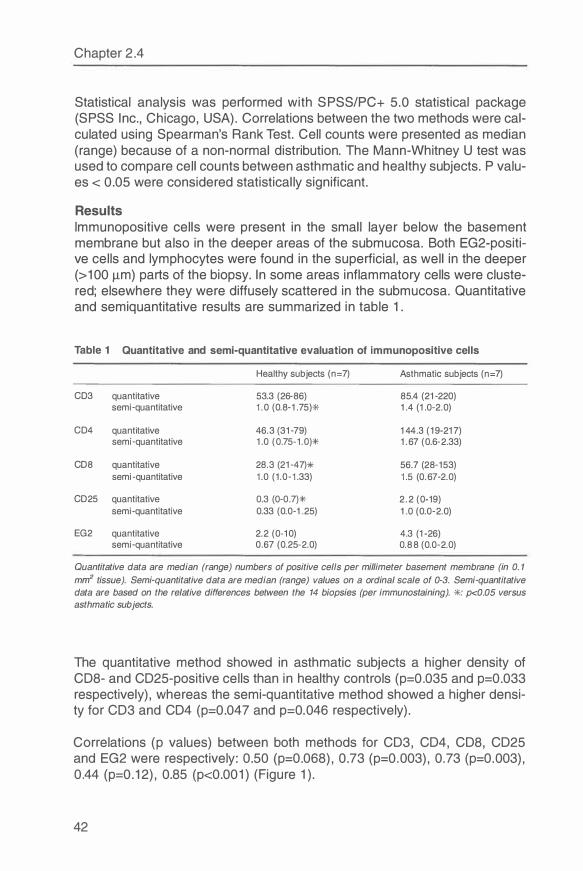
Chapter 2.4
Statistical analysis was performed with SPSS/PC+ 5.0 statistical package (SPSS Inc., Chicago, USA). Correlations between the two methods were calculated using Spearman's Rank Test. Cell counts were presented as median (range) because of a non-normal distribution. The Mann-Whitney U test was used to compare cell counts between asthmatic and healthy subjects. P values < 0.05 were considered statistically significant.
Results lmmunopositive cells were present in the small layer below the basement membrane but also in the deeper areas of the submucosa. Both EG2-positive cells and lymphocytes were found in the superficial, as well in the deeper (>100 µm) parts of the biopsy. In some areas inflammatory cells were clustered; elsewhere they were diffusely scattered in the submucosa. Quantitative and semiquantitative results are summarized in table 1.
Table 1 Quantitative and semi-quantitative evaluation of immunopositive cells
Healthy subjects (n=7) Asthmatic subjects (n=7)
CD3 quantitative 53.3 (26-86 ) 85.4 (21-220) semi-quantitative 1.0 (0.8-1 .75)* 1 .4 (1 .0-2.0)
CD4 quantitative 46 .3 (31-7 9) 1 44.3 (19-21 7 ) semi-quantitative 1 .0 (0.75-1.0)* 1 . 67 (0.6-2.33)
CD8 quantitative 28.3 (21-47)* 56 . 7 (28-153) semi-quantitative 1.0 (1.0-1.33) 1.5 (0.67-2.0)
CD25 quantitative 0.3 (0-0.7)* 2.2 (0-19) semi-quantitative 0.33 (0.0-1 .25) 1 .0 (0.0-2.0)
EG2 quantitative 2.2 (0-10) 4.3 (1-26 ) semi-quantitative 0.6 7 (0.25-2.0) 0.88 (0.0-2.0)
Quantitative data are median (range) numbers of positive cells per millimeter basement membrane (in 0. 1 mrrf tissue). Semi-quantitative data are median (range) values on a ordinal scale of 0-3. Semi-quantitative data are based on the relative differences between the 14 biopsies (per immunostaining). *: p<0.05 versus asthmatic subjects.
The quantitative method showed in asthmatic subjects a higher density of CDS- and CD25-positive cells than in healthy controls (p=0.035 and p=0.033 respectively), whereas the semi-quantitative method showed a higher density for CD3 and CD4 (p=0.047 and p=0.046 respectively).
Correlations (p values) between both methods for CD3, CD4, CDS, CD25 and EG2 were respectively: 0.50 (p=0.068), 0.73 (p=0.003), 0.73 (p=0.003), 0.44 (p=0.12), 0.85 (p<0.001) (Figure 1 ).
42
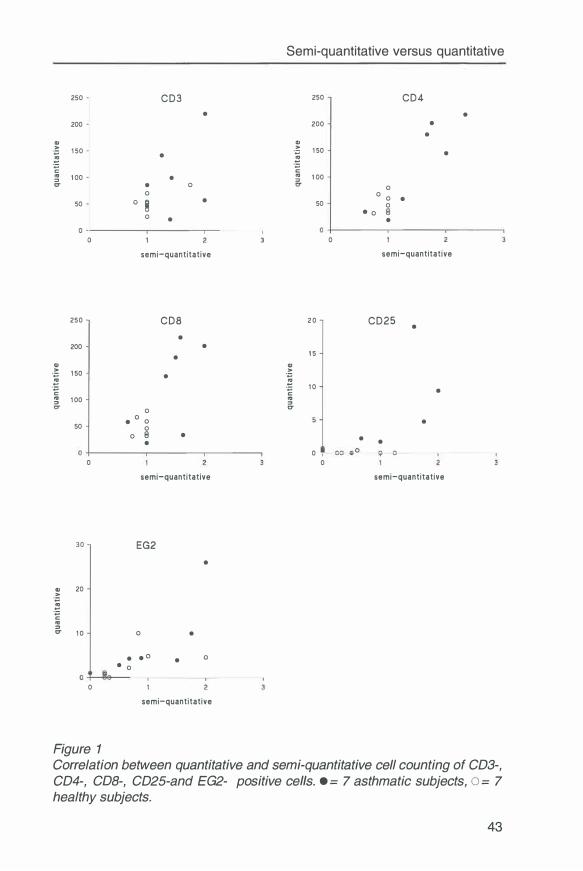
Semi-quantitative versus quantitative
250 CD3 250 CD4 • •
200 200 • •
i 1 50 • -� 1 50 •
-� IO 1 00 • ::,
IO 1 00 c::r • 0 0
0 50 0
8 •
0 •
0 0 • 50 0
• 0 • 0
0
semi-quantitative semi-quantitative
250 CDS 2 0 CD25 • •
200 • • 1 5
i Cl)
1 50 • -� -� 1 0 •
� 1 00 � 0 c::r
50 •
0 0 • 0
0 8 • • • • 0
0 0
semi-quantitative semi-quantitative
30 EG2
•
i 20
IO ::, c::r 1 0 0 •
• • o • 0 • 0
0
semi-quantitative
Figure 1 Correlation between quantitative and semi-quantitative cell counting of CD3-, CD4-, COB-, CD25-and EG2- positive cells. • = 7 asthmatic subjects, o = 7
healthy subjects.
43
Chapter 2.4
Discussion The present study showed that the quantitative and semi-quantitative way of evaluating cell density correlated well for CD4, CDS and EG2 immunostainings. The correlation between both methods for CD3 immunostaining was not significant, probably because the semi-quantitative method only used a narrow part of the scoring-scale (0.8-2.0), wheras the quantitative method showed a rather large range of cell numbers (21 to 220 cells per mm BM). The opposit trend was found in the evaluation of CD25-positive cells: the correlation was poor because the quantitative method detected mostly low cell numbers (see figure), whereas the semi-quantitative method used a relatively large part of the scoring possibilities (0-2). In general both methods corresponded well, despite the different areas and different scoring possibilities.
The results also show that the quantitative and semi-quantitative way of cell counting are complementary in discriminating asthmatic and healthy subjects. When low cell counts (CDS, CD25) were present, the quantitative method appeared to be more discriminative than the semi-quantitative one, whereas the opposite was true when high cell counts (CD3, CD4) were present. We speculate that in the presence of high cell numbers, the counting of positive cells is troubled by the fact that individual cells can not be easily discerned. In such circumstances a semi-quantitative estimation seems more valid. In the presence of low cell numbers (less than two positive cells per field of vision) the semi-quantitative method is less adequate because categories (0-3) are more difficult to define. In these circumstances the quantitative method has an advantage because of the use of an eyegrid for counting.
The counting of EG2-positive cells gave a very high correlation between the two counting methods. However, both methods failed to discriminate between asthmatic and healthy subjects. The high correlation can be explained by the fact that EG2-positive cells were easy to recognise and rather equally distributed between the superficial and deeper parts of the biopsies. The poor ability of EG2 to discriminate between asthmatic and healthy subjects may result from the fact that all our asthmatic subjects were in a stable condition and lacked an accumulation of activated eosinophils. Another explanation is that EG2 immunohistochemical staining may not discriminate sufficiently between resting and activated eosinophils (10, 11 ).
Determination of cell numbers in immunohistologically stained specimens has the problem that a gold standard is lacking. Consequently it is not possible to conclude that one of the methods is superior in evaluating cell density. We compared the value of both methods by investigating their ability to discriminate between asthmatic and healthy subjects. However, this ability does not necessarily correspond with the ability to measure the degree of inflammation in an individual subject. One explanation for the differences of both
44
Semi-quantitative versus quantitative
methods is the fact that semi-quantitative scoring was done in a larger part of the biopsy, including the deeper layers of the submucosa. In our opinion the presence of (activated) T lymphocytes in the deeper areas of a biopsy likely has biological significance, especially in asthmatic airway disease. We, therefore, use the semi-quantitative method to include clusters of inflammatory cells in the deep parts of the submucosa, an area in which quantitative cell counting often is troubled by crush artifacts, caused by the biopsy procedure.
We conclude that the semi-quantitative and quantitative examination of immunostained cells in airway biopsies of asthmatic and healthy subjects correspond reasonably well. The semi-quantitative method includes deeper and larger parts of the biopsy and seems more useful when high cell numbers are present. The use of the quantitative method is restricted to the superficial layers of a small representative part of the biopsy and seems more useful when low cell numbers are present, provided there is no uneven distribution in different areas of the biopsy. Depending on the aim of a study a choice can be made for one or both methods of cell counting.
References 1. Holgate ST, Wilson JR, Howard PH. New insights into airway inflammation
by endobronchial biopsy. Am Rev Respir Dis 1992; 145: S2-S6. 2. Holgate ST. Asthma: past, present and future. Eur Respir J 1993; 10: 1507-
20. 3. Haahtela T, Laitinen A, Laitinen LA. Using biopsies in the monitoring of in
flammation in asthmatic patients. Allergy 1993; 48: 65-9. 4. Azzawi, M. , Bradley, B. , Jeffery, P.K., Frew, A.J . , Wardlaw, A.J . , Knowles, G. ,
Assoufi, B. , Collins, J .V. , Durham, S. , and Kay, A.B. I dentification of activated T lymphocytes and eosinophils in bronchial biopsies in stable atopic asthma. Am Rev Respir Dis 1990; 142: 1407-13.
5. Bentley, A. M. , Menz, G., Storz, C. , Robinson, D.S. , Bradley, B. , Jeffery, P.K., Durham, S.R . , and Kay, A.B. I dentification of T lymphocytes, macrophages, and activated eosinophils in the bronchial mucosa in intrinsic asthma. Relationship to symptoms and bronchial responsiveness. Am Rev Respir Dis 1992; 146: 500-6.
6. Ying, S. , Durham, S.R. , Corrigan, C.J. , Hamid, Q. , and Kay, A.B. Phenotype of cells expressing mRNA for TH2 type (interleukin-4 and interleukin-5) and TH1 type (interleukin 2 and interferon gamma) cytokines in bronchoalveolar lavage and bronchial biopsies from atopic asthmatic and normal control subjects. Am J Respir Cell Mo/ Biol 1995; 12: 477-87.
7. Hamid, Q. , Azzawi, M. , Y ing, S. , Moqbel, R., Wardlaw, A.J . , Corrigan, C.J . , Bradley, B. , Durham, S.R. , Collins, J.V. , Jeffery, P.K. , and et al. Expression of mRNA for interleukin-5 in mucosal bronchial biopsies from asthma. J C/in Invest 87 1991: 1541-6.
45
Chapter 2.4
8. Ackerman, V, Marini, M , Vittori, E, Bellini, A, Vassali, G, and Mattoli, S. Detection of cytokines and their cell sources in bronchial biopsy specimens from asthmatic patients. Relationship to atopic status, symptoms, and level of airway hyperresponsiveness. Chest 1994; 105: 687-96.
9. NHLBI Workshop Summaries: Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis 1985; 132: 180-2.
10. Jahnsen FL, Brandtzaeg P, Halstensen TS. Monoclonal antibody EG2 does not provide reliable immunohistochemical discrimination between resting and activated eosinophils. J of lmmunol Methods. 1994; 175: 23-6.
11. Persson CGA, Erjefalt JS. Eosinophil lysis and free granules: an in vivo paradigm for cell activation and drug development. TiPS 1997; 18: 117-23.
46
Chapter 3
Nocturnal asthma: no nocturnal increase in inflammatory cells, but more severe airway wall inflammation both day and night
Nick ten Hacken, Wim Timens, Mieke Smith, Gineke Drok, Jan Kraan, Dirkje Postma
In press (European Respiratory Journal)
Abstract
Asthma at night is characterized by a nocturnal increase in airway obstruction and airway hyperresponsiveness for adenosine-5-monophosphate (AMP). Therefore, it has been hypothesized that nocturnal asthma results from an increase in airway wall inflammation at night. However, studies on inflammatory cells in BAL fluid and bronchial biopsies produce conflicting data. This study assesses the relationship between inflammatory cell numbers at night and nocturnal asthma in bronchial biopsies at 16 h and 04 h of 13 healthy controls, 15 asthmatic patients with PEF-variation � 15% and 10 asthmatic patients with PEF-variation > 15%. Subjects had not smoked for the last two years and did not use inhaled corticosteroids for the last four weeks. There was no significant increase at night in the number of CD3-, CD4-, CDS-, CD25-, AA 1 (tryptase)- and EG2- immunopositive cells in the submucosa. Numbers of EG2-positive cells in the two asthmatic groups was significantly higher than in healthy controls, both at 16 h (p<0.05) and 04 h (p<0.01 ). The number of EG2-, CD4- and CD25-positive cells at 04 h and at 16 h tended to be higher in asthmatics with a PEF variation > 15% as compared to asthmatics with PEF variation � 15%. We conclude that increased nocturnal airway obstruction is not caused by increased numbers of inflammatory cells in the bronchial submucosa at night. Apparently, these patients suffer from a higher overall severity of bronchial inflammation at night and day.
Introduction
Awakening at night due to asthma symptoms is very common: over 80% of subjects with asthma experience cough, wheeze and breathlessness at night (1 ). Asthmatic subjects with nocturnal symptoms have a larger circadian variation in airway diameter than asthmatic subjects without nocturnal symptoms (2,3). The term 'nocturnal asthma' is often used in these patients and this suggests a distinct disease entity. Until now, no convincing evidence is put forward that 'nocturnal asthma' has a unique pathogenesis (4,5). One of
47

Chapter 3
the hypotheses is that increased airway obstruction at night is caused by increased airway inflammation in this time period (5,6). Indeed, asthmatic patients with increased nocturnal airway obstruction are at night more hyperresponsive for adenosine-5-monophosphate (AMP) than at day-time, in contrast to asthmatic patients without increased nocturnal airway obstruction (7). Studies on BAL fluid in patients with 'nocturnal asthma' have produced conflicting results: Martin et al (8) and Mackay et al (9) found higher numbers of eosinophils at night than at day, whereas Jarjour and coworkers (10) and Oosterhoff et al (11, 12) found no differences. Further, two biopsy studies in patients with 'nocturnal asthma' showed the same number of inflammatory cells in the central airways at day and night time (9, 13), but a higher number of eosinophils in the alveolar tissue at night as compared to day time (13). In the present study we obtained bronchial biopsies at 16 h and 04 h of healthy controls, asthmatic patients with PEF variation � 15% and asthmatic patients with PEF variation > 15%. If increased nocturnal airway obstruction is caused by nocturnal worsening of airway inflammation, one would expect more inflammatory cells at 04 h than at 16 h, especially in asthmatics with PEF variation > 15%. On the other hand, if increased nocturnal airway obstruction is only an expression of more severe asthma, one would expect more inflammatory cells both at 04 h and 16 h in the asthmatics with PEF variation > 15%, as compared to the asthmatics with a PEF variation � 15%.
Materials and Methods
Study design - time schedule To study day-night changes in inflammatory cells we performed, in a randomized order, a bronchoscopy at 16 h and at 04 h, with an interval of seven to fourteen days. Four weeks before the first bronchoscopy inhaled corticosteroids were stopped. Two weeks before the first bronchoscopy subjects were characterized by peripheral blood eosinophils, serum total lgE, reversibility of FEV 1 after inhaling 400 µg salbutamol, PC20 methacholine and PC20 AMP. Three days before the first bronchoscopy, bronchodilators were withheld and PEF values were recorded at 08, 12, 16, 20, 24, and 04 h. PEF variation was defined as: (highest - lowest value) / mean of 6 measurements daily. Mean PEF variation was calculated as the average of the PEF variation measured during three days. Asthmatic subjects were divided on the basis of a mean PEF variation � or > 15%.
Subjects Subjects in the age of 18 to 45 years were recruited in our outpatient clinic or by advertisements in local newspapers. Asthmatic subjects were selected on: a history consistent with asthma; presence of atopy (positive intracutaneous tests against house dust mite or two other aero-allergens), FEV 1 > 1.5 I and > 60% predicted; PC20 methacholine � 9.8 mg/ml ; PC20 AMP � 80 mg/ml, no use of oral corticosteroids within 2 months before the study. Healthy volun-
48
Inflammatory cells
teers were selected on: no history of lung disease, FEV 1 > 1.5 I and > 85% predicted, no atopy and no airways hyperresponsiveness for methacholine or AMP. Subjects who smoked during the past 2 years, or with a respiratory infection during the past 4 weeks were excluded. Thirteen healthy volunteers and 25 asthmatic subjects participated in this study (Table 1 ). All subjects gave written informed consent. This investigation was approved by the medical ethics committee of the University Hospital.
Bronchoscopy and processing of the biopsies Bronchoscopy was performed using an Olympus 81 IT1 O flexible fiberoptic bronchoscope (Olympus Optical, Tokyo, Japan), according to the guidelines of the ATS (14). Biopsies were taken from the subcarinae of the left or right lower lobe using a fenestrated forceps (FB-21 C, Olympus, Tokyo, Japan). Biopsies were mounted in OCT and snap-frozen by immersing in isopentane (-80°C). Frozen sections of 4 µm thickness were immunostained for CD3, CD4, CD25 (Becton-Dickinson, San Jose, CA), COB (own laboratory), EG2 (Sanbio, Uden, The Netherlands) and AA 1 (DAKO, ITK, Denmark). An immunoperoxidase streptavidin-biotin method was used with hematoxylin as counterstain. In order to evaluate the bronchial biopsy architecture, sections were stained with Mayer's hematoxylin and eosin. Counting was carried out using a light microscope at a magnification of 400 x. Positive cells were counted in representative sections at a depth of 100 µm below an intact basement membrane (BM) with a cumulative length of 1000 µm, using an eyepiece graticule (cross-points each 25 µm at 400x). A representative part of the biopsy was chosen for evaluation on basis of (1) integrity of bronchial tissue, (2) thickness of the submucosa � 100 µm and (3) absence of smooth muscle or mucous glands. Counting was started at those locations that met best the above mentioned criteria. Counting was done twice by the same observer; the mean cell numbers were calculated and expressed as the number of positive cells per millimeter BM (0.1 mm2 tissue). Intra-individual reproducibility of counts of CD3-, CD4-, COB-, CD25-, EG2-, AA 1- immunopositive cells revealed a mean difference (Confidence Interval) of 10.4 (3.4, 17.4), -0.8 (-2.5, 0.9), -2.2 (-6.3, 1 .9), -0.05 (-0.15, 0.05), -1 .2 (-2.0, -0.35) and 2.9 (1.3, 4.5) respectively (p>>0.05). Intra-individual correlation of counts of CD3-, CD4-, COB-, CD25-, EG2-, AA 1- immunopositive cells were: 0.88, 0.99, 0.82, 0.99, 0.93, 0.84 respectively (p<<0.001 ).
Data analysis All analyses were performed with the SPSS/PC 6.01 software package (SPSS Inc., Chicago, IL). Values of p < 0.05 were considered statistically significant. The Student's t test was used to compare clinical variables between groups, on condition of a normal distribution . The Mann-Whitney U test was used to compare cell numbers between groups, and Wilcoxon's matched sign rank test was used to compare (paired) cell numbers at 16 h and 04 h
49
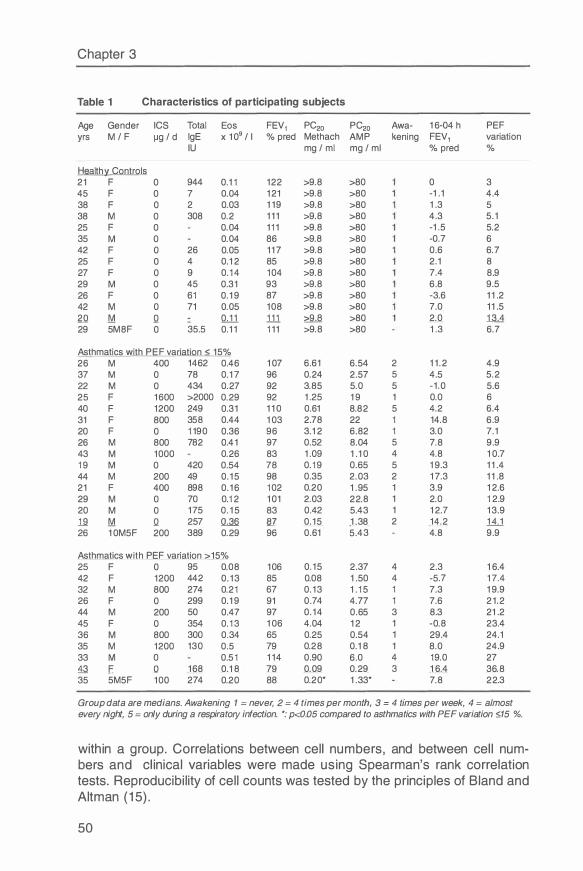
Chapter 3
Table 1 Characteristics of participating subjects
Age Gender ICS Total Eos FEV 1 PC20 PC20 Awa- 16 -04 h PEF yrs M / F µg / d lgE x 109 / I % pred Methach AMP kening FEV1 variation
IU mg / ml mg / ml % pred %
Health� Controls 21 F 0 944 0.11 122 >9.8 >80 0 3 45 F 0 7 0.04 121 >9.8 >80 -1 .1 4.4 38 F 0 2 0.03 119 >9.8 >80 1 .3 5 38 M 0 308 0.2 111 >9.8 >80 4.3 5.1 25 F 0 0.04 111 >9.8 >80 -1 .5 5.2 35 M 0 0.04 86 >9.8 >80 -0.7 6 42 F 0 26 0.05 11 7 >9.8 >80 0.6 6 . 7 25 F 0 4 0.12 85 >9.8 >80 2.1 8 27 F 0 9 0. 1 4 104 >9.8 >80 7 .4 8.9 29 M 0 45 0.31 93 >9.8 >80 6 .8 9.5 26 F 0 61 0.19 87 >9.8 >80 -3.6 11 .2 42 M 0 71 0.05 108 >9.8 >80 7 .0 11 .5 2Q M Q QJ.1 111 � >80 2.0 1M 29 5M8F 0 35.5 0.11 111 >9.8 >80 1 .3 6 . 7
Asthmatics with P E F variation < 15% 26 M 400 1462 0.46 107 6 .61 6 .54 2 11.2 4.9 37 M 0 78 0.1 7 96 0.24 2.57 5 4.5 5.2 22 M 0 434 0.27 92 3.85 5.0 5 -1.0 5.6 25 F 1600 >2000 0.29 92 1 .25 1 9 1 0.0 6 40 F 1200 249 0.31 110 0.61 8.82 5 4.2 6 .4 31 F 800 358 0.44 103 2.78 22 1 14.8 6 .9 20 F 0 1190 0.36 96 3.12 6 .82 1 3.0 7 .1 26 M 800 782 0.41 97 0.52 8.04 5 7 .8 9.9 43 M 1000 0.26 83 1 .09 1 .10 4 4.8 10.7 19 M 0 420 0.54 78 0.19 0.65 5 1 9.3 11 .4 44 M 200 49 0.15 98 0.35 2.03 2 1 7 .3 11 .8 21 F 400 898 0.16 102 0.20 1 . 95 1 3.9 12.6 29 M 0 70 0.12 101 2.03 22.8 1 2.0 12.9 20 M 0 175 0.15 83 0.42 5.43 1 12.7 13.9 19 M Q 257 Q,_.3fi fil 0.15 1 .38 2 14.2 1tl 26 10M5F 200 389 0.29 96 0.61 5.43 4.8 9.9
Asthmatics with PEF variation >15% 25 F 0 95 0.08 106 0.15 2.37 4 2.3 16 .4 42 F 1200 442 0.13 85 0.08 1 .50 4 -5.7 1 7 .4 32 M 800 274 0.21 6 7 0.13 1 .15 1 7 .3 1 9.9 26 F 0 299 0.19 91 0.74 4.7 7 1 7 .6 21.2 44 M 200 50 0.47 97 0.14 0.65 3 8.3 21 .2 45 F 0 354 0.13 106 4.04 12 1 -0.8 23.4 36 M 800 300 0.34 65 0.25 0.54 1 29.4 24.1 35 M 1200 130 0.5 79 0.28 0.18 1 8.0 24.9 33 M 0 0.51 114 0.90 6 .0 4 19.0 27 13 E Q 168 0.18 79 0.09 0.29 3 16 .4 36.8 35 5M5F 100 274 0.20 88 0.20* 1 .33* 7 .8 22.3
Group data are medians. Awakening 1 = never, 2 = 4 times per month, 3 = 4 times per week, 4 = almost every night, 5 = only during a respiratory infection. *: p<d).05 compared to asthmatics with PEF variation :£,15 %.
within a group. Correlations between cell numbers, and between cell num-bers and clinical variables were made using Spearman's rank correlation tests. Reproducibility of cell counts was tested by the principles of Bland and Altman (15).
50
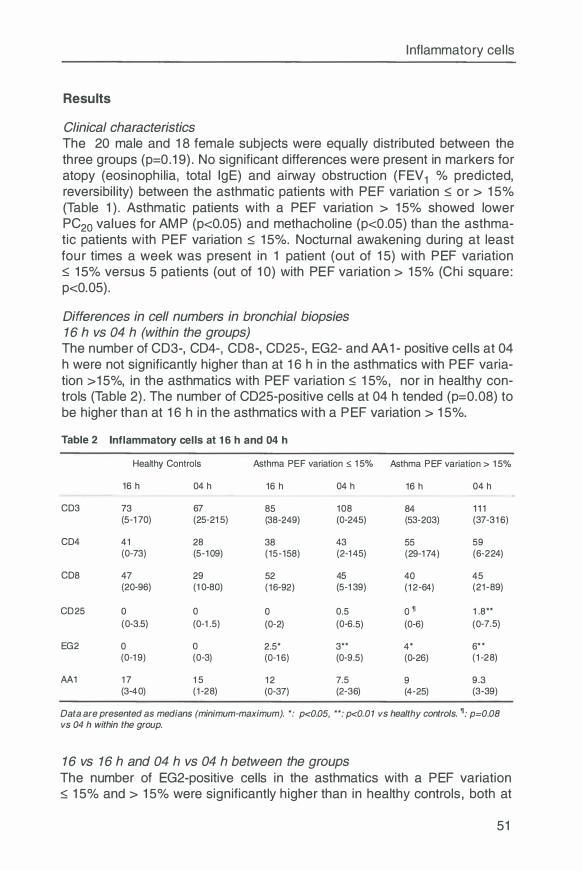
Inflammatory cells
Results
Clinical characteristics The 20 male and 18 female subjects were equally distributed between the three groups (p=0.19). No significant differences were present in markers for atopy (eosinophilia, total lgE) and airway obstruction (FEV 1 % predicted, reversibility) between the asthmatic patients with PEF variation ::; or > 15% (Table 1 ). Asthmatic patients with a PEF variation > 15% showed lower PC20 values for AMP (p<0.05) and methacholine (p<0.05) than the asthmatic patients with PEF variation ::; 15%. Nocturnal awakening during at least four times a week was present in 1 patient (out of 15) with PEF variation ::; 15% versus 5 patients (out of 10) with PEF variation > 15% (Chi square: p<0.05).
Differences in cell numbers in bronchial biopsies 16 h vs 04 h (within the groups) The number of CD3-, CD4-, CD8-, CD25-, EG2- and AA 1- positive cells at 04 h were not significantly higher than at 16 h in the asthmatics with PEF variation > 15%, in the asthmatics with PEF variation ::; 15%, nor in healthy controls (Table 2). The number of CD25-positive cells at 04 h tended (p=0.08) to be higher than at 16 h in the asthmatics with a PEF variation > 15%.
Table 2 Inflammatory cells at 1 6 h and 04 h
Healthy Controls Asthma PE F variation :;;; 15% Asthma PEF variation > 15%
16 h 04 h 16 h 04 h 16 h 04 h
CD3 73 67 85 108 84 111 (5-1 70) (25-215) (38-249) (0-245) (53-203) (37-316 )
CD4 41 28 38 43 55 59 (0-73) (5-109) (15-158) (2-145) (29-1 74) (6-224)
CDS 47 29 52 45 40 45 (20-96 ) (10-80) (16-92) (5-139) (12-64) (21-89)
CD25 0 0 0 0.5 0 � 1 .8** (0-3.5) (0-1 .5) (0-2) (0-6 .5) (0-6 ) (0-7 .5)
EG2 0 0 2.5* 3** 4* 6** (0-19) (0-3) (0-16 ) (0-9.5) (0-26 ) (1-28)
AA1 1 7 1 5 12 7 .5 9 9.3 (3-40) (1-28) (0-37 ) (2-36) (4-25) (3-39)
Data are presented as medians (minimum-maximum). *: p<0.05, **: p<0.01 vs healthy controls. �_. p=0.08 vs 04 h within the group.
16 vs 16 h and 04 h vs 04 h between the groups The number of EG2-positive cells in the asthmatics with a PEF variation ::; 15% and > 15% were significantly higher than in healthy controls , both at
51
Chapter 3
16 h and 04 h (Figure 1 ). The number of CD25-positive cells at 04 h in the asthmatics with a PEF variation > 1 5% was higher than in healthy controls. Inflammatory cell numbers did not significantly differ between the asthmatic patients with PEF variation � 1 5% and > 15%.
The relationship between clinical variables and inflammatory cells The number of inflammatory cells in biopsies of all asthmatic patients were not correlated with important clinical variables such as FEV 1 % predicted, PC20 Methacholine, PC20 AMP, and mean PEF variation. The 16-04 h difference in CD25-positive cells was not significantly correlated with the 16-04 h FEV 1 or PEF variation. The numbers of CD25-positive cells at 1 6 h and 04 h were correlated with peripheral blood eosinophilia at 1 6 h (rho=0.48, p=0.017) and at 04 h (rho=0.43, p=0.034) respectively.
Discussion This study demonstrated in the first place that the number of inflammatory cells in the bronchial wall of asthmatic patients at night is not higher than at daytime. Only CD25-positive cells tended (p=0.08) to be higher at night in asthmatics with a PEF variation > 15%. However, airway wall tissue of most asthmatics, and also of those with a PEF variation > 15%, contained very low numbers of CD25-positive cells. Therefore, we do not expect that a nocturnal increase in these cells is directly responsible for an increase in airway obstruction at night. This study further showed that EG2-, CD4- and CD25-positive cells at 04 h and at 1 6 h tended to be higher in asthmatics with a PEF variation > 15% than in asthmatics with a PEF variation � 1 5%. Together, these results suggest that patients with larger circadian variations in airway diameter probably are patients with a higher overall severity of bronchial inflammation. The increase in nocturnal airway obstruction does not seem to be the result of an increasing number of inflammatory cells in the bronchial submucosa at night.
Our results are in line with two other biopsy studies on bronchial inflammation in nocturnal asthma, despite the methodological differences of these studies (Table 3). Mackay et al. (9) for example did not find day-night differences in the number of lymphocyte subsets and eosinophils in biopsies of their subjects with nocturnal asthma. However, their patients were treated with inhaled corticosteroids and theophyllines, both agents theoretically being able to suppress nocturnal increases in inflammation. Moreover, their study lacked a control group of patients with non-nocturnal asthma. Kraft et al. (13) excluded patients with corticosteroid therapy, whereas theophyllines were permitted. Like our study they did not find day-night differences in inflammatory cells in biopsies from the central airways. If any conclusion was to be drawn, the number of eosinophils even seemed to be higher at daytime. In biopsies from the peripheral airways of patients with nocturnal asthma, they found more eosinophils at night than at daytime. However, 5 out of 11 pairs
52
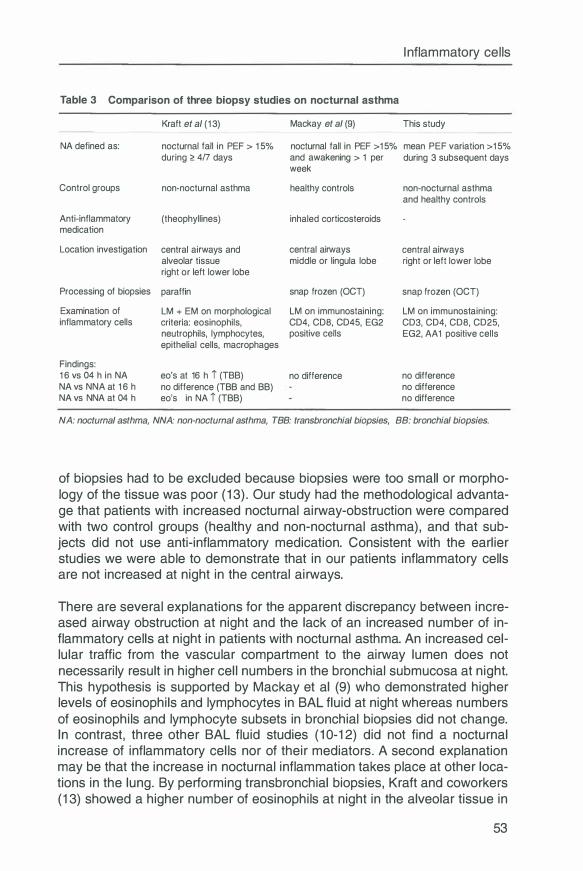
Table 3 Comparison of three biopsy studies on nocturnal asthma
Kraft et al (1 3) Mackay et al (9)
Inflammatory cells
This study
NA defined as: nocturnal fall in PEF > 1 5% nocturnal fall in PEF >1 5% mean PEF variation >1 5%
Control groups
Anti-inflammatory medication
Location investigation
Processing of biopsies
Examination of inflammatory cells
Findings: 1 6 vs 04 h in NA NA vs NNA at 1 6 h NA vs NNA at 04 h
during ;:::: 4/7 days and awakening > 1 per week
non-nocturnal asthma healthy controls
(theophyllines) inhaled corticosteroids
central airways and central airways alveolar tissue middle or lingula lobe right or left lower lobe
paraffin snap frozen (OCT)
LM + EM on morphological LM on immunostaining: criteria: eosinophils, CD4, CDS, CD45, EG2 neutrophils, lymphocytes, positive cells epithelial cells, macrophages
eo's at 16 h i (TBB) no difference no difference (TBB and BB) eo's in NA i (TBB)
during 3 subsequent days
non-nocturnal asthma and healthy controls
central airways right or left lower lobe
snap frozen (OCT)
LM on immunostaining: CD3, CD4, CDS, CD25, EG2, AA1 positive cells
no difference no difference no difference
NA: nocturnal asthma, NNA: non-nocturnal asthma, TBB: transbronchial biopsies, BB: bronchial biopsies.
of biopsies had to be excluded because biopsies were too small or morphology of the tissue was poor (13). Our study had the methodological advantage that patients with increased nocturnal airway-obstruction were compared with two control groups (healthy and non-nocturnal asthma), and that subjects did not use anti-inflammatory medication. Consistent with the earlier studies we were able to demonstrate that in our patients inflammatory cells are not increased at night in the central airways.
There are several explanations for the apparent discrepancy between increased airway obstruction at night and the lack of an increased number of inflammatory cells at night in patients with nocturnal asthma. An increased cellular traffic from the vascular compartment to the airway lumen does not necessarily result in higher cell numbers in the bronchial submucosa at night. This hypothesis is supported by Mackay et al (9) who demonstrated higher levels of eosinophils and lymphocytes in BAL fluid at night whereas numbers of eosinophils and lymphocyte subsets in bronchial biopsies did not change. In contrast, three other BAL fluid studies (10-12) did not find a nocturnal increase of inflammatory cells nor of their mediators. A second explanation may be that the increase in nocturnal inflammation takes place at other locations in the lung. By performing transbronchial biopsies, Kraft and coworkers (13) showed a higher number of eosinophils at night in the alveolar tissue in
53
Chapter 3
patients with nocturnal asthma. However, the contribution of these eosinophils to increased nocturnal airway obstruction remains uncertain. After all, two studies (10, 12) exploring the alveolar compartment with BAL fluid were not able to show higher levels of EON at night. Another explanation may be that increased degranulation or cellysis in the bronchial wall leads to increased airway inflammation at night without an increased number of inflammatory cells (16). However, there are as yet no studies available comparing numbers of eosinophils with levels of free ECP, EON or MBP in the submucosa.
It can be argued that our method to separate nocturnal from non-nocturnal asthmatics was not successful, thereby obscuring a real effect of increased inflammation at night. In a similar designed study in our hospital (7) a PEF variation � or > 15% was found to clearly separate the patients with symptoms of asthma at night, accompanied by an increase in airway obstruction, assessed with FEV 1 . In the present study, this cut-off point was less successful as evidenced by a similar nocturnal decrease in FEV 1 % predicted in both groups (Table 1 ). One explanation may be that the PEF variation was measured at home, while patients slept in the hospital before the 04 h bronchoscopy. Patients are probably less exposed to housedust in the hospital than at home. Also, the stress of being in a hospital and the anticipation of a nocturnal bronchoscopy may have resulted in altered sleep patterns. We have assessed PEF variation by subtracting the highest and the lowest value of 6 measurements (in three following days). Theoretically, the highest PEF value does not necessarily occur around 16 h; neither does the lowest PEF value have to occur around 04 h. Other (non-circadian) acute factors may influence PEF measurements, as exposure to smoke or an allergen at an alternative time point. Because of the above considerations we retrospectively divided our patients on basis of a 16-04 h FEV % predicted � 10% (n=16), or > 10% (n=9). This did not change the results. Thus, separating asthmatic patients on basis of an actual decline in lung function at night does not lead to other conclusions with respect to the presence and activation of inflammatory cells in the bronchial submucosa.
We conclude that increased nocturnal airway obstruction in patients with nocturnal asthma is not the result of an increased nocturnal presence of inflammatory cells in the bronchial submucosa. Because nocturnal increases in inflammatory cells and mediators in BAL fluid are not uniformly reported in the literature we have to be careful to draw definitive conclusions about the pathophysiology of nocturnal asthma. In our opinion, future research should focus on increases of cell traffic (from the vascular compartment, via the airway wall, to the airway lumen), cell activation and cell death at night.
Acknowledgments The authors thank Ors R. Douma, R. Meijer and S. Rutgers for their assistance during bronchoscopies at night.
54
Inflammatory cells
References 1 . Turner Warwick M. Epidemiology of nocturnal asthma. Am J Med 1 988;85:6-
8. 2. Clark T J. Diurnal rhythm of asthma. Chest 1 987;91 : 1 37S-41 S. 3. Hetzel MR, Clark T J. Comparison of normal and asthmatic circadian rhythms
in peak expiratory flow rate. Thorax 1 980;35:732-8. 4. Weersink EJ, Postma DS. Nocturnal asthma: not a separate disease entity.
Respir Med 1 994;88:4839-1 . 5. Postma DS, Oosterhoff Y, van Aalderen WM, Kauffman HF, Wempe JB,
Koeter GH. Inflammation in nocturnal asthma? Am J Respir Grit Care Med 1 994; 1 50:S83-6.
6. Oosterhoff Y, Timens W, Postma DS. The role of airway inflammation in the pathophysiology of nocturnal asthma. Clin Exp Allergy 1 995;25:91 5-2 1 .
7. Oosterhoff Y, Koeter GH, de Monchy JGR, Postma DS. Circadian variation in airway responsiveness to metacholine, and AMP in atopic asthmatic subjects. Am Rev Respir Dis 1 993; 1 47:51 2-7.
8. Martin RJ, Cicutto LC, Smith HR, Ballard RD, Szefler SJ. Airways inflammation in nocturnal asthma. Am Rev Respir Dis 1 991 ; 1 43:351 -7.
9. Mackay TW, Wallace WAH, Howie SEM, Brown PH, Greening AP, Church MK, Douglas NJ. Role of inflammation in nocturnal asthma. Thorax 1 994;49:257-62.
1 0. Jarjour NN, Busse WW, Calhoun WJ. Enhanced production of oxygen radicals in nocturnal asthma. Am Rev Respir Dis 1 992; 1 46:905-1 1 .
1 1 . Oosterhoff Y, Hoogsteden HC, Rutgers B, Kauffman HF, Postma DS. Lymphocyte and macrophage activation in bronchoalveolar lavage fluid in nocturnal asthma. Am J Respir Grit Care Med 1 995; 1 51 :75-81 .
1 2. Oosterhoff Y, Kauffman HF, Rutgers B, Zijlstra FJ, Koeter G, Postma DS. Inflammatory cell number and mediators in bronchoalveolar lavage fluid and peripheral blood in asthmatic subjects with increased nocturnal airways narrowing. J Allergy Clin lmmunol 1 995;96:21 9-29.
1 3. Kraft M , Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolar tissue inflammation in asthma. Am J Respir Grit Care Med 1 996; 1 54: 1 505-1 0.
1 4. NHLBI Workshop summaries: Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis 1 985; 1 32: 1 80-2.
1 5. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1 986; 1 :307-1 0.
1 6. Persson CGA, Erjefalt JS. Eosinophil lysis and free granules: an in vivo paradigm for cell activation and drug development. Ti PS 1 997; 1 8: 1 1 7-23.
55

Chapter 4
Vascular adhesion molecules in nocturnal asthma: a possible role for VCAM-1 in ongoing airway wall inflammation
Nick ten Hacken, Dirkje Postma, Froukje Bosma, Gineke Drok, Bea Rutgers, Jan Kraan, Wim Timens
Submitted
Abstract
Background: Increased airway inflammation at night is thought to be one of the underlying mechanisms in nocturnal asthma. Vascular adhesion molecules may be important for the recruitment of inflammatory cells in the process of asthmatic airway inflammation. Objective: To determine the possible role of vascular adhesion molecules in increased airway inflammation at night in subjects with nocturnal asthma. Methods: We obtained bronchial biopsies at 16 h and 04 h from 13 healthy controls, 15 asthmatic patients with PEF variation :::; 15% and 1 O asthmatic patients with PEF variation > 15%. Biopsies were snap-frozen and double-immunostained for CD31 in combination with P-selectin, E-selectin, ICAM-1 or VCAM-1. Results: No significant day-night differences in expression of adhesion molecules were found in any of the three groups. The percentage of VCAM-1 positive vessels in biopsies of asthmatic patients was higher than in biopsies of healthy controls: 4.5 vs 2.5 % (p<0.05) at 16 h and 11 vs O % (p<0.05) at 04 h. In asthma, VCAM-1 expression was correlated with the number of EG2-positive cells at 16 h (rho = 0.57, p < 0.01) as well as at 04 h (rho = 0.64, p < 0.01 ). Moreover, VCAM-1 expression was correlated with the number of CD25-positive cells at 16 h (rho = 0.43, p < 0.05) and at 04 h (rho = 0.41, p < 0.05). Conclusion: Increased nocturnal airway obstruction in asthma is not associated with an increased nocturnal expression of vascular E-selectin, P-selectin, ICAM-1 or VCAM-1. The relationship between vascular VCAM-1 expression and submucosal EG2- and CD25-positive cells, both at 16 h and 04 h, suggests a role for VCAM-1 in the ongoing airway wall in-flammation of asthma.
Introduction
Asthma at night is characterized by worsening of airway obstruction (1) and increased responsiveness for adenosine monophosphate (AMP) (2) at night. Several causes for nocturnal asthma have been suggested (3). Increased airway inflammation at night is an attractive explanation because of the increased responsiveness at night for the indirect stimulus AMP (4). Indeed, high-
57

Chapter 4
er numbers of eosinophils at night in BAL fluid (5,6) and transbronchial biopsies (7) have been reported in patients with nocturnal asthma. A higher number of eosinophils at night, at least when activated, may lead to swelling of the airway wall mucosa, epithelial damage and airway responsiveness at night. Thus it seems of importance to know which mechanisms are responsible for attracting and activating inflammatory cells. Vascular adhesion molecules are considered to play an essential role in the recruitment of inflammatory cells in asthma (8). Montefort et al (9) showed an increased expression of vascular ICAM-1 and E-selectin (but not VCAM-1) in bronchial biopsies of 6 atopic asthmatics 6 hours after allergen provocation, which correlated with an increased number of LFA positive cells in the epithelium and submucosa. In steady state conditions, Gosset et al (10) showed that bronchial biopsies of stable allergic asthmatics expressed more vascular E-selectin, ICAM-1 and VCAM-1 than healthy controls. Finally, Fukuda et al (11) demonstrated in bronchial biopsies a close relationship between IL-4 levels in BAL fluid and VCAM-1 positive vessels and eosinophils in the submucosa.
Because vascular adhesion molecules apparently are important for the recruitment of inflammatory cells, we examined their possible role in increased nocturnal airway inflammation. We investigated vascular P-selectin, Eselectin, ICAM-1 and VCAM-1 at 16 h and 04 h in bronchial biopsies of healthy controls and asthmatic patients with and without nocturnal airway obstruction.
Material and Methods
Subjects Subjects in the age of 18 to 45 years were recruited from our outpatient clinic or by advertisements in local newspapers. Healthy volunteers were selected on: no history of lung disease; FEV 1 > 1.5 I and > 85% predicted, no atopy and no airways hyperresponsiveness for methacholine or AMP. Asthmatic subjects were selected on: a history consistent with asthma; presence of atopy (positive intracutaneous tests against house dust mite or two other aero-allergens), FEV1 > 1.5 I and > 60% predicted; PC20 methacholine � 9.8 mg/ml ; PC20 AMP � 80 mg/ml, no use of oral corticosteroids within 2 months before the study. Subjects with smoking within the past 2 years, or with a respiratory infection within the last 4 weeks were excluded. This investigation was approved by the medical ethics committee of the hospital and all subjects had to give their written informed consent.
Study design Four weeks before the first bronchoscopy inhaled corticosteroids were stopped. Two weeks before the first bronchoscopy subjects were characterized by peripheral blood eosinophils, serum total lgE, reversibility of FEV 1 after inhaling 400 µg salbutamol, PC20 methacholine and PC20 AMP. Three days
58
Vascular adhesion molecules
before the first bronchoscopy, bronchodilators were withheld and PEF values were recorded at 08, 12, 16, 20, 24, and 04 h. PEF variation was defined as: (highest - lowest value) / mean of 6 measurements daily. A mean PEF variation of three days PEF variation was calculated. Asthmatic subjects were divided on the basis of a mean PEF variation being ::; or > 15%. The time point of the first bronchoscopy was randomized at 16 h or 04 h. Seven to fourteen days later the second bronchoscopy was performed at 04 h or 16 h respectively.
Bronchoscopy and processing of the biopsies Bronchoscopy was performed using an Olympus B 1 IT1 O flexible fiberoptic bronchoscope (Olympus Optical, Tokyo, Japan). Biopsies were taken from the subcarinae of the left or right lower lobe using a fenestrated forceps (FB-21 C, Olympus, Tokyo, Japan), according to the guidelines of the ATS (12).
Biopsies were mounted in Tissue Tel<® (Sakura, Tokyo, Japan) and snap-frozen by immersion in isopentane (-80°C). Serial sections were cut at a thickness of 4 µm. Every twenty fifth section was stained with Mayer's hematoxylin and eosin. The morphologically best and largest series were selected for immunostaining. In the double immunostaining, vessels were recognized by morphology in combination with immunostaining for a common vessel antigen: CD31 (lgG1 or lgG2b, Monosan). Labeling of anti-CD31 was performed by isotype specific biotinylated rabbit anti-mouse immunoglobulins and subsequently by streptavidin conjugated to alkaline phosphatase, providing a blue reaction product. Adhesion molecules were recognized by anti-CD62P (lgG1 , Monosan), anti-CD62E (lgG1 , Genzyme), anti-CD54 (lgG2a, A.W. Boyd, Royal Melbourne Hospital, Australia), anti-CD106 (lgG1 , Genzyme). Labeling of these anti-adhesion antibodies was performed by isotype specific goat anti-mouse antibody conjugated to peroxidase, using 3-amino-4-ethylcarbazole as a reagent, giving a reddish brown reaction product. In addition, in the same series, immunostainings for CD3, CD4 (BectonDickinson, San Jose, CA), CD8 (own laboratory), CD25, AA 1 (tryptase) and EG2 (Sanbio, Uden, The Netherlands) were produced with a standard immunoperoxidase streptavidin-biotin method and hematoxylin as counterstain.
Quantification of expression of vascular adhesion molecules Because sections were coded, the observer was not aware of the subject characteristics, nor the time points of obtaining biopsies. Sections were examined using a Zeiss light microscope at magnification 400 x. Complete sections were examined systematically, using an eye grid with crossings every 10 µm (at magnification 400 x). When less than twenty vessels were recognized in a section, a section of a second series (of the same biopsy) was quantified. The mean (st.dev.) number of vessels examined for expression of an adhesion molecule per subject per time point was: 40 (21 ). Because
59
Chapter 4
expression of adhesion molecules on CD31 positive vessels showed an irregular patchy pattern, vessels were scored positive whenever immunopositivity for an adhesion molecule was present. Sections were quantified twice, the mean results being entered for analysis. lmmunopositivity for an adhesion molecule was expressed as a percentage of CD31 positive vessels. The mean intra-observer differences (confidence interval) for E-selectin, P-selectin, ICAM-1 and VCAM-1 were: 0.6 (-0.9, 2.1 ), -1.0 (-3.1, 1.0), 3.5 (1.3, 5.6) and 0.4 (-0.4, 1.1 ), respectively. The mean intra-observer correlations for Eselectin, P-selectin, ICAM-1 and VCAM-1 were: 0. 78, 0.84, 0.80, 0.98 (p<0.001 ).
Quantification of CD3-, CD4-, COB-, CD25-, AA 1- and EG2-positive cells A representative part of the biopsy was randomly selected with as minimum requirements: (1) integrity of bronchial tissue, (2) thickness of submucosa (> 100 µm) and (3) absence of smooth muscle or mucous glands. Counting was carried out using an eyepiece graticule at a magnification 400 x. Positive cells were counted, in representative areas subtended by 100 µm of intact basement membrane (BM) and extending 100 µm into the submucosa. Totally, ten of these areas were counted, while counting was started at those locations which met best the above mentioned criteria. Data were expressed as the number of positive cells per millimeter BM (0.1 mm2 tissue).
Data analysis All analyses were performed with the SPSS/PC 6.0 software package (SPSS Inc., Chicago, IL). Chi-square test was used to compare the distribution of male and female subjects between groups. Student's t test for unpaired data was used to compare clinical data between groups, including logarithmically transformed measurements of PC20 AMP or methacholine, peripheral blood eosinophils and serum total lgE. All the other data were analyzed in a nonparametrical way, using Wilcoxon's test to compare between 16 h and 04 h values, and Mann Whitney U test to compare between groups at similar time points. Correlations between individual data sets were analyzed by Spearman's rank correlation test. Values of p < 0.05 were considered statistically significant.
Results
Clinical findings Thirteen healthy volunteers and 25 asthmatic subjects participated in this study (Table 1 ). Age and gender did not differ between the three groups. No significant differences were present in markers for atopy (eosinophilia, total lgE) and airway obstruction (FEV 1 at 16 h or 04 h, reversibility) between the asthmatic patients with PEF variation � or > 15%. However, asthmatic subjects with PEF variation > 15% more frequently woke up at night due to dys-pnea than asthmatic subjects with PEF variation � 15% (p<0.05). Also,
60
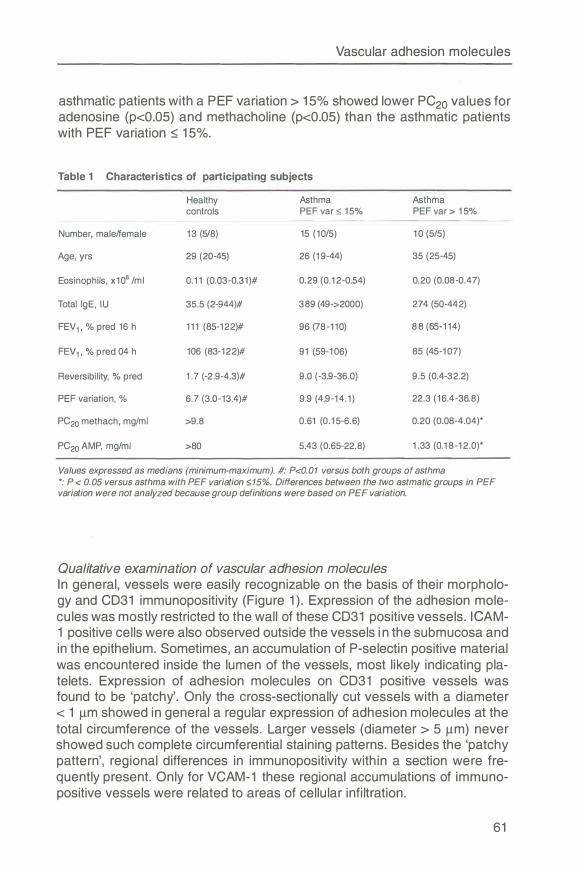
Vascular adhesion molecules
asthmatic patients with a PEF variation > 15% showed lower PC20 values for adenosine (p<0.05) and methacholine (p<0.05) than the asthmatic patients with PEF variation ::; 15%.
Table 1 Characteristics of participating subjects
Healthy Asthma Asthma controls PEF var :=; 15% PEF var > 15%
Number, male/female 13 (5/8) 15 (10/5) 10 (5/5)
Age, yrs 29 (20-45) 26 (19-44) 35 (25-45)
Eosinophils, x106 /ml 0.11 (0.03-0.31)# 0.29 (0.12-0.54) 0.20 (0.08-0.47)
Total lgE , IU 35.5 (2-944)# 389 (49->2000) 274 (50-442)
FEV1 , % pred 16 h 111 (85-122)# 96 (78-110) 88 (65-114)
FEV1 , % pred 04 h 106 (83-122)# 91 (59-106 ) 85 (45-107 )
Reversibility, % pred 1 . 7 (-2.9-4.3)# 9.0 (-3.9-36 .0) 9.5 (0.4-32.2)
PEF variation, % 6 . 7 (3.0-13.4)# 9.9 (4.9-14.1) 22.3 (16 .4-36.8)
PC20 methach, mg/ml >9.8 0.61 (0.15-6 .6 ) 0.20 (0.08-4.04)*
PC20 AMP, mg/ml >80 5.43 (0.65-22.8) 1 .33 (0.18-12.0)*
Values expressed as medians (minimum-maximum). #: P<0.01 versus both groups of asthma *: P < 0. 05 versus asthma with PEF variation :=; 15%. Differences between the two astmatic groups in PEF variation were not analyzed because group definitions were based on PEF variation.
Qualitative examination of vascular adhesion molecules In general, vessels were easily recognizable on the basis of their morphology and CD31 immunopositivity (Figure 1 ). Expression of the adhesion molecules was mostly restricted to the wall of these CD31 positive vessels. ICAM-1 positive cells were also observed outside the vessels in the submucosa and in the epithelium. Sometimes, an accumulation of P-selectin positive material was encountered inside the lumen of the vessels, most likely indicating platelets. Expression of adhesion molecules on CD31 positive vessels was found to be 'patchy'. Only the cross-sectionally cut vessels with a diameter < 1 µm showed in general a regular expression of adhesion molecules at the total circumference of the vessels. Larger vessels (diameter > 5 µm) never showed such complete circumferential staining patterns. Besides the 'patchy pattern', regional differences in immunopositivity within a section were frequently present. Only for VCAM-1 these regional accumulations of immunopositive vessels were related to areas of cellular infiltration.
61
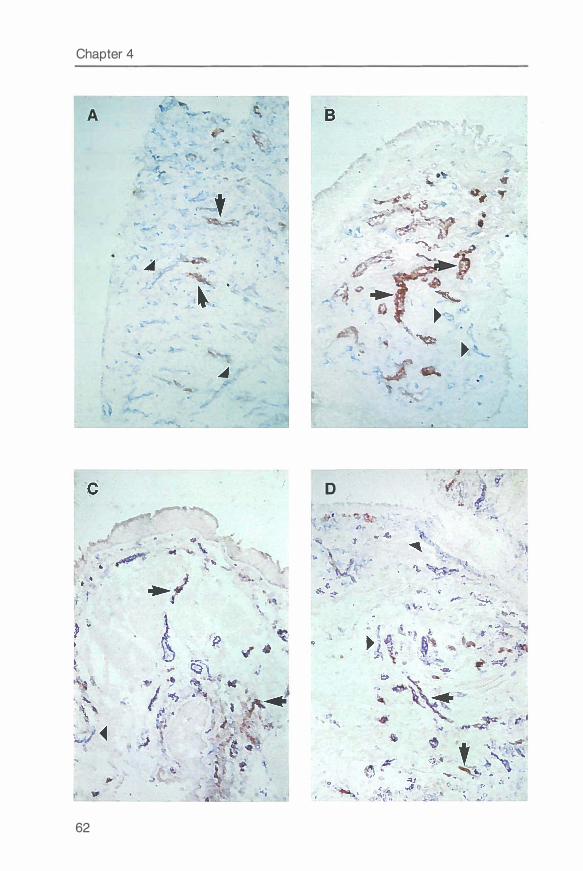
Chapter 4
D
62
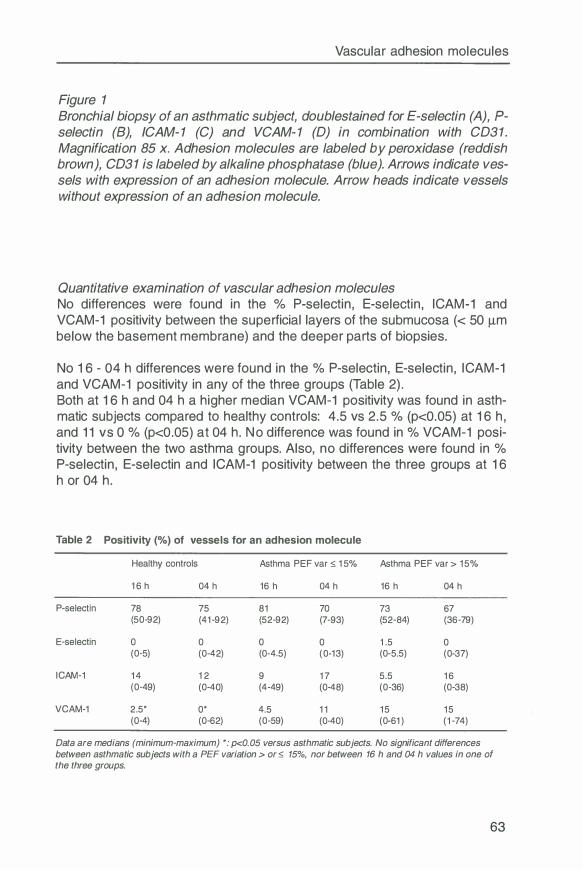
Vascular adhesion molecules
Figure 1 Bronchial biopsy of an asthmatic subject, doublestained for E-selectin (A), Pselectin (8), ICAM- 1 (C) and VCAM- 1 (D) in combination with CD31 . Magnification 85 x. Adhesion molecules are labeled by peroxidase (reddish brown), CD31 is labeled by alkaline phosphatase (blue). Arrows indicate vessels with expression of an adhesion molecule. Arrow heads indicate vessels without expression of an adhesion molecule.
Quantitative examination of vascular adhesion molecules No differences were found in the % P-selectin, E-selectin, ICAM-1 and VCAM-1 positivity between the superficial layers of the submucosa (< 50 µm below the basement membrane) and the deeper parts of biopsies.
No 16 - 04 h differences were found in the % P-selectin, E-selectin, ICAM-1 and VCAM-1 positivity in any of the three groups (Table 2) . Both at 16 h and 04 h a higher median VCAM-1 positivity was found in asthmatic subjects compared to healthy controls: 4.5 vs 2. 5 % (p<0.05) at 16 h, and 11 vs 0 % (p<0.05) at 04 h. No difference was found in % VCAM-1 positivity between the two asthma groups. Also, no differences were found in % P-selectin, E-selectin and ICAM-1 positivity between the three groups at 16 h or 04 h.
Table 2 Positivity (%) of vessels for an adhesion molecule
Healthy controls Asthma PEF var � 15% Asthma PEF var > 15%
16 h 04 h 16 h 04 h 16 h 04 h
P-selectin 78 75 81 70 73 67 (50-92) (41-92) (52-92) (7-93) (52-84) (36-79)
E-selectin 0 0 0 0 1 .5 0 (0-5) (0-42) (0-4.5) (0-13) (0-5.5) (0-37)
ICAM-1 14 12 9 1 7 5.5 16 (0-49) (0-40) (4-49) (0-48) (0-36) (0-38)
VCAM-1 2.5* 0* 4.5 11 15 15 (0-4) (0-62) (0-59) (0-40) (0-61 ) (1-74)
Data are medians (minimum-maximum) *: p<0.05 versus asthmatic subjects. No significant differences between asthmatic subjects with a PEF variation > or � 15%, nor between 16 h and 04 h values in one of the three groups.
63
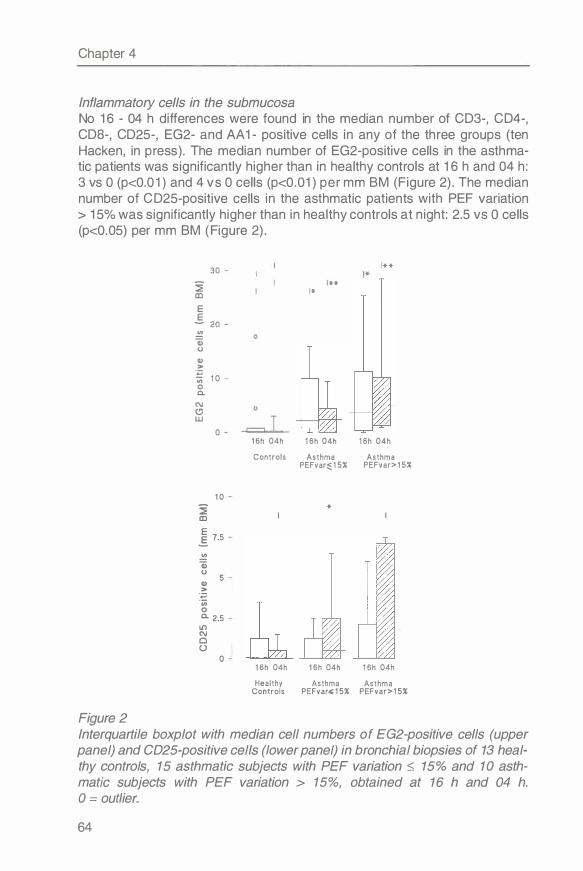
Chapter 4
Inflammatory cells in the submucosa No 1 6 - 04 h differences were found in the median number of CD3-, CD4-, CDS-, CD25-, EG2- and AA 1 - positive cells in any of the th ree groups (ten Hacken, in p ress) . The median number of EG2-positive cells in the asthmatic patients was significantly higher than in healthy controls at 1 6 h and 04 h : 3 vs 0 (p<0.0 1 ) and 4 vs 0 cells (p<0.01 ) per mm BM (Figure 2) . The median number of CD25-positive cells in the asthmatic patients with PEF variation > 1 5% was significantly higher than in healthy controls at n ight: 2.5 vs O cells (p<0.05) per mm BM ( Figure 2) .
Figure 2
� ID
E E
30
- 20
..!!! Q) (J
Cl) >
·;::; ·;;; 1 0 0 a.
C\I
Cl w 0
1 0
� ID
E E. 7.5
..!!! Q) (J
Cl) >
·;::; ·;;; 0 a. 2.5 It) C\I
0 (.)
0
** *
** *
1 6h 04h 1 6h 04h 1 6h 04h
Controls Asthma Asthma PEFvar� 1 5% PEFvar>1 5%
*
1 6h 04h 1 6h 04h 1 6h 04h
Healthy Asthma Asthma Controls PEFvar" 1 5% PEFvar>1 5%
Interquartile boxplot with median cell numbers of EG2-positive cells (upper panel) and CD25-positive cells (lower panel) in bronchial biopsies of 13 healthy controls, 15 asthmatic subjects with PEF variation :s; 15% and 1 O asthmatic subjects with PEF variation > 15%, obtained at 16 h and 04 h. O = outlier.
64
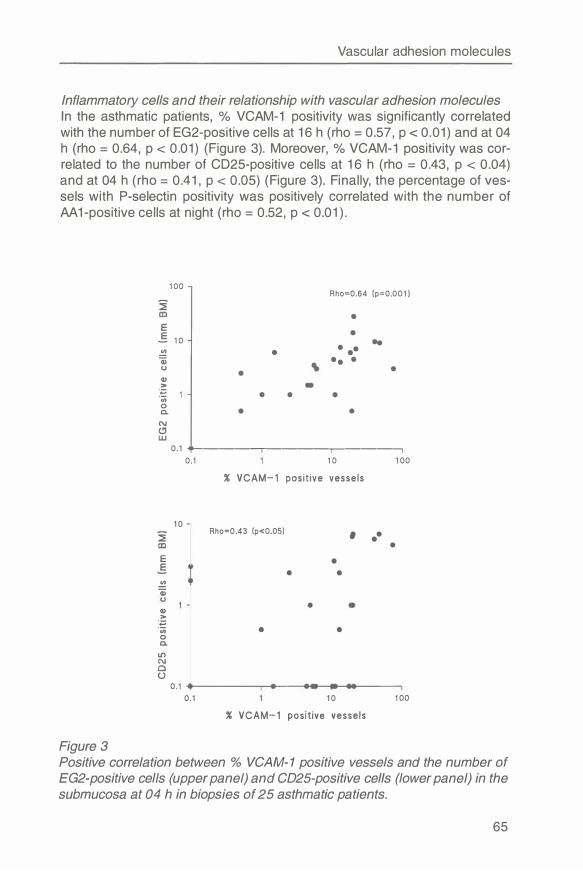
Vascular adhesion molecules
Inflammatory cells and their relationship with vascular adhesion molecules In the asthmatic patients, % VCAM-1 positivity was significantly correlated with the number of EG2-positive cells at 16 h (rho = 0.57, p < 0.01) and at 04 h (rho = 0.64, p < 0.01) (Figure 3). Moreover, % VCAM-1 positivity was correlated to the number of CD25-positive cells at 16 h (rho = 0.43, p < 0.04) and at 04 h (rho = 0.41, p < 0.05) (Figure 3). Finally, the percentage of vessels with P-selectin positivity was positively correlated with the number of AA 1-positive cells at night (rho = 0.52, p < 0.01 ).
Figure 3
1 00
� E
_§ 1 0 .!!? (U CJ
Q) > ;:;
'iii 0 0.
N (!J w
• •
• • •
Rho=0.64 (p=0.00 1 )
• •
• •• .. •• • • - •
•
0.1 ----�--------� 0.1 1 0 1 00
% VCAM- 1 posit ive vessels
1 0
� Rho=0 .43 (p<0.05) , •• • E •
.§ • • .!!? (U
Q)
.� 'iii • • 0 0.
It')
(.) 0.1
0 . 1 1 0 1 00
% VCAM- 1 posit ive vesse ls
Positive correlation between % VCAM-1 positive vessels and the number of EG2-positive cells (upper panel) and CD25-positive cells (lower panel) in the submucosa at 04 h in biopsies of 25 asthmatic patients.
65
Chapter 4
Discussion This study demonstrated that the vascular expression of P-selectin, E-selectin, ICAM-1 and VCAM-1 did not change at night in central airway wall biopsies of patients with PEF variation > 15%, nor in biopsies of patients with PEF variation � 15%. Also, the number of inflammatory cells in the submucosa were shown not to increase at night. Apparently, large circadian variations in airway diameter are not caused by an increased upregulation of vascular adhesion molecules leading to an increased number of inflammatory cells in the submucosa at night. This is not surprising because a prolonged vascular upregulation of E-selectin, ICAM-1 and VCAM-1 has been demonstrated for at least 12 to 48 hours after antigen stimulation (13,14). Therefore, detection of a circadian variation in expression of one of these adhesion molecules is less likely. An exception is P-selectin, which can be modulated within minutes to hours (14, 15) and is influenced by several mediators important in asthma (16). Interestingly, our asthmatic patients showed a positive correlation between the number of histamine containing mast cells (AA 1-positive cells) and the percentage P-selectin positive vessels at night. A previous study showed a higher level of circulating peripheral blood histamine in patients with nocturnal asthma at night (17), and histamine is known to induce Pselectin. However, vascular P-selectin expression did not increase at night in our asthmatic patients. Our observation that there is no increased expression of vascular adhesion molecules at night, supports the observation that there is no increased submucosal airway wall inflammation at night.
This study demonstrated a higher number of VCAM-1 positive vessels in asthmatic patients than in healthy controls, both at 16 h and 04 h. In our asthmatic patients, VCAM-1 expression correlated positively with the number of EG2-positive cells, probably because VCAM-1 causes adhesion and recruitment of eosinophils. Moreover, a higher percentage of vessels with VCAM-1 expression correlated with a higher number of CD25-positive cells. It may be hypothesized that CD25-positive cells release IL-4 which is able to cause an increase in vascular VCAM-1 expression. Our results are in line with those of Fukuda et al (11 ), who demonstrated a significant correlation between the amount of IL-4 in BAL fluid, the expression of vascular VCAM-1 and the number of submucosal eosinophils. Together with the latter study, the observed relationships between vascular VCAM-1 expression and submucosal EG2- and CD25-positive cells both at 16 h and 04 h in our study suggest a role for VCAM-1 in the ongoing airway inflammation in asthma, but not specifically so in nocturnal airway obstruction.
We have found similar expressions of vascular ICAM-1 , E-selectin and Pselectin in biopsies of asthmatic patients and healthy controls. This finding is not in line with Gosset et al (10), who showed higher vascular expressions of E-selectin and ICAM-1 to be associated with higher numbers of eosinophils
66
Vascular adhesion molecules
and leucocytes in biopsies of asthmatic patients. Probably our patients were not recently exposed to inhaled allergens, and too stable to find such a relationship. After all, in particular a higher vascular expression of E-selectin and ICAM-1 has been demonstrated after provocation with an inhaled allergen (9). Our results are in line with three other studies (11, 18, 19), demonstrating similar expressions of vascular ICAM-1 and E-selectin in asthmatic patients and healthy controls. Like in our study, the absence of upregulation in ICAM-1, E-selectin and P-selectin suggests that these adhesion molecules do not play an important role in patients with clinically stable asthma .
We conclude that asthma at night is not associated with an increased expression of vascular E-selectin, P-selectin, ICAM-1 or VCAM-1 at night in the submucosa of the central airways. The positive relationships between vascular VCAM-1 expression and submucosal EG2- and CD25-positive cells, both at 16 h and 04 h, suggest a role for VCAM-1 in the ongoing airway inflammation in asthma.
Acknowledgments The authors thank Ors R. Meijer, S. Rutgers and R. Douma for their assistance during bronchoscopies at night. The CD54 antibody was kindly donated by Dr. A.W. Boyd, Royal Melbourne Hospital, Australia.
References 1. Clark TJ . Diurnal rhythm of asthma. Chest 1987;91:137S-41S. 2. Oosterhoff Y, Koster GH, de Monchy JGR, Postma OS. Circadian variation
in airway responsiveness to methacholine, and AMP in atopic asthmatic subjects. Am Rev Respir Dis 1993; 147:512-7.
3. Busse WW. Pathogenesis and pathophysiology of nocturnal asthma. Am J
Med 1988;85:24-9. 4. Oosterhoff Y, Timens W, Postma OS. The role of airway inflammation in the
pathophysiology of nocturnal asthma. Clin Exp Allergy 1995;25:915-21. 5. Martin RJ, Cicutto LC, Smith HR, Ballard RD, Szefler SJ. Airways inflamma
tion in nocturnal asthma. Am Rev Respir Dis 1991 ; 143:35-17. 6. Mackay TW, Wallace WAH, Howie SEM, Brown PH, Greening AP, Church
MK, Douglas NJ. Role of inflammation in nocturnal asthma. Thorax 1994;49:257-62.
7. Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ . Alveolar tissue inflammation in asthma. Am J Respir Grit Care Med 1996;154: 1505-10.
8. Montefort S, Holgate ST, Howarth PH. Leucocyte endothelial adhesion molecules and their role in bronchial asthma and allergic rhinitis. Eur Respir J
1993;6:1044-54. 9. Montefort S, Gratziou C, Goulding D, Polosa R, Haskard DO, Howarth PH,
Holgate ST, Carroll MP. Bronchial biopsy evidence for leukocyte infiltration and upregulation of leukocyte endothelial cell adhesion molecules 6 hours after local allergen challenge of sensitized asthmatic airways. J Clin Invest 1994;93:1411-21.
67
Chapter 4
10. Gosset P, TillieLeblond I, Janin A, Marquette CH, Gopin MC, Wallaert B, Tonnel AB. Expression of E-selectin, ICAM-1 and VCAM-1 on bronchial biopsies from allergic and nonallergic asthmatic patients. Int Arch Allergy /mmuno/ 1995; 106:69-77.
1 1 . Fukuda T, Fukushima Y, Numao T, Ando N, Arima M, Nakajima H, Sagara H, Adachi T, Motojima S, Makino S. Role of interleukin-4 and vascular cell adhesion molecule-1 in selective eosinophil migration into the airways in allergic asthma. Am J Respir Cell Mo/ Biol 1996;14:84-94.
12. NHLBI Workshop summaries: Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis 1985; 132:180-2.
13. Wegner CD, Rothlein R, Gundel RH. Adhesion molecules in the pathogenesis of asthma. Agents Actions Suppl 1991 ;34:529-44.
14. Geng JG, Bevilacqua MP, Moore KL, McIntyre TM, Prescott SM, Kim JM, Bliss GA, Zimmerman GA, McEver RP. Rapid neutrophil adhesion to activated endothelium mediated by GMP1 40. Nature 1990;343:757-60.
15. Lawrence MB, Springer TA. Leukocytes roll on a selectin at physiologic flow rates: distinction from and prerequisite for adhesion through integrins. Cell 1991 ;65:859-73.
16. Larsen E, Celi A, Gilbert GE, Furie BC, Erban JK, Bonfanti R, Wagner DD, Furie B. PADGEM protein: a receptor that mediates the interaction of activated platelets with neutrophils and monocytes. Cell 1989;59:305-12.
1 7 . Szefler SJ, Ando R, Cicutto LC, Surs W, Hill MR, Martin RJ. Plasma histamine, epinephrine, cortisol, and leukocyte �-adrenergic receptors in nocturnal asthma. C/in Pharmacol Ther 1991 ;49:59-68.
1 8. Montefort S, Roche WR, Howarth PH, Djukanovic R, Gratziou C, Carroll M, Smith L, Britten KM, Haskard D, Lee TH, et al. lntercellular adhesion molecule-1 (ICAM-1) and endothelial leucocyte adhesion molecule-1 (ELAM-1) expression in the bronchial mucosa of normal and asthmatic subjects. Eur Respir J 1992;5:815-23.
19. Bentley AM, Durham SR, Robinson OS, Menz G, Storz C, Cromwell 0, Kay AB, Wardlaw AJ. Expression of endothelial and leukocyte adhesion molecules interacellular adhesion molecule-1, E-selectin, and vascular cell adhesion molecule-1 in the bronchial mucosa in steady state and allergen induced asthma. J Allergy Clin lmmuno/ 1993;92:857-68.
68
Chapter 5
Nocturnal asthma: not explained by circadian variations in Inducible Nitric Oxide Synthase
Nick ten Hacken, Dirkje Postma, Gineke Drok, Mieke Smith, Wilke Goers, Jan Kraan, Wim Timens
Submitted
Abstract Nocturnal asthma is thought to be the result of increased airway inflammation at night. Because nitric oxide (NO) may be involved in the pathogenesis of asthmatic airway inflammation, we hypothesized that inducible NO synthase (iNOS) expression is increased at night in bronchial biopsies of patients with nocturnal asthma. In order to test this hypothesis, we obtained biopsies at 16 and 04 h in 25 atopic asthmatics and 13 healthy controls, aged 18 to 45 years. lmmunohistochemical staining demonstrated that the expression of iNOS in the bronchial wall was not increased at night in the 1 O asthmatic patients with increased nocturnal airway obstruction (defined as PEF variation > 15%), nor in the other subjects. Inducible NOS positive cells in epithelium, endothelium and submucosa tended to be more frequently present in asthmatic patients than in healthy controls, both at 16 and 04 h. Inducible NOS immunoreactivity in the epithelium of asthmatic patients was very sparse and seemed located in migrating inflammatory cells and not in epithelial cells. With respect to inflammatory cells, more EG2-positive cells were found in asthmatic patients than in healthy controls (p<0.001 ), both at 16 and 04 h. No significant 16 - 04 h difference in EG2-positive cells was found in the asthmatic patients with PEF variation > 15%. Finally, epithelial and endothelial iNOS positivity at 04 h was accompanied by a higher degree of submucosal EG2-positivity (p<0.05). We conclude that nocturnal asthma can not be explained by circadian variations in iNOS expression. We suggest that increased expression of iNOS and EG2-positive cells represent a common underlying mechanism.
Introduction Asthma at night is characterized by frequent awakening due to dyspnea (1 ). The normal chronobiological rhythm in airway diameter and hyperresponsiveness is increased in these patients, leading to airway obstruction, wheezing, chest tightness, and coughing at night (2-4). The underlying mechanisms for this increased nocturnal airway obstruction are not clear (5-7). The
69
Chapter 5
higher responsiveness for adenosine-5-monophosphate (and not methacholine) at night as compared to day time in patients with asthma at night (8) suggests that nocturnal asthma results from increased airway inflammation at night. Indeed, the number of eosinophils and leucocytes in the bronchial lumen were found to be increased at night in subjects with nocturnal asthma, in contrast to subjects without a nocturnal increase in airway obstruction (9, 10). However, two other BAL fluid studies showed inflammatory cells were not to be increased at night, nor their mediators (11, 12). Two biopsy studies did not detect day-night differences in inflammatory cells of the central airways as well (10, 13). One explanation for these inconsistent findings may be that nocturnal increases in airway inflammation are only very modest and that the tools used until now were not sensitive enough to detect these relative small changes. Another possibility is that other inflammatory factors which were not investigated, are more important.
Nitric Oxide (NO) is a such a factor that may offer an alternative view on increased airway inflammation at night. Only recently, NO has been postulated to both reflect (14, 15) and mediate (16, 17) the underlying airway inflammation in asthma. A day-night variation in NO may exist because production of NO can be modulated within several hours under the influence of changing (micro)environmental factors, such as cytokines and corticosteroids (18). Interestingly, asthmatic patients with increased nocturnal airway obstruction have higher levels of IL-1 p in BAL fluid than patients without nocturnal airway obstruction (19), and interferon-y levels in serum are higher at night than at day time (20). Both these pro-inflammatory cytokines are able to stimulate the expression of inducible Nitric Oxide Synthase (iNOS), and to induce NO release within several hours. This effect may be augmented by the normally occurring dips in serum cortisol at midnight. Thus, for various reasons it is attractive to investigate the modulation of iNOS expression as an alternative factor in the pathogenesis of increased airway inflammation at night.
In the present study we hypothesize that the expression of iNOS is increased at night in asthmatic subjects with increased nocturnal airway obstruction, in contrast to subjects without nocturnal airway obstruction. To test this hypothesis, we obtained bronchial biopsies at 16 and 04 h in 25 atopic asthmatics and 13 healthy controls. Besides circadian variations in iNOS expression, other inflammatory variables were investigated in subjects with and without nocturnal airway obstruction.
Material and Methods
Study design Inhaled corticosteroids and cromolyns were stopped four and two weeks before the start of the study respectively. Characterization of the participating subjects took place within two weeks before the first bronchoscopy and con-
70
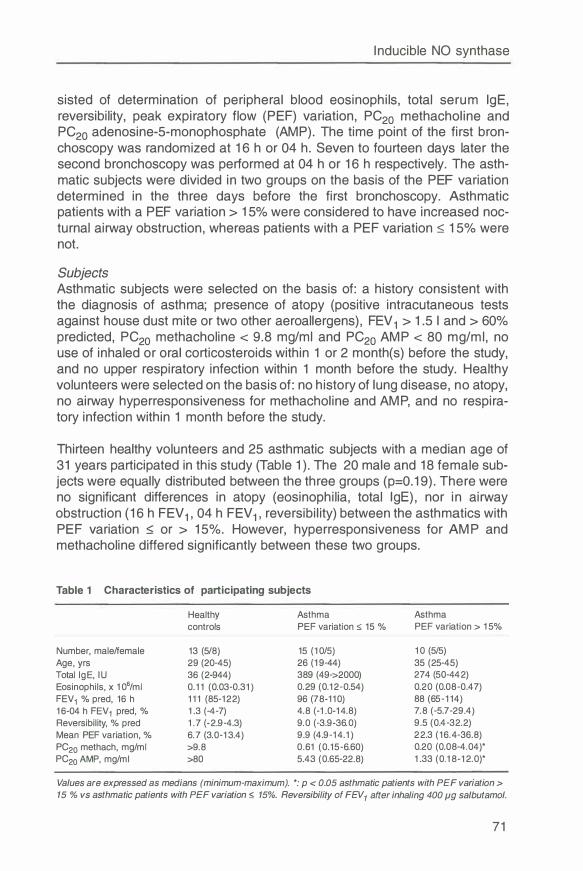
Inducible NO synthase
sisted of determination of peripheral blood eosinophils, total serum lgE, reversibility, peak expiratory flow (PEF) variation, PC20 methacholine and PC20 adenosine-5-monophosphate (AMP). The time point of the first bronchoscopy was randomized at 16 h or 04 h. Seven to fourteen days later the second bronchoscopy was performed at 04 h or 16 h respectively. The asthmatic subjects were divided in two groups on the basis of the PEF variation determined in the three days before the first bronchoscopy. Asthmatic patients with a PEF variation > 1 5% were considered to have increased nocturnal airway obstruction, whereas patients with a PEF variation :::;; 15% were not.
Subjects Asthmatic subjects were selected on the basis of: a history consistent with the diagnosis of asthma; presence of atopy (positive intracutaneous tests against house dust mite or two other aeroallergens), FEV 1 > 1.5 I and > 60% predicted, PC20 methacholine < 9.8 mg/ml and PC20 AMP < 80 mg/ml, no use of inhaled or oral corticosteroids within 1 or 2 month(s) before the study, and no upper respiratory infection within 1 month before the study. Healthy volunteers were selected on the basis of: no history of lung disease, no atopy, no airway hyperresponsiveness for methacholine and AMP, and no respiratory infection within 1 month before the study.
Thirteen healthy volunteers and 25 asthmatic subjects with a median age of 31 years participated in this study (Table 1 ). The 20 male and 18 female subjects were equally distributed between the three groups (p=0.19). There were no significant differences in atopy (eosinophilia, total lgE), nor in airway obstruction (16 h FEV 1 , 04 h FEV 1 , reversibility) between the asthmatics with PEF variation :::;; or > 15%. However, hyperresponsiveness for AMP and methacholine differed significantly between these two groups.
Table 1 Characteristics of participating subjects
Healthy Asthma controls PEF variation :;;; 15 %
Number, male/female 13 (5/8) 15 (10/5) Age, yrs 29 (20-45) 26 (19-44) Total lgE, IU 36 (2-944) 389 (49->2000) Eosinophils, x 106/ml 0.11 (0.03-0.31) 0.29 (0.12-0.54) FEV1 % pred, 16 h 111 (85-122) 96 (78-110) 16-04 h FEV 1 pred, % 1 .3 (-4-7) 4.8 (-1 .0-14.8) Reversibility, % pred 1 .7 (-2.9-4.3) 9.0 (-3.9-36.0) Mean PEF variation, % 6 .7 (3.0-13.4) 9.9 (4.9-14.1 ) PC20 methach, mg/ml >9.8 0.61 (0.15-6.60) PC20 AMP, mg/ml >80 5.43 (0.65-22.8)
Asthma PEF variation > 15%
10 (5/5) 35 (25-45) 274 (50-442) 0.20 (0.08-0.47) 88 (65-114) 7.8 (-5.7-29.4) 9.5 (0.4-32.2) 22.3 (16 .4-36 .8) 0.20 (0.08-4.04)* 1 .33 (0.18-12.0)*
Values are expressed as medians (minimum-maximum). *: p < 0.05 asthmatic patients with PEF variation > 15 % vs asthmatic patients with PEF variation :;;; 15%. Reversibility of FEV1 after inhaling 400 µg salbutamol.
71
Chapter 5
Lung function Lung volumes and forced ventilatory flows were performed according to standardized guidelines of the European Respi ratory Society (21 ) . FEV 1 was measured with a cal ibrated water-sealed spi rometer. Reversib i l ity of FEV 1 was tested after i nhal ing 400 µg salbutamol . PEF values were determined with a Wright min i peak flow meter. PEF values were recorded during three fol lowing days at 08, 1 2 , 1 6 , 20, 24, and 04 h. Bronchodi lators were withheld during these th ree days. Daily PEF variation was defined as: (highest - lowest value) / mean of 6 measurements. Mean PEF variation was calcu lated as the average of three daily PEF variations. Airway hyperresponsiveness was measured using a 2-minutes tidal breath ing method (22) . Doubl ing concentrations of 0.03 to 9.8 mg/ml methachol inebromide and 0.02 to 80 mg/ml AMP (both Sigma Chemical Co. , St. Louis, MO) were del ivered as an aerosol through a nebul izer (DeVilbiss Co. , Somerset, PA) . Solution output was 0. 1 3 ml/min. The challenge was discontinued when the FEV 1 had fal len by � 20% of the prechallenge level . PC20 values were calculated by l inear interpolation of the last 2 points of the log concentration response curve.
Bronchoscopy After obtaining IVC and FEV 1 , fiberoptic bronchoscopy was performed according to the guidelines of the American Thoracic Society (23) , by use of an Olympus B1 IT1 0 flexible fiberoptic bronchoscope (Olympus Optical , Tokyo, Japan). Biopsies were taken from the subcarinae of the left lower lobe and during the fi rst bronchoscopy and from the right lower lobe during the second bronchoscopy, using a fenestrated forceps (FB-21 C , O lympus, Tokyo, Japan) . The biopsies were snap-frozen by immersing in isopentane (-80°C) and stored at -80°C. In one asthmatic patient the second bronchoscopy was impossible because of persistent coughing and laryngospasm during introduction of the scope. Biopsies of one session lacked sufficient immunoreactivity, probably because of a techn ical fai lure.
Processing of the biopsies Frozen biopsies were cut serial ly, and divided in series of 25 sections (4 µm thickness) and stored at -20°C unti l use. Morphologically optimal tissue was selected on basis of a hematoxylin and eosi n (H&E) stained sl ide. Enzyme histochemical staining for NO synthase was performed by incubating the slides with a reaction m ixture consisting of 0. 1 mg/ml n itroblue tetrazol ium (in 0. 1 M phosphate-buffered sal ine pH 7.2) , 1 mg/ml NADPH diaphorase, and 0.3% Triton X-1 00 (pH 7.2) during 1 h at 37°C (modified from Kobzik (24)) . lmmunostaining for iNOS (Transduction Lab, Lexington, KY) was performed with polyclonal antibodies according to the prescriptions of the manufacturer, using goat anti-rabbit immunoglobul in antibodies conjugated to peroxidase as a second step, and 4-amino-3-ethyl-carbazole as substrate , with hematoxyl in as counterstain . Prel im inary experiments indicated that incubation with 1 : 1 00 anti-iNOS (in PBS/BSA 1 %) during 1 h at 20°c provided optimal
72
Inducible NO synthase
staining. Immune staining for CD4, CD8, tryptase and ECP was performed with Leu-3A (Becton-Dickinson, San Jose, CA), CDS (own laboratory), AA 1 (Dakopatts, Glostrup, Denmark) and EG2 (Sanbio, Uden, The Netherlands) respectively, using an immunoperoxidase streptavidin-biotin method, with hematoxylin as counterstain. Negative controls were acquired by omitting incubation with the primary antibodies or by incubation with species specific, isotype matched non-relevant antibodies.
Additional information on iNOS immunohistochemical staining iNOS immunostaining was performed with a polyclonal antibody that was purified by affinity chromatography and described by the manufacturer as highly specific in Western blotting, immunoprecipitation and indirect immunofluorescence. lmmunoblotting with this antibody using lung tissue indicated a specific signal at 130 kD. In human lung, this antibody showed a very specific staining of inflammatory and endothelial cells, and an absence of positive epithelial cells.
As results on iNOS immunohistology have been conflicting (24-27), we have performed additional experiments to obtain maximal sensitivity : 1) incubation of sections with increasing concentrations (1 :500, 1 :200, 1:100, 1 :50) of the anti-iNOS antibody , 2) incubation of sections overnight at 4 °C to include lowaffinity receptor binding, 3) potentiation of the second step with a three times repeated APAAP method (26). We also assessed whether any of the three methods combined improved the signal.
iNOS immunoreactivity was also tested with other polyclonal antibodies which were commercially available (Affinity Biological Reagents, U SA) or generous gifts (Dr H. Moshage, Dept. of Gastro-enterology, University Hospital Groningen, The Netherlands). lmmunoblotting of these antibodies with human lung showed also an intense signal at 130 KO. These antibodies gave moderate to intense immunohistochemically staining of normal lung tissue and more intense staining at sites of inflammation in concurrence with the polyclonal antibody of Transduction Laboratories. In this study we have used the purified polyclonal antibodies of Transduction Lab because of their higher specificity on sections.
Examination of the biopsies Sections were examined in a blinded fashion using a light microscope at 400x magnification. The architecture of the tissue was examined using routinely H&E stained sections. Sections were considered to be representative if the basement membrane had a continuous length of at least 100 µm, if the epithelium was at least partially present, and if the submucosa was at least 100 µm in depth. Staining of the anti-iNOS antibodies was compared with enzyme histochemical staining for NADPH diaphorase, and with controls.
73
Chapter 5
Because we expected day and night differences in the number of iNOS positive cells to be small and hard to detect, we compared the day and night sections of each patient two by two in a blinded fashion. These paired sections were later recoded as: more, equal or less immunopositive cells at night. In an intra-observer analysis, agreements in the weighted kappa (95% Cl) were high, i.e. in epithelium 1.00 (-0.85, 2.85), in endothelium 0.92 (0.10, 1.75), and in submucosa 0.83 (-0.37, 2.03).
iNOS positive cells were nominally scored in the epithelium and endothelium (-: not present, +: present), and ordinally scored in the submucosa (-: no, +:
a few, ++: several positive cells). In an intra-observer analysis, agreements in the weighted kappa (95% Cl) were high: e.g. in epithelium 1.00 (-0.64, 2.64), in endothelium 0.89 (0.09, 1.68), and in submucosa 0.91 (-1.11, 2.92).
CD3-, CD4-, CD8-, EG2- and AA 1- immunopositive cells in the submucosa were ordinally scored (0: no cells, 1: a few cells, 2: several cells, 3: many cells). In an intra-observer analysis the agreements in weighted kappa (95% Cl) were: 0.89 (0.55, 1.15) for CD3, 0. 71 (-1.52, 2.93) for CD4, 0. 77 (-1.49, 3.03) for CD8, 0.85 (0.47, 1.24) for EG2 and 0.88 (-0.51, 2.28) for AA 1.
Data analysis All analyses were performed with the SPSS/PC 6.0 software package (SPSS Inc., Chicago, IL). Values of p < 0.05 were considered statistically significant. Group differences of nominally scored variables (iNOS expression or daynight difference in iNOS expression ) were analyzed by the Chi-Square test. Group differences of ordinally scored variables (CD3, CD4, CDS, EG2, AA 1) were analyzed by the Mann-Whitney U test. Day-night differences of ordinally scored variables were analyzed by Wilcoxon Rank test within a group, or by Mann-Whitney U test between groups. Correlations between ordinal and ordinal, or ordinal and interval variables were analyzed by Spearman's rank test. Inter-observer and intra-observer agreement were analyzed by Cohen's kappa coefficient.
Results
NADPH diaphorase staining NADPH reactivity varied in biopsies of both asthmatic patients and healthy controls. Most epithelial (including glandular) and endothelial cells stained intensely, some inflammatory cells in the submucosa stained moderately or intensely, and most smooth muscle cells did not stain or only weakly (Figure 1 ). Epithelial cells stained intracellularly and most intensely at their apical site, but not in the brush border. Distribution and intensity of NADPH diaphorase positive cells did not differ between the three groups.
74
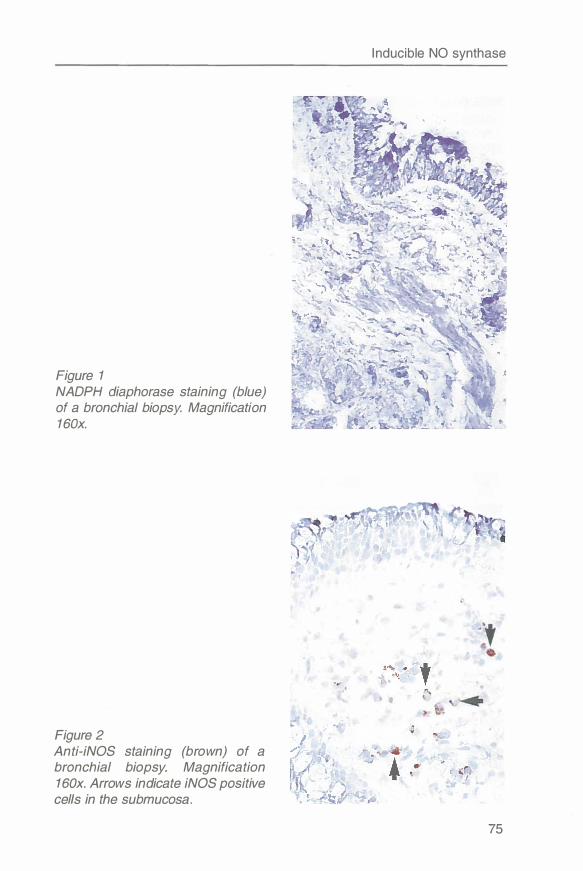
Figure 1 NADPH diaphorase staining (blue) of a bronchial biopsy. Magnification 160x.
Figure 2 Anti-iNOS staining (brown) of a bronchial biopsy. Magnification 160x. Arrows indicate iNOS positive cells in the submucosa.
Inducible NO synthase
75
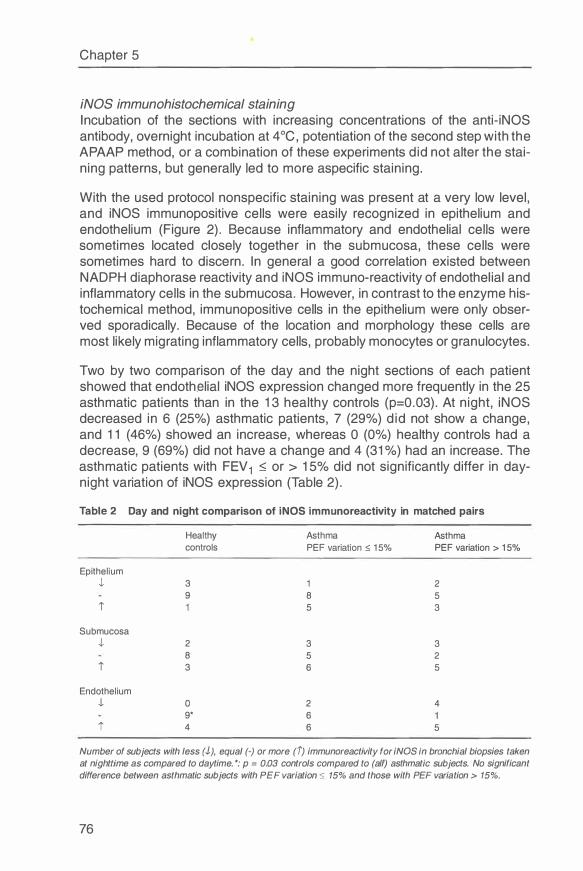
Chapter 5
iNOS immunohistochemical staining Incubation of the sections with increasing concentrations of the anti-iNOS antibody, overnight incubation at 4 °C, potentiation of the second step with the APAAP method, or a combination of these experiments did not alter the staining patterns, but generally led to more aspecific staining.
With the used protocol nonspecific staining was present at a very low level, and iNOS immunopositive cells were easily recognized in epithelium and endothelium (Figure 2). Because inflammatory and endothelial cells were sometimes located closely together in the submucosa, these cells were sometimes hard to discern. In general a good correlation existed between NADPH diaphorase reactivity and iNOS immuno-reactivity of endothelial and inflammatory cells in the submucosa. However, in contrast to the enzyme histochemical method, immunopositive cells in the epithelium were only observed sporadically. Because of the location and morphology these cells are most likely migrating inflammatory cells, probably monocytes or granulocytes.
Two by two comparison of the day and the night sections of each patient showed that endothelial iNOS expression changed more frequently in the 25 asthmatic patients than in the 13 healthy controls (p=0.03). At night, iNOS decreased in 6 (25%) asthmatic patients, 7 (29%) did not show a change, and 11 (46%) showed an increase, whereas O (0%) healthy controls had a decrease, 9 (69%) did not have a change and 4 (31 %) had an increase. The asthmatic patients with FEV 1 � or > 15% did not significantly differ in daynight variation of iNOS expression (Table 2).
Table 2 Day and night comparison of iNOS immunoreactivity in matched pairs
Healthy Asthma Asthma controls PEF variation � 15% PEF variation > 15%
Epithelium J, 3 2
9 8 5 i 5 3
Submucosa J, 2 3 3
8 5 2
i 3 6 5
Endothelium J, 0 2 4
9* 6 i 4 6 5
Number of subjects with less (J), equal (-) or more (i) immunoreactivity for iNOS in bronchial biopsies taken at nighttime as compared to daytime. *: p = 0.03 controls compared to (all) asthmatic subjects. No significant difference between asthmatic subjects with PEF variation � 15% and those with PEF variation > 15%.
76
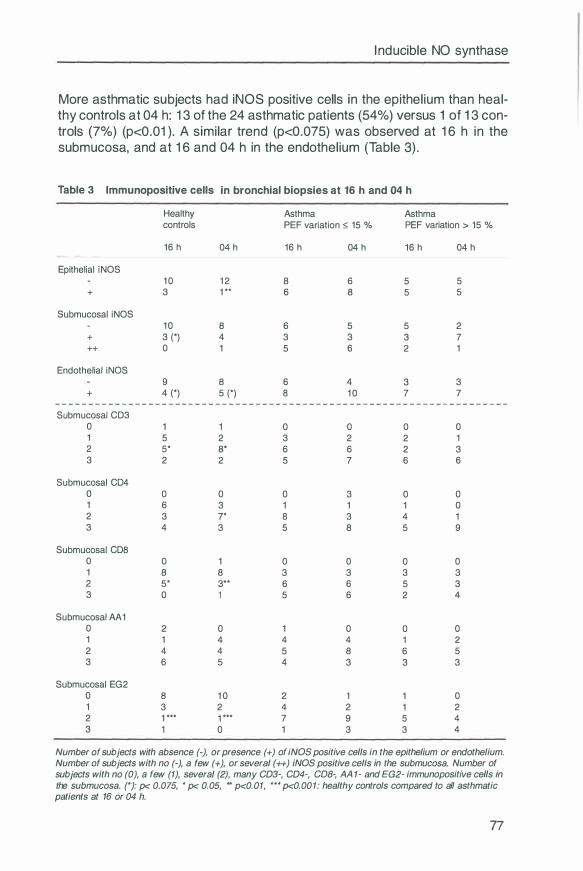
I nducible NO synthase
More asthmatic subjects had iNOS positive cells in the epithel ium than heal-thy controls at 04 h: 1 3 of the 24 asthmatic patients (54%) versus 1 of 1 3 con-trols (7%) (p<0.01 ). A simi lar trend (p<0.075) was observed at 1 6 h in the submucosa, and at 1 6 and 04 h in the endothel ium (Table 3) .
Table 3 lmmunopositive cells in bronchial biopsies at 16 h and 04 h
Healthy Asthma Asthma controls PEF variation � 15 % PEF variation > 15 %
16 h 04 h 16 h 04 h 16 h 04 h
Epithelial iNOS 10 12 8 6 5 5
+ 3 1 ** 6 8 5 5
Submucosal iNOS 10 8 6 5 5 2
+ 3 (*) 4 3 3 3 7 ++ 0 1 5 6 2 1
Endothelial iNOS 9 8 6 4 3 3
+ 4 (*) 5 (*) 8 10 7 7 - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Submucosal CD3
0 1 1 0 0 0 0 1 5 2 3 2 2 1 2 5* 8* 6 6 2 3 3 2 2 5 7 6 6
Submucosal CD4 0 0 0 0 3 0 0 1 6 3 1 1 1 0 2 3 7* 8 3 4 1 3 4 3 5 8 5 9
Submucosal CDS 0 0 1 0 0 0 0 1 8 8 3 3 3 3 2 5* 3** 6 6 5 3 3 0 5 6 2 4
Submucosal AA 1 0 2 0 1 0 0 0 1 1 4 4 4 1 2 2 4 4 5 8 6 5 3 6 5 4 3 3 3
Submucosal EG2 0 8 10 2 1 1 0 1 3 2 4 2 1 2 2 1 *** 1 *** 7 9 5 4 3 0 1 3 3 4
Number of subjects with absence (-), or presence (+) of iNOS positive cells in the epithelium or endothelium. Number of subjects with no (-), a few (+), or several (++) iNOS positive cells in the submucosa. Number of subjects with no (0), a few (1), several (2), many CD3-, CD4-, COB-, AA 1- and EG2- immunopositive cells in the submucosa. (*): p< 0.075, * p< 0.05, ** p<0.01, *** P<0,001: healthy controls compared to all asthmatic patients at 16 or 04 h.
77
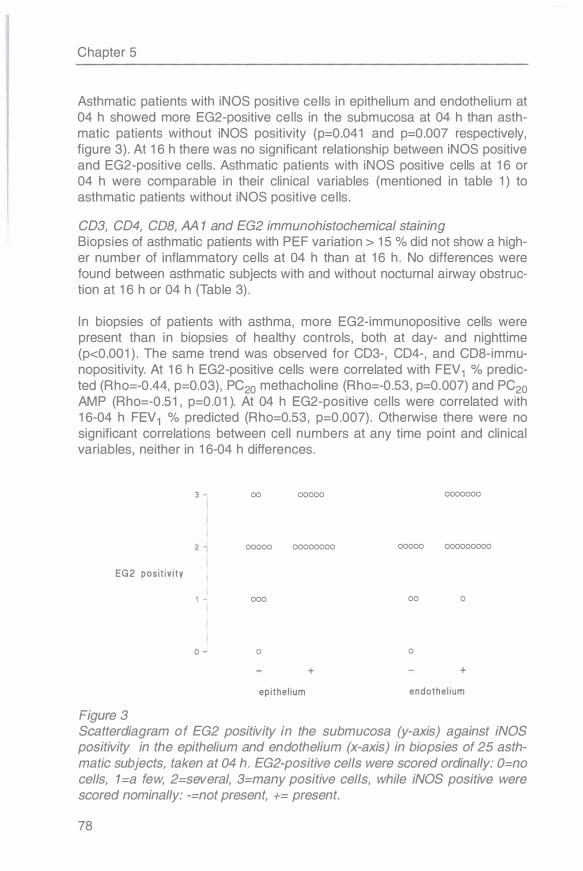
Chapter 5
Asthmatic patients with iNOS positive cells in epithelium and endothelium at 04 h showed more EG2-positive cells in the submucosa at 04 h than asthmatic patients without iNOS positivity (p=0.041 and p=0.007 respectively, figure 3). At 16 h there was no significant relationship between iNOS positive and EG2-positive cells. Asthmatic patients with iNOS positive cells at 16 or 04 h were comparable in their clinical variables (mentioned in table 1) to asthmatic patients without iNOS positive cells.
CD3, CD4, COB, AA 1 and EG2 immunohistochemical staining Biopsies of asthmatic patients with PEF variation > 15 % did not show a higher number of inflammatory cells at 04 h than at 16 h. No differences were found between asthmatic subjects with and without nocturnal airway obstruction at 16 h or 04 h (Table 3) .
In biopsies of patients with asthma, more EG2-immunopositive cells were present than in biopsies of healthy controls, both at day- and nighttime (p<0.001 ) . The same trend was observed for CD3-, CD4-, and CD8-immunopositivity. At 16 h EG2-positive cells were correlated with FEV 1 % predicted (Rho=-0.44, p=0.03), PC20 methacholine (Rho=-0.53, p=0.007) and PC20
AMP (Rho=-0.51, p=0.01 ). At 04 h EG2-positive cells were correlated with 16-04 h FEV 1 % predicted (Rho=0.53, p=0.007). Otherwise there were no significant correlations between cell numbers at any time point and clinical variables, neither in 16-04 h differences.
EG2 pos i t iv i ty
0
Figure 3
00 00000
00000 00000000
000
0
+
epithel ium
0000000
00000 000000000
00 0
0
+
endothe l ium
Scatterdiagram of EG2 positivity in the submucosa (y-axis) against iNOS positivity in the epithelium and endothelium (x-axis) in biopsies of 25 asthmatic subjects, taken at 04 h. EG2-positive cells were scored ordinally: 0=no cells, 1 =a few, 2=several, 3=many positive cells, while iNOS positive were scored nominally: -=not present, += present.
78
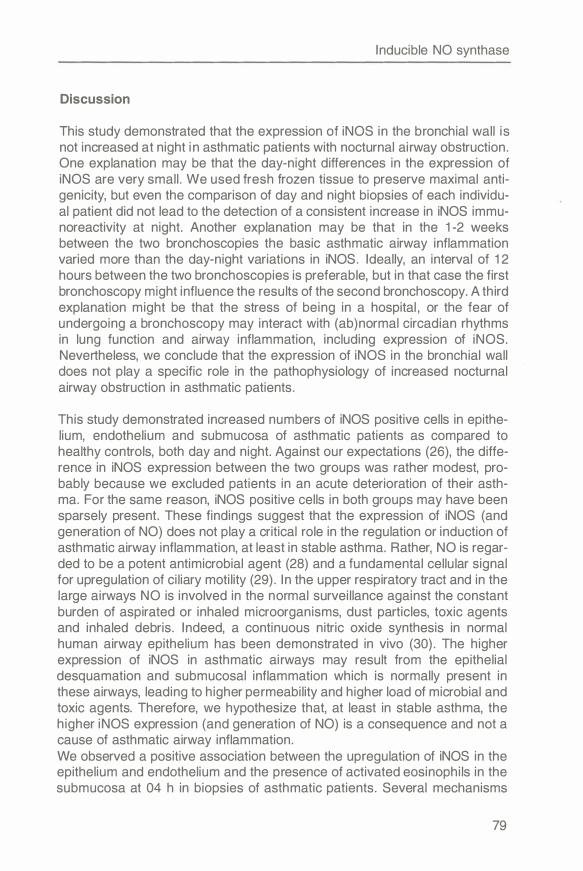
Inducible NO synthase
Discussion
This study demonstrated that the expression of iNOS in the bronchial wall is not increased at night in asthmatic patients with nocturnal airway obstruction. One explanation may be that the day-night differences in the expression of iNOS are very small. We used fresh frozen tissue to preserve maximal antigenicity, but even the comparison of day and night biopsies of each individual patient did not lead to the detection of a consistent increase in iNOS immunoreactivity at night. Another explanation may be that in the 1-2 weeks between the two bronchoscopies the basic asthmatic airway inflammation varied more than the day-night variations in iNOS. Ideally, an interval of 12 hours between the two bronchoscopies is preferable, but in that case the first bronchoscopy might influence the results of the second bronchoscopy. A third explanation might be that the stress of being in a hospital , or the fear of undergoing a bronchoscopy may interact with (ab)normal circadian rhythms in lung function and airway inflammation, including expression of iNOS. Nevertheless, we conclude that the expression of iNOS in the bronchial wall does not play a specific role in the pathophysiology of increased nocturnal airway obstruction in asthmatic patients.
This study demonstrated increased numbers of iNOS positive cells in epithelium, endothelium and submucosa of asthmatic patients as compared to healthy controls, both day and night. Against our expectations (26), the difference in iNOS expression between the two groups was rather modest, probably because we excluded patients in an acute deterioration of their asthma. For the same reason, iNOS positive cells in both groups may have been sparsely present. These findings suggest that the expression of iNOS (and generation of NO) does not play a critical role in the regulation or induction of asthmatic airway inflammation, at least in stable asthma. Rather, NO is regarded to be a potent antimicrobial agent (28) and a fundamental cellular signal for upregulation of ciliary motility (29). In the upper respiratory tract and in the large airways NO is involved in the normal surveillance against the constant burden of aspirated or inhaled microorganisms, dust particles, toxic agents and inhaled debris. Indeed, a continuous nitric oxide synthesis in normal human airway epithelium has been demonstrated in vivo (30). The higher expression of iNOS in asthmatic airways may result from the epithelial desquamation and submucosal inflammation which is normally present in these airways, leading to higher permeability and higher load of microbial and toxic agents. Therefore, we hypothesize that, at least in stable asthma, the higher iNOS expression (and generation of NO) is a consequence and not a cause of asthmatic airway inflammation. We observed a positive association between the upregulation of iNOS in the epithelium and endothelium and the presence of activated eosinophils in the submucosa at 04 h in biopsies of asthmatic patients. Several mechanisms
79
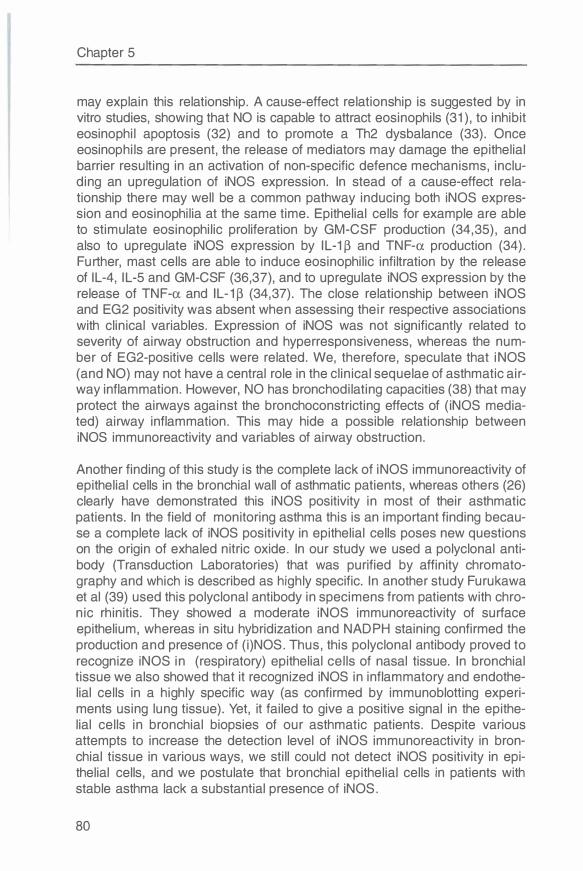
Chapter 5
may explain this relationship. A cause-effect relationship is suggested by in vitro studies, showing that NO is capable to attract eosinophils (31 ), to inhibit eosinophil apoptosis (32) and to promote a Th2 dysbalance (33). Once eosinophils are present, the release of mediators may damage the epithelial barrier resulting in an activation of non-specific defence mechanisms, including an upregulation of iNOS expression. In stead of a cause-effect relationship there may well be a common pathway inducing both iNOS expression and eosinophilia at the same time. Epithelial cells for example are able to stimulate eosinophilic proliferation by GM-CSF production (34,35), and also to upregulate iNOS expression by I L-1 � and TNF-a production (34). Further, mast cells are able to induce eosinophilic infiltration by the release of IL-4, I L-5 and GM-CSF (36,37), and to upregulate iNOS expression by the release of TNF-a and IL-1 � (34,37). The close relationship between iNOS and EG2 positivity was absent when assessing their respective associations with clinical variables. Expression of iNOS was not significantly related to severity of airway obstruction and hyperresponsiveness, whereas the number of EG2-positive cells were related. We, therefore, speculate that iNOS (and NO) may not have a central role in the clinical sequelae of asthmatic airway inflammation. However, NO has bronchodilating capacities (38) that may protect the airways against the bronchoconstricting effects of (iNOS mediated) airway inflammation. This may hide a possible relationship between iNOS immunoreactivity and variables of airway obstruction.
Another finding of this study is the complete lack of iNOS immunoreactivity of epithelial cells in the bronchial wall of asthmatic patients, whereas others (26) clearly have demonstrated this iNOS positivity in most of their asthmatic patients. In the field of monitoring asthma this is an important finding because a complete lack of iNOS positivity in epithelial cells poses new questions on the origin of exhaled nitric oxide. In our study we used a polyclonal antibody (Transduction Laboratories) that was purified by affinity chromatography and which is described as highly specific. In another study Furukawa et al (39) used this polyclonal antibody in specimens from patients with chronic rhinitis. They showed a moderate iNOS immunoreactivity of surface epithelium, whereas in situ hybridization and NADPH staining confirmed the production and presence of (i)NOS. Thus, this polyclonal antibody proved to recognize iNOS in (respiratory) epithelial cells of nasal tissue. In bronchial tissue we also showed that it recognized iNOS in inflammatory and endothelial cells in a highly specific way (as confirmed by immunoblotting experiments using lung tissue). Yet, it failed to give a positive signal in the epithelial cells in bronchial biopsies of our asthmatic patients. Despite various attempts to increase the detection level of iNOS immunoreactivity in bronchial tissue in various ways, we still could not detect iNOS positivity in epithelial cells, and we postulate that bronchial epithelial cells in patients with stable asthma lack a substantial presence of iNOS.
80
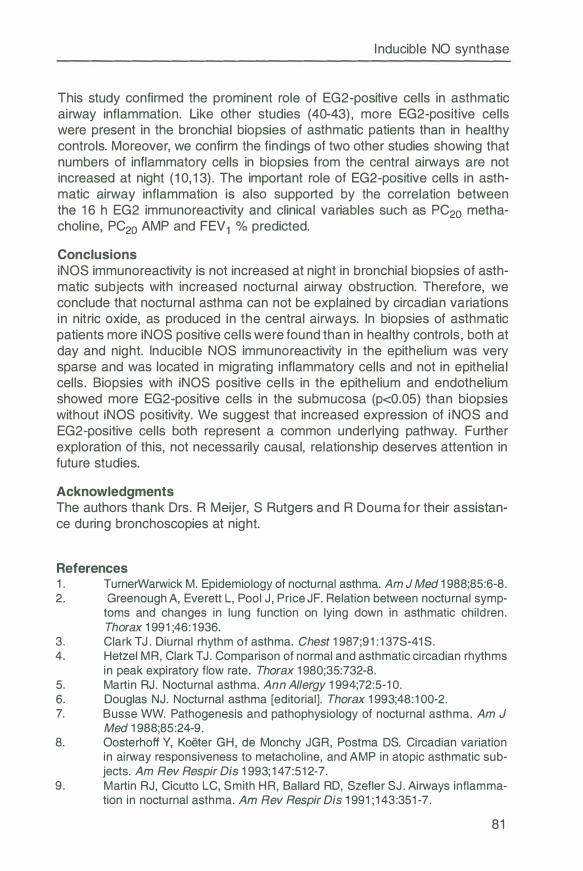
Inducible NO synthase
This study confirmed the prominent role of EG2-positive cells in asthmatic airway inflammation. Like other studies (40-43) , more EG2-positive cells were present in the bronchial biopsies of asthmatic patients than in healthy controls. Moreover, we confirm the findings of two other studies showing that numbers of inflammatory cells in biopsies from the central airways are not increased at night (10, 1 3) . The important role of EG2-positive cells in asthmatic airway inflammation is also supported by the correlation between the 1 6 h EG2 immunoreactivity and clinical variables such as PC20 methacholine, PC20 AMP and FEV 1 % predicted.
Conclusions iNOS immunoreactivity is not increased at night in bronchial biopsies of asthmatic subjects with increased nocturnal airway obstruction. Therefore, we conclude that nocturnal asthma can not be explained by circadian variations in nitric oxide, as produced in the central airways. In biopsies of asthmatic patients more iNOS positive cells were found than in healthy controls , both at day and night. Inducible NOS immunoreactivity in the epithelium was very sparse and was located in migrating inflammatory cells and not in epithelial cells . Biopsies with iNOS positive cells in the epithelium and endothelium showed more EG2-positive cells in the submucosa (p<0.05) than biopsies without iNOS positivity. We suggest that increased expression of i NOS and EG2-positive cells both represent a common underlying pathway. Further exploration of this, not necessarily causal, relationship deserves attention in future studies.
Acknowledgments The authors thank Ors. R Meijer, S Rutgers and R Douma for their assistance during bronchoscopies at night.
References 1 . TurnerWarwick M. Epidemiology of nocturnal asthma. Am J Med 1 988;85:6-8. 2. Greenough A, Everett L, Pool J, Price JF. Relation between nocturnal symp-
toms and changes in lung function on lying down in asthmatic children. Thorax 1 991 ;46: 1 936.
3. Clark T J. Diurnal rhythm of asthma. Chest 1 987;91 : 1 37S-41 S. 4. Hetzel MR, Clark T J. Comparison of normal and asthmatic circadian rhythms
in peak expiratory flow rate. Thorax 1 980;35:732-8. 5. Martin RJ. Nocturnal asthma. Ann Allergy 1 994;72:5-1 0. 6. Douglas NJ. Nocturnal asthma [editorial]. Thorax 1 993;48: 1 00-2. 7. Busse WW. Pathogenesis and pathophysiology of nocturnal asthma. Am J
Med 1 988;85:24-9. 8. Oosterhoff Y, Keeter GH, de Monchy JGR, Postma OS. Circadian variation
in airway responsiveness to metacholine, and AMP in atopic asthmatic subjects. Am Rev Respir Dis 1 993; 1 47:51 2-7.
9. Martin RJ, Cicutto LC, Smith HR, Ballard RD, Szefler SJ. Airways inflammation in nocturnal asthma. Am Rev Respir Dis 1 991 ; 1 43:351 -7 .
81
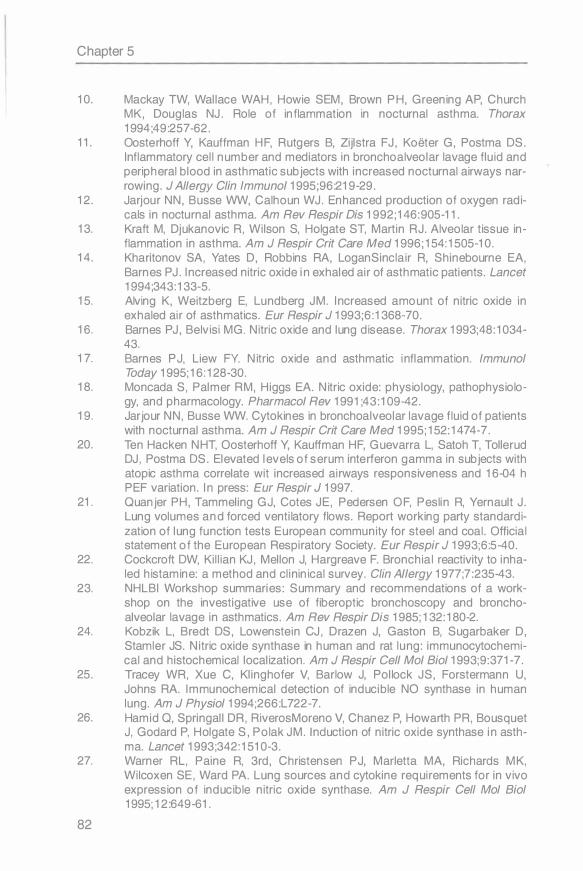
Chapter 5
10. Mackay TW, Wallace WAH , Howie SEM, Brown PH, Greening AP, Church MK, Douglas NJ . Role of inflammation in nocturnal asthma. Thorax 1994;49:257-62.
11. Oosterhoff Y, Kauffman HF, Rutgers B, Zijlstra FJ , Koeter G, Postma OS. Inflammatory cel l number and mediators in bronchoalveolar lavage flu id and peripheral blood in asthmatic subjects with increased nocturnal airways narrowing. J Allergy C/in lmmunol 1995;96:219-29.
12. Jarjour NN, Busse WW, Calhoun WJ. Enhanced production of oxygen radicals in nocturnal asthma. Am Rev Respir Dis 1992; 146: 905-11.
13. Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolar tissue inflammation in asthma. Am J Respir Grit Care Med 1996; 154: 1505-10.
14. Kharitonov SA, Yates D, Robbins RA, LoganSinclair R, Shinebourne EA, Barnes PJ . I ncreased nitric oxide in exhaled ai r of asthmatic patients. Lancet 1994;343:133-5.
15. Alving K, Weitzberg E, Lundberg JM. I ncreased amount of nitric oxide in exhaled ai r of asthmatics. Eur Respir J 1993;6:1368-70.
16. Barnes PJ , Belvisi MG. Nitric oxide and lung disease. Thorax 1993;48: 1034-43.
17. Barnes PJ, Liew FY. Nitric oxide and asthmatic inflammation. lmmunol Today 1995; 16: 128-30.
18. Moncada S, Palmer RM, Higgs EA. Nitric oxide: physiology, pathophysiology, and pharmacology. Pharmacol Rev 1991;43:109-42.
19. Jarjour NN, Busse WW. Cytokines in bronchoalveolar lavage fluid of patients with nocturnal asthma. Am J Respir Grit Care Med 1995; 152: 1474-7.
20. Ten Hacken NHT, Oosterhoff Y, Kauffman HF, Guevarra L, Satoh T, Tollerud DJ , Postma OS. Elevated levels of serum interferon gamma in subjects with atopic asthma correlate wi t increased ai rways responsiveness and 16-04 h PEF variation. I n press: Eur Respir J 1997.
21. Quanjer PH, Tammeling GJ, Cotes JE , Pedersen OF, Peslin R, Yernault J . Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests European communi ty for steel and coal. Official statement of the European Respiratory Society. Eur Respir J 1993;6:5-40.
22. Cockcroft OW, Ki l l ian KJ , Mellon J, Hargreave F. Bronchia l reactivity to inhaled histamine: a method and cl ininical survey. Clin Allergy 1977;7:235-43.
23. NHLBI Workshop summaries: Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis 1985; 132: 180-2.
24. Kobzik L, Bredt OS, Lowenstein CJ , Drazen J, Gaston B, Sugarbaker D, Stamler JS. Nitric oxide synthase in human and rat lung: immunocytochemical and histochemical localization. Am J Respir Cell Mo/ Bio/ 1993;9:371-7.
25. Tracey WR, Xue C, Klinghofer V, Barlow J, Pollock JS, Forstermann U, Johns RA. lmmunochemical detection of inducible NO synthase in human lung. Am J Physio/ 1994;266:L722-7.
26. Hamid Q, Springall DR, RiverosMoreno V, Chanez P, Howarth PR, Bousquet J, Godard P, Holgate S, Polak JM. Induction of nitric oxide synthase in asthma. Lancet 1993;342:1510-3.
27. Warner RL, Paine R, 3rd, Christensen PJ, Marietta MA, Richards MK, Wi lcoxen SE, Ward PA. Lung sources and cytokine requi rements for in vivo expression of inducible nitric oxide synthase. Am J Respir Cell Mo/ Biol 1995; 12:649-61.
82
Inducible NO synthase
28. Lyons CR. The role of nitric oxide in inflammation. Advances in Immunology 1 995;60:323-71 .
29. Thompson AB, Robbins RA, Romberger DJ , Sisson JH, Spurzem JR, Teschler H, Rennard SI . Immunological functions of the pulmonary epithelium. Eur Respir J 1 995;8: 1 27-49.
30. Guo FH, De Raeve HR, Rice TW, Stuehr DJ , Thunnissen FB, Erzurum SC. Continuous nitric oxide synthesis by inducible nitric oxide synthase in normal human airway epithelium in vivo. Proc Natl Acad Sci U SA 1 995;92:7809-1 3.
31 . Ferreira HHA, Medeiros MV, Lima CSP, Flores CA, Sannomiya P, Antunes E, De Nucci G. I nhibition of eosinophil chemotaxis by chronic blockade of nitric oxide biosynthesis. Eur J Pharmacol 1 996;31 0: 201 -7.
32. Beauvais F, Michel L, Dubertret L. The nitric oxide donors, azide and hydroxylamine, inhibit the programmed cell death of cytokinedeprived human eosinophils. FEBS Lett 1 995;361 : 229-32.
33. Taylor Robinson AW, Liew FY, Severn A, Xu D, Mcsorley SJ, Garside P, Padron J , Phillips RS. Regulation of the immune response by nitric oxide differentially produced by T helper type 1 and T helper type 2 cells. Eur J lmmunol 1 994;24:980-4.
34. Ackerman V, Marini M, Vittori E, Bellini A, Vassali G, Mattoli S. Detection of cytokines and their cell sources in bronchial biopsy specimens from asthmatic patients. Relationship to atopic status, symptoms, and level of airway hyperresponsiveness. Chest 1 994; 1 05:687-96.
35. Sousa AR, Poston RN, Lane SJ, Nakhosteen JA, Lee TH. Detection of GMCSF in asthmatic bronchial epithelium and decrease by inhaled corticosteroids. Am Rev Respir Dis 1 993; 1 47: 1 557-61 .
36. Ying S, Durham SR, Corrigan CJ, Hamid Q, Kay AB. Phenotype of cells expressing mRNA for TH2 type (interleukin-4 and interleukin-5) and TH1 type (interleukin-2 and interferon-gamma) cytokines in bronchoalveolar lavage and bronchial biopsies from atopic asthmatic and normal control subjects. Am J Respir Cell Mo/ Bio/ 1 995; 1 2:477-87.
37. Bradding P, Roberts JA, Britten KM, Montefort S, Djukanovic R, Mueller R , Heusser CH, Howarth PH, Holgate ST. lnterleukin-4, -5, and -6 and tumor necrosis factoralpha in normal and asthmatic airways: evidence for the human mast cell as a source of these cytokines. Am J Respir Cell Mo/ Biol 1 994; 1 0:471 -80.
38. Hagman M, Frostell CG, Hedenstrom H, Hedenstierna G. I nhalation of nitric oxide modulates adult human bronchial tone. Am Rev Respir Dis 1 993; 1 48: 1 474-8.
39. Furukawa K, Harrison DG, Saleh D, Shennib H, Chagnon FP, Giaid A Expression of nitric oxide synthase in the human nasal mucosa. Am J Respir Grit Care Med 1 996; 1 53:847-50.
40. Bradley BL, Azzawi M, Jacobson M, Assoufi B, Collins JV, I rani AM, Schwartz LB, Durham SR, Jeffery PK, Kay AB. Eosinophils, T-lymphocytes, mast cells, neutrophils, and macrophages in bronchial biopsy specimens from atopic subjects with asthma: comparison with biopsy specimens from atopic subjects without asthma and normal control subjects and relationship to bronchial hyperresponsiveness. J Allergy Clin lmmunol 1 991 ;88:661 -74.
41 . Bousquet J , Chanez P, Vignola AM, Lacoste JV, Michel FB. Eosinophil inflammation in asthma. Am J Respir Grit Care Med 1 994; 1 50:S33-8.
83
Chapter 5
42. Bentley AM, Menz G, Storz C, Robinson OS, Bradley B, Jeffery PK, Durham SR, Kay AB. Identification of T lymphocytes, macrophages, and activated eosinophils in the bronchial mucosa in intrinsic asthma. Relationship to symptoms and b ronchial responsiveness. Am Rev Respir Dis 1 992; 1 46:500-6.
43. Azzawi M, Bradley 8, Jeffery PK, Frew AJ, Wardlaw AJ, Knowles G, Assoufi B, Collins JV, Durham S, Kay AB. Identification of activated T lymphocytes and eosinophils in bronchial biopsies in stable atopic asthma. Am Rev Respir Dis 1 990; 1 42: 1 407-1 3.
84
Chapter 6
Decreased expression of eNOS at night in asthmatic subjects with large PEF variation
Nick ten Hacken, Dirkje Postma, Gineke Drok, Mieke Smith, Jan Kraan, Wim Timens
Submitted
Abstract
Nitric Oxide (NO) is thought to play an important role in asthmatic airway inflammation. Endothelial NO synthase (eNOS) is one of the constitutive enzymes involved in the production of NO. Recently eNOS has been reported to be subject to modest degrees of regulation. Therefore, we were interested in the (variable) presence of eNOS in bronchial tissue of asthmatic subjects. We investigated bronchial biopsies at 16 and 04 h from 13 healthy controls and from 25 asthmatic patients with a PEF variation ::; or > 15%. Biopsies were snap-frozen and double immunostained for eNOS in combination with a common vessel antigen (CD31 ). The degree of immunopositivity for eNOS was expressed as the percentage of CD31 positive vessels encountered in complete sections of a biopsy. The mean (sd) 16-04 h changes in % eNOS expression in healthy controls, asthmatic patients with mild and severe nocturnal airway obstruction were respectively: -17 (44), -14 (24) and +13 (27) %. The 16-04 h change in eNOS expression in asthmatic patients was significantly correlated with PEF variation: rho = 0.48 (p = 0.03). We conclude that patients with large swings in airway diameter lack the normally occurring increase in eNOS expression at night. Finally, we speculate about the causes and consequences of this aberrant circadian rhythm.
Introduction
Over the last years the interest in the role of Nitric Oxide (NO) in the pathophysiology of asthma has been a subject in many studies. At present, NO is considered to be one of the factors important for increased hyperresponsiveness (1) and asthmatic airway inflammation (2). Especially the role of inducible NO synthase (iNOS) has been the centre of attention in many in vivo and in vitro studies. Gradually, the paradigm has evolved that iNOS is up regulated in epithelial and inflammatory cells in asthmatic bronchi (3,4) and that it is responsible for the elevated NO values measured in exhaled air (5,6). Until now, only one biopsy study on iNOS has been published, showing an increased presence in the epithelium of asthmatic patients (7). In contrast to iNOS, relatively little attention has been given to the role of the constitutive
85

Chapter 6
NO synthases (cNOS), most likely because they can not be modulated by inflammatory factors, and because they are thought to be responsible for only relatively low amounts of NO production . However, new findings indicate that iNOS may be constantly present (8), whereas endothelial cNOS (eNOS) can be subject to modest degrees of regulation (9).
For this reason we were interested in the presence of endothelial cNOS in bronchial tissue of asthmatic subjects. The main question of this study was whether eNOS can be expressed in a variable way and how this may be related to clinical asthma. In a study on nocturnal asthma we obtained bronchial biopsies at 16 and 04 h from 13 healthy controls and from 25 asthmatic patients. We examined the presence of endothelial NO synthase and compared day and night values.
Materia l and Methods Thirteen healthy volunteers and 25 asthmatic subjects aged 18 to 45 years participated in this study (Table 1 ). Asthmatic subjects were selected on: a history consistent with asthma; presence of atopy (positive intracutaneous tests against house dust mite or two other aero-allergens), FEV1 > 1.5 I and > 60% predicted; PC20 methacholine :s; 9.8 mg/ml; PC20 AMP :s; 80 mg/ml; no use of oral corticosteroids within 2 months and no use of inhaled corticosteroids within 1 month before the study. Subjects with a history of smoking within the last 2 years, or with a respiratory infection within the last 4 weeks were excluded. The study was approved by the Medical Ethics Committee of the University Hospital Groningen, and all subjects gave their written informed consent.
Table 1 Characteristics of participating subjects
Number (male/female) Age, yrs Eosinophils, x106/ml F EV1 , % pred +Reversibility, % pred PEF variation, % PC20 methacholine, mg/ml PC20 AMP, mg/ml
Healthy controls
13 (5/8) 32 (8.4) 0.08 (0.03-0.31) 106 (14) 1 .5 (2. 1 ) 7 .5 (3.2) >9.8 >80
Asthmatic subjects
25 (15/10) 31 (9. 1 ) 0.25 (0.08-0.54)** 93 (13)* 11 (10)** 14.8 (8.2)** 0.54 (0.08-6 .61) 2.80 (0.18-22.8)
Values are expressed as means {sd). Eosinophils in peripheral blood and PC20 's are expressed as geometric means (range). *: P � 0.01, **: P� 0.001 versus healthy controls. t Reversibility of FEV1 % predicted on inhalation of 400 µg salbutamol.
Subjects underwent a bronchoscopy twice, in a randomized order at 16 or 04 h, with an interval of seven to fourteen days. Three days before the first bronchoscopy, bronchodilators were withheld and PEF values (Mini-Wright) were
86
Endothelial NO synthase
recorded at 08, 12, 16, 20, 24, and 04 h. PEF variation was defined as: (highest - lowest value) / mean of 6 measurements daily. Mean PEF variation was calculated as the average of the PEF variation measured during three days. Asthmatic subjects were divided on the basis of a mean PEF variation � or > 15%.
Bronchoscopy was performed using an Olympus B 1 IT1 O flexible fiberoptic bronchoscope (Olympus Optical, Tokyo, Japan). Biopsies were obtained from the subcarinae of the left or right lower lobe using a fenestrated forceps (FB-21 C, Olympus, Tokyo, Japan), according to the guidelines of the ATS (10). Biopsies were mounted in OCT and snap-frozen by immersion in isopentane (-80°C). Sections were cut with a thickness of 4 µm. Vessels were recognized by morphology in combination with staining for anti-CD31 (lgG2b, Monosan, Uden, The Netherlands) and labelling by isotype specific biotinylated goat anti-mouse immunoglobulins (SBA, Birmingham, AL, USA) and subsequently by streptavidin conjugated to alkaline phosphatase (DAKO, Glostrup, Denmark), providing a blue reaction product with Fast Blue 88. eNOS was recognized by anti-eNOS (lgG1, Transduction Lab, Lexington, Kentucky, USA) and labelled by isotype specific goat anti-mouse antibodies conjugated to peroxidase (SBA, Birmingham, AL, USA), using 3-amino-9-ethylcarbazole resulting in a reddish-brown reaction product. Whole sections were examined systematically in a blinded way, using an eye grid, at magnification 250 x. Vessels were scored positive, whenever immunopositivity for eNOS was present, and expressed as a percentage of CD31 positive vessels. Sections were quantified twice by the same observer (G.D.), the mean results being entered for analysis. The mean intra-observer difference (confidence interval) (11) was: 1.4 (-1.3, 4.1) %. The mean intra-observer correlation was: 0.93 (p<0.001 ).
Statistical analysis was performed on SPSS / PC 6.0 software package (SPSS Inc., Chicago, IL). The Student's t test was used to compare variables between groups, and Student's t test for paired values to compare between 04 and 16 h values within groups, on condition of a normal distribution. % eNOS positivity and 16-04 h change in % eNOS positivity showed normal distributions. Therefore, values are reported as means with standard deviations between brackets. Correlations between eNOS and clinical variables were performed using Pearson's rank test, also on condition of a normal distribution.
Results Expression of eNOS on CD31 positive vessels was found to be 'patchy' in asthmatic subjects as well as in healthy controls (Figure 1 ). No difference in the percentage of eNOS positive vessels was seen between the superficial layers of the submucosa (within 50 µm below the basement membrane) and the deeper parts of biopsies. eNOS expression did not differ significantly
87
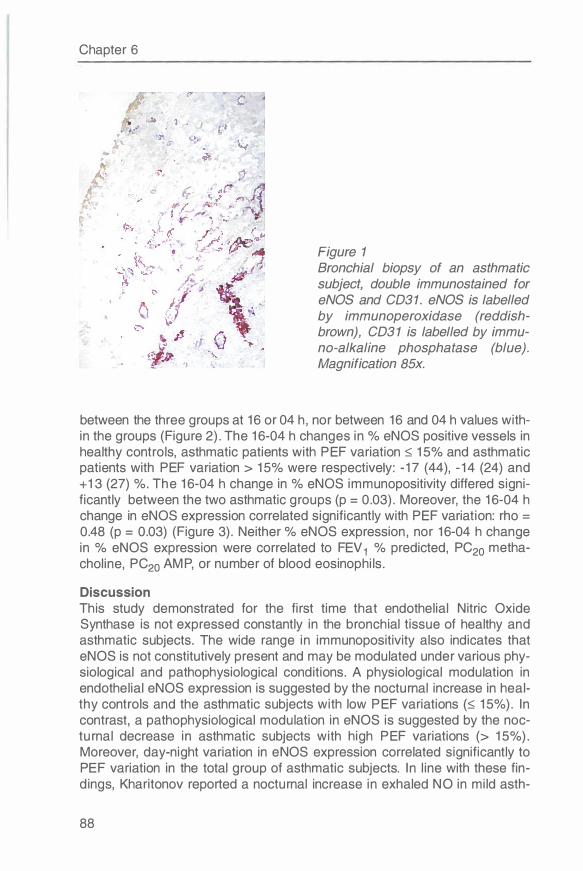
Chapter 6
Figure 1 Bronchial biopsy of an asthmatic subject, double immunostained for eNOS and CD31 . eNOS is labelled by immunoperoxidase (reddishbrown), CD3 1 is labelled by immuno-alkaline phosphatase (blue). Magnification 85x.
between the three groups at 16 or 04 h , nor between 16 and 04 h values within the groups (Figure 2). The 16-04 h changes in % eNOS positive vessels in healthy controls, asthmatic patients with PEF variation � 15% and asthmatic patients with PEF variation > 15% were respectively: -17 (44), -14 (24) and + 13 (27) %. The 16-04 h change in % eNOS immunopositivity differed significantly between the two asthmatic groups (p = 0.03). Moreover, the 16-04 h change in eNOS expression correlated significantly with PEF variation: rho = 0.48 (p = 0.03) (Figure 3). Neither % eNOS expression , nor 16-04 h change in % eNOS expression were correlated to FEV 1 % predicted, PC20 methacholine, PC20 AMP, or number of blood eosinophils.
Discussion This study demonstrated for the first time that endothelial Nitric Oxide Synthase is not expressed constantly in the bronchial tissue of healthy and asthmatic subjects. The wide range in immunopositivity also indicates that eNOS is not constitutively present and may be modulated under various physiological and pathophysiological conditions. A physiological modulation in endothelial eNOS expression is suggested by the nocturnal increase in healthy controls and the asthmatic subjects with low PEF variations (� 15%). In contrast, a pathophysiological modulation in eNOS is suggested by the nocturnal decrease in asthmatic subjects with high PEF variations (> 15%). Moreover, day-night variation in eNOS expression correlated significantly to PEF variation in the total group of asthmatic subjects. In line with these findings, Kharitonov reported a nocturnal increase in exhaled NO in mild asth-
88
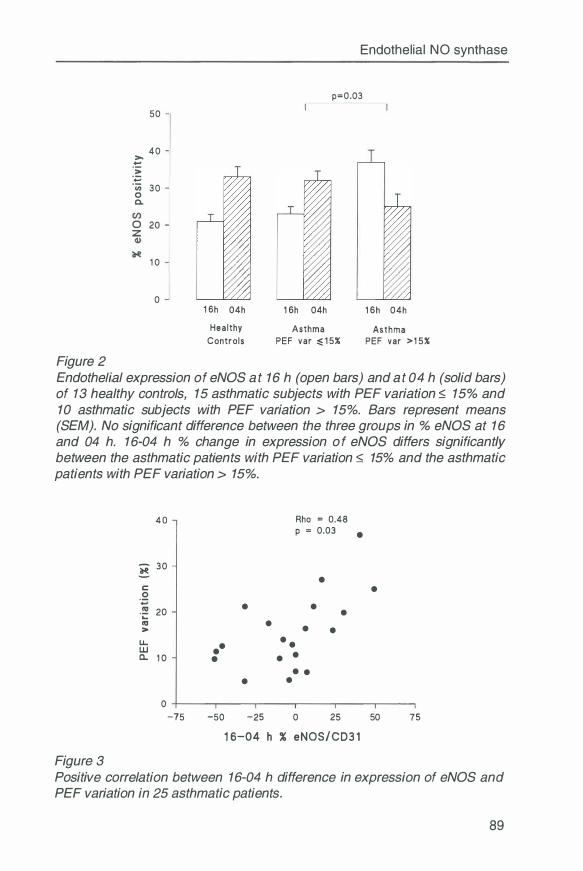
Figure 2
� ·;:
50
40
:� 30 0 C.
0 20 z
1 0
0 1 6h 04h
Hea l thy Controls
Endothelial NO synthase
p=0.03
1 6h 04h
Asthma PEF var � 1 5%
1 6h 04h
Asthma PEF var >1 5%
Endothelial expression of eNOS at 16 h (open bars) and at 04 h (solid bars) of 13 healthy controls, 15 asthmatic subjects with PEF variation :::; 15% and 10 asthmatic subjects with PEF variation > 15%. Bars represent means (SEM). No significant difference between the three groups in % eNOS at 16 and 04 h. 16-04 h % change in expression of eNOS differs significantly between the asthmatic patients with PEF variation :::; 15% and the asthmatic patients with PEF variation > 15%.
40 Rho = 0.48 p = 0.03 •
ii 30 •
C • . 2
20 • •
·.:::: • "' • • > •
LL •• • •
UJ • a.. 1 0 • • • • • •
0 -75 -50 -25 0 25 50 75
1 6-04 h % eNOS/CD3 1
Figure 3 Positive correlation between 16-04 h difference in expression of eNOS and PEF variation in 25 asthmatic patients.
89
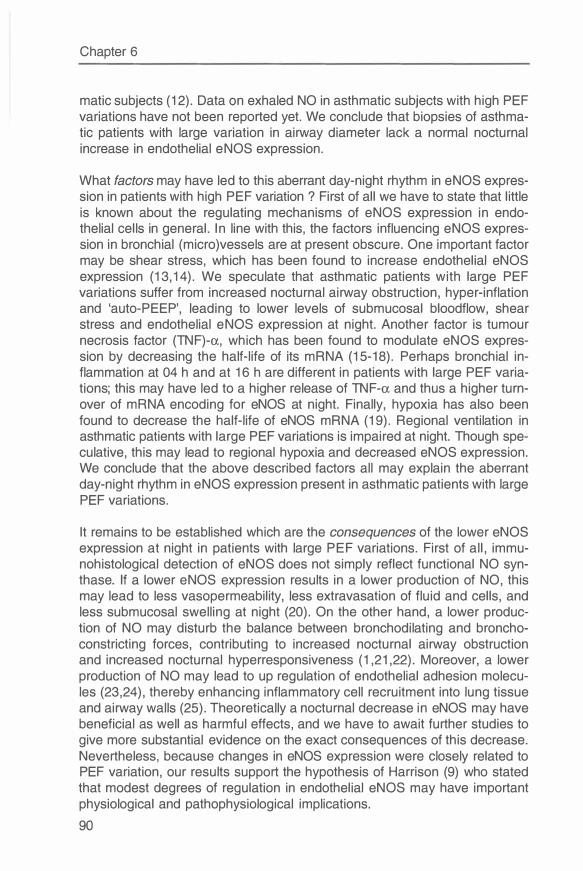
Chapter 6
matic subjects (12). Data on exhaled NO in asthmatic subjects with high PEF variations have not been reported yet. We conclude that biopsies of asthmatic patients with large variation in airway diameter lack a normal nocturnal increase in endothelial eNOS expression.
What factors may have led to this aberrant day-night rhythm in eNOS expression in patients with high PEF variation ? First of all we have to state that little is known about the regulating mechanisms of eNOS expression in endothelial cells in general. In line with this, the factors influencing eNOS expression in bronchial (micro)vessels are at present obscure. One important factor may be shear stress, which has been found to increase endothelial eNOS expression (13,14). We speculate that asthmatic patients with large PEF variations suffer from increased nocturnal airway obstruction, hyper-inflation and 'auto-PEEP', leading to lower levels of submucosal bloodflow, shear stress and endothelial eNOS expression at night. Another factor is tumour necrosis factor (TNF)-a, which has been found to modulate eNOS expression by decreasing the half-life of its mRNA (15-18). Perhaps bronchial inflammation at 04 h and at 16 h are different in patients with large PEF variations; this may have led to a higher release of TNF-a and thus a higher turnover of mRNA encoding for eNOS at night. Finally, hypoxia has also been found to decrease the half-life of eNOS mRNA (19). Regional ventilation in asthmatic patients with large PEF variations is impaired at night. Though speculative, this may lead to regional hypoxia and decreased eNOS expression. We conclude that the above described factors all may explain the aberrant day-night rhythm in eNOS expression present in asthmatic patients with large PEF variations.
It remains to be established which are the consequences of the lower eNOS expression at night in patients with large PEF variations. First of all, immunohistological detection of eNOS does not simply reflect functional NO synthase. If a lower eNOS expression results in a lower production of NO, this may lead to less vasopermeability, less extravasation of fluid and cells, and less submucosal swelling at night (20). On the other hand, a lower production of NO may disturb the balance between bronchodilating and bronchoconstricting forces, contributing to increased nocturnal airway obstruction and increased nocturnal hyperresponsiveness (1,21,22). Moreover, a lower production of NO may lead to up regulation of endothelial adhesion molecules (23,24), thereby enhancing inflammatory cell recruitment into lung tissue and airway walls (25). Theoretically a nocturnal decrease in eNOS may have beneficial as well as harmful effects, and we have to await further studies to give more substantial evidence on the exact consequences of this decrease. Nevertheless, because changes in eNOS expression were closely related to PEF variation, our results support the hypothesis of Harrison (9) who stated that modest degrees of regulation in endothelial eNOS may have important physiological and pathophysiological implications.
90
Endothelial NO synthase
References 1 . Nijkamp FP, Folkerts G . Nitric oxide and bronchial reactivity. Clin Exp Allergy
1 994;24:905-1 4. 2 . Barnes PJ, Liew FY. Nitric oxide and asthmatic inflammation. lmmunol
Today 1 995; 1 6: 1 28-30. 3. Barnes PJ, Belvisi MG. Nitric oxide and lung disease. Thorax 1 993;48: 1 034-
43. 4. Barnes PJ. NO or no NO in asthma ? Thorax 1 996;51 :21 8-20. 5 . Alving K, Weitzberg E, Lundberg JM. Increased amount of nitric oxide in
exhaled air of asthmatics. Eur Respir J 1 993;6: 1 368-70. 6. Kharitonov SA, Yates D, Robbins RA, LoganSinclair R, Shinebourne EA,
Barnes PJ. Increased nitric oxide in exhaled air of asthmatic patients. Lancet 1 994;343: 1 33-5.
7. Hamid Q, Springall DR, RiverosMoreno V, Chanez P, Howarth PR, Bousquet J, Godard P, Holgate S, Polak JM. Induction of nitric oxide synthase in asthma. Lancet 1 993;342: 1 51 0-3.
8. Guo FH, De Raeve HR, Rice TW, Stuehr DJ, Thunnissen FB, Erzurum SC. Continuous nitric oxide synthesis by inducible nitric oxide synthase in normal human airway epithelium in vivo. Proc Natl Acad Sci U S A 1 995;92:7809-1 3.
9. Harrison DG, Sayegh H, Ohara Y, Inoue N, Venema RC. Regulation of expression of the endothelial cell nitric oxide synthase. Clin Exp Pharm Physiol 1 996;23:251 -5.
1 0. NHLBI Workshop summaries: Summary and recommendations of a workshop on the investigative use of fiberoptic bronchoscopy and bronchoalveolar lavage in asthmatics. Am Rev Respir Dis 1 985; 1 32: 1 80-2.
1 1 . Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1 986; 1 :307-1 0.
1 2. Kharitonov SA, O'Connor BJ, Barnes PJ. Circadian variation in exhaled and nasal nitric oxide in normal and mild asthmatic subjects. Am J Respir Grit Care Med 1 997; 1 55:A825
1 3. Miller VM, Vanhoutte PM. Enhanced release of endothelium derived factor(s) by chronic increases in blood flow. Am J Physiol 1 988;255:H446-51 .
1 4. Uematsu M, Ohara Y, Navas JP, Nishida K, Murphy TJ, Alexander RW, Nerem RM, Harrison DG. Regulation of endothelial cell nitric oxide synthase mRNA expression by shear stress. Am J Physiol 1 995;269:C1 371 -8.
1 5. Peters RM. Pulmonary resection and gas exchange. J Thorac Cardiovasc Surg 1 984;88:872-9.
1 6. Ollerenshaw SL, Woolcock AJ. Characteristics of the Inflammation in Biopsies from Large Airways of Subjects with Asthma and Subjects with Chronic Airflow Limitation. Am Rev Respir Dis 1 992; 1 45:922-7.
1 7. Yoshizumi M, Perrella MA, Burnett JC, Jr., Lee ME. Tumor necrosis factor down regulates an endothelial nitric oxide synthase mRNA by shortening its halflife. Gire Res 1 993;73:205-9.
1 8. Mohamed F, Monge JC, Gordon A, Cernacek P, Blais D, Stewart DJ. Lack of role for Nitric Oxide (NO) in the selective destabilization of endothelial NO Synthase mRNA by Tumour Necrosis Factor". Arterioscler Thromb Vase Biol 1 995; 1 5:52-7.
91
Chapter 6
1 9. McQuillan LP, Leung GK, Marsden PA, Kostyk SK, Kourembanas S. Hypoxia inhibits expression of eNOS via transcriptional and posttranscriptional mechanisms. Am J Physiol 1 994;267:H1 921 -7.
20. lalenti A, lanaro A, Moncada S, Di Rosa M. Modulation of acute inflammation by endogenous nitric oxide. Eur J Pharmaco/ 1 992;2 1 1 : 1 77-82.
2 1 . Hagman M , Frostell CG, Hedenstrom H, Hedenstierna G. Inhalation of nitric oxide modulates adult human bronchial tone. Am Rev Respir Dis 1 993; 1 48: 1 474-8.
22. Kacmarek RM, Ripple R, Cockrill BA, Bloch KJ, Zapol WM, Johnson DC. Inhaled nitric oxide. A bronchodilator in mild asthmatics with methacholine induced bronchospasm. Am J Respir Grit Care Med 1 996; 1 53: 1 28-35.
23. Kubes P, Suzuki M, Granger DN. Nitric oxide: an endogenous modulator of leukocyte adhesion. Proc Natl Acad Sci U S A 1 991 ;88:4651 -5.
24. Gaboury J, Woodman RC, Granger DN, Reinhardt P, Kubes P. Nitric oxide prevents leucocyte adherence: role of superoxide. Am J Physio/ 1 993;265:H862-7.
25. Montefort S, Holgate ST, Howarth PH. Leucocyte endothelial adhesion molecules and their role in bronchial asthma and allergic rhinitis. Eur Respir J 1 993;6: 1 044-54.
92
Chapter 7
Exhaled Nitric Oxide is higher both at day and night in subjects with nocturnal asthma
Nick ten Hacken, Hester van der Vaart, Thomas van der Mark, Gerard Koeter, Dirkje Postma
Submitted
Abstract
Background: Nitric Oxide in exhaled air is thought to reflect airway inflammation. No data have been reported so far on circadian changes in NO in subjects with nocturnal asthma. Aim: To determine whether exhaled NO shows a circadian rhythm, inverse to the circadian rhythm in airway obstruction in subjects with nocturnal asthma. Methods: Six healthy controls, 8 individuals without nocturnal asthma (16-4 h PEF variation �15%) and 6 with (16-4 h PEF variation > 15%) participated. Smoking, use of corticosteroids, and recent respiratory infections were excluded. NO concentrations were measured at 12, 16, 20, 24, 4, 8 and 12 h, using the single breath method. At the same time points FEV 1 and PEF were measured. Results: Mean NO concentrations were significantly higher in subjects with nocturnal asthma than in subjects without nocturnal asthma and higher again than in healthy controls, at all time points. Mean NO levels over 24 hours correlated with 16-4 h PEF variation (r=0.61, p<0.01 ). Exhaled NO did not show a significant circadian variation in any of the three groups as assessed by cosinor analysis, in contrast to the FEV 1 in both asthma groups (p<0.05). At 4 h mean (SD) NO levels were higher than at 16 h in subjects with nocturnal asthma: 50 (20) vs 42 (15) ppb (p<0.05), otherwise all time points were similar. 16-04 h differences in NO and FEV 1 did not correlate. Conclusions: Subjects with nocturnal asthma exhale higher NO levels both at night and day, suggesting more severe airway wall inflammation. A circadian rhythm in exhaled NO was not observed. NO levels did not correspond to the circadian rhythm in airway obstruction. The small increase in NO at 4 h may indicate an aspect of inflammation, but is not associated with increased nocturnal airway obstruction.
Introduction
Nocturnal asthma is characterized by an increased circadian rhythm in airway patency, with in general maximal airway obstruction at 4 h and minimal airway obstruction at 16 h (1,2). The underlying mechanisms are only partially understood (3). One of the hypotheses is that airway inflammation is increased at night (4), probably resulting from a lack of counteracting mecha-
93
Chapter 7
nisms such as nocturnal dips in plasma cortisol and epinephrine (57). Biopsies from the central airways could not confirm a nocturnal increase in inflammatory cells (8,9). However, BAL fluid and transbronchial biopsies in one study group showed higher numbers of eosinophils in asthmatic subjects with increased airway obstruction at night as compared to those without (9, 10). This sug-gests that inflammatory changes inducing noctu rnal airway obstruction take place in a compartment that is unaccessible, for routine monitoring of inflammation.
Determination of exhaled NO (NO) has been suggested as a simple noninvasive way to investigate asthmatic airway inflammation (11, 12). It has been shown that exhaled NO is higher in asthmatics than in healthy controls, and that it decreases after administration of corticosteroids (13). Moreover, levels of exhaled NO are not changed by pharmacologically induced bronchoconstrictions (14). Recently it has been shown that measurements of exhaled NO are correlated to iNOS expression of alveolar macrophages and eosinophils in induced sputum (15, 16). Apparently, measurements of exhaled NO are suitable to detect upregulation of iNOS and activation of inflammatory cells in peripheral airways and alveolar tissues.
Since increased nocturnal airway inflammation has been shown to occur at night in peripheral airways of patients with increased nocturnal airway obstruction, we set out to measure exhaled NO in this study on nocturnal asthma. We hypothesized that subjects with nocturnal asthma would have a circadian rhythm in NO, inverse to the circadian rhythm in airway patency.
Methods and Materials
Subjects Non-smoking asthmatic patients and healthy controls with an age of 18-45 years were recruited at the outpatient clinic or by advertisements in local newspapers. All subjects gave written informed consent to participate in this study. The study protocol was approved by the university ethics committee.
Asthmatic subjects were selected based on: (1) a history consistent with the diagnosis of asthma; (2) a positive history of atopy and a positive Phadiatop (Pharmacia, Woerden, The Netherlands); (3) FEV 1 > 1.5 L and > 60% predicted; (4) PC20 methacholine � 9.8 mg/ml ; (5) no use of corticosteroids and no respiratory infection within 1 month before the study.
Healthy controls had: (1) no history of l ung disease; (2) no history of atopy and a negative Phadiatop; (3) less than 20% fall in FEV 1 after inhalation of methacholine in a concentration of 9.8 mg/ml; (4) no respiratory infection within 1 month before the study.
94
Exhaled Nitric Oxide
Study design After characterization, PEF was measured at home during seven subsequent days at 16 and 4 h. Asthmatic subjects were grouped in subjects with mean 16-4 h PEF variation :::; 15% (non-nocturnal asthma) and those with mean 16-4 h PEF variation > 15% (nocturnal asthma) . Thereafter, subjects were admitted to the hospital during 24 hours. Exhaled NO was measured at 12, 16, 20, 24, 4, 8 and 12 h. At the same time points PEF, FEV 1 , and blood pressure (RR) were measured. To reach maximal uniformity, all measurements were performed by one person (HvdV) .
Lung function Forced expiratory volume in one second (FEV 1 ) and reversibility on 400 µg salbutamol were measured using a pneumotachograph (Jaeger Masterscreen, Wuerzburg, Germany) , according to standardized guidel ines (17) . Hyperresponsiveness was assessed using a water-sealed spirometer (Lode, Groningen, The Netherlands) with increasing doubling concentrations of 0.03 to 9.8 mg/ml methacholinebromide (Sigma Chemical Co. ST. Louis, MO) , using a 2-minute tidal breathing method adapted from Cockcroft and coworkers (18) . At home, PEF values were measured with a Personal Best peak flow meter (GlaxoWellcome, Zeist, The Netherlands) at 16 and 4 h during seven subsequent days. During these days bronchodilators were withheld as much as possible. 16-04 h PEF variation was defined as: ( 16 - 4 hrs value) / (mean of 16 and 4 hrs value) . The mean PEF variation was calculated as the average of 7 days 16-4 h PEF variation.
Exhaled Nitric Oxide During admission to the hospital the participating subjects were offered a low protein diet (< 20 g/day) at 8 .30, 12.30 and 18.30 h and avoided heavy exercise. They rested fifteen minutes before each test. Single breath measurements of exhaled NO were performed following published guidel ines (19) , using a chemiluminescence analyzer (CLO 700 AL, Eco Physics, Switzerland) . Constant flow rates during the exhalation manoevre were targeted at 10 I/min. The mean value of three NO measurements were included for analyses. The lower detectable limit of the analyzer was 1 ppb with a resolution of ± 1 ppb. The sampling flow was 600 ml/min and the response time, including lag and rise time was <7 s. Repeated measurements within 1 O minutes showed a coefficient of variation in healthy and asthmatic subjects of 19 and 1 O %, respectively.
Data analysis All analyses were performed with the SPSS/PC 6.01 software package (SPSS Inc. , Chicago, IL) . Two-sided p-values < 0.05 were considered statistically significant. Parametrical analysis was performed using Student's t test for differences between groups at the same time point, and Student's paired t test for differences between 16 and 4 h values within a group after checking
95
Chapter 7
for normal distribution. Furthermore, the 12, 16, 20, 24, 4, 8 and 12 h measurements were analyzed in a longitudinal way by cosinor analysis (20). Correlations between NO and other variables in the total group of asthmatics were tested with a Pearson test and analyzed in a multiple regression model. In this model NO concentration was entered as the dependent variable, and age, gender, height, blood pressure, prior use of inhaled corticosteroids, FEV 1 and PC20 methacholine as independent variables.
Results
Clinical characteristics Six healthy controls, 8 asthmatics with PEF variation ::; 15% and 6 asthmatics with PEF variation > 15% participated in this study (Table 1 ). Systolic and diastolic blood pressures were higher, but not significantly, in the asthmatics with PEF variation > 15%. No cosine like rhythm in blood pressure was found in any of the three groups during 24 hours. Mean FEV 1 % predicted, post bronchodilator increase in FEV 1 and PC20 methacholine were similar in the two asthmatic groups. 16-4 h PEF variation at home correlated well with 16-4 h PEF variation in the hospital (r=0.77, p<0.001 ).
Table 1 Characteristics of participating subjects
Number, male/female Age, yrs Mean systolic pressure, mm Hg Mean diastolic pressure, mm Hg Inhaled corticosteroids, number Mean FEV 1 , % pred Reversibility, % pred PC20 methacholine, mg/ml 16-4 h PEF variation (hospital), % 16-4 h PEF variation (at home), %
Healthy controls
6 (2/4) 24 (1 .4) 111 (10) 78 (9) 0 96 (11) 3.0 (2.8) > 9.8 5.1 (5.9) 6.9 (1 .3)
Asthma PEF var ::; 15%
8 (1 /7) 22 (1 .8) 11 7 (4) 76 (6) 6 94 (12) 11 .4 (9.7) 0.58 (0.09-1 .3) 11 (8.0) 9.8 (4.3)
Asthma PEF var > 15%
6 (4/2*) 32 (9.5) 124 (14) 85 (12) 2 89 (27) 12.7 (6.7) 0.39 (<0.03-3.6) 21 (21 )* 22 (7 .2)*
Values expressed as means (SD). Mean FEV1 is the average of the FEV1 's at 7 different time points during one day. Reversibility of airway obstruction is expressed as the increase in FEV 1 % predicted after inhalation of 400 µg salbutamol. 16-4 h PEF variation (at home) is measured during 7 subsequent days. 16-4 h PEF variation (hospital) is measured during one day. *: P < 0.05 versus asthma with PEF variation ::;15%.
FEV 1 during 24 hours FEV 1 % predicted showed a significant cosine like rhythm in the two asthmatic groups (Figure 1 ), in contrast to the healthy controls. The peak and the nadir of this cosine function were at 16 h and at 4 h, in both groups. The amplitude of this cosine function was 5% in the asthmatics with PEF variation ::; 15%, and 8% in the asthmatics with PEF variation > 15%.
96
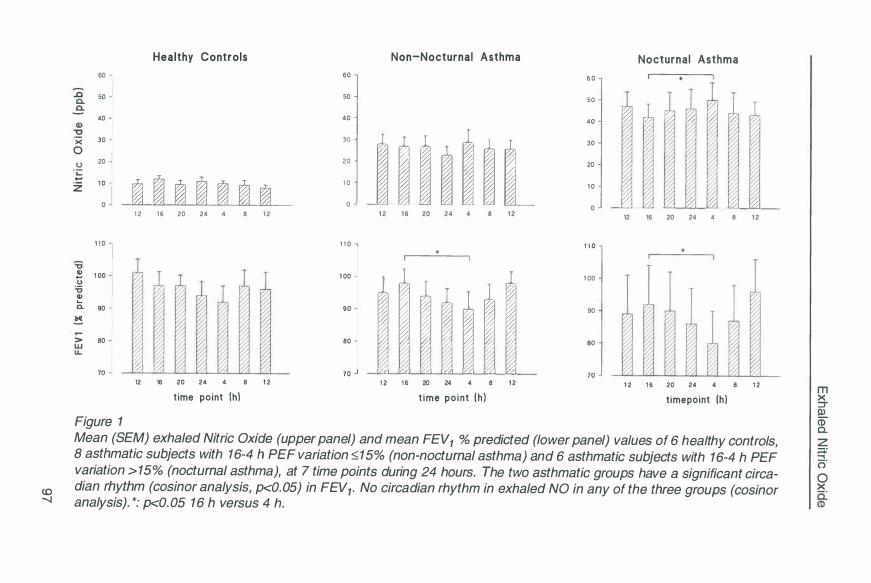
co --..J
60
.Q a.
50
Q) 40
·x 30
0
0 20
·5 z 1 0
1 1 0
� 1 00
� � c.. 90
� > 80 w
70
Figure 1
Healthy Controls
� � � � � � � 1 2 1 6 20 24 4 8 1 2
7
1/1 v 12 16 20 24 4 8 1 2
t ime point (h}
Non-Nocturnal Asthma 60
] 50
40 -l
'.i l l i l i l i 1 2 1 6 20 2 4 4 8 1 2
1 1 0 .. 1 00
i l 1 1 , 1 i 90
80
70 ...J V/I V/I Vll [i::::Q v,1 1',I V/I
1 2 1 6 20 24 4 8 1 2
t ime po in t ( h }
Nocturnal Asthma
6 0
:: J � l rd33 � � � v1 30
20
1 0
O j r½1 10! r½1 � 10! 10! � 12 16 20 24 4 8 1 2
1 1 0
1 00
90
80 "1 V/
1 2 1 6 20 24 4 8 1 2
t imepoint (h}
Mean (SEM) exhaled Nitric Oxide (upper panel) and mean FEV1 % predicted (lower panel) values of 6 healthy controls, 8 asthmatic subjects with 16-4 h PEF variation �15% (non-nocturnal asthma) and 6 asthmatic subjects with 16-4 h PEF variation > 15% (nocturnal asthma), at 7 time points during 24 hours. The two asthmatic groups have a significant circadian rhythm (cosinor analysis, p<0.05) in FEV1. No circadian rhythm in exhaled NO in any of the three groups (cosinor analysis). *: p<0. 05 16 h versus 4 h.
m X ::::r ll) m a. z ;::.:
o" 0 X
Chapter 7
Mean (SD) FEV 1 % predicted at 4 h was significantly lower than at 16 h in the asthmatics with PEF variation > 15%: 80 (25) vs 92 (31) % (p<0.05), as well as in the asthmatics with PEF variation ::;; 15%: 90 {16) vs 98 (12) % (p<0.05), and borderline so in healthy controls: 92 {12) vs 97 (11 ) % (p=0.07).
Exhaled Nitric Oxide
Differences between the three groups NO concentrations of the asthmatic subjects with 16-4 h PEF variation > 15% were higher than those of the asthmatic subjects with 16-4 h PEF variation ::;; 15% (p<0.05), and those of the healthy controls at all time points (p<0.01 ). Also, NO concentrations of the asthmatic subjects with 16-4 h PEF variation ::;; 15% were significantly higher than those of healthy controls at all time points (p<0.001 ). The mean (SD) NO concentrations of the 7 time points per group were: 46.0 (18.7) ppb for the asthmatics with PEF variation > 15%, 26.6 (12.6) ppb for the asthmatics with PEF variation ::;; 15%, and 9.9 (2.1) ppb for the healthy controls.
Variation during 24 hours Exhaled NO concentrations did not show a cosine like rhythm in any of the three groups (Figure 1 ). In the asthmatic subjects with PEF variation > 15% the mean (SD) NO concentration at 4 h was higher than at 16 h: 50 (20) vs 42 (15) ppb (p<0.029). There was no 16-4 h difference in the two other groups. Mean coefficients of variation of NO values at the 7 time points in asthmatics with PEF variation > 15%, asthmatics with PEF variation ::;; 15%, and healthy controls were: 15, 20, and 42%, respectively.
Relation to clinical variables The level of exhaled NO was significantly and positively correlated with 16-4 h PEF variation (Figure 2). Exhaled NO was not significantly correlated with any of the other clinical variables described in table 1. In a multiple regression model, the variation in exhaled NO was not explained by age, gender, height, blood pressure, prior use of inhaled corticosteroids, FEV 1 or PC20 methacholine. The 16-4 h difference in NO was not correlated to the 16-4 h difference in FEV 1 in any of the three groups.
Discussion This study confirmed that patients with increased PEF variability at home have an increased circadian rhythm in airway patency in the hospital, with the highest FEV 1 at 16 h and the lowest FEV 1 at 04 h {1,2). Despite an isolated increase in exhaled NO at 4 h in subjects with large PEF variations, we were not able to show an inverse cosine like rhythm in exhaled NO, neither was a significant correlation observed between exhaled NO levels and FEV 1 values. Subjects with nocturnal asthma exhaled significantly higher NO levels than subjects with non-nocturnal asthma during the whole day, suggesting an
98
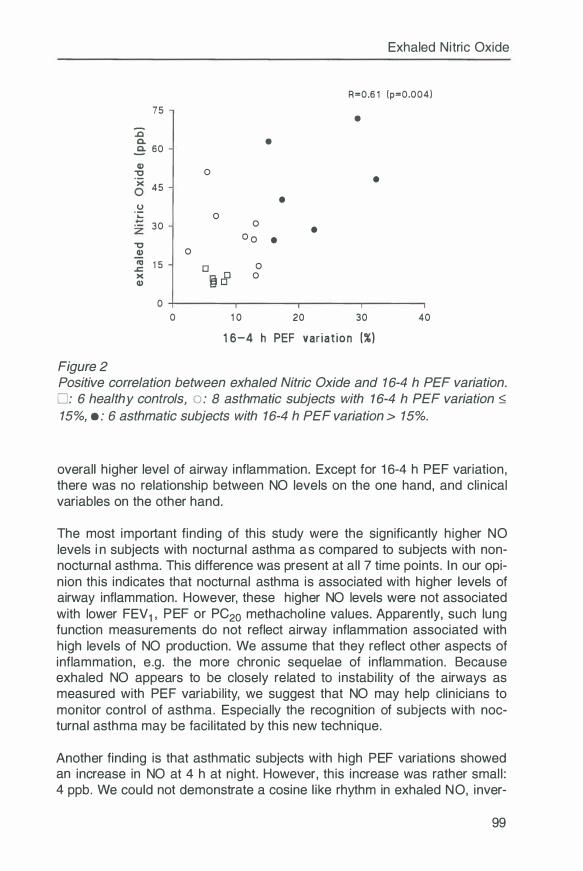
75
:c-C.
,E: 60
a, "'C ·x 45
0 'i:
30
"'C a, 0 "' 1 5 � >< a,
0 0
Figure 2
0
0 0
O o
0 □ � 8 0
1 0
•
• • •
20
Exhaled Nitric Oxide
R=0.6 1 (p=0.004)
•
•
30 40
1 6-4 h PEF var iat ion (%)
Positive correlation between exhaled Nitric Oxide and 16-4 h PEF variation. □ : 6 healthy controls, o : 8 asthmatic subjects with 16-4 h PEF variation �
15%, • : 6 asthmatic subjects with 16-4 h PEF variation > 15%.
overall higher level of airway inflammation. Except for 16-4 h PEF variation, there was no relationship between NO levels on the one hand, and clinical variables on the other hand.
The most important finding of this study were the significantly higher NO levels in subjects with nocturnal asthma as compared to subjects with nonnocturnal asthma. This difference was present at all 7 time points. In our opinion this indicates that nocturnal asthma is associated with higher levels of airway inflammation. However, these higher NO levels were not associated with lower FEV 1 , PEF or PC20 methacholine values. Apparently, such lung function measurements do not reflect airway inflammation associated with high levels of NO production. We assume that they reflect other aspects of inflammation, e.g. the more chronic sequelae of inflammation. Because exhaled NO appears to be closely related to instability of the airways as measured with PEF variability, we suggest that NO may help clinicians to monitor control of asthma. Especially the recognition of subjects with nocturnal asthma may be facilitated by this new technique.
Another finding is that asthmatic subjects with high PEF variations showed an increase in NO at 4 h at night. However, this increase was rather small : 4 ppb. We could not demonstrate a cosine like rhythm in exhaled NO, inver-
99
Chapter 7
se to the circadian rhythm in FEV 1 . Moreover, the 16-4 h change in NO was not correlated with the 16-4 h change in FEV 1 . Therefore, we assume that the small increase in NO at 4 h, but not at other time points, indicates an aspect of inflammation that is of less importance for the generation of increased nocturnal airway obstruction. Several factors may explain this increase in NO at 4 h. First, it may result from exaggerated nadirs in plasma cortisol at 24 h in subjects with nocturnal asthma (6), leading to enhanced transcription of DNA encoding for inducible NO Synthase. Second, it has been shown that the pro-inflammatory cytokines IL-1 � and interferon-y, both capable to stimulate NO production, are increased at 4h (21,22). Whatever the cause, we conclude that this nocturnal increase in NO was too small to solely explain the increased nocturnal airway obstruction in subjects with nocturnal asthma.
This study took all steps to minimize factors which might interfere with a possible circadian rhythm in NO. Participating subjects were offered a low protein diet to prevent a post prandial increase in serum L-arginine (23). They had to rest for at least 15 minutes prior to the test, because exercise has been found to decrease NO values (24). Also smoking and (intermittent) use of corticosteroids were excluded because of their down regulating effects on NO (11, 13,25). Diastolic blood pressure was measured together with NO, because hypertension was reported to be associated with low NO values (25). However, diastolic blood pressure did not show a circadian rhythm, and was not a variable contributing to the variance in NO. Finally, NO measurements were performed according to recently published guidelines (19), and special attention was paid to uniform expiratory flow rates and pressures. Using this protocol, repeated measurements of exhaled NO at short intervals (within 1 O minutes) have shown highly reproducible data.
This study recruited subjects with and without nocturnal asthma, based on 16 and 4 h PEF measurements at home during one week. In the hospital, FEV 1 and PEF decreased at night, both in subjects with nocturnal and non-nocturnal asthma. As expected, FEV 1 % predicted decreased more in the subjects with nocturnal asthma as compared to non-nocturnal asthma: 8 vs 12 %. In a multiple regression model we analysed potentially confounding variables on their effect on exhaled NO. Age, gender, blood pressure, inhaled corticosteroids prior to the study, FEV 1 , and PC20 methacholine did not contribute to the variation in NO. Therefore, an unequal distribution of the above factors is not responsible for the significant differences in NO between the two asthmatic groups.
Our study is partly in line with another study on day-night variations in exhaled NO. Kharitinov et al measured exhaled NO during 1 day, at intervals of 4 hours, in 4 healthy controls and 7 mild asthmatic subjects (26). Like our study
100
Exhaled Nitric Oxide
NO increased at 4 h at night in the same order of magnitude. Opposite to our study, the nocturnal increase in the latter study was positively correlated with the nocturnal decrease in FEV 1 , suggesting a pathophysiological relationship. However, the subjects in this study were not recruited based on circadian variations in airway obstruction, and none of them ever had nocturnal symptoms. Patel and colleagues measured between-day PEF variation and exhaled NO concentrations in 23 asthmatic subjects and 18 healthy controls during 12 weeks (27). They did not find a correlation between changes in exhaled NO and between-day PEF variation. Wempe et al demonstrated that inhaled corticosteroids resulted in a decrease in both within-day and between-day PEF variation, whereas �2-mimetics only influenced within-day PEF variation (28). Above studies indicate that within-day and between-day PEF variation are influenced by different pathophysiological mechanisms. Before drawing definitive conclusions, we have to await further (intervention) studies on the relationship between NO and PEF variability, especially in the field of nocturnal asthma.
This study has several theoretical, therapeutical and practical implications. First of all, our data suggest again (22,29,30) that nocturnal asthma is not caused by a circadian rhythm in airway inflammation. As suggested before, nocturnal asthma merely seems to reflect more severe airway inflammation (31-33). Thus, therapy should suppress airway inflammation maximally during the complete day. Measurements of exhaled NO may support measurements of within-day PEF variability to identify asthmatic patients with high levels of airway inflammation, who are at risk for nocturnal asthma. Finally, in the frame of standardization of NO protocols, it is not necessary to measure NO at fixed time points, as any time is good to show higher NO levels in those at risk for nocturnal asthma.
References 1 . Hetzel MR, Clark T J. Comparison of normal and asthmatic circadian rhythms
in peak expiratory flow rate. Thorax 1 980;35:732-8. 2. Greenough A, Everett L, Pool J, Price JF. Relation between nocturnal symp
toms and changes in lung function on lying down in asthmatic children. Thorax 1 991 ;46: 1 93-6.
3. Martin RJ. Nocturnal asthma. Ann Allergy 1 994;72:5-1 0. 4. Barnes PJ. Inflammatory mechanisms and nocturnal asthma. Am J Med
1 988;85:64-70. 5. Barnes P, FitzGerald G, Brown M, Dollery C. Nocturnal asthma and changes
in circulating epinephrine, histamine, and cortisol. N Engl J Med 1 980;303:263-7.
6. Kallenbach JM, Panz VR, Joffe Bl, Jankelow D, Anderson R, Haitas B, Seftel HC. Nocturnal events related to "morning dipping" in bronchial asthma. Chest 1 988;93:751 -7.
101
Chapter 7
7. Bates ME, Clayton M, Calhoun W, Jarjour N, Schrader L, Geiger KS, Sedgwick J, Swenson C, Busse W. Relationship of plasma epinephrine and circulating eosinophils to nocturnal asthma. Am J Respir Grit Care Med 1 994; 1 49:667-72.
8. Mackay TW, Wallace WAH, Howie SEM, Brown PH, Greening AP, Church MK, Douglas NJ. Role of inflammation in nocturnal asthma. Thorax 1 994;49:257-62.
9. Kratt M, Djukanovic R, Wilson S, Holgate ST, Martin RJ . Alveolar tissue inflammation in asthma. Am J Respir Grit Care Med 1 996; 1 54: 1 505- 1 0.
1 0. Martin RJ , Cicutto LC, Smith HR, Ballard RD, Szefler SJ . Airways inflammation in nocturnal asthma. Am Rev Respir Dis 1 991 ; 1 43:351 -7.
1 1 . Kharitonov SA, Yates D, Robbins RA, LoganSinclair R , Shinebourne EA, Barnes PJ. I ncreased nitric oxide in exhaled air of asthmatic patients. Lancet 1 994;343: 1 33-5.
1 2. Alving K, Weitzberg E, Lundberg JM. Increased amount of nitric oxide in exhaled air of asthmatics. Eur Respir J 1 993;6: 1 368-70.
1 3. Yates DH, Kharitonov SA, Robbins RA, Thomas PS, Barnes PJ . Effect of a nitric oxide synthase inhibitor and a glucocorticosteroid on exhaled nitric oxide. Am J Respir Grit Care Med 1 995; 1 52:892-6.
1 4. Garnier P, Fajac I , Dessanges JF, Dall'Ava Santucci J, Lockhart A, Dinh Xuan AT. Exhaled nitric oxide during acute changes of airways calibre in asthma. Eur Respir J 1 996;9: 1 1 34-8.
1 5. Ohuchi Y, I chinose M, Miura M, et al. Inducible nitric oxide synthase expression in asthmatic patients. [Abstract] Am J Respir Grit Care Med 1 996; 1 53:A800
1 6. Weng B, Holz 0, Mucke M, et al. Detection of inducible nitric oxide synthase (iNOS) in induced sputum of asthmatic subjects with and without inhaled corticosteroids. [Abstract] Eur Respir J 1 997; 1 0:31 8s
1 7. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault J. Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests European community for steel and coal. Official statement of the European Respiratory Society. Eur Respir J 1 993;6:5-40.
1 8. Cockcrott DW, Killian KJ , Mellon J, Hargreave F. Bronchial reactivity to inhaled histamine: a method and clininical survey. Clin Allergy 1 977;7:235-43.
1 9. Kharitonov SA, Alving K, Barnes PJ. ERS Task Force Report. Exhaled and nasal nitric oxide measurements: recommendations. Eur Respir J 1 997; 1 0: 1 683-93.
20. Nelson W, Tong Y L, Lee JK, Halberg F. Method for cosinor rhythmometry. Chronobiologia 1 979;6:305-23.
21 . Jarjour NN, Busse WW. Cytokines in bronchoalveolar lavage fluid of patients with nocturnal asthma. Am J Respir Grit Care Med 1 995; 1 52 : 1 474-7.
22. Ten Hacken NHT, Oosterhoff Y, Kauffman HF, Guevarra L, Satoh T, Tollerud DJ, Postma DS. Elevated serum interferon-y in atopic asthma correlates with increased airways responsiveness and circadian peak expiratory flow variation. In press: Eur Respir J 1 998.
23. Kharitonov SA, Lubec G, Lubec B, Hjelm M. L-Arginine increases exhaled nitric oxide in normal human subjects. Clin Sci (Goich) 1 995;VOL 88: 1 35
24. Persson MG, Wiklund NP, Gustafsson LE. Endogenous nitric oxide in single exhalations and the change during exercise. Am Rev Respir Dis 1 993; 1 48: 1 21 0-4.
1 02
Exhaled Nitric Oxide
25. Schil ling J, Holzer P, Guggenbach M, Gyurech D, Marathia K, Geroulanos S. Reduced endogenous nitric oxide in the exhaled air of smokers and hypertensives. Eur Respir J 1994;7:467-71.
26. Kharitonov SA, O'Connor BJ, Barnes PJ. Circadian variation in exhaled and nasal nitric oxide in normal and mild asthmatic subjects. Am J Respir Grit Care Med 1997; 155:A825
27. Patel M, Halpin DMG. Longitudinal relationship between peakflow £ exhaled nitric oxide concentrations in asthmatics and normal controls. [Abstract] Eur Respir J 1997;10:472s
28. Wempe JB, Tammeling EP, Postma DS, Auffarth 8, Teengs JP, Koster GH. Effects of budesonide and bambuterol on circadian variation of airway responsiveness and nocturnal symptoms of asthma. J Allergy C/in lmmunol 1992;90:349-57.
29. Oosterhoff Y, Hoogsteden HC, Rutgers 8, Kauffman HF, Postma DS. Lymphocyte and macrophage activation in bronchoalveolar lavage flu id in nocturnal asthma. Am J Respir Grit Care Med 1995;151 :75-81.
30. Oosterhoff Y, Kauffman HF, Rutgers B, Zijlstra FJ , Koster G, Postma DS. Inflammatory cell number and mediators in bronchoalveolar lavage flu id and peripheral blood in asthmatic subjects with increased nocturnal airways narrowing. J Allergy Clin lmmuno/ 1995;96:219-29.
31. Weersink EJ , Postma DS. Nocturnal asthma: not a separate disease entity. Respir Med 1994;88:483-91.
32. Postma DS, Oosterhoff Y, van Aalderen WM, Kauffman HF, Wempe JB, Koster GH. I nflammation in nocturnal asthma? Am J Respir Grit Care Med 1994; 150:S83-6.
33. Oosterhoff Y, Timens W, Postma DS. The role of airway inflammation in the pathophysiology of nocturnal asthma. Clin Exp Allergy 1995;25:915-21.
103

Chapter 8
Elevated serum interferon-y in atopic asthma correlates with increased airways responsiveness and circadian peak expiratory flow variation
Nick ten Hacken, Ytske Oosterhoff, Henk Kauffman, Lucille Guevarra, Toshihiko Satoh, David Tollerud, Dirkje Postma
In press (European Respiratory Journal)
Abstract
Interleukin (IL)-4, IL-5 and interferon-y (IFN-y) are thought to play an important role in chronic airway inflammation in asthmatic subjects. Increased airways responsiveness and nocturnal airway obstruction are important clinical manifestations of asthma. The aim of this study was to investigate whether IL-4, IL-5 and IFN-y values are elevated in atopic asthma and correlate with its clinical manifestations. Serum IL-4, IL-5 and IFN-y levels of 17 atopic asthmatics and eight nonatopic healthy subjects were determined at 16 and 04 h by a chemiluminescence enzyme-linked immunosorbent assay (ELISA) method. The clinical manifestation of asthma was determined by assessment of the degree of airway obstruction, airways responsiveness to methacholine and severity of nocturnal airway obstruction, defined as the mean circadian (16-04 h) peak expiratory flow (PEF) variation. Serum IL-4, IL-5 and IFN-y levels were significantly higher in asthmatic subjects as compared to healthy controls, both at 16 and 04 h. In asthmatic subjects serum I FN-y at both time points correlated significantly with the provocative concentration of methacholinebromide causing a 20% fall in forced expiratory volume in one second (PC20 methacholine) (rho = - 0.55) and with the mean 16-04 h PEF variation (rho = 0.53). In contrast, no relationship was found between the levels of IL-4 and IL-5 and the parameters of clinical manifestation of asthma. The results suggest that the serum level interferon-y is a reflection of the severity of airway inflammation in atopic asthma. More studies are needed to detect the cellular sources and to clarify the exact roles of interferon-y and other pro-inflammatory cytokines in asthma.
105
Chapter 8
Introduction Asthma is characterized as a chronic inflammatory disease of the airways. The presence of inflammation is associated with airways hyperresponsiveness to inhaled stimuli and the development of increased nocturnal airways obstruction [1 ]. Many different inflammatory cells are involved in asthma, including activated T-helper lymphocytes, eosinophils, mast cells and macrophages. These cells can synthesize and release cytokines, which are increasingly recognized to be important in chronic inflammation and play a critical role in orchestrating the inflammatory response. In this respect, emphasis has been laid on an imbalance between type 1 T-helper (Th1) and type 2 T-helper (Th2) cytokines in the development of allergic inflammation. Elevated levels of interleukin (IL)-4, an essential co-factor for immunoglobulin E (lgE) production, and IL-5, responsible for the final differentiation, activation and recruitment of eosinophils [2] , have been found in serum of patients with asthma [36]. lnterferon-y ( IFN-y) on the other hand inhibits Th2 mediated inflammation in atopic diseases. Both elevated [7 ,8] and non-elevated [4,6] serum levels of IFN-y have been reported in asthmatic patients.
Since little is known about the direct relationship between cytokine levels and the clinical manifestation of atopic asthma (the degree of airway obstruction, airways responsiveness to methacholine and severity of nocturnal airway obstruction defined as mean 16-04 h peak expiratory flow (PEF) variation), we determined the concentrations of IL-4, IL-5 and IFN-y in serum and bronchoalveolar lavage (BAL) fluid from subjects with atopic asthma and healthy controls in a study on nocturnal asthma [1 ] . The asthmatic subjects participating in this study were selected in order to obtain a wide range of circadian PEF variations, and measurements were performed at 16 and 04 h.
Materia l and Methods
Subjects Asthmatic subjects (nonsmokers) were selected on the basis of: 1) a history consistent with the diagnosis of asthma; 2) atopy, i.e. positive intracutaneous tests against house dust mite or two other of 12 tested common aeroallergens, expressed as histamine equivalent wheel size (HEWS) > 0.7 [9] ; 3) forced expiratory volume in one second (FEV 1 ) > 1 .5 L and > 70% predicted; postbronchodilator FEV1 (salbutamol 400 µg using a spacehaler) > 10%; 4) provocative concentration of methacholinebromide causing a 20% fall in forced expiratory volume in one second (PC20 methacholine) ::; 9.8 mg/ml; 5) no use of oral corticosteroids within 2 months, inhaled corticosteroids within 4 weeks or cromoglycates within 2 weeks before the study; and 6) no upper respiratory infection(s) within 1 month before the study.
Nonsmoking healthy volunteers had: 1) no history of lung disease or allergy;
106
Elevated serum interferon-y
2) no atopy, i.e. negative intracutaneous tests against 12 common aeroallergens (HEWS < 0.7); 3) no airways hyperresponsiveness to methacholine ( <10% fall in FEV 1 after inhalation of methacholinebromide in a concentration of 9.8 mg/ml); and 4) no upper respiratory infection(s) within 1 month before the study.
Study design IL-4, IL-5 and IFN-y were analysed in serum and bronchoalveolar lavage fluid, obtained during a previously published study on nocturnal asthma [1 ]. In this study FEV 1 , blood sampling and bronchoscopy were performed at 16 h (or 04 h), and repeated 7-14 days later at 04 h (or 16 h).
Three days before the first investigation, bronchodilators (Pragonists or ipratropiumbromide) were withheld and PEF values were recorded with a mini-Wright peak flow meter at 08, 12, 16, 20, 24, and 04 h. The 16-04 h PEF variation was defined as: (16 - 04 hrs value) / mean of six daily measurements. The mean 16-04 h PEF variation was calculated as the average of the 16-04 h PEF variation measured during 3 days. FEV 1 and airways hyperresponsiveness to methacholine, were assessed within 5 days before the first bronchoscopy. FEV 1 was measured with a calibrated water-sealed spirometer according to standardized guidelines [1 O]. Airways responsiveness to doubling concentrations of 0.03 to 9.8 mg/ml methacholinebromide (Sigma Chemical co. ST. Louis, MO) was measured using a 2 min tidal breathing method adapted from Cockcroft and coworkers, as described previously [11 ].
Thirty minutes before each bronchoscopy, FEV1 measurements were performed and blood samples were taken. Bronchodilator therapy was withheld 8 h before the pulmonary function tests. The bronchoscopy procedure has been described previously [1 ]. Briefly, ten aliquots of 20 ml sterile phosphate-buffered saline (PBS) of 37°C were instilled into the lateral segment of the right middle lobe and recovered by gentle suction (-40 cm H20) after each aliquot. The BAL fluid was collected in polypropylene cups and immediately placed in ice.
Laboratory techniques
Processing of BAL fluid The BAL-fluid recovered from the first two 20 ml aliquots of PBS instilled was processed separately and used for analysis of cytokines. The lavage fluid was filtered through a 100 µm pore filter of a venous infusion system (Curapharm, Medica B.V., Hospital Supplies, the Netherlands) to remove mucus, and centrifuged at 400xg at 4 °C for 5 minutes. The BAL supernatant was decanted from the cell pellet and stored at -80°C until further determination.
107
Chapter 8
Processing of blood samples Serum was acquired after coagulation of venous blood for 1 h at room temperature. The supernatant was centrifuged twice for 10 min at 2000xg and stored at -80°C until analysis. Serum total lgE was determined by a fluoro immunoassay (Kabi Pharmacia, Woerden, the Netherlands).
Determination of cytokines in serum and BAL fluid Levels of IL-4, IL-5 and IFN-y were determined by a chemiluminescence enzyme-linked immunosorbent assay (ELISA) in the laboratory of the Department of Environmental & Occupational Health at the University of Pittsburgh. Ninety six-well opaque microtiter plates (Microlite 1, Dynatech, Chantilly, VA) were coated with 100 µIs of diluted purified anti-cytokine monoclonal antibody (capture moAb, 1-4 µg/mL) in 0.1 M sodium bicarbonate (NaHCO3) coating buffer. Plates were incubated overnight at 4 °C, generally with gentle shaking, subsequently washed with 300 µls/well of PBS-Tween and blotted dry. Wells were blocked with 300 µls/well of 2.5% (w/v) bovine serum albumin (BSA)/PBS-Tween and washed with PBS-Tween. Recombinant standards and samples (diluted appropriately in 0.5-1 % BSA/PBS-Tween), were added (100 µls/well), in duplicate or triplicate wells and incubated overnight at 4°C with gentle shaking. Plates were then washed with PBS-Tween, and 100 µls/well biotinylated anti-cytokine monoclonal antibody (detecting moAb) diluted to appropriate concentration (20-400 ng/mL) with 0.5% BSA/PBS-Tween. After incubation at room temperature for 1 h with gentle shaking, plates were washed with PBS-Tween. Enzyme-labelled avidin or streptavidin in 0.5% BSA-PBS-Tween was added at 100 µls/well and incubated at room temperature for 50 min, with gentle shaking. Plates were then washed and 100 µIs Lumiphos 530 (Lumigen Inc., Southfield, Ml, USA) were added to each well. After incubating at room temperature for 25 min, light emission was read using microtiter plate luminometer (ML 1000, Dynatech Laboratories Inc., VA) and the data were analysed using BioCalc Data Analysis Software (Dynatech Laboratories Inc.). The CL-ELISA assays have been validated for accuracy and sensitivity using recombinant human cytokines, including W.H.O. standard recombinant cytokines. W.H.O. standards included: recombinant Human IFN-y (Catalogue No. Gg23-901-530; National Institute of Allergy and Infectious Disease, N IH, Bethesda, MD, USA); recombinant human IL-4 and recombinant human IL-5 (88/656 and 90/586, respectively; National Institute for Biological Standards and Control, Hertfordshire, UK). The assays were extensively tested using media and human serum samples spiked with mixtures of known quantities of recombinant cytokines. Each assay is highly specific for the cytokine of interest, with no detectable cross-reactivity with other cytokines. These studies confirmed the quality assurance data provided by the manufacturers of the monoclonal antibody pairs.
108
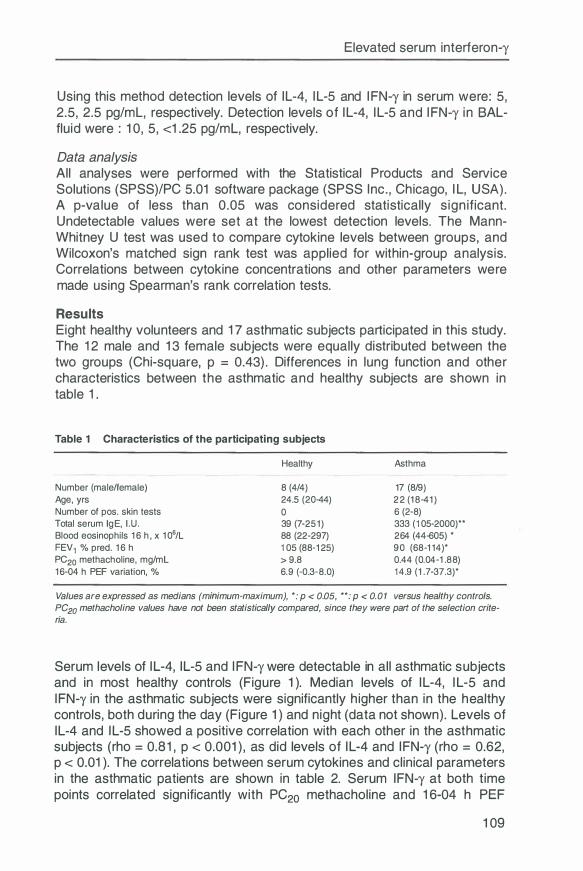
Elevated serum interferon-y
Using this method detection levels of IL-4, I L-5 and I FN-y in serum were: 5, 2.5, 2.5 pg/ml, respectively. Detection levels of I L-4, I L-5 and I FN-y in BALflu id were : 1 0, 5, <1 .25 pg/ml, respectively.
Data analysis All analyses were performed with the Statistical Products and SeNice Solutions (SPSS)/PC 5.01 software package (SPSS Inc . , Chicago, I L, USA) . A p-value of less than 0.05 was considered statistically s ign ificant. Undetectable values were set at the lowest detection levels. The MannWhitney U test was used to compare cytokine levels between groups, and Wilcoxon's matched sign rank test was applied for within-group analysis. Correlations between cytokine concentrations and other parameters were made using Spearman's rank correlation tests.
Results Eight healthy volunteers and 1 7 asthmatic subjects participated in this study. The 1 2 male and 1 3 female subjects were equally distributed between the two groups (Chi-square, p = 0.43) . Differences in lung function and other characteristics between the asthmatic and healthy subjects are shown in table 1 .
Table 1 Characteristics of the participating subjects
Number (male/female) Age, yrs Number of pas. skin tests Total serum lgE, 1 .U . Blood eosinophils 16 h, x 106/L FEV1 % pred. 16 h PC20 methacholine, mg/ml 16 -04 h PEF variation, %
Healthy
8 (4/4) 24.5 (20-44) 0 39 (7-251) 88 (22-297) 105 (88-125) > 9.8 6 .9 (-0.3-8.0)
Asthma
17 (8/9) 22 (18-41) 6 (2-8) 333 (105-2000)** 264 (44-605) * 90 (68-114)* 0.44 (0.04-1 .88) 14.9 (1 . 7-37 .3)*
Values are expressed as medians (minimum-maximum), *: p < 0.05, ,.,.: p < 0.01 versus healthy controls. PC20 methacholine values have not been statistically compared, since they were part of the selection criteria.
Serum levels of I L-4, IL-5 and I FN-y were detectable in all asthmatic subjects and in most healthy controls (Figure 1 ). Median levels of I L-4, I L-5 and IFN-y in the asthmatic subjects were significantly h igher than in the healthy controls, both during the day (Figure 1 ) and night (data not shown). Levels of IL-4 and I L-5 showed a positive correlation with each other in the asthmatic subjects (rho = 0.8 1 , p < 0.001 ) , as did levels of I L-4 and IFN-y (rho = 0.62, p < 0.01 ). The correlations between serum cytokines and clinical parameters in the asthmatic patients are shown in table 2. Serum IFN-y at both time points correlated sign ificantly with PC20 methacholine and 1 6-04 h PEF
1 09
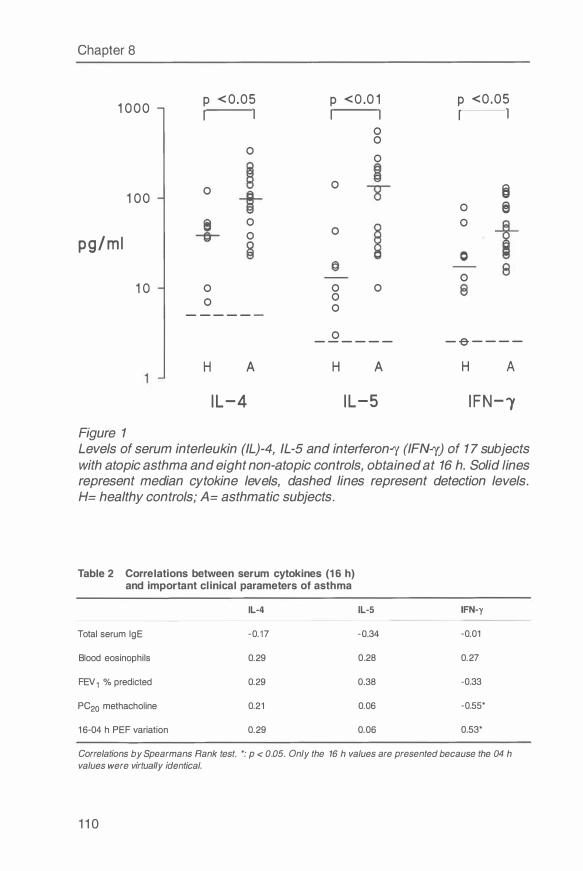
Chapter 8
1 000
1 00
pg/m l
1 0
Figure 1
p < 0 .05
I I
0
0
0
0
0
0
- - - - - -
H A
I L-4
p <0 .0 1 I I
0 0
0
0
0
0 0 0
0
0 - - - - - -
H A
I L-5
p <0 .05
I I
0
0
0
0
6 @)
- -e - - - -
H A
I FN-1
Levels of serum interleukin (IL)-4, IL-5 and interferon..ry (IFN..ry) of 1 7 subjects with atopic asthma and eight non-atopic controls, obtained at 16 h. Solid lines represent median cytokine levels, dashed lines represent detection levels. H= healthy controls; A= asthmatic subjects.
Table 2 Correlations between serum cytokines (1 6 h) and important clinical parameters of asthma
IL-4 IL-5 IFN-y
Total serum lgE -0.17 -0.34 -0.01
Blood eosinophils 0.29 0.28 0.27
FEV 1 % predicted 0.29 0.38 -0.33
PC20 methacholine 0.21 0.06 -0.55*
16-04 h PEF variation 0.29 0.06 0.53*
Correlations by Spearmans Rank test. *: p < 0.05. Only the 16 h values are presented because the 04 h values were virtually identical.
1 1 0
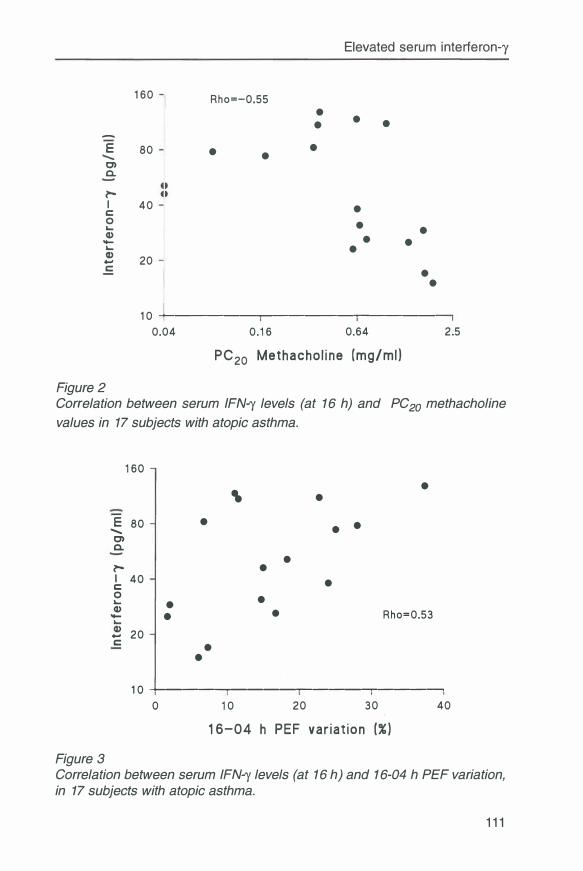
Elevated serum interferon-y
1 60
-
E 80 C) a. l'-1 40 C 0 ... Cl) -... ! 20 C
Rho=-0.55
• •
• • •
•
• • • •
•
• • • •
1 0 ---------------.-----0.04 0. 1 6 0.64
PC20 Methacho l i ne (mg/ml }
Figure 2
2.5
Correlation between serum IFN-y levels (at 16 h) and PC20 methacholine
values in 17 subjects with atopic asthma.
1 60 • ' •
E 80 • • ....... • C) a. • l'- • I 40 • C 0 • ... • Cl) • Rho=0.53 - •
20 -C • •
1 0 --+------.------.--------.--------, 0 1 0 20 30
1 6-04 h PEF var i a t ion (% )
Figure 3
40
Correlation between serum IFN-y levels (at 16 h) and 1 6-04 h PEF variation, in 17 subjects with atopic asthma.
1 1 1
Chapter 8
variation (Figure 2 and 3, respectively) . Otherwise , no significant correlations were found.
The median I FN-y level in serum of asthmatic patients was significantly higher during the night as compared to the day: 56 (range 1 6-223) pg/ml at 04 h vs 46 (range 1 5-1 28) pg/ml at 1 6 h (p <0.05) . Day-night changes of I FN-y in the asthmatic subjects did not correlate with day-n ight changes in PEF or FEV1 % predicted. The median I FN-y levels i n healthy subjects were not significantly different between day and n ight , and there were no significant differences in IL-4 and I L-5 levels between healthy and asthmatic subjects (data not shown) .
BAL-fluid levels of I L-4, I L-5 and I FN-y were frequently below the level of detection : in the eight healthy volunteers , levels below the detection l imit were found in none, four and eight subjects, respectively; and six, 1 2 and 1 4 of the 1 7 asthmatic subjects , respectively ( 1 6 h ) . Median (range) values of IL-4, I L-5 and I FN-y in the healthy volunteers were: 1 7 .5 ( 1 0-71 ) , 6 (5-24) and < 1 .25 (< 1 ,25) pg/ml, respectively ( 1 6 h). Median (range) values of I L-4, IL-5 and I FN-y in the asthmatic subjects were: 1 4 ( 1 0-442) , 5 (5- 1 43) and < 1 .25 (<1 .25-0.8) pg/ml, respectively ( 1 6 h). Median BAL-fluid levels of IL-4, I L-5 and I FN-y were not significantly d ifferent between healthy and asthmatic subjects at the different time points , nor between day and n ight values with in the healthy and asthmatic groups. The BAL-flu id levels of I L-4, I L-5 and IFN-y did not correlate with the PC20 methachol ine values, 1 6-04 h PEF-variation or FEV 1 % predicted.
Discussion This study demonstrated that the median levels of serum I L-4, I L-5 and I FN-y were sign ificantly h igher in the asthmatic group than in the healthy control group. Moreover, elevated serum levels of I FN-y in subjects with atopic asthma were correlated with an increased ai rways responsiveness to methacholine and a larger 1 6-04 h PEF variation . I n contrast, no relationship is found between serum levels of I L-4 and I L-5 and the parameters of cl in ical manifestation of asthma. Median levels of I L-4 and I L-5 in BAL-fluid were not different between asthmatic and healthy subjects, whereas the levels of I FN-y in BAL-fluid were mainly below the level of detection with the method used .
The finding of higher serum I FN-y levels are in l ine with the results of two other studies. Saito et al [8] showed a higher mean plasma concentration of I FN-y in patients with mite-sensitive asthma as compared to healthy controls. In addition , Corrigan et al [7] showed that serum I FN-y levels were elevated in patients with acute severe asthma and normal ized upon treatment. Un l ike the study of Corrigan , our patients did not suffer from a viral or bacterial a ir-
1 1 2
Elevated serum interferon-y
way infection as a potential cause for increased IFN-y production. The relationships of higher serum IFN-y levels with increased nocturnal airway obstruction and increased airways responsiveness to methacholine rather suggest that the increased serum IFN-y levels reflect an ongoing inflammatory process that determines the clinical manifestations of airway disease in atopic asthma. In ovalbumin-challenged mice it has been found that treatment with antibodies to IFN-y selectively abolished development of airway hyperresponsiveness, whereas antibodies to IL-5 inhibited BAL eosinophilia [12], suggesting that INF-y and I L-5 act on different phenomena. It has been reported that symptomatic asthma is associated with the production of additional cytokines, including tumour necrosis factor-a (TNF-a), granulocyte/macrophage colony stimulating factor (GM-CSF) and IL-6 [13] in BAL fluid, while the levels of GM-CSF in the bronchial epithelium decrease upon treatment with corticosteroids [14]. Unfortunately, measurements of IFN-y in BAL fluid in the present study were frequently below the level of detection, probably as a consequence of dilution. Nevertheless, the present results suggest that the serum IFN-y level can also be regarded as a reflection of the severity of airway inflammation in atopic asthma.
The higher serum levels of IFN-y in present asthmatic patients and their positive correlation with serum IL-4 levels apparently do not fit with the hypothesis that Th2 lymphocytes are upregulated and Th1 lymphocytes are suppressed in atopic asthma. It could be argued that the Th1/Th2-imbalance is responsible for the development of lgE-mediated inflammation. Once asthma is present, other factors may also contribute to the modulation of the severity of airway inflammation. Furthermore, serum cytokine levels probably do not reflect specifically the secretion by peripheral blood Th 1 or Th2 lymphocytes. IFN-y can also be produced by other cell types, including type 0 T-helper (Th0) and CD8 lymphocytes, granulocytes, eosinophils and macrophages, present in the bronchial wall, peripheral blood and other body compartments. It has been shown that the in vitro production of IFN-y by peripheral blood mononuclear cells is not increased in patients with asthma [4,6, 15]. We assume that the increased IFN-y values found in the serum of the present patients originated from cellular sources outside the vascular compartment. Interestingly, Krug et al [15] recently demonstrated a higher percentage of IFN-y producing T-cells in the BAL fluid of asthmatic subjects as compared to atopic and nonatopic controls. On the other hand, Ying et al [13] showed a significant lower number of CD3- and CD68-positive cells encoding messenger ribonucleic acid (mRNA) for IFN-y in the bronchial biopsies of atopic asthmatics as compared to healthy controls, but no information was presented on production of the protein. Up to now, no attention has been paid to cytokine signals in granulocytes and CDS-positive cells, nor to cytokine signals in the epithelial airway mucosa. This leaves open the possibility of an increased IFN-y production by inflammatory cells in the superficial layer of the bronchial wall.
113
Chapter 8
In contrast to other studies [3,6], serum IL-4 levels did not correlate with lgE, and serum IL-5 did not correlate with blood eosinophils. We have no clear explanation for our negative findings. It can be hypothesized that the indices of lgE-mediated inflammation are obscured by other inflammatory processes which are more related with the clinical manifestation of asthma.
This study also demonstrated higher levels of I FN-y in the serum at night than during the day in the asthmatic patients. The rise of IFN-y levels did not, however, correlate with day-night changes in PEF or FEV 1 . Thus, no evidence was found to suggest that increased nocturnal airway narrowing in atopic asthma is associated with increased cytokine production at night. This finding is in line with previous observations, showing that an increased nocturnal airway obstruction merely occurs in asthmatic subjects with signs of increased inflammatory cellular activation in the airways during the day [17].
In conclusion, elevated serum levels of IFN-y in subjects with atopic asthma were correlated with an increased airways responsiveness to methacholine and a larger 16-04 h peak expiratory flow variation. In contrast, no relationship was found between the levels of interleukin-4 and interleukin-5 and the parameters of clinical manifestation of asthma. The results suggest that the serum interferon-y level can be regarded as a reflection of the severity of airway inflammation in atopic asthma. Up to now, the origin of serum interferon-y is unclear. More studies are needed to detect the cellular sources and to clarify the exact roles of interferon-y and other pro-inflammatory cytokines in asthma.
References 1 . Oosterhotf Y, Hoogsteden HC, Rutgers B, Kauffman HF, and Postma DS.
Lymphocyte and macrophage activation in bronchoalveolar lavage fluid in nocturnal asthma. Am J Respir Grit Care Med 1 995; 1 51 :75-81 .
2. Kay AB. T lymphocytes and their products in atopic allergy and asthma. Int Arch Allergy Appl lmmunol 1 991 ;94: 1 89-93.
3 . Matsumoto T, Miike T, Yamaguchi K, Murakami M , Kawabe T, Yodoi J. Serum levels of soluble IL-2 receptor, IL-4 and lgE binding factors in childhood allergic diseases. Clin Exp lmmunol 1 991 ;85:288-92.
4. Hashimoto S, Amemiya E , Tomita Y, Kobatashi T, Arai K, Yamaguchi M , et al. Elevation of soluble IL-2 receptor and IL-4, and nonelevation of IFN gamma in sera from patients with allergic asthma. Ann Allergy 1 993;71 :455-8.
5. Matsumoto K, Taki F, Miura M, Matsuzaki M, Takagi K. Serum levels of soluble IL-2R, IL-4, and soluble Fe epsilon RII in adult bronchial asthma. Chest 1 994; 1 05 :681 -6.
6. Tang ML, Coleman J, Kemp AS. lnterleukin-4 and interferon gamma production in atopic and nonatopic children with asthma. Clin Exp Allergy 1 995;25:51 5-21 .
7 . Corrigan CJ, Kay AB. CD4 T lymphocyte activation in acute severe asthma.
114
Relationship to disease severity and atopic status. Am Rev Respir Dis 1 990; 1 41 :970-7.
Elevated serum interferon-y
8. Saito H, Hayakawa T, Mita H, Yui YS, Shida T. Augmentation of leukotriene C4 production by gamma interferon in leukocytes challenged with an allergen. Int Arch Allergy Appl /mmuno/ 1 988;87:286-93.
9. Brand PLP, Kerstjens HAM, Kauffman HF, de Monchy JGR, and the Dutch CNSLD Study Group. Interpretation of skin tests to house dust mite and relationship to other allergy parameters in patients with asthma and COPD. J
Allergy Clin lmmunol 1 993;91 :560-70 1 0. Rijcken B, Schouten JP, Weiss ST, Speizer FE, Van der Lende R. The rela
tionship of nonspecific bronchial reponsiveness to respiratory symptoms in a random population sample. Am Rev Respir Dis 1 987; 1 36:62-8
1 1 . Oosterhoff Y, Koeter GH, de Monchy JGR, Postma OS. Circadian variation in airway responsiveness to methacholine, propranolol and AMP in atopic asthmatic subjects. Am Rev Respir Dis 1 993; 1 47:351 -57
1 2. Hessel EM, Van Oosterhout AJM, Van Ark I, Van Esch B, Hofman G, Van Loveren H, Savelkoul HFJ, Nijkamp FP. Development of airway hyperresponsiveness is dependent on interferon-y and independent of eosinophil infiltration. Am J Respir Cell Mo/ Biol 1 997; 1 6:325-34
1 3. Broide DH, Lotz M, Cuomo AJ, Coburn DA, Federman EC, Wasserman SI . Cytokines in symptomatic asthma airways. J Allergy Clin Jmmunol 1 992;89:958-67
1 4. Sousa AR, Poston RN, Lane SJ, Nakhosteen JA, Lee TH. Detection of GMCSF in asthmatic bronchial epithelium and decrease by inhaled corticosteroids. Am Rev Respir Dis 1 993; 1 47: 1 557-61
1 5. Krug N, Madden J, Redington AE, Lackie P, Djukanovic R, Schauer U, et al. T cell cytokine profile evaluated at the single cell level in BAL and blood in allergic asthma. Am J Respir Cell Mo/ Bio/ 1 996; 1 4:31 9-26.
1 6. Ying S, Durham SR, Corrigan CJB, Hamid Q, Kay AB. Phenotype of cells expressing mRNA for TH2 type (interleukin-4 and interleukin-5) and TH1 type (interleukin-2 and interferon-y) cytokines in bronchoalveolar lavage and bronchial biopsies from atopic asthmatic and normal subjects. Am J Respir Cell Mo/ Bio/ 1 995; 1 2:477-87.
1 7. Postma OS, Oosterhoff Y, Van Aalderen WMC, Kauffman HF, Wempe JB, Koeter GH. Inflammation in nocturnal asthma? Am J Respir Grit Care Med 1 994; 1 50:583-86.
1 1 5

-
Chapter 9
Summary, discussion, conclusions and perspectives
9.1 Summary
In chapter 2. 1 -2.4 some methodological problems of obtaining, processing and evaluating bronchial biopsies were described. In chapter 3-5 the inflammatory data of our study on bronchial biopsies in nocturnal asthma were presented. Finally, in chapter 6-7 markers of inflammation in other body compartments were described, i.e. in exhaled air, serum and BAL fluid.
Chapter 2. 1 was directed to the problem of obtaining large and intact biopsies from the central airways. It is known that bronchial biopsies are rather small and that optimal biopsy technique is necessary to obtain high quality tissue samples, as sufficient length of intact basement membrane and sufficient depth of submucosal tissue are required. In this study, size and qualitative aspects of bronchial biopsies from non-asthmatic subjects, obtained by forceps of three different sizes (types FB-1 9C, FB-21 C and FB-35C) were compared. We concluded that bronchial biopsies obtained with forceps type FB-35C were the largest, but showed significant damage and crush artifacts. In contrast, biopsies obtained with forceps type FB-21 C were only slightly smaller and had more intact basement membrane, more submucosal depth and well preserved morphology. Therefore, forceps type FB-21 C was used in further studies of this thesis.
In chapter 2.2 inflammatory cell counts in sections of fresh frozen and glycol methacrylate (GMA)-embedded biopsies were compared. An important advantage of GMA embedding is its better morphology, although the main impression is that its lower antigenicity may be a problem. Indeed lower numbers of CD3-, CD4- and CDS-positive cells were counted in GMA-embedded biopsies as compared to snap-frozen biopsies. In addition, only a weak correlation between CD3-, CD4- and CDS-positive cell counts of both techniques was observed, which we we supposed to be caused by an ongoing loss of antigenic properties during storage of plastic-embedded tissue. An additional study confirmed that CD3-, CD4- and CDS-positive cell numbers decrease significantly within a few months after embedding in glycol methacrylate. Therefore, we recommended to process glycol methacrylate-embedded biopsies as soon as possible. Further, we considered frozen tissue to be preferred in the quantitative evaluation of inflammatory cells (like CD3, CD4, CDS, EG2) because of ease of the method and reliable cell counting. On the
1 1 7
Chapter 9
other hand, glycol methacrylate-embedded tissue shows superior morphology and seems attractive to study qualitative aspects as cell-cell and cellmatrix relationships.
In chapter 2.3 we evaluated the amount of tissue that is necessary to produce constant cell counts in frozen sections of bronchial biopsies. We formulated this question because immunopostive cells are present in varying densities in lung tissue, even within a section of a bronchial biopsy. CD4-, CDSand EG2-immuno positive cells in bronchial biopsies of five healthy and five asthmatic subjects were evaluated. Twenty successive areas of 0.1 x 0.1-mm submucosa were counted, and changes larger than 1 0 % were recorded. We demonstrated that the cumulative counting of 10 areas of 0.1 x 0.1-mm along 1 mm intact basement membrane is sufficient to obtain constant cell numbers (per area), provided that a proper selection of a representative part of the biopsy has been made. Also, it appeared that volume artefacts and presence of smooth muscle and glands were responsible for the observed changes in cell number above 10% after counting 1-mm basement membrane.
In chapter 2.4 the semi-quantitative and quantitative way of evaluating inflammatory cells in bronchial biopsies were compared. Fresh frozen airway biopsies of 7 asthmatic and 7 healthy subjects were immunostained for CD3, CD4, CDS, CD25 and EG2 antigen, and examined in a quantitative and semiquantitative way. This study demonstrated that both methods correlated in the evaluation of CD4-, CDS-, and EG2-immunopostive cells. The quantitative method showed a higher density of CDS- and CD25-positive cells in biopsies of asthmatic subjects as compared to healthy subjects, whereas the semi-quantitative method showed a relatively higher density of CD3- and CD4-positive cells. This partial agreement may be explained by the intrinsic features of the two methods. The semi-quantitative method includes the deeper and larger parts of the biopsy, and has the advantage that biopsies of lower morphological quality do not have to be discarded. In contrast, the quantitative method includes only small parts of the biopsy (generally the superficial layers) selected on basis of integrity of the tissue and absence of smooth muscles and glandular epithelium. We concluded that with high cell density the semi-quantitative method is more useful , whereas with low cell density the quantitative method may be preferred.
In chapter 3 we tested the hypothesis that bronchial biopsies of subjects with nocturnal asthma have more inflammatory cells at night than at daytime, in contrast to subjects without nocturnal asthma. We recruited 13 healthy controls, 15 atopic asthmatic patients with PEF-variation � 15% and 10 atopic asthmatic patients with PEF-variation > 15%. Bronchial biopsies were obtained at 16 h and 4 h, with an interval of 1-2 weeks. Bronchial biopsies were used to study inflammatory cells (chapter 3), vascular adhesion molecules
118
Summary, discussion, conclusions and perspectives
(chapter 4), iNOS expression (chapter 5) and vascular eNOS expression (chapter 6). The number of CD3-, CD4-, CD8-, CD25-, AA 1 (tryptase)- and EG2- immunopositive cells in the submucosa did not increase at night in any of the three groups. The number of EG2-positive cells in the two asthmatic groups was significantly higher than in healthy controls, both at 16 h and 04 h. The number of EG2-, CD4- and CD25-positive cells at 04 and at 16 h tended to be higher in asthmatics with a PEF variation > 15% as compared to asthmatics with PEF variation � 15%. We concluded that increased nocturnal airway obstruction is not caused by increased numbers of inflammatory cells in the bronchial submucosa at night.
Because vascular adhesion molecules are thought to be important for the recruitment of inflammatory cells in the process of asthmatic airway inflammation, we hypothesized in chapter 4 that adhesion molecules are expressed more extensively at night than at daytime in subjects with nocturnal asthma. Biopsies were double-immunostained for CD31 in combination with P-selectin, E-selectin, ICAM-1 or VCAM-1. We found no significant day-night differences in expression of adhesion molecules in any of the three groups. The expression of VCAM-1 in biopsies of asthmatic patients was significantly higher than in biopsies of healthy controls: 4.5 vs 2.5 % at 16 h and 11 vs 0 % at 04 h. In asthma, VCAM-1 expression was positively correlated with the number of EG2- and CD25-positive cells both at 16 h and 04 h, suggesting a role for VCAM-1 in the ongoing airway wall inflammation of asthma.
Because Nitric Oxide (NO) may be involved in the pathogenesis of asthmatic airway inflammation, we hypothesized in chapter 5 that the inducible form of NO synthase (iNOS) is upregulated at night in bronchial biopsies of patients with nocturnal asthma. Biopsies were immunostained with a polyclonal antibody against iNOS. We demonstrated that the expression of iNOS in the bronchial wall was not increased at night in the asthmatic patients with increased nocturnal airway obstruction, nor in the other subjects. Moreover, biopsies of asthmatic patients more frequently contained iNOS positive cells than those of healthy controls, both at 16 and 04 h. In contrast to reports in the literature, iNOS immunoreactivity in the epithelium was very sparse and seemed mainly located in migrating inflammatory cells and not in epithelial cells. Interestingly, epithelial and endothelial iNOS positivity at 04 h was accompanied by a higher degree of submucosal EG2 positivity. We concluded that nocturnal asthma can not be explained by circadian variations in iNOS expression and that increased expression of iNOS and EG2-positive cells probably represent a common underlying mechanism.
In chapter 6 the variable or constant presence of endothelial NO synthase in bronchial biopsies of subjects with and without nocturnal asthma was studied. Biopsies obtained at 16 and 4 h were double-immunostained for eNOS
119
Chapter 9
in combination with a common endothelial antigen (CD31 ). The degree of immunopositivity for eNOS was evaluated and expressed as the percentage of CD31 positive vessels encountered in complete sections of a biopsy. The mean (SD) 16-04 h changes in % eNOS expression in biopsies of healthy controls, asthmatic patients with mild and severe nocturnal airway obstruction differed significantly: -17 ( 44), -14 (24) and + 13 (27) %. Moreover, the 16-04 h change in eNOS expression in biopsies of asthmatic subjects significantly correlated with PEF variation. We concluded that patients with large swings in airway diameter lack the normally occurring increase in eNOS expression at night.
As Nitric Oxide in exhaled air may reflect airway inflammation we hypothesized in chapter 7 that subjects with nocturnal asthma show a circadian rhythm in exhaled Nitric Oxide, inverse to the circadian rhythm in airway obstruction. We measured NO concentration together with FEV 1 at 12, 16, 20, 24, 4, 8 and 12 h in 6 healthy controls, 8 asthmatics without and 6 asthmatics with increased nocturnal airway obstruction. Exhaled NO did not show a significant circadian variation in any of the three groups as assessed by cosinor analysis (in contrast to the FEV 1 in both asthma groups). However, exhaled NO concentration at 4 h was higher than at 16 h in subjects with nocturnal asthma; otherwise values at all time points were similar. Mean NO concentration was significantly higher in subjects with nocturnal asthma than in subjects without nocturnal asthma and higher again than in healthy controls, at all time points. Moreover, mean NO levels over 24 hours correlated with 16-4 h PEF variation in the asthmatic group. We concluded that subjects with nocturnal asthma exhale higher NO levels during the whole day, suggesting more severe airway wall inflammation than subjects without nocturnal asthma.
In chapter 8 we studied the relationship between important cytokines in serum and BAL fluid and clinical manifestation of atopic asthma. IL-4, IL-5 and IFN-y levels of serum and BAL fluid (obtained at 16 and 04 h) were determined in 17 atopic asthmatics and 8 non-atopic healthy subjects, participating in another study on nocturnal asthma. Serum IFN-y increased significantly at night in asthmatic subjects. Serum IL-4, IL-5 and IFN-y levels in asthmatic subjects were significantly higher than in healthy controls, both at 16 and 04 h. In asthmatic subjects, serum IFN-y at both time points correlated negatively with PC20 methacholine and positively with the mean 16-04 h PEF variation. In contrast, no relationship was found between the serum levels of IL-4 and IL-5 and the parameters of clinical manifestation of asthma. BAL fluid levels of IL-4, IL-5 and IFN-y were frequently below the level of detection, may be as a consequence of dilution. We concluded that serum IFN-y levels may indicate the severity of airway wall inflammation in subjects with atopic asthma. We suggested a.o. epithelial cells to be the cellular source of serum interferon-y.
120
9.2 Discussion
Findings
Summary, discussion, conclusions and perspectives
The findings reported in thesis on nocturnal asthma do not support the hypothesis that nocturnal asthma is resulting from increased airway wall inflammation at night. Biopsies from the central airways obtained at 1 6 and 4 h did not show a nocturnal increase in the density of inflammatory cells in the submucosa (CD3, CD4, CDS, CD25, AA 1 , EG2), expression of iNOS positive cells in epithelium, submucosa and endothelium, or expression of vascular adhesion molecules in the submucosa ( ICAM-1 , VCAM-1 , E-selectin, Pselectin). Our results are in line with the two recent biopsy studies showing no signs of a nocturnal increase in the density of inflammatory cells in the central airways of subjects with nocturnal asthma (1 ,2). With respect to other compartments, we demonstrated in exhaled air of subjects with nocturnal asthma a nocturnal increase in NO concentration, and in serum of mild to moderate severe asthmatics a nocturnal increase in IFN-y concentration. However, both exhaled NO and serum IFN-y showed relatively small increases, and there was no relation with the nocturnal decreases in PEF or FEV 1 . Therefore, a pathophysiologial relationship between circadian changes in inflammation and circadian changes in lung function is less likely.
Our findings do support the hypothesis that nocturnal asthma is resulting from increased airway inflammation in general (both at day and night). First of all, the degree of hyperresponsiveness for adenosine monophosphate and methacholine was found to be higher in subjects with increased nocturnal airway obstruction (in line with (3,4)). Secondly, the expression of CD4, CD25, EG2 and vascular VCAM-1 tended to be higher in the subjects with nocturnal asthma. Finally, exhaled Nitric Oxide concentrations of subjects with nocturnal asthma were higher than in subjects without nocturnal asthma and higher than in healthy controls, during the whole day.
Selection of subjects with nocturnal asthma This study selected somewhat milder asthmatic subjects with increased nocturnal airway obstruction than other research groups (1 ,2,58). Like other research groups, we prospectively divided the participating subjects based on PEF variation measured at home. However, different research groups use different criteria to set out PEF variation, ranging from 2 to 6 PEF measurements per day, during 3 up to 7 subsequent days. In our biopsy study, the participating subjects were classified according PEF measurements 6 times per day, during 3 subsequent days. In the hospital, our subjects with a PEF variation > 1 5% rather frequently showed a small nocturnal worsening of airway obstruction (Figure 1 A). It is possible that the normally occurring increase in airway obstruction at night was hampered because of an altered sleep pattern or increased circulating catecholamines, probably due to being in the
1 21
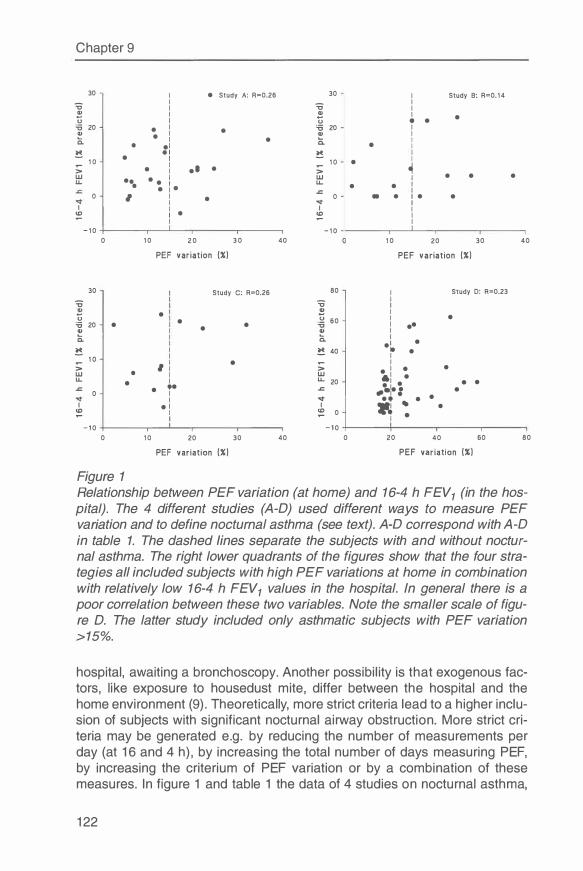
Chapter 9
30 I e Study A: R=0.26 30 I Study B: R=0. 1 4 � I � I
I I a, I � I e 0 I u • e '6 20 e
I e
'6 20 I � I a, I
e I e 0.. I 0. e e l e I � e t � e I I 1 0 I 1 0 e
� ;: e I e l e ;: w e
e I w I e e e
LI.. eee l e u. e e e �
0 I I e 0 • e t e e
I '<I' I I I I I � I e � I
I I - 1 0 - 1 0
0 1 0 2 0 3 0 40 1 0 20 30 40
PEF variation (%) PEF variation (%)
30 Study C: R=0.26 80 I Study D: R=0.23
� � I I
e a, I 0 -� 60 I e
'6 20 e e
e I ee e � � I
I 0. a. e l e
� � 40 • e I 1 0 e I ;: I ;:
e I e e
w e w 61 e LI.. e I LI.. 20
e l e e e � e ,e � e 0 I -•1e : I '<I' e • e e
I e l I ·�
• e
� I � 0 • I I - 1 0 - 1 0
0 1 0 20 30 40 0 20 40 60 80
PEF variation (%) PEF variat ion (%)
Figure 1 Relationship between PEF variation (at home) and 16-4 h FEV1 (in the hospital). The 4 different studies (A-O) used different ways to measure PEF variation and to define nocturnal asthma (see text). A-O correspond with A-O in table 1. The dashed lines separate the subjects with and without nocturnal asthma. The right lower quadrants of the figures show that the four strategies all included subjects with high PEF variations at home in combination with relatively low 16-4 h FEV1 values in the hospital. In general there is a poor correlation between these two variables. Note the smaller scale of figure D. The latter study included only asthmatic subjects with PEF variation >15%.
hospital, awaiting a bronchoscopy. Another possibility is that exogenous factors, like exposure to housedust mite, differ between the hospital and the home environment (9). Theoretically, more strict criteria lead to a higher inclusion of subjects with significant nocturnal airway obstruction. More strict criteria may be generated e.g. by reducing the number of measurements per day (at 16 and 4 h), by increasing the total number of days measuring PEF, by increasing the criterium of PEF variation or by a combination of these measures. In figure 1 and table 1 the data of 4 studies on nocturnal asthma,
122
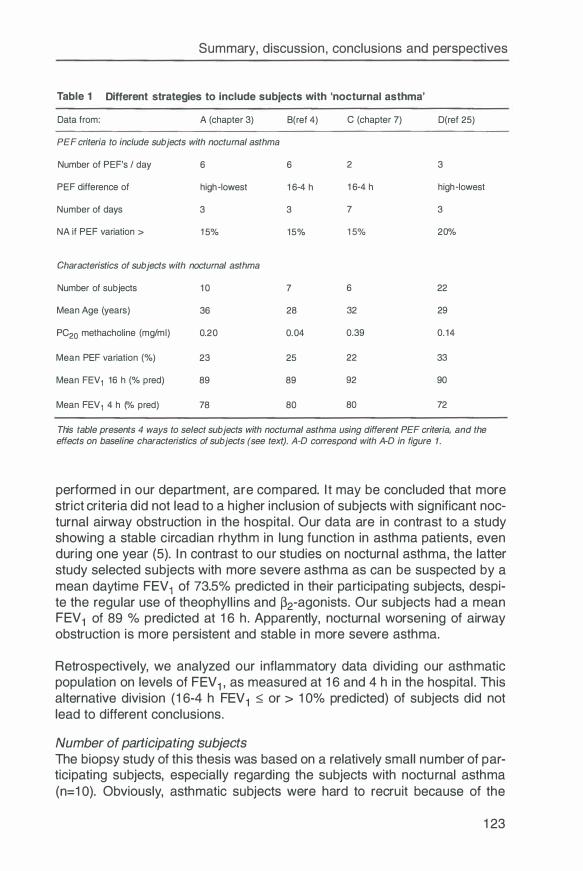
Summary, discussion, conclusions and perspectives
Table 1 Different strategies to include subjects with 'nocturnal asthma'
Data from: A (chapter 3) B(ref 4) C (chapter 7) D(ref 25)
PEF criteria to include subjects with nocturnal asthma
Number of PEF's / day 6 6 2 3
PEF difference of high-lowest 16-4 h 16-4 h high-lowest
Number of days 3 3 7 3
NA if PEF variation > 1 5% 15% 15% 20%
Characteristics of subjects with nocturnal asthma
Number of subjects 10 7 6 22
Mean Age (years) 36 28 32 29
PC20 methacholine (mg/ml) 0.20 0.04 0.39 0.14
Mean PEF variation (%) 23 25 22 33
Mean FEV 1 16 h (% pred) 89 89 92 90
Mean FEV 1 4 h (% pred) 78 80 80 72
This table presents 4 ways to select subjects with nocturnal asthma using different PEF criteria, and the effects on baseline characteristics of subjects (see text). A-O correspond with A-O in figure 1.
performed in our department, are compared. It may be concluded that more strict criteria did not lead to a higher inclusion of subjects with significant nocturnal airway obstruction in the hospital. Our data are in contrast to a study showing a stable circadian rhythm in lung function in asthma patients, even during one year (5). In contrast to our studies on nocturnal asthma, the latter study selected subjects with more severe asthma as can be suspected by a mean daytime FEV 1 of 73.5% predicted in their participating subjects, despite the regular use of theophyllins and �2-agonists. Our subjects had a mean FEV 1 of 89 % predicted at 16 h. Apparently, nocturnal worsening of airway obstruction is more persistent and stable in more severe asthma.
Retrospectively, we analyzed our inflammatory data dividing our asthmatic population on levels of FEV 1 , as measured at 16 and 4 h in the hospital. This alternative division (16-4 h FEV 1 � or > 10% predicted) of subjects did not lead to different conclusions.
Number of participating subjects The biopsy study of this thesis was based on a relatively small number of participating subjects, especially regarding the subjects with nocturnal asthma (n=10). Obviously, asthmatic subjects were hard to recruit because of the
123

Chapter 9
strict inclusion and exclusion criteria and the intensive study design (twice a bronchoscopy, stopping inhaled corticosteroids). The consequence of this low number of participating subjects is that negative findings (e.g. no nocturnal increase in inflammatory events), may be falsely negative. Richmond, making power calculations to establish the optimal sample size for a longitudinal analysis on inflammatory cell numbers in bronchial biopsies, estimated that approximate 15 subjects would be the optimal number to detect significant changes in inflammatory cell counts (a=0.05, �=0.20) (10). According to Sant et al (11 ), even 25 subjects are needed to detect in a longitudinal study a doubling difference in the number of EG2-positive cells (a=0.05, �=0.20). Apparently, high numbers of subjects are needed to detect rather small differences in inflammatory cell numbers. On the other hand, clinically relevant changes in airway wall inflammation have been detected with even low numbers of participating subjects, as has been demonstrated by numerous biopsy studies (2, 1218). Moreover, we also found significant differences with this number of individuals per group between healthy and asthmatic subjects.
eNOS, NO, interferon-y An interesting finding in this thesis are the significant day-night changes in vascular eNOS (chapter 6), exhaled NO (chapter 7) and serum interferon-y (chapter 8). At 4 h at night, exhaled NO and serum IFN-y were increased in subjects with nocturnal asthma, whereas vascular eNOS expression was relatively decreased. At night, it has also been shown that subjects with nocturnal asthma have an increased IL-1 � concentration and an increased production of oxygen radicals by inflammatory cells in BAL fluid (7,8). These results suggest that higher amounts of pro-inflammatory cytokines are released at night, contributing to higher levels of oxidative stress. Further, high amounts of pro-inflammatory cytokines may downregulate eNOS at a posttranscriptional level (19-21 ). We feel that much of the above results have to be reconfirmed, and that future research should focus on the cellular sources of pro-inflammatory cytokines and on the exact sides of NO production in the bronchial tree.
124
9.3 Conclusions
Summary, discussion, conclusions and perspectives
The most important observations of this thesis on nocturnal asthma may be summarized regarding the methodological questions:
1. Bronchial biopsies obtained with forceps type FB-21 C are only slightly smaller than biopsies obtained with forceps type FB-35C. Forceps FB-21 C should be preferred because it produces more intact basement membrane, more submucosal depth and well preserved morphology.
2. Inflammatory cell counts of fresh-frozen and plastic-embedded biopsies show a weak correlation because of an ongoing loss of antigenic properties during storage of plastic-embedded tissue. Therefore, we recommend to process plastic-embedded biopsies as soon as possible.
3. The cumulative counting of 10 areas of 0.1 x 0.1-mm along 1-mm intact basement membrane is sufficient to obtain constant cell numbers (per area).
4. The quantitative and semi-quantitative way of evaluating inflammatory cell density may correlate, but also differ significantly. With high cell density semi-quantitative evaluation is more useful, and with low cell density quantitative evaluation.
With regard to the biopsy findings:
5. The numbers of CD3-, CD4-, CDS-, CD25-, EG2- and tryptase positive cells are at night not higher than at day in asthmatic subjects with and without increased nocturnal airway obstruction. The former group tended to show a higher number of CD4-, CD25- and EG2-positive cells than the latter.
6. Expression of the vascular adhesion molecules E-selectin, P-selectin, ICAM-1 and VCAM-1 is at night not higher than at day in asthmatic subjects with and without increased nocturnal airway obstruction. VCAM-1 expression in asthmatic patients is significantly higher than in healthy controls, and is positively correlated with the number of EG2- and CD25-positive cells.
7. Expression of iNOS is at night not higher than at day in asthmatic patients with or without increased nocturnal airway obstruction. iNOS is more frequently expressed in asthmatic patients than in healthy controls. Epithelial cells express iNOS very sparsely, both in asthmatic and healthy subjects.
8. Vascular expression of eNOS is not constant. Expression of eNOS decreases at night in asthmatic subjects with PEF variation > 15%, opposite to subjects with PEF variation ::; 15%.
125
Chapter 9
Concerning exhaled Nitric Oxide:
9. Exhaled Nitric Oxide shows no circadian rhythm, inverse to the circadian rhythm in airway obstruction in subjects with or without nocturnal asthma. Exhaled NO concentrations are significantly higher in subjects with nocturnal asthma than in subjects without nocturnal asthma during the whole day.
With regard to cytokines in serum and BAL fluid:
10. Serum IL-4, IL-5 and IFN-y in asthmatic subjects are higher than in healthy controls, both at 16 and 4 h. Serum IFN-y concentration at night is higher than at day in asthmatic subjects. Serum IFN-y at 16 h and 4 h is negatively correlated with PC20 methacholine, and positively with 16-04 h PEF variation in asthmatic subjects.
Taking the most important data of this thesis into account we conclude that increased nocturnal airway obstruction in subjects with asthma is not the consequence of increased nocturnal inflammation in the central airways, but is an expression of more severe asthma.
126
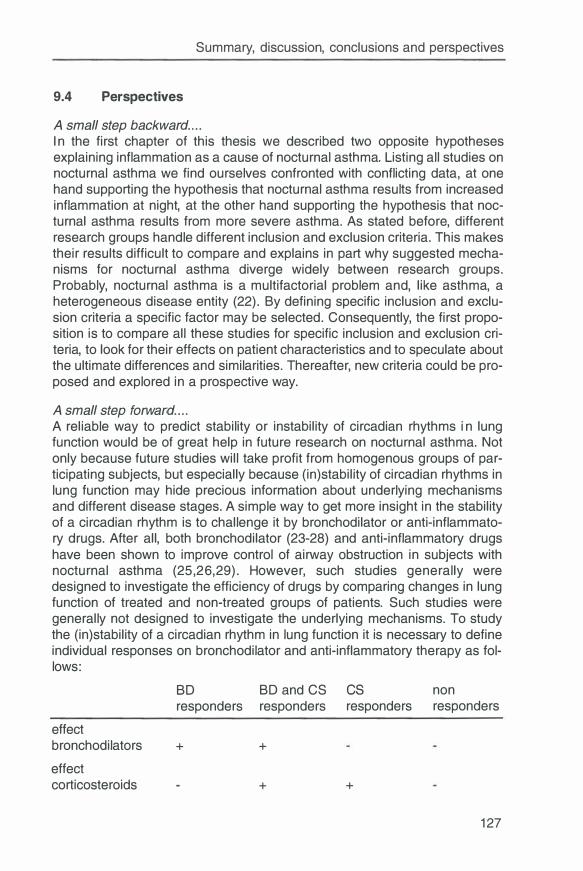
Summary, discussion, conclusions and perspectives
9.4 Perspectives
A small step backward .. . . I n the first chapter of this thesis we described two opposite hypotheses explaining inflammation as a cause of nocturnal asthma. Listing all studies on nocturnal asthma we find ourselves confronted with conflicting data, at one hand supporting the hypothesis that nocturnal asthma results from increased inflammation at night, at the other hand supporting the hypothesis that nocturnal asthma results from more severe asthma. As stated before, different research groups handle different inclusion and exclusion criteria. This makes their results difficult to compare and explains in part why suggested mechanisms for nocturnal asthma diverge widely between research groups. Probably, nocturnal asthma is a multifactorial problem and, like asthma, a heterogeneous disease entity (22). By defining specific inclusion and exclusion criteria a specific factor may be selected. Consequently, the first proposition is to compare all these studies for specific inclusion and exclusion criteria, to look for their effects on patient characteristics and to speculate about the ultimate differences and similarities. Thereafter, new criteria could be proposed and explored in a prospective way.
A small step forward . . . . A reliable way to predict stability or instability of circadian rhythms in lung function would be of great help in future research on nocturnal asthma. Not only because future studies will take profit from homogenous groups of participating subjects, but especially because (in)stability of circadian rhythms in lung function may hide precious information about underlying mechanisms and different disease stages. A simple way to get more insight in the stability of a circadian rhythm is to challenge it by bronchodilator or anti-inflammatory drugs. After all, both bronchodilator (23-28) and anti-inflammatory drugs have been shown to improve control of airway obstruction in subjects with nocturnal asthma (25,26,29). However, such studies generally were designed to investigate the efficiency of drugs by comparing changes in lung function of treated and non-treated groups of patients. Such studies were generally not designed to investigate the underlying mechanisms. To study the (in)stability of a circadian rhythm in lung function it is necessary to define individual responses on bronchodilator and anti-inflammatory therapy as follows:
8D 8D and CS cs non responders responders responders responders
effect bronchodilators + +
effect corticosteroids + +
127
Chapter 9
Of course such a division is quite artificial as the difference between responders and non-responders is an arbitrary one. Despite the methodological problems that can be anticipated, this division is in my opinion a fruitful way to deal with the heterogeneity of nocturnal asthma. It can be speculated that asthmatic subjects that show a complete abolition of their circadian rhythm in lung function after �2-mimetics have a low degree of airway inflammation, whereas those who show no significant or minor improvement suffer from a higher degree of inflammation. Theoretically, such an individual may become sensitive again for �2-mimetic therapy after treatment with corticosteroids, and migrate from the class of corticosteroid responders to the class of bronchodilator and corticosteroid responders. Another speculation is that the nonresponders on the right side of the above table suffer from i rreversible airway damage with airway remodeling. Future studies should therefore be focussing on the acute (reversible) and chronic (i rreversible) features of airway wall inflammation in these four groups.
Location of increased nocturnal airway obstruction An important question that has to be addressed in future research is whether increased nocturnal ai rway obstruction is settled in the large, intermediate or small airways. Because circadian variations in airway diameter are often small, the instrument that locates airway obstruction has to be sensitive and should not interfere with airway obstruction itself. Forced expiratory maneuvers therefore seem less valid because they lead to spirometer induced airway obstructions in susceptible individuals. Moreover, these maneuvers deliver mainly information about the airway resistance at the level of (sub)maximal inspi ration. Forced oscillation techniques measuring density dependence of pulmonary resistance have been proposed as a way to differentiate between peripheral and central airway obstruction, but this method failed to discriminate between normal subjects and patients with moderate airflow obstruction (30). Bronchoscopy measuring directly the peripheral airway resistance was able to detect a sevenfold higher resistance in stable asthmatics as compared to healthy controls, whereas spirometry detected no difference at all (31 ). However, this is a rather invasive procedure which also needs an esophageal balloon. Bronchography (32) has the advantage to visualize bronchi at the level of functional residual capacity, however the use of radio opaque contrasts will frequently lead to bronchospasm. With the improving qualities of HR-CT scan this seems an attractive technique to study in a non-invasive way the contribution of the small and large airways to (increased nocturnal) airway obstruction, without interfering with airway obstruction. HR-CT scan is able to visualize the bronchial tree from the first down to the sixt generation bronchi, whereas measurements of bronchi as small as 2 mm in diameter were found to be highly reproducible (33). HR-CT scan was able to detect small changes in the diameter of the large and small airways during exercise challenge followed by �-agonist induced bronchodilatations (34), as well as methacholine induced bronchoconstrictions (35).
128
Summary, discussion, conclusions and perspectives
Underlying mechanisms of increased nocturnal airway obstruction Not only the exact location but also the underlying mechanism of excessive airway narrowing is a challenging topic for future research in nocturnal asthma. An instrument to answer the simple question whether increased nocturnal airway obstruction results from an increase in the smooth muscle tone or from thickening of airway mucosa would be of great help. As far as known at present, such an instrument does not exist. Intuitively, forced oscillation techniques would be suitable to differentiate between changes in airway resistance due to smooth muscle contraction and airway wall thickening (36). However, these techniques are hardly sensitive enough to detect small circadian variations in airway diameter, and thus probably not sensitive enough to differentiate between underlying factors. Another way to differentiate is to investigate the effect of continuous positive airway pressure (CPAP) on circadian variations in the lung function (37). Theoretically, CPAP leads to relaxation of smooth muscle tone, without affecting mucosal thickening. However, interpretation of results will be difficult as CPAP also alters upper airway obstruction, snoring and sleep quality (38). Deep inspirations may also affect bronchomotor tone and retractile forces on the airways without altering mucosal thickening. In an elegant study, Liu in 1985 demonstrated that deep inspirations decrease airway resistance at 4 h more than at 16 h, in contrast to normal controls (36). They did not compare nocturnal asthmatics versus non-nocturnal asthmatics. Finally, with HR-CT scan it was demonstrated in asthmatic subjects that airway wall thickness (airway wall area) did not change after methacholine induced bronchoconstriction, in contrast to observations in healthy controls (35). However, HR-CT scan still has to be validated as an instrument to detect changes in airway wall thickness due to (nocturnal) changes in airway inflammation.
A new hypothesis for a new study If increased nocturnal airway obstruction is the expression of more severe airway inflammation the question remains how a circadian rhythm in airway diameter is mediated. The easiest explanation is that more severe airway inflammation leads to chronic thickening of airway mucosa and loss of airway diameter, superimposed on normally occurring circadian variations in bronchomotor tone. This mechanical explanation based on the ideas of Moreno (39) is not complete since more severe airway inflammation probably is accompanied by a continuous release of bronchoconstricting mediators and thus a tendency towards an increased bronchomotor tone contributing to increased airway narrowing. Apparently, at night there is a lack of counter regulating forces which protect the airway diameter at daytime. The most important broncho-protective mechanism in human airways is the �-sympathic nervous system, and indeed this system shows a circadian rhythm in serum (nor)epinephrine with a top at 16 h and a nadir at 4 h. Moreover, there are indications that severe asthmatic airway inflammation leads to a diminis-
129

Chapter 9
hed beta-adrenoceptor function of airway smooth muscle (40,41 ). Several components of asthmatic airway inflammation like bradykinin, pro-inflammatory cytokines, lipid mediators and reactive oxygen species have been suggested to impair the function of p-receptors (40,41 ). Therefore, it can be hypothesized that increased airway obstruction at night is caused by severe asthmatic airway inflammation, due to the combination of thickened airway wall mucosa, continuously increased smooth muscle tone, the physiological nocturnal nadir of serum (nor)epinephrine and an impaired P-adrenergic receptor function.
In this context it would be interesting to investigate in a prospective way the effects of inhaled corticosteroids on P-adrenergic function and expression in the bronchial wall of subjects with and without nocturnal asthma. In such a study the subjects with nocturnal asthma could be characterized in terms of responders and non-responders to p-mimetic and corticosteroid therapy. Genetic polymorphism for p-adrenoceptors could be studied in peripheral blood, thereby looking for the variant (Gly16) that is associated with nocturnal asthma (42). Impaired P-adrenergic receptor expression and activity could be explored in vivo by PET scanning of the lung (43,44), and by studying peripheral blood, bronchial washes or bronchial biopsies (45-47). Finally, the intimate relationship with increased airway inflammation could be studied in bronchial washes and biopsies focussing on inflammatory factors which potentially impair p-adrenergic receptor function. The above described study should compare day and night findings, because a significant nocturnal decrease of P-adrenergic receptor density and function in peripheral leucocytes has been demonstrated in the past (45).
In conclusion, this thesis about nocturnal asthma has answered some questions and provoked new ones. Most findings indicate that nocturnal asthma is the expression of more severe asthma. The next step is to study the exact relationship between more severe airway wall inflammation and the increased circadian rhythm in airway obstruction. Stability or instability of the circadian rhythm in airway obstruction might be investigated by looking to responses on bronchodilators and corticosteroids. From such studies, a better view on the relationship between airway wall inflammation and p-adrenergic receptor function may evolve, leading to understanding the development of nocturnal asthma.
References 1 . Mackay TW, Wallace WAH, Howie SEM, Brown PH, Greening AP, Church
MK, Douglas NJ. Role of inflammation in nocturnal asthma. Thorax 1 994;49:257-62.
2. Kraft M, Djukanovic R, Wilson S, Holgate ST, Martin RJ. Alveolar tissue inflammation in asthma. Am J Respir Grit Care Med 1 996; 1 54: 1 505-1 0.
130
Summary, discussion, conclusions and perspectives
3. Oosterhoff Y, Kauffman HF, Rutgers B, Zijlstra FJ, Koster G, Postma OS. Inflammatory cell number and mediators in bronchoalveolar lavage fluid and peripheral blood in asthmatic subjects with increased nocturnal airways narrowing. J Allergy C/in /mmuno/ 1 995;96:21 9-29.
4. Oosterhoff Y, Hoogsteden HC, Rutgers B, Kauffman HF, Postma OS. Lymphocyte and macrophage activation in bronchoalveolar lavage fluid in nocturnal asthma. Am J Respir Grit Care Med 1 995; 1 51 :75-81 .
5. Martin RJ, Cicutto LC, Ackerson LM. Stability of the circadian alteration in lung function in asthma. J Allergy Clin lmmunol 1 992;89:703-8.
6. Martin RJ, Cicutto LC, Smith HR, Ballard RD, Szefler SJ. Airways inflammation in nocturnal asthma. Am Rev Respir Dis 1 991 ; 1 43:35 1 -7.
7. Jarjour NN, Busse WW. Cytokines in bronchoalveolar lavage fluid of patients with nocturnal asthma. Am J Respir Grit Care Med 1 995; 1 52: 1 474-7.
8. Jarjour NN, Busse WW, Calhoun WJ. Enhanced production of oxygen radicals in nocturnal asthma. Am Rev Respir Dis 1 992; 1 46:905-1 1 .
9. Oosterhoff Y, Koster GH, de Monchy JGR, Postma OS. Circadian variation in airway responsiveness to metacholine, and AMP in atopic asthmatic subjects. Am Rev Respir Dis 1 993; 1 47:51 2-7 .
1 0. Richmond I, Booth H, Ward C, Walters EH. lntrasubject variability in airway inflammation in biopsies in mild to moderate stable asthma. Am J Respir Grit Care Med 1 996; 1 53:899-903.
1 1 . Sant JK, Willems LNA, Evertse CE, Hooijer R, Sterk PJ, van Krieken JHJM. Repeatability of measures of inflammatory cell number in bronchial biopsies in atopic asthma. Eur Respir J 1 997(in press).
1 2. Aalbers R, de Monchy JG, Kauffman HF, Smith M , Hoekstra Y, Vrugt B, Timens W. Dynamics of eosinophil infiltration in the bronchial mucosa before and after the late asthmatic reaction . Eur Respir J 1 993;6:840-7.
1 3. Trigg CJ, Manolitsas ND, Wang J, Calderon MA, McAulay A, Jordan SE, Herdman MJ, Jhalli N, Duddle JM, Hamilton SA, et al. Placebo controlled immunopathologic study of four months of inhaled corticosteroids in asthma. Am J Respir Grit Care Med 1 994; 1 50: 1 7-22.
1 4. Beasley R, Roche WR, Roberts JA, Holgate ST. Cellular events in the bronchi in mild asthma and after bronchial provocation . Am Rev Respir Dis 1 989; 1 39:806-1 7.
1 5. Bentley AM, Durham SR, Robinson OS, Menz G, Storz C, Cromwell 0, Kay AB, Wardlaw AJ. Expression of endothelial and leukocyte adhesion molecules interacellular adhesion molecule-1 , E-selectin, and vascular cell adhesion molecule-1 in the bronchial mucosa in steady state and allergen induced asthma. J Allergy Clin lmmunol 1 993;92:857-68.
1 6. Montefort S, Gratziou C, Goulding D, Polosa R, Haskard DO, Howarth PH, Holgate ST, Carroll M P. Bronchial biopsy evidence for leukocyte infiltration and upregulation of leukocyte endothelial cell adhesion molecules 6 hours after local allergen challenge of sensitized asthmatic airways. J C/in Invest 1 994;93: 1 41 1 -21 .
1 7. Finnerty JP, Lee C, Wilson S, Madden J, Djukanovic R, Holgate ST. Effects of theophylline on inflammatory cells and cytokines in asthmatic subjects: a placebo controlled parallel group study. Eur Respir J 1 996;9: 1 672-7.
1 8. Haahtela T, Laitinen A, Laitinen LA. Using biopsies in the monitoring of inflammation in asthmatic patients. Allergy 1 993;48:65-9.
131
Chapter 9
1 9. Yoshizumi M, Perrella MA, Burnett JC, Jr. , Lee ME. Tumor necrosis factor down regulates an endothelial nitric oxide synthase mRNA by shortening its halflife. Gire Res 1993;73:205-9.
20. Mohamed F, Monge JC, Gordon A, Cernacek P, Blais D, Stewart DJ. Lack of role for Nitric Oxide (NO) in the selective destabilization of endothelial NO Synthase mRNA by Tumour Necrosis Factor-a. Arteriose/er Thromb Vase Biol 1 995; 1 5:52-7.
21 . Harrison DG, Sayegh H, Ohara Y, I noue N, Venema RC. Regulation of expression of the endothelial cell nitric oxide synthase. C/in Exp Pharm Physio/ 1 996;23:251 -5.
22. Aas K. Heterogeneity of bronchial asthma. Subpopulations or different stages of the disease. Allergy 1981 ;36:3-1 4.
23. Petrie GR, Chookang JY, Hassan WU, Morrison JF, O'Reilly JFP, Shneerson JM, Tang OT, Ning AC, Turbitt ML. Bambuterol: effective in nocturnal asthma. Respir Med 1 993;87:581 -5.
24. Muir JF, Bertin L, Georges D. Salmeterol versus slowrelease theophylline combined with ketotifen in nocturnal asthma: a multicentre trial. French Multicentre Study Group. Eur Respir J 1992;5: 1 1 97-2000.
25. Weersink EJ, van Zomeren H, Koeter GH, Postma OS. Treatment of nocturnal airway obstruction improves daytime cognitive performance in asthmatics. Am J Respir Grit Care Med 1 997; 1 56: 1 1 44-50.
26. Dahl R, Pedersen B, Hagglof B. Nocturnal asthma: effect of treatment with oral sustained release terbutaline, inhaled budesonide, and the two in combination. J Allergy C/in lmmunol 1 989;83:81 1 -5.
27. Cox ID, Hughes OT, McDonnell KA. lpratropium bromide in patients with nocturnal asthma. Postgrad Med J 1 984;60:526-8.
28. Kraft M, Wenzel SE, Bettinger CM, Martin RJ. The effect of salmeterol on nocturnal symptoms, airway function, and inflammation in asthma. Chest 1 997; 1 11 : 1 249-54.
29. Beam WR, Weiner DE, Martin RJ. Timing of prednisone and alterations of airways inflammation in nocturnal asthma. Am Rev Respir Dis 1 992; 1 46: 1 524-30.
30. Guillemi S, Wright JL, Hogg JC, Wiggs BR, Macklem PT, Pare PD. Density dependence of pulmonary resistance: correlation with small airway pathology. Eur Respir J 1 995;8:789-94.
31 . Wagner EM, Liu MC, Weinmann GC, Permutt S, Bleecker ER. Peripheral lung resistance in normal and asthmatic subjects. Am Rev Respir Dis 1 990; 1 41 : 584-8.
32. Shioya T, Solway J, Munoz NM, Mack M, Leff AR. Distribution of airway contractile responses within the major diameter bronchi during exogenous bronchoconstriction. Am Rev Respir Dis 1 987; 1 35: 1 1 05- 1 1 .
33. Seneterre E, Paganin F, Brue! JM, Michel FB, Bousquet J . Measurement of the internal size of bronchi using high resolution computed tomography (HRCT}. Eur Respir J 1 994;7:596-600.
34. Paganin F, Vignola AM, Seneterre E, Brue! JM, Chanez P, Bousquet J . Heterogeneity of airways obstruction in asthmatic patients using High Resolution Computed Tomography. Chest 1 995; 1 07: 1 45s-6s.
35. Okazawa M, Muller N, McNamara AE, Child S, Verburgt L, Pare PD. Human airway narrowing measured using High Resolution Computed Tomography. Am J Respir Grit Care Med 1 996; 1 54: 1 557-62.
132
Summary, discussion, conclusions and perspectives
36. Liu YN, Sasaki H, Ishii M, Sekizawa K, Hida W, Ichinose M, Takishima T. Effect of circadian rhythm on bronchomotor tone after deep inspiration in normal and in asthmatic subjects. Am Rev Respir Dis 1 985; 1 32:278-82.
37. Wang CH, Lin HC, Huang TJ, Yang CT, Yu CT, Kuo HP. Differential effects of nasal continuous positive airway pressure on reversible or fixed upper and lower airway obstruction . Eur Respir J 1 996;9:952-9.
38. Chan CS, Woolcock AJ, Sullivan CE. Nocturnal asthma: role of snoring and obstructive sleep apnea. Am Rev Respir Dis 1 988; 1 37: 1 502-4.
39. Moreno RH, Hogg JC, Pare PD. Mechanics of airway narrowing. Am Rev Respir Dis 1 986; 1 33: 1 1 71 -80.
40. Nijkamp FP, Henricks PA. Receptors in airway disease. Am Rev Respir Dis 1 990; 1 41 :S 1 45-50.
41 . Barnes PJ. Beta adrenerg receptors and their regulation. Am J Respir Grit Care Med 1 995; 1 52:838-60.
42. Turki J, Pak J, Green SA, Martin RJ, Liggett SB. Genetic polymorphisms of the B2-adrenerg receptor in nocturnal and nonnocturnal asthma. J Clin Invest 1 995;95: 1 635-41 .
43. Visser TJ, Van Waarde A, Doze P, Elsinga PH, Van der Mark TW, Kraan J, Ensing K, Vaalburg W. Visualization of pulmonary B2-adrenoceptors in vivo, using the agonist [ 1 1 C]formeterol and positron emission tomography. Submitted 1 997.
44. Hayes MJ, Qing F, Rhodes CG, Rahman SU, Ind PW, Sriskandan S, Jones T, Hughes JMB. In vivo quantification of human pulmonary �-adrenoceptors: effects of �-agonist therapy. Am J Respir Grit Care Med 1 996; 1 54: 1 277-83.
45. Szefler SJ, Ando R, Cicutto LC, Surs W, Hill MR, Martin RJ. Plasma histamine, epinephrine, cortisol, and leukocyte beta adrenergic receptors in nocturnal asthma. Clin Pharmacol Ther 1 991 ;49:59-68.
46. Van Oosterhout AJ, Stam WB, Vanderschueren RG, Nijkamp FP. Effects of cytokines on beta adrenoceptor function of human peripheral blood mononuclear cells and guinea pig trachea. J Allergy Clin /mmuno/ 1 992;90:340-8.
47. Hamid QA, Mak JCW, Sheppard MN, Corrin B, Venter JG, Barnes PJ. Localization of B2-adrenoceptor messenger RNA in human and rat lung asing in situ hybridization: correlation with receptor autoradiography. Eur J Pharmacol 1 991 ;206: 1 33-8.
1 33

Abbreviations
ADP AEC AMP ATP ATS BAL
BM bNOS CD Cl cNOS ECP EON
eNOS ERS FEV1 FEV1 % pred GM-CSF H&E HEWS HLA
HR-CT ICAM lg iNOS IFN IL LFA
LPS LTC4 NA NANG NNA nNOS NO NOS PAF PBS PC20 AMP
PC20 methacholine
: adenosin diphosphate : 3-amino-9-ethylcarbazole : adenosine monophosphate : adenosine triphosphate : American Thoracic Society : bronchoalveolar lavage : basement membrane : brain NO synthase : cluster of differentiation : confidence interval : constitutive NO synthase : eosinophil cationic protein : eosinophil derived neurotoxin : endothelial NO synthase : European Respiratory Society : Forced Expiratory Volume in 1 second : FEV 1 as percentage of the predicted value : granulocyte monocyte colony stimulating factor : hematoxylin and eosin : histamine equivalent wheal size : human leucocyte antigen : high resolution computed tomography : intercellular adhesion molecule : immunoglobulin : inducible NO synthase : interferon : interleukin : leucocyte function associated molecule : lipopolysaccharide : leukotriene C4 : nocturnal asthma : non-adrenergic non-cholinergic : non-nocturnal asthma : neuronal NO synthase : nitric oxide : NO synthase : platelet activating factor : phosphate-buffered saline : provocative concentation of AMP required to produce a 20% fall in FEV 1
: provocative concentation of methacholinebromide required to produce a 20% fall in FEV 1
135
PEF PEF var PET PGD2 PMA
Th cell SD
SEM SPSS TNF VCAM
VLA
136
: peak expiratory flow : PEF variation : positron emission tomography : prostaglandin 02 : phorbol myristate acetate : T helper lymphocyte : standard deviation : standard error of the mean : statistical package for the social sciences : tumour necrosis factor : vascular cell adhesion molecule : very late (activation) antigen
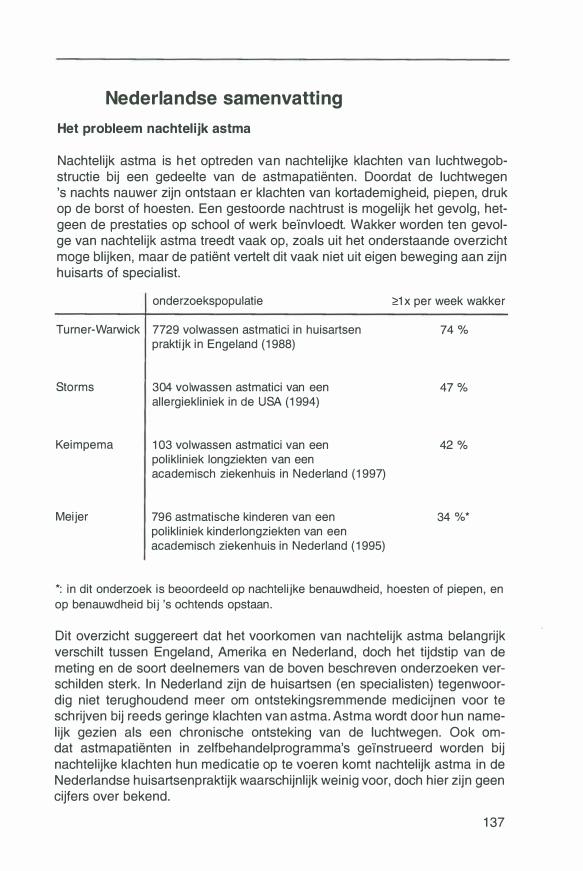
Nederlandse samenvatting
Het probleem nachtel ijk astma
Nachtelijk astma is het optreden van nachtelijke klachten van luchtwegobstructie bij een gedeelte van de astmapatienten. Doordat de luchtwegen 's nachts nauwer zijn ontstaan er klachten van kortademigheid, piepen, druk op de borst of hoesten. Een gestoorde nachtrust is mogelijk het gevolg, hetgeen de prestaties op school of werk be'invloedt. Wakker worden ten gevolge van nachtelijk astma treedt vaak op, zeals uit het onderstaande overzicht moge blijken, maar de patient vertelt dit vaak niet uit eigen beweging aan zijn huisarts of specialist.
onderzoekspopulatie
Turner-Warwick 7729 volwassen astmatici in huisartsen praktijk in Engeland (1 988)
Storms
Keimpema
Meijer
304 volwassen astmatici van een allergiekliniek in de USA (1 994)
1 03 volwassen astmatici van een polikliniek longziekten van een academisch ziekenhuis in Nederland (1 997)
796 astmatische kinderen van een polikliniek kinderlongziekten van een academisch ziekenhuis in Nederland (1 995)
�1 x per week wakker
74 %
47 %
42 %
34 %*
*: in dit onderzoek is beoordeeld op nachtelijke benauwdheid, hoesten of piepen, en op benauwdheid bij 's ochtends opstaan.
Dit overzicht suggereert dat het voorkomen van nachtelijk astma belangrijk verschilt tussen Engeland, Amerika en Nederland, doch het tijdstip van de meting en de soort deelnemers van de boven beschreven onderzoeken verschilden sterk. In Nederland zijn de huisartsen (en specialisten) tegenwoordig niet terughoudend meer om ontstekingsremmende medicijnen voor te schrijven bij reeds geringe klachten van astma. Astma wordt door hun namelijk gezien als een chronische ontsteking van de luchtwegen. Ook omdat astmapatienten in zelfbehandelprogramma's ge'instrueerd worden bij nachtelijke klachten hun medicatie op te voeren komt nachtelijk astma in de Nederlandse huisartsenpraktijk waarschijnlijk weinig voor, doch hier zijn geen cijfers over bekend.
1 37
Toegenomen ontsteking in de luchtwegen als oorzaak van nachtel ijk astma
Vele factoren zijn in het verleden genoemd als oorzaak voor de nachtelijke toename van luchtwegobstructie zoals:
- het prikkelen van de slokdarm door terugstromen van zure maaginhoud (reflux) ten gevolge van de liggende houding,
- de verminderde lichaamsactiviteit met daardoor een negatieve invloed van het onwillekeurige zenuwstelsel op de spierspanning in de luchtwegen,
- onvoldoende ophoesten en keelschrapen met daardoor opstapeling van slijm in de luchtwegen,
- de liggende houding waardoor de borstkas meer in een uitademingsstand staat,
- een nachtelijke toename van ontsteking in de luchtwegen, met daardoor een nachtelijke verdikking van het slijmvlies en een verkramping van spiertjes in de luchtwegen.
Nachtelijke toename van ontsteking in de luchtwegen als oorzaak voor nachtelijk astma vormt het centrale thema van dit proefschrift. Bestudering van luchtwegontsteking kan op een directe en I of indirecte wijze geschieden. lndirecte bestudering van ontsteking vindt plaats door de gevolgen ervan te meten, zoals door de bepaling van de aspecifieke (niet-allergische) overgevoeligheid van de luchtwegen. Aspecifieke overgevoeligheid uit zich bij een astmapatient door het optreden van hoesten, benauwdheid of piepen op de borst na inademen van mist, koude of rook. Dit gebeurt bij gezonde mensen niet. Meer directe informatie kan verkregen warden door de luchtwegen te spoelen en vervolgens de celrijke vloeistof op te vangen (broncho alveolaire lavage of BAL). De meest directe informatie wordt echter verkregen door het wegnemen van stukjes slijmvlies uit luchtwegen (bronchusbiopten), tijdens een zogenaamde kijkingreep (bronchoscopie).
In hoofdstuk 1 warden de voornaamste bevindingen van verschillende biopten BAL studies in het kader van nachtelijk astma op een rijtje gezet. De twee bioptstudies die op het moment van starten van dit onderzoek nog niet verschenen waren laten in de centrale luchtwegen geen dag-nacht verschillen in ontsteking zien. Wei zijn er BAL studies die een nachtelijk toename van ontsteking demonstreren bij patienten met nachtelijk astma i.t.t. patienten zonder nachtelijk astma. Daarentegen zijn er ook BAL studies die deze toename niet demonstreren maar juist aantonen dat patienten met nachtelijk astma zowel overdag als 's nachts in de luchtwegen meer ontsteking hebben dan patienten zonder nachtelijk astma.
138
Nederlandse samenvatting
Dit proefschrift onderzoekt met biopten uit de centrale luchtwegen of nachtelijk astma het gevolg is van een nachtelijke toename in luchtwegontsteking. Is dit niet het geval dan is nachtelijk astma mogelijk het gevolg van een ernstiger ontsteking in de luchtwegen, zowel overdag als 's nachts.
De resultaten
De hoofdstukken 2. 1 tot en met 2.4 beschrijven methodologische problemen die opgelost moesten warden v66r aanvang van de bioptstudie. Deze hoofdstukken beschrijven de voor- en nadelen van drie verschillende biopteurs (FB-19C, FB-21 C, FB-35C), van twee verschillende inbedmethodes (vries, plastic), van verschillende hoeveelheden luchtwegslijmvlies ter evaluatie van ontsteking (0.01-0.20 mm2) , en van twee verschillende manieren om de dichtheid van het ontstekingsinfiltraat vast te leggen (kwantitatief, semikwantitatief). In dit proefschrift werden de biopten uiteindelijk genomen met de biopteur FB-21 C, zij werden diepgevroren in Tissue Tek (-80°C), en het aantal ontstekingscellen werd op een kwantitatieve manier gescoord in 0.1 mm2 luchtwegslijmvlies.
Hoofdstuk 3 beschrijft de kenmerken van 13 gezonde- en 15 astmatische proefpersonen die deelnamen aan het bioptonderzoek. De astmatici werden ingedeeld in 1 0 patienten met- en in 15 patienten zonder nachtelijk astma op basis van een piekstroomvariatie > of :::; 15%. De piekstroom is de hoogste stroomsterkte van de lucht die tijdens een maximaal krachtige uitademing op een meter afgelezen wordt. Hoe lager de stroomsterkte is, hoe nauwer de luchtwegen zijn tijdens uitademen. De piekstroomvariatie in dit onderzoek was gebaseerd op piekstroommetingen thuis, gemeten gedurende 3 dagen, 6 x per dag, met behulp van een mini-Wright Peakflow meter. Voorwaarde voor deelname aan het onderzoek was de afwezigheid van een recent luchtweginfect, roken, en gebruik van ontstekingsremmende medicijnen (met name inhalatie corticostero'iden). Astmapatienten met een piekstroomvariatie groter dan 15% werden 's nachts vaker wakker en hadden een ernstiger aspecifieke overgevoeligheid van de luchtwegen dan astmapatienten met een piekstroomvariatie lager dan of gelijk aan 15%. Luchtwegbiopten die op 4 uur 's middags en 4 uur 's nachts genomen werden lieten geen dag-nachtverschil in het aantal ontstekingscellen zien, ook niet in de groep van astmapatienten met een hoge piekstroomvariatie. De voornaamste ontstekingscel in de luchtwegen van astmapatienten is de eosinofiele granulocyt, en ook in deze studie werd in vergelijking met gezonde controles een hoge dichtheid aan geactiveerde eosinofiele (of EG2 positieve-) cellen gevonden in de luchtwegbiopten. Astmapatienten met een toegenomen piekstroomvariatie neigden tot een groter aantal EG2 positieve cellen dan astmapatienten met een lage piekstroomvariatie, zowel overdag als 's nachts. Wij concluderen dat nachtelijk astma niet gepaard gaat met een nachtelijke toename van het aan-
139
tal ontstekingscellen in de centrale luchtwegen. Veeleer lijkt het erop dat nachtelijk astma een uiting is van een ernstiger ontsteking, zowel overdag als 's nachts. In hoofdstuk 4 t/m 6 bestuderen we andere aspecten van ontsteking in dezelfde patienten als hoofdstuk 3. In hoofdstuk 4 werden de adhesiemoleculen E-selectine, P-selectine, ICAM-1, en VCAM-1 bestudeerd. Deze adhesie- of kleefmoleculen bekleden de binnenkant van de bloedvatwand en warden belangrijk geacht voor het aantrekken van ontstekingscellen uit de bloedbaan. Vergelijkbaar aan de de dichtheid van ontstekingscellen, kon er geen dag-nachtverschil aangetoond warden in de aanwezigheid van deze adhesiemoleculen. Wei werd een correlatie gevonden tussen de aanwezigheid van VCAM-1 op de vaatwand en EG2 positieve cellen in het bronchusslijmvlies, zowel om 16 als om 4 uur. Dit sluit aan op recente bevindingen in de literatuur. In hoofdstuk 5 werd de aanwezigheid van een belangrijk ontstekingsenzym bestudeerd, namelijk het induceerbare stikstofmonoxyde synthase (iNOS). Een toegenomen nachtelijke vrijzetting van ontstekingseiwitten (cytokines) zou theoretisch kunnen leiden tot een toegenomen aanwezigheid van iNOS en stikstofmonoxyde (NO), hetgeen weer tot zwelling en ontsteking van de luchtwegen kan leiden. In de biopten konden wij echter geen dagnacht verschil in expressie van iNOS aantonen. In hoofdstuk 6 werd het constitutief (constant aanwezig) stikstofmonoxyde synthase van de vaatwand (eNOS) in de bronchusbiopten onderzocht. Astmapatienten met een hoge piekstroomvariatie toonden een nachtelijk daling in eNOS i .t.t. astmapatienten met een lage piekstroomvariatie en gezonde controles. eNOS expressie blijkt dus als constitutief enzym gedurende de dag te varieren. Er zijn diverse factoren en consequenties te noemen waarom patienten met nachtelijk astma een ander dag-nacht ritme in hun eNOS expressie hebben dan patienten zonder nachtelijk astma, doch een en ander blijft op dit moment nog speculatief. Ook hier concluderen wij dat nachtelijk astma, wat betreft de boven genoemde ontstekingsaspecten, niet gepaard gaat met een nachtelijke toename van onsteking.
In hoofdstuk 7 wordt de aandacht verlegd naar een indirectere maat voor luchtwegontsteking, namelijk het NO in de uitademingslucht. Om een grotere kans te hebben om patienten met nachtelijk astma te vinden, werd de piekstoom niet 3 dagen maar 7 dagen lang gemeten, en niet 6x maar 2x per dag, op 16 en 4 uur. Vervolgens werd tijdens een ziekenhuisopname van 1 dag, om de 4 uren de NO concentratie en de longfunctie gemeten bij 6 gezonde proefpersonen, 8 astmatici met een lage piekstroomvariatie (� 15%), en 6 astmatici met een hoge piekstroomvariatie (>15%). De astmatici met een hoge piekstroomvariatie lieten 's nachts een hogere waarde in de NO concentratie zien dan overdag: 50 versus 42 ppb. De gemiddelde NO waarde over de gehele dag van de astmapatienten met een hoge piekstroomvariatie was significant hoger dan van astmapatienten met een lage piekstroom-
140
Nederlandse samenvatting
variatie: 46 versus 27 ppb, en die waarden waren weer hager dan die van gezanden. Het verschil tussen de twee astmagraepen was aanzienlijk grater dan het dag-nacht verschil in NO binnen de graep astmapatienten met een hage piekstroamvariatie. Deze bevindingen suggereren dat de luchtwegantsteking bij patienten met nachtelijk astma gedurende de gehele dag meer uitgespraken is dan bij patienten zander nachtelijk astma.
In hoofdstuk 8 warden de resultaten besproken van cytakinemetingen in perifeer bloed en BAL vloeistof van patienten die deelnamen aan een andere studie over nachtelijk astma. Cytokines zijn boodschapper eiwitten die een sturende functie hebben bij ontstekingsprocessen zoals astma. De cytokines die belangrijk geacht warden voor het eosinofiele karakter van de astmatische ontsteking, namelijk IL-4 en IL-5, bleken verhoogd aanwezig te zijn in het serum van astmatici, zowel overdag als 's nachts. Tot onze verrassing was echter ook het serum interferon-y bij de astmatici verhoogd, een cytokine dat juist het easinofiele karakter van de astmatische ontsteking zou onderdrukken. Serum interferon-y bleek zowel om 16 uur 's middags als om 4 uur 's nachts positief gecorreleerd te zijn met de hoogte van de piekstroomvariatie en de ernst van de aspecifieke overgevoeligheid van de luchtwegen, terwijl serum IL-4 en IL-5 dit niet lieten zien. In deze cytokine studie hadden wij dus opnieuw geen aanwijzingen voor een nachtelijke toename in ontsteking als oorzaak voor de nachtelijke toename in I uchtwegobstructie.
lnterpretatie van resultaten
In hoofdstuk 9 wordt op basis van bovenstaande bevindingen geconcludeerd dat er meer argumenten zijn voor de hypothese dat nachtelijk astma een uiting is van een ernstiger ontsteking in de luchtwegen overdag en 's nachts, dan voor de hypothese dat nachtelijk astma het gevolg is van een nachtelijke toename in de luchtwegontsteking.
De voornaamste kritiek die op de studie gegeven kan warden betreft de insluitcriteria voor nachtelijk astma. Ondanks het feit dat de gemiddelde piekstroomvariatie thuis hoger was dan 15%, trad nachtelijk wakker warden slechts in 5 van de 1 O patienten op, en bleek de nachtelijke verslechtering van de longfunctie in het ziekenhuis gering. Dit laatste probleem bleek niet oplosbaar door de criteria voor nachtelijk astma strenger te maken. Het bepalen van een piekstroamvariatie over 7 i.p.v. 3 dagen, of een groepsindeling op basis van een piekstroomvariatie grater dan 20% i.p.v. 15%, leidt niet tot het vaker insluiten van personen met een belangrijke nachtelijke luchtwegobstructie in het ziekenhuis (lees 9.2). Het vinden van proefpersonen met een stabiel (toegenomen) dag-nacht ritme in de luchtwegobstructie
141

is blijkbaar niet goed mogelijk door het thuis meten van herhaalde piekstroommetingen. Om in de toekomst patienten in te sluiten met een stabiel dag-nacht ritme wordt het voorstel gedaan deze stabiliteit te toetsen met luchtweg verwijdende en ontstekingsremmende medicijnen. Tenslotte wordt gehypothetiseerd over de tot stand koming van het toegenomen dag-nacht ritme in luchtwegobstructie bij nachtelijke astmapatienten. Waarom hebben patienten met nachtelijk astma relatief meer luchtwegobstructie om 4 uur 's nachts dan andere astmapatienten, en ook gezonde controles ? Bij het hypothetiseren hierover wordt uitgegaan van de voornaamste bevinding van dit proefschrift namelijk dat patienten met nachtelijk astma geen dag-nacht ritme in luchtwegontsteking hebben, maar wel een hogere ontstekingsgraad overdag en 's nachts. De hypothese wordt voorgesteld dat de hogere ontstekingsgraad van de luchtwegen leidt tot een chronische vernauwing, welke de normaal optredende dag-nacht verschillen in luchtwegobstructie accentueert. Dit effect zou verder versterkt kunnen warden doordat een hogere ontstekingsgraad van de luchtwegen leidt tot een lagere gevoeligheid van de luchtwegen voor luchtweg verwijdende stoffen in de bloedbaan. Omdat deze luchtweg verwijdende stoffen (adrenaline en noradrenaline) een dieptepunt om 4 uur 's nachts hebben wordt het dag-nacht ritme van de luchtwegobstructie versterkt. Onderzoek op patienten met een stabiel dag-nacht ritme in de luchtwegobstructie zal in de toekomst duidelijk moeten maken of een toegenomen luchtwegonsteking met daardoor een lagere gevoeligheid voor luchtweg verwijdende stoffen de doorslaggevende factor is voor nachtelijk astma.
142
Dankwoord
DANKWOORD
Nachtelijke benauwdheid is een eenzame beleving. Daar waar gezonde personen 's nachts hun accu opladen, staan patienten met nachtelijk astma vaak 's ochtends gebroken op. Harold Horowitz heeft dit energie verslindende proces invoelbaar gemaakt met zijn gedicht 'Night attack' (zie voorin). Mijn doel was het om nachtelijk astma niet alleen invoelbaar, maar vooral begrijpbaar te maken.
lk dank dan ook het Nederlands Astma Fonds voor de geboden mogelijkheid om dit te onderzoeken. Het zijn echter ook de proefpersonen van dit onderzoek die een compliment verdienen. Zij lieten zich vrijwillig bloed afnemen, huidallergietesten verrichten, de luchtwegen vernauwen, en zelfs twee keer een bronchoscoop introduceren. De nachtelijke scopie heeft bij hen hopelijk niet tot nachtmerries of een geconditioneerd wakker warden op 4 uur geleid.
Goed onderzoek is niet mogelijk zonder een goed onderzoeksplan. Hiervoor hebben mijn voorgangers Johan Wempe, Ytske Oosterhoff, Els Weersink en Roel Aleva de basis gelegd, naast natuurlijk mijn beide promotores. Professor Dirkje Postma ben ik dankbaar voor het telefoontje naar Nijmegen 4 jaren geleden. Natuurlijk kon zij toen nog niet bevroeden wat allemaal nodig is om een weerbarstig karakter als het het mijne te moeten stimuleren, afremmen en bijsturen. Wetenschap bedrijven is een sociaal proces, en niemand is zich daar meer bewust van dan Dirkje. Beste Dirkje, ik hoop dat je in de toekomst nog vele jonge ( en soms wat oudere) personen de weg zult wijzen in wetenschappelijk niemandsland. Ook professor Wim Timens ben ik dankbaar voor het zijn van een steun en toeverlaat. Hij toonde mij de 'derde dimensie' van zijn vak, en ik ben er van overtuigd dat wij samen meer hebben gezien dan 'inflammatoire soep'. Beste Wim, ik hoop dat je ook bij vele anderen het heilige vuur voor het mooie vak immunopathologie zult ontsteken. Vergeef me als ik te vaak sprak over pathologische anatomie i.p.v. pathologie, en over longgeneeskunde i.p.v. longziekten.
Jan Kraan wil ik bedanken voor de bijstand die hij verleende met name in de begin periode van het onderzoek. Ook de analisten op het research laboratorium pathologie ben ik dankbaar voor hun geduld en toewijding. Mieke, Gineke en Bea waren zelfs bereid een verplichte vrije dag op te offeren voor het evalueren van het beruchte iNOS, vlak voor een groot congres. Sindsdien heeft de term 'deadline' meer betekenis voor ons. Bea, Mieke, Rob, Steven en Ronald kregen de twijfelachtige eer om de nachtelijke bronchoscopieen te mogen assisteren. Wij allen weten ondertussen dat een ziekenhuis, net als de eigen fysiologie, 's nachts anders functioneert dan overdag, tot en met het droogijs en de buizenpost toe. Overdag assisteerde het vaste personeel van de longbehandelkamer meestal bij de bronchoscopieen.
1 43
Daarbij moet speciaal Alie Smidt genoemd warden omdat zij tijdens het gehele project zorgvuldig waakte over de gewenste bronchoscopen en biopteurs. Naast de directe medewerkers aan het nachtelijk astmaproject ben ik dank verschuldigd aan de longartsen en arts-assistenten van afdeling longziekten van het AZG. In drukke periodes werd ik bijvoorbeeld zonder problemen vrijgesteld van belastende klinische en / of poliklinische taken. Tenslotte ben ik professor Gerard Koeter dankbaar. Op de achtergrond was hij steeds betrokken bij het onderzoek, en stelde mij in staat om naast het onderzoek als longarts te blijven functioneren. De secretaresses Petra, Erika en Christa waren mij ook welgezind en steunden mij waar mogelijk.
De leden van de Cara Research Groep in Groningen hebben verder bijgedragen aan mijn wetenschappelijke vorming. Een keer per week gedurende 4 jaren bij elkaar komen was niet alleen leerzaam maar ook gezellig. Je leert elkaars kracht en zwakheden kennen en dit geeft een extra band. Niets is zo leuk om (soms half voorbereid) een plan te lanceren, laagdrempelig te mogen reageren, een idee tot op het bot uit te kleden, en vervolgens weer op maat aan te kleden. Dit creatieve groepsproces is de kracht van de Groningse Cara Research Groep.
Miriam wil ik bedanken voor het accepteren van de 'partnerarme' periode van de afgelopen 4 jaren. Nu het s-je van de drs weggepoetst is, komt er vast weer meer tijd voor gezellige dingen.
Tenslotte ben ik mijn ouders dankbaar voor hun belangeloze liefde. Door de vrijheid die ik van hun kreeg heb ik mijn eigen weg kunnen vinden en is de verschijning van dit boekje uiteindelijk mogelijk geworden.
144
Related Documents